Collision with terrain at night involving Robinson R22 Beta II, VH-LYD, 25 km south-south-east of Kowanyama, Queensland, on 9 October 2025
Final report
Report release date: 06/05/2026
Investigation summary
What happened
On the evening of 9 October 2025, a Robinson R22 Beta II helicopter, registered VH‑LYD, was being operated by MDH Pty Ltd (MDH) 25 km south-south‑east of Kowanyama, Queensland.
The helicopter left Rutland Plains at around 1845 to guide ground vehicles tackling a bushfire. At around 1920 the pilot told the ground crew that it was getting too dark and set off to return to Rutland Plains Station.
Staff at the station lit the helipad for the arrival of the pilot. When the pilot did not return to the station, staff raised the alarm.
The following morning, the helicopter wreckage was found. The helicopter had collided with terrain. The pilot of VH-LYD was fatally injured in the accident, and the helicopter was destroyed.
What the ATSB found
The ATSB found that the pilot operated the helicopter at night. The helicopter was not equipped, and the pilot was unqualified, for flight at night. However, it was normal for company R22 pilots to exceed the limits of last light.
Instead of observing the legal limits, pilots chose their own limits, despite none of the company’s R22 pilots being qualified for night flight and none of its R22 helicopters being equipped for night flight. ATSB analysis of historical flight tracking data showed that on 39 occasions in the previous 6 months MDH pilots had flown beyond the legal minimums into night. Flying after last light was a tolerated and unmanaged risk on MDH properties.
In addition, the ATSB found that MDH did not require pilots to formally assess risk and did not provide tools or training to do so. This limited the ability of the company and its pilots to identify and understand operational hazards and their consequences.
What has been done as a result
MDH now requires its pilots to determine the official time of last light and has made it a clear responsibility of the pilot and the station manager to ensure aircraft are on the ground before last light.
Additionally, pre-flight planning now includes consideration of fatigue, including rest and duty times, and consideration of risk assessment criteria.
MDH has also implemented a pilot mentoring scheme to assist, mentor and supervise MDH pilots during aerial mustering operations. This includes a pre-season low level risk assessment and standardised mustering workshop, the first of which took place in March 2026.
Safety message
This accident is the fourth fatal accident of this type in the last 5 years. Flying after last light without appropriate equipment and qualifications is an unsafe practice. The acceptance of this activity is leading pilots to fatal accidents.
The ATSB’s Avoidable Accidents No 7 - Visual flight at night accidents provides further discussion about these practices and how they have contributed to accidents. The requirement to operate under daylight conditions, and plan to land 10 minutes before last light, provides a reliable method for ensuring there are sufficient external visual references available to safely operate an aircraft.
Pilots and the companies or landowners they work for, or contract to, must work together to avoid flight at night by unqualified, unequipped pilots. Development of risk management practices in any organisation should be an ongoing activity. It should develop an ability across all parties to document operational risks and codify learnings from operations.
The occurrence
On the evening of 9 October 2025, a Robinson R22 Beta II helicopter, registered VH‑LYD, was being operated by MDH Pty Ltd (MDH) at Rutland Plains, a cattle property in northern Queensland on the Gulf of Carpentaria (Figure 1).

Source: Queensland Globe
The pilot started the day’s flying just after 0600, aerial mustering in an area about 40 km south‑west of another company‑owned property, Dunbar Station, Queensland. In the afternoon, the pilot travelled to Rutland Plains to collect a colleague and conduct aerial reconnaissance for another muster planned for the following day. After leaving their colleague, the pilot flew to a nearby location to collect parts for equipment needed for the planned muster at Rutland Plains.
At around 1730, on the way to collect the parts, the pilot spotted a bushfire around 25 km south-south‑east of Rutland Plains station. The pilot advised crew at the station via radio and ground vehicles were dispatched to control the fire. Crew at the station recalled that after returning to Rutland Plains with the parts, the pilot flew to the fire to assist in guiding the ground vehicles through tracks and fences to the flame front.
The pilot and helicopter were limited to daytime operations. The pilot departed Rutland Plains for the fire at around 1845. The time of last light (the beginning of nighttime) at Rutland Plains on 9 October was 1852.
At around 1920, the pilot was providing airborne assistance to ground crew controlling the fire. Around that time the pilot announced over the radio that it was getting too dark, and the pilot needed to return to Rutland Plains. Hearing this, the crew at the station lit the helipad with the headlights of a vehicle to assist the pilot on their return.
At around 1935, crew at the station checked to see if the pilot had landed. Discovering that the helicopter had not returned, they tried contacting the pilot by radio. When radio contact was unsuccessful, they escalated the non-arrival within the company and sought information from a satellite tracking system on board the helicopter to establish its location. Tracking had stopped at 1929 around 7.5 km south-south‑east of the station (Figure 2).
Figure 2: Fire location and VH-LYD track
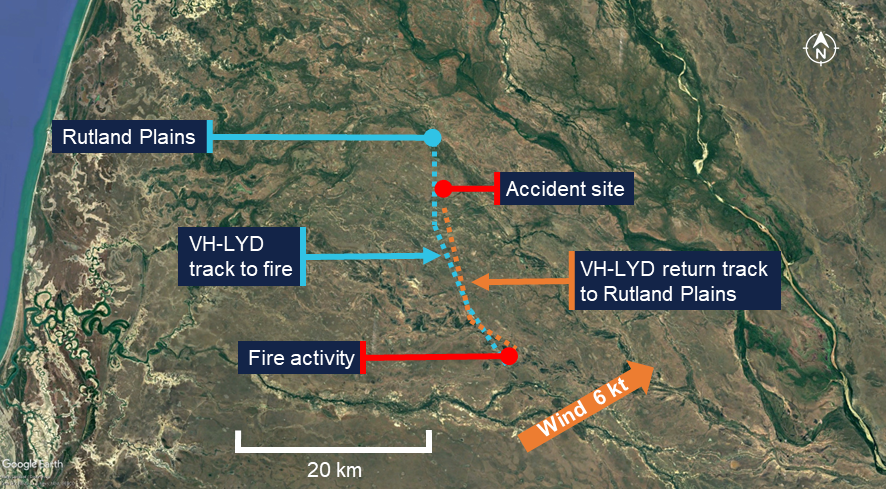
Source: Google Earth, BoM and SPOT Trace tracking data
Station crew conducted a ground search while company management contacted emergency services and the Joint Rescue Coordination Centre. A coordinated air search began just after midnight.
The following morning, helicopter wreckage was found by a station crew member from Rutland Plains and a helicopter pilot from a neighbouring property. VH-LYD had collided with terrain around 1.5 km north of the last satellite tracking point. The pilot was fatally injured in the accident, and the helicopter was destroyed by impact forces.
Context
Pilot information
The pilot held a valid Private Pilot Licence (Helicopter) (PPL(H)), which was issued in February 2023 and a mustering endorsement issued in April 2023. The pilot held a class 2 medical certificate which was valid to 31 August 2026.
The pilot commenced work in ground-based cattle operations with MDH Pty Ltd (MDH) in 2017 and transitioned to an aerial mustering role. The pilot had accumulated around 2,000 to 2,500 hours of flight time.
In November 2024, the pilot attended a Robinson Helicopter Company safety course. On 16 January 2025 they underwent a biannual helicopter flight review. In March 2025 the pilot attended an MDH leadership conference. In June 2025 the pilot completed refresher training and check flights in mustering techniques. There was no record of the pilot being trained or qualified to operate under night visual flight rules (NVFR) [1],[2] (see Night flight regulatory requirements).
It could not be determined if the pilot experienced a level of fatigue that would have impaired performance or decision‑making at the time of the accident (see Fatigue).
Helicopter information
VH-LYD was a Robinson Helicopter Company R22 Beta II helicopter, serial number 4471 (Figure 3). It was powered by a Textron Lycoming, O-360-J2A, 4-cylinder piston engine. VH-LYD was manufactured in the United States on 12 February 2010 and first registered in Australia on 19 May 2010. It was equipped and maintained to a day VFR standard. Its last 100-hourly maintenance was conducted on 24 September 2025. At the time of the accident VH-LYD had accumulated approximately 14,645 hours total time in service.
Figure 3: Exemplar Robinson Helicopter Company R22

Note: This exemplar image has been digitally altered by the ATSB. Source: MDH Pty Ltd
The R22 had 2 seats, with the pilot flying from the right seat, and each seat was fitted with a seatbelt and inertia reel shoulder strap. VH-LYD did not have doors fitted at the time of the accident.
Maintenance records and wreckage inspection both showed that VH-LYD was not equipped with instruments necessary for flight at night (see Night flight regulatory requirements).
Recorded information
The helicopter was not fitted with a flight data recorder or a cockpit voice recorder, nor was it required to be. During the accident flight, data was transmitted from a SPOT Trace[3] satellite tracking unit fitted to the helicopter, which could be used by MDH personnel to track the location of the helicopter during flight. The unit provided 5-minute time-stamped updates on the helicopter’s location, speed and altitude. The recorded data captured the accident flight until shortly before the impact with terrain.
The SPOT Trace units were fitted to all MDH R22 helicopters, and the ATSB sourced the preceding 6 months of fleet data for analysis purposes. The data covered 596 days of helicopter operation across 4 helicopters (see Night flight data analysis).
Wreckage and impact information
The ATSB did not attend the accident site. The site was mapped, documented and assessed by a team from the forensic crash unit of the Queensland Police Service (QPS). QPS recovered the wreckage of VH-LYD to a secure location in Cairns, Queensland, where it was examined by 2 ATSB investigators.
Site photographs and wreckage inspection indicate that VH-LYD was moving at high speed, around 90 degrees off track, at the time of the collision with terrain (Figure 4). The helicopter was significantly damaged by tree and ground impacts with the main rotor and transmission assembly separating from the helicopter. There were no pre-accident defects identified, and the engine was driving the main and tail rotor system at the time of the collision. The impact with terrain was not considered to be survivable.
Figure 4: VH-LYD accident site
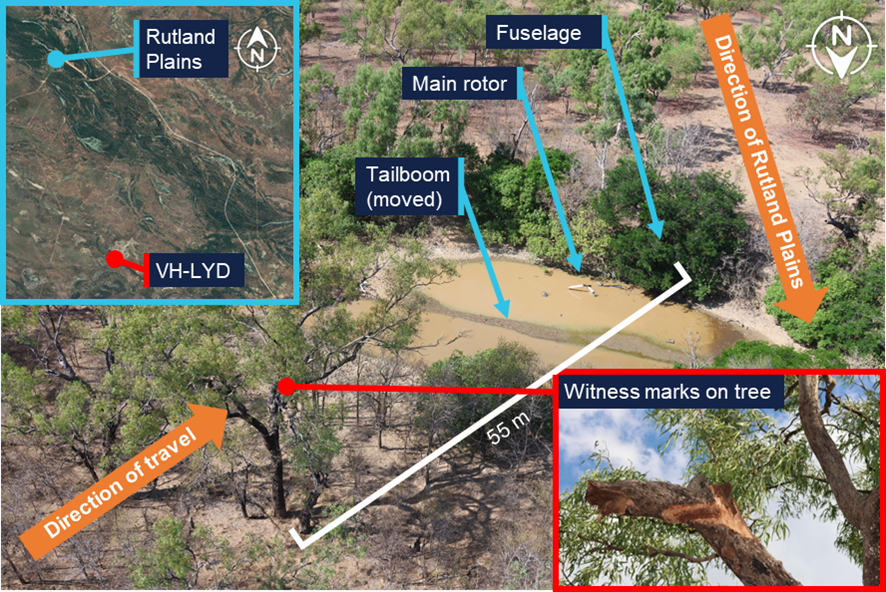
Source: Queensland Globe, Queensland Police Service, annotated by the ATSB
Meteorological and environmental information
Weather
A Bureau of Meteorology (BoM) aviation weather forecast for Kowanyama Airport (located around 20 km north‑west of Rutland Plains) for 9 October related the possibility of thunderstorms. Meteorological conditions recorded by the BoM weather station at Kowanyama Airport included distant lightning from around 1530, indicating that thunderstorms were reported within 30 NM (55 km) but not at the airport. Cloud developed through the day, with periods of scattered to broken cloud between 6,000 ft and 9,000 ft. No cloud was detected at Kowanyama Airport at the time of the accident.
No rainfall was detected throughout the day, and the wind had shifted from a variable easterly in the morning to a south-westerly wind of 6 kt from around 1730. Around that time the accident pilot reported to a colleague at Rutland Plains that dry storms[4] were building in the area, and that there was smoke, indicating a bushfire.
A witness who heard the departure of VH-LYD stated that on last light, shortly after the time the pilot departed Rutland Plains for the fire, cloud covered the area though there was still a visible horizon.
Light
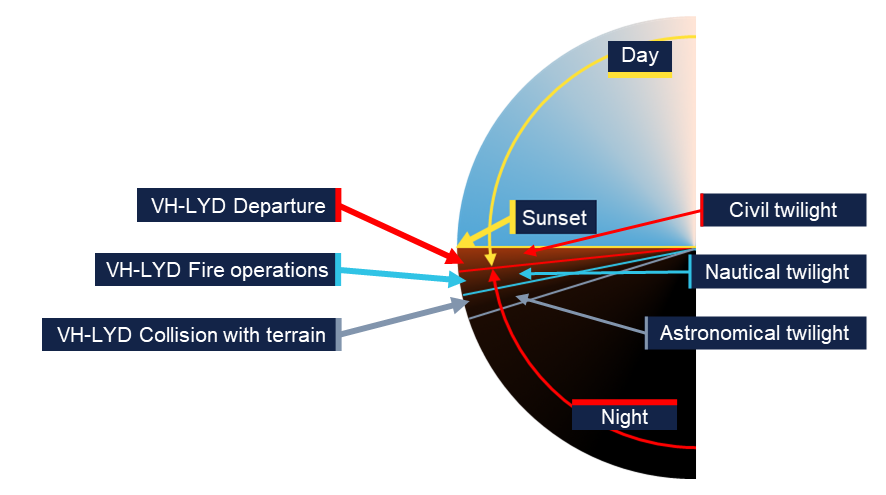
The period between sunset[5] and the geometric centre of the Sun’s disk reaching 6° below the horizon is called civil twilight (Figure 5). The end of civil twilight is otherwise known as last light. For aviation purposes last light is the boundary between night and day. The period when the geometric centre of the Sun is between 6° and 12° below the horizon is called nautical twilight. After that time, it is ordinarily, for all practical purposes, dark. This is especially so in areas devoid of artificial lighting.
Figure 5: Limits of day and night relative to the position of the Sun
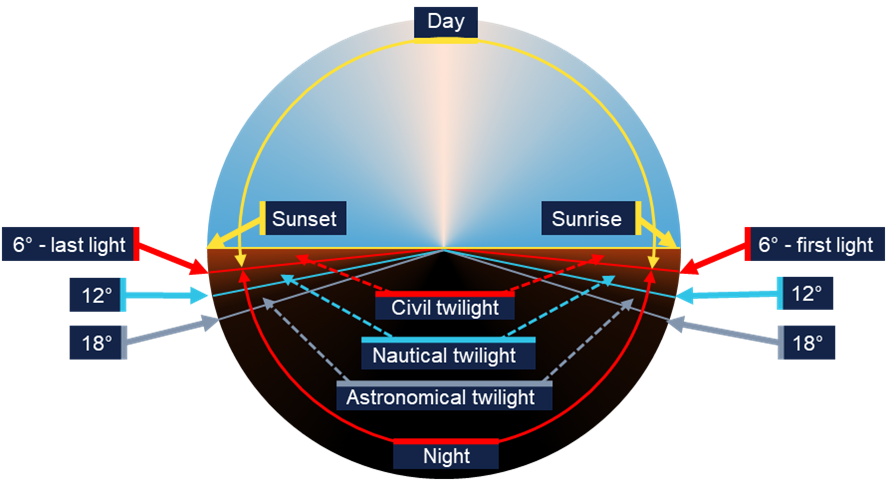
Source: Geoscience Australia, ATSB
The time of last light was readily available for any location in Australia from Airservices Australia’s national aeronautical information processing system (NAIPS). It could also be calculated using tables published in the aeronautical information package (AIP) at GEN Section 2.7 – First light and last light computations(Airservices Australia, 2024) or via Geoscience Australia’s calculator on its website.
On 9 October 2025 at the location of the accident near Rutland Plains Station, Queensland, sunset was 1831, the end of civil twilight was 1852 and the end of nautical twilight was 1917. Celestial illumination would have been limited by cloud and there was no moonlight as a waning gibbous[6] moon would not rise until 2045.
Smoke
The 6 kt (10.8 km/h) south-westerly wind, though light, is likely to have kept smoke away from the pilot’s return track to Rutland Plains Station. Moreover, the pilot was unlikely to have approached the fire through smoke, and the pilot departed the fire on a reciprocal track.
Operational information
Operator overview
MDH Pty Ltd was one of Australia’s largest beef cattle operations. It was a family business that owned 14 properties covering 3.36 million hectares. MDH’s aircraft and pilots were spread over Queensland and managed from Brightlands Station just south of Cloncurry, Queensland.
At the time of the accident MDH owned and operated 4 Robinson R22 helicopters, 1 Robinson R44 helicopter and 6 fixed wing aircraft. It had operated Robinson R22 helicopters since 1985. The chief pilot stated that at the time of the accident none of its R22 helicopters were equipped for night flight.
MDH had 4 helicopter pilots flying the R22s. Three of the pilots had Private Pilot Licences (Helicopter) and one had a Commercial Pilot’s Licence (Helicopter). All were endorsed for low‑level flight and mustering and none held a night visual flight rules rating.[7]
The helicopters were being operated by paid employees, aerial mustering for commercial beef cattle operations. As the helicopters were company‑owned, and were being operated over private land, those operations were conducted as limited aerial work operations under Part 138 of Civil Aviation Safety Regulations (CASR), which do not require the issue of an aerial work certificate by CASA. Part 91 of the Civil Aviation Safety Regulations (CASR) (2025b) also applied unless a specific requirement of Part 138 disapplied it. This meant MDH had to comply with the requirements of CASR Part 138 with respect to pilot fatigue and risk management of operations.
Operator procedures and oversight
MDH did not have, and was not required to have, a CASR Part 138 aerial work certificate for the R22 operations. Therefore, it was not required to provide the Civil Aviation Safety Authority (CASA) with a complete operations manual covering all requirements of the regulations for its proposed operations.
Instead of an operations manual detailing how operations were to be conducted, MDH had limited manuals and procedures for helicopter operations. An induction handbook for pilots carried information on administration and basic instructions with respect to flight operations. A statement at the head of the document required pilots to observe all applicable laws and rotorcraft flight manual limitations.
Pilots stated that the document matched their operations, and that the expectation of pilots not breaching regulations was observed. MDH held pre-season[8] safety meetings with the pilots. The last was 21 March 2025 in Brightlands. The meetings would cover operational elements, as well as a review of the pilot induction material to refresh procedures.
MDH had a senior pilot who was positioned in the induction handbook as the chief pilot. They were to be contacted for aircraft and pilot issues. The chief pilot stated that oversight of the pilots was conducted, when possible, by the chief pilot or another senior manager, though they were most often not co-located with the pilots.
The chief pilot would roster pilots by date, helicopter and location and build in rest days. They would also ensure that pilots’ tasks remained solely associated with flying. Ordinarily pilots would start at first light, but it was left to the pilots as to when their duty would end. Days rostered were documented and retained by the company, but duty hours worked by pilots were not.
The chief pilot acknowledged that there were occasions whereby pilots would have to use the helicopter for as long as possible and into twilight. They stated that they expected pilots to minimise their exposure to flight at night by landing near vehicles to get a lift home, or by staying at alternative accommodation. The chief pilot provided an example of setting this expectation to a pilot in mid-August 2025 after they exceeded last light by 35 minutes.
They also stated that pilots would assess whether there was enough light to continue flight, and the decision was at the sole discretion of the pilot. MDH’s pilots concurred with this, and all stated that the pilot in command was solely responsible for the operation of the helicopter and had final say in all decisions related to the operation of their helicopter.
There was one mention of daylight in the MDH induction handbook for pilots which concerned ferrying of aircraft. It stated:
A decision has to be made by the pilot if the daylight does not permit making the scheduled property in the afternoon to stay at a property and notify [management] that they did not make it.
Flight at night
Night flight AIP instructions and CASA guidance material
The CASA (2025f) Visual flight rules guide carried information on the regulations and requirements pertaining to night visual flight rules. It was a useful starting point for pilots and operators to ensure night flight was appropriately managed. In addition, advisory circular (AC) 61-05 Night VFR rating (CASA, 2022) was an important supporting document to the regulations and related notable hazards of night flight.
Untrained (and therefore unauthorised) pilots were not allowed to conduct flight at night. AIP ENR Section 1.2 – Visual Flight Rules, paragraph 1 Flight Rules, sub paragraph 1.1 The Visual Flight Rules (VFR), sub sub paragraph 1.1.2 stated:
1.1.2 Unless the pilot in command is authorised under CASR Part 61 to conduct a flight under the IFR or at night under the VFR and the aircraft is appropriately equipped for flight at night or under the IFR, a VFR flight must not be conducted at night.
The appropriate equipment mentioned was listed in CASR Part 91 manual of standards (MOS) (CASA, 2021). This included specific equipment such as:
- equipment for displaying the rotorcraft’s attitude
- radio communications system equipment
- navigation systems equipment, such as an approved GNSS
- navigation and cockpit lighting.
Furthermore, there were rules about fuel reserves, alternate aerodromes, and calculating and flying above lowest safe altitudes. Additionally, AC 139.R-01 v3.1 (CASA, 2024a) carried guidelines for helipad dimensions and markings for night operations which were in excess of those required for operations by day.
AIP ENR Section 1.2 – Visual Flight Rules, paragraph 1 Flight Rules, sub paragraph 1.1 The Visual Flight Rules (VFR), sub sub paragraph 1.1.3 stated:
1.1.3 For pilots not authorised to fly at night, it is recommended that they plan to arrive at the later of the destination aerodrome or alternate aerodrome at least 10 minutes before last light (allowing for any required holding).
The AIP instructions and associated CASA guidance material clearly indicate that the regulations precluded an untrained or unequipped pilot from flying at night. Additionally. there was a clear intention that pilots aim to land at least 10 minutes before last light (10 minutes before end of civil twilight).
Operator’s night flight practices
The ATSB interviewed 3 company R22 pilots and the chief pilot about practices related to night flight.
MDH did not roster pilots to fly after last light. To do so was against regulations. However, pilots reported that the requirement to land before last light was not always observed. They stated that while they would not plan to land after last light, at times, operational needs led them to do so.
On occasion, depending on the location and behaviour of the cattle, a muster could take longer than planned. In some locations where a holding yard was available, it was possible to re-plan and stop work without losing effort. Additionally, the option existed to land at the yards and return to the station in a vehicle rather than flying back to a station in fading light. However, that could delay the start of the following day’s muster and leave less time to manage overruns the next day.
In locations where cattle could not be held, ending the job before cattle were yarded up could lead to the loss of a day’s work. While there was no reported pressure on pilots to continue, pilots reported that they would do so rather than undo a day’s work. Exceeding last light was an accepted part of operations and pilots could make their own decisions about whether the light remaining was enough to finish the job and fly home.
The actual time of last light and 10-minute buffer was not used in pilot assessments, and pilots did not use the time of last light to delineate between night and day. Instead, pilots would weigh environmental factors such as sunset, cloud and available horizon against their own tolerance for risk. The distinction became one between dark with a discernible horizon and fully dark.
From time-to-time emergencies, such as fires, could crop up and require input or oversight from a pilot in a helicopter. There was no expectation on the part of MDH that pilots would fly after last light, no matter the reason. At the same time, it was reported that in an environment where the pilots were most often unsupervised, no-one would prevent a pilot from doing so. Individual accountability in pilot decision‑making was reported to be the only determining factor.
Night flight data analysis
The SPOT Trace data for MDH’s 4 R22 helicopters for the 6 months preceding the accident was analysed by the ATSB to identify night flight practices. The data was pruned to remove any points that did not indicate flight, then differenced with the time of civil twilight for that location. Matches close to last light were further refined by measuring the distance to the next spot and calculating time available to destination.
The tracking data (Figure 6) showed that in the 6 months preceding the accident, the 4 company helicopters operated on 596 days. Of the 596 days of operation, company helicopters were flown after last light on 39 occasions, around 6.5% of days of operation across the 4 helicopters. The level of exceedance ranged from under a minute up to 1 hour 34 minutes, with the average exceedance being 17 minutes. Eight of the late flights, including the accident flight, extended beyond nautical twilight.
Figure 6: Latest time flown after last light for 39 flights in company R22 helicopters
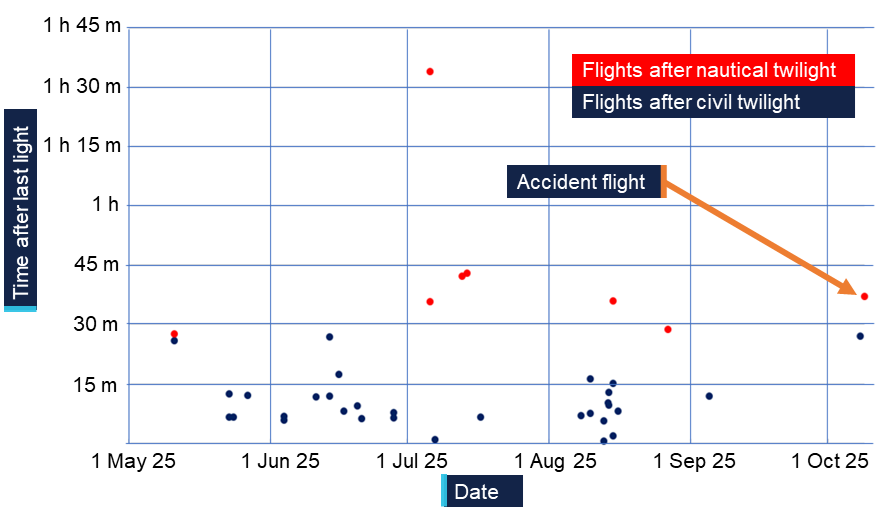
Source: SPOT Trace data
The largest exceedance of around 1 hour 34 minutes after last light took place in July 2025 in the vicinity of Mount Windsor Station, Queensland. While cloud cover is not known, the moon rose at 1404 and was approaching three quarters full at an altitude of 70° when the helicopter landed.
Operational risk management
Risk management regulatory requirements
MDH, as a limited aerial work operator, was required to comply with CASR 138.370 which required risk assessment and mitigation.
MDH had to ensure that, before beginning a task, a pilot had assessed the risk of an operation (Part 138 MOS 13.05). The pilot had to ensure that the operation could be conducted without unacceptable safety risk (Part 138 MOS 13.02).
Part 138 MOS at 13.04 instructed pilots to take specific notice of:
(a) the operation and its particular characteristics;
(b) the location of the operation and its particular characteristics;
(c) the aircraft to be used in the operation, its particular characteristics, and its performance;
(d) the qualifications and experience of the crew members to be used in the operation;
(e) the hazards, external to the aircraft, that may be met in the course of the operation.
Advice on risk management was available to operators in AC 138-05 v3.0 Aerial work risk management (2025a). It stated:
For limited aerial work operations, a risk assessment and mitigation process must be undertaken by the pilot in command (PIC) before an operation is conducted…
It is incumbent upon the operator … to ensure these procedures are carried out.
Annex A to AC 138-05 v3.0 was titled Sample risk assessment process - limited aerial work operator. It explained how to implement risk management to meet the requirements of the Part 138 Manual of Standards.
Operator’s risk management practices
MDH’s primary use of helicopters was aerial mustering. This activity was supported by training and operational documents. MDH provided training in aircraft knowledge, operational techniques and safety, which was suitable for conduct of its operations.
It had also outlined a pre-mustering assessment which pilots could use to discuss and manage mustering operations. The document contained some collected knowledge of hazards and prompts to identify powerlines and brief ground crew on safety around helicopters. However, it was essentially a task management document and did not address identification and management of risk.
The flight planning section of the pilot induction handbook also prompted identification of threats with respect to reconnaissance of known local hazards such as powerlines and dead trees. While this applied to managing safety during a flight, it did not constitute risk management. Risk management was where a pilot and organisation could decide if an operation could be conducted within the organisation’s safety performance criteria (CASA, 2025d).
The pilot induction handbook also contained a section called risk management which was a high-level outline of the pilots’ responsibilities with respect to weather, fatigue, mustering, aircraft handling, and sightseeing. It outlined some associated hazards but did not discuss risk management as an activity and no risk management plans were present. Specifically, there were no defined limits or organisational tolerance for risk. Additionally, there were no apparent tools or support for company pilots to formally identify and manage risks, to ensure that an operation could be conducted without unacceptable safety risk. This limited the guidance and support available to pilots undertaking novel or infrequently encountered activities such as fire spotting.
Fatigue management
Fatigue management regulatory requirements
As a limited aerial work operator CASR 138.150 required MDH to have a system for managing crew fatigue that met the requirements of the Part 138 Manual of Standards. The Part 138 MOS at 6.02 required compliance with an element of Civil Aviation Order 48.1. That element at paragraph 16.1 of CAO 48.1 put the onus on a pilot to not carry out a task if at any point during that task, they were likely to be fatigued.
The requirement for MDH was then to ensure that pilots had knowledge and frameworks to understand and measure fatigue and to support pilot decision‑making around fatigue.
While MDH was not required to comply with the rules for daylight aerial work operations from appendix 5A of CAO 48.1, it serves as useful guidance. CASA CAO 48.1 plain English guide (CASA, 2025c) stated:
• The maximum flight duty period (FDP) that can be assigned in 1 day is 14 hours.
• Following an FDP, you must be off duty for at least 10 hours.
• You cannot be assigned an FDP that starts 30 minutes before the start of morning civil twilight (MCT) or that ends later than the end of evening civil twilight (ECT).
• An FDP cannot be extended beyond the end of ECT, unless it is necessary to complete the duties associated with the last daylight flight.
The final provision was to allow a pilot to complete ground-based work after landing, not to continue flight.
Further guidance was available to flight crew members (FCM) in Civil Aviation Advisory Publication (CAAP) 48-01 (CASA, 2024b). Advice on meeting that requirement warned:
3.1.1.3 Reduced alertness may impact judgement. To manage the potential for poorer judgment and decision making associated with a fatigued FCM, CASA recommends involving a non-fatigued individual along with multiple methods for measuring alertness to assist the FCM when assessing fitness to fly.
Operator’s fatigue management practices
The pilot induction handbook contained advice to pilots on fatigue and stated:
Fatigue, or tiredness, can often be an issue in mustering operations where early mornings and long days are involved. Fatigue can have a profound effect on the performance of the mustering crew. Due to the high level of concentration required by the PIC, fatigue can set in earlier for the PIC than for the other crew members.
The accident pilot’s flight and duty times for the 7 days leading up to the accident are captured in Table 1.
Table 1: Pilot’s previous 7 days flight and duty
Date | Activity | Duty [1] | Flight Hours [2] | ||
Start | End | Total Hours [2] | |||
| 3/10/2025 | Time off | ||||
| 4/10/2025 | Travel | 10:00 | 15:30 | 5.5 | 4.1 |
| 5/10/2025 | Time off |
| |||
| 6/10/2025 | Muster | 6:36 | 18:27 | 11.9 | 5.2 |
| 7/10/2025 | Muster | 5:54 | 14:56 | 9.0 | 8.2 |
| 8/10/2025 | Muster | 5:45 | 19:47 | 14.0 | 10.3 |
| 9/10/2025 | Muster / Fire | 5:42 | 19:29 | 13.8 | 11.3 |
| Totals | 54.2 | 39.1 | |||
[1] A record of duty time was not available for the pilot. Duties have been calculated by adding 30 minutes to the beginning and end of flight time to allow for pre and post flight activities. [2] Total duty hours and flight hours are related in decimals of an hour | |||||
Source: Pilot’s roster and satellite tracking data from VH-LYD
In the 72 hours prior to the accident the pilot had flown 29.8 hours and completed an estimated 36.8 hours of duty. In the 2 days leading up to the accident the pilot had flown 21.6 hours and conducted an estimated duty of 27.8 hours. On both days the pilot’s duty exceeded daylight hours, with flight on 8 and 9 October being conducted at night. Additionally, the rest period between the duties was likely less than 10 hours.
While the fatigue regulations of an aerial work certificate holder did not apply to MDH, by way of example, this was outside of the fatigue limits for aerial work under day visual flight rules documented in Appendix 5A of CAO 48.1.
It was reported that the pilot’s accommodation was suitable for rest. Although the pilot had worked 2 long days leading up to the accident, the rest period earlier in the week potentially protected the pilot from an accumulation of fatigue. It is not possible to determine whether the pilot experienced a level of fatigue that would have impaired performance or decision‑making at the time of the accident.
Human factors
Fatigue
Fatigue can impact pilots in various ways. It can affect decision‑making, and CASA (2025e) states that fatigue at the end of a day, shift or flight, can lead people to persevere with a chosen course of action or ignore information which could contradict a decision to continue. Fatigue can diminish the ability of the eye to focus (Robson, 2008). It can also increase the risk of spatial disorientation, and lead to delayed response times as well as a range of pilot errors (ATSB, 2013).
Spatial disorientation
For day VFR pilots, spatial orientation is being aware of how they are orientated and moving in space with reference to external objects such as the surface of the Earth (Young, 2003). Spatial disorientation is loss of that awareness, ordinarily due to a loss of visual information, leading to an inability to correctly interpret aircraft attitude, altitude or airspeed in relation to the Earth or other points of reference (ATSB, 2013).
The mechanisms of spatial disorientation and dangers of flight at night, which by its very nature reduces available visual information, is discussed in detail in ATSB report Avoidable Accidents No.7 Visual flight at night accidents: what you can’t see can still hurt you (AR-2012-122) (ATSB, 2013).
Young (2003) describes the sensory systems that support spatial orientation. They include:
- The visual system (sight) tells us where things are and what is present. It makes use of peripheral vision to detect self-motion relative to objects and the ground. The central vision can detect objects of known size and character to provide distance and closing information.
- The vestibular system (balance and orientation organs in the ears) is the primary system for sensing body motion relative to gravity and acceleration. It supports the muscle commands that keep our eyes and head stable and keep us upright relative to gravity.
- Proprioception (the sense of movement) helps to sense orientation and acceleration through pressure on the skin. It will also generate an accurate estimate of the current position of the body to plan movements and predict the outcome of future actions (Tuthill & Azim, 2018).
Sight provides around 80% of the information, and the balance organs and sense of movement, providing around 10% of the information each, are prone to illusions and misinterpretation.
Poor visual cues are a feature of almost all spatial disorientation accidents. There are several well-known illusions that can affect pilots at night (ATSB, 2013):
- Somatogravic, the brain cannot differentiate between acceleration and a pitch-up event. In the absence of visual cues, the pilot can easily confuse the two states. A pilot response to an incorrect sensation can increase the confusion.
- Somatogyral, the pilot’s vestibular system responds to angular acceleration. Without visual cues, this can lead to an incorrect understanding of an aircraft’s angle of bank in a turn or level flight. In the absence of external visual cues, successful orientation relies on the use of appropriate flight instruments.
- Autokinesis is the phenomenon of a single point of light (a star or light from a distant station) appearing to move randomly in the visual field.
- Blackhole approach involves an approach to land at night where there is nothing to see between the aircraft and the intended landing site. The absence of peripheral visual cues, especially below the aircraft, can lead pilots to perceive the aircraft is high and initiate an aggressive descent to correct their perceived approach path. The result can be landing short or impacting terrain.
The helicopter manufacturer also highlighted the dangers of disorientation specific to rotary wing operations. Safety notice SN-18 in the Robinson Helicopter Company Pilot’s Operating Handbook for the R22 stated:
Flying a helicopter in obscured visibility due to fog, snow, low ceiling, or even dark night can be fatal. Helicopters have less inherent stability and much faster roll and pitch rates than airplanes. Loss of the pilot’s outside visual references, even for a moment, can result in disorientation, wrong control inputs, and an uncontrolled crash.
Related events
Accidents involving flight at night in an unequipped Robinson R22 by pilots unqualified for night flight are frequently repeated in Australia. Common features related in the accident investigation reports in Table 2 are summarised below.
Table 2: Investigations into similar events
| Investigation number | Title |
| AO-2023-058 | VFR into smoke on a dark night and collision with terrain involving Robinson R22, VH‑DLD |
| AO-2022-057 | Collision with terrain involving Robinson Helicopter Company R22 Beta, VH‑LOS |
| AO-2021-006 | Collision with terrain involving Robinson R22 Beta II helicopter, VH‑HKC |
| AO-2016-031 | Collision with water in dark night conditions involving Robinson R22, VH‑YLY |
| AO-2014-144 | Collision with terrain involving Robinson R22, VH‑YPC |
| AO-2011-087 | Collision with terrain, VH-YOL |
| AO-2011-051 | Controlled flight into water, VH‑RUR |
All these events involved pilots who were not qualified to fly at night. In addition, in all but one accident (AO-2014-144), the helicopters were unequipped for night flight. There was a general acceptance by pilots involved in these accidents that being unqualified and unequipped was not an impediment to flying at night.
One investigation report (AO-2014-144) noted that the pilot planned on landing with sufficient sunlight. In all other cases the flights were intentionally conducted after last light, or pilots did not discontinue the flight when presented with an opportunity to do so. In 2 accidents (AO-2023-058 and AO-2021-006), pilots departed locations with available accommodation into dark night conditions.
Many of the investigations related to hazards that would be easily detected or inconsequential in daytime but become difficult to detect and far more serious at night. Environmental conditions such as smoke (AO‑2023‑058) and cloud and rain (AO‑2022‑057, AO‑2021‑006, AO‑2016‑031, and AO‑2011‑051) were common features. Furthermore, in 3 of the accidents (AO‑2011‑087, AO‑2014‑144, and AO‑2016-031), lights inside the cabin from sources such as GPS, instrument lights and warning lights, were noted to interfere with vision outside of the helicopter by producing glare on the windscreen.
Several workarounds to support these activities were implemented by the pilots involved. These included turning off equipment to reduce glare (AO-2016-031 and AO-2014-144), flying at low level in an attempt to find ground references (AO-2023-061, AO-2021-006, and AO-2011-087), and lighting the helipad with vehicle headlights in anticipation of a late arrival (AO-2023-058).
All of the accidents took place while travelling between locations, as opposed to while conducting aerial work. All resulted in a high-speed collision with terrain or water and all but one of the accidents (AO-2011-051) resulted in fatal injuries.
Safety analysis
Flight at night
Witness statements and tracking data for VH-LYD on the night of the accident showed it was moving after last light and beyond nautical twilight. The last movement of VH-LYD was recorded at 1929, 37 minutes after last light (end of civil twilight at 1852) and 12 minutes after nautical twilight (1917) (Figure 7). Moonrise would not happen until 2045. The combination of cloud obscuring celestial light from stars, no artificial lighting on the ground, and no moonlight meant it was almost certainly very dark. This made the pilot susceptible to spatial disorientation and loss of control of the helicopter.
Source: SPOT Trace, ATSB
The pilot of VH-LYD did not have a night rating, and while there was evidence of the pilot previously operating at night, the pilot had not demonstrated competence or capability as part of a flight review or flight test.
The wreckage inspection showed it was highly unlikely that any mechanical failure of the helicopter contributed to the accident. The inspection also showed that VH-LYD did not have equipment required for flight at night such as an artificial horizon.
The extra risks inherent in visual flight at night are from reduced visual cues, and the consequent risk of spatial disorientation (ATSB, 2013). The accident site analysis showed that VH-LYD collided with a tree at high speed while travelling perpendicular to the direction required to reach Rutland Plains. While it is not possible to determine the exact nature of the disorientation affecting the pilot, being off track and too low at high speed indicated that the pilot was very likely disorientated and without visual references at the time of collision with terrain.
Contributing factor The pilot flew at night but was not qualified to fly at night and the helicopter was not equipped to be flown at night. |
Contributing factor It is very likely that the pilot became spatially disorientated, resulting in collision with terrain. |
Organisational acceptance
Risk management and decision‑making
The Civil Aviation Safety Regulations (CASR) Part 138 manual of standards explained that MDH Pty Ltd (MDH) had to ensure the pilot assessed that the operation could be conducted without unacceptable safety risk for the pilot and people on the ground in the context of the task. The accident occurred on the transit back from fire spotting and directing ground crew at night.
There was no evidence of a risk assessment being conducted or of risk assessment tools or training being made available to the pilot. To align with the manual of standards, the assessment would have had to include the aircraft used in the operation and the qualifications of the pilot. MDH did not have trained pilots or suitably equipped helicopters available. Had a risk analysis been conducted, mitigating the risk of the operation involving an untrained pilot in an unequipped helicopter at night was not possible without cancelling the flight.
Company pilots were making decisions about operations without input from the organisation, peers or risk management tools. The high level of pilot autonomy was reflected in interviews with the chief pilot, company pilots and employees. The consensus was that it was a pilot’s decision to fly and there was a position amongst pilots that it was not the place of others to tell a pilot to fly or not fly.
While the pilots reported no pressure to fly after last light, they stated that they would fly beyond last light to complete a task and not lose a day’s work for a mustering team. Pressure on decision‑making can come from various sources without being overt. Bearman and Bremner (2016) wrote that:
- Situational pressure can lead people to pursue a particular goal.
- People internalise values of the organisation they work for and value decisions that benefit the organisation.
- Social pressure can influence decisions to optimise the impression we present to others.
Perhaps due to situational and social pressure, the pilot of VH-LYD elected to use the helicopter to support fire operations after last light, and that was accepted by the pilot’s colleagues. This was consistent with accepted practices within their working environment.
Other factor that increased risk MDH did not require its R22 pilots to formally assess risk and did not provide tools or training to do so. This limited the ability of the company and those pilots to identify and understand operational hazards and their consequences. (Safety issue) |
Awareness of flight after last light
In MDH’s environment of animal management in remote areas, teams need to be flexible and be able to improvise solutions. Autonomy of crew is a large part of that. They also need to make best use of the resources available, and a helicopter is a valuable resource. Practices such as flying beyond last light, which is an unsafe practice, can develop to become normal operations. Especially if it provides positive outcomes without negative repercussions (CASA, 2017).
Analysis of 6 months of tracking data for 4 company R22 helicopters showed that over a combined total of 596 days of operation, on 39 occasions pilots landed after last light. There was evidence of exceedances in all company R22 helicopters. The average exceedance was just over 15 minutes. Combining the tracking data with pilot rosters showed that 3 of the accident pilot’s colleagues had flown after last light, reportedly for operational reasons.
The company was aware that the pilots were not trained nor equipped for flight at night and aware that last light was not always observed. The chief pilot stated that there were times that helicopters would be needed to be used as long as possible. Instead of observing the limits of last light, pilots would judge the available light by sight and operate to their own level of comfort.
Relying on individual pilot decision‑making is reflective of the Part 91 flight operations, however, the context for these flights were primarily aerial mustering and related aerial work activities for commercial cattle farming.
While these were considered limited aerial work operations by the regulations, MDH had the ability to influence pilots and set an organisational tolerance for risk. By ignoring an actual time for last light, a distinct and easy to measure limit became ambiguous and inconsistent. The company limit was not that pilots should observe last light, rather that they should not push on into the dark. However, MDH did not provide oversight or definition of this and expected pilots to manage it themselves.
Not preventing the activity normalised the deviation from a safe envelope of operations and indicated an acceptance of flight after last light. The only limit to the non-compliance became an individual pilot’s tolerance for risk. This meant the practice could easily extend to later times and different activities.
For the pilot of VH-LYD on 9 October 2025, flying at night to assist in firefighting was likely an easy step to take, especially in the absence of a formal consideration of risk. It is not possible to discern the factors that combined in the pilot’s decision‑making about the flight. Neither is it possible to separate that decision‑making from the general acceptance of flight after last light or the influence of the operating environment.
Within the operation, limited oversight and the absence of risk management, combined with an acceptance of flight after last light, created an increased and unmitigated risk of an accident at night by an untrained pilot in an unequipped company helicopter on MDH properties.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision with terrain at night involving Robinson R22 Beta II, VH-LYD, 25 km south-south-east of Kowanyama, Queensland, on 9 October 2025.
Contributing factors
- The pilot flew at night but was not qualified to fly at night and the helicopter was not equipped to be flown at night.
- It is very likely that the pilot became spatially disorientated, resulting in collision with terrain.
- Flying after last light by pilots without night ratings, in R22 helicopters not equipped for night flight, was a tolerated and unmanaged risk on MDH properties. This increased the risk of an accident in a company R22 at night. (Safety issue)
Other factors that increased risk
- MDH did not require its R22 pilots to formally assess risk and did not provide tools or training to do so. This limited the ability of the company and those pilots to identify and understand operational hazards and their consequences. (Safety issue)
Safety issues and actions
Accepted practice of exceeding last light
Safety issue number: AO-2025-063-SI-01
Safety issue description: Flying after last light by pilots without night ratings, in R22 helicopters not equipped for night flight, was a tolerated and unmanaged risk on MDH properties. This increased the risk of an accident in a company R22 at night.
Risk assessment not implemented
Safety issue number: AO-2025-063-SI-02
Safety issue description: MDH did not require its R22 pilots to formally assess risk and did not provide tools or training to do so. This reduced the ability of the company and those pilots to identify and understand operational hazards and their consequences.
Glossary
| AC | Advisory circular |
| AIP | Aeronautical information publication |
| CAAP | Civil Aviation Advisory Publication |
| CAO | Civil Aviation Order |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| FCM | Flight crew member |
| FDP | Flight duty period |
| MOS | Manual of standards |
| NVFR | Night visual flight rules |
| PIC | Pilot in command |
| QPS | Queensland Police Service |
| VFR | Visual flight rules |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- MDH Pty Ltd
- employees of MDH Pty Ltd
- accident witnesses
- Civil Aviation Safety Authority
- Queensland Police Service
- Robinson Helicopter Company
- maintenance organisation for VH-LDY
- Bureau of Meteorology
- recorded data from tracking units on company aircraft.
References
Airservices Australia. (2024). AIP Australia Part 1- General. online: Airservices Australia Retrieved from www.airservicesaustralia.com/aip/aip.asp
ATSB. (2013). Avoidable Accidents No. 7 Visual flight at night accidents: What you can’t see can still hurt you. (AR-2012-122). Canberra, ACT
Bearman, C., & Bremner, P. (2016). Don't just do something, stand there! National Emergency Response, 29(4), 12-17.
CASA. (2017, 15 May 2017). Safety in mind: Normalisation of deviance. Flight Safety. https://www.flightsafetyaustralia.com/2017/05/safety-in-mind-normalisation-of-deviance/
CASA. (2021). Part 91 (General Operating and Flight Rules) Manual of Standards
2020. Canberra, ACT: Civil Aviation Safety Authority
CASA. (2022). AC 61-05 v1.1 Night VFR rating. Canberra: Civil Aviation Safety Authority
CASA. (2024a). AC 139.R-01 v3.1 Guidelines for Heliports - Design and Operation. Canberra: Civil Aviation Safety Authority
CASA. (2024b). Civil Aviation Advisory Publication (CAAP) 48-01 v3.3. Canberra: Civil Aviation Safety Authority
CASA. (2025a). AC 138-05 v3.0 Aerial work risk management (D25/124220). Canberra, ACT: Civil Aviation Safety Authority
CASA. (2025b). CASR Part 91, General operating and flight rules - Plain English Guie v5.1. Canberra, ACT: Civil Aviation Safety Authority
CASA. (2025c). Civil Aviation Order 48.1 Fatigue Management Plain English Guide. Civil Aviation Safety Authority
CASA. (2025d). Safety behaviours: human factors for pilots 4th edition Resource booklet 8 Threat and error management. Civil Aviation Safety Authority. https://www.casa.gov.au/sites/default/files/2021-06/safety-behaviours-human-factor-for-pilots-8-threat-error-management.pdf
CASA. (2025e). Safety behaviours: human factors for pilots 4th edition Resource booklet 9 Human information processing. Civil Aviation Safety Authority.
CASA. (2025f). Visual Flight Rules Guide (8.2 ed.). Civil Aviation Safety Authority.
Flight Safety Foundation. (2025). Operational Risk Assessment. In Basic Aviation Risk Standard Aerial Mustering. Flight Safety Foundation.
Liu, Y., Tian, J., Martin-Gomez, A., Arshad, Q., Armand, M., & Kheradmand, A. (2024). Autokinesis Reveals a Threshold for Perception of Visual Motion. Neuroscience, 543, 101-107. https://doi.org/10.1016/j.neuroscience.2024.02.001
Robson, D. (2008). Night Flight (2nd ed.). Aviation Theory Centre.
Tuthill, J. C., & Azim, E. (2018). Proprioception. Current Biology, 28(5), R194-R203. https://doi.org/10.1016/j.cub.2018.01.064
Young, L. R. (2003). Spatial orientation. In P. S. Tsang, Vidulich, M.A. (Ed.), Principles and practice of aviation psychology (pp. 69-113). LEA Publishers.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- MDH Pty Ltd
- Cloncurry Air Maintenance
- Civil Aviation Safety Authority
- Bureau of Meterology
- Queensland Police Service
Submissions were received from:
- MDH Pty Ltd
- Civil Aviation Safety Authority
- Bureau of Meterology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] A night VFR rating ensures a pilot has the knowledge and skills necessary to safely operate and navigate an aircraft under visual flight rules at night.
[2] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[3] The SPOT Trace system allowed users to set tracking intervals and view the tracker’s GPS coordinates online in real time.
[4] A dry storm is a thunder storm that produces lightning but precipitation does not reach the ground.
[5] Geoscience Australia defines sunset as the instant in the evening under ideal meteorological conditions, with standard refraction of the Sun's rays, when the upper edge of the Sun's disk is coincident with an ideal horizon.
[6] A waning gibbous moon phase is the period between full moon and half-moon.
[7] A night VFR rating ensures a pilot has the knowledge and skills necessary to safely operate and navigate an aircraft under visual flight rules at night.
[8] In the north of Australia, cattle mustering ordinarily takes place in the dry season, from around April to November.
Occurrence summary
| Investigation number | AO-2025-063 |
|---|---|
| Occurrence date | 09/10/2025 |
| Occurrence time and timezone | 1929 Australian Eastern Standard Time |
| Location | 25 km south-south-east of Kowanyama |
| State | Queensland |
| Report release date | 06/05/2026 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Collision with terrain |
| Occurrence class | Accident |
| Highest injury level | Fatal |
Aircraft details
| Manufacturer | Robinson Helicopter Co |
|---|---|
| Model | R22 Beta |
| Registration | VH-LYD |
| Serial number | 4471 |
| Aircraft operator | MDH Pty Ltd |
| Sector | Helicopter |
| Operation type | Part 91 General operating and flight rules |
| Activity | General aviation / Recreational-Aerial work-Observation and patrol |
| Departure point | Rutland Plains Aircraft Landing Area, Queensland |
| Destination | Rutland Plains Aircraft Landing Area, Queensland |
| Injuries | Crew - 1 (fatal) |
| Damage | Destroyed |