On 24 October 2016, the operator (pilot) of a Lockheed Martin Stalker eXtended Endurance (XE) unmanned aerial system (UAS), configured in vertical take-off and landing (VTOL) mode,[1] prepared to conduct a demonstration flight at Mount Disappointment, Victoria.
Figure 1: VTOL Stalker XE
Source: Lockheed Martin Corporation. All rights reserved. Copyright 2017.
The previous day, the operator had loaded the latest autopilot software onto the aircraft’s main autopilot. One aim of the flight was to demonstrate the use of a particular radio frequency for the command and control communication link. The ground radio equipment incorporated a narrow beam width directional antenna.
The operator programmed a simple mission: launch segment to a first waypoint and one primary waypoint, which was a coordinate centred on the launch location, then a landing pattern and an alternate landing pattern.
The crew then conducted a physical inspection of the aircraft and ensured all was mechanically correct. They also completed the pre-flight checks. The operator then commanded the aircraft to launch. All four vertical-lift rotors were energised, and the aircraft lifted off the ground. At about 20 ft above ground level (AGL), the aircraft paused in accordance with normal procedures, to conduct an airborne check.
The aircraft then climbed to about 300 ft AGL, which was the programmed transition altitude, but did not transition to forward flight. As the aircraft climbed above the ground antenna, it flew into a null in the antenna pattern above the antenna where communication between the ground control station (GCS) and the aircraft was interrupted.
The aircraft hovered and, after about five minutes, the operator commanded ‘abort’ from the GCS. At that time, the operator observed that communication with the aircraft had been lost and repositioned the antenna to point directly at the aircraft. After observing continued lost link indications for about 30 seconds, the operator enabled the alternate radio datalink, restoring communication with the aircraft. However, the previously selected ‘abort’ command was unavailable for re-issue after the initial selection.
About 11 minutes after launch, the aircraft’s power failed, the vertical propellers stopped, and the aircraft pitched about 95 degrees nose down, descended vertically and collided with the ground.
The aircraft sustained substantial damage.
Vertical take-off and landing (VTOL) configuration
In the VTOL configuration, four vertical lift motors are fitted in addition to a conventional tractor motor/propeller. The aircraft takes off vertically and then transitions to horizontal flight at a set altitude. Following the period of horizontal (fixed-wing) flight, the aircraft transitions back to vertical flight for landing.
Transition altitude
The typical time needed to climb to departure altitude and transition to forward flight is less than 1 minute.
The transition altitude is specified by the operator and is usually 150-200 ft higher than any nearby obstacles. In this incident, the operator had selected 300 ft due to trees about 100 ft high in the vicinity. The lower the transition altitude, the less time is required in the VTOL configuration, which requires substantially more power (and therefore battery) than the more efficient forward flight.
Post-accident inspection
Following the accident, an inspection revealed that the aircraft’s negative main power cable was unsoldered and had separated from its pin in the main power connector, which was plugged into the aircraft’s battery. The operator’s investigation found that the connector had failed before the aircraft battery drained.
Loss of electrical power
The wiring in the VTOL aircraft configuration was designed to supply vertical climb power for 2 minutes and the system had been validation-tested for 3 minutes at that power setting. The battery connector wiring in the accident aircraft failed 11 minutes into flight, resulting in total loss of electrical power and loss of aircraft control.
Flight data
According to the recorded flight data, the data link was interrupted about 1 minute and 20 seconds after launch. Two seconds later, an aircraft software lost-link contingency response automatically issued a command to latch the current altitude command, navigate to the launch point, descend and land.
However, 1 second after the lost link contingency command was issued, an additional spurious command was issued. This inappropriate spurious command caused the aircraft to remain in an extended hover and prevented the operator from further affecting aircraft operation, even after re-establishing data link communications. Extended operations at hover power, well beyond electrical power supply system design limits, overheated the wiring and resulted in a connector failure causing interruption of the battery power supply and subsequent loss of aircraft control.
Software error
The system manufacturer found that an inappropriate spurious command issued by the aircraft software was due to a coding error in the VTOL software that had not been detected during testing.
Communications
Communication between the GCS and aircraft is not required for flight. If communication between the GCS and aircraft is lost during flight, the autopilot continues to fly the aircraft according to programmed contingency logic. If communications are lost for more than 5 seconds during the VTOL launch phase, contingency logic commands the aircraft to return to the launch point, descend and land.
Landing/emergency command options
Having commanded ‘abort’, the operator thought that the command would continue to be sent to the aircraft after communications were restored until the aircraft acknowledged receipt of the command. This did not occur. In the launch phase, the ‘abort’ command should cause the aircraft to navigate to the launch point and descend vertically to the ground.
No other appropriate commands were available to the operator.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Communication between the GCS and aircraft was lost for about 5.5 minutes during the launch phase, due to the aircraft flying into the null in the antenna pattern above the antenna.
A return to launch command was issued by the autopilot due to loss of communications, but was not completed, because a spurious command was issued due to a coding error.
After 11 minutes at vertical climb power, the high current overheated the wiring. The heat unsoldered the negative main power cable resulting in a total loss of electrical power.
The total loss of power resulted in a loss of control and the aircraft collided with the ground.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following safety action in response to this occurrence.
UAS manufacturer
As a result of this occurrence, Lockheed Martin has advised the ATSB that they are taking the following safety actions:
Software redesign
The software is undergoing testing, redesign and a review of contingency management in VTOL modes.
Safety message
This occurrence highlights the importance of UAS software testing to cover potential non-normal scenarios prior to release into operation.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 25 October 2016, an instructor was supervising students in the operation of a Lockheed Martin Stalker eXtended Endurance (XE) unmanned aerial system (UAS) (Figure 1) at the Avoca racetrack in Victoria.
Figure 1: Typical Stalker XE aircraft
Source: UAS manufacturer
At about 1700 Eastern Daylight-saving Time (EDT), the instructor reviewed the student’s programmed mission and proceeded through the ground control station (GCS) launch wizard application. The launch wizard functions as a pre-flight checklist and ensures that all systems are ready for flight and that the mission is valid. The student then armed the aircraft for launch, pulled the aircraft back on the bungee cord and released the aircraft in accordance with the normal bungee launch procedures.
After release, the aircraft tracked straight ahead for 10 seconds according to standard operation, then climbed and commenced a right turn towards the first programmed waypoint. After passing the first waypoint, the aircraft made another right turn towards the second waypoint. About 20 seconds into the flight, the aircraft entered an uncontrolled descent from about 225 ft above ground level and collided with the ground. The aircraft sustained substantial damage, and no one was injured.
Manufacturer’s investigation
Power failure
The aircraft was powered by a lithium polymer battery. A battery adapter cable was plugged into the aircraft’s battery. The adapter cable was connected to the aircraft’s main power cable via the main power (battery) connector. The main power cable was secured into a pocket at the back of the connector pin.
After the accident, the aircraft’s negative main power cable was found to have separated from its pin in the connector.
The battery connector consisted of two mating pairs of contacts. In normal operation, all current flow passed through spring contacts on the male plug to the female contact. Spring tension increased the mating area and generated pressure upon the surfaces.
A different Stalker XE aircraft also experienced a battery connector failure about one month prior to this incident. In both incidents, the failed battery connector pins had the following problems:
significant pitting and erosion of the outer quarter of the male contact
heat damage to the spring contact surface
loss of spring tension in most or all of the contact springs
minor pitting of the outermost edge of the female contact.
It was determined that the capacitive load of the electrical system caused inrush current,[1] and the operator payload and communication links increased both the capacitive load and the power draw. The contact damage from the inrush current initiated the failure process. Sustained current, which produced contact heating, then removed the contact temper[2] and significantly degraded the connection. The manufacturer was able to duplicate the unsoldering failures via this mechanism.
The connector failure was likely the result of multiple factors:
Inrush current produced pitting, erosion and metal splatter on other contact surfaces.
The erosion and splatter then produced localised areas of very high current density.
The current density resulted in localised hotspots that removed the spring contact temper, which produced very high resistance on that spring contact.
The load was then distributed across the remaining spring contacts, compounding the failure rate.
Eventually the connector resistance was high enough that the normal operating current heated the solder joint until the solder melted and the circuit was interrupted.
The first steps probably took many flight cycles to develop, while the last probably required only seconds to a few minutes of normal operating current.
The separation of the negative main power cable from its pin in the main power connector interrupted electrical power to all of the aircraft systems. This included the autopilot, motor and control surface servos.
Uncontrolled flight
The flight data stopped suddenly at 225 ft – the subsequent lack of data logging indicated a power interruption to the autopilot.
Once battery power was lost, all systems in the aircraft were inoperative and any subsequent ‘flight’ was uncontrolled. Due to the loss of electrical power to the motor and the autopilot, the aircraft was unable to glide to a safe landing.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The main power connector pins had sustained degradation from arcing and high temperatures due to inrush current, resulting in increased resistance.
During the initial climb, high current across the increased resistance of the main power connector heated the negative pin to a temperature high enough to melt the solder on the negative main power cable.
The separation of the negative main power cable from its pin in the main power connector interrupted electrical power to all aircraft systems, including the autopilot, motor and control surface servos.
Due to the total loss of electrical power, the aircraft was unable to maintain normal flight or conduct a safe glide landing, therefore collided with the ground.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following safety action in response to this occurrence.
Aircraft manufacturer
As a result of this occurrence, the aircraft manufacturer has advised the ATSB that they are taking the following safety actions with regard to Stalker XE aircraft:
All battery connectors are being replaced and sacrificial pigtails are being added to the connectors, to be replaced after a number of connections.
The aircraft battery circuitry is being modified to prevent arcing during connection and disconnection.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
The aircraft departed Denham for travel to Perth via a refuelling stop at Geraldton.
At about 0806 hours the aircraft crashed approximately 770 metres, bearing 347°M from the threshold of runway 21 at Geraldton, apparently out of control and with the stall warning audible throughout the final radio transmission.
Investigation Indicated that both engines had stopped prior to Impact due to fuel exhaustion. There were no Indications of fuel leaks, and an analysis of times flown by the aircraft preceding the crash revealed that the available fuel should have been exhausted at about the time the engines were reported to have stopped. Fuel was available at Denham but, for unknown reasons, was not utilised by the pilot.
The pilot did not lodge a flight plan with the Civil Aviation Authority nor was any evidence found in the wreckage to Indicate that the pilot had used a flight plan or fuel log enroute. No conclusive determination for the loss of control of the aircraft was reached, however, the proximity to the threshold of runway 21 and the configuration of the aircraft with the wheels down, suggests that the pilot may have been attempting to turn towards that runway for a glide approach and landing.
SIGNIFICANT FACTORS
The following factors were considered relevant to the development of the accident:
1. The aircraft departed Denham with Insufficient fuel for the flight to Geraldton. 2. The pilot was apparently unaware that the fuel state was Inadequate and did not refuel at Denham. 3. Both engines stopped due to fuel exhaustion. 4. Control of the aircraft was lost at a height which did not allow the pilot to recover.
On 8 October 2016 the ATSB was advised that the United States National Transportation Safety Board (NTSB) had commenced an investigation into a collision with terrain involving a Fokker DR-1 aircraft, registered N83WR. Initial investigation by the NTSB indicated that the aircraft experienced a partial engine power loss shortly after take-off.
As Australia is the State of Manufacture of the engine, on 11 October 2016 the ATSB requested to be appointed as an accredited representative to the NTSB investigation in accordance with clause 5.18 of Annex 13 to the Convention on International Civil Aviation Aircraft Accident and Incident Investigation. An ATSB investigator was appointed as accredited representative to the NTSB investigation on 12 October 2016. To facilitate support to the NTSB investigation, the ATSB also initiated an investigation under the Australian Transport Safety Investigation Act 2003.
On 7 September 2016, the pilot of a Jabiru J170-C aircraft, registered 24-5215, approached to land, or perform a ‘touch-and-go’ manoeuvre, on runway 09 at Yarram aerodrome, Victoria, as part of a solo training flight. The pilot mishandled the landing attempt and lifted off to perform a go-around. The aircraft was observed at 50 to 100 ft above the aerodrome in a left wing down 30° angle of bank prior to it entering a steep descent consistent with an aerodynamic stall. The aircraft collided with the terrain and the pilot was fatally injured.
What the ATSB found
The ATSB found that the aircraft was likely subject to mechanical turbulence at the threshold of runway 09 at Yarram aerodrome. Trees and hangars on the north-eastern perimeter of the aerodrome were known locally to cause turbulence in the last 50 ft of the approach when the wind gusted out of the east-northeast. This information was not published in the Airservices Australia En Route Supplement Australia entry for Yarram aerodrome. The pilot was also likely affected by physical and mental fatigue given their age, medical history and recent physical labour. Fatigue’s effect on attention, reaction time, and vigilance likely exacerbated the pilot’s mishandling of the landing attempt and the subsequent go-around.
Safety message
Pilots and flying school operators should ensure they have thorough knowledge of the effects of weather on the pilot’s destinations and plan accordingly prior to flight. They should also remain cognisant of the effects of fatigue on the individual at different stages of their life. All pilots need to take into account how lifestyle changes, age, medical history, and medication may affect their fatigue.
Safety analysis
Introduction
While landing on runway 09 at Yarram aerodrome, the pilot of Jabiru Aircraft Pty Ltd J170-C, 24‑5215, was unable to effect a safe landing, or ‘touch-and-go’ manoeuvre. The pilot then attempted to go-around but was unable to prevent a departure from controlled flight at low altitude. The departure from controlled flight was consistent with the aircraft entering an aerodynamic stall prior to colliding with terrain. This analysis will consider factors that potentially contributed to the accident.
Mishandled landing, go-around and subsequent aerodynamic stall
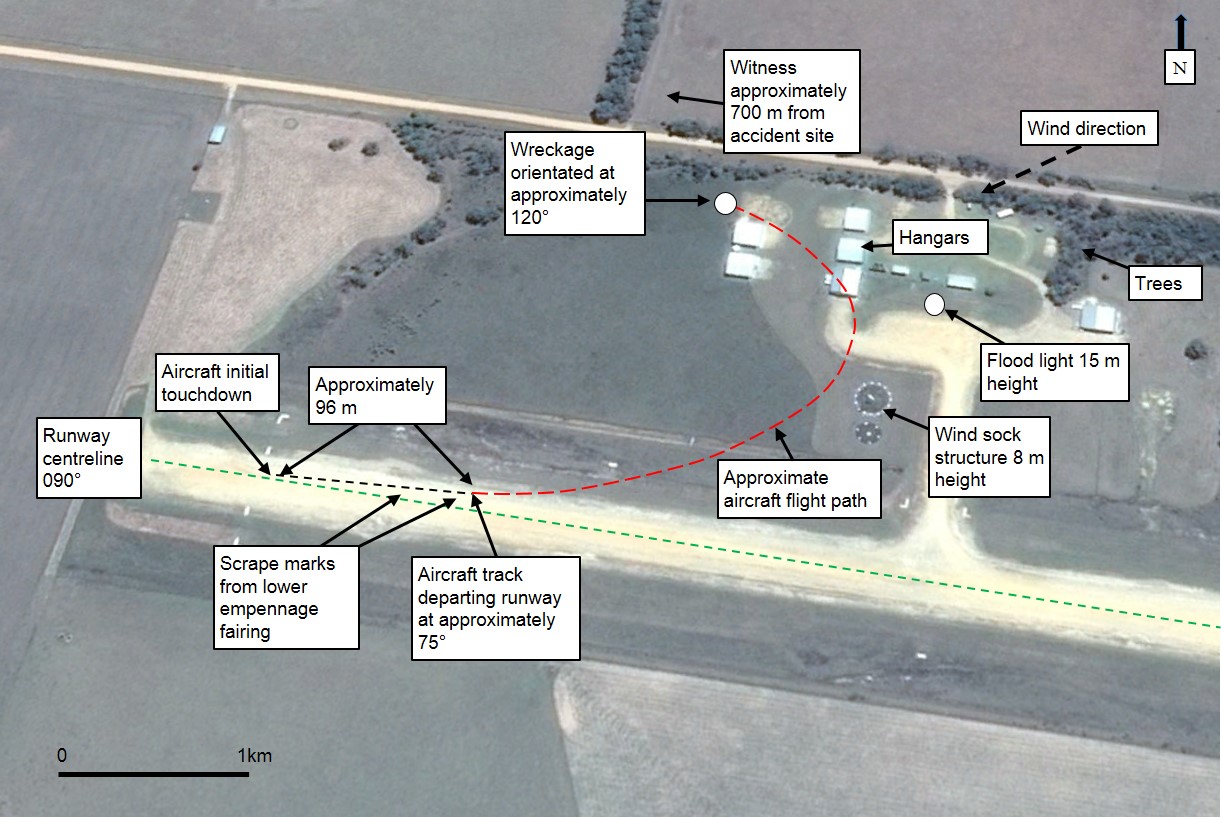
Examination of runway 09/27 shortly after the accident revealed aircraft tyre and empennage strike markings that indicated that the pilot had inadvertently mishandled an attempt to either land the aircraft or perform a ‘touch-and-go’ manoeuvre. The aircraft initially touched down on both main wheels but was 4 m to the left of the runway centreline, at a heading of 15° into the wind. The aircraft bounced and rolled on either one or both main wheels for approximately 96 m incurring two rear empennage strikes prior to lifting off. It is likely that the pilot was initially attempting to correct the landing or ‘touch-and-go’ attempt but then decided to lift off and go-around.
About this time, the witness heard the pilot apply a brief ‘burst’ of power and then saw the aircraft airborne at 50-100 ft height and in a left wing down 30° angle of bank. The aircraft continued to bank to the left prior to the left wing dropping, with the aircraft entering a nose down steep descent and then colliding with terrain.
Mechanical turbulence
The witness and other pilots with experience of the conditions at Yarram stated that, when approaching runway 09 with the wind from the north-east at between 10-15 kts, the final 10 ft prior to landing could be quite turbulent and become ‘a handful’ for an unaware or inexperienced pilot. It is likely that, given the conditions on the day, the aircraft was subject to mechanical turbulence at the threshold of runway 09. In addition to the pilot’s fatigue and level of experience (see below), it is likely this has resulted in the mishandled landing or ‘touch-and-go’ attempt.
At the time of the occurrence, the Airservices Australia’s En Route Supplement Australia did not indicate that a hazard such as mechanical turbulence could be experienced at Yarram aerodrome. Other locations such as Katoomba and Canberra specifically mention ‘turbulence and wind shear during winds above 15 kt’ and ‘during strong westerly winds TURB may be experienced in touch down area LDG RWY 35’ in the ‘Additional information’ sections. Highlighting the risk of an aircraft encountering mechanical turbulence during times when gusty north-easterly wind conditions are present could reduce the risk of a mishandling event during a critical phase of flight. It was unknown if the pilot was aware that these conditions could exist at Yarram.
Fatigue and experience
Researchers have stated that fatigue leads to lapses in attention, slowed reaction times, and reduced vigilance that can result in individuals overlooking or skipping tasks or parts of tasks. Researchers have also stated that older individuals still require the same amount of sleep as younger individuals but tend to get less due to increased nighttime awakenings. The decline in nightly sleep is accompanied by increased daytime fatigue (Battelle Memorial Institute, 1998). Researchers have also found that chronic pain is biologically linked to fatigue and 75 per cent of people with chronic musculoskeletal pain report having fatigue (University of Iowa, 2008).
The pilot was past retirement age and had a history of health and chronic pain issues including sleep apnoea. It was reported that the pilot had slept well leading up to the accident flight but had been physically fatigued through outdoor labour two days prior. There were a number of indicators of fatigue effecting the pilot’s performance, including not continuing to the Fish Creek navigational point, as well as neglecting to make a radio call on approaching Yarram aerodrome despite reminders in the cockpit to make the call and of the appropriate radio frequency.
Researchers have stated that experienced individuals will often make better decisions than inexperienced individuals due to their ability to recognise similar situations they have been in before and diagnose appropriate actions required to overcome problems quicker. They also state that an experienced individual will often be able to expend less cognitive effort in decision making as they do not need to do as much option evaluation as a novice, and thus will not experience as much decision, or cognitive, fatigue. The higher cognitive effort an inexperienced individual needs to solve a problem may further exacerbate the effects of any fatigue they may be experiencing (Wickens, Hollands, Banbury and Parasuraman, 2013).
The pilot did not have a great deal of flying experience given that they had recorded 191 hours total flying over a five-year period. This was their first solo cross-country navigation flight and the pilot had experienced an accident in a landing situation two years prior. It is likely that the pilot’s inexperience would have exacerbated the effects of the fatigue felt as discussed.
It is likely that, once the aircraft had been affected by mechanical turbulence, fatigue and experience level have led to the pilot’s inability to correct the aircraft’s departure from a controlled landing and controlled flight in time to prevent an aerodynamic stall and collision with terrain.
Aircraft maintenance logbook
During the engine examination, it could not be established when the accident aircraft’s engine had been certified and installed into the aircraft as this component change had not been recorded in the aircraft maintenance logbook. This action, while not contributing to the accident, increased safety risk as not recording component changes (such as the removal and installation of an engine) can result in an inability to trace changes to an aircraft’s life-limited components.
The occurrence
At about 1333 Eastern Standard Time on 7 September 2016, a Jabiru Aircraft Pty Ltd J170-C, registered by Recreational Aviation Australia (RAAus) as 24-5215, departed from Tooradin aerodrome, Victoria. The aircraft contained the pilot only.
The pilot planned to fly from Tooradin to the Latrobe Valley airport, Fish Creek, Yarram, Foster and then back to Tooradin as part of obtaining an RAAus solo cross-country navigation certificate endorsement. The endorsement syllabus required that the pilot perform either a full stop landing or conduct a ‘touch-and-go’[1] manoeuvre at Latrobe Valley airport and Yarram aerodrome. The pilot landed at Latrobe Valley at 1421 and stayed on the ground for about 25 minutes before proceeding with the flight.
At about 1544, the aircraft approached runway 09[2] at Yarram aerodrome, Victoria. A witness, who was also the Yarram Aerodrome Reporting Officer (ARO) and a pilot, was positioned about 0.7 km west of the accident site. The witness first heard and then saw the aircraft on final approach to runway 09 when it was about 500 m from the runway and at a height of about 300 ft. The witness stated that at this point, the aircraft and engine were both operating normally.
At that time, the witness was outside of their house in front of a machinery shed and adjacent to a shearing shed. The witness then walked into the shearing shed and, approximately 20 seconds later, heard a short application of power from the aircraft, like a ‘quick burst’. The witness thought that the pilot was possibly having some issues at the runway threshold as easterly and northerly winds may result in mechanical turbulence (refer to section titled Yarram aerodrome – Mechanical turbulence). On hearing the throttle ‘ease up’, the witness thought that the pilot must have decided to land further along the runway.
Subsequent examination of the dirt runway 09/27 showed marks where the aircraft attempted to either land or perform a ‘touch-and-go’. The first marks showed that both main wheels touched down about the same time, about 4 m to the left of the centre line. The aircraft then travelled on the right main wheel for about 54 m bouncing from the runway three times, missing runway cones and lights denoting the beginning of the landing area. The aircraft then rolled left and travelled on the left main wheel for 1.4 m before levelling out onto both main wheels, again bouncing, and then striking the lower empennage fairing once. The aircraft rolled right and travelled on the right main wheel for about 3.7 m, again striking the lower empennage prior to lifting off. During that sequence, the aircraft travelled about 96 m and about 15° to the left of the runway centre line. Neither wing tip nor nose wheel contacted the runway. In total, the aircraft bounced about eight times.
Following the quick power burst, the witness then looked out of the shed window and observed the aircraft in the air, away from the runway centreline in a 30° left angle of bank. The witness estimated the aircraft to be 50-100 ft above the ground. The aircraft continued to the left and the bank angle increased. The lower wing then dropped and the aircraft descended in a near to vertical attitude. The aircraft had turned 180° from the original flight path. The witness then lost sight of the aircraft as it went behind the trees at the western end of the aerodrome boundary, but they heard the aircraft impact the ground (Figure 1).
Figure 1: Overhead view of Yarram aerodrome incorporating runway 09/27 with the ATSB assessment of post lift-off flight path, runway markings, pertinent landmarks, wind direction, barriers pertinent to mechanical turbulence and wreckage site
The witness called out to their spouse, a registered nurse, and they drove to the aerodrome. The witness rang the emergency services on the way. Once at the site, they removed the pilot from the aircraft and began providing medical assistance while waiting for the emergency services to arrive. The pilot died from the injuries sustained in the accident. The aircraft was destroyed.
Personnel information
General information
The pilot held a valid RAAus Pilot Certificate, issued on 21 May 2013, and maintained the required medical standard. The pilot’s logbook included the following endorsements: human factors, high performance, nose wheel, passenger carrying, and RAAus flight radio.
The pilot’s logbook showed a total flying experience of 191.4 hours to the last recorded flight on 4 July 2016. The pilot’s total flying experience on the Jabiru J160 and J170 was 75.5 hours and 102.8 hours respectively. In the previous 90 days, the pilot had flown a total of 10.3 hours. The logbook also recorded 174 landings since July 2013.
Pilot training and experience
The pilot’s initial training took longer than the minimum 20 hours required, however, the pilot was reported as being conscientious and passionate. The pilot’s instructors stated that the pilot had been focussed on the cross-country endorsement for the previous two months and had successfully completed two navigation flights with an instructor. The pilot was considered competent to conduct the solo navigation flight and was reportedly very good at self-assessment and aware of their capabilities.
Two years prior to the occurrence, the pilot was involved in a landing accident at Tooradin aerodrome. When on final approach to runway 22, the Jabiru J170’s airspeed decayed and the aircraft stalled from a height of about 20 ft above ground level. The aircraft descended and when contacting the ground, the pilot applied full power and the aircraft bounced. The aircraft then yawed left and the left wing contacted the ground. It then rolled right, the nose contacted the ground, and continued rolling onto the right wing. The aircraft settled down onto the nose. The aircraft sustained substantial damage to the wings and fuselage. At that time, the wind was from the south-west at 5 kt and the pilot’s total flying experience was 125.2 hours, of which 100 hrs was on the Jabiru.
Go-arounds and turbulence
The pilot had conducted a considerable number of go-arounds and was considered ‘pretty good’. The instructor was confident that the pilot would make the appropriate decisions if an approach was unsuitable. The instructor also noted that when close to the runway, the Jabiru, like any high wing aircraft of a similar design, had a tendency to pitch-up when full flap and throttle were applied. Forward pressure on the control stick would have to be used to counteract this tendency. The pilot had practiced go-arounds in this configuration, and had also practiced crosswind circuits and go-arounds. Crosswinds at Tooradin were commonly experienced. The instructor reported that they had not experienced much turbulence at Yarram, but had so at Tooradin. After practice, the pilot handled the turbulent conditions well and had done a considerable number of circuits at Tooradin.
Recent history
On 4 September and 5 September, the pilot had slept from about 2100 until 0700, however, the sleep was reportedly disrupted due to the pilot being sore and tired due to physical labour. On 6 September, the pilot rested for the navigation endorsement flight the next day. The pilot reportedly went to bed at about 2100 and woke at 0700 on 7 September having slept well.
Medical information
Upon initial application as a student pilot with RAAus, the pilot signed the annual medical declaration on 3 December 2011. By signing the form, the pilot was affirming that their health was of a standard equivalent to that required for the issue of a private motor vehicle. On the date of the accident, the pilot held a current and appropriate medical authorisation.
The pilot had reportedly suffered from chronic pain and sleep issues for a number of years, including sleep apnoea. The pilot had had a major illness in the past and, at the time of the accident, was 72 years of age.
Aircraft information
The Jabiru Aircraft Pty. Ltd. J170-C is a two-seater, fibre-reinforced, light sport aircraft with a high wing and tricycle undercarriage. The aircraft was first registered on the RAAus aircraft register on 11 January 2007 and at the time of the occurrence, was fitted with a Jabiru 2200B 4-cylinder engine.
Meteorological information
The Bureau of Meteorology provided data recorded by the automatic weather station at Yarram. At the time of the occurrence (1544), the wind was from 080° at 13 kt gusting to 18 kt. This would have resulted in about a 5-7 kt left crosswind and a 12-17 kt headwind.[3]
Yarram aerodrome
Yarram was a registered aerodrome[4] maintained by the Wellington Shire Council. The aerodrome had two runways, runway 05/23 and runway 09/27. Runway 09/27 was constructed of yellow granitic sand and was 756 m in length. At the time of the accident, runway 05/23, a grass runway, was not in use due to surface water.
Mechanical turbulence
Any obstruction to the wind flow, including buildings and trees, can produce disturbed air that can manifest as mechanical turbulence. The intensity of mechanical turbulence is largely dependent on the wind speed, surface roughness, and atmospheric stability. The intensity increases as the wind speed and surface roughness increases, and when the airflow is forced by obstacles to diverge around, or converge through, gaps in barriers. For example, the Bureau of Meteorology (1988) stated that large scale disturbances to airflow may occur when strong winds strike a mountain range or large hill. Likewise, sometimes moderate winds of 15-20 kt may significantly disturb the airflow.
It was reported that mechanical turbulence due to trees and hangars on the north-eastern perimeter of the aerodrome could be experienced when operating on runway 09 (Figure 1). This occurred when there was a north-easterly wind, and could catch pilots by surprise, particularly if they were not expecting it.
A representative from the Yarram Aero Club stated that when landing on runway 09, turbulence could be experienced from about 50 ft and then, when at 10 ft, ‘things would be moving around quite a bit’. The representative also recommended that new users to the aerodrome should contact the ARO to ascertain the conditions. They also suggested a note in the Airservices Australia En Route Supplement Australia (ERSA) may bring attention to this phenomenon.
Radio broadcasts
The pilot had been trained on the use of the radio and was aware of the inbound and circuit broadcasts required when approaching an aerodrome. When departing from Tooradin, the pilot broadcast a departure call. However, the pilot did not make the required calls on the Yarram common traffic advisory frequency.[5] Examination of the aircraft post-accident found ‘post-it’ notes on the pilot’s flight plan with a script of the call and the required frequency showing the pilot had intended to make the calls.
Operational information
Flight route
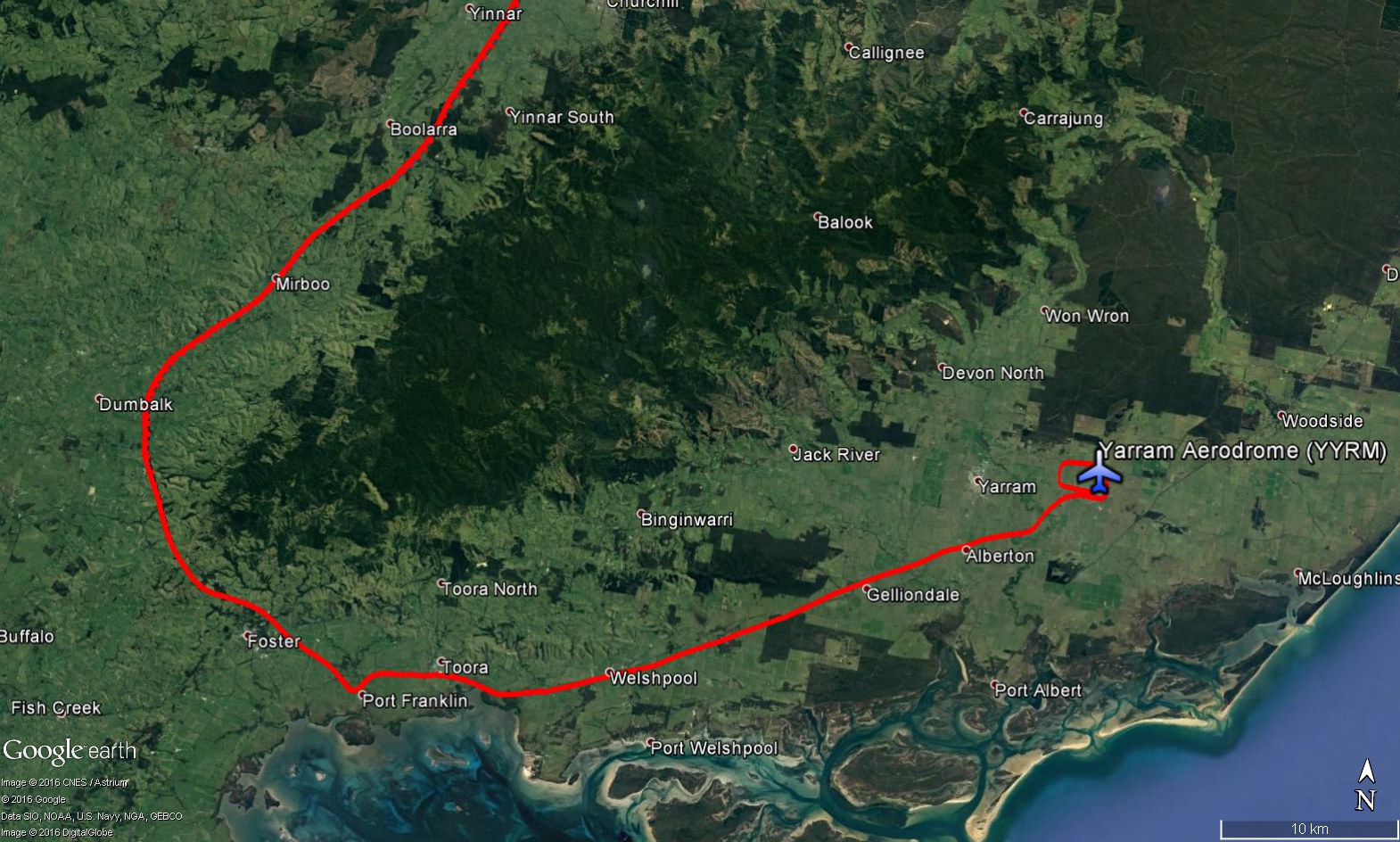
The pilot was conducting a solo navigation exercise from Tooradin to the Latrobe Valley airport, Fish Creek, Yarram, Foster and return to Tooradin requiring that they conduct either a full stop landing or a ‘touch-and-go’ manoeuvre at Latrobe Valley airport and Yarram aerodrome. A review of the data from a handheld GPS device recovered from the aircraft showed that the actual flight route was similar to that planned. However, the track from Latrobe Valley was more consistent with overflying Foster Township rather than Fish Creek Township (Figure 2). The aircraft then tracked around the mountain ranges to Yarram.
Figure 2: Google earth image overlayed with the aircraft’s actual flight route on the leg from Latrobe Valley to Yarram downloaded from the recovered handheld GPS unit bypassing Fish Creek – a required navigation point for the solo navigation exercise.
Source: Google earth, modified by the ATSB
Wreckage examination
On-site examination of the wreckage found that:
the aircraft travelled about 200 m from the lift-off point on the runway to where it came to rest
the aircraft collided with terrain in a left wing and nose down attitude
the wreckage trail was relatively short signifying a low speed, high angle of attack impact into soft muddy terrain
the wing flaps were in the full down position (as appropriate for landing or for a go-around from final approach)
the fuel quantity at the time of the accident could not be established due to the left wing and left-wing fuel cap being separated from the fuselage, however, the aircraft had a significant quantity of fuel in the right wing
debris was identified in the throat of the engine’s carburettor venturi, but these substances may have been sucked into the venturi during the accident sequence
fragments of the propeller were found displaced radially about 10-15 m either side of the wreckage.
The debris in the venturi, radial distribution of propeller fragments, as well as the distance the aircraft travelled after becoming airborne from the runway were all consistent with an engine producing thrust prior to the aircraft colliding with terrain.
Subsequent engine and instrumentation examination performed by the ATSB found no evidence of an engine, airframe or mechanical failure that may have contributed to the accident.
During the engine examination, the ATSB found that the aircraft’s engine had been replaced and had recently had an overhaul completed. However, the aircraft’s maintenance logbook did not state when the engine was certified and installed into the aircraft.
The aircraft maintenance logbook’s instruction page stated that where components were installed, removed, or replaced, complete details were to be recorded in Part 3 – modification and component change record. The RAAus technical manual stated that component changes must be recorded in the maintenance logbook and the logbook must have a section for this record titled ‘Modification and Components Record’. The logbook did have the appropriate section, however, a sheet for recording weight and balance changes had been pasted over it and component changes could not be recorded in this part.
The ATSB also found anomalies with the manufacturer’s instructions regarding certain aspects of the engine overhaul in their overhaul manual. These were subsequently identified and rectified by the manufacturer and no further action has been deemed necessary by the ATSB.
From the evidence available, the following findings are made with respect to the collision with terrain involving a Jabiru Aircraft Pty. Ltd. J170-C, Recreational Aviation Australia aeroplane, registered 24-5215, at Yarram aerodrome, Victoria on 7 September 2016. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
Upon reaching the threshold of runway 09 at Yarram aerodrome, the aircraft was likely subject to mechanical turbulence resulting in the mishandling of the landing or 'touch-and-go' attempt.
The pilot inadvertently mishandled the subsequent go-around leading to the aircraft's low altitude aerodynamic stall and collision with terrain.
Other factors that increased risk
Fatigue and level of experience likely affected the pilot's ability to respond to the demands required to correct the aircraft's departure from controlled flight during the landing attempt and subsequent go-around.
While locally known, the En Route Supplement Australia entry for Yarram aerodrome did not highlight the risk of an aircraft encountering mechanical turbulence on runway 09 during the gusty wind conditions present on the day, increasing the risk of a mishandling event during a critical phase of flight.
The aircraft’s maintenance logbook did not state when the engine was certified and installed into the aircraft resulting in an inability to trace changes to its life-limited components.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Yarram aerodrome reporting officer
Vice President Yarram Aero Club
Wellington Shire Council
Tooradin Flying School
Jabiru Aircraft Pty Ltd
Latrobe Valley Aero Club and Flying School
Civil Aviation Safety Authority
Recreational Aviation Australia
Victorian Police Coronial Support Unit
Victorian Police Force
Bureau of Meteorology
Directorate of Defence Aviation and Air Force Safety.
References
Battelle Memorial Institute (1998). An Overview of the scientific literature concerning fatigue, sleep, and the circadian cycle. Report prepared for the Office of the Chief Scientific and Technical Advisor for Human Factors, US Federal Aviation Administration.
Bureau of Meteorology. (1988). Manual of meteorology, part 2: Aviation meteorology. Canberra: Department of Administrative Services.
University of Iowa. (2008). Biological link between pain and fatigue discovered. ScienceDaily. Retrieved January 17, 2017 from
Wickens, C.D., Hollands, J.G., Banbury, S. and Parasuraman, R. (2013). Engineering psychology and human performance (4th Edition). Abingdon, UK: Routledge.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the next of kin, the Yarram aerodrome reporting officer, chief flying instructor, flying instructor and Level 2 maintainer at Tooradin Flying School, Wellington Shire Council, the aircraft manufacturer, the coroner’s representative, Recreational Aviation Australia and the Civil Aviation Safety Authority.
Submissions were received from the next of kin, the Yarram aerodrome reporting officer, Wellington Shire Council, the aircraft manufacturer, Recreational Aviation Australia and the Civil Aviation Safety Authority. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Safety issues and actions
Proactive safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
The Wellington Shire Council, as the operator of the Yarram Aerodrome, initiated an entry into the En Route Supplement Australia entry for Yarram aerodrome highlighting the risk of an aircraft encountering mechanical turbulence on runway 09 during the gusty wind conditions present on the day of the accident. In a letter dated 29 June 2017, Wellington Shire Council informed the ATSB that:
The draft report has identified mechanical turbulence as a risk factor which Council was not previously aware existed at Yarram Aerodrome. Council has initiated a new entry in ERSA in line with the draft report.
Processes for updating aeronautical information publications have also been examined and changes made whereby the aviation community will be formally consulted in the review and amendment of publications.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 13 April 2016, a Pilatus Britten Norman Turbine Islander (BN-2T) twin-turboprop aircraft, registered P2-SBC, departed from Tekin, West Sepik Province for Kiunga, in Western Province, Papua New Guinea (PNG). A pilot and 11 passengers were onboard the aircraft. While on approach to land, the aircraft impacted heavily into terrain, approximately 1,200m west of the runway. The aircraft was destroyed and there were no survivors.
The Accident Investigation Commission (AIC) of Papua New Guinea conducted an investigation into the accident in accordance with their obligations as the State of Occurrence under Annex 13 to the Convention on International Civil Aviation. The AIC requested technical assistance from the Australian Transport Safety Bureau (ATSB) to examine items recovered from the aircraft, including cockpit instruments and personal electronic devices. In providing this support, the ATSB commenced an external investigation under the Transport Safety Investigation Act 2003.
The ATSB has completed its examination of the recovered items. The results of the instrument examination along with a copy of the recovered data from the electronic devices was provided to the AIC.
The AIC has released the final investigation report into this accident, which is available at www.aic.gov.pg. Specific enquiries related to this accident should be addressed to the AIC by email at infor@aic.gov.pg, or in writing to:
Chief Executive Officer Accident Investigation Commission PO Box 1709 Boroko, NCD Papua New Guinea
On the morning of 20 March 2016, the pilot of a Cessna 182S aircraft, registered VH-PCO, conducted a private flight from Moorabbin Airport to Tooradin Airfield,[1] Victoria, with two passengers on board. The aircraft took off from runway 17 Right at Moorabbin, and the wind during the 21 NM flight was south-easterly at about 10 kt. The runway in use at Tooradin was 04 (Figure 1), and the pilot reported that the landing at the end of that flight was uneventful.
Figure 1: Tooradin Airfield
Source: Google earth, annotated by the ATSB
After landing at Tooradin, the pilot prepared to conduct a scenic flight to Wonthaggi, Wilsons Promontory and return, with three passengers on board. While on the ground at Tooradin, the pilot was concerned that the wind had increased since their arrival, therefore obtained an updated weather forecast and the actual weather at Tyabb, which was about 12 NM south-west of Tooradin. The pilot also obtained the latest weather report for Moorabbin, where the wind was from 120° at 11 kt, and runway 13 was in use.
Based on that information, the pilot assessed that it was suitable to go ahead with the planned flight, but also made the contingency plan to divert to Moorabbin if the strength of the crosswind at Tooradin was not suitable for a landing on their return.
The pilot reported that the flight was normal. At about 1320 Eastern Daylight-saving Time (EDT), the aircraft returned to Tooradin, and the pilot elected to join the circuit on a right downwind for runway 04. While on the downwind circuit leg, the pilot and the front seat passenger observed a windsock, which was located near the runway 04 threshold (near the helipad). The pilot stated that the windsock indicated that the wind was blowing straight down the runway, and elected to continue the approach.
After turning onto final approach, the pilot selected full flap (40°). When at about 300 ft above ground level, the pilot confirmed that the windsock still indicated a headwind, and continued the approach. The pilot reported that as the main wheels touched down, about 300 m beyond the runway threshold, the aircraft veered left off the runway onto the grass.
The pilot immediately commenced a go-around by applying full power and raising the aircraft’s nose in an attempt to clear aircraft parked on the grass ahead. The stall warning horn sounded, and the pilot assessed that the aircraft was not climbing and that its landing gear may collide with the parked aircraft.
The pilot therefore reduced the power to idle and the aircraft landed heavily to the north of the runway. The aircraft then struck three other aircraft that were parked on a grassed area between the runway and a sealed taxiway.
The aircraft sustained substantial damage and the pilot and passengers were uninjured (Figure 2).
Figure 2: Accident site showing damage to VH-PCO
Source: Country Fire Authority Victoria
Pilot experience and comments
The pilot had a total of 168.8 hours of aeronautical experience, including 5.4 hours in the Cessna 182S.
The pilot provided the following comments:
Prior to the flight, the pilot assessed the wind using the windsock to the north of the field and the torn windsock near the shipwreck. On final approach, the pilot referenced the windsock near the runway 04 threshold (near the helipad).
In hindsight, they should have retracted the flaps to 20° for the go-around.
There was no indication of a crosswind during the approach.
Weather observations
There was no automatic weather station at Tooradin. The nearest weather data recorded by the Bureau of Meteorology was at Moorabbin and Frankston, and the ATSB obtained the 1-minute weather data for those locations. The runway at Tooradin was situated adjacent to Western Port Bay, and the runway direction in use was 04. The pilot and an instructor at Tooradin reported that the wind at Tooradin was generally not the same as that experienced at Moorabbin.
Around the time of the accident, the wind at Frankston was varying in direction from 096° to 143°, from 6 to 10 kt, gusting to 15 kt. An instructor at Tooradin reported that throughout the day, the wind was about 7 to 9 kt, some of which was crosswind, as it was blowing at about a 45° angle to the runway.
The instructor also reported that the main windsock for the airfield was to the north of the field, and there were two windsocks on the southern side of the strip – one located near the helipad and the other, which was torn but still indicating accurately, adjacent to the shipwreck (Figure 1).
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following safety action in response to this occurrence.
Aircraft operator
Although the accident flight was a private flight, the aircraft operator, as a training organisation, has advised the ATSB that as a result of this occurrence, they are taking the following safety actions:
Improving the delivery of training in crosswind circuits and go-arounds
The aircraft operator is reviewing
what grade instructors are authorised to conduct training in crosswind conditions
which aerodrome the lessons are delivered at
the minimum crosswind component for the lessons
where it is delivered within the training syllabus
the contents of training notes and sequence briefing
how they allocate testing officer to ensure there is no student input.
The operator has also asked flight testing officers to emphasise crosswind and go-around techniques.
Presentation to company pilots
The operator has arranged for a senior airline captain to deliver a presentation to company pilots on stabilised approaches, selection of the touchdown zone, and appropriate responses to non-normal situations.
Carriage of airsick bags
Aircraft folders will be equipped with airsick bags, to reduce the effect a sick passenger may have on a pilot’s workload.
Review of Emergency Response Plan
While the operator assessed that their emergency response plan was effective in this incident, they have identified some improvements to be implemented.
Safety message
A report prepared by the US Aircraft Owners and Pilots Assocation, Cessna 182 Skylane Safety Highlights,stated that the number of accidents for the aircraft type was inversely proportional to the number of hours a pilot had accumulated, and the majority of accidents involved pilots with less than 400 hours’ total time. Landing was the most accident-prone phase of flight. The report also stated that the maximum demonstrated crosswind component for most Cessna 182 aircraft was 15 kt – most pilots should consider that as limiting until they are highly proficient in crosswinds. The aircraft’s Pilot Operating Handbook suggested procedures for landing in crosswinds, including that they should be performed with the minimum flap setting necessary for the field length.
The Flight Safety Foundation Approach-and-landing accident reduction tool kit
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
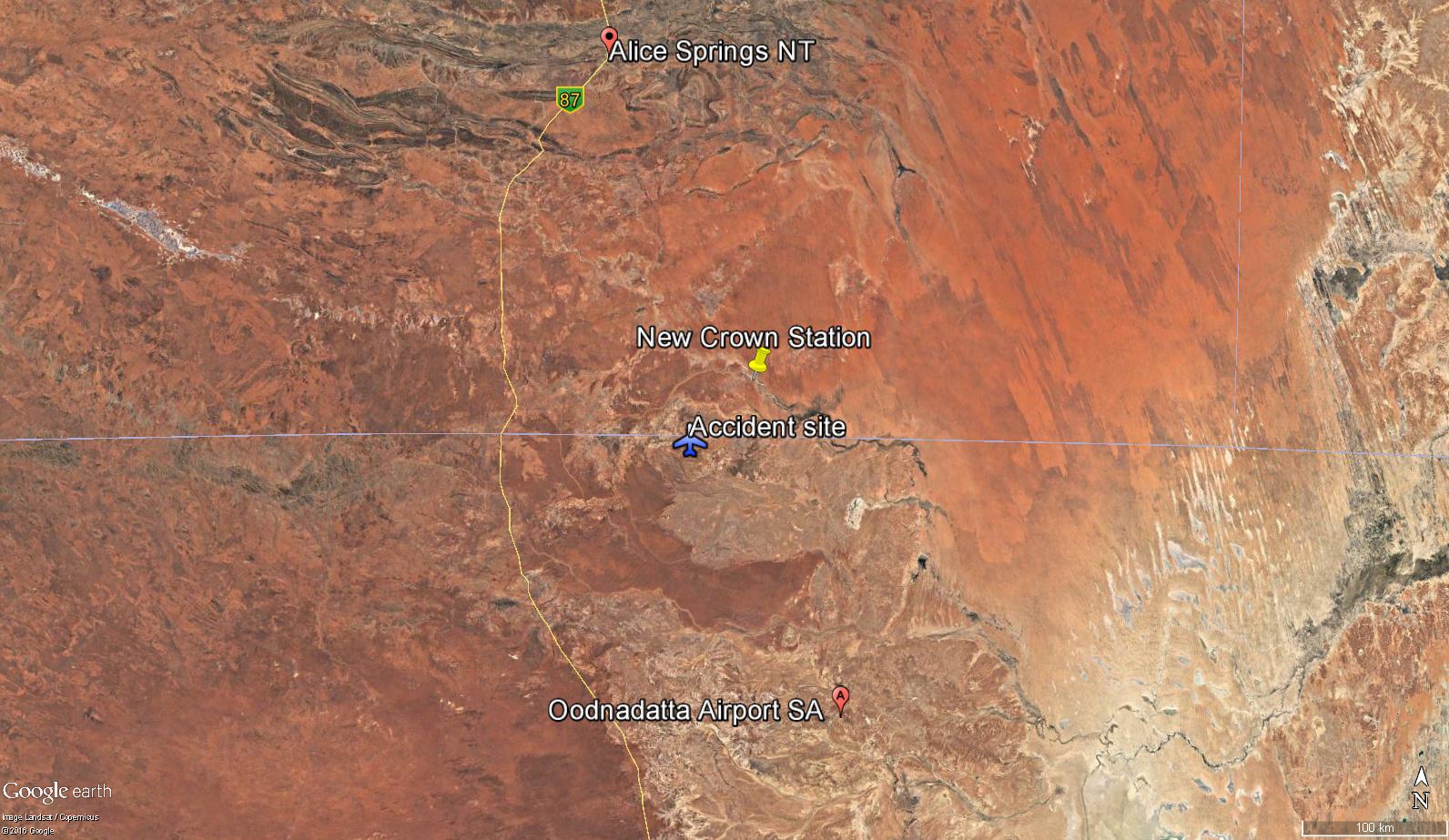
On 12 July 2016, the pilot of a Cessna 150 aircraft, registered VH-RXU, was conducting cattle spotting operations at New Crown Station, about 270 km south-east of Alice Springs, Northern Territory. The aircraft was observed conducting turning manoeuvres over the cattle at a reported altitude of about 500 ft.
A stockman recalled that, immediately preceding the accident, the pilot was directing them by radio to a breakaway herd of cattle in a nearby riverbed. The stockman observed the aircraft in a right turn moments before hearing it impact the ground, meters from their position.
For reasons that could not be determined, the pilot lost control of the aircraft and was unable to arrest the descent before the aircraft impacted the ground heavily. The pilot was the sole occupant on-board the aircraft and was fatally injured. The aircraft sustained significant damage.
What the ATSB found
The pilot lost control of the aircraft after commencing a right turn. While the actual events preceding the loss of control could not be concluded, the aircraft was likely operated at a slow airspeed with reduced stall margins. In the absence of other physical evidence, it was possible that control inputs made by the pilot induced a stall and incipient spin at an altitude that was not recoverable.
The pilot was not using the full lap/sash occupant restraint at the time of impact. The extent of injuries sustained by the pilot during the impact probably would have reduced if the sash portion of the restraint were used. This would likely have improved pilot survivability.
The fuel type used by the operator and pilot was not approved for use in VH-RXU. Although probably not contributing to the loss of control, it increased the risk of carburettor icing and formation of vapour in the fuel system.
What's been done as a result
The operator advised that since the accident, only the grade/type of fuel approved for use in the aircraft would be used.
Safety message
Turning manoeuvres at or close to the aircraft’s critical angle of attack, if mishandled, can lead to a stall that may result in the aircraft entering a spin. Recovery from this condition will take a considerable amount of altitude, dependant on the speed of response by the pilot and the use of appropriate control inputs.
Pilots need to assess the operational risks associated with not using full lap/sash restraints. The appropriate use of these restraints would prevent more serious deceleration injuries in the event of an accident.
To ensure engine performance, pilots and operators must ensure that the fuel used is of the correct grade/type for the aircraft, and is free of contaminants.
Context
Personnel information
Pilot
The pilot held a Private Pilot (Helicopter) and (Aeroplane) Licence and was qualified to fly the Cessna Aircraft Company C150G (C150) aircraft. The pilot was also endorsed on the Robinson R44 and R22 helicopter.
In 1998, the pilot completed a low-level safety course for which 10 hours flying was completed. The pilot did not hold a low-level flying or mustering endorsement, however, those endorsements were not required unless the aircraft was conducting spotting/mustering activities at an altitude lower than 500ft above ground level.
The pilot’s total aeronautical experience at the time of the accident could not be determined as the pilot’s logbooks were incomplete. The last recorded entry on 27 June 2016 indicated 2,676 total flying hours, of which 496 hours were on helicopters. The pilot’s logbook showed that from 1988, the pilot had predominantly flown single engine Cessna aircraft. The pilot last flew a C150 aircraft on the day prior to the accident, conducting aerial spotting operations.
Since obtaining a helicopter rating in 2014, the Robinson R44 helicopter was the primary aircraft flown. Although the operational characteristics of flying a helicopter would have differed from a fixed wing aircraft, there was no conclusive evidence that this adversely effected the pilot’s flying ability on the day of the accident.
A review of the pilot’s training records identified that the pilot had satisfactorily completed a biennial aeroplane flight review on 7 April 2014. The review was conducted under Civil Aviation Regulation (CAR) 1988, Part 5 in a Cessna 172 aircraft. Since that flight review, Civil Aviation Safety Regulation (CASR) Part 61 was introduced, and the pilot was overdue for a biennial flight review in accordance with those regulations.
On the day prior to the accident, while flying RXU, the pilot discontinued flying for the day after feeling a degree of motion sickness. The pilot reported this to the operator and discussed being more susceptible to motion sickness after having a medical procedure some years ago. The medical procedure was recorded in the pilot’s aviation medical file. A stockman and operator reported the pilot as appearing well on the morning of the accident.
The pilot held a valid Class 2 Aviation Medical Certificate with no restrictions.
Aircraft information
General information
The aircraft, VH-RXU, a C150, serial number 15066748, was manufactured in 1967 and entered the Australian register on 8 August 1968. The C150 is a single engine, all-metal, fixed tricycle-gear aircraft with a seating capacity of two.
Maintenance history
Review of the aircraft’s documentation showed it had a valid maintenance release with no open defects.
The aircraft logbooks show the last periodic inspection was conducted on 23 Sept 2015. At that time it had completed 6733.4 hours since manufacture.
The last periodic inspection identified some minor defects, which were rectified. Included in the maintenance tasks carried out during that inspection was the replacement of the seatbelts/lap sash occupant restraints and an airworthiness directive to test the stall warning system for which was certified as having no identified defects.
Meteorological information
Stockmen and ground crew operating in the area recalled the weather conditions as being fine with overcast cloud and a light to moderate breeze with some gusts. There were no ‘dust-devils’ reported in the area of operation.
Recorded meteorological information at Oodnadatta Airport, about 185 km to the south-east, indicated the temperature at 1130 was 13.0 °C. The wind was from the south-west at about 35 km/h and there was no recorded rain for the period. The area was under the influence of a high-pressure system with a recorded barometric pressure of 1023 hPa.
The elevation of the accident site was about 150 to 300 m above mean sea level.
While there were indications of light to moderate south-westerly winds with occasional gusts, the wind conditions were likely consistent with that experienced by the pilot during other in-flight manoeuvres. The wind was considered unlikely to have had an adverse effect the pilot’s ability to maintain control the aircraft during the right turn.
Wreckage information
Accident site
Photographic evidence provided to the ATSB indicated that the aircraft impacted the ground and slid approximately six meters before coming to rest upright, with the right-wing tip resting on the ground, and the left wing in the air. Despite significant damage, all major components remained attached to the aircraft, and the wreckage was not subjected to a post impact fire (Figure 2).
Figure 2: Photograph showing the accident site terrain and impact damage to the aircraft.
Source: SA police
Ground marks consistent with a left wheel and left-wing impact and sliding, was observed to the left of the wreckage. As a result of the ground impact, the pilot who was the sole occupant sustained fatal injuries.
There was no evidence of upward movement of the tailplane as would have been expected had the impact angle been steep. This indicates the aircraft’s nose impact angle was low (less than 45 degrees).
The left wing displayed a high level of impact damage to the lower outboard surface of the leading edge from the wing tip to approximately 1/3 its length (Figure 2). Crumpling and upward bending of the wing was evident behind the leading edge impact area and toward the wing root. It was probable that the left wing was part of the initial impact sequence of the aircraft. The right wing displayed significantly less damage, which was limited to the wingtip. Both wing fuel caps were in place and fuel seepage was observed from around the over-wing refill points.
Engine and propeller
From the evidence obtained from the accident site, there were no identified mechanical issues with the engine or propeller, that prevented normal operation of the aircraft. Bending and scratch marks on the propeller blades was consistent with the engine producing a level of power on impact.
Flightcontrols
The South Australia (SA) Police report indicated the control yoke was jammed in position. Operation of the ailerons, elevator, and rudder was not possible due to the impact damage. Continuity of the flight controls was not confirmed on-site. The flaps were in a partially extended position. The flap actuator extension was not measured, however, the flap indicator showed a position close to a 10-degree setting.
Fuel
On-site examination by the SA Police confirmed fuel was present in both aircraft wing tanks; however, the quantity could not be ascertained. The fuel appeared straw-coloured, and the samples taken did not show signs of particulate contamination. A combination of automotive unleaded fuel and aviation gasoline (Avgas) was identified in the fuel sample during testing. Traces of petroleum distillate were identified in the fuel samples. The operator indicated that no additives were used in the fuel. As such, the traces of distillate were considered fuel contamination. The fuel sample was identical to a drum fuel sample obtained from Mosquito airfield.
The operator advised that an unleaded fuel bulk storage tank was located at the homestead, and that the drum fuel supply at Mosquito airfield had been mixed with unleaded fuel and avgas in the ratio 2:1, (2 parts unleaded fuel to 1 part Avgas) to create a Mogas[2] variant. The operator advised that an Avgas drum fuel supply was sourced from a fuel distribution facility located at Alice Springs, and was normally used with the fixed wing aircraft.
Mogas utilisation
The operator advised Mogas was primarily used with the Robinson R44 helicopter but had been used in RXU on previous occasions. The C150 was capable of flying on Mogas fuel, with some countries providing approval for its use on the aircraft type. Where an Australian registered aircraft was to use Mogas, individual approval in the form of a supplemental type certificate was required. RXU did not have a supplemental type certificate issued for that purpose.
Due to variability of unleaded fuels used in Mogas, fuel volatility and susceptibility to carburettor icing and vapour locks was different from that of Avgas.
Carburettor icing
Mogas is generally higher in volatility than Avgas and will therefore absorb more heat from the mixing air when vaporising. This results in ice forming at higher ambient temperatures. As a consequence, the likelihood of carburettor icing while using Mogas is increased, with the onset of icing likely to occur at higher ambient temperatures and lower humidity than with Avgas.
Vapour lock
Vapour lock because of vaporisation of fuel is more critical with Mogas due to the increased volatility of the fuel. When engine shut down takes place, the engine compartment increases in temperature due to the sudden loss of cooling air flow and the thermal mass of the hot engine. If the engine is started shortly after, the fuel temperature in the engine compartment may be beyond its boiling point and therefore the risk of vapour lock is high.
A vapour lock in flight would result in an increased exhaust gas temperature, interrupted fuel supply, and rough running of the engine (similar to running too lean).
Survival aspects
In general, survival in the case of an aircraft accident depends on four separate aspects, the:
impact forces imparted on the aircraft occupants must be within human tolerance
occupants being restrained to prevent flail-type injuries
liveable space inside the aircraft being maintained
occupants having a means of escape.
Occupant restraints
The occupant restraints in RXU consisted of lap sash seatbelts. The seatbelts had a sash (shoulder) portion connected to the lap belt at an attachment buckle. The seatbelts were inspected by the SA police and were determined to be in a serviceable condition. Examination of the on-site evidence and injuries sustained by the pilot indicated the sash portion of the seatbelt harness system was not worn at the time of the accident.
Cessna aircraft information manuals recommended that for normal flight, the occupant adjust the harness tight enough to prevent excessive forward movement and contact with objects in the event of sudden deceleration. However, pilots sometimes disconnect or do not use the sash portion of the seatbelt harness during flight. This meant that the pilot’s upper torso was essentially unrestrained in the event of the aircraft decelerating quickly during an off-field forced landing, or impact with terrain.
The US National Transportation Safety Board published research paper SR 85-01 titled Impact Severity and Potential Injury Prevention in General Aviation Accidents. The paper highlighted the potential benefits of shoulder harnesses in reducing injury as follows:
There were five survivable accidents in which shoulder harnesses were worn by only one of two front‑seat occupants. A comparison was made of the relative injuries of each occupant. It was found in each case that injury severity was less for the occupant who wore the shoulder harness.
For example, in one accident each of two occupants sustained serious injuries, but the pilot, wearing a shoulder harness, sustained a broken leg and a slight concussion while the passenger without a shoulder harness sustained severe head injuries. The differences in the injuries in these comparisons were related to head and upper body injuries. Those persons who wore shoulder harnesses had markedly fewer head injuries.
The research also showed that if an aircraft occupant wore a shoulder harness, they increased their chances of survival by 20 per cent. Further, the chance of serious injury decreased by 32 per cent.
Liveable space
From photographs obtained of the wreckage, the occupied cabin area within the fuselage was compromised by the impact sequence. Figure 3 shows how the forward floor of the cabin under the instrument panel was crushed when the nose gear collapsed. The impact had buckled the floor under the seats, and the fuselage was breached behind the rear cabin bulkhead. The instrument panels had become dislodged and pushed rearward as a result of the nose impacting the ground. The cabin roof and wings had moved forward as a result of the nose section of the aircraft impacting the ground, reducing the cabin height. All of this damage reduced the survivable space within the cabin area.
Figure 3: Crush damage to accident aircraft compared to exemplar Cessna 150
Source: SA police modified by ATSB
Impact forces and pilot injury
A number of methods are available for measuring the impact forces an occupant is likely to experience during impact. While the outcome gives an appreciation of whether an accident is potentially survivable, the results should be interpreted with caution, as a number of variables do exist during an accident sequence. From the available data, the pilot would have sustained severe to fatal injuries as a result of the calculated impact forces.
The stall/spin condition
TheAerial Mustering Code of Practice[3] included a discussion on a specific stall/spin type of accident that had been observed in a number of low-level fatal accidents involving mustering operations. The common theme was a stall leading to the aircraft impacting terrain in a steep nose down pitch attitude. The sequence of events in these type of accidents followed a similar path to the accident aircraft.
Recovery from these stall/spin conditions required significant altitude. A figure of about 400 ft or more is often quoted. From an accident perspective, the strongest indication of a stall/spin is the steep nose down attitude, particularly when the aircraft was operating at low altitude. Without the spin entry, a Cessna stall typically will not drop the nose to a steep pitch down attitude.
Related/previous occurrences
The ATSB has investigated a number of accidents where a Cessna type aircraft have stalled and impacted terrain. Each of these accidents identify that, while the stalling characteristics of these aircraft types is benign, the stall condition is exacerbated through mishandling of the aircraft during the stall, which can result in entry into a spin. The stall/spin will result in a steep pitch down and rotation towards the stalled wing. Recovery from this condition will take a considerable amount of altitude, the magnitude of which is dependent on the speed of response by the pilot and the use of appropriate control inputs.
AO-2010-047: Cessna 172H, VH-RZV, Loss of control 30 June 2010, 21 km NNW of Cunnamulla, Queensland
While orbiting a water trough at about 500 ft, the pilot lost control of the aircraft. The aircraft impacted the ground and sustained serious damage.
The damage to RZV was consistent with the right-wing colliding with a tree branch followed by the aircraft impacting the ground inverted, with a steep nose-down attitude.
The pilot sustained serious injuries as a result of the impact and was unable to clearly recall the accident. The pilot reported that although he does not recall hearing the aircraft’s stall warning system, the most likely reason for the accident was an inadvertent stall. This probably occurred while the pilot was performing a steep turn with his attention divided between flying the aircraft and looking for cattle.
Investigation number 200506306: Cessna 150G, VH-KPQ, Loss of control 6 December 2005, 156 km north of Broken Hill, NSW.
At about 0835 Eastern Daylight-saving Time, the pilot was observed to circle some sheep at about 250 ft above ground level. Shortly after, ground mustering personnel noticed smoke nearby and found that the aircraft had impacted the ground and there was an intense fire. The pilot, who was the sole occupant of the aircraft, was fatally injured.
The aircraft wreckage was found approximately 400 m to the south-east from where the pilot was circling. The aircraft was upright with evidence of severe impact damage to the left wing, nose section and rear fuselage.
Examination of the aircraft, including the flight control systems and engine, did not reveal any evidence of pre-impact defects. Damage to the propeller indicated that the engine was operating at ground impact. The wing flaps observed in the retracted position.
The steepness of the angle of bank and the nose-down pitch attitude at the aircraft's point of ground impact indicated that the aircraft was in a steep left turn at that time. Those indications and the minimal forward movement of the aircraft after ground contact were consistent with the aircraft having stalled and slipped out of the turn. The lack of aircraft rotation at impact indicated that there had been insufficient time for the stall to develop into a spin, consistent with it occurring at low level.
The investigation concluded that the aircraft possibly stalled at a height from which the pilot was unable to recover.
Pastoralists & Graziers Association (PGA) of WA (Inc), Aerial Mustering Code of Practice, West Perth, Western Australia. Cited in ATSB B2005/0055.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the aircraft operator, Civil Aviation Safety Authority and the South Australia police.
Submissions were received from the aircraft operator, Civil Aviation Safety Authority and the South Australia police. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
The occurrence
On 12 July 2016, the pilot of a Cessna 150 aircraft, registered VH-RXU (RXU), was conducting cattle spotting operations at New Crown Station, about 270 km south-east of Alice Springs, Northern Territory (Figure 1). At about 0700 Central Standard Time,[1] the pilot departed the property to a remote runway called Mosquito airfield, about 60 km to the south. On arrival, the pilot was reported to have discussed the morning’s operations with two groups of stockmen.
Figure 1: Accident site location
Source: Google earth modified by ATSB
The stockmen were tasked with conducting ground-based mustering activities using motorbikes. The pilot of RXU was to assist with locating the cattle and directing the two mustering groups toward them. The property owner stated that ground based mustering supported by aerial spotting was preferred, as it did not stress the cattle as much as aerial mustering.
It was reported that the pilot and stockmen commenced mustering/spotting activities a short distance to the north of Mosquito airfield at about 0730. The pilot was reported to have been operating between the two groups for some time before one of the stockmen noted the aircraft leaving the area. The stockman assumed that the pilot departed the area for Mosquito airfield to refuel.
The operator reported that the original plan was to use a Robinson R44 helicopter for the days mustering but it became unserviceable. The drum fuel positioned at Mosquito airfield was intended for use with the Robinson R44. Consequently, the operator expected the pilot would return to New Crown homestead to refuel during the morning. However, it was determined that the pilot refuelled using the drum fuel at Mosquito airfield instead.
The stockmen reported the aircraft appeared to be operating normally on resuming spotting operations. Further, the pilot, who was in frequent radio contact with the stockmen, did not report having trouble with the operation of the aircraft.
The pilot continued spotting and directing the stockmen to cattle along a thickly wooded creek bed when some cattle broke away from the main cattle herd. Soon after, the stockman unexpectedly exited the creek bed and sought direction from the pilot back to the cattle. The stockman recalled observing the aircraft flying away from them before it commenced a right turn back toward the cattle herd.
The stockman turned the motorbike around to re-enter the creek bed when seconds later a loud ‘bang’ was heard. The stockman stopped and immediately looked toward the direction of the sound, observing the aircraft to have crashed about 30 m away.
The stockman radioed that the aircraft had crashed and immediately proceeded to the aircraft. The pilot had sustained fatal injuries.
From the evidence available, the following findings are made with respect to the loss of control and impact with terrain involving the Cessna Aircraft Company 150G, registered VH-RXU, that occurred 270 km SE Alice Springs, Northern Territory on 12 July 2016. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
While conducting a right turn at low altitude, the pilot lost control of the aircraft and was unable to recover before impacting terrain.
Other factors that increased risk
The pilot of the aircraft did not use the installed shoulder harness (sash), resulting in a greater risk of injury during the collision with terrain.
The use of unapproved fuels in aircraft increases the risk of engine performance related issues.
Safety analysis
Introduction
This analysis will examine the operational factors surrounding the accident involving VH-RXU (RXU). Evidence from witnesses and inspection of the aircraft wreckage indicate that the pilot most likely lost control of the aircraft while executing a right turn. A lack of direct evidence needed to determine the aircrafts final stages of flight meant a reliance was placed on examining:
accident site observations
witness accounts
the operation of the aircraft, and
stall/spin characteristics of Cessna aircraft.
While there was no conclusive evidence that the pilot lost control of the aircraft by aerodynamically stalling during the right turn, the aircraft’s nose-down, and left-wing low attitude on impact could indicate a partial recovery following a stall or early stages of a spin (incipient spin). The pilot may have attempted to recover from this abnormal flight condition, however the aircraft’s altitude was insufficient, and the aircraft impacted terrain. The analysis will consider the circumstances that preceded the event.
Flight during cattle spotting operations
Aircraft handling
The mustering operations required aerial cattle spotting in support of stockmen mustering cattle. Unlike other mustering operations that relied upon aircraft flying at low level (below 500 ft) to herd cattle, aerial spotting did not require the pilot to fly that low. The primary use of the aircraft was to identify cattle and direct the ground-based stockmen to them. It was therefore likely that the pilot was flying at about 500 ft before the accident.
Witnesses reported that while spotting, the pilot conducted a series of turns or orbits overhead to locate the cattle and direct the stockmen to them by radio. Moments before the accident the aircraft was observed in a right turn. The stockman considered this a deliberate manoeuvre by the pilot to reposition the aircraft back toward the creek bed, behind the ground mustering crew.
To facilitate the turn, it was likely that the pilot applied flap and increased the aircraft’s angle of bank. The application of the observed 10 degrees flap selection would have allowed the pilot to fly the aircraft at a lower airspeed while maintaining a margin above the stall. However, the introduction of bank and/or unbalanced control inputs would have decreased the stall margin. Consequently, an adequate airspeed through appropriate power application during increased bank angles was essential to maintain the stall margin.
Distraction during manoeuvring
It was possible that during the turn the pilot’s primary focus was on manoeuvring the aircraft back toward the direction of the creek bed attempting to reacquire the cattle. Research has shown that when a pilot becomes distracted, the tendency for not monitoring the aircrafts energy state and/or adding unbalanced control inputs is increased. This has the potential to induce a stall or entry into a spin from low altitude. In this case, it could have led to the pilot losing control of the aircraft. A review of similar accident investigations highlighted that this was particularly evident when conducting turns during mustering operations or when conducting other tasks that require the pilots attention to ground based activities.
It has been highlighted in other accident investigation reports that Cessna considers that the height required to recover the aircraft from the stall/spin condition is significant, and at least in the order of 400 ft. It was therefore important that the pilot monitors and maintains an appropriate margin above the stall during a turn, be cautious with manoeuvring, and was balanced with control inputs when flying at lower altitudes.
While the degree of manoeuvre that led to the loss of control of the aircraft could not be determined, it was possible that in an attempt to reacquire the cattle, the pilot’s control inputs induced a stall leading to a possible incipient spin and collision with terrain. Had a stall/spin condition occurred or been imminent, the aircraft’s low impact angle may indicate a partial recovery, or is indicative of the early stages of a spin.
Seatbelt use while conducting in-flight manoeuvres
A number of studies and accident investigations have examined the use and effectiveness of various occupant restraints. The ability for the occupant to sustain less life-threatening injuries relied upon the use and appropriate fitment of the seatbelt or harness restraint. Lap/sash or full harness restraints are shown to reduce the incidence of flail type injuries during an accident.
Although in this case, the likelihood of the pilot sustaining flail related injuries would have reduced if the sash portion of the seatbelt restraint had been used, it could not be determined if it would have changed the outcome of the accident.
This accident highlights the importance of the appropriate use of restraints by pilots and passengers during all phases of flight. This is particularly the case during aircraft operations at low altitudes where little time exists to refit the restraint in the event of an abnormal inflight condition or emergency.
The use of unapproved fuel
It was reported by the operator that the fuel primarily used in VH-RXU was Avgas, sourced from an authorised refuelling facility in drums. However, the fuel sample taken from RXU after the accident was identified as a combination of Avgas and unleaded fuel (referred to as Mogas by the operator). This was consistent with the drum contents at Mosquito airfield.
Research has shown that using Mogas can have an effect on the formation of vapour lock in the fuel system, and carburettor icing. Despite this, the pilot successfully climbed the aircraft after refuelling from Mosquito airfield and recommenced spotting operations. There were no reported difficulties with aircraft performance.
It was considered that, despite the known issues with the use of Mogas, it was unlikely that in this case it resulted in poor engine performance or contributed to a loss of aircraft control.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 21 March 2016, a Cessna 172L, registered VH-XZZ, disappeared from radar about 7 NM (13 km) north-east of Byron Bay, New South Wales (NSW). The pilot was the sole occupant and, despite initial search efforts, the aircraft was reported as missing.
The accident is being investigated by the NSW Police Force on behalf of the NSW Coroner. The ATSB did not initiate a separate accident investigation; however, on 14 June 2016, the police advised the ATSB that the wreckage had been located and video recorded by the Royal Australian Navy. In addition, the police requested ATSB assistance with their examination the video footage of the wreckage.
To facilitate this support, on 15 June 2016 the ATSB initiated an external investigation under the provisions of the Transport Safety Investigation Act 2003. The ATSB completed its review of the video footage and provided a report to the NSW Police Force on 30 August 2016.
Any enquiries as to the planning for, or conduct or progress of the Coroner’s investigation into this accident should be directed to the:
State Coroner’s Court of New South Wales 44–46 Parramatta Road Glebe NSW 2037
Phone: (02) 8584 7777
_________________
The information contained in this web update is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
On 12 May 2016, the pilot of a Robinson R22 Beta II helicopter, registered VH-WGB, was conducting aerial work at a property about 221 km east-north-east (ENE) of Port Hedland, Western Australia.
The pilot was observing two other helicopters engaged in aerial mustering for the benefit of the pilot’s own learning experience. The pilot’s attention was divided between flying the helicopter at about 200 ft above ground level and observing the mustering helicopters, which were operating between ground level and about 200 ft.
At about 1030 Western Standard Time (WST), while manoeuvring the helicopter to observe the mustering operation, the pilot commenced a level 180° turn to the left into wind. At the time the helicopter entered the left turn, it was flying at about 40 kt airspeed with about a 15 kt tailwind component.
Just prior to exiting the turn, the pilot felt the helicopter ‘kick’. The helicopter then yawed[1] rapidly to the right and pitched nose down. The pilot applied left pedal in an attempt to counteract the yaw, however, the helicopter did not respond normally to pedal[2] or cyclic[3] control inputs. The pilot also lowered the collective[4] and reduced the throttle. The helicopter pitch attitude[5] oscillated between a steep nose-down and a level attitude as the helicopter rotated towards the ground. As the helicopter neared the ground, the pilot applied aft cyclic, increased the throttle and raised the collective, which levelled the helicopter attitude and reduced the rate of descent.
The helicopter collided with the ground in a level attitude. The helicopter skids and seat collapsed following ground contact. During the accident sequence, the main rotor blades severed the tail boom. The pilot’s helmet struck the cyclic and the pilot sustained minor injuries. The aircraft was substantially damaged (Figure 1).
Figure 1: Accident site showing damage to VH-WGB
Source: Aircraft Operator
Pilot comments
The pilot provided the following comments:
the wind was steady at about 15 kt from the south-east with occasional gusts to 20 kt
the pilot was not sure what the ‘kick’ was, but thought it was due to the wind
the pilot did not recognise a low gravity (weightless) situation and may have applied incorrect cyclic technique, resulting in the main rotor striking the tail boom
the pilot thought that the tail boom was severed shortly after the kick because there was no response from the pedals to counteract the yaw and the helicopter immediately entered a nose down spiral
the pilot’s helmet was damaged during the collision, when it struck and broke the cyclic (Figure 2)
wearing the helmet probably prevented a more serious injury from occurring.
Figure 2: Damage to pilot’s helmet
Source: Helicopter pilot
Loss of tail rotor effectiveness
The United States Federal Aviation Administration (FAA) Helicopter flying handbook
The FAA Helicopter flying handbook chapter 11: Helicopter emergencies and hazards stated that loss of tail rotor effectiveness (LTE) is an uncommanded rapid yaw towards the advancing blade and is an aerodynamic condition caused by a control margin deficiency in the tail rotor. Tail rotor thrust is affected by numerous factors, including relative wind, forward airspeed, power setting and main rotor blade airflow interfering with airflow entering the tail rotor. There are several wind directions, relative to the nose of the helicopter which are conducive to LTE, including the following:
285–315°, which can lead to turbulent airflow from the main rotor disc interfering with the tail rotor
210–330°, which can lead to the development of unsteady airflow through the tail rotor.
The FAA handbook warns that a combination of factors in a particular situation can lead to more anti-torque required from the tail rotor than it can generate. In addition, low speed flight activities are a high-risk activity for LTE. The FAA handbook provided the following recovery technique for a sudden unanticipated yaw:
apply forward cyclic control to increase airspeed
if altitude permits, reduce power
as recovery is affected, adjust controls for normal forward flight.
The Robinson Helicopter Company advised that to avoid an unanticipated yaw, pilots should be aware of conditions (a left crosswind, for example) that may require large or rapid pedal inputs. They recommend practising slow, steady-rate hovering pedal turns to maintain proficiency in controlling yaw.
Low gravity (G) conditions
The FAA Helicopter flying handbook
The FAA handbook chapter 11 stated that semi-rigid rotor systems are especially susceptible to hazards from manoeuvres involving low accelerations of gravity (low-G or weightless) because the helicopter is designed to be suspended from the main rotor. In a low-G condition, such as abruptly pushing the cyclic forward, the helicopter airframe is not supported by the main rotor mast, which may allow the main rotor blades to exceed their normal flapping limits and contact the airframe.
The FAA handbook advised that in a low-G situation the pilot should first apply aft cyclic to return the lift and weight forces to balance and always adhere to the manufacturer’s manoeuvring limitations and advisory data.
The Robinson helicopter company issued safety notice SN-11 in October 1982, which stated:
Pushing the cyclic forward following a pull-up or rapid climb, or even from level flight, produces a low-G (weightless) flight condition. If the helicopter is still pitching forward when the pilot applies aft cyclic to reload the rotor, the rotor disc may tilt aft relative to the fuselage before it is reloaded.
ATSB comment
When the pilot manoeuvred the helicopter into wind, it flew through two relative wind directions conducive to an LTE event. The pilot commented that they entered the turn at about 40 kt airspeed, but was actively scanning between flying the helicopter and observing the aerial mustering activity. It is likely that during the turn, the airspeed combined with the relative wind direction to initiate an LTE event. The recommended actions to recover from an LTE include the application of forward cyclic to increase airspeed. This could place the helicopter into a low-G condition if an abrupt forward cyclic input is made, and increase the risk of striking the tail boom if the forward cyclic input is followed by an abrupt and/or large aft cyclic input.
Safety message
Loss of tail rotor effectiveness and low-G conditions
To avoid the conditions which could lead to main rotor blade/fuselage contact accidents, the Robinson R22 Pilot’s operating handbook recommends the following procedures for pilots:
maintain cruise airspeeds between 60 kt and less than 0.9 VNE[6], but no lower than 57 kt
use maximum power on revolutions per minute at all times during powered flight
avoid sideslip during flight and maintain in-trim flight at all times
avoid large, rapid forward cyclic inputs in forward flight, and abrupt control inputs in turbulence.
Effectiveness of helmets in helicopter operations
The United States Army referenced two United States Army Aeromedical Research Laboratory studies of helmet effectiveness in
. The first study from the period 1957–1960 found that fatal head injuries were 2.4 times more common among unhelmeted occupants of potentially survivable helicopter accidents than among occupants wearing the army’s APH-5 helmet. The second study from the period 1972–1988 found that the risk of fatal head injury was 6.3 times greater in unhelmeted occupants of potentially survivable helicopter accidents than among occupants wearing the army’s SPH-4[7] helmet.
In a separate study (report 98-18) the Army Aeromedical Research Laboratory reviewed 459 accidents in the period 1990–1996 where helmet visor use was verified. They found that visor use was attributed to preventing facial injury in 102 (22.2%) accidents and reducing injury in 13 (2.8%) accidents.
This accident highlights the effectiveness of wearing a helmet to prevent a more serious injury. ATSB report AO-2014-058 provides an account of a serious head injury to an R22 pilot who was not wearing a helmet. In a later ATSB report, AO-2015-134, the operator commented that the pilot of an R22 accident would have suffered more serious head injuries if he was not wearing a helmet.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.