On 23 November 2024, a Cessna 172F aircraft was being used to conduct a recency flight at Lismore Airport, New South Wales. On board was the pilot operating under a private pilot’s licence and a passenger with a recreational instructor rating. The pilot in command decided to conduct various configuration-based scenarios such as short field approaches and landings during the flight.
During a simulated short field landing scenario, the aircraft descended toward the runway and collided with a fence located at the beginning of the tarmac prior to the threshold of runway 15. The aircraft’s propeller, landing gear and engine cowling proceeded to strike the runway resulting in the aircraft rotating 180 degrees on the ground. During the rotation, the rear fuselage impacted the runway, and the aircraft slid on the bitumen for approximately 5 metres before coming to a stop.
The aircraft sustained substantial damage to the fuselage, wing, undercarriage and engine/propeller. The pilot and passenger were uninjured in the accident.
Figure 1: Propeller damage
Source: Aerodrome Operator, annotated by the ATSB
Safety message
Pilots must ensure that they are continually assessing both the aircraft’s profile and airspeed, especially during low-speed operations. Should the aircraft become unstable, conduct a missed approach.
This occurrence also highlights the importance of monitoring and assessing the landing area, taking into consideration all natural obstacles and infrastructure around the aerodrome.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
At about 1410 local time, a Cessna 152 aircraft with two crew from a local flight training facility was taxiing to the northern run-up bay at Moorabbin Airport, Victoria. The run-up bay is an area designated for pilots and engineers to perform high-power engine and pre-flight aircraft checks. The run-up bays were full and the Cessna queued behind a Piper PA-31 Navajo twin-engine aircraft that was positioned to conduct maintenance testing, involving high-power ground-running of the engines. A Piper PA-28 Cherokee was in the bay ahead of the Navajo, and another aircraft (a Cessna 172) was in the first bay before the Cessna 152 (Figure 1).
Figure 1: Position of the Cessna and Navajo aircraft immediately before occurrence
Source: Google Earth, annotated by the ATSB
By the time the pilot of the Cherokee had finished their checks and the aircraft vacated the bay, the pilot of the Cessna 152 (the Cessna) had already finished their checks and was given clearance to taxi behind the Cherokee to the runway.
As the Cessna started to taxi, the pilot of the Navajo increased the aircraft engines to full power as part of their engine inspection. The high intensity propeller wash[1] from the Navajo lifted the left wing of the Cessna, causing the aircraft to tip. Airport staff alerted the pilot of the Navajo to the incident, and they promptly shut down the aircraft engines. The Cessna sustained minor damage to the propeller and the wing tip of the aircraft as a result of the ground strike. No injuries were reported by the crew of the Cessna.
Safety message
Propeller wash from high-power engine tests can have serious consequences for light aircraft that can lead to loss of control and aircraft damage. Additionally, the propeller wash forces generated may result in flying debris which can cause damage to nearby people, equipment, or structures. To avoid this type of incident, pilots and ground crew must be vigilant of allowing safe distances to avoid propeller wash, particularly in congested apron areas. Flight and ground crews should also be aware of environmental conditions that can amplify the effects of propeller wash and always remain aware of their surroundings during operation or testing of an aircraft. This can include the re-evaluation of aircraft positioning during engine testing to prevent propeller wash from affecting nearby aircraft. Pilots taxiing in the vicinity of run-up areas should exercise caution, maintain situation awareness and avoid other aircraft conducting run-ups. Pilots are reminded to communicate directly to other aircraft if they believe an imminent safety risk exists to their operations.
About this report
Decisions regarding whether to investigate, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]The disturbed mass of air generated by the propeller of an aircraft.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2024-038
Occurrence date
24/09/2024
Location
Moorabbin Airport
State
Victoria
Occurrence class
Incident
Aviation occurrence category
Ground strike
Highest injury level
None
Brief release date
07/11/2024
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
152
Sector
Piston
Operation type
Part 142 Integrated and multi-crew pilot flight training
On 25 June 2024, a British Aerospace BAe 146‑300, registered VH‑SAJ, was being operated by ASL Airlines Australia on a freight flight from Sydney, New South Wales, to Brisbane, Queensland. On board the aircraft were the captain and first officer.
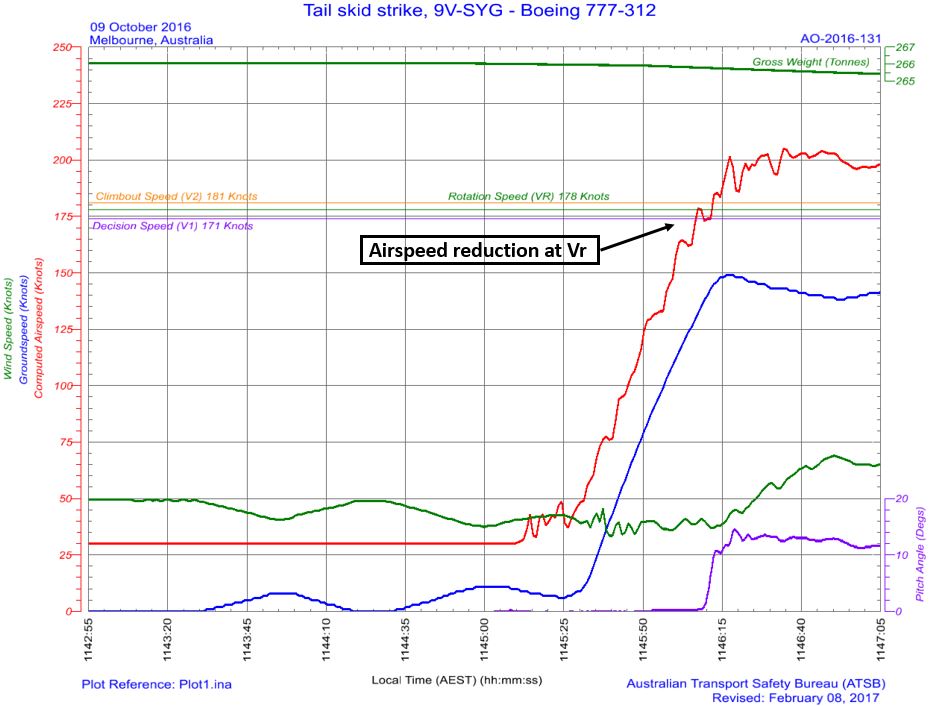
While on descent into Brisbane, the meteorological conditions worsened with visibility reducing to about 1,000 m in fog. The crew conducted an instrument approach for runway 19L, using the autopilot, and visually identified the high intensity approach lighting at about 220 ft. The first officer disconnected the autopilot at about 110 ft and made control inputs that resulted in an increasing aircraft pitch attitude with decreasing airspeed. The aircraft touched down with a high pitch angle and a vertical acceleration of about 2.4 g. The tail of the aircraft struck the runway, resulting in damage to the tail strike indicator and surrounding panels.
What the ATSB found
The ATSB’s investigation identified that the first officer likely became disoriented after disconnecting the autopilot and lost situation awareness. Consequently, they did not identify the increasing aircraft pitch attitude, decreasing airspeed, or low power setting and did not correct the resulting sink rate prior to touchdown. The captain prevented further rearward input by the first officer during the flare by placing their hand on the control column, likely reducing the severity of the tail strike.
It was also found that during the approach the captain became preoccupied with the remaining fuel on board and this likely limited their capacity to monitor other factors such as the first officer’s ability to undertake the approach and the undesired state of the aircraft during the flare. The ATSB also identified that the captain’s actions and communications during the approach likely increased the pressure on the first officer to commit to the landing.
Prior to joining the operator, the captain had predominantly flown single pilot operations in non‑jet aircraft. They had been promoted to the position of captain early, which resulted in a missed opportunity to gain valuable experience within a multi‑crew environment prior to commencing in the role. This limited multi‑crew experience likely reduced the captain’s capacity to include the first officer in the decision-making process during the approach or make an authoritative decision to assume the pilot flying role.
The ATSB identified that both the captain and first officer had been appointed to their respective positions despite not meeting the ASL Airlines Australia minimum experience requirements. This occurred without additional controls in place to manage the risk of lower experienced pilots and resulted in a reduction in the intended experience level on the flight deck for the incident flight.
What has been done as a result
Following an internal investigation by ASL Airlines Australia the following safety actions have been taken:
The upgrade or fleet transfer requirement of a minimum of 500 hours on a company type, or as deemed appropriate by the Director of Flight Operations contained in the operations manual was amended to a minimum of 500 hours on a company type, or similar type in terms of maximum take‑off weight as deemed appropriate by the Director of Flight Operations, Head of Training and Checking and Director of Safety.
Inexperienced flight crew that have been checked to line will not have their inexperienced status removed without a review of the candidate’s progress by the Director of Flying Operations or Head of Training and Checking.
The Planned Supervised Line Flying sectors for Captains – No Jet Experience listed in the OM‑D – Training and Checking Manual have been increased from 30 to 36 sectors.
Supervised Line Flying sectors for First Officers without previous jet experience has been increased from 30 to 36 sectors.
The Fleet Training Manager will review a candidate’s experience at the planning stage, and may elect to plan less, or more sectors, dependent upon the candidate’s progress.
Additional systems to track pilots with inexperienced status to avoid inadvertent rostering of inexperienced crew together.
The operator’s internal review identified an inconsistency between the operator’s standard operating procedures and the manufacturer’s recommendation with regard to which pilot (the pilot flying or the pilot monitoring) was to make an ‘attitude’ call when the aircraft pitch angle approaching landing increased above 5°.
The BAe 146 standard operating procedures manual has been updated and aligns with the manufacturer’s recommendation.
The operator’s internal review identified there was no policy stipulating that the captain must perform the landing when the weather conditions are below certain weather criteria.
A policy has been developed and incorporated into the operations manual that states the captain must conduct the approach and landing with visibility within 1,000 m and cloud within 100 ft of the minima unless the pilot in command is a company approved training or check pilot.
Safety message
Current shortages of aviation professionals, including pilots, have resulted in the need for operators to employ crew with less experience than has previously been expected. Operators are encouraged to review the employment and promotion processes for inexperienced crew, ensuring that additional training programs, or limitations on inexperienced crew and the pairing of less experienced crew during rostering are considered.
The occurrence
Overview
On 25 June 2024, a British Aerospace BAe 146‑300, registered VH‑SAJ, was being operated by ASL Airlines Australia on a freight flight[1] from Sydney, New South Wales, to Brisbane, Queensland. There were 2 flight crew on board. The captain was pilot monitoring, and the first officer (FO) was pilot flying. [2]
The aircraft departed Sydney at about 0415 with first light occurring at Brisbane at 0613. The forecast visibility for arrival at Brisbane was 10 km. While on descent to Brisbane, the meteorological conditions worsened with visibility reducing to about 1,000 m in fog. The crew conducted an instrument landing system (ILS) approach for runway 19L,[3] using the autopilot, and visually identified the high intensity approach lighting at about 220 ft.
The FO disconnected the autopilot at about 110 ft and made control inputs that resulted in an increasing aircraft pitch attitude with decreasing airspeed. The aircraft touched down with a high pitch angle and a vertical acceleration of about 2.4 g. The tail of the aircraft struck the runway, resulting in damage to the tail strike indicator and surrounding panels.
Cruise and descent
At about 0457, while the aircraft was in cruise at flight level[4] (FL) 270 and approximately 350 km to the south of Brisbane, air traffic control (ATC) advised the crew to expect runway 19L for their arrival.
At about 0505, cockpit voice recorder (CVR) data indicated that the captain obtained the automatic terminal information service (ATIS)[5] for Brisbane Airport. The meteorological conditions at that time were reported as a wind from 190° at 8 kt, visibility greater than 10 km with showers in the area, cloud few[6] at 500 ft, scattered[7] at 3,000 ft, and a temperature of 14°C (see Meteorological information). The captain then completed the take‑off and landing data (TOLD) card. This included calculated figures for fuel overhead the destination (Brisbane) of 2,400 kg and a minimum divert fuel of 1,700 kg.
The crew then conducted a briefing for the arrival into Brisbane and the ILS approach for runway 19L (see Airport information).
During the briefing, the FO noted the minima for the approach including a decision altitude (DA)[8] of 220 ft and visibility of 800 m, stating that conditions in Brisbane at the time were ‘showers and wet’.
At 0513, ATC advised the crew that the ATIS had been updated, and the cloud was now few at 200 ft, scattered at 3,000 ft and the temperature was 13°C. At 0519, when the aircraft was about 125 km south of Brisbane, ATC issued the crew with a clearance to descend to FL 130. A short time later, the captain commented on the cloud at 200 ft to the FO. The FO stated that they had 20 minutes of fuel, which was enough for a second approach if needed. The captain replied with ‘yeah, then we’re landing anyway’. The crew then completed the approach checklist.
The captain later advised that they believed their comment was a standard operational comment based on fuel limits.
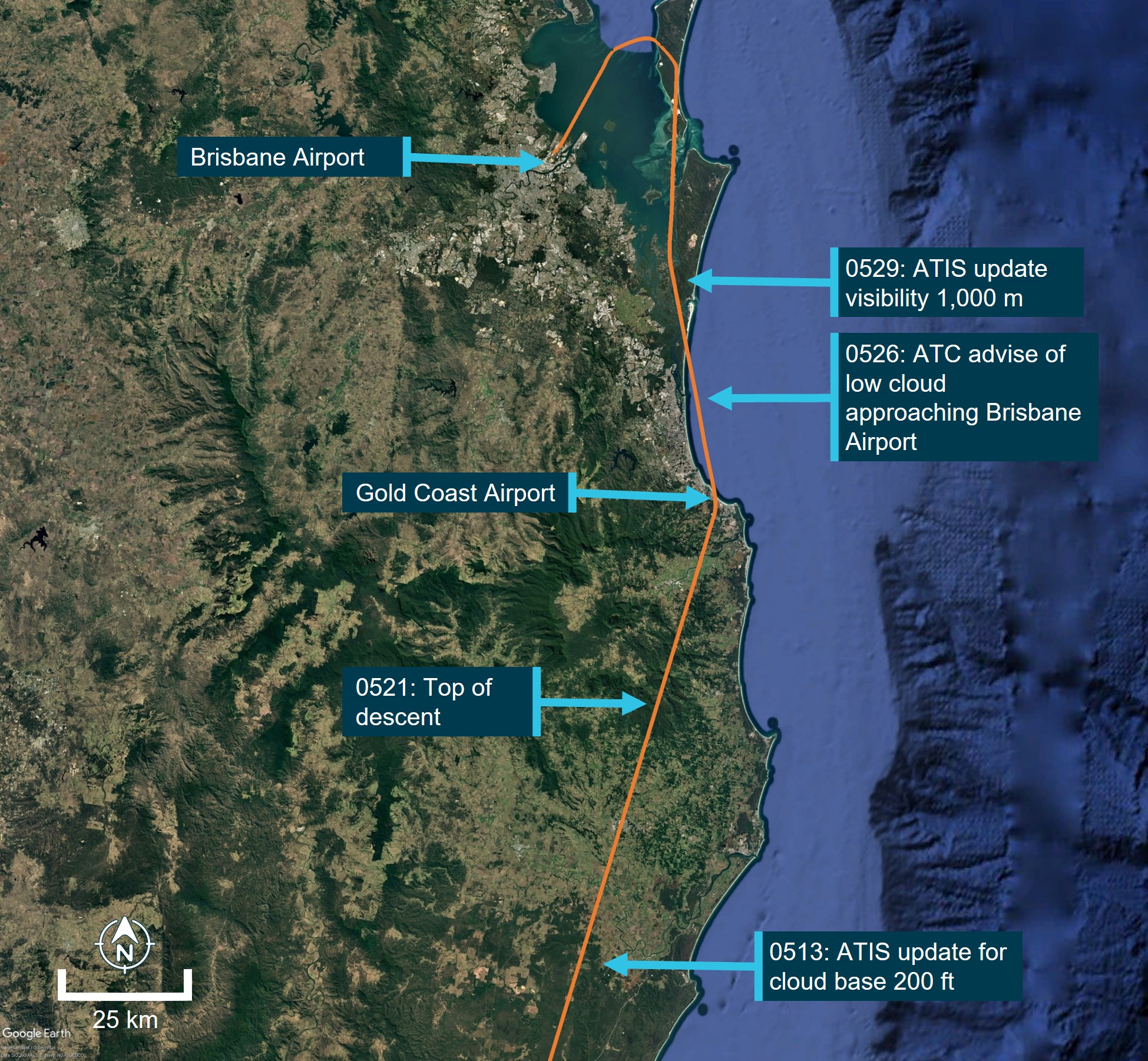
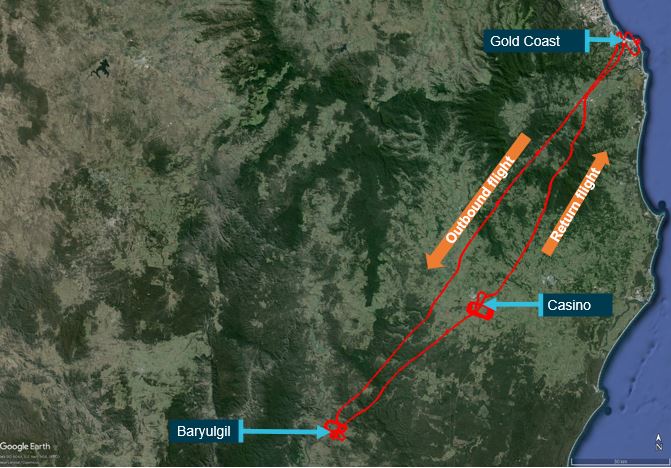
Figure 1: VH-SAJ flight track for arrival to Brisbane Airport
Source: Google Earth, annotated by the ATSB. *Flight was conducted in darkness
At 0521, the crew commenced the descent to FL 130. At 0525, ATC issued the crew with a further clearance to descend to 9,000 ft. A short time later, the crew were advised by ATC to expect the ILS approach for runway 19L.
At 0526, when the aircraft was about 67 km south-east of Brisbane, ATC advised the crew of low cloud south of the airport that was moving north and that they may be required to delay their arrival. On receipt of the meteorological information from ATC, the captain commented to the FO that they had ‘no fuel’. The FO proposed that they had sufficient fuel to complete 2 approaches, declare minimum fuel, and complete a third approach. The captain commented that they would just land from the second approach as they would ‘rather be on the ground’, expressing concerns about the paperwork involved.
Over the following 2 minutes, the captain and the FO continued to discuss the options for the approach with the captain stating that, given the fuel state, conducting a go‑around may result in a worse scenario as they expected the meteorological conditions at Brisbane to worsen. The crew did not discuss options for a diversion if they were required to undertake a go‑around due to the meteorological conditions. The closest suitable airport was the Gold Coast (see Gold Coast Airport meteorological conditions during flight).
At 0529, ATC advised that the visibility had reduced to 1,000 m in fog, with a cloud base of 200 ft and that low visibility procedures were in force with the high-intensity approach and runway lighting operating.
At 0530 the crew discussed the changing meteorological conditions. During this discussion, the captain stated that the conditions would only get worse and if they could see the high‑intensity approach lighting, then they were going to land. The FO agreed and stated that the captain should ‘call it when you see it’.
At about 0531, the aircraft passed through 11,000 ft and, a short time later, the crew initiated the additional approach checks. At 0533, the crew were cleared to continue the descent to 4,000 ft.
There were 3 aircraft ahead of VH-SAJ on approach to land on runway 19L at Brisbane Airport. At about 0532, the first of the 3 preceding aircraft landed and reported becoming visual with the runway at the minima.
Final approach
At 0534, ATC provided a clearance for the crew to undertake the ILS approach for runway 19L.
At 0536, the second aircraft in the sequence ahead of VH‑SAJ conducted a go‑around, later reporting to the ATSB that the combination of reduced visibility and low cloud prevented them from landing. At 0537, the captain of the third aircraft in the sequence declared to ATC, ‘should we, we will require an immediate diversion to the Gold Coast’. However, the third aircraft landed successfully.
The CVR indicated on hearing the transmission from the aircraft advising a go‑around, the captain stated ‘we haven't got the fuel for this’. The captain later stated that their comment was over concern should multiple go‑arounds be required.
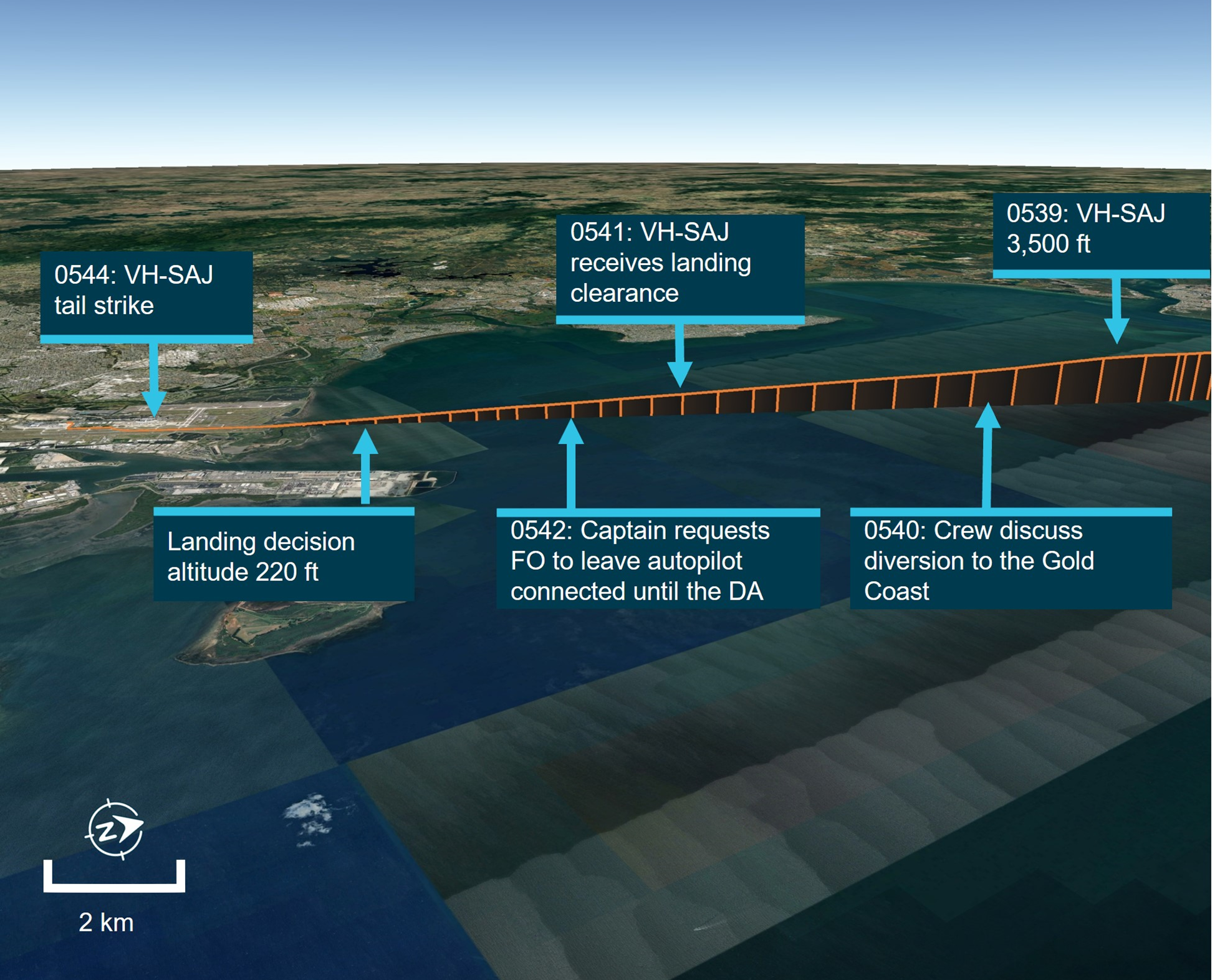
At about 0539, VH-SAJ became established on the ILS for runway 19L. At about 0540, approximately 4 minutes prior to landing, the captain stated to the FO that they did not have enough fuel to divert to the Gold Coast. The FO queried if it was possible to recalculate if there was sufficient fuel to conduct the diversion to the Gold Coast, to which the captain responded ‘not now on final, but let's try and get in’.
The captain later stated that they believed that it was not appropriate on final approach to calculate fuel for a diversion.
At 0541:28, the crew completed the landing checklist.
Landing
At 0541:45, the crew were provided with a landing clearance from ATC (Figure 2) and were advised that the runway visual range[9] was 1,200 m at the touchdown zone, 1,200 m at the runway mid‑point and 1,800 m at the end point of the runway.
Figure 2: VH-SAJ final approach to Brisbane Airport
Source: Google Earth, annotated by the ATSB. *Flight was conducted in darkness
At 0542:05, the captain instructed the FO to leave the autopilot connected until the aircraft reached 220 ft (the BAe 146‑300 minimum autopilot disconnect height is 60 ft). The captain later recalled to the ATSB that they did so to keep the aircraft on an accurate approach to the runway. The FO confirmed they would leave the autopilot engaged but also stated they would disconnect it should they require a go-around. In response, the captain stated ‘we don't want to go around. It’s gonna be a world of hurt’. The FO responded ‘but if we can't see, then we're gonna have to’.
The captain later responded after reviewing the draft report that their comment was over concern that a go‑around may lead to a more dangerous fuel critical situation and recalled at the time they considered similar occurrences that had occurred to other operators.
At 0542:40, the aircraft descended through 1,000 ft and was about 7 km from the runway threshold. At the same time, the captain advised the FO that the aircraft was stable, with the missed approach altitude set and armed.
At 0543:05 and about 600 ft, the captain announced they were visual with the high intensity approach lighting, the FO responded that they could also see the lighting, however ‘not super clearly’. At 0543:31 and about 350 ft, the captain instructed the FO to increase engine power.
At 0543:45, the aircraft reached the DA and the FO announced they could see the high intensity approach lighting. Four seconds later, the captain announced ‘there’s the runway’. The captain later recalled to the ATSB that they had more visibility than they had expected.
At 0543:57 the captain instructed the FO to disconnect the autopilot, which occurred at about 110 ft and an airspeed of about 128 kt. The airbrake[10] was extended and fully deployed as the aircraft passed 80 ft. Several pitch adjustments were made by the FO after the autopilot was disconnected. The FO later described that from the DA until landing, their workload increased ‘to a 9 or 10 out of 10’, they became ‘overwhelmed’ and that their scan pattern had broken down. The CVR indicated that neither the FO nor the captain commented on workload during the approach.
At 0544:01, both the captain and the FO announced becoming visual with the PAPI lights.[11] The FO later recalled they could make out the runway edge lighting, however could not see the touchdown point.
Just prior to touchdown, the captain instructed the FO ‘don’t come back too far’. The captain later recalled to the ATSB that the FO had levelled the aircraft shortly after disconnecting the autopilot and began to flare[12] too early. They recalled that the aircraft became high, slowed and then developed a high sink rate. From previous experiences they anticipated that the FO would attempt to pitch the aircraft up to arrest the sink rate. As a result, the captain placed their hand on the control column to prevent the FO from pulling back too far without verbalising their intention (see Operational policy and procedures). The FO also later recalled feeling the captain’s pressure on the control to prevent further rearward input.
The captain recalled to the ATSB that it was a common reaction for less experienced pilots to pull back and increase the pitch when the aircraft experienced a drop, and that this is discussed during their command training.
At 0544:11 the aircraft main wheels contacted the runway. The onboard flight data recorder captured a vertical acceleration of 2.4 g at initial touchdown, an aircraft pitch attitude of about 5.3°, and an airspeed of 105 kt (see Recorded information).
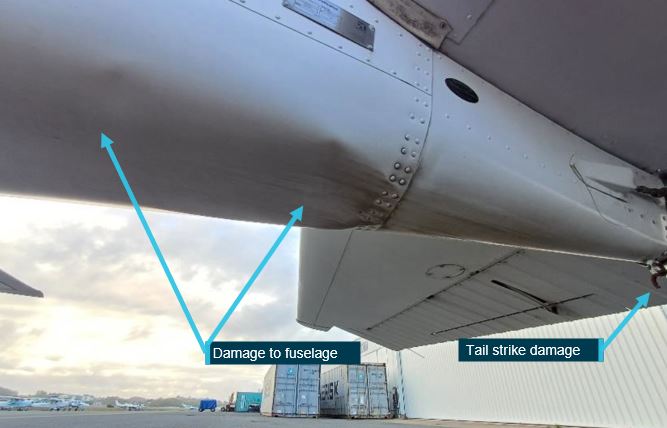
The crew were unaware of the tail strike until the damage was discovered on the post‑flight aircraft inspection. The tail contact with the runway damaged the tail strike indicator and surrounding fuselage skin panels (Figure 3).
Figure 3: VH-SAJ damage to tail strike indicator and surrounding panels
Source: ATSB
Context
Personnel information
Captain
Experience
The captain held an air transport pilot licence (aeroplane), issued in October 2017, and a valid class 1 aviation medical certificate. At the time of the incident, the captain had about 7,500 hours total aeronautical experience, of which about 5,400 hours was multi‑engine command. They had a total of 411 hours on the BAe 146, which included 198 hours as captain. The BAe 146 was the captain’s first jet aircraft rating, having previously flown smaller twin turboprop aircraft mostly in single pilot operations before commencing employment with the operator.
Operator training
The captain joined ASL Airlines Australia in November 2022 as a first officer. They completed their type rating on the BAe 146 aircraft in early 2023 and they were checked to line as a first officer in July 2023. In October 2023, they were assessed and recommended to undertake command training. At that time, their total BAe 146 time was 155 hours.
Their command training commenced in November 2023 and involved simulator training and command checks. During this training, the captain’s initial operator proficiency check (OPC) was assessed as unsatisfactory due to a breakdown in situation awareness during an instrument approach. Additional simulator training was provided, and the captain passed their OPC on 23 November 2023. The captain’s subsequent command simulator training was also assessed as unsatisfactory and was required to be retaken.
On 4 December 2023, the captain commenced supervised line flying sectors. The captain completed 19 sectors before being recommended to undertake their check to line on 19 December 2023. The captain’s check to line was assessed as unsatisfactory after the first sector. The captain was provided with additional simulator and ground school training support. The captain completed a further 8 supervised line flying sectors before being recommended to retake their line check. The captain successfully completed their line check on 15 February 2024.
The captain’s command training consisted of 31 sectors and 58 hours of flying.
First officer
Experience
The first officer (FO) held a commercial pilot licence (aeroplane), issued in March 2020, and a valid class 1 aviation medical certificate. The FO’s total aeronautical experience was about 1,090 hours, including about 113 hours as an FO on the BAe 146. Prior to their employment with the operator, the FO had flown for a general aviation operator, flying mostly smaller, single-engine aircraft and operating under visual flight rules.
Operator training
The FO joined ASL Airlines Australia in January 2024. They completed their type rating on the BAe 146 aircraft on 4 March 2024. They undertook 2 simulator sessions before successfully completing their OPC on 28 March 2024.
The FO commenced supervised line flying sectors in April 2024. The FO was assessed as achieving below the required standard in several areas including situation awareness, approach and landing. The FO undertook a simulator session on 8 May 2024 and an additional 16 supervised line flying sectors. The FO recalled that their simulator training included low visibility operations, but they had not previously landed an aircraft in foggy conditions.
On 28 May 2024 they were assessed as not proficient during their check to line. The FO was reassessed on 29 May 2024, 28 days prior to the incident and successfully completed their check to line.
The FO’s training consisted of 51 sectors and 90 hours of flying.
Fatigue
The ATSB considered the role of crew performance due to fatigue and found that, from the available evidence, fatigue was unlikely to have contributed to the incident (see Fatigue).
Aircraft information
General information
The BAe 146 (Figure 4) is a high‑wing cantilever monoplane with a T‑tail. It is powered by 4 Avco Lycoming ALF 502 turbofan engines mounted on pylons underneath the wings and had retractable tricycle landing gear.
The aircraft, serial number E3150, was a BAe 146‑300 series aircraft manufactured in 1989 and configured for air freight operations. It was first registered in Australia as VH‑SAJ on 24 October 2019. The last periodic inspection was completed on 12 June 2024 and on the day of the occurrence, the aircraft had accumulated 34,746 hours total time in service.
Figure 4: VH-SAJ BAe 146-300
Source: Jet photos, Cameron Roberts
Aircraft operator
At the time of the incident, ASL Airlines Australia (previously Pionair) held an air operator’s certificate issued by the Civil Aviation Safety Authority (CASA) on 14 May 2020 and valid until 1 December 2027, that authorised air transport in larger aeroplanes (CASR Part 121). ASL Airlines Australia operated a mixed fleet of aircraft that comprised 6 BAe 146s and 1 Boeing 737 aircraft, conducting mostly domestic air freight operations.
Airport information
Brisbane Airport
Brisbane Airport has 2 runways oriented 10°/190° magnetic (01L/19R and 01R/19L). At the time of the incident, aircraft departures and arrivals were taking place using runway 19L. The airport has a category 1 instrument landing system (ILS) on both runways. This landing system, combined with a 100% LED[13] category 1 lighting system,[14] including stop bar lighting, enables operations during low visibility events like fog.
Instrument approach
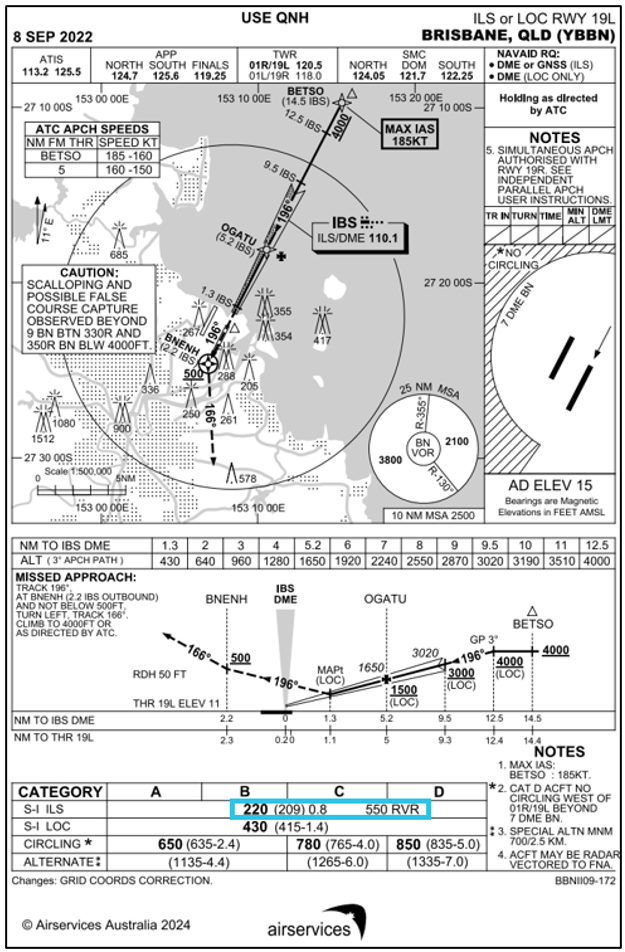
The crew of VH-SAJ were flying an ILS approach for runway 19L. The minima for the approach included a decision altitude8 of 220 ft, visibility of 800 m, and a runway visual range of 550 m (Figure 5).
Figure 5: Brisbane ILS runway 19L approach chart with landing minimums (blue box)
Source: Airservices Australia, annotated by the ATSB
Meteorological information
Predeparture briefing
The captain and FO were issued with a flight briefing package at 0057 that morning, which included the current terminal aerodrome forecast (TAF)[15] that was valid between 0000 on 25 June and 0400 on 26 June for Brisbane Airport.
At the time the flight briefing was issued, the TAF for Brisbane indicated:
active INTER[17] from 0000 through till 0400 for visibility of 3,000 m in showers of moderate rain and broken cloud at 1,500 ft.
Prior to their departure from Sydney, the crew checked the latest weather information for their arrival into Brisbane. The latest TAF had not extended the INTER period for showers beyond 0400.
Brisbane Airport meteorological conditions during flight
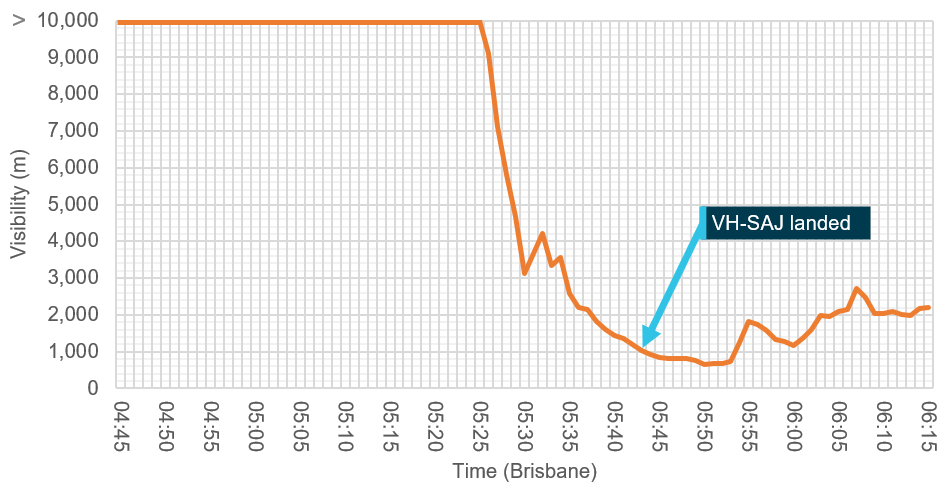
The aircraft departed Sydney Airport at 0415, one hour and 15 minutes after the scheduled departure time and had an estimated time of arrival in Brisbane at 0555. Over the period 0500 to 0525 the visibility at Brisbane Airport remained greater than 10 km. From 0525 to 0550 the visibility reduced from greater than 10 km to 660 m due to the formation of advected fog.[18] The recorded visibility at the time VH‑SAJ landed was 912 m (Figure 6).
Figure 6: Brisbane Airport visibility 0445 to 0615 on 25 June 2024
Source: Bureau of Meteorology, annotated by the ATSB
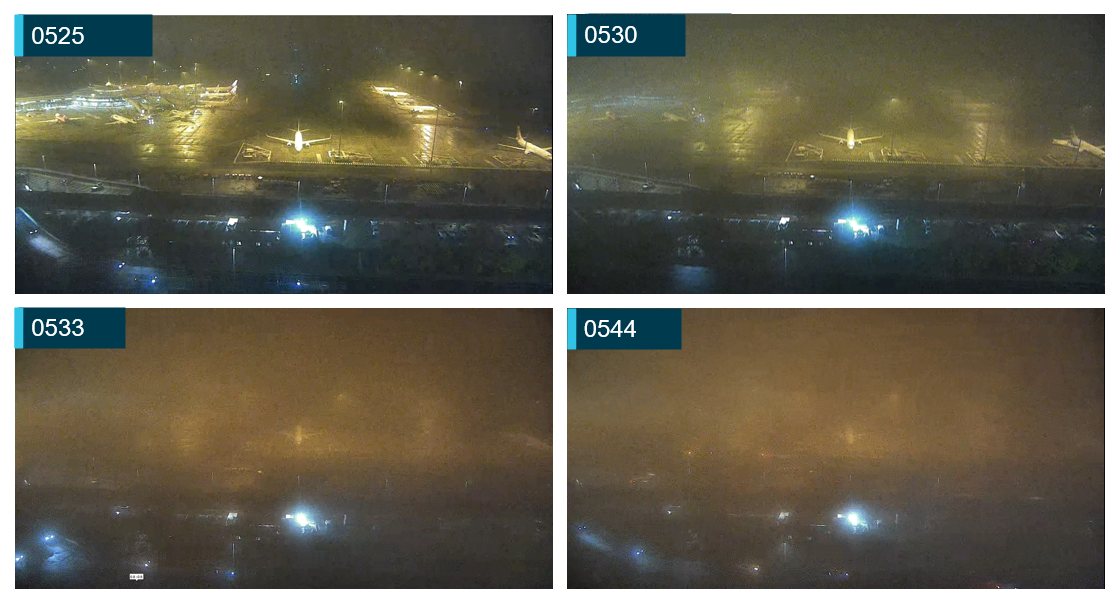
Closed circuit television (CCTV) recorded from the Brisbane air traffic control tower captured a progressive reduction in visibility that was consistent with the recorded meteorological information (Figure 7).
Figure 7: CCTV images from Brisbane Airport tower facing south
Source: Brisbane Airport Corporation, annotated by the ATSB
Gold Coast Airport meteorological conditions during flight
The closest alternate to Brisbane Airport was Gold Coast Airport which had a TAF issued at 0306 that contained an active TEMPO[19] for visibility of 4,000 m in showers of rain, with cloud scattered at 1,000 ft and broken at 2,000 ft.
At 0530, the Gold Coast meteorological aerodrome report (METAR) indicated visibility greater than 10 km and lowest cloud base of few at 6,100 ft. The subsequent METAR, issued at 0600, indicated visibility was still greater than 10 km with the lowest cloud base being scattered at 3,600 ft.
The Gold Coast Airport forecast was not issued to the crew as part of their flight briefing package and the crew did not obtain the Gold Coast Airport ATIS during the flight.
Recorded information
The aircraft was fitted with an L3[20] F1000 flight data recorder and L3 FA2100 cockpit voice recorder. Both units were transferred to the ATSB technical facilities in Canberra, Australian Capital Territory, for download.
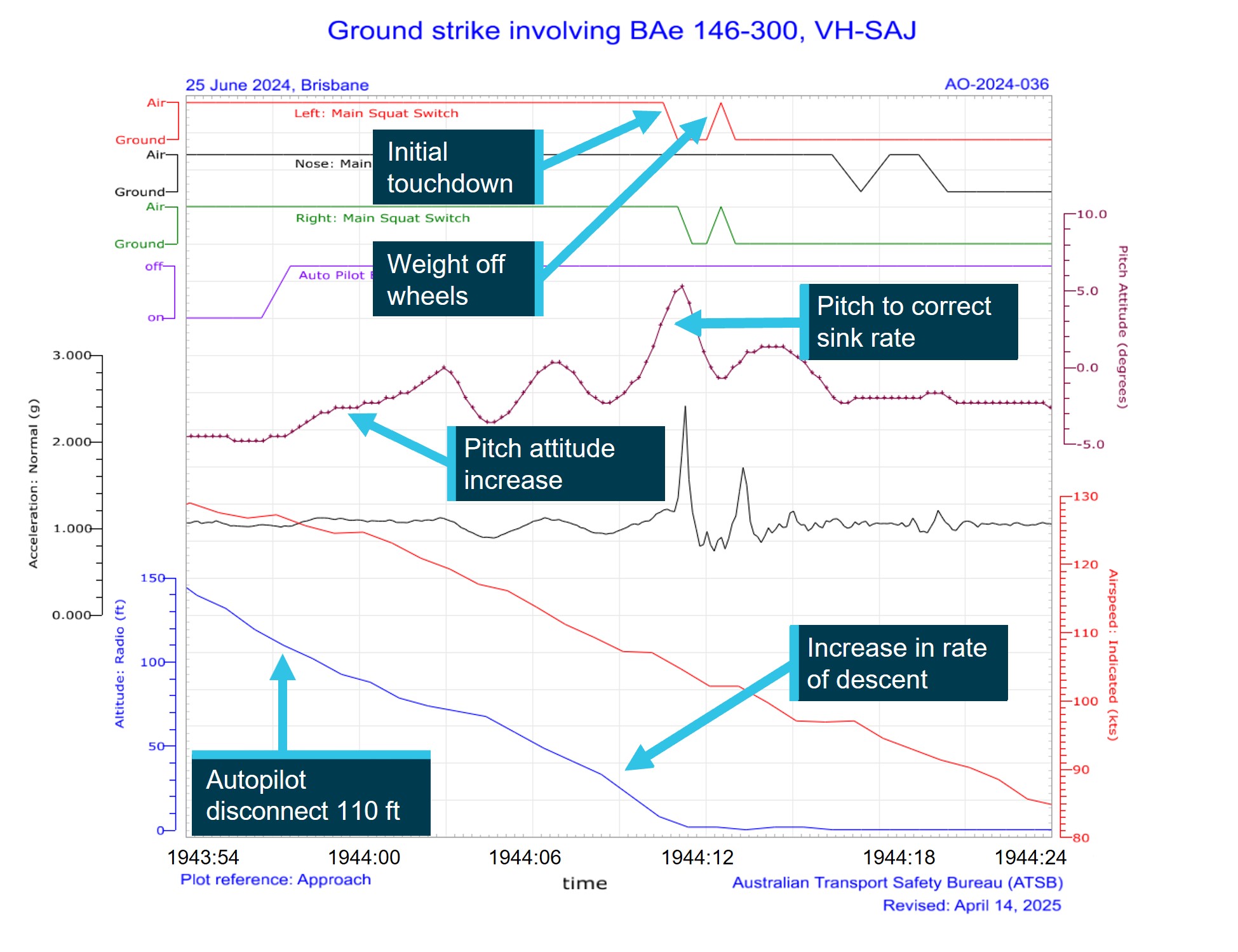
Recorded flight data during the approach phase indicated the aircraft was flown within the ASL Airlines Australia stabilised approach criteria. At a height of about 110 ft, approximately 13.5 seconds before the main gear touchdown, the data indicated the autopilot was disconnected. Immediately following the disconnection of the autopilot, over a period of 5 seconds, the aircraft pitch attitude increased from about −4.3° to about 0° (Figure 8). At the same time the aircraft speed reduced from about 128 kt to about 120 kt. The crew had calculated the aircraft landing reference speed (Vref)[21] to be 115 kt and the aircraft approach speed (Vapp)[22] to be 120 kt (Vref + 5 kt).
The airbrake was deployed at a height of 100 ft and was fully extended when the aircraft reached 80 ft. ASL Airlines Australia standard operating procedures manual for the BAe 146 advised that the airbrake should be deployed on final approach once the landing was assured.
Figure 8: Recorded flight data
Source: ATSB
At a height of about 65 ft, the aircraft decelerated through 117 kt with a pitch attitude of about −3.6° and an increasing rate of descent. Several further pitch attitude adjustments were recorded as the aircraft continued to descend.
At a height of about 30 ft, the pitch attitude decreased to about −2.3°, airspeed reduced to about 109 kt and the rate of descent increased. Shortly after, the pitch attitude increased to a maximum of about 5.3° coincident with main gear touchdown. The vertical acceleration at main gear touchdown was 2.4 g and the airspeed was 105 kt. The aircraft engine power throughout the landing sequence was about 37% N1[23] and there was no recorded increase in power prior to contact with the runway. About 4 seconds after the initial touchdown the main gear momentarily recorded a weight off wheels followed by a vertical acceleration of 1.7 g, indicating a possible bounce.
The aircraft manufacturer advised that a tail strike in a BAe 146‑300 would occur on a hard landing, when the main gear oleos[24] had fully compressed, at a pitch attitude of 6.9° or higher. The difference between the values provided by the manufacturer and the recorded data were likely due to a combination of the flight data recorder sampling rate for the pitch attitude parameter (4 times a second) and the overall system accuracy (+/− 1.34°).
Operational information
Flight plan
ASL Airlines Australia operations provided the flight plan as part of the flight briefing package. The flight would depart Sydney and climb to FL 270. The track would take the flight overhead Newcastle, Grafton, Lismore and the Gold Coast, before landing at Brisbane. The flight was scheduled to continue from Brisbane with a planned landing in Townsville before the crew would end their duty period in Cairns.
Fuel planning
On departure from Sydney, the onboard fuel load was recorded as 5,800 kg with a planned trip fuel of 3,332 kg, including taxi fuel. ASL Airlines Australia operations had planned the flight with an additional 30 minutes of holding fuel due to the forecast INTER, planned between midnight and 0400 in Brisbane, which was later cancelled. A delay due to an engine vibration warning light resulted in an additional fuel burn, however the crew determined that as the INTER had been removed, that they had sufficient fuel for the sector. After discussion with the engineering team, the warning light was deemed to be a faulty indicator and the aircraft cleared to depart.
The operator’s fuel policy required a fixed final reserve fuel of 30 minutes as well as an additional 15 minutes of holding fuel when no alternate was required. This was a provision for weather, GPS RAIM[25] outage, traffic, or beginning of daylight. A contingency fuel margin of 5% of the trip fuel was also required to compensate for unforeseen factors.
VH-SAJ landed in Brisbane with about 2,300 kg of fuel remaining, which equated to about 72 minutes of flight time that included the use of reserve fuel. The ATSB was advised that ASL Airlines Australia had undertaken an internal review of the flight and that this review determined that the aircraft had sufficient fuel to conduct a missed approach at Brisbane and then divert to the Gold Coast before having to utilise the final reserve fuel margin.
Weight and balance
The operator’s load and trim sheet records indicated the aircraft was within the weight and balance limitations for the intended flight.
Preflight briefing
At the beginning of the duty period, the operator’s policy was for flight crew to conduct a ‘big picture briefing’. This was an opportunity to discuss any significant factors that may affect the planned operation and to focus on underlying threats or unusual factors and to discuss any means of mitigating those threats.
During the big picture briefing conducted prior to flight, the captain and FO recalled that they discussed that they had not previously flown together, and the captain communicated that they were open to receiving any criticisms or concerns regarding their operating practices. The captain recalled assuming that the FO was new to the position, but they were unaware of the FO’s previous flying experience and were also unaware they had not previously landed in low visibility conditions.
Operational policy and procedures
Flight crew experience requirements
Legislative requirements to be qualified as pilot in command
Civil Aviation Safety Regulation (CASR) part 121.495 required the following pilot in command experience:
(1) A pilot is qualified as pilot in command for a flight of an aeroplane if:
(a) the pilot meets the minimum flying experience requirements specified, in accordance with subregulation (2), in the aeroplane operator’s exposition for the aeroplane; and
(b) the pilot has successfully completed command training that complies with regulation 121.565 for the aeroplane operator and an aeroplane; and
(c) the pilot is:
(i) if the aeroplane is an Australian aircraft—authorised to pilot the aeroplane during the flight as pilot in command under Part 61; or
(ii) if the aeroplane is a foreign registered aircraft—authorised to pilot the aeroplane during the flight as pilot in command by the aeroplane’s State of registry.
(2) For the purposes of paragraph (1)(a), the aeroplane operator’s exposition must include minimum flying experience requirements for all aeroplanes operated by the operator for Part 121 operations.
Operator’s documented requirements
The ASL Airlines Australia operations manual (OM-A) version 5.5, which was current when the flight crew were checked to their positions, contained the minimum experience requirements to be met before an FO could be considered for promotion to the position of captain (pilot in command). The stated experience requirements were:
• meet all regulatory requirements
• minimum of 3000 hours aeroplane
• minimum of 500 hours on a company type, or as deemed appropriate by the GMFO [General manager of flying operations]
• minimum of 500 hours multi-engine PIC [pilot in command] or ICUS [in command under supervision]
• Australian ATPL [air transport pilot licence] or CPL [commercial pilot licence] with exam credit in all required examination subjects may be acceptable if the company is able to arrange/conduct an ATPL flight test as part of the upgrade training program.
The OM-A also contained the minimum experience required for the employment of a first officer. The stated experience requirements were:
• minimum total time of 1000 hours
• minimum of 500 hours in multi-engine aircraft
• a current Australian CPL [commercial pilot licence] or ATPL [air transport pilot licence].
The OM-A permitted the employment or promotion of crew below the prescribed minimum hours in ‘exceptional circumstances’, with the specific approval of the director of flight operations (DFO). It stated:
All crew seeking positions as pilots with Pionair are to comply with the Australian CASR Part 61 requirements with respect to licencing. Flight crew experience criteria for the various categories are as detailed below. These criteria may be varied, with the specific approval of the Director of Flight Operations to cater for exceptional circumstances.
There was no definition of what would be considered ‘exceptional circumstances’ within the OM-A.
Incident flight crew engagement
Neither the captain nor the FO met the documented minimum requirements to hold their assigned positions at the time of the occurrence.
The FO had about 106 hours of multi-engine experience at the time of their engagement with ASL Airlines Australia and about 219 hours of multi‑engine experience at the time of the incident. The OM-A minimum multi-engine experience requirement for the position was 500 hours.
The captain completed their command check to line in February 2024. At that time, they had accumulated about 213 hours on the BAe 146, of which 155 hours were as FO and an additional 58.7 hours in command under supervision as part of their command training course. At the time of the incident, they had accumulated about 411 hours total flying in the BAe 146 as FO and captain. The minimum company type experience requirement for the position was 500 hours.
The DFO was interviewed by the ATSB and described the captain as having ‘significant operational experience in night freight operations and the ability to manage fatigue with appropriate rest which was a very important but often overlooked skill for a new captain.
The DFO also recalled that the FO had previously been an airline cadet (for a major carrier) and had performed well in their interview.
No evidence of the ‘exceptional circumstances’ that led to the promotion of the captain or the employment of the FO was provided or identified by ATSB. There was also no evidence that ASL Airlines Australia had considered and managed the risks associated with the engagement of flight crew that did not meet the stated minimum requirements.
The DFO explained that during the period after COVID‑19, other airlines were recruiting significant numbers of flight crew and that ASL Airlines Australia had less opportunity to recruit for experienced crew during that time.
The Australian Government’s Aviation White Paper released in 2024 cited that a shortage of aviation professionals, including flight crew, was worsening, with job vacancies having more than tripled since 2019. The report also identified the effect a pilot shortage has on regional airlines and smaller operators, as crew leave these organisations to progress their careers with larger airlines, resulting in a higher turnover and a pool of less experienced applicants during recruitment.
Rostering of ‘inexperienced’ flight crew
The ASL Aviation Australia OM-A contained a policy to prevent ‘inexperienced’ flight crew being rostered together for a flight. It stated:
A flight crew member is deemed to be 'inexperienced' following completion of a type rating or command course until achieving the following additional experience on the type in their respective flight crew role after a successful check-to-line:
a. 100 flying hours and 10 operational sectors, within a consolidation period of 60 days; or
b. 150 flying hours and 20 operational sectors (with no time limit).
The policy further stated:
The OCC [Operations Control Centre] must ensure that inexperienced flight crew are not rostered together. In exceptional circumstances on Day of Operations the Director of Flight Operations may approve a crew complement that does not meet the above minimum experience requirements. To ensure compliance with current Regulations the Director of Flight Operations must ensure that, at an absolute minimum, the above minimum hours and sectors have been met when considering a crew member’s total type experience (including line training).
The captain had accumulated 198 hours since their successful check to line in February 2024 and was not considered inexperienced.
The FO had accumulated a total of 113 hours total time on the BAe 146 including their line training. Since their successful check to line on 29 May 2024, they had flown about 25 hours and completed 15 sectors as FO and was still considered ‘inexperienced’ according to the operator’s policy.
The policy did not have a provision for crew members that had been promoted to their position below the operator’s minimum prescribed hours.
Operational restrictions for 'inexperienced' flight crew
CASA acceptable means of compliance guidance material regarding pilot experience, stated:
The operator should consider any operational restrictions to be placed on an 'inexperienced' crew member after the completion of the conversion training or post command line check. These considerations may include cross wind limits, aerodrome limits and weather minima limits if the operator assesses these limits as suitable for their operation.
ASL Airlines Australia reported that it did not have a policy that restricted ‘inexperienced’ FOs landing in adverse weather and raised concern that this would reduce the exposure of FOs to less than desirable weather conditions.
The ATSB interviewed the captains of 2 of the 3 aircraft that were on approach to Brisbane ahead of VH‑SAJ. These aircraft were being operated by the same CASR Part 121 operator. Both captains advised that the FO on board was originally the pilot flying for that sector. However, if the visibility was less than 2,000 m or if the cloud was within 200 ft of the minima,[26] their operator’s policy was that the captain was required to conduct the approach and landing. Both captains reported that as the visibility on the ATIS was reported as 1,000 m and the cloud height at 200 ft, both had assumed the pilot flying roles of their respective aircraft prior to landing in accordance with their operator’s captains only approach procedure.
The ATSB reviewed expositions from 6 CASR Part 121 operators and found that 5 out of 6 operators had restrictions on FO’s conducting take‑offs and landings in adverse weather conditions, including reduced visibility, low cloud and strong winds.
Responsibility for control of the aircraft
The ASL Airlines Australia OM-A stated:
The authority and responsibilities of the captain are crucial for the safe operation of an aircraft. The captain holds ultimate authority over the aircraft, maintains discipline, and is responsible for ensuring the safety of individuals and cargo onboard, as well as the overall safe operation of the aircraft.
During interview with the ATSB, the FO recalled that as the approach continued, they became uncomfortable with the reduced visibility and described feeling overwhelmed by the conditions. However, the cockpit voice recording indicated the FO did not advise the captain of this, and they continued the approach as pilot flying. The FO recalled that, in hindsight, they should have requested control handover to the captain when they started feeling uncomfortable. Additionally, the captain also reported that in hindsight they should have assumed control and landed the aircraft.
The ASL Airlines Australia OM-A required:
Handover of control from one pilot to another must always be conducted in a positive manner. To minimise confusion or operational risk, the PF must not relinquish control until the PM has advised that they have taken control of the aircraft. NOTE: The standard phraseology to be used for handover/takeover procedures is: "You have control" and "I have control".
• In non-normal situations or when required, the Captain must initiate the takeover procedure.
• If corrected responses are not achieved from control inputs, control should be handed over to another flight crew member.
• In critical phases of flight, Captains must be in a position to enable rapid takeover of controls.
Standard calls
ASL Airlines Australia operations manual B (OM-B) for the BAe 146 detailed the required standard calls for flight crew during an approach. Cockpit voice recorder information indicated that the crew missed several required calls (Table 1).
In addition to the standard calls, the ASL Airlines Australia OM-B for the BAe 146 stated that during landing the:
PF/PM must monitor the attitude – if the nose up attitude becomes excessive on the ADI the PF should stop the increase in pitch attitude and consider a go-around if necessary. Recommended attitudes at which an “attitude” call should be made by the PF are:
…
• BAe146-300: 5°
The cockpit voice recording indicated that no attitude call was made by the crew when the aircraft pitch attitude increased above 5° just prior to main gear touchdown.
Fatigue
General
Fatigue affects everyone regardless of skill, knowledge and training and its effects can be particularly dangerous in the transportation sector, including the aviation industry.
The International Civil Aviation Organization (ICAO, 2015) defined fatigue as a physiological state of reduced mental or physical performance capability resulting from sleep loss, extended wakefulness, circadian phase, and/or workload (mental and/or physical activity) that can impair a person’s alertness and ability to perform safety related operational duties. Fatigue can have a range of adverse influences on human performance. These include:
slowed reaction time
decreased work efficiency
increased variability in work performance
lapses or errors of omission (Battelle Memorial Institue, 1998).
Duty period and sleep obtained
ASL Airlines Australia exposition stated that when flight crew are rostered to begin a duty period between 0000 and 0459 and scheduled to fly 4 sectors, the maximum duty period is 9.5 hours. If both flight crew agree, the duty may be extended by 1 hour during the duty period.
The captain recalled not being rostered on for the previous 72 hours before they signed on for their duty period in Melbourne at about 0015. They reported that, on the Samn‑Perelli scale of alertness,[27] they felt fully alert, however at the time of the occurrence, reported they felt ‘okay, somewhat fresh’. The captain reported having about 5 hours sleep in the 24 hours prior to their duty period and about 12 hours of sleep in the past 48 hours.
The FO recalled not being rostered on for the previous 72 hours before starting their duty. They reported having about 9 hours sleep in the past 24 hours prior to their duty period and about 17 hours in the past 48 hours and that they felt ‘a little tired, less than fresh’ at the time of the occurrence.
The ATSB assessed that both crew had sufficient sleep opportunity prior to commencing their duty.
Adequate sleep is an obvious prerequisite for alertness during duty. The concept of adequate sleep however is subject to individual variability with inconsistencies in amount and quality.
Window of circadian low
The duty period required working through the time in the circadian body clock cycle when self‐rated fatigue and mood are worst (Salas & Maurino, 2010). According to ICAO (2015) there are 2 times of peak sleepiness within a 24‑hour cycle. The main peak is in the early morning between 0300‑0500 known as the window of circadian low (WOCL), another smaller peak is around 1500‑1700 known as the afternoon nap window (International Civil Aviation Organisation, 2015). For each individual this time can vary. The incident occurred at 0544 which was close to the WOCL, which would have had some impact on their alertness levels as seen in their subjective alertness ratings above.
However, the FO’s alertness was possibly heightened (Causse and others, 2024) due to their unfamiliarity with the unforecast conditions and as a result this would likely have counteracted any effect of fatigue.
Operator's biomathematical model of fatigue
The operator provided the ATSB with a summary of the June 2024 report from their fatigue management software which uses biomathematical modelling to predict fatigue risk from the roster times and duty periods. The results did not identify fatigue risk had occurred with either crew member. However, the model does not account for individual susceptibility or resilience to fatigue.
Fatigue summary
The ATSB considered the role of crew performance due to fatigue and found that the available evidence indicated that fatigue was unlikely to have contributed to the incident. However, the captain’s self-reported amount of sleep in the 24 hours prior to their duty period is below the guidelines for recommended hours (Hirshkowitz and others, 2015).
Related occurrences
Tail strike – Brisbane Airport, Queensland, 23 October 2008 (AO‑2008‑74)
On 23 October 2008 at 2357 Eastern Standard Time, a BAe 146‑300 aircraft, registered VH‑NJM, operating a freighter flight, had a tail strike on landing at Brisbane Airport, Queensland. The aircraft and crew had commenced duty earlier that evening at Adelaide, South Australia, and had flown via Sydney, New South Wales, to Brisbane. The aircraft and crew then did the reverse sectors back to Adelaide. It was only after landing at Adelaide that the crew became aware of the tail strike. Damage to the aircraft consisted of abrasion to the tail strike indicator through to the fuselage skin and abrasion to the fuselage skin. There was also damage to the aircraft’s structural frame under the tail strike indicator. The aircraft manufacturer had identified an increase in the number of BAe 146‑300 tail strikes and has recommended a number of procedural changes for flight crew. The aircraft operator has implemented those changes and issued notices to flight crew highlighting the risks and conditions for tail strike.
Tail strikes during landing involving Bombardier DHC-8 402, VH‑QOT and VH‑QOS, Brisbane Airport, Queensland, on 5 November 2013 and Roma Airport, Queensland, on 11 December 2013 (AO-2013-201)
On 5 November 2013 and 11 December 2013, 2 Dash 8‑400 aircraft, registered VH‑QOT and VH‑QOS, were being operated by QantasLink on scheduled passenger flights from Roma to Brisbane and Brisbane to Roma, Queensland, respectively. Both flights were crewed by a training captain, operating as pilot monitoring, and a trainee first officer, operating as pilot flying.
Although the 2 approaches utilised different flap settings, both were conducted using a propeller setting of 1,020 RPM. The early, initial and final stages of the approaches were unremarkable. Both training captains reported that as the aircraft approached the flare, they thought that the respective trainees had handled the approach well.
During landing, both trainees arrested the descent rate by raising the nose of the aircraft. In both cases the maximum pitch attitude was exceeded and the aircraft’s tail contacted the runway. Each aircraft sustained impact and abrasion damage to the fuselage skin and buckling of internal structures in the area of the tail strike sensor.
Safety analysis
Introduction
On 25 June 2024, a British Aerospace BAe 146‑300, registered VH‑SAJ, was being operated by ASL Airlines Australia on a freight flight from Sydney, New South Wales to Brisbane, Queensland. There were 2 flight crew on board. The captain was pilot monitoring (PM), and the first officer (FO) was pilot flying (PF).
While on descent to Brisbane, the meteorological conditions worsened with visibility reducing to about 1,000 m in fog. The crew conducted an instrument landing system (ILS) approach for runway 19L, using the autopilot, and visually identified the high intensity approach lighting at about 220 ft. The FO disconnected the autopilot at about 110 ft and made control inputs that resulted in an increasing aircraft pitch attitude followed by several corrections and continued decreasing airspeed. The aircraft touched down with a high pitch angle and a vertical acceleration of about 2.4 g. The tail of the aircraft struck the runway, resulting in damage to the tail strike indicator and surrounding panels.
This analysis will explore the operational considerations pertaining to flight crew experience and training, situation awareness, command decision‑making and crew communication.
Loss of situation awareness
The FO was new to their position with ASL Airlines Australia, having been checked to line 28 days prior to the incident. During their line training, the FO required additional simulator and supervised line flying sectors to achieve the required standard associated with situation awareness, approach and landing. At the time of the incident, the FO had accumulated a total of 113 hours of flying on the BAe 146.
The meteorological conditions at Brisbane at the time of the approach included reduced visibility due to the formation of advected fog. At the time the crew reached the ILS decision altitude (DA) for runway 19L, the visibility was recorded as 912 m. Although this exceeded the minimum required for the approach, the FO had only experienced flying in reduced visibility during their BAe 146 simulated training, and they had not previously landed an aircraft in foggy conditions. (The FO’s experience prior to employment with the operator had predominately been flying smaller single engine aircraft in visual meteorological conditions).
The presence of low cloud or fog can create a false visual reference which can result in a pilot orientating the aircraft to the fog layer, rather than the ground references (Federal Aviation Administration). The FO recalled that the low cloud and fog created a sight picture that they had not previously experienced in the aircraft and that following the transition to visual flying, their instrument scan pattern broke down as their attention shifted to outside the aircraft as they attempted to make sense of the landing environment.
Research by Garland et al, (1999) identified that high mental workload can negatively impact situation awareness, as only a subset of the available information can be processed and acted upon. Situation awareness can be defined as ‘the perception of the elements in the environment within a volume of time and space, the comprehension of their meaning and the projection of their status in the near future’ (Endsley, 1988) . The maintenance of a high level of situation awareness is a critical feature of a pilot’s role (Garland et al, 1999).
The combination of degraded visibility, potential visual illusion, high workload, and inexperience operating in similar meteorological conditions likely resulted in the FO losing situation awareness of the aircraft state. Consequently, the FO did not effectively manage the aircraft following the disconnection of the autopilot resulting in the aircraft initially becoming high on the approach.
A short time later, the FO likely became aware of the high profile and attempted to correct the height with several pitch attitude changes. However, the FO’s attention was outside the aircraft at this time and their instrument scan had broken down.
Consequently, they were likely not monitoring aircraft airspeed and did not command any change to the engine power settings. As a result, the airspeed reduced and the aircraft’s rate of descent increased. The FO likely identified the increased rate of descent as the aircraft neared the runway, as a large pitch attitude increase was recorded just prior to touchdown. However, these actions were not sufficient to arrest the high rate of descent and this, in combination with the high pitch attitude, resulted in the tail of the aircraft striking the runway surface.
Contributing factor
The first officer became disoriented after disconnecting the autopilot on short final and likely lost situation awareness. Consequently, they did not identify the increasing aircraft pitch attitude, decreasing airspeed, or low power setting and did not correct the resulting sink rate prior to touchdown.
Captain’s focus on remaining fuel
As a consequence of the unforecast reduction in visibility, with no original requirement to plan an alternative airport, the captain became increasingly concerned about the fuel state as the aircraft continued on the approach.
It was also an expectation of the captain that the visibility would deteriorate further, commenting to the FO that if they were to conduct a go-around this could potentially leave them in a worse situation. During the approach, the captain also made several remarks about committing to a landing including that if they could see the high-intensity approach lighting, then they were going to land. About 2 minutes prior to landing, the FO expressed concern regarding the autopilot usage stating that they would disconnect it should a go‑around be required. In response, the captain stated ‘we don't want to go around. It’s gonna be a world of hurt’.
Prior to their descent into Brisbane, the crew had calculated the minimum fuel to divert to the Gold Coast was about 1,700 kg. The aircraft landed at Brisbane with about 2,300 kg of fuel on board, indicating there was sufficient fuel to conduct a go-around at Brisbane and safely divert the aircraft to the Gold Coast.
The captain’s preoccupation with the aircraft fuel state, combined with the expectation of worsening conditions, led to an increased desire to land the aircraft on the first approach and avoid conducting a go‑around which they perceived would have resulted in an approach in conditions that would likely deteriorate further.
Contributing factor
The captain became preoccupied with remaining fuel. This combined with an expectation of worsening visibility resulted in a sense of urgency to land off the first approach.
Continued communication regarding fuel
Brisbane air traffic control (ATC) had alerted the crew to the approaching low cloud bank about 18 minutes prior to landing. From the time of the alert until the landing, the CVR recorded continued concern from the captain.
This concern included that they had ‘no fuel’ and ‘we haven't got the fuel for this’ as well as concern with the conditions stating, ‘the weather will only get worse’ and ‘if we can see the HIAL’s,[28] we’re going to land’.
About 4 minutes prior to landing, the FO asked if it was possible to calculate the fuel needed to divert to the Gold Coast, to which the captain responded ‘not now, on final, but let's try and get in’. Shortly after the FO discussed the go‑around procedure in preparation for the DA, to which the captain reinforced their intention to land.
Although there was continued communication regarding the fuel state and visibility, no discussion was recorded regarding diversion plans to an alternative airport until established on the final approach. Additionally, the crew did not proactively obtain the weather conditions for alternate aerodromes, in the event that they were required to conduct a go-around without a planned diversion, limiting the crew’s options to return to conduct a second approach in Brisbane, further exacerbating the expectation of landing off the approach.
In contrast, the crew of the preceding aircraft on the approach prior to VH‑SAJ, advised that there was sufficient time during descent to plan for a diversion on receipt of the weather changes. Subsequent ATC recordings indicated that this crew also advised ATC of their intention to divert to the Gold Coast, if a go-around was required.
The FO had no previous experience in a multi‑crew environment and had only recently been checked to line. According to Fabre (2022), when a newly appointed FO is paired with a captain that they consider as experienced, the captain’s opinion strongly influences the FO’s decision‑making and significantly increases the likelihood of the crew attempting a moderate to high-risk landing scenario. The FO’s limited experience in the position and in a multi‑crew environment likely meant they were more susceptible to the captain’s pressure to land and less likely to voice any concerns.
The continued verbal concern over landing off the approach compounded pressure on the FO, which likely compelled them to commit to a landing on reaching the DA.
Contributing factor
Repeated communications from the captain regarding the need to land off the first approach likely increased pressure on the first officer to commit to a landing.
Crew appointments
The ASL Airlines Australia operations manual outlined the minimum experience requirements for the appointment of captains and first officers. However, neither the captain nor the FO met these requirements at the time of their engagement, nor at the time of the incident.
In ‘exceptional circumstances’, the ASL Airlines Australia operations manual permitted the variance of the experience requirements with the specific approval of the director of flight operations.
There was no evidence that ASL Airlines Australia had considered the hazards associated with the appointment of pilots that did not hold the required level of experience, nor was any control put in place to manage the risks. Such controls could have included, but were not limited to, operational limitations for low experience crew. The ATSB reviewed expositions from 6 CASR Part 121 operators and found that 5 had restrictions on FOs conducting landings in marginal meteorological conditions, including reduced visibility and low cloud.
ASL Airlines Australia did not have such a policy, and it reported that having similar limitations could lead to FOs being promoted to captain without having acted as pilot flying in adverse weather conditions. However, the FO’s limited experience in marginal meteorological conditions likely contributed to the tail strike incident. Had a similar limitation been in place, it would likely have resulted in the captain assuming control when the crew were alerted to the low visibility at Brisbane Airport.
ASL Airlines Australia had a rostering policy that prevented crew who had not accumulated 100 hours in their positions from being rostered together. However, there was no consideration made for crew who had been provided early promotion to their positions. As a result, the captain, promoted early to their position and at the time of the occurrence had not yet attained the minimum experience requirements to hold the position, was paired with an inexperienced FO. Without administrative controls in the rostering policy to prevent unsuitable pairing of crew without requisite experience, the result was a reduction in the intended experience level on the flight deck for the incident flight.
Contributing factor
ASL Airlines Australia employed and promoted pilots earlier than the prescribed minimum experience hours without additional controls in place to manage the risk of lower experienced pilots on the flight deck. (Safety issue)
Captain’s multi-crew experience
The captain commenced with ASL Airlines Australia in November 2022, initially as a FO, before undertaking command upgrade training after 155 hours. They had held the position since February 2024 and had accrued 198 hours as a captain at the time of the incident. Prior to joining ASL Airlines Australia, the captain had not flown a jet aircraft and had mostly flown in single pilot operations. As discussed above in Crew appointments, the captain had been nominated for command upgrade training below the required 500 hours, and this reduced their opportunity:
to gain valuable exposure operating in a multi-crew environment
to model behaviour on experienced captains’ decision making
prior to commencing in the captain role themselves.
The missed opportunity to gain valuable multi-crew experience likely impacted the captain’s capacity to include the FO in the decision‑making process and limited the effectiveness of the crew during the approach. Although the captain was not the PF during the approach, the ultimate responsibility for the safety of the aircraft lay with them. The cockpit voice recording indicated that, although it was reasonable for the captain to assume the FO was competent in flying the ILS, they did not ask the FO if they were comfortable to continue the approach after being alerted to the low cloud, fog and changing weather conditions. Likewise, while the FO did not advise the captain that they were experiencing difficulties during the approach, the captain did not recognise other cues, such as the FO’s response when requested to disconnect the autopilot at the DA, their ability to clearly see the approach lighting on short final, or their obvious discomfort with the approach.
It is likely that the captain’s limited command multi-crew experience may also have reduced their ability to establish an appropriate ‘cockpit gradient’ following advice that the meteorological conditions at Brisbane Airport were deteriorating. The term ‘cockpit gradient’ describes the level of authority that exists between the crew members, and the way this authority influences communication and decision‑making. Although the pilot in command has ultimate responsibility in terms of decision‑making, depending on the cockpit gradient, other crew members can be either encouraged or discouraged from influencing these decisions through their own inputs.
A ‘steep’ cockpit gradient exists when the pilot in command has an overwhelming influence in decision‑making, with little input sought from other crew members. A steep gradient can ‘inhibit communication, coordination and the cross-checking of errors’ (Harris, 2011). The cockpit voice recording indicated a steep cockpit gradient existed during the approach phase, with the captain dismissing the FO’s request to recalculate diversion fuel or plans in the event of a go-around, thereby reducing the effectiveness of the decision‑making process.
The captain provided control input instructions to the FO during the final stages of the approach. Likely due to their limited experience in the captain role, they did not recognise that the approach would have been better handled by a more experienced crew member who had previously encountered comparable conditions. Consequently, no authoritative decision was made by the captain to assume the PF role or to command a go‑around when the aircraft entered an undesired state after autopilot disconnection.
Contributing factor
The captain’s limited command experience in a multi-crew environment likely reduced their capacity to include the first officer in the decision‑making process, consider the need to assume the pilot flying role or command a go-around when the aircraft entered an undesired state during landing.
Captain’s control input
The captain reported that as the high sink rate developed, they anticipated the FO’s reaction and placed their hand on the control column to prevent any further increase in the aircraft’s pitch during the landing. This likely reduced the severity of airframe damage caused by the tail strike.
ASL Airlines Australia procedures stated that any control handover must be conducted in a positive manner to minimise confusion and operational risk. The FO recalled feeling the captain’s pressure on the control column preventing further rearward input, but the captain did not verbalise their actions at the time. While the control column input from the captain may have prevented further damage to the aircraft, it also risked confusion about who was in control of the aircraft during a critical stage of flight.
Other finding
The captain prevented further rearward input by the first officer during the flare by placing their hand on the control column. While this action is not usually completed without the required takeover procedure it likely reduced the severity of the tail strike.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the ground strike involving British Aerospace BAe 146‑300, registered VH‑SAJ on 25 June 2024.
Contributing factors
The first officer became disoriented after disconnecting the autopilot on short final and likely lost situation awareness. Consequently, they did not identify the increasing aircraft pitch attitude, decreasing airspeed, or low power setting and did not correct the resulting sink rate prior to touchdown.
The captain became preoccupied with remaining fuel. This combined with an expectation of worsening visibility resulted in a sense of urgency to land off the first approach.
Repeated communications from the captain regarding the need to land off the first approach likely increased pressure on the first officer to commit to a landing.
ASL Airlines Australia employed and promoted pilots earlier than the prescribed minimum experience hours without additional controls in place to manage the risk of lower experienced pilots on the flight deck. (Safety issue)
The captain’s limited command experience in a multi-crew environment likely reduced their capacity to include the first officer in the decision‑making process, consider the need to assume the pilot flying role or command a go-around when the aircraft entered an undesired state during landing
Other findings
The captain prevented further rearward input by the first officer during the flare by placing their hand on the control column. While this action is not usually completed without the required takeover procedure it likely reduced the severity of the tail strike.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Employment and promotion of pilots earlier than company minimum hours
Safety issue description: ASL Airlines Australia employed and promoted pilots earlier than the prescribed minimum experience hours without additional controls in place to manage the risk of lower experienced pilots on the flight deck.
Additional safety action by ASL Airlines Australia
The operator’s internal review identified an inconsistency between the operator’s standard operating procedures and the manufacturer’s recommendation with regard to which pilot (the pilot flying or the pilot monitoring) was to make an ‘attitude’ call when the aircraft pitch angle approaching landing increased above 5°.
ASL Airlines Australia’s internal investigation of the occurrence will be incorporated into the relevant sections of the ASL Airlines Australia HF/NTS training.
A summary of the internal investigation will also be included in the operator’s internal safety publication.
Glossary
ATC
Air traffic control
ATIS
Automatic terminal information service
CAA
Civil Aviation Authority (UK)
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CCTV
Closed circuit television
CVR
Cockpit voice recorder
DFO
Director of flight operations
DA
Decision altitude
FO
First officer
ILS
Instrument landing system
LED
Light-emitting diode
METAR
Meteorological aerodrome report
OPC
Operator proficiency check
PAPI
Precision approach path indicator
PF
Pilot flying
PM
Pilot monitoring
TAF
Terminal area forecast
TEMPO
Temporary significant variation to prevailing conditions
WOCL
Window of circadian low
Sources and submissions
Sources of information
The sources of information during the investigation included:
ASL Airline Australia flight records from the occurrence aircraft
ASL Airlines Australia Operations Manuals and Standard Operating Procedures for the BAe 146
the captain and first officer of the occurrence aircraft
the director of flying operations, ASL Airlines Australia
Civil Aviation Safety Authority
BAE Systems
Airservices Australia
cockpit voice recorder and flight data recorder
Brisbane Airport Corporation CCTV images
the captains from the 2 preceding aircraft to VH-SAJ
Bureau of Meteorology
Flight Radar24
Google Earth
References
Australian Transport Safety Bureau. (2009). Tail Strike, Brisbane Airport, Queensland, on 23 October 2008, VH-NJM, British Aerospace BAe 146-300. Retrieved from /publications/investigation_reports/2008/aair/ao-2008-074
Australian Transport Safety Bureau. (2016). Tail strikes during landing involving Bombardier DHC-8 402, VH-QOT and VH-QOS, Brisbane Airport, Queensland, on 5 November 2013 and Roma Airport, Queensland, on 11 December 2013. AO-2013-201.
Causse. (2024). How a pilot's brain copes with a stress and mental load.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Director of Safety, ASL Airlines Australia
the captain
the first officer
Civil Aviation Safety Authority
Air Accidents Investigation Branch, United Kingdom
Part 121 aircraft operator (party with involvement)
Bureau of Meteorology
Airservices Australia.
Submissions were received from:
the captain
ASL Airlines Australia
Civil Aviation Safety Authority
Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The flight was operated under Civil Aviation Safety Regulations Part 121 (Air transport operations – larger aeroplanes).
[2]Pilot flying and pilot monitoring: procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[3]Runways are named by a number representing the magnetic heading of the runway. Parallel runways are represented by an L for left and R for right.
[4]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL).
[5]ATIS: an automatic service which broadcasts airport specific information on the aviation VHF radio frequencies.
[6]Few: 1–2 okta of cloud cover. An Okta is a unit of measurement used to describe the extent of cloud cover (1–8).
[7]Scattered: 3–4 okta of cloud cover. An Okta is a unit of measurement used to describe the extent of cloud cover (1–8).
[8]Decision altitude is a specified altitude in the precision approach at which a missed approach must be initiated if the required visual reference to continue the approach has not been established.
[9]Runway Visual Range: measured using an electronic instrument RVR is the maximum distance at which the runway, or lights or markers delineating it, can be seen from a position above a specified point on its centreline.
[10]BAe 146 airbrake forms part of the aircraft’s tail cone when in the closed position, two petals extend from the tail cone to provide aerodynamic resistance and slow the aircraft.
[11]Precision Approach Path Indicator (PAPI): a ground-based system that uses a system of coloured lights used by pilots to identify the correct glide path to the runway when conducting a visual approach. Four white PAPI lights on approach indicate the aircraft is too high.
[12]Flare: the final nose-up pitch of a landing aeroplane used to reduce the rate of descent to about zero at touchdown.
[13]Light-emitting Diode: a semiconductor diode which glows when a voltage is applied.
[14]Category 1 (CAT I) lighting system: a CAT I lighting system normally consists of a row of lights on the extended centre line of the runway extending over a distance of 900 m from the runway threshold.
[15]TAF: a statement of meteorological conditions expected for a specific period of time in the airspace within a radius of 5 NM (9 km) of the aerodrome reference point.
[16]Broken: 5–7 okta of cloud cover. An okta is a unit of measurement used to describe the extent of cloud cover (1–8).
[17]INTER: an intermittent deterioration in the forecast weather conditions, during which a significant variation in prevailing conditions is expected to last for periods of less than 30 minutes duration.
[18]Advection fog develops when warm moist air moves (advects) over a cooler surface resulting in the cooling of the air to below its dew-point temperature, and subsequent saturation and condensation.
[19]Tempo: used to indicate significant temporary variations from the prevailing conditions of 30 minutes or more but less than 60 minutes.
[20]L3: now L3 Harris Technologies, Inc. Melbourne, Florida, USA.
[21]Vref: reference landing speed calculated on the aircrafts gross weight for landing.
[22]Vapp: reference approach speed when the flaps are in landing configuration and the landing gear extended.
[23]N1: presents the rotational speed of the low pressure (low speed) engine spool.
[24]Oleo: an oleo strut is a pneumatic air–oil hydraulic shock absorber used on the landing gear of most large aircraft
[25]RAIM: receiver autonomous integrity monitoring – used to assess the integrity of individual signals collected by a GPS receiver.
[26]Minima: landing minima consist of both visibility and/or RVR, and cloud base elements.
[27]The self-report instrument utilised the Samn-Perelli Fatigue Checklist, which utilises a 7‑point scale ranging from “1 – Fully Alert, Wide Awake” to “7 – Completely Exhausted, Unable to Function Effectively” (Samn & Perelli, 1982).
On 6 February 2024, a student pilot and flight instructor conducted a dual training flight from Gold Coast Airport, Queensland, in a Cessna 172R aircraft, registered VH-EWW. On their return, the student received an initial air traffic control clearance to track direct to runway 32.
About 40 seconds later, the flight crew accepted an amended clearance to track to the shorter runway 35 at ‘best speed’. When VH-EWW was at 1,000 ft and 1.9 NM from the runway 35 threshold, the flight crew were cleared to conduct an approach and maintain ‘best speed all the way in to crossing the runway’. Unsure how to comply with that instruction, the instructor directed the student to reduce the throttle to idle and lower the aircraft’s nose.
The aircraft subsequently passed about 100 ft above the runway threshold at about 25 kt faster than the normal approach speed. As a result, the aircraft floated along the runway before it touched down and bounced once. During the landing roll, as the aircraft approached the end of the runway, the instructor took over control of the aircraft from the student. They attempted to brake and turn the aircraft onto a taxiway beyond the end of the runway. During the turn, the aircraft veered off the taxiway towards a ditch. In response, the instructor applied back pressure on the control column and full power to commence a go-around, during which the rear fuselage and tail struck the ground. A right circuit and landing to runway 32 was then conducted.
What the ATSB found
The ATSB found that the air traffic controller's request to maintain best speed to the runway, combined with the instructor's interpretation of the instruction, resulted in an excessively fast approach. Although the aircraft exceeded both the manufacturer’s approach speed and the operator’s stabilised approach speed, the instructor did not conduct a go-around prior to landing or while on the runway. This resulted in the aircraft landing long and fast.
The excessive landing speed also resulted in reduced braking effectiveness and a loss of control during the turn onto the taxiway. Following the loss of control, a go-around was initiated to avoid a drainage ditch, resulting in a ground strike and near collision with hangars located on the eastern boundary of the airport.
What has been done as a result
The aircraft operator reviewed the company’s standard operating procedures for stabilised and unstable approaches. They also reviewed training material and sequences for instructors and students, including human factors aspects regarding communication, decision making and assertiveness.
Finally, the operator and their instructor team discussed training challenges at Gold Coast Airport with a focus on non-standard air traffic control requests and clearances, including the refusal of clearances considered operationally unacceptable.
Safety message
Although not standard phraseology, air traffic controllers may ask pilots to maintain ‘best speed’. It is up to the pilot to determine what is best in this context and more generally advise if an instruction is unclear or cannot be complied with. An approach must be flown in accordance with the aircraft flight manual and operator’s procedures. Landing with excessive speed is likely to result in the aircraft floating, landing long on the runway, bouncing and/or ballooning, all of which increase the risk of a landing mishap.
When operating in visual meteorological conditions, if an approach is not stabilised by the height specified by the operator (or generally by about 500 ft above the ground), or becomes unstable after that point, a go‑around should be conducted. The Flight Safety Foundation’s briefing note Being prepared to go around, emphasises the importance of being go-around-prepared and go‑around‑minded. This includes being ready to conduct a go‑around during the approach if any desired flight parameter, such as aircraft configuration, vertical speed, airspeed, or attitude cannot be achieved.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 6 February 2024, a student pilot and flight instructor were conducting a dual training flight in a Cessna 172R aircraft, registered VH-EWW. The aircraft took off from Gold Coast Airport, Queensland, at about 1138 local time, and tracked to the locality of Baryulgil, New South Wales (NSW), where the flight crew conducted aerial work overhead. The aircraft then tracked to Casino Aerodrome, NSW, where the student conducted 5 circuits, before departing at about 1354 to return to Gold Coast Airport (Figure 1).
Source: Google earth overlaid with Airservices Australia radar data, annotated by the ATSB
At about 1419, when VH-EWW was about 10 NM south-west of Gold Coast Airport, the student pilot contacted Gold Coast Tower air traffic control. The student pilot advised that they were inbound and requested a clearance to enter controlled airspace. The aerodrome controller (ADC) issued the flight crew a clearance to track direct to the airport at 1,500 ft and advised them to expect runway 32. The ADC subsequently cleared the flight crew to descend to 1,000 ft. At that time, VH-EWW was 6.3 NM from the airport and tracking towards a right base leg[1] for runway 32.
About 40 seconds later, to facilitate sequencing with other aircraft, the ADC asked the VH-EWW flight crew whether they could ‘accept runway 35, best speed’. The student pilot reported looking at the instructor and shaking their head thinking the aircraft was too high and close to that runway. At that time, VH-EWW was 3.9 NM from the threshold of runway 35, which was 582 m long, and significantly shorter than runway 32, at 2,492 m (Figure 2). The student’s assessment was probably due to inexperience, having only landed on runway 35 once before. Had they been cleared to commence the approach from that position, a landing should have been readily achievable, with an approach profile of about 2.4°.
Figure 2: Gold Coast Airport showing runways 32 and 35
Source: Google earth, annotated by the ATSB
The instructor assessed that, as there was a headwind of about 14 kt, the aircraft could land safely on runway 35 from that position, and it would be a good opportunity for the student to practise landing on the shorter runway. The instructor therefore responded ‘affirm’ to the ADC. The ADC then issued a clearance to track for a straight-in approach to runway 35 at ‘best speed’ and advised the flight crew that they would shortly be cleared to descend.
Just over 1 minute later, the ADC cleared the flight crew to conduct a visual approach, and stated, ‘I need best speed all the way in to crossing the runway’. According to radar data, VH-EWW was then 1.9 NM from the runway 35 threshold, at about 1,000 ft and 90 kt ground speed.
The student and instructor later reported that, although on previous flights they had received air traffic control instructions to maintain best speed, these had been up to the commencement of an approach. They had not previously received a clearance for a visual approach and best speed to the runway, and were unsure what was expected.
In an attempt to comply with the clearance, the instructor advised the student to reduce the throttle to idle and lower the aircraft’s nose to maintain best speed. When the airspeed was below 110 kt, the student extended the flaps 10°. Further flap extension required a maximum airspeed of 85 kt. As the airspeed remained at or above 90 kt for the remainder of the approach, the flaps were not subsequently extended to the normal 30° landing configuration.
According to radar data, VH-EWW was about 1 NM from the runway 35 threshold, descending through about 500 ft at 95 kt ground speed, when the ADC cleared the flight crew to land and to ‘continue to taxi into GOLF’ (Figure 3 and Figure 4). This was to reiterate that they were cleared to continue through the runway 32 intersection. As VH-EWW approached the runway, the controller observed that the aircraft appeared to be faster than normal and, expecting the flight crew would conduct a go-around,[2] started planning to re-sequence the aircraft.
Figure 3: VH-EWW track showing positions of key air traffic control communications
Source: Google earth overlaid with Airservices Australia radar data, annotated by the ATSB
The aircraft crossed the runway 35 threshold at about 100 ft and 90 kt indicated airspeed (about 80 kt ground speed). The aircraft floated in ground effect just above the runway for a significant period before it briefly touched down and bounced/ballooned once. The instructor advised the student to continue the landing rather than go around. The instructor reported that this was based on their experience of normal operations on runway 32, which had sufficient runway length to decelerate following a fast approach and long float prior to touchdown. When the aircraft landed long on runway 35 and the student commenced braking, the wheels locked up. The instructor then took over control of the aircraft from the student and reported applying firm back pressure to the control column in an attempt to increase the weight on wheels to assist with the braking. However, the application of heavy braking still resulted in the brakes locking the wheels.
The instructor assessed that the aircraft was still travelling faster than expected. At this stage the aircraft was past the runway 32 intersection and rapidly approaching the end of the runway. Seeing this, the ADC stated, ‘turn up [taxiway] CHARLIE if need be’, to alert the flight crew that they could make a 20° left turn onto that taxiway, instead of a 66° right turn onto GOLF. The instructor heard the call but did not recognise the alternate option, as they were focused on making the turn onto GOLF (Figure 4).
Figure 4: Gold Coast Airport taxiways CHARLIE and GOLF, drainage ditch, hangars and VH-EWW track
Source: Google earth overlaid with Airservices Australia radar data, annotated by the ATSB
During the turn, the aircraft skidded left off the taxiway onto grass and towards a drainage ditch. The instructor then applied full power and back pressure on the control column to clear the ditch, which resulted in a ground strike, damaging the rear fuselage (Figure 5). Having observed the aircraft exit the taxiway, the ADC activated the crash alarm[3] to alert aviation rescue fire fighters.
Figure 5: Ground strike damage to VH-EWW
Source: Aircraft operator, annotated by the ATSB
Unaware of the ground strike, the instructor commenced a go-around, with the aircraft climbing towards a row of hangars. The instructor turned the aircraft slightly right towards the lowest roof to maximise the clearance from the buildings. The instructor reported that the stall warning horn[4] was sounding, and therefore they had to lower the aircraft’s nose to prevent a stall, but also maintain a high enough nose attitude for the aircraft to climb above the hangar (Figure 6). The instructor advised the ADC that they ‘just had to make an emergency go-around’.
Figure 6: Image from CCTV footage showing VH-EWW passing close above hangars
Source: Gold Coast Airport Limited, annotated by the ATSB
The ADC handed over aerodrome control duties to another controller, who advised the VH-EWW flight crew they had had a tail strike and confirmed they anticipated being able to conduct a normal approach and landing. The instructor then conducted a right circuit, with a left orbit on downwind as required by air traffic control for spacing, and landed on runway 32 at about 1434.
Context
Approach airspeeds
According to the Cessna 172R Pilot’s Operating Handbook (POH), the aircraft’s power-off stall speed was 47 kt with full (30°) flap and 51 kt with the flaps retracted. The handbook also provided the following approach speeds:
Table 1: Airspeeds for normal operation – approach
Approach
Indicated airspeed
Normal approach, flaps up
65–75 kt
Normal approach, flaps 30°
60–70 kt
Short field approach, flaps 30°
62 kt
Landing distance required
The automatic terminal information service current at the time of the accident broadcast the following: temperature 31 °C, QNH[5] 1008 hPa, wind from 010° (magnetic) at 15 kt. For runway 35, this equated to a headwind component of 14 kt and a crosswind of 5 kt. Gold Coast Airport aerodrome elevation is 21 ft above mean sea level. The calculated pressure altitude[6] was 171 ft and the density altitude[7] was 2,091 ft.
The pilot’s operating handbook provided a chart for calculating the landing distance required at the aircraft’s maximum weight. The distances were based on a short field landing technique with flaps 30°, power off, maximum braking, paved level dry runway, nil wind and 62 kt indicated airspeed at 50 ft above the ground. It also advised to decrease distances 10% for each 9 kt of headwind. Further, if landing with flaps up, increase the approach speed by 7 kt indicated airspeed and allow for 35% longer distances. There was no data for landing with flaps 10°, or for landing at a higher indicated airspeed.
At flaps 30°, sea level pressure altitude and 30 °C, the ground roll distance required was 177 m and the total distance required to clear a 50 ft obstacle (on the approach path) was 408 m. The beneficial effect of the 9 kt headwind reduced these distances to 159 m and 368 m respectively. If landing with the flaps retracted, the required approach speed was 69 kt, ground roll 215 m and distance to clear a 50 ft obstacle 496 m.
Speed control
The Airservices Australia Aeronautical Information Publication (AIP) listed standard air traffic control phraseologies, including for speed control. ‘Best speed’ was not a standard phrase however, the AIP also stated that clear and concise plain language should be used where no phraseology was available. In the section regarding speed control for arriving aircraft, the AIP stated that a clearance for a visual approach ‘terminates speed control’. Airservices Australia advised that this meant termination of previous speed instructions but did not preclude a controller issuing subsequent speed control instructions for sequencing. Further, speed control instructions to flight crew conducting visual approaches were frequently issued.
Additionally, the Airservices Australia Manual of Air Traffic Services section Speed control principles included ‘Do not vary the final approach speed’. That manual defined final approach as ‘That part of an instrument approach procedure which…commences at the specified final approach fix or point…ends at a point in the vicinity of an aerodrome from which…a landing can be made; or…a missed approach is initiated’. In response to the draft report, Airservices Australia reiterated that the term final approach only applied to aircraft conducting an instrument approach, therefore was not applicable when flight crew were conducting a visual approach.
The aerodrome controller issued the ‘best speed’ instruction to the VH-EWW flight crew to facilitate traffic flow. The controller estimated that had the flight crew conducted a normal approach, there would probably have been insufficient spacing for VH-EWW to land before an inbound Boeing 737. The controller reported that flight crew of training aircraft sometimes deliberately conducted very slow approaches. Further, that the approach speeds of similar aircraft to the Cessna 172 could vary by 20 to 30 knots, but the landing speed would be essentially the same. In issuing the instruction, the ADC expected that the flight crew would maintain a higher speed until the aircraft was a bit closer to the airfield than normal, and then reduce speed appropriately to make a safe landing.
The AIP Speed control section also included:
5.2 The pilot must request an alternative when an ATC-issued speed control instruction is unacceptable on operational grounds.
The instructor reported that during the approach, they wanted to help the ADC by getting in quickly, and not impeding the Boeing 737. After the incident, the instructor reported that in future they would be more assertive with air traffic control and advise they could not comply with maintaining best speed while conducting a normal approach.
Stabilised approach
The United States Federal Aviation Administration’s (FAA’s) Airplane Flying Handbook defined a stabilised approach as:
one in which the pilot establishes and maintains a constant-angle glide path towards a predetermined point on the landing runway. It is based on the pilot’s judgment of certain visual clues and depends on maintaining a constant final descent airspeed and configuration.
The handbook further stated that for a general aviation piston-engine aircraft, an immediate go‑around should be initiated if an approach became unstable below 300 ft above the ground. The handbook listed criteria for a stabilised approach. These included a criterion for airspeed. For a stable approach, the airspeed was to be within +10 and -5 kt of the recommended landing speed specified in the aircraft flight manual, 1.3 x stalling speed or an approved placard/marking.
The FAA fact sheet Stabilized approach and landing, described an optimum 3° glideslope. The fact sheet referenced a study that found unstable approaches with a glideslope greater than 3° often had high descent rates and approach speeds.
The operator of VH-EWW prescribed stabilised approach criteria in the operations manual. When operating in visual meteorological conditions[8] the criteria were, when below 300 ft:
in the landing configuration
on the correct flight path
only small changes in heading and pitch required to maintain the correct flight path
speed stabilised at not more than the reference landing speed[9] [in this case 61 kt with full flap and 66 kt with the flaps retracted] plus 10 kt and not less than the reference landing speed
sink rate of not more than 1,000 feet per minute
the power setting is appropriate for the aircraft configuration and is not below the minimum power for the approach as defined by the aircraft operating manual.
Safety analysis
When the aerodrome controller cleared the flight crew to conduct a visual approach and to maintain best speed until crossing the runway, their expectation was that the flight crew would initially maintain a higher airspeed, but reduce to normal final approach speed as required for a safe landing. However, the flight crew were uncertain how to comply with the instruction, having previously only been requested to maintain best speed up until the commencement of an approach. Despite that, the flight crew did not seek clarification from the controller, or advise that they were unable to comply with the speed requirement.
When the flight crew were issued the clearance to conduct a visual approach, the aircraft was at about 1,000 ft and 1.9 NM from the runway threshold. A stabilised approach is generally based on a 3° approach profile. In this case the aircraft’s flight path to the threshold was steeper at about 5° (to the horizontal). To achieve that flight path, and maintain what they interpreted as the required airspeed, the crew reduced the throttle to idle and lowered the aircraft’s nose. Those actions resulted in an approach airspeed significantly faster than that published in the POH.
The phrase ‘best speed’ used by the controller was not included in the standard air traffic control phraseology published in Airservices Australia’s Aeronautical Information Publication (AIP). However, controllers could use clear and concise plain language when a standard phrase did not exist. In this instance, the controller’s emphasis to maintain best speed until within the vicinity of the runway contributed to the aircraft’s excessive airspeed.
Based on published landing data, runway 35 was long enough for the aircraft to land at maximum weight, even using a normal landing technique with the flaps retracted. However, VH‑EWW’s 90 kt airspeed when it crossed the runway threshold was 15 kt higher than the upper limit of the flapless approach speed specified in the POH. Additionally, the aircraft’s approach speed exceeded the operator’s stabilised approach criteria for the airspeed to be not more than the reference landing speed (61–66 kt depending on flap setting) plus 10 kt, which should have prompted the flight crew to initiate a go-around.
The instructor’s expectation that they could remedy the effects of the fast approach on the runway, rather than having to go around, was based on usually landing on runway 32, which was more than 4 times the length of runway 35. The flight crew therefore continued the approach, resulting in the aircraft floating above the runway and landing a long way down the runway. Because of the higher airspeed (and possibly the extended flap) reducing the load on the wheels, when the aircraft landed brake application locked the wheels despite the instructor’s application of back pressure on the control column.
Although still travelling at speed, the instructor attempted to turn onto taxiway GOLF. The instructor did not identify the controller’s intent for them to make a much smaller left turn onto taxiway CHARLIE, while focused on trying to achieve the right-hand turn onto GOLF. The turn at speed resulted in the aircraft skidding off the side of the taxiway into grass.
The instructor’s application of full throttle and back pressure to avoid the aircraft nosing forward into a ditch resulted in the fuselage and tail striking the ground. Unaware that the ground strike had occurred, the instructor initiated a go-around from the grass. By that stage, the airspeed had reduced such that the stall warning indicated an impending stall. The instructor’s action to lower the aircraft’s nose prevented the stall but resulted in a low climb gradient and near collision with hangars.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the taxiway excursion, ground strike and near collision with terrain, involving Cessna 172R, VH-EWW, at Gold Coast Airport, Queensland, on 6 February 2024.
Contributing factors
The air traffic controller's requirement to maintain best speed to the runway, combined with the instructor's interpretation of the instruction, resulted in an excessively fast approach.
Although the aircraft exceeded the speed for a stabilised approach, the instructor did not conduct a go-around prior to landing or while on the runway.
The excessive landing speed resulted in reduced braking effectiveness and a loss of control during the turn onto the taxiway.
Following the loss of control, a go-around was initiated to avoid a drainage ditch, resulting in a ground strike and near collision with hangars located on the eastern boundary of the airport.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future.
The aircraft operator advised that the following safety actions had been taken:
The safety committee reviewed the company’s standard operating procedures for stabilised and unstable approaches. Company procedures and training were found to be aligned with the United States Federal Aviation Administration Private Pilot – Airplane Airman Certification Standards – Short field approach and landing speed tolerance (+10/-5 knots with gust factor applied) and the Civil Aviation Safety Authority’s Part 61 Manual of Standards Schedule 8, Table 1 Final approach speed tolerance (+5/-0 knots).
A review of training material and sequences for instructors and students, including human factors aspects regarding communication, decision making and assertiveness.
Discussions with the instructor team focused on training challenges at Gold Coast Airport for non-standard air traffic control requests and clearances, including refusal of clearances considered operationally unacceptable.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the student pilot, instructor and air traffic controller
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the student pilot, flight instructor and air traffic controller
the aircraft operator
Airservices Australia
the Civil Aviation Safety Authority.
Submissions were received from:
the aircraft operator
Airservices Australia.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The base leg of the circuit is at a right angle to the final approach leg.
[2]A go-around is an aborted landing of an aircraft that is on final approach or has already touched down.
[3]Crash alarm: an emergency is declared when an aircraft is experiencing problems and there is a reasonable certainty of a threat to the safety of the aircraft.
[4]The Cessna 172R Pilot’s Operating Handbook stated that the stall warning horn sounds between 5 and 10 knots above the stall in all configurations.
[5]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[6]Pressure altitude is the altitude corrected for non-standard pressure.
[7]Density altitude is pressure altitude corrected for temperature.
[8]Visual Meteorological Conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[9]Reference landing speed is usually defined as 1.3 x stall speed for the configuration.
Occurrence summary
Investigation number
AO-2024-004
Occurrence date
06/02/2024
Location
Gold Coast Airport
State
Queensland
Report release date
17/04/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Ground strike
Occurrence class
Accident
Highest injury level
None
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
172R
Registration
VH-EWW
Serial number
17280090
Aircraft operator
Flight One Australia Pty Ltd
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
On 7 December 2023, an Agusta A109E helicopter was conducting a marine pilot transfer operation. While landing on the ship Tai Keystone, the aircraft struck a handrail resulting in substantial damage to the tail rotor and minor damage to the vessel.
What the ATSB found
The ATSB found that the handrail had not been removed during the preparation of the helicopter landing site. It was also found that the ship’s crew was using an older version of a checklist which did not require their removal. This item was however included in the latest version of the International Chamber of Shipping Guide to Helicopter/Ship Operations checklist current at the time of the occurrence.
The ATSB also determined that the handrail would have been difficult for the helicopter pilot to detect as it had been painted in a colour which did not contrast with the colours used on the ship deck. This was not in accordance with the guidance for shipboard helicopter landing sites in the International Chamber of Shipping Guide to Helicopter/Ship Operations. Additionally, during the landing, the helicopter was not positioned correctly on the helicopter landing site. This resulted in the tail rotor being outside the obstacle free zone and striking the handrail.
It was also identified that the Civil Aviation Safety Authority Advisory Circular 139 Guidelines for heliports - design and operation did not include guidance material for the marking of objects, except for wind direction indicators, located on the helicopter landing site.
Finally, the Australian Maritime Safety Authority Marine Order 57 – Helicopter operations referenced an outdated version of the International Chamber of ShippingGuide to Helicopter/Ship Operations.
What has been done as a result
Taiwan Navigation Co. Ltd, have updated their helicopter/ship operation safety checklist to include the following checklist items:
the deck party is aware that a landing is to be made
the operating area is free of heavy spray or seas on deck
the side rails and, where necessary, awnings, stanchions and other obstructions have been lowered or removed
all personnel been warned to keep clear of rotors and exhausts
the ship operator will now be notified of updates to the International Chamber of ShippingGuide to Helicopter/Ship Operations when new versions are published.
Jayrow Helicopters have amended their procedures to ensure that helicopter pilots are provided with visual representation of each individual vessel helicopter landing site prior to departure. They were also developing a new pilot checklist that included a requirement to ensure no obstacles existed in the helicopter landing area.
The Australian Maritime Safety Authority noted the reference to the outdated guide and will include this for correction in a planned review of Marine Order 57.
Safety message
It is the responsibility of the pilot in command to ensure that a landing area is safe. Where possible, helicopter pilots should attempt to gather as much information about the helicopter landing site (HLS) prior to departure and conduct an inspection of the intended landing area before commencing an approach to land. Photographs and obstacle maps of the HLS can be a valuable source of information to assist helicopter pilots with threat identification.
Objects that present a threat to a landing helicopter that are retractable, collapsible or removable should be painted in an appropriate colour to ensure they are visible if forgotten or missed. The use of reflective tape or lighting also increases the visibility of these objects.
Additionally, vessel operators should ensure their procedures and the landing area on the ship are aligned with the relevant guidance material.
The occurrence
On 6 December 2023 at 2015 local time, the merchant vessel Tai Keystone, departed Hay Point, Queensland for Tachibana, Japan. The vessel’s route passed through the Great Barrier Reef via the Hydrographers Passage and due to its size (over 70 m in length), the Tai Keystone required a marine pilot[1] to assist navigating this route.
The Tai Keystone departed Hay Point with the marine pilot on board and reached the start of the compulsory pilotage area for Hydrographers Passage at about 0100 on 7 December. The vessel completed the passage at about 0730 and the marine pilot was relieved of duty. As the marine pilot did not expect to depart the vessel for several hours they left the ship’s bridge to obtain rest in the sleeping quarters.
At about 0830, an Agusta A109E helicopter, registered VH-RUA, departed Mackay, Queensland with just the pilot onboard. The pilot planned to land on the Tai Keystone to retrieve the marine pilot and then proceed to another ship, to conduct a second marine pilot retrieval, before returning to Mackay Airport.
The helicopter was flown north‑east from Mackay and at about 1012 the helicopter pilot attempted to establish communication with the Tai Keystone for the first landing however, this was unsuccessful. Another attempt to establish communication was successful at about 1027, 15 minutes prior to landing.
Due to slope landing limitations, the helicopter pilot requested information on the extent to which the vessel was rolling[2] and the master[3] of the ship advised it was between 3–5°. As this was at the helicopter operator’s limit of 5° for daylight operations, the helicopter pilot requested the marine pilot join the ship’s master on the bridge to give instructions to help reduce the ship’s roll.
The marine pilot arranged for the vessel’s heading to be changed to 340°, which reduced the roll to approximately 2°. The helicopter pilot was informed that the emergency crew was on standby, and that the master had given permission for the helicopter to land.
The helicopter pilot completed their pre-landing checks and, while at 300 ft on approach to the ship, conducted a visual inspection of the shipboard helicopter landing site (HLS).[4] They advised that, while they had not landed on this ship previously, this height was close enough to do an effective reconnaissance of the HLS. The pilot noted red manhole covers, where they would normally land the nose wheel, as the only obstacles inside the landing area. Having assessed that these did not present a threat as the helicopter could land clear of the manholes, they continued the approach.
At about 1042, the helicopter landed on the shipand as the wheels touched the deck, the tail rotor struck an upright handrail that was not identified by the pilot during the approach. The helicopter pilot reported hearing a shredding noise and an increase in the engine pitch before completing the emergency shutdown procedure.
The helicopter sustained substantial damage and was secured to the deck of the Tai Keystone,which then returned to Hay Point to assist with removal of the helicopter from the vessel.
Context
Helicopter Pilot
The pilot of the helicopter held a commercial pilot licence (helicopter) with a multi‑engine helicopter class rating. Their total flight experience at the time of the incident was 4,880 hours with 300.8 hours on the Agusta A109E and they had recently completed both a proficiency check and line check to a satisfactory standard. The helicopter pilot also held a current class 1 medical certificate.
Helicopter
The helicopter was an Agusta A109E, which was manufactured in 2001 and issued serial number 11129. It was registered in Australia in 2010 as VH-RUA and began operations with the operator in 2017. The Agusta A109E is a multi-engine helicopter with 2 Pratt & Whitney PW206-C engines driving a 4-blade main rotor and a 2-blade tail rotor.
The ATSB was provided aircraft flight data from the onboard spider track recording device. The data provided an updated aircraft position at a maximum of 15 second intervals.
Vessel
The merchant vessel Tai Keystone was a bulk carrier with an overall length of 228.41 m, it was built in 2017 and provided the unique ship identifier number 9789843 by the International Marine Organisation (IMO). The vessel was operated by the Taiwan Navigation Co Ltd and registered under the Panama flag.
The vessel had several hatch-covers, one of which was used as a shipboard HLS when needed (Figure 1).
Figure 1: Exemplar vessel for reference
Image source: ATSB investigation MO-2016-003 annotated by the ATSB
Handrails
Handrails or stanchions[5] are used as an extension of the ladders installed to gain access to the shipboard HLS (Figure 2). The handrails are removable and usually stowed when the ship is underway. They are normally only installed once the helicopter has landed and removed prior to its departure. The handrails were painted yellow and were about 2.5 cm in diameter by 1 m tall. It was reported that these types of handrails were not considered to be a common feature on vessels.
The marine pilot on board the ship advised they instructed the vessel’s crew to remove the handrails before the helicopter arrived. This request occurred prior to the marine pilot going to the sleeping quarters and when they returned to the bridge, they did not confirm whether this action had been completed.
Figure 2: Starboard[6] handrails (removed at the time of the occurrence)
Image source: helicopter pilot in command
The helicopter pilot reported that, after exiting the helicopter, they observed the vessel’s starboard‑side handrails were removed. However, the port‑side handrails that were struck were still installed (Figure 3).
Figure 3: Handrail positions
Image source: helicopter pilot in command
The HLS was predominantly painted in green with a yellow circle and a white ‘H’. The vessel’s name was also painted in white in the HLS. There was a permanent yellow ladder (Figure 2) leading up to the HLS and yellow painted walkway lines leading to the ladder, on the deck of the ship (Figure 4).
Figure 4: Struck handrail and damaged tail rotor
Image source: helicopter pilot in command
Communication
Once the marine pilot joined the master on the bridge, they advised the helicopter pilot that:
the wind was from 080° at 20 kt
the ship was not pitching
there was no sea spray
emergency crews were on standby
the helicopter had the master’s permission to land.
No information on obstacles was passed to the helicopter pilot.
Helicopter approach
The helicopter pilot advised that they commenced their approach from behind the Tai Keystone on the port[7] side of the vessel as it provided a clear view of the vessel from their position on the right side of the helicopter.
The pilot reported that once the helicopter was turned to align with the HLS, which occurred after they completed their reconnaissance, the instrument panel obscured the undershoot area of the HLS, so they could only see the landing area and not the entire hatch cover. They further advised that, due to the position of the manhole covers, they ensured that during the landing, the nose wheel was slightly back on the ‘H’ on the HLS (Figure 5). It was reported by both the helicopter and marine pilots that it was common for the helicopter tail rotor to hang over the edge of the hatch to avoid other obstacles, such as pipes and vents.
The helicopter pilot also advised that at 300 ft, a narrow yellow pole was almost impossible to detect. In addition, the ladder leading to the poles was painted yellow, there was yellow on the hatch, and yellow lines on the edge of the landing hatch (the yellow walkway) (Figure 4). They advised yellow was a very common colour on a ship and, on this occasion, impeded detection of the port‑side handrails during the approach.
Figure 5: Tai Keystone's helicopter landing site viewed from the bridge
Image source: helicopter pilot in command
Touchdown position
The Civil Aviation Safety Authority Advisory Circular 139 Guidelines for heliports – design and operation required that an HLS had a helicopter touchdown/positioning marking (TDPM) as follows:
The objective of touchdown/positioning marking (TDPM) is to provide visual cues which permit a helicopter to be placed in a specific position such that, when the pilot’s seat is above the marking, the undercarriage is within the load bearing area and all parts of the helicopter will be clear of any obstacles by a safe margin.
Where there was no limitation on the direction of touchdown/positioning, a touchdown/positioning circle (TDPC) should be used instead. The line width should be at least 1 m.
On this occasion, the helicopter was positioned with the pilot’s seat over the centre of the white ‘H’, rather than as required with the pilot’s seat above the yellow TDPC (Figure 5).
Marine pilot transfer procedures
Helicopter procedures
The operator’s exposition provided the following information on a typical transfer procedure:
…Descend to 500 ft for a recce[8] to confirm wind, obstructions and approach options.
It also stated that this could be amended to suit the variables of weather, pilot experience, type of ship and whether it is day or night.
The exposition also stated that:
• The safety of the helicopter remains at all times the responsibility of the helicopter pilot in command…
• On arrival overhead or approaching each ship a reconnaissance (recce) should be flown. During this recce or circuit, a careful assessment must be made of the relative wind over the deck with particular attention paid to possible obstructions such as stanchions and cranes, etc… For some transfers, several orbits or an approach with overshoot may be required to obtain sufficient information.
• Pilots should exercise caution on final to look for seamen or deck hands who may be in a position on the deck to approach the landing hatch from behind. Look for ladders and/or handrails during the recce and on final. They will have good intention in trying to assist the marine pilot exiting the helicopter but are often over enthusiastic and unaware of the dangers associated with the tail rotor. Therefore, attempt to keep the tail clear of ladders leading to the hatch from the surrounding deck…
The operator advised they did not maintain a database of ships that they regularly worked with, nor did they require the ship operators to provide a copy of the HLS certification. However, prior to each transfer the ship’s master was required to complete a form designed to identify hazards. If any hazardous items were identified, they were to be photographed and the images added to the form. These forms were provided to pilots prior to departure.
The ship’s master completed this form and did not identify any hazards that increased risk for this vessel. Specifically, they advised there were no obstructions higher than 30 cm on the landing hatch.
Vessel procedures
The Hay Point port procedures required that the ship’s master complete a form to show that the ship complied with the Hay Point port procedures. This form was completed and signed by the ship’s master on 19 November 2023 and indicated that there were no obstructions higher than 30 cm on the landing hatch. The form also indicated that the ship would comply with the International Chamber of Shipping Guide to Helicopter/Ship Operations, as per Marine Order 57 (see the section titled International Chamber of Shipping Guide to Helicopter/Ship Operations).
The vessel’s crew completed a helicopter/ship operation safety checklist on 7 December at 0925, prior to the helicopter’s landing. The checklist revision date was 2017 and referenced the International Chamber of Shipping Guide to Helicopter/Ship Operations, for further guidance. This checklist did not include an item to remove handrails/stanchions.
International Chamber of Shipping Guide to Helicopter/Ship Operations
The International Chamber of Shipping Guide to Helicopter/Ship Operations, fifth edition was published in June 2021, the checklist provided in the fifth edition of the guide included:
• Side rails and, where necessary, awnings, stanchions and other obstructions have been lowered or removed.
The guide also included the following additional considerations for helicopter operating areas.
Chapter 4.3.1 General guidance on markings
The recommended colours of the markings reflect current international standards and best practices and promote a standardised approach to helicopter landing area markings. But as the colour of the main deck may vary from ship to ship, there is some discretion in the selection of deck paint schemes, the objective always being to ensure that the markings show up clearly against the surface of the ship and the operating background.
Chapter 4.5 Additional considerations for helicopter operating areas
- Any handrails that exceed the height limitations set out in section 4.1.2 are made retractable, collapsible or removable and do not obstruct access/exit routes. These handrails should be painted in a contrasting colour scheme and procedures should be in place to retract, collapse or remove them before the helicopter arrives.
- Obstructions close to or inside the operating area, which may present a hazard to helicopter operations, need to be readily visible from the air and should be highlighted. Painting of obstructions should follow the scheme set out in Chapter 9 and Appendix E, as appropriate.
Chapter 9.5 Centreline/amidships helicopter landing/operating area plan included a procedure which should be followed when indicating obstructions on the operating area plan.
1. Red and white stripes should be used to mark the location of notifiable objects in either the central clear zone or the obstacle free sector for the breadth of the ship deck…
- Objects in the central clear zone of height exceeding 2.5 cm; and
- Objects around or outside the central clear zone but in the obstacle free sector described as the funnel of approach for the breadth of the ship’s deck of height exceeding 25 cm.
2. Yellow should be used for marking the position of objects in the forward and aft limited obstacle sectors for the width of the ship’s deck to which the attention of the helicopter pilot should be drawn.
The port‑side handrails were within the obstacle free sector (clear zone) (Figure 6). The clear zone is required to be free of obstacles that present a risk to the helicopter operation.
Figure 6: Landing area terminology
Image source: Civil Aviation Authority UK Civil Aviation Publication 437
Civil Aviation Authority of United Kingdom, Civil Aviation Publication 437
The Civil Aviation Authority (CAA) of United Kingdom published Civil Aviation Publication 437 (CAP 437) Standards for offshore helicopter landing areas. This publication has become an accepted worldwide source of reference for assessing offshore helicopter landing areas.
The CAP 437 provides the same guidance as the International Chamber of Shipping guide for handrails detailed above.
The Australian Civil Aviation Safety Authority published Advisory Circular (AC) 139 Guidelines for heliports design and operation. The AC guidance stated there should be no objects greater than 25 cm or that present a threat to the safe operation of the helicopter on the HLS. However, it did not discuss removable objects, nor a colour to ensure they were visible if accidently left in place.
Australian Marine Safety Authority, Marine Order 57
The Australian Marine Safety Authority, Marine Order 57 specifically defined the International Chamber of Shipping (ICS) guide as the Guide to Helicopter/Ship Operations,fourth Edition (2008), published by Marisec Publications, London, on behalf of the ICS. The fifth edition of this guide was released in June 2021, however Marine Order 57 was not amended to reflect the latest updated/improved document.
Safety analysis
The marine pilot advised that they detected the handrails installed on the helicopter landing site (HLS) and instructed a crew member to remove them prior to the helicopter arriving. The helicopter pilot also advised that only one set of handrails was in place when they landed. As such, it is possible that when the instruction was given to remove the handrails:
one set of handrails was installed, and these were not removed, or
2 sets of handrails were installed, and only one was removed.
The ship’s crew were using an outdated version of the International Chamber of Shipping Guide to Helicopter/Ship Operations checklist, which did not include a specific check for handrails or stanchions. While the ATSB could not identify if the checklist had been completed prior to the marine pilot detecting the installed handrails, it is likely that if the vessel was using the most current version, which included a specific item to check for handrails and stanchions, it would have required a member of the vessel’s crew to actively check the handrails and consequently they would have been removed.
The communication between the helicopter and vessel did not include information regarding obstacles, and because no obstacle information was passed to the helicopter pilot, they believed the HLS would be safe to land on. During the helicopter’s approach to the HLS, the helicopter pilot completed a reconnaissance at 300 ft, which provided an opportunity to identify the obstacle. However, as the handrails were an unusual method of accessing the HLS and due to their size, shape and colour, it is likely they would have been difficult to detect. Since the starboard‑side handrails were not installed, once the pilot aligned the helicopter with the final approach path to the landing site, there were no visual cues alerting them to the possibility that the port‑side handrails had not been removed.
The pilot of the helicopter stated they were aware of the red hatch cover obstacles inside the landing site and decided to avoid them by positioning the helicopter clear of the covers. Consequently, the aircraft was positioned with the pilot’s seat over the white ‘H’ instead of the yellow touchdown/positioning circle. This position put the tail rotor slightly outside the obstacle free sector and resulted in contact with the railing.
The International Chamber of Shipping guide provided guidance that removeable handrails should be painted in a contrasting colour scheme, however it did not identify what the colour should be contrasting with. The guide advised that:
objects in the forward and aft limited obstacle sector should be painted yellow (the handrails were not in this zone)
notifiable objects in the obstacle free sector exceeding 25 cm should be marked in red and white stripes.
However, despite the handrails being within the obstacle free sector, as they were removable, they were not notifiable objects. In addition, the HLS surface was painted green with yellow markings and, the environment surrounding the handrails, including the permanent ladder leading to the handrails, consisted of items which were also mostly painted in yellow. As such, the yellow handrails did not visually stand out to the helicopter pilot.
The helicopter operator’s exposition provided a warning for pilots relating to seamen installing the handrails prior to a helicopter landing. While the main concern was ensuring seamen did not enter the HLS, this indicated that handrails were a known threat. The helicopter pilots were not always provided with a visual representation of HLSs prior to departure. However, they did receive a form completed by the ship’s master which identified if obstacles were present. Often, the first time they saw the landing site was on arrival overhead the vessel, which limited the opportunity to assess possible threats. Despite this, because the handrails were not a notifiable object, it is unlikely that they would have been included in any guidance of the HLS.
The Civil Aviation Safety Authority published Advisory Circular (AC) 139 Guidelines for heliports ‑ design and operation however, when compared with the United Kingdom (UK) Civil Aviation Authority (CAA) Civil aviation publication (CAP) 437 Standards for Offshore Helicopter Landing Areas, it lacked guidance relating to the colour of obstacles inside the HLS clear zone. AC 139 did not encompass the most current guidance available.
As the Tai Keystone was using the guidance from the International Chamber of Shipping guide, despite it being an earlier version, the lack of information in AC 139 was not considered to have contributed to the incident.
The Australian Marine Safety Authority, Marine Order 57 specifically referenced the International Chamber of Shipping guide, however it referred to a superseded version.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the ground strike during a marine pilot transfer, involving an Agusta A109, VH-RUA and ship Tai Keystone, about 240 km north‑east of Mackay Airport, Queensland on 7 December 2023.
Contributing factors
During preparation for the helicopter’s arrival, the port side handrails were not removed.
Prior to the approach, the pilot did not detect the obstacle on the helicopter landing site.
During the landing, the pilot's seat was not positioned over the touchdown/positioning circle resulting in the tail rotor being outside the obstacle clear sector and striking the handrail.
An earlier version of the helicopter operations checklist was used by the crew of the Tai Keystone. That checklist did not include a requirement, present in the version current at the time of the incident, to remove handrails or stanchions from the helicopter landing site. [Safety issue]
The colour of the handrails did not comply with the guidance material provided by the International Chamber of Shipping guide, which increased the difficulty for the helicopter pilot to detect them.
Other factors that increased risk
The Civil Aviation Safety Authority Advisory Circular 139 Guidelines for heliports – design and operation did not include guidance material for the marking of objects, except for wind direction indicators, located on the helicopter landing site.
The Australia Maritime Safety Authority Marine Order 57 – Helicopter operations, defined the International Chamber of Shipping guide as the fourth edition published in 2008. This was not the latest improved/updated version of the guidance material.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the marine industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action..
Safety issue description: An earlier version of the helicopter operations checklist was used by the crew of the Tai Keystone. That checklist did not include a requirement, present in the version current at the time of the incident, to remove handrails or stanchions from the helicopter landing site.
Safety action not associated with an identified safety issue
Proactive safety action taken by Jayrow Helicopters
Action number:
AO-2023-059-PSA-03
Action organisation:
Organisation name: Jayrow Helicopters Pty. Ltd.
Action status:
Closed
Following this occurrence, Jayrow Helicopters amended their procedures to ensure that helicopter pilots were provided with images of each individual vessel helicopter landing site prior to departure. They were also developing a new pilot checklist that included a requirement to ensure no obstacles existed within the helicopter landing area.
Proactive safety action taken by Australian Maritime Safety Authority
Action number:
AO-2023-059-PSA-04
Action organisation:
Organisation name Australian Maritime Safety Authority (AMSA)
Action status:
Closed
AMSA noted the reference in Marine Order 57 to the 2008 edition of International Chamber of Shipping Guide, not the updated edition 2021. They advised that this outdated information would be noted for correction in its planned review of Marine Order 57.
Glossary
AMSA
Australian Maritime Safety Authority
CAA
Civil Aviation Authority (United Kingdom)
CASA
Civil Aviation Safety Authority
HLS
Helicopter landing site means an aerodrome, including a heliport, intended for use wholly or partly for the arrival, departure or movement of helicopters.
IMO
International Marine Organisation
TDPC
Touchdown/positioning circle
TDPM
Touchdown/positioning marking
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Australian Transport Safety Bureau. (2017). Contact with navigation buoy, Navios Northern Star, Torres Strait, Qld on 15 March 2016. MO-2016-003
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
helicopter pilot
helicopter operator
marine pilot
vessel operator
Tai Keystone Master
Civil Aviation Safety Authority
Australian Maritime Safety Authority
Submissions were received from:
the vessel operator
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Marine pilot is an expert in navigating a ship through specific waters.
[2]Roll: describes the degree to which the vessel tilts from one side to the other about the longitudinal axis.
[3]Master: the person who has command or charge of a vessel, but does not include a marine pilot.
[4]Helicopter landing site: means an aerodrome, including a heliport, intended for use wholly or partly for the arrival, departure or movement of helicopters.
On 31 August 2022, an Ayres Corporation S2R-T15, registered VH-IWI, was conducting aerial application operations. Around 100 m into a take-off roll, the pilot heard a bang as the left wing hit the ground and the aircraft performed a ground loop. No injuries were sustained.
Inspection revealed that the left main landing gear shock assembly had failed, with the left main landing gear folding outwards and contacting the bottom of the wing.
What the ATSB found
The ATSB examination identified that the lower tube of the left shock strut assembly failed at a fatigue crack, which led to the collapse of the left main landing gear and the aircraft wing to strike the ground. It is very likely that this lower tube was a part that Thrush Aircraft had instructed owner/operators to replace or modify in 1994 in accordance with a service bulletin. The reason the part was not replaced or modified was not identified.
Safety message
Manufacturers issue service bulletins to inform owners and operators about critical and useful information on aircraft safety, maintenance, or product improvement. The ATSB strongly encourages compliance with service bulletins pertaining to aircraft safety.
Additionally, on acquisition of an aircraft, it is important to review maintenance documentation to determine whether all the appropriate manufacturer issued instructions have been addressed.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 31 August 2022, an Ayres Corporation S2R-T15, registered VH-IWI, was conducting aerial application operations from Trangie Airport. The pilot was the only person on board.
Three application flights were scheduled for the day, and after performing the daily aircraft inspection, the pilot commenced the first flight at around 0800 local time. Once the first flight was complete, the pilot obtained fuel and chemical, and taxied back to the airstrip to commence the second flight. The aircraft was around 100 m into the take-off roll when the left wing struck the ground, resulting in the pilot’s view being obstructed with chemical, and the aircraft started to rotate. In an attempt to stop the aircraft, the pilot applied reverse thrust. After completing a ground loop, the aircraft came to rest near the left edge of the runway. No injuries were sustained.
Initial inspection revealed that the left main landing gear shock assembly had failed, with the left main landing gear folding outwards and contacting the bottom of the wing.
Context
Operational and maintenance history
VH-IWI was manufactured by the Ayres Corporation in 1980 and first registered in Australia on the 24 December that year. The aircraft was powered by a Pratt & Whitney PT6A -15AG engine. It had accumulated 14,474.5 hours total time in service. The last maintenance took place 2 days prior to the occurrence and the right landing gear was replaced in 2012.
The Ayres Corporation[1] had issued 2 service bulletins associated with the main landing gear shock strut assembly.[2] The first, SB-AG-31,[3] was issued in 1992 in response to failures that occurred in the upper tube. This service bulletin described a modification to strengthen the upper tube, adding 4 rosette welds to the existing 2 rosette welds.[4] An entry in the aircraft maintenance logbook indicated that shock struts were welded to comply with SB-AG-31.
The second service bulletin, SB-AG-36,[5] was issued in 1994 in response to failures that occurred in the lower tube and included strengthening the lower tube. SB-AG-36 described 5 methods to comply with the bulletin:
(1) replace shock assembly with P/N 50116-29 (new)
(2) replace shock assembly with P/N 50116-28F1 (re-worked)
(3) replace lower tube P/N 50116-12 with P/N 50116-12F (modified)
(4) replace lower tube P/N 50116-12 with P/N 50116-30 (new design)
(5) modify old lower tube P/N 50116-12
Option (5) described the removal of a plug from the top of the tube, removal of a 0.12” (3.0 mm) thick and 1 3/8” (34.9 mm) long reinforcing tube, insertion and welding (including rosette welds) of a 0.312” (7.9 mm) thick and 4.25” (108.0 mm) long reinforcing tube P/N 50116-100, and attachment of a plug by welding. No logbook record indicating compliance with SB-AG-36 was found. The current maintainer stated they were performing maintenance under the assumption that all previous maintenance had been performed according to the manufacturer’s instructions. The reason the lower tube was not replaced or modified when the service bulletin was issued was not identified.
The operator of VH-IWI acquired the aircraft in 2018. The maintainer commenced maintaining the aircraft in the 12 months leading up to the occurrence. They were not the maintainer of the aircraft when either SB-AG-31 or SB-AG-36 were issued.
ATSB technical examination
Examination of the damaged main landing gear shock strut assembly was conducted at the ATSB’s technical facilities. The overall condition of the assembly was aged, and the rubber shock biscuits were cracked (Figure 1).
Figure 1: Left main landing gear shock strut assembly
Schematic and photo showing the main landing gear shock struct assembly with components labelled. The assembly was dirty and the shock biscuit exhibited cracks.
Source: Thrush Aircraft (schematic), ATSB (photo and annotations)
The grease between the upper and lower tube was discoloured; however, there was fresh blue grease around the lubricator and within the lower tube near the point of fracture. A substantial amount of new grease appeared to have migrated out of the lower tube during the occurrence.
The left shock strut fractured at the hole where the lower steel tube attached to the slider plate (Figure 1). This allowed the bottom portion of the lower tube to separate from the remaining shock assembly. The fracture was consistent with fatigue cracking, followed by unstable crack growth and ductile overstress (Figure 2).
Figure 2: Fractured lower tube exhibiting characteristics of fatigue fracture followed by overstress
Fracture surface exhibiting characteristic of fatigue cracking followed by overstress.
Source: ATSB
The construction of the fractured lower tube consisted of a steel tube, around 3 mm thick and 400 mm long, reinforced inside with a smaller diameter section of tube, around 3mm thick and 35 mm long, over the region of the through-hole. The reinforcing tube was welded to the lower tube at the top end. There was no end cap on the lower tube, which was present on a more recently-manufactured lower tube. There were no rosette welds connecting the lower tube and the reinforcing tube. The upper tube of the left shock strut assembly was also examined; there were 6 rosette welds present on the upper tube.
There was a handwritten marking on the side of the lower tube (Figure 3) which was identified as the characters ‘50116T012 25[?]’, with an indistinct character at the end.
Figure 3: Marker writing on the lower tube
Writing on the lower tube written in black marker. The characters are 50116T012 25[?].
Source: ATSB
Advice from Thrush Aircraft
When asked about the writing on lower tube Thrush Aircraft informed the ATSB that first 5 characters represented a drawing number,[6] the 3 numbers to the right of the ‘T’ identified the component on that drawing. The drawing number, together with the component identifier, was considered the ‘part number’ and these numbers, 50116-012, were consistent with the designation of the pre-1994 lower tube design. Thrush Aircraft suggested the final 3 digits might be an employee or serial number.
A representative from Thrush Aircraft concluded that, based on the available evidence, the failure was consistent with the failures that prompted SB-AG-36.
Safety analysis
The ATSB examination identified that the lower tube of the left shock strut assembly failed at a fatigue crack. The crack had initiated from the hole where the lower tube attached to the slider plate and propagated around the circumference of the tube. The final fracture most likely took place early in the take-off roll which led to the collapse of the left landing gear and the aircraft wing striking the ground.
The dimensions of the reinforcing tube[7] and the writing on the side of the part were most consistent with the original part, noting that there was no plug. This part was to be replaced or modified to comply with SB-AG-36. It was not possible to determine the exact age of the lower tube. It is very likely that this lower tube was manufactured prior to 1994 and would need to have been replaced or modified to comply with the service bulletin.
The construction of the upper tube was consistent with SB-AG-31, which was issued 2 years before SB-AG-36.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the ground strike involving Ayres Corporation S2R-T15, registration VH-IWI at Trangie, New South Wales on 31 August 2022.
Contributing factors
A fatigue crack initiated in the lower steel tube of the left shock assembly, located at the hole where the lower tube connected to the slider plate. The fatigue crack grew until there was a final overstress failure of the lower tube during the take-off roll.
For reasons not identified, it was highly likely that the lower tube of the left landing gear shock assembly was not replaced or modified to comply with SB-AG-36, which was issued to prevent similar failures.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Maintenance Manual Model S2R-T15 Model S2R-T34, Serial Numbers T15-020 & Subsequent Numbers T34-091 & Subsequent Numbers, Thrush Aircraft Inc., 25 October 1990. Revised: 24 July 1991.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of the occurrence flight
maintenance organisation for VH-IWI
Civil Aviation Safety Authority
Thrush Aircraft
No submissions were received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] In 2003, Ayres Corporation’s assets were purchased by Thrush Aircraft, the current producer of the aircraft.
[2] The main landing gear shock strut reduces the landing loads transmitted from the landing gear to the fuselage.
[6] The drawing number together with the component identifier was considered the ‘part number’.
[7] The reinforcing tube was around 3mm thick and 35 mm long, while the pre-1994 reinforming was described as 0.12” (3.0 mm) thick and 1 3/8” (34.9 mm) long.
The Australian Transport Safety Bureau (ATSB) is investigating a pod strike involving a Singapore Airlines Cargo Boeing 747-412F freighter, 9V-SFO, at Sydney Airport, on 28 November 2019.
During the missed approach procedure, the no. 1 engine pod struck the ground.
As part of the investigation, the ATSB will interview the flight crew and other directly involved parties and obtain other relevant information, including recorded data.
A report will be released at the end of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant stakeholders so appropriate and timely safety action can be taken.
Discontinuation
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the ATSB to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation. The statement is published as a report in accordance with section 25 of the TSI Act, capturing information from the investigation up to the time of discontinuance.
Overview of the investigation
The ATSB commenced an investigation into an engine pod strike involving a Singapore Airlines Cargo Boeing 747-412F freighter, registered 9V-SFO, which occurred at Sydney Airport on 28 November 2019.
The flight crew were conducting an approach to runway 34L at night. The automatic terminal information service (ATIS) stated the wind was 040° at 15 kt (crosswind of 12 kt), and the latest weather observation reported the wind as 040° at 22 kt with gusts up to 32 kt. The flight crew stated they briefed for the threat of strong, gusty crosswinds. The captain was the pilot handling for the landing.
During the approach, the flight crew recalled experiencing moderate turbulence and undershoot shear below 300 ft. When passing 200 ft, the airspeed rapidly trended below the minimum approach speed, the first officer called ‘speed’ and the captain recovered the target speed.
As the aircraft entered the flare it drifted right of centreline, followed by a sudden uncommanded roll to the left. In response, the flight crew initiated a rejected landing manoeuvre, during which the number 1 engine pod struck the ground. After a second approach, the aircraft landed without further incident.
Engineering inspections identified damage to the number 1 engine fan cowl and thrust reverser skin panel. Following maintenance action, the aircraft returned to Singapore where it underwent further inspections. As a result, damage to the number 1 engine main gear box was identified as being beyond the serviceable limit and the engine was removed from service.
As part of its investigation, the ATSB:
interviewed the flight crew and examined their training records
analysed recorded data from the aircraft’s flight data recorder (FDR) and cockpit voice recorder (CVR)
reviewed Boeing’s flight data analysis and other documents
reviewed air traffic control recordings
examined engineering reports, documents, manuals and correspondence relating to the operator’s Boeing 747 operation
reviewed Bureau of Meteorology (BoM) weather forecasts and analysis
conducted significant analysis of potential wake turbulence
reviewed data related to the 2020 low-level windshear alert system trial at Sydney Airport
reviewed other investigations and references where similar themes had been explored.
Analysis of recorded data indicated that the aircraft was responding correctly to flight control inputs made by the pilot flying and that the inputs were appropriate for the environmental conditions. Research and analysis undertaken by the ATSB demonstrated that wake turbulence was not a factor.
Prior to the occurrence no windshear was forecast, broadcast by air traffic controllers, or detected by aircraft or ground systems. However, during the approach, the aircraft was affected by moderate undershoot shear and wind gusts during the landing. About 4 minutes after the occurrence, a Boeing 737 landed on runway 34R. That flight crew advised air traffic controllers they lost about 15 kt of airspeed during the flare due to moderate undershoot shear. Controllers subsequently broadcast to all aircraft there was moderate undershoot shear on runway 34R.
Following the incident, Singapore Airlines made minor procedural changes and enhanced its simulator training program by requiring demonstrated competency in all crosswind landing techniques.
Low-level windshear alerting systems
At low altitudes (below 1,000 ft) during critical stages of landing and take-off, windshear can present a significant hazard to aircraft. Low-level turbulence and windshear can be caused by many processes; however, regardless of the cause, a well-designed low-level windshear alerting system is capable of detecting operationally-significant windshear and turbulence in near real time.
In 2001, there was a windshear event involving a Boeing 737 at Brisbane Airport (ATSB investigation 200100213). The ATSB recommended that BoM expedite the development, testing, and installation of advanced weather radar systems to detect hazardous windshear in high-risk airport terminal areas. In response, the BoM advised that it would continue to derive the maximum operational utility from existing and future Doppler radar systems, as the cost of specialised radar systems was high and they were not fully suitable for general weather work. Additionally, BoM advised it would maintain knowledge of international research and development of experimental low-level windshear alert systems.
In 2007, there was a micro-burst event involving a Boeing 747 at Sydney Airport (ATSB investigation AO-2007-001). The investigation raised a safety issue, which stated that there was no ground-based automatic low-level windshear warning system at Sydney Airport. At that time, BoM and Airservices Australia initiated scoping activities and a proposed system was identified. A risk assessment identified that, with existing controls (including onboard windshear detection systems), the risk level was within the broadly acceptable range.
In 2013, meetings were held with industry to discuss the proposed solution. The airline participants agreed that unexpectedly encountering windshear did not pose a significant threat to aviation at Sydney Airport. The substantial expense of the proposed system, and environmental challenges associated with siting additional anemometers required by that system, were noted. Overall, it was concluded that the benefits of continuing with the proposed system were not sufficient to justify the cost at that time.
In 2020, Sydney Airport identified that the cost of a light detection and ranging (LIDAR) system had reduced significantly and did not have the same environmental impact. A LIDAR working group was established involving Sydney Airport, BoM, Airservices Australia, airlines and a pilot’s union to consider the implementation of the system, particularly given the benefits over other systems. In general, a ground-based LIDAR system is much better at detecting turbulence in clear air, whereas onboard systems are more effective for turbulence within detectable precipitation, such as rain. BoM advised the ATSB:
Scanning doppler lidar is able to observe turbulence in the atmosphere at smaller scales than is possible with existing anemometer and wind profiler assets at Sydney. As a result, automated alerts derived from the lidar data are able to capture transient and small scale turbulent features that are, by design, not typically represented in current aeronautical meteorology products such as the TAF and WS Warning. Integrating lidar observations into the turbulence forecast process for Sydney airport is therefore likely to result in improved turbulence and low level wind shear forecast quality.
A trial of a low-level windshear alerting system using a scanning doppler LIDAR system was conducted at Sydney Airport. The trial proved the effectiveness of the system to enhance awareness of turbulence and low-level wind shear when it occurs, and the working group is now considering implementation issues.
The ATSB strongly encourages the use of LIDAR systems at airports such as Sydney Airport where turbulence-related events have been known to occur.
Reasons for the discontinuation
Based on a review of the available evidence, the ATSB considered it was unlikely that further investigation would identify any new systemic safety issues or important safety lessons. Consequently, the ATSB has discontinued this investigation.
The evidence collected during this investigation remains available to be used in future investigations or safety studies. The ATSB will also monitor for any similar occurrences that may indicate a need to undertake a further safety investigation.
On 17 January 2018, at about 1700 New Zealand Daylight Time,[1] a Boeing 737‑800, registered VH-YIR and operated by Virgin Australia Airlines (Virgin), prepared to depart Auckland, New Zealand. The aircraft was operating scheduled passenger flight VA91 to Rarotonga, Cook Islands, with two flight crew, four cabin crewmembers and 135 passengers on board. Runway 05 right was in use and the wind direction and strength was from 040° true at 25 knots gusting to 38 knots. The captain was the pilot flying (PF) and the first officer was the pilot monitoring (PM).[2]
The flight crew prepared the take-off performance calculations and determined the take-off limit weight to be 76.7 t with an actual take-off weight of 75.0 t. The flight crew elected to use the 24,000 pound thrust rating for the reported weather conditions.
At about 1715, the PF commenced the take-off. During the take-off, the PF maintained a small amount of left aileron input for the crosswind. The aircraft accelerated to V1[3] and the automated V1 announcement sounded, shortly followed by the PM making the ‘rotate’ call at the rotation speed of 149 knots. During rotation, the PF felt a slight side-to-side movement of the aircraft’s tail, which he corrected with minor rudder input, and observed some fluctuation of the airspeed. The PF did not recall the PM announcing any variation in airspeed during the rotation. Just before the aircraft became airborne, the PF noticed the nose-up attitude of the aircraft was slightly higher than the target 8° pitch angle. The PM also recognised this and called out that the pitch attitude was high. As the main wheels left the ground, the flight crew felt a bump from the rear of the aircraft.
After the initial climb, the flight crew discussed the sequence of events and concluded that their observations were most likely the result of a tailstrike. The captain handed control of the aircraft to the first officer and called the cabin supervisor to verify their suspicion. The cabin crewmembers reported that there had been a very loud noise from the rear of the aircraft during take-off.
The captain then contacted air traffic control (ATC), informed them of the suspected tailstrike, requested a runway inspection and asked for the tower’s observations of the take-off.
The flight crew elected to stop the climb at 12,000 ft. Shortly after stopping the climb, ATC confirmed that the tower had not observed any abnormalities, and the runway inspection had identified no debris or damage to the runway.
The captain then called the Virgin ground operations duty manager to report the situation and seek input on whether an overweight landing be conducted or to continue a holding pattern to burn off fuel prior to return to Auckland. Subsequently, the captain elected to return to Auckland for an overweight landing. He then updated the cabin crew and made a passenger announcement advising of the intention to return to Auckland.
The aircraft returned to the airport where an overweight landing was conducted without further incident.
After shut-down, the captain monitored the off-loading of the bags and freight. The captain found that there were 10 fewer bags in the forward compartment of the cargo hold than detailed on the load sheet.
No persons were injured and the aircraft sustained minor damage in the incident.
Engineering inspection
An engineering inspection confirmed that the aircraft had sustained a tailstrike during the take-off. The damage was limited to a scratch on the tailskid shoe that was found to be within the allowable limits. An overweight landing check was completed and the aircraft was determined to be serviceable.
Recorded flight data
Analysis of flight data from the aircraft’s digital flight data recorder indicated the rotation occurred in gusty conditions with aircraft speed reducing during rotation. The data showed:
a reduction in airspeed of 7 knots (Figure 1), followed by a stagnation in airspeed (the groundspeed continued to increase over this period, indicating the change in airspeed was a result of the variation in headwind component, which reduced by up to 11 knots during rotation)
at lift-off, the pitch attitude of the aircraft was 10.55°
maximum pitch rate during the rotation was 3.5° per second
the average pitch rate during rotation was 2.4° per second
the aircraft was slow to lift-off the runway (6 seconds from the point of initial rotation).
Figure 1: VH-YIR take-off data
Source: ATSB
Flight crew training manual and Boeing guidelines
The operator’s 737 Flight Crew Training Manual provided the following guidance:
With a consistent rotation technique, where the pilot uses approximately equal control forces and similar visual cues, lift-off attitude is achieved in approximately 3 to 4 seconds.
A rotation rate of 2 to 3° per second is required to ensure adequate tail clearance is achieved on take-off.
At flaps 5 setting, the target attitude to achieve a 51 cm tail clearance to the runway is 8°.
Under gusty wind and strong crosswind conditions, do not rotate early or use a higher-than-normal rotation rate in an attempt to clear the ground and reduce the gust effect because this reduces the tail clearance margins (tail clearance).
The PM makes callouts based on instrument indications or observations for the appropriate condition. The PM should monitor engine instruments and airspeed indications during the take-off roll and announce any abnormalities.
Guidelines that relate to Boeing aircraft show that the following factors contribute to reduced tail clearance:
lateral control deflection
activation of flight spoilers, which reduces the amount of lift on the aircraft
average pitch rate above 2.5° per second
maximum pitch rate in excess of 4° per second.
Pilot’s comments
The captain stated that the runway in use had slowly rising terrain along the departure path, which created the visual illusion that the pitch attitude of the aircraft was lower than it actually was. He advised that this delayed his appreciation that the aircraft was approaching the pitch attitude where a tailstrike could occur.
The captain stated that during his initial training with the operator in 2012, a training captain had advised that he needed to increase the rotation rate on take-off. The captain advised that, because of this tail-strike, he has reduced his take-off rotation rate to ensure it is within the manufacturer’s recommended limits of 2 to 3° per second.
The captain also advised that, due to the crosswind conditions, significant control wheel input was required to keep the wings level. Even so, the aircraft became airborne with the right wing slightly lower than the left. The captain noted that in strong crosswind conditions, flight crews are required to make a quick decision on the compromise between keeping wings level and avoiding raising a spoiler, which has a corresponding loss of performance.
Operator’s comments
With respect to take-offs in strong crosswind conditions, the operator made the following comments:
The correct technique is as described below in the Boeing Flight Crew Training Manual:
Limit control wheel input to that required to keep the wings level. Use of excessive control wheel increases spoiler deployment, which has the effect of reducing tail clearance. All of these factors provide maximum energy to accelerate through gusts while maintaining tail clearance margins at lift-off.
In a swept wing jet aircraft additional momentary aileron input is often required after lift-off to maintain wings level until the control wheel can be neutralised and the aircraft direction controlled with rudder.
Training on crosswind take-offs is provided to pilots during each simulator session. The simulation is frequently conducted on a 30 m runway, which is more difficult than normal operations on a 45 m runway. Both take-off and landing simulations are conducted at maximum crosswind. Check and training captains assess that the correct procedures are used for the manoeuvres.
Crosswind technique is further reinforced during the supervised line training components of both intake and command upgrade training.
Safety analysis
Analysis of the flight data determined that, during rotation, as the aircraft continued to accelerate, a reduction in headwind resulted in an initial drop and then stagnation in airspeed until just after lift-off. The airspeed variations were reportedly not identified and called out by the PM, as required in the flight crew training manual. Stagnation in airspeed at rotation had a similar effect to that of rotating too early: reduced lift and an extended the take-off roll, as confirmed by the flight data. The continued rotation with the main landing gear remaining on the runway then resulted in a reduced tail clearance.
The flight crew training manual indicated that the recommended rate of rotation on take-off to achieve sufficient tail clearance is 2 to 3° per second, with a lift-off target attitude of 8°. The maintenance of take-off and initial climb performance is dependent on rotation at the correct airspeed and rate to the target attitude. Boeing data indicated that average rotation rates above 2.5° per second to 10° pitch attitude, impact tail clearance. Analysis of the flight data showed that the aircraft was rotating at an average of 2.4° per second up to lift‑off, at a pitch attitude of 10.55°. While the average rotation rate was towards the upper end of the recommended limit, it was not likely to have reduced the available tail clearance. Similarly, the maximum rotation rate of 3.5° was not considered to have contributed to the tailstrike.
Boeing data indicates that lateral control inputs can significantly reduce tail clearance on take-off. The small amount of left aileron input maintained during take-off to compensate for the crosswind was not considered to be sufficient to impact lift and consequently reduce tail clearance.
The minor discrepancy between the actual loading of the cargo hold and the load sheet was not significant and did not contribute to the tailstrike.
Following the occurrence event, the flight crew were proactive in gathering information from all available sources, which enabled them to make a complete assessment of the situation. They were decisive in their actions and kept cabin crew, passengers, ATC and ground staff up to date with clear communications.
Findings
This finding should not be read as apportioning blame or liability to any particular organisation or individual.
A decrease in the headwind component reduced the airspeed during rotation and extended the time required for VH-YIR to leave the runway, resulting in a reduced tail clearance and subsequent tailstrike.
Safety message
External factors can change flight conditions rapidly. How the crew plans for and mitigates threats can make the difference between an uneventful take-off or landing and one that results in a tailstrike. Boeing guidance shows that airspeed loss, lateral control deflection and a greater than average pitch rate can all contribute to reduced tail clearance. The risk of a tailstrike can be mitigated by using recommended take-off techniques. The Boeing Aero-magazine article Tail strikes: Prevention contains a number of useful recommendations on tailstrike prevention, which include stressing the importance of:
The role of the pilot monitoring to actively monitor and identify airspeed stagnation during the rotation phase to take-off target pitch attitude.
In gusty conditions, momentarily delay rotation to ensure that the aircraft starts rotation at an average speed above the rotate speed.
Adherence to the recommended average all-engine take-off rotation rate of 2 to 3° per second.
Following this tailstrike event, the flight crew made good use of resources and were proactive in assessing and resolving the situation. A safe outcome was achieved through the crew’s use of effective communication and by following practiced failure management procedures.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 9 October 2016, a Singapore Airlines Boeing 777-312 aircraft, registered 9V-SYG (SYG), was operating a scheduled passenger service from Melbourne Airport, Victoria, to Singapore with two flight crew, 16 cabin crew and 261 passengers.
The crew arrived on board the aircraft and commenced their standard pre-flight procedures. The captain was operating as pilot flying (PF) and the first officer operating as pilot monitoring (PM).[1] The captain commenced the flight deck pre-flight procedures while the first officer performed the exterior inspection. After completion of the external inspection, the first officer commented to the captain that while on the apron ‘they had difficulty walking straight due to the strong wind’. The flight crew received the automatic terminal information service (ATIS)[2] using the aircraft communication addressing and reporting system. ATIS W advised wind conditions at Melbourne Airport were 325°at 25 kt, gusting to a maximum of 45 kt, and turbulence had been reported in the control zone.
Both flight crew reviewed the load sheet and independently performed take-off performance calculations in accordance with normal procedures. The figures from these calculations were correctly programmed into the aircraft’s flight management computer. The flight crew stated that, in accordance with the operator’s standard operating procedures, they briefed the use of full climb thrust after becoming airborne to mitigate the strong and gusty wind conditions.
At about 1120 Eastern Daylight-saving Time (EDT), the aircraft was pushed back and taxi was commenced. The flight crew stated that while taxiing to the runway 34 holding point, they observed two aircraft on approach to runway 34 perform go-arounds. Both flight crew recalled hearing another aircraft query the tower controller if windshear was reported by the flight crew of the go-around aircraft. The tower controller stated, ‘no windshear, just unstable conditions’. Two aircraft departed prior to SYG with the tower controller again advising the departing aircraft that no windshear was reported. At about 1145, SYG was then cleared for take-off from the full length of runway 34.
During the take-off run, both flight crew recall observing airspeed fluctuations on the airspeed indicator due to wind gusts. Both flight crew stated that, in their opinion, they considered the aircraft’s acceleration rate to be normal during the take-off run. At the calculated rotation speed (Vr),[3] the PF initiated the aircraft rotation. During rotation, the PM observed a downward speed trend, below Vr on the ASI and called ‘SPEED’. The PF did not recall hearing this callout. The PF continued rotation, however, the aircraft did not achieve lift-off at the manufacturer’s stated lift‑off attitude (7 degrees). Flight data analysis shows the aircraft became airborne at 10.7 degrees pitch[4] attitude (see Flight data analysis).
After take-off, air traffic control contacted the flight crew alerting them of a ‘possible tail strike’. With no TAIL STRIKE caution message displayed on the engine indication and crew alerting system[5] the flight crew carried out the unannunciated tail strike non-normal checklist and determined the aircraft structural integrity was intact. The flight crew then referred to the operator’s supplementary procedures for further guidance.
An inspection of the runway identified contact marks, consistent with a tail skid contact. No metallic debris was observed on the runway. Air traffic control advised the flight crew that ‘only superficial concrete debris was found’ during the runway inspection. The captain communicated with the in-flight supervisor who reported back to the captain that cabin crew stationed at the rear of the aircraft heard a ‘loud bang’ during take-off.
The flight crew discussed all the available information and considered their options. With the aircraft pressurisation system indicating no abnormalities the captain made the decision to continue to the destination. This decision was supported by manufacturer’s recommended action to continue to operate normally in the case of an unannunciated tail strike in the B777-300 aircraft.
Subsequently, an uneventful landing was carried out in Singapore. Engineers conducted a post-incident inspection of the aircraft and found no damage to the aircraft fuselage. Damage was evident to the tail skid system with indications of a scraped tail shoe, compression of the crushable cartridge and one indicator pin extended (Figure 1).This damage indicated that a moderate energy skid contact had occurred during take-off.
Figure 1: Damage to tail skid
Source: Singapore Airlines, modified by the ATSB
Safety analysis
Flight data analysis
Analysis of the aircraft flight data showed multiple instances of airspeed stagnation from 77 kt computed airspeed through rotation initiation at 178 kt (Vr = 178 kt) and initial climb. Rotation was initiated at a computed airspeed of 178 kt (at Vr) at approximately 0.5 degrees per second initially before increasing to approximately 3 to 4 degrees per second. As rotation was initiated, the headwind component decreased 12 kt, the computed airspeed stagnated and reduced to 173 kt (Figure 2). Lift-off occurred at a pitch attitude of 10.7 degrees. The tail skid contact attitude is 8.9 degrees.
Figure 2: Flight data plot including computed airspeed, and rotation speed (Vr) and pitch attitude
Source: Aircraft operator analysed by ATSB
Wind and airspeed
After reaching rotation speed (Vr), the aircraft’s airspeed reduced by about 5 kt due to a reduction in headwind of about 12 kt.
Continued rotation
The PF reported not hearing the PM call of speed after the PF had rotated the aircraft. If the PF was aware of the speed reduction, the standard procedure, described in the operator’s Flight Crew Training Manual (FCTM), was to momentarily delay rotation. The PF reported that they thought the rotation was normal in the conditions.
Tail skid strike
The aircraft did not become airborne at the manufacture’s pitch attitude of 7 degrees, leading the PF to continue increasing the pitch attitude to 10.7 degrees where lift-off was achieved. This increased pitch attitude exceeded the 8.9 degrees attitude for where a tail strike will occur in the Boeing 777-300 aircraft.
Guidance to flight crew
The operator’s Flight Crew Operations Manual (FCOM) stated that the use of reduced thrust is standard procedure for take-off. The FCOM also listed the environmental conditions when take-offs with reduced thrust are not permitted.
The operator’s FCOM does not contain direct guidance regarding take-off thrust setting requirements in gusty wind and strong crosswind conditions. Guidance for considering the use of higher thrust settings and rotation speeds for take-offs under these environmental conditions is provided in the Flight Crew Training Manual (FCTM).
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The tail skid contact was a result of airspeed stagnation due to gusty atmospheric conditions which prolonged the time to lift-off, allowing the pitch attitude to exceed the tail skid contact attitude.
The use of a higher take-off thrust setting would most likely have reduced the required runway length and minimised the aircraft exposure to gusty atmospheric conditions during rotation and lift-off.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following safety action in response to this occurrence.
Flight Operations
As a result of this occurrence, Singapore Airlines has advised the ATSB that they are taking the following safety actions:
Action taken by Singapore Airlines
As a result of this incident, the aircraft operator issued circulars to all company flight crew directing operation towards Boeing’s recommendation of the use of higher thrust and rotation speed for take-off in gusty wind and strong crosswind conditions.
Safety message
This incident serves as a reminder to Boeing pilots that guidance material contained in manuals outside the FCOM should be considered in all aircraft operations. The use of a higher thrust setting as recommended by the Boeing FCTM would have reduced the required runway length and minimised the airplane exposure to gusty conditions during rotation, lift-off and initial climb. Boeing also states that the use of a higher take-off rotation speed, if take-off performance permits, can increase the tail clearance margin during the rotation.
While taking the above message into consideration, this incident provides an excellent example of flight crew managing a non-normal operation. Throughout the non-normal occurrence period, the flight crew communicated with each other, air traffic control and the cabin crew, which allowed all relevant information available to be gathered. The flight crew demonstrated effective crew resource management and decision making resulting in the flight being able to continue to destination without compromising safety.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 23 April 2016, a Virgin Australia Boeing 737-8FE aircraft, registered VH-YIW, operated as VA91 from Auckland, New Zealand to Faleolo Airport in Apia, Samoa, with the intent to conduct a return flight that day. The departure from Apia was planned to be completed before the arrival of an approaching tropical cyclone.
During the landing on runway 08, while correcting for a left drift from the runway centreline, the aircraft touched down in a nose-down, right wing-low attitude. This resulted in the right engine nacelle contacting the runway. The flight crew were not aware the nacelle strike had occurred, as the landing, while firm, was not assessed by the flight crew to be outside of normal landing parameters.
What the ATSB found
The ATSB identified that due to heavy rain, darkness and limited visual cues, the flight crew did not detect the aircraft's banked, nose-low attitude immediately prior to landing. Additionally, the subsequent routine flight crew and engineering inspections did not identify damage to the nacelle over the aircraft’s next four flights.
It was also found that the pilot flying was probably experiencing a level of fatigue that has been demonstrated to adversely influence performance.
What's been done as a result
Following this occurrence, the operator modified its aircraft external inspection procedures for flight crew and engineering staff. The flight crew training material was updated to reflect the inspection procedures in the flight crew operating manual, which stated that crew shall inspect the underside of engine nacelles. This action was supported by an internal flight operations update issued on 29 April 2016, re-emphasising that exterior inspections were to be conducted in accordance with the flight crew operating manual’s procedures.
The engineering daily inspection task card for pre‑flight inspections before extended operations was strengthened by issuing engineering technical advisories including the requirement to conduct checks of the underside surfaces of the engine nacelles during normal operation and also when there was indication of an increased likelihood of a nacelle strike on landing.
The operator also identified and implemented a number of improvements in the management of hazards associated with significant events, including cyclones.
Safety message
Detecting airframe damage, particularly to the underside of the engines, can be difficult due to the location not being within normal visual reference. Airframe damage in this location is more likely to be detected by thorough visual inspections of the lowest parts of the airframe before flight and during daily inspection.
While checking for damage in this inconspicuous location can be difficult, and influenced by an expectation that no damage is present, flight crew and engineers are reminded that damage can occur without flight crew awareness.
Safety issues and actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Virgin Australia Airlines Pty. Ltd.
The operator has modified its training in relation to flight crew external inspections to include a specific visual inspection of the underside of engine nacelles, as per the procedure outlined in the flight crew operations manual.
The operator has also modified the procedures for engineering external daily inspections to include a specific visual inspection of the underside of engine nacelles.
International roaming on the Virgin Australia International fleet has been introduced to enable automatic downland of QAR data immediately after shutdown at all Australian and International Airports.
Context
Aircraft information
General information
VH-YIW is a Boeing 737-8FE (B737) aircraft, powered by two wing‑mounted CFM-56-7B24/3, high bypass turbofan engines. In its configuration at the time of the occurrence, it was capable of carrying 176 passengers, and 6 crew.
Damage to aircraft
The right engine nacelle was damaged by briefly contacting the runway during the touchdown in an incident known as a ‘nacelle strike’ (Figure 1). The landing gear tyres also sustained some lateral or sideways wear damage during the event. Detailed inspection of the right engine identified that the:
lower right engine nacelle skin was holed by abrasion damage
lower surfaces of the right engine fan and reverser cowlings were damaged
right engine fan path abradable lining was worn (Figure 2).
Figure 1: VH-YIW No. 2 engine nacelle
Source: Operator’s investigation report, annotated by the ATSB.
Figure 2: VH-YIW right engine abradable lining.
The blue area shows where the rotating engine blades have contacted the abradable lining
Source: Operator’s investigation report, annotated by the ATSB.
The operator requested a design engineer to report on the potential damage. The report stated:
…the very minimal damage to the inner liner indicates that the energy of the impact was primarily absorbed by the cowl structure buckling as the initial contact occurred.
The design engineer’s report also concluded that:
…the continued flight with damage to the engine cowling posed no critical aerodynamic, structural or mechanical safety risk to the aircraft.
Personnel information
Qualifications and experience
The captain held an Air Transport Pilot Licence (Aeroplane) and had a total of about 10,000 hours’ flying experience, of which about 6,000 were on the Boeing 737 aircraft. The captain commenced flying with the operator in 2003 and held a valid class 1 aviation medical certificate.
The first officer (FO) held an Air Transport Pilot Licence (Aeroplane) and had a total of about 5,300 hours’ flying experience, of which about 1,100 were on Boeing 737 aircraft. The FO commenced flying with the operator in 2007 and held a valid class 1 aviation medical certificate.
Both flight crew had operated to Apia on many occasions, including at night and in rain.
Recent history
Both the captain and the first officer were based in Auckland. They both had the same duty periods during 20–24 April 2016, as indicated in Table 1. All times in this section are specified in the local time for the flight crew, which was or New Zealand Standard Time (NZST).[4]
Table 1: Actual duty time information for the flight crew for the period 20–24 April 2016
Date
Work activity
Duty start
Duty end
Duty time
Time free (of duty)
20 Apr 2016
Day off
21 Apr 2016
Day off
22 Apr 2016
Auckland–Apia–Auckland
1510
0205
10.9 hours
13.2 hours
23 Apr 2016
Auckland–Apia (pod strike)
1510
2300
7.8 hours
15.0 hours
24 Apr 2016
Apia–Auckland
1400
2050
6.8 hours
Source: Virgin Australia, modified by the ATSB.
The crew conducted flights from Auckland to Apia and return on the 22 April. Originally, they were scheduled to operate the flight from Auckland to Apia on 23 April, then overnight at Apia before operating a flight from Apia to Sydney on 24 April. Due to the approaching cyclone, the crew were unsure whether the flight on 23 April would be cancelled or their schedule would be changed to include a return flight (same as 22 April). After they awoke on 23 April they were advised that they would be conducting the same schedule as 22 April.
The flight to Apia on 23 April landed at 2007 NZST. The return flight was postponed due to the weather conditions and the crew stayed the night in Apia and operated the return flight to Auckland the next day.
The captain reported that he normally had 6–7 hours’ sleep a night and he had been sleeping normally up until the night of 22 April, after their flight arrived back in Auckland at 0135 on 23 April. On that night he reported getting 3–4 hours’ sleep (uninterrupted), waking at about 0700 because he often found it difficult to sleep beyond his normal waking time. He stated that he felt ‘okay’ during the flight to Apia on the 23 April.
The first officer reported that he normally had 7–8 hours’ sleep a night and slept normally in the nights prior to the 23 April flights, waking at about 1000 that morning after 7 hours’ sleep (uninterrupted). He said he felt alert at the beginning and towards the end of the flight to Apia on the 23 April, and okay during the middle part of the flight.
Both crew assessed that they were fit and appropriately rested to conduct the flight on 23 April. They also both reported eating normally prior to and during the flight.
The operator’s fatigue risk management system (FRMS) included the use of a biomathematical model and other processes to assess to suitability of planned duty periods. The minimum length of time off duty at home base was 12 hours, and the maximum planned duty period for a duty period with two sectors starting during 1300–1759 was 12.25 hours.
As part of its FRMS, flight crew could also take a short period of controlled rest at their flight deck seats during flights (for flights of over 3 hours under specified conditions). Neither pilot could recall taking a controlled rest during the flights on 22 or 23 April. Both pilots said they had previously used controlled rest on other flights to ensure they were alert on approach.
Meteorological information
A summary of the available and obtained weather information is shown in Figure 3.
Figure 3: Image of the flight and the weather information available at different times
Source: Google maps, annotated by the ATSB
Information available prior to the flight
The operator was aware of TC Amos, and had been monitoring its progress to assess its effect on company operations. The United States joint typhoon warning center (JTWC) issued advisory information (commonly known as ‘advisories’) at 1200 and 2100 on 22 April, and at 0000 and 0900 on 23 April. These advisories were numbered eleven to fourteen respectively.
The weather forecasts contained in the advisories had minor changes between the sequential forecasts, with the last being the most significant. Advisory No. 11, issued at 1200 on 22 April, forecast that TC Amos would be a category three cyclone located to the west of Samoa, and would be still approaching the island after the planned return flight had departed from Apia.
Advisory No. 12 was issued nine hours later, at 2100 on 22 April (Figure 4). It detailed that the tropical cyclone may turn right and pass to the south of Samoa and that TC Amos was due to pass the island at 0600 on 24 April, about one day after the proposed flights. However, the forecast expressed uncertainty on the direction of this turn. The advisory stated the next advice would be in 6 hours’ time, at 0300 on 23 April.
Based on the information from Advisory No. 12, the operator’s cyclone management team (CMT) convened and made operational decisions about flights that could be affected by TC Amos. The occurrence flight was planned on the basis that VH-YIW would have departed from Apia before the cyclone had a significant impact on the airport. All other flights to Apia were cancelled until after the cyclone’s passage, and overflying aircraft could not use Apia as a flight planning alternate airport.
Prior to departure, the flight crew were provided with a briefing package including information from Advisory No. 12. The package included information on the weather system associated with TC Amos, which was forecast to start influencing Samoa and the surrounding region during the time of the flight. The package indicated that for the estimated time of arrival for VH-YIW, the centre of TC Amos would be approximately 260 km west of Faleolo airport with forecast crosswinds at the airport expected to be about 20 kt (within the aircraft’s operational limit).
Figure 4 : JTWC Cyclone Advisory No. 12, issued 2100 on 22 April – the forecast provided to the flight crew. The four-digit number gives the date and hours in UTC (Z) when the cyclone was forecast to be in that location. The concentric circles are isotachs - lines of constant wind speed surrounding the cyclone
Source: JTWC, annotated by the ATSB.
The flight crew did not receive Advisory No. 13, issued at 0000. This forecast expected the cyclone would pass 80 km closer to Apia at about the same time as forecast in the previous advisory, with a 10 kt reduction in peak intensity, still providing adequate time for the return flight to be completed (Figure 5). Advisory No. 13 was assessed by the CMT as not altering any operational requirements and consequently was not passed to the flight crew.
At the time of the planned flights into and out of Samoa during the evening of 23 April, bands of heavy rain were expected in the vicinity of the airport, however the winds were forecast to be within the aircraft’s operational limitations.
Figure 5: JTWC Cyclone Advisory No: 13, issued 0000 23 April – the last forecast issued before the incident
Source: JTWC, annotated by the ATSB.
In-flight information
The aircraft took off from Auckland at 0433 and landed at Apia at 0807.
During the pre-flight briefing, the crew received the aerodrome forecast for Faleolo Airport. The forecast was issued on 22 April at 2148, and was valid from 0000 for the next 24 hours, unless it was amended or updated. Aerodrome forecasts are issued at scheduled times, or in response to significant weather changes. The aerodrome forecast issued at 2148 was re-issued at 0357 and was updated several times before the aircraft landed at 0807.
Forecast conditions, visibility reduction associated with rain showers and thunderstorms, required the operator to carry sufficient fuel to continue to an alternate aerodrome, and the carriage of holding fuel.
After departing Auckland, the flight crew obtained an amended aerodrome forecast. This forecast required the same operational restrictions, however identified the onset of possible thunderstorms to start three hours earlier than previously expected, at 0900.
The flight crew contacted Faleolo tower inflight and obtained the observed weather conditions from the controller prior to landing.
Information that became available after the flight
Cyclone Advisory No: 14 was issued at 0900 and advised that the cyclone was now moving twice as fast as previously forecast and was about 170 km west north-west of Apia at the time of landing.
Advisory 14 also detailed that TC Amos was expected to pass about 25 km north of Apia 14 hours earlier than first predicted (Figure 6). The forecast also indicated the airport would be exposed to sustained winds over 64 kt on the following morning (24 April) as the cyclone passed close by.
Figure 6: JTWC Cyclone Advisory No: 14, issued 0900 on 23 April – issued after landing
Source: JTWC, annotated by the ATSB.
Communication
During the flight, the crew requested and received numerous weather updates from the operator’s flight following service via the aircraft communication, addressing and reporting system.
The flight crew reported initial difficulty contacting air traffic control (ATC) at Faleolo tower using very high frequency radio. They were subsequently able to make contact with ATC using high frequency radio just prior to the top of descent. ATC provided surface observations at the airport to the crew, who asked to be updated on any weather changes throughout the descent.
The crew also coordinated with ATC for a missed approach clearance to FL140[5], instead of the normal 4,000 ft. This change was reportedly made to facilitate a diversion to Nadi if it became necessary.
Aerodrome information
General information
Faleolo runway 08/26, is about 3,000 m long and 45 m wide with 7 m sealed shoulders on each side. The control tower is located to the south of the parking apron at the eastern end of the runway. The runway has edge lighting, which was considered to be ‘quite bright’ by the occurrence flight crew, and runway centre-line lighting was not installed. There is a 150 m stop‑way before the threshold of the runway and the runway has a marked downhill slope from the threshold to about halfway along the runway, descending 49 ft.
Runway 08 was reportedly prone to what is referred to as ‘black hole effect’ at night (see the section titled Black hole approach). This phenomenon is particularly relevant when aircraft approach airports at night over the sea or unlit terrain.
The runway was equipped with a precision approach path indicator that provides vertical approach path information for crew as guidance to their height in relation to the runway.
Runway damage
During landing, the aircraft first contacted the runway at about 834 m along and to the left of the centreline of runway 08. The right main undercarriage was first to touch down, followed by the nose wheels, and then the left main undercarriage.
Recorded aircraft data indicated that the aircraft landed with a 5° yaw to the right, greater than10° of right roll, and nose-down attitude of more than 2°.
The impact damage visible on the runway due to contact with the nacelle was mostly due to paint transfer over a relatively localised area, and consisted only of superficial damage to the runway surface (Figure 7).
Figure 7: Runway 08 surface marks and nacelle paint transfer
Source: Operator, annotated by the ATSB
Flight recorders
The aircraft was equipped with a flight data recorder (FDR) and cockpit voice recorder (CVR). Due to the elapsed flight time between the occurrence and its detection, the CVR was overwritten. However, the occurrence was able to be downloaded from the FDR and analysed by the ATSB.
The FDR recorded that the autopilot was disengaged at 260 ft above ground level (AGL) and at about 240 ft AGL, the Take-Off Go-Around (TOGA) function was activated (which the flight crew reported as inadvertent), followed by the auto-throttle disconnection. The auto-throttle remained disengaged for the remainder of the flight.
Data indicated that the aircraft began to drift left of the centreline at about 20 ft AGL. At touchdown, the maximum recorded bank angle was 10.3° right wing-low, and the recorded pitch angle was about 2.5° nose-down. The corresponding vertical acceleration at touchdown was 1.95 G.
The recorded wind speed reduced from about 36 kt at 300ft AGL to about 22 kt at touchdown. The crosswind wind limits of the aircraft were not exceeded throughout the approach and landing. The recorded data also showed that the aircraft did not exceed the stable approach criteria during the approach and landed in the expected touchdown area, albeit laterally displaced to the left of the centreline.
Maintenance information
Engineering inspections
The aircraft was required to undergo a daily inspection and an additional ‘extended range operations’ inspection when the planned flight was more than 60 minutes’ flying time (at ‘one engine inoperative’ speed) away from the nearest airport suitable for emergency landing.
Daily inspection
The daily inspection task card required that an engineer perform:
…a visual check of the following components for obvious signs of damage, and indications of bird‑strike or foreign object damage...
The subsequent list included the:
…inlet cowl inner and outer surfaces.
Additionally, if other damage was found, the engineer was required to compare the damage with the limits in the applicable detailed inspection procedure. Following this event, the operator strengthened its inspection procedures. On 4 May 2016, the operator issued technical advisories to expand on this inspection item. The advice stated:
To fully achieve the inlet cowl outer surfaces inspection engineers must do a visual check on the underside surfaces of the inlet cowl.
The advisory was updated with more detail on 24 May 2016.
Extended range operations inspection
A different external inspection was also conducted using a different inspection schedule before every extended operations flight. Flights between Australia or New Zealand and Samoa were classified as extended range operations.
The extended range operations inspection includes an external walk around. This item required the engineer to ’carry out a walk around check for airframe condition and obvious damage by visually inspecting from the ground, and paying attention’ to a list of aircraft components, including engine inlets and fan blades.
Flight crew inspections
Flight crew are required to conduct a pre-flight external visual inspection before flight. This inspection is to ensure the aircraft is in sound operating condition from the previous flight and to identify any potential flight safety hazards.
Flight crew conduct pre-flight inspections in accordance with a documented procedure. The Flight Crew Operations Manual provided the procedure for the external inspection. This includes a diagram with the inspection sequence and the items to be inspected at each area of the aircraft. Following a nacelle strike in Dublin, Ireland in 2009 where the nacelle damage was not detected for the next two sectors, the aircraft manufacturer updated the inspection procedures.
Subsequently, the operator’s documented procedure in its Flight Crew Operations Manual was amended in October 2011 to include, for each engine, ‘Exterior surfaces (including the bottom of the nacelles)’.
The documented procedure was also supported by pilot training material that was intended to provide practical instruction on how to implement the procedure. However, the pilot training material had not been updated to include the specific requirement to inspect the bottom of the nacelles for damage.
Following the occurrence, the operator’s flight crew exterior inspection training package was updated to reflect the 2011 amendment in the Flight Crew Operations Manual, including the requirement to inspect the bottom of the nacelles.
Post-incident inspections
Two engineering daily inspections, one separate engineering extended range operations inspection, and two pre-flight inspections were carried out following the incident. Subsequent to this, various flight crew and engineers also inspected the aircraft during the pre-flight, daily and extended range operations inspections for the following three sectors.
The nacelle damage was not detected until the analysis of flight data prompted a subsequent inspection, about ten operating hours after the strike occurred.
Organisational information
Cyclone management team
The operator had a process, including a documented procedure, to activate its cyclone management team (CMT) if a cyclone was forecast to be within 370 km of an airport that would be used within the next 24 hours. The procedure also provided guidance on assessing the suitability of a landing airport in regard to the forecast wind strength.
During the CMT meeting at 2100 on 22 April, the team considered the identified risks to the operation. They determined that the flight was operationally safe with a number of added risk mitigators.
Following this occurrence, the operator identified and implemented a number of improvements in the management of hazards associated with significant events, including cyclones.
Flight dispatch and following
Prior to departure, flight crew are required to obtain all relevant operational information and are required to obtain inflight updates to ensure they have accurate and up to date information to assist with operational decision-making.
The operator maintained a flight dispatch and flight following function in which relevant operational information was collected and provided to flight crew.
Flight dispatch
Flight dispatch prepared and submitted operational flight plans on behalf of flight crew, who received an operational flight-briefing package before flight. The Group Operations Manual suite contained the Flight Dispatch Policy Manual. This contained guidance material and procedures for the Flight dispatch team to provide the following functions:
acquisition, collation and evaluation of NOTAM, meteorological and other operational information in support of flight-planning activities
The evaluation of navigational, meteorological, aircraft performance and flight-planning-related operational factors specifically associated with the dispatch and continuation of ‘extended range operations’
The provision of verbal pre-flight briefings and briefing updates to the flight crew of individual flights (upon request), to supplement the standard briefing documentation routinely provided to the crews.
Flight following
Flight following services were provided primarily to enhance and contribute to the safety of a flight. The occurrence flight met the criteria to receive a flight following service, including the provision of operationally critical information, such as that associated with tropical cyclones.
Flights that included sectors with extended diversion times had extra requirements, including special procedures for flight dispatch, the operations controller and the flight following function. Flight following is defined as an operational information service provided jointly by the duty operations controller and flight dispatcher to provide advice and information to assist in the safe and efficient conduct of extended range operations, including the provision of advice and information at the request of the captain, either before or during flight.
The occurrence flight was an extended range operation and as such, the flight dispatch division was also responsible for plotting current information on tropical cyclones on a display to assist with flight planning and flight following and to continually monitor and evaluate relevant operational information to assess its impact on extended range operations. Information on non-normal variances which may impact the continuation of the flight under extended range operations procedures shall be promptly communicated to the captain.
Approach to land
Go-around manoeuvre
The flight crew were required to maintain a stabilised approach from 1,000 ft above the aerodrome elevation until touchdown. If the approach became unstable during this segment, the crew were required to conduct the missed approach procedure.
The crew had planned, prepared and were ready to conduct a missed approach at Apia. They had briefed that if they initiated a missed approach procedure, the aircraft would be diverted to Nadi, Fiji instead of conducting another approach.
In the last four seconds of the approach, the flight path deviated sufficiently to require multiple flight control inputs to keep the aircraft on the desired flight path for landing.
The operator’s flight procedures stated that during this phase of flight:
…should it become apparent that the aircraft will touch down significantly short of the touch down aiming point, or beyond the end of the touch down zone (1000 m/3000 ft from the threshold or first third of the runway, whichever is less), the pilot flying shall initiate a go-around.
The aircraft remained within the touch down zone and over the runway prior to runway contact. A go-around was not required unless initiated by the flight crew at their discretion. The crew reported that they believed that the aircraft remained within the stabilised approach criteria for landing and were comfortable to continue to land.
Spatial disorientation
In 2007, the ATSB published a report An overview of spatial disorientation as a factor in aviation accidents and incidents.[6] The report identified several types of visual illusions that may impact a pilot’s ability to land an aircraft safely.
Runway shape and slope illusions
At a given altitude and distance from a runway, the slope of a runway will affect the amount of runway visible to a pilot. For a down-sloping runway such as Apia, this will result in less of the runway being visible. Pilots may perceive this lack of visibility as the flight path being below the correct approach path and as a result, the pilot may fly a higher-than-normal approach to achieve the runway visibility that would be present on a level runway.
Both flight crew identified this runway as having a significant down slope, which increased the difficulty of landing at Samoa. They also reported heavy rain on approach, which did affect visibility. However, both crew had a high level of experience operating into this airport and did not report any issues relating to the slope or visibility of this approach.
Black hole approach
A black hole approach is a term used by pilots to characterise an approach path at night with no visual cues between the aircraft and the intended runway on final approach to land. Black hole illusion occurs when darkness and an absence of visual cues, such as lights, may induce a false perception of altitude and/or attitude.
When the environment along the approach path is dark, with only the distant runway or airport lights providing visual stimuli, an illusory or false sense of height and/or attitude may be perceived. The absence of peripheral visual cues provides a false illusion of height to the pilot, often resulting in the inadvertent reaction to fly the aircraft lower than the normal approach path.
Runway centre line illumination
Runway lighting and, in particular, runway centre line and touchdown zone lighting accentuate approach rate cues and height appreciation. Runway 08 at Apia, did not have centre line lighting.
Bright runway lights may create the impression of being closer to the runway (hence on a steeper glide path). The crew reported that the runway lighting at the airport was particularly bright.
These visual illusions may affect a pilot’s ability to judge the correct time to initiate a flare to land.
Related occurrences
A number of similar nacelle strike events have been identified involving Boeing 737 aircraft. The conditions were not the same in all the occurrences, but they all had environmental phenomena present that increased pilot workload during landing.
Air Accident Investigation Unit Ireland investigation report No. 2011-007 Engine pod strike, Dublin Airport, Ireland, on 19 November 2009
On 19 November 2009, at 1245 UTC, a Boeing 737-8AS aircraft, registered EI-DAI was operating a scheduled flight from Rome’s Ciampino airport, Italy, to Dublin, Ireland. The weather at Dublin was forecast to be blustery during the day. The first officer (FO) was the pilot flying and the captain was the pilot monitoring.
On the leg to Dublin, a full briefing was carried out including flap selection, runway length with regard to flap setting, the landing chart and windshear. At Dublin the aircraft joined the approach traffic sequence for landing. There was a strong wind from the southwest, which the captain estimated as 70 kt at 3,000 ft. The captain rechecked the limits after the control tower provided a wind report and concluded that it was within limits. Although conditions were blustery the captain reported that the approach was normal given the conditions and the aircraft was configured ahead of normal and flown with plus 15 kt added due to wind.
At about 300 ft the aircraft was slightly left of the localiser. The captain called this out and the FO corrected it promptly. The captain said that the approach was normal until about 25 ft when the left wing dropped due to the wind. The captain assisted the FO with a control input.
According to the captain’s report, the aircraft was now steady on profile and a flare was initiated; the aircraft did not seem to descend and at this point the captain closed the thrust levers. Simultaneously, the left wing dropped again as the aircraft descended to the runway. The captain said that the aircraft landed quite benignly albeit with the left wing low. The captain reported that at no stage did he or the FO suspect ground contact.
Subsequently, a different crew operated the aircraft on the next two sectors to and from Poland. On arrival back in Dublin, the captain for these Polish sectors learned that a member of the public had reported the earlier nacelle scrape.
Transportation Safety Board of Canada investigation report A05A0161, wing ground strike, Halifax Airport, Canada, on 25 December 2005
On 25 December 2005, at 1924 Atlantic Standard Time,[7] A Boeing 737-700 aircraft, registered C‑GWJF, was on a scheduled passenger flight from Toronto, Ontario, to Halifax, Nova Scotia. About 10 minutes before landing, the crew was advised that another aircraft had just landed on runway 14, and that the pilots of that aircraft had reported that they had the runway lights visual at 250 ft above ground level (AGL). This was 50 ft above the decision height for the ILS approach to Runway 14.
Just before touchdown on runway 14 in low-visibility conditions, the aircraft rolled right and moved toward the right side of the runway. The aircraft then rolled to the left, and the left wing struck the runway. None of the passengers or crew members were injured, and the aircraft taxied to the terminal.
The aircraft touched down firmly on the left main landing gear at about 2,500 ft from the runway threshold, between the centreline and the right edge of the runway, with 16° of left bank. Concurrently, the left wing contacted the runway surface for about 0.5 second. The left main landing gear strut then extended to nearly full length, and the left bank increased to 18°. The left wing contacted the runway again for approximately 2 seconds, and simultaneously, the aircraft heading deviated left to 136°, or 8° left of the runway heading.
The aircraft settled onto both main landing gears five seconds after the left main gear made contact, approximately 3,550 ft beyond the runway threshold. After the nose gear touched down, heavy wheel braking was used to slow the aircraft. Eight seconds after nose gear touchdown, after being prompted, the pilot flying applied reverse thrust on both engines. Deployment of reverse thrust occurred approximately 5,300 ft beyond the runway threshold. The aircraft slowed to taxi speed with approximately 500 ft of runway remaining. The aircraft taxied uneventfully to the assigned gate at the terminal.
United Kingdom Air Accidents Investigation Branch investigation EW/2009/02/08, engine pod strike, Leeds Bradford Airport, UK, on 21 February 2009
On 21 February 2009, at 1401 UTC, a Boeing 737-33A aircraft, registered G-CELD, was landing on Runway 32 at Leeds Bradford Airport. As the aircraft approached the flare, at about 30 ft AGL, a speed loss of 10 kt occurred. The captain called ’speed slow’ and placed his hand near the throttles, with the FO applying a small amount of power.
The captain then felt the aircraft sink so applied a ’handful of power’, covering the FO’s hands as he did so, adding ’you’ll need more than that’. At some point after this, the FO thought he heard the captain say ’I have control’ to which he responded by taking his hands off the controls in accordance with the company standard operating procedures. The FO added that his ’feet remained on the rudder pedals as there was no time to remove them’. Both pilots then recalled a pronounced wing drop to the right, immediately prior to the aircraft touching down.
G-CELD encountered windshear at about 30 ft AGL and became unstable in the flare. As a result, and unbeknown to the crew at the time, the right engine nacelle contacted the runway. Inspection of the runway revealed a 15 m scrape mark on the threshold, with associated paint matching G‑CELD’s engine cowling.
An aftercast was obtained from the Meteorological Office. It stated that it was likely that there was no abnormal wind flow regime although the wind was strong and gusty. The gustiness was not abnormal, but reductions in speed of 10 to 15 kt over a short period of time/distance were likely.
United Kingdom Air Accidents Investigation Branch investigation EW/2009/11/09, Engine pod strike, Bristol Airport, UK, on 19 November 2009
On 19 November 2009, at 2124 UTC, a Boeing 737-8AS aircraft, registered EI-DAL, was on a scheduled flight from Dublin, Ireland to Bristol Airport. The crew were both based at Bristol and aware of the local conditions prevalent during strong crosswind approaches and landings on runway 27. The captain was the pilot flying, the runway surface was dry and it was dark.
During the landing flare, the captain de‑crabbed the aircraft at 15 ft and closed the thrust levers at about 10 ft. The aircraft experienced a wing drop to the left, which the captain corrected, quickly followed by a more severe wing drop to the right as the right main landing gear touched down.
Although the crew did not believe an engine had contacted the runway, the captain said to the FO he would have a look after they shut down.
The company engineers observed the landing and mentioned that it looked ’pretty scary’ and considered that the wingtip may have made contact with the runway. Whilst the passengers were disembarking, the engineers inspected the aircraft and found damage under the right engine. The damage was confined to the engine cowl and thrust reverser duct.
On 23 April 2016, a Virgin Australia Boeing 737-8FE aircraft, registered VH-YIW, was operating a scheduled passenger service as flight VA91 from Auckland, New Zealand to Faleolo Airport, Apia, Samoa. Due to tropical cyclone Amos (TC Amos) being predicted to arrive in the vicinity of Samoa in the early hours of the following morning, the operator planned for VH-YIW to conduct a return flight on the same day, using the same flight crew. The captain was the pilot flying and the first officer was the pilot monitoring.[1]
Before the flight, TC Amos was west of Samoa, moving eastward. At 2100 Coordinated Universal Time,[2] about seven and a half hours before the planned take-off, the operator’s cyclone management team (CMT) reviewed the weather information associated with the cyclone, and determined that the flight could continue with additional risk mitigation in place. Specifically, the aircraft was required to carry maximum fuel, to allow for 60 minutes’ holding fuel at Samoa and for possible diversion to an alternate landing at Nadi, Fiji. Furthermore, engineering coverage was required at Samoa, or an engineer had to be carried on board from Auckland.
Three hours later, at 0000, a new cyclone advisory was issued. There was no significant change to the cyclone forecast based on the new advisory. However, the updated information was not used when planning the flight, nor was it assessed by the CMT. The aerodrome forecast indicated that a night landing could be still be safely conducted at Apia.
The flight departed from Auckland at 0433. During the flight, the crew sought and received regular weather updates from the operator’s flight following service[3] (flight following). As part of the updates received, the crew obtained terminal area forecasts and meteorological aerodrome reports for Apia. The crew were not provided with the cyclone advisory that was issued at 0000, although it was assessed by flight following and available to the crew on request.
While planning for the descent, approach and landing, the crew decided they would not commence the descent until they had received a weather report from the aerodrome tower controller. The crew reported difficulty contacting the tower through standard very high frequency radio, and eventually made contact using the high frequency radio and obtained a weather report. Based on that report, the crew decided they would conduct one approach and if they could not land, they would divert to Nadi.
During the approach, the crew reported observing heavy rainfall on the aircraft’s weather radar display. The crew also reported that the conditions were not as turbulent as previously expected. On approach to land, the crew established visual reference with runway 08 at about 700 ft above ground level, and continued the approach. The captain disconnected the autopilot at 260 ft and then inadvertently activated the take-off/go-around (TOGA) function. He immediately realised, corrected this action and then deactivated the auto throttle as originally planned.
After about 20 seconds of manual flying on final approach, the aircraft started to drift left. The aircraft touched down about six seconds later. During those six seconds, both flight crew became aware of the aircraft’s left drift and the captain manoeuvred the aircraft to return to the runway centreline. At 0807, the aircraft landed on the right main landing gear wheels first, followed by the nose wheels, then the left main gear wheels. Flight data indicated that the aircraft was not pitched nose-up to flare for landing before touchdown. The crew taxied to the terminal and discussed the landing.
The weather conditions remained within the aircraft’s operating limitations, and were therefore suitable, during the approach and landing. While neither crew reported that it was a hard landing, the first officer considered it firmer than normal and consequently checked the landing data. Having only been informally shown how to access this information, the first officer recalled identifying the touchdown as 1.45 G landing with a 10° right roll. This alleviated his concerns of a hard landing and he communicated this to the captain.
Unknown to the crew, the right engine nacelle had briefly made contact with the runway during the landing and sustained damaged. There were no reported injuries as a result of the occurrence.
In preparation for the return flight, the captain and the engineer both conducted independent external pre-flight aircraft inspections in the heavy weather conditions. During this time, the weather deteriorated further and the crew postponed the return flight until the next day. The following day, and with a significant improvement in the weather, the captain and the engineer both conducted separate external pre-flight checks of the aircraft in preparation for the day’s flying. Neither inspection detected the right engine nacelle damage.
At least four separate external visual inspections were conducted on the aircraft between landing at Apia, and taking off the next day. No external airframe damage was detected or reported from either the crew or engineer before it departed.
Two days later, the operator’s flight data section detected the aircraft had encountered a designated hard landing with a significant angle of bank at Apia. Delays in uploading the data to the operator’s flight data system occurred due to the operator not having immediate data download capabilities at overseas ports. This data was uploaded on return of the aircraft from its overseas sectors to Australian ports. This, coupled with an Australian public holiday, meant a further day’s delay before the information was interpreted by the operator’s maintenance watch function. Subsequently, maintenance watch required the aircraft to undergo inspection on arrival from Port Moresby, Papua New Guinea into Brisbane, Queensland on 26 April.
Following the conduct of four sectors after the Apia landing, damage to the right engine nacelle was detected. Additional inspection identified lateral wear damage on the outer right landing gear tyre.
From the evidence available, the following findings are made with respect to the engine nacelle strike and continued operation involving a Boeing 737-8FE, registered VH-YIW and operated by Virgin Australia Airlines Pty. Ltd. that occurred at Faleolo Airport, Apia, Samoa on 23 April 2016. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
The aircraft drifted left during short final in heavy rain on an approach at night. The pilot flying started to correct the drift, however the aircraft was not flared and the wings were not level as it touched down. This led to the nose and right wing being low, resulting in an engine nacelle strike.
Due to heavy rain, darkness and limited visual cues, the flight crew did not detect the aircraft's banked, nose-low attitude immediately prior to landing which increased the likelihood of an engine nacelle strike.
The operator’s pre-flight external inspection procedure mandated that flight crew check under the engine nacelle for damage. This was not routinely done by flight crew and not included in the flight crew training material.
Although the operator had a maintenance task card for daily inspections of the Boeing 737, it did not contain a specific requirement to inspect underneath the engine nacelle. This contributed to the damage to the right engine nacelle not being identified during in post-occurrence maintenance inspections.
Other factors that increased risk
Due to limited sleep in the previous 24 hours, the captain was probably experiencing a level of fatigue that has been demonstrated to adversely influence performance.
Safety analysis
Introduction
The flight departed Auckland with an approaching tropical cyclone in the vicinity of Apia. At the time of departure, the effects of the tropical cyclone where not expected to adversely impact the safety of the flight.
The approach to land was conducted within the aircraft’s operational limitations at night and in heavy rain. During the touch down, the right engine nacelle momentarily contacted the runway.
Damage from the runway contact to the engine nacelle was not detected after landing or during any of the pre-flight and engineering inspections for four subsequent sectors.
The following analysis examines the weather information provided to the flight crew and the human factors associated with the approach leading to the nacelle strike. It further examines the visual inspection methods that should have provided opportunities to detect the aircraft damage.
Flight briefing and monitoring
TC Advisory No. 13 was not provided to the flight crew prior to departure or during the flight. The operator’s flight following service was in receipt of Advisory No. 13, which was available if requested by the crew.
However, the updated information contained in Advisory No. 13 did not contain any significant change from the previous forecast and was not deemed by flight following to contain operationally critical information and therefore was not actively provided to the flight crew. The flight crew utilised requested aerodrome forecasts and observed weather reports from Apia air traffic control to prepare the aircraft for landing in Samoa.
Human factors aspects
Fatigue
Fatigue can have a range of adverse influences on human performance, including slowed reaction time, decreased work efficiency, reduced motivational drive, increased variability in work performance and more lapses or errors of omission (Battelle Memorial Institute 1998), as well as various effects on decision making (Harrison and Horne 2000).
Sleep is vital for recovery from fatigue, with both the quantity and quality of sleep being important. Most people need at least 7–8 hours of sleep each day to achieve maximum levels of alertness and performance. Research has shown that obtaining less than 5 hours’ sleep in the previous 24 hours is inconsistent with a safe system of work (Dawson and McCulloch 2005), with some research indicating less than 6 hours sleep can increase risk (Thomas and Ferguson 2010, Williamson and others 2011). In addition to sleep, a number of other factors can influence fatigue levels, including time of day, time awake and the nature of work activities.
In this case, the captain reported having 3–4 hours’ sleep the night before the occurrence flight, and he had been awake for 13 hours at the time of the engine nacelle strike occurrence. He also stated that he did not feel fatigued, but most people generally underestimate their level of fatigue (Battelle Memorial Institute 1998). The first officer had significantly more sleep prior to the occurrence flight.
Overall, primarily due to restricted sleep in the previous 24 hours, it is likely the captain was experiencing a level of fatigue during the occurrence flight likely to have a demonstrated effect on performance. However, there was insufficient evidence to conclude he was experiencing a significant level of fatigue. In addition, it is difficult to conclude that the captain’s performance during the landing was influenced by fatigue. Other factors, such as reduced visual cues and environmental conditions, can explain the handling events, and the environmental conditions and context during the approach is likely to have elevated the crew’s arousal level.
The occurrence at Apia occurred during the first of two flights scheduled for the flight crew that day. Had the duty period proceeded as planned, it is likely that both flight crew would have been experiencing a higher level of fatigue towards the end of the second flight. However, both flight crew may have been able to enhance their alertness during that flight by taking controlled rest.
Overall, the flight crew’s scheduled flights on 23 April met the requirements of the operator’s fatigue risk management system. Nevertheless, this occurrence highlights the importance of ensuring that both flight crew and an operator adequately consider a flight crew member’s circumstances before extending duty periods.
Workload
Workload refers to the interaction between a specific individual and the demands associated with the tasks that they are performing. High workload leads to a reduction in the number of information sources an individual will search, and the frequency or amount of time these sources are checked (Staal 2004). It can result in an individual’s performance on some tasks degrading, tasks being performed with simpler or less comprehensive strategies, or tasks being shed completely (Wickens and Hollands 2000). An individual’s capacity to manage task demands at any point in time can be affected by a wide range of factors such as experience, training, task recency, familiarity with a situation and fatigue.
Neither pilot reported the workload during the approach as being too high to manage. They briefed for the approach and were actively monitoring the weather conditions, and they addressed the increased requirements for radar scanning successfully. However, final approach is normally known as a period of high workload for pilots, particularly at night. In this case, the workload was further increased by the changing weather conditions. The difficulty in communications with the tower, the crosswind, manual control of the aircraft and the potential influence of fatigue also added to this workload.
When the captain mistakenly selected take-off/go-around (TOGA) from the throttle controls instead of auto thrust disconnect, it had the effect of removing the flight director. This momentarily left the flight crew without a simple representation of pitch and bank angle guidance. With reduced visual cues due to the night-time conditions, rain and increasing crosswind on touchdown, the last 100 ft of the approach likely required the crew’s full attention to deal with the situation. Although the flight crew’s workload was undoubtedly higher than normal, the available evidence is not consistent with it being beyond the crew’s capabilities, and it is not possible to conclude that their elevated workload reduced their handling of the aircraft or their subsequent awareness of a nacelle strike.
Post-flight awareness of damage
The flight crew were aware that the landing had been non-standard and, after discussion with the captain, the FO obtained recorded data from the maintenance section of the on-board flight management computer. The FO’s interpretation of the data indicated that the landing had been conducted within normal parameters.
During the post-event investigation, the operator found that flight crew were not specifically instructed on how to interpret this data. Consequently, the FO did not understand the limitations in how the data was displayed, which led the flight crew to believe the landing was within acceptable limits, and alleviated any concerns they may have had with the landing. As a result, the flight crew did not alert the maintenance engineer of an increased likelihood of a hard landing or possible runway contact with the airframe.
Damage detection
Flight crew conduct an external inspection of the aircraft before every flight. As part of these inspections, the engines and surroundings are required to be examined. This includes an explicit requirement to inspect the underside of the nacelles for damage. This requirement was added to the operator’s procedures in 2011, adding to a previous requirement in 2005 to check that the engine exterior was not damaged.
At the time of the occurrence, however, the operator’s flight crew training package did not reflect the specific requirement to check for this damage. The captain conducted the planned return sector pre‑flight inspection at night, in heavy rain and wind. Although the environmental conditions were not optimal, the captain considered the inspection to be adequate. However, the flight did not proceed due to the weather and departed the next day, after an additional pre‑flight inspection, when conditions had eased. No flight crew inspections for the next four flights were effective in detecting the nacelle damage. Consistent with other occurrences investigated by the ATSB, this may have been influenced by an expectation that no damage was present. The operator has since amended its pilot training package to include the specific requirement to inspect the underside of the engine nacelles.
Additionally, a licensed engineer was required to conduct an external inspection before the first flight of a day and conduct a separate external inspection using a different inspection schedule before an aircraft conducted an extended range twin-engine operations (ETOPS) flight. Neither the daily external inspection, nor the ETOPS external inspection specifically required the underside of the nacelle to be visually inspected. Engineers were required to carry out a visual check of various components for ‘obvious signs of damage’. This included the inlet cowl outer surfaces and the abradable shroud.
While the lower surfaces of the nacelle were not specifically mentioned, the inspection requirements were broad in their requirements and not specific in their intent. This may have led to engineers not specifically inspecting under the engine nacelles. Since the occurrence, a specific requirement to inspect the nacelles’ underside has been added to engineers’ procedures.
A combination of rain, wind, and the position of the damage provided significant environmental challenges during the visual inspection.
Due to the positioning of the engines on a B737, the space between the underside of the nacelle and the ground is between 470 mm and 600 mm high, depending on the aircraft weight. While it is easy to inspect and access the sides of the nacelles, examining the underneath is more difficult. Tests by the operator showed that even when crouching down to view the underside of the nacelle from 2 m away, the area of damage was not visible. This meant anyone examining underneath the nacelle would have to be positioned close to the ground to obtain an adequate view of the area and any potential damage. No additional equipment, such as mirrors or waterproof clothing, were issued to flight crew to facilitate this level of inspection.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew of VH-YIW
Virgin Australia Airlines Pty. Ltd.
the flight data recorder from VH-YIW
United States Joint Typhoon Warning Center
United States National Transportation Safety Board.
References
Battelle Memorial Institute 1998, An overview of the scientific literature concerning fatigue, sleep,and the circadian cycle, Report prepared for the Office of the Chief Scientific and Technical Advisor for Human Factors, United States Federal Aviation Administration.
Dawson D & McCulloch K 2005, ‘Managing fatigue: It’s about sleep’, Sleep Medicine Reviews, vol. 9, pp. 365–380.
Harrison H & Horne JA 2000, ‘The impact of sleep deprivation on decision making: A review’, Journal of Experimental Psychology, vol. 6, pp. 236–249.
Staal MA 2004, Stress, cognition, and human performance: A literature review and conceptual framework, National Aeronautics and Space Administration Technical Memorandum NASA/TM‑2004-212824.
Thomas MJW & Ferguson SA 2010, ‘Prior sleep, prior wake, and crew performance during normal flight operations’, Aviation, Space, and Environmental Medicine, vol. 81, pp. 665–670.
Wickens CD & Hollands JG, 2000, Engineering psychology and human performance, 3rd edition,
Prentice-Hall International Upper Saddle River, NJ.
Williamson A, Lombardi DA, Folkard S, Stutts J, Courtney TK & Connor JL 2011, ‘The link between fatigue and safety’, Accident Analysis and Prevention, vol. 43, pp. 498–515.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the flight crew, Virgin Australia Airlines Pty. Ltd. and the Civil Aviation Safety Authority.
Submissions were received from Virgin Australia Airlines Pty Ltd. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.