The Civil Aviation Authority of Vanuatu (CAAV) investigated a fuel starvation and collision with terrain accident involving Britten-Norman Islander BN2A-20, YJ-AT2, 6 km east-south-east of Port Vila International Airport, Vanuatu, on 15 July 2024. The CAAV requested assistance from the Australian Government represented by the ATSB.
To facilitate this support and to provide the appropriate protections for the information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of the International Civil Aviation Organization Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
On 14 August 2025, the CAAV released its final report into this accident. This report is available here.
Any enquiries relating to the investigation should be directed to the CAAV.
The ATSB is investigating a wirestrike and collision with terrain involving an Air Tractor AT-502, registration VH-CJY, 19 km south-east of Lake Cargelligo Airport, New South Wales, on 18 July 2024.
During aerial agricultural spraying operations, the aircraft struck a wire and subsequently collided with terrain resulting in substantial damage. The pilot was fatally injured.
The ATSB deployed a team of transport safety investigators to the accident site with experience in aircraft operations, engineering, and human factors. As part of the onsite phase of the investigation, ATSB investigators examined the aircraft wreckage and other information from the accident site, interviewed witnesses and any involved parties, and examined maintenance records and any recorded data.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
The pilot, a New Zealand citizen, held a Civil Aviation Safety Authority Part 61 Commercial Pilot Licence (Aeroplane) with a single and multi-engine class rating with endorsements for retractable undercarriage, manual propeller pitch control, and low-level and instrument ratings. The pilot’s commercial licence was issued on 17 August 2023 in accordance with the Trans-Tasman Mutual Recognition Act 1997. The pilot held a Class 1 Aviation Medical Certificate with no restrictions, valid to 29 November 2024.
At the pilot’s last medical examination on 6 November 2023, the pilot reported having 251 hours of total aeronautical experience.
Aircraft information
VH-SQO was a Cessna Aircraft Company 172N 4-seat, single-engine, high (strut-braced) wing, all metal, unpressurised, fixed (tricycle) undercarriage aircraft. The aircraft was manufactured in the United States in 1978 and first registered in Australia on 29 August 1978. The operator had been the registered owner of the aircraft since the date of registry.
The current maintenance release was issued on 8 March 2024 and was valid until 8 March 2025 or 14,620.8 hours total time-in-service, whichever came first. At the time of take-off for the accident flight, the aircraft had accumulated 14,602.7 hours.
Meteorological information
Witnesses reported that on the morning of the accident, the weather was fine, clear and the temperature was cool, not cold. No wind or cloud cover was observed, and the conditions were described by a witness as being ‘almost perfect for paddock work’.
Wreckage examination
The ATSB’s onsite examination found that the aircraft impacted with terrain at about a 70° pitch down attitude, with ground impact marks directly under the nose showing no forward momentum (Figure 2). The aircraft’s flight controls and structure did not identify any pre‑existing faults or pre‑impact defects or failures. Additionally, one of the propeller blades showed significant rotational abrasion damage and chord-wise twisting indicating that the engine was driving the propeller under significant power at the time of impact.
To date, the ATSB has examined the aircraft wreckage, interviewed witnesses, and gathered electronic devices from the accident site. The investigation is continuing and will include consideration of the following:
evaluation of witness information
examination of the:
GPS device recovered from site
aircraft maintenance history
aircraft weight and balance, and performance
meteorological conditions
impact sequence and survivability
the conduct of similar flight operations
pilot qualifications, experience and medical information
regulatory requirements for fixed-wing aerial mustering.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Final report
Investigation summary
What happened
On the morning of 27 June 2024, the pilot of a Cessna Aircraft Company 172N, registered VH‑SQO, was assisting with mustering sheep at Mulgathing Station, South Australia. At about 0810 local time, a witness on a motorbike about 500 m away observed the aircraft dive down on what they presumed was a flock of sheep to an estimated height of about 50 ft above the ground before climbing rapidly, turning to the left and then descending towards the ground. The aircraft was destroyed, and the pilot who was the sole occupant was fatally injured.
What the ATSB found
The ATSB found that, while mustering sheep without the appropriate endorsement to do so, the pilot lost control of the aircraft leading to an aerodynamic stall and spin from an altitude that was not recoverable. Although not contributory, it was also found that the upper torso restraint part of the lap-sash seatbelt was not worn at the time of the accident. Further, the pilot was hired for a job advertised as aerial stock mustering but did not require an aerial mustering endorsement as the operator’s intention was that the role only involved aerial spotting.
What has been done as a result
The operator has advised that it is preparing a Safe Aerial Spotting & General Station Aviation Manual. It has also implemented a pilot mentoring program and initiated a third-party safety audit. It is also undertaking a review of its operations to ensure compliance with the Civil Aviation Safety Authority regulations as well as the safety and training standards for pilots.
Safety message
This accident highlights the importance of managing airspeed and bank angle to minimise the risk of an aerodynamic stall. This is particularly important when operating in close proximity to the ground, such as during take-off, landing and when conducing low-level air work, as recovery may not be possible. Low-level flying is a higher risk activity and mustering at low-level adds additional complexity and risk. It is important that pilots operate within the boundaries of their training and qualifications to ensure an adequate margin of safety is maintained.
The ATSB’s SafetyWatch initiative highlights broad safety concerns generated by its investigation findings, and fromoccurrence data reported by industry. One of the safety concerns is Reducing the severity of injuries in accidents involving small aircraft, which includes the appropriate fitment and use of seatbelts. This SafetyWatch notes that in several of its investigations, the ATSB has found injuries to aircraft occupants may have been avoided, or made less severe, through the appropriate use of multi-point harnesses.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
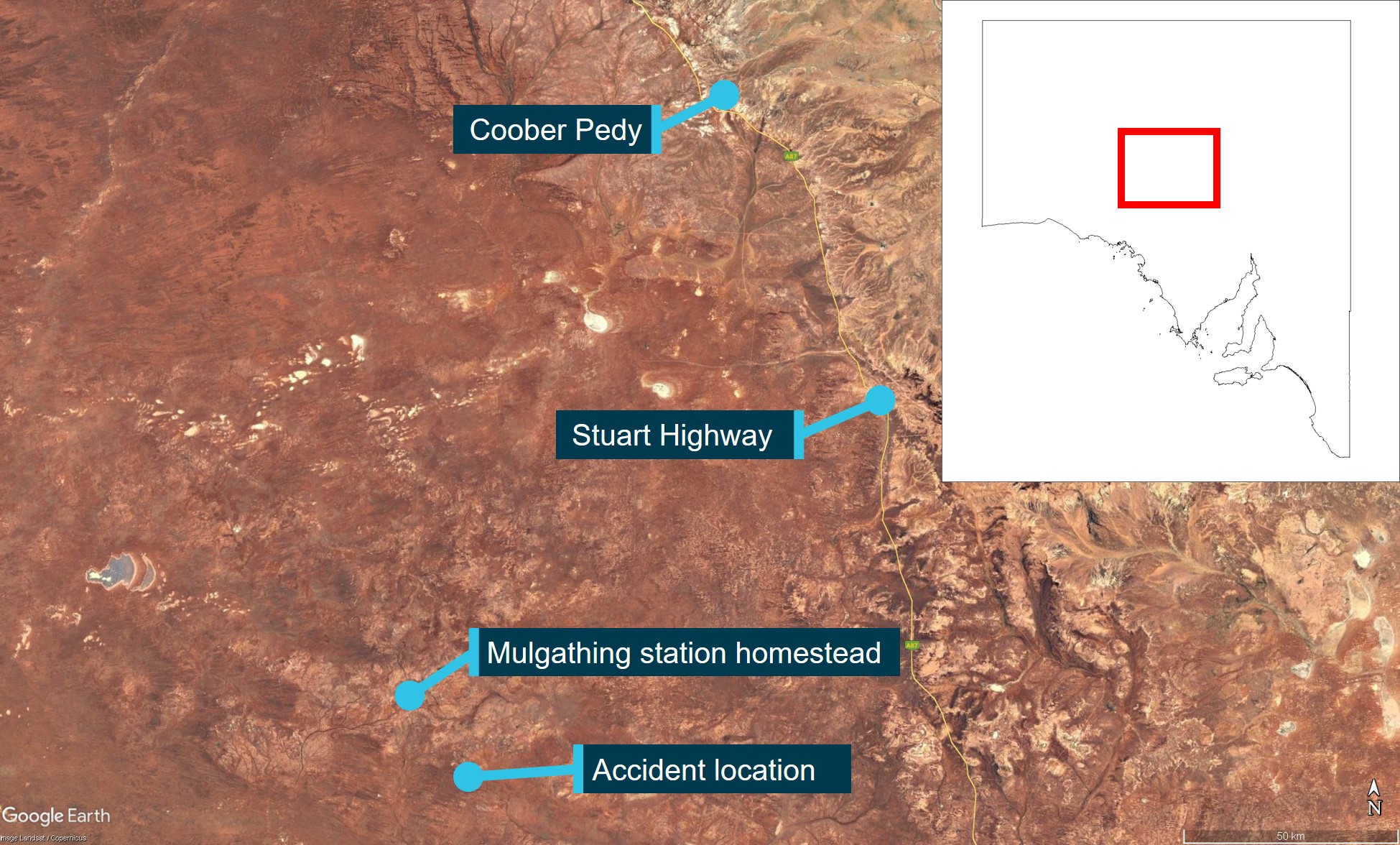
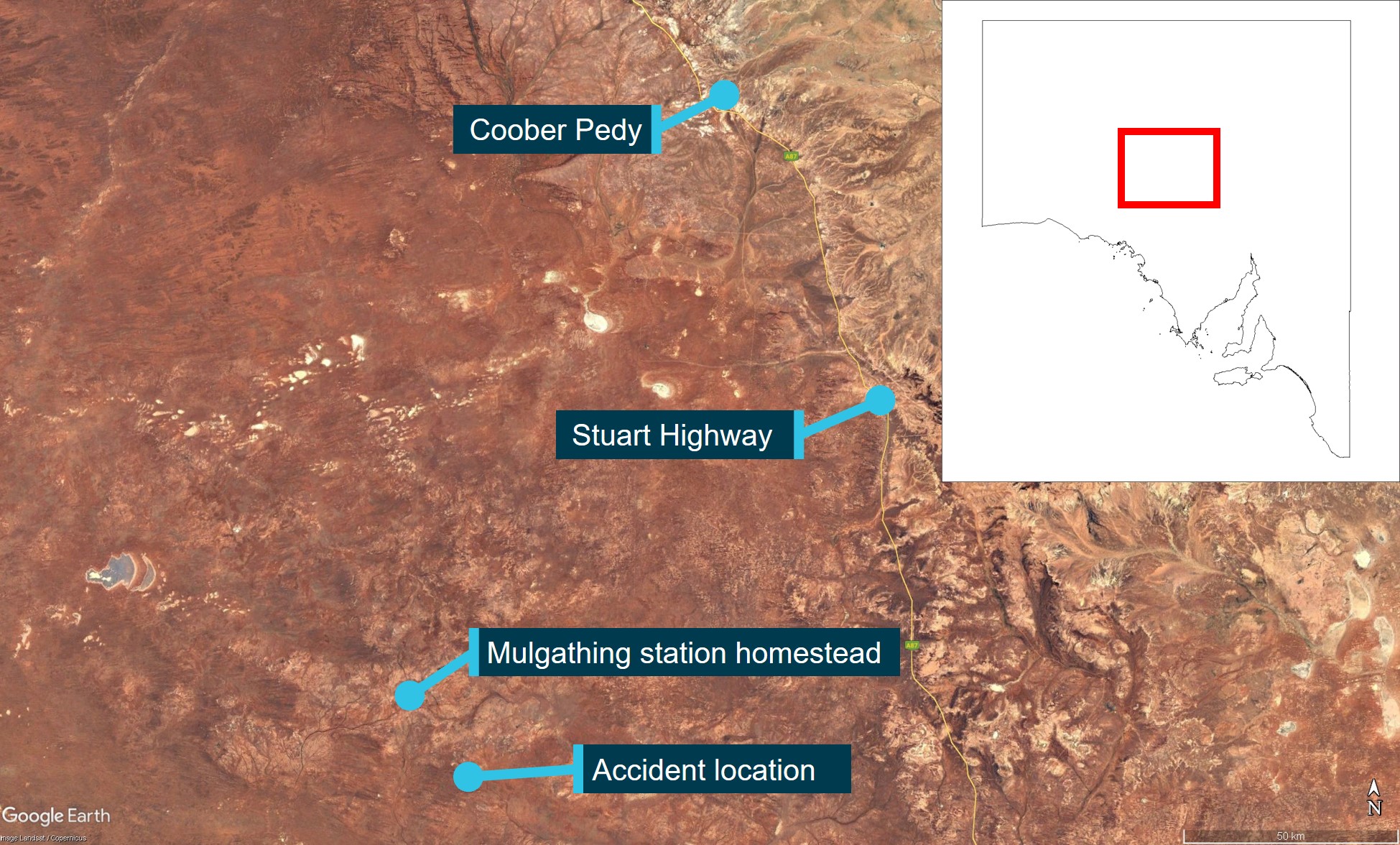
On the morning of 27 June 2024, the pilot of a Cessna Aircraft Company 172N, registered VH‑SQO, met co-workers for breakfast at about 0630 local time before a morning briefing on the task for the day, which involved mustering sheep at Mulgathing Station (owned by Jumbuck Pastoral (operator)), South Australia. At about 0700, the station manager, assistant manager and 4 station hands set off for a yard about 30 km south-east of the homestead (Figure 1). Meanwhile, the pilot drove to the airstrip about 5 minutes away, took off and flew towards the yard to rendezvous with the other workers.
The station manager and 4 station hands were marking[1] lambs in the yard while the pilot, in the aircraft, and the assistant manager (witness) on a motorbike, were rounding up stray sheep. At about 0810, the witness observed the aircraft flying overhead at about 300 ft above ground level looking for sheep when the pilot radioed to say they had found 2 flocks about 2 km away. The witness converged on one flock and observed the aircraft circling about 500 m away over what was presumed to be the second flock.
The witness radioed the pilot to ask if they needed help moving the sheep. The pilot responded that they thought they would be able to do it with the aircraft. The aircraft was then observed to continue circling to the left at a height the witness estimated to be 150–200 ft before diving at an angle of about 45° towards what was presumed to be the flock of sheep, to a height of about 50 ft. The witness estimated that the aircraft then climbed out at about a 60° nose‑up attitude to a height of about 250–300 ft, rolled to the left and descended nose-down towards the ground and impacted terrain. No bird activity was noted by the witness and they reported not hearing any changes in the engine noise during the accident sequence. While they were not certain of the actual angle of climb, they noted that it was steeper than the descent. The aircraft was destroyed, and the pilot who was the sole occupant was fatally injured.
Figure 1: Accident location with reference to Coober Pedy and the Stuart Highway
Source: Google Earth, annotated by the ATSB
Context
Pilot information
The pilot, a New Zealand citizen, held a Civil Aviation Safety Authority Part 61 Commercial Pilot Licence (Aeroplane) with a single and multi-engine class rating with endorsements for retractable undercarriage, manual propeller pitch control, and low‑level and instrument ratings. They did not hold an aeroplane aerial mustering endorsement. The pilot’s commercial licence was issued on 17 August 2023 in accordance with the Trans‑Tasman Mutual Recognition Act 1997. They had recorded 441.5 total flying hours in their logbook, dated 16 June 2024.
The pilot’s low‑level training was conducted on 1–3 December 2023 and their low‑level rating was issued on 3 December 2023, which was also their last flight review. The flight test was conducted in a Cessna 172 aircraft, with all elements of the low‑level rating with a single‑engine aeroplane endorsement assessed as satisfactory, including the approach and recovery from a stall in level flight and turning.[2] The instructor who conducted the pilot’s low‑level training noted that the role was for aerial spotting rather than mustering, therefore, the elements for the aerial mustering endorsement were not tested.
The pilot was employed by Jumbuck Pastoral to work at Mulgathing Station in December 2023. The pilot’s logbook showed 70 flights were conducted by the pilot at Mulgathing between January 2024 and the last logbook entry on 16 June 2024. These flights totalled 198.3 hours, all of which were conducted in VH‑SQO.
The pilot held a Class 1 Aviation Medical Certificate with no restrictions, valid to 29 November 2024. The pilot’s aviation medical examination indicated no reported medical conditions nor prescribed medications. Co‑workers reported the pilot was fit, healthy, did not drink alcohol excessively and did not smoke. On the morning of the accident, witnesses stated that the pilot demonstrated no abnormal behaviour.
Aircraft information
VH‑SQO was a Cessna Aircraft Company 172N 4‑seat, single‑engine, high (strut‑braced) wing, all metal, unpressurised, fixed (tricycle) undercarriage aircraft. The aircraft was manufactured in the United States in 1978 and assigned serial number 17270255. It was first registered in Australia on 29 August 1978. The operator had been the registered owner of the aircraft since the date of registry.
The current maintenance release was issued on 8 March 2024 and was valid until 8 March 2025 or 14,620.8 hours total time‑in‑service, whichever came first. At the time of take‑off for the accident flight, the aircraft had accumulated 14,602.7 hours. The maintenance release showed that required maintenance had been completed and no defects were recorded.
Meteorological information
There was no airport forecast for Mulgathing Station, however, the Bureau of Meteorology graphical area forecast issued at 0137 local time and current for the time of the accident forecast no cloud or weather below 5,000 ft and visibility greater than 10 km. This was consistent with witness accounts, which reported that, on the morning of the accident, the weather was fine, clear and the temperature was cool, not cold. No wind or cloud cover was observed, and the conditions were described by a witness as being ‘almost perfect for paddock work’.
Wreckage and impact information
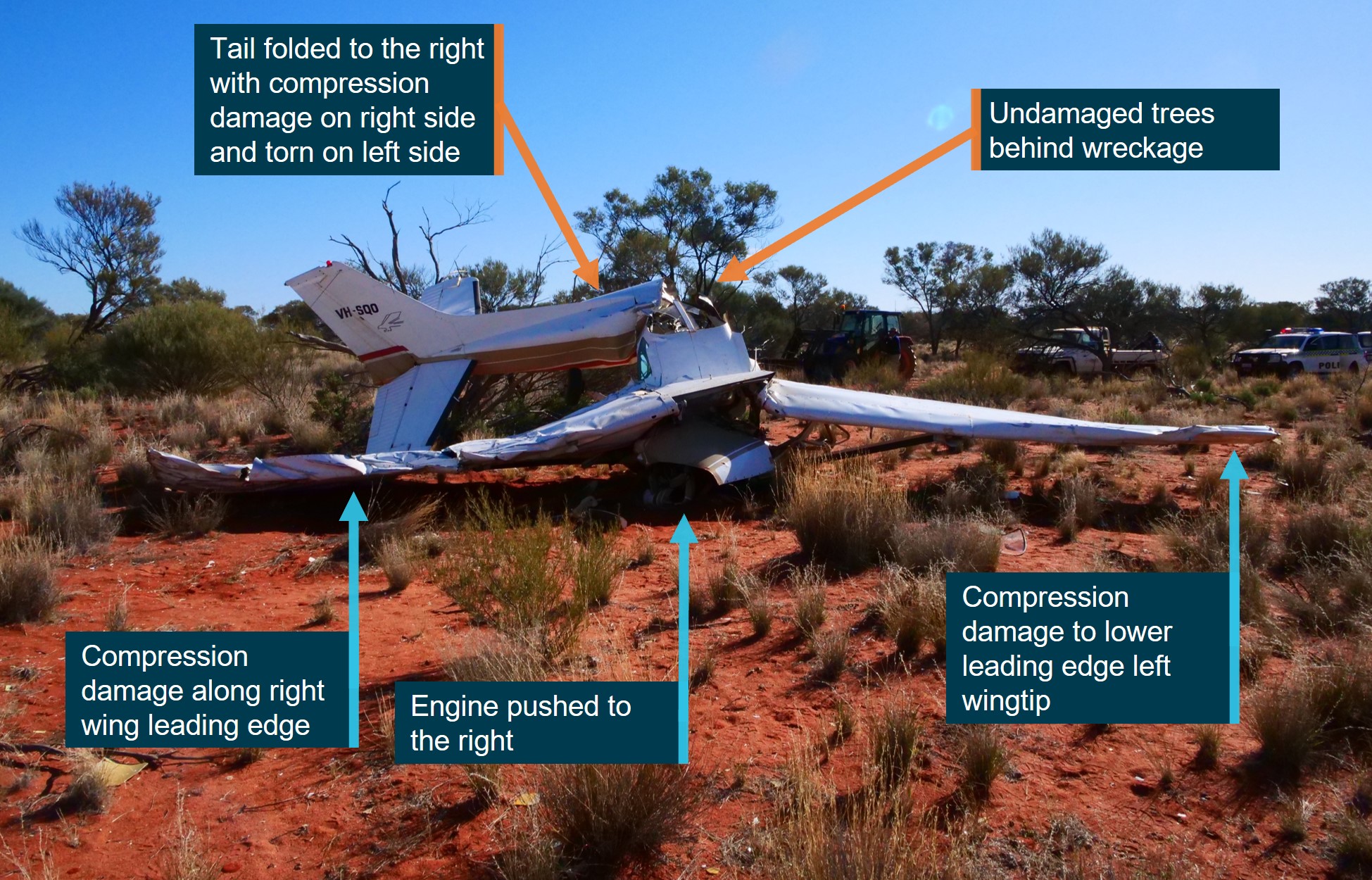
The ATSB’s onsite examination found that the aircraft impacted with terrain at about a 70° pitch down attitude with undamaged trees behind the wreckage. Ground impact marks were directly under the wreckage indicating no forward momentum.
The engine was deflected to the right of the longitudinal axis by about 25° (Figure 2). The crank case had fractured in overload, which separated the propeller from the engine. The underside of the left wingtip leading edge exhibited compression damage, which was also evident along the span of the right wing leading edge. The aft fuselage had folded towards the right with compression damage evident on the right side. The flaps were in the full retracted position.
Figure 2: VH-SQO accident site
Source: ATSB
The aircraft’s flight controls and structure did not identify any pre‑existing faults or pre‑impact defects or failures, and no evidence of a birdstrike was observed. Additionally, one of the propeller blades showed significant rotational abrasion damage and chord-wise twisting indicating that the engine was driving the propeller under significant power at the time of impact.
Examination of the fuel drum used to refuel the aircraft showed it had a water drain and filter in a clear bowl with uncontaminated fuel evident in the filter bowl. Although the fuel selector was found to be in an undetermined position due to the accident damage, there was a significant amount of fuel remaining in both tanks, a strong smell of fuel around the aircraft, and the fuel tank caps were observed to be locked in place.
Aerodynamic stall and spin
A wing generates lift as a result of the pressure differential created by airflow over the wing’s surface. The angle between the incoming or relative air flow and wing chord is known as the angle of attack (AoA). As the AoA increases, lift increases up to a certain angle, known as the critical AoA. At this point, the airflow over the upper surface of the wing becomes separated. This condition is referred to as an aerodynamic stall (or simply a stall) and results in a significant loss of lift and an increase in drag. Due to the sudden reduction in lift from the wing and rearward movement of the centre of lift, typically an uncommanded aircraft nose-down pitch results. Most general aviation aircraft typically have a critical AoA of around 16°. This critical AoA can be exceeded at any airspeed, any (pitch) attitude and any power setting. However, a high AoA combined with a low airspeed most commonly results in a stall condition.
A spin can result when an aircraft simultaneously stalls and yaws.[3] The yaw can be initiated by rudder application (through manipulation of the rudder pedals) or by yaw effects from a range of factors that include aileron deflection, torque and engine/propeller effects. A spin is characterised by the aircraft following a downward, corkscrew path and requires significantly more altitude for recovery compared to a wings level stall (Federal Aviation Administration, 2021).
The Cessna Aircraft Company Pilot’s Operating Handbook stated that the stall recovery height for the Cessna 172N is 180 ft. The handbook also stated that the recovery height for a one‑turn spin is 1,000 ft.
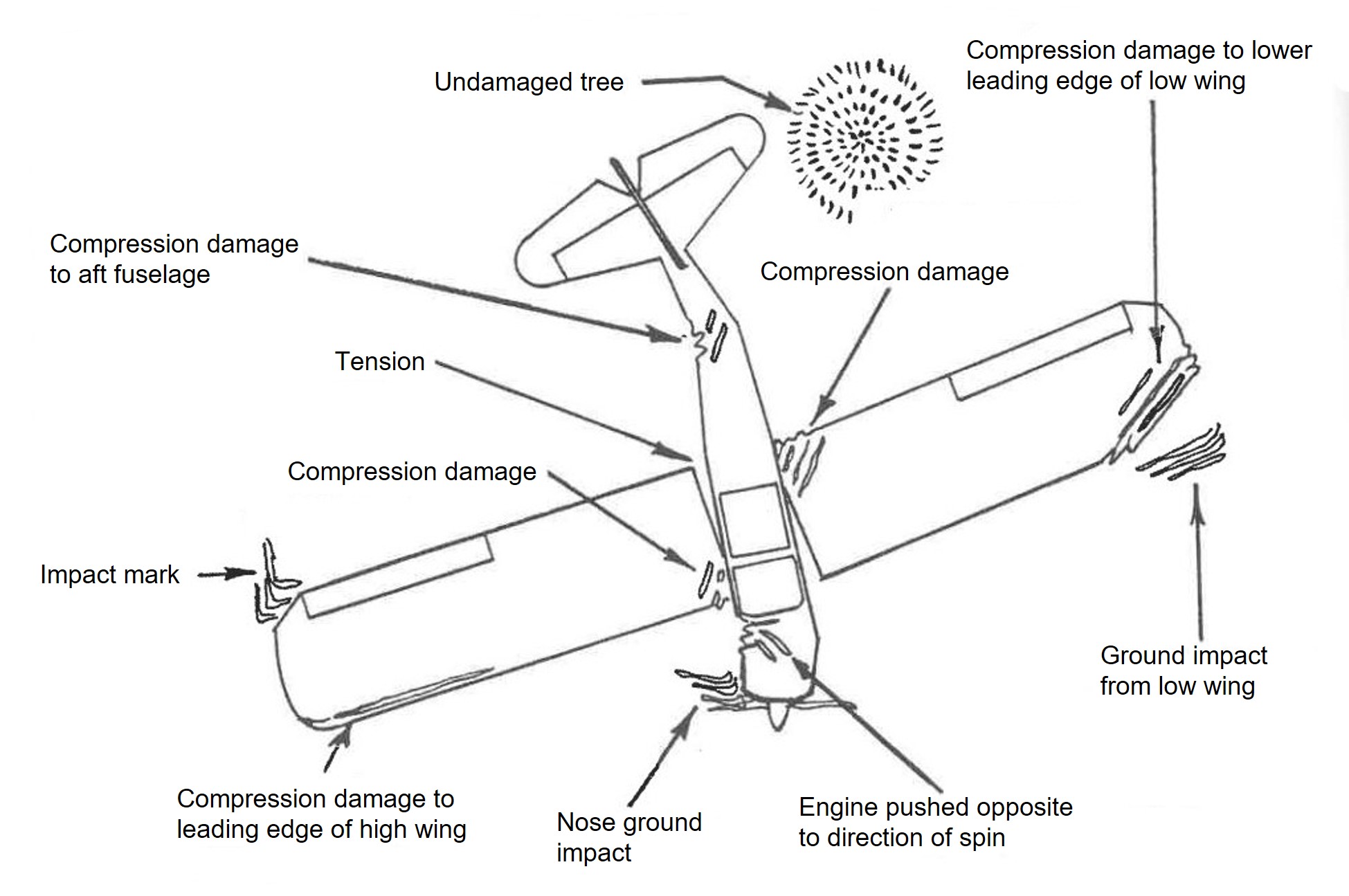
Wood and Sweginnis (2006), Aircraft Accident Investigation – 2nd edition, provides the following description of the wreckage from an aircraft that had spun into the ground, with reference to Figure 3:
There is little or no evidence of forward motion. Although the fuselage probably impacted at a steep nose down attitude, it is likely that there is evidence of a wing tip striking the ground before the nose. The down-going wing will normally strike the ground before the up-going wing, providing one clue as to the direction of the spin. Both the fuselage and the wings will probably have damage which reflects both a high sink rate and yaw. Tall thin objects on the ground, like trees and fence posts, are likely to penetrate the airplane almost from bottom to top, reflecting the almost vertical trajectory of the airplane. Undamaged objects may be found immediately behind the trailing edges, again indicating the vertical path of the airplane.
Aerial mustering is defined as the use of an aircraft to locate, direct and concentrate livestock. By definition, it is a hazard‑rich activity due to the inherent characteristics of the operation. Such hazards include manoeuvring at low-level, high workload, negative effects from weather, proximity to obstacles and the division of attention between flying and livestock management (Civil Aviation Safety Authority, 2015).
In addition to the aviation-specific definition for aerial mustering described above, in general terms, mustering livestock is usually a collaborative activity involving a ground-based team, typically using vehicles such as motorbikes, as well as personnel in the air, in either aeroplanes or rotorcraft. The role of the pilot in the overall mustering team could either be aerial spotting, or aerial mustering. The spotting role would involve the pilot searching for livestock and communicating their location to the ground team for them to round up. This is generally performed at a higher position and does not require the need to perform dynamic aircraft movements. This is somewhat different to aerial mustering, which, as defined by the Civil Aviation Safety Authority, would involve the intentional use of the aircraft to direct or concentrate the livestock. The ratings and endorsements a pilot had would limit which of these activities they could undertake.
Regulatory requirements
Since the introduction of Civil Aviation Safety Authority Civil Aviation Safety Regulations 1998 Part 61 in September 2014, an aeroplane aerial mustering endorsement was required to muster livestock with an aeroplane in Australia. Furthermore, an applicant for the aeroplane aerial mustering endorsement was required to hold a low-level rating with an aeroplane low-level endorsement. The mustering endorsement had additional elements and performance criteria to the low-level rating, which included demonstrating:
handling of the aeroplane up to the limits of the flight-manoeuvring envelope
coordinating and conducting an aerial mustering operation
an underpinning knowledge of critical operational conditions including aerodynamic stall and the safety hazards and risks of low‑level operations and methods of control.
To conduct aerial spotting a low‑level endorsement was required.
All aerial work operations in aeroplanes and rotorcraft are covered by Part 138 of the regulations. This includes operations that require an aerial work certificate as well as those that do not. However, if the aerial work is conducted over land owned or occupied by the person who is the registered operator of the aircraft or otherwise the owner of the aircraft, an aerial work certificate is not required. This is known as limited aerial work operations.
VH-SQO was owned by Jumbuck Pastoral and flying operations were conducted over their land.
Mustering observations
For the duration of the pilot’s time at Mulgathing Station, the pilot was observed by several staff members to have used a ‘dive‑bombing’ technique to muster sheep on multiple occasions. However, all staff members stated that they thought the procedure was normal operations for mustering and that the pilot was qualified to perform the activity. Following the accident, these staff became aware that the pilot was not qualified to conduct these aerial mustering manoeuvres.
Job application and role description
The pilot originally applied for a job with Jumbuck Pastoral at Bulgunnia Station, about 90 km east of Mulgathing. Although that application was not successful, Jumbuck Pastoral subsequently offered the pilot a similar job at Mulgathing Station. The job advertisement described the position as a pilot/station hand, stating that:
Your main duties while flying will be aerial stock mustering and supporting the crew on the ground during musters along with periodical property and stock inspections.
The qualifications required for the role were described as:
• Australian Commercial Pilots License (essential)
• Minimum 200 hours of total flying time (essential)
• Experience flying a Cessna 172 (essential)
• Low-Level Flying Endorsement (can be obtained if successful)
On 13 February 2025, in response to the draft report, the operator advised that the job description for the role involved aerial spotting only, to assist on‑ground mustering teams. It indicated that it had never required its aeroplane pilots to control or manoeuvre livestock directly. Instead, it relied on helicopter pilots for controlling stock movement when motorbikes could not be safely used on the ground for mustering cattle.
The operator also stated that the intention of the role was communicated to the pilot during their engagement with the company and the pilot was provided a copy of the Mulgathing Station Guide, which stated that:
Our mustering activities are supported by a Cessna 172 plane, with the pilot coordinating the muster below by relaying the location of stock in the paddocks. For those on 2-wheel motorbikes, stock visibility can be limited for a number of reasons, so having a pilot in the air assisting is an enormous help to ensure we muster paddocks cleanly and don’t leave any sheep behind. The terrain around the station can be tricky with a lot of rock, scrub and rough paddocks, so this is an added benefit.
Survival aspects
The aircraft impacted terrain with a 70° nose down attitude, which significantly compressed the liveable space within the cockpit. Injuries observed by first responders were consistent with those typically sustained from an aircraft accident. At the time of publication, the post‑mortem report was pending, however, the toxicology report indicated no presence of alcohol or drugs, and carbon monoxide[4] levels were also indicated to be within the normal range.
The pilot was not wearing a helmet at the time of the accident, nor were they required to. The pilot seat remained attached to the seat rails and was locked in a mid‑forward position. The pilot’s seat was fitted with a 3‑point lap‑sash belt and shoulder harness (upper torso restraint (UTR)). The pilot’s lap belt was reported to have been removed by the first responder to facilitate the pilot’s removal. The lap belt and clasp remained anchored to the floor and appeared to be in good condition. Inspection of the cockpit revealed that the UTR was stowed in the roof line.
When correctly worn, UTRs form an important part of the occupant protection system in aircraft, and the benefits in reducing the likelihood and severity of injuries is well established. A significant benefit of correctly fitted UTRs is the minimisation of body movement to prevent the body striking the aircraft structure in lateral and longitudinal impacts (Young, 1967). These findings are supported by research conducted by the United States National Transportation Safety Board (NTSB, 2011), which found that pilots who used lap belts only were nearly 50% more likely to be seriously or fatally injured compared with those who wore lap belts with UTRs.
With regards to the requirement for seatbelt usage in Australia, Civil Aviation Safety Authority Civil Aviation Safety Regulations 1998 Part 91.550 stated the following requirements:
• At all times during the flight, such a pilot must occupy a pilot seat, with the seatbelt [lap-sash belt] securely fastened.
• During take-off, landing or any other period that the pilot in command directs, each flight crew member required for the flight must occupy the flight crew member’s crew station with the seatbelt and shoulder harness securely fastened.
Safety analysis
Introduction
While mustering sheep on Mulgathing Station, South Australia, a Cessna Aircraft Corporation 172N, registered VH-SQO, was observed to dive towards a group of sheep before pulling out of the dive, rolling to the left, descending towards the ground and impacting terrain.
This analysis will focus on the examination of the factors that led to the pilot losing control of the aircraft at low-level while attempting to muster sheep. It will also consider the job advertisement for the pilot position and the use of upper torso restraints.
Loss of control
The aircraft was observed diving from about 150–200 ft to approximately 50 ft above the ground then pitching up at about a 60° nose-up attitude to about 250–300 ft with no observed change in the engine power setting, before banking to the left and descending to the ground. While there can be limitations to witness recollections, the key points made by the witness were that the angle of climb was steeper than the angle of descent, and that the exit height was greater than the entry. These aspects were consistent with a loss of control during the exit of the dive. The steep climb‑out from the dive likely resulted in a rapid decay of airspeed and increase in the angle of attack that made the aircraft susceptible to a power‑on stall/spin situation. Furthermore, the onsite examination showed that the aircraft impacted terrain in about a 70° nose-down attitude with no forward momentum with both the engine and tail sections deflected to the right.
Both the observations made by the witness and the condition of the wreckage were consistent with the aircraft stalling and entering a left spin. The Pilot’s Operating Handbook indicated that this occurred at a height from which the stall and spin was not recoverable, resulting in the impact with terrain.
Pilot qualifications
In order to undertake the activity of aerial mustering with an aeroplane, both a low-level rating and aerial mustering endorsement were required, however, the pilot did not possess the latter. During their time at Mulgathing Station, the pilot was observed on several occasions to dive towards sheep in an attempt to move them. This manoeuvre is considered to be aerial mustering. On the day of the accident, the pilot declined assistance from a colleague on a motorbike, stating their intention to move the sheep with the aircraft and they were subsequently observed conducting this manoeuvre.
Low-level flying is a higher risk activity and aerial mustering adds further complexity and risk as the pilot must divide their attention between flying the aircraft, monitoring the livestock on the ground and the effects of their flying on the livestock. Not having the additional training and experience that would have come with the aerial mustering endorsement likely left the pilot ill‑equipped to manage the challenges associated with mustering sheep. As they were not instructed in the appropriate techniques for mustering, this placed the pilot at an increased risk of experiencing a loss of control at low-level.
Job application and role
The pilot applied for, and was awarded, the job described as being a pilot/station hand. The job advertisement stated that the main flying duties would be ‘aerial stock mustering’. As mentioned above, from an aviation perspective this meant that the pilot was required to have an aeroplane aerial mustering endorsement. However, the qualifications specified for the role did not include such an endorsement, nor did the pilot have one. Instead, the qualifications listed were consistent with the operator’s intention for the role of aerial spotting requiring only a low-level rating, which the pilot had. It was unclear to what extent, if any, the description of ‘aerial stock mustering’ influenced the pilot’s actions.
Despite this, from the time they started the role, up until the day of the accident, they were observed mustering sheep using manoeuvres that were outside the scope of their qualifications and the operator’s intentions. Furthermore, although these actions were witnessed by several staff at the station, including the station manager, none of the staff reported being aware that the pilot was not qualified to perform aerial mustering.
Seatbelts
The onsite inspection found that the upper torso restraint was stowed in the roof line indicating that it was not used by the pilot. Although the pilot was only required to use the lap belt at the time of the accident, the aircraft was fitted with an over the shoulder sash belt and the benefits of using them are well documented. However, in this case, given the extent of damage to the aircraft, it was unlikely the upper torso restraint would have contributed to the survivability of the accident.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving a Cessna 172N, registered VH‑SQO, near Mulgathing, South Australia, on 27 June 2024.
Contributing factors
While in a steep climb-out after diving towards sheep, control of the aircraft was lost leading to an aerodynamic stall and spin from a height that was not recoverable.
Although the pilot held a low-level rating, they were conducting aerial mustering operations without the related qualification. Consequently, the pilot was not appropriately experienced to manage the challenges likely encountered during aerial mustering.
Other factors that increased risk
The operator had advertised for a pilot to conduct ‘aerial stock mustering’ operations, but did not require the qualifications to perform that activity as their expectation was that the role would only involve aerial spotting.
The upper torso restraint part of the lap-sash seatbelt was not worn on the accident flight.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Jumbuck Pastoral
On 13 February 2025, Jumbuck Pastoral advised the ATSB that it has undertaken the following safety action:
A Safe Aerial Spotting & General Station Aviation Manual is in the process of being prepared.
Implemented a mentoring program for pilots, particularly at Mulgathing Station.
A safety audit has been conducted by an external third party. This is currently before the Board.
It is undertaking a full review of its operations to ensure compliance with the Civil Aviation Regulations 1988 and Civil Aviation Safety Regulations 1998, as well as the safety and training standards for pilots.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
Jumbuck Pastoral
South Australian Police Service
maintenance organisation for VH-SQO
accident witnesses.
Submissions were received from:
Civil Aviation Safety Authority
Jumbuck Pastoral
South Australian Police Service.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Lamb marking refers to husbandry procedures including tail docking, castration of males, ear tagging, mulesing, and vaccination.
[2]For training purposes, these manoeuvres were performed above 3,000 ft.
[3]Yaw: the motion of an aircraft about its vertical or normal axis.
[4]Carbon monoxide is a colourless, odourless, tasteless, and poisonous gas that is produced as a by-product of burnt fuel. Exposure to a leak from the exhaust of an aircraft engine into the cabin can lead to elevated levels of carbon monoxide, which can impair cognitive function.
On 15 March 2024, a Bell 47G helicopter was conducting a post-purchase familiarisation flight at Nyngan, New South Wales. At 1200 local time, while hovering, the pilot commenced a practice left pedal clearing turn through the 180-degree position. The helicopter experienced weathercocking[1] followed by an unanticipated yaw. The wind was gusting 15‑20 knots.
The pilot detected that the yaw rate was increasing and climbed the helicopter to 30 ft, attempting to control the increased rate of rotation through the application of the opposite anti-torque pedal. The pilot then experienced a loss of control resulting in a hard landing. The left skid subsequently detached from the airframe and the main rotor blades contacted the ground resulting in damage to the tail rotor guard tube and a tail rotor frame crack.
The pilot detected leaking fuel from the fuel vents on top of the left fuel tank and a subsequent fire commenced at the base of the helicopter engine. The helicopter was destroyed by fire.
Figure 1: Helicopter damage – looking at the base of the helicopter
Source: Operator
Figure 2: Helicopter tail rotor damage
Source: Operator
Pilot’s comments
Based on the pilot’s account of the accident and assessment of the recovered aircraft, mechanical malfunctions were ruled out as a contributing factor.
The pilot advised that they may not have held an effective amount of pedal in an attempt to regain control. A better outcome could have been achieved by transitioning to forward flight allowing them to arrest the rotation speed through the use of the pedals in a controlled manner to improve directional stability.
Safety message
Unanticipated yaw is described by the European Union Aviation Safety Agency (EASA) as ‘an unanticipated or unintended rotation of the helicopter about the yaw axis. It occurs when the pedal input is not appropriate, and the helicopter suffers a sudden and unexpected yaw’.
A situational awareness of flight characteristics, weather conditions and recovery procedures are required when conducting low speed flight. The various wind directions can result in significantly differing rates of turn for a given pedal position. The most important principle for the pilot to remember is that the tail rotor is not stalled. The corrective action is to apply pedal opposite to the direction of the turn. Avoiding a loss of control may best be accomplished by pilots avoiding conditions which are conducive to unanticipated yaw. Appropriate and timely response is essential and critical. By maintaining an acute awareness of wind and its effect upon the helicopter, the pilot can significantly reduce exposure to an unanticipated yaw.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Weathercocking - a helicopter with its tail into wind is in an unstable position. The wind acts on the vertical fin and continuous and variable yaw control inputs are required to achieve precise control and counteract the tendency of the helicopter to turn into wind.
On 19 May 2024, a Tecnam P2600T aircraft was being operated on a flight from Salakanagara Tanjung Lesung airfield, Banten, Indonesia to Pondok Cabe Airport, Jakarta, Indonesia, with 3 people on board. At 1344 local time, on approach to Pondok Cable Airport at an altitude of 1,000 ft, the pilot declared a MAYDAY. Shortly after, the aircraft collided with terrain near a main road. All occupants were fatally injured.
The Indonesian National Transportation Safety Committee (NTSC) is investigating this occurrence.
NTSC has requested assistance from the ATSB to recover data from a damaged GPS unit. To facilitate this support and to provide the appropriate protections for the information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of the International Civil Aviation Organization Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
The ATSB has completed its work recovering the GPS data. A copy of the data and a report detailing the work undertaken by the ATSB was provided to the NTSC on 19 July 2024.
Any enquiries relating to the investigation should be directed to NTSC.
On 26 May 2024, a Cessna T210M, registered VH-MYW, was prepared for flight at Maitland Airport, New South Wales. The pilot planned to ferry the aircraft to Bankstown Airport, where the aircraft was to undergo maintenance. There was a pilot and one passenger on board.
During the approach, the engine stopped and while looking for a suitable landing place, the pilot saw a taxiway on the airport and decided to aim for that. To successfully reach the airport, the pilot elected to leave the flap retracted and gear up. This was done to reduce drag and achieve maximum glide range. Once the aircraft was assured of a landing on the airport, the gear was lowered. However, it did not successfully lock into place due to the limited time available before touchdown. The aircraft landed wheels-up resulting in minor damage and both occupants were uninjured.
What the ATSB found
The ATSB determined that, while the aircraft departed with sufficient fuel to complete the intended flight, it is likely that the amount of fuel reduced to a level that, in combination with unbalanced flight approaching Bankstown Airport, resulted in the engine being starved of fuel.
The ATSB also determined that the pilot's decision to carry non-essential crew placed the additional occupant at unnecessary risk of injury.
Safety message
Fuel starvation occurrences can often be prevented by conducting thorough pre-flight fuel quantity checks combined with inflight fuel management. Pilots are reminded to check fuel quantities prior to departure using a known calibrated instrument such as a dipstick. In addition, comparing the expected fuel burn with actual fuel remaining after a flight, will give a validated fuel burn for the aircraft and ensure the measuring equipment is accurate. Pilots should familiarise themselves with the Civil Aviation Safety Authority, Advisory Circular AC 91-15v1.1 Guidelines for aircraft fuel requirements, which provides further guidance for in‑flight fuel management.
Practising forced landings from different altitudes under safe conditions can help pilots prepare for an emergency situation, should one arise. Some components of the aircraft such as flap and gear, increase drag and reduce the glide range. Being familiar with emergency checklists and your aircraft’s systems will assist in an emergency when identifying and managing an engine failure.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 26 May 2024, a Cessna T210M, registered VH-MYW, was prepared for flight at Maitland Airport, New South Wales (NSW). The pilot planned to ferry the aircraft to Bankstown Airport, where the aircraft was to undergo maintenance. As the pilot had not previously operated to Bankstown Airport, they elected to carry a passenger, who was also a helicopter pilot, to assist with navigation and radio communication.
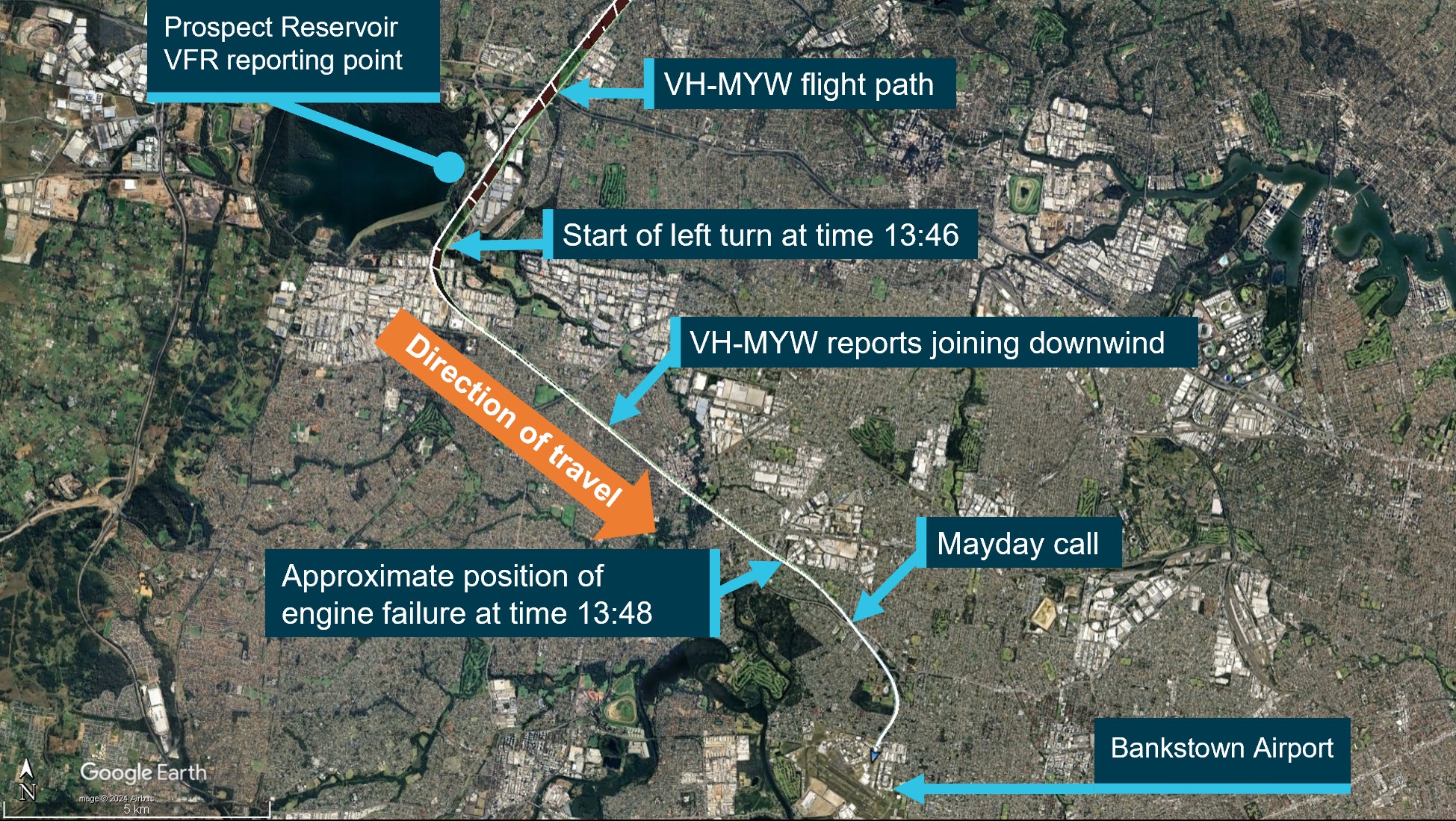
At 1313 local time, with the left fuel tank selected for take-off, the aircraft departed from runway 23[1] and tracked south. The pilot reported that about 4 minutes into the flight (while passing abeam Cessnock) they selected the fuller right tank, which they thought would reduce workload when entering Bankstown airspace. The aircraft entered the Visual Flight Rules (VFR) route[2] between Brooklyn Bridge and Prospect Reservoir at 1336 at approximately 2,000 ft.
Figure 1: Sequence of events
The image shows the sequence of events leading up to and during the forced landing, it highlights relevant places and reference times. Source: OzRunways flight data overlay on Google Earth.
The aircraft arrived overhead Prospect Reservoir at 1346 (Figure 1) and the aerodrome controller (ADC) instructed VH-MYW to maintain 1,500 ft and join the downwind leg of the circuit for runway 29R. An approximate 25° angle of bank turn was conducted to track toward a downwind join for runway 29R.
At 1347, the pilot reported joining downwind for 29R and the ADC instructed them to maintain 1,500 ft and provided them with updated Automatic Terminal Information Service (ATIS) [3] information ‘Foxtrot’. The pilot confirmed receipt of the new information by reading back the new QNH.[4]
The pilot recalled that, at about the time of that radio transmission, with the aircraft about 4.5 km north-west of Bankstown Airport, the propeller RPM increased, and they felt a braking sensation. They recalled that, in response they attempted to reduce drag on the propeller, changed fuel tank selection and briefly selected the electric fuel boost pump to ON. They then aimed to maintain glide speed while looking for a place to land.
At 1348, the pilot transmitted a MAYDAY call on the Bankstown Tower radio frequency stating they were having engine problems. The ADC advised that all runways were available, and they could track as required. The ADC continued to coordinate traffic to assist VH-MYW.
The pilot reported that while they were looking for a place to conduct a forced landing, they saw a taxiway on the airport and decided to try to land there. They advised that, during the approach the aircraft clipped the top of a tree and they raised the aircraft’s nose at the last minute to avoid a building on the airport perimeter. They decided not to deploy landing gear or flap until they were assured of reaching the airport.
At 1350, a helicopter operating in the area, reported that the aircraft had landed at the intersection of taxiway November 1 and taxiway Lima.
Both occupants of the aircraft were uninjured, and the aircraft sustained minor damage.
Context
Pilot
The pilot held a private pilot licence (aeroplane) issued in 2014 with a single‑engine class rating. They were appropriately endorsed to fly the Cessna 210 with design features for manual propeller pitch control and retractable undercarriage. The pilot also held a current class 2 aviation medical certificate.
They had accrued a total flight experience of approximately 222 hours, of which 15 hours were on the Cessna 210. In addition, they had previously flown other aircraft in this range including the Cessna 206 and Cessna 177. The pilot’s licence showed an entry for a single‑engine flight review conducted on 31 May 2023.
Weather
At the time of the incident, the Automatic Terminal Information Service information ‘Foxtrot’ was current, which indicated CAVOK[5] conditions, temperature 22°C, wind direction variable at 5 kt, and runway 29R in use for arrival and departures.
Aircraft
The aircraft was a Cessna Aircraft Company T210M manufactured in 1978 and issued serial number 21062277. It was powered by a fuel‑injected Continental Motors Inc TSIO-520-R piston engine driving a 3‑bladed, constant‑speed McCauley Propeller.
The aircraft was purchased from South Africa where it was previously registered as ZS-MYV and was shipped to Australia where it was reassembled and placed on the Australian register on 19 March 2021 as VH-MYW.
Maintenance
The aircraft was issued a maintenance release in November 2022 for private operations however, this expired in November 2023. At the time of the incident the aircraft was being ferried to Bankstown for completion of the maintenance required to return the aircraft to service.
As the maintenance release had expired, a special flight permit (SFP) was issued for the purpose of completing this ferry flight. The SFP was issued by the Civil Aviation Safety Authority (CASA) on 14 May 2024. The permit expired on 31 May 2024 and was subject to the following conditions:
Essential operating crew only to be carried.
Daily inspection and flight times are to be recorded on the Maintenance Release.
Day VFR, non-commercial operation by the most direct route practical and permitted by weather.
Operation shall be conducted in accordance with the approved flight manual / cockpit placards for the aircraft.
A copy of this SFP to be carried on-board and filed with the aircraft logbooks.
The permit also stated the flight was permitted to depart Maitland and arrive at Bankstown.
The last daily inspection signed on the aircraft maintenance release was completed on 2 November. The pilot advised that they had completed the daily inspection prior to the flight, but this was not recorded on the maintenance release.
The aircraft maintenance release also carried 2 endorsements for defects. These included the wing flaps not extending equally and hail damage. The flap defect was addressed by a third party, however, the hail damage was assessed by the aircraft owner in accordance with the CASA Airworthiness Bulletin 51-010 Assessment of hail damage.
Airworthiness Bulletin 51-010 recommended having a person who was appropriately qualified under Civil Aviation Safety Regulations 21.M to inspect the aircraft.
The pilot reported the aircraft had a tendency to fly right wing down. There was insufficient evidence available to the ATSB to determine whether either of the aircraft defects contributed to the flight characteristics described by the pilot.
Aircraft systems
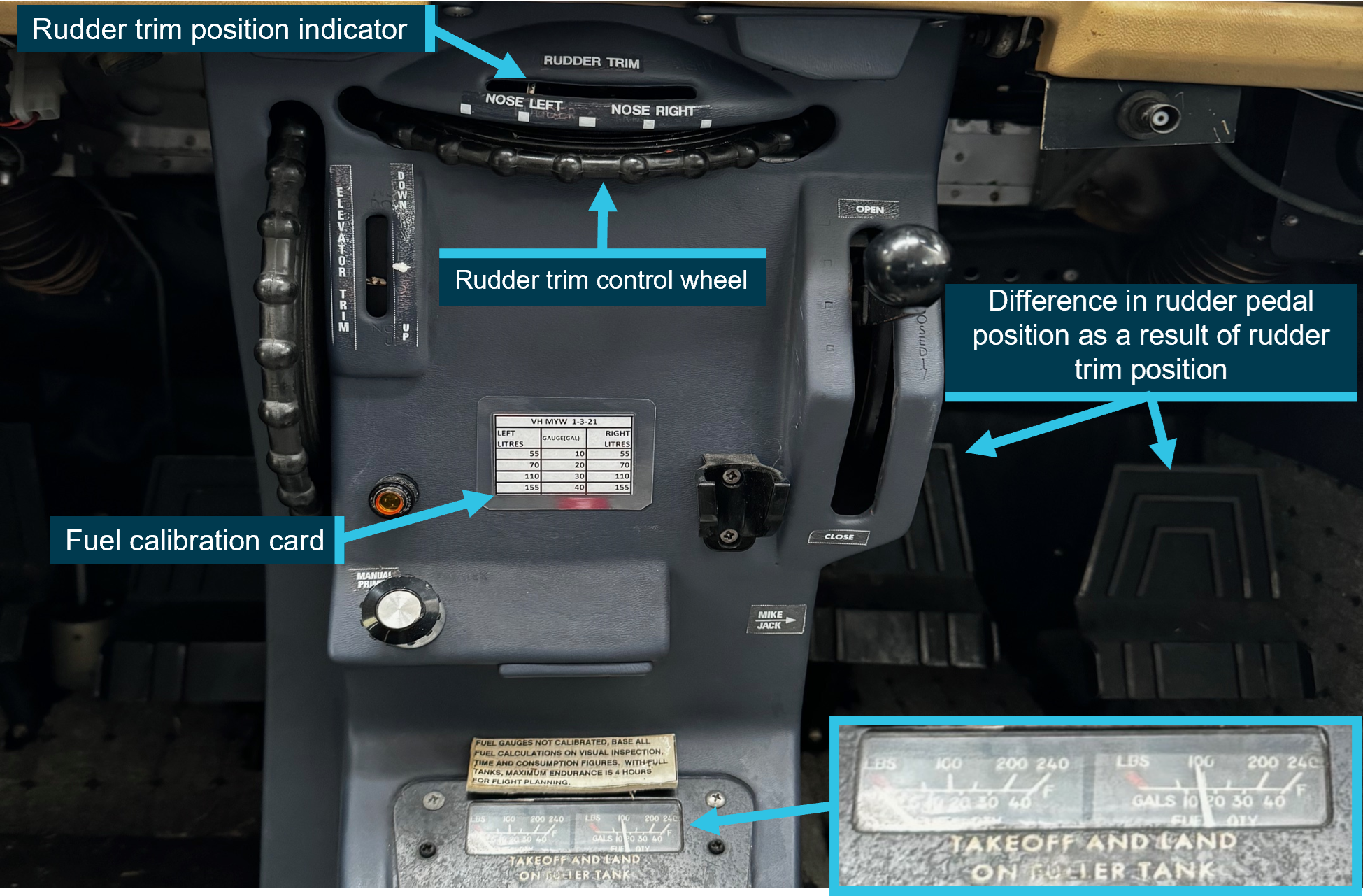
Trim
The aircraft was fitted with elevator and rudder trim. Rudder trimming was accomplished via a wheel mounted in the cockpit (Figure 2). Setting the rudder trim left of centre would result in the aircraft maintaining the nose left of the flight path and remaining in that position until the wheel was manipulated, or the rudder pedals were manipulated. To maintain the desired track with that trim configuration, the aircraft would need to be flown in an uncoordinated state with the right wing low.
The aircraft’s pilot operating handbook stated:
Unusable fuel is at a minimum due to the design of the fuel system. However, when the fuel tanks are ¼ full or less, prolonged uncoordinated flight[6] such as slips or skids can uncover the fuel tank outlets, causing fuel starvation and engine stoppage. Therefore, with low fuel reserves, do not allow the airplane to remain in uncoordinated flight for periods in excess of one minute.
Cessna advised this was originally added to the Cessna 210 model D owner’s manual and was carried through as the aircraft developed into different models. Cessna did not have the available data to assess the likelihood of uncoordinated flight contributing to fuel starvation.
The pilot stated the rudder trim had been set left of centre since the aircraft was re‑assembled in Australia and that the trim wheel was not manipulated in flight.
Figure 2: Aircraft control pedestal post-incident
The image shows the fuel gauge level and the rudder trim. The image was taken on 6 June 2024, several days after the incident. However, the person responsible for recovering the aircraft stated, no fuel was added prior to this photo and the trim was set as found on the day of the incident. Source: Engineer responsible for aircraft recovery.
Fuel system
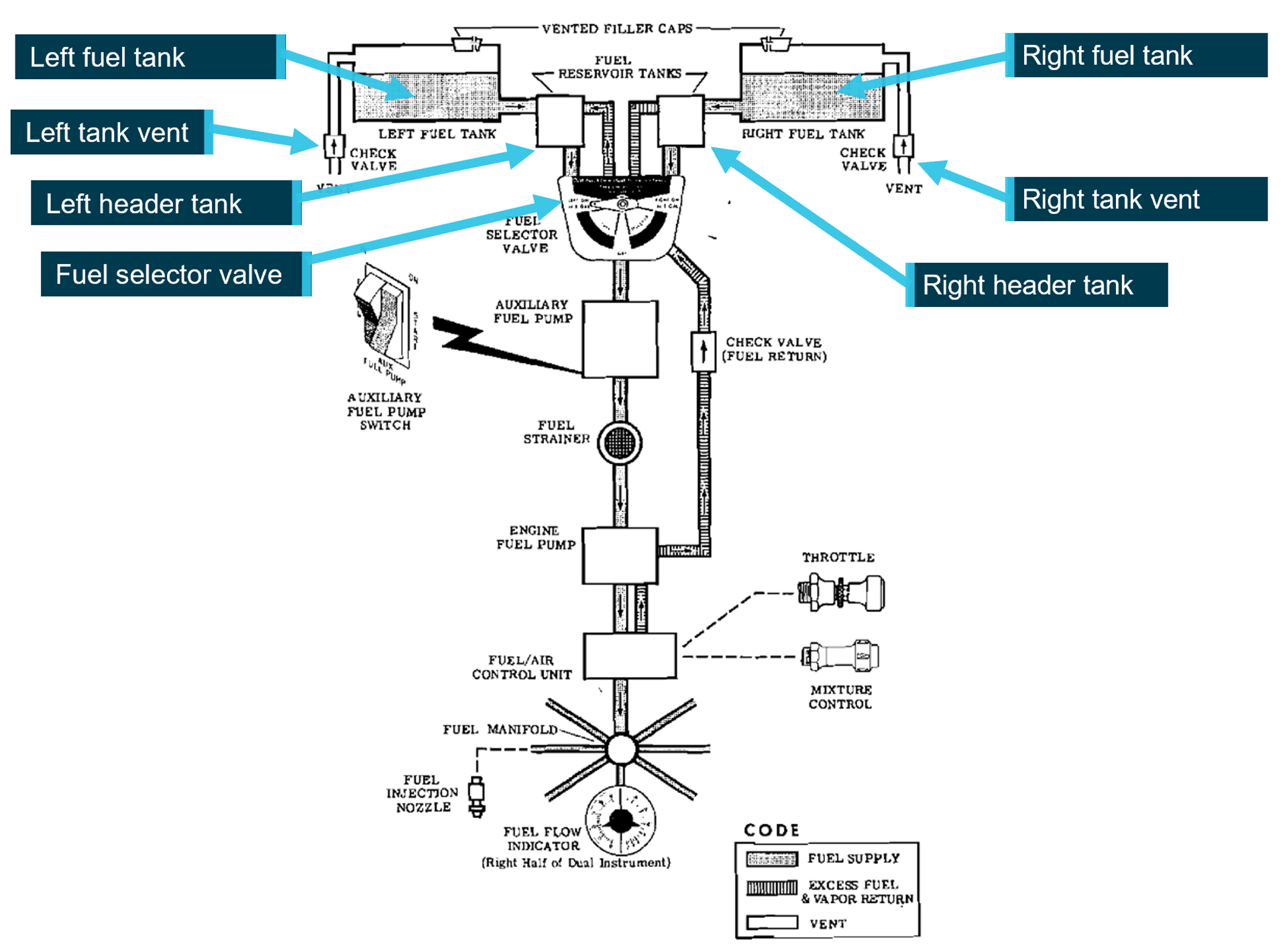
The Cessna 210 fuel system consists of a main fuel tank located in each wing. Each tank capacity is 171 L, of which 169 L is usable fuel. Each tank gravity fed a smaller fuel reservoir tank of approximately 1.9 L through fuel collector ports, which were located at the forward and aft inboard side of the main fuel tank (Figure 3Figure 3 and Figure 4).
Figure 3: Cessna 210M fuel schematic
Source: Cessna 210M pilot operating handbook, annotated by the ATSB
The fuel selector valve had 3 positions – left, right, and off – and so fuel could only be drawn from either the left or right tank. Cessna advised that at a low cruise power setting, if no fuel was being fed to the smaller fuel reservoir tank, it could supply fuel to the engine for between 1.5–3.5 minutes. The pilot advised that, at the time of the power loss the fuel selector was selected to the right fuel tank.
The fuel system has an engine-driven fuel pump and an auxiliary fuel pump, which is electrically driven. The pilot operating handbook states the following:
If it is desired to completely exhaust a fuel tank quantity in flight, the auxiliary fuel pump will be needed to assist in restarting the engine when fuel exhaustion occurs.
Cessna stated that during testing, the electric auxiliary fuel pump was required to operate for 4 seconds to restart the engine.
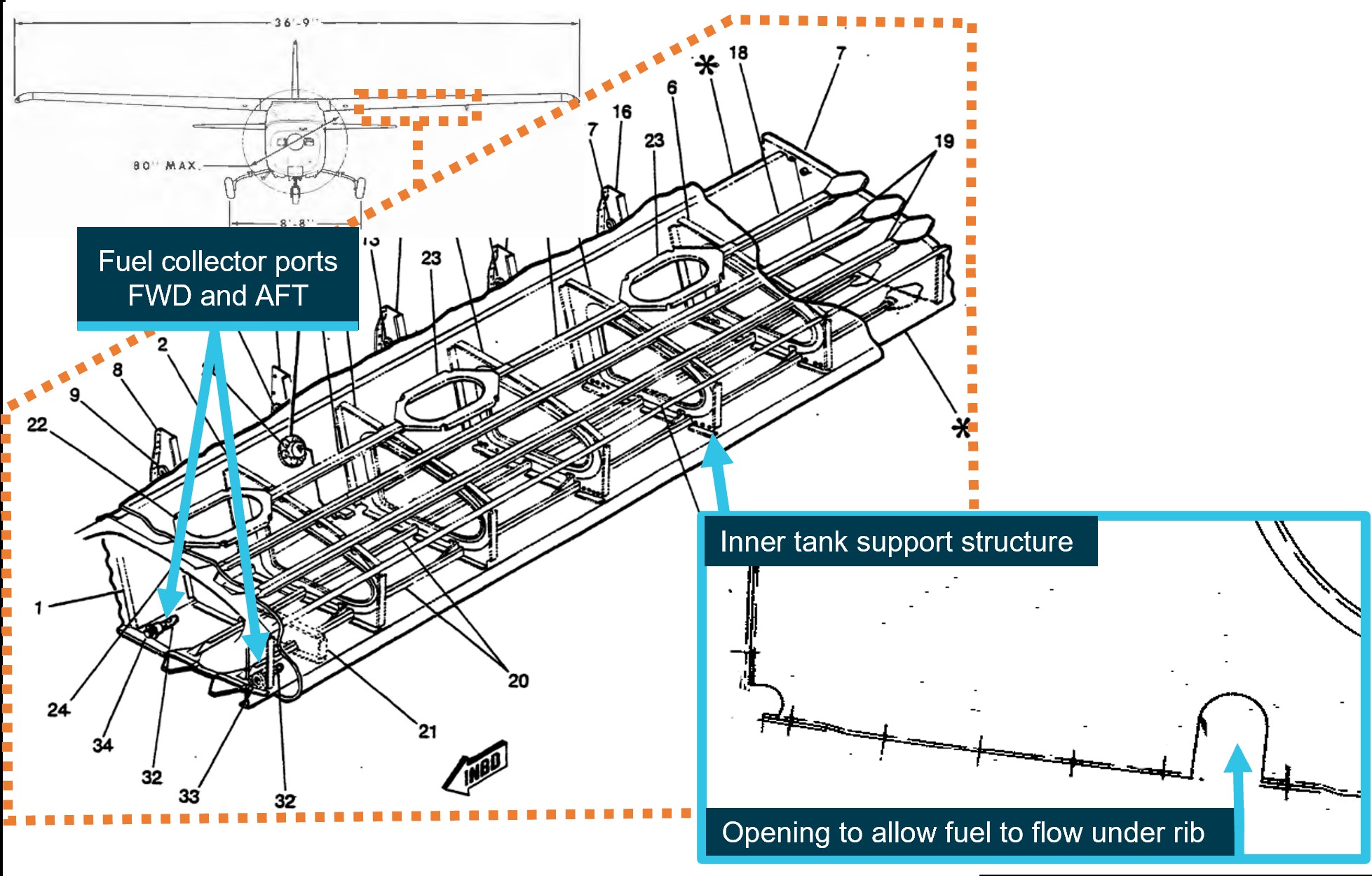
Figure 4: Fuel tank design
The above image shows the location of the fuel collector ports and the openings that are located in the rib support structure. The fuel cell image shown is for later serial numbers of the Cessna 210. However, it is the most descriptive image of fuel collector ports. Further images provided by Cessna show the aft collector port is located in a similar location to the above image. Source: Cessna 210 illustrated parts catalogue model 210 & T210 series 1981–1986, annotated by the ATSB.
The fuel tank design included an internal rib support structure (Figure 4). Each rib had an enlarged centre opening for fuel to freely flow through the tank, with small openings at the base of each rib, ensuring useable fuel could not become trapped. Cessna stated, ‘The small, if any, amount of fuel caught behind any structure would be part of the unusable fuel level determined during certification.’
Propeller
A control lever was used to set aircraft RPM by changing the propeller blade pitch. When the control lever is pushed inward, the propeller increases RPM (low blade pitch). When the control lever is pulled outward, the propeller RPM decreases (high blade pitch). This is achieved by a propeller governor which relies on engine oil pressure to move the propeller toward a high blade pitch (low RPM).
The combination of an internal spring and centrifugal force, twists the blades toward a low pitch (high RPM) setting when oil pressure at the propeller hub is relieved.
Engine Failure During Flight checklist
The pilot operating handbook provided the following checklist to be conducted in the event of an engine failure during flight:
airspeed – 85 [kt indicated airspeed] KIAS
fuel quantity – check
fuel selector valve – fuller tank
mixture – rich
auxiliary fuel pump – on for 3-5 seconds with throttle ½ open; then off
ignition switch – both (or start if propeller is stopped)
throttle advance slowly.
Flight data
The ATSB obtained flight data from an electronic flight bag (EFB) used by the pilot. The data provided aircraft position, time, altitude, and ground speed.
The flight data was analysed by the ATSB to obtain the approximate position when the engine stoppage occurred. This was determined to be at 1348 as there was a significant reduction in ground speed at that time.
Flight planning and fuel usage
The pilot reported that during the cruise, the manifold pressure was set near the top of the green (approximately 25 inches) and RPM at 2,200. A fuel flow reading was noted by the pilot of 14 gallons per hour (53 L/hr).
The pilot advised that they normally dipped the tank during the pre-flight inspection using the aircraft’s fuel dipstick. During the pre-flight they estimated 150 L of fuel on board, 60 L in the left tank and 90 L in the right tank (see the section titled Fuel system). Using that fuel quantity and recorded flight data, Table 1 details the expected consumption throughout the flight.
Table 1: Estimated fuel burn based on flight data
Sector
Start time
Block time
(min)
Estimated fuel burn (L) at 53 L/hr
Total
Comments
Departing Maitland
1313
0
5
145
Pilot stated, they departed on left tank (5 L allowed for taxi)
Abeam Cessnock
1317
4
4
141
Climbing phase, fuel burn was likely higher than 53 L/hr.
Near Warnervale
1325
8
8
133
Pilot stated, at approximately overhead Cessnock, they swapped to right fuller tank.
Brooklyn Bridge
1336
11
10
123
Prospect Reservoir
1346
10
9
114
Estimated engine stop
1348
2
2
113
Total
35
38
Totals have been rounded up
Post-incident inspection
The ATSB did not attend the site. A video of the aircraft, provided by 9News Australia showed fuel leaking from the right fuel tank vent. The aerodrome operator who attended the incident site stated that the fuel which leaked from the vent was no more than 2–4 litres, of which most was funnelled into a jerrycan. While the ATSB could not verify how long the fuel was leaking, based on the observations of the aerodrome operator, it was unlikely to have significantly affected the amount of fuel in the tank. There was no evidence of fuel leaking from the left tank.
Figure 5: Fuel leak from right tank vent
Source: 9News Australia
The aircraft was recovered, and an initial inspection was completed. The fuel level was checked using the on-board fuel gauges and dipstick. The left tank was estimated to hold between 0–5 L and the right tank was estimated between 40–50 L.
The aircraft’s damaged propeller was removed, and a suitable test propeller was fitted to the aircraft. The engine was started and was able to draw fuel from the remaining fuel in both tanks, the test continued for approximately 5 minutes on each tank. However, high power settings similar to in‑flight conditions were not tested.
The aircraft had undergone a fuel calibration and the placard above the fuel gauges was no longer relevant however, it was not removed (Figure 2). The placard was not considered to have contributed to the incident as the fuel on board was likely less than the 4 hours stated on the placard. The onboard fuel dipstick used was labelled C210 dipstick and was marked with the aircraft’s previous registration, ZS-MYV.
Related occurrences
Fuel management and fuel starvation incidents and accidents continue to occur with single and twin-engine aircraft. Examples of other ATSB investigations of similar occurrences include:
Fuel starvation and forced landing involving Piper PA-31-350, VH-HJE, 11 km south of Archerfield Airport, Queensland, on 7 April 2023 (AO-2023-017)
Fuel starvation and ditching involving Piper PA-28, VH-FEY, 15 km north-west of Jandakot Airport, Western Australia, on 20 April 2023 (AO-2023-021)
Fuel starvation and forced landing involving Pilatus Britten-Norman Islander BN2A, VH-WQA, Moa Island, Queensland, on 3 October 2022 (AO-2022-046).
Safety analysis
The pilot reported that, during approach to Bankstown Airport, they noted an increase in propeller RPM and could not maintain altitude. This behaviour was consistent with an engine failure, with the associated loss of oil pressure resulting in the propeller moving to a finer pitch (increased RPM). The post-incident aircraft inspection did not identify an engine malfunction, and the engine was able to run at low power on the remaining fuel in both tanks. As there was no evident malfunction of the engine, the most probable reason for the inflight power loss was fuel starvation.
The pilot reported that the aircraft departed with 90 L in the right tank and 60 L in the left tank (150 L total). They also advised the right tank was selected for most of the flight. If this was the case, there should have been approximately 61 L in the right tank and 51 L in the left tank. However, given the total fuel on board after the incident occurred (maximum 59 L), it was unlikely that approximately 91 L was burnt during the 35-minute flight. Therefore, it was unlikely that the amount of fuel the pilot stated was on board at the commencement of the flight was actually in the aircraft. Significantly however, there was sufficient total fuel on board for the flight.
The post-incident inspection revealed between 40–50 L remaining (which equated to approximately 1/4 full tank) in the right tank, with about 2–4 L reportedly leaking after the landing. The pilot operating handbook (POH) stated that if there was less than 1/4 fuel in the tank and the aircraft was in uncoordinated flight, the fuel pick-ups could uncover, and fuel starvation could occur.
The post-incident inspection also revealed between 0–5 L remaining in the left fuel tank. If the engine was being supplied from the left tank, during an uncoordinated left turn at Prospect Reservoir at 1346, it is possible the fuel drained away from the fuel pick-ups and the engine continued to draw fuel from the left header tank until 1348 when the engine stopped. This was consistent with Cessna’s advice that the header tank can supply fuel for 1.5–3.5 minutes at low cruise power.
In summary, irrespective of which tank was supplying the engine, the quantities of fuel remaining, when combined with the uncoordinated flight, were conducive to fuel starvation in accordance with the POH.
The pilot’s initial response during the emergency was largely focused on attempting to reduce drag created by the propeller, despite the aircraft not having this ability, and they did not complete the engine failure during flight checklist. If the checklist had been followed, the pilot would have increased the likelihood of restarting the engine in flight. During the extended period where the aircraft was resting on the ground and positioned right-wing low, it is likely the fuel remaining in the left tank drained into the left header tank. Even though this fuel was sufficient to run the engine at low power, it may not have been available during approach or sufficient for the power required in flight.
The pilot’s decision to minimise the aircraft’s drag during the glide, by keeping the gear up and flaps retracted, combined with managing the airspeed, resulted in the aircraft achieving the required performance to land safely inside the airport environment. However, due to the distance the aircraft needed to glide and obstacles that needed to be cleared, by the time the landing gear was selected down, there was not enough time to extend and lock in place before the aircraft collided with the ground resulting in a wheels-up landing.
Finally, the CASA special flight permit was issued for the purpose of ferrying the aircraft for maintenance. The conditions put in place were to minimise the consequences if an incident occurred during flight which was conducted outside of the normal aircraft operation. Although their reported purpose was to assist with navigation and radio communication, the pilot’s decision to allow a passenger to fly on board the aircraft unnecessarily exposed them to a risk of injury and consequently was another factor that increased risk.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel starvation involving Cessna T210M, VH-MYW, 4 km north-west of Bankstown Airport, New South Wales, on 26 May 2024.
Contributing factors
While the aircraft departed with sufficient fuel to complete the intended flight, low usable fuel quantities, in combination with probable uncoordinated flight approaching Bankstown Airport, resulted in the engine being starved of fuel.
Other factors that increased risk
The pilot's decision to carry non-essential crew placed the additional occupant at unnecessary risk of injury.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot
aerodrome operator
engineer responsible for aircraft recovery
aircraft manufacturer and insurer
Civil Aviation Safety Authority
Airservices Australia
OzRunways recorded data
video footage of the incident flight and other imagery taken on the day of the incident.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot
engineer responsible for aircraft recovery
Civil Aviation Safety Authority
aircraft manufacturer.
Submissions were received from the:
pilot
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[2]VFR route: A pre-defined laneway for aircraft traffic to remain clear of airspace and enter or exit high traffic areas such as Bankstown Airport.
[3]Automatic terminal information service: The provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is prefixed with a unique letter identifier and is updated either routinely or when there is a significant change to weather and/or operations. See Automatic terminal information service (ATIS).
[4]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[5]Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[6]Uncoordinated flight occurs when the aircraft skids or slips, this is most commonly associated with a turn, but a skid can occur when the ailerons and rudder are used in opposite directions during normal flight.
Occurrence summary
Investigation number
AO-2024-033
Occurrence date
26/05/2024
Location
4 km north-west of Bankstown Airport
State
New South Wales
Report release date
11/10/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing, Fuel starvation, Wheels up landing
On 16 April 2024, a pilot and passenger were conducting a private flight in an Aeropilot Legend 600 aircraft, south of Perth, Western Australia. During cruise, controllability issues were encountered which led the pilot to deploy the aircraft's emergency parachute.
The aircraft collided with trees prior to impacting the ground near Preston Beach. The pilot and passenger received minor injuries. An inspection of the aircraft identified that the vertical stabiliser had detached from the tail section of the aircraft.
Recreational Aviation Australia (RAAus) commenced an investigation in response to this accident. RAAus requested technical assistance from the ATSB to examine components from the aircraft. To facilitate that request, an investigation under the Transport Safety Investigation Act (2003) has been commenced.
Any enquiries relating to the accident should be directed to RAAus.
On 27 April 2024, a Grob - Burkhart Flugzeugbau G109B glider, registered VH-GUM, collided with terrain at Mount Beauty, Victoria. The pilot and passenger were fatally injured.
In response to this accident, Gliding Australia commenced an investigation. As part of its investigations, Gliding Australia requested technical assistance from the ATSB to examine video footage of the accident.
To facilitate this support and to provide the appropriate protections for the information, the ATSB initiated an investigation under the Transport Safety Investigation Act 2003.
The ATSB has concluded work on the supplied video footage and provided the results to Gliding Australia on 20 May 2024.
Any enquiries relating to the accident investigations should be directed to Gliding Australia.
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
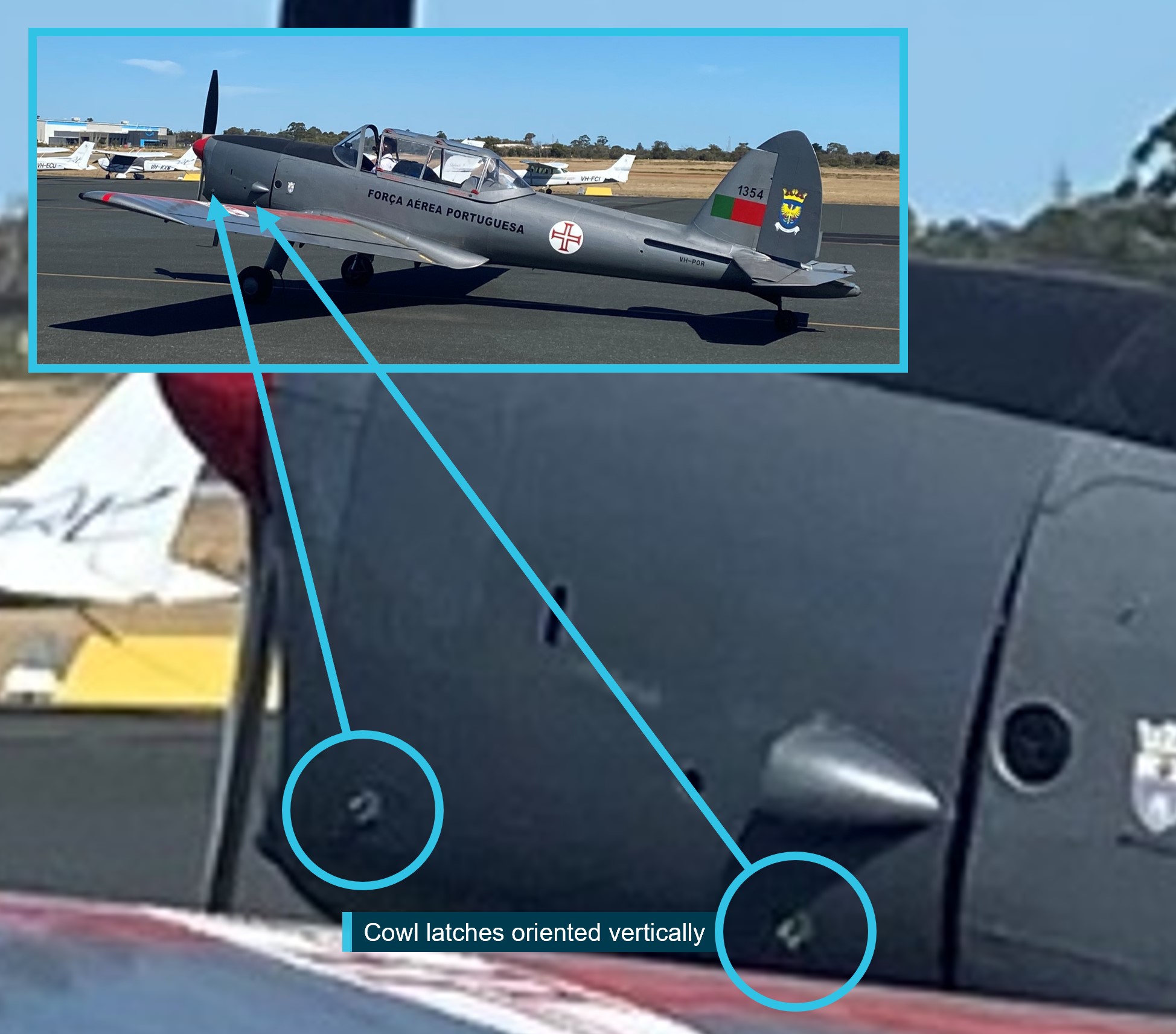
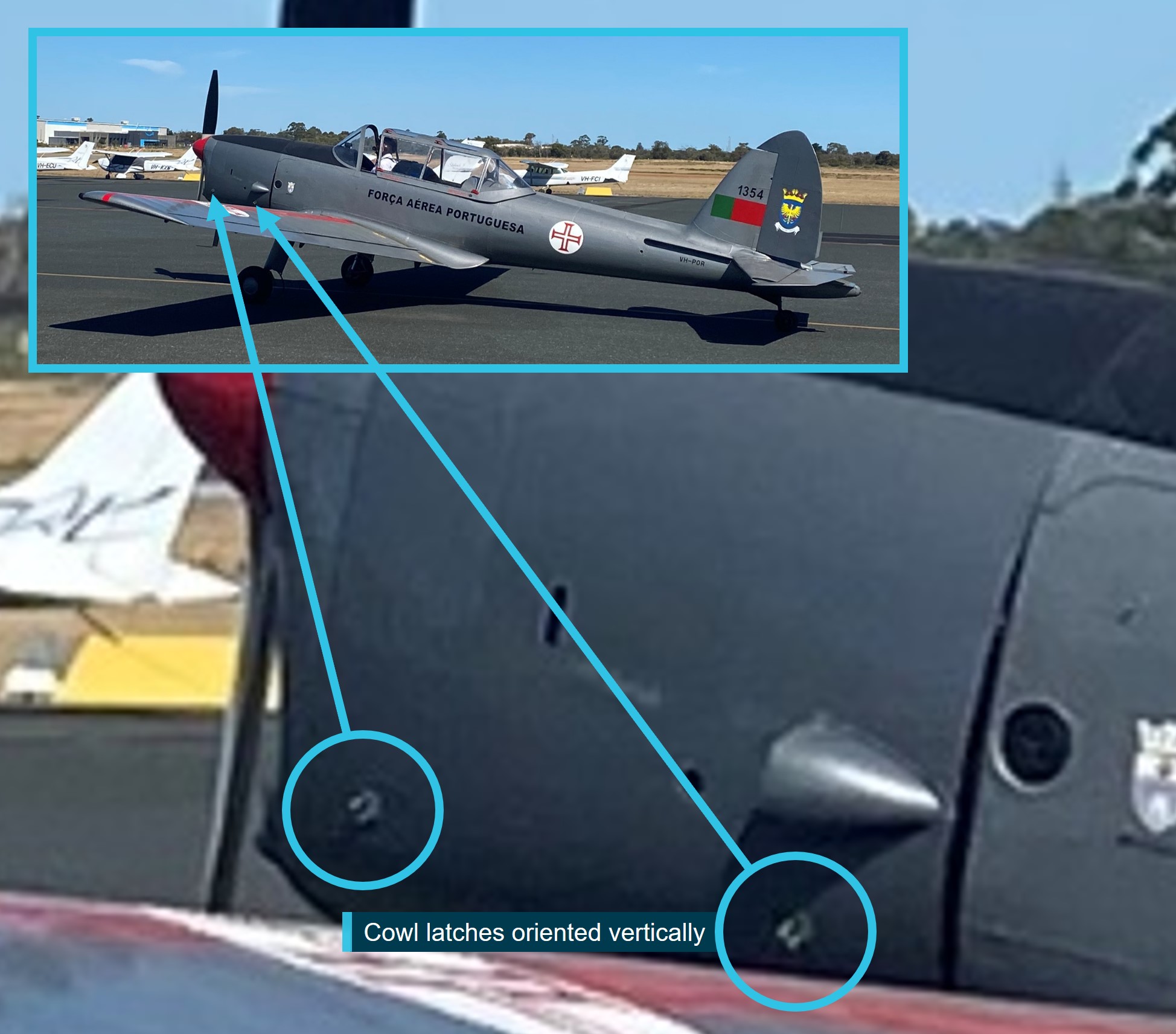
On the afternoon of 26 April 2024, the pilot (who was the sole occupant) of a DHC‑1 MK 22 Chipmunk, registered VH‑POR, commenced taxi for take-off at Jandakot Airport, Western Australia for a private flight. The weather was clear, with the wind about 10 kt from the north‑west.
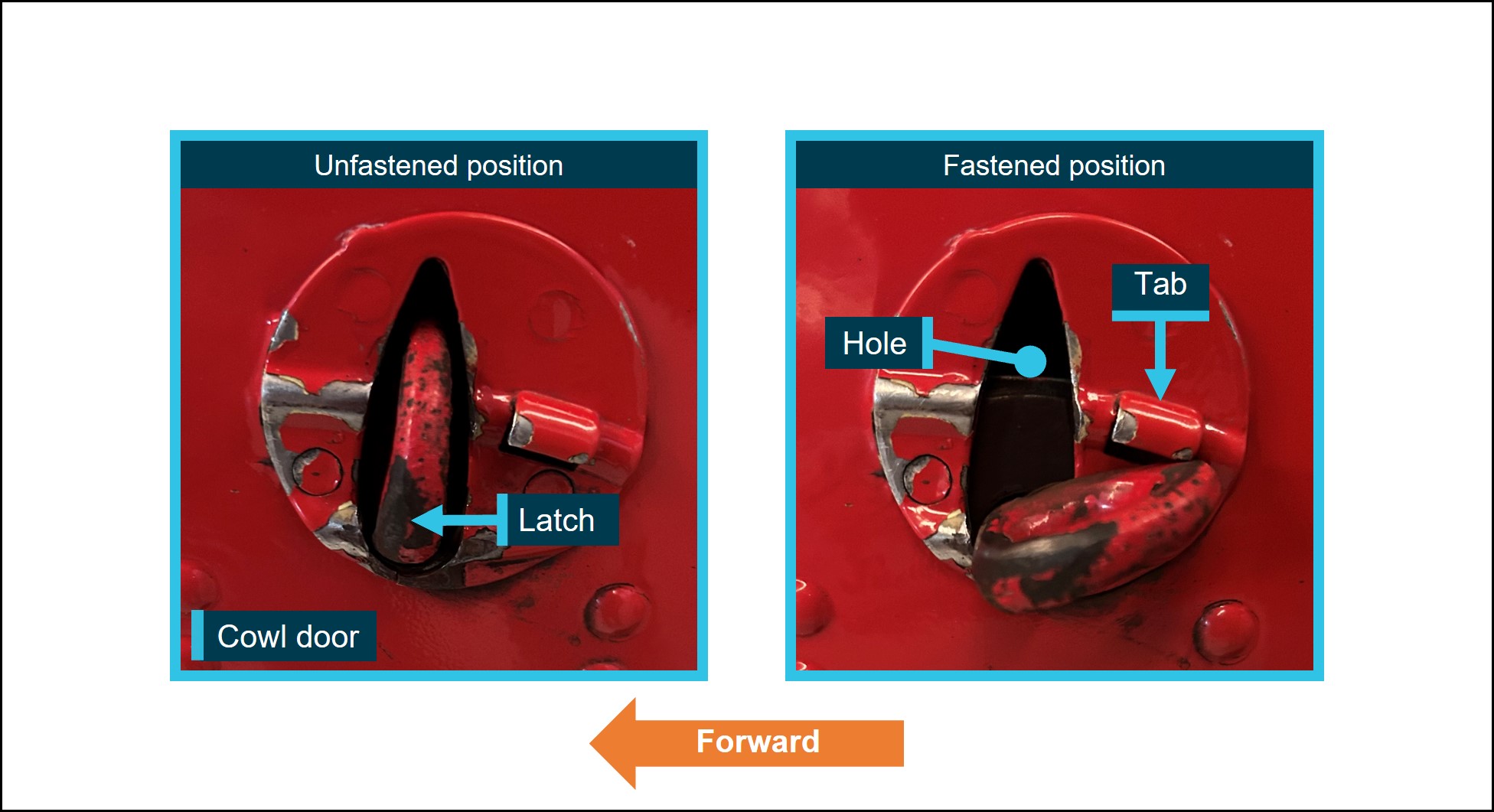
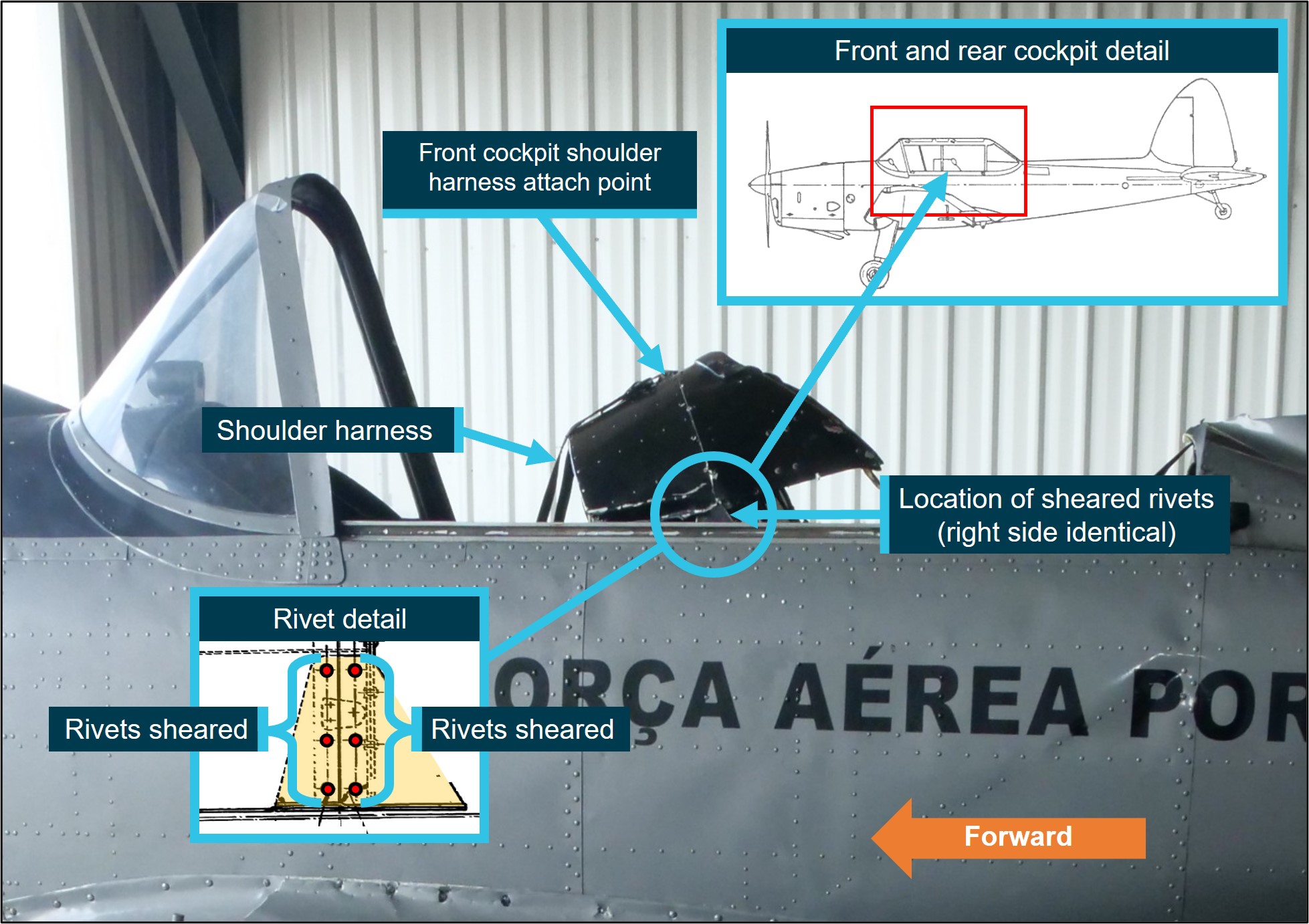
A witness on the southern apron took photographs of the aircraft taxiing past, which show the engine cowl latches on the left side were oriented vertically[1] (Figure 1).
The gap at the rear edge of the cowl is normally present when the cowl is closed fully.
Image source: Witness, annotated by the ATSB.
The pilot continued to taxi to the end of runway 24L and at 1313 was given clearance to take off. Camera footage recorded the aircraft commencing its take-off roll and becoming airborne about halfway along the runway’s length (Figure 2).
Image source: Google Earth, annotated by the ATSB.
One witness, located at the run-up bay, recalled seeing something ‘flapping’ on the aircraft during the take-off. This witness, and witnesses in a nearby building looking through a window, observed the aircraft roll to the left at low height near the end of runway 24L. There were no reports of an abnormal engine sound. At 1314:24, the pilot made a radio call stating ‘papa oscar romeo papa oscar romeo MAYDAY MAYDAY MAYDAY’.[2]
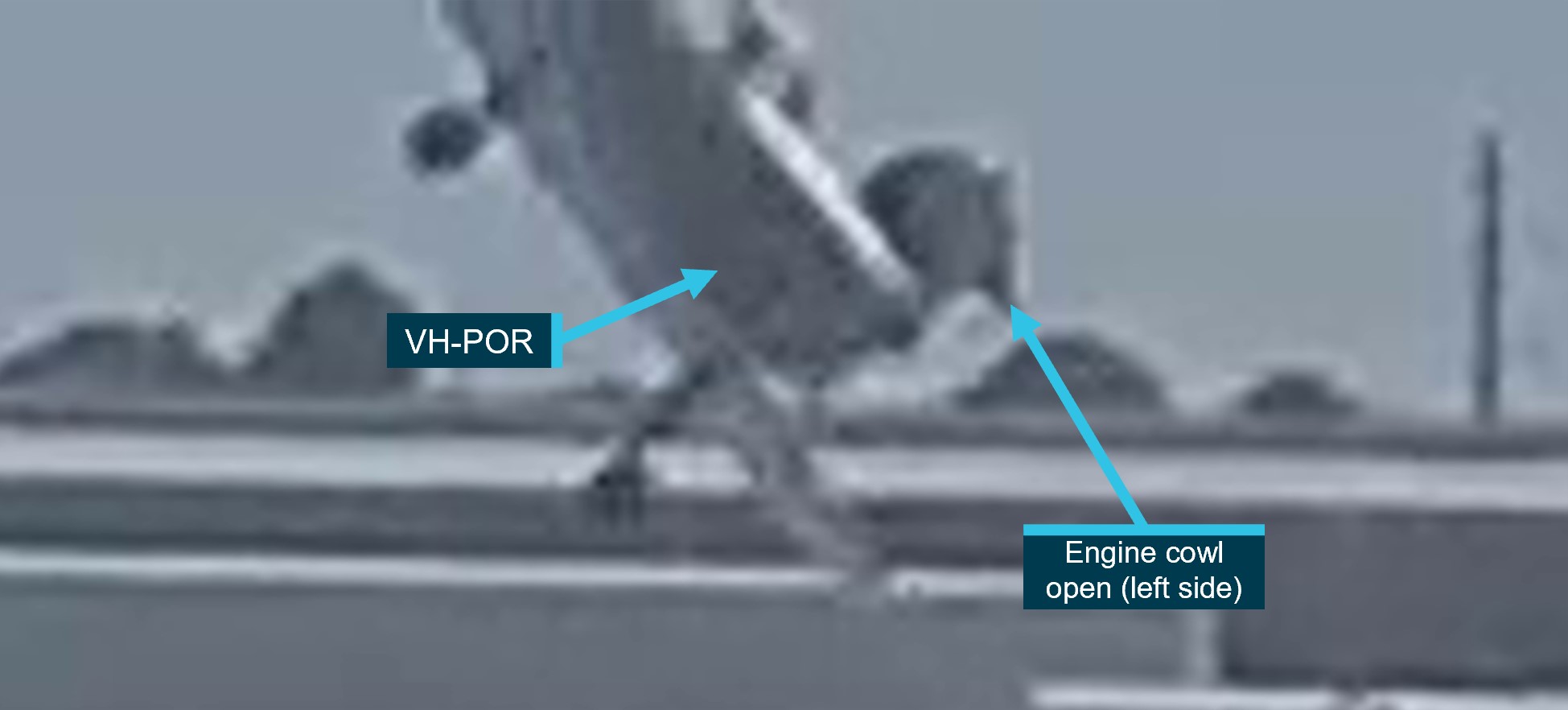
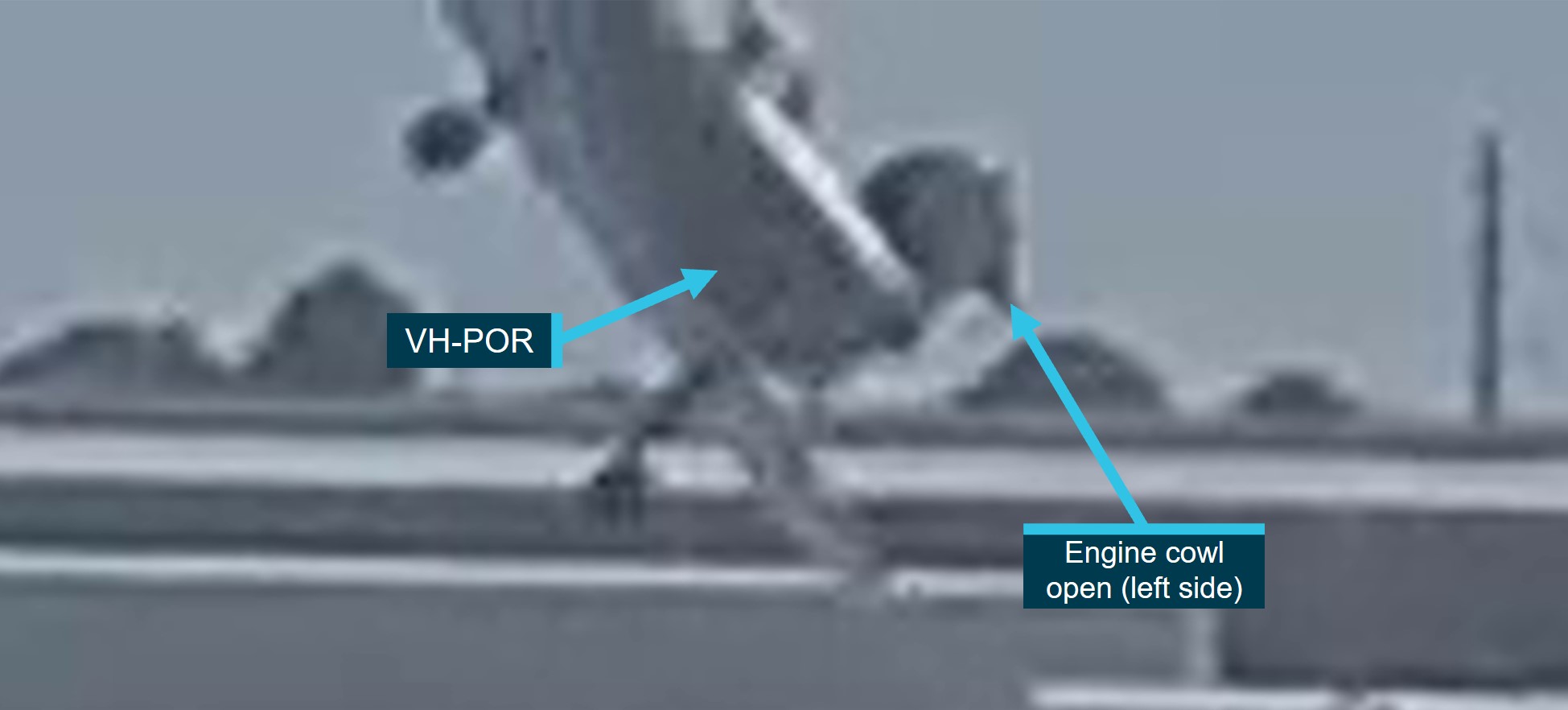
The camera footage showed the aircraft’s angle of bank increasing and the aircraft descending before colliding with terrain. A camera at a building about 180 m to the south‑east of the accident site recorded the engine cowling on the left side opening and closing in the seconds prior to the aircraft’s collision with terrain (Figure 3).
An instructor with a student pilot who had just landed recalled seeing the aircraft’s engine cowl open and the collision with terrain. The instructor and student taxied to a position adjacent to the accident site to provide assistance. The pilot was initially treated on‑site by Royal Flying Doctor Service personnel before being transported to hospital. Later, the pilot succumbed to injuries.
Context
Pilot information
The pilot was issued a private pilot licence (aeroplanes) by the United Kingdom Civil Aviation Authority in 1977. The pilot was issued with an Australian private pilot licence (aeroplanes) in 1978 and held a current Civil Aviation Safety Regulation Part 61 Private Pilot (Aeroplane) Licence. The pilot held a valid class 2 civil aviation medical certificate with no restrictions and was required to wear vision correction when flying.
The pilot had no reported significant medical conditions. Toxicology and post-mortem examination reports were not available at the time of publication.
At the time of the accident, the pilot had accumulated about 330 hours total aeronautical experience.
Aircraft information
General information
The DHC-1 MK 22 Chipmunk is a 2 seat, low-wing aircraft constructed predominantly from light aluminium alloy with fabric covered wings and control surfaces. The aircraft was designed for ab initio military flight training.
VH-POR was manufactured in Portugal under licence by Oficinas Gerais de Material Aeronautico (OGMA) in 1958. It was powered by a 4 cylinder de Havilland Gipsy Major 10 MK 2 engine driving a fixed-pitch wooden propeller. It was first registered in Australia in 2010 and the accident pilot had been the registration holder since 2018.
A periodic inspection and minor maintenance tasks were carried out on 22 March 2024. At the time of the accident, the aircraft had accumulated 2,082 flying hours.
Access to the engine is via a cowling door on either side. The cowl doors are hinged at the top and fastened by 2 latches at the bottom of each cowl. The latches are attached to the lower engine cowl and when in the vertical position pass through holes on the cowling doors (Figure 4, left). To fasten the cowl, the latches are pulled outboard, further compressing a pre‑compressed spring, and turned clockwise (1/4 turn) to the horizontal position. Releasing the latch fastens the cowl and the latches are held in place by the spring and prevented from turning counterclockwise by a tab (Figure 4, right).
The wreckage had been relocated to a secure hangar on Jandakot Airport prior to the arrival of ATSB investigators. Further, the accident site had been repatriated due to a significant fuel spill after the wreckage was relocated. Therefore, a detailed survey of the impact location was not possible. However, in addition to the 2 cameras showing the flight and accident, the ATSB obtained photographs of the site provided by first responders.
The ATSB examined the wreckage in the hangar. All major aircraft components were accounted for, and the propeller showed evidence that the engine was running at impact. Flight control continuity was established, and the wing flaps were assessed to have likely been in the retracted position at the time of impact.
Damage to the engine cowl latches was indicative of the latches being correctly fastened on the right side and unfastened on the left.
Further investigation
To date, the ATSB has:
examined the wreckage
recovered aircraft components associated with occupant restraints
interviewed relevant parties and eyewitnesses
collected aircraft, pilot, airport, and operator documentation
conducted preliminary analysis of video recordings and ATC transmissions.
The investigation is continuing and will include further:
examination of the aircraft components
review of aircraft and pilot documentation
analysis of the aircraft flight path, and impact forces.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[2]MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
Final report
Investigation summary
What happened
On 26 April 2024, the pilot (who was the sole occupant) of a DHC‑1 MK 22 Chipmunk, registered VH‑POR, taxied for take‑off from Jandakot Airport, Western Australia for a private flight. A witness took photographs of the aircraft taxiing past, which showed the engine cowl latches on the left side had not been secured.
After the aircraft took off, another witness near the runway recalled seeing something ‘flapping’ on the aircraft. This witness, and witnesses in a nearby building looking through a window, observed the aircraft turn to the left at low height near the end of the runway. The pilot declared a MAYDAY, and camera footage showed the aircraft’s angle of bank increasing and the aircraft descending before colliding with terrain.
An instructor, with a student pilot who had just landed, taxied to a position adjacent to the accident site to provide assistance. The pilot was initially treated onsite by Royal Flying Doctor Service personnel before being transported to hospital. Later, the pilot succumbed to injuries.
What the ATSB found
Prior to commencing taxi, the pilot did not detect that the engine cowl latches on the left side had been left unfastened. After take-off, the cowl was free to open and close in flight. Witness reports and camera footage show the engine cowl was opening and closing until the aircraft collided with terrain.
While likely distracted by the flapping engine cowl and experiencing a high cognitive workload, the pilot made a MAYDAY call while commencing a low‑level turn, likely in an attempt to return to land. During the turn, the aircraft’s angle of bank increased, and the aircraft aerodynamically stalled and collided with terrain.
When the aircraft collided with terrain, the upper structure between the front and rear cockpits, corresponding to the attach point for the front cockpit shoulder harness, was torn away from its mountings. Most noteworthy, all 12 rivets (6 per side) that attached the structure to the mountings had sheared. ATSB examination of the rivets using metallurgical equipment found that all of the rivets were of a non-conforming type, and half were estimated to be about one-third of the specification strength. This compromised the crashworthiness of the aircraft, however, the effect on survivability in this accident could not be determined.
What has been done as a result
To advise DHC‑1 Chipmunk maintainers and owners of the importance of ensuring modifications are carried out to the required specification, the ATSB issued a safety advisory notice (AO‑2024‑013‑SAN‑01) on 11 September 2024.
The Portuguese Office for the Prevention and Investigation of Accidents in Civil Aviation and Rail (GPIAAF) published information from the ATSB’s safety advisory notice (AO-2024-013-SAN-01) in its Civil Aviation Quarterly Bulletin Publication (issue
This accident illustrates the importance of pre-flight preparation to reduce the likelihood of an abnormal occurrence. In addition, pilots are reminded of the hazards that can lead to loss of control events, such as high angles of bank, especially at low heights, which should be avoided to reduce the risk of a stall/spin accident.
The modification carried out on the accident aircraft significantly compromised its crashworthiness. Maintainers and owners are reminded that when making modifications to any aircraft, that they are carried out to the required specification, or during maintenance returned to that specification.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the afternoon of 26 April 2024, the pilot (who was the sole occupant) of a DHC‑1 MK 22 ‘Chipmunk’, registered VH‑POR, commenced taxi for take-off at Jandakot Airport, Western Australia for a private flight. The weather was clear, with the wind about 10 kt from the north‑west.
A witness on the southern apron took photographs of the aircraft taxiing past, which show the engine cowl latches on the left side were oriented vertically[1] (Figure 1).
The gap at the rear edge of the cowl is normally present when the cowl is closed fully. Image source: Witness, annotated by the ATSB
The pilot continued to taxi to the end of runway 24L and at 1313 was given clearance to take off. Camera footage recorded the aircraft commencing its take-off roll and becoming airborne about halfway along the runway’s length (Figure 2).
One witness, located at the run-up bay, recalled seeing something ‘flapping’ on the aircraft during the take-off. This witness, and witnesses in a nearby building looking through a window, observed the aircraft turn to the left at low height near the end of runway 24L. There were no reports of an abnormal engine sound. At 1314:24, the pilot made a radio call stating ‘papa oscar romeo papa oscar romeo MAYDAY MAYDAY MAYDAY’.[2]
The camera footage showed the aircraft’s angle of bank increasing and the aircraft descending before colliding with terrain.
A camera at a building about 180 m to the south‑east of the accident site recorded the engine cowling on the left side opening and closing in the seconds prior to the aircraft’s collision with terrain (Figure 3).
An instructor with a student pilot who had just landed recalled seeing the aircraft’s engine cowl open and the collision with terrain. The instructor and student taxied to a position adjacent to the accident site to provide assistance. The pilot was initially treated onsite by Royal Flying Doctor Service personnel before being transported to hospital. The pilot succumbed to injuries 3 days later.
Context
Pilot information
The pilot was issued a private pilot licence (aeroplanes) by the United Kingdom Civil Aviation Authority in 1977. The pilot was issued with an Australian private pilot licence (aeroplanes) in 1978 and held a current Civil Aviation Safety Regulation Part 61 Private Pilot (Aeroplane) Licence. The pilot held a valid class 2 civil aviation medical certificate with no restrictions and was required to wear vision correction when flying.
The pilot had no reported significant medical conditions. Toxicology and post-mortem examination reports were not available at the time of publication.
At the time of the accident, the pilot had accumulated about 330 hours total aeronautical experience. In the 12 months prior to the accident, the pilot had flown about 5 hours, 3.5 hours of which was in VH‑POR. The pilot completed a flight review in December 2023, and their last flight prior to the accident was in January 2024. Both flights were in VH-POR.
Aircraft information
General information
The DHC-1 MK 22 Chipmunk is a 2 seat, low-wing aircraft constructed predominantly from light aluminium alloy with fabric covered wings and control surfaces. The aircraft was designed for ab initio military flight training. The Chipmunk was manufactured in Canada, the United Kingdom, and Portugal.
VH‑POR was manufactured in Portugal under licence by Oficinas Gerais de Material Aeronautico[3] (OGMA) in 1958 as a DHC-1 MK 20, and later modified to MK 22 specifications.[4] It was powered by a 4 cylinder de Havilland Gipsy Major 10 MK 2 engine driving a fixed-pitch wooden propeller. The aircraft operated in service with the Portuguese Air Force before being operated privately in the United States from 1979. It was first registered in Australia in 2010, and the accident pilot had been the registration holder since 2018.
A periodic inspection and minor maintenance tasks were carried out on 22 March 2024. At the time of the accident, the aircraft had accumulated 2,082 flying hours.
Access to the engine is via a cowling door on either side. The cowl doors are hinged at the top and fastened by 2 latches at the bottom of each cowl. The latches are attached to the lower engine cowl and when in the vertical position pass through holes on the cowling doors (Figure 4, left). To fasten the cowl, the latches are pulled outboard, further compressing a pre‑compressed spring, and turned aft (1/4 turn) to the horizontal position. Releasing the latch then fastens the cowl. The latches are held in place by the spring and prevented from unfastening by a tab (Figure 4, right). There was no evidence of pre‑impact damage to the engine cowl latches fitted to VH‑POR (see Wreckage and impact information).
Figure 4: DHC-1 Chipmunk cowl latch detail (exemplar aircraft, left side shown)
Image source: Supplied, annotated by the ATSB
Fuel line priming and carburettor flooding
A number of actions are required to start the engine of a DHC-1 Chipmunk, including to ensure the lines from the fuel pumps to the carburettor have been filled with fuel (primed). This is accomplished by the use of a hand lever on the rear fuel pump which is accessed via an opening on the left engine cowl. After this is accomplished, the carburettor is flooded[5] using a pull-wire that is accessed via another opening on the left engine cowl. The left engine cowl can be opened to allow direct access instead of using the access openings to perform these actions.
The upper structure between the front and rear cockpits of the DHC-1 Chipmunk, corresponding to the attach point for the front cockpit shoulder harness, had 2 mountings, called gussets (Figure 5 and Figure 6).
Image source: Alan K. Radecki, annotated by the ATSB
Figure 6: Modification H.268 gusset and rivet location (left side shown)
Image source: ATSB, de Havilland Support Ltd, annotated by the ATSB
In October 1966, modification H.268 was issued[6] to strengthen this structure. The modification was classified as ‘desirable’, and was applicable to DHC-1 Chipmunk marks 20 (which included Portuguese-manufactured aircraft), 21, 22, 22A and 23. The modification replaced the original aluminium alloy gussets with high-tensile steel. The modification required the forward row of rivets attaching the structure to the gussets to be part number SP85 mushroom head rivets, and the rear row to be part number AS2230 countersunk rivets. Later testing by the manufacturer subjected the front cockpit shoulder harness of a modified aircraft to a 22 G load, with no failures.
Information on the ATSB examination of relevant components of VH‑POR is presented in Wreckage and impact information.
Technical news sheet 154
On 29 March 1966, in the United Kingdom there was a fatal accident involving a DHC-1 MK 22 Chipmunk, registered G‑ARME. Following the investigation into the accident, Hawker Siddeley[7] issued technical news sheet TNS 154 in May 1967. Compliance with TNS 154 was classified as ‘mandatory’, to be carried out prior to 31 July 1967. The heading indicated that it was applicable to ‘CT(C1)’ series aircraft, meaning those in civilian (non-military) service. TNS 154 also stated that it was for English production Chipmunk aircraft. The ATSB was advised by de Havilland Support Ltd (DHSL) that since the 1990s, the Portuguese Air Force and military operators of DHC-1 Chipmunks in the United Kingdom have been briefed when new technical news sheets were issued.
The procedure to fulfil TNS 154 is summarised as follows. After gaining access to the gussets securing the upper structure between the front and rear cockpits to the fuselage, dimensional checks (diameter and edge distance) were to be made on the 3 bolt holes in each gusset. If either criterion was not met, the aircraft was required to have modification H.268 embodied. Additionally, each gusset was to be inspected for the presence of the correct number of securing rivets.
Applicability to Portuguese manufactured DHC-1 Chipmunks
All Chipmunk aircraft manufactured in Portugal had been originally built to MK 20 specifications. When issued in 1966, modification H.268 was applicable to Portuguese manufactured MK 20 Chipmunks and remained applicable when those aircraft were converted to MK 22 (civilian) specifications. When issued in 1967, TNS 154 was not applicable for MK 20 (military) aircraft but became applicable to any aircraft modified to MK 22 (civilian) specifications.
The available Portuguese records for VH‑POR did not include entries for modification H.268 or TNS 154. The records did however show that various modifications and civilian TNS inspection requirements had been carried out when VH-POR was operating in Portuguese Air Force service.
The aircraft manufacturer (OGMA) advised that it had no record of being advised about modification H.268 by Hawker Siddeley, and that it had received technical news sheet TNS 154 in 1997.
Additionally, the ATSB were advised[8] that the Portuguese Air Force held no records for aircraft serial number OGMA 44 (VH‑POR). However, of the 6 remaining DHC-1 Chipmunk aircraft still operating in Portuguese Air Force service in 2025, records indicate that:
no aircraft have records of modification H.268 being embodied
records showed inspections in accordance with TNS 154, and that modification H.268 was not needed.
In 1966, the Australian Department of Civil Aviation (DCA) issued airworthiness advisory circular AAC 1‑3 Chipmunk aircraft – crashworthiness. This document outlined 3 modifications that were considered by the DCA as ‘highly desirable’. The modifications were for the installation of inertia reel shoulder harnesses, energy absorbing seat inserts, and for the modification of the front cockpit shoulder harness mount point structure. For the latter, AAC 1‑3 stated that:
The structural shell which carries the front shoulder harness attachment is in itself quite rigid, but fails by tearing at its attachment to the aircraft upper longerons when subjected to a high load applied through the shoulder harness. A sheet aluminium alloy doubler running from the shoulder harness attach point down to the longeron bolts and using existing rivets and bolts will provide the reinforcement desired.
This modification could be seen in historical photographs of DHC-1 Chipmunk aircraft in Royal Aero Club service in Australia.
In response to TNS 154, an Australian airworthiness directive, AD/DHC-1/18, was issued in August 1967 and mandated that compliance to TNS 154 was required before 1 January 1968. In 2008, AD/DHC-1/18 was cancelled on the basis that ‘as all affected aircraft would have been inspected and modified by now, this AD is no longer required.’
VH-POR crashworthiness modification
No records from the aircraft’s time in the United States were available for examination. Maintenance records from the time the aircraft was registered in Australia were available to the investigation, along with incomplete records from the aircraft’s service in Portugal. There was no record available showing whether modification H.268 or the requirements of technical news sheet TNS 154 having been carried out on VH‑POR. Examination by the ATSB of the aircraft showed that modification H.268 had been embodied (the relevant mountings, or gussets, were steel as required by H.268) at an unknown time, and with non-conforming rivets (see Rivet examination).
Aerodrome information
Jandakot Airport is a certified, controlled airport. It had 3 asphalt runways:
06L/24R (in parallel with 06R/24L and 1,392-m long)
12/30 (1,508-m long).
The accident flight took off from runway 24L, which was only available from sunrise to sunset, and at all times the circuit direction was left (turns made in the circuit were to the left).
The wreckage had been relocated to a secure hangar on Jandakot Airport prior to the arrival of ATSB investigators. Further, the accident site had been decontaminated after the wreckage was relocated due to a significant fuel spill. Therefore, a detailed survey of the impact location was not possible. However, in addition to the 2 cameras showing the flight and accident, the ATSB obtained photographs of the site provided by first responders.
The ATSB examined the wreckage in the hangar. All major aircraft components were accounted for, and the propeller showed evidence that the engine was running at impact. The engine control pushrods in the engine compartment had been fractured by impact forces. Flight control continuity was established. The wing flaps were assessed to have likely been in the retracted position at the time of impact, which is a permissible setting for take-off.
Damage to the engine cowl latches was indicative of the latches being correctly fastened on the right side but unfastened on the left at the time of impact. The engine cowls and latches were otherwise undamaged.
Cockpit structure
The ATSB found that on impact the upper structure between the front and rear cockpits, corresponding to the attach point for the front cockpit shoulder harness, was torn away from its mountings (Figure 7). All 12 rivets (6 per side) that attached the structure to the mountings had sheared.
Figure 7: Detached upper structure showing harness attach point and location of sheared rivets
Upper structure has been placed in position for the photograph and is representative of its position immediately post-accident. Image source: ATSB, de Havilland Support Ltd (detail), annotated by the ATSB
The gussets fitted to VH‑POR were steel, rather than aluminium alloy, which indicated that modification H.268 had been embodied. This modification also required the use of part number SP85 and AS2230 rivets. Both types were required to be manufactured to British standard L.86, which was an aluminium alloy that included copper and magnesium.[10] The standard also specified that the rivets were to be anodised (a surface treatment) and coloured violet.
The sheared rivets and coatings from VH‑POR were examined and tested by the ATSB using metallurgical equipment. It was determined that:
The material composition of the rear row of rivets (countersunk) was consistent with pure or near-pure aluminium[11] and therefore a non-conforming specification. Testing indicated a significant reduction in strength, estimated to be about one-third of the strength of the specification rivets.
The material composition of the forward row of rivets (mushroom head) was consistent with an alloy consistent with L.86. The rivets were coated with a gold-coloured chromate conversion coating instead of violet anodising. ATSB testing indicated that the strength of the rivets met or exceeded literature values for L.86 alloy.
The presence of the non-conforming rivets significantly reduced the integrity of the structure retaining the front cockpit restraint, and thereby compromised the crashworthiness of the aircraft. This non-conforming modification may be present in other Chipmunk aircraft, in which case it would likely affect survivability in an accident.
To advise DHC‑1 Chipmunk maintainers and owners of the importance of carrying out this modification to the required specification, the ATSB issued a safety advisory notice (AO‑2024‑013‑SAN‑01) on 11 September 2024.
The ATSB attempted to determine the impact velocity and deceleration imparted on the aircraft’s structure during the accident. As there was no recorded data[12], calculations of deceleration during the impact were made using estimates of the aircraft’s velocity and angle of impact. Additionally, assumptions were required in the analysis resulting in a wide range of possible outcomes across the established threshold for human tolerance. As a result, the ATSB was unable to definitively determine whether the impact accelerations were within or exceeded the levels considered tolerable for human survival.
Similarly, it was not possible to determine whether the longitudinal force was greater than the force that the restraints were known to withstand in testing (22 G) and therefore not possible to determine whether the correct rivets would also have failed had they been fitted.
Flight path analysis
The pilot’s handbook and pilot’s notes for the Chipmunk state that normal take-off speed is 45 kt, climb speed is 70 kt, and stall speed is 47 kt with the wing flaps up. The ATSB estimated from camera footage of the accident flight that the aircraft’s angle of bank increased to about 55° during its turn while maintaining about 130 ft, immediately prior to the descent (Figure 8). It was not possible to accurately estimate its airspeed at this time.
Figure 8: VH-POR angle of bank during left turn after take-off
Image source: Supplied, annotated by the ATSB
The aerodynamic stall[13] speed of aircraft in a steady turn increases appreciably with an angle of bank greater than 30°, and at angles greater than 45° there is a rapid increase in stall speed. At 55° angle of bank, stall speed is increased by about 32%. The Chipmunk’s stall speed in a 55° steady turn while maintaining level flight would have therefore been about 62 kt.
Guidance on manoeuvring at low level
The 2024 Civil Aviation Safety Authority information card Preventing a stall at low level (2405.4903) provided tips for pilots including:
Manoeuvring at low level increases the chances of a low-level stall.
…
Remember that turns and any application of ‘G’ will increase the stall speed – sometimes dramatically.
…
Try to avoid using more than 30 degrees of bank in the circuit. Use coordinated controls.
The 2010 ATSB educational publication Avoidable Accidents No. 3 - Managing partial power loss after take-off in single-engine aircraft (AR-2010-055) noted that:
A turnback requires accurate flying during a period of high stress to prevent a stall and possibly a spin occurring. If an aerodynamic stall and or spin occurs, given that these circumstances are likely to be at low level, there is little likelihood of a successful recovery. With careful management and by being aware of the hazards that can lead to loss of control events, the risk of being involved in a stall/spin accident can be reduced.
During a non-normal or emergency event in-flight, and particularly in a critical phase of flight such as initial climb and final approach, there can be a high cognitive workload placed on the pilot. In such a situation, a pilot’s hierarchical priorities are to ensure the aircraft remains in controlled flight, navigate (such as to a suitable landing area) and, if time permits, communicate the nature of the emergency to air traffic control enabling them to respond appropriately. These hierarchical priorities are colloquially known as ‘aviate, navigate, communicate’.
Related occurrences
The ATSB was advised by DHSL of an occurrence in the United Kingdom where the left engine cowl of a DHC-1 Chipmunk opened in flight. The pilot of that aircraft reported that by sideslipping[14] the aircraft, the cowling slammed shut until the aircraft was straightened for touchdown when it opened again. The aircraft landed safely, and there was no reported damage to the cowling.
Additionally, a DHC-1 Chipmunk subject matter expert advised the ATSB of 3 other occurrences in Australia involving a Chipmunk where the left cowl opened in flight. The ATSB was able to obtain formal investigation records about one of these accidents (described below). On the other 2 occasions there were no reported issues with performance or controllability, and both aircraft landed safely. There was minor damage to the left cowl on one aircraft.
Accident involving DHC-1 MK 10 Chipmunk, VH-RFW at Bull Creek, Western Australia on 19 September 1959
On 19 September 1959, the pilot of a DHC‑1 MK 10 Chipmunk, registered VH‑RFW, had difficulty recovering from a spin during aerobatic manoeuvres and entered a dive, during which the left engine cowl opened then slammed shut. The investigation report did not state whether the cowl stayed shut or opened again. When the pilot applied power to return to Perth Airport, the engine did not respond, and the throttle lever was reportedly loose. The pilot elected to land at an emergency airstrip at Bull Creek. During landing the pilot inadvertently approached downwind and the aircraft overshot the runway, collided with trees and caught fire. The pilot survived and was treated for burns in hospital. The investigation found that the left engine cowl had been unfastened, and had damaged the throttle linkage as it slammed closed in flight.
Safety analysis
Engine cowl latches
In preparing the aircraft for flight, it is possible that the fuel line priming and carburettor flooding functions were carried out by opening the left engine cowl, rather than via the openings on it, and that the cowl was then left unsecured. Alternatively, the cowl might have been opened for another reason or left unfastened from previous activities. In any case, the pilot did not detect that the engine cowl latches on the left side had been left unfastened prior to boarding the aircraft and commencing taxi. After take-off, the cowl was free to open and close in flight.
Left turn after take-off
This accident, and the 1959 accident involving VH‑RFW, demonstrate that the engine cowl being free to open and close in‑flight can be hazardous. However, while by no means a benign event, there were 2 anecdotally reported occasions involving DHC-1 Chipmunks where the left engine cowl was not secured. With these, there were no reported performance or controllability issues, and the aircraft were able to be recovered safely. Nevertheless, in this case the engine cowl began flapping after take-off, and the pilot would have been likely distracted and experiencing a high cognitive workload while managing the in-flight emergency.
From the available evidence, there were no indications of pre-impact defects, configuration issues (other than the cowl being unfastened), or controllability issues. There were no engine issues, and it is very likely the aircraft’s engine controls had not been damaged in a similar way to the accident involving VH‑RFW. The reason for the pilot commencing a left turn after take-off could not be determined, though it is possible that the pilot was attempting to recover by conducting a circuit and returning to Jandakot Airport.
During the turn the pilot made a MAYDAY call, and the aircraft’s angle of bank then increased until reaching about 55°. The rapid increase in stall speed associated with higher angles of bank resulted in the aircraft aerodynamically stalling at a height where recovery was not possible.
While the pilot was appropriately licenced and had completed a flight review using VH‑POR about 4 months prior to the accident, the extent to which the pilot’s limited recent experience influenced their actions could not be established.
Non-conforming rivets and survivability
On an unknown date, potentially many years previously, rivets that did not conform to the design specification had been fitted to the mountings between the front and rear cockpits. Importantly, the attach point for the front cockpit shoulder harness was attached to this structure. Testing indicated a significant reduction in strength in half of the rivets (the aft 3 rivets on both sides), estimated to be about one-third of the strength of the specification rivets.
During the accident, all of the rivets securing the structure failed. However, it was not possible to establish whether the correct rivets would also have failed, and the impact deceleration alone may have been above expected human tolerance. Therefore, it was not possible to establish whether the presence of non-conforming rivets affected survivability in this instance. Regardless, the presence of non-conforming rivets was a latent threat to the aircraft’s crashworthiness and reduced the likelihood of an accident being survivable.
As complete records for the aircraft were not available, it was not possible to determine where or when the rivets had been installed. The 6 DHC-1 Chipmunk aircraft still operating in Portuguese Air Force service had been inspected but not modified, and this likely occurred after the aircraft manufacturer (OGMA) received TNS 154 in 1997. It is therefore likely that VH‑POR had not been inspected under TNS 154 in Portugal prior to 1979 when the aircraft was privately registered in the United States, and modification H.268 was likely carried out some time later. While the existing rivets would have been replaced when the H.268 modification was made, some or all may have been replaced again later.
This non-conforming modification may be present in other Chipmunk aircraft, in which case it would likely affect survivability in an accident.
Australian airworthiness directive
The Australian airworthiness directive relating to TNS 154, AD/DHC-1/18, was issued when the aircraft operating in Australia had been manufactured in England, and therefore meeting the stipulated applicability for TNS 154. The airworthiness directive was cancelled in 2008 (before VH‑POR was first registered in Australia) on the expectation that all aircraft by that time had been inspected and modified. Read strictly, the cancellation did not account for the possibility that an aircraft could have been inspected, met the dimensional criterion, and therefore not modified in accordance with H.268.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Oficinas Gerais de Material Aeronautico DHC-1 MK 22 Chipmunk, VH‑POR at Jandakot Airport, Western Australia on 26 April 2024.
Contributing factors
The pilot did not detect that the engine cowl latches on the left side had been left unfastened prior to commencing taxi. After take-off, the cowl was free to open and close in flight.
During a low level, high angle of bank turn, and while the pilot was likely distracted by the flapping engine cowl and experiencing a high cognitive workload, the aircraft aerodynamically stalled and collided with terrain.
Rivets that did not conform to the design specification had been fitted to mountings between the front and rear cockpits and significantly reduced the integrity of the structure retaining the front cockpit restraint. This compromised the crashworthiness of the aircraft; however, the effect on survivability in this accident could not be determined.
Safety advisory notice to DHC-1 Chipmunk maintainers and owners
SAN number:
AO-2024-013-SAN-01
SAN release date:
11 September 2024
The ATSB advises DHC-1 Chipmunk maintainers and owners to be aware that fitment of non‑conforming rivets where the upper structure between the front and rear cockpits attaches to the gussets on either side could significantly compromise the crashworthiness of the aircraft.
Those conducting work on aircraft must ensure modifications are carried out to the required specification, or during maintenance returned to that specification.
Proactive safety action taken by the GPIAAF
Action number:
AO-2024-013-PSA-01
Action organisation:
Gabinete de Prevenção e Investigação de Acidentes com Aeronaves e de Acidentes Ferroviários (GPIAAF)
Action status:
Closed
The Portuguese Office for the Prevention and Investigation of Accidents in Civil Aviation and Rail (GPIAAF) published information from the ATSB’s safety advisory notice (AO-2024-013-SAN-01) in its Civil Aviation Quarterly Bulletin Publication (issue
The ATSB would like to acknowledge the significant assistance provided by multiple DHC-1 Chipmunk subject matter experts during the onsite investigation phase and evidence collection activities.
National Archives of Australia B638, 6/659/133 - Accident at Bulls [sic] Creek on 19/9/1959: DHC‑1 A/C: VH‑RFW [includes photographs and plans], 1959 - 1960.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Air Accidents Investigation Branch (United Kingdom)
Civil Aviation Safety Authority
De Havilland Aircraft of Canada Limited
de Havilland Support Ltd
Gabinete de Prevenção e Investigação de Acidentes com Aeronaves e de Acidentes Ferroviários (Portugal)
Royal Aero Club of Western Australia
Transport Safety Board of Canada.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[2]MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
[3]Currently known as OGMA Indústria Aeronáutica de Portugal.
[4]The DHC-1 MK 20 was the export version of the original MK 10 manufactured for military service in the United Kingdom. For civilian use, aircraft were modified to MK 22 and other specifications.
[5]Flooding fills the carburettor float bowl by depressing its float and overriding the float’s normal function which is to shut off fuel flow to the carburettor bowl when it reaches a set level.
[7]Hawker Siddeley was the type certificate holder at the time.
[8]The Portuguese Office for the Prevention and Investigation of Accidents in Civil Aviation and Rail (GPIAAF) established contact with the Portuguese Air Force on the ATSB’s behalf and provided a response.
[9]Runway numbering: represents the magnetic heading closest to the runway orientation (for example, runway 24L is oriented 236º magnetic).
[10]International equivalences were Alloy Designation 2117, US specification AMS7222, and European specification ENAW-AlCu2.5Mg).
[11]The composition was not determined exactly; there was >99% aluminium with some alloying iron and silicon, consistent with 1000-series aluminium, although the specific alloy could not be determined.
[12]The aircraft was not fitted with flight or engine recording devices, and there was no requirement to do so.
[13]Aerodynamic stall occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16˚ to 18˚, and results in reduced lift.
[14]Sideslipping is a manoeuvre in which controls are deliberately crossed, for example to sideslip to the left, the aircraft is banked to left while right rudder is applied.
Occurrence summary
Investigation number
AO-2024-013
Occurrence date
26/04/2024
Location
Jandakot Airport
State
Western Australia
Report release date
25/03/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Aircraft preparation, Collision with terrain, Loss of control
On 11 April 2024, a flight instructor and student pilot were conducting a dual training flight under the instrument flight rules in a Beechcraft E55 aircraft, registered VH-OMD and operated by Fly Oz. The aircraft departed from Cowra Airport, New South Wales, and conducted instrument approaches to Goulburn and Canberra Airports, before returning to Cowra.
As the aircraft tracked over the Cowra non-directional beacon (NDB) to conduct a practise instrument approach to runway 15, the instructor simulated a failure of the left engine by moving the mixture lever to the idle cut-off position. The student continued the approach with the left engine inoperative and the propeller windmilling, then joined the circuit for runway 33 on the crosswind leg.
During the landing flare, the instructor initiated a go-around. The aircraft rapidly yawed and rolled to the left and impacted the ground in an almost vertical nose-down attitude before coming to rest inverted. The flight crew sustained minor injuries and the aircraft was substantially damaged.
What the ATSB found
The ATSB found that the instructor moved the left engine mixture lever to idle cut-off to simulate an engine failure over the navigation aid, and it was likely that they unintentionally did not subsequently move the lever to rich and ensure the engine was restarted and available for instant use, when attempting to set zero thrust on the downwind leg of the circuit. As a result, the instructor initiated a go-around below the minimum control speed, unaware the left engine was inoperative, resulting in an asymmetric loss of control.
The ATSB also found that Fly Oz's asymmetric training procedure involved failing one engine using the mixture control without confirmation the engine was subsequently restarted, rather than reducing throttle to simulate zero thrust in accordance with the Beechcraft E55 Airplane Flight Manual. The use of the throttle to simulate an engine failure ensures the engine is available for immediate use, whereas using the mixture control increased the risk of an undetected inoperative engine during descent and landing, and the associated loss of control.
What has been done as a result
Fly Oz amended its multi-engine training to simulate engine failures only using throttle at any height. It has also taken the following proactive safety action:
Following a simulated engine failure, zero thrust is to be set immediately after the student has completed the engine failure drills.
The instructor standardisation manuals were being updated to include a requirement that both the student and instructor confirm that the pitch, power and mixture controls are set back to normal 2‑engine configuration during checks on final. This is now a call out item, ensuring that both pilots are satisfied with the correct settings.
Safety message
In conventional twin-engine aeroplanes, loss of power on one engine can lead to a loss of directional control and an accident if there is insufficient height above the ground to recover.
Aircraft manufacturers’ procedures for one engine inoperative training should be followed in the first instance. In this case, the manufacturer required the throttle be used to simulate an engine failure. In addition to the manufacturer’s procedures, Civil Aviation Safety Authority guidance recommended using the throttle rather than the mixture to simulate an engine failure when at low level – such as asymmetric instrument approaches. This ensures power can quickly be restored if needed.
Accidents as a result of engine malfunctions in twin-engine aeroplanes are rare, but often fatal. As such, training to manage one engine inoperative flight is important, but should not introduce unnecessary risks.
The occurrence
On 11 April 2024, a student pilot and flight instructor were conducting a dual instructional flight in a Beechcraft E55 aircraft, registered VH-OMD and operated by Fly Oz. The flight was the student’s third multi-engine aeroplane navigation exercise. The flight was to be conducted under the instrument flight rules,[1] from Cowra, New South Wales (NSW), to Canberra, Australian Capital Territory, and return. As the flight was conducted almost entirely in visual meteorological conditions,[2] the student wore a view limiting device or ‘hood’, to simulate flying in cloud or poor visibility.
OzRunways[3] flight path data showed that the aircraft departed Cowra Airport at 1156 local time. En route to Canberra, the student conducted an instrument approach[4] to Goulburn Airport, NSW, but did not land there. The student then conducted an instrument approach to Canberra, landed and taxied to the general aviation apron. After a short break, and without shutting down the engines, the aircraft departed Canberra Airport at 1323 via a standard instrument departure. The aircraft climbed to 10,000 ft above mean sea level (AMSL), tracked via waypoint AVBEG and commenced a descent when 35 NM from Cowra (Figure 1).
Figure 1: VH-OMD track from Cowra to Goulburn, Canberra and return via AVBEG
Source: OzRunways data overlaid on Google Earth, annotated by the ATSB
At 1404, the aircraft passed over the Cowra non-directional beacon (NDB)[5] at about 3,600 ft AMSL (2,600 ft above ground level) and commenced the NDB approach to runway 15. The instructor then simulated an engine failure, by pulling the left engine mixture control lever to the idle cut-off position. In that position, no fuel would flow from the injectors to the engine, but the magnetos would continue generating spark, and the propeller blades would windmill[6] unless feathered.[7]
In response, the student conducted initial engine failure checks and identified that the left engine was inoperative. At that time, the flight crew did not complete the operator’s one engine inoperative procedure to either feather the left propeller or set zero thrust to simulate a feathered propeller (see the section titled Simulated one engine inoperative – Fly Oz procedures). The flight path data showed that, consistent with the simulated left engine failure, the aircraft deviated left of the published outbound track, and tracked outbound on the published inbound track for about 2 minutes, before starting to correct to the right (Figure 2).
Figure 2: VH-OMD track overlaid on published Cowra NDB approach
Source: OzRunways and Airservices Australia data overlaid on Google Earth, annotated by the ATSB
About 4 minutes after passing over the NDB, the aircraft commenced a left inbound turn and was established within the required 5° tolerance of the published inbound track about 5 NM from the threshold of runway 15.
The Cowra Airport common traffic advisory frequency (CTAF) was not recorded. However, the student reported making the standard radio calls, including broadcasting when inbound and on downwind, and using the word ‘asymmetric’ in their calls to alert others that they were practising one engine inoperative procedures. The instructor reported communicating with the pilots of 2 other aircraft operating in the circuit at the time. Those 2 aircraft were operating on runway 33, which was the most into wind runway. To sequence with the circuit traffic, the instructor advised the student they were now ‘visual’ and could lift the hood and track to join the crosswind leg of the circuit for runway 33.
The instructor thought that they had set zero thrust either when inbound on the instrument approach or on the downwind leg of the circuit, and recalled first asking the student whether they wanted zero thrust set. However, the student recalled prompting the instructor to set zero thrust on downwind. The instructor reported that their normal procedure for setting zero thrust was to bring the propeller pitch lever to the feather detent, then push the mixture lever forward to rich and gradually move the left throttle lever forward until the manifold pressure gauge read about 10 inches Hg.[8] The instructor reported that, although they usually moved the engine/propeller controls slowly, there would be a detectable yaw[9] associated with returning power to the inoperative engine.
The student and instructor both reported that the student’s normal downwind checks included checking both mixture levers were in the fully rich position, but neither could recall when the checks were done. The student recalled extending the landing gear either just before, or when turning onto, the base leg of the circuit. Neither the instructor nor the student recalled when the student extended the approach (15°) stage of flaps. After turning onto final, the student reported completing their pre-landing checks by pushing both pitch levers forward to the full fine position, checking they had 3 green lights, which indicated the landing gear was down and locked, and electing not to extend full (30°) flap for landing.
A review of recorded flight data identified that the aircraft crossed the runway threshold at 1416:01 aligned with the runway centreline. The instructor reported that the student commenced the flare[10] a bit high and therefore directed them to add some power to cushion the landing. The instructor further reported that when the student added power, the aircraft immediately yawed significantly to the left such that it was no longer aligned with the runway. In response, the instructor called for a go-around. The student could not recall being asked to add power and reported that the main landing gear touched down on the runway before the instructor initiated the go-around. However, the instructor recalled that the wheels did not touch down and that the go-around commenced about 30–50 ft above the runway.
OzRunways data showed that the aircraft started to deviate left of the runway centreline at 1416:14 at 69 kt ground speed, but there was insufficient recorded information to determine whether or not it touched down prior to that occurring. The instructor reported taking control of the aircraft from the student and verifying that both throttle levers were fully forward. Assessing that the yaw was due to left rudder input by the student, the instructor called for the student to let go of the controls and applied right rudder, but was unsuccessful in regaining control of the aircraft. A witness facing away from the runway heard what they assessed as one engine power up and turned to see the aircraft 10–20 ft above the runway, pitched 10–12° nose-up, and in a rapid left roll (Figure 3).
Figure 3: VH-OMD track along the runway, accident site and witness location
Source: OzRunways data overlaid on Google Earth, annotated by the ATSB
The aircraft collided with the ground in a nearly vertical nose-down attitude and came to rest inverted (Figure 4). The student and instructor sustained minor injuries and it is possible that their recollection of events may have been affected by trauma associated with the collision. The aircraft was substantially damaged.
The student was enrolled in Fly Oz’s commercial pilot licence (aeroplane), multi-engine aeroplane class and command instrument rating integrated flight training course. At the time of the accident, the student held a private pilot licence (aeroplane) and had accrued 247 hours of flying time, 11 of those in VH-OMD (all in the last 90 days), with 7 hours recorded as instrument flight time.
The instructor held a commercial pilot licence (aeroplane), with multi-engine aeroplane class and command instrument ratings, which they had attained at Fly Oz. The instructor had accrued 850 hours of flying time, of which 82.8 were in VH-OMD (70.3 of those in the last 90 days and 43.5 hours recorded as instrument flight time).
Aircraft information
General
VH-OMD was a Beechcraft E55 (serial number TE-970), manufactured in the United States (US) in 1974 and first registered in Australia in 1990. Fly Oz was not the registered operator[11] of VH‑OMD but hired the aircraft and had been using it for training and charter operations for about 6 months.
The aircraft was powered by 2 Continental IO-520-C 6-cylinder, horizontally‑opposed, fuel‑injected engines rated at 285 hp at 2,700 RPM and fitted with 2 Hartzell 3-bladed full‑feathering constant speed propellers (PHC-C3YF-2UF).
The maintenance release[12] current on the accident day showed that the aircraft was approved to operate under instrument flight rules and charter categories. The maintenance release was issued on 9 April 2024 with an aircraft total time in service of 4,622.1 hours. Since then, 2 flights totalling 8.8 hours flight time had been conducted prior to the accident day. There were no recorded defects or outstanding maintenance.
The aircraft departed with a take-off weight of 2,190 kg and operated within the approved weight and balance envelope during the flight, at mid-range centres of gravity.
Fuel system
The fuel system included multiple individual fuel cells with a total capacity of 651 L. The fuel cells had elastomeric liners capable of tolerating large deformation without rupture. In an impact, this reduced the likelihood of an explosive fuel-air mist compared with unlined metal tanks. The fuel selector was an OFF-ON-CROSSFEED arrangement for each engine with the selector panel located on the floor.
Each engine had a 2-speed electric (auxiliary) fuel boost pump, which could be selected at HIGH pressure, OFF or LOW pressure. High was used for providing fuel pressure to prime the engine before start and provided near maximum engine performance should the engine‑driven pump fail. The airplane flight manual (AFM) stated that the ‘high pressure position should not be selected while the engine is operating except in the event of engine driven pump failure since the high pressure mode supplies a greater pressure than can be accepted by the injector system for a reduced power condition’.
Front seats and restraints
The front seats were fitted with 4-point restraints, each consisting of 2 lap straps connected to the seat frame and 2 shoulder harness straps connected via a Y belt to an inertia reel attached to the upper cabin structure. The inertia reel was designed with a locking device that would secure the shoulder straps in the event of sudden forward movement or impact. The seats could be adjusted forward or aft, with the seat guides sliding along 3 seat rails: 2 main (aft) and 1 centre (forward) (Figure 5). The seat is retained at the desired adjustment by a spring-loaded locking pin engaging in one of the forward centre rail holes. Shims could be added to the inside of the guide to ensure locking pin alignment.
Left seat position depicted in image, right seat rails identical. Source: ATSB and Beechcraft, annotated by ATSB
Meteorological information
The Bureau of Meteorology graphical area and grid point wind and temperature forecasts covering Cowra Airport for the accident time predicted primarily clear skies, visibility greater than 10 km and a light northerly wind.
Consistent with the forecasts, Cowra Airport’s recorded meteorological conditions[13] at 1400 included wind at 3 kt from 010°, and at 1430 the wind was 5 kt from 310°. At both those times, there was no cloud, the temperature was 21 °C and QNH 1019 hPa.[14]
Recorded data
OzRunways[15] data from the student’s electronic flight bag application contained aircraft track, altitude and ground speed. The ATSB also obtained flight data from the aircraft’s Garmin electronic flight instrument (EFI), which included 40 data parameters. Figure 6 shows key parameters from the EFI data, with the following observations.
From 1404:07, after passing over the NDB, there were heading changes, yaw (evident as lateral accelerations) and a sudden left roll[16] followed by a 10–15 kt reduction in airspeed, consistent with a left engine power loss.
Between about 1408:12 and 1409:27, during the turn from the outbound to the inbound tracks of the NDB instrument approach, the aircraft descended, climbed and descended again, at vertical speeds exceeding 1,000 fpm. During that period the airspeed varied between about 120–150 kt, with left roll angles up to 34°.
The aircraft was on the downwind circuit leg between about 1413:26 and 1414:14, during which time there were no significant changes in lateral acceleration, roll, heading or performance (speed or height).
The aircraft crossed the runway threshold at 1416:01 at 98 kt airspeed aligned with the runway centreline. The last position recorded by the EFI was at 1416:09, at which time the aircraft’s nose had pitched[17] up 6.5°, the airspeed had reduced to 79 kt and the ground speed was 77 kt, indicating a 2 kt headwind. The OzRunways recorded ground speed at the same time was 76 kt.
The OzRunways data showed the aircraft started to deviate left of the runway centreline at 1416:14 at 69 kt ground speed, which would equate to an airspeed of about 71 kt for the same headwind component. The final OzRunways data point recorded before the fence, where the impact with terrain occurred, was at 1416:18 at a ground speed of 65 kt.
Figure 6: Selected parameters from the Garmin electronic flight instrument
Source: ATSB analysis of Garmin data
Site and wreckage
The aircraft impacted the ground nose-down and inverted about 75° from the horizontal, resulting in crushing of the 2 m‑long nose structure (Figure 7). It collided with a fence and came to rest about 66 m left of the runway centreline and about 700 m beyond the runway threshold. The landing gear was extended, and the flaps were in the approach position.
Both engines had folded backwards around the wing leading edge, which pulled the engine control cables such that the engine control levers were no longer representative of the pre‑impact positions. Damage to the wing leading edge resulted in fuel leaking, but there was no post-impact fire. The aircraft departed with full fuel, and had approximately 400 L of fuel remaining on board at impact. Both fuel selectors were set to ON. Flight control continuity was established.
The left propeller flange fractured resulting in the propeller assembly detaching from the engine crankshaft and coming to rest spinner-down embedded in the dirt. The propeller manufacturer advised that the damage to the blades was consistent with the propeller either windmilling or not rotating at impact. The left spinner was indented with the counterweight, showing that the propeller was in fine pitch and not feathered.
The right propeller remained attached to the right engine with evidence of being driven by significant engine power. Fence wire was wrapped around the engine and propeller, which had dug into the ground and first responders reported evidence of dirt having been flung from the hole by the rotating blades.
Examination of the left engine found no evidence of mechanical failure or any pre‑existing fault. The fuel filters and air induction system were clear. The spark plugs were removed with no evidence of fouling from oil or carbon deposits and there were no visible defects with the ignition leads. Borescope examination of the cylinders found no damage or abnormal appearance of the internal surfaces. The fuel distributor manifold was empty of fuel and the diaphragm was undamaged. When electrical power was applied to the starter motor, the engine turned over normally with no evidence of loss of compression in the cylinders.
The 2 front (crew) seats had separated from their track assemblies, although the shoulder harness inertia reels of both seats remained attached to the upper cabin structure. The instructor and student remained partially secured in their seats via the lap straps attached to the seat frame, The instructor came to rest in their seat outside the aircraft cabin following the opening of the cabin door during the accident sequence.
Damage and distortion to the seat rails and seat guides was consistent with forward and right forces sustained during the impact sequence. Both seats’ centre rails exhibited distortion and smearing on the forward edge from the locking pins being forced from their rail holes. The left seat locking pin was bent rearward, and the right seat alignment pin had sheared. Figure 8 shows spreading of one of the seat guides and the associated damage to the seat rails.
Figure 8: Spreading of one seat guide (left) and associated damage to the rails (right)
Source: ATSB
A post-impact photograph showed the left engine auxiliary pump in the high position (Figure 9). However, as the entire panel had come adrift, there was dirt adjacent to the switch, and most of the switches in the row beneath it had broken off, its post-impact position was not considered reliable evidence of its position at the time of the accident. The switch panel location was also consistent with injury to the student’s knee. Additionally, the student reported that the pump had been used only for priming prior to engine start then confirmed to be off and not used again during the flight. The metal fuel pump switches were also by design unlikely to be confused with the smaller plastic light switches in the row below and inadvertently selected. It was therefore unlikely to have been on prior to the accident.
Figure 9: Panel showing post-impact switch positions and disruption
Source: Fly Oz, annotated by the ATSB
Asymmetric flight
Asymmetric control
In conventional light twin-engine aeroplanes with one engine inoperative, asymmetric thrust will cause the aeroplane to yaw (rotate about its vertical axis) towards the inoperative engine. As a secondary effect of yaw, it will also roll. The yawing needs to be countered by deflection of the rudder and a small aileron deflection to raise the inoperative engine’s wing, in order to maintain balanced flight. At maximum power on the operative engine, the amount of rudder deflection needed increases as airspeed reduces, to a minimum control speed, below which the rudder is unable to maintain directional control.
Below the minimum control speed, the pilot must reduce power on the operative engine to reduce the asymmetric force, and/or lower the aircraft nose to increase airspeed, to prevent a loss of control. If directional control is lost, the aircraft will yaw and then roll and descend rapidly. Controlled flight may be recovered if enough height is available, by reducing power and lowering the nose.
Minimum control speed
The Civil Aviation Safety Authority’s (CASA) Civil Aviation Advisory Publication (CAAP) 5.23‑1(2) Multi-engine aeroplane operations and training, defined minimum control speed (VMC) as:
a speed that is associated with the maintenance of directional control during asymmetric flight. If the pilot flies below this speed the tail fin and rudder are unable to generate enough lift to prevent the aircraft from yawing. If uncorrected, the yaw causes roll, the nose drops, the aircraft rapidly assumes a spiral descent or even dive, and if the aircraft is at low altitude, it will impact steeply into the ground. This type of accident is not uncommon in a multi-engine aircraft during training or actual engine failure.
There is both a ground value (VMCG) and an airborne value (VMCA), but for simplicity, VMC usually refers to VMCA. The VMC is designated by the red radial on the airspeed indicator. The AFM specified VH-OMD’s VMCA as 79 kt indicated airspeed. That value is determined by US Federal Aviation Regulations (FAR) as the minimum airspeed at which it is possible to recover directional control of the aircraft within 20° heading change, and thereafter maintain straight flight, with no more than 5° of bank toward the operating engine following the sudden failure of one engine with:
take-off power on both engines
rearmost allowable centre of gravity
flaps in the take-off position
propeller windmilling in take-off pitch configuration.
However, the actual VMC will vary depending on the configuration, conditions and pilot technique (FAA, 2021). The CASA CAAP 5.23-1(2) stated that flight tests conducted in a Cessna Conquest aircraft, which had a published VMC of 91 kt, found that if the wings were held level instead of the inoperative engine wing raised 5°, the actual minimum control speed was 115 kt – an increase of 24 kt. Other light twin-engine aeroplanes would similarly show an increase in actual minimum control speed without bank towards the operative engine. The American Bonanza Society Air Safety Foundation advised that in Baron aircraft types (including the E55), actual VMC is about 15 kt higher than the published VMC if the wings are held level instead of the inoperative engine wing raised, and the slip/skid ball remains centred instead of deflected towards the operative engine.
At speeds below the actual VMC, with one engine inoperative and the other at take-off power, the aircraft will lose directional control – yaw, roll towards the inoperative engine and descend steeply.
Best rate of climb one engine inoperative airspeed
The best rate of climb speed with one engine inoperative (single-engine) (VYSE) is denoted by a blue line on the airspeed indicator and therefore also known as ‘blue-line speed’. It represents the single-engine best rate of climb speed at maximum weight. The AFM for VH-OMD specified the VYSE was 99 kt. Pilots often use blue-line speed as a safety margin above VMC for initiating a simulated engine failure and assume that if blue-line speed is maintained, there is sufficient margin above VMC to prevent an asymmetric loss of control.
Simulated one engine inoperative
Aircraft manufacturer’s procedures
The AFM emergency procedures section included the following procedure titled Determining inoperative engine:
The following checks will help determine which engine has failed.
1. DEAD FOOT – DEAD ENGINE. The rudder pressure required to maintain directional control will be on the side of the good engine.
2. THROTTLE. Partially retard the throttle for the engine that is believed to be inoperative; there should be no change in control pressures or in the sound of the engine if the correct throttle has been selected. AT LOW ALTITUDE AND AIRSPEED THIS CHECK MUST BE ACCOMPLISHED WITH EXTREME CAUTION.
Do not attempt to determine the inoperative engine by means of the tachometers or the manifold pressure gages. These instruments often indicate near normal readings.
The AFM further described the following procedure titled Simulated one engine inoperative:
Zero thrust (simulated feather)
Use the following power setting (only one engine at a time) to establish zero thrust. Use of this power setting avoids the difficulties of restarting an engine and preserves the availability of engine power.
The following procedure should be accomplished by alternating small reductions of propeller and then throttle, until the desired setting has been reached.
Propeller lever – RETARD TO FEATHER DETENT
Throttle lever – SET 12 in. Hg MANIFOLD PRESSURE
NOTE: This setting will approximate zero thrust using recommended one-engine inoperative climb speeds.
Fly Oz procedures
Fly Oz provided a document detailing its simulated engine failure procedure for the Beechcraft E55 aircraft. The procedure was for the instructor to reduce the mixture on one engine to idle cut‑off when above 1,000 ft. Once a student completed the initial checks, identified and verified the inoperative engine, the flight crew must decide whether to ‘fix’ the engine (if en route), or ‘feather’ the engine (‘at critical stages of flight’). If they elect to feather the engine:
… the student will articulate to the instructor which engine they determine has failed and the instructor will set zero thrust.
Fly Oz also provided a copy of their Multi Engine Training Approval Standardisation Manual, which it advised was written for operating Beechcraft Model 76 Duchess aircraft, but was also applicable to the Beechcraft E55. The manual included an Engine failure recovery sequence, describing the 3 stages of a student’s mastery in handling an engine failure. For that sequence, the instructor was to ‘fail an engine by closing the mixture’ [their emphasis]. This was followed by completing the ‘engine out checks’, identifying and verifying the failed engine, then either feathering or troubleshooting to ‘fix’ the failed engine. That procedure did not mention its applicability to asymmetric instrument approaches.
The standardisation manual also had an Asymmetric circuits one engine inoperative procedure, which included 2 notes:
• Never fail an engine below 500 ft AGL.
• Always use the throttle to fail engines in the circuit so you can immediately add power if required.
For that procedure, the instructor was to set zero thrust once the student had identified the correct engine to feather by touching the corresponding pitch lever. The asymmetric circuit procedure also mentioned conduct of an instrument approach and stated:
During an instrument approach a power setting of 20”MP [manifold pressure] with gear down should provide similar performance to the standard 15”MP with both engines operating. Gear should remain down if performance can be adequately maintained.
Additionally, the student or instructor was to include in the radio transmissions that they were ‘asymmetric’ to ‘allow other pilots to keep a safe distance and not try and push in on you in the circuit’.
Fly Oz also provided the ATSB with a copy of the Beechcraft Pilot Proficiency Program Instructor Standards Manual (American Bonanza Society, 2020), which it reported provided best practice guidance for operating the aircraft. The manual stated not to use the mixture to simulate an engine failure in single engine aircraft types. However, it did not stipulate how to simulate an engine failure in multi-engine aeroplanes, and included the following guidance on simulating zero thrust:
set the throttle to 10-12” MP, minimum governing RPM and mixture for ~ 6-7 GPH.
Fly Oz advised the ATSB that it was common industry practice in both flight training and CASA flight testing to use the mixture to shut down an engine particularly when above circuit height. They further advised that their interpretation of the Beechcraft E55 AFM was that it did not specify how a simulated engine failure should be initiated.
Guidance material
The US Federal Aviation Administration (FAA) publication Flying light twins safely (P-8740-066) advised pilots to ‘become thoroughly familiar with the AFM/POH recommended procedures’. Further, it recommended that simulated engine failures below 3,000 ft above ground level (AGL) should be accomplished by smoothly retarding the throttle (FAA, 2008). This was reiterated in the FAA’s Airplane Flying Handbook (FAA-H-8083-3C), Chapter 13: Transition to multiengine airplanes, which stated:
The FAA recommends that all in-flight simulated engine failures below 3,000 feet AGL, be introduced with a smooth reduction of the throttle. Thus, the engine is kept running and is available for instant use, if necessary. Smooth throttle reduction avoids abusing the engine and possibly causing damage.
The handbook also advised that the AFM/POH takes precedence, and that for engines equipped with dynamic crankshaft counterweights, it was essential to make throttle reductions smoothly.
The United Kingdom Civil Aviation Authority’s Aeronautical Information Circular (Pink) 2008-P-064 also advised pilots to refer to the engine manufacturer’s recommendations for simulating engine failures. It recommended that engine failures after take-off ‘should be simulated only by reducing power and never by complete shutdown of the engine until recommended minimum heights at paragraph 9.4 have been achieved’. The referenced paragraph 9.4 recommended minimum safe heights for complete shutdown of power plants for training purposes of 3,000 ft AGL for twin engine piston and turboprop aeroplanes with a maximum take-off weight not exceeding 5,700 kg.
Transport Canada’s Instructor Guide – Multi-engine class rating (TC, 2010), stated:
Actual engine shutdowns for training purposes are not recommended, as the training value is not worth the added safety risk and abuse of engines and airframe…
Simulate the engine failure by reducing the throttle to idle, while calling out "simulated". Complete the engine failure drill in accordance with the [pilot’s operating handbook] POH or the procedures outlined on the previous page.
When these checks have been completed, and you are ready to simulate feathering the propeller, adjust the manifold pressure and rpm to simulate by setting zero thrust. Consult the POH for zero thrust power settings prior to flight. Complete the engine securing items by referring to the appropriate emergency checklist.
The CASA CAAP 5-23-1(2) Multi-engine aeroplane operations and training advised instructors to consult the aircraft flight manual or pilot’s operating handbook for the recommended method of simulating an engine failure. It recommended:
Do not simulate an engine failure using procedures that may jeopardise the restoration of power. It is not recommended to simulate an engine failure at low level by selecting the mixture to idle cut-off or turn the fuel selector off. These procedures would be more appropriate at higher altitude.
Further, the CAAP stated:
6.5.4 Slowly closing the throttle is one of the methods used to simulate an engine failure. Although selecting idle cut-off may be kinder to an engine, the engine or aircraft manufacturer may not permit it. So slowly closing the throttle to idle or zero thrust is unlikely to harm the engine and allows for immediate restoration of power.
…
6.8.1 Flight instructors often simulate an engine failure by rapidly closing the throttle or moving the mixture control to idle cut-off. The latter method should never be used at low altitude.
American Bonanza Society Air Safety Foundation recommendation
The American Bonanza Society Air Safety Foundation recommended multi-engine instructors simulate an engine failure by smoothly reducing the throttle to idle, then block throttle movement on the simulated inoperative engine while the pilot receiving instruction (PRI) completes actions from the POH Engine failure in flight checklist. When the PRI gets to the checklist item ‘Propeller – Feather’, the instructor takes over the power controls and sets zero thrust in accordance with the BE55 POH/AFM.
The American Bonanza Society Air Safety Foundation recommended not simulating engine failure by turning off the fuel selector or pulling the mixture control to cutoff, consistent with FAA guidance.
Lycoming service bulletin
In April 1987, engine manufacturer Lycoming issued Service Bulletin No. 245D, Dynamic counterweight system detuning, which affected 9 Lycoming 6-cylinder engine models. The service bulletin explained that when the inertia force on an engine (which increases with engine speed), or the expansion force (manifold pressure), is suddenly changed, the engine counterweight system can ‘detune’. Damage to the counterweights, rollers and bushings could result, culminating in engine failure.
The service bulletin listed 4 operating conditions that could cause the counterweight system to detune: rapid throttle operation, high engine speed and low manifold pressure, excessive speed and power, and propeller feathering. The bulletin stated:
To avoid detuning during simulated engine failure, use the mixture control to shut off the engine and leave the throttle in normal open position until the engine has slowed down because of lack of fuel.
Fly Oz reported being unaware of the bulletin at the time of the accident. Additionally, Fly Oz reported that its procedures had been written for the Beechcraft 76 (Duchess) aircraft type, which were fitted with 4-cylinder Lycoming O-360 engines, and therefore not affected by the service bulletin. Finally, VH-OMD was not fitted with Lycoming engines and there was no comparable service bulletin or known issue associated with Continental engines.
Checklists
The student’s normal checklists are listed in the following tables.
The student described the flight as ‘quite busy’, that they were ‘learning a lot of things’, and ‘a little overwhelming but normal for that stage of flying’. The student rated their workload on final as moderate (about 6/10).
The instructor described that the student had been performing really well that day, asymmetric work and checks were good, and overall the student was a good pilot. The instructor also assessed that the student ‘got a bit distracted on the outbound’ leg of the approach, was a ‘little slow’ getting established on the inbound track, and there was some distraction due to circuit traffic operating on the opposite runway. The instructor reported that the student was ‘wrestling’ the aircraft on inbound or downwind, which prompted the instructor to ask whether the student wanted zero thrust set.
The instructor rated their workload as moderate (5/10) and reported that for every landing, they had their seat fully forward, feet on the pedals and was alert and ready to intervene if necessary.
Survivability
The student sustained a cut under the chin, a small fracture in the right hand, and lacerations to the left knee. The instructor had a deep laceration to the chin and one arm and bruising to the knees. Both sustained additional cuts and bruises, including bruising from the lap belt and shoulder harnesses.
The certification basis of the aircraft was US Civil Air Regulation 3. The certification standards required that for a standard weight person (77 kg), the seat must withstand flight, ground, and emergency load conditions. For the seats, the critical conditions were 9 G forward, 3 G upwards and 1.5 G sideways, with the seat attachments to withstand 133% of those requirements.
ATSB analysis of the wreckage and accident site found that the impact deceleration likely exceeded 30 G in a principally forward direction. This significantly exceeded the 9 G forward requirement and the 12 G requirement for the seat attachments. The stable collapse of the airframe structure forward of the occupants aided their survivability.
Similar occurrences
ATSB occurrences
The ATSB occurrence database contained 16 twin-engine aeroplane loss of control occurrences during simulated engine failures since 1978. Two of those occurred in the last 10 years and resulted in fatal accidents in which the loss of control resulted from a simulated engine failure using a method and/or height contrary to manufacturers’ guidance. Key findings of these 2 investigations are as follows.
Loss of control and collision with terrain involving Cessna 441, VH-XMJ, 4 km west of Renmark Airport, South Australia on 30 May 2017 (AO-2017-057)
The flight departed Adelaide, South Australia, at about 1524 local time and flew to the Renmark area for exercises related to the check flight, followed by a landing at Renmark Airport. After a short period of time running on the ground, the aircraft departed from runway 25 at about 1614.
The ATSB determined that, following a simulated failure of one of the aircraft’s engines at about 400 ft above the ground during the take‑off from Renmark, the aircraft did not achieve the expected single engine climb performance or target airspeed. As there were no technical defects identified, it is likely that the reduced aircraft performance was due to the method of simulating the engine failure, pilot control inputs or a combination of both.
It was also identified that normal power on both engines was not restored when the expected single engine performance and target airspeed were not attained. That was probably because the degraded aircraft performance, or the associated risk, were not recognised by the pilots occupying the control seats. Consequently, about 40 seconds after initiation of the simulated engine failure, the aircraft experienced an asymmetric loss of control.
The single engine failure after take‑off exercise was conducted at a significantly lower height above the ground than the 5,000 ft recommended in the Cessna 441 pilot’s operating handbook. This meant that there was insufficient height to recover from the loss of control before the aircraft impacted the ground. The 3 occupants were fatally injured.
The operator’s training and checking manual procedure for simulating an engine failure in a turboprop aircraft was inappropriate and increased the risk of asymmetric control loss.
Loss of control and collision with terrain involving Angel Aircraft Corporation 44, VH-IAZ, near Mareeba Airport, Queensland, on 14 December 2019 (AO-2019-072)
On 14 December 2019, 2 pilots were conducting a private flight in an Angel Aircraft Corporation Model 44 aircraft, registered VH-IAZ, at Mareeba, Queensland. An instructor seated in the right pilot seat was conducting a flight review of the pilot (and aircraft owner) in the left seat.
After the aircraft took off from Mareeba Airport, witnesses reported hearing one of the engines hesitating and backfiring, accompanied by a sooty smoke trail from the right engine. The aircraft operated in the training area until returning to the airport circuit area. Witnesses observed the aircraft touch down on the runway, accelerate and take off again. After take-off, the aircraft climbed to about 100–150 ft above ground level before entering a right descending turn. The aircraft was airborne for about 20 seconds before witnesses observed it rolling rapidly to the right and impacting terrain in a cornfield 475 m north of the runway. The pilots sustained fatal injuries and the aircraft was destroyed.
The ATSB found that shortly after take-off, the flight instructor very likely conducted a simulated failure of the right engine in environmental conditions and a configuration in which the aircraft was unable to maintain altitude with one engine inoperative. Power was not immediately restored to the right engine to discontinue the exercise and the pilots were unable to maintain altitude or heading, particularly with the aircraft banked towards the inoperative engine. The pilots did not reduce power and land ahead, as required by the Airplane Flight Manual, resulting in a loss of directional control and roll. The loss of control occurred at a height too low to recover and the aircraft impacted terrain.
United States occurrences
A search of the US National Transportation Safety Board’s (NTSB) database for investigations involving twin engine aeroplanes, with the words ‘engine’ and ‘simulated’ in the probable cause text, yielded 37 investigations since February 1989,13 of which occurred in the last 10 years. Two of those provide some context relevant to this occurrence:
Piper PA-34, N88AG, Miami, Florida, US on 11 September 2018
The flight instructor in the multi-engine aeroplane reported that the pilot under instruction was conducting a simulated instrument approach in visual flight rules conditions. The instructor placed the left engine fuel selector in the ‘off’ position to simulate an engine out, and the pilot under instruction initiated the left engine failure procedure by placing the engine and propeller levers in a simulated feathered zero-thrust configuration. The instructor became distracted by traffic and failed to place the left engine fuel selector back to the ‘on’ position.
With full flaps and the landing gear extended and while about 250 ft above ground level, the instructor terminated the simulated instrument approach and instructed the pilot to land visually; however, the airspeed decreased below safe limits, and the instructor directed the pilot to increase the airspeed. The pilot increased power on both engines; however, the left engine power did not increase, and the aeroplane rolled to the left about 45°. The instructor took the controls and applied right aileron and rudder, but the aeroplane settled down in a level attitude in a shallow lagoon on the left side of the runway.
Probable cause: The pilot under instruction’s failure to maintain the twin-engine airplane’s minimum control airspeed with one engine inoperative and the flight instructor’s distraction when reconfiguring the airplane following the simulated engine failure, which resulted in no power being available to the left engine and a loss of control during landing when the throttles were advanced to increase airspeed.
Cessna 402C, N2714B, Hyannis, Massachusetts, US on 26 April 2021
A flight instructor and a new-hire trainee pilot were practising instrument approach procedures in the multi-engine aeroplane. On climb-out, the flight instructor reduced power on the left engine to simulate an engine failure on take-off. The pilot then ran the memory items for an engine failure, which included turning the left engine auxiliary fuel boost pump to high. They then conducted an instrument approach. When the aircraft was about 50 ft above the runway, the flight instructor called for a 2-engine go-around. The pilot brought both throttles to full power and retracted the flaps and gear. The flight instructor reported that the aircraft yawed left, and the airspeed was about 80 kt, well under the aircraft’s best single engine rate of climb speed of 95 kt. The flight instructor took control of the aircraft and called for the gear to be extended. The aircraft landed hard and the nose and left main landing gear collapsed, resulting in substantial damage to the left engine and wing. Prior to exiting the aircraft, the pilot turned the left engine auxiliary boost pump from the high position to the off position.
The flight instructor reported that turning the boost pump to high while the engine was still operating could flood the engine with excess fuel and cause it to lose power. The instructor reported that they normally reminded pilots not to turn the pump to high during a simulated engine failure in flight, but neither flight crewmember recalled it being mentioned during the accident flight. Post-accident examination of the left engine revealed no mechanical discrepancies that would have precluded normal operation. As a result, it was most likely that when the boost pump was turned to high, it flooded the engine with excess fuel, resulting in loss of engine power while attempting to go around.
Probable cause: The flight instructor’s failure to confirm the position of the left engine’s auxiliary fuel boost pump switch during a simulated engine out procedure, which resulted in an excess amount of fuel in the engine and subsequent partial loss of power during a go-around/rejected landing. Contributing to the accident was the flight instructor’s failure to maintain control of the airplane, which resulted in a hard landing.
Engine control standardisation
VH-OMD was certified to the 1956 US Civil Air Regulations. The NTSB special study General Aviation Accidents involving fuel starvation 1970–1972 identified design-associated and pilot‑associated factors that influenced or caused ‘operational problems’ in fuel starvation accidents. As a result, the NTSB issued several recommendations. One was for the FAA to issue an advisory circular including ‘to warn certificated flight instructors of the danger associated with simulation of emergency engine failure by positioning the fuel selector valve to “off” or the mixture control to “idle cutoff”’. Another recommendation, A-74-38, was for the FAA ‘to amend the regulations to include specifications for standardizing powerplant control location, visual and tactile appearance, and mode of actuation’.
In 1976, in response to NTSB recommendation A-74-38 regarding fuel control standardization, the US General Aviation Manufacturers Association (GAMA) proposed to the FAA changes to FAR 23.777 through 23.781. It prescribed left to right throttle, propeller and mixture controls, landing gear to the left of the throttle or pedestal centreline, and flap to the right, and included recommended shapes and colours (Figure 10). The FAA’s General aviation (FAR 23) cockpit standardization analysis (FAA-NA-77-38) recognised that ‘increased standardization of cockpit systems can reduce cockpit workload, reduce the potential for habit interference when transitioning to another type aircraft, and provide for application of the best and most error‑resistant designs’ (FAA, 1978).
However, regarding the subsequent FAR amendment 23–33 1986, the FAA stated, ‘that color of control knobs is not a safety issue and will not adopt the proposed color requirement’. As a result, the recommended black throttle control knob and blue propeller control knob standard was not incorporated into FAR 23. A mixture lever was considered an ‘emergency control’ and therefore under FAR 23.1555(e)(2) must be red. The landing gear lever (left) and flap lever (right) requirement was incorporated in FAR 23.777 (f) and (g)).
Figure 10: Recommended control standardisation shapes and colours
Source: US Federal Aviation Administration
Figure 11 is a post-accident photo of VH-OMD’s engine control levers, which are all black, the throttle pair is in the middle and each pair has different shaped knobs. Additionally, the landing gear selector was to the right of the centre console and the flaps to the left. As VH-OMD was certified prior to the standardisation requirements, it was not required to comply with subsequent FARs.
In this case, as the instructor primarily flew VH-OMD, and it was the only twin engine aeroplane the student had flown (other than a simulator), habit interference was unlikely. However, the lack of colour differentiation in the levers, and particularly not having red mixture control levers, may have reduced the opportunity for rapid visual identification of the mixture lever position.
When overhead the Cowra Airport navigation aid at the commencement of an instrument approach, at about 2,600 ft above ground level, the instructor simulated a failure of the left engine. After the student conducted the instrument approach and had visually established the aircraft on final approach to the runway, the instructor initiated a go-around at a low height above the runway. Control of the aircraft was lost as it rapidly yawed and rolled left and impacted the ground in an almost vertical nose-down attitude, before coming to rest inverted.
Wreckage examination determined that the left engine was not producing power and the right engine was making significant power at impact. Additionally, there was no evidence of any defect in the left engine or airframe that could have contributed to the accident.
The following analysis will consider why the left engine was not operating at impact and why the go‑around was attempted with one engine inoperative. Additionally, operational procedures associated with simulated engine failures and related risk controls, including their potential to influence future operations will be discussed.
Left engine not restarted
The instructor followed their normal method of simulating an engine failure in accordance with the operator’s stated procedure for the aircraft type by moving the left engine mixture control lever to the idle cut-off position, thereby rendering the engine inoperative.
The required response was for the student to maintain directional control of the aircraft and complete the engine failure checks. Once the student had identified which engine was inoperative, they were to either complete troubleshooting checks to ‘fix’ the failed engine when en route or feather the propeller at a critical stage of flight.
In a training scenario, once the student had identified the inoperative engine correctly, the instructor would normally set zero thrust to simulate a feathered propeller. Their process for setting zero thrust included returning the mixture control to full rich, thereby restarting the engine. However, for reasons that could not be determined, zero thrust was not set at that stage, the mixture remained at idle cut-off with the left propeller windmilling.
The windmilling propeller increased drag and the likelihood of a loss of control, particularly during the left turn towards the inoperative engine. Although the student did not report experiencing a high workload, the approach was not flown within prescribed tolerances and included significant changes in airspeed and altitude. Given the benign weather and light winds at the time, these deviations were likely a result of pilot handling, not environmentally induced. The subsequent improvement in tracking accuracy evident when the aircraft turned to join the circuit, was consistent with the student lifting the hood and resuming flight with external visual reference.
Whether the instructor or student prompted the setting of zero thrust could not be resolved. Given that the instructor recalled setting zero thrust either on inbound or downwind and the student recalled this occurred on downwind, downwind was considered more likely as it was consistent with both recollections. There was no change in heading or increase in performance evident in the recorded data to indicate power was restored to the left engine on downwind, although any such change may have been negligible at the relatively low power settings.
As the manifold pressure would essentially read normally with the propeller windmilling, the stated practice of the instructor of moving the throttle lever forward to achieve the target manifold pressure for setting zero thrust would not confirm the engine was operating. It was for this reason that the Beechcraft E55 Airplane Flight Manual (AFM) cautioned against using manifold pressure indications to assess engine power. In the context of this accident, the observed (and expected) variation of manifold pressure with throttle movement supported an assessment that the engine had been restarted and was capable of normal operation.
Prompting and attempting to set zero thrust on downwind may have interrupted the student’s completion of the downwind checks, which should have included moving both mixture levers to the full rich position. Additionally, the student did not complete the previous checklist item of extending the landing gear, electing to defer doing so until turning onto the base leg and potentially interrupting the checklist flow. As the student had broadcast that they were operating in asymmetric configuration, they were not anticipating the conduct of a go-around. There was no check conducted by either crewmember, or required by procedure, that would verify the engine had restarted and was making power.
The initial small increase in power to the right engine and associated yaw prior to the go-around, as reported by the instructor, was not evident in the data. However, the recorded data showed the aircraft veered off the runway within 3 seconds of the initial deviation from the runway centreline, and the yaw and roll continued to impact. This was consistent with significant asymmetric thrust due to the left engine being inoperative, as evidenced by the absence of rotation when the propeller blades subsequently impacted the ground.
As there was also no evidence of any engine failure mechanism and although the mixture lever position prior to impact could not be determined, the ATSB found that the left mixture lever likely remained in the idle cut-off position from shortly after commencing the instrument approach and the engine was unintentionally not restarted.
Go-around and loss of control
The instructor was unaware they had not returned power to the left engine, and therefore when they instructed the student to commence a go-around, it was based on a belief that symmetrical power was available. This misunderstanding meant the instructor's initial actions in response to the left yaw were to verify the throttle levers were fully forward and to call for the student to let go of the controls, while attempting to correct with rudder. At that stage the only way to avoid the loss of control would have been to reduce power on the right engine and land.
The last recorded airspeed from the electronic flight instrument data, prior to the yaw was 79 kt, which was the published minimum control speed (VMC). The OzRunways data showed the ground speed reduced another 7 kt before the yaw commenced, and the airspeed likely similarly reduced. Additionally, the actual VMC may have been higher, as the wings were probably levelled for landing, rather than having the inoperative engine wing raised 5°, as required to achieve the optimum published VMC. As the aircraft was almost certainly below actual VMC when the go-around commenced, there was insufficient rudder authority to maintain control, and the loss of control occurred at a height too low to recover.
The low height at which the loss of control commenced, estimated to be about 20 ft above the runway, and the crushing of the aircraft’s structure on impact, contributed to the accident’s survivability. The impact forces exceeded the certification requirements of the seats, which detached from their rails, but the flight crew were initially restrained by 4-point harnesses. Significantly, as the aircraft was fitted with fuel cells, despite disruption to the wing leading edge and fuel slowly leaking post impact, there was no explosive fuel-air misting or post-impact fire.
Fly Oz simulated engine failure procedure
The Beechcraft E55 AFM included a procedure for simulating one engine inoperative. The procedure was to set zero thrust, which involved retarding the propeller lever to the feather detent and the throttle lever to set 12 inches of manifold pressure. The flight manual stated that the purpose of the procedure was to ‘avoid difficulties of restarting an engine and preserve the availability of engine power', which would be associated with cutting off the mixture and/or selecting the fuel off.
Fly Oz’s procedure for simulating an engine failure in the Beechcraft E55 aircraft was to move the mixture to idle cut-off to simulate an engine failure, when above 1,000 ft, which was contrary to the AFM procedure to use throttle. It was also contrary to guidance not to use mixture to simulate engine failures when below 3,000 ft above ground level from the aviation regulators in the United States, United Kingdom, and Canada. The Australian Civil Aviation Safety Authority’s guidance did not specify a height below which mixture cut-off should not be used. However, it advised not to simulate an engine failure ‘using procedures that may jeopardise the restoration of power’. Further, that slowly closing the throttle allows for immediate restoration of power.
As the conduct of an asymmetric instrument approach may include one or more legs of a circuit and end in a landing, there is a potential need for immediate restoration of power close to the ground. Therefore, the use of throttle to simulate an engine failure for conduct of an instrument approach could be inferred from the CASA guidance. The guidance also included the need to consult the aircraft flight manual for the manufacturer’s recommended method of simulating an engine failure.
Fly Oz’s Multi Engine Training Approval Standardisation Manual also included a procedure to simulate an engine failure that involved moving the mixture to idle cutoff. However, consistent with the AFM, it also contained a procedure that stipulated the use of throttle to simulate engine failures in the circuit (under which it included the conduct of asymmetric instrument approaches). Fly Oz stated that, while the manual had been written for a different aircraft type, it provided a description of the procedure applicable to VH-OMD. Despite that, on the day of the accident the instructor used the Fly Oz Beechcraft E55 specific procedure in use at the time and simulated the engine failure using the mixture control. That procedure did not contain a requirement or process to verify the engine was subsequently restarted and available for instant use.
This likely resulted in the inoperative engine being undetected by the flight crew, while operating at low power during the approach and landing. Ultimately this resulted in the loss of control during initiation of a go-around.
The ATSB occurrence database held 2 fatal accidents in the last 10 years that resulted from a loss of control following a simulated engine failure using a method and/or height contrary to guidance. Although there was no data available for the number of simulated engine failures conducted and by what method, the frequency of loss of control accident types and likelihood of fatality indicated that these posed a significant risk.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving Beech E55, VH-OMD, at Cowra Airport, New South Wales on 11 April 2024.
Contributing factors
The instructor moved the left engine mixture lever to idle cut-off to simulate an engine failure overhead the navigation aid, and it was likely that they unintentionally did not subsequently move the lever to rich and ensure the engine was restarted and available for instant use.
The instructor initiated a go-around below the air minimum control speed unaware the left engine was inoperative, resulting in an asymmetric loss of control.
Fly Oz's asymmetric training procedure involved failing one engine using the mixture control without confirmation the engine was subsequently restarted, rather than reducing throttle to simulate zero thrust in accordance with the Beechcraft E55 Airplane Flight Manual. This increased the risk of undetected asymmetric operation during descent and landing and the associated loss of control. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation, industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Operator’s procedure to use mixture to simulate engine failure
Safety issue description: Fly Oz's asymmetric training procedure involved failing one engine using the mixture control without confirmation the engine was subsequently restarted, rather than reducing throttle to simulate zero thrust in accordance with the Beechcraft E55 Airplane Flight Manual. This increased the risk of undetected asymmetric operation during descent and landing and the associated loss of control.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by Fly Oz
Fly Oz has taken the following proactive safety action:
Following a simulated engine failure, zero thrust is to be set immediately after the student has completed the engine failure drills.
The instructor standardisation manuals were being updated to include a requirement that both the student and instructor confirm that the pitch, power and mixture controls are set back to normal 2‑engine configuration during checks on final. This is now a call out item, ensuring that both pilots are satisfied with the correct settings.
Glossary
AFM
Airplane Flight Manual
AGL
Above ground level
AIP
Aeronautical information publication
AMSL
Above mean sea level
CAAP
Civil Aviation Advisory Publication
CASA
Civil Aviation Safety Authority
CTAF
Common traffic advisory frequency
EFI
Electronic flight instrument
FAA
(US) Federal Aviation Administration
FAR
Federal Aviation Regulations
METAR
Meteorological conditions at an aerodrome
NDB
Non-directional beacon
NSW
New South Wales
NTSB
(US) National Transportation Safety Board
QNH
The altimeter barometric pressure subscale setting used to indicate the height above mean seal level
TIS
Time in service
US
United States
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight instructor and student pilot
the maintainer of VH-OMD
Fly Oz
Civil Aviation Safety Authority
New South Wales Police Force
the aircraft, propeller and engine manufacturers
Bureau of Meteorology
OzRunways
accident witnesses
photographs and videos taken on the day of the accident and for subsequent examination
recorded data from the GPS unit on the aircraft.
References
American Bonanza Society, BPPP Instructor Standards Manual, Revision 10, July 2020.
Civil Aviation Safety Authority, Civil Aviation Advisory Publication 5.23-1(2) Multi-engine aeroplane operations and training, September 2015.
United Kingdom Civil Aviation Authority, Aeronautical Information Circular, 64/2008 (Pink 142) 17 July 2008. Accessed 10 May 2024: Pink 142.qxp (ead-it.com)
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the flight instructor and student pilot
Fly Oz
Civil Aviation Safety Authority
the maintainer of VH‑OMD
American Bonanza Society Air Safety Foundation
the aircraft, engine and propeller manufacturers.
Submissions were received from:
the flight instructor and student pilot
Fly Oz
Civil Aviation Safety Authority
American Bonanza Society Air Safety Foundation.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[2]Visual Meteorological Conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[3]OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[4]Instrument approach procedure: A series of predetermined manoeuvres by reference to flight instruments that provides specified protection from obstacles.
[5]NDB: a ground-based radio transmitter that provides a reference point to navigate by.
[6]Windmilling: a rotating propeller being driven by the airflow rather than by engine power, and results in increased drag at normal propeller blade angles.
[7]Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[8]Manifold pressure gauge measures the absolute pressure in the intake manifold of an engine, expressed in inches of mercury (in. Hg). Normal operating range (green arc) was 15 to 29.6 in. Hg.
[9]Yawing: the motion of an aircraft about its vertical or normal axis.
[10]Flare: the final nose-up pitch of a landing aeroplane used to reduce the rate of descent to about zero at touchdown.
[11]A registered operator is responsible for airworthiness and maintenance control of the aircraft (CASA).
[12]Maintenance release: an official document, issued by an authorised person as described in Regulations, which is required to be carried on an aircraft as an ongoing record of its time in service (TIS) and airworthiness status. Subject to conditions, a maintenance release is valid for a set period, nominally 100 hours TIS or 12 months from issue.
[13]METAR: a routine report of meteorological conditions at an aerodrome. METAR are normally issued on the hour and half hour. Winds use true north as the reference.
[14]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[15]OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It also provides the option for live flight tracking by transmitting the device’s position and altitude.
[16]Rolling: the movement of an aircraft about its longitudinal axis.
[17]Pitching: the motion of an aircraft about its lateral (wingtip-to-wingtip) axis.
Occurrence summary
Investigation number
AO-2024-011
Occurrence date
11/04/2024
Location
Cowra Airport
State
New South Wales
Report release date
22/08/2024
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Loss of control, Runway excursion
Occurrence class
Accident
Highest injury level
Minor
Aircraft details
Manufacturer
Beechcraft
Model
E55
Registration
VH-OMD
Serial number
TE-970
Aircraft operator
Fly Oz Cowra
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training