Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
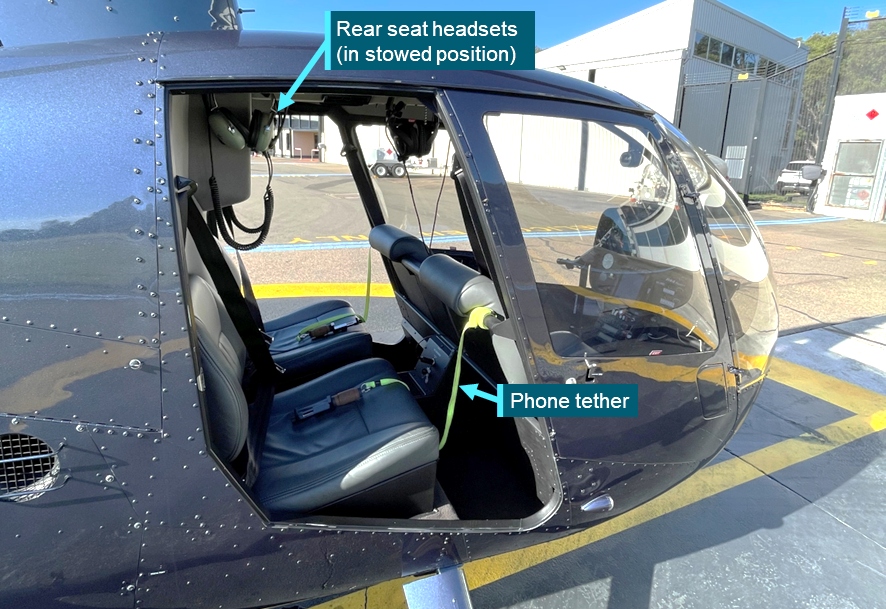
On the afternoon of 2 May 2026, a Robinson R44 Raven II helicopter was being prepared for a 30 minute ‘doors‑off’ sightseeing flight experience in Sydney, New South Wales, with 2 passengers in the rear seats. The flight was to be operated with the left and right rear doors removed from the helicopter, allowing passengers a wider view and an open-air experience. Both left and right front doors remained on the helicopter and the front left seat was vacant.
After receiving a video-based safety briefing, a ground crewmember boarded the passengers, tethered the passengers’ phones and provided a specific door-off briefing, which included use of the communication headsets and the need for keeping all parts of the body inside the cabin during the flight.
Figure 1: Helicopter in doors-off configuration
Source: Operator, annotated by the ATSB
The pilot reported that the departure from Sydney Airport was normal and the helicopter climbed to cruising height and tracked north to the city before following the harbour to North Head. After rounding the head and turning north, the pilot pointed out for interest another aircraft that was tracking parallel to the helicopter. At that moment, the rear right passenger placed their head through the open doorway for a better view. As the helicopter was travelling at around 80 kt indicated airspeed at that time, the slipstream immediately caught and pulled the passenger’s headset rearward, away from their head and leaving it hanging outside the helicopter cabin – retained by the connecting cable. The passenger was able to retrieve the headset using the cable, however the right ear cup cushion detached from the unit and was lost from the helicopter.
After the passenger re-donned the headset, the remainder of the flight was uneventful, and the helicopter sustained only minor scuffs and scratches from the headset contact.
Related occurrences
The US National Transportation Safety Board has undertaken several investigations into accidents and serious incidents resulting from loose objects striking a helicopter’s tail rotor.
WPR13CA071 – Headset lost from doors-off flight, striking tail rotor
WPR14CA363 – Jacket lost through open window, striking tail rotor
LAX03TA150 – Jacket lost through opened door, striking tail rotor
FTW86LA047 – Life vest lost through opened door, striking tail rotor
Advisory
The helicopter manufacturer published Safety Notice SN-30 in 1994 (revised in 2009) warning of the danger that loose objects present to the safety of flight – particularly with doors-off operations.
Safety message
While many helicopters (including the R44) can be approved for operation with one or more doors removed, doing so eliminates a key defence against objects and items being lost from the helicopter interior. As any item lost has the potential to strike and damage the tail and/or main rotors, doors-off flight inherently increases the operating risk environment, such that countering precautions must be taken.
While the operator’s existing operational procedures provided several sound physical and instructional defences against inadvertent passenger-related loss of items from the helicopter, this occurrence illustrates that it is indeed possible (and human) to ‘get caught up in the moment’ and briefly forget instructions given in briefings and during boarding. In this context, all helicopter operators providing doors-off flight experiences should consider whether further precautions may be applicable and desirable for their own operations.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2026-028
Occurrence date
02/05/2026
Location
20 km north-east of Sydney Airport
State
New South Wales
Occurrence class
Incident
Aviation occurrence category
Objects falling from aircraft, Passenger related
Highest injury level
None
Brief release date
27/05/2026
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R44 II
Sector
Helicopter
Operation type
Part 133 Air transport operations - rotorcraft
Activity
Commercial air transport - Non-scheduled - Joy flights / sightseeing charters
Departure point
Sydney Airport, New South Wales Sydney Airport, New South Wales
Destination
Sydney Airport, New South Wales Sydney Airport, New South Wales
The ATSB is investigating the fracture of a main landing gear wheel on a Saab 340B aircraft, registered VH‑VEF, at Melbourne Airport on 1 April 2026.
After a flight from Orange, New South Wales, to Melbourne, Victoria, a post-flight inspection identified that one of the aircraft's tyres had deflated and that a section of the wheel rim had fractured and separated. The separated piece was subsequently found on the lead-in to the aircraft's parking bay at Melbourne Airport.
Engineering inspections by the operator found evidence of fatigue cracking within the tyre bead seat area. The wheel had been recently overhauled by the supplier and had not previously been fitted to the operator's aircraft.
The ATSB has reviewed the wheel's overhaul records and will obtain a copy of the wheel supplier's investigation report into the occurrence. The fractured wheel, part number 5010488, was of the original design that was the subject to a number of in-service fractures, including two previous occurrences in Australia that were investigated by the ATSB (AO-2009-006 and AO-2019-047).
The wheel was redesigned by the manufacturer, and the original design was superseded in December 1995, however there was no requirement to remove the affected wheels from service. The aircraft operator advised the ATSB that they currently have 8 wheels of this design in service.
As a result of this occurrence the operator has ensured that no two of those wheels are on the same landing gear leg of any aircraft, and it has also elected to remove the remaining wheels from service, rather than continue to have them overhauled.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2026-071
Occurrence date
01/04/2026
Occurrence time and timezone
0741 UTC
Location
Melbourne Airport
State
Victoria
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Objects falling from aircraft
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Saab Aircraft Co.
Model
340B
Registration
VH-VEF
Serial number
340B-457
Aircraft operator
Vee H Aviation Pty Ltd
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the morning of 3 December 2025, the pilot of a Cessna Aircraft Company 340, with 4 passengers on board, departed Gnowangerup Airport for a private business flight to Jandakot Airport, Western Australia, under instrument flight rules (IFR).
After departure, as the aircraft was climbing through flight level 110 (11,000 ft above mean sea level), the left side cockpit window failed (Figure 1) and was ejected from the aircraft, which rapidly depressurised. The pilot assessed the situation, and after ensuring continued aircraft controllability, requested clearance to descend and traffic information from air traffic control. A descent to 8,000 ft followed and the aircraft was subsequently cleared for a direct track to Jandakot. With the aircraft stable, the pilot and passengers examined the exterior, and with no airframe or control surface damage evident, continued the flight to Jandakot, where the approach and landing were uneventful.
Figure 1: Failed left cockpit window
Source: Aircraft operator
Engineering information
The Cessna 340 is a 6-seat pressurised twin-engined aircraft with a maximum take-off weight of 2,717 kg. It was introduced in 1972, with production continuing until 1984, with 1,351 aircraft built. The 340 cockpit is framed with 4 acrylic (plexiglass) windows – 2 forward windscreens, each with adjacent side panel windows that have smaller, inward opening quarter vent panels. The initial design of the side windows with the vent panels has been found to be susceptible to cracking and in-flight failure, and in April/May 1982 Cessna introduced Service Kits SK340-26-1/2 and issued Service Information Letter ME82-18 for earlier build 340/340A aircraft. The letter and service kits provide instructions and equipment for the reinforcement of both pilot and copilot’s side windows by adding a diagonal brace (Figure 2) behind the quarter panel vent. This supports the larger window panel and reduces the pressurisation stresses that could lead to cracking or in-flight failure such as sustained in this incident. The service letter recommended compliance within the next maintenance period but not exceeding the next 200 flight hours.
Information from the aircraft owner advised that following the incident aircraft’s importation into Australia in mid-2021, the left and right window service kits had been procured, however due to pandemic-related delays, the kits had not yet been installed at the time of the occurrence.
Figure 2: Example of reinforced cockpit side window
Owners and operators of Cessna Aircraft Company 340 and 340A aircraft are advised to check their aircraft for the installation of cockpit side window reinforcing in accordance with Service Letter ME82-18. Where such reinforcing has not been installed, regular inspection of the windows and surrounds for evidence of cracking and degradation is recommended – particularly in areas around the quarter vent panel. Installation of Cessna Service Kit SK340-26-1/2 (or approved equivalent) is recommended.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2026-006
Occurrence date
03/12/2025
Location
5 km north-west of Katanning Airport
State
Western Australia
Occurrence class
Incident
Aviation occurrence category
Emergency/precautionary descent, Objects falling from aircraft, Windows
On 29 January 2026, a Saab 340 aircraft, registered VH‑VEZ, was operating a scheduled passenger service from Canberra Airport, Australian Capital Territory, to Newcastle Airport, New South Wales, with 3 crew members and 19 passengers on board. During take-off, the left inboard main landing gear wheel separated from the aircraft.
After coordinating with air traffic control (ATC) the crew returned the aircraft to Canberra where it landed without incident. The crew shut down both engines on the runway, and the aircraft was towed to the apron, where passengers later disembarked. The main wheel was subsequently located against an internal airport fence.
What the ATSB found
Examination of the components found that the left inboard wheel separated due to failure of the wheel bearings. Due to the degree of damage sustained by the bearing components, it was not possible to determine the cause of the bearing failure.
What has been done as a result
As a result of this occurrence, the aircraft operator conducted a fleet‑wide inspection of main wheel assemblies and nose wheel assemblies for any defects. No faults were found on any aircraft at the time of inspection.
In addition, the operator implemented a proactive change to its wheel bearing maintenance schedule.
Safety message
This occurrence highlights the importance of effective communication and decision‑making in managing unexpected aircraft malfunctions. After being advised by ATC that a wheel had separated from the aircraft, the crew initially focused on climbing the aircraft to the minimum safe altitude, before taking time to apply standard operating procedures to plan a return to Canberra Airport.
Communication and coordination with ATC enabled confirmation of the specific missing wheel and emergency services preparation. In combination, these actions maintained safety margins and resulted in a safe landing.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 29 January 2026, a Saab 340 aircraft, registered VH‑VEZ, was operating a scheduled passenger service from Canberra Airport, Australian Capital Territory, to Newcastle Airport, New South Wales, as flight FC201, with 3 crewmembers and 19 passengers on board. At 1548 local time, the aircraft taxied from the apron and conducted a take-off from runway 35.1
During the initial climb, air traffic control (ATC) advised the flight crew that a wheel had separated from the aircraft. In response, the crew requested and received clearance to maintain runway heading and climbed to the minimum safe altitude. They reviewed the quick reference handbook (QRH) for checklist items applicable to the event, however none were identified.
As the aircraft approached the limit of the Canberra Airport control area, the crew made the decision to return to the airport. They advised the cabin manager and ground staff of the decision. In coordination with ATC, the crew conducted a fly‑by of the control tower to allow for a visual inspection of the landing gear. Tower personnel confirmed that the left inboard main landing gear wheel was missing. The crew then commenced orbits on the eastern side of the airport to allow time for landing preparation, ensuring the landing performance calculations and briefing tasks were completed. They assessed that a normal landing configuration was most appropriate for the situation, and advised the cabin manager and passengers accordingly.
The crew notified ATC of their intention to return to land and emergency services were placed on standby. The captain declared a PAN2 while the first officer coordinated with company operations staff. The aircraft was subsequently positioned on an extended final approach to runway 35.
At 1611, the aircraft landed safely and was brought to a stop at the end of the runway (Figure 1). Airport emergency services reported no fire, smoke, or fluid leaks from the landing gear. The crew shut down both engines on the runway, and the aircraft was towed to the apron, where passengers were disembarked. Canberra Airport safety personnel located the main wheel against an internal airport fence on the eastern side of runway 35.
Figure 1: VH-VEZ left main landing gear with separated inboard wheel
Source: Aircraft operator
Context
Aircraft information
VH-VEZ was a Saab 340B, serial number 340B‑450. It was manufactured in Sweden in 1998 and was first registered in Australia on 18 November 2022. The aircraft was powered by 2 General Electric CT7‑9B turboprop engines, equipped with Dowty Aerospace R390/4‑123‑F propellers.
Main wheel assembly information
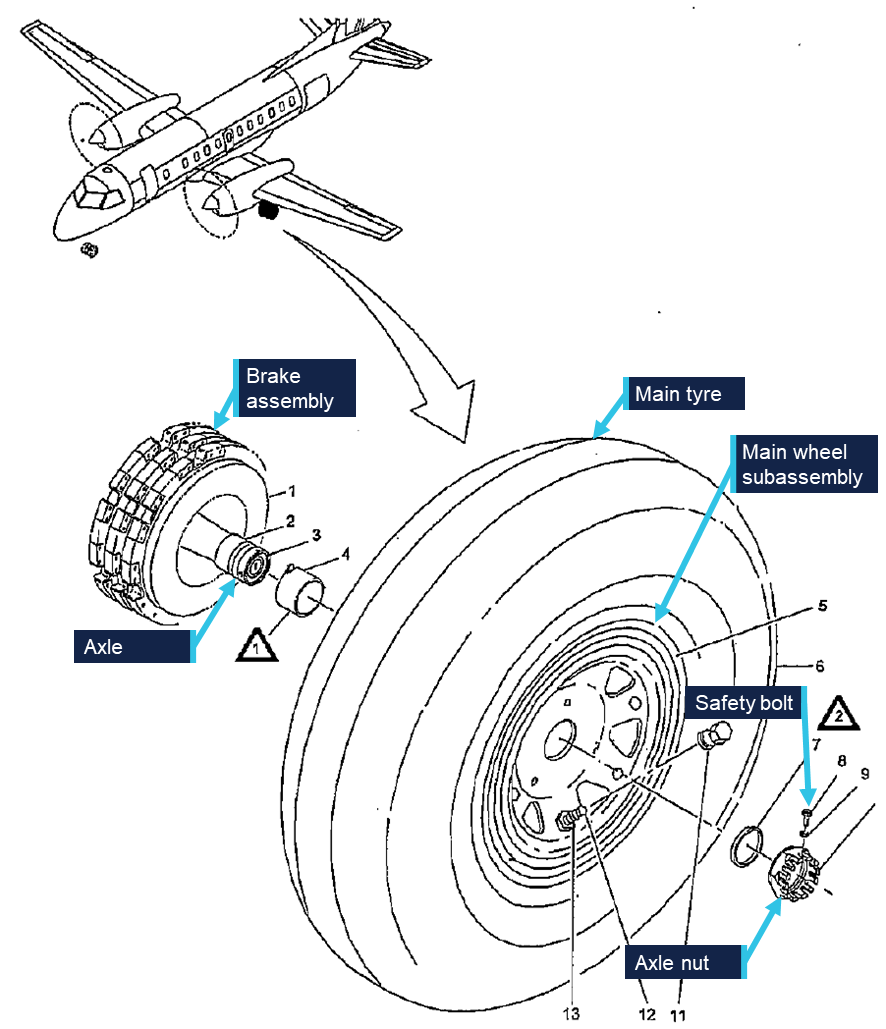
The Saab 340B main landing gear has an inboard and outboard main wheel, both with a brake assembly, attached to the main landing gear leg axle.
Main wheel assembly
An overview of a main wheel is shown in Figure 2. The main wheel assembly consists primarily of the tyre and the wheel subassembly; also referred to as the wheel hub. The main wheel assembly connects to the axle via an inboard and outboard tapered roller bearing, installed in the wheel subassembly as shown in Figure 2. The main wheel assembly is held onto the axle via a single axle nut and safety bolt.
Figure 2: Saab 340 main wheel assembly
Source: Saab Aircraft Maintenance Manual, annotated by the ATSB
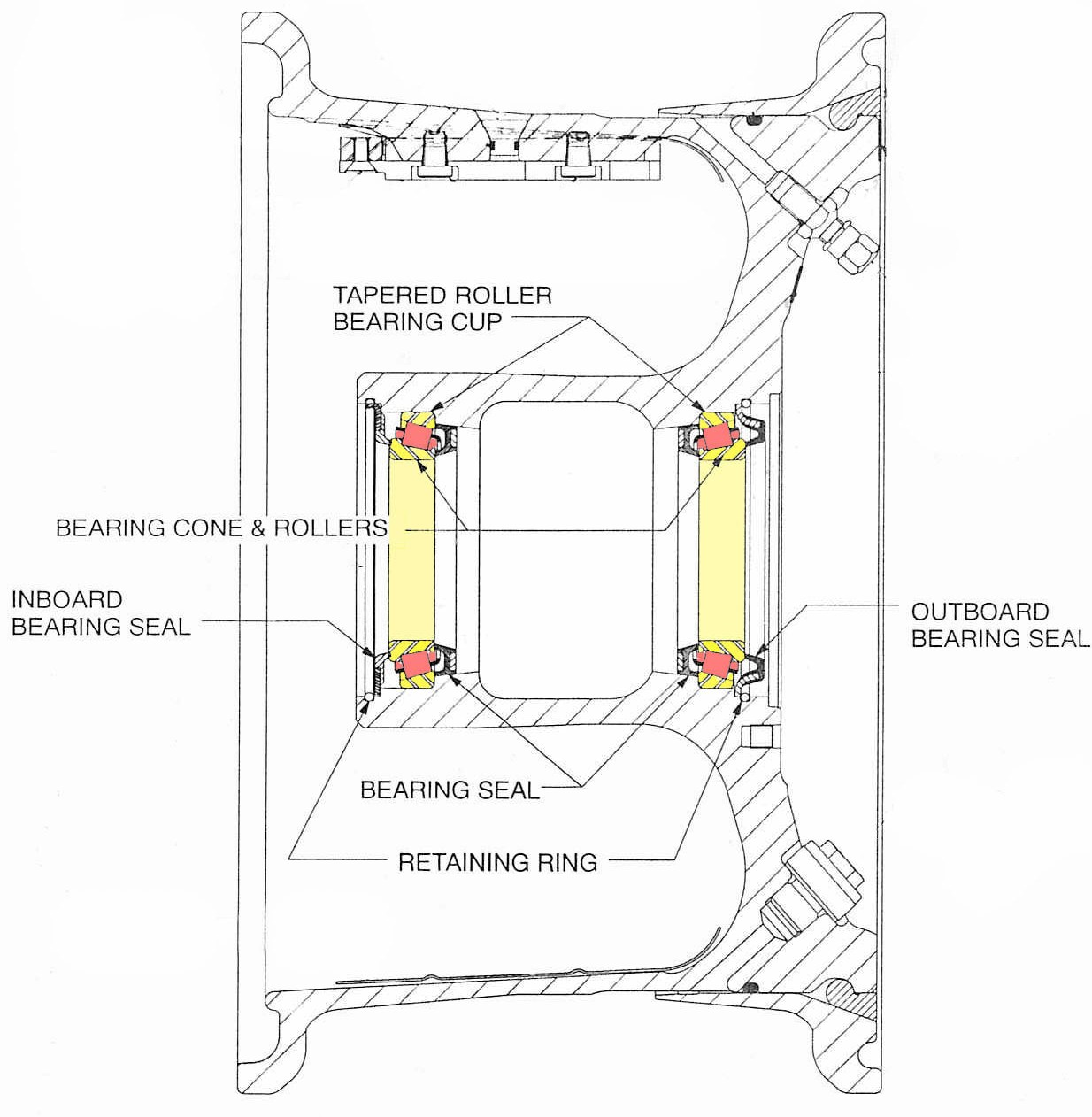
Figure 3: Wheel subassembly cross section with inner and outer bearings highlighted
Source: Meggitt Aircraft Braking Systems Component Maintenance Manual, amended by the ATSB
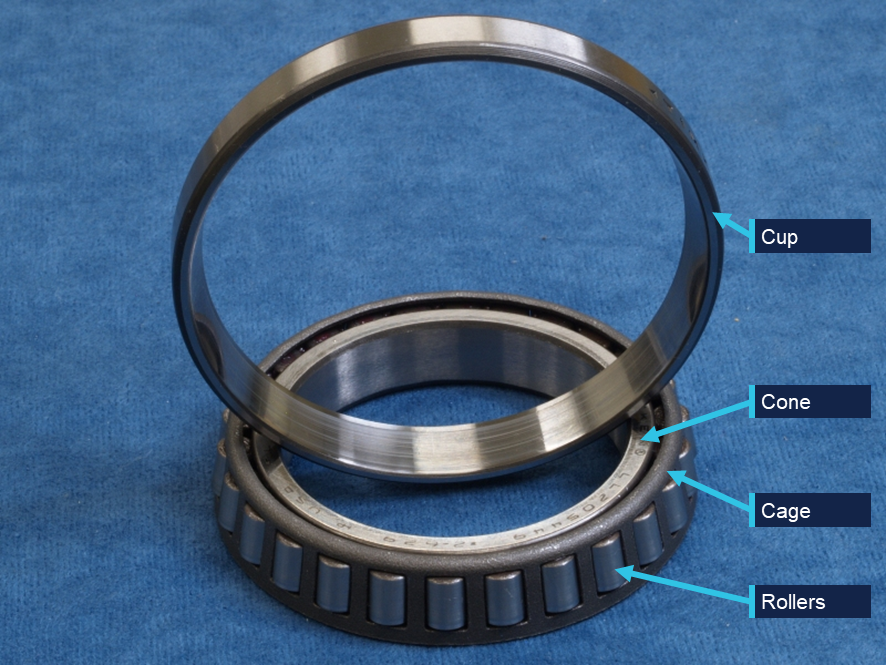
Each wheel subassembly bearing is comprised of a cup (outer race), cone (inner race), cage, and rolling elements (rollers) (Figure 4), held in place with a retaining ring. The bearing cups are shrink fitted into the wheel subassembly. Each bearing then has an inner and outer seal to protect it from contamination while preserving the grease lubrication. The cup or the cone-and-rollers can be replaced independently without changing the entire bearing.
Figure 4: Example bearing
Source: ATSB
Main wheel assembly examination
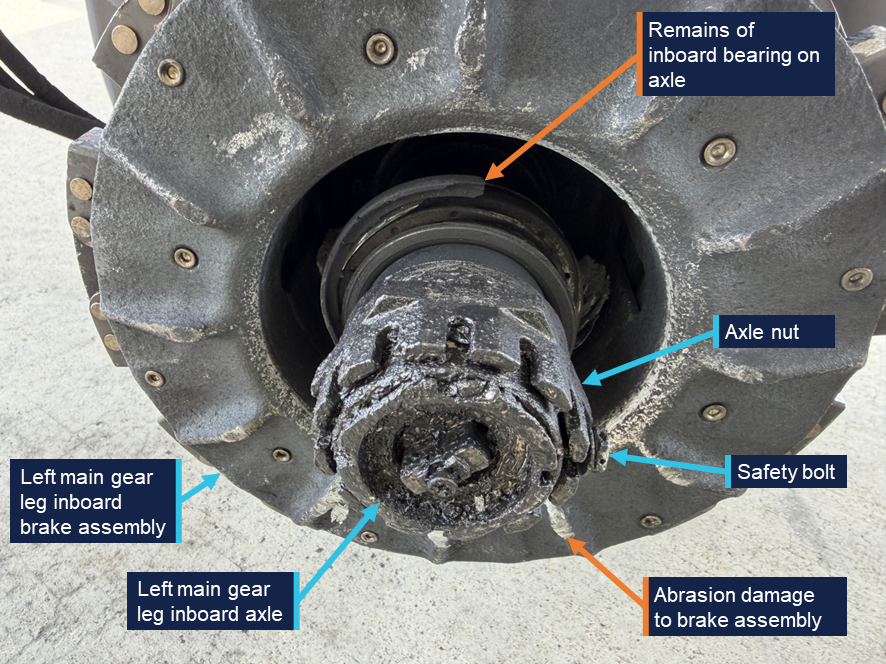
A post-incident inspection of the left main landing gear wheel and the main landing gear axle identified significant damage to both components. The axle nut and safety bolt remained in place on the axle (Figure 5). Remains of the inboard bearing were also identified on the axle, and there was visible abrasion to the brake assembly.
Figure 5: Left main gear leg inboard axle
Source: Aircraft operator, annotated by the ATSB
The tyre on the main wheel remained inflated and the fusible plug3 had not activated. The wheel face had sustained minor damage and the hub cap remained installed and was secured with safety wire. Grease residue was observed around the hub cap.
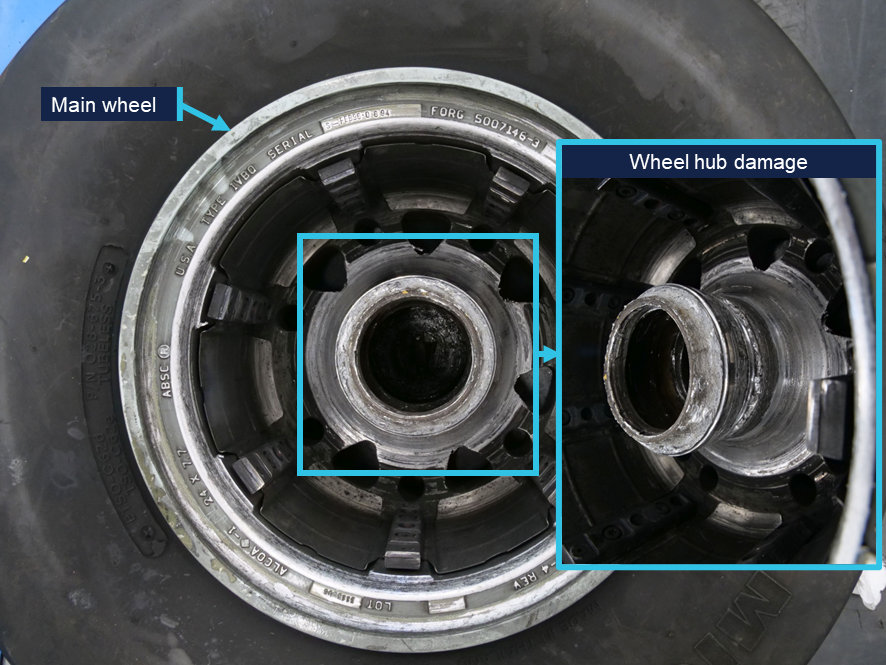
The inboard side of the wheel sustained significant damage (Figure 6). A circumferential fracture surface was visible on the inboard region of the hub encompassing the inboard bearing cone seat. The hub surfaces in proximity to the brake assembly when the wheel is installed exhibited deep rotational gouging and scoring.
Figure 6: Main wheel hub damage
Source: ATSB
Pieces of bearing material were found with the wheel, including 13 roller elements, fragments of the roller cages and bearing seals. The outboard cup remained installed in the wheel. All of the bearing races exhibited significant damage and smearing,4 including deformation from impact with loose rollers. Both cones had heat colouration as evidence of exposure to high temperatures.
The fractured sections of wheel hub also had evidence of heat damage. To the extent that could be established,5 the ATSB did not identify any evidence of progressive cracking or pre-existing defect that might have contributed to the fracture.
Main wheel assembly history
The main wheel assembly part number 5010488-2 and serial number APR93‑1167, was manufactured by the Aircraft Braking Systems Corporation (ABSC), now Meggitt Aircraft Braking Systems (MABS), in April 1993. The wheel was installed on VH‑VEZ on 11 December 2025 following an overhaul on 26 November 2025. Maintenance records documented the history of work on the wheel assembly in accordance with maintenance instructions. During those workshop visits, bearing cups and/or cone‑and‑rollers were replaced, however, the records did not specify whether the replaced components were installed in the inboard or outboard positions.
Component maintenance procedures
Service letter (SL) SL-GS-366 and component maintenance manual (CMM) 32-41-167 outlined the wheel inspection and overhaul schedules, and maintenance procedures for this type of wheel. The CMM stated that wheels are an ‘on condition’ part, meaning there was no defined service life and that inspections, tests and checks were used to determine the condition of the wheel and subcomponents with regard to continued serviceability.
Two key procedures given in the CMM include tyre change and overhaul.
Tyre change
The tyre change procedure was carried out when a tyre was worn to its tread limit. This involved removing the worn tyre, conducting a detailed visual inspection of the whole wheel assembly and non-destructive (eddy current or ultrasonic) inspection of specific areas. At each tyre change, the bearing cones, cups and rollers were cleaned, inspected and regreased prior to install. Parts were replaced when they failed to meet the inspection criteria within the CMM.
Overhaul
At an overhaul, wheels had to undergo a full tyre change inspection plus eddy current, ultrasonic or fluorescent penetrant inspection of the whole wheel. The SL stated that overhauls for fixed wing commercial aircraft wheels should be performed at maximum intervals of 5 tyre changes, or 1,500 cycles,8 whichever occurred first.
Operator’s maintenance process
The operator contracted an external maintenance organisation to conduct wheel tyre changes and overhauls for its Saab fleet. The operator advised the ATSB that the average cycles between tyre changes is 260, meaning that the wheel and bearings are inspected approximately every 260 cycles.
Previous occurrences
The aircraft manufacturer provided the ATSB with data on similar reported occurrences from global Saab 340B operators. Since 1997 there have been 14 reported occurrences relating to a main landing gear wheel departing the aircraft, one of which (AO-2008-046) was investigated by the ATSB, and 2 occurrences of bearing failures where the wheel did not depart the aircraft.
The aircraft manufacturer advised the ATSB that it had not identified any trends or variations related to loss of wheel or main wheel bearing failure occurrences. In 2008, the aircraft manufacturer released a service newsletter highlighting the importance of rotating the wheel while torquing the wheel axle nut to prevent axial play, which can result in bearing failures.
On 6 July 2008, a Saab 340B aircraft departed Orange for a scheduled flight to Sydney, New South Wales.
During take-off, the right outboard main wheel detached from the aircraft. The crew continued to Sydney where the aircraft landed without further incident.
Examination of the components identified that the wheel detachment occurred due to a failed wheel bearing. It was possible that the failure was related to a lubrication or setting (installation) issue, however the degree of damage sustained by the bearing components prevented a determination of the specific failure mechanism.
As a result of that occurrence, the aircraft operator implemented a range of safety actions, including a review of wheel bearing maintenance procedures, and an audit of main wheel axle nut torques across the fleet.
Safety analysis
As the aircraft rotated, the left inboard main landing gear wheel separated from the aircraft. Post-flight inspection of the aircraft identified that the axle nut remained secured on the end of the axle. As such, the potential mechanisms for wheel detachment were limited to a fracture of the wheel or bearing failure.
The level of damage to both bearings, and the absence of any identified pre-existing cracking or defect on the fractured hub pieces supported failure of the bearings as the initiating event. The hub fracture was assessed as secondary, the result of abnormal loading during continued wheel rotation with collapsed bearings.
The bearing failure allowed the wheel to move axially outward, pass over the axle nut, and separate once it was no longer restrained on the landing gear axle.
A bearing failure may have resulted from various initiating factors including:
material or manufacturing defect
improper installation
insufficient lubrication
corrosion
material fatigue
contamination by foreign material.
The condition of the bearing races and the other retained bearing fragments did not provide clear evidence as to an initiating event for the failure. Maintenance records indicated that the wheel was installed and maintained in accordance with the relevant maintenance instructions, and there was a history of replacement of the bearing components.
Additionally, all components were inspected during the overhaul on 26 November 2025 prior to being installed on VH-VEZ, and the wheel had subsequently completed 271 cycles on VH-VEZ. Taken together, they opposed failure being the result of an installation or maintenance error.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following finding is made with respect to the main landing gear wheel separation involving Saab 340, VH-VEZ, Canberra Airport, Australian Capital Territory, on 29 January 2026.
Contributing factors
During take-off, the left main landing gear inboard wheel bearings failed, resulting in the wheel separating from the aircraft. The cause of the bearing failure could not be determined.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Aircraft operator
In response to the occurrence, the operator conducted a fleet‑wide inspection of main wheel assemblies and nose wheel assemblies for any defects. No faults were found on any aircraft at the time of inspection.
In addition, the operator has elected to replace wheel bearings on-condition or at every second wheel overhaul, whichever occurs first.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
first officer
operator
aircraft manufacturer
aircraft component manufacturer.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
flight crew
operator
aircraft manufacturer
aircraft component manufacturer
Civil Aviation Safety Authority
Airservices Australia.
A submission was received from the operator.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
^Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
^PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
^The fusible plug is a safety device to prevent tyre explosion by deflating the tyre when a specific temperature is reached.
^Deformation of metal associated with shear loading.
^Not all of the separated wheel hub sections were recovered and there was limited deformation of the fracture surface.
^SL-GS-36 was first issued in July 1993. The most recent revision, version 7, was issued in January 2006.
^CMM 32-41-16 was first issued in April 1992. The most recent revision, revision 6, was issued in April 2014.
^A cycle is a completed take-off and landing sequence.
Occurrence summary
Investigation number
AO-2026-008
Occurrence date
29/01/2026
Occurrence time and timezone
1609 Eastern Daylight-saving Time
Location
Canberra Airport
State
Australian Capital Territory
Report release date
28/05/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Diversion/return, Landing gear/indication, Objects falling from aircraft
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Saab Aircraft Co.
Model
340B
Registration
VH-VEZ
Serial number
340B-450
Aircraft operator
Vee H Aviation Pty Ltd
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the afternoon of 12 November 2025, an instructor and student pilot departed Archerfield Airport, Queensland, for a navigational training flight in a Piper Aircraft Corporation PA-28R aircraft.
Following several hours of exercises, the flight was tracking east and transiting the Amberley Airport control zone at 1,500 ft when the entire upper engine cowling separated from its attachment points and flipped backward against the cockpit windshield, partially obstructing both pilots’ forward visibility.
Maintaining control of the aircraft and aware of their proximity to Amberley Airport, the crew immediately assessed the engine operation and aircraft handling – finding both unaffected. The crew called PAN PAN[1] to Amberley approach air traffic control and turned toward the aerodrome to conduct an approach to runway 15. After ATC advised of significant crosswinds for that runway and mindful of their very limited forward visibility, the crew re‑positioned for an approach to runway 04.
During the turn onto the base leg of the runway 04 approach, the cowling fractured into 2 sections, with the right side separating from the aircraft and the left side moving downward and away from the windshield, remaining attached to the aircraft. The final approach and landing were uneventful.
Engineering aspects
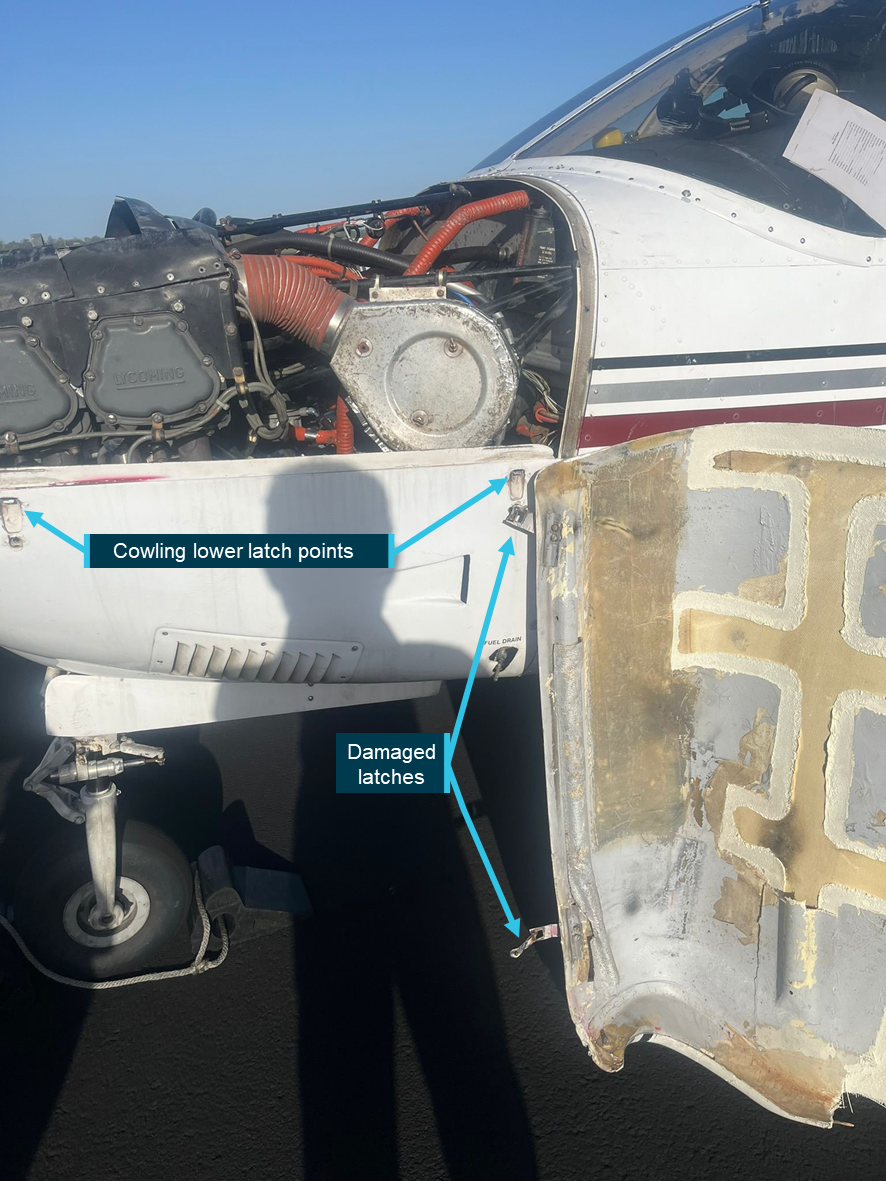
The PA-28 engine upper cowling is a shaped single-piece composite fibre structure that affixes to the lower cowling with 4 over-centre toggle style latches (2 on each side). The instructor reported that all latches were checked for security and tightness during the aircraft’s pre-flight inspection and noted that the flight had operated normally for around 3 hours before the separation. No defects or related issues were annotated in the aircraft’s maintenance release.
The reason/s for the cowl separation remain unknown.
Figure 1: Remaining cowl section and left separation points
Source: Supplied by operator, annotated by the ATSB
Safety message
The well-managed response to this significant in-flight emergency ensured the safe recovery of the aircraft and crew. The methodical approach to the problem assessment, decision-making and utilisation of ATC assistance is a good illustration of best-practice emergency management.
The unintended and sudden in-flight separation of cowlings or other airframe components has the potential to interfere with aircraft controllability, engine operation, or – in the worst-case scenario – cause pilot incapacitation should the components forcefully enter the cockpit through the windshield.
Maintenance attention and airworthiness inspections must have regard to the security and ongoing mechanical condition of all cowlings, panels and their fixtures.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-061
Occurrence date
12/11/2025
Location
8 km north-west of Amberley Airport
State
Queensland
Occurrence class
Serious Incident
Aviation occurrence category
Diversion/return, Fuselage/wings/empennage, Objects falling from aircraft
Highest injury level
None
Brief release date
23/12/2025
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-28R
Sector
Piston
Operation type
Part 142 Integrated and multi-crew pilot flight training
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
At around 1209 local time on 14 October 2025, a Eurocopter AS350, with only the pilot onboard, was carrying an externally slung load between 2 sites in regional Western Australia, located approximately 6 km apart. The load weighed around 800 kg, and was secured using 4 strops, each rated to carry 3,000 kg.
The helicopter was transiting at around 60 kt, about 1,000 ft above ground level. Approximately midway through the flight, with the load stable, the pilot heard a sudden loud thud and felt the helicopter vibrate. At the same time, without the pilot’s command, the helicopter pitched forward into a nose down attitude. The pilot attributed this to a large change in the aircraft’s centre of gravity. In response, they immediately jettisoned the load, which restored full control of the helicopter. The pilot continued the short flight to the intended destination and landed without further incident.
The jettisoned load was later located and inspection revealed that one of the lifting strops had been severed by jagged metal material contained in the load. This resulted in a sudden and significant shift in the load’s orientation beneath the helicopter, leading to the uncommanded pitch change.
Figure 1: Load and lifting strop condition post-occurrence
Image shows the load as it was found after being jettisoned and the condition of the severed lifting strop. Source: aircraft operator
Safety action
The operator has initiated a review of its risk assessment for sling load activities, which will incorporate information learned from this occurrence. It also produced internal recommendations to avoid loads from shifting in flight or damaging lifting equipment including:
using protective measures, such as rubber matting or edge protectors, wherever slings contact sharp or potentially abrasive surfaces
testing the structural integrity of loads prior to lifting, including an inspection process for loads that may have structural weaknesses, fatigue, or brittle components.
Safety message
This incident highlights the importance of detailed consideration when preparing external loads for lifting. The nature of aerial construction/deconstruction work can make it difficult for pilots to conduct a detailed inspection of the prepared load prior to each lift operation. Operators are encouraged to ensure effective risk control processes are in place for load preparation, especially with irregularly shaped loads. On this occasion the flight was operating in a remote area and the consequence of jettisoning the load was relatively benign. However, falling loads have the potential to cause catastrophic/fatal outcomes, and the risk must be appropriately mitigated.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 13 September 2025, the pilot of a Eurocopter AS 350 B2 helicopter was conducting aerial fire suppression operations over an active grass fire in regional North Queensland. The helicopter was about 500 ft above ground level, with about 50 kt airspeed and a laden water bucket. At about 1220 local time, the helicopter completed a turn and the pilot reported feeling a jolt and observed, via an external mirror, the water bucket and attached line falling from the helicopter. The bucket and line impacted the ground causing significant damage to the bucket but no other damage or injuries.
The pilot recalled that, at the time the bucket released from the helicopter, their hands were clear of the cyclic cargo release button and manual release handle. The pilot landed the helicopter immediately and advised the helicopter operator of the incident.
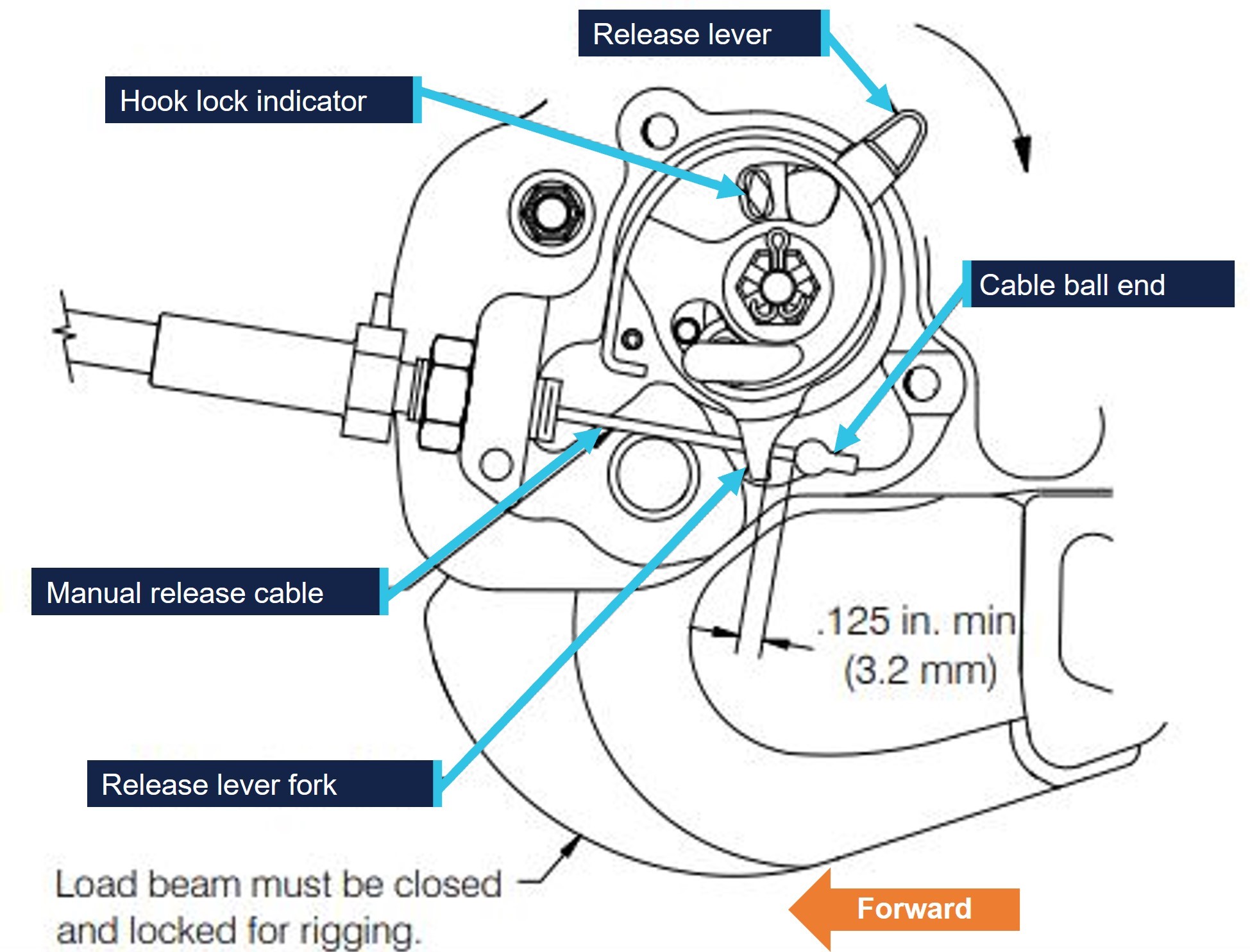
Shortly after landing the pilot conducted a post-flight inspection. There was no damage to the helicopter, however the pilot was able to replicate the cargo hook unintentionally opening by moving the assembly in certain directions (Figure 1 shows the type of cargo hook fitted). The pilot later determined that the manual release cable had been incorrectly rigged. They observed a loop in the manual release cable prior to the cable entering the cargo hook assembly that caused the cable to tension and triggered the opening of the cargo hook.
Figure 1: Cargo hook used by the operator’s AS350
Source: Onboard Systems, annotated by the ATSB
Safety message
The uncommanded release of an underslung load has the potential for fatal consequences, damage to property and the load itself. Another occurrence of an underslung load being released without pilot input from a Eurocopter AS 350 helicopter as a result of the incorrect rigging of the cargo hook manual release cable has been detailed by the ATSB (AB‑2024‑033).
Although the rigging mechanism of the manual release cargo hook cable is not visible to the pilot during a pre-flight inspection, pilots intending to conduct underslung operations are encouraged to check for correct rigging and, if possible, simulate the full range of cargo hook movement prior to flight to observe any abnormalities.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
On 18 June 2025, a Beechcraft King Air B200, registered VH-EEL, was on descent into Bankstown Airport, New South Wales, on a passenger transport flight with the pilot and 4 passengers on board when the pilot heard a whistling noise followed by the sound of an impact coming from the rear of the aircraft. There were no abnormal indications and the aircraft was flying normally, so the pilot continued the flight.
Shortly after, the pilot was unable to reach air traffic control via radio and switched to the aircraft’s alternative radio. Communication was re‑established and the aircraft landed safely. An external inspection of the aircraft found that the VHF antenna on top of the fuselage was missing, and the vertical stabiliser was damaged.
What the ATSB found
While the top of the antenna was not recovered, the aluminium antenna base showed evidence of moisture ingress. This resulted in the antenna failing and separating from the aircraft. The exact failure mechanism could not be determined – moisture could have been absorbed by the composite skin of the antenna, reducing its strength. Alternatively, observed corrosion could have weakened the bond between structural components within the antenna, reducing stiffness and allowing cracks to develop.
Safety message
While it is not clear whether pre-existing damage was observable during antenna inspections, this occurrence is a useful reminder on the importance of vigilance while conducting routine maintenance. In addition, it serves to demonstrate the value of redundancy in safety-critical systems.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the afternoon of 18 June 2025, a Beechcraft King Air B200, registered VH-EEL, departed from Dubbo Airport, New South Wales, on a passenger transport flight to Bankstown Airport. The flight was operated by CJ Aerospace with the pilot and 4 passengers on board. It was a clear day and the aircraft was flying in visual meteorological conditions.
At approximately 1523, the aircraft was about 30 NM (55 km) from Bankstown Airport and descending through 11,000 ft when the pilot heard a whistling noise coming from the back of the aircraft. After a few seconds, the pilot reported hearing the sound of an impact towards the rear of the aircraft. The aircraft’s airspeed was approximately 280 kt at the time. There were no abnormal indications in the cockpit and the aircraft was flying normally, so the pilot continued with the flight.
The aircraft had been previously cleared by air traffic control (ATC) to descend to 5,000 ft. However, after reaching this altitude it had not been cleared for further descent, which the pilot noted to be unusual. The pilot conducted a radio check with ATC but received no response. The pilot switched the aircraft’s active VHF radio from COM 1 to COM 2, and contact with ATC was subsequently re‑established. The rest of the approach and landing proceeded without incident and the aircraft landed at Bankstown Airport at 1534.
After landing, the pilot conducted an external inspection of the aircraft and found that the VHF antenna on top of the fuselage was missing, and the vertical stabiliser was damaged (Figure 1). Further information on the damage is in Aircraft information and Antenna examination.
Figure 1: Damage to the vertical stabiliser
Source: Jet Aviation
Context
Pilot information
The pilot held a Commercial Pilot (Aeroplane) Licence, issued in December 2019, with a multi‑engine aeroplane instrument rating. At the time of the occurrence, the pilot had approximately 1,980 hours total flying experience, of which 140 hours were accrued on the King Air B200.
Aircraft information
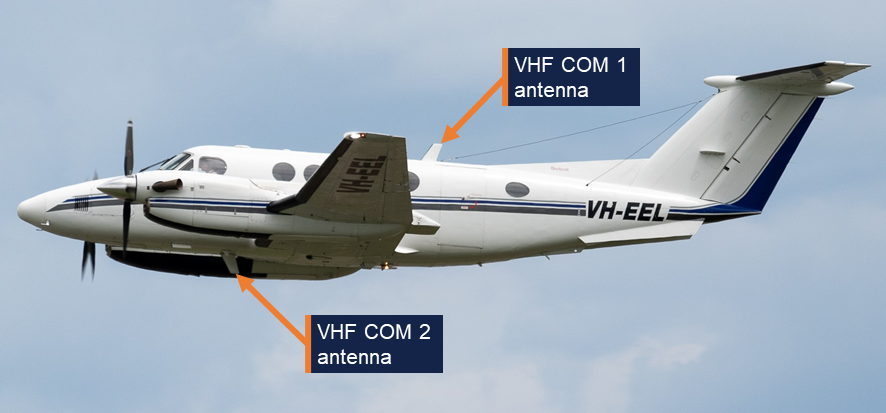
The Beechcraft King Air B200 is a pressurised, low-wing, twin turbine-engine aircraft. It has 2 VHF antennas: COM 1 is fitted on top of the fuselage, and COM 2 is underneath the fuselage (Figure 2). VH-EEL was manufactured in the United States in 2000 and registered in Australia in the same year. CJ Aerospace had been the registered operator of the aircraft since July 2021.
Figure 2: VHF antennas on VH-EEL
Source: CQ Plane Spotting
Aircraft examination
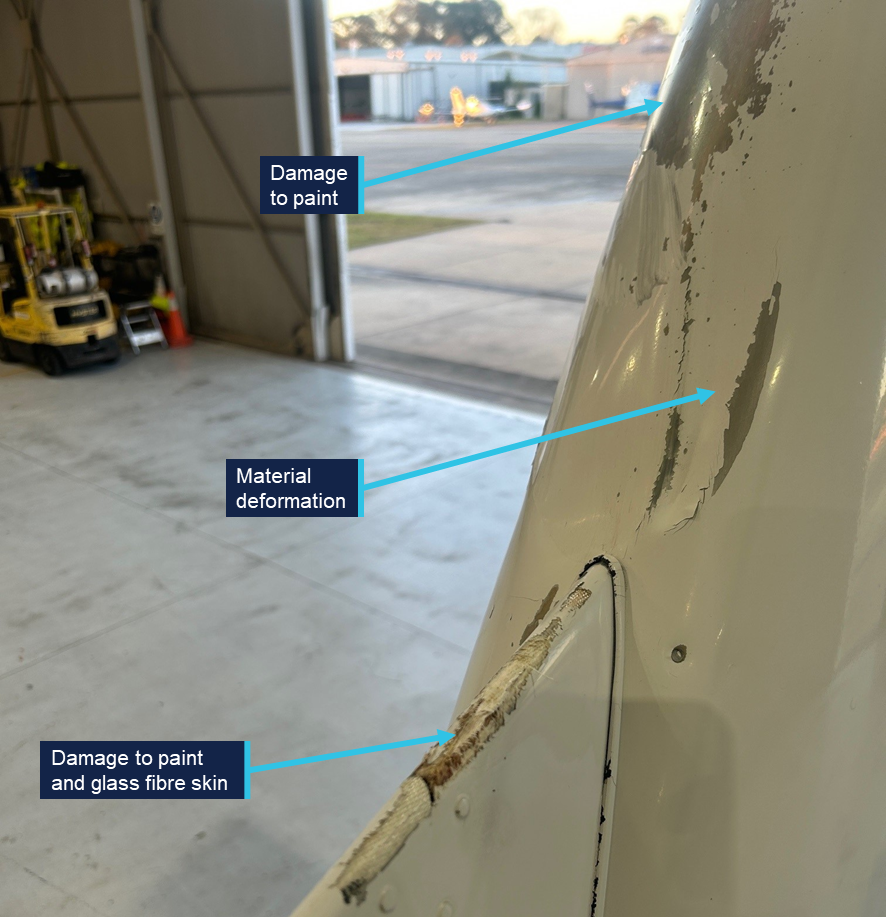
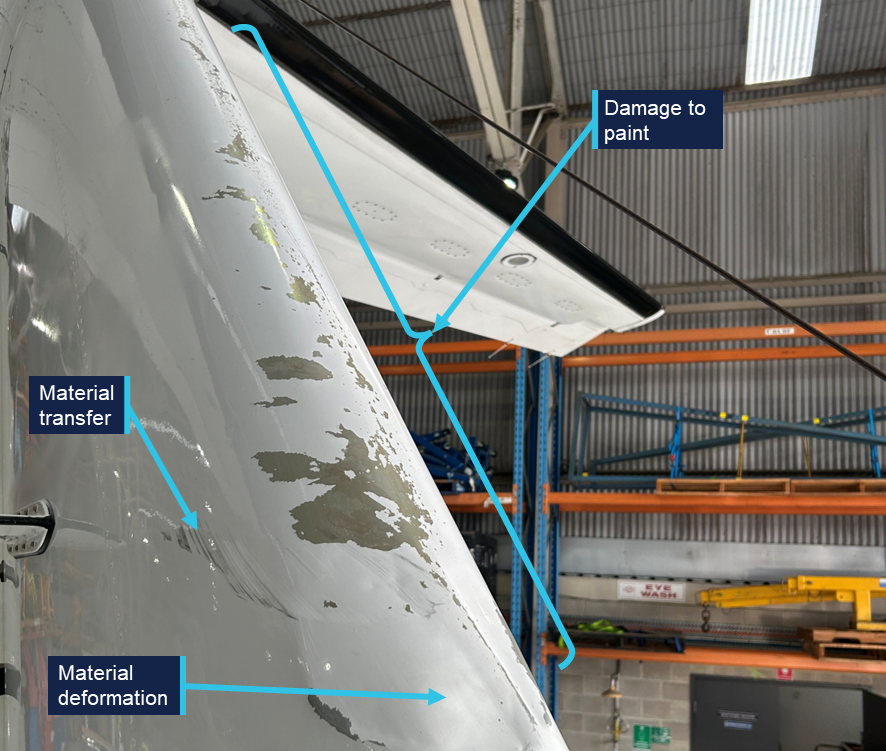
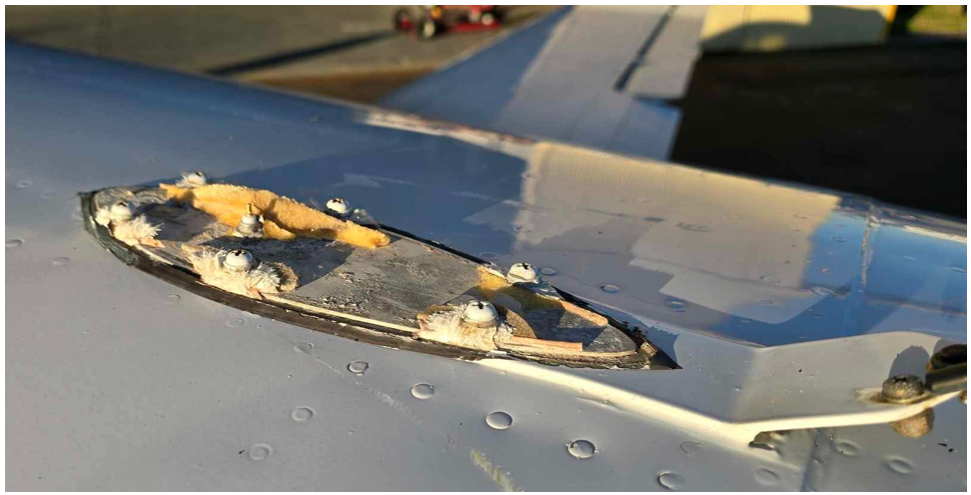
Following the occurrence, the aircraft was sent to a maintenance facility for examination and repair. The examination (not attended by the ATSB) identified that the leading edge of the vertical stabiliser had experienced deformation, and there was damage to the skin and paint on various parts of the empennage (Figure 3 and Figure 4). There also appeared to be some transfer of black material, possibly paint or rubber, onto the right side of the vertical stabiliser. The base of the antenna was still secured to the fuselage by 6 fasteners, but the glass fibre skin of the antenna had failed around each of the fasteners and separated from the aircraft (Figure 5).
Figure 3: Damage on the front of the empennage
Source: Jet Aviation, annotated by the ATSB
Figure 4: Damage on the right side of the empennage
Source: Jet Aviation, annotated by the ATSB
Figure 5: The antenna base still secured to VH-EEL
Source: Jet Aviation
Antenna examination
The detached antenna was not located. The antenna base was examined at the ATSB’s engineering facility in Canberra. The manufacturer’s label indicated that it was manufactured by the Trivec-Avant corporation. The part number was 18-40-01 and the serial number was 11514. The antenna was not original to the aircraft, and its installation date could not be determined. The Trivec-Avant corporation ceased operation in about 2011, and no technical drawings or other details could be obtained for the antenna. However, images of an antenna with the same part number were sourced online (Figure 6). It comprised a base and upper structure with an internal electrical antenna.
Figure 6: Exemplar VHF COM antenna
Source: majorjunque (eBay)
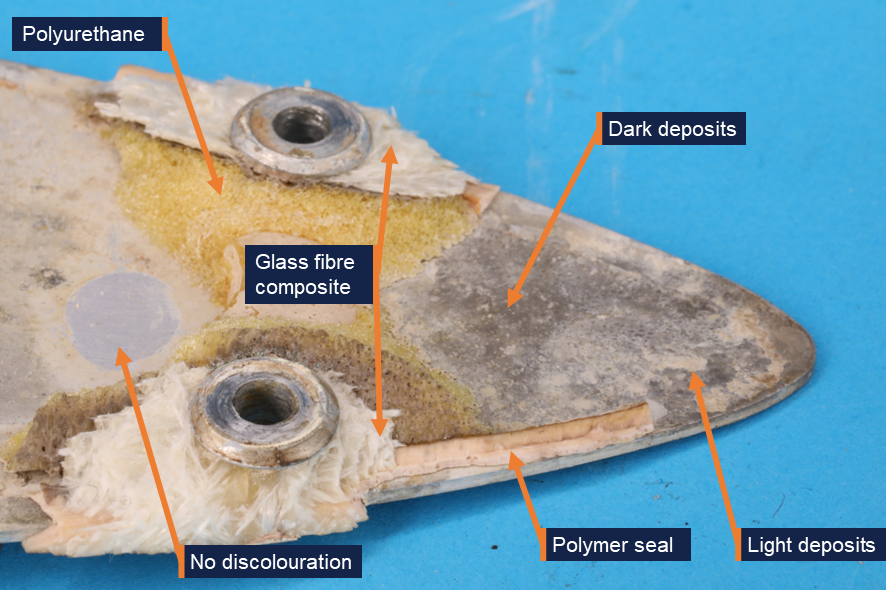
The antenna base from VH-EEL was an aluminium plate with 6 holes for fasteners and a central coaxial connection for the internal electrical antenna (Figure 7). A yellow foam adhered to the top face of the antenna was likely an expanding polyurethane product that was injected into the antenna during its construction in order to increase rigidity (Figure 8). Some fractured glass fibre composite material was observed around each of the fasteners. Fragments of a polymer seal were observed around the edges of the antenna base.
Figure 7: Antenna base from the aircraft
Source: ATSB
Both surfaces of the plate showed discoloration in several locations, identified as deposits on the surface of the metal (Figure 8). The deposits varied in colour. Samples of the dark-coloured and light-coloured deposits were scraped from the antenna using a plastic spatula and analysed for elemental composition using energy-dispersive X-ray spectroscopy (EDS). EDS analysis found that the composition of the light and dark deposits was very similar. Both predominantly contained aluminium, oxygen, and a smaller quantity of chlorine. The presence of chlorine indicated that the plate was exposed to salt water, resulting in corrosion of the aluminium plate, forming aluminium oxide.
Figure 8: Aft end of the antenna base, top face
Source: ATSB
The discolouration was not uniformly distributed over the base, and there were some regions, such as the one shown in Figure 8, where there was no evidence of deposits or discolouration. Similarly, while much of the base’s edge was discoloured, there were some regions underneath the polymer seal that appeared relatively unaffected (Figure 9).
Figure 9: Discolouration under the polymer seal, at the edge of the top face
Source: ATSB
Aircraft maintenance
The aircraft was maintained under a 4-phase inspection program over 800 flight hours or 24 calendar months. Each phase of routine maintenance was conducted sequentially every 200 hours. Inspection of the VHF antennas was conducted in Phase 3. The inspection required personnel to:
…inspect all external antennas for leading edge erosion and condition of base seals.
This was last performed on 18 October 2024 with no relevant findings recorded.
The aircraft manufacturer provided guidelines for corrosion control inspections, which were optional and to be used depending on the operating environment. Regarding antennas, the inspection stated the following:
ANTENNAS - Inspect antenna bases for proper sealing. Inspect antenna leading edges for severe erosion.
These inspections were also last carried out on 18 October 2024 with no relevant findings recorded.
Neither inspection specified whether antenna removal was necessary.
Similar occurrences
The aircraft manufacturer could not identify any previous instances of antenna separation in flight, but noted that ‘while it is rare, it is not unknown for antennas to crack at the fastener holes’.
Safety analysis
Based on the aluminium oxide and chlorine found on the surface of the VHF antenna base – a part of the antenna that should be fully enclosed and sealed – the antenna failed in flight due to pre-existing damage resulting from corrosion. The corrosion was almost certainly due to moisture ingress into the unit.
Since most of the antenna was not recovered, there was no way to determine the pathway through which moisture entered the antenna. Most of the seal surrounding the base had separated with the top half of the antenna. There was evidence of moisture under the seal in some regions, while some parts of the seal appeared to have prevented corrosion. The moisture under the seal could indicate a point of ingress, but it is possible that all the corrosion observed under the seals was due to moisture already inside the antenna, rather than evidence that the seal had been compromised.
Beyond the fact that the antenna cracked around the 6 fastener holes, the exact failure mechanism could not be determined. It is possible that corrosion weakened the bond between the polyurethane core and the base or skin of the antenna. This would have reduced the stiffness of the unit, allowing cracks to develop as it flexed during service. Alternatively, moisture could have been absorbed by the glass fibre composite skin, reducing its strength and increasing susceptibility to cracking.
Without an understanding of the mechanisms that led to moisture entering the antenna and the subsequent in-flight separation, it is not possible to determine whether any damage would have been externally visible during the relevant inspection 8 months before the occurrence. Cracking around the fastener holes might not have commenced at that point. Alternatively, damage could have been too small to detect or obscured by the paint.
One alternative possibility to pre-existing damage could not be entirely ruled out: a birdstrike or collision with a remotely piloted aircraft (RPA) could have resulted in antenna separation. However, very few birdstrikes occur above 10,000 ft, and most RPAs are not certified to fly that high. No in-flight RPA loss was reported. There was also no visual evidence of a birdstrike, and any contact with bird or RPA would likely have resulted in a loud bang precipitating the occurrence, rather than a whistling sound followed by the sound of an impact.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the antenna failure involving Beechcraft King Air B200, VH-EEL, 55 km west of Bankstown Airport, New South Wales, on 18 June 2025.
Contributing factors
During flight, pre-existing damage due to moisture ingress resulted in the VHF COM 1 antenna failing and separating from the aircraft.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot
CJ Aerospace
Textron Aviation (Beechcraft)
the aircraft maintenance organisation
the maintenance organisation that examined the aircraft following the occurrence
Civil Aviation Safety Authority
Flightradar24.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
CJ Aerospace
the aircraft maintenance organisation
Civil Aviation Safety Authority
Textron Aviation (Beechcraft)
National Transportation Safety Board (United States).
There were no submissions received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Occurrence summary
Investigation number
AO-2025-031
Occurrence date
18/06/2025
Occurrence time and timezone
1523 Australian Eastern Standard Time
Location
55 km west of Bankstown Airport
State
New South Wales
Report release date
15/05/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Avionics/flight instruments, Objects falling from aircraft
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Raytheon Aircraft Company
Model
B200
Registration
VH-EEL
Serial number
BB-1697
Aircraft operator
C J Aerospace Pty Ltd
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes
Activity
Commercial air transport-Non-scheduled-Passenger transport charters
On 27 August 2024, a Bell 206L-1 LongRanger helicopter with a single pilot on board was conducting a ferry flight with the doors removed, from Mitchell Falls campground to a coastal landing site on Nat Beach, Western Australia.
The helicopter departed at 0615 local time and climbed to an altitude of 1,800 feet AMSL. During the flight, the seat located in the rear row on the right side fell out of the helicopter. The pilot was unaware that the seat had fallen out until after the helicopter landed at Nat Beach and the pilot was preparing to pick up the passengers for the next flight.
The seat did not impact the tail rotor or stabilisers and there was no damage to the helicopter.
The helicopter had finished a 100 hourly maintenance inspection the day prior to the incident flight. It then conducted a ferry flight to Mitchell Falls with the doors on. The doors were removed at Mitchell Falls campground and the seat base was lost on the next flight (Figure 1).
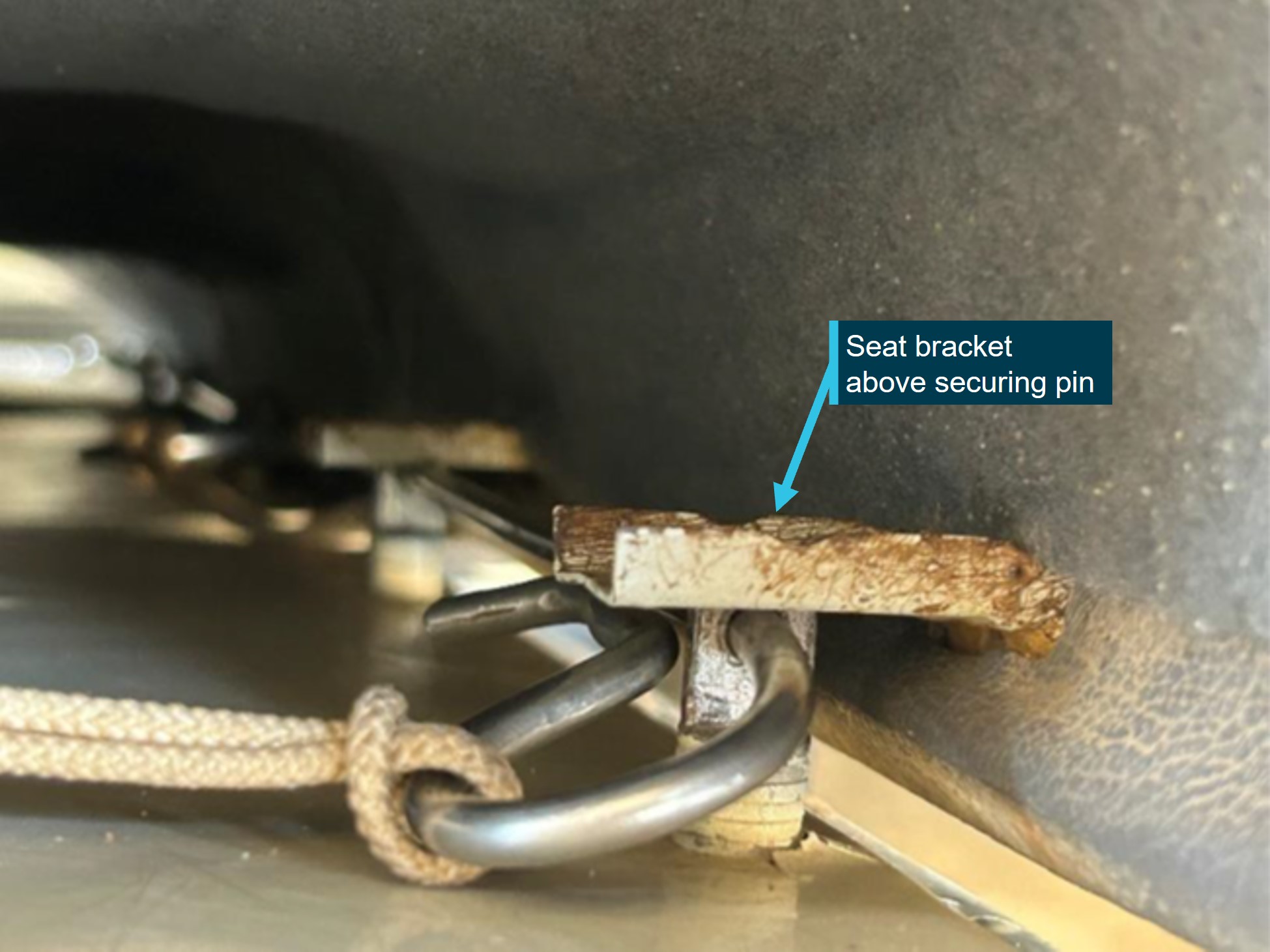
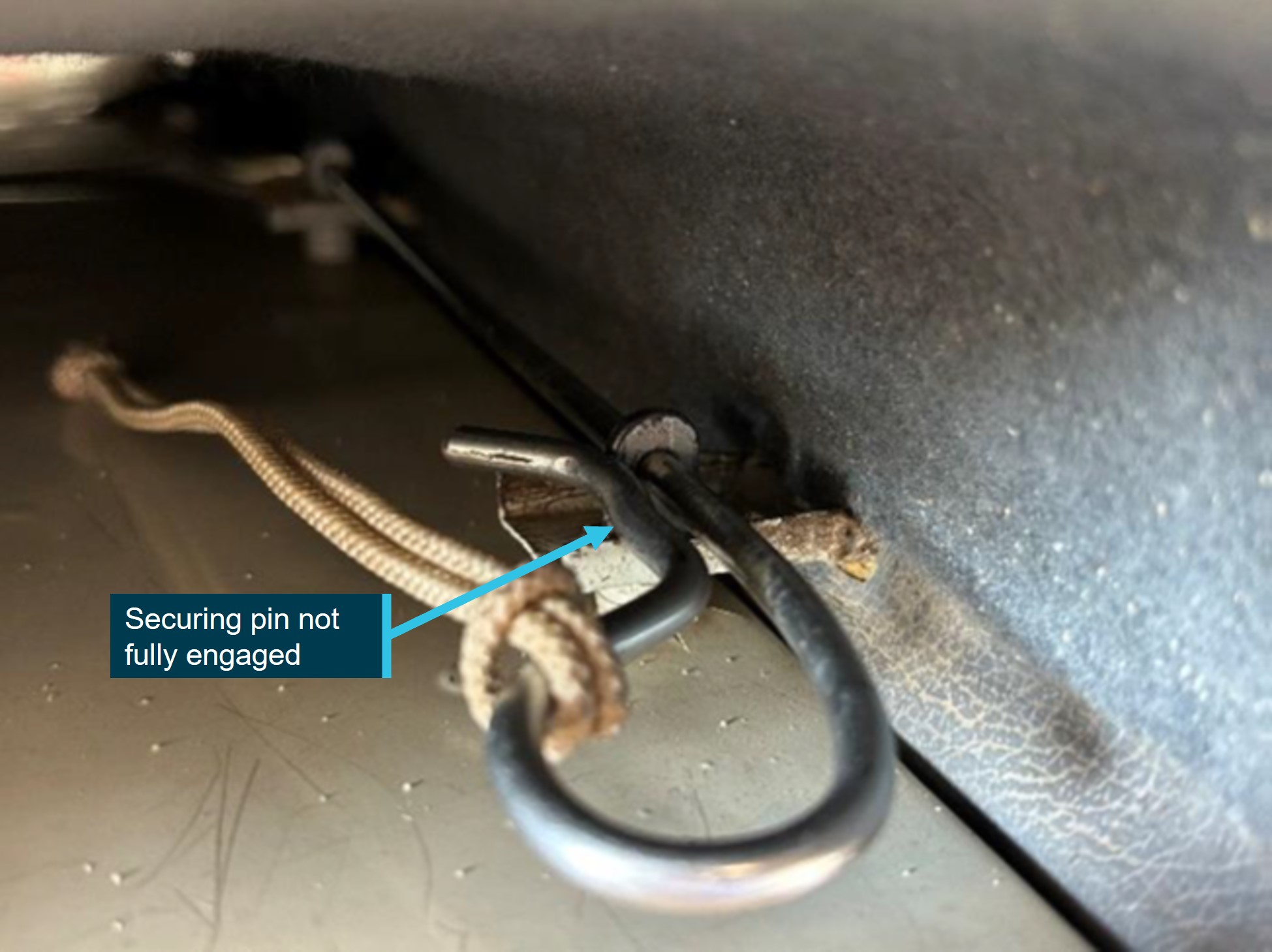
The operator’s internal investigation revealed that the seat had been incorrectly installed prior to release from the 100 hourly inspection. During installation, the brackets on the seat were most likely not installed fully onto the locating pins before the securing pin was installed (Figure 2), or the brackets missed the securing pin (Figure 3).
Figure 2: Incorrect installation – seat brackets not installed on locating pins
Source: Operator, annotated by the ATSB
Figure 3: Incorrect installation – securing pin not fully engaged
Source: Operator, annotated by the ATSB
Safety action
The Head of maintenance briefed the engineer who completed the 100 hourly inspection and reiterated to all engineering staff during a toolbox meeting the necessity of ensuring proper seat installation. The helicopter was inspected by the maintenance team and no damage was found. The Fleet Service Manager raised an alert relative to this occurrence to remind both pilots and engineers on the seat installation instructions.
Safety message
The Bell 206L rear seats are not standardised and have several different ways that they may be secured. Personnel installing seats need to be vigilant in understanding and double‑checking that seats are installed correctly, which usually requires a close visual inspection and a pull on the seat to check security, as seemingly minor tasks in nature can have a substantial impact.
Pilots accepting aircraft from maintenance should conduct a particularly thorough pre-flight inspection. Errors in maintenance can and do occur, and that first pre-flight inspection is a critical part in capturing those errors.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 10 December 2024 an Airbus AS350 B2 (Squirrel) was being operated on a multi-day ferry flight from Caloundra Airport, Queensland to Papua New Guinea (PNG). At about 1000 local time, the helicopter was landed at Gladstone Airport for fuel and then continued north for Cairns Airport. Abeam Rockhampton Airport and about 4 km from the airport control zone boundary, the left front door upper window became detached from the aircraft and was briefly observed by the crew member seated in the left side as falling down and away from the aircraft.
Following the incident the crew aerially searched the area for the window, however, were unable to find it in the dense bushland. Shortly after this the crew landed the aircraft to check for damage to the helicopter. No damage was found and the crew elected to continue to Cairns Airport where a spare window was fitted.
Figure 1: Airbus AS350 B2 left front door upper window before the incident
Source: Operator, annotated by the ATSB
After a repair in Cairns, the helicopter had a post-maintenance flight check before the planned departure.
The remainder of the flight to PNG continued without incident. The crew were reported to be startled by the loud noise that was created as the window detached from the helicopter, however, no injuries were sustained by the crew and no other damage to the helicopter was observed.
The operator advised that, in line with scheduled maintenance of the aircraft, some of the windows had recently been refitted after a period in storage. The operator’s internal review of the incident concluded that the seal on the left-hand door window was installed without sealant and in the incorrect orientation. Further, as depicted in Figure 1, the left front door upper window also displayed a bulge due to theincorrect orientationafter refit. This improper fit reduced the security of the window to stay in place permanently during flight. The review identified that an apprentice aircraft mechanical engineer fitted the window, however, the subsequent inspection and sign‑off process did not identify any problem with the installation.
Safety message
Attention to detail is critical for all aspects of aviation safety, as even small omissions can have serious safety implications. Maintenance manuals for manufacturer and operator procedures should be followed closely. Quality assurance checks to verify compliance following maintenance, and fostering a culture of vigilance in maintenance practices, is essential for preventing inadvertent errors.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.