On 2 December 2019, an Aeroprakt A22 Foxbat, recreational registration 24-4239, collided with terrain while conducting mustering 111 km SSW of Isisford, Queensland. The pilot sustained serious injuries.
In response to this accident, Recreational Aviation Australia (RAAus) commenced an investigation. As part of its investigations, RAAus requested technical assistance from the ATSB to download flight data from a Garmin GPS.
To protect the information supplied by RAAus to the ATSB and the ATSB's investigative work to assist RAAus, the ATSB initiated an investigation under the Transport Safety Investigation Act 2003.
The ATSB has concluded the examinations of the Garmin GPS and has provided the results of that work to RAAus on 7 February 2020.
Any enquiries relating to the accident investigations should be directed to RAAus at: www.raa.asn.au
At 1322 Eastern Standard Time, on 29 January 2020, a Cessna Aircraft Company U206G, registered VH-AEE and operated by Air Fraser Island with two pilots onboard, was being used for landing emergency procedure training on a beach aircraft landing area (ALA) on Fraser Island, Queensland.
Just after touching down, the aircraft veered significantly to the left, toward the sea. The training pilot took control of the aircraft and conducted a go-around. Once airborne it was identified that the rudder was jammed in the full‑left position and the pilot had to apply full opposite aileron to maintain control. The engine subsequently stopped and the aircraft collided with water. The pilots escaped the aircraft and swam to shore. The aircraft was destroyed.
What the ATSB found
The ATSB found that, following touchdown, a section of the nose landing gear attachment failed, resulting in the rudder becoming jammed in the full‑left position. Due to the aircraft’s significant deviation towards the water, a go-around was initiated. While there was only a short timeframe to make the decision to abort the landing, it resulted in flight over water with significantly reduced aircraft controllability that required uncoordinated flight control inputs to control the aircraft.
It was also identified that fuel starvation, due to either the uncoordinated flight or damage associated with the nose gear failure, led to the engine losing power at a height too low for recovery and the aircraft collided with water.
The ATSB also identified two safety issues associated with the Cessna 206 that, while not contributory to this accident, can lead to fatal consequences in the event of a ditching.
Firstly, the Cessna 206 procedure for ditching and forced landing stated that the flaps were to be extended to 40°. While that permitted the aircraft to land at a slower speed, it also significantly restricts emergency egress via the cargo door. However, there is no warning about that aspect in the ditching or forced landing pilot’s operating handbook emergency procedures.
In addition, the Cessna 206 with the cargo door does not meet the aircraft certification basis for the design of cabin exits, due to the complexity associated with opening the cargo door if it is blocked by the flaps. This significantly hampers emergency egress and has previously resulted in fatalities.
What has been done as a result
The ATSB has recommended that Textron Aviation take safety action to address the procedure for ditching and forced landing in the pilot operating handbook for the Cessna 206, to ensure pilots are aware that extending the flaps beyond 10° will significantly restrict emergency egress via the cargo door.
The ATSB also recommends that the United States Federal Aviation Administration and the Civil Aviation Safety Authority take safety action to address the certification basis for the design of the cargo door in the Cessna 206, as wing flap extension beyond 10° will block the forward portion of the rear double door, significantly hampering emergency egress.
In addition, and as a result of this accident, the operator has changed their procedures to specify that during emergency procedure training on the beach, no non-company vehicles are permitted to operate within the runway complex. They have also reassessed the company hazard register and included brake failures.
Safety message
This occurrence highlights the issue of evacuation through the cargo door when the flaps are extended in the Cessna 206. Pilots should be aware that lowering the flaps will block this exit and significantly increase the difficulty of opening the door. Consequently, all passenger pre‑flight briefings should include a practical demonstration of how to open a partially‑obstructed cargo door. Additionally, in the event that a ditching is required, pilots should consider not extending the flaps.
Furthermore, in 2009, research by the Transport Safety Board of Canada found that in the previous 20 years, where an aircraft had collided with water, 70 per cent of fatalities were caused by drowning. That statistic reflects the inherently disorientating nature of underwater exit from an often-inverted aircraft.
Transport Canada released TP 2228E-18 (04/2003), an ‘underwater egress’ safety guide which was forwarded to all Canadian operators of passenger carrying operations operating on water. This guide was to be provided to passengers before flight to increase their likelihood of survival in the event of a ditching.
The occurrence
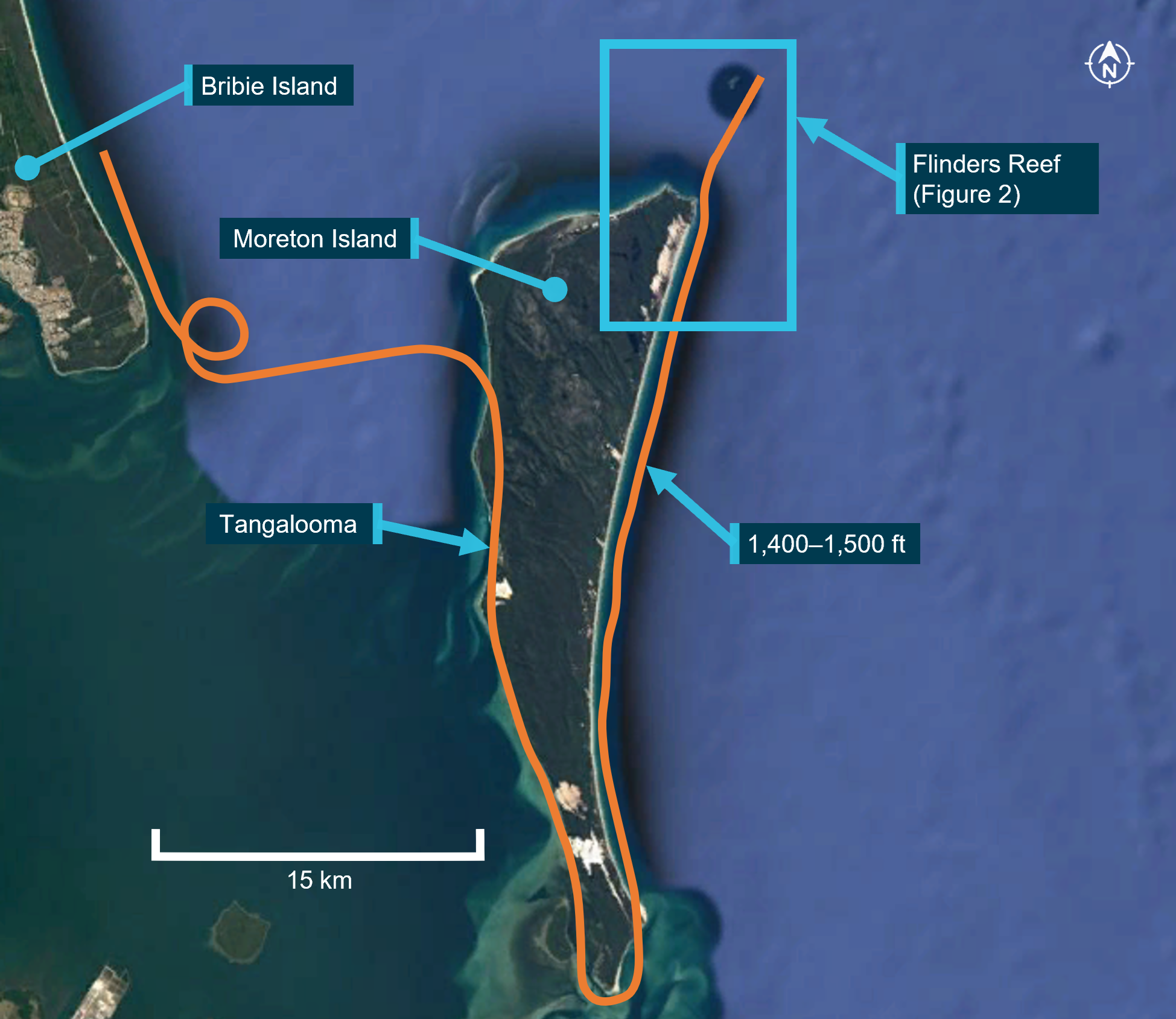
At 1322 Eastern Standard Time,[1] on 29 January 2020, a Cessna Aircraft Company[2] (Cessna) U206G aircraft, registered VH-AEE (AEE) and operated by Air Fraser Island, was being used for emergency procedure training at a beach aircraft landing area (ALA), south of Happy Valley, Fraser Island, Queensland (Figure 1). There were two pilots onboard, including a trainee pilot (trainee), who had just commenced flying with the company. The trainee was seated on the left and was flying the aircraft.
Figure 1: Accident location
Source: Google Earth annotated by ATSB
The crew were simulating failure of the left main wheel brake during the landing phase. Just after the aircraft touched down, the trainee heard a snapping noise and the aircraft immediately veered left, towards the sea. The training pilot reported that, on taking control of the aircraft, their[3] rudder pedals were ‘lying on the floor’. However, there was no change in the aircraft’s pitch or bank attitude, as would be expected if a major component of the landing gear had failed.
The training pilot immediately applied full power to conduct a go-around. The aircraft lifted off just before the water’s edge and struck a number of waves as it began to climb. The trainee advised that full aileron deflection was required to keep the wings level. The aircraft continued to climb to a height where the training pilot felt comfortable. They then lowered the nose to gain airspeed and reduced the flap, one stage at a time, to 20˚. The training pilot advised that as the airspeed increased above 70 kt they encountered difficulties controlling the aircraft’s roll, despite having full aileron deflection, so they reduced the power to maintain around 65–70 kt. About 150 m from the shore, they turned the aircraft north to parallel the beach. At that stage, the aircraft was maintaining a height of 150–300 ft above the water.
Both pilots then began to troubleshoot the control issues and identified that the flaps had raised symmetrically, and the rudder was jammed and fully deflected to the left. That control position resulted in significant uncoordinated flight (sideslip) to maintain control of the aircraft.
The training pilot advised the trainee that they were going to land back on the beach however, a short time later, estimated to be about 1.5 minutes after commencement of the go‑around, the engine stopped. The trainee advised there was about 5–6 seconds before the aircraft contacted the water. The training pilot had time to lower the nose and change fuel tanks from the right to the left tank, but not enough time to attempt to restart the engine.
After hitting the water, the aircraft remained upright, and the cabin quickly began to fill with water. Both pilots undid their seatbelts and the trainee tried unsuccessfully to open the single front pilot door (see the section titled Emergency egress in the U206). When the door could not be opened, the training pilot climbed over the seats into the rear cabin, kicked the cargo door to force it open, and then tried unsuccessfully to locate the trainee pilot in the aircraft. The training pilot then exited the aircraft via the cargo door.
Once outside, the training pilot could not locate the trainee so they re-entered the aircraft, which was then three quarters submerged. As the trainee could not be located, they exited a second time taking hold of a life jacket as it floated past. During this time, the trainee had opened and climbed out the pilot door window.
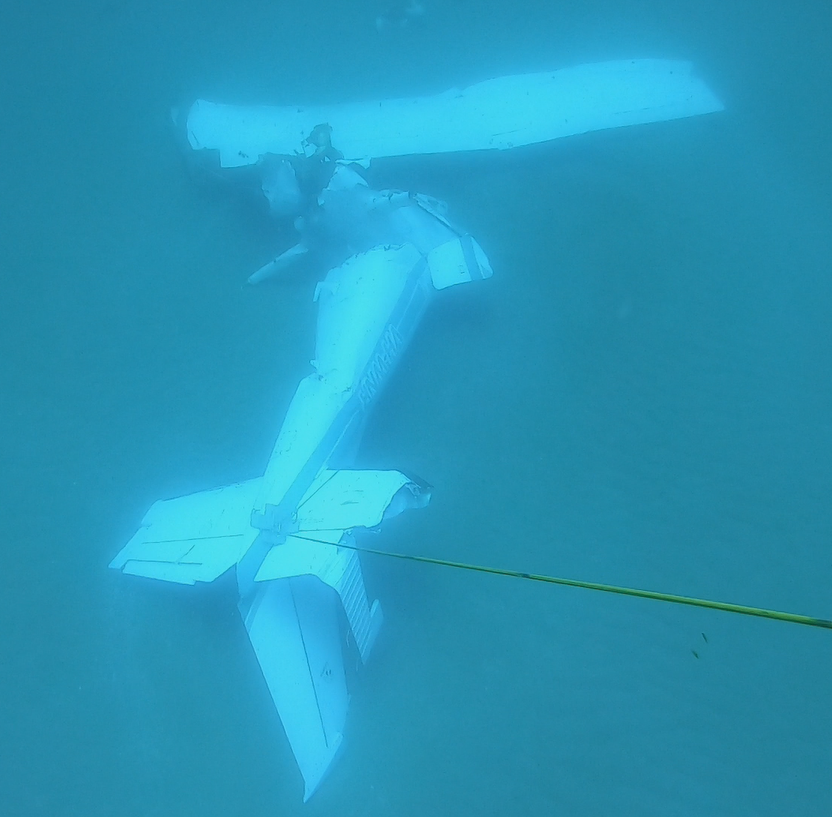
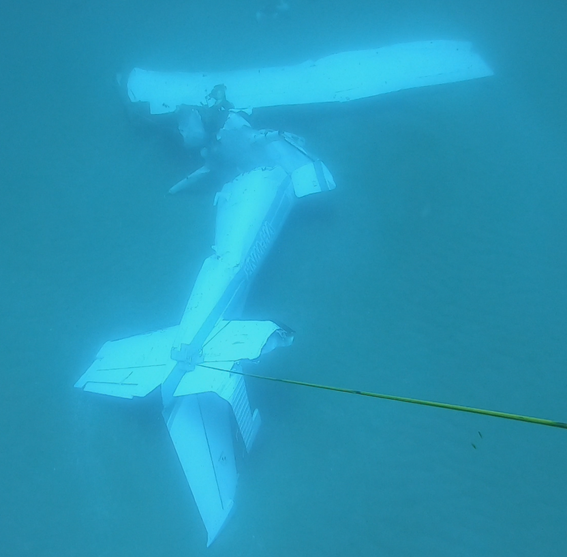
The training pilot then observed the trainee on the other side of the aircraft and after making them swim around the aircraft, put the life jacket on them. The training pilot subsequently put their arm through the life jacket and they both started swimming back to shore. They were met by a paramedic from the Happy Valley ambulance station who had entered the water to assist them to shore. Both pilots suffered minor injuries and the aircraft was destroyed (Figure 2).
It was reported that the aircraft’s nosewheel leg was found on the beach on the afternoon of the accident, approximately half-way between where the go‑around commenced and where the aircraft collided with water. The aircraft, without the engine, washed up on the beach the morning after the accident. At the time of writing, the engine had not been recovered (Figure 2).
The training pilot held a Commercial Pilot (Aeroplane) Licence with a Class 1 Aviation Medical Certificate. They had accrued over 10,200 hours of which around 5,000 hours were accumulated in the Cessna 206. At the time of the accident, they had been awake for around nine hours and advised feeling ‘fine’ on the day.
The trainee held a Commercial Pilot (Aeroplane) Licence with a Class 1 Aviation Medical Certificate. They had accrued around 500 hours flying. At the time of the accident, they had been awake for about nine hours and had self-assessed their fatigue level at ‘2: very lively’.[4]They advised that as part of their training they had completed the theory section of the emergency procedures training detailed in Civil Aviation Orders 20.11. They had previously been operating as a ground crew member on Fraser Island for the operator for several months and were proficient in the emergency procedure briefing for the aircraft and the use of life jackets.
Aircraft information
General details
The Cessna U206G is a single engine, six seat, high wing aircraft with fixed undercarriage. It is powered by a Teledyne-Continental Motors six-cylinder, horizontally opposed, fuel-injected piston engine with a constant speed propeller. The aircraft had modifications to improve the short take‑off and landing (STOL) capabilities.
AEE was manufactured in the United States in 1979 and first registered in Australia in the same year. The aircraft was maintained in accordance with the Civil Aviation Safety Authority (CASA) maintenance schedule, which required a periodic inspection every 100 hours or twelve months, whichever came first. It had undergone a periodic inspection on the 14 January 2020 and had a valid maintenance release. At the time of this inspection, the aircraft had accumulated about 13,725 hours in service. The operator advised they had purchased the aircraft two weeks prior to the occurrence.
Fuel system
The fuel system consists of left and right wing-mounted fuel tanks, which feed into separate fuel reservoir tanks. The pilot uses the fuel selector to select fuel from either the left or right reservoir tank. The fuel then passes from the selected reservoir tank into the engine through an auxiliary fuel pump, fuel strainer, engine driven fuel pump and fuel control unit.
The pilot operating handbook stated that, with a quarter tank or less, ‘prolonged uncoordinated flight such as slips or skids can uncover the fuel tank outlets, causing fuel starvation and engine stoppage’. This can occur with uncoordinated flight in excess of one minute.
The pilots reported they had departed Sunshine Coast Airport that morning with full fuel tanks. The trainee reported they had conducted approximately 1.5 hours flying before arriving at Hervey Bay Airport. The training pilot advised they had departed Hervey Bay Airport at approximately 1200. The accident occurred at approximately 1322. The training pilot reported that they had been changing fuel tanks every half hour. While the specific amount of fuel at the time of the accident could not be determined, based on the described flight sequences it is likely that each tank was about one third full.
Weight and balance
The aircraft was within the weight and balance limits at all stages of the flight.
Steering and brake system
The rudder pedals of both control positions are interconnected by torque tubes. The nose wheel steering system links the rudder pedals to the nose wheel steering arm, through a spring‑loaded steering bungee. This allows steering control on the ground using the rudder pedals and brakes. The steering bungee limits the turning of the nose wheel to 15-20°. Additionally, the nose wheel is locked straight ahead when there is no weight on the wheel.
The rudder system is also connected to the rudder pedals through the torque tubes. The torque tubes connect directly to the rudder via cables, and to a steering bellcrank, via pushrods, to form a closed loop system.
The brake system consists of a single disc, which has a hydraulically actuated brake, on each main landing gear wheel. The brake is operated by pressing the top of the rudder pedal. The right‑seat brakes are connected to the left-seat brakes by torque tubes located inside the rudder pedal torque tubes. Hence, applying the right brake on the right-seat pedal moves the right brake on the left-seat pedal, which then actuates the right brake master cylinder.
Stowable right-side pedals were an option on some models however, AEE had standard rudder pedals installed.
Damage to aircraft during accident sequence
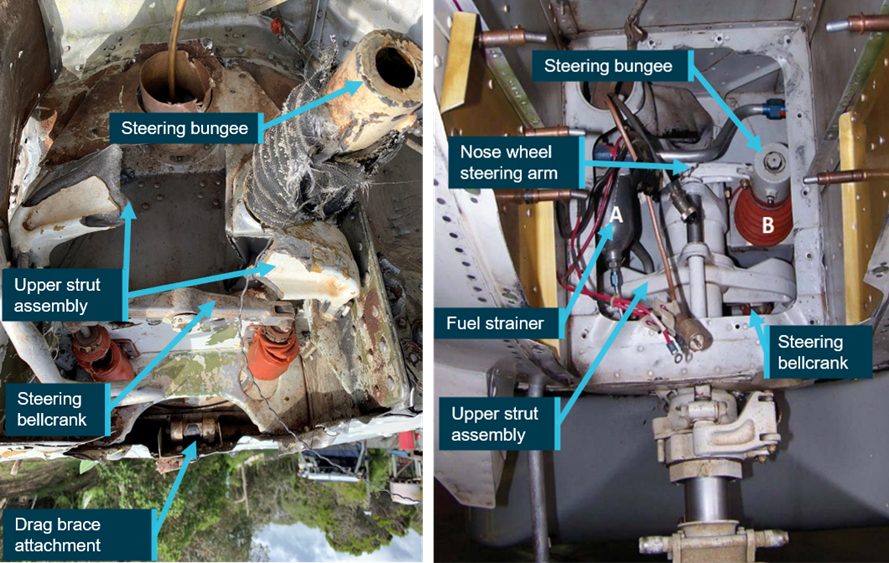
While the ATSB did not attend the accident site, a review of supplied images identified the following damage to the nose landing gear area (Figure 3 and Figure 4):
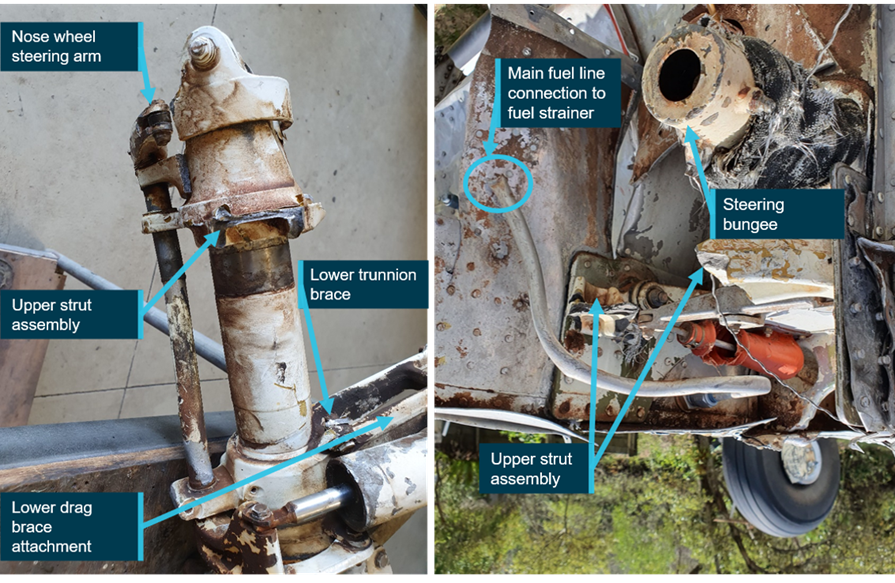
the nose wheel assembly had detached at the upper strut assembly and the steering bungee had separated
the drag link had fractured at both ends
both lower trunnion braces had fractured at their attachments
the fuel line to the fuel strainer had fractured and fuel strainer bowl was missing.
From the photographs of the aircraft, all fractures appeared to be overstress failures with no evidence of pre-existing damage. However, it could not be determined which failure occurred first.
The rudder cables were also found to be intact and connected at both the forward and aft cable ends.
Figure 3 : Nose landing gear area (image rotated 180˚) and exemplar C206 nose landing gear area
Source: Supplied, annotated by ATSB
Figure 4: Nose landing gear leg and front of aircraft showing the main fuel line (image rotated 180˚)
Source: Supplied, annotated by ATSB
Recorded information
The aircraft was not fitted with a recording device, nor was it required to be. A witness supplied video footage of the final portion of the flight. It showed that the aircraft was maintaining level flight before it suddenly lost altitude, which was consistent with both pilots’ recollection of events. It also showed the aircraft initially floated upright on the sea surface, which most likely assisted the pilots to evacuate the aircraft.
Weather conditions
The graphical area forecast for the area indicated visibility was greater than 10 km with scattered[5] cloud above 2,000 ft. The terminal area forecast for Hervey Bay, about 31 km west of the Happy Valley ALA, indicated the wind was from the east-north-east at 8 kt. The supplied video footage showed clear skies with a light sea chop. The training pilot advised the ocean was flat, with 1.2 m sets of waves with no wind. The current was running along the beach, from north to south.
Beach landing area
The operator used the criteria specified in Civil Aviation Advisory Publication 92-1(1) Guidelines for aeroplane landing areas to establish ALAs at various locations on the eastern beach on Fraser Island. These were set up, on the day, by trained ground crew. The pilots reported that the ALA was low on the beach with firm, hard sand. The ATSB did not attend the ALA after the accident and could not verify its condition.
Operator training
The operator regularly conducted sightseeing and passenger transfer flights from different locations along the eastern beach at Fraser Island. Their operations manual required that a passenger briefing be conducted prior to every passenger flight. This was to include the use of life jackets along with the location of, and the procedure to operate the emergency exit.
The operations manual had a section which outlined the training for the ground handling personnel. This section required that ground personnel be proficient in the use of all emergency exits in aircraft used in beach operations.
Newly employed pilots were required to complete pilot induction training, which included at least 15 hours of training in operating on the beach. In addition, pilots were required to undergo a beach-operations check every 90 days and a six-monthly route check.
The operator had a section in their operations manual which outlined their pilot training syllabus, covering all aspects of training. In the pilot induction training section, the syllabus specified that, along with other competencies, brake failure and asymmetric braking would be covered during the theory training, with no mention of simulated brake failure training in the practical syllabus. Despite this, the operator advised they always conducted simulated brake failures on the beach during the practical flying training. There was no information in the operations manual on how the brake failure simulation was to be conducted.
The operator advised they had devised their own method for brake failure training. To simulate the brake failure, after landing and with all three wheels on the ground, the flying pilot would apply full rudder on the side they were simulating as failed and then use the opposite brake to maintain directional control. That is, a simulated left brake failure required full deflection of left rudder pedal and the use of right brake to slow the aircraft and control direction and vice versa for simulation of right brake failure. The training pilot advised that they used this method, as the turning force associated with full brake application on one side was greater that the turning force created by the rudder and could result in the aircraft running off the side of the runway.
CASA had approved the operator’s operations manual, which included the operator’s pilot training syllabus. When questioned about the brake failure training being conducted by the operator, CASA stated ‘all pilots are taught basic “asymmetric brake failure recovery techniques” from an early stage in the flying training…’ but advised they had not observed the operator’s brake failure training method in the aircraft. They advised that brake failure training is normally conducted while taxiing rather than the landing phase of flight. CASA also advised that:
Due to the safety risks associated with the simulation of an asymmetric brake condition different training techniques may be used to simulate the failure that mitigate the safety risks, in the same way CASA expects flight training operators to manage the safety risks associated with flight training activities. As there was no guidance in the aircraft flight manual on the simulation of asymmetric brake failure the operator should have included clear guidance and procedures on how such activities were to be conducted.
The operator used Mahindra Airvan 8 (formerly GippsAero GA8 Airvan), Cessna 206 and 172 aircraft and advised that they conducted simulated brake failure training in all three aircraft types.
The ATSB sought Textron Aviation’s (type certificate holder for the Cessna 206) views on this type of simulated brake failure training. In response, they advised that they did not have an opinion about training.
A search of the ATSB database and CASA defect reporting service, between 2000 and 2020, did not identify any brake failures having been reported by the operator.
Effect of simulated brake failure training on nose wheel
In the Cessna 206 and 172, the nose gear steering is designed so the nose wheel is held with zero steering deflection while the gear strut is fully extended, regardless of rudder pedal deflection. Nose wheel steering is only available once the nose strut deflects and then it is only influenced by the steering bungee loads. The application of full rudder pedal deflection on the ground will only result in 15–20° of nosewheel deflection. However, for aircraft with direct nose gear steering linkages, such as the Airvan 8,[6] this could mean that the steering angles on the nose wheel could be much higher.
Aircraft design requirements account for fore/aft and side loads on the nose gear based on towing and tyre friction over a variety of hard surfaces. The friction properties of sand are likely to be low initially. However, if ploughing were allowed to develop the side loads on the nose wheel could be relatively high. For a wheel that can only turn 15–20°, this effect is not likely to develop to any great extent. However, for aircraft with direct steering linkages, the loads may increase significantly.
Differential braking is permitted and designed into the braking system. It does not produce any additional loads on the airframe other than side load on the nose gear, but this would be proportionally low. Therefore, stopping the aircraft with brakes from one wheel of the aircraft would not be damaging.
It was difficult to determine whether the side loads on the nose wheel would exceed the design requirements in the Airvan 8. As this was not the aircraft type involved in the accident, further consideration of this aspect was outside the scope of the investigation.
Operator training on accident flight
The training being conducted at the beach landing area consisted of flapless landings and simulated brake failures during landing. The crew advised that, as there was very little wind, they were taking off and climbing to 500 ft before conducting a teardrop turn to land back on the ALA in the opposite direction. They were conducting flapless landings when landing to the north and simulating a brake failure during the landing to the south. They advised they had conducted at least five simulated brake failure landings that day, with no problems encountered.
Operator’s safety management system
While not required by CASA, the operator had begun to introduce a safety management system (SMS) into their organisation in about 2013. This was incorporated into their operations manual which was divided into sections including one on the SMS and a section on specialised operations. The SMS section included procedures for a hazard identification process and included the statement ‘hazards can only be mitigated and controlled if their existence is known’.
The specialised operations section included information and procedures for beach operations. It identified that, due to operation in the harsh beach environment, special attention should be paid to the brakes in the pre-flight inspection. Despite this special attention and additional regular brake failure training, the operator had not identified brake failures as a hazard in their hazard register. CASA had approved the operations manual incorporating the SMS in 2015. However, they had not identified that the hazard register did not identify this aspect.
Go-around decision
The approach and touch down on the incident landing were reported to have been normal. The trainee pilot advised that, as they applied left rudder, but before applying the right brake, there was a snapping noise and the aircraft veered left. The training pilot advised that the aircraft veered left between 15–20˚.
They immediately called out ‘taking over’ and assumed control of the aircraft, with the trainee pilot removing their hands and feet from the flight controls. The training pilot assessed that their rudder pedals had collapsed forward, so they had neither rudder nor brake authority. They decided that, as they were heading for the water, which was about 40‑50 m away, and the aircraft was still moving at approximately 50–60 kt, the safest option was to apply full power and conduct a go‑around.
The trainee pilot stated that if they had continued on the ground ‘it would not have been a smooth impact’.
Federal Aviation Administration guidance
The Federal Aviation Administration’s (FAA) publication The art of aeronautical decision-making advises that aviation decision making can be broken down into three parts - to perceive, process and perform.
The FAA publication Airplane flying handbook Chapter 17 Emergency procedures advises that a pilot takes about 4 seconds to perceive and react to an emergency situation. In addition, ‘there are several factors that may interfere with a pilot’s ability to act promptly and properly when faced with an emergency’. These are listed as:
reluctance to accept the emergency situation
desire to save the airplane
undue concern about getting hurt.
It goes on to advise:
A pilot who is faced with an emergency landing in terrain that makes extensive airplane damage inevitable should keep in mind that the avoidance of crash injuries is largely a matter of: (1) keeping the vital structure (cabin area) relatively intact by using dispensable structure (i.e., wings, landing gear, fuselage bottom) to absorb the violence of the stopping process before it affects the occupants (2) avoiding forceful bodily contact with interior structure.
Emergency egress in the U206
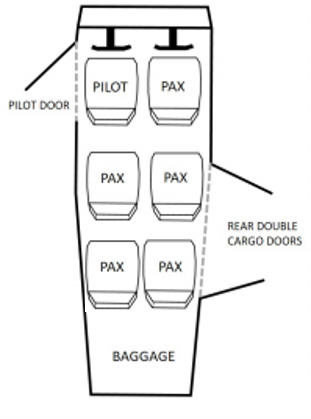
The U206[7] has a door adjacent to the left pilot’s seat and a double clamshell cargo/cabin door in the passenger compartment on the right, adjacent to the second and third seat rows (Figure 5).
Figure 5: Cessna U206 showing location of pilot door and double clamshell cargo/cabin door
Source: TSB investigation report A18W0129, adapted by ATSB to match occurrence aircraft
Operation of rear cargo doors
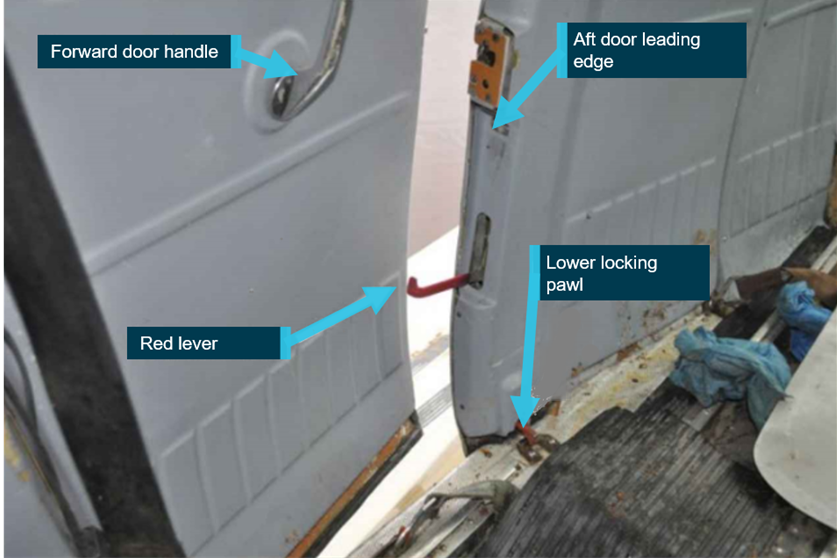
The forward door of the rear double cargo doors must be opened first to allow the aft door to open (Figure 7). The forward door handle is accessible for passengers in the middle row seats and is difficult to reach by passengers in the back-row seats. The forward door handle has three positions:
when the lever is horizontal (with the lever facing forward), the door is locked
turned clockwise 90° to the vertical position, the door is closed
turned clockwise another 30°, the door is open.
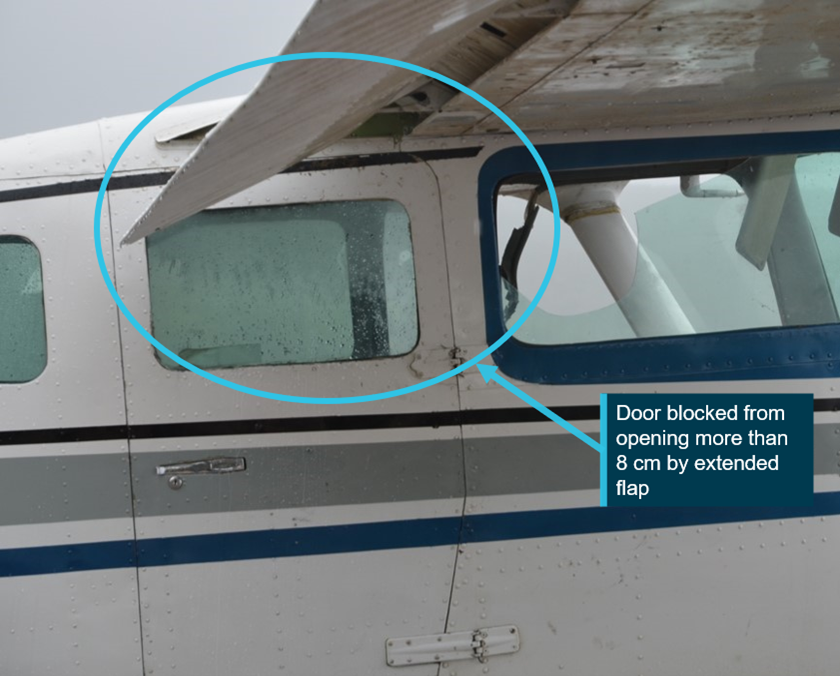
When the flaps are extended, the front half of the clamshell cargo door is blocked by the flap and can only be opened approximately 8 cm (Figure 6).
Figure 6: Cessna U206 with door unable to be opened more than 8 cm when flap is extended
Source: TSB investigation report A18W0129, annotated by ATSB
A red lever, mounted in the aft door leading edge, is used to unlatch the aft door (see Figure 7: Cessna 206 forward cargo door open showing red lever activated on the leading edge of rear door). However, this lever is in line with the backrest of the right middle row seat. As such, it is difficult to reach for the passenger occupying the middle seat and is again difficult to operate by passengers in the back-row seats.
In addition, when the red lever in the leading edge of the aft door, is lowered to the open position, it strikes the slightly open forward door, which prevents the aft door from opening. The lever must therefore be restowed before opening the aft door, being mindful that the aft door latch does not re-engage.
A service bulletin was subsequently released by Cessna to improve the red lever operation so that the lever automatically restowed (see Cessna service bulletin SEB91-4 Cargo door latch improvement in Australian requirements). Having to keep the forward door open to operate the lever in the forward edge of the aft door, adds to the difficulty of the procedure, especially when attempting to open the doors from the rear seats.
Figure 7: Cessna 206 forward cargo door open showing red lever activated on the leading edge of rear door
This image shows an aircraft where service bulletin SEB91-4 has not been incorporated and the red handle does not retract automatically. Before the door can be opened, the red lever is required to be restowed without the door relatching. This is not indicative of the accident aircraft. Source: TSB investigation report A18W0129, annotated by ATSB
In addition, when the doors on the aircraft are locked from the inside, neither the front nor the rear cargo door can be opened from the outside.
Emergency Procedures
The pilot operating handbook (POH) emergency procedures section provided checklist and amplified recommended actions to be taken in the event of an abnormal situation. In the ‘forced landings’ section, the procedure for ditching stated that flaps were to be extended to 40˚. In addition, it noted ‘evacuate through the cabin doors. If necessary, open window and flood cabin to equalise pressure so doors can be opened’.
There was no reference in this section to warn that the cargo door will be blocked if the flaps are extended. The procedures for other forced landings, with or without engine power, also stated that the flaps were to be extended to 40°. Again, there was no reference in that section to warn that the cargo door will be blocked if the flaps are extended.
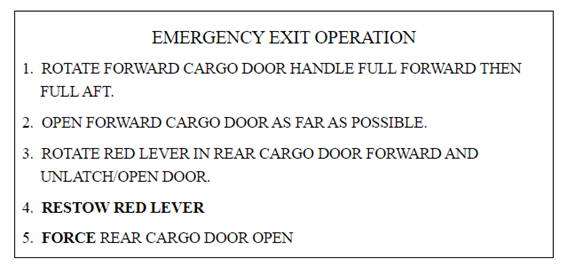
The amplified procedures section contained a brief description of the ‘cargo door emergency exit’, which included:
if the wing flaps are extended, open the doors in accordance with the instructions shown on the placard (Figure 8) which is mounted on the forward cargo door.
Figure 8: Cargo door emergency exit placard
Step 4 is not required in aircraft where Cessna service bulletin SEB91-4 has been incorporated.
Source: Cessna 206 pilot operating handbook
Federal Aviation Administration certification requirements
The Cessna 206 was first certified in 1963 under the United States (US) Federal Aviation Administration (FAA) Civil Aviation Regulation Part 3. Section 3.387 which stated:
Closed cabin airplanes carrying more than 5 persons shall be provided with emergency exits consisting of movable windows or panels or of additional doors which provide a clear and unobstructed opening….The exits shall be readily accessible, shall not require exceptional agility of a person using them….The method of opening shall be simple and obvious, and the exits shall be so arranged and marked as to be readily located and operated even in darkness.
There have been a number of revisions made to this standard over the years however, once an aircraft has been certified, the design standard under which it was certified continues to apply.
Australian requirements
In 1988, the Civil Aviation Authority (CAA),[8] released an airworthiness directive AD/Cessna 206/47 that required improved placarding of Cessna 206 emergency exits. Cessna subsequently released service bulletin SEB91-4 Cargo door latch improvement in March 1991, which recommended modifying the handle in the rear door half to include a spring to ensure that the handle would return to the stowed position.
That same year, the CAA issued AD/Cessna 206/47 amendment 2, which allowed SEB91-4 to be an alternate means of compliance to the required placards. In 2011, CASA subsequently issued amendment 3 to
which clarified which 206 models the AD applied to, as SEB91-4 had been incorporated at manufacture in some models and other models did not have the cargo door, however, SEB91-4 remained as an alternate means of compliance. AEE complied with this AD.
Transport Safety Board of Canada
In 2018, the Transport Safety Board of Canada (TSB) investigated a collision with water involving a float-equipped U206 (A18W0129). In this occurrence, the aircraft inverted upon impact and became submerged. The pilot and one passenger escaped through the forward door window. Three other passengers survived the impact and were found with their seatbelts undone, however, they did not escape the aircraft and subsequently drowned.
The TSB report noted ‘the rear double cargo doors have been identified as a risk to passengers in emergency situations for many years’. Further, the report documented some of the work which had been conducted to address the risk associated with the design of the cargo door, including:
In 1991, Cessna issued Service Bulletin SEB91-4 which provided a service kit to incorporate a spring assembly to automatically retract the handle on the leading edge of the rear half of the door to allow it to pass the front half of the door. It also included improved placarding to clarify the instructions on how to open the door in an emergency.
In 1998, Cessna resumed manufacturing the 206 with the 206H. This was certified under the US Federal Aviation Regulations[9] 23.807 legislation. Transport Canada determined that the 206H did not meet the requirements of the legislation, as the rear cargo door could not be considered an emergency exit as the means of opening was not ‘simple and obvious’. As a result of that assessment Transport Canada reduced the number of occupants permitted in the aircraft to five.
Between 1999 and 2003, Transport Canada, the FAA and Cessna worked on a design change to address this issue, which could be applied to the 206H, and retrofitted to the previous 206 models. No acceptable solution was found, and the matter was discontinued.
In 2005, Transport Canada proposed an airworthiness directive to address the issue of different models allowing different numbers of occupants, despite having the same design. However, following industry consultation, the proposal was withdrawn.
In response to the 2018 Canadian occurrence, TSB released an Aviation Safety Advisory A18W0129-D1-A1Cessna 206 emergency exit – blocked double cargo door with flaps extended, ‘to bring attention to the significant safety issue involving Cessna 206 series aircraft fitted with double cargo doors’.
Other action taken by regulatory bodies
November 1996
As a safety action in response to an accident in a Cessna U206 where a pilot and three passengers drowned when they could not escape the aircraft after it capsized during the take‑off run (A96Q0114), Transport Canada (TC) wrote to the FAA to express concern about the adequacy of the emergency exit in the Cessna U206 aircraft. In the letter, TC strongly recommended that should production of the U206 resume:
…the FAA require Cessna to incorporate a solution which eliminates the interference problem between the flaps and the emergency exit…
No action was taken by FAA in response to this letter.
March 2020
FAA released an Airworthiness Concern Sheet NOTC0041 asking for information from people who had experience using the 206 cargo door. They subsequently advised that 95 per cent of the respondents did not want action taken on the issue. They also advised that their research had shown that the biggest positive impact to safety was ensuring that pilots briefed their passengers on how to use the door. No further action was planned.
April 2020
Transport Canada released Airworthiness Directive CF 2020-10 which limited the number of seats in Cessna 206 aircraft to five, in other than the 206H and T206H models,[10] and aircraft which had not been modified to FAA supplemental type certificate (STC) SA1470GL (see Right side door below). Additionally, if passengers were seated in the rear row, they must have demonstrated the capability to operate the cargo door on the day of the flight. They must also have been briefed that the cargo doors were only to be used in an emergency if the front left cabin door was obstructed.
The same month, the Civil Aviation Authority of New Zealand released Continuing Airworthiness Notice 25-003 to alert operators of Cessna 206s in New Zealand to CF 2020-10.
August 2020
The European Union Aviation Safety Agency (EASA) released a Safety information bulletin 2020‑16 to alert European operators of Cessna 206s to CF 2020-10.
Cessna 206 exit modifications
Several organisations have developed solutions to ensure the cargo door can be opened easily in the event of an emergency. Some of these solutions have received approvals from the FAA and are commercially available. Some of these include:
Right side door
FAA STC SA1470GL approves a right-side door in the front cabin, which allows both egress for the front right passenger and emergency egress from the centre row seats in the cabin.
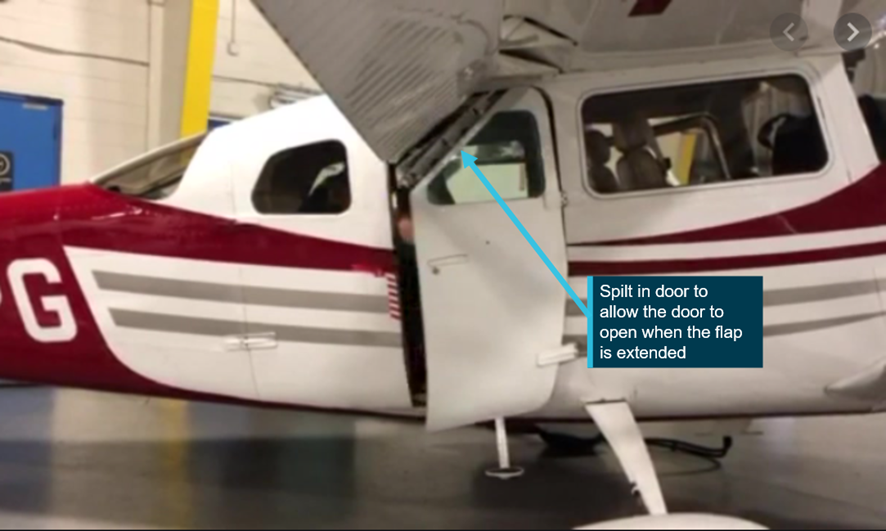
Installation of the Split Forward Cargo Door Window
Transport Canada have approved supplemental type certificate SA20-34. This allows for the forward cargo door to be split allowing the door to open when the flap is extended (Figure 9). This has also been approved in Europe under EASA STC 10074631 and the FAA under STC SA04550NY.
Figure 9: Cessna 206 split cargo/cabin door
Source: Coast Dog Aviation, annotated by ATSB
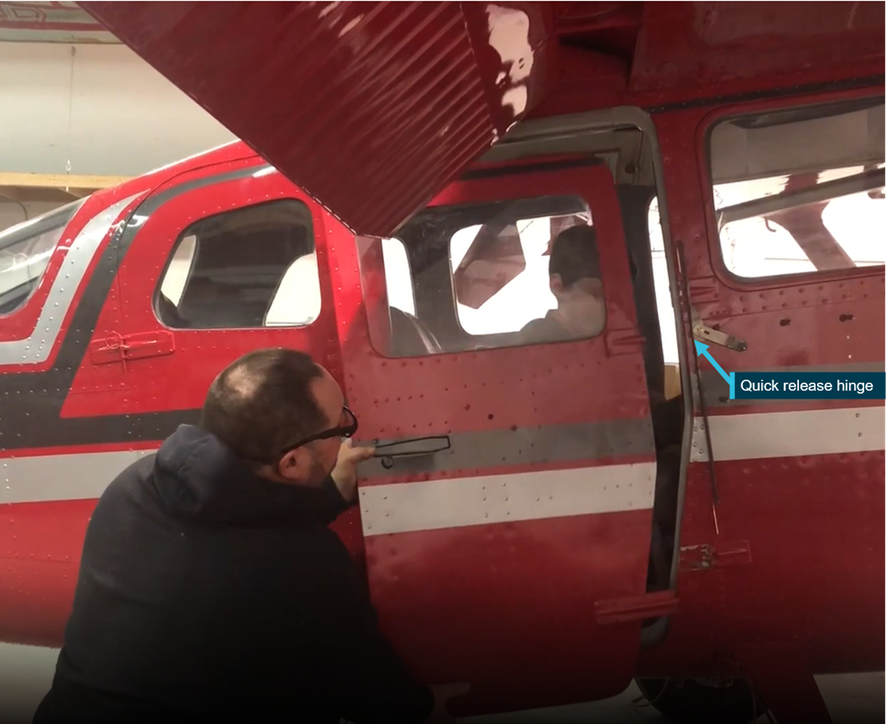
PDQ emergency egress system
At the time of writing this report, the manufacturer reported that the FAA were in the final stages of approval for supplemental type certificate ST02309AK. Under this approval a handle is installed which, when activated, allows the front cargo door to be released (Figure 10). This allows access to the red lever and the aft cargo door can then be opened.
Figure 10: Cessna U206 with emergency egress system
Source: Airframe Innovations
Similar occurrences
The ATSB conducted a search of aviation investigation databases, and other sources, to identify accidents involving Cessna 206 aircraft, where the impact was likely survivable however, difficulties opening the cargo door resulted in significant delays during the emergency egress, or the cargo door had not been opened. The following accidents were identified:
Table 1: Similar occurrences
Year
Injuries
Summary
Link
2018
5 persons on board (pob)
3 fatalities
During a landing on water, a float equipped U206G nosed over. The pilot and one passenger survived. The three remaining passengers, who received no injuries during the accident, were unable to escape the fuselage and drowned. The passengers were found with their seatbelts unfastened but had not opened the cargo door, which was blocked by 20˚ flap.
During a landing on water, the float equipped 206 nosed over. The flaps were extended blocking the cargo door. The pilot and three passengers escaped by bending the cargo door. The fourth passenger, found in her seat with the seatbelt on, likely died through injuries caused by the accident.
During cruise, the engine failed, and the pilot conducted a ditching into Lake Michigan. The pilot did not lower the flap; however, the cargo door had not been opened. The pilot survived. Two passengers were found outside the aircraft however, their life jackets had failed. Of the two passengers found inside the cabin, one had removed their seatbelt.
During the landing on water, the float equipped 206 flipped over. Contrary to instructions provided by the pilot, the passenger made their way to the rear of the aircraft, was unable to exit, and drowned.
TSB aviation occurrence A03Q0083
2001
5 pob
1 fatality
During the landing, the aircraft collided with a hole in the runway, nosed over and slid into a river. The pilot and three passengers escaped with minor injuries, however, one of the passengers drowned trying to escape the aircraft.
During the landing on water, the float‑equipped aircraft flipped as the landing gear had not been retracted. Two passengers were unable to exit the aircraft and drowned. The door handle was found in the upright closed position.
TSB Aviation investigation report A97C0090
1996
6 pob
4 fatalities
During the take-off on water, the aircraft capsized. The pilot and three passengers drowned in the rear of the aircraft, when the pilot could not open the cargo door. Two passengers escaped through the pilot door. There was evidence that an adult had attempted to open the cargo door.
During the landing on water, the float equipped 206 nosed over. The flaps had been extended to 20˚ and then raised to 10° during the accident sequence to prevent the flaps from blocking the cargo door. The pilot survived, however four passengers drowned when the cargo doors could not be opened.[1]
During the landing on a dam, the float‑equipped 206 nosed over as the landing gear had not been retracted. The pilot and one passenger survived, but three passengers were fatally injured.
In March 1999, at Pitt Island, New Zealand, a Cessna 206 had an engine failure and ditched in the sea. The pilot was aware of the issue with deployed flap blocking the rear doors and ditched the aircraft with the flaps retracted. Consequently, all the occupants escaped from the aircraft and swam to shore. (Transport Accident Investigation Commission New Zealand 99‑001)
On 29 January 2020, at about 1322, the flight crew of a Cessna U206G aircraft, registered VH‑AEE, were conducting simulated brake failure training on a beach at Fraser Island, Queensland. During the landing roll, directional control was lost, and the training pilot conducted a go-around. While the aircraft was flying parallel to the beach, with flight control issues, the engine stopped, and the aircraft collided with the water. Both pilots escaped the aircraft and swam to shore with minor injuries.
This analysis will examine the sequence of failure in the nose landing gear system, the decision to conduct a go-around and the engine stoppage. Further, it will analyse the brake failure training conducted by the operator and the interaction between the landing flaps and cargo door in the context of emergency egress.
Accident sequence
Both pilots reported having conducted several landings involving simulated brake failure, without incident. On this landing, just after touchdown, and as the left rudder was applied the trainee pilot heard a snapping noise, immediately followed by loss of directional control. Examination of the rudder control system after the occurrence established its continuity. As such, it is likely that a partial failure in the nose gear assembly compromised the interconnected rudder and steering controls. The training pilot reported the rudder was jammed in the full left position and use of the brakes was not possible as the right-seat pedals had collapsed.
Despite the nose landing gear being found on the beach between where the aircraft took off and where the collision occurred, it is likely the nose gear leg did not detach from the aircraft while the aircraft was on the ground as this would probably have resulted in the propeller striking the sand and stopping the engine.
Additionally, as the rudder probably jammed due to the partial failure of the nose gear assembly, if the nose gear detached during the take-off or initial climb, control of the rudder would likely have been restored. However, based on the account of the pilots, this did not happen.
Supplied images showed that the fuel strainer was missing, and the fuel line that fed the strainer was fractured. These components were in the nose gear bay and directly fed the engine fuel system. Loss of fuel supply at this location would have resulted in almost immediate engine stoppage. As the engine continued to provide power for approximately 1‑1.5 minutes after take-off, it is highly probable that the nose gear separated and fractured the fuel line, as the aircraft collided with the water.
Examination of the nose gear fracture surfaces revealed they were consistent with the attachments failing in overstress, with no indication of a pre-existing fault. It could not be established which part of the nose landing gear failed first nor why the training pilot’s rudder pedals were affected as described.
Engine failure and collision with water
The engine, and associated components, were not recovered for examination. However, as neither pilot reported issues with the engine before the accident, it is unlikely there was a coincidental mechanical issue with the engine.
The aircraft departed the Sunshine Coast Airport with full fuel and had been flying for approximately three hours, leaving less than half fuel remaining at the time of the accident. The fuel system could only be operated on one tank at a time. As the aircraft collided with water, the exact quantity of fuel in each tank at the time of the accident could not be confirmed, however if the fuel management had maintained roughly equal quantities of fuel, each tank would have been about one third full.
Following the go-around, the training pilot applied full right aileron to prevent the aircraft from rolling. This resulted in the aircraft being flown in a significantly uncoordinated state (sideslip), with right wing low. The pilot operating handbook stated that, with a quarter tank or less, ‘prolonged uncoordinated flight such as slips or skids can uncover the fuel tank outlets, causing fuel starvation and engine stoppage’. The aircraft was flown in an uncoordinated state for between 1‑1.5 minutes before the engine failed. If the fuel usage had not been equalised then it is possible the right tank contained quarter or less fuel, resulting in fuel starvation to the engine. It is also possible that the magnitude of the required sideslip permitted unporting of the fuel tank outlet at greater than one quarter capacity.
It is also possible, although considered less likely, that the damage to the landing gear in turn damaged the fuel strainer/fuel line during the final stages of the flight, again leading to fuel starvation.
Go-around decision
According to the United States Federal Aviation Administration, the typical time taken to realise there is a problem and react to it, is about 4 seconds. In that time frame, the pilot must perceive the problem, process the alternatives, and perform the selected action.
On this occasion, the decision to commence a go-around was influenced by the aircraft’s deviation towards water with little to no directional control or brake function. Taking into consideration that the flight crew were conducting training for emergency procedures (including multiple go-arounds), there may also have been a greater inclination to commence a go-around. While opting for a go‑around on this occasion was understandable, it resulted in flight over water with significantly reduced aircraft controllability.
The FAA’s guidance for emergency procedures advised that accepting there will be an accident may be the safest option and using the aircraft’s dispensable structure to absorb the ground/water impact forces will most likely reduce injuries. In this case, there was about 40‑50 m from when the pilots perceived they had no braking or directional control, to the water’s edge. Allowing the aircraft to continue to slow and using the aircraft structure to absorb the impact would, in hindsight, most likely have been the safest option.
Operator’s safety management system
The operator had determined that their aircraft were susceptible to brake failures because they were operated regularly on the beach. To mitigate this safety concern the operator ensured the brakes were inspected during the pre-flight inspections and conducted regular simulated brake failure training. However, the concern had not been formally documented in the operator’s hazard register.
The CASA booklet: SMS for aviation-a practical guide stated that if an operator identified a specific risk to their operation, appropriate mitigators should be identified and assessed. A risk analysis should be conducted to ensure the risk, after mitigators are applied, has been reduced to a level that is ‘as low as reasonably practicable’. Not documenting the brake failure hazard in the register was a missed opportunity to both:
assess the magnitude of the risk, taking in to account that apparent low likelihood of brake failure actually occurring
identify any hazards that simulated brake failure training introduced, including the potential for nose wheel damage.
ATSB assessment of the brake failure training, did not identify excess stresses on the Cessna U206 or 172 nose wheel. However, analysis of the stresses on the nose wheel in the Mahindra Airvan 8, also used by the operator, indicated if the nose wheel were fully deflected and the aircraft encountered soft sand, the additional side loads on the nose wheel system may induce damage.
Emergency egress
When the aircraft collided with the water, the extended flap prevented the front cargo door from opening fully. On this occasion, it is likely that when the training pilot kicked the doors open, the edge of it deformed the partially‑extended (20°) flap sufficiently to allow egress.
More generally, the Cessna U206 pilot’s operating handbook (POH) stated that 40° of flap were to be selected during ditching (and forced landings), creating a greater cargo door obstruction than occurred during this accident. Having the flap extended allows the aircraft to land at a slower speed, which has been shown to improve the chances of surviving a ditching. However, the POH emergency procedures did not identify that such a flap selection also prevents the forward cargo door from fully opening.
That situation may leave pilots unaware of the significant consequences of flap deployment. By contrast, at least one accident report shows that where the pilot has understood this issue and has not extended the flap during a ditching, the passengers have been able to readily exit the aircraft.
The aircraft’s certification criteria required that emergency doors be clear, unobstructed and capable of being opened with a simple and obvious method. This is particularly important in the event of ditching, due to the inherently disorientating nature of underwater egress. The Cessna U206 cargo door requires a number of sequential steps to open, and when the flaps are extended, this process is even more complicated. The inability to open the cargo door in this aircraft type has been shown in numerous accidents to have contributed to passengers being unable to exit the aircraft, resulting in fatalities.
Therefore, although the Cessna U206 with cargo door was certified, the method for opening the cargo door is not simple and in some flap configurations the forward door cannot be opened and therefore does not meet the emergency egress requirements.
Steps have been taken by regulators in an attempt to address the hazard presented by the rear double cargo door design, but to date, they have been ineffective at eliminating it. However, approved modifications are now available that remove the flap/door interference issue, despite this, to date no regulatory action has been taken to mandate the application of one of these modifications or remove the hazard by another means.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with water involving a Cessna Aircraft Company U206G aircraft, VH-AEE, near Happy Valley, Fraser Island, Queensland, on the 29 January 2020.
Contributing factors
Following touchdown, during a simulated brake failure exercise, a section of the nose landing gear attachment failed, resulting in the rudder becoming jammed in the full‑left position.
A go-around was initiated after directional control was lost on the ground. While there was only a short timeframe to make the decision to abort the landing, it resulted in flight over water with significantly reduced aircraft controllability.
It is most likely that fuel starvation led to the engine losing power at a height too low for recovery and the aircraft collided with water.
Other factors that increased risk
The 20° flap setting blocked the forward portion of the rear double cargo door, delaying the training pilot’s exit via the cargo door.
The Cessna 206 procedure for ditching and forced landing states that the flaps are to be extended to 40°. While that permits the aircraft to land at a slower speed, it also significantly restricts emergency egress via the cargo door. However, there is no warning about that aspect in the ditching or forced landing pilot’s operating handbook emergency procedures. (Safety issue)
Cessna 206 aircraft, that feature a rear double cargo door, do not meet the aircraft certification basis for the design of cabin exits. Wing flap extensions beyond 10° will block the forward portion of the rear double cargo door, significantly hampering emergency egress. This has previously resulted in fatalities. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The Cessna 206 procedure for ditching and forced landing states that the flaps are to be extended to 40°. While that permits the aircraft to land at a slower speed, it also significantly restricts emergency egress via the cargo door. However, there is no warning about that aspect in the ditching or forced landing pilot’s operating handbook emergency procedures.
Cabin exit design criteria (Issue owner: United States Federation Aviation Administration)
Safety issue description: Cessna 206 aircraft that feature a rear double cargo door do not meet the aircraft certification basis for the design of cabin exits. Wing flap extensions beyond 10° will block the forward portion of the rear double cargo door, significantly hampering emergency egress. This has previously resulted in fatalities.
Safety issue description: Cessna 206 aircraft that feature a rear double cargo door do not meet the aircraft certification basis for the design of cabin exits. Wing flap extensions beyond 10° will block the forward portion of the rear double cargo door, significantly hampering emergency egress. This has previously resulted in fatalities.
Additional safety action by Air Fraser Island
As a result of this accident, the operator has changed their procedures to specify that during emergency procedure training on the beach, no non-company vehicles are permitted to operate within the runway complex (the marked section of beach using bollards and witches hats identifying the area which has been identified as a suitable aircraft landing area.)
The operator has also reassessed the company hazard register and included brake failures.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew
Air Fraser Island
Civil Aviation Safety Authority
United States Federal Aviation Administration
Cessna Aircraft Company – Textron Aviation
the insurance company
video footage of the accident flight and other photographs
Transport Canada
Transport Safety Board of Canada.
References
Federal Aviation Administration, Airplane flying handbook FAA-H-8083-3B. US Department of Transportation, Federal Aviation Administration. Available on the FAA website www.faa.gov
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the flight crew
Air Fraser Island
Civil Aviation Safety Authority
Federal Aviation Authority
United States National Transportation Safety Bureau
Transport Safety Board Canada
Textron Aviation
Submissions were received from:
Air Fraser Island
Civil Aviation Safety Authority
Transport Safety Board Canada
Textron Aviation
The submissions from those parties were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 16 December 2019, a BRM Aero Bristell aircraft, recreational registration 24-8555, collided with terrain in Kanangra-Boyd National Park, near Oberon, New South Wales. The pilot was fatally injured.
In response, Recreational Aviation Australia (RAAus) commenced an investigation into the occurrence and requested technical assistance from the ATSB in the recovery of flight data from two instrumentation units – a Dynon SV-D1000 and Garmin aera 795; both of which were subsequently provided by NSW Police.
The ATSB successfully downloaded data from both devices, including flight path information and aircraft operational parameters. Figures 1 and 2 summarise this information.
Both instrumentation units were returned to NSW Police on 23 June 2020 and a technical report and all recovered data provided to RAAus on 24 June 2020.
With the completion of this work, the ATSB has concluded its involvement in the investigation of this accident. Any further enquiries in relation to the investigation should be directed to Recreational Aviation Australia.
The information contained in this update is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Figure 1: Flight paths from Garmin and Dynon units
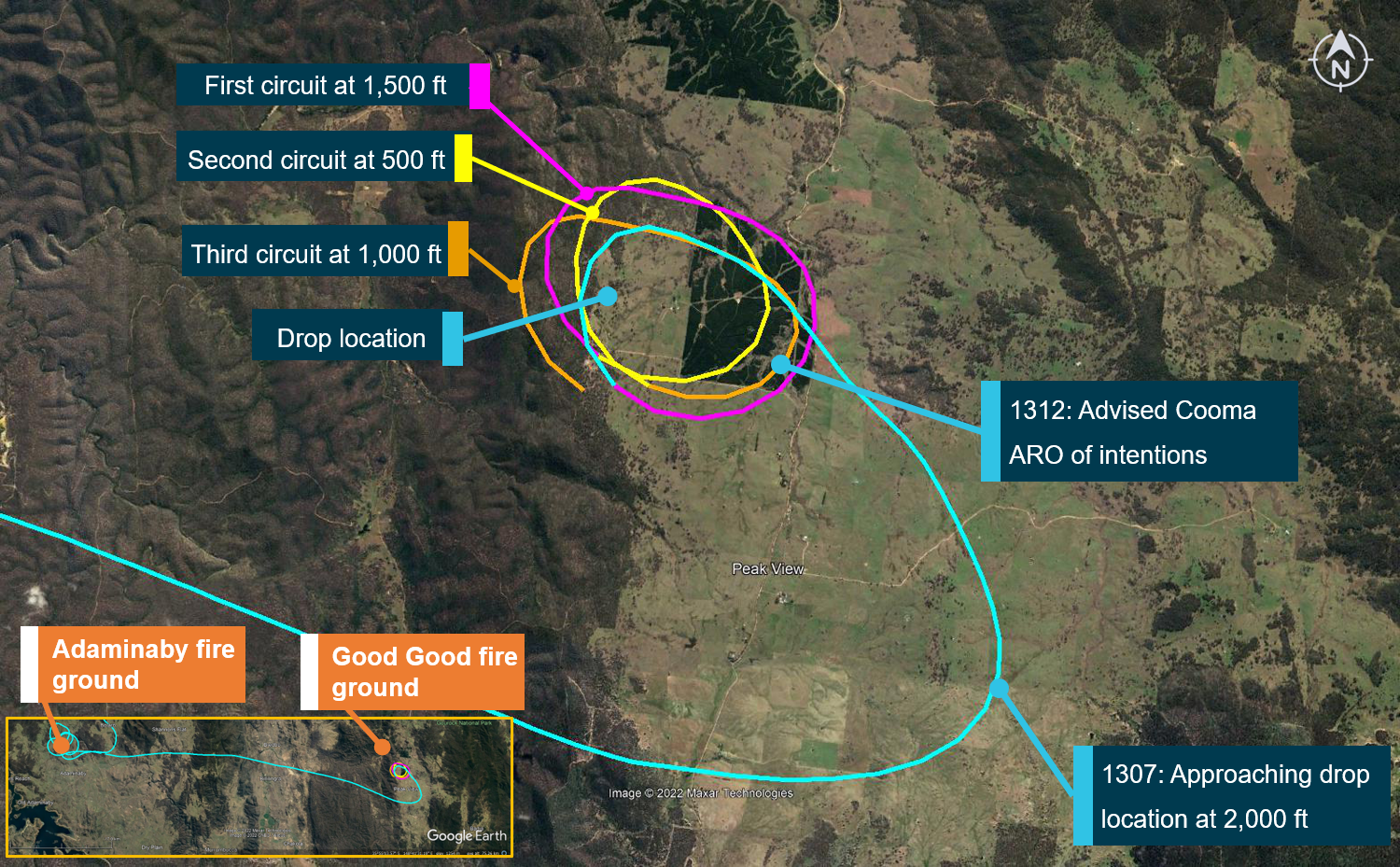
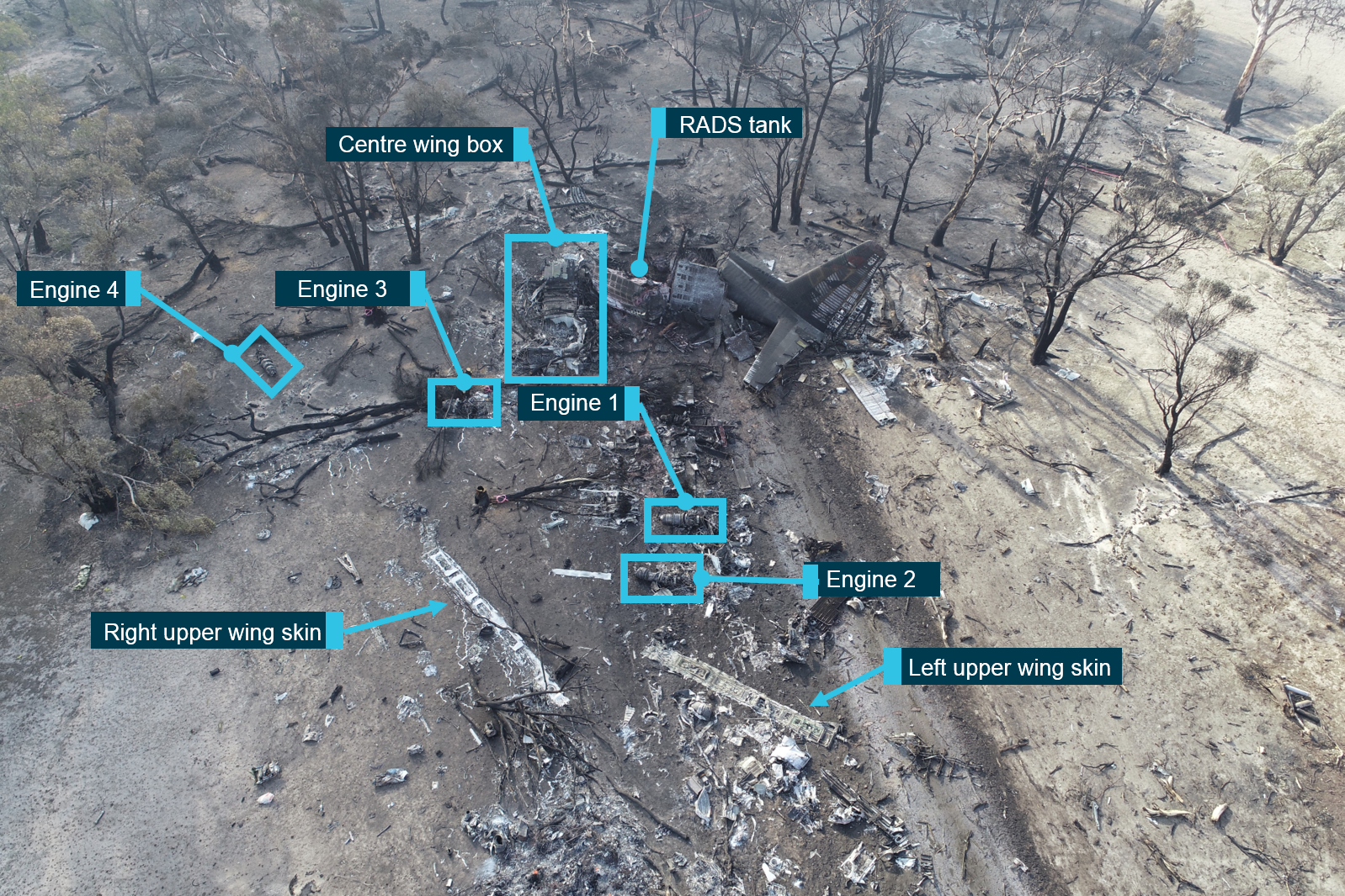
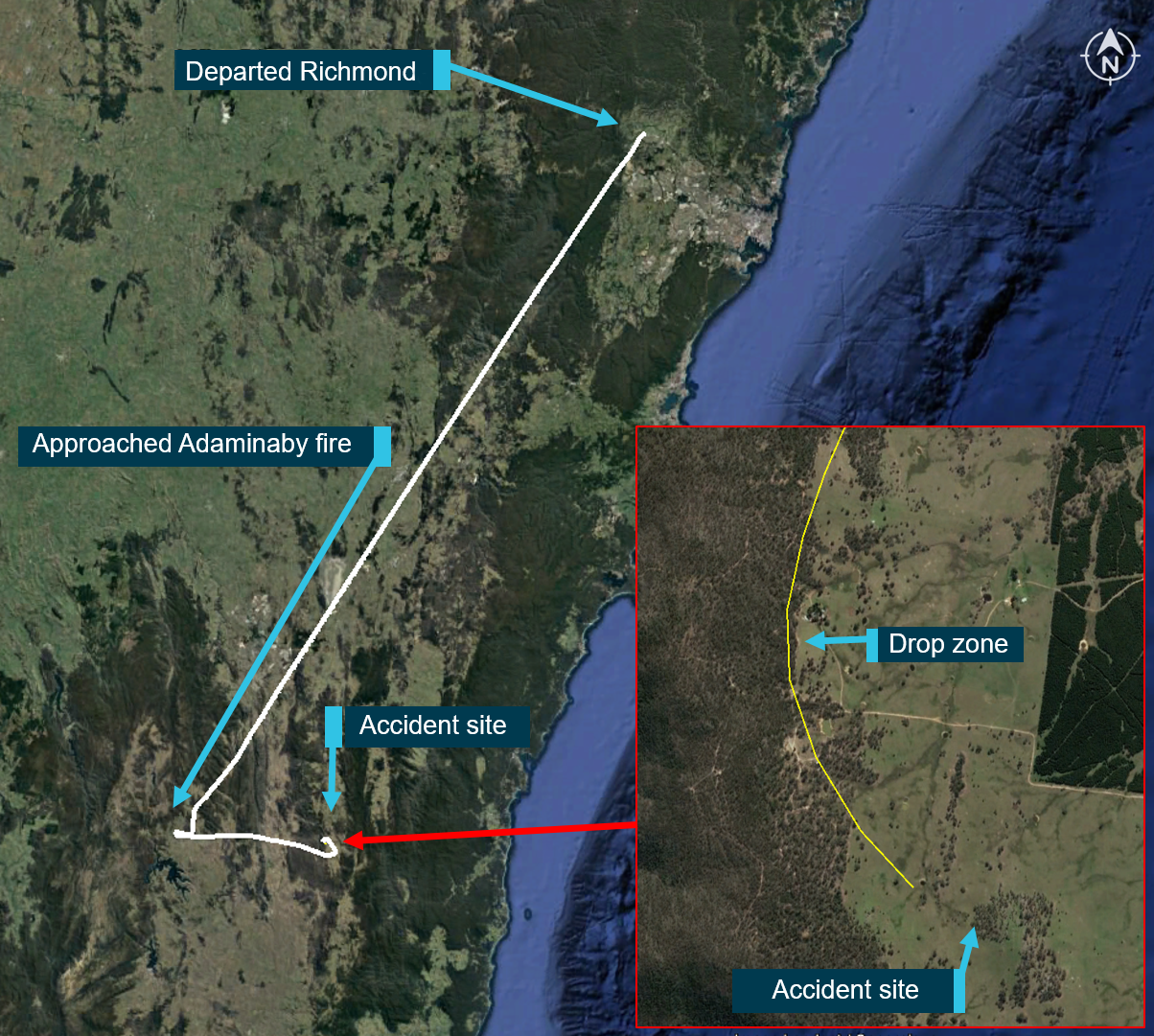
On 23 January 2020, the crew of a Lockheed Corporation (now Lockheed Martin) EC-130Q large air tanker, registered N134CG, were conducting bushfire control operations in the Snowy Mountains region of New South Wales. After assessing the initial fire-retardant drop site at Adaminaby as not suitable, the crew accepted an alternate tasking to the Good Good (Peak View) fire-ground.
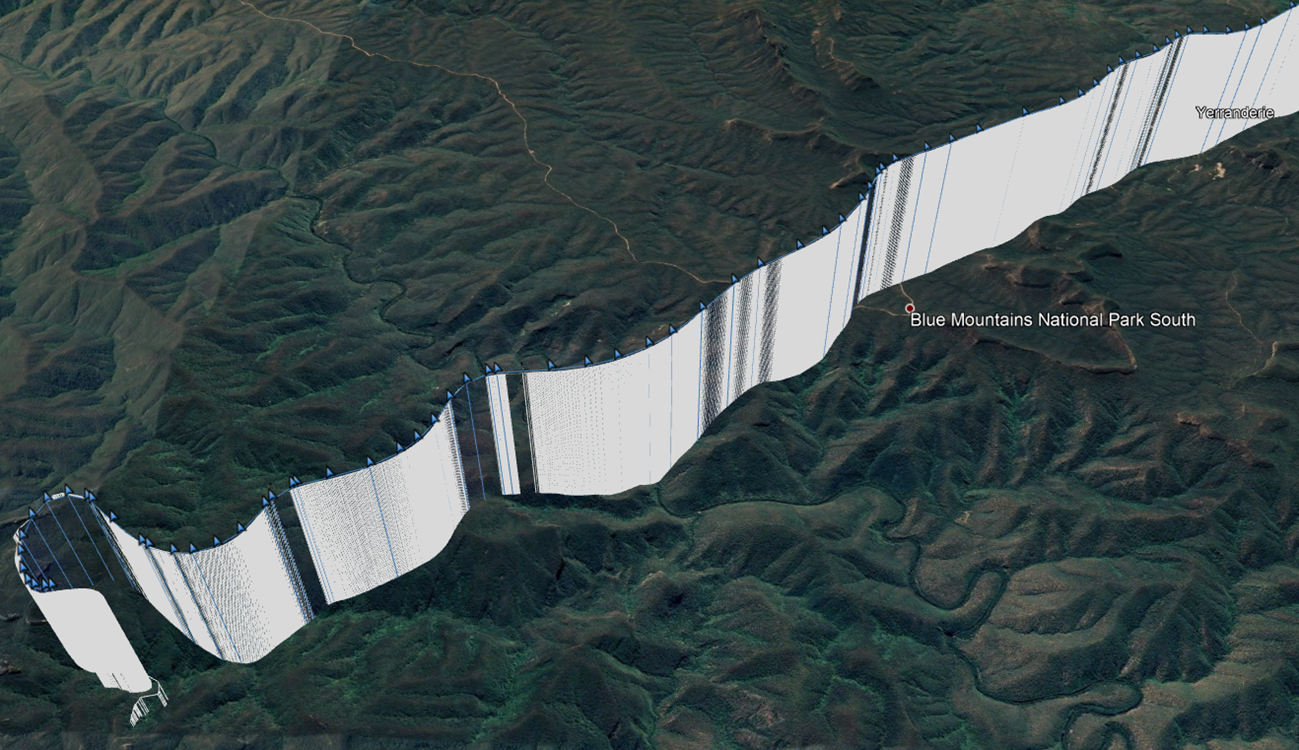
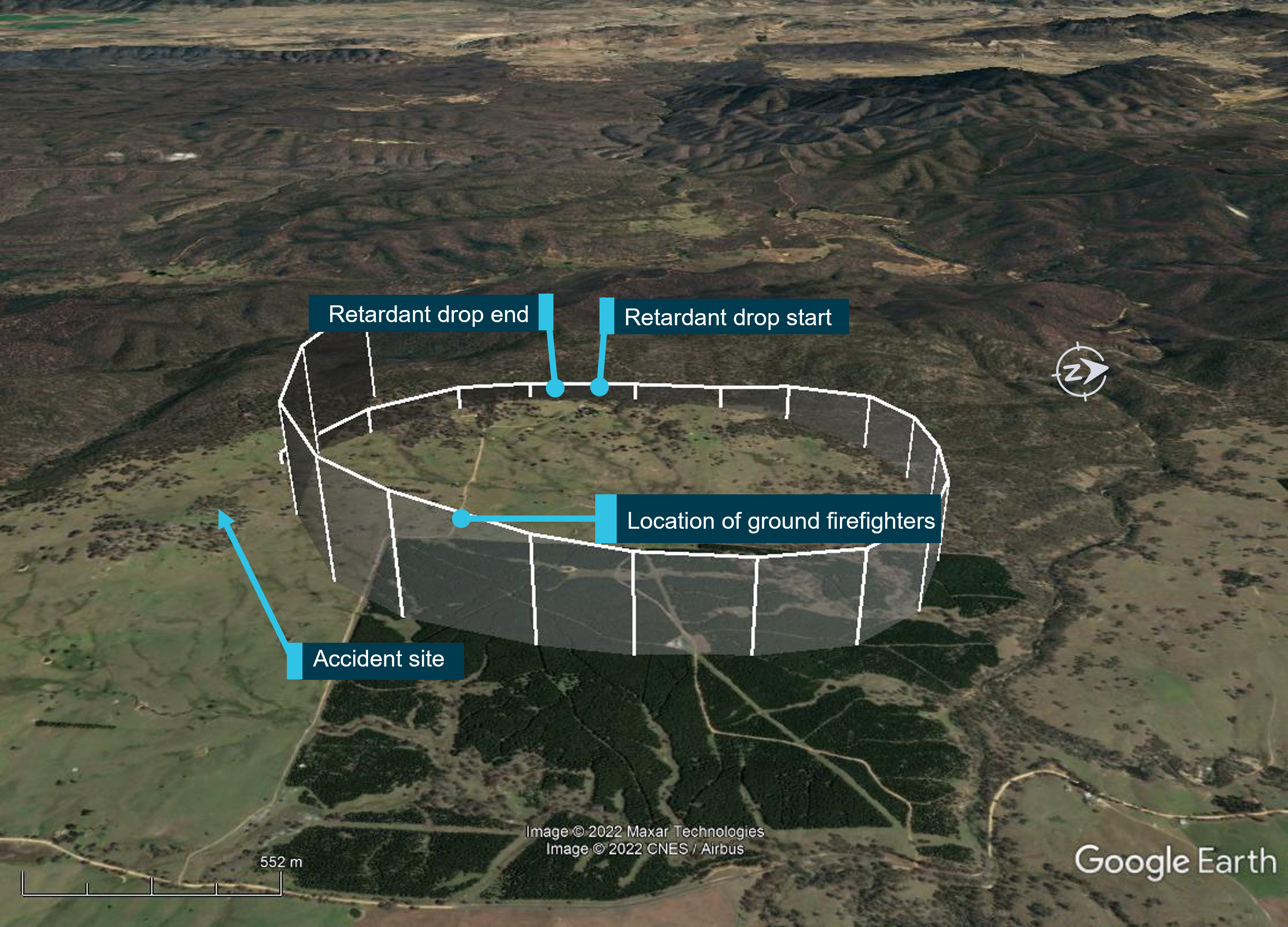
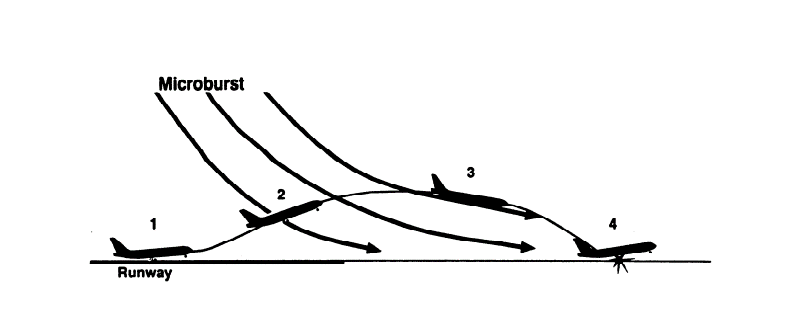
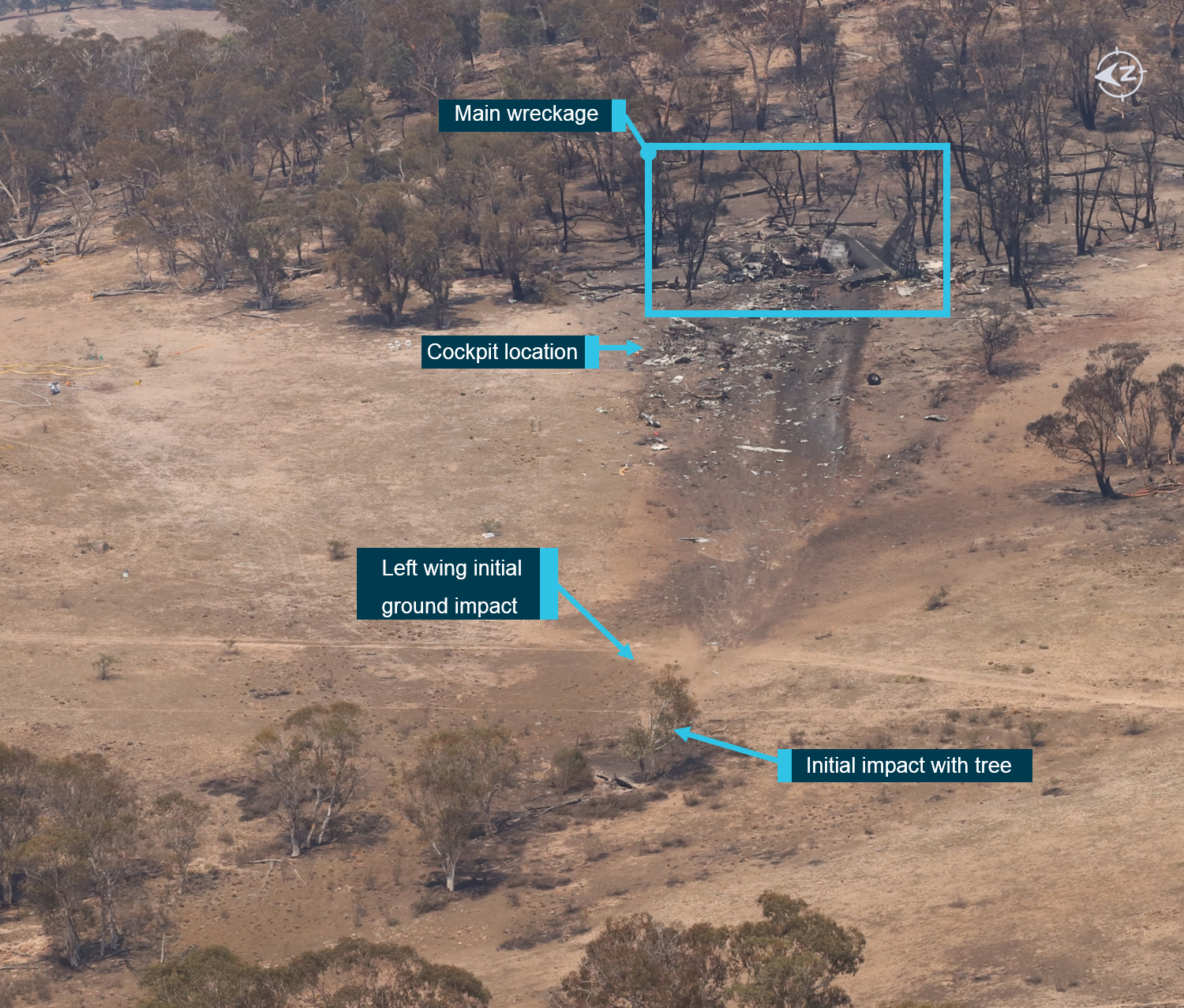
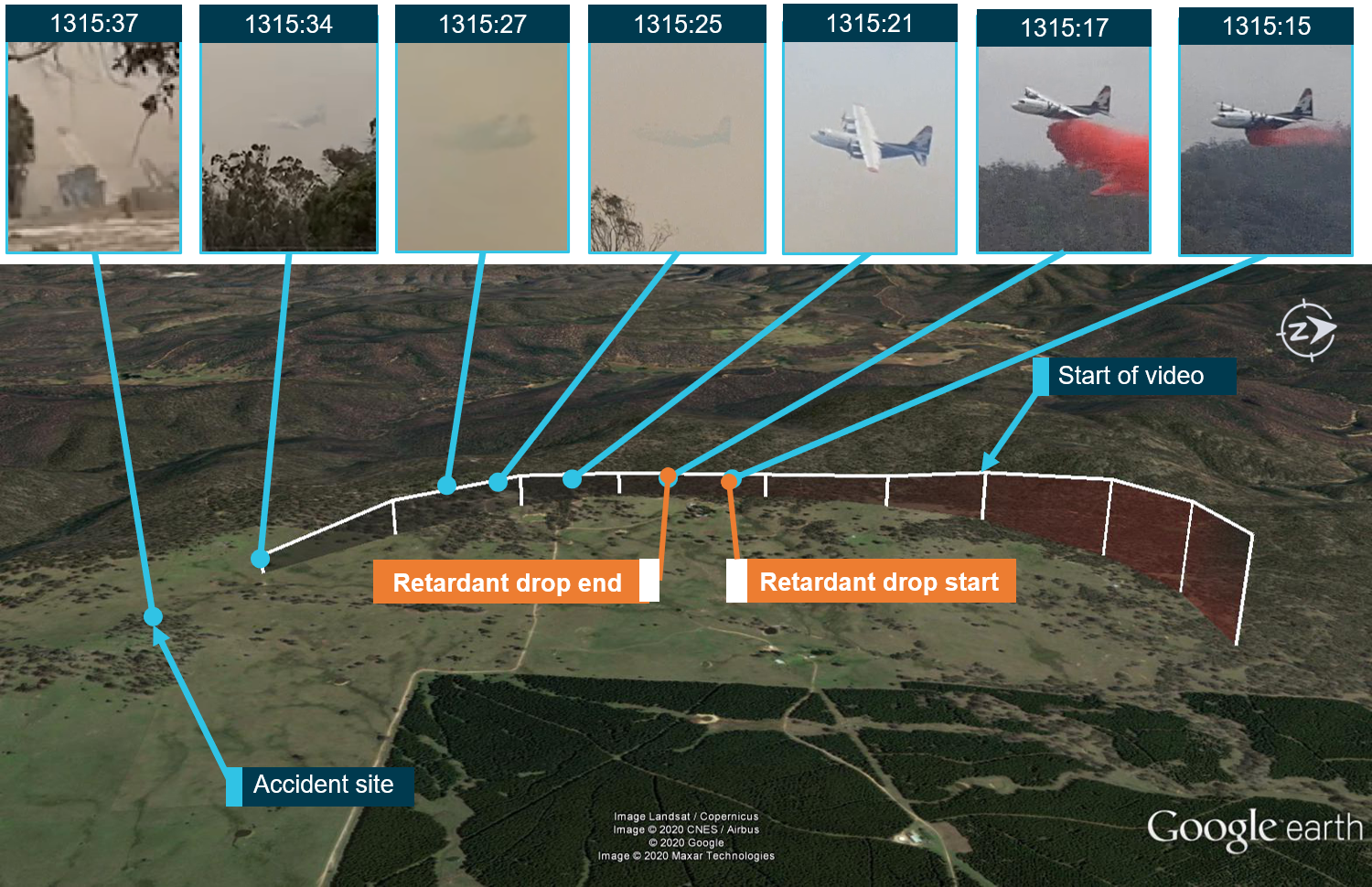
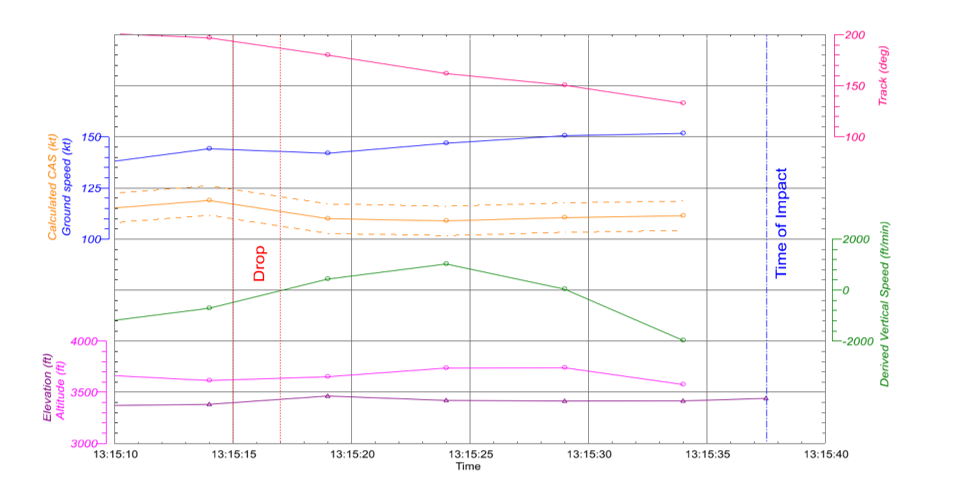
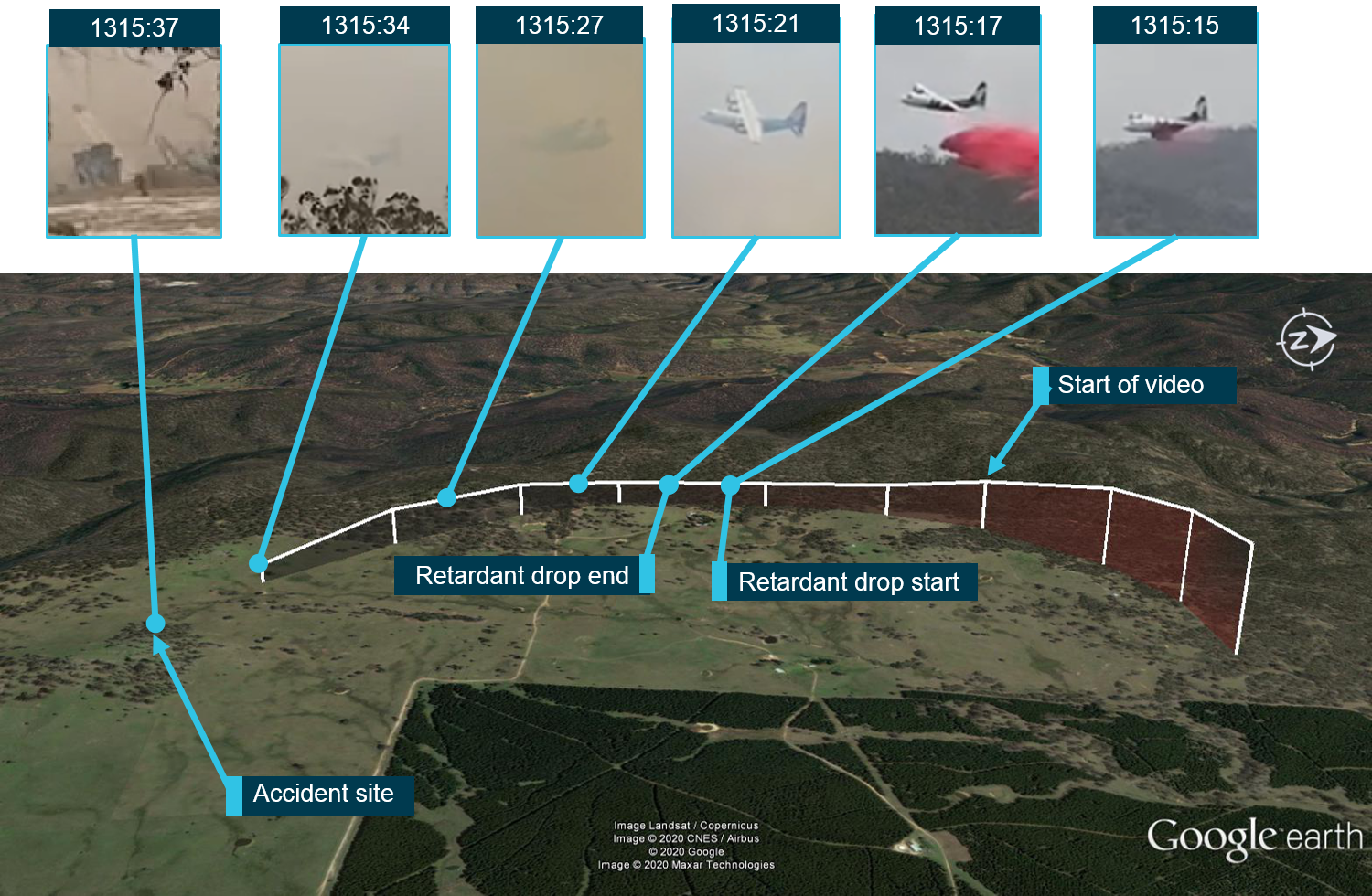
After conducting a partial retardant drop at Peak View, the aircraft was in a left turn and climbed for about 10 seconds to about 170 ft above the drop height. Following this, the aircraft was then observed descending. The aircraft was seen at a very low height above the ground, in a slight left bank, immediately followed by a significant left roll just before ground impact. The 3 crew were fatally injured and the aircraft destroyed.
What the ATSB found
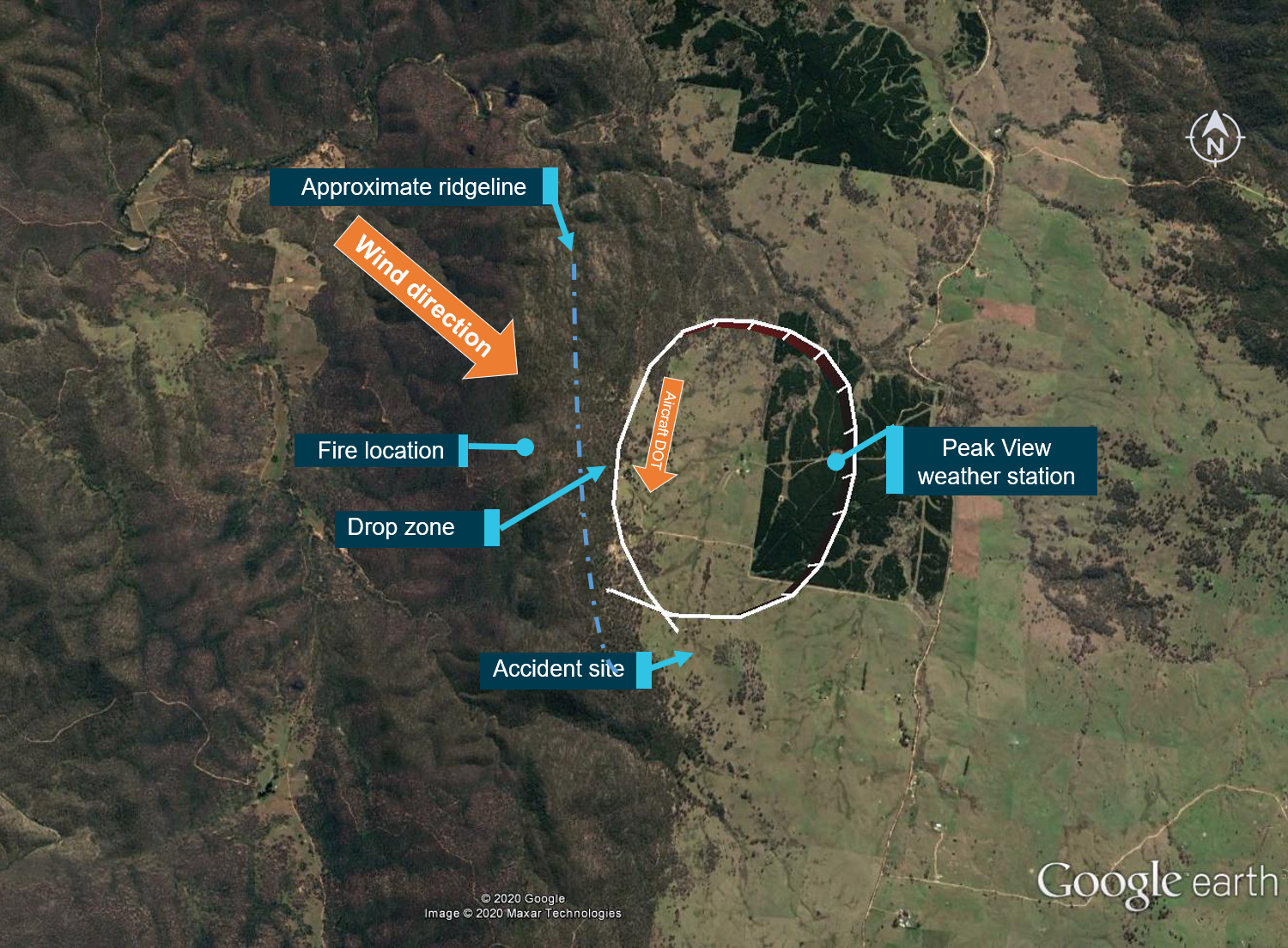
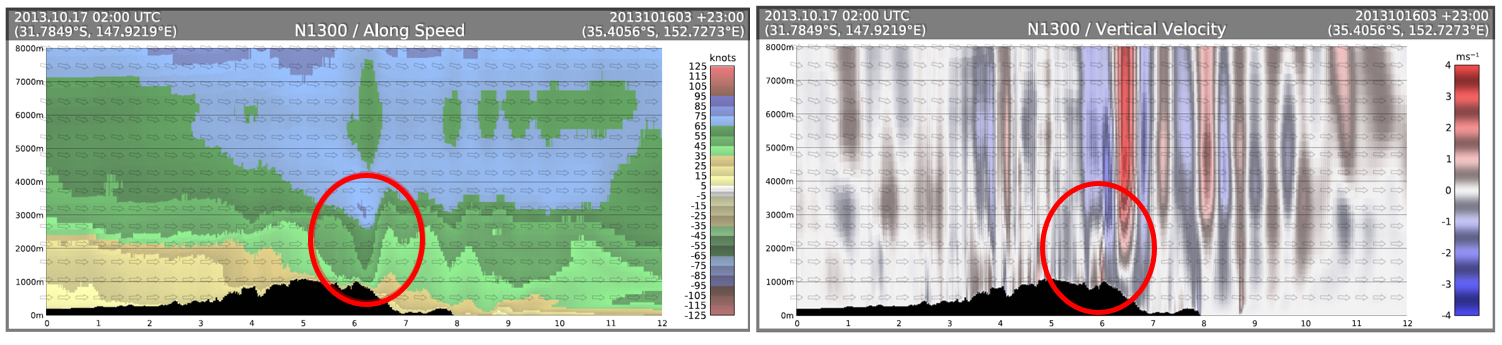
The ATSB found that the forecast and actual weather conditions present in the Snowy Mountains region were hazardous, with strong gusting winds and mountain wave activity, producing turbulence. This was likely exacerbated by the fire and local terrain. Subsequently, the ATSB determined that the conditions were conducive to windshear and downdraft development at a time when the aircraft was most vulnerable, with a low airspeed and at a low altitude.
Despite an awareness of these conditions and that all other fire‑control aircraft (including a Boeing 737 large air tanker) were not operating in the area at the time due to the weather conditions, the New South Wales Rural Fire Service (RFS) continued with their tasking of N134CG to Adaminaby without aerial supervision (birddog). In addition, they relied on the pilot in command to assess the appropriateness of the tasking but did not provide them all the available information to make an informed decision on flight safety. That information for the tasking to Adaminaby should have included details about actual hazardous environmental conditions, resulting in the cessation of local aerial operations, the birddog pilot declining the tasking due to the forecast weather conditions, and a report from the Boeing 737 crew that conditions precluded them from returning to the fire-ground.
The crew of N134CG were therefore very likely not aware that the birddog pilot had declined the tasking to the Adaminaby fire-ground, nor that the smaller fire-control aircraft had ceased operations in the area, due to the hazardous environmental conditions. While this was only one risk factor among others that would be considered by the crew when accepting a task, having this information would have allowed them to make a more informed decision about the weather conditions.
Nonetheless, the pilot in command of N134CG accepted the tasking to the Adaminaby fire‑ground, which was subject to hazardous environmental conditions. After assessing the conditions as unsuitable at Adaminaby, the crew accepted an alternative tasking to continue to the Good Good fire-ground, which had the same weather conditions. The acceptance of these taskings was consistent with the operator’s practices to depart and assess the conditions to find a workable solution rather than rely solely on a weather forecast, which may not necessarily reflect the actual conditions at the fire-ground.
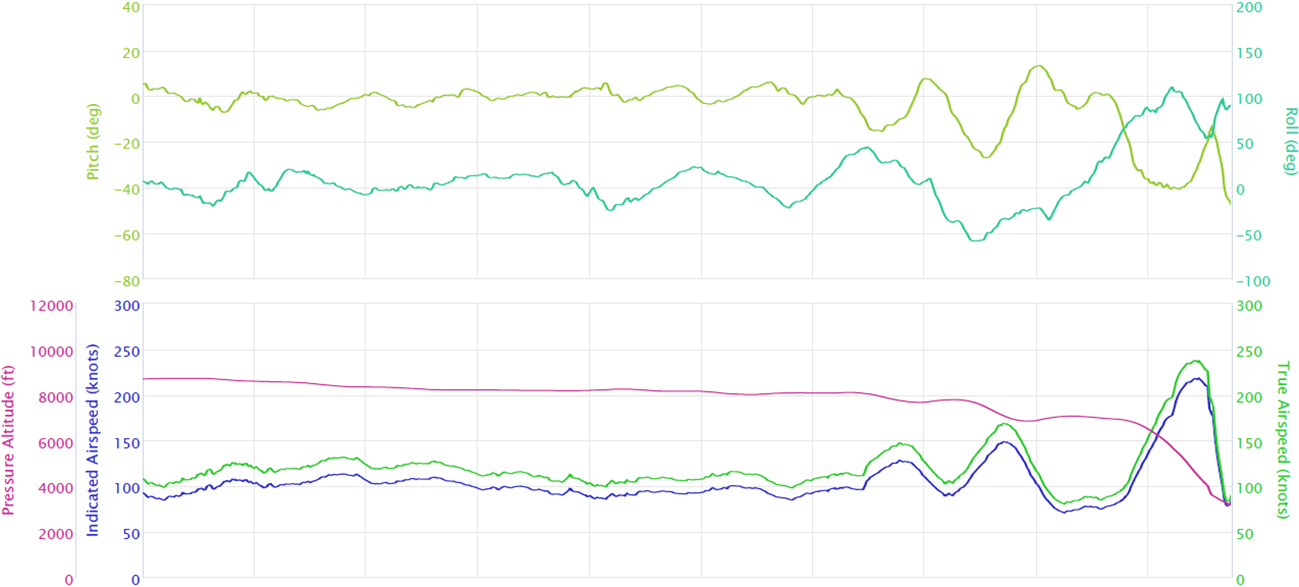
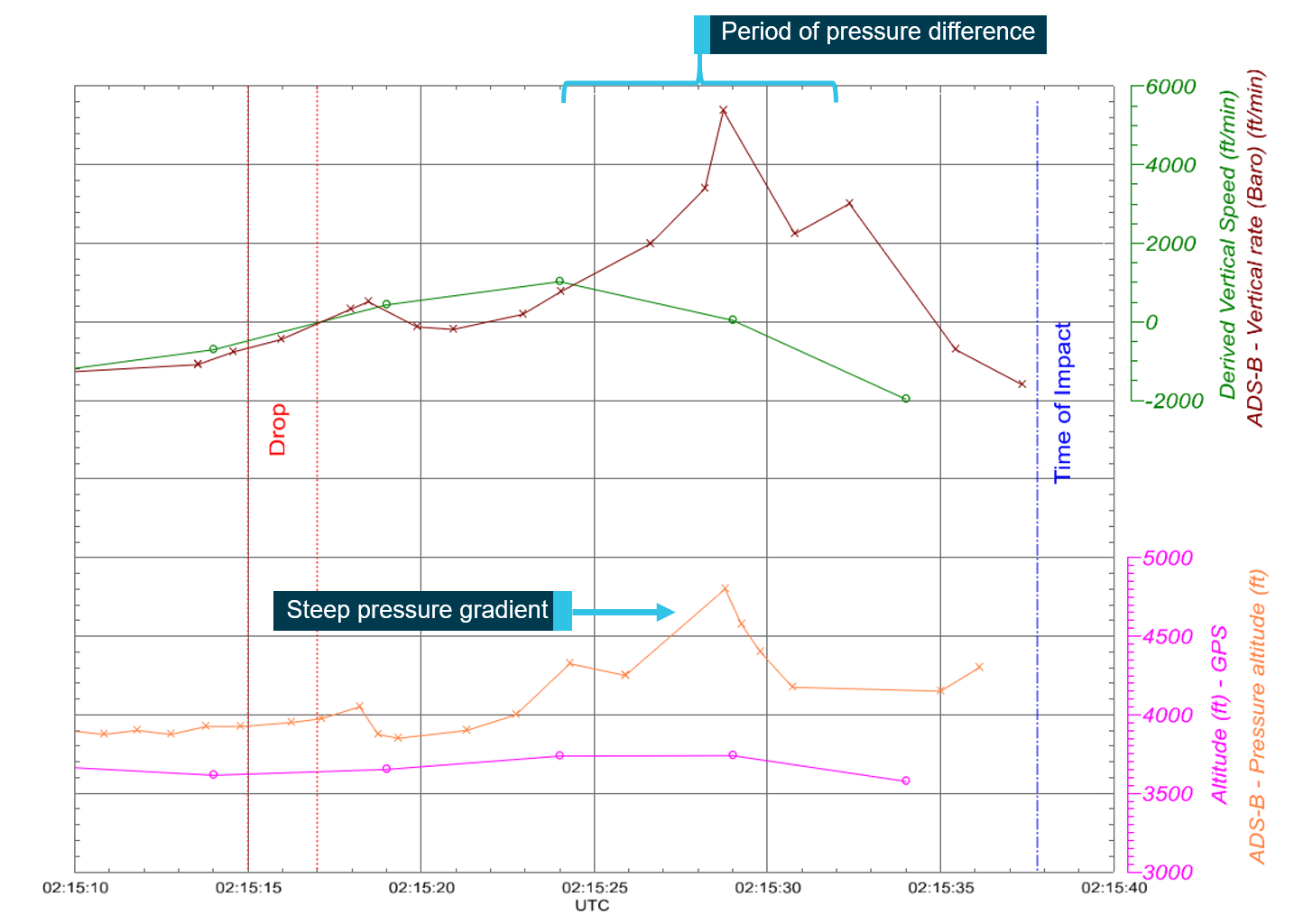
At the Good Good fire-ground, following a partial retardant drop and left turn, the aircraft was very likely subjected to hazardous environmental conditions including low-level windshear and an increased tailwind component. From a combination of witness video, and real-time position and flight path data, it was established that the aircraft’s climb performance degraded. Subsequently, while at a low height and airspeed, it was likely the aircraft aerodynamically stalled, resulting in a collision with terrain. In the limited time available, the remainder of the fire-retardant load was not jettisoned prior to the aircraft stalling.
The ATSB established that, while a safety management system was not required under Australian regulations at the time of the accident, Coulson Aviation's safety risk management processes did not adequately manage the risks associated with large air tanker operations. In particular, they had not conducted formal risk assessments of the hazards identified in their operations manual, and did not maintain a tool, such as a risk register, to track risk acceptance levels. Further, incident reports submitted through the safety reporting system were mainly related to maintenance issues, and therefore operational risks were less likely to be considered or monitored. This limited their ability to identify and implement control measures to manage the risks associated with their aerial firefighting operations.
It is critical that crews can differentiate between a low-risk and high-risk flight during the planning stage to establish the overall risk profile. While identifying it as a high-risk activity, Coulson Aviation had not identified a need for a pre-flight risk assessment for their firefighting large air tanker crews. This would have provided crews with predefined criteria to ensure consistent and objective decision-making with accepting or rejecting tasks, and include factors relating to crew, environment, aircraft and external pressures and factors.
There are a number of mitigators for windshear, including pilot training and procedures, and airborne detection systems. However, Coulson Aviation did not include a windshear recovery procedure in their C‑130 Airplane Flight Manual. Further, it was noted that a briefing on windshear recovery was incorporated into the training syllabus, but there was no requirement to conduct a simulator-based low-level windshear recovery scenario. Combined, these strategies could provide crews with the experience needed to recognise the symptoms of windshear and practice a recovery procedure. In addition, Coulson Aviation had not assessed their fleet of C-130 aircraft for fitment with a windshear detection system. This increased the risk of a windshear encounter and/or delayed response to an encounter.
While the New South Wales RFS was not an aviation organisation or directly responsible for flight safety, they were closely involved in the aerial operation, being responsible for determining the task objectives and selecting aircraft for the task. The ATSB found that the RFS had limited large air tanker policies and procedures for aerial supervision requirements and no procedures for deployment without aerial supervision. In addition, they did not have a policy or procedures in place to manage task rejections, nor to communicate this information internally or to other pilots working in the same area of operation. Such policies and associated procedures would provide frontline personnel with the required steps to effectively and safely manage taskings, and provide guidance for decision-making.
It was also identified that, while not applicable to the accident crew, the RFS procedures allowed aircraft operators to determine when pilots were initial attack capable. This was inconsistent with their intention for pilots to be certified by the United States Department of Agriculture Forest Service certification process.
While not contributing to the accident, the aircraft's cockpit voice recorder did not record the accident flight. This resulted in a valuable source of safety information not being available to the investigation, which not only increased the time taken to determine contributing factors to the accident but also limited the extent to which important safety issues could be identified and analysed.
What has been done as a result
As a result of this investigation, Coulson Aviation have incorporated a windshear recovery procedure into their C-130 Airplane Flight Manuals and plan to introduce simulator-based recurrent windshear training. Related to the consideration of risk in aerial firefighting operations, they have also implemented a pre-flight risk assessment to be completed by the pilot in command prior to the first tasking of the day. They will also be introducing a three-tier risk management approach, of organisational risk, operational risk, and tactical/mission risk, to be utilised during the upcoming fire season in Australia. Further, Coulson Aviation have updated their pre-flight procedures to incorporate a cockpit voice recorder system check before each flight. Lastly, the Retardant Aerial Delivery System software was reprogrammed so that the system will not require re-arming between partial load drops where less than 100% was selected.
The ATSB has issued 2 safety recommendations to Coulson Aviation. These are to further consider:
fitment of a windshear detection system to their C-130 aircraft to minimise the time taken for crews to recognise and respond to an encounter particularly when operating at low-level and low speed
incorporating foreseeable external factors into their pre-flight assessment tool to ensure the overall risk profile of a tasking can be consistently assessed by crews.
The New South Wales Rural Fire Service advised the ATSB that they intend to take the following actions in response to this accident:
Commissioned an independent report into the management of airspace in which aircraft are operating in support of fire-fighting activities.
Formalise and establish a ‘Large Air Tanker Co-ordinator’ role description, to be positioned on the State Air Desk during heightened fire activity.
Undertake an immediate audit, in conjunction with operators, of pilots qualified as initial attack capable and ensure appropriate records are accessible by RFS personnel.
Undertake detailed research to identify best practice (nationally and internationally) relating to task rejection and aerial supervision policies and procedures as well as initial attack training and certification.
Undertake a comprehensive review of RFS aviation doctrine to incorporate outcomes of the above-mentioned research into existing policies and procedures.
Promulgate the revised doctrine detailing the task rejection policies and procedures and aerial supervision requirements to all operational personnel, pilots/aircrew and other key stakeholders. This is to be reinforced at the aviation operators briefing held annually prior to the bushfire season.
Provide the National Aerial Firefighting Centre and national fire-fighting agencies with copies of the updated doctrine relating to these issues.
While the ATSB acknowledges the commitment to undertake reviews and research, at the time of publication, the New South Wales Rural Fire Service had not yet committed to adopting any safety action that would reduce the risk associated with the 3 identified safety issues to an acceptable level. As such, the ATSB has issued three safety recommendations to the RFS to take further action:
to address the absence of policies and procedures for personnel to effectively manage and communicate task rejections on the basis of operational safety concerns
to address the absence of policies and procedures regarding minimum aerial supervision requirements and the use of initial attack to assist frontline staff with making acceptable risk‑based tasking decisions
to address the ambiguity with the interpretation of ‘initial attack’ in the NSW and ACT Aviation Standard Operating Procedures with the intent of this requirement.
Safety message
As noted by the National Aerial Firefighting Centre, aerial firefighting has become a critical capability for the management and suppression of bushfires in Australia. To effectively achieve this, aircraft are flown at low altitudes and low airspeeds, often in challenging environmental conditions. This creates a high-risk environment, which requires a continued focus on risk mitigation.
Previous research conducted by the ATSB emphasised that any decisions made by tasking agencies during the management of an aerial campaigns (firefighting) could influence the level of risk of the operation. Therefore, if safety was to be maintained, this responsibility had to be shared between the tasking agency and the aircraft operator. This accident highlights the importance of having effective risk management processes, supported by robust operating procedures and training to support that shared responsibility.
While the identification of hazards is the initial step in safety risk management, conducting risk assessments, implementing risk mitigators, and having effective oversight of the process through a tool such as a risk register are critical aspects of this process. This provides the mechanism for organisations to consider the specific challenges associated with firefighting operations such as hazardous environmental conditions, and ensure they have the appropriate risk controls in place to support crew decision-making when conducting high-risk activities.
Further, the adoption of good systems for managing risk by the tasking agency could provide an effective additional layer of defences over and above that provided by each aircraft operator to protect against an incident or accident. This also ensures that one aspect of the operation does not compromise another aspect. This may include the development of procedures to support decision-making processes rather than personnel having to exercise judgement to the best of their abilities, based on their experience, skills and knowledge. This would include aspects such as tasking decisions, task rejection policies and procedures, and minimum aerial supervision requirements.
The occurrence
Overview
During the Australian ‘black summer’ of 2019-2020, the east coast experienced many severe bushfires. As part of the firefighting efforts, small and large aircraft were used for aerial fire suppression and intelligence gathering. The larger aircraft included large air tankers (LATs),[1] located at the Richmond Royal Australian Air Force (RAAF) Base, New South Wales (NSW). This included a United States-registered Lockheed Martin EC-130Q,[2] registered N134CG, operated by Coulson Aviation. On 23 January 2020, the aircraft was applying retardant for property protection in the Good Good fire-ground (near Peak View) in the Snowy Mountains region of NSW. While attempting to climb away after a partial fire-retardant drop, the aircraft collided with terrain. The 3 crew were fatally injured and the aircraft was destroyed.
Daily briefings at Richmond Base
On 23 January 2020, at about 0900 Eastern Daylight-saving Time,[3] the NSW Rural Fire Service (RFS) Richmond airbase manager (ABM)[4] had conducted a briefing with the crews of the air tanker and birddog[5] aircraft based there. The briefing included the current and anticipated fire activity and discussed fire-related weather conditions across the state. Following the briefing, the crews then remained on standby until they received a tasking from the RFS, with a contracted 15‑minute departure time following the completion of retardant loading.
The operator of two LATs at Richmond, Coulson Aviation, reported[6] that they had also conducted their daily safety management system call between management and crews, which would typically discuss the operations to be conducted on the day, and any reported issues encountered in the previous 24 hours. However, as there were no notes taken for the call, the details of the conversation were unknown.
Fire situation in the Snowy Mountains region
On the day, the Snowy Mountains region in NSW had a severe fire danger rating,[7] due to high temperatures, strong winds and forecast thunderstorms. This region included the Adaminaby and Good Good fire-grounds, which were both under the control of the RFS Cooma Fire Control Centre (FCC).[8]
At about 1100, the Cooma FCC incident controller[9] made a phone call to the RFS State Operations Centre.[10]A number of senior personnel from the State Operations Centre were involved in the conference call. They discussed the escalating fire danger at the Adaminaby fire‑ground, with rural properties under threat and concern the town would be impacted if containment lines did not hold. During that call, RFS personnel stated that there were strong winds, severe fire weather conditions, and that the smaller fire-control aircraft were not operating in the area due to the winds and poor visibility. There was also discussion as to whether a birddog aircraft had already departed to assess the conditions. However, a senior RFS officer stated they should send the Boeing 737 LAT aircraft irrespective, ‘as it can bomb by itself if need be’ and ‘not wait for the birddog assessment’.
Consequently, the State Operations Centre tasked 2 LATs[11] and a birddog to the Adaminaby fire‑ground: a Boeing 737 aircraft, registered N137CG, call sign ‘Bomber 137’ (B137); a Lockheed Martin C-130 aircraft, registered N134CG, call sign ‘Bomber 134’ (B134); and a Rockwell International 690-B aircraft (operating as a birddog). All 3 aircraft were based at the Richmond Base, about 316 km north-east of the Adaminaby fire-ground.
‘B137’ tasking to Adaminaby
Following the 1100 call, the tasking was communicated by the state air desk (SAD)[12] to the Richmond ABM. At 1120, the Cooma aerial operations manager log recorded that LATs were inbound, with no birddog. At about 1121, the crew of B137 had commenced taxiing at Richmond for another task to the north[13] when they were re-tasked to the Adaminaby fire-ground by the ABM. After the initial coordinates, location details, and information regarding the expected direction of the fire were provided, the pilot in command (PIC) of B137 requested details for the fire common traffic advisory frequency. The Richmond ABM was unable to provide these details immediately, but indicated the SAD ‘want to get them in the air and down there’. The ABM also advised the crew of the objective to ‘keep the fire out of Adaminaby’, that ‘the fire is burning towards the north-west’, that there were no other aircraft in the area, and that it ‘is very windy down there….take care’. The ABM further advised ‘the birddog won’t be down there’.[14] Therefore, the PIC was aware they would be operating as initial attack.[15] The aircraft subsequently departed at about 1127.
While en route, the crew contacted various fire centres to determine the correct ground-based contact, eventually communicating with the Cooma aviation radio operator (ARO), located at the Cooma FCC. At about 1155, B137 arrived overhead the Adaminaby fire-ground, but the crew were unsure of the actual planned location for the drop. After further discussion with the ARO, it was determined they were overhead the intended location.
Due to the weather conditions and ground-based fire-fighters in the planned drop area, the crew orbited for about 25 minutes. At interview, the PIC reported that, while assessing the conditions in the Adaminaby area, the aircraft encountered uncommanded rolls up to 45° angle of bank (due to wind) and they received a windshear[16] warning from the aircraft’s onboard systems.[17] The PIC elected to operate on the upwind side of the hills to avoid lee side mechanical turbulence.[18] They also reported that the wind speed at the Adaminaby fire-ground was 50 kt at 800 ft above ground level (AGL) and about 37 kt at the fire‑retardant drop height of 200 ft AGL. At about 1225, B137 departed the Adaminaby fire‑ground, having successfully deployed a retardant load.
After completing the retardant drop, the PIC reported that they advised the Cooma ARO to cancel all the aircraft operating in the area, although it was not clear if the ARO had received that message. They also sent a text message to the birddog pilot assigned to the Adaminaby fire‑ground indicating that the conditions were ‘horrible down there. Don’t send anybody and we’re not going back’. During B137’s return flight to Richmond, at about 1232, the PIC contacted the Richmond ABM and stated they were going ‘to put themselves on hold’, but would be available for other taskings. The ABM requested that they reload the aircraft with fire retardant in Canberra and return to Adaminaby. The PIC replied that they would not be returning to Adaminaby due to the weather conditions, as the ‘winds were getting too strong and the visibility is down’, and continued to Richmond. Subsequently, when the ABM communicated B137 PICs decision to the SAD, they indicated the weather was ‘fairly dicey…probably won’t go back’. There was some discussion as to the availability of other LATs to task to Adaminaby, however, the decision was made to wait for a report from B134 before any further tasking.
Birddog rejection of tasking
Meanwhile, at about 1137, the Richmond ABM contacted the SAD to confirm the dispatch of a birddog to Adaminaby. The birddog crew consisted of the birddog pilot and the LAT air attack supervisor.[19] The ABM had also noted in their log at 1130 and 1140 that they were intending to send the birddog to Adaminaby. The 1130 log entry also indicated that the incident air attack supervisor was not operating ‘due to extreme wind conditions’. By the time of the 1137 phone call, B137 had already departed Richmond as initial attack and B134 was being prepared for departure, with the expectation from the RFS that both LATs would do multiple retardant drops. The ABM and SAD discussed that the 2 LATs would beat the birddog to the fire‑ground, but it was considered unlikely ‘they will get through as [it] will be too windy for them’.[20]
The birddog pilot reported having experienced moderate to severe turbulence in the Snowy Mountains region about 2 weeks prior, which resulted in an uncommanded roll up to 30–40° angle of bank. This, combined with a downdraft, required the pilot to execute an escape manoeuvre. On receipt of the tasking to Adaminaby, the birddog pilot reviewed the weather and concluded that the conditions were forecast to be worse than previously experienced, and therefore declined the task. The RFS reported the SAD log recorded the birddog declining the task to Adaminaby at 1204.
At about 1209, the ABM had a conversation with the SAD and discussed that the birddog pilot was ‘questioning the weather conditions’. The SAD instructed the ABM to ‘get them on their way, and then turn them around’ (that is, rather than accept a rejection based on the forecast, they would prefer they re-assess the conditions in-flight). When the ABM communicated this to the birddog pilot, the pilot indicated to the ABM that B137 would arrive overhead Adaminaby shortly, and they could then report the actual conditions. At about 1235, following a report of the conditions from the PIC of B137, the ABM reportedly agreed that the birddog pilot had made an appropriate assessment to reject the task to Adaminaby.
The birddog pilot reported that they had not spoken to the crew of B134 following the receipt of the tasking on the day of the accident as they were both focussing on their pre‑flight planning, which was normal practice. Subsequently, the birddog pilot accepted an alternate tasking at 1259.
Figure 1 provides a timeline of the key communications regarding tasking allocation for B134, B137 and the birddog.
Figure 1: Timeline of tasking communications
Source: ATSB
‘B134’ tasking to Adaminaby
At about 1205,[21] while B137 was overhead the Adaminaby fire-ground, and about the same time the SAD logged the birddog rejection, B134 departed Richmond as initial attack. On board were the PIC, the copilot and flight engineer.
In response to the draft report, the RFS provided excerpts from the state operations controller (SOC) log.[22] entry was written in the log by the SOC following the accident.[23] The SOC noted having been advised that the birddog had indicated it was ‘not safe to fly’ and that B137 was not returning to the area until the conditions had eased. However, B134 would continue with the PIC to make the ‘decision of safety of bombing operations’. The RFS advised the ATSB that the SOC had the authority to cancel B134’s tasking, but instead allowed it to proceed, with the intention of gathering additional intelligence to assist in determining whether further aerial operations would proceed. The RFS further reported that this indicated an ongoing intelligence gathering and assessment process by the SOC.
At about 1235, while returning to Richmond, the PIC of B137 heard the PIC of B134 on the Canberra approach frequency and contacted them via their designated operating frequency. At that time, B134 was about 112 km north-east of Adaminaby, en route to the fire-ground (Figure 2). In this conversation, the PIC of B137 informed them of the actual conditions and that they would not be returning to Adaminaby. The PIC of B137 reported that they could not recall the specific details of the call, but that the conversation included that they were ‘getting crazy winds’ and ‘you can go take a look’ ’but I am not going back’. It was also noted that the PIC of B134 had asked several questions. It was reported by the majority of the operator’s pilots that, despite receiving information from another pilot, they would have also continued with the tasking under these circumstances, to assess the conditions themselves.
At about 1242, the crew of B134 contacted air traffic control to advise them of the coordinates they would be working at, provide an ‘ops normal’[24] call time, and confirm there was no reported instrument flight rules[25] aircraft in the area. About 5 minutes later, the Richmond ABM also attempted to contact the crew of B134 to confirm ‘ops normal’, firstly by radio, and then by text to the PIC’s mobile phone, but did not receive a response.
The automatic dependent surveillance broadcast (ADS-B) data showed that, after arriving at the Adaminaby fire-ground at about 1251, the crew of B134 completed several circuits at about 2,000 ft AGL.[26] At about 1255, the crew advised the Cooma ARO that it was too smoky and windy to complete a retardant drop at that location. The Cooma ARO then provided the crew with the approximate coordinates of the Good Good fire, about 58 km to the east of Adaminaby. The ARO further indicated that they had no specific requirements, but they could look for targets of opportunity, with the objective of conducting structure and property protection near Peak View.
Figure 2: Flight track of B134 (white line), timing and location of external communications, and key locations, with an inset detailing the circuits at Adaminaby
Source: Google earth, ADS-B data and radio calls, annotated by the ATSB
‘B134’ tasking to the Good Good fire-ground
At about 1259, the crew of B134 contacted air traffic control to advise that they had been re‑tasked to the Good Good fire-ground and provided updated coordinates. At about the same time, the RFS ground firefighters at the Good Good fire-ground, near Feeney’s Road in Peak View, contacted the Cooma FCC and requested additional assets for property protection. They were advised that a LAT would be passing overhead in about 10 minutes. The firefighters acknowledged the intention of a LAT retardant drop and advised the Cooma FCC they would wait in open country on Feeney’s Road, clear of any properties targeted for protection.
At about 1307, B134 arrived overhead the drop area (Figure 3). The drop area was located to the east of a ridgeline, with the fire on the western side of the ridgeline. The aircraft’s recorded track data (SkyTrac) showed that the crew conducted 3 left circuits, at about 1,500 ft, 500 ft and 1,000 ft AGL respectively, prior to commencing the drop circuit (Figure 4). At about 1312, after conducting about 2 circuits, they advised the Cooma ARO of their intention to complete multiple drops on the eastern side of the Good Good fire, and that they would advise the coordinates after the first delivery.
Figure 3: B134’s approach and circuits overhead the drop location; the inset shows the track from the Adaminaby to the Good Good fire‑ground
Source: Google earth and SkyTrac data, annotated by the ATSB
At 1315:15,[27] a partial retardant drop was conducted on a heading of about 190°, at about 190 ft AGL (3,600 ft above mean sea level). During the drop, about 1,200 US gallons (4,500 L) of fire retardant was released over a period of about 2 seconds. A ground speed of 144 kt was recorded at the time of the drop.
A witness video taken by ground fire-fighters captured the drop and showed the aircraft immediately after the drop in an initial left turn with a positive rate of climb, before it became obscured by smoke[28] While being intermittently obscured by smoke, the aircraft climbed to about 330 ft AGL (3,770 ft above mean sea level). At about this time, ATSB analysis of the video showed that the aircraft was rolling from about 18° left angle of bank to about a 6° right angle of bank. Following this, the aircraft descended and about 17 seconds after the completion of the partial retardant drop, it was seen at a very low height above the ground, in a slight left bank. Video analysis and accident site examination showed there was no further (emergency) drop of retardant. Throughout this period, the recorded groundspeed increased slightly to a maximum of 151 kt. Shortly after, there was a significant left roll just prior to ground impact.
Figure 4: Accident circuit and location of the firefighters and retardant drop
Source: Google earth and SkyTrac data, annotated by the ATSB
At about 1315:37, the aircraft collided with terrain and a post-impact fuel-fed fire ensued. The 3 crew were fatally injured, and the aircraft was destroyed.
A review of the Airservices Australia audio recording of the applicable air traffic control frequency found no distress calls were received by controllers prior to the impact.
The pilot in command’s (PIC) logbook, combined with the operator’s records for the accident aircraft showed that the PIC had a total flying experience of about 4,010 hours, which included 3,010.3 hours in the C-130 aircraft and 994 air tanker drops. The PIC had also accrued a further 1,616.8 hours as a flight navigator.
The PIC commenced work in Australia on 1 December 2019. In the 30 days prior to the accident, the PIC had flown about 32 hours. In the 72 hours prior, the PIC had flown 4.5 hours, all of which were in B134. The accident flight was the first flight of the day.
The PIC was initially trained as a navigator and pilot in the United States (US) Air National Guard. During this time, the PIC gained experience in firefighting operations through the modular airborne firefighting system (MAFFS)[29] program. The PIC joined Coulson Aviation in 2015 on a part-time basis, before being employed full-time in 2017.
Qualifications
The PIC held a current airline transport pilot certificate with ratings for multi-engine land airplane including the EC-130Q, issued by the US Federal Aviation Administration (FAA) on 13 October 2017. The PIC’s most recent flight instructor certificate with ratings for multi-engine and instrument aircraft was issued by the FAA on 6 April 2019. On 18 April 2019, the PIC’s latest ‘airplane pilot qualification card’ was issued from the US Department of Agriculture, Forest Service,[30] for the C-130 aircraft, which included the authorised missions of:
low level (below 500 ft above ground level)
mountainous terrain
airtanker initial attack.
An air tanker initial attack certification allowed a pilot to conduct fire retardant drops without the supervision of a birddog or air tactical (attack) supervisor.
At interview, other flight crew reported the PIC was ‘methodical’, ‘conservative’, who ‘always did his due diligence’ and was not considered to take unnecessary risks. It was also reported that Coulson Aviation pilots were not being paid per flight or by flying hours, and therefore that was not a motivational factor to accept a tasking. In addition, the PIC had recently resigned from the operator and accepted a US-based position.
Training
The PIC last completed training with Coulson Aviation in March and April 2019,[31] which included annual C-130 simulator training, controlled flight into terrain awareness and crew resource management courses. In addition, the PIC completed 2 assessed training flights in the C-130 on 14‑15 April 2019. The flight on 14 April included approach to aerodynamic stalls[32] in the circuit (with 50% flap) and drop (with 100% flap) configurations, and go-arounds with a full load (water). The flight on 15 April included drop planning (hazards, tactics, ingress, egress, and dry run) and an emergency on the drop run. The drop run emergency was a simulated ‘down air’ [downdraft]. All the assessed sequences, which included jettison of the load during a (simulated) emergency condition,[33] were recorded as satisfactory.
Copilot
The copilot had joined Coulson Aviation in September 2019, after 20 years in the US military, including experience flying the C-130. The copilot’s logbook combined with the operator’s records showed a total flying experience of about 1,744 hours, of which about 1,364 hours were on the C‑130. This was the copilot’s first fire season, and they commenced work in Australia on 1 December 2019. Since the start of the fire season, the copilot had flown about 85 hours, with about 28 hours in the last 30 days and about 4.5 hours in the 72-hour period prior to the accident.
The copilot held a current airline transport pilot certificate and ratings for multi-engine land aircraft, including the EC-130Q (second-in-command privileges only), issued by the FAA on 7 November 2019. The copilot also held a flight instructor certificate with ratings for single, multi‑engine and instrument aircraft, issued by the FAA on 14 August 2019.
The copilot’s C-130 check flight with the operator was completed on 12 September 2019, and was assessed as satisfactory against the qualification standards for second‑in‑command. On 13 September 2019, the copilot completed the crew resource management and controlled flight into terrain awareness courses and reviewed the US Department of Agriculture Forest Service’s air tanker pilot training video.
On 16 September 2019, the copilot was issued with an ‘airplane pilot qualification card’ from the US Department of Agriculture Forest Service for the C-130, which included the authorised missions of:
low level (below 500 ft above ground level)
mountainous terrain
airtanker SIC (second-in-command).
Flight engineer
The flight engineer joined Coulson Aviation in November 2019, after about 25 years in the US military. This was the flight engineer’s first fire season. The flight engineer held a flight engineer certificate with a rating for turbo-propeller powered aircraft, issued by the FAA on 20 November 2019. On the flight engineer application form, the flight engineer reported accruing about 4,050 hours on the C‑130. The flight engineer also held a mechanic certificate with ratings for airframe and powerplant, issued by the FAA on 2 June 2019.
The flight engineer’s check flight was completed with the operator on 20 November 2019. In addition to this flight, the flight engineer completed 2 air tanker drops under supervision in Australia on 12 January 2020. The flight engineer commenced work in Australia on 13 January 2020.
72-hour prior history
In Australia, each crew member’s roster cycle was 14 duty days followed by 2 rest days. The accident flight occurred on the PIC’s 9th day, and the copilot’s and flight engineer’s 11th day of their respective current duty periods.
Table 1, based on the operator’s records, details the crew’s sign-on and sign-off times for the 3 days before the accident. On 23 January 2020, the crew signed on at 0900.
Table 1: B134 crew working hours
20 January
21 January
22 January
23 January
Sign-on
1000
0800
1000
0900
Sign-off
1800
1700
1900
-
Duty time
8 hours
9 hours
9 hours
-
Information from the crew’s telephone and hotel records, in addition to work and flying duties, were used to determine their activities in the previous days. There were no indications of fatigue for the 3 crew members. However, there was insufficient information available to the ATSB about their sleep and non-duty activities to estimate fatigue levels with confidence.
Aircraft information
General information
The C-130 is predominantly an all-metal, high-wing aircraft, designed for military operations. The accident aircraft (Figure 5) was manufactured by the Lockheed Corporation (now Lockheed Martin Corporation) in 1981 and was powered by 4 Allison T56-A-15 turbopropeller engines, fitted with Hamilton Sundstrand 54-H60-91 4-blade propellers. The T56‑A‑15 is a constant speed engine, with a variable pitch propeller.
Previously owned by the US Navy, the aircraft was transferred to the US National Aeronautics and Space Agency in 1992 and later placed in storage. It was then re‑purposed for firefighting activities by Coulson Aviation and registered in the restricted category.[34] At that time, Coulson Aviation became the type certificate holder and assumed the responsibilities of the aircraft manufacturer for the entire aircraft and any modifications made.
Initially registered as N130CG in 2018, this was later changed to N134CG in April 2019. Modifications to the aircraft included the installation of an avionics package and firefighting tank system, known as the Retardant Aerial Delivery System XXL (RADS).
Figure 5: N134CG
Source: Coulson Aviation
Retardant Aerial Delivery System XXL
The RADS included a 4,000 US gallon (15,000 L) tank system located within the aircraft’s fuselage. The system was designed to deliver discrete quantities of retardant, dependant on the coverage factor[35] selected and the duration the doors remained open. This was controlled from the cockpit, with drop controls located on both the PIC and copilot yokes.
The drop quantity was manually controlled by the crew by setting the coverage factor and either selecting a pre-set percentage or setting 100%. The latter option allowed the crew to control the amount of retardant released by holding a button on the yoke until the desired amount was dispensed. The RADS system was designed that, if less than 100% volume was selected, the system would disarm after a partial load drop and the crew would need to re‑arm the system to complete further releases. It was reported that the crew on B134 normally selected 100%.
The system also included a guarded emergency dump (’e-dump’) switch, located in reach of all 3 crew members, which would fully open the doors and jettison the load in a period of about 2 seconds. Following an emergency dump, the doors would remain open until the RADS was reset by the crew.
Maintenance history
The aircraft had a total time-in-service of 11,888 hours and had accrued 683 hours of firefighting operations since the tanker conversion in 2018. The aircraft had a current certificate of airworthiness and was maintained in accordance with an FAA approved program.
N134CG arrived in Australia in November 2019. The last daily inspection conducted on 22 January 2020, at the end of flying activities the day before the accident, identified the propeller anti-icing system on engine number 2 was unserviceable, and rectification had been deferred in accordance with the minimum equipment list.[36]
In addition to a maintenance requirement to perform engine power efficiency checks at 150-hour intervals, the operator reported pilots were required to perform power checks before every take‑off. Operations were only permitted if a minimum performance requirement of 95% was met.
Weight and balance
The last weight and balance report for the aircraft, in April 2019, showed its basic empty weight was 75,794 lb (34,380 kg) and according to the RADS Airplane Flight Manual (AFM) supplement, the maximum take-off weight was 150,718 lb (68,365 kg). The aircraft flight and maintenance log indicated the PIC had the aircraft refuelled to a total of 34,000 lb (15,422 kg) at the completion of flying on 22 January 2020. The operational load monitoring system[37] indicated there was 35,514 lb (16,109 kg) of retardant on board prior to the accident drop, in addition to a 2,000 lb (907 kg) pallet of gel. This resulted in a take-off weight of about 147,308 lb (66,818 kg) and the centre of gravity being at the aft limit on departure from Richmond.
Using the operator’s reported fuel consumption for air tanker drop missions of 5,000 lb/h (2,268 kg/h) for a 70-minute flight, and the retardant drop of 10,764 lb (4,882 kg), the estimated post-drop weight was 130,656 lb (59,265 kg). The centre of gravity remained close to the aft limit. This was consistent with reports from the operator’s other crews that the location of the RADS tank in the aircraft meant there was no appreciable change in the centre of gravity following a retardant drop.
Aerodynamic stall
Stalling
An aircraft’s wing is said to be ‘aerodynamically stalled’ when the airflow over the wing separates from the wing; that is, the airflow no longer follows the contour of the top surface of the wing. This results in a rapid loss of lift, which balances the weight of the aircraft, and the aircraft will rapidly descend. An aerodynamic stall will also normally result in the nose of the aircraft pitching down, often with a left-wing drop.
The aerodynamic characteristics of an aircraft wing are such that the airflow will separate and the wing stalls when the angle of attack, the relative angle between the wing and the airflow, reaches a critical value. The C-130H did not have an angle of attack instrument, however, this could be referenced to an equivalent airspeed. The airspeed at which a stall occurs is not fixed to a single value, and varies depending on the flap setting, aircraft weight, and load factor.[38] The stall speeds are typically presented in the AFM (refer to section titled Aircraft performance).
The C-130 aircraft has 4 wing mounted engines driving propellers. The placement of the propellers forward of the wings results in the propeller slipstream providing a relative airflow over each of the wings in addition to the forward speed of the aircraft, which varies in strength with the power produced. This is known colloquially as a ‘blown lift’ wing and results in the stall speed lowering as power is increased. For the C-130, the published power-on stall speed with 50% flap is based on maximum power. Therefore, the stall speed will be higher when less than maximum power is applied. The higher power-off stall speeds are based on idle engine power.
Stall characteristics of the C-130
A C-130 discussion paper (Mizell, 2009), based on data obtained during US Air Force testing, described the aircraft as having a ‘very good natural stall warning... However, once in a stall, the plane becomes much less predictable’. In a clean (no flap) power-off stall:
The flying characteristics of the plane are very benign all the way up to full stall. A significant buffet was experienced 10 knots prior to stall. 3 knots above stall, a deterring buffet was experienced, giving a clear signal to the crew that stall was imminent. Immediately before stall, a yaw acceleration was detected by the data, but nearly imperceptible to the crew.
However, the 50% flap and 100% flap power-on stall ‘present a much larger hazard..’. Specifically, the paper noted that:
Similar to 0% flap, but with less buffet warning, the left-wing stalls first resulting in large, uncontrolled bank excursions and subsequent nose low attitudes. In some cases, the aircraft remained uncontrollable until the bank exceeded 100 degrees and the nose approached 75 degrees down. This caused massive altitude loss and overspeed of airframe components.
The approach to stall at 50% and 100% configurations also exhibited high descent rates.
The accident aircraft was not fitted with a stall warning system, nor was one required or available. However, according to the C-130 pilots consulted during the investigation, the aircraft had a noticeable pre-stall buffet through the rudder pedals and control column, and this was reported as being distinct from a turbulence-induced buffet, which could be felt throughout the aircraft. In addition, the flight controls become less effective at these lower speeds, described by pilots as ‘sluggish’ and ‘unresponsive’. The Lockheed Martin AFM also indicated that:
With flight idle power, stall warning buffet initially occurs at 4% to 15% above stall speed, depending upon configuration, and progresses to moderate or heavy buffet at the stall. The greatest stall warning airspeed margin exists in the take-off and approach configuration and less margin exists in the landing and cruise configurations. The stall of the C-130 is characterized by either a mild pitch down or a mild roll-off to the right or left depending on slightly unequal power settings.
Stall recovery
The Lockheed Martin AFM described the recovery actions for a stall as:
If in climbing or bank attitude, immediately drop the nose, level the wings, and apply power to limit loss of altitude. Move controls smoothly and avoid abrupt actions. Avoid diving the airplane and avoid abrupt or accelerated pull-up after recovery.
While the ATSB did not find a published procedure in the operator’s AFM (refer to section titled Operating documents) for stall symptoms and recovery actions, their C-130 pilots all reported that approaches to stall (start of the buffet) training[39] was conducted in the aircraft on an annual basis in various configurations. According to the operator’s Company Operations Manual (COM),[40] training for approaches to the stall were conducted in the clean, take-off and landing configurations.[41] The recovery procedure referred to both low altitude (ground contact imminent) and higher altitude (ground contact irrelevant) scenarios.
The C-130 pilots’ descriptions of the symptoms and recovery actions were consistent with the manufacturer’s published material, with some additions specific to their operation. These included the addition of load jettison and flying the aircraft towards their pre-briefed escape route from the release point. Although their recovery descriptions for a pre-stall buffet, following a fire-retardant drop, was to apply maximum power by pushing the power levers full forward, this was not a procedure that could be practically trained in the aircraft. The engine power was managed manually, therefore, pushing the power levers full forward during training could result in an over‑torque or over‑temperature condition for the engines. However, they reported they would apply as much power as needed and as quickly as possible in a real low-level stall situation.
Aircraft performance
Stall speeds
The aircraft stall speeds were contained in the respective performance charts in the Lockheed Martin AFM. The ATSB calculated the power-on and power-off stall speeds for an aircraft weight of 131,000 lbs (59,420 kg), in level flight and with 50% flap at 83 kt (IAS)[42] and 101 kt (IAS) respectively. This configuration and attitude were considered most representative of the aircraft state just prior to the observed descent (refer to sections titled Weight and balance, Wreckage and impact information, and Recorded information sections), noting that a pitch-up attitude, any bank angle above 0° and a decreasing flap setting would increase the stall speed. It was a standard operating procedure for the crew to calculate the power-off stall speeds at the take-off weight for 0-flap, 50% flap and 100% flap, for 0° and 45° angle of bank for each flight. A 25,000 lb (11,340 kg) weight reduction from a jettison of the remaining fire retardant would have reduced the power‑on stall speed to 76 kt.
Turbulence will also affect an aircraft’s stall speed. According to the Bureau of Meteorology, moderate turbulence is associated with a load factor increase of 0.5 to 0.99 G[43] with appreciable changes in attitude and/or altitude, while severe turbulence is associated with a load factor increase of 1.0 G to 1.99 G with large abrupt changes in attitude and/or altitude. Turbulence was forecast (refer to section titled Bureau of Meteorology forecasts) and likely experienced (refer to section titled Bureau of Meteorology analysis) at the accident location. Applying the moderate turbulence load factors as boundary conditions to the 50% flap power-on stall speed at 59,420 kg produced a range of 101-117 kt (IAS). Similarly, for severe turbulence, this produced a power-on stall speed range of 117-143 kt (IAS) at 59,420 kg.
Regarding turbulence, the airspeeds limitation section of the operator’s AFM stated that:
The aircraft should not be operated in conditions of severe turbulence [actual conditions] because gusts can be encountered that may impose excessive loads. However, if flight in severe turbulence cannot be avoided, flight should be in the range of 65 knots above the power-off stall speed (not to exceed 180 KIAS) for the operating gross weight.[44]
Emergency climb performance
The aircraft’s emergency climb performance with maximum power at 131,000 lb (59,420 kg) and 50% flap was about 1,500 ft/min. With a reduced weight from a jettison of the remaining fire retardant, the emergency climb performance would have increased to about 2,250 ft/min, representing a 50% improvement. This was the absolute best rate of climb that could have been achieved.
Meteorological information
Bureau of Meteorology forecasts
A Bureau of Meteorology graphical area forecast was issued at 0924 and was valid for the time of the flight. It forecast moderate mountain wave activity[45] above 3,000 ft above mean sea level (AMSL) and severe turbulence below 8,000 ft AMSL in the area of operation from Richmond to Cooma. This included the Adaminaby and Good Good fire-grounds. In addition, a SIGMET[46] issued at 0947, and valid for the flight, forecast severe turbulence[47] below 10,000 ft AMSL for the area. Of note, when commenting on the general nature of forecasts, some of the operator’s pilots indicated that they could be broad and cover a large area of the state, which may not accurately reflect the actual conditions over the fire-ground. The only operational limitation cited at interview by the pilots were related to thunderstorm activity.
The aerodrome forecast for the Cooma-Snowy Mountains Airport,[48] located 50 km south-west of the accident site was amended at 0948. It indicated wind speeds of 25 kt, gusting to 48 kt, with a mean wind direction of 300° from 1100 and visibility reduced to 8,000 m in light showers. Severe turbulence below 5,000 ft AGL was forecast from 0900-1500. A PROB30[49] for visibility reduced to 2,000 m in blowing dust and a broken[50] layer of cloud at 1,000 ft AGL was forecast for the period 1100–1700.
At 1012, the Richmond airbase manager (ABM) sent a text message to the air tanker and birddog pilots to advise them of an airport warning at Richmond for wind gusts in excess of 35 kt between 1000 and 1700.
Observations of the weather in the area
Other fire-control aircraft
On the day of the accident, several fire-control aircraft, primarily consisting of fixed-wing Air Tractors (single-engine air tankers) and Bell 206 helicopters, were operating from the Polo Flat airstrip, located 33 km south-west of the accident site. The Cooma Fire Control Centre (FCC) aviation radio operator (ARO) received reports of strong winds in the area from the fire-control pilots in the early morning. This included winds of 30-40 kt at 0839, 40-50 kt at 0902, and 52 kt at 0937. The ARO recorded in their operations log that, due to the weather conditions, all fire‑control aircraft had departed the area or landed by 1030.
In addition, the crew of B137 reported that the wind conditions at Adaminaby at about 1200 were 50 kt at 800 ft AGL and about 37 kt at 200 ft AGL.
Witness reports
Following the accident, the ATSB received multiple witness reports of the weather conditions at Peak View. They all consistently reported very strong winds from the north-west, with gusts up to 43 kt recorded at ground level. One resident noted that, although the prevailing wind was from the north-west, the direction and strength at ground level were also being influenced by the local terrain.
Glider pilots familiar with the area commented that, due to the local terrain, the area was often subject to turbulence and rotor conditions (refer to section titled Mountain wave activity). It was also a well-known area for mountain wave activity and that on the day of the accident it was a ‘terrible wave day’.
Weather station recorded conditions
About 12 minutes prior to the accident, the Cooma-Snowy Mountains Airport weather station indicated a wind speed of 25 kt, gusting to 39 kt, from a direction of 320°. The visibility was 6,000 m, with a QNH[51] of 1002 hPa, and temperature of 26 °C.
A personal weather station at Peak View, located about 1.3 km from both the drop and accident sites (Figure 6), recorded the conditions twice per hour. At about 1309 (7 minutes prior to the accident), the station recorded a mean wind of 15 kt from the west and a peak gust of 32 kt from the north, a temperature of 30 °C, and a QNH of 995 hPa.[52] At about 1330 (14 minutes after the accident), the station recorded a mean wind of 16 kt from the west and a peak gust of 42 kt from the north-west.
Figure 6: Accident circuit with predominant wind direction, direction of travel (DOT), and terrain
Source: Google earth, Peak View weather station and SkyTrac data, annotated by the ATSB
Bureau of Meteorology analysis
The Bureau of Meteorology analysed the conditions on the day and indicated that a cold front was approaching the accident location, with hot and strong north to north-westerly winds ahead of the front. High resolution weather model data indicated the winds at 5,000 ft AMSL were about 45 kt from the north-west, increasing in strength with height up to 80 kt from the north-west at 10,000 ft AMSL.
Gusting winds had produced some areas of blowing dust, which likely reduced visibility. Bushfire smoke in the area had also affected visibility. While nearby observations at the Cooma-Snowy Mountains Airport showed intermittent reductions in visibility, it was noted that measuring equipment may not have accurately reported visibility in smoke conditions. Therefore, it was likely that the actual visibility was lower than that reported by the instruments.
The strong winds over the terrain likely resulted in severe turbulence and mountain wave development. Satellite imagery of cloud formations confirmed the presence of mountain wave activity during the day. The conditions in the area at the time were generally favourable for mountain wave development, however, the Bureau of Meteorology were unable to determine the severity of this from the data available.
The Bureau of Meteorology considered that the conditions at the Cooma-Snowy Mountains Airport were likely representative of the general conditions experienced at the accident location. Further, their analysis of the weather conditions in the area was consistent with what was forecast on the day.
Accessing meteorological information
For operations in NSW, following the briefing with the Richmond ABM each morning, the crews would return to their own operational areas until they received a tasking from the RFS. On receipt of a tasking, crews would conduct their flight planning. It was reported that the operator’s crews used an electronic flight bag (their company issued iPad including the Foreflight app) to submit their flight plan to Airservices Australia, which also provided access to the required weather forecasts. While specific weather data access could not be confirmed, as the flight plan had been submitted, it was considered very likely that the crew of B134 would have also accessed the relevant weather information at that time.
In addition, the operator outlined that conditions at a fire could change rapidly, and when the fire was an hour or more flight time away, reported weather conditions were likely to be inconsistent with the actual conditions on arrival.
Weather systems: Mountain waves and windshear
Mountain wave activity
Mountain waves[53] are the result of flowing air being forced to rise up the windward side of a mountain range, then as a result of certain atmospheric conditions, sinking down the leeward side (ATSB, 2009). Immediately downwind of the range there is a strong downdraft followed quickly by an updraft, which produces the wave motion. According to Underdown and Standen (2003), mountain waves can develop when the wind direction is near perpendicular to a continuous mountain range and at a speed of 15 kt or more[54] at the summit, and increasing with height in a stable atmosphere. Aircraft may encounter severe turbulence in mountain wave systems.
Rotors or eddies can also be found embedded in mountain waves. Their formation usually occurs where wind speeds change in a wave or where friction slows the wind near to the ground. Often these rotors will be experienced as wind gusts or windshear (ATSB, 2009). According to the FAA (1997), localised gusts of 50 kt, with downdrafts greater than 1,500 ft/min, are not unusual in mountain wave systems. Although this phenomenon is usually forecast reasonably well by the Bureau of Meteorology, many local factors may also affect the formation of mountain wave activity.
When discussing the consequence on aircraft performance, the ATSB’s safety publication Mountain wave turbulence noted that (ATSB, 2009):
Many dangers lie in the effects of mountain waves and associated turbulence on aircraft performance and control. In addition to generating turbulence that has demonstrated sufficient ferocity to significantly damage aircraft or lead to loss of aircraft control, the more prevailing danger to aircraft in the lower levels in Australia seems to be the effect on the climb rate of an aircraft.
Study of mountain waves associated with bushfires
According to the Bushfire and Natural Hazards Cooperative Research Centre,[55] one of the most challenging situations in fire management was when relatively benign weather conditions were expected, but a severe fire eventuated. In December 2016, the centre released Hazard note issue 24: Fire escalation by downslope winds. The note, authored by specialists from the Bureau of Meteorology, investigated the meteorology of unexpected severe fire behaviour associated with mountain wave activity and identified 3 relevant bushfires. A detailed case study of the New South Wales (NSW) Blue Mountains fires of October 2013 was undertaken, focussing on 17 October at 1300. Of interest was the behaviour of the winds in the vicinity of the State Mine fire.
Figure 7 shows a cross-section of the horizontal wind speeds (left image) and vertical wind speeds (right image) along a section passing from the north-west to the south-east through the State Mine fire‑ground. The red circled region in the left image shows strong horizontal winds extending downwards towards the surface in the vicinity of the fire. Downwind (to the right) of the fire are oscillations (left image) in the wind speeds and alternating bands of ascending and descending air (right image), both of which are characteristic features of mountain waves. The note described mountain waves as:
Mountain waves are oscillations that can occur when the wind blows across a mountain or hill. They are somewhat similar to water flowing over a rock in a stream, but are much more complex because their existence and amplitude is sensitive to the atmospheric temperature structure (stability) and vertical variation of the wind (wind shear). They often lead to strongly accelerated flow attached to the lee slope of the mountain or hill, known as downslope winds…
Figure 7: North-west to south-east cross section of fire, illustrating horizontal (left image) and vertical (right image) wind speed changes, with the fire located near the number 6 on the horizontal axis
Source: Bushfire and Natural Hazards Cooperative Research Centre
While the purpose of the note was to consider the wind effect on the severity of a fire, this has potential implications for firefighting aircraft, particularly if low-level windshear was present. As a comparison, at position 1 on the horizontal axis (left image), the wind speed band of 45–55 kt would not be encountered until reaching a height greater than 8,000 ft (2,450 m) above the surface. However, at the fire-ground at position 6, these wind speeds could be encountered within a few hundred feet above the surface. The note also highlighted that this research revealed features at the location of the fire-ground that might not have been captured or possibly filtered out of broader‑scale forecasts.
Windshear
Windshear is defined by the Bureau of Meteorology (2014) as a ‘wind direction and/or speed change over a vertical or horizontal distance’. It is always present in turbulent air but can also occur without turbulence being present. This phenomenon becomes particularly significant when an aircraft is abruptly displaced from its intended flight path and substantial corrective action is required by the pilot. This is more so at lower levels and low speed, such as during take-off and landing. The hazards are a rapidly changing headwind and tailwind, strong side gusts, and a change in lift on the wings, all during a time when an aircraft is most vulnerable (Minor, 2000). Specifically, the Bureau of Meteorology (2014) noted that:
During the climb-out and approach phases of flight, aircraft airspeed and height are near critical values, rendering the aircraft especially susceptible to the adverse effects of wind shear.
Aircraft taking-off may be significantly affected by changes in headwind and tailwind components which create changes in the amount of lift experienced. A decrease in the vertical headwind component, or an increase in the tailwind component, will result in a reduction in airspeed, and in extreme cases the resulting loss of lift may be enough to cause the aircraft to stall or fly into the ground.
Likewise, the adverse effects on aircraft performance from low-level windshear was also discussed by Bowles (1990), when analysing airborne forward-looking windshear detection systems:
The hazard of windshear arises principally from its deceptive nature: In a windshear situation, from a microburst[56] or any other source, the pilot may be confronted with a performance-increasing headwind, followed a few seconds later by a powerful, performance-decreasing tailwind. To cope with the headwind, the pilot may take actions to prevent the plane from climbing. These actions are then compounded by performance loss caused by the tailwind and downdraft, so that it may be impossible to avoid ground impact.
Depending on crew action, a typical low altitude windshear may result in reduced airspeed and rate‑of-climb, which often result in significant altitude loss and possible ground impact. Full performance capability depends on two key factors: timely recognition and appropriate response.
Windshear controls
Aviation specific windshear research
In 1985, the FAA contracted a consortium of aviation specialists to study windshear. As a result of that work, a windshear training aid was developed. The aid provided an effective means of training crews to minimise the windshear threat through avoidance, cockpit recognition, and recovery techniques. This included the 1988 publication Pilot windshear guide (FAA advisory circular 00‑54). This outlined the limitations in pilot avoidance, with a reliance on visual indications, which can be complicated by marginal weather, and reports from other aircraft in high density traffic areas.
According to the advisory circular, between 1964 and 1986, there were at least 32 air transport accidents and incidents in which windshear was identified as a contributing factor, resulting in over 600 fatalities. There was also evidence to suggest that this figure was underestimated as it did not include undocumented ‘close calls’ and general aviation statistics.
Generally, the research showed that only 5 to 15 seconds may be available for the crew to recognise and respond to a windshear encounter. In describing a typical encounter shortly after take-off, with windshear encountered prior to a stabilised climb (Figure 8), for the first 5 seconds the take-off appeared normal, with early trends in airspeed, pitch attitude, vertical speed and altitude appearing normal. However, as airspeed decreased, pitch attitude was reduced, limiting performance capability, and resulting in a loss of altitude.
Figure 8: Effect of a windshear encounter on the aircraft flight path during take-off
Source: US Federal Aviation Administration
The timeframe mentioned above was consistent with windshear research reported by Tsukagoshi (1999) conducted following a 1993 Douglas DC-9-41 hard landing accident in Japan following windshear during the landing approach (while crossing the runway threshold in Japan). Following the occurrence, the Japan Federation of Flight Crew Unions established a project to obtain objective and quantitative data on flight crews’ reactions to windshear. The research was supervised by Dr Sado Horino from Kanagawa University, Japan, and was conducted on a DC-9 flight simulator at Northwest Aerospace Training Corporation near Minneapolis, US.
Eight DC-9 pilots completed 35 test approaches to land on the simulator. Windshear was encountered at random heights, from 50 ft to 900 ft. Of particular note, the results demonstrated that the average recognition time for a windshear encounter was about 5.5 seconds. Recognition time was defined as the time between the windshear encounter and when the pilot first moved the elevator control.
Windshear risk control systems
Windshear avoidance, based on pilot awareness and training, cannot be 100% effective. There are also limitations in recognition and recovery procedures, as this requires the aircraft to have entered the windshear condition, which can potentially exceed the aircraft’s performance capability, regardless of pilot actions. Therefore, ground-based and airborne detection systems have also been introduced to reduce the hazard of an inadvertent windshear encounter (Bowles, 1990).
Ground-based low-level windshear alerting systems were developed and introduced at selected airports, predominantly in the US. However, there were 2 prominent windshear accidents in the 1980s (a Pan Am Boeing 727 on 9 July 1982; and a Delta Airlines Lockheed L-1011 on 2 August 1985), which prompted the FAA, in 1988, to mandate the use of airborne windshear detection systems for passenger aircraft.
The initial airborne windshear detection systems were reactive systems, which relied on the aircraft performance instruments, combined with attitude, angle of attack and accelerometer inputs. According to FAA advisory circular 25-12, Airworthiness Criteria for the Approval of Airborne Windshear Warning Systems in Transport Category Airplanes, even reactive systems ‘provide a valuable service in the detection, timely annunciation, and confirmation of a potentially hazardous windshear condition generally in advance of human pilot recognition time’. With the development of digital signal processors in the 1990s, weather radar with forward-looking (predictive) windshear detection became possible and the first system was certified by the FAA in 1994. The requirement was to provide at least 10 seconds advance warning to the crew of a microburst. These systems used doppler weather radar and the moisture in the atmosphere to collect wind velocity data. Therefore, drier air would reduce the reflectivity and windshear warning time.
An article published by Honeywell Aerospace (2019), Radar Corner: Understanding Airborne Windshear Detection Systems, Part One, emphasised that ‘It is the advanced warning time that saves the aircraft’. This time allowed the pilot to increase engine power, and retract the flaps and landing gear, thereby increasing the aircraft’s energy state and climbing, so that the windshear encounter would occur at a higher, ‘more survivable altitude’. The article further indicated that, during studies evaluating windshear recovery manoeuvres, it was found that when a windshear recovery manoeuvre was delayed by 5 seconds, the average altitude loss increased by 300 ft.
Another study on Wind-Shear System Cost-Benefit Analysis (Hallowell and Cho, 2010) reviewed the effectiveness of various detection systems, as the FAA considered the options for managing aging systems and evaluating new systems. The study also considered windshear mitigation strategies, which were categorised into 3 groups: pilot recognition and recovery training, airborne (aircraft systems), and ground‑based systems.[57] While noting the difficulties in determining the effectiveness of pilot training in recognition and avoidance, for comparative purposes, this was estimated to be effective about 25% of the time. Conversely, while only measured in simulated environments, the effectiveness of predictive windshear (airborne) systems had often exceeded 95%, although this may be reduced in dry environments.
Notably, Hallowell and Cho (2010) identified that each of these categories provided their own advantages, with the greatest benefit achieved when multiple categories were combined. It also noted that air taxi and aerial work operations, which included firefighting aircraft, operated at low‑level and low‑speed outside the ground-based protection areas more frequently than air transport. Further, airborne systems including both reactive and predictive windshear systems, were not routinely available on air taxi, aerial work or general aviation aircraft.
While there are limitations to reactive and predictive systems, where these systems were fitted to firefighting aircraft, and warnings had activated in the low-level environment, several pilots reported at interview this had a positive effect on their management of the situation. In addition, in 2018, Lockheed Martin developed a civil-certified firefighting air tanker, which was a variant of the C-130J. The LM‑100J ‘FireHerc’ had numerous advanced features that provided increased situational awareness and modern safety features to protect and guide crews through challenging flight conditions. Of most relevance to this investigation was the inclusion of warning systems with visual and aural alerts for windshear detection.
The accident aircraft was not fitted with a windshear detection system as it was built in 1981, prior to such technology becoming available. Likewise, the operator’s other C-130 aircraft did not have this system. Retrofitted systems suitable for the C-130 have since become available.[58] However, the operator advised that they had not considered installing these systems into their C-130 fleet. Further, it was not required by regulation or contract to be installed.
On 10 July 2022, in response to the draft report, Coulson Aviation advised that aerial firefighting operate in very dry environments conducive to active fires. Therefore, with minimal or nil moisture present in the atmosphere it could be concluded that a forward-looking windshear detection system would provide little to no advance warning of a windshear event. They further indicated that their crews were highly experienced in recognising windshear events and crew reaction times would be as timely, if not quicker than a reactive-based system. The operator further advised that this statement was based on ‘rational conclusion’ based on experience supported by informed opinion. The ATSB was unable identify any research that supported this comment.
Lockheed Martin Airplane Flight Manual
The Lockheed Martin AFM contained a section on adverse environmental conditions, which defined windshear as ‘any rapid change in wind direction or velocity that results in an airspeed change of more than 10 knots’. Severe windshear was defined as ‘a rapid change in wind direction or velocity causing airspeed changes greater than 15 knots, or vertical speed changes greater than 500 fpm [ft/min]’.
The AFM also warned pilots that severe windshear, particularly those with downdrafts, could exceed aircraft performance capability. It was considered to be most dangerous at low levels when encountering a decreasing headwind (or increasing tail wind) such as during take-off and approach. At these times, the aircraft is at low-level and low speed, and the initial reaction of the aircraft will be a drop in indicated airspeed and a decrease in pitch attitude, resulting in a loss of altitude.
By 2010, the Lockheed Martin AFM had introduced a recovery procedure for severe windshear encountered during approach to land as:
1. Announce a go around.
2.Set maximum power and select a go around (G/A) flight director mode, if applicable. Best initial pitch attitude will be a function of the conditions. If ground impact is a concern, rotate above the G/A flight director cue, as necessary, to target threshold speed until safe altitude above the ground is reached.
3.The co-pilot will monitor and call sink rate (VVI/VSI) and airspeed as appropriate.
4.The navigator/engineer will monitor and call out radar altimeter.
5.If flaps are at 100%, transition to 50% flaps after assuring continued positive rate of climb at no lower than Obstacle Clearance Speed.
6.Do not retract the landing gear until recovery is complete with positive climb rate and increasing terrain separation.
7.When clear of the wind shear, adjust pitch and power for normal climbout.
8. When conditions permit, report the encounter with ATC.
Coulson Aviation’s Airplane Flight Manual and Company Operations Manual
On 10 July 2022, in response to the draft report, Coulson Aviation stated that the precursors that generally defined windshear would be routinely encountered in normal aerial firefighting operations due to the hot, dry, and windy conditions that lead to most bushfires. Therefore, the procedures, experience, and training to deal with, and respond to these conditions were in-built for their aerial firefighting operations. However, the ATSB noted that there was no windshear recovery procedure published in the operator’s AFM, nor did it contain a section on adverse environmental conditions.
The manual did contain a warning associated with the go-around procedure, which was described by the operator’s pilots as similar to the post-retardant drop climb out:
Retracting flaps from 100 percent to 50 percent will increase stall speed. Without proper power and attitude corrections, sink rate will also increase. This is particularly noticeable at lower than normal airspeeds. If safe altitude and airspeed are not attained, inadvertent touchdown and/or stall may occur.[59]
The COM contained information on windshear in the departure procedures section, which stated:
…wind shear may create a severe hazard for aircraft below 1,000 ft…the best defence is to avoid downdrafts altogether as it could be beyond you or your aircraft’s capability… If wind shear is encountered, prompt action is required. In the EC-130Q/L382G, the recovery requires full power and pitch attitude consistent with the maximum angle of attack for the aircraft.
The majority of the crew interviewed provided accounts of personal experiences with either a real or simulated windshear event in the low-level airdrop environment. It was noted that in-aircraft training was conducted by the operator for emergency scenarios with a focus on jettisoning the retardant. These descriptions were consistent with the manufacturer’s procedures for windshear recovery, with additional consideration of jettisoning the load if aircraft performance did not improve after maximum power was applied.
Coulson Aviation windshear training
A review of the operator’s C-130 simulator training syllabus noted there was no specific training item for a low-level windshear recovery scenario. The syllabus only noted that a briefing on recovery from windshear was to be conducted.
The operator conducted yearly training that consisted of ground school, simulator training, and in-aircraft flight training. Included in the ground school training were ‘consider the load’ discussions, where if there was an emergency or performance concern, they could jettison the load to improve aircraft performance. Further, in-aircraft training was conducted where each PIC completed a ‘consider the load’ scenario, with a focus on jettisoning the retardant. Any applicable emergency or non-normal event could be used for this purpose, which at times included a simulated ‘down air’ (downdraft) scenario.
At interview, it was noted by at least one pilot that the air drop[60] scenario was quite different between the firefighting and military scenarios, and that standardisation for completing these operations occurred through the operator’s yearly training sessions.
On 10 July 2022, in response to the draft report, Coulson Aviation indicated that the response to a downdraft was consistent with the windshear escape manoeuvre for most large aircraft, with the added protection of being able to jettison the load to increase aircraft performance. In addition, the operator emphasised that the majority of their C-130 crews were current or former military pilots, where windshear recovery training was conducted on a bi‑annual basis. Therefore, the operator considered their pilots to be ‘extremely familiar’ with the procedure.
Wreckage and impact information
Accident site
The accident site was located on slightly sloping, partially wooded terrain, near Peak View, 50 km north-east of the Cooma-Snowy Mountains Airport. The wreckage trail (Figure 9) was approximately on a heading of 100°, with the initial impact at an elevation of about 3,440 ft AMSL. The debris trail began at the lower end of the slope, with the wreckage distributed linearly over about 180 m.
Figure 9: Accident site overview showing the wreckage trail
Source: ATSB
Wreckage examination
The ATSB’s on-site examination of the wreckage, damage to the surrounding vegetation, and ground markings, all indicated that the aircraft initially impacted a tree in a left wing down attitude of about 55°, before colliding with the ground. An intense post-impact fuel-fed fire destroyed the aircraft. The ATSB’s on-site examination also found (Figure 10):
no pre-existing airframe issues
all major sections of the aircraft’s structure were identified and there was no evidence of an in‑flight break-up or pre-impact structural damage[61]
the cockpit and associated avionics were identified about two-thirds of the way along the wreckage trail
the cockpit and forward section of the airframe had separated from the fuselage, was inverted, and had been destroyed in the impact and fire
sections of the wing skin, leading edge spar, wing tips and portions of the wings were identified along the wreckage trail, having fragmented during the impact sequence, and sustained further damage during the fire
all flight control surfaces were identified, however, flight control continuity could not be established due to the impact and fire
the vertical and horizontal stabilisers had remained attached to the aft section of the fuselage
the 4 engines and 16 propeller blades were located on-site and some of the propeller blades remained attached to the propeller hubs, while others had detached through impact forces
there were varying degrees of damage observed across the 4 engines, likely due to the impact sequence of each engine, with the damage indicating the engines were rotating at impact.
The RADS tank remained upright, with no fire retardant identified between the drop area and the initial impact location. However, a large amount of retardant was located in the wreckage near the tank. The system was badly damaged, with the doors fragmented throughout the wreckage, and its operational state could not be established.
Figure 10: Main aircraft wreckage components
Source: ATSB
Aircraft configuration
The aircraft was equipped with 4 trailing edge flaps. All flaps had separated from the aircraft during the impact sequence. On-site measurements of the flap screw jacks indicated the flaps were set at 50% at impact. This was consistent with the expected setting following a retardant drop. Due to the extent of damage, the elevator, aileron, and rudder trim settings could not be established.
Fuel testing
Fuel samples were retained from the 2 fuel tankers that last serviced the aircraft and from the refuelling storage tank at Richmond. The fuel samples were independently tested by a commercial fuel company for correct specifications, with nil abnormal indications found. In addition, there were no reports of fuel quality concerns with any other aircraft using the same fuel source.
Engine and propeller examinations
With the assistance of the Australian Army, the engines, partial remnants of the reduction gearboxes, and propeller assemblies and blades were transported to a secure hangar at Richmond Royal Australian Air Force (RAAF) Base for further examination. The engine manufacturer attended the inspections, where it was confirmed that all engines were rotating at impact, and there were no noted pre‑existing issues. As power changes were controlled by changes to the propeller blade pitch while maintaining a constant engine speed, the engine power levels were determined from the blade pitch angle at impact.
During the propeller hub assembly inspection, measurements of the internal components were recorded. The ATSB consulted the propeller manufacturer to determine the propeller blade angles at impact, and establish engine power levels. The propeller manufacturer concluded the following:
The calculations indicate that, based on the operating conditions estimated by the ATSB,[62] all the propellers were absorbing power from their respective engines and were producing positive thrust. The horsepower computed for each of the four engines are within the normal operating range for the T56 engine installed on this aircraft.
Recorded information
General information
The aircraft was not fitted with a flight data recorder, nor was it required to be by Australian or US regulations. However, there were devices on board that recorded information relevant to the flight path, as well as data that was transmitted in real time. Further, 2 firefighters located near the accident had videoed the aircraft. An analysis of these sources are presented below.
Witness video
Two firefighters were located on Feeney’s Road (800 m from the accident site), and both videoed the aircraft during the retardant drop. One video was taken in the landscape orientation and had a duration of 18 seconds. This video captured the drop and stopped as the aircraft was descending). The other video was taken in the portrait orientation and was 37 seconds in duration. It captured the aircraft descending into the drop zone and ended after the aircraft impacted with terrain. Collectively, the videos captured the aircraft from 10 seconds prior to the retardant drop, the drop, and the 5 seconds after the drop when the aircraft became obscured by smoke and was only intermittently visible (Figure 11). From the witness video, it was unclear if the aircraft flew behind the smoke, or entered the smoke. Seventeen seconds after the drop, the aircraft was seen at low-level, followed by the collision with terrain and post-impact fire.
The videos were analysed by the ATSB using commercial camera tracking software[63] to estimate the aircraft’s flight path and attitude. The RAAF Aircraft Research and Development Unit also analysed the video to evaluate the aircraft attitude. These analyses indicated that:
at 1315:15 (commencement of the drop), the aircraft was at a left bank angle of 10°, with a pitch of 0°
at 1315:17 (end of the drop), the aircraft was at a left bank of 17° and a pitch-up of 6°
at 1315:21, the aircraft reached its maximum left bank of 31°and maximum pitch-up of 12°
at 1315:22 and 1315:23, the aircraft was obscured by smoke and the attitude could not be determined
at 1315:25, the aircraft was at a left bank of 18° and a pitch-up of 8°
at 1315:26, the aircraft was at a left bank of 5° and a pitch-up of 6°
at 1315:27, the aircraft was at a right bank of 6° and pitch-up of 5°.
From 1315:27 the aircraft was obscured by smoke, and the attitude could not be determined using SynthEyes. The general attitude could be determined from basic photogrammetry at limited points from this time.
Figure 11: Aircraft attitude and approximate flight path at key times
Source: Google earth and SkyTrac data, annotated by the ATSB
For about 10 seconds after the completion of the drop, a positive rate of climb was achieved, with the aircraft climbing about 170 ft (to 3,770 ft AMSL) from the drop height. Following this, the aircraft was then observed descending. At 1315:34, the aircraft was seen at a very low height above the ground, in a slight left bank, immediately followed by a significant left roll just before ground impact. The elevation of the terrain, while undulating, also increased by about 40 ft from the drop site to the accident site.
The footage was also used to review aircraft control and configuration changes, such as flap positions and aileron movement. Shortly after the drop, the flap position was assessed as being 100%, consistent with the operator’s AFM supplement drop procedure. However, further assessments could not be made due to limitations with the video quality, visibility, and aircraft attitude. At various points in the video, both left and right aileron movement could be seen, but actual deflections could not be determined.
The videos also provided a general understanding of the low-level wind conditions at the time, with significant audible and visual movement of the surrounding trees and smoke, and blowing dust at ground level. It was also noted that there was no video evidence of any retardant being dropped between the initial drop location and the impact site.
Operational load monitoring system
Aerial firefighting contract requirements in the US required the aircraft be fitted with an operational load monitoring system (OLMS), predominantly for monitoring aircraft loading during operation. The OLMS was located behind the centre wing section in the fuselage and recorded data at a rate of 32 Hz (32 times per second). This recording device had no impact or fire protection, and was destroyed in the accident sequence.
Six months of historical data for B134 was made available to the ATSB, to allow for a comparison of the available accident flight data with previous flights. This review identified that the pitch and angle of bank data was not recorded correctly by the OLMS. Therefore, only the flap retraction timing and duration, and the vertical speed (rate of climb/descent) could be compared. While there was no comparable data available for flights with the entire accident crew, a review of the PIC’s recent flights and comparison with other crews indicated that the flap retraction was generally initiated between 2.5 and 5.5 seconds (with an average of 3 seconds) after the drop was completed. It also showed that the actual flap retraction from 100% to 50% flap took about 4-5 seconds and was completed, on average, about 7-8 seconds after the drop.
The rate of climb post‑drop varied between 500 ft/min and 2,400 ft/min, with the majority of the flights between 1,100‑1,500 ft/min. These variations were possibly related to weather patterns, terrain limitations, and the operational requirements, which were unique to each drop.
SkyTrac and automatic dependent surveillance broadcast (ADS-B) data
Aerial firefighting contracting requirements in Australia required the aircraft to be fitted with a tracking capability. The aircraft was fitted with SkyTrac, a system that could transmit the aircraft’s position in real-time, and was monitored by the NSW Rural Fire Service (RFS). The SkyTrac unit was recovered from the wreckage and transported to the ATSB’s technical facility for examination and download. The Canadian Transportation Safety Board assisted in the conversion of the downloaded data.[64] The SkyTrac unit recorded data at 5 second intervals.
Data broadcast by the automatic dependent surveillance broadcast (ADS-B) equipment fitted to the aircraft for air traffic control purposes was also obtained from various providers. This system determined the aircraft’s position using GPS and then broadcast this information, along with pressure altitude,[65] ground speed,[66] and other data, at regular intervals. ADS-B data was transmitted every 0.5 seconds, however, not all transmissions were available, with gaps of up to 5 seconds during the accident flight. Aside from the difference in recording intervals, the data provided for the common parameters across both sources was identical.[67] Table 2 shows the parameters recorded by SkyTrac and ADS-B.
Table 2: SkyTrac and ADS-B recorded parameters
SkyTrac
ADS-B
· time
· time
· latitude and longitude (position)
· latitude and longitude (position)
· ground speed
· ground speed
· track
· track
· GPS altitude (AMSL)
· pressure altitude
· vertical rate of climb/descent
Airspeed calculations
Using the ground speed from the SkyTrac and ADS-B data, and the weather observations from Peak View, the wind speeds of 15, 30 and 40 kt from the north-west were used to estimate the aircraft’s true airspeed.[68] These values were consistent with a review of the aircraft ground speed in the drop planning circuits. These circuits showed a periodic variation consistent with the aircraft flying into, and then with, the wind, and indicated that the wind speed was likely of a magnitude of 20-40 kt from a north‑westerly direction during their drop planning circuits.
The calculated true airspeed values were then converted to a computed calibrated airspeed (CAS)[69] using temperature and pressure data also from Peak View. The airspeed calibration charts in the operator’s C-130 AFM showed that there was a negligible difference between the CAS and indicated airspeed at the airspeed range being considered. Therefore, the CAS was equivalent to the indicated airspeed that would have been presented to the crew on the airspeed indicator.
The data showed a limited increase in the ground speed from 144 kt at the start of the drop, to 149 kt during the post-drop climb-out period, to a maximum of 151 kt just prior to the collision with terrain. However, the CAS (Figure 12) can be seen to be significantly lower, and with a much smaller increase during the climb. In the last 15 seconds of the available data, the calculated CAS was between 100 and 123 kt.
Vertical speed
From the SkyTrac data, a positive rate of climb was recorded for the 10 seconds following the drop, with the aircraft climbing to about 170 ft above the drop height, which was consistent with the witness video. The derived vertical speed,[70] while noting its limitations (as described above for the operational load monitoring system), increased from zero at the end of the drop to about 1,000 ft/min in the 8-10 seconds after the drop, then decreased to about 0 over the next 5 second period. At the last data point, the aircraft was descending at about 2,000 ft/min.
Aircraft track
From both SkyTrac and ADS-B data, the retardant drop was conducted on a track of about 190°. The aircraft was then turned through 160° as the climb rate peaked, with the last recorded track of 133°, about 3 seconds prior to impact.
The recorded ground speed, calculated CAS, track, derived vertical rate, and altitude for the last 30 seconds of flight is shown in Figure 12.
Figure 12: Recorded flight path data, derived airspeed, and rate of climb for the last 30 seconds of flight
Source: SkyTrac and Geoscience Australia digital elevation data, annotated by the ATSB
Low pressure spike
Prior to the drop, the ADS-B pressure altitude was, on average, about 250 ft above the SkyTrac GPS altitude (Figure 13), which was consistent with the QNH on the day. It was noted that there was a small increase in the ADS‑B pressure altitude immediately following the drop. This was consistent with the RADS tank doors closing on previous drops, but this returned to about a 250 ft difference with the GPS-based SkyTrac altitude.
However, at about 1315:24, the ADS-B pressure altitude and the vertical rate began to diverge significantly, with a low atmospheric pressure spike at about 1315:29. This was identified by an abrupt increase in both the pressure altitude[71] and barometric vertical speed. In comparison, the SkyTrac GPS-based derived vertical speed showed a smaller increase, which correlated with the SkyTrac altitude.
As there were several data points associated with this spike, this was considered more likely to be associated with a real event, rather than an erroneous reading. The abrupt rise and fall in these parameters suggested the aircraft encountered a region of low pressure, relative to the surrounding air, with a steep pressure altitude gradient during the climb‑out.
The reason for the localised pressure change could not be determined by the ATSB. Aircraft configuration changes (the RADS tank doors opening or closing, and flap changes) were excluded based on a review of the historical OLMS data. Several other potential factors were considered, including localised turbulence, wind gusts, terrain effects, temperature changes, and fire driven changes associated with smoke plumes. However, limitations in the available evidence prevented a determination.
Figure 13: Comparison of SkyTrac and ADS-B altitude and vertical rate data showing the low-pressure spike
Note: ADS-B pressure altitude shown as recorded references the international standard atmosphere QNH rather than actual QNH.
Source: ADS-B and SkyTrac, annotated by the ATSB
Cockpit voice recorder
The cockpit voice recorder (CVR) fitted to the aircraft was a solid-state memory Universal Avionics Model CVR-30B, part number 1603-02-03 (Figure 14). CVRs are designed on an endless loop principle, with the oldest audio continuously overwritten by the most recent audio. In this case, the CVR recorded crew and cockpit audio for a duration of at least 30 minutes. While the aircraft was not required to be fitted with a CVR under the US or Australian regulations, it was a contract requirement with the US Department of Agriculture, Forest Service (USFS).
Figure 14: N134CG cockpit voice recorder
Source: ATSB
The CVR was recovered from the aircraft and transported to the ATSB’s technical facility in Canberra on 25 January 2020 for examination and download. Thirty‑one minutes of audio data was successfully downloaded. However, the audio was from a previous flight when the aircraft was operating in the US. No audio from the accident flight was recorded on the CVR.
Inertia switch
The power supply to the CVR was fitted with an inertia switch. Inertia switches are designed to stop the recording function by removing power to the CVR when a pre-set deceleration force was detected. The recovered audio was of crew training flights undertaken on 7 May 2019 near Sacramento McClellan Airport, California. The audio included 4 landings conducted as part of that training. The recording ceased immediately after the fourth landing, and the post-landing taxi and engine shutdowns were not recorded. It was likely that the inertia switch was activated during this landing and consequently disconnected power to the CVR.
Pre-flight testing
Following installation in an aircraft, supplemental material related to the operation of the CVR must be attached to the approved AFM. The supplement for the accident aircraft indicated that the CVR conducted a self-test at power up, and the status of the system would be presented to the crew on the CVR control unit, located on the copilot side console. A CVR system check for crew was also included in the operator’s AFM supplement, but was not included in their pre-flight checklists. None of the operator’s C-130 flight crew interviewed were aware of the need to check this system status prior to flight.
CVR maintenance
A review of the aircraft’s maintenance logs indicated that the underwater locating beacon attached to the front of the CVR was replaced on 24 December 2019. This was a self-contained, replaceable unit, and a full maintenance service check was not required with this replacement. A maintenance check was conducted yearly, and had last been performed in February 2019.
Medical and pathological information
Pilot in command
The PIC held a first-class medical certificate that was issued on 5 September 2019 by the FAA, with a limitation to wear corrective lenses. The PIC’s aviation medical records were provided for the period 2013 to 2019. Overall, these examinations reported no significant medical conditions or abnormal physical findings. Of note, the PICs last electrocardiogram (ECG),[72] conducted as part of their annual medical examinations, showed indications of an inter-atrial conduction delay,[73] while previous ECGs noted sinus bradycardia.[74] Otherwise, the ECGs were considered normal and were ‘cleared’ by the FAA medical officer.
The PIC was reported to be fit and active, with no known medical conditions. On the morning of the accident flight, the PIC’s behaviour appeared normal and there was no evidence to indicate any concerns regarding their general health. While limited, the post‑mortem examination did not identify any pre‑existing medical conditions that could have contributed to the accident nor detect any commonly used drugs or alcohol. Due to limited blood samples, carbon monoxide testing could not be conducted.
Copilot
The copilot’s most recent first-class medical examination was issued on 17 July 2019 with no limitations. The copilot’s aviation medical records were provided for 2018 and 2019. The records reported no significant medical conditions or abnormal physical findings. The records noted that they were taking prescribed medication to lower blood cholesterol and reduce the risk of heart disease. The copilot’s last ECG noted several common anomalies,[75] but it was ‘cleared’ by the FAA medical officer.
The post-mortem examination identified narrowing and areas of calcification[76] in both the left anterior descending artery and right coronary artery of the heart. However, the muscle layer of the heart showed no identifiable scarring and there was no indication of an acute coronary artery occlusion (blockage). While no other evidence of significant natural disease was identified, the examination concluded that, the significance of the narrowing, in the absence of any evidence to indicate a blockage in the heart, was unclear. In addition, toxicology testing did not detect the presence of any alcohol, or common medications and illicit drugs. Carbon monoxide testing could not be conducted due to the lack of a suitable sample material.
Flight engineer
The flight engineer’s most recent second-class medical examination was issued on 27 August 2019 with no limitations. From their 2019 aviation medical records, there were no reported medical conditions or abnormal physical findings that could have affected aircraft operations. While limited, the post‑mortem examination did not identify any pre‑existing medical conditions that could have contributed to the accident. The toxicological analysis identified traces of a commonly used over-the-counter antihistamine. Carbon monoxide testing could not be conducted due to the lack of suitable sample material.
Aviation medical specialist
The ATSB engaged an aviation medical specialist to review the crew’s aviation medical records and post-mortem examinations. Noting the limited evidence that could be collected from the examinations due to the nature of the accident, the specialist concluded that:
As best as could be determined, there was no suggestion of in-flight incapacitation.
The copilot’s examination identified that 2 of the arteries in their heart showed evidence of narrowing and calcification, but there was no pathological evidence of acute coronary occlusion. The copilot had been taking prescribed medication to treat elevated cholesterol levels for several years. This medication was approved for use by flight crew in both the US and Australia. Further, the copilot’s blood pressure readings and last ECG tracing were all within normal limits.
The detection of the antihistamine and the reported concentration could not be used to determine with any certainty if the flight engineer was using the medication at the time of the accident or during non-flying periods. This was considered an ‘incidental’ finding.
While any exposure to carbon monoxide from the fires could not be determined in this case, limited research on a small cohort of ground fire-fighters many years earlier, determined that carboxyhaemoglobin[77] levels of around 6% were indicative of fire-ground exposures. This level, had it been present in the crew, was not likely to have caused in‑flight incapacitation.
Test and research
Reconstruction flight
On 24 January 2021, at about 1300, the operator reconstructed the flight path from the drop location to the accident site. The intention was to record the perspective and challenges of the terrain, while acknowledging the lack of bushfire smoke and environmental conditions. The flight was in a Cessna Citation 550 (business jet), with the Director of Flight Operations on board. They flew the path twice, firstly at 3,665 ft AMSL and then at 3,610 ft AMSL (noting the accident flight path was at about 3,600 ft AMSL). They noted that, as they turned toward the drop exit and were flying towards the accident site, they experienced an airspeed decay, even as engine power was increasing. While this was not considered ‘extreme’ on the day, it was ‘a bit surprising’. Further, they stated that the path flown by the crew of B134 from the drop to the accident site was into slightly rising terrain.
At the time of the flight, the METAR[78] for the Cooma-Snowy Mountains Airport recorded wind was 13 kt at 250°, with the direction varying between 200° and 290°. However, at 1143, a SPECI[79] recorded winds of 15 kt gusting to 29 kt at 260°, and the aerodrome forecast issued from 1200 indicated winds of 14 kt gusting to 25 kt at 270°.
C-130 simulator testing
Purpose
A series of tests were undertaken in a simulator representative of the accident aircraft, the RAAF C-130J-30 full flight mission simulator. The purpose of the testing was to determine if, and under what conditions, wind speeds representative of the strength and prevailing direction reported on the day of the accident could potentially affect aircraft performance. In particular, if the airspeed of the simulator could decay to the power‑on stall speed given the accident flight profile, of a climbing turn from 200 ft AGL. In addition, tests were also conducted to evaluate the effect following a weight reduction of 25,000 lbs (11,340 kg), from a jettison of the remaining fire retardant.
The testing was performed by RAAF Aircraft Research and Development Unit C-130 qualified test pilots (QTPs), supported by the simulator fidelity manager, under the direction of the ATSB. There were no recordings available of the accident crew’s actions. Therefore, the testing was limited to attempting to replicate the known flight path and aircraft attitude, with crew inputs (configuration and power setting changes) described as typical by the operator’s crew. The accident site and drop location were in the simulator database, which enabled a recreation of the accident flight profile from the start of the drop to be used for the tests. The intent was not to recreate the accident flight in full, or review the crew’s potential response to the situation, but focussed on the aircraft performance in the environmental conditions.
Aircraft differences
Access to a C-130H model simulator was limited, with none located in Australia and restrictions imposed by the COVID-19 pandemic. However, a C‑130J model simulator was offered to the ATSB. The C-130H (accident aircraft) and the C-130J were both listed on the same FAA Type Certificate. A discussion of the differences and limitations was held with the RAAF’s Aircraft Research and Development Unit chief of flight test, which considered the airframe, engines, aircraft controls, wings, aircraft systems and modelling limitations. The primary differences with respect to the aircraft were that the C-130J simulator had:
a longer airframe affecting some aircraft handling qualities
significant upgrades to the propulsion units
stall speeds likely to be slightly lower
aural and visual stall warnings, tactile stall warning (stick shaker) and stall avoidance (stick pusher) systems (not installed on the H model).
As control effectiveness was not being tested, the differences in aircraft handling qualities were of little impact to the proposed assessment. Similarly, an equivalent thrust level could be used to determine the necessary power settings, and limited to the available C-130H levels. To characterise the potential differences in stall speeds, a series of tests were completed, documented in the Results below. The stick shaker and stick pusher functions were both turned off during testing.
Simulator limitations
The ATSB also considered the limitations of the simulator, noting that they are designed for flight training, with the following being of most importance:
it had a pre-programmed stall characteristic of a 50° left wing drop
the stall was not considered to be well modelled
complex weather phenomena such as mountain waves and rotors could not be modelled
pre-programmed windshear models had a tailwind of 60 kt
wind gusts could be modelled, but the timing of the gusts could not be controlled.
As the test objectives were to characterise the flight profile with wind speeds that could reduce the airspeed to the stall speed, the pre‑programmed stall behaviour and modelling did not impose any limitations on the assessment. As the pre-programmed windshear model was in excess of the planned test conditions, the simulator fidelity manager developed a method to simulate windshear using the wind gradient tool. This resulted in the wind magnitude changing linearly, proportional to the altitude increase. This also required the test runs to commence in level flight at the drop height of 200 ft AGL, rather than from a descent profile to avoid a pre-drop windshear disrupting the climb-out test profile. A consequence of this methodology was that, on the occasions the simulator entered a pre-stall sink, it exited the windshear condition, which allowed it to recover airspeed and fly-away.
Test summary
The planned test criteria included constant winds of increasing strength, windshear of increasing strength, followed by the addition of turbulence[80] and gusts to each of these base conditions. Three thrust settings were calculated, based on the calculated true airspeeds (refer to section titled SkyTrac and automatic dependent surveillance broadcast (ADS-B) data) and propeller blade angles (refer to section titled Engine and propeller examinations) considered to provide reasonable boundary conditions.
Fourteen test profiles were developed, which included:
Three initial tests to establish the equivalent power settings, and comparison of the stall values against the C-130J and C130H flight manuals. It also included the development of the flight profile for the QTPs to practice using the pitch changes, bank angles and heading changes provided by the ATSB.
Eight profiles were planned for the QTPs to fly the accident profile under various wind conditions. These conditions included constant wind speed environments of varying strengths, windshear environments of varying strength, followed by the addition of turbulence and wind gust profiles.
Three profiles were developed to test the effect on the stall speed of a reduction of 25,000 lbs, simulating the emergency dump of the remaining fire retardant.
Multiple flight runs were then undertaken for each test profile by 2 QTPs.
Results
The RAAF simulator for the C-130J-30 demonstrated stall speeds comparable to those published for the C-130H at the approximate weight of the accident, 131,000 lb (59,420 kg), in the unaccelerated level flight condition. The power-off stall speeds were 98 kt (simulator) and 101 kt (C-130H), and power-on stall speeds were 82 kt (simulator) and 83 kt (C-130H).
The simulator provided useful insight into the potential for a significant loss of airspeed to occur when a combined maximum wind speed (mean wind plus gust) of 50 kt was used as the control variable. Although this was greater than the surface wind speed recorded at Peak View of 43 kt, it was consistent with the pilot reports from the smaller fire-control aircraft earlier on the day of the accident.
The key outcomes from the simulator testing were:
A constant strong (40 kt) north-westerly wind resulted in a small loss of airspeed during the climb-out, with minimum airspeeds of about 113 kt IAS, and a ground speed of about 160 kt. There were no aural stall warnings activated, the pilots reported no indications of any pre‑stall buffet or other warnings, and was a notably higher ground speeds than the accident flight.
A moderate (15 kt) north-westerly wind, combined with a 15 kt windshear, a 25 kt windshear and a 35 kt windshear during the climb-out resulted in an airspeed decay to between 98 kt and 104 kt, with intermittent aural stall warnings. The pilots also reported the controls were less responsive in the higher wind speed scenarios, indicative of approaching the stall.
A moderate (15 kt) north-westerly wind, with +10 kt gust and +25 kt windshear during climb‑out produced similar ground speeds to the accident flight. This consistently resulted in the airspeed decaying into the stall speed region between power-on (82 kt IAS) and power‑off (98 kt IAS) with repeated stall warnings. The minimum airspeed was in the range 84–98 kt IAS and the ground speed was in the range 141–151 kt.
When simulating an emergency dump of the remaining fire retardant, the rapid weight reduction, if made after the aural stall warning activation,[81] but prior to aerodynamic stall, reduced the stall speed. The simulator exited the stall warning/pre-buffet stall regime and improved the performance as expected.
Aerial firefighting in Australia
Overview
The National Aerial Firefighting Centre (NAFC) was formed by the Australian States and Territories in 2003 to provide a cooperative national arrangement for combating bushfires by facilitating the coordination and procurement of specialised firefighting aircraft.
The NAFC contracted aircraft on behalf of all the states and territories, with leasing arrangements allowing for aircraft to be moved around the country to address the prevailing bushfire risk. For each aircraft, a state or territory then assumed primary responsibility, and managed the operation and deployment of that aircraft.
As detailed in the National Aerial Firefighting Strategy 2021–26 (National Aerial Firefighting Centre, 2021), firefighters operate in an escalating risk environment frequently challenged by ‘changing fuel, vegetation and vulnerabilities’. At the same time, they strive to meet the community, government, and media expectations for protecting lives, properties, and the environment. This has resulted in:
…situations where aerial assets can provide effective support are increasing, and with them, community expectations. Meeting these expectations is a risk. Aerial firefighting has grown from ‘just another tool in the toolbox’ to a point where the community expect firefighting aircraft over every fire (especially ‘their’ fire).
Consequently, aerial firefighting has become a critical capability for the management and suppression of bushfires in Australia. To effectively achieve this, aircraft are flown at low altitudes and low airspeeds, often over inhospitable terrain with reduced visibility from smoke. This creates a high-risk environment, which ‘requires an enduring focus on training, compliance, and risk mitigation’ (National Aerial Firefighting Centre, 2021).
Operating environment and limitations
In 2020, although born out of the 2019-2020 bushfires, an inquiry into Australia’s national natural disaster coordination arrangements was conducted. The final report, Royal Commission into National Natural Disaster Arrangements, was published in October 2020. The report noted that the effectiveness of aerial firefighting was dependent on a number of factors including the distance and time to travel to the fire-ground, the type of aircraft used, pilot skill, weather conditions, fire‑fuel type, intensity and size of the fire, type of suppressant use, and the tactics employed to respond to the fire. Specifically, the report identified the following limitations:
Aircraft alone are not a solution to fighting bushfires. Interaction between aircraft and fire crews is necessary to bring a fire fully under control…
…poor weather conditions can limit and sometimes prevent the use of aircraft. For example, requirements for pilots to maintain visibility of terrain can limit the use of aircraft in severe conditions (eg low visibility in heavy smoke or cloud); and turbulence caused by strong winds and the terrain can make operating aircraft unsafe, especially at low altitude.
Poor weather conditions can also restrict the effectiveness and use of aerial firefighting. For example, during the 2019 SA [South Australian] Cudlee Creek and Kangaroo Island fires, weather conditions prevented all attempts by aircraft, including LATs, from containing the forward spread of the fires. Furthermore, extreme weather conditions experienced periodically throughout the 2019-2020 bushfire season meant there were a number of days when aerial firefighting could not be employed.
Activity
According to research conducted by the ATSB (2020), A safety analysis of aerial firefighting occurrences in Australia, the number of occurrences per financial year increased steadily between 2016–17 and the bushfire season 2019-20. However, data collected by the NAFC and presented in the Australian and New Zealand National Council for fire and emergency services’ (AFAC) 2019-20 annual report, estimated that aerial firefighting activity for the 2019-20 season was around 4 times higher than previous seasons. Given the increased activity, the rising trend in the number of occurrences could be expected and probably did not indicate a significant increase in the risk per flight.
In addition, the ATSB research report identified that half of all reported aerial firefighting occurrences and four fifths of more severe aerial firefighting occurrences were operational in nature, typically terrain collisions, with around one quarter of the more severe occurrences associated with aircraft control. Further, there were 2 fatal accidents between August 2018 and the report publication in May 2020, whereas the previous 17 years only had 3 fatal accidents.
While there have been various deployments and trials of larger aircraft over many years, the current LAT program including the use of C-130 aircraft was evaluated during the 2014-2015 bushfire season. Since commencing operations in Australia in 2015, these LATs have been operating between North America and Australia over alternate bushfire seasons.
On 1 June 2022, in response to the draft report, the RFS reported that the 2019-2020 bush fire season was unprecedented, which meant that a large contingent of aerial resources was required for firefighting, personnel and resource movement, and for surveillance and reconnaissance missions. The RFS acknowledged that aircraft were particularly valuable for fires in difficult terrain or fast-moving fires that were too dangerous for ground personnel to confront.
Over the season, there were 317 aircraft engaged in firefighting activities including 2 very large air tankers (VLATs)[82] and 4 LATs. Together, the LATs and VLATs completed a total of 1,708 missions and dropped more than 24 million litres of fire suppressant. This represented the largest contingent of VLAT and LAT used in Australia to date.
The RFS further noted:
The season also challenged assumptions about how agencies fight fires - techniques and strategies that worked in previous seasons often did not work as well in the 2019-20 season. The scale of the fires stretched the capacity of fire authorities with many ignitions started by lightning in remote and rugged terrain, quickly spreading to the point where suppression was extremely difficult.
For the 2019-2020 season, the RFS contracted one C-130 and one Boeing 737 from Coulson Aviation via a service agreement subject to the NAFC contract.
Coulson Aviation
General information
Coulson Aircrane Ltd. was a privately-owned company based in British Columbia, Canada. The company had been involved in aviation for over 36 years, operating both fixed-wing and rotary‑wing aircraft. The company's operations included helicopter logging, forest fire suppression, power-line construction, airliner passenger, transport, and other industrial heavy lift operations. Coulson Aviation (USA) Inc. was a subsidiary of Coulson Aircrane Ltd., and contracted rotary and fixed-wing aircraft to the US and Australia.
Coulson Aviation (Australia) PTY Ltd. was formed in 2010 to support Coulson Aircrane's long-term commitment in Australia. The company provided aircraft personnel for Coulson’s rotary and fixed‑wing aircraft operating under contract in Australia for the 2019-2020 bushfire season through the National Aerial Firefighting Centre (NAFC). At the time of the accident, they had a fixed‑wing fleet in Australia consisting of two C-130 aircraft and one Boeing 737 aircraft. They also provided crews for the NSW Rural Fire Service (RFS) Boeing 737, which had previously been purchased from Coulson Aviation in 2019. Following the Australian bushfire season, the aircraft and crews returned to North America for heavy maintenance and recurrent training prior to the US season.
B134 was contracted on an absolute availability requirement. This included standing charges, paid on an hourly availability, with additional charges for flight time (to account for fuel and other costs). Flight time charges were paid regardless of the fire retardant or suppressant being used.
Operating documents
Coulson Aviation maintained a suite of documents, which provided the necessary information for conducting operations in Australia and for operating the C-130 aircraft including N134CG. These were:
Company operations manual (COM): The COM contained the procedures, instructions and information required by CASA necessary to enable the operations personnel, including crews, to perform their duties safely and ensure the safe conduct of flight operations. The COM was for Australian operations only and applied to both fixed-wing and rotary-wing aircraft.
Airplane flight manual (AFM): Coulson Aviation, as the type certificate holder, developed their own C-130 AFM for FAA acceptance and approval. The manual was derived from the 1989 US Naval Air System Command document for the EC‑130Q. It detailed the recommended procedures for normal and emergency operations, operating limitations, aircraft systems and equipment, weight and balance, and the aircraft performance that should be achieved when operating in accordance with these procedures. The AFM was approved by the FAA in 2013 with a supplement for the RADS later approved in 2016, and a supplement for an avionics upgrade, which included the CVR installation, approved in 2018.
The FAA advised the ATSB that, for restricted category/military surplus aircraft, the original equipment manufacturer (in this case, Lockheed Martin) did not usually provide any support to the operator, or issue amendments or offer a subscription service, as would normally occur for transport category aircraft. Rather, the source for documents and manuals was normally the military service, although Lockheed Martin may have originally prepared the manuals for the military.
While the COM contained some procedures applicable to all aircraft operations, at least one of the operator’s C-130 PICs did not consider this manual as the reference document for operating the aircraft. Instead, they considered the AFM and checklists were the appropriate source.
Retardant drop procedures
The operator’s RADS AFM supplement outlined the operating limitations and configuration for the retardant drop procedure. This included 100% flap selection, the landing gear retracted, and airspeed lower and upper limits of 118 kt and 170 kt respectively.
At interview, the operator’s pilots reported the targeted parameters for the C-130 drop were 200 ft above ground level (AGL) and an indicated airspeed target of 120 kt. On completion of the drop, the climb-out procedure was for the PIC to increase power and request the copilot retract the flaps to the 50% position, while the flight engineer monitored and called the engine parameters (temperature and torque). The operator’s crews also reported that they typically targeted 150 kt during the climb-out, with an initial climb to at least 500 ft. The crews who had previously flown with the accident PIC, indicated there was about a 2-3 second period from the completion of the drop to the start of the flap retraction when flying with the PIC.
Where the retardant drop was conducted without a birddog or aerial supervision (refer to section title Aerial supervision), prior to conducting the drop, the LAT crew conduct a number of assessment circuits at various altitudes. These circuits were for drop planning purposes, and as outlined in the COM, would include identifying hazards, the retardant drop plan, entry and exit strategies, as well as a dry run at 500 ft AGL and 150 kt.
Safety management system
Coulson Aviation had introduced a safety management system (SMS) in 2013. At the time of the accident, it was not mandated under either the CASA[83] or FAA regulations, although it was required under the USFS contract. The International Civil Aviation Organization (ICAO, 2018) defined SMS as:
A systematic approach to managing safety, including the necessary organizational structures, accountability, responsibilities, policies and procedures.
It is designed to continuously improve safety performance through the identification of hazards, the collection and analysis of safety data and safety information, and the continuous assessment of safety risks. The SMS seeks to proactively mitigate safety risks before they result in aviation accidents and incidents.
An SMS comprised 4 components: safety policy and objectives, safety risk management, safety assurance, and safety promotion. The component of most relevance to this investigation was safety risk management, which included hazard identification, and safety risk assessment and mitigation.
From an Australian perspective, the NAFC indicated that an operator with an SMS would be highly regarded, but it was not compulsory. If an operator had an SMS, a requirement was included in their contract, to ensure the operator maintained the same safety standard throughout the contract period. The NAFC also indicated that they would not review or evaluate the SMS, with the expectation, if required for safety regulation purposes, that this would be undertaken by CASA. A review of CASA records found that, while surveillance had been conducted on the operator, these did not include an audit of the SMS, nor was it required as the system was not mandated.
The operator’s SMS manual outlined the company’s safety policy, processes, and procedures for implementing the SMS and safety management plan. It also included information regarding safety oversight, which included their safety reporting processes.
Safety risk management process
ICAO (2018) described the safety risk management process as:
… a key component of safety management and includes hazard identification, safety risk assessment, safety risk mitigation and risk acceptance. SRM [safety risk management] is a continuous activity because the aviation system is constantly changing, new hazards can be introduced, and some hazards and associated safety risks may change over time. In addition, the effectiveness of implemented safety risk mitigation strategies must be monitored to determine if further action is required.
The process allows validation of decisions, evaluation of the results, and provides an opportunity to assess the need for further risk mitigation. Where risks cannot be reasonably eliminated, risk management enables the tasking to be accomplished by controlling risks to acceptable levels.
The operator’s safety and risk management processes were detailed in the COM and were described as:
…safety management processes provide a structure for Coulson to exercise its appropriate duty of care to minimise the risks involved.
…provide a formal mechanism that are designed to capture all aspects of safety performance, conformance with approved procedures, continued improvement of procedures, regulatory compliance and operational risks that have the potential to adversely affect the operation.
Risk management is a structured approach to managing uncertainty related to a threat or hazard through a sequence of activities including risk assessments, strategies developed to manage the threat and mitigation of risk...
Hazard identification
According to ICAO (2018), a hazard can be considered as a dormant potential for harm, which is present in one form or another within the system or its environment. Therefore, hazard identification is the first step in the safety risk management process. The intention is to proactively identify hazards before they lead to accidents, incidents, or other safety‑related occurrences. Hazard identification may also consider hazards that are generated outside of the organisation and outside their direct control, such as weather (ICAO, 2018).
The COM stated that ‘Coulson acknowledges that a certain element of risk exists in all aspects of its business’ and that ‘the implementation of a comprehensive safety system can greatly assist in reducing risk’. As part of their fatigue risk management system, the COM outlined the potential hazards crews may encounter in all types of operations (Table 3).
Table 3: Some hazards identified in the Company Operations Manual
· Unfamiliarity or low experience with the type of operation
· Operations at low altitude
· Lack of experience in operating under specific operational conditions
· Operations in reduced visibility
· Lack of familiarity with, or low experience on, specific aircraft equipment
· Operations at high density altitude
· Operations in high wind or turbulent conditions, particularly if accompanied by high ambient temperatures
· Operations at high ambient temperatures
· Operations in areas of mountainous or hilly terrain
· Contact of flight crew with high-demand clients
In addition to the hazards identified above, the ATSB’s review of the COM found numerous references to other hazards. The fire-bombing procedures made references to factors such as prevailing winds (particularly with mountain flying), turbulence and downdrafts associated with either mountain or fire generated conditions, and visibility. Further, the training and checking, and standard operating procedures sections for fixed-wing aircraft also referred to windshear.
Hazards are detectable through many sources including reporting systems, inspections, audits, brainstorming sessions, and expert judgement. These sources are categorised as being either formal or informal methods and can be used to detect hazards at all levels of an organisation. The operator’s SMS used both informal and formal methods for hazard identification. This included a safety reporting system where all employees were encouraged to report issues, hazards and incidents that affected flight or ground safety. Further, the operator had a daily SMS conference call at the start of the day, which discussed the previous days operations, and the operations to be conducted that day. Present on the call were senior management, the safety manager, and the crew. They would discuss the current status of the crew and aircraft, any reported issues, and would often end with a relevant safety message or topical discussion. On 10 July 2022, in response to the draft report, the operator reported that this process allowed the group to tactically manage the risks in a dynamic environment providing an opportunity to discuss actual or emerging hazards and risks in an open and supportive environment.
Safety reporting system and daily SMS calls
The operator’s safety reports for the period 2019 and 2020[84] were provided to the ATSB. A review of these 32 reports found that around 60% were related to maintenance issues, while only 9% were operationally focused. These operational events included aircraft separation issues and retardant overload events. While previous years’ data was unavailable, the operator had conducted yearly SMS reviews, and these summaries were provided for the earlier period. Although the individual reports were not available, based on these summaries, it was likely the previous years’ safety reports followed a similar reporting pattern, with a majority being maintenance related.
During the investigation, several of the operator’s crew provided the ATSB with accounts of previous windshear encounters they had experienced:
In the previous firefighting season, while conducting structure protection, they encountered a windshear event, which resulted in an uncommanded bank angle of 80°. The crew recovered the situation by flying the planned exit into an area of lower terrain (valley).
In the season of the accident, while climbing out after completing a drop, the airspeed fluctuated ‘quite a bit’ (10 kt) and the aircraft sank slightly, while being ‘tossed around’. This was while working with the birddog. After this encounter, the decision was made not to return to the drop area.
On the day of the accident, the crew of B137 received a windshear warning and uncommanded bank angles up to 45° in the Adaminaby area.[85]
These encounters were not recorded in the operator’s safety reporting system, nor were any other weather-related incidents found in the reports provided to the ATSB. Neither the former[86] nor current safety manager recalled any such reports in the system. At interview, one pilot reported that the online SMS program was used for issues that were considered applicable across the company. Issues that could be resolved within the small group of fixed-wing pilots, or could be taken directly to the chief pilot, noting they spoke on a daily basis, would not necessarily be included in the system.
In addition, the ATSB reviewed the daily SMS call notes from 2018 to 2020. While limited in detail, the topics most frequently discussed were maintenance issues. In the days preceding the accident, the hot and severe weather conditions were noted. These were the only occasions where the weather conditions were noted in the calls. In response to the draft report, the operator advised that they considered the incident reporting numbers discussed above were mitigated by the daily SMS calls’ impact on flight risk awareness.
Risk assessment
A risk assessment is a process where sources of potential harm (hazards) and the chances of an adverse event happening due to the hazard were identified, analysed, and evaluated (CASA, 2021). This evaluation was expressed in terms of likelihood and consequence, and should highlight the risks to be considered before and while carrying out an operation.
Organisations should have multiple layers of controls or defences in place (CASA, 2014) to manage their identified hazards. Risk assessments should be carried out across all levels of an organisation and at different stages in the operation. These could consist of a formal, documented process or a continuous ongoing mental assessment carried out by a pilot, or a combination of both. Examples of a formal risk assessment may include an operational risk assessment conducted by the operator to consider and evaluate the risks associated with the type of work being undertaken, and pre-flight risk assessments, conducted by the PIC and associated with a specific tasking. An example of continuous processes could include in-flight tactical[87] risk assessments.[88]
The operator’s SMS manual stated that, if a risk assessment was required, the SMS manager would conduct and document the process by completing the risk management worksheet. The associated risk matrix categorised the risk as either acceptable, mitigable or unacceptable, although there was no guidance on how to categorise the risk. These risk assessments only applied to the safety reports and change management processes that were captured in the operator’s online SMS program. At interview, both the former and current safety managers indicated there was no formal risk assessments conducted on the identified operational hazards, such as those listed in the COM.
Prior to the accident, the operator had voluntarily initiated the International Standard for Business Aircraft Operations audit phase II,[89] which was conducted between December 2019 and March 2020. This audit identified significant growth since the stage 1 audit completed in 2017, and that the SMS had not fully matured to be as effective as it could be. Of note, it identified that the operator could not provide a process for assessing risk potential in terms of likelihood and severity.
After the safety risks have been assessed, the appropriate risk controls can be implemented. ICAO (2018) noted that:
It is important to involve the “end users” and subject matter experts in determining appropriate safety risk controls. Ensuring the right people are involved will maximize the practicality of safety risk chosen mitigations. A determination of any unintended consequences, particularly the introduction of new hazards, should be made prior to the implementation of any safety risk controls.
In response to the draft report, Coulson Aviation stated that aerial firefighting was conducted within an ‘unforgiving, dynamic, and complex operational and meteorological environment’. Consequently, they considered aerial firefighting lends itself to a more tactical approach to risk identification and mitigation.
Risk register
Safety risk management activities should be documented, including any assumptions underlying the probability and severity assessment, decisions made, and risk controls implemented (ICAO, 2018). A tool such as a risk register could be used to ensure identified hazards were tracked and mitigated as part of a formal risk management process of prioritisation, documentation, and assessment. The register could include the hazard, potential consequences, assessment of the associated risks, and any controls put in place to manage the risk. This not only allowed for ongoing tracking and monitoring of the identified hazards, but also (ICAO, 2018):
…becomes a historical source of organizational safety knowledge which can be used as reference when making safety decisions and for safety information exchange. This safety knowledge provides material for safety trend analyses and safety training and communication. It is also useful for internal audits to assess whether safety risk controls and actions have been implemented and are effective.
At the time of the accident, the operator did not maintain a risk register, or any alternate means to track the identified hazards and associated controls, as part of their SMS.
Assessing pre-flight risk
Flight risk assessment tool
Aerial firefighting activities, like other aerial work operations, are subject to elevated risks. A 2014 National Transportation Safety Board study of agricultural (aerial work) accidents in the US found the following:
…the mission priorities…present pilots with unique hazards, challenges and constraints, some of which cannot be completely eliminated. For example, pilots must manoeuvre their aircraft at very low altitude over terrain and must therefore accept an elevated risk of terrain and obstacle collisions, as well as having limited time to safely respond to an aircraft mechanical anomaly or recover from an inadvertent aerodynamic stall.
Risk management is a decision-making process by which pilots can systematically identify hazards, assess the degree of risk, and determine the best course of action. Effective risk management involves good decision-making that allows a pilot to identify personal attitudes that are hazardous to safe flying, apply behavioural modification techniques, recognize and cope with stress, and effectively use all resources. Risk management strategies can help pilots apply a systematic process that can help them resist pressures that can adversely affect their decision-making and performance and can help them mitigate other hazards that could adversely affect the safety of flight.
The study also concluded that risk management guidelines and best practices specific to agricultural aircraft operations were necessary tools to help operators and pilots mitigate the unique risks associated with their operations. In addition to the safety risk management processes discussed above, another such tool was a flight risk assessment tool (FRAT). In 2016, the FAA Safety Team released their FRAT with the introduction:
When implementing a Safety Management System (SMS), one of the most critical components to develop is a Flight Risk Assessment Tool (FRAT). Because every flight has some level of risk, it is critical that pilots are able to differentiate, in advance, between a low-risk flight and a high risk flight, and then establish a review process and develop risk mitigation strategies. A FRAT enables proactive hazard identification, is easy to use, and can visually depict risk. It is an invaluable tool in helping pilots make better go/no-go decisions and should be a part of every flight.
Every flight has hazards and some level of risk associated with it. It is critical that management and pilots are able to differentiate, in advance, between a low-risk flight and a high-risk flight using a risk assessment tool that allows pilots, managers and dispatchers to see the risk profile of a flight in its planning stages. When the risk for a flight exceeds the defined acceptable level, the flight will be further evaluated and risk decisions made by appropriate leadership.
The USFS (Forest Service Manual: Aviation Management Handbook) also recognised that risk management was a critical component of their SMS, and the identification of new hazards, determination of risk levels and effectiveness of mitigations ‘must be collaborated’ from the local level to aviation staff in their headquarters. Noting this, they discussed the different types of risk assessments, which included a ‘time critical risk assessment’:
Time critical risk assessment is the tool that pilots and managers use to assess actual risks specific to the day of flight. The product representing a time critical risk assessment is a Flight Risk Assessment Tool (FRAT)… While completing a FRAT, if an emerging hazard or higher than expected risk level is identified, the Aviation Manager (for example a helicopter manager, flight manager, project aviation manager, pilot in command), must follow up with the appropriate management level before a mission commences.
A FRAT was an efficient and structured process that allowed for a consistent and objective evaluation of flight risks, and could be adapted to manage the unique risks present for a specific operation or tasking. The tool established the risk profile for an individual flight and prompted the pilot or operator to take appropriate mitigation actions. It also allowed for better visibility by the operator, as to crew decisions made in accepting or rejecting tasks. However, it should be noted that a FRAT cannot anticipate all the hazards and corresponding risks that may emerge during a flight.
The FRAT could incorporate factors relating to the crew, such as operational experience and fatigue; environmental conditions, both at the airport and en route; aircraft factors, such as equipment serviceability; and any external pressures or factors, such as task rejection by another pilot or operator. Each of these factors was then assigned a numerical risk value and a total risk score was calculated. Based on this score, the risk profile was determined using predefined criteria for acceptable levels of risk, elevated levels of risk that required mitigation such as escalation to a more senior pilot, or task rejection.
The operator’s COM acknowledged the risks associated with their operations, stating ‘the combination of terrain, weather, fire occurrence patterns, and visibility can make firebombing extremely challenging’. The COM also required their rotary-wing pilots conducting firefighting activities using night vision goggles to complete a pre-flight risk assessment. However, the operator relied on the LAT crews to conduct their normal pre-flight planning and make their own assessment of the suitability of a tasking, without the need for a formal pre‑flight risk assessment. The former safety manager also confirmed that, while the LAT operation was considered high risk, there was no FRAT available for the crews.
Accident flight estimated risk profile
Following the change in safety managers in 2020, the operator introduced a FRAT into their LAT operations, with the criteria for an acceptable level of risk (score <30), a level of risk that required mitigation or escalation (30–39), and a ‘no-go’ level of risk (40+). Using this tool, the ATSB calculated a score within the range that required mitigation or escalation for the accident flight. However, the ATSB noted that the FRAT did not consider factors such as a weather‑related task rejection by another pilot, in this case, by the birddog pilot. Task rejection was a potential risk indicator for a FRAT, as explained in the US FAA advisory circular 135-14B for helicopter air ambulance operators:
Declined HAA [helicopter air ambulance] Flight Requests. The operator must establish a procedure for determining whether another HAA operator has declined the flight request under consideration and if so, for what reason (weather, maintenance, etc.). If applicable, the reason for the declined flight must be factored into the required risk assessment process, i.e., do not include a declined flight due to a maintenance issue or pilot not available. This could be as simple as asking the requestor whether or not this specific flight request has previously been made and declined and why.
Similarly, the Helicopter Association International’s FRAT tool included the risk factor of ‘Flight Turned Down By Other Operators Due to Weather’, which had the highest risk score of all the example factors.
Civil Aviation Safety Authority
When operating in Australia, Coulson Aviation aircraft were operated under a short-term air operator certificate authorisation issued by CASA, involving the use of foreign aircraft under relevant legislation and national aviation authorities. The certificate permitted aerial work including aerial spotting (fire and flood), dropping (water and fire retardant), and other activities such as search and rescue and surveillance.
As part of this process, CASA required Coulson to have a Company Operations Manual (COM) for Australian operations. CASA required Coulson Aviation to comply with their COM, which included reference to the FAA approved AFM. In these circumstances, CASA relies on the FAA approval process, and has no role in reviewing the AFM.
CASA had conducted 5 surveillance events in the past 5 years across 3 different short-term AOCs for this operator. All events were level 2[90] operational checks and no safety findings were raised. No CASA surveillance events were performed on Coulson during the 2019-2020 firefighting season. The short-term AOCs were not included in CASA’s national surveillance selection process, and therefore no level 1[91] surveillance activities were conducted.
New South Wales Rural Fire Service
General
The NSW Rural Fire Service (RFS) was the lead combat agency for bushfires in NSW. They worked closely with other agencies to respond to a range of emergencies including bush and grass fires, bushfire mitigation, structure fires, search and rescue, motor vehicle accidents, and storms that occurred within rural fire districts. The RFS was primarily made up of volunteers, with paid staff members managing day-to-day operations, Fire Control Centres (FCCs), and operational support, among other roles. There were many roles involved in the RFS emergency management response; for simplicity, only those roles applicable on the day of the accident are discussed below.
The multiagency state-wide response to large bushfire emergencies were overseen and coordinated by the State Operations Centre, located at NSW RFS Headquarters in Sydney Olympic Park (Sydney). The State Operations Centre provided a variety of specialised resources to the FCCs, including but not limited to, aviation resources. The state operations controller (SOC), located in the State Operations Centre, maintained an overall awareness of the firefighting effort across the state, and ensured resources were allocated as needed. The State Operations Centre also contained the state air desk (SAD), which was the state level multiagency team responsible for coordination of aircraft operations.
FCCs were the administrative and operational base of each rural fire district or zone. The coordination and management of local brigade responses to fires and other incidents was undertaken through the incident management team, led by the incident controller. For each emergency response, an incident controller was responsible for that response, including the objectives, operations, and application of resources. Where necessary, an aviation unit was established to manage and support deployment of aviation resources within the rural district, including an aviation radio operator (ARO).
The LATs were based at an airbase overseen by an airbase manager (ABM). The ABM was responsible for the supervision and coordination of airbase personnel and the layout and operation of the airbase. They operated as a liaison for the RFS SAD, and could be from another organisation.
Aircraft management procedures
The RFS maintained a suite of documents, which detailed the procedures for managing aerial firefighting. The 2 primary documents for air tanker operations were the NSW and ACT Aviation Standard Operating Procedures (operating procedures), which outlined the basic procedure of all air tanker operations, and the Operating guidelines for air tanker operations (operating guidelines), which provided further details specifically for the LAT program.[92] The preface to the operating procedures stated it was ‘produced to assist all members…in the safe, efficient, and effective management and use of aircraft for operational purposes’. This should be read in conjunction with other relevant documents, ‘which may contain more comprehensive information, specification and overarching operational and incident management procedures’. Additional procedures and forms were contained in the Operational management procedures and Incident management procedures.
While the RFS were responsible for coordinating aircraft and conducted training on various aviation aspects, they did not claim to be aviation experts. Therefore, it was possible that the frontline staff may have had a limited understanding of the operational capabilities and constraints for the varied aircraft used. The ATSB noted that there was limited information contained in any documentation provided to the frontline staff regarding the capabilities and constraints of each aircraft type within the LAT category. Where a LAT was requested by an incident management team, the asset was selected based on availability, location, and response time, rather than aircraft type. There was no distinction of capability between LAT aircraft types aside from information related to tank capacity, delivery system, and cruise capability. It did not contain any performance capability information related to operating conditions. However, the documents acknowledged that, ‘it is essential that all personnel seek specialist advice when planning or conducting air operations’. It also stated that ‘any agency members, contractors or air crew may decline to carry out tasks for which they are unfamiliar, unprepared or consider unsafe’.
On 1 June 2022, in response to the draft report, the RFS acknowledged that aerial ‘operations are risky, made more so as weather conditions deteriorated. However, when assessing tasking decisions, the RFS must balance this against the risk posed by fire to civilians and [ground] fire fighters… with the ability of aerial operations to achieve far greater gain’ than ground-based firefighting. Further, they considered that the tasking of large air tankers ‘may be sufficiently safe in circumstances that were not necessarily safe for other aircraft.’ They also indicated that ‘B134 had greater flight capability than other aircraft’ used by the RFS and was able to make a different assessment of risk. ‘Therefore, conditions that may have been unsafe for other aircraft, including B137, may not have been so for B134.’
Aerial supervision
The air attack supervisor (AAS) was a tactical command position, which ensured that aerial operations were consistent with the procedures and incident controller’s intent. This included maintaining communications with relevant incident management team personnel, and coordinating ground and air communications to achieve these objectives.
An incident AAS would be in an independent local aircraft overseeing the fire-ground, responsible for coordinating the aviation assets over an incident. They were responsible for coordinating the smaller aircraft and overall strategy, and in place when there were 3 or more aircraft operating on an incident. When LATs were involved, the incident AAS would normally communicate to another AAS onboard the birddog aircraft (LAT AAS).
A LAT AAS was located in the birddog aircraft, and coordinated the LAT movement with the incident AAS. Their role included briefing the LAT crew on the specific assignment, identify hazards, tactics and manage communications with the incident AAS. In practice, the LAT AAS established contact with the assigned LAT crews as they approached the relevant fire-ground to provide this information.
Requirements
When discussing aerial supervision for air tanker firefighting operations, the RFS operating procedures stated the following requirements:
Generally, Air Tanker Suppression operations, training flights and evaluation flights should not be undertaken without the supervision of an authorised AAS [air attack supervisor]. The AAS provides tactical aircraft coordination with the Incident AAS and/or IMT [incident management team] and directs the firebombing aircraft to critical areas of a fire for suppressant or retardant drops.
The only exception to the above may be in the event that an Air Tanker has an ‘initial’ attack’ certified crew on board who understand the mission requirements, Agency Air Tanker Procedures and there are operational advantages to the LAT commencing operations prior to an AAS arriving.
Operational advantages, while not defined or outlined in any documentation, were described at interview as including aspects such as the faster LAT transit times,[93] when a birddog was not available due to resourcing constraints, or a crew specific concern such as fatigue or exceeded duty times. There were no further requirements or considerations in either the operating procedures or guidelines regarding aerial supervision for LATs, or its use when an AAS was not available due to an operational safety concern. It was also noted that there was no policy, procedure or guidance identified in the provided documentation for tasking air tankers with initial attack certified crew in the case where a birddog pilot, and therefore the associated AAS, had rejected the tasking.
On 1 June 2022, in response to the draft report, the RFS advised that it was always their intention to send a birddog when possible. However, due to the constantly changing circumstances on the day, this was not possible to do. The decision to deploy the LATs without the birddog was based on an evaluation of the available information at the time and the unavailability of the birddog. In addition, the RFS stated that prohibiting LATs from operating if a birddog had not assessed the conditions, or if it was considered unsafe for smaller aircraft to operate would have severe impacts on firefighting operations across the state, and the resultant safety of people and property on the ground.
Initial attack certification recognition
The ATSB was unable to find a definition for the term ‘initial attack certified’ within the RFS documentation and sought clarification from the RFS. The RFS advised that it was their intention to recognise the initial attack certification endorsed by the US Forest Service (USFS). Broadly, this certification required a minimum flight time as a PIC in the specified aircraft type; a minimum flight time conducting low-level retardant drops; ground school training on relevant aspects such as hazard identification, ingress and egress strategies, and communications; and the satisfactory completion of 25 supervised drops.
In addition, the RFS advised that they did not maintain a register of initial attack certified pilots, and did not confirm the crew were initial attack certified when issuing the tasking. Rather, they relied on the individual aircraft operators for ensuring pilots held and maintained the necessary licences and certification. When the ATSB discussed the initial attack certification with Coulson Aviation, they also noted that this had not been defined by the RFS. Therefore, they utilised their own internal training framework to determine when a PIC was capable of operating without aerial supervision. One such example cited was the PIC of the Boeing 737 (B137) who had received the requisite internal training, but had not yet completed the required number of supervised drops to gain the USFS certification.
Tasking large air tankers
The operating procedures, and more so the operating guidelines, detailed the process for the tasking and mission management of air tankers. This included what aspects were to be considered when tasking an air tanker, the request and approval process, and dispatch. The ATSB noted that some functions during this process could be completed by multiple RFS positions. However, for simplicity, only those roles applicable on the day of the accident are discussed below.
Considerations and request
The operating procedures noted that air tankers could provide large volumes of suppressant, and careful planning and supervision was needed to ensure this was used effectively. The first step involved the incident controller (incident management team in the FCC) advising the intent to consider a tanker to the SAD, and outlining a strategy in conjunction with the SAD who could provide ‘guidance on availability and suitability’.
When considering tasking air tankers, the operating procedures stated the incident controller was to consider the following:
incident objectives
threats (life/property, assets, forests)
a proposed strategy
prevailing and/or forecast weather conditions
the likely period of deployment or loads [suppressant/retardant] required
the terrain and fuel (grass, urban, forest) type
possible risks and safety issues
time of day (last light considerations)
the mission alternatives.
A similar list of considerations was also included in the operating guidelines (for both air tanker and birddog taskings), with the addition of the elapsed time for the aircraft to arrive onsite. The operating guidelines stated that these considerations were a ‘risk assessment’. However, there was no further guidance on assessing each of these considerations.
Approval
The SAD would then brief the SOC. The SAD would provide advice on the availability, competing priorities, strategies, and load requirements for the LAT. The SOC then decided on the mission approval. Following that approval, the SAD would advise the LAT airbase manager (ABM) of the approval and mission objectives.
In this case, the Cooma incident controller did not request the tasking of the LATs. Rather, the decision to task a LAT was determined during the 1100 conference call discussing the fire situation at Adaminaby with senior personnel from the State Operations Centre (which included the RFS Commissioner and Deputy Commissioner). On that 3.5-minute conference call, while aware that the smaller fire-control aircraft were not flying due to the weather conditions, it was decided to send the LATs. They were unsure if a birddog had been launched to assess the conditions due to the known visibility and weather conditions, but determined that rather than wait for the birddog assessment, they could send a LAT ‘as it can bomb by itself if need be, if the opportunity presents’. The tasking decision was then communicated to the SAD, who then communicated the tasking for B137, B134, and the birddog from Richmond airbase to the Richmond ABM.
While the tasking on the day did not follow the RFS procedure outlined above, it was very likely that the LATs and birddog would have still been tasked if the above procedures had been followed.
Dispatch
The LAT ABM then conducted a pre-mission briefing with the crew, providing the required tasking details. The RFS operating guidelines indicated that these details would include, at a minimum, the latitude and longitude, a geographic location (referencing a map or chart), the incident air attack supervisor’s contact details, communication details for the incident controller radio channel and fire location’s common traffic advisory frequency, information on any aircraft working in the same location, and the type of load product.
Generally, the birddog with an aerial attack supervisor would arrive at the fire-ground ahead of the LATs. Given that the smaller birddog aircraft would generally fly slower than a LAT, it was common for the birddog to depart before the LATs. However, where there was an urgency to dispatch aircraft due to the rapid spread or the impending impact of the fire, and the crew were appropriately certified, it was standard practice to launch the LATs at the same time, or ahead of, tasking the associated birddog.
Re-tasking
Generally, re-tasking would be managed through the SAD in consultation with the incident management team and the LAT AAS, noting that the LAT crew would take on the AAS role when flying initial attack operations. On the day of the accident, the re‑tasking from the Adaminaby fire‑ground to the Good Good fire-ground was managed by the Cooma incident management team, who were in direct contact with the crew via the Cooma aviation radio operator (ARO). This re-tasking was considered within scope, as both fires were being managed by the Cooma team, and therefore, they could direct the crew as necessary at the local level.
Task rejections
The ATSB were provided with an example of a previous occasion where a task was stopped in‑flight, while operating in Australia. In that case, an aircraft had a number of warnings activated, and the crew elected not to continue. This decision was communicated among the other crews involved in the tasking, who were in continual contact with each other, and the task was subsequently stopped by the AAS.
For the tasking related to the accident, a task rejection had been made on the ground by the birddog pilot (due to weather-related safety concerns) and no communication had been established with other crews. The birddog pilot reported that they had not conveyed the decision to the crew of B134, but expected the RFS personnel would relay this information in their continued coordination of the tasking, or cancel the tasking.
A review of the available radio recordings provided by the RFS found no evidence to indicate that the birddog pilot’s rejection of the tasking had been communicated to the LAT crews (B134 and B137) by either the Richmond ABM or the SAD. In addition, the Cooma ARO, who could reasonably be expected to be in contact with the crews, reported that they were not aware of the birddog rejection. However, it was noted that not all radio communications were recorded.
At interview, mixed responses were received from pilots regarding their expectations on task rejections. All were consistent in that, there was a need to be informed of, and the reason for, the rejection decision, so this could be factored into their decision-making, in line with their company policies and procedures. Others stated that a weather-related rejection should result in cancellation of the tasking. The operator indicated that while a birddog can provide valuable risk mitigations, when the PIC is initial attack trained, they do not consider it to be a requirement. However, for a tasking without the birddog, the reason for this would need to be factored into the PIC’s pre-flight planning.
In addition, the birddog pilot had also reported that, after making the decision to reject the tasking based on the weather conditions, an air attack supervisor had advised them that the smaller fire‑control aircraft had earlier ceased operations due the wind conditions. The birddog pilot further stated that this information was generally not passed on to the pilots by the RFS.
The ATSB reviewed the available RFS documentation and procedures. No policy or procedure was in place to support the ABM or SAD’s management and communication of a task rejection by any of the crews operating in the tasking area that day or involved in the task.
In response to the draft report, the RFS stated they were of the view that ultimate responsibility for assessing risk, and accepting or rejecting a task, was the responsibility of the PIC. For the RFS to make such assessments on behalf of the PIC would constitute a shift in RFS responsibility.
United States firefighting practices
For comparison, the ATSB reviewed the aerial firefighting practices currently in place in the US. This was particularly relevant as many of the LAT operators worked in both the US and Australia, and the NSW RFS reviewed the practices from the US Department of Agriculture, Forest Service (USFS) when implementing their current LAT program.
Task rejections
The USFS placed a significant focus on managing risk exposure. They outlined their safety expectations in a statement of intent, placing emphasis on implementing:
…strategies and tactics that commit responders only to operations where and when they can be successful…[and that] understanding and acceptance that intense fire behaviour may mean we can’t protect values at risk under all circumstances…this direction also requires greater focus on identification of unnecessary exposure.
These expectations were then supported in the USFS Forest Service Manual – Aviation Management Handbook, which included the following statement:
Pilots and aviation users are expected to make sound decisions, including cancelling a flight, when conditions or circumstances may cause undue risk…
Forest Service employees perform challenging work in very high-risk and dynamic environments that are not always predictable. This responsibility can only be realized through participation of every employee. Safety is the first priority, and leadership at all levels must foster a culture that encourages employees to communicate unsafe conditions, policies, or acts that could lead to accidents without fear of reprisal...
The USFS 2019 Standards for Airtanker Operations detailed the processes and procedures to be followed by staff, supervisors, specialists, and managers when planning, administering and conducting airtanker operations. When discussing aviation safety, one aspect considered was task rejections or a ‘turn down’. Notably, the document stated:
Every individual (government and contracted employees) has the right and obligation to report safety problems affecting his or her safety and has the right to contribute ideas to correct the hazard. In return, supervisors are expected to give these concerns and ideas serious consideration. When an individual feels an assignment is unsafe, he or she also has the obligation to identify, to the degree possible, safe alternatives for completing that assignment. Turning down an assignment is one possible outcome of managing risk.
A “turn down” is a situation where an individual has determined he or she cannot undertake an assignment as given and is unable to negotiate an alternative solution. The turn down of an assignment must be based on assessment of risks and the ability of the individual or organization to control or mitigate those risks. Individuals may turn down an assignment because of safety reasons…
The standards further indicated that those individuals who turned down a task were to directly advise their supervisor. That supervisor would then communicate this information to others associated with the management of fire control activities. In addition, when a tasking had been turned down and the supervisor then asked another individual (resource) to perform the task:
…he or she [the supervisor] is responsible to inform the new resource that the assignment had been turned down and the reasons why. Furthermore, personnel need to realize that a “turn down” does not stop the completion of the assigned operation. The “turn down” protocol is an integral element that improves the effective management of risk, for it provides timely identification of hazards within the chain of command, raises risk awareness for both leaders and subordinates, and promotes accountability.
Proper handling of turn downs provides accountability for decisions and initiates communication of safety concerns within the incident organization.
Task rejections, including those related to weather, was also recognised within the Alaskan USFS Forest Service Handbook – Flight Operations Handbook: 33.1 - Forest Service Flight Operations, as follows:
If a flight is cancelled or refused by one operator or pilot because of weather or other operating conditions, the flight will be postponed until the weather improves. Forest Service employees shall not “shop” for an operator that will make the trip when another operator has refused.
Aerial supervision
The USFS Standards for Airtanker Operations outlined the circumstances and minimum supervision required based on the following situations:
number of aircraft assigned to an incident
drops conducted in high traffic areas
low light conditions
use of the modular airborne firefighting system or very large air tankers
airtanker flight crews not initial attack carded
combination of different types of aircraft operating simultaneously
use of foreign aircraft
periods of marginal weather, poor visibility or turbulence
night operations
if requested by the airtanker, birddog or others involved.
It also noted that initial attack certified pilots were authorised to drop retardant without the supervision of a birddog and/or AAS. However, the standard stated that:
Aerial supervision resources must be launched together with the airtanker on the initial order to maximize safety, effectiveness, and efficiency of incident operations. Incidents with 3 or more aircraft over/assigned will have aerial supervision over/assigned the incident.
Likewise, The US National Wildfire Coordinating Group[94] document,
, stated that ‘a safe aviation operation depends on accurate risk assessment and informed decision making’. It further indicated that, often, incident response flights were conducted under adverse flight conditions, and this complexity dictated the level of supervision required to conduct aerial operations safely and effectively. While noting factors similar to those listed above, it outlined:
There is no way to define an exact trigger point for adjusting, downsizing, or completely suspending aviation operations. The factors listed below [similar to those listed above] should be evaluated to determine whether additional Aerial Supervision resources are needed, or tactical/logistical missions need to be modified/suspended.
The standard further stated that, in some cases, the aerial supervisor would be required to shut down or suspend operations. In this case, ‘air operations must not proceed until risk mitigations are in place’.
, stated that a FRAT was required for every flight conducted for the USFS. They also recommended that a FRAT sheet be used when planning a mission and that this should be updated as necessary. The tool, provided as an appendix to the standards, contained the following note:
Because the overall cumulative score is a composite of individual flight, environmental, and operational values, it may not fully emphasize a heightened level of risk that may be associated with an individual category. For example, extremely adverse weather in itself, exclusive of the other categories, may alone merit the suspension of operations. Conditions also change over time and distance, therefore, this tool should be used periodically throughout a mission as conditions change to assure that individual or overall risks have not measurably increased.
Lessons learnt from aerial campaign management
In response to 3 accidents involving helicopters undertaking locust control operations in 2004, the ATSB commenced a research investigation (B2004/0337) into the practices used by Government organisations to contract aerial operators. While focused on locust control, the report findings were also applicable to fire control, other pest management, and emergency service operations. Collectively referred to as ‘aerial campaigns’, these types of operations were generally conducted in relatively hazardous environments that also had the potential to be high-risk environments characterised by:
a significant community need for the operation, possibly urgent
requiring the coordination of significant numbers of resources and organisations
a degree of irregularity or unpredictability as to when the operation will be required and the size the operation
requiring aerial operations with a relatively high hazard level
a regularly changing operational environment throughout the course of the campaign.
The report identified that organisations that contracted aerial operators were directly involved in the management of significant parts of the aerial campaign, such as assigning tasks and briefing pilots. Therefore, decisions made in the management process had the capacity to influence the level of risk of the operations. If safety was to be maintained, that capacity had to be monitored and managed: leaving responsibility for safety to another party that was not managing the overall campaign would not be effective.
In addition, the organisational complexity of aerial campaigns and the subsequent coordination effort required may lead to a diffusion of responsibility among the parties involved. This complexity was further increased when staff from different organisations were working together towards a joint outcome.
The report concluded that, while the aerial component of the operation was provided by an aerial contractor, the campaign control organisation was in a central position to understand the big picture. The adoption of good systems for managing risk by the contracting organisation could provide an effective additional layer of defences over and above that provided by each operator to protect against an incident or accident. An effective overall management system could ensure that no one aspect of the operation compromised another aspect.
Similar occurrences
This accident was the first occurrence of a collision with terrain involving a LAT in Australia. However, the ATSB identified another C-130H firefighting weather‑related accident, and a windshear encounter during firefighting operations in the US where the retardant was not jettisoned. A summary of these reports is provided below.
US Air Force Aircraft Accident Investigation Board investigation
On 1 July 2012, the crew of a US Air Force Lockheed Martin C-130H aircraft was conducting wildland firefighting operations near Edgemont, South Dakota, US. While following a lead aircraft (birddog) and positioning for a fire-retardant drop, both aircraft encountered a microburst.
The pilot of the lead aircraft conducted a ‘show me’ run,[95] and shortly after, the crew of the C-130 established a 0.5 NM (1 km) trail formation for the first drop. About 7 minutes later, while setting up for the second drop, the C-130 was in about a 1 NM (1.9 km) trail formation when the lead aircraft hit a ‘bad sinker’, resulting in a loss of altitude and airspeed. The lead aircraft came within 10 ft of the ground, and the pilot called ‘I got to go around’. One second later, the C-130 crew also elected to go-around, and 16 seconds after, they called ‘E-dump, E-dump’. Despite completing an emergency dump of the remaining retardant, the C-130 collided with terrain shortly after, fatally injuring 4 crew and seriously injuring 2 crew.
The investigation found that an inadequate assessment of the operational conditions resulted in the aircraft impacting the ground after flying into a microburst. In addition, it was established that there was a failure to communicate critical operational information from the lead aircraft and air attack crew to the C-130 crew, and there was conflicting guidance concerning thunderstorm avoidance.
The USFS and Department of the Interior maintained an aviation safety reporting system as part of its safety program and published a yearly safety summary. On average, it was noted there were about 8 weather-related events reported in the database yearly, with an incident of significance to this investigation described below.
On 17 June 2017, the flight crew of a British Aerospace BAe-146 aircraft were conducting firefighting operations in northern New Mexico, US. The pilot reported that, during a fire-retardant drop, they experienced significant ‘down air’, which resulted in them coming close to terrain. While slowing the aircraft through 130 kt when about 500 ft above the planned drop height, ‘the bottom fell out’ resulting in a loss of about 10 kt airspeed and 300 ft altitude. The pilot applied engine power and manoeuvred the aircraft toward lower terrain, but they did not achieve the expected climb performance and passed just above the tree line. The pilot indicated that the event took less than 10 seconds, and while they should have jettisoned the load in hindsight, they did not consider this at the time as they were focused on flying the escape manoeuvre.
About midday on 23 January 2020, a Lockheed Martin C-130 aircraft, call sign ‘Bomber 134’ (B134), departed the Richmond Royal Australian Air Force Base, New South Wales (NSW) on a firefighting tasking to Adaminaby. On arrival at Adaminaby, the crew determined that the conditions were unsuitable for a fire-retardant drop and were subsequently re-tasked to the Good Good fire near Peak View. Shortly after conducting a partial drop, and while in a left turn, the aircraft stopped climbing. The pitch attitude reduced, followed by a slight right wing down attitude. Shortly after, the aircraft was observed left wing down at low-level before colliding with terrain. The 3 crew were fatally injured and the aircraft was destroyed.
The extent of the impact damage and post‑impact fire meant the ATSB was unable to verify the operation of every aircraft system. However, there were no known defects that would have affected the aircraft’s serviceability, with the only item noted relating to the propeller anti-icing system on engine number 2, with rectification deferred in accordance with the minimum equipment list. There was no evidence of pre-impact structural damage, and detailed examination showed all engines were operational and producing power at the time of impact.
The ATSB established that the crew were appropriately qualified to perform the flight and there was no evidence of fatigue. While the post-mortem examination identified abnormalities with the copilot’s heart, there was no pathological evidence of scarring or a blockage suggesting a pre‑existing heart condition. Although elevated blood cholesterol levels increase the risk of coronary heart disease, the copilot had been appropriately treated for several years prior to the accident, and their blood pressure readings and last electrocardiogram were all within normal limits. In addition, ATSB research into pilot incapacitation occurrences (AR-2015-096) emphasised that multi-pilot operations provide a safety net if one crew member becomes incapacitated and that such events had a minimal effect on flight. Therefore, noting the medical information above and that the copilot was not the pilot flying, it was considered very unlikely that they had experienced a heart‑related condition that contributed to the accident.
This analysis will examine the environmental conditions and how this influenced the aircraft’s degraded performance and subsequent stall. The tasking process, management of task rejections, and the crew’s awareness of such on the day will also be discussed. It will also consider the risk management of large air tankers, the use of a flight risk assessment tool, and the aerial supervision and initial attack certification requirements in place. Further, the impact of limited recorded flight data and cockpit voice recordings, along with the benefits of on-board windshear systems will also be discussed.
Hazardous weather conditions
The Bureau of Meteorology graphical area forecasts for the area of operation contained strong winds, mountain wave activity and severe turbulence, which extended from Richmond to the Adaminaby and Good Good (at Peak View) fire‑grounds. The Cooma-Snowy Mountains Airport (50 km from the accident site) aerodrome forecast also indicated gusting winds nearing 50 kt and reduced visibility from blowing dust. These forecasts were consistent with the Peak View weather station recordings, witness reports, and video of the actual conditions. The ATSB’s analysis of the aircraft’s ground speed from the automatic dependent surveillance broadcast (ADS-B) data also showed that the wind speed was likely of a magnitude of 20-40 kt from a north‑westerly direction during their drop planning circuits at Peak View.
Overall, the Bureau of Meteorology concluded that the actual conditions in the accident area were consistent with the forecasts. This was reinforced by the pilot reports in the morning, which resulted in the smaller fire-control aircraft ceasing operations due to winds of about 50 kt. In addition, the pilot in command (PIC) of the Boeing 737 (B137) reported similar winds and experiencing a windshear warning and uncommanded roll when at Adaminaby. Of note, the birddog pilot had rejected the tasking to Adaminaby as the forecast conditions were worse than what they had experienced 2 weeks prior, where they were subjected to moderate to severe turbulence and downdrafts.
At Peak View, the crew had followed their procedures and conducted a number of circuits over the drop location, which was on the eastern side of a ridgeline. As the crew had elected to conduct the drop, this would indicate that they had assessed the meteorological conditions during these circuits as suitable to continue. However, the lowest circuit height of 500 ft may not have been low enough for the crew to accurately assess the conditions at the drop height and identify any localised terrain or fire effects.
The low-pressure spike recorded in the ADS-B data potentially indicated the aircraft had been subjected to localised weather effects, but due to limited information the reason for this could not be conclusively determined. The drop was located on the lee side of a ridgeline, an area prone to turbulence and potential development of mountain waves. However, while mountain waves were confirmed by the Bureau of Meteorology analysis to be present across the Snowy Mountains region at the time of the accident, the severity of this could not be ascertained from the available information. In addition, the drop was in an area noted by local glider pilots to be subject to turbulence and rotor conditions.
Strong winds and mountain waves are considered hazardous conditions due to their ability to generate strong downdrafts that may adversely affect an aircraft’s climb performance. They may also create windshear, which is of particular significance when it results in an increased tailwind component, with a subsequent reduction in airspeed. At the same time, moderate to severe turbulence would increase the stall speed.
In addition, the presence of a large fire will produce smoke and heat plumes, and potentially fire‑driven winds, that is likely to exacerbate the forecast conditions. The Blue Mountains fire case study suggested the possibility of fires drawing strong winds down closer to the surface than might otherwise be forecast.
Therefore, the environmental conditions in the accident area were conducive to windshear and downdraft development at a time when the aircraft was most vulnerable, with low airspeed and low height.
Tasking continuation by the Rural Fire Service
In the 1100 conference call between the Cooma incident controller and several senior personnel from the State Operations Centre, they discussed the severe fire weather conditions and escalating fire threat at Adaminaby. They also acknowledged that the smaller fire-control aircraft (which included the incident air attack supervisor), had stopped operations due to strong winds, with pilots reports of winds up to 52 kt and limited visibility. In that same conference call, a senior NSW Rural Fire Service (RFS) officer indicated that they should send B137 rather than wait for a birddog assessment. That is, they elected to send the LATs as initial attack to determine if they could work the fire-ground, rather than wait for an assessment prior to re-starting aerial operations. Following this, the State Operations Centre tasked 2 large air tankers (LATs), and subsequently the birddog, from Richmond to Adaminaby knowing the conditions were marginal, and that the LATs would arrive prior to the birddog.
During the initial crew tasking, the Richmond airbase manager (ABM) had mentioned the wind conditions to the crew of B137 and advised them to ‘take care’. Similarly, subsequent calls made between the ABM and the state air desk (SAD) at 1137 and 1209 discussed the adverse environmental conditions and that the birddog pilot was questioning the suitability of the weather. When the birddog pilot rejected the tasking, based on operational safety concerns, there was an expectation from them and the operator’s pilots that the tasking for the LATs would be cancelled, or at least reconsidered. This was consistent with the normal practice for a ‘turn down’ in the United States (US), and the need for aerial supervision in marginal weather conditions as outlined in the US Department of Agriculture, Forest Service (USFS) Standards for Airtanker Operations and Forest Service Handbook. However, despite an awareness of the hazardous environmental conditions, the earlier withdrawal of the smaller fire-control aircraft and the birddog pilot rejection, the tasking was continued, and this information was not relayed to either B137 or B134 crews.
Subsequently, following the drop at Adaminaby, the PIC of B137 reportedly advised the RFS Cooma aviation radio operator to cancel all aircraft operating in the area and indicated to the ABM (at about 1232) that they would not be returning due to the weather. While the crew of B134 had already been tasked and were en route to Adaminaby, this was another opportunity for the RFS to reassess the suitability of the tasking. In addition, the RFS, having received information that further operations in the Adaminaby area were unsuitable for LAT operations, did not communicate this information to the Cooma aviation radio operator or B134. In response to the ATSB draft report, the RFS noted that, while the State Operations Controller was aware of these rejections, they elected to allow B134 to continue, for further intelligence gathering purposes.
It was recognised that RFS personnel may have a limited understanding of aviation operations and therefore, there was a reliance on aircraft operators and crew to manage safety. However, in this case, the crew were not provided with a full awareness of the situation, with no knowledge of the birddog pilot rejection or that the smaller fire‑control aircraft were no longer flying. In addition, while B134 had been in contact with B137 and received advice on the conditions, this was unknown to the RFS at the time.
While some RFS personnel considered it unlikely that the LATs would be able to achieve the planned objectives due to the weather conditions, they continued with the tasking, relying on the crews to independently assess the conditions and cancel the tasking while airborne. As highlighted in the ATSB’s research into aerial campaign management, leaving the responsibility of safety to another party (the operator and crew in this instance) who are not managing the overall campaign is not effective. When there is a high-level decision to proceed with a tasking despite known elevated risk factors, providing information on those risks would allow crews and operators to make more informed decisions.
Crew awareness of task rejection
As discussed above, the smaller fire-control aircraft had ceased operations in the area earlier that day, which had been acknowledged by the RFS personnel from the State Operations Centre in the 1100 conference call. Also, the birddog pilot had rejected the tasking to Adaminaby, unaware that the smaller aircraft had stopped flying at that time. The birddog pilot indicated that it was not routine to talk to the other pilots about taskings. Therefore, they did not communicate with the crew of B134 that they had declined the tasking, but expected the RFS personnel would relay this information.
In addition, there was no indication in the available radio calls or at interview that the cessation of operations earlier that day or the birddog pilot task rejection was communicated to the crew of B134 by any RFS personnel. It was noted that this information was not required to be passed on in any of the tasking or dispatch procedures. While not directly communicated to the crew, there was the potential that they may have been monitoring the radio call between the SAD and the Richmond ABM at 1209, shortly after they had departed. However, there was no clear statement of the rejection in that call, rather, they only discussed the birddog pilot’s uncertainty about the weather conditions.
Therefore, while known to RFS personnel, it was very unlikely that the crew of B134 were aware that the birddog pilot had rejected the tasking, or that the smaller fire‑control aircraft were no longer operating in the area, due to the hazardous environmental conditions. While this was only one risk factor among others that would be considered by the crew, having this information would have allowed them to make a more informed decision about the weather conditions and task acceptance.
Nevertheless, as the tasking to Adaminaby for B134 had been provided prior to the assignment of the birddog, it was likely the crew expected to be departing as initial attack. In which case, even if they were aware of this information, it was possible that they may have still departed to self‑assess the conditions, particularly given the fire-ground was at least 45 minutes away. However, as this was an individual judgement, it could not be established how this information alone would have influenced their decision on the day.
Task acceptance by the crew
The weather forecasts applicable at the time of the flight contained mountain wave activity and severe turbulence, which extended from Richmond to both the Adaminaby and Good Good fire‑grounds. While the crew’s access to weather information on the day could not be determined, the usual practice of filing a flight plan through the operator’s electronic flight bag provided access to the required forecasts. They had also attended the morning RFS briefing with the Richmond ABM in which the weather conditions across the state were discussed. In addition, the PIC was one of the recipients of the ABM’s text message for the weather alert for Richmond in the morning prior to the tasking.
Although the PIC of B137 was made aware by the ABM at the time of the initial tasking that there no other aircraft operating at Adaminaby, they were not aware of the reason for this. Therefore, it was plausible that the crew of B134 were also not aware of this information and were not able to factor in the actual conditions to their decision when accepting the initial tasking to Adaminaby. Further, as discussed above, they were very likely unaware of the birddog pilot’s rejection of the task. Irrespective, it was reasonable to conclude that the crew of B134 were at least aware of the forecast conditions for the area of operation before departing Richmond.
While both the operator’s and manufacturer’s documents stated that flight was prohibited in known severe turbulence, this did not prevent crews from departing when severe turbulence was forecast. The only weather-related operational limitations were associated with thunderstorm activity. Therefore, it was considered normal practice to accept a tasking in these forecast conditions. Most of the operator’s LAT pilots interviewed indicated a preference to depart and assess the actual conditions to determine if they could find a workable solution rather than rely solely on a forecast, which could cover a large area and time frame, and may not necessarily reflect the actual conditions at the fire‑ground.
When B134 was en route to Adaminaby, the PIC of B137 (returning to Richmond) discussed the actual conditions with the PIC of B134, and advised they were not returning. Although B134 continued to Adaminaby, the crew discontinued the task once there as they experienced similar conditions. Despite this, knowing the decision made by the PIC of B137 and the forecast conditions for the area, the crew of B134 accepted the alternate tasking to the nearby Good Good fire‑ground, consistent with company practice. Circuits were conducted at Good Good, as per the standard retardant drop planning, to identify the asset for protection and the suitability for a drop. While the details of the assessment were unknown, the crew elected to continue with the retardant drop. Ultimately, the decisions to accept the initial and alternate tasking, and proceed with the retardant drop by the crew exposed the aircraft to a situation where it experienced degraded performance following the drop.
Degraded aircraft climb performance
Witness video, ADS-B and SkyTrac data showed that, following the completion of the drop, the aircraft climbed about 170 ft over a period of about 10 seconds, which was comparable to previous climb rates from the operational load management system. It was reported by the operator’s pilots that, at this stage of the flight, they would be targeting an airspeed increase from the drop at 120 kt indicated airspeed (IAS) to 150 kt IAS, while climbing from the drop height of 200 ft to at least 500 ft above ground level. However, during this period, the ATSB calculated a calibrated airspeed (CAS) range of between 100 and 123 kt (comparable to the IAS), which indicated the airspeed likely stagnated or reduced over this period.
Following this initial 10 seconds, the climb ceased, and altitude appeared to be maintained for about 3 seconds before the aircraft began to sink with an estimated descent rate increasing to 2,000 ft/min. The CAS also continued to stagnate after the initial 10 seconds. The reduction in vertical speed and estimated airspeed stagnation occurred at the time it would be expected that the engine power would be increasing. This increase in power would either translate to an increased height (while maintaining IAS) or maintained altitude (with an increase in IAS). Of note, the ATSB had established that there were no indications of mechanical or technical failures with the aircraft.
After the drop, the aircraft was turned from a predominant crosswind to a predominant tailwind, based on the recorded mean wind direction. This would have resulted in an initial slight decrease in the IAS. At the same time, as previously established, there were strong gusting winds, turbulence, and mountain wave activity present at the time of the accident, and these conditions were conducive to windshear.
If there was an additional increase in this tailwind component from windshear, this would have resulted in a further reduction of the airspeed. There would also be a corresponding decrease in pitch attitude and rate of climb, with a subsequent loss in altitude, as highlighted in the Lockheed Martin C-130 Airplane Flight Manual (AFM), and by the Bureau of Meteorology (2014) and Bowles (1990). These descriptions were consistent with the ATSB’s analysis of the recorded information. The witness video showed that the maximum pitch-up angle occurred 4 seconds after the completion of the drop and from this point it decreased. Likewise, the aircraft initially had a rate of climb up to 1,000 ft/min, but this also decreased, and the aircraft descended.
For comparison, the simulator testing showed that a strong constant mean wind during the climb‑out resulted in a small loss of IAS, but a significantly higher ground speed than was seen in the accident sequence. However, scenarios that used a moderate (15 kt) mean wind with gusts and windshear between 15 kt and 35 kt (similar to the total wind speeds recorded on the day), produced similar ground speeds to the recorded accident data. They also consistently resulted in the IAS decaying into the stall speed region, with minimum speeds between 84 kt and 98 kt.
In addition, observations made on the reconstruction flight noted an airspeed decay when they turned and were flying toward the accident site, even though the engine power was increasing. This was consistent with the glider pilot comments that there could be localised effects in this area due to the terrain. On the day of the accident, while the reason could not be determined, the ADS‑B data recorded a low‑pressure spike, which also had the potential to result in decreased aircraft performance.
The intensity of the environmental conditions (including mountain wave activity, strong gusting winds and turbulence) and therefore the windshear, could not be determined. However, the ATSB’s analysis of the available recorded data showed that the aircraft’s performance had degraded during the climb-out, consistent with encountering windshear, while concurrently turning into an increased tailwind, based on the mean wind direction. This was supported by the C‑130 simulator testing. With the limitations of the available recordings, and the absence of a cockpit voice recorder, it could not be determined if the crew had identified the conditions or initiated a recovery procedure. As cautioned in the Lockheed Martin AFM, severe windshear could exceed aircraft performance capability.
Stall at low altitude
About 10 seconds after the completion of the drop, the aircraft had climbed to about 330 ft above ground level but then ceased climbing, and the altitude was maintained for a few seconds. Although the aircraft was in a nose-up attitude, the aircraft was sinking and developed a high sink rate up to 2,000 ft/min. This was followed by a significant left roll just prior to impact. This was consistent with the stall characteristics as outlined in the C-130 discussion paper (Mizell 2009), where the approach to the stall in this configuration exhibited high descent rates, before the left wing stalled resulting in a large angle of bank excursion.
The ATSB calculated the power-on stall speed, with 50% flap and at the post-drop weight, as 83 kt. Consideration was also given to the potential effect of turbulence, which increased the stall speed to between 101-117 kt for moderate turbulence and 117-143 kt for severe turbulence. Noting that the ATSB derived CAS for the accident flight was between 100 and 123 kt in the last 10 seconds of the available data, this presented a significant overlap with the calculated stall speeds. It was also noted that, in the simulator test scenario that was most consistent with the accident flight, the IAS consistently decayed into the stall speed region with repeated stall warnings activated.
In the absence of the cockpit audio recording, it was unknown if the PIC, as the pilot flying, had initiated a response to the stall. Despite this, in consideration of the observed high sink rate followed by a significant left-wing roll, and the overlap in the stall speed and CAS, it was likely that the aircraft aerodynamically stalled at a height that was insufficient to recover before colliding with terrain.
Coulson Aviation risk management of large air tankers
While there was no regulatory requirement at the time of the accident, Coulson Aviation had implemented a safety management system (SMS), it was a contract requirement in the US, and which was viewed favourably by the National Aerial Firefighting Centre. However, as the system was not mandated, it was not assessed by the Civil Aviation Safety Authority or the Federal Aviation Administration. The ATSB acknowledges that any operator’s SMS will evolve and mature with time. However, significant events like accidents need to be used to explore whether their SMS is operating in a way that can assure the highest level of safety given the nature of their operations.
Acknowledging the element of risk associated with firefighting operations, the ATSB reviewed the safety risk management component of the SMS. Although the operator’s SMS manual outlined that the online SMS program would record the identified hazards, this was limited to submitted incident reports, and did not contain previously identified hazards. Although, the Company Operations Manual had detailed several operational hazards, the current and previous safety managers indicated that no risk assessments for the identified hazards associated with the LAT operations had been conducted. However, it was noted that risk assessments were included in the SMS manual, but these only applied to safety reports and change management contained within the online SMS program. While some of these hazards may have been discussed during the daily SMS conference call, this process was not formalised.
Without formal operational risk assessments of the recognised hazards applicable to the LAT operation, there was no identified risk mitigation strategies nor was there any assurance that the risks were at an acceptable level. For example, windshear and downdrafts had been recognised as a potential hazard in the Company Operations Manual. However, as no formal assessment for the C-130 aircraft had been conducted, there was no opportunity to formally identify and assess potential risk mitigators, such as those discussed by Hallowell and Cho (2010).
As noted by ICAO (2018), safety risk management activities such as operational risk assessments should be documented. Both the current and previous safety managers indicated that the operator did not have a risk register as part of their SMS, or an alternative process, at the time of the accident. This limited their ability to track, monitor, and mitigate the identified hazards, and assess the effectiveness of any risk controls.
Another important element of safety risk management was the use of reporting systems for hazard identification. The ATSB’s review of the operator’s safety reporting system found that there were few reports related to flight operations, and there were no reports of weather-related incidents. This was despite several of the crews interviewed having recalled encountering windshear during firefighting operations, which affected the aircraft. Given the operator’s draft report response comments that they considered the incident reporting numbers were mitigated by the daily SMS calls, it was likely they relied on this informal process for flight risk awareness, rather than incident reporting. Although the weather conditions were mentioned in the days prior to the accident, there was minimal detail of the discussions recorded in the daily SMS conference calls. Therefore, as there was limited information on operational issues recorded in the SMS, there was limited ability to conduct risk assessments of any identified hazards, to gain an understanding of their potential impacts on operations and mitigate the associated risks, or to perform any safety trend analysis.
As established above, aerial firefighting operations were subjected to elevated risks. Therefore, the supporting risk management practices should consider risk assessments at all levels of the organisation and all stages of the operation. Acknowledging that the risks cannot be entirely eliminated, an operational risk assessment would have provided an opportunity to identify the need to establish acceptable risk levels associated with firefighting taskings. While elevated risks were individually identified, there was no clear process for pilots to review or assess all the factors collectively and consistently. Instead, the operator’s risk management process relied predominately on crews conducting their individual, undocumented risk assessments for each task as part of their normal pre-flight planning and tactical assessment during flight. In particular, there was no identification of the need for a risk-based decision‑making framework to support pilot decision‑making when accepting potentially high-risk taskings.
The operator’s voluntary audit had identified significant growth in the company since the initial audit 2 years earlier, but it also noted that the SMS had not yet fully matured. While it was recognised there was no requirement for Coulson Aviation to have an SMS in Australia, the ATSB identified that there was very limited oversight of the identified hazards. Without operational risk assessments for the LAT operations or a method to monitor identified hazards, associated risk assessments, or risk mitigation, this limited Coulson Aviation’s ability to manage the risks related to their LAT operation.
Pre-flight risk assessment tool
As noted by the US National Transportation Safety Board, effective risk management involves good decision-making. These skills are important in most work domains but are especially critical in high-risk settings when individuals may be functioning under time pressure and stress, such as firefighting operations.
The LAT operation was a 15-minute notice standby tasking arrangement, which could send the aircraft to any location within the bounds of the tasking authority. The retardant drop task was a response to a possibly urgent threat that involved low-level, low-speed operations in a potentially hazardous and challenging environment. This made it a comparatively high-risk activity, in addition to which pilots were also responding to an external tasking agency, a potential source of external pressure.
At the start of each day, the RFS conducted a briefing for the LAT and birddog crews, which provided an overview of the weather, likely areas of operation, and fire conditions. However, on receiving a tasking, crews were still required to conduct their own flight planning specific to the area of operation, in a timely manner, to determine what was an acceptable level of risk.
The only consideration provided at interview as no-go criteria by the Coulson Aviation crews was a thunderstorm. Consequently, there could be several flight planning factors, which individually were not a no-go criterion, but collectively elevated the risk to higher-than-normal for the LAT operation. There could also be additional external factors, such as task rejections or cancellations by other pilots, which could elevate the risk if they were known to the LAT crew.
While acknowledging that LAT operations had inherent risks, Coulson Aviation had not introduced a pre-flight risk assessment tool for their LATs. Instead, there was a reliance on the PIC to assess the acceptability of the task based on their assessment of the conditions. However, this process may not have necessarily detected the cumulative effect of several indicators of elevated risk.
On the day of the accident, there were multiple pre-flight risk indicators, which included:
forecast strong winds, severe turbulence, and mountain waves in the area of operation
operating in mountainous terrain
the Richmond Airport weather warning sent to the LAT crews by the ABM prior to the Adaminaby tasking
the cessation of the smaller fire-control aircraft due to the actual weather conditions in the Snowy Mountains
the birddog pilot’s rejection of the task following assessment of the forecast weather conditions for the area compared with a previous experience
the copilot and flight engineer were in their first firefighting season
potential pressure to respond to the bush-fire risk to the town of Adaminaby.
While it could not be determined if all factors were known to the crew of B134, or their assessment of each factor, none of the above risk indicators were likely to be individually sufficient for the PIC to reject the task. However, when assessed collectively against pre-defined criteria, they would have produced an elevated score, as identified in the ATSB’s estimate of the accident flight risk profile using the operators recently introduced pre-flight risk assessment tool. However, it was noted that this tool did not include weather-related task rejections, considered one of the highest risk indicators for helicopter operations by the Helicopter Association International.
While there was no regulatory requirement at the time, the use of a pre-flight risk assessment tool was a contract requirement with the USFS. A 2014 NTSB study of aerial work accidents outlined that risk management guidelines and best practices specific to aerial work aircraft operations included a pre-flight risk assessment tool. These help operators and pilots mitigate the unique risks associated with their operations, in particular, when the operation is often conducted in high‑risk circumstances. As emphasised by both the US Federal Aviation Administration (FAA) and USFS, every flight has some level of risk. Therefore, it is critical that crews can differentiate between a low-risk and high‑risk flight during the planning stage to establish the overall risk profile. Risk management strategies, such as a pre-flight risk assessment tool, can assist pilots with applying a systematic process that helps them resist pressures that can adversely affect their decision-making and identify risks that could affect the safety of the flight.
In this case, the availability of such a tool would have assisted the PIC with making a more informed go/no-go decision for the initial tasking to Adaminaby. This almost certainly would have resulted in the PIC identifying the elevated risk associated with the tasking, and having to consider implementing risk mitigations, or escalation of the decision-making, if not rejection of the task. In addition, the PIC was reported to be conservative, therefore, the knowledge of the cessation of aerial operations due to strong winds and limited visibility and followed by subsequent weather‑related rejections due to safety concerns, would have likely increased the risk above an acceptable level.
Rural Fire Service aerial supervision requirements
Although it was acknowledged that the RFS was not an aviation operator, they were responsible for tasking a variety of aerial assets, with substantially different operating capabilities, often in high pressure situations in challenging environmental conditions. It could be foreseen that there will be community expectations that the RFS respond to fire threats, and use all available aerial assets to achieve the planned objectives. Accordingly, the tasking agency needs to define the acceptable level of risk for the overall operation, to provide an effective additional layer of defence above that provided by the aircraft operator. Such systems and policies have been implemented in firefighting operations in the US.
Operationally, the tasking-related risk assessment noted in the RFS Aviation Standard Operating Procedures (operating procedures), predominantly focused on the use of the aircraft to manage the fire threat rather than ensuring the safe use of those aircraft. The RFS had identified considerations to ensure the effective use of LATs, and acknowledged that certain task environments had higher risks. However, there was no guidance provided to frontline RFS personnel on how to assess these risks as part of the tasking process, such as those noted by the USFS and the US National Wildfire Coordinating Group.
For example, the RFS tasking considerations included weather as a potential threat, but there was no further guidance around how to assess the environmental conditions, or under what circumstances taskings should be considered acceptable or not acceptable. For the tasking to Adaminaby, it was noted in the 1100 conference call and various logs that the weather conditions were hazardous and that no aircraft were flying in the area due to the wind and visibility conditions. Despite this, there was an expectation that the LATs had greater flight capabilities and the pilots could make their own assessment of the conditions. Therefore, the decision was to send the LATs, and see if an opportunity presented itself that allowed for their assistance.
However, if the RFS had implemented policies and supporting procedures applicable to minimum aerial supervision requirements, similar to those in place in the US, this would have provided guidance to the front-line staff to assist with tasking decision making. For example, the USFS documents outlined the requirement for aerial supervision in marginal weather, including limited visibility and turbulence, and further, where the aerial supervisor suspended operations, they must not proceed with further taskings until risk mitigations are in place. If such policies were in place, it was likely that RFS personnel would have identified the higher risk environment, and therefore the need for aerial supervision on this tasking. In turn, this would have likely identified that an initial attack deployment was not suitable in the elevated risk environment.
The operating procedures indicated that aerial supervision was generally required for LAT firefighting operations unless the crew were initial attack certified and there were operational advantages to commencing operations prior to aerial supervision arriving. Those advantages included considering the speed differential between a birddog and LAT, or when a birddog was not available due to resourcing constraints, such as diversion to another tasking. However, there was no differentiation between the use of an initial attack deployment where aerial supervision was not available, in comparison to the rejection or cessation of a tasking due to safety concerns.
While the initial deployment of B137 ahead of the birddog could reasonably be accepted as meeting an operational advantage, the departure of the smaller fire-control aircraft and subsequent rejection of the birddog should have resulted in reconsidering the use of ‘initial attack’. However, there was no supporting procedure or guidance on the use of ‘initial attack’ deployment in these elevated risk circumstances, such as when the task was rejected by the birddog due to safety concerns. In the case of the accident, this rejection occurred shortly prior to B134 departing Richmond, and there would have been sufficient opportunity to reassess the task, and potentially redirect the LAT elsewhere, prior to their arrival overhead Adaminaby.
Policies and procedures on aerial supervision should include consideration of the known factors that elevate risk associated with aerial firefighting tasks, and would ensure the RFS have minimum aerial supervision requirements in place for each tasking circumstance. It would also include policies and procedures for the deployment of LATs without aerial supervision (initial attack), and in what circumstances this would be acceptable. In order to make acceptable risk‑based tasking decisions, these considerations need to be enshrined in policies and procedures, to assist with time-critical decisions during the fire season by frontline staff. The RFS personnel would have to assess that the tasking meets the minimum aerial supervision requirements prior to approaching operators with taskings, to ensure the taskings can be conducted within their defined, accepted risk levels.
Rural Fire Service management of task rejections
The ATSB’s 2004 research into aerial campaign management stated that organisations that contracted aerial operations (such as the RFS) were directly involved in the management of significant parts of the aerial campaign and were in a central position to understand the big picture. Decisions made during this process had the capacity to influence the level of risk of the operations.
It could be reasonably expected that there will be situations in which tasks are declined for safety reasons. While the RFS Aviation Standard Operating Procedures and the Operating Guidelines for Air Tanker Operations outlined some initial considerations regarding the tasking of LATs, there was no further policies or procedures following the initial tasking process to support the ongoing task. Consequently, there was no process in place to support RFS frontline personnel on managing a task rejection by crews or operators.
These policies and procedures would detail when task rejections should be considered as a risk indicator, such as when flights were declined due to weather-related safety concerns. For comparison with the USFS Standards for Airtanker Operations, this may also include communication of this information to other crews, reassessment of the tasking, incorporation of appropriate mitigations, or cancellation of the task. They should also encourage pilots and operators to communicate unsafe conditions without fear of reprisal.
On the day of the accident, neither the Richmond ABM nor the SAD communicated to either of the LAT crews or the birddog pilot tasked to Adaminaby, information regarding the smaller fire-control aircraft ceasing operations due to unsuitable weather. Nor did they communicate the task rejection by the birddog pilot to the crew of B134 shortly prior to take-off from Richmond (noting this occurred about the time B137 was overhead Adaminaby). The LAT AAS (who would have been on board the birddog) also did not communicate this to the LAT crews, as their communication role did not commence due to the birddog aircraft not departing. In addition, this rejection was not communicated by RFS personnel to the Cooma Fire Control Centre aviation radio operator, who could reasonably be expected to be in contact with the LAT crew as they were operating as initial attack, and they were the appropriate local ground contact to coordinate the task. While acknowledging the LAT’s, birddogs, and the smaller fire‑control aircraft have different capabilities and performance limitations, this was relevant information (specifically, reported strong winds and limited visibility, and the rejection based on safety concerns) that could reasonably have been communicated to the crews. As previously discussed, there was an expectation from the birddog pilot and the operator’s pilots that the RFS would either relay this information to them so it could be included in their decision-making processes, or the task would be cancelled by the RFS.
The subsequent rejection of further tasking by B137 as the conditions were worsening and reportedly unsuitable for LAT operations, was also not communicated by either the ABM or SAD to the crew of B134 nor to the Cooma incident management team. In addition, shortly after this rejection, the ABM and SAD discussed sending an alternative LAT to Adaminaby. None of these rejections resulted in a reassessment or cancellation of the tasking for B134 to Adaminaby. Rather, the RFS allowed B134 to proceed with the intention of gathering additional intelligence to assist in determining whether further aerial operations would proceed. Subsequently, the Cooma aviation radio operator was also unaware of this rejection of further tasking by B137, or their assessment of the conditions when providing the secondary tasking to the B134 crew.
As outlined above, while some crews were initial attack certified and could operate without aerial supervision, the RFS operating procedures indicated that this was only to occur when there were operational advantages prior to an air attack supervisor (AAS) arriving. However, the operating procedures did not reference any circumstances, such as in the case of the accident flight, where a tasking had been rejected due to safety concerns, such as unsuitable weather. While initial attack crews were trained to conduct operations without the AAS, continuing a tasking where the local AAS had departed or grounded due to weather concerns, and/or the birddog pilot (and therefore LAT AAS) rejected the tasking, appeared outside of the intended scope of ‘initial attack’ deployments.
As the task rejections were on the basis of weather or fire-ground safety concerns, which equally applied to B134, appropriate policies and procedures regarding task rejection should have resulted in the initial tasking to Adaminaby being cancelled following the rejections. There were 2 opportunities for this. The first was at the time of the birddog rejection when B134 was departing Richmond, which, at the very least (noting the RFS understanding of differing capabilities between the birddog and the LATs) should have resulted in communication of that information to allow the LAT pilots to make their own more informed risk assessment. The second was when B134 was transiting over the Canberra region and the RFS received advice from B137 which indicated that it was not suitable for LAT operations. Task cancellation would have also been consistent with the RFS intended use of initial attack and the general operating principles in the US.
While the RFS was not an aviation organisation or directly responsible for flight safety, they were closely involved in the aerial operation, being responsible for determining the task objectives and selecting the aircraft category for the task. Policies and associated procedures for task rejections would provide RFS personnel with the required steps to effectively and safely manage taskings, and provide guidance for decision-making. It would allow for consideration of a rejection by other crews, resulting in clear communication from RFS personnel of crew rejection decisions both internally, and to all aircraft on the tasking, and additional risk treatments being implemented up to task cancellation. A policy would also provide all RFS personnel with an objective mechanism to cancel taskings on the basis of safety.
Retardant load not jettisoned
Although the aircraft was obscured by smoke at various points, the witness video showed no further retardant dispersal after the initial drop, nor was any found between the drop area and the accident location. At the site, the operational state of the retardant aerial delivery system could not be determined due to the damage sustained, but a large amount of retardant was found in the wreckage near the tank.
However, as there was only about 10 seconds between the climb performance degrading and the likely stall, there was limited time available for the crew to identify and respond to the situation. Past research shows pilot recognition time of windshear can be expected to be about 5 seconds, and the emergency dump function would take a further 2 seconds. However, in the absence of the cockpit audio recording, it could not be determined if the crew had considered or called for an emergency dump of the remaining load. Therefore, for reasons undetermined, the remaining 11,340 kg of retardant was not jettisoned during the accident sequence.
The ATSB established that jettisoning the remaining load would have lowered the stall speed and optimised the aircraft’s climb performance. This was also confirmed from the simulator testing. Nonetheless, it was not possible to determine if jettisoning the remaining load, taking into account the time available, and typical recognition and response times, would have prevented the collision with terrain. The outcome of the US Air Force C-130 accident, where the crew did jettison the load, is an example of when this action may not be sufficient to avoid a collision with terrain.
Windshear recovery procedure and training
It is acknowledged throughout the aerial firefighting industry that they operate in a challenging environment with elevated risk conditions. Windshear was a known phenomenon, which could be exacerbated by fire-associated winds that may be difficult to forecast and could be influenced by local terrain effects. Most of the operator’s crews interviewed reported encountering a windshear event during firefighting operations. The FAA study published in 2010 identified 3 categories of windshear mitigators: ground-based alerting systems, pilot training, and airborne detection systems.
Large air tanker firefighting operations were generally conducted away from airports often over inhospitable terrain. Therefore, it would be unlikely the ground-based systems, or weather-based monitoring from airports would be available for windshear alerting during a retardant drop.
The Lockheed Martin C-130 AFM had been updated prior to 2010 to include a section on adverse environmental conditions, which included a windshear recovery procedure. Although the FAA had approved the Coulson Aviation C-130 AFM in 2013, the operator had used an earlier version (1989) of a military document to develop the manual. This was consistent with comments provided by the FAA to the ATSB, where the documents and manuals for military surplus aircraft would normally be sourced from the military rather than the manufacturer. Therefore, the windshear recovery procedure was not included in the Coulson Aviation C-130 AFM.
While both the departures and standard operating procedures sections of the Company Operations Manual provided basic windshear recovery guidance for the C-130, it was not presented as an emergency procedure, nor did it consider any specific requirements for firefighting activities, such as the potential jettison capability offered by the retardant aerial delivery system. In addition, while this manual was applicable to all aircraft types, it was specifically developed for Australian operations only, although the company operated internationally. At least one of the operator’s C-130 pilots stated that they did not consider this manual to be the reference document for operating the aircraft, rather, the AFM and checklists were the appropriate source. This was consistent with the purpose of an AFM, which was to provide the procedures for operating the aircraft.
Although the PIC of B134 had completed an in-flight training scenario in 2019 that incorporated a simulated downdraft, the training generally focussed on responding to an emergency on the drop run, rather than specific to windshear. While a windshear encounter could be simulated airborne in the aircraft, it was not possible to replicate the effect on aircraft performance. Therefore, this would not provide pilots with the performance instrument indications that would be typically experienced. However, the operator provided their C-130 pilots with annual simulator training. While it was noted that a briefing on windshear recovery was incorporated into the training syllabus, there was no requirement to conduct a simulator-based low-level windshear recovery scenario as part of initial or recurrent training. This could provide crews with the experience needed to recognise the symptoms of windshear and practice a recovery procedure.
The operator also noted that most of their crews were former or current military pilots and would have received windshear training on a bi-annual basis when serving members. However, for those pilots no longer in the military, no recurrent training was provided by the operator to maintain proficiency in windshear recovery. Further, it was also recognised that the air drop scenario conducted in the military differed somewhat from a retardant drop. Most notably was the inclusion of the retardant aerial delivery system and capability to conduct an emergency dump to improve aircraft performance.
Research conducted on behalf of the FAA found that there was only about 5-15 seconds available for pilots to recognise and respond to a windshear encounter. Japanese research into pilot reactions to windshear on landing approach found that about 5.5 seconds was the average time to recognise a windshear event. As such, when in a low airspeed and low height scenario associated with a retardant drop, recognition and reaction to a significant windshear event must be prompt to avoid a collision. However, as no cockpit audio recording was available for the accident flight, it could not be determined if the crew had recognised that they very likely experienced a windshear event and/or had initiated a recovery. Despite this, an effective training program, using a combination of theory and practice, could provide pilots with the necessary skills and experience to recognise and respond to a low-level windshear encounter with minimal delay.
In multi-pilot operations, effective crew coordination and performance depends on the crew having a shared mental model of the task. This mental model is founded on operating procedures (ICAO, 2015). Such procedures are designed to help reduce variation within a given process and ensure operations are performed correctly. Without formal procedures, pilots are required to exercise judgement to the best of their abilities, based on their experience, skills and knowledge. Together, a recovery procedure specific to the nature of the operation supported by training, should provide pilots with a shared mental model of the symptoms and recovery actions for a windshear encounter.
Windshear system not fitted
Where it has been recognised that pilot awareness and training are not 100% effective for windshear avoidance, advanced warning systems are designed to detect and confirm the hazardous condition prior to the encounter. This provides additional time for the crew to increase the aircraft’s energy state and climb, so that any windshear encountered is at a higher, safer altitude. Alternatively, reactive systems alert the crew that they are experiencing windshear so that they can respond immediately, thereby minimising the time required for the crew to identify the situation before responding. These systems are particularly relevant to aerial firefighting aircraft, where there is an increased risk of encountering windshear, which is most hazardous in the low-level low‑speed environment where they regularly conduct operations. As noted by some pilots interviewed, the fitment of such a system was reported to have had a positive effect on their management of a windshear encounter.
While a birddog pilot could provide advanced warning of a windshear condition, there may not be enough time for the LAT crew to respond and avoid the encounter. In the 2012 US Air Force C‑130H accident, the birddog aircraft was about 1 NM (about 2 km) ahead when a warning was provided. This was insufficient for the C-130 crew to prevent a collision with terrain after experiencing low‑level windshear, despite conducting an emergency retardant jettison. It was also noted that LATs deployed as initial attack, such as in the case of the accident, will not have aerial supervision, or an aircraft providing a ‘show me’ run.
Airborne forward-looking, or predictive, windshear detection systems have been developed in response to commercial aviation accidents and have been shown to be around 95% effective (in simulator studies). It is acknowledged that the bushfire environment will be dry (low relative humidity) and the effectiveness of a forward-looking system may be reduced. However, the Lockheed Martin FireHerc aircraft, a civilian-certified aerial firefighting tanker is fitted with a windshear warning system. This would suggest these systems offer an enhanced level of safety for firefighting operations, in particular where operations are at low level in windshear prone environments, which would assist pilots in the early identification and/or potential avoidance of windshear, minimising any loss of aircraft performance. In addition, reactive systems are considered capable of confirming potentially hazardous windshear conditions in advance of human pilot recognition time. The activation of the warning on B137 at Adaminaby, and the crew’s subsequent response and adjustment of the drop location indicated a standard response to a windshear warning in aerial firefighting operations.
B134 and the operator’s other C-130 aircraft were not fitted with any windshear warning systems as these were not available at the time of manufacture and there was no regulatory or contract requirement to have them. The operator also indicated that they had not considered installing windshear detection systems into their C‑130 fleet when they were re‑purposed for firefighting activities.
Given the local weather conditions, the fact that B134 was very likely subjected to windshear, and the activation of the warning on B137 in similar environmental circumstances, it was possible that the crew of B134 would have also received a warning. If a warning had triggered, it was reasonable to expect that the crew would have responded. In addition, if this had occurred during the drop planning phase, it would have also assisted the crew in their hazard assessment and identification that the location was possibly unsuitable before committing to the drop run. If it had occurred during, or following the drop at Peak View, it would have provided immediate identification to all crew of the situation, assisting with timely recognition and response.
However, in the absence of an airborne system, windshear detection is reliant on the pilot’s assessment of the conditions based on the information available and their interpretation of that information. Without any known weather phenomena or reports from that location, detection is likely to be reactive, and dependent on the crew identifying a loss of aircraft performance. The recovery is subject to timely recognition and response, which could take 5 to 15 seconds and potentially result in further altitude loss. In this case, there was only 10-15 seconds and 330 ft between the degradation in climb performance and the impact.
Either a reactive or a predictive windshear detection system may have warned the crew of B134 of the actual or impending windshear and allowed for an earlier response. However, given the limited time and height available, it could not be determined if this would have been sufficient to have reduced the performance loss and prevent the accident. Despite this, research conducted on behalf of the FAA indicated that the risks associated with a windshear encounter would be reduced through a combination of pilot training and the use of on-board systems.
Initial attack certification
The NSW and ACT Aviation Standard Operating Procedures stated that aerial supervision was generally required for air tanker firefighting operations, except for those crew who were ‘initial attack certified’. While the RFS documentation did not define the requirements for this, their intention was to recognise the US Department of Agriculture, Forest Service (USFS) certification and for operators to ensure crews held this certification. However, without a definition, or any reference to the USFS certification in the procedures, this allowed individual operators to determine when pilots were initial attack capable, without necessarily having the official USFS certification. This was consistent with Coulson Aviation’s understanding, where they determined if a pilot was initial attack capable based on their internal training framework, rather than relying on the USFS certification. Despite this, this did not influence the development of the accident as the PIC of B134 held the initial attack certification from the USFS.
Standard operating procedures, among other risks controls, are fundamental for safe operations. They provide a common ground for users by ensuring consistency and predictability across all aspects of an operation. However, if procedures are not clearly defined, this results in a risk control not being applied as intended, lessening their effectiveness in managing safety. In this case, an individual operator may assess the capability of their pilots as satisfactory based on their own training, but it may not necessarily reflect the same requirements as that achieved through the USFS certification process.
Lack of recorded data
While the aircraft was not required to be fitted with a cockpit voice recorder (CVR) under the Australian or US regulations, it was a contract requirement in the US.
As detailed in the AFM supplement, when power was applied to the CVR, the system conducted a self-test, and the status of that test was presented to the crew. However, the CVR did not record the accident flight as a result of the inertia switch activating on a previous flight about 8 months prior. Subsequently, the aircraft was operated on multiple flights by several crews in the intervening period with the CVR in an unserviceable condition. It was very likely that the inertia switch had not been reset during that time as the checklist being used in B134 did not include the requirement for the crew to check the status of the CVR. None of the operator’s C‑130 crew interviewed were aware of this requirement.
While this had no influence on the accident, the CVR being inoperable resulted in a valuable source of information not being available to the investigation. This increased the time taken to determine the contributing safety factors, and restricted the extent to which important safety issues could be identified and analysed. The benefits of flight recorders were further outlined in the ATSB publication Black box flight recorders, which highlighted recorders, such as the CVR, could be an invaluable tool to assist in identifying the factors behind an accident. The CVR captured more than crew communications, it also captured the audio environment in the cockpit, which could include radio transmissions, aural alarms, switch activations and engine noise.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Lockheed EC-130Q, registered N134CG (call sign B134), that occurred near Peak View, New South Wales, on 23 January 2020.
Contributing factors
Hazardous weather conditions were forecast and present at the drop site near Peak View, which included strong gusting winds and mountain wave activity, producing turbulence. These conditions were likely exacerbated by the fire and local terrain.
The Rural Fire Service continued the B134 tasking to Adaminaby when they learned that no other aircraft would continue to operate due to the environmental conditions. In addition, they relied on the pilot in command to assess the appropriateness of the tasking to Adaminaby without providing them all the available information to make an informed decision on flight safety.
The pilot in command of B134 accepted the Adaminaby fire-ground tasking, which was in an area of forecast mountain wave activity and severe turbulence. After assessing the conditions as unsuitable, the crew accepted an alternate tasking to continue to the Good Good (Peak View) fire-ground, which was subject to the same weather conditions. The acceptance of these taskings were consistent with company practices.
Following the partial retardant drop and left turn, the aircraft was very likely subjected to hazardous environmental conditions including low-level windshear and an increased tailwind component, which degraded the aircraft’s climb performance.
While at a low height and airspeed, it was likely the aircraft aerodynamically stalled, leading to a collision with terrain.
Coulson Aviation's safety risk management processes did not adequately manage the risks associated with large air tanker operations. There were no operational risk assessments conducted or a risk register maintained. Further, as safety incident reports submitted were mainly related to maintenance issues, operational risks were less likely to be considered or monitored. Overall, this limited their ability to identify and implement mitigations to manage the risks associated with their aerial firefighting operations. (Safety issue)
Coulson Aviation did not provide a pre-flight risk assessment for their firefighting large air tanker crews. This would provide predefined criteria to ensure consistent and objective decision-making with accepting or rejecting tasks, including factors relating to crew, environment, aircraft and external pressures. (Safety issue)
The New South Wales Rural Fire Service had limited large air tanker policies and procedures for aerial supervision requirements and no procedures for deployment without aerial supervision. (Safety issue)
The New South Wales Rural Fire Service did not have a policy or procedures in place to manage task rejections, nor to communicate this information internally or to other pilots working in the same area of operation. (Safety issue)
Other factors that increased risk
The B134 crew were very likely not aware that the 'birddog' pilot had declined the tasking to Adaminaby fire-ground, and the smaller fire-control aircraft had ceased operations in the area, due to the hazardous environmental conditions
In the limited time available, the remainder of the fire-retardant load was not jettisoned prior to the aircraft stalling.
Coulson Aviation did not include a windshear recovery procedure or scenario in their C‑130 Airplane Flight Manual and annual simulator training respectively, to ensure that crews consistently and correctly responded to a windshear encounter with minimal delay. (Safety issue)
Coulson Aviation fleet of C-130 aircraft were not fitted with a windshear detection system, which increased the risk of a windshear encounter and/or delayed response to a windshear encounter during low level operations. (Safety issue)
The New South Wales Rural Fire Service procedures allowed operators to determine when pilots were initial attack capable. However, they intended for the pilot in command to be certified by the United States Department of Agriculture Forest Service certification process. (Safety issue)
Other findings
The aircraft's cockpit voice recorder did not record the accident flight, which resulted in a valuable source of safety information not being available. This limited the extent to which potential factors contributing to the accident could be identified.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Rural Fire Service task rejection management
Safety issue number: AO-2020-007-SI-01 Safety issue description: The New South Wales Rural Fire Service did not have a policy or procedures in place to manage task rejections, nor to communicate this information internally or to other pilots working in the same area of operation.Safety issue description: The New South Wales Rural Fire Service did not have a policy or procedures in place to manage task rejections, nor to communicate this information internally or to other pilots working in the same area of operation.
Rural Fire Service aerial supervision requirements
Safety issue number: AO-2020-007-SI-02 Safety issue description: The New South Wales Rural Fire Service had limited large air tanker policies and procedures for aerial supervision requirements and no procedures for deployment without aerial supervision.
Initial attack certification
Safety issue number: AO-2020-007-SI-07 Safety issue description: The New South Wales Rural Fire Service procedures allowed operators to determine when pilots were initial attack capable. However, they intended for the pilot in command to be certified by the United States Department of Agriculture Forest Service certification process.
Coulson Aviation’s risk management processes
Safety issue number: AO-2020-007-SI-05 Safety issue description: Coulson Aviation's safety risk management processes did not adequately manage the risks associated with large air tanker operations. There were no operational risk assessments conducted or a risk register maintained. Further, as safety incident reports submitted were mainly related to maintenance issues, operational risks were less likely to be considered or monitored. Overall, this limited their ability to identify and implement mitigations to manage the risks associated with their aerial firefighting operations.
Windshear procedures and training
Safety issue number: AO-2020-007-SI-06 Safety issue description: Coulson Aviation did not include a windshear recovery procedure or scenario in their C‑130 Airplane Flight Manual and annual simulator training respectively, to ensure that crews consistently and correctly responded to a windshear encounter with minimal delay.
Windshear warning systems
Safety issue number: AO-2020-007-SI-04 Safety issue description: Coulson Aviation fleet of C-130 aircraft were not fitted with a windshear detection system, which increased the risk of a windshear encounter and/or delayed response to a windshear encounter during low level operations.
Pre-flight risk assessment tool
Safety issue number: AO-2020-007-SI-03 Safety issue description: Coulson Aviation did not provide a pre-flight risk assessment for their fire-fighting large air tanker crews. This would provide predefined criteria to ensure consistent and objective decision-making with accepting or rejecting tasks, including factors relating to crew, environment, aircraft and external pressures.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by Coulson Aviation
The ATSB has been advised of the following proactive safety action taken by Coulson Aviation in response to this accident:
The Retardant Aerial Delivery system (RADS) software was reprogrammed so that the system would not require re-arming between partial load drops where less than 100% volume was selected.
Updated their pre-flight procedures to incorporate a cockpit voice recorder system check in their abbreviated checklist before each flight.
Glossary
ABM
Airbase manager, responsible for the supervision and coordination of airbase personnel and the layout and operation of an airbase.
ADS-B
Automatic dependent surveillance broadcast
AFM
Airplane Flight Manual. The aircraft manufacturer, Lockheed Martin, produced a C-130 AFM for military operations. When introducing the aircraft to the civilian register, the FAA required the operator to produce an AFM, meeting the FAA requirements. The operator’s AFM was based on the US Navy flight manual, but incorporated procedures and limitations for the intended use of the aircraft.
AGL
Above ground level
AMSL
Above mean sea level
ARO
Aviation radio operator
ATC
Air traffic control
B134
A Lockheed Martin C-130H aircraft, registered N134CG, a large air tanker with the callsign ‘Bomber 134’.
B137
A Boeing 737 aircraft, registered N137CG, large air tanker with the callsign ‘Bomber 137’.
Birddog
Birddog aircraft were used to lead large air tanker aircraft across the fire‑ground and provide guidance on the release of the water or fire suppressant (retardant or gel). The birddog crew consisted of a birddog pilot and a large air tanker air attack supervisor (LAT AAS).
CAS
Calibrated airspeed
CASA
Civil Aviation Safety Authority
COM
Company Operations Manual (Coulson Aviation). The COM was developed to contain the procedures, instructions and information required by CASA for the conduct of operations in Australia.
CVR
Cockpit voice recorder
ECG
Electrocardiogram
FAA
Federal Aviation Administration (US)
FCC
A Fire Control Centre forms the administrative and operational base of the rural fire district or zone. The coordination and management of local brigade responses to fire and other incidents was undertaken through the Fire Control Centre.
FRAT
Flight risk assessment tool
GPS
Global positioning system
IAS
Indicated airspeed
ICAO
International Civil Aviation Organization
Incident controller
The incident controller was responsible for all aspects of an emergency response, and managed the response, including the objectives, operations, and application of resources of the FCC.
Incident management team
The coordination and management of local brigade responses to fire and other incidents was undertaken through the incident management team, led by the incident controller.
Incident AAS
Incident air attack supervisor
LAT
Large air tanker. An aircraft with a minimum suppressant/retardant capacity of 3,000 US gallons (11,356 L).
LAT AAS
Large air tanker air attack supervisor (onboard the birddog aircraft)
MAFFS
Modular airborne firefighting system
NAFC
National Aerial Firefighting Centre. Formed by the Australian States and Territories in 2003, NAFC provided a cooperative national arrangement for combating bushfires by facilitating the coordination and procurement of specialised firefighting aircraft.
NSW
New South Wales
OLMS
Operational load monitoring system
PIC
Pilot in command
RAAF
Royal Australian Air Force
RADS
Retardant aerial delivery system XXL
RFS
Rural Fire Service (NSW)
SAD
State air desk. The state level multi agency team located in the State Operations Centre responsible for coordination of aircraft operations.
SMS
Safety management system. A systematic approach to organisational safety encompassing safety policy and objectives, risk management, safety assurance, safety promotion, third party interfaces, internal investigation and SMS implementation.
SOC
State operations controller roles was to maintain overall awareness of the firefighting effort across the state ensuring information and warnings are being distributed and resources are being allocated where needed. The SOC was located within the State Operations Centre.
State Operations Centre
State Operations Centre was located at NSW RFS Headquarters in Lidcombe and allows the RFS and its partners to effectively oversee and coordinate incidents. The staff within the Centre monitor developments, analyse their potential and provide a variety of specialised resources to the incident management teams and firefighters on the ground.
TAS
True airspeed
US
United States
USFS
US Department of Agriculture, Forest Service
Sources and submissions
Sources of information
The sources of information during the investigation included:
Coulson Aviation
Coulson Aviation current and former personnel
other C-130 crews and maintenance staff
New South Wales Rural Fire Service
Lockheed Martin
a number of witnesses
Royal Australian Air Force
Defence Flight Safety Bureau
the Bureau of Meteorology
ATSB aviation medical specialist
Rolls Royce
Hamilton Sundstrand
National Aerial Firefighting Centre
CAL FIRE
Airservices Australia
United States Federal Aviation Administration
United States Department of Agriculture, Forest Service
Canadian Transportation Safety Board
next-of-kin
video footage of the accident flight
recorded data from automatic dependent surveillance broadcast (ADS-B), SkyTrac and historic data for the operational load monitoring system.
Australian Transport Safety Bureau (2004) Risks associated with aerial campaign management: Lesson from a case study of aerial locust control. Retrieved from /publications/2005/aerial_locust_control/
Australian Transport Safety Bureau (2015) Pilot incapacitation occurrences 2010-2014. Retrieved from /publications/2015/ar-2015-096/
Bowles, R. L. (1990) Reducing Windshear Risk Through Airborne Systems Technology. Proceedings of 17th Congress of the International Council of the Aeronautical Sciences, pp 1603-1630.
International Civil Aviation Organization (2015). Model advisory circular for air operator's: Standard Operating Procedures for Flight Deck Crewmembers, Montreal: ICAO.
Mosier, KL, Fischer, U, Cunningham, K, Munc, A, Reich, K, Tomko, L, and Orasanu, J (2012) Aviation decision making issues and outcomes: Evidence from ASRS and NTSB reports, Proceedings of the Human Factors and Ergonomics Society Annual Meeting, 56(1):1794-1798.
Tsukagoshi, H. (1999) Another look at windshear accidents. Proceedings of the International Society of Air Safety Investigators annual seminar, pp 67-86.
US Air Force (2012) Aircraft accident investigation, C-130H3, T/N 93-1458, Edgemont, South Dakota, 1 July 2012. United States Air Force Aircraft Accident Investigation Board Report.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Coulson Aviation
New South Wales Rural Fire Service
Coulson Aviation personnel
Lockheed Martin
Royal Australian Air Force Aircraft Research and Development Unit
the Bureau of Meteorology
ATSB aviation medical specialist
National Aerial Firefighting Centre
Civil Aviation Safety Authority
United States National Transportation Safety Board
the birddog pilot.
In addition, the draft report was sent to the NSW State Coroner for information.
Submissions were received from:
Coulson Aviation
New South Wales Rural Fire Service
Royal Australian Air Force Aircraft Research and Development Unit
the Bureau of Meteorology
Civil Aviation Safety Authority
the birddog pilot.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Interim report
Report release date: 24/09/2020
This interim report details factual information established in the investigation’s evidence collection phase and has been prepared to provide timely information to the industry and public. Interim reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this interim report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Fire situation in the Snowy Mountains region
On 23 January 2020, the Snowy Mountains region in New South Wales (NSW) had a severe fire danger rating,[1] due to high temperatures, strong winds and forecast thunderstorms. This region included the Adaminaby and Good Good fire-grounds, which were both under the control of the Cooma Fire Control Centre (FCC).
At about 1100 Eastern Daylight-saving Time,[2] the Cooma FCC incident commander made a call to the NSW Rural Fire Service (RFS) State Operations Centre, to discuss the escalating fire danger at the Adaminaby fire-ground. During that call, it was noted that the smaller firefighting aircraft were not flying in the area due to strong winds and poor visibility. Consequently, a birddog[3] and two large air tankers (LAT) were tasked by the State Operations Centre to the Adaminaby fire-ground: a Rockwell International 690-B aircraft; a Boeing 737 aircraft, registered N137CG, call sign ‘Bomber 137’ (B137); and a Lockheed EC130Q[4] aircraft, registered N134CG, call sign ‘Bomber 134’ (B134). All three aircraft were based at Richmond Royal Australian Air Force (RAAF) Base, NSW, about 316 km north-east of the Adaminaby fire-ground.
‘B137’ tasking to Adaminaby
At about 1121, B137 had commenced taxiing at Richmond for a task when the crew were re‑tasked to the Adaminaby fire-ground. The aircraft subsequently departed at 1127, with the crew having been notified by the Richmond airbase manager[5] that there was no birddog in the area, and that it ‘is very windy down there’.
The birddog pilot had experienced moderate to severe turbulence in the Snowy Mountains region about 2 weeks prior to the day of the accident. On receipt of the tasking to Adaminaby, the birddog pilot reviewed the weather and concluded that the conditions were forecast to be worse than previously experienced, and therefore declined the task. In addition, as B137 was already en route to Adaminaby, the crew of that aircraft would be able to provide a report to the birddog pilot and other crews of the actual conditions.
At about 1155, B137 arrived overhead the Adaminaby fire-ground. At interview, the pilot in command (PIC) of B137 reported the wind speed at the Adaminaby fire-ground was 50 kt[6] at 800 ft above ground level (AGL), and about 37 kt at the retardant drop height of 200 ft AGL. While assessing the conditions in the Adaminaby area, the crew reported experiencing uncommanded aircraft rolls up to 45° angle of bank (due to wind) and a windshear[7] warning from the aircraft on‑board systems. The PIC of B137 elected to operate on the upwind side of the hills to avoid lee‑side mechanical turbulence.[8] At about 1225, B137 departed the Adaminaby fire‑ground, having successfully deployed a retardant load.
After completing the retardant drop, the B137 crew sent a text message to the birddog pilot assigned to the Adaminaby fire-ground indicating that the conditions were ‘horrible down there. Don’t send anybody and we’re not going back’. They also reported to the Cooma FCC that the conditions were unsuitable for firebombing operations. During B137’s return flight to Richmond, the Richmond air base manager requested that they reload the aircraft in Canberra and return to Adaminaby. The PIC replied that they would not be returning to Adaminaby due to the weather conditions.
‘B134’ tasking at Adaminaby
While B137 was still at the fire-ground, at about 1205, B134 departed Richmond with the PIC, co‑pilot and flight engineer on board.
At about 1235, the PIC of B137 had a conversation with the PIC of B134 on their designated operating frequency, to inform them of the actual conditions, and that they would not be returning to Adaminaby. At that time, B134 was about 112 km north-east of Adaminaby, en route to the Adaminaby fire-ground.
At about 1242, the crew of B134 contacted air traffic control (ATC), advising them of the co‑ordinates they would be working at, provided an ‘ops normal’[9] call time, and confirmed there was no reported instrument flight rules[10] traffic in the area. About 5 minutes later, the Richmond air base manager also attempted to contact B134 to confirm ‘ops normal’, firstly by radio, and then by text to the PIC’s mobile phone, but did not receive a response.
The automatic dependent surveillance broadcast (ADS-B) data showed that after arriving at the Adaminaby fire-ground (Figure 1), the crew of B134 completed several circuits at about 2,000 ft AGL.[11] At about 1255, the crew contacted the air operations officer at the Cooma FCC by radio and advised them that it was too smoky and windy to complete a retardant drop at that location. The Cooma air operations officer then provided the crew with the location details (co‑ordinates) of the Good Good fire, about 58 km to the east of Adaminaby, with the objective of conducting structure and property protection near Peak View.
Figure 1: Flight path overview (in white), including the times and locations of where the crew of B134 was in communication with others
Source: Google earth and ADS-B data, annotated by the ATSB
‘B134’ tasking at the Good Good fire-ground
At 1259, the crew of B134 contacted ATC, to advise them that they had been re‑tasked to the Good Good fire-ground for a retardant drop and provided the updated co‑ordinates. At about the same time, the RFS ground firefighters at the Good Good fire-ground, near Feeney’s Road in Peak View, contacted the Cooma FCC and requested additional assets for property protection. They were advised that a LAT would be passing overhead in about 10 minutes. The firefighters acknowledged the intention of a LAT drop, and advised the Cooma FCC they would wait in open country on Feeney’s Road, clear of the properties targeted for protection.
At about 1307, B134 arrived overhead the drop area (Figure 2). From the aircraft’s recorded tracking data, the crew conducted three left circuits, at about 1,500 ft, 500 ft and 1,000 ft AGL respectively, prior to commencing the drop circuit.
At 1315:15,[12] the retardant drop was conducted on a heading of about 190° and at about 190 ft AGL (3,595 above mean sea level (AMSL)) with a drop time of about 2 seconds. During the drop, about 1,200 US gallons (4,500 L) of fire retardant was released. Witness video footage and images showed that at the commencement of the drop, the aircraft was at an approximate bank angle of 10°, with the flaps set at 100 per cent. A ground speed of 144 kt was recorded at the time of the drop.
Figure 2: B134’s approach and circuits overhead the drop location, and the position of the firefighters
Source: Google earth and Skytrac data, annotated by the ATSB
The ATSB’s analysis of the witness videos found that, at the completion of the drop at 1315:17, the aircraft was observed to be banked about 17° to the left (Figure 3). About 4 seconds after the drop at 1315:21, the aircraft had a pitch-up attitude of about 12°, with an increase to about 30° angle of bank. Over the next 1.5 seconds, the aircraft’s angle of bank and pitch attitude reduced to about 22° and 10° respectively. The aircraft then became obscured by smoke.[13]
While being intermittently obscured by smoke, a positive rate of climb was achieved for about 10 seconds, with the aircraft climbing to about 330 ft AGL (3,770 ft AMSL) at 1315:27. Just prior to this, from about 1315:25, a right roll was observed on the video. The video captured the aircraft at about an 18° left angle of bank at 13:15:25, and then at about a 6° right angle of bank at 13:15:27. At the same time, the aircraft pitch attitude had decreased to about 6°. Following this, the aircraft was then observed descending. A further 7 seconds after this, at 1315:34, the aircraft was seen at a very low height above the ground, in a left bank. Throughout this period, the recorded groundspeed increased slightly to a maximum of 151 kt.
Shortly after, at about 1315:37, the aircraft collided with terrain and a post-impact fuel-fed fire ensued. The three crew were fatally injured and the aircraft destroyed.
A review of the Airservices Australia audio recording of the applicable air traffic control frequency found no distress calls were received by ATC prior to the impact.
Figure 3: Aircraft attitude and approximate flight path at key times
Source: Google earth, witness videos and Skytrac data, annotated by the ATSB
Context
Operator
Coulson Aviation are a USA (US) based operator, with US registered aircraft and US licensed crew contracted to Australia for the 2019/2020 fire season through the National Aerial Firefighting Centre. At the time of the accident, Coulson Aviation had a fixed wing fleet in Australia consisting of two C130 aircraft, and one Boeing 737 aircraft. They also provided flight crews for the NSW RFS Boeing 737 which had previously been purchased from Coulson Aviation in 2019.
The RFS subsequently contracted one C130 and one 737 from Coulson Aviation via a service agreement subject to the National Aerial Firefighting Centre contract. Following the Australian fire season, the aircraft and crews then return to North America for heavy maintenance and recurrent training prior to the US fire season.
Crew information
Pilot in command
Qualifications and experience
The PIC was initially trained as a navigator and pilot in the United States Air National Guard. During this time, the PIC gained experience in firefighting operations through the modular airborne firefighting system (MAFFS)[14] program. The PIC subsequently joined the operator in 2015 on a part-time basis, before being employed full-time in 2017.
The PIC’s logbook, combined with the operator’s records for the accident aircraft showed that the pilot had a total flying experience of about 4,010 hours, which included 3,010.3 hours in the C130 aircraft, and 994 air tanker drops. The PIC had also accrued a further 1,616.8 hours as a flight navigator.
The PIC held a current airline transport pilot certificate with ratings for multi-engine land aircraft including the EC130Q, issued by the US Federal Aviation Administration (FAA) on 13 October 2017. The PIC’s most recent flight instructor certificate with ratings for multi-engine and instrument aircraft was issued by the FAA on 6 April 2019. On 18 April 2019, the PIC’s latest airplane pilot qualification card was issued from the US Department of Agriculture, Forest Service,[15] for the C130 aircraft, which included the authorised missions of: Low level (below 500 ft above ground level); Mountainous terrain; and Airtanker Initial Attack. An air tanker initial attack qualification allows a pilot to conduct fire retardant drops without the supervision of a birddog or air tactical supervisor.
The PIC’s most recent first-class medical examination was on 5 September 2019, with the certificate issued with a limitation to wear corrective lenses.
Training
The PIC’s training with the operator in March and April 2019[16] included annual C130 simulator training, controlled flight into terrain awareness, and crew resource management. In addition, the PIC completed two assessed training flights with the operator in the C130 on 14‑15 April 2019. The training flight on 14 April included approach to stalls in the circuit (50 per cent flap) and drop (100 per cent flap) configurations, and go-arounds with a full load. The flight on 15 April included drop planning (hazards, tactics, ingress, egress and dry run) and an emergency on the drop run. The drop run emergency was a simulated ‘down air’ [downdraught] with the comment ‘Jettison for down air’. All the assessed sequences, which included jettison of the load during an emergency condition,[17] were recorded as satisfactory.
Co-pilot
The co-pilot had joined the operator in September 2019, after 20 years in the military, including experience flying the C130. This was the co-pilot’s first fire season. The co-pilot’s logbook combined with the operator’s records showed a total flying experience of about 1,744 hours, of which about 1,364 were on the C130. The co-pilot held a current airline transport pilot certificate and ratings for multi-engine land aircraft, including the EC130Q (second-in-command privileges only), issued by the FAA on 7 November 2019. The co-pilot also held a flight instructor certificate with ratings for single, multi-engine and instrument aircraft, issued by the FAA on 14 August 2019. The co-pilot’s most recent first-class medical examination was issued on 17 July 2019 with no limitations.
The co-pilot’s check flight with the operator was completed on the C130 on 12 September 2019, and was assessed as satisfactory against the qualification standards for second-in-command. On 13 September 2019, the co-pilot completed the operator’s crew resource management and controlled flight into terrain awareness courses, and reviewed the US Department of Agriculture Forest Service’s air tanker pilot training video.
On 16 September 2019, the co-pilot was issued with an airplane pilot qualification card from the US Department of Agriculture Forest Service for the C130 aircraft, which included the authorised missions of: Low level (below 500 ft above ground level); Mountainous terrain; and Airtanker SIC (second-in-command).
Flight engineer
The flight engineer joined the operator in November 2019, after about 25 years in the US military. This was the flight engineer’s first fire season. The flight engineer held a flight engineer certificate with a rating for turbo-propeller powered aircraft, issued by the FAA on 20 November 2019. On the flight engineer application form, the flight engineer reported accruing 4,050 hours on the C130 aircraft. The flight engineer also held a mechanic certificate with ratings for airframe and powerplant, issued by the FAA on 2 June 2019. The flight engineer’s most recent second-class medical examination was issued on 27 August 2019 with no limitations.
The flight engineer’s check flight was completed with the operator on 20 November 2019. In addition to this check flight, the FE completed two air tanker drops with a supervising flight engineer in Australia on 12 January 2020.
72 hour prior history
The PIC and co-pilot commenced work in Australia on 1 December 2019 and the flight engineer on 13 January 2020. Each crew member’s roster cycle was 14 duty days followed by two rest days. The operator’s records show they signed on between 0800 and 1000, and signed off between 1700 and 2100, with their duty times varied between 7.5 and 12 hours per day.
The accident flight occurred on the PIC’s 9th day, and the co-pilot’s and flight engineer’s 11th day of their respective current duty periods.
Table 1, based on the operator’s records, details the crew’s sign on and sign off times for the 3 days before the accident. On 23 January 2020, the crew signed on at 0900.
Table 1: B134 crew working hours
20 January
21 January
22 January
Sign on
1000
0800
1000
Sign off
1800
1700
1900
Information from the crew’s telephones and hotel records, in addition to work and flying duties, were used to determine their activities in the previous days. There were no indications of fatigue for the three crew members. However, there was insufficient information available to the ATSB about their sleep and non-duty activities to estimate fatigue levels with confidence.
Aircraft information
General information
The C130 is predominantly an all-metal, high-wing aircraft, designed for military operations. The accident aircraft (Figure 4) was manufactured in 1981 and was powered by four Allison T56-A-15 turboprop engines, fitted with Hamilton Sundstrand 54-H60-91 four blade propellers. The T56‑A‑15 is a constant speed engine, with a variable pitch propeller.
Previously owned by the US Navy, the aircraft was transferred to the US National Aeronautics and Space Agency (NASA) in 1992 and later placed in storage. It was removed from storage, re‑purposed for firefighting activities by the operator and registered in the restricted category.[18] Initially registered as N130CG in 2018, its registration was later changed to N134CG in April 2019. The modifications included the installation of an avionics package and firefighting tank system, known as the Retardant Aerial Delivery System XXL (RADS).
Figure 4: N134CG
Source: Coulson Aviation
Maintenance history
The aircraft had a total time-in-service of 11,888 hours and had accrued 683 hours of firefighting operations since the tanker conversion in 2018.
N134CG arrived in Australia in November 2019. The aircraft had a current certificate of airworthiness, and was maintained in accordance with an FAA approved program. The last daily inspection conducted on 22 January 2020, at the end of the day’s flying activities the day before the accident, identified the propeller anti-icing system on engine number 2 was unserviceable, and rectification had been deferred in accordance with the minimum equipment list.[19]
In addition to a maintenance requirement to perform engine power efficiency checks at 150-hour intervals, the operator reported pilots were required to perform power checks before every take off, with operations only permitted if a minimum performance requirement of 95 per cent was met.
Retardant Aerial Delivery System XXL
The Retardant Aerial Delivery system (RADS) included a 4,000 US gallon (15,000 L) tank system located within the aircraft’s fuselage. The system could deliver discrete quantities of retardant, dependant on the duration that the doors remained open. It was controlled from the cockpit, with drop controls located on both the PIC and co-pilot yokes.
The drop quantity could be controlled either as a pre-set percentage by the crew, or alternatively, if selected at 100 per cent, the crew could control the amount of retardant released by holding the button until the desired amount was dispensed. The RADS system was designed that, if less than 100 per cent volume was selected, the system would disarm after a partial load drop, and the crew would need to re-arm the system to complete further releases. It was reported that the crew on B134 normally selected 100 per cent volume and released the drop button once the desired amount had been dispensed.
The system also included a guarded emergency dump switch, located in reach of all three crew members, which would fully open the doors and jettison the load in a period of about 2 seconds. Following an emergency dump, the doors would remain open until the RADS was reset by the crew.
Weight and balance
The last weight and balance report for the aircraft, in April 2019, showed its basic empty weight was 75,794 lb (35,380 kg) and according to the RADS flight manual supplement, the maximum take-off weight was 150,718 lb (68,365 kg). The aircraft flight and maintenance log entry for 22 January 2020 indicated the PIC had the aircraft refuelled to a total of 34,000 lb (15,422 kg) at the completion of flying the previous day. The operational load monitoring system[20] indicated there was 35,514 lb (16,109 kg) of retardant on board prior to the drop, in addition to which the aircraft carried a 2,000 lb (907 kg) pallet of gel. This resulted in a take-off weight of about 147,253 lb (66,826 kg) and centre of gravity at the aft limit.
Using the operator’s reported fuel consumption for air tanker drop missions of 5,000 lb/h (2,268 kg/h) for a 70 minute flight, and the retardant drop of 10,764 lb (4,882 kg), the estimated post-drop weight was 130,656 lb (59,265 kg). The centre of gravity remained close to the aft limit, which was consistent with the reports from the operator’s other crews that the location of the RADS tank in the aircraft meant there was no appreciable change in the centre of gravity following a retardant drop.
Meteorological information
Bureau of Meteorology forecasts
A Bureau of Meteorology graphical area forecast was issued at 0924 and was valid for the time of the flight. It forecast moderate mountain wave activity[21] above 3,000 ft AMSL and severe turbulence below 8,000 ft AMSL in the area of operation from Richmond to Cooma. This included the Adaminaby and Good Good fire-grounds. In addition, a SIGMET[22] issued at 0947, and valid for the flight, forecast severe turbulence[23] below 10,000 ft AMSL for the area.
The aerodrome forecast for the Cooma-Snowy Mountains Airport,[24] located 50 km south-west of the accident site was amended at 0948. It indicated wind speeds of 25 kt, gusting to 48 kt, with a mean wind direction of 300° from 1100 and visibility reduced to 8,000 m in light showers. Severe turbulence below 5,000 ft AGL was forecast from 0900-1500, and a PROB30[25] for visibility reduced to 2,000 m in blowing dust and a broken[26] layer of cloud at 1,000 ft AGL was forecast for the period 1100–1700.
At 1012, the Richmond air base manager sent a text message to the air tanker and birddog pilots to advise them of an airport warning for wind gusts in excess of 35 kt between 1000 and 1700 at the Richmond base.
Observations of the weather in the area
Other fire control aircraft
On the day of the accident, several fire-control aircraft, primarily consisting of fixed-wing Air Tractors and Bell 206 helicopters, were operating from the Polo Flat airstrip, located 33 km south-west of the accident site. The Cooma FCC received reports of strong winds in the area from the fire-control pilots in the early morning. This included winds of 30-40 kt at 0839, 40-50 kt at 0902, and 52 kt at 0937. All fire-control aircraft had departed the area or landed by 1030.
Additionally, the flight crew of B137 reported that the wind conditions at Adaminaby at about 1200 were 50 kt at 800 ft AGL, and about 37 kt at 200 ft AGL.
Witness reports
Following the accident, the ATSB received multiple witness reports of the weather conditions at Peak View. They all consistently reported very strong winds from the north-west, with gusts up to 43 kt recorded at ground level. One resident noted that, although the prevailing wind was from the north-west, the direction and strength at ground level were also being influenced by the local terrain.
Weather station recorded conditions
About 12 minutes prior to the accident, the Cooma-Snowy Mountains Airport weather station indicated a wind speed of 25 kt, gusting to 39 kt, from a direction of 320°. The visibility was 6,000 m, with a QNH[27] of 1002 hPa and temperature of 26 °C.
A personal weather station at Peak View, located about 1.3 km from both the drop and accident sites (Figure 5) recorded the conditions twice per hour. At about 1309 (7 minutes prior to the accident), the station recorded a mean wind of 15 kt from the west and a peak gust of 32 kt from the north.[28] At about 1330 (14 minutes after the accident), the station recorded a mean wind of 16 kt from the west and a peak gust of 42 kt from the north-west.
Figure 5: Accident circuit with predominant wind direction and terrain
Source: Google earth and SkyTrac data, annotated by the ATSB
Bureau of Meteorology analysis
The Bureau of Meteorology analysed the conditions on the day and indicated that a cold front was approaching the accident location, with hot and strong north to north-westerly winds ahead of the front. High resolution weather model data indicated the winds at 5,000 ft AMSL were about 45 kt from the north-west, increasing in strength with height up to 80 kt from the north-west at 10,000 ft AMSL. They reported that their analysis of the weather conditions in the accident area was consistent with what was forecast on the day.
The Bureau of Meteorology considered the conditions on the day were favourable for mountain wave development, and satellite imagery of cloud formations confirmed their presence in the general area of the accident. However, they were unable to determine the severity of the mountain wave activity from the data available.
Recorded information
Cockpit voice recorder
Cockpit voice recorders (CVR) are designed on an endless loop principle, where the oldest audio is continuously overwritten by the most recent audio. The CVR fitted to the aircraft was a Universal Avionics Model CVR-30B, part number 1603-02-03 (Figure 6). This solid-state memory CVR recorded crew and cockpit audio for a recording duration of at least 30 minutes. While the aircraft was not required to be fitted with a CVR under US or Australian regulations, it was required under contract requirements in the US.
Figure 6: N134CG cockpit voice recorder
Source: ATSB
The CVR was recovered from the aircraft and transported to the ATSB’s technical facility in Canberra, Australian Capital Territory, on 25 January 2020 for examination and download. The CVR was successfully downloaded, and the recording downloaded contained 31 minutes of audio. However, the audio was from a previous flight when the aircraft was operating in the US. No audio from the accident flight was recorded on the CVR.
Inertia switch
The power supply for the CVR was fitted with an inertia switch. Inertia switches are designed to stop the recording function by removing power to the CVR when a pre-set deceleration force is detected. The recovered audio was of crew training flights undertaken on 7 May 2019 near Sacramento McClellan Airport, California. The audio included four landings conducted as part of the training in the aircraft on that day. The recording ceased immediately after the fourth landing, and the post-landing taxi and engine shutdowns were not recorded. It was likely that the inertia switch was activated during this landing and consequently disconnected power to the CVR.
Pre-flight testing
Following a CVR installation in an aircraft, supplemental material related to the operation of the CVR must be attached to the approved airplane flight manual. The supplement for the aircraft indicated the CVR conducted a self-test at power up, and the status of the CVR would be presented to the crew on the CVR control unit, located on the co-pilot side console. A CVR system check was not included in any of the operator’s checklists, and none of the operator’s flight crew were aware of the need to check this system status prior to flight.
Flight data
The aircraft was not fitted with a flight data recorder, nor was it required to be by Australian or US regulations. However, contracting requirements in the US required the aircraft be fitted with an operational load monitoring system, which was located behind the centre wing section in the fuselage. This recording device had no impact or fire protection and was destroyed in the accident sequence.
The aircraft was also fitted with SkyTrac, a tracking system that can transmit the aircraft’s position in real-time. This system was able to be monitored by the NSW RFS, and generally had an update rate of about 1 minute. The SkyTrac unit was recovered from the wreckage and transported to the ATSB’s technical facility for examination and download. The SkyTrac unit recorded data at 5 second intervals.
Data broadcast by the ADS-B equipment fitted to the aircraft for ATC purposes was also obtained from various providers. ADS-B data is transmitted nominally every 0.5 seconds; not all transmission were available, with gaps of up to 5 seconds during the accident flight. Table 2 shows the parameters recorded by SkyTrac and ADS-B.
Table 2: SkyTrac and ADS-B recorded parameters
SkyTrac
ADS-B
time
time
latitude and longitude
latitude and longitude
groundspeed (GPS)
groundspeed
altitude (GPS)
pressure altitude
track (GPS course)
track
vertical rate of climb/descent
A detailed review of the available recorded data is ongoing and will be included in the ATSB’s final investigation report.
Witness video
Two firefighters were located on Feeney’s Road (800 m from the accident site), and videoed the aircraft during the retardant drop and subsequent accident. Overall, the video footage had a duration of 37 seconds. It captured the aircraft from 10 seconds prior to the drop, the drop, and 4 seconds after the drop, when the aircraft became obscured by smoke, and was only intermittently visible. Eleven seconds after being obscured by the smoke, the aircraft was seen at low level, followed by a collision with terrain and post-impact fire. The ATSB’s analysis of this footage is continuing and will be included in the final investigation report.
Wreckage and impact information
Accident site
The accident site was located on slightly sloping, partially wooded terrain, near Peak View, 50 km north-east of Cooma-Snowy Mountains Airport. The wreckage trail (Figure 7) was approximately on a heading of 100°, with the initial impact at an elevation of about 3,440 ft AMSL. The debris trail began at the lower end of the slope, with the wreckage distributed linearly over about 180 m.
Figure 7: Accident site overview showing the wreckage trail
Source: ATSB
Wreckage examination
The ATSB’s on-site examination of the wreckage, damage to the surrounding vegetation, and ground markings, indicated that the aircraft initially impacted a tree in a left wing down attitude, of about 55°, before colliding with the ground. An intense post-impact fuel-fed fire destroyed the aircraft. The ATSB’s on-site examination (Figure 8) also found:
no pre-existing airframe issues
all major sections of the aircraft’s structure were identified and there was no evidence of an in‑flight break-up or pre-impact structural damage[29]
the cockpit and associated avionics were identified about two-thirds of the way along the wreckage trail
the cockpit and forward section of the airframe had separated from the fuselage, was inverted, and had been destroyed in the impact and subsequent fire
sections of the wing skin, leading edge spar, wing tips and portions of the wings were identified along the wreckage trail, having fragmented during the impact sequence, and sustained further damage during the resultant fire
all flight control surfaces were identified, however, due to the impact and fire, flight control continuity could not be established
the four engines and 16 propeller blades were located on-site and some of the propeller blades remained attached to the propeller hubs, while others had detached through impact forces
there were varying degrees of damage observed across the four engines, likely due to the impact sequence of each engine, with the damage indicating the engines were rotating at impact.
The RADS tank remained upright (Figure 8), along with the aft section of the fuselage, with the vertical and horizontal stabilisers attached. There was no retardant identified between the drop area and the initial impact location, however, a large amount of retardant was located in the wreckage near the tank. The system was badly damaged, with the doors fragmented throughout the wreckage, and its operational state could not be established.
Figure 8: Main aircraft wreckage components
Source: ATSB
Aircraft configuration
The aircraft was equipped with four trailing edge flaps. All flaps had separated from the aircraft during the impact sequence. On-site measurements of the flap screw jacks indicated the flaps were set at 50 per cent at impact. This was consistent with the expected setting following a retardant drop. Due to the extent of damage, the elevator, aileron and rudder trim settings could not be established.
Fuel testing
Fuel samples were retained from the two fuel tankers that last serviced the aircraft and from the refuelling storage tank at Richmond. The fuel samples were independently tested by a commercial fuel company for correct specifications, with nil abnormal indications found. In addition, there were no reports of fuel quality concerns with any other aircraft using the same fuel source.
Engine and propeller examinations
With the assistance of the Australian Army, the engines, partial remnants of the reduction gearboxes, propeller assemblies and blades were transported to a secure hangar at Richmond RAAF Base for further examination.
The engine manufacturer attended the engine inspections, where it was confirmed that all engines were rotating at impact, and there were no noted pre-existing issues. As power changes are controlled by changes to the propeller blade pitch while maintaining a constant engine speed, the engine power levels were determined from the blade pitch angle at impact.
During the propeller hub assembly inspection, measurements of the internal components were recorded. The ATSB consulted the propeller manufacturer to determine the propeller blade angles at impact and establish engine power levels. The propeller manufacturer concluded the following:
The calculations indicate that, based on the operating conditions estimated by the ATSB, all the propellers were absorbing power from their respective engines and were producing positive thrust. The horsepower computed for each of the four engines are within the normal operating range for the T56 engine installed on this aircraft.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk.
The ATSB has been advised of the following proactive safety action taken by Coulson Aviation in response to this accident:
The Retardant Aerial Delivery system (RADS) software was reprogrammed so that the system will not require re-arming between partial load drops where less than 100 per cent volume is selected.
Updated their pre-flight procedures to incorporate a cockpit voice recorder system check before each flight.
Ongoing investigation
To-date, the ATSB has interviewed Coulson Aviation pilots and key personnel, NSW RFS personnel involved in the large air tanker and aviation operations, witnesses, C130 and other aerial firefighting pilots, and key personnel in overseas aerial firefighting operations. In addition, the ATSB has conducted a detailed examination of the aircraft, engines and propellers; reviewed recorded RFS radio calls; and engaged C130 subject matter experts.
The investigation is continuing and will include consideration of the following:
ongoing analysis of recorded data, including the on-board systems and witness videos
aircraft performance and handling characteristics
review and analysis of environmental influences
operating policies and procedures
aircraft maintenance history
cockpit instruments examination
crew health and medical history
similar occurrences.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
This interim report details factual information established in the investigation’s evidence collection phase and has been prepared to provide timely information to the industry and public. Interim reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this interim report is released in accordance with section 26 of the Transport Safety Investigation Act 2003.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Sequence of events
On 23 January 2020, at about 1205 Eastern Daylight-saving Time,[1] a Lockheed EC130Q (C‑130) aircraft, registered N134CG and contracted to the New South Wales (NSW) Rural Fire Service, departed Richmond RAAF Base, NSW. The crew had been tasked with a fire retardant drop over the ‘Adaminaby Complex’ bush fire.
After approaching the Adaminaby complex fire, the drop was unable to be completed and the aircraft was diverted to a secondary tasking, to drop retardant on the ‘Good Good’ fire (Figure 1). Witnesses reported seeing the aircraft complete a number of circuits, prior to completing the retardant drop. The drop was conducted on a heading of about 190°, at about 200 ft above ground level, with a drop time of approximately 2 seconds. The crew released about 1,200 US gallons (4,500 L) of fire retardant during the drop.
Figure 1: Flight path of N134CG (white)
Source: Google Earth, Aireon and RFS tracking data, annotated by the ATSB
Witness videos taken of the aircraft leading up to the accident showed a number of passes conducted at varying heights prior to the retardant drop. Following the retardant drop (Figure 2), the aircraft was observed to bank left, before becoming obscured by smoke[2] after about 5 seconds. A further 15 seconds after this, the aircraft was seen flying at a very low height above the ground, in a left wing down attitude. Shortly after, at about 1316, the aircraft collided with terrain and a post-impact fuel-fed fire ensued. The three crew were fatally injured and the aircraft was destroyed.
Figure 2: Overview of the drop zone (red fire retardant) and accident location
Source: ATSB
A review of the Airservices Australia audio recording of the applicable air traffic control frequency found no distress calls were made by the crew prior to the impact.
Wreckage and impact information
The accident site was located on slightly sloping, partially wooded terrain, about 50 km north-east of the Cooma-Snowy Mountains Airport. The wreckage trail (Figure 3) was approximately on a heading of 100°, with the initial impact at an elevation of about 3,440 ft above mean sea level.
The ATSB’s on-site examination of the wreckage, damage to the surrounding vegetation, and ground markings indicated that the aircraft initially impacted a tree in a left wing down attitude, before colliding with the ground. The post-impact fuel-fed fire destroyed the aircraft. The examination also found that an emergency dump of the fire retardant had not been activated.
The engines, propellers, and several other components have been retained by the ATSB for further examination.
Figure 3: Aircraft impact and wreckage
Source: ATSB
Aircraft information
The Lockheed C-130 is predominantly an all-metal, high-wing aircraft, largely designed for military operations. The aircraft was manufactured in 1981 and was powered by four Allison T56-A-15 turboprop engines, fitted with Hamilton Sundstrand 54-H60-91 four blade propellers. Previously owned by the United States Navy, the aircraft was re-purposed for firefighting activities and registered as N134CG in 2018 (Figure 4). The modifications included the installation of an avionics package and firefighting tank system known as Retardant Aerial Delivery System XXL (RADS).
The RADS included a 4,000 US gallons (15,000 L) tank system located within the aircraft’s fuselage. The system was capable of delivering discrete quantities of retardant, dependent on the duration that the doors remained open. It was controlled from the cockpit, with drop controls located on both the pilot and copilot yokes. The system also included an emergency dump switch, which, when activated, fully opened the doors and jettisoned the load. The doors remained open until the RADS was reset by the crew.
N134CG arrived in Australia in November 2019, but had previously operated in the country during the 2018‑2019 fire season. The aircraft was designated as a ‘large air tanker’.
Figure 4: N134CG
Source: Coulson Aviation
Meteorological information
A Bureau of Meteorology graphical area forecast, issued at 0924 and valid for the time of the flight, forecast moderate mountain wave activity above 3,000 ft (above mean sea level) in the area of operation from Richmond to Cooma, and included the Adaminaby and Good Good fire grounds. A SIGMET[3] issued at 0947 forecast severe turbulence below 10,000 ft.
The aerodrome forecast for the Cooma-Snowy Mountains Airport[4] was amended at 0948, and indicated wind speeds of 30 kt, gusting to 48 kt, with a mean wind direction of 320°. It also included blowing dust and visibility of 2,000 m, with severe turbulence below 5,000 ft above ground level.
The weather observations recorded at the airport about 11 minutes prior to the accident, indicated a wind speed of 25 kt, gusting to 39 kt, from a direction of 320°, with visibility reduced to 6,000 m.
Cockpit voice recorder
Cockpit voice recorders (CVR) are designed on an endless loop principle, where the oldest audio is continuously overwritten by the most recent audio. The CVR fitted to the aircraft was a Universal model CVR-30B, part number 1603-02-03, serial number 1541. This model of recorder used solid-state memory to record cockpit audio and had a recording duration of 30 minutes.
The CVR was recovered from the aircraft and transported to the ATSB’s technical facility in Canberra, Australian Capital Territory, on 25 January 2020 for examination and download. The CVR was successfully downloaded, however, no audio from the accident flight had been recorded. All recovered audio was from a previous flight when the aircraft was operating in the United States.
Further investigation
The investigation is continuing and will include consideration of the following:
engine, gearbox and propeller component examinations
aircraft maintenance history
aircraft performance and handling characteristics
impact sequence
analysis of numerous witness reports
review and analysis of the available recorded data, including witness videos, aircraft tracking data, audio recordings and any onboard systems
review and analysis of environmental influences
the crew's qualifications, experience and medical information
the nature of aerial fire-fighting operations
operating policies and procedures
exploring the possible reasons why the CVR did not record the accident flight
similar occurrences.
The ATSB will continue to consult with the engine and airframe type certificate holders. Accredited representatives from the United States National Transportation Safety Board (NTSB) have been appointed to participate in the investigation.
Acknowledgments
The ATSB acknowledges the support of the NSW Police Force, NSW Rural Fire Service, NSW Fire and Rescue, the Australian Defence Force, and those involved with facilitating safe access to an active fire ground and supporting the ATSB’s on-site investigation team.
_________
The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this preliminary report. As such, no analysis or findings are included.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 22 January 2020, at about 1530 Eastern Standard Time,[1] a Cessna 182Q, registered VH‑WNR, took off from Caloundra aerodrome, Queensland. The pilot was conducting a private sightseeing flight with one passenger on board.
The aircraft flew south to the light aircraft lane at Woorim on Bribie Island, climbing to transit to Moreton Island. At 1606, the pilot reported on the Brisbane air traffic control (ATC) frequency that the aircraft’s position was overhead Tangalooma resort, Moreton Island, at 2,500 ft. He also stated that his intention was to track south to the end of Moreton Island and then north up the eastern side of the island.
Recorded radar data at 5-second intervals indicated that, from about 1613, the aircraft flew north along Moreton Island’s eastern coastline at 1400–1500 ft above mean sea level (AMSL) with a groundspeed of 100–110 kt (Figure 1). The wind at the time was about 19 kt from the north-north-east, so the aircraft’s airspeed would have been about 120–130 kt.
Figure 1: Preliminary representation of the flight path of VH-WNR
Source: Google Earth, modified by the ATSB.
At 1624, the aircraft passed the northern tip of the island at about 1,100 ft in a shallow descent (about 160 ft/minute). It then continued north-east towards Flinders Reef, 6 km away (Figure 2), at a similar airspeed and descent rate.
Figure 2: Preliminary representation of the flight path of VH-WNR, near Flinders Reef
Source: Google Earth, modified by the ATSB.
The aircraft’s descent rate began to increase from 1625:09. At 1626:26, the pilot made a MAYDAY[2] call on the Brisbane ATC frequency, without identifying the nature of the problem. At this time, the aircraft was east of Flinders Reef and descending at about 1,400 ft/minute through 300 ft with a groundspeed of about 115 kt. The air traffic controller attempted to establish contact with the pilot; however, no further transmissions from the aircraft were received.
The aircraft’s transponder continued to transmit. Later analysis of the recorded radar data indicated that the aircraft probably continued north-east for 15–20 seconds after the MAYDAY call before colliding with water. There were no witnesses.
An aerial and marine search was initiated. The aircraft was located on the ocean floor on 29 January 2020, north-east of Flinders Reef. The pilot and passenger have not been located.
Context
Pilot information
The pilot was reported to have flown in Africa and Australia decades earlier. He then had an extended break from flying and resumed in late 2019. After conducting 13.5 hours flying training he was reissued a Private Pilot Licence (Aeroplane) on 17 October 2019 with a class rating for single engine aeroplanes.
The pilot held a Class 2 Aviation Medical Certificate that was issued on 17 October 2019 and valid until 17 October 2021.
The available information from the pilot’s records indicated that he had about 1,700 hours total aeronautical experience and had previously held night VFR[3] and instrument ratings. He was also reported to have significant experience on the Cessna 182 type and had flown VH‑WNR several times over the previous week, including around Moreton Island. His last flight prior to the accident flight was on 19 January.
Aircraft information
The aircraft (Figure 3) was manufactured in 1978 and was first registered in Australia in the same year.
The aircraft was fitted a Continental O-470-U piston engine, installed new in December 2013. It had been operated for approximately 742 hours before the accident flight.
The aircraft was operated by a flying school. It was privately hired to the pilot for the flight.
The aircraft’s last periodic (100 hourly) inspection was conducted on 21 August 2019 and the last maintenance release was issued on the same date. At the time of the accident, the aircraft had about 3,318 hours total time in service and 73 hours time in service since the previous periodic inspection.
The last maintenance conducted on the aircraft was on 21-22 January 2020, when the alternator and regulator were replaced to rectify an electrical defect reported by another pilot on 20 January.
Figure 3: Cessna 182, registered VH-WNR, in 2019
Source: Aircraft operator.
Site and wreckage
The wreckage was located in about 30 m of water. The engine and propeller were found about 10 m away from the main wreckage.
The Queensland Police Service (QPS) took underwater video footage of the wreckage on 29–30 January 2020. The ATSB examination of the video footage identified that the aircraft was destroyed by impact with water (Figure 4). Damage to the cabin indicated that the impact was unlikely to be survivable. One of the front seats was found floating some distance from the wreckage, and the other front seat was not located. Both of the front seats’ seat belts were found to be attached to the airframe and latched. All major aircraft components were accounted for in the video footage.
On 6 February, with assistance from the QPS and the Queensland National Parks and Wildlife Service, the ATSB recovered some aircraft components including the engine, propeller and instruments for examination. No pre-existing defects were identified during workshop examinations of the engine and propeller.
The ATSB identified that the only item on the aircraft that was likely to record any data was a J.P. Instruments EDM-700 engine monitoring recorder. The ATSB recovered the instrument and obtained data from it. Further analysis will be required to determine whether the data is relevant to the accident flight.
Figure 4: Wreckage of VH-WNR on ocean floor
Source: Queensland Police Service.
Meteorological information
Relevant aviation weather forecast(s) indicated good visual flying conditions would have existed at the time of the flight.
The nearest weather station to the aircraft’s flight path was at Cape Moreton, at the northern end of Moreton Island and a height of 328 ft AMSL. Observations taken at 1600 and 1630 showed the wind speed was 19 kt, gusting to 24 kt. No precipitation was recorded. The temperature at 1630 was 27.1 °C, dew point 24.9 °C and QNH 1,009.5 hPa. Other nearby weather stations recorded similar observations.
Satellite images taken at 1620 and 1630 indicated no significant cloud in the vicinity of the northern end of Moreton Island. The 1630 METAR (meteorological aerodrome report) for Brisbane Airport, 29 NM south-west of Cape Moreton, reported few cloud at 2,000 ft and broken cloud[4] at 27,000 ft.
A pilot, who was flying over Bribie Island at about 1600, recalled the visibility over Tangalooma on Moreton Island was clear.
Further investigation
The investigation is continuing and will include further examination and analysis of the:
recovered components including engines and propellers
aircraft’s maintenance and operational records
video footage of the wreckage
pilot qualifications, experience and medical history
recorded radio, radar and engine monitoring data.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 22 January 2020, a Cessna 182Q, registered VH-WNR, took off from Caloundra Aerodrome, Queensland. The pilot was conducting a private sightseeing flight with one passenger on board. At 1624, the aircraft passed the northern tip of Moreton Island at about 1,200 ft in a shallow descent towards nearby Flinders Reef.
The aircraft’s descent rate began to increase with no significant changes to direction or speed. At 1626:26, the pilot made a MAYDAY call identifying the aircraft but not its position or nature of the emergency. At this time, the aircraft was east of Flinders Reef and descending at about 1,400 ft/min through 300 ft with a groundspeed of about 115 kt. The aircraft continued north-east for 15–20 seconds after the MAYDAY call before colliding with water.
On 29 January 2020, the aircraft was located on the ocean floor to the north-east of Flinders Reef, about 45 m from the estimated point of impact with water. The pilot and passenger were not located.
What the ATSB found
The nature of any in-flight emergency or abnormal situation, and any effect it had on the pilot’s ability to control and configure the aircraft for ditching, could not be established.
ATSB analysis found that the engine’s power was reducing over the last part of the flight, over a period of about 100 seconds. At the time of the accident, the weather conditions were conducive to carburettor icing. These conditions are common in the region. However, a conclusion regarding the possible influence of carburettor icing on the development of the accident could not be drawn with any certainty.
The ATSB also found that the pilot had descended over water beyond the glide range of a suitable landing area twice on a previous flight, limiting the options for a forced landing in the event of an emergency.
Safety message
Although it could not be determined whether the aircraft’s descent out of glide range was intentional, pilots are reminded that the operation of single engine aircraft over water should at all times be conducted with consideration of the aircraft’s glide distance to a suitable landing area.
The occurrence
On 22 January 2020, at about 1530 Australian Eastern Standard Time,[1] a Cessna 182Q, registered VH‑WNR, took off from Caloundra Aerodrome, Queensland. The pilot was conducting a private sightseeing flight with one passenger on board. The flight was being conducted under visual flight rules (VFR).[2] Weather observations and the short-term forecasts for the area indicated that good visual flying conditions existed at the time of the flight.
The aircraft flew south to the VFR route[3] at Bribie Island, climbing to transit at 3,500 ft to Moreton Island. At 1606, the pilot reported on the Brisbane Centre air traffic control (ATC) frequency that the aircraft’s position was overhead Tangalooma at 2,500 ft. The pilot broadcast their intention to track south to the southern end of Moreton Island and then north up the eastern side of the island.
Recorded radar data at 5-second intervals indicated that, from about 1613, the aircraft flew north along Moreton Island’s eastern coastline at 1,400–1,500 ft above mean sea level with a groundspeed of 100–110 kt (Figure 1). The wind was about 19 kt from the north-north-east, meaning the aircraft’s airspeed would have been about 120–130 kt.
Figure 1: Flight path of VH-WNR on the accident flight
Source: Google Earth, modified by the ATSB
At 1623, the aircraft commenced a shallow descent (about 162 ft/min) from 1,500 ft. At 1625, the aircraft passed Cape Moreton at the northern tip of the island at about 1,300 ft and continued north-east towards Flinders Reef, at a similar airspeed and descent rate (Figure 2).
Figure 2: Flight path of VH-WNR, near Flinders Reef
Source: Google Earth, modified by the ATSB
At 1625:09, the aircraft passed through an altitude of 1,200 ft and the descent rate began to increase with a concurrent reduction in engine power. At 1626:26, the pilot made a MAYDAY[4] call on the Brisbane Centre ATC frequency, identifying the aircraft’s callsign but not its position or the nature of the emergency. At this time, the aircraft was east of Flinders Reef and descending at about 1,400 ft/min through 300 ft with a groundspeed of about 115 kt. The air traffic controller attempted to establish contact with the pilot; however, no further transmissions from the aircraft were received.
The aircraft’s transponder continued to transmit. Analysis of the recorded radar data indicated that the aircraft continued north-east for 15–20 seconds, while still descending, after the MAYDAY call. There were no witnesses.
An aerial and marine search was immediately initiated. The aircraft was located on the ocean floor on 29 January 2020, north-east of Flinders Reef (Figure 2). The pilot and passenger were not located.
The pilot was reported to have flown aircraft overseas and in Australia decades earlier. Logbook records showed that the pilot had an extended break from flying and resumed in late 2019. After conducting 13.5 hours of flight training, the pilot was issued a Civil Aviation Safety Regulation Part 61 Private Pilot (Aeroplane) Licence on 17 October 2019 with a class rating for single engine aeroplanes.
The pilot held a Class 2 Aviation Medical Certificate that was issued on 17 October 2019 and valid until 17 October 2021, with a condition requiring reading correction be available when exercising the privileges of the licence. A review of the pilot’s medical records and interview with a close family member identified no significant medical conditions.
The pilot’s logbook records showed about 1,700 hours total aeronautical experience and previous night VFR[5] and instrument flight rules[6] experience. The pilot was also reported to have significant experience on the Cessna 182 type and had flown VH‑WNR 6 times over the previous fortnight, including around Moreton Island (see also Previous flights in VH-WNR). Prior to the accident flight, the pilot’s last logged flight was on 19 January 2020.
Aircraft information
General
The Cessna 182Q is a high-wing, all-metal, unpressurised aircraft with a fixed landing gear. The accident aircraft had a single, Continental O-470-U reciprocating piston engine driving a constant-speed propeller. The engine ignition system comprised two magnetos that provided a self-generated charge to the engine spark plugs and was independent of the aircraft electrical system.
An engine driven alternator supplied electrical power to aircraft systems. The alternator was also used to charge the battery and was controlled by a voltage regulator. A battery supplied power for engine starting and was a reserve source of power in the event of alternator failure.
VH-WNR (Figure 3) was manufactured in 1978 and was first registered in Australia in the same year. The aircraft was privately hired by the pilot for the flight.
Figure 3: VH-WNR in 2019
Source: Aircraft operator
Maintenance history
At the time of the accident, VH-WNR had about 3,318 hours total time in service and had flown about 73 hours since the previous periodic inspection (100 hourly), which was conducted on 21 August 2019. The engine was installed new in December 2013 and had accumulated about 742 hours time in service.
During a flight on 19 January 2020,[7] the aircraft began to experience electrical issues over a period of about 3 minutes, resulting in the loss of some aircraft systems including the radio and transponder. After landing, engineers identified that the aircraft charging system was unserviceable and the battery had discharged. The battery was charged for the return flight to Caloundra. A new voltage regulator and alternator were fitted and the battery was charged again. On the morning of 22 January 2020, 6–7 ground runs were carried out to test and adjust the replaced components before the aircraft was released to service.
Weight and balance
According to a witness, the pilot visually checked the aircraft’s fuel quantity prior to the accident flight with the aid of a dipstick, which showed there was 135 L on board. A correction was made to the fuel record, which had been incorrectly annotated as 130 L. This amount was more than sufficient fuel for the intended flight.
Based on witness observations as well as estimates of fuel and occupant weights, the aircraft was likely within its weight and balance limits for the entire flight.
Meteorological information
The nearest weather station to the flight path of the aircraft was at Cape Moreton, at the northern end of Moreton Island, 328 ft above sea level. Observations taken at 1600 and 1630 both showed the wind speed at 19 kt from 030°, gusting to 24 kt, with no recorded precipitation.
Satellite images taken at 1620 and 1630 indicated visual meteorological conditions in the vicinity of the northern end of Moreton Island. The 1630 meteorological aerodrome report for Brisbane Airport, about 53 km south-west of Cape Moreton, stated the cloud cover as ‘few’ at 2,000 ft and ‘broken’ at 27,000 ft.[9]
Another pilot was conducting a training flight in the vicinity of Bribie Island shortly before the accident. That pilot described the conditions and visibility as good for VFR operations with some low-level turbulence. Above 1,000 ft the conditions were smoother with a north-westerly wind at about 18 kt.
Wreckage and impact information
Wreckage location
Immediately after the accident, after being advised by Airservices Australia that contact was lost with VH-WNR, the Queensland Police Service (QPS) and the Australian Maritime Safety Authority (AMSA) commenced an aerial and marine search operation. That evening, floating debris from the aircraft was found and recovered. The following day the marine search focused on a position near Flinders Reef, but the aircraft could not be located.
At the request of the QPS, the ATSB analysed the supplied radar data and refined the estimated position of the aircraft on 28 January 2020. The wreckage was located by the QPS on the morning of 29 January 2020, about 45 m from the supplied coordinates in about 30 m of water. The engine and propeller were found about 10 m north-east of the main wreckage. The QPS took underwater video of the wreckage on 29–30 January 2020.
Partial wreckage recovery
On 6 February, with assistance from the QPS, specialists from the New South Wales Police Force and the Queensland National Parks and Wildlife Service, the ATSB recovered various aircraft components including the engine, propeller and instruments for detailed examination.
Wreckage examination
ATSB examination of the underwater video identified that the aircraft was likely destroyed by collision with water at a moderately high speed (Figure 4). Damage to the aircraft cabin from the collision with water indicated that it was unlikely to be survivable. There was no evidence of fire.
All major aircraft components were accounted for, and there was no evidence of pre-impact defects or structural failure. As far as could be established, cockpit switch positions were configured as expected for normal flight.
The flap control and right flap were found in the ‘up’ position. The left flap was observed to be displaced towards the down position from disruption caused during accident sequence to the adjacent wing structure. One of the front seats was found floating some distance from the wreckage, and the other front seat was not located. The seatbelts for both front seats were found to be attached to the airframe and latched.
The carburettor heat control, used to prevent or recover from engine icing, was in the ‘off’ position. However, due to the disruption of the wreckage, this may not have been indicative of its position prior to the accident.
Figure 4: Wreckage of VH-WNR on the ocean floor
A weight, rope and buoy had been attached to the aircraft tail by the divers.
Source: Queensland Police Service
Engine examination
The engine was disassembled and examined at a Civil Aviation Safety Authority (CASA) approved overhaul facility under the supervision of the ATSB. Apart from impact and submersion damage, the engine was generally in good condition. Some components such as the magnetos, alternator and voltage regulator were extensively damaged by their immersion in seawater and their function could not be tested. No pre-existing defects were evident, and there was no evidence of fire or overheating (Figure 5).
Figure 5: Corrosion damage to the magnetos
Source: ATSB
Propeller examination
The propeller was disassembled and examined at a CASA-approved overhaul facility under the supervision of the ATSB. No pre-existing defects or irregularities were identified. The propeller could not be functionally tested because of internal damage that occurred during the accident sequence.
The propeller blades were observed to be progressively bent out of plane (Figure 6), in a manner indicative of low but non-zero power. The pitch change lugs on all three blades were sheared off, with the direction of the fracture surface smearing being consistent with the blades being forcibly rotated towards low (fine) pitch, which is an indication of low power or windmilling.
Preload plates are fitted to each propeller blade at their base, within the propeller hub. Each blade pitch change lug transverses through a cut-out in the plates. Using damage signatures made by the propeller blade pitch change lugs onto the preload plates (Figure 6, inset), and estimating the propeller speed from the known velocity of the aircraft in the moments prior to impact, an estimate of power and the blade angle at impact was made using established datums with the assistance of the propeller manufacturer. These calculations were limited in accuracy as the preload plates are not indexed (such as with a key or slot), and so during assembly there could be slight variations with their position. The results of the calculations indicated that the propeller was rotating under low power, and with a blade angle at or near the low pitch stop.
Figure 6: VH-WNR propeller blade bending and inset image of example preload plate damage signatures
Source: ATSB
Recorded data
Accident flight radar data
Airservices Australia provided radar data for the accident flight. This data combined primary surveillance radar (PSR) and secondary surveillance radar (SSR) data into a single, smoothed track. PSR has a shorter range than SSR, and is generally less reliable, but it is used to enhance the accuracy of SSR tracks and provide position information when SSR is not available.
Position data for the accident flight was generally recorded at 5‑second intervals, and occasionally at a 4- or 6-second interval. It included Mode C altitude data that was obtained from the aircraft static system referenced to the standard atmospheric pressure (1,013.25 hPa) and rounded to the nearest 100 ft. The aircraft’s average groundspeed between data points was derived from the position and time data.
The approximate position the aircraft collided with water was determined from the system track by extrapolating the estimate of groundspeed and a fitted altitude curve to sea level.
Engine monitoring recorder
The ATSB identified that the only item on the aircraft that was likely to record any data was a J.P. Instruments EDM-700 engine monitoring recorder. The ATSB recovered the instrument, however the recorded data it contained did not include the accident flight.
Additional information
Previous flights in VH-WNR
In the weeks prior to the accident, the pilot flew VH-WNR on the following 6 return flights from Caloundra Aerodrome, with available aircraft tracks shown in Figure 7:
1 hours on 8 January as a proficiency check with an instructor (radar data not available)
8 hours with one passenger on 11 January (radar data not available)
8 hours with two passengers on 14 January (radar data not available)
4 hours with two passengers on 15 January (blue line)
2 hours with two passengers on 17 January (orange line)
1 hours with two passengers on 19 January (red line).
Figure 7: Accident pilot’s previous flights in VH-WNR
Source: Google Earth, modified by the ATSB
On the 15 January flight, the pilot transited between Bribie Island and Moreton Island at about 2,000 ft and 80–90 kt groundspeed. The flight profile was broadly similar to the accident flight past Cape Moreton towards Flinders Reef (Figure 8). On the return leg, the pilot flew from Flinders Reef direct to Bribie Island at about 1,800 ft.
Figure 8: Previous flights and the accident flight compared
Source: Google Earth, modified by the ATSB
ATSB analysis indicated that two segments of the 15 January flight, including between Moreton Island and Flinders Reef, were further from land than the aircraft was capable of gliding with no engine power. Although complete analysis of glide distances was not feasible, the ATSB estimated that the aircraft was also flown near or beyond the limits of its glide range to land on other flights in this area. During the accident flight on 22 January, the aircraft similarly reached a point further from glide distance to land about halfway between Moreton Island and Flinders Reef.
On the 19 January flight, when the aircraft was approaching Moreton Island, the Brisbane Centre controller attempted to contact the pilot to advise that the aircraft was 2 NM west of Moreton Island at 3,900 ft (that is, they had entered controlled airspace by climbing above 3,500 ft in that area). After receiving assistance from the pilot of another aircraft in the area, the pilot of VH-WNR made contact with the controller, who explained the problem. The pilot apologised and stated that the entry to controlled airspace was unintentional, and they confirmed they were now at 3,000 ft approaching the eastern side of the island. The controller reminded the pilot to keep at or below 3,500 ft on the way back to Caloundra. On that flight, the pilot did not descend when travelling along the eastern side of Moreton Island.
As noted in The occurrence, during the accident flight on 22 January, the pilot contacted Brisbane Centre to report they were at 2,500 ft approaching Moreton Island. There was no requirement for the pilot to make a call on that frequency in that area while they remained at or below 3,500 ft.
Analysis of thrust required
A performance analysis was carried out on the last minutes of the accident flight based on the radar data, documented performance characteristics of the aircraft type (such as lift and drag coefficients), and estimates of aircraft weight. The analysis calculated the propulsive power that would be required for the aircraft’s estimated airspeed and altitude. For the section of flight analysed, the aircraft was flown with likely minor changes in heading and pitch, for which the radar data was considered sufficiently accurate. The analysis provided an estimate of the thrust power, not engine power, as efficiencies and other power losses were not calculated.
The analysis relied on the following assumptions:
Thrust opposed drag along the longitudinal axis of the aircraft.
The aircraft was not accelerating longitudinally (as indicated by the relatively constant groundspeed).
The aircraft was not banking, slipping, or accelerating vertically (turbulence).
Wing flaps were retracted.
Wind did not vary.
The analysis indicated that there was a reduction in thrust during the last 100 seconds of the flight.[10] At the end of the recorded data, due to the flight path being flown, the thrust power required by the aircraft was approximately zero.
Speech analysis
The ATSB conducted a basic speech analysis on the pilot’s ATC and Caloundra Aerodrome common traffic advisory frequency (CTAF)[11] radio transmissions. The pilot’s response times, delay between microphone keying and speaking, microphone un-keying delay, duration to annunciate the aircraft callsign, average speech rate, and voice pitch were analysed. The analysis was inconclusive regarding whether there were any changes to the pilot’s speech during the accident flight.
Carburettor icing
According to the CASA Visual Flight Rules Guide:
Carburettor icing is of particular concern because, unlike airframe icing, the risk of ice build-up in the carburettor can be high even with no visible moisture and an OAT [outside air temperature] of up to 38°C.
Carburettor icing occurs when the air temperature adiabatically decreases sufficiently to condense water vapour and for the localised air temperature to reduce below freezing. Ice builds up as the chilled condensed water makes contact with localised surfaces, such as the butterfly valve and the venturi walls. Carburettors experience additional cooling because of the evaporation of fuel. Furthermore, the risk of carburettor icing is significantly increased at partial power settings (for example, when power is reduced during descent), because of the cooling effect of a partly-closed throttle.
The effect of carburettor icing on aircraft may result in reduced power output, poor engine performance, rough running and in extreme cases engine failure. The onset of this may be evidenced by an unexplained drop in manifold pressure.
The pilot’s operating handbook (POH) for VH-WNR was not recovered. A reviewed sample of Cessna 182Q POHs required pilots who suspect carburettor icing to apply full throttle and set the carburettor heat control to ‘on’ until the engine ran smoothly.
To assist pilots in anticipating the potential for carburettor icing, CASA published a carburettor icing probability chart (Figure 9). The temperature recorded at Cape Moreton at the time of the accident was 27.1 °C, and the dewpoint 24.9 °C. This gave a dewpoint depression of 2.2 °C. The intersection between the resulting temperature and dewpoint lines was just inside the shaded area where ‘serious’ icing under descent power is possible.
Figure 9: Carburettor icing probability chart with local observations
Source: CASA, annotated by the ATSB
An ATSB review of temperature and dewpoint observations for the south-east Queensland region showed that, over a 12-month period, carburettor icing conditions are frequent.
Previous ATSB investigations found to be, or potentially be, related to carburettor icing include:
AO-2018-050, Wirestrike and collision with terrain involving Cessna 172RG, VH-LCZ, Parafield Airport, South Australia, on 3 July 2018
AO-2016-059, Engine failure involving Piper PA-28, VH-IPO, Mangalore Airport, Victoria, on 16 June 2016
AO-2014-149, Collision with terrain involving Van's Aircraft RV-6, VH-TXF near Mudgee Airport, NSW on 14 September 2014
AO-2012-078, Collision with terrain - Robinson R44, VH-HOU, 93 km S Alice Springs Airport, NT, 10 June 2012.
Flights over water
Civil Aviation Regulation (CAR) 258 (Flights over water) stated:
The pilot in command of the aircraft must not fly over water at a distance from land greater than the distance from which the aircraft could reach land if the engine… were inoperative.
The Aeronautical Information Publication (AIP) stated in ENR 1.1 (section 11.11) that CAR 258 did not apply to charter, aerial work or private operations if each occupant was wearing a life jacket, unless they were exempted from doing so under Civil Aviation Order (CAO) 20.11 (Emergency and life saving equipment and passenger control in emergencies). CAO 20.11 paragraph 5.1.1 (a) stated that a single engine aircraft must carry a life jacket for each occupant when the aircraft was operated over water at a distance from land greater than that it could reach with its engine inoperative. In such cases, paragraph 5.1.7 also stated that each occupant shall wear a life jacket, but this was not required for occupants of aeroplanes during flight above 2,000 ft.
The operator stated that the pilot was briefed to transit between Bribie Island and Moreton Island (a distance of about 15 km) at 3,500 ft using the VFR route. The operator also stated that, after some previous flights, it briefed the pilot that its preference for the pilot was to not operate on the northern side of Cape Moreton.
The operator stated that it encouraged the pilot to take life jackets on board the aircraft, which was done on previous flights. However, witnesses reported that no life jackets were taken on the accident flight.
Carriage of emergency locator transmitter
The aircraft was fitted with a deceleration-activated emergency locator transmitter (ELT), which was not serviceable at the time of the accident. The carriage of an ELT was not required for flights within 50 NM of the origin. A personal locator beacon was carried on board the aircraft at the time, in the glove box of the aircraft.
Cessna 182 emergency procedures
Engine failure
The POH for the Cessna 182Q contained an emergency procedure for an engine failure in flight. For this scenario, pilots were required to establish a best glide speed of 70 kt with the wing flaps retracted, and to identify a suitable landing area (Figure 10).
Figure 10: Cessna 182Q maximum glide distance chart
Source: Cessna, annotated by the ATSB
Ditching
The POH procedure for ditching included transmitting a MAYDAY message over the radio, unlatching the cabin doors, and establishing a level attitude during descent. If engine power was available, the flaps were to be set to 20–40° and the aircraft established in a 60 kt and 300 ft/min descent. In an engine failure situation, the glide speed and configuration should be 70 kt with flaps up or 65 kt with 10° of flap.
The aircraft’s flight path was not indicative of uncontrolled flight, and no pre-existing defects with the aircraft could be identified. Other than a likely gradual loss of engine power, discussed below, there was no evidence of engine overheating, fire, loss of control, or other in-flight emergencies. However, as the entire aircraft could not be recovered, it was not possible to verify the operation of all aircraft systems.
The existence of secondary surveillance radar data for the aircraft almost to its collision with water, as well as the reception of the MAYDAY call, indicated that the aircraft’s electrical systems were receiving power. However, it was not possible to determine whether this was battery or alternator power. In any case, electrical power was not necessary for flight or ditching.
Analysis of the radar data showed there was likely a gradual reduction in thrust (and therefore engine power) during the last 100 seconds of the flight, and that this correlated with the increasing descent rate. The impact signatures on the propeller and propeller pitch change lugs were also consistent with a low level of engine power or windmilling at impact. Although the power reduction may have been due to pilot action, no reason for doing so at this point in the flight could be identified.
The aircraft maintained a moderately high speed until radar contact was lost at about 180 ft. Had the engine been inoperative, the radar data would have indicated a significantly steeper descent profile.
Regardless, a gradual reduction in engine power should not necessarily lead to very serious consequences. If detected early enough, with a suitable emergency landing area within range, a pilot could attempt to land. If no such landing area was available, a pilot could attempt a forced landing or ditching.
In this case, the aircraft maintained course away from suitable landing areas at a speed well above the aircraft’s best glide speed. The pilot may have been initially unaware of the gradual reduction in power and resulting descent. Although this would have been indicated on the aircraft’s instruments, the constant-speed propeller would maintain engine and propeller speed, and a gradual power loss would result in little or no change in sound and feel.
The MAYDAY call shortly before the impact indicated that the pilot was not totally incapacitated. However, in the absence of other evidence, a partial incapacitation could not be excluded.
The aircraft’s final position on the sea floor close to the last radar position strongly indicated that it continued along the established flight path without turning or, more critically, reducing descent rate and speed for a ditching. Furthermore, examination of the video footage of the wreckage on the sea floor showed the flaps were likely up at impact and that the aircraft had been significantly disrupted by a relatively high-speed collision with water.
In summary, the nature of any in-flight emergency or abnormal situation, and any effect it had on the pilot’s ability to control and configure the aircraft for ditching, could not be established.
Descent over water beyond glide range
On 15 January 2020, the pilot descended over water beyond the maximum glide distance of a suitable landing area for a Cessna 182Q during two segments of that flight. However, there was insufficient evidence to determine if an emergency landing on Moreton Island was possible had the pilot been able to turn the aircraft and establish the optimal glide speed. Nevertheless, flight outside of the glide range of a suitable landing area limits the opportunities for recovery in the event of an engine failure or other emergency. The same situation occurred on the accident flight, although the extent to which this was intentional could not be determined.
Carburettor icing
Carburettor icing can be insidious in its development and have serious consequences. Weather observations taken at Cape Moreton at the time of the accident, and plotted on the carburettor icing probability chart, showed that carburettor icing was possible. The plotted point was just inside the serious icing range at descent power and adjacent to the light icing range in cruise or descent power.
The likely reduction in power in the last 100 seconds of recorded flight could plausibly have been due to carburettor icing. However, carburettor icing conditions are frequently encountered in the region, and prevention and management of carburettor icing is easily done through use of carburettor heating. As the pilot had significant experience on the Cessna 182, they would very likely have been familiar with the use of carburettor heating. Due to wreckage disruption during the impact sequence, the position of the carburettor heat control during the accident flight could not be established. Overall, a conclusion regarding carburettor icing could not be drawn with any certainty.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with water involving Cessna 182, registered VH-WNR, 6 km north-west of Moreton Island, Queensland, on 22 January 2020.
Contributing factors
After passing the northern end of Moreton Island at 1,200 ft, the aircraft continued descending away from the island at about 110 kt groundspeed, with no significant change in direction and with reducing engine power. The pilot broadcast a MAYDAY when passing 300 ft; however, for reasons that could not be determined, the flight path and speed of the aircraft did not significantly change after this point until it collided with water.
Other factors that increased risk
The pilot had descended over water beyond the glide range of a suitable landing area twice on a previous flight, limiting the options for a forced landing in the event of an emergency.
At the time of the accident, the meteorological conditions were conducive to carburettor icing. However, such conditions are common in the region, and able to be easily managed with the aircraft’s carburettor heat control.
Other findings
From the limited evidence available, no pre-existing aircraft defects could be identified.
Glossary
AMSA Australian Maritime Safety Authority
ATC Air traffic control
CASA Civil Aviation Safety Authority
POH Pilot’s operating handbook
PSR Primary surveillance radar
QPS Queensland Police Service
SSR Secondary surveillance radar
VFR Visual flight rules
Sources and submissions
Sources of information
The sources of information during the investigation included:
another pilot who flew VH-WNR
the aircraft operator
Civil Aviation Safety Authority
Queensland Police Service
the maintenance provider
Hartzell propeller
Airservices Australia
Bureau of Meteorology.
References
National Aeronautics and Space Administration 1973, Point and path performance of light aircraft, Contractor report NASA CR-2272.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the aircraft operator
the maintenance provider
Civil Aviation Safety Authority
US National Transportation Safety Board
Hartzell propeller.
Submissions were received from the aircraft operator, the Civil Aviation Safety Authority, and Hartzell propeller. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Sequence of events
On 14 December 2019, two pilots were preparing to conduct a flight review[1] in an Angel Aircraft Corporation Model 44 aircraft, registered VH-IAZ (IAZ) (Figure 1). The aircraft was owned and operated by the pilot under review, who was to occupy the left seat. The right-seat pilot had a Grade 1 flight instructor rating. The flight was to be conducted as a private flight and the right-seat pilot was the pilot in command for the flight.
Figure 1: VH-IAZ (when formerly registered as VH-IOZ)
Source: Provided to the ATSB
Closed circuit television footage from Mareeba Airport, Queensland, showed the aircraft taxi and park outside a hangar at 0922 Eastern Standard Time.[2] A witness observed the left-seat pilot in the aircraft conducting engine run-ups between 0915 and 0930. The aircraft engines were then shut down.
At 1046, the pilots taxied the aircraft from outside the hangar towards the runway intersection. In recorded radio transmissions, the left-seat pilot broadcast on the common traffic advisory frequency that IAZ was taxiing for runway 28.[3]
At 1054, the left-seat pilot broadcast that IAZ was entering and backtracking the runway and 4 minutes later, that the aircraft had commenced the take-off roll on runway 28. Witnesses heard the aircraft during the take-off roll and reported that it sounded like one of the engines was hesitating and misfiring. An aircraft maintainer at the airport observed the aircraft take off and reported seeing black sooty smoke trailing from the right engine. He then watched the aircraft climb slowly and turn right towards the north. Another witness who heard the aircraft in flight reported that it sounded normal for that aircraft, which had a distinctive sound because the engine’s exhaust gases pass through the propellers.
Once airborne, the pilot broadcast that they were ‘making a low-level right-hand turn and then climbing up to not above 4,500 [feet] for the south-west training area.’
About 2 minutes later, the right-seat pilot broadcast that they were just to the west of the airfield in the training area at 2,500 ft and on climb to 4,000 ft, and communicated with the pilot of a helicopter operating in the area.
After 8 minutes in the training area, the left-seat pilot broadcast that they were inbound from the training area and 2 minutes later, that they were joining crosswind for runway 28. No further transmissions were heard from the aircraft.
Witnesses then saw the aircraft touch down on the runway and take off again, and heard one engine ‘splutter’ as the aircraft climbed to between 300 and 450 ft above ground level. At about 1115, the aircraft was observed overhead a banana plantation beyond the end of the runway in a right descending turn, before it suddenly rolled right. Witnesses observed the right wing drop to near vertical and the aircraft collided with terrain in a cornfield. Both pilots were fatally injured, and the aircraft was destroyed.
Weather and environmental information
At 1115 EST, the temperature was 34 ºC, the dewpoint 15 ºC, and the wind from 266º at 6 kt gusting to 9 kt. There was no cloud and the QNH[4] was 1012 hPa.
The aerodrome elevation was 1,650 ft and with the given temperature and QNH, the density altitude[5] was 4,440 ft.
Recorded data
The aircraft was not equipped with a flight data recorder or cockpit voice recorder, nor was it required to be. A witness reported watching the aircraft track on OzRunways,[6] but the ATSB has not yet obtained any recorded data for the flight.
Aircraft information
The Angel Aircraft Corporation Model 44 was an eight-seat, twin-engine aircraft with retractable tricycle landing gear. It was designed for short take-off and landing distances, long endurance and the ability to carry a heavy payload. The aircraft was powered by two Lycoming IO-540-M1C engines with Hartzell three-blade constant speed feathering[7] HC-E3YR-2ALTFC pusher propellers mounted aft of the engines.
IAZ was manufactured in the United States in 2008 with serial number 004. It was first registered in Australia in January 2010 as VH-IOZ, deregistered in November 2017 and reregistered as VH-IAZ in March 2019. The aircraft was approved to operate under the instrument flight rules[8] and in the charter category.
The factory-rebuilt right engine was installed in May 2017 and had run for a total of 2.2 hours before the accident flight. The factory-overhauled left engine was installed in June 2016 and had run for a total of 12.7 hours prior to the accident flight.
On 10 December 2019, two new spark plugs were fitted to cylinder No. 3 on the right engine and one spark plug was replaced on cylinder No. 1 on the left engine due to magneto drops during ground runs. The engines were subsequently ground run satisfactorily.
The last maintenance release[9] (MR) was issued on 30 April 2019 and the aircraft had 1,803.5 hours total time in service. No daily inspection or additional flight time was recorded on the MR.
Operational information
The pilot under review (left seat) had accrued over 20,000 flying hours, approximately 300 of which were in IAZ.
The right-seat pilot held an air transport pilot licence and had accrued approximately 5,000 hours of aeronautical experience. He had not previously flown IAZ.
Wreckage and impact information
Examination of the aircraft wreckage indicated that the aircraft impacted terrain right wingtip first, then nose, followed by the left wingtip. The aircraft then pivoted about the left wing and the fuselage came to rest upright (Figure 2).
Figure 2: Accident site
Source: ATSB
Continuing investigation
The investigation is continuing and will include examination of the following:
recovered components including engines and propellers
the aircraft’s maintenance and operational records
aircraft and site survey data
pilot qualifications, experience and medical history
regulatory requirements for flight reviews
previous research and similar occurrences.
______________
The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this report. As such, no analysis or findings are included in this report.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 14 December 2019, two pilots were conducting a private flight in an Angel Aircraft Corporation Model 44 aircraft, registered VH-IAZ, at Mareeba, Queensland. An instructor seated in the right pilot seat was conducting a flight review of the pilot (and aircraft owner) in the left seat.
The aircraft took off from Mareeba Airport at 1058 Eastern Standard Time,[1] after which witnesses reported hearing one of the engines hesitating and backfiring, accompanied by a sooty smoke trail from the right engine. The aircraft operated in the training area until returning to the airport circuit area at 1112. Witnesses observed the aircraft touch down on the runway, accelerate and take off again. After take-off, the aircraft climbed to about 100-150 ft above ground level before entering a right descending turn. The aircraft was airborne for about 20 seconds before witnesses observed it rolling rapidly to the right and impacting terrain in a cornfield 475 m north of the runway. The pilots sustained fatal injuries and the aircraft was destroyed.
What the ATSB found
Based on the witness reports of abnormal engine sounds and because the instructor had planned to conduct a simulated engine failure after take-off, the ATSB assessed whether the accident occurred following a simulated or real engine failure.
Examination of the fuel system found that two of the fuel injectors in the right engine showed evidence of partial blockage by corrosion particles. Such blockage would have resulted in the over-fuelling of the other injectors and the engine running overly rich; reducing the maximum power available from that engine. There was, however, no evidence of a complete power loss, with both engines producing power at the time of impact.
The ATSB found that shortly after take-off, the flight instructor very likely conducted a simulated failure of the right engine in environmental conditions and a configuration in which the aircraft was unable to maintain altitude with one engine inoperative. Power was not immediately restored to the right engine to discontinue the exercise and the pilots were unable to maintain altitude or heading, particularly with the aircraft banked towards the inoperative engine. The pilots did not reduce power and land ahead, as required by the Airplane Flight Manual, resulting in a loss of directional control and roll. The loss of control occurred at a height too low to recover and the aircraft impacted terrain.
The instructor had limited experience in multi-engine aeroplanes with retractable landing gear and only one short flight in the Angel 44 aircraft several years earlier. Therefore, the instructor was likely unfamiliar with the time necessary for the landing gear and flaps to retract (significantly longer than other aircraft the instructor had flown) and the associated detrimental effect that extended flaps and landing gear had on the aircraft’s single-engine climb performance. This likely influenced the decision to initiate a low-level simulated engine failure and diminished the instructor’s ability to interpret and manage the situation.
Additionally, the pilot (in the left seat) had not flown for 3 years prior to the accident flight, which likely resulted in a decay of skills at managing tasks such as an engine failure after take-off. The pilot probably over-estimated their self-assessed competency for the planned task and did not demonstrate proficiency at a safe height before the low-level simulated engine failure.
The ATSB found that the right-side altimeter was probably set to an incorrect barometric pressure, resulting in it over-reading the aircraft’s altitude by about 90 ft.
The aircraft had not been flown regularly for more than 2 years and the engines had not been preserved in accordance with the manufacturer’s procedures. Both engines had mild internal corrosion and the right engine had signs of water contamination within the fuel system, including in the engine‑driven fuel pump and fuel injection servo. Corrosion particles in the fuel injection servo likely originated from the fuel tank. These particles lodged in two of the fuel injection nozzles and contributed to the right engine running overly rich, backfiring and a reduction in maximum power available.
Safety message
Flight reviews
Flight reviews that are conducted without the oversight of a training organisation remove the opportunity to include training. Due to the known limitations of self-assessed competency, pilots who choose this option should have recent demonstrated proficiency in all of the required exercises.
Simulated engine failures
In light twin-engine aeroplanes, loss of power on one engine shortly after take-off poses a high risk due to low altitude, low airspeed and generally limited single-engine climb performance. The asymmetric thrust can lead to a loss of directional control that, if mishandled, will likely result in an accident due to insufficient height above the ground to recover.
The regulatory requirement to use simulators for conducting engine failure after take-off exercises has eliminated the risk for those aircraft where simulators are available. However, where simulators are not available, there is still a requirement to perform the exercise in the aircraft. In those situations, it is essential to understand the risks and ensure effective controls are in place to prevent the simulation turning into a loss of control at low level, where recovery will probably not be possible. Consideration of these risks should include:
the method of simulating engine failure
instructor/check pilot training, experience and proficiency specific to the aircraft make and model
ensuring the pilot/student has first demonstrated the ability to maintain asymmetric control at a safe height and understands handling one engine inoperative flight and associated risks
thorough pre-flight briefing including minimum control speed, configuration including flaps and landing gear, safe intentional single-engine speed, one engine inoperative climb performance and limitations
ensuring the aircraft is in a configuration and at an airspeed at which climb with one engine inoperative is possible
criteria for aborting the procedure including airspeed, height above terrain/obstacles, directional control and bank angle
effect of, and time required to restore power to the simulated inoperative engine
understanding when a reduction in power and landing ahead may be ultimately necessary to avoid a loss of control.
Attempting to continue flight with one engine inoperative in a multi-engine aeroplane when directional control cannot be maintained, carries a high risk of an accident and fatal injuries.
Airframe and engine preservation
If an aircraft is not flown regularly, the airframe and engine/s should be preserved in accordance with the manufacturer’s procedures. Incorrect or inadequate preservation can increase the likelihood of in-flight failures, with the associated safety risks.
The sources of information during the investigation included the:
aircraft maintainer
witnesses
aircraft, engine and propeller manufacturers
Bureau of Meteorology
Civil Aviation Safety Authority
Queensland Police and forensic pathologist.
References
Arora et al., (2011). Self vs expert assessment of technical and non-technical skills in high fidelity simulation. The American Journal of Surgery, 202, 500-506.
Arthur Jr, W; Bennett, Jr, W; Stanush, PL and McNelly, TL 1988, Factors that influence skill decay and retention: A quantitative review and analysis. Human Performance 11(1) 57-101.
Campbell, K. S., Mothersbaugh, D. L., Brammer, C., & Taylor, T. (2001). Peer versus self assessment of oral business presentation performance. Business Communication Quarterly, 64(3), 23-42.
Civil Aviation Safety Authority 2002, Even worse than the real thing. Flight Safety Australia, March-April 2002.
Dunning, D., Heath, C., & Suls., J. M. (2004). Flawed self-assessment. Implications for health, education and the workplace. Psychological Science in the Public Interest, 5(3), 69-106.
Federal Aviation Administration 2016, Airplane Flying Handbook FAA-H-8038-3B. US Department of Transportation, Federal Aviation Administration, Flight Standards Service.
Raaijmakers et al., (2017). Effects of self-assessment feedback of self-assessment and task-selection accuracy. Metacognition and Learning, 14, 21-42.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the aircraft maintainer
the aircraft, engine and propeller manufacturers
the certificate of airworthiness issuer
the Civil Aviation Safety Authority
the US National Transportation Safety Board
the UK Air Accidents Investigation Branch.
Submissions were received from:
the aircraft manufacturer
the certificate of airworthiness issuer
the Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
The occurrence
On 14 December 2019, at 1046 Eastern Standard Time,[2] an Angel Aircraft Corporation Model 44 aircraft, registered VH-IAZ (Figure 1), commenced taxiing at Mareeba Airport, Queensland. On board the aircraft were two pilots. The pilot in the left seat (‘the pilot’) owned the aircraft and was undertaking a flight review,[3] which was being conducted by the Grade 1 flight instructor in the right seat (‘the instructor’). The planned flight was to operate in the local area, as a private flight and under visual flight rules.[4]
Figure 1: VH-IAZ (when formerly registered as VH-IOZ)
Source: Aircraft maintainer
As the aircraft taxied towards the runway intersection, the pilot broadcast on the common traffic advisory frequency (CTAF)[5] that VH-IAZ was taxiing for runway 28.[6] The pilot made another broadcast when entering and backtracking the runway, then at 1058, broadcast that the aircraft had commenced the take-off roll.
Witnesses who heard the aircraft during the take-off reported that it sounded like one of the engines was hesitating and misfiring. An aircraft maintainer who observed the aircraft take off, reported seeing black sooty smoke trailing from the right engine. The maintainer then watched the aircraft climb slowly and turn right towards the north. Another witness who heard the aircraft in flight soon afterwards, reported that it sounded normal for that aircraft, which had a distinctive sound because the engines’ exhaust gases pass through the propellers.
Once airborne, the pilot broadcast that they were ‘making a low-level right-hand turn and then climbing up to not above 4,500 [feet] for the south-west training area.’
About 2 minutes later, the instructor broadcast that they were just to the west of the airfield in the training area at 2,500 ft and on climb to 4,000 ft, and communicated with a helicopter pilot operating in the area. After 8 minutes in the training area, the pilot broadcast that they were inbound to the aerodrome.
At 1112, the aircraft’s final transmission was broadcast by the pilot, advising that they were joining the crosswind circuit leg for runway 28.
Witnesses then saw the aircraft touch down on the runway and continue to take off again, consistent with a ‘touch-and-go’ manoeuvre, and heard one engine ‘splutter’ as the aircraft climbed to an estimated 100–150 ft above ground level. At about 1115, the aircraft was observed overhead a banana plantation beyond the end of the runway, banked to the right in a descending turn, before it suddenly rolled right. Witnesses observed the right wing drop to near vertical and the aircraft impacted terrain in a cornfield. Both pilots were fatally injured and the aircraft was destroyed (Figure 2).
Figure 2: Accident site showing the take-off direction, initial impact point and fuselage resting position
During a planned flight review, VH-IAZ touched down on the runway at Mareeba Airport and after accelerating, took off again. About 20 seconds after take-off, the aircraft rolled rapidly to the right and impacted terrain, fatally injuring the pilot and instructor.
Although post-mortem examination identified coronary atherosclerosis in the pilot and instructor, which increased the risk of incapacitation, there was no evidence that this occurred. The nature of the loss of aircraft control was consistent with the aircraft slowing to below the minimum control speed and as such, a medical event affecting the pilot flying was unlikely.
The following analysis will consider the operational factors associated with the development of the accident.
Development of the accident
Engine failure scenario
After the aircraft took off, witnesses observed it climb to 100–150 ft above ground level (AGL) and one witness heard an engine splutter. The aircraft was seen to turn and bank to the right, descend slowly then suddenly roll right wing down and impact the ground. Due to the low height reached and the abnormal engine sounds reported by witnesses, the ATSB analysed whether the loss of control occurred following an actual engine failure or an intentional simulated one.
Actual engine failure
Neither pilot declared an emergency on the common traffic advisory frequency, which would be expected following an actual engine failure but not a simulated one. In any case, however, there was very limited time available to make such a call.
Technical examination of the engines did not reveal any pre-impact failure that would have prevented the left engine from producing full power, and although the right engine was likely running overly rich,[22] there was no indication of an uncommanded power loss or complete engine failure.
Had the right engine actually failed shortly after take-off, when a witness heard spluttering, the immediate pilot actions called for the fuel mixture, propeller pitch and throttle levers to be pushed fully forwards, the landing gear and flaps selected up, and once the failed engine had been identified (as the right-hand engine) the right propeller feathered by moving the right pitch lever to the fully aft position. All of which could have been achievable within a few seconds.
However, at the accident site, the right propeller pitch lever was fully forward in the full fine pitch position, the propeller was not feathered and damage to the right propeller blades indicated that the right engine was making low power (and driving the propeller). These aspects were also consistent with the right engine’s tachometer indication and mid-range throttle lever position; collectively suggesting a deliberate reduction in right engine power.
While an attempt to resolve or reduce rough engine operation may have involved movement of the right fuel mixture lever aft to a position lean of full rich, moving the right throttle lever aft would be very unlikely to do so. In this manner, the right throttle lever position was inconsistent with an attempt to resolve a partial power loss. Notably, witnesses reported similar engine sounds on the first take-off of the flight, after which there was no indication that the pilots had attempted or needed to resolve any partial loss of power, nor considered it an issue that required a return to land.
Simulated engine failure
Unlike for an actual engine failure, feathering a propeller following a simulated engine failure after take-off is not recommended. Emulating the reduced drag from feathering is often accomplished by moving the throttle lever from idle to a ‘zero thrust’ position once the student or pilot has identified the correct simulated failed engine. This was consistent with the right throttle lever mid-range position.
In further support of the most likely scenario leading up to the loss of control being an intentional simulated failure of the right engine, was the requirement for a pilot to demonstrate management of a simulated engine failure after take-off as part of the flight review standards. Simulation of an engine failure by rapidly retarding the throttle was also consistent with the witness report of an audible ‘splutter’. Additionally, the flight instructor’s hand-written plan included a simulated engine failure after take-off, following a short-field landing, which had very likely just been conducted.
Aircraft performance
Given the density altitude at the time of the occurrence, the aircraft had minimal climb performance in the optimal one engine inoperative configuration, which included the propeller of the inoperative engine feathered, and the landing gear and flap retracted. However, while either the landing gear or flap were extended, the aircraft would not maintain altitude with one engine inoperative.
While the landing gear and flaps were probably selected up after take-off, the landing gear took 14 seconds to fully retract and gear retraction paused while the flaps retracted. Additionally, as the aircraft yawed and banked to the right, the right main landing gear would have experienced the greatest resistance and therefore would have been last of the three wheels to retract – principally as a result of gravitational forces and the inward landing gear retraction design. The extended right main landing gear would have increased the asymmetric drag and therefore the amount of rudder input required to counteract the yaw.
Therefore, commencing the simulated engine failure before the landing gear was fully retracted, likely resulted in the aircraft having insufficient performance to maintain altitude and reduced its ability to accelerate or maintain airspeed.
Response to simulated engine failure
With the aircraft unable to maintain altitude with one engine inoperative until the gear and flaps were fully retracted, a descent was necessary to maintain airspeed. Attempting to maintain altitude would have caused the airspeed to decrease. At the low height at which the simulated engine failure was commenced, this provided very limited time for the pilots to interpret the situation and abort the simulated engine failure exercise by restoring full power to the inoperative engine.
The fact that the aircraft was observed to turn and bank right and slowly descend, indicated that directional control was not achieved following the simulated engine failure.
The emergency procedure specified in the Angel 44 Airplane Flight Manual (AFM) for an engine failure after take-off with the landing gear and flaps extended, was to maintain control of the aeroplane and land straight ahead. There was, however, no obstacle-free area ahead for landing, because the simulated engine failure was commenced after a touch-and-go landing, in which the aircraft became airborne close to the end of the runway.
The next steps in the AFM emergency procedure were to be conducted after retraction of the landing gear and flaps. These required the pilot to maintain directional control and airspeed at or above the best rate of climb with one engine inoperative airspeed (‘blue-line speed’). The procedure stated that if below the published minimum control speed (VMC or ‘red-line speed’), ‘reduce power on the operative engine as required to maintain lateral and directional control.’
As the aircraft turned and banked right, towards the inoperative engine, the actual minimum control speed increased significantly above the red-line speed, due largely to the bank angle. Therefore, increased airspeed was needed to regain directional control; to be achieved by lowering the aircraft nose. The aircraft was then at very low height above the ground with the decreasing airspeed rapidly approaching the actual minimum control speed, which was significantly higher than the red-line speed and may also have exceeded the blue-line speed.
Without adequate height above terrain available to descend and increase airspeed, when airspeed reduction below the actual minimum control speed was imminent, preventing a ‘VMC roll’ required the pilots to reduce power on both engines and land ahead. However, the aircraft departed controlled flight with no indication of a reduction in power on the left engine or an attempt to land. Once the aircraft departed controlled flight, there was insufficient altitude available to effect a recovery before the aircraft collided with terrain. The aircraft was at a height where reducing power and landing ahead would have resulted in a landing beyond the aerodrome confines and almost certain collision with vegetation. Landing ahead with the aircraft under control would almost certainly have resulted in a safer outcome. Despite this, it can be a difficult decision for a pilot to make, particularly when faced with a simulated, rather than actual engine failure.
The Angel 44 flight manual did not specify a safe altitude for conducting simulated engine failures, nor was it required to. The aircraft almost certainly did not reach the Civil Aviation Safety Authority’s (CASA’s) recommended minimum height of 400 ft AGL at which to simulate an engine failure. Even with the right-side (instructor’s) altimeter likely reading about 90 ft above the actual barometric altitude, it would have been indicating an altitude 190 to 240 ft above the aerodrome elevation when the simulated engine failure commenced.
Instructor experience and proficiency
The instructor had almost no experience in the aircraft make and model, and limited opportunity to prepare for the flight. While the accident flight had initially been discussed two weeks prior, there was no evidence that the instructor obtained a flight manual or had any information specific to the aircraft make and model. Given that the pilot owned the aircraft and had over 300 hours experience in it, the instructor may have assumed that the pilot was competent in the aircraft and would not have to intervene, particularly as the flight review was not to include training, as it was being conducted as a private flight. Had the instructor known the pilot had not flown for over 3 years however, it could be expected that the instructor would consider pilot recency when planning the flight.
On the morning of the accident flight, the pilot and instructor had the opportunity to discuss the flight for around 20 minutes at the airport then about 30 minutes in the aircraft prior to taxiing, however, it could not be known what was discussed during that time. During the 14 minutes that the aircraft was airborne before re-joining the aerodrome circuit, the pilot had demonstrated several items of the planned flight review. There was insufficient time for the instructor to also gain proficiency at operating the aircraft during the short flight.
The Angel 44 aircraft was included in the multi-engine aeroplane class rating as CASA considered that it did not have any unusual performance or handling characteristics. It also required the same standard actions in response to an engine failure as other aircraft in the same class. Although the instructor had the previous day demonstrated proficiency at managing engine failures after take-off in a twin-engine aeroplane with fixed landing gear, it had been nearly two years since the instructor had last flown one with retractable landing gear (the Piper PA-34). The Angel 44’s landing gear took twice as long to retract as that aeroplane’s, during which time it would not maintain altitude with one engine inoperative. With inexperience in the Angel 44 and limited preparation for the flight, the instructor was likely unaware how long the landing gear took to retract and the resultant negation of effective climb performance.
Pilot proficiency
The pilot had demonstrated proficiency in handling simulated engine failures in the Angel 44 and other aircraft types over many years and thousands of hours of flying experience. Additionally, because this was the only aircraft of its type in Australia, when it was operated by a charter company, the pilot had CASA approval to conduct check flights for company pilots in the aircraft—including managing simulated engine failures. Significantly however, the pilot had not flown at all for over 3 years before the accident.
Research shows that skills decay significantly after 1 year and then continue to do so, particularly for procedure-based tasks such as managing an engine failure after take-off. This decay probably increased the pilot’s workload and the time taken to complete the required actions following simulation of the engine failure, and likely affected the pilot’s ability to interpret the situation and act to prevent a loss of control.
Research has also established that people are generally poor at assessing their own competency. Under the general competency requirements, pilots must be competent for the planned flight. A meta-analysis showed that in general, people overestimate their abilities and performance – this can stem from being too optimistic and a belief they are above average (Dunning, Heath & Suls, 2004). In the medical industry, surgeons were found to be able to self-assess ability in technical skills, but less able to assess their own non-technical skills (Arora et al., 2011).
The pilot may not have appreciated the likelihood of skill decay and over-estimated their ability to manage a simulated engine failure. Regular demonstrated proficiency, including in abnormal and emergency procedures, is required in commercial aviation settings, which reduces the reliance on self-assessed competency.
To regain a level of proficiency following the absence from flying, it would have been prudent to spend time conducting familiarisation at a safe height prior to attempting low-level asymmetric exercises. As the aircraft was airborne for 14 minutes prior to the simulated engine failure, there was limited time for the pilot to become proficient.
Aircraft preservation
The aircraft’s engines exhibited levels of internal corrosion inconsistent with their service life. In the years preceding the accident, the aircraft went through several periods of limited to no operation. While the aircraft’s maintainers reported that the engines had been run on several occasions, there was no indication that prescribed periodic storage maintenance practices had been conducted. Additionally, the engine manufacturer advised that ground running the engines was not a substitute for flying and had the potential to worsen corrosion. Further, storing the aircraft with fuel tanks less than full increased the potential for water to enter the fuel system components.
The corrosion in the fuel system of the right engine indicated that the engine had been run with water contamination in the fuel. This may have occurred in April 2019 when the fuel contamination was found, or during engine ground runs conducted by the aircraft’s maintainers. Where water contamination is evident, in addition to draining the fuel tank, it is necessary to disconnect the fuel lines before running the engine to ensure water is not introduced to the engine fuel system.
There was no evidence that inadequate engine preservation directly contributed to the accident, however, the corrosion-related debris located in the fuel system likely resulted in the right engine running overly rich, producing black smoke and backfiring, as well as a probable reduction in maximum power available. It is also likely that the service life of the engines would have been adversely affected, which had the potential to increase the risk of premature engine performance issues.
Pilot medical status, qualifications and experience
The 73-year-old pilot’s Class 1 aviation medical certificate had expired in February 2017. Although the pilot had attended a general practitioner and completed a Class 2 medical examination on 12 August 2019, the requirements to be issued with a medical certificate had not been completed at the time of the accident.
The pilot held a commercial pilot licence (aeroplane) and had accrued over 20,000 flying hours, approximately 300 of which were in VH-IAZ. When purchasing the aircraft, the pilot had completed aircraft type training in the Angel 44 aircraft with the manufacturer in the United States (US). The pilot had operated the aircraft for commercial passenger-carrying charter flights and had previously been authorised by the Civil Aviation Safety Authority (CASA) to perform training in it, although that authority had lapsed.
In 2015, the pilot had completed flight instructor and instrument rating proficiency checks, but those ratings were no longer current. The pilot had last flown in June 2016, in VH-IAZ (which at the time was registered VH-IOZ). Also in 2016, the pilot had completed a flight review, valid for 2 years, which expired in February 2018.
Instructor medical status, qualifications and experience
The 63-year-old instructor had a valid a Class 1 medical certificate, and was in the process of renewing it, as it was due to expire in January 2020.
The instructor held an air transport pilot licence (aeroplane), current multi-engine aeroplane class, instructor and instrument ratings, and had accrued 5,029.5 hours of aeronautical experience.
According to the instructor’s logbooks, most of the recorded 976 hours of multi-engine command time was obtained in Vulcanair (formerly Partenavia) P68 C and Britten-Norman Islander aircraft, both aircraft types having fixed (non-retractable) landing gear. The instructor had also recorded limited hours in several multi-engine aeroplanes with retractable landing gear, including Piper PA34, PA31 and Cessna 421 aircraft. The instructor’s most recent experience in an aeroplane with retractable landing gear was in January 2018, when the instructor conducted flight training in a Piper PA34 aircraft.
From available evidence, the instructor’s only Angel 44 experience was ‘a circuit’ in VH-IAZ with a senior pilot on board, about 4 years prior to the accident flight. At that time, the instructor was assessed as ‘not ready’ to be employed as a charter pilot operating the aircraft.
The day before the accident flight, the instructor had satisfactorily completed a multi-engine instructor rating proficiency check[7] in a P68 C aircraft with the chief flying instructor (CFI) of a flight training school based at Mareeba Airport. The CFI reported that the proficiency check involved the instructor giving a briefing on asymmetric operations and a pre-flight briefing on single-engine (simulated one engine inoperative) circuits. The flight included upper airwork in the training area near Mareeba followed by simulated engine failures in the aerodrome circuit including after take-off, which were initiated between 400 and 500 ft above ground level (AGL).
The CFI reported that the instructor came across as quite professional, with handling skills slightly above average and ‘really good’ non-technical skills.
Post-mortem and toxicology results
Post-mortem examination established that both pilots received severe, non-survivable injuries as a result of the accident.
The examination also found that the pilot had 75 per cent narrowing of one of the major coronary arteries and the instructor had 75 per cent narrowing of two of the major coronary arteries. The instructor also had significant heart enlargement with thickening of the major heart chamber and stiffening and hardening of the aortic heart valve. However, neither the pilot nor the instructor had any features to indicate a recent heart attack.
The forensic pathologist reported that:
both pilots had a sufficient degree of coronary artery narrowing (atheroma) that is associated with a significant increase in the possibility of a potentially lethal heart rhythm disturbance that might render a pilot (or passenger) unconscious or have onset of chest pain or shortness of breath that might incapacitate a pilot.
It is possible that this may have led to some level of incapacitation of either the pilot or the instructor during the accident flight, however, this can be neither confirmed nor excluded on the basis of autopsy examination.
Toxicology results included the presence of a blood pressure lowering medication in the pilot’s blood, which was consistent with that prescribed by the pilot’s general practitioner.
Aircraft information
Angel 44, VH-IAZ
The Angel Aircraft Corporation Model 44 is an eight-seat, twin-engine aeroplane with retractable tricycle landing gear (Figure 1). It was designed as a utility aircraft, with short take-off and landing capability. The aircraft is powered by two Lycoming IO-540-M1C engines with ‘pusher-configuration’ aft-mounted Hartzell three-blade constant speed feathering propellers.[8]
The occurrence aircraft, serial number 004, was manufactured in the US in 2008. It was the only Angel 44 aircraft in Australia, where it was first registered in January 2010 as VH-IOZ. It was deregistered in November 2017 for sale and international export. The sale did not proceed, and the aircraft was re-registered, this time as VH-IAZ, in March 2019. VH-IAZ was approved to operate under instrument flight rules[9] and in the charter category and was fitted with dual flight controls. The aircraft had a maximum gross weight for take-off and landing of 2,630 kg (5,800 lb).
Aircraft maintenance history
The aircraft was to be maintained as per the CASA maintenance schedule, with a periodic inspection required every 100 hours or 12 months, whichever came first. Table 1 details the recent maintenance and operational history of VH-IAZ.
Table 1: Recent maintenance and operational history
Date
Flight hours
Description of event
28 June 2016
0.2
Left engine replaced due suspect oil analysis – factory overhauled engine fitted. Maintenance release issued.
29 June 2016
0.9
Flight
4 September 2016
0.9
Flight
12/14/15 October 2016
5.1
Three flights over 3 days
22 February 2017
0.5
Flight
30 May 2017
0.5
Right engine replaced, no reason for change noted – factory overhauled engine fitted
13 September 2017
0.5
Periodic inspection and maintenance release issued and flight
30 September 2017
0.6
Flight (last recorded flight hours)
1 November 2017
Airworthiness Directive 2017-0788 Identification of connecting rods with non-conforming small end bearings, which referenced Lycoming service bulletin 632B, carried out on left engine (not applicable to right engine) and other minor maintenance tasks.
14 November 2017
VH-IOZ removed from Australian register
29 March 2019
Aircraft registered as VH-IAZ
26 April 2019
Certificate of airworthiness issued
30 April 2019
Current maintenance release issued.
Right fuel tank water contamination – both fuel tanks drained, flushed, 70 litres AVGAS[10] uploaded into the fuel tanks, ground run carried out and fuel lines flushed.
5 December 2019
‘All fuel drains removed, cleaned of wasp nests and refitted. Both tacho cables removed, lubed, flushed outer cables, refitted and ops check off.’
10 December 2019
Two new spark plugs fitted to right engine No. 3 cylinder due magneto drop, ground run okay.
14 December 2019
Accident flight: nothing recorded on maintenance release, no daily inspection signed. No flight hours recorded since 30 September 2017.
Source: Aircraft maintainer
The two licenced aircraft maintenance engineers who maintained VH-IAZ reported that the aircraft had been ground run a few times since it was last flown, but not to a specified schedule. These ground runs were not recorded, nor were they required to be.
The last recorded flight time was on 30 September 2017 and no flights had been recorded since the aircraft was reregistered in March 2019.
A certificate of airworthiness is issued when CASA, or an authorised person, has assessed that the aircraft complies with applicable airworthiness requirements and has been satisfactorily maintained, ensuring the aircraft is in a condition for safe operation. VH-IAZ was issued with a certificate of airworthiness on 26 April 2019. This involved a review of the aircraft logbooks and continued airworthiness requirements, a visual inspection of the aircraft, and verification that engine and airframe serial numbers were in accordance with the documentation.
The authorised person reported that, at the time of the inspection, they were aware the aircraft had not been flown for some time. Therefore, the authorised person sought confirmation from the maintainers that the engine fuel components had been assessed for serviceability and that the engine internals had been checked for evidence of corrosion. Following discussion with the maintainers, the authorised person was satisfied these items had been addressed and did not identify any issues regarding the engines’ serviceability.
The current maintenance release, issued on 30 April 2019, recorded that the aircraft had accrued 1,803.5 hours total time in service. Records show that evidence of water contamination was found in the right engine fuel system at that time. Therefore, both fuel tanks were drained and flushed, filters were cleaned, and the fuel lines were flushed. After draining the tanks, 70 L of fuel was uploaded into them. They were then stored until the accident flight with significantly less fuel than the total capacity of 840 L. No flights, or additional maintenance, had been recorded on the maintenance release and the required daily inspection had not been endorsed prior to the accident flight.
Weight and balance
The aircraft was operating within the approved weight and balance envelope during the flight, at a take-off weight of 2,344 kg (5,169 lb) and a centre of gravity (CG) forward of mid-range.
Hydraulic system
The hydraulic system operates the nose, left main and right main landing gear and flaps. Hydraulic pressure is provided to the gear and flap control valves by an electric pump located in the nose of the aircraft. The landing gear and flaps were held up by hydraulic pressure and when fully extended, the landing gear was locked down by a mechanical stop and springs.
The Airplane Flight Manual (AFM) stated:
9.4.8 It is normal for the landing gears not to retract simultaneously. Since all 3 landing gears are interconnected hydraulically, the gear requiring the least pressure will retract first, then the next, and the one requiring the most pressure will be last.
9.4.9 When the landing gear and flap operations are selected simultaneously, their systems are interconnected. Since the flaps require less pressure, they will retract first. A check valve in the gear pressure line prevents the gear from going back down while the flaps are moving.
According to the aircraft manufacturer and pilots who had flown the aircraft, the landing gear took about 14 seconds to move from the extended (down) to fully retracted (up and locked) positions when selected up. As the gear and flap systems were interconnected, this time would increase if the flaps were selected up while the gear was retracting. If hydraulic pressure is lost, the landing gear will free-fall down and be locked over centre by springs.
Engine preservation
Unprotected surfaces in the engine, including cylinder walls, valves and fuel system components are susceptible to corrosion from moisture that naturally occurs in aviation fuels and the atmosphere. It is widely acknowledged that aircraft located in humid regions, and near the ocean and lakes, are at a greater risk of damaging corrosion than those in dry, low humid areas.
When a six-cylinder engine is stationary, generally at least one valve will be open in four of the six cylinders. With the day/night heating and cooling cycle, there is an exchange of air via the inlet or exhaust systems. If the air is warm and humid when it flows in and the engine then cools down, the water vapour can condense in the cylinders. This accumulation of moisture on the surfaces can lead to corrosion. Similarly, air exchange via the crankcase breather results in condensation in the oil. This can lead to formation of acidic compounds that promote surface corrosion.
In-service engines will generally self-purge the moisture through the combustion process and heating of the lubricating oil, which will provide a degree of protection to this corrosion. Engines in aircraft that are not flown frequently, and those that have flown less than 50 hours in total, are especially susceptible to corrosion. In this instance, effective storage procedures are required to ensure that the serviceability of the engine is maintained.
Storage procedures
The aircraft maintenance manual detailed three storage procedures when the aircraft is not expected to be flown for a period. For all three storage methods, the pitot[11] tube should be covered.
Flyable storage procedures – where the aircraft is not expected to be flown for an indefinite period but is kept in a condition to ‘fly quickly’ included:
Turn each engine by hand at least 5 revolutions each week to redistribute the oil and ensure the engine does not ‘end up in the same place each time.’
Keep fuel tanks as ‘full’ as possible.
The aircraft wheels should be chocked and the aircraft tied down securely, if stored outside.
After 30 days, the aircraft should be flown for at least 30 minutes, or ground run until the oil reaches operating temperature.
Short-term storage procedures – where the aircraft is not expected to be flown for a period of up to 3 months included:
The engine is to be inhibited by spraying a small amount of corrosion inhibitor through the spark plug holes and oil filler tube.
Cover exhausts, pitot, static and cowl openings.
Lock landing gear retraction linkage.
Disconnect or remove the battery.
Long-term storage procedures – where the aircraft is not expected to be flown for an extended indefinite period included:
The aircraft should be stored inside or under some type of cover if possible.
Replace the engine oil with a defined lubricating mixture and fly the aircraft for 15-30 minutes, then spray the lubricating mixture into the cylinders and replace upper spark plugs with blanks. Respray the cylinders and interior of the engine at least every 6 months.
An alternate method is as per short-term storage, but de-inhibit the engine and run it every 90 days, before reapplying corrosion inhibitor.
The engine manufacturer, Lycoming, also had procedures for corrosion prevention in engines that will be inactive for a period up to 30 days. These were similar to the aircraft maintenance manual procedure for short-term storage, in that the engine is sprayed with corrosion preventative oil. In addition, the engine manual had the note:
Ground running the engine for brief periods of time is not a substitute for the following procedure; in fact, the practice of ground running will tend to aggravate rather minimise this corrosion condition.
Lycoming Service Letter L180B Engine preservation for active and stored aircraft reinforced the requirement for short-term storage, of up to 30 days, and long-term storage practices, particularly in humid environments. Long-term storage also included the use of a desiccant,[12] which should be inspected at least every 15 days.
Further, CASA airworthiness bulletin 85-021 Piston engine low utilisation maintenance practices reinforces following the manufacturer’s procedures to prevent corrosion.
The fuel injector manufacturer, Precision Airmotive also published short- and long-term storage requirements in their operation and service manual. In addition, this manual stated:
A complete overhaul is mandatory regardless of any FAR [US Federal Aviation Regulation] operational category when the injector or fuel system component has been subjected to severe environment such as but not limited to…contaminated fuel such as water, rust sand, etc.
Recorded data
The aircraft was not equipped with a flight data recorder or cockpit voice recorder, nor was it required to be.
Post-accident examination and assessment
Accident site
The accident site was located in a cornfield about 475 m north of the runway at Mareeba Airport. Based on an analysis of the wreckage and ground marks, it was evident that the aircraft impacted terrain right wingtip first, while travelling in a northerly direction. The nose landing gear impacted the ground about 33 m beyond the initial impact point, after the right wing had fractured and collapsed under the weight of the aircraft. At that point, the fuselage was at, or slightly over, vertical, and the cockpit folded under and to the left.
The aircraft then slid on its left wing at about mid-span, until the left wingtip dug into the terrain, resulting in the fuselage lifting and clearing a section of corn, before coming to a halt, upright, and 67 m from the initial impact point.
An assessment of the area beyond the runway identified that obstacle-free forced landing areas were limited to a road which ran perpendicular to the runway (Figure 2).
On-site examination
From the accident site examination, there was no evidence of an in-flight breakup or discontinuity of the flight controls that may have contributed to a loss of aircraft control. The rudder trim lever was in the neutral position and the elevator trim was fully forward in the down position.
The left altimeter QNH was set to 1013[13] and the right altimeter QNH was set to 1009. Due to the design of the selector, these settings were unlikely to have moved during impact. An aerodrome forecast service for Mareeba Airport was available from the Bureau of Meteorology, which included forecast QNH. Additionally, an Aerodrome Weather Information Service was available by phone or VHF radio, which provided actual QNH. However, it could not be determined whether the pilots accessed either service prior to the flight.
Landing gear and flaps
The landing gear selector was in the up position. The nose landing gear was fully or almost fully retracted, the right main landing gear was partially extended, and the left main landing gear was extended and on the mechanical (down) lock. However, the electric pump for the hydraulic system detached from the aircraft when the nose impacted the ground. This removed the hydraulic pressure required to hold the landing gear and flap up. After that, the main landing gear (and flap) was able to free-fall. As such, the main landing gear was either retracted and free-fell down during the impact sequence, or was not fully retracted before impact. From the observed flight path, the aircraft was airborne for about 20 seconds; for approximately 5 of those seconds after take-off, the landing gear remained extended. This left a maximum of about 15 seconds for all three wheels to retract to the up-and-locked position. As it took about 14 seconds for the landing gear to retract, and longer as the flaps also retracted (see section Hydraulic system), it was probable that the landing gear had not fully retracted prior to impact.
The normal take-off flap position was 20 degrees extension. At the accident site, the flap was extended 5-15 degrees, however, the associated paint transfer mark on the fuselage indicated that the flap was likely up or almost fully up prior to impact and was pushed down in the accident sequence. The flap selector lever was at about a 45-degree angle, indicative of the flaps selected in the fully extended position, but due to disruption of that part of the panel during the impact sequence, it was not indicative of the actual flap position.
Engines and propellers including controls and indications
Both of the fuel mixture levers were fully forward in the ‘rich’ position, with the fully aft position denoted ‘lean’. The propeller pitch levers were both fully forward in the full fine position, denoted ‘Hi RPM’, with the fully aft position denoted ‘feather’. The left throttle lever was fully forward in the ‘open’ position, with the aft position denoted ‘close’. The right throttle lever was at mid-travel and was likely at that position prior to impact, as the lever had been bent to the right during the impact sequence. That position was consistent with the right engine tachometer, which was stuck at about 1,300 RPM and was likely in that position immediately prior to impact.
For both a normal take-off and in response to an (actual) engine failure after take-off, the expected lever positions would be all six levers in the fully forward position.
Initial on-site examination found no evidence of pre-impact mechanical, electrical or other catastrophic failure to either engine or propeller assembly. The propeller blades indicated that both engines were making power at impact, with the right engine operating at lower power than the left. The propellers and engines were taken to specialist facilities for further examination.
Propeller examination
Chord-wise scoring and leading-edge damage was present on both propellers, consistent with the propellers operating under engine power (not windmilling) during the impact sequence.
The left propeller had all three tips missing, one of which was severed twice and another had twisted during separation. This was consistent with the left engine producing significant power at the time of impact. The right propeller blade tips had not detached.
The location of the pusher-propellers and impact sequence, including the materials the blades passed through, likely affected the blade damage signatures. The right blades typically showed less substantial markings from having passed through soil, vegetation and the fuselage. The left propeller blades had more damage, due to impact with the airframe including the wings.
Engines and fuel system examination
There was no evidence of catastrophic failure of the engines or fuel system components. All magnetos and spark plugs were tested and found serviceable.
Mild corrosion was evident in cylinder bores of both engines. While the internal corrosion was consistent with inadequate preservation and storage of the engines, it was unlikely to have contributed to significant power loss or engine failure.
There was no evidence of water contamination in the left engine fuel system. The right engine-driven pump and right fuel injection servo unit carried a black residue – consistent with water contamination. For this to occur, the right engine would have to have been run with water contamination in the fuel.
When tested, the fuel injector nozzles from cylinders No. 2 and 4 on the right engine had reduced flow due to particulate contamination. Partially obstructed fuel injectors had the potential to contribute to the unaffected cylinders running overly rich. This was consistent with carbon deposition observed in the No. 2 and No. 4 cylinder exhaust and witness reports of a dark sooty trail emitting from the right engine on the first take-off of the flight.
ATSB examination found the particulates were consistent with iron-oxide (corrosion). The contamination and deposits in the right engine had the possibility to reduce engine efficiency and performance, but the broader effect on the flight could not be determined.
Weather and environmental information
At 1115 EST, the temperature at Mareeba Airport was 34 ºC, the dewpoint 15 ºC, and the wind from 266º (westerly) at 6 kt gusting to 9 kt. There was no cloud and the QNH was 1012 hPa.
The aerodrome elevation was 1,650 ft and with the given temperature and QNH, the density altitude[14] was 4,440 ft.
Planned flight
Purpose
The purpose of the flight was to conduct a flight review so the pilot could exercise the privileges of a multi-engine aeroplane class rating.
Preparation
The ATSB obtained evidence to determine what opportunities the instructor had to gain familiarity with the aircraft prior to the flight. On 30 November 2019, the pilot contacted the instructor to ask whether they could do this flight review. The instructor responded being happy to do the review and would be qualified to do so following completion of an instructor rating renewal (proficiency check). The instructor anticipated needing about 1 hour on the ground to become familiar with the aircraft and reported having flown it previously, with an experienced pilot. On December 10, the instructor arranged to conduct the instructor rating renewal on December 13 and confirmed with the pilot that they would do the flight review on December 14.
Documents that the instructor carried immediately before and/or during the accident flight included information about the P68 C aircraft flown the previous day for the instructor rating renewal and regulations pertaining to flight reviews. There was no information about the Angel 44 aircraft.
Pre-flight planning
On the morning of the accident flight, the pilot departed from a friend’s house at about 0800. A witness saw the pilot conducting engine run-ups in VH-IAZ at about 0915 and closed-circuit television (CCTV) footage showed the aircraft taxi and park near the maintainer’s hangar at 0922.
CCTV footage showed the pilot and instructor walking past the hangar together in a westerly direction at 0950, both carrying flight bags. About 21 minutes later, they walked east towards the parked aircraft. It is probable that the plan for the flight was discussed between them during that time, and as they walked to the aircraft, the pilot can be heard to say ‘right circuit’, which was the circuit direction for runway 28. Another 35 minutes elapsed before the aircraft commenced taxiing.
In-flight exercises
Table 2 shows a transcription of a document found at the accident site, confirmed to be in the instructor’s handwriting. The aircraft registration, model and date were written across the top of the page, followed by the numbers ‘10-58’ and ‘10-44’. The pilot broadcast rolling on runway 28 at 1058, consistent with the instructor logging the time the aircraft became airborne. The second time (1044) may have been the engine start time, as the aircraft commenced taxiing at 1046.
The document listed items that were required to be demonstrated for a multi-engine flight review. Of the standards required to demonstrate competency for a flight review, the list represented what could be considered a bare minimum of the required procedures (see section Flight reviews). Of the listed exercises, some had been ticked, presumably to indicate they were complete. The item ‘Missed approach’ was ticked. The next item on the list was a short-field landing, which was consistent with witnesses observing the aircraft touch down just before commencing the second take-off, rather than a missed approach, where it would not be expected to touch down. A simulated engine failure after take-off was next in the sequence, which was to be followed by a single-engine approach and landing. A diagram that the instructor had drawn on the same document as the list, showed a missed approach followed by an engine failure after take-off in a single circuit pattern.
Table 2: Transcribed copy of handwritten plan for the flight
IAZ ANGEL 44 14/12/19
10-58 10-44
Short field take-off
Stall and recovery
✓
Steep turn
✓
500’ turn
✓
1 full circuit
Missed approach
✓
Short field landing
Engine failure take-off (EFATO)
Single engine approach and land
Source: Retrieved from the accident site by Queensland Police, transcribed by ATSB
Flight reviews
Flight instructor requirements
The instructor held grade 1 training and multi-engine aeroplane training class rating endorsements and was authorised to do the flight review in accordance with Civil Aviation Safety Regulations (CASR) including 61.1175. However, the instructor was not authorised to include any training, as the review was not being conducted under the oversight of a training organisation.
General competency requirement
To operate an aircraft, pilots are required to be competent. CASR 61.385 Limitations on exercise of privileges of pilot licences—general competency requirement, included:
1. The holder of a pilot licence is authorised to exercise the privileges of the licence in an aircraft only if the holder is competent in operating the aircraft to the standards mentioned in the Part 61 Manual of Standards for the class or type to which the aircraft belongs, including all of the following areas:
a) operating the aircraft’s navigation and operating systems;
b) conducting all normal, abnormal and emergency flight procedures for the aircraft;
c) applying operating limitations;
d) weight and balance requirements;
e) applying aircraft performance data, including take-off and landing performance data, for the aircraft.
Flight review requirements
CASR 61.745 Limitations on exercise of privileges of aircraft class ratings—flight review, required a pilot to complete a flight review within the previous 24 months to exercise the privileges of a rating, in this case a multi-engine aeroplane class rating. As the pilot had not completed a flight review within the 24 months prior to the accident flight (or completed CASA medical requirements), the instructor was the pilot-in-command for the flight.
The CASA publication Flight crew licensing—Flight reviews, described a flight review as an opportunity to receive training that refreshes your flying skills and operational knowledge.
It stated that the instructor is responsible for designing appropriate content for your flight review. A flight review should include training, so it is not just an assessment.
It explained that if the review includes training, it must be done under an approved training organisation.
However, while CASA strongly encourages pilots to include training within their flight reviews, flight reviews could be conducted as a private flight, not under the oversight of a training organisation, as long as training was not included.
The publication further stated that the requirements of a flight review are met when the instructor conducting the review is satisfied you have demonstrated competency for the rating according to the Part 61 Manual of Standards (MOS).
If on initial assessment, the instructor deemed that the pilot needed training, that would then have to be conducted with the oversight of a training organisation.
CASR 61.400 Limitations on exercise of privileges of pilot licences—flight review, required the pilot to demonstrate in the flight review, that they are competent in each unit of competency mentioned in the Part 61 MOS for the rating.
Relevant standards
Of particular relevance to this occurrence, the Part 61 MOS standards required to demonstrate competency for a multi-engine aeroplane class rating flight review, included:
2.6 FR-MEAC.6 – Manage non-normal and emergency conditions
(a) manage a simulated engine failure in the take-off segment;
(b) manage a simulated partial engine failure;
(c) manage a simulated complete engine failure and execute a simulated asymmetric approach and landing;
(d) manage aircraft system malfunctions.
CASA does not provide a definition of the ‘take-off segment’ or what maximum height above the runway this extends to. However, CASA guidance recommends that instructors consider not conducting simulated engine failure in the take-off segment exercises below 400 ft (see Simulated engine failures after take-off).
Comparison flight review requirements
The US Federal Aviation Regulations also required a flight review every 2 years with an instructor, with some exemptions. A US flight review must consist of a minimum of 1 hour of ground training and 1 hour of flight training. The FAA did not permit flight reviews to be conducted without including training. The US Federal Aviation Administration (FAA) advisory circular (AC) 61-98D – Currency requirements and guidance for the flight review and instrument proficiency check, provided the intent of a flight review as ‘a training event in which proficiency is evaluated.’ The AC advised that flight reviews should always include abnormal and emergency procedures.
Regarding instructor qualifications, the FAA AC advised that:
For aircraft in which the flight instructor is not current or with which he or she is not familiar, he or she should obtain recent flight experience or sufficient knowledge of aircraft limitations, characteristics, and performance before conducting the review.
Additionally, US Federal Aviation Regulation 61.195 stipulated that a flight instructor may not give training in a multi-engine aeroplane, unless they have at least 5 flight hours of pilot-in-command time in the specific make and model aeroplane.
Transport Canada provides several means for private pilots to remain current and proficient, including a biennial component, of which one option is a flight review conducted by an instructor. The alternative options to a flight review include attending a seminar or completing on-line study.
The European Union Aviation Safety Agency’s multi-engine piston rating for aeroplanes was valid for 1 year. To revalidate the rating, a pilot must pass a proficiency check with an approved examiner, in a multi-engine piston (single-pilot) aeroplane or an approved simulator. During the rating validity period, the pilot must have completed at least one route sector of a single-pilot multi-engine aeroplane with an examiner.
Multi-engine class rating and the Angel 44
The Angel 44 aircraft was included in the multi-engine aeroplane class rating. This means that CASA assessed it as not having unusual performance or handling characteristics compared with other light (under 5,700 kg) twin-engine aeroplanes. International Civil Aviation Organization Annex 1 recommended (2.1.3.1.1) that class ratings should be established for aircraft for single-pilot operations which have ‘comparable handling, performance and other characteristics.’
The last pilot to fly the aircraft prior to the accident flight had about 30 hours of experience in it. That pilot reported that the controls were all familiar but slightly unusual. Having previously conducted a simulated engine failure after take-off at about 500 ft above the ground, the pilot reported that the aircraft handled normally when the yaw was corrected, the standard actions performed and blue-line speed (see section Key speeds below) was maintained. While that pilot would not recommend a pilot flew it without any training, the pilot’s expectation was that any commercial multi-engine rated pilot should be able to manage a circuit with both engines operative.
A pilot with extensive experience flying Angel 44 aircraft advised that the aircraft was more ‘docile’ than other twin-engine aeroplanes and had less propeller torque effect due to the geometry of the engines and propellers. That pilot reported that during take-off, unlike other twin-engine aeroplanes, it yaws right (rather than left), so left rudder is needed to keep straight. However, with one engine inoperative, it is the same as other twin-engine aeroplanes in that opposite rudder (to the inoperative engine) is used to counteract the yaw. That pilot confirmed that the initial actions following an engine failure are the same as for other twin-engine aeroplanes.
The experienced pilot further commented that if a pilot was new to the aircraft, it would take several hours in the aircraft to be competent and 5 to 12 hours to get comfortable with it. The pilot advised that in the US, although the regulations require an instructor to have 5 hours before they can instruct in an aircraft, insurers generally require 12 hours experience in the aircraft make and model.
Asymmetric flight
Asymmetric control
In light twin-engine aeroplanes, with one engine inoperative, the asymmetric thrust will cause the aeroplane to yaw (rotate about its vertical axis) towards the inoperative engine. As a secondary effect of yaw, it will also roll. The yawing needs to be countered by deflection of the rudder and a small aileron deflection to raise the inoperative engine wing in order to maintain straight flight or ‘directional control’. The amount of rudder deflection needed increases as the operative engine power increases and airspeed reduces, to a minimum control speed, below which the rudder is ineffective in maintaining directional control. Angle of bank has a large effect on the minimum control speed, and if the aeroplane is banked towards, instead of away from the inoperative engine, the minimum control speed increases significantly.
Below the minimum control speed, the pilot must reduce power on the operative engine to reduce the asymmetric force, and/or lower the aircraft nose to increase airspeed, to prevent a loss of control. If directional control is lost, the aircraft will yaw and then roll rapidly. While controlled flight can be recovered if enough height is available, reducing power and lowering the nose when close to the ground may result in a landing. The US FAA Airplane Flying Handbook Chapter 12 stated:
Landing under control is paramount. The greatest hazard in a single-engine take-off is attempting to fly when it is not within the performance capability of the airplane to do so. An accident is inevitable.
Performance requirement
Subsection 8 of Civil Aviation Order 20.7.4 required multi-engine aeroplanes below 5,700 kg to be able to climb at a gradient of 1 per cent, or to maintain height, as follows:
8.1 Multi-engined aeroplanes engaged in charter operations under the Instrument Flight Rules or aerial work operations under the Instrument Flight Rules must have the ability to climb with a critical engine inoperative at a gradient of 1% at all heights up to 5 000 feet in the standard atmosphere in the following configuration:
(a) propeller of inoperative engine stopped;
(b) undercarriage (if retractable) and flaps retracted;
(c) remaining engine(s) operating at maximum continuous power;
(d) airspeed not less than 1.2 VS [stalling speed].
8.2 Multi-engined aeroplanes (other than those specified in paragraph 8.1) must have the ability to maintain height at all heights up to 5 000 feet in the standard atmosphere in the configuration specified in subparagraphs 8.1 (a), (b), (c) and (d).
Key speeds
Three key ‘V’ speeds critical to understanding the accident flight were specified in the Angel 44 AFM. They are stalling speed, best rate of climb speed with one engine inoperative, and minimum control speed.
These reference V speeds are published for specific configurations and the actual V speeds will be different in any other configuration. The ATSB investigation considered the published V speeds and the likely actual V speeds associated with the aircraft’s probable configuration when the loss of control occurred.
The aircraft configuration was:
approximately 5,100 lb (2,313 kg) weight
CG slightly forward of mid-range
flaps up or nearly up
landing gear partially retracted
15 degrees right wing down angle of bank
left engine at full power
right engine between idle and 1,300 RPM
right propeller not feathered.
Stalling speed
Stalling speed (VS) is defined as the minimum steady flight speed at which the aeroplane is controllable in a given configuration. VSO is the stalling speed in the landing configuration.
The AFM specified VSO as 57.5 kt calibrated airspeed (KCAS)[15] for the aircraft in 1G flight at maximum gross weight, most forward CG, power off and in the landing configuration (flaps and landing gear fully extended).
However, an aircraft will stall when the critical angle of attack is exceeded, regardless of airspeed. To this end, the AFM provided a table from which to derive stalling speeds including:
at weights less than the maximum gross weight
flap at 0°, 20° and 37° (fully extended)
landing gear up and down
0°, 15°, 30°, 45° and 60° angle of bank
aft CG.
The stalling speed in the probable configuration at the point of loss of control was about 68 KCAS. Flight testing for aircraft certification found that full power (on both engines) reduced stalling speed by about 12 kt. Therefore, the stalling speed with 1,300 RPM on the right engine may have been 4–6 kt lower, that is, 62–64 kt.
As increase in power reduces the stalling speed, asymmetric thrust will also produce asymmetric stall characteristics, with the inoperative engine side wing stalling at a higher airspeed than the operative engine wing.
The AFM also stated that when recovering from single-engine stall, an altitude loss of 800 ft could be expected.
Best rate of climb speed with one engine inoperative
The best rate of climb speed with one engine inoperative (single-engine) (VYSE) is marked on the airspeed indicator with a blue radial line and is therefore also known as the ‘blue-line speed’. In the Angel 44 aircraft it was a thick line or ‘sector’ marked from 90–92 KIAS (Figure 3). This represented the single-engine best rate of climb speed at maximum weight, with the lower value of 90 KIAS for 5,000 ft AMSL and the higher value of 92 KIAS for sea level. According to the AFM, the single engine best rate of climb is established in the following configuration:
gear and flaps up
the critical (left) engine[16] feathered [note that the flight test data detailed in the next section states that the right engine was the critical engine but that the difference was not significant]
full power on the right engine
the inoperative engine wing up about 1°.
The AFM Climb performance summary table specified single-engine climb performance in feet per minute (fpm) and the associated best rate of climb speed. These were provided for gross weights of 5,800 lb (2,631 kg) and 4,800 lb (2,177 kg) and altitudes at the associated international standard atmosphere (ISA) temperatures from sea level to 20,000 ft AMSL.
Interpolating from the AFM table for the 4,500 ft density altitude (at 100 ft above ground level on the accident flight) and the aircraft weight (which was less than maximum weight), the single engine climb rate was approximately 169 fpm at a single engine best rate of climb speed of 89 KIAS. Note this equates to a climb gradient of about 1.87 per cent. Therefore, a positive rate of climb could have been expected on the accident flight if the aircraft had been configured for the best rate of climb as above.
However, compared with the configuration for best single engine climb performance, at the time of the loss of control on the accident take-off, the landing gear was probably not fully retracted, the right engine was probably simulated inoperative and the propeller was not feathered (although an engine speed of 1,300 RPM may have been selected to simulate the reduced drag from a feathered propeller) and the right wing was banked down about 15 degrees rather than up 1 degree. Therefore, the aircraft was not configured to achieve the expected rate of climb. Moreover, in the environmental conditions and with the landing gear extended, the aircraft was almost certainly unable to maintain altitude. This was specified in the AFM, which warned:
The airplane will not maintain altitude at most weights, altitudes and temperatures with gear or flaps extended.
Figure 3: Airspeed indicator from VH-IAZ showing red-line (VMC) and blue-line (VYSE) speeds
Source: VH-IAZ annotated by ATSB
Minimum control speed
Definition
The CASA Civil Aviation Advisory Publication (CAAP) 5.23-1(2) Multi-engine aeroplane operations and training, defined minimum control speed (VMC) as:
a speed that is associated with the maintenance of directional control during asymmetric flight. If the pilot flies below this speed the tail fin and rudder are unable to generate enough lift to prevent the aircraft from yawing. If uncorrected, the yaw causes roll, the nose drops, the aircraft rapidly assumes a spiral descent or even dive, and if the aircraft is at low altitude, it will impact steeply into the ground. This type of accident is not uncommon in a multi-engine aircraft during training or actual engine failure.
Flight test and published figure
Minimum control speed (VMC) is published in the AFM and obtained from testing in a specific configuration. There is both a ground value (VMCG) and an airborne value (VMCA), but for simplicity, VMC usually refers to VMCA. VMC is marked with a red line on the airspeed indicator, and often referred to as ‘red-line speed’ (Figure 3).The AFM specified the aircraft’s minimum control speed (VMC) as 65 KIAS and stated:
This is the minimum speed at which the airplane is controllable with takeoff power on one engine, the other engine suddenly made inoperative, 5° bank toward the operating engine, takeoff flaps (20°), and the landing gear retracted.
At the time of the Angel 44’s certification, VMC was tested in accordance with US Federal Aviation Regulations (FAR) 23.149 Minimum control speed. This has since been replaced with FAR 23.2135 Flight characteristics - Controllability, which includes:
(c) VMC is the calibrated airspeed at which, following the sudden critical loss of thrust, it is possible to maintain control of the airplane. For multiengine airplanes, the applicant must determine VMC, if applicable, for the most critical configurations used in takeoff and landing operations.
The aircraft manufacturer provided details about the VMC flight testing for the aeroplane. Because aircraft weight does not appreciably affect VMC but does affect VS, it is conducted at a light weight (and aircraft loaded to aft CG) to demonstrate that VMC does not exceed 1.2 VS1[17] (which was 69 KCAS).
There were two steps to determining VMC. These were conducted in the take-off configuration with flap extended 20° and landing gear down, full power on the left engine, right engine inoperative and propeller windmilling in the fully fine pitch setting.
Step 1: The aircraft was gradually slowed until directional control (heading) could not be maintained with the right wing raised 5°. This was done at various altitudes and extrapolated to sea level. For the Angel 44 aircraft, the VMC obtained was about 61 kt and the published VMC value was 65 kt.
Step 2: Engine cuts were performed (by pulling the mixture control) at 65 kt. The ability to maintain control (heading) and not allow speed to decay below 61 kt was verified.
The flight data computed VMC obtained from testing decreased linearly from 65 kt at mean sea level to 54 kt at 10,000 ft, so at 5,000 ft the VMC would be 60 kt.
The manufacturer advised that the pusher-propeller configuration significantly reduced some of the asymmetric effects of single-engine operation. While the amount of yaw was still large, the amount of roll was much less (than for a normal ‘tractor’ propeller aeroplane).
Actual minimum control speed
The published VMC is for the specified configuration. The actual VMC that a pilot will experience in flight varies depending on weight, altitude, rudder, thrust settings, configuration and, most significantly, on bank angle. Flight testing is generally not performed at bank angles other than with the inoperative engine wing raised 5°, as it is not required. Therefore, there is limited published data to show the effect of different configurations.
The CASA CAAP 5.23-1(2), stated that flight tests conducted in a Cessna Conquest aircraft, which had a published VMCA of 91 kt, found that if the wings were held level instead of the inoperative engine wing raised 5°, the actual minimum control speed was 115 kt – an increase of 24 kt. Further, the testing found that lowering the wing towards the failed engine (instead of raising it), increased the minimum control speed by about 3 kt per degree of bank.
Other light twin-engine aeroplanes would similarly show an increase in actual minimum control speed with bank.
In the accident flight, witnesses assessed the aircraft’s bank angle during the right turn at 15–30 degrees. That is, 20–35 degrees in the wrong direction of bank from the published VMC. The density altitude, some power on the right engine and flap retracted, would have reduced the actual VMC but would not diminish the bank angle effects. Additionally, as the right main landing gear was likely last to retract, due to the forces during the right turn, it would have further compounded the asymmetric drag, increasing the actual VMC.
The US FAA Airplane Flying Handbook Chapter 12 – Transition to multiengine airplanes, stated:
The first consideration following engine failure during takeoff is to maintain control of the airplane. Maintaining directional control with prompt and often aggressive rudder application and STOPPING THE YAW is critical to the safety of flight…At least 5° of bank should be used initially to stop the yaw and maintain directional control. This initial bank input is held only momentarily, just long enough to establish or ensure directional control.
At speeds below the actual VMC, the aircraft will lose directional control – yaw and then roll towards the inoperative engine. Transport Canada’s Instructor Guide: Multi-engine class rating (TP 11575) stated:
It cannot be too strongly emphasized that control will be regained only by a reduction in power of the good engine or by increasing airspeed through a change in pitch attitude, or both.
VYSE as a safety margin above VMC
In the accident flight, banking towards the inoperative engine significantly increased the actual VMC to the extent that it probably exceeded the VYSE (blue line) speed (90-92 KIAS). This is important as pilots often use blue-line speed as a safety margin above VMC for initiating a simulated engine failure and assume that if blue-line speed is maintained, there is sufficient margin above red-line speed (published VMC) to prevent an asymmetric loss of control.
However, for aircraft certification, the configurations used to determine the VMC (red-line) and VYSE (blue-line) speeds are different. For VMC, the inoperative engine propeller is windmilling and wing raised 5°, the landing gear is down and the flaps are extended 20°. For VYSE, the inoperative engine propeller is feathered, and wing raised 1°, the landing gear and flaps are retracted. Even with the propeller feathered and landing gear and flaps retracted, if the pilot turns towards the inoperative engine, actual VMC can exceed VYSE. As it is essential to achieve and maintain an airspeed above actual VMC in order to maintain directional control, understanding the effect of bank angle is vital to maintaining asymmetric control; particularly during take-off.
Rudder trim
Rudder deflection will be needed to control the yaw for the duration of the asymmetric flight. The rudder force that the pilot must apply can be reduced by adjusting the rudder trim. In the accident flight, the rudder trim was in the neutral position at the time of impact, however there was limited time to adjust the rudder trim before the loss of control and impact with terrain.
Engine failure procedures
The AFM contained the following emergency procedure for engine failure during take-off:
After Airborne, Gear and Flaps Still Extended:
a. Airplane Control……………….MAINTAIN
b. Action……………………….….LAND STRAIGHT AHEAD
WARNING
The airplane will not maintain altitude at most weights, altitudes and temperatures with gear or flaps extended.
If airspeed is below 65 KIAS, reduce power on operative engine as required to maintain lateral & directional control.
After Gear & Flaps Retracted:
a. Airplane Control……………...…MAINTAIN
b. Airspeed…………………...........VYSE OR GREATER
c. Throttle (inoperative engine)…..CLOSE
d. Propeller (inoperative engine)…FEATHER
e. Throttle (operative engine)…….AS REQUIRED
f. Enroute Checklist……………….COMPLETE AS ABLE
Point a. Airplane Control, is maintained with use of rudder to counteract yaw and aileron to raise the inoperative engine wing 5°. The warning that ‘if airspeed is below 65 KIAS…’ only applies in the demonstrated VMC configuration. If the inoperative engine wing is not raised 5°, a speed higher than 65 KIAS will be needed to maintain directional control.
Consistent with the warning in the published procedure, the FAA Airplane Flying Handbook stated:
When operating near or above the single-engine ceiling and an engine failure is experienced shortly after lift-off, a landing must be accomplished on whatever essentially lies ahead…
Remaining airborne and bleeding off airspeed in a futile attempt to maintain altitude is almost invariably fatal. Landing under control is paramount. The greatest hazard in a single-engine takeoff is attempting to fly when it is not within the performance capability of the airplane to do so. An accident is inevitable.
The manufacturer reported that on take-off, the Angel 44 aircraft accelerates to the 90 kt take-off safety speed ‘pretty quickly.’ In case of engine failure below that speed, a pilot would need to lower the aircraft nose and descend to achieve the required speed.
The Angel 44 AFM did not contain guidance for conduct of simulated engine failures (after take-off), provide a safe intentional single-engine speed,[18] or specify a safe altitude at which to conduct them. At the time of the aircraft certification, it was not required to provide this information.
Simulated engine failures after take-off
Civil Aviation Safety Authority guidance for simulated engine failures
Civil Aviation Advisory Publication (CAAP) 5.23-1(2) – Multi-engine aeroplane operations and training was produced by CASA in part, to provide advice on multi-engine training following ‘a number of multi-engine aeroplane accidents caused by aircraft systems mismanagement and loss of control by pilots, flight instructors and persons approved to conduct multi-engine training’.
The CAAP specified risks associated with multi-engine training as:
inappropriate management of complex aircraft systems
conducting flight operations at low level (engine failures after take-off)
conducting operations at or near VMCA or VSO with an engine inoperative[19]
errors
asymmetric operations including:
inadequate pre-take-off planning and briefing
decision making
aircraft control
performance awareness and management
operations with feathered propellers
missed approaches and go-arounds
final approach and landing
stalling.
To mitigate these risks, it suggests that:
Instructors should consider not simulating engine failures below 400 ft above ground level (AGL) to provide a reasonable safety margin. The use of simulators has reduced the perils of this activity. Other mitigating factors are:
• well trained instructors
• complete knowledge of the theoretical factors involved during asymmetric operations
• proven procedures, provided these are strictly adhered to
• comprehensive pre-flight and pre-take-off planning and briefings
• ongoing training
• situation awareness
• flying competency.
Section 6.5 of the CAAP, Simulating engine failures, advised instructors to ‘be aware of the implications and be sure of their actions,’ before simulating an engine failure. Further, that they ‘must ensure that the aircraft is not in a dangerous situation to start with, such as the aircraft is flying too slow, too low, is in an unsuitable configuration or hazardous weather (wind, ice or visibility) is present. There is no benefit introducing more risks than the emergency being trained for.’
A CASA subject matter expert provided the following comments regarding simulated engine failures after take-off.
The risk of not doing practice engine failures after take-off exceeded the risk of doing them. However, CASA had not conducted a risk assessment and were not required to do so by legislation for historical regulations.
The suggested 400 ft AGL minimum height in CAAP 5.23-1(2) is general in nature and not specific to a particular aircraft type. This suggested minimum is consistent with a common point in the take-off path utilised in the certification. [US Federal Aviation Regulation 23.2120 for level 3 (7-9 passengers) low speed (VNO and VMO less than or equal to 250 KCAS)[20] aeroplanes requires a 1 per cent climb gradient at 400 ft above the take-off surface with the landing gear retracted and flaps in the take-off configuration. This was not in effect at the time VH-IAZ was certified and no similar criteria then applied to the aircraft. Based on data provided in the AFM, in the accident environmental conditions, and in the stated configuration, VH-IAZ would have met (and exceeded) this criterion.]
Simulating engine failures after take-off is necessary because it is representative of what may occur. At lower density altitudes the operative engine will have better performance and the aircraft will have better climb performance.
Conducting these at a higher altitude such as 3,000 or 5,000 ft AGL would still not ensure recovery in all instances, such as from a VMCA departure. However, altitude provides an opportunity to regain speed [by lowering the aircraft nose and descending].
The drills and hand and muscle movements should be practised at height then that skill and muscle memory taken to the after-take-off scenario, where there is potential for the ‘startle effect’. Conducting engine failures after take-off invokes an emotional response necessary to train for a real engine failure at low height above the ground.
The competency check must be done in the environment where the skill is going to be used.
US Federal Aviation Administration
The US Federal Aviation Administration (FAA) Flying light twins safely brochure included the following training recommendation:
Low-altitude engine failure is never worth the risks involved. Multiengine instructors should approach simulated engine failures below 400 feet AGL with extreme caution, and failures below 200 feet AGL should be reserved for simulators and training devices.
included the following guidance regarding altitude and speed for simulating engine failures.
When training in an airplane, initiation of a simulated engine inoperative emergency at low altitude normally occurs at a minimum of 400 feet AGL to mitigate the risk involved and only after the student has successfully mastered engine inoperative procedures at higher altitudes. Initiating a simulated low altitude engine inoperative emergency in the airplane at extremely low altitude, immediately after liftoff, or below VSSE creates a situation where they [sic] are non-existent safety margins.
US National Transportation Safety Board
Due to a number of fatal accidents in the US where pilots did not maintain control following a loss of power in one engine while flying multi-engine aeroplanes, the US National Transportation Safety Board issued safety alert SA-081 – Maintain airplane control with one engine inoperative. It stated:
These accidents demonstrate that having a multiengine rating alone may not be enough to avoid the risk of loss of aircraft control with one engine inoperative (OEI), especially if engine failure occurs during a critical phase of flight.
Recommendations in the safety alert included:
• Be thoroughly familiar with the recommended procedures and checklists for OEI operations—particularly the memory checklist items—in the airplane flight manual and pilot operating handbook.
• Ensure that you have a multiengine rating and establish multiengine proficiency.
• Seek training in any new multiengine airplane model you fly to ensure that you fully understand the relationship between OEI and VMC for each phase of flight and the proper recovery techniques for that airplane.
Flight training organisations
Based on the assessment that a large number of simulated engine failures after take-off are conducted every day in Australia without incident, the ATSB spoke to flight instructors from several flight training organisations to see what risk controls were used. Instructors usually used 400 ft AGL as a minimum height but would start higher until the student was proficient. The aircraft would be accelerated to the manufacturer-recommended minimum safe intentional one-engine inoperative speed or blue-line speed before simulating the engine failure. As soon as the student either did not maintain heading or airspeed, the instructor would restore power and discontinue the exercise.
Related occurrences
Training accidents
A review of the ATSB occurrence database revealed that in the 10 years between 2008 and 2017, there were 24 accidents for twin-engine, VH-registered, aircraft under 5,700 kg[21] conducting training or checking. Of these, three involved an asymmetric simulated engine failure on take‑off or climb.
The only fatal training accident during that period occurred on 30 May 2017. An inductee pilot undergoing a proficiency check, a chief pilot conducting the check and a CASA flying operations inspector observing the flight were on board a Cessna 441 (Conquest II) aircraft. Shortly after take-off from Renmark Airport, South Australia, a simulated engine failure was conducted at about 400 ft above the ground. The expected single-engine climb performance and airspeed were not achieved, and the exercise was not discontinued. Consequently, about 40 seconds after initiation of the simulated engine failure, the aircraft experienced an asymmetric loss of control, from which recovery was not made.
The aircraft impacted the ground, all on board were fatally injured and the aircraft was destroyed. (ATSB investigation AO-2017-057). The investigation’s safety message was:
Conducting a simulated engine failure after an actual take-off is a high-risk exercise with little margin for error. For that reason, Cessna recommended practicing this sequence in the [Cessna] 441 aircraft at a height of 5,000 ft above ground level to allow the opportunity for recovery in the event that control is lost.
A review of past accidents indicates that, while accidents associated with engine malfunctions are rare, training to manage one engine inoperative flight (OEI) after take‑off is important. The ATSB recommends that such training should follow the manufacturer’s guidance and, if possible, be conducted in an aircraft simulator. If the sequence is conducted in the aircraft close to the ground, then effective risk controls need to be in place to prevent a loss of control as recovery at low height will probably not be possible. Such defences include:
• defined OEI performance criteria that, if not met, require immediate restoration of normal power
• use of the appropriate handling techniques to correctly simulate the engine failure and ensure that aircraft drag is minimised/OEI performance is maximised
• ensuring that the involved pilots have the appropriate recency and skill to conduct the exercise and that any detrimental external factors, such as high workload or pressure, are minimised.
The two other asymmetric training accidents were:
On 23 December 2010, a flight instructor and student pilot departed Camden Airport, New South Wales on an instrument training flight in a Piper PA-30 (Twin Comanche) aircraft. Shortly after take-off, the instructor simulated an engine failure by moving the mixture control on the right engine rearwards at 400 ft above the ground. In response, the student reduced the engine control/s on the left engine. Shortly after, the airspeed decayed, and the aircraft stalled. The aircraft rolled abruptly, with the right wing dropping to a 120° angle and the aircraft entered a spin. The instructor regained control of the aircraft at about 10 ft above ground level, with the aircraft in a relatively level attitude. As the nose of the aircraft was raised the airframe began to shudder, indicating that a stall was imminent. Consequently, the instructor elected to reduce the throttles to idle and land the aircraft. The aircraft subsequently impacted the ground resulting in minor injuries to the instructor. The student was not injured. (ATSB investigation AO-2010-111).
On 10 July 2009, a flight instructor and student were conducting asymmetric circuit refresher training in a Beechcraft Aircraft 76 at Bunbury Airport, Western Australia. During a go-around from a practice asymmetric landing, the flying pilot flared too high and bounced on one wheel. While the instructor said ‘I have control’, the student pilot applied power on the good engine, and (under 50 ft above the ground) the aircraft yawed right then impacted the ground in a flat attitude. The aircraft was seriously damaged but there were no reported injuries (ATSB occurrence number 200904058).
Engine failure and malfunction occurrences
For the same 10-year period (2008-2017) and types of aircraft, there were 405 actual engine failures or malfunctions reported to the ATSB. Of these, 43 per cent were in the take-off/climb phases of flight. Only 9 resulted in accidents (2%), but 78 per cent of accidents were in the take-off/climb phases of flight. Five accidents followed a single engine failure on take-off or climb that resulted in asymmetric thrust:
On 6 February 2009, a Piper PA-31 aircraft was on a business flight departing from Darwin, Northern Territory. During the initial climb, the right engine gradually lost power. The aircraft failed to climb, and the pilot shut the engine down and feathered the propeller. The aircraft did not maintain altitude and subsequently the pilot landed the aircraft on water. The pilot and five passengers walked to shore in knee deep water (ATSB occurrence number 200900366).
On 23 March 2010, a Piper PA-30 was conducting a ferry flight to the United States. During the initial climb from San Francisco Airport, the left engine failed at 60 ft above the ground. The aircraft veered left and lost height until it struck the ground. The aircraft was seriously damaged but the pilot was not injured (ATSB occurrence number 201001978).
On 15 June 2010, a Piper PA-31P aircraft, with a pilot and a flight nurse on board departed Bankstown Airport, New South Wales for a repositioning flight to Archerfield Airport, Queensland in preparation for a medical patient transfer flight. While the aircraft was climbing to 9,000 ft the right engine sustained a power problem and the pilot subsequently shut down that engine. Following the engine shut down, the aircraft’s airspeed and rate of descent were not optimised for one engine inoperative flight. As a result, the aircraft descended to a low altitude over a suburban area and the pilot was then unable to maintain level flight, which led to a collision with terrain. Both occupants were fatally injured and the aircraft was destroyed (ATSB investigation AO-2010-043).
On 14 November 2010, a Piper PA-31 aircraft was being operated on a passenger charter flight from Marree, South Australia. During the climb, at 2,500 ft, the pilot detected an unusual noise in the right engine followed by a gradual decrease in engine performance. The pilot returned to Marree Airport, however during the turn back the aircraft was unable to maintain altitude and elected to conduct a forced landing about 22 km south-east of the airport. The pilot did not feather the right engine as he assessed that the right engine was still producing some power. The aircraft was substantially damaged, however, the passengers and crew were able to exit the aircraft safely (ATSB investigation AO-2010-094).
On 8 March 2015, the pilot of an Aero Commander 500 aircraft taxied for a charter flight from Badu Island to Horn Island, Queensland, with five passengers. The pilot commenced rotation and the nose and main landing gear lifted off the runway. Just as the main landing gear lifted off, the pilot detected a significant loss of power from the left engine. The aircraft yawed to the left, which the pilot counteracted with right rudder. He heard the left engine noise decrease noticeably and the aircraft dropped back onto the runway. The pilot immediately rejected the take-off; reduced the power to idle, and used rudder and brakes to maintain the runway centreline. Due to the wet runway surface, the aircraft did not decelerate as quickly as expected and the pilot anticipated that the aircraft would overshoot the runway. To avoid a steep slope and trees beyond the end of the runway, he steered the aircraft to the right towards more open and level ground. The aircraft collided with a fence and a bush resulting in substantial damage. The pilot and passengers were not injured (ATSB investigation AO-2015-028).
Risks associated with simulated and actual engine failures
While the risks associated with practice engine failures have mostly been eliminated for large air transport category aeroplanes through the use of simulators, accidents continue to occur worldwide as a result of simulated engine failures after take-off in flight in smaller (under 5,700 kg) multi-engine aeroplanes. The ATSB was unable to find any analyses or studies that had been conducted into the relative benefits versus risks of conducting simulated engine failures after take-off.
The above data on Australian accidents and incidents from 2008 to 2017 was used in the ATSB investigation into the fatal accident at Renmark in 2017 (described above) to conclude:
A review of the ATSB occurrence database identified that there were three accidents during asymmetric training/checking flights in the last 10 years, with this accident being the only one with a fatal outcome.
Over the same time period there were nine accidents associated with actual engine failures/malfunctions in ‘small’ aeroplanes like the Cessna 441, four of which followed a single engine failure on take-off/climb that resulted in asymmetric thrust but no injuries. One of the accidents was fatal and followed an engine failure at an altitude of about 7,500 ft. The nine accidents represented two per cent of the total number of engine failure/malfunction occurrences. However, 78 per cent of the accidents occurred during the take-off/climb phase of flight despite only 43 per cent of the total engine failures occurring during that flight phase.
The data indicates that while accidents associated with engine malfunctions are rare, training to manage OEI flight after take-off is important.
At present there is insufficient information available to accurately assess the accident rate associated with simulated engine failures, compared to the accident rate of actual engine failures occurring after take-off. Specifically, there is no data collected about the number of times asymmetric exercises are conducted in aircraft in Australia, in either flight training or company-based training and checking, which means the exposure is unknown.
Without knowing the exposure rate and how the training exercises are being conducted, including whether they accurately represent the conditions of a real engine failure, the ATSB could not determine whether the benefits of conducting simulated engine failures at low level outweighed the risks. Further research in this area is required to answer that question.
Skill decay
A pilot’s technical and non-technical skills decay when they are not used. To mitigate against this, pilots are subject to recency requirements to assess, practise and retain their skills.
Childs and Spears (1986) suggest that cognitive and procedural elements of flying skills decay more rapidly than control-oriented skills. Pilots whose skills had decayed, had difficulty correctly identifying cues and classifying situations, but once a situation was correctly classified, they remembered what to do.
Casner and others (2014) noted that hand-eye skills were quite resistant to forgetting, but decay was more significant for ‘…the set of cognitive skills needed to recall procedural steps, keep track of which steps have been completed and which steps remain, visualize the position of the aircraft, perform mental calculations, and recognize abnormal situations.’ In addition, skill decay is more significant for procedural tasks with many steps and where the steps must be recalled in a specific order (Wisher and others 1999).
Simulated engine failures are predominantly procedural tasks, which require a set of actions to be completed. They are an abnormal situation and have serious consequences if not managed appropriately. These require well-rehearsed, proficient physical and mental skills as well as rapid cognition of the situation and decision making.
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
From the evidence available, the following findings are made with respect to the collision with terrain involving an Angel Aircraft Corporation Model 44 aircraft, registered VH-IAZ, which occurred near Mareeba Airport, Queensland, on 14 December 2019.
These findings should not be read as apportioning blame or liability to any organisation or individual.
Contributing factors
The flight instructor very likely conducted a simulated engine failure after take-off in environmental conditions and a configuration in which the aircraft was unable to maintain altitude with one engine inoperative.
Having not acted quickly to restore power to the simulated inoperative engine, the pilots did not reduce power and land ahead (in accordance with the Airplane Flight Manual procedure) before the combination of low airspeed and bank angle resulted in a loss of directional control at a height too low to recover.
The instructor had very limited experience with the aircraft type, and with limited preparation for the flight, was likely unaware of the landing gear and flap retraction time and the extent of their influence on performance with one engine inoperative.
Other factors that increased risk
The pilot had not flown for 3 years prior to the accident flight, which likely resulted in a decay in skills at managing tasks such as an engine failure after take-off and in decision-making ability. The absence of flying practice before the flight review probably affected the pilot’s ability to manage the asymmetric low-level flight.
The aircraft had not been flown for more than 2 years and had not been stored in accordance with the airframe and engine manufacturers’ recommendations. This very likely resulted in some of the right engine cylinders running with excessive fuel to air ratio for complete combustion and may also have reduced the expected service life of both engines’ components.
The right-side altimeter was probably set to an incorrect barometric pressure, resulting in it over-reading the aircraft’s altitude by about 90 ft.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 6 July 2019, a Brumby Aircraft Brumby 610 Evolution amateur-built aircraft, recreational registration 24-8552, collided with terrain near Leigh Creek, South Australia. The pilot and single passenger were fatally injured.
In response to this accident, Recreational Aviation Australia (RAAus) commenced an investigation and subsequently requested technical assistance from the ATSB in the recovery of flight data from a Dynon EFIS and Garmin GPS.
To protect the information supplied by RAAus to the ATSB and the ATSB's investigative work to assist RAAus, the ATSB initiated an investigation under the Transport Safety Investigation Act 2003.
Flight path data was successfully recovered from a Garmin GPSMap 495 – a representation of which is shown as Figure 1. This data was provided to RAAus investigators on 6 February.
Data was not recoverable from the Dynon FlightDEK-D180 (combined electronic flight instrument system and engine monitoring), and RAAus was advised on 29 May 2020.
Figure 1: Recovered Flight Data representation
Source: Google Earth, track by ATSB
This concludes the ATSB involvement in the investigation of this accident.
Any enquiries relating to the accident investigations should be directed to RAAus at: www.raa.asn.au.
_____________
The information contained in this update is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
On 20 October 2019, an I.C.P. Savannah aircraft, recreational registration 19-7429, collided with terrain near the Emkaytee aerodrome, Northern Territory. The pilot was fatally injured.
In response to this accident, Recreational Aviation Australia (RAAus) commenced an investigation. As part of its investigation, RAAus requested technical assistance from the ATSB.
The ATSB initiated an investigation under the Transport Safety Investigation Act 2003 and assisted RAAus by downloading flight data from the aircraft’s Dynon Electronic Flight Instrument System (EFIS) The Dynon EFIS was successfully downloaded. However, the data logging functionality of the device was not enabled. No flight data was retrieved from the device.
With the completion of the examinations and data recovery, the ATSB has concluded its involvement in the investigation of this accident. Any enquiries relating to the accident investigations should be directed to RAAus at: www.raa.asn.au
At about 0640 Eastern Standard Time on 20 September 2019, a Mooney M20J aircraft, registered VH-DJU, departed Murwillumbah, New South Wales for a private flight under visual flight rules to Taree, New South Wales. On board were the pilot and one passenger.
At 0717, when DJU was 45 NM north of Coffs Harbour, the pilot contacted air traffic control and requested a clearance to transit the Class C controlled airspace at 6,500 ft. Air traffic control advised that a clearance was not available at that altitude and that, due to cloud conditions, a visual transit of the airspace would only be possible at an altitude not above 1,000 ft. The pilot then advised that the flight would descend to ‘not above 1,000 ft’.
The aircraft continued on a direct track to Taree and at 0724 the pilot reported that the aircraft was operating outside controlled airspace in clear conditions at 4,100 ft and would remain on that track. The aircraft was then climbed to 4,500 ft and at 0732, commenced a descent in the vicinity of high terrain.
The aircraft did not arrive at Taree as expected so a search was initiated. The aircraft was found to have collided with terrain about 26 km west of Coffs Harbour Airport. The two persons on board were fatally injured and the aircraft was destroyed.
What the ATSB found
The ATSB found that the pilot was not provided clearance to transit Class C airspace due to the trainee controller’s conservative assessment that workload would not allow it although there was no conflicting traffic, meteorological factor or limiting air traffic control instructions or procedures. The trainee’s supervisor accepted the assessment as an alternate transit option was provided to the pilot. Additionally, the information subsequently provided by air traffic control likely resulted in the pilot deciding to descend the aircraft from 6,500 ft instead of other available safe options. This descent exposed the flight to increased risk.
The ATSB also found that the pilot was not carrying suitable navigation equipment and had most likely not obtained the required weather forecasts. These factors reduced the pilot's ability to manage the flight path changes and identify the high terrain. This led to the aircraft being descended toward the high terrain in visibility conditions below that required for visual flight, resulting in controlled flight into terrain.
The pilot had also not completed the required flight reviews or proficiency checks. This resulted in the pilot not possessing the required licence to undertake the flight and likely led to a deterioration in the knowledge and skills required for effective flight management and decision‑making.
What has been done as a result
Following the occurrence, Airservices Australia (Airservices) provided additional training for air traffic controllers focussing on clearance issues, workload assessments, and coordination with other traffic units where decisions affect the other unit. An information and education package was developed for controllers regarding the provision of advice and information to pilots not subject to a clearance.
Performance checks and unit reviews were also undertaken to provide assurance that airways clearances were consistently issued in accordance with documented procedures. Airservices also included additional content in on‑the‑job instructor professional development sessions to ensure trainees’ capability is commensurate with actual workload to optimise performance.
Safety message
The safety risks of visual pilots flying into non-visual conditions are well documented. This continues to be a recurring factor in aircraft accidents and has been the focus of numerous previous ATSB reports and publications.
This accident also emphasises the importance of pilot and flight preparation. Ensuring that all required training is completed assists a pilot to both develop and maintain the necessary skills to manage challenges that may be encountered during a flight, such as inclement weather or inadvertent entry into non-visual conditions. Further, confirming that appropriate operational information is obtained and readily available ensures that a pilot is well prepared to anticipate in‑flight complications and successfully manage unforeseen challenges.
The accident also illustrates the significant influence that air traffic control can have on the conduct of a flight.
The occurrence
At about 0640 Eastern Standard Time[1] on 20 September 2019, a Mooney M20J aircraft, registered VH-DJU, departed Murwillumbah, New South Wales for a private flight under visual flight rules (VFR)[2]to Taree, New South Wales. On board were the pilot and one passenger.
After departing Murwillumbah, the aircraft climbed to 6,500 ft above mean sea level (AMSL) on a direct track to Taree (Figure 1).
At 0717 when the aircraft was 45 NM north of Coffs Harbour Airport, the pilot contacted Brisbane Centre air traffic control (ATC) and requested a clearance to transit Class C controlled airspace (see the section titled Airspace and airways clearances) on a continuation of the direct track to Taree at an altitude of 6,500 ft. The air traffic controller advised the pilot that a clearance to enter controlled airspace was not available at 6,500 ft and provided the option to request clearance through the underlying Coffs Harbour Class D controlled airspace.
Figure 1: Aircraft track (yellow) on 20 September 2019
Source: Google Earth, annotated by ATSB
The pilot subsequently contacted the Class D controller in the Coffs Harbour air traffic control tower and requested a clearance. In response, the tower controller contacted the Brisbane Centre Class C controller to discuss and coordinate the aircraft’s transit. Following that discussion, at about 0721, the tower controller advised the pilot that due to the extensive cloud cover, ‘the only way’ to transit that airspace under the VFR would be at an altitude not above 1,000 ft. The pilot responded that the aircraft would descend to ‘not above 1,000 ft’.
Recorded air traffic surveillance data indicated that at about this time, the pilot manoeuvred the aircraft slightly further laterally away from the Class C airspace however, during the descent, it briefly entered that airspace without a clearance.
The aircraft then continued on a direct track outside controlled airspace (OCTA) towards Taree and at 0724, the pilot advised the tower controller the flight was ‘currently 4100 in clear and we’re OCTA’. In the context of the preceding discussion regarding the extent of the cloud, the ATSB assessed the pilots reference to ‘in clear’ was an indication that the aircraft was operating in clear weather conditions at an altitude of 4,100 ft at that time. The pilot also advised that the flight would continue on that track and that a clearance request would be made upon reaching the airspace boundary (the aircraft’s track intersected further Class D controlled airspace to the south of Coffs Harbour). The tower controller acknowledged this and asked that the pilot report entering controlled airspace.
A review of recorded air traffic control surveillance data showed that after the pilot reported that the flight was operating in clear conditions, the aircraft was climbed to about 4,500 ft in Class G uncontrolled airspace and continued on a direct track until 0732. At that time, the aircraft commenced a descent, which continued until the last recorded position about 1 minute later. The aircraft was last recorded descending through an altitude of 3,564 ft at a ground speed of 165 kt. No further position or radio broadcasts were received from the aircraft.
In response to the aircraft not arriving at Taree as expected, a search was initiated. Although the search was initially hampered by rain and low cloud in the vicinity of the aircraft’s last known position, the aircraft was located, having impacted terrain at an elevation of 2,920 ft. The wreckage was positioned in line with the last recorded track and about 2.8 km south of the last recorded position. The two persons on board were fatally injured and the aircraft was destroyed (Figure 2).
The pilot obtained a Civil Aviation Regulation 1988 Regulation 5 (CAR 5) Private Pilot Licence (Aeroplane) in 1982. For that licence, the pilot held endorsements for single engine aircraft below 5,700 kg maximum take-off weight, manual propeller pitch control, retractable undercarriage, tail wheel undercarriage and operation in controlled airspace. The pilot had never held an instrument rating.
The pilot was reported to have kept an up to date logbook but it was not found at the accident site or located during the investigation. An earlier logbook provided to the ATSB, contained two entries, including one relating to the conduct of a flight review in January 2010. The pilot had declared a total aeronautical experience of 1,006 hours at their last medical examination in November 2017.
Licencing and flight reviews under CASR Part 61
In September 2014, the Civil Aviation Safety Authority (CASA) introduced new flight crew licencing regulations, Civil Aviation Safety Regulation 1998 (CASR) Part 61. As part of the transition to the new licencing system, pilots could continue to exercise the privileges of their CAR 5 licence until 31 August 2018. Between September 2014 and 31 August 2018, pilots were required to make an application for a new Part 61 licence in conjunction with their next required flight review or proficiency check.
From 1 September 2018, CASA ceased recognising CAR 5 licences and a pilot was required to hold a CASR Part 61 licence in order to conduct a flight.
Prior to conducting a VFR private flight, CASR Part 61 required an aeroplane flight review (AFR), or other specified proficiency check, to have been undertaken within the previous 2 years.
The CASA Flight reviews information sheet provided the following guidance on the purpose and benefits of flight reviews:
A flight review is an opportunity to receive training that refreshes your flying skills and operational knowledge. Pilots undertake flight reviews to ensure they continue to be competent flying particular types of aircraft or exercising the privileges of an operational rating.
After gaining a qualification, it is normal for some skills to deteriorate over time. A flight review ensures your piloting skills remain - or are brought back up - to standard.
During an AFR, a pilot is required to demonstrate competency as outlined in the Part 61 manual of standards. The AFR also serves as an opportunity for a pilot to receive training to attain the required standards.
The manual of standards included the following competencies which were relevant to the management of hazards associated with the accident flight:
2.2 3 (d) perform diversion procedure
2.5 5 (a) perform basic flight manoeuvres using full instrument panel
2.7 7 (a) recognise and manage threats and errors during pre-flight planning and in-flight;
(b) maintain effective lookout and situational awareness;
(c) assess situations and make appropriate decisions;
(d) set priorities and manage tasks;
(e) maintain effective communication with stakeholders;
(f) communicate effectively using aeronautical radio.
4 (c) obtaining, interpreting and applying meteorological and aeronautical information;
(d) navigation and flight planning for day VFR operations;
(j) hazard identification and risk management;
(m) hazardous weather;
Prior to the introduction of CASR Part 61, flight reviews were only required to be recorded in a pilot’s logbook. After the introduction of CASR Part 61, flight reviews and proficiency checks were required to be recorded in a pilot’s licence, logbook and with CASA. As the pilot’s current logbook was not recovered during the investigation, the date of any flight review after January 2010 and before September 2014 could not be determined.
However, CASA did not hold any record of an application for a flight review or equivalent proficiency check after September 2014. The ATSB contacted flying training organisations at Murwillumbah Airfield and Gold Coast Airport, where the pilot’s previous aircraft was maintained, and the pilot was reported to have regularly visited. None of these organisations held training records for the pilot.
Based on the available information, the ATSB concluded that the pilot had not met the CASR Part 61 flight review requirements and, as such, did not hold the required licence to undertake the flight.
Fatigue
The ATSB collected information about the pilot’s 72 hours of activity prior to the accident. A review of that evidence identified that it was unlikely that the pilot was experiencing a level of fatigue known to affect performance.
Medical and pathological information
The pilot held a Class 2 medical certificate valid until November 2019.
Two prescription medications belonging to the pilot were found in the wreckage and the pilot’s toxicology report confirmed the presence of both medications. The use of one of those medications was not recorded in the pilot’s medical file held with CASA. It is unlikely that this medication adversely affected the pilot’s performance during the accident flight.
CASR Part 67 describes the requirements for aviation medical certification. One of the criteria for exercising the privilege of a Class 2 medical certificate is that the use of ‘any over‑the‑counter or prescribed medication or drug… that causes the person to experience any side effects likely to affect the person to an extent that is safety‑relevant’ is prohibited.
Further, medical certificate applicants are required to answer ‘every question asked by the examiner that the examiner considers necessary to help…CASA decide whether the applicant meets the relevant medical standard’. They are obliged to notify CASA of changes in medical conditions that impair their ability to ‘do an act authorised by the license’.
The following extracts from CASA-developed brochures are particularly relevant to pilot medical examinations.
Designated aviation medical examiners (DAMEs) and pilots together should foster a culture where it is likely that pilots will feel comfortable disclosing medical problems, even if they may impact on their ability to maintain an aviation medical.
Your DAME…will expect you to answer both written and verbal questions, honestly and fully...
Under the clinical practice guidelines for DAMEs, certain risk assessment protocols allowed them to take into account the pilot’s need for medication use when assessing if the applicant met the relevant medical standard. A CASA brochure states ‘only 0.29 percent of all initial and renewal medical certificates were refused by CASA during 2016-2017’.
Aircraft information
The Mooney M20J is a four seat, piston-engine aircraft with a two-blade variable-pitch propeller and retractable tricycle landing gear. VH-DJU (serial number 24-1075, Figure 3) was manufactured in 1981 and first registered in Australia in 2005.[3]
Figure 3: The aircraft, VH-DJU
Source: Previous aircraft owner
The pilot purchased the aircraft on 6 July 2019, about 3 months prior to the accident, and had flown about 31 hours in the aircraft. The most recent entry on the maintenance release was 11 days prior to the accident (9 September 2019) and showed that the aircraft had accumulated 3,295 hours total time‑in‑service.
At the last scheduled maintenance inspection, in December 2018, the required inspections and test of the pitot-static system[4] to maintain the aircraft’s approval for instrument flight rules (IFR)[5]operation were not undertaken. However, as a condition of purchasing the aircraft, the pilot of the accident flight required that the test and inspections be carried out. In April 2019, this was carried out and at the time of the accident the aircraft was equipped and approved for IFR operation (Figure 4).
Figure 4: Composite image of the instrument panel
Source: Supplied
The aircraft was equipped with an autopilot capable of maintaining a selected heading and navigation track. The autopilot did not have an altitude hold function or ability to manipulate the vertical flight profile.
Two smartphones and a tablet computer were recovered from the wreckage. Neither smartphone contained an electronic flight bag or other aviation application. The tablet computer was found packed in an overnight bag indicating that it was not used during the flight.
Date-expired air navigation charts for the area encompassing the flight were found stowed in a flight bag indicating that they were not being used at the time of the accident. No paper flight plan or other flight planning notes were located in the wreckage.
Global Navigation Satellite System units
Passengers who had flown with the pilot reported that the pilot routinely used a Garmin Aera 500 Global Navigation Satellite System (GNSS)[6] unit carried in their lap. The aircraft was also equipped with a Garmin GTN650 GNSS unit.
Aera 500
The Aera 500 unit carried by the pilot was not approved as a sole means of navigation. However, the unit did present useful information relating to the progress of the flight. This included topographical and airspace information. The unit had a terrain function that required a valid 3D GNSS position solution and a valid terrain and obstacle database to operate properly. Terrain information was advisory only and could include:
display of altitudes of terrain and obstructions relative to the aircraft’s altitude
pop-up terrain alert messages issued when flight conditions meet parameters set within the terrain system software algorithms
forward looking terrain avoidance alerts
The ATSB recovered data from this unit indicating that it was in use at the time of the accident. However, it could not be established which mode was selected at the time of the accident or whether the terrain function was operable and the status of any user and system inhibitions.
GTN650
The GTN650 unit fitted to the aircraft operated as both a radio communications unit and an IFR‑approved GNSS unit. The unit was capable of operating in different modes, which could display a significant amount of information relating to progress of the flight. This included the selected track, any deviation from this track, topographical, and airspace information.
Like the Aera 500, the GTN650 had a terrain function. The unit provided similar advisory information and alerts as the Aera 500 unit with similar limitations. The previous owner of the aircraft, a flying instructor, advised the ATSB that at the time of the pilot’s purchase of the aircraft, the pilot declined familiarisation training with the GTN650 unit as the Aera 500 would be used. It could not be determined if the pilot subsequently undertook user training for the GTN650 unit.
The ATSB was not able to recover any data from the GTN650 unit to determine if it was used during the accident flight.
Terrain in the accident vicinity
At the time of the request to transit Class C airspace, the aircraft was about 10 NM north of Grafton (Figure 5). The area to the north of and surrounding Grafton was low-lying coastal terrain with elevations generally below 1,000 ft AMSL. However, the line of hills associated with the Coast Range, between the aircraft’s position and a track toward the coast and Coffs Harbour, rose to elevations in excess of 1,000 ft AMSL.
Figure 5: World Aeronautical Chart extract showing terrain in the vicinity of the aircraft’s track
Source: ATSB
Along a direct track toward Taree, the aircraft’s path passed over a region where the Great Dividing Range extended near to the coast at Coffs Harbour. This area included the mountain range encompassing Dorrigo National Park. The topography within this region was substantially more rugged and elevated than the terrain further north, rising in excess of 3,000 ft AMSL.
The terrain over which the aircraft was flying at the time of the descent from 4,500 ft was within this mountain range. The highest obstacle near the aircraft’s track were two towers on Mount Moombil at 3,950 ft, 400 m east of the track. Immediately south of Mount Moombil was a broad valley, which rose on the southern side to a ridge. The highest point of the ridge was 3,018 ft.
Meteorology
Airservices Australia (Airservices) did not hold any National Aeronautical Information Processing System (NAIPS)[7] login records for the pilot for that, or any past, flights. A review of the pilot’s
personal electronic devices identified that there were no aviation flight planning or aviation weather applications and no weather documentation relevant to the accident flight was found in the wreckage.
The ATSB obtained relevant weather information from the Bureau of Meteorology (BoM).
BoM information
Graphical area forecast
The graphical area forecast for the accident region forecast the following cloud conditions for the time of the accident (all heights AMSL):
Satellite images (Figure 6) for the area just prior to the accident time showed generally clear conditions between Murwillumbah and Grafton. South of Grafton and throughout the area encompassing the high terrain west of Coffs Harbour, the images showed extensive cloud coverage. Further along the intended route towards Taree, the cloud coverage reduced near the coast, but persisted inland.
Figure 6: Meteorological satellite image extract for 0730 on 20 September 2019
Source: Bureau of Meteorology, annotated by ATSB
Analysis
The BoM provided the following analysis of meteorological conditions for the Coffs Harbour region on the morning of the accident:
On the 19th of September 2019, the analysed mean sea level pressure (MSLP) chart for 1800 UTC (4 am AEST 20th September) showed a strong, slow-moving high-pressure system over the Tasman Sea extending a ridge over eastern New South Wales. A coastal trough situated north of Coffs Harbour, whilst an approaching cold front was moving east through Central Australia at approximately 30 knots.
At the time of the incident the region was covered in widespread broken low cloud. With bases generally between 2000 - 3000ft above mean sea level, this most likely resulted in cloud on ground around Mount Moombil. Recent rainfall over the area with persistent onshore flow likely increased the low-level moisture within the air mass, creating saturated conditions.
The top of the broken low cloud layer was approximately 3,000 (±1,000) ft AGL [above ground level] with a second cloud layer, few to scattered in its extent and at approximately 8,000 (±1,000) ft AGL.
Automatic terminal information service
At the time of the accident, the Coffs Harbour automatic terminal information service detailed the following weather information:
wind: Variable at 5 kt
visibility: Greater than 10 km
cloud coverage: Few at 1,500 ft and broken at 2,500 ft[9]
temperature: 17° C
Witness
A witness located about 10 km south‑east of the accident site stated that cloud was ‘down to the ground’ at the base of the mountain from 0700 until 0830 on the morning.
Visual meteorological conditions
Visual meteorological conditions (VMC) are the minimum meteorological conditions in which flight is permitted under the VFR – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft. Additionally, when operating VFR at or below 2,000 ft above the ground or water, the pilot must be able to navigate by visual reference to the ground or water.
The VMC requirements for aeroplanes vary for different classes of airspace (Table 1).
Table 1: Visual meteorological conditions
Airspace
Flight visibility
Distance from cloud
Additional conditions
Class C below 10,000 ft AMSL
5,000 m
1,500 m horizontal
1,000 ft vertical
ATC may permit operations in weather conditions that do not meet this criteria (special VFR)
Class D
5,000 m
600 m horizontal
1,000 ft vertically above; or 500 ft vertically below
ATC may permit operations in weather conditions that do not meet this criteria (special VFR)
Class C & D Special VFR
1,600 m
Clear of cloud
Operate within the requirements of Civil Aviation Regulation 157 Low flying.
Class G below 10,000 ft (subject to below)
5,000 m
1,500 m horizontal
1,000 ft vertical
Class G at or below (whichever is the higher) of:
(a) 3000 ft AMSL;
(b) 1000 ft AGL
5,000 m
Clear of cloud and in sight of ground or water
Radio must be carried and used on the appropriate frequency
Source: Aeronautical Information Publication ENR 1.2
Airspace and airways clearances
Coffs Harbour airspace
Coffs Harbour Airport is situated within Class D terminal airspace (Figure 7). This airspace was controlled by an air traffic controller situated within the Coffs Harbour control tower. The Class D airspace extended to the north and south‑west at ground level to a 7 NM boundary. West of the airport, the airspace extended about 6 NM and further west of this boundary, the controlled airspace base was the overlying Class E airspace at 8,500 ft.[10] To the north and south‑west, the airspace fanned out at increasing distances from Coffs Harbour. The base of the airspace also progressively stepped up at increasing distances to a maximum altitude of 4,500 ft at about 22 NM.
Overlying the Class D airspace was Class C en route airspace, which continued up from 4,500 ft to overlying Class A airspace at flight level (FL) 180.[11] The Class C airspace was controlled by an air traffic control position situated in Brisbane. At the time of the accident, this position was occupied by a trainee controller (trainee) in the first week of on-the-job training and under the supervision of an on-the-job training instructor (OJTI). The trainee and OJTI were managing both the sector of Class C and uncontrolled Class G airspace overlying and surrounding Coffs Harbour (Grafton) combined with a second sector of Class C and Class G airspace (Newell) extending to the west over the New England region.
The base of the Class C airspace also fanned out and progressively stepped up at further distances from Coffs Harbour Airport. At a distance of about 30 NM, where the pilot of DJU requested to enter the airspace, the base of the Class C airspace was 5,500 ft. Outside of these boundaries was Class G uncontrolled airspace that extended up to the base of overlying Class A airspace at FL 180.
Within Class C airspace, aircraft were identified and controlled using automatic dependent surveillance broadcast (ADS-B) or radar surveillance data. IFR aircraft were positively separated from both IFR and VFR aircraft. VFR aircraft were provided traffic information about other VFR aircraft. The controllers had access to relevant weather forecasts and observations, but as they were physically located in Brisbane, they could not see the actual weather conditions.
In addition, Class C controllers provided pertinent operational information to IFR aircraft as well as to VFR aircraft upon request within the Class G airspace.
Within Class D airspace aircraft were not identified and controlled using surveillance data, and separation between aircraft was provided as follows:
IFR flights were separated from other IFR and special VFR flights,[12]
IFR flights were provided traffic information for VFR flights,
VFR flights were provided traffic information on other VFR flights, and
special VFR flights were separated from other special VFR flights in conditions less than VMC.
The Class D controller at Coffs Harbour Airport had access to weather forecasts, observations and could observe the prevailing weather conditions for the airspace. In addition, the control tower was fitted with a tower situation awareness display (TSAD). This displayed ADS-B and radar aircraft position information to enhance controller awareness but was not used for traffic management or separation.
Flight notification
The pilot was not required to and did not submit a flight plan prior to departure.
As the pilot intended to operate in the Class C airspace, notification of the flight was to be provided to ATC as per Airservices’ Aeronautical Information Publication (AIP) requirements. The pilot provided this notification when the aircraft was 10 NM north of Grafton (about 4 minutes prior to reaching the airspace boundary), with detail of the intended track and a clearance request to transit the Class C airspace.
Traffic
At the time of the Class C clearance request, there was no other traffic below 10,000 ft in the Coffs Harbour airspace, nor were there any impending arrivals or departures during the time the aircraft would have transited the airspace. Within the remaining airspace being managed by the trainee and OJTI, there were five other aircraft being provided an air traffic service.
Additionally, in the minute prior to receiving the request from VH-DJU, the trainee had completed handling a flight following request from a VFR aircraft.
Class C clearance request
The pilot requested a clearance to proceed from a position 10 NM north of Grafton (14 NM from the airspace boundary) direct to Taree at an altitude of 6,500 ft. This track passed within the Class C airspace for a distance of about 7 NM (2 minutes and 50 seconds at the aircraft’s speed).
On receiving the clearance request, the trainee assessed that workload and priorities would not permit a clearance at the requested level, and that the transit would be better facilitated through the underlying Class D airspace. The trainee then advised the pilot accordingly, providing the option to request clearance for the Class D airspace. The trainee or OJTI did not contact the Class D controller prior to initially proposing the pilot contact that controller. The OJTI felt that it was more effective for the pilot to contact the Class D controller directly rather than coordinating the request.
Workload assessment
The Airservices investigation report into the accident identified the following:
Sampling of Grafton sector controller performance assessment reports and daily training records included debriefing and coaching comments emphasising to trainees and controllers to be cautious with issuing clearances below A080 through the [Coffs Harbour] airspace. These comments are intended to highlight the known complications of transiting aircraft with processing IFR departures and arrivals. Techniques including the use of alternative clearances for departing and overflying aircraft are also emphasised during training and checking together with options for transiting aircraft to climb/descend to transit the airspace to manage the traffic scenarios. Assessing the options available with regard to the traffic picture is also emphasised during training and checking.
While acknowledging the complexities during training and checking is appropriate, this may unduly influence decision-making particularly in trainees and inexperienced controllers as they gain confidence and familiarity with new airspace volumes. In these cases, perceived workload may be prioritised ahead of an appropriate assessment of the current and projected traffic disposition.
The OJTI assessed that the workload at the time of the clearance request was low, but the trainee being new to the role may have perceived the workload as higher. The OJTI also stated that while the trainee’s decision was conservative, it was appropriate. The OJTI felt no intervention was required as the pilot had been provided a suitable option. The OJTI further stated that 6,500 ft was a level that created separation difficulties with Coffs Harbour arrivals and departures and given the limited size of the airspace this can very quickly create a significant workload issue.
Class C airspace infringement
After being advised that a Class C clearance was not available, the aircraft entered the Class C controlled airspace without clearance. After entering the controlled airspace, the pilot descended the aircraft before exiting the airspace about 1 minute later (see the section titled Class D clearance request and communications below).
The trainee did not attempt to contact the pilot of the aircraft during the airspace infringement. The OJTI noted that this airspace infringement did not cause any separation or traffic management concerns.
Class D clearance request and communications
The direct track to Taree from the pilot’s position did not intersect the northern sections of the Class D airspace and therefore a clearance was not required on the direct track at or below 4,500 ft. However, the track did intersect the southern section of the airspace beyond Coffs Harbour.
The pilot requested a clearance with the Class D controller for a transit at 6,500 ft on a direct track to Taree. This flight path would have transited the Class C airspace and the Class D controller, queried whether the pilot wanted to remain at 6,500 ft. The pilot stated being ‘happy to remain at 6,500 ft’ and the controller, unaware of the previous Class C clearance request, instructed the pilot to contact the Class C controller for a clearance through that airspace.
The Class D controller then contacted the trainee to advise that the pilot would be calling them to request the clearance through the Class C airspace and that they wanted to transit at 6.500 ft. The Class D controller informed the trainee that a VFR transit would be difficult. During this discussion between the controllers, the pilot again contacted the Class C controller for the clearance.
The trainee advised the pilot that the Class D controller had been in contact and instructed the pilot to again contact that controller.
At 0721, the pilot again contacted the Class D controller. The Class D controller advised that a clearance through the Class D airspace would only be available ‘about not above 1,000 ft’ and the pilot responded that the flight would descend to that level. The Class D controller asked the pilot to report entering the airspace at the 7 NM boundary. While a change in track was required to enter the airspace at the 7 NM boundary, no tracking instruction or guidance was provided to the pilot. The pilot did not voice any concerns about the advice provided by the Class D controller.
At 0724, about 10 minutes prior to the accident, the pilot contacted the Class D controller and advised that the flight was operating outside controlled airspace, in clear conditions at 4,100 ft AMSL, would remain on that track and request a clearance upon reaching the airspace boundary. No clearance was issued by the tower controller, but the controller acknowledged the request and instructed the pilot to report entering controlled airspace. No further broadcasts were heard from the aircraft.
Seventeen minutes later, at around the time the controller expected the pilot to enter controlled airspace (and about 7 minutes after the accident had occurred), the Class D controller tried contacting the pilot twice without receiving a response.
Uncertainty phase not declared
Aircraft to the west of Coffs Harbour were known to disappear from the TSAD (as DJU did about 1 minute prior to the accident) due to the effect of the surrounding terrain. It was also common for VFR aircraft to be uncontactable by Coffs Harbour ATC when operating in Class G airspace in that area. The controller reported that, as the pilot had advised that the flight was operating in clear conditions at 4,100 ft, they held no concern for the progress of the flight. Consequently, no uncertainty phase was declared with respect to the flight.[13]
Fatigue
The ATSB found no indicators that increased the risk of the controllers experiencing a level of fatigue known to affect performance.
Future Coffs Harbour airspace reclassification
Prior to the accident, Airservices commenced the Airspace Modernisation Program. This program will reclassify the Class C airspace above Coffs Harbour to Class E. At the time of writing, the timeframe for the completion of this program was not available.
Undertaking a VFR transit of the Class E airspace will not require a clearance.
Recorded flight data
The aircraft was not required to be and was not fitted with flight data recorders.
Airservices provided ADS-B and radar surveillance data relating to the flight. The data captured the flight from soon after departure at Murwillumbah until about 2.8 km north of the accident site (Figure 8).
Figure 8: Recorded flight path near accident site (towers on Mt Moombil not depicted)
Source: Google Earth annotated by ATSB
From 0722 until 0724, the aircraft descended from its cruising altitude of 6,500 ft to 4,100 ft. At this time, the pilot reported operating in clear conditions. About 2 minutes later, the aircraft climbed to 4,500 ft.
The aircraft remained at 4,500 ft until 0732 when a descent commenced and continued until the last recorded position at 0733:50. The descent rate averaged about 850 ft per minute with a groundspeed between 165 kt and 175 kt. The observed wind was almost directly across the descent track at 10-20 kt. According to the aircraft’s previous owner, this descent profile was consistent with maintaining a cruise engine power setting.
During this descent, the aircraft passed a saddle about 400 m west of the summit of Mount Moombil. On top of the summit were two towers, 538 ft high. The aircraft passed about 386 ft below the top of these towers and continued descending across a broad valley. Throughout the descent, no significant variations in either aircraft track, speed or descent rate were recorded.
Data recovered from the pilot’s Aera 500 GNSS unit was similar to the surveillance data until 3 minutes prior to accident (about 1 minute before the final descent) when the recorded data ended. The ATSB’s examination of the unit determined that the data loss was most probably the result of power supply interruption during the accident sequence, before that data was recorded to the non-volatile memory.
Accident site and wreckage
The accident site was located at an elevation of 2,920 ft in heavily wooded, steep terrain within Dorrigo National Park (Figure 9).
Figure 9: Aircraft wreckage
Source: ATSB
The path made by the aircraft through the vegetation continued for about 65 m from the first identified aircraft component to the ground impact point (Figure 10). Tree-impact marks and the impact crater showed that the aircraft entered the vegetation in a wings-level attitude on a continuation of the previously recorded descent angle of about 2°.
Examination of the wreckage found that the aircraft entered the vegetation at relatively high speed with the flaps and landing gear retracted. No pre-impact faults were identified, but the examination was limited by the extensive damage. The serviceability of the flight instruments and associated systems could also not be verified. Both fuel tanks ruptured, and an odour of fuel was present. The engine separated from the fuselage and the engine controls were severely disrupted during the accident sequence, which prevented determination of their positions. Damage to the propeller indicated that it was being driven by the engine at the time of the accident. The accident was not survivable.
Figure 10: Final descent path of the aircraft
Source: ATSB
Similar occurrences
The safety risks of visual pilots flying into non-visual conditions are well documented and continue to represent a significant factor in aircraft accidents and fatalities.
A large amount of reference material is available to pilots for guidance on avoiding VFR flight into adverse weather as well as recovering a flight should inadvertent IMC entry occur, including by seeking the assistance of ATC. The United States Aircraft Owners and Pilots Association Air Safety Institute website VFR into IMC provides an online course, videos and reference materials to assist pilots in avoiding and managing these scenarios. The following articles also provide valuable guidance on the subject.
On the morning of 20 September 2019, while en route from Murwillumbah to Taree, New South Wales, a Mooney M20J, registered VH-DJU (DJU) descended into an area of low visibility and high terrain near the town of Dorrigo. During this descent, the aircraft collided with steep, forested terrain within Dorrigo National Park.
A review of the pilot’s medical records, post‑mortem toxicology results and recorded data indicated that it was very unlikely that the pilot became incapacitated during the flight. While examination of the wreckage was limited by extensive damage, no defects or anomalies were identified that contributed to the accident. As such, this analysis focuses on the examination of the operational factors that led to the aircraft’s collision with terrain while being operated under the visual flight rules (VFR).
Class C clearance request
At 0717, about 4 minutes prior to reaching the Class C airspace north of Coffs Harbour, the pilot notified the controller (in Brisbane) of their intended track and requested clearance to transit the airspace. The intended transit would be short (7 NM, less than 3 minutes) and there was no other aircraft in the Class C or D airspace overlying Coffs Harbour, or any impending departures or arrivals there.
The aircraft was cruising at 6,500 ft and the pilot reported being ‘happy’ at that altitude, indicative of the visibility and conditions at the time. Based on the Bureau of Meteorology (BoM) analysis of the cloud conditions, the ATSB assessed that a VFR transit of the airspace at or above 6,500 ft was possible.
At the time the transit clearance request was made, the trainee controller (trainee) controlling the Class C airspace was managing five aircraft across two airspace sectors and had just completed handling another request. The trainee assessed that the workload would not allow the clearance requested for DJU and advised the pilot that it was not available and to contact the Coffs Harbour control tower to transit via the underlying Class D airspace.
The supervising on-the-job training instructor (OJTI) felt that the trainee’s perception of workload was higher than it actually was, but it was a conservative assessment and appropriate given the trainee’s experience (within the first week of on-the-job training). In any case, the OJTI was satisfied with the trainee’s handling of the request as the decision to not provide a clearance was not considered unsafe and the pilot had been provided with an appropriate alternative.
The trainee and the OJTI also reported considering that the requested 6,500 ft transit may create separation difficulties with aircraft departing Coffs Harbour Airport under instrument flight rules. However, at the time there was no traffic expected to or from the airport. Additionally, a review of the available evidence indicated that there were no meteorological factors, traffic control instructions or procedures that prevented the pilot of DJU being provided with a clearance.
When DJU subsequently infringed Class C airspace as it descended, the trainee took no action and the OJTI felt the infringement did not present any traffic management issues. This indicates that the clearance requested could have been accommodated without any significant increase in controller workload.
Acceptance of the ATC option to seek a clearance through Class D airspace resulted in the pilot deviating from their intended plan and commenced a sequence of events that ultimately culminated in the accident. However, it is also important to recognise that the pilot had other available safe courses of action that were not utilised (discussed further below) and the ultimate outcome could not have been anticipated.
Decision to descend
When communicating with the Coffs Harbour tower controller to transit the Class D airspace, the pilot reported being ‘happy at 6,500 ft’. An assessment of the BoM cloud conditions analysis indicated that visual meteorological conditions (VMC) allowed the flight to progress at and above that altitude or below about 2,000 ft, but extensive cloud cover probably prevented VMC flight between those two levels. The analysis also indicated that it was possible to proceed in VMC around the Class C controlled airspace at or above 6,500 ft. Conditions also permitted a diversion or descent to the north of Grafton to proceed coastal beneath the cloud layers south to Taree.
In response to the pilot’s request, the Class D controller advised that ‘…the only way you could transit this airspace VFR would be around… not above one thousand [feet]’. The pilot responded that the flight would descend to ‘not above 1,000 ft’ and commenced a descent from 6,500 ft.
The controller had also requested that the pilot report at the 7 NM airspace boundary to receive a clearance but had not provided any tracking information. Given the aircraft’s position at the time, the pilot would have had to change track to reach that boundary.
At altitudes less than 1,000 ft along a track between the aircraft’s position and Coffs Harbour Airport and more significantly, along a continuation of the direct track to Taree, terrain clearance was not possible. However, the pilot did not voice any concerns with the advice provided and the flight descended on the direct track to Taree.
While it was the pilot’s decision to descend from 6,500 ft and continue along the direct track instead of other available safe options, this decision was likely influenced by the information provided by the controller. The descent took the aircraft toward both significant cloud and high terrain, increasing risk to the flight.
Pre-flight preparation
Although out-of-date, the aeronautical charts carried by the pilot showed the high terrain west of Coffs Harbour. However, the pilot was not using the charts at the time of the accident. Additionally, an electronic flight bag program was not used to provide topographical information. The pilot was heavily reliant on the global navigation satellite system units for situational awareness, but the limitations of these units may have prevented them from displaying adequate terrain information.
There was no evidence that the pilot obtained weather information prior to departure or during the flight, nor was any weather information found in the wreckage. As the weather encountered during the flight was similar to forecast, this information would have provided the pilot with advance notice of the likely conditions and supported more effective decision-making.
In summary, the pilot probably did not have an adequate understanding of the weather conditions or awareness of the topography west of Coffs Harbour. These factors reduced the pilot's ability to manage the flight path changes and identify the high terrain into which the aircraft was descending.
Flight into unsuitable conditions
The BoM analysis indicated that conditions across the mountain range west of Coffs Harbour at the time of the accident were below the minimum stipulated for VMC. This is consistent with the account of a witness located 10 km south‑east of the accident site.
About 8 minutes after reporting that the aircraft was operating in clear conditions, surveillance data showed that the aircraft commenced a descent. Given the weather conditions in this area, it is possible that the pilot initiated this descent to remain clear of cloud (to comply with the VFR) as it is a pilot’s responsibility to ensure VFR flights operate in accordance with VMC.
During the descent, the aircraft passed about 400 m to the west of and about 386 ft below the top of two towers at the summit of Mount Moombil. At or after that time, no significant change in flight path was recorded, which suggests that the aircraft had encountered poor visibility and/or these towers were not sighted.
The aircraft’s path through the vegetation to the final impact point was a continuation of the previous descent angle and track. This indicates that the flight was under control until the collision and that the pilot was unable to identify the high terrain in the aircraft’s path in sufficient time to take avoiding action.
Flight reviews
An aeroplane flight review (AFR) is required every 2 years for a pilot to exercise the privileges of a flight crew licence. A current logbook was not located during the investigation, a previous logbook contained the only recorded flight review undertaken by the pilot, in January 2010. As the pilot had not undertaken an AFR since the introduction of CASR Part 61 in September 2014, by September 2018, the pilot’s CAR 5 licence was no longer valid, and the pilot was not licensed in accordance with Part 61.
As some piloting skills deteriorate over time, flight reviews serve as valuable opportunities for pilots to ensure that these skills remain at, or return to, the required standard. Furthermore, a number of the competencies required to be demonstrated during a flight review were relevant to the challenges faced by the pilot during the accident flight. Any deterioration in these skills would have diminished the pilot’s ability to effectively manage these challenges. Therefore, undertaking the required regular training would very likely have assisted the pilot in the management of the flight. However, insufficient data was available to identify whether the uncompleted flight reviews contributed to the accident.
Mandatory medical disclosure
Toxicological examination identified that one of the medications that the pilot was using was not recorded in the pilot’s medical file held by CASA. However, the ATSB found no evidence that the pilot’s actions and decision making was impacted by this medication or a medical condition.
Nevertheless, it is important to declare all medications to address risks that could affect performance. While it is acknowledged that some pilots may be concerned about not meeting medical certificate requirements if they declare using medications or have a medical condition, pathways exist for managing certain medical conditions while maintaining a medical certificate.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
From the evidence available, the following findings are made with respect to the collision with terrain involving Mooney M20J, VH-DJU, which occurred 26 km west of Coffs Harbour Airport, New South Wales on 20 September 2019.
The pilot was not provided with a clearance to transit Class C airspace despite no limiting meteorological factors. Instead, the Class C controller provided the option to seek a clearance at a lower altitude with an increased risk of encountering poor weather.
The limited information provided by the Class D controller to enter that airspace probably led to the pilot’s decision to descend into a hazardous area instead of other available safe options.
The pilot was not carrying appropriate navigation equipment and had most probably not obtained weather forecasts. This reduced the pilot's ability to manage the flight path changes and identify the high terrain.
The aircraft was descended into an area of high terrain in conditions below that required for visual flight, leading to controlled flight into terrain.
Other factors that increased risk
The pilot had not undertaken required recurrent flight reviews or proficiency checks to maintain currency or obtain the licence required to undertake the flight. This probably led to a deterioration in the knowledge and skills required for safe flight management and decision making.
Although there is no evidence that it contributed to this occurrence, the pilot was taking an undisclosed medication. The disclosure and recording requirements for a pilot’s medical certificate aim to address the risks associated with medications or conditions that could affect performance.
Safety action
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Additional safety action Airservices Australia
Following the occurrence, Airservices Australia implemented the following proactive safety actions:
Classroom briefings and simulator exercises were completed by all New England controllers focussing on clearance issue techniques and workload assessment, as well as coordination with other units, where decisions taken will affect the other unit.
Performance checks and unit reviews were undertaken to provide assurance that airways clearances were consistently issued in accordance with documented procedures.
An information and education package was developed for controllers regarding the provision of advice and information to pilots not subject to a clearance.
Inclusion of additional content to the on-the-job-instructor professional development sessions on ensuring the trainee’s capability is commensurate with actual workload to optimise performance.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 6 September 2019, at 1430 Eastern Standard Time,[1] the pilot of a Bell Helicopter Company UH-1H helicopter registered VH‑UVC (UVC) departed Archerfield Airport, Queensland, on a private flight with four passengers for Bankstown, New South Wales.
Following a refuelling stop at Coffs Harbour, New South Wales, the pilot made contact with Williamtown air traffic control (ATC), while north-east of Broughton Island and requested clearance to track south via the visual flight rules (VFR) coastal route. The initial radio calls between the pilot and Williamtown ATC, occurred about 6 minutes prior to the published time of last light. The radio calls indicated that the helicopter was being affected by turbulence and as a result the pilot was having difficulty maintaining a constant altitude. In response, the controller issued a clearance for the aircraft to operate between 2,400 and 3,500 ft.
Once past Anna Bay, and about 11 minutes past published last light, UVC was observed on Williamtown ATC radar to make a left turn to the south, depart the coastal route and head offshore, on a direct track to Bankstown Airport. The turn likely resulted in the pilot losing visual cues and encountering dark night conditions.
The helicopter continued to track offshore to the south-west for about 90 seconds, maintaining between about 2,500 and 3,200 ft before commencing a rapidly descending, left spiral turn. It disappeared from Williamtown radar coverage about 12 minutes after published last light. Attempts by the controller to contact the pilot were unsuccessful and authorities were subsequently advised of a missing helicopter.
On 25 September 2019, wreckage from the destroyed helicopter was located in about 30 m of water, 5 km south‑west of Anna Bay. Two of the five persons on board the helicopter were confirmed to have received fatal injuries. The bodies of the pilot and two of the passengers were not found but they were presumed to have similarly not survived the accident.
What the ATSB found
The ATSB found that the pilot continued to fly after last light without the appropriate training and qualifications, and then into dark night conditions that provided no visual cues. That significantly reduced the pilot's ability to maintain control of the helicopter, which was not equipped for night flight.
Once visual references were lost, the pilot likely became spatially disorientated and lost control of the helicopter, resulting in a collision with water.
Further, the pilot did not disclose on-going medical treatment for significant health issues to the Civil Aviation Safety Authority. That prevented specialist consideration and management of the on‑going flight safety risk the medical conditions and prescribed medications posed.
Safety message
Various ATSB research and investigation reports refer to the dangers of flying after last light without the appropriate qualifications and experience. The ATSB report, Avoidable Accidents No. 7, highlights the risks of visual flight at night. Risks include, reduced visual cues, increased likelihood of perceptual illusions, and spatial disorientation.
A VFR flight in dark night conditions should only be conducted by a pilot with instrument flying proficiency as there is a significant risk of losing control if attempting to fly visually in such conditions. If day VFR‑rated pilots find themselves in a situation where last light is likely to occur before the planned destination is reached, a diversion or precautionary landing is probably the safest option. Air traffic control assistance with available landing options is also available.
This accident also highlights the importance of aviation medical certificate holders reporting relevant conditions and medications to their Designated Aviation Medical Examiner. A full understanding by the Civil Aviation Safety Authority’s aviation medical specialists of a pilot’s medical conditions, and use of medications, enables management of the risk for both the individual and flight safety overall.
On 6 September 2019, at 1430 Eastern Standard Time,[2] the pilot of a Bell Helicopter Company UH-1H helicopter registered VH‑UVC (UVC) departed Archerfield Airport, Queensland, with four passengers on board. The pilot was conducting a private flight for the purpose of repositioning the helicopter to Bankstown Airport, New South Wales (NSW).
Witnesses at Archerfield advised that the intent was for UVC to be self-sufficient in terms of fuel requirements during the transit to Bankstown. Pre-flight preparation included the loading and filling of a plastic 400 litre fuel storage tank and a 205 litre drum. A portable, battery‑operated transfer pump and hose was to be used to transfer fuel from the on-board storage into the helicopter’s fuel tanks, when on the ground. Basic maintenance was also completed in preparation for the flight.
At about 1600, the pilot landed at Coffs Harbour, NSW to refuel the helicopter. A nearby helicopter operator who witnessed UVC land, reported that fuel was transferred from the 400 litre tank until it was empty, and then from the 205 litre drum. The refuelling operation drained the available battery power and the pilot sought assistance from the operator, who supplied a battery power pack to complete the refuelling. Shortly after, the operator noted that fuel was overflowing from the helicopter’s fuel tank filling port and called out that the tank was full. The partially‑emptied drum was then reloaded into UVC, and the battery pack returned to the operator.
During the refuelling stop, one of the passengers called a Bankstown operator to advise that they were in the process of refuelling. Arrangements had been made with the operator to provide hangar space for UVC. The operator was awaiting their arrival to assist moving the helicopter into the hangar. Following refuelling, the pilot departed Coffs Harbour at about 1648.
At 1652 the passenger advised the Bankstown operator via text message that they were on their way to Bankstown. The operator was aware of the time it would take to fly to Bankstown and that an arrival after last light was now likely. The operator contacted the passenger via a text message and queried whether they were ‘night VFR’ - a reference to whether the flight could continue at night under the visual flight rules (VFR).[3] The response from the passenger was that the pilot ‘is’ night VFR rated.
At 1755, the pilot made contact with Williamtown Tower, requesting clearance to track south via the VFR coastal route (Figure 1). The pilot also requested a climb to a higher altitude, to take advantage of more favourable winds. In response, the Williamtown Tower controller advised them to contact Williamtown Approach (Approach) for clearance.
At 1757, the pilot of UVC contacted Approach and requested a clearance. At 1758, the Approach controller identified UVC’s position as 7.4 km to the north-east of Broughton Island (Figure 1), and advised the pilot they could operate at whatever altitude was required provided it was not below 2,400 ft.[4] The pilot responded with a request to operate between 3,000 and 3,500 ft. UVC was cleared to track coastal southbound at a block altitude between 3,000 and 3,500 ft.
At 1759, following an inquiry from the Approach controller, the pilot advised that Bankstown was the intended destination. At 1800, the pilot was advised that if any further track or altitude changes were required, to inform Air Traffic Control (ATC) accordingly. While no response was required, the pilot did not acknowledge the transmission.
Published last light for Anna Bay, NSW was 1801. At this time the controller again contacted UVC to offer alternative tracking if required. The pilot responded requesting to remain on the eastern side of the R578A Williamtown restricted area. The controller clarified this request and in response, the pilot advised that if the track was not available, they would continue on the VFR coastal route. The pilot was then cleared to track as required for Bankstown Airport. The track clearance was acknowledged by the pilot at 1802.
Figure 1: Williamtown airspace map with VH-UVC’s position at various times
Source: Airservices Australia, annotated by the ATSB
A final text message from the passenger was received by the Bankstown operator at 1804 advising that UVC was approaching Williamtown.
At 1805, the Approach controller contacted the pilot to confirm that operations were normal, having observed that UVC’s altitude had dropped to 2,700 ft. The pilot acknowledged the loss of altitude, commenting on a wind gust affecting the helicopter. The controller responded by providing clearance for the pilot to operate between 2,400 and 3,500 ft. This was acknowledged by the pilot who also commented on the turbulent conditions that were being experienced. The controller acknowledged the conditions and made a further offer of assistance should it be required.
UVC was then observed on Williamtown ATC radar to make a left turn to the south, depart the VFR coastal route and head offshore. Automatic Dependent Surveillance - Broadcast (ADS-B)[5] data supplied by Aireon, indicated that the helicopter’s position at the beginning of the turn, at 1811:23, was 2.3 km west-south-west of Anna Bay[6] (Figure 2).
The turn offshore was witnessed by two recreational fishers who were located on Stockton Beach, about 2 km to the west of Birubi Point, Anna Bay. They described seeing a helicopter track overhead in a westerly direction, then turn out to sea, heading in a south-westerly direction. They reported that the helicopter sounded loud, and its lights were observed until it disappeared from sight, following a turn to the east.
The helicopter continued to track offshore to the south-west for about 90 seconds, maintaining an altitude of between 2,568 and 3,168 ft, before commencing a rapidly descending left turn. ADS-B data showed that the aircraft commenced this descent from 2,968 ft at 1812:55 which was about 12 minutes after published last light. At 1813:12, a short, loud but indistinct transmission, that may have originated from UVC was recorded by Williamtown ATC. The last Aireon ADS-B data point identified the aircraft passing an altitude of 93 ft at 1813:18. UVC disappeared from the Williamtown ATC radar display at 1813:26.
Figure 2: Flight path of VH-UVC following the VFR coastal route passing Anna Bay and the turn offshore
Source: Google and ADS-B data (Aireon), annotated by the ATSB
Two attempts by the Approach controller to contact the pilot at 1813:17 and 1813:27 were unsuccessful. The controller then broadcast advice to the pilot that surveillance identification had been lost and to immediately check altitude. Further advice of the area’s QNH[7], the lowest safe altitude in the area, and an instruction to climb immediately, were broadcast. The controller followed that transmission with several more unsuccessful attempts to contact the pilot. There was no response and at 1815 the Approach controller contacted the Australian Maritime Safety Authority’s, Joint Rescue Coordination Centre and notified them of the missing helicopter.
The initial search for UVC, using a fixed wing aircraft and several rotary wing aircraft, was hampered by poor weather and sea conditions. The search was concentrated in the vicinity of reported oil slicks and floating wreckage several kilometres to the south west of Birubi Point. The search was suspended after several days when the likelihood of locating survivors had passed.
An extended sea and aerial search for the helicopter was continued by the NSW police and later, with assistance from the Royal Australian Navy. Wreckage from the destroyed helicopter was located on 25 September 2019, 5.3 km to the south west of Anna Bay, in about 30 m of water.
Two of the five persons on board the helicopter were confirmed to have received fatal injuries. The bodies of the pilot and two of the occupants were not found but they were presumed to have similarly not survived the accident.
The pilot held Private and Commercial Pilot licences (Helicopter) and was qualified to fly by day under the Visual Flight Rules (VFR). The pilot also held a single-engine helicopter class rating and a gas turbine engine design feature endorsement. The pilot last conducted a single-engine helicopter flight review on 25 October 2018 that was valid until 31 October 2020. A Class 1 Aviation Medical Certificate issued by the Civil Aviation Safety Authority (CASA), valid until 26 April 2020, was also held.
The pilot’s logbook indicated a total of 1,440.5 hours total flying experience, of this about 103 hours were on the UH-1H. In the previous 90 days, 9 hours were accrued with 1.8 hours on the UH‑1H. A review of flying‑related documents showed that the pilot:
commenced flying on 9 September 2011
completed his Private Pilot Licence (Helicopter) on 10 April 2013
completed his low level (Helicopter) flying training on 13 June 2013
completed his Commercial Pilot Licence (Helicopter) on 26 June 2015.
The pilot completed their endorsement on the UH-1H on 26 October 2018 and was appropriately qualified to operate VH-UVC (UVC). The pilot was not qualified or trained to fly at night. At the time of gaining their Private and Commercial Pilot Licences (Helicopter) there was no requirement for night or instrument flight training. An examination of the pilot’s logbook found no evidence of night flying or instrument flying experience.
Pilot’s medical history
The pilot was being treated for significant health issues and sought regular medical support from a non‑aviation medical specialist from January‑March 2019. Following a break in treatment, the pilot again visited the specialist on 3 September 2019. While being treated, the following medications were prescribed:
valdoxan
olanzapine
naltrexone
diazepam
Valdoxan and olanzapine have the potential for producing a sedating side-effect, requiring management of the dosage amount. During medical reviews with their specialist, the pilot did not report feelings of sedation in the morning or during the day. The diazepam was prescribed three days before the accident, with a planned review at a subsequent appointment.
A witness reported that in the week of the accident the pilot disclosed that they had slept for a full day, waking briefly in the evening, then slept through to the following morning. No explanation was offered as to what prompted this. The pilot’s treating specialist last saw the pilot on 3 September 2019 and was unaware of the reported sleep episode. The specialist’s opinion was sought on possible reasons, and the ATSB’s assessment of their comments was that it was unlikely to have been the result of any of the prescribed medicines taken at their specified dosages.
As the pilot’s body was not recovered following the accident, the ATSB was unable to gain any further medical information from a post-mortem examination or toxicological assessment.
72-hour history
The ATSB was unable to gather sufficient information to complete a 72-hour history, primarily due to the pilot living alone. However, in the 24-hour period prior to the accident, the pilot:
exchanged text messages with a family member around midnight
accessed the National Aeronautical Information Processing System to gain location briefings that included weather related information at 0200
briefly met up with a family member around 0745 on the morning of the accident.
With the limited information available, it was not possible to determine, whether at the time of the accident, the pilot was operating with a level of fatigue known to affect performance. However, from the available history, the pilot had about five hours of sleep opportunity the night before the accident.
Aviation medical certificates
A current medical certificate is required to exercise the privileges of a pilot licence. A Class 1 medical certificate is required to exercise the privileges of a commercial pilot licence and a Class 2 medical certificate is required for a private pilot licence.
When applying to renew a medical certificate, pilots are required to update their medical history by providing details of medications they have taken or have been prescribed. Additionally, pilots are required to provide information relating to any medical procedures, medical issues or symptoms that required the input of a medical specialist.
On completion of an examination by a Designated Aviation Medical Examiner (DAME) a report is submitted to the CASA to assess whether a medical certificate can be issued or whether further information or tests are required.
In the course of renewing their medical certificates, the accident pilot did not disclose medical conditions under treatment, or the medications that had been prescribed.
For the awareness of flight crews, CASA publicises a limited list of approved medications,[8] along with a list of medications that are considered hazardous to aviation. Medications that assist sleep are considered as hazardous. Medications that are considered as hazardous can only be used with the express clearance of the CASA or a DAME.
The ATSB sought advice regarding the medications that had been prescribed to the pilot of UVC from a subject matter expert (SME) in aviation medicine. The SME advised the ATSB that diazepam, olanzapine and naltrexone:
Were absolutely incompatible with flying with respect to CASA guidelines, as were the conditions for which they had been prescribed.
and for valdoxan:
(restrictions) would be imposed for conditions requiring valdoxan, but only after 1-3 months grounding and then with a written clearance from a [treating specialist], DAME and treating GP. CASA would require on‑going medical audit and only a restricted medical certificate would be issued.
The SME further advised that, based on the pilot’s medical history and occurrence information, medical incapacitation from a heart attack, seizure, other underlying condition or known medications were unlikely to have contributed to the accident.
Aircraft information
General information
UVC was a Bell Helicopter Company UH-1H, S/No 5144, manufactured in the United States of America in 1966. The UH-1H is a medium size, single engine utility helicopter with a two‑bladed main rotor system. Standard configuration included dual controls, seating capacity for 13 persons, including two crew members, and skid type undercarriage. UVC was placed on the Australian Civil Aircraft Register on 2 October 2018 and was issued with Special Certificate of Airworthiness No. 13L1817 in the Limited[9] category on 17 October 2018.
The Special Certificate of Airworthiness specified that the aircraft was to be operated:
in accordance with the operating limitations contained within the approved Army Model UH-1H Helicopter Operator’s Manual
by day under the Visual Flight Rules unless the aircraft was appropriately equipped for night or instrument flight.
Aircraft records
UVC’s Log Book Statement[10] specified that maintenance releases were to be issued for periods of 150 hours time-in-service or 12 months, whichever occurred earlier. Maintenance reference data for UVC was the UH-1 series, military services Inspection Planning Guide from the Interagency Committee for Aviation Policy (ICAP[11]).
The maintenance release, current at the time of the accident, was issued on 16 October 2018 for day VFR operations at an aircraft time in service of 6,693.0 hours.
The current maintenance release with flight hour information for UVC was not recovered from the helicopter following the accident. An estimate of the aircraft time in service was derived from the pilot’s logbook to determine UVC’s operating time since the issue of the maintenance release. It was estimated that prior to departure from Archerfield, UVC’s total time in service was about 6790.0 hours.
At 6,743.0 airframe hours a 50-hour inspection was required, involving:
visual inspections
mounting hardware torque checks
rotor drive train oil system maintenance.
Additionally, a voltage regulator inspection was required to be performed by 16 April 2019.
Maintenance history
Following arrival in Australia, the helicopter was assembled and refurbished. The refurbishment included maintenance actions for the initial issue of the certificate of airworthiness, systems checks and post-maintenance testing. Maintenance records indicated that on completion of the refurbishment, flight testing that included dynamic balancing of the main rotor system and confirmation of correct flight control stick forces was conducted. Additional and on-going maintenance requirements were annotated on the maintenance release.
Prior to departure from Archerfield, a 10-hour/14-day inspection was performed, and a clearing endorsement was entered on part 1 of the maintenance release. An image of the maintenance release showing the clearing endorsement was provided to the ATSB.
The image also showed that the 50-hour inspection due at 6,743.0 hours, and the voltage regulator inspection due on 16 April 2019, had not been endorsed on the maintenance release as having been completed. An image of part 2 of the maintenance release, where maintenance can be certified, was not provided. The aircraft logbook did not contain details of maintenance activity beyond UVC’s refurbishment and maintenance release issue on 16 October 2018.
The ATSB was unable to verify if the required maintenance had been performed as the aircraft’s maintenance release was not recovered from the wreckage.
Aircraft systems
Flight control system
UVC was equipped with a hydraulically‑assisted flight control system which could be operated by either the pilot or co-pilot. The system included the cyclic and collective control systems, allowing operator inputs to the main rotor system, and tail rotor pedals for control of the tail rotor.
With hydraulic assistance power removed, the pilot would experience higher than normal forces to move the cockpit controls, and moderate feedback would be felt when the controls were moved. However, full main and tail rotor system control would still be available and control movements would result in a normal helicopter response.
Figure 3: Layout of Bell Helicopter Company UH-1H with major components labelled
Source: Bell Helicopter Company, annotated by the ATSB
Hydraulic system
The hydraulic system consists of a single hydraulic pump supplying pressure to the hydraulic servo cylinders connected to mechanical linkages in the helicopter’s flight control system. When the cockpit controls are moved, pressurised hydraulic fluid enters the cylinders reducing the force for control movement.
In the event of a hydraulic system malfunction, feedback forces from the main rotor are prevented by irreversible (check) valves in the hydraulic servo cylinders. This allows the pilot to continue making the required control system inputs. In the event of a hydraulic power failure, the pilot should land a soon as practicable in an area that will permit a run-on landing.[12]
Aircraft modifications
UVC was a standard UH-1H helicopter with no recorded airframe modifications, however a tablet device (Figure 4) was mounted on the pilot’s side instrument panel. From reference to an image of UVC’s cockpit and the UH-1H Operator’s Manual it was determined that the pilot’s side, attitude indicator and directional gyro may have been removed to accommodate the device or were obscured once the device was installed. A second attitude indicator was mounted in the left side instrument panel.
To accommodate the tablet installation, the pilot’s airspeed and turn and slip indicators were relocated to new positions below the tablet device. While the UH-1H Operator’s Manual did not specify the instruments that were required for VFR flight, relocation of instruments was permitted.
Figure 4: VH-UVC instrument panel
Source: Niza Villanueva, annotated by the ATSB
UH-1H helicopter limitations
The Operator’s Manual for Army Model UH-1H helicopters, specified that intentional flight into severe or extreme turbulence or into thunderstorms was prohibited. Other limitations for UVC were a gross weight limitation of 4,309 kg, and a never exceed limit of 112 kt indicated airspeed. This limiting airspeed varied slightly with aircraft gross weight and atmospheric conditions.
Wreckage information
Search for helicopter and wreckage field
A Royal Australian Navy vessel tasked to assist the search, located the helicopter wreckage field about 3.5 km offshore, in about 30 metres of water. NSW police divers located parts from the helicopter and provided the ATSB with a series of location coordinates from a GPS‑enabled dive camera. The positions of the helicopter parts were mapped to show their relative positions on the ocean floor (Figure 5).
Figure 5: Map showing relative positions of helicopter wreckage on the ocean floor relative to UVC’s flight path
Source: Google using Aireon data for UVC flight path and NSW police supplied positions of wreckage items, annotated by the ATSB.
The heaviest items, including the main rotor system and the engine, were located within 10 metres of each other. Other debris and parts of the cabin were also nearby. The tailboom was located about 51 metres to the south-east of the engine’s position.
Helicopter wreckage
The engine, main rotor system and tailboom were identified in underwater imagery recorded by the Royal Australian Navy during the search for the helicopter. The imagery showed that the tailboom was missing the vertical fin, tail rotor gearbox, tail rotor, and the synchronised elevators (Figure 3).
Imagery of the main rotor system showed both main rotor blades attached to the rotor head and the transmission mast connected to the upper reduction gearbox section of the transmission assembly. The lower section of the transmission assembly that included the mount casing and tail rotor drive section was not identified.
One of the main rotor blades appeared to be largely straight with damage to the outboard section. In contrast, the opposite blade was significantly damaged. The blade tip section was missing and there was evidence of blade deformation in bending. The ‘D’ section leading edge main spar, was visible and portions of the blade aerofoil section between the blade leading and trailing edges were missing. It is likely that both blades were rotating when they struck the water.
The swashplate, main rotor system (Figure 3) and pitch control mechanism were also present. Additionally:
the transmission and main rotor blade system had detached from the fuselage during the accident sequence
there was no evidence of a flight control system fault
significant disruption of other sections of the helicopter was evident
the damage was consistent with a high-speed impact with water.
The engine was located on the ocean floor in the vicinity of the main rotor system and the cockpit and cabin remains (Figure 5). The engine was intact, with the exception of the exhaust pipe. It was not possible to determine the integrity of the engine, or its serviceability from available imagery, however no obvious defects were identified.
Figure 6: Engine from VH-UVC located within the wreckage field
Source: NSW police, annotated by the ATSB.
Other helicopter parts that were identified included:
remains of the cockpit area
both cockpit seats
fragments of cabin structure
sections of the undercarriage
items of portable refuelling equipment.
Other pieces of the helicopter were present however identification was limited by the clarity of the water and some items had become partially buried by sand. On Monday 16 September 2019 a member of the public provided NSW police with a small honeycomb panel. It had washed ashore between Kingsley Beach and Little Kingsley Beach, located about 2 km to the south-east of Anna Bay.
Two other pieces were found and reported to NSW police on 18 September 2019. They were also of honeycomb construction (Figure 7) and were found at separate locations on Stockton Beach, NSW. The construction and paint colour of the panels were similar to structural panels used in UVC, however no features specifically linking the items to UVC were identified.
A portion of helicopter main rotor blade washed ashore at Blinky Beach on Lord Howe Island, NSW and was reported to police on Friday 17 January 2020. The blade was constructed from an aluminium composite material, measured 800 mm by 340 mm and was painted matt black. It bore a sticker that read ‘bh Fort Worth Texas’, which identified the section as belonging to a Bell Helicopter.
Figure 7: Items of honeycomb construction found on Stockton Beach, probably from UVC
Source: NSW police
Tailboom assessment
UVC’s tailboom was retrieved by NSW police divers and made available to the ATSB for examination. The tailboom (Figure 8), without the vertical fin, synchronised elevators, tail rotor gearbox and tail rotor assembly (Figure 3), had separated at the fuselage rear bulkhead due to overstress failure of the rear fuselage structure.
Figure 8: VH-UVC tailboom following recovery from the ocean floor
Source: NSW police, annotated by the ATSB
Internally, the remains of the synchronised elevator control system and the tail rotor pitch control systems were present. Failures of the control tubes and cables were attributed to overstress. Examination of the tailboom did not identify any pre-existing defects likely to have influenced the accident sequence.
The tail rotor drive train from the rear fuselage tailboom junction to the 42° gearbox was also present. Compression damage to the tailboom driveshaft cover was consistent with water impact. Drive shaft coupling imprints were noted on the cover (Figure 9). The imprints were consistent with the driveshaft not rotating at the time of impact. However, rotational damage signatures were also present at either end of the recovered tail rotor drive train. Additionally, multiple contact marks were evident on the side of the boom in the vicinity of the synchronised elevator attachment points. Those marks were consistent with repeated movements of the elevators.
The aircraft was fitted with a Mode S transponder that broadcast ADS-B data. This information included the position and altitude of the aircraft and was received by Airservices Australia as well as other third‑party ADS‑B receivers (Aireon and Flightradar24).
Two mobile devices with the OzRunways electronic flight bag application installed were on board. The application provided the option for live flight tracking by transmitting the device’s position and altitude. ADS-B and OzRunways data was obtained and analysed by the ATSB.
Both the Aireon and OzRunways data was compared and found to be consistent, however the Aireon data has been used in this report as it provided higher fidelity for altitude information over the final flight segment. The data was transmitted at five second intervals and a track line was produced by joining each data point with a straight line. Variations between these data points were not captured.
VH-UVC flight path
From Broughton Island UVC tracked past Yacaaba Head, Fingal Bay then Morna Point (Figure 10). Once past Anna Bay, the pilot commenced a left turn away from the coast, aligning with a direct track to Bankstown (Figure 11 and 12). The turn and subsequent track were inside the Williamtown military control zone area boundary. The helicopter tracked offshore to the south‑west for about 90 seconds before commencing a rapidly‑descending, left turn followed by a collision with the ocean surface.
Figure 10: Townships along the VFR coastal route once UVC passed Broughton Island
Source: Google using ADS-B data (Aireon), annotated by the ATSB
Figure 11: Overhead view of UVC flight path showing turn to seaward and spiral descent
Source: Google and ADS-B data (Aireon), annotated by the ATSB
Figure 12: Side view of UVC flight path showing turn to seaward and spiral descent
Image description: The flight path is provided for illustrative purposes. The altitudes as presented originate from raw data and have not been corrected for atmospheric conditions.
Source: Google and ADS-B data (Aireon), annotated by the ATSB
The variation in UVC’s flight parameters over the final 30 minute period is presented in a graphical format (Figure 13) with key events presented in an overhead view (Figure 14). The rate of change of altitude and track, before and after last light, where the pilot appeared to be attempting to maintaining a constant altitude, were averaged and compared. For the period after last light and prior to the turn away from the coast:
the average variations in altitude increased by a factor of 2 compared to daylight operation.
excluding what appeared to be a deliberate turn by the pilot at about 1809, the average variations in track increased by a factor of 3 compared to daylight operation.
Figure 13: UVC flight parameter variation over the final 30 minutes
Source: ADS-B data (Aireon) with ATSB analysis
Figure 14: UVC flight path from Broughton Island
Source: Google and ADS-B data (Aireon), annotated by the ATSB
Once past Anna Bay, UVC’s flight path from the turn to seaward to the spiral descending turn was further examined. The flight path is presented in a graphical format in (Figure 15) with key aspects noted below:
at 1811:23, UVC commenced a left turn which continued until 1811:56, aligning with the direct track to Bankstown Airport
from 1811:27 to about 1812:24, the altitude increased by about 550 ft
a right turn commenced at 1811:56, continuing until 1812:15. Ground speed decreased during this time period
a turn to the left commenced between 1812:15 and 1812:20
from 1812:20 to 1812:24 the track changed to the left by about 21⁰
from 1812:24 to 1812:50 there were ground speed and altitude changes, with a continuing left turn
from 1812:50 to 1812:55 the turn rate and altitude increased
from 1812:55 there was a rapid loss of altitude and rapid changes in track and ground speed, consistent with a loss of control. The average rate of descent after the loss of control was calculated to be about 7,500 feet per minute, peaking at 11,636 feet per minute at 1813:18
Based on wind speeds recorded at WLM it is estimated that in the last 14 seconds of the descent, UVC’s VNE[13] limit was exceeded by up to 45 kt.
Figure 15: UVC flight parameter variation over the final 150 seconds of flight
Source: ADS-B data (Aireon) with ATSB analysis
Air traffic services
The pilot submitted a flight plan for the Archerfield to Coffs Harbour leg. A flight plan was not submitted for the Coffs Harbour to Bankstown leg, however, there was also no requirement for one.
The pilot’s first contact with Williamtown Air Traffic Control (WLM ATC) was a request for an airways clearance at 1755. When issuing the requested clearance, the controller asked whether UVC had a CAR174B exemption[14], which would allow UVC to operate at a lower minimum altitude at night. On receiving no acknowledgement, the Approach (APP) controller advised the pilot that 2,400 ft was the lowest altitude that could be offered. There was no indication provided to the controller in the radio exchange that the pilot was not qualified to continue the flight after last light.
At 1800:27 and 1800:56 WLM ATC offered the pilot of UVC alternate tracking and at 1801:41 cleared the pilot to manoeuvre as required for tracking to Bankstown. At 1805:41, the APP controller issued a safety alert advising the pilot to ‘check altitude’ when UVC dropped to 2,700 ft, which was below the clearance altitude of 3,000 ft. The pilot reported turbulent conditions and in response the controller re‑cleared the pilot to operate from the lowest safe altitude of 2,400 ft to 3,500 ft. At 1806:09 the controller requested the pilot to advise if anything further was needed.
The turn offshore at 1811:23 was observed on WLM radar. An indistinct transmission, which was assumed by ATC to be from UVC, was heard at 1813:12, about 17 seconds after the loss of control had likely occurred (Figure 15). UVC was observed on radar in a rapid descent from about 2,900 ft, disappearing from WLM radar coverage at 1813:26. By 1813:27, the APP controller had alerted the Tower controller of the unfolding situation, and made two standard radio calls seeking a response from UVC.
A detailed alert to UVC specifying that identification had been lost, and a low altitude warning to check altitude, was made at 1813:32 by the APP controller. The alert also included the area barometric pressure, the lowest safe altitude, and an instruction to initiate an immediate climb. There was no response from UVC and a further five radio calls were made to contact the pilot by WLM ATC controllers.
At 1824:13, in response to a request from the APP controller, the pilot from one of the WLM departing aircraft called UVC on the 121.5 emergency frequency and reported that no response was received.
The ATSB engaged the services of an ATC subject matter expert (SME) to review the controller’s interaction with the pilot of UVC. The SME concluded that:
The actions of WLM ATC throughout the flight of UVC were in accordance with the published rules and procedures for an aircraft operating Night VFR. In addition, WLM ATC offered alternative and flexible clearances to meet the needs of the pilot in command.
Operational information
Flight endurance
CASA regulatory requirements specify that pilots of helicopters conducting private flights under the VFR are to carry a fixed fuel reserve of 20 minutes flight time. The pilot in command is required to ensure that this fuel reserve remains unused on landing unless an emergency is declared. Pilots are also required to refer to operational information such as current weather reports and forecasts for the route to be flown and to plan the flight using that information.
The witness at Coffs Harbour noted that prior to departure, the helicopter’s fuel tank had been filled to overflowing and a quantity of fuel remained in the 205 litre drum. The UH-1H operations manual stated that the useable fuel quantity was 781.6 litres or 1,362 lbs of fuel. UVC’s fixed fuel reserve requirement was calculated to be 195 lbs of fuel.
The distance from Coffs Harbour to Bankstown via a coastal route to Anna Bay and then direct track to Bankstown, was calculated to be about 250 nautical miles. A flight in nil wind conditions, allowing for climb and descent, at an indicated airspeed of 95 kt would have required about 1,570 lbs of fuel. The fuel quantity required for UVC to transit from Coffs Harbour to Bankstown using forecast winds was calculated to be about 1,265 lbs.
Provided the forecast conditions had continued, the pilot of UVC would have required an intermediate refuelling stop or to declare a fuel emergency prior to arrival at Bankstown. Any holding or diversion would likely have required a landing before Bankstown to prevent airborne fuel exhaustion.
Pilot access to weather information
The pilot accessed the National Aeronautical Information Processing System (NAIPS) using the OzRunways electronic flight bag application at 0200 and 0202 on 6 September 2019. Requests were made for location briefings and NOTAM[15] information for Archerfield, Coffs Harbour and Sydney.
A forecast for the intended route was not requested, nor were Head Office NOTAMs or SIGMETs.[16] The pilot did not access further weather information through NAIPS. However, it could not be established whether the pilot, or one of the passengers, sourced further updates enroute via other means.
Night VFR (Helicopter) qualification and training
For VFR flights conducted at night, a Night Visual Flight Rules (NVFR) rating and helicopter NVFR endorsement are required. Training for the rating and endorsement covers theory and practise in the areas of basic instrument flight, navigation aid training and procedures in the event of abnormal situations. In addition, human factors and non-technical skills awareness and application, specific to the night flying environment are covered.
A minimum of 10 hours night flying experience is necessary, of which at least five hours are required to be in a helicopter or approved flight simulation training device. These night hours must include dual flight, solo night circuits, and cross-country flights. Three hours of dual instrument time in a helicopter or approved flight simulation training device is also required.
CASA regulatory requirements specify that a pilot who does not hold a NVFR rating, or instrument rating, is not permitted to depart on a flight before first light or after last light, and is also not permitted to depart unless the estimated time of arrival at the destination is at least ten minutes before last light.
Decision making
Flight under the VFR requires minimum conditions of visibility and distance from cloud. Variation from the expected weather conditions enroute may not enable a pilot to reach the planned destination under this ruleset. That, in turn, will require a timely decision to land or divert when things are not going to plan. However, the human tendency to continue with a course of action is documented in various research studies.
The American Psychological Association defines plan-continuation bias as:
‘The tendency of people to continue with an original course of action that is no longer viable’. An example would be an airline pilot who unexpectedly encounters bad weather at the scheduled destination but decides to land anyway rather than divert to another location. Plan-continuation bias tends to be particularly strong towards the end of the activity and has been theorized to result from the interaction of such factors as cognitive load, task demands, and social influences.
Errors associated with plan-continuation have been recognised in the analysis of a number of aircraft accidents previously (NTSB, 1994; Batt and O’Hare, 2005; Dismukes, Berman and Loukopoulos, 2007).
In the ATSB research investigation report B2005/0127, addressing general aviation pilot behaviours in the face of adverse weather, Batt and O’Hare (2005) identified that the halfway point of a flight may feel like a psychological ‘turning point’ for pilots.
The focus of the pilot’s thoughts and attention will shift gradually from the point of departure to the planned destination…as the flight progressed, the chances of a VFR into IMC encounter increased until they reached a maximum of 27.6% during the final 20% of the flight distance. This pattern suggests that an increasing tendency on the part of pilots to ‘press on’ as they near their goal.
Options available to day VFR pilot’s experiencing reduced visual cues include contacting air traffic control for assistance or conducting a precautionary landing. The ATSB’s ‘Don’t push it, LAND It’ safety messaging, jointly developed and supported by the Civil Aviation Safety Authority and the Australian Helicopter Industry Association, encourages helicopter pilots to exercise this option.
Weight and Balance
Weight and balance information was derived from maintenance records, witness statements and images provided to the ATSB. Additionally, estimated and known weights of the pilot, passengers, baggage, equipment and fuel on board were used to calculate UVC’s weight and centre of gravity. It was estimated that the weight of UVC on departure from Coffs Harbour was 3,808 kg, which was below the Operator’s Manual gross weight limit of 4,309 kg.
The occupant seating positions were established from information provided by witness and from on-board images that occupants exchanged with ground-based parties following their departure from Coffs Harbour. UVC’s longitudinal and lateral balance was found to be within limits from Coffs Harbour to Anna Bay.
Helicopter – basic operational equipment for flight under the night VFR
In addition to the equipment requirements for day VFR operations, Civil Aviation Order, CAO 20.18 specifies that a helicopter may only be operated under the night VFR, if it is equipped with instruments that include an attitude indicator and a heading indicator (directional gyroscope).
Further, for night VFR flights conducted over land or water where the helicopter’s attitude cannot be maintained by the use of external visual surface cues from lights on the ground or celestial illumination, a helicopter is to be:
equipped with an approved automatic pilot or automatic stabilisation system, or
operated by a qualified two pilot crew, each with access to the flight controls.
Helicopter emergency procedures
The Operator’s Manual for Army Model UH-1H helicopters provides guidance for pilots in the event of system malfunctions or loss of function. In the event of a partial power loss, or if the engine is no longer operating (Figure 16), an auto rotational descent[17] and landing is required.
Likewise, the pilot would initiate an auto rotational descent in response to:
a drive train or tail rotor failure
an engine to transmission main drive shaft failure
a transmission free wheel unit disengagement.
Figure 16: Airflow through the main rotor system during an auto rotational descent
Image description: During an autorotation, the upward flow of relative wind permits the main rotor blades to rotate at their normal speed.
Source: FAA Helicopter Flying Handbook
The descent is typically conducted at a specified forward airspeed for the helicopter type and characterised as a controlled descent. For the UH-1H helicopter a typical auto rotational rate of descent is about:
1,600 feet per minute with an indicated airspeed of 52 kt for minimum rate of descent, or
2,060 feet per minute with an indicated airspeed of 82 kt for maximum glide distance.
A loss of tail rotor control or drive to the tail rotor, is manageable provided adequate airspeed is maintained, as directional stability will be provided by the helicopter’s vertical fin. The UH-1H helicopter requires airspeeds above 30-40 kt to maintain directional control with a loss of tail rotor drive. Other tail rotor malfunctions, including stuck pedals (fixed tail rotor pitch settings), require 40‑70 kt airspeed be maintained.
When performing an auto rotational descent to a suitable landing site, a pilot has a choice in the angle of descent, varying from vertical to maximum horizontal range. Pilots are trained to perform auto rotational descents and auto rotational capability is a certification requirement for helicopters.
Meteorological information
Forecast weather
Graphical Area Forecast (GAF)
The flight from Coffs Harbour to Bankstown occurred within the Graphical Area Forecast[18] New South Wales – East that was valid from 1500 to 2100. Forecast conditions included:
average conditions of greater than 10 km visibility with areas of scattered[19] cumulus and stratocumulus cloud at altitudes between 4,000 and 8,000 ft
widespread blowing dust reducing visibility to 5,000 m
scattered showers of rain reducing visibility to 4,000 m with associated scattered cumulus and stratocumulus cloud from 3,000 to 5,000 ft and broken cumulus and stratocumulus cloud from 5,000 to above 10,000 ft
isolated smoke over the land reducing visibility to 4,000 m and isolated heavy smoke over the land north of Taree reducing visibility to 2,000 m
isolated thunderstorms over the sea reducing visibility to 3,000m with associated isolated cumulonimbus clouds from 3,000 to above 10,000 ft
moderate mountain wave activity forecast above 4,000 ft
severe turbulence forecast below 10,000 ft with moderate turbulence north of Taree
The GAF also noted that moderate turbulence[20] is implied in cumulus, stratocumulus and altocumulus cloud and severe turbulence[21] is implied in cumulonimbus cloud.
Significant Meteorological Information Advisory (SIGMET)
The Bureau of Meteorology (BoM) issued a Significant Meteorological Information Advisory at 1436 for severe turbulence below 10,000 ft valid from 1500 to 1900. The area affected by the SIGMET covered the entire flight from Archerfield to Bankstown.
Grid Point Wind and Temperature
The Grid Point Wind and Temperature forecast valid at the time of the flight indicated the average wind south of Coffs Harbour was 25 kt from the north‑north‑west at 2,000 ft.
Mean Sea Level Pressure chart
The Mean Sea Level Pressure chart showed a trough and frontal system approaching the Williamtown area on the afternoon of the flight. These systems were moving west to east and had an associated tight pressure gradient.[22]
Williamtown TAF
The BoM provided an aerodrome forecast (TAF)[23] for Williamtown Airfield, located about 21 km to the west of the accident location. Due to the weather front passing through the area, the TAF was amended several times. An updated TAF for Williamtown was issued at 1534 and was valid from 1600 on the 6 September 2019 to 1600 the following day. The forecast conditions were:
wind 20 kt, gusting 35 kt from 320° with CAVOK[24] conditions
from 1600, moderate to severe turbulence below 5000 ft until 1800
from 1800:
wind 27 kt, gusting 48 kt from 290°, visibility 9,000 m in blowing dust with light showers of rain, cloud scattered 4,000 ft and broken cloud[25] at 12,000 ft
a 40 per cent probability of visibility reducing to 4,000 m in blowing dust until midnight
severe turbulence below 5,000 ft.
Williamtown Aerodrome warning
On the afternoon of the flight there were two aerodrome weather warnings in place for Williamtown. The weather warnings were valid from 1800 to 2200. The first warning released at 1306 was for wind gusts in excess of 41 kts. A later warning released at 1345 added visibility reduction in blowing dust to the wind gust warning.
Actual weather
The BoM provided a summary of the conditions in the area at the time of the accident and stated that broad scale severe turbulence was likely to have been present. A tight pressure gradient near the frontal system generated strong and gusty west to north-westerly winds. Generally, significant west to north-westerly wind crossing the mountains to the west of the Newcastle area would have caused mechanical turbulence in the area, particularly downwind of the ranges. Strong north westerly winds were observed following the passage of the trough (ahead of the front).
The Bureau of Meteorology (BoM) provided the ATSB with the SPECI[26] and METAR[27] data from Williamtown at the time of the accident (Table 1).
Table 1: Williamtown observations
Type
Time
Wind
Visibility (m)
Cloud
Temp (°C)
QNH (hPa)
SPECI
1745
310°, 15‑26 kt
9,999
SCT070, SCT078
30
997
METAR
1800
310°, 14 kt
9,999
BKN072
30
997
SPECI
1810
300°, 15‑29 kt
9,999
BKN070 OVC081
30
997
METAR
1830
290°, 19 kt
9,000
OVC072
29
997
Although SPECI and METAR reports indicated visibility in the area was unlimited, comments between Williamtown Approach and Tower controllers at 1753 made reference to visibility to be about 6‑7 km with dust. Also of note are the overcast cloud conditions from 1810.
The BoM also provided the ATSB with one-minute interval data recorded by the Williamtown Automatic Weather Station. The one-minute cloud data from Williamtown showed that the cloud cover started to build from 1728, was likely overcast by 1751 and considered as overcast by 1802.
Visibility at Williamtown reduced markedly from 35.7 km at 1742 to 8.34 km by 1811. SPECI reports are only issued when weather conditions fluctuate about or below specified criteria. Visibility reductions only trigger a SPECI when the visibility is below an aerodrome’s highest alternate minimum visibility or 5,000 m, whichever is greater. As such, the one-minute visibility data indicating 8.34 km was not low enough to trigger a SPECI.
Last light
For aviation purposes, night is defined as the period of darkness between the end of evening civil twilight (last light) and the beginning of the following morning civil twilight (first light). At last light, in ideal conditions, there will be enough light from the sun for large objects to be seen, but no detail.
Published last light[28] for the Anna Bay area, on the day of the accident was 1801, however the presence of cloud cover, dust and masking terrain to the west would have resulted in last light occurring earlier.
Additionally, although the moon was high on the horizon, with the lunar disc 52 per cent illuminated, any celestial lighting was likely obscured by the overcast conditions.
Data from a privately‑owned weather station located about 4 km to the north‑east of the accident site was provided to the ATSB. The data, which included ambient lighting levels, showed that by 1750, the ambient light had degraded to 19 lux[29], reducing to 4 lux by 1800. By 1820, the available light had reduced to zero. By comparison, at 1700 the lux level was 2,055 while in full daylight, the lux levels were about 10,750.
Once UVC passed Broughton Island various townships were present along the VFR coastal route that may have provided sources of lighting for the pilot’s reference (Figure 10).
Spatial disorientation
Spatial orientation defines the natural human ability to maintain body orientation and/or posture in relation to the surrounding environment (physical space) at rest and during motion. The FAA’s Medical Facts for Pilots provides the following:
Humans are designed to maintain spatial orientation on the ground. The three-dimensional environment of flight is unfamiliar to the human body, creating sensory conflicts and illusions that make spatial orientation difficult, and sometimes impossible to achieve. Statistics show that between 5 to 10 % of all general aviation accidents can be attributed to spatial disorientation, 90 % of which are fatal.
Spatial disorientation is defined by Benson (1999) as where ‘the pilot fails to sense correctly, the position, motion or attitude of the aircraft or of him/herself’ with respect to the ground. For pilots flying under the VFR, seeing the horizon is crucial for orientation of both the pilot’s sense of pitch and bank of the aircraft (Gibb et al, 2010). In conditions of low visibility where the horizon may not be visible to the pilot, they can become rapidly disorientated.
Spatial disorientation is also often simply described as an inability to determine ‘which way is up’, although the effects of disorientation can be considerably more subtle. It occurs when the brain receives conflicting or ambiguous information from the sensory systems. It is likely to happen in conditions in which visual cues are poor or absent, such as in adverse weather or at night. Spatial disorientation presents a danger to pilots, as the resulting confusion can often lead to incorrect control inputs and resultant loss of aircraft control.
Pilots obtain information about their orientation from:
The visual system (eyes), which can obtain information from a range of cues outside the aircraft and relevant flight instruments inside the aircraft
The vestibular system, which consists of the balance organs located in the inner The semicircular canals provide information about angular or rotational accelerations in the vertical (yaw), horizontal (pitch) and longitudinal (roll) axes, and the otolith organs provide information about linear accelerations
The somatosensory system, which includes a range of receptors in the muscles, tendons, joints and skin that sense gravity and other pressures on the Such perceptions are often known as the ‘seat of the pants’ aspect of flying.
The visual system generally provides about 80 per cent of a person’s raw orientation information, with the remainder provided by the vestibular and somatosensory systems, both of which are prone to misinterpretation and illusions during flight (Newman 2007). Although the visual system can overcome these limitations, the risk of spatial disorientation is significantly increased if the relevant visual cues are absent, ambiguous or not attended to.
Benson (1999) outlined that spatial disorientation would typically occur within 60 seconds of all visual cues being removed, while another United States study showed a loss of control by non‑instrument rated pilots would occur, on average, about 180 seconds after the loss of all visual cues (Bryan, Stonecipher, & Aron, 1954).
A range of factors can influence the extent to which a pilot may experience or be able to recover from spatial disorientation. Common factors include limited or ambiguous visual cues outside the cockpit, not directing sufficient attention to the flight instruments due to workload or distraction, and not being proficient in instrument flying skills.
The risk of experiencing spatial disorientation can be managed effectively in the absence of external visual cues by reference to suitable aircraft instrumentation. However, controlled flight by sole reference to cockpit instruments is a separate, and complex, learned skill from those skills associated with flight in visual conditions.
Newman (2007) reported that spatial disorientation is affected by
pilot factors such as fatigue, medication and workload
aircraft factors that include single pilot operations, the presence or otherwise of an autopilot or stability augmentation system, and serviceable cockpit instrumentation
operational factors, that include pressing on into instrument meteorological conditions[30] without an instrument rating
environmental factors that are related to time of day (flight after last light) and ambient weather conditions.
A further consideration is the likelihood that the lack of training and qualifications makes the day VFR‑rated pilot susceptible to spatial disorientation following the loss of visual cues when flying in dark night conditions.
Newman (2007) also commented on the inherent instability of a helicopter increasing pilot workload and the likelihood for spatial disorientation. The Flight Safety Australia (2015) article, Workload and Helicopters includes the following about piloting a helicopter.
Piloting a helicopter is a complex, continuous, multi-task operation…This means helicopter pilots face a high workload in day-to-day flying…Workload also varies temporarily, according to weather (IMC, wind/turbulence) and environment (terrain, obstacles, wires).
Compared to fixed wing aircraft, helicopters are dynamically unstable and require constant pilot input to maintain controlled flight (Fay, 1976; Prouty, 2004). Depending on design, they can be fitted with stability control systems or an autopilot to assist the pilot and reduce workload.
Vestibular system illusion
A false sensation of rotation is an illusion generated by the vestibular system involving the semicircular canals, that can lead to spatial disorientation and result in loss of control. It is commonly referred to as the ‘graveyard spiral’. The FAA’s Medical Facts for Pilots describes how under conditions of unreliable or unavailable visual references, the false sensation of rotation is:
…associated with a return to level flight following an intentional or unintentional prolonged bank turn. For example, a pilot who enters a banking turn to the left will initially have a sensation of a turn in the same direction. If the left turn continues (~20 seconds or more), the pilot will experience the sensation that the airplane is no longer turning to the left. At this point, if the pilot attempts to level the wings this action will produce a sensation that the airplane is turning and banking in the opposite direction (to the right).
If the pilot believes the illusion of a right turn (which can be very compelling), he/she will re-enter the original left turn in an attempt to counteract the sensation of a right turn. Unfortunately, while this is happening, the airplane is still turning to the left and losing altitude. Pulling the control yoke/stick and applying power while turning would not be a good idea–because it would only make the left turn tighter. If the pilot fails to recognize the illusion and does not level the wings, the airplane will continue turning left and losing altitude until it impacts the ground.
With appropriate training and experience, pilots who become disorientated when flying in compromised visual conditions are able to recognise illusions and utilise cockpit instruments to restore their orientation.
Related Occurrences
Between 2010 and 2019 the ATSB investigated 11 fatal accidents, involving aircraft flown after last light in dark night conditions, that resulted in a collision with water or terrain. Loss of control was a factor in five of them, with spatial disorientation found to have contributed to three of the five. Of the 11 accidents, five involved pilots who were qualified to fly an aircraft at night. Six of the accidents involved helicopters, two of which were flown by pilots who were qualified to fly at night. The remaining four accidents involved non-night qualified, day VFR‑rated pilots. Four related occurrences are presented below.
On the evening of 27 July 2011, the owner-pilot of a Robinson Helicopter Co. R22 helicopter, registered VH-YOL was conducting a local flight from Big Rock Dam to Brooking Springs homestead near Fitzroy Crossing, Western Australia. The pilot was reported missing, and the wreckage of the helicopter was located the following day, 14 km north-west of Fitzroy Crossing township. The helicopter was seriously damaged, and the pilot sustained fatal injuries. The ATSB found that the pilot was operating at night without the appropriate training or qualifications in a helicopter that was not suitably equipped.
On 15 August 2011, the pilot of a Piper PA‑28‑180 Cherokee aircraft, registered VH-POJ, was conducting a private flight transporting two passengers from Essendon to Nhill, Victoria under the VFR. The flight was arranged by the charity Angel Flight to return the passengers to their home location after medical treatment in Melbourne. Global Positioning System data recovered from the aircraft indicated that when about 52 km from Nhill, the aircraft conducted a series of manoeuvres followed by a descending right turn. The aircraft subsequently impacted the ground at 1820 Eastern Standard Time, fatally injuring the pilot and one of the passengers. The second passenger later died in hospital as a result of complications from injuries sustained in the accident.
The ATSB found that the pilot landed at Bendigo and accessed a weather forecast before continuing towards Nhill. After recommencing the flight, the pilot probably encountered reduced visibility conditions approaching Nhill due to low cloud, rain and diminishing daylight, leading to disorientation, loss of control and impact with terrain.
On 18 August 2011, an Aérospatiale AS355F2 (Twin Squirrel) helicopter, registered VH-NTV, was being operated under the VFR in an area east of Lake Eyre, South Australia. At about 1900 Central Standard Time, the pilot departed an island in the Cooper Creek inlet with two film crew on board for a 30-minute flight to a station for a planned overnight stay. It was after last light and, although there was no low cloud or rain, it was a dark night.
The helicopter levelled at 1,500 ft above mean sea level, and shortly after entered a gentle right turn and then began descending. The turn tightened and the descent rate increased until, 38 seconds after the descent began, the helicopter impacted terrain at high speed with a bank angle of about 90°. The pilot and the two passengers were fatally injured, and the helicopter was destroyed.
The ATSB found that the pilot probably selected an incorrect destination on one or both of the helicopter’s global positioning system (GPS) units prior to departure. The ATSB concluded that, after initiating the right turn at 1,500 ft, the pilot probably became spatially disoriented. Factors contributing to the disorientation included:
dark night conditions
high pilot workload associated with establishing the helicopter in cruise flight and probably attempting to correct the fly-to point in a GPS unit
the pilot’s limited recent night flying and instrument flying experience
the helicopter not being equipped with an autopilot.
On 7 April 2016, the pilots of two Robinson R22 helicopters flew from Mossman, Queensland, to various fishing locations to the north with a passenger in each helicopter. Late in the afternoon, on the return flight to Mossman the pilots encountered weather and winds that slowed their progress and required them to refuel at Cooktown. The pilots departed Cooktown at last light and as the flight progressed, the light available from the sun continued to decrease and there was no moon. There were also patches of cloud and rain in the general area.
Shortly after passing Cape Tribulation, in dark night conditions one of the helicopters registered VH-YLY, collided with the sea. The passenger was injured in the accident but was able to reach the shore and notify emergency services. A search was initiated and the missing helicopter was located about 400 m offshore in about 10 m of water. The pilot was not located. The ATSB found that the pilot of VH-YLY, who was only qualified to operate in day VFR conditions, departed on a night flight and continued towards the destination in deteriorating visibility until inadvertently allowing the helicopter to descend into water.
While on a positioning flight to Bankstown, New South Wales, Bell Helicopter Company UH-1H registered VH‑UVC entered a descending turn, about 12 minutes after last light, resulting in a collision with water near Anna Bay, New South Wales.
The pilot was not qualified, and the helicopter was not equipped, to operate at night. At the time of the accident, dark night conditions and moderate to severe turbulence were likely present. No evidence was found of a mechanical defect with the helicopter that may have contributed to the accident.
The following analysis will discuss the continuation of the flight after last light, and the reasons for the subsequent loss of control. The analysis also considers the pilot’s medical history.
Flight after last light
Due to the departure time from Archerfield Airport, and the need to refuel enroute, there was insufficient time to reach Bankstown before published last light. Considering the prevailing weather conditions, last light probably passed prior to the published end of evening civil twilight, as the helicopter approached Broughton Island.
Recognising that the pilot could have identified prior to departing Coffs Harbour that the flight could not be completed in daylight, given the inherent utility of a helicopter, there were also opportunities to land at a beach, or other suitable areas, prior to reaching Broughton Island. After this point, the pilot would have required suitable ground lighting to avoid obstacles during landing. An option available to the pilot at this point was to contact Williamtown air traffic control for assistance and a possible landing at Williamtown Airfield.
The pilot’s decision to continue the flight at night may have been influenced by self-induced pressure to complete the flight for business and personal reasons. It is also possible that plan‑continuation bias influenced the pilot’s decision. As the flight passed the halfway point and progressed closer to the destination the pilot may have become increasingly committed to continuing with the original plan. Consequently, deciding to turn back or divert may have become increasingly difficult.
Loss of visual cues
As the flight progressed after last light visual cues may have been available to the pilot from ground‑based lighting close to the aircraft’s track and there may have been a horizon or silhouette of terrain to the west.
However, about 10 minutes after published last light UVC commenced a left turn, departed the coastal route, and tracked offshore. The position of the helicopter at this point was about 2 km to the west of Anna Bay. As the helicopter tracked over a featureless sea with overcast conditions blocking out celestial lighting, the pilot likely lost any remaining visual cues and encountered dark night conditions.
Loss of control
Flight profile
The aircraft’s flight path after last light showed increasing variations in track and altitude. Considering that turbulent conditions were likely present for the whole flight from Coffs Harbour it is likely that the reduced visual cues encountered by the pilot affected their ability to control the helicopter.
UVC’s track following the turn offshore was aligned with a direct track to Bankstown and was inside the Williamtown military control zone, which shared a lateral boundary with the R578A restricted area. As such, it is likely that the pilot was attempting to track directly to Bankstown, rather than follow the R578A restricted area boundary as previously requested.
From 1812:55 UVC entered a descending and tightening left spiral turn. Information derived from ADS-B data indicated that between UVC’s last two recorded positions the helicopter’s descent rate was in excess of 11,500 feet per minute and the aircraft’s airspeed was in excess of 150 kt. The magnitude of those parameters significantly exceeded the operational limitations published in the Operator’s Manual and, together with the characteristic spiralling turn, supported a loss of control of the helicopter at that point.
Helicopter systems assessment
Compression damage to the tailboom driveshaft cover was consistent with the upper surface of the tailboom impacting the ocean surface. Further, witness marks on the driveshaft cover indicated that the tail rotor drive train was stationary at the time of impact. However, there was also physical damage consistent with rotation and continuity of the tail rotor drive train. As such, it was considered likely that the tailboom detached from the helicopter prior to impact, decoupling the tail rotor drive and allowing the boom to rotate to an inverted position prior to impact.
Considering that the loss of control commenced about 1.2 km from the wreckage field and the tailboom was found only about 51 meters away from the main wreckage of the helicopter, it is likely the tailboom separation from the helicopter occurred very close to the helicopter’s impact point and did not contribute to the loss of control.
The vertical fin and synchronised elevators detached from the tailboom and were not identified in underwater wreckage imagery provided to the ATSB. From the available information, it was not possible to determine when these components separated from the tailboom. However, as there was no evidence of pre-existing defects, it is considered more likely that they separated in the final moments due to the forces associated with contacting the water or as a result of dynamic loading effects associated with flight in turbulent conditions at very high airspeed.
The ATSB considered whether a system failure or malfunction influenced the development of the accident. Due to the location and condition of the wreckage the ATSB was unable to examine the helicopter’s powerplant, rotor and flight control systems. As a result, the helicopter’s flight path after 1812:55 was analysed in order to determine if it was consistent with a system fault.
The three possible faults considered were a loss of drive to the main rotor, loss of thrust from the tail rotor or loss of hydraulic power. The Operator’s Manual advised that in the event of a loss of drive to the main rotor system an autorotational descent is required. A loss of tail rotor thrust or failure of the hydraulic system requires the pilot to maintain an airspeed above 30‑70 kt and to position the aircraft for a run on landing at a suitable flat location.
The left turn initiated at 1812:55 was inconsistent with a track to a suitable landing site due to the proximity of Stockton beach to the right of the helicopter’s track and a mayday call was not made, as would be expected in this situation. In addition, the helicopter’s airspeed prior to 1812:55 was above that required to counter both a loss of tail rotor drive and hydraulic failure.
The airspeed and descent rate were also inconsistent with an autorotational descent or approach to a suitable landing site. It is therefore considered likely that the aircraft control and propulsion systems were serviceable and did not compromise the operation of the helicopter.
Spatial disorientation
When the pilot turned offshore near Anna Bay it is likely that the absence of celestial lighting and ground references resulted in dark night conditions being encountered. In addition, moderate to severe turbulence was likely present. The lack of external visual cues would have required the pilot to reference the aircraft’s flight instruments to maintain control of the helicopter.
The primary instrument for maintaining control, or to recover from an unusual attitude, is the attitude indicator. In UVC the pilot’s attitude indicator was not available to the pilot due to the location of a tablet on the instrument panel. The tablet was not located in the wreckage, as a result the screen brightness settings and their potential influence on the pilot’s night vision could not be determined.
A second attitude indicator was located on the left side instrument panel however, it would have been difficult for a pilot with no instrument training to effectively use that instrument given its cross‑cockpit position.
The pilot was not trained or experienced in maintaining control of the helicopter with sole reference to the flight instruments. Research has shown that pilots not proficient in maintaining control of an aircraft with sole reference to the flight instruments will become spatially disorientated and lose control of the aircraft within 1 to 3 minutes after visual cues are lost.
The helicopter’s inherent instability coupled with the turbulence conditions and lack of an auto pilot probably made it more difficult to control UVC and may have increased the pilot’s susceptibility to spatial disorientation. In addition, the pilot’s reduced sleep opportunity the night before the accident, the elapsed flight time since departure from Archerfield and the workload associated with the turbulent conditions may have increased their level of fatigue, increasing the likelihood of disorientation.
The helicopter’s spiralling descent flight profile after 1812:55 was consistent with spatial disorientation influenced by limitations of the vestibular system and absence of visual cues. The absence of external visual references also prevented the pilot from regaining control of UVC before it collided with the water.
Reporting of medication and medical conditions to the Civil Aviation Safety Authority
To assess and manage flight safety risk, the Civil Aviation Safety Authority (CASA) uses Designated Aviation Medical Examiners (DAMEs) as a point of contact for pilots renewing their medical certificates. The renewal process relies on self-reporting by the pilot of any medical conditions or treatments. Specifically, pilots are required to advise their DAME, and ultimately CASA, of any medications, medical procedures, medical conditions or symptoms that required the assessment a medical specialist.
The pilot, who was under the care of a non‑aviation medical specialist in the month prior to their most recent medical certificate renewal process, did not disclose to their DAME the medical conditions that were being treated nor details of the medications that were prescribed.
The pilot’s treating specialist reported that the sedating characteristics of the prescribed medications were known, and the dosages were carefully monitored, albeit based on pilot self‑reports. The specialist further reported that the dosage was appropriate for the pilot and did not impact on the pilot’s decision-making ability or physical functioning.
While the specialist’s clinical assessment was not in question, the input of CASA aviation medicine specialists was necessary to determine whether the pilot remained eligible to be issued with an aviation medical certificate.
Pathways exist for managing certain medical conditions that do not preclude a pilot from maintaining an aviation medical certificate. However, disclosure of medical information is essential to enable CASA to manage any on-going flight safety risk for both the individual and flight safety overall.
Findings
From the evidence available, the following findings are made with respect to the collision with water involving Bell UH-1H helicopter, VH-UVC, 5 km south-west of Anna Bay, New South Wales, on 6 September 2019. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
The pilot continued to fly after last light without the appropriate training and qualifications, and then into dark night conditions that provided no visual references. That significantly reduced the pilot's ability to maintain control of the helicopter, which was not equipped for night flight.
The pilot likely became spatially disorientated, resulting in a loss of control and collision with water.
Other factors that increased risk
The pilot did not disclose on-going treatment for significant health issues to the Civil Aviation Safety Authority. That prevented specialist consideration and management of the on‑going flight safety risk the medical conditions and prescribed medications posed.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Aireon
Airservices Australia
Bureau of Meteorology
Civil Aviation Safety Authority
FlightRadar24
maintenance organisation for VH-UVC
medical and air traffic control specialists
New South Wales police service
OzRunways
a number of witnesses
References
ATSB (2013), Avoidable Accidents No. 7. Visual flight at night accidents: What you can’t see can still hurt you, ATSB, Canberra, Australia.
Batt, R, and O’Hare, D (2005), General Aviation Pilot Behaviours in the Face of Adverse weather, Australian Transport Safety Bureau, Aviation Research Investigation Report B2005/0127.
Benson, A (1999) Spatial disorientation – general aspects. In J Ernsting, AN Nicholson, DJ Rainford (Eds.) Aviation medicine. Butterworths & Co. Ltd, London:
Bryan L, Stonecipher J, and Aron K (1954) 180-degree turn experiment, 54(11):1-52, University of Illinois Bulletin.
Dismukes, RK, Berman BA and Loukopoulos LD (2007), The limits of expertise: Rethinking pilot error and the causes of airline accidents, Ashgate Publishing Limited, Hampshire, England
Fay, J (1976), The Helicopter. History, Piloting and How it Flies, David and Charles, London.
Federal Aviation Administration (2019), Helicopter Flying Handbook, U.S. Department of Transportation, FAA-H-8083-21B
Federal Aviation Administration, Medical facts for pilots,AM-400-03/1, Civil Aerospace Medical Institute
Flight Safety Australia (2015), Workload and helicopters, Civil Aviation Safety Authority, Australia,
Newman DG (2007), An overview of spatial disorientation as a factor in aviation accidents and incidents, Australian Transport Safety Bureau, Aviation Research and Analysis Report B2007/0063.
NTSB (1994), A review of flight crew involved, major accidents of U.S. air carriers, 1978 through 1990, NTSB/SS-94/01, Washington, D.C. 20594
Prouty RW (2004), Helicopter Aerodynamics, Eagle Eye Solutions, Lebanon, USA.
Flight Safety Foundation (1997), ‘Inadequate visual references in flight pose threat of spatial disorientation’, Human Factors & Aviation Medicine, 44(6).
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
medical specialists
Bureau of Meteorology
Civil Aviation Safety Authority
maintenance organisation for VH-UVC
Williamtown air traffic controllers
air traffic control specialist.
Submissions were received from:
Bureau of Meteorology
a medical specialist
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.