On 26 November 2016, at about 0908 Eastern Standard Time (EST), a Bombardier DHC-8-402 aircraft, registered VH-QOV (QOV), operating scheduled passenger flight QF2320 from Brisbane, commenced descent to Bundaberg Airport, Queensland (Qld). At about the same time, a Eurocopter MBB-BK 117 helicopter, registered VH-EHQ (EHQ) was being prepared to depart Bundaberg. The crew of EHQ had been tasked to conduct a visual flight rules (VFR) flight to search for potential wreckage from a trawler missing off the Qld coast.
Bundaberg is a non-controlled airport with a common traffic advisory frequency (CTAF). A CTAF is a designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled aerodrome. Bundaberg is also equipped with an aerodrome frequency response unit (AFRU) with a pilot activated light (PAL) option. When a pilot transmits on the correct frequency, the AFRU will provide an automatic response, either ‘Bundaberg CTAF’ (if the frequency has not been used in the previous five minutes) or a beep-back. At night, or at other times of low natural light levels, transmitting three one second pulses, one second apart, on the frequency will activate the runway lighting and the transmission will change to the aerodrome name and CTAF with either ‘runway lights on’ or ‘no runway lights’. At other times, this action will activate the precision approach path indicator (PAPI).
At 0912, three one second pulses were broadcast on the Bundaberg CTAF. This resulted in the AFRU correctly responding automatically, ‘Bundaberg Aerodrome no runway lighting’. Two seconds later a single one second pulse was also broadcast on the CTAF. The next recorded CTAF broadcasts were those made by the flight crew of QOV while on approach to Bundaberg. Broadcasts were made at 27 NM, 10 NM and 5 NM and on each occasion the flight crew received the AFRU beep-back. No responses from other aircraft were heard.
While QOV was on final approach to Bundaberg, EHQ taxied for departure from a position to the east of runway 32. The helicopter taxied a short distance, took off and once airborne commenced a left turn tracking initially towards Hervey Bay.
During EHQ’s departure, the flight crew of QOV received a traffic advisory (TA)[1] from their aircraft’s traffic alert and collision avoidance system (TCAS).[2] On receipt of the TA, the flight crew of QOV attempted to sight the traffic causing the alert. After a few seconds, they identified a helicopter, later determined to be EHQ, in their 2 o’clock[3] position around 1.5 NM, and around 1,000 ft below their aircraft. The helicopter was clear of their projected flight path and accordingly the flight crew continued the approach, landing without further incident.
After landing, the flight crew of QOV made two broadcasts on the CTAF to identify the helicopter. These were unsuccessful and they requested, on area frequency, if air traffic control knew the identity of the helicopter. The pilot of EHQ heard this exchange and subsequently identified themselves also advising they had not heard the earlier broadcasts made by the flight crew of QOV.
Pilot comment VH-EHQ
The pilot of EHQ provided the following comments:
The flight was routine, preparations for the flight were not rushed with normal pre-departure checks conducted. They recalled completing normal communication checks including ensuring all frequencies were set correctly and at appropriate volumes. They also recalled hearing an aircraft broadcast on the air traffic control area frequency, and a response from the AFRU when the PAPI was activated. They did not hear any other broadcasts made by the flight crew of QOV.
Normally, when departing from a location similar to the one they did on the day of the incident, the pilot advised they would make a taxi call and a call departing on the CTAF. They recalled making these calls but could not recall if an AFRU response was received.
During the left turn after departure, the crew of EHQ sighted QOV on final approach, clear of their projected flight path.
After departure, they heard the flight crew of QOV on area frequency attempting to determine the identity of the helicopter. They identified themselves and subsequently checked their communications set up, with nothing abnormal found.
Captain’s comment VH-QOV
The Captain of QOV provided the following comments:
They had made all of the necessary CTAF broadcasts, receiving the AFRU response, and did not receive any broadcasts made by EHQ.
They were surprised upon receipt of the TA, but had quickly visually identified the traffic and confirmed it was not on a conflicting flight path.
Safety Analysis
The ATSB reviewed all available recordings from air traffic control and the Bundaberg CTAF. All broadcasts made by the flight crew of QOV and the AFRU responses were recorded. There were no identifiable recordings of broadcasts made by the pilot of EHQ. The ATSB was not able to determine why the broadcasts reportedly made by the pilot of EHQ were not transmitted on the CTAF or why the crew were not able to hear the broadcasts made by the flight crew of QOV. It is probable that the pilot did not correctly configure and operate the helicopter’s communications system.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
It is probable the pilot of EHQ did not correctly configure and operate the helicopter’s communications system for CTAF operations while departing Bundaberg airport and they did not detect the error.
Safety action
As a result of this occurrence, the pilot of EHQ has advised they now transmit on the CTAF and activate the lighting to confirm they have the correct radio frequency and volumes selected.
Safety message
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry.
One such concern is Safety around non-controlled aerodromes, which highlights that it is difficult for pilots to detect another aircraft through visual observation alone. The ATSB has identified that insufficient communication between pilots operating in the same area is the most common cause of safety incidents near non-controlled aerodromes.
This incident highlights the fundamental importance of effective communication, particularly during operations at a non-controlled aerodrome. The Civil Aviation Safety Authority (CASA) has produced several publications and resources that provide important safety advice related to operations in the vicinity of non-controlled aerodromes. Relevant guidance and explanatory material provided by CASA includes the following:
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 25 August 2016, a Robinson R44 helicopter, registered VH-EYD (EYD), departed from Bankstown Airport on a training flight to Camden Airport, New South Wales. On board were a student pilot and a flight instructor. After completing exercises in the Camden area, the helicopter returned towards Bankstown.
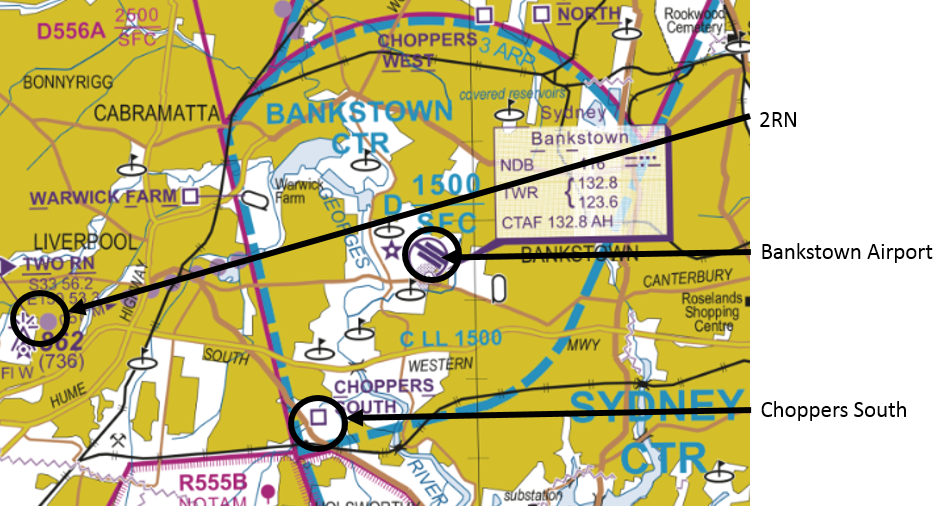
According to air traffic control (ATC) audio data, at about 1607 Eastern Standard Time (EST), the instructor of EYD contacted the Bankstown aerodrome controller (ADC), advising that they were at inbound reporting point 2RN at 1,000 ft (Figure 1). The ADC instructed EYD to track via, and report at, ‘Choppers South’ reporting point at 500 ft. EYD then tracked via Choppers South at 500 ft, but the instructor omitted to advise ADC when they were overhead that point.
Figure 1: Extract of Sydney Visual Terminal Chart
Source: Airservices Australia – annotated by ATSB
At about 1610, the solo student pilot of a Cessna 152 aircraft, registered VH-MRC (MRC), who was conducting circuit training at Bankstown Airport, contacted the ADC and stated that MRC was on the downwind circuit leg, and requested clearance to depart the control zone on the upwind circuit leg. The ADC instructed the pilot of MRC to ‘go around from base, maintain 1,000 ft and depart on upwind’.
The pilot of MRC asked the ADC to repeat the instruction and then read back ‘MRC going around from base and depart at 1,000 ft’. The pilot of MRC then continued their approach, descending on the base leg and final approach to about 300 ft above the runway before commencing a go-around. At about 1613, passing about 500 ft on climb, the pilot of MRC advised the ADC that they were going around and departing at 1,000 ft upwind.
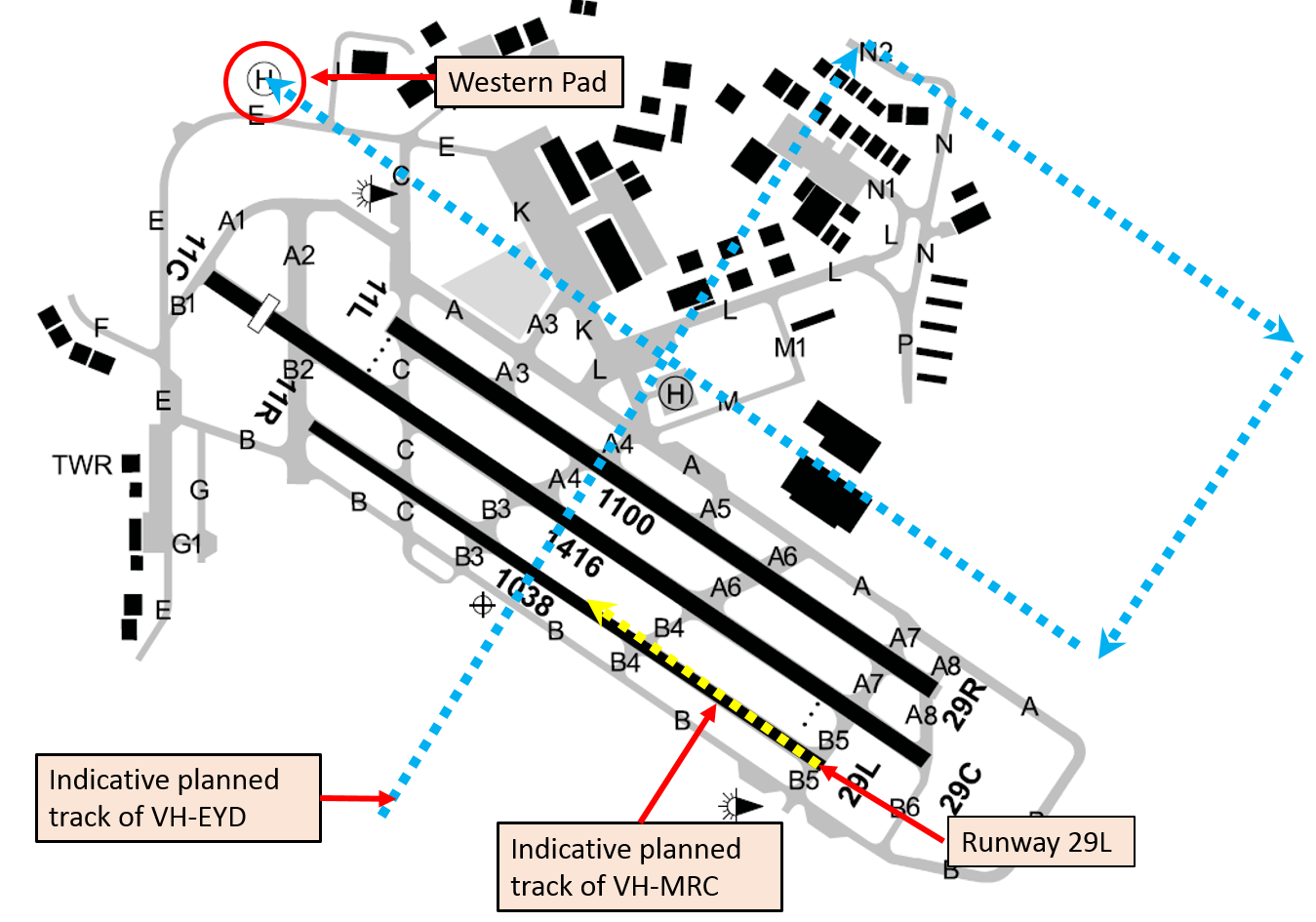
The ADC reported that they sighted MRC about mid-way along the runway, lower than the assigned altitude of 1,000 ft, and also sighted EYD about 200 m away at about the same altitude (Figure 2). The ADC immediately issued a safety alert[1] to the pilot of MRC advising of a helicopter (EYD) to their left crossing midfield at 500 ft. The ADC then issued a safety alert to EYD advising of the Cessna (MRC) in the go-around.
The instructor of EYD had already sighted MRC and commenced a right turn to increase separation. On receiving the safety alert, the pilot of EYD continued the right turn to pass behind MRC. EYD landed at the western helipad without further incident. MRC departed to the training area, before returning to land at Bankstown Airport, also without further incident.
Figure 2: Indicative aircraft tracks
Source: Airservices Australia – annotated by ATSB
Aerodrome control and radio frequencies
There were two Tower frequencies and two ADC positions at Bankstown, with ADC1 having responsibility for arrivals and departures on runways 29 right/11 left and 29/11 centre; ADC2 was responsible for the training circuit with runway 29 left/11 right.
The two Tower frequencies at Bankstown were combined at the time of the incident, and one controller occupied the ADC position. When combined, pilots of aircraft operating on either the circuit Tower frequency or the arrivals and departures Tower frequency would have been able to hear transmissions on the other frequency. Although the pilots of MRC and EYD had different radio frequencies selected, they were combined such that the transmissions made on both frequencies could be heard on either frequency.
Pilot comments
Pilot of MRC
The pilot of MRC was a student with 41 hours of aeronautical experience, six of which were solo. They provided the following comments:
They had not departed from the circuit runway to the training area previously and were not sure how to do so or what to expect from ATC.
Their understanding of a go-around was to descend as if on a normal approach to the runway, discontinue the approach on final at about 300 ft, apply full power and commence a climb, and diverge to the left of the runway.
They misunderstood the ADC’s instruction, but were unsure why the controller had not noticed the aircraft descending on base and final before it commenced the go-around.
They were not aware of the Choppers South arrival procedure until after the incident.
If the instruction had been sequenced differently, with the direction to maintain 1,000 ft first, it would have made the ADC’s expectations clearer.
Controller comments
The ADC commented that if the pilot of MRC had maintained 1,000 ft there would not have been a separation issue. Having issued the instruction to maintain 1,000 ft, the ADC turned their focus to monitoring other aircraft and communicating with the pilots of other aircraft in the control zone.
The controllers have a liaison role with local flying schools, which involves visiting them and talking to the students, and they also invite students to the tower during quiet periods. This liaison fosters a safer working relationship between pilots and air traffic control.
Go-around
Aeronautical Information Package (AIP) En Route (ENR) 1.1 – 16.4 stated:
At Class D aerodromes with parallel runways where contra-rotating circuit operations are in progress, if ATC instructs, or a pilot initiates a go around, the pilot must:
commence climb to circuit altitude
position the aircraft on the active side and parallel to the nominated duty runway, while maintaining separation from other aircraft and
follow ATC instructions or re-enter the circuit from upwind.
The Manual of Air Traffic Services defined a go-around as a ‘procedure in which the pilot discontinues the approach immediately and rejoins for another circuit, or proceeds as directed by ATC’.
The ADC commented that when they issued the instruction to go around, they expected the pilot of MRC to terminate their approach and maintain 1,000 ft while continuing to fly the circuit geographically.
En Route Supplement Australia
The ERSA entry for Bankstown included the following under the heading Class D:
‘CAUTION: HELICOPTERS OVERFLY RUNWAYS MIDFIELD AT 500FT.’
Operator comments
The operator of MRC provided the following comments:
Helicopter pilots inbound via Choppers South should be aware that crossing a training circuit runway is inherently risky as a go around can occur at any time and is obviously more likely to occur with low time student pilots who are more likely to not have their approach to land stabilised.
It is also very likely that during their initial solo circuit training students will be more likely to be focussing on the preceding traffic they are following and will be less likely to see crossing helicopter traffic in their peripheral vision.
Bankstown is a very busy training environment, which can have sudden increases in traffic volume. ATC needs to be aware of this as it is very difficult for student pilots to monitor traffic and radio calls and make broadcasts when conjoined frequencies are in operation, and there is a heavy traffic load.
It is, and it always will be, company policy to safely fly the aeroplane first, navigate to the southern side of the runway and then communicate their intentions/actions.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Operator of VH-MRC
As a result of this occurrence, the operator of MRC has advised the ATSB that they are taking the following safety actions:
Amended operations manual
The operator of MRC is proposing to amend their operations manual to read:
Unlicensed solo pilots are not permitted to request circuits on arrival or when inbound to Bankstown. Unlicensed solo pilots may only depart the training circuit after they have demonstrated proficiency in the procedure to an instructor and a note has been made in the training record to that effect
Safety message
The Civil Aviation Safety Authority booklet, Class D airspace, advises pilots that when operating in Class D airspace, they must sight and maintain separation from other aircraft. Pilots and ATC have a dual responsibility to maintain situational awareness of other traffic.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 31 May 2016 at 1018 Eastern Standard Time (EST), Virgin Australia Airlines flight VA1615, an Embraer ERJ 190 aircraft, registered VH-ZPJ (ZPJ), departed Melbourne Airport on a scheduled passenger service to Mildura Airport, Victoria. On board the aircraft were 2 flight crew, three cabin crew and 81 passengers. The aircraft captain was the pilot flying (PF) and the first officer was the pilot monitoring (PM).[1]
About 40 NM from Mildura and just prior to ZPJ leaving controlled airspace, air traffic control (ATC) passed the flight crew traffic information about two aircraft operating above 10,000 ft to the west of Mildura Airport. In addition, there was also a public transport flight inbound to Mildura from Broken Hill and a light twin-engine aircraft inbound to Mildura on a converging track to ZPJ. The PM on board ZPJ contacted the light twin-engine aircraft and confirmed they would arrive at Mildura after ZPJ. The estimated arrival time for the public transport flight at Mildura was also later than the estimate for ZPJ, and consequently the flight crew on board ZPJ did not consider any of the traffic passed to them by ATC would conflict with their own arrival.
The aircraft operating to the west of Mildura were a GippsAero GA10 aircraft, registered VH-XGY (XGY), conducting spin testing supported by a Gippsland Aeronautics GA-8 ‘chase plane’, registered VH-XGA (XGA), from the same company.
ZPJ joined the Mildura Airport circuit on the crosswind leg for a left visual circuit to land on runway 09.
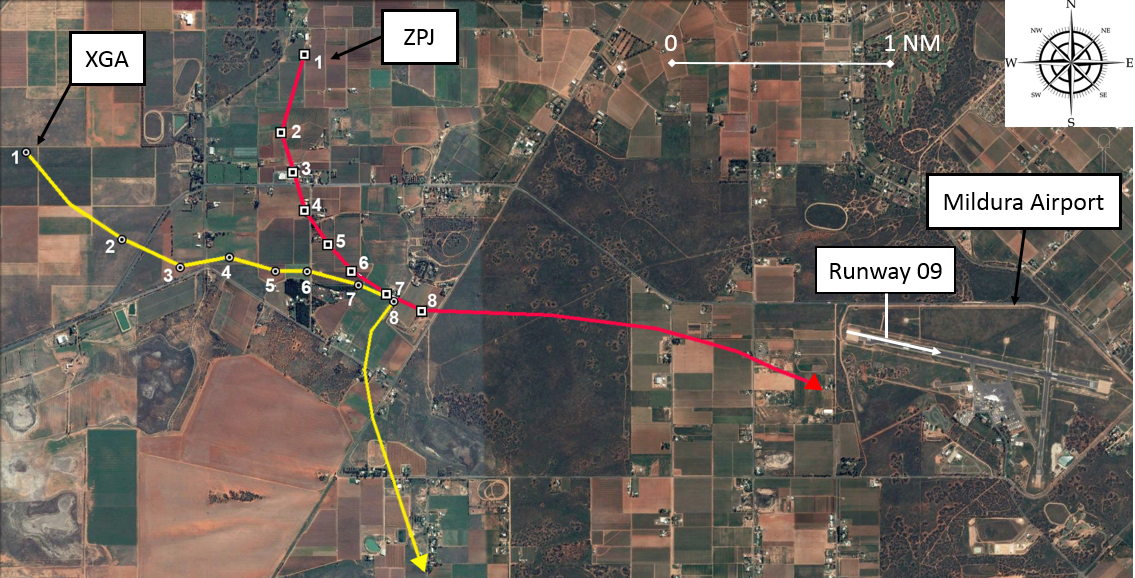
On the base leg of the circuit, the flight crew on board ZPJ heard their traffic collision alert system (TCAS) announce a traffic advisory (TA) aural alert (see TCAS limitations on approach). They glanced at their TCAS display to check the relative position of the traffic, which indicated it was to their right (position 1 in Figure 1). The flight crew looked out the right window of the flight deck and identified the traffic to their right and high against the skyline. The traffic appeared to them to be stationary in the windscreen relative to their own aircraft and with a high closure rate (from TCAS data the aircraft were 1.25 NM apart at the time of the TA alert).[2]
The PM on board ZPJ contacted the other traffic on the radio and requested their intentions. The other traffic was XGA, which was leading XGY back to Mildura Airport for a straight-in approach to runway 09. When the pilot of XGA responded that they were tracking for a straight-in approach to runway 09, the PM assessed they were on a collision course on their present track. They also recognised that there would be a potential risk of collision if both aircraft performed a go-around to the south of the main runway. Therefore, the PM responded to the pilot of XGA to immediately turn and remain south of the airport. The pilot of XGA identified ZPJ ahead of them on approach to runway 09 and responded that they would discontinue their approach and manoeuvre to the south of the airport.[3]
The PF on board ZPJ decided to discontinue their approach to land on runway 09, as they were too late for their turn onto final and therefore not in a stabilised condition.[4] However, the PM indicated to the PF that they could not execute a go‑around manoeuvre because there was another aircraft joining the circuit on crosswind (the light twin-engine aircraft). The PF decided that continuing the approach to land was not an option and therefore executed the go‑around to the south of runway 09, maintained separation from the other traffic on crosswind and then landed from the subsequent circuit. During the go-around manoeuvre, the aircraft’s TCAS detected XGA pass about 200 ft above and 0.125 NM behind ZPJ (position 7 & 8 in Figure 1).
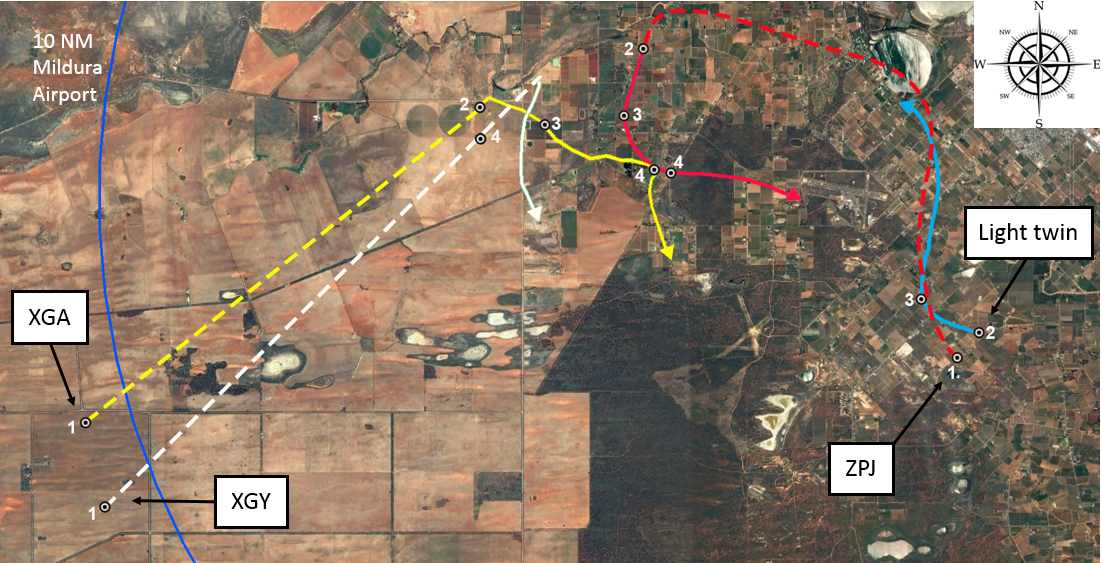
Figure 1: Traffic conflict between ERJ 190 (VH-ZPJ) and GA-8 (VH-XGA)
Source: Google earth, annotated by ATSB based on Virgin Australia Airlines TCAS data (numbers indicate the relative positions of the conflict aircraft at the same time)
Airspace
Class E airspace
A Class E controlled airspace corridor extends from Melbourne to overhead Mildura Airport with a lower limit of FL 125.[5] In Class E airspace, instrument flight rules (IFR) traffic, such as ZPJ, require a clearance. Visual flight rules (VFR) traffic, such as XGA and XGY, do not require a clearance, but should monitor the Class E airspace air traffic service frequency. In Class E airspace, IFR flights are separated from other IFR flights and receive traffic information on VFR flights as far as practicable. ZPJ left Class E airspace on descent to Mildura about 37 NM from Mildura Airport, at which point ZPJ entered Class G airspace for the remainder of the flight.
Class G airspace
Class G airspace is non-controlled airspace. IFR and VFR traffic are permitted without a clearance and there is no separation service provided by ATC. Mildura Airport is a non-controlled aerodrome with a discrete common traffic advisory frequency (CTAF), which is a different frequency from the surrounding Class G airspace area frequency. About 10 NM to the north-west of Mildura Airport is Wentworth Aerodrome. Wentworth uses the same CTAF as Mildura.
Radio broadcasts at non-controlled aerodromes
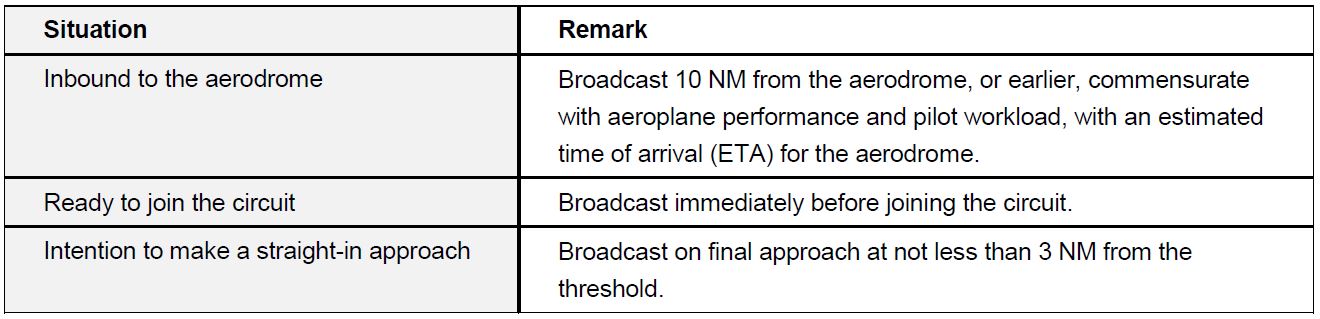
The following Table 1 indicates the non-controlled aerodrome radio broadcast requirements for inbound aircraft in accordance with the aeronautical information publication (AIP).
Table 1: Summary of broadcasts required for inbound aircraft at non-controlled aerodromes
Incident flight radio broadcasts
During the spin testing of XGY, XGY was classified as ‘lead’ aircraft and XGA as ‘in-trail’. The pilot of XGA set one of their two radio frequencies to their company frequency, for communication with XGY, and the other to area frequency, for communication with other traffic if required. While operating on the area frequency, the pilot of XGA heard a broadcast from ZPJ that they were inbound to Mildura from Melbourne, and a broadcast from another public transport aircraft inbound to Mildura from Broken Hill. On completion of the spin testing, XGA assumed the lead from XGY at about 10,000 ft and 11–12 NM from Mildura Airport. Shortly after the lead change, the pilot of XGA changed from area frequency to the Mildura CTAF.
The pilot of XGA made a 10 NM broadcast on CTAF, which included their position, altitude and intentions for a 5 NM straight in approach for final approach to runway 09. They received an immediate response from the public transport aircraft tracking from Broken Hill, who provided an estimated time of arrival for their 5 NM final approach position for runway 09. The pilot of XGA responded with a revised estimate for their arrival on the ground at Mildura Airport, which was the same time as the other aircraft’s estimate for their 5 NM final position. At the end of this exchange, XGA, with XGY in-trail, was about 7 NM from Mildura Airport tracking to the north-east to intercept a 5 NM final position, at 140–150 kt airspeed, descending at about 2,000 ft per minute. The pilot of XGA heard no radio broadcasts from ZPJ on CTAF and assumed they had already landed.
XGA made a right turn onto final approach for runway 09 at about 3,200 ft, 4.5 NM[6] from the runway threshold. Shortly after the turn, the pilot of XGA heard a broadcast requesting their intentions from ZPJ. Following the initial exchange of broadcasts with ZPJ, the pilot of XGA visually identified ZPJ about 2 NM ahead on approach to runway 09. They recognised that ZPJ had right-of-way and made a broadcast that they were ‘breaking off’ their approach to runway 09 and turning south.
The PM duties on board ZPJ included managing the radio communications with other traffic. During the approach to join the circuit, and subsequently while flying the circuit, the captain was preoccupied with PF duties and did not comprehend all the radio broadcasts. However, the PM made several CTAF broadcasts, which started at 42 NM from Mildura at 01:06:35. The last broadcast before entering the Mildura circuit was just prior to ZPJ crossing overhead runway 09 to join crosswind at 01:15:27. The next CTAF broadcast made by ZPJ was at 01:18:16, after they turned base. The flight crew received a TA at 01:18:31 and subsequently made a broadcast to challenge the intentions of XGA at 01:18:43.
Incident aircraft geometry
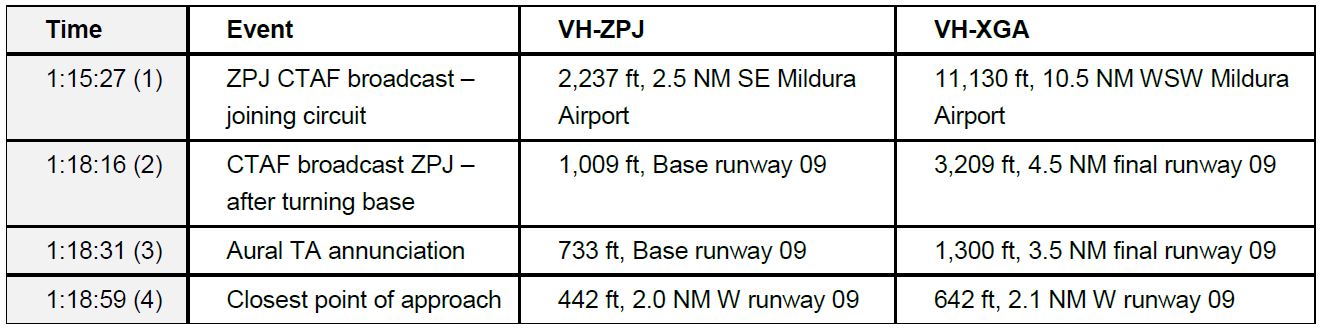
The following Table 2 indicates the positions of ZPJ and the conflict aircraft XGA. Figure 2 depicts the geometry of traffic in the vicinity with numbering in accordance with Table 2. The positions of the aircraft are based upon TCAS data from ZPJ.
Table 2: Aircraft geometry
Figure 2: Aircraft geometry from Table 2
Source: Google earth, annotated by ATSB based on Virgin Australia Airlines TCAS data.
TCAS limitations on approach
The traffic alert and collision avoidance system (TCAS) II, will display traffic to the flight crew as: other traffic, proximate traffic, traffic advisory,[7] or resolution advisory.[8] However, only traffic advisories and resolution advisories trigger an aural alert to the flight crew.
The collision avoidance system logic is based on the concepts of sensitivity level (SL), threshold time (tau) for issuing a traffic alert or resolution advisory, and protected volume of airspace around the TCAS equipped aircraft. The higher the SL, the greater the volume of protected airspace. As SL reduces, the volume of protected airspace reduces and TCAS functions may become inhibited.
Tau is an approximation of the time, in seconds, to the closest point of approach of another aircraft. This forms the basis for the alerting functions and therefore the volume of protected airspace. Therefore, a reduction in the TCAS SL reduces the volume of protected airspace by reducing the value of tau.
Below 1,000 +/-100 ft above ground level, the TCAS SL reduces from SL3 to SL2. For the ERJ 190 this equates to 900 ft when on descent and 1,100 ft when on climb. From SL3 to SL2 the tau reduces from 25 seconds to 20 seconds and resolution advisories are inhibited. Below 500 +/-100 ft above ground level, TCAS aural alerts are inhibited. For the ERJ 190 this equates to 400 ft when on descent and 600 ft when on climb. Close to the ground, the windshear and ground proximity warning system alerts have a higher alert priority.
The PM on board ZPJ commented that during the visual circuit they changed the focus of their scan from inside the cockpit to outside the cockpit. They suspect that XGA was probably displayed as other traffic on their TCAS before they received the TA alert. However, there are no company procedures specific to the use of TCAS at non-controlled aerodromes. Company procedures emphasise the importance of flight crew maintaining a ‘constant lookout when operating within a CTAF’, and use positive altitude separation or alternatively coordinate a track deviation with conflict aircraft.[9]
Limitations with visual sighting
Three limitations to sighting other traffic, of interest to this incident, are:
alerted search versus unalerted search
lack of relative motion on collision course
effects of complex backgrounds
Alerted search versus unalerted search
Traffic alerts may come from radio calls or TCAS at a non-controlled aerodrome. Knowing where to look has been shown to improve visual detection of other traffic. The PF on board ZPJ was alerted to the potential conflict by TCAS, and then visually identified XGA. The pilot of XGA was alerted to the potential conflict following ZPJ’s radio broadcast on the base circuit leg, and then visually identified ZPJ.
Lack of relative motion on collision course
The PF on board ZPJ commented that when they visually sighted XGA, the aircraft appeared to be stationary in the windscreen, which indicated a potential collision course. In this case ZPJ would also appear stationary to the pilot of XGA. Lack of relative motion against a background reduces the probability of visual detection.
Effects of complex backgrounds
When the PF on board ZPJ visually identified XGA, XGA was above the horizon (higher altitude relative to ZPJ) and against a background of sky. For the pilot of XGA, ZPJ was lower and against a background of terrain. The pilot of XGA was therefore required to detect the contrast between the aircraft and terrain to detect ZPJ. A terrain background may create a complex background and reduce the probability of visual detection.
Safety analysis
The AIP directs pilots to the minimum required radio broadcasts when operating at non-controlled aerodromes and the pilots of ZPJ and XGA complied with these requirements. However, it is likely that the pilot of XGA was not on the Mildura CTAF when the PM on board ZPJ made a broadcast that they were joining the Mildura circuit. When the pilot of XGA switched to the Mildura CTAF they were initially occupied with communicating with another public transport aircraft inbound from the north and considered this aircraft to be their only potential conflict. It could not be determined why the flight crew on board ZPJ did not comprehend the presence of a potential conflict from this radio traffic. However, the flight crew of ZPJ had previously dismissed these two aircraft (XGA and XGY) as a potential conflict for their arrival.
After ZPJ turned onto the base leg for runway 09, the PM made a base radio broadcast. It could not be determined why the pilot of XGA did not comprehend the presence of a potential conflict from this broadcast. However, the investigation could not rule out the possibility that other aircraft operating at Mildura or Wentworth made broadcasts which interfered with one or several of the broadcasts made by ZPJ or XGA.
Shortly after the base leg radio broadcast from the PM in ZPJ, the flight crew were alerted to the presence of XGA by a TCAS TA aural alert. At this time ZPJ was below 900 ft and therefore TCAS resolution advisory was inhibited. However, the TCAS visual display of the relative position of XGA cued their visual search and facilitated a quick identification. XGA appeared to the flight crew on board ZPJ as stationary against a background of sky. Therefore, to the pilot of XGA, ZPJ was probably against a more complex background with no relative motion, contributing to the difficulty for the pilot of XGA to detect ZPJ before they were alerted by the radio call by ZPJ.
The radio broadcast from the PM on board ZPJ directed to the ‘traffic inbound to Mildura from the west’ alerted the pilot of XGA to the presence of other traffic and cued them to search for the conflict. The PM on board ZPJ then directed the pilot of XGA to ‘turn immediately away to the south’ to avoid a potential collision either during their turn onto final approach or in the event that both aircraft attempted a simultaneous go-around manoeuvre on the south side of runway 09.
After receiving an acknowledgement from the pilot of XGA, the flight crew on board ZPJ turned their attention to the execution of their go-around manoeuvre as their turn onto the final leg of the circuit was late due to their preoccupation with monitoring XGA. However, during their turn to join the upwind circuit leg for runway 09 on the south side of the runway, XGA continued to converge to a closest point of 0.125 NM behind and about 200 ft above ZPJ before making an abrupt turn to the south. This was the result of the intention of the pilot flying XGA to join the upwind leg of the circuit to the south of runway 09, before they realised that ZPJ was also conducting a go-around from their approach.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The pilot of XGA was probably not monitoring Mildura CTAF when the PM on board ZPJ broadcast joining the Mildura circuit.
The flight crew of ZPJ did not detect the broadcast from XGA that they were intending to join a straight in approach to runway 09.
After a separation strategy was agreed, XGA continued to close on ZPJ to a closest point of approach of 0.125 NM behind and 200 ft above ZPJ when ZPJ started their go-around.
Both aircraft made the required broadcasts on the CTAF.
The flight crew on board ZPJ were cued to the conflict by their TCAS traffic advisory alert.
The pilot on board XGA was cued to the conflict by the radio broadcast from ZPJ.
Safety message
Despite compliance with the radio broadcast requirements, a traffic conflict occurred in an environment with limited manoeuvring options for a high-capacity public transport aircraft. This incident highlights the importance of an alerted search to the successful identification of potential conflict traffic. Further information is available from ATSB Research report: Limitations of the See-and-Avoid Principle.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns relates to safety around non-controlled aerodromes.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 9 August 2016, at about 0930 Western Standard Time, a Cessna 210N aircraft, registered VH-NLV (NLV), departed Kununurra Airport for a scenic charter flight to Mitchell Plateau aircraft landing area (ALA), Western Australia (WA), with a pilot and five passengers on board.
Shortly before 1100, the pilot of NLV tracked for a straight-in approach to runway 06 at Mitchell Plateau ALA.
At that time, the pilot of a Gippsland Aeronautics GA-8 aircraft, registered VH-BFL (BFL), prepared to taxi at Mitchell Plateau ALA, for a scenic charter flight to Kalumburu, WA, with four passengers on board.
When about 5 NM from the ALA, the pilot of NLV broadcast on the CTAF, advising they were on a 5-mile final for runway 06 at Mitchell Plateau, and did not receive a response.
The pilot of BFL reported that they broadcast a taxi call, a call prior to entering runway 16/34 to taxi to runway 06 and prior to entering runway 06. The pilot inadvertently made those broadcasts company frequency instead of CTAF.
When at about 1 NM on final approach to runway 06, the pilot of NLV broadcast again on the CTAF and did not receive a response.
As the pilot of NLV flared the aircraft for landing, they sighted BFL taxi onto runway 06. After landing, the pilot of NLV braked more heavily than normal and moved to the left of the runway to increase the separation between the two aircraft.
As BFL entered runway 06, the pilot sighted NLV in the landing roll and also moved to their left. The pilots assessed that the aircraft passed within 2 m of each other at taxi speed and neither aircraft moved outside the runway strip. The aircraft were not damaged and no injuries were sustained.
Pilots are encouraged to prioritise their attention carefully and appropriately as they near non-towered aerodromes. An effective lookout for other aircraft, supported by communication with traffic in the vicinity, should be a high priority.
On 9 August 2016, at about 0930 Western Standard Time (WST), a Cessna 210N aircraft, registered VH-NLV (NLV), departed Kununurra Airport for a scenic charter flight to Mitchell Plateau aircraft landing area (ALA), Western Australia (WA), with a pilot and five passengers on board.
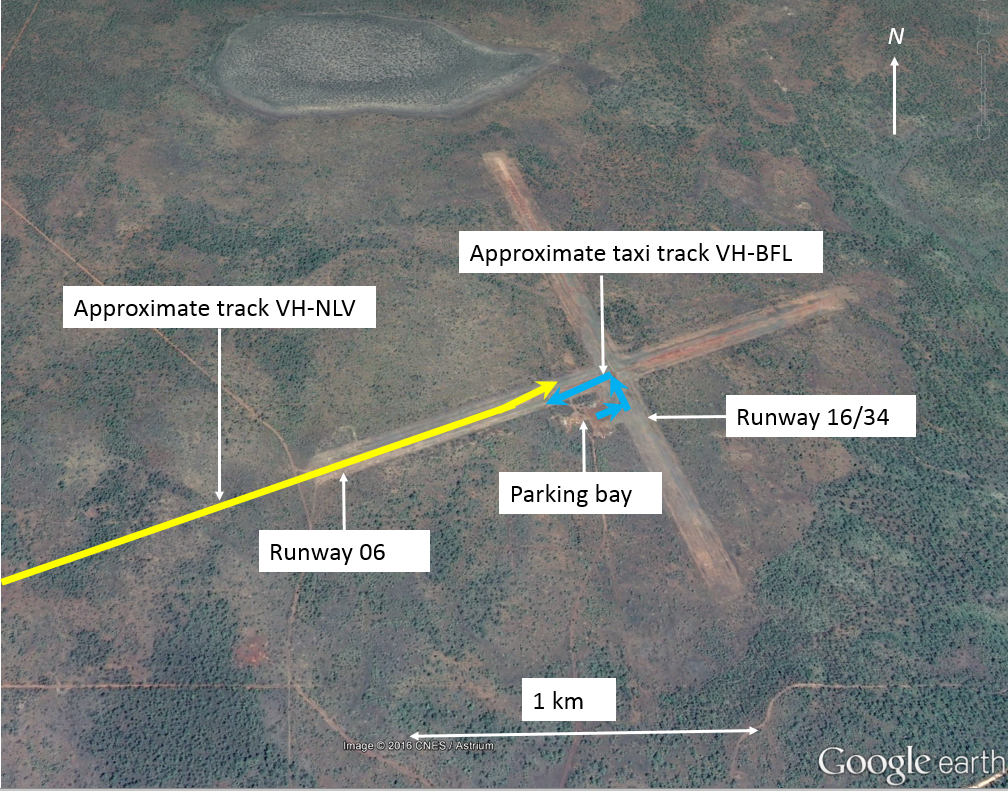
Shortly before 1100, after completing orbits overhead Mitchell Falls, about 9 NM south-west of Mitchell Plateau ALA, the pilot of NLV positioned the aircraft to track for a straight-in approach to runway 06 at Mitchell Plateau ALA (Figure 1).
Figure 1: Mitchell Plateau ALA showing approximate aircraft tracks
Source: Google earth – annotated by ATSB
At that time, the pilot of a Gippsland Aeronautics GA-8 aircraft, registered VH-BFL (BFL), prepared to taxi at Mitchell Plateau ALA, for a scenic charter flight to Kalumburu, WA, with four passengers on board. Prior to taxiing, the pilot of BFL selected a company frequency on the aircraft’s radio and communicated with the pilot of another aircraft. After that communication, the pilot pressed the radio’s frequency select button in an attempt to switch to the North Kimberley common traffic advisory frequency (CTAF). However, the pilot did not detect at that time that the CTAF had not been selected and the radio remained tuned to the company frequency.
When about 5 NM from the ALA, the pilot of NLV broadcast on the CTAF, advising they were on a 5-mile final for runway 06 at Mitchell Plateau, and did not receive a response. When about 3 NM from the runway, the pilot of NLV sighted an aircraft (BFL) on the parking bay at the ALA, with the beacon on, indicating that the aircraft’s engine was running.
The pilot of BFL reported that they broadcast a taxi call and a call advising that BFL was entering runway 16/34 to taxi to runway 06, and subsequently broadcast prior to entering runway 06 to backtrack to the runway threshold. The pilot inadvertently made those broadcasts company frequency instead of CTAF and did not receive any response.
When at about 1 NM on final approach to runway 06, the pilot of NLV broadcast again on the CTAF and did not receive a response. From the aircraft’s position, the parking bay and adjacent taxiway were obscured by a line of trees, and the pilot was unable to see BFL.
As the pilot of NLV flared the aircraft for landing, they sighted BFL turn left and taxi onto runway 06. The pilot of NLV assessed that if they conducted a go-around the aircraft may be unable to climb fast enough to avoid the aircraft on the runway and could not diverge from the runway direction due to the trees beside the runway, therefore the pilot elected to land. After landing, the pilot of NLV braked more heavily than normal and moved to the left of the runway to increase the separation between the two aircraft.
As BFL entered runway 06 to backtrack, the pilot sighted NLV in the landing roll and also moved to their left. The pilots assessed that the aircraft passed within 2 m of each other at taxi speed and neither aircraft moved outside the runway strip. The aircraft were not damaged, and no injuries were sustained.
Pilot comments
Pilot of VH-NLV
The pilot of NLV commented that during the flare, they considered conducting a go-around, but assessed that due to the high outside temperature, the aircraft may not have adequate climb performance to pass at a safe height above BFL.
Pilot of VH-BFL
The pilot of BFL had been in the airport terminal for about 2 hours before the incident. They commented that as the CTAF covered a large area, normally they would have very good awareness of other aircraft operating there. As they had not been listening to the radio during the time in the terminal, they were not aware of NLV. The pilot recalled looking for aircraft as they taxied onto runway 06, but did not see NLV.
The pilot also commented that due to a delay on the ground, they were keen to get away, and that may have contributed to not noticing that the radio was still on the company frequency.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following safety action in response to this occurrence.
Operator of VH-BFL
As a result of this occurrence, the operator of BFL has advised the ATSB that they are taking the following safety actions:
Flight crew briefing
The operator is proposing the following briefing for new flight crew regarding radio procedures:
mentally confirm the required frequency
visually confirm the required frequency is set as active, and the correct COM is selected on the audio panel
aurally check by activating the squelch.
In addition, company pilots will be reminded to be mindful of the impact that stress (such as that due to delays) can have on their performance, to recognise the signs and symptoms of stress, and to return to the basics of good airmanship if/when they find themselves under stress and pressure.
Safety message
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is safety around non-towered aerodromes.
Pilots are encouraged to prioritise their attention carefully and appropriately as they near non-towered aerodromes. An effective lookout for other aircraft, supported by communication with traffic in the vicinity, should be a high priority.
The ATSB report Limitations of the See-and-Avoid Principle outlines the major factors that limit the effectiveness of un-alerted see-and-avoid. Insufficient communication between pilots operating in the same area is the most common cause of safety incidents near non-controlled aerodromes.
Most occurrences reported to the ATSB at non-towered aerodromes involve conflicts between aircraft, or between aircraft and ground vehicles. In particular, active runways should be approached with caution. The ATSB publication A pilot’s guide to staying safe in the vicinity of non-towered aerodromes, stated that a large number of the conflicts between aircraft involved:
ineffective communication between pilots operating in close proximity
the incorrect assessment of other aircraft’s positions and intentions
relying on the radio as a substitute for an effective visual lookout
failure to follow published procedures.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
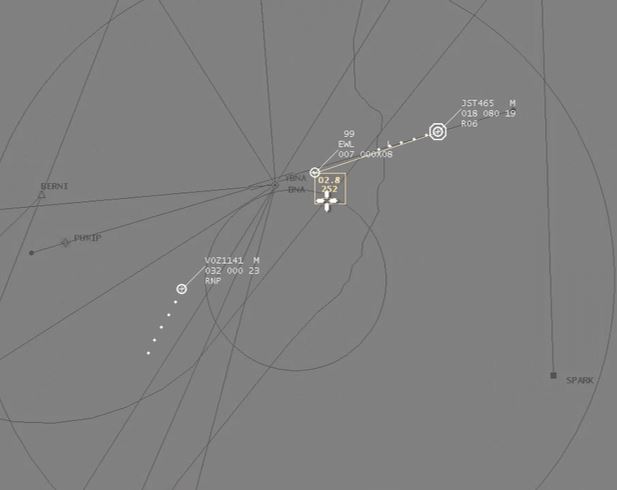
On 14 January 2016, whilst taking-off from Ballina/Byron Gateway Airport, Airbus A320, registered VH-VQS (VQS) and operated by Jetstar Airways, came in close proximity to Beech Aircraft Corporation BE-76 Duchess, registered VH‑EWL (EWL). The Duchess was conducting navigation training in the vicinity of the runway and was noticed by the flight crew of VQS during the take‑off roll and below the maximum speed from which they could stop. The take-off was continued and while manoeuvring to maintain separation from EWL, the crew of VQS received master warning/caution alerts regarding the aircraft’s configuration. The crew also commenced flap retraction at low altitude and turned contrary to operator-prescribed departure procedures before departing for Melbourne. There were no injuries or damage to equipment recorded during the occurrence.
Your browser does not support the video tag.
What the ATSB found
The ATSB found that despite an increase in passenger numbers and a mixture of traffic, Ballina/Byron Gateway Airport operated without the support of air traffic information and/or services. While recognising that a direct comparison between airports is difficult, Ballina also experienced a higher number of incidents relating to communication and separation issues compared to airports with similar traffic levels. The ATSB also found that a number of non‑standard operating practices and procedures led to a breakdown of crew resource management and the ability to adequately manage the dynamic situation by the crew of VQS. Finally, the ATSB found that the level of communication between the crews of VQS and EWL was inadequate to develop a shared mental model of what each crew was intending to do to ensure separation.
What's been done as a result
Following a recommendation by the Civil Aviation Safety Authority (CASA), the operator of Ballina/Byron Gateway Airport implemented a certified air/ground radio service (CA/GRS) to provide weather services and traffic information at the airport. This service commenced in March 2017 and operates daily between 0800 and 1800 local time. The CASA Office of Airspace Regulation is planning a post‑CA/GRS implementation review in mid-2017 to assess its effectiveness.
Additionally, Jetstar Airways have proposed to increase their annual audit schedule of common traffic advisory frequency operations, reviewed their jump seat policy when operating in such aerodromes to assist in distraction management, and altered their training matrix to further include exercises pertaining to levels of assertion and upwards managing by first officers.
Safety message
Operations at non‑controlled airports remain a safety watch priority for the ATSB. This occurrence highlights that traffic separation in that environment relies on a clear and shared plan between involved aircraft.
Adherence to standard operating practices and procedures promotes a shared understanding of crew’s actions by making them ordered and predictable to the other pilots. As well as reducing the likelihood of task omission or duplication during times of high workload, standardised practices and procedures decrease the mental demand on flight crew when carrying out a set of complex steps, allowing for better processing of unexpected events.
Appendices
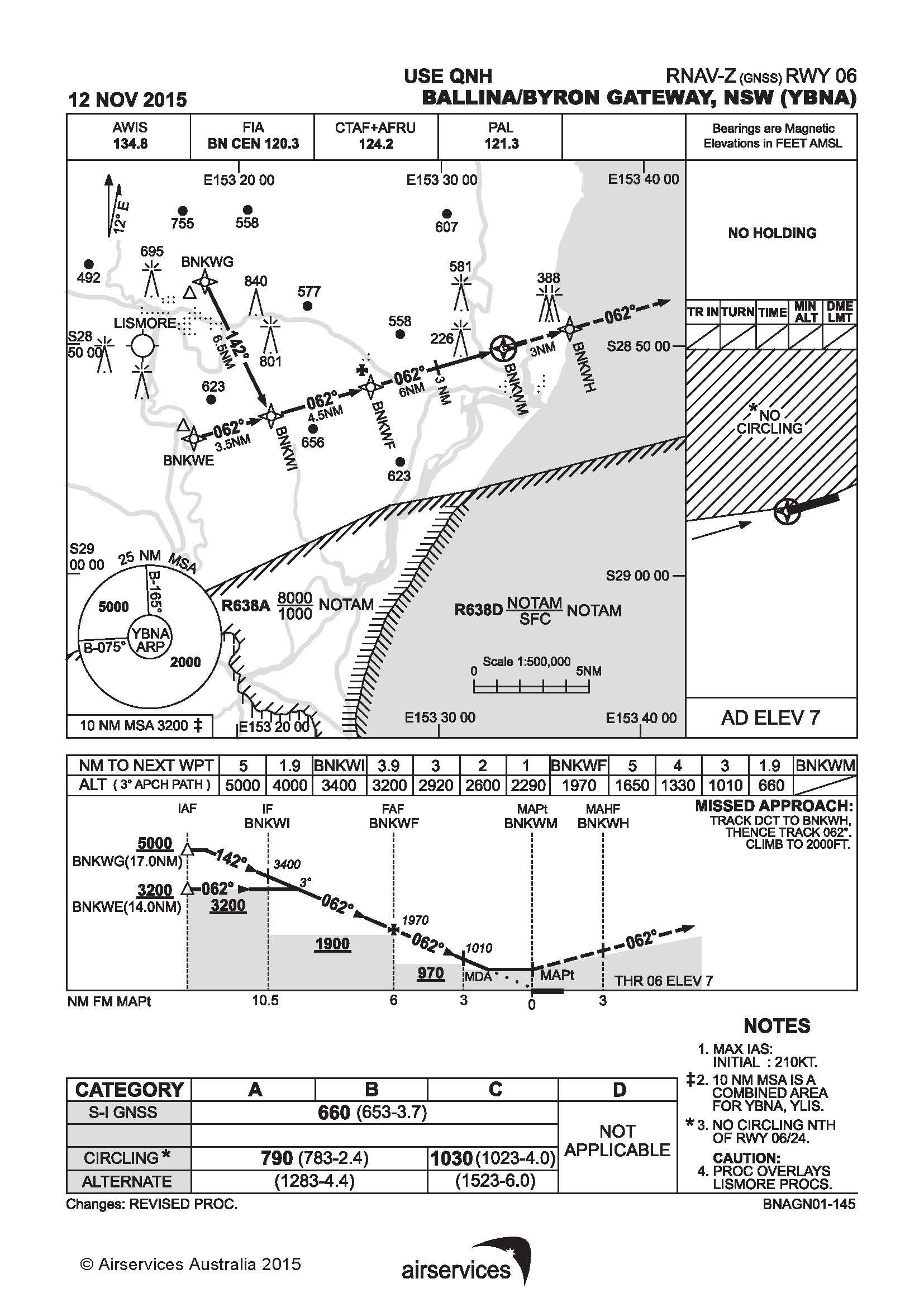
Appendix A- RNAV-Z (GNSS) approach runway 06
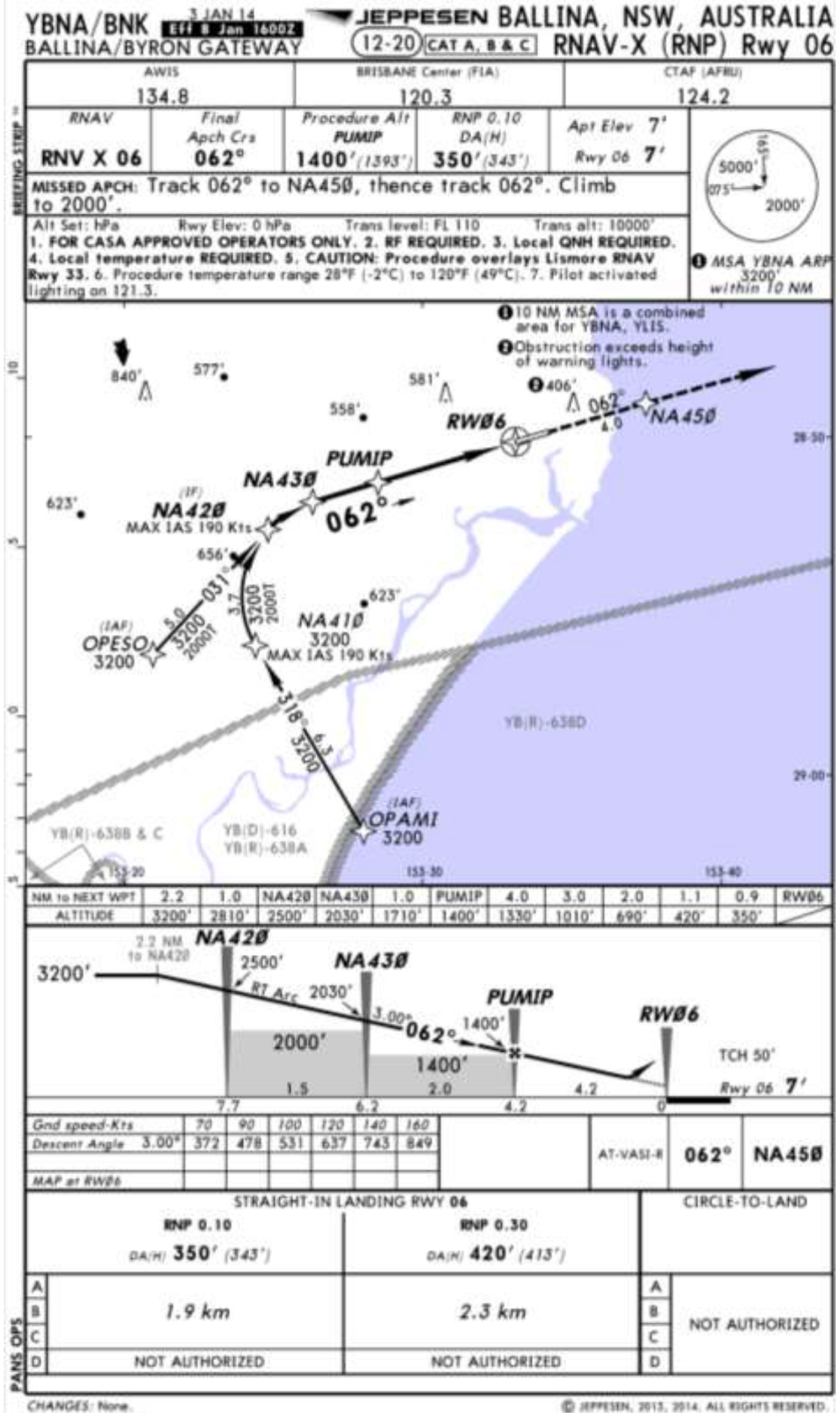
Appendix B –RNAV- X (RNP) approach runway 06
Safety issues and actions
The safety issue identified during this investigation is listed in the Findings and Safety issues and actions sections of this report. The Australian Transport Safety Bureau (ATSB) expects that all safety issues identified by the investigation should be addressed by the relevant organisation(s). In addressing those issues, the ATSB prefers to encourage relevant organisation(s) to proactively initiate safety action, rather than to issue formal safety recommendations or safety advisory notices.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Air traffic facilities at Ballina/Byron Gateway Airport
Despite a steady overall increase in passenger numbers and a mixture of types of operations, Ballina/Byron Gateway Airport did not have traffic advisory and/or air traffic control facilities capable of providing timely information to the crews of VH-EWL and VH-VQS of the impending traffic conflict. It is likely the absence of these facilities, which have been shown to provide good mitigation at other airports with similar traffic levels, increased the risk of a mid-air conflict in the Ballina area.
Safety analysis
Introduction
On departure from Ballina/Byron Gateway Airport (Ballina airport), New South Wales an Airbus A320 commenced take-off while a Duchess BE-76 was conducting instrument approach training in close proximity and nearing the missed approach point for the same runway. The A320 crew noticed the Duchess before reaching the V1 decision speed, however the take-off was continued. During manoeuvres shortly after take-off to remain below the altitude of the Duchess, the crew of the A320 received master warning/caution alerts and commenced flap retraction at a low altitude. The A320 was then turned in a direction contrary to the prescribed noise abatement departure procedure.
The following analysis will examine the operating environment at the non-controlled Ballina airport, and the human performance factors involved in the occurrence.
Air traffic facilities
At the time of the occurrence, Ballina airport was a non-towered (non‑controlled) airport with no traffic control or advisory services.
Passenger numbers at Ballina airport had increased steadily over a number of years to in excess of 486,000 per annum by September 2016. That increase in passenger numbers occurred in the context of the airport also having a mix of non-passenger transport services (see the section titled Passenger numbers and traffic movements).
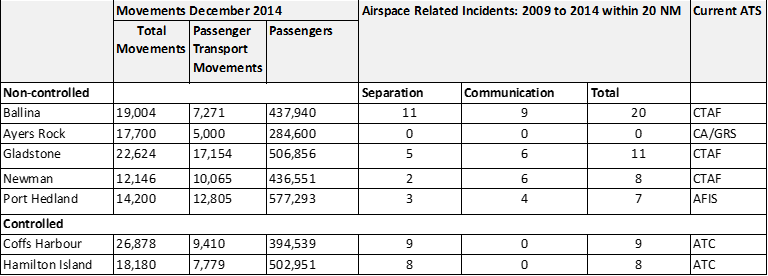
Direct comparisons of occurrence data between airports can be problematic due to differences in the levels and types of traffic that operate in the associated airspace, and the variance in incident reporting by operators. However, compared with other non‑controlled aerodromes, in the period 2009–2014 no other Common Traffic Advisory Frequency (CTAF) airspace had a higher total number of separation and communication incidents than Ballina airport. Ballina had approximately double the number of those incidents compared to the next highest similar airport. In addition, the two CTAFs with a high ratio of non‑passenger transport movements (Ballina and Gladstone) recorded the highest number of separation/communication incidents.
The data also supports that the availability of a certified air/ground radio service or an aerodrome flight information service, neither of which were available at Ballina, reduces the separation/communication risk. Non‑controlled airports equipped with a certified air/ground service, such as Ayers Rock, Northern Territory recorded little if any separation/communication incidents. Like Ballina, Ayers Rock also facilitated passenger transport movements and a large number of visual flight rules traffic. Similarly, airports equipped with an aerodrome flight information service, such as Port Headland, Western Australia recorded approximately 65 per cent fewer incidents compared with Ballina. Of note, in the period examined, Ballina recorded 26 per cent fewer aircraft movements, but approximately 32 per cent greater overall passenger numbers.
The ATSB also examined the broader suitability of the airspace surrounding Ballina airport. This included consideration of comments made in the Civil Aviation Safety Authority (CASA) Supplementary Airspace Review for Ballina conducted in July 2015, and additional information sought from CASA and Airservices Australia (Airservices) during the investigation. Airservices and CASA commented that since 2009 no aircraft separation incidents were recorded above 5,000 ft above mean sea level within 20 NM (37 km) of Ballina airport in Class G airspace. They also stated that existing radar or radar-like surveillance around Ballina is currently limited to 5,000 ft and this was unlikely to improve in the near future.
In response to a recommendation of the 2015 CASA review, Airservices examined the introduction of Class E airspace below Class C airspace in the vicinity of Ballina. Airservices determined that there would be no significant safety benefit to support the establishment of Class E airspace below Class C airspace. Airservices also identified that introducing Class E airspace would provide pilots with less time to comply with CTAF requirements when entering or leaving Class E airspace. CASA also consulted with passenger transport operators that regularly used Ballina Airport and determined that they also did not support the lowering of Class E. CASA did not recommend any changes to the existing airspace architecture at that time.
CASA is planning a post implementation review in mid-2017, which will, in part, assess any airspace risks since the introduction of the Certified Air/Ground Service. CASA will also continue to monitor aviation activity and incident reports around Ballina to determine if any changes in the volume or complexity of aviation activity generate the need for further airspace review.
Development of the occurrence
Take-off preparation
When the flight crew of A320, VH‑VQS (VQS) entered and backtracked for departure on runway 06 the estimate provided by the pilots of Duchess, VH‑EWL (EWL) indicated that there was about 5 minutes gap between the aircraft. Additionally, as the crew of VQS entered the runway EWL was sighted on a long final approach and the crew assessed that sufficient separation would be maintained between the two aircraft during the take-off. Once VQS was lined up however, its crew could no longer visually assess EWL’s position, as it was behind them.
The captain of VQS was operating as pilot flying for the departure from Ballina. As such, the first officer (FO) was providing the pilot monitoring support duties of, including managing radio communications. However, while entering and backtracking the runway for take‑off, the captain repeatedly communicated with the crew of a second, more distant aircraft, a Boeing 737 registered VH-VUE (VUE) on the CTAF.
The captain’s assumption of control of the radios was not conducted as part of a normal handover/takeover procedure, nor communicated to the FO beforehand. Although there are indications that the captain’s actions were an attempt to expedite a separation plan with the crew of VUE, the additional task increased their workload close to the time of departure. Furthermore, taking control of the radios without informing the FO was contrary to established crew resource management principles and removed the FO from the ‘loop’ regarding the division of responsibility for cockpit tasks.
The captain reported a level of frustration in relation to coordinating separation with the crew of VUE, which was also consistent with the CTAF audio recordings. It is likely that the captain’s increased workload and frustration was a distraction that led to their attention becoming focused on organising a separation plan from VUE, at the expense of maintaining an awareness of the position of the more proximal EWL. Focused attention occurs when an individual becomes fixated on one source of information or task, to the exclusion of other available information (Harris, 2011).
Initial take-off roll
The time required to confirm that adequate separation existed from VUE delayed the take‑off by VQS and reduced the separation from EWL. As the crew of VQS were unable to see EWL once lined up, assessing whether the delay created a traffic conflict essentially relied on radio communication.
The instructor in EWL believed that VQS would hold in the lined-up position until EWL completed the missed approach. However, the captain of VQS intended to depart prior to EWL reaching the missed approach point but did not convey that intent to the pilots of EWL. Had the pilots of EWL been advised of the intended take‑off, it is likely that on seeing VQS delayed in the lined‑up position, they would have perceived VQS as a traffic conflict threat. This would have provided an opportunity for the pilots of EWL to communicate with the crew of VQS and establish a different separation plan.
The FO reported not expecting the captain to commence take-off and, as such, did not transmit the take-off ‘rolling’ call to alert other traffic of the impeding take-off until after the VQS was already moving. This was contrary to normal practice, where the radio call was carried out prior to advancing the thrust levers. Based on the estimate provided by the crew of EWL, at the commencement of the take‑off roll there was about 2 minutes before EWL arrived overhead the runway threshold. However, given position estimates are only required to be updated when considered to be more than 2 minutes in error, the time and therefore separation between the two aircraft may have been significantly less.
The instructor in EWL reported only realising that the crew of VQS intended to take‑off on noticing the aircraft moving. The instructor reacted by getting the student pilot to look up and confirm the instructor’s interpretation of the situation. Shortly after, the instructor heard the take-off call by the crew of VQS. Although the instructor reported being satisfied with continuing the approach, had the take-off call taken place prior to VQS moving, the instructor in EWL would have had time to alert the crew of VQS early in the take‑off. This would have reduced the risk of a traffic conflict.
The captain commenced the take-off without first confirming that the FO was ready and before the FO completed the take-off radio call. Additionally, the use of Take-Off/Go-Around thrust was also decided and actioned by the captain without communicating with the FO. This was contrary to the pre-flight briefing where a FLEX temperature take‑off was discussed, calculated and entered into the aircraft systems.
The actions to commence the take-off that was contrary to plan was possibly motivated by the desire to expedite the take-off due to concern with the proximity of EWL. However, doing so reduced the shared understanding of what the captain was intending to do, and made managing these unexpected actions more difficult. They were also indicative of an elevated cockpit gradient. It is likely that these non-standard practices and procedures resulted in the FO experiencing a series of unexpected actions over a short period of time. This resulted in surprise, distraction and increased workload for the FO.
Research shows that surprise is a response to an unexpected action that results from a mismatch between one’s mental expectations and what is actually happening (Rivera and others 2014). If a pilot is not expecting something to go wrong, the level of surprise can result in taking no action, or the wrong action (Martin and others 2012). As the FO was surprised by the decision to commence the take‑off, it is likely their ability to recognise and respond to the traffic conflict was affected. As a result, there was no opportunity for the FO to question the decision to continue the take‑off. Instead, the FO focussed on supporting the captain. While there is insufficient evidence to determine whether this contributed to the development of this occurrence, avoiding distraction and a breakdown in shared crew mental modelling reduces the risk of a breakdown in standard operating procedure.
Take‑off and initial climb
The captain of VQS became aware of EWL’s proximity after observing it on the traffic alert and collision avoidance system (TCAS) at approximately 100 kt during the take‑off roll. While that was below the V1 decision speed and sufficient runway was available, there was no indication that actions associated with a rejected take-off were initiated by the captain. Furthermore, when the captain advised the FO of the traffic and requested proximity information, the FO did not encourage the captain to stop the take‑off.
Jetstar Airways guidance material advised that above 100 kt and nearing V1 the captain should give preference to continuing the take‑off, unless there was a major technical malfunction. In that context, the unexpected proximal traffic would probably not have been previously considered, nor pre‑briefed, by the crew as a reason to abort the take‑off. Additionally, the increased acceleration associated with the use of Take‑Off/Go‑Around thrust, and the exchange between the flight crew assessing the displayed position of EWL, would have provided limited time to assess and initiate a rejected take‑off.
Use of the RAISE model (see the section titled Levels of assertion) provides a method to recognise and identify a threat, assess the level of threat and then decide which step to use to achieve the appropriate level of assertion. Although there was no indication that the FO supported a rejected take‑off, it is likely that the FO’s ability to express an appropriate level of assertion to encourage the captain to stop was impeded by the available time.
The captain advised that, given the available runway length, they were concerned about aborting the take‑off and felt that the best course of action was to become airborne and remain below EWL’s altitude and until sufficient lateral separation was established. That option provided a means of separation between the two aircraft. However, as EWL was by now close to the missed approach point at low altitude, it required VQS to level off shortly after take‑off. That, in turn led to non‑standard handling of the aircraft and the activation of a number of master warning/caution alerts.
Findings
From the evidence available, the following findings are made with respect to the traffic management occurrence involving Airbus A320, registered VH-VQS and operated by Jetstar Airways, and a Beech Aircraft Corporation Duchess BE-76, registered VH-EWL that occurred at Ballina/Byron Gateway Airport, New South Wales on 14 January 2016. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
Despite a steady overall increase in passenger numbers and a mixture of types of operations, Ballina/Byron Gateway Airport did not have traffic advisory and/or air traffic control facilities capable of providing timely information to the crews of VH-EWL and VH-VQS of the impending traffic conflict. It is likely the absence of these facilities, which have been shown to provide good mitigation at other airports with similar traffic levels, increased the risk of a mid-air conflict in the Ballina area. [Safety Issue]
In addition to conducting the pilot flying role, the captain of VH-VQS assumed control of the radio to ensure separation with the incoming aircraft VH-VUE. This increased the captain's workload, resulting in reduced positional awareness of the more proximal VH-EWL and a subsequent traffic conflict with that aircraft.
Other factors that increased risk
The non-adherence to standard operating procedures by the captain of VH-VQS, although possibly influenced by a desire to expedite the take-off, was consistent with a steep cockpit authority gradient. This resulted in a lack of crew shared understanding and distraction, removing the opportunity for the first officer to identify the impending traffic conflict.
Despite a positive separation plan between VH-VUE and the two other aircraft, no such plan was established between the pilots of VH-EWL and the crew of VH-VQS. This led to the pilots of VH-EWL expecting VH-VQS to remain in the line-up position until after VH-EWL had completed the missed approach and therefore not perceived as a conflict threat.
The radio call to inform Ballina/Byron Gateway traffic that VH-VQS was rolling was transmitted after the take-off roll had commenced. This limited the opportunity for the instructor in VH-EWL to process the situation and ensure adequate separation.
The decision by the crew of VH-VQS to remain below VH‑EWL’s operating altitude after take‑off, although intended to assure adequate separation until sufficient lateral separation was established, resulted in non‑standard handling of the aircraft and the activation of a number of master warning/caution alerts.
Context
Ballina/Byron Gateway Airport
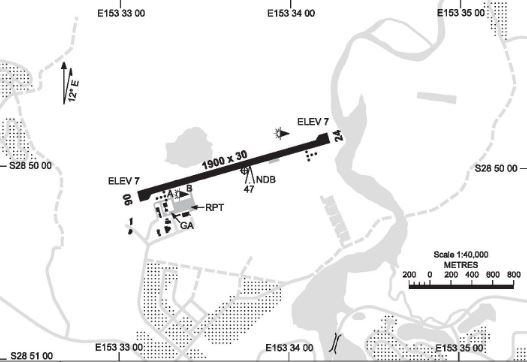
Ballina/Byron Gateway Airport (Ballina airport) was a certified aerodrome with a single, sealed 1,900 m long and 30 m wide runway. The runway was orientated in a 062°/242° magnetic (north‑east/south‑west) direction with an elevation of 7 ft above sea level. The airport did not have taxiways parallel to the runway for use when positioning aircraft for departure or after arrival. Therefore, aircraft were often required to backtrack on the runway prior to take‑off and after landing. The airport had GPS‑based instrument approaches and a non-directional beacon ground-based navigation aid. Runway 06 was designated as a right-hand traffic pattern and circling to the north of runway 06/24 was not permitted for aircraft conducting instrument approaches. These requirements were due to the higher terrain to the north of the runway (Figure 2).
Figure 2: Navigational chart depicting the Ballina airport runway and position of the regular public transport (RPT) apron areas. Note there are no taxiways running parallel to the runway
Source: Airservices Australia
Traffic services
At the time of the occurrence, Ballina airport did not have a control tower and was not supported by air traffic control and/or traffic advisory facilities. It was equipped with a fire command centre and provided fire and rescue services when high-capacity aircraft were operating at the airport.
Civil radar around Ballina was capable of tracking aircraft that were equipped with a transponder above about 5,000 ft. Military radar and automatic dependant surveillance broadcast systems were not used by civil air traffic services in the Ballina area.
Airspace and traffic separation
Airspace above Ballina was classified as class G (non-controlled) below 8,500 ft. Above this altitude, the airspace changed to class C (controlled), where air traffic information and separation control were provided. Restricted airspace is located approximately 5 NM (9 km) south of the airport, which is activated by a notice to airmen when military high-speed jet aircraft were using that airspace and/or live-firing exercises where underway.
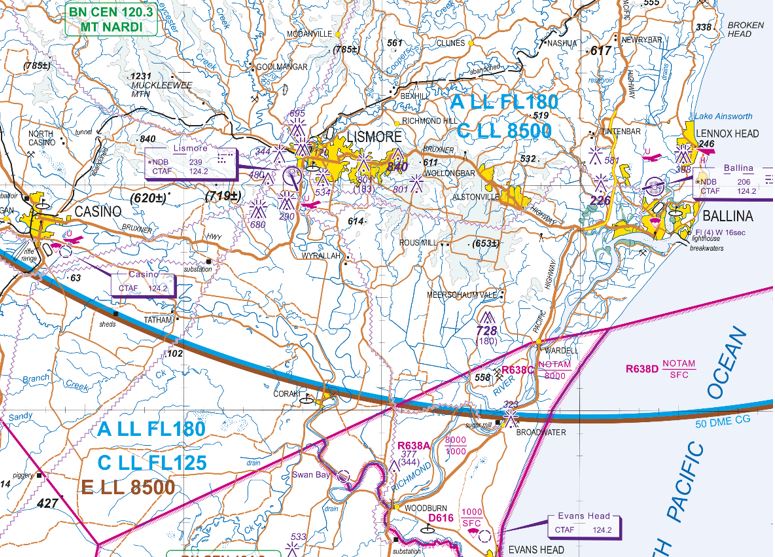
As well as prescribed traffic patterns for aircraft to follow in the immediate vicinity of the runway, the primary method of traffic separation at Ballina airport was visual. This relied on flight crew being able to use ‘see and avoid procedures’, which were stipulated in various regulations and guidance material for non-controlled aerodromes. See and avoid also relies on voice communication using the Common Traffic Advisory Frequency (CTAF). Due to their close proximity, the Ballina airport CTAF was shared with Casino and Lismore airports. As such, a pilot using this frequency would be affected by all radio transmissions from traffic at any one of these airports (Figure 3).
Figure 3: An extract of the Visual Terminal Chart of the Ballina area. The Casino and Lismore airports are depicted and share the CTAF of 124.2 MHz with Ballina airport. Also depicted in magenta are the restricted areas to the south Ballina, and the lower limit of the class C controlled airspace overhead those airports of 8,500 ft (in blue)
Source: Airservices Australia
Passenger numbers and traffic movements
An aeronautical study of activity at Ballina airport by the Civil Aviation Safety Authority’s (CASA) Office of Airspace Regulation[8] was released in July 2015. Using statistical data from the Bureau of Infrastructure, Transport and Regional Economics for the period 2009‑2014, the study identified an average increase in passenger numbers at Ballina airport between 2009 and 2014 of six per cent per annum. Over the same period, the number of regular public transport movements increased by an average of four per cent per annum.
More recent data from Airservices Australia (annualised to September 2016) identified that, while the number of air transport movements had remained constant, there has been a five per cent increase in passenger numbers to 486,600. That is consistent with the increased use of larger aircraft, such as the Airbus A320, Boeing 737‑800 and large turboprop aircraft.
The CASA study also identified that the total number of aircraft movements increased initially by five per cent per annum until 2013 and then by 12 per cent per annum. One-third of the projected 12 per cent increase was attributable to greater regular passenger transport services. The remaining increase was attributable to a mixture of VFR[9] traffic, including training flights (including aircraft conducting circuit training), helicopter operations, private and charter operations and intermittent parachute operations.
The CASA study also found that, when compared with other airports with similar traffic levels, Ballina recorded the highest number of reported safety incidents between 2009 and 2014 relating to separation and communication issues, and almost double the number of reported incidents as the next highest airport (Table 1). The study also noted that a direct comparison between airports was difficult as ‘…every aerodrome is different and supports different levels and mixes of air traffic.’
More recent data detailing the aviation activity at Ayers Rock, Port Hedland and Ballina for the year ending September 2016 is shown in Table 2. Of note, both the total movements and air transport movements at Ballina had reduced from the year ending December 2014, while the passenger numbers increased.
Table 1: Number of reported separation and communication incidents for similar airports
Source: Airservices Australia and ATSB data provided to the Office of Airspace Regulation
Table 2: Aviation activity at Ayers Rock, Port Hedland and Ballina airports for the year ending September 2016
Total movements
Air transport movements
Passenger numbers
Ayers Rock
18,200
5,500
365,100
Port Hedland
12,282
10,485
424,741
Ballina
12,200
6,300
486,600
Source: Airservices Australia
Certified air/ground radio service
A certified air/ground radio service (CA/GRS) is an aerodrome radio information service that provides pilots with weather and traffic information. CASA Advisory Circular AC 139-27 Guidelines for certified air/ground radio services stated that:
The primary purpose of a CA/GRS is to enhance the safety of air transport operations by the provision of relevant traffic information. A CA/GRS is beneficial in that the pilot receives traffic information in specific terms for their flight(s), which enhances their ability to see and avoid potentially conflicting traffic.
The CA/GRS also provides an automated aerodrome information service that broadcasts the:
preferred runway
wind direction and speed
runway surface conditions
atmospheric pressure at sea level (QNH)
temperature
cloud base and visibility
weather information
aerodrome operational information.
A CA/GRS does not provide definite traffic separation, as would occur at a controlled aerodrome. Instead, it provides relevant information to assist pilots organise their own separation.
The CA/GRS includes a certified air/ground radio operator who meets the training and qualifications requirements to hold the regulatory approval to carry out this role. The system also contains a minimum list of service facilities and documentation required by CASA. These facilities and documentation requirements included:
a workstation with full view of the circuit area and manoeuvring area
a very high frequency transmitter/receiver operating on the CTAF or broadcast area frequency
an automatic aerodrome information service on a separate very high frequency transmitter
meteorological instrumentation that complies with Bureau of Meteorology standards for aviation use
current aeronautical documents, including notices to airmen, appropriate to instrument flight rules and visual flight rules operations within the vicinity of the aerodrome or broadcast area
a telephone
local CA/GRS operating procedures
an aerodrome emergency plan.
At the time of the occurrence, Ballina airport did not have CA/GRS. Recent reviews of the airspace around Ballina by the CASA Office of Airspace Regulation identified a complex mix of air traffic and strong growth in overall passenger and operating traffic numbers. The reviews also examined the frequency and type of safety occurrences comparable to other non-controlled aerodromes.
The CASA report titled Supplementary Airspace Review of Ballina Byron Gateway of July 2015 recommended that the operator of Ballina airport implement a CA/GRS before the end of June 2016 to reduce the airspace risk. It also noted that CASA should continue to monitor movement numbers at Ballina with a view to designating Ballina as a controlled aerodrome as soon as the risk to traffic warranted.
In September 2016, the ATSB was informed by the operator of Ballina airport that approval had been granted for the implementation of a CA/GRS at Ballina by Airservices Australia and CASA. Certified air/ground radio operations commenced in March 2017 from the airport’s fire command centre’s facilities.
Aircraft systems
Traffic alert and collision avoidance system
The Airbus A320 is equipped with a traffic alert and collision avoidance system (TCAS) designed to detect transponder-equipped traffic within a 30-40 NM (56‑74 km) radius and up to 9,900 ft above and below the aircraft (referred to as intruders). Depending on the phase of flight, and the level of sophistication of the intruding aircraft, the TCAS categorises the intruder(s) depending on the potential for conflict and/or collision. The category of the intruder determined which symbol would be used to represent the traffic on the flight crew’s navigation displays (ND). In certain emergency situations the TCAS would offer instructions to the pilot through aural alerts and visual alerts on the navigation and primary flight displays to avoid a collision.
The intruder categories were represented as follows (Figure 4):
Proximate ‐ no collision threat existed but the intruder was in the vicinity of the aircraft (closer than 6 NM (11 km) laterally and ±1200 ft vertically). The pilot would see a white filled diamond symbol on their ND depicting the position of the intruder.
Traffic advisory (TA) ‐ a potential collision threat existed, however the closest point of separation was about 40 seconds away on the current projected flight paths. The pilot would see an amber filled circle on their ND, as well as receiving an aural alert.
Resolution advisory (RA) ‐ a real collision threat existed and the closest point of separation was approximately 25 seconds away or less. The pilot would see a red filled square on their ND and receive vertical speed orders on their primary flight display and a series of aural alerts.
Other intruders ‐ no collision threat existed and any non-proximate traffic with 30 NM (56 km) and a defined vertical range was depicted. The pilot would see a white outline diamond on their ND depicting the position of the intruder.
Relative altitude - in all categories the pilot would receive indications on their ND of the relative altitude of the intruder in hundreds of ft.
Vertical speed arrow - in all categories, if the intruder was climbing or descending at greater than 500 ft per minute, the pilot would see an up or down arrow on their ND.
No bearing intruder - If the bearing of a suspected TA or RA intruder was not available, it was displayed in amber or red in digital form at the bottom of the ND
Figure 4: Typical Airbus A320 navigation display depicting the various representations of TCAS intruders. The number of each representation accords with the numbered list above
Source: Airbus
TCAS inhibit
Depending on the aircraft’s altitude, some of the TCAS advisories and alerts were inhibited. In particular:
All intruders flying below 380 ft above ground level (AGL) when the own aircraft altitude is below 1,700 ft AGL.
All RA alerts when the own aircraft was below 1,100 ft AGL and climbing, and below 900 ft AGL on descent. In this case, the RA was converted into a TA.
All TA aural messages when the own aircraft is below 600 ft AGL in climb, and below 400 ft AGL on descent.
During take-off, all RA alerts are converted into TA alerts and all TA aural alerts are inhibited.
Aircraft alerting systems
The Airbus A320 is equipped with various sensors throughout the aircraft to monitor key parameters. These sensors feed their respective data into two System Data Acquisition Concentrators, which in turn process the data and feed it to two flight warning computers (FWCs). The FWCs check for discrepancies in the data and then display the data on the electronic centralised aircraft monitor system (ECAM). In the event of a fault, the FWCs generate the appropriate warning messages and sounds. More vital systems are routed directly through the FWCs such that failures in those systems can still be detected even with the loss of both System Data Acquisition Concentrators. The whole system can continue to operate even with a failure of one of the concentrators and one FWC.
Failures are classed by importance, ranging from level 1 failures to level 3 failures. In the event of simultaneous failures the most critical failure is displayed first. The warning/caution hierarchy is as follows:
Level 3 failures: Warnings reflecting situations that require immediate crew action and that place the flight in danger. These are enunciated with a red master warning light, a warning (red) ECAM message and a continuous repetitive chime or a specific sound or a synthetic voice. The chime can be silenced by pressing the master warning push button.
Level 2 failures: Cautions showing failures that require crew attention, but not immediate action and with no direct consequence to flight safety. Level 2 failures are shown to the crew through an amber master caution light, a caution (amber) ECAM message and a single chime.
Level 1 failures: Cautions, failures and faults that lead to a loss of system redundancy and require monitoring but present no hazard. Level 1 failures are enunciated by a caution (amber) ECAM message but produce no aural warning.
Gear not down and locked master warning
In the event that the system detects the thrust levers being retarded outside a defined take-off thrust parameter and the landing gear is not down while at a low altitude, the system classifies the condition as a level 3 failure. In this case the red master warning activates to alert the crew of the condition.
Autothrottle disengage master caution
If the thrust levers are retarded after the application of take-off/go-around thrust, the autothrottle system disengages and the system generates a level 2 failure message. This activates the amber master caution alerts to notify the crew of the condition.
Take-off performance
Take-off performance is typically calculated for each flight to allow for variations such as runway length, aircraft weight and environmental conditions. To assist with these calculations, Jetstar Airways (Jetstar) provided crews with a computer tablet loaded with a program known as ‘Flysmart’, into which a series of parameters could be entered before each flight. This program then generated an optimum take-off solution including the:
optimum flap setting
maximum speed in which the take-off can be rejected and remain within the runway confines (V1)
optimum speed in which to commence the take-off rotation (VR)
optimum speed to maintain in the event the take‑off is continued after the loss of thrust on one engine (V2).
To allow for minor fluctuations in temperature and/or barometric pressure between calculation of take-off performance and actual take-off time, pilots would typically increase the outside air temperature value by 1 °C and decrease the barometric pressure value by 1 hPa. This was a conservative measure designed to alleviate the need to recalculate performance data once taxiing had commenced.
Manufacturers and operators of transport category aircraft emphasise the importance of the decision to stop or continue the take-off in the event of a problem before reaching V1. The Airbus recommendations and Jetstar training matrixes in such cases included a list of reasons to reject the take-off before V1. This list was divided into reasons to reject below 100 kt for Airbus aircraft (80 kt for Boeing aircraft) and when above 100 kt but before V1. The rationale behind the two lists of reasons was that at higher speed it was only desirable to reject for critical conditions that affect the immediate safety of flight and that the take‑off could be continued for less serious faults.
The Jetstar Flight Crew Training Manual contained the following guidance to assist crews in the decision to reject the take‑off:
…To assist in the decision-making process, the take-off is divided into low and high-speed regimes, with 100 kt being chosen as the dividing line. The speed of 100 kt is not critical but was chosen in order to help the Captain make the decision and to avoid unnecessary stops from high speed:
Below 100 kt, the Captain will seriously consider discontinuing the take-off if any ECAM warning/caution is activated.
Above 100 kt, and approaching V1, the Captain should be “go‑minded” and only reject the take-off in the event of a major failure, sudden loss of thrust, and any indication that the aircraft will not fly safely, any red ECAM warning, or any ECAM caution listed below:
- F/CTL SIDESTICK FAULT
- ENG FAIL
- ENG REVERSER FAULT
- ENG REVERSE UNLOCKED
- ENG 1(2) THR LEVER FAULT
…
To ensure these reasons for continuing or rejecting a take-off were highlighted in the crew’s mind, and that all crew members shared the same mental model, it was compulsory to brief these reasons and required actions before every take-off.
The decision to stop or continue the take-off in the event of an impending traffic conflict before V1 was not covered in these reasons, either below or above 100 kt.
FLEX temp/take-off/go-around
The calculated performance data also included a temperature known as a ‘FLEX’ temperature, which could be programmed into the aircraft to provide a reduced take‑off power setting. With the exception of specific environmental conditions and certain runway conditions listed in the Jetstar manuals, reduced power take-off settings were encouraged whenever available to decrease engine wear and fuel burn while still meeting the required take-off parameters.
Once the FLEX temperature was calculated and entered into the aircraft’s systems, the desired thrust setting was achieved by the pilot pushing the thrust levers into the FLEX detent of the thrust lever quadrant at the commencement of the take-off roll. This signalled the autothrottle system to set the desired power. Alternatively, the pilot could push the thrust levers beyond the FLEX detent into the take-off/go-around detent. This would cancel the reduced thrust and provide maximum available engine thrust for the environmental conditions.
Standard operating procedures
Standard operating procedures encompass such things as the standardised and coordinated order in which a series of steps are undertaken (scan action flows) and checklists to ensure that the required steps are completed correctly. These scan action flows and checklists are described in the Jetstar Flight Crew Training Manual, Flight Crew Operations Manual amplified and supplementary procedures and the Quick Reference handbook.
In order to achieve a balanced workload and encourage a shared crew mental model, the standard operating procedures were typically divided into areas of responsibility. This ensured that each crew member was aware of their actions dependent on the phase of flight, and increased their ability to predict other crew members’ actions. This awareness and predictability increased the likelihood that a deviation from standard operating procedures would be detected.
In two pilot operations, the areas of responsibility were typically divided into the pilot flying role (PF) and pilot monitoring roles (PM). The PF was primarily responsible for guidance of the aircraft in the air and, on some aircraft, while taxiing. The PM was responsible for monitoring the aircraft’s progress and carrying out supplementary support tasks, such as the activation of switches at the PF’s request and communicating on the radio. Crew resource management principles dictate that during all phases of flight, each crew member has a clear understanding of the role for which they are responsible.
In the event that these areas of responsibility need to change, it is essential that this be communicated clearly. In the event of a complete change from PF to PM, standard phrases such as ‘handing over’ and ‘taking over’, or ‘you have control’ and ‘I have control’ are commonly used. In the event that the roles are partially amended, the area amended is clearly communicated such as ‘your radios’ or ‘I have the radios’.
A clear understanding of each crew member’s area of responsibility reduces duplication, omissions, and/or the risk of a loss of shared mental model.
Crew resource management
Crew resource management is a skill developed by flight crew through training that focuses on using all available resources to assist decision making while avoiding or managing error (Harris, 2011). It is underpinned by good communication and appropriate use of available resources, including those outside of the flight deck, such as air traffic control.
Cockpit gradient
The term ’cockpit gradient’ describes the relative level of authority that exists between various crew members, and the way this authority influences communication and decision making. It is widely accepted that the pilot in command has ultimate responsibility in terms of decision making. However, depending on the cockpit gradient, other crew members are encouraged or discouraged from influencing these decisions through their own inputs.
A ‘level’ cockpit gradient is where all crew members have equal weighting in their input and influence towards a decision. However, care must be taken to ensure the gradient is not too ‘flat’ and it is clear as to who is ‘in charge’.
A ‘steep’ cockpit gradient is when the pilot in command has an overwhelming influence in decision making, with little input sought from the other crew members. A steep gradient can ‘inhibit communication, coordination and the cross‑checking of errors’ (Harris, 2011).
Levels of assertion
In order to standardise and provide a graduated method in which a junior crew member, such as a first officer, communicates pertinent information to a more senior crew member, a number of acronyms have been developed. These are designed to enable junior crew to pass information in a way that emphasises its importance and the associated level of concern. In particular, they also include any observed deviations from standard operating procedures. For example, Jetstar has adopted the acronym ‘R.A.I.S.E’, which emphasises the importance of:
R - Relay information: "There's a strong tailwind here on base."
A - Ask a question: "Do you think you should start the final turn early?"
I - The 'I' statement: "I am concerned that we'll cross over to the other runway path."
S - Solution statement: "Increase your bank angle."
E - Emergency statement: "Captain, you must act now!"
If the situation is still unresolved, then the pilot-not-flying must take control of the aircraft using the phrase "I have control".
Depending upon the urgency of the situation, it may be necessary to skip some stages, or enter the process at a later stage.
On 14 January 2016, Airbus A320, registered VH-VQS (VQS) and operating as Jetstar 465 taxied for departure runway 06[1] at Ballina/Byron Gateway Airport, New South Wales. The flight was a scheduled passenger service originally scheduled to depart for Melbourne, Victoria at 1330 Eastern Daylight-saving Time[2] but had been delayed until 1404 by previous schedule disruptions. The flight crew consisted of a captain, who was pilot flying (PF) and a first officer (FO) who was pilot monitoring (PM).[3] Both had been called out as part of a reserve duty and had operated the previous flight from Melbourne.
As VQS taxied, a Beech Duchess BE-76, registered VH-EWL (EWL), was conducting navigation aid training in the Ballina area. EWL had commenced a practice RNAV Z instrument approach (appendix A) for runway 06, with the intention of conducting a missed approach manoeuvre from a point approximately 660 ft above the landing threshold. EWL had an instructor and a student on board, with the student pilot hand flying the practice approach and responsible for communicating on the radio. As part of the exercise, the student was using a hood that inhibited vision outside the cockpit, simulating a reduced visibility approach, while the instructor maintained a visual lookout. The approach was also conducted with a simulated single engine failure.
At 1406, while VQS was taxied towards the holding point prior to entering runway 06, the instructor of EWL reported being on a 5 nautical mile (9 km) final passing 2,000 ft and estimating the missed approach point at 1412.[4] The captain of VQS confirmed with the pilots of EWL that they intended to conduct a missed approach rather than land and, at 1407, the FO broadcast that they were entering the runway and backtracking. The FO reported that, as the aircraft backtracked, EWL was sighted on a long final approach and that the captain and FO were confident of maintaining adequate separation during the take-off. The instructor in EWL reported expecting the crew of VQS to delay commencement of the take‑off until EWL was in the missed approach. However, the captain of VQS advised that the intent was to depart prior to EWL reaching the missed approach point. That intention was not conveyed to the pilots of EWL.
As VQS taxied and EWL was conducting the practice approach, a third aircraft, a Boeing B737‑800, registered VH-VUE (VUE) and operating as Virgin 1141, approached the Ballina area from the south with the initial intention of carrying out an RNAV X instrument approach and landing on runway 06 (appendix B). All three aircraft communicated on the Common Traffic Advisory Frequency (CTAF)[5] in order to coordinate separation assurance between the aircraft. During this process, the crew of VUE elected to discontinue tracking for the RNAV X approach, and instead join the traffic pattern from overhead the runway at 3,000 ft before conducting a visual circuit to runway 06. As part of the communication, the instructor in EWL also agreed to conduct a left turn on reaching the missed approach point to assist with separation. Additionally, the crew of VQS agreed to remain below 2,000 ft on departure until clear of VUE.
Once VQS had entered the runway, there were no further exchanges on the CTAF between the crew and EWL. However, there were exchanges between the crews of VQS and VUE to confirm that VUE would be maintaining 3,000 ft and that VQS would not climb above 2,000 ft on departure until both aircraft had adequate separation. These radio exchanges contributed to the decision by the crew of VQS to hold in the line-up position for 41 seconds while EWL continued the approach. Both the captain and FO of VQS were heard transmitting on the CTAF. Although the PF making radio calls was contrary to that role (see the section titled Standard operating procedures), the FO indicated that the captain’s reason for making the transmissions as PF may have been to expedite understanding of the intentions of the crew of VUE.
At 1410, the captain of VQS commenced the take-off roll and shortly after the FO transmitted an ‘all stations’ radio call to announce the take-off. Although the crew had previously calculated and briefed the use of a reduced thrust take-off power setting as per standard operating procedure, the captain actually selected take-off/go-around (TOGA) power. By using TOGA,the engines were commanded to provide the maximum available thrust for the environmental conditions (see the section titled Take-off performance). The FO stated that the commencement of the take‑off at that time and the selection of TOGA thrust were unexpected. However, as TOGA thrust was in excess of that required for take-off, the FO did not challenge this selection. Additionally, the FO assessed that the initiation of the high‑energy take‑off limited the opportunity for further discussion on the position of EWL.
As EWL was on short final and approaching the missed approach point over the landing threshold of runway 06, the instructor noticed VQS commence the take-off roll and then heard the associated radio call from the FO of VQS on the CTAF. The instructor told the student to look up from under the hood because it was felt that VQS should not be commencing take‑off. There were no radio exchanges between the two aircraft at that time and the instructor recalled that EWL was just short of the runway as VQS rotated. The instructor stated that they were satisfied with continuing as planned and that they did not lose sight of, nor overtake VQS.
The captain of VQS stated that as the aircraft accelerated towards 100 kt, they noticed a proximate traffic symbol on the navigation display (see the section titled Traffic alert and collision avoidance system). This symbol indicated an aircraft approximately 400 ft above and directly behind VQS, which the captain believed to be EWL. The captain pointed this out to the FO and sought confirmation of the position of the traffic while continuing with the take‑off. The FO reported that in response, after rotation, the FO assessed the traffic alert and collision avoidance system (TCAS)[6] display and advised the captain that the aircraft was about ‘1 mile’ (nautical mile, 1.9 km) behind and 400 ft above their aircraft. The captain advised not being happy to fly through EWL’s level.
VQS rotated at approximately 134 kt, which coincided with the calculated maximum speed at which the crew could initiate a rejected take-off and stop the aircraft within the runway confines (see the section titled Take-off performance). Neither the captain nor the FO reported discussing rejection of the take‑off following identification of the TCAS traffic and the captain recalled that, given the length of the runway, they did not want to abort. Calculations by Jetstar Airways identified that had the take-off been rejected just prior to V1[7], the aircraft could have been stopped 239 m from the runway end.
The captain of VQS rotated the aircraft to an initial take-off pitch angle of approximately 10° and after lift‑off, the FO commenced retracting the landing gear. At approximately 150 ft above the runway, the pitch angle was reduced to 5° and the rate of climb reduced to approximately 600 ft per minute. The captain reported taking this action in order to avoid flying through EWL’s level until adequately laterally separated.
As a result of the lower pitch angle and TOGA thrust setting, the airspeed rapidly increased towards 200 kt, which was the maximum flap limit speed for the take‑off configuration selected (CONFIG 2). The FO recalled calling ‘speed’ in order to alert the captain of the impending flap overspeed and that the captain reacted by retarding the thrust levers to idle power. The captain then called for the FO to retract the flap to the CONFIG 1 position, which had a higher maximum limiting speed. The FO carried out this action.
The aircraft master warning activated due to the thrust lever being retarded below take-off thrust while the landing gear was not down and locked and the aircraft was at a low altitude. The master caution also activated as a result of the autothrottle system disengaging when the thrust was manually reduced (see the section titled Aircraft alerting systems).
The crew of VQS stated that on assessing that the aircraft was clear of EWL and accelerating away (Figure 1), they manually re-established a normal climb out pitch attitude and thrust setting. At approximately 1,700 ft VQS conducted a right turn to intercept the outbound track, which was contrary to the left turn stipulated in the Jetstar Airways departure procedures. The remaining flight to Melbourne was normal.
Figure 1: A screenshot of the radar display depicting the positions of VQS (JST 465) and EWL in the vicinity of Ballina. VUE (VOZ 1141) is also seen approaching from the south-west
Source: Airservices Australia, modified by the ATSB
The sources of information during the investigation included:
the flight crews of VH-VQS and VH-EWL
flight data from VH-VQS
Jetstar Airways
Airservices Australia radar data
the Civil Aviation Safety Authority
the Ballina/Byron Gateway Airport operator.
References
Harris D 2011, Human Performance on the Flight Deck, Ashgate Surrey, England.
Martin WL, Murray, PS, Bates, PR 2012, The Effect of Startle on Pilots During Critical Events: A Case Study Analysis, Proceedings of the 30th EAAP Conference: Aviation Psychology & Applied Human Factors, Sardinia, Italy, pp. 388–394.
Rivera, JR, Talone, AB, Boesser, CT, Jentsch, F and Yeh, M 2014, Startle and Surprise on the Flight Deck: Similarities, Differences and Prevalence, Proceedings of the Human Factors and Ergonomics Society 58th Annual Meeting, Chicago, IL United States, pp. 1047–1051.
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the flight crew of VH-VQS, Jetstar Airways, the pilot instructor of VH-EWL, the Ballina/Byron Gateway airport operator, the Civil Aviation Safety Authority, Airservices Australia and the accredited representative of the French Bureau d'Enquêtes et d'Analyses (BEA).
Submissions were received from the first officer of VH‑VQS, Jetstar Airways, the Ballina/Byron Gateway airport operator, the Civil Aviation Safety Authority and Airservices Australia. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Early on the morning of 11 November 2015, a Watco freight train, 4K26, was travelling southbound on the Frenches to East Northam rail line in Western Australia. The train was travelling at about 60 km/hr along a section of track as it approached a left corner, approximately 3 km north of Northam (Figure 1). As the train rounded the corner, the driver saw a hot air balloon in close proximity to the rail tracks. The driver observed that the balloon was low to the ground and inside the rail corridor,[1] to the left side of the track (Figure 2).
Figure 1: Location of incident with rail line (white) showing direction of travel of the train, the approximate width of the rail corridor (yellow), the direction of travel of the hot air balloon (orange dashed line) and the approximate position of the hot-air balloon (red mark)
Source: Google maps. Modified by ATSB
Figure 2: View from train driver’s cabin as the train rounded the corner with the approximate position of the fences (yellow) either side of the rail line marking the rail corridor
Source: Watco driver’s video, modified by ATSB
The driver estimated that the balloon was approximately 200–300 m in front of the train and applied full service brakes. However, the driver realised there would be insufficient distance for the train to come to a complete stop before passing the balloon. At the same time as applying the brakes, the driver also sounded the train’s horn to warn the balloon that the train was approaching. The driver slowed the train to about 20 km/hr as it passed the balloon.
Figure 3: Picture from the train driver’s cabin just before the train passed the balloon’s position with the approximate position of the fence on the left side (yellow)
Source: Watco driver’s video, modified by ATSB
The Kavanagh Balloons E-300, registered VH-LPG, had taken off east of Northam earlier in the morning for a scenic flight, with the pilot and 16 passengers on board. The pilot’s initial intention was to land in a paddock to the west of the rail line. However, the prevailing wind meant that this was not an option. Instead, they elected to land in the paddock east of the railway line, as the pilot judged it to be the most suitable location in the area. Also, flying to an alternative landing site may have unnecessarily impinged on fuel reserves with the prevailing winds and weather conditions on the morning.
The pilot crossed the rail line from the south-west to the north-east at a height of approximately 50–60 ft, and then descended to around fence top height. The pilot’s intention was to land inside the paddock, just after the fence line at the edge of the rail corridor. As the train came around the corner, the hot air balloon was on descent to the paddock. When the train passed the balloon, the pilot reported the basket was just above fence height and moving away from the rail tracks. The balloon crossed over the fence and landed in the paddock without incident.
Pilot comments
The pilot of the balloon made the following comments in relation to the event:
Crops in the centre of the paddock and a powerline limited the available landing space, which meant the pilot was landing close to the fence.
The pilot had landed in the same paddock on many occasions without problems.
The pilot did not recall hearing the train horn or brakes until the train passed the balloon.
Train driver and observer comments
The train driver and observer made the following additional comments:
The driver and observer saw the balloon in the distance, however due to the winding track it was not possible to see the location of the balloon relative to the track, until the train came around the bend.
They were unable to discern the direction of travel of the balloon.
When they saw the balloon, they believed a collision was likely.
They suggested that an awareness of the train schedule by balloon operators may avoid a similar event.
Proactive safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Balloon operator
The balloon operator is amending the Low Flying Operations section of their Operations Manual to include the following:
A minimum height of 50 feet shall be maintained when the flight path of the balloon will cause it to cross over a road reserve or rail corridor.
Safety message
Rail corridors are areas where access is strictly controlled as the presence of non-authorised or unexpected personnel and/or vehicles may pose a danger to the safety of rail operations and personnel. Trains require significant distance to come to a complete stop and may not be able to avoid colliding with an obstruction that is on, or near, the tracks.
Operators of balloons or other aircraft that may fly at low-level in the vicinity of rail tracks should consider and minimise risks when operating in these environments.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 15 August 2015, the student pilot of a Cessna 172 aircraft, registered VH-MJK (MJK) conducted a solo flight from Emkaytee aeroplane landing area (ALA) to Bathurst Island Airport, Northern Territory (Figure 1). There the student pilot completed touch-and-go circuits for about 30 minutes on runway 15.
Figure 1: Image showing Bathurst Island, Darwin and Emkaytee airports
Source: Google earth – annotated by the ATSB
At about 1210 Central Standard Time (CST), a Cessna 404 aircraft, registered VH-ANM (ANM) and operated by Hardy Aviation, departed from Darwin Airport, Northern Territory, on a scheduled flight to Bathurst Island, with a pilot and five passengers on board. The pilot broadcast when inbound and about 15 NM from Bathurst Island Airport on the common traffic advisory frequency (CTAF) of 126.5 MHz, and did not receive any response. At about 1220, the aircraft joined on the downwind leg of the circuit for runway 15 at 1,000 ft above ground level and broadcast joining the circuit. As the aircraft turned onto base, the pilot sighted MJK also on base, at the same height, closer to the runway and estimated it was about 150 m away (Figure 2).
The pilot of ANM immediately manoeuvred the aircraft to the west to increase separation between the two aircraft. After unsuccessfully trying to contact the pilot of MJK on the CTAF, the pilot of ANM briefly selected frequency 126.7 MHz to try to communicate with the pilot of MJK, but again did not receive a response. The pilot of ANM observed MJK conduct a touch-and-go, and kept that aircraft in sight, while overflying and re-joining the circuit on the crosswind leg.
After the touch-and-go, when upwind of the runway at about 500 ft above ground level, the pilot of MJK sighted ANM. ANM was then to the left, above MJK at 1,000 ft, and turning onto the downwind leg. The pilot of MJK then saw that the radio was selected to frequency 126.6 MHz. The pilot checked their flight plan, noted that the correct frequency was 126.5, and immediately changed the radio to that frequency. The pilot of MJK then broadcast a departure call on the CTAF. The pilot of ANM then contacted the pilot of MJK, who advised that the radio had been on the wrong frequency.
Figure 2: Bathurst Island Airport showing approximate aircraft tracks and relative positions
Source: Google earth – annotated by the ATSB
The pilot of ANM continued the approach, and landed at Bathurst Island, and MJK returned to Emkaytee without further incident.
The radar data provided to the ATSB by Darwin air traffic control, indicated the aircraft came within about 100 ft vertically and 0.6 NM at the closest proximity (Figure 3).
Source: Department of Defence – annotated by the ATSB
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Operator of VH-ANM
As a result of this occurrence, the operator of VH-ANM advised the ATSB that they have taken following safety action:
Notice to company pilots
The Chief Pilot distributed a notice to all company pilots advising them of the incident. The notice stated that the Tiwi Islands continue to be a hot spot for traffic, and reminded pilots to be ‘doubly aware’ when operating in the area.
Safety message
The pilot of MJK commented that there were three important learnings from this incident:
crosscheck the selected frequency against the flight planning notes
ensure the selector reaches the detent when selecting a radio frequency
listen for the ‘beep-back’ response from the CTAF to verify the correct frequency has been selected.
An aerodrome frequency response unit (AFRU) identifies correct radio frequency selection at non-towered aerodromes. The AFRU automatically responds to a transmission on the CTAF either with a pre-recorded voice message, if no transmission has been received in the previous five minutes, or with a beep-back.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
The pilot of the outbound aircraft, VH-WJQ, reported that he had passed a single engined light aircraft which was tracking inbound at the same altitude of 7,500ft. The inbound aircraft, VH-PDF, just before the incident, was still on the area frequency and had not yet obtained a clearance into the control area. The Approach Radar Controller noticed a transponder return, indicating an aircraft inbound at 6,200ft.
There was no need to advise the pilot of the outbound aircraft as the indicated vertical separation was 1,300ft. When the inbound aircraft came onto the control frequency to ask for a clearance, it became apparent that this aircraft was also at 7,500ft. The controller realised that the transponder of VH-PDF was suspect and asked the pilot to switch the height mode off. The pilot of VH-PDF did not see the outbound aircraft.
As the aircraft approached the holding point for runway 19, the Tower Controller issued a line up clearance. A Boeing 767 aircraft was on base for runway 19. The controller then judged that the sequence may be too close and told the taxiing aircraft to hold short of the runway. The crew of this aircraft were taxiing over the holding point and managed to stop just beyond the marked line.
The controller then had the option of sending around the Boeing 767, now on a two mile (3.7km) final approach, or asking the crew to accept a slightly infringed flight strip. The crew of the Boeing 767 decided to continue the approach and landed safely.
The crew of VH-KDJ taxied the aircraft for departure from runway 18. Calls were made on both the area and Mandatory Traffic Advisory Frequency (MTAF). From this it was ascertained there were two other aircraft operating in the area. Initially both were to use runway 18, but one of these advised he would land on 36 instead. This did not cause any problems for the crew of VH-KDJ, and they were still able to use runway 18.
Engine power was applied for take-off and as the roll started, they transmitted a call that they were rolling. The pilot of the aircraft using runway 36 called them and said there was another aircraft, of which they were not aware, taking off in the opposite direction. The take off in VH-KDJ was rejected at low speed and the two aircraft did not get close.
The conflicting aircraft on runway 36 was a Jabiru which was being flown on circuits. It was subsequently learned that the radio on the Jabiru was defective. A carrier wave could be heard when the pilot tried to transmit a message, but the pilot's voice could not be heard.
Significant Factor
The following factor was considered relevant to the development of the accident: