In-flight door failure involving Sling 4, about 11 km east of Dochra, New South Wales, on 15 December 2024
What happened
On 15 December 2024, the pilot of an amateur built Sling 4 was conducting a local private scenic flight from Maitland Airport, New South Wales, with 2 passengers on board. At 1130 local time, while on descent passing through about 2,400 ft above mean sea level, the right gullwing door of the aircraft adjacent to the front passenger detached and separated from the fuselage. The pilot immediately reduced the aircraft’s speed and conducted a safe landing at Maitland Airport. There were no injuries to the pilot or passengers.
Post-incident inspection of the aircraft identified that the detached door had impacted the left elevator counterweight arm resulting in minor damage (Figure 1).
Figure 1: Damage to left elevator counterweight arm caused by impact from the detached door

Source: Owner of aircraft
The pilot advised that they had upgraded the standard door latch fittings with ones that had a larger post to provide increased strength and durability for more security (Figure 2).
Figure 2: Latching mechanism (pilot side shown, passenger side was identical)
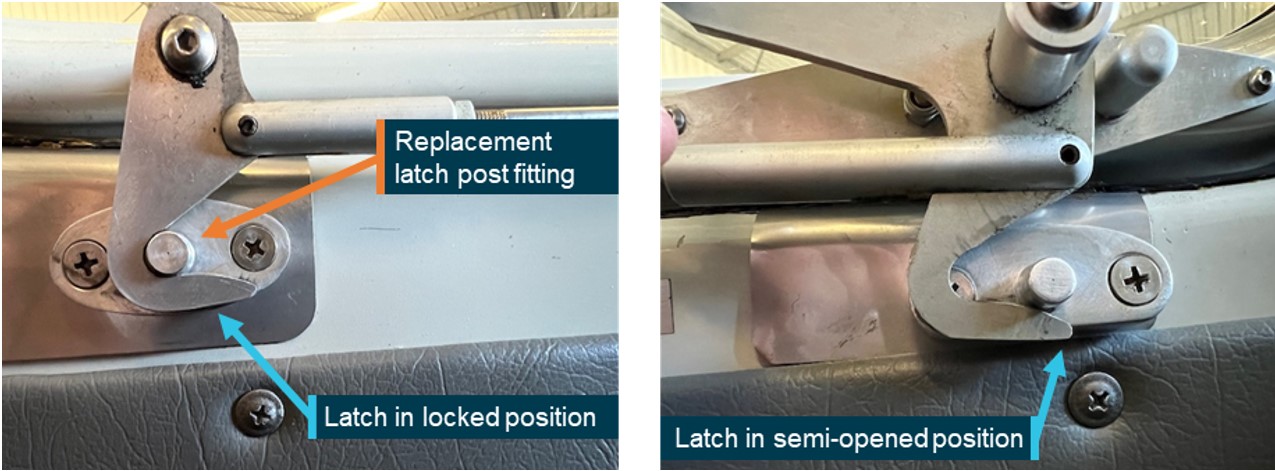
Source: Owner of aircraft
The passenger sitting beside the door during the descent described resting their arm on the door and reported that they unwittingly released the door latching mechanism. The airstream pressure exerted sufficient force to separate the open door from the aircraft. The location of the detached door remains unknown, however it is believed to have landed in an unpopulated area.
Safety message
The incident highlights the potential for inadvertent passenger actions to interfere with aircraft systems. Specific briefings for passengers seated next to doors to provide awareness of the door mechanisms before and during flight should be a part of standard operating procedures.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2024-052 |
| Occurrence date | 15/12/2024 |
| Location | About 11 km east of Dochra |
| State | New South Wales |
| Occurrence class | Serious Incident |
| Aviation occurrence category | Objects falling from aircraft |
| Highest injury level | None |
| Brief release date | 17/01/2025 |
Aircraft details
| Manufacturer | Amateur Built Aircraft |
|---|---|
| Model | Sling 4 |
| Sector | Sport and recreational |
| Operation type | Part 91 General operating and flight rules |
| Departure point | Maitland, NSW |
| Destination | Maitland, NSW |
| Damage | Minor |