
Confirm Registration
<?UMBRACO_MACRO macroAlias="ConfirmRegistration" />
Aviation Incident Reporting Summary information
Australia’s aviation industry has a world-leading safety reporting culture. This is the result of many pilots and flight crew openly reporting incidents and accidents to the ATSB – sharing knowledge and information for the continual improvement of aviation safety.
All accidents and incidents are reportable to the ATSB under the Transport Safety Investigation Act 2003. The ATSB receives on average around 17,000 aviation occurrence reports every year from pilots and flight crew. Information provided with these occurrences are recorded in a database, and are used for the sole purpose of improving aviation safety.
When lodging an accident or incident notification, the pilot or flight crew involved may have their Aviation Reference Number (ARN) recorded in the occurrence information retained by the ATSB. In the absence of further analysis of the occurrence, retaining information about an individual present at the time of an occurrence does not mean they contributed to the occurrence happening. In contrast, having identifying information in relation to multiple occurrences can be indicative of an individual who is safety orientated and willing to report.
It is important to note the ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. It it is not a function of the ATSB to apportion blame or provide a means for determining liability.
Requesting an Aviation Incident Reporting Summary
To receive an Aviation Incident Reporting Summary covering information referencing you in an occurrence, an ARN holder must submit a completed Aviation Incident Reporting Summary Request form. The form must be submitted by the individual to whom the information relates and it must be accompanied by a certified true copy of the applicant's licence. The copy must be certified by a person prescribed under the Statutory Declarations Regulations 1993(Opens in a new tab/window) and be annotated as follows: I certify this to be a true copy of the original sighted by me.
The certification must include the name and signature of the person certifying the copy, together with the prescribed capacity, under the Statutory Declarations Regulations 1993, in which they are doing so.
A request for an Aviation Incident Reporting Summary will normally be actioned within five working days from the date the application is received by the ATSB.
Requests for an Aviation Incident Reporting Summary will not be accepted from parties other than the identified flight crew licence ARN holder. Similarly, the result of the check will only be provided directly to the applicant.
Submit an online Aviation Incident Reporting Summary request form.
Limitations on use
The ATSB considers the use of the information provided in an Aviation Incident Reporting Summary inappropriate for all purposes other than the improvement of aviation safety.
The ATSB strongly advises against the use of an Aviation Incident Reporting Summary for employment selection purposes, as the involvement, or a lack of involvement, in safety occurrences does not truly qualify an individual’s airmanship.
If applying for a position overseas and the organisation wants a letter of verification of your flight crew licence, as the issuer of your licence, CASA can issue a Flight Crew Licence (FCL) Verification Letter.
Legal limitations
In accordance with the applicant's rights under the Privacy Act 1988(Opens in a new tab/window), the ATSB will take all reasonable steps to assist with requests for an Aviation Incident Reporting Summary. The Commonwealth of Australia, and the ATSB, do not accept any liability if a person is inaccurately identified or the information contains other errors of fact or interpretation.
Request an Aviation Incident Reporting Summary
Submit an online Aviation Incident Reporting Summary request form.
| Once submitted, please allow a minimum of five (5) working days for your AIRS to be emailed to you. |
Investigation levels
Information on ATSB investigation levels can be found here: Occurrence investigation levels | ATSB
Aviation Safety Digest
Known colloquially as the 'Crash Comic', the 150 issues of the Aviation Safety Digest provided valuable information and advice to help promote aviation safety in Australia.
The digest was published by ATSB predecessor agencies, the Department of Civil Aviation's Accident Investigation and Analysis Branch, which became the Air Safety Investigation Branch, and then the Bureau of Air Safety Investigation, from 1953 to 1986. It was then published by the Department of Aviation through to 1988 and then the Civil Aviation Authority through until 1991.
Scanned copies of the Digest were made available on the ATSB website in 2018 in the interest of preserving history and making accessible the many still-relevant safety lessons contained within.
Issue 01 - July 1953
(8.93 MB)
Issue 02 - October 1953
(9.3 MB)
Issue 03 - January 1954
(13.82 MB)
Issue 04 - April 1955
(2.92 MB)
Issue 05 - February 1956
(11.29 MB)
Issue 06 - June 1956
(11.18 MB)
Issue 07 - September 1956
(11.96 MB)
Issue 08 - December 1956
(11.27 MB)
Issue 09 - March 1957
(11.16 MB)
Issue 10 - June 1957
(11.62 MB)
Issue 11 - September 1957
(9.39 MB)
Issue 12 - December 1957
(11.23 MB)
Issue 13 - March 1958
(12.64 MB)
Issue 14 - June 1958
(12.28 MB)
Issue 15 - September 1958
(13.78 MB)
Issue 16 - December 1958
(12.99 MB)
Issue 17 - March 1959
(12.67 MB)
Issue 18 - June 1959
(12.62 MB)
Issue 19 - September 1959
(12.77 MB)
Issue 20 - December 1959
(11.86 MB)
Issue 21 - March 1960
(12.07 MB)
Issue 22 - June 1960
(11.46 MB)
Issue 23 - September 1960
(11.86 MB)
Issue 24 - December 1960
(9.5 MB)
Issue 25 - March 1961
(11.16 MB)
Issue 26 - June 1961
(11.4 MB)
Issue 27 - September 1961
(10.11 MB)
Issue 28 - December 1961
(10.42 MB)
Issue 29 - March 1962
(9.45 MB)
Issue 30 - June 1962
(9.54 MB)
Issue 31 - September 1962
(11.24 MB)
Issue 32 - December 1962
(10.38 MB)
Issue 33 - March 1963
(10.88 MB)
Issue 34 - June 1963
(10.47 MB)
Issue 35 - September 1963
(10.63 MB)
Issue 36 - December 1963
(10.74 MB)
Issue 37 - March 1964
(10.94 MB)
Issue 38 - June 1964
(10.59 MB)
Issue 39 - September 1964
(11.71 MB)
Issue 40 - December 1964
(11.89 MB)
Issue 41 - March 1965
(12.51 MB)
Issue 42 - June 1965
(10.64 MB)
Issue 43 - September 1965
(13.42 MB)
Issue 44 - December 1965
(13.88 MB)
Issue 45 - March 1966
(13.54 MB)
Issue 46 - June 1966
(12.81 MB)
Issue 47 - September 1966
(10.88 MB)
Issue 48 - December 1966
(12.71 MB)
Issue 49 - March 1967
(11.04 MB)
Issue 50 - May 1967
(9.99 MB)
Issue 51 - July 1967
(11.04 MB)
Issue 52 - September 1967
(10.75 MB)
Issue 53 - November 1967
(11.14 MB)
Issue 54 - January 1968
(10.32 MB)
Issue 55 - March 1968
(11.42 MB)
Issue 56 - May 1968
(10.99 MB)
Issue 57 - July 1968
(10.91 MB)
Issue 58 - September 1968
(12.71 MB)
Issue 59 - November 1968
(12.21 MB)
Issue 60 - January 1969
(11.76 MB)
Issue 61 - March 1968
(10.83 MB)
Issue 62 - May 1969
(10.45 MB)
Issue 63 - July 1969
(13 MB)
Issue 64 - September 1969
(11.84 MB)
Issue 65 - November 1969
(10.54 MB)
Issue 66 - January 1970
(11.12 MB)
Issue 67 - March 1970
(11.07 MB)
Issue 68 - May 1970
(12.7 MB)
Issue 69 - July 1970
(12.07 MB)
Issue 70 - September 1970
(12.2 MB)
Issue 71 - November 1970
(12.4 MB)
Issue 72 - January 1971
(14.22 MB)
Issue 73 - March 1971
(16.4 MB)
Issue 74 - May 1971
(15.21 MB)
Issue 75 - July 1971
(13.36 MB)
Issue 76 - November 1971
(14.42 MB)
Issue 77 - January 1972
(14.64 MB)
Issue 78 - March 1972
(14.68 MB)
Issue 79 - May 1972
(12.27 MB)
Issue 80 - July 1972
(13.02 MB)
Issue 81 - September 1972
(12.2 MB)
Issue 82 - November 1972
(13.22 MB)
Issue 83 - February 1973
(12.27 MB)
Issue 84 - April 1973
(12.7 MB)
Issue 85 - June 1973
(11.31 MB)
Issue 86 - September 1973
(13.49 MB)
Issue 87 - 1974
(12.98 MB)
Issue 88 - 1974
(11.6 MB)
Issue 89 - 1974
(12.74 MB)
Issue 90 - 1975
(11.9 MB)
Issue 91 - 1975
(12.95 MB)
Issue 92 - 1975
(12.26 MB)
Issue 93 - 1975
(12.67 MB)
Issue 94 - 1976
(13.33 MB)
Issue 95 - 1976
(12.61 MB)
Issue 96 - 1976
(14.44 MB)
Issue 97 - 1977
(13.73 MB)
Issue 98 - 1977
(14.37 MB)
Issue 99 - 1977
(13.63 MB)
Issue 100 - 1977
(14.61 MB)
Issue 101 - 1978
(12.3 MB)
Issue 102 - 1978
(11.62 MB)
Issue 103 - 1978
(11.41 MB)
Issue 104 - 1978
(12.39 MB)
Issue 105 - 1979
(11.95 MB)
Issue 106 - 1979
(14.59 MB)
Issue 107 - 1979
(13.52 MB)
Issue 108 - 1979
(12.43 MB)
Issue 109 - 1980
(12.94 MB)
Issue 110 - 1980
(13.22 MB)
Issue 111 - 1980
(11.7 MB)
Issue 112 - 1981
(12.32 MB)
Issue 113 - 1982
(11.11 MB)
Issue 114 - 1982
(9.04 MB)
Issue 115 - 1883
(8.99 MB)
Issue 116 - 1983
(10.22 MB)
Issue 117 - 1983
(12.24 MB)
Issue 118 - 1983
(11.98 MB)
Issue 119 - 1984
(13.46 MB)
Issue 120 - 1984
(13.29 MB)
Issue 121 - 1984
(14.35 MB)
Issue 122 - 1984
(12.79 MB)
Issue 123 - 1985
(14.71 MB)
Issue 124 - 1985
(13.68 MB)
Issue 125 - 1985
(13.99 MB)
Issue 126 - 1985
(15.16 MB)
Issue 127 - 1985
(13.46 MB)
Issue 128 - 1986
(14.83 MB)
Issue 129 - 1986
(16.07 MB)
Issue 130 - 1986
(15.54 MB)
Issue 131 - 1986
(14.8 MB)
Issue 132 - 1987
(12.79 MB)
Issue 133 - 1987
(14.48 MB)
Issue 134 - 1987
(14.51 MB)
Issue 135 - 1987
(16.72 MB)
Issue 136 - 1988
(19.6 MB)
Issue 137 - 1988
(12.32 MB)
Issue 138 - 1988
(13.18 MB)
Issue 139 - 1988
(9.67 MB)
Issue 140 - 1989
(10.14 MB)
Issue 141 - 1989
(10.36 MB)
Issue 142 - 1989
(13.69 MB)
Issue 143 - 1990
(11.35 MB)
Issue 144 - 1990
(11.52 MB)
Issue 145 - 1990
(10.07 MB)
Issue 146 - 1990
(11.72 MB)
Issue 147 - 1990
(12.8 MB)
Issue 148 - 1991
(11.43 MB)
Issue 149 - 1991
(13.28 MB)
Issue 150 - 1991
(14.51 MB)
Special edition - Agricultural Operations
(14.52 MB)
Special edition - The Human Factor
(19.54 MB)
Special edition - Visual Flight
(19 MB)
Corporate Plan 2018–19

This Corporate Plan sets out the ATSB’s purpose – to improve transport safety – and its strategies for achieving that purpose. The Plan also sets out the ATSB’s key deliverables and associated performance criteria. It has been prepared consistent with paragraph 35(1)(b) of the Public Governance, Performance and Accountability Act 2013 and the relevant provisions of the Transport Safety Investigation Act 2003 (the TSI Act), which establishes the ATSB. It also incorporates the Minister for Infrastructure and Transport’s Statement of Expectations (SOE) as notified under Section 12AE of the TSI Act.
The TSI Act provides that the ATSB’s primary purpose is to improve the safety of aviation, rail and marine transport through accident investigation, data analysis and safety education. It must do so independently while cooperating with the other organisations that share responsibility for transport safety, including counterpart organisations in other countries. Successive governments have indicated that, in carrying out its role, the ATSB should give priority to the safety of the travelling public.
To accomplish its primary purpose, the ATSB must take into account the known and projected environmental challenges associated with continuing growth, emerging technologies and safety trends across the aviation, rail and marine transport sectors. In response, the ATSB is preparing a Vision Statement 2025 that will provide a roadmap for the ATSB into the future, driving safety action in a rapidly changing transport environment. I will release the Vision Statement during the current year.
In my capacity as Chief Commissioner and Chief Executive Officer, I am fully committed to maintaining the ATSB’s reputation as a world leading safety investigation body. Consistent with this commitment, I will work collaboratively with the relevant authorities to ensure the ATSB is appropriately resourced to fulfil its legislative duties and positioned to meet the expectations of our stakeholders and the broader travelling public.
Greg Hood
Chief Commissioner
28 August 2018
Major Accident Contact
This contact form is intended for use during Major Accident Response scenarios. If you need to contact the ATSB, please visit the contact page.
.: EXERCISE ONLY - EXERCISE ONLY :.
At 11.35am today (15 September 2022) a twin-engine airliner operated by ‘No Fuss Airlines’ made an emergency landing at Long Green Grass Airport, Western Australia.
Smoke and flames were seen coming out of the right engine, as well as parts of the aircraft have detached up upon landing (landing gear and part of the right wing). The ATSB understands multiple people have been injured, however no further information as to the health status of any individual passenger is currently available to the ATSB.
The ATSB is appealing for witnesses to the accident to contact them on their Major accident witness hotline and will be publicising a 1800 992 986 number which will be forwarded to Services Australia to log initial calls.
ATSB investigators will follow up with witnesses as soon as possible after the event.
Contacting the ATSB:
Select the 'REVIEW AND SUBMIT' button above, then the 'SUBMIT FORM' button.
Investigation phases
All occurrence investigations progress through a series of phases in accordance with the ATSB’s investigation methodology to ensure a rigorous and comprehensive investigation report with evidence-based findings that lead to improvements in transport safety.
Evidence collection
During the evidence collection phase, investigators build a detailed picture of the occurrence or other transport safety matter being investigated. Evidence gathered may include:
- site observations and mapping, including recording wreckage distribution and witness marks
- relevant components and wreckage, materials and recorded data (including on-board flight, voyage and event recorders, GPS, images, video, system equipment data, and voice recorders) for subsequent analysis
- human performance information such as work and rest patterns and time awake, workload, perceptual limitations, communications, and social norms
- testing or procuring test and examination reports such as fuel quality-tests, toxicology, functional tests, manufacturer’s test procedures, simulation studies, meteorological analyses
- interviews with involved parties, witnesses and subject matter experts
- operational records such as logbooks, technical logs, maps or charts, trip reports, weather observations, job sheets, repair records, training records and performance checks, and audit reports
- technical documentation such as procedures and manuals, training manuals, maintenance manuals, troubleshooting guides, design drawings and system safety assessments, and
- data on similar occurrences in Australia and overseas and other occurrence data.
Examination and analysis
ATSB investigators use the collected evidence to build a detailed understanding of the circumstances surrounding the occurrence (or other transport safety matter) being investigated. This involves evidence interpretation, safety factors analysis, risk analysis and analysis review activities, as shown in the following diagram:
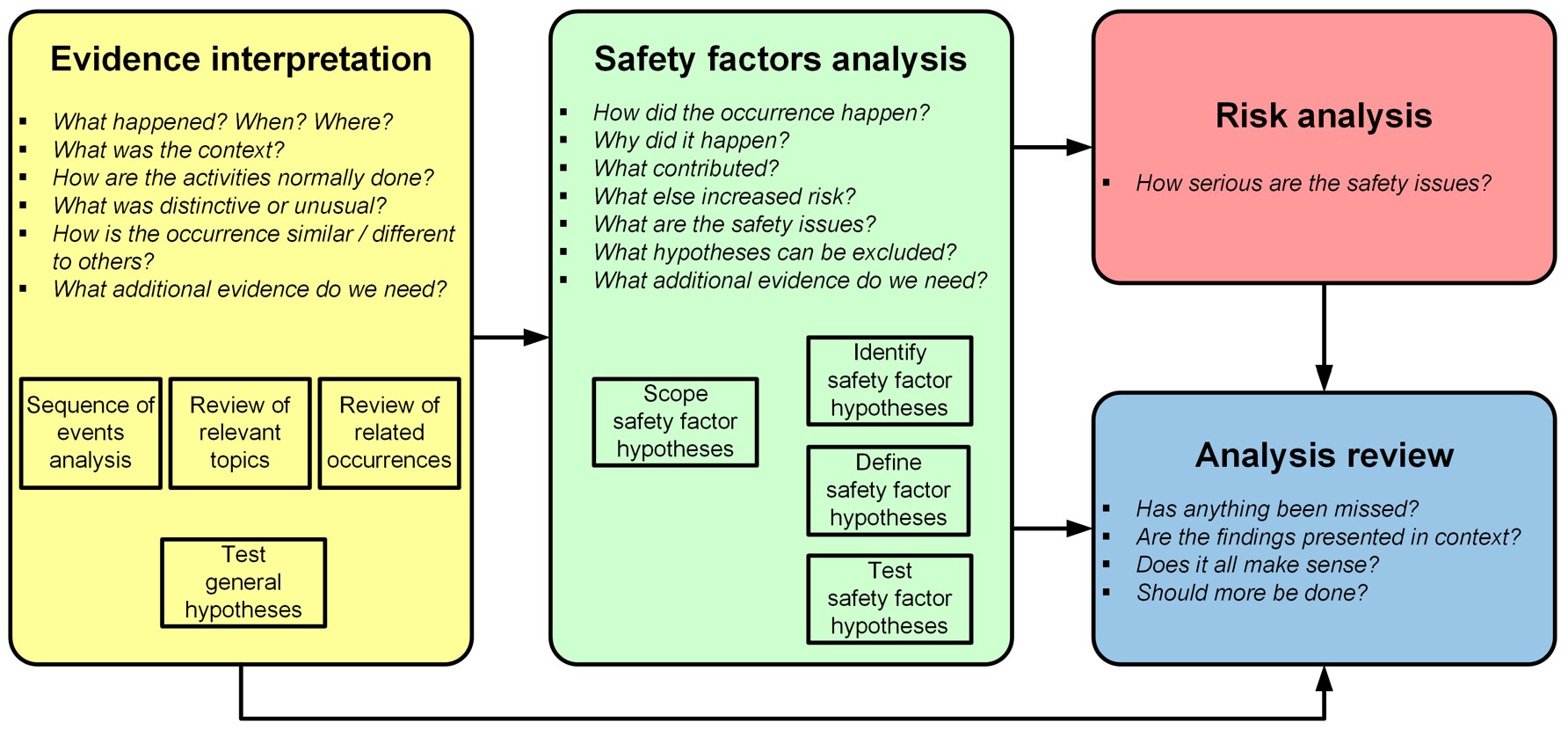
Evidence interpretation involves a series of activities to review, examine, organise and interpret the collected evidence and convert this evidence into formats that assist the analysis of safety factors. ATSB investigators may:
- undertake detailed data analysis
- create simulations and reconstruct events
- examine company, vehicle, regulator and other records
- examine wreckage and test components and system in the ATSB’s technical facilities
- research scientific literature related to human factors or other topics associated with the evidence
- review specialist reports (such as meteorology, component examination, post-mortem report and toxicology reports) and consult with relevant experts
- conduct further interviews
- determine the sequence of events
- review related occurrences, and
- compare evidence from multiple sources to look for similarities, differences, patterns and trends.
Examination and analysis requires evaluating complex sets of data, and the available evidence can be vague, incomplete and or contradictory. The review of the evidence may prompt the collection of more evidence, which in turn needs to be analysed and examined, potentially adding to the length of an investigation.
Once the examination and interpretation of the evidence about a topic is complete, the investigation team will develop and test a series of hypotheses to determine the contributing factors and other factors that increased risk. This involves conducting test for existence and influence, and evaluating the relevance and credibility of the reasons and evidence that support and oppose each hypothesis.
During the examination and analysis phase, the investigation team convenes one or more safety factor reviews with ATSB management. These are rigorous internal reviews of the progress of the investigation, its findings, scope and schedule. A safety factor review involves the investigation team presenting their evidence and analysis to reach consensus on the investigation findings. Once consensus is achieved on all the findings, the safety analysis section of the draft report can begin.
Final report: Drafting
Most ATSB reports contain the following sections:
- Investigation summary—a summary of the occurrence (or other transport safety matter), the findings and any safety action taken as a result, as well as any broader safety messages.
- The occurrence—a description of the sequence of events related to the occurrence and, if relevant, the consequences in terms of injuries and damage.
- Context—description of evidence collected during the investigation that is necessary to help the reader understand the occurrence and safety analysis, or the broader safety issues for research purposes.
- Safety analysis—a demonstration of how the evidence justifies the investigation findings
- Findings—a list of contributing factors, other factors that increased risk and other findings identified during the investigation and discussed in the safety analysis.
- Safety issues and actions—a summary of the safety issues that were identified during the investigation and details of what safety action has been taken, or is planned to be taken, by relevant parties to address those issues.
During the drafting of the report it may be necessary to return to the evidence collection or examination and analysis phases of an investigation. There will often be significant overlap in time between the evidence collection, examination and analysis and final report drafting phases.
Final report: Internal review
Final ATSB investigation reports undergo a rigorous internal review process to ensure the report adequately and accurately reflects the evidence collected, analysis, and agreed findings of the Safety Factor Review. Final investigation reports also undergo other technical and administrative reviews to ensure the reports meet national and international standards for transport safety investigations.
If a review identifies any issues with a report, such as information that needs to be expanded or findings that need to be modified, investigators will look to collect new evidence or conduct additional examination and analysis of existing evidence.
Final report: External review
To check factual accuracy and ensure natural justice, Directly Involved Parties (DIPs) are given the opportunity to comment on the final report before it is approved to ensure their input to the investigation has been accurately reflected.
DIPs are individuals or organisations outside the ATSB who possess direct knowledge of the circumstances surrounding the incident or accident.
Draft reports are provided to DIPs under Section 26(1)(a) of the Transport Safety Investigation Act 2003. Under Section 26, the report may only be copied and disclosed for the purpose of taking safety action or providing comment to the ATSB. Anyone who receives a copy for these purposes is also bound by the confidentiality requirements.
Disclosure of the draft report in any other circumstance may constitute a criminal offence.
ATSB draft reports may contain information that is subject to change as a result of internal and external review and consideration of further evidence. In its draft form, copying or disclosing the report may unjustly affect reputations. This in turn could potentially impede and discourage the crucial, future free flow of safety information to the ATSB.
The external review process is consistent with international transport safety investigation conventions, including those published by the International Civil Aviation Organization(Opens in a new tab/window), International Maritime Organization(Opens in a new tab/window) as well as the Transport Safety Investigation Act 2003(Opens in a new tab/window). DIPs are provided from five to 28 working days to provide their comment and present evidence in support of their comments. This timeframe can be extended to allow DIPs based overseas to provide comment.
Final report: Approval
Following the external review process, the report is approved by management before being sent to the ATSB Commission for final approval. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release.
Final report: Dissemination
Once an ATSB report is approved, it is prepared for public release and approved safety issues and recommendations are formally communicated to the relevant parties.
The report is then released publicly on the ATSB website and shared on social media, to ATSB subscribers via email and with the media. For certain investigation releases the ATSB may also produce an explanatory video(Opens in a new tab/window).
The progress of safety action to address ATSB recommendations is tracked and communicated, on an ongoing basis, via the ATSB website.
Witness contacting the ATSB
If you have witnessed an incident or accident – or have information that could be of relevance to an ATSB investigation – please call 1800 992 986 or (+61) 2 6257 3193.
Alternatively, complete an online witness form.
Major Accident Info
This contact form is intended for use during Major Accident Response scenarios. If you need to contact the ATSB, please visit the contact page.
The ATSB has been advised of .... The ATSB is investigating this accident.
Police and emergency services are on site.
We understand multiple people are injured.
Concerned family and friends need to <operator's> hotline to be kept informed as to the wellbeing of the passengers on board the flight.
• (Within Australia): 1800 XXX XXX
• (International callers) +61 X XXXX XXXX
The ATSB has deployed a team of investigators to the accident site.
While on-site the investigators will be:
- examining the wreckage for evidence
- interviewing witnesses and survivors as well as people involved in the aircraft operation
- examining documentation relating to the airworthiness, maintenance history, company operation, flight crew qualification, air traffic records
- recovering the flight data recorder and cockpit voice recorder to download in our Canberra facilities.
Other investigators will be called in, depending on what is found during the initial stages. ATSB staff back in our offices are also collecting relevant data from other sources that may also shed some insight into the nature of this accident.
To help us with our investigation, we are asking witnesses to complete the form below or call the ATSB on 1800 992 986.
We will be releasing more information as it come to hand.
We will publish a preliminary investigation report within the next month, detailing what factual information has been obtained so far.
Contacts:
- Family and friends – please contact <Operator's> hotline: 1800 XXX XXX
- Media outlets – to receieve email updates on this investigation, please send your contact details to: media@atsb.gov.au
- Witnesses – please contact the ATSB on 1800 992 986 or complete the below form
- Overseas investigation agencies – please contact the ATSB on +61 2 6257 XXXX or via email: atsbinfo@atsb.gov.au
- National Emergency Call Centre (DHS) 1800 992 986
If you or anyone you know needs help:
- Lifeline(Opens in a new tab/window) on 13 11 14
- Kids Helpline(Opens in a new tab/window) on 1800 551 800
- MensLine Australia(Opens in a new tab/window) on 1300 789 978
- Suicide Call Back Service(Opens in a new tab/window) on 1300 659 467
- Beyond Blue(Opens in a new tab/window) on 1300 22 46 36
- Headspace(Opens in a new tab/window) on 1800 650 890