Loss of control, Guimbal Cabri G2, Redcliffe Airport, Queensland, on 28 April 2021
BRIEF
| Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. |
What happened
On 28 April 2021, at 0830 Eastern Standard Time,[1] a flight instructor and student pilot were conducting circuit training in a Guimbal Cabri G2 helicopter at Redcliffe Airport, Queensland.
The student completed one circuit before the instructor took over control of the helicopter to demonstrate another circuit. The instructor reported the controls felt slightly unusual and initially thought that may be due to the crosswind or their own control inputs at the time. The instructor turned the helicopter onto the crosswind then downwind legs of the circuit, before levelling off at 800 ft.
When the instructor attempted to level the helicopter, it did not respond to cyclic inputs and initially maintained the angle of bank (about 20° to the right), before a small increase in angle of bank and a significant nose-down pitch. The cyclic was full aft and left and the helicopter did not respond to instructor inputs.
The helicopter entered a nose-down descending right turn and the instructor broadcast a MAYDAY[2] call. While moving the cyclic, the instructor regained control of the helicopter and conducting a shallow approach back to the airfield with no further control issues.
Post-flight inspection of the helicopter revealed the left cyclic locking collar was not secure, allowing the cyclic to disengage (Figure 1). The dual controls had been removed and reinstalled the previous day for a private flight. The position of the left cyclic locking collar was not noted prior to the flight and the right side cyclic was serviceable throughout.
Figure 1: Dual controls showing the left cyclic control locking collar
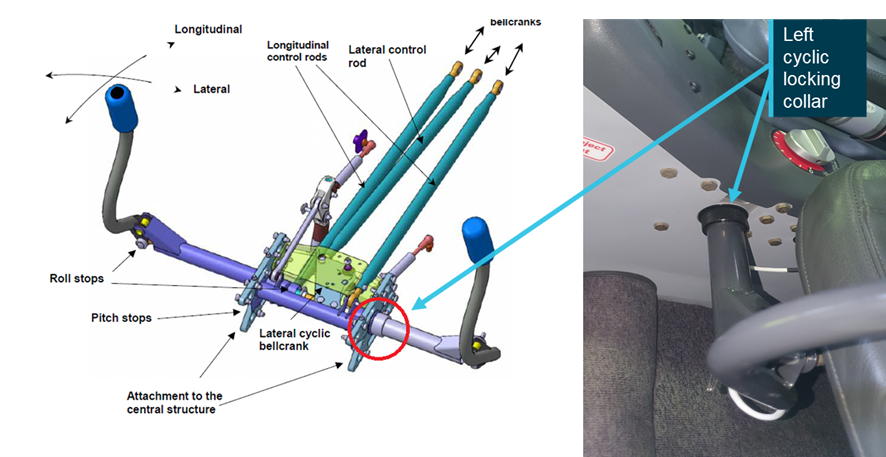
Source: Aircraft operator
Safety action
As a result of this occurrence, the aircraft operator advised the ATSB of the following proposed safety action:
- removal and installation of dual controls by engineers instead of pilots
- redesign of the dual control sign in/out register to mitigate confusion
- consider dual check sign-off for installation of dual controls
- raising a company safety alert to highlight the importance of removing distraction while engaged in safety critical tasks.
The operator assessed that the pilot installing the dual controls may have been distracted, as they were concurrently explaining the installation process to another pilot.
Safety message
This occurrence reinforces the importance of a thorough inspection of all visible flight control components and attachment points following maintenance and before flight.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
__________
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2021-015 |
| Occurrence date | 28/04/2021 |
| Location | Redcliffe |
| State | Queensland |
| Occurrence class | Serious Incident |
| Aviation occurrence category | Loss of control |
| Highest injury level | None |
| Brief release date | 02/06/2021 |
Aircraft details
| Manufacturer | Guimbal |
|---|---|
| Model | Cabri G2 |
| Sector | Helicopter |
| Operation type | Flying Training |
| Departure point | Redcliffe, QLD |
| Destination | Redcliffe,QLD |
| Damage | Nil |