Loss of control and forced landing involving Bell 206B3 helicopter, VH-ZMN, 18 km north-east of Perth Airport, Western Australia, on 19 January 2013
Summary
What happened
On 19 January 2013, a Bell 206B3 helicopter was being operated on an aerial filming task over hilly terrain on the north-eastern outskirts of Perth, Western Australia. The weather was fine with east to north-easterly winds of 10 to 15 kt.
After hovering and manoeuvring at about 500 ft above ground level to allow the camera operator to record footage of a truck accident, the pilot conducted a right orbit to complete filming and depart the area. The pilot had initiated the turn when the nose of the aircraft moved left, then suddenly and rapidly to the right as the helicopter yawed and developed a rotation of about five revolutions.
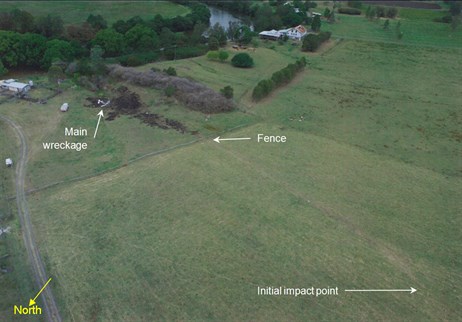
The pilot regained some control close to the ground, but assessed that the performance of the helicopter was insufficient to avoid a forced landing. In an area with a number of obstacles the pilot selected a clearing and managed the available energy to perform a low-impact landing. The slope was such that the helicopter immediately rolled over with the engine still operating, but importantly for occupant survivability did not catch fire. The pilot and camera operator sustained minor injuries while the helicopter was seriously damaged.
What the ATSB found
The ATSB found that when the pilot turned to the right to commence the orbit, the helicopter was exposed to a crosswind from the left while at an airspeed around the 30 kt threshold value for susceptibility to loss of tail rotor effectiveness (LTE), precipitating an unanticipated right yaw and temporary loss of control. The pilot regained sufficient control for a forced landing, but he did not use full left pedal as recommended for loss of tail rotor effectiveness, resulting in a likely delay in recovery.
What's been done as a result
The helicopter operator advised that as a result of the accident they conducted an internal investigation and implemented a number of safety actions in relation to LTE training and aerial work guidelines. In addition, the camera operators were issued with flight suits and helmets, and the operator advised the television station of the option to fit an externally-mounted gimbal camera that would allow the camera operator to remain seated and permit left or right orbits during filming operations.
Safety message
Aerial photography from most helicopters at relatively low airspeed and height, over hilly terrain in variable winds, is a challenging task with an inherent risk of LTE. In those circumstances, where visual cues can be misleading, pilot attention to airspeed, height and orientation to local wind is critically important. And, as demonstrated in this occurrence, LTE can be preceded by momentary strong yaw in the opposite direction, a characteristic which is counter-intuitive and has the potential to be confusing for the pilot.
As well as understanding how LTE can occur, pilots should be familiar with the recommended recovery techniques and apply them immediately to the fullest extent possible in the situation.
Occurrence summary
| Investigation number | AO-2013-016 |
|---|---|
| Occurrence date | 19/01/2013 |
| Location | 18 km north-east of Perth Airport |
| State | Western Australia |
| Report release date | 01/08/2013 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Loss of control |
| Occurrence class | Accident |
| Highest injury level | Minor |
Aircraft details
| Manufacturer | Bell Helicopter Co |
|---|---|
| Model | 206 |
| Registration | VH-ZMN |
| Serial number | 3591 |
| Sector | Helicopter |
| Operation type | Aerial Work |
| Departure point | Perth TV Stations, WA |
| Destination | Perth TV Stations, WA |
| Damage | Substantial |