On 18 January 2026, firefighting aircraft, ground personnel and assets were conducting firefighting operations at Wabonga – The Razor fireground, 58 km west of Mount Hotham, Victoria.
There were 2 helicopters and 3 fixed wing aircraft conducting firebombing and 1 helicopter conducting rappelling operations, being coordinated by an air attack supervisor (AAS) in a Eurocopter AS350 helicopter, callsign Firebird 303. There were also 2 large air tankers (LATs) operating on the Razor ridge south of the fireground, being coordinated by a LAT AAS in a fixed wing aircraft, callsign Birddog 376.
At about 1421, the pilot of a Bell 212 helicopter, callsign Helitak 368, reported broadcasting on the fire common traffic advisory frequency when about 5 NM (9 km) south of the fireground and inbound for rappelling operations. The pilot recalled being cleared to enter the fireground by the AAS. While the AAS could not recall issuing the clearance, they recalled checking there was no conflict with the large air tankers. As all the other aircraft were entering the fireground from the north, the AAS expected Helitak 368 to track east and remain clear of the fireground before holding and entering from the north, but did not communicate that to the pilot of Helitak 368.
About 90 seconds before Helitak 368 crossed the Razor ridge, a PZL M18B aircraft, callsign Bomber 359, left its holding position north of the fireground to conduct a drop at the southern end of the fireground, having been cleared by the AAS.
Shortly after crossing the Razor ridge, the crew of Helitak 368 sighted Bomber 359 ahead on a conflicting track. The Helitak pilot conducted a left descending turn to increase separation between the aircraft. At about the same time, Bomber 359 commenced a drop, then climbed and departed the area.
The pilot of Bomber 359 was unaware of the incident. The pilot of Helitak 368 elected to continue tracking northwards through the fireground and did not report the incident to the AAS.
What the ATSB found
The ATSB found that the air attack supervisor did not provide tracking instructions to the Helitak 368 pilot when approaching the fireground. Additionally, the Helitak pilot believed that they had separation assurance and were clear to conduct rappelling operations, resulting in a separation issue with an aircraft conducting firebombing operations.
The ATSB also found that, despite communications on the fire common traffic advisory frequency, the pilots of both Helitak 368 and Bomber 359 were unaware they were on a conflicting track. However, upon sighting the aeroplane, the pilot of Helitak 368 took action to maintain safe separation.
Additionally, the ATSB found that the pilot of Helitak 368 did not advise the air attack supervisor of the separation issue and continued to track north through the fireground, with no assurance of positive separation with other aircraft in the fireground.
What has been done as a result
The Victorian Department of Energy, Environment and Climate Action (DEECA) advised that the findings and contributing factors in this report would be further analysed, and lessons learned through this investigation reinforced through future Victorian aviation pre‑season briefings and incorporated into Victorian training and case study material. Lessons learned would also be shared with the Victorian aviation sector and with national counterparts via the National Aviation Firefighting Centre (NAFC) Aviation Safety Group to enhance collective safety awareness with the broader sector.
DEECA also advised that it would focus learnings on mandatory escalation of separation issues and supervisory control recovery following airspace conflicts to inform doctrine enhancements to interagency aviation operating procedures. Specifically, accident and incident response procedures and the management of aircraft at incidents.
Safety message
Aerial firefighting is a critical capability for the management and suppression of bushfires in Australia. To effectively achieve this, multiple aircraft are flown at low heights above the ground and varying airspeeds, often in challenging environmental conditions. The low operating heights, conditions, and high traffic density increase the complexity of flight crew tasks.
Maintenance of situational awareness of other aircraft operating in the vicinity is significantly enhanced by radio communications, aided by the presence of an air attack supervisor issuing directed communications and tactically separating aircraft. However, the effectiveness of radio communications can be affected by factors such as the number of aircraft operating on a fire common traffic advisory frequency and by terrain shielding.
The last line of defence to avoid midair collisions under visual flight rules is for pilots to see‑and-avoid other aircraft, noting that the limitations of see-and-avoid are well‑documented, particularly where visibility may be reduced by smoke. It is therefore vital that pilots involved in firefighting operations understand where other aircraft are operating and immediately communicate any issues so that all have a common mental model of the fireground.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
Background
On 18 January 2026, firefighting aircraft as well as ground personnel and assets were conducting firefighting operations at Wabonga – The Razor (Razor) fireground, 58 km west of Mount Hotham, Victoria. This was the third day of operations at the fireground, and as the wind and turbulence had eased, it was the first day large air tankers (LATs) had been deployed to the area. It was also the first day conditions were suitable for helicopters to be used to rappel[1] ground crews into the fireground.
During the morning, the following aerial assets were operating at the fireground:
2 Sikorsky (heavy) helicopters (Helitak 369 and Helitak 290) conducting long line waterbombing
2 Eurocopter AS350 B3 (light) helicopters (Firebird 303 and Firebird 312) with a pilot and air attack supervisor (AAS), alternating with only 1 helicopter at the fireground at a time
1 Bell 412 (medium) helicopter (Helitak 332) conducting rappelling operations
2 Bombardier DHC-8-400 LATs, Bomber 390 and Bomber 391, with a SOCATA TBM700 aircraft operating as a LAT Birddog[2] (Birddog 376)
3 fixed wing single engine air tankers (SEATs), Bomber 358, Bomber 359, and Bomber 363
Firescan (fire intelligence gathering) aircraft (usually twin-engine turbo-propeller aircraft) were also present at times.
All aircraft were operating on a discrete fire common traffic advisory frequency (Fire‑CTAF)[3] 128.90, identified for radio communications as the ‘Razor spur fire’. Communications on the Fire-CTAF were not recorded (normally and on the incident day), nor were they required to be.
The AAS was responsible for the safe and efficient tactical coordination of aircraft operations and with directing the firebombing aircraft to ensure there was separation between aircraft. However, the aircraft were operating under visual flight rules,[4] with the pilots ultimately responsible for separation with other aircraft, using ‘see-and-avoid’ principles.
The firebombing helicopters (Helitaks) were filling up from a water source referred to as the ‘dip’, north-west of the fireground. The SEATs were refuelling and filling with retardant at Mansfield aircraft landing area (ALA) 50 km to the west of the fireground. The dip was then being used as the inbound entry point to the fireground. After reporting when passing the dip, the aircraft were joining a holding pattern or ‘stack’, north of the fireground. To ensure separation, the Helitaks were joining the stack below 3,000 ft above mean sea level (AMSL) and the SEATs were joining above 3,500 ft, with all aircraft conducting left circuits. The AAS was then clearing the aircraft into the fireground, with the SEATs primarily dropping retardant on the western side of the fire (in an easterly direction) and the Helitaks dropping water on the northern and eastern side, with aircraft making left circuits to enter, drop, and exit the fireground. The AAS reported that they sighted each aircraft prior to clearing them into the fireground.
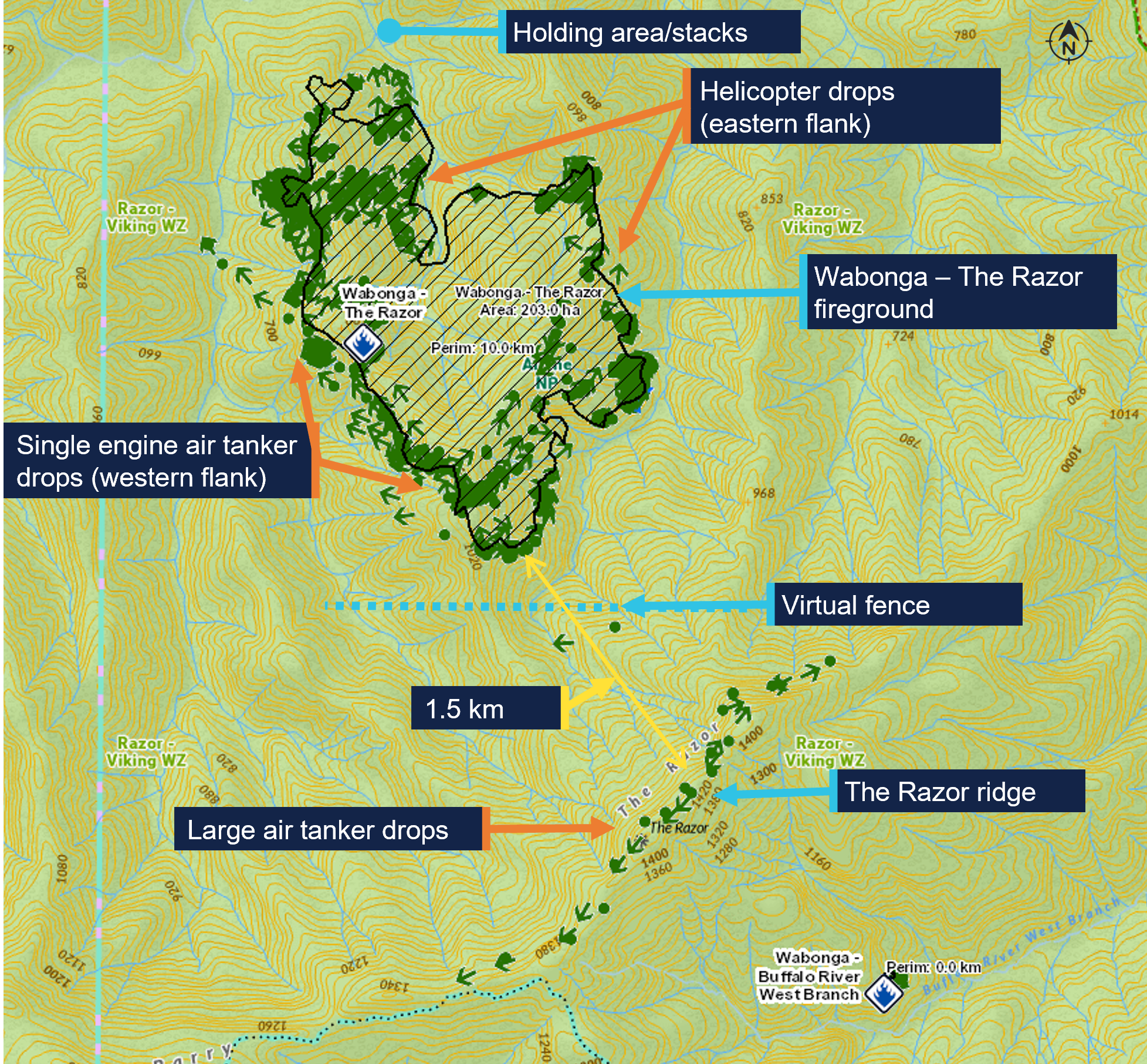
The LATs and LAT Birddog were dispatched from Avalon Airport, Victoria, dropping retardant on the Razor ridge south of the fireground, and then proceeded to Albury Airport, New South Wales, to refuel and reload retardant. The LATs were operating at altitudes not below 3,500 ft and were separated from the SEATs and Helitaks by a ‘virtual fence’ about 500 m north of the ridge (Figure 1).
Figure 1: Wabonga – The Razor fireground map showing firebombing drops, the holding area and virtual fence
The green dots are the drops over the 5-day duration of the fire 16–20 January 2026. Source: DEECA, annotated by the ATSB
What happened
On 18 January 2026, at 0948 local time, a PZL M18B aircraft, VH-VWF, operating as a SEAT with callsign Bomber 359, departed from the pilot’s base at Benambra Airport, 93 km east of the fireground. Between 1014 and 1359, the pilot conducted 5 drops at the Razor fireground, returning to Mansfield ALA after each drop to refill.
Meanwhile, a Bell 412 helicopter, callsign Helitak 333, which had been tasked for rappel operations, left 5 rappelers and a rappel dispatcher at Snowy Range Mountain Airport, 28 km south of the Razor ridge, while the helicopter departed to get maintenance on a radio issue. A Bell 212 helicopter, VH-KHO, callsign Helitak 368, was then tasked to collect the rappelling crew and conduct the rappelling operation. The pilot of Helitak 368 had not previously operated at the Razor fireground and was not expecting to operate there that day. Helitak 368 departed Latrobe Valley Airport at 1331 and arrived at Snowy Range Mountain Airport at 1404, departing for the fireground with the rappelling crew 11 minutes later.
Also at 1404, Bomber 359 left Mansfield for the fireground with its sixth load. When 5 NM (9 km) from the fireground, at about 1419 based on tracking data, the pilot reported broadcasting on the Fire-CTAF that they were inbound and tracking for the dip. Bomber 359 then entered the stack at 1421:30 and held there, awaiting clearance from the AAS (in Firebird 303) to enter the fireground and conduct a drop.
The pilot of Helitak 368 also reported broadcasting on the Fire-CTAF when inbound about 5 NM south of the fireground, at about 1421 based on tracking data. The pilot reported handing over ‘flight following’[5] to the AAS and requesting a clearance from them to enter the fireground. The Helitak pilot reported that they would have included in the request to enter the fireground that they were also seeking clearance to enter for reconnaissance and insertion of the rappelling crew. The helicopter then commenced descent from about 5,000 ft AMSL.
The rappel dispatcher in Helitak 368 recalled that the pilot made a 10-NM call and then a 5‑NM call, saying words to the effect of ‘We are 5 miles out. Are we ok to approach?’ and confirming what aircraft were in the area. The dispatcher reported writing the aircraft callsigns on the helicopter window and recalled the AAS saying they could enter the area. The dispatcher also recalled being aware from the communications that a bomber was in the vicinity, but did not know where the reporting points being referred to were.
The AAS recalled Helitak 368 reporting being inbound from the south and reported that this was the first time an aircraft had entered the fireground from that direction. They recalled checking that the LATs were clear of the Razor ridge and would not conflict with Helitak 368 but could not specifically recall clearing Helitak 368 into the fireground.
The AAS advised that it was likely they had instructed Helitak 368 to hold to the north of the fireground while the SEATs were conducting drops on the western side of the fire. They reported that they had expected Helitak 368 to follow lower terrain east of the fireground before holding to the north with the other aircraft but did not specifically instruct the pilot of Helitak 368 to do so. The AAS was typically operating north-east of the fire, away from the SEAT and helicopter water/retardant dropping circuits, and did not see Helitak 368 entering the fireground from the south. The first time the AAS recalled sighting Helitak 368 was after the incident, when it was holding to the north. The pilot of Firebird 303 could not recall Helitak 368 being cleared into the fireground from the south.
At 1422:30, recorded track data showed that Bomber 359 left the stack and tracked south‑west towards the drop target, near the virtual fence at the southern edge of the fire. The Bomber 359 pilot, AAS and Firebird 303 pilot expressed confidence that Bomber 359 would not have left the stack to commence a drop without first receiving AAS clearance, which the AAS would not give until they had sighted the aircraft and ensured the area was clear of ground personnel. However, they could not recall the clearance being given.
At 1423:55, Helitak 368 crossed the Razor ridge at about 4,700 ft AMSL, tracking approximately north-north-east and immediately commenced descending and tracking north into the fireground to conduct reconnaissance for the rappel crew insertion. The elevation of the ridge was about 4,600 ft, with most of the fireground about 2,000–3,000 ft AMSL. The pilot of Helitak 368 reported that they did not expect to encounter any other aircraft, as they believed they had been cleared into the fireground. At the time Helitak 368 crossed the ridge, Bomber 359 was about 4 km to the north-west, from where it commenced a left turn before lining up for a drop at an altitude of about 4,000 ft, tracking approximately east (Figure 2).
Figure 2: Relative positions of Bomber 359 and Helitak 368 at 1423:55
Source: DEECA, overlaid on Google Earth, annotated by the ATSB
The rappel dispatcher reported sighting a bomber pointed out by the rappel crew leader and directing the Helitak 368 pilot to go left to increase separation. The Helitak pilot reported that they then observed a ‘yellow’ bomber in their 10 o’clock position slightly below their altitude on a reciprocal track. On sighting the aeroplane, they immediately conducted a descending left turn (Figure 3).
Figure 3: Relative positions when Helitak 368 turned left at 1424:25
Source: DEECA, overlaid on Google Earth, annotated by the ATSB
Based on the recorded data for Helitak 368, the helicopter turned left to track west about 30 seconds after crossing the ridge, and Bomber 359 commenced the drop in an easterly direction about 5 seconds later. The pilot of Bomber 359 reported that they would have broadcast both ‘on the drop’ and ‘off the drop’ on the Fire-CTAF. After the drop, Bomber 359 climbed and conducted a left climbing turn before returning to Mansfield. The closest proximity between the 2 aircraft occurred at 1424:45, with Helitak 368 about 400 ft below and 500 m horizontally from Bomber 359 (Figure 4).
Figure 4: Closest proximity of Bomber 359 to Helitak 368 at 1424:45
Source: DEECA, overlaid on Google Earth, annotated by the ATSB
The pilot of Helitak 368 reported checking with and receiving confirmation from the onboard rappel dispatcher that they had received a clearance to enter the fireground and conduct reconnaissance operations. The pilot also reported attempting to say something like ‘that was close’ on the Fire-CTAF but thought they may not have successfully transmitted that communication while focused on returning the aircraft to normal operations.
At 1425:10, Helitak 368 conducted a left orbit then tracked northwards through the fireground. The pilot reported that they did not conduct rappel operations and instead exited the fireground to the north, to ensure they remained clear of other aircraft. At about 1429, Helitak 368 joined the stack at the northern end of the fireground, conducted 2 left orbits over the next 7 minutes, then departed the fireground to refuel at a refuelling site, about 11 km to the north-east.
The Bomber 359 pilot had not seen or heard Helitak 368 and was unaware of any separation issue. The first time the Bomber 359 pilot recalled hearing the Helitak 368 pilot on the Fire-CTAF was when Helitak 368 was holding north of the fireground and the pilot advised they were ‘fuel critical’ and needed to depart the fireground to refuel.
The AAS and Firebird 303 pilot were also unaware of the incident as the Helitak 368 pilot did not communicate it to them. Shortly after Helitak 368 left the fireground to refuel, the AAS in Firebird 303 handed over to the AAS in Firebird 312 and Firebird 303 departed the fireground to refuel.
Helitak 368 subsequently re-entered the fireground from the north and conducted rappelling operations. At 1939, Helitak 368 returned the rappelling crew to Heyfield and arrived at Latrobe Valley Airport at 2001.
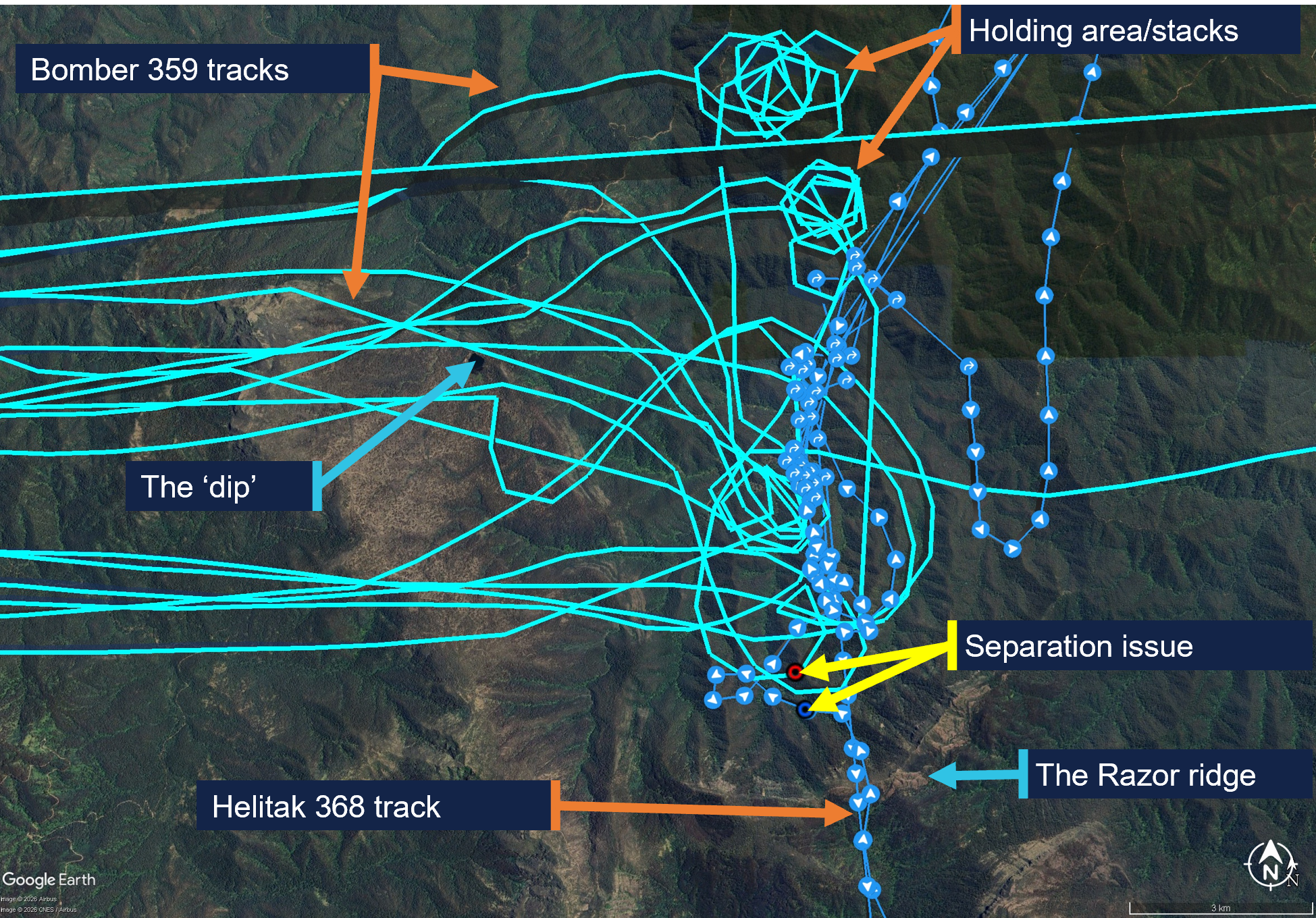
The pilot of Bomber 359 completed 9 loads that day before ferrying the aircraft to Benambra. Figure 5 shows the tracks for Helitak 368 and Bomber 359 at the Razor fireground on 18 January 2026.
Figure 5: Helitak 368 and Bomber 359 tracks for 18 January 2026 showing key locations
Source: DEECA, overlaid on Google Earth, annotated by the ATSB
Reporting of the occurrence
On 19 January 2026, the operator of Helitak 368 reported the incident as a ‘near miss’ to the Department of Energy, Environment and Climate Action of Victoria (DEECA). Unsure whether the operator had reported the incident to the ATSB as required, on 20 January, DEECA reported the incident to the ATSB as a ‘near miss’ between Helitak 368 and an unknown aircraft.[6] The Helitak 368 pilot reported having a seen a yellow aircraft and having later spoken to the pilot of Bomber 360 (a yellow Air Tractor 802 aircraft),[7] however Bomber 360 was not operating at the Razor fireground on 18 January. DEECA reviewed the available data and identified Bomber 359 (red and white livery) as the most likely aircraft involved in the reported occurrence. The ATSB investigation commenced on 2 February. The AAS was notified of the event on 29 January. The operator of Bomber 359 was made aware of the occurrence on 23 January and subsequently advised DEECA on 27 January that their pilots had no knowledge of the event. This limited the ability of those involved to recall the events.
Context
Personnel and aircraft information
Bomber 359
The pilot of PZL M18B, VH-VWF, callsign Bomber 359, held a Commercial Pilot Licence (Aeroplane), a class 2 aviation medical certificate, and had been conducting aerial firefighting operations since 1997. The pilot had accrued 13,501 hours total flight time, 103 of which were in the last 90 days. Of the total flight time, 3,987 hours were on the PZL M18 aircraft type, 75 of which were in the last 90 days.
The incident occurred on the pilot’s third day operating at the Razor fireground, which they described as ‘very technical’ with ‘cliffs, steep escarpments, tumbling air and severe turbulence’, and a complex mix of aerial assets.
The pilot reported that the AAS was ‘doing really well’ and the pilot of Firebird 303 was very experienced and was helping manage the AAS’s workload by assisting with communications.
The Bomber 359 pilot also reported that pilots of inbound aircraft could hear communications from the AAS, but generally not from other aircraft until they were within the fireground, due to terrain shielding. Further, pilots entering from north of the fireground would have been unable to see aircraft in the south due to smoke.
The pilot rated their fatigue as 1/7[8] and fatigue was not considered to be a factor in the occurrence.
Helitak 368
Pilot
The pilot of Bell 212, VH-KHO, callsign Helitak 368, held a Commercial Pilot Licence (Helicopter), a class 1 aviation medical certificate, and had about 2,500 hours total flight time, 600 of which were conducting aerial firefighting operations. The pilot had accrued 190 flight hours on the Bell 212 aircraft, 80 of which had been in the previous 90 days.
The pilot’s self-assessed fatigue score was 1/7 and fatigue was not considered to be a factor in the occurrence.
Rappel dispatcher
The rappel dispatcher was serving their fifth year as a flightcrew member, with 2 years as a rappeler followed by 3 years as a rappel dispatcher in firefighting operations. The rappel dispatcher was seated in the rear section of the helicopter cabin facing rearwards, attached to a ‘wander lead’ mounted to the cabin roof and connected to a harness.
The DEECA Helicopter Rappel Operations Manual stated that the rappel dispatcher was responsible for:
the pre-flight preparation of the helicopter for a rappel operation
the conduct of aerial reconnaissance of the fire area and selection of a suitable deployment location in consultation with the pilot and rappel crew leader
the safe dispatch of rappelers and rappel equipment from the helicopter to the ground.
The pilot advised that in the aircraft, the dispatcher assisted in reducing the pilot’s workload by managing firefighting agency radios. Additionally, the dispatcher monitored the external environment while maintaining constant communication with the pilot.
Rappel crew leader
The rappel crew leader was seated in the rear of Helitak 368 at the right-side door, facing forwards. The rappel crew leader, as the ‘mission commander’, was responsible for conducting a mission briefing with the pilot, air operations manager and other relevant personnel.
The rappel crew leader was dispatched to the Razor fire by the district duty officer at 1205. The details they received included a ground contact, command and fireground radio communication channels and a grid reference for the fireground. Before Helitak 333 departed Heyfield, the state air desk provided the Fire-CTAF and AAS callsign (Firebird 303).
The rappel crew were picked up during a ‘hot change’ at Snowy Range Mountain airport, in which the helicopter was not shut down. Once airborne, the rappel crew leader relayed the communications channels, fire location, Fire-CTAF, AAS and other aircraft details to the pilot of Helitak 368.
Rappel operation
The pilot reported that they were tasked to conduct reconnaissance of the fireground for a suitable insertion point for the rappel crew. They expected that if there were aircraft that could conflict with the rappel operation, the AAS would have told them to remain south of the area until the bombers finished their drops.
The pilot reported that the task was to get crew into the proposed site and they wanted to ‘get in and get that job done’, and that the reconnaissance would take about 5 to 10 minutes.
The dispatcher reported that their assigned task was to liaise with another rappel crew already on the ground and either assist where they were or go elsewhere on the fireground. They reported that rappel aircraft were ‘awkward to deal with’, as rather than joining the firebombing circuit, ‘we just appear and want to go straight through and do our thing straight away’. Additionally, when they first arrive at a fireground, although they would hear bomber pilots broadcasting (for example, ‘off the dip’, or ‘on the drop’), they would not necessarily know where the dip site or drop targets were.
Firebird 303
Air attack supervisor
The air attack supervisor was in an Airbus AS350 B3 helicopter, VH-PXX, callsign Firebird 303. The AAS had substantial firefighting experience in other roles, and this was their second season as an AAS. The incident day was the AAS’s fifth consecutive day as AAS and third day at the Razor fireground, with a similar traffic mix to the previous days, although the conditions had been unsuitable for LATs or rappel crews on the previous days.
The AAS assessed their workload as 7–8 out of 10 due to the number (up to 12 aircraft) and different types of aircraft operating in the fireground during the day. They self‑assessed their fatigue at the time as about 3–4 out of 7.
The DEECA Air Attack Supervisor Manual described the AAS role as being:
primarily responsible for the safe and efficient tactical coordination of aircraft operations when fixed and/or rotary wing firebombing aircraft are operating on a fire.
The AAS duties included ensuring safety standards were maintained at all times. The AAS was also required to establish and maintain communications with the fire aircraft.
The AAS described their role as primarily being a safety role ensuring safety between aircraft and other aircraft, and between aircraft and people on the ground and secondly, coordinating the effective use of the aircraft to suppress bushfires.
The AAS responsibilities also included reporting accidents and incidents. The AAS manual specified notification procedures, which included the requirement to notify the incident controller and State Air Desk in the event of an aircraft occurrence. The Interagency Aviation Operating Procedure – Victoria, Management of aircraft at incidents, included a standdown matrix with the requirements for standing down resources in accordance with interagency procedure and that a standdown may be required as a result of an incident or near miss.
The AAS training included strategies to tactically separate firebombing aircraft from each other, segregating fixed and rotary wing aircraft, and scaling requirements for large and heavy aircraft. While this did not include separate strategies for helicopters conducting rappel operations, the same principles of situation awareness and clear communications for the tactical separation of aircraft applied.
Pilot
The Firebird 303 pilot had accrued over 3,000 hours in the AS350 aircraft type and more than 8,000 hours total flight time, about 40% of which was in firefighting operations.
Air operations manager
The air operations manager’s responsibilities involved coordinating all operational components of the air operation, including the conduct of required briefings.
The air operations manager did not recall communicating with the pilot of Helitak 368 or the AAS, but ensured the rappel crew leader made the pilot aware that there were 2 Fire‑CTAFs in use (at different firegrounds). As Helitak 368 was dispatched by the state air desk, and transported the same rappelling crew that had been in Helitak 333, essential details were provided to the pilot by the rappel crew leader.
Meteorological information
The Bureau of Meteorology forecast for the area at 5,000 ft AMSL included north to north-easterly winds up to 14 kt, visibility greater than 10 km and, for the time of the incident, broken[9] cumulus/stratocumulus clouds with bases at 5,000 ft and tops at 9,000 ft (all AMSL).
The AAS reported that the visibility was ‘really good’ and the flying conditions were good, with no cloud that day. Weather over the previous 2 days included turbulence and south‑easterly winds that had prevented insertion of ground crew. On the day of the incident, the winds remained easterly but had abated and one rappelling crew had already deployed on the ground.
Safety analysis
The pilot of Helitak 368 had not previously been to the fireground and was unaware of the operational tactics in place where aircraft were holding and entering the fireground from the north. The air attack supervisor (AAS) was aware Helitak 368 intended to conduct rappelling operations, and expected Helitak 368 would track east of the fireground and enter from the stack in the north, however, they did not specifically instruct the pilot of Helitak 368 to do so. While the AAS could not recall clearing Helitak 368 to enter the fireground, the pilot believed they had been cleared to do so. Additionally, they also assumed that the AAS had assured they would not conflict with other aircraft and could commence their reconnaissance and rappelling task from the south.
As a result of the misunderstanding, Helitak 368 tracked north through the fireground, without the AAS’s awareness, and unexpectedly sighted and came into proximity with Bomber 359 on a drop run.
Any clearances issued by the AAS for Helitak 368 to enter the fireground and for Bomber 359 to conduct a drop would have occurred within a 3-minute period and been broadcast on the fire common traffic advisory frequency (Fire-CTAF) that both aircraft were monitoring. Additionally, Bomber 359’s pilot also broadcast twice (on and off the drop) during the run for their retardant drop. However, neither of the pilots were aware of the presence or of the increasing proximity of the other aircraft. While the reason for this could not be conclusively determined, there are several potential factors which may have limited the crew’s ability to identify the presence of the other. There were a number of other aircraft operating in the fireground with the associated additional communications on the Fire-CTAF in that period. The ability of the pilots of both aircraft to hear all Fire‑CTAF communications may also have been affected by terrain shielding. Further, as the pilot of Helitak 368 was unaware of the operational tactics to be used, it is likely that they would not have been aware of the locations of the reporting points and geographical references in the communications and may not have understood that Bomber 359 was operating in their vicinity.
Although the external communication was ineffective at alerting the Helitak 368 pilot to a potential conflict, the rappel dispatcher sighted Bomber 359, and instructed the Helitak 368 pilot to go left. When the pilot sighted the aeroplane, they manoeuvred the helicopter to increase separation. The 2 aircraft passed within about 500 m horizontally and 400 ft vertically of each other.
The pilot of Helitak 368 did not alert the AAS to the incident but continued to track through the fireground. This increased the risk of a subsequent separation issue, as the AAS still had an expectation that Helitak 368 was flying to the east of the firebombing area. However, no subsequent separation issues were reported.
As the AAS was unaware of the incident at the time, the required post‑incident actions, which would have included advising the incident controller and may have involved a standdown of personnel, were not conducted.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the separation issue involving Bell 212, VH-KHO, and PZL M18B, VH-VWF, 58 km west of Mount Hotham Airport, Victoria, on 18 January 2026.
Contributing factors
The air attack supervisor did not provide tracking instructions to the Helitak 368 pilot when approaching the fireground. Additionally, the Helitak pilot believed they had separation assurance and were clear to conduct rappelling operations, resulting in a separation issue with an aircraft conducting firebombing operations.
Despite communications on the fire common traffic advisory frequency, the pilots of both Helitak 368 and Bomber 359 were unaware they were on a conflicting track. However, upon sighting the aeroplane, the pilot of Helitak 368 took action to maintain safe separation.
Other factors that increased risk
The pilot of Helitak 368 did not advise the air attack supervisor of the separation issue and continued to track north through the fireground, with no assurance of positive separation with other aircraft in the fireground.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Department of Energy, Environment and Climate Action
The Victorian Department of Energy, Environment and Climate Action (DEECA) advised that the findings and contributing factors in this report would be further analysed, and lessons learned through this investigation reinforced through future Victorian aviation pre‑season briefings and incorporated into Victorian training and case study material. Lessons learned would also be shared with the Victorian aviation sector and with national counterparts via the National Aviation Firefighting Centre (NAFC) Aviation Safety Group to enhance collective safety awareness with the broader sector.
DEECA also advised that it would focus learnings on mandatory escalation of separation issues and supervisory control recovery following airspace conflicts to inform doctrine enhancements to interagency aviation operating procedures. Specifically, accident and incident response procedures and the management of aircraft at incidents.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilots and operators of the involved aircraft
air attack supervisor
rappel dispatcher
rappel crew leader
air operations manager
recorded tracking data
Department of Energy, Environment and Climate Action
Civil Aviation Safety Authority.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilots and operators of the involved aircraft
air attack supervisor
air operations manager
rappel dispatcher and rappel crew leader
Department of Energy, Environment and Climate Action
Civil Aviation Safety Authority.
Submissions were received from:
air attack supervisor
rappel crew leader
the operator of VH-KHO
Department of Energy, Environment and Climate Action.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Civil Aviation Safety Regulations Part 138 MOS defined rappelling as an aerial work Class D external load operation that involves a person exiting or entering an aircraft in flight using a rope or ladder attached to the helicopter.
[2]Birddog is used to assess the fireground and determine the most appropriate flight path to facilitate LAT integration with other aircraft.
[3]Discrete radio frequencies are allocated for Victorian firefighting operations, which the state air desk assigns to respective firegrounds.
[4]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[5]Flight following during flight: requirement to communicate position and intentions every 30 mins to nominated person and to advise of any changes, diversions and pick-ups. Failure to communicate activates search and rescue action.
[7]DEECA stated that there are psychological factors in witness recall, whereby individuals can rely on stereotypical associations when reconstructing events. Such associations are a normal aspect of human memory and can result in familiar or expected characteristics being recalled in place of the observed features (e.g. yellow for a bomber aircraft).
[8]Samn-Perelli fatigue scale: A self-assessed 7-point fatigue scale where 1 is ‘fully alert and wide awake’ and 7 is ‘completely exhausted, not able to function’.
[9]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘broken’ indicates that more than half to almost all the sky is covered.
Occurrence summary
Investigation number
AO-2026-006
Occurrence date
18/01/2026
Occurrence time and timezone
1424 Eastern Daylight-Saving Time
Location
58 km west of Mount Hotham Airport
State
Victoria
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Separation issue
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
PZL Mielec
Model
M18B
Registration
VH-VWF
Serial number
1Z027 26
Aircraft operator
Alpine Airwork
Sector
Piston
Operation type
Part 138 Aerial work operations
Activity
General aviation / Recreational-Aerial work-Firefighting
Departure point
Benambra aircraft landing area, Victoria
Destination
Benambra aircraft landing area, Victoria
Injuries
None
Damage
Nil
Aircraft details
Manufacturer
Bell Helicopter Co
Model
212
Registration
VH-KHO
Serial number
31181
Aircraft operator
Kestrel Aviation Pty Ltd
Sector
Helicopter
Operation type
Part 138 Aerial work operations
Activity
General aviation / Recreational-Aerial work-Firefighting
On 12 June 2025, a student pilot conducting a solo navigation flight in a Piper PA-44 was returning to Jandakot Airport, Western Australia, at the same time a Cessna 172 was approaching the airport from the training area. Air traffic control (ATC) directed the pilot of the faster PA-44 to overtake the C172 as they approached the circuit area. However, the PA-44 did not pass the C172 prior to joining the circuit and, consequently, ATC amended their instruction to the pilot of the PA-44, instructing them to ‘follow the Cessna’ and instructed the C172 pilot to join downwind and land first.
Despite that instruction, the pilot of the PA-44 continued to overtake the C172 as per the previous instruction, by accelerating, descending and turning inside the C172.
What the ATSB found
The ATSB found that the PA-44 pilot did not identify the final part of the amended instruction to ‘follow the Cessna’, likely due to receiving an unexpected cockpit traffic alert at the time the approach clearance was issued. Consequently, the PA-44 pilot passed the C172 as per the original clearance, resulting in reduced separation between the 2 aircraft.
The ATSB also found that, although a key element of the revised approach clearance, the pilot’s incomplete readback was not corrected by the controller as the Manual of Air Traffic Services did not explicitly require sequencing instructions to be read back. This was a missed opportunity to resolve the situation and, more generally, provided no assurance that this safety-critical aspect had been correctly understood.
What has been done as a result
Following the incident, the operator of both aircraft completed a presentation to students regarding compliance with ATC instructions and conducted a flight with the incident pilot to assure circuit rejoin procedures and to regain their confidence. Similar flights were also conducted with other student pilots at the company. Additionally, the operator and Airservices have engaged to better understand the challenges with student training at Jandakot.
In addition, Airservices Australia advised that the Air Traffic Management Standards and Senior Air Traffic Services Specialists conducted a review, and will investigate a change to Manual of Air Traffic Services 9.2.2.13.2 and the respective Aeronautical Information Publication reference (GEN 3.4 – 37) to include the instruction ‘follow’ in the list of items requiring readback.
Safety message
This incident highlights the importance of ensuring that all parties have an accurate situational understanding, especially when plans change. Sequencing of aircraft is a safety critical component of assuring separation and needs to be unambiguous for all. For flight crew, they should seek confirmation from controllers if they are unsure of what is required of them or if the picture doesn’t look right. Similarly, if there is any doubt, ATC should confirm that pilots have a correct understanding of sequencing requirements.
The occurrence
At 1124 local time on 12 June 2025, a pilot conducting a navigation flight in a Piper Aircraft Inc. PA-44-180 (PA-44) aircraft, registered VH-KZJ, was inbound to the circuit area at Jandakot Airport, Western Australia. The flight was the third solo flight for the pilot in a twin-engine aircraft, and their first time operating VH-KZJ. At the same time, a Cessna 172 (C172) aircraft, registered VH-ZER, was also inbound to Jandakot Airport, with an instructor and student on board after conducting a training flight.
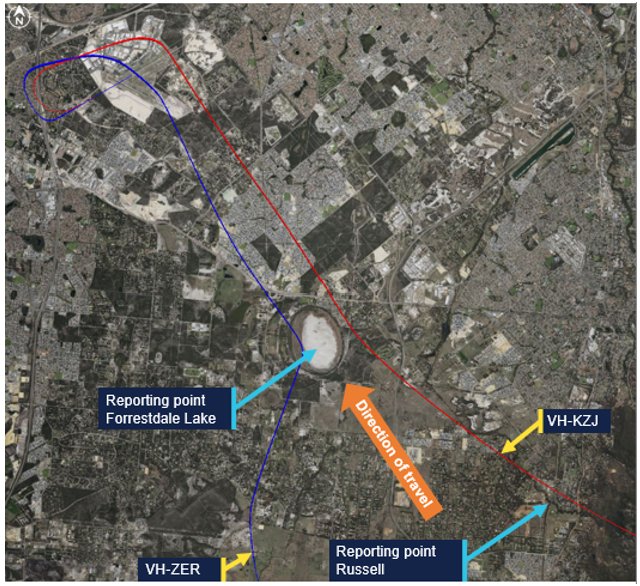
The runway in use at Jandakot was 06L[1] and local procedures required aircraft to contact air traffic control (ATC) at specified approach points (in this instance Oakford and Russell) then track to Forrestdale Lake. From there, aircraft were to fly overhead the airport at 1,500 ft above mean seal level (AMSL) towards the north and join the circuit as directed by Jandakot Tower (Figure 1).
As the PA-44 was passing the inbound reporting point Russell, ATC passed traffic information on the C172 inbound to the circuit area via the Forrestdale Lake inbound reporting point (Figure 1). With the PA-44 being the faster aircraft, ATC instructed the PA-44 pilot to overtake the C172 on the right which was acknowledged by the PA-44 pilot by a callsign response. The pilot then reported at Forrestdale Lake with the C172 in sight. Both aircraft were at 1,500 ft.
Figure 1: Aircraft inbound tracks
Source: Google Earth with fight radar tracking, annotated by the ATSB
Despite the ATC instruction to overtake the C172, the pilot in the PA-44 reduced the engine power to circuit power, which resulted in the aircraft slowing down. As such, the PA-44 did not overtake the C172 prior to joining the downwind leg of the circuit.[2]
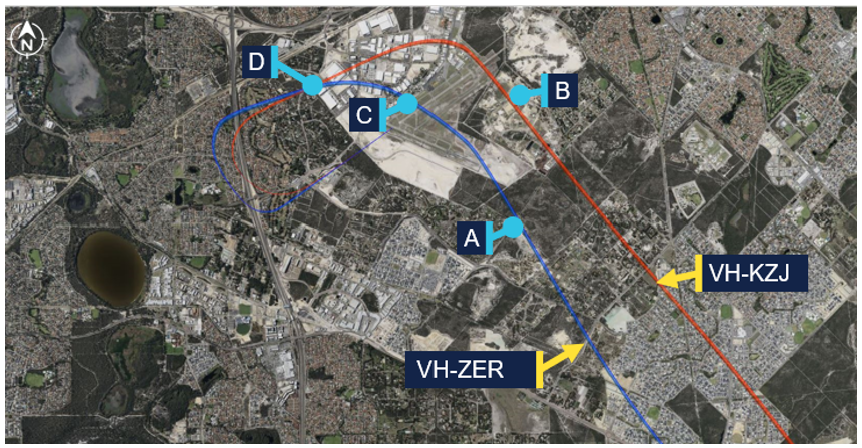
Observing that the PA-44 had not overtaken the C172 as they had anticipated, the controller changed their sequencing plan to have the C172 land first. The table below details the exchange between the pilots and controller and Figure 2 shows where these calls were in relation to the flight paths.
Table 1: Communication
Time
From
To
Transcript
A
1127:55
Controller
C172
ZER make a left turn, join late downwind RWY 06L maintain 1,500
C172
Controller
Take a left turn join late downwind 06L and maintain 1,500 ZER
B
1128:13
Controller
PA-44
KZJ join downwind from that heading, cleared visual approach and follow the Cessna out to your left joining late downwind, high mid downwind
ZER that twin has cut you off they’re low in your 12 o’clock
C172
Controller
Yeah we’ve got the company twin, we’ll make number two to them ZER
Controller
C172
ZER thanks
Figure 2: Aircraft track with ATC clearances
Source: Google Earth with fight radar tracking, annotated by the ATSB
The pilot in the PA-44 reported that, as ATC was issuing its approach clearance, the traffic advisory system (TAS) in the aircraft began audibly alerting. The pilot later advised they were not familiar with the TAS and had never heard the audible alert before. They reported that as their attention was focused on the alert, they did not hear the sequencing part of the instruction to ‘follow the Cessna’. As such, they did not repeat this part of the instruction during the readback of their clearance and believed they were still cleared to pass the C172.
They further advised they had always previously been required to read back the complete sequencing instruction and as they were not prompted for any further readback on this occasion, did not consider that they had not heard the instruction correctly.
The PA-44 continued to overtake the C172 on downwind by descending and accelerating, and then turning inside the C172. The pilot recalled that they thought the sight picture of the close overtake ‘did look a bit odd’, but did not consider questioning the controller.
The instructor in the C172 was also an instructor of the pilot in the PA-44. When hearing their student’s interactions with ATC, they were concerned that the pilot may not have understood the intention of ATC. As such the instructor ensured they maintained visual contact with the PA-44 throughout the sequence.
Both pilots reported that they could see the other aircraft for the duration of the incident.
Context
Pilot details
The pilot of the Piper Aircraft PA-44 held a private pilot licence (aeroplane) and had a class 1 aviation medical certificate. They were undergoing training to obtain their commercial pilot licence (aeroplane) and had a total of 128 hours of flying experience, of which 22 were on the PA-44. They had flown 37 hours in the previous 90 days.
The instructor of the Cessna Aircraft Company 172 (C172) held a commercial pilot licence (aeroplane) with a class 1 aviation medical certificate. They held an instructor and instrument flight rating. They had a total of 1,200 hours of flying experience, of which 390 were on the C172. They had flown 155 hours in the previous 90 days.
Aircraft details
The Piper Aircraft Inc PA-44-180 is 4-seat, low-wing, retractable-undercarriage aircraft with 2 piston engines. VH-KZJ was equipped with the Garmin G1000 avionics suite and optional traffic advisory system (TAS).
The Cessna Aircraft Company 172S is a 4-seat, high-wing, fixed-undercarriage aircraft with one piston engine.
Training
The operator advised that VH-KZJ was the only aircraft in its fleet fitted with the optional traffic advisory system (TAS) with the avionics suite (G1000) and it does not provide formal syllabus training on the TAS. A general awareness was provided during a dual flight, where the TAS system test was conducted as part of the PA-44 (G1000) Normal Checklist – After Start Checklist.
Provision of separation in Class D airspace
In accordance with Aeronautical Information Publication Enroute 1.4-13 as both aircraft were operating under Visual Flight Rules (VFR) in Class D airspace there was no requirement for Air Traffic Control (ATC) to provide separation.
Readback requirements
Airservices Safety net – operating in Class D airspace highlighted the importance of correct readbacks from pilots to prevent frequency congestion. As part of this guidance, it referred pilots to Aeronautical Information Publication (AIP) General (GEN) 3.4.
AIP GEN 3.4 6.6 General Phrases provided the following phraseology when a pilot was assigned and required to maintain separation with a sighted aircraft:
when a pilot is assigned and required to maintain separation with a sighted aircraft ATC are to use the phrase FOLLOW (or MAINTAIN OWN SEPARATION WITH [AND PASS BEHIND]) (aircraft type or identification) [instructions or restrictions].
Manual of Air Traffic Services (MATS) pilot readback requirements stated:
Obtain a readback in sufficient detail that clearly indicates a pilot’s understanding of and compliance with all ATC clearances, including conditional clearances, instructions and information which are transmitted by voice.
MATS further stated that readback discrepancies must be immediately corrected by the controller.
The controller later advised that the ‘follow the’ instruction was not required to be read back as part of the [key elements] readback requirements in MATS (Figure 3), and therefore there was no reason to correct the incomplete readback. Airservices Australia later confirmed it does not require ‘follow the’ type instructions to be read back.
Figure 3: Manual of air traffic services
Safety analysis
When the air traffic controller identified that the PA-44 had not overtaken the C172 as expected, they amended the PA-44 pilot’s approach clearance to require them to follow it as the second aircraft in the landing sequence. However, when the amended clearance was issued, the pilot’s attention was focused on the aural alert from the traffic advisory system and they did not identify the final part of the instruction to ‘follow the Cessna’. Consequently, and despite recognising that the sight picture was ‘looking a bit odd’, the PA-44 pilot passed the C172 as per the original clearance, resulting in reduced separation between the 2 aircraft.
Contributing factor
The PA-44 pilot did not identify the final part of the amended instruction to ‘follow the Cessna’. Consequently, the PA-44 pilot passed the C172 as per the original clearance, resulting in reduced separation between the 2 aircraft.
Having missed the requirement in the amended clearance to follow the C172, the PA-44 pilot did not include the sequencing information in their readback. Although this was a key element of the revised approach clearance, the pilot’s incomplete readback was not corrected by the controller as they considered that the pilot was not required to read back that instruction. This was a missed opportunity to resolve the situation.
Contributing factor
Although a key element of the revised approach clearance, the pilot’s incomplete readback was not corrected by the controller as they considered that the pilot was not required to read back the ‘follow the Cessna’ instruction.
Safe circuit pattern operation relies on all the involved pilots having a common understanding of the aircraft sequence. Additionally, overarching guidance in the Manual of Air Traffic Services (MATS) required controllers to ‘obtain a readback of sufficient detail that clearly indicates pilots’ understanding of and compliance with all ATC clearances.’ Despite that, MATS did not explicitly require sequencing instructions to be read back as a ‘Key element’ of the approach clearance, providing no assurance that this safety-critical aspect had been correctly understood.
Contributing factor
The Manual of Air Traffic Services did not explicitly state that sequencing instructions were required to be read back by a pilot, providing no assurance that this safety-critical aspect had been correctly understood. (Safety issue)
Finally, the situation awareness maintained by the instructor in the C172 ensured that adequate separation was maintained between the 2 aircraft as the situation developed, possibly preventing a more serious outcome.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the separation occurrence involving Piper PA-44, VH-KZJ, and Cessna 172, VH-ZER, near Jandakot Airport, Western Australia, on 12 June 2025.
Contributing factors
The PA-44 pilot did not identify the final part of the amended instruction to ‘follow the Cessna’. Consequently, the PA-44 pilot passed the C172 as per the original clearance, resulting in reduced separation between the 2 aircraft.
Although a key element of the revised approach clearance, the pilot’s incomplete readback was not corrected by the controller as they considered that the pilot was not required to read back the ‘follow the Cessna’ instruction.
The Manual of Air Traffic Services did not explicitly state that sequencing instructions were required to be read back by a pilot, providing no assurance that this safety-critical aspect had been correctly understood. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The Manual of Air Traffic Services did not explicitly state that sequencing instructions were required to be read back by a pilot, providing no assurance that this safety-critical aspect had been correctly understood.
Glossary
AIP
Aeronautical information publication
AMSL
Above mean sea level
ATC
Air traffic control
MATS
Manual of Air Traffic Services
TAS
Traffic Advisory System
VFR
Visual Flight Rules
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilots of both aircraft
the air traffic controller
Airservices Australia
ADS-B data for both aircraft
the operator of both aircraft.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilots of both aircraft
the air traffic controller
Airservices Australia
the operator
Civil Aviation Safety Authority.
Submissions were received from:
the air traffic controller
Airservices Australia
the operator.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[2]The leg of the circuit pattern where the aircraft is flying parallel to the runway but opposite to the direction of landing.
Occurrence summary
Investigation number
AO-2025-033
Occurrence date
12/06/2025
Location
Near Jandakot Airport
State
Western Australia
Report release date
04/12/2025
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Operational non-compliance, Separation issue
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-44-180
Registration
VH-KZJ
Serial number
4496462
Aircraft operator
Airflite Pty Ltd
Sector
Piston
Operation type
Part 142 Integrated and multi-crew pilot flight training
Departure point
Jandakot Airport, Western Australia
Destination
Jandakot Airport, Western Australia
Damage
Nil
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
172S
Registration
VH-ZER
Serial number
172S10855
Aircraft operator
Airflite Pty Ltd
Sector
Piston
Operation type
Part 142 Integrated and multi-crew pilot flight training
On the afternoon of 13 June 2025, a Pilatus PC‑12, registered VH‑NWI and operated by Armada Aviation, was being used to conduct a charter air transport flight from Essendon Airport, Victoria, to Launceston Airport, Tasmania. On board were a pilot and 4 passengers.
During the approach to Launceston, the aircraft deviated left from the final approach course and intercepted the extended centreline of the adjacent taxiway. The aircraft then continued towards the taxiway where a Cessna 152 (C152) was holding for departure. Approaching the taxiway, the pilot conducted a low-level right then left turn to realign with the runway, before commencing a missed approach. During the manoeuvre the aircraft passed in close proximity to the C152. Following the missed approach, the aircraft conducted a visual circuit and landed without further incident.
What the ATSB found
The ATSB found that the final approach was conducted in clear conditions almost directly into the sun, exposing the pilot to glare. Subsequently, the pilot misidentified the taxiway as the runway and aligned the aircraft with the taxiway's extended centreline. The pilot then corrected the aircraft's flight path at a low level rather than conducting an immediate missed approach. During the manoeuvre the aircraft passed in close proximity to an aircraft on the taxiway.
It was also found that after identifying that the approaching aircraft was aligned with the taxiway, the instructor on board the aircraft on the taxiway made a radio broadcast, likely alerting both the pilot and air traffic control to the situation.
What has been done as a result
Armada Aviation circulated a notice to its aircrew advising them of hazards associated with a visual approach, such as sun glare. Additionally, it made the following changes to its operating procedures:
Updated the final decision to proceed to landing to include a requirement that the runway was confirmed and clear by 400 ft above ground level, or the approach minima.
Added a top of descent safety briefing to ensure pilots brief other risks associated with the visual approach segment following an instrument approach, including lighting configuration and sun position.
Updated the checklist of the final phase of flight to include checking that the runway was confirmed and clear.
Safety message
Sun glare can reduce a pilot’s visual effectiveness even when meteorological visibility is good. When flying visually in such conditions, pilots should crosscheck against available flight and navigation instruments in conjunction with external indicators, such as airport lighting, to verify that the aircraft is on the intended flight path.
If a discrepancy is identified below an appropriate stabilised approach height, an immediate missed approach should be conducted. Low-level manoeuvring outside of the published approach and associated obstacle clearance increases the risk of collision with terrain or objects on the ground.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 13 June 2025, a Pilatus PC-12, registered VH‑NWI and operated by Armada Aviation, was being used to conduct a charter air transport flight from Essendon Airport, Victoria, to Launceston Airport, Tasmania (Figure 1). On board were a pilot and 4 passengers.
Figure 1: Occurrence flight
Source: Google Earth annotated by the ATSB
At 1511 local time, the aircraft commenced the instrument approach procedure for runway 32L[1] at Launceston. The weather at the time was predominately clear skies with few[2] clouds at 3,000 ft, variable wind up to 5 kt and visibility greater than 10 km.
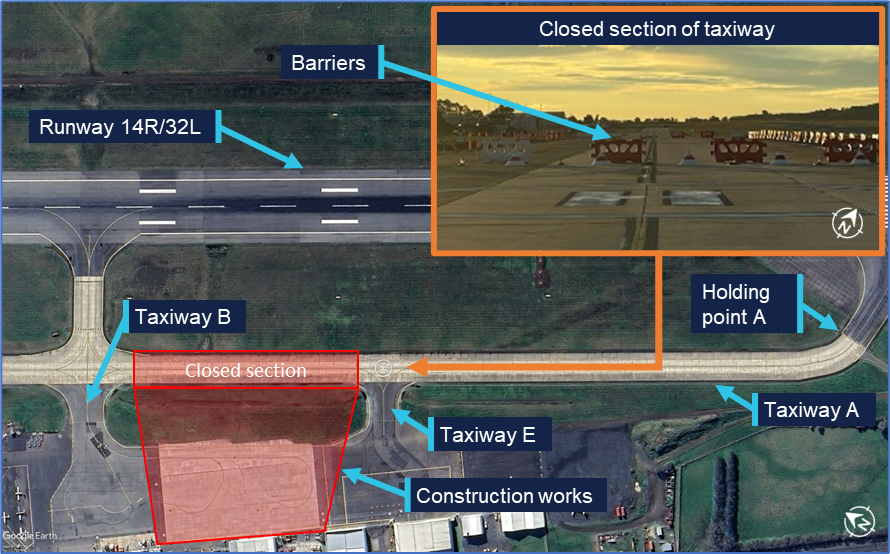
At approximately the same time, the occupants (instructor and student) of a Cessna 152 (C152) on the ground at Launceston contacted air traffic control (ATC) to request taxi clearance for departure on a training flight. Due to the closure of a section of the taxiway (see Figure 4 and the section titled Construction works), the C152 was required to backtrack the runway and vacate onto taxiway A at the runway 32L threshold. The aircraft then turned 180° on the taxiway and stopped with the nose of the aircraft at holding point A. At 1515, the C152 reported to ATC that they had completed the taxi and were clear of the runway.
By this time VH‑NWI was established on the final segment of the approach, approximately 7 NM (13 km) from the runway. Shortly thereafter, ATC cleared the aircraft to land, later reporting that at this time they observed the aircraft established on the final approach. The pilot reported that throughout the final approach, they were looking into the sun and consequently they ‘couldn’t really see much at all’.
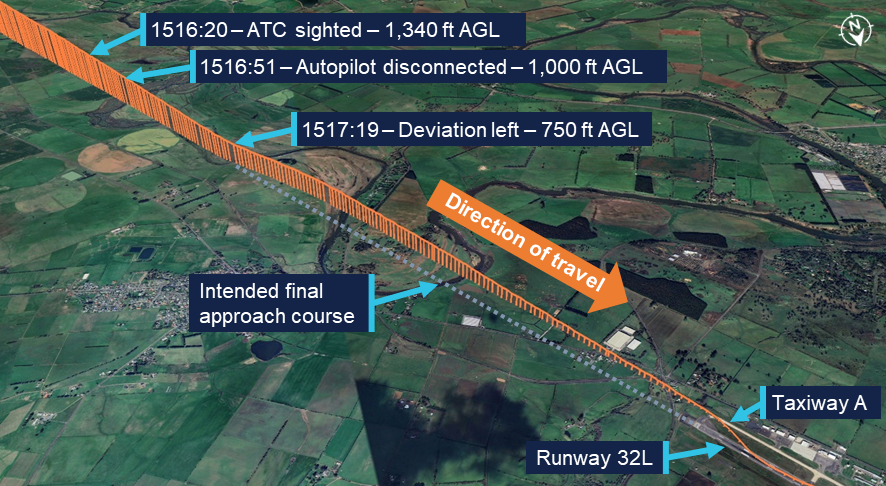
ATC reported again sighting the aircraft when it was approximately 4 NM (7 km) from the runway. At this point the aircraft was approximately 1,340 ft above ground level (AGL) and still aligned with the final approach course (Figure 2).
Figure 2: Final approach flight path
Recorded altitude resolution ± 12.5 ft, over underlying terrain elevation, rounded to nearest 5 ft. Source: ADS-B flight data overlaid on Google Earth, annotated by the ATSB
The pilot advised that, during the approach, they used the autopilot to manage the aircraft’s flight path until approximately 1,000 ft AGL. At this point they disconnected the autopilot and transitioned to looking outside. The pilot recalled that they were still looking into the sun and only seeing one feature on the ground that stood out. Identifying it as the runway, they began visually flying the aircraft towards it. Recorded flight data showed that at approximately 750 ft AGL, the aircraft began to deviate left until it intercepted the extended centreline of taxiway A. From this position the aircraft continued to descend towards the taxiway. At 1519, when the aircraft was approximately 120 ft AGL, weather cameras at the airport recorded images showing both the aircraft on final and the C152 at the holding point (Figure 3).
Figure 3: Weather camera images at 1519
Combination of 2 images: Left image camera bearing 135° (SE) at 1519:04, right image camera bearing 225° (SW) at 1519:02. Source: Bureau of Meteorology, annotated by the ATSB
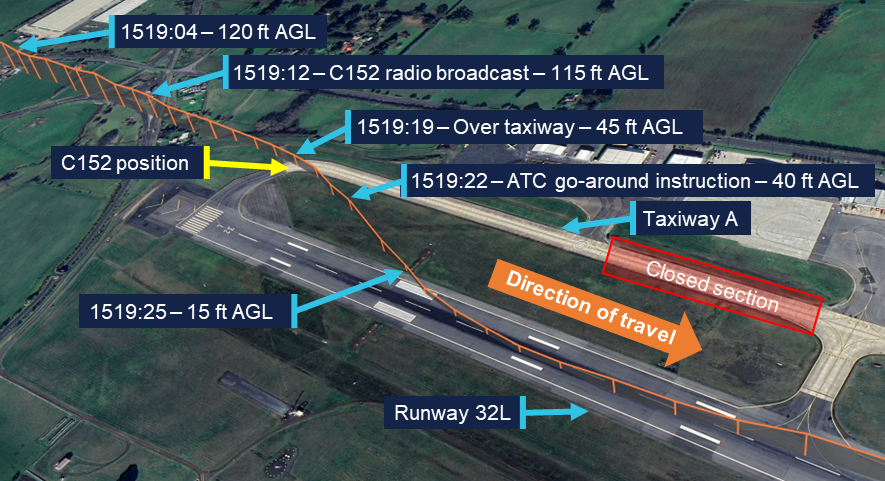
The instructor on board the C152 recalled that upon looking for the approaching aircraft, they saw that it was lined up with the taxiway. At 1519:12, they made a radio broadcast on the Launceston Tower frequency advising ‘He’s landing on the taxiway’. Following the call, VH-NWI passed above and behind them. It then reappeared on their left side, after conducting a right, then left, turn to align with the runway.
A review of flight data showed that VH-NWI continued to descend as it tracked the taxiway extended centreline until 1519:16, at which point it commenced a right turn (Figure 4). During the turn, the aircraft passed over the taxiway at a height of approximately 45 ft AGL, 15 m behind holding point A, at which the C152 was positioned. Subsequently, the aircraft descended further as it flew over the grassed area between the taxiway and the runway before turning left to align with the runway centreline. During the realignment manoeuvre, the aircraft descended to approximately 15 ft AGL.
Figure 4: Low-level manoeuvre and missed approach
Recorded altitude resolution ± 12.5 ft, over underlying terrain elevation, rounded to nearest 5 ft. Source: ADS-B flight data overlaid on Google Earth, annotated by the ATSB
The pilot recalled that when not far from the runway environment they became aware that they were approaching the taxiway and in response turned the aircraft towards the runway. They further reported that they were not aware of the C152 at the holding point. While they recalled hearing a radio broadcast as they were moving towards the runway, they did not know who had made it.
ATC reported that upon hearing the broadcast from the C152 they observed VH-NWI on short final lined up with taxiway A, after which it immediately made a right turn to align with the runway. At 1519:22 they instructed the pilot to go around.[3] The pilot later reported that they heard the instruction from ATC, by which time they had decided to initiate a missed approach. Flight data recorded that the aircraft commencing a climb away from the runway at 1519:31. Following the missed approach, the pilot conducted a visual circuit and the aircraft landed without further incident. Subsequently, the C152 departed.
Context
Pilot
The pilot held an air transport pilot licence (aeroplane) issued in 2013 and a class 1 aviation medical certificate. They had accumulated 4,251 flight hours, of which 659 hours were operating the Pilatus PC‑12. In the previous 90 days, the pilot had accumulated 26 hours, all in the PC‑12. They completed an instrument proficiency check in January 2025.
The pilot reported that they had flown into Launceston Airport a number of times previously, both during the day and at night. They did not recall any prior occasion where sun glare had been an issue during final approach.
Aircraft
VH-NWI was a Pilatus PC‑12, powered by a Pratt & Whitney PT6A‑67B turbine engine driving a 4‑bladed, variable pitch Hartzell propeller. The aircraft was manufactured in 1995 and first registered in Australia in 2002. It was subsequently registered with the operator in 2014.
At the time of the incident, the aircraft had accumulated 8,674 hours total time in service. The aircraft was being maintained in accordance with the operator’s system of maintenance and the PC‑12 maintenance manual. The last periodic inspection was conducted in April 2025, and the maintenance release showed no outstanding items.
Launceston Airport
Runway environment
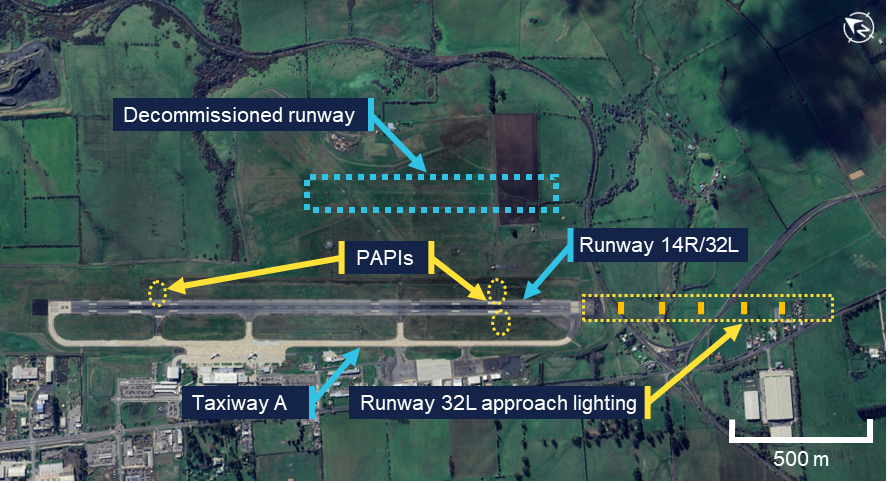
Launceston Airport had a single grooved asphalt runway 14R/32L (Figure 5). The runway was 45 m wide and approximately 2 km long with a runway heading of 313°. The airport had previously operated a parallel grass runway 14L/32R which had been decommissioned however, the remaining runway had not been renamed to remove the left / right designation. The En Route Supplement Australia (ERSA) provided information on Launceston Airport and identified the single operational runway and the decommissioned runway.
Access to the ends of the runway was via taxiway A located on the western side. The taxiway was 23 m wide and ran the length of the runway. The taxiway surface was a lighter colour compared to that of the asphalt runway.
Figure 5: Launceston Airport runway environment and lighting
Source: Google Earth, annotated by the ATSB
Aerodrome and approach lighting
Launceston Airport was equipped with runway edge lighting, approach lighting, taxiway lighting and precision approach path indicator (PAPI)[4] systems. Approach lighting was installed leading to runway 32L with a PAPI on both sides of the runway. Runway 14R had no approach lighting, and a single PAPI on the left of the runway. When activated, the intensity level of each lighting component could be set between 1–6, with 1 being the lowest intensity, and 6 being the highest. During tower hours, this setting was controlled by ATC via a panel in the control tower. Outside tower hours the settings were preset.
On the day of the occurrence, all aerodrome lighting was initially inactive. At 1331 local time, the PAPIs for both runway 14R and 32L were activated at an intensity setting of 5. At 1506, 13 minutes prior to the occurrence, the runway edge lighting, taxiway lighting and the approach lighting for runway 32L were activated with an intensity setting of 4. At the same time, the intensity of the PAPIs was reduced to 4. Airservices advised that this intensity setting was selected due to decreasing ambient light associated with winter conditions at that time of day.
The pilot could not recall whether the airport lighting was on during the first approach. During the second approach and landing, they recalled that the lighting was on and thought that it looked dim and was difficult to see.
Construction works
At the time of the incident construction works were being conducted in the area adjacent to the southern apron. These works required the closure of taxiway A between taxiway B and taxiway E (Figure 6). Barriers, unserviceability markers and lighting was deployed at the ends of the closed section of taxiway to prevent access. The presence of works and the taxiway closure were advised both via NOTAM[5] and the airport’s automatic terminal information service (ATIS).[6] The pilot reported being aware that the taxiway was closed.
Figure 6: Airport construction works
Source: Google Earth, inset supplied, annotated by the ATSB
Sun effect during the approach
Sun position
At 1517, the time that the aircraft began to deviate from the final approach course, the sun was positioned 10° to the left of the runway heading and 12° above the horizon.
Glare
Glare occurs when unwanted light enters the eye. Direct glare comes directly from a light source whereas veiling glare occurs when light is reflected from crazing[7] or dirt on the windscreen. The ATSB research report Limitations of the See-and-Avoid principle examined the effect of glare on pilots stating:
It has been claimed that glare which is half as intense as the general illumination can produce a 42 per cent reduction in visual effectiveness when it is 40 degrees from the line of sight.
When the glare source is 5 degrees from the line of sight, visual effectiveness is reduced by 84 per cent (Hawkins 1987). In general, older pilots will be more sensitive to glare.
Direct glare from the sun and veiling glare reflected from windscreens can effectively mask some areas of the view.
The pilot reported that the aircraft was equipped with a tinted sun visor. They had placed this between their eyes and the sun during the approach however this did not sufficiently reduce the direct glare. Consequently, they reported that for most of the final approach, when not required for power adjustments, they held their right hand in front of their face to block the sun.
They further reported that the windscreen was not crazed or dirty and that the aircraft had been recently washed. They were wearing reading correction glasses which did not provide glare protection and were not wearing any headwear that could be used to shield the sun.
Stabilised approach criteria
The operator’s procedures defined criteria for stabilised approaches. If an approach was not stable below 300 ft above aerodrome elevation, an immediate missed approach was required to be conducted. These criteria included that:
From 500 ft AGL on the descent, the aircraft shall be:
- on the correct flight path with only small changes in heading and pitch required to maintain the correct flight path
- the indicated airspeed is not more than Vref [landing reference speed] (-0/+ 10 kts)
- the aircraft is in an acceptable landing configuration
- sink rate is no greater than 600 fpm [feet per minute]; if an approach requires a sink rate greater than 1000 fpm, a special briefing should be conducted
- power setting is appropriate for the aircraft configuration and is not below the minimum power for approach as defined by the aircraft operating manual
- all briefings and checklists have been completed.
Safety analysis
The pilot conducted the final approach segment in clear conditions with the sun low in the sky and 10° to the left of runway heading. This exposed them to direct sun glare during the approach. To reduce the effect of the glare they used the aircraft’s visor and their right hand to block the sun. However, some glare remained, and their raised hand likely impacted their view of the runway and associated lighting. Consequently, the pilot misidentified the taxiway as the runway and aligned the aircraft with the taxiway centreline.
During the subsequent segment of the approach, the aircraft’s navigation instruments were likely indicating that the aircraft was to the left of the intended flight path. However, the pilot was looking outside during this time and therefore did not detect the deviation. Furthermore, they did not observe the C152 positioned on the taxiway, likely due to the continued reduced visibility throughout the approach.
The instructor on board the C152 broadcast over the radio after identifying that the approaching aircraft was aligned with the taxiway. Shortly after this broadcast, the aircraft commenced a turn towards the runway. While continuation to landing on the taxiway would likely have resulted in the aircraft passing over the C152, it would probably have resulted in a collision with obstacles associated with the airport’s construction works. As the aircraft commenced its turn toward the runway after the broadcast was made, it is likely that the broadcast contributed to the pilot’s recognition of the situation. However, they advised that they remained unaware that there was an aircraft on the taxiway.
During the manoeuvre, the aircraft passed behind and in close proximity to the C152. Conducting such a manoeuvre carried a risk of collision with both the C152 and other objects on the ground. Moreover, this manoeuvre was not in accordance with the operator’s stabilised approach criteria where only small heading changes were permitted below 500 ft above ground level (AGL). Upon recognising that the aircraft was not on the intended flight path, an immediate missed approach was required to be conducted. The broadcast from the C152 instructor also alerted air traffic control (ATC) to the situation, prompting them to instruct the pilot to discontinue the landing.
Consideration was given to whether the designation of the landing runway at Launceston Airport as the left runway may have led the pilot to misidentify the taxiway as the left of 2 parallel runways. However, this was not reported by the pilot. Furthermore, they had prior experience operating at the airport and were therefore familiar with the runway layout.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the passing in close proximity to an aircraft on a taxiway during approach involving a Pilatus PC‑12, VH‑NWI, Launceston Airport, Tasmania, on 13 June 2025.
Contributing factors
The final approach was conducted in clear conditions almost directly into the sun, exposing the pilot to glare. Subsequently, the pilot misidentified the taxiway as the runway and aligned the aircraft with the taxiway's extended centreline.
The pilot corrected the aircraft's flight path at a low level rather than immediately conducting a missed approach. During the manoeuvre, the aircraft passed in close proximity to an aircraft on the taxiway.
Other findings
After identifying that the approaching aircraft was aligned with the taxiway, the instructor on board the aircraft on the taxiway made a radio broadcast, likely alerting both the pilot and air traffic control to the situation.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future.
Safety action by Armada Aviation
Armada Aviation circulated a notice to its aircrew advising them of hazards associated with a visual approach, such as sun glare. Additionally, it made the following changes to its operating procedures:
Updated the final decision to proceed to landing to include a requirement that the runway was confirmed and clear by 400 ft above ground level, or the approach minima.
Added a top of descent safety briefing to ensure pilots brief other risks associated with the visual approach segment following an instrument approach, including lighting configuration and sun position.
Updated the checklist of the final phase of flight to include checking that the runway was confirmed and clear.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and operator
the pilot and operator of the aircraft on the taxiway
Bureau of Meteorology
Launceston Airport
Airservices Australia
recorded data from the electronic flight bag (EFB) on the aircraft.
References
Australian Transport Safety Bureau (ATSB) (2004). Limitations of the see-and-avoid principle, /sites/default/files/media/4050593/see_and_avoid_report_print.pdf, ATSB, accessed 13 June 2025
Hawkins, F.H. (1987). Human Factors in Flight, Gower, Aldershot.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot and operator
the pilot and operator of the aircraft on the taxiway
Launceston Airport
Airservices Australia
Civil Aviation safety Authority.
Submissions were received from:
the operator.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, or R as required for left or right when there are parallel runways.
[2]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered.
[3]Missed approach / go-around: a standard aircraft manoeuvre that discontinues an approach to landing.
[4]Precision Approach Path Indicator (PAPI): a ground-based system that uses a system of coloured lights to visually identify the correct glide path to the runway when conducting an approach.
[5]Notice to Airmen (NOTAM): a notice containing information or instructions concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to persons concerned with flight operations.
[6]Automatic terminal information service (ATIS): the provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is updated either routinely or when there is a significant change to weather and/or operations.
[7]Crazing: Small, thin cracks or lines that can develop on the surface of an aircraft window.
On 31 October 2023, several active fires were burning in the Tenterfield area of New South Wales (NSW). By that afternoon, up to 21 NSW Rural Fire Service (RFS) aircraft, including 3 large air tankers and their lead plane (birddog) were deployed to the area to assist with fire control. Concurrently, Queensland (Qld) Fire and Emergency Services (QFES) had deployed aerial assets to an adjacent fireground on the NSW/Qld border.
The crews of the NSW RFS birddog and the large air tankers reported multiple incidents of being unable to communicate and coordinate with other aircraft at the firegrounds. Multiple occurrences of unsafe aircraft proximity were also reported.
What the ATSB found
The ATSB identified that as the fire activity increased in the early afternoon, the state operations controller (SOC) proactively dispatched 3 large air tankers to the region without a target and without coordinating with the local incident management team to ensure they could be effectively integrated into the existing local incident plan. The SOC likely assumed that the large air tankers would be coordinated by the air attack supervisor (AAS) in the Tenterfield area when they arrived. However, most likely due to the communication breakdown, the AAS was not aware the air tankers were inbound. Further, when they arrived, the AAS was about to depart the fireground for fuel and did not advise the incoming Birddog AAS (dispatched with the large air tankers) of the known traffic in the area.
The ATSB also identified that the NSW RFS had inadequate guidance to ensure there was consideration given to the continuity of aerial supervision if the AAS was required to depart the fireground. There was also no mechanism to assess whether increased aerial supervision was required when aircraft numbers and/or fire complexity increased.
In addition, the NSW RFS had no procedure to ensure that fire common traffic advisory frequencies (Fire-CTAFs) were reliably known by state air desk personnel. As a result, when the 3 large air tankers were dispatched to the area, they were provided with incomplete Fire‑CTAF information.
In combination, this resulted in the large air tankers having no target information, incomplete traffic information and operating on the incorrect frequency. Additionally, NSW RFS and QFES were operating in proximity on the NSW/Qld border with, initially, no communication or coordination.
The ATSB also identified safety issues associated with the inconsistent understanding within the NSW RFS state air desk of the threshold required to action task rejection procedures when safety concerns were raised. Also as there was no procedure for implementing a temporary restricted area, there was an increased risk of an air proximity event with aircraft not associated with firefighting operations.
What has been done as a result
Following the events that occurred near Tenterfield on 31 October 2023, the NSW RFS introduced extensive systemic-level safety improvements to its operations.
This included the introduction of a policy to ensure that pilots in command of large air tankers receive a briefing from the incident management team regarding incident strategy prior to departure. It has also developed new procedures for state air desk and incident management team (IMT) liaison, and structured communication loops between the IMT and air attack supervisors.
Further, NSW RFS has issued a directive that requires regular assessment of operational complexity, environmental conditions and the number of aircraft dispatched to a fireground to ensure that aerial supervision arrangements remain appropriate.
Issues around the implementation of a temporary restricted area (TRA) and recording Fire‑CTAF information have also been addressed.
In addition, the National Aerial Firefighting Centre (NAFC) developed the national cross‑border airspace management guideline (released in January 2024), which involved all jurisdictions. This guideline established common procedures for frequency alignment, air desk-to-air desk liaison, cross-border tasking triggers, and shared TRA/TFR activation.
Refer to the section titled Safety issues and actionsfor a full list of proactive safety actions taken.
Safety message
As noted by the National Aerial Firefighting Centre, aerial firefighting is a critical capability for the management and suppression of bushfires in Australia. To effectively achieve this, multiple aircraft are flown at low altitudes and varying airspeeds, often in challenging environmental conditions. This creates a high-risk environment, which requires a continued focus on risk mitigation.
As previously identified in ATSB investigation AO-2020-007, at a large fireground it is likely there will be personnel and assets from multiple organisations and jurisdictions interacting. In this scenario, non-standard procedures and practices may result in unforeseen risks emerging. It is therefore critically important for tasking agencies to take the lead, with the support of stakeholders, in developing the quality and safety standards they require for the firefighting effort to mitigate operational risks.
Further, the adoption of robust systems for managing risk by the tasking agency provides an additional layer of defence, above that provided by each aircraft operator. This also ensures that one aspect of the operation does not compromise another. This may include the development of procedures to support decision-making processes rather than personnel having to exercise judgement based on their experience, skills and knowledge. This includes tasking decisions, task rejection procedures, and minimum aerial supervision requirements.
Summary video
The occurrence
Introduction
Aerial firefighting is a critical capability for the management and suppression of bushfires in Australia. To effectively achieve this, multiple aircraft often operate together over inhospitable terrain at low altitudes and varying airspeeds with reduced visibility from smoke. This hazardous environment ‘requires an enduring focus on training, compliance, and risk mitigation’ (National Aerial Firefighting Centre (NAFC), 2021).
After firefighting operations in the Tenterfield area of New South Wales (NSW) on 31 October 2023, the ATSB received multiple reports of proximity incidents between firefighting aircraft dispatched to the area and initiated an investigation, including a detailed review of the flight data (see the section titled Recorded data).
Following interviews with key personnel, a review of communications, dispatch and communication procedures, and written submissions from operators involved on the day, the ATSB identified several risks associated with communications and coordination between the state air desk and the incident management team and between the state air desk and the aircraft dispatched to the fireground. As such, these risks became the focus of the investigation. The proximity incidents were considered consequential to these risks.
Background
In the days leading up to 31 October 2023, extreme fire weather,[1] critically dry fuels, and multiple simultaneous fire escalations combined across the Tenterfield, Inverell, and Glen Innes Severn Local Government Areas (LGA). The NSW Rural Fire Service (NSW RFS) advised this created one of the most challenging operational environments encountered during the 2023 fire season.
By midday on 31 October, the RFS State Operations Centre reported 93 active incidents across NSW, including 77 bush and grass fires, with 25 still to be contained. There were also 6 concurrent Section 44[2] bushfire emergency declarations, one of which covered the Inverell/Tenterfield LGAs.
To meet these escalating demands, 617 personnel, 167 appliances, 39 heavy plant units and 45 aircraft were deployed across the state. Despite this, resourcing remained critical.
The Tenterfield LGA recorded 10 active fires, many of which escalated during the afternoon under the influence of strong winds and critically dry fuels. By evening, 6 fires had reached Emergency Warning level, and 8 Emergency Alerts were issued, including for new ignitions, such as the Christies fire on the NSW/Qld border.
The key fires in the LGA included:
Benders Creek Fire – made significant afternoon runs, jumped the New England Highway (closing the road), and escalated to Emergency Warning with a Seek Shelter message.
Sawyers Creek Fire – breached containment, crossed the Bruxner Highway and threatened properties west of Tenterfield.
Frost Road Fire – escalated from Watch and Act to Emergency Warning during the day as it crossed Woodside Road and threatened the Sunnyside area.
Ogilvie Drive Fire (Tabulam) – crossed the Clarence River, destroyed several structures and forced Emergency Alerts for downstream communities.
Christies Fire (Jennings/Wallangarra) – ignited in Queensland, crossed into NSW and impacted the towns of Wallangarra (Queensland) and Jennings (NSW), resulting in property losses, power outages, and residents sheltering in place under direct fire impact.
An incident management team (IMT) (see the section titled Incident management team) had been established at Glen Innes, NSW, to coordinate firefighting activities in the region. There were many roles involved in the NSW RFS response; for simplicity, only the most relevant roles applicable on the day, in the regions involved, are discussed in this report.
The IMT included an incident controller (IC), responsible for the overall fire management, an air operations manager (AOM), responsible for coordination of aviation resources, and 2 air attack supervisors (AAS) (see the section titled Air attack supervisor) operating in helicopters over the firegrounds, conducting tactical aircraft coordination.
As part of the daily morning briefing at the IMT, aerial crews deployed to the Tenterfield area were advised that there were 3 fire common traffic advisory frequencies (Fire‑CTAFs)[3] (see the section titled Fire common traffic advisory frequencies) and were provided the corresponding boundaries in use that day (Figure 1). These frequencies were allocated to help with communication in anticipation of the high number of aircraft expected to be operating in the area. The Fire-CTAFs in operation were the:
northern area containing Jennings (118.65)
southern area containing Tenterfield (123.65)
western area (124.45).
Although the 3 Fire-CTAFs had been issued by the NSW RFS state air desk (SAD) (see the section titled State air desk) in Sydney the previous evening, the personnel manning the SAD on the morning of 31 October 2023 were only aware of the southern Tenterfield Fire-CTAF (123.65).
Figure 1: Map of NSW Fire-CTAFs in the Tenterfield area on 31 October 2023
Source: NSW RFS, annotated by the ATSB
In total, there were up to 18 aerial assets deployed by the NSW RFS to the region throughout the morning.[4] The AAS in Firebird 254 (FB254), a Eurocopter AS350, was assigned to the area encompassing Fire-CTAF 123.65 and was primarily focused on 2 fires west of Tenterfield – Frost Road (purple section in Figure 2) and Donnybrook State Forest (blue section in Figure 2). They were coordinating up to 14 aerial assets, including single engine air tankers (SEATs) and helicopters.
Figure 2: Zoomed in map of active fires released at 1600
Note: Fire mapping data was only provided at 4-hour intervals. There was no imagery provided for 1400. The above map was released at 1600; and was indicative of fire activity between 1400–1500 – the NSW RFS personnel on the ground were not aware of the extent of the fire at Christies. Source: NSW RFS annotated by the ATSB
While not associated with the proximity events of the day, a second AAS was operating in a helicopter, callsign Firebird 279 (FB279), around 27 km north-east of Tenterfield at a fireground near Ogilvie (Figure 1). They were operating on the northern Fire-CTAF (118.65) coordinating 2 helicopters at the Ogilvie fire. That AAS later reported that they could not hear any radio transmissions being made later in the day, when aircraft were operating in the Jennings area, most likely due to terrain shielding.
In the late morning and early afternoon, a forecast wind change occurred, and the fires to the west of Tenterfield made a faster than anticipated run towards the town and the airport. This increased the workload for personnel in the IMT, specifically the AOM, as there was a possibility that the Tenterfield air base, where major RFS assets were based, would come under threat from the fire. The AAS was also allocating assets to try to contain this fire to the west of the main highway.
At 1329, during a teleconference[5] between the operations control centre in Sydney and the IC at Glen Innes, the IC advised there was a new fast‑moving grass fire in the Scrub Road area (red section in Figure 2) with 20–30 properties under threat. They advised they had one aircraft and 2 ground firefighting units but no other resources available to fight this fire. In response, the NSW RFS state operations controller (SOC) (see the section titledState operations controller) advised that one large air tanker (LAT),[6] already operational, could be diverted to the area. They also advised there was a possibility a second LAT could be made available, and that the IC could consider using those assets and reprioritising other assets already at the fire, if deemed necessary, which the IC noted.
Approximately 20 minutes later, without further consultation with the IC or personnel at the IMT, the SOC ordered the dispatch of 3 LATs – callsigns Bomber 210, Bomber 164 and Bomber 132, and a lead aircraft (Birddog 123)[7] to the Tenterfield area. The SOC advised the IC in a second conference call when discussing the Frost Road (purple section in Figure 2) and Donnybrook (blue section in Figure 2) fires that ‘we have 3 LATs that have been tasked to you in Tenterfield, and I understand the AASis liaising with the AOM in the IMT’. The IC did not conduct any further follow up with the AOM regarding the LATs.
The LATs and Birddog crews were (verbally) dispatched to the Scrub Road fire by the state air desk in Sydney and were provided with the southern area Fire-CTAF of 123.65. As the 2 adjacent Fire-CTAFs were not known to the state air desk, the LATs and Birddog crews were not advised of these. In addition, they were not provided with specific target information but were instructed to coordinate with the AAS in FB254 upon their arrival. The Birddog AAS reported that they were also not verbally informed that Bomber 132 had been tasked to the fire (although this was included in the tasking information, the tasking information could not be downloaded in flight).
Shortly after, the state air desk operations manager (SADOM) sent a text message via mobile phone to the Glen Innes AOM advising that 3 LATs had been dispatched. However, the text message did not include an estimated time of arrival for the LATs or any intended targets. Although it was common practice for the AOM to pass details of arriving aircraft to the AAS, they could not specifically recall doing so, and the AAS in FB254 later reported being unaware that the LATs had been dispatched.
Bomber 164 and Birddog 123 departed from Dubbo, NSW, and Bomber 210 departed from Coffs Harbour, NSW, at about the same time. During their flights, dispatch details were received, however due to the lack of internet reception at altitude, this could not be downloaded. About 30 minutes later, Bomber 132 departed from Richmond, NSW. The Birddog crew were in communication with the Bomber 164 crew on the NSW RFS assigned LAT frequency (130.55). Birddog 123 also communicated with Bomber 210 via the LAT CTAF[8] on Bomber 210’s arrival.
Concurrently, the QFES was conducting firefighting operations at the ‘Christies’ fire. The NSW AOM and AAS were aware that these fires had been burning for several days and were aware QFES would be managing these fires. However, they had not considered the implications for their operations of aerial assets operating on the Queensland (Qld) side of the border.
At 1400,[9] the Christies fire started to threaten the Wallangarra/Jennings area on the border of Qld and NSW. QFES continued to refer to this fire as the ‘Christie’s’ fire, with NSW RFS referring to this fire as the ‘Jennings’ fire. Neither agency initially recognised that this was the same fire. Subsequently, QFES dispatched 6 aircraft, including a large air tanker,to the border area. These aircraft were operating on a different QFES assigned Fire-CTAF, 122.65.
There was no coordination between the NSW RFS and QFES regarding border operations at that time, and so NSW RFS personnel (SAD and the IMT) were unaware these aircraft had been dispatched.
Birddog 123 arrived at the Scrub Road fire, broadcasting on the 123.65 Fire-CTAF, at around 1450. The Birddog AAS contacted the AAS in FB254, who, unaware that the birddog and LATs had been dispatched, was about to depart the Frost Road fireground to refuel. Prior to departing, they told the Birddog AAS they could head north of the Donnybrook fire, where a new fire had just started to develop and was running toward the Jennings township, and find a target. A review of flight data confirmed that FB254 was on the ground at Tenterfield Airport between 1454 and 1504.
Bomber 164 and Bomber 210 arrived around 7 minutes after the Birddog, which was about an hour after the AOM was advised via text message that they had been dispatched. The Birddog AAS advised the ATSB that to ensure separation with aircraft at the fireground, Bomber 164 and Bomber 210 were kept about 28 km to the west and south-west of the fireground, not lower than 6,000 ft above ground level (AGL).
The FB254 AAS reported that, following refuelling at Tenterfield Airport, the helicopter was tasked to assist with a report of ground crews under threat from fire. A review of flight data confirmed that shortly after becoming airborne again, FB254 movements were consistent with a search and rescue pattern around 19 km south of the Scrub Road fire. While the AOM could not specifically recall tasking FB254 to assist the ground crews, they advised it was likely they had tasked them, as they were responsible for tasking aerial assets to respond to triple 0 calls or requests from ground crews.
The Birddog AAS reported that they attempted contacting other aircraft in the area around the Scrub Road fire and made a couple of low runs with the intention of putting a retardant line to protect 2 properties on the southern edge of this fire. Once satisfied the area was suitable, they contacted the crew of Bomber 210, advising them to enter the area, and briefed them accordingly. However, the Birddog AAS reported that as Bomber 210 was on their final run to drop their retardant, they received a call from personnel within the IMT advising them not to drop the retardant and instead move further north towards Jennings to targets of higher priority. The ATSB could not verify when the Birddog was instructed to go north, or who issued that instruction.
Neither the IMT personnel nor the FB245 AAS advised the Birddog AAS that the Jennings area was operating on a different Fire-CTAF. Therefore, when the Birddog and the LATs headed north towards Jennings, they remained on 123.65 instead of 118.65, which was being utilised by other aircraft in the Jennings area on the NSW side of the border (Figure 3).
Figure 3: Aerial traffic in the Tenterfield area at 1500
Image shows aircraft active in the specified area between 1455 and 1505. A 10-minute duration was used noting some only transmit positional information at a rate of 2 minutes, and with low level work some transmissions may not be captured. 5 aircraft were identified as being on an airfield (FB254 (AAS), Cessna 182 (private), HT297, HT468 and FB717). Source: NSW RFS map, data from ADSB and NAFC, annotated by the ATSB
Over the next hour, Bomber 210, Bomber 164 and Birddog 123 (operating on their discrete frequency) transited in and out of the northern Fire-CTAF 118.65, with the Birddog AAS also using the 123.65 Fire-CTAF. They also entered the Qld Fire-CTAF (122.65), unaware they were on a different frequency to other aircraft operating in this area. The LATs and Birddog crews reported multiple proximity events with other aircraft, citing other flight crews not communicating and not being visible on TCAS,[10] as the primary reasons for these events (see Transponder analysis).
Birddog 123 reported that they contacted the SAD multiple times on their mobile phone throughout the afternoon, advising of difficulty identifying and contacting aircraft in the area. In response, the SAD provided the Birddog with mobile telephone numbers for the pilots assigned to the fireground so that the Birddog could contact them directly. Confirmation of the Fire-CTAFs in use did not occur during these telephone calls.
Personnel on the SAD had access to flight tracking software Tracplus,[11] which was used as a strategic situational awareness tool. It was not actively monitored and was not used to assess airspace congestion. Despite that, the SAD operations manager viewed Tracplus and noticed that the airspace appeared congested, and that Qld aircraft were operating in proximity to NSW RFS aircraft on the border.
That observation prompted contact with the Qld SAD at 1525 (NSW time) to advise of NSW aerial operations taking place near the border. However, unaware of the northern Fire-CTAF in use, initially only Fire-CTAF 123.65 was relayed to the Qld SAD. In response, the Qld SAD advised the NSW SAD that Qld aircraft were operating on Fire‑CTAF 122.65. There was no evidence that that information was passed to any NSW RFS personnel at the firegrounds.
Around 1530, Bomber 132 arrived at the fireground, and the crew contacted the Birddog 123 AAS. Until then, the Birddog AAS was unaware that the third LAT had been dispatched. There were no reports of proximity events involving Bomber 132 and it largely held at a higher altitude to the west of the fireground, due to having significant endurance and no specific targets allocated.
At around 1600, the Glen Innes AOM advised the NSW SAD that there were 3 Fire‑CTAFs in use, and provided the specific frequencies.
Subsequently, the NSW SAD relayed that information to the Qld SAD, to enable QFES aircraft to coordinate with NSW RFS aircraft on 118.65. However, the Fire-CTAF information was not passed to the 3 LATs and Birddog already at the fireground.
Shortly afterwards, while operating near Jennings, the pilot of Birddog 123 detected the QFES Birddog (125) on TCAS. By chance Birddog 125 was a company aircraft, and the 2 pilots knew each other personally. The pilot of Birddog 123 was therefore able to contact the other pilot by mobile telephone. During the subsequent discussion between them, it became clear that there were aerial assets, including LATs, operating at fires on either side of the border.
The pilot of Birddog 123 reported that they subsequently advised the NSW RFS SAD that conditions were dangerous due to a lack of coordination and communication. Additionally, after the LATs completed their drops – one effective, one partially effective, and one ineffective – the Birddog AAS advised the NSW RFS LAT coordinator and SOC that they would not be returning to the fireground until communication issues were resolved.
This was not recognised as a task rejection (see the section titled Task rejection procedures) by either the large air tanker tasking coordinator (LATCO) or the SOC. As such, no records were made of the conversation and neither the LATCO nor the SOC took any action to ensure the communication concerns were addressed. Additionally, the safety concerns were not passed on to aircraft already at the fireground, nor the subsequent Birddog and LAT crew dispatched to the fire approximately one hour later.
Context
Personnel from multiple agencies were involved in the firefighting operations in the Tenterfield area on 31 October 2023. These included the New South Wales (NSW) Rural Fire Service (RFS), NSW National Parks and Wildlife Service and pilots and air crew of various aircraft operators contracted to NSW RFS. Later in the afternoon, as fires on the Queensland side of the border converged with fires in NSW, personnel from Queensland Fire and Emergency Services (QFES) were also involved.
New South Wales Rural Fire Service
The NSW RFS was the lead agency for fighting bushfires in NSW. They worked closely with other agencies to respond to a range of emergencies, including:
bush and grass fires
bushfire mitigation
structure fires
search and rescue (SAR)
motor vehicle accidents
storm response in rural districts.
The RFS was primarily made up of volunteers, with paid staff members managing day‑to‑day operations, incident management teams (IMTs) and operational support, among other roles. There were many roles involved in the RFS emergency management response; for clarity, only those roles applicable on the day are discussed below.
State operations centre
When required, the multi-agency, statewide response to large bushfire emergencies was overseen and coordinated by the state operations centre, located at NSW RFS headquarters in Sydney.
State operations controller
The state operations controller (SOC), located in the state operations centre, maintained overall command of the firefighting effort across the state, and allocated resources as needed.
State air desk
The state operations centre also contained the state air desk (SAD), which was the state level multi-agency team responsible for coordination of aircraft operations. When activated, the SAD provided ‘advice, dispatch services and logistical support in response to a request for aviation resource/s in accordance with available information and contractual arrangements’. The 2 key positions for aerial assets were the:
state air desk operations manager (SADOM), who was responsible for ensuring that aircraft and aviation support resources were dispatched and coordinated to incidents. The SADOM was to maintain ‘a strategic overview to ensure the safe, effective and efficient management of aerial and logistical support assets’.
large air tanker tasking coordinator (LATCO) who coordinated ‘the tasking of LAT resources on days of heightened fire danger/activity in consultation with the state operations controller’.
The NSW RFS advised that the scale of activity on 31 October 2023 placed the NSW RFS State Operations Centre and SAD under significant pressure.
Personnel in the State Operations Centre were required to manage high levels of incident reporting, resourcing requests, and inter-agency coordination across 6 concurrent Section 44 declarations. This included prioritising the movement of out‑of‑area strike teams, coordinating logistics for remote firegrounds and supporting Incident Management Teams (IMTs) that were themselves under strain.
The SAD also faced exceptional demand as numerous firegrounds across northern NSW required aviation support simultaneously.
Incident management team
The coordination and management of a regional response to fires and other incidents was undertaken through an IMT located in proximity to the fires. The IMT for the fires in the Tenterfield area on the day was established at Glen Innes, NSW. Personnel at the IMT were responsible for management of all firefighting activities including:
answering triple 0 fire calls for the area and deploying assets to respond to those calls
coordinating ground crews
coordinating aerial assets
managing all logistics for aerial and ground crews, including fuel, food and breaks.
Incident controller
At the IMT, the incident controller (IC) had overall command of all ground and aerial firefighting activities in their allocated region.
The Glen Innes IC’s intent on the day, outlined in an incident action plan,[12] was to hold fires within proposed containment lines, monitor fire progression and protect assets on the eastern and southern sides of the fire. The IMT was managing 10 separate fires in the Tenterfield area on 31 October 2023.
Air operations manager
The IC relied on the air operations manager (AOM) to coordinate all aerial activities, as the AOM had more specific training in aerial firefighting. NSW RFS procedures stated that an:
AOM shall be activated during a major incident and/or when five or more aircraft are required in relation to an incident.
The incident AOM advised that they worked closely with the air attack supervisor (AAS), located overhead the fireground, to ensure they had enough resources, and to ensure the employed strategy was working. During interviews after the event, both the AOM and AAS stated that they had sufficient aerial assets on the day to fight the fires, and the addition of LATs did not assist the task.
The AOM assessed that due to the:
fire complexity
number of aviation assets dispatched to the region
available resources in the centre
they ‘were completely task saturated on the day’.
The AOM had been involved in firefighting for over 20 years and, after obtaining extensive experience in many different areas, had trained and qualified in the AOM role in 2018. They advised this was one of the busiest shifts they had encountered. The SADOM later reported that the IMT was ‘certainly busy’, and in hindsight ‘we should have got them more resources’.
Air attack supervisor
The AAS was a tactical command position, controlling the overall firefighting strategy for aircraft at a fireground. They ensured that aerial operations were consistent with procedures and the incident action plan. This included maintaining communications and providing intelligence about the fires to relevant IMT personnel and organising aircraft at the fireground. NSW RFS procedures stated ‘an AAS should be considered where there were 2 or more aircraft’ and was required ‘when there are 3 or more aircraft operating on the one incident’.
While all aircraft assigned to a fireground were ultimately responsible for their own separation, using ‘see‑and‑avoid’ principles, the AAS was required to:
brief pilots, in the air and on the ground, on specific assignments including identification of ground personnel, hazards, tactical information, and communication links; and to ensure safety standards were maintained at all times.
On the incident day, the number and mix of helicopters, small and large aeroplanes and the convergence of different fire fronts presented a complex aerial firefighting operation.
The AAS in FB254 was managing:
Donnybrook fire – 4 single engine air tanker (SEATs) aeroplanes – 3 of which were floatplanes collecting water from a nearby lake and 1 returning to Tenterfield for loading, along with 1 firebombing helicopter
Frost Road fire – several firebombing helicopters working with ground crews
south-east of Tenterfield – 2 helicopters collecting intelligence on the fire conditions.
These aircraft were geographically separated and, where applicable, a stack was applied, with:
established exit and entry points so that all aircraft working on a fire were operating in the same direction
entry and exit lanes at different altitudes
standard radio communication procedures to ensure separation
different aircraft types assigned different altitudes.
The AAS had extensive firefighting experience and had been performing the AAS role for around 23 years. The AAS self-assessed that they were not overloaded, stating that while it was busy, they were not at saturation point and it was not the worst fireground they had experienced. The AOM also assessed that the AAS was managing their workload well and no evidence was identified that the AAS lost situation awareness. Further, there were no reports of any communication or separation issues prior to the arrival of the LATs.
Operational procedures
The RFS maintained a suite of documents, which detailed the procedures for managing aerial firefighting. The 2 primary documents for air tanker operations were the:
interagency aviation standard operating procedures, which outlined the basic procedure for all air tanker operations
NSW RFS operating guidelines for air tanker operations (operating guidelines), which provided further details specifically for the LAT program.
Additional procedures and forms were contained in the operational management procedures, incident management procedures and the air attack supervisor manual.
Aerial supervision
Supervision continuity
The NSW RFS procedures contained no information on ensuring continuity of the AAS role when the AAS was required to depart the fireground for rest or to refuel. The AAS, and others interviewed, described that if the AAS was required to depart, they would leave aircraft strategically separated, and they would also ask a senior pilot to ‘keep an eye on things’ while they were gone.
The United States Department of Agriculture (US Forest Service) advised the ATSB that, while not documented, where an AAS needed to depart (for fuel or a scheduled rest break), a replacement AAS would be pre-arranged to ensure an adequate handover. If no replacement was available, they would reduce either the complexity of the aerial firefighting strategy, or the number of aircraft at the fireground.
Number of aircraft under supervision
The NSW RFS procedures also contained no information on a maximum number of aircraft to be controlled by one AAS nor information on specific trigger points on when to review the ongoing supervision arrangements.
There is no way to define an exact trigger point for adjusting, downsizing, or completely suspending aviation operations. The factors listed below should be evaluated to determine whether additional Aerial Supervision resources are needed or tactical/logistical missions need to be modified/suspended.
• Complexity of aviation operations • Communications • Topography • Firefighter and public safety • Poor visibility • Wind/turbulence • Fire behaviour • Aircraft performance • Aircraft incident/accident.
NSW RFS released a memo after this fire activity, which stated:
the SAD is to liaise regularly with the Air Operations Manager (AOM) and AAS responsible for 3 or more aircraft to confirm aerial supervision arrangements remain appropriate. In particular, consideration should be given to the allocation of additional AAS platforms' taking into account:
• the number of aircraft tasked • the number of fires burning and their proximity to each other • size of the area of operations • other complexities such environmental factors (e.g. weather, visibility).
Birddog operation
When LATs were dispatched to a fire, they would generally be accompanied by a separate birddog aircraft. In those circumstances, a LAT air attack supervisor (LAT AAS) in the birddog aircraft coordinated the LAT movement with the incident AAS. Their role included briefing the LAT crew on the specific assignment, identifying hazards, tactics and managing communications with the incident AAS.
The NSW RFS air tanker guidelines indicated that an incident AAS was pivotal to LAT operations, stating:
the Incident AAS is to ensure all incident aircraft are advised of the proposed air tanker mission and agreed airspace and communication arrangements are established.
Prior to the Birddog arriving over the fire, the Incident AAS will identify and assign an altitude following discussion with the Birddog.
The Incident AAS aircraft will orbit at this level and operate as a communication link between the ground crews and Birddog while maintaining a strategic overview and coverage of the operation.
This will allow the Birddog aircraft to focus on mission objectives and coordinating the air tanker(s).
The guidelines further stated that:
When an Incident AAS is not established at an Incident, the LAT AAS will assume the Incident AAS roles and responsibilities.
The RFS advised that this model adapted supervisory functions to available resources, fleet composition, and the dynamic nature of domestic fireground operations.
In contrast, the Western Australia (Department of Fire and Emergency Services) LAT guidelines stated that:
In the absence of a Primary AAS during fuel cycles, etc. the BDOG [birddog] AAS is not permitted to undertake duties conducted by the Primary AAS. An arriving LAT shall not enter the stack or the ‘holding area’ until permission is given by the Primary AAS PIC.
Large air tanker dispatch approval procedures
The NSW inter-agency aviation standard operating procedures noted that air tankers could provide large volumes of suppressant, and careful planning and supervision was needed to ensure this was used effectively.
The NSW RFS air tanker guidelines stated that for a LAT and/or birddog to be dispatched, an aircraft request form from the incident controller (IC) was required, outlining a strategy in conjunction with the SAD who could provide ‘guidance on availability and suitability’. The request was then subject to approval by the state operations controller (SOC).
When considering tasking air tankers, the operating procedures stated the IC and SOC were to consider the following:
• incident objectives • threats (life/property, assets, forests) • terrain and fuel types (forest/grassland/urban interface) • prevailing and/or forecast weather and flying conditions, including turbulence & visibility • effectiveness of alternate capacity aircraft and/or ground units • elapsed time for aircraft to arrive ‘on site’ • time of day (last light); and • suppressant / retardant quantity required.
Following SOC approval, the SAD would advise the LAT airbase manager of the approval and mission objectives.
According to the NSW RFS operational management procedure ‘dispatch of aviation resources’:
Any dispatch of aviation resources must always be supported by an appropriately approved aircraft/aviation equipment request form.
The operational management procedures further noted that:
It is acknowledged that the tasking of aviation resources can have a range of specific requirements not covered directly in this tasking procedure. In the event the SAOM [state air desk operations manager] or the SDAO [state duty aviation officer] believes there is valid reason to initiate dispatch outside of these guidelines (including dispatching a different resource to what was requested, or a compelling reason to dispatch another aircraft in addition to the area contract aircraft), they must first contact the State Duty Operations Officer (SDOO), State Operations Controller (SOC) or Manager aviation and advise the reasons for operating outside of the guidelines and gain approval for this variation BEFORE the dispatch is allocated.
The reasons and approval for dispatch outside of these guidelines should be documented within the ‘decision notes’ area of the air desk dispatch module in ARENA.[13]
NSW RFS later advised that:
No decision notes were kept in ARENA, if the aircraft were directed to attend by the SDOO or SOC this was captured in the Air Tanker Dispatch form and SAD/SOC log books.
In response to the draft report, NSW RFS advised the ATSB that:
RFS doctrine explicitly provided the SOC and State Duty Operations Officer discretion to deploy aircraft outside the standard request workflow in rapidly escalating situations or where there was an immediate threat to life or property.
In addition, it advised:
that SOC-initiated tasking on the day was consistent with approved doctrine and that the absence of formalised integration triggers reflected procedural maturity at the time, not non-compliance.
Since the occurrence, NSW RFS has strengthened integration processes through revised Standard Operating Procedures (SOPs) and targeted training. These changes explicitly address the interface between SOC-initiated tasking and IMT coordination, ensuring that Large Air Tanker (LAT) tasking is both procedurally supported and operationally integrated.
Large aircraft tanker tasking on 31 October 2023
On the incident morning, the IMT requested one LAT with a birddog to assist with fire suppression. The request form was completed by the AOM, with the form detailing:
the specific target intended for the LAT
the entry and exit paths mapped out
appropriate Fire-CTAF.
This request was approved by the SOC. The LAT arrived at the fireground a short time later and after discussions with the AAS around drop sites, successfully completed a drop.
Later that afternoon, a decision to task 3 additional LATs was made by the SOC and relayed to the Glen Innes IC during the 1352 conference call discussing the fire situation in the Tenterfield area with senior personnel from the State Operations Centre. However, the ARENA dispatch form for all 3 LATS listed the AOM as the requesting officer.
The incident controller, air operations manager, air attack supervisor, state air desk operations manager and large air tanker coordinator logbooks were provided to the ATSB, none of which detailed the decision to send the 3 LATs on 31 October 2023.
The SOC did not maintain an operational logbook for 30 and 31 October 2023. They recorded some notes in their personal notebook, however, they were not of sufficient detail for the SOC to later recall key events or decisions made on 31 October 2023, including the rationale for dispatching 3 unrequested LATs to the Tenterfield area.
In response to the draft report the NSW RFS advised the ATSB that:
The NSW RFS Operational Management Procedure – State Operations Controller (OMP) in force at that time, did not impose a universal requirement for all senior personnel to maintain a formal operational logbook. Rather, it required that the SOC was ‘responsible for ensuring a record is maintained of significant decisions taken, the rationale for those decisions, and to whom, when and how they were communicated.’
In addition, the recorded emergency conference calls constitute an important complementary record. These recordings capture significant decisions, the rationale underpinning them, and the details of communication including who was informed, when, and how. Taken together, the SOC’s notebook and the conference-call recordings demonstrate compliance with the OMP requirement to maintain a record of significant decisions, even if that record was not in the form of a formal logbook.
While recorded conference calls did provide operational context and captured significant decisions, the rationale for the dispatch of 3 LATs remained unclear. The LAT dispatch forms also did not capture any decision-making notes.
Additionally, the dispatch form, received by the birddog AAS after departure, did not contain detail of specific target/s or information on the 3 Fire-CTAFs in use. It also had incomplete detail of the known aircraft already operating in the area (the intelligence gathering aircraft were not identified). At the time, there was no documented requirement for flight crew to wait for a dispatch form prior to departure.
Despite the IC not requesting the LATs, no personnel from the SAD, the IMT or the fireground queried the LATs dispatch. Multiple personnel interviewed stated that LATs were often dispatched by the SAD without a request from the fireground. Those personnel further stated that dispatch in that manner was often a hindrance as the LATs did not have specific targets, and the incident plan was regularly disrupted to accommodate them, which reduced overall firefighting effectiveness.
In this instance:
B164 ‘dropped wherever they could as they were running out of fuel’
B210 departed for Coffs Harbour after completing a partially effective drop retardant
B132 ‘completed an effective drop’ before returning to Richmond.
Task rejection procedures
The NSW RFS task rejection procedure provided guidance for the rejection of an aviation dispatch/tasking as follows:
Flight crew or operators may reject an aviation tasking when:
• there is a violation of regulated safe aviation practices; • weather and environmental conditions make the activity unsafe; • there is insufficient information to safely plan or undertake the activity; or • they lack the necessary qualification or experience.
There is an obligation on individuals to ensure any concerns or a decision to reject a tasking are notified as soon as possible.
Equally, there is an obligation on an IMT and/or SAD to ensure all aircraft and operators assigned to a particular incident are advised of any tasking rejection as soon as possible.
The NSW RFS held a task rejection register, which had 19 task rejections recorded for 2023.
When interviewed 12 months after the Tenterfield fires, neither the LATCO nor SOC could recall specific details of the call with the AAS in Birddog 123, in which they reported voicing safety concerns about coordination and communication. However, at the time neither recognised the concerns raised as a task rejection. They further reported that they needed to hear the words ‘task rejection’ from crew before actioning the task rejection procedures.
The SAD operations manager stated that in hindsight it was probably not recognised because no one said, ‘I task reject this’ and that ‘we should have paused and taken it as a task rejection’. Additionally, the SOC advised that it was the first or second season after the task rejection arrangements had been implemented, and that improvements were probably required to ensure that task rejections were more explicit.
Other NSW RFS personnel advised that crew relaying safety concerns would prompt them to ask the crew if they were rejecting a task. Another LATCO, who was not on shift that day, reported that if a crew advised they were not returning to a fireground due to safety concerns, that would prompt them to action the task rejection process.
In addition to the Birddog’s concerns, the B210 crew reported that on return to their base at Coffs Harbour, they advised the SAD that their intentions were not to return to the fire until the communications problems were resolved. The LATCO reported being unaware of that, and there were no records in any logbooks or ICON[14] of that conversation.
At about 1800 on 31 October 2023, B210 was re-tasked back to the fireground with a different birddog. Recorded calls to the SAD confirmed that B210 sought clarification from the SAD that communication issues have been resolved. When the SAD operator advised that they did not know, B210 advised the operator that ‘we had to shut it down because too many aircraft were not communicating’. They reported advising the SAD that they would load but remain on the ground until they received confirmation from their birddog, when they arrived at the fireground, that the operation was safe to continue.
Following the occurrence, the NSW RFS sent a memo to all operators reminding them to raise any risks or concerns and to reject an aviation tasking if they felt it necessary.
Airspace procedures
Fire common traffic advisory frequencies
On the evening prior to the incident, anticipating significant aerial assets, the AOM based at the Glen Innes IMT requested, and was issued, 2 additional fire common traffic advisory frequencies (Fire-CTAFs) to the earlier assigned 123.65 by the SAD (Figure 1). While there was likely a verbal handover between SAD shift personnel following the frequency allocation, it was not possible to determine what information was shared.
There was also no requirement for a map of the Fire-CTAF divisions to be recorded or displayed at the SAD, although it was reported that this had occurred on previous occasions. Personnel manning the SAD on 31 October 2023 had no visual representation of the Fire-CTAF divisions and assumed the only Fire-CTAF in use in the Tenterfield area was the southern Fire-CTAF 123.65.
In addition, aircraft request and aircraft dispatch forms only prompted one Fire-CTAF to be recorded.
Temporary restricted area
To prevent aircraft entering airspace associated with an active fireground, a temporary restricted area (TRA) could be requested through the Civil Aviation Safety Authority’s (CASA) Office of Airspace Regulation. NSW RFS had a 24/7 contact number for CASA to facilitate such a request.
The NSW RFS interagency aviation standard operating procedures stated that:
ICs may require additional airspace restrictions or provide additional NOTAM advice to pilots during incident operations. This requirement may be due to complex incident operations, working environment, level of activity or interference from other traffic. The IC/OIC is required to contact the SAD [state air desk] or the hiring agency to seek advice.
The emergency services inter-agency standard operating procedures stated that:
Airservices Australia (ASA) provide a Temporary Flight Restriction (TFR) for bush fires on Area Forecasts specifying non fire traffic to remain clear at a five (5) nautical mile radius and not below 3,000 feet above ground level (AGL) of observed fires.
However, CASA advised that the emergency services inter-agency standard operating procedure was outdated, and, although published in the Airservices Australia (Airservices) Aeronautical Information Publication (AIP), was advisory only, and there was no requirement for aircraft to remain clear of bushfires unless a TRA had been implemented.
NSW RFS had no further guidelines or procedures in place regarding when a TRA should be implemented, or who was responsible for implementing one. The NSW RFS did not request a TRA for the Tenterfield area on 31 October 2023.
Wake turbulence separation
Wake turbulence[15] is produced by heavy aircraft with the most turbulent air being produced by aircraft flying slowly at high angles of attack, which is typical of a LAT during a fire-retardant drop. Wake turbulence can result in a dangerous situation for smaller aircraft flying directly into a larger aircraft’s wake.
NSW RFS had no minimum wake turbulence separation (time or distance) requirement in its procedures, and the responsibility for separating LATs with other aircraft operating at the fireground was assigned to the Birddog crew (LAT AAS).
According to the NSW RFS LAT guidelines:
The Birddog is to establish flight paths to avoid creating hazards to other aircraft at the fire and drop zone along with persons or property on the ground with consideration to potential wake turbulence created by the air tanker.
The United States Forestry Service (USFS), which oversees extensive aerial firefighting operations across the US, has a minimum wake turbulence separation of 2 minutes when very large air tankers (VLATs) are operating, but there was no minimum separation standard when LATs are operating.
While not specifically a wake turbulence procedure, the WA aerial fire suppression procedures always required a 5 NM (9 km) separation between LATs and other aircraft:
All firebombing aircraft shall be cleared from the sector prior to the LAT entering the stack from its 5 NM holding position at a pre-determined nominal entry level of not above 1,500 ft [above ground level] AGL.
There must be a minimum horizontal separation of 5 NM from:
• the sector the LAT is operating in
• all other aircraft operating below 2,500 ft AGL.
The ATSB notes that procedures from other jurisdictions are shaped by their own operating context and may not be directly transferable or suitable for the NSW operational environment.
Cross-border procedures
Queensland Fire and Emergency Service (QFES) had a similar command structure to NSW RFS. On the incident day, the state operations centre, including a SAD was established in Brisbane. Similar to the incident management teams established by NSW RFS, QFES established a regional operations centre (ROC) to oversee the Wallangarra fire,[16] at Charlton, Qld. An incident AAS was in a helicopter over the fireground at Wallangarra supervising QFES aerial assets at the fire on the Queensland side of the border.
There were no documented procedures for either QFES or NSW RFS for cross‑border fires regarding aviation assets. However, NSW RFS had established cross‑border arrangements in place with both Victoria and the Australian Capital Territory.
On the day, at around 1525 (NSW time), the NSW SAD advised the Qld SAD of 3 LATs inbound to Jennings. The Qld SAD advised NSW of the Qld 122.65 Fire-CTAF in use. It could not be ascertained why this information was not provided to the 3 NSW LATs and Birddog.
At 1555 (NSW time), the NSW SAD advised the Qld SAD of the NSW 123.65 Fire-CTAF which was passed to the Qld incident controller. About 15 minutes later, the Qld SAD received updated advice from the NSW SAD that the correct frequency for the area was 118.65.
Recorded data
The ATSB sourced flight track data between 0800–1800 on 31 October 2023, based on geographic location, as in the area outlined in red in Figure 4. The reviewed data included information sourced[17] from:
National Aerial Firefighting Centre (NAFC) ARENA[19] recordings.
Figure 4: ATSB data search area
The red border outlines the area assessed. The Qld/NSW border is marked in orange. Source: ATSB
The ASA-processed radar data provided positional information at 5‑second intervals. Where available, the ADS-B data was generally captured at 1‑second or better intervals. The NAFC data, which could be transmitted at any selected interval, with an interval no greater than 120 seconds, varied between 15 seconds and 120 seconds. Data from all sources was combined for the analysis.
Identification of proximity events
Where data was not captured at 1‑ second intervals, positional data was interpolated, based on great circle arcs between recorded points. This allowed for determination of approach points between aircraft, noting that where gaps are large (up to 2 minutes for the 19 NAFC only dataset) and aircraft are manoeuvring, these paths may not accurately reflect aircraft movement. Distances between aircraft at each point were then calculated using the same method.
The data review identified 205 instances of unique pairs of aircraft operating within 1,000 m of each other over the reviewed period. This was indicative of the nature of aerial firefighting operations, where aircraft are typically managed through established altitude, lateral, and time-separation procedures. As such, proximity alone does not indicate an elevated collision risk.
Limitations of the data for aircraft operating at low levels meant there may have been more instances where aircraft were in close proximity to each other which were not captured.
Of the 4 reported incidents reviewed, 2 were positively identified in the data analysis. The third event could not be identified, however, potentially involved a private aircraft without an active transponder. Analysis of the available data for the fourth event identified a few potential conflicts, but due to data limitations could not positively identify the aircraft involved.
Transponder analysis
Reporters raised concerns that firefighting helicopters had transponders turned off. An analysis was conducted of the 52 aircraft with active transponders (either in the ADS-B or NAFC data set), to determine the time elapsed between received data points, and identify periods of missing data greater than 5 minutes. The ATSB reviewed the data and could find no evidence of any firefighting helicopters turning transponders off during flight. (For further information on the data review see Appendix.)
Safety analysis
Introduction
In the days leading up to 31 October 2023, extreme fire weather,[20] critically dry fuels and multiple simultaneous fire escalations combined across the Tenterfield, Inverell, and Glen Innes Severn Local Government Areas (LGAs). The NSW Rural Fire Service (NSW RFS) advised this created one of the most challenging operational environments encountered during the 2023 fire season.
On 31 October 2023, the Tenterfield LGA recorded 10 active fires, many of which escalated during the afternoon under the influence of strong winds. Up to 17 New South Wales (NSW) Rural Fire Service (RFS) aircraft were deployed in the Tenterfield area in support of firefighting activities. The aircraft had been separated geographically and by different operating altitudes, and there were also 3 separate fire common traffic advisory frequencies (Fire-CTAFs) in use. While the airspace was busy, the involved air attack supervisor (AAS) reported that the activity was manageable, and there were no reported aircraft separation or communication/coordination issues.
In the early afternoon, a birddog aircraft and 3 large air tankers (LATs) were dispatched to the Tenterfield area, with incomplete operational information provided to both the involved crews and the receiving personnel. That led to the LATs and birddog arriving unexpectedly and transiting through the busy airspace on incorrect frequencies, resulting in multiple communication issues with other aircraft.
This analysis will examine the safety risks associated with the deployment of the LATs, together with airspace issues and state cross‑border coordination.
Large air tanker dispatch
Operational coordination
The state operations controller (SOC) ordered the dispatch of the birddog aircraft and 3 large air tankers (LATs) to the Tenterfield area without consultation with the incident management team (including the air operations manager (AOM)) on how the LATs would be effectively integrated into the existing incident plan. While there were provisions for the SOC to instigate the dispatch of the LATs, this bypassed the normal provision of operational tasking information and resulted in the LATs being dispatched without specific targets or correct airspace information. Additionally, their specific arrival time was unknown by the receiving personnel.
Contributing factor
Three large air tankers (LATs) were tasked to the Tenterfield fireground by the state operations controller without consultation with the incident management team. That resulted in the LATs being dispatched without targets or correct airspace information and receiving personnel being unaware of their arrival time.
Incident plan integration
While NSW RFS had documented procedures outlining the process when the incident management teams (IMTs) requested a LAT, there was no documented procedure specifying what communication and coordination needed to occur when the state air desk (SAD) proactively dispatched a LAT/s.
On the day, this resulted in the LATs being dispatched with no consideration for how they would be incorporated into the already established incident plan at the fireground/s and no clear consideration of their intended target/s. There was also no apparent consideration of whether the incident AAS had capacity to incorporate the LATs when they arrived. In this instance the AAS was required to depart the fireground to refuel as the LATs arrived.
While acknowledging that the SAD has a greater understanding of available aircraft resources across the state during an emergency than local IMTs do, procedures requiring coordination with the IMT prior to dispatch ensures that:
the incident AAS is on scene and has capacity to coordinate the LATs when they arrive
there is a suitable plan to utilise the LATs when they arrive at a fireground
LAT crews have all the required operational information.
Contributing factor
The New South Wales Rural Fire Service did not have a procedure for ensuring that when large air tankers were dispatched by the state air desk their tasking was coordinated with the incident management team and integrated into the existing incident plan. (Safety issue)
Fire common traffic advisory frequency usage
Despite the fire common traffic advisory frequencies (Fire-CTAFs) being allocated by the state air desk the evening prior, personnel on the state air desk were not aware that there were 3 Fire‑CTAFs in use on 31 October 2023.
While it was normal practice to display a pictorial map of Fire-CTAF boundaries at the state air desk, there was no documented requirement to do so. This resulted in the 3 LATs and their birddog being dispatched with incomplete airspace information provided to their crews.
Contributing factor
The New South Wales Rural Fire Service had no procedure to ensure that fire common traffic advisory frequencies (Fire-CTAFs) were reliably known by state air desk personnel. This resulted in aircraft being dispatched with incomplete Fire-CTAF information. (Safety issue)
Fireground communication
While the AOM was aware that LATs had been dispatched around 60 minutes prior to their arrival, they had not been made aware of the LATs’ anticipated arrival time or intended target/s. It is possible that due to their workload on a day of high fire complexity, they did not pass what they knew of the LAT tasking to the incident AAS.
Shortly after the Birddog and LATs arrived at the fireground, the AAS was required to depart the fireground to refuel and then tasked by the AOM to a search and rescue task around 19 km south of the Scrub Road fireground. This meant that while there was an AAS in the birddog aircraft, there was no supervision of the remaining aircraft at the fireground following the arrival of the LATs.
Contributing factor
Possibly due to their workload, the air operations manager likely did not pass what they knew of the large air tanker tasking to the incident air attack supervisor (AAS) and subsequently tasked the AAS away from the fireground on an emergency task.
The incident AAS was not aware that the LATs had been dispatched and was about to depart the fireground to refuel when they arrived. As such, they had no opportunity to plan and coordinate the LATs’ arrival.
Prior to departing, the AAS did not provide the birddog crew with an overview of the known traffic situation. In addition, while it was reasonable that they assumed that LAT and birddog crews had been informed of the multiple Fire-CTAFs in operation, this was a missed opportunity for that information to be passed on.
Contributing factor
Due in part to the air attack supervisor (AAS) not expecting the large air tankers, and being unaware they had incomplete dispatch information, the AAS did not provide traffic or Fire-CTAF information to the birddog AAS prior to departing the fireground.
Aerial supervision
NSW RFS required an incident AAS to be in place when 3 or more aircraft were operating at a fireground. However, an AAS would have to leave the fireground for scheduled rest breaks or, as on the day, to refuel, and there was no documented procedure for consideration of ongoing supervision when this occurred. On the day, this resulted in no AAS being made available to replace the incident AAS when they were required to depart the fireground.
Contributing factor
Despite a New South Wales Rural Fire Service requirement for an air attack supervisor (AAS) to be in place when 3 or more aircraft were operating, when the AAS was required to depart the fireground there was no planned replacement AAS to supervise the multiple aircraft in the area.
There was a provision in the NSW RFS large air tanker (LAT) guidelines for the LAT AAS in the birddog aircraft to assume the incident AAS role in the absence of an incident AAS, but there was no guidance or procedure to assess their capacity to do so. On the day, there was no evidence that the LAT AAS was expected to take over the incident AAS role and it was unlikely they would have had capacity to do so, while already coordinating 3 LATs.
Additionally, there was no consideration or trigger points for increasing the number of supervisors when the number of aircraft increased at a fireground or when the complexity of fire activity increased. Although the NSW RFS ground firefighting span of control principle was that no more than 8 assets should be under one individual’s control, similar limits were not applied to aerial operations. As such, the NSW RFS had no documented means of ensuring there was adequate supervision when aerial assets were operating.
Contributing factor
The New South Wales Rural Fire Service procedures required an air attack supervisor when 3 or more aircraft were deployed to a fireground. However, there was:
no assurance aerial supervision would remain adequate as aircraft numbers and/or fire complexity increased
inadequate guidance for consideration of suitable supervision when the AAS was required to depart the fireground. (Safety issue)
Task rejection
The birddog crew reported having numerous conversations with the state air desk relaying concerns around communication issues and congested airspace including advising that the conditions were ‘dangerous’. LAT Bomber 210 also reported advising the state air desk they would not be returning to the fireground until communication issues were resolved. Neither of these conversations were recognised by the state air desk as task rejections and, as such, the task rejection procedures were not implemented. However, on the day, this did not have an adverse effect on the replacement birddog and LAT, as by the time they were re-tasked, the traffic levels had reduced and the state air desk had information on the Fire-CTAFs.
Both the LAT tasking coordinator (LATCO) and SOC stated in interview that unless the term ‘task rejection’ was specifically stated, they did not necessarily action the procedure, which was inconsistent with the understanding of other senior state air desk personnel interviewed. This indicated an under appreciation of the importance of the procedure by senior management at the NSW RFS.
The NSW RFS task rejection register verified that the task rejection procedure had previously been followed multiple times, indicating that state air desk personnel were aware of, understood, and actioned this procedure.
As previously identified in ATSB investigation AO-2020-007 (Collision with terrain involving Lockheed Martin EC-130Q, N134CG 50 km north-east of Cooma-Snowy Mountains Airport (near Peak View), New South Wales, on 23 January 2020), communication of identified unsafe conditions to other operating crews and to personnel on the state air desk is critically important to ensure everyone has the same situation awareness, and that this information can be factored into flight crews and state air desk personnel’s decision‑making process and risk assessments.
Other factor that increased risk
There was an inconsistent understanding within New South Wales Rural Fire Service state air desk of the threshold required to action task rejection procedures. Consequently, reports of unsafe conditions on the fireground were not promptly actioned. (Safety issue)
Temporary restricted area
The NSW RFS did not have a procedure for implementing a temporary restricted area (TRA), including a trigger for when one should be implemented. As a result, despite anticipating multiple firefighting aircraft in the area, neither the state air desk nor personnel in the IMT considered implementing one on the day. The ATSB review of flight data identified that 27 non-essential aircraft transited through the Fire-CTAFs, with no way of verbally communicating with firefighting aircraft. Of these aircraft, 8 were also not transmitting a secondary surveillance radar output, so were not visible on firefighting aircraft’s traffic avoidance systems.
Other factor that increased risk
The New South Wales Rural Fire Service did not have a procedure to implement a temporary restricted area to reduce the risk of an air proximity event with aircraft not associated with firefighting operations. (Safety issue)
Wake turbulence
While NSW RFS procedures considered wake turbulence separation between lighter aircraft from LATs, it relied on the incident or birddog AAS to provide separation between the LATs to other aircraft. However, the procedures did not require an incident AAS to always be present.
When large air tankers are completing drops, their configuration creates significant wake turbulence and aircraft within the wake turbulence zone may be subject to a loss of control in flight. Given these operations almost always occur at low level, there is an increased risk that there may not be sufficient altitude for affected aircraft to recover.
Other factor that increased risk
The New South Wales Rural Fire Service did not have an effective means to manage wake turbulence separation for aircraft operating in the vicinity of the large air tankers, increasing the risk of an unrecoverable loss of aircraft control. (Safety issue)
Cross-border coordination
Queensland Fire and Emergency Service (QFES) and the NSW Rural Fire Service (RFS) did not have documented procedures for how aircraft from both states would conduct joint cross-border firefighting. As a result, while there were some discussions at the state air desk level once the concerns were identified, NSW RFS and QFES aerial assets initially operated in proximity without any coordination, and on different radio frequencies.
On the day, the NSW RFS state air desk and the Glenn Innes IMT were aware of fires on the Qld border and, at some point, both QFES and NSW RFS were also aware of each other’s aerial assets. However, initially neither agency considered that aerial assets on either side of the border may conflict.
Contributing factor
Neither the New South Wales Rural Fire Service or Queensland Fire and Emergency Service had established cross-border coordination procedures for aerial firefighting activities to ensure reliable aircraft communication and separation. (Safety issue)
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the coordination and communication breakdown during aerial firefighting operations near Tenterfield, New South Wales, on 31 October 2023:
Contributing factors
Three large air tankers (LATs) were tasked to the Tenterfield fireground by the state operations controller without consultation with the incident management team. That resulted in the LATs being dispatched without targets or correct airspace information and receiving personnel being unaware of their arrival time.
The New South Wales Rural Fire Service did not have a procedure for ensuring that when large air tankers were dispatched by the state air desk their tasking was coordinated with the incident management team and integrated into the existing incident plan. (Safety issue)
The New South Wales Rural Fire Service had no procedure to ensure that fire common traffic advisory frequencies (Fire-CTAFs) were reliably known by state air desk personnel. This resulted in aircraft being dispatched with incomplete Fire-CTAF information. (Safety issue)
Possibly due to their workload, the air operations manager likely did not pass what they knew of the large air tanker tasking to the incident air attack supervisor (AAS) and subsequently tasked the AAS away from the fireground on an emergency task.
Due in part to the air attack supervisor (AAS) not expecting the large air tankers, and being unaware they had incomplete dispatch information, the AAS did not provide traffic or Fire-CTAF information to the birddog AAS prior to departing the fireground.
Despite a New South Wales Rural Fire Service requirement for an air attack supervisor (AAS) to be in place when 3 or more aircraft were operating, when the AAS was required to depart the fireground there was no planned replacement AAS to supervise the multiple aircraft in the area.
The New South Wales Rural Fire Services procedures required an air attack supervisor (AAS) when 3 or more aircraft were deployed to a fireground. However, there was:
no assurance aerial supervision would remain adequate as aircraft numbers and/or fire complexity increased
inadequate guidance for consideration of suitable supervision when the AAS was required to depart the fireground.(Safety issue)
Neither the New South Wales Rural Fire Service or Queensland Fire and Emergency Service had established cross-border coordination procedures for aerial firefighting activities to ensure reliable aircraft communication and separation. (Safety issue)
Other factors that increased risk
There was an inconsistent understanding within New South Wales Rural Fire Service State Air Desk of the threshold required to action task rejection procedures. Consequently, reports of unsafe conditions on the fireground were not promptly actioned. (Safety issue)
The New South Wales Rural Fire Service did not have a procedure to implement a temporary restricted area to reduce the risk of an air proximity event with aircraft not associated with firefighting operations. (Safety issue)
The New South Wales Rural Fire Service did not have an effective means to manage wake turbulence separation for aircraft operating in the vicinity of the large air tankers, increasing the risk of an unrecoverable loss of aircraft control. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action
Safety issue description: The New South Wales Rural Fire Service did not have a procedure for ensuring that when large air tankers were dispatched by the state air desk their tasking was coordinated with the incident management team and integrated into the existingincident plan.
Safety issue description: The New South Wales Rural Fire Service had no procedure to ensure that fire common traffic advisory frequencies (Fire-CTAFs) were reliably known by state air desk personnel. This resulted in aircraft being dispatched with incomplete Fire-CTAF information.
Safety issue description: The New South Wales Rural Fire Services procedures required an air attack supervisor (AAS) when 3 or more aircraft were deployed to a fireground. However, there was:
no assurance aerial supervision would remain adequate as aircraft numbers and/or fire complexity increased
inadequate guidance for consideration of suitable supervision when the AAS was required to depart the fireground.
Safety issue description: There was an inconsistent understanding within New South Wales Rural Fire Service state air desk of the threshold required to action task rejection procedures. Consequently, reports of unsafe conditions on the fireground were not promptly actioned.
Safety issue description: The New South Wales Rural Fire Service did not have a procedure to implement a temporary restricted area to reduce the risk of an air proximity event with aircraft not associated with firefighting operations.
Safety issue description:The New South Wales Rural Fire Service did not have an effective means to manage wake turbulence separation for aircraft operating in the vicinity of the large air tankers, increasing the risk of an unrecoverable loss of aircraft control.
Safety issue description: Neither the New South Wales Rural Fire Service or Queensland Fire and Emergency Service had established cross-border coordination procedures for aerial firefighting activities to ensure reliable aircraft communication and separation.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by New South Wales Rural Fire Service
Governance and oversight
The NSW RFS established the Aviation Services Directorate in March 2025 to centralise governance, safety oversight and operational policy for all aviation activities. This created a single accountable structure linking doctrine development, training, and operational delivery. The Directorate provides leadership on strategic planning, resource coordination and risk management, supported by specialist functional areas, such as Fixed Wing Operations, Rotary Wing Operations, Aviation Business and Aviation Safety.
The Aviation Safety Governance Committee was also formalised to provide cross‑directorate oversight of aviation safety performance indicators, monitor Aviation Safety Management System (ASMS – see below) outcomes, and ensure compliance with both Civil Aviation Safety Authority and National Aerial Firefighting Centre frameworks.
Quarterly safety assurance reviews now integrate training, audit results, and operational performance data. These mechanisms ensure lessons are captured and directly inform continuous improvement cycles, reinforcing transparency and leadership accountability.
Aviation Safety Management System
The NSW RFS developed a formal Aviation Safety Management System (ASMS), following extensive consultation, to provide a structured, agency-wide framework for managing aviation risk, aligning with Civil Aviation Safety Regulations Part 138, ICAO Annex 19 and the Civil Aviation Act 1988.
The ASMS was approved by the Commissioner in October 2025 and defines governance, accountabilities and assurance processes across all aviation activities. It also integrates hazard reporting, contractor oversight, safety performance indicators, investigation management, and continuous improvement mechanisms.
The ASMS is administered by the Aviation Safety Manager and overseen by the Aviation Safety Committee, providing structured oversight of safety performance, trend analysis, and corrective action tracking. Safety data is captured in the NSW RFS Safety Hub (DoneSafe platform) and monitored through quarterly governance reviews.
Through the ASMS, the NSW RFS has strengthened coordination with the Civil Aviation Safety Authority, National Aerial Firefighting Centre and contracted operators, embedding consistent reporting standards and assurance pathways.
Training, simulation and assurance
Ongoing investment in the Aviation Centre of Excellence has enabled integration of advanced simulation, scenario-based learning, and operator workshops. Between 2024 and 2025, new modules were developed focusing on supervision under stress, airspace deconfliction and communications reliability.
Pre-season briefings for 2024–25 and 2025–26 incorporated updated doctrine and safety lessons from recent reviews. Annual operator briefings (beginning July 2025) provided a structured forum for information exchange between NSW RFS, contractors, and partner agencies.
These briefings have also included joint industry engagement with the Aerial Application Association of Australia (AAAA), the Australian Helicopter Industry Association (AHIA), and the National Aerial Firefighting Centre (NAFC), promoting shared understanding of emerging risks, standardisation of safety practices, and alignment of operational expectations across jurisdictions and sectors.
Audit and assurance results are reviewed by the Aviation Safety Governance Committee and directly inform training updates.
Glossary
AAS
Air attack supervisor
ADS-B
Automatic dependent surveillance broadcast
AGL
Above ground level
AIP
Aeronautical information publication
AOM
Air operations manager
ARENA
National system for supporting the use of aircraft for fire and emergency response
CASA
Civil Aviation Safety Authority
Fire-CTAF
Fire common traffic advisory frequency
IC
Incident controller
ICON
Incident control online
IMT
Incident management team
LAT
Large air tanker
LAT AAS
Large air tanker air attack supervisor
LATCO
Large air tanker tasking coordinator
LGA
Local Government Areas
NAFC
National Aerial Firefighting Centre
QFES/QFD
Queensland Fire and Emergency Services/Queensland Fire Department
RFS
Rural Fire Service
SAD
State air desk
SADOM
State air desk operations manager
SAR
Search and rescue
SEAT
Single engine air tankers
SOC
State operations controller
TCAS
Traffic collision avoidance system
TFR
Temporary Flight Restriction
TRA
Temporary Restricted Area
Sources and submissions
Sources of information
The sources of information during the investigation included:
New South Wales Rural Fire Service
Queensland Fire and Emergency Service/Queensland Fire Department
the involved flight crews
Airservices Australia
National Aerial Firefighting Centre
AgAir
Careflight
Coulson Aviation
Field Air
United States Department of Agriculture (Forestry Service).
Western Australia Department of Fire and Emergency Services and Department of Biodiversity, Conservation and Attractions (2023) ‘Western Australia fire suppression procedures 2023-2024’.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
New South Wales Rural Fire Service
Queensland Fire Department
NSW National Parks and Wildlife Service
Coulson Aviation
Ag Air
Field Air /Conair
Civil Aviation Safety Authority
National Transportation Safety Board
United States Forest Service
incident air attack supervisor
air operations manager
incident controller
state air desk operations manager
large air tanker coordinator
state operations controller
large air tanker air attack supervisor (birddog).
Submissions were received from:
Coulson Aviation
New South Wales Rural Fire Service
Queensland Fire Department
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Appendix
Identification of relevant aircraft
The ASA data included any aircraft that had transited the selected geographic area at any altitude. Commercial flights were identified and excluded, as were any other flights above 10,000 ft; these tracks showed the aircraft flying directly overhead, well above the operational firefighting area.
In addition, the NSW RFS provided a list of aircraft potentially active in the area throughout the day, which was data matched against the tracked aircraft, correlating registration with firefighting callsigns.
The data analysis identified 67 aircraft operating in the area of interest, which consisted of a mix of large and small aeroplanes and helicopters. Of these, 40 aircraft were identified as aerial firefighting assets from NSW RFS and Queensland (Qld) Fire and Emergency Services (QFES).[21] The remaining 27 aircraft were not associated with firefighting operations. Of these 27 aircraft, 8 did not have a transponder return or a matched flight plan and were only identified through primary radar returns in the data provided by ASA. As such, identifying details for these aircraft could not be obtained.
Of the 67 identified aircraft:
19 were contained in the NAFC data set only
19 were contained in both ADS-B and NAFC data sets
1 had both NAFC and radar returns
13 were contained in the Airservices ADS-B data set only[22]
15 had radar data only.
A total of 117 instances were identified where there were gaps of 5 minutes or longer between recorded data points. Of these, 53 were related to time between flights, where the aircraft was on the ground at an airport or aerodrome and 59 were related to the aircraft transiting in and out of the selected area of interest.
The remaining 5 instances related to 3 aircraft:
One instance of a privately operated Cessna 210, where the transponder was activated about 9 km from Tenterfield Airport (last recorded about 1 hour 42 minutes before arriving at Tenterfield).
One instance of a privately operated Cessna 182, where the transponder was activated about 20 km from Tenterfield Airport (last recorded about 1 hour 16 minutes before arriving at Tenterfield).
Three instances of a NSW RFS fixed-wing aircraft with missed returns of 9 minutes, 16 minutes and 5 minutes respectively. These all correlated with the aircraft operating in the same area, at low level (below 2,100 ft AMSL).
In the case of the missed returns from the NSW RFS aircraft in the reviewed data set, this was likely due to terrain and/or aircraft shielding between the aircraft and the receiver. ADS-B receivers require line-of-sight. For periods when an aircraft is operating at low level, this increases the likelihood there was no line of sight to a receiver due to terrain shielding. This may not reflect receipt of the transmission in a secondary, nearby aircraft. Aircraft that are operating in line of sight of the aircraft transmitter, if fitted with an appropriate receiver, may still receive transmissions, although again with potential shielding depending on their respective orientation and relative positions. It was also noted that multiple other aircraft operating below 3,000 ft had short (less than 2 minutes) periods of no recorded transmissions in the reviewed data set, again indicative of terrain shielding.
There was no evidence of any firefighting helicopters turning transponders off during flight.
Alternatively, in addition to potential shielding between aircraft, given the density of aircraft operating, and potential for electronic flight bag limitations, these limitations may lead to missed transmissions. It was outside the scope of the analysis to review the electronic flight bags, transponders and collision avoidance devices in use by these aircraft.
[1]The Australian Fire Danger Rating System uses a combination of weather forecasting and information about vegetation that could fuel a fire, to provide an indication of the consequences of a fire, if one was to start. The ratings are medium, high, extreme and catastrophic. Extreme indicates dangerous fire conditions.
[2]Section 44 of the Rural Fires Act (1997) allows the commissioner to take charge of bush firefighting operations and bush fire prevention in any part of NSW.
[3]The NSW RFS was allocated discrete radio frequencies, which it could assign to fire grounds.
[4]There was some discrepancy between flight data and aircraft-related documentation, noting that aircraft operating at low altitudes may not have appeared on data sources. Additionally, throughout the afternoon, different aircraft entered and exited the area assessed by the ATSB. As such, the exact number of aircraft in a particular area changed throughout the day.
[5]Teleconference calls between the state operations centre and the Glen Innes IMT were recorded.
[6]Large air tanker (LAT): multi‑engine aircraft that carries up to 15,000 L of water or fire retardant. Often converted from large cargo, passenger or military aircraft.
[7]Birddog 123 was a small jet aircraft (Cessna 525 Citation) used to assess the fireground, determine the best flightpath, lead the air tankers across the fireground and show them where to drop with a smoke generator. It was crewed by a pilot and an air attack supervisor (LAT AAS).
[8]LAT CTAF is a discrete frequency used by the LATs.
[9]NSW RFS was operating on Eastern Daylight-saving Time, while Qld aircraft were operating on Eastern Standard Time, which was one hour behind NSW. Unless stated otherwise, all times in the report have been converted to Eastern Daylight-saving Time.
[10]TCAS: traffic collision avoidance system is a form of aircraft airborne collision avoidance system. It uses transponders which operate independently of ground-based equipment, to provide advice to flight crews on potential conflicting aircraft.
[11]Tracplus: used satellites to track aircraft and relay their position and other associated data every 3 minutes.
[12]Incident action plan (IAP): a document used to define and communicate the incident objectives, strategies and resources, and other information relevant to the control of an incident.
[13]ARENA: a web-based national aviation management system developed and maintained through the National Aerial Firefighting Centre. ARENA effectively acted as a single access point for tracking and event data relating to aerial firefighting.
[14]ICON: incident control online – NSW RFS operational management system.
[15]Wake turbulence: turbulence from wing tip vortices that result from the creation of lift. Those from large, heavy aircraft are very powerful and persistent and are capable of causing control difficulties for smaller aircraft either following or below.
[16]Qld QFES identified the fire at Christies as the ‘Wallangarra’ fire.
[17]Consideration was given to sourcing ADS-B data from commercial sources, however, sufficient data was available in the Airservices data set for the work that was completed.
[18]ADS-B:Automatic Dependant Surveillance Broadcast is a system in which electronic equipment on board an aircraft automatically broadcasts the precise location of the aircraft via a digital data link.
[19]ARENA: a web-based national aviation management system developed and maintained through the National Aerial Firefighting Centre. ARENA effectively acted as a single access point for tracking and event data relating to aerial firefighting.
[20]The Australian Fire Danger Rating System uses a combination of weather forecasting and information about vegetation that could fuel a fire, to provide an indication of the consequences of a fire, if one was to start. The ratings are medium, high, extreme and catastrophic. Extreme indicates dangerous fire conditions
[21]QFES was subsequently renamed the Queensland Fire Department.
[22]One of these aircraft was matched to a NSW RFS firefighting asset that had not been captured in the NAFC dataset.
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the ATSB to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation.
Overview of the investigation
Just after midnight on 5 April 2023, a Boeing 737-838, registered VH‑VXH, was being operated by Qantas on a passenger air transport flight from Darwin, Northern Territory to Melbourne, Victoria. An Airbus A320, registered VH-VGV, was being operated by Jetstar on a passenger air transport flight from Sydney, New South Wales, to Darwin.
A temporary restricted area (TRA) was in place between 2130–0530 each night due to Royal Australian Air Force (RAAF) air traffic control services not being available in the airspace around Darwin Airport below 8,500 ft. As a result, aircraft flight crews were required to coordinate their own separation when arriving and departing the airport. Flight crews were also required to gain permission from the RAAF Darwin flightwatch prior to operating within the TRA. With the TRA in place, Airservices Australia was responsible for managing the airspace above 8,500 ft through its Brisbane Centre.
At 0009:56, the 737 first officer (FO) contacted the Darwin flightwatch and received permission to operate within the TRA. Darwin flightwatch also advised of opposite direction traffic inbound to Darwin (this referred to the A320 and another subsequent flight).
At 0013:43, the 737 FO contacted Brisbane Centre and advised that the aircraft was taxying at Darwin Airport and would depart using runway 11. The Brisbane Centre controller acknowledged the FO’s radio call and advised of the 2 inbound aircraft, giving details of the arrival routes (both were VEGPU SEVEN standard arrivals from the south-east and landing on runway 29). The A320 was due to land at Darwin Airport at about 0027:00.
The flight crew of the 737 recalled considering the inbound traffic and believed there was sufficient spacing to safely depart ahead of the A320 using runway 11 (the reciprocal to runway 29).
At 0016:16, the 737 flight crew commenced the take-off from runway 11 and, at 0018:04, the captain made a departure call on the Darwin flightwatch frequency. Shortly after, the Darwin flightwatch controller queried when the 737 would commence a turn and stated the A320 was now 30 NM to the south. At 0018:37 the 737 captain responded they were conducting the PALGA SEVEN standard instrument departure and they would contact Brisbane Centre shortly to get a clearance to enter the overlaying airspace.
At 0019:22, and climbing through 4,500 ft, the 737 captain contacted the A320 flight crew directly on the Darwin flightwatch frequency and offered to level off at 7,000 feet to maintain separation. By this time, the flight crew of the A320 had the 737 displayed on the aircraft’s Traffic Collision Avoidance System (TCAS) and believed the aircraft did not present a conflict. At this time, the aircraft were about 26 NM apart on converging courses, with the A320 at 8,500 ft. The A320 FO replied on the Darwin flightwatch frequency that the 737 could continue the climb.
At 0019:42, the 737 captain contacted Brisbane Centre to advise the aircraft had departed Darwin. The Brisbane Centre controller informed the 737 captain they could expect a clearance to enter the overlaying airspace on a heading of 060° and further stated, ‘suggest left heading 060 now’. The 737 captain confirmed the heading. The 737 commenced a left turn onto a heading of 060° at about 0020:00, with the aircraft about 20 NM apart. The tracks diverged and the aircraft crossed the same level a few seconds later.
At about 0022:06, the lateral separation between the 737 and the A320 decreased to its closest point of approach of about 10.6 NM, with vertical separation reducing to about 4,500 ft (Figure 1).
Figure 1: 737 and A320 locations at 0019:46, 0021:06 and 0022:06
Source: Airservices Australia, annotated by the ATSB
The ATSB received an initial occurrence report on 5 April 2023 and commenced an investigation on the same date. As part of the investigation, the ATSB interviewed the 737 flight crew, A320 flight crew, and the Brisbane Centre air traffic controller, and reviewed:
data from the 737 and A320 quick access recorders
weather information
recorded air traffic control audio and surveillance data
information provided by the aircraft operators and air traffic control services.
The investigation identified the following:
The practice of activating daily TRAs at Darwin Airport commenced in July 2022 due to controller availability preventing the delivery of a continuous approach control service. The RAAF advised that daily TRAs were planned to continue to be utilised at Darwin Airport until approximately the first quarter of 2024.
Both flight crews described an increased level of workload associated with the Darwin Airport TRA that was similar in complexity to common traffic advisory frequency (CTAF) procedures.
Although experiencing increased workload the crews felt that there was no concern regarding separation in this instance.
The 737 flight crew elected to depart from runway 11 for noise abatement and operational reasons, believing there would be adequate separation between the 737 and the arriving A320.
At the time the 737 departed, the automatic terminal information service for Darwin Airport stated the preferred runway was runway 29. The windspeed and direction recorded at the time was 2-3 kts from between 150–191° magnetic, which favoured runway 11.
The A320 and 737 flight crews coordinated their separation on the Darwin flightwatch frequency and were sufficiently aware of each other’s position, level and track to maintain separation.
Neither the 737 or A320 flight crew received a TCAS alert or advisory.
The Brisbane Centre controller recalled having concerns about the proximity of the 2 aircraft; however, the controller recalled not knowing the actual separation between the 2 aircraft due to the scale of the display.
The Brisbane Centre controller’s decision to turn the 737 was to provide increased separation; however, this purpose was not communicated to the 737 flight crew.
The lateral and vertical separation between the 737 and A320 at the closest point of approach met the separation standards required had the airspace been controlled at the time. It is probable the same separation standards would have been met had the 737’s flightpath continued without the turn.
Reasons for the discontinuation
Based on a review of the available evidence, the ATSB considered that there was no safety-related separation issue in this instance and it was unlikely that further investigation would identify any systemic safety issues or important safety lessons. Consequently, the ATSB has discontinued this investigation.
The evidence collected during this investigation remains available to be used in future investigations or safety studies. The ATSB will also monitor for any related occurrences that may indicate a need to undertake a further safety investigation, noting the potential for increased risk in terminal airspace that is made non-controlled for certain periods.
Occurrence summary
Investigation number
AO-2023-015
Occurrence date
05/04/2023
Location
Near Darwin Airport
State
Northern Territory
Report release date
29/06/2023
Report status
Discontinued
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Discontinued
Mode of transport
Aviation
Aviation occurrence category
Separation issue
Occurrence class
Incident
Aircraft details
Manufacturer
The Boeing Company
Model
737-838
Registration
VH-VXH
Serial number
33478
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
Departure point
Darwin Airport, Northern Territory
Destination
Melbourne Airport, Victoria
Aircraft details
Manufacturer
Airbus
Model
A320-232
Registration
VH-VGV
Serial number
4229
Aircraft operator
Jetstar Airways Pty Ltd
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 21 October 2021, at 0743 local time, a Beech Aircraft B200 aircraft, registered VH-WXB, departed Roma Airport on a passenger charter flight to Brisbane West Wellcamp Airport (Wellcamp), Queensland. At 0806, a Saab 340B aircraft, registered VH-ZLV, departed Brisbane Airport on a scheduled passenger service flight to Wellcamp. Both aircraft were operating under instrument flight rules, and both estimated their time of arrival at the airport to be at 0827.
Prior to each aircraft leaving controlled airspace, the Brisbane Centre air traffic controller passed traffic information to VH-WXB and VH-ZLV in 2 separate broadcasts with an updated arrival time for each aircraft. The pilots of both aircraft made a number of calls on the common traffic advisory frequency to organise separation at the non-controlled aerodrome, however, at about 0828, VH‑WXB conducted a 180° left turn on the active side of the circuit, crossing in front of VH-ZLV. This resulted in the separation between the aircraft reducing to 300 ft vertically and 1,000 m horizontally. As VH-WXB commenced the left turn, VH-ZLV’s traffic alert and collision avoidance system (TCAS) announced a traffic advisory (TA), shortly followed by a resolution advisory (RA). The pilot flying immediately disconnected the autopilot and followed the RA instructions and climbed the aircraft until they were clear of conflict. At about the same time, the pilot of VH-WXB received a TCAS TA and commenced a visual lookout.
The flight crew of VH-ZLV advised VH-WXB they had received a TCAS RA. Further communication occurred between the pilots of the 2 aircraft to confirm and visually identify each other’s position in the circuit and ensure separation. Both aircraft landed safely at Wellcamp Airport.
What the ATSB found
The ATSB found that the pilots of both aircraft had an incorrect mental model of the positions of the other aircraft and neither had positively sighted the other aircraft before the conflict. The flight crew of VH-ZLV broadcast an incorrect position of their aircraft when approaching the circuit, which probably resulted in the pilot of VH-WXB misidentifying VH-ZLV for another aircraft on their TCAS.
This misunderstanding affected the pilot of VH-WXB’s decision to fly opposite the downwind circuit direction while in a descent. The pilot then conducted a 180° left turn in front of VH‑ZLV, as they thought that aircraft was further ahead on the downwind leg. Further, the flight crew of VH-ZLV also did not effectively monitor the radio, resulting in them having an incorrect mental model of VH-WXB’s position, and not identifying it as a threat. As neither the crew in VH‑ZLV and the pilot in VH-WXB had positively sighted the other aircraft, alerted see-and-avoid was limited and the last line of defence was the TCAS, which prevented a potential collision.
What has been done as a result
As a result of this occurrence the operators advised the ATSB of the following actions:
The operator of VH-WXB:
will ensure there is an increased buffer between a regular public transport (RPT) flight and their aircraft by orbiting at a waypoint further out, to ensure that the RPT flight is on final approach when they join the circuit
have briefed their pilots of the event and communicated the need to adhere to the procedures written in CAAP 166 - Operations at Non-Towered Aerodromes. Further, they advised their pilots that when traffic congestion is anticipated, actions such as conducting orbits to allow greater spacing in traffic sequencing should be considered
have discussed the traffic congestion issue with the flight training school based at Wellcamp and have agreed that during the scheduled arrival times of RPT aircraft, the training school will limit the number of their aircraft flying within the area.
The operator of VH-ZLV:
has included operations at, and in the vicinity of, non-towered aerodromes as a focus item in the periodic aircrew check cycle
will use this occurrence internally as a human factors case study for operations around common traffic advisory frequency airports.
Safety message
The ATSB’s SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported by industry. One of the priorities is safety around non-controlled aerodromes. Insufficient communication between pilots is the most common cause of safety incidents near non-controlled aerodromes. Pilots should ensure that the location and intention of surrounding traffic is well understood, and their intentions are clearly communicated while maintaining a visual lookout.
Safe operation at any aerodrome requires pilots to use sound judgement and to follow standard procedures and CASA guidance. Using standard procedures at non-towered aerodromes, unless otherwise stated in the En Route Supplement Australia (ERSA), assists pilots in maintaining situational awareness and separation from other aircraft.
Developing and maintaining situational awareness is essential for the conduct of safe flight, particularly at non-towered aerodromes. In addition to radio communication, systems such as ADS-B and TCAS are valuable sources of information to assist pilot’s situation awareness and decision making.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 21 October 2021, at 0743 local time, a Beech Aircraft B200 aircraft, registered VH-WXB (WXB) and operated by Air Charter Coordinators, departed Roma Airport, Queensland on a passenger transport flight to Brisbane West Wellcamp Airport (Wellcamp), Queensland. On board were the pilot and 8 passengers.
At 0806, a Regional Express Saab 340B aircraft, registered VH-ZLV (ZLV), departed Brisbane Airport, Queensland on scheduled passenger service flight ZL5662 to Wellcamp (Figure 1). On board were 2 flight crew, one cabin crew and 9 passengers. The captain was the pilot monitoring (PM), and the first officer was the pilot flying (PF).[1] Both aircraft were operating under the instrument flight rules.[2]
Figure 1: Locations of Brisbane and Roma Airports in reference to Brisbane West Wellcamp Airport
Source: Google Earth, annotated by ATSB.
Prior to each aircraft leaving controlled airspace, the Brisbane Centre[3] air traffic controller passed traffic information to the pilot of WXB and the flight crew of ZLV on 2 separate broadcasts at 0811 and 0820, respectively. The controller advised the pilot of WXB that ZLV was inbound to Wellcamp from Brisbane with an estimated time of arrival of 0829, and advised the flight crew of ZLV that WXB was inbound for Wellcamp with an estimated time of arrival of 0830.
At 0821 the pilot of WXB made a broadcast on the Wellcamp common traffic advisory frequency (CTAF)[4] advising that they were 30 NM west of the airport, on descent, inbound for Wellcamp via waypoint LUKEY.[5] The stated intention was to make a left turn and to join right base for runway 12 (Figure 2), with an estimated time of arrival of 0827. About 1 minute later, the PM of ZLV made a radio call advising traffic they were 20 NM east of Wellcamp, at 8,000 ft, descending shortly to join crosswind for runway 12, with an estimated arrival time of 0827.
As WXB and ZLV approached the airport there were 5 other aircraft operating in the CTAF area. There were 2 Diamond DA 40’s associated with a flight training school operating in the circuit for runway 12, VH‑YNH and VH‑EQV and another DA 40, VH-YTK, which was outbound from Wellcamp via Toowoomba to the north-east operating at 4,600 ft. In addition, a Beech Aircraft 58, VH‑CLE, that was inbound for Toowoomba from the west and another Beech Aircraft B200, VH‑WXN, that was inbound to Wellcamp, 3 minutes behind WXB.
At 0823:56, the pilot of VH-YNH broadcast on the CTAF they were entering and rolling for take-off on runway 12 to conduct circuit training. At 0824:26, the flight crew of ZLV responded to this call, advising they were 11 NM to the east leaving 8,000 ft with the intention to join downwind behind VH-YNH. About 30 seconds later, the pilot of the second DA 40 VH-EQV, which was in the circuit ahead of VH-YNH, advised the pilots of both ZLV and WXB that they were downwind in the circuit for runway 12 for a touch-and-go.[6]
At 0825:07, the pilot of WXB advised the pilots of both ZLV and the DA 40s, that they were 6 NM west of LUKEY, with the intention to soon make a left turn to join a wide right base circuit leg and again advised their estimated arrival time was 0827.
The pilot of VH-EQV responded and advised the pilot of WXB they would be on final when WXB and ZLV joined the circuit and would stay out of their way.
The pilot of WXB then contacted the crew of ZLV at 0825:43 (Figure 2 - positions 1) and advised them they were about to make a left turn at LUKEY and then join the circuit on the base leg for runway 12 at time 0827 and asked if ZLV would be happy if WXB went number 1[7] to them.
Figure 2: Aircraft flight paths and positions during different CTAF broadcasts – WXB in yellow, ZLV in blue, EQV in green and YNH in pink, with numbering showing where each aircraft was at the time of the broadcasts
Source: Google Earth, annotated by ATSB based on FlightRadar24 data.
The crew of ZLV acknowledged the request and incorrectly advised that they were positioned on a very early downwind (rather than their actual crosswind position) and would reduce their airspeed and track second to WXB.
The pilot of WXB, thinking that ZLV was already established in the circuit on downwind rather than on an early crosswind, responded and advised they would track as number 2 to ZLV and join the circuit behind them on downwind. The PM of ZLV acknowledged the broadcast.
At 0826:40, the pilot of VH-YNH made a downwind broadcast on the CTAF and advised they would be making a full stop landing.
At 0827:37 (Figure 2 - positions 2), the pilot of WXB broadcast on the CTAF that they were continuing on an easterly heading, passing 3,500 ft on descent to 3,000 ft (circuit altitude), and would be shortly making a left turn to join downwind behind ZLV. The pilot then continued their descent through 3,500 ft, opposite to the circuit direction on the downwind leg.
At about 0828 (Figure 2 – TCAS RA/TA) WXB made a left turn and crossed ZLV’s path from left to right, resulting in a separation of 300 ft vertically (WXB at 3,000 ft and ZLV at 3,300 ft) and 1,000 m horizontally between the 2 aircraft. As this occurred, the crew of ZLV heard their traffic alert and collision avoidance system (TCAS)[8] announce a traffic advisory (TA)[9], shortly followed by a resolution advisory (RA).[10] In response, the PF immediately disconnected the autopilot and following the RA instructions, climbed the aircraft until they were clear of conflict. Around the same time as ZLV’s TCAS alert, the pilot of WXB received a TCAS TA while they were conducting the 180° turn onto downwind.
At 0828:49 (Figure 2 - position 4), the PM of ZLV made a broadcast on the CTAF to ask the aircraft to the south of the field (WXB) to identify themselves. The pilot of WXB responded and advised they were now mid-downwind and asked the pilot of ZLV to confirm their aircraft was positioned on the base leg (Figure 2 - positions 4 and 5).
At the time of this broadcast, VH-YNH was on the base leg and VH-EQV was on the final leg of the circuit. The PM of ZLV advised they were on the downwind leg of the circuit, and had received a TCAS RA. The pilot of WXB then asked the PM of ZLV to confirm their aircraft’s altitude and the PM advised they were abeam (to the left) WXB. The pilot of WXB, who had not visually sighted ZLV at that stage, then advised they would widen out their circuit and come in behind ZLV. The PM again advised WXB they were to the left of them on downwind and were about to commence their descent back to circuit height.
The pilot of WXB again requested ZLV’s level, to which the PM responded 3,100 ft and the pilot of WXB suggested they would track as number 1. After assessing the risk of another potential conflict between the 2 aircraft on base, the PM of ZLV requested WXB climb clear of the circuit. WXB responded and advised they now had ZLV visual and would track as number 2 to them. The pilot of WXB then made a left turn to reposition behind ZLV.
Both aircraft landed safely at 0833 and 0835 respectively.
Animation 1: Aircraft flight paths and positions during different CTAF broadcasts - WXB in orange, ZLV in blue, and YNH in red.
Source: ATSB based on FlightRadar 24 data
Context
Pilot information
VH-WXB
The pilot held a commercial pilot licence (aeroplane) (CPL(A)) and had a total flying time of 5,556 hours, having flown 88.6 hours in the previous 90 days. The pilot was familiar with Wellcamp and had been operating out of the airport since it opened in 2014.
VH-ZLV
The captain held an air transport pilot licence (aeroplane) and had a total flying time of 4,703 hours, and had flown 148 hours in the previous 90 days. The captain was familiar with Wellcamp and had operated there often in the previous 3 years.
The first officer held a CPL(A) and had a total flying time of 3,361 hours, with 154 hours accrued in the previous 90 days. The first officer was also familiar with Wellcamp and had operated there regularly for the previous 2 years.
Pilot reports
VH-WXB
The pilot of WXB reported that they were aware that ZLV would be joining the circuit at the same time. The pilot also stated that they had ZLV visual most of the time and the only time ZLV was not visual to the pilot of WXB was when the left turn was conducted with the intention of positioning behind ZLV on downwind. However, they also advised that, because of the traffic congestion, they were entirely reliant on their TCAS screen to determine the location of ZLV.
The pilot of WXB reported seeing ZLV to the left of WXB’s position on the TCAS screen, just before they turned to join downwind. They reported that they intended to make 2 more broadcasts to ZLV to verify their position and any other information they could collate, but they were unable to do so because the CTAF was too congested.
Once the pilot thought it was safe to do so, they turned left to join the downwind leg.
The pilot’s TCAS screen was congested with numerous aircraft. For the pilot to identify the aircraft they were required to touch the aircraft symbol on the screen to obtain the callsign, level, and closing speed. It was unknown if the pilot did this.
VH-ZLV
The flight crew both recalled the traffic information providing an estimated arrival time for WXB of 0830, prior to switching over to the CTAF.
The crew reported overflying Toowoomba at 5,600 ft to maintain 1,000 ft separation with outbound traffic, VH-YTK. As a result, the crew reported they were 600 ft higher on their normal descent profile into Wellcamp. Once they were clear of VH-YTK, about halfway between Toowoomba and Wellcamp, they commenced their descent.
They determined that the safest course of action, which was not standard procedure, was to descend while on the early crosswind and downwind legs, as they were limited on where they could conduct a descending orbit without interfering with the Toowoomba circuit traffic, or encroaching Oakey airspace to the north or the training area to the south of the field (Figure 3). They also reported that the dead side/non-active side[1] of the circuit was also an area they could not orbit in due to training aircraft frequently operating in there to avoid interfering with incoming and outgoing high-performance aircraft.
After organising separation with WXB and making circuit position broadcasts on the early crosswind and downwind legs, the flight crew thought separation with WXB had been effectively organised and focused their attention on circuit spacing with VH-YNH and configuring the aircraft for landing.
The flight crew did not recall hearing any broadcasts from WXB about joining downwind, and neither pilot saw WXB visually or on the TCAS until it crossed their flightpath ahead from left to right.
Airspace
The airspace surrounding Wellcamp is non-controlled Class G airspace up to 8,500 ft. About 6 NM to the east of Wellcamp is Toowoomba Airport and about 9 NM to the north-north-west is Oakey Army Aviation Centre (Oakey). There are also other aircraft landing areas (ALAs) within a 10 NM radius of Wellcamp, including Wyreema, Colanya, Argyle and Southbrook (Figure 3).
All the above-mentioned airfields and ALAs, including Oakey, operate on the same CTAF when the Oakey airspace is inactive.
Within the airspace surrounding Wellcamp there are identified Danger Areas[2] to the south and west, including a flight training area up to 6,000 ft.
Figure 3: Brisbane Visual Navigation Chart depicting the airport locations and surrounding airspace
Source: Airservices, annotated by ATSB.
In 2019, the Office of Airspace Regulation (OAR) within the Civil Aviation Safety Authority (CASA), completed a review of the airspace within 10 NM of Wellcamp. At the time of the review, the flight training school had not established operations at Wellcamp.
The 2019 airspace review found that the airspace surrounding Wellcamp was fit for purpose, however the following recommendations were made:
Recommendation 1: The OAR should monitor the traffic growth at Wellcamp over the next two years, including the integration of flight training operations based at Wellcamp. If appropriate, another review should be conducted post-implementation of flight training at Wellcamp.
Recommendation 2: The OAR should continue to liaise with other business areas of CASA regarding the commencement of flight training at Wellcamp to ensure that the airspace remains fit for purpose.
A further review of Wellcamp was scheduled to commence in February 2023. However, this review was delayed due to unscheduled changes to priorities. The OAR expects that a review of Wellcamp will be included in a Brisbane basin aeronautical study and is scheduled to commence late 2023.
Brisbane West Wellcamp Airport
Brisbane West Wellcamp Airport is a certified aerodrome located 8 NM west of Toowoomba CBD. It was opened in 2014 and consists of one runway orientated 12/30. The airport services a variety of operations including regular public transport, charter, freight, flight training and aero‑medical aviation services.
The En Route Supplement Australia (ERSA)[3] details local traffic regulations and procedures for the airport. These included stipulating the use of published departure procedures whenever practicable to avoid Oakey military Restricted Airspace. Additionally, due to high terrain to the north‑east of the airport, left circuits are to be flown to runway 30 and right circuits to runway 12.
Operations at non-controlled aerodromes
Guidance provided by CASA[4] (2019) defined that an aircraft was in the vicinity of a non‑controlled aerodrome if it was:
within airspace other than controlled airspace
within a horizontal distance of 10 NM from the aerodrome (reference point), and
at a height above the aerodrome (reference point) that could result in conflict with operations at the aerodrome.
Radio Broadcasts
When operating in the vicinity of non-controlled aerodromes on the shared CTAF, as per Regulation 166C of Civil Aviation Regulations (1988), pilots were required to make a broadcast whenever it was reasonably necessary to do so to avoid a collision, or the risk of collision, with another aircraft.
Further guidance from CASA Advisory Circular 91-10 V1.1 to pilots on the recommended positional broadcasts in the vicinity of non-controlled aerodrome for inbound aircraft is provided at Table 1. It does advise pilots may use their discretion in the number and type of broadcasts they make.
Table 1: Recommended positional broadcasts in the vicinity of a non-controlled aerodrome
Source: CASA 91-10 (2021)
[1] NOTE: Some distances above refer to the runway threshold and others refer to the aerodrome reference point. Pilots should be aware that a global positioning system (GPS) indication of 3 NM from and aerodrome may not be 3 NM from the runway threshold.
Circuit and arrival procedures
A circuit pattern is a conventional standard path for coordinating air traffic that are taking off or landing on a runway. A circuit pattern consists of 5 legs – upwind, crosswind, downwind, base and final (Figure 4).
The Civil Aviation Safety Authority (CASA) Visual Flight Rules Guide states the following regarding standard circuit procedures at non-controlled airports, such as Wellcamp:
The standard aerodrome traffic circuit pattern facilitates an orderly flow of traffic and is normally a circuit pattern made with all turns to the left. When arriving at an aerodrome to land, a pilot will normally join the circuit upwind, crosswind (mid-field), or downwind (before mid-downwind). Landings and take-offs should be made on the active runway or the runway most closely aligned into wind. Aerodromes that have right-hand circuits are listed in ERSA. Circuit information may also be published or provided by aerodrome operators in other sources of aeronautical information.
The CASA (2019) guidance provided the following caution on arrival into non-controlled aerodromes:
Pilots should not descend into the active side of the traffic circuit from above because of the difficulty of seeing – and being seen by – aircraft directly below the aircraft’s flight path.
The guidance noted that pilots joining the circuit on the downwind leg at a midfield position should enter the circuit at approximately 45° to the downwind leg and give way to aircraft already established in the circuit.
The guidance further noted that joining the circuit on base is not a standard procedure and increases the risk of traffic conflict and/or landing on a closed runway. It is recommended that pilots join the circuit on either crosswind or downwind.
ZLV joined the circuit on the early crosswind leg and WXB joined the downwind leg after conducting a 180° turn on the active side of the circuit.
Figure 4: Arrival procedure for a non-controlled airport (left direction circuit). The circuit direction was right at Wellcamp
Source: CASA Visual Flight Rules Guide.
CTAF congestion at Wellcamp
All pilots involved in the incident reported the CTAF can often be quite congested with many calls being over‑transmitted. The flight crew of ZLV reported the CTAF congestion on the day of the incident was manageable and was not a factor in the incident. However, the pilot of WXB reported the CTAF was highly congested. At the time of the incident there were 5 aircraft operating on the CTAF.
In the 3 minutes and 6 seconds from when WXB and ZLV started communicating with each other on the CTAF to just after the incident occurred, 16 broadcasts were made on the CTAF. These had an average length of time of 8 seconds and an average gap of 4 seconds between each broadcast.
Traffic alert and collision avoidance system
Both aircraft in this incident were equipped with a TCAS. In addition to traffic alerts, the TCAS also provides pilots with visual traffic information on a screen. The screen displays other aircraft that are operating in their proximity, and as a result, pilots are able to make decisions based on the displayed information, reducing the risk of collision. The TCAS in WXB only issued traffic advisories and not resolution advisories.
See-and-avoid
When operating in non-controlled airspace, there is no separation service provided by ATC and pilots must rely on their own separation through radio communication with see‑and‑avoid as the last defence.
There are 2 characteristics of see-and-avoid, unalerted and alerted. Unalerted see-and-avoid relies entirely on the pilot sighting another aircraft with no other assistance, while alerted see‑and‑avoid exists when a pilot has been alerted to the existence and approximate location of other traffic. The primary tool of alerted see-and-avoid is radio communication between aircraft and traffic information provided by the air traffic controller. Other tools include ADS-B IN and electronic flight bags that receive traffic information through mobile network or ground-based receivers and TCAS, which provides its own traffic surveillance function.
In the absence of a traffic alert, the probability of a pilot sighting a threat aircraft before impact is low, whereas alerted see-and-avoid can be 8 times more effective.
Reported incidents at Brisbane West Wellcamp and Toowoomba Airports
Since 2016, the ATSB has received 17 airspace occurrence reports that occurred within a 30 NM radius of Wellcamp and Toowoomba Airports (Refer to Appendix A – Separation and TCAS events within the circuit area at Wellcamp and Toowoomba for further details).
Fourteen of the occurrences involved separation issues with the involved aircraft either receiving or not receiving a TCAS alert. Eight of these occurrences occurred at or near Wellcamp, including 6 within the circuit area. Only one of these occurrences involved an aircraft turning inside another aircraft already established in the circuit, during circuit operations. The other 6 were at or near Toowoomba, with 3 occurring within the circuit area.
Two of the occurrences were classified as near collisions. In one, the crew of a Beechcraft B300 observed a glider cross their flightpath near Wellcamp. In the other a Bell 412 was on approach for Toowoomba when a Piper PA-38 crossed their track.
A loss of separation was also reported between a Cessna 182 and a de Havilland DHC-8 25 NM (46 km) east of Toowoomba, where the Cessna182 climbed above its assigned altitude.
Safety analysis
Incorrect mental models
Mental models are a form of cognitive structure that enables an individual to effectively interact with their environment by organising knowledge into meaningful patterns (Reynolds & Blickensdefer, 2009). An individual, when performing a task will develop a mental model of what they think will occur during the task being completed. Their mental model is based upon the information available to them at the time.
VH-WXB
The flight crew of ZLV advised the pilot of WXB that they were on early downwind (Figure 2 - position 1), when they were actually on early crosswind for runway 12. At the time of this broadcast, there were 2 other aircraft in the circuit: VH-EQV on mid-downwind and VH-YNH on mid-crosswind.
The pilot of WXB recalled seeing ZLV to the left of their position on their TCAS screen at about the same time as when they broadcast that they were continuing on an easterly heading (Figure 2 - position 2). However, a review of recorded flight data identified that ZLV was not to the left of WXB until after the 2 aircraft had crossed paths and it was VH-YNH to the left of WXB at this time. The pilot of WXB also stated that they had ZLV visual most of the time and the only period that ZLV was not visual to them was when the pilot was conducting the left turn to position behind ZLV on downwind.
After WXB crossed ZLV’s track and was in communication with the flight crew of ZLV, the pilot asked the crew to confirm ZLV was on base. At the time of this broadcast, VH-YNH was on base (Figure 2 - position 5) and ZLV was to the left of WXB on downwind.
The pilot of WXB's description of when they first became aware of ZLV on their TCAS screen and their common traffic advisory frequency (CTAF) broadcasts after crossing ZLVs flight path, suggested the pilot of WXB had sighted VH-YNH and not ZLV visually or on the TCAS screen. The advice from the crew of ZLV that their aircraft was on early downwind when they were on crosswind, would have likely also confirmed the pilot’s assumption that VH-YNH was ZLV and the pilot possibly assumed VH-EQV was VH-YNH.
The decision by the pilot of WXB to fly opposite to the traffic direction on downwind while descending to circuit height, before turning left, across ZLV’s flight path indicates that it is likely that the pilot had not identified ZLV either visually or on the TCAS.
VH-ZLV
Both flight crew members of ZLV recalled WXB’s field estimate was 0830, which was initially given to them by the air traffic controller. However, after they transferred over to the CTAF, the pilot of WXB broadcast their new arrival time of 0827 on 2 separate occasions, including a broadcast directly to ZLV. This was the same estimated arrival time as ZLV. It is evident that the flight crew of ZLV were aware of the potential arrival time conflict as a discussion occurred between the pilot monitoring and the pilot of WXB, for the flight crew to slow down ZLV to go in number 2 to WXB.
Due to the earlier incorrect positioning call from the flight crew of ZLV, leading the pilot of WXB to believe that ZLV was already established in the circuit on downwind, the pilot of WXB advised the flight crew that they would track number 2 to ZLV and join the circuit behind them on downwind. The pilot monitoring of ZLV acknowledged the broadcast.
The pilot monitoring did not recall hearing anymore broadcasts from the pilot of WXB, after they had organised that WXB would track behind them, until after the TCAS resolution advisory was received. The pilot of WXB had made one other broadcast prior to this, just before they conducted the 180° turn onto downwind, that included intentions to descend and to shortly join the circuit via a left turn (Figure 2 - positions 2). If the flight crew of ZLV had of been effectively monitoring the CTAF, this transmission should have been a trigger for them to look for WXB and respond to confirm their mental model. At this time, ZLV was 1,300 ft higher than WXB (4,800 ft vs 3,500 ft) and in the process of conducting a right turn onto early downwind, making sighting of a lower aircraft more difficult.
It is possible that after organising separation with WXB and agreeing that WXB would go number 2 behind them, the crew thought that WXB was aware of their position and therefore discounted WXB as a threat. Believing adequate separation had been organised, focus switched to VH-YNH and configuring the aircraft for landing.
The flight crew’s ineffective monitoring of WXB’s broadcasts and their incorrect mental model meant that they were now dependent on either visually acquiring WXB or the TCAS detecting them.
Neither crew had positively sighted the other aircraft
The pilot of WXB recalled having ZLV in sight both visually and on the TCAS screen prior to the left turn to join the circuit. If the pilot of WXB had accurately identified ZLV’s location, it is very unlikely that they would have assessed that it was safe to turn left in front of ZLV and cross their flight path. Therefore, the pilot of WXB probably did not identify ZLV visually or on the TCAS until the completion of the left turn when both aircraft were on downwind.
The flight crew of ZLV, reported that while they were on early downwind, they did not hear any broadcasts from WXB about joining the circuit. The first indicator they had that WXB was in the vicinity of their aircraft was when they received a TCAS traffic alert followed shortly after by an RA. They recalled, during their initial communications with WXB, being unsure where WXB was planning to join the circuit, which was why they were initially happy for WXB to go first. After organising separation with WXB, they reported being under the impression that WXB would slow down and join the circuit behind them either on downwind or base. They did not recall seeing WXB on the TCAS prior to the RA. The pilot flying recalled seeing WXB visually for the first time when the aircraft crossed their flight track from left to right.
Separation in a CTAF is dependent on pilots organising their own separation through radio communication, as well as conducting standard circuit procedures. Neither crew positively identified the other aircraft’s location while in, and prior to joining, the circuit, so the potential conflict was not recognised.
Conducting standard circuit procedures provides the best opportunity and risk control for aircraft to maintain separation. Finally, if available, it is also important to follow TCAS RA information. In this instance, it prevented a potential collision.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the separation issue involving a Saab 340B, registered VH-ZLV, and a Beech Aircraft B200, registered VH-WXB that occurred at Brisbane West Wellcamp, Queensland on 21 October 2021.
Contributing factors
The flight crew of VH-ZLV broadcast an incorrect position of their aircraft when approaching the circuit. This probably resulted in the pilot of VH-WXB misidentifying it for another aircraft in the circuit and influenced their decision to conduct a non‑standard circuit entry contrary to the traffic flow.
The flight crew of VH-ZLV did not effectively monitor the radio, resulting in them having an incorrect mental model of VH-WXB’s position and thus not perceiving VH-WXB as a threat.
The pilot of VH-WXB manoeuvred their aircraft opposite to circuit traffic direction while descending into the active side of the circuit in the vicinity of the airport resulting in a conflict with VH-ZLV.
Neither flight crew identified the other aircraft visually or on their TCAS, leading to VH-WXB turning in front of VH-ZLV and resulting in the crew of VH-ZLV receiving a TCAS RA.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Air Charter Coordinators
As a result of this incident the operator of VH-WXB advised the ATSB that they:
will ensure there is a 4-minute buffer between a regular public transport (RPT) flight’s time in the circuit and theirs by holding[1] at LUKEY, to ensure that the RPT flight is on final approach when they join the circuit
have briefed their pilots of the event and communicated the need to adhere to the procedures written in CAAP 166 - Operations at Non-Towered Aerodromes. This included advice that when traffic congestion is anticipated, actions such as conducting orbits to allow greater spacing in traffic sequencing should be considered
have discussed the traffic congestion issue with the training school based at Wellcamp and have agreed that during the scheduled arrival times of RPT aircraft, the training school will limit the number of their aircraft flying within the area.
Safety action by Regional Express Pty Ltd
The operator of VH-ZLV advised the ATSB of the following actions:
operations at, and in the vicinity of, non-towered aerodromes have been included as a focus item in the periodic aircrew check cycle
this occurrence will be used internally as a human factors case study for operations around common traffic advisory frequency airports.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Reynolds, R., & Blickensderfer, E. (2009). Crew Resource Management and Shared Mental Models: A Proposal. Journal of Aviation/Aerospace Education & Research, 19(1), 15-24. https://doi.org/10.15394/jaaer.2009.1380
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the flight crew of VH-ZLV
the pilot of VH-WXB
the aircraft operators
the Civil Aviation Safety Authority
Submissions were received from:
the pilot in command of VH-ZLV
the Civil Aviation Safety Authority
Regional Express Pty Ltd
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Separation and TCAS events within the circuit area at Wellcamp and Toowoomba
Year
Location
Occurrence type
Aircraft 1
Aircraft 2
Overview
2014
Toowoomba
Airborne collision alert system warning | Issues
de Havilland DHC-8
Unknown helicopter
During initial climb, the de Havilland DHC-8 crew received a TCAS RA on a helicopter operating within the vicinity. The helicopter did not track as previously advised by its crew.
2014
Toowoomba
Near collision
Bell 412
Piper PA-38
Passing 400 ft on approach, the pilot of the Bell 412 observed the Piper PA-38 cross in front in close proximity. The pilot of the 412 contacted the crew of the PA-38 which subsequently conducted a missed approach.
2016
Brisbane West Wellcamp
Issues
Cessna 172
Saab 340
Passing 300 ft on climb, the Cessna 172 crew turned to maintain separation with the Saab 340 on final approach to the reciprocal runway.
2016
Brisbane West Wellcamp
Airborne collision alert system warning | Issues
Bombardier DHC-8
Beech B200
The crew of the Bombardier DHC-8 conducted a missed approach into Brisbane West Wellcamp to maintain separation with the Beech B200 on approach into Toowoomba.
2020
Toowoomba
Airborne collision alert system warning | Issues
Beechcraft B200
Diamond DA 40
During initial climb, the pilot of the Beechcraft B200 received a TCAS TA on the Diamond DA 40 and turned to increase separation. It was determined the pilot of the DA 40 was found to be on the incorrect frequency.
2020
Brisbane West Wellcamp
Airborne collision alert system warning
Saab 340
Diamond DA 40
During approach, the crew of the Saab 340 received a TCAS RA on the Diamond DA 40 in the circuit area.
2020
Brisbane West Wellcamp
Airborne collision alert system warning | Issues
Socata TB-10
Beechcraft B300
During circuit operations, a Socata TB-10 turned inside the Beechcraft B300 that was already established on downwind. The crew of the B300 received a TCAS RA and manoeuvred to maintain separation. No radio calls were heard from the TB-10.
2021
Brisbane West Wellcamp
Issues
Airbus A350
Diamond DA 40
During approach to runway 12, the Airbus A350 closed on the slower preceding Diamond DA 40 on approach to the reciprocal runway 30. The crew of the DA 40 were concerned with the horizontal separation and amended their approach to increase separation. The instructor completed a short field landing that damaged the main landing gear tyres and vacated the runway with the A350 on short final.
2021
Brisbane West Wellcamp
Airborne collision alert system warning
Beechcraft B200
Unknown aircraft
As the Beechcraft B200 joined the circuit, the pilot received a TCAS RA on another aircraft operating in the circuit.
Source: ATSB
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Holding procedure: a predetermined manoeuvre which keeps an aircraft within a specified airspace whilst awaiting further clearance.
[1] Dead side/non-active side: the area on the opposite side of the runway to where the circuit is flown.
[2] Danger area: an airspace of defined dimensions within or over which activities of potential danger to aircraft flying over the area may exist.
[3] En Route Supplement Australia (ERSA): a directory for Australian aerodromes that includes details of an aerodrome and details of available air traffic and ground services, navigation aids and public facilities and any special procedures.
[1] Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR).
[3] Brisbane Centre is one of 2 major centres – the other being in Melbourne. From Brisbane Centre, Airservices manages the airspace over the northern half of Australia, representing around 5% of the world’s total airspace. Brisbane Centre’s flight information region (FIR) neighbours include Indonesia, East Timor, Papua New Guinea, Fiji, New Zealand, and the USA.
[4] A common traffic advisory frequency (CTAF): a designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled airport or within a broadcast area.
[5] A waypoint is a specified geographical location used to define an area navigation route or the flight path of an aircraft employing area navigation.
[6] Touch-and-go landing: a procedure whereby an aircraft lands and takes off without coming to a stop.
[7] Sequence numbers specify the landing sequence position of an aircraft with respect to any preceding traffic.
[8] Traffic alert and collision avoidance system (TCAS): a type of airborne collision avoidance system (ACAS).
[9] Traffic advisory (TA): an alert issued by an airborne collision avoidance system (ACAS) when the detected traffic may result in a conflict. Pilots are expected to initiate a visual search for the traffic causing the TA.
[10] Resolution advisory (RA): a manoeuvre, or a manoeuvre restriction, calculated by an airborne collision avoidance system (ACAS) to avoid a collision. Pilots are expected to respond immediately to an RA unless doing so would jeopardize the safe operation of the flight.
On the afternoon of 16 September 2021, a Virgin Australia Airlines Boeing 737-8FE (B737) aircraft, registered VH-YIO, was conducting a scheduled passenger service from Sydney Airport, New South Wales (NSW), to Ballina Byron Gateway Airport (Ballina Airport), NSW. At the same time, a Cessna Caravan 208 (Caravan) aircraft, registered VH-YMV, taxied for a private instrument flight rules flight from Ballina Airport to Sunshine Coast Airport, Queensland.
While the B737 was on final approach to land on runway 24, the Caravan was taxied onto the runway and a take-off was commenced towards the approaching B737. The flight crew of the B737 conducted a missed approach to avoid the Caravan, during which they received a traffic collision avoidance system traffic advisory. At the closest point of approach, the lateral separation between the 2 aircraft decreased to approximately 0.9 NM with vertical separation reducing to about
700 feet. At the time of the incident, the aircraft were operating within the airport’s broadcast area and were both receiving a surveillance flight information service (SFIS).
What the ATSB found
The ATSB’s investigation identified that the Caravan pilot had an incorrect mental model of the traffic scenario, believing the B737 would land behind them on runway 06, rather than runway 24. The Caravan pilot had been provided with traffic information by the Ballina Airport SFIS controller, but the controller had not specified the landing direction of the B737 and the pilot had not sought this information.
The scenario was further compounded by the flight crew of the B737 not hearing the initial communications from the Caravan pilot, or the SFIS controller's response, and the flight crew remained unaware of the Caravan until just prior to it entering the runway. The Caravan pilot did not see the B737 approaching from the opposite direction and took-off directly towards it, resulting in the flight crew of the B737 to conducting a missed approach. No safety alert was issued by the SFIS controller as they were concerned that doing so would result in over transmitting communications from the aircraft in conflict.
The ATSB also found that the SFIS had been implemented in an area with known surveillance coverage limitations, resulting in the SFIS controller having no displayed positional information for the Caravan until it reached an altitude of about 1,500 feet. Consequently, the controller was solely reliant on radio communications for situation awareness during the period of conflict between the Caravan and B737, significantly reducing their ability to provide appropriate traffic and avoidance advice.
What has been done as a result
Although reportedly an outcome of a post‑implementation review, rather than a response to this occurrence, Airservices Australia (Airservices) advised that there was an intention to install additional technology to improve surveillance coverage in the vicinity of Ballina Byron Gateway Airport by March 2023, but that timeline was dependent on a number of factors.
Noting the indefinite timeframe, in order to support Airservices’ intended action, including complying with a related recommendation issued by the Civil Aviation Safety Authority in its Ballina airspace review, the ATSB issued a safety recommendation to Airservices to address this surveillance limitation in a timely manner.
Safety message
Safety around non-controlled airports is an area of focus for the ATSB and a SafetyWatch priority. Pilots can reduce the likelihood of similar incidents occurring by communicating directly with aircraft on the common traffic advisory frequency when services such as a surveillance flight information service are provided. Additionally, pilots and controllers alike should ensure critical information is communicated and understood in order to maintain the accuracy of shared mental models.
The ATSB also strongly encourages the fitment of ADS‑B transmitting, receiving and display devices as they significantly assist the identification and avoidance of conflicting traffic. The continuous positional information that ADS‑B provides can highlight a developing situation many minutes before it becomes hazardous – a significant improvement on both point‑in‑time radio traffic advice and ‘see‑and‑avoid’. The ATSB also notes that ADS‑B receivers, suitable for use on aircraft operating under both the instrument or visual flight rules, are currently available within Australia at low cost and can be used in aircraft without any additional regulatory approval or expense.
The occurrence
On the afternoon of 16 September 2021, a Virgin Australia Airlines Boeing 737-8FE (B737) aircraft, registered VH‑YIO (Figure 1), was conducting a scheduled passenger service from Sydney Airport, New South Wales (NSW), to Ballina Byron Gateway Airport (Ballina Airport), NSW. There were 2 flight crew, 4 cabin crew and 47 passengers on board. The captain was pilot flying (PF) and the first officer (FO) was pilot monitoring (PM).[1]
Figure 1: VH-YIO
Source: Supplied
At 1332:33 Eastern Standard Time,[2] when the B737 was approximately 44 NM to the south of Ballina Airport, the FO made an initial positional broadcast on the Ballina Airport common traffic advisory frequency (CTAF) [3] (see the sections titled Broadcast area and Common traffic advisory frequency). This broadcast was acknowledged by the Ballina surveillance flight information service (SFIS) controller (see the section titled Surveillance flight information service).
At 1335:15, the B737 FO made another broadcast on the Ballina CTAF advising that the aircraft was now 27 NM south of Ballina Airport and would land on runway 24 at an estimated time of 1345.
Meanwhile, the pilot of a Cessna Caravan 208 (Caravan) aircraft, registered VH-YMV prepared for a private instrument flight rules (IFR) flight from Ballina Airport to Sunshine Coast Airport, Queensland. The pilot was the only person on board and the purpose of the flight was to reposition the Caravan to the Sunshine Coast for parachute operations.
The Caravan pilot had flown a different aircraft from Sunshine Coast Airport to Ballina Airport earlier that day. On arrival at Ballina Airport, the pilot undertook a prefight inspection of VH-YMV and readied the aircraft for the flight.
At 1338:00, the B737 FO made a further broadcast on the Ballina CTAF advising that the aircraft was now 15 NM south‑east of Ballina Airport and would be positioned for a 10 NM final to land on runway 24 at a time of 1345.
At 1341:17, the Caravan pilot made a taxi broadcast on the Ballina CTAF advising that the aircraft would depart from runway 06 for an IFR flight to the Sunshine Coast. At the time, the weather recorded by the aerodrome weather information service (AWIS) indicated a few clouds at 2,600 feet above ground level, visibility greater than 10 km and a 12-17 knot wind from a 160-170° direction. The pilot recalled listening to AWIS and noting a crosswind. Although this wind direction favoured a departure from runway 24, the pilot recalled observing the windsock, assessing it favoured a departure from runway 06, and hence electing to do so. The aircraft was parked on the general aviation apron and the pilot chose to take-off from the intersection of taxiway A and runway 06, which involved a short taxi to the hold point with no backtracking along the runway.
At 1341:27, the SFIS controller responded to the Caravan pilot’s broadcast and provided the pilot with traffic information on the B737 and a Jetstar Airbus A320 (A320), registered VH-VQK, that was also inbound to Ballina Airport (Figure 2). The SFIS controller stated:
Yankee Mike Victor squawk 4547. Traffic [is] Velocity 1141, 737, shortly turning onto a 10 NM final, followed by Jetstar 464 an Airbus 320 currently 20 NM to the south-west and they're tracking for a right downwind runway 24. They'll be crossing centreline at about time four five.
Figure 2: At 1341:51, the pilot of the Caravan advised the SFIS controller that they had copied the traffic and correctly read back the transponder squawk code. Figure 2: A320 and B737 locations at 1341:27
Source: Google Earth, annotated by the ATSB
The flight crew of the B737 did not recall hearing the Caravan pilot’s taxi broadcasts or the SFIS controller’s responses to the taxi broadcast on the CTAF and were unaware of the presence of the Caravan. The SFIS controller noted that the B737 flight crew had not responded to the Caravan pilot’s taxi broadcast but did not confirm if they were aware of the Caravan (see the section titled SFIS procedures).
The B737 continued the approach for Ballina Airport and, at 1341:57, made a left turn onto a 10 NM final for runway 24.
Meanwhile, the Caravan pilot had formed the belief that the B737 would land on runway 06 based on their earlier observation of the runway windsock. The pilot had also misunderstood the traffic information provided by the SFIS controller as meaning that the B737 was on approach for runway 06, not runway 24, and hence believed that the Caravan could depart ahead of the arriving B737 without causing a conflict. The pilot recalled conducting a visual check for traffic before entering the runway but did not see the B737 that was on final approach to land on runway 24 (see the section titled Human factors).
At 1343:28, the pilot of the Caravan made a broadcast on the CTAF stating that the aircraft was entering and rolling runway 06 (Figure 3).
Figure 3: Caravan and B737 locations at 1343:28
Source: Google Earth, annotated by the ATSB
The SFIS controller heard the Caravan pilot’s ‘entering and rolling’ broadcast and was aware of the developing conflict between the Caravan and the B737. However, the SFIS controller elected not to issue a safety alert (see section titled Safety alert).
The ‘entering and rolling’ broadcast was the first transmission the flight crew of the B737 recalled hearing from the Caravan pilot and when they first became aware of the Caravan. At 1343:36, the B737’s FO made a broadcast on the CTAF stating that the B737 was on a 5 NM final approach for runway 24. Neither the Caravan pilot nor the SFIS controller responded to this broadcast.
At about 1344:00, the Caravan pilot commenced the take-off directly towards the approaching B737.
At 1344:15, the B737’s FO made a further broadcast on the CTAF querying the Caravan’s location. At 1344:19, the Caravan’s pilot responded stating that the aircraft had just become airborne from runway 06 (Figure 4). The B737’s FO immediately replied asking if the Caravan pilot could see the B737, which was now on a 3 NM final for runway 24. At 1344:36, the Caravan pilot confirmed sighting the B737, and its FO then requested the Caravan pilot to commence a turn. The Caravan pilot did not respond to the FO’s broadcast, but the pilot did initiate a turn to the right shortly after becoming airborne.
Figure 4: Caravan and B737 locations at 1344:19
Source: Google Earth, annotated by the ATSB
At 1345:06, the captain of the B737 initiated a missed approach and, a short time later, the flight crew sighted the Caravan ahead of their aircraft, travelling in a northerly direction. During the missed approach, the flight crew received a traffic collision avoidance system[4] traffic advisory[5] generated by the Caravan’s proximity. The flight crew maintained visual contact with the Caravan and repositioned the B737 for a left circuit to land on runway 24.
A review of recorded flight data indicated that the closest point of approach occurred at 1346:12 as the lateral separation between the 2 aircraft decreased to approximately 0.9 NM with vertical separation reducing to about 700 feet (Figure 5).
Figure 5: Caravan and B737 tracks and relative distances
Source: Google Earth, annotated by the ATSB
The Caravan pilot set course north for Sunshine Coast Airport and communications with the aircraft were transferred to the Brisbane Airport approach controller at 1349:26. The B737 landed at Ballina Airport at about 1359:00.
Context
Personnel information
B737 flight crew
The captain held an air transport pilot licence (ATPL) (aeroplane) and had a total flying time of 15,719 hours, having flown 25 hours in the previous 90 days. The captain was familiar with Ballina Airport and had operated there in both turboprop and jet aircraft over a 20-year period.
The FO held an ATPL (aeroplane) and a total flying time of 8,607 hours, having flown 72.3 hours in the previous 90 days. The FO was also familiar with Ballina Airport having operated there in both turboprop and jet aircraft throughout their career. The FO’s last flight to Ballina Airport took place on 11 May 2021.
Caravan pilot
The pilot held a commercial pilot licence (aeroplane) and a total flying time of 1,008 hours, having flown 50 hours in the previous 90 days. The pilot was familiar with Ballina Airport and had last flown into the airport approximately 3 months prior to the incident flight.
Controller
The surveillance flight information service (SFIS) controller had experience in both tower and en route air traffic environments prior to commencing in the SFIS controller role. The controller was based in the Airservices Australia Brisbane Centre and had undertaken SFIS endorsement training in August 2021, before the SFIS service commenced on 12 August.
Ballina Byron Gateway Airport
Ballina Byron Gateway Airport is situated approximately 3 NM from the city of Ballina, NSW. The airport has an elevation of 7 feet above mean sea level (AMSL) and a single sealed runway, orientated in a 062°-242° magnetic direction (Figure 6). The airport had global positioning system (GPS)‑based instrument approaches and a non-directional beacon ground-based navigation aid.
Figure 6: Ballina Byron Gateway Airport
Source: Airservices Australia
Airspace and traffic services
Ballina Airport was located within non‑controlled Class G airspace, which extended from the ground surface to 8,500 feet AMSL. The airport did not have a control tower and was not supported by an air traffic control separation or sequencing service (that is, a non-controlled airport).
Overlying the non‑controlled airspace was Class C controlled airspace which extended up to flight level (FL) 180,[6] and controlled Class A airspace above that. An air traffic information and separation service was provided within the Class C airspace and a separation service was provided within the Class A airspace. A restricted area existed approximately 5 NM south of the airport (the aircraft involved in this incident were clear of this area).[7]
The non‑controlled airspace surrounding Ballina Airport was available for use by aircraft operating under visual flight rules and instrument flight rules. The primary method of traffic separation at Ballina Airport was visual and relied on pilots using ‘alerted see-and-avoid’[8] practices.
A broadcast area (BA) was in place within an approximate radius of 15 NM from the airport and a surveillance flight information service (SFIS) was provided to aircraft operating within the BA during defined periods (see the section titled Surveillance flight information service).
Broadcast area
Surrounding Ballina Airport was a BA that mandated the carriage and use of radio equipment for aircraft operating within a radius of 15 NM of the airport, from surface level to 8,500 feet, excluding penetrating arcs of circles for Lismore Airport and Gold Coast control area steps (Figure 7).
Figure 7: Ballina Airport broadcast area
Source: Google Earth, annotated by the ATSB
The broadcast area was expanded from 10 NM to 15 NM on 28 January 2021 to ‘reduce residual airspace risk’. The expansion of the BA occurred following a separation incident involving a Jetstar A320 and a Jabiru aircraft that occurred about 13 NM from Ballina Airport on 28 November 2020 (see ATSB investigation AO-2020-062).
The broadcast area required all pilots to make mandatory positional broadcasts when entering or operating within the defined lateral and vertical limits of the BA on the Ballina Airport CTAF. Pilots were also required to acknowledge calls from aircraft departing or landing whose operations were in conflict with their own, and should announce when in receipt of a call indicating that their aircraft may be in conflict when operating outside of the circuit area.
Common traffic advisory frequency
The Ballina Airport CTAF was a designated radio frequency on which pilots made positional broadcasts when operating in the vicinity of the airport. The Ballina Airport CTAF was shared with neighbouring airports and aeroplane landing areas at Casino, Lismore and Evans Head.
A surveillance flight information service, detailed in the following section, was provided on the CTAF to aircraft operating within the Ballina Airport BA.
Surveillance flight information service
A surveillance flight information service (SFIS) was provided to aircraft operating within the Ballina Airport BA between 2200-0800 Coordinated Universal Time [9] (1 hour earlier during Eastern Daylight-saving Time[10]) or as notified by notice to airmen.
The SFIS utilised available surveillance data, and broadcasts on the airport’s CTAF, to provide all visual flight rules (VFR) and instrument flight rules (IFR) aircraft with a full traffic information and alerting service. The information provided by the SFIS controller contained advice on conflicting traffic. However, the SFIS was not a separation or sequencing service and pilots remained responsible for seeing and avoiding other aircraft.
The service was provided by a dedicated Airservices Australia air traffic controller located at the Brisbane Centre. Pilots made broadcasts and reported to the SFIS controller (callsign ‘Ballina Information’) on the Ballina Airport CTAF.
The SFIS commenced on 12 August 2021 and replaced the previously established certified air/ground radio service (CA/GRS).The CA/GRS was provided at Ballina Airport from March 2017 to the commencement of the SFIS service in August 2021 and was delivered by a certified air/ground radio operator (CA/GRO) located at the airport.
SFIS procedures
Airservices Australia procedures required the SFIS controller to communicate specific details when passing traffic information to aircraft. This information was to include the traffic’s intentions, the traffic’s reported position and estimate. The SFIS controller was also procedurally required to provide traffic information to aircraft in class G airspace when an aircraft was expected to arrive with less than 10 minutes separation time from aircraft departing from the same airport.
During this occurrence, the SFIS controller provided traffic information to the Caravan pilot that did not include the B737’s estimated landing time and runway number. The controller stated that as the pilot’s communications appeared to be ‘competent’ and ‘confident’, it had not been considered necessary to emphasise the B737’s landing direction. Similarly, when the B737’s flight crew did not respond to the Caravan pilot’s taxi broadcast, the controller did not consider it necessary to confirm they were aware of the Caravan because, according to their SFIS training, they were not required to follow-up communications for aircraft already on the CTAF (as was the case for the B737).
Safety alert
A safety alert comprises advice provided to a pilot when the SFIS controller becomes aware that an aircraft is in a position that places it in unsafe proximity to terrain, obstructions, active restricted or prohibited areas, or another aircraft. In cases where an aircraft is in close proximity to another, a safety alert should be issued by the controller unless the pilot had advised that action to resolve the situation was being taken, or the other aircraft was in sight. A safety alert could be issued in all classes of airspace both within and outside surveillance coverage.
However, on the day of the occurrence, the SFIS controller did not issue a safety alert to either the B737 or the Caravan after its pilot reported entering and rolling runway 06 although it was apparent to the controller that a conflict would result. The controller advised that their reason for not doing so was due to a concern that the alert could result in the over transmission of radio communications from either aircraft.
Technical systems
Secondary surveillance radar
Secondary surveillance radar utilises ground stations (interrogators) and transponders on board aircraft.
A transponder is a receiver/transmitter which transmits an automatic reply upon receiving an interrogation request. A manual ‘ident’ transmission can also be initiated by the pilot. The information that may be transmitted by a transponder is dependent on the ‘mode’ of equipment fitted to an aircraft:
Mode A transponders transmit an identifying code only
Mode C transponders transmit an identifying code and altitude (based on standard pressure)
Mode S transponders transmit an identifying code, altitude (based on standard pressure) and permit data exchange
The signal from the transponder is received by the ground station and combined with the aircraft’s position established via radar (range and bearing). This information is then relayed to air traffic control where it is displayed on the controller’s console screen.
Automatic dependant surveillance broadcast
Automatic dependent surveillance broadcast (ADS-B) utilises electronic equipment on board an aircraft to automatically broadcast the aircraft’s precise location, and other parameters, via digital data link (ADS-B OUT). The data is then used by air traffic control and other aircraft to depict the aircraft’s position, and other information, on a display without the need for radar.
The system uses GPS data to determine the aircraft’s position then transmits the position, and other parameters (such as identity, altitude and speed), at rapid intervals. These transmissions are received by dedicated ADS-B ground stations and the information is then relayed to air traffic control and displayed on the controller’s console screen.
The transmissions can also be received by other aircraft with the capability to receive and displayed this information (ADS-B IN). Both the B737 and Caravan were fitted with ADS-B OUT equipment. Neither aircraft was fitted with ADS-B IN equipment, nor were they required to be.
Surveillance coverage
The SFIS was a surveillance-based service that utilised secondary surveillance radar (SSR) and ADS-B information, in combination with pilot broadcasts made on the CTAF, to provide pilots with traffic information and alerts.
Documents developed by Airservices Australia before implementing the Ballina Airport SFIS contained a list of ‘critical components’ necessary for the service. Although ‘adequate surveillance coverage’ was one of these critical components, Ballina Airport had no ADS-B ground station and the surrounding area had significant limitations in SSR and ADS-B coverage. Surveillance coverage charts produced by Airservices Australia indicated that, near the airport, the SSR and ADS-B coverage did not commence until about 1,500 feet above ground level (Figure 8).
Figure 8: SSR and ADS-B coverage within the vicinity of Ballina Airport
Source: Airservices Australia, annotated by the ATSB
The hazards and risks associated with the surveillance coverage limitations were identified by Airservices Australia prior to the implementation of the SFIS and documented as:
Limited surveillance coverage may lead to unintended aircraft proximity (Airprox), inadequate separation assurance (ISA), or loss of separation (LOS) occurrence.
Airservices Australia conducted a risk assessment and rated the initial risk as moderate. However, its pre-implementation risk treatment did not reduce the risk any further. Residual risks associated with the surveillance coverage limitations were formally accepted and the SFIS was implemented with the risks unaddressed. These limitations meant the Caravan’s positional information was not displayed on the SFIS controller’s console screen until it reached an altitude of about 1,500 feet, which occurred about 100 seconds after take-off was commenced.
Previous events
A search of the ATSB occurrence database found that during the period from the implementation of the SFIS (12 August 2021) to the date of the incident (16 September 2021), there was one reported occurrence and no reported separation issues within 20 NM of Ballina Airport.
Regulatory oversight
The Airspace Act 2007 assigned the administration and regulation of Australian administered airspace to the Civil Aviation Safety Authority (CASA). As part of this function, CASA was required to undertake regular reviews of airspace to determine if existing classifications were appropriate, air navigation services and facilities were suitable, there was safe, efficient, and equitable use of airspace, and identify any associated risk factors.
On 15 December 2022, CASA publicly released a final Ballina airspace review. The review identified 3 areas of concern:
Frequency congestion
Heightened risk of separation incidents
Situational awareness
As a result, the review made 9 recommendations (Table 1).
Table 1: Ballina airspace review recommendations
No.
Recommendation
1
CASA should prepare a Request For Change (RFC) to separate the Lismore and Casino Common Traffic Advisory Frequency (CTAF) from the Ballina CTAF by 16 June 2022.
2
Evans Head Airport should be allocated the common CTAF (126.7 MHz) by 16 June 2022.
3
CASA should direct AA to install an Automatic Dependent Surveillance - Broadcast (ADS-B) ground station in the vicinity of Ballina to improve surveillance as soon as practicable but no later than April 2023. The ground station should, as far as is practical, provide ADS-B surveillance capability to the runway surface.
4
CASA should explore a suitable regulatory framework that can safely authorise sport and recreational aircraft and pilot certificate holders to operate in the controlled airspace associated with Ballina where pilot certificate holders meet CASA specified competency standards and the aircraft are appropriately equipped.
5
CASA’s Stakeholder Engagement Division (SED) should conduct additional safety promotion programs in relation to Ballina operations as soon as practicable. The programs should include, but are not limited to the following key elements:
a. reinforce the mandatory radio calls required when operating within the Ballina MBA in the interim, pending the establishment of controlled airspace, and
b. later, provide guidance as to how a Sport Aviation Body might develop a suitable scheme and make application to CASA for approval, under the regulatory framework identified in recommendation 4.
6
Uncertified aerodromes and flight training areas around Ballina should be promulgated in aeronautical publications to increase pilot situational awareness.
7
As an interim action pending the completion of Recommendation 8, CASA should make a determination to establish a control area around Ballina Byron Gateway Airport with a base which is as low as possible, and direct AA to provide services within the control area. The services should be provided during all periods of scheduled Air Transport Operations and include an Approach Control Service to aircraft operating under the Instrument Flight Rules (IFR), separation between IFR aircraft, VFR traffic information to all aircraft, and sequencing of all aircraft to and from the runway. CASA and AA should jointly explore opportunities to detect non-cooperative aircraft or vehicles in the immediate vicinity of the runway. The services should be established as soon as practicable but no later than 30 November 2023.
8
CASA should make a determination that Ballina Byron Gateway Airport will become a controlled aerodrome with an associated control zone and control area, and direct Airservices Australia (AA) to provide an Aerodrome Control Service1 to the aerodrome. That service should be established as soon as practicable but no later than 13 June 2024.
9
CASA should prepare and finalise an Airspace Change Proposal (ACP) for a control zone and control area steps in preparation for the implementation of Recommendations 7 and 8.
Source: Airspace Review of Ballina – 2022 with minor amendments by the ATSB
On 16 June 2022, recommendation 1 and 2 were implemented resulting in Lismore, Casino and Evans Head being separated from the Ballina Airport CTAF. Recommendation 3 was due for implementation by April 2023 and proposed the installation of an ADS-B ground station in the vicinity of Ballina Airport to provide surveillance coverage to the runway surface.
The ATSB undertook a detailed assessment of CASA’s role in the oversight of the airspace surrounding Ballina Airport following a separation occurrence involving an Airbus A320-232 and a Jabiru that took place on 28 November 2020 (see investigation AO-2020-062).
Human factors
The ATSB investigation considered a range of human factors that could have influenced the decisions and actions of the pilots and controller involved. No indicators that increased the risk of any of the individuals experiencing a level of fatigue known to influence performance were found. The following factors, however, were found to have possibly had an influence:
shared mental models
situation awareness
confirmation bias
Mental models
According to Methieu et al (2000), mental models are internally organised knowledge structures that allow individuals to understand and interact with their environment. Mental models are said to be ‘shared’ when the models of individuals overlap – the greater the overlap the greater the similarity of understanding.
In scenarios involving the movement of aircraft within the airspace system, it is anticipated that pilots and air traffic controllers will have a high degree of shared mental model overlap. However, when communication is ineffective, and critical information and assumptions are not shared, the degree of shared mental model overlap is decreased, coordinated decision making is degraded, and safety defences are eroded (Bearman et al 2010).
The mismatch of mental models was evident in the lead up to this incident. Critical traffic information and assumptions were not shared between the SFIS controller, the Caravan pilot, and the B737 flight crew. This resulted in each party holding a different mental model of the traffic scenario.
Situation awareness
Situation awareness (SA) is best conceptualised as a 3-stage process:
task related features or cues are acquired and interpreted by the individual
information is integrated and comprehended within the context of the task to derive meaning for the individual
the individual anticipates the future state of the system (Wiggins 2022)
The accuracy of an individual’s SA directly influences their decisions.
The SFIS controller, the Caravan pilot and the B737 flight crew all held incomplete information on the traffic scenario and the intended actions of the others involved. As a result, their capacity to accurately predict the future traffic state was compromised and their decision-making impacted accordingly.
Confirmation bias
Confirmation bias involves an individual seeking out information that confirms an assumption and rejecting, ignoring, or explaining away information that conflicts with the held assumption (Wiggins 2022). Based primarily on their assessment of the windsock, the Caravan’s pilot incorrectly believed that the B737 was on final approach for runway 06 and not runway 24. It is therefore possible that the pilot’s confirmation bias influenced the visual check before entering the runway with the B737 on final approach from the opposite direction going undetected.
Safety analysis
The incident
On 16 September 2021, a Boeing 737, VH-YIO (B737), was approaching runway 24 to land at Ballina Byron Gateway Airport when a Cessna Caravan 208, VH-YMV (Caravan), commenced a take-off on the reciprocal runway. The B737’s flight crew conducted a missed approach during which the lateral separation between the 2 aircraft decreased to approximately 0.9 NM with vertical separation reducing to about 700 feet. At the time of the incident, the aircraft were operating within the airport’s broadcast area, and both were receiving the associated surveillance flight information service (SFIS).
Communications
The SFIS controller had not included the B737’s estimated time of landing and runway direction when providing traffic information to the Caravan pilot. In addition, the Caravan pilot had formed the belief that the B737 would land on runway 06 (based on observing the runway windsock), and then interpreted the traffic information provided by the controller incorrectly as it confirmed their incorrect mental model. The pilot did not seek to validate this assumption by communicating directly with the B737’s flight crew or by querying the information provided by the controller.
The scenario was further compounded by the B737’s flight crew not hearing the Caravan’s taxi broadcasts or the SFIS controller’s responses. Those taxi transmissions commenced 40 seconds before the B737 turned onto final approach for runway 24. The ATSB was not able to determine why the flight crew did not hear the exchange. In any case, they were not aware of the Caravan until the ‘entering and rolling’ broadcast made by its pilot.
The SFIS controller knew the B737’s flight crew had not acknowledged the Caravan pilot’s taxi broadcast but recalled from SFIS training that follow-up communications were not necessary for aircraft already on the common traffic advisory frequency (CTAF). Consequently, the controller decided not to confirm that the flight crew were aware of the Caravan, and an opportunity to address the evolving situation was missed. This resulted in the B737’s flight crew remaining unaware of the Caravan and the latter’s pilot continued to incorrectly believe the B737 would land in the opposite direction.
The Caravan pilot’s incorrect mental model also led them to believe the Caravan could take-off ahead of the landing B737, using runway 06, without any conflict. The pilot recalled conducting a visual check prior to entering the runway; however, their likely confirmation bias and reduced situation awareness possibly resulted in not sighting the approaching B737. Consequently, the Caravan was taxied onto the runway and a take-off commenced directly towards the B737.
Safety alert
The SFIS controller recognised the impending conflict between the two aircraft after hearing the Caravan pilot’s ‘entering and rolling’ broadcast but decided not to issue a safety alert because of concerns of over transmitting communications from the Caravan or the B737. However, between the ‘entering and rolling’ broadcast and confirmation that the Caravan pilot had sighted the B737, there was a total of 53 seconds during which time no transmissions were made on the CTAF. A safety alert issued during this time would probably have ensured the pilots on both aircraft were fully aware of the conflict.
Surveillance coverage limitations
Prior to the implementation of the Ballina Airport SFIS, Airservices Australia had identified a hazard associated with a critical component of the service that could lead to unintended aircraft proximity events. As the secondary surveillance radar and automatic dependent surveillance broadcast (ADS-B) coverage near the airport did not commence until about 1,500 feet above ground level, ADS-B equipped aircraft operating below this height may not be displayed on the SFIS controller’s console screen. Airservices Australia formally accepted the risk associated with the surveillance coverage limitations and the SFIS was implemented with this critical component compromised.
The limitation in coverage resulted in the SFIS controller having no positional information on the Caravan during the period of conflict until the aircraft reached an altitude of about 1,500 feet about 100 seconds after taking off. During this period, the controller was solely reliant on radio communications for situation awareness and had reduced options for providing any avoidance advice necessitated by the situation.
The heightened risk of separation incidents in the vicinity of Ballina Airport was identified in the Civil Aviation Safety Authority’s (CASA’s) Ballina airspace review, which was published in December 2022. Recommendations contained in that review document included the installation of an automatic dependent surveillance broadcast (ADS-B) ground station in the vicinity of Ballina Airport to enable ADS-B surveillance capability to the runway surface. The review document contained 8 other recommendations designed to incrementally transition Ballina Airport to a controlled aerodrome service with an associated control zone and control area steps by 13 June 2024. Such an aerodrome control service would have prevented the traffic conflict between the B737 and the Caravan.
Both this separation occurrence and that detailed in AO-2020-062 involved high-capacity transport aircraft using the primary defence of alerted see‑and‑avoid. Noting the known limitations of this principle, and the increasing and complex mix of traffic, the ATSB considers that timely implementation of the recommendations detailed in CASA’s airspace review document would significantly improve safety at Ballina Airport.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the separation occurrence involving Boeing 737-8FE, VH-YIO (B737) and Cessna Caravan 208, VH-YMV (Caravan) at Ballina Byron Gateway Airport, New South Wales on 16 September 2021.
Contributing factors
Based on an assessment of the windsock only, the Caravan pilot wrongly assumed that the B737 would land behind them on runway 06 and not present a conflict for their departure. This incorrect mental model of the traffic was not corrected prior to the conflict as the surveillance flight information service controller did not specify that the B737 would land on runway 24 and the pilot did not confirm the runway direction with the controller or with the B737’s flight crew.
The B737’s flight crew did not hear the Caravan pilot’s taxi broadcast or the surveillance flight information service controller's response, who also did not confirm if the flight crew were aware of the Caravan. Consequently, the flight crew was unaware of the Caravan until its pilot made a broadcast before entering the runway.
The visual check by the Caravan’s pilot before entering the runway did not identify the B737 on final approach to land on runway 24, possibly due to confirmation bias and degraded situation awareness resulting from the pilot’s incorrect mental model of the traffic.
The Caravan’s pilot commenced a take-off directly towards the approaching B737 resulting in its flight crew conducting a missed approach to avoid the Caravan.
Other factors that increased risk
The surveillance flight information service controller did not issue a safety alert after the Caravan entered the runway and commenced taking off towards the approaching B737 due to concerns that issuing an alert would result in over transmitting communications from either aircraft.
The surveillance flight information service (SFIS) had been implemented in an area with known surveillance coverage limitations, resulting in the SFIS controller having no displayed positional information for the Caravan until it reached an altitude of about 1,500 feet. Therefore, during the period of conflict between the Caravan and B737, the controller was solely reliant on radio communications for situation awareness, reducing their ability to provide appropriate traffic and avoidance advice. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The surveillance flight information service (SFIS) had been implemented in an area with known surveillance coverage limitations, resulting in the SFIS controller having no displayed positional information for the Caravan until it reached an altitude of about 1,500 feet. Therefore, during the period of conflict between the Caravan and B737, the controller was solely reliant on radio communications for situation awareness, reducing their ability to provide appropriate traffic and avoidance advice.
Glossary
ADS-B Automatic dependant surveillance broadcast
AMSL Above mean sea level
ATPL Air transport pilot licence
BA Broadcast area
CA/GRO Certified air/ground radio operator
CA/GRS Certified air/ground radio service
CTAF Common traffic advisory frequency
FO First officer
GPS Global positioning systems
IFR Instrument flight rules
KM Kilometres
NM Nautical miles
NSW New South Wales
PF Pilot flying
PM Pilot monitoring
SA Situation awareness
SFIS Surveillance flight information service
SSR Secondary surveillance radar
VFR Visual flight rules
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew of VH-YIO and pilot of VH-YMV
the SFIS controller
Virgin Airlines Australia
Avdata
OzRunways
Civil Aviation Safety Authority
Airservices Australia
Bureau of Meteorology
Experience Co Limited
References
Wiggins M 2022, Introduction to human factors for organisational psychologists, Taylor & Francis Group, Milton
Bearman C, Paletz S, Orasanu J & Thomas M 2010, The breakdown of coordinated decision making in distributed systems, Human factors, Vol. 52, pp. 173-188
Mathieu J, Heffner T, Goodwin G, Salas E & Cannon-Bowers J 2000, The influence of shared mental models on team process and performance, Journal of applied psychology, vol 85, pp. 273
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the flight crew of VH-YIO and pilot of VH-YMV
the SFIS controller
Virgin Airlines Australia
Airservices Australia
Experience Co Limited
Civil Aviation Safety Authority.
Submissions were received from:
Airservices Australia
Experience Co Limited
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] Eastern Standard Time (EST): Coordinated Universal Time (UTC) +10 hours.
[3] A common traffic advisory frequency is a designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled airport, or within a broadcast area.
[4] A traffic collision avoidance system (TCAS) interrogates the transponders of nearby aircraft and uses this information to calculate the relative range and altitude of this traffic. The system provides a visual representation of this information to the flight crew as well as issuing alerts should a traffic issue be identified.
[5] A traffic advisory (TA) is an alert issued when the detected traffic may result in a conflict (the closest point of separation is about 40 seconds away on the current projected flight paths). Pilots are expected to initiate a visual search for the traffic causing the TA.
[6] Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 180 equates to 18,000 ft.
[7] The restricted area was activated by a notice to airmen when military jet aircraft were operating within the area and/or live-firing exercises were taking place.
[8] Pilots are responsible for sighting conflicting traffic, and avoiding a collision, having been alerted to the presence of
traffic in their immediate vicinity. This is principally achieved via radio communications.
[9] Coordinated Universal Time (UTC): the time zone used for aviation. Local time zones around the world can be expressed as positive or negative offsets from UTC.
[10] Eastern Daylight-saving Time (EDT): Universal Coordinated Time (UTC) +11 hours.
On 29 June 2021, a NSW Trains XPT was operating passenger service run ST24, between Albury and Sydney in NSW. At around 1325, ST24 passed through a worksite (504.500 km) at approximately 100 km/h. At the time the train passed through the worksite, ongoing repairs required that a speed limit of 40 km/h should have been in place.
No injuries or damage resulted from the incident.
What the ATSB found
During the process of preparing the track to allow ST24 to run through the worksite, the Australian Rail Track Corporation (ARTC) Protection Officer (PO) did not impose the required 40 km/h temporary speed restriction when fulfilling the Track Occupancy Authority (TOA) that had been in place to protect the worksite from trains entering the area. The speed restriction should have been applied using the Condition Affecting the Network (CAN) process.
When it came time to fulfil the TOA, the PO was away from the worksite where the repairs occurred. They were removing protection at the Wagga Wagga end of the TOA while also completing tasks associated with fulfilling the TOA. The PO was likely distracted by performing these competing tasks and did not inform the ARTC Network Controller (NC) of the need to place a temporary speed restriction on the track.
After the TOA was fulfilled and train ST24 was permitted to run at track speed, the PO realised the omission but was unable to successfully make contact with the NC in time to prevent the train passing through the worksite. As the train neared, the PO was still trying to contact the NC and did not use emergency stop handsignals.
The PO was using a new electronic form (eTAP) and system to fulfil the TOA. It was the first time they had used this system to fulfil a TOA when there was a CAN warning required for a temporary speed restriction. During the TOA fulfilment, the PO incorrectly answered one of the assurance questions about whether there was a CAN and consequently, the NC was not advised of the need for a temporary speed restriction to be applied. The NC acted on the electronic message from the PO and fulfilled the TOA and allowed ST24 to run unrestricted. The eTAP system, used at Track Occupancy Authority (TOA) fulfilment, does not include a key safeworking requirement contained in the ARTC Network Rules for confirming and repeating back safety critical information prior to acting on it.
The initial training for this new system was delivered to the PO while they were a PO1 level, meaning they did not possess the technical competency to implement a TOA. The PO may not have absorbed the content of the training because they did not possess the technical competency at the time of delivery. The ARTC training was delivered to a group of POs, irrespective of their competence level. There was no evidence of a competence assessment being applied to the PO after the training to confirm their ability to use the new system.
What has been done as a result
ARTC has separated the training modules for eTAP to ensure the content delivered is specific to the competency levels of the trainees. ARTC will undertake a review of the relevant Rules and Procedures applicable to TOA Fulfilment being ANWT 304 and ANPR 701, including ANGE 204.
Safety message
When introducing new technology, training regimes should include competency assessments, and content tailored for the workers and their required application of the technology. Training should include practical use of the technology under different scenarios, and include managing foreseeable errors, to promote familiarisation and understanding.
The occurrence
An ARTC civil workgroup from Wagga Wagga was assigned a task to straight rail the redundant Shepherds siding on the Main South rail line between Bomen and Harefield (figure 1) in the Riverina region of NSW. This task involved welding the rails to remove the redundant switches that serviced the old siding. The work group, consisting of six civil team members, left Wagga Wagga at approximately 0730 and arrived at the worksite around 0830.
Figure 1: Shepherds Siding
Source: Google images
The work was delayed by the absence of a team of signal electricians who were required to dismantle the disused points. The signal electricians arrived on site at approximately 1000 and the work then proceeded.
At approximately 1149 that day, NSW Trains XPT passenger service ST24, departed Albury for a scheduled service to Sydney. At approximately 1307, ST24 arrived at Wagga Wagga on time and departed at approximately 1309.
Shortly after leaving Wagga Wagga, ST24 stopped for a short period of time waiting for authorisation to continue its journey. The delay was required to allow workers to move off the track ahead, at the worksite in Shepherds Siding (504.500 km). At this point, the work was not yet complete, and the rail had not been welded together. The rail was held together with a device called a Robel clamp, which holds each end of the unwelded rail in place and allows for the passage of rail traffic until the weld is completed.
The worksite was being protected using a Track Occupancy Authority (TOA) which excluded trains for a specified period. At approximately 1320, once the track was clear, the Protection Officer (PO) fulfilled the TOA and handed the track back to the Network Controller (NC), who then authorised ST24 to proceed on its journey towards Sydney.
Just after they fulfilled the TOA, the PO realised they had forgotten to place a Condition Affecting the Network (CAN) 40 km/h speed limit warning on the section of track through the worksite. The PO unsuccessfully attempted to contact the NC on the regular phone line to inform them of the error.
At approximately 1325, ST24 passed through the worksite at Shepherds Siding travelling at 100 km/h. The PO managed to contact the NC on the emergency phone line just as ST24 entered the worksite and requested the verbal CAN warning, reducing speed to 40 km/h, for all subsequent rail traffic. The PO was then stood down and transported to Wagga Wagga ARTC provisioning centre for mandatory drug and alcohol testing, returning negative results.
Context
Location and rail network information
Shepherds Siding was an intermediate siding attached to the single main line between the crossing loops of Bomen and Harefield, located between 504.234 km and 504.940 km (figure 2). The siding was being removed as it was no longer operational. The rail network at this location is a single line, bi-directional system, which allows trains to run in either direction under the authority of the engineered signal control system.
Figure 2: Incident location
Source: Geoscience, annotated by OTSI
Environment
The Bureau of Meteorology showed the weather as recorded at Wagga Wagga (approximately 16 km from Shepherds Siding) was a minimum temperature of 4.7° C, and a maximum of 15.7° C. No rainfall was recorded in the 24-hour reporting period. Weather and environmental conditions were not considered a factor in this incident.
Parties Involved
NSW Trains
ST24 and the rest of the XPT fleet at the time of the incident were operated by NSW Trains, under the operating name of NSW TrainLink. NSW Trains was an agency of Transport for NSW[1].
Australian Rail Track Corporation (ARTC)
ARTC was a statutory corporation fully owned by the Government of Australia. ARTC was the Rail Infrastructure Manager (RIM) that manages the Main South rail line from Macarthur on the outskirts of Sydney to Melbourne. ARTC was an accredited operator and since September 2004 has held a 60-year lease of the interstate and Hunter Valley rail lines of NSW.
Trains were managed and controlled by ARTC Network Controllers at the Junee Control Centre, NSW.
eTAP
eTAP was a mobile device application designed as a tool for use by POs and Network Controllers to communicate safety critical information in the ARTC NSW Network. It was used to establish, monitor, and fulfill TOA, Look Out Working and Working in Corridor requests. The eTAP application replaced, to a large extent, the verbal exchange between the NC and the PO when applying for, authorising, and ending work on track.
The eTAP solution did not replace the need for verbal communication between the PO and NC when reporting or managing emergency conditions or CANs.
ARTC investigated engineering solutions to mitigate some of the error-inducing factors resulting from applying work on track rules and decided to trial the 4Tel / John Holland Rail Electronic Track Work (ETW) System to determine its suitability for roll out across the ARTC network.
The ETW application was originally designed by John Holland Rail (JHR) & 4Tel to assist Rail Safety Workers in their daily roles and ultimately, create safer outcomes on the NSW Country Regional Network (CRN).
The initial ARTC trial was undertaken between May and July 2018 on the section between Wolseley and Mile End in South Australia on the interstate rail corridor. This trial only focused on use for the application of TOAs.
Based on the success of the initial trial, the scope of the trial was extended to include the ARTC Hunter Valley network in August 2018. A risk assessment workshop was conducted in March 2019 to assess and validate the performance of the application.
The workshop had 23 participants, of which one was an active worker from an infrastructure team, a work group leader from Coffs Harbour. Other participants included four network controllers, and staff from various business areas including safety, IT and management.
Network rules and procedures
The relevant ARTC Network Rules and Procedures applicable to this incident are:
ANWT 300 – Planning work in the rail corridor. This rule sets out the requirements for planning work in the rail corridor and assessing it for the necessary safety requirements.
ANWT 304 – Track Occupancy Authority. This rule describes the requirements for authorising, issuing, managing and ending occupation of the track for a specified period to allow work to occur.
ANPR 701 – Using a Track Occupancy Authority. This procedure describes the steps to take to authorise, issue, manage and end occupation of the track for a specified period in order allow work to occur.
ANGE 206 – Condition Affecting the Network. This rule describes the requirements for reporting and responding to unsafe conditions on the rail network.
ANGE 204 – Network Communication. This rule describes the universal requirements for spoken and written communication in the ARTC Network.
Robel clamp
A Robel rail clamp was a device used to link rail ends in a safe and secure manner until permanent connection by welding is complete (figure 3). The clamp was used by the civil workgroup at Shepherds Siding to temporarily secure the rail for the low speed, up to 80 km/hr, passage of rollingstock, prior to completion of permanent joining works.
Figure 3: Robel clamp
Source: Robel.com
Protection Officer
A PO1 is the base level of Protection Officer certification in a group of four certification levels from PO1 to PO4. As a PO moves through the grades, they are able to implement more complex methods of protection.
The PO involved in this incident had approximately two years of experience in that role. They had worked for 12 months as a PO1, followed by completing four months of supervised training before qualifying as a PO2. The PO had carried out a variety of protection work in this time.
The PO attended a briefing on the eTAP system in February 2020 that included the requirements for requesting, managing and fulfilling a TOA, but as a PO1 they were not authorised to implement this method of protection at the time. The PO received no further instruction on the application and learned its use on the job when promoted to a PO2.
The PO was removing protection for the southern end of the TOA at the time of fulfilling the TOA due to the make-up of the work group. The workers in the team were needed at the site for the task being performed, so the PO was absent from the worksite when the TOA was fulfilled.
Network Controller
The NC at the Junee Control Centre had been in the rail industry since November 2020, when they commenced as a trainee NC, progressing through the traineeship in April 2021. The NC had been operating as an authorised NC in the Junee Control Centre for approximately four months.
Safety analysis
The work being undertaken
The workgroup was in the process of installing and welding a closure rail in a section of track after removing a redundant switch to a disused siding. This entailed cutting the track to disconnect the disused infrastructure and joining the main line rails to form a continuous rail. Once the track was cut, it was plated together using bolts and clamps, and the join would then be welded together.
The workgroup encountered some delays in performing this task due to the late arrival of the signal electricians at the worksite, who were delayed by a meeting in the Wagga Wagga depot that ran overtime. The signal electricians arrived approximately 90 minutes late to the worksite. The signal electrician’s role was to disconnect the points to allow the civil team to cut the track and weld it back together.
Just prior to the incident, the work had not yet progressed to the point where welding had commenced. The join was secured using a Robel clamp until the welding could occur. By this time, the worksite protection arrangement being used for this work, a TOA, was due to end because a passenger train, the Sydney bound XPT service ST24, was scheduled to arrive at Bomen and travel through the section.
Fulfilling the Track Occupancy Authority (TOA)
The rules of ending, or fulfilling, the TOA meant the below activities had to be undertaken in the following order:
Removal of people, tools, and equipment from the track
Removal of trackside protection including railway track signals and red flags or lights
Informing the NC of these activities and confirming the track is fit for service, or alternatively, of any conditions or restrictions that need to apply.
The NC then removes blocks on the protecting signals for the TOA and trains are allowed to run, subject to any conditions or restrictions.
As the expiry time for the TOA was approaching, the PO was advised that the work was not complete because the welding had been delayed by the late arrival of the signal electricians. As the rail was held in place by a clamp a temporary speed restriction would be necessary. The track certifier in the work group spoke with the PO and advised that a 40 km/h speed restriction was required.
Removal of Track Occupancy Authority (TOA) protection
Due to the makeup of the team, the PO needed to go to the Wagga Wagga end of the TOA to remove the protection, as there were no other available workers to perform this task. The protection was approximately 500 m away from the worksite. Another team member went to the northern end of the TOA to remove the protection there. The remaining team members were required at the worksite to complete the work activity in order to make the track safe for train running.
Ten minutes prior to leaving the worksite, the PO had a conversation with the track certifier about the need to impose a temporary 40 km/h speed restriction. However, at the time of fulfilling the TOA, the PO was likely focused on removing the protection and associated tasks with fulfilling the TOA so overlooked the application of the speed restriction.
The ARTC Network Rule ANWT 300 Planning work in the rail corridor states:
Protection Officer
A worksite must have a Protection Officer (PO).
A Protection Officer’s primary duty is to keep the worksite and workers safe.
The Protection Officer must be satisfied other work will not interfere with protection duties.
In this case the PO was performing another task, being the Qualified Worker removing the protection for the TOA which is permitted under the ARTC Network Rules. It meant that the PO was absent from the worksite, and their attention was on both removing the protection and fulfilling the TOA in order to allow the passage of a high-priority passenger service.
Temporary speed restriction and fulfilling the TOA via eTAP
A temporary speed restriction is applied through Network Rule ANGE 206 Condition Affecting the Network (CAN), it states:
Warning Rail Traffic
The Network Control Officer must give written warning using a CAN form to rail traffic crews if:
• temporary speed restrictions have been reported and no signs erected.
While at the Wagga Wagga end of the TOA, the PO attempted to gain an extension of time for the TOA but was refused by the NC as the northbound XPT was due to run, then the southbound XPT needed to run after that. These were two high-priority, long-haul passenger trains, and effort is always made to avoid delays to these services.
The unsuccessful attempt to extend the TOA did not result in any discussion between the PO and the NC about the reason for the extension, i.e., that the work was incomplete, and the track was not suitable for normal line speed. This conversation focused on the train running after the XPT trains, and on when another TOA was expected to be taken.
The NC asked the PO if the existing TOA would be handed back at the expected time and the PO answered that it would. There was no mention of any speed restriction or other condition. The reduced speed would have affected the train running time as any trains travelling through the section would have required a written CAN issued to the driver, and the train would have had to slow down over the worksite.
After the unsuccessful attempt to extend the TOA, the PO made arrangements to restore the line for rail traffic and fulfil the TOA.
The PO had arranged the TOA utilising the eTAP application on their mobile phone. They also used eTAP to fulfill the TOA when handing back the track. The PO selected ‘Yes’ in response to the question “Is the track suitable for line speed operations?” in the fulfillment assurance checks, instead of selecting ‘No’.
If No was selected, then the application would have directed the PO to call the NC and advise the details of the temporary speed restriction. The PO stated at interview that they had never used the eTAP application to impose a temporary speed restriction after fulfilling a TOA. This was the first time the PO had fulfilled a TOA that required a CAN warning for a speed restriction.
Operation of XPT train ST24
Shortly after fulfilling the TOA on eTAP, the PO realised their error and unsuccessfully attempted to contact the NC before the XPT arrived at the worksite. At this time, the NC was dealing with a report of children trespassing in the rail corridor and another request for work on track access from a different work group at Harefield using Absolute Signal Blocking. When the PO was unable to contact the NC on the regular phone line, they called the emergency Network Control number notifying the NC of the error. The NC answered the emergency call but by this time the train had already left Bomen.
By the time the NC was aware of the need for the CAN warning, ST24 had passed the PO at the Wagga Wagga end of the TOA and was travelling through the worksite.
ST 24 passed through the worksite at approximately 100 km/h, 60 km/h over the intended speed of 40 km/h. The driver reported seeing the workers beside the track and so sounded the train horn and received acknowledgement from the workers before passing through the site.
It was possible for the PO to stand to the side of the track and use the emergency stop handsignal to alert the driver to stop. The PO did not attempt to use handsignals to stop the train.
ARTC introduction of eTAP app-based solution
ARTC undertook a trial of the eTAP solution prior to full implementation.
Prior to initiating the trial, ARTC established the following criteria to determine the success or failure of the trial. These were:
It had to be a functional electronic system
It had to reduce the time it took to issue a TOA (with an aim of 50%)
The trial had to contain zero safe working errors attributed to the application
It had to be positively taken up by the workforce
At least 200 TOA events needed for validity of trial.
Figure 4: eTAP screen shot for TOA fulfillment on PO device
Source: Australian Rail Track Corporation
Using eTAP, a NC could issue TOA information electronically to a PO. The PO could then review and confirm the information and location on the device before verification and acceptance. This process replaced the previous paper form and verbal read out/read back communication.
At the time of fulfillment of a TOA, a PO checks off assurance questions in the eTAP application (figure 4). If there is no CAN identified (as indicated by the PO’s answers to the assurance questions) then the PO can complete the fulfilment of the TOA electronically. The NC then completes their work to fulfil the TOA by using the fields on their screen (figure 5). However, if any CAN are identified (as indicated by the PO’s answers to the assurance questions) then the application requires the PO to call the NC and verbally complete the fulfilment of the TOA.
Figure 5: eTAP screen shot for TOA fulfillment on Network Controller workstation
Source: Australian Rail Track Corporation
eTAP was designed to improve safety and efficiency outcomes for POs and NCs, by enhancing decision making through the provision of more information and electronic delivery.
Through a review into the establishment of worksite protection on its network, ARTC identified several common factors which had the potential to result in errors during the issue of a TOA. The most common factors identified were;
Inadequate communication
Incorrect planning
Incorrect form compilation
Incorrect graphing
Incorrect location
Lack of area knowledge
Failure to identify the correct location of trains within the limits of a work authority
Incorrect or inadequate use of blocking facilities.
The risks to track workers from one or more of these factors, led ARTC to explore controls to mitigate these errors. ARTC identified the 4Tel/John Holland Rail ETW System (eTAP) as a potential solution to trial. A trial was conducted in South Australia on the ARTC west network control centre between 9 May 2018 and 9 July 2018.
At the conclusion of the trial, ARTC determined that the eTAP electronic system had met the criteria successfully. In August 2018, ARTC recommended to continue utilising the eTAP electronic system in the trial location and to introduce its use throughout the entire ARTC interstate and Hunter Valley NSW networks.
ARTC risk assessment for the introduction of eTAP
ARTC conducted a risk assessment workshop on 28 March 2019 which explored potential risks involved with the introduction of the eTAP system into the NSW ARTC controlled network. The makeup of the risk assessment team included one operational infrastructure worker, a team leader from Coffs Harbour NSW.
The risks identified in the workshop included:
System availability
Confusion for the Network Controller using two systems
Inadequate worksite protection
Lack of interface between the eTAP app and the Phoenix signalling system
IT security of devices
Functionality of the eTAP application
Failure of the device in the field.
The ARTC risk assessment did not contemplate a failure mode whereby the PO would return the track to service without imposing a temporary speed restriction to ensure safe operation of rail traffic. The potential for this human error was not identified by the risk assessment team. The composition of the risk assessment team did not include representation from people who could provide input on using the application from the PO perspective.
An ARTC Human Factors and Safety Risk Assessment was completed in November 2019 (prior to introduction of eTAP into the ARTC network) by an external organisation (RGB Assurance). The risk assessment included the risk of a PO answering the Assurance Questions incorrectly and this was identified including recognition of Current and Planned Controls to reduce the likelihood of that risk.
The current and planned controls included the correct application of rules and procedures and training in the use of the eTAP application. Despite recognising the risk and having these controls in place, the incident still occurred.
When the eTAP application is used to fulfil the TOA, it replaces with an electronic form, the use of a paper form and a conversation with the NC unless the PO ticks a box on the electronic form that indicates a conversation with the NC is required. The use of the eTAP electronic form replicates the conventional fulfilment process but uses a different media. It is arguable that removing the conversation between the PO and the NC at TOA fulfilment may reduce the safety performance of the rule. The conversation with the NC is an opportunity to confirm the situation during the fulfillment process and possibly address any risks during transition back to full operations.
The flow of information using the eTAP system follows the same path as conventional safeworking communication, but in this case, it has eliminated the explicit need to have a conversation and therefore the confirm and repeat back provision for safety critical messages under the ARTC Network Rule ANGE 204 Network Communication. The rule states:
Confirmation of communication
The receiver must confirm the content of a message by repeating the message back to the sender, if the communication is about:
• a Proceed Authority, or
• an instruction not to proceed, or
• a work on track authority, or
• a work on track method, or
• Train Running Information, or
• special working, or
• a Condition Affecting the Network (CAN).
The receiver must not act on the communication until the sender confirms that the message has been repeated correctly.
The requirement to repeat back in the ARTC Network Rule for network communication regarding work on track authority is not obviated or overridden by the use of an electronic device to transmit and receive safety critical information. However, the adoption of this technology has led to a possible reduction in the performance of safeworking because it limits when a conversation with the NC is required. It relies on the correct completion of an e-form to identify when a conversation with the NC should take place.
The human factors aspects of using an electronic form to replace what was a verbal exchange between the NC and PO during the TOA fulfilment were not addressed in the design and implementation of the new eTap. For example, there is no repeat back or prompting involved in the eTAP application during the TOA fulfilment.
If an error is made during the TOA fulfillment process, it remains contained within the information transmitted electronically to the NC and acted upon without question or validation by the NC. That is what happened in this incident where a train was permitted to run in excess of the desired track speed because the e-form was incorrectly completed and there was no required conversation between the PO and the NC which might have detected the error.
Possible enhancements to the eTAP system such as, an additional prompt to confirm that the track is fit for normal speed prior to the completion of the fulfillment message to the NC, were not examined during the risk assessment process to overcome this issue.
ARTC did consider reverting to verbal communications for TOA fulfilment rather than relying on the eTAP system, but this was rejected by the ARTC risk assessment team as counter to the aims of the eTAP implementation.
Rollout of eTAP to the Wagga Wagga district
The PO involved in the incident identified at interview that the eTAP solution was implemented in their district some time before the incident, but they could not be sure when. Evidence provided by ARTC indicated the briefing associated with the roll out of eTAP took place in February 2020.
At this time the PO was a PO1 and was therefore not trained in the rules and procedures for TOA and unable to implement a TOA. The PO indicated that they may not have absorbed this element of the briefing, as it was not relevant to their level of certification at the time.
The PO stated that the briefing was a Power Point presentation only with no opportunity to try out the test device to become familiar with it and the process. According to the PO, the presentation consisted of 93 slides that were rushed through. They said that there was an exercise about TOA fulfilment at the end of the presentation, however that exercise was not applicable to them at the time, being only a PO1.
There was no record of any competence assessment of these exercises for the PO involved in this incident.
No additional training was offered for someone moving between the PO grades to provide assurance that they were competent in the use of the eTAP system. Noother training took place with the PO prior to them becoming a PO2 and therefore able to use the eTAP system for TOA. Their knowledge was gained on the job not from a structured learning program.
The Robel clamp
The track was being held together by a Robel clamp while awaiting permanent joining via a weld. At interview, the ARTC work supervisor advised that a Robel clamp with a safety lock fitted and used, is safe for trains to travel up to 80km/h.
The 40 km/h temporary speed restriction was requested by the track certifier to protect the edge of the unwelded rail joint from wheel damage by passing trains. This speed reduction is consistent with the ARTC engineering standards for this type of join. Irrespective of the engineering performance of the Robel clamp, the speed restriction required for XPT train ST24 was 40km/h and the train travelled at 100km/h over the join, 60km/h above the required speed.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the overspeed of XPT train ST24 at Harefield on 29 June 2021.
Contributing factors
The Protection Officer answered “no” to the assurance question on eTAP which asked whether there were any Conditions Affecting the Network (CAN). As a result, the Protection Officer fulfilled the Track Occupancy Authority (TOA) without initiating a temporary speed restriction.
The work group task allocation meant the Protection Officer had to leave the worksite, to remove protection while also completing actions to fulfill the Track Occupancy Authority (TOA). It is likely the Protection Officer was distracted while performing these competing tasks.
A further delay in communicating the Condition Affecting the Network (CAN) occurred when the Protection Officer’s call to the Network Controller on the regular phone went unanswered, and a follow up call was required on the emergency phone line to try and stop the train after the Protection Officer realised the error.
The Protection Officer did not attempt to use hand signals to stop the train when it approached the worksite.
The eTAP system, used at Track Occupancy Authority (TOA) fulfilment, did not include a key safeworking requirement contained in the ARTC Network Rule ANGE 204 for confirming and repeating back safety critical information. (Safety issue)
The eTAP roll out did not include an effective training regime, as the briefing was not targeted to the appropriate level of competence of the trainees. The Protection Officer involved was not trained or competent in the rules and procedures for Track Occupancy Authority (TOA) at the time of the eTAP briefing. There was no competence assessment for the use of the application for the Protection Officer involved. (Safety issue)
Glossary
ARTC Australian Rail Track Corporation
CAN Condition Affecting the Network
DIP Directly Interested Party
JHR John Holland Rail
NC Network Controller
PO Protection Officer
RIM Rail Infrastructure Manager
TOA Track Occupancy Authority
XPT Express Passenger Train
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Interview with the ARTC Protection Officer
Interview with the ARTC Civil team leader
Interview with the ARTC Network Controller
Audio recordings from ARTC Junee control centre
eTAP implementation presentation
ARTC Risk assessment report for implementation for eTAP.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Australian Rail Track Corporation
Office of the National Rail Safety Regulator
NSW Trains
Any submissions from those parties will be reviewed and, where considered appropriate, the text of the draft report will be amended accordingly.
Submissions were received from:
Australian Rail Track Corporation
Office of the National Rail Safety Regulator
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] A NSW Government agency constituted by the Transport Administration Act 1988 1A Section 3C.
On the morning of 28 November 2020, a Jetstar Airways Airbus A320, registered VH-VGP (VGP), was conducting an approach to land at Ballina Byron Gateway Airport, New South Wales (NSW). At the same time, a Jabiru J230D, registered 24-7456 (7456), was conducting a private flight from Heck Field, Queensland, to Evans Head, NSW. About 12 NM south-west of Ballina Airport, the flight paths of the two aircraft inadvertently intersected. The crew of VGP received a traffic collision avoidance system (TCAS) traffic advisory alert prior to passing beneath 7456. The vertical separation between the two aircraft reduced to about 600 ft. Both the pilot of 7456 and the flight crew of VGP observed no lateral separation between the two aircraft.
What the ATSB found
The ATSB’s investigation identified that the pilot of 7456 was not aware of the presence of VGP, or that the two aircraft were converging, until having passed above VGP. The flight crew of VGP were also unaware of the presence of 7456 until they were alerted to the impending conflict by the aircraft’s TCAS. The ATSB also found the pilot of 7456 did not set the aircraft’s transponder to broadcast altitude data. Consequently, the TCAS on board VGP was unable to provide the flight crew with the necessary information to positively avoid the potential collision. The flight crew of VGP were unable to sight the aircraft until just before the flight paths intersected. The vertical separation between the two aircraft was influenced by chance alone as the flight crew of VGP and the pilot of 7456 were not aware of the altitude of the opposing aircraft.
The ATSB also found that the most recent regulatory review of the airspace surrounding Ballina Byron Gateway Airport, and subsequent periodic reviews, had not specifically considered the risks associated with aircraft transiting the airspace without taking off or landing at the airport (such as 7456).
What has been done as a result
The Ballina Airport broadcast area was expanded to a radius of 15 NM in January 2021 and an Airservices Australia surveillance flight information service (SFIS) began operating in August 2021. The SFIS provided traffic information to aircraft operating within the broadcast area on the airport’s common traffic advisory frequency.
The Civil Aviation Safety Authority (CASA) has advised that the current Ballina Airport airspace review (due for release in February 2022) utilises data that includes transiting aircraft. Additionally, CASA has developed an airspace risk modelling system (ARMS) that should provide an enhanced capability to consider transiting aircraft. CASA also advised that an initiative by the Australian Government to increase the uptake of automatic dependent surveillance broadcast (ADS-B) equipment in general aviation would result in improved aircraft detection.
While the proposed CASA actions have the potential to address the safety issue, this will largely depend on the conclusions of the current Ballina Airport airspace review and the effectiveness of the new ARMS. As such, the ATSB will monitor and assess their effect on the safety issue.
Safety message
Communication and self-separation in non-controlled airspace is one of the ATSB’s SafetyWatch priorities. Pilots can guard against similar issues to those highlighted by this incident by:
making the recommended broadcasts when in the vicinity of a non-controlled aerodrome
actively monitoring the common traffic advisory frequency while maintaining a visual lookout for other aircraft
ensuring transponders, where fitted, are selected to transmit altitude information.
The occurrence
On the morning of 28 November 2020, a Jetstar Airways Airbus A320-232 aircraft, registered VH‑VGP (VGP) (Figure 1), was conducting a scheduled passenger service from Melbourne Airport, Victoria, to Ballina Byron Gateway Airport (Ballina Airport), New South Wales (NSW). There were two flight crew, five cabin crew and 163 passengers on board. The captain was pilot flying (PF) and the first officer (FO) was pilot monitoring.[1]
Figure 1: VH-VGP
Source: Supplied
At about 1122 Eastern Daylight-saving Time,[2] when VGP was approximately 40 NM to the south‑west of Ballina Airport, the FO made a positional broadcast on the Ballina Airport common traffic advisory frequency (CTAF).[3] This CTAF was also used by two neighbouring airports and several neighbouring aircraft landing areas (ALAs) (see the section titled Common traffic advisory frequency).
On receipt of the broadcast from VGP, the Ballina Airport certified air/ground radio operator (CA/GRO) (see the section titled Certified air/ground radio service) responded. The CA/GRO confirmed that the flight crew were aware of two other passenger services, an Airbus A320 aircraft departing to the south from runway 06 at Ballina Airport, and a Boeing 737 inbound to Ballina Airport from the south.
At about the same time, a Jabiru J230D aircraft, registered 24-7456 (7456) (Figure 2), was conducting a private visual flight rules flight from Heck Field ALA, Queensland, to Evans Head ALA, NSW. There was one pilot and one passenger on board. At 1124:49, the pilot of 7456 made a broadcast on the shared CTAF, addressed to Lismore traffic, advising that the aircraft was 4 NM to the east of Lismore at 5,300 feet and descending. The flight crew of VGP did not respond to (or recall hearing) this broadcast.
Figure 2: 24-7456
Source: Andrei Bezmylov
Meanwhile, VGP continued tracking towards Ballina Airport via the waypoint[4] OPESO, descending to an altitude of about 3,200 feet in preparation for the required navigation performance[5] approach for runway 06. Prior to crossing the OPESO waypoint, the flight crew of VGP received a traffic collision avoidance system (TCAS) proximate traffic alert for an unidentified aircraft at an unspecified altitude in the 11 o’clock[6] position relative to VGP (see the section titled Traffic collision avoidance system). Unbeknown to the flight crew of VGP, the proximate traffic was 7456 tracking in a southerly direction towards Evans Head (Figure 3).
Figure 3: VH-VGP and 24-7456 tracks
Source: Google Earth, annotated by the ATSB
The pilot of 7456 did not recall hearing the earlier CTAF broadcast from VGP and was unaware that the two aircraft were on converging tracks. 7456 was fitted with a transponder that could transmit the aircraft’s altitude (see the section titled Transponder). However, 7456’s transponder was selected ‘ON’ (not ALT) and was not transmitting the altitude of the aircraft.
Without the altitude information, the TCAS on board VGP could only display the relative bearing and distance of 7456.
The flight crew of VGP attempted, unsuccessfully, to visually acquire the proximate traffic (visibility was greater than 10 km and there was no cloud at the time). The crew later reported experiencing ‘tunnel vision’ while conducting the visual search. They did not attempt to contact the traffic on the CTAF.
At 1128:18, VGP’s flight crew received a TCAS traffic advisory. The flight crew maintained their visual scan and continued with the approach to runway 06.
At 1128:38, the flight crew of VGP made a broadcast on the shared CTAF and advised Ballina traffic, and the Boeing 737 aircraft in the vicinity, that VGP had just passed waypoint OPESO. The pilot of 7456 did not respond to, or recall hearing, this broadcast.
The data obtained from VGP’s quick access recorder and the OzRunways program used by the pilot of 7456, indicated that, at 11:28:41 and 12 NM south-west of Ballina Airport, the tracks of VGP and 7456 intersected, with vertical separation between the two aircraft reducing to about 600 ft. The flight crew of VGP sighted 7456 just prior to passing below the aircraft. The pilot of 7456 sighted VGP shortly after passing above the aircraft. Both the pilot of 7456 and the flight crew of VGP observed no lateral separation between the two aircraft (Figure 4).
Figure 4: : Recorded flight paths of VH-VGP and 24-7456
Source: Google Earth, annotated by the ATSB
At 1128:59, the flight crew of VGP contacted the crew of the Boeing 737 inbound to Ballina Airport on the shared CTAF to advise that they had experienced a traffic advisory, and the involved aircraft was headed in the direction of the Boeing 737.
A short time later, VGP landed at Ballina Airport while 7456 continued on to Evans Head ALA.
The captain held an Air Transport Pilot Licence (ATPL) (Aeroplane) and had a total flying time of 13,935 hours, having flown 66.5 hours in the previous 90 days. The captain was familiar with Ballina Airport but had not operated there often. The captain’s last flight to Ballina Airport took place in June 2019.
The FO held an ATPL (Aeroplane) and a total flying time of 4,830 hours, having flown 10.5 hours in the previous 90 days. The FO was somewhat familiar with Ballina Airport having operated there twice before the incident flight. The FO’s last flight to Ballina Airport took place the day prior to the incident.
Pilot 24-7456
The pilot held a recreational pilot certificate and a total flying time of 775 hours, having flown 56 hours in the previous 90 days. The pilot was familiar with Ballina Airport and transited the surrounding airspace about eight times a year. The pilot reported being unfamiliar with the radio phraseology commonly used by passenger transport flight crew, including reference to waypoints such as OPESO.
Ballina Byron Gateway Airport
Ballina Byron Gateway Airport is a certified airport situated approximately 3 NM from the city of Ballina, NSW. The airport has an elevation of 7 feet above mean sea level (AMSL) and a single sealed runway orientated in a 062°-242° magnetic direction (Figure 5). The airport had GPS‑based instrument approaches and a non-directional beacon ground-based navigation aid.
Figure 5: Ballina Byron Gateway Airport
Source: Airservices Australia
Airspace and traffic services
Ballina Airport was located within non‑controlled Class G airspace which extended from the ground surface to 8,500 feet AMSL. The airport did not have a control tower and was not supported by air traffic control (a non-controlled airport).
Overlying the non‑controlled airspace was Class C controlled airspace which extended up to flight level (FL) 180,[7] and controlled Class A airspace above that. An air traffic information and separation service was provided within the Class C airspace and a separation service was provided within the Class A airspace. A restricted area existed approximately 5 NM south of the airport (the aircraft involved in this incident were clear of this area).[8]
The non‑controlled airspace surrounding Ballina Airport was available for use by aircraft operating under visual flight rules and instrument flight rules. No separation service was provided to aircraft operating in this airspace with pilots responsible for making themselves aware of nearby aircraft and maintaining self‑separation.
The primary method of traffic separation at Ballina Airport was visual and relied on pilots using ‘alerted see-and-avoid’[9]practices. A broadcast area was in place requiring aircraft to use a radio on the Ballina Airport CTAF when operating within a 10 NM radius of the airport.
Common traffic advisory frequency
The Ballina Airport CTAF was a designated frequency on which pilots made positional broadcasts when operating in the vicinity of the airport. The Ballina Airport CTAF was shared with neighbouring airports and ALAs Casino, Lismore and Evans Head to assist traffic coordination and enhance the situational awareness of pilots operating within the surrounding airspace (Figure 6).
Figure 6: Shared common traffic advisory frequency
Source: Airservices Australia, annotated by the ATSB
When operating within the Ballina Airport broadcast area, pilots were required to make mandatory transmissions when arriving or departing from the airport, and when flying through the broadcast area.
When operating outside of the Ballina Airport broadcast area, but within the vicinity of the other non‑controlled airports on the shared CTAF, pilots were required to make a broadcast whenever it was reasonably necessary to do so to avoid a collision, or the risk of collision, with another aircraft. There were also several recommended positional broadcasts (Table 1).
Table 1: Recommended positional broadcasts in the vicinity of a non-controlled airport
Recommended calls in all circumstances
Situation
Broadcast
The pilot intends to take-off
Immediately before, or during taxiing
The pilot is inbound to an aerodrome
10 NM from the aerodrome, or earlier, commensurate with aeroplane performance and pilot workload, with an estimated time of arrival for the aerodrome
The pilot intends to fly through the vicinity of, but not land at, a non-controlled aerodrome
10 NM from the aerodrome, or earlier, commensurate with aeroplane performance and pilot workload, with an estimated time of arrival
Recommended calls dependent on traffic
Situation
Broadcast
The pilot intends to enter a runway
Immediately before entering a runway
The pilot is ready to join the circuit
Immediately before joining the circuit
The pilot intends to make a straight-in approach
On final approach at not less than 3 NM from the threshold
The pilot intends to join on base leg
Prior to joining on base
During an instrument approach when:
a. departing final approach fix or established on final approach segment inbound
b. terminating the approach, commencing the missed approach
Including details of position and intentions that are clear to all pilots (both instrument flight rules and visual flight rules)
The aircraft is clear of the active runway(s)
Once established outside the runway strip
Source: Civil Aviation Advisory Publication 166-01 V4.2 (Feb 2019) with minor amendments by the ATSB
Certified air/ground radio service
At the time of the incident, Ballina Airport was one of two airports in Australia to have a certified air/ground radio service (CA/GRS) in operation.
According to CASA’s guidelines for a CA/GRS, the primary purpose of the service was to enhance the safety of passenger operations by providing all pilots with information to enhance their ability to see-and-avoid potentially conflicting traffic.
The information provided to pilots included:
frequency confirmation
traffic information on first call
airport weather
other advice to facilitate aeronautical safety and efficiency
The Ballina Airport CA/GRS commenced operations in March 2017 in response to the increasing number of aircraft movements at the airport. The service was delivered by the airport operator, via a third-party contractor, and had formal CASA approval. The service was delivered by a certified air/ground radio operator located at the airport.
At the time of the incident, the service was provided to all aircraft operating within the Ballina Airport broadcast area of 10 NM, during passenger service operations (greater than 30 seats) between the hours of 0800-1800 local time.
The CA/GRS did not provide a traffic separation service to aircraft as would occur at airports located within Class D or higher airspace (controlled airports).
Regulatory oversight
The Airspace Act 2007 assigned the administration and regulation of Australian administered airspace to the Civil Aviation Safety Authority (CASA). As part of this function, CASA was required to undertake regular reviews to determine if:
existing classifications of ‘volumes of airspace’ were appropriate
existing air navigation services and facilities provided to volumes of airspace were appropriate
there was safe and efficient use of airspace, and equitable access to that airspace for all users
any identifiable risk factors were present
Ballina airport airspace review
At the time of this occurrence, CASA had last completed a review of the airspace surrounding Ballina Airport in July 2015. The purpose of that airspace review was to examine the airspace classification within 20 NM of the airport from ground level to 8,500 feet AMSL.
The objective of the review was to assess the risk levels for passenger transport operations to determine if the airspace classification was appropriate and whether an air traffic service was required. The options considered during the review included upgrading the airspace to Class D or higher classification (a controlled airport).
The Australian Airspace Policy Statement (AAPS) contained airspace review criteria thresholds for volumes of airspace around airports (Table 2). If an airport met or exceeded any of the thresholds for a classification, then CASA was required to undertake a review of the volume of airspace in question. This review was to consider public, industry and agency comments, forecast future traffic levels, and any significant risk mitigators before finalising an airspace determination.
Table 2: Airspace criteria thresholds AAPS 2015
Class B
Class C
Class D
Service provider
ATC
ATC
ATC
Total annual aircraft movements
750,000
400,000
80,000
Total annual PTO aircraft movements
250,000
30,000
15,000
Total annual PTO passengers
25 million
1 million
350,000
Source: Civil Aviation Safety Authority
The 2015 airspace review found that the Ballina Airport exceeded the AAPS passenger criteria threshold for Class D airspace with 437,940 passenger movements recorded in 2014. However, it also found that both passenger transport aircraft movements and total aircraft movements for 2014 were significantly below the Class D trigger criteria. Therefore, CASA decided not to upgrade Ballina to a controlled airport on the basis that:
Considering the total aircraft movements, total passenger transport aircraft movements, stakeholder feedback and aviation safety incident reports CASA considers Class D or higher would currently be a disproportionate response to the identified airspace issues at Ballina.
The ATSB noted that, in reaching that conclusion, the airspace review had not assessed risks associated with aircraft transiting the airspace surrounding Ballina Airport without taking off or landing at the airport (that is, transiting aircraft such as 24-7456 was in this occurrence). While the review included analysis of reportable events near Ballina Airport from 2009 to 2014, it did not specifically consider the involvement of transiting aircraft in those events or the influence such aircraft may have on future separation events to properly assess the risks involved. Of the 11 separation events in the area that the review identified, 6 involved a passenger transport service. However, while CASA advised that all of these occurrences were considered, the review did not identify that 2 of those 6 also involved a conflict with a transiting aircraft.
The review primarily focused on aircraft movements (the total number of take-offs and landings at an airport) specified in the AAPS threshold criteria. Movement data for Ballina Airport was sourced from Airservices Australia (Airservices) and the Bureau of Infrastructure, Transport and Regional Economics.
While Airservices had some data on transiting aircraft, it was not readily available as computational analysis of this data was required to extract information on aircraft operating under the visual flight rules and/or aircraft operating without a flight plan. Notwithstanding these difficulties, data for transiting aircraft was available, but not obtained or analysed in the 2015 review.
In March 2020, CASA commenced another review of the airspace, but following the expansion of the Ballina Airport broadcast area, decided to defer its finalisation. At the time of writing, a final report had not been released.
Periodic assessments
In addition to the 2015 airspace review, CASA conducted periodic risk assessments of Ballina Airport and the surrounding airspace. The information considered for these assessments included:
aircraft and passenger movements
incident reports
IFR to VFR traffic ratios
stakeholder feedback
previous risk assessments.
Records provided by CASA indicated eight documented risk assessments between July 2015 (when the 2015 airspace review was published) and the time of the incident. The last of these assessments was completed in June 2020. The analysis recorded within these assessments primarily focused on aircraft and passenger movements. There was no reference to transiting aircraft, either in terms of occurrences involving such aircraft or overall numbers/movements.
Comments included in this assessment stated that passenger transport aircraft and passenger numbers had declined at the airport, probably due to the impact of COVID-19,[10] but passenger numbers continued to exceed the AAPS 2018 threshold by 19 per cent. The assessment indicated three reported incidents had occurred in the vicinity of the airport but provided no detail about those incidents. The last periodic assessment concluded that the risk level was lower than that of the previous assessment.
Previous events
A search of the ATSB database identified that between 1 January 2010 and 28 November 2020, there were 20 separation events involving passenger transport services (including this incident) within a radius of approximately 20 NM of Ballina Airport below 8,500 feet AMSL (Table 3). Of those 20 events, seven involved a conflict between an aircraft transiting the airspace and a passenger transport service approaching or departing from Ballina Airport (Table 4). Two of these events occurred prior to the publication of the 2015 CASA airspace review.
Table 3: Ballina separation events involving passenger transport services
Year
Total
Not involving transiting aircraft
Involving transiting aircraft
2020
1
0
1
2019
4
3
1
2018
4
2
2
2017
2
2
0
2016
2
2
0
2015
1
0
1
2014
0
0
0
2013
1
0
1
2012
0
0
0
2011
3
2
1
2010
2
2
0
Total
20
13
7
Source: ATSB
Table 4: Separation events involving passenger transport service and transiting aircraft
Year
Aircraft 1
Aircraft 2
Overview
2020
Airbus A320
Jabiru J230D
During approach, the crew of the Airbus A320 received a TCAS TA on the Jabiru J230 on a crossing path.
2019
Airbus A320
Cessna 180
During approach, an Airbus A320 came into close proximity with the Cessna 180. No radio broadcasts were heard from the light aircraft.
2018
Boeing 737 & Airbus A320
Diamond DA40
During approach, a Boeing 737 and Airbus A320 came into close proximity with a Diamond DA40. There were no radio broadcasts identified from the crew of the DA40.
2018
Jetstream Series 3206
Aerospatiale Ind AS350B2
During approach, the crew of a Jetstream Series 3206 observed an Aerospatiale AS.350 helicopter on a reciprocal track. Both aircraft turned to increase separation. The crew of the 3206 did not hear any radio broadcasts from the AS.350.
2015
Airbus A320
Cessna 182
During approach, the crew of an Airbus A320 coordinated separation from a Cessna 182 that was in the vicinity. However, the pilot of the Cessna 182 did not follow their broadcast intentions, resulting in the crew of the Airbus A320 conducting a missed approach.
2013
Airbus A320
Unknown
During take-off, the crew of the Airbus A320 heard a broadcast from an aircraft transiting through Ballina airspace. The crew subsequently observed a TCAS return but were unable to sight the inbound aircraft.
2011
Airbus A320
Piper PA20
While an Airbus A320 was in a holding pattern an instrument flight rules aircraft in the vicinity did not track as expected. The A320 was turned early to ensure that separation was maintained.
Source: ATSB
Aircraft systems
Traffic collision avoidance system
A traffic collision avoidance system (TCAS), as fitted to VGP, interrogates the transponders (see the section titled Transponder) of nearby aircraft and uses this information to calculate the relative range and altitude of this traffic. The system provides a visual representation of this information to the flight crew as well as issuing alerts should a traffic issue be identified. These alerts include:
Proximate traffic – an alert issued when an aircraft is within a range of less than 6 NM and 1,200 ft, or a range of 6 NM if the traffic is not transmitting altitude information. Depicted as a white filled diamond on the navigation display (ND)
Traffic advisory (TA) – an alert issued when the detected traffic may result in a conflict (the closest point of separation is about 40 seconds away on the current projected flight paths). Depicted as an amber filled circle on the ND and an aural alert. Pilots are expected to initiate a visual search for the traffic causing the TA (the operator’s procedures required flight crew not to perform a manoeuvre based solely on a TA).
Resolution advisory (RA) – a manoeuvre, or a manoeuvre restriction, calculated by the TCAS to avoid a collision (the closest point of separation is approximately 25 seconds away or less). Depicted as a red filled square on the ND and vertical speed orders on the primary flight display. A series of aural alerts will also sound. Pilots are expected to respond immediately to an RA.
Due to its method of operation, a TCAS cannot detect aircraft that are not equipped with a transponder (or switched off). Additionally, the system is unable to issue an RA for traffic that is not fitted with an altitude reporting transponder (mode C or S), or in circumstances where the mode C or S transponder on board the conflicting traffic is not transmitting altitude information (as was the case with 7456).
Transponder
A transponder is a receiver/transmitter which transmits an automatic reply upon receiving an interrogation request. A manual ‘ident’ transmission can also be initiated by the pilot. The information transmitted by a transponder is dependent on the ‘mode’ of equipment fitted and the mode of transmission selected by the pilot.
The transponder fitted to 24-7456 was capable of operating in mode 3A and 3C. In mode 3A (ON) the equipment would transmit the configured transponder code only. In mode 3C (ALT) the equipment would transmit the aircraft’s altitude in addition to the configured transponder code.
The pilot of 24-7456 had elected to set the transponder to mode A only so the altitude of the aircraft was not being transmitted. The pilot incorrectly believed there were no requirements relating to the use of modes 3A and 3C.
The Aeronautical Information Publication (AIP) contained information on the operation of aircraft transponders. AIP ENR 1.6 paragraph 7.1.2 stated:
Unless advised otherwise by ATC, pilots of Mode 3A or Mode S transponder equipped aircraft operating in Australian airspace must activate their transponders, and where a Mode C capability is also available it must be activated simultaneously with Mode 3A.
Note: Pilots must ensure that transponders and ADS-B transmitters are activated and the altitude function is selected as:
a. primary radar coverage only exists within 50NM of major airports and the remainder of the ATS surveillance system relies on SSR transponder and ADS-B transmitter information, and b. TCAS relies on transponder information for its pilot alerting and collision avoidance functions.
AIP GEN 1.5 paragraph 7.1.2 stated:
Pilots of transponder-equipped aircraft should ensure their transponder is switched to ON/ALT (Mode C) at all times.
Human factors
The ATSB investigation considered a range of human factors that could have influenced the decisions and actions of the pilots involved. No indicators that increased the risk of any of the individuals experiencing a level of fatigue known to influence performance were found. The following factors, however, were likely to have had an influence.
cognitive tunnelling
human visual system limitations.
Cognitive tunnelling is an inattentional blindness where an individual becomes overly‑focused on some variable other than the present environment (Mack & Rock 1998). Cognitive tunnelling may also impact an individual’s decision-making processes (Bell et al 2005). The comments by VGP’s flight crew about ‘tunnel vision’ after they received the TCAS TA was a reference to this factor.
Limitations associated with the human visual system include:
empty field myopia – in an empty field, such as blue sky, the eye will focus at around 56 cm which may reduce the chance of identifying a distant object
a lack of relative motion when on a collision course – the human visual system is less effective at detecting stationary objects than moving objects. Because of the geometry of collision flightpaths, from each pilot’s point of view, the converging aircraft will grow in size while remaining fixed at a particular point in the windscreen
visual angle – an approaching aircraft at high speed will present a small visual angle until a short time before impact. Limitations associated with visual acuity mean this small visual angle may make it impossible for a pilot to detect the aircraft in time to take evasive action (Hobbs 1991).
All these limitations impair the effectiveness of ‘see-and-avoid’ practices, the primary method of self-separation in uncontrolled airspace, which requires pilots to conduct a visual search to ‘see-and-avoid’ potentially conflicting traffic.
An ‘unalerted’ search is one where reliance is entirely on the pilot searching for, and sighting, another aircraft without prior knowledge of its presence. On the other hand, an ‘alerted’ search is one where the pilot is alerted to another aircraft’s presence, typically via radio communications or aircraft based alerting systems. An alerted search is likely to be eight times more effective than an unalerted search (Hobbs 1991).
On 28 November 2020, the flights paths of Airbus A320, VH-VGP, and Jabiru J230D, 24-7456, intersected about 12 NM south-west of Ballina Byron Gateway Airport, with the vertical separation between them reducing to about 600 ft. The aircraft were outside the airport’s broadcast area and within non‑controlled Class G airspace. That meant that the pilots were responsible for safe separation using radio communications and collision avoidance aids to support ‘see-and-avoid’ practices.
Communications and collision avoidance aids
The flight crew of VGP did not recall hearing the broadcast from 7456 prefixed with ‘Lismore traffic’ on the common traffic advisory frequency (CTAF). That prefix (a different airport to their destination, Ballina) probably did not trigger their auditory attention. In any case, they were not aware of 7456 until alerted to a conflict by the aircraft’s traffic collision avoidance system (TCAS).
Similarly, the pilot of 7456 did not recall hearing broadcasts from VGP on the CTAF. Additionally, the pilot was not familiar with phraseology commonly used in passenger transport operations, including reference to instrument approach waypoints such as OPESO. That probably contributed to the pilot not registering those broadcasts and being unaware of the presence of VGP before the incident.
The pilot of 7456 incorrectly selected mode 3A (instead of the required 3C) on the aircraft’s transponder resulting in altitude data not being transmitted. As the aircraft approached VGP, its TCAS issued the conflict alert and, subsequently, a traffic advisory alert with the relative bearing and distance of 7456. However, the TCAS could not indicate the approaching aircraft’s altitude or provide a resolution advisory, significantly disadvantaging the flight crew in managing the situation.
See-and-avoid
The circumstances and the restrictions imposed on the available electronic aids, particularly TCAS functionality, were impediments to effectively applying see-and-avoid practices.
Since the pilot of 7456 was not aware of VGP, seeing and avoiding it depended on the success of ‘unalerted’ visual searches by the pilot. Although visibility was greater than 10 km with no cloud in the area, any searches were unsuccessful as the pilot only sighted VGP after passing above it.
On the other hand, VGP’s TCAS alerted the flight crew to 7456. However, their ‘alerted’ search was unsuccessful in part due to the limitations associated with the human visual system and the absence of altitude data. Additionally, the effects of cognitive tunnelling, together with the rapid sequence of events following the TCAS alerts, possibly resulted in them not considering options such as contacting the approaching aircraft via radio on the CTAF. With no TCAS resolution advisory manoeuvre available, they continued visually searching, sighting 7456 moments before it passed and too late to take any action to avoid a potential collision.
Therefore, the vertical separation of about 600 ft when the aircraft passed was entirely fortuitous.
This incident, together with previous events involving transiting aircraft shows that separation occurrences, with potentially serious consequences, can and do occur (Table 4) in the airspace encompassing the approach and departure flight paths of large transport aircraft operating at Ballina Airport.
Airspace classification
The objective of the 2015 Civil Aviation Safety Authority (CASA) review of the airspace surrounding Ballina Byron Gateway Airport was to assess the level of risk posed to passenger transport services and determine if the airspace classification was appropriate. The review considered total aircraft movements (including passenger transport aircraft) at the airport, some reportable events near the airport and stakeholder feedback and determined that a Class D or higher airspace classification was not appropriate. Significantly, transiting aircraft movements were not considered, primarily due to difficulty in extracting this data.
However, the review had not specifically considered the risks associated with aircraft transiting the airspace without taking off or landing at Ballina Airport. Recognising that such a consideration at the time of the review would have only identified 2 occurrences associated with transiting aircraft, additional occurrences in the intervening years indicate that the risk of a proximity event in these circumstances may be significant. However, opportunities to consider such risk events in the periodic risk assessments of the airspace since the 2015 review had not been taken.
Capturing these tangible risks through the airspace review and periodic assessment mechanisms would result in a more accurate and realistic risk assessment. Such a risk assessment would, in turn, better inform an assessment of the appropriate airspace classification.
When operating in non-controlled airspace (such as the current Class G airspace around Ballina), whether under the instrument or visual flight rules, pilots hold responsibility for separation from other aircraft. A review of past occurrences indicates that self-separation using broadcast traffic advice has been a largely reliable procedure.
The ATSB does however note that the effectiveness of the current pilot-separation method relies on individual pilots:
recognising a potentially unsafe situation
formulating an effective separation plan that often requires coordination with the occupants of the other involved aircraft.
While on this occasion one of the involved aircraft was equipped with TCAS, this process is almost exclusively reliant on individual human actions without other mechanisms potentially acting as a safeguard and/or safety redundancy, and as such subject to human error, even when it involves experienced pilots. Furthermore, such errors often increase under high workload associated with, for example, instrument flying approach procedures, low experience or a busy airspace environment.
Of note, the airspace surrounding Ballina Airport accommodates a complex mix of aircraft types and operations, including high-capacity passenger transport, while also being located close to several other non‑controlled airports.
In that context, while the available evidence in this investigation does not support a conclusion that the present self‑separation system is unsafe, there is an opportunity to potentially reduce safety risk further.
The ATSB therefore supports systemic enhancements to the overall air traffic system that have been assessed by regulatory and air traffic specialists, in keeping with their obligations as providing a net overall safety increase. Key examples of such enhancements include:
the increased use of controlled airspace and ADS‑B aircraft surveillance data (both by air traffic services and in‑cockpit)
improved monitoring of air traffic movements (both quantity and complexity) to assist the identification of increasing risk areas.
With respect to this occurrence, had the aircraft been operating in controlled airspace the crew of VGP would have, at a minimum, received traffic information from air traffic control on 7456 and may have been positively separated.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the separation occurrence involving Airbus A320-232, VH-VGP and Jabiru J230D, 24-7456 about 12 NM south‑west Ballina Byron Gateway Airport, New South Wales on 28 November 2020.
Contributing factors
The mode of the transponder on board 24-7456 was not selected to transmit altitude data, which resulted in VH-VGP’s traffic collision avoidance system (TCAS) not indicating the approaching aircraft’s altitude or providing a resolution advisory.
The pilot of 24-7456 did not recall hearing broadcasts from VH-VGP and remained unaware of the other aircraft until passing above it.
The flight crew of VH-VGP did not recall hearing the broadcast from 24-7456 when it was near Lismore and remained unaware of the aircraft until receiving a TCAS alert. However, they did not know the approaching aircraft’s altitude, did not attempt to make radio contact and only sighted it moments before the aircraft passed.
The vertical separation between the aircraft when their flight paths inadvertently intersected reduced to about 600 ft, which was entirely fortuitous as the pilots of neither aircraft had been able to manage aircraft separation in the circumstances.
Other factors that increased risk
The Civil Aviation Safety Authority review and periodic risk assessments of the airspace surrounding Ballina Byron Gateway Airport did not include data for aircraft transiting the airspace without using the airport. Therefore, the risk associated with occurrences such as this one were not specifically considered when assessing the appropriate airspace classification. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The Civil Aviation Safety Authority review of the airspace surrounding Ballina Byron Gateway Airport did not include data for aircraft transiting the airspace without using the airport. Therefore, the risk associated with occurrences such as this one were not specifically considered when assessing the appropriate airspace classification.
Glossary
AIP Aviation information publication
ALA Aircraft landing area
AMSL Above mean sea level
ATC Air traffic control
ATSB Australian Transport Safety Bureau
CA/GRS Certified air/ground radio service
CASA Civil Aviation Safety Authority
CTAF Common traffic advisory frequency
EDT Eastern daylight-saving time
FDR Flight data recorder
FL Flight level
FO First officer
NM Nautical mile
NSW New South Wales
PF Pilot flying
PM Pilot monitoring
RA Resolution advisory
SFIS Surveillance flight information service
TA Traffic advisory
TCAS Traffic collision avoidance system
UTC Coordinated universal time
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew of VH-VGP and pilot of 24‑7456
the CA/GRO and CA/GRS service provider
Jetstar Airways
Ballina Byron Gateway Airport
Avdata
Bureau of Infrastructure and Transport Research Economics
Civil Aviation Safety Authority
Airservices Australia
References
Bell, M, Facci, E, & Nayeem, R 2005, Cognitive Tunnelling, Aircraft-Pilot Coupling Design Issues and Scenario Interpretation Under Stress in Recent Airline Accidents, 2005 International Symposium on Aviation Psychology, 45-49
Hobbs A 1991, Limitations of the See-and-Avoid Principle, Australian Transport Safety Bureau
Mack A & Rock I 1998, Inattentional blindness, MIT Press Cambridge MA
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to:
the crew of VH-VGP and pilot of 24-7456
Jetstar Airways
Ballina Byron Gateway Airport
Civil Aviation Safety Authority
Airservices Australia.
Submissions were received from:
the crew of VH-VGP
Civil Aviation Safety Authority
Airservices Australia
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Preliminary report
Report release date: 01/03/2021
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 28 November 2020, a Jetstar Airways Airbus A320-232 aircraft, registered VH-VGP (VGP), was conducting a regular public transport (RPT) flight from Melbourne Airport, Victoria, to Ballina Byron Gateway Airport (Ballina Airport), New South Wales (NSW). At about 1122 Eastern Daylight-saving Time,[1] when VGP was approximately 40 NM to the south-west of Ballina Airport, the flight crew made a broadcast on the common traffic advisory frequency (CTAF).[2] This CTAF is shared with two neighbouring airports and several neighbouring aircraft landing areas (ALAs) including Evans Head (Figure 1).
Figure 1: CTAF Airports
Source: Airservices Australia, annotated by the ATSB
On receipt of VGP’s broadcast, the Ballina Airport certified air/ground radio operator (CA/GRO) (see Certified air/ground radio service section) contacted the flight crew of VGP. The CA/GRO confirmed that the flight crew were aware of an RPT A320 aircraft departing to the south from runway 06 at Ballina Airport, and an RPT Boeing 737 inbound to Ballina Airport from the south.
At about the same time, a Jabiru J230D aircraft, registered 24-7456 (7456), was conducting a private visual flight rules flight from Heck Field ALA, Queensland, to Evans Head ALA, NSW. At 1124:49, the pilot of 7456 made a broadcast on the CTAF, addressed to Lismore traffic, advising that the aircraft was 4 NM to the east of Lismore at 5,300 feet and descending. The flight crew of VGP did not respond to, or recall hearing, this broadcast.
Meanwhile, VGP continued its track towards Ballina Airport via the waypoint[3] ‘OPESO’, descending to an altitude of about 3,200 feet in preparation for the required navigation performance[4] approach for runway 06. Prior to crossing the OPESO waypoint, the flight crew of VGP received a traffic collision avoidance system (TCAS) proximate traffic alert for an unidentified aircraft at an unspecified altitude in the 11 o’clock[5] position relative to VGP (see Traffic collision avoidance system section). Unbeknown to the flight crew of VGP, the proximate traffic was probably 7456 tracking in a southerly direction towards Evans Head (Figure 2).
Figure 2: VH-VGP and 24-7456 tracks
Source: Google Earth, annotated by the ATSB
The pilot of 7456 had not heard the earlier CTAF broadcast from VGP and was unaware that the two aircraft were on converging tracks. 7456 was fitted with a transponder that could transmit the aircraft’s altitude. However, 7456’s transponder was selected ‘ON’ (not ALT) and was not transmitting the altitude of the aircraft (without the altitude information, the TCAS on board VGP could only display the relative horizontal position of 7456).
At that time, there was no cloud and visibility was greater than 10 km. The flight crew of VGP attempted, unsuccessfully, to visually acquire the proximate traffic, but did not attempt to contact the traffic on the CTAF.
At 1128:17, VGP’s flight crew received a TCAS traffic advisory. The flight crew maintained their visual scan and continued with the approach to runway 06.
At 1128:38, the flight crew of VGP made a broadcast on the shared CTAF and advised Ballina traffic, and the Boeing 737 aircraft in the vicinity, that VGP had just passed waypoint OPESO. The pilot of 7456 did not respond to, or recall hearing, this broadcast.
The data obtained from VGP’s quick access recorder and the OzRunways program used by the pilot of 7456, indicates that, at approximately 12 NM south west of Ballina Airport, the tracks of VGP and 7456 intersected, with vertical separation between the two aircraft reducing to about 600 feet. The flight crew of VGP sighted 7456 just prior to passing below the aircraft. The pilot of 7456 sighted VGP shortly after passing above the aircraft. Both the pilot of 7456 and the flight crew of VGP observed no lateral separation between the two aircraft (Figure 3).
Figure 3: Recorded flight paths of VH-VGP and 24-7456
Source: Google Earth, annotated by the ATSB
At 1128:59, the flight crew of VGP contacted the crew of the Boeing 737 inbound to Ballina Airport on the shared CTAF to advise that they had experienced a traffic advisory, and the involved aircraft was now headed in the direction of the Boeing 737.
A short time later, VGP landed at Ballina Airport while 7456 continued on to Evans Head ALA.
Context
Airspace
Ballina Airport is located within uncontrolled Class G airspace. Overlying this airspace is Class C controlled airspace with a base of 8,500 feet above mean sea level.
The airspace surrounding Ballina Airport is available for use by aircraft operating under visual flight rules and instrument flight rules with significant recreational and sport aviation activity in the area. Ballina Airport is also serviced by several low and high capacity regular public transport operators.
Common traffic advisory frequency
The Ballina Airport CTAF is a designated frequency on which pilots make positional broadcasts when operating in the vicinity of the airport. The Ballina Airport CTAF is shared with neighbouring airports and ALAs in order to aid with traffic coordination and enhance the situational awareness of pilots operating within the surrounding airspace.
Pilots are required to make a CTAF broadcast whenever it is reasonably necessary to do so to avoid a collision, or the risk of collision, with another aircraft. Recommended positional broadcasts are listed in the table below (Figure 4)
Figure 4: CTAF recommended positional broadcasts
Source: Civil Aviation Safety Authority, modified by the ATSB
Certified air/ground radio service
Ballina Airport is one of only two airports in Australia to have a certified air/ground radio service (CA/GRS) in operation. A CA/GRS is a radio information service that is operated at a non-controlled airport and is provided by the airport operator.
The Ballina Airport CA/GRS commenced operations in March 2017 in response to the increasing number of aircraft movements at the airport. The purpose of the service is to provide pilots with operational information relevant to the airport to aid with decision making. The information provided includes:
frequency confirmation
traffic information on first call
airport weather
other advice to facilitate aeronautical safety and efficiency.
At the time of the incident, the service was provided to all aircraft operating within a designated broadcast area of 10 NM, during RPT operations (greater than 30 seats) between the hours of 0800-1800 local time.
Traffic collision avoidance system
A traffic collision avoidance system, as fitted to VGP, interrogates the transponders[6] of nearby aircraft and uses this information to calculate the relative range and altitude of this traffic. The system provides a visual representation of this information to the flight crew as well as issuing alerts should a traffic issue be identified. These alerts include:
Proximate traffic – an alert issued when an aircraft is within a range of less than 6 NM and 1200 feet, or a range of 6 NM if the traffic is not transmitting altitude information.
Traffic advisory (TA) – an alert issued when the detected traffic may result in a conflict. Pilots are expected to initiate a visual search for the traffic causing the TA.
Resolution advisory (RA) – a manoeuvre, or a manoeuvre restriction, calculated by the TCAS to avoid a collision. Pilots are expected to respond immediately to an RA unless doing so would jeopardise the safe operation of the flight.
A TCAS cannot detect aircraft that are not equipped with a transponder. Additionally, the system is unable to issue a RA for traffic that is not fitted with an altitude reporting transponder (mode C or S), or in circumstances where the mode C or S transponder on board the conflicting traffic is not transmitting altitude information—as was the case with 7456.
Further investigation
The investigation is continuing and will include the examination of:
airspace density levels
airspace suitability
flight crew actions
CA/GRS procedural design and application
future Ballina airspace plans
TCAS and recorded flight data
CTAF recordings.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the morning of 4 November 2019, an Airbus A320-200 aircraft, registered VH-VQG (VQG), was operating a scheduled passenger flight from Sydney, New South Wales, to Sunshine Coast, Queensland (Qld). As the aircraft was on final approach to land, a proximity event occurred with an Aero Commander 500 aircraft, registered VH-UJS (UJS), which was departing Sunshine Coast Airport on the reciprocal runway. The two aircraft paths converged, until the pilot of UJS conducted a right turn and increased the separation between them. The flight crew of VQG continued the approach and UJS continued to Maryborough, Qld, without further incident. The time of the incident was outside the operating hours of Sunshine Coast Airport air traffic control tower and it was therefore operating as a non-controlled aerodrome.
What the ATSB found
The ATSB found that important radio broadcasts made on the common traffic advisory frequency (CTAF) were not heard by the flight crew of VQG and the pilot of UJS regarding each other’s position and intention. These included the inbound broadcasts made by VQG and the take-off broadcast made by UJS. In addition, the flight crew of VQG determined the most suitable runway based on the radio-transmitted aerodrome weather information service. However, this was either recorded incorrectly or heard incorrectly such that the chosen runway was the less favourable of the two options for the wind direction. This resulted in the aircraft approaching the opposite runway to other aircraft at the time. Finally, the pilot of the departing aircraft did not confirm the location and intention of the inbound aircraft prior to commencing take-off, as it was assumed the inbound aircraft would use the most suitable runway for the conditions.
Safety message
When operating in uncontrolled airspace and around non-towered aerodromes, it is important to ensure that the location and intention of surrounding traffic is well understood and communicated prior to commencing take-off or landing.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is safety around non-controlled aerodromes. The ATSB SafetyWatch page provides information and resources about staying safe around non-controlled aerodromes. In addition, the ATSB booklet A pilot’s guide to staying safe in the vicinity of non-controlled aerodromes outlines many of the common problems that occur at non-controlled aerodromes, and offers useful strategies to keep yourself and other pilots safe.
The Civil Aviation Safety Authority has also produced a resource booklet ‘be heard, be seen, be safe’ which is in relation to radio procedures in uncontrolled airspace, and highlights that radios must always be used in conjunction with a safe ‘see-and-avoid’ procedure.
The occurrence
What happened
On the morning of 4 November 2019, the flight crew of an Airbus A320-200 aircraft, registered VH-VQG (VQG) and operated by Jetstar Airways, were conducting a scheduled passenger flight from Sydney, New South Wales, to Sunshine Coast, Queensland (Qld).
Prior to commencing the descent, both flight crewmembers of VQG independently listened to the Aerodrome Weather Information Service (AWIS) for Sunshine Coast Airport. Both reported hearing that the wind was from 230° (Magnetic) at 6 or 7 kt and recorded it on the take-off and landing data card. Based on those wind conditions, they assessed that runway 18 would be the most suitable runway for landing as it was the most into wind. The flight crew noted that the wind direction from the AWIS differed from the aerodrome forecast and routine aerodrome weather report[1] they had obtained prior to the flight, which was 340° True (329° Magnetic), but assessed that was reasonable for a coastal aerodrome. The flight crew then calculated the landing data using their electronic flight bag[2] software. In accordance with normal procedures, they assessed that for the aircraft landing weight and runway length available they could safely land with a tailwind of up to 10 kt if necessary.
At 0622 Eastern Standard Time (EST),[3] the flight crew of VQG contacted Brisbane Centre air traffic control (ATC) to advise that they were on descent to flight level 130[4] and on approach to Sunshine Coast Airport. As this was outside Sunshine Coast ATC Tower operating hours, the airspace was Class G (uncontrolled) and pilots of aircraft in the vicinity of the airport were communicating on the common traffic advisory frequency (CTAF).[5] Pilots conducting flights under the instrument flight rules (IFR) were also required to report to Brisbane Centre on a different frequency. Brisbane Centre provided a traffic information service to IFR flights about other conflicting IFR aircraft and observed (known) visual flight rules flights. Therefore, the VQG flight crew had one radio on the CTAF and another on the Brisbane Centre frequency, which allowed them to hear both frequencies.
At about 0625, the first officer (FO) who was the pilot monitoring (PM),[6] broadcast on the CTAF stating they were 30 NM south of the field, at an altitude of 10,500 ft and were tracking for a left circuit for runway 18[7] with an estimated arrival time of 0636 at Sunshine Coast. About 2 minutes later the PM made a similar broadcast on the CTAF, with updated altitude and position, again stating their intention to land on runway 18. During that time, the flight crew of VQG were also communicating with the pilot of another aircraft operating to the south of Sunshine Coast Airport who agreed to hold to the south of the field until VQG had landed.
A few minutes later, at about 0631, the PM made a third broadcast on the CTAF stating their altitude, position and intention to land on runway 18.
About 25 seconds later, the pilot of an Aero Commander 500 aircraft, registered VH-UJS (UJS) and operated by General Aviation Maintenance as a freight charter flight, broadcast on the CTAF that he was taxiing for runway 36 at Sunshine Coast Airport. The planned flight was from Sunshine Coast to Maryborough, Qld. Shortly after, the pilot of UJS also contacted Brisbane Centre stating that UJS was taxiing for runway 36. Brisbane Centre responded, advising of the inbound aircraft (VQG) that was turning onto final for approach from the north-east, ‘landing about 36’.[8] Brisbane Centre did not stipulate the runway being used by VQG, nor were they required to. The pilot of UJS later reported that he had observed other aircraft using runway 36 while he was refuelling at Sunshine Coast Airport, and that it usually takes him around 3 minutes on average from start up with his radios on, to being airborne.
At about the same time, the PM of VQG was communicating on the CTAF with the pilot of an aircraft (VH-XTU) to the north of the airport, which was identified by the flight crew of VQG as a potential conflict as per the operator’s ’Ten, Ten, One’ rule.[9] Also at that time, Brisbane Centre was attempting to contact VQG flight crew, regarding the taxiing call made by UJS, however contact was delayed as VQG was communicating on the CTAF with VH-XTU.
On entering the runway, the pilot of UJS visually checked to the south where he believed VQG was approaching from. After not visually sighting VQG, the pilot of UJS commenced take-off without making direct contact with VQG on the CTAF and confirming their location, making a ‘rolling’ (for take-off) broadcast on the CTAF at 06:33:30.
As this broadcast was being made, Brisbane Centre was still attempting to contact VQG, and the flight crew of VQG later reported not hearing the take-off broadcast made by UJS. After the communication with Brisbane Centre was established and finished, a different aircraft broadcast on the CTAF for about 20 seconds.
Once that broadcast finished, the PM of VQG broadcast on the CTAF that they were on final approach[10] for runway 18 and asked the pilot of UJS if he was holding short of the runway. The pilot of UJS responded that they were airborne, had VQG sighted and would track to VQG’s left (make a right turn). Table 1 shows a summary of the relevant radio broadcasts made on the CTAF and Brisbane Centre frequencies.
Table 1: Summary of the relevant CTAF and Brisbane Centre (shaded) radio broadcasts made by the pilots of aircraft VH-VQG and VH-UJS
Time
Frequency
Summary
0625:36
CTAF
VH-VQG first inbound broadcast
0627:11
CTAF
VH-VQG second inbound broadcast
0631:28
CTAF
VH-VQG third inbound broadcast
0631:53
CTAF
VH-UJS makes taxiing broadcast at Sunshine Coast airport
0632:24
Brisbane Centre
VH-UJS makes taxiing call, Centre informs them of inbound VH-VQG ‘turning onto final for approach’ ’about 8 miles north-east’ ’landing about 36’
0632:45 – 0633:18
CTAF
VH-VQG coordinating with VH-XTU, who was on the runway 18 Zulu approach. VH-XTU advised that they would be breaking off at the final approach fix for a circuit.
0632:58
Brisbane Centre
Centre informs VH-VQG of VH-UJS taxiing
0633:30
CTAF
VH-UJS makes ‘rolling’ broadcast from runway 36
0633:30
Brisbane Centre
Centre attempts to contact VH-VQG
0633:38
Brisbane Centre
Centre attempts to contact VH-VQG
0633:40
Brisbane Centre
VH-VQG responds they are communicating with VH-XTU on CTAF, Centre confirms they are also aware of VH-UJS, and VH-VQG responds ‘affirm’
0634:06
CTAF
Another aircraft is broadcasting their position and intention
0634:35
CTAF
VH-VQG broadcasts they are turning 5 mile final runway 18 and queries if VH-UJS is holding short of the runway
0634:48
CTAF
VH-UJS responds ‘negative, airborne’ and that he had VH-VQG sighted and would track to their (VH-VQG’s) left
Source: Airservices Australia and AvData, summarised by the ATSB
Within seconds, a short-term conflict alert (STCA) for the two aircraft was presented on the Brisbane Centre display (Figure 1). The two aircraft passed each other with a recorded separation of 0.7 NM horizontally and 265 ft vertically.
Figure 1: The position of the aircraft in the area in relation to Sunshine Coast Airport, and the alerts that were displayed to Brisbane Centre for the two aircraft VH-UJS and VH-VQG. The aircraft to the north, VH-XTU, is also shown.
Source: Airservices Australia, annotated by the ATSB
The flight crew of VQG discussed conducting a missed approach as a result of the proximity event. However, they assessed it was safer to continue with the approach due to the other aircraft in the area that they had already de-conflicted with, and although there was a tailwind, it was assessed as within tolerance. At about 0637, VQG landed at Sunshine Coast Airport and UJS continued to Maryborough without further incident.
In this occurrence, VQG was fitted with a functional traffic collision avoidance system (TCAS).[11] However, it was inhibited (as a standard) such that when the aircraft was on descent and below 900 ft the system did not generate a resolution advisory (RA)[12] or an aural alert and all traffic, including UJS, was marked as a traffic advisory only.
Safety analysis
The pilots from both aircraft did not hear some of the important radio broadcasts made by the other aircraft regarding their location and intention and did not establish direct communications with each other until after UJS was airborne. The pilot of UJS likely did not have his radio on at the time the flight crew of VQG made their inbound radio broadcasts, therefore missing the opportunity to understand that they were intending on landing on runway 18. There was about 97 seconds between the taxi and take-off broadcasts made by UJS, reducing the amount of time available to determine the location and intention of VQG. The flight crew of VQG did not hear the rolling broadcast made by the pilot of UJS, which occurred at the same time as Brisbane Centre was contacting VQG on the Centre frequency.
It was noted that the flight crew of VQG recorded the aerodrome wind direction as 230° (Magnetic) when planning their approach. However, local aerodrome wind direction was reported as 329° (Magnetic). It is unknown if the flight crew of VQG misheard the airport weather information recording or if the recording was incorrect, as a copy of the recording was unable to be obtained. The incorrect wind information obtained or understood by the flight crew of VQG led them to plan their approach on the least favourable runway for the wind direction at the time, and in conflict with other aircraft operating in and out of the airport.
The pilot of UJS believed that VQG would be landing on runway 36, as it was the most suitable for the wind conditions at the time and other aircraft operating at the airport had been using runway 36. This resulted in the pilot of UJS relying on unalerted see and avoid, to de-conflict with the inbound VQG. This occurred after UJS became airborne and the reciprocal trajectory of VQG was observed.
Findings
From the evidence available, the following findings are made with respect to the separation issue between two aircraft, VH-UJS and VH-VQG, where VH-UJS took off from runway 36 while VH-VQG was landing on opposing runway 18, resulting in reciprocal paths for the two aircraft before the pilot of VH-UJS conducted a right turn to increase separation from VH-VQG.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Important radio broadcasts on the CTAF were not heard by the flight crew of VH-VQG and the pilot of VH-UJS regarding each other’s positions and intentions, leading to them continuing to use reciprocal runways.
The flight crew of VH-VQG assessed runway 18 as the most into wind runway based on information obtained from the aerodrome weather information service, however this information was either recorded incorrectly or heard incorrectly such that runway 36 was instead more favourable. This resulted in the aircraft approaching the opposite runway to what was being used by other aircraft at the time.
The pilot of VH-UJS commenced take-off without confirming the location and intention of VH-VQG, assuming that they would be landing on runway 36, which had been used by previous landing and departing aircraft.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.