At 0944 Eastern Standard Time on 19 October 2004, the Gyroflug Speed Canard aircraft departed Bundaberg, Qld, on a private flight to Parafield, SA, with a planned refuelling stop at Bourke, NSW. At about 1145, the pilot, who owned the aircraft and was the only occupant, radioed another pilot who was operating in the St George, Qld, area and advised that he was feeling dizzy, faint and disoriented, and was having difficulty lining up the aircraft to land on the St George runway. The aircraft remained airborne in the vicinity of St George for approximately 90 minutes. At about 1335, the aircraft impacted terrain 20 km south-west of St George, and the pilot sustained fatal injuries.
There was no evidence that the aircraft was not capable of normal operation at the time of the accident.
During a routine aviation medical examination in 2003, the pilot was diagnosed with diabetes.
The pilot apparently became incapacitated during flight and was unable to manoeuvre the aircraft to a successful landing.
It could not be established why the pilot became incapacitated, however a diabetes-related condition could not be ruled out.
On 17 November 2004, the helicopter manufacturer advised that it had contacted the emergency locator transmitter (ELT) manufacturer concerning the ELT antenna coaxial cable connectors. The ELT manufacturer had undertaken to test coaxial cable connectors with a 30 lb. tension load. Connectors held in stock by the helicopter manufacturer would also be tested. The helicopter manufacturer advised that it was converting to the new 406 MHz capable ELTs. The antenna connector for the new installation would be crimped by the helicopter manufacturer. The style of crimping used by the helicopter manufacturer has been tested and could typically withstand in excess of 100 lb tension. The helicopter manufacturer believed that those actions would prevent failures of the type that occurred to the ELT installation in the occurrence helicopter.
ATSB
A summary of this accident report will be included in a future edition of CASA's Flight Safety Australia magazine.
Analysis
ANALYSIS
The investigation found that there was no evidence of a pre-existing defect in the helicopter that may have contributed to the occurrence, nor was there any evidence of a medical condition that could have affected the pilot's ability to control the helicopter. Consequently, the investigation concluded that in the prevailing environmental conditions, the accident was consistent with pilot spatial disorientation. This analysis examines the development of the occurrence and highlights a significant risk associated with night VFR operations.
The pilot departed for Eurella homestead 6 minutes after civil twilight in moonless, overcast, and probably showery conditions that were likely to restrict visibility to less than the required 5 km. Except for the homestead lights, the ground lighting or celestial illumination required by the Aircraft Flight Manual was not available. Although the pilot had flown at night on two recent occasions (23 and 26 August 2004), those flights did not fully satisfy the night VFR recency requirements and were probably over a well lit area. Given the pilot's limited recent and overall helicopter night flying experience, and the forecast weather conditions, it is unlikely that the pilot planned to conduct the return flight at night. The pilot had probably used the helicopter to move cattle and that task may have taken longer than expected. The proximity of the homestead, the local knowledge of his passenger, the night VFR capability of the aircraft and access to GPS information may have influenced the pilot to attempt the return flight.
The track information recovered from the hand-held GPS showed manoeuvring after 1830 that suggests that the pilot, probably using GPS information, made several attempts to track to the homestead, but was unable to do so. It is likely that during the manoeuvring the pilot was at a low altitude, attempting to maintain visual contact with surface features, possibly with the assistance of the landing lights. Such visual contact would have enabled control of the helicopter and clearance from terrain. In the absence of a consistently discernable horizon, any visual contact with the homestead lights would not have enabled the pilot to determine the helicopter's attitude. Prior to the impact, the pilot may have lost visual contact with the surface due to cloud and/or rain and become spatially disorientated.
The pilot may have attempted to control the helicopter by reference to the flight instruments. However, he had not logged any instrument flight time in a helicopter and had not been exposed to significant night-flight away from metropolitan areas. The relative instability of the helicopter and the different operating environment meant that the pilot's considerable aeroplane night and instrument flight experience was not directly transferable to night VFR helicopter operations. Consequently, spatial disorientation could have developed rapidly.
Flying the helicopter at a low altitude at night with cloud and/or showers in an area with little lighting was a very demanding task with little margin for error. However, once the helicopter became airborne after civil twilight, there were few options available to the pilot. The pilot's lack of helicopter instrument flight experience would probably have precluded consideration of climbing to the lowest safe altitude and tracking to an aerodrome with an instrument approach. Given that the adverse weather was widespread, diversion to another location while maintaining external visual reference was also an unlikely option.
A landing at a location other than the homestead was an option. It is possible that the accident occurred when the pilot became spatially disorientated in the adverse conditions while attempting to land the helicopter. However, it is also possible that, unable to communicate with the homestead, the pilot avoided an out-landing due to the consequent difficulty in reaching the homestead without transport.
Illumination of the clutch light as indicated by the stretched filament may have resulted from clutch operation during flight or from disruption during the impact. If the clutch light had illuminated during flight it may have distracted the pilot and contributed to spatial disorientation.
As a result of the separated ELT antenna cable, the search and rescue effort was significantly affected. However, in this case, the nature of the impact and the extent of injury to the occupants indicated that the search and rescue effort would not have influenced their survivability.
The circumstances of this occurrence highlight the risk of spatial disorientation during night VFR operations and reinforce the significance of the cautions included in the helicopter manufacturer's safety notices SN-18 and SN-26.
SIGNIFICANT FACTOR
The pilot departed after civil twilight in conditions where a natural horizon was probably not discernible and consistent visual reference to surface features was not likely.
Factual information
FACTUAL INFORMATION
History of the flight
On 8 September 2004, the owner/pilot of a Robinson Helicopter Company R44 Raven II helicopter, registered VH-JWX, conducted a private flight under the visual flight rules (VFR) from Coffs Harbour, NSW to Eurella Station, Qld. The flight included a landing at Roma, Qld where the pilot refuelled the helicopter with 180 L of Avgas from the bulk underground fuel storage supply.1 The pilot then continued to Eurella Station, located approximately 54 km west of Roma, arriving at 1705 Eastern Standard Time. The pilot shut down the engine and the property owner boarded the helicopter for a pre-arranged local flight. The pilot made several attempts to start the engine, during which it backfired a few times. Once started, the engine seemed to function normally.
The helicopter departed the homestead at 1725 in a northerly direction. A person on an adjoining property about 7 km north of Eurella homestead saw the helicopter operating to the east late in the afternoon. He reported that the helicopter conducted a number of take-offs and landings in what appeared to be the same general area over a period of about 30 minutes. He saw the helicopter depart in a southerly direction at about 1830.
The next reported sighting was by a person at Eurella homestead who, in poor light conditions, saw what appeared to be the helicopter's landing light to the north of the homestead. The light moved toward the west of the homestead. Soon after, that person again saw the light to the west and expected the helicopter to land at the homestead within a few minutes. However, she became concerned when the helicopter did not arrive and telephoned an employee of the property owner to report her concern. The employee contacted the Australian Search and Rescue organisation (AusSAR) and search action was initiated. The helicopter was located the following morning in open, rolling country, 3 km west of Eurella homestead. The two occupants were fatally injured, and the helicopter was destroyed.
Search and rescue
AusSAR reported that it was notified at 1947 that the helicopter was overdue. Weather conditions were unsuitable for an air search, but a surface search was initiated. AusSAR advised that no ELT signal was received on 8 September by satellite or by aircraft at high altitude passing within 130 km of Eurella Station. An ELT signal was detected on two satellite passes early on the morning of 9 September. The signals were identified as originating from separate locations; one approximately 22 km to the south-west, and the other approximately 22 km to the south-east, of Eurella Station. However, those signals were not merged by the satellites as coming from the same source, so they were of little assistance in the search. Local aircraft were tasked to begin a search at daylight on 9 September and the wreckage was located at 0708 by the crew of a search aircraft. Accident site information
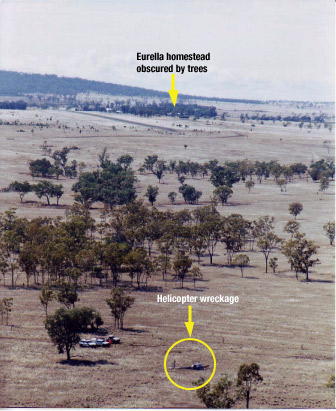
The accident site elevation was about 30 m below the ground elevation at the homestead. The homestead was not visible from the accident site.
Figure 1: Aerial view of the accident site
GPS track information
The helicopter was fitted with a fixed global positioning system (GPS) receiver, and also a handheld GPS receiver mounted in a cradle on the instrument panel. The fixed receiver did not contain a non-volatile memory card, but the handheld unit did. Track and ground-speed data for the occurrence flight was retrieved from the non-volatile memory card. Altitude information was not retained in the memory card.
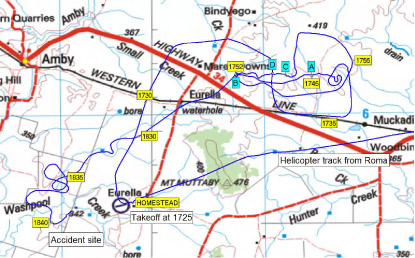
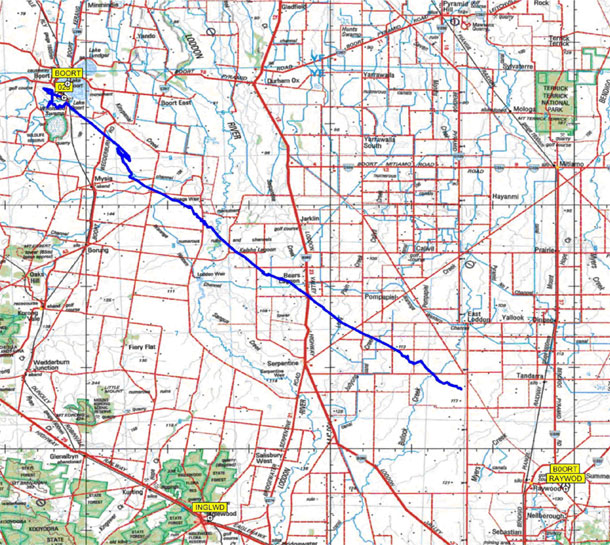
Figure 2 displays the GPS recorded track of the helicopter overlaid in blue on a 1 in 250,000 scale topographical map of the area. The local times that the helicopter was at various locations are depicted.
Figure 2: GPS track overlay, with the landing sites A, B, C and D
The GPS data showed that the helicopter landed five times during the flight. Those positions are depicted on the map and are described as follows:
Position A
The helicopter landed at 1742 and departed at 1745. There was a water tank adjacent to that location.
Position B
The helicopter landed at 1749 and departed at 1752.
Position C
The helicopter landed at 1800 and departed at 1802.
Position D
The helicopter landed at 1805 and departed at 1807.
Position B
The helicopter returned to position B at 1823 and departed at 1827.
The data indicated that, after the helicopter departed position B at 1827, it initially tracked almost directly toward the homestead, but that the track then veered south-west. That track was clear of the high ground indicated by the 400 m contour near Mt Muttaby, as depicted on the chart at Figure 2. There are distinct features in the helicopter's track after 1830, indicating that the pilot turned toward the homestead on four separate occasions between 1830 and 1840, only to turn away each time. The accident occurred on the fifth occasion that the helicopter's recorded track turned in the approximate direction of the homestead.
Subsequent to the occurrence, an employee from Eurella Station found that cattle had been moved from the paddock that included positions A, C, and D, to an adjoining paddock. Those paddocks were linked by a gate adjacent to position B. The employee recalled that the property owner had intended to move the cattle to the adjoining paddock and that the gate adjacent to position B was the gate through which he would have expected the cattle to be moved.
Pilot information
The pilot held an air transport (aeroplane) pilot licence and a command multi-engine instrument rating. He had extensive aeroplane flying experience, including regular public transport turbo-jet aircraft and corporate turbo-jet aircraft operations in Australia and overseas. His aeroplane flying experience exceeded 10,000 hours and included 1,418 hours of night flight and 711 hours of instrument flight.
The pilot obtained a private pilot (helicopter) licence on 23 September 1998 and had about 582 hours helicopter experience. He obtained a night VFR (helicopter) rating on 12 September 2000 and since that date had recorded about 11 hours helicopter night flight. Almost all of the logged flights were in the Sydney metropolitan area. Helicopter night flying recorded by the pilot in the two years prior to the occurrence was 0.4 hours on 23 August 2004 and 0.6 hours on 26 August 2004. That night flying most likely occurred during the latter stages of flights to the Sydney metropolitan area.
There was no record of the pilot having received any specific training in operating helicopters in remote areas or dark night conditions where there was little or no ambient lighting. No helicopter instrument flight time was logged.
The pilot held a valid medical certificate. Post-mortem and toxicology examinations did not reveal any pre-existing condition that might have affected the pilot's ability to safely conduct the flight.
Helicopter information
The pilot purchased the helicopter new in early August 2004. At the time of the occurrence the helicopter had operated for 34.1 hours. The maintenance release was valid and the documentation indicated that all applicable maintenance and regulatory requirements had been met.
The helicopter was equipped and certified for night VFR operations. Instrumentation included an airspeed indicator, artificial horizon, sensitive pressure altimeter, turn coordinator, horizontal situation indicator, global positioning system indicator, and vertical speed indicator.
The helicopter was equipped with twin landing lights in the lower nose section. The lights were fitted with 100 watt spot globes and, according to the Aircraft Flight Manual, were 'set at different angles to increase the pilot's field of vision'. Both lights were activated by the one switch which was mounted on the cyclic control centre post.
A row of eight amber warning lights located at the top of the flight instrument panel included a clutch warning light. A further six warning lights were positioned at the top of the centre pedestal.
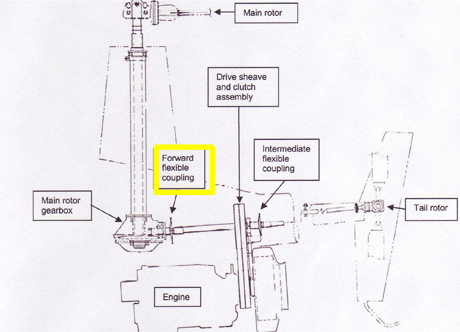
The helicopter's engine was coupled to the rotor drive system via four double-stranded vee-belts. After engine start, an electric actuator would tension the belts when the pilot engaged the clutch switch. The actuator sensed belt tension and was automatically energised when the tension was less than required. The clutch warning light would illuminate whenever the clutch actuator circuit was activated. The Aircraft Flight Manual included a note regarding the clutch in Section 3, Emergency Procedures. The note stated that stretching of the belts often resulted in illumination of the clutch warning light for brief periods as the drive actuator readjusted belt tension. The note also included actions that the pilot should take after 7 or 8 seconds of illumination of the clutch light. One of those actions was to pull the clutch circuit breaker.
The helicopter was fitted with a Pointer (TSO-C91A) Model 3000-10 emergency locator transmitter (ELT). The unit was located on the left side of the rear fuselage.
The total flight time from Roma until the time of the occurrence was about 1 hour 35 minutes. Assuming a fuel usage rate of 60 L per hour, approximately 95 L would have been consumed during that time. On that basis, approximately 95 L should have remained at the time of the occurrence.
Wreckage information
opposite to the helicopter's direction of travel at impact. The impact severely crushed most of the cabin area and deformed the fuselage and tail boom structures. Two distinct main rotor blade impact marks on the ground forward and to the right of the initial nose impact position, and the damage to the main rotor blades, indicated that the rotor blades were being driven by the engine at impact. The tail-rotor system was intact and there was no evidence that the fuselage was yawing at impact. There was no indication that the helicopter had struck any of the trees in the vicinity of the impact site.
The left fuel tank ruptured during the impact sequence and was empty. The right fuel tank was also empty. With the helicopter lying on its left side, the right fuel tank vent line was at the lowest part of the tank and would have allowed fuel to drain out. There was a strong smell of Avgas in the vicinity of the wreckage on the day after the accident.
The hydraulic system switch was found in the ON position.
Instrument panel light globe and instrument examination confirmed that electrical power was available to the instruments. There was no evidence of malfunction of any of the instruments.
The six warning lights at the top of the centre pedestal were destroyed by impact forces, preventing an assessment being made of their status at impact. The eight warning lights at the top of the flight instrument panel were intact. Examination of those light globes revealed stretching of the clutch warning light filament. Stretching indicates that the filament was hot and that electrical power was applied to the globe when it was subject to forces during the impact sequence. It was not possible to determine the length of time that the globe had been illuminated. Filament stretch was not evident in any of the other seven warning light globes from the top of the instrument panel.
Damage to the landing light globes prevented any assessment being made regarding their status at the time of the occurrence. The damage to the landing light switch indicated that it was in the ON position at impact.
The circuit breaker panel was destroyed by impact forces. The clutch actuator fuse was serviceable. The wreckage examination did not reveal any fault in the clutch system. Although the circuit breaker panel was destroyed, the evidence of electrical power to the clutch warning light indicates that the circuit breaker was engaged, and therefore the system was powered at the time.
The coaxial cable from the ELT unit to the external antenna had separated at the connector to the antenna base on the inside of the antenna mounting panel. The separation of the coaxial cable trapped the transmitted signal within the fuselage compartment. That rendered the ELT unit ineffective and prevented satellite detection of the signal. The separation of the cable appeared to have been as a result of impact forces. As a result, the search and rescue effort was significantly affected.
Specialist examination of the ELT revealed that it had activated upon impact and, when connected to a suitable antenna, was capable of transmitting a normal signal.
The engine was test run after removal from the wreckage and operated normally. The hydraulic pump and three hydraulic servos that formed part of the main rotor flight control system were removed from the wreckage for functional testing. The tests were conducted at the helicopter manufacturer's facility in the USA and supervised on behalf of the ATSB by a representative from the US National Transportation Safety Board. The tests confirmed that the hydraulic system components met the specifications for normal operation.
Meteorological information
Documents found in the helicopter included an Area 41 weather forecast valid from 0900 to 2100 on the day of the occurrence and the Roma terminal area forecast (TAF) valid from 1200 to 2400 on the day of the occurrence.
The area forecast indicated that the weather in the vicinity of Eurella Station would include areas of rain with locally moderate falls, scattered showers and isolated thunderstorms. The Roma TAF indicated that between 1500 and 2400 there would be 60 minute periods in which the visibility would be 2 km in heavy rain, with broken cloud2 at 700 ft.
An analysis by the Bureau of Meteorology indicated that during the late afternoon on the day of the occurrence, a surface trough was located from Camooweal to St George, with cold south-west winds to its west and northerlies to its east. The surface trough combined with an upper level trough over the southwest of the state to bring a large cloud band with widespread rain and isolated thunderstorms to the interior. The analysis of satellite imagery and synoptic reports, concluded that there was a high probability of rain in the Eurella Station area around the time of the occurrence, and most likely greater than 5 oktas of cloud cover. However, because the nearest weather radar station was about 200 km distant at Charleville, the amount of cloud cover in the area of the occurrence could not be confirmed.
Persons at and near Eurella Station variously reported that the weather conditions during the day of the accident were windy, with heavy cloud and showers.
Astronomical information
According to information published on the Geoscience Australia website, sunset and twilight times at Eurella Station on the day of the occurrence were:
Other information on the website indicated that the moon set at 1409 and was 79 degrees 31 seconds below the horizon at 1830 that evening.
Helicopter night VFR
The pilot's night VFR (helicopter) rating authorised him to act as pilot in command of private or aerial work flights at night under the VFR. Once issued, a night VFR rating remained permanently valid. To exercise the privileges of the rating, a pilot needed to complete a 1-hour night flight during the previous 12 months and one take-off and landing at night during the previous 6 months. There was no requirement for the holder of a night VFR rating to have any recent instrument flight time prior to conducting a flight at night.
A pilot operating under the VFR at night was required to operate in visual meteorological conditions that included a minimum of 5 km visibility. The Aircraft Flight Manual, Section 2, Limitations, included the following statements:
VFR operation at night is permitted when landing, instrument, and anti-collision lights are operational. Orientation during night flight must be maintained by visual reference to ground objects illuminated solely by lights on the ground or adequate celestial illumination.
At the time of the occurrence there was a 1,000 watt flood light on each of the northern and western walls of Eurella homestead, as well as lights in other buildings. However, there were many trees in the vicinity of the homestead, some of which were higher than the homestead roof. Depending on the altitude and position of the helicopter, the trees could have prevented those lights being seen from the helicopter (Figure 1). There was no other lighting in the general area, including at the airstrip adjacent to the homestead. The homestead lights, in effect, formed a 'point' source of light.
Spatial Disorientation
Spatial disorientation refers to a situation in flight in which the pilot fails to sense correctly the position, motion or attitude of the aircraft. When the condition is fully developed, the pilot is unable to tell which way is 'up'.
The risks of non-instrument rated pilots flying in conditions in which they are not able to orientate the aircraft by visual reference have been well known for over 50 years. During testing conducted on a group of non-instrument rated pilots, the average time before loss of control of the aeroplane, after visual reference was lost, was 178 seconds.5
US FAA Advisory Circular 60-4A, Pilot's Spatial Disorientation, was published in 1983 and was intended to inform pilots of the hazards associated with disorientation caused by loss of visual reference with the external environment. It included the following information:
Tests conducted with qualified instrument pilots indicate that it can take as much as 35 seconds to establish full control by instruments after the loss of visual reference with the surface.
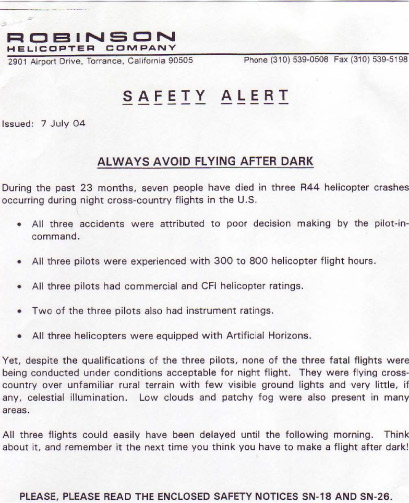
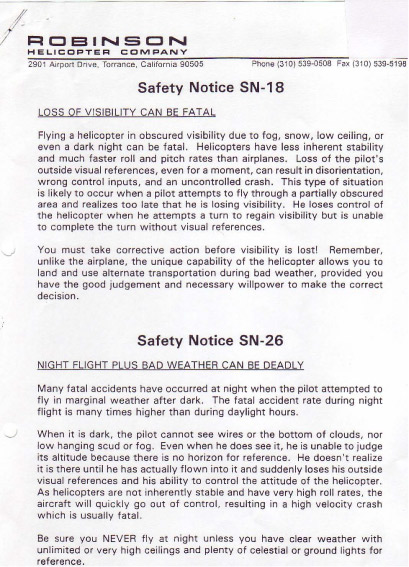
The helicopter manufacturer issued a safety alert and safety notices (SN) as a result of various occurrences and incidents, and included those notices in the Aircraft Flight Manual Section 10, Safety Tips. Two of the notices related to night flight - SN-18 Loss of Visibility Can Be Fatal, and SN-26 Night Flight Plus Bad Weather Can Be Deadly (see Appendix A). Safety notice SN-18 stated in part:
Helicopters have less inherent stability and much faster roll and pitch rates than airplanes. Loss of the pilot's outside visual references, even for a moment, can result in disorientation, wrong control inputs, and an uncontrolled crash.
Appendix A
1.On the day of the occurrence, other aircraft were refuelled from the Roma bulk fuel storage. The ATSB received no reports of fuel quality related problems involving those aircraft.
2. Forecast cloud was explained as 'few'-1 to 2 oktas (okta - a unit of visible sky area representing one-eighth of the total area visible to the celestial horizon), 'scattered'- 3 to 4 oktas, 'broken'- 5 to 7 oktas and 'overcast'- 8 oktas.
3. Sunset is defined as the instant in the evening under ideal meteorological conditions, with standard refraction of the sun's rays, when the upper edge of the sun's disk is coincident with an ideal horizon.
4. Ending of evening civil twilight is defined as the instant in the evening when the centre of the sun is at a depression angle of six degrees below an ideal horizon. In the absence of moonlight, artificial lighting or adverse atmospheric conditions, the illumination is such that large objects may be seen, but no detail is discernible.
5. Bryan, L.A., Stonecipher, J.W. & Aron, K. 1954. 180-degree turn experiment. University of Illinois Bulletin. 54(11), 1-52.
Summary
On 8 September 2004, the owner/pilot of a Robinson Helicopter Company R44 Raven II helicopter, registered VH-JWX, conducted a private flight under the visual flight rules (VFR) from Coffs Harbour, NSW to Eurella Station, Qld. The flight included a landing at Roma, Qld where the pilot refuelled the helicopter with 180 L of Avgas from the bulk underground fuel storage supply. The pilot then continued to Eurella Station, located approximately 54 km west of Roma, arriving at 1705 Eastern Standard Time. The pilot shut down the engine and the property owner boarded the helicopter for a pre-arranged local flight. The pilot made several attempts to start the engine, during which it backfired a few times. Once started, the engine seemed to function normally.
For reasons that could not be determined, the aircraft commenced a slight left angle of bank and drifted left after lift-off at a height from which the pilot was unable to recover prior to striking trees to the left of the runway.
Analysis
Preparation for take-off
The pilot was qualified, appropriately endorsed and reported to be fit and well for the flight. The available aircraft and maintenance documentation, results of the recent 50-hourly inspection and subsequent engine ground run, and the successful 2-hour flight to El Questro indicated that there were no known pre-existing aircraft anomalies that might have contributed to the occurrence.
Although it was reported that the pilot most likely observed the El Questro Aircraft Landing Area (ALA) in June 2003, the investigation was unable to determine the means by which the pilot satisfied himself prior to arriving on 28 August 2004 that the ALA was suitable for his operation in accordance with the requirements of Civil Aviation Regulation 92. The runway width and length satisfied the guidance provided by Civil Aviation Advisory Publication (CAAP) 92-1(1) for the aircraft. While the tree that was initially struck by the aircraft may have infringed the lateral transitional slope, the pilot had indicated his acceptance of the suitability of the ALA for his operation and had landed without incident on 28 August 2004.
The results of the fuel tests, and the large number of other aircraft that had also used the Broome fuel supply without any reported problems, indicated that the quality of that fuel supply had not contributed to the development of the occurrence. The reported conduct by the pilot of the left underwing fuel drain test and observed presence of the pilot underneath the right wing tended to suggest that the pilot had completed the fuel drain and sump checks. That supported the consistent reports from all witnesses that the aircraft's engines sounded 'normal' throughout the take-off, and decreased the likelihood that water or other particulate contamination of the aircraft's fuel supply to the engines had any effect during the take-off.
The pilot's extensive and recent experience in the operation of this type of aircraft, and apparent intimate knowledge of its systems and procedures, would have reduced the likelihood of the pilot omitting to unlock the aircraft's controls prior to commencing the take-off. In any case, the ability of the pilot to fly the aircraft from the runway meant that the control column and optional rudder gust locks were unlocked at that time. Therefore, the pilot should have been able to react to the reported initially slight left bank after take-off.
The Broome engineer's report that the engines had started and run normally after the 50-hourly inspection, and the lack of any indication by the pilot during his stay at El Questro of any problems affecting the flight to El Questro indicated that the aircraft probably did not have a recurring engine starting problem. The action by the pilot to continue the engines start, taxi and take-off without interruption indicated that the pilot was unconcerned by the reported initial difficulty starting the left engine, or by the 'frequency vibration' that was reported by the passenger witnesses at the runway 32 parking area. In addition, given the history of extensive efforts by the pilot during the flight to Australia to at all times ensure the serviceability of the aircraft, it was likely that the pilot would have attended to any engine(s) start or after-start anomaly as soon as it became evident. The investigation concluded that the start and after-start passenger witness reports probably resulted from observations that were accepted as 'normal' by the pilot and also by the pilot witness who was also located at the runway 32 parking area.
Take-off
The action to conduct a rolling take-off was consistent with an attempt by the pilot to minimise the potential for damage to the propeller blades and underside of the aircraft as a result of the dislodgement from the runway surface of pebbles and other potentially damaging debris. The investigation considered whether the pilot may have attempted to lift off the runway earlier than normal in an attempt to minimise the possibility of such damage. However, this was considered unlikely given the report from the pilot witness, that the lift-off appeared to reflect other twin-engine aircraft take-offs that he had observed, and the approximation of the length of the take-off roll to that predicted by the Pilot's Operating Handbook (POH) performance charts.
The reports from the witnesses at the runway 32 parking area that there had been no smoke or fumes observed emanating from the aircraft and that nothing fell from it during the take-off, corroborated the results of the after-accident runway inspection. That, along with the identification of all control surfaces at the accident site, and the distribution of the aircraft wreckage, indicated that there had been no aircraft break-up or detachment of the aircraft's control surfaces prior to the impact with the trees and ground.
There was no evidence of any pre-existing failure or anomaly in either engine or their supporting assemblies or components that were able to be tested, that might have adversely influenced the performance of the engines during the take-off. In addition, the nature of the damage to the propellers and propeller hubs was consistent with the delivery of comparable amounts of power to both propellers from within the engines' upper operating range at the time of ground impact. There was no evidence of an enduring power failure of either engine during the take-off.
The investigation considered a number of possible factors that could have had the potential to affect the lateral control of the aircraft. Those factors included: the possibility of a lateral weight imbalance; an aerodynamic influence on the performance of the aircraft; and whether the pilot might have either intentionally or inadvertently manoeuvred the aircraft to the left of the runway immediately after lift-off.
Given that all of the baggage was observed being stowed in the aircraft cabin, there was minimal potential for the baggage distribution on take-off to have adversely affected the lateral control of the aircraft. The pilot's high and recent experience operating the aircraft minimised the possibility that he might have neglected to check the correct engine fuel selections on the three occasions (at least) required by the POH during the flight to El Questro. Similarly, had the pilot inadvertently mis-selected the engines' fuel supply, the nature of the aircraft checks meant that it was unlikely that a mis-selection would remain undetected by the pilot for the duration of the flight to El Questro. Therefore, it was considered that the potential for a lateral fuel load imbalance, and therefore aircraft weight imbalance to have developed during the flight to El Questro was minimal.
In any case, given the short taxi to runway 32 from the parking area and the rolling take-off, any disparity that may have existed in the lateral fuel distribution for the take-off was estimated to have been within 50 pounds of that for the landing at El Questro. That meant that the pilot would have been aware of the potential for any associated aircraft roll during the take-off and would have been ready to compensate. In addition, as indicated in the POH, the relatively benign nature of the ambient conditions and reported 'normal' appearance of the take-off ought to have allowed the pilot to control the aircraft even had there been a lateral fuel imbalance.
The aerodynamic factors with the potential to have affected the lateral control of the aircraft included the effects of asymmetric or 'split' flap and a wing stall. The damage to the left flap meant that, in the first instance, the investigation could not discount that split flap might have occurred during the lift-off. However, given that the right flap was confirmed retracted at ground impact, the only possibility was that the left flap might have self-extended. In that case, the aircraft would have rolled to the right after lift-off. That was not consistent with the witness reports that the aircraft banked to the left after lift-off before striking the trees to the left of the runway. On that basis, the investigation discounted that split flaps had occurred.
It was considered most likely that the experienced and proficient pilot would have raised the nose wheel at 95 knots indicated air speed (KIAS) and lifted the aircraft from the runway at 100 KIAS in accordance with the procedures recommended in the POH.
The pilot witness's description of the take-off and initial slight left bank after take-off could be construed as normal manoeuvring. In that case and given the reported lack of a very steep pitch angle after take-off, it ought to have been difficult for the pilot to have stalled the aircraft. In addition, the pilot's high experience and proficiency in the aircraft, and intimate knowledge of its systems meant that it was highly unlikely that he might have: allowed the speed to decrease to between about 88 to 93 KIAS in order for the stall warning to have activated; to have then reacted inappropriately, or not at all to that warning; to have finally not, or inappropriately, reacted to any developing mild and then increasing aerodynamic buffet; and, instead allowed a continuing reduction in airspeed until reaching about 83 KIAS whereupon the aircraft stalled. On that basis, it was concluded that an aerodynamic stall had most likely not occurred.
Given the pilot's predominant recent experience during the flight to Australia of landing and taking off from major or international aerodromes, the occurrence take-off was potentially his first from an airstrip and surface such as that at the El Questro ALA for some time. In addition, as a result of the pilot having landed the aircraft on runway 14, the take-off from runway 32 was potentially his first opportunity to have comprehended the relative proximity of the trees to the left of the runway. That comprehension was probably only possible during the conduct of the occurrence take-off and may have influenced the pilot's awareness of the need to maintain the aircraft overhead the runway centreline during the take-off.
The absence of bird or other animal remains along the runway surface, and the reported absence of any thermal activity or dust devils, indicated that the pilot most likely was not required to intentionally manoeuvre the aircraft as a result of those potential influences on the take-off. Also, the nature of the pilot's recent flying experience, the number and variety of the exotic locations visited during his flight to Australia, the pilot's age and total flying experience, and his probable desire to not compound any apprehension on the part of the passenger meant that it was most unlikely that the pilot was performing the early stages of any sort of intentional low-level manoeuvre.
The investigation could not discount that the pilot might have been momentarily distracted during the lift-off from the runway to the extent that the aircraft developed an unintended slight left bank and drift. The probable small amount of time for the pilot to have reacted once he perceived any unintended movement of the aircraft would have minimised the possibility for the pilot to have avoided impacting the trees to the left of the runway.
Summary
There was no documentary, physical or witness evidence identified during the investigation that indicated that an anomaly or failure in the aircraft or its systems contributed to the development of the occurrence. In addition, there was no evidence to indicate that the reported slight left bank after lift-off from the runway was the result of a lateral imbalance of the aircraft, an aerodynamic effect or an intentional control input by the pilot. However, the investigation was unable to determine whether the pilot might have been distracted during the lift-off by an unidentified event to the extent that he did not notice or was unable to react to any unintentional left bank and drift of the aircraft in sufficient time to prevent the aircraft impacting the trees to the left of the runway.
CONCLUSIONS
Findings
Pilot
The pilot was qualified and appropriately endorsed for the flight.
The pilot was reported to have 975 hours experience flying the Cessna 421 B and C models over the preceding 10-year period and at least 2,100 total flying hours.
The pilot held a valid Class 2 medical certificate.
The pilot was reported to be fit and well and in good spirits prior to the flight.
There was no evidence of any pre-existing medical disease, sudden illness or incapacitation that may have affected the pilot's ability to control the aircraft.
Aircraft
Export Certificate of Airworthiness number 3588/04 was issued for the Swiss-registered aircraft by Swiss regulatory authorities on 27 February 2004.
The quality of the fuel that was supplied from the Broome supplier was not a factor in the occurrence.
There was sufficient fuel onboard the aircraft to complete the flight to Broome.
The aircraft weight and balance was estimated to be within the published limits at the time of the take-off.
The ability of the pilot to lift the aircraft from the runway meant that the control column lock and optional rudder gust lock were unlocked at that time.
There was no break-up of the aircraft or detachment of the aircraft's control surfaces prior to the impact with the trees and ground at the accident site.
There was no evidence of any pre-existing failure or anomaly in either engine or their supporting assemblies or components.
Comparable amounts of power were being delivered to both propellers from within both engines' upper operating range when the aircraft impacted the ground.
Other findings
Witness reports indicated that, shortly after lift-off from the runway, the aircraft banked and drifted to the left slightly, before striking the trees to the side of the runway and impacting the ground.
There was no evidence that the ambient conditions contributed to the circumstances of the occurrence.
The pilot indicated that the El Questro ALA was suitable for his operation.
There was no distress radio transmission by the pilot.
Based on the available evidence, it was considered most unlikely that the pilot was performing the early stages of any sort of intentional low-level manoeuvre.
The investigation could not discount that the pilot might have been momentarily distracted during the lift-off, resulting in the development of an unintentional slight left bank and drift of the aircraft.
The relative proximity of the trees to the left of the runway would have adversely affected the time available for the pilot to have reacted to the development of any unintentional left bank and drift.
The destruction of the aircraft cockpit and cabin from the combined effects of the impact forces and post-impact fire rendered the accident non-survivable.
On 30 August 2004, shortly before 1200 Western Standard Time, the owner-pilot of a twin-engine Cessna Aircraft Company 421C Golden Eagle (C421) aircraft, registered HB-LRW, commenced his take-off from runway 32 at El Questro Aircraft Landing Area (ALA). The private flight was to Broome, where the pilot intended resuming the aircraft delivery flight from Switzerland to Perth. The available documentation indicated that the flight segments en route to Australia had all been to international or major aerodromes.
The pilot of a Cessna Aircraft Company 210 (C210) and his two passengers in the runway 32 parking area witnessed the take-off. Those witnesses reported that the C421 pilot carried out a pre-flight inspection of the aircraft prior to boarding for the take-off. During that inspection, he was observed preparing for and conducting a fuel drain check under the left wing, and to have removed some weed-like material from the right main wheel. He then loaded a small amount of personal luggage into the aircraft cabin, before he and the sole passenger boarded.
The C210 pilot witness, who reported having observed a number of twin-engine aircraft operations at another aerodrome, did not comment on the nature of the pilot's start and engines run-up checks. The passenger witnesses reported that the pilot of the C421 made a number of unsuccessful attempts to start the left engine, before reverting to starting the right engine. He then started the left engine and moved the aircraft clear of the C210 in order to conduct his engine run-up checks. The passenger witnesses reported that during those checks they heard a 'frequency vibration' as the C421 pilot manipulated the engines' controls.
The witnesses at the parking area reported that the C421 pilot taxied the aircraft onto the runway and applied power to commence a rolling take-off.2 They, together with a hearing witness3 located to the north of the ALA indicated that the engines sounded 'normal' throughout the take-off. Witnesses who observed the take-off reported that the aircraft accelerated away 'briskly'. The pilot witness stated that the take-off roll and lift-off from the runway appeared similar to other twin-engine aircraft take-offs that he had observed.
The witnesses at the parking area also stated that, shortly after lift-off from the runway, the aircraft banked slightly to the left at an estimated 10 to 15 degrees angle of bank and drifted left before striking the trees along the side of the runway and impacting the ground. There was no report of any objects falling from the aircraft, or of any smoke or vapour emanating from the aircraft during the take-off. The aircraft was destroyed by the impact forces and post-impact fire. The pilot and passenger were fatally injured.
Personnel information
The 60-year-old pilot was appropriately licensed and held the relevant aircraft and other endorsements to conduct the flight. It was reported that the pilot had accumulated more than 975 hours experience flying the Cessna 421 B and C model aircraft over the preceding 10 year period and had at least 2,100 total flying hours. The pilot had flown about 50 to 60 hours in the aircraft since March 2004 and held a valid Class 2 medical certificate. He last underwent an electro cardiogram examination (ECG) in support of the revalidation of his medical certificate, on 22 September 1999. That included an annotation by the consulting doctor that the ECG was 'normal'. The pilot's family indicated that the pilot's personal logbook would have been in the aircraft at the time of the accident.
The passenger had accompanied the pilot for the majority of the flight from Switzerland to Australia, but was reported to have been a little nervous about take-offs and landings.
The pilot and passenger arrived at the El Questro ALA at about 1330 on 28 August 2004 and landed on runway 14. They were reported to have spent the next two days relaxing in the tourist resort and homestead. During that time, the pilot was observed by staff to have retired for bed by about 2200 and appeared from his room by about 0930 each day. During his stay the pilot ate regularly, drank alcohol only socially, and recounted many of his experiences during the delivery flight to staff and other guests. That did not include the discussion of any difficulty starting the aircraft engines, of any anomalies during the after-start checks and procedures, or during the flight to El Questro. The pilot was reported to be fit and well and in good spirits on the morning of the accident.
Aircraft information
General information
All of the aircraft's original maintenance documentation was reported to be on board the aircraft for the flight to Australia and was subsequently destroyed in the post-impact fire. The loss of the aircraft's maintenance documentation and historical records precluded a thorough review of the aircraft's documentation concerning compliance with applicable airworthiness directives and service bulletins. Aircraft and engine maintenance and airworthiness-related issues were reconstructed from available secondary documentation, including: pilot and other relevant party e-mails and facsimile messages, and data from international regulatory and other agencies.
Forward limit: 152.59 ins at 7,450 lbs or less and 147.14 ins at 6,100 lbs or less with a straight line variation between those points
Manufacturer
Cessna Aircraft Company
Model
421C Golden Eagle
Serial number
421C-0633
Registration
LB-LRW
Year of manufacture
1979
Export Certificate of Airworthiness
Certificate number 3588/04 i ssued in Switzerland on 27 February 2004
Allowable centre of gravity limits (measured aft of the reference datum)
Aft limit: 157.95 inches (ins) at 7,450 lbs or less
Centre of gravity at occurrence
157.5 ins (estimated)
E-mail correspondence from the pilot dated 16 September 2003 indicated that the aircraft was equipped with the Robertson Short Take-off and Landing (R-STOL) Kit. That kit included the following changes to the configuration of the aircraft:
Replacement of the existing trailing-edge split flaps with R-STOL slotted flaps for use with the flaps extended 10°. The effect was to reduce the aircraft stall speed and the best single-engine climb speed.
Introduction of a scissors-type aileron bell crank that allows symmetrical aileron droop with extension of the flaps. This had the effect of further reducing the aircraft stall speed.
Introduction of a spring/cable flap/elevator interconnect to minimise pitch trim changes with flap extension or retraction.
In this instance, and as discussed in the wreckage examination discussion at page 13, and the asymmetric or 'split' flap discussion at page 19, the aircraft flaps were retracted. In that case, the R-STOL kit would have had no effect on the aircraft take-off performance, and the aircraft's performance would have been in accordance with a standard C421C in a flaps retracted configuration.
The aircraft's take-off weight and centre of gravity were estimated by the investigation to be within the limits published in the C421C's Pilot's Operating Handbook (POH). The POH also included a Normal Take-off Distance prediction chart. Application of the estimated aircraft take-off weight and reported ambient conditions for a normally configured C421C to that chart resulted in a predicted take-off roll that approximated the estimated take-off distance reported by the witnesses located at the runway 32 parking area.
Aircraft history
The aircraft was manufactured in the United States (US) and was US-registered until 1992, when it was exported to Switzerland. It was operated in Switzerland in the private category until purchased by the pilot in December 2003. E-mail correspondence from the pilot and dated 4 December 2003 indicated that a Swiss maintenance organisation would commence a 'new annual/200-hours check' on 10 December 2003. The available aircraft maintenance records indicated that the total aircraft flight hours were 3,192 hours 40 minutes as at 10 December 2003. That corresponded with the initial entry made by the pilot in the aircraft maintenance record after a flight in the aircraft on 2 March 2004. The last entry in the aircraft's maintenance record, that was available to the investigation, was a total of 3,233.6 aircraft flight hours at Ahmedabad, India on 9 August 2004.
A number of aircraft anomalies or maintenance requirements needed resolution while the aircraft was en-route from Switzerland to Australia. They included:
In Malta, where an approved maintenance facility:
replaced leaking right engine push rod tube seals
replaced a faulty left engine vacuum pump
identified a leaking right main landing gear oleo and disassembled the landing gear oleo and installed new packings and 'o' ring seals before reinstalling the oleo on the aircraft.
In Cyprus, where a crack was discovered in the right engine crankcase that necessitated the replacement of that engine.
In the United Arab Emirates and Oman, where a number of attempts were made by local engineering companies to resolve a problem with the operation of the aircraft's landing gear. That ultimately required the replacement of a selector valve and hydraulic line.
In addition, the pilot established communications with a twin-engine Cessna owners group in an effort to fault analyse ongoing problems with:
the left and right hydraulic pumps that supplied the necessary hydraulic pressure to extend and retract the landing gear, and
the right alternator warning light, which was reported to commence flickering after about 30 minutes flight time. That anomaly was reported to have commenced in July 2004.
The resolution or otherwise of those two anomalies was not documented by the pilot.
On arrival in Australia, a 50-hourly inspection of the aircraft was carried out by a Broome aircraft maintenance company on 26 August 2004. The total airframe hours at the time of that inspection were not noted on the inspection work sheet. At the conclusion of the inspection, a company engineer carried out a ground run of the engines with the pilot accompanying him in the right front seat. The engineer reported that during that ground run, both engines started on the first attempt and ran normally without any anomalies being noted.
The available right engine documentation indicated that it had been certified by a US Federal Aviation Administration-approved maintenance organisation. In addition, the documentation confirmed that the engine complied with all of the engine manufacturer's service bulletins and service letters that affected the engine up to and including 17 May 2004.
The details of the propellers, including their relationship to their respective engines, were determined from examination of the pilot's e-mail correspondence and the aircraft sales brochures, and included:
A Bureau of Meteorology (BoM) post-accident assessment of the wind at the ALA at the time of the accident was that it would have been a light southerly at around 5 kts. An estimation of the ambient temperature and humidity at the ALA was not included in the BoM assessment. The BoM indicated that any difference between the BoM estimation of the prevailing wind and that reported by any witnesses could have been due to local topographical effects at the site. The BoM advised that a possible influencing factor on the aircraft's take-off could have been the presence of a dust devil9, but that the presence of that phenomenon would also require confirmation by any witnesses at the scene of the accident.
The witnesses at the landing area estimated that the wind affecting the runway was south-easterly at 5 to 10 kts at the time of the take-off. There were no dust devils reported in the vicinity of the runway at that time, and another pilot who was conducting charter work in the vicinity of the landing area indicated that there was minimal thermal activity.
Aerodrome and communications information
Aerodrome
The El Questro ALA, designation YEQO, is located at 16°00.5'S, 127°58.5'E and is at an elevation of 300 ft above mean sea level. The dirt runway is aligned south-east (runway 14) to north-west (runway 32) and is 1,400 m long and about 15 m wide. Windsocks are located at the northern side of the threshold to runway 14 and at the tourist resort homestead, which is located about 1 km south-east of the landing area.
The manager of the tourist resort indicated that when making bookings with the resort, visiting pilots generally included that they were 'self-fliers'. That was the case with the occurrence pilot. In addition, it was reported that the pilot telephoned the resort manager on the morning of 28 August 2004 and nominated a SARTIME10 for his arrival at El Questro. During that call, the pilot confirmed that he was comfortable with the location and details of the ALA. Other twin-engine aircraft of similar size to the C421 Golden Eagle were reported by the resort manager to have operated to, and continue to operate to, the El Questro ALA.
It was reported that in mid-March each year, just prior to the commencement of each tourist season, resort staff conducted a routine inspection of the runway and environs. As a result of those inspections, any newly growing vegetation was cleared from the runway and its surrounds, runway markers were repainted as required and other actions were undertaken by resort staff as and when required. In addition, the resort manager stated that he routinely consulted with aircraft operators who regularly fly to the resort, in order to confirm the ongoing suitability of the ALA for aircraft operations.
Communications
The charter pilot indicated that just prior to 1200, he exchanged a number of radio transmissions with the pilot of an unknown aircraft on frequency 126.7 Mhz in order to coordinate that pilot's take-off from the ALA. The charter pilot reported observing a plume of smoke from the vicinity of the ALA shortly thereafter, and that he did not hear a distress radio transmission. There was no facility at the ALA to record pilots' radio transmissions.
Wreckage information
The impact forces and post-impact fire sustained by aircraft structures in occurrences of this type can result in erroneous control position indications. In general, the position of the flight controls after impact cannot be relied upon as evidence of the aircraft's pre-impact configuration.
Overview of accident site and aircraft wreckage
The accident site was located on level ground, alongside a dry creek bed about 106 m to the left of the runway centreline and abeam a point on the runway about 888 m from the runway 32 threshold. A photograph of the general location of the accident site is at Figure 1. Groupings of rocks were located about the site and the surrounding light scrub was interspersed with isolated larger Boab and other trees.
Figure 1: General location of the accident site
A number of trees to the left of the runway were struck by the aircraft before it impacted the ground. Those trees were oriented along a line at about 15° to the left of the runway heading. Laser range equipment was used to measure the distances of those tree strikes from the aircraft wreckage. Trigonometry was then applied to the laser ranges in order to estimate the height of the strikes above ground level as follows:
The initial tree strike was to a tree located about 66 m to the left of the runway centreline and at an estimated height of about 8.2 m (27 feet (ft)).
The final tree that was struck prior to ground impact was located about 97 m from the runway centreline. That tree was struck at an estimated height of about 10.7 m (36 ft). The location of the left-wing tip and remnants of the left navigation light in the immediate vicinity of that tree indicated that tree strike had been by the left wing.
The aircraft impacted the ground about 33 m beyond the last tree, in a left-wing low attitude and cartwheeled counter-clockwise. The right wing and tail then struck the ground. During the impact sequence, the right engine separated from the airframe mounts and was thrown about 26 m from the main wreckage and the tail section separated from the aircraft. The main wreckage came to rest upright, with the nose of the aircraft facing south-east. All structural components and flight control surfaces were accounted for in the vicinity of the impact point. A severe post-impact fire destroyed the majority of the aircraft's fuselage, wings, tail section, cockpit and cabin, and damaged the left engine. The right engine sustained minor fire damage from a scrub fire that was started by the aircraft fire. A photograph of the aircraft wreckage is shown at Figure 2.
Figure 2: Aircraft wreckage
Wreckage examination
The investigation conducted a post-accident inspection of runway 32 from the threshold of the runway to a point on the runway abeam the ground impact point. That inspection found no evidence of any: bird or other animal remains; gouges, scrapes or other abnormal ground marks; or the presence of any detached aircraft items or components.
Very few ground impact scars or marks were able to be examined at the accident site due to them having been partially obliterated by the vehicles and personnel involved in the initial firefighting and rescue response. However, a number of rocks located in the dry creek bed had evidence of propeller impacts at substantial propeller revolutions per minute (RPM).
Both wing structures were destroyed by the fire. The right-wing forward attachment point was intact, and the aft spar was fractured in overload consistent with upward loads in excess of design limits. The left-wing structure had separated at the wing spar outboard of the engine nacelle, having also failed in overload due to the ground impact.
The fire severely damaged the aircraft fuel system. Both wing tanks were destroyed, and their associated auxiliary pumps were severely damaged. The left- and right-over-wing filler caps were secure. Damage during the impact, and the post-impact fire precluded the recovery of a fuel sample from the wreckage.
Both of the engines' air boxes and both turbocharger compressor turbines, together with their associated valves were fire damaged. On-site examination of the turbochargers did not reveal any anomalies, or foreign object, or other damage that might have adversely affected their operation. Deformation damage to the right engine's exhaust system was consistent with engine operation at ground impact. The left and right engines were recovered from the accident site and transported to an authorised overhaul facility for subsequent inspection under the supervision of the Australian Transport Safety Bureau (ATSB).
All six propeller blades separated from their respective hubs during the ground impact. Four intact propeller blades and segments from the remaining two blades were recovered from the accident site for subsequent technical examination.
Both engine propeller hubs flanges displayed indications of rotation at high RPM at the time of ground impact and were recovered from the accident site for subsequent technical examination. Severe impact damage to the propeller static stops prevented any determination of the propeller pitch settings at the time of ground impact. All of the propeller counterweights were recovered and examined on site. That examination identified overload of the threaded inserts, to the extent that a number of the counterweights had separated from their housing. That corroborated the earlier evidence of high engine RPM at the time of ground impact.
All of the cockpit and cabin seats and structures, along with the seat belts and their attachments, were destroyed by the fire. Most of the cabin fittings and cockpit, including instrumentation and switches were also destroyed. The nature of the damage to the switches was such that their position prior to the ground impact could not be ascertained. The control columns and flap actuator were destroyed in the fire and the engine controls, and the cockpit instruments and radios were severely damaged. While that prevented the examination of most of the instruments, the attitude indicators and annunciator panel were recovered for subsequent technical examination.
Pre-impact flight control continuity was confirmed for the elevator and rudder control surfaces. Flight control continuity was evident for the ailerons, from the cockpit controls aft to the point where the wing impact damage occurred. A continuity check of the engine controls was not possible as a result of the fire damage. The nature of the damage to the right flap indicated that it was retracted at the time of ground impact. The more extensive damage to the left flap precluded a definitive assessment of its position at ground impact. The landing gear was fully extended. The tyres were destroyed by the fire. The severe disruption of the tail structure rendered the determination of the aircraft trim measurements inconclusive.
Examination of components recovered from the wreckage
The left and right engines were disassembled and inspected at an authorised overhaul facility under the supervision of the ATSB and with the engine manufacturer's representative in attendance. That inspection found no evidence of internal mechanical failure within either engine, or of their associated accessories or components that would have prevented the normal operation of either engine prior to the accident.
Technical examination of the propellers and propeller segments indicated multiple high-energy hard object impact signatures on all blade surfaces. Several of those impacts were of sufficient force to have caused ductile shear of the outer airfoil sections. In addition, there was backward curling or loss of material from the blades' leading edges, with associated chordwise scoring and gouging across the airfoil sections. That was consistent with each propeller being actively driven by a comparable amount of power from within the respective engine's upper operating range at the time of ground impact.
Both engine propeller hubs sustained similar multiple fractures to their aluminium alloy housings that was consistent with ductile overload during the accident sequence. There was no indication of any pre-impact cracking or manufacturing defects. The propeller hubs were exposed to gross bending loads through the blade sockets, which was assessed as being consistent with the magnitude of the impact forces that damaged the propellers.
The technical examination of the primary attitude indicator proved inconclusive due to the extensive heat damage to the instrument. There was evidence of rotational scoring to the inside of the secondary attitude indicator's instrument case and to the gyro armature, which indicated that pneumatic drive was available to the aircraft's vacuum instruments at the time of ground impact.
The filaments from the annunciator panel globes were distorted and encased in molten glass as a result of the fire. That prevented the analysis of whether any of those lights had been illuminated at the time of ground impact.
Medical and pathological information
A review of the pilot's aviation-related medical records and the results of the pilot's postmortem examination found no evidence of any pre-existing medical disease, sudden illness or incapacitation that may have affected his ability to control the aircraft.
Fire
There was no report by the witnesses to the take-off, or evidence, of an in-flight fire. The tourist resort volunteer fire-fighting crew responded to the accident site and scrub fires.
The source of the intense post-impact fire was fuel that had spilled from the ruptured wing fuel tanks. The ignition source of the fire could not be confirmed but was likely the hot engine exhausts.
Survival aspects
The emergency locator transmitter (ELT) was destroyed in the post-impact fire. There was no report from the charter pilot, or from the search and rescue authorities to indicate that the ELT had activated on ground impact.
The destruction of the cockpit and cabin from the combined effects of the impact forces and fire rendered the accident non-survivable.
Tests and research - aircraft fuel
The last recorded refuel of the aircraft was the addition of 594 litres of aviation gasoline 100 at Broome on 27 August 2004. It was reported that the pilot refuelled the aircraft's tanks to capacity. The investigation team quarantined a sample of that fuel for subsequent analysis by an approved National Association of Testing Authorities facility. That analysis indicated that the fuel:
was clear and bright
was free from water and sediment
conformed to specification for aviation gasoline 100.
Examination of the Broome fuel supplier's records confirmed that 18 other aircraft were refuelled from that source after the occurrence aircraft on that day. There were no reports from the pilots of those aircraft of any fuel-related problems.
There were no aircraft refuelling facilities at El Questro.
Additional information
Use of aerodromes
Civil Aviation Regulation 92 places responsibility for ensuring that an aircraft landing area is suitable for landing or take-off with the pilot in command. In addition, the regulation requires the pilot to have regard to the prevailing weather conditions and other circumstances affecting the proposed landing or take-off. The determination by a pilot of which other circumstances should be considered is not stated in that regulation.
Civil Aviation Advisory Publication (CAAP) 92-1(1): Guidelines for Aeroplane Landing Areas includes guidance on the factors that may be considered by a pilot when determining the suitability of a potential landing area. While there was no evidence that the pilot had considered the requirements of the CAAP prior to planning his arrival at the El Questro ALA, the investigation applied the minimum landing area physical characteristics recommended by the CAAP to the pilot's take-off from runway 32 until the point at which the aircraft first struck a tree to the left of the runway. That examination determined the following relevant recommended parameters for the take-off:
minimum runway width - 15 m
required runway length - about 624 m
suitable lateral transitional slope, which the CAAP notes could allow for a desirable area of increased lateral clearance during the take-off and may reduce wind shear if near tall trees - maximum obstacle height of about 7.2 m at 66 m from the runway centreline.
The pilot's family indicated that the pilot had operated at a gravel airstrip in the south-west of Western Australia on a number of occasions over the previous 3 years. In addition, the family reported that the pilot drove to El Questro in June 2003 and, during that visit, most likely observed the ALA.
Preparation for flight
The pilot submitted a flight notification to Airservices Australia on the morning of the accident, for a 2 hours 15 minutes flight under the Visual Flight Rules from El Questro to Broome. The investigation estimated that 740 lbs of fuel remained after the reported 2-hour flight from Broome to El Questro, and the POH stated that 50 lbs of fuel was required for 'taxiing for take-off'. That, and the endurance nominated by the pilot in the flight notification, indicated that sufficient fuel was carried for the planned flight to Broome.
The POH stated that the aircraft equipment included a control column lock that restricted control column movement and held the ailerons in a neutral position and the elevators at about 10° trailing edge down. The aircraft manufacturer indicated that the design of the control column lock was such that, if inadvertently left engaged by a pilot, the aircraft would be unable to take-off. The available documentation indicated that an optional rudder gust lock was also included in the aircraft equipment. The POH stated that engagement of that lock required the rudder to be centralised and the elevators to be moved to the fully 'down' position. Disengagement of the rudder lock was possible either manually during the aircraft pre-flight, or automatically as the elevator was moved up through the 6° 'down' position. Due to the damage to the aircraft, the investigation was unable to confirm the position of these locks.
Manufacturer data
The POH promulgated the necessary checks to be carried out by the pilot when operating the aircraft. That included confirmation of the selection of the left and right engines to the left and right main fuel tanks respectively as part of the following checks: before start, before take-off and during the descent. In addition, the POH stated that:
A take-off with one main tank full and the opposite tank low on fuel creates a lateral unbalance. This is not recommended since gusty air or premature lift-off could create a serious control problem.
The published take-off technique included the requirement for the pilot to raise the nose wheel at 95 kts indicated air speed (KIAS) and lift the aircraft from the runway at 100 KIAS. In addition, the POH included a description of the aircraft stall including that:
the stall characteristics are conventional
there is an aural stall warning device that operates at 5 to 10 KIAS above the stall in all configurations
the stall is preceded by a mild, aerodynamic buffet, which increases in intensity as the stall is approached
the power-on stall occurs at a very steep pitch angle, either with or without flaps extended
it is difficult to inadvertently stall the aircraft during normal manoeuvring.
Stall speeds were published in the POH for a number of aircraft configurations. None of those configurations reflected the aircraft's take-off configuration. At the estimated aircraft weight and with wings level, the maximum stall speed for the published configurations was calculated as 83 KIAS. The increase in stall speed at 15° angle of bank for all published configurations was about 2 KIAS.
The manufacturer's Pilot Safety and Warning Supplements identified a rare, but potentially serious problem known as 'split wing flaps'. Split or asymmetric wing flaps may result from a mechanical failure in the flap system and cause the flap position on one wing to differ from that of the opposite wing flap. The result is a tendency for the aircraft to roll in the direction of the retracted flap. Depending on the experience and proficiency of a pilot, the manufacturer indicated that any rolling tendency caused by a split flap situation may be controlled with opposite aileron. In addition, there was the potential for a pilot to apply differential power in a multi-engine aircraft to assist in managing the condition. This is discussed further in the Analysis under 'Take-off'.
Only those investigation areas identified by the headings and subheadings were considered to be relevant to the circumstances of the occurrence.
A take-off commenced by a pilot without pausing an aircraft in a stationary position on a runway, or decreasing the speed of an aircraft on arriving at a runway intended for use for a take-off.
A witness that heard, but did not observe the take-off.
On 14 November 2003, the pilot submitted an application to the Australian Civil Aviation Safety Authority (CASA) to reserve an Australian aircraft registration in anticipation of registering the aircraft in Australia. That reservation was granted by CASA.
Based on the 50-hourly inspection that was carried out in Broome on 26 August 2004 being conducted within the potential 10-hour extension period that had been authorised by the Swiss regulatory authorities. That was between 50 and 60 hours after an annual/200 hours check that was reported as being commenced in Switzerland on 10 December 2003, and included the 2.0 hour flight to El Questro ALA.
Derived from e-mail correspondence from the pilot dated over the period 16 September 2003 to 24 August 2004 and the available aircraft and engine documentation.
Derived from the right engine Export Certificate of Airworthiness of 19 May 2004 and e-mail correspondence from the pilot dated 29 July to 19 August 2004.
Precise date not available.
A miniature whirlwind with the potential to be of considerable intensity, and to pick up dust and perhaps other items and carry them some distance into the air.
The time nominated by a pilot for the initiation of Search and Rescue action if a report has not been received by the nominated unit.
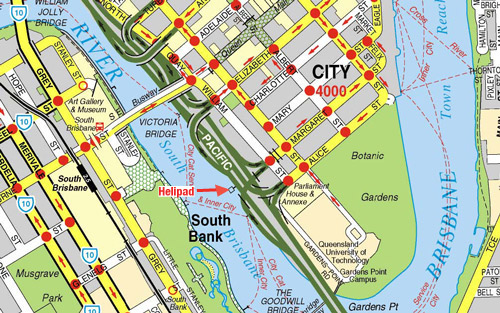
On 11 November 2005, CASA advised that is was considering a review of Civil Aviation Advisory Publication (CAAP) 92-2(1) - Guidelines for the establishment and use of helicopter landing sites, which would take into account issues including helipad load bearing capability, including how such information is relevant to owners and users of helipads, the differences in deck-imposed loads for wheel compared to skid equipped helicopters, and whether the load bearing capability of a helipad should be painted on the landing surface.
CASA also advised that it represented Australia on the International Civil Aviation Organization Aerodromes Panel which has established a Heliport Design Working Group to review the design standards for helicopter landing sites. Recommendations from the working group, which are expected in mid 2006, may assist in a review of the CAAP.
On 18 October 2005, the Queensland Government advised that it had undertaken significant action to review and enhance its management and operation of its helicopter landing sites in Queensland since the accident. Those measures included:
closure and removal of the helipad from the Brisbane River;
the conduct of an audit of Queensland Government owned helicopter landing sites;
establishment of a project within the Department of Public Works assisted by a whole of government reference group to develop comprehensive guidelines for administration of Queensland Government helicopter landing sites, in consultation with the Civil Aviation Safety Authority; and
engagement of a consultant to prepare the guidelines, due for completion in December 2005.
On 9 January 2006, the Queensland Government advised that:
… the consultant appointed to develop guidelines for the management of government helicopter landing sites has been given an extension until 25 January 2006 to complete the guidelines. Following review by the Committee and government consideration, it is anticipated that the guidelines will be finalised and adopted during the first quarter of 2006.
Analysis
ANALYSIS
The circumstances of the accident are consistent with dynamic rollover occurring after the right wheel penetrated the helipad surface and acted as a pivot point about which the helicopter rolled. As the helicopter rolled, the main rotor blades contacted the walkway. Because the timing and order of the events that occurred during the rollover were not available, a detailed analysis of the accident sequence was not possible. However, the pilot's response of applying opposite cyclic control, but not lowering the collective pitch control when the helicopter began to roll was not the most effective method of preventing the development of the rollover. Whether the rollover may have been prevented and/or the consequences limited had the pilot lowered the collective pitch control was not able to be determined.
The pilot did not establish before the landing that the load capability of the helipad was appropriate to the requirements. He appeared to have two bases to support his decision to operate the Agusta A109C onto the helipad. One was that neither the helipad owner, nor CASA, had told him that he could not. Such reasoning was inadequate and demonstrated a low level of risk awareness. The second was that other helicopters of operating weight similar to the Agusta A109C had used the helipad. That reasoning was also inadequate because it did not take into account that those helicopters were skid-equipped, and would not subject the helipad deck to the point loads that would exist with the Agusta A109C. It demonstrated an inadequate level of knowledge.
The location of the deck failure was where the plywood would be subject to the greatest bending for a given load, and consequently, where a failure was most likely to occur. The potential for a similar failure would have been present since changes were made to the plywood sheeting size and grade. However, variability between factors such as helicopter wheel positions, dynamic movement of the helipad, and the pilot's flight control inputs would have changed the effect on the deck of each landing. It is likely that the crack in the underside of the plywood in the area of the deck opposite the failure location was an example of the effect of those factors during a previous landing by the helicopter.
Documentation regarding maintenance of the helipad indicated that the installation of the smaller size sheeting most likely occurred during repairs that were completed in September 2000. At that time, other than by way of the design drawings prepared in 1984, full-width plywood sheeting was not specifically addressed either by the oversighting government department or the contractor conducting the repairs.
The strength of the helipad deck compared with the load imposed by the helicopter can be demonstrated from the following information:
Decking design load
73 kg (evenly distributed on each 600 mm x 400 mm panel)
Calculated static load on each helicopter main wheel
928 kg (spread over the tyre footprint, which approximates a point load of 66 MPa)
Decking design stress
5.138 MPa
Measured strength of plywood from failed deck
61 MPa
Strength of marine grade plywood
40 MPa
It is apparent that the strength of the plywood used in the decking (61 MPa) was approximately 12 times greater than required by the design (5.138 MPa). By comparison, the load applied by each main wheel (928 kg) was approximately 13 times greater than the design load (73 kg per panel).
It is unlikely that the helipad owner calculated the load bearing capability of the helipad with respect to specific helicopters that used the helipad, or their type of landing gear. In particular, the reason for the 2,000 kg load limit, as advised to users of the helipad, appears to be unsubstantiated. The potential for the plywood to be subjected to point loads by helicopter wheels, was not taken into account during the design of the replacement deck. Together with the dynamic movement of the deck by wind and wave action, that effect would have significantly increased the effective ratio of wheel loading to deck design load.
The load limit issues, the installation of plywood deck sheeting of size inappropriate given the existing supporting structure, and the poor condition of some areas of the deck indicated shortcomings in the maintenance and management oversight of the helipad.
Prior to April 2004 there was apparently no awareness within the helipad owner's organisation of the significance of helicopter landing gear configuration to the load bearing capability of the helipad. Nor were there indications that the owner was aware of CAAP 92-2(1), or the guidance it contained. It is likely that those issues were unrecognised due to a lack of aviation technical expertise within the helipad owner's organisation.
CONCLUSIONS
Factors
Management and maintenance of the helipad did not encompass all the aspects necessary to ensure that the actual load bearing capability of the helipad, including for skid and wheel type landing gear equipped helicopters, was known.
The actual load bearing capability of the helipad was less than that required for safe use by the Agusta A109C helicopter.
The pilot did not check before the flight, whether the helipad was capable of safely accepting the loads imposed by the Agusta A109C helicopter.
On 30 July 2004, at about 1120 Eastern Standard Time, an Agusta A109C helicopter, registered VH-ZZN, was being operated on a private flight from the Gold Coast to Brisbane Airport via the Brisbane River Helipad. The pilot and two passengers were on board. The intention was to disembark one of the passengers at the helipad, without shutting-down the engines, and then to continue the flight to Brisbane Airport.
The pilot reported that he established the helicopter in a low hover above the helipad and was satisfied that it was correctly positioned above the painted white landing circle. He then allowed the wheels to settle on the helipad, with the right side of the helicopter facing the river bank. The pilot said that he kept his left hand on the collective pitch control lever and his feet on the tail rotor pedals. He then gripped the cyclic control with his knees so that he could open the cockpit door with his right hand. He leaned out and checked that the helicopter was centrally positioned in the landing circle and that the right main wheel was not causing any visible stress to the helipad surface. He then applied the parking brake and closed the door before telling the passenger to disembark through the right cabin door.
The pilot recounted that when the passenger was safely clear of the helicopter, he applied a small amount of collective pitch control in preparation for lift off. He then felt the helicopter lurch and begin to roll right. The pilot immediately applied full left cyclic pitch control and maintained the collective pitch control position. However, the helicopter continued to roll rapidly right and the main rotor blades struck the walkway safety rails. The helicopter came to rest inverted between the helipad and the riverbank, with the forward fuselage against the junction between the helipad and the connecting walkway.
The helicopter was not fitted with a flight data recorder or cockpit voice recorder, nor was it required to be by relevant aviation regulations. Consequently, there was no information available regarding the events or timing of the accident sequence, including the rate of helicopter movement and any control inputs made by the pilot.
Injuries to persons
The pilot and passenger received minor injuries but were able to egress from the helicopter unassisted.
Damage to the helicopter
The helicopter was substantially damaged during the rollover sequence. Contact with the walkway destroyed the main rotor blades and damaged the forward fuselage. The fuselage was partly immersed in water. There was no fire.
Debris from the helicopter was found up to 200m from the helipad, both on and adjacent to the pedestrian/bikeway on the riverbank. There was potential for debris to have been thrown onto the adjacent road complex.
Other damage
Initial examination of the helipad revealed that the helicopter's right main wheel had broken through the deck sheeting on the edge of the white painted landing circle (Figure 1). See also page 7, 'Helipad examination'.
The helicopter's main rotor blades caused substantial damage to the walkway linking the pontoon to the riverbank.
Figure 1: The helicopter as it came to rest. The arrow points to the location of the deck surface failure
Pilot in command
The pilot, who was the chief pilot of the organisation that operated the helicopter, held a valid commercial pilot licence (helicopters). His total flying experience (all rotary wing) was 1,720 hours, of which approximately 250 hours were on the Agusta A109C type (all on VH-ZZN). The pilot had operated onto the Brisbane River Helipad on numerous occasions since 1 July 2003 in Hughes 500 and McDonnell Douglas 600 type helicopters, and on 19 occasions in the Agusta A109C type2.
Aircraft information
The Agusta A109C was a twin turbine-engine helicopter capable of carrying up to seven passengers. Its maximum operating weight with an internal load was 2,720 kg. The helicopter was equipped with a retractable landing gear, which comprised a nose wheel and two main wheels.
The estimated weight of the helicopter at the time of the accident (including approximately 300 L aviation turbine fuel) was 2,471 kg. Under those conditions, and taking account of the centre of gravity position, the static load on each main wheel was about 930 kg. According to documentation provided by the operator, there were no outstanding maintenance requirements for the helicopter at the time of the accident. The pilot reported that the helicopter was operating normally in the period prior to the accident.
Brisbane River Helipad
The 9.4 m square helipad was owned and administered by the Queensland State Government. It was located adjacent to the northern bank of the Brisbane River at the end of Margaret Street in Brisbane City (Figure 2). It was mounted on a tethered floating pontoon that was linked to the riverbank by an 11 m walkway. Safety rails approximately one metre high were attached to either side of the walkway. There was a pedestrian pathway and motor vehicle road infrastructure along the riverbank adjacent to the helipad.
Figure 2: The Brisbane River Helipad location
Documentation relating to the operation and maintenance of the helipad was contained in separate files that were administered by various Queensland State Government departments and branches of departments during the period 1981-2004. Through most of that time, operational control and maintenance responsibility for the helipad were held by separate departments, with maintenance aspects being handled predominantly by the department that had responsibility for maritime safety and/or harbours and marine. No record was found on the files of the original design criteria for the helipad, including the helicopter type(s), operating weights, and type of landing gear (skid or wheels) for which it was intended to be used.
Helipad examination
The helipad deck (Figure 3) consisted of 1,200 mm x 2,400 mm plywood sheeting nailed to 100 mm x 75 mm hardwood joists 600 mm apart. The joists were attached to a series of aluminium 'I' beams mounted on two pontoons. The longer (2,400 mm) sides of the plywood sheets had tongue and groove edges and butted over the approximate mid-point of every alternate joist. The shorter (1,200 mm) sides of the plywood sheets did not have tongue and groove edges and were not structurally connected. There was no supporting structure beneath those sides except at the midpoint position at the location of a joist. The central area of the helipad surface (where the helicopter landed) appeared to have been in relatively good condition.
Figure 3: After removal of the wreckage. Individual plywood decking sheets are evident. The arrow points to the location of the deck failure
Figure 4: Location of the deck failure and its relationship to the supporting framework
The location of the deck failure coincided with the corner of one of the plywood decking sheets (Figure 4). The nature of the failure was consistent with the right wheel of the helicopter bearing down on the plywood sheet midway between two adjacent joists, and near the edge of the sheet. The edge formed the shorter (1,200 mm) side of the sheet and was not structurally connected to the adjacent sheet edge.
Specialist examination concluded that the final failure occurred at the point of highest bending moment between the joists. The individual layers within the decking sheet all failed at the point of highest bending, suggesting that the plywood adhesive and the timber layers had not deteriorated due to water ingress.
Laboratory tests carried out on samples taken from the failed section of the deck revealed a bending strength of 61 megapascals (MPa). The size of the test samples was smaller than stipulated by the standard. However, that bending strength exceeded the bending strength of marine grade plywood3.
Examination of the underside of the deck revealed a significant longitudinal crack on the side of the deck opposite the failed section. The deck upper surface at that location showed no sign of damage. The crack displayed damage to the lower layers of the plywood midway between two longitudinal joists. The cracking was not adjacent to the edge of a plywood sheet and was not observed when the helipad was inspected in April 2004. Specialist assessment of the damage concluded that it was likely to have been caused by a point loading in the order of 1,200 kg.
Some areas of the deck on the river and upstream sides of the helipad were significantly degraded due to water ingress into the layers of the plywood, probably as a result of wave action. Examination of those areas indicated that both the ply adhesive and the wood itself had deteriorated significantly. Deterioration of that nature was consistent with continuous contact with, or immersion in, water for an extended period. Those areas, however, were not related to the occurrence.
Helipad load bearing capability
There were numerous references in the helipad owner's documentation regarding the pad's load bearing capability. The earliest of those appeared in drawings that were completed in 1984 for the installation of a new deck consisting of plywood sheets mounted on aluminium support beams (Drawing No. BN-5-43-1). The design strength of the replacement deck was based on a pressure of 3 kilopascals (kPa) evenly distributed over the entire deck area, although the origin of the selected value was not clear. A pressure of 3 kPa is equivalent to 306 kg evenly spread over each square metre of decking. The layout of the plywood sheets over the aluminium support beams resulted in a design panel size of 600 x 400 mm (0.24 sq.m), equivalent to 73 kg evenly distributed on each design panel. The designer's calculations showed that this loading would create a bending stress of 5.138 megapascals (MPa) in the plywood decking, which was well within the allowable working stresses for the F114 grade structural plywood selected for the repairs. There was no indication in the documentation that the design of the repairs included any consideration for point loads, such as would be experienced from wheel equipped helicopters.
In May 1982, a request to land a helicopter weighing up to 3,630 kg on the helipad was refused because 'it would be unsafe to place this weight on the helipad'. However, there was no supporting documentation for that statement.
A July 1997 document authorising a private operator to use the helipad included the statement that the applicant 'should be aware that there is a load limit for the HLS [helicopter landing site], and aircraft in excess of 1,400 kg should not access the HLS'. There was no information regarding the origin of that figure.
In late 1996, the Queensland Government commissioned a feasibility study by a town planning consultant on the future options for the helipad. The study, completed in late 1997, noted that there was:
… no evidence at hand which would indicate it's [the helipad's] safe load capabilities but it appears to be beyond the operation of the Queensland Emergency Services helicopter - a Bell 412 with a maximum take-off weight approaching 5,400 kg - but comfortably accommodates most small to medium-sized turbo driven helicopters in use in the region. The practical limit appears to be approximately 3,000 kg.
There was no supporting evidence to indicate how that conclusion was reached.
In March 1997, there was internal correspondence regarding the establishment of a deed of indemnity that was to apply to users of the helipad. A deed was developed and in early 1999 was sent to users of the helipad for signature. In June 1999, in response to a request to use the helipad, a list of 'requirements that apply to the use of the helipad' was included, for the first time, in the covering letter to the deed. Those requirements included the following:
1. The helicopter landing site is intended for the use by helicopters within the "small" utility class only i.e. helicopters up to 2,000 kg in mass, and 2. The permittee, or their nominated pilot, are responsible for ensuring that the helicopter landing site is in suitable condition before intended use.
There was no indication in the documents regarding the origin of those 'requirements'. Subsequently, there were other instances where prospective users of the helipad were provided with a copy of the requirements when they were asked to sign the deed of indemnity.
In April 2004, a helicopter operator not associated with VH-ZZN contacted the helipad owner requesting confirmation that an Agusta A109C helicopter could land on the helipad. The operator noted that the weight of the Agusta A109C was between 2,000 and 3,000 kg and that, because the helicopter was equipped with wheel instead of skid type landing gear, a 'wheel footprint' of about '1,200 kg per mainwheel' would exist. A reply was sent to the operator advising that the helicopter weight exceeded the 2,000 kg limit that formed part of the standard terms of use for the helipad. The operator replied, noting that skid equipped helicopters weighing greater than 2,000 kg, such as the AS350 Squirrel5, had landed on the helipad.
In May 2004, the Civil Aviation Safety Authority (CASA) contacted the helipad owner regarding the helipad. CASA requested the weight restrictions and the conditions of use of the helipad, and asked whether the weight limit was clearly marked on the helipad. That request, along with the earlier questions and information regarding the suitability of the helipad for the Agusta 109 helicopter, generated activity by the helipad owner including the proposal that a safety audit of the helipad be conducted as a matter of priority.
The justification for the proposed audit was that there may be safety issues associated with the helipad that were not being adequately addressed, such as appropriate usage and signage, and the proximity of the helipad to pedestrian and motor vehicle traffic adjacent to the helipad. At the time of the accident, those issues had not been progressed.
Helipad maintenance history
The helipad owner conducted major maintenance on the helipad in 1984, 1997, 2000 and 2004. In the intervening periods, minor maintenance was conducted. The maintenance activities generally involved work on the flotation pontoons, mooring chains, and the walkway linking the pontoon to the riverbank, and the helipad deck. For the purposes of this report, however, discussion of maintenance activities will focus on the helipad deck.
The drawings for the helipad prepared in 1984 (Drawing No. BN-5-43-1) indicated nominal deck dimensions of 9,400 mm x 9,400 mm and specified a series of hardwood plywood 'rot proofed' decking sheets 9,400 mm x 1,200 mm, with minimum stress grade F11.
At the commencement of the work phase of the repairs conducted in 1984, the contractor proposed standard size plywood sheeting 2,400 mm x 1,200 mm for the decking but that was deemed not acceptable by the helipad owner because the sheet size was not in accordance with the drawing specifications. Subsequently, a special order of 9,400 mm x 1,200 mm plywood sheeting was obtained. The repairs to the helipad, including the installation of the new 9,400 mm long plywood decking sheets on aluminium support beams, were completed in March 1985.
The major maintenance undertaken on the helipad in 1997 included the replacement of two plywood decking sheets and painting of the deck. The documentation indicated that the replacement plywood sheets were 9,400 mm long.
Inspection of the helipad in May 2000 revealed that, in addition to other items requiring rectification, most of the plywood decking was badly deteriorated and beyond repair. On 4 May 2000, the company that subsequently won the contract to conduct the repairs was asked to provide a price:
… to replace any damaged structural plywood sheeting of the deck of the helipad (both a price to replace each sheet and a price to replace all the sheeting). The plywood shall [be] in accordance with Drawing No. BN-5-43-1 and classified as Marine Grade Structural Plywood.
The contractor provided a price to remove and replace all sheets/deck and to coat all surfaces with a product that he stated would waterproof all surfaces and provide total protection to the pontoon/helipad for many years. The contractor was awarded the contract on 16 May 2000. Aside from the reference contained in drawing No. BN-5-43-1, the documents did not refer to the plywood decking sheet size. Documents dated early September 2000 indicated that the rectification works had been inspected as being completed. There was no confirmation in those documents regarding the grade of plywood or sheet size used on the deck.
Another inspection of the helipad was conducted in December 2003. Among the defects identified were four areas of deck sheeting that had loosened, and that the deck needed repainting. The pontoon was removed from the river in March 2004 and the repairs undertaken. There was no reference to any plywood deck panels or supporting beams being replaced during that work. The helipad was returned to service on 21 April 2004.
Operator's information regarding the helipad
The helicopter operating company's operations manual included a register of helicopter landing sites that were used by the company, and pertinent details regarding those sites. The Brisbane River helipad was included in that register. The register details included a caution note regarding river craft during approach and departure, and local pedestrian traffic during approach termination. The register contained no information regarding the load capability of the helipad.
An email dated 1 December 2003 was sent by the helipad owner to the company operating the helicopter regarding access by that operator to the Brisbane River Helicopter Landing Site. The email stated that the deed of indemnity applying to the operator was attached to the email along with:
a copy of the cover sheet that accompanies the Deed of Indemnity as this cover sheet provides details of access restrictions etc.
However, the investigation was unable to establish conclusively that details of the access restrictions had been attached to the email. The deed of indemnity, signed by the helicopter pilot under the company seal, was returned to the helipad owner by facsimile on 1 December 2003 under the signature of the company operations manager.
The pilot reported that he had not sought any information from the helipad owner regarding the load capability of the helipad and claimed that he was not aware that the helipad had a load rating. He stated that he had never seen any document regarding a load rating for the helipad and that the helipad owner had never advised him of a weight limit for operating on the helipad. His rationale for not seeking information regarding the load capability of the helipad was that both the helipad owner and CASA were aware that he was operating the helicopter onto the helipad and neither organisation had advised him against such operations. He had therefore presumed that it was safe to land on the helipad.
The pilot believed that a Bell 412 helicopter operated by the helipad owner had landed on the helipad, and that 'countless other helicopters of larger sizes' than the Agusta 109 had operated onto the helipad. (Personnel involved in the operation of the helipad owner's Bell 412 helicopters reported that they had never operated the Bell 412 helicopter type onto the Brisbane River helipad. No record was found to indicate that any helicopter larger than the Agusta 109, or any other wheel equipped helicopter, had landed on the helipad.)
Operator's procedures
The operator advised that its standard procedures for operating onto a marine helipad included the following after-landing checks:
• visually determine if the helicopter is actually centred on the heli-pad; • visually observe the deck of the pad to make sure [sic] it is holding the aircraft well; and • Apply the handbrake and allow passenger(s) disembarkation.
The pilot reported that he followed those procedures for all landings on helipads with both wheel and skid equipped helicopters, and did so on this occasion. In the case of the Agusta A109C, it was necessary to open the door to view below, and fore and aft of, the helicopter. When he checked after landing whether the right main wheel was causing any stress to the helipad surface, it was as part of his standard practice and not because he was unsure as to whether the deck would support the helicopter.
Regulatory aspects
The Civil Aviation Safety Authority issued the Civil Aviation Advisory Publication (CAAP) 92-2(1), in January 1996 titled Guidelines for the establishment and use of helicopter landing sites (HLS). The CAAP included the following introductory statement:
The information contained in this publication is advisory only. There is no legal requirement to observe the details as set out. The Civil Aviation Regulations detail the legal requirements that must be complied with in relation to use of areas for takeoff and landings by a helicopter. While there may be a number of methods of ensuring that the requirements of the Civil Aviation Regulations are met, this CAAP sets out criteria which ensures compliance with the regulations. The CAAP must be read in conjunction with the Civil Aviation Regulations.
The following text appeared under the heading 'Purpose of this CAAP':
Civil Aviation Regulation 92 (1) states that: "an aircraft shall not land at, or take-off from, any place unless: … (d) the place …. is suitable for use as an aerodrome for the purposes of the landing and taking off of aircraft; and, having regard to all the circumstances of the proposed landing or take-off (including the prevailing weather conditions), the aircraft can land at, or take-off from, the place in safety."
Regulation 92 (1) does not specify the method of determining which "circumstances", other than the prevailing weather conditions, should be considered in any particular case. These matters are the responsibility of the pilot in command and, in some circumstances, are shared with the aircraft operator. These guidelines set out factors that may be used to determine suitability of place for the landing and taking off of helicopters. Experience has shown that, in most cases, application of these guidelines will enable a take-off or landing to be completed safely, provided that the pilot in command: • has sound piloting skills; and • displays sound airmanship.
Under the heading 'Factors that should be considered prior to using an HLS', the CAAP stated, in part, that:
The pilot of the helicopter operating to, from or at an HLS should ensure that: • the HLS is clear of all: - persons, other than persons essential to the helicopter operation; and - objects and animals likely to be a hazard to manoeuvring the helicopter, other than objects essential to the helicopter operation; and • no person outside the helicopter, other than a person essential to the operation is within 30 m of the helicopter; and • appropriate permission from the owners and authorities has been given.
The CAAP also listed recommended criteria for two types of HLS - Basic and Standard.
The CAAP defined a basic HLS as 'a place that may be used as an aerodrome for infrequent, opportunity and short-term basis for all types of operation, other than RPT, by day under helicopter VMC6'. The criteria for a basic HLS included that it should be large enough to accommodate the helicopter safely and should have a surface capable of withstanding the static and dynamic load imposed by the helicopter.
The CAAP defined a standard HLS as a place that may be used as an aerodrome for helicopter operations by day or night. The recommended criteria for a standard HLS were more comprehensive than those for a basic HLS.
Documents from the helipad owner revealed that in 1992 the question arose as to whether the helipad complied with the then Civil Aviation Authority (CAA) regulations. In 1994, that issue was raised again and there was concern that if the helipad was moved a further 11 metres away from the riverbank to comply with CAA regulations, such action could conflict with the requirements of the Harbours Act.
The consultant undertaking the feasibility study commissioned in late 1996 advised the helipad owner at that time that the CAA requirement impacting on the distance of the helipad from the riverbank had been removed, and that it was now up to the pilot to determine the suitability of a particular location for landing.
The consultant's report, completed in October 1997, expanded on the advice given in late 1996 and discussed some aspects of CAAP 92-2(1). The study noted that 'the type of HLS to be authorised for use at this site under the Civil Aviation Regulations is a little obscure but would appear to fit the 'Marine HLS' model'. The study concluded that the 'existing facility' did not conform to the Marine HLS criteria due to the proximity of the adjacent infrastructure. The study did not address the basic or standard HLS load bearing criteria contained in the CAAP. There was no evidence on the files examined that there had been any follow-up by the helipad owner regarding the criteria of the helipad against those of the CAAP.
Dynamic rollover
A phenomenon known as dynamic rollover can occur during helicopter operations. It arises when the helicopter is placed in a situation where it is pivoting or rolling around a wheel or skid that is in contact with a fixed object.
Dynamic rollover can occur during or prior to the hover when any part of the helicopter acts as a pivot and the helicopter exceeds a critical angle of roll. This angle is dependant upon control limits and, in most helicopters, is in the order of 15 degrees.
Rough ground or obstructions that pin a wheel or skid to the ground can contribute to dynamic rollover. Several rollover accidents have been caused by hitting an obstruction with the landing gear or by attempting a take-off with an obstruction next to the gear.
Regardless of rotor design, actions needed to correct a roll rate are the same and should be instinctive: simultaneously reduce collective and adjust cyclic to maintain lateral trim.7
Once started, dynamic rollover cannot be stopped by application of opposite cyclic control alone. For example, if the right skid or wheel of a helicopter contacted an object and became the pivot point while the helicopter started to roll to the right. Even with full left cyclic applied, the main rotor thrust vector and its moment would follow the aircraft as it continued rolling to the right. Quickly applying down collective is the most effective way to stop the development of dynamic rollover. The phenomenon can occur in both skid and wheel equipped helicopters, and all types of rotor systems.8
Dynamic rollover has been identified in Australia9 and overseas as a contributing factor in helicopter accidents.
The helicopter manufacturer advised that the critical dynamic rollover angle for the A109C had not been determined. The static lateral rollover limit for the helicopter was 27.8 degrees at minimum flight weight (the most critical condition). The maximum slope from which the helicopter was able to takeoff and land with adequate safety margins was 10 degrees.
1. Only those investigation areas identified by the headings and subheadings were considered to be relevant to the circumstances of the occurrence. 2. The Hughes 500 and McDonnell Douglas 600 were small utility type helicopters whose normal maximum operating weights were less than 2000 kg. Both were equipped with skid type landing gear. 3. Table B1 of AS/NZS 2272 1996 Plywood Marine stated that 'The stress grade of plywood manufactured to this standard is a minimum of F14. The sectional properties, if required, shall be calculated by the method specified in AS/NZS 2269'. Table 4.1 of AN/NZS 2269 Plywood-Structural stated that the characteristic bending strength of F14 plywood was 40 MPa. 4. 'Stress grade' refers to the classification of a piece of timber to indicate, for purposes of structural design, a set of basic working stresses and stiffness appropriate to that piece. The grade is designated by a number preceded by the letter F eg. F8. The letter stands for "force" and the number is the amount of stress, in megapascals, that the timber will withstand without bendin beyond acceptable limits in a test situation. 5. It was reported that a single-engine Eurocopter Squirrel helicopter, which had a maximum all-up weight of 2,100 kg and a twin-engine Eurocopter Squirrel helicopter, which had a maximum all up weight of 2,540 kg had operated onto the Brisbane River Helipad. However, the operating weights of the helicopters on those occasions were not established. 6. Visual Meteorological Conditions (VMC) define the in-flight conditions (visibility and distance from cloud) under which aircraft should operate to conduct flight under the visual flight rules (VFR). 7. Rotorcraft Dynamic Rollover. A new look at the problem. Flight Safety Australia, April 1999. 8.Rotorcraft Flying Handbook (FAA-H-8083-21) 2000, Federal Aviation Administration, Flight Standards Service. 9.ATSB report 200300982.
Summary
The pilot landed the helicopter on the Brisbane River Helipad to disembark a passenger. As the pilot prepared to lift off, the right main wheel penetrated the pontoon deck, causing the helicopter to capsize. The circumstances were consistent with dynamic rollover. The pilot did not lower the collective pitch control (the recommended response to dynamic rollover) when the helicopter began to roll.
The helipad consisted of a plywood deck mounted on a framework that formed a floating pontoon moored to the river bank. Prior to the flight the pilot had not checked the load bearing capability of the deck, but assumed that the helipad was capable of accepting the Agusta 109 helicopter. Examination revealed that the point load imposed by the main wheels of the helicopter was close to the tested strength of the plywood pontoon decking material. The additional dynamic load effects due to helicopter movement, and wind and water action, were likely to have increased the loads on the deck surface, causing failure of the plywood.
Documentation relating to the management and maintenance of the helipad revealed that the actual load bearing capability had never been established. Potential users of the helipad had been advised of a load limit of 2,000 kg, although the origin of that figure was unknown. The pilot claimed that he was not aware of that limit.
The engineering drawings for the deck called for plywood sheets that extended the full width of the deck. However, smaller sheets were used when the deck surface was last replaced. That had the effect of introducing weaker areas where sheet ends butted together but were unsupported. The deck failure occurred at one of the sheet ends.
As a result of this occurrence, The Australian Transport Safety Bureau (ATSB) draws to the attention of Australian operators of Hiller UH-12E helicopters, the difficulties associated with inspecting the horizontal stabiliser spar tube assembly.
The ATSB has also advised the Civil Aviation Safety Authority of the difficulties associated with inspection of the horizontal stabiliser spar tube assembly and will circulate copies of this report to all Australian operators of Hiller UH-12E helicopters.
Factual information
FACTUAL INFORMATION
On 15 June 2004, a Hiller Aviation UH-12E helicopter, registered VH-HMT, crashed during an agricultural operation, after the pilot reported a loss of tail rotor authority. The pilot was not injured in the accident. The horizontal stabilizer was found about 150 m from the wreckage site, indicating that it had separated from the helicopter in-flight. The operator reported that damage to the stabiliser and the tail rotor blades was consistent with the separated stabiliser coming into contact with the tail rotor blades, as it was still connected to the helicopter by the taillight wiring. The operator reported that an engineering examination found no evidence of tail rotor system failure.
The horizontal stabiliser spar tube failed in the area where the tube passes through a collar in the doubler attached to the inner stabiliser rib (refer to figure 1).
Figure 1: Horizontal stabiliser and detail of the spar tube and doubler.
Helicopter
The helicopter was manufactured in 1978 and had accumulated 6,903.50 hours time in service at the time of the accident. In September 2002, at 6,386.25 hours in service, it sustained major damage following a sudden main rotor stoppage. The helicopter was rebuilt and had since accumulated approximately 517.20 hours in service. It was maintained in accordance with the maintenance requirements applicable at the time and had a valid Maintenance Release. It had flown approximately 31 hours since the last periodic inspection, a 100 hourly inspection completed in May 2004.
Horizontal stabiliser
The operator advised the Australian Transport Safety Bureau (ATSB) that the horizontal stabiliser is not a serial numbered item and its time in service since new was not known. The stabiliser was fitted to the helicopter when it was acquired from its previous owner. During the helicopter rebuild in September 2002, the stabiliser was inspected in accordance with the 100 hourly component inspection guide and the Hiller UH-12E maintenance manual, before being re-installed. The component inspection guide required the stabiliser tube to be inspected for corrosion and security and the maintenance manual detailed the spar tube inspection requirements and wear limits. No anomalies with the horizontal stabiliser were reported at that time.
Spar tube failure
The failed horizontal stabiliser was forwarded to the ATSB for detailed examination. That examination revealed that the stabiliser spar tube fractured as a result of fatigue cracking. The crack initiation occurred at a number of locations where the tubing had been reduced in wall thickness by wear. It was apparent that the wear of the tubing was associated with small scale repeated movement between the stabiliser tube and the doubler attached to the stabiliser's inner rib. There was no evidence of any pre-existing defect present.
A search of the ATSB, United States National Transportation Safety Board and Federal Aviation Administration databases found no reported events involving an in-flight separation of the horizontal stabiliser on similar helicopter types.
Summary
The Australian Transport Safety Bureau did not conduct an on-scene investigation of this occurrence.
In July 2006, the Robinson Helicopter Company issued Safety Notice SN-40, titled "Post crash Fires". That Safety Notice states:
There have been a number of cases where helicopter or light plane occupants have survived an accident only to be severely burned by fire following the accident. To reduce the risk of injury in a post-crash fire, it is strongly recommended that a fire-retardant Nomex flight suit, gloves, and hood or helmet be worn by all occupants.
Conclusions
3 Conclusions
3.1 Findings
There was no witness or mechanical evidence to indicate any problems with the flight controls, fuel system or engine prior to the event.
Failure of the forward flex plate resulted in drive to the main rotor gearbox being partially disconnected.
The failed forward flex plate coupling punctured one or both the helicopter fuel tanks and the stainless steal engine compartment firewall.
The helicopter settled heavily and impacted with terrain.
The helicopter was destroyed by impact forces and a post-impact fire.
Egress from the helicopter was hampered by the unusual attitude of the cabin which caused extended exposure of the survivor to the post-impact fire.
3.2 Significant factors
One of the two bolted joints linking the flex plate to the main rotor gearbox yoke in the forward flexible coupling was previously assembled incorrectly, resulting in a lack of clamping force and subsequent fatigue failure of the flex plate and loss of drive to the main rotor gearbox.
Analysis
2 ANALYSIS
2.1 Helicopter
The initiating event in the occurrence sequence was the failure of the flex plate in the forward flexible coupling. That event was the source of the loud noise that the passenger reported hearing. Once the plate failed, the clutch shaft yoke was retained at one end only. As a result, the diameter of the yoke and flex plate effectively doubled, allowing those rotating components to contact and puncture the fuel tanks and the horizontal stainless steel fire wall, as observed in the wreckage examination. Fuel leaking from the punctured tanks and firewall, would have fed directly into the engine compartment. The evidence indicates that the fuel then contacted either a hot engine component or some other source of ignition, which could have resulted in the helicopter being on fire before impact. The soot pattern on the ground confirmed that fuel from the punctured tanks was being ejected from the helicopter at first impact with the ground. The fuel may have ignited while the helicopter was still airborne or flash back could have occurred after impact.
One of the bolted joints in the forward flexible coupling had been assembled incorrectly, resulting in a lack of clamping force and subsequent fatigue failure of the flex plate in the forward flexible coupling and loss of drive to the main rotor gearbox.
The build records and digital photographs supplied by the manufacturer showed that the assembly of this joint at the factory had been correct.
Examination of the maintenance history of the helicopter revealed that, while maintenance had been performed on the drive system on a number of occasions since factory assembly, there was no recorded documentary evidence found that any subsequent maintenance had been performed on the particular bolted joint where the failure occurred. The stated procedure employed by the engineer who carried out AD/R22/51 was appropriate and consistent with accepted practices and did not require disassembly of the bolted joint that failed.
Examination confirmed that both tail rotor blades failed as a result of contact with the ground during the impact sequence.
At the time of the incident the helicopter was being operated close to the ground with low forward air speed. That would have left the pilot with little time to respond effectively to failure of a critical flight system such as the main rotor drive system.
The manner in which the failure of the forward flex plate occurred resulted in an unusual emergency situation for the pilot. As well as the obvious noise and out of balance caused by the still rotating but partially separated forward flexible coupling, symptoms would have included a failure of the drive to the main rotor gearbox resulting in decreasing main rotor speed and a nose-left yaw. That was consistent with some of the symptoms normally associated with an engine failure. However, in this case the engine had not failed and initially would have presented the pilot with additional and potentially confusing symptoms. Those symptoms would have included an initial indication of engine overspeed, and continuing tail rotor drive.
The normal response to an engine failure, and also relevant in this case, would be for the pilot to lower the collective control in order to recover any loss of main rotor RPM. The pilot would then allow the helicopter to enter an autorotation descent. If there was insufficient height for the descent to stabilise, main rotor RPM would not have recovered before the pilot commenced the touchdown phase of the autorotation. Low main rotor RPM during the touchdown phase would have decreased the possibility for the pilot to reduce the helicopter's rate of descent and carry out a safe touchdown. It is evident that fatigue cracking in the flexplate initiated at the bolthole and propagated under the washers of the bolted joint towards the edge of flexplate. It was also evident from the fracture surface features that crack growth had occurred over a number of flights prior to the accident flight. Because cracking occurred under the washers in the bolted joint, the opportunity to detect cracking by a pre-flight visual inspection would have been limited to the detection of a crack at the edge of the flexplate arm.
The reliability of a general visual inspection (for example, a pre-flight inspection) is affected by lighting, the ability to get close to the component (proximity), and dirt and dust from the operating environment. Reliable detection of a specific defect would require a directed detailed inspection.
2.2 Survival
The crush damage observed to the right side of the cabin structure showed that impact forces were greater on the right side of the helicopter than the left. As a result, the pilot, who occupied the right seat, was subjected to higher impact forces than the passenger in the left seat. The impact forces in this accident were not directly aligned with the helicopters fore-aft and vertical axes. Hence, the level of protection afforded by the seat/harness combination was reduced and probably contributed to the injuries sustained by the pilot. The extent of the post-impact fire precluded any definite conclusions as to what, if any, material may have been carried under the pilot's seat.
When the helicopter came to rest on its right side, the seat in which the passenger was trapped was in an elevated position and was severely affected by the fire. It was also likely that the difficulty the passenger experienced in escaping from the helicopter was due, at least in part, to him being suspended by the safety harness. The time it took the passenger to release himself contributed to the extent of his burn injuries.
The passenger, although seriously injured himself, walked approximately 8 km to summon help. Unfortunately, due to the accident site's remote location, the pilot succumbed to his injuries before medical assistance could reach him.
2.3 Communication equipment
No record of fitment of a fixed Emergency Locator Transmitter (ELT) could be found in the logbooks for the accident helicopter and no ELT unit remnants for either a fixed or personal unit were identified within the main wreckage. Given the intensity of the post-impact fire, it was probable that, had a fixed ELT been fitted, it would have only operated for a very short period of time before being destroyed.
If the pilot was carrying a personal ELT at the time, it is possible that it separated from his person either during the impact or during egress from the wreckage and was destroyed in the subsequent fire. In addition, if the occupants carried a satellite telephone, it may have reduced the time taken to summon assistance.
At about 1100 Central Standard Time on 30 May 2004, a Robinson R22 Mariner II helicopter, registered VH-MIB, crashed and caught fire while being operated on a fence inspection flight at Tobermorey Station, NT. The pilot sustained fatal injuries, and the passenger was seriously injured. The passenger reported that the purpose of the flight was to inspect a fence line bordering the property and then to conduct cattle mustering operations. The helicopter was refuelled to full tanks prior to departure. The weather was fine and sunny, with a slight breeze from the south-east. The passenger reported that while overflying a section of the fence line about 45 km south of the homestead at 30 to 40 ft above ground level, the pilot initiated a turn back to the left to enable a closer look at a particular section of fence. Part way through the turn there was a loud bang from behind the cabin, followed by "horrendous vibration" and the helicopter immediately began to yaw left and descend. The ground marks showed that the tail rotor blades contacted the ground first and then the forward section of the helicopter's right skid struck the ground, disrupting the front section of the cabin. The helicopter then came to rest on its right side and fire rapidly spread to engulf the cabin area.
The pilot was able to free himself from the helicopter through the broken front section of the cabin, but the passenger experienced difficulty undoing his safety harness and remained trapped. He was eventually able to free himself and joined the pilot at some distance from the wreckage. The passenger reported that he assessed the pilot to be badly injured and directed him to a nearby water hole. The passenger then walked to a water bore approximately 8 km from the accident site, where he met other station personnel. The pilot was deceased when medical assistance arrived at the accident site some hours later.
The passenger reported that he had flown in the helicopter several times. During the last few flights before the accident, and during the accident flight itself, he had detected a vibration that he considered abnormal. The passenger advised the investigation that he had conveyed these concerns to the pilot, who advised that he conducted a good check of the helicopter and was satisfied that there were no problems.
1.2 Wreckage examination
Examination of the wreckage by the Australian Transport Safety Bureau (ATSB) investigation team at the accident site (Figure 1) confirmed that the helicopter was yawing left and moving forward when it struck the ground. The tail rotor blades contacted the ground first. The helicopter then contacted the ground slightly nose down and heavily onto the right skid, causing it to separate from the helicopter. The ground impact marks showed that the helicopter continued to yaw left though about 180 degrees after it struck the ground, before coming to rest on its right side. The majority of the cabin and engine bay, including the entire floor area and cabin structure beneath the pilot and passenger seat positions were destroyed by fire.
The extent of fire damage meant that a complete examination of the helicopter was not possible. Some aluminium components such as tubing in the flight control system had been destroyed. However, all steel components in the control systems for the main and tail rotor were identified and damage to all of these components was consistent with impact forces or fire. The main rotor blades exhibited damage consistent with low rotor energy at impact. Both tail rotor blades had fractured approximately 1/4 span outboard of the rotor hub centre drive (Figure 2). The failed section of one blade was found adjacent to the main wreckage. The failed section of the other blade was found subsequently about 70 m from the main wreckage. Both blade sections were taken to the ATSB laboratories for further examination.
Figure 2: Tail rotor damage
All of the engine drive system components were identified within the wreckage. The flex plate for the forward flexible coupling of the main rotor drive system was fractured at one of the two attachment points to the main rotor gearbox yoke (Figure 3 and 4). The flex plate, including the clutch shaft, were retrieved from the accident site, for further examination. The flex plate for the intermediate flexible coupling was intact and showed evidence of rotational damage consistent with partial drive system power at impact. The rear flex plate and coupling components were also found intact.
Figure 3: Forward flexible coupling as found in wreckage
Figure 4: Components of failed forward flexible coupling
The fuel system and engine ancillaries were destroyed by the fire. There were vertical cuts puncturing the inside wall of the right fuel tank and the horizontal stainless-steel firewall above the engine. The cuts in the right tank and the firewall aligned with the forward flex plate plane of rotation (Figure 5). The left fuel tank was destroyed by fire.
Figure 5: Flex plate puncture of stainless-steel firewall above engine.
1.3 Personnel information
The pilot held a commercial pilot (helicopter) licence and was appropriately endorsed on the R22. He was issued with a private pilot (aeroplane) licence in 1974 and a commercial pilot (helicopter) licence in 1990. The pilot was issued with a commercial pilot (aeroplane) licence in 1995. He held a stock mustering rating and a valid class 1 medical certificate. He completed a flight review in the occurrence helicopter on 19 April 2004. At the time of the accident, the pilot had approximately 10,400 hours aeronautical experience. He flew 31 hours in the occurrence helicopter between 17 and 30 May 2004.
1.4 Medical and pathological information
Postmortem and pathology reports did not indicate that the pilot was suffering from any condition that might have affected his performance during the flight. The most significant injuries sustained by the pilot were the result of impact forces rather than fire.
1.5 Fire
There was a fire affected area (sooting) on the ground that extended up-slope from the wreckage (Figure 6). The sooting formed a swirl pattern of decreasing radius in the direction the helicopter was yawing when it contacted the ground.
Figure 6: Sooting pattern adjacent to wreckage (arrow indicates approximate direction of flight at impact)
1.6 Survival aspects
Three-point lap/sash type safety harnesses were fitted to both seating positions in the helicopter. The passenger reported that both he and the pilot had their harnesses fastened during the flight. Fire damage precluded a detailed assessment of the seats and performance of the crush zones beneath them as well as the seat belt harnesses.
Severe crush damage to the lower cabin bulkhead was evident immediately behind the pilot's seat. (Figure 1).
Following the accident, no Emergency Locator Transmitter signal was received (refer section 1.7.6). There was no mobile telephone coverage in the area and the passenger reported that they did not carry any other communications aids, such as a portable satellite telephone.
1.7 Helicopter information
1.7.1 Helicopter data
The helicopter was manufactured in August 2002 as Serial No 3357M. The most recent maintenance release for the helicopter could not be located. It was reported to have been kept in the helicopter. If so, the maintenance release would have been destroyed in the post-impact fire. Based on other maintenance records and information contained in the pilot's personal diary, the total time in service of the helicopter on 30 May 2004 was estimated to have been 506 hours.
1.7.1 Main and tail rotor drive system
In the R22 helicopter, power to drive the main and tail rotors was transmitted from the engine to the rotor drive train via a multiple Vee belt drive and clutch system. A shaft transmitted power forward from the clutch to the main rotor gearbox and aft to the tail rotor gearbox (Figure 7).
Figure 7: Main components of main and tail rotor drive systems2
A forward flexible coupling, which includes a flex plate, connected the drive shaft to the main rotor gearbox. The tail rotor drive system also included an intermediate and a rear flexible coupling. Yoke assemblies at the end of each drive shaft section connected the shaft to the flex plate via bolted joints (Figure 8). The purpose of these flex plates was to accommodate small differences in shaft axial alignment during drive shaft rotation. The flex plates and the bolted joints were critical elements in drive system integrity.
Figure 8: Components of the forward flexible coupling
The helicopter manufacturer published procedures for assembling and aligning the drive system components, including the allowed tolerances. The design loads of components could be exceeded if those tolerances were not met.
1.7.3 Helicopter manufacture
The helicopter arrived in Australia partly disassembled for ease of shipment. The main drive system components within the engine compartment were assembled during manufacture and not subsequently disturbed for this method of international shipment.
In order to assist the investigation, the manufacturer supplied the investigation with the itemised build records, which included digital photographs of the rotor drive system, for the occurrence helicopter. Those records were reviewed as part of the laboratory analysis of the flexible coupling failure. The review of the build records and photographs for the forward flexible coupling in the occurrence helicopter showed that NAS6605-6 bolts had been used, and a spacer washer had been included in each bolted joint and one thin washer had been installed under the nut, with a palnut (locking nut) fitted to each. The build records showed that the build-up of the bolted joint at the time of manufacture of the helicopter was correct and in accordance with the assembly procedures.
The 'Daily or Preflight Checks' section 4-2 and 4-3 of the manufacturers Pilot's Operating Handbook identified the requirement for a visual check of the flex coupling to ensure there are 'No cracks and 'Nuts tight'. Also required is a check of the yoke flanges for cracking. It further advised, in part, that 'During the following inspection, check the general condition of the aircraft and also look for any evidence of leakage, discolouration due to heat, dents, chafing, galling, nicks, corrosion and especially for cracks. Also check for fretting at seams where parts are joined together. Fretting of aluminium parts produce a fine black powder, while steel produces a reddish brown or black residue'.
1.7.4 Maintenance history
Maintenance records indicated that an Australian certificate of airworthiness for the helicopter was issued on 11 October 2002, after assembly in Australia, following manufacture and acceptance flights in the US. At that time, the total time in service was 5.1 hours. A summary of subsequent maintenance conducted on the helicopter is as follows. All references to drive system adjustments and/or maintenance have been included.
11 March 2003. Total time in service 55.1 hours. 50 hourly engine inspection
27 March 2003. Total time in service 98.5 hours. 100 hourly inspection. Maintenance carried out included adjustment of the engine sheave alignment.3
30 June 2003. Total time in service 198.2 hours. 100 hourly inspection. Maintenance carried out included checking and adjustment of the engine sheave alignment and intermediate flex plate shimming to within limits.
15 September 2003. Total time in service 296 hours. 100 hourly inspection.
17 February 2004. Total time in service 384.1 hours. Civil Aviation Safety Authority Airworthiness Directive (AD) R22/51 'Main Rotor Clutch Shaft', dated 12 November 2003, was incorporated. AD/R22/51 was applicable to all R22 helicopters. It required disassembly of the main rotor yoke (A907) to the clutch shaft joint (A166) (see Figure 6) and inspection of the shaft and yoke for damage including fretting4 of bolt holes, cracking in the area of the bolt holes, and the presence of an unapproved jointing compound in the mating surfaces. The helicopter maintenance worksheet indicated that no fretting was evident but that the incorrect jointing compound had been used. The worksheet stated that the AD had been complied with and that the clutch shaft and yoke were reassembled in accordance with the maintenance manual. The worksheet also recorded that a duplicate inspection of the clutch shaft installation and the yoke (A907) assembly had been performed. The licensed aircraft maintenance engineer who carried out the AD reported that he disconnected the yoke (A907) from the forward flex plate, but did not disconnect the flex plate from the main rotor gear box yoke (A908). He stated that he did not perform any maintenance on the bolted joints at the connection between the main rotor gear box yoke and the flexible coupling.
27 March 2004. Total time in service 396 hours. 100 hourly inspections. Maintenance carried out included engine sheave alignment.
12 May 2004. Total time in service 476.1 hours. 100 hourly inspections.
The documentation showed that maintenance had been performed on 27 March 2003, 30 June 2003, and 17 February 2004 in the vicinity of the forward flexible coupling that, while it did not specifically necessitate bolt removal, provide opportunities for the forward flexible coupling bolts to be disturbed.
A review of the diagrams contained in the manufacturer's Maintenance Manual and the Illustrated Parts Catalogue (IPC) revealed a difference in the specifications of the parts in the bolted joints. Notes contained within the IPC explained that bolts of different grip lengths and washers of different thickness were to be used in the flex plate bolted joints to expose between two and four threads beyond the end of the nut. A table comparing the different specifications between the Maintenance Manual table and the IPC is provided in section 4.1.3 of the ATSB technical analysis report attached as Appendix 1.
The manufacturer advised that the bolt length identified in the Maintenance Manual was for use in an earlier version of the manual and was out of date. Corrective action to update this information was scheduled by the company for November 2005, but at the time of writing of this report had not been accomplished.
The manufacturer advised that the company did not publish any warning to maintenance organizations about the discrepancy in bolt length between the Maintenance Manual and the Illustrated Parts Catalogue. The discrepancy was not considered by the manufacturer to be critical in that the use of either a NAS6605-5 or a NAS6605-6 bolt with the appropriate combination of spacer and washers would give the correct clamp up for proper joint integrity. In the few cases where the -5 bolt did not allow proper installation of the B330-16 palnut, the problem would be self-evident. The manufacturer believed that any engineer performing the installation where the bolt was too short to install a palnut would install a longer bolt or make inquiries to resolve the problem.
1.7.6 Emergency locator transmitter
The maintenance records indicate that the helicopter was imported from the US and subsequently operated by various owners without a fixed Emergency Locator Transmitter (ELT) unit being fitted. This fact was noted on the maintenance releases issued at 5.1 airframe hours total time in service (TTIS) on 11 October 2002 and 98.5 hours TTIS on 27 May 2003, which required the pilot to observe the requirements of CAR 252 and carry a personal ELT. No further entries of this nature were found on maintenance releases issued after this date, nor could evidence be found in the aircraft logbooks that an ELT had been fitted. A search for both a fixed and personal ELT within the wreckage and surrounding accident site was conducted but nothing was found. The passenger stated that the pilot normally carried a personal ELT on him. No personal ELT was identified among the pilots clothing or personal effects and no emergency signal was received by AusSAR from that location on the day.
1.8 Specialist examination of the failed components
The forward flex plate and the broken sections of the tail rotor blades were subject to detailed examination by the ATSB. The report on those examinations and analysis of the failures is attached as Appendix 1.
The metallurgical evidence confirmed that the failure mode of both tail rotor blades was very similar and was the result of contact with the ground during the impact sequence. The rocky material embedded in the blade tips provided clear evidence that the blades had struck the ground while rotating. The blade that was found about 70 m from the wreckage was thrown that distance as the result of tail rotor rotational energy.
The specialist examination found that the flex plate in the forward flexible coupling fractured as a result of the propagation of a fatigue crack at one of the bolted connections between the plate and main rotor gearbox yoke. Final fracture of the flex plate occurred during operation and not as a result of the collision with the ground. No crack growth or wear damage was observed at the three remaining boltholes. Examination of the bolt installed at the failure location revealed that extensive fretting wear had occurred around the entire circumference of the bolt, in the region adjacent to the flex plate and the regions adjacent to the reinforcing plates. Fretting wear was also evident on the washer surface adjacent to the bolt head.
The bolted joint at the flex plate failure location was found to have a single thin washer under the bolt head and nut, and no spacer washer between the yoke and flex plate. This spacer and washer combination was different from that specified by the manufacturer for use with a NAS6605-6 bolt.
Only those investigation areas identified by the headings and subheadings were considered to be relevant to the circumstances of the accident.
Diagram with permission of Robinson Helicopter Company.
Drive Vee belts sometimes stretch when new and adjustments are then necessary to maintain the correct drive system alignment. Engine sheave alignment is part of that adjustment process.
The AD defined major fretting as 'any evidence of the machining marks in any of the bolt holes being partly or fully obliterated'.
Summary
The crew of the Robinson R22 helicopter were undertaking a fence line inspection at about 30 to 40 ft above ground level. The crew had initiated a turn back along the fence line for a closer look at a particular section of fence. During the turn, a loud bang was heard, and the helicopter began to rotate quickly before striking the ground.
Both occupants were able to exit the helicopter unaided after it came to rest but sustained serious injuries and burns as a result of a post-impact fire. The pilot subsequently died of his injuries.
The investigation found that one of the bolted joints linking the forward flexible coupling flex plate to the main rotor gearbox drive shaft yoke had been assembled incorrectly. This resulted in subsequent fatigue failure of the flex plate and loss of drive to the main gearbox. Control of the helicopter was then lost at a height from which it was difficult to recover.
The crew of the Robinson R22 helicopter were undertaking a fence line inspection at about 30 to 40 ft above ground level. The crew had initiated a turn back to the left, along the fence line for a closer look at a particular section of fence. During the turn, a loud bang was heard, and the helicopter began to yaw quickly before striking the ground.
Both occupants were able to exit the helicopter unaided after it came to rest but sustained serious injuries and burns as a result of a post-impact fire. The pilot subsequently died of his injuries.
Examination of the helicopter wreckage revealed that both tail rotor blades had failed due to contact with the ground. In addition, the flex plate in the forward flexible coupling of the main rotor drive was found fractured at one of the two attachment points to the main rotor gearbox yoke. The tail rotor blades and several components from the main rotor drive were recovered for detailed analysis in order to resolve the mechanism of fracture and the sequence of failure.
The flex plate in the forward flexible coupling fractured due to the propagation of a fatigue crack at one of the bolted connections between the plate and main rotor gearbox yoke. Final fracture of the flex plate occurred during operation and not because of the collision with the ground. There was no crack growth or wear damage evidence at the three remaining boltholes. Examination of the bolt installed at the failure location revealed that extensive fretting wear had occurred around the entire circumference of the bolt, in the region adjacent to the flex plate and the regions adjacent to the reinforcing washers. Fretting wear was also evident on the washer surface adjacent to the bolt head. This type and degree of wear damage was indicative of operation with insufficient clamping force in the bolted joint.
A review of the manufacturer's original build-sheets for the forward flexible coupling in the occurrence helicopter revealed that NAS 6605-6 bolts were used, and a spacer washer had been included in each bolted joint and one thin washer had been installed under each nut with a palnut (locking nut) fitted to each.
Examination of the forward flexible coupling retrieved from the accident site, found that the bolted joint had been assembled with a washer and spacer combination that was different from that identified by the manufacturer's original build records. These differences indicated that it was likely that the joint had been disassembled and reassembled during a maintenance action subsequent to assembly in the manufacturer's facility.
The Australian Transport Safety Bureau did not conduct an on scene investigation of this occurrence. The information presented below was obtained from information supplied to the Bureau.
The pilot of the Robinson Helicopter Co R22 Alpha reported that on 23 May 2004 while operating at Scott Creek Station, he hot re-fuelled the helicopter from a bulk fuel tank installation in preparation for mustering. During the into-wind transition from the hover to forward flight, the helicopter rolled rapidly to the right and impacted the ground. The pilot sustained minor injuries and the helicopter was destroyed. He reported that the fuel hose had disconnected from the bulk fuel outlet. It was likely that the helicopter had become entangled with the re-fuelling hose and pump during the departure.
The Australian Transport Safety Bureau did not conduct an on scene investigation of this occurrence. The report presented below was derived from information supplied to the Bureau.
The Piper PA 32R-301 aircraft, registered VH-WMC, was intended to be flown on a return charter flight from Winton to Boulia in Queensland. The flight was to familiarise the pilot in command with the route and the facilities at Boulia Aerodrome. The aircraft load, which comprised 300 litres of fuel and six adults, including the pilot in command and the aircraft owner, placed the aircraft approximately 67 kg above the maximum allowable take-off weight. The weather was bright and clear with a light easterly wind, and an ambient temperature of approximately 15 degrees C.
The pilot in command reported that all pre-flight checks and engine indications were normal, and that the elevator trim was set rearward of the neutral position, in accordance with the Aircraft Operating Manual. One stage of flap was selected and they were using runway 14 at Winton. The initial take-off roll was normal and rotation was initiated at about 80 knots. The pilot reported that the aircraft became airborne and then veered to the left of the runway centreline. The pilot lowered the nose of the aircraft slightly in an attempt to gain airspeed and increase aircraft control, but it veered right and travelled beyond the edge of the runway towards the aerodrome boundary fence. Throughout this period, the aircraft became airborne but did not fly out of ground effect. In a further attempt to increase speed, the pilot retracted the landing gear. However, the aircraft settled onto its lower fuselage and collided with the aerodrome boundary fence.
On the day before the accident, the pilot in command completed three circuits as a refamiliarisation exercise in the aircraft type. The aircraft owner, also a pilot, accompanied the pilot in command and occupied the right cockpit seat. No other persons were on board the aircraft. At the owner's suggestion, the pilot in command set the elevator trim close to the full forward position before takeoff. The owner reported that the pilot in command handled the aircraft satisfactorily.
The Aircraft Operating Manual stated that for a normal takeoff, the elevator trim should be set slightly rearward of neutral, and that the aircraft should be accelerated to 74 to 80 knots, depending on its weight, before backpressure on the control wheel was applied to rotate the aircraft to the climb attitude. From the information provided, it is likely that a combination of the different trim setting, the rear centre of gravity position, and the higher aircraft weight for the accident takeoff, compared with the flight the previous day, resulted in the aircraft assuming a high nose-up attitude after becoming airborne. The resultant drag lead to the control difficulties reported by the pilot and prevented the aircraft accelerating to the normal climb speed.
On 31 March 2004, at 0600 Eastern Standard Time, the Robinson R22 helicopter with one pilot on board departed on a ferry flight to commence mustering operation from a property approximately 15 minutes flying time to the north-north-east. The pilot reported that he landed at the property and picked up a passenger who was going to show him the paddocks, fences and laneways.
At about 1000, after mustering cattle into a small paddock, the pilot made an approach to land beside a fence. The pilot indicated that the weather was fine with good visibility. The wind was from an easterly direction at 5 kts and the temperature was 25 degrees C. He reported that he saw a powerline and aimed to land adjacent to a point where the powerline changed direction. However, he did not see a third wire, which the helicopter struck at a height of about 30 ft. The helicopter spun into the ground and landed on a barbed wire fence. The helicopter sustained substantial damage to the tail boom, lower vertical fin and tail rotor blades. The two occupants escaped with minor injuries.
The Australian Transport Safety Bureau did not conduct an on scene investigation of this occurrence. The report presented below was derived from information supplied to the Bureau.
On 8 March 2004 at about 1550 Eastern Summer Time, a glider impacted the ground in Western Victoria. The pilot was fatally injured. Following the accident, the Victorian Coroner's office forwarded a global positioning system (GPS) navigation unit and a data logging unit from the glider to the Bureau for examination.
The GPS unit was able to be interrogated and data for the accident flight was downloaded (Fig 1). The data recovered from the GPS showed that the glider departed from Boort and appeared to be tracking towards Raywood. The track stopped at a position coincident with the reported accident site.
No altitude data was recorded by the GPS unit, therefore only the track of the glider was able to be displayed on a map.
The data logging unit sustained impact damage. The unit was connected to a computer with the applicable interrogation software installed. However, when an attempt was made to download the data, the unit returned an error signal, and no data was able to be downloaded.