Collision with terrain involving Liberty Aerospace XL-2, VH-XLK, 9 km north-east of Braidwood, New South Wales, on 6 August 2019
Preliminary report
Preliminary report published: 8 October 2019
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
What happened
On 6 August 2019, at 1103 Eastern Standard Time,[1] a Liberty XL-2, registered VH-XLK (XLK), departed Moruya Airport, for a rural property near Braidwood, New South Wales (Figure 1). The pilot was the sole occupant and had been flying in company with another pilot and his aircraft on a social, multi-day touring flight of the New South Wales hinterland, alpine and southern coast regions.
The accompanying pilot landed his aircraft on a private landing area at the Braidwood property about 15 minutes prior to the arrival of XLK. That pilot advised the pilot of XLK that the landing area was undulating and not suitable for his aircraft type. At about 1126, witnesses on the ground (which included the accompanying pilot) observed XLK circling the landing area. On the second orbit, the aircraft was observed to slow and begin to lose height. At about 500 ft above ground level, and after crossing the marked end of the landing area, the left wing dropped and the aircraft entered a steep rotating descent. The pilot was unable to recover control of the aircraft before it impacted terrain.
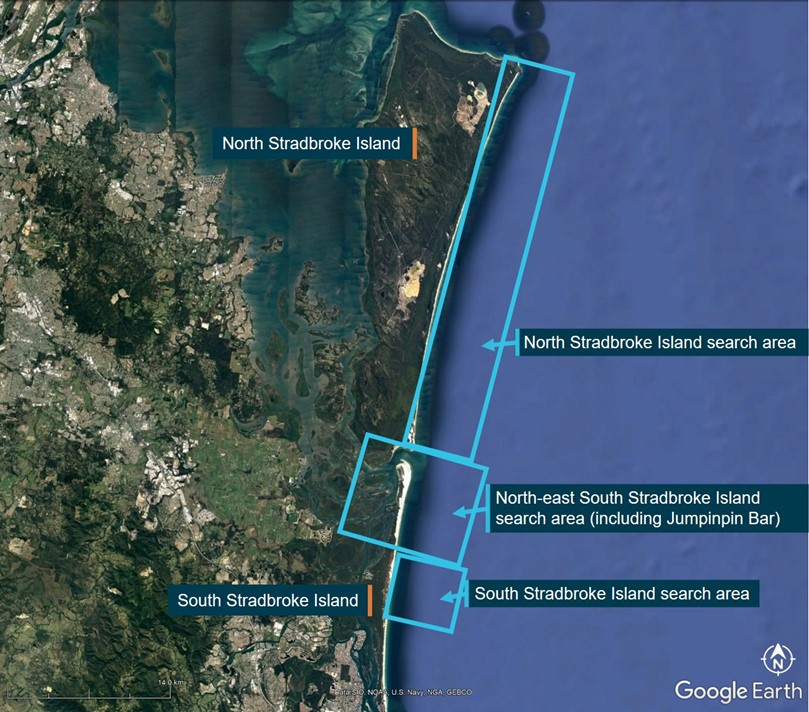
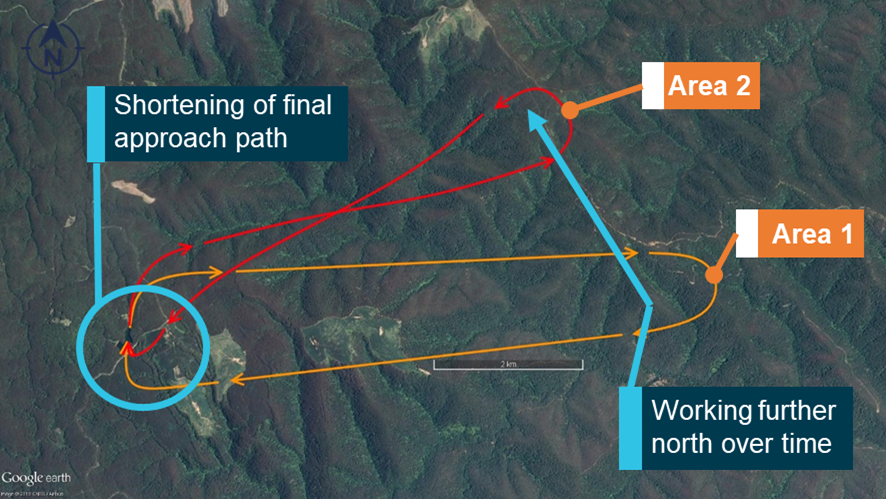
Figure 1: Aircraft’s flight path and accident site location
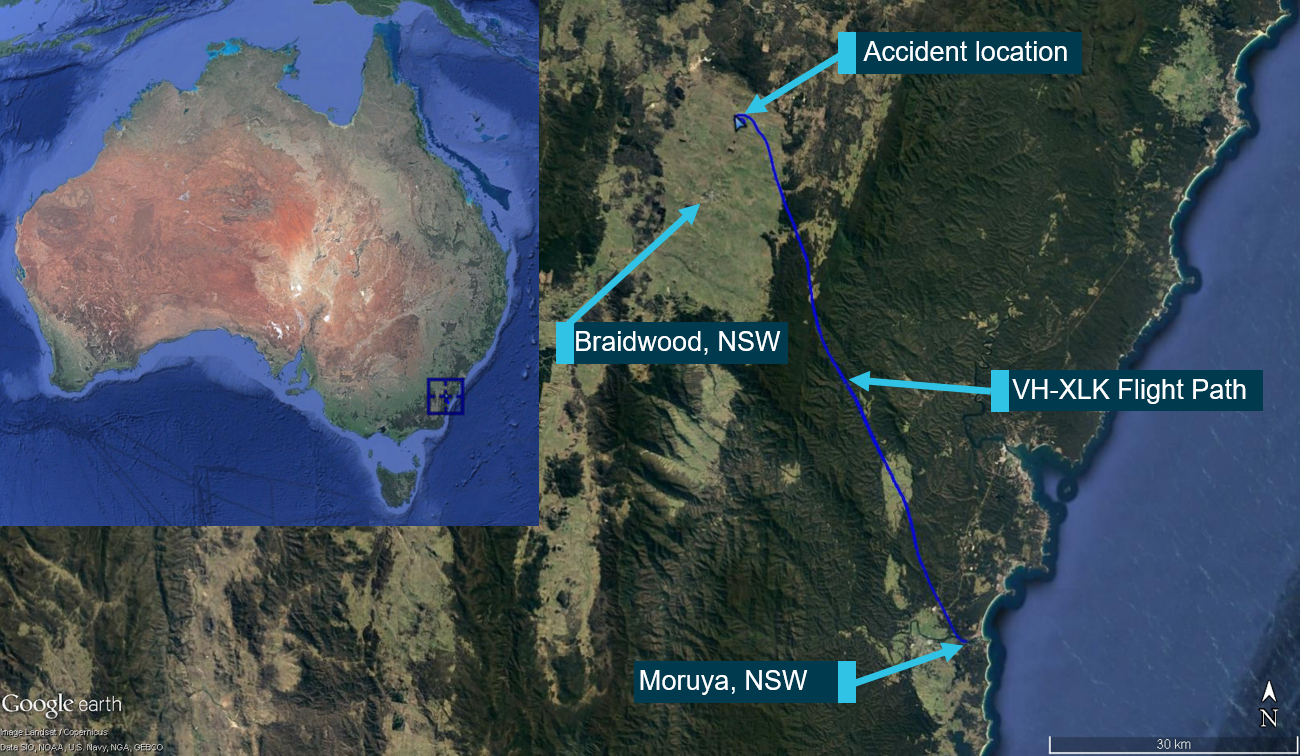
Source: Google Earth. Modified by the ATSB
The witnesses at the landing area were first to arrive at the scene, however the pilot had sustained fatal injuries. The aircraft was destroyed.
Site and wreckage examination
The accident site was located in relatively flat and open farmland, approximately 9 km north-east of Braidwood (Figure 2). The ATSB conducted an examination of the site and wreckage and identified that the:
- ground impact marks indicated that the aircraft had impacted terrain nose‑down, upright, with counter‑clockwise rotation
- left wing separated from the airframe on impact with the terrain
- flaps were in the retracted position.
No pre-impact defects were identified with the engine, flight controls or aircraft structure. The internal cabin fuel tank had ruptured and a quantity of fuel had leaked into the soil. There was no fire.
A damaged electronic flight bag was recovered from the accident site and an engine control unit was removed from the aircraft and taken to the ATSB’s technical facility in Canberra for examination.
Figure 2: Accident site

Source: ATSB
Further investigation
The investigation is continuing and will include:
- analysis of the downloaded data from the engine control unit and other electronic devices
- examination of the aircraft flight instruments and a stabiliser trim component
- examination of the pilot’s qualifications, experience and medical history
- assessment of the aircraft’s flight performance characteristics
- examination of aircraft maintenance and operational records.
_______________
The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this update. As such, no analysis or findings are included.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2019
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |

__________
Final report
Safety summary
What happened
On 6 August 2019, at 1103 Eastern Standard Time, a Liberty XL-2, registered VH-XLK, departed Moruya Airport, New South Wales, for a rural property near Braidwood. The pilot was the sole occupant and had been flying in company with another pilot.
The accompanying pilot landed their aircraft on a private landing area at the Braidwood property about 15 minutes prior to the arrival of VH-XLK. That pilot advised the pilot of VH-XLK by phone that the landing area was undulating and not suitable for the Liberty XL-2 aircraft type. At about 1126, witnesses on the ground observed VH-XLK circling the landing area with a slowing airspeed.
On the second orbit, at about 400 ft above ground level, and after crossing the marked end of the landing area, witnesses observed the left wing drop and the aircraft entered a steep rotating descent. The pilot was unable to recover control of the aircraft before it impacted terrain. The pilot sustained fatal injuries and the aircraft was destroyed.
What the ATSB found
Recorded data showed that the pilot was circling the landing area at a height of 200–400 ft. The ATSB also found that the aircraft departed controlled flight after slowing and turning downwind with no flap selected. The left wing stalled, and this resulted in the aircraft entering into an upright spin, at an altitude that limited an effective recovery.
An airworthiness directive requiring an inspection of the engine exhaust muffler had not been completed, however this did not contribute to the accident.
Safety message
The accident highlights the need for pilots to minimise the risk of aerodynamic stall, particularly when in proximity to the ground, such as during take-off and landing. Turning manoeuvres at or close to the aircraft’s critical angle of attack, if mishandled, can lead to a stall that may result in the aircraft entering a spin. Pilots can limit their risk of losing control in flight by maintaining situational awareness of the aircraft state while conducting turns, maintaining adequate airspeed through appropriate power application during increased bank angles, and by selecting altitudes to operate at that provide sufficient height to recognise and recover from a stall.
In addition, aircraft owners should ensure that required maintenance and airworthiness directives are completed and recorded as they become due, to avoid invalidating the aircraft maintenance release and potentially increasing risk to flight safety.
Appendices
Appendix A – Related occurrences
The following ATSB accident investigations are drawn from investigation reports published between 2010–2019. The common theme from these fatal accidents is the loss of control of the aircraft following an aerodynamic stall, with a resultant steep pitch attitude and insufficient altitude to enable recovery before impacting terrain.
ATSB investigation AO-2010-079[14]
On 18 October 2010, a Cessna 172S aircraft, registered VH-VSK, was operating at low level near Durham Downs Homestead, Queensland. A pilot and one passenger were on board. The pilot was assisting a ground party locate two horses. The aircraft was seen manoeuvring at low level before radio and visual contact was lost. A search later found that the aircraft had impacted terrain near a dry creek bed. Both occupants received fatal injuries and the aircraft was seriously damaged.
The aircraft's impact attitude was consistent with a loss of control following aerodynamic stall. The operating status of the aircraft’s stall warning system could not be determined.
ATSB investigation AO-2012-059[15]
On the morning of 29 April 2012, the owner-pilot of a Cessna 150 aircraft, registered VH- UWR was aerial stock mustering on a cattle station about 55 km north-east of Bourke, New South Wales. The aircraft was observed circling over an area (where cattle were not moving) then in a steep descent followed by the sound of an impact. The aircraft was seriously damaged, and the pilot sustained fatal injuries.
The ATSB found that, while manoeuvring at low level, the pilot inadvertently allowed the aircraft to aerodynamically stall, resulting in a high rate of descent and collision with terrain. There was insufficient information about pilot control inputs to establish the factors that precipitated the stall.
ATSB investigation AO-2012-149[16]
On 9 November 2012, a student and instructor departed Gold Coast Airport, Queensland for a training flight in a SOCATA TB 20, registered VH-HBB, to Lismore Airport, New South Wales. On their fifth circuit, and while making a left turn from downwind to base, the left wing dropped steeply. A recovery was commenced, but the aircraft collided with terrain. Both occupants received fatal injuries.
The ATSB found that while making the left turn, an aerodynamic stall occurred, resulting in a significant left-wing low and nose-down attitude in close proximity to the terrain. The instructor was unable to prevent the stall from occurring due to either insufficient warning or available time to react. Although it appeared that a stall recovery was commenced, the aircraft stalled at an altitude from which they were unable to fully recover to controlled flight before the aircraft collided with the terrain.
ATSB investigation AO-2013-051[17]
On 17 March 2013, the owner-pilot of an amateur-built scale-replica Spitfire aircraft (VH-VSF) was participating in an air display at Parafield Airport, South Australia. The pilot completed the display with a slow speed pass at 400 ft with the landing gear and some wing flap extended. Towards the end of this pass the pilot radioed the tower to coordinate a landing and accepted runway 21 Left with an 11 kt crosswind.
By now the pilot had turned right and the Spitfire was near the extended runway centreline and 1 km from the runway threshold at a slow speed. A left turn was then observed and, soon after, a wing dropped, and the aircraft entered a steep descent. The aircraft crashed in a factory car park, fatally injuring the pilot and substantially damaging the aircraft.
The ATSB found that while coordinating a landing clearance with air traffic control and flying a low-level circuit with a close downwind and base in turbulent conditions, the pilot inadvertently allowed the airspeed to decay. In the subsequent turn (downwind) to adjust the circuit the aircraft aerodynamically stalled, descended steeply, and impacted the ground.
ATSB investigation AO-2014-192[18]
On 29 December 2014, a Cessna 172S aircraft, registered VH-PFT, departed Cambridge Airport, Tasmania to photograph yachts participating in the 2014 Sydney Hobart race. On board the aircraft were the pilot and a photographer.
At about 1815 the aircraft commenced low-level photographic runs on yachts to the east of Cape Raoul. Shortly after completing a run on one yacht at a height of about 50 ft, the aircraft entered a steep climbing turn. The aircraft had almost completed a 180° turn when the upper (right) wing dropped sharply while the aircraft’s nose pitched down to almost vertical. The aircraft impacted the water’s surface in an almost vertical nose down attitude with wings about level. Both aircraft occupants were fatally injured, and the aircraft was seriously damaged.
As a result of the steep climbing turn, the aircraft’s upper wing aerodynamically stalled, resulting in a rapid rotation out of the turn. The steep pitch attitude indicated that, because of the stalled upper wing, the aircraft entered a spin. There was insufficient height for the pilot to recover the aircraft.
ATSB investigation AO-2016-074[19]
On 12 July 2016, the pilot of a Cessna 150 aircraft, registered VH-RXU, was conducting cattle spotting operations at New Crown Station, about 270 km south-east of Alice Springs, Northern Territory. The aircraft was observed conducting turning manoeuvres over the cattle at a reported altitude of about 500 ft.
While conducting a right turn at low altitude, the pilot lost control of the aircraft and was unable to recover before impacting terrain. The pilot was the sole occupant on-board the aircraft and was fatally injured.
While the actual events preceding the loss of control could not be concluded, the aircraft was likely operated at a slow airspeed with reduced stall margins. In the absence of other physical evidence, it was possible that control inputs made by the pilot induced a stall and incipient spin at an altitude that was not recoverable.
__________
- ATSB Investigation report AO-2010-079, Collision with terrain – Cessna 172S, 2 km NNE Durham Downs, Queensland, 18 October 2010.
- ATSB Investigation report AO-2012-059, Collision with terrain involving Cessna 150, VH-UWR, 55 km NE of Bourke, NSW, 29 April 2012.
- ATSB Investigation report AO-2012-149, Loss of control involving SOCATA TB 20, VH-HBB, 3 km south of Lismore Airport, NSW on 9 November 2012.
- ATSB Investigation report AO-2013-051, Loss of control involving scale replica Spitfire, VH-VSF, near Parafield Airport, South Australia on 17 March 2013.
- ATSB Investigation report 2014-192, Collision with terrain Cessna 172 VH-PET, Maingon Bay (9 km south of Port Arthur), Tasmania, 29 December 2014.
- ATSB Investigation report AO-2016-074 Loss of control and collision with terrain, Cessna 150, VH-RXU 270 km SE Alice Springs, Northern Territory, on 12 July 2016.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- Civil Aviation Safety Authority
- New South Wales Police Service
- aircraft manufacturer
- maintenance organisation for VH-XLK
- Bureau of Meteorology
- witnesses to the accident (including pilot of the accompanying recreational aircraft)
- recorded data from an electronic flight bag on the aircraft.
References
Australian Transport Safety Bureau 2005. Dangerous Distraction: An examination of accidents and incidents involving pilot distraction in Australia between 1997 and 2004. Aviation Research Investigation B2004/0324.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the:
- Civil Aviation Safety Authority
- Bureau of Meteorology
- US National Transportation Safety Board (NTSB)
- maintenance provider
- the pilot of the accompanying recreational aircraft.
Submissions from those parties were reviewed and, where considered appropriate, the draft report was amended accordingly.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk.
CASA guidance on spin avoidance
Due to an increase in spin type accidents across a broad range of light aircraft types in the training environment, CASA released guidance material in the form of advisory circular (AC) 61-16 v1.0 (Spin avoidance and stall recovery training) in April 2020.
The AC provided detailed guidance for pilots, flight instructors, flight examiners and flight training organisations. Several of the key points for the safe conduct of advanced stalling and spinning exercises from the AC stated that all pilots should be aware of:
- Training in spin avoidance must include the recognition of symptoms associated with slow flight and approach to the stall through to recovery from stall with a wing drop
- Recognise and manage changes in aircraft energy state
- Spin avoidance training where a wing may drop at the stall should be undertaken through scenario-based in-flight manoeuvres:
- Approach configuration descending turns (base to final turn) …
- Turns in slow flight.
The occurrence
Events prior to the accident flight
On 4 August 2019, the pilot of a Liberty XL-2, registered VH-XLK, departed Camden Airport, New South Wales, on a private flight to Adaminaby Airstrip to attend a social function. The pilot met a friend, who was flying a recreational aircraft, at the airstrip. That night, both pilots stayed at Adaminaby before departing the next day to fly around the local area before heading to Merimbula.
On arrival at Merimbula Airport on 5 August, the pilot refuelled VH-XLK with about 73 L of aviation gasoline and then continued in company with the other aircraft to Moruya Airport, where both pilots stayed the night. They met some aviation friends for dinner before retiring back to their accommodation early in the evening.
On 6 August 2019, both pilots planned to fly to a property located 9 km to the north-east of Braidwood to meet friends that owned the property (Figure 1). This was the first time an aircraft would use the freshly prepared landing area on the property. The pilot of VH-XLK then intended to continue on to Camden Airport later that day.
Figure 1: Aircraft’s flight path and accident site location
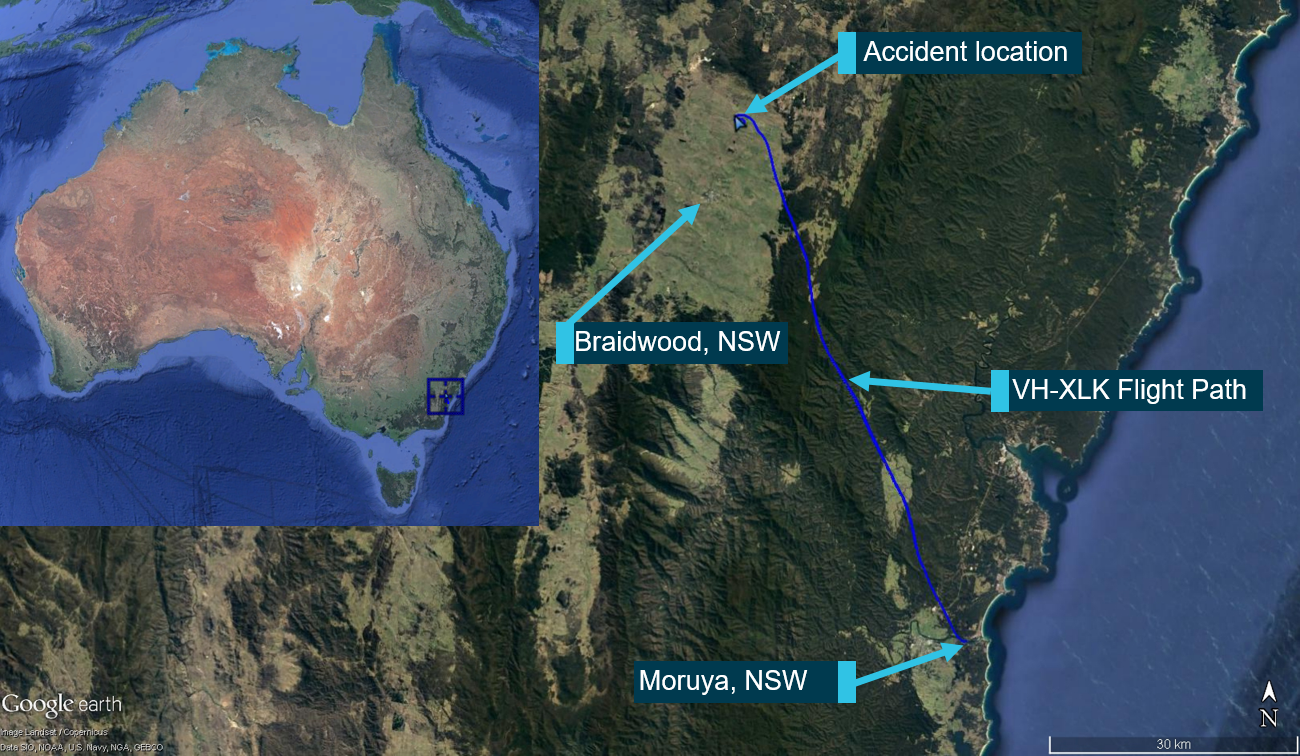
Source: Google Earth, modified by the ATSB
Accident flight
Due to the performance differences between the two aircraft, the pilot of the slower recreational aircraft departed Moruya first at about 1030 Eastern Standard Time[1] and arrived in the vicinity of the Braidwood landing area at about 1110. After surveying the landing area, the recreational pilot made a landing to the east. The slower aircraft was designed for landing on unprepared areas, having a different landing gear configuration and high propeller clearance from the ground.
The landing area was oriented in an east-west direction, and the recreational pilot reported that they landed with a left quartering tailwind, uphill to the east. After landing there, the recreational pilot believed that the runway was not suitable for the Liberty XL-2 (VH-XLK).
VH-XLK departed Moruya at about 1103 and had sufficient fuel to either land at Braidwood, or to continue to Camden Airport. The recreational pilot recalled that, prior to VH-XLK’s arrival overhead the Braidwood landing area, they called the pilot of VH-XLK by mobile phone to advise that the runway was not suitable for the Liberty XL-2.
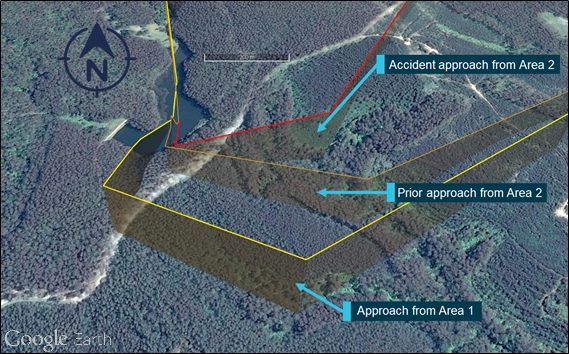
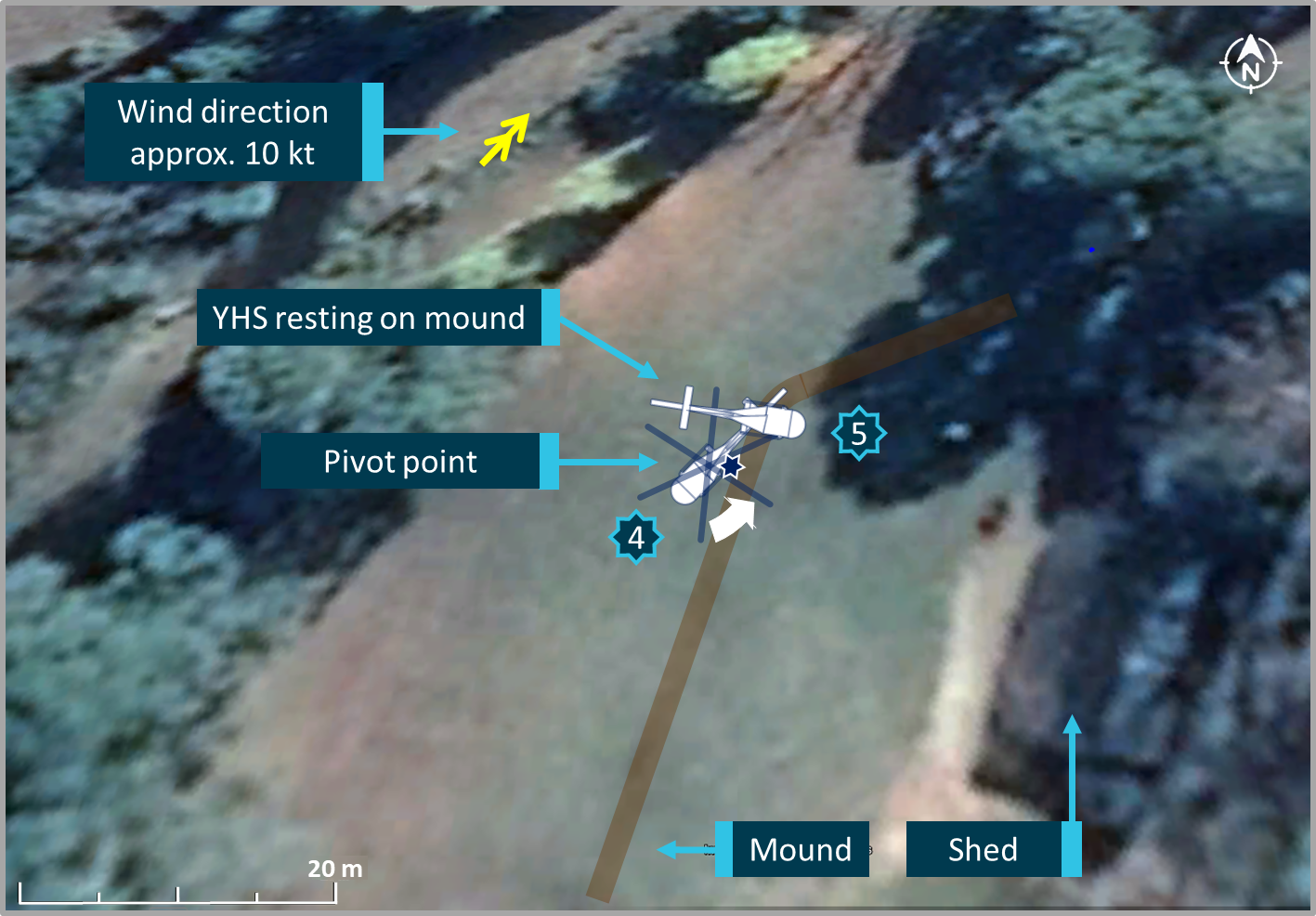
Recorded data showed that VH-XLK approached the landing area (Figure 2) from the south-east and overflew the property homestead at about 1123, before turning left to circle around the landing area. A witness reported that the aircraft appeared to be slowing and descending and that the engine noise was a lot less noticeable overhead the landing area than when it first approached the property. The witness also stated that the aircraft appeared to be ‘hanging off the prop’, describing VH-XLK having a slowing speed and nose-high attitude. The recorded data indicated an inconsistent airspeed and height during the first orbit overhead the Braidwood landing area (Figure 5).
Figure 2 : VH-XLK flight path approaching the Braidwood landing area
Flight data overlay of Braidwood aircraft landing area, with final 15 seconds recreated from witness accounts and highlighted for reference.
Source: Google Earth, modified by the ATSB
As VH-XLK approached the western end of the landing area, it began a left turn to track close to the western threshold of the runway on a slow descent, at about 400 ft above ground level. At about 1127, after passing over the western threshold and travelling in a southerly direction, a further left turn was initiated.
Witnesses described that, during this left turn, the left wing of VH-XLK dropped and the aircraft pitched nose-down while rotating to the left. The aircraft then entered a steep, rotating, counterclockwise descent around the longitudinal axis for one rotation before impacting the flat, open farmland adjacent to the landing area.
Witnesses to the accident arrived promptly to assist, however the pilot was fatally injured.
__________
Context
Pilot information
General information
The pilot obtained a recreational pilot certificate in March 2008 and achieved a cross country endorsement in May 2008. In July 2010, the pilot purchased VH-XLK and in December 2010 obtained a Private Pilot Licence (Aeroplane).
The pilot completed their last aeroplane flight review on 8 December 2018. They had about 654 hours total flying experience, with about 548 hours in VH-XLK. This included 22 hours flight time in the 2 weeks prior to the accident, and 4.1 hours during the 2 days prior to 6 August.
Stall and spin recovery training
The pilot had previously been taught theoretical and practical stall recovery techniques, including recovery from an entry into a spin, during their initial flying training. A part of the pilot’s last aeroplane flight review required the pilot to demonstrate competency in the recognition of stall signs and symptoms, and the recovery from incipient stalls and spins.
Medical and recent history information
The pilot’s last medical examination was on 10 August 2018 for a class 2 medical certificate. This medical certificate placed restrictions on the exercise of the pilot’s licence and required that distance vision and reading correction was to be worn whilst exercising the privileges of the licence.
Post-mortem examination identified that there was no evidence of pre-existing natural disease and that the pilot most likely succumbed to impact-related injuries. Toxicological testing identified low levels of a cough suppressant, however no other drugs or medications were detected. Further specific testing for carbon monoxide did not indicate elevated levels.
The recreational pilot reported that the pilot of the accident flight had significant sleep opportunity on the nights of 4 August and 5 August, but did not know how much sleep the pilot actually obtained. On the morning of 6 August both pilots had breakfast before heading to Moruya Airport.
Weather information
The aerodrome forecast (TAF)[2] for Goulburn Airport (62 km north of the Braidwood landing area) for the period from 0900 included clear conditions with a wind of 12 kt from 290°. The TAF for Canberra Airport (58 km west of the landing area) for the period from 1000 indicated conditions of broken cloud at 500 ft above ground level with clear visibility and wind of 4 kt from 040°, improving to clear conditions with a wind of 12 kt from 330° by 1200.
The weather observation (METAR) [3] for Goulburn at 1200 indicated a wind of 13 kt from 270° with clear visibility and no cloud. One-minute weather observations for Braidwood racecourse, about 8 km from the accident site, for the period from 1122 to 1132 indicated an average wind of 2.3 kt with a maximum gust of 5.4 kt (recorded at 1126). The recorded winds during this period varied from 330° to 030°.
Witness reports identified the wind direction as being from the north-west, and the recreational pilot reported that the wind direction and strength produced a quartering tailwind from the left when approaching to land towards the east at the landing area. They estimated the wind at the landing area to be about 5–7 kt, and they also noted that they had experienced no turbulence during their flight.
The ATSB considered that the recreational pilot’s weather observations provided a reasonable and timely local representation of the weather below 1,000 ft above ground level. These observations were broadly consistent with the Bureau of Meteorology (BoM) forecasts and the observations at ground level. All the weather sources confirmed that the conditions and visibility were conducive to flight under visual flight rules.[4]
Aircraft information
General
The Liberty XL-2 aircraft is a single engine, two seat, low wing aircraft mostly used as a private touring aircraft, or as a primary flight trainer. The fuselage is made from composite fibreglass and carbon, with metal wings. The limited propeller ground clearance and relatively small tyres make it less suited to rough field operations and more suited to prepared runway surfaces.
The aircraft is powered by a Continental IOF-240-B engine with a full authority digital engine control (FADEC), fuel injection control system, which produces 125 hp and a cruise speed of about 125 kt. The FADEC system is a solid state, computer controlled electronic ignition and fuel injection system, allowing the electronic control unit (ECU) to adjust the fuel to air ratio, and other engine parameters, to adapt to the operating conditions and obtain peak engine performance, and to promote reduced pilot workload and better fuel economy.
Airworthiness and maintenance
The aircraft involved in the accident, serial number 0106, was manufactured in 2008. In February 2009, the aircraft had 19.6 hours total time and was issued with an Australian certificate of airworthiness in the normal category[5] and was registered as VH-XLK.
The aircraft’s last maintenance release[6] (MR) was issued by a maintenance provider at Bankstown on 30 November 2018, at which time the aircraft had 766.5 hours total time in service.
At the time of the accident (6 August 2019), the last entry on the MR was recorded on 5 August 2019 and showed an aircraft total time in service of 822.6 hours. VH-XLK was operated for an additional three additional flights, totalling 1.1 hours, until the time of the accident.
The MR was issued in the instrument flight rules[7] category, however an entry by the issuing maintenance organisation advised that VH-XLK was restricted to night visual flight rules as the electrical, instrument and radio periodic inspection had not been completed at the time of MR issue.
The MR indicated a requirement for an oil and filter change to be conducted every 50 flight hours; that is by 816.5 hours with tolerance of +/- 5 hours. There was no certification on the MR to indicate that this had occurred before the accident flight.
Airworthiness Directive (AD) FAA AD 2009-08-05R1 was required to be completed every 50 hours of service or every 12 calendar months, whichever came first. The AD required a check for cracking in the exhaust muffler system, and was due on 30 November 2019 or at 816.5 flight hours (whichever came first), as annotated on VH-XLK’s MR. The AD stated, that should cracking be identified, then it must be replaced as it had potential to allow carbon monoxide to enter the aircraft cabin through the cockpit heating system.
On 19 July 2019, while returning from another journey, the AD became due on VH-XLK (50-hour requirement). The aircraft continued to operate for another 6.1 hours and 10 flights, until the time of the accident. There was no certification on the MR to indicate that the AD inspection was conducted.
Stall warning system and stall speed
VH-XLK was equipped with a stall warning system. The stall warning capability was provided through a lift switch (stall sensor) mounted in the left-wing leading edge, and electrically connected to an aural warning device located behind the instrument panel. The stall warning system was designed to produce an audible tone about 5–10 kt above the airplane stalling speed to warn the pilot of an impending stall, and to enable them to take avoiding action.
The stall speeds listed in the XL-2 Flight Manual varied according to aircraft configuration and the bank angle, as shown in Table 1.
Table 1: Liberty XL-2 stall speeds

Source: Liberty XL-2 Flight Manual, Section 5 Performance
Site and wreckage information
Accident site
The accident site was located about 150 m to the south of the western threshold of the landing area in relatively flat and open farmland, about 9 km north-east of Braidwood (Figure 1).
Witnesses reported that the aircraft was travelling in an easterly direction when it impacted the ground. Ground scars indicated that the aircraft impacted terrain in an upright, nose‑down, left wing low attitude, consistent with counter‑clockwise rotation around the longitudinal axis.
Wreckage examination
The wreckage was distributed over a relatively small area, with all of the major aircraft components accounted for at the site (Figure 3).
Examination of the wreckage identified:
- the flight control system was assessed for control continuity with no pre-existing defects identified
- fragments of the wood propeller blades, and propeller slash marks, were located at the point of impact
- the propeller blades showed evidence of rotation damage consistent with engine operation at impact
- the engine, empennage and right wing were located about 20 m from the initial impact point
- the left wing had separated from the fuselage and was located a short distance from the initial impact point
- the flaps were in the retracted position, consistent with the observed position of the electric flap actuator.
Figure 3: Accident site

Source: ATSB
Impact signatures were consistent with witness reports, indicating that the left wing struck the ground first, followed by the propeller, engine and then the fuselage. The wing ground strike resulted in compression damage to the left lower fuselage below the gull door at the wing root location, and subsequent separation of the left wing from the fuselage.
Creases and tears in the carbon fibre panels behind the cabin area were also as a result of the ground impact (Figure 4).
No pre-impact defects were identified with the engine or aircraft structure. The internal cabin fuel tank had ruptured and a quantity of fuel had leaked into the ground. Fuel was observed in the fuel filter bowl, free of contamination. There was no post impact fire.
Figure 4: VH-XLK rear fuselage section showing compression damage to composite structure and creasing at empennage junction

Source: ATSB
Component examinations
Several components were taken from site for further examination by the ATSB, including:
- airframe fuel filter
- static system alternate air valve
- stall warning vane and annunciator unit
- horizontal stabiliser actuator.
Fuel supply to the engine is from the fuel tank located in the pilot and passenger seat back, via a ‘gascolator’ or airframe fuel filter assembly. The filter contained residual fuel with no blockages or inhibiting obstructions to prevent normal operation.
The alternate static air selector valve was found on the accident site to be in the ‘OFF’ or normal position and its function and sealing was checked for serviceability. Physical examination showed that the unit was intact, although had sustained some impact-related damage to the associated tubing. The unit was tested, and no faults were identified with its correct operation.
The stall sensor assembly was externally damaged with the mounting flange showing signs of significant distortion. However, the internal micro-switch operated correctly with a loud, audible response from the annunciator unit, indicating that the annunciator likely would have provided warning to the pilot if the lift switch was appropriately positioned.
It was not possible to confirm whether the lift switch was appropriately positioned, and this is not usually checked or required to be checked during periodic maintenance. However, pilots are required to confirm that the stall warning is working (will make a noise) prior to flight.
The stabilator trim actuator was identified on-site in the fully extended position (pitch-up trim), and free of external defects. However, due to the impact forces, continued electrical power post-accident, and the compressed cockpit area, it was not possible to confirm the pre-impact trim actuator position.
Recorded information
Engine data
An engine data storage card was retrieved from the aircraft’s engine control unit for examination. The memory card was designed to store all engine data between overhauls, and the data was ordinarily extracted with a card reader. The data recovered from the card installed in VH-XLK did not contain any valid date or time data, and it stored insufficient detail to identify the accident flight.
Electronic flight data
A damaged iPad was recovered from the accident site. The pilot utilised the iPad to run an electronic navigation program, but the damage to the device precluded any on-device data download. However, the software provider was able to supply remotely stored data. The recorded data included time, latitude, longitude and altitude, recorded at 5-second intervals.
The ATSB used the recorded data to derive a groundspeed, and then calculated the true airspeed (KTAS) using an estimated wind of 310° at 6 kt as witnessed by the previous landing pilot. Calibrated airspeed (KCAS) was then calculated by correcting true airspeed for pressure changes in altitude. The indicated airspeed (KIAS) was then calculated by applying the flight manual calibration differences at certain speeds for the Liberty XL-2, taking into consideration the position errors associated with installation. KIAS is the speed that would be indicated to the pilot in the aircraft.
The height above ground was calculated by comparing the recorded altitude at each position with the landing area elevation of 2,132 ft.
Figure 5 shows the derived airspeed and height above ground level for the last 3 minutes of the flight. However, constraints on the buffering of the in-flight data meant that the last 15 seconds of flight Figure 5 (data after 1126:51) were considered less reliable.
Figure 5: VH-XLK flight profile
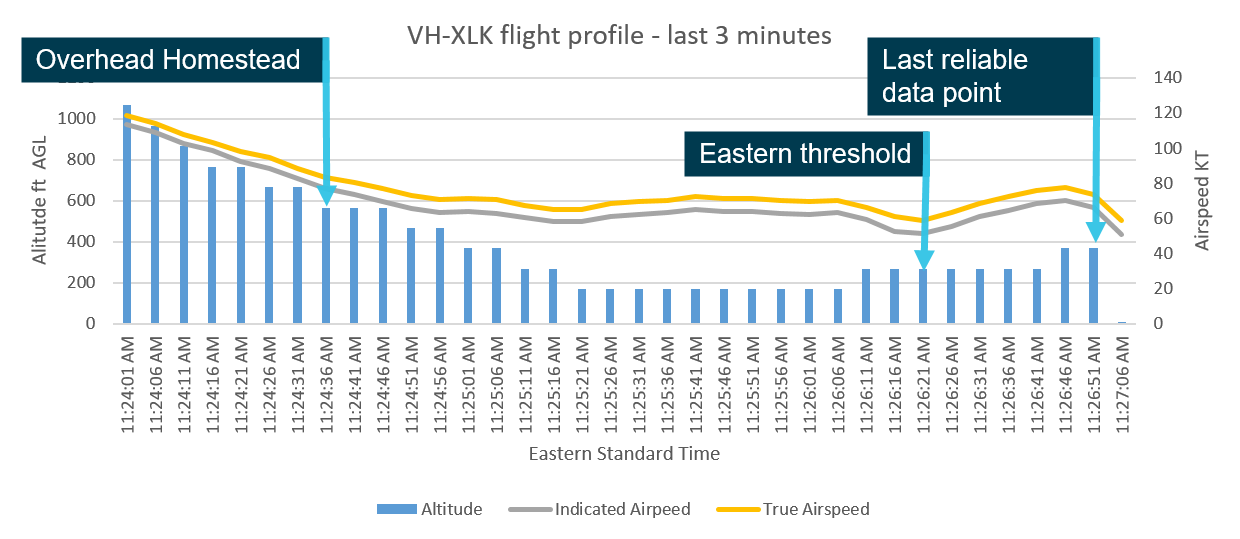
Analysis of 5-second flight data with ground speed corrected for observed wind (6 kt). True airspeed corrected for elevation and indicated airspeed corrected for installation. Altitude was recorded to the nearest 100 ft, and this figure was subtracted from the elevation of the landing area (2,132 ft).
Source: ATSB
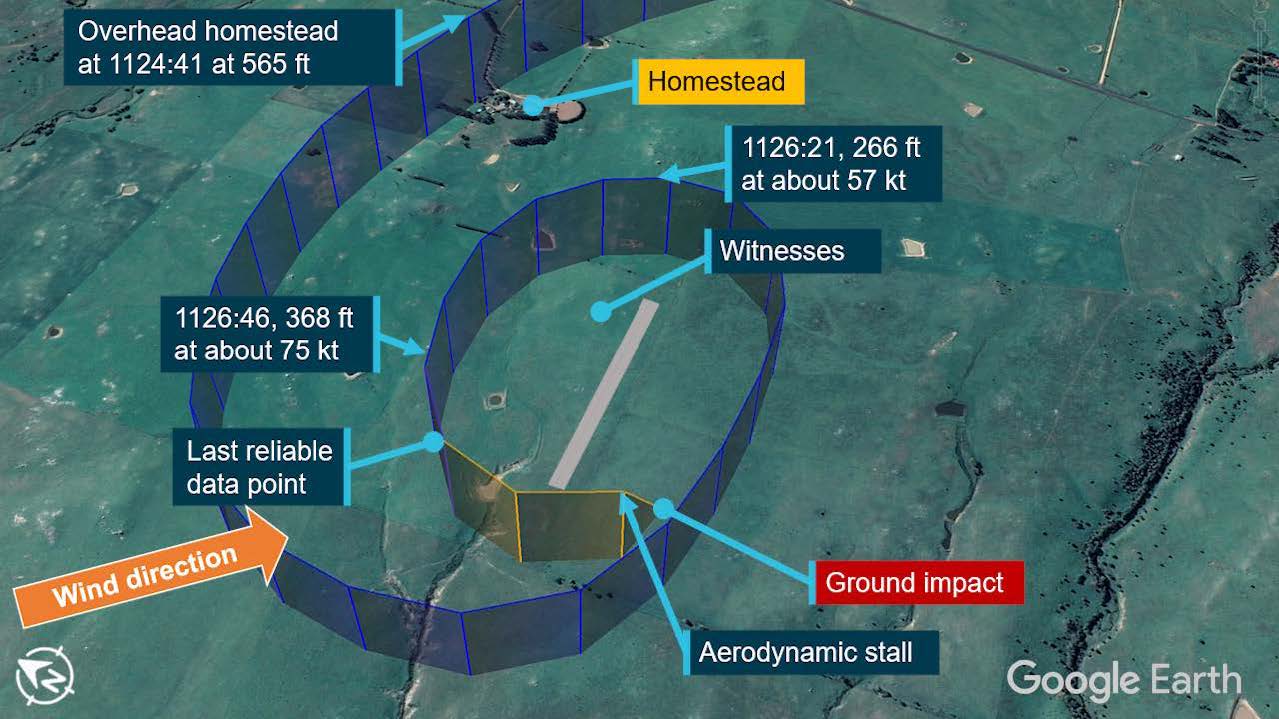
VH-XLK descended to fly overhead the landing area, and at 1125:21 the altitude stabilised at about 2,300 ft, which was about 170 ft above ground level. From 1125:21 to 1126:41 the altitude increased to about 2,400 ft, which was about 270 ft above ground level.
During the descent, at 1124:41, airspeed reduced below 80 KTAS (about 73 KIAS). After levelling out about 1125:21, the estimated speed was about 65 KTAS (about 58 KIAS), and it then increased up to 72 KTAS (65 KIAS) before decreasing to about 59 KTAS (51 KIAS) at 1126:21. It then increased to about 78 KTAS (70 KIAS) at 1126:46, but was decreasing again by the time of the last reliable data point (1126:51).
At 1126:21, VH-XLK commenced a left turn over the eastern end of the landing area. Based on the recorded and estimated parameters, this turn had an estimated bank angle of about 15–20°, which continued up until the last reliable data point (1126:51). At this point the recorded altitude was 2,500 ft (about 400 ft height above ground) and the estimated airspeed was 74 KTAS (66 KIAS). Based on witness reports, the aircraft continued the left turn after this point, which meant it would have been turning towards a downwind direction, with decreasing airspeed, when the loss of control occurred.
Survival aspects
Examination of the aircraft confirmed the correct function of the pilot’s safety harness. Although the harness was cut by emergency services, the belt tongues were secure in the belt buckle. The passenger seatbelt was found securely fastened.
The upward opening, gull doors on each side of the aircraft were open (gas strut operated), however the door locks were in the closed/locked position. The open doors were most likely due to airframe distortion during the accident sequence. The windscreen was broken with little remaining, the left gull door transparency was substantially damaged, and the right gull door transparency was intact.
The accident impact forces imparted on the aircraft cockpit was considered by the ATSB to be not survivable.
Weight and balance information
The standard empty weight of the XL-2 is about 1174 lbs (438.2 kg), however VH-XLK was fitted with a ‘factory rework kit’ which enabled the aircraft to be flown at the increased weight of 1750 lbs (793.8 kg) maximum take-off weight. Aircraft manuals, navigation equipment, travel bags and other personal items were located in the wreckage.
An assessment of the aircraft’s weight and balance during the flight was made based upon the aircraft’s basic weight, estimated fuel, the weight of the pilot and an estimate of the baggage carried. The weight of the aircraft was calculated to have been within weight and balance limits throughout the flight.
Aircraft landing area information
The landing area is located to the south-west of the homestead, in open undulating farmland running almost east-west in orientation. The landing area was freshly marked with painted tyres and had not previously been used by any aircraft prior to the day of the accident.
The landing area ran uphill to the east, with a southerly transverse (side) slope from left to right and was about 540 m long. It was unevenly sloped in the initial sections with a number of undulating steps. The landing area had an elevation of 2,132 ft, and the surrounding area varied by about 100 ft in altitude.
The surface contained depressions, grass tufts and rocks, and was not suited to smaller aircraft tyres, such as those fitted to the VH-XLK.
The landing area met the requirements of Civil Aviation Advisory Publication (CAAP) 92-1 (Guidelines for aeroplane landing areas) for the conduct of the operations of the Liberty XL-2 and was suitable in terms of runway distance required and landing area width.
Additional information
The aerodynamic stall
A wing generates lift when the airflow around the upper and lower surfaces results in a pressure difference between those surfaces. At a certain angle of attack,[8] which is a characteristic of the wing design, the flow over the upper surface of the wing separates from the surface (Figure 6). This condition is known as an aerodynamic stall (or simply a stall) and results in a rapid reduction in the lift generated.
Figure 6: Angle of attack increase to stall
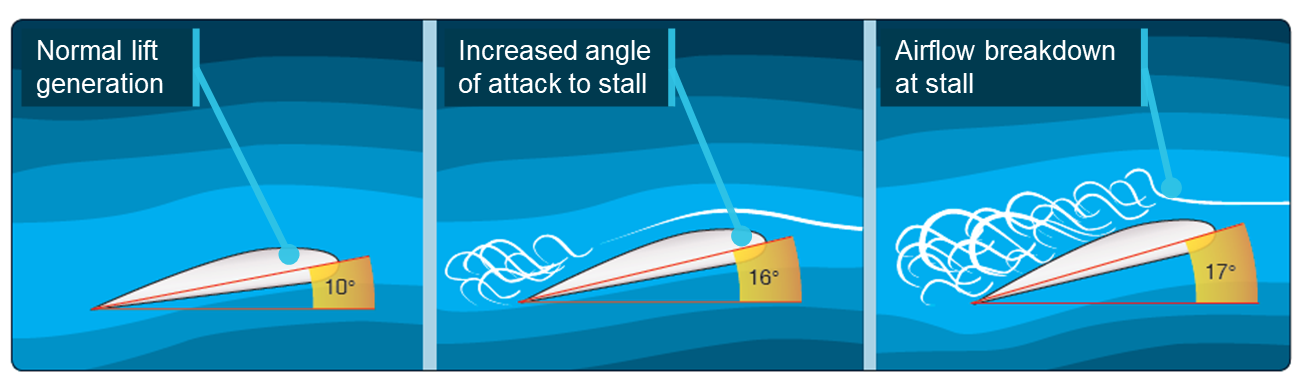
Source: United States Federal Aviation Authority publication FAA-H-8083-3A – Critical angle of attack and stall, annotated by the ATSB
A wing drop occurs when an aircraft approaches the stall and one wing stalls before the other. This signals a loss of symmetrical lift across both wing surfaces, and can be exacerbated by unbalanced flight. The loss of lift on one wing will induce a rolling and pitching moment, that if not immediately addressed by the application of the appropriate recovery actions, will likely result in entry to a spin.
The US Federal Aviation Administration (FAA) Airplane Flying Handbook[9] provides guidance on basic pilot skills and knowledge essential for piloting aeroplanes. The handbook contains a section on stalls that states:
If an uncoordinated turn[10] is made, one wing may tend to drop suddenly, causing the airplane to roll in that direction.
The handbook also described aircraft behaviour during a cross-control stall, when aileron and rudder inputs are applied in opposite directions during a turn, as follows:
In a cross-control stall, the airplane often stalls with little warning. The nose may pitch down, the inside wing may suddenly drop, and the airplane may continue to roll to an inverted position. This is usually the beginning of a spin… It is imperative that this type of stall not occur during an actual approach to a landing, since recovery may be impossible prior to ground contact due to the low altitude.
Depending on timely action and pilot input, the aircraft may require several hundred feet of altitude to effect a safe recovery.
Spins and spin recovery
An aerodynamic spin is a sustained spiral descent, in which one or both aircraft’s wings are in a stalled condition.[11]
A spinning aircraft (Figure 7) will descend more slowly than one in a vertical or spiral dive and it will have a lower airspeed. The pitch angle can also vary considerably from significant pitch down, to a relatively flat attitude, depending on the aircraft type.
Spinning ceases only when opposing forces and moments overcome the rotation. The pilot must recover by applying the recommended spin recovery technique. Due to rotational inertia, spin recovery is not instantaneous. It may take several turns of the applied technique before the recovery technique is effective.
Spins are recoverable when correct recovery technique is taken and there is enough altitude and therefore time to recover.
Figure 7: Spin entry and recovery
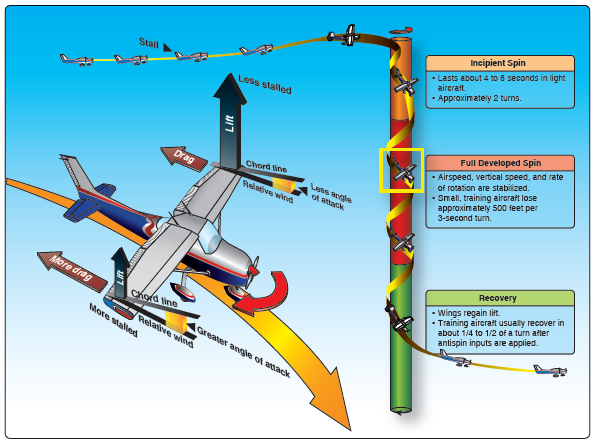
Source: United States Federal Aviation Authority publication FAA-H-8083-3A– Spin entry and recovery
Aircraft flight manual procedures about spins
The Liberty XL-2 flight manual, section 3, described the recovery from unintentional spins as follows:
If an inadvertent spin occurs, use the following recovery procedure:
• Throttle - idle
• Ailerons neutral
• Rudder pedals – Apply and hold full opposite rudder
• Control stick – forward to break stall
• Neutralize rudder – make smooth pull-up from the resulting dive
• Throttle – Adjust for straight and level flight
In addition to the inadvertent spin guidance, section 2 of the Liberty XL-2 flight manual (limitations) stated:
No aerobatic manoeuvres, including spins, are authorized.
Additional guidance material about spins and stalls
A large amount of guidance material has been published for pilots regarding the nature of spins and stalls, such as the guidance material provided by the US FAA mentioned above, a 2008 Civil Aviation Authority (NZ) publication titled Spin Avoidance and Recovery stated:
The majority of unintentional spins occur at altitudes too low for recovery.
The publication discussed how aircraft enter unintentional spins and how in a low-speed descending turn, the aircraft is vulnerable by being at low speed with a higher angle of attack and therefore closer to the stall. This coupled with a reducing or low airspeed can provide the conditions to start a spin.
In the event of a spin, pilots must immediately recognise the spin, its direction, know what to do in the correct order and correctly execute the procedure the first time. In most cases, there is only about 3 seconds to do all this. The minimum altitude loss for a text-book recovery will be about 1,000 to 1,500 ft. At low heights above ground level, there will be little opportunity to recover.
The criticality of immediate and correct pilot input will reduce recovery time and minimise the required altitude to recover, thereby reducing the risk of collision with terrain.
At the time of the accident, CASA had published some guidance material about stalls and spins in its Flight instructor’s manual, as well as educational articles in its Flight Safety magazine. However, it had not published an advisory circular or similar document on stalls and spins. It published an advisory circular on spin avoidance and stall recovery training in April 2020 (see Safety action).
Low flying
Flight below 500 ft above ground level is subject to different sets of visual cues and references, and therefore different techniques. Often slow flight can be involved in low level flight and, as a result, attitude, trim settings, control loads and aerodynamic control effectiveness, and power settings, may all be quite different to what the pilot is familiar with or has experienced before. Accordingly, sustained operational flight at low level requires specific training and testing for competence.
Related occurrences
The recent CASA advisory circular on spin avoidance and stall recovery training stated:
Stall - spin related accidents continue to account for approximately one-quarter of all fatal general aviation accidents worldwide, including many during dual flight training. Most unintentional spins other than during dual instruction, occur at altitudes too low for recovery, generally on climb after take-off and turns onto final approach.
The ATSB has investigated a number of accidents where light general aviation aircraft have stalled and impacted terrain. Each of these investigations identified that the stall condition is exacerbated through mishandling of the aircraft during the stall, which can result in entry into a spin. The stall/spin will result in a steep pitch down and rotation towards the stalled wing. Recovery from this condition will take a considerable amount of height, the magnitude of which is dependent on the reaction time of the pilot, and the use of appropriate recovery technique.
A summary of eight of these investigations, that have similar characteristics to the accident near Braidwood on 6 August 2019, is located in Appendix A.
__________
- Aerodrome Forecasts (TAF): are a statement of meteorological conditions expected for a specific period of time in the airspace within a radius of 5 NM (9 km) of the aerodrome reference point.
- METAR: a routine aerodrome weather report issued at routine times, hourly or half-hourly.
- A set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
- An airworthiness categorisation that applies to aircraft which are intended for non-acrobatic operation, having a seating configuration (excluding pilot seats) of nine seats or less, and a maximum take-off weight (MTOW) of 5700 kg or less, or 2,750 kg or less for rotorcraft.
- An official document, issued by an authorised person as described in Regulations, which is required to be carried on an aircraft as an ongoing record of its time in service (TIS) and airworthiness status. Subject to conditions, a maintenance release is valid for a set period, nominally 100 hours TIS or 12 months from issue.
- A set of regulations that permit the pilot to operate an aircraft to operate in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
- Angle between the wings cord line and the relative airflow.
- US Department of Transportation Federal Aviation Administration 2004, Airplane Flying Handbook.
- An uncoordinated (or unbalanced) turn is one where a sidewards acceleration (force) is felt during the turn due to a sideslip.
- Aerodynamic stall: occurs when the airflow separates from the wings upper surface and becomes turbulent. It occurs at high angles of attack, typically 16–18° and results in reduced lift and increased drag.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision with terrain involving Liberty Aerospace XL-2, VH-XLK, 9 km north-east of Braidwood, New South Wales, on 6 August 2019. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
- After arriving at the landing area, the pilot circled the landing area at a height of 200–400 ft above ground level.
- Soon after the pilot turned downwind at low airspeed with no flap selected, the aircraft’s left wing aerodynamically stalled. This resulted in the aircraft entering into an upright spin, at an altitude that limited an effective recovery.
Other factors that increased risk
- An airworthiness directive requiring an inspection of the engine exhaust muffler had not been completed and the aircraft was overdue for an oil change. These overdue maintenance items rendered the maintenance release invalid, which should have prevented further flight until rectified.
Safety analysis
Introduction
Evidence from witnesses and the available flight data indicated that control of the aircraft was lost while the pilot was executing a slow speed turn downwind. The witnesses then observed the aircraft’s left wing drop and the aircraft enter an upright spin. The examination of the wreckage confirmed that the aircraft impacted terrain in a nose-down, left wing low attitude, consistent with the aircraft being in the early stages of a spin.
The local meteorological conditions around the time of the accident suggested that a meteorological event, such as a sudden and large wind gust that might contribute to a loss of control, was unlikely to have occurred. In addition, the available evidence indicated that the engine was operating at impact and there was no evidence to suggest any impediment to normal engine operation. There was also no evidence to indicate a problem with the aircraft’s flight controls or weight and balance leading to the loss of control.
This analysis will consider the circumstances that preceded the event, including navigation data and witness reports. It also considers some maintenance aspects associated with the aircraft.
Flight over the landing area
Aircraft handling
Flight profile data provided by the navigation software manufacturer indicated the aircraft’s height to be ranging from 200–400 ft above ground level (AGL) as the pilot circled the area prior to the loss of control. The aircraft’s speed and altitude fluctuated, commensurate with holding a reduced power setting and interchanging speed for altitude.
In slow speed situations, the selection of partial flap would allow the pilot to fly the aircraft at a lower airspeed, while maintaining a greater margin above the stall.[12] However, the flaps were confirmed to be in the retracted position at the accident site.
The stall handling characteristics of most light, general aviation aircraft suggest that a significant wing drop, as reported by the witnesses, may be due to an unbalanced turn at slow speed, leading to entry to a spin. In this case, the left wing most likely aerodynamically stalled, rolling the aircraft left and pitching the aircraft nose down. The aircraft then entered a left spin with a near vertical attitude and completed one rotation before impacting terrain.
Enabling a recovery from the stall
It has been highlighted in other accident investigation reports and guidance material that the height required to recover most light general aviation aircraft from a stall/spin condition is in the order of at least 400 ft. By operating the aircraft below 500 ft while circling the landing area, the pilot reduced an important safety margin.
It is also important that a pilot monitors and maintains an appropriate margin above the stall speed during a turn, is cautious with manoeuvring, and remains balanced with control inputs when flying at lower altitudes.
Pilot intentions
It is unclear what the pilot’s intentions were after arriving overhead the landing area. The pilot of the accompanying aircraft reported that they had advised the pilot of VH-XLK that the surface of the landing area was not suitable for VH-XLK to land. It is possible that the pilot of VH‑XLK was assessing the landing area to make up their own mind or was potentially just conducting an overflight of the property. In either case, flight below 500 ft above ground level, unless they were conducting a precautionary search and landing or were in the process of landing (after conducting a suitable circuit or approach), reduced the available time and altitude to recover from an emergency situation, such as a stall or spin.[13]
In addition, regardless of their intention, it is likely that the pilot’s focus of attention was looking outside the aircraft at the landing area. Accordingly, they may well have not been allocating sufficient attention to monitoring the aircraft’s airspeed and/or energy state and controlling the aircraft. A substantial body of research has shown the significant effects that distraction can have on pilot performance (ATSB 2005).
Effectiveness of the stall warning
A stall warning should provide adequate warning to the pilot prior to the onset of stall symptoms during flight. The stall warning system fitted to the XL-2 was designed to provide aural warning of impending stall conditions about 5 kt above the expected stall speed.
Analysis of the stall warning system components identified that it was most likely functional at the time of the accident. However, it is unknown if and for how long this warning may have sounded. Likewise, the pilot’s reaction to the warning before the aircraft stalled is also unknown.
Stall speed can be reduced by the application of flap and is recommended while conducting sustained slow speed flight. Although it is possible the pilot may have been using some flap during the early part of the circling, it is very unlikely any flap was selected prior to commencing the final turn (downwind), given that the flaps were retracted at impact.
Summary
The introduction of bank and/or unbalanced control inputs decreases the margin between slow flight and the stall. Maintaining adequate airspeed through appropriate power application during increased bank angles is essential to maintain a controllable airspeed and margin above the stall, especially in slow speed flight, without height loss.
If the pilot was evaluating the suitability of the landing area for their aircraft, the conduct of a precautionary search and landing by overflying the landing area at progressively lower heights, and then climbing back to circuit height each time, would have reduced the risk of a loss of control.
Taking into consideration the time required to recognise and react to a stall/spin event, and recovery height requirements, VH-XLK was most likely at an altitude that would have precluded a safe spin recovery prior to impacting terrain.
Maintenance overrun
VH-XLK departed Moruya with maintenance requirements that were due prior to the flight. This included an airworthiness directive (AD) specifying a muffler inspection, and an engine oil and filter change. The aircraft had been flown on 10 previous occasions with the muffler AD pending completion.
The operation of the aircraft beyond the maintenance requirements resulted in the maintenance release ceasing to be valid; this should have prevented further flight in the aircraft until the actions were completed (or an exemption obtained).
The overdue maintenance did not contribute to the accident. There was no indication of an engine problem. In addition, although the overdue muffler inspection increased the potential of carbon monoxide gas entering the cockpit, there was no indication that the pilot was affected by carbon monoxide.
__________
- The use of flap would also lower the nose attitude and increase forward visibility.
- In addition, flying a normal circuit pattern, oriented with reference to the intended landing area, assists in the conduct of normal procedures and minimises the potential for omissions or distractions.
Purpose of safety investigations & publishing information
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2020
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
Occurrence summary
| Investigation number | AO-2019-040 |
|---|---|
| Occurrence date | 06/08/2019 |
| Location | 9 km north-east of Braidwood |
| State | New South Wales |
| Report release date | 26/11/2020 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Collision with terrain |
| Occurrence class | Accident |
| Highest injury level | Fatal |
Aircraft details
| Manufacturer | Liberty Aerospace Incorporated |
|---|---|
| Model | XL-2 |
| Registration | VH-XLK |
| Serial number | 0106/2008 |
| Sector | Piston |
| Operation type | Private |
| Departure point | Moruya Airport, New South Wales |
| Destination | Nerriga Road, Braidwood, New South Wales |
| Damage | Destroyed |