Aircraft loading-related occurrence involving Airbus A330-303, VH-QPD, Sydney Airport, New South Wales, on 17 December 2017
Final report
Safety summary
What happened
On 17 December 2017, a Qantas A330 aircraft, registered VH-QPD, was being loaded with freight in preparation for an international passenger flight from Sydney, New South Wales to Beijing, China. After landing in Beijing, the operator’s freight agent identified that the aircraft had been loaded incorrectly. As a result, the aircraft exceeded its maximum take-off weight on departure from Sydney by 494 kg.
What the ATSB found
A decision by the flight crew to uplift additional fuel for the flight to Beijing led to a reduction in the aircraft’s freight capacity. This required the operator’s load control department to re-issue the ‘load instruction report’ for the flight. The re-issued report required that a 2,005 kg freight pallet be replaced with a lighter unit weighing 1,130 kg.
The required cargo variation was not actioned by the loading supervisor as electronic messages associated with the revised loading instruction were acknowledged without being correctly interpreted. That action was probably influenced by the supervisor’s experience that load changes were accompanied by verbal advice, and that did not occur on this occasion.
In addition, the loading irregularity was not immediately reported, as required by the operator’s procedures.
What's been done as a result
As a result of this, and other freight loading occurrences, Qantas have updated the technology used by staff directly involved in freight operations. The update involved the introduction of handheld scanning devices that automate much of the freight confirmation and mobile communication process using printed barcode and scanning technology. The hand scanners were implemented at most domestic and international Qantas ports by June 2019.
Qantas also advised that in order to reduce the potential for communication errors between those responsible for loading the aircraft, an amendment to their Weight and Balance Manual was implemented on 1 September 2019. The changes formalised communication associated with loading changes.
Safety message
This incident highlights a loading error that led to a maximum take-off weight exceedance during the conduct of a high-capacity passenger flight from Sydney to Beijing. Planning and loading of freight within this sector is often conducted in a time-pressured environment where delays can lead to scheduling issues. Effective communication between all parties responsible for aircraft loading can assist in reducing errors in such an operating environment.
Findings
From the evidence available, the following findings are made with respect to the loading-related occurrence involving an Airbus A330-303, registered VH-QPD on 17 December 2017. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
- An operational requirement for additional holding fuel resulted in the issuing of a revised load instruction to carry less cargo. This instruction was not actioned and led to a heavier freight pallet remaining on board the aircraft, instead of being exchanged for a lighter unit. The aircraft subsequently departed Sydney 875 kg above the weight listed in the revised load sheet and 494 kg above the aircraft's maximum take-off weight.
- The required cargo variation was not actioned by the loading supervisor as electronic messages associated with the revised loading instruction were acknowledged without being correctly interpreted. That action was probably influenced by the supervisor’s experience that load changes were accompanied by verbal advice, and that did not occur on this occasion.
Other factors that increased risk
- The loading irregularity was not immediately reported, which was not in accordance with the operator’s procedures for international airports, therefore delaying any assessment of the hazard presented by the exceedance of the aircraft’s maximum take-off weight.
Safety analysis
Introduction
The following analysis discusses the factors surrounding the incorrect freight pallet being loaded onto the Qantas A330, which resulted in an exceedance of the aircraft’s certified maximum take-off weight (MTOW) on departure.
Maximum take-off weight exceedance
An operational requirement for additional holding fuel resulted in the issuing of a revised load instruction to carry less cargo. This instruction was not actioned and led to a heavier pallet of freight remaining on board the aircraft, instead of being exchanged for a lighter unit. The aircraft subsequently departed Sydney 875 kg above the weight listed in the revised load sheet and 494 kg above the aircraft's maximum take-off weight.
The heavier freight was positioned in the underfloor hold close to the aircraft’s centre of gravity. This limited the potential for control of the aircraft to be affected. Further, the flight crew did not report any control or performance anomalies. While the outcome was benign in the case of QF107, the operational risk level is increased when any significant addition of freight and/or passengers remains unaccounted. Continued operation of an aircraft that has exceeded its certificated weight may lead to unaccounted structural damage and pose a safety risk.
Load instruction report not actioned
Although the presence of an electronic message of a cargo variation was acknowledged by the loading supervisor, as confirmed through pressing ‘OK’ on the iPad, it was not correctly interpreted. This led to the required cargo variation not being actioned. The lack of accompanying verbal advice from load control or the ramp office personnel meant that the usual prompt for the loading supervisor of a significant change to the aircraft cargo configuration did not exist. This variation from normal practice probably influenced the actions of the loading supervisor on this occasion.
Additionally, as the freight had been loaded and the forward cargo doors locked by the time the new electronic messages were received, it is possible that the messages were perceived as not relevant.
Reporting delay
A number of factors were identified that led to a three-week delay in the operator identifying, and subsequently reporting to the ATSB, that the aircraft MTOW limits had been exceeded when QF107 departed from Sydney.
The freight agent in Beijing did not immediately report the loading irregularity, as required by the Qantas procedures for international airports. Additionally, the initial occurrence report did not identify the ULD irregularity as a serious risk. This limited the ability of the company to understand and address the circumstances associated with the loading error.
Another factor identified by the operator’s investigation was the significant backlog of occurrence notifications awaiting processing. The backlog, in combination with a corporate shutdown period, led to the delay in identifying the significance of the MTOW breach and its subsequent reporting to the ATSB. Although there was no consequence associated with this occurrence, reporting delays can lead to an increased safety risk with regard to continued operation of an overstressed aircraft and/or identification of deficiencies in the loading process.
Context
Aircraft information
The A330-303 is a wide-body aircraft with underfloor cargo hold areas used for the carriage of baggage and freight (Figure 3). As is typical of most wide-body aircraft, all of the freight in the main cargo hold area is contained within a unit load device (ULD) (Figure 4). Specialised loading equipment is required with trained operators to ensure that the correct freight is loaded and positioned in accordance with the load instruction report (LIR).
The freight loading of wide-body aircraft is generally considered more complex than the loading of smaller, narrow-body aircraft in which freight is predominantly handled manually. The Airbus A330-303 aircraft cargo area consists of a forward and rear hold. Position 24P, which was associated with the loading of the incorrect ULD, is located in the forward hold as shown in Figure 5.
Figure 3: Typical A330-300 cargo hold

For reference only – internal detail of the A330‑300 rear cargo hold.I
Source: ATSB
Figure 4: Sample unit load devices being loaded into an A330 forward hold

Source: ATSB, image digitally altered to remove aircraft operator logos
Figure 5: A330-300 series cargo hold showing the position of location 24P (shaded red) within the forward hold

Source: Qantas, edited by ATSB
Freight management system
To facilitate communication between those responsible for loading a departing aircraft, Qantas used an electronic freight management system. The system provided a direct means of sending data or messages between staff at the load control office, the ramp and the ramp office. Once an aircraft’s departure load was determined, the freight was configured and an electronic copy of the LIR sent from the load control office to the loading supervisor’s portable electronic tablet.
The LIR was also sent to the ramp office where it was automatically printed for hard-copy distribution to ramp personnel. The ramp office was staffed by the ground services coordinator, whose role was to provide liaison between the load control office and ramp staff, at the aircraft.
Any additional announcements or instruction from the load control office were also sent to the loading supervisor’s tablet via this system. If a LIR was re-issued, Qantas procedures required the load control office to make contact with ramp staff.
Qantas reported that loading supervisors often received messages on their iPad while using the freight loading application. Though not necessarily directly related to the loading task, all messages received from load control were related to the specific flight being worked on. To use the application on the iPad, loading supervisors were required to ‘log in’ to a specific flight, in order to progressively record the ULDs loaded onto that aircraft.
Aircraft loading procedures
The LIR assigned a specific location to each container or pallet in order to maintain the calculated weight and balance of the aircraft. It was the responsibility of the loading supervisor on the ramp to ensure that each item of allocated freight was loaded and secured in the correct position.
The procedures describing the loading supervisor’s responsibilities are contained in the Qantas Ramp Operations Manual. Section 5.2.2.2 of the manual describes the specific operating procedures that the loading supervisor was required to follow when loading a departing aircraft, including:
When loading, the Loading Supervisor and in-hold operators are all responsible for confirming that the following details are checked and in accordance with the LIR:
• Flight Number and Date
• Destination
• ULD numbers (containerised aircraft), where the ULD numbers are noted on the LIR.
After finalising the load, section 5.2.2.3 of the Ramp Operations Manual required the loading supervisor to record the final load, including any variations to the planned load on the LIR before a final ‘ramp clearance’ is given to the load control office.
In the event that an LIR was re-issued, Section 5.7.2.4 of the Ramp Operations Manual indicated that the load control office would make contact with the loading supervisor or ramp staff. Section 5.5.3.2 of the Ramp Operations Manual required that:
If a subsequent edition of the LIR is received during the loading process the Loading Supervisor must instruct the team to cease loading until the next edition LIR has been received and distributed to ALL relevant operational team members.
The operator’s Weight and Balance manual specified that:
Load Control (are) to make contact with and Notify Ramp in the event that an LIR needs to be re-issued.
Load Instruction Report – Edition 2
When Edition 2 of the LIR for flight QF107 was issued by the load control office, a copy of the LIR was automatically printed in the ramp office. The officer responsible within the load control office contacted the ramp office by telephone and spoke to the ground services coordinator, advising of the new edition LIR.
Qantas advised the ATSB that they were unable to establish the person on duty within the ramp office at that time. Nor could that they establish why the message that a new LIR had been released was not conveyed directly to the loading supervisor and his team at the aircraft.
Loading supervisor
The loading supervisor performs an integral role during the loading of an aircraft. The main tasks of the loading supervisor include managing ramp staff during aircraft-loading activities and ensuring that freight, goods and other luggage are appropriately loaded on a departing aircraft. The loading supervisor responsible for loading QF107 had about 15 years of experience in aircraft freight operations. In relation to this loading occurrence, the loading supervisor advised the ATSB that he:
- had no clear recollection of the QF107 freight-loading irregularity. This was largely due to the high number of aircraft he had subsequently loaded and the latency period between the incident flight and the time it was reported.
- had no clear recollection that an Edition 2 LIR had been released, requiring an exchange in the freight pallet at position 24P from the 2,005 kg unit to the 1,130 kg unit.
- indicated that in his experience, ramp staff were always verbally contacted whenever the load control office released a new edition LIR. The announcement arrives from personnel within the ramp office, or via a radio or telephone call from the load control office.
- advised that messages were often received on the iPad that were not necessarily directly related to the current task.
Load control officer
The load control officer had about 16 years of experience in aircraft loading and freight operations and the following comments were provided to the ATSB:
- Contact with the loading supervisor or ramp staff was accomplished through various means including a messaging system on the loading supervisor’s portable tablet device (iPad), a phone call, or ground-to-ground radio contact.
- When a new Edition LIR is released from the load control office, it must be acknowledged by the loading supervisor on their iPad.
- When the Edition 2 LIR was issued, the freight management system was programmed to change the colour of position 24P from ‘green’ to ‘white’. That colour change would have been displayed on the loading supervisor’s iPad when he logged back into the system. It would have also required the loading supervisor to ramp clear position 24P again, despite already completing that task minutes earlier.
- The load control officer’s understanding was that the ground services coordinator within the ramp office would deliver a printed copy of the new edition LIR to the loading supervisor once Edition 2 had been released.
Ground services coordinator
Qantas advised the ATSB that they could not identify the duty officer (ground services coordinator) within the ramp office when Edition 2 of the load instruction report was released. The ATSB was therefore unable to interview that person to discuss the occurrence.
Communication and actions
The loading supervisor reported that he had always been verbally contacted by the load control officer via radio or telephone if an aircraft load plan had changed while he was on the ramp, and he had never previously simply been issued a change via iPad with no accompanying verbal notification. Therefore, his expectation was that if a change occurred in this case, it would be accompanied by a call.
Since this occurrence, Qantas has formalised a procedure for verbal communication to accompany any changes in the load instruction report (refer to section titled Safety issues and actions).
Operator’s investigation
The operator’s agents noted a discrepancy with the palletised freight during the evening of 18 December when the aircraft was unloaded in Beijing. The contents of the offload instruction report indicated that ULD PMC42559QQ (1,130 kg) should have been within the forward hold of the aircraft. The ATSB received an occurrence notification of the maximum take-off weight exceedance on 10 January 2018, approximately 3 weeks after the incident had occurred. The Qantas investigation into this occurrence detailed a number of factors that led to the reporting delay.
Operator’s notification procedures
In their investigation report of this loading occurrence, Qantas indicated that their procedures for international airports contained various options when addressing an operational incident. The response and level of escalation was dependant on the identified level of safety risk. The risks were categorised from Very Low through to Extreme. Incidents that led to a breach in the MTOW limits qualified as a Medium Risk requiring an immediate escalation to the company authorities. The Qantas procedures for international airports required that when an irregular load was identified, such as a misplaced ULD, an internal report was to be lodged within a 12-hour period.
The Qantas investigation established that the freight personnel in Beijing had not realised the aircraft MTOW limits had been exceeded by the ULD discrepancy. As such, the occurrence report was not identified as an occurrence notifiable to any authority. On 19 December 2018, two days after the occurrence had been identified, an internal notification report was lodged into the Qantas reporting system. The report was titled, ‘Miss Handle of Cargo’.
Due to a combination of the corporate Christmas shutdown period, the classification level of the notification, and a significant backlog of other accumulated notifications, the report relating to the MTOW exceedance remained in triage within the internal Qantas reporting system and unattended for another 10 days. On 9 January 2018, the significance of the ULD discrepancy was identified by a quality assurance manager who realised the aircraft’s MTOW had been exceeded. The occurrence report was then internally escalated and the ATSB was notified.
Previous loading-related occurrences
A search of the ATSB occurrence database was conducted for ’Aircraft loading’ occurrence types involving high-capacity, Australian-registered aircraft, throughout the years 2010 to 2019. The search returned 1,135 Aircraft Loading occurrences[3] over the 10-year reporting period. Nearly all of these reported occurrences involved passenger-carrying operations. They were further defined into three broad categories (displayed in Figure 6):
- Loading Related with 408 occurrences
- Dangerous Goods[4] with 752 occurrences
- Other with 18 occurrences.
Occurrence types identified as Loading Related have the potential to affect the aircraft weight and/or balance, aircraft structural integrity, aircraft performance and its flight characteristics. In the reporting period, there were 25, or about 6 per cent, of the notifications that described an impact on aircraft performance involving centre of gravity and/or maximum take-off weight. Of the 408 Loading Related occurrences within the 10-year reporting period, 12 investigations were commenced by the ATSB.[5] Most of the loading occurrences had minimal impact on the safety of operations and there were either people, processes, procedures, and/or engineering equipment to control the risks to the aircraft.
Figure 6: Aircraft Loading occurrence types over the period 2010 to 2019 (left chart), and (right chart), a subset of the Loading Related occurrence types with a descriptor breakdown
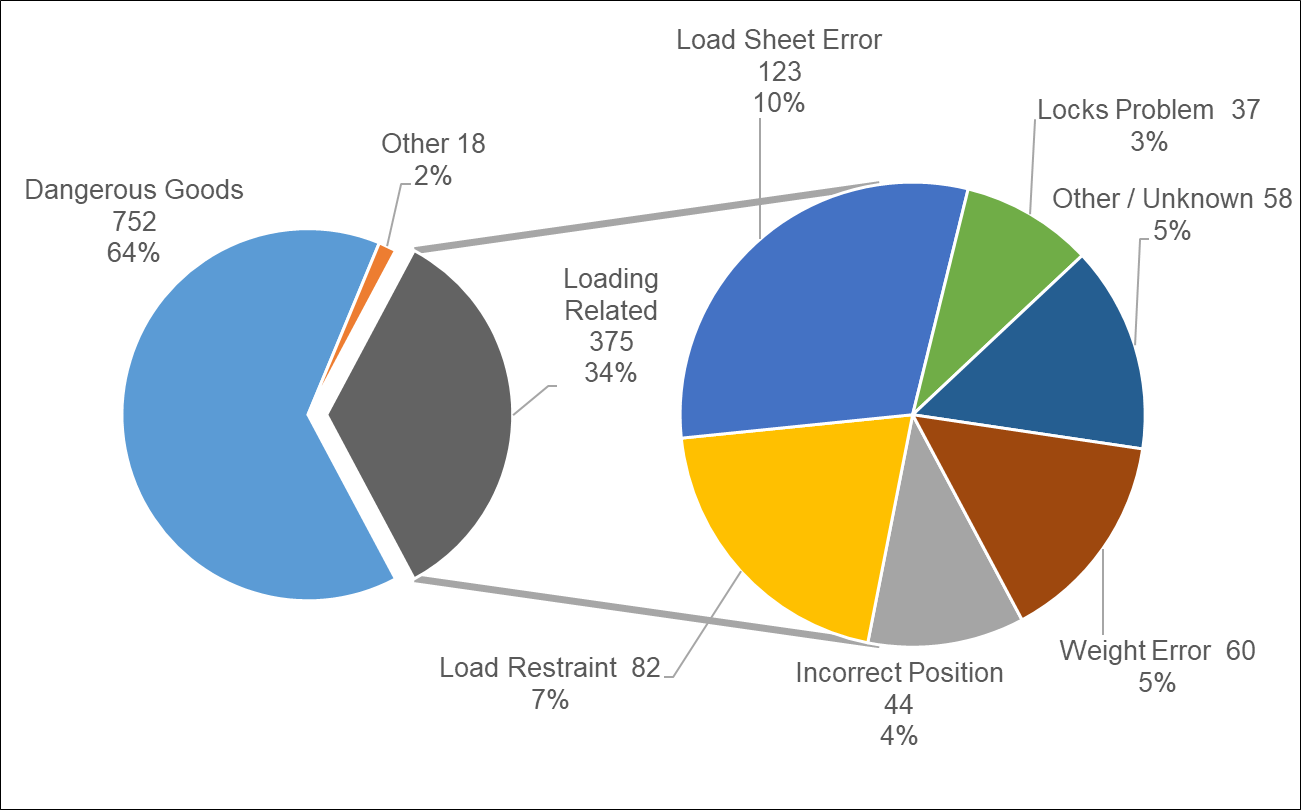
Image source: ATSB
Further derivation of the Loading Related data revealed 123 occurrences attributable to ‘Load Sheet Errors’ that included unaccounted freight, receipt of a new load sheet after take-off, incorrectly recorded weights of baggage and freight items, and calculation of the weight of children as adult passengers.
There were 82 occurrences coded as ‘Load Restraint’ mostly relating to securing of containers and pallets. Some also related to bags not being secured with webbing. For the 60 occurrences relating to an aircraft ‘Weight Error’, most were the result of either non-manifested containers, pallets or bags being loaded. The most significant ‘Weight Error’ involved additional and unaccounted baggage that constituted an additional 1,600 kg of weight to the aircraft. The 44 ‘Incorrect Position’ occurrences related to passengers in the wrong seating location or baggage and freight being loaded into the incorrect position within the hold.
There were 37 occurrences coded as a ‘Locks Problem’. Containers and pallets are positioned in the hold using a series of electronically controlled rollers, which are then locked into place using retractable latches integrated into the floor or wall of the aircraft. These latches, called cargo locks, stop containers and pallets from moving while the aircraft is in flight or when taxiing.
__________
- More than one occurrence type can be coded to an occurrence, for example an undeclared and unrestrained Dangerous Good may also classified as Loading Related with an associated Load Restraint descriptor. The Level 4 descriptors are incorporated primarily to value add for the purposes of statistical and research analysis.
- Occurrence types coded as Dangerous Goods and Other include situations where freight such chemicals or batteries were undeclared and had been discovered while unloading the aircraft, had spilled or were incorrectly packed and stowed.
- ATSB ‘Loading Related’ investigations: AO-2010-034, AO-2012-004, AO-2014-110, AO-2014-145, AO-2015-088, AI2015-139, AO-2016-119, AO-2016-145, AO-2016-177, AO-2017-012, AO-2017-018, AO-2017-019
The occurrence
What happened
On 17 December 2017, an Airbus A330-303 aircraft, registered VH-QPD and operated by Qantas Airways, was being prepared for passenger flight QF107 from Sydney, New South Wales, to Beijing, China (Figure 1). The loading of baggage and freight into the lower hold of the aircraft was conducted as part of pre-departure operations. The aircraft departed from the international terminal at Sydney Airport at 1346 Eastern Daylight-saving Time.[1] After landing in Beijing, the operator’s freight agents identified that the aircraft had been loaded incorrectly. An incorrect freight pallet resulted in the aircraft exceeding its maximum take-off weight on departure from Sydney.
Figure 1: A330 aircraft VH-QPD

Source: Anthony Filippousis
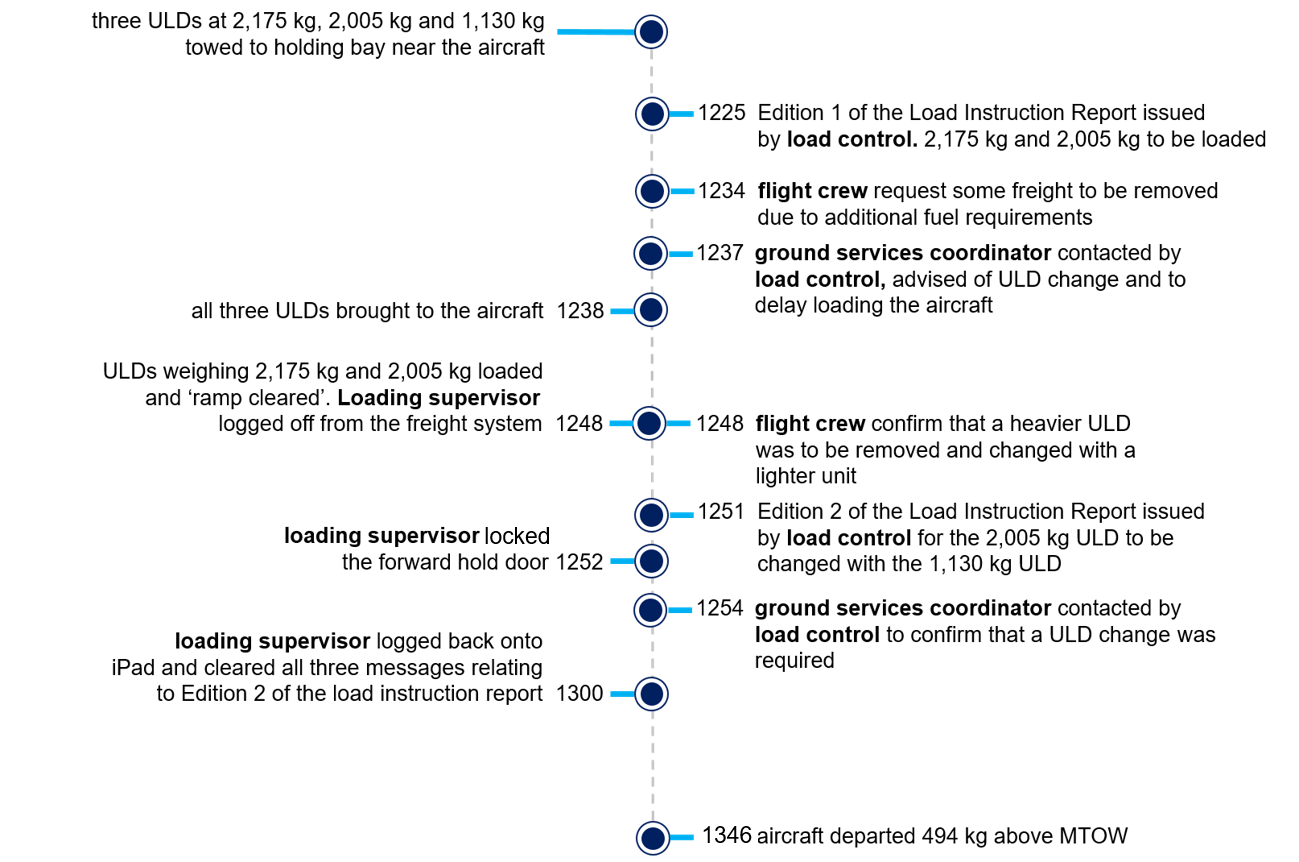
Aircraft loading sequence of events
The following sequence of events describes the primary actions and decisions during the freight-loading process prior to the departure of QF107 from Sydney. The sequence of events is further summarised in Figure 2.
Preparations for loading the aircraft typically commenced about two hours prior to departure. These included finalisation of passenger numbers, freight planning, fuel uplift and aircraft departure weight calculations. The freight that had been prepared for transport to Beijing on QF107 included three unit load devices (ULDs).[2] All three ULDs were weighed and assigned a unique identification number as follows:
- PMC42476QF at 2,175 kg
- PMC41566QF at 2,005 kg
- PMC42559QQ at 1,130 kg.
The pallets were then towed to a holding bay near the aircraft.
At 1210, the operator’s staff within the load control office determined that the aircraft’s maximum take-off weight (MTOW) would be exceeded if all three ULDs were loaded into the hold. Load control determined that only two of the three ULDs could be sent on QF107. PMC42476QF at 2,175 kg and PMC41566QF at 2,005 kg were selected. The provisional flight plan was subsequently issued to the operating flight crew for review.
At 1225, approximately 75 minutes prior to the scheduled departure time, Edition 1 of the load instruction report (LIR) was sent from the load control office to the ramp staff allocated to load the aircraft. The ULDs PMC42476QF at 2,175 kg and PMC41566QF at 2,005 kg were identified in the LIR to be loaded into the aircraft. The loading supervisor accessed Edition 1 of the LIR using his portable electronic tablet (iPad).
At 1234, the operating flight crew contacted the load control office with a request to remove some cargo from the aircraft due to the requirement to carry an additional fuel reserve for the flight to Beijing. In order for the aircraft to depart below its MTOW, load control elected to switch a heavier ULD with a lighter unit. The resultant changes to aircraft take-off weight required the release of another LIR (Edition 2), detailing that:
- PMC42476QF at 2,175 kg was to remain as originally planned and to be loaded within the rear hold of the aircraft at position 31P.
- PMC41566QF at 2,005 kg was to be removed and replaced with the lighter weight unit, PMC42559QQ at 1,130 kg, within the forward hold at position 24P.
At 1237, the load control officer contacted the ground services coordinator to advise that a ULD change had been requested by the operating flight crew and to delay loading the ULDs pending release of Edition 2 of the LIR.
At around 1238, all three ULDs were brought by tug from the holding bay to the aircraft. By 1248 PMC42476QF at 2,175 kg and PMC41566QF at 2,005 kg were loaded and secured into their respective positions on board the aircraft, in accordance with Edition 1 of the LIR.
At 1248, the operating flight crew contacted the load control office to confirm the final fuel upload data, also confirming that a change to a lighter ULD would be required to offset the weight of the additional fuel.
At 1250, the load control officer ‘locked out’ the flight within the freight management system. Just prior to the freight management system lock out, the loading supervisor at the aircraft accessed the system and both loaded ULDs were ‘ramp cleared’, indicating they had been loaded and secured into their respective positions. The loading supervisor then logged off from the system, and directed the tug driver to return the remaining ULD (PMC42559QQ at 1,130 kg) back to the freight terminal.
At 1251, Edition 2 of the LIR was entered into the freight management system with three accompanying electronic messages from the load control office:
1. Flight Locked by Load Control. Please contact Load Control.
2. Edition has changed
3. 24P has changed Ref: PMC41566QF to PMC42559QQ
Cargo Weight: 2005 to 1130
At 1252, shortly after the release of Edition 2 of the LIR, the loading supervisor locked the forward hold door of the aircraft.
At 1254, the load control officer contacted the ground services coordinator in the ramp office to confirm that Edition 2 of the LIR had been released with a requirement for the heavier ULD to be exchanged with the lighter unit.
At 1300, the loading supervisor at the aircraft logged back into his iPad and resumed using the freight management software. All three messages advising that Edition 2 of the LIR had been issued, that a ULD change was required, and that he was to contact Load Control, were displayed on the tablet device. The supervisor acknowledged the electronic messages and tapped the ‘OK’ button, clearing them from the system. Despite the electronic acknowledgement, the supervisor did not change the ULD configuration at Position 24P.
The final load sheet provided to the operating flight crew incorporated the ULD change from Edition 2 of the LIR, where the 1,130 kg ULD had been loaded to Position 24P, when in fact the heavier 2,005 kg ULD remained on the aircraft. Calculations showed that with the heavier unit in place the aircraft take-off weight was 233,494 kg, which was 875 kg above the planned take-off weight and 494 kg above the aircraft’s MTOW.
The flight crew were unaware of the load discrepancy during the flight. There were no reported handling or control issues encountered during take-off and no associated abnormal indications were received.
Figure 2: Sequence of events for this loading event
__________
- Eastern Daylight-saving Time (EDT): Co-ordinated Universal Time (UTC) +11 hours.
- Unit load devices (ULDs) are pallets or containers used to transport bulk freight in aircraft. The PMC code identified the occurrence ULDs were a pallet design.
Safety issues and actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Freight management
Qantas advised that an internal project to address freight discrepancies and loading errors was commenced in June 2018 and was completed in June 2019. The project involved the replacement of the loading supervisors’ portable electronic tablets (iPads) with handheld scanning devices. The new devices provide an automated freight confirmation and mobile communication process using printed barcode and scanning technology. The vast majority of domestic and international Qantas ports are using the scanners to validate freight before loading onto an aircraft.
Internal occurrence reporting
A change to the Qantas international airports occurrence notification form has been made. The completion of the ‘Loading Related Incident’ field within the form is now mandatory.
Load control to loading supervisor communication
To reduce the potential for communication errors between load controllers, ramp staff and loading supervisors, an amendment to the Qantas Weight and Balance Manual was incorporated on 1 September 2019. The amendment stated:
The preferred methods of contacting the Loading Supervisor when notifying of a LIR/LGR new edition or any other urgent message are:
1. Directly via phone, VHF radio or FM Messenger to First Load requiring a positive response that the message has been understood, not just read, e.g. “have you received the changes in EDNO 2?”,
2. Via Ramp office or Duty Manager, explicitly stating the Loading Supervisor MUST be notified.
CAUTION: If at any point you are unsure that the Loading Supervisor will not or has not received and understood the message, lock out the First Load application by setting the Load Control status to LO or LL until contacted.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Qantas Airways.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the loading supervisor, and the load controller, Qantas Airways and the Civil Aviation Safety Authority.
Submissions were received from Qantas Airways and the Civil Aviation Safety Authority. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2020

Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
Occurrence summary
| Investigation number | AO-2018-003 |
|---|---|
| Occurrence date | 17/12/2017 |
| Location | Sydney Airport |
| State | New South Wales |
| Report release date | 18/06/2020 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Loading related |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Airbus |
|---|---|
| Model | A330-303 |
| Registration | VH-QPD |
| Serial number | 0574 |
| Aircraft operator | Qantas Airways |
| Sector | Jet |
| Operation type | Air Transport High Capacity |
| Departure point | Sydney, New South Wales |
| Destination | Beijing, China |
| Damage | Nil |