The ATSB is investigating a weather event involving a balloon display of multiple tethered balloons at Wangaratta Racecourse, Victoria, on 11 April 2026.
During a static balloon display, multiple tethered balloons encountered a sudden change of wind conditions.
One of the tether ropes for an Amateur-built GUS-69, registered VH-XUP, failed and the balloon became airborne before colliding with terrain resulting in injuries to a person on the ground.
The tether rope on a Kavanagh Balloons D-77, registered VH-CZX, was placed under extreme tension and the basket became briefly airborne before landing hard, resulting in injuries to an additional person on the ground.
The ATSB has commenced the examination and analysis of the initial evidence collected. To date, the ATSB investigation has included interviewing witnesses and involved parties, reviewing recorded data, and the collection of other relevant information. The continuing investigation will include examination of operational documentation and components from the site.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2026-070
Occurrence date
11/04/2026
Occurrence time and timezone
19:15 Australian Eastern Standard Time
Location
About 6.5 km north-north-west of Wangaratta Airport
State
Victoria
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Cabin injuries, Collision with terrain, Ground operations - Other, Hard landing, Turbulence/windshear/microburst
Occurrence class
Accident
Highest injury level
None
Aircraft details
Manufacturer
Amateur Built Aircraft
Model
GUS-69
Registration
VH-XUP
Serial number
GUS-01
Sector
Balloon
Operation type
Part 131 Balloons and hot air airships
Activity
General aviation / Recreational-Sport and pleasure flying-Other sport and pleasure flying
Departure point
Near Wangaratta Racecourse, Victoria
Injuries
None
Aircraft details
Manufacturer
Kavanagh Balloons
Model
D-77
Registration
VH-CZX
Serial number
D77-549
Sector
Balloon
Operation type
Part 131 Balloons and hot air airships
Activity
General aviation / Recreational-Sport and pleasure flying-Other sport and pleasure flying
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the evening of 6 July 2025, a Saab 340 was being used to conduct a scheduled air transport flight to Sydney Airport, New South Wales. On board were 2 flight crew, 1 cabin crew and 27 passengers. The captain reported that the weather around Sydney at the time included developed thunderstorms and that holding and diversions had been in effect. They further reported that arrivals had recently been resumed as storms had passed and that, on final approach, weather radar indicated that the nearest storm cell was no closer than 19 km to the north.
When the aircraft was about 19 km west of Sydney, the automatic terminal information system (ATIS)[1] was revised to advise that the wind had increased from 20 kt from the west to include gusts of up to 40 kt. Consequently, air traffic control (ATC) changed the active runway to runway 25.[2] The aircraft was the second to be sequenced for an approach to the revised runway, following an Airbus A320. Passing about 14 km from the airport on final approach, the Saab crew heard a broadcast from the A320 crew that they were conducting a windshear escape[3] (Figure 1).
At the time, the A320 was approximately 9 km ahead. Hearing that the preceding aircraft had encountered windshear, the Saab crew discussed their windshear escape procedure and decided to continue the approach, waiting to hear more details about the nature of the windshear.
Figure 1: Aircraft flight path
Source: Flightradar24 overlaid on Google Earth, annotated by the ATSB
Approximately 2 minutes later, ATC advised the Saab crew that the A320 had encountered severe undershoot windshear.[4] The crew assessed that they were passing the position the A320 had first detected the windshear at this time. Shortly afterwards, when at approximately 700–800 ft, the captain reported that they observed a decrease in airspeed and an abnormal power indication consistent with windshear. The captain called for a windshear escape which the crew initiated. Throughout the subsequent climbing manoeuvre, they conducted a series of power, airspeed and configuration changes until confident they were no longer affected by windshear.
Two subsequent aircraft landed on runway 25 without any further reported windshear encounters, after which arriving aircraft were again sequenced for runways 34L/34R. Following the windshear escape, the aircraft was re-sequenced for runway 34L and landed without further incident.
Safety message
Low-level windshear is a serious threat to the safety of departing and landing aircraft. If windshear is encountered, rapid and large control inputs may be required and in severe cases, the effect of windshear may exceed the performance capabilities of the aircraft. Flight crew should use all available indicators to avoid areas of known windshear on the intended flight path. These include the presence of thunderstorm cells, and reports from pilots of other aircraft and air traffic control.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Automatic terminal information service: the provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is updated either routinely or when there is a significant change to weather and/or operations.
[2]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L or R as required for left or right when there are parallel runways.
[3]Windshear: a change in wind speed and/or direction over a short distance. A windshear escape is a pilot recovery technique used when an inadvertent windshear encounter is experienced.
[4]Undershoot windshear: a rapid decrease in the headwind component of the wind.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-029
Occurrence date
06/07/2025
Location
5 km east of Sydney Airport
State
New South Wales
Occurrence class
Incident
Aviation occurrence category
Missed approach, Turbulence/windshear/microburst
Highest injury level
None
Brief release date
25/08/2025
Aircraft details
Manufacturer
Saab Aircraft Co.
Model
340B
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
At 1021 on 7 April 2025, a Bankstown Helicopters Robinson R44 helicopter, registered VH‑EWM (EWM), with a pilot and 2 passengers on board, departed from Bankstown Airport, New South Wales, for a local scenic flight around Sydney Harbour. Shortly after 1028, as EWM was entering the Parramatta River helicopter lane behind an EC120 helicopter, the occupants of EWM experienced a sudden onset of turbulence followed by an uncontrolled descent.
In response, the pilot applied full collective, which resulted in a low rotor speed condition as the helicopter descended towards the water. The pilot was able to manoeuvre the helicopter and complete a forced landing on the river shoreline.
What the ATSB found
The ATSB found that it is likely that EWM entered the rotor wake from a preceding heavier EC120 helicopter, which resulted in the control difficulties, an uncontrolled descent, low rotor speed warning and the forced landing.
What has been done as a result
Following review of the draft report, the Civil Aviation Safety Authority undertook proactive safety action to improve existing guidance about helicopter wake vortices in Advisory Circular 91-16. The updated advisory circular was released on 17 July 2025 and can be found at the link: AC 91-16 v1.2 - Wake turbulence.
Safety message
Flight tests have demonstrated that helicopter wake turbulence is comparatively larger and less predictable in its behaviour than for aeroplanes of the same weight. Helicopter rotor vortices can descend, remain level or climb, and the duration of their persistence can increase significantly in conducive weather conditions. The United States Helicopter Safety Team website recommends remaining 3 rotor disks clear of a hovering or taxiing helicopter and allowing 3 NM and/or 2 minutes for the rotor wake from a preceding helicopter to dissipate.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
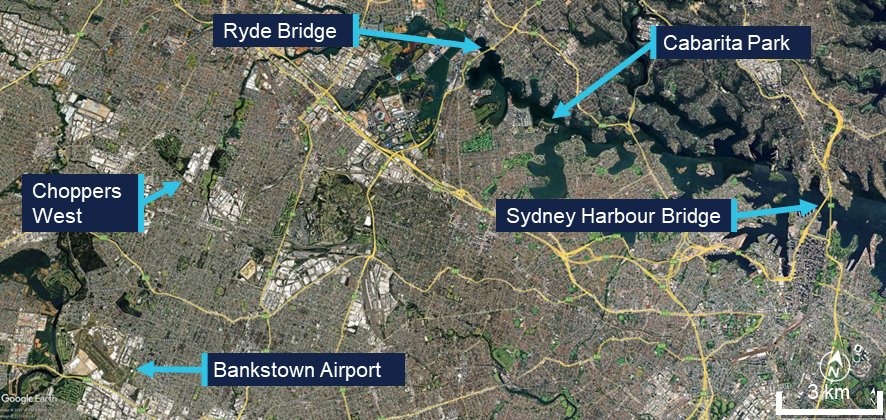
At 1021 local time on 7 April 2025, a Bankstown Helicopters Robinson R44 Raven 1 helicopter, registered VH‑EWM (EWM), with a pilot and 2 passengers on board, departed from Bankstown Airport, New South Wales for a local scenic flight around Sydney Harbour. Bankstown Tower air traffic control (TWR) cleared EWM to depart via ‘Choppers West’, which was a standard procedure for helicopters departing to the north when runway 29 was active at Bankstown.
The pilot reported that they climbed to about 1,000 ft above mean sea level.[1] The pilot’s plan was to join the Parramatta River on the west side of the Ryde Bridge and descend to 500 ft to follow the helicopter lane[2] along the south side of the river to Sydney Harbour (Figure 1).
Figure 1: Key locations
Source: Google Earth, annotated by the ATSB
About 1 minute after EWM departed, an Airbus EC120B helicopter departed Bankstown, also following the Choppers West departure. Shortly after the EC120 departed, TWR advised the EC120 pilot that there was ‘R44 traffic 1 NM ahead’, to which the EC120 pilot reported that they had the traffic sighted. Bankstown TWR then advised the pilot of EWM that they were not receiving their transponder data, which the pilot acknowledged. The pilot of EWM then turned their transponder off and on in an attempt to transmit transponder information, but no data was received from it throughout the incident flight.
As the 2 helicopters tracked north towards the Parramatta River, the EC120 flew to the west of EWM and passed it before reaching the river. The EC120 then turned right to join the Parramatta River helicopter lane, tracking towards the Ryde Bridge and Sydney Harbour, and passed over the Ryde Bridge at a recorded radar altitude of 600 ft.
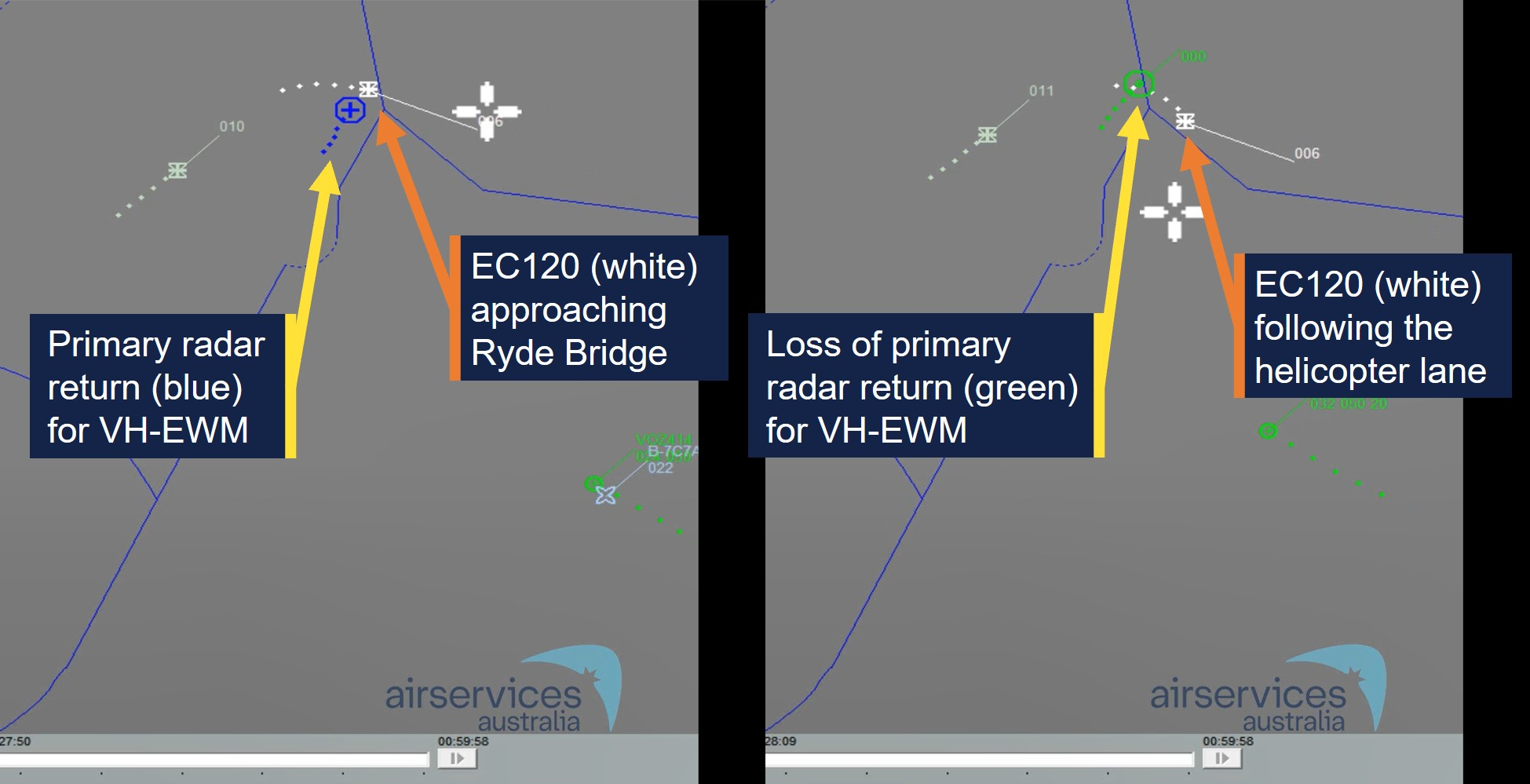
The pilot of EWM reported that they descended the helicopter to 500 ft as they approached the river. Just before the pilot turned EWM right to join the helicopter lane, another larger helicopter (the EC120) suddenly appeared in front of them (Figure 2). The pilot of EWM estimated the EC120 was about 500–600 ft (150–180 m) in front of them and about 100 ft above them. While there was no recorded altitude for EWM, primary radar data indicated that EWM entered the lane about 9 seconds behind the EC120.[3] Primary radar data for EWM was lost about 10 seconds later, just after 1028, indicating it had descended below radar coverage.
Figure 2: Primary radar return (left) and loss of primary radar return (right) for VH‑EWM
Source: Airservices Australia, annotated by the ATSB
The pilot of EWM made a radio broadcast that they were entering the helicopter lane as they crossed the Ryde Bridge behind the EC120. They then experienced what they described as very strong turbulence from a vertical motion in the atmosphere. A passenger later described it as ‘like heavy turbulence … rolling left and right’ followed by ‘diving towards the water’.
The pilot noted that the helicopter was descending through 400 ft and responded by raising the collective lever.[4] However, the helicopter continued descending towards the water as it tracked behind and below the EC120. A passenger recalled the pilot announced ‘brace for impact’ as the helicopter approached the water. The pilot applied full collective to avoid the water, which caused the rotor speed to decay sufficiently for the low rotor speed warning horn to activate. They also reported feeling that they could not escape what they believed to be the rotor wake from the EC120. The pilot then sighted a suitable forced landing area at Cabarita Park and, using the helicopter’s remaining airspeed and rotor speed, manoeuvred the helicopter to the shoreline for a landing.
Following the landing, the pilot rolled the engine throttle back to idle and proceeded through their after‑start checks and confirmed normal operations on the ground. The pilot then conducted a hover check and again confirmed normal operations. The pilot attempted radio contact with their operations base but received no reply. They then conducted a return flight to Bankstown without further incident.
Context
Pilot information
The pilot held a commercial helicopter pilot licence, issued on 26 November 2024, with a single‑engine helicopter class rating and low‑level rating. The pilot held a class 1 aviation medical certificate with no restrictions and expiration date of 30 May 2025. The pilot had accumulated about 112 hours flying experience and the incident flight was the pilot’s first commercial flight.
Helicopter information
The incident helicopter, EWM, was a piston‑engine 2‑bladed Robinson Helicopter Company R44 Raven 1 with a maximum take‑off weight of 1,089 kg. The weight and balance data provided by the operator indicated it was within limits for the flight.
The Airbus EC120B was a turbine-engine 3‑bladed helicopter with a maximum take‑off weight of 1,715 kg. Therefore, the EC120 was about 57% heavier than EWM at their respective maximum take‑off weights.
The maintenance release for EWM indicated the helicopter was operated by Bankstown Helicopters in the operational category of Part 133 Air Transport. The maintenance release current at the time of the incident was issued on 3 April 2025 at 4,349 hours total time in service with an expiry date of 3 April 2026 or 4,400 hours. A maintenance test flight was certified on the maintenance release as conducted on 3 April with ‘nil defects evident.’
After the incident, the operator’s maintenance organisation inspected the helicopter and found no defects. As the flight hours remaining on the helicopter were close to the next overhaul, the operator elected to remove the helicopter from service and have the maintenance organisation complete the overhaul.
Meteorological information
The METAR[5] recordings for Bankstown Airport at 1000 and 1030 indicated that the wind was westerly at a speed of 9 kt at 1000 and 7 kt at 1030. No cloud was detected. These conditions were consistent with the Bankstown Airport forecast for 8 kt westerly winds. The pilot reported their assessment of the weather was 5 kt of variable wind and CAVOK[6] conditions, but when they encountered the turbulence over the Ryde Bridge it felt like 40 kt of wind.
Rotor wake turbulence
In 1996, the United States Federal Aviation Administration (FAA) produced a report on the subject of Flight test investigation of rotorcraft wake vortices in forward flight. They used a laser doppler velocimeter to measure the vortices and small probe aircraft to test the actual flying conditions. Smoke generation was used to visualise the wake vortices for the probe aircraft. Their investigation concluded that:
The measured vortex circulation diminished with decreasing airspeed for helicopter airspeeds below 40 knots. At these lower speeds, the wake vortex structure begins to break down and changes to a distinct downwash.
Vortex duration depends strongly on ambient weather conditions and a variance of 300% was observed on those days most conducive[7] to vortex persistence and duration compared with those observed on typical days.
Typically, helicopters with higher gross weight, larger rotor diameters, and larger numbers of rotor blades generated vortices of larger core diameters.
Probe tests revealed that helicopter vortices did not descend in the same predictable manner as for fixed‑wing aircraft. Some vortices descended; some remained level; and some initially descended, levelled off, and then ascended above the altitude of the generating helicopter.
Figure 3: Rotor wake vortices visualised with smoke generators
Visualisation of the wake vortices behind an S‑76A helicopter in forward flight with smoke generators from the FAA (1996) flight tests. Source: Reddit
Meiris (n.d.) provided an article for the United States Helicopter Safety Team website, on the subject of Avoiding helicopter wake turbulence. The article referenced the FAA 1996 flight test report and provided the following recommendations:
As a result of these findings and the studies conducted regarding helicopter downwash in a hover, a few guidelines have been developed to increase awareness around helicopter wake turbulence:
• For hovering flight or a hover taxi, stay three rotor diameters away.
• For forward flight, a minimum of 3 nm [NM] separation is recommended, especially from larger helicopters. The investigation we discussed previously discovered that even at 3nm [NM], the planes encountered uncommanded pitch and roll oscillations.
• Leave 2 minutes for the rotor vortices to dissipate behind a helicopter in forward flight.
Related occurrences
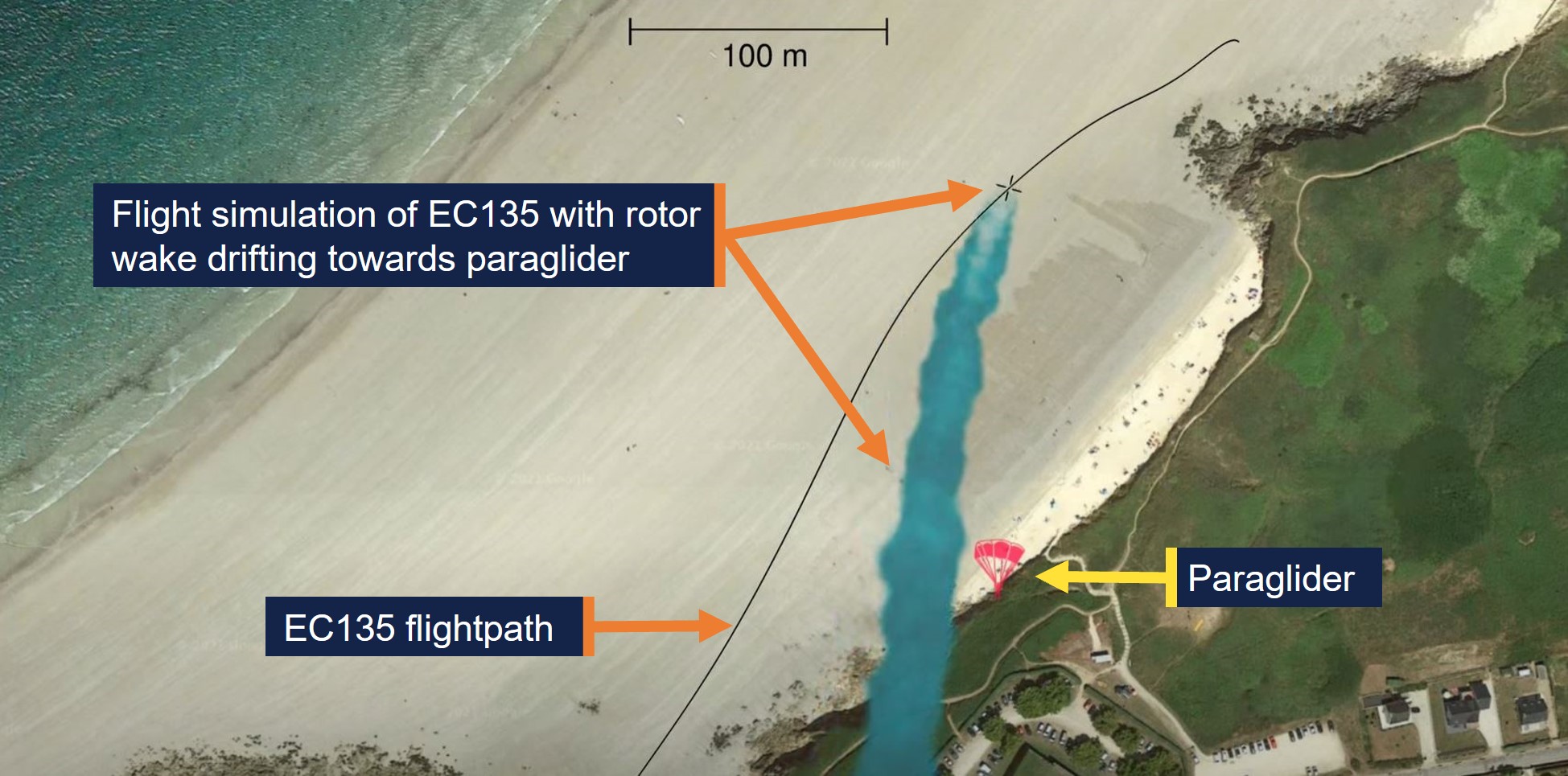
The French Bureau of Enquiry and Analysis for Civil Aviation Safety investigation BEA2019-0234, Accident to a paraglider involving the Airbus - EC135 - T2 PLUS registered F-HTIN, examined a fatal paraglider accident in 2019. The paraglider’s wing collapsed after encountering the rotor wake from an Airbus EC135 helicopter, which drifted with the wind from the helicopter’s flightpath onto the paraglider (Figure 4).
Figure 4: Simulation of rotor wake drifting onto the paraglider
Source: YouTube – Bureau of Enquiry and Analysis for Civil Aviation Safety, annotated by ATSB
The 2022 United States National Transportation Safety Board investigation WPR22LA072 found that the pilot of a Cessna 120 attempted a go‑around about 20 seconds behind the passage of a Bell UH‑1H helicopter. During the go‑around the Cessna encountered wake turbulence, resulting in a loss of control and collision with terrain (Figure 5). The report indicated light wind conditions of 4 kt at the airport.
Figure 5: Loss of control accident from rotor wake
Source: YouTube – Aviation Safety Network, annotated by ATSB
Safety analysis
Primary radar data and the pilot’s report indicated that EWM entered the Parramatta River helicopter lane and passed over the Ryde Bridge about 9 seconds behind and slightly below the EC120 helicopter. At this point, EWM encountered heavy turbulence, an uncontrolled descent and a low rotor speed when the pilot applied full collective to avoid a collision with the water.
The uncontrolled descent and low rotor speed condition resulted in the pilot conducting a forced landing on the shoreline of the Parramatta River.
The incident occurred under relatively calm wind conditions and EWM operated in a serviceable condition for the return flight. Subsequent maintenance inspections of the helicopter found no fault. Furthermore, EWM passed overhead the Ryde Bridge in sufficient proximity to a preceding heavier 3‑bladed helicopter to be subject to a rotor wake induced upset. Therefore, the ATSB concluded that the sudden onset of turbulence and uncontrolled descent were likely the result of EWM encountering rotor wake turbulence from a preceding EC120 helicopter.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the wake turbulence encounter and forced landing involving Robinson R44, VH-EWM, about 15 km north‑east of Bankstown Airport, New South Wales, on 7 April 2025.
Contributing factors
It is likely that the incident helicopter entered the rotor wake from a preceding heavier helicopter, which resulted in control difficulties, an uncontrolled descent, low rotor speed warning and a forced landing.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by the Civil Aviation Safety Authority
Following review of the draft report, the Civil Aviation Safety Authority undertook proactive safety action to improve existing guidance about helicopter wake vortices in Advisory Circular 91-16. The updated version of the advisory circular was released on 17 July 2025 and can be found at the link: AC 91-16 v1.2 - Wake turbulence.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Airservices Australia
Civil Aviation Safety Authority
the operator and maintenance organisation for VH-EWM
the pilot and passengers of the incident flight
References
Bureau of Enquiry and Analysis for Civil Aviation Safety. (2021). Accident to a paraglider involving the Airbus - EC135 - T2 PLUS registered F-HTIN on 11 May 2019 at Le Conquet (Finistère).https://bea.aero/fileadmin/user_upload/BEA2019-0234.en.pdf
Federal Aviation Administration. (1996). Flight test investigation of wake vortices generated by rotorcraft in forward flight (DOT/FAA/CT-94/117). https://apps.dtic.mil/sti/tr/pdf/ADA318103.pdf
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
the maintenance organisation for VH-EWM
the operator and pilot of the incident flight.
No submissions were received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]All heights in the report are altitudes unless stated otherwise.
[2]The helicopter lane from Ryde Bridge to Sydney Harbour Bridge was contained within Restricted Area R405A.
[3]Radar data did not display speed for the helicopters, but this would correspond to a separation of 556 m at 120 kt.
[4]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor and engine power. Collective input is the main control for vertical velocity.
[5]METAR: a routine report of meteorological conditions at an aerodrome. METAR are normally issued on the hour and half hour.
[6]Ceiling and visibility okay (CAVOK): Visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[7]Studies have shown that atmospheric turbulence hastens wake breakup, while other atmospheric conditions can transport wake horizontally and vertically (FAA, 2023).
Occurrence summary
Investigation number
AO-2025-018
Occurrence date
07/04/2025
Location
About 15 km north-east of Bankstown Airport
State
New South Wales
Report release date
18/07/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Control issues, Forced/precautionary landing, Turbulence/windshear/microburst, Warning devices
On 13 November 2024, a Boeing 737 departed Sydney, New South Wales on a scheduled passenger flight to Brisbane, Queensland.
Just prior to descent, the flight crew, aware of potential upcoming turbulence, turned the seatbelt sign on, and made a standard announcement for all passengers to return to their seats and to fasten their seatbelts.
Around 4–5 minutes after the seatbelt sign was turned on, as the aircraft passed FL330,[1] the aircraft encountered severe turbulence for approximately 45–60 seconds.
One passenger, who was already in the toilet prior to the seatbelt sign being turned on, did not return to their seat before the turbulence encounter. Another passenger, with a small child, ignored the seatbelt sign and cabin crew requests to be seated and proceeded with the child to the second toilet where they remained during the turbulence encounter. The door to this toilet was damaged during the turbulence, likely from passenger impact, and was unable to be opened. An off-duty pilot assisted removing the door to access the 2 passengers inside. All 3 passengers sustained minor injuries and were provided with first aid by cabin crew.
The flight crew declared a medical PAN PAN[2] to air traffic control and the aircraft landed in Brisbane without further incident. Ambulance staff treated the injured passengers at the gate.
Context
Turbulence
Turbulence is caused by the irregular movement of air and often cannot be seen and is responsible for the abrupt sideways and vertical jolts that passengers often experience during flights.
Cabin safety
While turbulence is normal and occurs frequently, severe turbulence can cause passengers and cabin crew who are not wearing their seatbelts to be thrown around without warning. About 20 in‑flight turbulence injuries are reported in Australia each year. Some of these injuries are serious and have resulted in broken bones and head injuries.
Almost all turbulence injuries involve people who are not properly seated and do not have their seatbelt fastened. A securely fastened seatbelt is the best defence against injuries. It should be fastened low and tight around the waist.
Safety message
When the seatbelt sign is on, passengers are required by law to have their seatbelt fastened for their own safety. Even when the seatbelt sign is off, passengers should continue to keep their seatbelt fastened, as pilots or cabin crew do not always have enough time to warn passengers to fasten their seatbelts before turbulence hits.
Cabin crew are trained to ensure passengers are safe at all times, and are aware of the dangers of in-flight turbulence. It is for this reason that passengers should follow any requests by cabin crew – including fastening seatbelts, securing carry-on baggage, or returning to seats when asked.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1] Flight Level: at altitudes above 10,000 ft, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 330 equates to 33,000 ft.
[2] PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2024-045
Occurrence date
13/11/2024
Location
67 km east of Tenterfield
State
New South Wales
Occurrence class
Serious Incident
Aviation occurrence category
Turbulence/windshear/microburst
Highest injury level
Minor
Brief release date
15/01/2025
Aircraft details
Manufacturer
The Boeing Company
Model
737
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 9 October 2024, VH-ZMW, a Beech Aircraft B200, was conducting an air transport flight with 6 persons on board, from Toowoomba to Normanton, Queensland. The aircraft departed and, approximately 30 minutes into the flight, entered a thunderstorm. The pilot diverted the aircraft to Roma, Queensland, where it was assessed by an engineer. The aircraft sustained minor damage, and the passengers and pilot were uninjured.
What the ATSB found
The ATSB found that although the pilot delayed the initial departure, reviewed the available weather information, and discussed their plan with more experienced colleagues, the aircraft entered a thunderstorm resulting in minor damage to the aircraft.
The ATSB also found that as the airborne weather radar had been incorrectly installed, its effectiveness at detecting cloud was reduced and was providing misleading information, which degraded the pilot's in-flight assessing and planning.
In addition, the pilot’s fuel planning using the company software included a fixed reserve that was less than the value detailed in the company’s exposition.
Finally, prior to departure the pilot informed the passengers of possible turbulence and kept the seatbelt sign on throughout the flight. This briefing and decision‑making likely contributed to the safety of the passengers when turbulence was experienced.
What has been done as a result
The operator rectified the incorrect installation of the weather radar. While the operator already provided weather radar theory training, it was not specific to the device installed on the aircraft. A Garmin training course is now provided to company pilots.
The flight planning software has also been reviewed to ensure the correct parameters are used as per the operator’s exposition.
Additionally, even though fatigue was not considered a safety factor, the operator has introduced a new fatigue reporting tool and monitoring system for rostering.
Safety message
This incident highlights how quickly weather conditions can change and, where possible, remaining visual can provide better identification of the weather. Using equipment such as airborne weather radar, can provide pilots with better situational awareness. However, the equipment is only useful if it is installed correctly, and the pilot has previously used and become knowledgeable with operating it before they’re required to use it to assist with navigating weather.
Areas of known weather should be avoided by 20 NM (37 km) and weather radar should not be used for penetrating areas of known weather. Instead, it should be used at longer range to plan around the precipitation returns.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry.
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
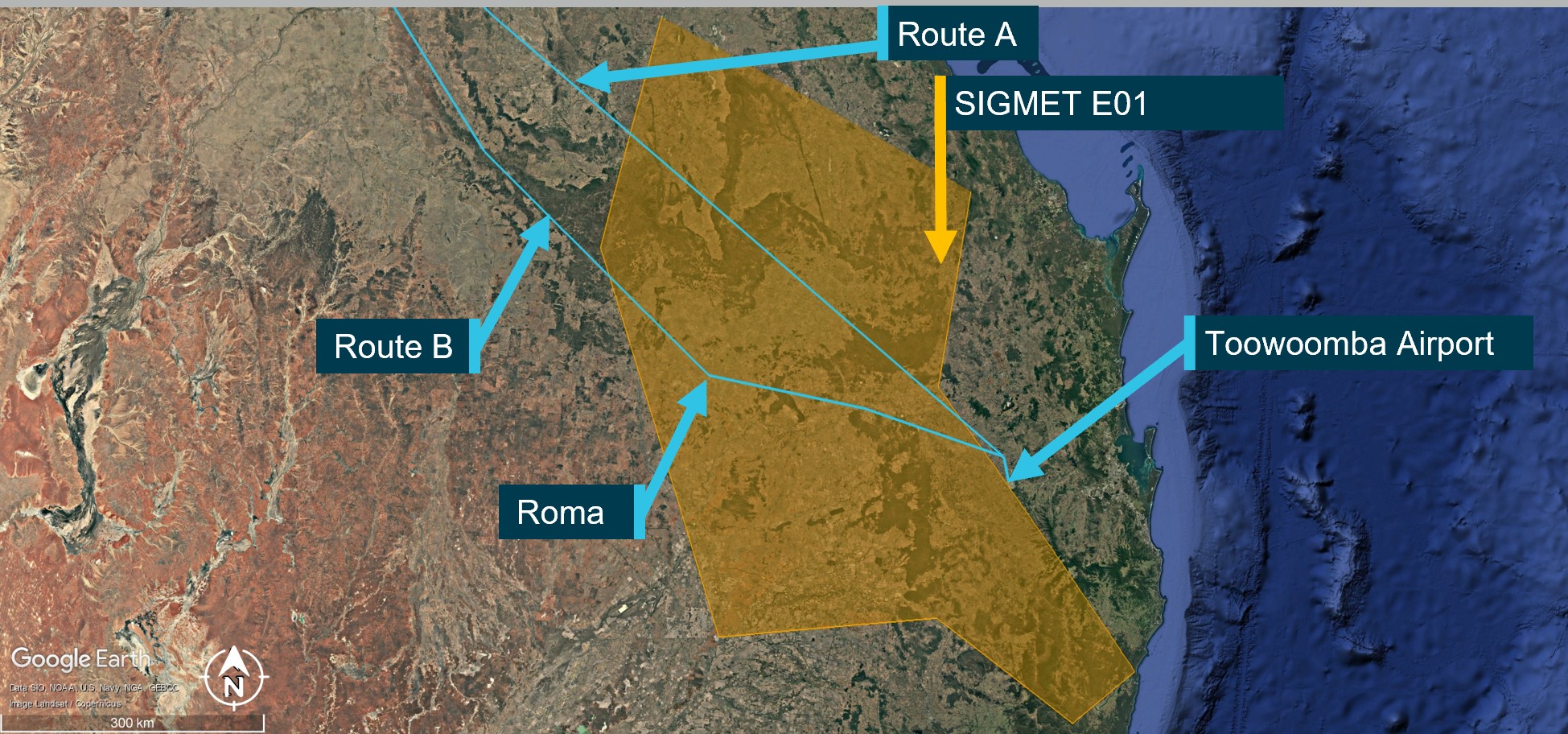
On 9 October 2024, a Beechcraft B200, registered VH-ZMW and operated by Austrek Aviation, was being prepared for a passenger transport flight with a pilot and 5 passengers from Toowoomba Airport to Normanton Airport, Queensland. At 1138 local time, the pilot submitted a flight plan to air traffic services for a direct route to Normanton (route A) (Figure 1), intending to depart at 1600.
During the pilot’s preparations, they identified that thunderstorm activity was likely along the intended flight path. Consequently, they reported accessing multiple weather forecasts and observations via their electronic flight bag (EFB), which was running a flight planning application. Additionally, they used the Bureau of Meteorology weather radar to obtain an indication of likely thunderstorm activity in the area. The pilot also reported discussing the weather with their more experienced colleagues. At 1517, they revised the flight plan to route B, to overfly Roma Airport and then to Normanton, which was assessed as a more suitable route around the thunderstorm activity.
Figure 1: Planned flight routes
Source: Flight route submission provided by AirServices Australia, recreated and annotated by the ATSB overlaid on Google Earth
The pilot delayed departure due to a passing thunderstorm in the vicinity of Toowoomba. The pilot advised that prior to departure at 1620, they provided a briefing to the passengers, which included the possibility of encountering turbulence. Additionally, they kept the seatbelt sign on throughout the flight.
At 1624, the pilot reported to air traffic control (ATC) that they were taxiing for departure at Toowoomba. The controller advised that the pilot of another aircraft, approximately 20 NM (37 km) north‑west of Toowoomba, was currently deviating around multiple cloud build-ups[1] and asked what their intentions on departure were concerning the deteriorating weather in the area. The pilot opted to further revise their flight plan at this time and requested to fly directly to LIKTO waypoint[2] (Figure 1) rather than tracking north to the MESED waypoint as planned. Additionally, they advised that they would initially level at an altitude of 4,000 ft to remain clear of cloud until they could climb without entering it. On departure, the pilot estimated they would reach LIKTO at 1654.
At 1634, approximately 20 NM (37 km) north-west of Toowoomba, passing 10,900 ft on climb and clear of cloud, the pilot requested and received clearance to deviate 10 NM (18.5 km) right and left of the flight plan track to avoid cloud. They then turned onto a more northerly heading (Figure 2). The pilot later reported that they were able to maintain visual conditions up to the intended cruise level of FL 240.[3] Reaching FL 240 at 1645, the pilot observed a return on the weather radar to the right of the aircraft’s intended flight path, which they associated with a thunderstorm cell. Consequently, they deviated to the left toward the Toowoomba to LIKTO direct flight track. At this time another Beechcraft B200 departed Dalby Airport and climbed to an altitude of 4,000 ft, tracking for Roma Airport. This aircraft also reported an expected LIKTO arrival of 1654.
Figure 2: VH-ZMW actual flight track
Source: Google Earth, annotated by the ATSB
Expecting that FL 260 would provide smoother conditions for the passengers, the pilot obtained ATC approval to climb. At approximately 1648, as they captured the new altitude, they entered what the pilot later described as ‘wispy cloud’, which the sun could be seen through.
With the aircraft operating at 150 kt indicated airspeed, the pilot noted that the outside air temperature at this time was −23°C and that the aircraft had begun to accumulate ice (see the section titled Icing). With the ice vanes for the air inlet on the engine cowl open (see the section titled Anti-Icing and de-icing equipment), the aircraft was operating near its altitude limit. As the pilot did not feel comfortable attempting to climb higher to exit the icing conditions, they instead requested to descend.
At about this time, the turbulence increased and the autopilot disconnected showing multiple failure annunciations. In response, the pilot manually flew the aircraft. They also attempted to adjust the weather radar to find the best route. However, due to the turbulence, they had difficulties adjusting the settings using the equipment’s touch screen.
At 1654 on descent and passing through approximately 18,500 ft, and still experiencing turbulence, the pilot of VH‑ZMW contacted the pilot of the other Beechcraft B200, who had deviated to the north of LIKTO due to the weather in that area. Based on the discussion with that pilot, the pilot of VH-ZMW elected to track north. At 1656, the pilot of VH-ZMW contacted ATC and obtained a clearance to divert to Roma Airport to land and assess if they could continue to Normanton safely. They then tracked toward the other B200 location, which they observed on their traffic display.
The pilot later reported that between entering cloud at FL 260 and becoming visual at approximately 1705 at 4,000 ft they encountered turbulence, updrafts, downdrafts, icing, and observed lightning flashes. They also stated that they remained in control of the aircraft at all times.
At 1735, after landing at Roma Airport, the pilot endorsed the maintenance release with a possible lightning strike during a severe weather event. The subsequent engineering inspection did not identify any lightning strike damage however, there was minor damage observed to the leading edges of the aircraft’s wings and radome.[4] There were no injuries to the pilot or passengers.
Context
Pilot
The pilot held a commercial pilot licence (aeroplane) and a valid class 1 aviation medical certificate. They had completed an instrument proficiency check in a multi-engine aircraft and held the required design feature endorsements for the B200 aircraft. They had also completed an operator proficiency check flight on 23 September 2024.
The pilot had a total flight experience of 1,691.3 hours, of which 609.8 were on B200 type aircraft. The pilot had also accrued 190.3 hours of instrument flight experience and had completed a theory course in weather radar principles and operations on 8 August 2023.
Prior to the incident, they reported having 9.5 hours of sleep in the previous 24 hours and described feeling fully alert and wide awake.
Aircraft
VH-ZMW was a Beech Aircraft Corporation B200, manufactured in the United States in 1993 and issued serial number BB1460. It was registered in Australia on 9 June 2010 and registered with the operator on 9 October 2019. The aircraft could be operated by a single qualified pilot and was powered by 2 Pratt & Whitney PT6A-42 turbine engines driving 4‑blade Hartzell propellers.
Weather radar
The aircraft was equipped with an airborne weather radar capable of detecting and displaying areas of precipitation along the intended flight path. The device fitted to VH-ZMW had a 12-inch antenna, allowing a maximum weather avoidance range of 320 NM (593 km).
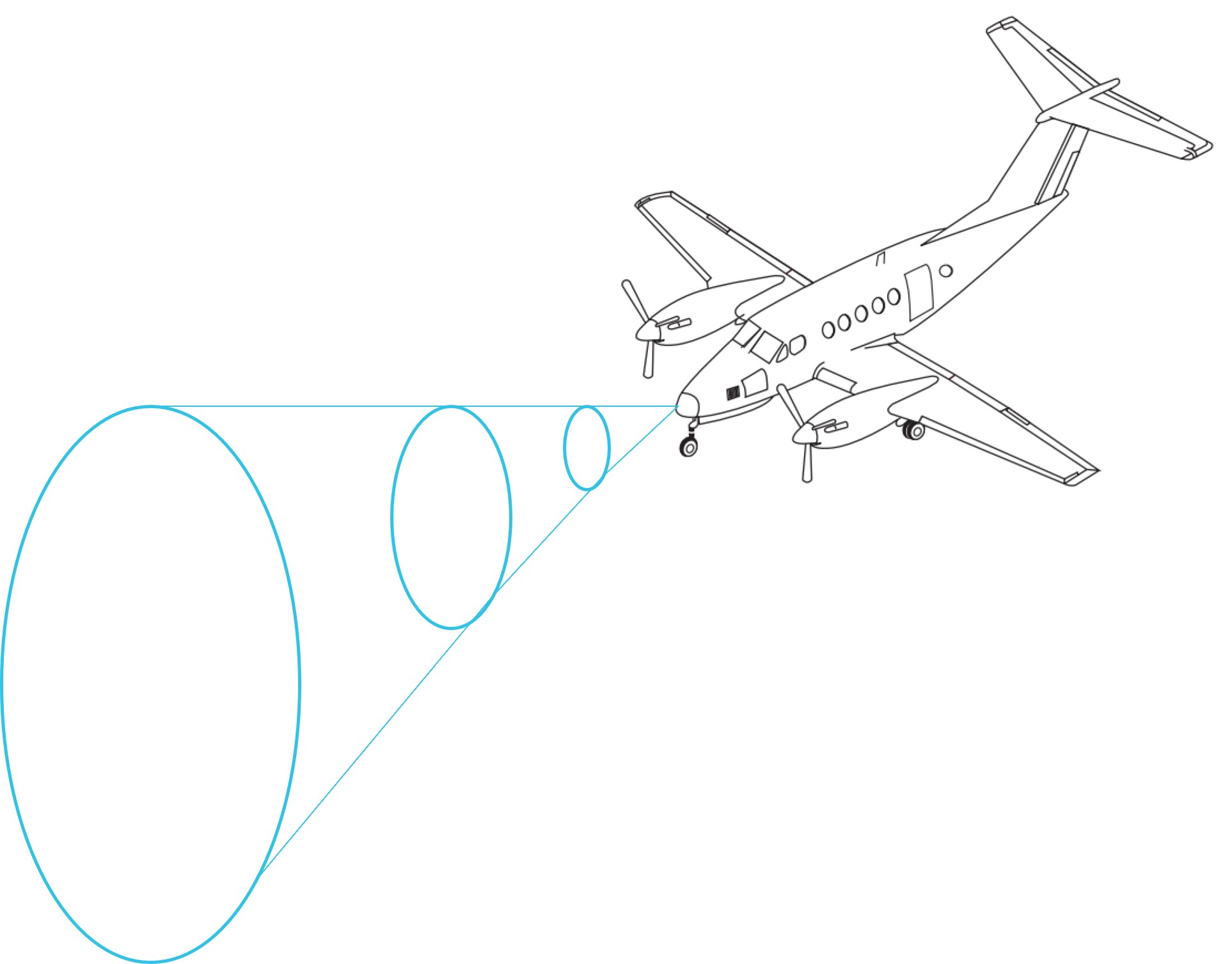
A weather radar detects moisture by sending out a microwave pulse beam that is reflected by moisture such as precipitation, and solid objects such as terrain. The return beam is captured by the weather radar antenna and presented to the pilot. As the initial radar beam leaves the aircraft, it expands the further it is from the aircraft (Figure 3).
Figure 3: Radar beam expansion
Source: Aircraft image from FlightSafety International–Super King Air 200/B200 pilot training manual 2002
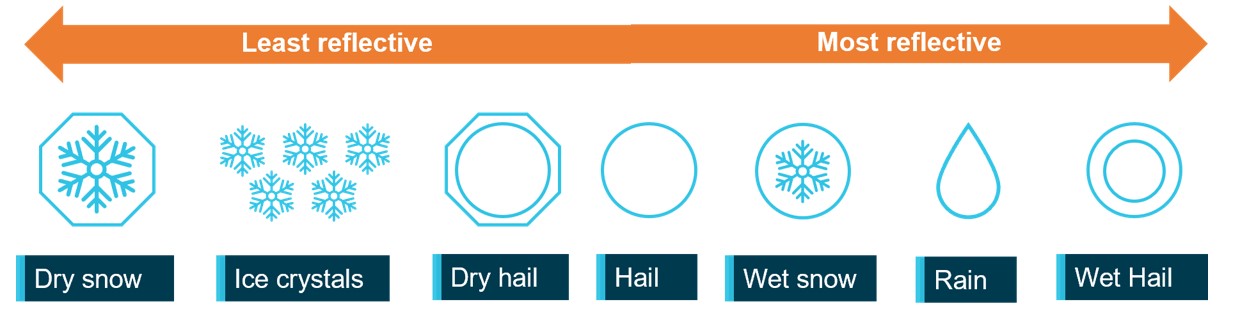
The reflectivity of precipitation is dependent on the type of precipitation, which itself is affected by the outside air temperature (Figure 4). Lower air temperatures, where the precipitation has not yet frozen, results in good reflectivity and useful information presented to the pilot. However, frozen materials are less reflective and can be misrepresented or undetected. The weather radar training course stated that the least reflective areas occur below −20°C.
Figure 4: Reflectivity of precipitation types
ATSB’s recreation of a similar image from the weather radar training video. Source: ATSB
As the temperature of precipitation within a cloud decreases with altitude, the proportion of liquid water in the atmosphere will also decrease. That will generally reduce the reflectivity within the cloud. This means that a thunderstorm does not have the same reflectivity over its altitude range with the lower/middle altitudes of the cloud having much better visibility to weather radar.
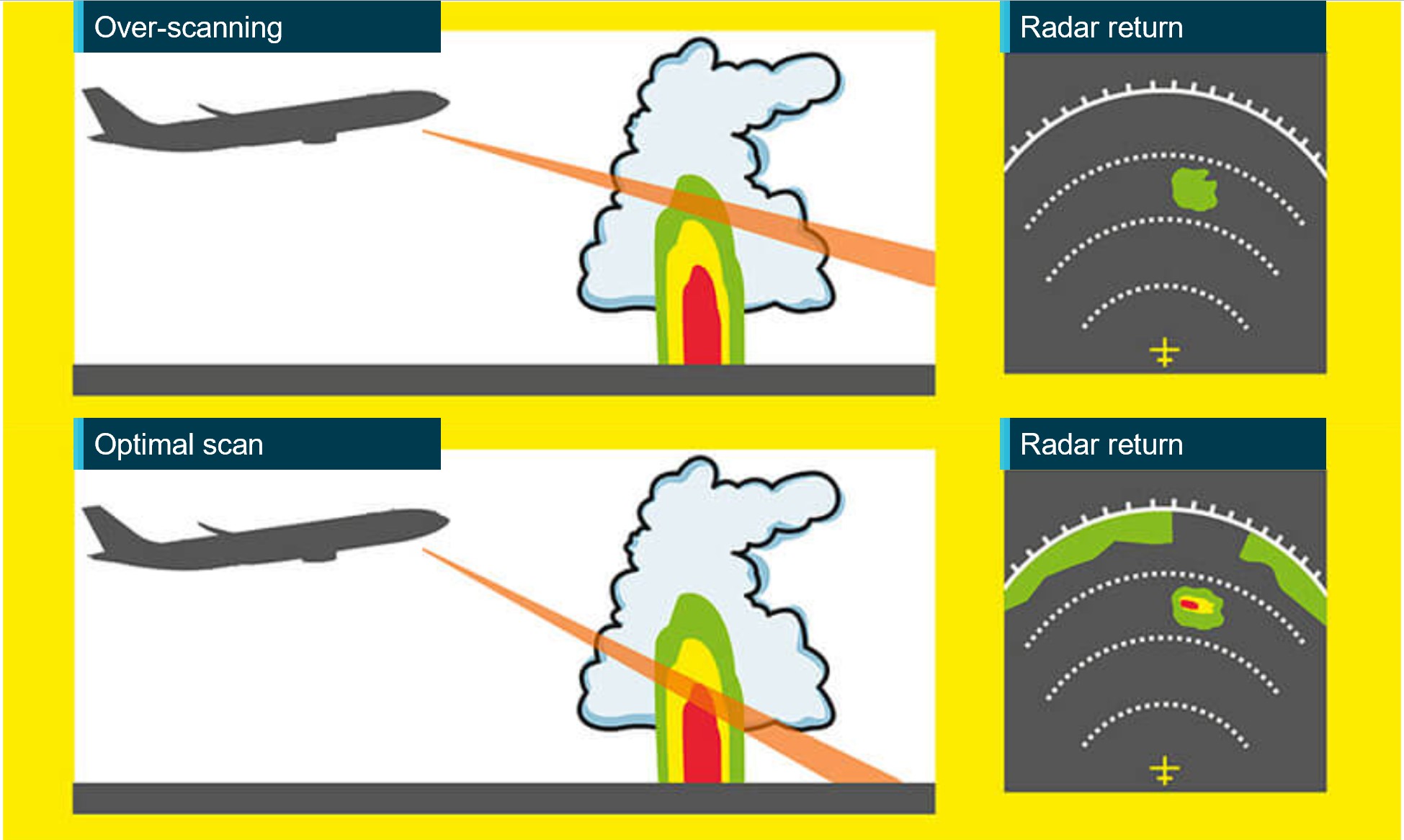
The weather radar automatically pans left and right multiple times per minute to continually refresh the information provided to the pilot. The pilot can adjust the beam position by tilting the antenna up or down, with the maximum tilt angle of 15°, both up and down. If the radar beam is tilted too low, it can return terrain which can be misinterpreted as weather, this is known as ground clutter. To reduce ground clutter, the manufacturer advised the best practise is to set the tilt angle so ground returns are visible, then slowly tilt the radar up until the ground clutter is minimised.
Over-scanning occurs when the weather radar tilt angle is set too high, providing an inaccurate radar return (Figure 5).
Figure 5: Over-scanning
Source: Optimum use of weather radar, Safety first | July 2016 - Airbus S.A.S, annotated by the ATSB
When the pilot in command was asked about their technique for determining the best tilt angle, they described a similar method. They could not recall the exact tilt setting used on the day however, stated that they believed it was set at a 1° up tilt.
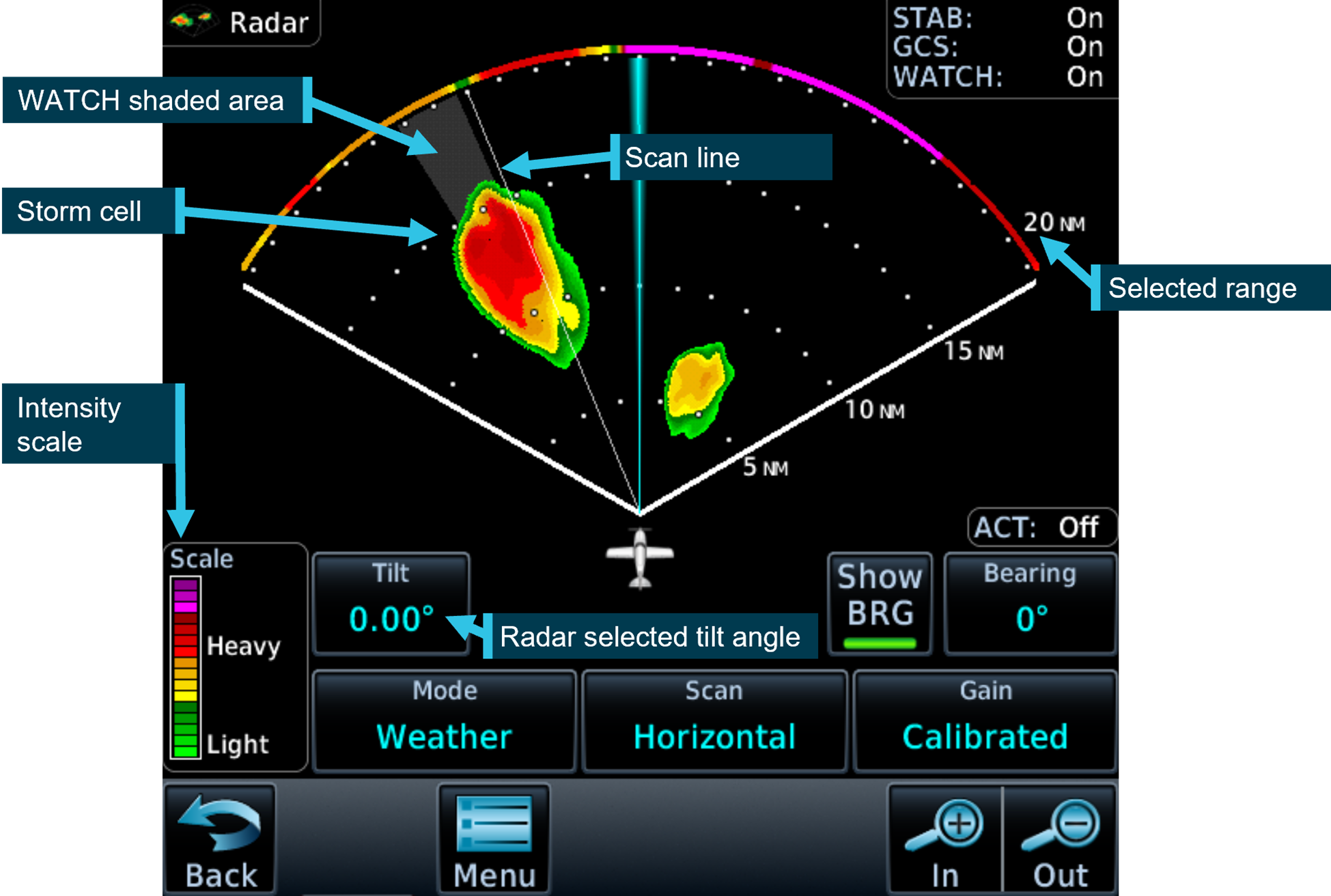
If the radar detects a return, it is displayed to the pilot in different colours, dependent on the intensity of the return (Figure 6).
Figure 6: Garmin GTN 700 series weather radar
Source: Garmin GTN700 series manual, annotated by the ATSB
The weather radar has multiple options and settings to assist the pilot under different circumstances. The pilot reported that during the occurrence flight the range was set to 80–100 NM (148–185 km) and the following settings were used:
Table 1: Weather radar settings
Radar optional setting
Active (ON/OFF)
Description
Altitude compensation tilt
ON
Automatically adjusts the tilt during climb and descent to keep centre of beam at same altitude (75% of selected range). The manufacturer recommend turning this setting off once reaching desired altitude.
WATCH
(default position is ON and pilot did not recall changing this setting)
Weather attenuated colour highlight (WATCH), highlights areas that are likely associated with radar shadow.[5]
Weather messages
ON
Provides alerts when presence of heavy precipitation beyond the currently displayed range and 80 to 320 NM from aircraft present position. Messages appear when the detected weather is within 10° of current heading.
Antenna stabilisation
ON
Corrects for pitch and roll changes, it keeps radar beam relative to horizon as aircraft attitude changes.
The pilot’s guide stated the following:
The GWX weather radar should be used to avoid severe weather, not for penetrating severe weather. The decision to fly into an area of radar targets depends on target intensity, spacing between targets, aircraft capabilities, and pilot experience.
The weather radar training video stated that intense returns should be avoided by at least 20 NM (37 km).
The aircraft flight manual made the following statement regarding the use of weather radar:
Airborne weather avoidance radar is, as its name implies, for avoiding severe weather – not for penetrating it… Thunderstorms build and dissipate rapidly. Therefore, do not attempt to plan a course between echoes[6]…Remember that while hail always gives a radar echo, it may fall several miles from the nearest visible cloud and hazardous turbulence may extend to as much as 20 miles from the echo edge, avoid intense or extreme level echoes by at least 20 miles; that is, such echoes should be separated by at least 40 miles before you fly between them…
The operator’s exposition provided similar guidance to company pilots:
To minimise the risk of exceeding aircraft structural limitations due to thunderstorm turbulence,
the pilot in command should:
• ensure the aircraft does not take-off when thunderstorms are active within 10 NM of the aerodrome
• avoid thunderstorms enroute by diverting by a minimum of 10 NM upwind or 20 NM downwind
• the pilot in command must either hold or divert to an alternate aerodrome if a thunderstorm is within 20 NM of the destination aerodrome.
Forecast and reported areas of turbulence should be avoided whenever possible.
Weather radar installation
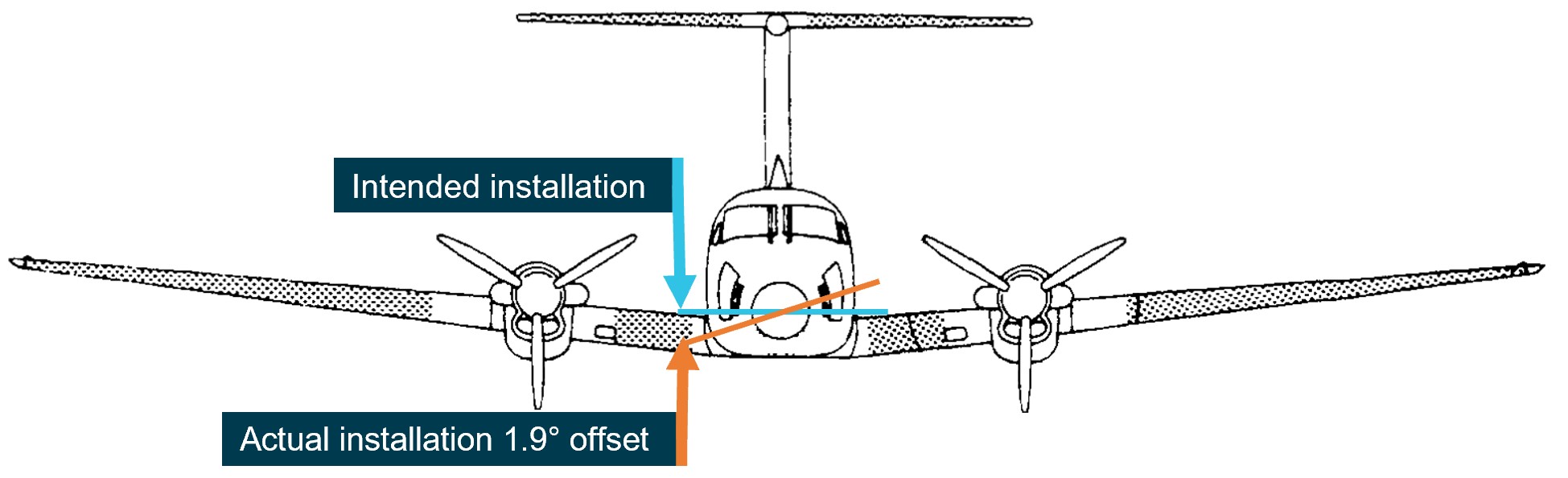
The operator advised that, as part of an aircraft upgrade, the weather radar was installed approximately 3 weeks prior to the occurrence. During the installation, it was inadvertently mounted into position offset from the lateral aircraft axis by approximately 1.9° right side low, rather than level (Figure 7).
Figure 7: Installation of the weather radar on VH-ZMW
Source: VH-ZMW flight manual, annotated by the ATSB
This meant that, with the aircraft level, when the radar panned to the maximum left position, it was tilted up 1.9° and at the maximum right position, it was tilted down 1.9°. This resulted in ground clutter appearing on the right side of the radar when the left side was clear (Figure 8).
Figure 8: Weather radar ground clutter on VH-ZMW
Source: Operator, annotated by the ATSB
Effect on the weather radar returns
Using the return from 10 NM (18.5 km) in front of the aircraft as an example, for a correct installation, the beam scanned a vertical range of approximately 8,300 ft. Therefore, if the tilt was 0° approximately 4,150 ft would be scanned below the aircraft and 4,150 ft would be scanned above the aircraft.
Based on the pilot’s recollection that the tilt angle was set at 1° up tilt, the following would be true at approximately 10 NM (18.5 km) from the aircraft’s position at FL 260:
Table 2: Minimum and maximum radar scan altitudes
Aircraft altitude = FL 260
Left scan 1.9° up from centre
Centre scan 1° above aircraft attitude
right scan right 1.9° below centre
Maximum altitude scanned
FL 330
FL 310
FL 290
Minimum altitude scanned
FL 250
FL 230
FL 210
The table shows approximate values for an aircraft at FL 260, a 12-inch antenna, the radar set at a 1° up tilt and does not consider the curvature of the earth.
Autopilot
The aircraft was equipped with an autopilot that could manipulate the aircraft in pitch, roll, and yaw. The autopilot maintained lateral and vertical navigation based on the pilot’s mode selection.
The autopilot could be disconnected by pressing the autopilot ‘AP’ button on the device or by pressing the ’AP DISC / TRIM INT’ on the control yoke. Additionally, the manufacturer’s pilot’s guide stated:
Automatic disengagement may occur due to a failure within the … system, loss of both GPS and air data inputs, strong turbulence, or exceeding the engagement attitude limits.
Anti-icing and de-icing equipment
The aircraft was capable of flying into known icing conditions and was equipped with multiple anti‑icing[7] and de-icing[8] devices. The aircraft limitations required a minimum airspeed for sustained flight in icing conditions of 140 kt.
There was a pitot tube located on each side of the aircraft nose, and they were both equipped with individually‑selectable heating elements. The heated surface prevented ice from building up and blocking the pitot tube. Additionally, the stall warning vane was equipped with a heating element.
The propeller blades were equipped with electrically‑heated de-ice boots that loosened the attachment point of any ice build-up along the propeller blade. The ice was then detached due to forces associated with the rotating propeller. In the ‘AUTO’ position all electrical heating was provided to one propeller for 90 seconds and then cycled to the other propeller for 90 seconds.
De-ice boots were located on the leading edge of the wings and horizontal stabiliser. They were pneumatically inflated by bleed air[9] from the engines. The selector switch was spring loaded to the OFF position and could be selected to either single or manual. With single selected, the distributor valve opened to inflate the wing boots for approximately 6 seconds, it then deflated the wing boots and inflated the horizontal stabiliser boots for approximately 4 seconds, this completed the cycle. With manual mode selected, all boots inflated simultaneously and remained inflated until the switch was released.
There were 2 levels of windshield heat – normal and high. When normal mode was used, heat was applied to the majority of the windshield area. When high was selected, a higher level of heat was applied to a smaller area of the windshield.
Ice vanes in the air inlet of the engine cowl were required to be extended for operations in ambient temperatures of 5°C and below, when flight free of visible moisture could not be assured. When the ice vanes were extended, it introduced a sharp turn in the engine inlet air resulting in any moisture or frozen materials continuing undeflected, due to their momentum, and being discharged overboard. This reduced the amount of moisture entering the engine. When the ice vanes were in their extended position, the aircraft’s engine performance was reduced.
The pilot reported using the available anti-icing and de-icing equipment during the flight due to the accumulation of ice, which was observed to be building rapidly.
Turbulence
The aircraft flight manual specified a turbulence penetration speed of 170 kt. The flight manual also included the following caution for turbulent air penetration:
For turbulent air penetration, use an airspeed of 170 knots. Avoid over-action on power levers. Turn off autopilot altitude hold. Keep wings level, maintain attitude and avoid use of trim. Do not chase airspeed or altitude. Penetration should be at an altitude which provides adequate manoeuvring margins when severe turbulence is encountered.
Weather
Graphical area forecast
At 1417, a graphical area forecast (GAF) was issued for the south Queensland area. It was valid between 1500 and 2300, which included the planned and actual departure time. The GAF predicted occasional[10] cumulonimbus cloud (CB) from 4,000 ft extending above 10,000 ft. It also stated that CB implied severe icing and severe turbulence.
Icing
Ice can accumulate at temperatures below 0°C in visible moisture such as cloud and rain. According to the Bureau of Meteorology, the highest risk of ice accumulation is between 0°C and −15°C. However, ice can accumulate at temperatures as low as −40°C. The Bureau of Meteorology’s–Hazardous Weather Phenomena Airframe Icing stated:
The rate of ice accumulation is directly proportional to the amount of supercooled liquid water present. In clouds, the worst-case scenario is most likely to occur in towering cumulus and cumulonimbus because of their vertical extent, the abundant supply of moisture and the large droplet size found in them.
Severity classification
The Bureau of Meteorology classified icing into different severities, depending on the rate at which it accumulated:
• Trace is used when the rate of accumulation is slightly greater than rate of sublimation (the process of ice changing directly to vapour, bypassing the liquid phase).
• Light means the rate of accumulation may create a problem if flight is prolonged in the environment (i.e more than one hour). Occasional use of de-icing/anti-icing equipment is used.
• Moderate means the rate of accumulation is such that even short encounters become potentially hazardous, and use of de-icing/anti-icing equipment or diversion is necessary.
• Severe means the rate of accumulation is such that de-icing/anti-icing equipment fails to reduce or control the hazard, and thus an immediate diversion is necessary.
The Bureau of Meteorology classified turbulence intensity into categories dependent on perceived effect on the aircraft and occupants:
• Light is associated with momentary slight erratic changes in attitude and/or altitude. Rhythmic bumpiness. Airspeed fluctuations of 5–14 kt. G–loading of 0.15 to 0.49.
• Moderate is associated with appreciable changes in attitude and/or altitude. Pilot remains in control at all times. Rapid bumps or jolts. Airspeed fluctuations of 15–24 kt. G-loading of 0.50 to 0.99.
• Severe is associated with large abrupt changes in attitude and/or altitude. Momentary loss of control. Airspeed fluctuations greater than 25 kt. G-loading of 1.00 to 1.99.
• Extreme is associated with a very difficult to control aircraft. May cause structural damage. Airspeed fluctuations of greater than 25 kt. G-loading of greater than 2.00.
SIGMET
SIGMET[11] E01 was issued at 1416 and was valid between 1416 and 1630. It identified frequent[12] thunderstorms with hail. The top of the storms was stated as FL 450 and the storms were moving east-north‑east at 15 kt. SIGMET E01 covered the area west of Toowoomba Airport and the intended flight path went through the affected area (Figure 9).
Figure 9: SIGMET area
Source: Bureau of Meteorology provided SIGMET E01, ATSB annotated and re-created the SIGMET co-ordinates on Google Earth.
The SIGMET validity period for thunderstorm activity was no longer than 4 hours or the time specified. SIGMET E01 was valid for 2 hours and 14 minutes. The Bureau of Meteorology stated that the shorter validity period was an indication that the forecast weather phenomena was expected to have ceased by the end time stated. The pilot obtained and reviewed this SIGMET, which was available prior to their departure.
A follow-up SIGMET was issued at 1641, 10 minutes after the aircraft became airborne. It also identified frequent thunderstorms with hail in the area. Air traffic control provided the new SIGMET information to the pilot at 1653 after the aircraft had already entered significant weather.
Ground‑based weather radar
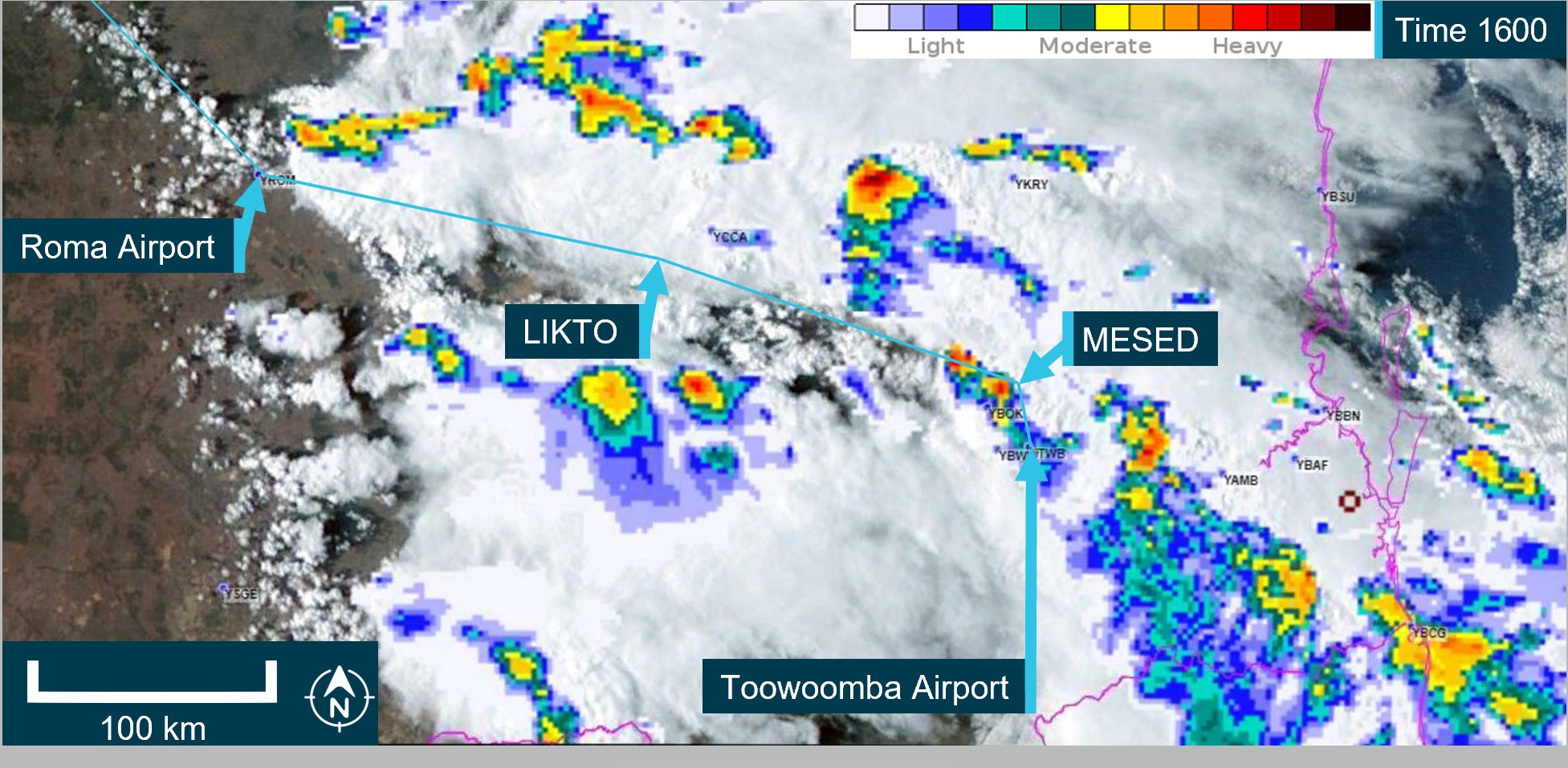
The Bureau of Meteorology provided the ATSB with ground-based weather radar images at different intervals throughout the flight. The ground-based weather radar available to the pilot prior to departure, showed that, apart from the storm activity in the vicinity of Toowoomba (that the pilot delayed the departure for), moderate level precipitation could be avoided by 20 NM (37 km) along the planned departure route (Figure 10).
Figure 10: 1600 Ground‑based weather radar
The image shows the route B flight path at 1600 which was the planned departure time. It is a combination of satellite and weather radar. Source: The Bureau of Meteorology provided weather radar and satellite image, ATSB overlaid on Google Earth and annotated.
Flight data
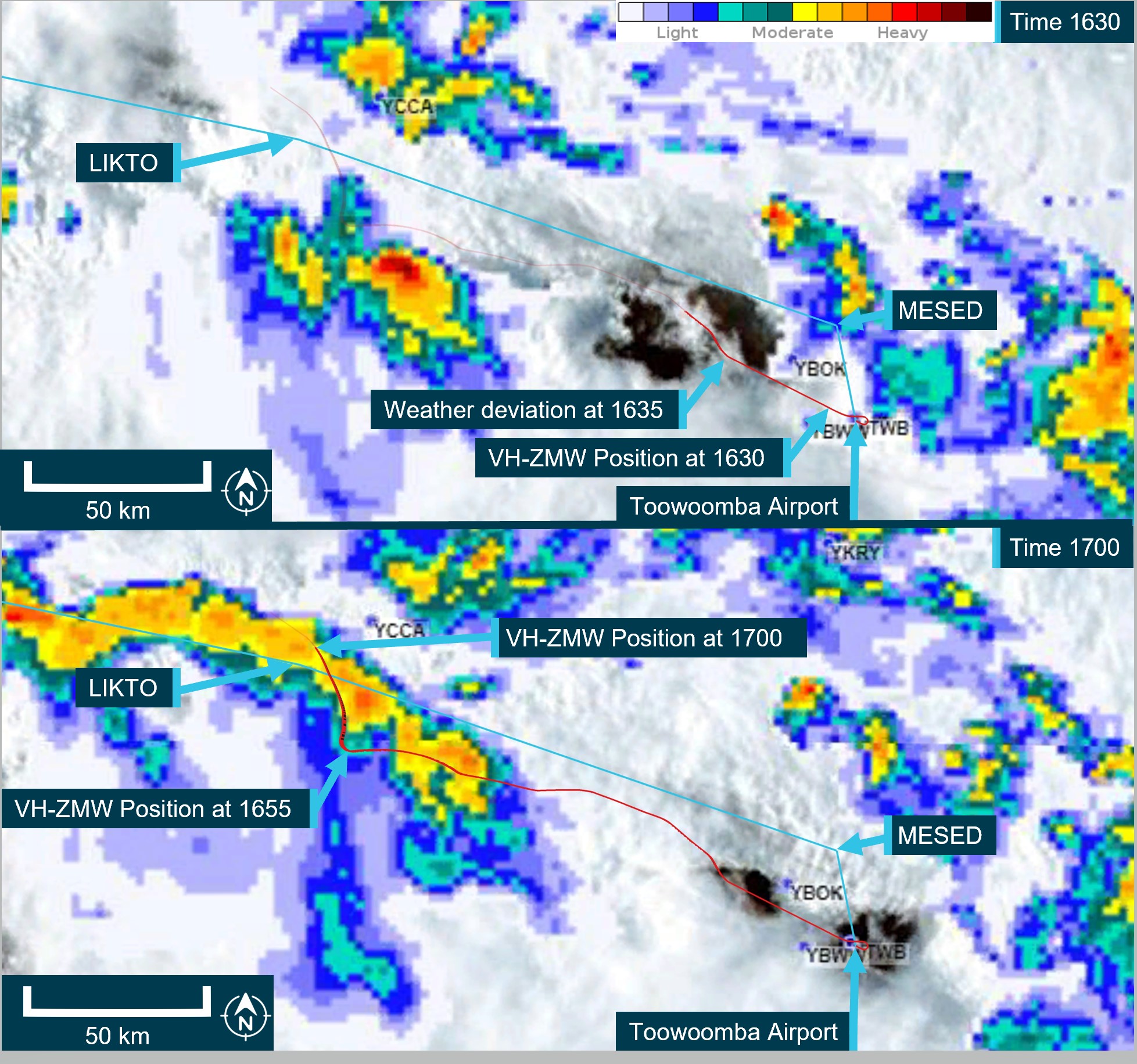
The ATSB obtained flight data information from the aircraft’s on-board recorder, the pilot’s EFB, and third‑party ADS-B recorded information. The ATSB used this data to determine the aircraft’s position, altitude, and speed at different times throughout the flight. This data was overlaid on the weather radar information provided by the Bureau of Meteorology (Figure 11). At 1630, there was less than 20 NM between intense weather returns. However, this was after the aircraft had departed.
Figure 11: Ground - Based weather radar at 1630 and 1700
The image shows the route B flight path in blue with the actual aircraft flight path in red. It is a combination of satellite and weather radar. Source: The Bureau of Meteorology provided weather radar and satellite image, ATSB overlaid on Google Earth and annotated. Flight data provided by ADS-B exchange.
Flight planning
Flight route
The En Route Supplement Australia (ERSA) outlined the flight planning requirements for flights departing from Toowoomba Airport. It stated that when departing west, flights should plan via the MESED waypoint then to LIKTO. This was consistent with the flight plan the pilot submitted to ATC prior to departure.
The pilot later reported to the ATSB that it was normal to request the next tracking point after MESED when there was no requirement for traffic avoidance and Oakey military airspace was not active. Several recent flights completed by VH-ZMW showed that the aircraft did not initially track via the MESED waypoint.
Fuel planning
The company used fuel planning software to plan company flights. The ATSB reviewed the fuel plan calculated for this flight (Table 3).
Table 3: Fuel plan
Phase of flight
Minutes
Litres (lbs)
Climb
20
150 (264)
Cruise
184
1158 (2038)
Alternate
22
188 (331)
Trip fuel
204
1308 (2302)
Contingency fuel
20
130 (230)
Final reserve
30
164 (289)
Additional fuel
0
0
Holding
30
148 (260)
Approach
0
Taxi
51 (90)
Fuel required
307
1990 (3503)
Margin
–8
–42 (–75)
Endurance
300
1947 (3428)
As the aircraft planned to arrive at Normanton after last light, the aircraft was required to carry alternate fuel but was not required to carry both alternate and holding fuel. This was to ensure that if the aerodrome lighting could not be activated, there was sufficient fuel available to divert to a suitable airport.
The company exposition required that the flight plan include contingency fuel[13] and final reserve fuel.[14] The exposition stated that for the B200 aircraft, the final reserve fuel was 198.8 L (350 lbs). However, the software was using an incorrect lesser figure for the final reserve fuel of 164 L. As the pilot had added the extra holding fuel, the deficiency of 35 L was not an issue for this flight.
In addition, the pilot advised that they had planned to fly overhead Hughenden, and if their in-flight fuel replanning indicated that they required more fuel, they had planned that they would land and refuel.
Related occurrence
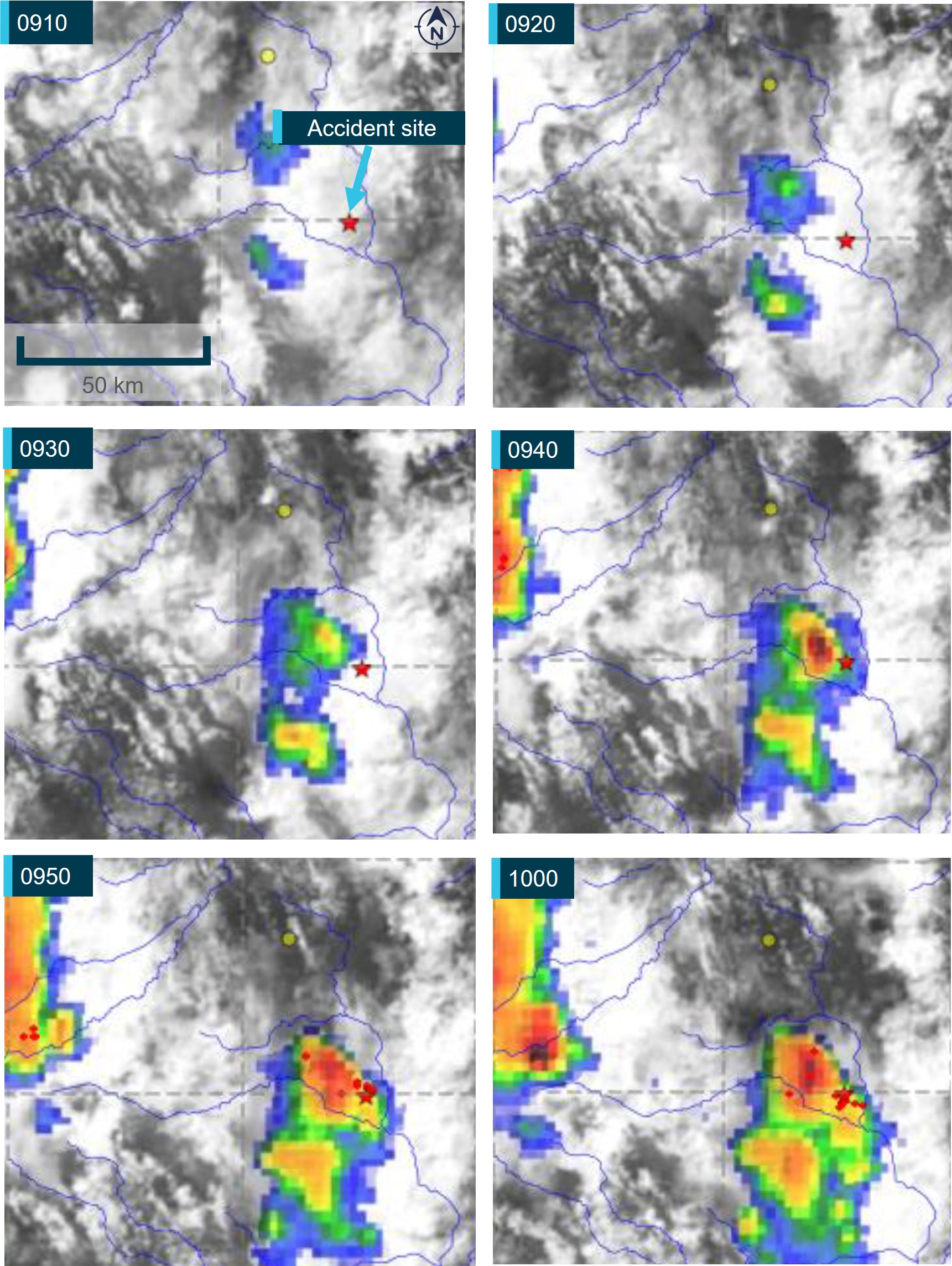
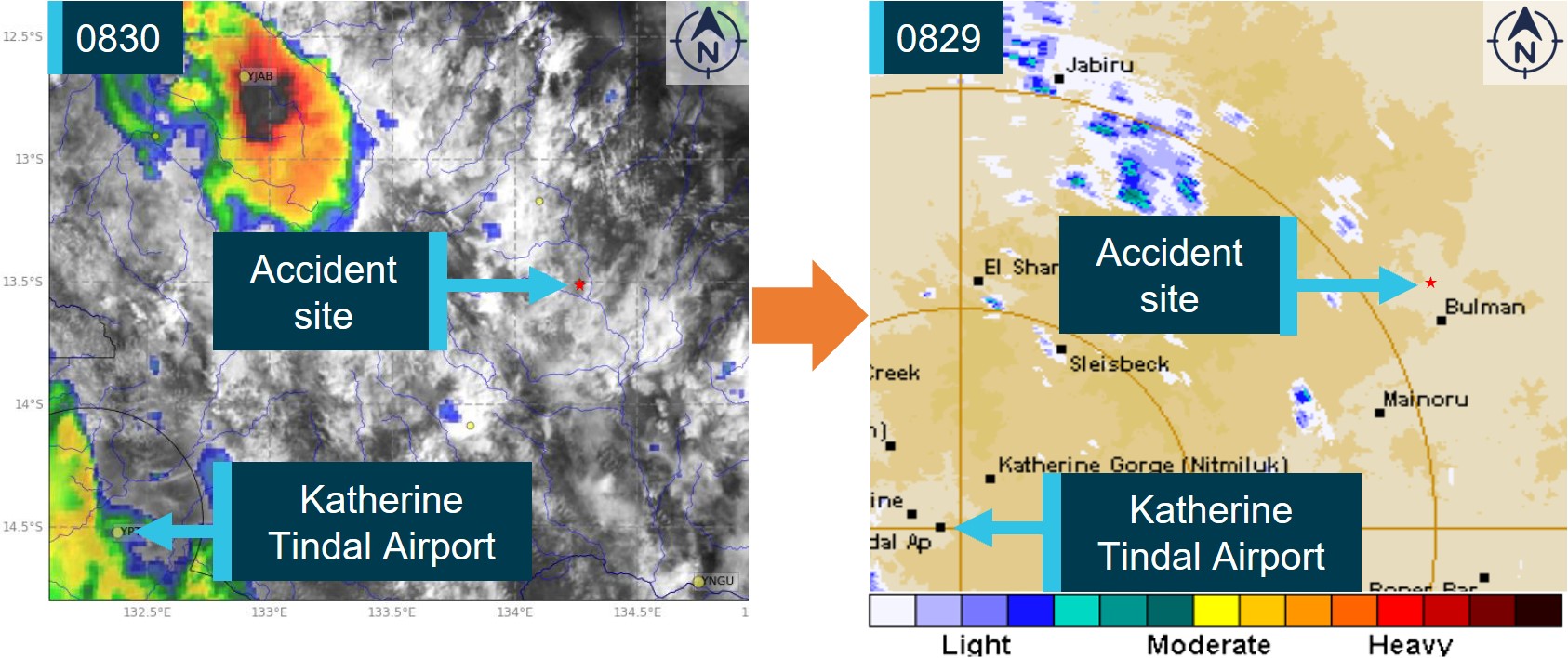
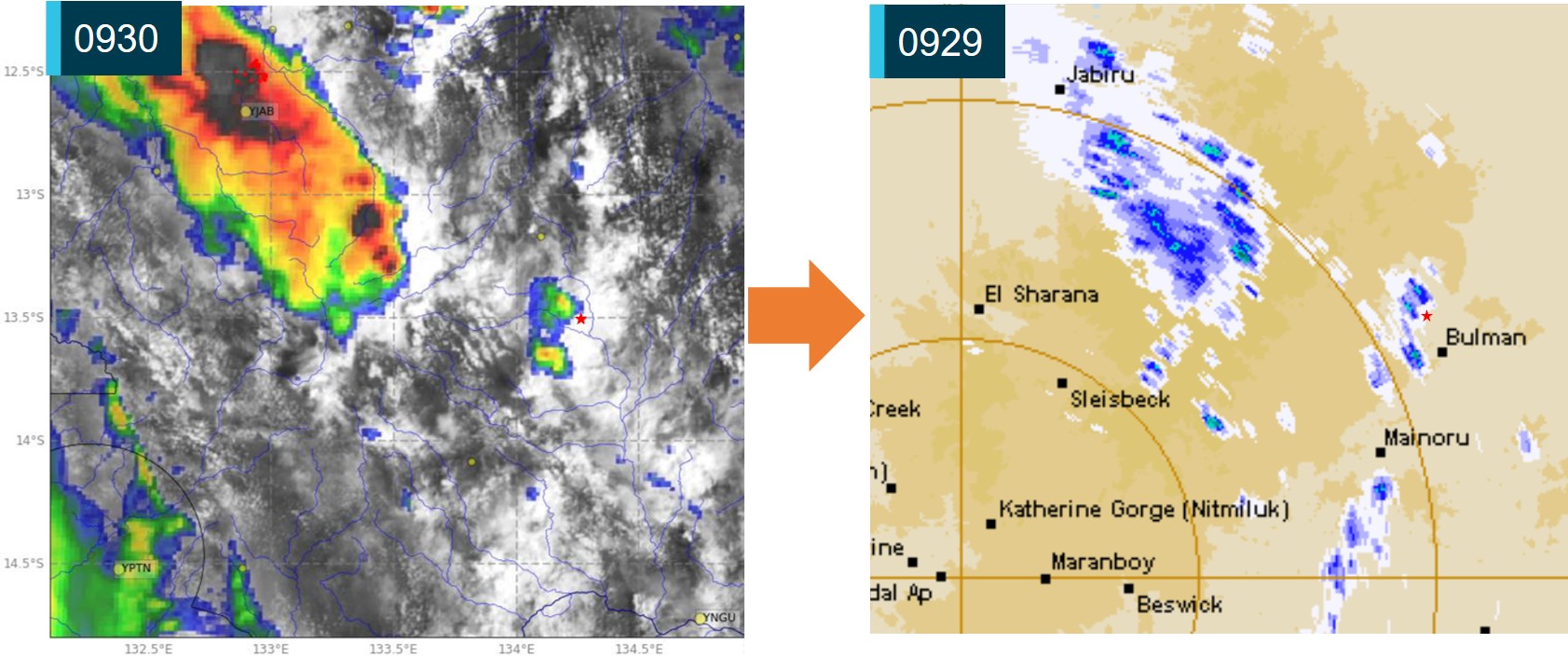
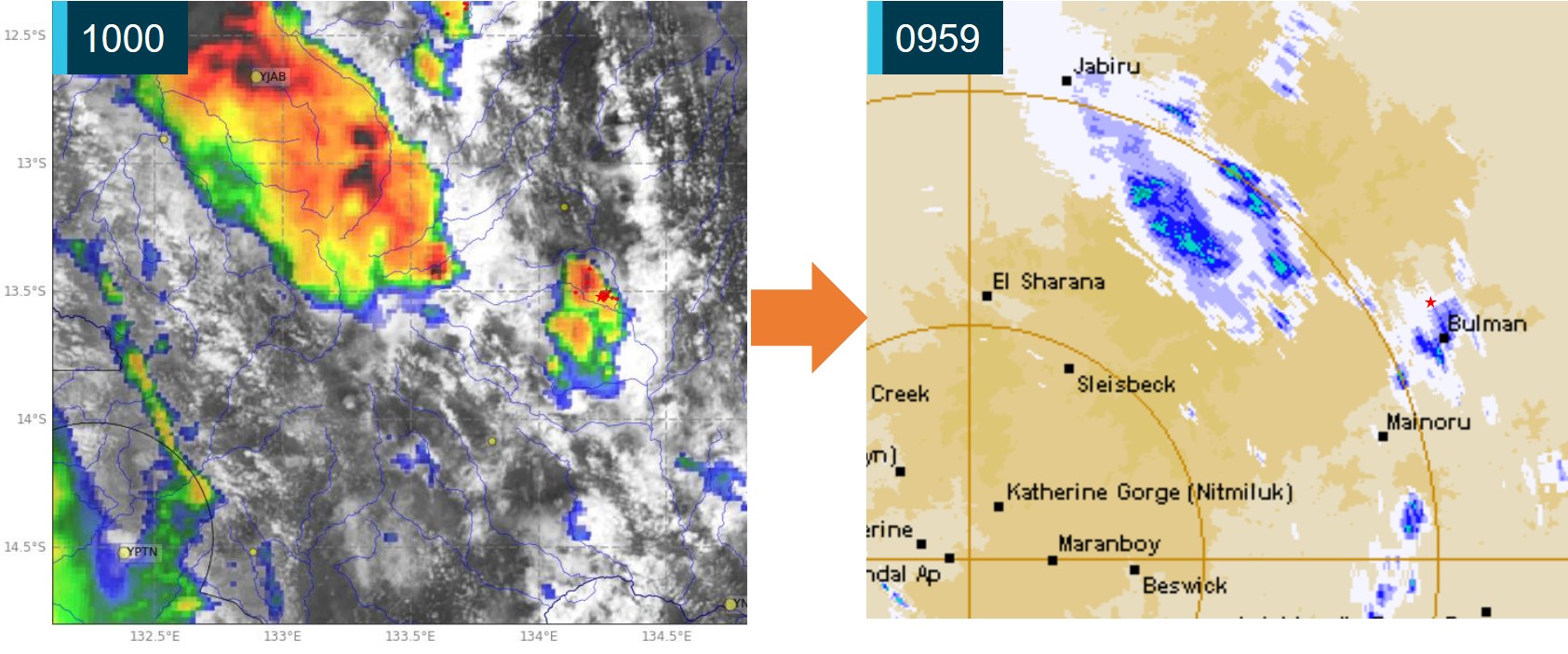
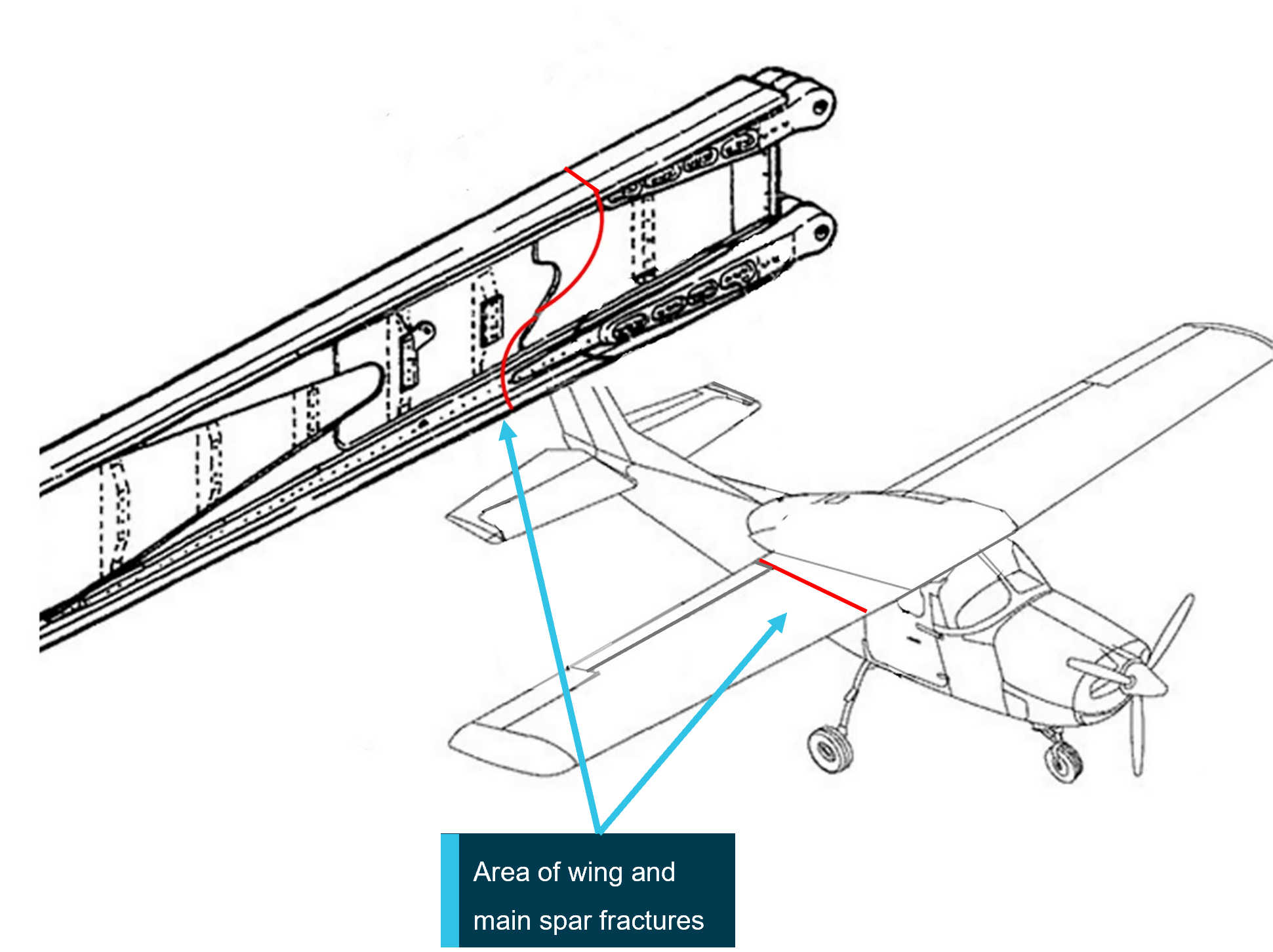
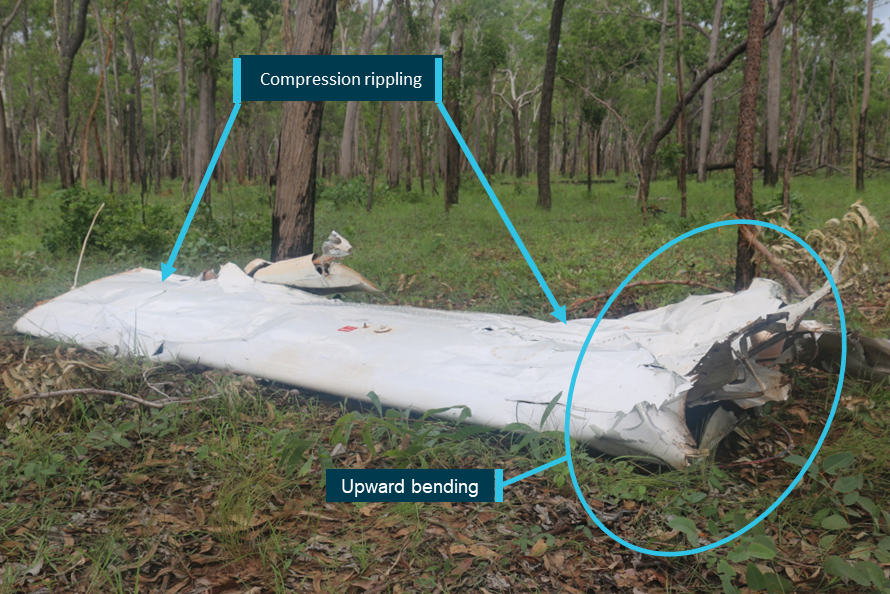
In-flight break-up involving Cessna 210N, VH-TFT, 237 km east-north-east of Katherine, Northern Territory, on 24 December 2022 (AO-2022-067).
Upon arrival overhead the Bulman region, the aircraft likely entered an area of strong convective activity from a rapidly developing thunderstorm, which probably resulted in exposure to a combination of severe turbulence and reduced visibility for the pilot.
It is probable that a combination of turbulence encountered from the thunderstorm, airspeed, and control inputs led to the excessive structural loading and in-flight separation of the right wing from the fuselage before the aircraft collided with terrain.
Safety analysis
Before departing, the pilot utilised multiple sources of information to assist with their decision‑making, resulting in them delaying their departure to avoid encountering a thunderstorm. The SIGMET received indicated that the forecast frequent thunderstorms were due to dissipate around the aircraft’s departure time. However, the graphical area forecast still showed occasional thunderstorms were forecast. The ground-based weather radar at 1600 showed that moderate precipitation could be avoided by 20 NM (37 km) along the planned route after the thunderstorm overhead Toowoomba had passed. As they taxied at 1620, the pilot was informed that there was significant build-up of cloud in the area they planned to fly through.
The route flown by the pilot took them in a direction towards that developing cloud, the effects of which were also visible on the ground-based weather radar prior to departure. During climb, the pilot remained in visual conditions until FL 260. However, once they entered cloud at FL 260, they were reliant on the weather radar, which had been installed incorrectly, to identify and avoid thunderstorms.
The incorrect installation resulted in increased ground clutter on the right side of the screen. This meant that using the recommended method for setting the tilt resulted in a higher initial baseline tilt angle. This most likely resulted in the radar beam scanning the tops of the clouds rather than the most reflective areas within a storm. This would have been exacerbated on the left side due to the increased tilt on that side.
In addition, the outside air temperature at FL 260 was −23°C, resulting in less reflective precipitation within the clouds. As it was likely that the weather radar was over-scanning and therefore, the weather radar returns presented to the pilot would not have indicated where the most active storms were. This likely resulted in the severity of the storms in the area not being visible to the pilot.
It is likely that the pilot’s in-flight assessing and planning was influenced by the airborne weather radar information, and they did not remain clear of thunderstorms by the recommended 20 NM (37 km). The ADS-B data overlaid on the ground-based radar along with the pilot’s recollection of visible lightning, turbulence, and icing are all consistent with flying into a thunderstorm.
Although the aircraft had sufficient fuel on board for the planned flight, the final reserve figure used during planning was less than the figure stipulated in the operator’s exposition. While it did not contribute to this incident, it did increase the risk of landing below the final reserve fuel.
Finally, the pilot’s pre-flight safety briefing to the passengers, which included the potential for encountering turbulence, and their decision to keep the seatbelt sign on, reduced the likelihood of passenger injuries when the aircraft encountered turbulence.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the flight into a thunderstorm involving Beech Aircraft B200, VH-ZMW, 108 km west‑north‑west of Toowoomba, Queensland on 9 October 2024.
Contributing factors
During the cruise the aircraft entered a thunderstorm, resulting in minor damage to the aircraft.
As a result of incorrect installation, the aircraft’s weather radar provided misleading information to the pilot. This reduced its effectiveness at detecting significant weather.
Other factors that increased risk
The pilot’s fuel planning, using the company software, included a final reserve that was less than the operator’s requirement.
Other findings
Prior to departure, the pilot informed the passengers of possible turbulence and kept the seatbelt sign on throughout the flight. This briefing and decision‑making likely contributed to the safety of the passengers when turbulence was experienced.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Austrek Aviation
the operator identified and implemented an enhanced radar manufacturer training course for its pilots, specific to the installed GWX 70 radar
the incorrect antenna installation has been rectified
the flight planning software has been reviewed to ensure that the parameters are as specified in the company exposition
although fatigue was not considered to be a safety factor in the occurrence, the company has adopted the use of the Samn-Perelli Seven Point Scale fatigue reporting tool, for sign‑on and sign‑off to improve monitoring of pilot fatigue due to roster patterns.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot
the operator’s safety manager
Bureau of Meteorology
Garmin manuals and online weather radar training video
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
the operator
Civil Aviation Safety Authority
Textron Aviation
United States National Transportation Safety Board
A submission was received from:
the operator
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Build-ups: a general term describing convective activity and maturing clouds that are developing into thunderstorms.
[2]Waypoint: a geographical location referenced by a 5-letter identifier used for navigating.
[3]Flight Level: the aircraft altitude above sea level when the atmospheric pressure is equal to 1013 hPa. FL 240 equates to 24,000 ft.
[4]Radome: protective nose area of the aircraft which houses the airborne weather radar.
[5]Radar shadow: when the radar beam encounters precipitation, it is reflected before it can penetrate the weather fully. This leaves some areas unscanned and consequently will appear free of weather to the pilot but have the potential to be areas of heavy precipitation.
[6]Echoes: The radar returns that are displayed to the pilot.
[7]Anti-icing: devices that attempt to prevent the accumulation of ice on the aircraft.
[8]De-icing: devices that attempt to remove accumulated ice from the aircraft.
[9]Bleed air: compressed air taken from the engine to be used for other system purposes.
[10]Occasional: Well-separated features which affect, or are forecast to affect, greater than 50% but not more than 75% of an area.
[11]SIGMET: Significant Meteorological information provides a concise description concerning the occurrence or expected occurrence, in areas over which meteorological watch is being maintained, of en-route weather phenomena that are potentially hazardous to aircraft.
[12]Frequent: An area of thunderstorms with little or no separation between adjacent storms and covering more than 75% of the affected area.
[13]Turbine-engine aircraft – 5% of the flight fuel (not less than 5 minutes at holding speed at 1,500 feet above the destination aerodrome).
[14]Turbine-engine aircraft – fuel required to fly at 1,500 ft above aerodrome elevation for 30 minutes and must be remaining on completion of landing at the destination (or destination alternate).
On 4 May 2024, a Boeing 737, operated by Qantas Airways Limited, departed Sydney, New South Wales for a scheduled passenger carriage flight to Brisbane, Queensland. In the latter stages of descent, the aircraft entered a band of approaching cloud. While the flight crew expected some turbulence associated with the entry to cloud, after passing 11,400 ft about 36 km south‑east of Brisbane, the aircraft experienced unanticipated severe turbulence. Three cabin crew were unrestrained and suffered various injuries during the occurrence. Two received minor injuries, including a facial injury and concussion, whilst the third was seriously injured with a fractured ankle.
What the ATSB found
The ATSB found that the captain did not inform the cabin crew about the expected turbulence during descent, likely due to not being aware of its severity. This resulted in 3 unrestrained cabin crew being injured during severe turbulence.
Following the turbulence, the captain instructed all passengers and crew to return to their seats and fasten seatbelts. However, 2 cabin crew and 2 passengers remained unrestrained in the rear galley to assist the seriously injured crew member during landing. When the flight crew were informed of this, the captain repeated the instruction that everyone besides the injured crew member was to return to their seats for landing. Assuming the cabin would be secured after the repeated instruction, the flight crew proceeded with the landing, unaware that 4 crew and passengers remained unrestrained. Qantas 737 standard operating procedures relied on the customer service manager to inform the flight crew if the cabin crew had not secured the cabin for landing.
A crew member who had sustained a concussion returned to work before seeking medical treatment. The ATSB found that the operator did not have a procedure to ensure that crew were assessed for fitness for duty after a significant injury.
What has been done as a result
Qantas has updated the integrated operation control procedures for requesting medical assistance for cases where any crew member or passenger is significantly injured. Updated protocols now mandate that a doctor will immediately be required to assess the fitness of cabin crew members prior to commencing any further work‑related duties. Additionally, the operator will arrange immediate medical assessment following any turbulence or unplanned aircraft movement classified as moderate or severe with injuries or unrestrained crew.
Safety message
Effective coordination and communication among all crew members is critical in managing turbulence and ensuring cabin safety. This coordination should extend beyond pre‑flight briefings to include continuous communication throughout the flight, particularly during periods of increased workload and operational complexity.
Collaboration between the flight and cabin crew helps ensure the timely completion of service‑related tasks while minimising the risk of injury during known or anticipated encounters with turbulence.
Flight crew rely on clear and timely communication from the cabin crew to maintain awareness of the condition in the cabin. When there is a different understanding of the state of the cabin, there is an increased risk delayed responses or misaligned decision‑making which may lead to safety being compromised.
Aircraft are more likely to experience the effects of weather and wake turbulence during the descent, approach, and landing phases of flight, highlighting the importance of effective communication procedures to promote cabin safety and minimise the risk of injury to passengers and crew.
The occurrence
On 4 May 2024, a Boeing 737, registered VH‑VYK, being operated by Qantas Airways Limited as QF520, departed Sydney, New South Wales on a scheduled flight to Brisbane, Queensland. The aircraft departed Sydney at 1202 local time and was scheduled to arrive in Brisbane at 1335. On board was the flight crew, comprised of the captain and first officer (FO), a customer service manager (CSM) supported by 3 cabin crew members, and 143 passengers.
Prior to departing Sydney for Brisbane, the captain recalled briefing the CSM about leaving the seatbelt sign on for the departure from Sydney due to weather, however neither the captain nor the CSM could recall any specific details regarding the weather conditions in Brisbane.
Descent into Brisbane
At about 1300, the flight crew commenced their descent into Brisbane while approaching Lismore, New South Wales. As the aircraft continued descent towards Coolangatta, Queensland, the captain visually observed cloud over Moreton and Stradbroke islands, but recalled no weather radar indications that identified precipitation normally associated with increased turbulence.
After passing 30,000 ft above mean sea level (AMSL) at 1303, the captain, who was pilot monitoring, recalled performing the ‘prepare cabin’ public announcement (PA), and the cabin crew commenced securing the cabin for landing. About 6 minutes later, the captain contacted the CSM to enquire about the amount of time the cabin crew required to complete their cabin preparations. At about 15,000 ft AMSL, the aircraft entered a thick layer of stratiform[1] cloud with minimal turbulence observed initially by either the flight or the cabin crew. The CSM advised the captain the preparations would take about 2 minutes. About 2 minutes later, the captain turned on the seatbelt sign and announced the ‘seatbelts PA’.
Immediately after the captain turned on the seatbelt sign, the CSM and the 2 cabin crew members in the aft galley completed their duties as per the procedures. The CSM made a PA while standing in the forward galley, then checked and locked their assigned lavatory. The 2 cabin crew members in the rear galley got out of their jump seats to verify that the lavatories were vacant before locking them.
At about this time, the captain observed a cumulus[2] cloud embedded in the stratiform layers. However, there was no radar return consistent with increased turbulence, and the cloud did not appear to be overly concerning in terms of turbulence risk from their shape or size.
After descending below 12,000 ft AMSL at 1311, the aircraft encountered a severe turbulence event less than one minute after the seatbelt sign was illuminated, while 3 cabin crew were unrestrained. The CSM recalled observing the right 2 primary (R2P) cabin crew member at the rear galley rising off the floor and colliding with the aircraft's ceiling. They immediately fell back to the floor, landing on their right ankle. The R2P felt a crushing sensation as they landed on their ankle and experienced intense pain and was unable to move.
Events in the cabin
The CSM contacted the captain to inform them that the R2P was injured and that some passengers were standing. The captain responded with instructions that all passengers and cabin crew must remain seated. Following this interaction, the CSM made a public announcement to remind passengers to stay seated and to request assistance from the cabin crew if needed. The captain contacted the operator’s Brisbane airport coordinator to advise that there was an injured cabin crew member and medical assistance would be required on arrival in Brisbane. Queensland Ambulance service records showed that a request for an ambulance was received at 1315.
Although being instructed to remain seated, the CSM immediately moved to the rear of the aircraft to assist the injured R2P in the aft galley. There, they observed the injured R2P lying on the floor while a passenger was holding their leg. Another passenger, who identified themselves as a doctor, offered to assist with providing first aid. Meanwhile, another cabin crew member, the left two primary (L2P), was supporting the R2P’s head.
At this point, the CSM advised the L2P and the passengers that the captain had instructed everyone to return to their seats. However, they were unwilling to leave the R2P unattended. The CSM instructed the L2P to advise the captain of the situation. The CSM then retrieved the physician's kit from the front of the cabin. At this point, the passenger seated in 3F advised the CSM that they were a travelling cabin crew member and were able to assist.
The L2P contacted the captain to advise that all the occupants located in the rear galley were still unrestrained. However, the captain did not recall receiving requests for additional time to address the situation. The captain reiterated that all uninjured occupants must return to their seats as the aircraft was in the final stages of the approach and would be landing soon.
The CSM subsequently returned to the rear galley with the physician’s kit and the off‑duty cabin crew from 3F, who subsequently relieved the passenger who was holding the R2P’s leg. While the CSM was attempting to provide first aid and preparing a splint with the assistance of the travelling doctor, a passenger seated in 30D yelled, ‘we’re about to land’. Shortly after at 1322, the aircraft landed in Brisbane with 4 unrestrained passengers and cabin crew in the rear galley. The flight crew taxied the aircraft to its assigned gate, arriving at 1328, with paramedics in attendance at 1338.
Context
Flight crew information
Captain
The captain held an Airline Transport Pilot (aeroplane) Licence with an instrument rating and a Class 1 aviation medical certificate. They had 23,177 flight hours, including 15,005 hours on the Boeing 737, and had logged 165 hours on the 737 in the last 90 days.
The captain reported sleeping 7 hours the night before the occurrence. They were awake for 8 hours and 45 minutes at the time of the occurrence and reported feeling ‘responsive, but not at peak’.
First officer
The first officer held an Airline Transport Pilot (aeroplane) Licence with an instrument rating and a Class 1 aviation medical certificate. They had 10,163 flight hours, including 1,717 hours on the Boeing 737, and had logged 152 hours on the 737 in the last 90 days.
The first officer reported sleeping 7 hours the night before the occurrence. They were awake for 8 hours and 45 minutes at the time of the occurrence and reported feeling ‘somewhat fresh’.
Cabin crew
The cabin crew on board was comprised of a complement of 4 members, with their assigned jump seats located in the forward and aft galleys. Each cabin crew member was responsible for one of the 4 main cabin doors (Table 1) during critical phases of flight, with their assigned jump seat (Figure 1) located immediately next to their assigned door. The cabin crew were under the supervision of the customer service manager (CSM) who was responsible to the captain for administration of in‑cabin service and liaison with the crew for all service and safety related matters.
Table 1: Cabin crew door assignment
Cabin Door
Cabin crew assignment
Left one (L1)
Customer service manager (CSM)
Right one (R1)
Right one primary (R1P)
Left two (L2)
Left two primary (L2P)
Right two (R2)
Right two primary (R2P)
Figure 1: 737 Cabin layout, doors and assigned jump seats for cabin crew
Source: Qantas, annotated by the ATSB
Cabin crew injuries
R2P
The R2P had been in the process of taking their seat when the turbulence occurred. They rose into the air during the turbulence, struck their head on the ceiling, and landed heavily on their feet. R2P immediately fell to the galley floor and told L2P that they were injured, possibly with a broken bone. They were later diagnosed in the hospital with a fracture involving 2 breaks in the ankle and another break in the leg, which required surgery.
CSM
The CSM sustained minor injuries due to striking aircraft fixtures while standing unsecured during the turbulence. The CSM self‑assessed their injuries and applied first aid the following day after noticing minor pain, including discomfort in their lower back and right shoulder blade. They also became aware of facial pain 2 days after the event.
L2P
The L2P sustained a head injury, due to striking the ceiling or other aircraft fixtures during the event but did not initially believe they were injured. They had several rostered days off after the event. They returned to work on 11 and 12 May and were made aware by co‑workers that they were displaying symptoms of possible injury. On 16 May, 12 days after the turbulence event, they were diagnosed with concussion after a consultation with their general practitioner.
Aircraft
The aircraft was registered as VH‑VYK in Australia on 11 January 2006, serial number 34183. The Boeing 737‑800 is a twin‑engine, narrow‑body commercial aircraft in the 737 Next Generation series, used for short to medium‑haul routes. It had a seating capacity of 174 passengers, with Qantas configuring its aircraft with 12 business class seats in a 2‑2 layout and 162 economy class seats. It is powered by two CFM56‑7B turbofan engines.
The passenger address system broadcasts announcements throughout the cabin, and the interphone facilitates communication between the flight and cabin crew.
Weather radar
The weather radar system fitted to the Boeing 737 detects and locates various types of precipitation bearing clouds along the flight path of the aircraft and gives the pilot a visual indication in colour of the cloud’s intensity. The radar antenna sweeps a forward arc of 180°. The radar indicates a cloud’s rainfall intensity by displaying colours contrasted against a black background. Areas of heaviest rainfall appear in red, the next level of rainfall in amber, and the least rainfall in green (Figure 2).
Figure 2: Example depiction of 737 weather radar returns on pilot's navigational display
Source: Qantas, annotated by the ATSB
The turbulence mode displays normal precipitation and precipitation associated with turbulence. When the radar detects a horizontal flow of precipitation with velocities of 5 or more metres per second toward or away from the radar antenna, that target display becomes magenta. These magenta areas are likely associated with heavy turbulence.
The captain did not recall identifying areas of turbulence on the weather radar on descent or report that they were experiencing any difficulties operating the weather radar. Neither the captain nor the operator reported that the weather radar fitted to the aircraft was unserviceable during this occurrence.
Post‑event maintenance
Aircraft data was collected for use by the operator’s maintenance operations control, and engineering. The aircraft health monitoring (AHM) section collected and analysed data from aircraft components and systems post‑event to assess their condition and identify any potential overstressing of components. The operator’s AHM and flight data analysis showed that the event did not exceed tolerances, and no additional inspections were required.
Meteorological information
Brisbane Airport weather
The TAF for Brisbane Airport predicated winds from 100° at 10 kt with visibility more than 10 km in light rain showers and scattered cloud at 3,500 ft from 1200–2000 local time. Table 2 shows the automatic terminal information service (ATIS)[3] report at the time of departure.
Table 2: Brisbane Airport automatic terminal information service (abridged)
The TAF for Gold Coast Airport predicted winds from 100° at 10 kt with visibility more than 10 km in light rain showers and scattered cloud at 2,000 ft. There was a significant intermittent variation from the prevailing conditions from 1300–2200 local time. For up to 30 minutes at a time during this period, the visibility was forecast to reduce to 4 km in rain showers with broken[5] cloud at 1,500 ft.
Graphical area forecast
The flight transited through a region contained in the graphical area forecast for Queensland south, covering subdivisions A and A2 (Figure 3). Table 3 shows the forecast conditions for the duration of the descent into Brisbane Airport which was issued at 0815 local time.
Figure 3: Graphical area forecast Queensland south
Source: Australian Bureau of Meteorology, annotated by the ATSB
Table 3: Graphical area forecast Queensland south
Area
Surface visibility and weather
Cloud
Turbulence
A
Visibility greater than 10 km
Scattered[6] cumulus/stratocumulus clouds between 2,500–8,000 ft AMSL
Scattered altocumulus/altostratus clouds from 8,000 ft to above 10,000 ft
Broken cumulus cloud between 2,000–9,000 ft
Moderate turbulence associated with stratocumulus and altocumulus clouds
A2
Visibility 3 km in scattered showers of rain
Visibility 1 km in isolated thunderstorms with rain showers
Isolated towering cumulus cloud from 2,000 ft to above 10,000 ft
Broken stratus cloud between 800–2,000 ft
Broken cumulus cloud from 2,000 ft to above 10,000 ft
Moderate turbulence associated with cumulus cloud
Severe turbulence associated with thunderstorms, cumulonimbus and towering cumulus clouds
Turbulence reporting
In accordance with the requirements of regulation 91.675 of CASR (Civil Aviation Safety Regulations 1988) and instructions contained in the Aeronautical Information Publication Australia, a special air report must be provided to air traffic control whenever turbulence meeting the following specifications is encountered:
Moderate: Changes to accelerometer readings of between 0.5 g and 1.0 g at the aircraft’s centre of gravity. Moderate changes to aircraft attitude and/or altitude may occur but aircraft remains under positive control. Usually small changes in airspeed. Difficulty in walking. Loose objects moved about.
Severe: Changes to accelerometer readings greater than 1.0 g at the aircraft’s centre of gravity. Abrupt changes to aircraft attitude and/or altitude may occur; aircraft may be out of control for short periods. Usually large changes of airspeed. Loose objects tossed about.
The flight crew could not recall whether a special air report was provided to air traffic control and the turbulence event was classified as moderate in a post‑flight conference call between the captain and Qantas personnel. The operator defined moderate turbulence as ‘causing rapid bumps or jolts without appreciable changes in aircraft altitude or attitude.’ The description elaborated that unsecured objects are dislodged, and walking is difficult.
Recorded data
The operator’s internal investigation report detailed flight data and showed that over a 4‑second period, at an altitude of approximately 11,100 ft, the aircraft recorded:
vertical G went from +1.2G to -0.06G (negative) to +1.35G to +0.61G to +1.59G.
pitch attitude changed from -2.4deg to -0.7deg over 1 sec.
Operator procedures
Dispatch weather briefing
For the operator’s domestic sectors, a flight plan, textual weather, and notice to airmen (NOTAM)[7] were provided in a briefing package to flight crew via an electronic application installed on their iPads. The briefing information included graphical area forecasts, additional weather, turbulence information and weather radar overlay imagery. Figure 4 shows a weather radar overlay issued at the time of departure. For operator domestic flights under 90 minutes, the crew did not receive a flight watch service[8] from the operator’s flight dispatch during the flight and consequently, any hazard alerts or amended terminal forecasts (TAF)[9] were only provided by air traffic control.
Prior to departure from Sydney, the flight crew conducted their pre‑flight planning and reviewed the weather briefing package. The crew recalled that the weather briefing package contained forecast light showers and some cloud in the vicinity of Brisbane and that the forecast weather for departure at Sydney was worse.
Figure 4: Brisbane Airport weather radar overlay on 4 May at 1200 local time (time of departure)
Source: Qantas, annotated by the ATSB
Cabin preparation for landing
The Qantas Flight administration manual (FAM) specifies that the flight crew make the ‘prepare cabin’ public announcement (PA) for cabin crew to commence cabin preparations at 20,000 ft or no lower than 10,000 ft above the destination airport. This PA can be performed at a higher altitude when considering descent profile, arrival procedures, weather and workload management. The customer service manager will then confirm receipt of the PA by directly contacting the flight crew.
The Qantas Cabin crew operation manual (CCOM) states the timing of this announcement should provide the cabin crew at least 10 minutes to secure the cabin and occupants for landing prior to the illumination of the seatbelt sign. After receipt of the ‘prepare cabin’ PA, all activity by the cabin crew shall be safety‑related only and no new service duties may be initiated.
Additionally, the FAM stated, ‘should contingencies occur that impact on the planned preparation time, every effort should be made to advise the cabin crew of these changes.’
In the case of the occurrence, the CSM recalled that the captain advised them that they would prepare the cabin earlier for a ‘bit of weather’. The prepare cabin PA was performed after passing 30,000 ft and the seatbelt sign was illuminated less than 10 minutes later following a further discussion with the CSM relating to the progress of the cabin preparations.
Anticipated turbulence on descent
In the event that turbulence is anticipated on descent, the Qantas FAM stated that:
Where turbulence is anticipated during descent, the flight crew should consider the 10 minutes requirement to prepare the cabin for landing. Cabin crew are to be alerted to anticipated turbulence as early as possible to enable them to complete their duties.
Any time the seatbelt signs are illuminated for turbulence, a PA must be made by the crew.
Securing cabin for landing
Cabin secured for landing
The CCOM specified that when the seatbelt sign is illuminated at the conclusion of the 10 minutes, the CSM will make the following PA:
All customers and crew must now be seated for landing with their seatbelt fastened
The cabin crew will subsequently perform the following procedures:
• ensure passengers are seated
• verify lavatories are vacant
• conduct a simultaneous galley secure check
• return to jump seats and secure within one minute
• after one minute, the CSM initiates a callback from their jump seat to the other cabin crew, to advise that the cabin was secure
• perform silent [safety] review.
Cabin unsecured for landing
Approximately one minute after the seatbelt sign is illuminated, the CSM will initiate a callback from their designated jump seat. Each cabin crew member will respond with ‘door number, name, cabin secured for landing’. If the cabin is not secured for landing, the CSM will inform the flight crew. In this case, the CCOM stated the ‘the CSM will assess the situation and inform the flight crew regarding the status of the cabin.’ This allows alternative actions before the no contact period, which commences when the landing gear is extended for landing. The cabin crew are not to contact the flight deck under any circumstances during this period.
In this case, the captain stated they would have ensured that passengers and cabin crew assisting the injured member were seated before landing had they been informed the cabin was not secure.
Use of cabin secure notifications in Australian airlines
The ATSB also reviewed the cabin secure procedures of 7 similar Part 121 passenger air transport operators in Australia. Of those, 4 operators employed a positive signal to confirm cabin security during normal operations, while 3 did not.
In the past 20 years, the ATSB identified 26 occurrences involving unrestrained occupants on landing, based on historical occurrence data. None of these resulted in fatalities, serious injuries, or minor injuries. Of these 26 occurrences, only 4 could potentially be linked to the absence of a positive cabin secure signal.
Anticipated turbulence procedure
If the flight crew anticipates turbulence, the following procedure from the CCOM will apply:
When the flight crew become aware of anticipated turbulence, they will liaise with the CSM advising the time and likely duration of the anticipated turbulence.
The CSM will relay this information to the members of the cabin crew to enable them to prioritise their duties by securing carts, galleys, items of service equipment, cabin and galley curtains, and the passenger cabin, based on time available.
A PA may be made by the flight crew to the passengers and cabin crew advising that cabin service is to cease as there is a likelihood of turbulence and the following actions will be initiated (Table 4):
Table 4: Crew actions during anticipated turbulence
Action
Description
Seatbelt sign illumination
Must be illuminated by the flight crew no later than one minute prior to anticipated turbulence.
Cabin crew seated
Cabin crew to be seated in their jump seat within one minute of seatbelt signs illumination
Seatbelt announcement
Flight crew announces, ‘all passengers and crew to be seated and fasten seatbelts.’
Call back procedure
CSM initiates call back to ensure all cabin crew are seated and have assessed the cabin condition.
Cabin crew call back response
Cabin crew respond to CSM with, ‘door number, name, seated and secured,’ or if cabin or crew are not secure, cabin crew report this to CSM during the call back.
Confirming security
If secure, CSM calls flight crew via interphone to confirm, ‘passengers and crew are secure’, as well as any other relevant information
Unanticipated turbulence
Unanticipated light turbulence
If it is deemed necessary to illuminate the seatbelt signs for unanticipated light turbulence, the flight crew will perform the ‘seatbelts’ PA announcing, ‘all passengers and crew must be seated and fasten seatbelts.’
The CCOM states the following will then apply:
Cabin crew are to prioritise their duties by securing carts, galleys, items of service equipment and the passenger cabin and initiate crew actions for anticipated turbulence…..
When the captain illuminated the seatbelt sign prior to the turbulence encounter, they performed the ‘seatbelts’ PA. They stated they did this as a precautionary measure as this was their normal practice if there is the possibility of some turbulence.
Unanticipated turbulence posing an immediate hazard
In the event of unanticipated turbulence that poses an immediate safety hazard, the flight crew must select the seatbelt signs on and announce the ‘turbulence’ PA:
All passengers and crew be seated and fasten seatbelts immediately.
Following this announcement, the CCOM issues the following instructions:
Cabin crew will lock carts in position and secure themselves in the nearest seat or wedge themselves in the aisle.
If circumstances permit, the CSM will initiate the call back procedure, ascertain the condition of the cabin and relay this information to the flight crew.
Cabin crew incapacitation
In the event of a cabin crew member’s incapacitation, the CCOM calls for first aid to be administered, and the CSM and captain to be notified as soon as practicable. The CSM would then reassign the duties of the incapacitated crew member to an assist crew member, if available. If the incapacitation results in a crew complement less than the minimum required, the CSM, in consultation with the captain, will determine whether any additional off‑duty crew members are available to assume the role of the incapacitated cabin crew for landing.
The timing of the incapacitation placed concurrent procedural demands on the CSM and disrupted the cabin secure procedures. The CCOM procedures were sequential instructions designed to achieve consistent performance and reduce the potential for miscommunication and non‑conformances.
Injury response tool
The Qantas Group injury response tool specified the actions the crew must follow if an injury has occurred inflight. In this case, the injury response tool directed crew to seek immediate doctor advice via telephone for a turbulence event and for a head blow or head strike which fell under the classification as a ‘specific circumstance’. Consequently, the crew would be required to cease work immediately.
However, as neither co‑workers nor the injured crew recognised the symptoms of a concussion in the L2P or a facial injury in the CSM, they were not triaged according to the Group injury response tool. The operator stated that this likely occurred due to the injury response tool process relying on the self‑assessment of injuries which may not be immediately apparent.
Integrated operations controls procedures
The integrated operations control (IOC) was the central point of contact during any kind of disruption or incident on a Qantas aircraft. At the time of this occurrence, the IOC incident notification communications protocol contained in the operations control procedure (Figure 5) included contact with the on‑call doctor in cases of severe turbulence regardless of whether there were reported injuries. The IOC notification process for a ‘significant passenger/crew injury or illness’ event did not include contact with the Qantas on‑call doctor.
As the turbulence in this event was deemed post‑event by flight crew as moderate, contact with the on‑call doctor was not required under the process.
Figure 5: Qantas incident notification communications protocol version 11, March 2024
Source: Qantas
Research into turbulence detection
There are occasions where it can be challenging to identify turbulence. The US National Transportation Safety Board conducted 10 case studies (National Transportation Safety Board, 2021) of accidents between 2019–2020 that involved turbulence and embedded convection and determined that:
Embedded convection may not be easily detected by onboard or ground‑based weather radar, and when not visible outside the aircraft windows, this class of convective activity can act as a hidden source of severe turbulence encounters within an otherwise benign‑looking cloud mass.
Research into turbulence related injuries
From 2009 through 2018, the US National Transportation Safety Board (NTSB)[10] found that turbulence‑related accidents accounted for more than a third of all Part 121 accidents. The accident data revealed that the most common phase of flight associated with turbulence‑related accidents in Part 121 operations was during the en route descent, which accounted for 36.0% of accidents.
Further analysis indicated that cabin crew accounted for 78.9% of serious injuries, with the majority occurring in the aft section of the aircraft cabin. Passengers accounted for 21.1% of serious injuries, while no flight crew members were seriously injured (National Transportation Safety Board, 2021).
The distribution of cabin crew injuries found most occurring in or near an aft galley (Figure 6), which likely reflects that the service‑related duties of cabin crew often require them to spend more time working unrestrained in the galley area. The most commonly reported cabin crew activities at the time of serious injury were:
preparing the cabin for landing (39.2%)
conducting cabin service (13.4%)
preparing for cabin service (9.3%).
During this occurrence, the R2P and L2P sustained the most severe injuries while unrestrained in the aft galley as they prepared the cabin for landing, which is consistent with research on turbulence‑related injuries.
Figure 6: Location of cabin crew at time of turbulence‑related serious injury, 2009–2018
Source: National Transportation Safety Board
Safety analysis
Crew communication
During the descent into Brisbane, the captain commenced cabin preparations earlier than usual, using standard protocols to account for known weather conditions en route. Although the graphical area forecast indicated the possibility of moderate to severe turbulence, the captain did not observe weather radar returns or receive any other pilot reports indicating the presence of moderate to severe turbulence during the descent.
Approximately 5–6 minutes after initiating cabin preparations, the aircraft entered stratiform cloud and the captain contacted the customer service manager (CSM) to check on the cabin crew’s progress. The purpose of this communication was to provide the captain with information to guide the timing of the seatbelt sign illumination. However, the captain did not provide any weather‑related information to the CSM during this interaction, leaving the cabin crew unaware of any increased likelihood of turbulence.
Two minutes later, the seatbelt sign was illuminated, accompanied by the ‘seatbelt’ public announcement (PA). The captain then observed an approaching cumulus cloud along the flight path but determined it did not pose an immediate hazard based on a visual assessment and the lack of radar indications. As a result, the captain did not perform the ‘turbulence’ PA, which would have prompted the cabin crew to immediately secure themselves in the nearest seat or wedge themselves in the aisle to prepare for the turbulence encounter.
Although the captain contacted the CSM to confirm the time remaining to prepare the cabin, the absence of indications to the subsequent severity of the turbulence limited the captain's perception of the possible threat. Therefore, additional precautions were not considered. The captain followed normal descent procedures, however, did not discuss any additional weather‑related information in communications with the CSM.
As a result, the cabin crew, who relied on information from the flight crew, were unprepared for the turbulence encounter. This situation underscores the difficulties posed by unexpected turbulence, as the procedures for managing in‑flight turbulence rely on the flight crew's ability to predict or avoid these situations.
Contributing factor
The captain did not communicate to the cabin crew about the expected turbulence, likely as a result of the captain not knowing the severity of the turbulence.
Crew unrestrained during severe turbulence
When the seatbelt sign was illuminated during the descent, cabin crew members were required to perform several duties whilst being unrestrained. In the moments immediately preceding the turbulence encounter, the CSM and R2P recalled checking their assigned lavatories as part of securing the cabin for landing.
Cabin crew were required to complete their assigned duties within one minute of the seatbelt sign being illuminated, which was also the case for unanticipated light turbulence. The captain performed the ‘seatbelts’ PA when the seatbelt sign was illuminated, which indicated unanticipated light turbulence to the cabin crew members. However, the cabin crew did not recall hearing this PA and remained unaware of the increased risk of turbulence as the aircraft approached a cumulus cloud.
Because the turbulence event occurred less than one minute after the illumination of the seatbelt sign, which was accompanied by the ‘seatbelt’ PA, the cabin crew did not have sufficient time to ensure they were seated and restrained prior to the aircraft being affected by turbulence. The injuries sustained during the encounter reflect research showing that cabin crew members face a higher risk of turbulence‑related injuries, especially during the descent phase of a flight when they are preparing for landing (National Transportation Safety Board, 2021).
Contributing factor
Three cabin crew were unrestrained while performing duties during unanticipated severe turbulence resulting in all 3 receiving injuries.
Cabin management
After the turbulence event, the CSM and left 2 primary (L2P) turned their attention to the right 2 primary (R2P) who was laying on the floor of the aft galley and was unable to move due to their injury. The turbulence event occurred in the latter stages of the descent, which meant there was little time to provide first aid to the R2P and complete the required preparations for landing. The CSM, L2P and the passengers assisting the R2P were reluctant to return to their assigned seats despite the clear instructions from the captain to do so.
The situation in the aft galley disrupted the procedural flow and meant that the CSM and L2P became focused on providing first aid rather than returning to their seats to complete the callback and silent review prior to landing. Interruptions often lead people to forget to resume their tasks, while multitasking can further complicate the situation by increasing the overall workload within a limited timeframe (Loukopoulos & Barshi, 2009). In this case, the CSM and L2P had to balance providing first aid and securing the cabin. High stress levels are also known to cause errors(Kim & Hyun, 2022), which likely contributed to the CSM prioritising providing first aid over securing themselves and the cabin for landing.
The CSM subsequently lost situational awareness with respect to the phase of flight and the sequence of the standard operating procedures. As a result of being situated in the aft galley, the CSM likely missed audible cues, such as the extension of the landing gear.
The captain did not recall receiving any requests for more time to prepare the cabin for landing. Additionally, the single aisle cabin configuration of the Boeing 737 offered limited options for accommodating the R2P anywhere other than the aft galley. After repeated instructions for everyone to be seated for landing, the captain was confident that all uninjured occupants had complied.
The decision of the CSM and L2P to remain unrestrained in the aft galley during a critical phase of flight increased the risk of incapacitation to additional cabin crew, which could have further compromised their ability to manage a landing‑based emergency effectively if one was to happen. Additionally, the 5 occupants in the aft galley created a potential obstruction to emergency exits, increasing the likelihood of delays or complications if they needed to enact an emergency evacuation.
Other factor that increased risk
Although the captain had instructed that the uninjured passengers and crew needed to be seated, 3 cabin crew and one passenger were unrestrained for landing due to being preoccupied with administering first aid to the injured cabin crew member. This increased the risk of injury to the unrestrained occupants and had the potential to compromise a safe emergency evacuation if required.
The aircraft landed with the CSM, L2P, R2P and 2 passengers unrestrained in the aft galley. The flight crew was made aware by the CSM that the injured cabin crew member was unsecured and unable to be made secured for landing and instructed the CSM to ensure everyone else was secure for landing. While this instruction was communicated to those people unsecure in the cabin, the instruction was not followed as described above. The CSM attempted to inform the flight crew by instructing the L2P to communicate with them. However, the captain again instructed that everyone who could be secured needed to be, as they were landing. As such, the flight crew assumed all cabin occupants would be secure apart from the injured R2P crew. At this stage, the cabin crew operating procedures requiring the CSM to inform the flight crew if the cabin was not secure broke down as there was no further communication that the cabin was not secure.
The captain stated that if they had known that 4 uninjured occupants were still unrestrained in the aft galley, they would have taken appropriate action to ensure they had returned to their seats prior to the final approach to land. The lack of a positive signal increased the likelihood that flight crew would be unaware of unrestrained occupants during the approach and landing phases of flight.
While the lack of a positive cabin secure signal played a role in this occurrence, the available data does not indicate it as a significant ongoing risk.
Other factor that increased risk
The Qantas 737 procedures did not require flight crew to receive positive confirmation that the cabin was secure for landing. This increased the risk that occupants and objects were not secure for landing.
Post‑flight medical assessment
Shortly after arrival at the gate at Brisbane airport, the R2P was attended to by ambulance personnel. However, the CSM and L2P, who were also injured during the event, did not receive any follow‑up medical assessments or treatment. This situation arose due to procedural gaps, which relied on crew members to self‑assess and report a significant injury to receive a medical assessment.
While the CSM self‑diagnosed a minor injury and reported it the following day, the L2P was unaware of their injury. As a result, the L2P operated on multiple flights while experiencing symptoms of an undiagnosed concussion, until some days later when co‑workers noticed signs of a possible injury.
Other factor that increased risk
A crew member with undiagnosed concussion from the accident flight operated on subsequent flights without receiving appropriate medical attention.
The Qantas integrated operations control protocols did not mandate contacting the on‑call doctor in cases where a passenger or crew member was significantly injured. Although the protocol required consultation with the on‑call doctor in cases of severe turbulence, this turbulence event was classified as moderate, and no medical consultation was either required or requested. Additionally, the Qantas group injury response tool also relied on crew members self‑assessing their injuries to determine if medical treatment would be required, but an injured crew member may not realise the extent of their injury at the time.
In the cases of a concussion, symptoms may include impairments in neurocognitive functioning, primarily affecting attention, concentration, memory, and judgment or problem‑solving (Ryan & Warden, 2003). Returning to work with an undiagnosed concussion likely compromised the L2P’s ability to perform safety‑critical tasks. A subtle incapacity due to an undiagnosed injury could negatively impact operational safety, particularly during emergencies.
Other factor that increased risk
Qantas lacked a procedure to ensure cabin crew fitness was assessed after a significant injury. This increased the risk that a crew member could continue to operate while being unfit for duty. (Safety issue)
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the turbulence event and cabin crew injury involving Boeing 737, VH‑VYK, 36 km south‑east of Brisbane Airport, Queensland, on 4 May 2024.
Contributing factors
The captain did not communicate to the cabin crew about the expected turbulence, likely as a result of the captain not knowing the severity of the turbulence.
Three cabin crew were unrestrained while performing duties during unanticipated severe turbulence resulting in all 3 receiving injuries.
Other factors that increased risk
Although the captain had instructed that the uninjured passengers and crew needed to be seated, 3 cabin crew and one passenger were unrestrained for landing due to being preoccupied with administering first aid to the injured cabin crew member. This increased the risk of injury to the unrestrained occupants and had the potential to compromise a safe emergency evacuation if required.
The Qantas 737 procedures did not require flight crew to receive positive confirmation that the cabin was secure for landing. This increased the risk that occupants and objects were not secure for landing.
A crew member with undiagnosed concussion from the accident flight operated on subsequent flights without receiving appropriate medical attention.
Qantas lacked a procedure to ensure cabin crew fitness was assessed after a significant injury. This increased the risk that a crew member could continue to operate while being unfit for duty. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Qantas lacked a procedure to assess cabin crew fitness after a serious injury. This increased the risk that a crew member could continue to operate while being unfit for duty.
Glossary
AHM
Aircraft health monitor
AMSL
Above mean sea level
ATIS
Automatic terminal information service
CCOM
Cabin crew operations manual
CSM
Customer service manager
FAM
Flight administration manual
IOC
Integrated operations control
L1
Left one
L2
Left two
L2P
Left two primary
NOTAM
Notice to airmen
NTSB
National Transportation Safety Board
PA
Public announcement
R1
Right one
R1P
Right one primary
R2P
Right two primary
TAF
Terminal area forecast
Sources and submissions
Sources of information
The sources of information during the investigation included:
the captain of the accident flight
the customer service manager on the accident flight
the R2 primary cabin crew member on the accident flight
Kim, J. Y., & Hyun, S. (2022). Study on Factors That Influence Human Errors: Focused on Cabin Crew. International Journal of Environmental Research and Public Health, 19(9), 5696.
Loukopoulos, L. D., & Barshi, I. (2009). The multitasking myth : Handling complexity in real-world operations. Taylor & Francis Group. Taylor & Francis Group.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the captain of the accident flight
the customer service manager on the accident flight
the L2 primary cabin crew member on the accident flight
the R2 primary cabin crew member on the accident flight
Qantas Airways Limited
Civil Aviation Safety Authority
Bureau of Meteorology.
Submissions were received from:
the L2 primary cabin crew member on the accident flight
the R2 primary cabin crew member on the accident flight
Qantas Airways Limited
Civil Aviation Safety Authority
Bureau of Meteorology
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Stratiform: clouds that exhibit extensive horizontal development (in contrast to the vertical development of cumuliform clouds).
[2]Cumulus: a principal cloud type, forming in the low levels of the troposphere, characterised by flat bases and dome or cauliflower‑shaped upper surfaces. Small, separate cumulus are associated with fair weather but may grow into towering cumulus or cumulonimbus.
[3]Automatic terminal information service (ATIS): the provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts.
[4]Few is a meteorological term used in aviation to describe cloud coverage that occupies 1 to 2 oktas (eighths) of the sky.
[5]Broken cloud is a meteorological term used in aviation to describe cloud coverage that occupies 5 to 7 oktas (eighths) of the sky.
[6]Scattered cloud is a meteorological term used in aviation to describe cloud coverage that occupies 3 to 4 oktas (eighths) of the sky.
[7]NOTAM: Notice to Airmen (NOTAM) is a notice containing information or instructions concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to persons concerned with flight operations.
[8]Flight watch service: a flight watch service provides updated weather information to pilots en route.
[9]Terminal forecast (TAF): a TAF is a coded statement of meteorological conditions expected at an aerodrome and within a radius of 8 kilometres of the aerodrome reference point.
[10]National Transportation Safety Board. (2021). Preventing Turbulence‑Related Injuries in Air Carrier Operations Conducted Under Title 14 Code of Federal Regulations Part 121.
Occurrence summary
Investigation number
AO-2024-032
Occurrence date
04/05/2024
Location
36 km south-east of Brisbane Airport
State
Queensland
Report release date
27/05/2025
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Cabin injuries, Turbulence/windshear/microburst
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
The Boeing Company
Model
737-838
Registration
VH-VYK
Serial number
34183
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 24 December 2022, the pilot of a Cessna 210N aircraft, registered VH-TFT and operated by Katherine Aviation, was conducting a charter flight under the visual flight rules to transport a single passenger from Gove to Katherine, Northern Territory. The aircraft departed Gove at 0814 local time, with an estimated arrival time to Katherine Tindal Airport of 1024. When the aircraft did not arrive, and contact was unable to be made with the pilot, search and rescue activities were initiated by the authorities. At 1204 the following day a wreckage field was found near to the intended flight track at a remote location in East Arnhem, approximately 237 km east-north-east of Katherine. The pilot and passenger sustained fatal injuries.
What the ATSB found
Upon arrival overhead the Bulman region, the aircraft likely entered an area of strong convective activity from a rapidly developing thunderstorm, which probably resulted in exposure to a combination of severe turbulence and reduced visibility for the pilot.
It is probable that a combination of turbulence encountered from the thunderstorm, airspeed, and control inputs led to the excessive structural loading and in-flight separation of the right wing from the fuselage before the aircraft collided with terrain.
It could not be determined with certainty why the pilot flew in close proximity to the storm, however, it is possible that they were in the process of diverting or turning back when the break-up occurred and/or the severity of the storm was not apparent.
What has been done as a result
Shortly following this accident, Katherine Aviation advised that it had:
provided tracking and communication devices for their pilots that enabled real-time satellite‑based tracking and monitoring of their fleet. The devices allowed messages to be exchanged between the company and their pilots in the absence of a mobile telephone signal.
presented the theory component of their wet season training material to their company pilots and updated their exposition with the requirement that all pilots were to complete the briefing program on an annual basis.
developed flight assessment tools to provide their pilots with better decision-making capability when planning for operations during marginal weather.
Safety message
During the Northern Territory wet season, rapidly developing and frequent thunderstorms with associated severe turbulence present pilots with a challenging and hazardous operating environment. Identifying and maintaining adequate clearance from thunderstorms is critical to flight safety.
The United States Federal Aviation Administration recommends that thunderstorms be avoided by at least 20 NM. Weather radar and satellite imagery can assist planning and in‑flight storm avoidance, provided their limitations are understood.
A careful study and understanding of the relevant Bureau of Meteorology (BoM) forecasts, including the graphical area forecasts (GAF), when flight planning will also assist in avoiding hazardous weather. As shown in the example below, GAFs detail the forecast prevailing weather and other weather phenomena over a broad area for a 6-hour period. The forecast is set out in a tabular format, with the first row detailing the forecast prevailing conditions and the subsequent rows forecasting the presence, and effect, of other weather phenomena.
Of note, this format does not mean that the prevailing (first row) conditions and subsequent rows will necessarily co‑exist. Pilots should keep this in mind and the BoM advises that it is not always practical for GAFs to detail the specific timing and likely locations of weather phenomena.
Source: BoM
Contacting the duty BoM forecaster via the phone number on the relevant GAF is the best way for pilots to assess the viability of a planned route, particularly if the forecast is marginal and the weather is changing. The BoM’s online Knowledge Centre for pilots can further assist understanding of the meteorological information that is necessary for safe operations in the wet season.
A range of other education resources are also available for pilots to understand the unique weather challenges of operating during the wet season, including the Civil Aviation Safety Authority’s (CASA) annual Flying in the wet season seminars. CASA also has available online a range of educational resources for managing severe weather-related scenarios.
The occurrence
On 24 December 2022, a pilot from Katherine Aviation was assigned to operate a Cessna 210N aircraft, registered VH-TFT, on a passenger transport flight from Gove Airport to Katherine Tindal Airport, Northern Territory under the visual flight rules[1] (Figure 1).
At about 0730 local time, a Katherine Aviation operations staff member called the pilot advising of a potential delay to the sole passenger’s arrival for the scheduled 0800 departure. With the pilot in attendance, the aircraft was refuelled by the Gove Airport refueler at 0735. The passenger arrived at about 0800 and boarded the aircraft with the pilot.
The pilot’s radio transmissions were recorded on the Gove common traffic advisory frequency (CTAF). The transmissions indicated that at 0812 the aircraft was taxied for engine run-up checks and the take-off roll commenced shortly after at 0814. A witness observed the aircraft depart from runway 31 at about this time. At 0818, a final transmission was recorded on the CTAF, in which the pilot advised that VH-TFT was passing an altitude of 1,700 ft on climb to 8,500 ft and tracking direct to Katherine. No further radio communications from the pilot were identified. At 0841, the operations staff member received a text message from the pilot advising their expected arrival time of 1024 at Katherine Tindal Airport.
At 1058, when the aircraft had not arrived as scheduled, the staff member called the pilot’s mobile phone without answer and then sent a follow-up text message. When no response was received, they checked with another company pilot stationed at Gove, who confirmed that VH-TFT had not returned to Gove. Several station properties were then contacted along the expected route to check whether VH-TFT had been sighted. At around midday, search and rescue officials were contacted by Katherine Aviation advising that VH-TFT was overdue.
Search and rescue
A search and rescue response was commenced by the Australian Maritime Safety Authority’s Joint Rescue Coordination Centre (JRCC), with an airborne search commencing at 1344. The JRCC requested mobile phone tracing records that enabled the search to be refined around the Bulman area (Figure 1). The JRCC advised there was no signal received from the aircraft’s emergency locator transmitter to assist with locating the aircraft.
On 25 December 2022 at 1204, a debris field was sighted from a search aircraft in a remote area of medium-density bushland in East Arnhem. The accident location was 237 km east-north-east of Katherine, approximately 7 km north of the planned track and 18 km north of Bulman. At 1354 first responders arrived at the accident site and confirmed that both occupants were fatally injured and the aircraft was destroyed. There were no known witnesses to the accident.
Figure 1: Satellite view showing the planned direct track, the location of the accident site and its proximity to Bulman
Source: Google Earth, annotated by the ATSB
Context
Pilot and passenger information
Pilot information
The pilot commenced their flight training in June 2021 and obtained a commercial pilot licence (aeroplane) on 24 January 2022. After further flight training, the pilot obtained a multi‑engine aircraft instrument rating that was issued on 19 February 2022. The pilot had accrued 23.6 hours of instrument flying, the last of which was 1.9 hours during the conduct of the instrument rating assessment flight on 19 February 2022. No further instrument hours were recorded in the pilot’s logbook. The pilot held a Class 1 aviation medical certificate, valid until 13 May 2023, with no restrictions and no declared medical conditions.
The pilot’s first commercial flying role commenced in August 2022 with Katherine Aviation, based in Katherine, Northern Territory. On 11 August 2022 the pilot commenced line training through the operator’s in-command-under-supervision (ICUS) program, operating Cessna 210 aircraft under the supervision of either a senior base pilot or the head of flying operations. During that period, the pilot flew to remote communities and station properties throughout the Big Rivers, Top End and East Arnhem regions,[2] including on 3 occasions to the airfield at Bulman. The operator’s training records showed that the pilot undertook 14 ICUS flights totalling 53.1 hours, and passed their company line check on 20 September 2022. The pilot remained in Katherine and completed an additional 76.1 hours conducting passenger‑carrying charter flights under the visual flight rules (VFR) to predominantly remote locations within the Northern Territory.
On 1 December 2022, the pilot relocated to the operator’s base in Gove, East Arnhem and accrued a further 45.2 flight hours prior to the accident day.
The pilot’s logbook and operator’s records showed the pilot had a total flying experience of 364.3 hours, 180.8 of which were in Cessna 210 aircraft. In the 30 and 90 days prior to the accident, the pilot had flown 53.7 and 99.1 hours exclusively in Cessna 210 aircraft.
72-hour history
The operator provided the pilot’s accommodation in Gove. Table 1 summarises the pilot’s flight and duty times for the previous 3 days. The pilot did not fly on 21 or 22 December 2022. On 23 December 2022 they accrued 5.7 hours on a flight to Lake Evella, Groote Eylandt and Elcho Island.
Table 1: Summary of pilot’s duty and flight times
Date
21 December 2022
22 December 2022
23 December 2022
Duty time
0 hours
0700 – 1300 (6 hours)
0730 – 1815 (10.8 hours)
Flight time
0 hours
0 hours
5.7 hours
The ATSB was unable to establish the pilot’s sleep routine in the 3 days prior to the accident, as the pilot lived alone at their Gove accommodation. A company pilot reported that during those 3 days, they saw the pilot intermittently in the office at Gove Airport. They also socialised together as part of pre-Christmas celebrations during the evenings of 22 and 23 December 2022, with each event concluding between 2000 and 2030. No concerns were noted by the co‑worker on the accident pilot’s wellbeing during that period.
At 0615 on the morning of the accident, the pilot sent a text message to the Gove Airport refueller requesting that the aircraft be refuelled. Software login records showed that at 0659 the pilot had commenced their pre-flight flight planning from the airport company office. At about 0735 the refueller met with the pilot while the aircraft was being refuelled. They commented that the pilot did not show any indications of fatigue.
Passenger information
The passenger was being transported to Katherine for a period of respite care over the Christmas and New Year period and was scheduled to return to Gove on 4 January 2023. Katherine Aviation advised that the flight on 24 December 2022 was the third attempt to depart Gove, with the 2 previous attempts being cancelled due to unsuitable weather.
Aircraft information
General overview
The aircraft was manufactured by the Cessna Aircraft Company as a model 210N in the United States in 1979 and was first registered in Australia in 1989. It had seating for 6 people including the pilot and had a high‑cantilever wing with retractable tricycle landing gear. It was powered by a Teledyne Continental IO-520-L46B 6-cylinder engine operating a Hartzell variable-pitch, 3‑blade propeller.
The wing construction comprised a forward spar, main spar, conventional formed sheet-metal ribs and aluminium skin. The inboard section of each wing, forward of the main spar, was sealed to form an integral fuel tank. The aircraft fuel tanks held a combined total capacity of 341 L, of which 337 L was useable. Both wings attached to the central wing spar carry-through structure, which was the primary structural design element for carrying lateral and bending flight loads.
Aircraft maintenance
The maintenance records showed that the aircraft had accrued about 15,100 total flight hours. The engine had been factory overhauled and fitted on 27 March 2022, subsequently accruing 273.5 hours. The propellor had accrued 1,201.8 hours since overhaul.
The aircraft was maintained in accordance with Schedule 5 requirements prescribed by the Civil Aviation Safety Authority (CASA). Schedule 5 is a generic maintenance program developed by CASA that is required to be completed every 100 flight hours or 12 months, whichever comes first.
The most recent scheduled maintenance was a 100-hourly inspection completed on 27 October 2022 at 15,004.9 hours total time in service. During that maintenance, the following detailed inspections for cracking of the wing were completed with no defects found:
Federal Aviation Administration Airworthiness Directive (FAA AD) 2012-10-04– Inspection for cracking of the main spar lower cap
Cessna Special Inspection Document (SID) operation 33 – Inspection of the wing lower spar cap
SID operation 35 – Inspection of the carry through spar lower surface
SID operation 37 – Inspection of the wing spar carry through attachment lugs.
The maintenance release current at the time of the accident was issued in the night visual flight rules and charter categories. It was found in the aircraft wreckage with the daily inspection certified for the day of the accident. There were 3 minor defects listed on the maintenance release that had not been certified as rectified, however they were not considered to have influenced the development of the accident. The defects were:
rear navigation light inoperative
early peaking of exhaust gas temperature in the number-5 cylinder
fuel gauge flickering.
The maintenance release indicated that VH-TFT was due for a 100-hourly inspection at 15,104.9 hours. As the aircraft had less than 5 hours remaining prior to commencement of the accident flight, Katherine Aviation operations personnel arranged with the pilot to exchange VH‑TFT with another Cessna 210 for the return to Gove.
Meteorological information
Wet season
Although variable from year to year, weather in the Northern Territory can generally be divided into the dry season from May to September and the wet season from October to April. In the context of Northern Territory aviation operations, most of the hazardous weather occurs during the wet season. This is a period of unstable atmospheric conditions where tropical cyclones and active monsoon troughs may produce heavy rainfall for prolonged periods, squally winds, and thunderstorms.
Thunderstorms are a very frequent and widespread hazard during the wet season. They are common during the late afternoon and early evening, with a secondary peak in the early morning. They often spread out to form sheets of altostratus and cirrostratus clouds late in their life cycle, bringing steady overnight rain and low cloud persisting into the morning. As a thunderstorm is growing, updrafts in the core can reach over 100 kt. These updrafts can exist alongside downdrafts of similar strength as rain starts to fall out of the storm, resulting in potential for severe turbulence and loss of aircraft control if flying into such conditions (BoM, 2012).
General weather conditions
The Bureau of Meteorology (BoM) advised that, on the morning of 23 December 2022, tropical cyclone Ellie crossed the coastline west of Darwin and tracked south. Later that evening, Ellie was downgraded to a tropical low, however, heavy rain and strong to damaging winds were expected to impact large parts of the greater Northern Territory the next day.
Aerodrome forecasts for Gove and Katherine Tindal
The BoM produces aerodrome forecasts (TAFs) that state the expected meteorological conditions in the airspace within an 8 km radius of the aerodrome reference point. TAFs were available for both Gove and Katherine Tindal Airports for the proposed flight.
Gove Airport conditions after 0830 and until 1130 were predicted to be clear with visibility greater than 10 km, northerly winds at 10 kt, no cloud ceiling below 10,000 feet above ground level (AGL) and no other weather phenomena.
The prevailing weather conditions at Katherine Tindal Airport were forecast to be above the day VFR alternate minima for the entire validity period of the TAF. Notably, the prevailing cloud ceiling was predicted to improve after 0930. However, deteriorating conditions below the alternate minima were predicted for periods up to 1 hour during the expected arrival time of the aircraft. Specifically, thunderstorms, low visibility (1,000 m), strong winds up to 35 kt, and a cloud ceiling at 500 ft AGL were forecast. These conditions required the pilot to plan for at least 60‑minutes holding fuel on arrival at Katherine Tindal, or to plan for an alternate destination aerodrome to land.
Graphical area forecast
The Graphical Area Forecast (GAF) provides information on weather, cloud, visibility, icing, turbulence and freezing level in a graphical layout with supporting text. They are produced for 10 areas across Australia and are broadly state-based (BoM, 2017). Cloud amount is given using the following descriptions (BoM 2018):
For cumulonimbus and towering cumulus, cloud amount is described as:
isolated – individual features which are forecast to affect up to 50% of an area
occasional – well-separated features which are forecast to affect greater than 50% but not more than 75% of an area
frequent – little or no separation between adjacent features forecast to affect greater than 75% of an area.
Embedded is added to these coverage quantifiers to indicate cumulonimbus or towering cumulus clouds are embedded in layers of other cloud and cannot be readily recognised, regardless of whether or not they are protruding from the layer.
Weather coverage is described as:
isolated – individual features which are forecast to affect up to 50% of an area
scattered – well-separated weather features which are forecast to affect greater than 50% but not more than 75% of an area
widespread – features with little or no separation forecast to affect greater than 75% of an area.
When thunderstorms, cumulonimbus or towering cumulus are forecast, it implies severe icing and severe turbulence will be present. Forecast cumulus, stratocumulus and altocumulus imply moderate turbulence. All heights referred in the GAF are above mean sea level (AMSL) (BoM, 2017).
The GAF for the Northern Territory issued at 0135 on 24 December 2022, valid from 0830 to 1430, divided the territory into several areas (Figure 2). Gove was in area A, Katherine in area B and the accident occurred about 25–35 km into area B.
Figure 2: GAF for the Northern Territory with the track from Gove to Katherine Tindal Airport highlighted (upper image) and accompanying weather features (lower table)
Source: Bureau of Meteorology, annotated by the ATSB
For the planned flight in area A, the GAF predicted visibility greater than 10 km when no other weather was present. Visibility was forecast to reduce in 2 weather phenomena, each with isolated coverage of up to 50% of area A. These were moderate showers of rain reducing visibility to 3,000 m, and thunderstorms with moderate rain reducing visibility to 1,000 m. Forecast clouds associated with these phenomena were:
moderate rain – isolated towering cumulous clouds covering up to 50% of the area of reduced visibility with bases at 3,000 ft to above 10,000 ft, scattered stratus clouds covering 25–50% of the area with bases at 1,000 ft and cloud tops at 3,000 ft and broken cumulous clouds covering more than 50% of the area from 3,000 ft to above 10,000 ft.
thunderstorms with moderate rain – broken stratus clouds covering more than 50% of the area from 1,000 ft to 3,000 ft, and isolated cumulonimbus clouds covering up to 50% of the area from 3,000 ft to above 10,000 ft.
In area B, broken cloud, covering more than 50% of the area was forecast from 1,000 ft to above 10,000 ft. Visibility was forecast to be greater than 10 km except in scattered light rain reducing visibility to 8,000 m in 50–75% of the area, scattered moderate showers of rain, reducing visibility to 2,000 m in 50–75% of the area, and isolated thunderstorms with heavy rain, reducing visibility to 500 m in up to 50% of the area. Clouds associated with these weather phenomena were forecast to be:
light rain – overcast alto-cumulous and alto-stratus covering 100% of the area from 8,000 ft to above 10,000 ft.
moderate showers of rain – occasional towering cumulus clouds covering 50–75% of the area from 2,000 ft and to above 10,000 ft. Broken stratus clouds from 500 ft to 2,000 ft and broken cumulus clouds from 2,000 ft to above 10,000 ft covering more than 50% of the area.
thunderstorms of rain – isolated cumulonimbus clouds covering up to 50% of the area from 2,000 ft to above 10,000 ft, and broken stratus clouds covering more than 50% of the area from 500 ft to 2,000 ft.
Grid-point wind and temperature
Grid-point wind and temperature (GPWT)[4] forecasts are issued by the BoM every 3 hours for low‑level operations and display mean wind speed, direction and temperature for a range of altitudes. ATSB’s review of the GPWT chart that was issued at 0330 (local) and valid at 0930 (local) showed a wind direction of 340° and speed of 18 kt at an altitude of 8,500 ft.[5]
En route weather
Analysis of satellite imagery[6], conducted by the BoM, indicated that from 0900 convective cloud developed to the west of the accident site. The cloud developed into thunderstorms with the first observations of lightning recorded between 0940 and 0950. The satellite imagery in the vicinity of the accident site is shown in Figure 3 and the montage in Figure 4. The imagery shows the development of the weather system near the accident location from 0900 to 1000. The system persisted for several hours after 1000. The BoM estimated that the cloud tops in the vicinity of the accident site were between 38,000 ft and 46,000 ft AMSL.
The BoM further advised that the thunderstorms near the accident site may have resulted in severe turbulence,[7] severe icing[8] and wind shear with outflows of strong and gusty winds, not only in the immediate vicinity but also at some distance away from the storm. An automated weather station near Bulman recorded 12.4 mm of rainfall between 0930 and 1030 that morning. The development of the severe weather was consistent with the forecast for isolated thunderstorms in the Northern Territory GAF issued by the BoM at 0135.
The ATSB queried the BoM on whether the term embedded (EMBD) should have been added to the GAF considering the forecast for extensive cloud cover and isolated thunderstorms. The BoM advised that the term embedded indicates that a pilot may encounter cumulonimbus or towering cumulus clouds that they may not be able to readily recognise due to them being contained within other cloud layers.
In their analysis of the satellite imagery the BoM identified that the thunderstorms were not embedded due to discrete scattered to broken convective cloud rather than an overcast, poorly separated layer of cloud as would more likely occur in a rain band. The Bureau further advised that although the forecast prevailing conditions were for extensive cloud cover in area B, there was still a moderate to high likelihood that the convective clouds would have been visible to the pilot. This means that the top, or prevailing weather, row and subsequent weather rows may not necessarily co-exist. Put another way, conditions in area B at any location or point in time would be either the prevailing conditions or one of the subsequent rows in the forecast.
The forecast for area B covered a substantial portion of the Northern Territory, for a 6-hour period, with unstable atmospheric conditions. BoM advised that the predicted coverage was a worst case forecast for each weather row in area B, with conditions predicted to develop at different times and places throughout the period. For example, thunderstorms were predicted to cover up to 50% of area B at some point in time during the validity period of the forecast.
The BoM also advised that it was not practical to include additional detail of the specific timing and likely locations of weather phenomena in the GAF product in scenarios like those predicted for area B. To account for this, in cases where convective weather is forecast, pilots are encouraged to call the meteorologist who produced the GAF for details on the weather phenomena likely to be encountered for a specific route and time period.
A comparison of the overhead satellite imagery and the Katherine–Tindal weather radar is also shown at Figure 5 to Figure 7. After the flight had departed Gove, the data at 0830 that morning identified that while significant thermal activity had developed to the north-west of the planned route, the immediate area along the planned track near to Bulman was clear of rain. At 0930 to 1000, the weather radar identified light to moderate rain, along with increased convective activity, signalling the development of a thunderstorm. The BoM identified that limitations exist to the accuracy of weather radar information, particularly as distances increase from the radar head. As the flight progressed toward Bulman, it remains possible that the weather radar did not completely display the extent of the weather system to the pilot. Optimal coverage of weather radar information is described by the BoM:
Generally, the optimal coverage area extends to approximately 200km away from the radar. Beyond this distance some rainfall echoes may be displayed on the radar image, however these echoes will be from clouds higher up in the atmosphere and will not directly correspond with conditions experienced on the ground.
OzRunways and AvPlan were 2 electronic flight bag (EFB) applications authorised by Katherine Aviation. Each application can display rain radar information to assist pilots with weather‑related decision‑making. The operator reported that it was expected that its pilots would access weather radar information in flight, however they identified that this was dependent on cellular data availability.
It was not possible to determine whether the pilot accessed the weather radar information prior to, or during the accident flight. Furthermore, the location of the accident site surrounding Bulman was beyond the optimal coverage range of the BoM radar. Therefore, as discussed above, even if this information was accessed by the pilot, the rain intensity detected by the BoM weather radar on approach to Bulman may not have accurately represented the conditions at the time.
Figure 3: Weather satellite imagery showing cloud and convective cloud activity relative to the accident site at 0900 on 24 December 2022
The white areas are scattered to broken clouds, and the colours provide an indication of the vertical development of the cloud with temperatures ranging between −35 to −70 ºC. The colours provide an indication of the vertical development of the cloud and in general terms, the colder the cloud top temperature, the higher the top of the cloud. Source: Bureau of Meteorology, annotated by the ATSB
Figure 4: Montage of satellite imagery showing the rapid build-up of convective activity near the accident site from 0910 to 1000 on 24 December 2022
Red dots in the above images at 0940, 0950 and 1000 are recorded lightning strikes. The accident site is represented by a red star. The white areas are scattered to broken clouds, and the colours provide an indication of the vertical development of the cloud. Source: Bureau of Meteorology, annotated by the ATSB
Figure 5: Broad area comparison of satellite/convective activity (left) and rain radar data (right) near to the accident site at 0830 on 24 December 2022
Source: Bureau of Meteorology, annotated by the ATSB
Figure 6: Broad area comparison of satellite/convective activity (left) and rain radar data (right) near to the accident site at 0930 on 24 December 2022
Source: Bureau of Meteorology, annotated by the ATSB
Figure 7: Broad area comparison of satellite/convective activity (left) and rain radar data (right) near to the accident site at 1000 on 24 December 2022
Source: Bureau of Meteorology, annotated by the ATSB
Operational information
Flight planning
The planned track between Gove and Katherine was over remote sections of the Northern Territory in class G non-controlled airspace and, closer to Katherine, RAAF Tindal controlled airspace. Katherine Aviation required its pilots to produce an internal company flight plan using an electronic flight planning tool within one hour prior to departure. The planning tool was also used to access en route and destination weather data, through Airservices Australia’s National Aeronautical Information Processing System (NAIPS).[9] Login files identified that NAIPS was accessed by the pilot’s personal and company accounts 3 times on the morning of the accident flight; at 0659, 0702 and 0712.
The NAIPS records showed that a GPWT forecast had been accessed during these periods, however, due to software limitations it could not be confirmed whether a GAF was accessed by the pilot.
A review of the pilot’s previous flights identified that meteorological information, including the GAF, was used by the pilot for their flight planning. The operator indicated that their pilots were required to submit their flight documents to the senior base pilot at the conclusion of each flight. Documents included the flight plan, passenger information, fuel receipts and meteorological information. Although the loose-leaf flight plan printouts were not located at the accident site, based on previous work practice, the required weather forecasts, including the departure and destination TAFs, were probably accessed by the pilot on the morning of the accident flight.
It was a company requirement that a flight notification be lodged with Airservices prior to departure. This could be accomplished using the NAIPS website, the EFB software, or by telephone if internet access was not available. Airservices advised that a flight notification was not lodged for the accident flight.
During a telephone conversation at about 0730 on the morning of the accident flight, the pilot was reported to have stated to a Katherine Aviation operations staff member that the weather was ‘a bit iffy’. The staff member further stated that pilots were encouraged by Katherine Aviation to remember that there was always the option to divert or return. The pilot had taken off and then turned back, due to unsuitable weather, on a flight a few days prior to the accident.
Requirements for flight under visual flight rules
Visual meteorological conditions are the minimum conditions in which a VFR flight is permitted. These conditions ensure pilots have sufficient visibility to control the aircraft and maintain visual separation from terrain and other aircraft.
The rules require that pilots operating below 10,000 ft have a minimum of 5,000 m flight visibility. Pilots also need to maintain 1,500 m horizontal and 1,000 ft vertical separation from cloud when above the higher of 3,000 ft AMSL or 1,000 ft AGL in non-controlled airspace. When operating at or below the higher of 3,000 ft AMSL or 1,000 ft AGL, the pilot must remain clear of cloud and in sight of the ground or water.
En route
The flight was expected to track directly from Gove to Katherine Tindal Airport. A loose-leaf form used by the operator for engine trend monitoring was located at the accident site. The document was damaged and incomplete, however it identified that the pilot had conducted trend monitoring when the aircraft was stabilised in cruise at 146 kt airspeed and at an altitude of 8,500 ft. Taking into account the climb performance of the aircraft, a forecast 18 kt wind speed at 340°, the cruise speed and a direct track to Katherine, the ATSB assessed that the aircraft would pass north of Bulman and over the accident site at about 0930.
Operational staffing
Due to the approaching Christmas and New Year shutdown period, most Katherine Aviation staff were on leave, including the head of flying operations (HOFO) in Katherine and the senior base pilot at Gove. With only 2 flights scheduled for 24 December 2022, 2 staff remained on duty comprising of a senior pilot and an operations staff member, both in Katherine. The senior pilot had prepared another Cessna 210 aircraft for transfer back to Gove, while waiting for TFT to arrive.
Fuel
The aviation refueller at Gove reported receiving a text message from the pilot at about 0615, requesting full fuel (169 L) in the left wing tank and the right wing tank to be filled to the indicator tab (127 L), totalling 296 L. The fuel receipt showed that 211 L of Avgas 100 low lead fuel was uploaded to the aircraft between 0735 and 0745. Based on the Pilot’s Operating Handbook (POH), 4 L was unusable, therefore there was 292 L usable fuel on board at startup, equating to 210 kg using a specific density of 0.72 for Avgas. Previous flight logs showed the pilot allowed 5 L (3.6 kg) for taxiing. This was consistent with the passenger/cargo manifest located at the accident site, which listed 207 kg fuel on board at take-off.
Weight and balance
The passenger/cargo manifest included a loading summary, which calculated the take-off weight including occupants, cargo and fuel for the aircraft to be 1,415 kg, which was less than the aircraft’s maximum take-off and landing weight of 1,724 kg. The associated weight and balance assessment normally completed by the pilot was not located in the wreckage and the passenger’s seating position was unknown.
Based on the weights listed in the manifest and the information provided in the POH, the ATSB assessed that the aircraft was in the mid-range of the aircraft’s centre of gravity envelope, whether the passenger was seated in the front or centre row. Records from previous flights also showed that the pilot routinely switched between left and right tanks to maintain lateral balance. Therefore, the aircraft was almost certainly within the weight and balance limits throughout the flight.
Design limitations
The Cessna 210N is certified as a normal category aircraft. The airspeed and load limits defined in the Cessna 210N POH are defined in Table 2.
Table 2: Cessna 210N airspeed and load limitations
Never exceed airspeed (VNE)
200 kt (red line on the airspeed indicator)
Maximum structural cruising airspeed (VNO)
165 kt (green line on the airspeed indicator)
Manoeuvring airspeed (VA)
125 kt at 1,724 kg
113 kt at 1,428 kg
101 kt at 1,134 kg
Maximum flight load factors (g)
+3.8 g to −1.52 g (flaps up)
+2.0 g (flaps down)
Manoeuvring airspeed (VA) is the maximum airspeed at which full control travel can be used without exceeding the design load factor. The manoeuvring speed decreases with aircraft weight. Factoring the take-off weight and TFT’s fuel usage, the ATSB calculated that the manoeuvring airspeed at the time of the accident was about 111 kt.
The 4 forces acting on an aircraft in flight are lift, weight, thrust and drag. The ratio of lift force to the aircraft weight is the load factor. Load factors are defined in terms of g-loading, which is a measure of the forces acting on the aircraft structure to produce the accelerations involved in changing speed and direction in flight. In straight and level flight, lift force and aircraft weight are balanced, so the load factor is 1 g. Aircraft structural limits are based on aircraft weight and the load factor, which can be affected by any one or combination of the following:
full control movements above VA which can occur while manoeuvring, as a result of disorientation, or during recovery from an unusual attitude.
windshear, turbulence or gusts – severe turbulence is defined as variations in vertical acceleration greater than 1 g.
An aircraft must be operated within its flight envelope[10] to prevent structural damage, or aerodynamic stall.[11] Exceeding the flight load limit below VA results in a stall, whereas exceeding the flight load limit at a speed above VA can produce structural damage.
Accident site and wreckage examination
Wreckage location
The ATSB initiated a field-based investigation following notification from the JRCC that the aircraft wreckage had been located. ATSB investigators attended the accident site on 29 and 30 December 2022. It was situated within the East Arnhem wilderness region with medium‑density trees and largely flat terrain. The nearest aerodrome was located at Bulman, approximately 18 km south.
Site examination
The ATSB’s onsite examination identified that the right wing and its detached wing tip were the first components in the wreckage trail. The wing tip and right wing were located 370 m and 300 m respectively from the primary point of ground impact, indicating they had separated from the aircraft during flight (Figure 8).
Figure 8: Aerial view of the accident site showing the spread of wreckage
Source: ATSB
Severed tree branches and ground scars were consistent with the aircraft having a trajectory of approximately 35° down from horizontal immediately before colliding with terrain. Almost complete fragmentation of the aircraft structure had occurred on impact leading to aircraft components spreading over about 80 m from the primary ground contact point. The propellor, engine, left wing, carry-through structure, empennage, nose gear and cabin components were all identified in the wreckage trail.
The orientation of the wreckage trail was in a north-east direction, which was about 180° to the intended flight track to Katherine Tindal. The tail and empennage section had broken into several pieces and was partially reassembled to ensure that all the extremities and flight control mass balance weights were identified. Excluding the right wing and wing tip, all key components of the airframe were identified in the wreckage trail with no pre-impact defects identified. The left wing remained attached to the intact wing carry-through structure. The landing gear was assessed to be retracted at impact and the flaps were assessed to be in the retracted position.
Both wing tank filler caps remained fitted to their respective fill ports. There was no remnant smell of fuel in the wreckage when it was examined although there had been significant rain through the region prior to ATSB’s examination of the wreckage. Additionally, yellowing of the small grasses and vegetation surrounding the accident site was consistent with chemical burning, likely from the release of fuel when the aircraft impacted terrain.
Separated right wing
Onsite examination of the right main wing spar identified that it had fractured diagonally, about 30–60 cm from the fuselage attachment points (Figure 9–Figure 11).
The right wing showed extensive permanent deformation and tearing of the internal structure with associated compression rippling to the upper skin. The damage was indicative of substantial upward bending forces applied to the wing prior to its failure and separation from the aircraft. The wing structure at the point of failure contained a permanent deflection of about 30° in the upward direction. The internal main fuel tank had been ruptured during the break-up, with no residual fuel remaining.
The inboard end of the right wing spar remained attached to the fuselage carry-through structure. Examination of the fracture surfaces from the right wing spar presented evidence of ductile overstress. Wood fibres and soil were also embedded throughout the main spar surfaces. The onsite assessment did not identify any regions of fatigue cracking or other pre-existing damage that might have weakened the spar caps, straps, or web structure of the wing.
Black contact marks on the wing tip surfaces indicated that it had probably impacted the rubberised leading-edge protection on the tail during the break-up sequence.
The inboard end of the right wing spar and the corresponding fracture surfaces from the separated right wing were retained for further detailed examination at the ATSB technical facilities in Canberra.
Figure 9: The right wing as it was found approximately 300 m from the main wreckage
Source: ATSB
Figure 10: The right wing showed compression rippling of the upper skin surface and permanent deformation from exposure to upward bending
The wing was permanently deformed by about 30° in the upward direction at the point of failure. Source: ATSB
Figure 11: Illustration of the Cessna 210 and the wing and main spar fracture location
Source: Textron – annotated by the ATSB
Engine
The engine had separated from the airframe and was found several metres from the initial impact point. The engine was examined externally for any type of pre-impact mechanical failure with none identified.
Exhaust system
Only small portions of the exhaust system from the engine were located at the accident site. The left side of the exhaust system containing the muffler section and heater shroud had been liberated from the engine and was not found at the accident site. It is possible they were obscured by debris or buried under the soil within the impact crater. The firewall area that housed the cabin heater inlet was destroyed and unable to be assessed for integrity.
The chief engineer for Katherine Aviation indicated they were unaware of any pre‑existing issues with the exhaust system from VH‑TFT and that it was inspected every 100 hours.
Propeller
The propeller hub had separated from the engine crankshaft due to overstress fracture under predominantly bending loads. One propeller blade had fractured from the hub at its base. All blades had sustained forward bending and rotational abrasion damage from passing through sand/soil. One of the blades displayed chord-wise twisting and compound bending. The damage signatures produced on collision with the terrain were consistent with an operating engine (Figure 12).
Figure 12: Propeller assembly after removal from the ground impact site
Source: ATSB
Emergency locator transmitter
The emergency locator transmitter (ELT) installed in the aircraft was an Artex 406 transmitter fitted to a fixed mounting bracket within the aft fuselage. It was required to be switched to the ARM position for flight so that the g-switch would provide impact-activation in the event of an accident.
The ELT from the aircraft was located within the wreckage trail. The switch was set to the armed position and the front panel light had illuminated, indicating that the inertial switch had activated on impact as designed. Although the unit was likely transmitting, the antenna had been severed, preventing the signal from propagating sufficiently to be received by overflying aircraft and/or satellites.[12]
Technical examination
A limited number of items from the accident site were retained as evidence for further review by the ATSB. They included operational documentation, electronic devices and physical components that were subsequently transported to the ATSB’s technical facilities.
Electronic devices
It was a Katherine Aviation requirement for all pilots to use an electronic flight bag (EFB). The pilot used the OzRunways application on an iPad device. The ATSB’s review of the pilot’s OzRunways account identified a portion of a previous flight to Groote Eylandt on 23 December 2022. The account contained no flight data from the accident flight on 24 December 2022.
The ATSB’s examination of the iPad and 2 mobile phones retrieved from the accident site was completed to establish if electronic data regarding the conduct of the flight could be recovered. Access to the severely damaged passenger’s phone was achieved, however there was no data relating to the accident flight stored on that device. Data recovery from the pilot’s phone and iPad was unsuccessful.
Flight instruments
Portions of 2 flight instruments were recovered from the accident site – a gyroscope from the artificial horizon and the front face of the vertical speed indicator.
Disassembly and examination of the gyroscope identified rotational scoring from contact with the rotor’s housing. The scoring damage indicated that the aircraft’s vacuum system and artificial horizon were likely operating.
Examination of the front face of the vertical speed indicator identified a defined witness mark that was consistent with the needle striking against the instrument face on ground impact. The witness mark showed a descent rate of 2,000 ft per minute. However, because the mark was at the limit of the instrument range, the descent rate of the aircraft may have been higher than indicated when it collided with terrain.
Right wing main spar
A red-brown product was adhered to much of the spar fracture surfaces and was likely a mixture of soil and impacted vegetation. Detailed examination of the main spar fragments identified features typical of ductile overstress. There was deformation and angular tearing throughout the spar cap, shear web and strap structure.
Overstress fracture in ductile materials (including the alloys comprising the wing component) occurs when the structure is loaded beyond its ultimate limit. Several rivets that had secured the straps to the spar cap had sheared during the break-up. The examination did not identify any evidence of pre-existing damage such as fatigue cracking, corrosion or other defects (Figure 13 and Figure 14).
Figure 13: Fractured right wing main spar as received at the ATSB’s technical facilities
Source: ATSB
Figure 14: Close-up of the lower spar cap outboard fracture surfaces
Only ductile overstress features and associated deformation was present through the spar structure fracture surfaces. Source: ATSB
Post-mortem and toxicology information
General
The pilot was described by co-workers and next of kin as active with a high level of health and fitness. They were a non-smoker.
Pilot results
A post-mortem examination conducted on the pilot found they sustained fatal injuries during the impact sequence. Toxicological analysis[13] identified the presence of alcohol and carboxyhaemoglobin (COHb). However, due to chemical changes that occur post‑mortem there was significant doubt over the validity of these results. That is, they were not reliable indications that the pilot was exposed to either alcohol or carbon monoxide prior to the accident.
Passenger results
A post-mortem autopsy examination was performed on the passenger, which found that they sustained fatal injuries during the impact sequence. Toxicology testing was not conducted.
Survivability
The accident was not survivable. Although a product of the accident dynamics, had an ELT signal been received by the search and rescue satellite system this would have resulted in earlier location of the accident site by the search authorities.
Organisational information
General
Katherine Aviation was established in 2006. It held an Air Operator’s Certificate (AOC) and operated 15 Cessna 210, 6 Beechcraft Baron BE58, and 4 Cessna 172 aircraft. At the time of the accident it employed 20 pilots and was the registered operator of VH-TFT. It operated from 6 locations, with Katherine Tindal Airport being their main base, and Gove being one of 5 remote bases. The company conducted operations under Civil Aviation Safety Regulations (CASR) Part 135.[14] It flew to communities and townships throughout the Northern Territory, and its services included general charter, patient transfer, freight and mail delivery, and scenic flights.
Katherine Aviation had a CASA-approved exposition that defined its procedures, activities, and conditions. It did not, and wasn’t required to under the regulations, have a safety management system.
In December 2023, following sale of the business and its assets, Katherine Aviation ceased all charter operations and in January 2024 it cancelled its AOC, de‑registering as an authorised aviation operator.
Key personnel
Katherine Aviation’s key personnel were the chief executive officer (CEO), who was also the head of aircraft airworthiness and maintenance control (HAAMC), and a separate head of flying operations (HOFO). The HOFO commenced their aviation flying career with Katherine Aviation and after several years as a line pilot and performing other duties within the company, was appointed as the HOFO in May 2021. The HOFO role described in the company Exposition was to manage and ensure the safety of flight operations. Duties also included the employment and induction of new pilots into the company, ground training and checking pilots to line.
Line pilots
The organisation’s minimum requirements for pilots was a multi-engine instrument command rating with at least 5 flight hours operating a Cessna 210. Once located at a remote base, it was general practice that a senior base pilot provided supervision, mentoring and advice. Senior base pilots reported to the HOFO.
The HOFO and other company personnel stated that there was never any pressure applied to line pilots to complete a flight. They advised that the company supported the decision of a pilot if they elected to cancel a flight due to bad weather. The HOFO also advised it was an accepted, though not formalised practice, for pilots to depart and ‘go have a look’, when the forecast weather was unfavourable.
In-command-under-supervision training
Katherine Aviation required all pilots joining the company to complete line training as part of their induction. The training program was conducted in-command-under-supervision (ICUS) and provided assurance to the operator that, following a series of reviews, a pilot was proficient to conduct line operations. The HOFO reported that it typically took 25–60 ICUS flight hours before new pilots were checked to line. Elements from the ICUS program included:
aircraft knowledge (aircraft speeds and limitations, pre-flight inspections)
flight planning requirements
flight component (taxi, climb, cruise, circuit and landing)
weather management
passenger briefings
rules and procedures.
The operator advised that competency surrounding weather management and avoidance was assessed during ICUS flights. There was no formal weather examination during the training period, and pilots were expected to deviate, or descend early, to ensure the aircraft did not enter cloud.
Weather hazard management
On 13 October 2022, the operator held a safety meeting, which the pilot attended in preparation for the upcoming wet season. According to the meeting minutes, senior pilots discussed their personal accounts and experiences from flying during a wet season. The minutes from the meeting also identified that the HOFO had addressed the attending pilots, reiterating that:
‘…no pressure to get the job done exists, and that pilots will be supported in their decision making.’
Katherine Aviation had created a specific internal training presentation on the hazards that exist in the Northern Territory during the wet season. That presentation was not delivered at the pilot safety meeting, however it was available for pilots to review on the internal computer network. The operator did not have a record of the accident pilot reviewing the presentation. The training presentation commenced with the following introductory statement:
This course is aimed at providing you with some specific information and guidance to help with decision making processes during the wet season. If you are new to flying in the NT then it is likely that you may not have experienced flying in a wet season. Wet season presents some extreme weather patterns that add to the complexities of planning and carrying out a flight. It is important that you are aware of some of these challenges and are suitability equipped to manage these situations whilst you are flying in the NT.
The presentation included advice on wet season weather phenomena, flight planning, flight into marginal visual meteorological conditions, guidance on the safe operation and control of an aircraft when in turbulence and when to turn back. It also included a case study and lessons learned from a Cessna 210 in-flight break-up that occurred during the 2017 Northern Territory wet season (see the section titled Related occurrences).
Procedure for severe weather
The wet season training identified that it was likely for turbulence to be encountered when flying during a wet season. The presentation offered the following guidance:
• When encountering turbulence your priority is always to CONTROL THE AIRCRAFT
• Determine the intensity of the turbulence
• If the turbulence is of adequate intensity, begin to make corrective actions but do this slowly, (any abrupt changes to control inputs and power can increase G-loading on the aircraft)
• If descending – slowly revert to level flight to reduce airspeed
• Ensure you keep the wings level and do not “chase” attitude adjustments
• Slowly reduce power as appropriate to a minimum of 18 inches to reduce airspeed
• Allow the aircraft to decelerate to below the appropriate turbulent penetration speed for its weight (if applicable)
• If needed, ensure the aircraft is below gear extension speed and lower the gear
• Continue flight or descent in this configuration until you are clear of the turbulence
• DO NOT initiate quick roll manoeuvres or large turns. This may significantly increase G-loading on wings. G-loading limits are assessed on vertical movements of pressure and are not applied to twisting moments on wings. A twisting moment on the wing caused by rapid rolling movements (usually associated with someone attempting to “chase” an attitude) will apply further stresses to the aircraft. If a turn is required to attempt to manoeuvre away from a high turbulence area, ensure that it is made slowly and with minimum bank angle.
• CB’s and developed thunderstorms should be avoided by up to 10-15 nm or more. Some may need to be avoided by up to 40 nm or more!
• If you are diverting around a thunderstorm and it is turbulent then you are probably too close!
Additionally, section 2.19.3 of the operator’s exposition described procedures when encountering severe weather:
To minimise the risk of exceeding aircraft structural limitations due to thunderstorm turbulence, the pilot in command should:
• Ensure the aircraft does not take-off when thunderstorms are active within 10 nm of the aerodrome
• Avoid thunderstorms enroute by diverting by a minimum of 10 nm upwind or 20 nm downwind
• The pilot in command must either hold or divert to an alternate aerodrome if a thunderstorm is in 20 nm of the destination aerodrome.
Forecast and reported areas of turbulence should be avoided whenever possible. If turbulence is anticipated or encountered, the pilot in command should:
• ensure all persons, loose articles and cargo are secured
• maintain turbulence penetration speed or manoeuvring speed (VA)
• maintain attitude control and accept altitude changes and speed variations whilst keeping the attitude within safe limits.
Decision making and perceived pilot pressure
The pilot was described by their co-workers and the HOFO as professional and meticulous with their selection of speed and power settings when operating the Cessna 210 aircraft. They reported that the pilot exercised good en route decision‑making during the ICUS program, particularly in the avoidance of weather. A few days prior to the accident, the pilot turned back during a flight when en route weather conditions were unfavourable. In that instance, the pilot called the operations department and advised of the decision to cancel the flight. The decision not to push on was reflected by the company’s stance on turnback and cancellation decisions during periods of adverse weather.
Perceived (or self-induced pressure) is specific to each pilot and may come from a range of sources. It may not be evident or easily identifiable by the pilot. Not every flight will result in potential for pilots to experience pressure; some pilots may not have experienced pressure due to the flights they have been involved in, and some pilots may not feel pressure in circumstances where other pilots do. In their research, Bearman (2014) reported that outback pilots are more likely to undertake risky behaviour to meet commercial imperatives and gain approval from their management. The desire for career progression by accumulating flight time was also an identified factor to influence risky behaviour for outback pilots.
On the day of the accident, conditions existed that may have led the pilot to experience a level of self-perceived pressure to proceed with the flight. These included:
The aircraft was expected in Katherine for a 100-hourly scheduled maintenance. If the flight had returned to Gove, then it is likely that insufficient hours would remain on the aircraft’s maintenance release to return to Katherine, potentially requiring a maintenance engineer to travel to Gove and complete the necessary maintenance.
The flight was described in the booking as a patient transfer flight. This was the third time that Katherine Aviation had attempted to transfer the passenger for respite care. The previous flights earlier that week had been cancelled due to bad weather.
The accident pilot was seeking to further their commercial flying career. The operator reported that the pilot was always keen to be assigned flight taskings to build flight time.
Balancing the potential for the above conditions, Katherine Aviation had no expectations for company pilots to depart or continue with a flight when confronted with adverse weather conditions. This expectation was outlined in the company Exposition and was supported by statements provided by operational personnel that pilots were accepted if they elected to cancel, divert or turn back. While it could be demonstrated that some aspects of self-perceived pressure were present, there was insufficient evidence available for the ATSB to determine the influence of each of these on the pilot’s decision‑making related to the accident flight.
Recorded data
Radar data
The Royal Australian Air Force (RAAF) provided air traffic control (ATC) recordings from Darwin and Tindal radar towers for the period of the accident flight. A review of the ATC data was completed and VH-TFT was not detected by the radar. In their analysis of the radar coverage, RAAF ATC confirmed that an aircraft operating at an altitude of 8,500 ft overhead the accident site would not have been detected by the Tindal radar system.
Telephone records
A single text message was sent from the pilot’s phone to the operator at 0841, advising of the planned 1024 arrival time to Katherine. Mobile phone call charge records for the pilot and passenger’s mobile phone devices were provided by a telecommunication network provider for the period 0900 to 1130. The data identified that from 0900 as the flight progressed, network connections were established with the cellular towers at Ramingining, Gapuwiyak, Alyangula, Numbulwar, and then to Bulman. The pilot’s phone first came into the detectable range of the Bulman cellular tower at 0914 and the passenger’s phone into range of the Bulman tower at 0915.
At 0929 both phones were again briefly detected on the Ramingining cellular tower, approximately 150 km north of the accident site. The provider advised that mobile networks were designed for ground coverage. Connection to a network from within an aircraft while en route can be unpredictable and may be affected by variables such as climatic conditions, aircraft altitude and radio network traffic within the region. The Ramingining tower connection suggests that the aircraft may have been at a higher elevation and possibly closer to the planned cruise altitude of 8,500 ft, rather than at significantly lower altitudes.
At 1001 the passenger’s phone signal ceased its connection with the Bulman tower, however the data identified that the pilot’s phone remained connected to the cellular network. The passenger’s phone was severely damaged during the accident sequence and had likely stopped operating upon impact with the terrain. In contrast, the pilot’s phone remained relatively undamaged.
Recording devices on VH-TFT
The aircraft was not equipped with either a cockpit voice recorder or a flight data recorder, nor was it required to be. Further, there was no active flight tracking equipment fitted to the aircraft, which may have otherwise been used by the operator to track the aircraft and to assist search authorities to locate the occupants. The was no other device or system fitted to the aircraft that provided flight data.
Onboard recording devices have long been recognised as an invaluable tool for investigators in identifying the factors behind an occurrence and assisting with the identification of important safety issues. However, in many cases, investigations involving light aircraft are hampered by a lack of data about the circumstances that led to the occurrence. This contrasts with the investigation of occurrences involving larger transport aircraft that are required to be fitted with a flight data recorder and cockpit voice recorder.
Two recent ATSB investigations benefited greatly from the availability of recording devices. Although not crash protected, they greatly assisted in determining the contributing safety factors and enabling safety advice to be provided to the aviation industry:
VFR into IMC, loss of control and collision with terrain involving Airbus Helicopters EC130 T2, VH-XWD, near Mount Disappointment, Victoria, on 31 March 2022(AO-2022-016),
Loss of control and in-flight break-up involving Robinson R66, VH-KFT, near Hawks Nest, New South Wales, on 26 October 2023(AO-2023-051). Ongoing at the time of writing.
Related occurrences
A search of the ATSB occurrence database identified 5 other fatal accidents involving structural break-up for the Cessna 210 series aircraft in Australia (Table 3). Of these:
One accident from 1976 (Cessna 210L) and one from 2017 (Cessna 210B) were attributed to significant aerodynamic loading, the source of which could not be established with certainty.
The 2019 in-flight break-up and separation of the right wing from a Cessna 210M was identified to be from the fatigue cracking and fracture of the wing carry-through spar. Weather was not a factor to that accident.
Exposure to severe weather was identified to be contributory for 2 accidents, one in 2011 (Cessna 210M) and the other in 2017 (Cessna 210L). These accidents and a serious incident from 2019 involving severe turbulence are briefly discussed below.
Table 3: Cessna 210 in-flight break-ups – Australia
Date
Investigation agency accident ID
Aircraft detail
General location
Detail
11 June 1976
Commonwealth of Australia Department of Transport AAIR 197600023
On 7 December 2011, the owner-pilot of a Cessna 210M was conducting a private flight under visual flight rules from Roma to Dysart in Queensland. Thunderstorms with associated cloud, rain and severe turbulence were forecast for the area. About 30 minutes into the flight, the outer sections of the wings and parts of the tail separated. The aircraft collided with terrain, fatally injuring the pilot.
The ATSB established that the aircraft was structurally sound before the wing and tail sections separated. No aircraft system defects were identified. Ground-based weather radar showed thunderstorms in the vicinity of the accident site, and recorded engine data showed cruise power setting was maintained until recording ceased. Although the precise circumstances leading up to the accident were not known, a combination of aircraft airspeed with the effects of turbulence and/or control inputs generated stresses that exceeded the design limits of the aircraft structure.
On 23 October 2017, a Cessna 210L with 2 pilots on board was conducting a charter flight from Darwin to Elcho Island, Northern Territory. When the flight was diverted to avoid adverse weather, the aircraft entered an area of strong convective activity and rapidly developing precipitating cells, which resulted in it experiencing severe turbulence and possibly reduced visibility for the pilots. While flying in these conditions, a combination of airspeed, turbulence and control inputs probably led to excessive loading on the aircraft’s wings, which separated from the fuselage in-flight before it collided with terrain.
The ATSB found that the pilots had limited experience flying in the ‘build-up’ to the wet season in the Darwin area. Although pairing a supervisory pilot with a pilot new to the company was likely to reduce risk in other instances, in this case it did not adequately address the weather-related risks because neither pilot had experience flying in the region during the wet season.
A serious incident was investigated by the ATSB following the report of passenger injuries and structural damage from exposure to severe turbulence during a charter flight.
On 25 November 2019, a Cessna 210M with four passengers was being flown from Darwin to Tindal, Northern Territory. Soon after departure, the pilot diverted 5 NM right of the planned track to avoid a large storm cell that was 5 NM left of track. Shortly after, the aircraft encountered sudden and sustained severe turbulence.
During the turbulence, the aircraft airspeed could not be controlled for several minutes through changing power settings, and for the most part the airspeed could not be held below 155 kt. For extended periods, the pilot had no control over bank angle, height, or heading. At one stage, the airspeed dropped below 140 kt, and the pilot lowered the landing gear in order to create drag and slow the aircraft down. ATSB’s analysis of the radar data showed that the aircraft ground speed reached 210 kt, a maximum descent rate of 5,000 ft per minute.
International accidents
A search of the accident report databases held by both the Transportation Safety Board of Canada (TSB) and the United States National Transportation Safety Board (NTSB) identified several instances over a 25-year period where the Cessna 210-aircraft type has sustained structural failure during flight (Table 4). There were 8 fatal accidents identified and categorised as private operations and one other categorised as a charter operation. The accidents were further categorised to similarly themed primary and secondary contributing factors, these included: manoeuvring in excess of VA, loss of control, spatial disorientation, continued flight into instrument meteorological conditions and severe weather.
Table 4: Cessna 210 in-flight break-ups – International
Date
Investigation agency accident ID
Aircraft detail
General location
21 Jan 1997
US NTSB CHI97FA056
Cessna 210N
Highland, Michigan
28 July 1997
Canada TSB A97Q0158
Cessna 210L
Milan, Quebec
18 June 2001
Canada TSB A010O165
Cessna 210L
Lake Lavieille, Ontario
4 December 2002
US NTSB FTW03FA057
Cessna 210L
Harrison, Arkansas
7 April 2005
US NTSB LAX05FA132
Cessna T210L
Tranquillity, California
12 August 2007
US NTSB MIA08FA027
Cessna T210N
Bloomfield, Kentucky
7 September 2010
US NTSB CEN10FA520
Cessna T210
Mountain Home, Arkansas
17 November 2014
US NTSB CEN14FA064
Cessna T210M
Cedaredge, Colorado
25 March 2017
US NTSB ERAFA17136
Cessna T210
Hayden, Alabama
Analysis
Introduction
On the morning of 24 December 2022, a Cessna 210N, registered VH-TFT, operated by Katherine Aviation, departed Gove Airport for a charter flight under the visual flight rules (VFR) to Katherine Tindal Airport. The flight departed with one pilot and one passenger on board. After the aircraft did not arrive and contact was unable to be made with the pilot, search and rescue activities were initiated by authorities. A distributed wreckage field was found the following day at a remote location in East Arnhem, approximately 237 km east-north-east of Katherine. Both occupants of the aircraft were fatally injured.
Examination of the accident site and recovered wreckage identified that the aircraft had sustained an in-flight break-up involving separation of the right wing. No pre-existing aircraft defects that had the potential to influence the accident were identified. The emergency locator transmitter fitted to the aircraft had activated from the accident sequence, however physical disruption between the unit and its antenna prevented an alert signal being received by the search authority.
The availability of flight data generally assists in the determination of contributing factors in accidents investigated by the ATSB. In this instance additional data may have provided time‑referenced positional information, airspeed, altitude and heading. Notwithstanding, weather satellite information was gathered that identified the formation of a rapidly developing thunderstorm near to Bulman during the time period the aircraft likely transited the region. The following analysis will examine the flight into adverse weather, the accident time, development of the structural break-up, and aspects related to the operator’s wet season training.
Time of the accident
The ATSB reviewed the aircraft performance, planned flight information and the available telecommunication records to determine a likely accident time. Based on the expected direct flight route conditions and aircraft speed, the aircraft should have arrived overhead the accident site at about 0930. However, the ATSB’s review of the available telecommunication records identified that the passenger’s mobile phone ceased its connection with the Bulman cellular tower at 1001 probably due to damage sustained during the accident sequence.
While there was insufficient information to ascertain the likely accident time more accurately than somewhere between about 0930–1000, possible reasons for the additional flight time to that planned included that the aircraft was slowed en route or diverted due to weather, including possibly being flown beyond Bulman and then turned back towards Gove.
Flight into adverse weather
This was the pilot’s first commercial aviation role and was also their first period operating through a Northern Territory wet season. They had completed their line training with the operator in September 2022 during the dry season and after deployment from Katherine had flown for approximately 3 weeks from the operator’s base in Gove. During that period, they had turned back previously due to unsuitable weather. This showed that the pilot had decision‑making experience flying in convective weather.
The ATSB considered it likely that, while completing flight planning earlier that morning, the pilot had accessed the graphical area forecast (GAF) that described the predicted weather en route to Katherine. Supporting that was the pilot’s previous flight planning records, where all the necessary information had been obtained and documentation completed. The pilot had mentioned in conversation to the Katherine Aviation operations staff member on the morning of the accident that the weather ‘appeared to be a bit iffy’, which also supported that the pilot had obtained and assessed the en route weather forecast.
Though most Katherine Aviation staff were away on leave that day, including the Gove senior base pilot and Head of Flying Operations, there were operational staff in place and on duty at the Katherine Aviation main base for consultation to assist with decision‑making surrounding the conduct of the flight. Additionally, Bureau of Meteorology staff who had produced the forecast remained available as an informed source to provide weather advice.
The prevailing cloud coverage along the flight route near to Bulman were predicted in the GAF to cover between 5 and 7 oktas, with an effective ceiling of 1,000 ft above mean sea level (AMSL). There were no breaks predicted between subsequent cloud layers, with cloud tops predicted to be the same as each subsequent cloud base to above 10,000 ft AMSL. These forecast conditions were unsuitable for a flight under the VFR at an altitude of 8,500 ft. However, BoM analysis of satellite imagery identified that the forecast overcast conditions were not present in the Bulman region in the lead up to the accident.
Increasingly severe weather conditions were predicted to develop from the prevailing cloud coverage during the validity period of the GAF. Visibility was expected to between 500 m and 2,000 m from rain showers, which was significantly below the required visual meteorological conditions. Towering cumulus and cumulonimbus clouds were also forecast to develop from cumulus cloud cells at different times and locations throughout area B during the forecast period.
A review of the available satellite imagery identified that the prevailing cloud coverage around the Bulman region rapidly formed into convective clouds as the aircraft approached the area. The thermal activity depicted in the satellite imagery within the Bulman area was accompanied by lightning strike detections at 0940, which confirmed that the towering cumulus and cumulonimbus clouds had further developed into a thunderstorm. This would have led to areas of moderate to heavy rain, with significantly reduced visibility as forecast in the GAF.
Depending on the proximity to these weather phenomena, it is also likely that the aircraft encountered severe turbulence associated with the convective action. Furthermore, because the satellite imagery confirmed that the prevailing overcast conditions did not exist in the Bulman region in the lead up to the accident, there was probably sufficient separation between the convective cloud formations associated with the developing thunderstorm to have been visible to the pilot. However, the severity of the conditions may not have been visually apparent.
The operator’s procedures required a 20 NM downwind separation from thunderstorms and it was expected practice that a flight was to be diverted upon encountering such phenomena. If severe turbulence was encountered, pilots were to slow the aircraft and to avoid rapid manoeuvres. It was not possible to determine the pilot’s precise actions during this final period of the accident flight. Had they been using the weather radar application on the iPad during the flight, it is possible that the extent of the developing storm near to Bulman was not evident due to the storm’s significant distance from the weather radar head. This may have led to the pilot not perceiving the potential severity of the storm as they approached the Bulman region.
In summary, upon arrival into the Bulman region, the aircraft likely entered an area of strong convective activity from a rapidly developing thunderstorm which probably resulted in exposure to a combination of severe turbulence and reduced visibility for the pilot.
In-flight break-up
The position of the right wing and its control surfaces relative to the remainder of the aircraft at the accident site indicated that an in-flight break-up had occurred. All other control surfaces remained with the aircraft up until the collision with terrain. The main wing spar was critically important to carry the aerodynamic loads encountered during flight. Bending and shear loads were transmitted from the wing spar into the fuselage via the carry-through structure. Without any redundant load paths, aeroelastic upward bending and then fracture of the main spar led to the wing separation and an immediate loss of control. There was only evidence of overstress and associated deformation on the fracture surfaces, with no pre-existing defects or damage that might have otherwise reduced its overall structural integrity.
The single wing separation indicates that the aircraft was likely subject to asymmetric loading at the time of the in-flight break-up consistent with the aircraft being manoeuvred. The limited distance between the separated wing and the primary accident site also indicates that the break‑up occurred at an altitude considerably lower than the initial cruise altitude. The direction of the wreckage trail was toward Gove. It was therefore possible that the aircraft had been, or was being, turned back to Gove prior to the break-up.
Had the aircraft entered an area of reduced visibility this would have likely created an increased risk of the pilot losing visual cues and experiencing spatial disorientation. The pilot’s last recorded flight under instrument flight was about 10 months prior when they obtained their multi-engine endorsement. Though the pilot was rated for flight into instrument meteorological conditions, it was likely that the pilot’s instrument flying proficiency had reduced during the intervening period.
Other previously investigated Cessna 210 accidents have identified structural failure and in-flight wing separation to be associated with conditions that were present near Bulman on the day of the accident. One serious incident from the Northern Territory during the 2019 wet season, also investigated by the ATSB, identified that upon coming within 5 NM of a developed thunderstorm, the pilot was unable to control the aircraft’s attitude, airspeed and descent rate. Although the aircraft was able to be landed, the investigation determined that the structural limits of the airframe were likely approached during that flight.
Based on the available evidence, the ATSB concluded that the most likely explanation for the in‑flight break-up of VH-TFT is that, while operating above the manoeuvring speed, the pilot applied a control input and/or the aircraft encountered severe turbulence that resulted in overloading and separation of the right wing.
Wet season training
New pilots employed by Katherine Aviation were given weather avoidance training during the ICUS period. Supporting that training, Katherine Aviation had specific information contained within its exposition for pilots to avoid thunderstorms as part of their operational requirements. Specifically, while en route pilots were to divert by a minimum of 10 NM upwind or 20 NM downwind of such weather systems. Pilots were to also slow the aircraft to the manoeuvring or turbulence penetration speed (VA) when turbulence from these weather systems was encountered. Due to limited available information, the ATSB was unable to assess the degree those requirements were being applied by the accident pilot prior to the in-flight break-up of VH‑TFT.
In addition to the formal operational requirements, Katherine Aviation had developed a training package that detailed the unique hazards of flying during the wet season. It described the procedures to help pilots mitigate the hazards when operating in that environment. The briefing contained specific advice on wet season weather phenomena that included: flight planning, flight into marginal visual meteorological conditions, safe operation and control of an aircraft when in turbulence, and advice on when to cancel the flight.
The pilot attended a company safety briefing prior to the commencement of the 2022 wet season, where elements of decision making were discussed, including first-hand accounts from senior pilots of their own wet season experiences.
Although the slide pack was not presented at the briefing it was made available for pilots to review after the meeting. Katherine Aviation did not require the training material to be reviewed by its pilots. The absence of a requirement for the training material to be reviewed may have been a lost opportunity for Katherine Aviation to ensure its pilots were further prepared to safely operate during the top end wet season.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the in-flight break-up involving a Cessna Aircraft Company 210N, registered VH-TFT, that occurred 237 km east‑north‑east of Katherine, Northern Territory on 24 October 2022. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
Upon arrival in the Bulman region, the aircraft likely entered an area of strong convective activity from a rapidly developing thunderstorm, which probably resulted in exposure to a combination of severe turbulence and reduced visibility.
It is probable that a combination of turbulence from the thunderstorm, airspeed above the aircraft manoeuvring speed, and control inputs led to the excessive structural loading and in‑flight separation of the right wing from the fuselage before the aircraft collided with terrain.
Safety actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are provided separately on the ATSB website, to facilitate monitoring by interested parties. Where relevant, the safety issues and actions will be updated on the ATSB website as further information about safety action comes to hand
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by Katherine Aviation
Wet season training
On 11 February 2023, Katherine Aviation formally presented its wet season training material to its company pilots. In August 2023, the Katherine Aviation Exposition was updated with the requirement that all pilots were to complete the training on an annual basis.
Flight monitoring
Katherine Aviation advised that, in January 2023, it commenced providing satellite tracking and communication devices for its pilots that enabled real-time satellite-based tracking and monitoring of its fleet. The devices allowed text messaging to be exchanged between the company and its pilots in the absence of a mobile telephone signal.
Operational control
Katherine Aviation advised that it had developed flight assessment tools that were required to be completed by its pilots prior to the conduct of any flights. The requirement to complete the assessments was identified in the August 2023 update to the Katherine Aviation Exposition. The tools were targeted to provide its pilots with better decision-making tools during planning for marginal weather.
A marginal weather decision-making chart was also developed to assist pilots assess the daily conditions. The requirement was communicated during a pilot safety meeting and the flowchart was displayed at all Katherine Aviation bases. Both charts are displayed below.
Glossary
AD
Airworthiness Directive
AGL
Above ground level
AMSL
Above mean sea level
ATC
Air traffic control
BoM
Bureau of Meteorology
CB
Cumulonimbus
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CEO
Chief Executive Officer
CTAF
Common traffic advisory frequency
EFB
Electronic flight bag
ELT
Emergency locator transmitter
EMBD
Embedded
FAA
Federal Aviation Administration
GAF
Graphical area forecast
GPWT
Grid-point wind and temperature
HAAMC
Head of aircraft airworthiness and maintenance control
HOFO
Head of flying operations
ICUS
In-command-under-supervision
JRCC
Joint Rescue Coordination Centre
NAIPS
National Aeronautical Information Processing System
POH
Pilot’s Operating Handbook
RAAF
Royal Australian Air Force
TAFs
Terminal area forecasts
VFR
Visual Flight Rules
Sources and submissions
Sources of information
The sources of information during the investigation included:
Katherine Aviation
Civil Aviation Safety Authority
Northern Territory Police Service
Textron Aviation (Cessna)
Airservices Australia
Royal Australian Air Force
Australian Maritime Safety Authority
Northern Territory Health
Bureau of Meteorology
Champagne PC Services
Telecommunication network provider
OzRunways
witnesses.
References
Australian Transport Safety Bureau. (2013). A review of the effectiveness of emergency locator transmitters in aviation accidents. AR-2012-128
Bureau of Meteorology, Graphical Area Forecast & AIRMET User Guide, Version 2.0 July 2018, Commonwealth of Australia
Bureau of Meteorology, Graphical Area Forecast User Guide, A guide for the transition from ARFORs to GAF, Version 1.2 20 October 2017, Commonwealth of Australia
Bureau of Meteorology, Aeronautical Services Handbook, Amendment 213, 1 December 2022, Commonwealth of Australia 2020
Federal Aviation Administration, Advisory Circular No. 00-24C (2013), Thunderstorms, U.S. Department of Transportation
Michalski, D.J., and Bearman, C. (2014). Factors Affecting the Decision Making of Pilots who Fly in Outback Australia. Safety Science, 68, 288-293
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Katherine Aviation
Bureau of Meteorology
Civil Aviation Safety Authority
Airservices Australia
Australian Maritime Safety Authority.
A submission was received from the Bureau of Meteorology.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions in which they have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[2]The Northern Territory is administered through 6 defined regional areas: 1. Darwin, Palmerston and Litchfield, 2. Top End, 3. East Arnhem, 4. Big Rivers, 5. Central Australia, and 6. Barkly.
[3]Cloud cover: cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[5]The wind direction and speed at an altitude of 8,500 ft was calculated by interpolating the wind speed and direction that was provided in the GPWT at altitudes of 7,000 ft and 10,000 ft.
[6]Satellite images were processed by the Bureau of Meteorology from the geostationary meteorological satellite Himawari-8 that was operated by the Japan Meteorological Agency.
[7]Turbulence intensity is specified according to the perceived effect upon aircraft and occupants. Severe turbulence produces large abrupt changes in attitude and/or altitude and momentary loss of control. Unsecured objects are tossed about and occupants violently forced against seatbelts. www.bom.gov.au/aviation/data/education/turbulence.pdf
[8]Severe icing: the rate of accumulation is such that de-icing/anti-icing equipment fails to reduce or control the hazard to the aircraft, and thus an immediate diversion is necessary. www.bom.gov.au/aviation/data/education/icing.pdf
[9]The National Aeronautical Information Processing System (NAIPS) is a multi-function, computerised, aeronautical information system. It processes and stores meteorological and NOTAM information as well as enables the provision of briefing products and services to pilots and the Australian Air traffic Control platform. About NAIPS (airservicesaustralia.com)
[10]Flight envelope: the range of combinations of speed, altitude, angle of attack etc., within which an aircraft is aerodynamically stable.
[11]Aerodynamic stall: occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16˚ to 18˚, and results in reduced lift.
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 24 December 2022, a pilot from Katherine Aviation was assigned to operate a Cessna 210N aircraft, registered VH-TFT (TFT), on a charter flight from Gove Airport to Katherine-Tindal Airport, Northern Territory. The fight was arranged to transport a single passenger who was scheduled to be in Katherine over the Christmas period.
At about 0730 local time the aircraft was refuelled with 211 litres of Avgas 100LL. At about 0800 the passenger arrived at the airport in preparation for the flight. Radio transmissions recorded on the Gove common traffic advisory frequency (CTAF) indicated that, at 0812, the aircraft was being taxied for engine run-up checks, and at 0814 the pilot advised that the aircraft had commenced the departure roll on Runway 31. At 0817 a final transmission was recorded on the CTAF indicating that TFT had departed Gove on a direct track to Katherine-Tindal Airport and was on climb to a cruising altitude of 8,500 ft.
At 0841 the operator received a text message from the pilot advising an expected arrival time at Katherine-Tindal Airport of 1024. As the aircraft tracked toward Katherine, mobile phone tower tracing records identified that the aircraft first came into the detectable range of the Bulman cellular tower at 0914.
At 1044 the operator called the pilot’s mobile phone and then at 1058 sent a text message seeking confirmation that the flight had arrived at its destination. When the operator did not receive a response, they checked with another company pilot who was stationed at Gove who confirmed that TFT had not returned to the departure airport. The operator then contacted several station properties along the expected route to check whether TFT had been sighted. At around midday, the operator contacted search and rescue officials and advised that TFT was overdue.
An airborne search and rescue response for the aircraft was commenced by the Joint Rescue Coordination Centre (JRCC) that afternoon. On 25 December 2022, at about 1345, a debris field was located by a search aircraft in a remote area of medium-density bushland, approximately 237 km east-north-east of Katherine (Figure 1). Both occupants were fatally injured and the aircraft was destroyed.
Figure 1: Satellite view of the Northern Territory showing the location of the accident site
Source: Google Earth, annotated by the ATSB
Context
Site and wreckage
The ATSB initiated a field-based investigation following notification from the JRCC that the aircraft wreckage had been located. ATSB investigators attended the accident site on 29 and 30 December 2022. The ATSB’s on-site examination of the wreckage and accident site identified that:
the right wing and its wing tip (which was not attached to the wing) were the first major components in the wreckage trail
the right wing was located approximately 300 m before the primary point of ground contact, indicating that it had separated from the aircraft fuselage during flight (Figure 3)
severed tree branches and ground scars were consistent with the aircraft having a trajectory of approximately 35° down from horizonal immediately before colliding with terrain
almost complete fragmentation of the aircraft structure had occurred on impact with trees and the terrain
aircraft components were spread over a distance of 80 m from the primary ground contact point. The propellor, engine, left wing, carry-through structure, empennage, nose gear and cabin components were all identified in the wreckage trail
the general orientation of the wreckage spread was in a north-east direction, opposite to the intended flight path to Katherine-Tindal
all major sections of the aircraft’s structure were accounted at the accident site
flight control continuity was established where possible
the wing flaps were assessed to have likely been in the retracted position
the landing gear was likely in the retracted position
there was no cockpit voice or flight data recorder, nor was there a regulatory requirement for them to be fitted to an aircraft this size
the aircraft was not fitted with ADS-B out or in-flight satellite tracking equipment and the aircraft was beyond the range of air traffic control radar.
Figure 2: Aerial view of the accident site showing the spread of wreckage
Source: ATSB
Figure 3: As found position of the right wing approximately 300m from the main wreckage
Source: ATSB
Wing inspection
The right wing and its wing tip were the first items located in the wreckage trail. On-site examination of the main wing spar identified that it had fractured diagonally, about 30‑60 cm from the inboard fuselage attachment points (Figure 4).
Figure 4: Illustration of the Cessna 210 and the wing and main spar fracture location
Source: Textron – annotated by the ATSB
Examination of the right wing showed extensive permanent deformation of the wing surface with associated compression rippling to the upper skin. The damage was indicative of substantial upward bending forces applied to the wing prior to its failure and separation from the aircraft (Figure 5).
The inboard end of the right wing-spar remained attached to the fuselage carry-through structure. The left wing remained attached to the carry-through and was located within the primary wreckage area. Examination of the fracture surfaces from the right wing-spar identified evidence of ductile overstress. The on-site assessment did not identify any regions of fatigue cracking or other pre‑existing damage that might have weakened the spar caps, straps, or web.
The outboard tip section from the right wing was found about 70 m from the right wing. Black contact marks on the tip surfaces indicated that the outboard tip impacted the rubberised leading-edge protection on the tail during the break-up sequence.
The inboard end of the right wing-spar and the corresponding fracture surfaces from the separated right wing were retained for further detailed examination at the ATSB technical facilities in Canberra.
Figure 5: Separated right wing assembly showing damage associated with significant upward bending forces
Source: ATSB
Propeller assembly
On-site inspection of the propeller identified that the propeller hub had separated from the engine crankshaft due to overstress fracture under predominantly bending loads. One propeller blade had fractured from the hub at its base. All of the blades had sustained forward bending and rotational abrasion damage. One of the blades displayed chordwise twisting and compound bending. The damage signatures indicated that the engine was likely to have been driving the propeller with significant power when the aircraft collided with terrain.
Figure 6: Propeller assembly as removed from the ground impact crater
Source: ATSB
Aircraft
VH-TFT was a 210N, manufactured in the United States in 1978 by the Cessna Aircraft Company and first registered in Australia in 1989. The aircraft was capable of seating six-people including the pilot and had been designed with a high cantilever wing and a single-engine operating a variable-pitch three-blade propeller. The aircraft was equipped with retractable tricycle landing gear.
The operator’s maintenance records indicated that the aircraft had accrued about 15,100 total flight hours. The most recent scheduled maintenance was a 100-hourly inspection that was completed in accordance with the Civil Aviation Safety Authority maintenance Schedule 5, about 2 months (95 flight hours) prior to the accident. A number of detailed wing inspections were conducted during the last 100 hourly. They included:
Federal Aviation Administration Airworthiness Directive 2012-10-04 (inspection for cracking of the main spar lower cap)
Cessna Special Inspection Document (SID) operation 33 – Inspection of the wing lower spar cap
SID operation 35 – Inspection of the carry through spar lower surface
SID operation 37 – Inspection of the wing spar carry through attachment lugs.
A maintenance release was issued in the night visual flight rules and charter operational categories. The current maintenance release was found in the aircraft wreckage with the daily inspection certified on the day of the accident. No defects or overdue maintenance were recorded on that document.
Weather and environmental information
The Bureau of Meteorology (BoM) advised that, on the morning of 23 December 2022, the day prior to the accident, tropical cyclone Ellie crossed the coastline to the west of Darwin and tracked to the south. Later that evening, Ellie was downgraded to a tropical low, however heavy rain and strong to damaging winds were expected to impact large parts of the greater Northern Territory top-end.
BoM analysis of satellite imagery[1] indicated that on the morning of 24 December 2022, convective cloud started to develop along the expected flight path of the aircraft, near to the accident site. At around 0900, the cloud development strengthened into thunderstorms, with the first observations of lightning recorded between 0940 and 0950. The satellite imagery in the vicinity of the accident site is shown in Figure 7 and Figure 8. That imagery showed the formation of a thunderstorm near to the accident site from about 0910 and its progression through to 1000. The system persisted for several hours after that initial formation.
The BoM further advised in their analysis of the weather conditions that a thunderstorm could result in severe turbulence, severe icing and wind shear with outflows of strong and gusty winds, not only in the immediate vicinity but also at some distance away from the storm. An automated weather station at Bulman, approximately 20 km to the south of the accident site, recorded 12.4 mm of rainfall between 0930 and 1030 that morning.
The development of the severe weather was consistent with the forecast conditions in the Northern Territory Graphical Area Forecast (GAF) that was issued by the BoM at 0135. In the region of the aircraft’s expected flight path the GAF predicted cloud coverage between 5 and 7 oktas[2] at the accident site location around the time of the accident, with an effective ceiling of 1,000 feet above ground level (AGL). There were no breaks predicted between subsequent cloud layers, with cloud tops predicted to be the same as each subsequent cloud base to above 10,000 ft AGL. Further, areas of heavy and moderate rain were predicted with reduced visibility between 500 and 2,000 metres from convective clouds including towering cumulous and cumulonimbus, each with associated severe turbulence.
Figure 7: Weather satellite imagery showing cloud and convective activity over the region of the accident site at 0900. Subsequent changes in convective activity (within the boxed region) are further highlighted in Figure 8
Source: Bureau of Meteorology, annotated by the ATSB
Figure 8: Close-up montage of satellite imagery and convective activity overhead the accident site from 0910 to 1000
Red dots in the above images at 0940 Central Standard Time (CST), 0950 CST and 1000 CST are recorded lightning strikes. The accident site is represented by a red star.
Source: Bureau of Meteorology, annotated by the ATSB
Pilot information
The pilot commenced their flight training in June 2021 and in late January 2022 they obtained a commercial pilot license (aeroplane). The pilot obtained a multi-engine aircraft instrument rating in February 2022. The pilot also held a Class 1 aviation medical certificate, valid until May 2023.
The pilot commenced flight training with Katherine Aviation in August 2022, completing 14 proficiency flights in a Cessna 210 during the induction period and passing the company line check on 20 September. The pilot was then employed by the operator, completing passenger‑carrying charter flights from Katherine-Tindal to remote locations within the Northern Territory top-end (totalling 76 hours). At the start of December, the pilot was restationed to the operators base in Gove, East Arnhem, completing an additional 45 hours until the day of the accident. They had recorded a total of 364 flying hours before the accident flight.
Witness information
The expected track for the flight between Gove and Tindal-Katherine was over remote sections of the Northern Territory. No witnesses to the accident have been identified.
Audio information
Examination of the recorded CTAF radio transmissions for Gove on 24 December 2022 revealed 3 transmissions from the pilot:
during the ground run-up checks
during taxi for departure
shortly after take-off.
No additional recordings regarding the operation of the flight have been identified.
Further investigation
To date, the ATSB has examined the accident site and wreckage, interviewed personnel associated with the operation of the aircraft, collected meteorological and air traffic control radar data, and reviewed the aircraft maintenance and pilot records.
The investigation is continuing and will include further review of the:
aircraft wreckage and recovered electronic devices
environmental influences including analysis of the meteorological data
pilot qualifications, experience, and training
operator training policies and procedures
passenger records
similar occurrences in Australia and internationally.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB acknowledges the assistance provided by the Bureau of Meteorology, Airservices Australia, the Northern Territory Police Force and Heli-Muster Pty Ltd in supporting the ATSB’s onsite team, and for providing information through the evidence collection phase of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Satellite images were processed by the Bureau of Meteorology from the geostationary meteorological satellite Himawari-8 that was operated by the Japan Meteorological Agency
[2] Cloud cover observations are measured in oktas (eighths). A completely clear sky is recorded as zero okta, while a totally overcast sky is 8 oktas. Any trace of blue on an otherwise cloudy sky is recorded as 7 oktas.
Occurrence summary
Investigation number
AO-2022-067
Occurrence date
24/12/2022
Location
237 km east-north-east of Katherine
State
Northern Territory
Report release date
30/10/2024
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, In-flight break-up, Turbulence/windshear/microburst
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
210N
Registration
VH-TFT
Serial number
21063448
Aircraft operator
KATHERINE AVIATION PTY LTD
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
On 25 November 2019, a Cessna 210M, registered VH-SJW and operated by Mistar Holdings, was conducting a charter flight with four passengers from Darwin to Tindal, Northern Territory. Soon after departure, the pilot diverted 5 NM right of the planned track to avoid a large storm cell that was 5 NM left of track. About 10 minutes after departure, while maintaining 3,500 ft, the aircraft encountered sudden and sustained severe turbulence. Control of the aircraft was lost for over 3 minutes, and three passengers sustained minor injuries.
After landing at Tindal and inspecting the aircraft for potential damage, the pilot ferried the aircraft to Millingimbi. At Millingimbi, the pilot picked up four more passengers for a charter to Galiwin’ku (Elcho Island). The pilot reported the incident to the operator that evening. Upon receiving notification of the turbulence encounter, the operator grounded VH-SJW at Galiwin’ku, pending an engineering inspection.
What the ATSB found
At 10 NM from the thunderstorm, the pilot did not have sufficient separation to ensure safe passage.
Following the incident, the inspection carried out by the pilot was not sufficient to ensure the airworthiness of the aircraft beyond doubt. Flying another charter flight without an aircraft inspection by a qualified person exposed the operator, the pilot, and the passengers to elevated risk. In addition, the operator did not have guidance to direct pilots to seek advice or peer support following abnormal events.
What has been done as a result
The operator has developed case studies for pilots, emphasising weather avoidance and management of abnormal events. These have been integrated into proficiency checks to ensure solid understanding of theory, and practical application of weather avoidance, escape and post encounter management.
Safety message
The primary protection against thunderstorm related turbulence is avoidance. In this case, 10 NM was not far enough. Operators, pilots and passengers can work together to avoid flying in adverse weather. For instance, by starting a day’s flying early it can be completed before weather becomes a problem in the afternoon.
A pilot with the best intentions may make a suboptimal decision after experiencing an abnormal event. Operators can provide guidance to assist pilots to make good decisions in these situations, by providing peer support and emphasising the importance of reporting abnormal events in a timely manner. Early reporting reduces pressure in operations, allowing ample time to make alternative arrangements.
To support continuous improvement in performance, pilots should regularly review operational documents and industry advice, to build on experience, and develop a comprehensive knowledge of issues and strategies available.
The investigation
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
Planned flights
On 25 November 2019, at 1119 Central Standard Time,[1] a Cessna 210M, registered VH-SJW and operated by Mistar Holdings, departed Galiwin’ku (Elcho Island), Northern Territory, for a passenger charter flight with the pilot and three passengers on board. The flight had a planned stopover in Darwin, to collect another passenger, before continuing on to Tindal. From Tindal, the pilot planned to fly to Millingimbi empty, collect passengers, and return to Galiwin’ku (Figure 1). The flights were being conducted under visual flight rules (VFR).
The pilot briefed the passengers that seatbelts were to be worn at all times, and that they should be tight. The pilot visually checked the passenger’s seat belts before departure.
Figure 1: Charter flight route for VH-SJW
Source: Google Earth, annotated by the ATSB
Turbulence encounter
As per the forecast, on approach into Darwin Airport, the pilot noticed a large thunderstorm to the south of the city crossing the intended departure track. After landing at Darwin, the passengers disembarked and had about a 30-minute break before boarding the aircraft again.
The pilot accepted a departure delay from air traffic control (ATC) of 28 minutes. The air traffic controller recalled that multiple aircraft were requesting diversions due to storm activity. During this time, the pilot reviewed graphical area forecasts issued by Airservices Australia, and used Bureau of Meteorology weather radar to track the progress of the storm cell.
The aircraft departed Darwin at 1418 and the pilot was cleared to depart via VFR route 4. The pilot had identified that the storm cell was about 5 NM left of the planned track, so requested a diversion of 5 NM right of track to provide a 10 NM separation from the weather. ATC approved the pilot’s request. One of the passengers photographed the weather after they diverted (Figure 2).
Figure 2: Photograph taken by right centre row passenger
Source: Supplied by passenger aboard VH-SJW
About 10 minutes after take-off, the pilot reported maintaining an altitude of 3,500 ft. At about this time, and shortly after the photograph was taken, the aircraft was subjected to sudden severe turbulence.[2] The mobile phone used to take the photograph fell under the pilot’s rudder pedals with the first significant drop in altitude. The pilot’s checklist and an iPad were also loose in the cabin.
The pilot was wearing a four-point harness and the passengers, seated in the centre and rear rows, all wore lap belts. There was no facility for the pilot and passengers to communicate over an intercom. Due to the high noise environment in the aircraft cabin, the pilot could only communicate with passengers using hand signals. As a result, the passengers were not warned of potential turbulence, or instructed to check their seatbelts were tight, and stow loose items.
The pilot reported tightening their own harness and initially aimed to climb to 4,500 ft, hoping to climb over the turbulence. This strategy changed in order to retain visual meteorological conditions.
Turbulence penetration speed[3] for the Cessna 210M was 119 kt. The pilot stated that, during the incident, airspeed could not be controlled through changing power settings, and for the most part the airspeed could not be held below 155 kt. For extended periods, the pilot had no control over bank angle, height, or heading. At one stage, the airspeed dropped below 140 kt, and the pilot lowered the landing gear in order to create drag and slow the aircraft down.
The backrest of the centre row of seats in VH-SJW could be folded forwards for access to the rear row of seats, which was standard. One centre row passenger found it difficult to brace against the moveable seat back, and though wearing a seatbelt, reported not being sufficiently secure. This passenger’s neck was injured in the incident.
The turbulence encounter lasted about 3.5 minutes. Radar at Darwin recorded the aircraft’s highest groundspeed as 210 kt, and rate of descent at one point to be 5,000 ft/minute with a lowest altitude of 1,200 ft.
The pilot gave the passengers a ‘thumbs-up’ indication when control was returned and continued to Tindal Airport in mild turbulence and rain.
After landing
The aircraft landed at Tindal Airport at 1538, and the passengers disembarked 5 minutes later. The passengers reported that the pilot asked if they were okay but said the pilot did not de-brief them on the incident other than to say that it was normal turbulence. The pilot did not report the turbulence encounter to the operator or the ATSB.
A passenger stated that the group was distressed by the incident, and, with no debriefing or advice, they went directly to their accommodation. In retrospect, the passenger believed the group should have instead gone to hospital to be checked over. Three of the passengers later visited hospital for shoulder and neck injuries, and one case of damage to a pre-existing leg injury.
Recognising the potential for damage to the aircraft from the turbulence encounter, the pilot reported conducting a thorough daily inspection at Tindal. The pilot spent a total of 31 minutes on the apron at Tindal before departing for Milingimbi at 1614. At Milingimbi, the pilot met four passengers and flew them to Galiwin’ku.
At Galiwin’ku, the pilot told the operator’s base manager about the turbulence encounter. The base manager advised the pilot to contact the head of flight operations (HOFO). The pilot did so and the HOFO instructed the base manager to ground the aircraft and ordered an engineering inspection of the aircraft for flight under abnormal loads. An engineer carried out the inspection the following day and returned the aircraft to service after finding no defects.
Context
The pilot
The pilot of VH-SJW held a commercial pilot licence (aeroplane) and had 802 hours’ aeronautical experience, with 550 hours as pilot in command, and had flown in the region for the operator for 11 months. Upon commencement with the operator in December 2018, the pilot underwent a course of training designed to bridge the gap between commercial licence training and commercial operations in general aviation. This included exposure to decision making around adverse weather.
Weather information
Meteorological conditions over the northern half of Australia are favourable for thunderstorms from October through to March. Abundant moisture and instability is present through most of the Wet Season. During this time, low pressure lies across northern and central Australia, giving rise low-level convergence and vertical motion necessary for thunderstorm development. During these months, thunderstorms during the afternoon are a common occurrence due to the convergence of sea breezes with an east to south-easterly synoptic wind regime (Figure 3).
The convective cloud bases can be very high (sometimes up to 15 000 feet), with very severe downdraughts from the cloud base to the surface. For this reason, flights should never be conducted under or through precipitation (including virga) from towering cumulus or cumulonimbus clouds.
Figure 3: Mechanism of local storm generation
Source: ATSB
The weather forecast for Darwin received by the pilot before departure stated:
PROB30 TEMPO 2505/2514 VRB20G45KT 1000 THUNDERSTORMS WITH MODERATE RAIN BKN010 SCT025CB
That translated as a 30 per cent probability of thunderstorms for periods of at least 30 minutes but less than 60 minutes, and wind variable in direction with gusts up to 83 km/h (45 kt), accompanied by low cloud and rain with low visibility around Darwin from 1430 local time onwards. Tindal shared similar predicted conditions although any thunderstorms were expected for periods of less than 30 minutes.
The routine report of meteorological conditions at Darwin Airport at the time VH-SJW was readying for departure stated:
This translated as surface wind from the north-west at 18 km/h. Visibility was 10 km or greater, with showers in the vicinity of the airport. Cloud at 4,500 ft covered up to one half of the sky, and the layer included embedded cumulonimbus. The air temperature was 34 °C and the pressure (QNH) was 1,008 hPa. Additionally, a trend forecast was included with the report, warning of the expectation of periods of thunderstorms. These would have low cloud at 1,000 ft covering three quarters of the sky and cumulonimbus at 2,500 ft covering up to half the sky, bringing rain with variable wind gusting from 35 to 83 km/h, and reduced visibility of 1,000 m.
The pilot used information from a Bureau of Meteorology high-resolution Doppler radar, located 5.5 NM to the east of Darwin, to aid awareness of the weather conditions. There are, however, limitations to that technology. Heavy rain closer to the radar will absorb energy and reduce the displayed intensity of other cells behind it. Additionally, the image is a composite of the last 6 to 10 minutes of data and shows where the weather was, not where it is. A cell could be much closer and more intense than displayed.
Figure 4 shows satellite images that captured the build-up of thunderstorm activity on the day. In the first frame at 1230 Darwin (YPDN) is relatively clear of cloud. After VH-SJW arrives in Darwin, the next hour shows significant build-up of cloud on VH-SJW’s intended track to Tindal (YPTN).
Figure 4: Satellite images of thunderstorm development at the time
Source: Bureau of Meteorology annotated by ATSB
Procedures and guidance
In August 2019, the operator amended its operations manual with a section titled ‘Adverse weather operations’. This section required pilots to avoid thunderstorms by 20 NM during the cruise phase of flight. The pilot had signed to confirm receipt of the operations manual amendment on the day it was issued. The operator also created a training program to support the amendment. The pilot had not received the training before the incident flight.
The safety message of ATSB report AO-2017-102,[4] an investigation of a fatal turbulence penetration event involving a Cessna 210 in the Northern Territory, stated that diversions of 10 NM may not be sufficient. That report was presented by an ATSB investigator in the pre-season Top-End safety briefing hosted by the Civil Aviation Safety Authority in Darwin on 9 October 2019. The operator’s pilots on Galiwin’ku (Elcho Island) could not attend, and instead got together to watch the 2018 briefing which was available via the internet.
In interview, the HOFO stated that pilots were encouraged to report incidents, and in some cases, such as for birdstrike, there were written requirements and instructions for reporting and managing the event. Even though the operator provided pilots with extensive guidance on avoidance of adverse weather, the HOFO stated that there was no formal guidance for the actions for pilots to follow after encountering severe turbulence.
Safety analysis
Anticipating and avoiding turbulence
The primary tool for reducing the risk of turbulence encounters of this type is avoidance of the associated weather phenomenon. Advice existed for the pilot in the operations manual that a 20 NM separation was required. A previous ATSB investigation report stated that 10 NM separation may not be enough, and a recent seminar repeated the message. Unfortunately, partially due to the reality of remote area operations, the pilot missed these recent reminders.
By diverting 5 NM right of track, and being 10 NM from the cell, the pilot was still too close to the weather phenomenon. Although the extent of loss of control was unexpected, some turbulence could be reasonably foreseen.
The pilot was well secured by wearing a harness, yet the passengers and cabin were not sufficiently prepared. The brief before flight stated that seatbelts were to be worn at all times, and that they should be tight, and the pilot conducted a visual check before departure. During flight when turbulence is anticipated or encountered, these instructions should be repeated with instruction to stow all loose items. In this case, an inability to communicate via intercom with the passengers while airborne limited the pilot’s ability to prepare the cabin.
Post incident reporting
A loss of control due to weather is an immediately reportable matter for an air transport operation under Regulation 2.3 (3)(s) of the Transport Safety Investigation Act 2003. In accordance with section 18 of this Act, the occurrence must be reported as soon as is reasonably practicable to the ATSB by telephone and a follow up written report must be made within 72 hours. The requirement to ensure a report is made resides with all responsible persons having knowledge of the occurrence.
The pilot did not report the turbulence encounter to the operator until after the last flight. From that point, the pilot and operator both had a responsibility to report the encounter to the ATSB. The encounter was reported by the operator 7 days after it occurred. It is important for preservation of perishable evidence that occurrences are reported as soon as practicable.
Operational support and management of risk
During the turbulence encounter and loss of control, the pilot was sure that no airframe limitations were exceeded. If the limitations were not exceeded, the pilot was not legally required to cease operations in that aircraft. However, when encountering such a high level of turbulence, the aircraft instruments may not present an accurate picture of what the aircraft experiences. It was reasonable to assume that airframe limitations could have been exceeded.
A pilot may not recognise or appreciate the implications of an abnormal event until a much later time. An objective view from a peer or senior person can lead pilots to make better decisions after an abnormal event.
Without formal guidance as to next steps following an encounter with severe turbulence, the pilot did not report the incident, or seek outside input into decision-making. Subsequently, the pilot prescribed a suboptimal inspection for the circumstances. The pilot did recognise the potential for damage, and inspected the aircraft to the extent that a pilot could. Licenced aircraft maintenance engineers are qualified to inspect aircraft for abnormal flight loads, yet the pilot did not consider such an inspection was necessary. Although the later engineering inspection found no defects, continuation of flight without an appropriate inspection exposed the pilot, operator, and passengers to additional, avoidable risk.
The operator demonstrated active risk management by grounding the aircraft to ensure its airworthiness after receiving a report of the occurrence. This set a visible benchmark of risk tolerance, which if supported by formal guidelines, would clearly set the operator’s expectations of its pilots.
Even in remote areas, pilots are not expected to manage the safety of a flight on their own, and facilities exist for pilots to enlist support and seek alternative solutions. Operators should ensure that there are well-communicated and structured solutions in place.
On the operational level, reporting issues as early as possible gives an operator time to develop alternative solutions for customers, which takes any acquired operational pressure away from the pilot. This supports pilots in cautious decision-making.
Another tool to assist in pilot decision-making is passenger debriefing. It is an opportunity for the pilot and passengers to process the occurrence and develop strategies for next steps and future avoidance.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the turbulence encounter and loss of control involving VH-SJW on 25 November 2019.
Contributing factors
Although the pilot diverted 5 NM right of track to avoid a large storm cell that was 5 NM left of track, the 10 NM separation from the storm was not sufficient and the aircraft encountered severe turbulence, resulting in a loss of aircraft control.
Other factors that increased risk
The operator provided no formal guidance to pilots with respect to immediate reporting of abnormal events, and the pilot did not make an immediate report.
The pilot flew another passenger charter flight in the incident aircraft before reporting the turbulence encounter and loss of control to the operator. Upon receiving the notification, the operator immediately grounded the aircraft for a precautionary airframe inspection.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot of VH-SJW
passengers aboard VH-SJW
Mistar Holdings (operator of VH-SJW)
Department of Defence (air traffic control provider)
Bureau of Meteorology
Civil Aviation Safety Authority.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of VH-SJW
Mistar Holdings
Bureau of Meteorology
Civil Aviation Safety Authority
Department of Defence.
Submissions were received from the Bureau of Meteorology and Mistar Holdings (safety action only). The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 28 November 2016, at about 1656 Coordinated Universal Time (UTC),[1] a China Eastern Airlines Airbus A330-243, registered B-5821, operating flight MU-777, departed Kunming, China, for Sydney, New South Wales. On board were 14 crew and 213 passengers.
As the aircraft approached Sydney, the flight crew commenced descent from flight level (FL) 370.[2] The flight crew advised the cabin crew of the descent and illuminated the seatbelt signs. The cabin crew manager announced to the passengers that the aircraft was on descent to Sydney and that as the seatbelt sign had been illuminated they needed to fasten their seatbelts. The cabin crew proceeded to check that passengers had their seatbelts fastened, starting from the front rows and moving towards the back of the cabin.
During descent, the flight crew diverted 5 NM from the flight route due to thunderstorms. Once clear of weather, they received instructions to descend via waypoint[3] BOREE.
At 0248 UTC at FL 230, about ten minutes after the seatbelt sign had been illuminated, the aircraft experienced a severe turbulence event which lasted about 30 seconds. The flight crew commenced the turbulence checklist as per the quick reference handbook (QRH), starting with ‘ignition on’, but as the turbulence had stopped, the rest of checklist was not completed. They checked the flight instruments and engine indications, which were normal, so the flight was continued to Sydney.
Prior to the event, the cabin crew manager was at the back of the cabin checking seatbelts and observed four passengers without a seatbelt, one of whom was standing and reaching for their baggage. During the turbulence event, the cabin crew manager struck their back on a seat armrest. A cabin crewmember in front of the cabin crew manager fell to the ground. Two of the passengers without seatbelts struck their head on the ceiling. After the event, all cabin crewmembers returned to their seats.
After landing, at around 0314 UTC, a cabin crewmember informed the flight crew that there were eleven people who were injured, including three cabin crew. The aircraft sustained minor damage to the interior cabin above row 42, 64, 65, and 68 (Figure 1).
Figure 1: Damage to cabin (row 42, and 68 passenger service unit)
Source: Operator (annotated by the ATSB)
Captain’s comments
The captain provided the following comments:
On approach to Sydney, the crew did not receive any reports regarding turbulence. They did observe other aircraft divert to avoid the thunderstorms.
Once they completed the diversion around the thunderstorms, there was no further weather on the radar.
During the descent, there was some cloud scattered, but no dangerous weather, because they had diverted from the thunderstorms 5–8 minutes earlier.
The turbulence they experienced was different to any turbulence they experienced before, as it was very short, but very strong.
As the turbulence event was very short, they did not report it to ATC.
During the turbulence, there was little change in airspeed or rate of descent.
The flight crew did not realise that there were any issues within the cabin until after landing. Normally, they would be notified by the cabin crew if there were injuries.
The flight crew did not make any announcement to passengers, nor cabin crew about the turbulence, as they did not have any warning.
Cabin crew manager comments
The cabin crew manager provided the following comments:
The seatbelt sign had been switched on about 10 minutes before the turbulence.
The cabin crew were preparing the aircraft for landing, and ensuring that passengers had their seatbelts on, when the turbulence event occurred.
The cabin crew did not notify the captain until after landing as the cabin crew manager was injured and they were aware the flight crew were preparing for landing.
The cabin crew had to keep encouraging passengers to fasten their seatbelts during the flight.
Flight data
The aircraft manufacturer provided the ATSB with a report of the data extracted from the digital flight data recorder (DFDR). The data shows that when the aircraft encountered the turbulence, the vertical G[4] loadings varied between -0.20 G and 1.8 G and the lateral G loadings varied between -0.07 G and 0.12 G (Figure 2). The calculated longitudinal wind varied between around 15 kt tailwind and 5 kt headwind and the lateral wind varied between 20 kt right and 5 kt left. The vertical wind reached a maximum of about 3,100 feet per minute updraft (Figure 3). During the turbulence, the autopilot stayed engaged and the load factors experienced during the turbulence did not exceed the limits of the aircraft.
The rapid changes to wind speed and direction confirm the aircraft encountered turbulence conditions.
Figure 2: G Loadings during turbulence
Source: Airbus
Figure 3: Wind variation during turbulence
Source: Airbus
Bureau of Meteorology report
The Bureau of Meteorology (BoM) provided the ATSB with a report detailing the weather at the time of the incident, including conditions, the weather forecast, warnings, and satellite and radar imagery.
The report showed that there were light winds between 20 to 30 kt from FL180 to FL450. There was no significant weather at the time of the turbulence.
It is likely that the turbulence encountered was the result of developing thunderstorms in the area.
Clear air turbulence
Clear air turbulence (CAT) is defined as sudden severe turbulence occurring in cloudless regions that causes violent buffeting of aircraft.
CAT can be serious, because it is not shown on weather radar, meaning it is difficult for pilots, air traffic controllers, and weather forecasters to detect. It can also occur when no clouds are visible. It is common at high altitudes, especially in the vicinity of jetstreams.
Previous occurrences
A search of the ATSB database found the following occurrences where aircraft encountered clear air turbulence resulting in injuries on board:
On 27 October 2000, a Boeing 747 encountered clear air turbulence en route from Sydney to Osaka, Japan (ATSB investigation 200005031). Although the weather forecast indicated thunderstorms within 110 NM of the flight route there was no turbulence forecast. When the CAT stuck, the seatbelt sign was not illuminated, and people were moving about the cabin. Two passengers sustained broken ankles.
On 10 May 2013, a Bombardier DHC-8 encountered clear air turbulence about 49 NM north of Townsville, Queensland (ATSB investigation AO-2013-084). The turbulence lasted about 10 seconds. The crew did not observe any cloud and the weather radar did not show any significant weather for the entire flight. Two cabin crew members who were standing at the time sustained head injuries, one of whom was knocked unconscious. Two flight crew sustained minor injuries when objects were thrown around the flight deck.
Safety analysis
The aircraft encountered unforecast CAT about ten minutes after the seatbelt sign had been illuminated for the descent into Sydney. The cabin crew were preparing the cabin for landing. A number of passengers and members of the cabin crew, towards the back of the aircraft, who were not wearing seatbelts, were injured during the CAT event. They sustained head, neck, hand, back, and abdominal injuries.
Finding
This finding should not be read as apportioning blame or liability to any particular organisation or individual.
The aircraft encountered CAT. The cabin crew and passengers who were injured during the turbulence did not have seatbelts fastened, despite the seatbelt sign being switched on.
Safety message
A clear air turbulence encounter can be a surprising experience for both crew and passengers. A safety bulletin published by the ATSB Staying safe against in-flight turbulence, noted that almost all turbulence injuries involved people who are not properly seated and do not have their seatbelt fastened. This incident is a timely reminder of the importance of having the seatbelt fasted when the seatbelt sign is switched on and to pay attention to instructions given by the cabin crew, so that injuries during a turbulence encounter can be minimised.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 10 October 2016, a QantasLink Bombardier DHC-8-402, registered VH-LQM, conducted a scheduled passenger flight from Melbourne, Victoria, to Canberra, Australian Capital Territory. On board the aircraft were two flight crew, two cabin crew and 70 passengers. The captain was the pilot flying (PF) and the first officer was the pilot monitoring (PM).[1]
During the pre-flight briefing at Melbourne Airport, the flight crew noted there was severe turbulence and severe mountain wave turbulence in the area forecast[2] and SIGMET[3] for their descent and approach to Canberra. They briefed the cabin crew to be prepared for a quick cabin service and that the seat belt sign would be activated early on the approach due to the forecast turbulence.
The aircraft departed from Melbourne at about 1158 Eastern Daylight-saving Time (EDT) and climbed to a cruising level of FL 210.[4] The flying conditions were smooth at FL 210 and the flight was issued with the POLLI FOUR ALPHA standard arrival route into Canberra, which started at waypoint POLLI, to the south west of Canberra (Figure 1). The flight crew instructed the cabin crew to prepare the cabin for landing several minutes before the top of descent. However, the flying conditions continued to be smooth during the descent, so the flight crew waited until about FL 130 before activating the seatbelt sign. This was shortly after passing waypoint POLLI.
Between waypoints GOMAN and HONEY, the aircraft descended below FL 110 and the PF reduced the aircraft speed to 210 kt, which is the best speed for turbulence penetration. The PM estimated that the tailwind component reduced from about 70 kt to about 40 kt after the descent below FL 110. At this point, the aircraft was tracking about 060° and passing in and out of cloud over the Brindabella Ranges, which has ridgelines orientated north-south to the south-west of Canberra.
During the descent, the flight crew did not observe any weather radar indications of potential turbulence or visible indications from the shape or movement of the clouds. Between waypoints HONEY and DALEY at about 7,000 ft AMSL, while passing through a small cloud, the aircraft dropped abruptly. The flight crew reported that everything in the flight deck became airborne, the autopilot disengaged, and the PF struck the left side of their head on the overhead air-vent and light, which dislodged their headset. The captain handed control over to the first officer while they refitted their headset and re-established communications, then resumed their flying pilot role and reset the autopilot.
The flight crew continued the approach to land at Canberra without further incident and notified Canberra air traffic control of their severe turbulence encounter on the approach. After the aircraft landed, the PM contacted the cabin crew to check if there were any cabin injures to report. The cabin crew indicated they were uninjured and made a public address to the passengers to check for injuries. The PM then called their company to inform them the aircraft was unserviceable after a severe turbulence incident, and also noticed the captain’s minor injuries.
During the disembarkation of the passengers, the cabin crew informed the first officer that one passenger had hit their head on the overhead baggage locker. The first officer then asked a company ground agent to contact the emergency services so the passenger could be checked. However, the passenger declined treatment. The emergency services arrived and checked the captain. The captain was then advised by the company to visit a doctor where they were diagnosed with minor injuries.
Figure 1: POLLI FOUR ALPHA arrival track of VH-LQM
Source: Google earth, annotated by ATSB
Flight data recorder
The flight data recorder showed that as the aircraft descended through about 7,800 ft the aircraft was in a stable descent maintaining 210 kt and heading 042°. As the aircraft descended through about 7,300 ft the airspeed peaked at about 240 kt and the vertical acceleration oscillated rapidly between a maximum of +1.6G,[5] minimum of -1G, then maximum of +1.6G before returning to +1G.
Maintenance inspection
After landing, the captain raised a defect report in the maintenance technical log for the severe turbulence encounter. Inspections were then conducted for the severe turbulence assessment. No defects were found, and the aircraft returned to service on 12 October 2016.
Weather forecast
The weather forecast for the Canberra area, issued for the period from 0840 to 2200 EDT on 10 October 2016 included severe turbulence below 12,000 ft and severe mountain wave turbulence above 5,000 ft. The wind was forecast as follows:
10,000 ft, from 300° at 60 kt
7,000 ft, from 300° at 45 kt
5,000 ft, from 290° at 30 kt.
Mountain waves
Mountain waves may be experienced on the lee-side of mountain ranges as smooth undulating airflow or may contain turbulence in the form of breaking waves and rotors (Figure 2). They typically form when the wind direction is close to perpendicular to a ridge line (+/-30°), the wind speed is at least 15 kt[6] and increases with height, and there is stable air above the crest of the ridge with less stable air above that and a stable layer below the ridge. The formation of clouds on the lee-side may indicate turbulent flying conditions. Further information can be found in the ATSB website safety publications: Mountain wave turbulence.
Figure 2: Mountain wave turbulence
Source: US Federal Aviation Administration
Flight crew harnesses
The aircraft’s flight crew seats are fitted with five point harnesses. The harness consists of a lap belt, a rotary buckle, a crotch strap, two shoulder straps and inertia-reel assembly with emergency locking retractors and cable control assembly (Figure 3). At the time of the turbulence, both flight crewmembers had the five points of their harnesses fitted, but with their shoulder harnesses in the AUTOMATIC position. In the AUTOMATIC position, the shoulder harness inertia-reel permits the occupant to move forward slowly, but locks when the straps are pulled at 1.5G and remains locked until the force is removed. In the MANUAL position, the shoulder straps are locked. The shoulder harness is primarily intended to mitigate forward movement of the torso and head.
The lap belt combined with the crotch strap are the primary means of restraint for turbulence encounters and exposure to negative-G forces. The crotch strap is also referred to as the ‘negative-G strap’ and its purpose is to reduce upward movement of the lap belt during negative-G aircraft motion. The length of the crotch strap should be adjusted such that no slack exists in the strap when the lap belt is properly positioned in the pelvic region. In this position, the crotch strap will resist the upward pull from the shoulder harness in negative-G.
When the aircraft encountered the negative-G turbulence, the captain felt the aircraft drop from underneath them and struck their head on the overhead air-vent and light. The captain and first officer reported that they had their lap belts tightened to ‘firm but comfortable’. The first officer reported that they may have hit their head on the ceiling of the flight deck, but received no injuries. The captain reported that some crotch straps do loosen during flight. The captain also advised that they had set their seat height so their eyes were lined up with height bar markers on the screen. They estimated that provided them with about 20-25 cm head clearance.
Figure 3: Aircraft flight crew harness
Source: Operator
Safety analysis
The flight crew had briefed and prepared the aircraft for flight in forecast severe turbulence.
As the aircraft tracked from waypoint HONEY to DALEY, it entered the lee-side of the Brindabella Ranges, tracking towards the north-east with a strong tailwind component. The wind was forecast to be 30 kt at 5,000 ft, increasing to 45 kt at 7,000 ft and within 30° of perpendicular to the ridgeline, at this location. Therefore, the abrupt encounter with turbulence was probably the result of mountain wave activity.
During the encounter, the flight crew described their movement relative to the aircraft as vertical when the aircraft dropped from underneath them. The primary method of restraint for negative-G is the lap belt supported by the crotch strap. If there is slack in the lap belt, this will permit the body to move up relative to the lap belt, and if there is slack in the crotch strap, this will permit the lap belt to move up if it is pulled upwards by the shoulder harness. The captain reported that the crotch strap can loosen with occupant movement and the aircraft was subject to minor fluctuations in G before the turbulence incident. Therefore, the captain’s injury was probably the result of some measure of slackness in their crotch strap.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The severe turbulence incident was probably an encounter with mountain wave activity in the lee-side of the Brindabella Ranges.
The captain was probably insufficiently restrained by their crotch strap to prevent them striking their head during the encounter with turbulence.
The flight crew were prepared for the risk of an encounter with severe turbulence during the descent and approach to Canberra.
Safety message
This incident highlights the importance of flight crew preparation for entry into an area of forecast turbulence and the importance of ensuring the correct adjustment of all harness straps. The captain planned to activate the seat belt sign early on the descent into Canberra and briefed the cabin crew accordingly. On descent into Canberra, all personnel were seated, the seat belt sign was activated and the aircraft speed reduced to turbulence penetration speed before the encounter with severe turbulence, which minimised the risk of injury to personnel and damage to the aircraft. However, despite the precautions taken by the crew, the captain received minor injuries.
Further information on flight crew harnesses can be found in United States Federal Aviation Administration Advisory Circular 21-34: Shoulder harness – safety belt installations.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.