Boeing 737-476, VH-TJF, Canberra Aerodrome, on 15 December 2002
Summary
At about 1020 Eastern Summer Time on 15 December 2002, a Boeing 737-400 (737) aircraft, registered VH-TJF, departed runway 35 at Canberra Airport for Melbourne. As the aircraft was rotated, the handling pilot felt that the pitch control was unusually stiff. The crew informed air traffic control of the problem and climbed the aircraft to a safe altitude in order to conduct a controllability check. The crew declared an urgency emergency phase as a precaution. The aircraft subsequently landed at Canberra Airport, at about 1115, with airport emergency services in attendance.
The operator’s maintenance personnel could not reproduce the problem on the ground. After investigation and replacement of the system B flight control module an assessment flight was conducted the following day to Melbourne Airport. That flight determined that the defect was still present and the aircraft was relocated to the operator’s maintenance facility in Melbourne for further investigation.
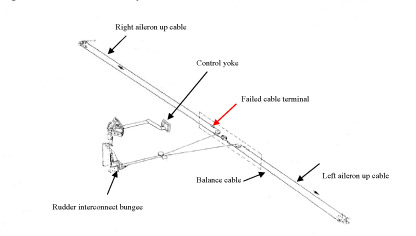
After an extensive investigation by the operator, the elevator binding was reproduced and found to be due to an incorrectly located elevator control cable. The control cable was hooked over the lip of a J shaped floor support beam, beneath the aft galley. The angular deflection of the cable over the floor support beam was such that the cable would only bind intermittently. The cable was repositioned and re-rigged in accordance with the manufacturer’s aircraft maintenance manual. An assessment flight was conducted and it confirmed that the defect was no longer evident.
A scheduled maintenance inspection on the 737 was completed on 13 December 2002. A review of the aircraft’s technical log indicated that on three of the eleven sectors flown since that inspection, reports of heavy and binding flight controls were noted. During the scheduled maintenance inspection completed on 13 December 2002, several flight control cables had been disconnected to carry out a modification that required the removal of the flight control columns. One of those cables was found, during the operator’s subsequent investigation, to be hooked over the aft galley floor support beam. The scheduled maintenance inspection did not require the floor panels to be removed and therefore did not allow a complete inspection of the cables after the modification was completed. Although there was no reported work carried out on the control cable system in that area, several maintenance work cards detailed maintenance near that area.
The operator conducted tests to determine how the cable might have become hooked over the J section floor support beam. With normal operating tension on the cable, a force of approximately 30 kg was required to place the cable over the beam. With only slight tension on the cable and the cable clamped, it could be readily placed over the beam. The test also determined that with the aft galley installed, as was the case, access to the location where the cable was hooked over the floor support beam was very limited.
The manufacturer’s aircraft maintenance manual contained instructions for maintaining a light tension on control cables that were disconnected but not removed. The instructions detailed the installation of cable clamps on the affected cables, to ensure that the cables do not unwind on their cable drums or become displaced from their pulley guides. If the cables were between rig pin locations, then rig pins were to be installed through the applicable cable drum or quadrant.
The aircraft manufacturer indicated that during certification of the 737, tests were performed to determine if an untensioned cable during emergency operations of the flight controls would interfere or hang up on adjacent structure. The manufacturer determined that the J section of the floor support beam did not present a risk.
The operator conducted an inspection of other 737 aircraft and found that two other configurations existed. One installation was the same as the incident aircraft but the cable was located within a plastic tube. The other installation had the floor support beam facing in the opposite direction (J section tail of the beam facing away from the cable). The manufacturer determined that the configuration of the incident aircraft was in accordance with the design drawing for the aircraft and that the floor support beam location was limited to the operator’s fleet.
Occurrence summary
| Investigation number | 200205893 |
|---|---|
| Occurrence date | 15/12/2002 |
| Location | Canberra, Aerodrome |
| State | Australian Capital Territory |
| Report release date | 16/09/2004 |
| Report status | Final |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Flight control systems |
| Occurrence class | Serious Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 737 |
| Registration | VH-TJF |
| Serial number | 24431 |
| Sector | Jet |
| Operation type | Air Transport High Capacity |
| Departure point | Canberra, ACT |
| Destination | Melbourne, Vic. |
| Damage | Nil |