On 21 September 2006 at 2356 Eastern Standard Time, the US National Transportation Safety Board (NTSB) notified the Australian Transport Safety Bureau (ATSB) of an accident involving a foreign registered and operated Grumman G-73T, Turbo Mallard, aircraft, which occurred on 19 December 2005 near Watson's Island, US (see www.ntsb.gov and DCA06MA010). The NTSB requested assistance from the ATSB to obtain information relating to the operation of Turbo Mallard aircraft in Australia.
The ATSB appointed an accredited representative to participate in the investigation into the occurrence, in accordance with clause 5.23 of Annex 13 to the Convention on International Civil Aviation. To protect the information supplied by the NTSB to the ATSB and the investigative work undertaken to assist the NTSB, the ATSB initiated an investigation under the Transport Safety Investigation Act 2003.
The ATSB accredited representative coordinated the exchange of airworthiness information from an Australian operator of Mallard aircraft. That operator had modified an aircraft by fitting turbine engines.
The NTSB is responsible for the final investigation report regarding this occurrence.
The aircraft stalled at a height from which the pilot was unable to effect recovery.
Analysis
The absence of witnesses to the accident, and of an emergency radio broadcast from the pilot meant that there was no information available to the investigation about the pilot's situation immediately prior to the accident. However, the low-level manoeuvring carried out by the pilot overhead the sheltering sheep, and interaction via radio with the driver of the four-wheel drive vehicle was consistent with the pilot attempting to disturb the sheep from their position.
The steepness of the angle of bank and the nose-down pitch attitude at the aircraft's point of ground impact indicated that the aircraft was in a steep left turn at that time. Those indications and the minimal forward movement of the aircraft after ground contact were consistent with the aircraft having stalled and slipped out of the turn. The lack of aircraft rotation at impact indicated that there had been insufficient time for the stall to develop into a spin, consistent with it occurring at low level. It was likely that there was insufficient time for the pilot to recover before impacting the ground. Given the variety of opinion relating to the use of wing flap during mustering operations, the investigation was unable to determine the degree of influence that the lack of flap had on the development of the accident.
The pilot's probable focus on the sheltering sheep, together with the need to operate the UHF radio may have distracted the pilot from the primary task of flying the aircraft. In addition, any sensory illusion as a result of the pilot moving his head during the low-level manoeuvring, or inadvertent movement of the flight controls could have resulted in an unintentional increase in the aircraft's angle of bank. In either case, it was likely that the pilot was initially unaware that the aircraft was in such a steep turn, or that the airspeed was insufficient for the angle of bank. The stall warning probably sounded before the stall, but given warnings were often activated during aerial mustering, it may not have had a significant effect on the pilot's awareness of the impending stall.
A possible influence on the development of the stall was a decrease in available engine power. However, the damage to the propeller indicated that the engine was developing power at ground impact, there were no identified engine defects, there was adequate fuel on board and the pilot had flown for about 1.5 hours without any apparent performance degradation prior to the accident. That evidence indicated that the engine was capable of performing normally. Notwithstanding that evidence, the use of a mix of aviation gasoline and unleaded petrol, and the estimated dewpoint depression at about the time of the accident, meant that the investigation could not discount the possibility of the formation of carburettor icing. The result in that case was the possible loss of some engine power.
During the pilot's 18 years experience operating the Cessna 206, he would have become accustomed to the relatively large amount of engine power available during aerial mustering manoeuvres in that aircraft. The investigation considered whether the pilot might have unwittingly expected the same performance from the Cessna 150. However, the pilot had operated the Cessna 150 on aerial mustering operations for over 15 months, and it was concluded that the pilot would most probably have been aware of, and adjusted to that performance difference between the aircraft types during that time.
Although the pilot's flight reviews included the practice of stall recovery in turns, and the pilot had been mustering for 18 years, the lack of an aerial stock mustering permission meant that the pilot had not completed formalised training in all of the competencies inherent in the award of that permission. As a result, there was the potential that the pilot may have acquired and, over time, reinforced perhaps inappropriate responses to some of the risks inherent in the mustering environment. The completion by the pilot of the aeronautical experience requirements of Civil Aviation Order 29.10 would have provided some assurance that he had acquired the appropriate knowledge and skills necessary to manage the risks inherent in the low-level, low-speed, and high workload mustering environment.
On 6 December 2005, the owner-pilot of a single-engine Cessna Aircraft Company 150G, registered VH-KPQ, was conducting aerial mustering operations on a family-owned station, 156 km north of Broken Hill, NSW. The pilot, who was the sole occupant, had departed a station airstrip at about 0710 Eastern Daylight-saving Time to coordinate the movement of sheep from an 18,000-acre paddock to shearing shed yards near the homestead. The paddock had medium to dense coverage of 2.5 m high scrub and was generally flat. Aerial mustering activity that day involved flying a north to south pattern progressively from the east to the west and directing ground-based mustering personnel to the location of the sheep. Those personnel were using two motorbikes and a four-wheel drive vehicle in the muster. All of the musterers were communicating with ultra-high frequency (UHF) radio.
At about 0835, the four-wheel drive vehicle was being used to move a few sheep along when the driver lost sight of them. The driver advised the pilot by UHF radio and shortly after the aircraft circled above the area a number of times at about 250 ft above ground level (AGL), but the pilot was reported to have not seen the sheep. The driver then sighted the sheep in thick scrub that the vehicle was unable to penetrate and advised the pilot of the situation. The pilot requested that the driver reverse and drive onto a nearby track. The driver asked the pilot to report when the sheep moved away from the scrub. There was no response. Shortly after the driver noticed smoke nearby and found that the aircraft had impacted the ground and there was an intense fire. The pilot was fatally injured.
The other musterers were in different areas of the paddock and did not observe the aircraft's descent and impact with the ground. No one heard an emergency radio broadcast from the pilot. One of the musterers observed the pilot's take-off from the station airstrip and heard the engine a number of times during the mustering before the accident and reported that it sounded normal.
Wreckage and site information
The aircraft wreckage was found approximately 400 m to the south-east from where the mustering vehicle was operating. The aircraft was upright with evidence of severe impact damage to the left wing, nose section and rear fuselage. There was evidence of intense fuel-fed fire damage to the cabin area and left wing. The main wreckage, approximately 8 m from the first ground impact mark, contained all the aircraft parts except for the nosewheel, which was found nearby. The ground impact marks and damage to the left wing indicated that the initial impact with the ground was the outer leading edge of the left wing. In addition, the minimal damage to the shrubs surrounding the initial ground impact marks indicated that the aircraft impacted the ground with a steep left angle of bank between 70 and 80 degrees. The damage to the wing, and the nose impact position also indicated that the aircraft impacted in a nose down attitude with a high descent rate. There was no evidence of rotation.
Examination of the aircraft, including the flight control systems and engine, did not reveal any evidence of pre-impact defects. Damage to the propeller indicated that the engine was operating at ground impact. The wing flaps were found in the retracted position.
Pilot information
The pilot commenced flight training in 1987 and flew 18 hours in a Cessna 150 and 32 hours in a Cessna 172. The pilot purchased a Cessna 206 and completed his flight training in that aircraft. He was issued with a private pilot (Aeroplane) licence in 1988. There was no evidence of any low level or aerial stock mustering permission (the relevant regulations are outlined below).
Family members reported that the pilot used the Cessna 206 primarily for aerial mustering on pastoral properties that he owned in regional NSW. About 18 months prior to the accident, the pilot purchased the station north of Broken Hill and in August 2004, purchased the Cessna 150 primarily for mustering on that station.
The pilot's logbook was full and did not contain any entries after 1 October 2004. He had logged 36.5 hours flying the Cessna 150 over the station north of Broken Hill and a total of 2,041 hours. Although there were no flights logged by the pilot after 1 October 2004, family members reported that the pilot continued to fly the Cessna 206 and the Cessna 150 after that date.
The pilot's most recent flight review was competed on 24 April 2004 in his Cessna 206. The instructor who conducted the review reported that the pilot was competent and that the review had included steep turns and stall recovery. Steep turns were practiced at 3,000 ft AGL and between 45 and 60 degrees angle of bank. Stall recovery was practiced at 3,000 ft AGL and included recovery from a stall during a steep climbing turn with low power.
The pilot's logbook indicated that the pilot had completed stall and steep turn training in a Cessna 150 during his initial training in 1987/1988. There was no record of any stalls or steep turn training in a Cessna 150 since.
The Civil Aviation Safety Authority (CASA) issued the pilot with a Class 2 Medical Certificate on 30 June 2004 that was valid to 30 June 2006. That certificate contained a restriction requiring the pilot to wear distance vision correction and to have reading correction available during flight.
The pilot had been involved in mustering activities that included about two hours aerial mustering in the Cessna 150 per day during the previous two weeks. Two days before the accident the pilot did some aerial mustering in the Cessna 150 and then flew the Cessna 206 to a station in the Hay area. He was reported to have worked on the station until about 2030, before going to bed at 2300. The next morning the pilot awoke at 0600 and departed at 0830 for Wagga Wagga aerodrome, landing at 1000. At 1500, the pilot departed for the station north of Broken Hill via Hay and Broken Hill, arriving home at about 2000. The pilot worked in the sheep yards until returning to the homestead at 2130. Family members reported that the pilot was tired and had a sore shoulder for which he took a non-prescription painkiller. He retired to bed shortly after.
On the day of the accident, the pilot woke at about 0615 and at about 0630 flew the Cessna 206 from the airstrip near the homestead to another station airstrip where the Cessna 150 was hangered. It was reported that he was in good spirits and appeared well rested.
At the time of writing this report, the postmortem report was not available. There was no evidence of any physiological condition that may have contributed to the accident.
Aircraft information
The Cessna 150G was a two-seat, high wing aircraft equipped with a Continental O-200A engine rated at 100 HP (74.6 kW). The aircraft was fitted with a pneumatic aural stall warning system that activated 4 to 8 kts before the stall was reached. That was the only aural warning known to be fitted to the aircraft.
The pilot operated the Cessna 150 on a mixture of 10% aviation gasoline (Avgas) and 90% unleaded automotive petrol as authorised by a flight manual supplement. The flight manual supplement stated that when using automotive fuel, the onset of carburettor ice may occur earlier than with Avgas under the same atmospheric conditions. Two days before the accident, the aircraft fuel tanks were reportedly filled from clean drum stock in the hangar using a hand-pump that included an in-line filter. On the morning of the accident, the pilot was observed conducting his pre-flight checks, including of the aircraft's fuel system drains.
In addition to the aviation radios, a UHF transceiver was fitted to the aircraft for use during mustering operations. The audio output from that transceiver was wired into the aircraft's phones jack, and there was a hand microphone. The pilot was reported to use an aviation headset.
The pilot's Cessna 206 was a six-seat high wing aircraft equipped with a Continental IO-520F engine rated at 300 HP (223.7 kW).
Meteorological information
The applicable aviation area forecast was valid from 0800 and predicted isolated showers and thunderstorms with broken 2 cloud at 10,000 ft. The wind at 2,000 ft was expected to be from the north-west at 20 kts. Turbulence was forecast to be moderate in the broken cloud and after 1200, light to moderate below 9,000 ft.
Automatic weather observations at 0830 from the nearest Bureau of Meteorology (BoM) site at Broken Hill recorded scattered cloud at 9,500 ft and a surface wind from the south-west at 10 kts. The temperature was 26 degrees, the dewpoint was 14 degrees and the barometric pressure was 1003 hPa. There was a report of a thunderstorm and 0.2 mm precipitation between 0730 and 0800. The BoM advised that the Broken Hill observations were representative of the weather conditions at the accident site.
One of the ground-based musterers reported that at the time of the accident, the wind was a light south-westerly and it was overcast and humid.
The 0830 Broken Hill temperature and dewpoint depression3 was plotted on a Carburettor icing - probability chart. That chart predicted moderate icing at cruise power, or serious icing at descent power in those conditions.
Current regulations
Civil Aviation Order 29.10 defines aerial stock mustering as 'the use of aircraft to locate, direct and concentrate livestock whilst flying below 500 feet above ground level'. The aeronautical experience requirements for a pilot to engage in mustering operations include that the pilot must complete 5 hours low flying training and an exam to confirm pilot proficiency, followed by 10 hours operational training. That training included:
level, climbing and descending turns and recovery from the stall at up to 60 degrees angle of bank
slow flying and the methods of losing height at low level
steep climbing and descending turns away from and returning to a ground reference.
Aerial stock mustering
Aerial mustering of stock in aeroplanes such as the Cessna 150 usually involves low-level flight including steep turns at low airspeed to allow the pilot to monitor the location and movement of stock, and to guide ground-based personnel accordingly. It was reported that the pilot usually conducted aerial mustering at an estimated height of between 150 and 200 ft AGL, but if sheep found cover in dense scrub, the pilot would sometimes fly lower and apply power over the sheep to encourage them to move.
Turns are a significant risk during aerial mustering in aeroplanes due to the reduction in vertical lift component and significant increase in stall speed4 with bank angles over 60 degrees. To maintain height in a turn at a constant airspeed requires an increase in lift, which produces an increase in drag that necessitates an increase in engine power. Depending on the angle of bank and the conditions, maximum engine power may not be sufficient to prevent a descent.
The use of small angles of flap reduces the stall speed and lowers the nose angle for a particular airspeed. Although one low-level flying expert indicated that use of flap was advantageous during low-speed turns, opinion amongst pilots with experience in low-level operations regarding the use of flap during those operations varied.
One of the ground-based musterers reported that he heard a buzzer twice in the background of some of the pilot's UHF radio transmissions. That included while the aircraft was circling shortly before the accident. He also reported hearing the same buzzer during the pilot's previous mustering operations. An experienced aeroplane mustering pilot and instructor reported that it was common for the stall warning to activate in the steeply banked turns used during aerial mustering operations.
A number of potential sensory illusions can result in mustering pilots inadvertently applying excessive bank angles during turns. If a pilot's head is orientated into a turn (such as looking at the ground or stock) and is then quickly rotated away, the pilot's vestibular balance system can produce a sensation that the aircraft is underbanked. A visual illusion that the aircraft is skidding out of a turn can occur when turning from downwind to upwind while looking at the ground, also giving the sensation that the aircraft is underbanked.
When pilots are paying very close attention to stock by moving their head during a turn, they may tend to move the flight controls in sympathy with head-body movement. This can lead to inadvertent overbanking. Distractions during a turn, such as looking for stock or using a radio, can also increase the risk of inadvertently steepening the turn and/or allowing the airspeed to decay.
Only those investigation areas identified by the headings and sub headings were considered to be relevant to the circumstances of the occurrence.
Five to seven eighths of the sky obscured by cloud.
Dew point depression is calculated by subtracting the dewpoint from the ambient temperature.
Stall speed is the airspeed at which the stalling angle of attack (angle between effective wing chord line and relative airflow) occurs resulting in rapid decrease in lift
Summary
On 6 December 2005, the owner-pilot of a single-engine Cessna Aircraft Company 150G, registered VH-KPQ, was conducting aerial mustering operations on a family-owned station, 156 km north of Broken Hill, NSW.
At about 0835 Eastern Daylight-saving Time, the pilot was observed to circle some sheep at about 250 ft above ground level. Shortly after, ground mustering personnel noticed smoke nearby and found that the aircraft had impacted the ground and there was an intense fire. The pilot, who was the sole occupant of the aircraft, was fatally injured.
The aircraft wreckage was found approximately 400 m to the south-east from where the pilot was circling. The aircraft was upright with evidence of severe impact damage to the left wing, nose section and rear fuselage.
Examination of the aircraft, including the flight control systems and engine, did not reveal any evidence of pre-impact defects. Damage to the propeller indicated that the engine was operating at ground impact. The wing flaps were found in the retracted position.
The steepness of the angle of bank and the nose-down pitch attitude at the aircraft's point of ground impact indicated that the aircraft was in a steep left turn at that time. Those indications and the minimal forward movement of the aircraft after ground contact were consistent with the aircraft having stalled and slipped out of the turn. The lack of aircraft rotation at impact indicated that there had been insufficient time for the stall to develop into a spin, consistent with it occurring at low level.
The investigation concluded that the aircraft stalled at a height from which the pilot was unable to effect recovery.
At about 1425 Western Standard Time1 on 22 October 2005, the pilot of an Air Tractor Inc AT-602 (AT-602) aircraft, registered VH-NIT, was fatally injured when his aircraft impacted terrain, approximately 150 m south of the Ballidu airstrip, WA. Figure 1 depicts the township of Ballidu, the airstrip, the approximate flight path of the aircraft and the location of the accident site.
Figure 1: Ballidu townsite, airstrip and accident site2
The pilot had not operated the AT-602 prior to the day of the accident. The series of flights that day were for familiarising the pilot with the aircraft's handling characteristics, and were carried out under the supervision of the company owner/chief pilot.
The chief pilot reported that the aircraft was fully fuelled before the first in the series of flights. That flight had included ground taxying operations, take-offs, landings and general aircraft handling, including simulated spray runs along the strip and practice operating the hopper door. The accident occurred during the second flight of the day.
During those flights, the pilot returned to the operating pad several times, during which the chief pilot asked the pilot how he was progressing and, when necessary, replenished the contents of the hopper. The chief pilot reported that the aircraft was being operated with about 200 L of water in the hopper, which was the minimum quantity to prevent the hopper's seals from drying out. He recalled that he had replenished the hopper several times that day.
A number of witnesses sighted the aircraft flying over the airstrip at low altitude and saw water drop from the underside of the aircraft. The witnesses observed the aircraft gain a small amount of height before the nose of the aircraft suddenly pitched downwards and the aircraft descended steeply towards the ground.
Witnesses
The witnesses that reported either seeing or hearing events associated with different portions of the flight immediately prior to the accident included:
Three witnesses that were located at two separate positions, who observed water dropping from the underside of the aircraft and recalled that the nose of the aircraft pitched steeply upwards after completion of that drop, with the aircraft gaining a small amount of height.
The chief pilot, who sighted the aircraft climbing out as it flew past his hangar, but recalled that the nose attitude did not appear abnormally high. He did not recall hearing any unusual noises from the aircraft engine or propeller.
A witness who sighted the aircraft as it flew abeam her location and recalled that the nose of the aircraft was at a level attitude, before the nose 'dropped'. The sound from the aircraft appeared normal and at a constant level until the witness heard the sound of an impact.
A witness who was familiar with dropping operations and was watching the aircraft as it approached the airstrip. From the aircraft's position relative to the airstrip and the location of the runway thresholds, he surmised that the pilot was making a practice water drop. The aircraft disappeared from his view as it descended to what he perceived to be the drop zone before reappearing again, having made what he presumed to be either a water drop or a dummy water drop. The witness recalled that the aircraft was climbing steeply, but that the nose attitude of the aircraft was close to horizontal, before pitching steeply down towards the ground. The witness recalled hearing an unusual noise from the aircraft's engine or propeller as the aircraft started to descend, which he described as being similar to the noise when a pilot reversed the propeller's pitch on landing, or made a significant change to the power setting of the engine.
A witness who was adjacent the airstrip and thought that the aircraft's engine sounded as if it was not producing much power as the aircraft started to climb away, when compared to water drops that he witnessed earlier that day.
Two residents close to the site of the accident who heard the noise of an aircraft approach and then an increase in engine noise, similar to when a pilot applies power to enter a climb or the noise that the aircraft makes after it lands. A few seconds of silence followed, and the residents recalled thinking that the aircraft must have landed. They then heard the sound of an impact and immediately realised that the aircraft had crashed.
All of the eyewitnesses were consistent in their recollection of the aircraft's final descent towards the ground, recalling that the nose of the aircraft suddenly and violently pitched downwards, and the aircraft descended steeply towards the ground.
Accident site and wreckage examination
The sandy scrub-type terrain in the vicinity of the accident site was flat, with gently upwards sloping terrain on approach to the site. Bushes and small trees, approximately 3 to 5 m high, covered the immediate area and a power line, supported by power poles about 10 m high, ran east to west along a road adjacent the airfield boundary.
Examination of the wreckage and analysis of impact loads through the structure of the aircraft indicated a slightly right wing low, almost nose-level (zero) pitch attitude on impact with terrain. The characteristics of the impact were consistent with a high rate of vertical descent and low forward speed. Damage to the vegetation in the vicinity of the accident site indicated a steep final flight path towards the ground, with the main wreckage located about 23 m along the wreckage trail from the initial point of impact. Figure 2 shows the initial impact point relative to the main aircraft wreckage.
Figure 2: Terrain impact point and aircraft wreckage
All structural components and flight controls were accounted for at the accident site. The aircraft was intact prior to impact with terrain. The main landing gear collapsed on contact with the ground and the fuel tanks ruptured during the impact sequence. There was evidence that a significant quantity of fuel had spilled from each of the tanks.
There was no evidence of bird strike or collision with other obstacles prior to the initial contact with terrain.
Weather
Witnesses at Ballidu recalled that the weather conditions around the time of the accident were generally fine with light south-westerly winds.
The Bureau of Meteorology reviewed the available weather data for the afternoon of the accident. That review indicated the presence of south-westerly surface winds and little or no cloud in the Ballidu area at the time of the accident.
The closest official meteorological recording station was at Dalwallinu, about 40 NM to the north-west. At the time of the accident, Dalwallinu recorded a south-westerly wind at 8 to 10 kts and a temperature of about 23 degrees C.The Bureau of Meteorology assessed that, under the prevailing conditions, similar weather would have been experienced at Ballidu around the time of the accident.
Aircraft
The AT-602 was manufactured as a single-seat, specialist type aircraft designed for agricultural and fire fighting (water dropping) operations. That aircraft model had been issued an airworthiness certificate by the US Federal Aviation Administration (FAA) as a Restricted Category3 aircraft, for use in special purpose operations. As the airworthiness certificate was issued by a recognised National Airworthiness Authority, that certification was accepted by the Civil Aviation Safety Authority (CASA) for operating that aircraft type on the Australian aircraft register.
The aircraft was manufactured in the US during 2000 and exported to Australia. It was placed on the Australian aircraft register in December of that year. The aircraft was exported from Australia in April 2002 and placed on the aircraft register of New Zealand. In December 2004, the aircraft was re-imported to Australia and placed on the Australian aircraft register as VH-NIT.
An aircraft Maintenance Release was issued on 22 July 2005 following the last period of scheduled maintenance. The maintenance release recorded 58.7 hours operation since that time. During that period, no defects were recorded on the maintenance release. The aircraft had accumulated approximately 1,650 hours since manufacture.
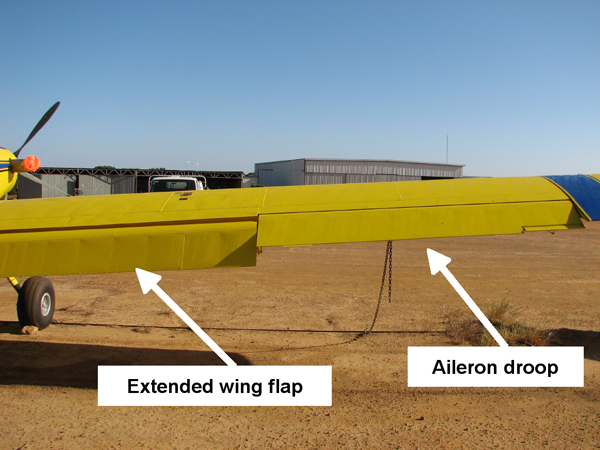
The AT-602 was equipped with an electrically operated Fowler flap system that also incorporated an aileron interconnection, which symmetrically drooped the ailerons as the flaps extended. The motion of the aileron interconnection was non-linear, in that most of the aileron droop occurred during the first 15 degrees of flap extension. Full flap extension for the AT-602 was 30 degrees, with an associated aileron droop of 10 degrees. Figure 3 illustrates the flap extension and aileron droop in an AT-602.
Figure 3: AT-602, showing extended wing flap and aileron droop
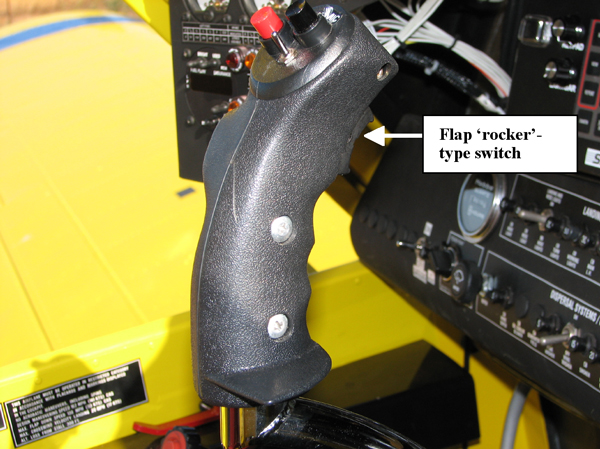
The flaps were actuated by a 'rocker'-type switch4 on the control stick (Figure 4). That switch enabled the pilot to extend the flaps between 0 and 30 degrees. The flaps could also be activated by a control switch mounted adjacent to the engine and propeller control levers on the left side of the cockpit (Figure 5).
Damage to the wing flaps was consistent with their being in an extended position at the time of impact.
Figure 4: Control stick for a similarly-equipped AT-602, showing flap 'rocker' switch
Figure 5: Flap control switch adjacent engine controls
The aircraft was configured for water dropping operations and was equipped with a 630 US Gallon capacity fibreglass hopper (2,385 L). A manually-controlled fire-bomber dump door was fitted to the base of the hopper. Activation of the cockpit drop handle opened the dump door and allowed the hopper contents to drop from the aircraft.
The aircraft manufacturer's FAA-approved Airplane Flight Manual (AFM) recommended using 10 degrees of flap and an airspeed of 109 kts on approach and load release during water dropping operations.
The AFM indicated a wings-level stall speed for the AT-602 at an operating weight of 4,173 kg of 76 kts CAS5 (flaps up) and 61 kts CAS (flaps down). The AFM indicated that the maximum altitude loss from a wings-level stall was 300 ft.
At the time of the accident the aircraft's operating weight was estimated to be approximately 3,500 kg.
Engine
The aircraft was equipped with a Pratt and Whitney Canada PT6A-60AG (PT6A) turboprop engine.
The logbooks and maintenance records indicated that the engine had accumulated approximately 1,650 hours since new.
The engine was shipped to the engine manufacturer for disassembly and examination under the direct supervision of the Canadian Transportation Safety Board. The final report from that examination was not available at the time this interim report was written.
Pilot details
The pilot held a Commercial Pilot (Aeroplane) Licence and a Grade 1 Agricultural Rating, and had previously performed water dropping operations in the operator's reciprocating-engine aircraft. A review of the pilot's logbook indicated approximately 6,736 hours total aeronautical experience, including about 400 hours water dropping operations in the reciprocating-engine PZL "Dromader" D-18 aircraft.
Civil Aviation Regulation 5.22 enables CASA to prescribe the aircraft endorsements that must be held by the holder of a flight crew licence. Civil Aviation Order 40.1.0 requires the holder of a flight crew licence to hold an endorsement to operate certain types of aeroplane and provides for aircraft with similar design features to be grouped into aircraft classes.
The pilot recently completed training for, and was issued with a class endorsement on Ayres Turbo (PT6)-type aircraft. The Ayres Turbo (PT6) aeroplane class endorsement includes the Ayres S2R "Thrush" and Air Tractor AT (400, 401, 402, 502, 602 and 802) aircraft types equipped with a PT6A turbine engine.
Protective equipment/survivability
The pilot was not wearing a protective helmet.
The aircraft was fitted with a metal frame seat with a mesh-fabric seat cover and a four-point restraint harness. Vertical impact forces distorted the base of the seat frame.
Testing and examination of recovered components
The jackscrew for the flap actuator was found along the wreckage trail and had separated from the aircraft during the impact sequence. The jackscrew remained attached to the actuator gearbox, but had fractured in the vicinity of the ACME-threaded nut assembly connecting the jackscrew to the flap actuator arm. The jackscrew and ACME-threaded nut were submitted for technical examination.
Laboratory examination of those components revealed a bending overload failure as a consequence of impact forces. The extension of the jackscrew was consistent with the wing flaps being fully extended at the time of the impact with terrain.
The aircraft was equipped with a cockpit instrument that monitored the quantity of fuel consumed by the aircraft's engine. That instrument contained a non-volatile memory and so was recovered from the aircraft for subsequent examination. That examination revealed a total fuel consumption of 227 L and a quantity of 772 L remaining.
An elevator pushrod had fractured at the eye-end bearing fitting and was recovered from the accident site for analysis. Examination of that component did not reveal any evidence of a pre-existing material anomaly. The fracture surface exhibited characteristics consistent with gross structural overload and component failure during the accident sequence.
A number of cockpit instruments were recovered for laboratory analysis. Examination of the instrument face from the airspeed indicator revealed witness marks from the instrument's indicator needle. Those marks indicated that, at the time the indicator needle contacted the face of the instrument, the needle was indicating between 45 and 55 knots.
Other instruments that were recovered for subsequent laboratory examination included the: engine Ng (gas-generator speed), oil temperature and pressure gauges; and propeller RPM and engine torque gauges. No witness marks were evident on those instruments.
Indicator globes from the aircraft's annunciator panel were recovered and analysed for evidence of any filament stretch that could indicate the illumination of the lights at the time of ground impact. The following indicator globes were examined:
Propeller beta - illuminates when propeller blade angle is in the "beta" range6.
Fuel filter - illuminates when the fuel filter is partially blocked.
Low fuel quantity - illuminates in a low fuel condition.
Air filter - illuminates to indicate restricted airflow to the engine's air inlet.
Chip detector - indicates metal particles in contact with detector terminals and the possibility of other metal particles in the engine lubricating oil. A brittle fracture was observed in that filament.
There was no evidence in any of the examined indicator globes of filament stretch, or illumination of any of the associated indicator lights at the time of the aircraft's impact with the ground.
The aircraft was equipped with an emergency locator transmitter (ELT), which separated from its mounting bracket during the impact sequence. Although the ELT was armed, it did not automatically activate. The ELT activated normally when tested after the accident.
Fuel sample testing
A sample of fuel was recovered from one of the ruptured fuel tanks. Testing of that sample indicated a blend of diesel and aviation turbine fuel. Particulate matter within the fuel sample was consistent with contamination of the fuel with bacterial organisms.
Propeller examination
The engine was equipped with a five-bladed Hartzell Propeller Inc., HC-B5MP-3C constant speed propeller that was fully feathering and reversible in pitch.
The propeller was recovered from the accident site and examined under the direct supervision of investigators from the Australian Transport Safety Bureau (ATSB). When reconstructed as a set, all of the propeller blades showed a progressive and marked increase in axial twist and rearward, out-of-plane bending around the sequence of rotation. That damage indicated a steep angle of impact with terrain (ie low horizontal speed, high vertical speed) and a rapid cessation of rotation.
The pitch change mechanism for the propeller blades was damaged during the accident sequence and each of the blades showed evidence of moving independently during the terrain impact sequence. Witness marks on the hub of the propeller blades indicated blade rotation beyond the assembly limit of -11 degrees.
There was no evidence to indicate that the propeller was operating in the beta or reverse blade angle range at the time of the collision with terrain.
Ongoing investigation
The investigation is continuing, including in the following areas:
assessment of engine operation at the time of the accident, pending the results of the examination/testing performed under the supervision of investigators from Canadian Transportation Safety Board
examination of survivability issues associated with the accident
the assessment of aircraft handling characteristics and operational factors associated with the accident flight, including the aircraft's configuration immediately prior to the loss of control.
The 24-hour clock is used in this report to describe the local time of day, Western Standard Time (WST), as particular events occurred. Western Standard Time was Coordinated Universal Time (UTC) + 8 hours.
Aerial photograph reproduced by permission of the Department of Land Information, Perth, Western Australia, Copyright Licence 33/2006 www.dli.wa.gov.au
The Restricted Category certification was on the basis of airworthiness complying with US Federal Aviation Regulation 23, excluding those sections deemed inappropriate for the special purpose use of agricultural spraying, dusting and seeding and for the special purpose use of forest and wildlife conservation (fire fighting).
That switch was installed subsequent to the manufacture of the aircraft and following the aircraft's initial importation to Australia, in accordance with Engineering Order ADG-AT602-EO2125.
CAS is calibrated airspeed and is the indicated airspeed corrected for instrument and position errors. At those speeds, the AFM indicated that the calibrated airspeed is within about 1 knot of the indicated airspeed.
Beta refers to operation of the propeller blade at fine blade angles, during which the propeller blade angle (and consequently thrust) is directly controlled by movement of the power lever. In this operating range, the propeller does not operate at a constant speed and propeller blade angle is coordinated with fuel flow, according to the power lever position. The beta operating range extends from just below flight idle on the power lever, through ground idle and reverse.
Summary
At about 1425 Western Standard Time on 22 October 2005, an Air Tractor AT-602 aircraft, registered VH-NIT, impacted terrain approximately 100 metres south of the perimeter fence of Ballidu aerodrome, WA. The pilot was carrying out a series of familiarisation flights. He was the sole occupant of the aircraft and was fatally injured.
Witnesses recalled that the aircraft had dropped a quantity of water at low level over the aerodrome. Soon after that drop, the nose of the aircraft pitched steeply towards the ground and the aircraft descended into terrain.
The aircraft impacted terrain in a slightly right wing-low, almost nose-level attitude at a high vertical rate of descent, but with low forward speed.
Examination of the wreckage did not identify any anomaly that could have affected the normal operation of the aircraft during the accident flight. Examination of the engine indicated that it was producing power at the time of terrain impact.
Toxicology testing revealed that the pilot had ingested cannabis. Specialist medical advice was that the results of the toxicology testing would be consistent with the pilot using cannabis sometime during the 24 hours prior to the accident.
The physical and witness evidence was consistent with the pilot losing control of the aircraft at low altitude, most probably as the result of an inadvertent aerodynamic stall. There was insufficient altitude to recover the aircraft to level flight.
The pilot undertook a flight for which he was not qualified, and for which the helicopter was not equipped.
The helicopter was flown at about 30 ft above the ground in dark night conditions.
The pilot became disorientated at a height from which recovery was not possible before the helicopter impacted the ground.
Analysis
The overriding survivor, witness and physical evidence was that the helicopter's engine was operating normally up to and including at the time of ground impact. On that basis, the investigation concluded that the performance of the engine had not contributed to the development of the occurrence.
Application of the requirements of the Aeronautical Information Publication (AIP) to the time of last light at Yalda Downs meant that a pilot in command who did not hold a night Visual Flight Rules (VFR) rating should have planned to arrive at Yalda Downs no later than 1816. In addition, the reported thin layer of cloud in this instance suggested that the planned arrival time should probably have been adjusted to earlier than 1816. The reported time of departure from Border Downs of 1800, and normal time interval for the planned flight to Yalda Downs of 1 hour 15 minutes, meant that the occurrence pilot attempted a flight for which:
he was not qualified
the equipment standard of the helicopter was not adequate.
Each increased the likelihood, and therefore risk that the pilot might become disoriented in the dark night conditions, resulting in a situation from which he was unable to recover.
The content of the approved flight manual (AFM) meant that the pilot ought to have been aware of the risk of his becoming disoriented when operating the helicopter in dark night conditions. The reported operation of the helicopter at about 30 ft above ground level minimised the time available for the pilot to recover from any disorientation before impacting the ground. In addition, it was likely that the climbing right U-turn eroded the already marginal outside references that the pilot may have gained as a result of identifying the lights and road as he passed north abeam Calindary. As indicated to pilots in the Safety Notices in the AFM, the likely result was that the impact with the ground was almost inevitable.
The action of the pilot to request successive property owners along the planned route to illuminate their homesteads' external lighting could have been interpreted to have had the secondary benefit of acting as a replacement for the flight notification requirements for flight through a Designated Remote Area. However, that was not an approved means of providing flight notification, and was based on the assumption that each of those property owners would be at home and respond to the pilot's radio transmissions.
That lack of a formal flight notification, and the apparent omission by the pilot to carry an Emergency Locator Transmitter meant that, had the accident not been observed by the witnesses at Calindary, the subsequent search and rescue effort could have been delayed. Any delay in locating the survivor had the potential to have:
adversely affected the survivor's subsequent recovery from his injuries
significantly complicated the survivor's injuries
diminished the survivor's chances of survival.
Factual Information
At about 1800 Central Standard Time on 6 October 2005, a Robinson Helicopter Company model R22 Beta helicopter (R22), registered VH-HUZ, departed Border Downs, NSW on a private flight to the pilot's property at Yalda Downs, NSW with the pilot and one passenger on board. The helicopter subsequently crashed near a homestead at Calindary Station (Calindary), fatally injuring the pilot and seriously injuring the passenger.
A hearing witness1 at Border Downs who was also a pilot and endorsed to fly the R22, had previously flown the occurrence helicopter. He reported that the helicopter 'sounded completely normal' during the take-off and departure from Border Downs. He indicated that the normal time interval for the flight to Yalda Downs was about 1 hour 15 minutes.
Witnesses at a number of properties along the route flown by the pilot reported that, as the flight progressed, the pilot requested by radio for each of them to illuminate their external homestead lights. The reason given by the pilot for those requests included, earlier in the flight, for the pilot to 'get his bearings' and, as the helicopter approached Calindary, to assist the pilot to identify two sets of power lines that crossed the main west to east road about 1 and 3 kms west of the property respectively. In response to the pilot's request, the property owners at Calindary reported that they parked their vehicle on top of a sand embankment that was about 100 m south of the main road. The vehicle's spotlights, and a third hand-held spotlight, were illuminated in the direction of the helicopter's anticipated approach.
The pilot advised the property owners by radio that he had sighted their spotlights. The property owners reported that they suggested to the pilot that he should land at Calindary and use one of their vehicles to return to Yalda Downs by road. The pilot declined that suggestion and indicated that, after picking up the road from Calindary to Yalda Downs, he would continue with the flight. The property owner estimated that the helicopter was below 30 ft above ground level (AGL) at that time, and described the helicopter's 'powerful white lights' as being visible 'down amongst the trees'. The survivor indicated that the pilot manoeuvred the helicopter in order for the helicopter's landing lights to criss-cross the road.
One of the witnesses at Calindary, with extensive experience flying aeroplanes, stated that there was nothing abnormal about the sound of the helicopter or its engine as it passed the vehicle's position, or immediately prior to the ground impact.
The survivor stated that, shortly after passing Calindary, the road appeared to merge with the surrounding bush and the pilot turned the helicopter to visually reacquire the road. The property owners at Calindary reported that the helicopter commenced a climbing right U-turn, before returning in a westerly direction and descending at an estimated angle to the horizon of 20 to 30 degrees. The survivor indicated that, during the turn and until the impact with the ground:
he heard no abnormal noises from the helicopter
he did not observe the illumination of any warning lights in the cockpit
there was no apparent apprehension or degree of panic displayed by the pilot.
At about 1921, the helicopter impacted a sand hill a number of times and was destroyed by the impact forces and post-impact fire.
The pilot held a private pilot (helicopter) licence, was endorsed to fly the R22 and was reported to have about 9,000 hours flying experience. The pilot did not hold a night Visual Flight Rules (VFR) rating. The requirements of Civil Aviation Regulation (CAR) 174C(1) included that the pilot was required to have held that rating in order to conduct a flight at night under the VFR.
The pilot last undertook a medical examination in order to renew his Class 2 Medical Certificate in January 2002. There was no evidence that:
the pilot finalised the administrative requirements for the renewal of that certificate
the pilot held a valid Class 2 Medical Certificate at the time of the occurrence
the Civil Aviation Safety Authority (CASA) had given the pilot permission to continue flying without a current medical certificate.
CAR 5.04(1) required that:
Without the permission of CASA, the holder of a flight crew license must not perform a duty authorised by the license if the person does not hold a current medical certificate that is appropriate to the license.
That meant that on the day of the accident, the pilot should not have been performing the duties that were authorised by his license.
The helicopter was first registered in Australia on 3 May 2005 and was reported to have flown about 130 to 140 hours since its delivery flight to Yalda Downs on 1 August 2005. An examination of the helicopter's maintenance records found that the helicopter was certified for day VFR flight and equipped and maintained in accordance with existing regulations and approved procedures. The helicopter was not equipped for flight under the night VFR, nor was it installed with an Emergency Locator Transmitter (ELT)2.
The helicopter's weight and centre of gravity were estimated to have been within the prescribed limits at the time of the occurrence.
It was reported that the pilot would have refuelled the helicopter to capacity from the aviation gasoline fuel source at Yalda Downs prior to departing for Border Downs earlier that day. A witness at Border Downs indicated that the pilot did not refuel the helicopter at that location. It was estimated that at the time of the accident, about 24 L of fuel remained on board the helicopter. That would have been sufficient for the remainder of the planned flight to Yalda Downs.
A Bureau of Meteorology (BoM) examination of the forecast weather and meteorological observations from the Tibooburra Automatic Weather Station3 indicated that there was no significant weather, no low-level cloud, and no reduction in visibility in the region of Tibooburra at the time of the occurrence. The investigation determined that the times of sunset, and of the end of civil twilight for the relevant locations along the planned west to east route included:
Location
Sunset
End of Civil Twilight
Border Downs
1810
1834
Calindary
1804
1828
Yalda Downs
1802
1826
The pilot was reported to have accessed a private weather source via the internet prior to the departure from Border Downs. The available information from that source included the observed surface wind for a number of locations in the general vicinity of the flight and the weather forecast and times of sunrise and sunset for Broken Hill. Sunset for Broken Hill on the day of the occurrence was published by that source as 1809.
A witness at Border Downs reported the weather as being 'good', with a wind of about 10 to 15 kts from the west-south-west, and a cloud base of above 1,500 ft AGL. The weather at the accident site at the time of the accident was reported by witnesses to include: a light north-westerly wind; a 50% overcast layer of thin cloud, with a high base; good visibility; and no horizon. Witnesses reported that it was 'pretty dark, as in black'.
Examination of the NSW Police and other photographic evidence indicated a low angle of impact with the sand hill at a relatively high speed, which compromised the integrity of the helicopter's cockpit area. That was consistent with the reported 85 m wreckage trail and witness reports of the helicopter's approach towards the ground.
The damage to the helicopter's landing skids and engine mount frame was consistent with a slightly nose-down, right angle of bank at ground impact. One of the main rotor blades separated from the main rotor head at its hinge bolt attachment point, consistent with static overload as a result of the blade's impact with the ground. The damage to that main rotor blade confirmed that the main rotor was rotating at that time. The tail boom appeared to have failed in overload and separated from the main wreckage following the initial impact with the ground. The relatively minor torsional shear indications evident on the tail rotor driveshaft, and the nature of the damage to the tail rotor blades, indicated that the tail rotor had ceased rotating prior to its impact with the ground.
Based on the available information, there was no evidence that material failure or component malfunction had contributed to the development of the occurrence.
At the time of writing this report, the pilot's post mortem report was not available to the investigation team.
There was no report by the witnesses to the occurrence of an in-flight fire. The source of the post-impact fire was from fuel that had spilled from the ruptured helicopter fuel tanks. The ignition source of the fire could not be confirmed, but was most likely from the hot engine exhaust.
CAR 252A specified that a pilot in command of an aircraft that was not an exempted aircraft4 may only begin a flight if the aircraft either:
was fitted with an approved and functioning ELT, or
carried an approved and readily accessible portable ELT that was in working order.
The helicopter was not an exempted aircraft and it was reported that the pilot normally carried a portable ELT during flight. The survivor indicated that he had not observed a portable ELT in the helicopter prior to or during the occurrence flight, and the item was not identified by the NSW Police amongst the wreckage of the helicopter, or at the site of the accident. AusSAR5 reported that an emergency signal was not identified at or about the time of the accident.
The flight was within the central Australian mainland component of the Designated Remote Area that was promulgated in Appendix III to Civil Aviation Order 20.11. That required the carriage of sufficient survival equipment for sustaining life appropriate to the area being overflown, and either the submission of a SARTIME6 flight notification to Air Traffic Services (ATS) or for a pilot in command to leave a flight note with a responsible person. It was reported that the pilot and passenger carried sufficient clothing in case the decision was made to remain overnight at Border Downs. ATS records indicated that a SARTIME was not submitted to that agency, and a flight note was not left at either Border Downs or Yalda Downs for the occurrence flight. Witnesses at Yalda Downs indicated that the first confirmation that the pilot intended to return that night was via a radio call from the pilot at about 1900 to 1915, indicating that '[he] would be late [arriving at Yalda Downs]'.
The Aeronautical Information Publication (AIP) requires that:
Unless the pilot in command holds a Command Instrument Rating or night VFR (NGT VFR) rating and the aircraft is appropriately equipped for flight at night, a VFR flight must not depart from an aerodrome:
before first light or after last light; and
unless the ETA [Estimated Time of Arrival] is at least 10 minutes before last light after allowing for any required holding.
Last light was interpreted by the AIP to equate to the end of civil twilight 7. In addition, the AIP alerted pilots to the potential for the presence of cloud cover to the west of an aerodrome, and a number of other variables to adversely affect a flight arriving at its destination near the end of daylight. Sunset was highlighted as 'having no relevance when calculating daylight operating times for the VFR pilot.'
The AIP also placed altitude restrictions on the operation of an aircraft under the night VFR. That included that a pilot should not operate an aircraft under those rules at a height lower than the published lowest safe altitude (LSALT) for the route, or a height that was calculated in accordance with the requirements of the AIP, except under certain prescribed circumstances. Depending on the calculation methodology applied by a pilot, the LSALT for the route Border Downs to Yalda Downs was at least 2,020 ft above mean sea level (equivalent to about 1,500 ft AGL at Calindary).
The Approved Flight Manual for the helicopter included a number of Safety Notices that were relevant to the operation of the helicopter at night. Those notices included that:
Flying a helicopter in obscured visibility due to fog, snow, low ceiling, or even dark night can be fatal.
Loss of the pilot's outside visual references, even for a moment, can result in disorientation, wrong control inputs, and an uncontrolled crash.
…[the pilot] loses control of the helicopter when he attempts to turn to regain visibility but is unable to complete the turn without visual references.
[pilots should] be sure you NEVER fly at night unless you have clear weather with unlimited or very high ceilings and plenty of celestial or ground lights for reference.
A witness who heard, but did not observe the takeoff.
Crash-activated radio beacon that transmits an emergency signal that includes the position of a crashed aircraft.
The closest station to the site of the accident, being about 49 NM north-north-west of that location.
Exempted aircraft means high capacity regular public transport or charter aircraft, single seat or turbo-jet powered aircraft, or balloons, airships or gliders.
Australian Search and Rescue - in general terms, AusSAR coordinates the response to aviation SAR incidents across Australia.
The time nominated by a pilot for the initiation of Search and Rescue action if a report has not been received by the nominated unit.
Period at sunset when the sun's centre is between 0°50' and 6° below the horizon.
Summary
The helicopter with the pilot and one passenger onboard, was returning to Yalda Downs Station from Border Downs Station after last light. As it overflew Calindary Station homestead, which is approximately 46 km west of the intended destination, the helicopter was observed to gain height and conduct a right turn. The helicopter then descended and impacted the ground about 500 m from the homestead. The helicopter was destroyed by impact forces and the post-impact fire. The pilot was fatally injured and the passenger sustained critical injuries.
The accident is consistent with the pilot becoming incapacitated, the aircraft departing controlled flight and subsequently impacting terrain. The possible nature of, or reasons for, any incapacitation could not be determined by the investigation.
Analysis
Examination of the aircraft wreckage and accident site indicated that the aircraft impacted terrain at a steep angle and at high speed. In addition, the investigation concluded that the engine was producing power at the time of the accident.
The recorded Air Traffic Services (ATS) radar data indicated that the autopilot was engaged prior to the aircraft entering a steep left descending turn. The abruptness of the turn and the high rate of descent indicated that the autopilot was no longer controlling the aircraft. The autopilot could be disconnected by either pressing the electric trim switch or manually overriding the controls. The pilot was familiar with the route being flown and would be unlikely to have deliberately diverted from the intended flightpath. There was no significant weather in the area at the time of the accident, so the pilot would not have had to alter his heading to maintain visual flight.
If the pilot had deliberately disconnected the autopilot and manoeuvred the aircraft, the resultant flight path would probably not have been as abrupt as the recorded ATS radar data indicated. Therefore, the autopilot was probably disconnected by the pilot making an unintentional control input.
The investigation was unable to determine the reason for the sudden control input, but the circumstances are consistent with pilot incapacitation. The pilot was the only occupant of the aircraft who could manipulate the controls with the autopilot disconnected. The passenger, due to the usual seating arrangements, would have been unable to render assistance to the pilot, or assumed control of the aircraft, prior to the accident, if the pilot had become incapacitated.
Factual Information
History of the flight
At about 0855 Eastern Standard Time1 on 24 September 2005, a Raytheon Aircraft Company Beechcraft A-36 Bonanza, registered VH-BKM, took off from Murwillumbah, NSW, on a private flight to Coonabarabran, NSW, with one passenger, who was the pilot's wife, under the visual flight rules. The pilot had not submitted a flight plan or nominated a SARTIME2 and there was no requirement to do so. The pilot and passenger regularly flew return flights from Coonabarabran to Murwillumbah in this aircraft.
The aircraft was subsequently reported to be missing on 28 September 2005, and a search was commenced. The wreckage of the aircraft was located on 29 September 2005. The aircraft had impacted a heavily timbered hill on a private property 'Millera', located approximately 35 km east of Tenterfield. The aircraft had been destroyed by impact forces and a post-impact fire (Figure 1), and both occupants were fatally injured.
Figure 1: View of impact crater looking north-west
Operational Information
The pilot was 71 years old and held both commercial and private pilot licences for aeroplanes and had a valid Class 2 medical certificate. He held a pilot's licence for over 50 years and had previously owned and operated an aerial agricultural business. He had a total aeronautical experience of approximately 13,000 flying hours.
The aircraft had been owned and operated by the pilot for the previous 14 years. Maintenance records indicated that the aircraft had a valid maintenance release which was issued on 27 January 2005 and was valid for 12 months. The aircraft maintenance release was unable to be located in the wreckage, however the estimated total time in service of the aircraft at the time of the accident was 3,231 hours. The engine had been rebuilt and fitted to the aircraft in April 1992.
The aircraft was fitted with a two-axis autopilot which included separate roll and pitch engagement, altitude hold and automatic and manual electronic pitch-trim. The autopilot could be disconnected by pressing down on an electric pitch-trim switch on the control wheel, or by manually overriding the controls. The aircraft was fitted with a single control wheel.
Prior to the flight to Murwillumbah the aircraft was refuelled at Coonabarabran, from a fuel bowser owned by the pilot. Witnesses reported that the aircraft had been refuelled to its maximum capacity. Fuel records for the fuel supplied to the bowser indicated that the fuel sample in the supply truck was clear and free of sediment. The local aero club had been supplied with 400 L of fuel from the pilot's bowser and had not reported any problems with the fuel.
Performance calculations were used to estimate the fuel burn from Coonabarabran to Murwillumbah and from Murwillumbah to the accident site. These calculations indicated that approximately 140 L of fuel would have been on-board the aircraft at the time of the accident. Discolouration of tree foliage at the accident site and the extent of the post-impact fire confirmed that there was fuel in the aircraft when the accident occurred. Weight and balance calculations showed that the aircraft was within centre of gravity limits for the final flight.
Information provided by the Bureau of Meteorology indicated that a low-pressure trough was present to the west of Tenterfield on the morning of the accident. The weather forecast and actual observations indicated that the flight was conducted under visual meteorological conditions. Witnesses reported clear weather in the vicinity of the accident site.
The pilot had not submitted a flight plan for the flight or contacted air traffic control for an area QNH3 and was not required to do so. The recorded Air Traffic Services (ATS) radar data indicated that the aircraft was operating on a transponder code of 12004.
A review of recorded radar data indicated that the aircraft had been maintaining a stable heading and altitude for most of the flight, which was consistent with the autopilot having been engaged.
The aircraft had then descended from a cruising altitude of about 6,300 ft above mean sea level (AMSL) to a final recorded altitude of about 3,800 ft AMSL at a rate of approximately 5,000 ft/ min. The accident occurred at an approximate elevation of 1,000 ft AMSL.
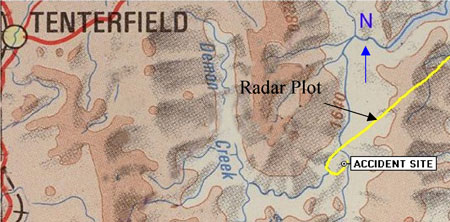
The recorded radar data of the aircraft's flight path was superimposed on a topographical chart that indicated that the aircraft had made a sudden left turn over the area of the accident site (Figure 2).
Figure 2: Radar plot of final segment of flight
There were no recorded radio transmissions from the aircraft prior to departure from Murwillumbah, or during the flight. The aircraft was fitted with a fixed emergency locator transmitter; however, it was destroyed at impact and was not capable of transmitting a distress signal.
Wreckage and impact information
The aircraft wreckage was fragmented and damage to the aircraft structure was consistent with a high-speed impact. There was no evidence of an in-flight breakup, birdstrike or in-flight fire prior to the accident and a technical examination of the engine and propeller indicated that they were producing power at the time of the accident.
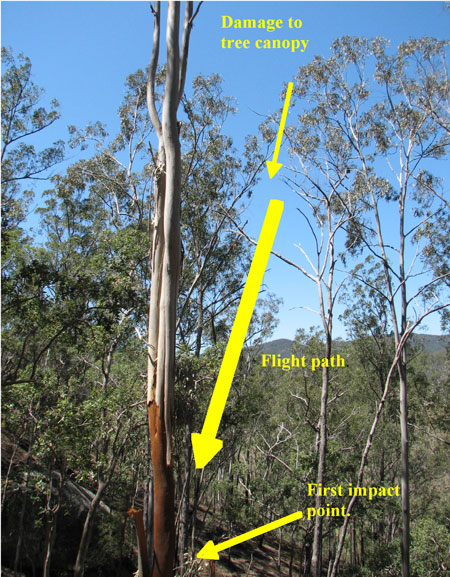
Ground contact marks indicated that the aircraft impacted the ground in a left wing-low, nose-down attitude. Damage to the tree canopy in the vicinity of the impact crater indicated an impact angle of 72 degrees to the horizontal (Figure 3). The aircraft's direction of flight at the time of the accident was estimated to be 290 degrees Magnetic.
Figure 3: Tree canopy damage
Post-mortem medical examination was unable to determine if the pilot had experienced any incapacitation prior to the accident. The pilot's medical records indicated that he was taking regular medication to control blood pressure and that he recently had undergone a minor surgical procedure to remove skin cancers but there was no evidence that either had a bearing on the accident.
Witnesses reported that the passenger normally travelled in the second row of seats, which faced rearwards. The passenger would occupy the seat diagonally across from the pilot (Figure 4) and only communicate with the pilot occasionally during a flight. There was no evidence of the passenger having any aeronautical experience.
Figure 4: Seating configuration of aircraft
The 24-hour clock is used in this report to describe the local time of day, Eastern Standard Time (EST), as particular events occurred. Eastern Standard Time was Coordinated Universal Time (UTC) + 10 hours.
The time nominated by a pilot for the initiation of search and rescue action if a report has not been received by the nominated time.
QNH is the altimeter subscale barometric pressure setting to provide altimeter indication of altitude relative to mean sea level. Area QNH is representative of the QNH of any location within a particular area.
A transponder is a receiver/transmitter which will generate a reply signal upon proper interrogation of an air traffic control radar signal.
Summary
On the morning of 24 September 2005, a Raytheon Aircraft Company Beechcraft A-36 Bonanza, registered VH-BKM, was being flown by the owner pilot on a private flight from Murwillumbah, NSW, to Coonabarabran, NSW, with one passenger. The pilot had not submitted a flight plan or nominated a SARTIME and there was no requirement to do so.
The aircraft was reported to be missing on 28 September 2005, and a search was then commenced. The wreckage of the aircraft was located on 29 September 2005. The aircraft had impacted a heavily timbered hill on a private property 'Millera', located approximately 35 km east of Tenterfield. The aircraft had been destroyed by impact forces and a post-impact fire and both occupants were fatally injured. Witnesses reported clear weather in the vicinity of the accident site.
The recorded radar data indicated that the aircraft was maintaining a stable heading and altitude which was consistent with the autopilot having been engaged. The aircraft then descended from a cruising altitude of 6,500 ft above mean sea level (AMSL) to a final recorded altitude of 3,800 ft AMSL, at a rate of approximately 5000 ft/min.
The pilot was 71 years old and held both commercial and private pilot licenses for aeroplanes with a valid Class 2 medical. The maintenance records indicated that the aircraft had a valid maintenance release which was issued on 27 January 2005.
Weight and balance calculations showed that the aircraft was within centre of gravity limits for the final flight. Discolouration of tree foliage at the accident site and the extent of the post-impact fire indicated that fuel was present when the accident occurred.
The accident is consistent with the pilot becoming incapacitated, the aircraft departing controlled flight and subsequently impacting terrain. The possible reasons for any incapacitation could not be determined.
The pilot performed a manoeuvre that resulted in a loss of control at a height and speed that was insufficient to permit recovery before the aircraft hit the ground.
Analysis
The pilot was reported to have conducted a similar low-level manoeuvre to that which preceded the accident on several previous occasions. On that basis, the investigation team considered that it was unlikely that the passenger was at the controls of the aircraft at the time of the accident. The manoeuvre left little or no margin for error and required sound judgement and skill. Although the pilot may have possessed those skills, no evidence was found of his ever having undertaken the appropriate check to assess those skills and obtain approval to conduct low-level aerobatic manoeuvres.
Repetition of the manoeuvre over a period of time may have led to the pilot gaining a false sense of security and may have led to the pilot becoming complacent about the inherent dangers involved with such manoeuvres. The manoeuvre performed by the pilot earlier that day at another location was commenced from a 'high-speed' flypast. The associated energy would have allowed the aircraft to convert speed to height and climb higher and attain a greater altitude for recovery than the manoeuvre performed during the accident flight. That manoeuvre was commenced from a take-off roll that did not use the full runway length available. When combined with a tailwind component, it was unlikely that the aircraft attained adequate airspeed to safely complete the intended manoeuvre by the end of the strip. It was also possible that the pilot was unaware of the windshear or had not considered its affect on the aircraft's climb performance.
Although the aircraft appeared to have stopped spinning to the right just before impact, the pilot had insufficient height to avoid a collision with the ground. Had the stall warning been operating, it could have provided the pilot with an earlier indication of the stall condition and thus enabled him to initiate a recovery earlier in the development of the manoeuvre.
The affect of the pilot's medical condition on his judgement or decision-making could not be determined. However, some aspects of the pilot's behaviour were not consistent with compliance with rules and regulations or good airmanship. These included conducting low-level aerobatics without approval, ignoring concerns expressed by peers, operating with an unserviceable stall warning indicator and ignoring weight and balance limitations. Furthermore, the pilot flew the aircraft knowing that he was suffering from a medical condition that was being reviewed by the Civil Aviation Safety Authority (CASA) and having been advised by CASA that he was not to fly until the results of the review were known. Disregard for the rules governing the conduct of flight and the operation of the aircraft removed safety defences that were established to prevent this type of accident.
On 15 May 2005 at 1535 Central Standard Time, an American Champion Corporation Citabria 7GCAA aircraft, registered VH-TUF (TUF), took off on a local flight from a private airstrip at Stonefield, SA. On board were the pilot and a passenger, who was also a licensed pilot. Dual controls were installed in the aircraft. The aircraft was observed by witnesses at the airfield to pull up into a steep climb after becoming airborne, before apparently stalling and impacting the ground. Both occupants were fatally injured. The aircraft was destroyed by impact forces and a post-impact fire (see Figure 1).
Figure 1: View of the wreckage looking west
The pilot had been at the Stonefield airstrip during the weekend with other pilots and aviation enthusiasts. On the morning of the accident, the pilot had conducted a short flight in TUF, which included a flypast at a nearby airstrip that was witnessed by two experienced commercial pilots. They described observing the aircraft flying at 'high speed', approximately 20 ft above ground level (AGL) over a taxiway, before pulling up into a vertical climb. The pilot then performed a stall turn and the aircraft was observed to enter a spin or spiral before recovering at a height of about 200 ft and continuing on its original heading.
After returning to Stonefield airstrip, the pilot was required to transport a passenger to Parafield Airport, SA. While at Parafield, the pilot arranged for the aircraft to be refuelled with 62 L of AVGAS. The refueller reported to investigators that that quantity of fuel filled the tanks2. After returning to Stonefield airstrip again, the accident pilot was reported to have undertaken a flight with another pilot in a different aircraft, during which the accident pilot had demonstrated a number of aerobatic manoeuvres to the other pilot. The accident pilot then undertook a further flight in TUF with the same passenger as the previous flight, and demonstrated a number aerobatic manoeuvres again.
After discussion with other people at Stonefield, the accident pilot decided to conduct a further local flight, and the same passenger from the previous two flights was invited as a passenger again. Witnesses observed the passenger in the rear seat and the pilot in the front seat. After engine start-up, the pilot performed a turn on the ground of more than 360 degrees before taxying on the north-east strip without performing an engine run-up. The aircraft engine was heard increasing in RPM prior to the aircraft commencing a downwind take-off into the north-east. After becoming airborne, the aircraft was observed to remain at approximately 10 ft AGL until it reached a fence line to an adjoining property at the end of the strip. At about this point, the aircraft was observed to enter a near vertical climb. At an estimated height of 500 ft AGL, the aircraft appeared to aerodynamically stall in the vertical attitude, before entering a right hand spin. The aircraft completed one and a half turns in the spin, before it appeared to almost recover just before impacting the ground.
Personnel information
The pilot was 63 years old and held both commercial and private pilot licences for aeroplanes. He had successfully completed an Aeroplane Flight Review in August 2004. The pilot had a total of 2,848 hours experience, 2,746 hours of which was as pilot in command in single-engine fixed-wing aircraft. The pilot was an experienced aerobatic pilot in New Zealand. He did not hold a low-level aerobatic approval from the Australian Civil Aviation Safety Authority (CASA).
The pilot had undergone medical treatment for a terminal illness and, at the time of renewal of his Class 1 medical certificate, informed his Designated Aviation Medical Examiner (DAME) of this illness. At the time of that examination, the pilot's Class 1 medical certificate had expired. However, his Class 2 medical certificate was not due to expire until December 2005.
The DAME did not reissue either the Class 1 or Class 2 medical certificate and referred the matter to CASA. An assessment by CASA medical staff confirmed that the pilot's medical condition precluded him from flying as pilot in command. The pilot appealed to CASA regarding that adverse assessment and was advised verbally and in writing by CASA of his obligations under Civil Aviation Safety Regulations 67.2653 and 67.2704 until the outcome of the review of that appeal was known.
Although a review of the assessment was commenced, CASA did not cancel or suspend his Class 2 medical certificate while that review process was being completed. CASA advised the Australian Transport Safety Bureau (ATSB) that it was normal procedure to only cancel or suspend a certificate after all specialist medical information was received and all options to mitigate safety risks to air navigation were considered. During the period his medical condition was under review, the pilot logged more than 20 hours in aircraft as pilot in command.
In addition to the flights made on the day of the accident, the pilot had flown to Stonefield from Parafield during the previous day. Prior to this, the pilot had worked during the days at his own business conducting non-aviation activities and was reported to have been well rested.
Several pilots reported that the pilot had regularly performed a similar low level aerobatic manoeuvre to that which preceded the accident. A chief flying instructor who had known the pilot, reported that he had observed the pilot perform this type of low-level aerobatic manoeuvre several times in the past. During the investigation, he advised investigators that he was concerned about the safety of the manoeuvre and had warned the pilot about the dangers of performing it.
Aircraft information
A 100-hourly maintenance check was completed on the aircraft 3 days prior to the accident, at which time the aircraft had recorded 2,451.14 total time in service (TTIS). The maintenance release was unable to be located and was probably burnt in the wreckage. As a result, the time flown subsequent to that check could not be accurately determined.
Weight and balance calculations made using estimated fuel and occupant weights, determined that the aircraft may have been as much as 20 kg over the maximum all up weight, and that the centre of gravity (CoG) was rearward of the aerobatic limit, but within the normal operating range.
Meteorological information
There was no terminal aerodrome forecast for the private airstrip. However, the area forecast indicated that the wind at 2,000 ft was 150 degrees true at 15 kts. Other pilots who flew into Stonefield that day reported that the ceiling and visibility was acceptable for visual flight and that the wind was a southerly at 8 to 10 kts at ground level. However, at 500 ft AGL, the wind was reported to be a southerly at approximately 30 kts. The temperature was reported to be 19 to 20 degrees Celsius.
Wreckage information
The aircraft struck the ground in a 40-degrees nose-down attitude with the left wing low, and came to rest facing the southwest, 22 m from its initial impact point. Damage to the propeller indicated the propeller was rotating at impact. The aircraft was destroyed by severe impact forces and a post-impact, fuel-fed fire.
Two persons attempted, unsuccessfully, to extinguish the fire with hand-held fire extinguishers. The fire was subsequently contained by local fire fighters. The accident was not survivable.
The engine was removed and examined at an approved engine overhaul facility under supervision of the ATSB. No anomaly or defect was found in the engine and it was determined that the engine was capable of normal operation prior to the accident.
The stall warning system on the aircraft was examined. The wing-mounted air vane switch that actuated a warning horn/light in the cockpit was found to have one of the electrical leads disconnected, rendering the stall warning system inoperative. The lead had been safely secured and appeared to have been deliberately disconnected. Subsequent testing of the stall warning system found that when wired correctly, it was capable of functioning normally. The investigation was unable to determine when, or by whom, the stall warning system was deactivated. The stall warning device gives an indication to the pilot of an impending aerodynamic stall condition.
There was no evidence of any other mechanical defect that could have contributed to the accident.
Medical and pathological
Results of post-mortem and toxicologic testing of the pilot did not reveal any evidence of any sudden incapacitating condition that could have contributed to the accident.
Fuel
A small sample of fuel was taken from the aircraft wreckage, however, this fuel was contaminated by fire fighting agents, and could not be used as a reliable pre-fire indicator of fuel quality. The aircraft had been refuelled at Parafield earlier that day, but the batch from the tanker was unable to be tested, as it had been mixed with a new batch of fuel. The investigation determined that fuel from the batch from which TUF had been refuelled had also been used to refuel more than 12 other aircraft. There were no reports of fuel contamination or fuel related problems from those operators.
Aircraft manufacturer's information
The aircraft manufacturer was asked to comment on aspects of the aircraft's performance and handling. Their test pilot reported that:
flight above gross weight would decrease take-off performance and increase stall speed
In respect to the exceedance of the rearward aerobatic CoG datum, the test pilot reported that:
the CG [centre of gravity] exceeded the aft aerobatic limit… but was within the normal category of 18.2. I do not feel this contributed to the pilot's ability to control or recover the aircraft.
The manufacturer reported that:
the decision to conduct a low altitude aerobatic maneuvre [sic] with insufficient airspeed resulted in the subsequent stall/spin.
Only those investigation areas identified by the headings and subheadings were considered to be relevant to the circumstances of the occurrence.
Full tanks 147 L.
Essentially, this regulation requires a pilot in the accident pilot's circumstances to be cleared by a DAME before exercising the privileges of a licence.
This regulation places the onus on a pilot not to exercise the privileges of a licence if the pilot is aware that he or she has a medically significant condition.
Summary
On 15 May 2005, at 1535 Central Standard Time, an American Champion Corporation Citabria 7GCAA aircraft registered VH-TUF, with a pilot and passenger, took off from Stonefield private airstrip in South Australia for a local private flight. Shortly after becoming airborne, the aircraft crashed. Both occupants were fatally injured. The aircraft was destroyed by impact forces and a post impact fire.
After start up, the pilot performed a turn on the ground of more than 360 degrees before taxying on the north-east strip. The aircraft engine was heard powering up on the strip into the north-east and shortly after became airborne. After becoming airborne, the aircraft was observed to remain approximately 10 feet above the strip, and remained at that height until the end of the strip. At about this point, the aircraft was observed to enter a near vertical climb. At an estimated height of 500 feet above ground level, the aircraft stalled in the vertical position, before entering a right hand spin. The aircraft completed one and a half turns in the spin before it appeared to recover. At the point where the aircraft appeared to have recovered from the spin, it impacted the ground.
The investigation determined that the aircraft on the accident flight was 20kg over maximum all up weight (MAUW). The increased weight would have the effect of increasing the stall speed of the aircraft, thereby reducing its performance. It was also determined that the pilot took off north-east with a quartering down wind component, and attempted a vertical climb with a wind gradient of approximately 30kt and at 500 feet from the south, above ground level. This wind gradient would have significant impact on the aerodynamic performance of the aircraft, and the pilot may not have achieved the height he intended before it stalled.
The Australian Transport Safety Bureau did not conduct an on-scene investigation of this occurrence.
REPORTED INFORMATION
At about 1610 central standard time on 18 April 2005 the pilot of a Cessna Aircraft Company Cutlass, registration VH-LCZ commenced the takeoff at Warooka Aeroplane Landing Area (ALA), SA. The private flight, with one pilot and two passengers, was the last of a number of planned flights that day from Warooka to Wedge Island ALA. The pilot estimated that his aircraft was about 10 kg (22 lbs) below the maximum allowable take-off weight for the aircraft. The aircrafts centre of gravity (c.g.) was not reported.
The pilot elected to take off towards the south, which resulted in a right crosswind that he described as `steady, but with a bit of swing to it. The pilot indicated that the take-off run to the south was `normal, and that he lifted the aircraft off from the runway at 60 kts indicated airspeed (KIAS) with the intent of establishing the climb at the aircraft best angle of climb speed of 67 KIAS. That was in order to avoid a house and powerlines at the southern end of the airstrip.
As the aircraft became airborne the pilot retracted the landing gear, which swings downward approximately 2 ft as it starts retracting. The pilot reported that almost immediately, the aircrafts stall warning unit activated. In response, he `lowered the nose of the aircraft towards the cruise attitude. The aircraft lost height and impacted the ground and subsequently slid to a stop on its belly. The occupants were not injured. The aircraft was substantially damaged.
The aircrafts Information Manual (manual) stated that the wing flaps should be set at zero degrees for normal takeoffs, and that the landing gear should not be retracted unless there was insufficient remaining runway to allow a wheels-down forced landing. In addition, the manual included that the aircrafts stall warning unit provides a continuous warning tone to the pilot at 5 to 10 kts above the aircrafts stall speed. With zero flap, and at zero angle of bank and maximum take-off weight, that speed was 46 KIAS at the most rearward c.g. and 50 KIAS at the most forward c.g.
ATSB COMMENT
Given the reported take-off weight and nature of the load, it was likely that the aircrafts centre of gravity approached the rearward limit. In that case, a takeoff conducted in the normal take-off configuration would have meant that the stall warning unit would most likely have activated in between 51 to 56 kts indicated airspeed (KIAS).
The safety margin between the lift-off speed and the stall speed may have been eroded by the effect of any `swing in the wind during the retraction of the landing gear, and the potential for any increase in drag associated with the retraction of that gear. The relative proximity of the aircraft to the ground when the stall warning unit activated minimised the possibility for the pilot to recover the aircraft before it impacted the ground.
The Australian Transport Safety Bureau did not conduct an on-scene investigation of this occurrence. The report presented below was prepared principally from information supplied to the Bureau.
REPORTED INFORMATION
On 8 March 2005, the Gippsland Aeronautics Pty Ltd GA-8 aircraft, registered VH-FGN, was carrying emergency relief supplies from Muelaboh to Patek in Aceh Province, Indonesia, as part of the Tsunami relief effort. The aircraft occupants comprised the pilot and one passenger.
A level, 700 m long and 7 m wide portion of a bitumen-sealed roadway formed the designated landing area for the operator's relief flights into Patek. The landing area was not marked with runway markings.
The operator reported that the pilot misidentified the commencement of the landing area, and that the aircraft touched down about 400 m short of the commencement of that area.
There was debris adjacent to the part of the road where the aircraft landed.
During the landing flare, the aircraft's left wingtip struck some of that debris, and a 1 m portion of the left wingtip was dislodged. The impact yawed the aircraft to the left, and the right wingtip then contacted the ground.
The landing gear collapsed, and the aircraft came to rest to the left of the sealed roadway, about 100 m from where the left wingtip initially struck the debris.
The two occupants were uninjured and were able to exit the aircraft unaided.
The pilot held an Australian Commercial Pilot (Aeroplane) Licence and was endorsed to fly the GA-8 aircraft. The operator provided induction training for the pilot at the commencement of his duties in Aceh Province. The training included one landing at Patek. The accident occurred four days after the pilot commenced duties in Aceh Province. During those four days, the pilot had performed two take-offs from Patek and had landed there twice before the accident flight.
There was no evidence that environmental, mechanical, operational or other factors contributed to the circumstances of the accident.
The operator reported that as a result of the occurrence, it will conduct a risk analysis before the commencement of any new operations such as those conducted at Aceh Province. The operator also reported that it would include a special training module in its Operations Manual for pilots assigned to operations in Aceh, and that procedures for aircraft operating on roads would also be included in its Operations Manual.
Summary
On 8 March 2005, the Gippsland Aeronautics Pty Ltd GA-8 aircraft, registered VH-FGN, was carrying emergency relief supplies from Muelaboh to Patek in Aceh Province, Indonesia, as part of the Tsunami relief effort. The aircraft occupants comprised the pilot and one passenger.
At about 1326 Eastern Daylight-saving Time on 7 March 2005, the pilot of a Cessna Aircraft Company 310R, registered VH-FIN, commenced take-off from runway 30 right at Tamworth on a ferry flight to Scone, NSW. Witnesses reported that the pilot initially maintained the runway heading, as cleared by air traffic control (ATC). When the aircraft was between 800 and 1,000 ft above ground level (AGL) and while making a shallow banked turn to the left, the pilot broadcast to ATC that he was experiencing 'control difficulties'. Upon or shortly after reaching an early downwind position the aircraft was observed to enter a steep nose-down descent. While there were some inconsistencies in the available witness reports, it appeared that the aircraft may have rolled about its longitudinal axis at some stage on the final descent. The aircraft impacted the ground in a cleared paddock about 4 NM west-south-west of Tamworth airport, fatally injuring the sole occupant pilot of the aircraft. The aircraft was destroyed by the impact forces and post-impact fire.
The pilot was appropriately licensed and rated, held a valid class 1 medical certificate and was reported as being fit to fly. The results of postmortem examination and toxicology screening found no evidence of any physiological factor that may have impaired the pilot's performance during the occurrence flight.
The aircraft was maintained under a Civil Aviation Safety Authority (CASA) approved maintenance system. The aircraft had been subject to scheduled maintenance by a CASA approved maintenance facility immediately prior to the accident. The aircraft had a current maintenance release and there were no recorded defects at the time of the accident.
The investigation calculated the aircraft's weight and balance based on fuel load records and estimated fuel burn rates for previous operations, including engine runs relating to the maintenance activity completed immediately prior to the occurrence flight. The investigation estimated that at the time of the occurrence, the aircraft was operating below the maximum permitted take-off weight and within the stipulated centre of gravity limits.
The Automatic Terminal Information Service (ATIS) current at the time of the occurrence, reported that the wind was variable at eight knots with occasional crosswind of eight knots, CAVOK1, temperature 27°C and a calculated mean sea level pressure datum (QNH) of 1019 hPa.
The wreckage trail extended over a distance of about 232 m. Ground impact marks and other physical evidence indicated that the aircraft struck the ground in an upright slightly right wing low, 35 to 50 degrees nose-down attitude, and that both engines were developing significant power at the time of impact.
During the on-site examination of the wreckage, investigators located a tool that would normally not be expected to be carried on the aircraft. Metallurgical analysis showed no evidence that the tool had been trapped within or had in any way interfered with the control systems of the aircraft.
The pilot did not specifically transmit a distress call to ATC during the occurrence. The pilot advised that the aircraft was subject to 'control difficulties', that he was 'losing direction of the aircraft' and that the autopilot was 'not on'.
The aircraft was equipped with a Cessna 400B Nav-O-Matic Autopilot System. The autopilot controller recovered from the site showed evidence of thermal damage to a wire within the controller, consistent with current overload (Figure 1). That damage was inconsistent with post-impact fire damage. The ATSB is awaiting data from the manufacturer and other specialist agencies regarding the effect of the damaged wire on autopilot operation.
Figure 1: Damaged wire within the autopilot controller
The ongoing investigation will include examination of:
the aircraft's autopilot and electric pitch trim systems
the inspection requirements for wiring to critical systems
the degree of autopilot system training provided during aircraft endorsement training.
CAVOK is defined as visibility of 10km or more, no cloud below 5,000 ft or below the highest minimum sector altitude whichever is greater, no cumulonimbus clouds and no precipitation, thunderstorm, shallow fog, low drifting snow or dust devils.
Summary
At about 1326 Eastern Daylight-saving Time on 7 March 2005, the pilot of a Cessna Aircraft Company 310R, registered VH-FIN, took off from runway 30 Right at Tamworth Airport, for Scone, NSW. Approximately 1 minute after becoming airborne, the pilot reported flight control difficulties. At about 1329, the aircraft impacted the ground in a cleared paddock about 7 km west-south-west of the airport. The pilot was fatally injured, and the aircraft was destroyed by the impact forces and post-impact fire.
Examination of the aircraft's mechanical flight control systems, autopilot and electric trim system did not reveal any evidence of pre-impact malfunction. Those results, however, were inconclusive due to the extensive impact and fire damage. A bent hand tool found in the wreckage was not implicated in the development of the accident.
A periodic maintenance inspection carried out in the days before the flight resulted in the rudder trim tab being set at the full right position and possibly aileron and elevator trim tabs being set at non-neutral positions prior to the flight. There were indications that the pilot was rushed and probably overlooked the rudder and aileron trim tab settings prior to take-off. The aircraft flight path reported by witnesses was found to be consistent with the effect of abnormal rudder and/or aileron trim tab settings.
The investigation found that aircraft operating checklists produced by aircraft operators did not always include the autopilot and electric trim procedures located in the supplements of aircraft operating handbooks/flight manuals. At the time of the accident, the training and guidance generally provided to pilots did not emphasise the management of flight control difficulties including autopilot and electric trim related difficulties.
Following the accident, the aircraft operator and the maintenance provider advised that they had reviewed and amended some procedures. The Civil Aviation Safety Authority advised that a Civil Aviation Advisory Publication titled Multi-engine Aeroplane Operations and Training will be issued by July 2007 and that three items have been forwarded to the Safety Promotion Branch for consideration/action.
On 6 January 2005, the pilot of an Air Tractor AT-802A aircraft, registered VH-BQN, was spraying insecticide on a cotton crop on Wynella Station, 41 km south of Dirranbandi, Qld. The aircraft departed the station airstrip at about 2005 Eastern Standard Time to commence spraying operations and impacted the ground at 2035. The pilot was fatally injured, and the aircraft was destroyed by fire.
There was no evidence that the aircraft was not capable of normal operation at the time of the accident. The pilot had substantial agricultural and general flying experience but had only recently completed night agricultural flight training. The accident occurred after the end of nautical twilight, there was no moon, and there was a band of cloud over Wynella station. There was virtually no ground lighting in the area. Post-mortem examination identified severe atherosclerotic narrowing of all three coronary arteries.
The lack of recorded and witness information, and the destruction of the cockpit by fire, prevented the investigation from conclusively identifying the factors that contributed to the development of the accident. However, the combination of pilot inexperience in night agricultural operations and the dark night conditions increased the risk of an accident.