Although this investigation report highlights a low incidence of accidents and incidents involving insecure canopies in Lancair Legacy aircraft, the potential consequences of such occurrences have generated discussion among Lancair Legacy owners, builders and pilots. In particular, the ATSB is aware of a discussion paper, available on the United States Lancair Owners & Builders Organization website at www.lancairowners.com, which examines a number of canopy-related accidents and incidents in this type, and reviews the pilot actions in each case in response.
As highlighted in its investigation report, the ATSB reiterates the importance of owners, operators and pilots of aircraft with canopies reviewing the adequacy of their existing measures that are intended to ensure canopies are securely latched before flight (such as pre-take-off checks and warning systems), and the actions in case of inadvertent canopy opening during take-off. In this respect, and without endorsing any particular recovery procedure, the above Lancair discussion paper could be expected to enhance that review.
Summary
What happened
On 18 September 2013, the pilot of an amateur-built Lancair Legacy aircraft, registered VH-ALP, was taking off from runway 32 at Geraldton Airport, Western Australia. Late in the take-off roll the canopy came open – the pilot continued the take-off and manoeuvred at low level for a landing. During the approach the aircraft undershot the runway, touched down across a road then collided with the airport perimeter fence and caught fire. The aircraft was destroyed and the pilot sustained injuries that were later fatal.
What the ATSB found
The ATSB found that the pilot conducted the take-off with the canopy down but inadvertently unlatched. As the aircraft accelerated the aerodynamic loads on the canopy increased and resulted in it suddenly lifting up to a partially open position. The pilot did not reject the take-off and during the subsequent manoeuvring for landing, likely encountered control, performance and forward visibility difficulties associated with the open canopy. This adversely affected the pilot’s capacity to conduct a normal approach.
Safety message
The ATSB advises owners, operators and pilots of aircraft with canopies to review the adequacy of their existing measures that are intended to ensure canopies are securely latched before flight (such as pre-take-off checks and warning systems), and the actions in case of inadvertent canopy opening during take-off.
Where possible in abnormal situations, pilots should take time to assess the nature of the abnormality to rectify the situation or mitigate the effects.
In the early evening of 23 September 2013, the student pilot of a Cessna Aircraft Company 182R aircraft, registered VH‑AUT, was conducting solo night circuit consolidation training at Hamilton Airport, Victoria. On the fourth circuit the pilot made a radio call indicating he was aborting the landing. Witnesses observed the aircraft climb, then turn to the right and descend, followed by a collision with terrain. The aircraft was destroyed by the impact and post‑impact fire and the pilot was fatally injured.
What the ATSB found
The ATSB found that following an aborted landing during circuit training in dark night conditions, the solo student pilot lost control of the aircraft, resulting in a collision with terrain. There was insufficient evidence to determine the reason for the loss of control.
The student pilot’s post-mortem examination identified a cardiac condition capable of causing incapacitation and their medical history included another condition that, if having effect at the time, had the potential to have contributed to the development of the accident. The Civil Aviation Safety Authority (CASA) was unaware of either condition.
In addition, the aircraft’s flaps were found to have been in the fully-extended position at impact, which was not consistent with either the operator’s or manufacturer’s procedures for a go-around. The ATSB was unable to determine when the flaps were extended and to what extent the misconfiguration influenced the accident.
Safety message
This accident highlights the importance of the shared responsibility by holders of aviation medical certificates, examining physicians and CASA to report, assess and manage medical and other conditions as they might affect the issue/renewal of those certificates. A full understanding by CASA of an aviation medical certificate applicant’s current and prior medical conditions, and use of medications, informs the consideration and development of appropriate risk controls to ensure continued safe flight. This can include the applicant continuing in, or recommencing their participation in the industry.
The ATSB investigation team has completed the on-site phase of its investigation into the collision with terrain involving a Cessna 206 aircraft, registered VH‑WAV, about 156 km south-east of Croydon, Queensland on 15 September 2013. The investigation team examined the area used by the pilot for the take-off, the accident site and wreckage, and interviewed an eyewitness to the accident.
The site evidence and witness report indicated that, during take-off from an unsealed access road to a council work camp, the aircraft’s left wing struck a tree. The wingtip and aileron separated before the aircraft impacted terrain, fatally injuring the pilot and passenger. The aircraft was seriously damaged,1(Figure 1).
Figure 1: Aircraft wreckage
Source: ATSB
The investigation is continuing and will include consolidation of the site evidence, a review of witness reports, consideration as to the suitability of the access road for the take-off and examination of the aircraft’s records and pilot history.
A final investigation report is expected to be published by the end of February 2014.
_________
1. The Australian Transport Safety Regulations 2003 definition of ‘serious damage’ includes the destruction of the transport vehicle.
________________
The information contained in this web update is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this web update. As such, no analysis or findings are included in this update.
Summary
What happened
At about 1200 on 15 September 2013, the pilot-owner of a Cessna 206, registered VH-WAV, landed on a public road to repair a truck at a work camp. At about 1516, during take-off from a different, curved road, the aircraft’s left wing struck a tree at a height of about 30 ft. The wingtip and aileron separated before the aircraft impacted terrain, fatally injuring the pilot and passenger. The aircraft was destroyed.
What the ATSB found
The distance available from where the pilot increased power for take-off was much shorter than the distance advised in the aircraft’s pilot operating handbook under the prevailing conditions.
There was no apparent reason for the pilot to attempt a take-off from that location when a more suitable location was nearby. It is most likely that the pilot misjudged the distance available, the prevailing conditions and their effect on the aircraft’s performance, or had a false recollection of the relative layout of the two roads and thought that there was more take-off room available beyond the curve. However, it is also possible that the pilot’s judgement of the available distance, or his decision-making capability, was affected by a serious medical condition and/or prescribed medications that had not been reported to the Civil Aviation Safety Authority (CASA) until after the pilot’s previous medical certificate had expired.
In addition, the ATSB found that the pilot’s seat had broken from its mounts, probably as the result of heavy, unsecured cargo striking it during the accident sequence. This could have had a detrimental effect on the survivability of the accident.
Safety message
The accident highlights the importance of carefully considering all relevant factors that could affect the suitability of a particular landing and take-off area. These include: aircraft weight and engine power; wind direction, speed and gusts; ambient air pressure and temperature; surface slope, material, and condition; other physical characteristics of the area such as its length and width; and the height and location of surrounding obstacles.
Though no link with the accident was established, flying without a valid medical certificate, or omitting to report a diagnosed condition or treatment to a Designated Aviation Medical Examiner or to CASA, can lead to such an impairment being undetected or its effect underestimated.
Unrestrained cargo poses a significant risk to the survivability of aircraft occupants. Pilots should take care to ensure that all cargo is adequately restrained to prevent movement during flight and improve survivability in the event of an accident.
On 30 March 2012, a Europa XS amateur-built aircraft collided with terrain shortly after takeoff from Caboolture Airfield, Queensland. The pilot, who was the sole occupant, was fatally injured.
The Australian Transport Safety Bureau (ATSB) did not investigate the accident, which was investigated by the Queensland Police Service (QPS) on behalf of the Queensland Coroner. On 20 June 2013, the Queensland Coroner requested ATSB assistance with the review of the coroner’s investigation and advice of any potential additional lines of enquiry or other expert review before the matter proceeded to inquest.
To facilitate this support, the ATSB initiated an external investigation under the provisions of the Transport Safety Investigation Act 2003. A report on the results of the ATSB’s review of the coroner’s investigation was provided to the Queensland Coroner on 6 September 2013.
Any enquiries as to the planning for, or conduct of the Coroner’s Inquest into this accident should be directed to the Queensland Coroner’s Office at:
Queensland Courts Office of the State Coroner Brisbane Magistrates Court 363 George Street Brisbane QUEENSLAND 4000
On 14 January 2012 at approximately 0930 (local time), a ‘GT Kruza’ gyroplane (registration G-762) with a pilot and student passenger on-board, departed Mangalore Aerodrome, Victoria, for a one hour training flight. At around 1130 later that morning, a member of the public identified the wreckage of the gyroplane, which had impacted terrain a short distance from the aerodrome. Both occupants had sustained fatal injuries. There were no witnesses to the accident.
The Victorian Police Service was responsible for investigating this accident; assisted by investigators from the Australian Sports Rotorcraft Association (ASRA). From an assessment of the accident site, ASRA investigators determined that the gyroplane had impacted terrain at high speed with a near-vertical nose-down attitude. The rotor system had detached from the airframe during the impact sequence and lay several metres from the majority of the wreckage. There was no evidence of fire.
A preliminary inspection of the gyroplane’s flight controls found that the rotor head torque tube had fractured through the central section where it adjoined the rotor head torque bar. Upon closer examination, ASRA investigators identified evidence of possible pre-existing cracking within the torque bar at the point of failure, and in consideration of the critical nature of this component in the flight control system, ASRA staff sought assistance from the Australian Transport Safety Bureau (ATSB) in the formal technical examination and analysis of the torque bar failure. Assistance was also sought in the examination and possible data recovery from a GPS unit and personal mobile telephone being carried on board the gyroplane.
The following conclusions were drawn from the examinations performed:
Fracture of the rotor head torque tube was directly associated with the development of fatigue cracking that had initiated from stress concentration effects around a clamping bolt hole that passed, by design, through the centre of the tube.
The level of surface fretting and evidence of movement between the tube and torque bar suggested a level of inadequate clamping force between the components.
There was no evidence of loosening of the clamping bolt locking nut.
There was some evidence to suggest that the tightness/security of the clamping bolt nut had been checked at some time before the accident.
No data was able to be recovered from either the Blackberry mobile phone or the Garmin GPSmap 295 device.
Further information:
The investigation into the circumstances of this accident was conducted by the Victorian Police Service, supported by the Australian Sports Rotorcraft Association. The involvement of the Australian Transport Safety Bureau was limited to the technical examinations summarised within the associated report.
Requests for further information regarding the occurrence should be directed to the Victorian Police Service or ASRA.
On 27 June 2013, a Cirrus SR22 aircraft, registered VH-CKS, collided with a tree that was adjacent to the private airstrip at Boxwood, Victoria. The pilot of the aircraft was attempting to land on the unlit airstrip after last light. As a result of the collision, the pilot lost control and the aircraft continued for a short distance before impacting terrain inverted. The pilot was fatally injured, and the aircraft destroyed
What the ATSB found
The pilot was appropriately licensed to operate the visual flight rules category aircraft at night and had passed a number of airports in the vicinity, all of which were appropriate for a night landing. However, consistent with a degree of self-imposed pressure to get home after a series of business commitments and prior to a 1-month period away from home, the pilot bypassed these airports and continued to their property airstrip. This airstrip did not meet the physical, lighting and obstacle clearance requirements for night operations.
The final approach to land was made after last light, with a family member positioned in a motor vehicle ‘at the end of the strip’. The vehicle’s headlights were intended to illuminate the upwind end of the strip, facing the oncoming aircraft. However, this lighting was inadequate and provided insufficient guidance for the approach and landing. This increased the risk of a collision with terrain.
Safety message
Night landings at inadequately lit airstrips are inherently dangerous and increase the risk of a collision with terrain. The requirements for the conduct of operations at night, including lighting, pilot qualifications, aircraft equipment and systems and aerodrome equipment are intended to reduce this risk.
It is likely that, had these risk controls been given effect, this accident would not have happened.
Cirrus SR22, VH-CKS
Source: ATSB
Safety analysis
Introduction
The aircraft was capable of normal operation until the collision with the tree. Similarly, there was no operational reason for the attempted night landing on the ill-equipped property airstrip when there was a suitable aerodrome 30 km away. This analysis will focus on the pilot’s decision to continue the flight to, and attempt a night landing on the property airstrip.
Landing on an unlit airstrip at night
There were indications of a conscious decision by the pilot to land at their property’s airstrip, knowing that the lighting was inadequate. Likely influencing the pilot was a degree of self-imposed pressure to get home after a series of business commitments and prior to a 1-month period away from home.
Given the decision to continue to the property airstrip, the pilot planned his final approach using two pre-selected waypoints and with vehicular headlights illuminating the airstrip. This contrasted with the pilot’s recorded night flying experience, which showed that all previous night landings were on licenced aerodromes that were equipped with appropriate runway and obstruction lighting.
It was concluded that the pilot was either unaware of or accepted the risks associated with the night approach and landing at Boxwood. In addition to the influence of any self-imposed pressure to get home, the potential for the pilot to have accepted these risks may have also been influenced by confidence that his experience and ability, aircraft equipment and his local knowledge would be sufficient to conduct the landing.
Navigation
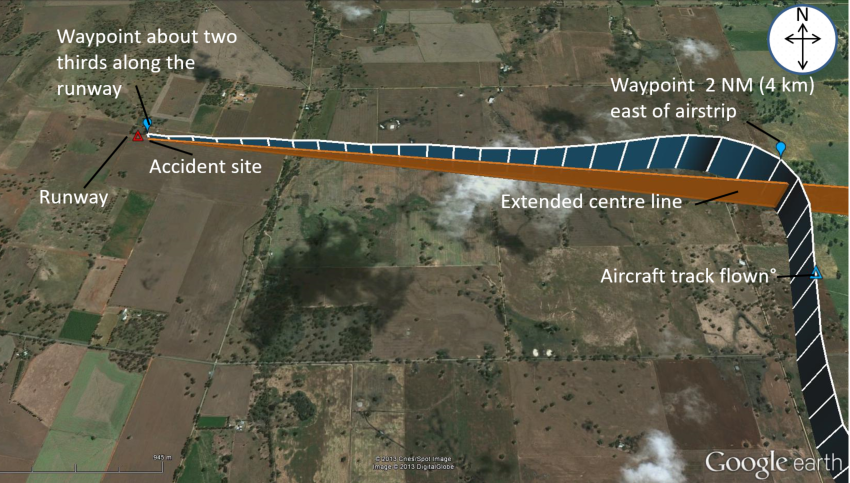
The approach was consistent with reliance by the pilot on the provision of lateral and vertical guidance from the course deviation and vertical speed indications on the aircraft’s primary flight display. In this context, although the decent path was relatively constant, the turn onto final was commenced overhead the 2 NM (4 km) waypoint, resulting in the aircraft overshooting the extended centre‑line. As a result, the aircraft was to the north of the intended track to the airstrip and required the pilot to track back to the centreline during the remainder of the approach. This increased the risk that, given the inadequate lighting, the aircraft would strike the trees north‑adjacent to the airstrip.
The use of Global Positioning System-derived waypoints for the final approach may have given the pilot a false sense of accuracy and an expectation that a single-point light source was adequate for the attempted night approach and landing. In contrast, the only means of judging the latter stages of the approach, flare and touchdown was by the aircraft’s landing light. Together with the closer‑than‑recommended location of the trees to the runway, this sole reliance on the landing light increased the risk of the pilot not comprehending the trees in time to take avoiding action.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Airservices Australia
the Bureau of Meteorology
the Civil Aviation Safety Authority (CASA)
the maintenance provider
the United States National Transportation Safety Board (NTSB)
the aircraft manufacturer
a family member at Boxwood
Victorian Police.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the family member, the aircraft manufacturer, CASA and the NTSB.
Submissions were received from some of the parties to the investigation. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Context
Pilot information
The pilot held a Commercial Pilot (Aeroplane) Licence, a valid Command Instrument Rating (Single-engine aeroplanes) and a valid Class 1 Medical Certificate. This certificate required the pilot to wear distance vision correction and to have reading correction available during flight.
The pilot renewed his instrument rating on 25 May 2013. The pilot’s application for renewal indicated that a significant proportion of his flying since his last renewal was at night, reportedly associated with business travel.
At the time of the accident, the pilot had accumulated a total of 633 flying hours, including 101 hours of night flying. The pilot had flown the accident aircraft for a total of 267 flight hours, 34 hours of which were at night. During the last 90 days the pilot accumulated 59 flying hours.
The pilot was reported to have intended to fly the aircraft to Boxwood for several days previous, but work commitments detained him in Melbourne. On return to Boxwood, the pilot was scheduled to depart on a 1-month period away from home.
The pilot’s post-mortem examination and toxicological testing found no underlying factor that might have contributed to the accident.
Aircraft information
The Cirrus SR22 aircraft was manufactured in 2005, was appropriately registered and had a valid Certificate of Airworthiness and current aircraft Maintenance Release with no recorded defects. The aircraft was approved for instrument and night flight in the charter category, and had accumulated about 1,788 flight hours.
The aircraft was equipped with a factory-fitted advanced cockpit ‘glass panel’ instrument display that consisted of 2 Avidyne integrated flight displays (flat screens) mounted side-by-side (Figure 1). The left screen was referred to as the Primary Flight Display (PFD) and the more centrally mounted screen as the Multi-Function Display (MFD). The brightness of the screens is controlled manually for night operations.
Information displayed on these glass panel displays included from a Stormscope, Active Traffic Awareness, Jeppesen Chartview, an Embedded Terrain Awareness Warning System and a CMax engine and fuel monitoring system. Conventional analogue flight instruments were located on the lower left of the instrument panel and indicated the aircraft’s airspeed, attitude and altitude.
The PFD screen was divided laterally to depict flight information on the upper part of the screen and azimuth information on the horizontal situation indicator, which formed the lower part of the display. Within this lower display, a horizontal deviation indicator displayed any left or right deviations from a selected course.
A vertical deviation indicator on the PFD directed the pilot to adjust the rate of descent in order to fly a constant descent path. This provided the pilot with a form of descent guidance between waypoints.
The MFD had a pilot checklist, approach chart and map function, which allowed the selection of chart images to show the aircraft’s progress on a ‘moving-map’ display. The type, scale and orientation of these images could be selected manually by the pilot.
Figure 1: Aircraft instrument panel showing the Primary Flight Display (left screen), the Multi-Function Display (right screen) and analogue instruments during a daylight flight
Source: A pilot that had flown VH-CKS
Wreckage
The aircraft impacted terrain in a nose-down attitude of approximately 70° – 90° with significant forward speed. Both wings were breached from impact forces and all of the remaining fuel on board leaked from the damaged integral wing fuel tanks. There was no evidence of fire (Figure 2).
An examination of the wreckage identified no pre-existing mechanical defect that may have contributed to the accident. Consistent with there being no report from the pilot of a problem with the aircraft, there was evidence that the engine was producing power prior to the impact.
Figure 2: Aircraft wreckage showing the trees adjacent to the airstrip, one of which was struck by the aircraft (looking back along the direction of the approach)
Source: ATSB
The aircraft’s primary structure and flight control surfaces were identified at the accident site. Flight control continuity was established with no pre-impact defects identified. Furrowing of the horizontal stabilisers and elevators and impact damage to the elevator leading edges was consistent with their striking tree branches during flight. In addition, portions of tree branches were embedded in the lower centre wing section, between the left and right main landing gear.
The aircraft’s two batteries remained secure in the aircraft and had retained voltage. The instrument panel was severely disrupted and the MFD and PFD were liberated from the panel by impact forces. Both units included memory storage devices that stored engine and flight information and were recovered for examination in the Australian Transport Safety Bureau’s technical facilities in Canberra, Australian Capital Territory.
Recorded electronic data
The MFD had a compact flash card and the PFD two non-volatile memory chips that recorded engine and flight information, including data from the flight to Boxwood that night. Data was downloaded from those devices with assistance from the United States National Transportation Safety Board.
The recovered flight information included the aircraft’s speed, track, altitude and a number of engine parameters. The flight data also included a number of waypoints, including one on the extended runway centreline about 2 NM (4 km) east of the airstrip, and another about two thirds along the runway (Figure 3).
Figure 3: Approach flight path
Source: Google Earth and GPS track data overlaid by ATSB
The recorded data showed that at 1806:08 the aircraft was at 1,600 ft above mean sea level on a northerly heading on what appeared to be a base leg. The aircraft was then turned onto about 267° for the final leg of the approach. The aircraft was flown through the 2 NM (4 km) waypoint before the turn, which positioned it to the north of the extended centreline. This required a number of heading corrections by the pilot to regain track to the final waypoint. The aircraft maintained a steady descent path and airspeed of 93 kt toward the last waypoint.
At 1808:01, all recordings ceased, indicating the likely time of impact.
Weather
The nearest available Bureau of Meteorology aerodrome forecasts[4] were for Benalla and Shepparton Airports, 30 and 40 km respectively from Boxwood. The forecasts for those airports at the time of the pilot’s arrival at Boxwood predicted partly cloudy conditions and nil wind.
Airstrip details
The airstrip was oriented in an approximately east–west direction. It was constructed from hard‑packed earth and was about 760 m long with an upslope of 2°‑3° in the direction of landing. There was rising terrain to the west of the strip and a power cable about 10 m above ground level situated about 200 m to the east of the strip. A line of trees north-adjacent and parallel to the strip was about 30 m (98 ft) high.
There were no markers or lighting associated with the airstrip.
It was reported that the pilot’s previous landings at Boxwood were all in daylight. The airstrip did not conform to the physical dimensions for night operations as recommended in Civil Aviation Advisory Publication 92-1(1) Guidelines for aeroplane landing areas, nor did the single set of vehicle headlights meet the recommended minimum night lighting requirements.
In contrast, the aerodromes at Benalla and Shepparton were suitable night destinations for the flight. The pilot was reported to have previously landed at Benalla when returning to the Boxwood area after dark.
From the evidence available, the following findings are made with respect to the collision with terrain involving Cirrus SR22 aircraft, registered VH-CKS, which occurred at Boxwood, Victoria on 27 June 2013 and should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
The pilot attempted a landing at Boxwood after last light, knowing that the lighting was inadequate.
The single-point light from vehicle headlights did not provide adequate guidance for an approach and landing at night.
The airstrip did not meet the physical and obstacle clearance requirements for night operations.
The occurrence
The pilot departed Moorabbin Airport, Victoria at 1723 Eastern Standard Time[1] on 27 June 2013 on a private flight in a Cirrus SR22 aircraft, registered VH-CKS. The night visual flight rules[2] flight was to an airstrip on a private property at Boxwood, about 40 km east-north-east of Shepparton Airport, Victoria.
A family member reported that at about 1750, the pilot made contact by mobile phone and advised where to position a vehicle on the airstrip to provide guidance for a landing. In accordance with the family member’s understanding of those instructions, the vehicle was positioned at the western end of the airstrip facing east towards the aircraft’s expected approach path. The vehicle’s headlights were selected to high beam and flashed to ensure identification. The family member observed the aircraft’s landing light travel from south to north before turning west towards the airstrip. During that period, mobile phone communication was maintained between the pilot and family member and the pilot confirmed that the vehicle headlights were visible. The conversation with the pilot was reported to be normal with no indication of any problems.
Last light[3] for Boxwood on 27 June 2013 was 1737. The private airstrip was not illuminated by fixed or portable lighting. The pilot attempted the approach and landing at about 1806‑1808. There would have been no celestial light, such as from the moon, at that time.
As the aircraft approached the airstrip, the family member saw from the aircraft’s landing light that the aircraft was not aligned with the extended runway centre-line. As the aircraft continued the approach the family member advised the pilot that the aircraft appeared to be too close to the trees north-adjacent to the airstrip. The pilot appeared to continue the approach until the aircraft collided with a tree adjacent to the airstrip. The aircraft rolled to the left and impacted terrain coming to rest inverted. The pilot was fatally injured and the aircraft destroyed.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 13 June 2013, at about 1924 Eastern Standard Time, a Bell 412 helicopter, registered VH‑EMZ (EMZ), departed Horn Island, Queensland on a training flight to Prince of Wales Island, Torres Strait. On board the helicopter was the pilot flying (PF) who was under instruction, a training pilot, and a crewman. The PF conducted a practice approach using the ‘Nightsun’ to illuminate the ground below the helicopter.
At 400 ft AGL, and about 0.6 NM from the targeted landing area, the training pilot noted that the indicated airspeed (IAS) was 60 kt with a 500 ft/min rate of descent and the GPS showed a ground speed of 45 kt. The PF looked outside to confirm that the profile and sight picture were correct for a visual approach and adjusted the Nightsun beam onto the landing site. The training pilot also looked out of the cockpit and when he looked back inside the cockpit he observed a high rate of descent of about 800 ft/min and he called ‘rate of descent’. The training pilot also observed that the IAS was below 35 kt and called ‘go around’. The training pilot reported that there was no immediate response so he repeated the call to ‘go around’.
The PF reported commencing a go-around and responded ‘going around’. The training pilot reported that he felt the collective move. The helicopter entered an incipient vortex ring state and impacted the ground heavily. The crew were uninjured, and the helicopter was substantially damaged.
On 19 May 2013, the pilot of a Pietenpol Air Camper commenced pre-flight checks in a paddock behind his home in St Leonards, about 9 km north of Launceston Airport, Tasmania. The pilot was taking a passenger on a scenic flight around Launceston.
The pilot had operated the aircraft from the paddock in the past, but not for a few years. Prior to landing in the paddock, a week earlier, the pilot had surveyed the area by car.
The aircraft was operating normally and became airborne at about 35 knots indicated airspeed. The pilot held the aircraft low, aiming to clear a fence at the end of the paddock. Nearing the fence, the pilot heard a loud noise, and the nose of the aircraft jolted to the right.
The airspeed quickly decreased, as the pilot attempted to hold the wings level. After initially climbing to about 10 ft, the aircraft impacted the ground, breaking the landing gear. The aircraft skidded on its nose and then pitched over onto its back, breaking the propeller.
Both the pilot and the front seat passenger exited the aircraft without injury. On surveying the accident site, the pilot realised the aircraft’s landing gear had caught the top wire of an electric fence he had not been aware of, located a short distance before the paddock’s main fence.
When not operating from a designated landing area, pilots should ensure the area is suitable. A thorough survey of the area to be used for take-off and landing should be completed prior to use.
On 13 April 2013, an Indonesian registered B737-800 aircraft collided with water on approach to Denpasar Airport, Indonesia.
As the accident took place in Indonesia, the Indonesian National Transportation Safety Committee (NTSC) is responsible for investigating this occurrence, consistent with Indonesia’s obligations as State of Occurrence under Annex 13 to the Convention on International Civil Aviation Aircraft Accident and Incident Investigation (Annex 13).
The NTSC requested ATSB assistance to seek weather and visibility reports from Australian flight crews operating into Denpasar close to the time of the accident. To facilitate this support, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of Annex 13 and, in order to protect the information supplied by the NTSC, commenced an external investigation under the Transport Safety Investigation Act 2003. The ATSB completed its work as accredited representative on 26 April 2013.
The National Transport Safety Committee of Indonesia is responsible for releasing the investigation report.
National Transportation Safety Committee Ministry Of Transportation Republic Of Indonesia Transportation Building 3rd Floor Jalan Medan Merdeka Timur No. 5 Jakarta Pusat 10110 Indonesia
On 24 March 2013, a Vans RV-12 amateur-built aircraft collided with terrain shortly after take-off from Lismore Airport, New South Wales. The pilot was fatally injured.
The NSW police service was responsible for investigating the accident on behalf of the state Coroner. On 10 April 2013, investigating officers contacted the ATSB and requested assistance with the recovery of data from the aircraft’s Dynon Avionics Skyview system. The display unit and control module were subsequently sent to the ATSB for examination and an investigation was initiated under the provisions of the Transport Safety Investigation Act 2003.
The ATSB liaised with the manufacturer of the display unit and was able to successfully disassemble and download flight data stored on the unit. The flight data contained the accident flight, however the flight data ended moments before the aircraft collided with terrain. An archive file, containing the downloaded flight data is released as Appendix A to this report and contains four comma-separated value (.csv) files. Attention is directed to the Data Limitations section of the main report, should any analysis of the recorded information be undertaken.
The ATSB report and the associated data were prepared by the ATSB to assist the NSW police investigation. The ATSB report, including the referenced data files, has been released under section 25 of the Transport Safety Investigation Act 2003 (the Act). Per section 27(1) of the Act, this report and the appended data files are not admissible in evidence in any civil or criminal proceedings. The device containing the original data was returned to the NSW Police Service on 13 November 2013.