On the afternoon of 10 October 2014, the pilot of an amateur-built One Design DR-107 aircraft, registered VH-EGT, was performing low-level aerobatic manoeuvres. The manoeuvres were being performed to the east of Goolwa Airport, South Australia.
Witnesses described the aircraft performing a series of similar manoeuvres. Each involved a vertical climb and tumbling manoeuvre followed by a vertical dive and a low altitude recovery.
Witnesses reported that, during recovery from the last vertical dive, the aircraft collided with terrain. The aircraft was destroyed by the impact and the pilot was fatally injured.
What the ATSB found
The ATSB found no evidence of pilot incapacitation or a mechanical fault with the aircraft that could have contributed to the accident. There was insufficient evidence to determine why the recovery was not accomplished above the pilot’s minimum authorised aerobatics height.
The Civil Aviation Safety Authority (CASA) recommends that pilots performing low-level aerobatics undertake regular peer reviews due to the high level of skill and fine safety margins involved. The ATSB found no evidence of the pilot undertaking a peer review of their aerobatic performance in the 15 months prior to the accident.
Finally, the ATSB identified a safety issue that CASA does not require builders of amateur-built experimental aircraft to produce a flight manual, or equivalent, for their aircraft following flight testing. Without a flight manual, the builder, subsequent owners and other pilots do not have reference to the operational and performance data necessary to safely operate the aircraft.
What’s been done as a result
In response to the identified safety issue, the ATSB has issued a safety recommendation to CASA to take action to require builders of amateur-built experimental aircraft to produce a flight manual, or equivalent, for their aircraft following flight testing.
Safety message
This accident highlights the risks inherent in performing low-level aerobatics. Applying the recommendations in CASA civil aviation advisory publication CAAP 155-1(0) Aerobatics will reduce these risks. Specifically, pilots are encouraged to always maintain minimum approved heights above the ground when performing aerobatics and to engage in regular peer reviews.
Owners of amateur built experimental aircraft are also encouraged to ensure a comprehensive and accurate flight manual, or equivalent, is available for reference by themselves, subsequent owners and other pilots who may fly the aircraft.
Amateur-built One Design DR-107 aircraft, registered VH-EGT
Source: FlightAware
The occurrence
On the afternoon of 10 October 2014, the pilot of an amateur-built One Design DR-107 (DR-107) aircraft, registered VH-EGT (EGT), was performing low-level aerobatic manoeuvres to the east of Goolwa Airport, South Australia. The aerobatics were observed by a number of witnesses and described as consisting of a series of repeated manoeuvres. Specifically, the aircraft was seen to conduct a number of vertical climbs and tumbling manoeuvres, followed by a vertical dive and a low altitude recovery.
Witnesses observed that as the aircraft started to recover from a vertical dive it collided with terrain. The two witnesses furthest from the aircraft reported that the aircraft was rolling or spiralling while in the final vertical dive. By contrast, the two closest witnesses reported the aircraft was not rolling or spiralling during the final vertical dive.
The collision occurred at about 1430 Central Daylight-saving Time[1] in a paddock to the east of Goolwa Airport (Figure 1). Emergency services received a telephone call from a witness to the accident at 1431. Police, fire and ambulance personnel arrived at the accident site by 1443. The aircraft was destroyed by the impact and the pilot was fatally injured.
Figure 1: Goolwa Airport showing the location of the aircraft wreckage and witness locations. The runway is oriented basically north/south
The pilot held a Private Pilot (Aeroplane) Licence, issued in March 1983, with the appropriate aircraft endorsements to operate a DR-107-type aircraft. The pilot also held a valid and unrestricted Class 2 Aviation Medical Certificate, issued by the Civil Aviation Safety Authority (CASA).
The pilot’s last recorded biennial aeroplane flight review was on 4 September 2013. Entries in the pilot’s logbook recorded a total flying experience of 993 hours to 20 September 2013. There were no further entries in the pilot’s logbook after this date. The pilot had logged a total of 201.8 hours in EGT to 20 September 2013. From that date, entries in EGT’s maintenance release indicated the pilot flew the aircraft for a further 16.8 hours. It could not be determined if the pilot flew any aircraft other than EGT after 20 September 2013.
In November 1990 the pilot was assessed as competent, by a CASA Approved Testing Officer, to recover from spins in a Cessna 152-type aircraft and to perform basic aerobatic manoeuvres. The manoeuvres included loops, aileron rolls, slow rolls, barrel rolls and stall turns.
In order for CASA to grant a low-level aerobatics approval, pilots were required to demonstrate proficiency at progressively lower levels. The pilot was granted progressively lower low-level aerobatics approvals as follows:
in August 2009, the pilot was found competent to recover from inverted spins and to perform low-level aerobatics down to 500 ft above ground level[2]
in August 2011, the pilot was found competent to perform low-level aerobatics down to 330 ft and to perform non-aerobatic manoeuvres down to 100 ft.
In August 2013 CASA renewed the pilot’s low-level aerobatics approval for a further 2 years. The pilot’s continued competence to perform low-level aerobatics was not re-assessed prior to this renewal.
The pilot exceeded the recommended minimum recent experience for low-level aerobatics contained in Civil Aviation Advisory Publication (CAAP) 155-1(0) Aerobatics.
Aircraft information
General
The aircraft was a single seat, low wing, fixed gear, amateur-built[3] aircraft designed for competition aerobatics (Figure 2). Entries in the aircraft’s logbook indicated that the pilot commenced construction of the aircraft as an amateur builder in October 2003. The aircraft was completed in March 2008. A CASA authorised person issued a special certificate of airworthiness in the experimental category on 13 March 2008.
Figure 2: Amateur-built One Design DR-107 aircraft, registered VH-EGT
Source: FlightAware
The last entry in the aircraft’s maintenance records was the removal, by the pilot,[4] of the propeller and engine in September 2013. The pilot removed the engine and propeller from the aircraft for overhaul following a propeller overspeed. There was no record of the engine and propeller overhaul or subsequent installation in the aircraft. There was also no record of the last annual inspection performed on the aircraft.
On 14 January 2014, the pilot issued a maintenance release that was valid for 12 months. This allowed the aircraft to be operated privately under the day visual flight rules.[5] The aircraft flew for 16.8 hours between 14 January 2014 and the accident. No defects or unserviceable equipment endorsements were recorded on the maintenance release.
Aircraft weight and balance
The pilot, as builder of the aircraft, determined the aircraft’s empty weight and balance limits and produced a weighing summary document in March 2008. The empty weight was recorded to be 475 kg. The ATSB found no record of a maximum take-off weight (MTOW) in the aircraft’s records or the CASA aircraft file. No flight manual or placards relating to the aircraft’s weight and balance were found.
The kit supplier of the plans and building materials for the aircraft specified an empty weight of 322 kg and a MTOW of 517 kg. The aircraft’s weighing summary contained an aerobatic weight of 610 kg, which is 93 kg above the kit supplier’s listed MTOW. CASA allowed builders of amateur-built experimental aircraft to nominate their own MTOW. However, builders are required to demonstrate that their aircraft are safe to fly at their nominated MTOW during flight testing. Logbook entries indicated that the aircraft was test flown at approximately 610 kg on 1 and 2 June 2008.
The aircraft designer determined that the aircraft was capable of withstanding a flight load factor of plus or minus 10 g[6] at a weight of 454 kg. Operations at weights above this required a corresponding decrease in the maximum flight load factor. This included a corresponding reduction in the aircraft’s maximum manoeuvring speed (VA).[7] The ATSB determined that the manoeuvring speed on the aircraft’s airspeed indicator was marked appropriately for a 610 kg aerobatic weight. The VA marking on the airspeed indicator, in the absence of a flight manual, indicated the application of a reduced flight load factor limit.
The ATSB surveyed DR-107 owners on the Australian civil aircraft register to place the aircraft’s MTOW in context with other aircraft of the same type. Reported empty weights varied from 408 kg to 493 kg. MTOWs varied from 550 kg to 669 kg. One responder stated that their aircraft did not have a MTOW.
Flight manuals
The ATSB found no evidence that a flight manual or equivalent placarding was produced for the aircraft. A flight manual documents emergency procedures, systems information, operational and performance data necessary to safely operate an aircraft. For certified aircraft,[8] a flight manual is produced by the aircraft manufacturer for use by any pilot who flies the aircraft. For an amateur-built experimental aircraft, the builder of the aircraft is considered the manufacturer.
As each amateur-built aircraft is unique, CASA requires the builder to test their aircraft following construction. The purpose of flight testing is to determine that the aircraft is safe to fly and to determine the aircraft’s flight limits and performance characteristics. CASA recommends, but does not require, builders of amateur-built experimental aircraft to produce a flight manual for their aircraft following flight testing.
The ATSB’s survey of DR-107 owners indicated that half of the responders did not have a flight manual. The owners without a flight manual were not the builders of their aircraft, having purchased their aircraft from the builder or a subsequent owner.
Meteorological information
The Bureau of Meteorology did not provide observations or forecasts for Goolwa Airport. The area forecast[9] covering Goolwa Airport indicated that a trough would pass over the airport from the south-west at around the time of the accident. Low altitude winds were forecast to change from the north-west to the south-west as the trough passed.
Weather observations from nearby Victor Harbour and Hindmarsh Island indicated that the trough passed Goolwa at least 2 hours before the accident.
Witnesses at Goolwa Airport reported that the weather was fine and sunny with good visibility at the time of the accident. Witnesses also reported a ‘strong wind’ coming from the south-west. Due to low terrain to the south-west of Goolwa Airport, the presence of mechanical turbulence was considered unlikely.
Wreckage and impact information
On-site examination
The accident site was in a flat, recently harvested paddock adjacent to Goolwa Airport. The aircraft collided with terrain approximately 400 m east of the northern end of runway 01/19.[10] The wreckage trail was approximately 45 m long on a bearing of 115°. The length of the wreckage trail, combined with the initial ground impact mark and damage to the aircraft, indicated an impact at relatively high vertical and horizontal speed. Ground impact marks and aircraft damage further indicated that the aircraft collided with terrain in a wings level, slightly nose down pitch attitude (Figure 3).
Figure 3: Initial ground scar
Source: ATSB
Fuel soaked soil was identified under the wreckage, indicating that the aircraft’s fuel tank contained fuel prior to its disruption during the impact sequence. No evidence was found of any fault with the aircraft that could have contributed to the accident.
Propeller ground impact marks, blade dispersion and damage was consistent with the engine operating under power at the time of the accident. Witness reports of engine noise were consistent with the engine operating normally up to the collision with terrain. There was no evidence of an in-flight fire or break-up.
The aircraft was not fitted with a fixed emergency locator transmitter, nor was it required to be by regulation.
Medical and pathological information
The forensic pathologist who conducted the post-mortem examination concluded that the pilot succumbed to injuries sustained during the impact sequence. No abnormalities were identified that could have led to pilot incapacitation.
Toxicology results did not identify any substances that could have impaired the pilot’s performance.
Operational information
Aerobatic manoeuvres
Witnesses reported that the pilot was performing low-level aerobatic manoeuvres on the day of the accident, including vertical dives. Vertical dives meet the definition of an aerobatic manoeuvre contained in CAAP 155-1(0). There was insufficient evidence to determine the height at which the pilot was recovering from the vertical dives.
The ATSB was unable to determine the reason why the pilot was performing low-level aerobatics. However, the pilot had previously performed air show aerobatic routines and may have been practicing for an upcoming performance.
An experienced aerobatic pilot pointed to the possibility that the aircraft was in a spin,[11] which may have become an inverted spin during the final descent. While there was insufficient evidence to confirm that proposition, such a development would have required additional time, and therefore height, to recover the aircraft to level flight.
The ATSB obtained video evidence of the pilot performing aerobatic manoeuvres at Goolwa Airport significantly below 330 ft 1 week prior to the accident. This was below the height that the pilot was permitted to engage in aerobatic flight.
Peer reviews
Due to the ‘high level of skill and fine safety margins’ in low-level aerobatics, CAAP 155-1(0) part 7.28.1 strongly suggested pilots undertake regular peer reviews of their aerobatic performance. In this respect, Part 7.28.2 of the CAAP stated:
The peer review process is intended to provide an independent assessment by a similarly qualified person or persons on the way the pilot conducts the activity and to identify any incorrect techniques or practices that the pilot may have developed over time. It is not intended to be a flight test for the renewal of the permission, but an opportunity for constructive discussion with other practitioners with a view to enhancing the safety of a pilot’s performance.
CAAP 155-1(0) recommended a maximum of 15 months between reviews. The ATSB was unable to find any evidence of the pilot undertaking a peer review of their aerobatic performance in the 15 months before the accident.
The fatal/serious injury accident rate across the period of the study was significantly higher for amateur-built aircraft (average 1.27 per 10,000 hours) than it was for similar factory-built aircraft (average 0.22). The fatal and serious injury accident rate was more than 5.5 times higher for amateur-built aircraft compared to factory-built during private operations.
Similar to the total accident rate, the fatal/serious injury accident has reduced from 1988-1999 to 1999-2010, but the reduction has been significantly greater for amateur-built aircraft. In the second half of the period of study from 1999-2010, the fatal/serious injury accident rate was more than 3.5 times higher for amateur-built aircraft.
Those results were consistent with the findings of the United States National Transportation Safety Board (NTSB) safety study NTSB/SS-12/01 The Safety of Experimental Amateur-Built Aircraftavailable at NTSB website. The abstract of that study noted that:
Experimental amateur-built (E-AB) aircraft represent nearly 10 percent of the U.S. general aviation fleet, but these aircraft accounted for approximately 15 percent of the total—and 21 percent of the fatal—U.S. general aviation accidents in 2011…
The NTSB study also stated that:
Areas identified for safety improvement include expanding the documentation requirements for initial aircraft airworthiness certification, verifying the completion of Phase I flight testing, improving pilots’ access to transition training and supporting efforts to facilitate that training, encouraging the use of recorded data during flight testing, ensuring that buyers of used E-AB aircraft receive necessary performance documentation, and improving aircraft identification in registry records.
As a result of their safety study, the NTSB made a number of recommendations to the United States Federal Aviation Administration (FAA) that were aimed at improving the safety of amateur-built aircraft. These included recommendations that the FAA:
Revise 14 Code of Federal Regulations 21.193, Federal Aviation Administration Order 8130.2G, and related guidance or regulations, as necessary, to require applicants for an airworthiness certificate for experimental, operating amateur-built aircraft to submit for Federal Aviation Administration acceptance a flight test plan that will (1) ensure the aircraft has been adequately tested and has been determined to be safe to fly within the aircraft’s flight envelope and (2) produce flight test data to develop an accurate and complete aircraft flight manual and to establish emergency procedures and make a copy of this flight test plan part of the aircraft’s certification file. (A-12-29)
…
Revise Federal Aviation Administration Order 8130.2G, and related guidance or regulations, as necessary, to require the review and acceptance of the completed test plan documents and aircraft flight manual (or its equivalent) that documents the aircraft’s performance data and operating envelope, and that establishes emergency procedures, prior to the issuance of Phase II operating limitations. (A-12-32)
The FAA responded to these NTSB recommendations on 24 September 2012 and advised that they were ‘creating a cross organizational Amateur-Built Safety Team to review the current guidance and policy for amateur-built certification and operation.’ At the time of writing, no further safety action had been reported to the NTSB.
Related occurrences
A review of the ATSB occurrence database identified three potentially similar accidents that occurred during aerobatic manoeuvres. Of these, two involved amateur-built aircraft. One of the occurrences was preceded by a loss of engine power during take-off. There was insufficient information available on the circumstances of the other two occurrences to determine if they were substantially similar to this accident.
While performing aerobatic manoeuvres the pilot did not fully recover the aircraft from a vertical dive before colliding with terrain. The ATSB did not find any evidence of pilot incapacitation or a fault with the aircraft that could have contributed to the accident. The weather conditions were also considered unlikely to have influenced the development of the accident. Additionally, the pilot was qualified to perform low-level aerobatics down to 330 ft and the aircraft type was appropriate for the aerobatic manoeuvres being performed that day.
This analysis will consider the possible reasons why aerobatic flight was continued below 330 ft. In addition, the safety benefit of aerobatic peer reviews and provision of aircraft flight manuals for amateur built experimental aircraft will be discussed.
The occurrence
The accident site ground impact marks and aircraft damage indicated that the aircraft was in a slightly nose low, wings level attitude at impact. Additionally, the ATSB determined that the aircraft collided with terrain with a high vertical and horizontal speed. This evidence is consistent with witness reports indicating that the aircraft appeared to be pulling out of a dive when it collided with terrain.
There was insufficient evidence to determine why the recovery was not accomplished above the pilot’s minimum aerobatics height of 330 ft. It is possible that the pilot either intentionally or inadvertently delayed the recovery of the aircraft during the vertical dive.
Misjudgement of the height that recovery was initiated
The ATSB was unable to determine the intended lowest height of the aerobatics on the day of the accident. However, evidence was provided to the ATSB that the pilot performed aerobatic manoeuvres significantly below 330 ft 1 week prior to the accident.
It is possible that the pilot was completing the aerobatic manoeuvres below 330 ft on the day of the accident. If this occurred, a misjudgement of the recovery initiation height may have resulted in insufficient remaining height above terrain for the pilot to recover the aircraft from the vertical dive before impacting terrain.
Inadvertent late initiation of the recovery
Raising the aircraft’s pitch attitude from vertical nose-down to close to horizontal while maintaining the wings level required active inputs by the pilot and flight control authority. Consequently, pilot incapacitation or a fault with the aircraft’s flight controls were considered unlikely. Momentary incapacitation of the pilot or an intermittent aircraft fault that distracted the pilot and delayed initiation of the recovery; however, could not be ruled out.
Witness descriptions of the aircraft rolling or spiralling were consistent with the aircraft being in a spin during the final descent. However, the two closest witnesses described the aircraft descending vertically without spinning. Additionally, observations of the attempted recovery and accident site ground impact marks indicated that the aircraft was not in a spin when it collided with terrain. If the aircraft had inadvertently entered an inverted spin at some stage during the vertical dive, additional height would have been required to recover the aircraft to level flight. In that case, the possibility that there was insufficient height available to fully recover the aircraft could not be ruled out.
Aerobatics peer review
The ATSB found no evidence of the pilot undertaking a peer review of their aerobatic performance in the 15 months prior to the accident. A peer review, as suggested by Civil Aviation Advisory Publication 155-1(0) Aerobatics has the potential to help a pilot maintain safety margins in low-level aerobatic routines, and may have assisted the pilot avoid inadvertently breaching their minimum approved aerobatics height. However, there was insufficient evidence to determine if the non-completion of the peer review influenced the development of the accident.
Aircraft flight manual
The Civil Aviation Safety Authority did not require amateur-built experimental aircraft to have a flight manual or equivalent placards. The ATSB found no evidence that a flight manual or equivalent placarding was produced for the aircraft following flight testing. The lack of a flight manual was unlikely to have influenced this accident due to the pilot's familiarity with the aircraft. This familiarity was a result of their experience building, test flying and operating the aircraft.
However, as evidenced by the recommendations made to the United States Federal Aviation Administration by the National Transportation Safety Board, not having a flight manual increases the risk associated with amateur-built experimental aircraft operations. Without a flight manual the builder, other pilots and especially subsequent owners do not have reference to operational and performance data necessary to safely operate the aircraft. Given that accidents involving amateur-built aircraft occur at a significantly higher rate than comparable factory-built aircraft, a requirement to document important operational information would be a valuable safety enhancement.
Findings
From the evidence available, the following findings are made with respect to the collision with terrain involving One Design DR-107 aircraft, registered VH-EGT, which occurred near Goolwa Airport, South Australia on 10 October 2014. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
The aircraft collided with terrain while the pilot was attempting to recover from an aerobatic manoeuvre at low level.
Other factors that increased risk
Although suggested by Civil Aviation Advisory Publication 155-1(0) Aerobatics, the pilot probably did not undertake a peer review of their aerobatic performance in the preceding 15 months to the accident.
The Civil Aviation Safety Authority did not require builders of amateur-built experimental aircraft to produce a flight manual, or equivalent, for their aircraft following flight testing. Without a flight manual the builder, other pilots and subsequent owners do not have reference to operational and performance data necessary to safely operate the aircraft. [Safety issue]
Sources and submissions
Sources of information
The sources of information during the investigation included:
an experienced aerobatic pilot
the Bureau of Meteorology
the Civil Aviation Safety Authority (CASA)
the South Australian Police and Forensic Science SA
the One Design DR-107 designer
a number of other One Design DR-107 aircraft owners.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the experienced aerobatic pilot, the Sport Aircraft Association of Australia and CASA.
Submissions were received from the experienced aerobatic pilot, the Sport Aircraft Association Australia and CASA. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 3 April 2016, the pilot of a de Havilland DH-82 aeroplane, registered VH-BJE, conducted a 30‑minute scenic flight from Redcliffe Airport, Queensland, with one passenger on board. The weather was fine, with wind was from the east-northeast at less than 8 kt, no precipitation, and the runway was dry.
On returning to Redcliffe, the pilot elected to join the circuit on a mid-field crosswind leg for runway 07. The pilot reported that the approach was normal.
As the aircraft landed, the pilot reported the tail was slightly higher than normal, but the aircraft’s speed was normal. The aircraft wheels touched down at the pilot’s aiming point, about half way along the grass strip to the right of the sealed runway. The pilot reported that the wheels seemed to dig in. The aircraft nose pitched down, the propeller struck the grass runway, and the aircraft rolled over forwards, coming to rest inverted (Figure 1).
The pilot and passenger were uninjured. The aircraft sustained substantial damage.
Figure 1: Accident site showing damage to VH-BJE
Source: Ron Ennis – modified by the ATSB
Pilot comments and experience
At the time of the accident, the pilot had a total of 259.3 hours of aeronautical experience, including 7.9 hours on the aircraft type. The pilot held tailwheel and aerobatic endorsements, obtained in an American Champion/Bellanca Citabria aircraft.
The pilot commented that the ground was a bit soft where the wheels had touched down, but that they had landed there twice previously that day without incident. In future, the pilot would land with a slightly higher nose attitude.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
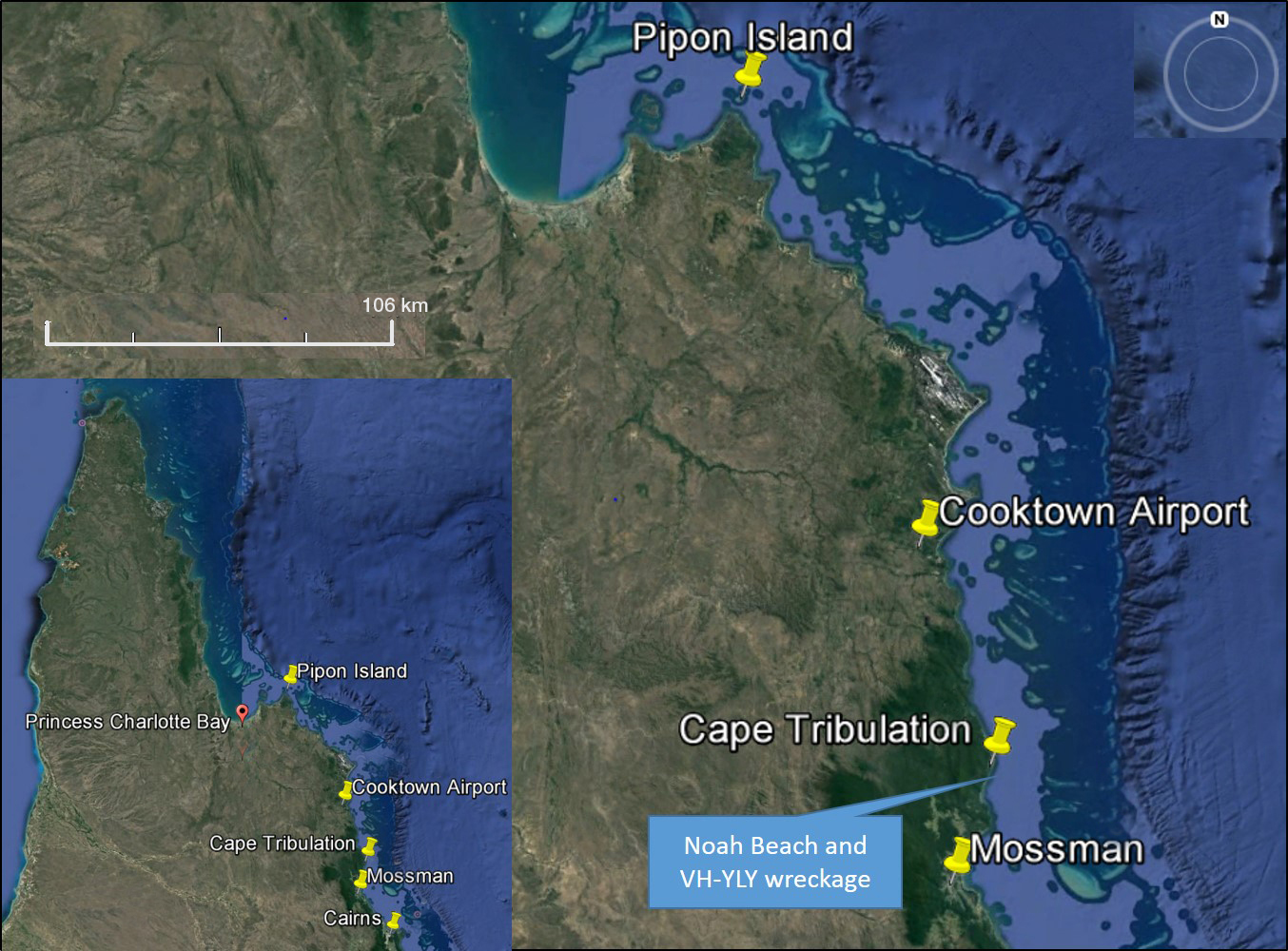
On 7 April 2016, the pilots of two Robinson R22 helicopters flew from Mossman, Queensland to various fishing locations to the north with a passenger in each helicopter. Late in the afternoon, the pilots commenced the direct return flight to Mossman. However, the pilots encountered weather and winds that slowed their progress and required them to refuel at Cooktown.
The pilots departed Cooktown at last light intending to track via the coast to Mossman. As the flights progressed, the light available from the sun continued to decrease and there was no moon. There were also patches of cloud and rain in the general area.
Shortly after passing Cape Tribulation, in dark night conditions, one of the helicopters, registered VH-YLY (YLY), collided with the sea. The passenger was injured in the accident but was able to reach the shore and notify emergency services. Unaware of the accident, the occupants of the other helicopter continued to Mossman.
A search was initiated and the missing helicopter was located on 9 April 2016 in about 400 m offshore in about 10 m of water. The pilot was not located.
What the ATSB found
The ATSB found that the pilot of YLY, who was only qualified to operate in day-VFR conditions, departed on a night flight and continued towards the destination in deteriorating visibility until inadvertently allowing the helicopter to descend into water.
The ATSB also identified the following other factors that collectively increased risk:
an unapproved modification attached to the skids of YLY
exceedance of weight and balance limitations
non-carriage of life jackets
incomplete operational information
overdue calibration checks of the helicopter pitot-static system and altimeter.
Safety message
To avoid the usually fatal consequences of losing visual reference, day-VFR pilots need to plan to arrive at their destination at least 10 minutes before last light and to have a realistic ‘plan B’ to use when it becomes apparent that the intended flight cannot be completed in daylight. A further consideration for pilot decision-making about flying conditions is the degree to which passengers are also exposed to risk.
Key messages from the ATSB Avoidable Accidents series report No.7 highlight that some nights and some terrain are darker than others, and inadvertently flying into instrument meteorological conditions is also harder to avoid at night. Pilots need to be mindful of similar messages provided in pilot operating handbooks that refer to risks associated with loss of visibility and night flight in bad weather.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
surviving occupants of the two helicopters
Cairns Forensic Crash Unit, Queensland Police
the Bureau of Meteorology
the Civil Aviation Safety Authority (CASA)
Airservices Australia
Geoscience Australia
References
ATSB (2013), Avoidable Accidents No. 7. Visual flight at night accidents: What you can’t see can still hurt you, ATSB, Canberra, Australia.
Robinson Helicopter Company (Rev. 1994), Safety Notice SN-13 Do not attach items to the skids.
Robinson Helicopter Company (Rev. 1994), Safety Notice SN-18 Loss of visibility can be fatal.
Robinson Helicopter Company (Rev. 1994), Safety Notice SN-26 Night flight plus bad weather can be deadly.
Robinson Helicopter Company (2001), Safety Notice SN-37 Exceeding approved limitations can be fatal.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the other R22 pilot and CASA.
Submissions were received from the other R22 pilot and CASA. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
The occurrence
On the morning of 7 April 2016, the pilot of a Robinson Helicopter Company R22 helicopter, registered VH-YLY (YLY) flew from Mareeba to Mossman, Queensland, to join the pilot of another R22 for a fishing trip (Figure 1). Both pilots were qualified to operate the helicopters on private‑category operations by day under the visual flight rules[1].
The two pilots departed Mossman at about 0800 EST[2] with a passenger in each of the two‑seat helicopters. The pilots tracked north to Cooktown to refuel then continued northward to Pipon Island, landing at various coastal locations so they and the passengers could do some fishing. At one of the landing sites the pilots were able to fill the helicopter fuel tanks from a drum of fuel.
By the time the helicopters arrived at Pipon Island, the occupants had caught between 20 and 30 kg of fish, which were carried in a non-standard container attached to the left skid of YLY. After spending some time at Pipon Island, the pilots departed separately somewhere between 1600 and 1700 to return to Mossman. The pilots had used GPS route information and local weather conditions, rather than the required aviation Area Forecast,[3] to decide that they had sufficient fuel and daylight to make it to Mossman, a direct-track distance of 148 NM (274 km).
Figure 1: Location of Pipon Island with Cooktown and Mossman destinations showing position of VH-YLY accident site south of Cape Tribulation. The inset shows Cape Tribulation relative to far north Queensland
Source: Google Earth and modified by ATSB
During the return flight, squalls and headwinds of about 20 kt were encountered that slowed progress and necessitated a landing at Cooktown to refuel. Relative to the other helicopter, YLY was slower likely due to the aerodynamic drag of the skid‑mounted container, the additional weight of the fish, and doors-off operation.
Recorded fuel transaction information showed the time of fuel uplift at Cooktown occurred at 1836. Given last light for Cooktown was calculated to be 1838 (based on ideal conditions), night conditions existed by the time the pilots were ready to depart. Neither pilot was qualified to fly at night or in low visibility conditions that would require instrument flying. Additionally, the helicopters were not equipped with an artificial horizon instrument and lacked other equipment required for flight at night under Australian regulations.
The passenger in YLY reported he was concerned about the available light and weather conditions and queried the pilot’s intention to continue the flight after Cooktown. Without elaborating, the pilot indicated he intended to continue and the flight (direct-track distance of 60 NM) would only take 45 minutes. None of the pilots or the passengers reported any specific reason to arrive at Mossman that evening. The pilots did not discuss staying in Cooktown.
Both helicopters departed Cooktown at about 1840. A witness who observed the departure reported it was getting dark, which was consistent with it being after last light and no moonlight (local moon-set was 1811). Due to the slower speed of YLY, the other helicopter drew ahead. Every 10 minutes or so, the pilot of the lead helicopter, who was the more experienced pilot, checked in with the pilot of YLY by radio.
According to the pilot in the lead helicopter, and as had been discussed, they flew close to the coast intending to keep an outline of the mountains as a visual reference. In ‘bad conditions’, the proposed method was to ensure the altimeter was accurate relative to sea level and use it to fly not below 250 ft above the water. If the conditions got ‘really bad’, in that it got too dark and the outline of the mountains or sight of the water was being affected, the plan discussed between the pilots was to land on a beach. The pilot of the lead helicopter advised they had done this on previous occasions due to bad weather, though only in daylight.
The coastal route between Cooktown and Mossman has few settlements and from halfway, most of the coastline is part of the Cape Tribulation section of the Daintree National Park. It is a remote area and, as such, there is little or no ground lighting.
Initially, the weather conditions were reported to be clear but about 15-20 minutes into the flight, the pilot of the lead helicopter encountered small squalls with a bit of cloud. After passing Cape Tribulation, the pilot of the lead helicopter radioed the pilot of YLY who advised he had just passed the cape and did not report any difficulties.
The passenger in YLY recalled that at one stage the helicopter descended close to the water before the pilot corrected and climbed. He further stated that visibility decreased until it was dark and the pilot dimmed the cockpit lights to reduce glare off the windscreen. The passenger recalled passing the Cape Tribulation campgrounds and was aware that there were people on the beach as indicated by campfires and a spotlight being waved at the passing helicopters.
To the passenger, it got ‘really dark’ and concerning so he suggested landing on the beach. The pilot did not respond verbally but it appeared to the passenger that they might be descending to land. Suddenly the passenger saw the ocean more clearly followed almost immediately by a ‘massive bang’ as the helicopter impacted the water.
When the passenger regained consciousness, he was strapped into the helicopter on the ocean floor. He was able to release himself, reach the surface, and tread water in a heavy swell. Injuries to a leg and arm restricted swimming but the tide carried him to the beach where he was able to make contact with campers and notify the authorities. Campers had heard an impact and already reported it to police.
About 10 minutes after the radio call near Cape Tribulation, the pilot in the lead helicopter tried unsuccessfully to contact the pilot of YLY. He recalled that, at the time, there was light cloud, mist, showers, and strong winds. The lead pilot said he was concerned about YLY and wanted to turn back but was prevented by limited time, strong winds, and marginal visibility. So the pilot continued to Mossman.
A search was mounted but the missing pilot was not found.
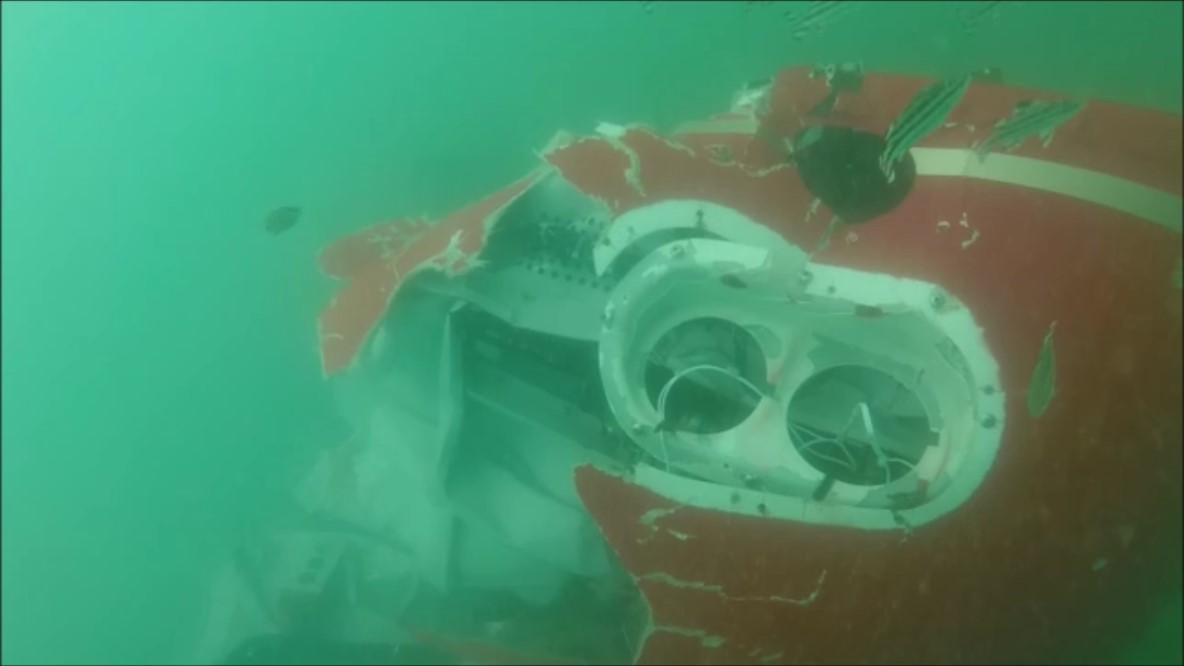
Queensland Police with the assistance of specialist divers located the empty wreckage about 400 m seaward of Noah Beach. The wreckage was not recovered but divers examined the wreckage and recorded underwater video imagery, which was provided to the ATSB (Figure 2).
Figure 2: Underwater image of VH-YLY showing significant damage to the nose and belly panel of the helicopter particularly to the right forward section and loss of the cockpit upper portion
Extensive damage to the right side of the helicopter, including the pilot’s seat belt fitting found torn from its mount, indicated a significant right‑side impact with the water. The main rotor blades and transmission were present and similarly damaged. The tailboom was not identified in the footage and it likely became detached during the accident sequence. The damage to the helicopter and rotor system was consistent with powered flight into the water.
A maintenance release had been issued for YLY authorising VFR Day operation only. A check calibration of the aircraft pitot-static system and altimeter was due in October 2015 and had yet to be certified as complete. As such, the accuracy of the airspeed indicator, vertical speed indicator and altimeter was not assured. A review of the helicopter logbooks did not find any reference to installation of the container to the left skid.
Based on the reported loading of YLY, on departure from Cooktown for Mossman the helicopter was estimated to be at least 35 kg over the maximum gross weight limitation. Although there was no weight and balance data for the skid-mounted container, the longitudinal and lateral centre of gravity were estimated to be outside limits on departure or as fuel was consumed.
Although some of the flying that day included flight over water, the pilots and passengers did not wear life jackets. This was contrary to the regulatory requirement for the occupants of single‑engine aircraft being operated beyond gliding/autorotation distance of land and while below 2,000 ft.
According to the applicable area forecast required for flight planning, in the area of operation east of the ranges and coast, there would be isolated showers with associated low cloud and reduced visibility. The wind was expected to be from the east to south-east at 15 to 20 kt. From 2300, isolated areas of low cloud were expected east of the ranges and coast. This was broadly consistent with the aerodrome forecasts for Cooktown and Cairns, except that the showers and low cloud were due at Cairns from 1700.
The closest official weather observation site to the accident location was at Low Isles, 15 NM (28 km) to the south. At the approximate time of the accident, the wind was from the south-east at 20 kt. No precipitation was recorded during the hour before and after the accident. The extent of cloud coverage was not measured at the site.
The recorded imagery from the Cairns weather radar showed a small area of light rain inland near Cape Tribulation and patches of light to moderate rain off the coast no closer than 15 NM (28 km).
For aviation purposes, night is defined as the period of darkness from last light (end of evening civil twilight) to first light (beginning of morning civil twilight). At last light, in ideal conditions, there will be enough light from the sun for large objects to be seen but no detail. As time passes, light from the sun further diminishes to reach a point where it is insufficient to allow a horizon to be seen at sea level. This point (end of evening nautical twilight) at Cape Tribulation was calculated to be 1919 but high terrain to the west would tend to make it effectively earlier.
The time of the accident was estimated to be 1930, which was about 10 minutes after end of evening nautical twilight.
From the evidence available, the following finding is made with respect to the collision with water of a Robinson Helicopter Company R22 helicopter, registered VH-YLY that occurred near Cape Tribulation, Queensland, on 7 April 2016. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factor
The pilot of YLY, who was only qualified to operate in day-VFR conditions, departed on a night flight and continued towards the destination in deteriorating visibility until inadvertently allowing the helicopter to descend into water.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 21 March 2016, at about 1200 Eastern Standard Time (EST), the pilot of a Robinson R22 helicopter, registered VH-RGY, prepared to conduct a private ferry flight from Richmond Airport to Bow Park Station, Queensland. The pilot was the only person on board. The helicopter had been parked at the airport for 12 days, with the doors on.
As the pilot rolled the throttle on to start the helicopter’s engine, the pilot discovered the adhesive holding the foam cover of the throttle twist grip had deteriorated and become like grease (Figure 1). The pilot then slid the cover forwards on the collective[1] control to grip the steel column.
Figure 1: Cockpit of VH-RGY
Source: Pilot
After starting the engine, the driver of the vehicle that had taken the pilot to the airport radioed to tell the pilot that the pilot’s drink bottle was still in the vehicle, and that they would meet the pilot with the drink bottle at the airport exclusion fence.
The pilot reported that they looped the bungee cord fitted to the helicopter over the collective control. The pilot then exited the helicopter, leaving the engine running and the rotor blades turning, and walked about 4 m to the fence. Within about 30 seconds, the pilot heard the helicopter engine RPM increase, and turned and ran back towards the helicopter. The pilot and driver then observed the helicopter rotate away from the direction of the pilot, lift up, into and over the fence and land on its side on the other side of the fence, damaging the fence.
The helicopter sustained substantial damage (Figure 2). The pilot, who was outside of the helicopter was uninjured.
Figure 2: Damage to VH-RGY (after removal from accident site)
Source: Queensland Police Service
Pilot comments
The pilot reported that they had not had any issues with the adhesive before, despite operating in temperatures over 40 °C, but they did not usually have the doors on. However, even though the temperature was about 35 ⁰C on the day of the accident, the helicopter had been parked for 12 days with the doors on, and the temperature inside the cabin was much hotter. Additionally, there had been rain during the period the helicopter was parked at the airport, increasing the humidity inside the cabin. The pilot believed that the temperature (and possibly combined with high humidity) inside the helicopter must have exceeded the adhesive’s limit. The pilot was unsure whether the adhesive, which had been applied during a rebuild of the helicopter about two years earlier, was the approved adhesive for the grip.
The pilot assessed that because the grip had slid forwards on the collective control, the bungee cord may not have been far enough over the steel column, and it then slid further forwards, allowing the collective to rise, and the helicopter then lifted off.
Adhesive for grip
The R22 Illustrated Parts Catalogue specified Part Number B270-15 Adhesive to be used to install the grip. The specified adhesive was clear, and was manufactured by 3M, with part number 2262. According to the Technical Data for 3M Plastic Adhesive 2262, when the adhesive was tested for ‘plus 7 days’ at 140 °F (60 °C), it failed ‘in adhesion to the indicated substrate (steel)’.
Given the helicopter was parked for over 7 days, with doors on and in hot and humid conditions, this testing suggests that if the approved adhesive was used on the collective grip, it was likely to fail.
Helicopter manufacturer comments
A representative from Robinson Helicopter Company (RHC) advised that the bungee cord was not an RHC installation, nor part of the type design. The post-accident photo (Figure 1) shows that the collective friction knob was in the OFF position, which indicates that the pilot had not applied it. (When tightened to the ‘locked’ position, the collective friction knob is designed to prevent the collective from moving from the position it was locked in.) However, they emphasised that the safest way to prevent similar incidents is to never leave the flight controls unattended while the engine is running.
They had received no other reports of similar events with the grip adhesive. They also commented that a thorough pre-flight check would likely alert the pilot to any issue with the collective grip.
Safety message
Pre-flight checks are designed to ensure the helicopter is capable of operating correctly. To ensure safety of flight, any discovery of an unservicability should be dealt with before flight.
Leaving any vehicle unattended with the engine running carries considerable risk. The Normal Procedures in the R22 Pilot’s Operating Handbook (POH) includes the caution: ‘Never leave helicopter flight controls unattended while engine is running.’ The POH also includes a number of important safety tips and notices. One safety notice with relevance to this accident is Safety Notice 17, which includes the following text:
NEVER EXIT HELICOPTER WITH ENGINE RUNNING
Several accidents have occurred when pilots momentarily left their helicopters unattended with the engine running and rotors turning. The collective can creep up, increasing both pitch and throttle, allowing the helicopter to lift off or roll out of control.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
The owner and maintainer of a Piper PA-23 aeroplane, registered VH-BIQ, who was also a pilot, had received a special flight permit (from a person authorised by the Civil Aviation Safety Authority to issue such permits) to ferry the aircraft from Mareeba, Queensland, to Darwin, Northern Territory, for a 100-hourly inspection.
On the morning of 5 March 2016, the pilot conducted a local flight from Mareeba Airport, to check everything was functioning normally on the aircraft, in preparation for the planned flight to Darwin. The pilot reported that the aircraft performed normally during the take-off and climb to about 2,500 ft above mean sea level (AMSL). However, witnesses reported that at least one engine was running roughly during taxi and take-off, and that the aircraft appeared to climb poorly after take-off. After departing the airport, the pilot reported performing a number of in-flight checks of the aircraft, including retracting and extending the landing gear.
At about 1200 Eastern Standard Time (EST), the aircraft was returning to the airport when the pilot observed the left engine revolutions per minute (RPM) decrease from about 2,300 RPM to 2,000 RPM, which was still above idle power. The pilot conducted a series of actions to try to rectify the power loss, including checking the fuel mixture and full range of the throttle, but the aircraft descended rapidly. As the aircraft continued to descend, the pilot set the aircraft attitude to maintain an airspeed of 70 kt, which was the nominated glide speed for the aircraft.
As the aircraft descended to about 200 ft above ground level, the pilot realised that the landing gear was extended. The pilot reduced the power to idle and conducted a forced landing. The aircraft collided with cane fields, crossed a road and collided with a tree, resulting in substantial damage (Figure 1). The pilot, who was the only occupant of the aircraft, initially exited the aircraft without injury. A small quantity of fuel in the cross-feed line ignited briefly, but the flame quickly extinguished. After assessing that there was then minimal risk of a fire, the pilot returned to the aircraft and in the process sustained a minor injury.
Pilot comments
The pilot provided the following comments:
The temperature was 33 °C, with light rain falling, and the aerodrome was at an elevation of 1,560 ft AMSL. These conditions may have contributed to the aircraft being unable to maintain altitude even while the right engine continued to produce normal power. The pilot also elected not to feather the left propeller as the engine was still producing some power. The extended landing gear created substantial drag and further reduced the aircraft’s ability to maintain altitude.
Some debris may have been present in the fuel that blocked the injectors, resulting in partial loss of power. It was possible that fuel had dried out in the distributor valve, creating a gum, which was then loosened and picked up in the fuel.
Figure 1: Accident site showing damage to VH-BIQ
Source: Aircraft owner
Safety message
The partial or complete failure of one engine in a light twin-engine aircraft can present a number of issues for a pilot to manage. Immediate actions include maintaining control of the aircraft, while assessing the aircraft’s ability to climb or maintain altitude, and configuring the aircraft for maximum available performance.
Reducing the drag by retracting landing gear and flaps, and by feathering the propeller of the failed engine, need to be considered as they may assist in maintaining altitude, but may be extended for approach and landing.
The aircraft’s ability to maintain altitude depends on the pilot’s timely and correct actions, as well as factors that affect aircraft performance such as heat, high humidity and altitude. The local conditions and aircraft configuration may reduce the capability of the aircraft such that a forced landing is the only option available. In this situation, good decision making such as selecting a suitable landing site as soon as possible, which way to turn and avoiding manoeuvring at low level, is essential.
Pilots need to be situationally aware at all times, and be able to impose good judgement and well developed skills to accomplish the flight objectives. Pilot actions or inactions may reduce perceived safety margins and increase the probability of adverse operational events. The CASA training resource Safety Behaviours: Human Factors for Pilots includes guidance for pilots in situational awareness, decision making, threat and error management and airmanship.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 27 February 2016, a Jabiru Aircraft, recreational registration 55-3692, collided with terrain at Medlow Bath, New South Wales. The pilot, the sole occupant, died as a result of the accident.
NSW police is the organisation responsible for investigating this accident. As part of their investigation, they had requested that Recreational Aviation Australia (RA-Aus) provide some technical assistance related to the aircraft and engine. As part of their involvement, RA-Aus requested that the Australian Transport Safety Bureau (ATSB) assist with the examination of the engine.
To protect the information supplied by RA-Aus to the ATSB and the ATSB's investigative work to assist them, the ATSB initiated an investigation under the Transport Safety Investigation Act 2003.
The Jabiru 2200J engine was disassembled and examined at a facility at Bankstown Airport on 8 April 2016 in the presence of a number of interested parties, including the Australian Transport Safety Bureau, NSW Police, the Civil Aviation Safety Authority, and the manufacturer. The examination did not identify any anomalies that may have contributed to the development of the accident. No further assistance was provided to RA-Aus, and further enquiries should be directed to the NSW police as the investigating agency.
On 14 February 2016, at about 0945 Eastern Standard Time (EST), the pilot of a Cessna R182 aeroplane, registered VH-PFZ, was returning to a private airstrip near Ingham aircraft landing area (ALA), Queensland. The pilot, who was the only person on board, had just completed a routine one-hour property inspection and decided to complete the flight with some practice touch and go circuits.
The pilot reported that the weather was fine, with minimal wind and a temperature of about 30 °C.
The pilot approached the circuit with the aircraft in the same configuration used for the inspection flight. This was with 20 inches of manifold pressure, the propeller set at 2,000 revolutions per minute (RPM), and the landing gear retracted.
The pilot joined downwind for runway 22 as per their normal procedure, and conducted their downwind checks. However, they inadvertently omitted one of the checks. Although they extended the landing gear, they did not return the pitch control to the HIGH RPM (full fine) position. The pilot continued with the approach, and selected full flap, but again omitted the pre-landing checks on final approach. This oversight left the pitch control lever at about 2,000 RPM.[1]
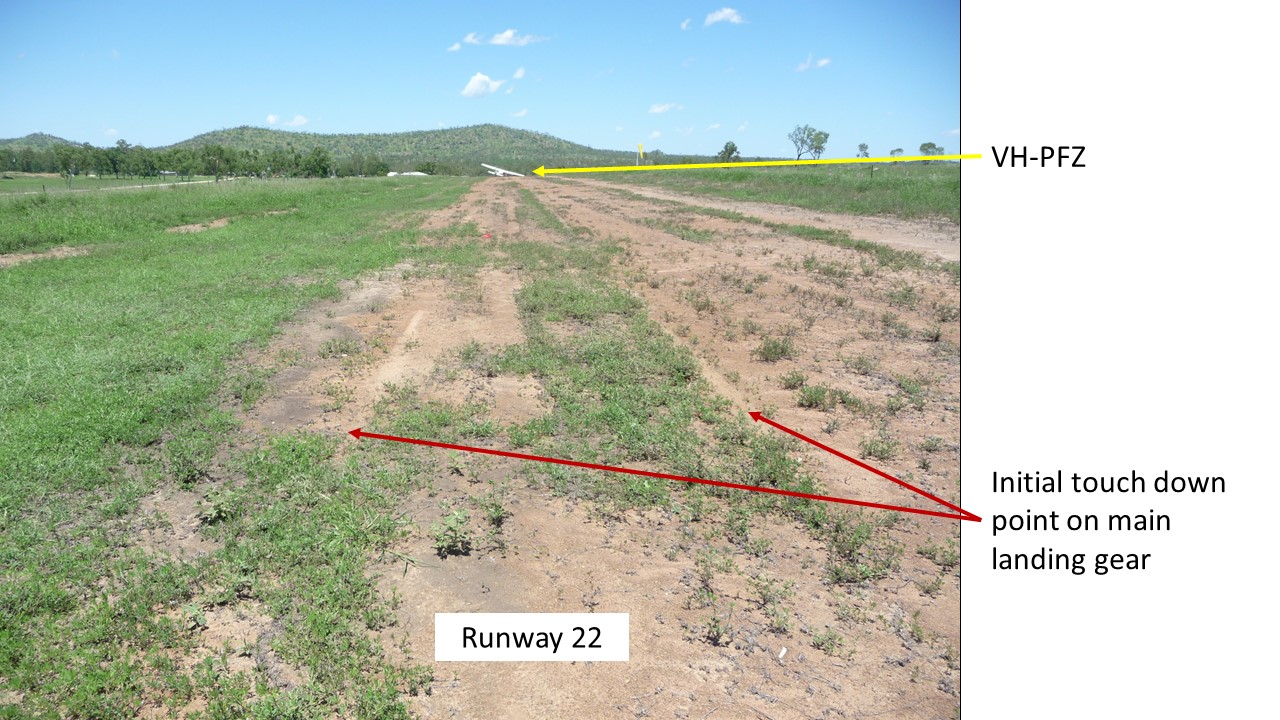
The pilot described the approach and initial touchdown as a little faster and higher than normal, with the touchdown point about 300 m into the 1,100 m airstrip (Figure 1).The aircraft ballooned slightly. At about 10-15 ft above ground level, the pilot commenced a go-around and applied full throttle, with the propeller remaining at 2,000 RPM. With an airspeed of 64 kt, the pilot assessed there was sufficient airspeed to climb out, so retracted all of the flap and then the landing gear.
Figure 1: Initial touchdown point on runway 22, and VH-PFZ (far end)
Source: Pilot
However, the aircraft began to sink, and the nose dropped. Moments later, the main landing gear struck the ground. This second ‘touchdown’ was about 265 m beyond the first, (about 565 m along the airstrip). The pilot attempted to keep the nose of the aircraft raised. However, the propeller struck the ground and the pilot realised that the nose wheel had retracted, so closed the throttle. The aircraft continued to skid along the runway. The propeller stopped rotating when the aircraft had travelled about another 77 m. The aircraft then continued to slide sideways, and the right main landing gear retracted (Figure 2). The pilot was not injured, but the aircraft sustained substantial damage.
Figure 2: VH-PFZ showing retracted nose wheel and right landing gear, and damaged propeller
Source: Pilot
Pilot experience and comments
The pilot had attained almost 4,000 hours of flight experience, 2,800 of which were in VH-PFZ.
The pilot reported that there had been no particular issues affecting the flight on the day, the weather was good, and the inspection flight had been enjoyable. However, the temperature was 30 °C, which increased the density altitude.[2] The pilot could not attribute any particular reason for the checklist oversight.
The pilot reported that during their early flying training, when they had been training for a go-round, they had been instructed to retract all the flap with their right hand, then immediately move their right hand onto the landing gear selector, and retract the landing gear. The pilot commented that ‘the flap travelling up reduced the lift being produced, and the landing gear retracting reduced the drag. These two actions balance out each other.’ The pilot qualified this statement by stating that this technique should only be attempted once a positive rate of climb has been achieved. On this occasion this had not occurred.
The pilot consulted the aircraft’s performance charts post-accident. With the correct propeller (2,400 RPM) and manifold pressure settings, the aircraft delivers the maximum brake horsepower (BHP).[3] For any of the take-off configurations (see POH data below), it is a requirement to have the propeller in the full fine position of 2,400 RPM. The charts do not cater for propeller settings of 2,000 RPM. The pilot reasoned that landing further along the runway than normal may have contributed to a slight rushing of the go-round sequence. It is possible, that this mindset also contributed to retracting the flap and landing gear prior to achieving a positive rate of climb.
The pilot also reported that possibly being too comfortable in the aircraft, and the reliance on its performance, had created an expectation that all would be well.
The pilot summarised that engine RPM was insufficient to produce enough thrust to maintain altitude and climb at the critical point of change in aircraft configuration, while retracting the flap and landing gear.
Cessna R182 Pilot operating handbook (POH)
Information from a generic 1981 Cessna R182 pilot operating handbook stated that the propeller control should be moved to HIGH RPM (full fine) prior to landing.
Climb speed – 59 KIAS until all obstacles are cleared.
Landing gear – RETRACT after obstacles are cleared
Wing Flaps – RETRACT slowly after reaching 70 KIAS.
ATSB comment
The pilot could not recall any particular reason as to why the pre-landing check (propeller control to HIGH RPM (full fine)) was overlooked on two occasions in the circuit.
Although the aircraft could have landed safely in this configuration, attempting to climb with the propeller still at 2,000 RPM created a chain of events from which the pilot did not recover.
The pilot’s decision to retract the flaps all at once, followed immediately by the landing gear, prior to obtaining a positive rate of climb at a low altitude also decreased the aircraft’s performance. The elevation of the airport was 1,100 ft above mean sea level. This, coupled with a warm day of around 30 °C, translated to a higher density altitude,2 resulting in reduced performance.
Safety message
Although the pilot did not recall any distraction which could have led to the omission of the checklist item on both the downwind and final approach checklists, this omission fits a familiar pattern.
Any change of routine or even cognitive thoughts can distract a pilot from an essential checklist item. Research conducted by the ATSB found that distractions, or a change in routine, were an everyday part of flying, and that pilots generally responded quickly and efficiently. The report, Dangerous Distraction: An examination of accidents and incidents involving pilot distraction in Australia between 1997 and 2004 speaks to these issues.
This research commented that pilot distractions in the study did not always occur in response to non-normal tasks. In fact, the research indicated that distraction can occur when pilots are conducting normal routine tasks.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 6 November 2015, the pilot of a Robinson R22 helicopter, registered VH-NCL, prepared to conduct a private flight with one passenger on board, from Newman Airport in Western Australia.
At about 0830 Western Standard Time (WST), the helicopter lifted off to about 10 ft above ground level, and the pilot commenced hover-taxiing. As the helicopter started to move forwards, it encountered a gust of wind from behind and sank rapidly. The helicopter landed heavily, then bounced and rotated rapidly to the right. During the accident sequence, the main rotor blade severed the tail, and the helicopter sustained substantial damage (Figure 1). The pilot and passenger were not injured.
Figure 1: Accident site showing damage to VH-NCL
Source: Airservices Australia - Aviation Rescue Fire Fighting
Loss of tail rotor effectiveness
Loss of tail rotor effectiveness (LTE) causes a yaw to the right in helicopters with a counter-clockwise rotating main rotor. When operating at airspeeds below 30 kt, a tailwind may result in an uncommanded turn, if the tail rotor is unable to provide adequate thrust to maintain directional control. To reduce the onset of LTE, the United States Federal Aviation Administration (FAA) Helicopter Flying Handbook, advises pilots to:
Avoid tailwinds below an airspeed of 30 knots. If loss of translational lift occurs, it results in an increased power demand and additional anti-torque pressures.
To recover from LTE:
If the rotation cannot be stopped and ground contact is imminent, an autorotation may be the best course of action. Maintain full left pedal until the rotation stops, then adjust to maintain heading.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 28 January 2016, the pilot of a Cessna Aircraft Company C208 Caravan amphibian aircraft, registered VH-WTY, was flying 10 passengers on a charter flight over the Great Barrier Reef, Queensland. Before returning to Hamilton Island, the flight was scheduled to stop for about 90 minutes at Chance Bay, Whitsunday Island, about 11 km north-east of Hamilton Island Airport. During the attempted water landing, the aircraft bounced twice on the water’s surface. The pilot then initiated a go-around and the aircraft bounced a third time. While attempting to climb out of the bay, the aircraft clipped trees and collided with terrain. The pilot and all passengers safely exited the aircraft with minor injuries. The aircraft was destroyed.
What the ATSB found
The ATSB found that the aircraft was flown beyond the aircraft landing area northern boundary before the first bounce off the water. This, combined with the delay in initiating a go-around, reduced the options and margins available for a safe outcome.
The engine operating limitations contained in the float operations pilot operating handbook supplement were also not consistent with other publications and may have influenced the power level applied by the pilot during the go‑around.
What's been done as a result
The float manufacturer-published pilot operating handbook supplement was amended with respect to engine operating limits.The operator advised they have taken action to enhance or update existing procedures and checklists for their float plane operations.
Safety message
Charter seaplane operations present unique challenges, particularly in relation to the water landing environment. Variable sea conditions and the possibility of sharing the landing area with marine vessels and people mean that every landing has the potential to be markedly different.
A go-around is a normal procedure and a safe option whenever landing conditions are not satisfactory. However, it is important to consider aircraft performance and local conditions when planning an escape route, including conducting ‘mental rehearsals’ of standard procedures. In addition, making an early decision to conduct a go-around significantly reduces the associated risk.
VH-WTY at Chance Bay earlier on 28 January 2016
Context
Pilot information
The pilot commenced flying in November 2008, was issued a Private Pilot Licence (Aeroplane) in July 2010 and a Commercial Pilot Licence (Aeroplane) in June 2012. The commercial licence was endorsed with a class rating for single-engine aircraft and design feature endorsements for floatplane,[3] manual propeller pitch control, retractable undercarriage and gas turbine engine. The pilot held a class 1 aviation medical certificate with no restrictions, and also held a valid boat driver’s licence to allow operation as pilot‑in-command of floatplanes, when operated on the water. The pilot commenced flying with the operator in May 2014.
To be a charter pilot on single-pilot, single-engine floatplane aircraft (Beaver and C208 Caravan as operated by the operator), under day VFR operations, the company required a pilot to have the following minimum qualifications and experience:
Commercial Pilot Licence(Aeroplane)
type or class endorsement
minimum of 50 hours on type or equivalent type
minimum of 250 water landings.
The pilot had accrued about 1,350 hours of total flying experience, which included 483 water landings across several aircraft types, including the company‑operated Cessna Aircraft Company C208 Caravan (C208 Caravan), and de Havilland Canada DHC‑2 (Beaver). The pilot also flew the company land‑based GippsAero GA8 Airvan.
Table 1 shows the total number of water landings conducted by the pilot in WTY at Whitehaven Beach and Chance Bay, and Table 2 shows the number of water landings conducted by the pilot, in WTY in the last 90 days. In total on the C208 Caravan, the pilot had accrued about 230 hours and 165 water landings.
The pilot advised he had conducted one go-around during line operations. This was carried out about 18 months previously, in the Beaver at Whitehaven Beach. In addition, all of the pilot’s training flights into Chance Bay had been conducted in the Beaver.
Table 1: Pilot-conducted water landings in VH-WTY for Whitehaven Beach and Chance Bay
Whitehaven Beach
Chance Bay
Dual (ICUS)
34
0
Solo
117
14
Total
151
14
Table 2: Water landings by pilot in VH-WTY in last 90 days. Figures in brackets show water landings conducted in other aircraft types
November 2015
December 2015
January 2016
Total
Whitehaven Beach
18 (2)
29 (6)
20 (4)
67 (12)
Chance Bay
5
1
5
11
Reef / other
9 (1)
9 (8)
9 (8)
27 (17)
The pilot had conducted five water landings at Chance Bay during January 2016, all in WTY. This included two landings on 24 January 2016, and one at about 1205 on 28 January 2016, prior to the occurrence landing at about 1515.
The pilot's training records also show a ‘line check proficiency report’, conducted on 13 November 2015, which included water landings at Hardy Reef and Whitehaven Beach. The report identified that this line check was conducted with a ‘light load’. The comments section of the report included the following:
after splash-n-go at Hardy, slow to feed in full PWR once airborne, speeds ok, just need to get the power in faster with heavier loads in confined spaces.
The pilot passed the proficiency check and there was no record of any further training, or dual flights, being conducted.
In summary, at the time of the occurrence, the pilot was suitability qualified and authorised to operate the C208 Caravan in Chance Bay. Drug and post-incident alcohol testing did not identify any substance that could have impaired the pilot’s performance.
Sleep and work history
On the day of the occurrence the pilot woke up at about 0530, and arrived at work at 0645. He undertook three flights totalling 3.3 hours of flying. The occurrence took place at 1515, therefore meaning he had been at work for about 7.5 hours, and awake for about 8.5 hours. The pilot flew for approximately 5 hours the previous day and had two days off prior to that.
The pilot reported that he usually obtained about 8 hours of sleep per night and that he was healthy and not overly-tired at the time of the occurrence. There was no evidence that the pilot was experiencing a level of fatigue known to affect performance at the time of the accident.
Operator information
The operator had been the sole general aviation service provider for the privately owned Hamilton Island Resort since June 2010. They operated a fleet of 16 aircraft, which included light helicopters and fixed-wing aircraft. Hamilton Island was the main operating base for charter flights and tours to Hayman Island, Whitsunday Island and the Great Barrier Reef. The Civil Aviation Safety Authority (CASA) issued an air operator’s certificate (AOC) that permitted charter flights and specified aerial work applications.
Civil Aviation Regulation (CAR) 215 Operations manual required an operator to provide an operations manual for the use and guidance of operations personnel. The operator’s operations manual was prepared in accordance with CASA guidelines, was reportedly available to all personnel, and was last updated in 2011. In July 2017, the operator submitted to CASA, and had accepted, a revised operations manual which included a description of a safety management system (SMS) that was to be implemented. There is currently no requirement for a SMS for this type of operation. However, CASA encouraged all operators to develop and maintain an SMS.
Aircraft information
General
VH-WTY (WTY) was an unpressurised, single-engine, high wing, turboprop amphibian aircraft that could accommodate up to 14 people, operated by a minimum crew of one. WTY was manufactured in the United States in 2010 and was powered by one Pratt & Whitney Canada (PWC) PT6A‑114A turboprop engine. The aircraft had Wipaire Inc. (Wipaire) floats fitted on 1 June 2011. WTY was first registered in Australia on 18 July 2011. At the time of the accident, WTY had accumulated about 1,510 hours’ time in service.
A periodic inspection was completed on 27 November 2015 and WTY was issued with a maintenance release that was valid for 12 months or 100 hours. At the time of the accident the maintenance release was current and no defects or endorsements were recorded. The aircraft log book identified that no significant items of maintenance had been carried out since the last periodic inspection. The pilot reported that they had no concerns with aircraft serviceability at the time of the accident and review of the engine data log[4] identified no anomalies.
Engine operating limits
The engine operating limits were published in the Cessna Caravan model 208 G1000 pilot’s operating handbook (POH) and the Wipaire POH supplement[5] for amphibian floatplane operations. The engine was operation-limited by factors including torque, temperature or gas generator revolutions per minute (RPM), as well as propeller RPM, and was determined by whichever limit was reached first. With respect to torque, the maximum was advised to be 1,865 ft-lb. A torque of 1,970 ft-lb was permitted as long as the propeller RPM was set to ensure the maximum-rated 675 shaft horsepower was not exceeded. The Cessna POH torque indications description stated that ‘the redline varies from 1865 to 1970 ft-lb depending on prop RPM’.
Transient limitations for engine parameters including torque, gas generator RPM and propeller RPM are available for periods requiring increased engine performance. Table 3 shows the published transient torque available and its time limitation.
Table 3: Maximum transient torque available and associated time limitations
Manufacturer publication
Maximum torque (ft-lb)
Time limitation (seconds)
PWC Maintenance Manual
2,400
20
Cessna Caravan POH
2,400
20
Wipaire POH supplement
2,200
2
While increasing power during the initial stages of the go-around, the pilot recalled that the indicated torque was at the ‘second red line’, which he advised was about 1,970 ft-lb and an over-torque for the propeller condition. A review of the engine data log indicated a recorded maximum torque value of 1,882 ft-lb.
Several Caravan pilots were asked about their understanding of available transient power and all quoted 2,200 ft-lb or 2,400 ft-lb for the time limit of 2 seconds. The occurrence pilot advised that he was aware of the availability of transient torque but could not recall the specific figures. It was reported that while the availability of transient power may have been mentioned during training, it is generally not demonstrated due to increased risk of engine damage. The operator has since included a copy of the flight manual engine limitation section in the daily engine trend record folders in the aircraft, and also in a quick reference guide that included other performance and operational guidance from the flight crew operating manual. The purpose was to serve as memory prompts for pilots on documents frequently handled by them.
The ATSB advised Wipaire of the apparent discrepancy with their POH supplement engine limitations section regarding the transient torque and time available limit. A revised Wipaire POH supplement, with a transient torque of 2,400 ft-lb for 20 seconds, was issued on 22 December 2016, which was in line with the engine manufacturer’s limits. See the section titled Safety issues and actions.
Weight and balance
The occurrence flight was one of several standard tours offered by the operator. Therefore, a typical payload was available for each tour. The available payload considered aircraft basic weight and standard fuel burn for each leg, among other details. The operator advised that passengers reported their weight at the time of booking and this figure was recorded on the flight manifest. A computer program was utilised by the operator to determine the aircraft’s position in the weight and balance envelope for each flight. A review of the operator-supplied data indicated that WTY was within weight and balance limitations at the time of the collision with terrain.
Chance Bay
Chance Bay is located at the south-east point of Whitsunday Island (Figure 1) and is separated from Whitehaven Beach by a strip of land about 1,400 m wide. Whitsunday Craig is about 350 m elevation and is about 2.5 km to the west of the bay. The terrain falls away from Whitsunday Craig over a distance of 1-1.6 km and consists of undulating hills with rock formations near the water surface.
Chance Bay is characterised by surrounding terrain, being semi-circular in shape (Figure 3). The height of the terrain surrounding the bay is generally from about 35 to 80 m. The ridge line (marked in red) varies from about 60 m elevation in the west to about 50 m at the eastern end of the island. The lowest point (saddle) in this ridge line is about 30 m elevation and is located about 280 m inland from the main beach.
Figure 3: Chance Bay overview showing local features and elevations
Source: Google Earth, modified by the ATSB
For most of the year the Whitsunday area experiences south-easterly winds and Whitehaven Beach is the preferred tour destination for operators. It was reported that for about 20 per cent of the year, the winds shifted to be predominantly from the north, which produced conditions that are unsuitable for floatplane operations at Whitehaven Beach. During these periods, Chance Bay was the alternative landing area for local operators. Chance Bay was also identified as a preferred marine vessel anchorage in northerly winds.
Aeroplane landing areas
Civil Aviation Regulation 92 (CAR 92) defined the requirements for use of aerodromes, including those which are authorised and registered. Other places, if suitable, may be used for the purposes of the landing and taking-off of aircraft. In all cases, CAR 92 identified the responsibilities of both the pilot in command and the operator and required:
…and, having regard to all the circumstances of the proposed landing or take-off (including the prevailing weather conditions), the aircraft can land at, or take-off from, the place in safety.
CASA also published the Civil Aviation Advisory Publication (CAAP) 92-1 (1) Guidelines for aeroplane landing areas[6] to set out factors that may be used to determine the suitability of a place for the landing and taking-off of aeroplanes.
Chance Bay and Whitehaven Beach were identified as ‘regular aircraft landing areas’ that had been defined in accordance with Schedule 7 of the Great Barrier Reef Marine Park Authority (GBRMPA) – Plan of Management 2008. The operator maintained a company register of its authorised aeroplane landing areas (ALA) for floatplanes, which were approved for use by the chief pilot. Whitehaven Beach and Chance Bay were included in this register and were identified as meeting the ‘minimum standard for a landing area…as specified in CAAP 92-1(1)’. Each operator‑registered ALA consisted of an area map showing the ALA boundary and a written guide detailing operational and other information unique to that ALA.
The ALA was the preferred landing area for each location. However, the operator advised that it was possible to occasionally land outside the ALA. This allowed aircraft to land further from the beach, before the ALA, when location conditions and/or proximity of other vessels required it.
CAAP 92-1(1) provided guidance on various aspects of water alighting areas in terms of water channel width, depth and length. No specific dimensions were provided for the length of a water landing area, however the CAAP indicated that the length of the water channel was to be equal to or greater than that specified in the aeroplane’s flight manual. If the distances in the flight manual were un-factored, with allowance for degradation in aeroplane performance due to the prevailing conditions, then 15 per cent was to be applied to the distance. The CAAP included guidance for the calculation of approach and take-off area obstruction splays, however the supplied diagram only applied to floatplanes up to 2,000 kg maximum take-off weight. Both floatplane types operated by the company were above that weight.
The company operations manual specified that aircraft landing areas and water alighting areas were to comply with the CAAP. In addition, the company operations manual gave consideration to degradation in aircraft performance, in that any take-off distance was to be increased by a factor of 15 per cent and landing distance increased by 43 per cent. When these factors were applied to the C208 Caravan aircraft flight manual data, for operations on float landing gear, the take-off distance required was 1,256 m and the landing distance 926 m.
Operator’s aircraft landing area details
The operator’s ALA register included a map showing details for Chance Bay (refer to Appendix A), which was a marine chart showing bathymetric data for the water areas. Topographical information included 100 m contours and a spot height at the eastern end of Whitehaven Beach. The northern ALA boundary was about 950 m from the beach and the southern boundary, depending on the approach flown, was between 1,500 m and 2,300 m from the beach.
The operator’s published guide for Chance Bay ALA included, in part, the following points:
…
Operations will not take place without prior approval from chief pilot when winds exceed 20 kts[7]
Strong[8] northerly winds will produce severe turbulence and down drafts.
…
Chance Bay can be very difficult to work out of. Ensure you fly over the area before landing. Always observe the ALA limits. Ensure you always allow yourself an escape route…Note: Very important to set up an undershoot approach and plan escape route at this location.
A number of pilots who were interviewed by the ATSB all described the approach into Chance Bay as being a ‘dead end landing’ due to the terrain surrounding the cove. Therefore, the importance of setting up an undershoot approach[9] and to plan an escape route for the location was also reinforced. Further, any decision to go‑around was to be made early.
The operator advised their preferred departure or go-around route was a right turn over water, through the approximately 130 m clearance between the south-eastern most tip of Whitsunday Island and the northern tip of Moon Island (Figure 4). The terrain on either side of this route is less than 20 m above mean sea level. Flying straight ahead, over the saddle, was not the preferred departure path, but it was an option shown to company pilots. If a go-around was initiated early, the right turn departure was the safest option and allowed a water landing in the event of a precautionary or emergency situation. The pilot reported utilising either departure track, as dictated by the conditions at that time. Refer to Appendix B for the Chance Bay ALA containing hand written notes and annotations that were in addition to the company register.
Figure 4: Typical approach path at Chance Bay showing preferred and optional departure and/or go-around path. Also noted is the location of the ALA boundary and the pilot defined decision point.
Source: Google Earth, modified by the ATSB
The pilot had nominated a decision point (aiming point) for his operations into Chance Bay (refer Figure 4 and Appendix B). This point was devised in conjunction with the company senior floatplane pilot as a line between easily identifiable topographical features, being a point of land below Whitsunday Craig and the southern tip of Moon Island, about 1,500 m from the beach. The pilot described the decision point as, ‘if you’re not happy with what you see in front of you, if you’re not stabilised, you go‑around’.
From the decision point onward, the pilot could not use the preferred departure path to conduct a go‑around (‘preferred departure / go-around’ identified in Figure 4). However, the option to conduct a straight ahead go-around remained, or a turning departure over the terrain to the right of the bay, if initiated early enough to ensure terrain clearance.
A calculation of the climb performance of the C208 Caravan in the go-around configuration revealed that the aircraft was capable of climbing at 800 ft per minute when a straight ahead go‑around was conducted. That climb rate was dependent upon the aircraft being established in the correct configuration.[10] The point at which the aircraft could no longer theoretically out-climb the terrain was almost coincident with the shoreline. Therefore, in practical terms, to provide an adequate margin above terrain, an aircraft conducting a straight ahead go‑around would have to be established in the climb configuration before that point.
In summary, the ALA, as defined in the operations manual, was appropriate for conducting operations in the Caravan, when adhering to the ALA boundaries, nominated decision point and escape routes. Company guidance indicated that operations could be conducted outside of the ALA when operationally required, however the operator’s preference was to land further away from the beach and undertake a longer taxi into the bay, rather than landing between the ALA and the beach.
Guidance material from international regulators
When landing at an airport, the pilot can expect the runway surface will be flat and free of obstacles. In contrast, the United States Federal Aviation Administration (FAA) published a Seaplane, Skiplane, and Float/Ski equipped Helicopter Operations Handbook (2004),[11] which stated that water landings have no defined runway and are subject to wind and sea state affecting the landing surface. It is also common for floatplane pilots to share their landing areas with marine vessels and people.
The Civil Aviation Authority of New Zealand[12] published the Takeoff and Landing Performance booklet, which detailed factors that affect aircraft performance and included the following advice:
plan to clear obstacles on the climbout path by at least 50 ft
always nominate a decision point where you will discontinue the approach if things are not going as expected
even after having worked out your aircraft's take-off or landing performance, it is prudent to add a contingency to allow for other factors that you may have overlooked.
The United Kingdom Civil Aviation Authority (UKCAA)[13] published the Civil Aviation Publication (CAP) 793 Safe operating practices at unlicenced aerodromes. This CAP highlighted the importance of the pilot being ‘well aware of the performance characteristics of their aircraft and the aerodrome dimensions’ and that their ‘operating practices should be appropriate and proportionate to the activity’. In addition, the UKCAA published a Safety Sense Leaflet series which included guidance for strip flying and aeroplane performance. These leaflets included recommendations to:
use maps to determine accurate elevations
check the strip is long enough and add a 30 per cent margin for safety
remember that aeroplane performance figures are obtained using a new aeroplane, flown by an expert pilot under specific conditions
be clear about your go / no go decision process
consider surrounding terrain—if there are hills nearby, check that you will have a rate or angle of climb sufficient to out-climb terrain. Even a moderate wind may cause significant down draughts.
In combination, the guidance material recommended that a pilot should examine their intended landing area thoroughly before landing. This allows the pilot to choose the best landing area and plan a safe, conservative path for a go-around should the landing need to be aborted. The landing area should also include a predetermined ‘aiming point’ to assist with the decision to commit to land or initiate a go-around. In this case, the ALAs published in the company register defined the boundary only.
Recorded engine and video data
Data was recovered from the on-board digital data acquisition system, which received information directly from a Garmin G1000.[14] This system recorded a number of different engine operating parameters along with airspeed, altitude and temperature. The data was extracted and validated by the engine manufacturer.
The propeller speed and gas generator (engine) speed data was analysed in conjunction with video footage from several of the passengers. From this data it was possible to plot the flight path in relation to the landing area and bounce locations (Figure 2).
The data from the engine logger correlated with the video evidence and indicated that the established approach path aimed for an initial touchdown beyond the northern boundary of the ALA, leading to the pilot overflying the ALA before the aircraft touched down. Airspeed data showed that the aircraft was operating close to the stall speed when the go‑around commenced, and that the airspeed did not significantly increase, or reach the airspeed for the optimal go‑around climb configuration, before the aircraft impacted terrain.
Operational information
Go-around
Whenever landing conditions are not satisfactory, a go-around should be initiated.[15] The pilot can then bring the aircraft around for another landing or continue to an alternate site. A go-around is also known as a balked landing and can be initiated either before or after an aircraft has touched the water (in this case). A go‑around is considered a normal procedure and, although it is not often required, with appropriate training, planning and preparation it should not result in increased risk.
The company operations manual required that pilots adhere to the manufacturer’s POH, any associated supplements and the CASA-approved company checklists for normal and emergency procedures. The aircraft checklists included the abbreviated normal procedures published in booklet form and a control wheel flip card, and were required to be carried on every flight. In addition, the operations manual required pilots to demonstrate proficiency in recall of the checklists at no less than 12-month intervals.
The operations manual procedures for take-off stated ‘all water take-offs shall be with 20˚ flap set’. The manual recommended initial climb speeds were 80 kt for flaps 20°, 85 kt for flaps 10° and 95 kt for flaps retracted. The procedures for a balked landing were contained within the normal procedures and operations sections of the manual. It outlined that the aircraft needed to achieve an indicated airspeed of 81 kt in the climb out.
Consistent with the Wipaire POH supplement, the operator’s procedure for a baulked landing commenced with flaps 30 (as configured for landing) and throttle advanced to take-off power. The following step in the checklist was to retract the flaps to 20 degrees to achieve the maximum rate of climb.
Meteorological information
Hamilton Island area
Hamilton Island is part of the Whitsunday Islands archipelago and is located approximately 900 km north of Brisbane. The weather is classified as subtropical with year-round warm temperatures averaging 23˚C in winter and 30˚C in summer. The wet season occurs typically December to February with humid days, averaging around 75 per cent, which are often broken by tropical showers.
Weather conditions and wind velocity
The Bureau of Meteorology (BoM) forecast for the area indicated the presence of variable north-westerly winds, up to 5,000 ft, of about 10 kt. Information from the radiosonde trace from Townsville and the marine forecast indicated that the surface winds were about 10 kt from the north-north-east. BoM observations at Hamilton Island between 1500 and 1530 indicated a wind of about 14 kt from the north-west.
The BoM advised there are local effects at Hamilton Island Airport which can affect velocity in the synoptic situation that was present on the day. The BoM advised that the wind direction at Chance Bay at the time of the occurrence was likely to have been about 10 kt from the north‑west. In addition, BoM indicated that it was unlikely that turbulence due to the nearby terrain would have been present at Chance Bay due to the wind strength in the lowest part of the atmosphere. However, light turbulence could not be excluded.
Witnesses positioned on marine vessels in Chance Bay reported north-west variable winds of about 10 kt, gusting to 15 kt. They described the sea surface as ‘smooth’.
The pilot reported observing, during the pre-landing flyover, evidence of ‘bullets’ coming from the north-west on the surface of the water within Chance Bay. Bullets were described by several pilots as a phenomena associated with wind gusts contacting the water surface and creating visually darker patches. Riley (2009) indicated that these phenomena result from a combination of terrain and atmospheric conditions, including:
winds, of 15 kt or greater, predominantly blowing from the south-east over water then encountering the terrain of the Whitsunday Islands and being forced aloft
an inversion between about 500 to 2,000 m in a stable atmosphere.
The combination of the inversion and stability of the atmosphere compresses the airflow and increases its velocity. The stability of the atmosphere forces the air to descend on the leeward side of the terrain. When the increased velocity air encounters the sea surface it forms the bullets, which poses problems to mariners and to aircraft operating on the water.
The BoM report indicated that, while there was an inversion layer present at approximately 1,500 m, the 10 kt wind velocity was below that expected for the formation of bullets. Additionally, according to the Beaufort wind scale, for whitecaps to appear the wind must be 11-16 kt. FAA H‑8083-23 Seaplane Operations Handbook indicated that ‘when the wind increases to a velocity of 12 knots, waves will no longer maintain smooth curves. The waves will break at their crest and create foam – whitecaps’.
Several pilots with experience operating in Chance Bay advised that the area can be affected by turbulence and/or down drafts.[16] This turbulence most likely resulted from Whitsunday Craig being in the path of west to north‑westerly winds and the airflow ‘wrapping around’ the southern coast of the island. In addition, it was reported the turbulent air became more pronounced as you proceeded further into the bay. The pilots advised that these conditions reduced the approach and departure options and necessitated the adjustment of procedures to suit different aircraft performance.
In summary, while accurate weather observations for Chance Bay were not available, witness videos showed some areas of possible wind gusts, with the appearance of darker patches of water on the surface. In these patches, no lifting of water and almost no whitecaps are seen, indicating wind at or below 12 kt. Wind direction on the day was consistent with possible turbulence, the severity being dependent on the wind velocity. The pilot reported the conditions on this flight were similar to those of earlier in the day, with perhaps a slight increase in wind velocity. The pilot also advised that he had previously conducted operations in Chance Bay in windier conditions.
Wind gusts and aircraft handling
Several floatplane pilots (including a flight instructor) advised of the importance of flying through a wind gust and landing the aircraft on the water when in smoother air. It was also reported that a pilot should avoid rushing to land before a wind gust.
The accident pilot described his understanding of the standard procedure when encountering a gust, which included:
reducing power by a small amount to counter the increased lift associated with entering the wind gust, then
increasing the power to control aircraft descent resulting from the reduced lift when exiting the wind gust.
This procedure is the correct technique for flying the DHC-2 Beaver aircraft. However, a flight instructor indicated that the use of power to counter the effects of winds gusts on landing in the C208 Caravan was not appropriate due to the increased mass of the aircraft, and had advised the pilot of this during initial C208 Caravan training, when this incorrect technique had been observed. It was reported that best practice for flying through a gust in a Caravan is through manipulation of the flight controls rather than increasing or decreasing power, which has a slower response time.
The pilot indicated that he elected to delay the landing, in order to fly through the wind gust, and used the alternating power technique previously mentioned. After exiting the first gust, the pilot observed a second wind gust, and delayed the landing further, using the same alternating power technique.
The recorded engine data was inconsistent with the pilot’s report of altering engine power as he flew through wind gusts. It was not possible to determine the level of influence of the reported wind gusts had on the aircraft bounces, or if general aircraft handling technique contributed in this instance.
Site and wreckage
The ATSB did not attend the accident site but did interview the pilot, the operator, several witnesses, passengers and accident site visitors. In addition, the ATSB reviewed supplied images and video footage. Video footage from the flight and information from the pilot did not indicate any issues with aircraft operation prior to the collision with terrain. However, video footage and engine data were consistent with the engine not having been fully shut down before the pilot exited the aircraft.
WTY collided with trees and then the terrain, part-way up the ridge about 150 m from the eastern end of Chance Bay main beach. WTY was located at an elevation of about 40 m and the height of the ridge was about 50 m. The aircraft came to rest upright and in dense foliage (Figure 5). WTY was described as being oriented facing back toward the bay, which was consistent with the aircraft being in a right turn and the flight path being disrupted during the collision with terrain. The pilot reported there was no evidence of fuel leak and there was no pre- or post‑impact fire.
The float landing gear (pontoons) had splayed outwards and upwards until they were aligned with the fuselage, which, together with the nature of the foliage, may have provided some cushioning effect to the fuselage during the impact with terrain. Both wings remained attached to the fuselage, but the impact sequence had forced the wings rearwards. As a result, the flaps and the trailing edge of both wing root ends had entered the cabin, however there were no reports of passenger injuries associated with this. The position of the flaps was consistent with being fully-extended (30˚), which corresponded with an image of the flight control pedestal showing the flap selector lever near to ‘full’.
It was reported that the pilot’s door (forward left) was utilised for evacuation, as exit via the rear cabin left passenger door was hindered by foliage. One passenger also reported a drop of a few feet, from the pontoon to the ground, due to the aircraft position on top of foliage. Egress to the ground was via the pontoon and then all persons on board assembled a short distance from the aircraft before the group walked to Chance Bay main beach.
Figure 5: VH-WTY wreckage, located in dense foliage
Source: Gordon Simmons
Survivability
Civil Aviation Order (CAO) 20.11 defined the requirements for emergency and life-saving equipment and passenger control in emergencies. The below paragraphs review the CAO requirements relevant to this operation and the overall emergency response.
Forced landing preparation
Pre-impact actions have the potential to reduce the severity of a collision with terrain. The operator’s published pre-impact actions included, but were not limited to:
activating the emergency locator transmitter (ELT)[17]
briefing passengers, including their requirement to adopt the brace position
configuring the aircraft and engine, including turning off fuel selector and battery master switch, among other actions
transmitting a mayday call giving position and intentions.
The pilot reported that the requirement for a forced landing was not considered during the go‑around attempt.
Briefing
The operator advised that passengers were shown a generic briefing video on the bus, while being transferred to the airport. If passengers made their own way to the airport, then a briefing video was shown to them upon their arrival.
The pilot provided a safety briefing to the passengers at the aircraft, just prior to departure from Hamilton Island. This briefing was specific to the aircraft type.
Seatbelts
The aircraft was fitted with lap-sash seatbelts in the passenger seats and five-point harnesses in the pilot and co-pilot seats. The pilot explained the seat belt operation to the passengers, and the requirement to keep them fastened for the duration of the flight, prior to boarding the aircraft. Additionally, the pilot reported visually checking the passengers’ seat belts prior to departure from Hamilton Island. Video footage of several passengers, from just prior to take-off, showed their seatbelts were fastened. In addition, audio from the footage included the pilot advising them to keep seatbelts fastened.
While flying over Chance Bay and setting up for landing, the pilot reminded the passengers to make sure their seatbelts were fastened for landing. Some of the passengers interviewed also recalled the pilot advising them to check their seatbelts prior to the landing at Chance Bay.
The United States’ National Transportation Safety Board (NTSB) published safety report SR 85-01 General aviation crashworthiness project: Phase 2 - Impact Severity and Potential Injury Prevention in General Aviation Accidents. In terms of the potential benefits of shoulder harnesses (specifically, some form of upper body restraint), the safety report commented on the extent of any injuries in case of an accident, as follows:
There were five survivable accidents in which shoulder harnesses were worn by only one of two front‑seat occupants. A comparison was made of the relative injuries of each occupant. It was found in each case that injury severity was less for the occupant who wore the shoulder harness.
For example, in one accident each of two occupants sustained serious injuries, but the pilot, wearing a shoulder harness, sustained a broken leg and a slight concussion while the passenger without a shoulder harness sustained severe head injuries. The differences in the injuries in these comparisons were related to head and upper body injuries. Those persons who wore shoulder harnesses had markedly fewer head injuries.
The NTSB research also showed that if an aircraft occupant wore a shoulder harness, they increased their chances of survival by 20 per cent. Further, the chance of serious injury was decreased by 32 per cent. The FAA published Advisory Circular (AC) 21-34 Shoulder Harness – Safety Belt Installations in 1993. This AC described the various forms of shoulder harnesses and detailed the safety benefits of correct installation and use. Pilot and passenger survivability on WTY was likely enhanced through correct utilisation of the available seat belts.
Pilot emergency training
The pilot had completed the flight crew emergency procedures training within the previous 12 months, as was required by CAO 20.11. This CAO did not require training and demonstration of aircraft-related procedures such as emergencies and shut down process.
Life jackets
Each passenger was provided with a pouch-style life jacket prior to the flight departing Hamilton Island, as required by the regulations. The pilot provided a safety brief and demonstration on how to wear and use the passenger life jackets. The pilot wore his own vest‑style life jacket, which also contained the pilot’s PLB in a pouch.
Safety equipment
The aircraft was fitted with a fixed ELT, which self-activated during the collision with terrain. In addition, the operator required that each pilot equip themselves with a personal locator beacon (PLB) that was suitable for overwater operations. The pilot reported activating his PLB once everyone had evacuated the aircraft.
There was also a satellite phone on board the aircraft due to the occasional requirement for extended offshore operations. The pilot used this phone to contact the operator and advise of the accident.
Emergency response
The Australian Maritime Safety Authority (AMSA), reported that the aircraft’s ELT beacon was detected at about 1519 and a search and rescue phase was initiated by Australia’s Joint Rescue Coordination Centre (JRCC). In addition, the ELT beacon was detected by several aircraft flying in the area and they advised air traffic control, who subsequently passed the information on to the JRCC at about 1528. The JRCC monitored and coordinated the search and rescue phase. The pilot’s PLB was not detected by the AMSA.
As the ELT was registered, the JRCC’s first attempt to contact the operator was at 1526. It was reported that the operator was initially unsure of the JRCC’s report of ELT activation as the flight following of WTY had been cancelled. At about 1528, the operator advised the JRCC they had dispatched one of their helicopters to Chance Bay. At 1543, the operator advised the JRCC that the pilot had contacted them via the satellite phone.
Several vessels were moored in Chance Bay and those on board who witnessed the accident contacted the local volunteer marine rescue (VMR) via marine radio. The VMR Mackay log indicated they received the first notification at about 1515 and subsequently advised VMR Whitsunday. VMR Mackay monitored the situation until advised that all persons on board the aircraft had arrived at Hamilton Island at about 1616.
Related occurrences
A review of the ATSB occurrence database from 1969 to February 2016 identified only one other aviation occurrence in Chance Bay. This, and other similar occurrences are detailed below.
The pilot of a de Havilland Beaver floatplane registered VH-BVA was conducting a charter positioning flight from Hamilton Island Marina to Chance Bay, Whitsunday Island. He had landed at Chance Bay seven times in the previous two days. Weather conditions recorded at the Hamilton Island automatic weather station indicated a 7 - 10 knot wind from the north‑west. Witnesses in Chance Bay said that the surface wind in the bay was 2 - 5 knots and the water surface was smooth, but not glass. The pilot said that he commenced a straight-in approach to Chance Bay but elected to go‑around due to the increased number of vessels moored in the bay since the previous flight. During the subsequent landing the left wing of the aircraft collided with the rear mast of an anchored ketch resulting in substantial damage to both. There were no injuries to the pilot or the three occupants of the ketch.
The investigation found that the technique employed by the pilot to achieve the intended touchdown was not appropriate for floatplane operations. In response, the operator revised the floatplane operations section of their operations manual. In addition, an experienced floatplane pilot provided a report to the operator regarding company floatplane operations. Recommendations from that report included:
additional theoretical and practical training and checking for company floatplane pilots
development of a company-specific pilot training guide; and
review and amendment as required of the company floatplane authorised landing area guide
On Sunday, 26 July 1998, at about 1324 local time, a Cessna A185E floatplane, VH-HTS, crashed onto a ridge forming the southern shore of Calabash Bay NSW. The accident occurred during a go-around manoeuvre following an unsuccessful landing approach to the Berowra water alighting area. All on board suffered fatal injuries and the aircraft was destroyed.
The investigation found that the circumstances of the accident were consistent with uncontrolled flight into terrain. The decision by the pilot to carry out a go-around into a confined area surrounded by steep-sided terrain was the culminating factor in a combination of local factors, organisational deficiencies and inadequate safety defences. Local factors included a lack of formal procedures to provide safe methods of operation, and commercial pressures. Organisational deficiencies were also identified, concerning the management and conduct of charter operations carried out by that company.
The sources of information during the investigation included:
interviews with the pilot, passengers, operator, other pilots and a flight instructor
engine data
aircraft, engine and float manufacturers
the Bureau of Meteorology
the Australian Maritime Safety Authority.
References
Clarke, S, 1996, The effect of habit as a behavioural response in risk reduction programmes, Safety Science, vol. 22, no.1-3, pp.163-175
Klein, G 1999, Sources of Power How People Make Decisions. MIT Press.
Orasanu and Martin, L, 1998, Errors in Aviation Decision Making: A Factor in Accidents and Incidents, Human Error, Safety and Systems Development Workshop 1998
Reason, J, 1997, Managing the Risks of Organizational Accidents, Ashgate Publishing Limited, Aldershot, England
Riley, Malcolm 2009 Afloat Magazine Bullets
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
Draft reports were provided to the pilot, the operator, the pilot’s flight instructor, the Civil Aviation Safety Authority, Transportation Safety Board of Canada, National Transportation Safety Board (United States), the aircraft, engine and float manufacturers, Australian Maritime Safety Authority and Airservices Australia.
Submissions were received from the pilot, the operator, the engine manufacturer and the Civil Aviation Safety Authority. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
The occurrence
On 28 January 2016 the pilot of a Cessna Aircraft Company Caravan 208 amphibian aircraft, registered VH-WTY (WTY) was conducting a series of charter flights in the Whitsunday region of Queensland.
The pilot was conducting his third flight of the day when the aircraft departed Hamilton Island Airport at about 1415 Eastern Standard Time[1] with 10 passengers on board. The tour included a scenic flight over the Great Barrier Reef for about 50 minutes before heading to Chance Bay, on the south-east tip of Whitsunday Island, about 11 km north east of Hamilton Island Airport (Figure 1). Following a water landing at Chance Bay, the group was to spend 90 minutes at the beach before a short flight back to Hamilton Island. The tour was originally planned to include a landing at Whitehaven Beach, however wind conditions at the time required the water landing be altered to Chance Bay.
Figure 1: Google Earth overview showing Whitsunday Island location
Source: Google Earth, modified by the ATSB
Radar surveillance data showed WTY approach Whitsunday Island from the north and conduct an orbit about 2 km north of Whitehaven Beach at about 1510, before heading toward Whitehaven Beach. WTY flew over the southern end of Whitehaven Beach and the strip of land that separates it from Chance Bay. At about 1515, after crossing Chance Bay beach in a southerly direction, WTY descended below radar surveillance for the remainder of the flight.
The pilot advised that he flew WTY over the western end of Chance Bay’s main beach in order to conduct a visual pre-landing check of the bay. The pilot noted the positions of various vessels moored in the bay to determine the best taxi path to the beach. During this fly-over, the pilot also noted the sea state and observed evidence of wind gusts on the water surface. The pilot then initiated a right downwind turn toward the landing area. The approach was from the south with the intent to land in the most suitable location within the designated landing area and then taxi to the beach.
The pilot reported setting up for landing at about 50 ft above the water and then delayed the landing in order to fly through an observed wind gust. Passenger video footage indicated that, during the subsequent landing, WTY bounced three times on the surface of the water (Figure 2). After the second bounce, with WTY getting closer to the beach and terrain, the pilot increased engine power and initiated a go‑around. The third bounce, which occurred almost immediately after the second, was the most pronounced and resulted in the aircraft rebounding about 30 to 50 ft above the water. While increasing power, the pilot perceived that the torque was indicating red, suggesting an over-torque for the selected propeller configuration. Noticing that the climb performance was less than expected with the flaps at 30˚, the pilot stopped increasing power and reduced the flap to 20˚.
As the aircraft climbed straight ahead towards a saddle, climb performance was still below the pilot’s expectations and he assessed that WTY would not clear the terrain. In response, the pilot turned right to avoid the surrounding rising terrain.[2] WTY clipped trees during this turn, before colliding with terrain and coming to rest in dense scrub about 150 m from the eastern end of the main beach, near the top of the ridge. The pilot promptly advised the passengers to exit and move away from the aircraft. Some of the 11 people on board suffered minor injuries but all were able to quickly leave the aircraft. There was no post-impact fire.
Figure 2: Aircraft track toward Chance Bay main beach, showing approximate bounce locations and VH-WTY final position
Source – Basemap – State of Queensland, modified by ATSB
The aircraft’s fixed emergency beacon self-activated during the collision with terrain and was detected by the Australian Maritime Safety Authority (AMSA), resulting in a search and rescue response being initiated by the Joint Rescue Coordination Centre (JRCC) Australia. The pilot reported also activating his personal locator beacon, however this was not detected by AMSA. In addition, the pilot used the company satellite phone to advise the operator of the occurrence and current status of all on board. At about the same time, several witnesses who were located in Chance Bay made their way to the aircraft before assisting everyone down to the beach. A tourist boat was utilised to transfer the pilot and passengers to Hamilton Island, arriving at about 1600. From there, one passenger was transferred by helicopter to Mackay for further treatment.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety actions in response to this occurrence.
Engine operating limits
Wipaire Inc. published an amendment to the pilot operating handbook supplement for the Cessna 208 amphibian on 22 December 2016. The engine operating limits now identify that a transient torque of 2,400 ft-lb is available for 20 seconds, which is consistent with the engine manufacturer’s recommendations.
Aircraft operator
The operator advised they have enhanced/updated existing procedures and checklists for their float plane operations. Among other things, this included provision of engine limitation figures, including transient power, on documents used by pilots, as well as revision of the Chance Bay ALA guidance, incorporating detailed orographic information in addition to that included on the Whitsunday visual terminal chart.
Pilot details
Pilot details
Licence details:
Commercial Pilot Licence (Aeroplane), issued June 2012
Endorsements:
Single Engine Aeroplane; Tail wheel undercarriage; Manual Propeller Pitch Control; Retractable Undercarriage; Floatplane; Gas turbine engine
Ratings:
Nil
Medical certificate:
Class 1, valid to March 2016
Aeronautical experience:
Approximately 1,350 hours
Last flight review:
May 2015
Findings
From the evidence available, the following findings are made with respect to the collision with terrain involving amphibian Cessna Aircraft Company C208 Caravan aircraft, registered VH-WTY that occurred at Chance Bay, 11 km north-east of Hamilton Island airport, Queensland, on 28 January 2016. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
The aircraft's initial touches with water were past the nominated decision point and beyond the northern boundary of the ALA, which reduced the safety margins available for a successful water landing or go-around.
The pilot initiated a go-around without using all available power and the optimal speed, turned towards higher terrain and placed the aircraft in a down‑wind situation, which ultimately resulted in the collision with terrain.
Other findings
The aircraft was equipped with lap-sash seatbelts, which have been demonstrated to reduce injury, and the use of emergency beacons and satellite phone facilitated a timely response to the accident.
Safety analysis
The pilot of VH-WTY was conducting a tourist flight in the Whitsunday area with 10 passengers on board, that included landing in Chance Bay. During a go‑around that followed an aborted approach to the water landing site, the aircraft collided with terrain.
The pilot was appropriately qualified to conduct the flight and there was no evidence that an aircraft‑related issue contributed to the occurrence. This analysis will examine the operational aspects associated with the attempted landing and decision to go‑around, which preceded the collision with terrain.
Development of the accident
Terrain surrounding the Chance Bay water landing area poses two significant operational landing hazards:
significant mechanical turbulence/downdrafts in adverse wind conditions
go‑around options reduce to zero the further an aircraft approaches in to the bay.
Both of these hazards were identified in the operator’s aircraft landing area (ALA) guidance, with specific emphasis on the need to operate within the ALA limits and maintain an escape route.
On this occasion, the pilot delayed touching down on the water until he assessed that he was past a wind gust. While that decision was motivated by a desire to avoid unsuitable landing conditions, it resulted in the aircraft first touching down beyond the ALA and significantly closer to the terrain surrounding Chance Bay than recommended. That situation was further aggravated by two further bounced water contacts as the approach was continued towards the beach, before the go‑around was initiated.
Continuation beyond the nominated decision point removed the preferred option to abort the landing and turn right to depart Chance Bay over water. However, despite progressing further into the bay, the option to conduct a missed approach straight-ahead over the saddle remained.
A straight-ahead departure from the go‑around point was within the documented performance capabilities of the Caravan in the optimal configuration, however the pilot assessed that the aircraft was not climbing as expected and would not clear the terrain. This resulted in the decision to turn away from the saddle, exposing the aircraft to higher terrain to the east of the beach. The turn also positioned the aircraft downwind, which also adversely affected the climb profile. These factors combined to result in the accident.
The pilot had recent familiarity with Chance Bay, having flown there 11 times in the past 90 days in WTY, including on the morning of the accident. The pilot had also been shown and had used, the straight-ahead departure over the saddle toward Whitehaven Beach. However, the pilot had not conducted a go‑around in any aircraft at Chance Bay during line operations, nor conducted a go‑around in the Caravan with a loaded aircraft weight.
This may have influenced his knowledge and judgement around the expected performance of the aircraft, including not using the available transient power or the correct go‑around airspeed, and the distance required to safely conduct a go‑around. Despite this, flying well beyond the decision point and persisting with conditions that were not conducive for a safe landing meant that the decision to conduct a go‑around was made late in the approach. The late decision reduced the options and margins available for a safe outcome and ultimately led to the ground collision.
Approach and landing is the most common phase of flight for aviation accidents, accounting for approximately 65 per cent of all accidents. A Flight Safety Foundation study[18] of 16 years of runway excursions determined that 83 per cent could have been avoided with a decision to go‑around. The study identified that just over half of the landing excursions followed a fully stable approach; in these instances the flight became unstable only during landing.
Whenever landing conditions are not satisfactory, a go‑around should be initiated. A go‑around is considered a normal procedure, however, they can present challenges, especially when initiated late in the approach or during landing. Good flight preparation includes completing a mental rehearsal before departure and prior to the approach to land. By having plans and procedures in place, the pilot will reduce their workload during critical stages of flight and also in the event of any emergencies. Recurrent training into ‘challenging’ environments is helpful in maintaining consistent operational procedures and identifying any non‑standard practices.
Safety equipment and procedures
The pilot reported that the preparation for a forced landing was not considered during the go‑around attempt. As such, no pre‑impact preparation was conducted or briefed to the passengers. The pilot did however, maintain control of the aircraft during a rapidly changing sequence of events. Continued pilot control, the crashworthiness of the aircraft, combined with all persons on board wearing shoulder-restraint seatbelts, likely resulted in minimal injuries being sustained, even without impact preparedness. The characteristics of the foliage contacted may also have cushioned the impact.
The pilot did not completely shut down and secure the aircraft before evacuating, which increased the risk of a post-impact fire. However, the passengers were consistent in their recollection of the pilot’s prompt and effective handling of the aircraft evacuation and relocation of everyone to a safe distance from the aircraft.
Cancelling flight following prior to landing increased the risk of delay to an emergency response. However, the self-activation and detection of the emergency locator transmitter resulted in prompt initiation of a search and rescue coordination. Use of the satellite phone also provided the means for communication with the operator’s main base.
The occurrence highlighted the importance of emergency training, available equipment and defined safety‑related procedures combining to increase safety to all on board the aircraft.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Occurrence summary
Investigation number
AO-2016-007
Occurrence date
28/01/2016
Location
11 km north east Hamilton Island Airport (Chance Bay)
On the morning of 28 December 2015, a DH82A Tiger Moth, registered VH-UZB, departed Pimpama Airfield, Queensland for an adventure flight. The pilot had assessed the weather as suitable, with a headwind of 10‑15 kt straight down the intended take-off airstrip.
Shortly after take-off, the pilot manoeuvred at low level, to remain over the clearest terrain for the climb out. At an altitude of between 200 and 300 ft, the engine power unexpectedly reduced. In response, the pilot made a left turn during which the aircraft entered an incipient spin. The pilot reported attempting to recover from the spin, however, the aircraft collided with terrain. The passenger was fatally injured, and the pilot sustained serious injuries. The aircraft was substantially damaged.
What the ATSB found
The ATSB examined the aircraft’s engine, its components and fuel system, but was unable to determine the reason for the partial power loss. The investigation also found that when the aircraft entered the spin, there was insufficient height to recover before ground contact.
Safety message
The partial power loss of an aircraft’s engine presents a more complex scenario than a complete power loss, where a forced landing is inevitable. The scenario is further complicated when the partial loss occurs shortly after take-off. Further, in a partial power loss situation, the power may continue to deteriorate and/or stay at the same reduced level and/or return to normal.
Prior to take-off, pilots should consider options and actions in the event of a partial power loss. Factors to consider should include their piloting skills, experience, conditions on the day and the aircraft type-specific characteristics to decide a height below which a forced landing straight ahead is required, should a partial or complete power loss occur. Self-briefing on this subject before take‑off reduces the decision-making load if a power loss does occur.
When an emergency landing is required, flying the aircraft in a controlled manner, wings level and at the recommended glide speed has a better survivability outcome than when control of the aircraft is lost.
DH82A Tiger Moth, registered VH-UZB
Source: Supplied
Context
Pilot information
The pilot held a commercial pilot (aeroplane) licence and was endorsed to operate the Tiger Moth aircraft. The pilot’s logbook showed a total flying experience of 1,111.4 hours to the last recorded flight on 21 December 2015, of which 23.8 were on tail-wheel aircraft, including 7.6 hours on the Tiger Moth. All the pilot’s Tiger Moth experience was in UZB. The pilot had last completed a single‑engine aeroplane flight review on 22 December 2014, which was valid until 31 December 2016. The pilot held a tail-wheel design feature endorsement and an aerobatic flight activity endorsement.
Medical information
The pilot held a valid Class 1 Aviation Medical Certificate without restrictions. His last medical examination was conducted on 30 January 2015 and was valid until 30 January 2016. The pilot stated that he was well rested and in good health on the morning of the occurrence.
Tiger Moth training
The pilot held a current single-engine aircraft rating and a tail-wheel undercarriage endorsement, so no additional training was required by the Civil Aviation Safety Authority (CASA) to operate the Tiger Moth.
The operator’s operations manual indicated that initial training to conduct adventure flights consisted of 5 hours on type, conducted over four flights. The training could however, be tailored depending on previous experience. Flight reviews, medical and licence currency requirements were to be maintained in accordance with those applicable to charter operations. In addition, pilots were also required to have flown the aircraft type within 60 days prior to conducting an adventure flight.
The operator’s insurance certificate (valid between 14 January 2015 and 14 February 2016) attached to the operations manual, indicated that, for adventure flights, pilots were to be approved by the company director subject to having a commercial pilot licence and 25 hours tail-wheel experience (as applicable for tail-wheel aircraft).
The pilot commenced employment with the operator about 4 weeks prior to the accident. Before conducting adventure flights, the pilot received 3.7 hours of training, from the aircraft owner and operator, in the accident aircraft, at Pimpama. The training included:
general handling
slipping and skidding turns
aerial work
stalls and spins
emergency procedures, including:
full and partial engine failures
glide approaches
engine failures on take-off.
Organisational and management information
The operator company, PDRL, was established in 2008 and specialised in warbird adventure flights. They operated under a number of trading names, including Gold Coast Aerobatic Adventures. Their primary base of operation was in the Hunter Valley, New South Wales with the operation at Pimpama established in 2015. The accident pilot was the sole pilot operating at Pimpama and had been operating from that location since November 2015. The aircraft operated by PDRL were operated in the Limited Category[8] under the administration of the Australian Warbird Association Limited (AWAL).
The PDRL operations manual detailed how its warbird operations in limited category aircraft were to be conducted to ensure compliance with the regulations and AWAL policies. This included operations involving VH-UZB and noted the accident pilot as one of the operator’s pilots. The manual specifically stated that the over-arching philosophy was that aircraft should be operated as if they were in the charter category, though recognising the specific requirement for limited category aircraft.
After the accident, AWAL conducted an audit of the operator in March 2016, at its New South Wales facilities. The audit included a review of the operator’s facilities and operations as well as an aircraft inspection. The audit identified a number of required administrative corrective actions, but overall the results of the audit were deemed ‘acceptable’.
CASA requirements
Civil Aviation Regulation (CAR) 1988 subregulation 166A(2)(f) requires that a pilot conducting a take‑off from an uncontrolled aerodrome maintain the same track as the take-off until the aircraft is 500 ft above the terrain, unless as per subregulation 166A(4) it is necessary to avoid terrain.
Aircraft information
General
The DH82A Tiger Moth is a two-seat, single-engine biplane with a tailskid and fixed undercarriage. The accident aircraft VH-UZB (Figure 1), serial number 291, was manufactured in the United Kingdom in 1941 and had accumulated 7,986.4 hours total time in service at the time of the accident. The aircraft was powered by a Gipsy Major series 1 four-cylinder piston-engine, engine serial number 150.
Figure 2: DH82A Tiger Moth, registered VH-UZB
Source: Supplied
The Special Certificate of Airworthiness issued to VH-UZB in the Limited Category on 20 May 2015 required that the aircraft be operated in accordance with the Royal Australian Air Force (RAAF) Publication No. 416, Pilot’s Notes for Tiger Moth Aircraft. A copy of the publication was found in the aircraft at the accident site. These notes did not provide details of any crosswind take-off limitations. The aircraft was fitted with several placards that listed the relevant operating limitations. A summary of those limits are listed at Table 1.
Table 1: Relevant operating limits and speeds for VH-UZB
Condition
Limit (RPM)
Speed (kt)
Normal full throttle
2,100
Take-off
2,100
Climbing
2,100
56
Cruise 1,900-2,050 RPM
2,100
74
Stall
39
A review of industry‑accepted pilot handling notes for the aircraft found a maximum crosswind component listed as 10 mph (8 kt) in Tiger Moth Type Conversion Syllabus.[9]
Tiger Moth aerodynamic characteristics
First flown in 1931, the Tiger Moth has high overall drag[10] in comparison to more modern aircraft. The aircraft operates at relatively slow speeds and its light weight results in low inertia. Therefore, in order to maintain airspeed after a reduction in engine power, the attitude of the aircraft needs to be adjusted more quickly and by a greater amount than more modern aircraft.
The Civil Aviation Authority (CAA) of NZ accident report 03/2955 (ZK-DHA) noted that a rate one[11] level turn commenced at about 56 kt will reduce the airspeed to 52 kt. Steeper turns require full power to initiate and maintain the turn at a safe margin above the stall speed (which increases with the angle of bank in a level turn). An engine failure will require an immediate lowering of the nose to avoid stalling and loss of control.
Another CAA of NZ accident report ‑ 06/4477 (ZK-BAR) stated that, from a test flight and research into Tiger Moth spin characteristics, it was determined that in a spin the aircraft airspeed is usually low and the descent rate was high. In a spin, the Tiger Moth typically rotated once every 2‑3 seconds and descended at 4,000 feet per minute - one full turn equated to a height loss of about 200 ft. That investigation report also noted that recovery from a spin, if done quickly, correctly and precisely, would require about half a turn to stop. The aircraft would recover in a dive with airspeed increasing rapidly, resulting in further height loss. Therefore, any spin entered during climb-out after take-off or from circuit height (1,000 ft AGL) makes a recovery highly unlikely before collision with terrain. An analysis of accident records showed that a considerable number of stall/spin accidents commenced from relatively low altitude.
A RAAF test pilot in a discussion[12] of the Tiger Moth’s spin characteristics noted that during incipient spin recovery, the rapid yaw and roll ceased within half a turn of application of the recovery technique. The test pilot found that the height loss from the commencement of recovery from the incipient stage to wings level, climbing flight at 58 kt was about 250 ft. Flight testing also identified that rotation associated with a fully developed spin ceased within one turn, once recovery was initiated and that 300 ft was lost during recovery to the same parameters. These height losses were based on the time from initiation of recovery and did not take into account the height lost during the time taken to recognise and react to the situation.
Maintenance history
In 2009, at 7,884 hours total time in service, the accident aircraft was refurbished and an overhauled engine was installed. The last recorded maintenance was an oil change and tappet inspection. Prior to that a periodic inspection and maintenance release issue was performed on 13 April 2015 at 7,936.8 hours total time in service.
Fuel
The aircraft was operated using Mogas.[13] It was reported that unleaded 91 and 95 was used and mixed with a cylinder head lubricant. The RAAF Publication No. 416 pilot notes contained within UZB’s flight folder recommended a 73 octane fuel. Within industry it was accepted that the Gipsy Major engine runs better on lower octane fuel more suited to automotive specifications rather than the higher octane aviation fuel. Therefore, utilising automotive fuel was not unusual. The ATSB did not find any documentation that the use of a fuel additive, while common industry practice, was approved. However, there was no evidence that the use of Mogas or the fuel additive was linked to the partial power loss.
The total fuel on board prior to the flight was reported to be about 60 L, sufficient for the planned flight. This equated to about three-quarters of the fuel tank’s capacity. The pilot indicated that he generally departed with the fuel tank about three-quarters full and returned with the tank about half full.
Meteorological conditions
The ATSB gathered weather information from a number of sources to get an accurate representation of the weather at the time of the occurrence.
Bureau of Meteorology
The Bureau of Meteorology provided the ATSB with a report on the weather conditions in the vicinity of the occurrence location. For the period between 0900 and 0930 on 28 December 2015, the following was noted:
From exposed maritime locations (The Seaway and Banana Bank), winds were from the south-southeast and about 20 kt, gusting to 25-27 kt.
From locations on the Moreton Bay coast (Redland and Brisbane Airport), the winds were from the south-east at 10-12 kt gusting to 17 kt.
From the inland location of Beaudesert, the winds were from the south-southwest at 12 kt gusting to 15 kt.
At 0900, the recorded temperature at Beaudesert was 23.7oC
Private weather representations
A private weather station about 4 km north of Pimpama Airstrip provided an unverified representation of the likely wind conditions on the morning of the accident. Between 0840 and 1000, it recorded winds between 8‑13 kt, gusting up to 15 kt, and coming generally from the south‑southeast.
The website Windyty.com[14] provided an unverified representation of the wind conditions experienced in the vicinity of the accident site. At 0900, the wind was recorded as 19 kt from a south-south-easterly direction.
Observed weather
The pilot reported that there was about 10-15 kt of wind and it would gust every now and then, but overall was relatively constant. The wind direction was from the south-east, ‘down the cross strip’. The wind speed was consistent with a brief view of the windsock, recorded by the video camera during the take-off roll.
The Westpac Lifesaver helicopter was first to arrive on scene at about 1002. The pilot of the helicopter reported that it was very windy and gusty, with gusts to 30-35 kt from about a southerly direction. The helicopter pilot also stated that, when on the ground at the accident site, it did not feel as windy compared with the conditions above tree level and that it was ‘certainly’ less than 30 kt.
Summary of weather conditions
The proximity of the personal weather station and its consistency with the pilot’s weather observations suggest it provided a more accurate representation of the weather than the Bureau of Meteorology observations. Based on these sources, the wind at ground level at the time of the flight was probably 8-19 kt coming from the south-east and gusty. It is likely that the wind above tree level was stronger.
Recorded information
The aircraft was fitted with a Garmin portable video recorder mounted underneath the upper right wing and facing rearwards. The video recorder separated from the aircraft during the accident sequence and was subsequently located near the accident site.
The recorded files were downloaded. The memory card contained a flight on 16 December 2015, a damaged file and a file that contained a recording for approximately 1 hour after the accident. The accident flight file did not record correctly to the memory card, probably due to a power disruption during the impact, and had to be repaired. The accident flight video file was 6 minutes and 43 seconds long and ended a few seconds prior to the impact. It is likely the recording of the last few seconds of the flight was stored in random access memory prior to being recorded onto the memory card and was lost with the power disruption during the impact.
A summary of the events in the accident flight recording is detailed in Table 2.
Table 2: Summary of the accident flight recordings
Time (EST)
Event
0900
Recording starts – Engine running, pilot returns chocks to hangar and then takes his seat in aircraft
0901:40
Taxi commences
0903:15
Aircraft lines up for take-off – about 100 m in from the runway threshold (Figure 1)
0905:55
Take-off roll commences – windsock visible during ground roll, indicates a southerly wind of 10-15 kt
0906:11
Lift-off
0906:13
Left turn commences
0906:23
Right turn commences
0906:36
Aircraft heading towards the south-east
Pilot observed looking outside the cockpit.
0906:38
Engine RPM starts to reduce
After the reduction in engine RPM, the video shows the pilot looking inside the cockpit in the direction of the instrument panel. The pilot’s and passenger’s hand and any movements of the controls could not be observed in the video.
0906:43
End of flight recording – height between 200-300 ft
A frequency analysis of the recorded engine and propeller noise indicated that the engine was operating at around normal take-off RPM of 2,010 RPM until 0906:38 when RPM reduced to 1,740 over the last 4 seconds of the recording. The RPM did not appear to have stabilised at the time the video recording stopped. The reason for the reduction in engine RPM could not be determined from the video and frequency analysis.
Site and wreckage information
The accident site was located about 850 m east of where the aircraft began the take-off and about 7 m west of a group of tall trees (Figure 3). The initial ground impact mark was about 2 m east of the aircraft nose and co-located with propeller slash marks. The aircraft was orientated to the east, and was upright.
Impact marks were identified on the underside of the upper left wing (Figure 4) and significant tree debris were located in the vicinity of the left wing. There was evidence of freshly broken branches in the trees to the east of the accident site. There was minimal damage to the right wing.
The examination of the aircraft identified:
all parts of the aircraft were present at the accident site
there were no observable pre-accident defects to the airframe
propeller slash marks and the damage to the propellers indicative of the engine driving the propeller at the time of impact (Figure 5)
the aircraft impacted the ground in a steep nose-down attitude with little forward velocity
the damage to aircraft, the trees and location of the aircraft wreckage was consistent with a collision with terrain while spinning to the left.
Figure 3: Accident site
Source: ATSB
Figure 4: Tree impact marks on underside of upper left wing
Source: ATSB
Figure 5: VH-UZB damaged propeller
Source: ATSB
Fuel system
The fuel tank was located between the upper wings and had a capacity of 86 L. Fuel was gravity-fed from the tank to the engine. The fuel exiting the tank passed through a matrix of 21 - 1/8 inch (3 mm) diameter holes to trap larger contaminates. Any finer contaminates were captured by the fuel filter. The filters were examined and found to be relatively clear from debris.
The fuel tank ruptured during the accident and there was evidence of post-accident fuel leakage. A fuel sample was recovered from the fuel tank and found to be visually contaminant free. A water contamination test was conducted on-site and returned a negative result.
A vent with a ball mechanism was installed on the upper surface of the fuel tank to allow air to enter the tank as fuel was used. The vent and ball mechanism was examined on-site and found to be clear of debris and serviceable.
A cork float connected to a visual fuel quantity gauge was located within the fuel tank. The float was inspected and found to be intact and in good condition.
A fuel shut-off valve was located immediately below the fuel tank. The valve was mechanically connected to a lever located in the pilot compartment. The video of the flight showed the flight shut-off valve was open throughout the flight up to and including in the last frame of the recording. Previous testing identified that if the engine was operating at 2,050 RPM and the valve was turned off, the engine would stop in about 16 seconds.
Engine and engine systems examination
Engine
The engine was disassembled and examined at an engineering facility under the supervision of the ATSB. The examination found that there was no evidence of a catastrophic engine failure. In addition, the examination identified:
impact damage to the rocker covers and exhaust system
the number 1 cylinder exhaust valve was bent and stuck, most likely due to impact damage
the engine rotated freely by hand with all cylinders (apart from number 1) having correct compression
the number 4 piston had a full thickness crack through the piston pin boss (Figure 6). The crack may have been pre-existing or a result of the impact. As the crack had not propagated to the point of failure, it did not lead to the power loss.
the spark plugs appeared normal
the engine carburettor in line filter was clean
the valve guide clearances were within the documented tolerance. The cylinder number 4 exhaust valve was stiff in comparison to the other valves, although still free to move.
There were no mechanical defects identified that would have led to a sudden reduction in engine power.
Figure 6: Number 4 piston with full thickness crack in piston pin boss
Source: ATSB
Component examination
The magnetos were bench-tested, under the supervision of the ATSB. Both magnetos were found to be serviceable for normal engine operation.
The carburettor was disassembled and inspected. The float chamber was refilled with fuel and the fuel level was measured and found to be within limits. The freedom of movement of the mechanism was also checked and found to be serviceable. Some cracks in the varnish of the cork float were identified (Figure 7). Such cracking can allow the ingress of fuel into the float and affect both the dimensions and buoyancy of the float within the carburettor. Fuel-affected cork floats have been found to be a contributing factor in a number of other engine malfunctions involving Gipsy Major engines.
Consequently, the ATSB conducted testing of the float to determine if the cracks allowed fuel to penetrate the float. The cork float dimensions and weight were measured and recorded. The float was then immersed in unleaded petrol for a total of 26 hours. There were minor changes in the float dimensions and a minor increase in weight, however, these changes were not considered significant enough to have resulted in the observed power loss.
Following review of the draft report, de Havilland Support Ltd (the aircraft type certificate holder, provided advice that it could take many months for the cork to become impregnated with fuel to a point where engine performance was affected. As a result of this new information, the ATSB conducted additional testing on the float, in consultation with de Havilland Support (Figure 8).
The ATSB found that over a period of 101 days the float increased in weight by about 0.89 grams (from 39.41 to 40.30 grams), a 2.4 per cent increase in weight. When the cork float was re‑weighed approximately 16 months after the beginning of the test it weighed about 40.55 grams (a 2.91 per cent increase in weight). This final weight could not be verified, as a portion of the fuel had evaporated, and the cork had not been submerged for a period of time.
As part of the initial draft report review process, de Havilland Support advised that from practical experience cork floats with aluminium alloy rivets, such as the one in VH-UZB, will generally weigh between 36 and 40 grams. The final weight of the tested float was 0.55 grams more than the upper weight range.
The aircraft type certificate holder and the ATSB assessed that the increase in weight, while low, had the potential to affect the buoyancy of the float. However, the degree of any resultant effect on carburettor operation could not be determined.
Figure 7: Carburettor float chamber and cracked cork float
Source: ATSB
Figure 8: Carburettor cork float testing
Source: ATSB
Survival aspects
Examination of the aircraft, first responder observations and witness statements confirmed the correct function of the safety harnesses. Video footage of the flight showed that the pilot, seated in the rear, was wearing a helmet made of hard material and a 4-point harness. The passenger, seated in the front, was wearing a soft leather helmet and a 4-point harness.
The impact forces sustained to the forward section of the aircraft and passenger compartment were not considered survivable.
The aircraft was not fitted with an emergency locator transmitter (ELT) nor was a portable ELT carried. Carriage of an ELT was not required under Civil Aviation Regulation 1998 Section 252A, subsection 2.[15]
Managing partial power loss in single engine aircraft
The ATSB report Managing partial power loss after take-off in single-engine aircraft identified 242 reported occurrences (between 1 January 2000 and 31 December 2010) involving single-engine aircraft sustaining a partial engine power loss after take-off. In two-thirds of these, the pilot turned back toward the aerodrome. Four fatal accidents and one serious injury accident involved loss of control after a turn back due to the aircraft entering an aerodynamic stall and spin, followed by a collision with the ground. The report highlighted that a turn back requires accurate flying during a period of high stress to prevent a stall and possibly a spin. If a stall or spin does occur, there is little likelihood of recovery before collision with the terrain.
The research suggested that the following initial actions should be performed when responding to a partial loss in power:
lower the nose to maintain the aircraft’s glide speed
time permitting, conduct basic initial engine trouble checks as per a total engine failure in accordance with the aircraft manufacturer’s advice
Fly the aircraft to make a landing. If a turn is conducted, be mindful that an increase in elevator input to maintain a desired descent path will reduce the margin to the stall. Also, keep the aircraft in balance to minimise the rate of descent in the turn. Having a planned minimum turning height is recommended; CASA suggests a minimum height of 200 ft above ground level. Below your planned minimum turning height, if continued climb to a safer altitude is possible, it should be done with level wings. With insufficient remaining power to climb, landing ahead is the only option.
re-assess landing options throughout any manoeuvres
land the aircraft.
Unintentional spins
The CAA of New Zealand’s publication Spin Avoidance and Recovery[16] states: ‘The majority of unintentional spins occur at altitudes too low for recovery.’ The publication discusses how aircraft enter unintentional spins and methods to recover from a spin.
When in a low-speed climbing turn, the aircraft is already vulnerable by being at low speed with a nose-up attitude and therefore close to the stall. Low-energy, low-powered aeroplanes, such as the Tiger Moth, in this situation will suffer some performance loss during a turn. To compensate, the nose of the aircraft should be lowered, otherwise the speed will further diminish.
Increased rudder application in the direction of the turn without increasing bank will result in a skidding turn. This coupled with a reducing or low airspeed can provide the conditions to start a spin.
With a high nose-up attitude, high power setting and low speed, the immediate priority following an engine failure after take-off is to lower the nose and preserve existing airspeed. In most cases, there is little option but to land ahead. Attempting to turn back to the runway or to a limited landing area will increase the risk of a loss of control.
In the event of a spin, pilots must immediately recognise the spin, its direction, know what to do in the correct order and correctly execute the procedure the first time. In most cases, there is only about 3 seconds to do all this. The minimum altitude loss for a text-book recovery will be about 1,000 to 1,500 ft. At low heights above ground level, there will be little opportunity to recover.
Shortly after take-off, and at a height of about 150 ft above the ground, the Tiger Moth’s engine began to run rough and lose power. The pilot banked the aircraft to the right towards a clear area to avoid the residential area directly ahead. During the landing roll, the aircraft came into contact with a number of trees and was substantially damaged. The pilot and two passengers were uninjured.
Examination of the carburettor found that the carburettor’s cork float had two large blisters in the fuel proof varnish. Further examination indicated that the larger of these blisters was binding against the float chamber housing walls. This could have resulted in either an excessively rich or lean mixture, leading the engine to run rough and stop.
During the investigation, several experienced Tiger Moth operators were contacted to ascertain their experience with this type of problem. These operators advised that they were aware of several incidents where the varnish surrounding the cork float had cracked and the cork float had then absorbed fuel. However, none had any previous experience of the varnish blistering in this manner.
Immediately after take-off, the Tiger Moth was observed to have a partial, intermittent power loss. When at the upwind end of the runway, a climbing left turn was made. The aircraft then stalled and descended. The aircraft collided with terrain and both occupants were fatally injured. The aircraft was destroyed by the impact forces and a post-impact fire.
Examination found the varnish coating on the carburettor float was darker than normal and had blistered away from the float, allowing the blister to contact the float bowl and interfere with the free movement of the float. Tests on exemplar floats found that the coating blistered when exposed to elevated temperatures, which may have been similar to temperatures inside the carburettor during the post-impact fire.
The investigation determined that the partial engine power loss was probably the result of a partial blockage of the aircraft’s fuel cock.
ATSB occurrence 200806008 (VH-FBO)
The pilot reported that the airstrip was experiencing ‘powerful’ standing waves[17] with ground winds appearing to be strong. While on approach, the aircraft appeared ‘out of wind’ and turbulence and control difficulties were experienced. As a result, the pilot aborted the landing and commenced a go-around, with less than full power being applied. During this time, the pilot was reportedly focusing on the ground winds and it was possible that the control column was moved rearward. With likely windshear also being experienced, the aircraft’s airspeed diminished and the aircraft entered a spin. The aircraft collided with terrain and the pilot received serious injuries.
Civil Aviation Authority (CAA) of NZ 06/4477 (ZK-BAR)
While in level flight, between 500 and 800 ft above ground level, the Tiger Moth entered a left climbing turn and then stalled and spun towards the ground. No unusual engine noise was reported and if such had occurred, a pilot’s first visible and expected reaction would be to lower the nose to maintain airspeed and establish a glide. The aircraft impacted the ground and caught fire.
The examination of the wreckage indicated that the impact was in a steep nose-down attitude with the right main-planes striking the ground first following by the left main-planes. The aircraft then rebounded backwards pivoting around the right main-plane tips.
Examination of the CAA of NZ database showed that there had been three fatal Tiger Moth accidents in the previous 12 years resulting from a low altitude stall/spin. These were:
Registration
Injuries
Pilot experience on type
Details
ZK-BGP
2 fatal
33 hours
Stalled from less than 500 ft, spun, then caught fire.
On the morning of 28 December 2015, a de Havilland DH82A Tiger Moth, registered VH-UZB, was prepared to conduct a 20-minute local adventure flight[1] operated by Gold Coast Aerobatic Adventures. The aircraft was to depart from and return to Pimpama Airfield near the Gold Coast, Queensland, with the pilot and one passenger.
The pilot arrived at the airfield at about 0800 Eastern Standard Time[2] and drove onto the airfield to check the windsock. He assessed the wind as being straight down the cross strip from the southeast. Based on the wind direction, he elected to conduct the take-off towards the southeast on the cross strip (Figure 1). He also assessed that, due to the forecast conditions, there would be some mechanical turbulence[3] during the flight. The pilot reported that the weather was forecast to deteriorate later in the day but he considered the conditions for the period of the adventure flight were suitable. While the cross strip was shorter than the main landing strip, it was adequate for the Tiger Moth and the pilot had reportedly used the cross strip many times for both take-off and landing.
At about 0815, the passenger and a relative arrived at the airstrip. They observed the pilot in the process of getting the aircraft out of the hangar. They went over and spoke with him while he inspected and prepared the aircraft for the flight. The pilot and passenger discussed the wind, with the pilot commenting that it would assist with take-off and landing. The pilot continued to prepare the aircraft and added about 20 L of fuel to the fuel tank, providing a total of about 60 L, sufficient for the planned flight.
The pilot assisted the passenger into the front seat of the aircraft and secured his 4-point harness. He then explained the operation of the intercom and stressed to the passenger the importance of not operating the controls.[4] The pilot then completed the pre-engine start actions.
The pilot hand swung the propeller to start the engine with wheel chocks in place (the Tiger Moth is not equipped with a starter motor). After starting the engine, the pilot climbed into the rear seat[5] of the aircraft and completed the checklist items and engine run-ups. The run-ups and magneto checks were conducted and the engine was running normally. At about 0900, after setting the engine throttle to idle, the pilot exited the aircraft, turned on the on-board video recorder and removed the wheel chocks.
After getting back in the aircraft and fastening his harness, the pilot taxied the aircraft to the take‑off strip. The aircraft was stopped about halfway between the end of the take‑off airstrip and the intersection of the two strips (Figure 1). The pilot reported that he elected to take-off from this location because the grass at the departure end of the runway was significantly longer than the part that he would use. The aircraft was equipped with a skid instead of a tailwheel, so the pilot exited and manually positioned the aircraft in the take-off direction.
At about 0906, the pilot commenced the take-off, with the aircraft becoming airborne 17 seconds later. About 2 seconds after it was airborne, at a height of approximately 20-40 ft above ground, the pilot commenced a left turn. After a substantial turn to the left, the pilot made a right turn back to the approximate take-off heading (Figure 1). The pilot stated that these turns allowed additional time to climb out over clear terrain before overflying trees.
Figure 1: Flight path of the aircraft
Source: Google Earth, modified by the ATSB. The yellow dotted line indicates the aircraft’s taxi, the blue line the ground roll and the pink the flight path, based on analysis of the on-board video recording (the recording stopped before the accident).
The yellow dotted line indicates the aircraft’s taxi, the blue line the ground roll and the pink the flight path, based on analysis of the on-board video recording (the recording stopped before the accident).
About 27 seconds after lift-off, when the aircraft was travelling approximately parallel to the take‑off strip, the pilot observed a change in engine noise and a reduction in engine RPM.[6] He reported that he retarded and then fully advanced the throttle but the engine only returned to a similar lower power condition.
The pilot assessed that, as the aircraft still had partial power, he would make a left turn and return to the airfield to land. Following review of the draft report, the pilot reported that following his decision to return to the airfield, the aircraft’s performance deteriorated further so he attempted to perform a forced landing in a cleared area. Soon after he started the turn, the aircraft aerodynamically stalled[7] and began to enter a left spin. The pilot recalled applying full right rudder in an attempt to stop the spin, however, the aircraft collided with the ground.
At 0916, about 9 minutes after the accident and after regaining consciousness, the pilot, who was trapped in the aircraft, called emergency services to request assistance. Emergency services arrived at the airfield at 0935 but there was a delay in locating the accident site. A rescue helicopter subsequently located the aircraft 45 minutes after the pilot’s phone call. The passenger received fatal injuries and the pilot sustained serious injuries. The aircraft was substantially damaged.
The sources of information during the investigation included the:
Air Accidents Investigation Branch (AAIB) UK
Australian Warbirds Association
Bureau of Meteorology
Civil Aviation Authority of New Zealand
Civil Aviation Safety Authority (CASA)
Flight crew
Operator
Witnesses
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the AAIB, Australian Warbirds Association, CASA, de Havilland Support, the owner/operator of Gold Coast Aerobatic Adventures, the pilot, the airstrip maintenance provider and the next of kin of the passenger.
Submissions were received from the AAIB, Australian Warbirds Association, CASA, de Havilland Support, the owner/operator of Gold Coast Aerobatic Adventures, the pilot and the airstrip maintenance provider. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Safety analysis
Introduction
Shortly after take-off, the aircraft had a partial engine power loss. In response, the pilot elected to return to the landing area. During the subsequent left turn, the aircraft stalled and entered a spin, at a height from which recovery was not possible before the collision with terrain.
The ATSB established that the pilot was appropriately qualified to be conducting the flight. The pilot had limited experience on the aircraft type, however, it was not possible to determine whether that contributed to the development of the accident as the management of this emergency would have challenged most pilots. While there was 8-19 kt of wind and gusty conditions, it did not exceed any aircraft- or industry-accepted limitations.
This analysis will examine the power loss and the potential reasons for the subsequent loss of control.
Engine power loss
The video audio analysis corroborated the pilot’s account that at a height of about 200 ft above ground level (AGL), the engine RPM began to reduce. The pilot reported that in an attempt to recover engine power, he retarded the throttle to idle and then advanced the lever back to full power. There was no apparent change to the reduced power level after the throttle was advanced.
The reported continued low power level after the pilot advanced the throttle indicated that the throttle had not ‘rolled back’ and had not been inadvertently interfered with by the passenger. The aircraft was refuelled prior to the flight and there was no evidence of fuel contamination. The engine, its components and fuel system were examined.
Observed cracking of the carburettor cork float varnish raised the possibility of the float being impregnated with fuel to the extent that the performance of the carburettor may have been affected. Testing of the carburettor mechanism and additional submersion testing of the float conducted during the investigation indicated that this was possible, however the likelihood was difficult to assess.
There was an anomaly with the number four exhaust valve clearance, however it was within the manufacturer’s specifications and there was insufficient evidence to determine if it contributed to the partial power loss. There were no other defects identified that would explain the partial power loss.
Loss of control
A partial engine power loss presents a more complex scenario to a pilot than a complete engine power loss. Following a complete engine failure, a forced landing is the only option whereas in a partial power loss, pilots are faced with making the difficult decision of whether to continue flight or to conduct an immediate forced landing. ATSB research found that the two-thirds of pilots who experience a partial power loss after take-off elect to return to the landing area. The pilot of VH‑UZB (UZB) similarly elected to return to the airfield.
In the event of a complete power loss, CASA suggests keeping wings level below 200 ft AGL and landing ahead. At the time of the partial power loss, UZB was just above this height and the pilot assessed that he had the option to return to the airfield. This accident highlights the decision‑making challenges during critical stages of flight, especially when faced with an unusual problem and the importance of pre‑briefing the intended actions if faced with a power loss during take‑off.
A number of scenarios could have led to the loss of control in the turn, these include:
The higher winds above tree height may have resulted in an illusion of slipping when the pilot turned the aircraft downwind. This may have resulted in the pilot increasing the rudder input, leading to an out-of-balance turn and entry to the spin.
The wind was reported to be gusting (gusts during the turn could have increased the angle of attack sufficiently to result in a stall/spin).
There may have been a sufficient loss of airspeed due to the power loss and turn to reduce the airspeed below the stall speed. The design of the Tiger Moth as a biplane with struts and wires creates higher drag than a monoplane.
The speed reduced below the stall speed as the nose may not have been lowered sufficiently after the partial loss of power.
Previous tests, research and accident data indicates that recovery from a spin is difficult to achieve below 1,000 ft. The aircraft was about 200-300 ft above ground level when the spin occurred and therefore recovery was not considered possible.
Immediately after take-off, the pilot conducted two low-level turns, despite the requirement to maintain the take‑off track until 500 ft above terrain. These turns were reportedly to provide additional time to climb out over clear terrain prior to overflying trees. However, banking during the climb resulted in a reduced climb rate. It was not possible to determine whether the increased altitude that could have been obtained by climbing straight ahead would have assisted in managing the power loss. However, even without the manoeuvring, the aircraft could not have gained sufficient height in 23 seconds (flight time prior to the power reduction) to recover from the spin.
While the pilot’s initial actions in deciding to return to the airfield were understandable, they introduced an additional risk of a loss of control. The best survivability outcome if an emergency landing is required for any reason is by flying:
the aircraft in a controlled manner
with wings level
at the recommended glide speed
using available headwinds, to reduce the touchdown speed.
Findings
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving a DH82A Tiger Moth aircraft, VH-UZB, near Pimpama, Queensland, on 28 December 2015. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
Shortly after take-off, for reasons that could not be determined, the aircraft experienced a partial engine power loss at low altitude.
In response to the partial power loss, the pilot elected to return to the airfield. During the subsequent manoeuvring, the aircraft stalled and entered a spin that was unrecoverable in the available height.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.