At about 0825 Eastern Standard Time on 9 January 2019, an Insitu ScanEagle X200 (X200) unmanned aircraft system was launched to conduct ‘beyond visual line of sight’ aerial survey work in the Woleebee Creek area of Queensland. The flight crew consisted of two pilots and two ground crew.
Shortly after launch, one of the ground crew observed the X200 pitch up and then enter an aerodynamic stall. The flying pilot commenced the emergency procedures for a stall-spin, however the X200 self-recovered before the checklist was completed. At about the same time the pilots received an alert indicating an airspeed sensor failure and initiated the associated emergency procedure checklist.
Before visual sight was lost, the ground crew observed the X200 oscillating in pitch as it continued to fly to the programmed first waypoint. While the flying pilot was executing the emergency procedures checklist, the X200 entered a second aerodynamic stall. Following self‑recovery from a low height above terrain, the X200 commenced a climbing orbit. Shortly after, the X200 entered a third aerodynamic stall, this time from a height that was insufficient for recovery, and collided with terrain. There was no post-impact fire and the X200 was destroyed. There were no reported injuries to people or damage to infrastructure. A post-incident inspection of the X200 identified a partial blockage in the pitot system.
What the ATSB found
The investigation found that the blockage in the pitot-static system resulted in unreliable airspeed data being supplied to the autopilot. Unreliable airspeed data led to the X200 entering an aerodynamic stall at a height that was insufficient for recovery.
During the pre-flight checks, there were opportunities for the erroneous airspeed indications to be identified. However, they were not recognised by the crew or flagged by the ground control station.
What's been done as a result
Following the occurrence, the manufacturer revised their procedures to reduce the risk of aircraft being affected by a pitot blockage. Additionally, all of the operator’s pilots underwent refresher training. This included emergency procedures simulator experience.
The X200 manufacturer revised their procedures to provide support to pilots and ground crew in correct assembly of the articulated turret, identifying anomalies (on the ground and in-flight), and steps for aircraft recovery in the event of a departure from normal flight. In addition, updates to the operational software would ensure any spurious on‑ground anomalies were alarmed, to prevent the X200 being launched with an unidentified issue.
Safety message
This occurrence highlights the importance of confirming the significance of any unexpected observations during the pre-flight checks, to minimise the risk of the aircraft departing with an unserviceability. In addition, providing pilots and ground crew with the reasoning behind specific checks and procedures can enhance their ability to identify anomalies and perform the appropriate corrective actions in a timely manner.
Insitu ScanEagle X200
Source: Insitu Pacific
The occurrence
What happened
On the morning of 9 January 2019, the Insitu Pacific (the operator) crew prepared to conduct a 4‑hour ‘beyond visual line of sight’ survey flight, in the Woleebee Creek area, about 350 km west‑north‑west of Brisbane, Queensland. The flight was being conducted by an Insitu ScanEagle X200 (X200).
The crew consisted of two remote pilots[1] (one acting as mission controller/pilot in command and one acting as pilot flying) and two ground crew (who were also qualified remote pilots).[2] The two pilots for this flight were located in the ground control station (GCS).[3] Headsets were worn by all crew members, to enable effective communication. All crew reported to being ‘refreshed’ and looking forward to the day’s flight.
The X200 was launched at 0825 Eastern Standard Time.[4] The crew described the launch as ‘textbook’. The secondary ground crew member maintained visual contact with the X200, typically done until advised by the pilots that they had video feedback from the on-board camera.[5] He reported that, about one minute after launch, the X200 pitched up ‘quite high’, before entering an aerodynamic stall.[6] He immediately advised the pilot flying (PF) with the standard phrase ‘wings level, wings level, you’re stalling’. At this time, the primary ground crew member also observed the X200 in a ‘left-hand spin’ and advised the PF ‘you’ve stalled, wings level, wings level’.
At the same time, the GCS identified the stall condition and projected the ‘stall-spin’ emergency procedures checklist to the display. The PF commenced the checklist items, however the X200 self‑recovered before the checklist was completed. The ground crew reported the X200 recovered ‘low to the ground’ and then commenced a climb to return to the programmed flight altitude.
At about the time of the recovery from the first stall, the GCS initiated the warnings and emergency procedures checklist for an ‘airspeed failure’. Upon the mission controller’s direction, the PF commenced the airspeed failure checklist. The ground crew reported that following a ‘steep’ climb, the X200 was then observed to be ‘porpoising’ (oscillating in pitch) while it continued to the first programmed waypoint. Shortly after this, the X200 flew beyond visual sight of the ground crew.
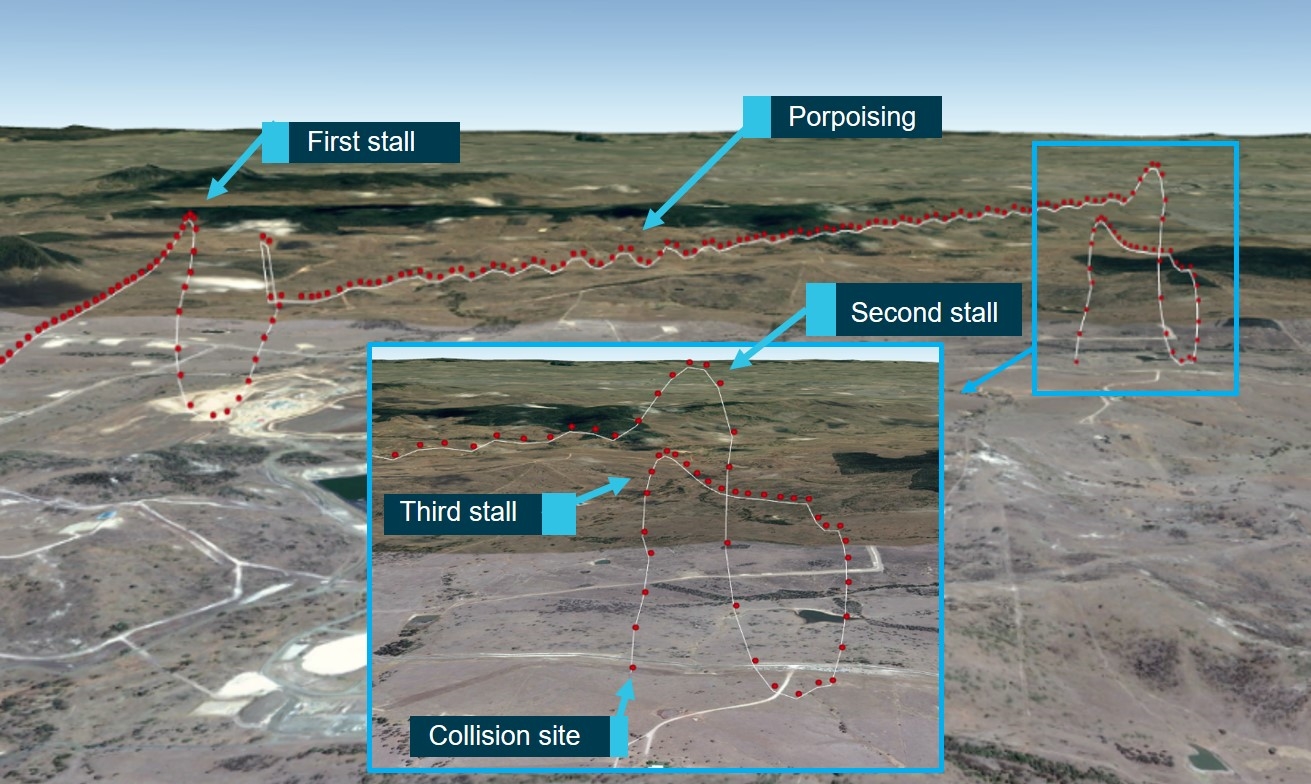
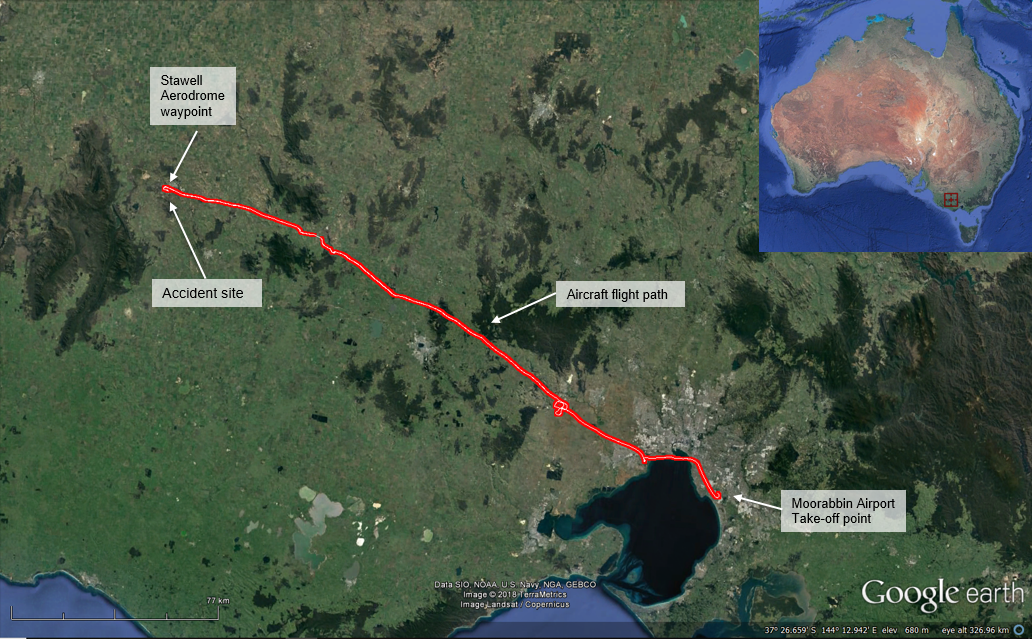
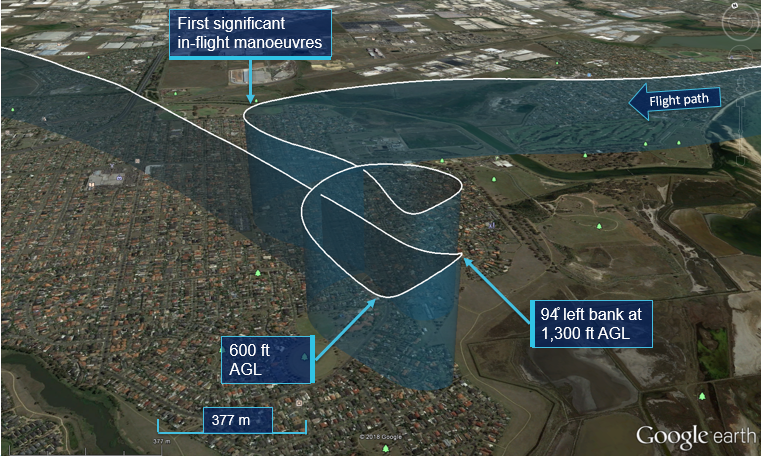
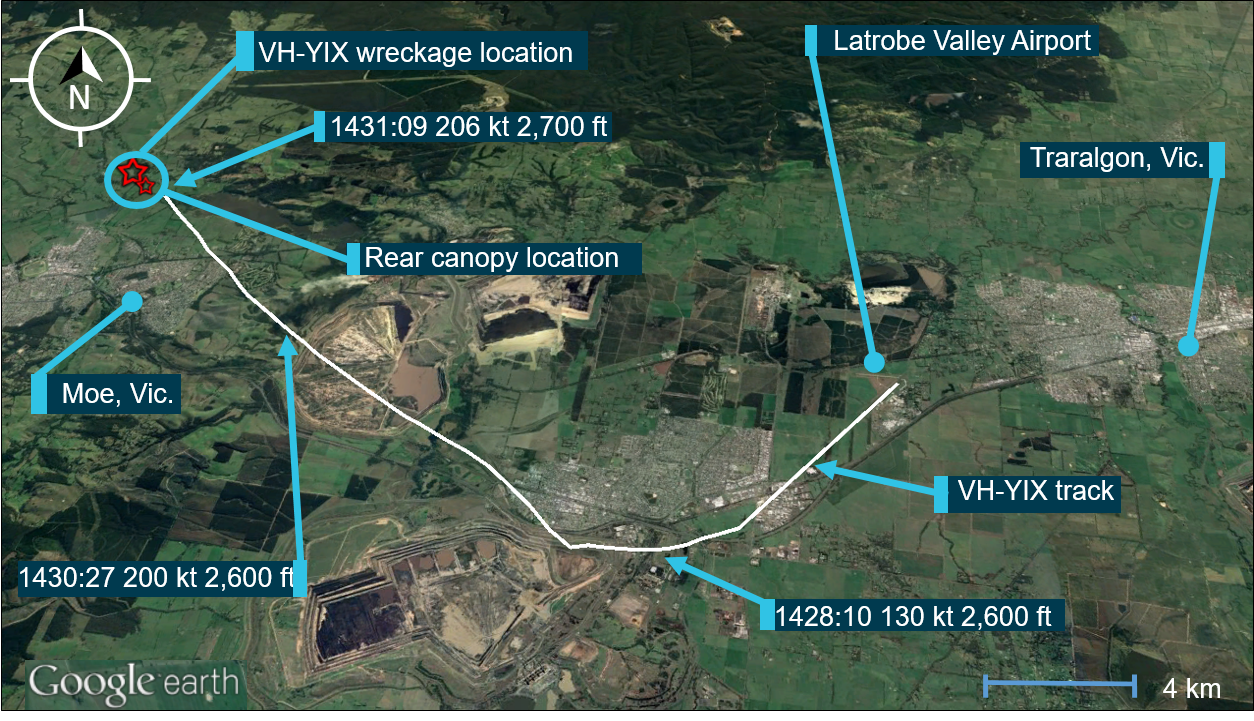
Telemetry data showed that, about 90 seconds after the first stall, the X200 entered a second stall. The X200 self-recovered again, at about 150 ft above the ground, and commenced a climbing orbit. After about 30 seconds, the X200 entered a third stall and impacted the ground eight seconds later. The mission controller advised the ground crew that the X200 had been lost. Total flight time was less than four minutes and distance from the launch site to the collision with terrain location was about 4.75 km (Figures 1 and 2).
Figure 1: X200 flight path
Source: Insitu Pacific and Google Earth, modified by the ATSB
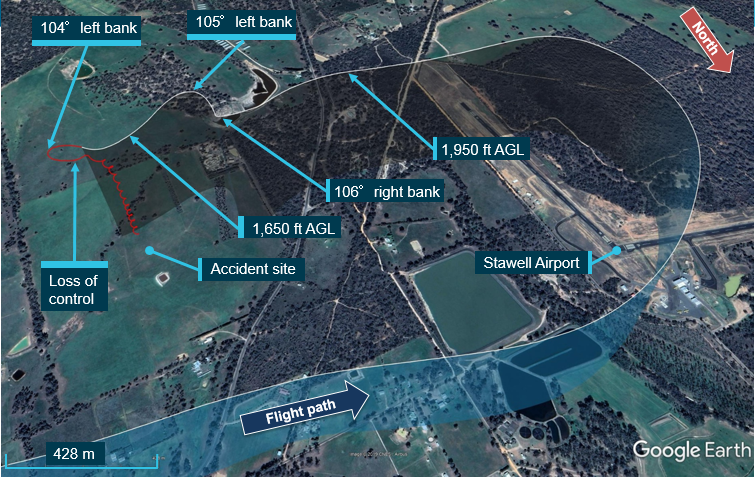
Figure 2: X200 flight profile
Source: Insitu Pacific and Google Earth, modified by the ATSB
Post-accident recovery and inspection
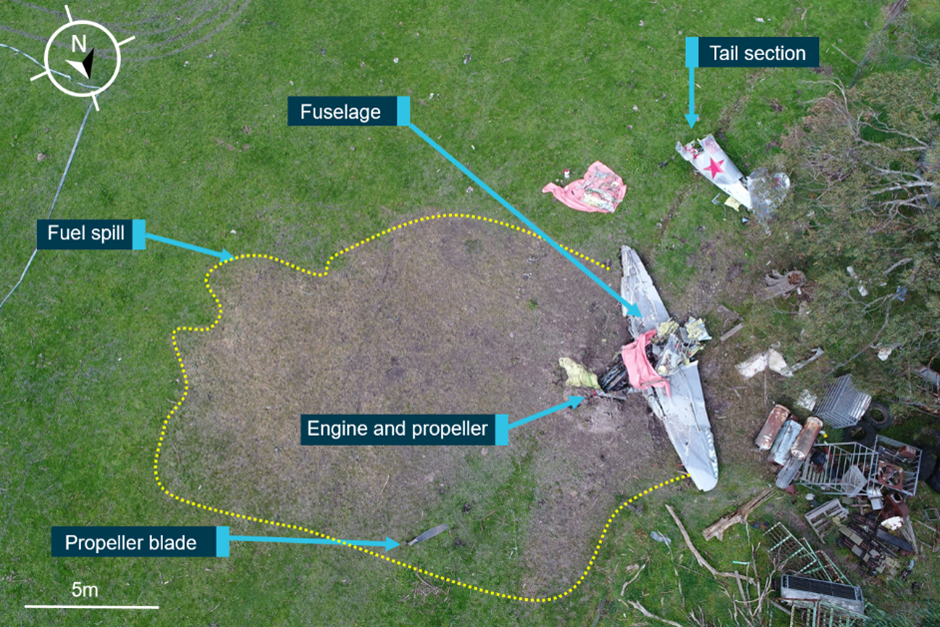
The aircraft impacted the ground near vertically, there was no post-impact fire and the X200 was destroyed. There was no evidence of in-flight break-up or collision with vegetation or infrastructure prior to the impact. In addition, there were no reported injuries. The operator conducted an examination of the occurrence X200 and identified a partial blockage in the pitot system, which was subsequently confirmed by the manufacturer. The blockage appeared to be a combination of a section of O-ring debris and grease.
Flight operations
The Civil Aviation Safety Authority (CASA) issued the operator with an authorisation to operate the X200 beyond visual line of sight, within a defined area. Some of the authorisation’s requirements included:
all remote pilots were to hold a CASA authorisation
a mode C transponder[7] was to be operational, and transmitting accurate barometric altitude, on all flights
a primary and secondary ‘fail safe’ mode to ensure that, in the event of data-link loss, the X200 did not depart the area of operation and would land at a pre-determined location
air traffic control at Brisbane was to be advised of the intended operation 15 minutes prior to launch, and the crew were to maintain standard airspace radio procedures for the duration of the flight
the operator was to ensure a current Notice to Airmen (NOTAM)[8] was active for each operation
the X200 was only to be operated in visual meteorological conditions.
In addition to the CASA authorisation, the operator’s procedures included:
no flight over populous areas
operations were conducted at altitudes intended to avoid agricultural and passenger aircraft.
Remote pilots underwent a 10-week course prior to being endorsed to operate the X200. This course included a theory component and time in the simulator. The pilots recalled that ‘airspeed failure’ was included in the course, however they felt that particular emergency procedure wasn’t focussed on as ‘heavily’ as others.
The accident site was located within the defined operational area, which was in accordance with the authorised requirements.
Aircraft information
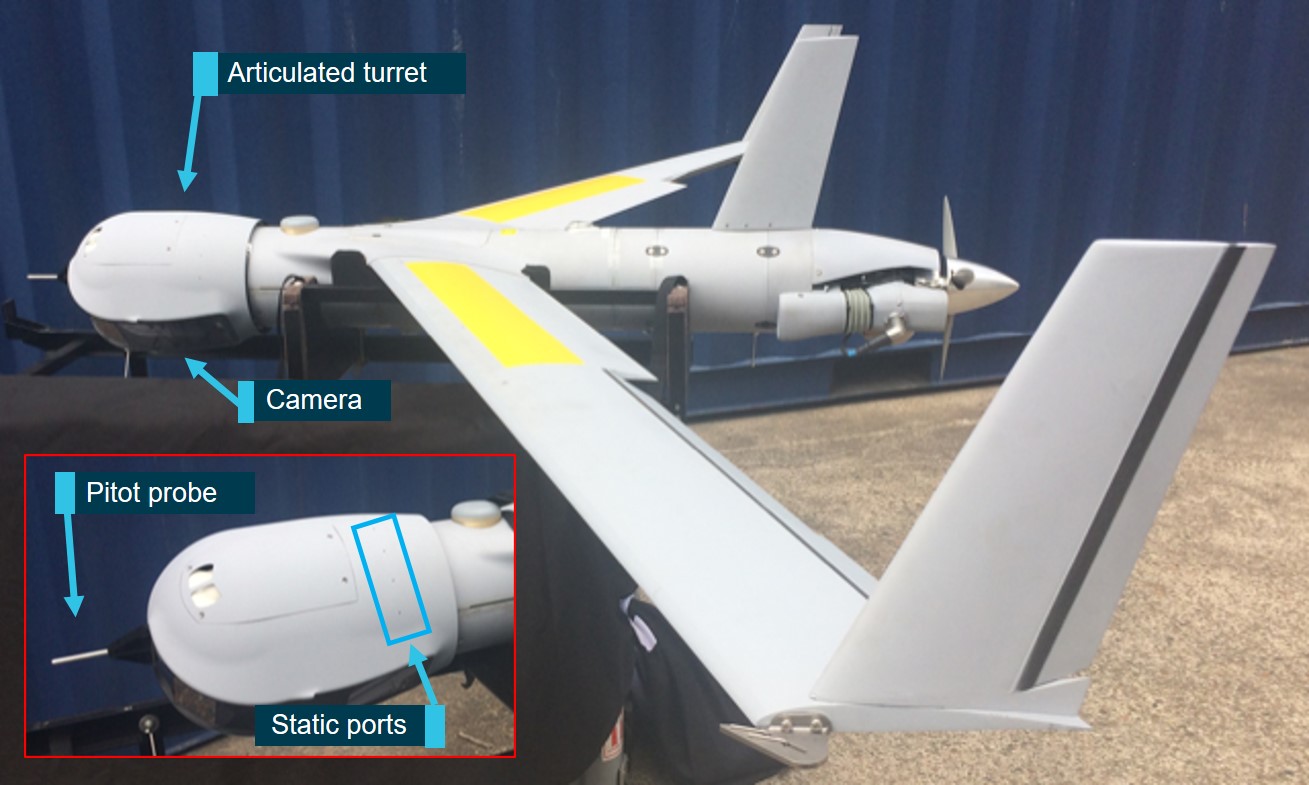
The ScanEagle is a small, long-endurance, low-altitude unmanned aerial system (UAS) built by Insitu, a subsidiary of Boeing, and is used for defence and civilian applications (the X200 variant). The X200 (Figure 3) has a wingspan of 3.1 m, a length of 1.6 m, maximum take‑off weight of about 23 kg and a typical cruise speed of 50-60 kt.
The nose module (payload) on the X200 is interchangeable, depending on the type of mission being flown, and was supplied by the payload manufacturer. The payload fitted to the X200 at the time of the occurrence consisted of a camera assembly located in an articulated turret (turret). The camera could be directed through a defined fore/aft arc and the turret rotated through 360˚.
The pilot controls the X200 entirely through the aircraft autopilot from launch until recovery. The aircraft’s flight path is controlled by position, altitude and airspeed commands through the remote pilot station computer (part of the ground control station), which is then sent to the aircraft autopilot. The pilot does not have a control yoke, or equivalent, that links directly or indirectly to the aircraft control surfaces.
Typically, once the X200 has launched, the pilot commands it through a pre-planned sequence of locations and orbits around each location of interest. At the completion of the flight’s activities, the pilot would position the aircraft in preparation for the recovery phase using the same method of control. In this instance, the emergency procedure checklist actions involved the pilot utilising additional X200 autopilot control laws in order to negate the erroneous airspeed information.
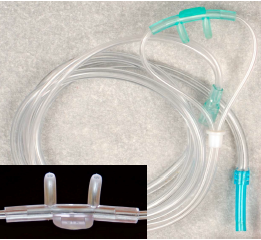
Figure 3: X200 with articulated turret
Source: Insitu Pacific, modified by the ATSB
Pitot-static system
The pitot-static system senses ram air pressure through the pitot probe (on the forward face of the payload) and static air pressure through the static ports (on each side of the payload). The two pressures are used to calculate true airspeed (TAS) and barometric altitude (Alt). The autopilot uses this data to calculate the minimum and maximum airspeed in relation to the weight of the X200 and to maintain controlled flight.
The pitot and static tubes for the X200 were routed from the pitot probe and static port through the turret and connected to the pitot-static tubing in the fuselage. If not correctly oriented during assembly, the tubes could become pinched, blocked or damaged with turret operation. Obstructed pitot-static tubes have the potential to cause incorrect TAS and Alt calculations, affecting autopilot operation.[9] In addition, the TAS and Alt indications to the pilots would also be unreliable. The manufacturer alerted X200 operators to this potential condition in November 2017, via both a service advisory and an operational advisory. Damage sustained to the X200 during this occurrence prevented testing for possible turret interference.
The service advisory (SA) provided expanded procedures for pitot and static tube routing and connection, and inspection procedures if an anomaly was identified during pre-flight checks. A review of the X200 maintenance records showed the turret had been installed as per the SA in July 2018. Since then, it had been operated for about 80 hours, without indication of turret interference.
The operational advisory (OA) included:
information about how to identify and troubleshoot different types of incorrect TAS and Alt indications on the ground and in-flight
a pre-flight function test to identify incorrect TAS and Alt indications shown on the ground control station (GCS) program
in-flight emergency procedures to normalise the incorrect TAS and Alt indications and avoid loss of controlled flight.
The function test was to be completed before every flight and the OA provided examples of how anomalies with the pitot-static tubing may appear on the GCS display. Where inspection and routing of the pitot-static tubes did not rectify the anomaly, the turret was to be replaced prior to next flight. The OA procedures had been incorporated into the GCS program at the time of the occurrence.
In addition, the payload manufacturer identified a quality issue with the turret assembly procedures that had the potential to induce a blockage in the pitot system. The operator identified that the occurrence X200 was affected by this quality issue, consisting of excess grease and O‑ring debris forming the pitot-system partial blockage. The X200 manufacturer published procedures to inspect (and, if required, clean) turrets that were in-service and prior to fitment. The operator examined the remainder of their fleet with these revised procedures, with no further occurrences identified.
Pre-flight checks
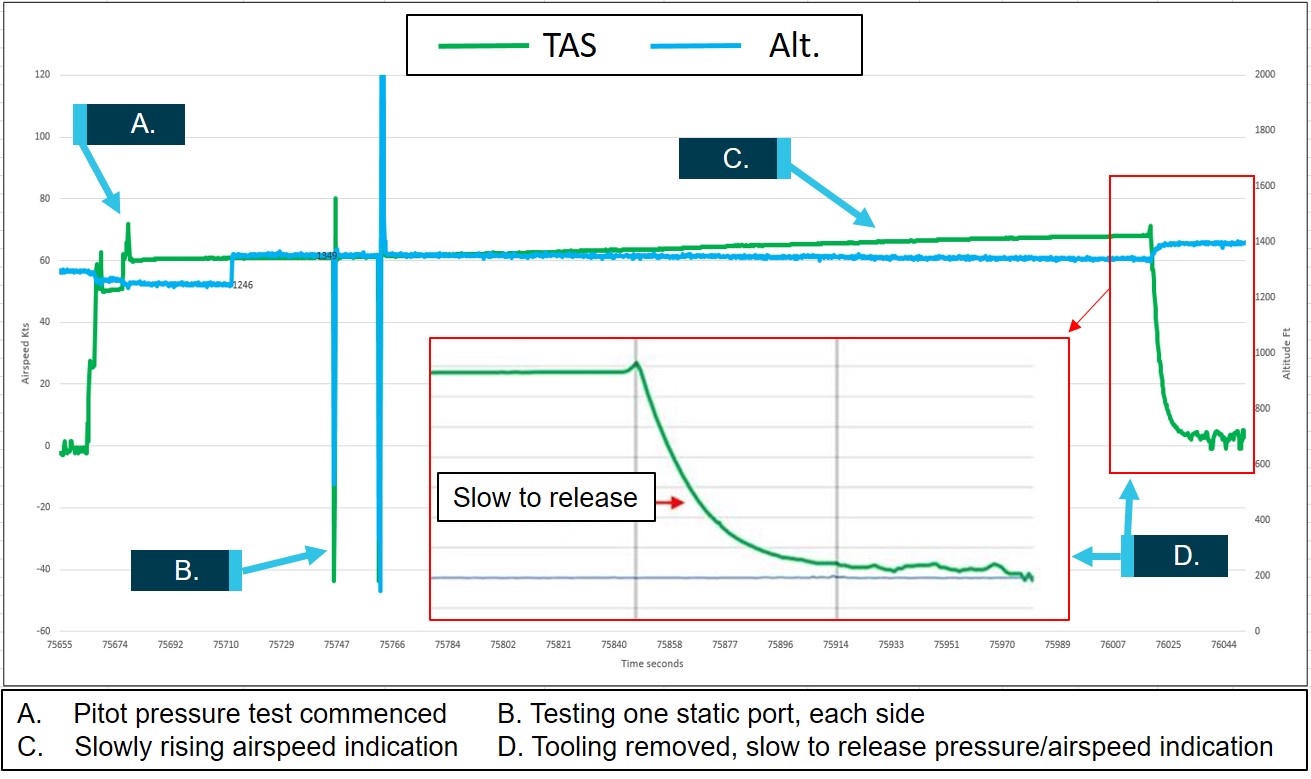
As part of the pre-flight procedures, the primary ground crew conducted an inspection of the X200 while the secondary ground crew readied the launcher and recovery systems. At the same time the pilots, located in the GCS, conducted their pre-flight systems checks, which included a function test of the pitot-static system (Figure 4). This test included the primary ground crew fitting a sealed clear tube to the pitot probe, which increased pressure in the system and simulated an airspeed indication associated with forward flight (equivalent to TAS). The procedure stated that any reduction in pressure (TAS) indicated on the GCS during the test, equal to or greater than the specified limits, was indicative of a system leak that required rectification prior to flight.
During the test, a slow rise of about 10 kt TAS occurred, while the indicated altitude remained steady. The OA detailed that if the TAS ‘increases slowly without turret movement or pressurisation of the pitot-static system’, this was an indication of a blockage in the pitot-static system. As per the OA, turret movement had the potential to induce a restriction in the pitot system tubing, which could ‘clear’ with subsequent movement. The pitot system was pressurised and the turret was being operated for part of this test and as such, the rise in TAS as a possible indication of a blockage may have been difficult to identify. Following this occurrence, a revised OA amended the criteria for the slow increase in TAS to show ‘at any time’ during the procedure, removing any ambiguity surrounding pitot pressurisation and turret movement during the tests.
With no pitot system leak identified by the pilots, the tooling was removed. At this time, the pilot flying (PF) commented that the TAS was ‘slow to release’ (return to pre-check indication). The primary ground crew member reported that he heard this comment however, he took no action as he wasn’t aware of the significance of this indication. The pilot pre-flight checklist identified that slow to release pressure was indicative of a blockage in the pitot system.
Following completion of the crew’s pre-flight checks, the GCS continued with the system self‑checks, while the crew met outside for a pre-mission brief, as per their standard procedure. During the time the crew were outside, the GCS self-check indicated an anomaly within the pitot‑static system. In this instance, there was an increase over time in TAS, while the Alt decreased. For this indication, the procedures required an inspection of the pitot-static system prior to launch. However, this indication was not flagged or latched.[10] Therefore, when the pilots returned to the GCS, there was nothing to alert them to this additional indication of a pitot system anomaly.
Figure 4: Pitot pressure test indications
Source: Insitu Pacific, modified by the ATSB
All subsequent pre-flight checks were described as normal. Weather conditions at the time were recorded as overcast conditions, 22˚C, a wind speed of about 6 kt and were described by the crew as ‘ideal’.
Autopilot and the occurrence flight
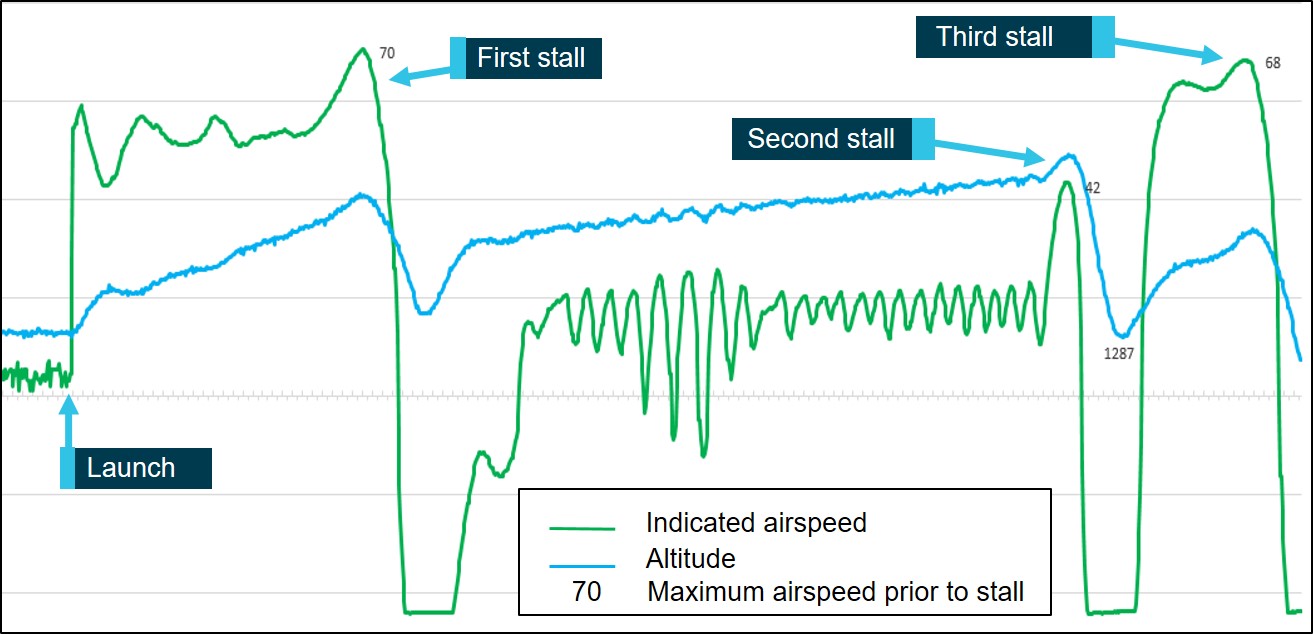
The X200 autopilot control loops rely on airspeed to control altitude. The target airspeed for the occurrence flight was 53 kt. Recorded data shows that following launch, the TAS reached 70 kt. This resulted in the autopilot commanding a rapid pitch up to try to arrest the perceived high TAS. The pitch attitude was too great for the actual airspeed, which resulted in the X200 entering an aerodynamic stall. Stall recovery took 12 seconds, with an altitude loss of 579 ft (at a rate of 48 ft/s), before the X200 began to climb back to the programmed flight altitude.
Erratic TAS is one of the parameters that can lead to a stall-spin in the X200. Flight data showed that erratic TAS was present from launch, before the turret was unlocked and operated. This was consistent with a blockage of the pitot system, rather than turret interference.
The erratic TAS also resulted in the porpoising flight profile following the first stall and recovery. Following about 80 seconds of porpoising flight, the data showed another rapid increase in TAS. The autopilot likely commanded the X200 to increase pitch attitude, which again resulted in an aerodynamic stall and rapid reduction in height. Within 12 seconds, the X200 had again self‑recovered from the stall, but at a much lower altitude than the first recovery. The second stall required 778 ft for self-recovery (at 64.83 ft/s rate of altitude loss).
This was followed by another extreme increase in TAS, leading to the third stall. This stall was at a similar rate to the second stall. Recovery was again initiated but only 591 ft was available and the X200 collided with terrain, about 9 seconds later (Figure 5).
Figure 5: Flight data showing erratic indicated airspeed and altitude
Source: Insitu Pacific, modified by the ATSB
Safety analysis
Following launch, the Insitu ScanEagle X200 (X200) twice entered an aerodynamic stall and self‑recovered. The X200 entered a third stall, this time at a lower height, and did not recover prior to collision with terrain. The analysis will examine the pre-flight indications of the pitot system blockage and its effect on the flight.
Pre-flight checks
The pre-flight checks provided three opportunities for anomalies in the pitot static system to be detected. There was a slow rise in TAS, which was indicative of an anomaly in the pitot system. The pressurisation of the pitot system and movement in the turret during the pitot-static function test, however, may have meant that the slow rise in TAS and the physical blockage was not obvious. The slow reduction in TAS after the pressure test was an indication of a pitot system blockage. This was noted by some of the crew, however the significance of this indication was not recognised.
The ground control station (GCS) system self-checks showed an additional indication of a pitot system anomaly, however it was not observed by the crew, as they were carrying out other duties at the time. At the completion of the self-checks, there was no ‘flag’ or other indication on the GCS that the pitot system irregularity had occurred. This resulted in the indications of pitot system anomaly not being identified by the crew or flagged by the GCS, resulting the X200 being launched with a blockage in the pitot system.
Unreliable airspeed data
The X200 autopilot uses true airspeed (TAS) and altitude (Alt) data to maintain controlled flight. The blockage in the pitot system resulted in unreliable airspeed data being provided to the autopilot, affecting calculation of TAS. While there remained the possibility that the turret interference may also have been present, it could not be determined as contributory in this occurrence. Flight data showed that erratic (TAS) data was present from launch, before the turret was unlocked and operated. Subsequent movement of the turret may have alleviated any turret‑induced restriction in the pitot system but due to the presence of the identified blockage, the airspeed data was unreliable even without any turret interference.
Following launch, the autopilot interpreted the TAS as increasing and increased the pitch (nose up) to maintain target airspeed. This resulted in the X200 nose-up attitude being too great for the actual airspeed and led to an aerodynamic stall. The X200 self-recovered and recommenced the climb to operating altitude.
Following recovery from the first stall, flight data showed the TAS was oscillating by up to 30 kt, resulting in the ‘porpoising’ flight profile, indicative of the autopilot trying to maintain controlled flight using unreliable airspeed data. A rapid 30 kt increase in TAS likely led to the autopilot increasing pitch attitude, resulting in the second aerodynamic stall. Again, the X200 self-recovered, however at a much lower altitude. A third rapid TAS increase followed shortly after, leading to the final stall, with insufficient height available for recovery.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Erroneous airspeed system indications during the pre-flight checks were not identified by the crew or flagged by the ground control station, resulting in the X200 being launched with an unserviceable pitot-static system.
A blockage in the pitot-static system resulted in unreliable airspeed data being supplied to the autopilot.
Unreliable airspeed data led to the X200 entering an aerodynamic stall at a height that was insufficient for recovery.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
The operator
As a result of this occurrence, the operator advised the ATSB that the following safety actions, in cooperation with the X200 and payload manufacturers, have been undertaken:
Pilot training
Following the occurrence, all of the operator’s remote pilots underwent refresher training with a focus on identification and emergency procedures regarding incorrect true airspeed (TAS) and/or barometric altitude (Alt) indications. The training consisted of theory (including ‘how’ the system works and symptoms of pitot-static blockage) and several hours’ simulator experience of failures and use of emergency procedures. Feedback from the pilots following this training was positive. In addition, the ATSB was advised that the X200 manufacturer will amend the ab-initio pilot training to highlight pitot-static system anomalies and associated pre- and in-flight procedures.
Training and enhanced procedures can provide ‘reasoning’ behind the steps. This can assist pilots and maintainers in their understanding of indications and events, prompting effective actions and timely resolution.
The manufacturer
Documentation and procedures
The X200 manufacturer published a revised Operational Advisory (OA) on 18 February 2019. One amendment in this revised publication was the inclusion of an image from the occurrence X200, showing the Ground Control Station indication for ‘slow to release’ pitot pressure. The criteria for the slow increase in TAS was also amended to ‘at any time’ during the procedure, removing any ambiguity surrounding pitot pressurisation and turret movement during the tests.
In addition, the revised OA included an additional caution (in red text) warning that the ‘TAS error exceeds launch limit alarm is disabled for pre-flight pitot-static system checks. Therefore, it is critical to monitor the TAS-ALT-Tachometer plot throughout the on ground phase for any abnormal TAS or Alt signatures’. The operator reported that the X200 manufacturer advised a ‘latching system alarm’ would be incorporated into the next software release (scheduled for mid-2019) to alert the crew where the TAS has exceeded a threshold during on-ground checks.
Further, the manufacturer revised their procedures for assembly of the turret and provided a reworked procedure to X200 operators to reduce the risk of in‑service aircraft being affected by a pitot blockage.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
What happened
On 24 November 2018, at about 0800 Central Standard Time,[1] a Robinson R22 helicopter, registered VH-KZV, collided with terrain about 125 km east-north-east of Alice Springs Airport. The pilot was fatally injured and the passenger was seriously injured. The helicopter was substantially damaged.
The pilot held a private helicopter pilot licence and was employed by a cattle station for general flying duties, which included cattle mustering. On the morning of the accident, the pilot and passenger were tasked to assist with the recovery of a motor vehicle, located about 63 km east-north-east of Ambalindum Station (departure point). A station hand assisted them with preparing the helicopter for departure. The station hand could not recall the actual time of departure, but estimated it was between 0730 and 0745.
At about 0811, the pilot’s Spot Tracker device transmitted its location in SOS mode.[2] A local helicopter company in Alice Springs was subsequently tasked by the Joint Rescue Coordination Centre to transport a paramedic to the reported location and conduct a search and rescue. In addition, Ambalindum Station dispatched two employees by road to investigate. The search helicopter pilot located the wreckage of the R22 at the reported location, and the paramedic subsequently attended to the accident pilot and passenger. At about 1045 the paramedic found the pilot deceased and the passenger in a serious condition. The rescue helicopter departed to collect the two station employees who were enroute to assist with the emergency response. The rescue helicopter pilot and the paramedic, with the assistance of the two station employees, retrieved the passenger and transported him to Ambalindum Station for treatment by a retrieval doctor, before transporting him to Alice Springs Hospital for further medical attention.
Figure 1: Robinson R22 helicopter, VH-KZV, main wreckage site
Source: ATSB
The ATSB attended the accident site on 26 and 27 November 2018. The helicopter’s clock had stopped at about 0756. The helicopter had impacted the ground on a downslope, in an easterly direction, and continued down the slope, producing debris as it struck rocks and trees, before crossing a dry creek bed. The helicopter came to rest on the far side of the creek bed, in a southerly direction, with the port side of the helicopter resting against the upslope of the far bank. The main rotor disc struck and separated the rear section of tailcone as a consequence of the accident sequence. Significant torsional deflection of the tail rotor driveshaft intermediate flexible coupling indicated that it was rotating when the strike occurred.
The ATSB found no pre-existing defect with the rotors, transmission, sprag clutch, drive belts or flight controls, which would have prevented normal operation. The main fuel tank had sufficient fuel for flight. A fuel test on site and at the point of departure did not identify any visual contaminates, including water. In addition, fuel samples were collected from the helicopter and departure point fuel pump, for future chemical analysis testing if required. The engine and a majority of the airframe was retrieved from the accident site and transported to Alice Springs. The engine was then removed from the wreckage and transported to Brisbane for further examination under the supervision of the ATSB. Several components and cockpit warning lamps were retained for examination.
Weather and terrain
The accident site was within the MacDonnell Ranges at an elevation of about 1,850 ft, 31 km east of Ambalindum Station. At the time of the accident the weather forecast included moderate turbulence throughout the area. At 0800 the Alice Springs Airport recorded a wind speed of 18 kt, with gusts to 29 kt, from 330 degrees, and a temperature of 29 °C. The Arltunga weather station, located about 40 km west of the accident site, recorded two observations each day. At 0800 it recorded a wind speed of 14 kt[3] from 360 degrees, and a temperature of 30 °C.
Engine tests and inspections
On 8 and 9 January 2019, inspections and tests were conducted on the recovered engine. Representatives from the workshop, Civil Aviation Safety Authority, insurance company and helicopter owner were present.[4] No fault was identified that would have prevented normal engine operation. Damage to the engine cooling fan and the presence of dirt inside the number 2 cylinder indicated the engine was operating at the time of initial impact. Scoring damage to the V-belt actuator was identified. The helicopter manufacturer advised the ATSB that the identified damage was consistent with the upper sheave rotating on contact with the actuator as the structure distorted on impact and that the actuator was in the extended position.[5]
Further investigation
To date, the ATSB has examined the wreckage, interviewed witnesses, consulted with the helicopter manufacturer and collected weather data and analysis from the Bureau of Meteorology.
The ATSB will conduct further enquiries into:
flight planning
the weight and balance of the helicopter
examination of individual components and warning lamps
analysis of data recording devices
pilot training and qualifications.
The information contained in this update is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this update.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the morning of 24 November 2018, the pilot and passenger of a Robinson R22 helicopter, registered VH-KZV, were tasked to assist with the recovery of a motor vehicle near Quartz Hill, located about 63 km east-north-east of Ambalindum Station (departure point), Northern Territory. They were also intending to visit some water bore sites.
After departing, they landed at one bore site before continuing towards Quartz Hill. Shortly after entering the MacDonnell Ranges, the helicopter collided with terrain on a downslope (125 km east-north-east of Alice Springs Airport). The pilot was fatally injured and the passenger received serious injuries. The helicopter was destroyed.
What the ATSB found
The ATSB found that the collision with terrain was very likely the result of the helicopter encountering a strong downdraft while low flying on the lee side of higher terrain in the MacDonnell Ranges. In addition, the ATSB identified a number of factors of increased risk.
Other factors of increased risk included that it was very likely the helicopter was overloaded and beyond the forward centre-of-gravity limit, which would have reduced the helicopter’s power margin and flight control available to the pilot. Secondly, there was moderate turbulence forecast at the time of the accident and the pilot did not check the weather forecast prior to departure. Thirdly, the pilot had an elevated level of alcohol in his system, which was capable of impairing his performance, and increased the likelihood of risk-taking behaviour and mishandling the helicopter in an emergency. Lastly, the helicopter’s emergency locator transmitter was selected ‘OFF’, disabling the automatic crash-activation of an emergency signal.
Safety message
It is important for all pilots to understand that flight planning and prescribed operating limits are safety barriers designed to provide a reasonable margin of safety. Thorough pre-flight planning is essential for avoiding hazardous weather conditions. It is not only important to obtain the relevant weather information to develop a mental picture of the conditions that may be encountered, but also to assess and understand how it relates to the planned flight.
Further, as the helicopter weight and balance has the potential to influence the handling characteristics, it is critical that the loading remains within the prescribed operating limits for the entire flight. Otherwise, as the safety margin steadily erodes, even an experienced pilot may not be able to recover from a rapidly developing unsafe condition.
At low altitude, there is a lower margin for error due to obstacle avoidance. Recognising the risks and hazards of low-level flying, it should be avoided when there is no operational requirement, even if a pilot has been trained and approved to conduct low-level operations. Further information is available from the ATSB publication: Avoidable Accidents No. 1 – Low-level flying.
This accident is also a reminder that blood-alcohol can persist the day after significant alcohol consumption, and the residual effects of alcohol may impair performance, especially in demanding situations.
The occurrence
On the morning of 24 November 2018, the pilot and passenger of a Robinson R22 helicopter, registered VH-KZV, were tasked to assist with the recovery of a motor vehicle near Quartz Hill, located about 63 km east-north-east of Ambalindum Station (departure point), Northern Territory. The pilot was employed by the Ambalindum cattle station for general flying duties, which included cattle mustering and inspecting water bore sites. As such, the pilot was also intending to visit some water bore sites.[1]
At about 0715 Central Standard Time,[2] the pilot refuelled the helicopter with the remaining contents of a fuel drum. A station-hand assisted with preparing the helicopter for departure, which included providing the pilot and passenger with a 20 L drum filled with diesel fuel. The station‑hand reported that this was stored at the passenger’s feet (tail rotor pedals position). He also reported that the weather appeared to be fine for the departure.
At 0732, the pilot’s global positioning system device was powered on while the helicopter was on the concrete helipad in front of the station homestead’s facilities. At 0737, the helicopter departed from the helipad and conducted an air transit to the worker’s accommodation block. The helicopter was on the ground next to the accommodation for 2.5 minutes before it departed from Ambalindum Station. The helicopter flew on a direct track at a height of between 500 and 1,000 ft across relatively open and flat terrain to a bore site, which was located near the boundary of the more rugged terrain of the MacDonnell Ranges.
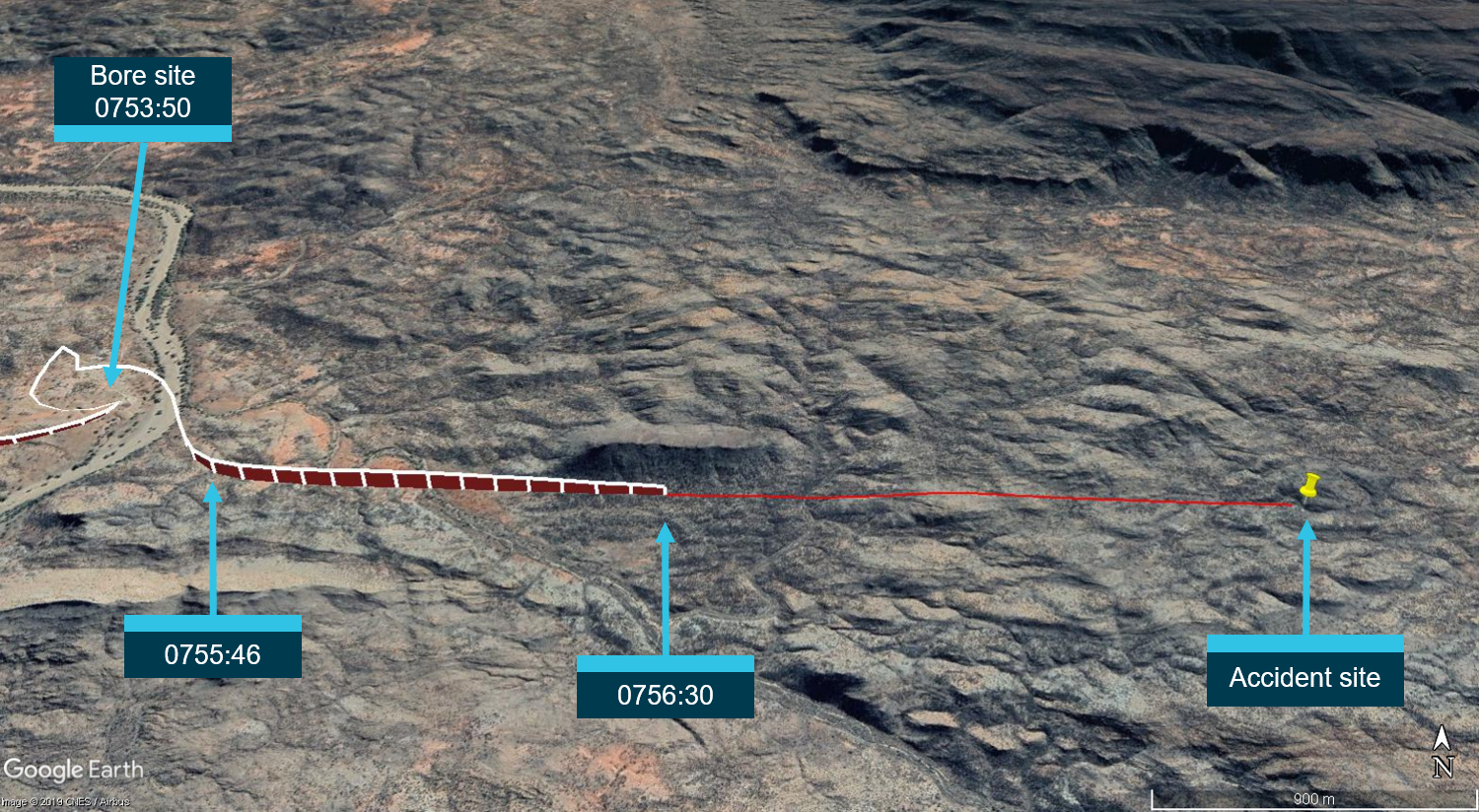
The pilot and passenger stopped at the bore site[3] for 2 minutes and departed at 0753:50. On departure, the helicopter was levelled off at about 150 ft above ground level, which was below the peaks of the surrounding terrain as it tracked into the MacDonnell Ranges. The last recorded data point was at 0756:30, at which time the helicopter was about 142 ft above ground level with a ground speed of 79 kt. About 56 seconds later (based on the ground speed), the helicopter collided with terrain.
The passenger could not recall any details of the flight, but remembered activating the pilot’s Spot Tracker[4] device after the accident. At 0811, it transmitted its location in SOS mode. A helicopter company in Alice Springs was tasked by the Australian Maritime Safety Authority’s Joint Rescue Coordination Centre (JRCC) to transport a paramedic to the location and attempt a search and rescue (SAR). Ambalindum Station, which was also notified of the activation of the Spot Tracker device, dispatched two employees, the general manager and a station-hand, by road to investigate.
The SAR pilot located the helicopter wreckage at the reported location (Figure 1) and dropped the paramedic nearby to attend to the accident pilot and passenger. The SAR pilot then ferried the two station employees to the accident site. At about 1040, the paramedic found the pilot fatally injured and the passenger seriously injured. The SAR pilot and paramedic, with the assistance of the station employees, retrieved the passenger and transported him to Ambalindum Station for treatment by a retrieval doctor, before moving him to Alice Springs Hospital for further medical attention. The helicopter was destroyed.
The pilot was issued with a Private Pilot Licence (Helicopter) on 10 June 2014 with an endorsement for the Robinson R22 helicopter (R22) under the Civil Aviation Regulations 1988 Part 5 (CAR 5) licencing system. He held a Class 2 aviation medical certificate with an expiration date of 2 February 2020, with the restriction of ‘Reading Correction to be available whilst exercising the privileges of his licence’. His last flight review was completed in February 2018.
On his employment application letter to Ambalindum Station in January 2018, the pilot reported having a total flying experience of 10,000 hours in gyrocopters, 350 hours in the (amateur-built) Cicaré CH-7 helicopter and 800 hours in the R22. At the time of his last medical examination in February 2018, he reported having accrued 800 flying hours. The pilot’s personal diary indicated he had accumulated about 470.5 hours in his current job, which suggested he had about 1,270 hours in the R22.
Validity of qualifications
On 1 September 2014, the Civil Aviation Safety Regulations 1998, Part 61 pilot licencing system was introduced to replace the CAR 5 system. Part 61 included licencing, ratings and endorsements, and provided pilots with a 4‑year period to transfer a CAR 5 licence to a Part 61 licence. In the period 27–29 October 2014, the pilot received low-level and aerial mustering flying training, with an endorsement made by the approved training officer in the pilot’s logbook and on a copy of Appendix II to Civil Aviation Order (CAO) 29.10 (2006): Air service operations – aircraft engaged in aerial stock mustering operations – low flying permission.
On 3 December 2014, the Civil Aviation Safety Authority (CASA) issued the pilot with an approval to conduct aerial stock mustering operations in helicopters under CAO 29.10 subparagraph 6(a). However, subsection 6 of this order was amended on 1 September 2014 by Civil Aviation Order (Flight Crew Licencing) Repeal and Amendment Instrument 2014 (No. 1). The amendment stated that ‘A pilot must not engage in aerial mustering operation unless the pilot is authorised under Part 61 of the Civil Aviation Safety Regulations 1998 to conduct an aerial mustering operation in that kind of aircraft’. Therefore, an approval under CAO 29.10 could no longer be granted. The equivalent authorisation under Part 61 was a low-level rating and mustering endorsement, in accordance with the Part 61 Manual of standards.
During the transition period, the pilot made an application for a Part 61 licence, but with evidence of a mustering endorsement conducted after 1 September 2014 in accordance with CAO 29.10, rather than the Part 61 Manual of standards. Therefore, his Part 61 licence was not issued and he was advised by CASA to resubmit his application with completed forms 61-2I: Notification of issue of CASR Part 61 Operational Rating, and 61-1507: Low-level rating flight test. Completed copies of these forms were required to provide evidence that his CAO 29.10 training complied with the Part 61 Manual of standards requirements for a low-level rating and mustering endorsement. However, CASA did not receive a copy of these forms and never issued the pilot with a Part 61 licence. The pilot was required to hold a Part 61 licence from 1 September 2018 for his licence to be valid.
72-hour history
The pilot’s diary indicated that the accident occurred on his third day of work after 5 days leave. There were no flying hours recorded 2 days prior to the accident, but there was an entry of ‘Chopper going…4 hours’ the day prior to the accident, which suggested this was flight time. There was no indication from his diary or from his colleagues that he was working excessive hours in the week prior to the accident.
The evening prior to the accident, the pilot and station-hands had a ‘few’ alcoholic drinks before and after dinner, and then retired to their private rooms. The evening drinks were reported to be a normal habit and that nothing unusual occurred.
Helicopter information
General description
The helicopter was a two-seat Robinson R22 Beta 2 powered by a Textron Lycoming 4-cylinder O-360-J2A engine. It was manufactured in the United States in January 2010 and registered in Australia in February 2010. It was acquired by the owners on 2 August 2018.
Drive system
The engine has a V-belt sheave bolted directly to its output shaft. V-belts transmit power to the upper sheave, which has an overrunning clutch contained in its hub. The inner shaft of the clutch transmits power forward to the main gearbox, which drives the main rotors, and aft to the tail gearbox, which drives the tail rotors. Flexible couplings are located at the main gearbox input and at each end of the tail rotor drive shaft.
The V-belts are tensioned for flight after engine start by raising the upper sheave. An electric actuator, located between the drive sheaves, raises the upper sheave when the pilot engages the clutch switch. The actuator senses belt tension and automatically switches off when the V-belts are properly tensioned.
Fuel system
The helicopter was fitted with two fuel tanks, a main and an auxiliary, located behind the main rotor mast. Total usable capacity is 100 L (main – 64 L, auxiliary – 36 L). The auxiliary tank is interconnected with the main tank and with its base elevated relative to the base of the main tank, so that the auxiliary will empty first.
Maintenance
The helicopter was issued with its last maintenance release[5] on 12 October 2018, when it completed its last 100-hourly inspection, with 7,000 hours’ time-in-service. Additional work during the 100-hour inspection included replacing the number 1 cylinder, two tail rotor pitch change levers and re-rigging the main rotor flight controls. The maintenance organisation reported that the helicopter had completed four 100-hourly inspections since the last 2,200-hour major overhaul. The organisation’s licenced aircraft maintenance engineer (LAME) had completed the last two of those four inspections (since it was acquired by the new owners) and indicated that the helicopter was overall in good condition.
On 23 November 2018, the day before the accident, the LAME[6] went to Quartz Hill to replace the electric actuator fitted to the helicopter. The actuator and V-belts were replaced, followed by a cooling fan balance. No maintenance release was provided to record the work, but the pilot reported to the LAME that the helicopter had accumulated about 15 hours since the last 100‑hourly inspection. The LAME returned to Alice Springs with the understanding that the pilot would phone that evening with the actual hours but did not hear from him.
Meteorological information
When transporting the passenger from the accident site to Ambalindum Station, the SAR pilot asked him what happened. Neither the SAR pilot nor the paramedic were certain of the passenger’s reply and the passenger had no recollection of the conversation. However, the paramedic recalled words to the effect that the ‘wind lifted them up’, that the pilot had said to him (passenger) ‘look at this [expletive]’, ‘and we were lifted up in the air’. The SAR pilot recalled the passenger indicated that the accident pilot had told him they ‘better pull-up to get a bit more height/air to make it safer’.
Planning
The station homestead had a local Wi-Fi network, so that the workforce could use their personal electronic devices, and computers located in the office area. The general manager for the company, who was at the station at the time, reported that the office computers were for management staff and not a common access area. The pilot would have been granted access to use them for flight planning purposes, but he had not requested access and the manager was not aware of him ever using them. The ATSB reviewed the pilot’s iPad and iPhone. A review of applications and browsing history on the iPad and iPhone found no evidence that either was used to access any aviation-related applications or aviation-related services (such as the Bureau of Meteorology) on either the day of, or day prior, to the accident. However, both were in use in the week of the accident.
Weather forecast
The Bureau of Meteorology graphical area forecasts valid between 0230 and 1430 on 24 November included moderate turbulence below 7,000 ft above mean sea level throughout the area. The aerodrome forecast for Alice Springs Airport[7] (about 125 km east-north-east of the accident site), issued at 0249 and valid from 0330 24 November to 0330 25 November, reported CAVOK[8] conditions, but with a wind of 18 kt, gusting to 28 kt, from 320°. In addition, the remarks included moderate turbulence below 5,000 ft above mean sea level from 0630.
Reported weather conditions
On 24 November, the recorded aerodrome weather report for Alice Springs Airport between 0600 and 0730 indicated a wind direction of 330–340° at about 15 kt. However, at 0758, SPECI[9] conditions were recorded with a wind speed of 18 kt, gusting to 29 kt. The Arltunga weather station, located about 40 km east of the accident site, recorded a wind speed of 14 kt[10] from a direction of 360°, QNH 1015 hPa[11] and a temperature of 30 °C, at 0800.[12] The Ambalindum Station personnel interviewed by the ATSB reported that the weather was fine and clear in the morning at the station.
The SAR pilot reported that engine start in his Bell 206 at Alice Springs Airport was at 0940. He reported that the weather was turbulent all the way out to the accident site, and estimated it was moderate to severe in the ranges with a wind speed of 20 kt, gusting to 40 kt. He reported that, on arrival at the accident site he encountered a strong downdraft at about 100 ft above ground level.
The SAR pilot also stated that he took three approaches to land due to the turbulence at the accident site with the paramedic but could not remember what occurred when he subsequently ferried the station‑hand and general manager into the site. The paramedic recalled only one approach to land, but the station-hand recalled they took three approaches to land, that the helicopter was being thrown around and that the SAR pilot had warned him about downdrafts. The general manager recalled they took one approach but was aware that the pilot was concerned about the flying conditions.
The station-hand recalled that, while on the ground at the accident site, he felt the wind tunnelling down the ravine. He reported that it was cycling from ‘nothing, to heavy wind to slight breeze, then nothing’. In consideration of the weather forecast and reports, the ATSB requested analysis from the Bureau of Meteorology for the likelihood of mountain or lee wave activity in the area at the time of the accident.
Bureau of Meteorology analysis
The Bureau of Meteorology reported the following:
The mean sea level pressure chart for the morning of the accident showed a deep trough and low-pressure system moving into the central and southern parts of the Northern Territory from Western Australia. Conditions ahead of the trough saw moderate to fresh north-east to north-west winds. The synoptic pattern was conducive to moderate turbulence, and, particularly after sunrise, gusty and turbulent flow was anticipated as the stronger winds from aloft mixed to the surface.
At the ridge-top level of the ranges north of Alice Springs, approximately 2,000 ft to 4,000 ft above mean sea level, the winds observed at 0830 on 24 November were 25 kt. The strong north to north-west winds, being perpendicular to the ranges, were conducive to mechanical turbulence, especially in the lee of the ranges. The height of the ridge being over 1,000 ft, and the strength of the winds perpendicular to the ridge being over 25 kt, indicated the necessary requirements for the occurrence of mountain waves.
The aerological diagram showed the wind strength increasing with height above the height of the ridge, as well as instability in the atmosphere above ridge-top level. However, no evidence was found for mountain waves in the cloud patterns observed on the satellite imagery. Therefore, the occurrence of mountain waves remained inconclusive.
The breaking of an inversion layer can also be associated with moderate turbulence. The onset of gusty conditions at Alice Springs Airport at 0758 indicated the overnight inversion would have broken by then, with stronger winds aloft mixing down. Broadscale moderate turbulence was especially likely at that time.
Terrain-induced turbulence
According to the United States Federal Aviation Administration (2016) Pilot’s handbook of aeronautical knowledge, ground topography can break up the flow of the wind and create wind gusts that change rapidly in direction and speed. While the wind may flow smoothly up the windward side of higher terrain, on the leeward side it attempts to follow the contour of the terrain and is increasingly turbulent. The stronger the wind, the greater the downward pressure and turbulence. The downdrafts can be severe in valleys due to the effect of the terrain. Hence, it is recommended to avoid flying in this area when strong winds are present or likely to occur. Figure 2 depicts the potential wind conditions on the lee (right) side of terrain.
Figure 2: Potential wind conditions on the lee side of terrain
Source: Federal Aviation Administration (2012)
Recorded information
The ATSB examined the pilot’s iPad, iPhone, GoPro camera and GPS devices. There was no evidence that the iPhone was in use at the time of the accident and no location data was available to create a flight path.[13]
Global positioning system data
Data was recovered from the pilot’s GPS device. The flight profile on the day before the accident (23 November) revealed the pilot had been flying back-and-forth along a dry riverbed at low‑level (below 200 ft) near Quartz Hill. The helicopter then tracked back‑and‑forth between Quartz Hill and Ambalindum Station. The last sector recorded an arrival time at Ambalindum Station helipad of 1815.
For the accident flight, the first recorded data point was from the helipad at 0732 (Figure 3).[14] After transiting to the workers’ accommodation block, the helicopter departed at 0740 for the bore site.
Figure 3: Departure from the homestead
Source: Google earth, annotated by the ATSB
Figure 4 shows that, about 2 minutes after taking off from the bore site, at 0755:46, the helicopter was levelled off at about 150 ft above ground level and then entered the MacDonnell Ranges. The final data point, recorded at 0756:30, was located at a height of about 142 ft, with a ground speed of 79 kt,[15] on a direct track towards the accident site. Based on this ground speed, the ATSB estimated that the time between the last data point and the accident site was 56 seconds.
Figure 4: GPS track from the bore site to the accident site
Source: Google earth, annotated by the ATSB
GoPro data
The GoPro camera did not hold a recording of the accident flight. However, a total of 69 videos and 25 images were recovered, dated from 1 January 2012 to 15 June 2016. The time and date of the GoPro can be set manually or by Wi-Fi. It could not be determined if the recorded dates were correct, but the files included videos of the accident pilot flying an R22 from a different operator. It was therefore likely that the files were from his previous employment.
The video files showed the pilot engaged in low flying and cattle mustering activities throughout the time period. They included low-level contour flying between mustering tasks, along a river and along a dry riverbed (see Figure 5 example). Mustering videos included manoeuvring the R22 at up to 50° angle of bank with indeterminable pitch changes, coupled with skidding or side-slipping[16] within about 1–2 rotor diameters of the ground.
Figure 5: Example of low flying in previous employment
Source: ATSB
Wreckage and impact information
Accident site
The accident site was in the MacDonnell Ranges at an elevation of about 1,850 ft, 31 km east of Ambalindum Station. The helicopter impacted the ground on a downslope, in an easterly direction, and continued down the slope. It then came to rest on the far side of the riverbed in a southerly direction, with the left side resting against the upslope of the far bank.
The ATSB noted there was higher terrain, orientated east-west, immediately to the north of the initial point of impact. This was the reported direction for the prevailing wind at the time of the accident.
Impact sequence
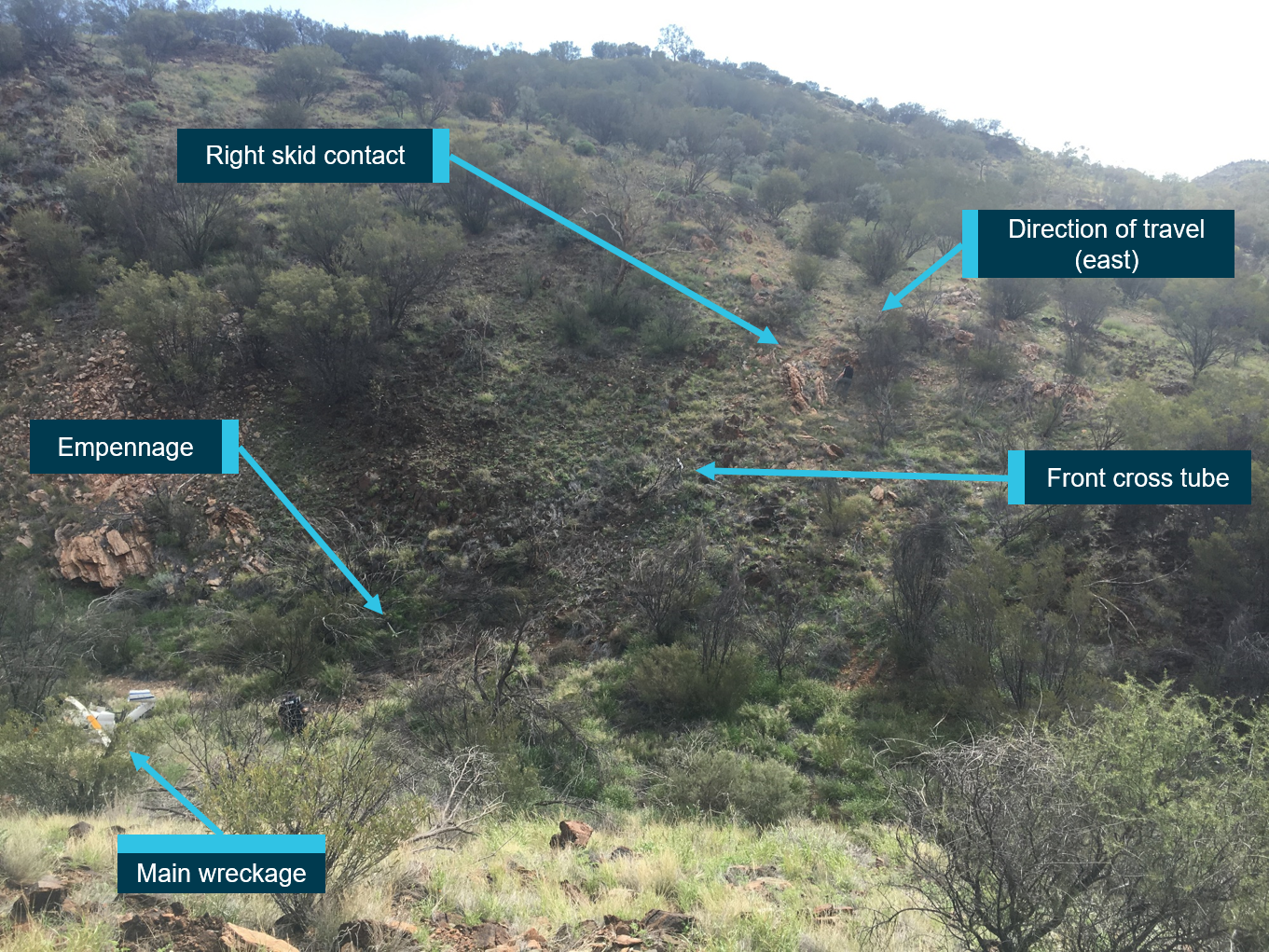
The impact sequence started with the main rotor severing the upper branches of a small tree, indicating 10–15° right bank, before the tail stinger struck a rock and was separated from the tailcone. A tail rotor blade then separated after impacting a tree branch at about the same time as the right skid contacted the ground adjacent to protruding rocks (Figure 6), which were struck by the underside of the helicopter. About half way down the slope the helicopter passed through a tree, which fragmented the cabin plexiglass and removed the front landing skid cross-tube.
Just prior to crossing the riverbed, the main rotor disc struck and separated the tail rotor driveshaft and empennage from the airframe. The empennage was located just prior to crossing the riverbed, to the right of the accident path. The driveshaft was found on the far side of the riverbed to the right of the accident path and beyond the main wreckage.
Figure 6: Impact sequence
Source: Alice Springs Helicopters, annotated by the ATSB
Wreckage examination
The helicopter’s clock had stopped at about 0756 and the engine hour-meter indicated 6,893.36 hours. The helicopter was fitted with an impact activated emergency locator transmitter (ELT), which was found selected to the ‘OFF’ position.[17] In addition to the pilot and passenger, the helicopter was loaded with:
a double-barrelled shotgun and bolt action rifle with ammunition
two six-packs of beer (no evidence that any were consumed)
empty 20 L drum (perforated, but strong diesel fuel odour)
empty 10 L water container (used for testing water flow rate at bore sites)
bore test equipment (data logger)
two webbing straps and a bag of lifting equipment
between one-third and two-thirds fuel contents in the main fuel tank and unusable fuel in the auxiliary fuel tank.[18]
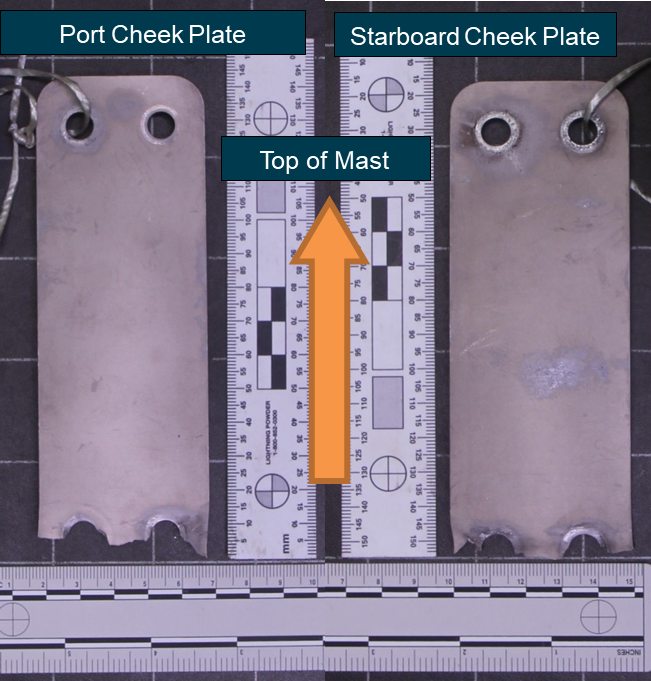
The ATSB found no pre-existing defects with the rotors, drivetrain or flight controls, which would have prevented normal operation. The tail rotor driveshaft was folded by the main rotor strike. It was also noted to have been pulled apart at the intermediate and aft flex couplings (Figure 7). This indicated a loss of energy from the main rotor system occurred at some time prior to the main rotor striking the tailcone.[19] A fuel test on-site and at the point of departure did not identify any visual contaminates or water.
Figure 7: Tail rotor driveshaft
Source: ATSB
The engine and a majority of the airframe was retrieved from the accident site and transported to Alice Springs Airport where further inspections of the drivetrain and engine components were performed. No pre-existing defects were found to prevent normal operation. The engine was then removed from the wreckage and transported to Brisbane for further examination under the supervision of the ATSB.
Engine tests and inspections
On 8 and 9 January 2019, tests and inspections were conducted on the recovered engine. No fault was identified that would have prevented normal operation of the engine. Damage to the engine-cooling fan and the presence of dirt inside the number 2 cylinder indicated the engine was operating at the time of initial impact.
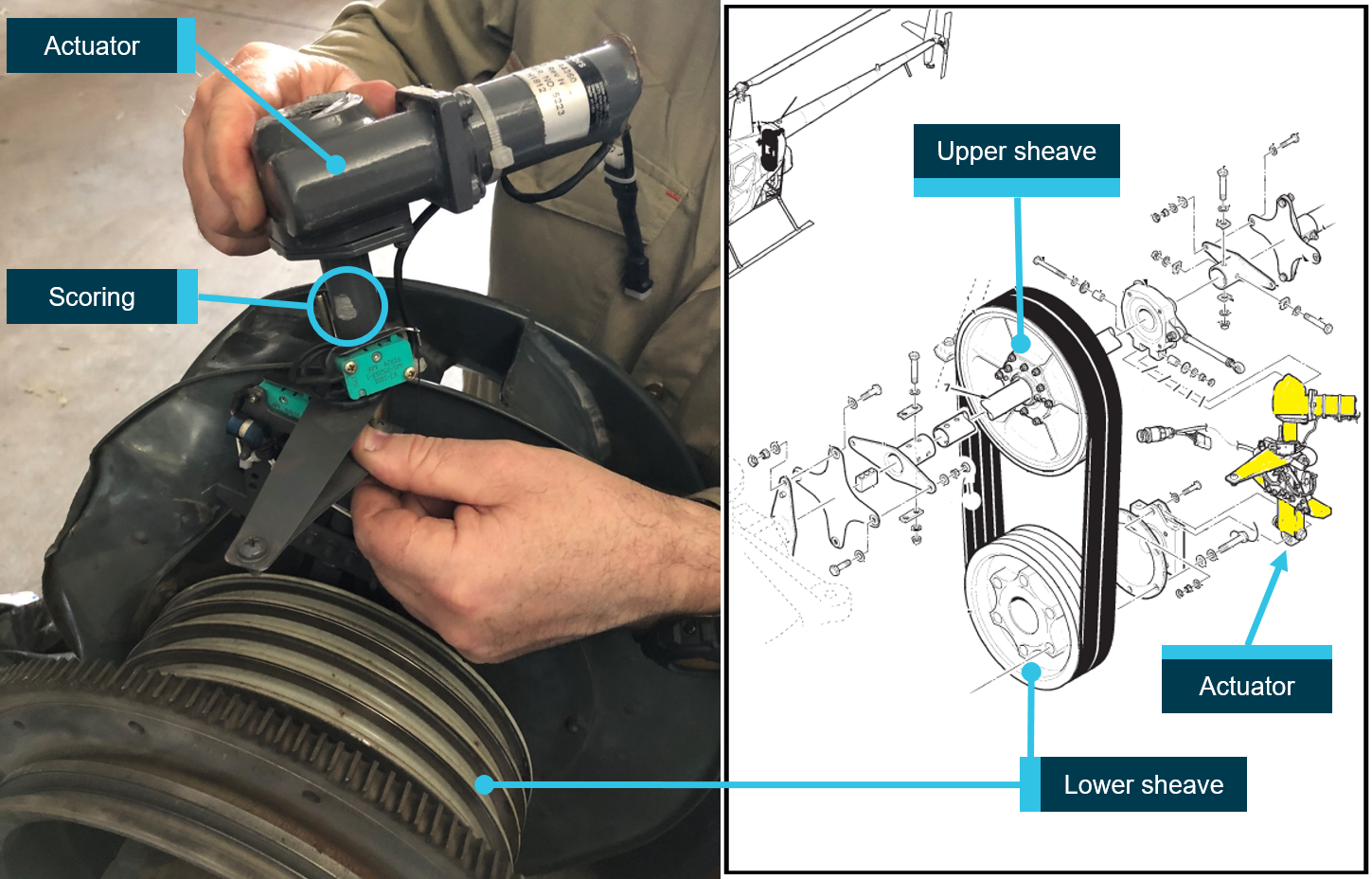
The V-belts were found intact and scoring damage to the V-belt actuator was identified. Robinson advised the ATSB that the length of the actuator indicated it was extended in the normal position for flight and that the scoring was consistent with the upper sheave rotating on contact with the actuator as the helicopter’s structure distorted on impact (Figure 8). This indicated that the engine was driving the V-belts and upper sheave at impact.
Figure 8: Scoring to the clutch actuator
Source: ATSB
The lower third section of the engine-cooling fan exhibited ‘gathering’ of metal in the direction of fan rotation. This suggested that the engine was producing power at the time of impact. The exhaust was crushed and the carburettor throttle arm bent, resulting in the throttle butterfly valve being forced towards the full closed position. It was concluded that the damage to the engine components likely resulted in engine stoppage shortly after the initial ground impact.
Medical and pathological information
A post-mortem examination was conducted on the pilot at Royal Darwin Hospital. The forensic pathologist concluded that the pilot received multiple injuries, sustained during the impact sequence, which resulted in his fatality. A sample of bloodstained chest cavity fluid and urine contents were submitted for toxicological analysis.
The pilot’s toxicology results included 0.20 per cent alcohol detected in the bloodstained chest cavity fluid and 0.14 per cent alcohol detected in the urine. The forensic pathologist confirmed that the bladder was intact, but that fermentation with microbiologically generated alcohol might be an issue as decomposition had started.[20] Therefore, he advised seeking assistance from a subject matter expert for interpretation of the alcohol results. The ATSB consulted with the forensic scientist who conducted the toxicology, and engaged a forensic and aviation pathology consultant.
The forensic scientist reported that during their routine screen of the chest cavity fluid, they noted the presence of a number of compounds that are typically indicative of decomposition. She reported that alcohol can be produced during decomposition, ‘however the high alcohol levels observed for this case (especially in the urine, which is typically less prone to post-mortem alcohol production) don’t appear to suggest extensive post-mortem production of alcohol’.
The consultant reviewed the material, including the correspondence with the forensic pathologist and forensic scientist, and provided an interpretation for the alcohol results. She reported that, for the bloodstained chest cavity fluid, ‘the possibility that some of this level is not the result of ethanol [alcohol] ingestion prior to death but the result of decomposition changes in the blood occurring after death, exists. It is however, still a significant level… Urine is less susceptible to the effects of decomposition than blood and chest fluid, particularly in the absence of injury [intact bladder] suggesting that the finding is a significant indicator of ingested alcohol’.
According to the consultant, blood alcohol levels greater than 0.05 per cent have the effect of lowering caution, worsening of judgement and reasoning. Higher levels of around 0.1 per cent may affect these more and impair coordination and reaction time. Blood alcohol levels generally decrease at a rate of 0.01 per cent per hour. If the pilot was drinking heavily the evening prior to the accident flight, his blood alcohol level could still have been elevated during the flight such as to affect his piloting performance. It is possible that heavy drinkers may develop some tolerance to the effects of alcohol.
The consultant concluded that the time required to retrieve the pilot resulted in sub‑optimal collection of specimens on which to perform the analysis. Both samples showed the presence of considerable amounts of alcohol, but the precise level of blood alcohol could not be ascertained. However, given the measured levels and degree of decomposition [early stages], ‘it is highly likely that alcohol was present in blood at a level capable of impairing pilot performance’.
Survival aspects
The accident occurred at about 0757 at a remote location. The main rotor tree strike, and ground impact marks, suggested the initial impact was in a relatively level attitude and survivable. However, about half way downslope, the helicopter passed through a tree, resulting in the fragmentation of the plexiglass and separation of the landing skid front cross‑tube from the airframe, which compromised the liveable space of the cabin. This exposed the pilot and passenger to multiple injuries as the helicopter continued on its trajectory over rocky terrain and across a dry riverbed, before coming to rest upslope on the far side.
The pilot and passenger seats were both fitted with lap and shoulder restraints (three-point lap‑sash seatbelts). The seat harnesses were found in various conditions. The pilot’s shoulder harness was cut away by first responders and his lap belt was found unbuckled. The passenger’s lap strap had completely pulled through its clasp, leaving the clasp inside the buckle without a strap attached. The occupants were not wearing helmets and both were found with head injuries.
Emergency locator transmitter
The helicopter was fitted with an ELT in the transmission bay area, above the horizontal firewall. The ELT had a protected 3-position toggle switch. The three selections were OFF, ARM and ON. The ELT was found by the ATSB to be in the OFF position. Therefore, it could only be activated by an individual accessing the device and selecting it to the ON position. The passenger reported that he was intermittently conscious following the accident and that the pilot did not regain consciousness.
In the ARM position, the ELT will automatically activate if the deceleration is sufficient in magnitude and direction. The examination of the accident site did not indicate that the helicopter was subject to either a high vertical or horizontal deceleration. In 2013, the ATSB published a review of the effectiveness of ELTs in aviation accidents, and found that even in a high deceleration impact they only activated 40–60 per cent of the time in the ARM mode.
Search and rescue sequence
Ambalindum Station staff were provided with a Spot Tracker device. The Spot Tracker is a personal tracking device, which sends a GPS location signal at a set time interval. In addition to the routine signal, the device has a button for an SOS signal to provide an alert for emergency assistance. The pilot was carrying his device on the flight, but the passenger was not. The passenger could not recall why he did not have his device. However, at about 0811, the passenger was able to activate the pilot’s Spot Tracker in SOS mode.
The Spot Tracker service contacted the station owners and the JRCC. The SAR pilot was contacted by the station owners and then by the JRCC who also activated the paramedic. The paramedic met the SAR pilot at their Alice Springs Airport hangar.
The SAR pilot achieved engine start at 0940, and the paramedic arrived at the scene of the accident at about 1040, while the SAR pilot was ferrying the station personnel to the site.
The station-hand and general manager were left at the site while the pilot ferried the paramedic and passenger to Ambalindum Station, where a trauma doctor was waiting. Weather storm cells started to develop after arrival at Ambalindum Station and at 1350, the SAR pilot ferried the trauma doctor with the passenger to Alice Springs. His triage at Alice Springs Hospital was recorded as occurring at 1500.
Helicopter performance
The ATSB used the Arltunga weather station to calculate the accident site pressure altitude and density altitude, which were 1,796 ft and 4,000 ft respectively. According to the R22 Pilot’s operating handbook (POH), the helicopter was capable of producing at least maximum continuous power, and likely take-off power, under these conditions.
Weight and balance
The published maximum all-up-weight limit for the R22 was 622 kg.[21] However, there was no record of how much fuel was on board at departure and the fuel contents at the accident site was based on visual estimates. Therefore, the ATSB calculated the weight and balance progressively from full main tank contents to empty main tank contents. The calculations included the pilot and passenger’s weights, 20 L of diesel fuel at the passenger’s tail rotor pedals position, and 20 kg for the additional articles.
The results provided in Table 1 indicated that at full main tank fuel, the helicopter’s operating weight was above the limit for maximum all-up-weight, and the centre-of-gravity (‘Arm’) was beyond the forward limit. At the reduced fuel load of 1/3–2/3 main tank fuel observed at the accident site, the helicopter’s operating weight was still above the maximum all-up-weight and the centre-of-gravity was further forward of the forward limit.
A negative weight margin indicates a higher weight than the maximum all-up-weight, and a negative arm indicates a centre-of-gravity position forward of the forward limit. The range of the centre-of-gravity was 160 mm from the aft limit to the forward limit.
Table 1: Weight and balance
Main tank contents
All-up-weight (kg)
Weight margin (kg)
Arm (mm)
Full
659
-37
-37.7
Two-thirds
643
-21
-46.2
One-third
626
-4
-48.2
Empty
613
9
-55.9
The high all-up-weight of the helicopter would result in a high power requirement under normal flight conditions. This would have reduced the power margin available for contingency situations, such as an emergency climb. As stated in the United States Federal Aviation Administration (2012) Helicopter flying handbook ‘Excessive weight reduces the flight performance in almost every respect’.
Robinson had published a caution in the R22 POH for loading the helicopter near the forward centre-of-gravity limit, as follows:
CAUTION: Fuel burn causes the CG [centre-of-gravity] to move forward during flight. Always determine safe loading with empty fuel as well as with takeoff fuel. Payload may be limited by forward CG as fuel is burned.
The caution provided by Robinson was consistent with the advice published by the United States Federal Aviation Administration in their Helicopter flying handbook, which provided the following information for a centre-of-gravity forward of the forward limit:
A forward CG may occur when a heavy pilot and passenger take off without baggage or proper ballast located aft of the rotor mast. This situation becomes worse if the fuel tanks are located aft of the rotor mast because as fuel burns the CG continues to shift forward.
The handbook further indicated that the position of the centre of gravity will influence the handling characteristics of the helicopter. The fuselage acts as a pendulum suspended from the rotor, and when the centre of gravity is directly under the rotor mast, the fuselage should remain horizontal. If the centre of gravity is beyond the forward limit, the nose of the helicopter will tilt down. Consequently, a pilot would have to apply aft cyclic control to raise the nose and balance the helicopter. However, as fuel is consumed and the centre of gravity continues to move forward, a pilot could rapidly lose rearward cyclic control. In this condition:
A pilot may also find it impossible to decelerate sufficiently to bring the helicopter to a stop. In the event of engine failure and the resulting autorotation, there may not be enough cyclic control to flare properly for the landing.
The GPS data indicated the pilot flew the approach and departure to the bore site, just prior to the accident, in a northerly direction, which was into wind. In a headwind, the forward centre-of-gravity may be less noticeable to the pilot as the cyclic is displaced forward of the nil wind position, thereby providing a greater aft cyclic range than in a nil wind or tail wind condition.
Strong winds and turbulence
Robinson has published a safety notice (SN-32) in the R22 POH on the subject of flight in strong winds or turbulence.[22] The safety notice included the following information:
Flying in high winds and turbulence should be avoided. If turbulence is encountered, the following procedures are recommended:
1. Reduce power and use a slower than normal cruise speed. Mast bumping is less likely at lower airspeeds.
2. For significant turbulence, reduce airspeed to 60–70 knots.
3. Tighten seat belt and rest right forearm on right leg to minimize unintentional control inputs. Some pilots may choose to apply a small amount of cyclic friction to further minimize unintentional inputs.
4. Do not overcontrol. Allow aircraft to go with the turbulence, then restore level flight with smooth, gentle control inputs. Momentary airspeed, heading, altitude, and RPM excursions are to be expected.
5. Avoid flying on the downwind side of hills, ridges, or tall buildings where turbulence will likely be most severe.
Employment of the pilot
In early 2018, the pilot was employed by Hewitt Cattle Australia, the owners of Ambalindum Station and the accident helicopter, in accordance with their recruitment process. This included the pilot’s submission of a résumé with referee details and relevant aviation qualification documents. The documents included a copy of his CAR 5 private pilot licence, dated 10 June 2014, and a copy of his CAO 29.10 Appendix II and log book endorsements for low flying and mustering training, dated 29 October 2015. It was agreed that the pilot’s completion of a flight review would satisfy the employer’s requirements.
The pilot’s application was vetted by his prospective employer and their insurance company. This included a check of his log book to verify he had completed the flight review as agreed. Although the pilot did not hold a commercial licence, CASA confirmed that aerial mustering may be conducted as a private operation over land occupied by the owner of the aircraft with the appropriate licence, rating and endorsement.
At the time, the pilot submitted his documents to his prospective employer, his CAR 5 licence was still valid and there was about 7 months remaining until the end of the transition period to the Part 61 licence. It was considered unlikely that the discrepancy associated with his low flying and mustering training would have been identified by anyone who did not have an intimate knowledge of the Part 61 licencing system.
While flying in the MacDonnell Ranges, Northern Territory, VH-KZV collided with terrain on a downslope. The pilot was fatally injured and the passenger received serious injuries. The helicopter was substantially damaged. The time of the accident was within a period of a weather forecast for moderate turbulence in the area.
The on-site wreckage examination and additional testing of the engine found no evidence of a pre‑existing defect to prevent normal operation of the helicopter. Therefore, it was almost certain that the engine was operating and driving the rotors at initial impact.
This analysis will discuss the pilot’s flight planning and loading of the helicopter, the likelihood that his performance was impaired by alcohol, and the operational state of the helicopter’s emergency locator transmitter (ELT).
Collision with terrain
The pilot’s global positioning system device track data, recovered from the accident site, indicated the helicopter levelled-off at about 150 ft above ground level on entry to the MacDonnell Ranges. This flight profile was maintained to the last recorded data point (less than 1 minute before the accident) at which stage the helicopter was about 142 ft above terrain. On review of the track data for the previous day, and GoPro camera footage of previous work experience, the pilot appeared to have a habit of manoeuvring his helicopter to contour fly along dry riverbeds. The helicopter’s track from the bore site was towards rugged terrain with dry riverbeds and not a direct track towards their destination of Quartz Hill. Therefore, it was very likely the pilot was operating the helicopter at low-level and possibly engaged in contour flying, just prior to the accident.
The meteorological conditions at the time of departure were reported as fine, but moderate turbulence was forecast for the period of the accident flight. The final track of the helicopter placed its path on the lee side of higher ground for the prevailing winds. At about that time there was a change in weather conditions recorded at Alice Springs Airport, indicating stronger winds aloft were mixing with the surface winds. The Bureau of Meteorology’s analysis indicated that these winds could have generated at least moderate mechanical turbulence, with the potential for strong downdrafts in the lee of higher terrain. This was consistent with what was experienced by the search and rescue pilot on arrival at the scene of the accident site and suggestive of the comments made by the passenger during his retrieval.
In consideration of the track data, meteorological conditions, accident site and wreckage, it was likely the helicopter encountered a downdraft when low flying in the MacDonnell Ranges with insufficient height to recover, resulting in the collision with terrain.
Flight planning
Ambalindum Station was equipped with an office and computers that had internet access. However, the employer’s general manager reported that the pilot did not use, or request to use, the office computers for flight planning. Further, the ATSB found no evidence on either the pilot’s iPad or iPhone to indicate he had accessed any flight planning data in preparation for the accident flight.
Consequently, the pilot was most likely unaware of the forecast conditions of moderate turbulence and strong winds for his area of operation. Prior knowledge of potentially hazardous meteorological conditions at low-level may have resulted in him selecting an alternate flight path and/or higher altitude to mitigate the associated risks.
Helicopter performance
ATSB calculations of the loading of the helicopter indicated it was likely overweight, with a centre‑of-gravity beyond the forward limit, for the entire accident flight. However, the performance charts in the pilot’s operating handbook did not provide results beyond the published limits, and therefore, the performance of the helicopter under the actual conditions could not be determined.
The engine was capable of producing sufficient power for normal flight in the overloaded condition, which was evidenced by the fact that the helicopter had taken off and had been flying for about 20 minutes. However, a downdraft would increase the power required if the pilot attempted to recover lost height during an uncommanded descent. In this situation, the power required by the rotors could rapidly exceed the power available from the engine, resulting in a loss of power margin and a forced descent.
The location of the fuel tanks, behind the main rotor mast, meant that the centre-of-gravity would move forward in-flight as fuel was consumed. This would reduce the range of aft cyclic movement available to the pilot, used to flare and decelerate the helicopter. The into-wind approach and departure, flown to the bore site just prior to the accident, likely increased the available aft cyclic range compared with a nil wind or tail wind condition. Therefore, the pilot may not have been aware of the reduction in aft cyclic control that had already occurred.
After departure from the bore site, the helicopter’s track towards the accident site resulted in a wind direction from the left rear quarter (left of the nose between 90–130°). Any rearward component of wind, combined with a reduction of aft cyclic control, would have severely compromised the ability of the pilot to reduce the forward speed of the helicopter.
It was possible that the downdraft would have exceeded the capability of the helicopter loaded within the prescribed limits. However, without knowledge of the actual direction and strength of the downdraft encountered, it could not be determined if the overloaded condition and forward centre‑of-gravity contributed to the collision with terrain. Despite this, if hazardous weather was encountered at low-level, the combination of a reduced power margin and aft cyclic control would reduce the response available, thereby increasing the risk of a collision with terrain.
Impaired pilot performance
Research conducted for the ATSB (Newman, 2004) into alcohol and human performance highlighted that:
In simple terms, alcohol impairs human performance…
It has detrimental effects on cognitive functions and psychomotor abilities. Risk taking behaviour may result, and a full appreciation of the consequences of a planned action may not be possible… Adverse effects can also persist the day after alcohol ingestion, with reductions in alertness, concentration and vestibule-ocular function, and increases in anxiety all being reported…
Alcohol has been shown to impair registration, recall, and organisation of information, leading to increased reaction times and/or a greater number of errors…
…performance has also been found to suffer most when an unexpected or unanticipated event occurs.
The pilot’s toxicology report results indicated an elevated level of alcohol in his urine. The toxicologist, and forensic and aviation pathology consultant, concluded that the level of alcohol present was unlikely to be solely the result of decomposition. The consultant also indicated that it was highly likely there was sufficient alcohol present in his blood at a level capable of impairing his performance and that an elevated level of alcohol has the effect of lowering caution, worsening judgement and impairing coordination and reaction time, although heavy drinkers may develop some tolerance to these effects.
The ATSB noted that the evidence of previous low flying suggested his actions may have been normal behaviour and not influenced by alcohol. Therefore, it could not be concluded that his elevated level of alcohol contributed to the accident but considered that it increased the likelihood of risk-taking behaviour and mishandling the helicopter in an emergency.
Emergency locator transmitter
Emergency locator transmitters are radio beacons carried on most aircraft so that in the event of an accident in a remote location, the aircraft wreckage and its occupants can be located quickly by search and rescue (SAR) operations. Finding the aircraft wreckage quickly not only increases the chance of survival of the occupants, but also reduces the risk to pilots of SAR aircraft who commonly need to operate in marginal weather conditions and over mountainous terrain (ATSB 2013).
The inspection of the wreckage found that the emergency locator transmitter (ELT) was selected OFF, rather than ARM. The ARM mode would provide an impact-activated signal. The ELT was located in the transmission area and while selected OFF, it required an individual to access it and select the ON mode for it to transmit a signal. However, the pilot did not regain consciousness following the accident and therefore the ELT was never activated. If not for the pilot’s Spot Tracker device, it was possible that the search and rescue response may not have commenced for some time after the accident, delaying medical treatment for the passenger.
ATSB research into the effectiveness of ELTs in aviation accidents (ATSB, 2013) established that they functioned as intended in about 40-60 per cent of accidents in which their activation was expected. In the accidents where it did not work effectively or at all, the ATSB found that this was due to the ELT not being armed before flight, incorrect installation or flat batteries, a lack of water or fire protection, damage to the ELT during the impact sequence, or the way in which the aircraft came to rest after the impact. Activation of the ELT in the ARM mode requires a high deceleration. Examination of the accident site and wreckage suggested it was possible that the ELT would not have activated in the ARM mode, but this could not be verified. Therefore, it could not be concluded that the OFF-mode selection of the ELT would have hindered a response to the accident, but not having it selected to ARM was considered to increase the risk of a delayed response.
Findings
From the evidence available, the following findings are made with respect to the collision with terrain involving a Robinson R22, registered VH-KZV, 125 km east-north-east of Alice Springs Airport, Northern Territory, on 24 November 2018. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
It was very likely that the pilot was operating the helicopter at low-level when it encountered a downdraft with insufficient height to recover, resulting in a collision with terrain.
Other factors that increased risk
The pilot did not consult any weather forecast data before departure, which increased the risk of him selecting a flight path through the MacDonnell Ranges that was not appropriate for the forecast wind conditions and turbulence.
It was very likely that the helicopter was overweight on departure and the centre-of-gravity was beyond the forward limit for the entire flight, which increased the risk of the pilot experiencing reduced control authority over the helicopter.
It was very likely the pilot's blood alcohol content was capable of impairing his performance, which increased the likelihood of risk-taking behaviour and mishandling the helicopter in an emergency.
The impact-activated emergency locator transmitter fitted to the helicopter was selected off, which increased the risk of a delayed emergency response.
Other findings
There was no fault found with the helicopter to prevent normal operation. It was almost certain the engine was operating and driving the rotors when it collided with terrain.
The pilot’s Private Pilot Licence (Helicopter), and low-level and aerial mustering qualifications had not been transferred to the Civil Aviation Safety Authority’s new licencing system and therefore, were not valid at the time of the accident.
Pilot details
Pilot details
Licence details:
Private Pilot Licence – Helicopter (invalid from 1 September 2018)
Endorsements:
R22 (invalid from 1 September 2018)
Ratings:
Nil
Medical certificate:
Class 2, valid to 2 February 2020
Aeronautical experience:
Approximately 1,270 hours in the R22
Last flight review:
February 2018
Proactive safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence:
Operator safety management improvements
Subsequent to the accident, Hewitt Cattle Australia (HCA) elected to contract out the majority of its aviation operations to Air Operator Certificate holders, including all rotary operations.
Through their recently appointed a work health and safety manager, they commenced a review of their aviation safety system. A third party aviation expert consultant was engaged to lead the review. As a result of that review, HCA developed further improvements to their aviation safety system in order to enhance the safety standards, which included the development of:
An aviation safety management system, which borrows elements contained in Civil Aviation Advisory Publication SMS-01 v1.1: Safety management systems for regular public transport operations.
An aviation safety management manual, which is based on the recommended framework contained in the International Civil Aviation Organization’s safety management manual, and incorporates best practice from the Flight Safety Foundation basic aviation risk standard, and the International Association of Oil and Gas Producers aircraft management guidelines. The manual has been tailored for HCA’s operations, with a specific focus on the areas of safety policy, risk management procedures, hazard and occurrence reporting, ‘just culture’, and assurance, specifically focused on the audit of service providers and suppliers.
A revised safe operating procedure for pilots, which is integrated with the HCA safety management system (in which pilots operating HCA aircraft have been inducted). This includes a number of additional requirements designed to decrease the likelihood of similar accidents in the future, including: pilot minimum experience requirements based on industry best practice; the basic aviation risk standard pilot runway and helicopter landing site assessment process; a process for the conduct of an abbreviated risk assessment by pilots; safety occurrence reporting requirements; Civil Aviation Safety Authority drug and alcohol training for pilots (which pilots operating HCA aircraft have undertaken); adverse weather policy; approved and prohibited flying activities; and restriction on carriage of passengers.
The aviation safety management manual creates a framework to allow for open reporting of safety occurrences based on the ‘just culture’ philosophy. This is aimed at shaping the behaviour and the culture of pilots to ensure that activities, which are not in line with HCA’s expectations, are less likely to occur. HCA considers that this cultural shift is important as the remote and expansive location of its aviation operations affect management’s ability to constantly view and assess a pilot’s general and specific flight conduct. The manual also provides a process for monitoring and auditing the currency of pilot training, ratings and endorsements on HCA’s training management system.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Alice Springs Helicopters
Bureau of Meteorology
Civil Aviation Safety Authority
Forensic and aviation pathology consultant
Forensic Science South Australia
Hewitt Cattle Australia employees
Northern Territory Police
Robinson Helicopter Company
Royal Darwin Hospital
St John Ambulance – Northern Territory.
References
Australian Transport Safety Bureau 2019, AO-2016-156: In-flight break-up involving Robinson R44, VH-ZNZ, 41 km NW Mossman, Queensland, on 18 November 2016, ATSB, Canberra.
Australian Transport Safety Bureau 2013, AR-2012-128: A review of the effectiveness of emergency locator transmitters in aviation accidents, ATSB, Canberra.
Federal Aviation Administration 2016, Pilot’s handbook of aeronautical knowledge, chapter 12: weather theory (FAA-H-8083-25B), US Department of Transportation, Oklahoma City United States.
Federal Aviation Administration 2012, Helicopter flying handbook (FAA-H-8083-21A), US Department of Transportation, Oklahoma City United States.
Wagtendonk WJ 2011, Principles of helicopter flight, 2nd edn, Aviation Supplies & Academies, Inc. Washington United States.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to Alice Springs Helicopters, Bureau of Meteorology, Civil Aviation Safety Authority, the forensic and aviation pathology consultant, Forensic Science South Australia, Hewitt Cattle Australia, Northern Territory Police, Robinson Helicopter Company, Royal Darwin Hospital, St John Ambulance Northern Territory and the United States National Transportation Safety Board.
Submissions were received from Hewitt Cattle Australia, the Civil Aviation Safety Authority, and Forensic Science South Australia. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 31 October 2018 a Titanium Explorer Autogyro, registered G-0014, collided with terrain approximately 1 km south‑east of Orange Airport, New South Wales. The pilot and passenger sustained fatal injuries. The rotors and masthead were found some distance from the main wreckage, having separated at the cheek plates (Figure 1). The cheek plates sit on either side of the collapsible mast and are designed to secure the mast in the upright position during operation.
The Australian Sport Rotorcraft Association commenced an investigation into this accident and requested technical assistance from the ATSB to examine the cheek plates and their fracture surfaces. Specifically, the ATSB was requested to determine the direction of fracture progression through the plates and to identify any factors that may have contributed to their failure.
To facilitate this work, the ATSB initiated an external investigation under the Transport Safety Investigation Act 2003.
Results
The ATSB examination undertook physical, microscopic and chemical analysis of the cheek plates. These examinations found that the plates had failed due to ductile overstress, commencing at the leading edge and progressing to the trailing edge (when oriented in the direction of travel). The plate’s dimensions and chemical composition were in accordance with manufacturer’s specifications and there was no evidence of any pre-existing defects.
Figure 1: Port and starboard cheek plates as supplied to the ATSB
Source: ATSB
With the completion of the component examinations, the ATSB has concluded its involvement in the investigation of this accident. Any further enquiries in relation to the investigation should be directed to the Australian Sport Rotorcraft Association.
______________
This report has been released in accordance with section 25 of the Transport Safety Investigation Act 2003.
On 29 October 2018, Lion Air Flight JT610, a scheduled domestic service from Jakarta to Pangkal Pinang, Indonesia, collided with water in the Java Sea, north of Jakarta, about 13 minutes after take-off. The aircraft, a Boeing 737 MAX 8, registered PK-LQP, was destroyed and all 189 passengers and crew on board were fatally injured.
As the accident occurred in Indonesia, the Indonesian National Transportation Safety Committee (NTSC) was responsible for investigating this occurrence. In accordance with Annex 13 to the Convention on International Civil Aviation, the ATSB appointed an accredited representative to the NTSC investigation. The ATSB provided specialist expertise to support the NTSC in downloading and analysing the flight data recorder (FDR) and cockpit voice recorder (CVR) from the aircraft.
The ATSB has concluded its support of this investigation. On 25 October 2019, the NTSC released the final investigation report into this occurrence and it is available at http://knkt.dephub.go.id/knkt
Any enquiries regarding the investigation and report should, in the first instance, be directed to the NTSC.
On 31 October 2018, an Aeropro 3K, registration 24-7502, collided with terrain 65 km north of Wentworth in NSW. The pilot and passenger were fatally injured.
Recreational Aviation Australia (RAAus) commenced an investigation of this accident and requested technical assistance from the Australian Transport Safety Bureau (ATSB) to download the flight data from a Dynon data logging unit.
To protect the information supplied by RAAus to the ATSB and the ATSB's investigative work to assist RAAus, the ATSB has initiated an investigation under the Transport Safety Investigation Act 2003.
Any enquiries relating to the accident investigations should be directed to RAAus at: www.raa.asn.au.
Updated: 26 March 2019
The ATSB has completed its work attempting to download the recorded data from the Dynon SkyView SV‑D1000 unit supplied by RAAus. A report detailing the work undertaken by the ATSB was provided to RAAus on 15 March 2019.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
What happened
On 5 October 2018, at about 1120 Eastern Daylight‑saving Time,[1] a Bristell Light Sport Aircraft, registered VH-YVX, departed Moorabbin Airport, Victoria, with a pilot and passenger onboard. The purpose of the flight was a navigation exercise in support of the pilot’s commercial pilot training requirements. The passenger held a student pilot licence, but his aviation medical certificate was not current.
At about 1240, following an overfly of the intended waypoint at Stawell Airport, the aircraft was observed by witnesses to conduct a 180° turn towards the east at about 1,500 ft above ground level (Figure 1). Following the turn the aircraft was observed to commence a number of manoeuvres before entering a spin. The pilot was unable to recover control of the aircraft before it impacted terrain.
Figure 1: Aircraft’s flight path and accident site location
Source: Google earth, with Airservices surveillance radar data. Modified by the ATSB
A witness at the aerodrome notified emergency services about the accident. Two other witnesses at the aerodrome utilised an aircraft to locate the accident site and guided the emergency services to its location. The pilot and passenger sustained significant injuries and were airlifted to hospital. The aircraft was destroyed.
Site and wreckage examination
The ATSB conducted an examination of the accident site and wreckage (Figure 2). This examination identified that the:
aircraft was located in relatively flat and open farmland, which was about 1.7 km south‑east of Stawell Airport
ground impact marks indicated that the aircraft had impacted terrain in a relatively flat, upright, counter clockwise spin
flaps were in the retracted position
elevator trim was in a neutral position.
No pre-impact defects were identified with the flight controls or aircraft structure.
A panel‑mounted avionics unit was removed from the aircraft and taken to the ATSB’s technical facility in Canberra for examination. The stored information was successfully downloaded and included numerous flight and engine parameters recorded during the accident flight.
Figure 2: Accident site of Bristell Light Sport Aircraft, registered VH-YVX
Source: ATSB
Ongoing investigation
The investigation is continuing and will include:
interviews with parties involved in the accident
analysis of the downloaded data from the avionics unit and other electronic devices
examination of the pilot’s qualifications, experience and medical history
assessment of the aircraft’s flight performance characteristics
examination of aircraft maintenance and operational records
examination of the training organisation records and procedures.
___________________
The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this update. As such, no analysis or findings are included in this update.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 5 October 2018, a BRM Aero Bristell light sport aircraft (LSA), registered VH-YVX, departed Moorabbin Airport, Victoria, with a pilot and passenger on board. The purpose of the flight was a navigation exercise in support of the pilot’s commercial pilot training requirements. Following an overfly of the intended waypoint at Stawell Airport, the aircraft was observed by witnesses to conduct a number of aerobatic‑type manoeuvres before control was lost. The pilot was unable to recover control of the aircraft before it impacted terrain. The occupants sustained significant injuries and the aircraft was destroyed.
What the ATSB found
The ATSB determined that, contrary to the aircraft’s limitations and the pilot’s qualifications, aerobatic manoeuvres were conducted during the flight, and immediately prior to the loss of control. The aircraft experienced an accelerated aerodynamic stall and entered into an upright, fully‑developed spin. Although the pilot did not consistently apply the manufacturer’s recommended spin recovery technique, recovery from a fully‑developed spin may not have been possible in the aircraft type.
The avionics system fitted to the accident aircraft had data storage capability and also backup storage capability by way of a secure digital (SD) card which could be fitted to the avionics system. An SD card was not fitted as standard equipment when Bristell aircraft were delivered to operators from new. Further, the operator was not aware of the additional memory card storage capability and had not installed SD cards in any of their Bristell fleet.
What's been done as a result
Following a number of fatal spin‑related accidents involving BRM Aero Bristell aircraft in Australia and overseas, the Civil Aviation Safety Authority (CASA) reviewed the flight test data supplied by the aircraft manufacturer against the ASTM standard for which the manufacturer self‑certifies compliance. CASA found that there was not enough information in the initial and follow-up test data to provide them with assurance that the aircraft type meets the required standards for spin recovery. At the time of writing the final investigation report, the manufacturer and CASA were still in discussion.
The operator conducted a fleet-wide installation of SD cards to all aircraft capable of storing data.
Safety message
Aerobatic flight should not be undertaken by pilots who have not been adequately trained, as it requires specialist techniques and methods to maintain control of the aircraft during significant manoeuvring. Further, aircraft manufacturers that prohibit aerobatics in certain aircraft types do so because the aircraft has not been designed and/or tested to ensure these manoeuvres can be conducted safely. This accident clearly demonstrates the catastrophic consequences when the hazards of aerobatic flight are not managed.
Aircraft data recording systems can be a readily accessible tool for both flying training, maintenance and safety investigation. Aircraft owners should make themselves aware of the data recording capability of their aircraft and ensure that the systems are fully functioning and backing up information.
Safety issues and actions
Proactive safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Civil Aviation Safety Authority
During the investigation, the ATSB became aware that the Civil Aviation Safety Authority (CASA) was reviewing the BRM Aero Bristell LSA aircraft certification testing against the ASTM standards. At the time of writing, there was insufficient information available to assure CASA that the Bristell LSA aircraft met the required standard for spin recovery. Consequently, CASA has requested further information from the aircraft manufacturer.
The operator
The operator conducted a fleet-wide installation of SD cards to all aircraft capable of storing data.
Context
Pilot information
General information
The pilot attained a Private Pilot Licence (Aeroplane) on 13 August 2018 and had about 160 hours of flying experience. At the time of the accident the pilot was undergoing training for the issue of a Commercial Pilot Licence (Aeroplane) qualification. The pilot was not trained or endorsed to conduct aerobatics.
Medical information
The pilot held a current Class 1 Aviation Medical Certificate with a requirement to conduct additional assessments as directed by the Civil Aviation Safety Authority. The pilot confirmed being well-rested on the day of the flight, with no medical issues.
Stall and spin recovery training
According to the pilot’s instructor, the pilot had been taught theoretical and practical stall recovery techniques, including recovery from an incipient spin. The pilot’s training records indicated that the pilot had demonstrated the correct incipient spin recovery technique to their instructor and flight examiner on several occasions.
Aircraft information
General
The BRM Aero Bristell is a light sport aircraft (LSA). It is an all-metal, low-wing monoplane of semi-monocoque construction with side-by-side seating and dual flight controls. It is driven by a 4-cylinder, 4-stroke, normally aspirated piston engine, driving a composite three-blade constant-speed propeller. It has a maximum all up weight of 600 kg (Figure 4).
Figure 4: Exemplar BRM Aero Bristell LSA aircraft
Source: Aircraft operator with permission
VH-YVX Airworthiness and maintenance
BRM Aero Bristell LSA serial number 284 was manufactured in 2017 and registered in Australia as VH-YVX.
At the time of the accident, the aircraft was:
operating on a special Certificate of Airworthiness in the light sport aircraft (LSA) category
approved for private operations/flight training
maintained in accordance with the manufacturer’s maintenance schedule
operating under a current maintenance release with no outstanding defects or maintenance. It indicated that the aircraft had about 928 flight hours since new.
Approved aircraft manoeuvres
The aircraft operating instructions (AOI) section 2.9 had approved manoeuvres listed as follows:
• Steep turns not exceeding 60° bank
• Lazy eights
•Chandelles
• Stalls (except whip stalls).
The section also had the following warning:
Aerobatics and intentional spins are prohibited.
The same warning is also included as a placard on the cockpit instrument panel (Figure 5).
Figure 5: Depiction of placard attached to the instrument panel
Source: Bristell LSA operating instructions
Section 2.10 of the AOI identified the maximum manoeuvring load factors as +4.0 to -2.0 G.
Integrated instrument and avionics system
The aircraft was fitted with a Garmin G3X avionics system, which was an integrated flight instrumentation, position, navigation and communication system.
Recorded flight data
The G3X unit had a flight data logging feature which automatically stored flight and engine data to its memory module. A secure digital (SD) card can also be fitted as a backup memory storage that can be easily removed from the aircraft so that the flight data can be downloaded for operational and maintenance monitoring purposes. A data file was created each time the system was powered on with an SD card inserted, or each time an SD card was inserted after power on.
A 2 GB SD card can store over 1,000 hours of flight data or up to 1,000 files (whichever comes first). The SD card is normally located in a receptacle on the right upper face of the unit. However, an SD card was not provided with the aircraft when it was first supplied from the manufacturer. It was therefore at the owner’s discretion if they wished to utilise the recording feature. No SD card was installed at the time of the accident.
Stall warning and angle of attack display
When the angle of attack (AOA) system identifies an exceedance in the calibrated caution alert threshold, an intermittent audible warning will be heard. The tone will increase in frequency until it reaches the AOA stall warning threshold, at which point the audible warning will change from intermittent to continuous.
In conjunction with the audible warning, the AOA system will display a change from a solid green to yellow in the caution level. It flashes from yellow to red when it reaches the stall warning threshold (Figure 6).
Figure 6: Angle of attack on the primary flight display
Source: Garmin G3X Pilot’s Guide, modified by the ATSB
Regulatory definition and requirements for aerobatic flight
Definition of aerobatic flight
Civil Aviation Safety Regulations 1998 (CASR) Dictionary, Part 1 Definitions defined aerobatic manoeuvres as those that involve:
(a) bank angles that are greater than 60˚; or
(b) pitch angles that are greater than 45˚, or are otherwise abnormal to the aircraft type; or
(c) abrupt changes of speed, direction, angle of bank or angle of pitch.
Regulatory requirements for aerobatic flight
To conduct aerobatic manoeuvres, pilots are required to have an aerobatics flight activity endorsement entered on their pilot’s licence. To obtain this endorsement, a pilot is required to have received training and demonstrated competency in all the course units mentioned in CASR Part 61 Manual ofStandards. That training includes recovery from unusual attitudes and spins.
CASR 61.065 prohibits the conduct of any activity for which the licence holder is not authorised. In addition, CASR subpart 61.S Flight activity endorsements stated the requirements for aerobatic endorsements. These included an initial aerobatic endorsement that would authorise the pilot to conduct aerobatic manoeuvres in an aeroplane above 3,000 ft above ground level (AGL). Subsequent endorsements were necessary for aerobatic activities at lower altitudes.
information and guidance on safety issues related to aerobatic flight, including in respect of the aircraft, pilot and regulations
an explanation of spin recovery techniques
advice on the importance of ensuring sufficient height to recover from an aerobatic manoeuvre by 3,000 ft AGL (or the lower limit of the pilot’s approval).
In particular, section 7.3.2 of the CAAP stated:
It is highly probable that the consequence of an error or failure during low-level aerobatics will be fatal to the participants.
Aerobatics are not permitted over populous areas or public gatherings without the written permission of CASA.
Spins and spin recovery
Overview
An aerodynamic spin is a sustained spiral descent in which one or both an aircraft’s wings are in a stalled condition,[3] with the outside wing producing more lift and less drag than the other wing. The associated forces sustain the rotation and keep the aircraft in the spin. A spinning aircraft will descend more slowly than one in a vertical or spiral dive and it will have a lower airspeed, which may oscillate. The pitch angle can also vary considerably from significant pitch down to a relatively flat attitude.
Intentional spins are normally entered from a stall in straight and level flight, via the application of full back elevator and full rudder in the intended direction of rotation at the moment of the stall. The circumstances of a spin entry during aerobatic manoeuvring can be very different. If for example, aerobatic manoeuvres are incorrectly conducted, an unintentional consequence can be a flick roll[4] and entry into a spin.
Incipient spin
When entering a spin, an aircraft motion through the air is irregular at first. This is a transition phase from the stall and is known as incipient spin. Though the nature of the incipient spin is heavily dependent on the aircraft type and the manner of entry, recovery may be more rapid and require less control input in this stage compared with recovery from a developed spin.
Developed Spin
After a number of rotations and depending on the aircraft loading, type and control inputs, an aircraft in an incipient spin may settle into a regular rotating descent known as a developed spin. A developed spin is typified by reduced oscillations when compared to an incipient spin and the axis of rotation becomes vertical. The spin may steepen (nose down) or flatten (nose more horizontal) as it continues.
Recovery from an unintentional spin
The BRM Aero Bristell LSA AOI, section 3.7 described the recovery from unintentional spins as follows:
There is no[t] an uncontrollable tendency of the airplane to enter into a spin provided the normal piloting techniques are used.
Unintentional spin recovery technique:
1. Throttle - idle
2. Lateral control - ailerons neutralized
3. Rudder pedals - full opposite rudder
4. Rudder pedals - neutralize rudder immediately when rotation stops
5. Longitudinal control - neutralize or push forward and recover dive.
Spinning ceases only when opposing forces and moments overcome auto-rotation. Since yaw coupled with roll powers the spin, the pilot must forcibly uncouple them by applying the recommended spin recovery technique. Due to rotational inertia, spin recovery is not instantaneous. It may take several turns of the applied technique before recovery control forces finally overcome the spin stabilising forces and rotational inertia. Spins are only recoverable when the cumulative effects of the interacting variables favour recovery and there is enough altitude and therefore time to recover. Generally speaking, recovery from an incipient spin will take less time than a recovery from a fully developed spin. It is therefore vital that the correct recovery technique is implemented as soon as possible.
Pilot and passenger recollection of the attempted spin recovery
The pilot stated that the aircraft did not provide him with an aural or visual warning of an impending stall leading up to or during the accident sequence. When asked about the recovery technique following entry into a spin, the pilot confirmed that full opposite rudder was not maintained. Rather, the pilot initially applied opposite rudder to the spin and then reversed the control and noted that the spin rate increased. The pilot then moved the rudder back to the full opposite rudder position.
Analysis of the recorded data showed that the engine power was only slightly reduced following entry into the spin. Power was reapplied and then reduced to idle about 14 seconds after the spin commenced.
The passenger did not have a full recollection of the event but recalled the plane going pitch-up to a vertical position and then one rotation. The passenger remembered then saying ‘opposite rudder power down’ to the pilot before passing out prior to impact.
Although the passenger did not recall an audible warning when interviewed by the ATSB, they did mention hearing a beeping sound when discussing the event with their family a short time after the accident.
Light sport aircraft certification standards for spin recovery
Aircraft in the LSA category are certified to the ASTM International[5] standards. The certification process is conducted and self-certified for compliance by the manufacturer themselves, rather than by the regulating aviation authority from the state of manufacture. The LSA process relies on the manufacturer declaring that the aircraft meets all the construction and flight requirements of the LSA standards identified by them in the statement of compliance.
Aircraft certification standards for spin testing
ASTM F2245 standard specification for design and performance of light sport aeroplanes, section 4.5.9 states:
4.5.9 Spinning:
4.5.9.1 For airplanes placarded “no intentional spins,” the airplane must be able to recover from a one turn spin or a 3-s[econd] spin, whichever takes longer, in not more than one additional turn, with the controls used in the manner normally used for recovery.
In some aircraft not approved for spinning, recovery may not be possible if the spin progresses to the developed stage.
The standard has various requirements, for example the light sport aircraft category for non-aerobatic aircraft requires the aircraft manufacturer to prove the aircraft type can recover from a one-turn spin.
CASA assessment of BRM Aero Bristell LSA spin testing
The LSA category relies solely on the aircraft manufacturer declaring that each individual aircraft meets/complies with the standard(s) that they have indicated within the statement of compliance. Each individual aircraft must have its own statement of compliance issued and signed by the aircraft manufacturer that the particular aircraft meets the identified standards. Manufacturers are not required to submit test data, or show compliance to those standards, to CASA or any other regulator.
Following a number of fatal accidents involving Bristell aircraft entering into and not recovering from spins in Australia and overseas, CASA assessed the Bristell LSA self-certification testing documentation against the ASTM certification test standards.
CASA found that there was insufficient information in the initial test data to provide assurance that the aircraft type met the ASTM standards for spin recovery. As a result, CASA requested more certification testing data from the manufacturer. The manufacturer conducted further certification flight tests in the Bristell LSA and provided that data, including video recordings of each flight sequence to CASA. CASA’s assessment of the new flight-testing data and further information supplied by the manufacturer was that it still did not confirm that the aircraft met the required ASTM standard for spin recovery.
Post-accident CASA guidance on spin avoidance
Due to an increase in spin‑related accidents across a broad range of light aircraft types in the training environment, CASA produced guidance material in the form of an advisory circular (AC) 61-16 v1.0 titled Spin avoidance and stall recovery training. The AC highlights:
…the risks associated with advanced stalling training when conducted in aircraft that are not certified for intentional spinning. It clarifies the difference between wing drop at the stall and the incipient phase of a spin and provides background for the interpretation of aircraft flight manual manoeuvre limitations with respect to spinning. It also provides guidance on acceptable methods of training and testing stalls with a wing drop and spin avoidance.
The AC provides detailed guidance for pilots, flight instructors, flight examiners and flight training organisations. The AC states that:
The key messages in this AC that are critical for the safe conduct of advanced stalling and spinning exercises, and that all pilots instructors, operators and flight examiners should be aware of are:
• A spin must not be induced in aircraft not certified or approved for intentional spinning
• A spin must not be induced without the pilot in command holding a spinning flight activity endorsement
• Aircraft flight manual limitations and any special procedures before conducting any exercise which may result in a spin
• The need to comply with aeroplane centre of gravity limits
• Wing drop at the stall for the purposes of spin avoidance training must not be induced by application of pro-spin rudder and the induction of a spin
• Training in spin avoidance must include the recognition of symptoms associated with slow flight and approach to the stall through to recovery from stall with a wing drop
• Recognise and manage changes in aircraft energy state
• Spin avoidance training where a wing may drop at the stall should be undertaken through scenario-based in-flight manoeuvres:
- Approach configuration descending turns (base to final turn)
- Go-around from approach configuration (significant change in trim state)
- Climbing turns in departure configuration (trim changes during flap retraction and turns)
- Engine failure after take-off (potential out of trim condition)
- Turns in slow flight.
Site and wreckage examination
The ATSB conducted an examination of the accident site and wreckage (Figure 7). The examination identified that:
the aircraft was located in relatively flat and open farmland, about 1.7 km south‑east of Stawell Airport
ground impact marks indicated that the aircraft had impacted terrain in a relatively flat, upright, counterclockwise spin
the flaps were in the retracted position
there was evidence of a significant amount of fuel at the accident site and the airframe fuel filter bowl was full of fuel and free of contaminants
the propeller blades showed rotation damage consistent with engine operation at a low power setting at impact
elevator trim was in a neutral position
no pre-impact defects were identified with the flight controls or aircraft structure
all aircraft components were accounted for at the accident site.
A Garmin G3X (G3X) panel‑mounted avionics unit was removed from the aircraft for detailed examination at the ATSB’s technical facility in Canberra.
Figure 7: Aircraft accident site
Source: ATSB
Recorded information
G3X avionics system flight data download
The ATSB inspected the G3X unit and identified that it was visually undamaged. There was no SD card fitted to the unit. On return to Canberra, the unit was powered up with an SD card fitted (Figure 8). Data files associated with the accident flight were successfully downloaded from the memory module to the card.
Figure 8: G3X avionics unit being downloaded, showing memory card position
Source: ATSB
Flight data summary
The downloaded data recorded 86 parameters for the duration of the accident flight, from the initial taxi until impact with terrain. The flight data indicated that the aircraft and engine were operating normally throughout the flight with no anomalies identified within the data or aircraft operating systems.
Position verification
The GPS position was verified to be accurate within 2 metres by utilising the aircraft’s:
track on the parking bay, taxi ways and runway at Moorabbin Airport
track during the touch-and-go on the runway at Bacchus Marsh Airport
final position at the accident site.
Significant aircraft manoeuvres
The data recorded that at about 1230, while the aircraft was overhead the built‑up area shown in Figure 2, it was operated significantly outside of its allowable flight envelope. This included banking to 94° while manoeuvring between 600‑1,300 ft above a populated area.
At 1319, the recording captured a 91° roll to the left followed by a pitch down to 40°. The data also recorded a climbing right turn to 91° angle of bank at 1323, followed by a pitch down to 38° then a rolling left pull out turn. Whilst pulling out, the instrumentation system recorded a peak normal acceleration of 4.4 G. That loading exceeded the aircraft’s positive load limit of 4 G.
From 1340, there was significant variation in the magnitude of pitch, roll and load factor, consistent with additional aerobatic manoeuvring during the final minute of the flight (Figure 9).
At 1340:36, while the aircraft was operating at:
about 90 kt indicated airspeed
a pitch-down angle of about 50°
high angle of attack and positive load factor
it abruptly pitched down to 90° and rolled significantly to the left. That behaviour was consistent with the aircraft experiencing an accelerated aerodynamic stall.[6]
Subsequent variation in the recorded parameters indicated that the aircraft then entered a counter-clockwise upright spin at a rotation rate of about one full turn every 1.5 seconds and a vertical descent rate of over 3,000 ft/min at the time of impact.
The engine power level remained at a constant high setting prior to the spin entry.
Figure 9: Last 60 seconds of recorded flight data parameters prior to the accident
Source: ATSB
Weight and balance information
The aircraft weight was calculated as being about 17 kg over the maximum allowable limit at take‑off from Moorabbin Airport, but within the balance limits. However, the aircraft was within the weight and balance limits at the time of the accident, when the weight was adjusted for 1 hour 20 minutes of fuel consumption.
Previous accidents
BRM Aero Bristell registered 24-7954, Clyde North, Victoria
This accident was investigated by Recreational Aviation Australia. The accident investigation report is not a publically available document.
On 3 August 2017, during a training flight, a student pilot was conducting stall recovery training under supervision of an instructor at an altitude of 3,500 ft AGL. Following entry into the stall, the right wing dropped and, despite the correct instructed actions, the student pilot mishandled the stall recovery by applying opposite aileron. Although this is an intuitive response to raise the wing, it exacerbated the stall and the aircraft entered a spin.
The instructor took over control of the aircraft from the student and initiated the correct spin recovery technique using ailerons neutral and opposite rudder. Despite having 3,000 ft remaining, the instructor was unable to regain control of the aircraft before it impacted the terrain. The student pilot was fatally injured, and the instructor sustained serious injuries.
On 14 June 2019, during a flight with two occupants, recorded data showed that the engine power was reduced as the aircraft maintained about 3,200 ft with reducing airspeed. The aircraft then rapidly lost height and impacted the ground about 30 seconds later. The aircraft was destroyed and the two occupants were fatally injured.
The on-site examination indicated that the aircraft impacted the ground at a high vertical rate, in a nearly level attitude, whilst rotating anticlockwise about the yaw axis.
At the time of writing the accident was still under investigation by the Irish Aircraft Accident Investigation Unit.[7]
The sources of information during the investigation included:
the pilot and passenger
witnesses and first responders to the accident
the aircraft operator and manufacturer
Civil Aviation Safety Authority
Airservices Australia
Victoria Police.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the pilot and passenger, the aircraft operator and manufacturer and the Civil Aviation Safety Authority.
Submissions were received from the pilot and passenger, the aircraft operator and manufacturer and the Civil Aviation Safety Authority. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
The occurrence
What happened
On 5 October 2018, at about 1220 Eastern Daylight‑saving Time,[1] a Bristell light sport aircraft, registered VH-YVX, departed Moorabbin Airport, Victoria, with a pilot and passenger on board. The purpose of the flight was a navigation exercise in support of the pilot’s commercial pilot training requirements. The passenger held a student pilot licence, however their aviation medical certificate was not current. Photographs taken during the flight indicated that the passenger operated the aircraft for brief periods, but the ATSB assessed that this did not contribute to the development of the accident.
Automatic Dependence Surveillance Broadcast and on-board flight and GPS data recorded the aircraft position and attitude throughout the flight (see the section titled Recorded information). The data showed the take-off and flight over the northern part of Port Phillip Bay, followed by the commencement of significant manoeuvring overhead a built-up area to the west of Melbourne (Figures 1 and 2).
Figure 1: Aircraft’s flight path and accident site location
Source: Google Earth, modified by the ATSB
Figure 1 details the flight path of the aircraft in the area labelled as ‘Detail A’ in Figure 1. The data showed that the pilot conducted significant manoeuvres including steep climbs, descents and turns in excess of 90° angle of bank over a built-up area and at heights between 600‑1,300 ft above ground level (AGL).
In discussing that segment of the flight, the pilot stated that a 360° turn was conducted over the house of someone the pilot knew in the area. The pilot did not recall conducting any aerobatics or significant manoeuvring at that time.
Figure 2: Detail A – Recorded data of the aircraft flight path over a built-up area
Source: Google Earth, modified by the ATSB
The aircraft then continued to Bacchus Marsh Airport where the pilot conducted a circuit followed by a touch-and-go landing. The aircraft then continued in a north‑west direction until overhead Stawell Airport (Figure 3).
At about 1240, three witnesses at Stawell Airport observed the aircraft overfly the airport before commencing a 180°turn back towards the south‑east. Following that turn, the aircraft was observed to commence a number of significant manoeuvres including steep climbs and turns described as aerobatic in nature. The aircraft was then observed to abruptly enter a flat spin (see the section titled Spins and spin recovery) and descend out of view.
Analysis of the recorded data identified that, after passing overhead the airport, manoeuvres far in excess of the aircraft’s performance limitations were conducted. Based on the magnitude of the recorded pitch and roll values, the manoeuvres were classified as aerobatic. Further data analysis established that while the aircraft was pitching and rolling out from a diving left steep turn, it experienced an accelerated aerodynamic stall[2] while rolling at an indicated airspeed of about 93 kt. The aircraft subsequently flick-rolled and entered a fully developed upright spin at an altitude of about 1,650 ft AGL. The aircraft maintained the spinning descent until it impacted terrain.
The pilot stated that, immediately prior to the accident, a turn of no more than 50° angle of bank was conducted in the process of lining up for a practice circuit and landing at Stawell Airport when ‘the back end of the aircraft slid out’ and control was lost. The pilot also stated that the accident occurred prior to reaching the airport.
When provided with detail of the recorded flight data and other accounts, the pilot was unable to reconcile the difference between their recollection of the event and that of the witnesses and the recorded data. Figure 3 shows the aircraft track, manoeuvring and spin. The red portion of the flight track is the point at which the GPS lost signal and position data was no longer recorded. This was likely due to a combination of the aircraft’s rapid movements and the GPS antenna position. From that point onwards, position data was calculated using groundspeed, bearing and barometric altitude data.
Figure 3: Detail B – Aircraft operation in the vicinity of Stawell Airport
Source: Google Earth, modified by the ATSB
A witness at Stawell Airport notified emergency services about the accident. Two other witnesses at the airport used an aircraft to locate the accident site and guided the emergency services to the location by flying overhead. The pilot and passenger sustained serious injuries and were airlifted to hospital. The aircraft was destroyed.
Private Pilot Licence (Aeroplane), issued 13 August 2018
Endorsements:
Manual Propeller Pitch Control
Ratings:
Single engine aeroplane
Medical certificate:
Class 1 and 2, valid to 19 October 2018
Aeronautical experience:
about 160 flight hours
Findings
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving a Bristell LSA aircraft, registered VH-YVX, in Stawell Victoria on 5 October 2018. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
While conducting aerobatics, the aircraft experienced an accelerated aerodynamic stall and entered into an upright spin that continued until impacted terrain.
The pilot conducted aerobatic manoeuvres without aerobatic training, in an aircraft which prohibited such manoeuvres.
Other factors that increased risk
During the accident flight, the pilot conducted aerobatics at low altitude over a built-up area in contravention to safe practices and the regulations. Had an unrecoverable loss of control occurred there was a significantly increased risk of injuries or fatalities to people on the ground.
A regulatory review of the aircraft type’s self-certification flight test data and documentation by the Civil Aviation Safety Authority (ongoing at the time of writing) did not provide assurance that the aircraft type met the required standard for spin recovery.
Other findings
The aircraft's avionics system, while capable of storing data, was not fitted with a memory card. The memory card serves as a back-up for stored data, which can be a readily accessible tool for both flying training and safety investigation.
Safety analysis
Introduction
Examination of the aircraft and recorded flight data identified that there were no mechanical defects that contributed to the accident. Further, a review of the meteorological conditions as described by witnesses and the pilot indicated that weather was not a factor.
Evaluation of the flight data also established that the pilot engaged in aerobatic manoeuvres during the course of the flight, including just prior to the loss of control in the vicinity of Stawell Airport. This analysis will discuss the development of the accident in that context.
Aerobatic limitations
The Bristell light sport aircraft (LSA) operating instructions prohibit excessive angles of bank, aerobatics and intentional spins. This was clearly defined and the information relating to spin avoidance was also presented by way of a placard in the cockpit.
Civil aviation regulations stipulate the types of manoeuvres that are considered to be aerobatic. It also sets out the pilot training and endorsements requirements before aerobatics are to be conducted. The framework provided by these rules ensures that this hazardous activity can be performed with an acceptable level of safety.
When interviewed, the pilot demonstrated an awareness of the aircraft limitations and the requirements relating to aerobatics. Further, the pilot did not have any training or endorsements in aerobatics and did not apply for or receive permission from CASA to undertake aerobatics over a populous area. Despite that, manoeuvres meeting the definition of aerobatics were carried out during the accident flight in the form of abrupt changes in flight parameters and excessive bank and pitch.
Aerobatic manoeuvring and loss of control
Aerobatics were first conducted above a built-up area at 600‑1,300 ft above ground level (AGL), and with a maximum bank angle of 94°. Had an unrecoverable loss of control occurred over such a populated area, in addition to the likely fatality of the occupants, there was a significantly increased risk of injuries or fatalities to people on the ground.
Additional aerobatics were conducted mid-flight between Bacchus Marsh and Stawell airports, with one exceeding the aircraft’s flight load limitations. The aircraft was then observed by witnesses to overfly Stawell Airport before again commencing significant pitch and bank manoeuvres. During one of these manoeuvres, the aircraft experienced an accelerated aerodynamic stall and entered into an upright spin at an altitude of about 1,650 ft AGL. This progressed into a fully developed spin that continued until the aircraft impacted terrain.
Due to the accelerated nature of the spin entry and the already nose-down and banked attitude, the entry to the spin would probably have been abrupt and disorientating. The pilot reported not maintaining the correct spin recovery technique with respect to rudder input. Despite that, as discussed further below, even with immediate and sustained application of spin recovery control inputs, recovery from the spin may not have been possible.
The pilot’s account of the aircraft manoeuvring during the flight, including immediately before the loss of control, did not align with either the flight data or the witness statements. The passenger only recalled fragments of information about the flight and did not recall what happened before the aircraft entered the spin.
The ATSB assessed that the recorded flight data was accurate. It clearly indicated that the aircraft was operated significantly beyond the allowable limits of both the aircraft and the pilot’s qualifications, with catastrophic consequences.
Aircraft spin certification and characteristics
Non‑aerobatic aircraft in the LSA category, such as the Bristell LSA, are certified to the ASTM International standards. As such, the aircraft is required to demonstrate the ability to recover from a one‑turn or 3‑second spin, whichever was longer, in not more than one additional turn. Recovery from a multiple-turn, fully developed spin is not required to be demonstrated.
As a consequence, there is no assurance that, even if the normal spin recovery technique was applied, that recovery from a fully developed spin is possible in the Bristell LSA aircraft.
In response to a number of fatal accidents involving Bristell aircraft entering and not recovering from spins in Australia and overseas, the Civil Aviation Safety Authority (CASA) assessed the Bristell LSA type certification testing documentation against the ASTM certification test standards. CASA found that there was insufficient information in the initial flight test data to provide assurance that the aircraft type met the ASTM standards for spin recovery. As a result, CASA requested more certification testing data from the manufacturer. The manufacturer conducted further certification flight tests in the Bristell LSA and provided that data, including video recordings of each flight sequence to CASA. CASA’s assessment of the new flight-testing data and other information provided after that point still did not confirm that the aircraft met the required ASTM standard for spin recovery. At the time of writing, CASA and the manufacturer were still in discussion.
In the context of this accident, as the aircraft was operated significantly outside its operating limitations, it was not possible to identify if a safety issue surrounding aircraft spin and recovery characteristics of the Bristell LSA exists.
Avionics memory and data use
There are many advantages to having recording devices installed in aircraft. These include the use of downloaded data to monitor:
student pilot performance
third party aircraft usage
engine health trends and aircraft limitation exceedances.
They also provide a significant source of evidence during the investigation of aircraft accidents.
The avionics system fitted to the accident aircraft had data storage capability and also backup storage capability by way of a secure digital (SD) card which could be fitted to the avionics system. An SD card was not fitted as standard equipment when Bristell aircraft were delivered to operators from new. Further, the operator was not aware of the additional memory card storage capability and had not installed SD cards in of their Bristell fleet. As a result, had the avionics unit memory module been damaged, then important recorded data associated with this accident could have been destroyed.
The ATSB encourages operators and owners of aircraft to, wherever possible, use on board recording capability to capture the available data parameters.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
The pilot of a Cessna 208B aircraft, registered VH-FAY (FAY), was contracted by the aircraft operator to ferry FAY from Jandakot Airport, Western Australia to Mississippi, United States. On the morning of 27 September 2018 local time, the aircraft departed Saipan International Airport, Northern Mariana Islands, for a planned flight to New Chitose Airport, Hokkaido, Japan. After climbing for about an hour, the aircraft levelled off at flight level (FL) 220.
After 2 hours 20 minutes flight time, the pilot contacted Tokyo Radio flight information service at the first mandatory reporting position. The aircraft passed the next reporting point at the same altitude, 1 hour 20 minutes later, but the pilot did not contact Tokyo Radio as expected. Tokyo Radio made repeated attempts to communicate with the pilot, without success. Having received no communications from the pilot for 4.5 hours, two Japan Air Self‑Defense Force (JASDF) aircraft intercepted FAY. The pilot did not manoeuvre the aircraft in response, in accordance with international intercept protocols.
After about 30 minutes, the JASDF pilots observed FAY descend into cloud. The aircraft descended rapidly and disappeared from radar less than 2 minutes later. Within 2 hours, search and rescue personnel located the aircraft’s rear passenger door. No other aircraft parts were located and the pilot was not found.
What the ATSB found
While the aircraft was in the cruise on autopilot, the pilot almost certainly became incapacitated and did not recover. About 5 hours after the last position report, without pilot intervention to select fuel tanks, the aircraft’s engine stopped, likely due to fuel starvation. This resulted in the aircraft entering an uncontrolled descent into the ocean.
The cause of incapacitation could not be determined. While a medical event could not be ruled out, the pilot was operating alone in an unpressurised aircraft at 22,000 ft and probably using an unsuitable oxygen system, which increased the risk of experiencing hypoxia and being unable to recover.
What's been done as a result
The aircraft operator amended their operations manual to include additional guidance for international ferry flights. They also created an oxygen use guide and a specific risk assessment for positioning (ferry) flights.
Safety message
Operating unpressurised aircraft above 10,000 ft requires careful oxygen management and planning. Where an increased risk of hypoxia exists, good risk management practices should be used for flight planning. Because the effects of hypoxia can be insidious, training in recognition of early symptoms of hypoxia can increase the time available to react, descend and resolve any issues. The Flight Safety Australia (2014) article Do not go gentle: the harsh facts of hypoxia provides further information, including anecdotal experiences of hypoxia.
VH-FAY with full survey equipment installed
Source: Sid Mitchell, Aviation Spotters Online
Safety analysis
Introduction
After departing Saipan and climbing for about an hour, the aircraft levelled off at flight level (FL) 220. An hour later, the pilot made a mandatory position report on HF radio and then no subsequent communications. About 5 hours after the position report, while maintaining FL 220 and the flight planned route, the aircraft descended to the ocean. No wreckage other than a part of the aircraft door was recovered and the pilot was not found, limiting the evidence available.
The analysis will consider reasons for the pilot’s lack of any further communication and the aircraft’s subsequent descent. The investigation identified some operational factors that increased the pilot’s risk of experiencing hypoxia. These factors are explored in detail below.
Pilot incapacitation
The absence of any communication by the pilot after reporting at position TEGOD was almost certainly a result of pilot incapacitation. He did not make any further mandatory position reports, or respond to repeated attempts by Tokyo Radio to communicate on HF radio. The pilot had several alternative means of communication available in case of HF radio failure or failure of the aircraft’s electrical system. He would have been able to communicate using one of those means if not incapacitated, as demonstrated by having successfully sent messages from his standalone Garmin device prior to reaching TEGOD.
Additionally, the pilot did not respond in accordance with international intercept protocols, either by rocking the aircraft wings or turning, when intercepted by two Japan Air Self-Defence Force (JASDF) aircraft. The JASDF pilots were unable to see into the cockpit to confirm whether the pilot of VH-FAY was visibly incapacitated.
No evidence was available from which to determine the cause of incapacitation. The two most likely mechanisms for incapacitation were due to the pilot experiencing a medical event or hypoxia. Although the pilot had a valid medical certificate and was reportedly in good health, a medical event could not be ruled out. Similarly, the pilot’s last communications with Tokyo Radio were not of adequate sound quality to determine whether the pilot was affected by hypoxia at that time. In any case, there was ample time after TEGOD for the pilot to experience hypoxia and be unable to recover at the cruise altitude, before the aircraft reached the next reporting point.
With the pilot incapacitated, the aircraft continued on autopilot. The aircraft’s track and altitude were consistent with the flight director selected to hold flight level (FL) 220 and to follow the GPS programmed track.
Fuel starvation and uncontrolled descent
About 5 hours after the pilot’s last transmission, the JASDF aircraft radar showed FAY start to descend at an increasing rate, which was indicative of engine power loss. In the absence of pilot intervention, the power loss would have resulted from either engine failure or fuel starvation. An engine failure could not be ruled out, however this would had to have occurred in addition to pilot incapacitation, and the likelihood of both these events occurring in the same flight was considered to be low. The engine power loss was therefore considered more likely to have resulted from fuel starvation.
The estimated fuel used at the commencement of the descent was significantly less than the total fuel carried. However, as the pilot almost certainly became incapacitated relatively early in the flight, he would therefore not have been able to manually alter the fuel state after that point. It was possible to have starved the engine of fuel around the descent point by switching to the right tank and using some or all of the ferry tank (and venting some). However, this would have resulted in a fuel imbalance that was not evident in photos of the aircraft taken shortly before its descent. Given that the estimated fuel used was approximately equal to the usable fuel in the wing tanks, it was more likely that the wing tanks were selected for the duration and this usable fuel was exhausted, leaving the ferry tank full.
The aircraft’s last computed descent rate was below the dive speed for the aircraft, and was therefore indicative of an uncontrolled descent, rather than an in-flight breakup. There was no recorded data of the aircraft’s collision with the water, however the descent profile and wreckage indicated that the collision with water was not survivable.
Increased risk of experiencing hypoxia
In exploring the potential reasons for pilot incapacitation, there were several operational factors identified that increased the pilot’s risk of experiencing hypoxia and being unable to recover.
The pilot elected to fly solo at FL 220 where, without adequate oxygen supply, the time of useful consciousness (TUC) was in the order of 5-6 minutes. This was limited compared to FL 180, for example, where the TUC was two to three times longer.
The pilot had undertaken a hypoxia awareness course and reportedly knew the initial symptoms that presented in himself, which would aid in identifying and mitigating against the risk of hypoxia. However, particularly above FL 180, impairment and incapacitation can occur quickly, with little or no warning, rendering a person unable to take action to recover. The pilot also had a pulse oximeter to monitor blood oxygen saturation, but had been observed on a previous flight to use it intermittently rather than continuously. Given the limited TUC, had the pilot followed a similar regime on this flight, it may have resulted in insufficient time to alert the pilot to decreasing saturation levels. The pilot elected not to have a second pilot on board, as offered by the operator, which would have provided an additional risk control in assisting to identify the signs of hypoxia in each other and enable recovery action, as illustrated by previous occurrences. This would be especially pertinent at altitudes where there is limited TUC.
There was adequate oxygen on board for the flight, however the pilot was probably using a nasal cannula connected to the pilot’s electronic pulse-demand system (EDS) at all flight levels, as indicated by the fact that the Cessna mask was unused by the time the aircraft was in Saipan, despite having flown above FL180. This increased the risk of reduced oxygen-blood saturation levels.
The pilot had also indicated his intention to connect the EDS to the aircraft system without the in-line regulator that was required to ensure the EDS operated within its limits. At FL 220, this had the potential for the pilot to receive inadequate oxygen supply or for the EDS to be rendered inoperative, resulting in higher oxygen consumption than anticipated. However, it is noted that the pilot had the Cessna mask available which, if used with the aircraft system, would have mitigated this risk.
Findings
From the evidence available, the following findings are made with respect to the uncontrolled flight into water involving a Cessna Aircraft Company 208B, registered VH-FAY, that occurred 260 km north-east of Narita International Airport, Japan, on 27 September 2018. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
During the cruise between Saipan and New Chitose, the pilot very likely became incapacitated and could no longer operate the aircraft.
The aircraft’s engine most likely stopped due to fuel starvation from pilot inaction, which resulted in the aircraft entering an uncontrolled descent into the ocean.
Other factors that increased risk
The pilot was operating alone in the unpressurised aircraft at 22,000 ft and probably not using the oxygen system appropriately, which increased the risk of experiencing hypoxia and being unable to recover.
Context
Pilot information
According to information provided by the aircraft operator, the pilot had accrued over 13,600 hours of aeronautical experience and had conducted more than 200 ferry flights for various companies. The pilot held a valid US First Class Medical Certificate issued on 19 March 2018, with the restriction of vision correction. The 66 year-old pilot was reported by acquaintances to be a non-smoker, in good health for his age, and there was no evidence of any underlying medical conditions. In the nights before FAY departed from Saipan, the pilot had reportedly not slept well, but there was insufficient evidence to determine whether he could have been experiencing a level of fatigue that would affect performance.
The pilot was a Norwegian/American dual citizen with a United States (US) Airline Transport Pilot Licence issued in January 2018. For the ferry flight, a Certificate of Validation was issued by the Civil Aviation Safety Authority (CASA) on 14 September 2018 for a Commercial Pilot Licence (Aeroplane). This included the conditions that the flight ‘must be conducted in accordance with [the aircraft operator’s] operations manual and CASA legislative requirements pertaining to the flight planned route.’ In January 2018, the pilot had ferried another Cessna 208B aircraft, VH-FHY (FHY) from Canada to Perth, WA.
Aircraft information
VH-FAY (FAY) was a Cessna Aircraft Company C208B aircraft manufactured in the US in 2001. At that time, the aircraft was issued with a Certificate of Airworthiness and an associated Airplane Flight Manual.[5]
The aircraft was fitted with a Honeywell TPE331-12JR engine and a Hartzell Propeller Inc. HC-B4TN-5QL/LT10891NK (De-ice) propeller under a Supplemental Type Certificate (STC). Also under an STC, the aircraft had been fitted with an improved landing gear axle. This increased the maximum landing weight from 3,856 to 4,082 kg and the maximum take-off weight (MTOW) from 3,969 to 4,110 kg. Flight Manual Supplements (FMS) to the Airplane Flight Manual had been issued for each of these modifications.
FAY was fitted with a Garmin GTN 750 GPS. Among other options, the aircraft’s autopilot could be selected to ‘Altitude hold’, and lateral navigation mode could be selected to capture a GPS programmed flight plan.
The aircraft’s last Maintenance Release[6] was issued on 7 September 2018 following completion of extensive maintenance in preparation for overseas operations. It was valid for 14 months or 230 hours. At issue, the aircraft had 9,269.8 hours total time in service and was approved in the aerial work category and for flight under the instrument flight rules (IFR).[7]
On the morning of 27 September, prior to departure from Saipan, the aircraft had a total of 9291.7 hours in service.
Survey equipment
The aircraft was usually used for aerial survey work and had been fitted with an electromagnetic (EM) loop system under an Engineering Order[8] (EO) and an associated FMS had been issued. The system consisted of a copper cable loop suspended around the aircraft and supported by nose, wingtip and tail stingers with a transmitter mounted in the cabin. A receiver (bird) could be towed behind the aircraft on a cable, extended and retracted using a winch. The cable, bird and its cradle, and wingtip stingers had been removed in preparation for the ferry, and the tail stinger had been shortened but was still fitted to the aircraft. EM equipment in the cabin had also been removed, except for some fixed cables.
As the equipment was fitted under an EO, the aircraft had a Special Certificate of Airworthiness (CoA) that limited aircraft operation to the restricted category, for the purpose of aerial surveying.
The FMS for the EM loop limited the aircraft to a maximum operating airspeed of 161 kt and a maximum operating altitude of 20,000 ft, however, most of the equipment had been removed from the aircraft for the ferry. The design holder of the EM loop system advised the ATSB that exceeding the altitude limit had no safety implications in that configuration.
Although the aircraft was permitted to operate in IFR conditions, flight into known icing conditions was prohibited.
Ferry fuel tank and special flight permit
An aircraft that is not operated in accordance with its Type Certificate (and approved Supplementary Type Certificates) is not permitted to operate in foreign countries without a Special Flight Permit (SFP) and the approval of all countries the aircraft flies over or into.
For the ferry, FAY had been fitted with a ferry fuel tank under an engineering order with an associated FMS. The ferry fuel tank fitment meant that the aircraft no longer met the design requirements for the aircraft. Therefore, the aircraft was required to operate under an SFP. An SFP was issued on 6 September 2018 by a person authorised by CASA to issue SFPs, but not to issue overweight approvals.
The aircraft Type Certificate Data Sheet (TCDS) stated that the aircraft was structurally satisfactory for ferry flight up to 130 per cent of the TCDS MTOW (which equates to 11,375 lb or 5,160 kg). However, without overweight approval, the aircraft was required to be operated not above the STC MTOW of 9,062 lb (4,110 kg). The ferry tank FMS stated that ‘the ferry tank may only be able to be partially filled to stay within the aircraft 9062 lbs MTOW.’
Weight and balance
The load sheet indicated that on departure from Saipan, the aircraft’s take-off weight was 4,430 kg and it was loaded within the centre of gravity and structural limits.
Journey logs
The pilot completed journey logs for each flight sector, which included a daily inspection certification, take-off, landing and flight times, and fuel information. The pilot had also recorded engine condition trend monitoring information including the exhaust gas temperature (EGT) and RPM percentage. These are depicted in Table 1.
Table 1: Trend exhaust gas temperature (EGT) and engine RPM
Date
EGT (°C)
RPM (%)
15 September
657
100.5
16 September
658
100.4
17 September
658
100.2
Source: Aircraft operator
Operating the engine at 100.2 to 100.9 per cent was within the normal continuous engine speed allowable range. The FMS for the engine specified the maximum EGT as 650 °C. The engine manufacturer advised that operating at an average EGT of 658 °C relative to 650 °C increased fuel flow by about 5 lb (2.8 L) per hour under the conditions of the accident flight. The aircraft operator’s head of airworthiness and maintenance control advised that no inspection was needed for the recorded temperature exceedances, which could be avoided if the pilot reduced RPM to 100 per cent.
The journey logs were sent to the operator each day, however they were not reviewed during the ferry flight.
Communications
Radio equipment
The aircraft was fitted with the following equipment:
two VHF radios
one HF radio
a Spidertracks GPS connected via a switch on the instrument panel to a hot bus straight to the aircraft battery, so it would continue to operate in case of electrical failure
one Artex G406-4 emergency locator transmitter fitted with a G shock and remote panel switch
a satellite phone was installed in the aircraft, docked and with Bluetooth connection
four personal locator beacons (MT410G) and one Kannad marine sport emergency position indicating radio beacon were on board, all of which needed to be manually activated.
The pilot had a Garmin inReach system from which he could send and receive messages, navigate and track flights and ‘if necessary, trigger an SOS to get emergency help from a 24/7 global monitoring via the 100% global Iridium® satellite network.’
Push to talk
When the company licenced aircraft maintenance engineer (LAME) arrived in Saipan, the pilot advised him that the pilot-side push-to-talk (PTT) button had only been working intermittently and reported that he had been using the co-pilot-side PTT. The LAME cleaned and tested the button, which the pilot then verified was transmitting correctly.
Recorded data
GPS data
The on-board Spidertracks and Garmin GPS devices recorded the aircraft’s position and geometric altitude at 2-minute intervals. The recorded altitude of all sectors flown from Jandakot Airport to the last recorded position is shown in Figure 4. About half of the first leg, from Jandakot to Alice Springs, was flown at FL 210 before descending to FL 130, which was also the cruise altitude on the following sector to Weipa. On the flight from Horn Island to Saipan, having conducted a climb to FL 200, the pilot then made a descent over Papua New Guinea, possibly to avoid weather near Mount Hagen, before climbing and then maintaining FL 200.
The geometric altitude for the occurrence flight from Saipan showed a gradual descent from top of climb at 23,412 ft to the last recorded position at 22,770 ft. This was consistent with the aircraft flying into reducing temperature and barometric pressure. The corresponding radar data recorded pressure altitude at intervals of about 10 seconds and showed a constant altitude at 22,000 ft AMSL.
The pilot sent several messages from the Garmin device after departing Saipan and before the aircraft reached reporting point TEGOD. The last position recorded by the Spidertracks and Garmin devices was at 0626 UTC at FL 220. The aircraft took less than 2 minutes to descend from FL 220 to the ocean and there were no GPS recorded points below that altitude.
Figure 4: Geometric altitude of all flight sectors
Source: Spidertracks analysed by ATSB
Radar and ADS-B data
Japanese air traffic services recorded mode C radar and automatic dependant surveillance broadcast (ADS-B) data from FAY. Secondary surveillance radar (SSR) returns depend on an aircraft transponder’s reply to an interrogation from the ground. In response to a mode C interrogation, the aircraft transmits an encoded return with the aircraft’s selected SSR code and pressure altitude.
Radar data recorded the aircraft’s position (in X and Y coordinates) from the ground radar site and pressure altitude (referenced to 1013 hPa and quantised to the nearest 100 ft) at approximately 10-second intervals. ADS-B data transmitted from FAY’s GPS included the aircraft’s altitude within about 25 ft.
The aircraft was recorded by radar at 22,000 ft at 0627:36 and there were five valid radar returns after that. The data showed that the aircraft descended from 22,000 to the last recorded position of about 11,500 ft in 62 seconds, with an increasing descent rate of up to 22,000 and 23,000 ft/min. That descent rate was less than the dive speed (VD)[9] for the aircraft (250 kt calibrated airspeed), which corresponded to a vertical descent rate of about 25,300 ft/min.
Recorded audio transmissions
The ATSB obtained recorded audio of the pilot’s transmissions on HF radio to Tokyo Radio and VHF transmissions while tracking across Australia. Comparative analysis of these was carried out with the aim of determining whether the pilot was likely to have been using a nasal cannula and/or affected by hypoxia in the final transmission. Indicators of hypoxia include timing of microphone keying, voice onset time and fundamental frequency range of the pilot’s voice, but these could not be measured due to the noise in the HF channels. The pilot’s communications with Tokyo Radio at TEGOD included some hesitation and a misstated time, but the tempo of the pilot’s next transmission appeared normal and he corrected the time error. The ATSB was unable to make any conclusions based on the recorded audio.
Fuel
The aircraft was fitted with left- and right-wing tanks, which held a combined total of 1,257 L (2,225 lb) of usable fuel. The ferry tank held 924 L (1,635 lb) of usable fuel. The ferry tank was fitted under an engineering order with an associated FMS.
Based on the journey log and fuel dockets, the aircraft ferry and wing tanks were filled in Saipan on 18 September. Although the pilot had taxied the aircraft for maintenance, the fuel was likely close to full on departure. The LAME in Saipan had seen the pilot conduct a pre-flight fuel sample drain from the aircraft and check for contaminants, on the morning prior to departure.
There was no published fuel flow data for flight at FL 220, but the pilot reported an in-flight fuel consumption rate of 163 L/hr (288 lb/hr), which would have been relatively constant for the 6.4 hours in cruise. The aircraft took about 1 hour from taxi to reaching top of climb at 22,000 ft. The operations manual specified a planned fuel burn rate of 450 lb/hr in the climb and the design holder for the engineering orders estimated a taxi and climb fuel consumption of 353 lb. Given the pilot had previously started the aircraft and taxied for maintenance, an estimated fuel consumption for the taxi and climb was 400 lb. Based on these figures, the estimated total fuel used at the last recorded position was 1,241 L (2,196 lb), which was approximately the combined volume of the wing tanks.
Fuel transfer and imbalance
The fuel transfer protocol detailed in the ferry tank FMS was to conduct the take-off and climb to altitude using both aircraft main fuel tanks and, when established in the cruise, turn the left-wing tank selector to off, as fuel in the ferry tank could only be transferred to the right-wing tank. Two electric ferry tank pumps could be selected with different flow rates – 440 lb/hr (low) and 600 lb/hr (high). There was no gauge to indicate fuel quantity remaining in the ferry tank, and the pilot was required to monitor the fuel quantity of the right-wing tank to ensure fuel was transferring as planned and that fuel was not venting overboard.
The FMS specified 200 lb as the maximum permitted fuel imbalance between the left and right tanks. When more severe sideslip is maintained (due to imbalance), the unusable fuel quantity increases. In this occurrence, if the left tank selector was set to off at the top of climb and the right tank was used until empty, it was possible to have a 900 lb imbalance.
In August 1998, the Cessna Aircraft Company conducted flight tests at the request of the US National Transportation Safety Board to determine controllability of the Cessna 208B at various airspeed and lateral fuel imbalance combinations. A Cessna 208B aircraft was flown to a maximum 600 lb imbalance, at airspeeds between 70 and 120 kt at flap settings of 0° and 20°. The maximum control wheel deflection attained was about 28°, of the maximum available 55° control wheel deflection. Control deflection versus lateral imbalance curves were derived from the test. The ATSB extrapolated the data and found that for a 900 lb imbalance, at the aircraft’s likely airspeed, this equated to a control wheel deflection of +14°-17° and right aileron travel of +5-7°.
The aircraft manufacturer (now Textron Aviation) advised the ATSB that the autopilot servo was capable of driving the ailerons to the travel limits of 25° +4°/-0° up and 16° +1°/-0° down in the hangar. This indicated that if the aircraft had a fuel imbalance of 900 lb, there was adequate aileron control to maintain level flight at the aircraft’s likely airspeed, however the autopilot force required to maintain this was not assessed. Photos from the JASDF of FAY in the final 30 minutes of the flight did not show any visible aileron deflection.
Weather
During the last 30 minutes of the flight, the aircraft was observed to be situated between two layers of cloud. The weather conditions that the aircraft likely encountered at FL 220 included strong south-westerly winds averaging about 50 kt, temperature about -15 °C and moderate turbulence. Moderate icing and light rain were present in cloud.
Supplemental oxygen
Because of reduced atmospheric pressure, operation of unpressurised aircraft in Australia above 10,000 ft requires supplemental oxygen.
Flight crew oxygen requirements
Australian Civil Aviation Order (CAO) 20.4 – Provision and use of oxygen and protective breathing equipment, stated:
A flight crew member who is on flight deck duty in an unpressurised aircraft must be provided with, and continuously use, supplemental oxygen at all times during which an aircraft flies above 10 000 feet altitude.
CAO 108.26 – System specification – oxygen systems included that portable oxygen units may be used to meet the crew or passenger breathing requirements and that:
…flight crew members may use nasal cannula manufactured under the name “Oxymizer”, subject to the following conditions… (b) the flight crew members must use the nasal cannula only during private, aerial work, or charter, operations; (c) the aircraft must not operate above 18 000 feet altitude.
Further, it stated that ‘Dispensing units provided in an aircraft operating above flight level 180 must be designed to cover the nose and mouth.’
Aircraft oxygen system
The aircraft was fitted with a 13-port oxygen system with a 3.312 cubic metre (116.95 cubic foot) capacity oxygen cylinder located in the fuselage tail cone. The cylinder had been tested and maintained in accordance with requirements, was within its 15-year life limit and had been filled with aviator breathing oxygen (ABO) prior to the aircraft’s departure from Jandakot.
Oxygen from the cylinder was first reduced to 70 PSI by a pressure regulator and then by two altitude-compensating regulators located between the pressure regulator and oxygen supply lines, which automatically varied the flow of oxygen to the masks with changes in altitude. A remote shut-off valve in the overhead console was used to shut off the supply of oxygen to the system when not in use. A cylinder pressure gauge was located on the overhead console above the pilot’s (and copilot’s) seat.
A microphone-equipped Cessna mask with a vinyl plastic hose and flow indicator was stored under the pilot’s seat. It was observed to be in its packaging (unused) when the aircraft was in Saipan.
On-demand system
The pilot had a battery-operated Mountain High (MH) Pulse-Demand™ Electronic Delivery System (EDS) O2D1 (single-person) model (Figure 5). The EDS unit supplied a measured pulse of oxygen at the beginning of each inhalation and was oxygen-compensating (increasing flow with altitude). The unit had audible and illuminating flow fault and apnoea alarms. A representative from Mountain High advised that although the ceiling of the MH EDS is 25,000 ft, at 22,000 ft it is at the maximum flow rate requirement for oxygen.
Figure 5: Mountain High Pulse-Demand Electronic Delivery System O2D1
Source: Mountain High
Cannula
The pilot preferred to use a nasal cannula for oxygen delivery and he intended to use it for the ferry flight. This was consistent with the supplied oxygen mask being unused before departing Saipan, despite two previous sectors above 18,000 ft. The pilot had also sent a message on the previous sector, indicating that he was using the cannula at 19,000 ft.
The ATSB could not establish the cannula model used for the ferry, however the MH EDS manual stated ‘Use only the supplied MH EDS cannula, as other cannulas may not work properly with the EDS.’ The standard MH nasal cannula (Figure 6) differed from the Oxymizer specified in CAO 108.26, which had a reservoir that stored oxygen during the exhalation then added it to the delivery during inhalation to increase oxygenation. Mountain High advised that the risks of wearing a cannula are:
it is ineffective if the pilot has nasal congestion, is eating, talking or mouth-breathing
it can come away from the nose, which would also trigger the apnoea alert.
Figure 6: Mountain High nasal cannula
Source: Mountain High
In-line regulator
The EDS was required to be operated with an oxygen inlet pressure between 16 and 20 PSI, which could be achieved with an in-line regulator (Figure 7). The MH EDS manual indicated that the flow of oxygen would be unnecessarily high between 20-30 PSI. The manual also included the warning that higher pressure ‘will not only compromise the performance of the EDS, but is likely to damage the internal breathing sensor, rendering your EDS unit inoperable.’ MH advised that pressures above 30 PSI would cause the valve to open up and result in the EDS working like a constant flow system. In this situation, the apnoea alert would sound out constantly until the oxygen supply was nearly depleted.
The pilot did not have an in-line regulator for the flight. At altitudes above 17,000 ft, the aircraft’s system provided oxygen at 21.55 ± 2.5 PSI, which was higher than the EDS inlet pressure range. At 20,000 ft, this increased 24.45 ± 2.5 PSI. There was no data for the output pressure at 22,000 ft.
Figure 7: In-line regulator to connect EDS to aircraft oxygen outlet
Source: Mountain High
Mountain High aluminium cylinders
In his briefing before the aircraft departed Jandakot, the chief pilot understood that the pilot intended to plug his EDS directly into the aircraft system without an in-line regulator and was concerned about its effectiveness. Therefore, to ensure the pilot had an independent oxygen supply, the operator provided two MH aluminium (AL682) cylinders fitted with MH regulators, each of which had a maximum volume of 0.68 cubic metres (24.1 cubic feet) and a ‘typical volume’ of 0.63 cubic metres (22.1 cubic feet). The cylinders were filled with ABO and secured behind the copilot’s seat, which the pilot could reach if he slid his seat backwards.
Flight above FL 180
The MH EDS manual advised that pilots operating above 18,000 ft should have a supplementary oxygen cylinder gauge and an emergency backup oxygen system. The manual also provided full cylinder duration figures up to its ceiling of 25,000 ft and cylinder duration graphs from which to calculate usable oxygen for altitudes up to 18,000 ft.
The FAA pilot safety brochure Oxygen equipment: Use in General Aviation Operations stated that the use of cannulas was restricted by US Federal Aviation Regulations to 18,000 ft ‘because of the risk of reducing oxygen-blood saturation levels if one breathes through the mouth or talks too much.’
The aircraft operator’s operations manual approved the use of the MH EDS O2D2 and MH standard aviation nasal cannula up to FL 180, above which pilots were required to use a constant flow mask.
Pulse oximeter
To aid in identifying the symptoms of hypoxia, the pilot had a pulse oximeter, which showed blood oxygen saturation levels based on reading from the finger. On a previous flight the pilot was observed only to use the oximeter intermittently.
The US Federal Aviation Administration (FAA) cautions against relying on pulse oximeters as the sole indicator of hypoxia because by the time the oxygen saturation levels fall, it may result in a level of hypoxia sufficient to cause impairment. Further, the haemoglobin oxygen saturation in blood passing through the finger may not reflect oxygen available to the brain.
Pilot’s oxygen usage
An oxygen management plan from the pilot was not provided to the operator, however there were three sources of oxygen available to the pilot – the aircraft oxygen system and two aluminium cylinders, which were all filled prior to departure from Jandakot. It was not known which source the pilot used and when, but only one cylinder remained behind the copilot’s seat prior to the aircraft departing Saipan. This suggests the pilot had used one cylinder during the flights to Saipan. The pilot had not refilled the aircraft or portable oxygen cylinders since commencing the ferry.
The ATSB estimated whether the pilot had sufficient oxygen to complete the sector. This was based on the time at various altitudes flown for all sectors up to the last recorded aircraft position, and the expected endurance of the available oxygen, filled to typical pressures, according to the manufacturer’s documentation. The estimation was also based on using the available equipment as follows:
oxygen was used at all altitudes above 10,000 ft
the nasal cannula was used with the MH cylinders at all flight levels
the aircraft system was used with a mask or cannula, with or without the EDS.
The pilot’s actual equipment usage may have varied from these assumptions and it is acknowledged that oxygen usage can vary significantly between individuals, especially with on‑demand systems. However, it represented realistic usage scenarios and approximate endurance for the available oxygen. Even when conditions of highest usage were considered, there should have been several hours of oxygen remaining at the completion of the sector to Japan.
Hypoxia
Hypoxia is the absence of an adequate supply of oxygen to the tissues. Hypobaric hypoxia is the most common form in aviation and is associated with breathing air at low barometric pressure. A deficiency in alveolar oxygen exchange due to low oxygen tension (partial pressure) of inspired air leads to inadequate oxygen supply to the blood and reduced oxygen available to the tissues.
Hypoxia can be prevented by pressurising the aircraft cabin or by breathing supplemental oxygen. However, hypoxia can still occur in unpressurised aircraft if, for example, the supply equipment fails and/or does not provide an adequate concentration of oxygen or if the supply is not managed appropriately. In an aviation context, acute hypobaric hypoxia is the ‘most serious single physiological hazard during flight at altitude.’ [10]
Signs and symptoms of hypobaric hypoxia include:
darkening and restriction of the visual field and loss of peripheral vision
increased heart rate, hyperventilation and light-headedness
syncope (fainting/unconsciousness, pallor, sweating, nausea and vomiting)
cyanosis (bluish colouration of the skin, nail beds and mucous membranes)
impairment of mental performance and neuromuscular control, slowed reaction time
muscular spasms.
From 15,000 to 20,000 ft ‘there is a loss of critical judgment and willpower…the subject is usually unaware of any deterioration in performance or indeed of the presence of hypoxia; it is this that makes the condition such a potentially dangerous hazard in aviation.’ Above 20,000 ft these symptoms and signs become more pronounced. Involuntary jerks of the arms, loss of consciousness and convulsions occur, and after several minutes, death.
Physical activity, cold, illness and certain drugs increase the onset speed and severity of hypoxia.
US FAA Advisory Circular AC_61-107B Aircraft operations at altitudes above 25,000 feet mean sea level or Mach numbers greater than .75 indicated that while the signs of hypoxia can be detected in an individual by an observer, signs are not a very effective tool for hypoxic individuals to use to recognize hypoxia in themselves. The circular carried the following warning:
A common misconception among pilots is that it is easy to recognize the symptoms of hypoxia and to take corrective action before becoming seriously impaired. While this concept may be appealing in theory, it is both misleading and dangerous for crewmembers.
Above this altitude, complete incapacitation can occur with little or no warning. All senses fail, and a pilot will become unconscious within a very short period of time. No stimuli such as the radio will be able to help a pilot suffering from hypoxia, especially [rapid onset] fulminant hypoxia, above 5,500 meters (18,000 feet).
A less common form of hypoxia in an aviation context is anaemic hypoxia, caused by carbon monoxide poisoning. This is most commonly associated with piston engine aircraft, in drawing air for cabin heating over a damaged or defective exhaust system. Turbine engines produce up to two orders of magnitude lower carbon monoxide emissions than piston engines and utilise compressor bleed air as opposed to an exhaust heat exchanger. In addition, in 1984, the US National Transportation Safety Board investigated the possible effect of engine oil bleed air contamination on pilot incapacitation, from Garrett TPE 331 engines. It was concluded that such contamination was not likely to occur.
Time of useful consciousness
The FAA circular referenced above (AC_61-107B) defined the time of useful consciousness (TUC) as ‘the period of time from interruption of the oxygen supply, or exposure to an oxygen-poor environment, to the time when an individual is no longer capable of taking proper corrective and protective action.’ There are significant variations in TUC between individuals, and it does not mean that everyone will be capable of performing complex tasks in a challenging environment for the duration.
The circular included a graph showing decreasing TUC with increasing altitude (Figure 8). At 22,000 ft, the TUC was 10 minutes, or 5-6 minutes following rapid decompression. However, it goes on to caution that slow decompression is as dangerous as, or more dangerous than, a rapid decompression, as the resultant hypoxia may be unrecognized by the pilot. The circular also carried the warning: ‘The TUC does not mean the onset of unconsciousness. Impaired performance may be immediate.’
Figure 8: Times of useful consciousness versus altitude
Source: FAA AC 61-107B
Pilot exposure and training for high altitude flying
There was evidence from previous flights that the pilot had some exposure to operating at higher altitudes. The pilot also held a valid US type rating for a Bombardier Challenger aircraft which had a service ceiling above FL 250. Under US Code of Federal Regulations Part 61.31 (g), this required completion of ground theory training including the effects, symptoms and causes of hypoxia and any other high-altitude sickness. The pilot had completed theoretical hypoxia awareness training and reported being aware of his own initial signs of hypoxia.
Altitude-induced decompression sickness
Flying unpressurised aircraft above 18,000 ft can not only induce hypoxia, but also result in altitude-induced decompression sickness (DCS). This is the formation of nitrogen bubbles in different areas of the body due to exposure to reduced barometric pressure. According to the FAA pilot safety brochure on decompression sickness, in most cases of DCS, the bubbles form in the joints, but in 10-15 per cent of cases, neurological manifestations occur. These can include similar symptoms to hypoxia such as confusion, seizures and unconsciousness.
While most cases occur at or above 25,000 ft, the risk of DCS increases with exposure to altitudes above 18,000 ft.
Oversight of the ferry flight
The aircraft operator’s Air Operator Certificate (AOC) was for aerial work and as such, it was not a regulatory requirement to have a formal safety management system. Despite this, the aircraft operator had implemented a health, safety and environmental operating management system (HSE-OMS) that applied to their aviation activities, most of which were low-level survey operations.
FAY was routinely ferried to new surveying locations with its specialised equipment installed. Although ferry flights were classed as private operations, they were normally carried out by company pilots, operating under the AOC. The flights were conducted in accordance with the standard operating procedures and the chief pilot was responsible for operational matters affecting the safety of flying operations. However, following the successful ferry of FHY from Canada to Western Australia by the contract pilot 6 months earlier, the operator elected to re‑engage the contract pilot to ferry FAY to the US.
Risk assessment for the ferry flight
The operator initially conducted a gap analysis to identify any changes that had occurred since the ferry of FHY. It identified several actions, including the need to audit the pilot’s qualifications, conduct a familiarisation flight and briefing on the aircraft and fitments, and for flight monitoring by company staff.
At the planning stage of the FAY ferry, the primary concerns of the operator were around managing:
long sectors over water – fatigue, lack of alternate landing areas and distance from search and rescue assistance
single-pilot operation – the operator required their own ferry flights to be conducted with two crewmembers, but the contracted ferry pilot preferred to operate alone
routing – including consideration of security in countries to be overflown.
In accordance with the HSE-OMS, the operator then conducted a risk assessment for the ferry flight. The operator’s risk matrix guidelines included:
The Risk Matrix must be used with good judgment, applying the following recommendations:
- Make use of the experience of several people, with a broad range of experience and backgrounds.
- Within the defined context, the relevant hazards should be identified and documented in the hazard libraries.
- For an identified hazard, the potential consequences (severity) are determined first. A hazard can have a consequence in several categories…
- Risk must be assessed in the context of an activity as hazards manifest themselves differently in different environments or conditions…
The aviation manager reported that he had done the risk assessment based on what the company had experienced in previous ferries and general risk assessment from their operations. The quality assurance manager and flight operations administrator were involved in the assessment process. He also obtained input from the company’s aviation specialist in Canada, who had been involved with the risk assessment for the previous ferry (of FHY). The assessment report was then provided through to their HSE manager.
The HSE manager commented that normally they would get flight operations personnel involved; he, the chief pilot, the aviation manager, a ferry pilot, and a couple of other pilots would form a team. However, the HSE manager had been on vacation during the ferry risk assessment and had not been involved in the process.
The risk assessment identified 32 hazards including one relating to hypoxia:
Unconscious pilot due to oxygen starvation [resulting in] uncontrolled flight into terrain.
It was initially rated as moderate and assessed as unlikely to occur. The nominated control to reduce risk was that there was an oxygen system fitted to the aircraft, with no resultant change to the risk rating (or likelihood). Consideration of specific operational or technical factors that could contribute to hypoxia were not included in the risk assessment. Nor was any form of pilot incapacitation other than hypoxia.
Nearly half of the identified hazards nominated the pilot’s experience (having conducted over 200 ferry flights, including multiple recent Pacific crossings) as one of, or the only risk control. The assessment did not detail whether the pilot had considered the hazards or associated risks, or how he proposed to mitigate them. However, the day before FAY departed Jandakot, the ferry pilot reviewed the risk assessment in conjunction with the operator and suggested additional risks, including road transport, ‘poor decision making due client pressure,’ and access to food and medical support. The chief pilot and a senior company pilot later outlined to the ATSB that they assessed the pilot as being ‘quite organised and competent’, albeit with a clear preference for doing things his own way.
Aircraft operator and pilot agreement
The contract between the pilot and aircraft operator for the ferry detailed the responsibilities of each party, and stipulated how the aircraft was to be operated, including the requirement to adhere to standard operating procedures as specified in the operations manual.
The ‘International Operations’ section of the operations manual included requirements for approvals, permits and documentation associated with travelling to foreign countries as well as flight planning, flight following and emergency equipment. In the agreement between the aircraft operator and the contract pilot, most of these responsibilities had been assigned to the pilot to manage. Of significance, the section stated that ‘In general, the Chief Pilot will manage an overseas operation. Close liaison between the aircrew and the Chief Pilot or their delegate is essential.’
The chief pilot had commenced with the operator on 28 August 2018, two weeks before FAY departed Jandakot on the ferry flight. The chief pilot had previously conducted ferry flights for a different operator, but was inexperienced on the C208 aircraft type. Additionally, because the ferry was assigned to a contract pilot, the chief pilot reported having been informed that he was not required to have involvement in the conduct of the operation, other than briefing the ferry pilot prior to departure.
Along with the risks inherent to the type of operation, the aircraft operator had considered the additional threats posed by financial incentive to complete the ferry as expeditiously and cost-effectively as possible. To this end, the contract included that the pilot would be paid for any days delayed on the ground to reduce pressure to continue the flight in adverse conditions. The pilot was responsible for fuel, oil and other en-route costs such as accommodation and food.
Pre-flight briefing and familiarisation flight
The day before the ferry flight departed from Jandakot, the pilot completed an aircraft familiarisation flight with a senior company pilot experienced in ferry flights, and a briefing with the chief pilot. The familiarisation flight focused on aircraft handling and use of the ferry tank fuel. The chief pilot’s briefing was primarily about the aircraft’s minimum equipment list and safety equipment. These measures had been identified in the gap analysis but not included in the risk assessment.
When the chief pilot briefed the ferry pilot, he was concerned about the pilot’s intention to connect his EDS unit to the aircraft oxygen system without the requisite regulator. To address the concern, he provided the pilot with the two portable oxygen cylinders that were appropriate for use with the pilot’s equipment. The risk assessment did not include the pilot’s oxygen management plan and further risk assessment was not done to assess the effect of the additional oxygen sources.
Flight following
The gap analysis indicated that company operations staff would be responsible for flight following. As required by the contract, the pilot sent the flight plan and journey logs to the operator each day, however they were not reviewed by the operator until after the aircraft disappeared from radar. The logs showed the pilot consistently operated the aircraft engine above the exhaust gas temperature (EGT) limit of 650 °C. Additionally, on the first sector to Alice Springs, the aircraft was flown at 21,000 ft and the final sector from Saipan was at 22,000 ft. Operations staff did not contact the pilot about exceeding the 20,000 ft limit.
Flight plan
The flight plan that the aircraft operator obtained, which was submitted for the planned flight from Saipan to New Chitose Airport, showed the flight planned altitude as FL 250, total estimated elapsed time of 10 hours and 15 minutes and (fuel) endurance of 9 hours and 30 minutes. The discrepancy with the planned flight time exceeding the endurance may have been a transposition error by the pilot, however neither this, the lack of alternates, nor the planned altitude in excess of the 20,000 ft limit was identified or amended prior to departure.
The flight plan obtained by Japan Civil Aviation Bureau was sent from Honolulu at 0507 UTC on 26 September, before the aircraft departed Saipan. That flight plan had a planned cruising level of FL 220 and a total estimated elapsed time of 8 hours and 53 minutes.
Summary of operational oversight
The aircraft operator had processes in place to identify and manage the risks associated with the ferry flight. This included conducting a gap analysis and risk assessment, familiarisation flight and pre-flight briefing, which identified the potential issue with pilot’s intended use of the oxygen system.
The operator also relied on the pilot’s extensive ferry experience to bring level of safety to the ferry flight. However, many of the risk controls relied solely on the pilot’s experience and did not provide any detail on the steps the pilot had taken to manage those risks. The flight also took place outside of the company’s standard procedures and without the normal level of oversight from operations personnel, both of which could have provided an additional opportunity to identify and manage the hazards associated with the ferry flight.
Previous occurrences
ATSB research publication Pilot Incapacitation – Analysis of medical conditions affecting pilots involved in accidents and incidents (2007), reviewed occurrences recorded by the ATSB from 1 January 1975 to 31 March 2006. It identified three cases of hypoxia, which was 3 per cent of the medical/incapacitation events. One of those was a Beech Super King Air aircraft (VH-SKC) near Burketown, Queensland on 4 September 2000. The ATSB investigation report (200003771) assessed that the incapacitation of the pilot and seven passengers was probably due to hypobaric hypoxia due to operating at high cabin altitude and not receiving supplemental oxygen. The report also identified that all the fatal accidents where medical conditions or incapacitation occurred were single-pilot operations where there was no second pilot on board who could assume control of the aircraft and prevent an accident.
The ATSB investigated an incapacitation event involving a Raytheon Aircraft Super King Air 200, VH-OYA, which occurred on 21 June 1999 (199902928). As the aircraft climbed through 10,400 ft, the pilot inadvertently selected the ‘bleed air off’, which prevented the aircraft from pressurising. As the aircraft reached the planned cruising altitude of FL 250, the aircraft deviated from the assigned track and the pilot was observed repeatedly attempting to program the GPS. Shortly afterwards, the pilot lost consciousness. The passenger in the co‑pilot seat took control of the aircraft and conducted an emergency descent, during which the pilot regained consciousness. The investigation findings included that hypobaric training did not provide an effective defence to ensure the pilot (or passengers) would identify the onset of hypoxia.
ATSB investigation AO-2014-134: Flight crew incapacitation involving a Reims F406, VH-EYQ near Emerald Airport, Qld on 1 August 2014. The pilot and navigator were planning to conduct a survey operation at FL 240. The aircraft was unpressurised but fitted with an oxygen system. Having selected the oxygen supply on and donned oxygen masks, passing about FL 180, the pilot noticed the blood saturation level reporting on his oxygen pulse meter was 77 per cent instead of above 90 per cent. In a hypoxic state, the pilot worked to rectify a problem with his oxygen system connection with assistance from the navigator and air traffic control. In this case, the pilot subsequently commented that his hypoxia awareness training had aided his appreciation of his symptoms and effects of hypoxia.
On 23 September 2012, a Metro 3 aircraft, VH-SEF, failed to pressurise on climb (ATSB investigation AO-2012-127). Passing FL 140, the captain started to feel the effects of hypoxia, donned an oxygen mask, and the first officer took over flying the aircraft and conducted an emergency descent to 10,000 ft.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Aircraft operator
As a result of this occurrence, the aircraft operator has advised the ATSB that they are taking the following safety actions:
Risk assessment and standard procedures
The aircraft operator reviewed their risk assessment processes and the standard operating procedures for conduct of ferry flights. As a result, they amended the guidance for international ferry operations in their operations manual including: maximum sector length, fuel planning, mandating two-crew operations, oxygen planning, management and training, operating altitude limitations, and use of contract pilots.
Oxygen use guide
The aircraft operator also created an oxygen use guide and a specific risk assessment for positioning (ferry) flights.
The occurrence
What happened
The pilot of a Cessna 208B aircraft, registered VH-FAY (FAY), was contracted to ferry the aircraft from Jandakot Airport, Western Australia (WA), to Greenwood, Mississippi in the United States (US). The pilot planned to fly via the ‘North Pacific Route’ (Figure 1).
At 0146 Coordinated Universal Time (UTC)[1] on 15 September 2018, the aircraft took off from Jandakot Airport, WA, and landed in Alice Springs, Northern Territory at 0743. After landing, the pilot advised the aircraft operator that the aircraft had a standby alternator fault indication. In response, two company licenced aircraft maintenance engineers went to Alice Springs and changed the alternator control unit, which fixed the problem.
Late the next morning, the aircraft departed Alice Springs for Weipa, Queensland, where the pilot refuelled the aircraft and stayed overnight.
On the morning of 17 September, the pilot conducted a 1-hour flight to Horn Island, Queensland. About an hour later, the aircraft departed Horn Island with the planned destination of Guam, Micronesia. While en route, the pilot sent a message to the aircraft operator advising that he would not land in Guam, but would continue another 218 km (118 NM) to Saipan, Northern Mariana Islands. At 1003, the aircraft landed at Saipan International Airport.
The next morning, the pilot refuelled the aircraft and detected damage to the propeller anti-ice boot. The aircraft was delayed for more than a week while a company engineer travelled to Saipan and replaced the anti-ice boot.
Figure 1: North Pacific Route
Source: Aircraft operator – annotated by ATSB
At 2300 UTC on 26 September, the aircraft departed Saipan, bound for New Chitose Airport, Hokkaido, Japan. Once airborne, the pilot sent a message from his Garmin device, indicating that the weather was clear and that he had an expected flight time of 9.5 hours.
About an hour after departure, the aircraft levelled out at flight level (FL) 220.[2] Once in the cruise, the pilot sent a message that he was at 22,000 feet, had a tailwind and the weather was clear. This was followed by a message at 0010 that he was at FL 220, with a true airspeed[3] of 167 kt and fuel flow of 288 lb/hr (163 L/hr).
At 0121, while overhead reporting point TEGOD (Figure 2), the pilot contacted Tokyo Radio flight information service[4] on HF radio. The pilot was next due to report when the aircraft reached reporting point SAGOP, which the pilot estimated would occur at 0244. GPS recorded track showed that the aircraft passed SAGOP at 0241, but the pilot did not contact Tokyo Radio as expected. At 0249, Tokyo Radio made several attempts to communicate with the pilot on two different HF frequencies, but did not receive a response. Tokyo Radio made further attempts to contact the pilot between 0249 and 0251, and at 0341, 0351 and 0405.
Figure 2: VH-FAY GPS recorded track
Source: Aircraft operator, Google Earth – annotated by ATSB
About 4.5 hours after the pilot’s last communication, two Japan Air Self-Defense Force (JASDF) aircraft intercepted FAY. The pilot did not respond to the intercept in accordance with international intercept protocols, either by rocking the aircraft wings or turning, and the aircraft continued to track at FL 220 on its planned flight route. The JASDF pilots were unable to see into the cockpit to determine whether the pilot was in his seat or whether there was any indication that he was incapacitated. The JASDF pilots flew around FAY for about 30 minutes, until the aircraft descended into cloud.
At 0626 UTC, the aircraft’s GPS tracker stopped reporting, with the last recorded position at FL 220, about 100 km off the Japanese coast and 589 km (318 NM) short of the destination airport. Radar data showed that the aircraft descended rapidly from this point and collided with water approximately 2 minutes later. The Japanese authorities launched a search and rescue mission and, within 2 hours, searchers found the aircraft’s rear passenger door (Figure 3). The search continued until the next day, when a typhoon passed through the area and the search was suspended for two days. After resuming, the search continued until 27 October with no further parts of the aircraft found. The pilot was not located.
The sources of information during the investigation included the:
Aircraft operator and maintainer
Aircraft engineer and design holder
Japan Transport Safety Board
Civil Aviation Safety Authority
Bureau of Meteorology
Honeywell
Textron Aviation
United States National Transportation Safety Board.
References
Campbell RD, Bagshaw M 2002, Human performance and limitations in aviation, Blackwell Science Ltd.
Gradwell DP, Rainford DJ 2006, Ernsting’s aviation medicine, Edward Arnold (Publishers) Ltd London, Chapter 3.
Newman, DG 2004, Flying fast jets: Human factors and performance limitations, CRC Pres LLC.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the aircraft operator, aircraft maintainer, aircraft insurance assessor, Civil Aviation Safety Authority, Japan Transport Safety Board, US National Transportation Safety Board, Textron Aviation, Honeywell, Thomson Design and Mountain High.
Submissions were received from the Japan Transport Safety Board, Honeywell, aircraft insurance assessor, aircraft operator, Thomson Design and Mountain High. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
What happened
On 7 September 2018, a Yakovlev Aircraft Factories YAK-9UM aircraft, registered VH-YIX (Figure 1), was being operated on a private flight from Latrobe Regional Airport, Victoria. The pilot/owner of the aircraft was the sole occupant.
The aircraft departed the airport at about 1425 Eastern Standard Time.[1] Recorded air traffic control data showed that the aircraft initially tracked from the airport to the west toward Morwell, climbing to about 2,600 ft and heading north-west near Moe.
Several witnesses described seeing the aircraft conducting aerial manoeuvres to the north of Moe and video footage from a witness showed the aircraft in a steep spiralling dive shortly before it collided with terrain (Figure 2). Other witnesses described seeing the aircraft moments prior to the accident with the engine ‘not revving very loudly’, and ‘making popping noises’. The aircraft was destroyed, and the pilot was fatally injured.
On-site examination of the wreckage and surrounding ground markings indicated that the aircraft impacted terrain in a right-wing low, nose‑down attitude. The tail of the aircraft separated from the fuselage during the accident sequence. Both wings, the forward fuselage and the cockpit were substantially disrupted and compressed from vertical impact forces. An extensive area surrounding the accident site was contaminated with fuel that was released when the wing tanks ruptured. The degree of propeller damage observed on-site was consistent with the engine producing a level of power at the time of impact.
The ATSB recovered a number of components from the accident site for further examination. The aircraft was not equipped with a flight data recorder or cockpit voice recorder, nor was it required to be.
Figure 2: VH-YIX aerial picture of accident site
Source: ATSB
Ongoing investigation
The investigation is continuing and will include consideration of the:
pilot’s qualifications, experience and medical history
recovered aircraft components
maintenance documentation
operational documentation
witness interviews
electronic devices recovered from the aircraft.
__________
The information contained in this update is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this web update. As such, no analysis or findings are included in this update.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 7 September 2018, the pilot of a Yakovlev 9-UM (YAK 9) aeroplane, registered VH-YIX, departed Latrobe Regional Airport, Victoria for a local private flight. The aircraft was observed by witnesses to the north of Moe, Victoria performing aerobatic manoeuvers. A short time later the aircraft impacted the ground in a steep nose‑down attitude, fatally injuring the pilot and destroying the aircraft.
What the ATSB found
The ATSB found that the aircraft entered a spin at low altitude from which it was not possible to recover. There was no evidence of pilot incapacitation, or a mechanical fault with the aircraft that contributed to the accident.
The pilot had limited experience and recency in the YAK 9 and had not previously conducted aerobatics in the aircraft. He was therefore likely unaware of its unique handling characteristics and not adequately prepared to conduct the solo aerobatic flight.
The ATSB also identified a number of other factors that, while not contributory, increased safety risk. These included inadequate aircraft maintenance and operation without important flight and maintenance documentation.
Safety message
This accident highlights the inherent risks associated with performing low-level aerobatics in high performance aircraft. Pilots engaged in such flights are encouraged to observe minimum approved operating heights above the ground, commensurate with their ability and qualifications, and to engage in regular flight reviews and/or flight instruction.
Pilots should also ensure that careful preparation and planning is undertaken prior to each flight and that all documentation, checklists and required manuals are appropriately stored and accessible within the aircraft.
Findings
From the evidence available, the following findings are made with respect to the collision with terrain involving the Yakovlev 9-UM (YAK 9), registered VH‑YIX, which occurred 19 km west‑north‑west of Latrobe Regional Airport, Victoria on 7 September 2018. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
While conducting aerobatic manoeuvers, the aircraft entered a spin and impacted terrain.
The pilot initiated aerobatics lower than his flight activity endorsement permitted and well below the height required to safely recover the YAK 9 from a spin.
The pilot had limited experience and recency in the YAK 9 and had not previously conducted aerobatics in the aircraft. He was therefore likely unaware of its unique handling characteristics and not adequately prepared to conduct the solo aerobatic flight.
Other factors that increased risk
The rear canopy was unsecured before take-off and consequently separated from the aircraft during flight. This increased the risk of damage to aircraft structure, distraction of the pilot and possibly adverse handling qualities.
Post-accident examination of the aircraft identified incomplete maintenance practices, including inadequate airframe anti‑corrosion measures and insecure primary flight controls and seat fasteners.
The aircraft was operated without the maintenance release or the flight manual, which deprived the pilot of important operational and maintenance‑related information.
Context
Pilot information
Qualifications
The pilot held a Commercial Pilot Licence (Aeroplane), issued in March 1983. At the time of the accident, the pilot held the appropriate aircraft ratings and endorsements to operate the YAK 9. The pilot had undertaken an aeroplane flight review with an instructor in a twin-engine Cessna 310, about two weeks prior to the accident.
In August 1997, the pilot conducted spin training in a basic aerobatic training aircraft. At that time, the pilot also received an aerobatic endorsement. This qualification permitted the pilot to perform basic aerobatic manoeuvres such as loops, aileron rolls, slow rolls, barrel rolls and stall turns. The endorsement contained an altitude restriction which required the pilot to have completed any aerobatic manoeuvre by 3,000 ft above ground level.
Experience
The pilot was a relatively experienced private aircraft operator, and had operated a number of ex‑military, high-performance warbird aircraft. The pilot had logged over 2,000 flight hours in multiple aircraft types, and had flown about 100 hours in warbird aircraft. The pilot had recorded a total of 1.9 hours in VH-YIX as at 29 March 2018, however it was reported that a number of additional flights were undertaken in the aircraft but not recorded in the pilot’s logbook. The instructor who had overseen all of the pilot’s operation of the aircraft estimated that the pilot’s experience in the YAK 9 was about 5‑6 hours.
As part of transitioning to operate high-performance warbird aircraft, the pilot had voluntarily undertaken a significant number of instructional flights in warbird aircraft since 2011. Flight training records and instructor interviews indicated that the pilot normally required debriefing in a number of areas after these flights. Basic warbird aircraft handling issues were identified as the most prevalent debriefing points. However, the use of checklists and correct procedures were also identified a number of times. Several different instructors noted in the pilot’s training records that he needed to fly often to retain currency and consistency in operating warbird aircraft.
The pilot had conducted aerobatics in a number of high-performance warbird aircraft in the two years prior to the accident, however he had not flown the YAK 9 in over 3 months, and had not previously conducted aerobatics in the aircraft.
Medical
The pilot conducted an aviation medical examination on 10 July 2018 and was issued a Class 2 aviation medical certificate on 31 July 2018. Limitations placed on the pilot’s medical certificate required distance vision correction to be worn whilst flying and reading correction to be available whilst exercising the privileges of the licence. A review of the previous five years of medical files did not identify any medical concerns. The post-mortem examination found no evidence of any medical conditions that may have affected the pilot’s performance.
The pilot was reported to be excited about the return of the YAK 9 to Latrobe Regional Airport, and took a flight bag when departing for the airport that morning. However, family members reported that the pilot was uncertain if he would fly the aircraft that day.
Aircraft information
General
The YAK 9 is a two-seat, low-wing, aerobatic[2] aircraft with retractable landing gear. At the time of design, it was intended to perform the role of an advanced wartime aerial combat platform. Manufactured with front and rear flight controls, the primary flight controls are located in the front cockpit section with independent, secondary flight controls located in the rear passenger cockpit.
VH-YIX was manufactured in Russia in 1996 and exported to the United States shortly after construction without an engine. A Special Airworthiness Certificate issued for the purpose of experimental exhibition was granted on 20 February 2004 to allow the aircraft to operate in the United States. Logbook entries indicate that an Allison V-12 liquid‑cooled engine was installed and on 12 April 2004, the aircraft had flown 1.5 hours. The aircraft was imported to Australia and was placed on the Australian civil aircraft register on 19 July 2004, as VH-YIX.
Handling characteristics
As part of dive recovery, most aircraft require the application of rearward pitch control input to raise the nose and ease out of a dive. Experienced YAK 9 pilots reported that the aircraft exhibited a divergent pitch control that was more pronounced when it had a rearward centre of gravity. This characteristic, which is different to most other warbird aircraft, meant that the effort required to pull back on the control stick reduced as the airspeed increased during a high-speed dive. That behaviour increases the possibility of the pilot over-controlling the aircraft with excessive pitch-up input. This, in turn, increases the risk of unintentionally entering a high‑speed stall by exceeding the wing’s maximum angle of attack[3] and entering a spin.[4]
The YAK 9 flight manual emphasises the need for smooth and deliberate control inputs for aerobatics. A high-speed stall occurs when the airflow over one or both wings of an aircraft detaches and becomes turbulent due to a high angle to the relative airflow.[5] At this point the addition of a yawing force, most typically due to an out of balance condition, begins to rotate the aircraft into a spin. These forces will continue until control input from the pilot stops them. High‑performance aircraft like the YAK 9 transition into a fully developed spin quicker and more forcefully than a typical light training aircraft. It is essential during recovery from a spin to have sufficient altitude to effect the recovery. Experienced YAK 9 pilots stated that, depending on pilot experience, 5-7,000 ft is required to safely recover the aircraft from a developed spin.
The YAK 9 flight manual states that recovery from a spin (Figure 3) also requires considerable forward control stick movement to hold the aircraft in a dive until the speed builds up. It also warns pilots not to energetically over-control the elevator during dive recovery as the aircraft may ‘wing rock’, which is a symptom of impending stall. Should too much rearward control stick application continue, then the aircraft may re-enter a stalled state that may lead to a further spin.
It is an Australian regulatory requirement that the aircraft maintenance history is documented in the aircraft and engine logbooks. A review of the aircraft’s logbooks indicated that the YAK 9 was operated in Australia for about 106 hours before the aircraft was damaged in a landing incident at Tyabb, Victoria, in September 2015. The aircraft underwent a significant repair process, which was completed on 21 October 2016. The aircraft logbook indicated that, as part of the repair the:
rudder and port aileron had been removed, repaired, recovered and refitted
fin and port wingtip had been repaired
engine was removed, bulk stripped and refitted
propeller was overhauled and propeller blades replaced
centre and rear cockpit canopy transparencies were removed and replaced.
An independent inspection of the flight control system was undertaken relating to the rudder and port aileron refit.
Following the purchase of the aircraft from the original owner, a maintenance provider conducted a periodic inspection, and a maintenance release was issued on 20 December 2017. The aircraft’s total time in service was 107.9 hours when it became registered to the pilot on 22 January 2018.
Entries in the maintenance release[6] indicated that it flew a further 15.9 hours before the day of the accident. The last recorded entry on the aircraft maintenance release was dated 29 May 2018 and listed a total time in service of 122.8 hours with no recorded outstanding maintenance or defects. It was reported by the ferry pilot that prior to departing Boonah, there were no outstanding recorded maintenance or defects.
It was originally reported that the Yak 9 was relocated to Queensland for maintenance, however the only maintenance performed on the aircraft during its time at Boonah related to checking the security of coolant hoses. It was subsequently reported that the aircraft was primarily flown to Queensland to attend, and conduct a display at, an air show.
Requirements for the carriage of a documents in flight
The Civil Aviation Regulations 1988 (CAR) require that the pilot-in-command of an aircraft carries, as a minimum on the aircraft during flight, the maintenance release and the flight manual (if any).
Paragraph 139 (1) (c) of the (CAR) also directs that an aircraft shall not commence a flight unless there is a valid maintenance release or other approved document in force, covering the period of the proposed flight. This is to ensure that the pilot-in-command:
is informed of any defects in the aircraft
is able to determine that all required maintenance on the aircraft has been completed and certified
can determine that no maintenance requirement will become due during the time of the proposed flight.
Pilots familiar with operation of the YAK 9 reported that there was little provision to store flight documents in the cockpit. When preparing to land the aircraft, it was common for a pilot to open/slide the forward canopy rearward to allow for a better view of the landing area during the final turn for landing. On a previous occasion, opening the forward canopy in flight resulted in the loss of the aircraft maintenance release and the aircraft checklist. At that time, the maintenance release was re-issued by an approved maintenance organisation.
A similar situation occurred when the aircraft arrived at Dubbo, on its return flight to Latrobe Regional Airport on the day of the accident. As a consequence, the aircraft departed Dubbo without the maintenance release or checklist. The instructor reported that on arrival at Latrobe Regional Airport, he asked the maintenance provider to arrange a replacement maintenance release for VH-YIX. However, before a maintenance release could be reissued, the aircraft departed the airport without an aircraft checklist or current maintenance release.
In the case of VH-YIX, the aircraft checklist was incorporated into, and formed part of the flight manual. Neither the flight manual nor the maintenance release were located at the accident site.
Rear canopy
The rear canopy of the YAK 9 can be secured from the rear seat inside the cockpit, or prior to flight from the front seat. Securing the rear canopy from the front seat requires the front seat pilot to face backwards in order to lock the rear canopy in place, prior to resuming the control seat.
The YAK 9 pre-flight checklist specifically requires that in single seat operations, prior to starting the engine, the rear seat must be properly prepared by securing the seatbelt assembly to prevent interference with the aircraft’s controls, and the rear canopy is also to be locked in place prior to taxi. It is not possible to secure the rear canopy once seated from the front seat.
Wreckage and impact information
On-site examination
The accident site was in a flat grazing paddock, 19 km west-north-west of Latrobe Regional Airport. The aircraft collided with terrain close to the fence line of two properties.
Figure 4: Major features of the wreckage at the accident site
Source: ATSB
The site inspection confirmed the presence of all the major flight control surfaces including trim tabs, the tailplane, fuselage and wings.
Fuel burns to grass were identified forward of the aircraft’s orientation. This was the result of the highly compressed wing structure rupturing the main leading edge fuel tanks, allowing fuel to escape on impact, chemically burning vegetation adjacent to the accident site.
The lack of wreckage trail, high compression of the aircraft structure and close proximity of the majority of the aircraft pieces indicated an impact at a high vertical speed with little forward movement.
Figure 5: Right wing structure impact damage
Source: ATSB
Ground impact marks and aircraft damage indicated that the YAK 9 collided with terrain in about a 30° right wing low, and 30° nose‑low attitude (Figure 5). This attitude and wreckage distribution was consistent with the wreckage pattern of an aircraft established in, or partially recovering from, a spin.
One propeller blade separated from the aircraft at impact and the other two sustained damage consistent with the engine operating under low power at the time of the accident. Witness reports of engine popping and backfiring prior to impact were consistent with the engine operating in a dive with a reduced power setting. The inspection of the engine and its controls did not reveal any defect that may have prevented its operation. The availability of fuel, serviceability of the ignition and engine control systems and a lack of structural defects, indicated that all systems appeared serviceable during the flight.
In combination with the propeller blade damage, it is likely that at the time of impact with terrain, the engine was operating, however at a low power setting.
The flight controls were present and accounted for at the site. Examination of the systems did not reveal any pre-existing defects that may have inhibited normal operation.
Some anomalies were noted within the wreckage during the ATSB’s on-site phase of the investigation, these included:
the rear canopy was not accounted for within the wreckage at the accident site - it was subsequently located by a land owner in a nearby paddock
one of the rear seat rudder control balance cables and pulley had detached from the airframe
internal corrosion was identified within the compromised structure of the welded steel fuselage
unsecured fasteners in the forward and rear seats
rear-seat seatbelt assembly unbuckled and unsecured.
Rear canopy
The rear passenger canopy was located approximately 500 m to the south-east of the impact site. The proximity of the canopy in relation to the accident site, in combination with the recorded radar track of the aircraft during the final moments of the flight, indicated that the canopy most likely separated from the aircraft during the vertical descent.
Assessment of canopy photographs identified that the canopy was relatively intact, sustaining only minor damage upon separation from the aircraft and some further damage on impact with the ground. The canopy’s transparency contained two large cracks on the left and right side; originating at the forward corners of the canopy frame and extending rearward. The transparency was contained within its alloy frame. The forward part of that frame, identified as the canopy bow, had buckled in a rearward manner, likely due to impact with the ground (Figure 6). There was no evidence that the rear canopy contacted the aircraft structure, including the flight controls, following detachment.
Figure 6: Forward looking view of the rear canopy
Source: Insurance assessor image with ATSB annotations
Rear rudder control assembly
The YAK 9-UM is a tandem two-seat aircraft. Each seating position has independent rudder cables running from the rudder, through a series of pulleys, to the rudder pedals. To balance the movement of each rudder pedal position in each seat, a balance cable ran between the left and right rudder pedals. This ran through a series of pulleys to ensure that if one rudder pedal was depressed then the other would raise. Each rudder control, for both the forward and rear seating positions, was independent of each other. This means that in the event of a failure in one, the other would function appropriately.
On-site wreckage examination identified that the passenger right-side rudder balance cable pulley had separated from its mount within the airframe structure. The castellated nut, washer and accompanying split pin that would normally secure the pulley bolt to the airframe tube were not able to be located and there was no evidence that the fastener had failed due to force associated with the impact sequence (Figure 7).
Figure 7: Rear right rudder pulley, found away from the airframe.
Source: ATSB
An additional anomaly was noted with the left-side rudder pulley. Although the castellated nut was present on the bolt threads to that pulley, no split pin had been fitted. Furthermore, even if one had been fitted, the fastener arrangement would not have prevented loosening of the castellated nut (Figure 8).
Figure 8: Left side rear rudder balance cable bolt and castellated nut
Source: ATSB
Internal corrosion within tubular structure
During the on-site examination of the wreckage, corrosion was noted inside a number of airframe tubes. The rear cockpit‘s rudder balance cable pulley structure also had evidence of internal corrosion. The pilot’s seat rear mount cross-member had separated from the tubular side frames of the forward cockpit, revealing further evidence of internal corrosion. Internal corrosion was also found in the tubular steel structure of the fuselage. It was noted that there was little provision for applying and draining corrosion-inhibiting products to the internal surfaces of the tubes.
Further examination
ATSB identified other anomalies during the on-site examination of the wreckage. There was evidence of incomplete maintenance activity, with further examples of missing split-pins, in the rear-seat mounting bolts and nuts. A split-pin was also missing from the pilot’s seat lower mounting bolt securing nut, which was engaged by several threads, with the locking portion of the nut disengaged.
The rear seat was found outside the aircraft near the tailplane with the individual straps of the seatbelt assembly loose. The position of the seat indicated that significant force/s had been applied to it, raising the possibility that the rear seatbelt assembly became unclipped during the impact sequence.
However, the instructor who flew the aircraft to Latrobe Valley earlier that day reported that, on arrival, he removed a bag that had been secured via the harness to the rear seat and left the seatbelt undone in preparation for a planned 1630 flight with the pilot. If that harness was not secured by the pilot prior to the accident flight, the straps may have fouled the control stick and inhibited full and free movement in flight. From the available evidence, it was not possible to determine if that occurred.
On 7 September 2018, a Yakovlev 9-UM (YAK 9), VH-YIX was flown from Boonah Queensland, to Latrobe Regional Airport, Victoria. The relocation of the aircraft was undertaken by two separate pilots, with a handover conducted at Dubbo Airport, New South Wales. One of the pilots, an instructor, flew another aircraft from Latrobe Regional Airport to Dubbo. On arrival at Dubbo the pilots swapped aircraft for their respective return flights.
Prior to landing at Dubbo in the YAK 9, the pilot from Boonah opened the forward cockpit canopy in-flight to provide greater visibility for the landing. It was reported that the resultant turbulent airflow from the open canopy ejected a number of aircraft documents from inside the cockpit. After landing at Dubbo, the instructor was advised of the loss of the aircraft checklist, maintenance release, Certificate of Registration, and Special Certificate of Airworthiness from the aircraft.
The instructor conducted an uneventful flight back to Latrobe Regional Airport in the YAK 9, and landed at about 1155 Eastern Daylight-saving Time.[1] He refuelled the aircraft with 341 litres of aviation gasoline and parked the aircraft on the Latrobe Valley Aero Club hardstand at 1244.
One of the aircraft’s owners (the pilot) met the instructor on arrival. The pilot told the instructor that his intention was to conduct some taxi practice prior to a pre-arranged instructional flight scheduled for 1630 that afternoon.
The instructor and the pilot discussed the absence of the checklist and other required documents. The instructor reported that they agreed that the aircraft should not be flown, but taxiing would be acceptable, provided the aircraft’s operating temperatures were monitored. The instructor then proceeded inside the aero club to prepare another student for a training flight.
Sometime later, the instructor heard the pilot attempting to start the YAK 9. After numerous starting attempts, the instructor went outside to assist the pilot to apply the correct starting sequence.
At about 1420, the pilot began to taxi the aircraft, which was witnessed by two aircraft engineers standing outside a hangar at the northern end of runway 21. The aircraft was taxied along to the run-up bay. The witnesses observed that the rear canopy of the aircraft was open and that the pilot appeared to conduct routine engine checks. A short time later, the aircraft entered runway 21, the pilot applied power and commenced to take-off.
The instructor, who was walking across the tarmac from the aero club, recalled observing the take-off roll of the YAK 9 and noted that the aircraft used more than double the normal length of runway before it lifted off. The instructor then noticed that the rear canopy was not secure.
He attempted to contact the pilot from within the aero club by radio to advise him that the rear canopy was not secure. The instructor made several broadcasts but did not receive a response from the pilot. However, another pilot in the area responded to the instructor’s radio call, which confirmed that the radio call had been broadcast.
The YAK 9 initially maintained runway heading as it continued to climb. At 1428, it was identified by military radar turning off runway heading to the west at about 130 kt (Figure 1). The aircraft climbed to about 2,600 ft above mean sea level (AMSL). About 4.6 km to the south‑west of Latrobe Regional Airport, it was observed on radar to level out.
Figure 1: Flight track of VH-YIX
Source: Google Earth with annotations by ATSB
At 1431:09, the aircraft was about 18 km to the north-west Latrobe Regional Airport at about 2,800 ft, and travelling at 206 kt groundspeed when the pilot began to conduct what ground witnesses assessed as aerobatic manoeuvers. Radar contact with the aircraft was lost during those manoeuvres. The aircraft briefly reappeared on radar at 1431:34, at about 3,100 ft, (2,900 ft above ground level) with a groundspeed of 157 kt. This was the last contact received by radar, and showed a 49 kt reduction in groundspeed during the 25-second period when the aircraft was not visible on radar.
Figure 2: Video captured by a witness with overlayed ATSB analysis
Source: Witness footage with ATSB analysis and annotations
Witnesses in the Moe region, who were actively watching the aircraft from the ground, observed the YAK 9 conduct a series of what appeared to be aerobatic manoeuvers. One witness described what appeared to be a roll followed by a loop. They stated that as the aircraft came out of the bottom of the loop, the aircraft appeared to conduct an abrupt left turn before it began spiralling towards the ground. Video taken by another witness showed the aircraft in a spinning, steep nose‑down attitude prior to disappearing from view (Figure 2). These four frames were captured over 0.48 seconds.
At about 1432, the aircraft impacted terrain in a paddock about 3 km north of Moe, in a flat, slightly right‑wing and nose-low attitude, with little to no forward movement (Figure 4). The aircraft was destroyed, and the pilot was fatally injured.
VH-YIX departed Latrobe Regional Airport, Victoria at about 1428 and climbed to 2,600 ft before turning to the north and accelerating to over 200 kt north of Moe. The pilot then began to conduct manoeuvres identified by witnesses as being consistent with aerobatics. A short time later the aircraft impacted the ground in a steep nose‑down attitude, fatally injuring the pilot.
This analysis will discuss the development of the accident, including the pilot’s qualifications and readiness for the flight. Aspects of the aircraft maintenance and associated documentation will also be detailed.
Development of the accident
Aerobatic manoeuvres
Witness reports indicated that the pilot was performing manoeuvres consistent with aerobatics, including loops and rolls, immediately prior to an abrupt loss of control.
Analysis of video footage provided by a witness indicated that VH-YIX was established in a spin when the aircraft disappeared from view below 1,000 ft above ground level (AGL). The aircraft damage and localised nature of the accident site confirmed that the aircraft collided with terrain in a right wing‑low and nose‑down attitude at high vertical speed and with little forward movement. That impact signature was consistent with the aircraft established in a spin.
Analysis of radar coverage in that area identified that an aircraft operating below about 1,800 ft above mean sea level would be below radar coverage, and therefore not identifiable on radar. The absence of radar identification of the aircraft during the latter part of the flight therefore indicated that the pilot was operating significantly below his approved 3,000 ft AGL aerobatic limit. More importantly, the aircraft was also well below the altitude that experienced YAK 9 pilots advised was required to safely recover from a spin. As such, and consistent with the observed impact signature, the spin was probably unrecoverable in the height available.
The pilot was qualified to perform basic aerobatics above 3,000 ft AGL, and the aircraft type was appropriate for the aerobatics conducted. However, while the pilot had experience conducting aerobatics, he had limited experience and recency in the YAK 9 and had not previously conducted aerobatics in the aircraft. He was therefore likely unaware of its handling characteristics during such manoeuvres. Specifically, the possible pitch control sensitivities required during aerobatic manoeuvres or spin recovery in the YAK 9.
Additionally, as there was no flight manual/checklist available to the pilot, he was unable to refer to important operational information such as operating airspeeds/limitations during the flight.
In summary, the ATSB concluded that the pilot was probably not adequately prepared to conduct a solo aerobatic flight in the YAK 9.
Canopy
Numerous witnesses recalled that the rear canopy of the YAK 9 was not secure prior to take-off. Consequently, this allowed in flight air loads to slide it fully rearward along its guide rails and ultimately detach it from the aircraft. There was no evidence that the canopy struck any other part of the aircraft as it departed the airframe.
While it remains unknown if an open rear canopy may have a detrimental effect on airflow over the rear control surfaces of the YAK 9, it is unlikely to have been sufficient to cause a loss of control as it was open from the commencement of the take-off. However, the canopy’s departure from the airframe was probably sudden and could well have distracted the pilot. Given the proximity between the canopy and the wreckage location and the flightpath of the aircraft however, it was considered likely that the canopy detached during the spinning vertical descent.
Aircraft maintenance
Defects
Examination of the rear rudder balance cable pulleys identified that the associated fasteners were not correctly secured. Specifically, the required split pins were not fitted and this led to detachment of one of the castellated nuts. Despite that, the design of the pulleys is such that the bolt shank is unlikely to migrate from its installation during operation as cable tension from the rudder control is likely to keep the rudder pulley bolt in place during service.
In addition, wreckage examination also identified unsecured rear seat mounting bolts and an unsecured pilot’s seat mounting nut.
Finally, significant corrosion was identified within the steel fuselage frame. The nature and progression of the corrosion was not at a magnitude to be visually identifiable on the external airframe, however it may have presented a significant future risk to aircraft operation. Russian accredited representatives advised that internal tube anti‑corrosion measures are not applied to the YAK 9, and that no internal surfaces are coated during manufacture.
These observations, while not considered to have contributed to the accident, indicated that maintenance had not been performed on the aircraft to an acceptable standard. That had the potential to affect the future airworthiness of the aircraft.
Documentation
The loss of the maintenance release approaching Dubbo Airport meant that the written means to convey relevant maintenance information or defects was unavailable to both the instructor and the accident pilot. While this did not influence the development of the accident, operation without this document increases the risk that maintenance may be overdue, or that a defect may compromise the safety of the aircraft.
Additional details
Pilot details
Licence details:
Commercial Pilot Licence (Aeroplane) issued April 2010
The sources of information during the investigation included:
witness interviews
the pilot’s previous flight instructors
interviews with YAK 9 pilots
the aircraft logbooks and maintenance documentation
the aircraft flight manual and documentation
Airservices Australia and Department of Defence radar data
the Civil Aviation Safety Authority pilot licence and aircraft documentation
the pilot logbook
video and audio information related to the flight.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Civil Aviation Safety Authority, Airservices Australia, Department of Defence, National Transport Safety Bureau, Interstate Aviation Committee, the maintenance provider and the pilot’s recent flying instructor and a subject matter expert in the YAK 9.
A submission was received from the pilot’s recent flying instructor. The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Occurrence summary
Investigation number
AO-2018-061
Occurrence date
07/09/2018
Location
19 km WNW, Latrobe Regional Airport (near, Tanjil South)
On the afternoon of 17 August 2018, the pilot of a Kawasaki Heavy Industries BK117 helicopter, registered VH-JWB, was conducting fire-bombing operations approximately 9 km west of Ulladulla, New South Wales (NSW).
The pilot was on the third flight for the day and was conducting repeated water bombing of a fire on Plot Road, Woodburn, NSW. On the fifth fire-bombing circuit, at this location, the pilot filled the slung Bambi Bucket (bucket) without incident from a nearby dam and departed towards the fire area. Shortly after, the aircraft diverted off course, the bucket and longline became caught in trees and the helicopter collided with terrain. The pilot was fatally injured and the helicopter was destroyed.
What the ATSB found
The ATSB found that it was likely the pilot suffered an incapacitating medical event. As a result, the pilot unintentionally diverted off track, leading to the bucket becoming tangled in the trees and causing the helicopter to collide with terrain.
The pilot’s post-mortem identified a focus of acute inflammatory change in the heart muscle, a condition known as lymphocytic myocarditis. This condition is capable of causing sudden impairment or complete incapacitation. The pilot is unlikely to have known they suffered from this condition. There are no risk factors for the development of this condition and it cannot be detected by medical screening.
The pilot’s post-mortem also identified coronary heart disease which is also capable of causing sudden impairment and incapacitation. This condition was being effectively managed by medication.
Despite the pilot suffering from these two heart-related conditions, there was insufficient evidence to determine if they contributed to the accident.
The ATSB also determined that the pilot was known to use an over the counter medication for the treatment of hay fever that, although labelled as non‑sedating, was not approved for use while conducting flying operations.
Finally, the pilot did not wear the upper torso restraint correctly. Although on this occasion the accident was unsurvivable, the use of such a shoulder harness restraint generally reduces the likelihood of fatal head injuries.
Safety message
Pilots are reminded that some medical conditions may be undetectable by the normal aviation medical screening process. Pilots should remain vigilant for any medical symptoms which may be the precursor to a more serious medical event.
Pilots should also exercise caution when using over-the-counter medications as their availability does not mean they are automatically safe for use while conducting aviation activities.
The occurrence
On 17 August 2018, a Kawasaki Heavy Industries BK 117 (BK 117),[1] registered VH-JWB (JWB), was performing aerial work in the Ulladulla area, New South Wales (NSW). The operator had been tasked by the NSW Rural Fire Service (RFS) to support fire-fighting activities in the Bombaderry area, near Nowra, on 15 August 2018, then in the Ulladulla area from the afternoon of 16 August 2018 (Figure 1). The fire-bombing operations were being flown out of the Milton Showground during the day, with the fire-bombing aircraft flown back to Nowra, for overnight parking.
Figure 1 - Accident location
Source: Google Earth, annotated by the ATSB
On the morning of 17 August 2018, JWB departed Nowra for the Milton Showgrounds. The pilot was the sole occupant and conducted a number of flights that day, refuelling from the showground at 1030 Eastern Standard Time[2]
In the afternoon, JWB and another BK 117, VH-FHB (FHB), were tasked to assist ground‑based fire crews extinguish fires near Plot Road, Milton (Figure 2). Both helicopters were operated with a Bambi Bucket[3] (bucket) on a longline.[4] The operation involved flying circuits between the fire area and a nearby dam, where the buckets were re‑filled with water.
Figure 2 - Area of operations
Figure 2 shows the area of operations with circuit direction arrows that are indicative of the average track of JWB during the previous 4 circuits.
Source: Google Earth, annotated by the ATSB
At 1400 the RFS Air Attack co-ordinator conducted an ‘operations normal’ radio call with all aircraft operating in the Ulladulla fire area. The pilot of JWB responded normally and did not report any difficulties.
At about 1407, the pilot of FHB observed JWB’s pilot fill the bucket at the dam before releasing a small quantity of water, consistent with normal operations. JWB then departed the dam in a south‑easterly direction towards the fire.
The pilot then moved FHB over the same dam to fill its bucket. On completion of filling the bucket, the pilot looked for JWB but could not sight the helicopter.
A witness on Plot Road, approximately 100 m east of the accident site, observed JWB tracking in a north-easterly direction, contrary to the established flight pattern. A number of witnesses in the same area then observed the bucket and longline become tangled in trees at the edge of a clearing, and the helicopter collide with terrain (Figure 3). The pilot was fatally injured and the helicopter was destroyed.
The pilot was a New Zealand citizen who had flown in several countries and had experience on numerous helicopter types. They held a valid Commercial Pilots Licence (Helicopter) that was initially issued by the Civil Aviation Authority of New Zealand, in June 1987 and then converted to an Australian licence by the Civil Aviation Safety Authority in October 1998.
The pilot held a Class 1 aviation medical certificate, valid until 5 June 2019, with a restriction requiring reading correction to be available whilst exercising the privileges of the licence.
The pilot’s logbook, combined with the operator’s flying record, showed a total flying experience of approximately 7,750 hours. The pilot had approximately 1,300 hours experience operating the BK117 and in excess of 3,000 hours of longline experience.
The pilot last completed an aerial application rating proficiency check on 9 August 2018, which was valid until 31 August 2020, and included Bambi Bucket operations. The pilot was qualified to conduct helicopter fire operations and had a low-level rating and a sling operations endorsement. The pilot’s logbook contained evidence of fire operations first being conducted in 1997. The pilot obtained an Agricultural Pilot (Helicopter) Rating Grade 2 from the Civil Aviation Safety Authority Australia in March 2003.
Fatigue assessment
The ATSB assessed whether the pilot may have been fatigued at the time of the accident. The pilot’s start times, rest time available, accommodation facilities, environmental factors and workload associated with the task were all reviewed. From the evidence available it was considered unlikely that the pilot was experiencing a level of fatigue known to affect performance.
Meteorological information
Bureau of Meteorology data was available from an automatic weather station located on the coast at Ulladulla, approximately 9 km east of the accident site. One-minute observations at the time of the accident indicated that the wind was from the south-east, between 8‑10 kt.
The other pilot operating in company with JWB at the time of the accident similarly reported the wind to be about 10 kt from the south‑east, which was roughly in the direction of the up-wind leg of the fire-bombing circuit.
Visibility was estimated to be in excess of 5 km by another pilot operating in the same area. Photographs taken shortly after the accident were consistent with that visibility assessment. Other pilots reported that the conditions were good for fire-bombing operations, with no turbulence or visibility issues.
Aircraft information
General
The Kawasaki Heavy Industries BK117 helicopter is a multi-purpose, twin-engine, skidded, medium helicopter with ten seats in the basic configuration.
Airworthiness and maintenance
The helicopter was built in 1994 and operated in Japan before being imported to Australia in 2015. A Certificate of Airworthiness inspection was completed on 24 September 2015. JWB had a current maintenance release, issued on 5 September 2017 and was valid for a period of 300 hours or 12 months, whichever occurred sooner.
The helicopter was maintained in accordance with an approved System of Maintenance. A general maintenance review was conducted on the helicopter’s history since being imported into Australia. This review did not identify any anomalies with the aircraft’s maintenance. At the time of the accident, there were no outstanding defects or maintenance requirements.
Weight and Balance
It was calculated that at the time of the accident the aircraft’s weight and balance were within the operational limits for the helicopter.
Engines
The helicopter was powered by two Lycoming (now Honeywell) LTS101-750B-1 engines. The engines were initially examined on site by the ATSB and also subject to detailed disassembly and technical examination by the manufacturer (see the section titled Wreckage examination).
Hydraulic System
The hydraulic system consists of two independent subsystems of which construction, function and performance are identical.
Bambi Bucket
JWB utilised a Bambi Max bucket that is a lightweight, low‑power draw, quick‑operating multiple drop valve Bambi Bucket. The bucket was attached to the helicopter cargo hook via a 130 ft longline. The pilot controlled the bucket using a push button switch mounted on the cyclic.[5]
Cargo Hook
JWB was fitted with an Indraero Siren Equipment cargo hook. The hook allows external cargo to be released via a collective[6] ‑mounted electrical switch. In addition, a foot‑activated manual release lever was located to the right of the pilot’s tail rotor pedal. This lever was used to release cargo in the event of an emergency or failure of the electrical release system.
During the course of the investigation, the ATSB was informed that the pilot sometimes operated with the circuit breaker for the electrical hook release pulled. The operator advised that the company procedure was to fly with the circuit breaker in and the electrical hook switch armed during flight. Additionally, even if the pilot had flown with this circuit breaker pulled, they would still have had the foot‑activated manual release lever available in the event of an emergency.
Operational information
The pilot of FHB commented during interview that each time JWB was overhead the fire‑bombing area there was a substantial level of clearance between the bucket and the trees. This pilot estimated that water was consistently dropped from JWB at about 6‑9 m above the trees.
None of the ground or airborne crews heard any radio transmissions from JWB immediately before the accident. During water bombing operations it is standard practice to make a radio call when leaving the circuit for any reason, to inform other airborne assets of the helicopter’s tracking.
Ground fire-fighting crews were also operating in the immediate area. Those personnel advised that there were no other spot fires in the immediate area. Additionally, the crew of the air attack helicopter reported to the ATSB that when they came into land at the accident location minutes after the accident, they did not see any fire in the area that may have caused JWB to turn away from the circuit.
Fuel
JWB and the other helicopters on task, had all refuelled using Jet A1 fuel from the same onsite tanker based at the Milton Showgrounds. In addition, other helicopters operating in the area were using fuel from the same source and there were no reported issues with fuel quality. Fuel records confirmed the fuel on-board the tanker conformed to the relevant specification.
JWB had refuelled twice from the tanker on the day of the accident with the last refuel of 435 litres conducted approximately 2 hours and 20 minutes prior to the accident. Considering the helicopter’s fuel consumption rate, there was adequate fuel onboard at the time of the accident.
Wreckage and accident site information
Accident site
The accident site was located 9 km west of Ulladulla, New South Wales. The wreckage of JWB was approximately 200 m from the average circuit path and the aircraft final track was estimated to be 90° off the circuit direction (Figure 2).
The main cabin of the helicopter was found inverted in a clearing with the bucket and longline still attached (Figure 3). The bucket and longline were caught in a 22 m tall tree at the edge of the clearing.
Rub marks from the longline were found on the trunk of the tree that the bucket was hanging from. These marks indicated the bucket snagged the tree at least 13 m down from the top of the tree.
In the later part of the circuit the helicopter bucket would normally have a minimum of 6–9 m clearance above the treetops. Taking this into account, and the tree contact 13 m below the canopy, the bucket was at least 19–22 m lower than expected when it snagged the tree and brought the helicopter down.
Figure 3 - Accident site and wreckage
Source: ATSB
The bucket, while suspended from the tree, still contained a large quantity of water. After removal, examination of the bucket showed that the cable required to operate the drop valve had broken at the attaching point to the motor, either during the accident sequence or as the bucket was removed from the tree. However, during post‑accident repairs the main valve was tested and found to be serviceable.
Wreckage examination
The ATSB examined the wreckage and did not identify any pre-existing aircraft defects that may have contributed to the accident sequence. The aircraft and all its components were accounted for at the accident site. There was no evidence of fire.
There was extensive damage to the fuselage with heavy vertical compression evident. One main rotor blade detached, while the other three remained attached to the head, with varying degrees of damage due to contact with the airframe and terrain. The vertical fin, including the tail rotor assembly, intermediate and tail rotor transmissions, fractured from the tail boom at the lower section of the vertical fin. The horizontal and vertical stabilisers had been struck by the main rotor blades multiple times.
Consistent with normal firefighting operations, the pilot door was not fitted at the time of the accident. The cabin doors were forced from their closed position due to impact forces.
All flight controls were observed to be connected at the time of the accident and did not indicate any pre-existing defects. There was no visible damage to the cockpit controls.
Several circuit breakers in the overhead panel were found in the ‘tripped’ position, including the cargo hook, annunciator warn and main rotor RPM warning. However, due to the nature of the accident sequence, these circuit breakers may have tripped due to impact forces.
The serviceability of the cargo hook mechanical release mechanism was verified after disconnecting the cargo hook from the helicopter. This was necessary due to the damage at the hook end of the actuating cable.
The ATSB tested the hook assembly electrically with the use of another BK117 and it was found to be serviceable. The hook was cycled a number of times and released and relatched without any anomalies observed.
Each engine assembly was examined on-site and found to be complete, with no evidence of pre‑accident defects that influenced the accident.
Both engines were removed from the wreckage and shipped to the manufacturer in the United States for detailed examination under the supervision of the United States National Transportation Safety Board.
The disassembly and examination of the engines identified that the type and degree of damage was indicative of both engines rotating and operating normally at the time of impact. No pre‑existing conditions were noted that would have affected their operation.
Examination of the tandem hydraulic unit assembly showed three of the four filter bypass indicators in the ‘popped’ condition. An examination of the filters in each location showed them to be clear of blockages and debris. Consequently, the ‘popped’ indicators were probably impact related. The fluid level indicators for each reservoir showed that both systems had adequate fluid to operate.
While moving the wreckage upright, approximately 100 litres of fuel leaked from JWB. This fuel was clear in appearance and indicated sufficient fuel on-board for use.
Recorded information
The aircraft was not fitted with a flight data recorder or a cockpit voice recorder and neither were required.
A Spidertracks system was installed in the helicopter. Spidertracks provides a real-time flight tracking service using satellite communications. The device reports position and groundspeed at a pre-set time interval, in this case every 2 minutes.
The last recorded point for JWB was at 1408 (Figure 2). At that time, the helicopter was departing the dam, where it had just taken on water, and was heading towards the fire ground. This was consistent with previous circuits.
Medical and pathological informational
Post-mortem examination
The forensic pathologist who conducted the post-mortem examination concluded that the pilot succumbed to injuries sustained during the accident sequence. The examination also identified a widespread area of acute lymphocytic myocarditis, likely of viral origin, and ischaemic (coronary) heart disease. The examining pathologist noted that the myocarditis and/or coronary heart disease found during the post-mortem may have caused sudden incapacitation.
The post-mortem also identified injuries to the pilot’s left arm and both hands. Specialist opinion was that this injury pattern evidence was inconclusive in determining whether the pilot was manipulating the flight controls at the time of the accident.
No witness marks were identified during the examination to indicate the pilot was wearing the available upper torso restraints over the shoulders and the time of the accident.
Finally, toxicological examination identified that a level of 5 per cent carboxyhaemoglobin was present in the pilot’s blood (see the section titled Carbon monoxide below). No other substances were identified that were likely to have impaired the pilot’s performance.
Lymphocytic myocarditis
Lymphocytic myocarditis (myocarditis) is an inflammatory change in the heart muscle, usually caused by an acute viral infection. Acute viral myocarditis can involve a period with mild early symptoms which can be followed by chest pain, heart rhythm abnormalities, heart failure, or sudden cardiac death. Myocarditis may also have a sudden onset with no early mild symptoms. The signs and symptoms of myocarditis vary, depending on the cause of the disease. Common myocarditis signs and symptoms include:
chest pain
rapid or abnormal heart rhythms (arrhythmias)
shortness of breath, at rest or during physical activity
fluid retention with swelling of the legs, ankles and feet
fatigue
other signs and symptoms of a viral infection, such as headache, body aches, joint pain, fever, sore throat and/or diarrhoea
The ATSB engaged two external aviation medicine specialists (consultants A and B), to provide advice regarding the pilot’s health, medications and medical conditions in relation the accident sequence.
The consultants advised that the standard aviation medical examination procedure would not have detected myocarditis. Myocarditis cannot be detected by medical screening, and there are no risk factors for the development of viral myocarditis. The only avenue for prevention is for pilots to self-monitor for any symptoms or signs of illness prior to and during each flight.
Advice was sought from the medical consultants as to the likelihood of the pilot having symptoms of the condition based on the post-mortem report. Consultant A, in conjunction with a cardiologist, reported that the presence of a focus of acute myocarditis in the pilot was a finding ‘likely to have functional significance for the risk of sudden impairment or sudden complete pilot incapacitation.’ Consultant A also stated that viral infections of all kinds are often characterised by quite severe illness developing suddenly, sometimes with early mild symptoms. They also advised that the risk of cardiac arrhythmia due to viral myocarditis and the apparent cessation of pilot control inputs were strongly suggestive of severe and sudden loss of situational awareness and/or loss of consciousness occurring as a result of myocarditis in the final moments of the flight.
Consultant B reported that it was possible the myocarditis was an incidental finding in the post‑mortem and did not cause any symptoms. However, they also advised that it was equally possible the pilot was suffering some medical incapacitation from this condition, however there was no evidence for this prior to the flight.
Coronary heart disease
Coronary heart disease describes a condition where narrowing of the coronary arteries by fatty deposits in the artery walls, or hardening of the arteries, causes a reduction of the blood to the heart muscle, reducing the oxygen supply. If this condition causes a blockage to one of the major arteries supplying blood to the brain, a stroke can occur. Depending on the part of the brain affected, sudden incapacitation and the inability to operate an aircraft may result.
Common symptoms of this disease include:
chest pain
dizziness
shortness of breath
decreased ability to function normally
The ATSB medical consultants advised that the pilot had undergone an aviation medical examination, including an electrocardiogram, by an aviation medical examiner three months prior to the accident and was found to be fit to fly. In addition, consultant A advised that the pilot’s medical examination and medical certification processes were appropriate and took into account the effective management of cardiovascular risk factors.
Opinion was sought from the consultants on the potential for the condition to have influenced the accident. They commented that coronary artery disease of the level found at post-mortem is often found in healthy people and can be regarded as part of the normal degenerative process of aging. The presence of calcification indicated that the pilot’s heart disease was longstanding and would not necessarily have caused symptoms.
Consultant A also commented that coronary artery narrowing without evidence of inadequate blood supply was reported at post-mortem, but the changes were longstanding and unlikely to have caused symptoms.
Observed behaviour
Several people were interviewed as part of the investigation who had contact with the pilot on the day of the accident and during the days immediately preceding the accident. With one possible exception, all commented that the pilot was generally well and in good spirits.
Following a lunch break on the 16 August, the pilot was observed having difficulty writing down the latitude and longitude of a new task location. The pilot was passed the latitude and longitude three times over the radio and the pilot was observed to write part of the numbers correctly, part incorrectly or just stop writing mid sequence. The latitude and longitude was described as being passed via the radio very clearly.
The observer knew the pilot in a professional capacity and had witnessed the pilot landing, taking off and attending briefings that day and the previous day with no indications the pilot was having any difficulties. The observer made comment that, when the pilot had difficulty writing down the latitude and longitude, nothing in the pilot’s movement, speech or facial expression appeared unusual.
With regard to this observation of apparent impairment, consultant A commented that it may have been associated with myocarditis-related arrythmia or transient ischaemic attack.
Consultant B commented that this apparent episode of confusion was non-specific and while it could be attributed to myocarditis, or the effects of heart disease, it could also have been unrelated.
Medication
During the wreckage examination four prescription medications and one over the counter antihistamine medication were found with the pilot’s possessions. It was confirmed with the pilot’s designated aviation medical examiner (DAME) that all four prescription medications had been taken by the pilot for a number of years and were consistent with their age and health. It was reported by a family member that the pilot did not suffer any side effects from the prescription medications.
Opinion was sought from medical consultant A, in conjunction with an aviation cardiologist, whether the medications could have influenced the accident. The potential for side effects such as sedation and drug interactions, were all considered and excluded by these specialists. The potential for cardiac irregularity due to an interaction between one of the antihypertensive drugs and the antihistamine was also assessed as very unlikely.
The antihistamine medication was for the treatment of hay fever and the pilot’s DAME was not aware of its use. The active ingredient of this medication is listed in the CASA guidance as prohibited. It was reported that the pilot was known to suffer from hay fever and used this medication to treat the symptoms.
Medical opinion regarding the possible sedating side effects of this medication was that, while some people experience sedation when taking this non-sedating antihistamine, this was recognisable on taking the first dose. The pilot was known to have been taking this medication regularly, so any adverse effects on the day of the accident were considered unlikely.
Carbon monoxide
Carbon monoxide (CO) is a colourless, odourless and tasteless gas. It is the by-product of the incomplete combustion of materials containing carbon. The Agency for Toxic Substances and Disease Registry (2012) stated that CO is produced from both human-made and natural sources.
When inhaled, CO is absorbed into the bloodstream where it readily binds with the haemoglobin to form carboxyhaemoglobin (COHb). The binding affinity of CO for haemoglobin is 200-300 times stronger than that for oxygen. Therefore, CO reduces the oxygen carrying capacity of the blood.
An individual’s COHb levels increase as the duration and intensity of the CO exposure increases.
Normal levels of carbon monoxide and effects
There have been a considerable number of studies examining CO exposure, though very few regarding such exposure in helicopters.
Hampson et al. (2007) cited various publications that indicated that there were differing views regarding the correlation between COHb levels and a patient's clinical symptoms.
Further, when comparing the COHb levels detected in individuals, Rathore and Rein (2016) highlighted that it was important to note that ‘both the concentration and length of time are key distinguishing factors. It is vital to note however that individuals exposed to the same source simultaneously can exhibit differing levels of COHb’. Taking this into consideration, when discussing the normal levels of CO contained in an individual’s blood, Consultant B stated that:
Normal levels of carbon monoxide in non-smokers are less than 2-3%. Smokers may have elevated levels around 3-5% or even as high as 9%, depending on number of cigarettes smoked and time since last cigarette smoked.
A police forensic pharmacologist involved in a previous ATSB investigation[7] reported similar levels, where a non-smoker’s maximum COHb level would be around 5 per cent, while smokers could have levels up to 10 per cent and up to 16 per cent for heavy smokers.
While the research shows some variability in what was considered to be the normal production of CO without occupational exposure, generally less than 3 per cent COHb saturation was considered normal for non-smokers. For smokers, levels up to 10 per cent, or even more were expected.
Recognising the potential for variability, physical symptoms and cognitive effects of CO exposure generally start to occur at COHb levels of around 10 per cent. These include headaches, nausea, dizziness, confusion, and disorientation.
ATSB report AO-2017-118 contains further details on the effects of CO.
Possible sources
Aviation fuels contain carbon so exhaust gasses are a source of carbon monoxide that can potentially enter the cabin during flight. Piston engines produce the highest concentrations of CO, however turbine engines also produce CO (Salazar).
Based on the configuration of the helicopter, with the engines above and behind the cabin as well as the cabin doors closed, it was considered unlikely for significant exhaust gasses to enter the cabin, even with the pilot door removed.
Carbon monoxide is also produced during combustion from bushfires. Studies have been conducted regarding the effect of the smoke on firefighters on the ground, however there is no data in relation to pilots conducting airborne firefighting. One study conducted by Reinhardt and Ottmar (2004) found 5‑10 per cent of firefighters exceeded exposure standards for respiratory irritants, of which carbon monoxide is one, while attending bushfires.
In a study conducted by MacSween et al (2019) it was noted that emissions and subsequent exposure levels were highly variable over the duration of a burn. Carbon monoxide levels present during fire-fighting activities depend on numerous variables, including fuel properties, temperature, moisture, ventilation of the area and proximity to the fire (De Vos, et al, 2008). The pilot was operating at varying altitudes and proximity to the fire and considered to be further from the fire source than ground-based firefighters.
The pilot’s smoking history was also examined. The pilot had been a non-smoker for more than 20 years and it was considered by consultant B to not be a factor in the elevated levels of CO found in the toxicology.
In summary, the source of the pilot’s slightly elevated CO could not be determined.
Medical opinion
The forensic pathologist, who performed the post-mortem, considered the level of carbon monoxide found in the pilot’s blood was unlikely to have had an effect on the pilot’s ability to fly the helicopter.
Consultant B reviewed the results of the CO testing and the post-mortem report. Taking into account the circumstances of the accident and the CO level found in the pilot’s toxicology, they similarly concluded it was extremely unlikely that the level of CO in the pilot’s blood would have affected their operation of the helicopter.
Survival aspects
Due to the inverted nature of the accident and resulting vertical compression of the fuselage, the accident was not considered survivable.
It was noted, however, that evidence from the first responders showed the upper torso restraint (UTR) was worn incorrectly. The UTR was fastened around the pilot’s waist rather than over the shoulders, meaning the upper torso was unrestrained. A photograph from a previous flight also showed the pilot with the UTR being worn in the same manner as found in the accident flight.
examined medical conditions and incapacitation events between 1 January 1975 and 31 March 2006. This report concluded that the majority of pilot incapacitation events do not involve a chronic or pre-existing medical condition. That is, they are largely unforeseeable events, often involving acute illnesses or injury. Of the 10 accidents that resulted in fatalities, all involved single-pilot operations and in half of these, heart conditions were identified as a significant contributing factor.
The ATSB safety education publication Pilot incapacitation occurrences 2010–2014 (AR‑2015‑096) documents recent pilot incapacitation occurrences in high capacity air transport, low capacity air transport, and general aviation to help educate industry about the causes and risks associated with inflight pilot incapacitation. Part of the safety message reminded pilots to assess their fitness prior to flight. Assessment of fitness includes being aware of any illness or external pressures they may be experiencing.
ATSB investigation AO-2015-145: Flight crew incapacitation – Lake Macquarie Airport, NSW, on 15 December 2015
On the morning of 15 December 2015, a SOCATA TBM 700, aircraft, registered VH-YZZ, departed Gold Coast Airport, Queensland for Lake Macquarie Airport, New South Wales. On board were the pilot and one passenger.
The flight to Lake Macquarie was uneventful. However, when the aircraft was just about to land on the runway the pilot started to feel ‘woozy’ and, shortly afterwards, lost consciousness. The aircraft impacted the runway, bounced and impacted the runway a second time before the pilot regained consciousness. The pilot and passenger were not injured during the accident and exited the aircraft. Medical tests and monitoring after the accident found that the loss of consciousness was due to a previously undiagnosed heart condition.
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Kawasaki Heavy Industries BK117, VH-JWB, which occurred 9 km west of Ulladulla, New South Wales, on 17 August 2018.
Contributing factors
While conducting fire-bombing operations, the pilot likely experienced an incapacitating event resulting in deviation off track, entanglement of the bucket in trees and subsequent collision with terrain.
Other factors that increased risk
The pilot had acute lymphocytic myocarditis which is known to affect heart rhythm and/or blood pressure. This can cause dizziness, impaired consciousness, and incapacitation.
The pilot had coronary heart disease which is known to reduce the supply of blood to the heart muscle. This can cause chest pain, dizziness, shortness of breath and possible incapacitation.
The pilot used an over-the-counter medication for the treatment of hay fever that, although labelled as non‑sedating, was not approved for use while conducting flying operations.
The pilot did not wear the upper torso restraint correctly. Although this accident was unsurvivable, the absence of such a shoulder harness restraint generally increases the likelihood of fatal head injuries.
Safety analysis
Introduction
During daytime fire-bombing operations the aircraft deviated off track without making a radio call, flew too low and caught the bucket in trees resulting in a collision with terrain.
Site and wreckage examination did not identify any defects or anomalies that might have contributed to the accident. The following analysis will focus on possible reasons why the aircraft diverted off track as well as medical and survivability aspects.
Pilot incapacitation
The pilot of JWB was familiar with the area of operations and the conditions on the day, having flown several circuits in the area that afternoon. No weather or mechanical issues were identified during the course of the investigation that could have influenced the accident.
The absence of any communication by the pilot after filling the bucket for the final time was unusual as it was standard practice to make a radio call when leaving the circuit for any reason and was a simple action to perform.
At any time during the flight the pilot had the option to dump the water and/or release the bucket and longline in total from the aircraft hook should circumstances have required it. However, this action was not completed by the pilot. Had the observed flight deviation been the result of the pilot responding to a mechanical issue, dumping the water and/or releasing the bucket would have increased the aircraft performance and made dealing with a mechanical malfunction easier.
If the pilot was attempting an emergency landing, then it would be expected that they would have tracked for one of the nearby suitable landing areas and, depending on the emergency, dumped the water and/or released the bucket and made a radio call. The area the accident occurred in was not a suitable emergency landing site due to the slope of the terrain and surrounding obstacles. In addition, the pilot did not perform any of the expected actions associated with an emergency. Therefore, it was considered unlikely that the pilot was attempting an emergency landing at the time of the accident.
The on-site assessment indicated that JWB was at least 19–22 m lower than expected at the time the bucket caught in the trees. The bucket and longline contacted the tree at least 13 m below the top of the tree. The pilot was aware of terrain having completed four circuits in the area and was on the fifth at the time of the accident. In addition, the pilot had been observed flying with a substantial level of clearance between the bucket and the trees on previous circuits.
With the pilot’s extensive experience working with a longline and at low level, as well as several standard pilot actions that were missing, it is unlikely that the pilot knowingly diverted off track, did not make a radio call and flew significantly lower than was safe resulting in the bucket snagging in the trees and the helicopter colliding with terrain.
In the absence of any mechanical issue, and considering the significant, unannounced tracking and height deviation from the normal operating procedure, the evidence indicated that the pilot probably suffered an incapacitating event. Due to this event the pilot unintentionally diverted off track, was unable to make a radio call and was unable to react to the low altitude of the helicopter. This led to the bucket becoming tangled in the trees and caused the helicopter to collide with terrain.
Possible sources of incapacitation
Although 5 per cent carboxyhaemoglobin was present in the pilot’s blood, the level was considered by medical specialists to be too low to have affected the pilot’s ability to operate the helicopter. Recognising the potential for individual variability, the conclusions of the specialists were consistent with research that indicated about 10 per cent carboxyhaemoglobin was generally required to produce adverse effects. As such, it was considered unlikely that carbon monoxide was the source of pilot incapacitation.
Lymphocytic myocarditis
Both medical consultants engaged by the ATSB agreed that myocarditis may have a sudden onset with no initial mild symptoms. In addition, the signs and symptoms of myocarditis vary depending on the cause of the disease and can include sudden incapacitation.
However, the consultants’ opinion differed in relation to the strength of the link between this specific condition and the outcome of the flight. Consultant A stated that the presence of a focus of acute myocarditis in this pilot was a finding likely to have functional significance for the risk of sudden impairment or sudden complete pilot incapacitation. However, consultant B concluded that it was possible that the pilot was suffering some medical incapacitation from myocarditis or heart disease or other causes that were not identified.
Due to the variation between the specialist conclusions, the ATSB was unable to determine if the effects of myocarditis contributed to the accident.
Coronary heart disease
Both medical consultants commented that the level of coronary heart disease found at the post‑mortem examination was likely typical of a large proportion of the population of similar age to the pilot and was not known to produce symptoms.
The pilot had undergone and passed a Class 1 aviation medical within 3 months prior to accident which included an electrocardiogram.
Due to the pilot’s current effective management of their cardiovascular risk factors and a lack of any other evidence linking this condition to the outcome of the flight, it was considered unlikely to have influenced the accident.
Over the counter medication
During the examination of the wreckage, the ATSB found an over-the-counter antihistamine in the pilot’s possessions, and it was reported that the pilot regularly took this medication for the treatment of hay fever. The Civil Aviation Safety Authority (CASA) provides guidance on medications that are approved, hazardous and prohibited for flight. CASA notes that just because a medication is available over the counter does not mean it is automatically safe for aviation. CASA also recommends that a pilot should always consult their designated aviation medical examiner or CASA about the safe use of medication.
The active ingredient of this medication is listed in the CASA guidance as prohibited in aviation. While the label stated it was non-sedating, it is classed by CASA as a sedating antihistamine. ATSB medical consultant A commented that the sedating effects of this medication would be recognisable on taking the first dose. The pilot had been taking this antihistamine for some time and had not reported any side effects. Therefore, any adverse effect on the day of the accident was considered unlikely.
Upper torso restraint
The pilot was found to have not been wearing the upper torso restraint correctly at the time of the accident. The ATSB medical consultant commented that had this been an un-inverted impact, or an impact with significant longitudinal aircraft deceleration, the absence of the shoulder harness restraint would have increased the likelihood of head injuries, with possible fatal consequences in an otherwise survivable accident.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Civil Aviation Safety Authority (CASA)
operator
pilot’s and crew of other helicopters airborne in the area
New South Wales Police Service and Rural Fire Service
aircraft and engine manufacturers
maintenance organisation for VH-JWB
Airservices Australia
next of kin
medical consultants
accident witnesses
recorded data from Spidertracks
References
Civil Aviation Safety Authority’s aviation medicine guidance, Medication, available from the CASA website.
De Vos, A. Reisen, F. Cook, A. Devine, B & Weinstein, P. (2008). Respiratory Irritants in Australian Bushfire Smoke: Air Toxics Sampling in a Smoke Chamber and During Prescribed Burns. Arch Environ Contam Toxicol (2009). 56:380-388.
Hampson, N.B. & Hauff, N.M. (2007). Carboxyhemoglobin levels in carbon monoxide poisoning: do they correlate with the clinical picture? The American Journal of Emergency Medicine, 2008(26), 665-669.
MacSween, K. Paton-Walsh,C. Roulston, C. Guerette, E. Edwards, G. Reisen, F. Desservettaz, M. Cameron, M. Young, E & Kubistin, D. (2019). Cumulative Firefighter Exposure to Multiple Toxins Emmitted During Prescribed Burns in Australia. Exposure and Health.
Rathore, O. & Rein, G. (2016). Carbon Monoxide Toxicology: Overview of Altitude Effects on the Uptake and Dissociation of COHb and Oxygen in Human Blood. Retrieved from RFImpactAltitudeCOToxicology.ashx (nfpa.org)
Salazar, G.J. Federal Aviation Administration. (n.d.). Carbon Monoxide: A Deadly Menace. Retrieved from CObroforweb (faa.gov)
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
The Australian Transport Safety Bureau was an accredited representative to assist the South African Civil Aviation Authority (SACAA) for their investigation of a General Dynamics Convair 340, registered ZS-BRV, which collided with a building near Wonderboom Airport, South Africa, on 10 July 2018.
During the initial climb, smoke was observed emanating from the left engine. The aircraft subsequently collided with a building. One person on board the aircraft was fatally injured and 18 people were injured. One person on the ground was fatally injured and two people sustained serious injuries.
The SACAA’s Accident and Incident Investigations Division has completed the investigation and the final report is now available. Any enquires relating to the investigation should be directed to the SACAA at: www.caa.co.za