On 12 November 2015, a pilot was mustering cattle in a Robinson R22 helicopter, registered VH-HWJ, at a property about 90 km south of McArthur River Mine, Northern Territory.
At about 1400 Central Standard Time (CST), as the helicopter approached the cattle yards, it descended rapidly and collided with a tree and terrain. The helicopter landed on its side and sustained substantial damage (Figure 1). The accident occurred about 200 m prior to the cattle yards. The pilot sustained serious injuries and was unable to recall the sequence of events.
Figure 1: Accident site showing damage to VH-HWJ
Source: Helicopter operator
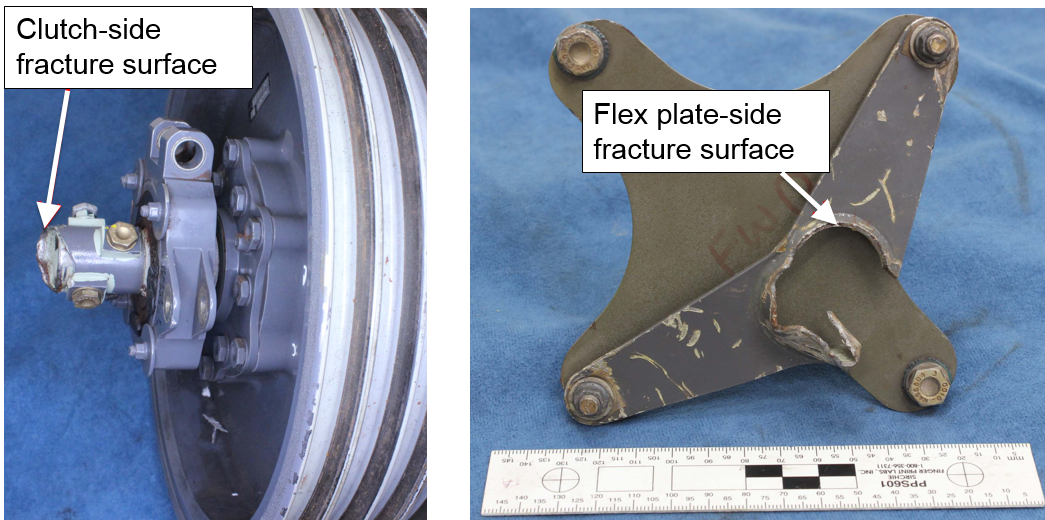
Analysis of fractured yoke
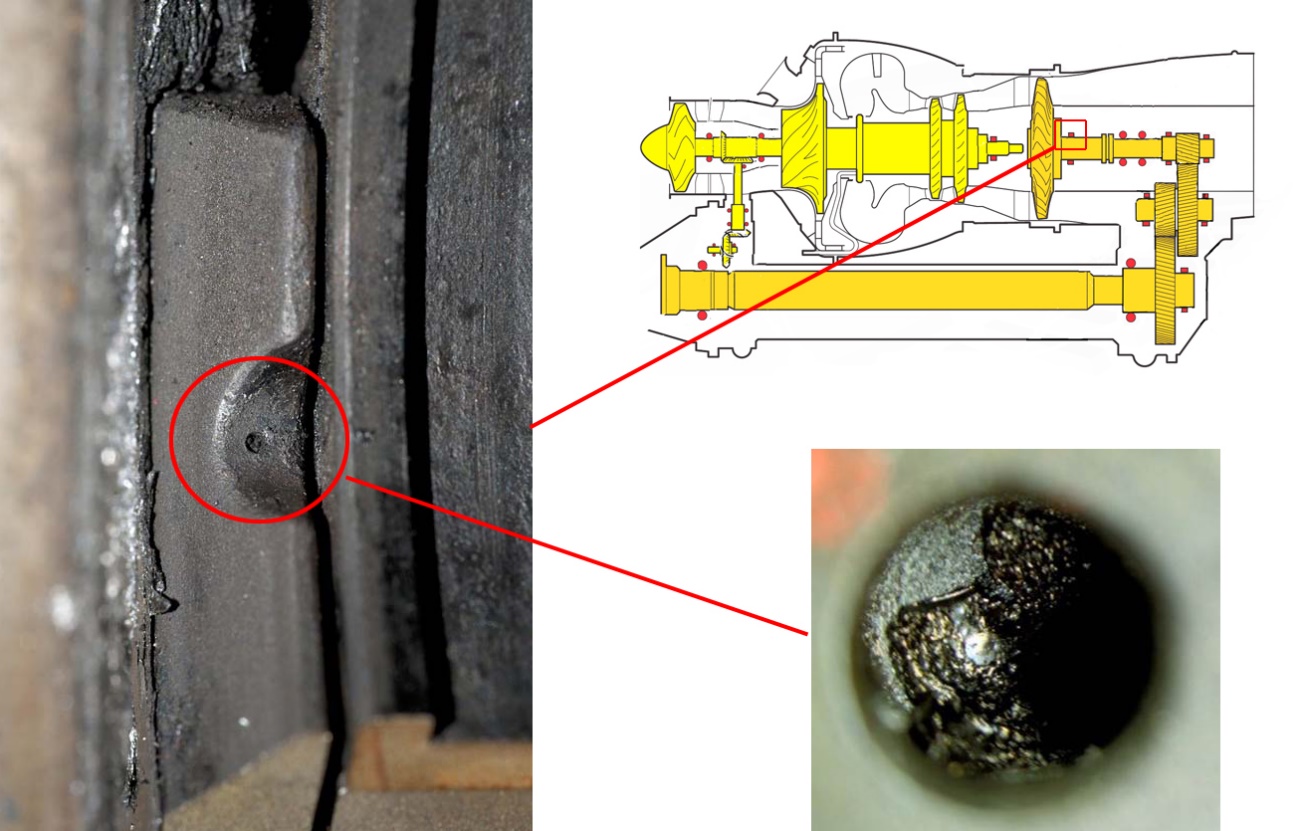
The yoke connecting the clutch shaft to the rearward flex plate was found to have fractured at the connection to the shaft (Figure 2). The ATSB conducted analysis to determine whether the yoke failure may have contributed to the accident, or occurred as a result. The analysis found no evidence of fatigue damage in the yoke, and no other signs of pre-existing damage. The helical fracture was consistent with torsional overstress inducing failure in the yoke.
Figure 2: Fracture surfaces
Source: ATSB
Weather
The weather at McArthur River mine was recorded at 1200 and 1530. At 1200, the wind was from 340° at 5 kt and the temperature was 36 °C. At 1530, the wind was from 160° at 4 kt and the temperature was 38 °C. The direction of the helicopter relative to the wind at the time of the accident could not be determined. The ambient temperature at the time of the accident was about 37 °C. Although the influence of the temperature on the accident is unknown, high ambient temperatures adversely affect helicopter performance.
Operator comments
Subsequent to a previous accident, the operator mandated the wearing of helmets for all pilots. The operator commented that although the pilot sustained head injuries, the outcome might have been worse if the pilot had not been wearing a helmet.
ATSB comment
The ATSB was unable to determine the cause of the accident.
Safety message
US military research[1] analysed helicopter accidents that were at least partially survivable. It found that occupants not wearing a protective helmet were significantly more likely to sustain severe and fatal head injuries. The US National Transportation Safety Board (NTSB) also acknowledged that the use of head protection can reduce the risk of injury and death. The NTSB issued Safety Recommendation A-88-009, recommending that crewmembers of emergency medical services helicopters wear protective equipment including helmets.
The ATSB investigation report (AO-2014-058) into an accident involving a Robinson R22 helicopter where the pilot sustained a serious head injury, reminded pilots and operators to consider the benefit of occupants wearing helmets to reduce the risk of head injury in the event of an emergency landing.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
At about 1730 AEDT[1] on 7 November 2015, the owner-pilot of an Airbus Helicopters (Eurocopter) EC135 T1, registered VH-GKK, departed Breeza, New South Wales, on a private flight to Terrey Hills, New South Wales. The flight was conducted under the visual flight rules and there were two passengers on board.
About 40 km to the south-west of the Liddell mine, the pilot diverted towards the coast, probably after encountering adverse weather conditions. Witnesses in the Laguna area observed the helicopter overfly the Watagan Creek valley in the direction of higher terrain. The helicopter was then observed to return and land in a cleared area in the valley.
After 40 minutes on the ground, the pilot departed to the east towards rising terrain in marginal weather conditions. About seven minutes later and approximately 9 km east of the interim landing site, the helicopter collided with terrain. A search was initiated about 36 hours later. The helicopter wreckage was found at about 1840 on 9 November 2015. The pilot and two passengers were fatally injured.
What the ATSB found
The ATSB found that the pilot departed an interim landing site under the visual flight rules in marginal weather conditions. The pilot likely encountered reduced visibility conditions leading to loss of visual reference leading to the collision with terrain.
The ATSB also found that the fixed, airframe-mounted emergency locator transmitter had been removed and that personal locator beacons which required manual activation were carried instead. While in this accident it did not affect the outcome for the occupants, the lack of activation, combined with the absence of flight notification information, delayed the search and rescue response.
Safety message
Weather-related general aviation accidents remain one of the most significant causes of concern in aviation safety and the following safety messages are key:
Avoiding deteriorating weather or instrument meteorological conditions (IMC)[2] requires thorough pre-flight planning, having alternate plans in case of an unexpected deterioration in the weather, and making timely decisions to turn back or divert.
Pressing on into IMC conditions without a current instrument rating carries a significant risk of encountering reduced visual cues leading to disorientation. This can easily affect any pilot, no matter what their level of experience. In the event of inadvertent entry into IMC, pilots are encouraged to contact air traffic control for assistance.
ELTs and PLBs are key safety devices that may become inhibited in a crash. In light of their respective limitations, it is worth considering the use of both.
The pilot was issued with an Australian Private Pilot (Helicopter) Licence in January 1989, following acceptance of a licence issued in the United Kingdom in 1988. At the time of the accident, the pilot held endorsements for two types of piston-engine helicopter and three types of turbine-engine helicopter, including the EC135 type that the pilot was operating.
In 1991, the pilot was issued a Night VFR[8] Helicopter rating and in 1992, the pilot completed low flying training. Between 2005 and 2008, the pilot was approved by the Civil Aviation Safety Authority (CASA) to give endorsement or conversion training in EC-135 helicopters. The pilot did not hold an instrument rating[9] and there was no indication that he had sought to obtain one. This limited the pilot to visual flight operations.
The pilot’s logbook recorded a total aeronautical experience of 2,654 hours, which included 1,256 hours on the EC135 helicopter type. This included a total of 5 hours of simulator experience, 7.5 hours instrument flight time, and 8.1 hours in command at night. No night experience was logged since September 2010, so the pilot did not appear to meet the night-VFR recency requirements.
The most recent helicopter flight review was conducted by a CASA Flying Operations Inspector (FOI) in March 2014. This included a pre-flight assessment of the pilot’s interpretation and application of meteorological reports. It also included a bad weather navigation exercise and diversion. The FOI assessed that the pilot performed to a satisfactory standard overall, and displayed average flying skills and a high level of technical knowledge about the helicopter.
The pilot held a Class 2 Civil Aviation Medical Certificate that was due to expire in May 2016. He was required to wear distance vision correction and to have vision correction available for reading. Post-mortem and toxicological examination found no underlying medical disorder likely to lead to incapacitation of the pilot, however the medical examiner could not exclude hypertension as contributing to the accident.
A search of the ATSB database yielded notifications regarding two significant occurrences involving the pilot and VH-GKK: a weather-related event in December 2004 and a wire strike in November 2012. This earlier event is described in a book published by the pilot. As the book relates, the pilot became caught in cloud at low level over water then climbed to a safe altitude to continue in cloud with reference to a GPS[10] moving map. The pilot advised air traffic services of the situation and sought information about the extent of the weather. Approaching land displayed on the moving map, the pilot slowed down and gradually descended until the coastline became visible. According to the book, to cope with this type of situation the pilot was night-rated and regularly practised flying on instruments, and the helicopter was equipped with an autopilot and instrumentation.
In the wire strike event, the helicopter was damaged and was subsequently operated in that condition for a short duration. This was investigated by CASA, as were other events:
August 2006: main rotor blade contact with trees resulting in main rotor damage
May 2012: operations at an aerodrome in close proximity to aircraft on the ground with risk of collision or damage from downwash
Although the pilot disputed the investigation findings, CASA undertook counselling in 2006 and licence suspension in 2013. Following the flight review conducted by a CASA FOI in March 2014, CASA reinstated the pilot’s licence.
The ATSB did not identify a connection between the incident history and the flight into terrain.
Visual flight rules
The basic principle for VFR operations is for pilots to ensure that the flight is conducted in visual meteorological conditions (VMC), which provides for sufficient flight visibility and clearance from cloud. In non-controlled airspace (Class-G) and for operations at/below 1,000 ft above ground level (AGL), the general requirement is for 5,000 m visibility and clearance from cloud.
In the case of helicopters operated below 700 ft AGL, the minimum required visibility can be decreased to 800 m if certain conditions are met. The pilot must be operating during the day only and at a speed that allows adequate opportunity to see any obstructions or air traffic in sufficient time to avoid a collision.
Unless a pilot holds a current instrument or night visual flight rules rating, a departure must not take place unless the estimated time of arrival for the destination (or alternate destination) is at least 10 minutes before last light.[11] However, the presence of cloud cover or poor visibility, may cause daylight to end at a time earlier than the time stated.
For a night-VFR flight, a pilot must be at or above the lowest safe altitude in conditions that provides at least 5,000 m visibility and specified clearance from cloud. In this case, the weather conditions were not suitable for night VFR so the pilot was restricted to daylight conditions.
Calculations based on an average groundspeed of 120 kt, taken from the approximate departure time from the interim landing site, indicated that an arrival at the Terrey Hills base would have occurred about 15 minutes before last light.
Aviation-specific meteorological forecasts and warnings
Overview
The Bureau of Meteorology (BoM) produces observations, forecasts, warnings and advisories that are essential for safe and efficient aviation operations. For flight planning, aviation users were advised to obtain the applicable aviation meteorological products from Airservices Australia, the official provider of the Aeronautical Information Services. These products could be obtained through:
Airservices NAIPS Internet Service (free registration required)
Airservices AVFAX (free registration required)
Airservices Pilot Briefing Services (free-call telephone)
Third party websites and apps with access to NAIPS.
In addition, the BoM provided an unofficial copy of aviation meteorological products on their website and nominated a phone number on some forecasts for users requiring more information.
The pilot was not registered to access NAIPS or AVFAX directly and there was no indication that the pilot utilised the Airservices Pilot Briefing Service to obtain weather forecasts or reports on the day of the accident. The pilot did have mobile devices with internet access and was registered to use at least one app that provided aeronautical information sourced from NAIPS. That app did not record any details of the data obtained by a user.
On a ‘Useful data’ sheet dated 2013, the pilot noted the BoM website address and phone numbers as the only entries under the heading of weather. The ATSB did not have information about the pilot’s internet use and there was no record of the pilot calling the BoM on the day of the flight to Breeza.
Before departure from Terrey Hills, the pilot could have used a home computer or mobile device to access aviation forecasts and reports through the app or the BoM website. From then on, wherever there was mobile internet data available, the pilot could have used a mobile device to access weather information.
At the time of the occurrence, the BoM produced three general types of routine forecasts applicable to general aviation: an area forecast for a defined geographical region and aerodrome forecasts (TAF) [12] and trend forecasts (not relevant to the occurrence flight) for specified aerodromes/airports. The bureau generally issued these forecasts for a set validity period but would issue an amended forecast if there was a change to the expected weather conditions during the validity period.
The bureau also issued warnings if they became aware of un-forecast deterioration (AIRMET) and if there was significant weather expected (SIGMET). In addition to being available on demand from aeronautical information providers, these warnings were broadcast on relevant air traffic service frequencies.
It is noted that at the time of the occurrence, aviation meteorological forecasts were presented in a textual format. In November 2017, the area forecast was replaced with a Graphical Area Forecast and Grid Point Wind and Temperature Forecasts to make it easier to interpret and use the information.
Following is a summary of the decoded text of the relevant aviation-specific forecasts and warnings issued by the BoM. The times have been converted from UTC to AEDT.[13]
Area forecasts 7 November 2015
The direct track from Terrey Hills to Breeza and return was within the eastern half of Area 20 which covers north-eastern NSW. On the day of the flight, the initial Area 20 forecast was issued at 0253 and was valid from 0400 to 1600. This was the forecast valid in the period before the pilot’s departure from Terrey Hills.
Between 0400 and 1600, in the eastern half of Area 20, isolated thunderstorms were forecast from 0700 and isolated showers from 1000. There would be areas of broken low cloud and isolated fog/mist but these were expected to clear by 1100. As a surface trough moved up the coast from near Williamtown during the period, broken low cloud and light showers/drizzle were expected to form behind it. This low cloud would be between 1,000 and 3,000 ft AMSL but would lower to 500 ft in showers/drizzle. (There was also other cloud forecast at or above 3,000 ft but this was not relevant to the occurrence.)
For the critical locality of Murrurundi Gap, 53 km south-east of Breeza and close to the direct track, there would initially be broken cloud on the ground but in the period from 0900 to 1100 this would become scattered cloud at 6,000 ft (3,700 ft above ground) with light showers of rain.
The initial area forecast was superseded by an amended forecast issued at 0828, which was itself superseded by an amended forecast issued at 1439. Another amended forecast was issued at 1549, which was the forecast valid for the return flight from Breeza.
In the overviews of all three amended area forecasts, isolated thunderstorms and rain showers were still forecast in the eastern half of the area throughout the period. The areas of broken low cloud that had been forecast to clear by 1100 were now forecast to redevelop after 1700. In the amended forecasts issued at 1439 and 1549, broken low cloud would be expected from the start of the respective validity periods over the sea/coast south of Williamtown Airport (near Newcastle) and in rain showers, and this would extend inland from 1600. From 2100, isolated fog and mist would be expected over land. From 2200, broken cloud would be on the ground at Murrurundi Gap.
Based on the forecast issued at 1549, by the time the pilot departed Breeza at 1730, there would be broken cloud between 1,000 ft and 8,000 ft over the sea and coast south of Williamtown Airport and extending. There would also be broken cloud between 2,000 ft and 5,000 ft with higher scattered cloud over the ranges and slopes that pilot intended to fly over in the latter part of the flight. Thunderstorms and rain showers may also have developed on or near the intended track with associated visibility down to 2,000 m and severe turbulence in the thunderstorm.
Aerodrome forecasts 7 November 2015
The pilot was operating between his private helipad at Terrey Hills and a private property at Breeza, neither of which are served by aerodrome forecasts (TAFs). In the case of such flights, pilots can refer to TAFs for aerodromes in the vicinity of the intended route. As well as providing a more localised forecast, these TAFs can inform contingency planning. The heights referenced in TAFs are heights above the aerodrome reference point (ground).
Although Sydney International Airport is the closest airport to Terrey Hills with a TAF (or equivalent), the TAF for RAAF Base Richmond, located 40 km to the west of the pilot’s helipad, would be a useful reference. Other TAFs of interest for this flight would be for Maitland and Scone aerodromes for the en route phase and Tamworth Airport for the arrival and departure at Breeza.
The TAFs issued early in the day for Richmond forecast light showers of rain and few cloud at 1,000 ft and broken at 2,000 ft. Although the cloud was due to lift after 1300 to 2,500 ft and 3,000 ft respectively, intermittent periods of broken cloud at 1,000 ft with rain showers up to 1500 and after 2000 were forecast.
Amended Richmond TAFs were issued at 1030, 1544, 1609 and 1734. Based on the 1544 and 1609 TAFs that were valid about an hour before the pilot’s intended departure from Breeza, the weather in the Terrey Hills local area could have been light showers of rain with scattered cloud at 1,500 ft and broken cloud at 2,500 ft. From 1700 onwards, there would be temporary periods up to 60 minutes duration where the cloud would be broken at 1,000 ft with rain showers.
The initial TAF for Maitland was issued at 0450 and was valid from 0600 to 1900. The cloud was scattered at 2,000 ft with rain showers. From 1100 onwards, there would be intermittent periods where the cloud would be broken at 1,000 ft with drizzle and visibility reduced to 4,000 m.
An amended Maitland TAF was issued at 1137 and was valid from 1300 to 0100 the next day. The conditions were the same as the initial forecast until 1900 when the intermittent periods would extend to temporary periods. Another amended TAF was issued at 1919 to include a 30% probability of a thunderstorm.
The TAF for Scone was issued at 0451 and was valid from 0600 to 1900. For the periods that the pilot was airborne, the cloud was forecast to be scattered at 1,000 ft and 4,000 ft with light showers of rain.
The TAFs for Tamworth were issued at 0942 and 1535. These were essentially the same and advised of scattered cloud at 5,000 ft and rain showers until 2300, when the cloud would change to ‘few’ at 1,000 ft.
Warnings 7 November 2015
An AIRMET[14] issued at 1543 indicated that isolated thunderstorms were observed at Richmond, NSW. An amended area forecast was subsequently issued at 1549 as described above.
Forecasts and warnings 6 November 2015
Given it was reported to the ATSB that the pilot intended to conduct the flight the day before but cancelled due to warnings of storms in the Hunter Valley, the ATSB reviewed the relevant forecasts and warnings issued by the BoM for the day before.
The area forecast for Area 20 issued early in the day forecast isolated thunderstorms throughout the area until 1600 when they were expected only in the Hunter Valley and northward. Broken low cloud would be on the ranges/slopes and sea/coast but would clear by 1300. Any isolated fog and mist was to clear by 0900.
For the critical locality of Murrurundi, broken cloud was forecast to be on the ground with light showers of rain until it improved between 1000 and 1200. From 1000 onwards, there would be temporary periods up to 60 minutes duration of thunderstorms with broken cloud on the ground.
The TAFs issued for Richmond forecast possible foggy conditions that would clear by 0900 followed by benign conditions for the rest of the day. For Maitland, Scone, and Tamworth, the morning conditions included a risk of fog, and scattered low cloud with light showers of rain. By late morning, intermittent or temporary periods of thunderstorm activity could be expected at the three locations until evening.
Assessment of the weather conditions
7 November 2015
To assess the weather conditions encountered by the pilot on the return flight to Terrey Hills, the ATSB obtained and integrated the following data:
helicopter position from radar data
forecast for Area 20
weather radar imagery and observations from the BoM
witnesses in the vicinity of the interim landing site
private weather station data in vicinity of the interim landing site.
Weather radar images from Lemon Tree Passage (located on the southern shores of Port Stephens) recorded significant rainfall returns over Richmond at 1548. As the thunderstorm moved to the north-east, the weather radar images showed that it developed from a single isolated return into a wide band of rainfall extending 50 km in a north-west / south-east direction.
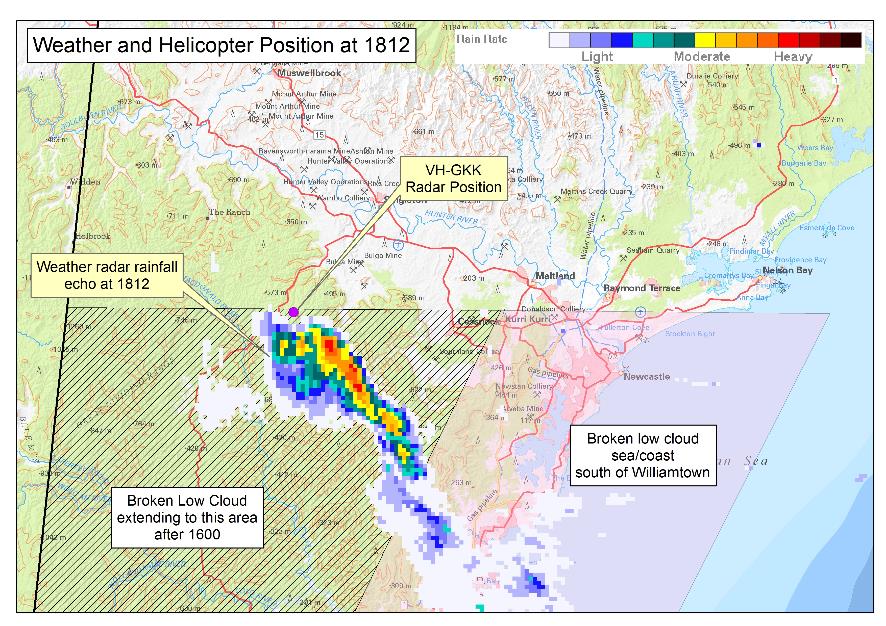
By 1812, the rain/storm band had moved north-east to be evident 100 km west and south-west of Williamtown Airport. At the same time, the helicopter was identified at a position that is just north of the weather band (Figure 7).
As the rain/storm band continued to move to the north-east, the helicopter moved to the southeast and was identified at 1818 at a position that correlates with the leading edge of the rain/storm band.
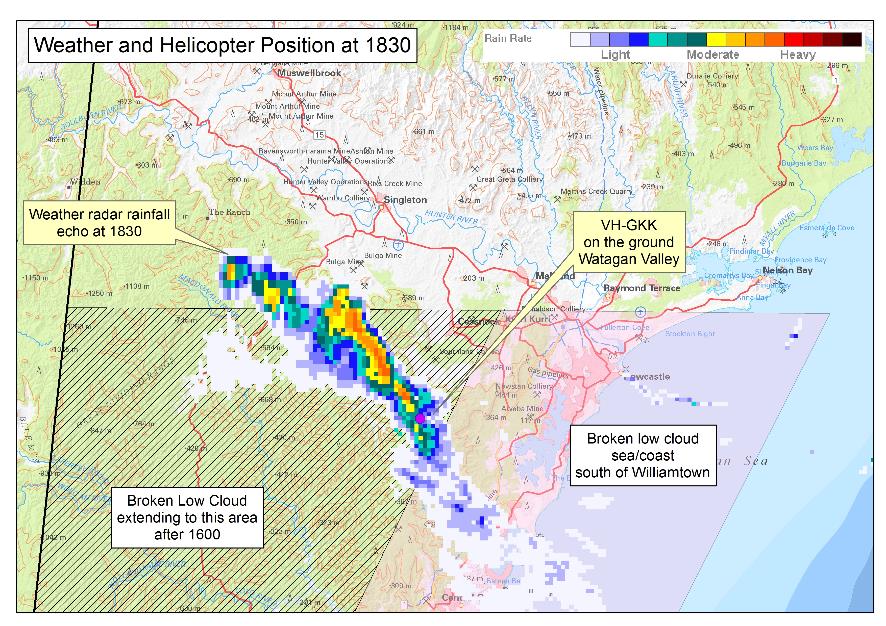
By 1822, the leading edge of the rain/storm band had encircled the identified position of the helicopter. At 1830, the rain/storm band was over the Watagan Creek valley location where the pilot landed the helicopter (Figure 8).
Figure 7: Composite weather image and position of VH-GKK at 1812
Source: Background image Geoscience Australia, Weather image Bureau of Meteorology, annotated/modified by ATSB.
Figure 8: Composite weather image and position of VH-GKK at 1830
Source: Background image Geoscience Australia, Weather image Bureau of Meteorology, annotated/modified by ATSB.
Witnesses in the Watagan Creek valley area recalled that on the afternoon of the accident, a storm had approached from the south-east with dark clouds and rain moving in. By 1600 the weather had started to deteriorate further, with low cloud in the valley. Between 1830 and 1845, around the time when the helicopter landed in the valley, the witnesses reported that there was heavy rain and reduced visibility in the area. One witness, who advised he was a pilot, later reported that the conditions did not appear conducive to VFR flight.
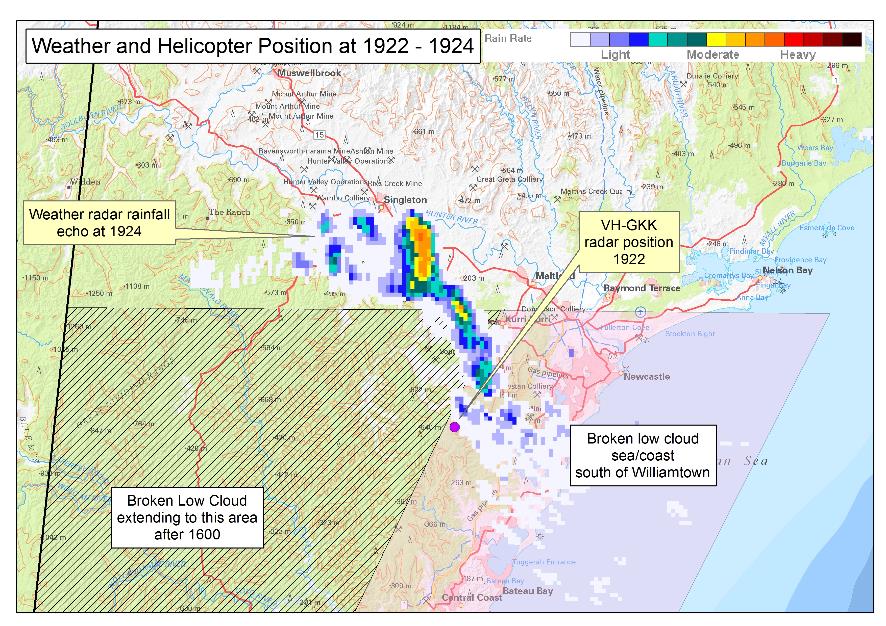
By 1912, the intense elements of the rain/storm front had moved away from the interim landing site but there was still light activity to the east and south-east. When the helicopter was last identified at 1922:50, it was in the vicinity of the light precipitation activity that had moved up the coast and adjacent ranges (Figure 9).
Figure 9: Composite weather image 1922-1924 and position of VH-GKK
Source: Background image Geoscience Australia, Weather image Bureau of Meteorology, annotated/modified by ATSB.
The data recorded by a local private weather station situated at the eastern end of the Watagan Creek valley reflected conditions that were conducive to cloud and fog, including fluctuations in ambient light and rainfall throughout the afternoon and early evening. That recorded data also indicated that there was a change in the ambient lighting. Between 1852 and 1909, the ambient lighting improved but by 1915 the lighting had returned to previous, darker conditions and no further improvements in ambient lighting up to, and beyond, the time of the accident were recorded.
Last light for Terrey Hills was calculated as 1954, although the presence of cloud cover or poor visibility will cause daylight to end at a time earlier than the time stated. Pilots are advised to make allowance for this when flight planning or when confronted with such factors when an estimated time of arrival nears the end of daylight. It should be noted that the parameters used in compiling times of last light do not include the nature of the terrain surrounding the location, or the presence of other than a cloudless sky and unlimited visibility at the destination location.
Aircraft and maintenance
The helicopter was powered by twin Turbomeca engines and was configured for seating five people. The helicopter was manufactured in 1999 and was registered in Australia the same year. Since new, the helicopter had been operated for about 1,400 hours.
The aircraft was equipped with all of the required instrumentation for flight under the VFR, Night VFR, and IFR, but was not being maintained to IFR specifications. Since manufacture, the helicopter had been fitted with a 3-axis autopilot and Garmin GNS[15] 430 and GNS 530 units. These avionics were integrated and provided the capability to navigate IFR conditions in various autopilot modes. The GNS 530 could display terrain information or provide a Terrain Awareness and Warning System (TAWS), depending on the installed hardware and configuration. The status of the unit fitted to VH-GKK was not established.
The helicopter was also equipped with an auxiliary battery providing ground power for camping and photography equipment.
The helicopter was maintained primarily by the owner-pilot who held a CASA instrument of approval to perform and certify specific aspects of maintenance. There were no anomalies identified in the maintenance records.
Following a 12-monthly inspection, the owner-pilot issued a maintenance release in April 2015 for a period of 12 months and 200 hours of operation. No defects were recorded and maintenance due during the validity period was signed off. Since April 2015, some minor work had been recorded in the logbook, including removal of the fixed Emergency Locator Transmitter (ELT).
Two personal locator beacons (PLBs) were on board and both were found at the accident site within their respective cases. The PLBs were an appropriate regulatory substitute for the fixed unit that had been removed prior to the accident. Neither of the PLBs demonstrated evidence of manual or attempted activation.
At the time of the accident, the aircraft had been operating below its maximum gross weight and the centre of gravity was within the flight manual limits.
Wreckage and impact information
Accident site assessment
The helicopter wreckage was distributed in a linear pattern along a distance of approximately 90 m on a heading of 143 degrees magnetic. The first items in the trail were parts from the tail, which indicated that the helicopter entered the tree canopy in a slightly nose up attitude. Tree upper limb damage about 40 metres from the start of the wreckage trail indicated that the helicopter was not banking during entry.
Along the wreckage trail, the trees were about 34 m high and a number of these had upper trunks and branches that were damaged, which was indicative of a relatively level trajectory. As the helicopter passed through the tree canopy, the helicopter cockpit and cabin progressively disintegrated.
All of the helicopter major subassemblies were identified at the accident site. A fragment of one of the main rotor blade tips was found 80 m to the west of the main wreckage along with remnants of tree-top foliage and light branches. There was insufficient evidence to determine how the foliage was dislodged.
The ATSB examined the wreckage and did not identify any pre‑existing aircraft defects that may have contributed to the accident sequence.
Data download
The ATSB recovered various aircraft components with recorded data stored from the accident site. The helicopter was not equipped with a flight data recorder or cockpit voice recorder, nor were they required to be fitted in accordance with Australian regulations. The Garmin GNS 430 and 530 units did not record flight parameters.
The two engine control units recovered from the accident site recorded engine power parameters and related parameters such as collective pitch. To establish the functionality of the engines, the ATSB arranged for the Bureau d'Enquêtes et d'Analyses (BEA) to work with the engine manufacturer in France to download data from the engine control units. This data showed that the engines were operating normally up to the time of the accident. A failure message, typically generated as a result of this type of accident, was recorded at the same time by both units, approximately 7 minutes after electrical power was turned on, prior to departure from the interim landing site.
The warning unit recovered from the accident site monitors the status of critical operating systems and provides warnings in case of abnormalities such as engine fire, fuel low level, battery malfunction, and low main rotor RPM. The ATSB downloaded data from the warning unit and arranged for the data to be decoded by the BEA and another independent agency. There were no anomalous recorded warnings from engine start until the end of the recorded data. At that point, the warning unit recorded autopilot and main rotor RPM decay warnings that were attributed to the collision with terrain.
The data recorded by the engine control units and the warning unit was not as comprehensive as that recorded by a flight data recorder and does not provide sufficient evidence that all of the helicopter systems were operating normally. However, based on the available data, it is almost certain that the engines were operating normally.
Mobile electronic devices
The ATSB recovered three mobile phones, three cameras, and one iPad from the accident site. The pilot’s iPhone was undamaged and had logged the last phone call at 0828 on the morning of the flight. A weather app was installed, but no data was available to indicate usage.
Another iPhone, belonging to the pilot’s wife, was undamaged and logged the last phone and text activity at 0935 on the morning of the flight. The phone belonging to the other passenger was too damaged to recover any data.
The stored data on the cameras was reviewed and images recorded during the return flight were retained and used in developing the sequence of events and weather information. The iPad did not have a SIM card and no information useful to the investigation was identified.
Emergency locator transmitters
Civil Aviation Regulation (CAR) 252(A) requires the carriage of an emergency locator transmitter (ELT) on most flights in Australian airspace. This requirement can be satisfied by an ELT that is mounted on the helicopter and activates automatically when it senses an excessive force, such as a ground impact. An alternative means of compliance is the carriage of a portable personal locator beacon (PLB) that is activated manually.
On activation, an ELT or PLB transmits on two frequencies, one of which can be detected by orbiting satellites that transmit a signal to search and rescue coordinators. The other frequency can be picked up by overhead aircraft for detection and homing in on the activated beacon, or can be used by crews to alert relevant authorities.
The ATSB research report AR-2012-128: A review of the effectiveness of emergency locator transmitters in aviation accidents states that search and rescue personnel were alerted to aviation emergencies in a variety of ways including radio calls and phone calls and that ELT activation accounted for the first notification in only about 15 percent of incidents. To the date of the research report reference, ELT activations have been directly responsible for saving an average of four lives per year.
The research report noted that both fixed ELTs and personal portable beacons have limitations that include degraded signalling capability when the ELT aerial is damaged in a serious accident, and lack of activation when the impact force is not aligned with the orientation of the ELT or when the occupant is unable to activate a PLB due to injury. GPS-equipped ELTs significantly increase the accuracy of positional information and newer ELTs, incorporating 3-axis g-switches may improve the likelihood of activation upon impact. Carriage of a PLB in place of, or as well as a fixed ELT will be of most safety benefit if it is carried on the person.
Additionally, developments in tracking technology now allows for GPS supported or combined GPS/cellular network supported products enabling real time monitoring of an aircraft’s movements, with the provision of scheduled updates to nominated parties and immediate notification in case of an emergency. Automatic alert signals can also be provided in the event of loss of power or sudden change in altitude with the ability to manually activate in the event of an emergency.
Visual flight into Instrument Meteorological Conditions
Accident data
The safety risks of VFR pilots flying from VMC conditions into instrument meteorological conditions (IMC)[16] are well documented. This has been the focus of numerous ATSB reports and publications, as VFR pilots flying into IMC represent a significant cause of aircraft accidents and fatalities. In 2013, the ATSB Avoidable Accidents series was re-published. One of these publications, the booklet titled Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions outlined that:
In the 5 years 2006–2010, there were 72 occurrences of visual flight rules (VFR) pilots flying in instrument meteorological conditions (IMC) reported to the ATSB…About one in ten VFR into IMC events result in a fatal outcome.
Additionally, a study conducted by the United States National Transportation Safety Board (2005) found that ‘about two-thirds of all general aviation accidents that occur in instrument meteorological conditions (IMC) are fatal’.
Wiggins and O’Hare (1995) explained that when pilots are not trained or qualified to fly in IMC and find themselves in these conditions, ‘the result will almost inevitably involve loss of control of the aircraft resulting in a fatal crash’.
Loss of visual cues and spatial disorientation in low visibility conditions
In a discussion of spatial disorientation, Benson (1999) defined the experience as follows:
Spatial disorientation is…[where] the pilot fails to sense correctly the position, motion or attitude of the aircraft or of him/herself [resulting in] errors in perception by the pilot of their position, motion or attitude with respect to their aircraft...
Gibb et al. (2010) explain that seeing the horizon is ‘crucial for orientation of the pilot’s sense of pitch and bank of the aircraft.’ In conditions of low visibility, the horizon may not be visible to the pilot, during which time they can become rapidly disorientated.
Extensive research on spatial disorientation indicates that loss of control will likely occur between 60 seconds (Benson, 1983 in Gibb et al., 2010) and 178 seconds (Newman, 2007) after the loss of visual reference. This is the case even when the aircraft is in straight and level flight at the time vision is lost, and is shorter still if the aircraft is in a turn. Gibb et al. (2010) state that ‘spatial disorientation accidents have fatality rates of 90–91 percent, which indicates how compelling the misperceptions can be’.
Related occurrences
ATSB investigation AO-2008-063 Controlled flight into terrain – Scone, New South Wales on 14 September 2008
On 14 September 2008, a Cessna Aircraft Co. U206A aircraft, registered VH-JDQ, with a pilot and two passengers on board, was on a private flight under the visual flight rules (VFR) from Bankstown, NSW to Archerfield, Qld with a planned stop at Scone, NSW. The aircraft was reported missing when it did not arrive at Archerfield as expected later that day.
Australian Search and Rescue were notified and, during the subsequent search, the wreckage of the aircraft was located the following day on top of a 3,800 ft ridge in rugged terrain, approximately 56 km (30 NM) north-north-east of Scone Airport. All three occupants were fatally injured and the aircraft was destroyed.
The weather in the area at the time of the occurrence was not suitable for VFR flight and included low cloud, rain showers and high winds. Inspection of the accident site indicated that the aircraft was tracking towards Scone prior to impact with terrain.
ATSB investigation AO-2009-077 Visual flight into instrument meteorological conditions – Dorrigo, New South Wales on 9 December 2009
On 9 December 2009, at about 1120 Eastern Daylight-saving Time, the pilot of a Bell Helicopter Company 206L-1 LongRanger, registered VH-MJO, was conducting a visual flight rules fire‑fighting support flight in the area of Dorrigo, New South Wales with one passenger on board. Shortly after takeoff, the pilot encountered reduced visibility conditions due to low cloud. Subsequently, all visual reference with the horizon and the ground was lost. The pilot attempted to land, but the helicopter impacted the ground in an uncontrolled state and with significant vertical force. The passenger was fatally injured and the pilot was seriously injured. The helicopter was seriously damaged.
The investigation found that after the pilot established the hover, the helicopter entered the rapidly fluctuating cloud. The pilot lost visual reference and became spatially disoriented and the helicopter impacted the ground in an uncontrolled state. The at times rapidly-moving fog or low cloud in the vicinity of the helicopter landing area (HLA) increased the risk of visual operations encountering instrument meteorological conditions at the HLA.
ATSB investigation AO-2011-100 VFR flight into dark night conditions – Horsham, Victoria on 15 August 2011
On 15 August 2011, the pilot of a Piper PA-28-180 Cherokee aircraft, registered VH-POJ, was conducting a private flight transporting two passengers from Essendon to Nhill, Victoria under the VFR. The flight was arranged to return the passengers to their home location after medical treatment in Melbourne.
Global Positioning System data recovered from the aircraft indicated that when about 52 km from Nhill, the aircraft conducted a series of manoeuvres followed by a descending right turn. The aircraft subsequently impacted the ground at 1820 Eastern Standard Time, fatally injuring the pilot and one of the passengers. The second passenger later died in hospital as a result of complications from injuries sustained in the accident.
The ATSB found that the pilot landed at Bendigo and accessed a weather forecast before continuing towards Nhill. After recommencing the flight, the pilot probably encountered reduced visibility conditions while approaching Nhill due to low cloud, rain and diminishing daylight, leading to disorientation, loss of control and impact with terrain.
ATSB investigation AO-2016-031 Collision with water – Cape Tribulation, Queensland on 7 April 2016
On 7 April 2016, the pilots of two Robinson R22 helicopters flew from Mossman, Queensland to various fishing locations to the north with a passenger in each helicopter. Late in the afternoon, the pilots commenced the direct return flight to Mossman.
Shortly after passing Cape Tribulation, in dark night conditions, one of the helicopters registered VH-YLY, collided with the sea. The passenger was injured in the accident but was able to reach the shore and notify emergency services. The pilot’s body was not located.
The ATSB found that the pilot, who was only qualified to operate in day-VFR conditions, departed on a night flight and continued towards the destination in deteriorating visibility until inadvertently allowing the helicopter to descend into water.
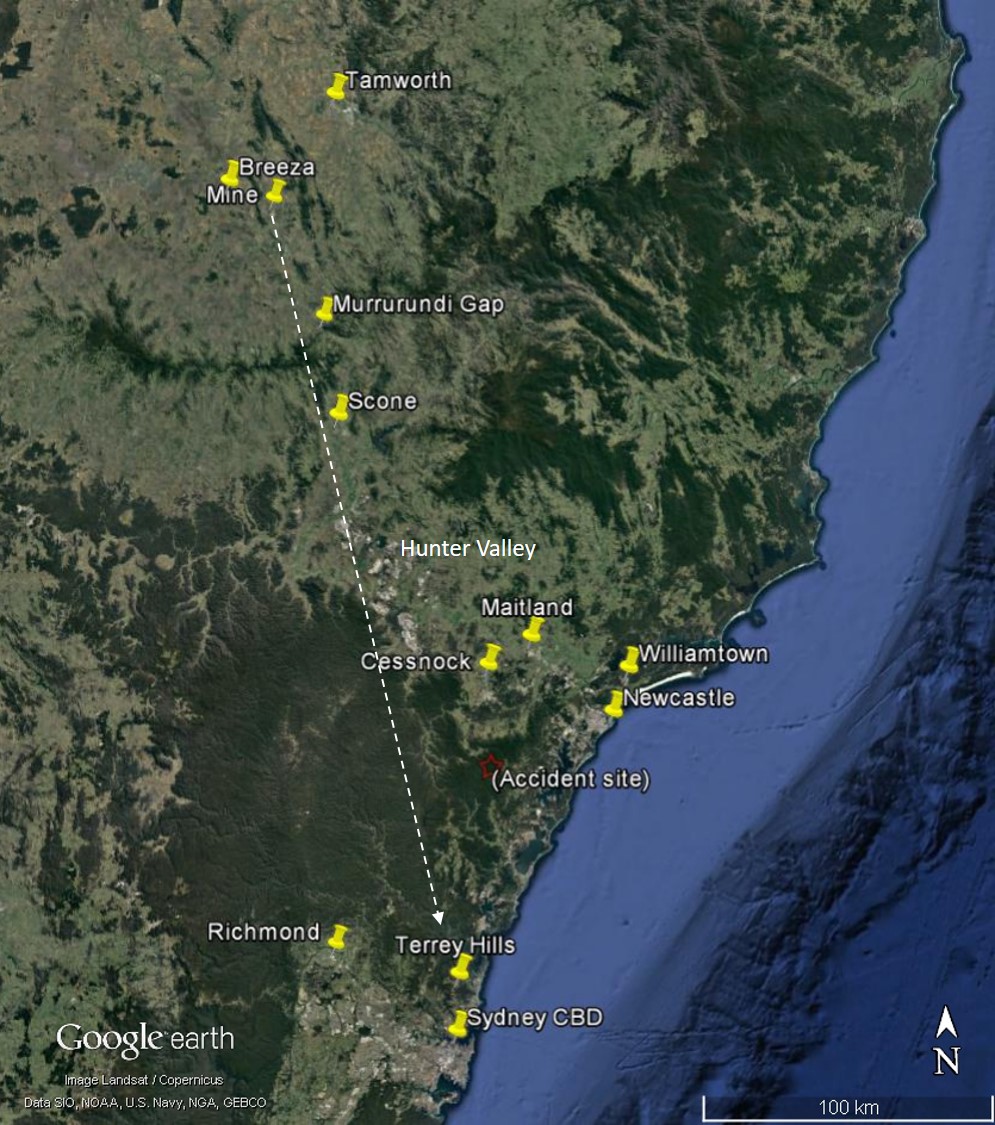
On 7 November 2015, the owner-pilot of an Airbus Helicopters EC135 T1,[3] registered VH‑GKK, made arrangements to fly from a private helipad at Terrey Hills, 17 km north of the Sydney Harbour Bridge, to Breeza, 44 km south-west of Tamworth, New South Wales. Based on a direct track, the distance was 146 NM (270 km). The flight was originally intended for the day before, but was reportedly postponed due to severe storm warnings for the Hunter Valley, which was on the direct track.
This was a private flight under the visual flight rules (VFR)[4] for the pilot and his wife to attend an event near Breeza (Figure 1). They indicated that they might return to Terrey Hills later that day, or possibly the next. The pilot’s wife was also a qualified helicopter pilot.
Figure 1: Area of operation with dashed line representing nominal return track
Source: Background image Google Earth, annotated by ATSB.
The pilot did not submit a flight notification to Air Traffic Services and, as the flight was conducted under the VFR and outside controlled airspace, there was no requirement to do so. There was no record that the pilot accessed aviation-specific meteorological forecasts and reports in preparing for the flight. Given that there were multiple means of access to those products and other sources of weather information, the pilot may have obtained the weather through these sources.
There was limited recorded data available for the flight from Terrey Hills to Breeza. VH-GKK departed Terry Hills sometime after 0940 and arrived at Breeza at about 1100. It was arranged for an acquaintance, who was a documentary filmmaker, to join the pilot and his wife for the return flight. Their return track would take them over the Werris Creek coal mine where their intent was to film the mine and surrounds.
It appears that the pilot was hoping to leave at about 1700 but there was a delay associated with the event. Witnesses recalled that the helicopter lifted off at about 1730 and headed in a south-easterly direction, toward the general location of the mine. The weather at Breeza was warm and sunny, with predominantly clear skies and light winds.
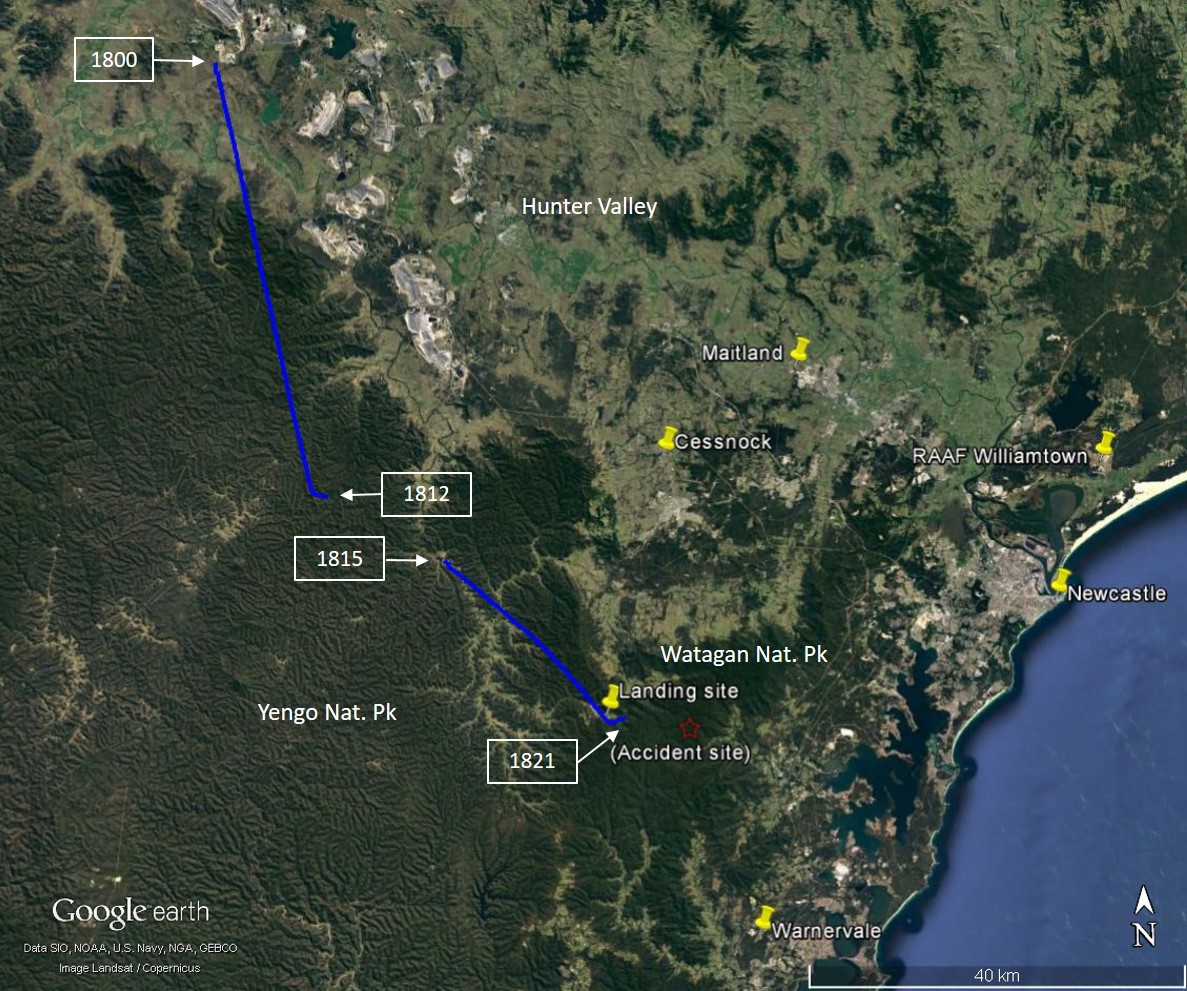
Based on photos recovered from the filmmaker’s camera, the pilot departed at 1735 and tracked to Werris Creek coal mine then southward in the general direction of Terrey Hills. At 1800, air traffic control radar detected the helicopter in the vicinity of the Liddell mine in the Hunter Valley, which was about the halfway point. On initial detection, the helicopter was at 2,800 ft above mean sea level,[5] before climbing to 3,500 ft as it approached higher terrain. It had an average groundspeed of 116 kt and the pilot was maintaining a consistent track in the general direction of Terrey Hills (The radar data recorded between 1800 and 1821 is depicted in Figure 3).
From 1811, the radar data shows a descent and at 1812, the pilot made a turn to the left to track in a more easterly direction. Shortly after, the radar return dropped out when the helicopter was at 2,700 ft with a groundspeed of 125 kt.
Three minutes later, the helicopter reappeared on radar 13 km south-east of the last position, at 1,900 ft with a groundspeed of 146 kt. The pilot then maintained a consistent south-easterly track in the general direction of Warnervale, located near the coast. A photo taken from inside the helicopter at 1817 (Figure 2), shows that low clouds and darkening skies were being encountered during this time.
The south-easterly track continued for about 6 minutes and covered 25 km until the pilot made a left turn onto an easterly track. At this point the helicopter was at 1,800 ft and in the vicinity of the eastern end of the Watagan Creek valley. The radar return dropped out soon afterwards.
Figure 2: Image of weather conditions recorded at 1817 looking towards the Watagan Mountains
Source: Recovered camera. Copyright: Not to be reproduced.
Figure 3: Radar data (in solid blue line) of the helicopter track on 7 November 2015 before the interim landing with times and accident site
Source: Background image Google Earth, annotated/modified by ATSB
Witnesses reported that the helicopter crossed the valley and continued in an easterly direction, in conditions they described as overcast with low clouds and rain.
At about 1830, witnesses observed the helicopter return to the valley from the east. The pilot landed the helicopter in an open area within the valley in conditions that witnesses reported as including low cloud, reduced visibility and moderate to heavy rain. One of the passengers took photos of this interim landing site, with two pictures showing the weather conditions at 1901 and 1910 respectively (Figure 4 and Figure 5). During the period that the helicopter was on the ground, the available ambient light varied with the overcast conditions and there was low cloud and drizzle in the area.
Figure 4: Image of VH-GKK at the interim landing site at 1901, facing eastward with obscured, rising terrain in the background
Source: Image retrieved from passenger camera. Copyright: Not to be reproduced.
Figure 5: Image of VH-GKK at the interim landing site at 1910
Source: Image retrieved from passenger camera. Copyright: Not to be reproduced.
The witnesses noted that the helicopter remained on the ground for about 40 minutes before departing at about 1915. By 1920, the helicopter was observed over a property to the east of the Watagan Creek valley, tracking east toward timbered, rising terrain. The witness reported that the heavy rain had abated to drizzle and the visibility remained low.
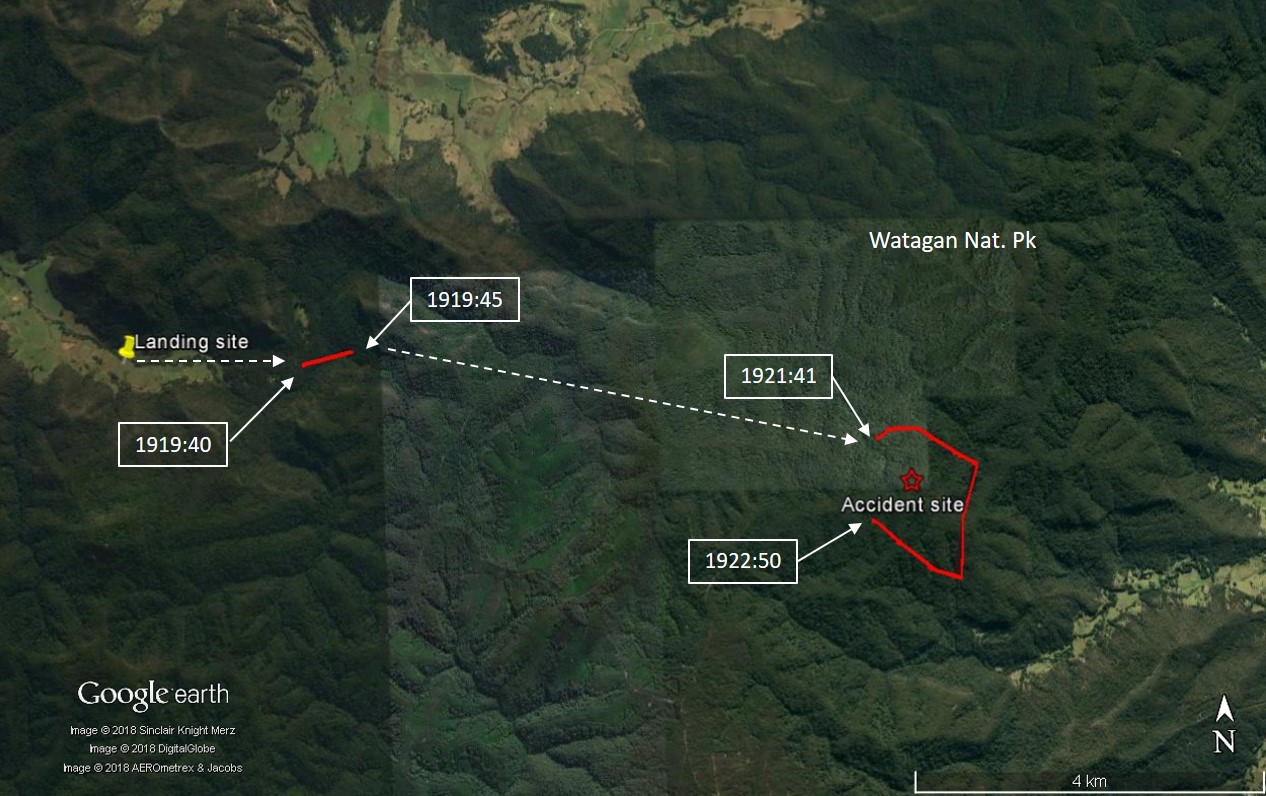
The helicopter reappeared on radar for a couple of returns at 1919:40 and 1919:45, about 2 km east of the interim landing site. Nothing more is known about the helicopter flight path until 1921:41, when it reappears on radar a further 6 km to the east (Figure 6). The pilot then made consecutive right turns to reverse track from a north-easterly to north-westerly direction while climbing from 1,700 ft to 2,100 ft. Radar detection was lost after 1922:50 and there was no further available data about the flight path.
While the flight was intended to reach Terrey Hills that day, it was also understood by relatives of the passengers that it might not return that evening. As a result, the following day, no immediate concerns were raised with authorities despite the fact the pilot and passengers had not arrived at Terrey Hills. The alarm was raised about 36 hours later, after it became apparent that they were overdue. The pilot of the helicopter had not logged a search and rescue time (SARTIME)[6] with Airservices Australia, nor was a flight note[7] left with a nominated other.
An aerial search for the missing helicopter began at 0930 on 9 November 2015. The wreckage was located in heavily timbered, hilly terrain within the Watagans National Park later that day. The pilot and the two passengers were fatally injured.
The helicopter had collided with terrain near the top of a ridge on a south-easterly heading and close to the last recorded radar detections at an elevation of 1,340 ft. The time of the accident could not be precisely established but was estimated to have occurred by 1925.
Figure 6: Radar data (solid red line) of the helicopter track after the interim landing with nominal intermediate tracks (dashed white lines) and times
Source: Background image Google Earth, annotated/modified by ATSB.
The ATSB did not have access to recorded data that showed the helicopter flight path or key operational parameters, at, or immediately before the collision with terrain. There were no witnesses to, or video of, the accident sequence. As such, the ATSB was reliant on recorded engine parameters and system warnings along with interpretation of aircraft wreckage, the accident site and weather data, to determine the characteristics of the collision with terrain.
The following analysis examines the known flight path and considers elements that may have influenced the decision to depart the interim landing site and continue the flight. The analysis also examines safety considerations associated with VFR pilot decision making and the carriage of emergency locator transmitting devices.
Pre-flight weather assessment
Although the pilot did not have a NAIPS account for access to aviation weather forecasts/reports, the pilot might have accessed equivalent weather information from other sources or referred to available non‑aviation weather information.
Based on the Area 20 forecast and aerodrome forecasts (TAFs) available before the pilot’s departure from Terrey Hills, it would have been apparent that the flight to Breeza and return could be affected by isolated thunderstorms, and low cloud with light showers/drizzle near the coast south of Williamtown. Although the weather for the flight to Breeza was not reported to have presented a problem, the return flight was later in the day and the type of forecast weather was associated with a moist, unstable air mass.
If the Area 20 forecast issued about an hour before the intended departure from Breeza was taken into consideration, it would be apparent that the flight could be affected by isolated thunderstorms, and low cloud south of Williamtown that would have extended inland. The TAFs for aerodromes adjacent to the route were relatively benign, but the TAF for Richmond indicated that the weather in the Terrey Hills area could have temporary periods of low cloud and rain.
The forecasts were generally consistent with the conditions that developed in the area. The thunderstorm-related activity on the pilot’s intended route was more extensive than the isolated descriptor in the forecast might indicate. However, this type of weather was not precluded by the forecast and local conditions across a forecast area will vary.
Collision with terrain
Data downloaded from the engine control and warning units indicated that there was no problem with the operation of the engines or other monitored helicopter systems up to the point of collision with terrain. There was also no radio transmission from the pilot, either heard or recorded, to advise of any problem. This was consistent with examination of the helicopter wreckage and review of the helicopter logbooks that did not identify any airworthiness concerns. Although these items of evidence are not conclusive, it is unlikely that there was a problem with the helicopter.
The ATSB accessed and analysed a variety of sources of meteorological data to ascertain the weather at the time of the accident. There was low cloud, drizzle and reduced visibility in the area. Although the conditions were marginal for VFR, there was likely to be some variability and it was not possible to establish if the weather in the latter stages of the flight allowed the pilot to operate clear of cloud and with a minimum of 800 m visibility, as per the helicopter visual meteorological conditions (VMC) requirements.
The last recorded radar data showed that the pilot conducted a series of right turns with a change of direction from south‑east to north-west. During the turns, the pilot climbed from 1,700 to 2,100 ft, which correlated to an increase in height above terrain from about 350 to 750 ft.
It is almost certain that the pilot made the right turns in response to the weather conditions and it is possible that the pilot lost visual contact with the ground and climbed to ensure that he maintained terrain clearance. Given the weather conditions, at the point the radar returns dropped out, it is unlikely that the pilot was able to remain in VMC. It is possible that pilot was reversing track to return to the interim landing area.
Nothing more is known about the helicopter’s flight path until it collided with terrain shortly afterwards on a south-easterly bearing and close to the last recorded radar position. This bearing and position are consistent with a continuation of the original flight track; however, the ATSB could not determine if that was the pilot’s intention.
In the period from the last recorded radar return prior to the collision with terrain, the pilot descended about 700 ft. The ATSB was unable to determine if the pilot was taking advantage of a break in the cloud to descend visually or trying to descend through cloud to establish visual reference to the ground.
If the pilot had been descending through cloud in order to establish visual reference to the ground, this behaviour may have been consistent with the pilot’s experience in 2004, as related in the book published by the pilot. Although the book related the pilot’s descent in cloud until visual reference was established at low altitude, the context in this case was different. Instead of flying over water and coastline, the pilot was contending with terrain that was undulating, uniformly textured, and relatively high.
To fly visually in this environment with low visibility is difficult, as the situation requires that the pilot maintain reference to the ground to maintain control, avoid terrain, and avoid low cloud and other areas of reduced visibility. The pilot had GPS receivers and moving map displays to assist with navigation, and flight instruments and autopilot with IFR capability, but that equipment was of limited use if the pilot was attempting to maintain visual reference. Based on the data available to the ATSB, it was not possible to determine whether the accident was a result of controlled flight into terrain or loss of control due to spatial disorientation.
Assessment of local conditions
It was not possible to establish if the manoeuvring before the collision with terrain indicated the pilot was attempting to return to the previous landing area or attempting to find a way through to the destination. Whatever the pilot’s intentions, at the time of the accident the pilot probably found himself in a situation where he was unable to negotiate the weather conditions with visual reference to the ground. In that context, the ATSB considered the pilot’s decision to lift off from the interim landing site and to continue the flight.
The ATSB was unable to identify all of the aspects relevant to the pilot’s decision to depart from the interim landing site but it is likely that the pilot was influenced by the following situational factors:
an apparent improvement in the local weather
the expected flight time to the destination meant that the expected time of arrival was getting increasingly closer to last light
the distance from the interim landing site to lower terrain was relatively short
the pilot may have been unaware of the actual weather along the prospective route or had reasonable expectations of navigating the weather conditions.
In considering a departure from the interim landing site, the pilot was able to assess the weather visible from the location and had the capability to access forecast and actual weather information via mobile devices. Although the pilot’s phone was not used, there were other devices available, and internet use for those devices could not be established.
The pilot’s decision to depart the interim landing site can be interpreted as likely taking advantage of a break in the severity of the local weather to proceed as far as the weather would allow. If the pilot had reached the lower terrain near the coast, there was a greater likelihood of being able to continue the flight to the destination or land at an airport with access to accommodation.
Once airborne, the pilot would have been in a position to assess the in-flight visibility and cloud and rain in the intended direction of travel. In another occurrence investigation,[17] the ATSB has found that the ‘continuation of flight towards an area of low cloud and rain was likely influenced by the inherent challenges of assessing low visibility conditions, particularly without instrument flying proficiency.’ This finding was based on the following references.
The United States National Transportation Safety Board (2005) found that ‘reduced-visibility weather represents a particularly high risk to [general aviation] operations’ and that ‘weather may…test the limits of pilot knowledge, training, and skill to the point that underlying issues are identified.’
Wiegmann and Goh (2000) explained that:
One reason why pilots may decide to continue a VFR flight into adverse weather is that they make errors when assessing the situation. That is, pilots are seen to engage in VFR flight into IMC [instrument meteorological conditions] because they do not accurately assess the hazard (i.e., the deteriorating weather conditions).
The previously mentioned United States National Transportation Safety Board report (2005) added that in these cases, pilots who might appear to intentionally engage in risky behaviour may actually be making choices that they mistakenly believe to be safe:
Even if pilots are able to correctly assess current weather conditions, they may still underestimate the risk associated with continued flight under those conditions, or they may overestimate their ability to handle that risk.
Wiggins and O’Hare (1995) further explained how errors in assessment can take place, acknowledging that weather-related decision making can be highly complex and therefore more prone to errors:
Because of the variable nature of operations in the aviation environment, weather-related decision making is often considered a skill that cannot be prescribed during training. Rather it is expected to develop gradually through practical experience. However, in developing this type of experience, relatively inexperienced pilots may be exposed to hazardous situations with which they are ill‑equipped to cope.
ATSB Aviation Research and Analysis Report B20070063, An overview of spatial disorientation as a factor in aviation accidents and incidents, stated that pilots should not attempt to fly into instrument meteorological conditions under the VFR. Pilots should develop a plan prior to take-off on what to do if the weather en route is different from that expected, or deteriorates. This plan should consider a requirement to divert or turn back prior to entering instrument meteorological conditions. However, this depends on a pilot correctly assessing the weather conditions. The United States National Transportation Safety Board (2005) noted that targeted weather-related training programs have had some success in teaching pilots to recognise and respond to deteriorating weather conditions.
Additionally, Wiggins and O’Hare (2003) evaluated the effectiveness of a cue-based training system called Weatherwise, which was designed to equip VFR pilots with the skills to recognise and respond to the cues associated with deteriorating weather conditions during flight. VFR pilots were more likely to use the cues following the training, with subsequent improvements in their weather-related decision-making. The Weatherwise program was made available to pilots by the Civil Aviation Safety Authority (CASA). Additionally, CASA produced a Weather to Fly education program which focuses on topics such as the importance of pre-flight preparation, making decisions early, and talking to ATC.
The ATSB was unable to determine the pilot’s understanding of the weather conditions ahead of him prior to entering an area of low visibility conditions. However, the pilot had demonstrated an awareness of the risk posed by the weather and the need to maintain visual reference by diverting from the original track from Breeza then turning back from the first attempt to cross the high terrain.
Until the conditions improved, the only safe option available to the VFR pilot was to leave the helicopter at the interim landing site or transit to another landing area in the valley as the conditions permitted.
Weather-related general aviation accidents remain one of the most significant causes for concern in aviation safety; the often-fatal outcomes of these accidents are usually all the more tragic because they are avoidable.
In the 5 years 2006–2010, there were 72 occurrences of visual flight rules (VFR) pilots flying in instrument meteorological conditions (IMC) reported to the ATSB. Seven of these resulted in fatal accidents, causing 14 fatalities. That is, about one in ten VFR into IMC events result in a fatal outcome.
Flying into IMC can occur in any phase of flight. However, a 2005 ATSB research publication General Aviation Pilot Behaviours in the Face of Adverse Weather concluded that the chances of a VFR into IMC encounter increased as the flight progressed, with the maximum chance occurring during the final 20 per cent of the flight distance.
The dangers of flying VFR into IMC have been recognised for a long time, yet VFR pilots still fly into deteriorating weather and IMC. This publication describes recent weather-related general aviation accidents and incidents that show that weather alone is never the only factor affecting pilot decisions that result in inadvertent IMC encounters. It has been produced solely with the intention of encouraging all pilots, no matter what their experience level, to develop the knowledge and skills required to avoid unintentional operations in IMC.
One of the key messages is for pilots to avoid deteriorating weather by conducting thorough pre-flight planning and to have alternate plans in case of an unexpected deterioration in the weather and making timely decisions to turn back or divert.
This principle applies to all aircraft operations, even though helicopters are inherently more flexible in terms of availability of landing areas and manoeuvrability. All pilots need to have a relevant and effective contingency plan that is based on the best available information in weather forecasts and reports.
Location of aircraft in an emergency
The pilot was operating with two Personal Locator Beacons (PLBs) and no fixed Emergency Locator Transmitter (ELT). Unlike a fixed ELT, the PLBs were not fitted with a ‘g’ switch and would require manual activation to transmit information. In this case, the occupants were fatally injured in the accident and no position information was transmitted from the beacons.
ATSB report AR-2012-128: A review of the effectiveness of emergency locator transmitters in aviation accidents references an Australian Maritime Safety Authority (AMSA) recommendation that occupants of an aircraft proactively activate an ELT (or PLB in this case also) when flying in dangerous weather conditions. This would greatly increase the likelihood of establishing the exact position of the aircraft if required. AMSA would need to be notified once the dangerous phase of the flight was complete and the ELT/PLB has been switched off. Activating a beacon under such circumstances requires an active decision on the part of the pilot. Additionally, in the event of inadvertent entry into IMC, pilots are encouraged to contact air traffic control for assistance, however on this occasion, no radio calls from the pilot to air traffic control were on record.
The severity of an accident potentially restricts fixed or portable ELTs to be reliably activated due to impact forces that can render the units inoperable, with research noting that they save about four lives a year. Furthermore, search and rescue operations also place others at risk and a degree of uncertainty exists until a missing aircraft is located. The removal of the fixed ELT with the potential for self-activation, for manually operable PLBs was in accordance with the regulatory requirements. On this occasion, the absent transmission coupled with the uncertainty of when the group would return to Terrey Hills, delayed the search and rescue response.
Benson, AJ, 1999a, “Spatial disorientation – general aspects”, in J Ernsting, AN Nicholson & DJ Rainford (Eds.), Aviation Medicine (3rd ed.), Oxford, England, Butterworth Heinemann, pp. 419-436.
Gibb, R, Gray, R and Scharff, L, 2010, Aviation Visual Perception: Research, Misperceptions and Mishaps, Ashgate Publishing Limited, Surrey, United Kingdom.
Wiegmann, D and Goh, J, 2000, Visual Flight Rules (VFR) Flight into Adverse Weather: An Empirical Investigation of Factors Affecting Pilot Decision Making, Federal Aviation Administration research DTFA 00-G-010, Illinois, United States.
Wiggins, M and O’Hare, D, 1995, “Expertise in Aeronautical Weather-Related Decision Making: A Cross-Sectional Analysis of General Aviation Pilots”, Journal of Experimental Psychology: Applied Vol. 1 No. 4, pp. 305-320.
Wiggins, M and O’Hare, D, 2003, “Weatherwise: Evaluation of a cue-based training approach for the recognition of deteriorating weather conditions during flight”, The Journal ofHuman Factors and Ergonomics Society, pp.337-345.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Civil Aviation Safety Authority and the German Federal Bureau of Aircraft Accident Investigation.
Submissions were received from both organisations. A review of those submissions did not result in any amendment to the text of the report.
Findings
From the evidence available, the following findings are made with respect to the collision with terrain involving Airbus Helicopters EC 135 T1, VH-GKK, that occurred near Cooranbong, NSW on 7 November 2015. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factor
The pilot departed an interim landing site for Terrey Hills under the visual flight rules with a high risk of encountering forecast cloud and reduced visibility. Due to the likely presence of cloud, the pilot probably experienced a loss of visual reference leading to a collision with terrain.
Other findings
The personal locator beacons carried in lieu of a fixed emergency locator transmitter were required to be activated in the case of an accident. While in this accident it did not affect the outcome for the occupants, the lack of activation, combined with the absence of flight notification information, delayed the search and rescue response.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 6 November 2015, at about 1829 Eastern Daylight Saving Time, the pilot of a Cessna Aircraft Company 310R registered VH‑BWZ, on a private flight from Moorabbin to Mildura, Victoria lost control of the aircraft near Mildura Airport and collided with terrain. The pilot was fatally injured and the aircraft destroyed.
What the ATSB found
Witnesses reported that when on final approach to land at Mildura, at low altitude, the aircraft yawed to the left, dropped its left wing and rapidly lost altitude. A number of factors contributed to the loss of control. The aircraft’s left engine was found to have been starved of fuel and at the time of the accident was not producing power. The left propeller was found to be towards fine pitch, not feathered (rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in-flight engine failure or shutdown), and the flaps and landing gear were fully extended, consistent with a normal landing configuration. In that configuration with the engine not producing power, the aircraft’s performance would have degraded to the extent that altitude could not be maintained.
The ATSB was unable to ascertain why the left engine was starved of fuel, nor could it be determined when the engine was starved of fuel. The ATSB did establish that it was likely the aircraft was carrying a substantial amount of fuel on board for continued flight and that the left engine and left propeller were capable of normal operation.
Several components recovered from the aircraft were tested. Some abnormalities were identified, however, it was unlikely that these contributed to the accident. No mechanical defects were identified that may have contributed to the accident. However, examination of the aircraft was limited due to the extent of the damage resulting from the post-impact fire.
It was likely that the combination of the inoperative left engine with the propeller in the fine pitch and the right engine at high power resulted in asymmetric thrust. Whilst at low altitude in a landing configuration with asymmetric thrust, the pilot lost control of the aircraft.
Safety message
In situations such as an inoperative engine condition, the aircraft’s landing gear, flaps and or propeller management can potentially impose increased drag impacting significantly on the aircraft’s performance. Low airspeed in critical phases of flight such as take-off and landing can further exacerbate the situation. Pilots need to train, maintain their skills and constantly monitor aircraft systems to be prepared for abnormal flight situations, especially during critical phases of flight where greater attentional focus is required.
While ATSB research has found that the rate of power loss accidents in multi-engine aircraft occur less than that in single-engine aircraft, they are more likely to be fatal and overwhelmingly due to the potential for loss of control. In particular, the approach phase of flight is considered riskier due to lower altitudes and lower available aircraft energy.
This accident has emphasised the adverse consequences of aircraft configuration on performance with one-engine inoperative, particularly when at low altitudes. It reinforced the importance of pilots remaining well versed in engine failure response procedures and being aware of the drag penalties associated with varying configurations. It also highlighted the challenges associated with recognising an asymmetric condition when in a descent or at a low power setting. When faced with an inoperative engine in a multi-engine aircraft, attention to both aircraft control and performance is crucial for safe flight.
The occurrence
On 3 November 2015, the pilot of a Cessna Aircraft Company 310R, registered VH-BWZ, departed Mildura, Victoria on a private flight to Latrobe Valley. The pilot had intended to return to Mildura the next day, however, due to poor weather, he elected to fly to Moorabbin. On 5 November, the pilot was again unable to return to Mildura due to poor weather and took the opportunity to have some minor maintenance performed on the aircraft while at Moorabbin where a wire was repaired to the tachometer.
On 6 November, at about 1650 Eastern Daylight-saving Time,[1] the pilot departed Moorabbin for Mildura, operating under instrument flight rules.[2] Despite the pilot having some difficulties shortly after departing, including a transient transponder code issue, navigating in poor weather and reporting a ‘downward force on the aircraft’, the pilot appeared to resolve these issues and stated to air traffic control (ATC) an intention ‘to continue to Mildura’. ATC subsequently issued vectors to depart Melbourne airspace for Mildura.
The flight between Melbourne and Mildura appeared to continue uneventfully. Airservices Australia surveillance radar data showed the aircraft tracking direct from Melbourne to Mildura at an altitude of 6,000 ft until radar services were no longer available.
While en route, the pilot sent several text messages, and telephoned the Mildura automatic weather information service and a family member. During this latter communication, the pilot indicated that he experienced difficulties while departing Moorabbin, however, the pilot did not state any specific mechanical defects or problems with the aircraft. The pilot was reported to have sounded normal during that conversation.
At about 1814, the pilot made a broadcast on the Melbourne Centre ATC frequency that the aircraft was 38 NM (70 km) from Mildura, at top of descent. No further broadcasts were made by the pilot on this frequency. It was unknown if the pilot made a call on the Mildura common traffic advisory frequency as broadcasts were not recorded.
Several witnesses situated to the south and east of Mildura Airport observed the aircraft approaching from the north, consistent with being on final approach to runway 18. One witness described the aircraft to be flying ‘in a nose-up attitude or yawing’.[3] At about 1829, when about 1.9 km north-north-east from the runway at low altitude, several witnesses described the aircraft as yawing left, the left wing dropping, the aircraft then rotating in an anti-clockwise direction and rapidly lose altitude before colliding with terrain.
The aircraft collided with steel trestles mounted on wooden poles that were strung with heavy gauge single strand wires, used to support grape vines. The aircraft came to rest on four strands of 11,000 volt high tension (HT) power lines that were strung across the property from the road. A post impact fuel-fire ensued. The pilot, the sole occupant, was fatally injured and the aircraft destroyed.
Pilot information
The pilot held a Private Pilot (Aeroplane) Licence issued on 25 June 2006. The pilot was endorsed on the Cessna 310 in September 2012 and last completed a multi-engine flight review in December 2013, valid until December 2015. The pilot was also the owner of VH-BWZ.
Extracts from the pilot’s logbook found at the accident site showed a total flying experience of about 511 hours. The pilot’s experience on the Cessna 310 was estimated at about 113 hours, based on a combination of entries on the aircraft’s maintenance release and the pilot’s logbook. It appeared that the pilot had not flown in the period February to October 2015. However, on 14 October 2015, the pilot completed an instrument landing system endorsement for the private instrument rating with a Civil Aviation Safety Authority (CASA) approved testing officer. During the endorsement, the pilot was subjected to several simulated one-engine inoperative exercises in the approach phase-of-flight. The testing officer reported that the pilot’s response to these exercises were considered ‘normal’.
The pilot held a valid Class 2 Medical Certificate with the requirement for reading correction to be available while exercising the privileges of the licence. While a post-mortem medical examination found that the pilot had a mild heart enlargement, there was no evidence of any pre-existing conditions identified that may have contributed to the accident.
The investigation included an assessment of whether the pilot may have been experiencing a level of fatigue known to have an effect on performance. Consideration was made of the pilot’s sleep obtained, time awake at the time of the occurrence, time on task, potential workload and environmental factors. However, given the limited data available in relation to the pilot’s sleep history in the 72 hours prior to the accident and the nature of the individual actions leading up to the accident, there was insufficient evidence to determine whether fatigue contributed to the accident.
Aircraft information
The aircraft was maintained by a provider approved by CASA. About 4 months prior to the accident, a periodic inspection was conducted and the aircraft was released to service. The maintenance provider reported that during the pre-maintenance engine run check the autopilot was operated while holding the elevator trim wheel. This test established that, while the autopilot was operating the trim could be arrested manually, establishing that the elevator trim could be overridden if unintentionally activated.
The aircraft’s fuel system consisted of two main tanks located on the tip of each wing and two auxiliary tanks located within each wing. The combined usable capacity was about 100 US Gallons (378 L) for the two main tanks, and 63 US Gallons (238 L) for the auxiliary tanks. The main tanks were integrally sealed aluminium tanks, which were vented to the atmosphere. Each auxiliary fuel tank consisted of two interconnected bladder-type fuel cells that were located between the wing spars in the outboard section of each wing.
Two fuel selectors, one for each engine, were located on the floor in between the pilot and co-pilot seats. These allowed selection of main tank fuel, auxiliary fuel, cross-feed and no fuel through the wing selector valves located in each respective wing.
Meteorological information
The Mildura aerodrome forecast, issued at 1613 and valid between 1700 on 6 November to 0500 on 7 November 2015 indicated that conditions were forecast as CAVOK[4] with a wind direction of 210° at 10 kt. The Bureau of Meteorology provided the ATSB with data recorded by the automatic weather station at Mildura which indicated at the time of the accident (1829), the wind was 220° at 11 kt gusting to 12 kt.
Wreckage and impact information
The aircraft was found in a left-wing, nose-down attitude and had come to rest on four strands of 11,000 volt HT power lines that were strung across the nearby property from the road. Ground scars of ruts, and soil and vegetation built up on one side of the landing gear and wings, indicated that the aircraft was rotating in an anti-clockwise direction during the impact sequence. The aircraft was destroyed by the impact forces and a post impact fuel-fed fire. The ATSB examined the wreckage and found:
The landing gear was down and flaps fully extended.
Continuity of all flight controls was established.
The elevator, rudder and aileron trims were found in the neutral position.
There was nil evidence of a pre-impact structural failure or in-flight fire.
All fuel caps were identified in the wreckage in a closed locked position. The left wing main fuel tank was found attached to the left wing tip, while the right main tank had separated from the wing and had been thrown forward about 10 m. Both were significantly melted, consistent with the fuel-fed fire. The outer section of the right auxiliary fuel tank had fractured and separated due to the impact forces, and was found forward of the main wreckage, also significantly melted (Figure1). The inner section of the right wing auxiliary fuel tank did not burn and contained an adequate quantity of fuel to obtain a sample. That sample was field tested and found to be consistent with aviation fuel of a suitable quality. In contrast, the left auxiliary fuel tank displayed only some degree of melting. In consideration of the left wing-down attitude at the time of impact, it was unlikely that the left auxiliary fuel tank contained a significant quantity of fuel.
Figure 1 : Aircraft wreckage with evidence of fire and right wing auxiliary fuel tank in the foreground
Source: ATSB
The right engine propeller blades were towards the fine pitch[5] and displayed significant bending, torsional twisting and chord wise (across the width of the blade) scratching. The bolt holes of the engine crankshaft propeller flange, where the propeller mounted to the crankshaft with bolts and locating dowels, were elongated opposite to the direction to the crankshaft rotation. This was consistent with the right engine producing significant power when colliding with terrain.
The left engine propeller displayed no evidence of torsional bending or chord wise scoring, nor was the engine crankshaft propeller mount flange distorted. The angle of the propeller blades were consistent with being towards the fine pitch. In addition, one HT power line was found routed through the left propeller arc and engine cowling, then under the wing and through the landing gear. There was no evidence of the HT power line or the single strand wires used to support the grape vines being wrapped around the engine crankshaft. Similarly, there was evidence of arcing and mechanical abrasion on one of the propeller blades from contact with a HT power line while in-flight. This was limited to the leading edge of the propeller blade only. Collectively, these elements indicated that at the time of the collision the left engine was not producing power nor was the propeller producing thrust.
The cockpit and cabin were severely fire damaged, consistent with a significant fuel-fed fire supplied from the right inboard section of the auxiliary fuel tank.
The fuel selectors located in the cockpit were melted. Examination of the wing fuel selector valves, operated through push pull rods from the cockpit, showed that the right valve was selected to the right main fuel tank. In that position, the right engine received fuel from the right main fuel tank. The left wing fuel selector valve was in between the left auxiliary and cross-feed positions. The ATSB could not establish if that valve position was:
representative of the tank selection during normal operations,
selected in response to a left engine issue, or
a result of the impact sequence.
For each engine, the fuel line between the engine and fuel control unit and the engine and the wing were disconnected by the ATSB. The right engine fuel lines contained fuel. In contrast, no fuel was observed in the fuel lines of the left engine. No mechanical defects were identified that may have prevented normal operation of the left engine.
The source of ignition that led to the fire could not be established, however, the aircraft battery, damaged aircraft electrical wiring, hot engine and turbo charger, HT power lines and collision with steel were all possible sources of ignition. No mechanical defects were identified that may have contributed to the accident.
The left engine and propeller were recovered from the wreckage and transported to a CASA approved overhaul facility for detailed inspection under the supervision of the ATSB. The autopilot pitch and roll servos, and elevator trim actuator were also removed and sent to the United States for inspection under the supervision of the Federal Aviation Administration (FAA) and aircraft manufacturer. These components were tested in accordance with the manufacturer’s system of maintenance (refer to section titled Test and research).
Test and research
Left engine fuel system
The left engine fuel control fuel filter and fuel manifold top cap were removed and examined. No foreign object debris or fuel was identified in either component.
Left engine and propeller examination
Left engine internal components used to achieve normal engine operation, including the crankshaft, connecting rods, pistons, pushrods, cylinders, valves, camshaft, bearings and gears were inspected and found to have continuity. External accessories such as the fuel pump, magnetos, propeller governor and fuel injector were inspected and tested for correct operation. Other components such as the turbo charger and associated components were visually inspected.
The left propeller was also disassembled and inspected. Witness marks of the propeller blade situated in the cuff and bearing race damage found within the propeller established that, at the time of the collision, the propeller was towards the fine pitch position. Nothing was identified from those inspections or tests that may have prevented normal engine or propeller operation.
Autopilot pitch and roll servo, and elevator electric trim actuator
The servo drive motor for the autopilot pitch mode operated when power was applied. When an over voltage is detected in the system, the unit should trip the autopilot off-line and stop the motor; this function was inoperative. The motor clutch assembly was tested and slipped at 17 in lb in the clockwise direction and 21 in lb in the anti‑clockwise direction. The specification for this unit is 14 ±1 in lb in either direction. The actuator mount clutch on the capstan did not breakaway until 70 in lb in both directions. The specification for this clutch to slip is 20 ±2 in lbs.
The servo drive motor for the autopilot roll mode and the electric elevator trim actuator were also tested. Some minor breakout torque discrepancies were identified, however, were not considered significant.
Operational information
Fuel quantity
The pilot’s personal fuel records showed that 219.69 L was uplifted at Latrobe Valley on 4 November. The ATSB could not determine if that fuel was placed in the main and/or auxiliary fuel tanks. However, a witness at Latrobe Valley reported observing the main fuel tanks full. There were no fuel records identified to indicate any fuel uplift at Moorabbin.
The combined flight time from Latrobe Valley to Moorabbin and Moorabbin to Mildura was about 110 minutes, excluding taxi time. A pilot that had previously flown the aircraft reported that it had an average fuel burn rate of 60 litres per hour per engine (120 litres per hour total).
The Cessna Aircraft Company’s Pilot Safety and Warning Supplements, dated 1 June 1998, stated that:
Many twin engine Cessna airplanes incorporate auxiliary fuel tanks to increase range and endurance. These tanks are usually bladder type fuel cells located symmetrically in the outboard wing areas and contain no internal fuel pumps. When selected, the fuel from these tanks is routed to the engine driven fuel pump.
If the auxiliary fuel tanks are to be used, the pilot must first select main tank (tip tank) fuel for at least 90 minutes of flight with use of 63-gallon auxiliary fuel tanks. This is necessary to provide space in the main fuel tanks for vapour and fuel returned from the engine driven fuel pumps when operating on the auxiliary fuel tanks. If sufficient space is not available in the main tanks for this returned fuel, the tanks can overflow through the overboard fuel vents. Since part of the fuel from the auxiliary fuel tanks is diverted back to the main tanks instead of being consumed by the engines, the auxiliary tanks will empty sooner than may be anticipated. However, the main tank volume or quantity will be increased by the returned fuel.
As the ATSB was unable to establish the amount of total fuel on-board the aircraft when it departed Latrobe Valley or Moorabbin, or the pilot’s fuel management practices, the fuel remaining in each tank at the time of the accident could not be determined.
Asymmetric operations
The aircraft was fitted with two Teledyne Continental IO-520-MB piston engines and two three‑bladed McCauley propellers. Both engines rotated clockwise as viewed from the pilot’s seat.
When discussing the differences between single-engine and multi-engine aircraft, the FAA Airplane Flying Handbook (2016) stated that:
The basic difference between operating a multiengine airplane and a single-engine airplane is the potential problem involving an engine failure. The penalties for loss of an engine are twofold: performance and control. The most obvious problem is the loss of 50 percent of power, which reduces climb performance 80 to 90 percent, sometimes even more. The other is the control problem caused by the remaining thrust, which is now asymmetrical. Attention to both these factors is crucial for safe OEI [one-engine inoperative] flight.
The majority of light multi-engine aircraft such as the Cessna 310 have two wing-mounted engines that produce symmetrical propeller thrust during normal operation. One-engine inoperative operations on these aircraft result in asymmetric thrust and drag due to the offset position of the engines from the aircraft’s centreline. This results in a tendency for the nose of the aircraft to yaw in the direction of the inoperative engine. The extent of the yaw may vary depending on which engine becomes inoperative. The engine whose failure would most adversely affect an aircraft’s performance and handling qualities is termed the ‘critical’ engine. As the Cessna 310 engines turn in a clockwise direction, the left engine is the critical engine.
The asymmetric yawing tendency may be countered through the application of rudder and aileron control inputs. However, the minimum control speed of 80 kt[6] for the Cessna 310 must be achieved to ensure that the rudder and aileron retain sufficient control authority to maintain directional control of the aircraft. The Cessna 310 Pilot’s operating handbook stated that, the aircraft is controllable at this speed, but performance is so far below optimum that continued flight near the ground is improbable. Consequently, the handbook indicated that a more suitable recommended safe single-engine speed was 92 kt. At this speed, altitude could be maintained more easily with the landing gear retracted and the propeller feathered[7]. This speed is similar to the all engines landing approach speed of 93 kt with full flaps selected.
In addition, the CASA Civil Aviation Advisory Publication 5.23-1(2) stated that the majority of engine failures were not instantaneous. For example, if an engine failed as a result of fuel starvation or low fuel pressure, the engine will usually cough and splutter before stopping. However, the FAA recognised that:
An engine failure in a descent or other low power setting can be deceiving. The dramatic yaw and performance loss will be absent. At very low power settings, the pilot may not even be aware of a failure.
Pilot actions
The Cessna 310 Pilot’s operating handbook states that, following an engine failure, the pilot’s first consideration is to maintain control of the aircraft and ensure the airspeed remains above the minimum control speed. It then states that the pilot needs to identify the inoperative engine, adjust the operative engine as required, and perform a number of checks relating to fuel flow, tank selection and quantity; engine oil pressure and temperatures; magneto switches and mixture. If the engine does not re-start, the pilot must ‘secure’ or shutdown the engine, which includes feathering the propeller. The FAA flying handbook highlighted that completely securing a failed engine may not be necessary or even desirable depending upon the failure mode, altitude, and time available.
Aircraft performance degradation
The aircraft manufacturer advised that the Cessna 310 had a single-engine climb rate of about 375 feet per minute (at sea level and at maximum landing weight). However, with drag penalties of an unfeathered windmilling[8] propeller, landing gear extended and full flap, the aircraft’s single-engine climb performance would degrade. Under these conditions, one-engine inoperative performance would result in a descent at 875 feet per minute.
Various other sources have also highlighted these adverse consequences on aircraft single-engine performance. For example, Multi-Engine Pilot Manual by Jeppesen Sanderson (1992) stated:
It is important that the pilot be familiar with the correct order for drag reduction following an engine failure. Normally, a windmilling propeller contributes the greatest amount of drag, followed by full flaps, extended landing gear, and the control deflections required to stop the airplane from turning. Since it is considered unwise to immediately feather an engine before it has been positively identified, drag is normally reduced by first retracting flaps and gear. Next, the failed engine is identified and the propeller is feathered. However, the specific order of drag reduction may vary between types of twin‑engine airplanes, so the manufacturer’s recommendations should be followed.
Generally, the landing gear is not extended during the approach until the airplane is established at approach airspeed and the pilot is positively assured of reaching the desired runway. This timing is important since the extension of the landing gear adds sufficient drag to create a 300 to 500 f.p.m. [feet per minute] rate of descent without power reduction.
The wing flaps should be used as little as possible, preferably not at all until the landing gear is extended and the landing is assured.
The FAA Airplane Flying Handbook (2016) stated:
A single-engine go-around must be avoided. As a practical matter in single-engine approaches, once the airplane is on final approach with landing gear and flaps extended, it is committed to land on the intended runway, on another runway, a taxiway, or grassy infield. The light-twin does not have the performance to climb on one engine with landing gear and flaps extended. Considerable altitude is lost while maintaining VYSE[9] and retracting landing gear and flaps. Losses of 500 feet or more are not unusual. If the landing gear has been lowered with an alternate means of extension, retraction may not be possible, virtually negating any climb capability.
The CASA Civil Aviation Advisory Publication 5.23-1(2) stated:
A windmilling propeller causes the largest component of drag on an aircraft that suffers an engine failure. If the propeller is not feathered following an actual failure…the aircraft’s climb performance cannot be guaranteed. In many cases, it is likely that the aeroplane will only be able to maintain a descent.
Multi-engine power loss accidents
An ATSB research report, Power loss related accidents involving twin-engine aircraft (Research and analysis report B2005/0085), found that power loss accident rates in twin-engine aircraft were almost half of the rate for single-engine aircraft.[10] However, a power loss accident in a twin‑engine aircraft was more likely to be fatal and overwhelmingly the result of in-flight loss of control. Of the 58 accidents identified between 1993 and 2002 that resulted in damage following the power loss, seven accidents occurred during the approach phase of flight. Three of these involved a loss of control, including one fatal accident. Given the approach phase was a relatively small portion of the overall flight, this was considered a more risky time, with low altitude and only a little more energy available than during the take-off phase.
From the evidence available, the following findings are made regarding the collision with terrain involving a Cessna Aircraft Company 310R, registered VH-BWZ, which occurred 1.9 km north-north-east of Mildura Airport, Victoria, on 6 November 2015. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
For undetermined reasons the left engine was starved of fuel, which resulted in a loss of power during flight.
The left engine’s loss of power while the aircraft was in a landing configuration resulted in the pilot being unable to maintain aircraft control and the aircraft subsequently collided with terrain.
Safety analysis
Introduction
When on final approach to runway 18 at Mildura, witnesses reported seeing the accident aircraft at low altitude yaw to the left, followed by the left wing drop where the aircraft rapidly lost altitude. The aircraft subsequently impacted powerlines before colliding with terrain. The pilot was fatally injured, and the aircraft destroyed. The ATSB examined air traffic control recorded data, the aircraft wreckage, the pilot’s training and medical records, postmortem and toxicology reports, aircraft maintenance history and witness interviews. Aircraft components, including the left engine, left propeller and aircraft auto-pilot servo units were recovered from the wreckage for further examination.
The pilot was appropriately qualified to conduct the flight and was declared medically fit. Despite having relatively low flying hours on the aircraft type and twin-engine aircraft operations, the pilot demonstrated proficiency about one month prior to the accident where he completed an instrument landing system endorsement for the private instrument rating in the accident aircraft. During that endorsement he was subject to several simulated one-engine inoperative exercises during the approach phase for the ILS endorsement.
Four months prior to the accident, the maintenance provider performed a simple operational test of the autopilot and held the elevator trim wheel, proving that the elevator electric trim could be overridden manually. The ATSB did identify some anomalies with the auto-pilot elevator clutch assembly but could not determine if those abnormalities were pre-existing or were a result of the collision with terrain The ATSB did not consider the identified abnormalities factors contributing to the accident.
Examination of the left engine and propeller determined the engine was not producing power nor was the propeller producing thrust. This was most likely due to fuel starvation to that engine. No mechanical defects were identified that may have contributed to the occurrence. However, the examination of the wreckage was limited due to the extent of the fire damage sustained to the aircraft.
The following analysis will examine fuel starvation of the left engine and the subsequent power loss. The adverse consequence of this on aircraft performance, combined with the aircraft’s configuration, will also be discussed.
Left engine and fuel
Disassembly, inspection and examination of the left engine, left engine accessories and the left propeller at the accident site and during the post onsite detailed examination did not identify any mechanical defects or abnormalities that may have prevented normal engine or propeller operation.
However, examination of the engine fuel system identified no fuel in the left engine fuel manifold and supply fuel lines, which is situated between the wing fuel selector and the engine. The right fuel manifold and supply fuel line did contain fuel.
The aircraft departed Latrobe Valley with both main fuel tanks full, a total of at least 378 L of usable fuel on board. The flight time from Latrobe Valley to Mildura via Moorabbin was about 110 minutes. Based on that data and in consideration of an average fuel burn of 2 litres per minute, there should have been at least 158 litres of fuel remaining on board when the aircraft reached Mildura, not taking into account any fuel in the auxiliary fuel tanks. On that basis, it is likely that the aircraft had a significant amount of fuel on board at the time of the accident and the left engine had been starved of fuel.
The severe disruption of the left and right main fuel tanks and the right auxiliary fuel tank, including burning and melting indicated that those tanks held a significant amount of fuel at the time of the collision. In contrast, the left auxiliary fuel tank did not display the same level of disruption, including burning and melting of the aluminium structure or bladder fuel cell indicating that it is likely the left-wing auxiliary fuel tank did not have a significant quantity of fuel at the time of the accident.
The position of the wing fuel selector valves during flight was inconclusive as it could not be determined if the pilot had selected the fuel selector to the position found during the wreckage examination, or whether it was a result of the accident sequence.
The reason for the starvation of fuel to the left engine and the disparity of fuel quantity between the left and right auxiliary fuel tanks could not be quantified or determined due to the damage to the aircraft from impact forces and post impact fire.
Asymmetric condition
Witnesses observed the aircraft yawing to the left prior to loss of aircraft control and evidence located at the accident site showing the aircraft rotating in an anticlockwise direction during ground impact sequence was consistent with asymmetric thrust. It was likely the inoperative engine (which was the critical engine), with its propeller towards the fine pitch and the opposite engine at high power, resulted in an asymmetric thrust condition. To maintain control of the aircraft and counteract asymmetric thrust the pilot needed to apply rudder and if necessary the aileron to counteract the forces generated from the drag of the non-performing engine and high thrust from the performing engine. Rudder and aileron input also increases drag and contributes to the decay of airspeed.
Aircraft performance degraded
The ATSB could not determine when the engine failed, nor could it be determined if or when the pilot was aware of the failure. At the time of impact, the aircraft landing gear and flaps were fully down, the flight control trim devices were in the neutral position and both propellers were towards the fine pitch, consistent with a normal landing configuration. In this configuration, combined with the left engine not producing power the drag penalties were such that altitude could not be maintained.
It is possible that the pilot may have been in the initial stages of responding to the engine failure and was not in a position to secure the engine, which included feathering the propeller. Further, it is not known if the landing gear and flap positions were selected prior to the asymmetric condition in preparation for a normal landing or after, as the pilot may have believed an engine inoperative landing onto the runway could be assured. Irrespective, in this configuration the aircraft’s performance would have degraded to the point at which altitude could not be maintained to assure a landing.
This accident highlights the adverse consequences of aircraft configuration on one-engine inoperative performance, particularly when at low altitudes. It further demonstrates the challenges of asymmetric operations and the importance of pilots being aware of the drag penalties and associated consequences.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Airservices Australia
a number of witnesses
Textron Aviation
the Civil Aviation Safety Authority
United States Federal Aviation Administration
Victoria Police.
References
Jeppesen Sanderson Inc 1992, Multi-Engine Pilot Manual, Jeppesen Sanderson, Colorado.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Civil Aviation Safety Authority, Airservices Australia, Textron Aviation, the aircraft maintenance provider, National Transportation Safety Board and the operator of the aircraft.
Submissions were received from the Civil Aviation Safety Authority. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the afternoon of 2 November 2015, a Eurocopter AS350-BA helicopter, registered VH-SFX, was performing a low-altitude aerial weed spotting operation over dense forest in the Whyanbeel Valley, Queensland. On board the helicopter were the pilot, a navigator and two aerial spotters.
While conducting the work, the helicopter yawed twice in an uncommanded manner. In response, the pilot climbed and increased the helicopter’s forward airspeed and attempted to return to his base of operations. Subsequently, the engine failed, which required the pilot to conduct an autorotation and emergency landing.
The passengers adopted the brace position and the helicopter landed heavily with the skids digging into the uneven terrain and breaking off. The navigator in the front seat received minor injuries and the pilot received serious back injuries from the impact forces.
What the ATSB found
The ATSB found that the emergency landing was handled in a competent and proficient manner. The pre-departure briefing gave the passengers the necessary knowledge to prepare for the emergency by adopting the brace position and exiting the helicopter only when it was safe to do so.
Analysis of the engine identified that the aircraft lost power due to a front bearing failure in the turbine module. The failure was due to an accumulation of coke particles in an oil jet. The ATSB was unable to conclude specifically why the coke particles had formed.
The severity of the engine failure was increased through the fracture of the power turbine shaft and the subsequent separation of the turbine disc. This was due to a lack of adhesive on the splined nut that was threaded to the rear of the power turbine shaft.
A service information bulletin issued by the helicopter manufacturer in 2010 recommended that AS350 helicopter operators consider the safety benefits of installing energy-absorbing seats. Had these seats been installed, the forces imparted to the pilot during the accident sequence may have been reduced.
What's been done as a result
The engine manufacturer (Safran Helicopter Engines) has amended their procedure manual to include systematic cleaning of the power turbine front bearing assembly oil jet and oil jet supply pipe. Safran HE have initiated a number of training and process changes to ensure the adhesive bonding between the power turbine and the rear nut is maintained during service.
Safety message
This investigation highlights that responding to an emergency in a timely and proficient manner can minimise the consequences of an accident. Similarly, providing emergency procedures briefings enables passengers to react appropriately in an emergency.
In this occurrence, the reason for the engine oil jet coking leading to the engine failure was not specifically determined. However, a range of factors can affect engine oil coking. These factors should be considered to ensure normal ongoing engine operation.
Context
Pilot training and experience information
The pilot held a valid Commercial Pilot (Helicopter) Licence that was issued on 6 January 2004 and a valid Class 1 Aviation Medical Certificate. The pilot’s last flight review was issued on 17 February 2014 and was valid until 29 February 2016.
The pilot had a total flying experience of about 6,200 hours, of which over 3,000 hours were in the AS350 series helicopter. This included a substantial amount of experience conducting low-level operations. In the previous 90 days, the pilot had flown 9 hours on type, and in the previous 24 hours the pilot had flown 6 hours on type. The pilot reported feeling rested and alert prior to the occurrence flight.
Helicopter information
The helicopter was a Eurocopter AS350-BA helicopter, manufactured in 1981 and first registered in Australia on 16 June 2005. At the time of the occurrence, the airframe had accumulated approximately 10,518 hours total time in service (TTIS).
Wreckage and impact information
The on-site examination found that the helicopter struck the ground tail rotor first, with the skids subsequently digging into the uneven terrain and separating from the fuselage (Figure 2).
The engine had sustained damage consistent with a high-energy failure. The power turbine separated from the disc and the containment shield was twisted and deformed. The exhaust duct was bulged and puncture marks from internally liberated engine debris was evident (Figure 3).
Figure 2: VH-SFX at the accident site
Source: ATSB
Figure 3: View of the helicopter engine at the accident site
Source: ATSB
Engine information
The helicopter was powered by a Turbomeca[3] Arriel (model 1B) engine, located above and to the rear of the passenger compartment. The Arriel 1B engines feature a modular design with the major modules consisting of an axial and centrifugal compressor, an annular combustion chamber, a two-stage axial turbine, a single-stage axial power turbine and a reduction gearbox (Figure 4). This occurrence related to a failure within the power turbine.
Figure 4: General arrangement of a Turbomeca Arriel 1B turboshaft engine showing the locations of the major sub-components
Source: Turbomeca, modified by the ATSB
Power turbine information
Gases from the two-stage axial turbine are directed downstream to the power turbine. The power turbine disc and shaft is a cantilevered design supported by front and rear bearings (Figure 5). Surrounding the power turbine is a containment shield to prevent high-energy engine debris from exiting the engine in the event of a blade fracture or disc separation from the shaft. The fractured turbines blades did not penetrate the containment shield in this occurrence.
Figure 5: General arrangement of the power turbine showing the relative location of the major parts including the guide vanes, labyrinth seal, power turbine shaft, rear nut, and the front and rear bearings
Source: Turbomeca, modified by the ATSB
Engine examination
The engine was removed from the helicopter and a preliminary examination was completed at the engine manufacturer’s facilities in Sydney, New South Wales. The power turbine shaft assembly of the engine was subsequently transported to the manufacturer’s facilities in France. The assembly was inspected in detail under the supervision of the French aviation investigation agency, the Bureau d'Enquêtes et d'Analyses pour la sécurité de l'aviation civile (BEA). The examination determined that:
The power turbine disc had fractured in overstress and separated from the power turbine shaft (Figure 6). The power turbine disc sustained a complete loss of power and the turbine blades had separated from their respective stations. Fracture of many of the blade inter-recesses within the disc had also occurred.
The front bearing of the power turbine shaft had totally seized (Figure 7). Evidence of roller skidding, metal contamination and gross overheating was found within the bearing assembly. The accumulation of hardened coking products and varnish deposits from oil degradation was also found within the rolling elements.
As a result of extreme frictional heating, the oil-air labyrinth seal, just forward of the front bearing, had melted and fused with the power turbine shaft.
Metallurgical analysis of the power turbine shaft showed that it had been exposed to temperatures in excess of 1,300C. That temperature was several hundred degrees above the normal maximum operating temperature of the engine.
Examination of the oil jet and surrounding oil ducts to the front bearing of the power turbine shaft identified that the jet outlet was blocked with an accumulation of coke particles (Figure 8).
Examination of the splined nut that was threaded to the rear of the power turbine shaft assembly revealed evidence that it had tightened. The location of the nut determined the position of the shaft and any potential axial preload of the shaft bearings. No evidence was found of the adhesive that was required to have been applied between the threads on the rear shaft and the nut (Figure 9).
Figure 6: Cross-section through the power turbine assembly from the engine showing that the disc had separated from the shaft and the blades had fractured
Source: Turbomeca, modified by the ATSB
Figure 7: The seized front bearing and labyrinth seal, showing blackening from severe heat distress, flattening of the rollers, deformation of the cage and sealing fins
Image source: Turbomeca, modified by the ATSB
Figure 8: Close up of the blockage (circled) at the oil jet to the front bearing, as positioned in the general arrangement view
Image source: Turbomeca, modified by the ATSB
Figure 9: Cross-section of the rear splined nut contacting the rear bearing inner race
Source: Turbomeca
Power turbine rear nut adhesive bonding
The engine manufacturer had intended for an adhesive to be used in order to secure the rear nut into position. The adhesive was only applied during maintenance at a Turbomeca overhaul facility when the power turbine was overhauled.
Failure to adequately bond the nut could result in a tightening of the rear nut when abrupt changes in torque occur, leading to axial displacement of the turbine shaft in excess of the designed amount. This displacement would result in contact between the turbine shaft and the front bearing inner race, resulting in frictional heating, and damage to the turbine shaft.
The engine examination identified that the rear nut fitted to the rear of the power turbine shaft had not been adhesively bonded, as required.
Oil coking
The observed coking of the front bearing and its oil jet duct was likely a result of the engine oil exposure to abnormally high temperatures in the area. While there were clogging inspection procedures of the power turbine rear bearings, no preventative maintenance actions existed that allowed for the identification of coking within the front bearing.
Coking is an artefact from exposure to abnormally high temperatures that leads to oxidation and chemical breakdown of the oil. Coking can form as a thin-film layered deposit (as was the case in the oil duct) or in thicker clumps (which resulted in the clogging of the oil jet). It forms within the oil distribution channels and pipes, and can shed from the wall surface leading to reduced or obstructed oil flow. Determining the initiating source of coke formation is difficult as it can be attributed to a combination of influences, including:
operational conditions such as hot shutdown
design traits such as abrupt changes in oil flow direction and areas of low fluid velocity that can lead to reduced oil flow rates
low-drainage areas resulting in conductive or convective oil temperature increases post-shutdown
reductions in cross-sections such as scavenge ports that increase the likelihood of blockage
prolonged aircraft inactivity leading to moisture absorption of coke deposit.
The manufacturer of Arriel engines had published guidance for the thermal stabilisation of engines at shutdown. The guidance involved throttling the engine back until the engine was at ground idle for at least 30 seconds prior to shutdown. Stabilising an engine after operation allows for the temperature to reduce and thermally balance, while maintaining sufficient oil-scavenging capability and oil flow rates to minimise the potential for coke formation. Non-compliance with the manufacturer’s stabilisation recommendations may lead to coking.
The helicopter operator’s manual referred to the correct shutdown procedure in the AS350 flight manual. However, an appendix to the operator’s manual included a checklist that referred to a two-minute idle time before shutdown. The engine manufacturer advised that a two-minute shutdown would not adversely affect the formation of coke particles.
The engine manufacturer reported that a design trait of the power turbine is that the fluid velocity is lower at the bottom of the oil jet duct to the front bearing. For a given volume, this trait can lead to increased convective heating of the oil and depending on the temperatures in that region, may lead to coking.
In the period January 2000 to September 2015, there were 13 cases of Arriel engine deterioration in the power turbine shaft front bearing due to oil jet clogging. However, this is the only accident that has resulted in the failure of the turbine shaft.
Engine maintenance
The most recent significant maintenance involved removal of the engine from the airframe for repair after it sustained foreign object damage in February 2015 (7,786 hours TTIS). The centrifugal compressor and gas generator were replaced in May 2015. The engine was not operated during this period.
The last scheduled engine maintenance was performed on 30 October 2015 (8,060 hours TTIS), two days prior to the accident. Among the maintenance actions performed at that time, a clogging check of the gas generator rear bearing was conducted along with an inspection of the oil return line strainer. No anomalies were recorded in the maintenance documentation. The helicopter subsequently accumulated an additional 5 hours flight time up until the accident. There was no overdue maintenance requirements or declared defects.
Oil and filter analysis program
The helicopter operator had been monitoring the internal health of the engine components by participating in a spectrometric oil and filter analysis program (SOAP). That program relied on detecting the type and quantity of wear-material products within the engine oil and oil filter. The wear-material is generated from the breakdown mechanisms of internal engine components. SOAP checks were recommended by the engine manufacturer at intervals not exceeding 100 hours of service.
The most recent oil sample was collected and analysed approximately 10 hours prior to the engine failure. The previous sample to that was taken approximately 100 hours prior to the failure. Those checks indicated no unusual trends or signs that internal damage had been developing.
Emergency Procedures
The AS350 flight manual defined the emergency procedures for the illumination of the ‘ENG CHIP’ chip detector light and an autorotation landing. As per the AS350 flight manual, upon the Illumination of the ‘ENG CHIP’ caution light the pilot was required to:
“Land as soon as possible: land at the nearest site at which a safe landing can be made.”
A successful autorotation is dependent on the pilot’s airmanship and the helicopter’s speed and altitude relative to the airspeed-height envelope.
Airspeed-height envelope
The airspeed-height envelope defines a region within the helicopter’s flight envelope where there is insufficient energy (height and/or airspeed) for a successful autorotation to be completed. Section 5.1 of the AS350 flight manual defines the airspeed-height envelope for the helicopter. The envelope is determined using the density altitude and weight of the helicopter. The resulting envelope outlines the avoidance zone (Z); operating in the avoidance zone as defined in the FAA Rotorcraft Flying Handbook (FAA-H-8083-21A) ‘“may not allow enough time or altitude to enter a stabilised autorotative descent.’
Helicopters are not restricted from conducting operations in the avoidance zone, however, a pilot should always evaluate the risk of the manoeuvre versus the operational value.
In this case, the helicopter was equipped with a Garmin GPSMAP 195 portable device capable of storing track data for flights. During the operational portion of the flight, the helicopter was inside the avoidance zone. This was due to the aircraft being required to travel at a low airspeed and altitude such that the aerial spotters were able to identify the noxious plants.
The GPS track data for the accident ended while the aircraft was still airborne. At the time of the last track point, the aircraft was approximately 295 ft above the terrain travelling at approximately 65 kts groundspeed. This was outside the avoidance zone defined as per the flight manual.
Survival aspects
The passengers had received the pre-departure briefing and adopted the brace position. The navigator in the front seat received minor injuries and the pilot received serious back injuries from the impact forces. No objects were located underneath the front or rear seats.
Helicopter seating
The helicopter was fitted with the original seats installed by the manufacturer (Figure 10). The rear passenger seats had deformed during the accident and likely absorbed some of the energy during the impact. The seat-belt attachments remained intact during the accident sequence. There was no observable deformation to the front seats of the helicopter.
In 1999, the helicopter manufacturer released a service letter (SL No. 1424-25-99) to inform all helicopter operators of the optional availability of redesigned seating for the pilot and copilot. The improved seat design increased the strength of the seat and attachments, and depending on the installed option, introduced energy-absorbing seat installations.
The manufacturer also published a service bulletin (EC SB AS350 No. 25.00.57) recommending the installation of the energy-absorbing seats on AS350 helicopters. A European Aviation Safety Authority (EASA) safety information bulletin, SIB 2010-05, reiterated the safety benefits associated with the installation of energy absorbing seats.
According to the EASA SIB, the modification of the helicopter in accordance with the SL would:
increase the pilot and co-pilot’s seat strength and crashworthiness and thus to provide an increased level of protection to the occupants in case of impact during an accident.
Figure 10: VH-SFX front seats (left) and rear passenger seats (right)
Emergency equipment
The helicopter was fitted with an emergency locator transmitter (ELT) that could be activated by a switch on the instrument panel, an emergency position indicating radio beacon, and a first aid kit. Just prior to touchdown the pilot activated the ELT. After the landing, two passengers proceeded on foot to search for persons/households to contact emergency services. About 30-45 minutes after the accident occurred, the passengers were met by emergency services, who were responding to the ELT transmissions. The pilot received medical treatment onsite and was transported to hospital for further treatment. There were no other communication devices available, such as a satellite phone, for contacting emergency services.
The sources of information during the investigation included the:
Safran Helicopter Engines (formerly Turbomeca)
Airbus Helicopters (formerly Eurocopter)
the Civil Aviation Safety Authority
the aircraft operator
the pilot
the passengers.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the pilot, the passengers, the aircraft operator, the Civil Aviation Safety Authority, Airbus helicopters, Safran Helicopter Engines ,and the Bureau d'Enquêtes et d'Analyses pour la sécurité de l'aviation civile (BEA).
Submissions were received from the pilot, the aircraft operator, Safran Helicopter Engines, the Civil Aviation Safety Authority and the BEA. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
The occurrence
On 2 November 2015, a Eurocopter AS350-BA helicopter, registered VH-SFX, was performing aerial work to identify noxious plants in dense forest within the Whyanbeel Valley (Figure 1), Queensland (Qld). The nature of the aerial work required the helicopter to operate at a low altitude and airspeed. On board the helicopter was the pilot, a navigator and two aerial spotters. The base of operations was in Mossman, Qld.
At approximately 1620 Eastern Standard Time,[1] during the fourth flight of the day, the helicopter momentarily yawed twice within a short period in an uncommanded and unusual way. The pilot, concerned with the uncommanded movements, ceased the operation, climbed and increased the helicopter’s forward airspeed. The pilot then elected to head back towards the base of operations (approximately 11km away) and, if required, land along the way if a suitably safe area along the flight path presented.
Shortly after, the chip detector light[2] illuminated on the instrument panel, prompting the pilot to search for a suitable landing area. As the helicopter continued to climb through approximately 200 ft, the engine stopped producing power.
The pilot identified the most suitable area to land, given the limited available height and airspeed, and commenced an emergency autorotation. The identified area was uneven, overgrown with plants, and surrounded by tall trees. During the landing sequence, the skids of the helicopter dug into the terrain and were broken off. The helicopter came to rest about 10 m after first touching down. The passengers received nil to minor injuries and waited until the rotor blades had ceased turning before evacuating the helicopter. The passengers then assisted the pilot who had received serious back injuries. The helicopter was substantially damaged.
Figure 1: The helicopter’s GPS track, arriving in the area of operations, its flight path around the forested terrain in the Whynabeel valley, and the accident site
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
The engine manufacturer (Safran Helicopter Engines) has amended their practices to include:
Periodic cleaning of the power turbine front bearing assembly oil jet and oil jet supply pipe. This reduces the occurrence probability for oil jet clogging by removing any accumulated deposits from these locations.
Degreasing of the threaded surfaces prior to application of the adhesive bonding and assembly of the parts. Maintenance and overhaul personnel have been informed of the importance of degreasing the surfaces before bonding the nut to the power turbine shaft.
Safran Helicopter Engines is also studying the use of heating equipment to obtain a more repeatable polymerization.
Findings
From the evidence available, the following findings are made with respect to the engine failure involving a Eurocopter AS350BA helicopter, registered VH-SFX that occurred in the Whyanbeel Valley, Queensland on 2 November 2015. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
The helicopter lost power due to a failure of the Arriel 1B engine. The failure was a result of coke particles that had clogged the front oil jet from the power turbine shaft, preventing oil flow, and leading to a total seizure of the front bearing. The specific source that led to the coke formation and oil clogging of the front oil jet could not be determined.
The rear-splined rear nut had not been adhesively bonded to the power turbine shaft, as required. When the front bearing failed, the lack of adhesive led to a progressive tightening of the nut and additional frictional heating of the shaft from contact with the static engine components. The consequential reduction in material strength from the heating allowed the power turbine shaft to fracture and the disc to separate, further increasing the severity of the engine failure.
Other factors that increased risk
The helicopter was not fitted with energy absorbing front seats, which may have reduced the risk of injury to occupants during an accident.
Other findings
The ATSB found that the emergency landing was handled in a competent and proficient manner. The decision by the pilot to increase forward airspeed and altitude, after the uncommanded and unusual yaw movements, removed the helicopter from within the avoidance zone and likely prevented serious injuries to the passengers.
Safety analysis
Introduction
While conducting aerial weed spotting operations at low level, the helicopter’s engine failed necessitating an emergency landing into unfavourable terrain. The ground impact resulted in substantial damage to the helicopter. The pilot received serious injuries and the passengers sustained nil to minor injuries.
This analysis will examine why the engine failed, why an impending failure was not detected, the pilot’s handling of the emergency, and how occupant injuries can be reduced in the event of a hard landing.
Engine failure
The uncommanded yawing of the helicopter was the result of the engine failing from a seizure of the front bearing to the power turbine. The failure commenced rapidly when the oil supply to the front bearing became obstructed due to clogging of the bearing’s oil jet by the accumulation of coke particles (a solid residue from the breakdown of the engine oil).
During this period of transient engine operation, it is likely that the abrupt changes in torque from the power turbine and the lack of adhesive, led to a progressive tightening of the rear nut (fitted to the rear of the shaft). The tightening resulted in an axial coupling between the front bearing, stop, and labyrinth seal. That contact generated additional frictional heating and a further temperature rise within the shaft.
The combined effects of the front bearing seizure and the axial coupling of the components led to excessive heating and a subsequent critical reduction in mechanical properties for the shaft. Consequently, the turbine shaft was unable to sustain the operating stresses and it eventually fractured at the interconnection with the disc.
Oil coking
Coke formation is influenced by a range of complex factors (as mentioned in the coke formation section). The engine had been removed from the aircraft due to foreign object damage early in 2015 and spent several months out of operation. The ATSB was not able to determine if coke deposits were present at this point in time. Similarly, it was unknown if inactivity had impacted on moisture absorption of any coke deposits. The manufacturer has subsequently added an additional operation in their maintenance procedures which include the systematic cleaning of the turbine shaft front bearing assembly oil jet and oil jet supply.
While non-compliance with the stabilisation time before engine-shutdown can result in coke formation, the operator’s procedures, included a stabilisation time of not less than 30 seconds and it was reported that flight crew followed these procedures. As such, the ATSB was unable to determine to what extent (if any) the compliance with stabilisation times affected the formation of coke particles.
The service history of the Arriel-series engine indicates there have been multiple instances of deterioration of the turbine shaft front bearing as a result of the front oil jet clogging. The geometry around the oil jet was such that in the event of front bearing degradation due to clogging, temperature rises in this area would occur. This induced variations in the oil fluid velocity and led to conditions that were favourable to coking and the formation of hardened deposits. The use of the manufacturer specified oil and continuous monitoring for metal particles should have limited the effect of this phenomenon. However, the metal particle detection checks (SOAP) were not intended for assessing the presence of coke particles, but rather the breakdown of engine components. In this instance, clogging of the oil jet likely occurred before the breakdown of the engine components. The ATSB was unable to determine to what extent the geometry of the area affected the formation of coke particles.
Due to the complex combination of factors that can affect coke formation, the ATSB was unable to determine a specific source that led to the coke formation and oil clogging of the front oil jet.
Adhesive bonding of the power turbine rear nut
The engine manufacturer had intended for an adhesive be used in order to secure the rear nut into position. The adhesive was only applied during maintenance at a Turbomeca overhaul facility when the power turbine was overhauled. The engine examination identified that the rear nut fitted to the rear of the power turbine shaft had not been adhesively bonded, as required.
The engine would still have ceased operating if the appropriate adhesive had been present on the rear splined nut. However, the likelihood of the shaft failing would have been reduced and the failure sequence less severe. The failure sequence would likely have been extended, allowing greater time for the pilot to respond to the failing engine.
Flight operation
The operation necessitated the helicopter to operate at a low altitude and airspeed. At the time of the uncommanded yaw movements and subsequent ‘ENG CHIP’ light illumination, the helicopter was inside the avoidance zone. According to the helicopter operating manual, an ‘ENG CHIP’ light illumination necessitates the pilot to land the helicopter ‘as soon as possible’. This should be interpreted as soon as safe landing is possible. The pilot immediately increased airspeed and altitude and brought the aircraft out of the avoidance zone. This allowed the pilot to conduct a successful autorotation when the engine failed.
At the time, the helicopter was over densely forested and steep terrain, making it unsuitable for a safe landing. The pilot had elected to head back towards the base of operations (approximately 11 km away) and land if there was a suitably safe area along the flight path. Given the location of the helicopter and the surrounding terrain, returning to a known safe landing area (the base of operations), with the possibility of identifying a safe landing area during transit, provided an appropriate option in the difficult circumstances.
The pilot’s actions while responding to the emergency situation likely prevented serious injuries to the passengers.
Helicopter seating crashworthiness
The rear passengers had adopted the brace position prior to the impact and the seats had absorbed some of the energy from the hard landing. These passengers received nil injuries. Similarly, the passenger in the front seat braced for the landing and received only minor injuries.
The helicopter was fitted with the original front basic seats installed when it was manufactured. The basic seats complied with the minimum performance standard of the applicable certification bases.
As aerospace technology and design has evolved since the original certification, new certification rules have been enacted to better protect the occupant’s safety in the event of an accident. The manufacturer of the helicopter had installation options available to operators to install energy-absorbing seats. Energy absorbing seats reduce the amount of energy transferred to their occupants in the event of an accident.
In the case of this accident, there was not enough information on the impact forces and dynamics to determine whether energy-absorbing seats would have reduced the injury severity to the pilot.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 29 May 2015, at about 1145 Eastern Standard Time (EST), a Victa 115 Airtourer aircraft, registered VH-MUV (MUV), departed from Leongatha Airport, Victoria, for crosswind circuit training, with an instructor and student on board.
The student pilot was flying the first circuit. The instructor reported that the circuit was normal and the approach was stable up to about 100 ft above ground level (AGL) when the student put the final stage of flap out. As the aircraft flared to land on runway 22, a strong gust of wind blew the aircraft off the runway centreline to the left and the aircraft bounced hard. The student initiated a go-around, applying full power, with the aircraft still drifting further to the left. As the aircraft was not climbing, the instructor called “taking over” and the student handed over control of the aircraft. The instructor lowered the nose of the aircraft to gain airspeed.
The aircraft continued to drift further away from the runway centreline. The student noticed the flaps were in the down position and, thinking that it would assist and without checking with the instructor, retracted the flaps to the up position. The aircraft descended and about 100 m past the threshold of runway 22, the aircraft collided with the airport perimeter fence. After a further 20 m, the aircraft flipped over the fence and came to rest upside down. The instructor and student exited the aircraft quickly through the broken canopy, as fuel was gushing from the fuel tanks. The instructor and student pilot received minor injuries and the aircraft was substantially damaged (Figure 1).
Figure 1: VH-MUV inverted after flipping over the airport perimeter fence
Source: Aircraft operator
Instructor comment
The instructor reported that the purpose of the flight was to instruct the student in crosswind landing techniques and then to conduct further flight training in the training area. The instructor indicated that, as they were planning to conduct 2 hours of flight training, the aircraft had full fuel on board and was near the aircraft maximum take-off weight.
The instructor described the wind as gusting between 15 to 22 kt at 270 degrees, with a crosswind component of between 10 to 15 kt.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following safety action in response to this occurrence.
Flight training organisation
As a result of this accident, the flight training organisation advised the ATSB that they are taking the following safety actions:
The instructor has been briefed on the importance of making sure students understand not to touch any of the aircraft’s controls when the instructor is in control of the aircraft.
The instructor has been briefed on the handing over and taking over procedures with the emphasis on handing over and taking over controls procedures.
Safety message
It is important in flight training to have a positive exchange of flight controls. The US Federal Aviation Administration (FAA) has found that numerous accidents have occurred due to a lack of communication or misunderstanding regarding who had actual control of the aircraft, particularly between students and flight instructors. The FAA publication Aviation Instructor’s Handbook, includes a section on the Positive Exchange of Flight Controls. The handbook provides guidance to use for the positive exchange of flight controls (Figure 2).
Figure 2: FAA Positive exchange of Flight Controls
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Late in the afternoon of 7 October 2015, a pilot prepared the Robinson 44 helicopter, registered VH-ZWA (ZWA), for a solo training flight. The local flight from Darwin Airport, Northern Territory, was to consolidate the pilot’s knowledge of the local area, and become more familiar with the helicopter, as it was the pilot’s first day in a new job. Earlier in the day, the chief pilot had conducted an acceptance flight with the pilot in ZWA.
The pilot refuelled the helicopter and conducted a pre-flight inspection, before boarding, and completing the pre-start checklist.
The pilot then conducted the following engine start checklist from memory.
Engine start (main actions)
engaged the starter until it fired
engaged the clutch and turned the alternator on
when the clutch light went out, increased the rotor RPM to 79%
conducted a magneto check; and noted that all warning lights were out
began to increase the rotor RPM toward 100% and turned the governor on
Just as the pilot was about to conduct the next checklist item, a low rotor horn check[1], the pilot reported that the helicopter yawed slightly to the left. The pilot quickly checked that the pedals were neutral and put some ‘weight’ on the collective to confirm that it was fully down.
However, the helicopter continued to yaw left rapidly, through about 90° (Figure 1). The pilot applied full right pedal but the helicopter did not respond and continued the yaw, through about 180°, before falling onto its right side. The pilot, who sustained minor injuries, quickly exited the helicopter and the helicopter was substantially damaged (Figure 2).
Pilot experience
The pilot held a Commercial Pilot Licence (H) and a Private Pilot Licence (A). The pilot had logged about 340 hours in helicopters, with about 16 hours of these in the Robinson R44 and about 15 hours in the Robinson R22 helicopter.
Apart from the acceptance flight earlier that day, and a check flight a couple of weeks earlier, the pilot had not flown a R44 for more than three years. The pilot’s most recent helicopter experience was in a MD 520N helicopter. Although the pilot had flown two separate one-hour flights in the last three weeks, the pilot stated they were not current nor experienced on the R44. The pilot reported that flying opportunities had been limited, and spread out over about 4-5 years. During this time, the pilot had also worked as a helicopter support person and as a teacher of commercial helicopter theory subjects.
Figure 1: Skid marks made by VH-ZWA yawing to the left
Source: Operator
Figure 2: VH-ZWA on right side showing damage to main rotor and cabin
Source: Operator
Pilot comments
The pilot arrived from interstate at 0100 on the morning of the accident, ready to start the new job. They signed on for duty at 1000 after 7 hours of sleep. After completing some paperwork, the pilot underwent a one-hour company acceptance flight with the chief pilot. This flight was conducted in ZWA.
After a lunch break, more paperwork was completed before the chief pilot suggested the pilot go for a solo flight, to consolidate their knowledge of the local area and become more comfortable with the R44. The pilot reported feeling a little uncomfortable conducting the solo, but reasoned that it would be a good opportunity to gain some more practice. In addition, the pilot stated being slightly fatigued, and affected by the extra pressure of ‘new employee expectations’.
The pilot made a number of comments regarding different factors of the occurrence, these included:
at the time of the accident, not understanding why the helicopter turned to the left, or yawed so rapidly, particularly after full right pedal had been applied. The pilot later reflected that the pedals must not have been as neutral, as first thought and that this had allowed the yaw leading to the resultant loss of control
suggesting the left yaw may have been from the collective lock being jammed under the collective just enough for the control to feel fully down, but actually have sufficient play to allow the yawing movement.
felt that the helicopter falling onto the right side was consistent with dynamic rollover
Operator comments
The operator acknowledged that the new pilot had low total flying hours and low time on the R44 helicopter. This was combined with only 1.9 hours of flying logged in the last 90 days. Although two recent dual checks had been carried out, the additional solo practice was suggested to allow the pilot some consolidation time. In hindsight, the company realised that the pilot required even more dual time prior to being authorised for any solo practice.
A post-accident engineering inspection did not reveal any mechanical defects with ZWA.
ATSB comment
The ATSB did not conduct an onsite investigation to this accident. The pilot reported not being aware of making any errors during the engine start, but noted that a helicopter is unable to move if the collective is fully down.
In researching several databases for like occurrences, the ATSB found a Robinson 44 accident with similarities, in the United Kingdom. In this accident, the helicopter yawed to the left and fell onto the right side during an engine start. The UK Air Accidents Investigation Branch (AAIB) commented that a rapid yaw to the left could be induced, if too much left pedal is applied at the point of governor engagement, due to the effectiveness of the tail rotor.
The fact that the pilot’s most recent helicopter experience was on a MD 520N, also supports this possibility. The MD520N does not have a traditional tail rotor; it is fitted with a NO Tail Rotor (NOTAR) system, and requires very little pilot input on the pedals. It is probable that the pilot defaulted to this more relaxed pedal pressure during the accident flight.
Other R44 accidents, with relatively inexperienced solo pilots at the controls, were attributed to the pilot’s lack of recency, or inexperience, managing the different handling characteristics of the helicopter, due to the weight shift, which occurred without a person occupying the left seat.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Operator
As a result of this occurrence, the aircraft operator has advised the ATSB that they are taking the following safety actions:
Operations manual amendment
All pilots recruited with under 500 hours total time and / or 30 hours in the previous 90 days, must fly with a Grade 1 instructor. This flight is to assess the pilot’s practical and mental status. The Grade 1 instructor is to provide a report on the flight to the Chief Pilot prior to the new pilot undergoing company induction.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 28 June 2015, at about 1500 Central Standard Time (CST), a Robinson R22 helicopter, registered VH-RBO, took off from a property near Daly Waters, Northern Territory, for a local flight, including inspection of bores on the property. The temperature was about 30°C with a south-easterly wind at 10-15 kt. After flying for about 20 minutes, the pilot, who was the sole occupant of the helicopter, landed to open a gate and put out a bucket of chain. The pilot selected the governor off, then exited the helicopter, leaving the engine running. The pilot then re-boarded the helicopter and took off.
After a further 5 to 10 minutes of flight, when at about 100 ft above ground level, and an airspeed of 40 kt, the pilot conducted a turn to the south. The low rotor revolutions per minute (RPM) warning horn sounded. The pilot immediately wound the throttle fully open, and lowered the collective[1] to try to regain rotor RPM. The helicopter continued to descend. The pilot attempted to flare[2] the helicopter when low to the ground. The main rotor blades collided with tree branches. The helicopter landed heavily, the skids dug in to the soil and the helicopter rolled onto its side.
The pilot sustained minor injuries and the helicopter was substantially damaged (Figure 1).
Figure 1: Accident site
Source: Aircraft engineer
Pilot comments
The pilot was unsure whether the engine was running normally when the helicopter touched down, and could only recall hearing the rotor RPM warning horn. The pilot was focused on looking outside the helicopter at an earth tank and a mob of cattle and not inside at the instruments. The pilot reported that it was their normal procedure to switch off the governor when exiting, and then select it back on when returning to the helicopter. However, on this occasion, the pilot could not recall specifically switching it back on.
Engineering report
A 100-hourly maintenance inspection and the replacement of two cylinders was completed on the morning of the accident flight. The pilot and an engineer then conducted a flight of about 20 minutes duration, during which the helicopter performance and all indications were normal.
An initial inspection of the helicopter following the accident found the following:
No oil on the exterior of the engine or helicopter to indicate any oil line failure.
Fresh oil droplets on the right skid and a smear on the right strut. Immediately adjacent to the helicopter there was a small oil spill on the ground, probably from impact damage.
The fuel tanks still contained a substantial amount of fuel, which was leaking out down the mast.
Fuel from the drum was checked with no contamination found. The helicopter was fuelled with premium unleaded petrol.
Icing was found to have been unlikely.
Drive belts were still on and intact.
Clutch engagement position appeared normal.
Main rotor blades were buckled and damaged, partly from falling onto a fence, but were still attached to the hub.
Main rotor blades were evidently not turning fast when they hit the ground.
The engine was running on impact.
The governor switch was in the OFF position. The engineer turned on the master switch, and the governor light (GOV OFF) illuminated.
The engineer removed the main rotor blades and rolled the helicopter upright. The bottom spark plugs were removed and cleaned of oil, and then replaced. The engineer then started the engine and a positive oil pressure indicated. The engine was ground run for about 30 seconds and the magnetos, temperatures and pressure indicated normally.
Safety message
The Robinson Helicopter Company Safety Notice SN-24 states that rotor stall due to low RPM causes a very high percentage of helicopter accidents. These mostly occur close to the ground during take-off and landing. Safety Notice SN-10 reminds pilots to have their ‘reflexes conditioned so they will instantly add throttle and lower collective to maintain RPM in an emergency’.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the Australian Transport Safety Bureau (ATSB) to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation.
On 6 October 2015, the ATSB commenced an investigation into a collision with terrain involving a Cessna 172, registered VH-IMY, 27 km NW of Landor Racecourse, Western Australia, which occurred on 3 October 2015.
The ATSB was unable to establish sufficient information to draw any specific conclusions regarding the circumstances of the accident, but is satisfied that there are unlikely to be any broad systemic safety issues associated with the accident that could affect future transport safety. On that basis, the ATSB determined that there was limited safety benefit in continuing to direct resources at this investigation when compared with other priorities and elected to discontinue this investigation.
On 17 September 2015, at about 1330 Eastern Standard Time (EST), the pilot of a Cirrus SR22 aircraft, registered VH-OPX (OPX), conducted a short flight from Moree Airport, New South Wales, to a private airstrip about 6 NM to the north. The pilot was the sole occupant of the aircraft.
The aircraft approached the airstrip from the south, and the pilot elected to overfly the runway at the eastern end, then turn left and join the circuit on a left downwind for runway 09. The pilot had observed the wind at Moree Airport to be from a southerly direction at about 15 kt, and therefore anticipated having a crosswind for the landing at the airstrip.
The pilot reported that the circuit and approach were normal. On final approach, the pilot extended full flap, and commenced the flare at an airspeed of about 80-90 kt. To align the aircraft with the runway, the pilot reported applying almost full left rudder and right aileron due to the crosswind.
The right main landing gear touched down first, and the aircraft bounced back into the air. The pilot immediately applied full power to initiate a go-around. However, the left wing dropped and the aircraft yawed to the left. The aircraft’s left wing and propeller then collided with a dam wall (Figure 1). The aircraft stopped abruptly and spun around. The engine separated from the aircraft and came to rest about 20 m away, the tail broke off and the nose landing gear collapsed. The pilot suffered minor injuries, and the aircraft sustained substantial damage (Figure 2).
Figure 1: Accident site
Source: Google earth – annotated by the ATSB
Figure 2: Damage to VH-OPX
Source: NSW Police Force
Pilot experience
The pilot held a private pilot licence and had about 1,400 hours of aviation experience, with 80 hours experience in the Cirrus aircraft. The pilot had not flown into that airstrip before the accident flight.
Airstrip information
Prior to conducting the flight to the private airstrip, the pilot contacted the owner and obtained information about the runway condition.
The runway was about 850 m long – unsealed for about 150 m at the western end, then sealed with bitumen for about 700 m. The runway was situated east-west, and the pilot elected to land towards the east. The aircraft initially touched down on the dirt, just prior to the start of the sealed part of the runway, which was slightly beyond where the pilot anticipated it to land.
As the aircraft overflew the runway, the pilot looked for, but did not see, a windsock by which to verify the conditions at the airstrip. The owner of the airstrip reported that there were three windsocks located at various positions near the runway.
Wind
The Bureau of Meteorology provided the ATSB with the wind recorded at Moree Airport. Table 1 depicts the calculated downwind and crosswind components based on the runway direction of 090° magnetic (101° true) of the airstrip 6 NM north of Moree. As seen in the table, at 1334, a significant wind gust of 22 kt from 242°, would have equated to a downwind component of 17 kt and a crosswind of 15 kt. If the aircraft had encountered similar conditions during the landing, this may have affected the pilot’s ability to control the aircraft.
Table 1: Wind direction, speed, gusts and calculated downwind and crosswind components
Safety message
This incident highlights the importance of the identification and management of risks associated with operating into unfamiliar airfields. Pilots should carefully assess the environmental conditions, runway surface and surrounds before attempting to land at an airfield.
The Civil Aviation Safety Authority Out-N-Back video Aircraft landing areas and precautionary search and landing, stated: ‘A precautionary inspection of an unfamiliar airstrip before landing is a logical and effective way to satisfy yourself that you have chosen a suitable landing area for your aircraft, and for your skill level’. This airborne inspection includes assessing the wind velocity and direction, and whether any terrain surrounding the field may affect a go-around.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 17 September 2015, the pilot of an Air Tractor 502B aircraft, registered VH-FNX, was conducting aerial application (spraying) operations on a property about 23 km to the west of Hay Aerodrome, New South Wales. The spray application area consisted of a block of nine adjoining paddocks, separated by combination of irrigation channels and access roads that allowed for movement of plant and equipment. There was a single paddock included in the spray application area that joined the larger block at the eastern end, separated from the other paddocks by an irrigation channel. The pilot planned to spray the group of paddocks as a single block (Figure 1).
Figure 1: Spray application area - a block of nine paddocks with another adjoining paddock at the eastern end
Source: Google earth (supplied by the agricultural company and annotated by the ATSB)
As per normal procedure, while en route to the spray application area, the pilot had made a broadcast on UHF Channel 25 advising that spraying operations were about to commence, and also, the area where that would occur. UHF Channel 25 was monitored by employees on the property, and used for general communications.
At the time the pilot made the broadcast, there was a tractor operating in the southern part of the spray application area, and the tractor driver responded to the pilot’s broadcast. The pilot determined that although the tractor was inside the spray application area, there was no likelihood of an immediate conflict with the spraying operations. Due the southerly wind, the pilot intended to commence spraying runs along the northern edge of the block and gradually work toward the south. The pilot advised the tractor driver that they would be able to safely continue in that southern area, without creating any conflict for spraying operations, for about an hour. Without hearing any other responses to the broadcast, the pilot switched to a different UHF frequency (Channel 20), in accordance with their normal practice.
The pilot commenced spraying operations at about 1100 Eastern Standard Time (EST). The pilot was flying a left hand racetrack pattern, in an east-west direction; moving the pattern further south with each spray run. After a short time, the pilot departed the spray application area to reload with more chemical mixture at a nearby property.
The pilot then returned to the spray allocation area, and resumed spraying operations at about 1130. The pilot did not make another UHF radio broadcast upon the resumption of spraying operations.
At about 1145, as part of the continual southerly movement of the race-track spray pattern, the pilot was conducting a spray run in an easterly direction, along a roadway that divided some of the paddocks inside the spray application area. The pilot intended to continue the run, across the irrigation channel, and along the southern boundary of the eastern most paddock in the spray area (Figure 2).
During this run, the pilot reported seeing a white Toyota Hilux Double Cab utility vehicle turn onto an irrigation channel crossing ahead of the aircraft (Figure 2). However, the Hilux appeared to the pilot to be slowing to a stop, short of the intersection/irrigation channel crossing. The pilot assumed that the driver of the Hilux had seen the aircraft, and was stopping to allow the aircraft to continue its run over the channel crossing.
Figure 2: Layout of accident site, showing path of the aircraft, path of the tractor and Hilux along the irrigation channel bank, the south-eastern border of the spray application area, and the point where the collision occurred
Source: Google earth (supplied by the agricultural company and annotated by the ATSB)
Confident that the vehicle was stopping, the pilot continued the spray run and, as per normal routine, checked the spray pressure gauge, and momentarily looked to each side of the aircraft to confirm that no spray nozzles were blocked. As the pilot then turned their attention forward again, and commenced a short climb to clear the raised channel bank,[1] they saw that the Hilux had not stopped, but had continued along the road, turned right, and was climbing up over the raised channel bank. (Note: the agricultural company report advised that the tractor was ahead of the Hilux and already moving down the other side of the channel bank at this stage – refer section titled ‘Movement of Hilux’).
The pilot immediately stopped the spray and continued to climb, but was unable to clear the Hilux. The left wheel of the aircraft struck the tray headboard of the Hilux. As the vehicle and aircraft were both heading east, the aircraft struck the Hilux from behind.
Following the collision, the pilot climbed the aircraft to a higher altitude. The pilot checked that the aircraft was handling normally, including a brake pressure check, to confirm that the landing gear was still attached. The pilot saw that the driver had exited the vehicle, so made a broadcast on UHF Channel 25, advising farm personnel of the accident and requesting assistance for the driver. The driver of the vehicle responded to that broadcast. The pilot then flew back to the loading area and conducted a fly-by to enable the support crew to inspect the landing gear, prior to an uneventful landing.
The pilot was unhurt, but the driver of the vehicle sustained a shoulder injury.
Subsequent inspection of the aircraft revealed that the parts of the left landing gear were damaged, particularly in the area where the leg of the landing gear attaches to the aircraft structure. The vehicle was substantially damaged in the collision, particularly the tray headboard and roof structure on the passenger side of the cabin area (Figures 3 and 4).
Figure 3: Rear view showing damage to the Hilux headboard
Source: Agricultural company
Figure 4: Roof structure damage on passenger side
Source: Agricultural company
Movement of the Hilux
The Hilux driver had been attending to other tasks on another property (unrelated to the spraying operations) during the morning of the accident, but was aware of the spraying operations. Although the driver commented that notification regarding the spraying operations from the agricultural company was not provided until relatively late, the driver had been emailed about the spraying the day before, and the topic was again discussed on the phone on the morning of the accident. The driver was planning to assist with the logistics associated with moving the tractor from its location inside the spray application area to another part of the property. The tractor driver was relatively new to the property, so the Hilux driver intended to coordinate the move, and provide guidance to the tractor driver.
While en route to the property to coordinate movement of the tractor, the driver heard the pilot’s broadcast on UHF Channel 25 regarding commencement of spraying operations. The driver recalled hearing that the pilot intended to start spraying at the northern boundary of the spray application area. The Hilux driver attempted to respond to the broadcast, but was unable to establish contact, perhaps because the vehicle was still some distance away at the time. In any case, the Hilux driver was aware that the tractor driver had responded to the pilot’s broadcast.
As they prepared to move the tractor, the Hilux driver noted that the aircraft appeared to be still operating in the northern part of the spray application area (having returned from a chemical mixture reload). With that in mind, and because the planned route of the tractor and Hilux was along the south-eastern perimeter of the spray application area, the driver believed this would keep them clear of the spraying operation. Furthermore, the Hilux driver was of the impression that the pilot was operating to the north to accommodate movement of the tractor. The Hilux driver therefore elected not to contact the pilot as they were moving the tractor, because they believed that the move could be conducted safely without disrupting the pilot.
The Hilux driver was proceeding slowly, so as to monitor the progress of the tractor ahead. The driver’s attention was on the tractor as it turned right towards the east, to negotiate the raised channel crossing.
Following the tractor, the Hilux driver turned right to cross the channel. Near the top of the crossing, the aircraft collided with the vehicle from behind. The driver was unaware of the approaching aircraft until hearing the sound of the engine immediately before the collision.
Pilot and driver comments
The pilot commented that with the benefit of hindsight, it was unwise to assume that the Hilux driver had seen the aircraft and was travelling slowly for that reason. The pilot and driver both commented that the accident highlighted the importance of effective communication.
Agricultural company investigation
The agricultural company conducted a Workplace Health and Safety investigation into the accident. In general terms, contributing factors identified by the investigation related substantially to ‘assumptions’ and ‘ineffective communication’.
The agricultural company investigation also identified that the Pesticide Application Management Plan (PAMP)[2] had expired at the end of June 2015. Notwithstanding expiry of the document, the investigation report identified some areas where, in the opinion of the investigator, PAMP instructions were not effectively applied. The report also noted that the PAMP did not require that aerial application operators use the same UHF channel as that used by farm employees, apart from a broadcast announcing spraying intentions. The report identified that this channel mismatch potentially hindered timely and effective communication.
Notification to the driver: The agricultural company reported that the Hilux driver had been emailed about the spray operations the day before the accident; and that the spray job was again discussed on the telephone the following morning.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following safety action in response to this occurrence.
Agricultural company
As a result of this occurrence, the agricultural company (in consultation with contracted aerial application operators) has indicated their intent to revise and re-issue the PAMP, to better identify procedures, roles and responsibilities, in the interests of safety improvement. The agricultural company investigation report made a number of recommendations with respect to the PAMP. These recommendations are broadly summarised as follows:
Issue the 2015/2016 PAMP as soon as possible (noting that the 2014/2015 PAMP had expired).
Provide more specific instructions regarding roles and responsibilities, including the responsibilities of managers, farm employees and pilots engaged in aerial application operations (including communication requirements).
Promulgate specific requirements with respect to buffer zones separating equipment and aircraft, and define responsibilities related to the application of those buffer zones.
Improve relevant signage at property entry points notifying (and reminding) staff and visitors of spraying operations, movement restrictions and communication requirements.
Require farm employees and pilots engaged in aerial application operations to operate on the same UHF channel.
Include relevant procedures in property site instructions to provide for safe movement of farm employees, visitors and equipment when spraying operations are planned.
Safety message
This accident highlight the importance of effective communication by all parties involved with aircraft operations. Effective communication substantially reduces the risk of a misunderstanding, reduces the likelihood that false assumptions will prevail, and allows for timely action to reduce the likelihood of any confliction in the first instance.
ATSB Research and Analysis Report AR-2015-031 Aerial application safety: 2014 to 2015 year in review, provides statistical data regarding aerial application accident rates, and summarises a number of accidents that occurred during aerial application operations. The report includes a section that highlights the importance of communication and coordination of operations. Although the report deals primarily with inter-pilot communication, the same message relates to all parties involved with aerial application operations. The report includes a lesson learnt:
Communication is important in parts of aerial agriculture and firefighting operations, including planning to convey information to relevant parties, and during the operation to reiterate the plan and notify parties of any new information arising during the task. Do not rely on other pilots communicating, and always scan for other aircraft even when you are at remote locations.
Organisations with responsibility related to the safe conduct of aerial application operations should ensure that all staff are familiar with planned operations (including being advised in a timely manner), and that all associated responsibilities are clearly documented and understood. Relevant documents should be regularly reviewed and updated, and the associated procedures and instructions consistently applied. Risk assessments should address the importance of effective communication.
The accident also highlights the manner in which assumptions can elevate risk. Pilots are encouraged to exercise caution, and not assume that the actions of others will necessarily be based upon a common understanding. If any doubt exists with respect to the intentions of others, pilots should adopt a safe course of action in the first instance. This is particularly important where the margin for error is small, such as in aerial agriculture operations.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.