On 18 November 2013, an ICP Savannah aircraft, registration 24-7787, collided with terrain near Moomba, South Australia. The pilot and sole occupant was fatally injured.
Recreational Aviation Australia (RA-Aus) is assisting the South Australian Police Service with their investigation of this accident. RA-Aus requested technical assistance from the Australian Transport Safety Bureau (ATSB) in the download of data from a portable Global Positioning System (GPS) navigation device from the aircraft. To facilitate this work and provide appropriate protections for the recovered data, the ATSB initiated an investigation under the Transport Safety Investigation Act 2003.
The AvMap Navigation GPS unit recorded the parameters date, time, latitude, longitude and altitude at a 5 second frequency. A total of 7 flights were successfully recovered from the unit including the accident flight. This data was provided to RA-Aus on 14 January 2014.
______________
Released in accordance with section 25 of the Transport Safety Investigation Act 2003.
On 9 December 2013, the pilot/owner of an amateur-built Stoddard-Hamilton Glasair III aircraft, registered VH-USW and operated in the ‘experimental’ category, was conducting a local flight from Jandakot Airport, Western Australia with a passenger on board.
Shortly after take-off, when about 2 km from the airport, the aircraft’s engine stopped without warning. During the ensuing forced landing onto a sports oval, the aircraft’s left wing detached from the fuselage after striking a metal goal post. Fuel from the ruptured left wing fuel tank ignited as the aircraft tumbled across the ground.
The pilot and passenger sustained serious burns and were taken to hospital. The aircraft was destroyed by impact forces and an intense post-impact fuel-fed fire.
Photograph of Stoddard-Hamilton Glasair III, VH-USW
Source: Aircraft owner
What the ATSB found
During the aircraft’s construction, modification of the electronic ignition system incorporated a single point of failure in the intended dual system, increasing the risk of the simultaneous failure of both systems and a total loss of engine power. In addition, the connector plug used for the modification was inappropriate for the in-line installation, increasing the risk of its disconnection and disabling the ignition system.
Examination of the engine found that the single wiring harness for the ignition system was disconnected from the connector plug. However, due to the level of impact and fire damage sustained by the aircraft, the ATSB was unable to conclusively establish if this occurred inflight, resulting in the total engine power loss, or during the early stages of the impact sequence.
Safety message
The aviation industry has long recognised the need for redundant systems, particularly those relating to safety-critical components. The ATSB cautions that, even if unintended, the incorporation of a single point of failure into such systems during construction or modification can eliminate all levels of redundancy. In this case, damage to the aircraft’s modified single wiring harness resulted in the failure of an otherwise redundant system, with near-fatal consequences.
Context
Pilot information
The pilot held a Private Pilot (Aeroplane) Licence that was issued on 12 March 1990 and a valid Class 2 Aviation Medical Certificate.[4] The pilot had a total flying experience of 3,265 hours, of which 114.6 hours were conducted in the Glasair III aircraft. In the previous 90 days, the pilot had flown 10.2 hours and they last completed an aeroplane flight review on 1 November 2013. This review was carried out in a Van’s Aircraft RV-8 and included a practice forced landing.
Aircraft information
General
The Stoddard-Hamilton Glasair III is a kit-built, all-composite aircraft (primarily fibreglass/resin and carbon fibre/resin) with a low-wing and retractable undercarriage. Consistent with its construction in the United States (US), an experimental amateur-built certificate of airworthiness was issued by the US Federal Aviation Administration (FAA) on 19 July 2000. The aircraft was subsequently purchased by the present owner/pilot and imported into Australia, where it was registered on 1 October 2008 as VH-USW. A special certificate of airworthiness designating the aircraft in the Experimental airworthiness category, and for operation as an amateur-built aircraft, was issued by a Civil Aviation Safety Authority (CASA) authorised person on 22 January 2009.
Engine and propeller
The aircraft was fitted with a six-cylinder, direct-drive, horizontally-opposed, air-cooled Textron Lycoming engine, model number IO-540-K1B5, serial number L-25612-48A. The engine drove a two-bladed Hartzell, constant-speed propeller, model HCCZYK-1BF.
Maintenance
A review of the aircraft’s logbook and other related documentation indicated that USW was maintained in accordance with an approved CASA maintenance schedule. The last periodic inspection was conducted on 11 March 2013, at which time the aircraft’s total time in service was 223.2 hours. The aircraft last flew on 12 November 2012 and had undergone several ground runs following maintenance since that time.
Recent maintenance was carried out on the aircraft’s Light Speed Engineering Plasma I capacitor discharge ignition (CDI) electronic ignition system. This included the removal of the aircraft’s two CDI modules for upgrade by the manufacturer before they were refitted to the aircraft and ground tested satisfactorily.
The power feed to each system was also modified during that maintenance to enhance the independence of the two CDI systems. It was reported that a wire that led from the main power bus to the voltmeter switch was temporarily disconnected (see the section Engine monitoring and recording) and that the wire was not reconnected prior to the occurrence. The aircraft had not flown in the intervening period.
Alternator V-belt
The aircraft’s maintenance records indicated that a notched alternator V-belt was fitted to the engine in about January 2000 and had not been replaced. The engine manufacturer specified that, following fitment of a new belt, the belt should be checked for correct tension 25 hours after installation. It was unknown if this had been conducted.
Routine maintenance inspections were certified as conducted in the intervening 14-year period. According to the FAA and CASA maintenance schedules, these inspections included an inspection of the V-belt. The pilot indicated that when inspected, no problems were identified with the condition of the belt. According to the belt manufacturer, the belt had an acceptable storage life of 8 years, even if stored for this time on the drive under tension. Examination of the alternator belt tensioning arm showed a single, circular witness mark that coincided with the under-head washer on the bolt. Consistent with the maintenance records, this indicated that the alternator belt had likely not been replaced since initial installation during the construction of the aircraft.
Further, in order to prevent ‘belt set’,[5] the manufacturer recommended that tension be removed from the belt if storage time before re-use was greater than about 6 months. Depending on a number of factors including drive design, storage environment and maintenance practices, serious belt damage may occur when starting this type of belt if ‘set’ had occurred and/or the belt had lost tension. The maintenance records for USW indicated a maximum storage time of just over 6 months. As such, there would have been no need to remove tension from the belt.
Electronic ignition system
During the aircraft’s construction, the engine was modified by replacing its dual magneto system and corresponding aircraft-type spark plugs and leads with the Plasma I capacitor discharge ignition (CDI) system (electronic ignition system). This system was originally designed to operate as a single CDI system and used dual-lead coils and automotive spark plugs and leads.
In normal operations, six-cylinder engine ignition timing on the Plasma I was achieved by a trigger coil system. As part of this system, a trigger plate mounted on the front of the engine crankcase contained three trigger coils and precisely-placed interrupter trigger bolts fastened to the ring gear support assembly (flywheel). This assembly is attached to the propeller hub. As the flywheel rotates, the trigger coils sense the trigger bolts and produce an electrical signal each time successive bolts pass the coils. This provides an indication of crankshaft position (timing) and allows the determination of the engine revolutions per minute (RPM) via wiring to the individual CDI modules located beneath the instrument panel in the cockpit. Timing, RPM and manifold pressure information is integrated by the CDI modules to optimise the timing of the spark in each cylinder.
Aircraft builders were supplied with a trigger plate assembly and were responsible for connecting a short wiring harness from the trigger plate to the pre-manufactured CDI module cable. The manufacturer’s diagram recommended that the wiring harness be attached using a suitable connector. The manufacturer also recommended a soldered joint connection as a preference. These connections were based on a single electronic ignition system installation.
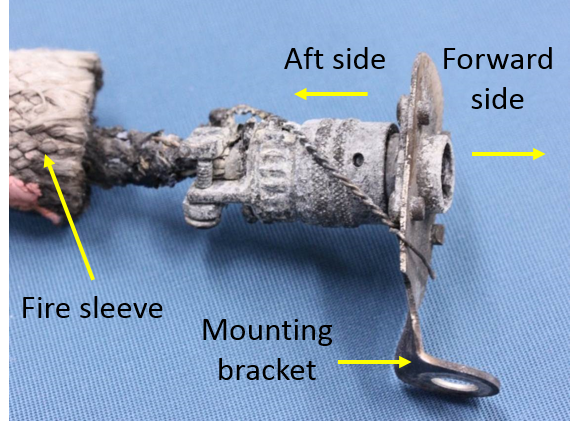
The aircraft’s ignition system was further modified by the aircraft builder to include a second CDI module and an auxiliary battery. The addition of an auxiliary battery was recommended by the manufacturer and independently powered the second system. The aircraft’s two CDI systems were intended by the builder to operate independently, providing redundancy in the event that one of the duplicated elements failed. To duplicate the wiring for the two CDI modules, the builder split the single wiring harness from the trigger plate into two using a MILSPEC connector plug.[6] This plug was designed to be attached to a metal box or a panel, such as a firewall. However, in USW, it was mounted onto a homemade, right-angled bracket that was fastened to the front of the engine crankcase (Figure 3). The connector plug and associated wiring were in an in-line arrangement.
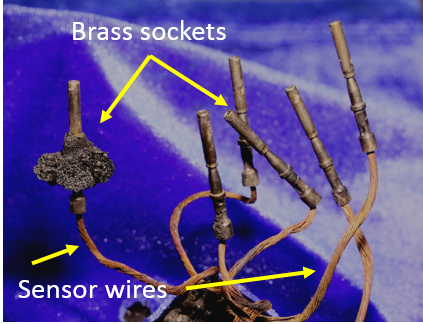
On the aft side of the connector plug in USW, the duplicated wires were clamped to relieve stresses from wire tension and were collectively shrouded in fire sleeving (Figure 3), which went to each CDI module. On the forward side of the plug, the single set of wires from the trigger plate was inside two plastic sleeves and their ends inserted into brass sockets, which were crimped for security (Figure 4). The sockets were then pushed into the forward side of the connector plug through a rubber sealing grommet and held in place in the cylindrical, plastic insulator by plastic clips. There was no means on this type of connector for relieving any stresses placed on the wires.
Figure 3: Bracket-mounted connector plug and fire sleeve
Source: ATSB
Figure 4: Sensor wires and brass sockets
Source: ATSB
Light Speed Engineering Plasma II and III ignition systems, such as the direct crank sensor installation, are now available as a dedicated dual system, with two independent wiring harnesses originating from the sensor plate and connecting directly to each CDI module. No intermediate plug, such as the connector plug used on USW, is required.
Engine monitoring and recording
The aircraft was fitted with a Vision Microsystems Inc. VM 1000 engine management system and an EC 100 electronic checklist and caution advisory system. The VM 1000 was normally used to display engine and aircraft system parameters during a flight. Additionally, when the engine RPM increased above 1,500 RPM, the VM 1000 automatically recorded the minimum and maximum values for various operating parameters for the flight. The system also had a built-in warning system whereby any out-of-tolerance parameter flashed on the display.
The recorded data for the occurrence flight was retrieved from the VM 1000 following the accident. This data showed a voltmeter reading of zero for the flight. This was consistent with the reported disconnection of the wire between the main power bus and voltmeter switch, which had been selected to indicate main bus voltage. The remaining values, including engine oil pressure and temperature, ammeter and fuel flow and pressure gave no indication of the reason for the engine failure.
The EC 100 operated in conjunction with the VM 1000 and alerted the pilot to abnormal conditions or trends in the engine operating parameters. The pilot could not recall a warning of a problem with the engine, but had reportedly mentioned to witnesses immediately after the accident that an unspecified engine warning had been received. The passenger reported not paying any particular attention to the warning display during the flight.
Fuel system and selection
The fuel was carried in integral fuel tanks located in each wing, with a reported total capacity of 114 L in each tank. A fuselage header tank located between the engine firewall and the cockpit had a total capacity of 25 L. Additionally, USW was fitted with optional wingtip tanks, but the pilot reported that they were empty for the flight.
A four-position fuel selector was located on the centre console near the pilot’s right knee. To prevent inadvertent selection, a button on the selector had to be raised in order to select the OFF position. The pilot reported selecting the left fuel tank for the flight.
The pilot also reported a previous temporary fuel starvation event with the header tank selected. In that instance the engine had coughed and surged, providing sufficient warning for the pilot to change tanks.
Meteorological information
The automatic terminal information service[7] at Jandakot Airport indicated a 14 kt (26 km/h) surface wind between 140° and 200° (south-south-easterly to south-south-westerly) and a temperature of 27 °C at the time. A nearby surveillance camera showed smoke from the post-impact fire being blown from the south-west.
Wreckage and impact information
An examination of the wreckage found that the aircraft’s right wingtip clipped a tree on the southern boundary of the oval before the left wing was sheared off at the wing root by the collision with a tubular, metal goal post. This impact ruptured the left-wing fuel tank and severed aircraft wiring from the fuselage into the left wing. Images from a nearby surveillance camera showed that the fuel ignited shortly after the collision with the goal post (Figure 5).
Figure 5: Security camera image of the fire (looking south-south-east)
Source: Channel 7
Damage to the aircraft was consistent with witness descriptions and the surveillance images depicting the aircraft tumbling before coming to rest with the fuselage, attached right wing and tailplane inverted. The engine, upper engine cowling, engine mounts and header tank were orientated in an upright position. The upper engine cowling was in situ and intact, with the engine still attached to the firewall assembly via the support frame. The damage to the propeller blades and strike marks on the ground were consistent with the propeller rotating at impact but the engine producing no power (Figure 6 inset).
The impact and fuel-fed fire destroyed the cockpit and severely damaged the composite airframe. This included the destruction of components of the electronic ignition and fuel systems, limiting or preventing examination of these parts.
Figure 6: Aircraft wreckage and propeller damage (see inset)
Source: ATSB
Fire
Shortly after colliding with the ground, a significant fire commenced that was initially fed by fuel from the ruptured left-wing tank. The right wing and header tanks were also breached during the impact sequence. The fire was subsequently extinguished by local fire authorities. The aircraft was destroyed in the fire and the occupants received serious burn injuries. The investigation was unable to identify the ignition source(s) for the fire; however, disruption of the aircraft’s wiring while still powered provided a potential ignition source for the fire.
The emergency procedures section of the Glasair III owner’s manual detailed the actions in the event of an engine failure, in particular, once committed to landing. These included the requirement for the aircraft’s alternator, master and ignition switches to be selected to OFF. In addition, the FAA Airplane Flying Handbook stated that:
Deactivation of the airplane’s electrical system before touchdown reduces the likelihood of a post-crash fire. However, the battery master switch should not be turned off until the pilot no longer has any need for electrical power to operate vital airplane systems.
In this instance, due to the difficult approach and landing area constraints, the pilot lowered the flaps and undercarriage to assist with controlling the aircraft’s landing speed and prevent an overshoot. As the undercarriage required electrical power to extend, the pilot elected to leave the aircraft’s electrical system on for the landing. This was consistent with the FAA guidance.
Survival aspects
The pilot reported that he and the passenger most likely escaped the burning wreckage during the break-up of the fuselage as the aircraft tumbled across the oval. This dislodged the seatbelt attachment points from the fuselage and released the pilot and passenger from the wreckage.
Tests and research
Engine examination
The engine was recovered from the wreckage and transported to an approved overhaul facility for technical inspection under the supervision of the ATSB. The examination found no evidence of internal mechanical failure of the engine that would have prevented normal operation prior to the occurrence.
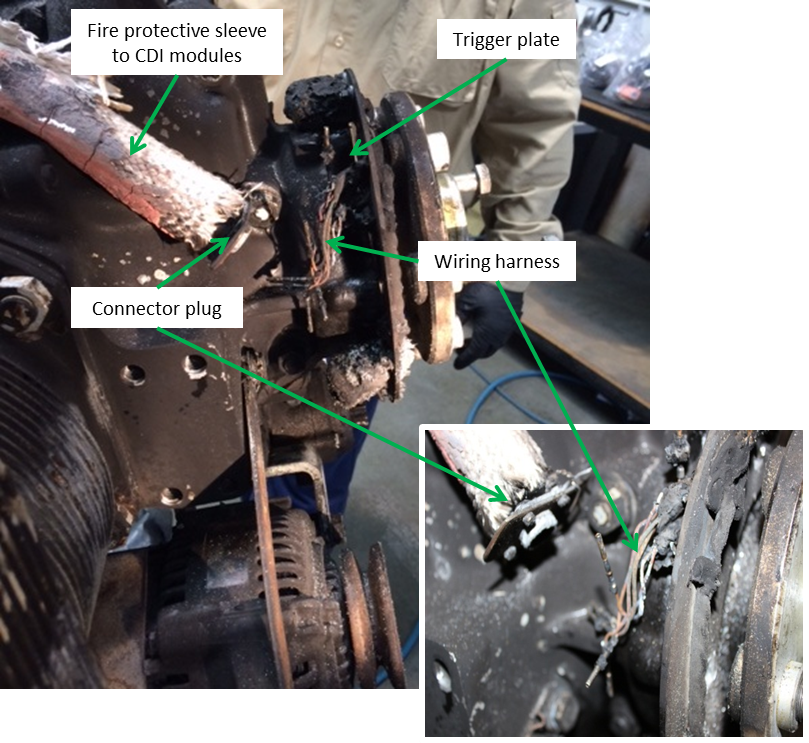
The wires from the engine timing trigger plate for the aircraft’s electronic ignition system were found disconnected from the connector plug and displaced in the direction of engine rotation (Figure 7). In addition, there was no evidence of the alternator V-belt. Whether the belt failed or dislodged from the drive prior to or during the accident sequence, or was consumed in the postimpact fire could not be determined.
The remaining components from the aircraft’s ignition system and the alternator were removed from the engine. Together with the already-removed flywheel, these items were transported to the ATSB technical facilities in Canberra, Australian Capital Territory for further examination.
The wires for each of the trigger coils on the engine timing trigger plate were resistance tested and found within manufacturer’s specifications. A check for short circuiting between the wires was also conducted, with nil evidence found. This indicated that the trigger coils were capable of functioning prior to the occurrence.
Examination of the pins and brass sockets on the forward side of the connector plug showed damage consistent with the wiring harness being forcefully and unevenly disconnected either inflight or during the early stages of the impact sequence. However, no witness marks were identified on the two flywheel trigger bolts to indicate contact with another part of the engine or its accessories. This and the fire damage to the plastic insulation on the wiring harness meant that there was insufficient evidence to conclude that they had contacted a trigger bolt.
System redundancy and single points of failure
On 22 June 2001, the pilot of an amateur-built Quickie Aircraft Corporation Q2 aircraft reported that their aircraft’s engine stopped during the climb. The pilot attempted a forced landing at the departure aerodrome. The pilot reported that, as the aircraft approached the runway, they ‘encountered sink’ and undershot the runway. The aircraft collided with a boundary fence before coming to rest. The pilot reported that the switch for the aircraft’s ignition system had failed. The aircraft was fitted with a dual magneto ignition system but had a single ignition selector switch. The pilot indicated that not being able to select the individual ignition systems reduced the redundancy of the system (ATSB occurrence 200103043).
Downer (2009) described system redundancy as follows:
An element is redundant if it contains backups to do its work if it fails; a system is redundant if it contains redundant elements. This can mean having several elements that work simultaneously but are capable of carrying the ‘load’ by themselves if required…
Describing the advantages of system redundancy, Dekker (2011) highlighted that:
…redundancy is the best way to protect against hazard…safety-critical systems usually have multiple redundant mechanisms…it protects them against the failure of a single component or part that could directly lead to a bad outcome.
The October 2014 edition of the Sport Aircraft Association of Australia Airsport magazine included an article on the occurrence involving USW and the aircraft’s electronic ignition system. Specifically, the article discussed that, while the ignition system was well-built, with redundancies in place, the wiring from the trigger plate was a potential common point of failure that, if damaged, would result in a sudden and total power loss. The article further suggested a number of strategies to help manage this risk, including the installation of a hybrid ignition system (one magneto and one electronic ignition system) and/or ensuring the wiring was protected from mechanical damage. The manufacturer of the ignition system fitted to USW noted the benefits of having a dual electronic ignition system. In particular, dual ignition would provide enhanced performance and reliability when compared with traditional (two magnetos) or hybrid ignition systems. Regardless of the solution adopted by builders, the manufacturer reinforced that, in order to address the risk of a single point of failure, it is crucial that dual electronic ignition systems operate independently.
The US Federal Aviation Administration Advisory Circular 25.1309-1A (System design and analysis) suggests that in any safety-critical system, the failure of a single element, component or connection should be assumed, regardless of the probability. However, such single-point failures should not compromise the safety of a flight or significantly reduce the aircraft’s capability or a crew’s ability to cope with the resultant failure. A single point of failure can simultaneously eliminate all levels of redundancy (Berk 2009).
From the evidence available, the following findings are made with respect to the engine failure at about 1,000 ft shortly after take-off, and subsequent collision with terrain in a nearby sports oval involving an amateur-built Stoddard-Hamilton Glasair III aircraft, registered VH-USW, near Jandakot Airport, Western Australia on 9 December 2013. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
The aircraft's engine stopped without warning and, with very few landing options available and a number of obstacles on short finals to the intended landing area, the forced landing resulted in a collision with terrain.
Other factors that increased risk
Modification of the aircraft’s electronic ignition to an intended dual system during aircraft construction incorporated a single point of failure, increasing the risk of the simultaneous failure of both systems and a total loss of engine power.
The connector plug for the aircraft’s electronic ignition system was inappropriate for an in-line installation, increasing the risk of the single wiring harness becoming disconnected and disabling the ignition system.
The alternator V-belt fitted to the aircraft exceeded the manufacturer's storage life of 8 years, increasing the risk of belt failure.
Other findings
Although the initiator and timing of the disconnection could not be conclusively determined, the single wiring harness for the aircraft’s electronic ignition system was found disconnected from the connector.
Safety analysis
The loss without warning of engine power at about 1,000 ft shortly after take-off, combined with the surrounding built-up area and obstacles, presented the pilot with very few landing options. The loss of the left wing from the collision with the goal post contributed to the aircraft tumbling across the sports oval, increasing the severity of the occupants’ injuries and aircraft damage.
The extensive damage from impact forces and the post-impact, fuel-fed fire precluded examination of a number of the aircraft’s fuel system components. However, the pilot’s description of the symptoms associated with a previous loss of engine power from fuel starvation, and the amount of fuel on board so shortly after take-off, indicated that fuel-related issues were not a factor in the sudden engine power loss.
While the engine examination identified no internal mechanical failure or abnormality that would have precluded normal operation, the single wiring harness to the aircraft’s electronic ignition system was found disconnected.
This analysis will discuss the aircraft’s electronic ignition system and the possible reasons for, and timing of the disconnection of the wiring harness. It will also consider the suitability of the associated connector plug and discuss the risks to aircraft systems of single points of failure.
Electronic ignition system installation
During construction, the aircraft was fitted with a single electronic ignition system that was then modified by the builder of the aircraft with the addition of a second ignition module. The installation was intended by the builder to create a dual system that would provide for redundancy. That is, in the event of one system failing, the other would continue to operate. However, the modification retained the original single wiring harness from the engine timing trigger plate to the connector plug, incorporating a single point of failure in the intended dual system.
Cessation of the engine timing signal, such as from the disconnection of the single wiring harness, would result in the loss of timing signals to both ignition modules and failure of the ignition system. Without an ignition source, the engine would stop operating.
The alternator V-belt and the engine timing trigger bolts on the flywheel were the only two moving components within the vicinity of the single wiring harness and connector plug with the potential to disconnect the harness. The still rotating propeller meant that, dependent on the presence of an operational alternator belt, these components may still have been rotating at impact. However, the unavailability of the alternator belt for examination prevented any conclusion on its pre-impact condition or contribution to the disconnection of the harness. Regardless, the continued use of the V-belt, which had been stored under tension for longer than the manufacturer’s acceptable storage life, increased the risk of belt failure.
As with the difficulty determining the contribution, if any, of the V-belt to the occurrence, the lack of witness marks on the two flywheel trigger bolts and the fire damage to the plastic insulation on the wires precluded a conclusion that the wiring harness had contacted a trigger bolt.
In any case, examination of the connector plug and sensor wire sockets showed that the wiring harness was forcibly disconnected prior to the fire. However, given the number and nature of the multiple impacts with terrain during the accident sequence, the timing of the disconnection could not be established.
Suitability of the wiring harness connector plug
The connector plug and associated wiring forward and aft of the plug were an in-line installation. The connector allowed duplication of the wiring for the intended dual ignition system and provided clamping on the aft side of the plug to relieve wire tension. The clamping was not repeated forward of the plug, where the single wiring harness from the engine timing trigger plate had disconnected.
The wiring on the forward side of the plug relied on friction and an internal, plastic locking mechanism to retain the sensor wires and sockets in position. The limited support provided on the forward side of the plug increased the risk of the wiring harness disconnecting from the in-line installation.
Single point of failure
The aviation industry has long recognised the need for redundant systems, particularly those relating to safety-critical components. Incorporating a single point of failure into such systems during construction or modification can eliminate all levels of redundancy. In this case, the loss of the single wiring harness resulted in failure of an otherwise redundant system, with near-fatal consequences.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and passenger of VH-USW
the Licenced Aircraft Maintenance Engineer and electrical technical expert for VH-USW
Light Speed Engineering
a number of witnesses
the Civil Aviation Safety Authority.
References
Berk J 2009, Systems Failure Analysis, ASM International Ohio.
Dekker S 2011, Drift into failure: from hunting broken components to understanding complex systems, Ashgate Publishing Surrey.
Downer J 2009, When Failure is an Option: Redundancy, reliability and regulation in complex technical systems, Discussion Paper No. 53, Centre for Analysis of Risk and Regulation London.
Federal Aviation Administration 2004, Airplane Flying Handbook, Chapter 16: ‘Emergency procedures’, United States Department of Transportation.
Federal Aviation Administration 1988, System design and analysis, Advisory Circular AC 25.13091A.
George A 2014, ‘Engine failure Glasair III’, Airsport, October 2014, pp. 14–15.
Gates Facts Extended Storage of Belt Drives and Analyze Your Way to Longer Lasting, Better Performing V-belt Drives.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the pilot and passenger of VH-USW, the aircraft’s electrical technical expert, Light Speed Engineering, the Civil Aviation Safety Authority and the United States National Transportation Safety Board.
A submission was received from Light Speed Engineering. The submission was reviewed and where considered appropriate, the text of the report was amended accordingly.
The occurrence
On the afternoon of 9 December 2013, the pilot/owner of an amateur-built Stoddard-Hamilton Glasair III aircraft, registered VH-USW (USW) and operated in the ‘experimental’ category, conducted a preflight inspection in preparation for a local flight from Jandakot Airport, Western Australia. The pilot reported that the aircraft’s wingtip fuel tanks were empty, the main tanks were full and 25 L was uploaded into the header tank. The pilot and passenger then boarded the aircraft and taxied for the flight.
The flight was the first since the aircraft’s electronic ignition system had undergone maintenance. While the ignition system was engine ground-run tested by a Licenced Aircraft Maintenance Engineer as part of that maintenance, the pilot elected to perform the engine run-up checks twice as a precaution. The pilot reported that the engine operated as normal.
At about 1434 Western Standard Time,[1] the pilot advised Jandakot Tower air traffic control that they were ready for departure and was subsequently cleared to take off from runway 24 Right (R). After take-off, the aircraft was climbed to 1,000 ft and a shallow right turn commenced toward Fremantle. The pilot and passenger stated that at about 1436 the aircraft’s engine suddenly stopped without warning and the pilot broadcast on the Jandakot Tower radio frequency that they had experienced an engine failure. The pilot reported that, while there was insufficient altitude to conduct the engine failure ‘trouble checks’,[2] they moved the two toggle switches for the aircraft’s ignition system to OFF and ON again in an attempt to re-start the engine, but with no effect.
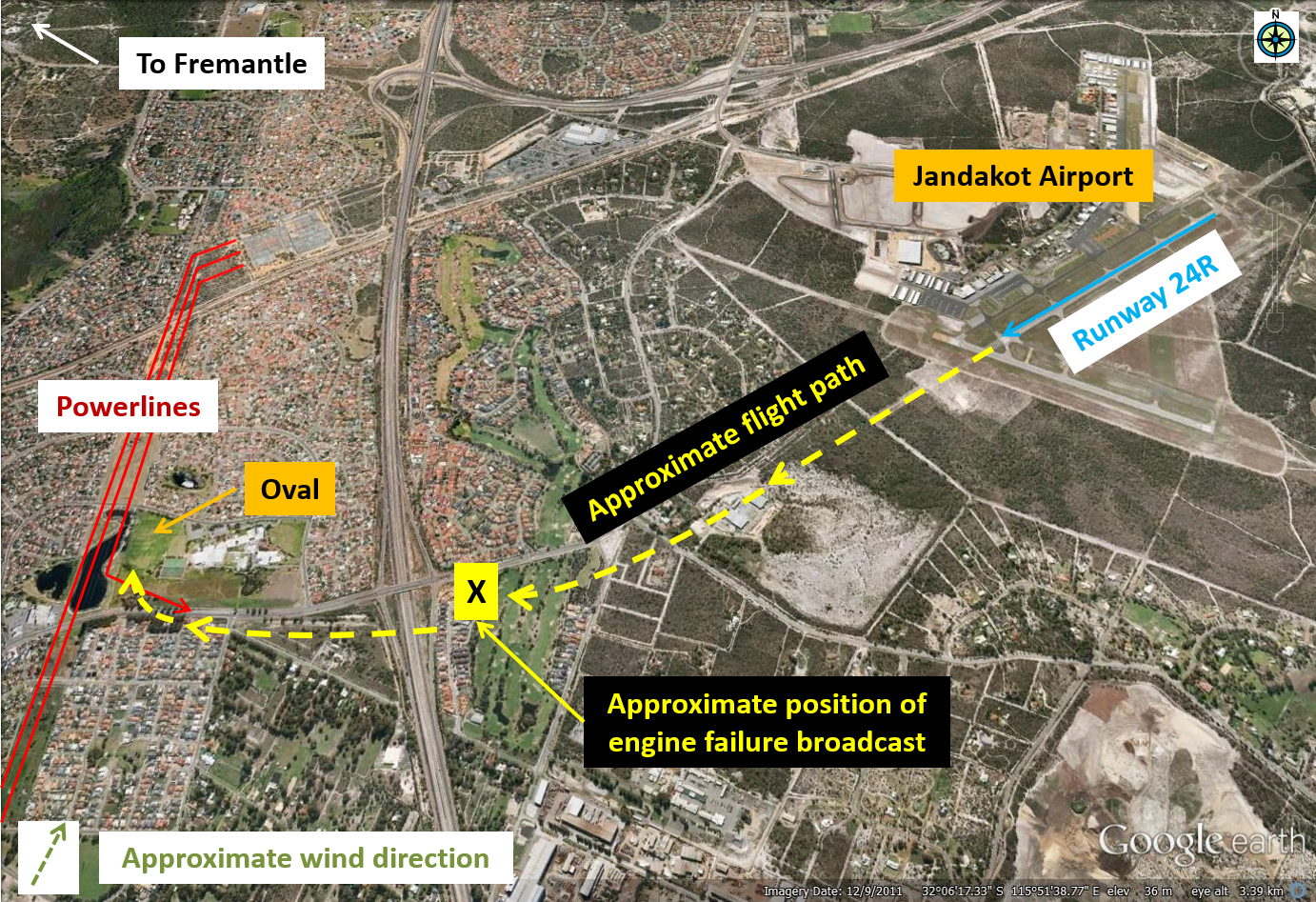
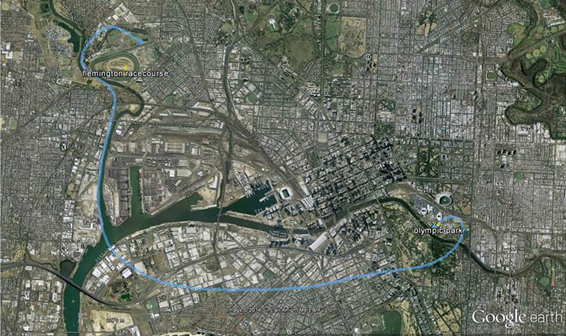
The pilot focused on flying the aircraft and looking for a suitable landing area. With very few options available, the pilot, who was aware of powerlines in the vicinity (Figure 1), manoeuvred the aircraft for a forced landing in a nearby grassed area (Lakelands Reserve Oval). It was reported that the propeller was windmilling during the descent.[3]
Figure 1: Approximate flight path and forced landing area
Source: Google earth, modified by the ATSB
Approaching the landing area, the pilot observed a powerline along the flight path and dived abruptly to pass beneath that line. At the same time, the pilot lowered the undercarriage and flaps to control the aircraft’s airspeed and avoid overshooting the oval. The pilot elected not to turn the aircraft’s electrical system off for the landing to ensure that the undercarriage lowered completely.
After flying under the powerline, the aircraft lightly clipped a tree bordering the oval before colliding with a metal goal post. The pilot reported not seeing the goal posts until it was too late to avoid the collision (Figure 2). The pilot recalled hearing the sound of the impact then next remembered lying on the ground and seeing the passenger nearby and the aircraft wreckage on fire. The pilot helped the passenger to move away from the wreckage and remove burning clothes items.
Figure 2: Three-strand powerline on late approach to the landing area and the impacted tree and goal post (looking back along the direction of travel)
Source: ATSB
Witnesses in the vicinity heard the sound of an impact and saw a fireball and the burning aircraft tumbling across the oval before coming to rest. A number of people rushed to assist and found the two occupants clear of the burning wreckage. They moved the occupants further away and administered first aid until emergency services personnel arrived.
The pilot and passenger both sustained serious burns and were taken to hospital. Emergency services extinguished the fire, but the aircraft was destroyed by the impact forces and intense fuel fed fire.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 1 December 2013, an Aérospatiale AS350B2 helicopter, registered VH-HRQ (HRQ), was on a return flight to Davis Base, Antarctica, with a pilot and two passengers on board. HRQ was one of two helicopters that were tasked to take a scientist and two field training officers to a penguin rookery at Cape Darnley. The helicopters refuelled during the return flight at a fuel cache on the Amery ice shelf, before departing to the south‑east for their next refuelling stop.
As a result of a rapid reduction in visual cues, the pilot of HRQ maintained about 150 ft above ground level. The pilots of both helicopters discussed the reduced surface definition and loss of visible horizon along their flight path and elected to return to the fuel cache until the weather improved. During the turn back to the fuel cache, HRQ descended and impacted the ice shelf. The pilot and two passengers were seriously injured, and the helicopter destroyed.
What the ATSB found
The ATSB found that the pilot did not detect the descent during the turn back to the fuel cache. The ATSB concluded that, after initiating the right turn, the pilot probably became spatially disoriented. Factors contributing to the disorientation included a loss of visual cues as a result of the change in weather conditions, and a breakdown of the pilot’s scan of his flight instruments, resulting in collision with terrain.
What's been done as a result
Following this accident the operator introduced new helicopters equipped with an autopilot and other equipment to reduce pilot workload. They also introduced simulator training that is administered by an experienced Antarctic pilot, a situation awareness course, and training on the use of the autopilot in the new helicopters and limitations of the radar altimeter. The operator has also amended their operational documentation to prescribe minimum settings for radar altimeters, discuss the use of the autopilot in low visibility environments, and provide decision-making guidance in relation to early avoidance of, and action on encountering inadvertent white-out conditions.
Safety message
This accident provides a timely reminder to flight crews of the importance of monitoring the flight instruments when encountering areas of reduced visual cues. The risks associated with flight in these conditions have been highlighted on the ATSB website as a SafetyWatch priority, along with a number of strategies to help manage the risk and links to relevant safety resources.
On 11 May 2013, the pilot of a Pacific Aerospace Fletcher FU24-950 aircraft was conducting aerial agricultural spraying activities near North Rawajitu, Lampung, Indonesia, when the aircraft collided with terrain. The pilot was fatally injured and the aircraft destroyed.
The National Transportation Safety Committee (NTSC) of Indonesia is responsible for investigating this accident. The aircraft carried an Ag-Nav GPS-based guidance and track monitoring system which the NTSC downloaded using conventional techniques. The normal download yielded data prior to the accident flight. The NTSC requested specialist assistance from the Australian Transport Safety Bureau (ATSB) to recover any accident flight data from the Ag-Nav system non-volatile memory chips that may not yet have been written to the unit's normal file system.
In accordance with clause 5.23 of Annex 13 to the Convention on International Civil Aviation (ICAO Annex 13), and to provide for the necessary protections of the Ag-Nav information, the ATSB appointed an Accredited Representative to assist the NTSC and initiated an investigation under the Australian Transport Safety Investigation Act 2003.
Download, examination and correspondence with the unit's manufacturer yielded no additional data beyond that retrieved in Jakarta. The latest available data from the Ag-Nav unit was found to be on 10 May 2013 consequently no accident flight data was available to assist the NTSC investigation team.
A report detailing the download and data examination was provided to the NTSC on 29 October 2013.
All inquiries regarding the investigation into this accident should be forwarded to the National Transportation Safety Committee of Indonesia.
National Transportation Safety Committee Ministry Of Transportation Republic Of Indonesia Transportation Building 3rd Floor Jalan Medan Merdeka Timur No. 5 Jakarta Pusat 10110 Indonesia
On 6 November 2013, the pilot of a Robinson R44 helicopter, registered VH‑UGC, was conducting a private flight from Latrobe Valley to Mount Buller, Victoria, with three passengers onboard.
At about 1425 Eastern Daylight-savings Time, the helicopter arrived overhead the Mount Buller Township. Two orbits at about 500 ft above ground level (AGL) were conducted to assess the landing area (helipad), the wind conditions and confirm the outside air temperature.
The pilot then commenced an approach to the helipad. When in an out-of-ground-effect hover, he conducted a power check at 21 inches hg manifold pressure. He then reduced the engine power to 18 inches hg and reported that, when about 30 m from the helipad, the helicopter became a bit unstable. He then raised the collective, but the engine appeared to lose power. He attempted to increase the power, but the engine appeared not to respond.
As the front of the helicopter’s skids were about to touch down, the pilot applied full forward cyclic, and reported experiencing mast bump. In response, he raised the collective lever. The low rotor revolutions per minute (RRPM) horn then sounded and the pilot reported the helicopter felt as if it was going to fall backwards. The helicopter rolled onto its side and came to rest about 9 m down an embankment. The helicopter was substantially damaged and the passengers were uninjured.
To maintain a steady hover, an increase in the weight of the helicopter requires more engine power. Increases in altitude and temperature reduce air density, and consequently the engine’s ability to produce power. Mount Buller helipad was at an elevation of 5,400 ft above mean sea level. The pilot reported that the helicopter was at a gross weight of about 1,048 kg when it landed.
On 2 November 2013, the pilot of a Bell 206L-1 helicopter, registered VH-VDZ, was conducting passenger-carrying charter operations between Olympic Park oval and Flemington Racecourse, Melbourne, Victoria. At about 1830 Eastern Daylight-saving Time, the pilot prepared to reposition the helicopter from one of the temporary helipads at Olympic Park. There were no passengers on board.
As the pilot lifted the helicopter into a hover it started rolling about the right skid, which was in contact with the ground. The helicopter rapidly rolled further right until the main rotor blades struck the ground. A large amount of main rotor and other high energy debris was released from the helicopter and impacted a nearby marquee, a number of vehicles and a helicopter on an adjacent helipad. The pilot sustained minor injuries.
What the ATSB found
The ATSB found that the pilot did not identify and react to the helicopter’s right-skid low attitude in sufficient time to prevent the helicopter rolling over. In addition, an unsecured ballast bag was positioned on the left front floor of the helicopter, increasing the risk of injury to occupants. Further, the helicopter’s dual flight controls were removed to facilitate the flights. The person who removed the controls did not have the training or authorisation to conduct the maintenance procedure. The left cyclic stub cover was not installed, leaving the stub exposed. This resulted in the potential for the ballast bag to inhibit movement of the pilot’s cyclic control due to fouling of the left cyclic stub.
The ATSB identified safety issues relating to the availability of first aid and emergency response equipment at the oval and the proximity of the helipads to the perimeter fence and public access areas. Each increased the risk of injury to bystanders in the event of an accident.
What's been done as a result
For subsequent operations at the Olympic Park oval for the remainder of the event, the charterer positioned firefighting equipment at each helipad and first aid equipment was made available nearby. In addition, the helipads were repositioned further from the passenger marquee, and passengers were not loaded or unloaded if helicopters were in the process of landing or taking-off from adjacent helipads. Operations at the Olympic Park oval ceased following the 2013 carnival.
Safety message
This accident highlights the importance of coordinated control inputs by pilots during lift-off to control any roll, and if necessary smoothly lowering the collective in coordination with cyclic input to re-establish the helicopter’s weight evenly on the ground before any roll becomes excessive. The importance of properly securing any equipment, particularly if stowed in aircraft cockpits, and of the correct removal and re-fitting of dual flight controls to prevent any obstruction or fouling of the controls is emphasised.
In addition, this accident is a reminder of the risks involved when operating helicopters in public areas. Although the likelihood of a helicopter accident on the ground that results in injuries was found by the ATSB to be low, in the event of an accident, high energy rotor and other debris can travel large distances. Where possible, operators should consider larger distances around helicopter landing areas, in particular when operating close to public areas.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot of the helicopter
charterer of the helicopter
owner of the helicopter
Civil Aviation Safety Authority (CASA).
References
Wagtendonk, WJ 1996, Principles of Helicopter Flight, Aviation Supplies & Academics, Inc. Washington, USA.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the CASA, the aircraft owner, the charterer of the helicopter and the pilot.
Submissions were received from CASA, the charterer of the helicopter and the pilot. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Context
The charterer[2] secured the services of other operators in support of the passenger-carrying charter flights that day. This provided additional capacity to move passengers between Olympic Park oval and Flemington Racecourse during peak periods.
Personnel information
Pilot
The pilot held a Commercial Pilot (Helicopter) Licence and was endorsed on the Bell 206 (B206) helicopter. The pilot also held a valid Class 1 Aviation Medical Certificate.
The pilot indicated that, at the time of the accident, they had a total aeronautical experience of about 1,020 flying hours, which included about 50 hours flying B206 Jetranger helicopters and about 22 hours flying the B206 Longranger. The pilot’s most recent check flight was conducted on 21 January 2013 in a Robinson R44 helicopter. The pilot was not approved for pilot-permitted maintenance on the B206 in relation to the removal of flight controls (see Conduct of the flights and Dual flight controls).
A review of the pilot’s training file identified that sections relating to the pilot’s ab-initio training, B206 endorsement and recurrent training were incomplete. The pilot’s former employer reported that these sections were missing.
The pilot attended operational briefings 1 week prior to the passenger-carrying charter flights from Olympic Park that day. The briefings, conducted by the charterer’s chief pilot, included preferred routes, airspace boundaries, radio frequencies and other flight procedures. These included passenger loading and helicopter positioning.
Charterer’s chief pilot
The charterer’s chief pilot held the appropriate approvals and endorsements to fulfil their role. Although endorsed to fly the B206 helicopter, the chief pilot was not approved for pilot-permitted maintenance on the B206 in relation to the removal of flight controls.
For the purposes of the contract with Olympic Park for the conduct of flights between Olympic Park oval and Flemington, the charterer undertook a project management role, providing, through its chief pilot and other staff, oversight from both locations throughout the day.
Marshallers
The marshallers stated that they acted in a similar capacity during the previous year’s events. They were reported to have attended a specific ground crew briefing conducted by the charterer’s chief pilot 1 week prior to the event. It was also reported that, on the morning prior to commencing the passenger-carrying charter operations, an additional briefing session was conducted at Olympic Park oval for all operational personnel. The charterer stated that the marshallers had completed first aid training and were instructed on the use of emergency equipment, such as fire extinguishers.
Aircraft information
General information
VH-VDZ (VDZ) was a Bell Helicopter Co. 206L-1/C30P (Bell 206L-1), and was manufactured in the United States in 1981 (serial number 45693). It was first registered in Australia on 20 September 1991 and had accumulated about 6,159 hours total time in service at the time of the accident. The helicopter had been appropriately modified to incorporate a single Rolls-Royce 250-C30P turboshaft engine under a supplemental type certificate.
In the charter role, VDZ had seating for a pilot in the front right seat and six passengers. It was certified for day and night charter operations under the day/night Visual Flight Rules[3].
VDZ was installed with a handheld fire extinguisher.
Maintenance History
Examination of the helicopter’s current maintenance release indicated that it was maintained to a night Visual Flight Rules standard in the charter category. At the time of the accident, all of the scheduled maintenance recorded on the maintenance release had been completed. No maintenance entries were identified on the maintenance release in relation to the removal or installation of the dual flight controls.
Weight and balance
A minimum weight of 170 lb (77 kg) was required in the cockpit to operate the Bell 206L-1. This meant that, due to the reported pilot weight of about 65 kg, supplemental ballast was required for flights in VDZ where no passenger or crew occupied the front left seat. This took the form of a ballast bag (see the section Conduct of the flights), which was placed in the left of the cockpit.
The aircraft’s weight and longitudinal centre of gravity (CofG) at the time of the accident was calculated to be within limits. The lateral CofG was slightly to the right of the helicopter’s centreline.
Meteorological information
Photographic evidence and witness observations indicated a light wind at the time of the accident and that it crossed the helicopter from left to right. Weather observations by the Bureau of Meteorology at a nearby airport recorded that, at about the time of the accident, the wind was from the south at 12 kt.
The Bell 206L-1 flight manual stated that satisfactory stability and control was demonstrated in relative winds of 17 kt from the side of the helicopter. The pilot reported that meteorological conditions at the time did not adversely affect the operation of the aircraft and that the crosswind was within the helicopter’s normal operating limits.
Operational information
Planned operations
In preparation for the flying activities the charterer assessed the Olympic Park helicopter landing site. This enabled the charterer to draft a suite of event-specific documents that was issued to operational crew during a pre-event briefing. This included to all pilots involved in the charter operations on the day of the accident. The documents included information on the locations of the helipads, the passenger access points and hazards at each site, the preferred flight routes and altitudes and relevant emergency procedures.
Prior to the event, representatives of the charterer had meetings with the Victorian Racing Club and the Melbourne and Olympic Park Trust. These meetings reviewed the operational procedures and other requirements surrounding the proposed aviation activities. It was reported that this included items of the charterer’s risk management plan and safe work method statement.
The charterer’s risk management plan identified nine key risks to the operation. The risk areas that were pertinent to the accident included personnel error/fatigue and passenger safety and loading. In order to treat these risks, the charterer required that operational crew had regular breaks, including for meals, passengers were briefed before entering the operational area and all passengers were escorted to and from the helicopters by trained ground crew.
In addition to the risk management plan, the charterer’s safe work method statement[4] established the means to protect the public from hazards associated with operating helicopters from Olympic Park in support of the Spring Racing Carnival 2013. The identified hazards included the potential for members of the public to be struck by a helicopter, be exposed to hazardous and noisy environments, and that a helicopter may be damaged as a result of interference. A number of control measures were imposed by the charterer to reduce the associated risk. These included:
providing a suitable physical barrier such as high visibility fence bunting around the helicopter landing site
attaching warning signs to the fencing
restricting public access by utilising security and ground crew
trained ground crew present during all helicopter operations
locating the helipads away from roads and footpaths
24-hour security at access points
access to first aid facilities, equipment and trained personnel
suitable communications equipment and emergency contact details.
Conduct of the flights
Although the charterer had been conducting spring racing carnival passenger transfer flights for a number of years, it was the pilot’s first time operating the flights. As such, the charterer’s chief pilot elected to accompany the pilot on their first passenger transfer flight from Olympic Park to Flemington. The purpose of the flight was to familiarise the pilot with the designated route and procedures discussed during the pre-event operational briefings. Dual flight controls were fitted to the left pilot’s position as the charterer’s chief pilot would occupy that seat for the flight (see the section Dual flight controls). The charterer reported that the chief pilot did not intend to use, nor used the dual controls during the flight.
The charterer’s chief pilot assessed the pilot’s operation of the helicopter and compliance with the prescribed procedures during the familiarisation flight as ‘satisfactory’. After the familiarisation flight, the charterer’s chief pilot exited the aircraft and the dual flight controls were removed from the left pilot’s position. Removal of the dual flight controls allowed for the possible carriage of an additional passenger during the day’s operations and eliminated the risk of a front seat passenger inadvertently bumping the flight controls.
The pilot reported that a 20 kg supplemental ballast bag was placed on the front left seat during the return leg of the first flight after the familiarisation flight as there were no passengers. The pilot indicated that for all subsequent flights, the ballast bag was positioned unsecured on the front left cockpit floor, regardless of whether there were passengers or not.
The charterer advised that as many passengers were expected to be transferred to and from the spring racing carnival using multiple helicopters, they had developed a specific procedure for passenger loading. This included that:
prior to boarding, passengers were staged at a marquee, given a safety briefing, weighed, and then included on a passenger manifest
passengers were then re-briefed and escorted to the helicopter by the marshallers.
During loading or unloading of passengers, it was normal practice for other helicopters to operate from the adjacent helipads.
A number of return passenger flights were conducted from Olympic Park that morning before a scheduled lunch break. This break also allowed pilots to refuel the helicopters and rest prior to recommencing operations later that afternoon. The pilot of VDZ reported refuelling the helicopter to a total fuel load of 400 lb prior to commencing their last return passenger-carrying flight to Olympic Park before the accident.
The pilot reported that the helicopter operated normally that day.
Emergency response
The charterer had an emergency response plan that was included in the briefing documents issued to operational staff. The plan documented a number of procedures should an aircraft accident be observed. These included for the observer to:
phone for assistance from off-site emergency services, including police, fire and ambulance
render assistance if able or safe to do so
utilise available emergency response first aid equipment and fire extinguishers.
There was no ground-based emergency response equipment readily available at the Olympic Park landing site at the time of the accident.
Helicopter landing site information
Civil Aviation Regulation (CAR) 92 stated that an aircraft shall not land at or take off from any place unless it was ‘suitable for use as an aerodrome for the purposes of the landing and taking-off … having regard to all the circumstances of the proposed landing or take-off’.
, which was current at the time of the accident, provided detailed guidelines for the establishment and use of helicopter landing sites (HLS). A basic HLS was defined as ‘a place that may be used as an aerodrome for infrequent, opportunity and short-term basis for all types of operations, other than RPT [Regular Public Transport], by day under helicopter VMC [Visual Meteorological Conditions].’ The CAAP also recommended that helicopter pilots and operators should ensure that:
…no person outside the helicopter, other than a person essential to the operation, is within 30 metres of the helicopter.
The charterer’s operations manual stated that pilots had to comply with the CAAP. According to the landing site criteria in the CAAP, the landing site at Olympic Park oval was consistent with a basic HLS.
Before conducting helicopter operations, pilots and operators needed to ensure that neither the helicopter nor its rotor downwash constituted a hazard to other aircraft, persons or objects (Civil Aviation Orders 95.7 (paragraph 3.2)). In this regard, it was reported that security personnel and ground staff were employed to restrict public access at the Olympic Park HLS.
As the information contained in CAAP 92-2(1) was not a requirement, other operators were queried by the ATSB regarding the use of HLSs for operations away from their base. Those operators stated that, prior to conducting charter operations requiring the use of HLSs, an in-flight survey of the intended landing site was conducted. Where possible, a ground survey was also undertaken to confirm the suitability of the site.
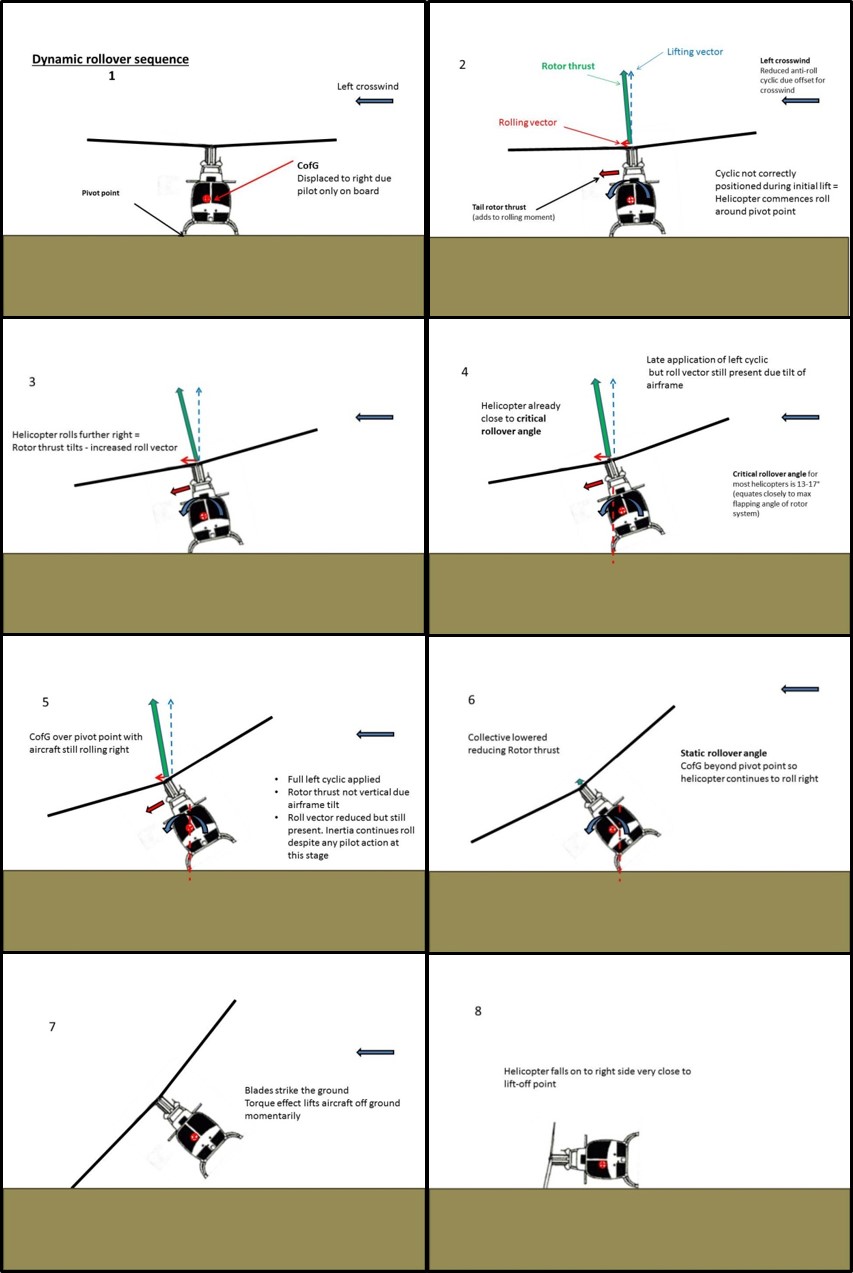
Dynamic rollover
General
Static rollover occurs when a helicopter is pivoted about one of its landing skids or wheels and the helicopter’s CofG passes outside the in-contact skid or wheel. Once in this position, removal of the original force that raised the helicopter to that angle will not stop the helicopter from rolling further. This angle is termed the ‘static rollover angle’.
A rotors-running helicopter resting with one landing skid or wheel on the ground may, without appropriate pilot input, commence rolling. Under certain circumstances, this roll cannot be controlled and the helicopter rolls over. This condition is known as ‘dynamic rollover’ and is a function of the interaction between the:
horizontal component of the total rotor thrust (or lift) acting about the point of ground contact
weight of the aircraft, initially acting between the helicopter’s skid-landing gear or wheels. This second, counter-rolling moment decreases the greater the roll.
The angle beyond which it is impossible to stop an already-rolling helicopter from further roll is termed the ‘critical angle’.
The principles of dynamic rollover are well-known to helicopter pilots as they are covered during their ab initio and recurrent pilot training. A number of pre-conditions are necessary before a helicopter can sustain dynamic rollover. Depending on the type of helicopter, the roll characteristics may differ but, if not controlled early, the condition is generally catastrophic.
Recovery from dynamic rollover is by smoothly lowering the collective lever while controlling any tendency to roll in the opposite direction with cyclic. Alternatively, some publications suggest that, if normal in-flight rotor rpm is available and a safe take-off is possible, it may be appropriate to lift from the ground. These publications caution that, if a safe take-off is not possible, further application of collective lever only aggravates the situation and worsens the roll.
In general, the application of smooth collective inputs is more effective in avoiding rollover problems than using the cyclic control.
Normal take-off in the Bell 206L-1
The procedure normally used by pilots to lift to the hover (commonly termed ‘pick-up’) is to scan to the front of the helicopter in preparation to establish the necessary hover attitude. A distant object forward of the helicopter is used as a heading reference as the collective lever[5] is slowly raised.
Although initially still on the ground, as the collective lever is raised the pilot controls any tendency to roll/drift and/or yaw[6] with the cyclic control[7] and tail rotor pedals respectively. As the helicopter becomes lighter on the skids and breaks from the ground, the pilot assesses and then makes appropriate control inputs to maintain ground position and heading and control any roll. The pilot applies additional collective lever to lift the helicopter further from the ground and cyclic to establish the hover attitude, thereby maintaining the helicopter’s position over the ground. The tail rotor pedals are used to control heading.
The amount and number of tail rotor pedal and cyclic control inputs during lift-off depends on variables such as the helicopter’s CofG, the slope of the landing area, the wind direction and speed relative to the helicopter, the presence of any turbulence, pilot inputs and so on. Given these variables, appropriate pilot input to control the helicopter during lift-off is crucial.
Viewed from above, the Bell 206L-1 has a counterclockwise rotating main rotor system. This generally requires the application of left tail rotor pedal to counter the right yaw and left cyclic control input to counter any right drift and control any roll during lift-off. The action of countering the right drift can normally be expected to result in the helicopter hovering in a left skid-low attitude. The aim is to make a clean break from the ground with no drift or yaw and with any roll under control before adopting the hover attitude at the appropriate height.
Dynamic rollover in helicopters with counterclockwise rotating main rotors
A number of factors influence the critical angle in helicopters with counterclockwise rotating main rotors such as the B206L-1. These include:
The rate of any roll. The faster any roll allowed to develop by the pilot, the smaller the critical angle. Controlled application of collective lever allows the pilot time to make adjustments for drift, roll or yaw.
Which skid (or wheel in other helicopter types) is in contact with the ground or other object. When this contact is via the right skid, the normal tendency to drift right during lift-off exacerbates any roll. This reduces the critical angle.
Left crosswind at lift-off. A left crosswind results in the main rotor blades ‘flying up’ on the left of the helicopter, adding to the tendency to roll and drift right.
A lateral CofG to the right of the helicopter’s centre-line. Should the pilot raise the collective lever to lift-off without appropriately controlling any drift, a lateral CofG to the right of the helicopter’s centre-line adds to the tendency to drift right during lift-off. If the right landing skid remains in contact with the ground this tendency to drift right will, without appropriate pilot input, result in right roll.
Sloping ground. A take-off from sloping ground requires careful application of cyclic to control roll around the upslope landing skid. In this instance, too little cyclic can result in the helicopter rolling down the slope. Too much into slope cyclic can contribute to the helicopter rolling up the slope.
Failure to address any uncompensated roll with one landing skid or wheel in contact with the ground or other object can result in the helicopter quickly approaching its critical rollover angle. If the roll does not abate, exceedance of the helicopter’s static rollover angle follows. Recovery is not possible and the helicopter rolls over.
Figure 2 illustrates the various forces acting on VDZ during the attempted pick-up to the hover and a representation of the approximate rollover angles relative to the helicopter’s lateral CofG. The perception from the preceding discussion, and representation at Figure 2, may be that dynamic rollover in helicopters with counterclockwise rotating main rotors only occurs to the right. This is not the case. For example, consider a lift-off with the right landing skid down slope. If the pilot applies too much into slope cyclic during lift-off, or maintains too much into slope cyclic after the right skid breaks the ground, the helicopter may roll left, up the slope.
Figure 2: Dynamic rollover of VH-VDZ showing the forces acting on the helicopter during the attempted lift-off and a representation of the approximate rollover angles relative to the helicopter’s lateral CofG
Source: ATSB
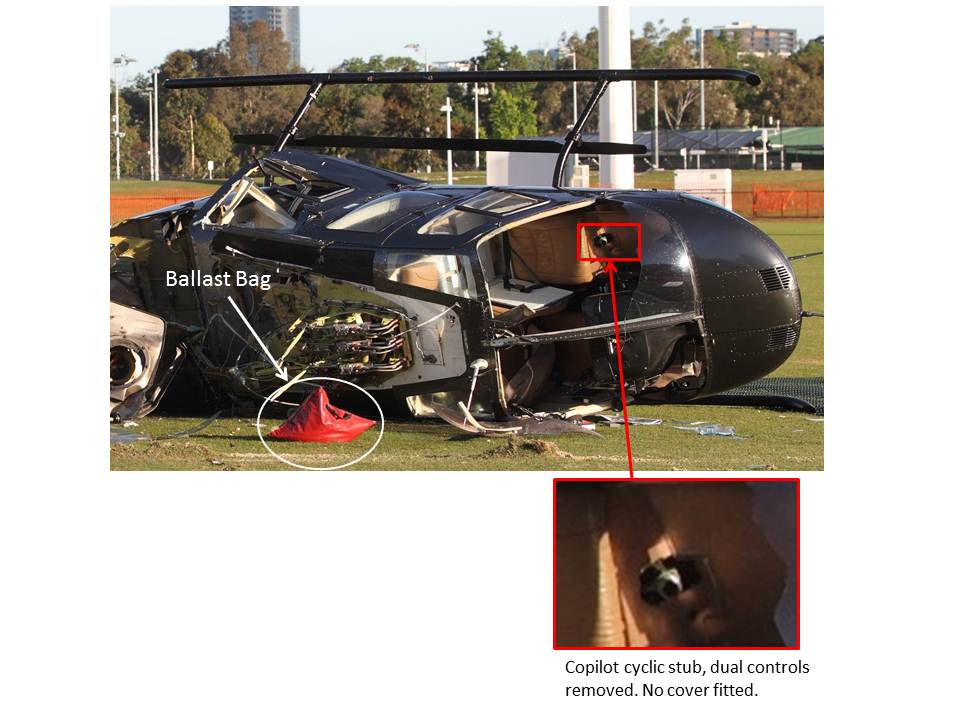
Dual flight controls
The pilot reported that, on completion of the familiarisation flight, the dual flight controls were removed from the left pilot’s position by the charterer’s chief pilot. This included removing the left cyclic and collective controls and isolating the tail rotor pedals. Later, the charterer’s chief pilot reported that, although they removed the collective control and isolated the tail rotor pedals, the pilot removed the cyclic control while remaining secured in their seat. The ATSB could not reconcile the respective pilots’ differing recollections of this action.
As the helicopter was still running during the removal of the controls, the pilot remained at the primary (right) flight controls with their seatbelt harness fastened. The cyclic control and collective lever stub covers were not fitted after removal of the respective flight controls. Figure 3 shows the exposed stub of the left cyclic control. Examination of the wreckage identified the dual flight controls and control stub covers in the rear baggage compartment of VDZ.
CAR 1988 Schedule 8 permitted pilots to conduct basic maintenance such as the replacement of seatbelts or harnesses and batteries on Class B aircraft, such as VDZ. However, fitment and removal of dual controls was not permitted under that schedule. This required specific approval by CASA under CAR 1988 sub regulation 42ZC Maintenance on Australian aircraft in Australian territory, and may entail supporting conditions, such as the requirement for training and required the issue of a certificate of approval.
In the case of VDZ, approved pilot maintenance training and the subsequent issue of a certificate of approval would have ensured instruction on the removal of the dual controls, disconnection of the dual tail rotor pedals and fitting of the control stub covers in accordance with the manufacturer’s procedures. The pilot reported that, as no training was provided to them for fitting or removing the dual flight controls, another pilot with the appropriate authority fitted the dual flight controls prior to what became the familiarisation flight with the charterer’s chief pilot.
In 1993, Bell Helicopter Co. (formerly Bell Helicopter TEXTRON) issued an Operations Safety Notice in response to reports of binding of cyclic controls through possible contact between the copilot’s[8] cyclic control assembly (stub) and objects located on the cockpit floor. The safety notice stated that:
…INSTALLATION OF CYCLIC AND COLLECTIVE STUB SAFETY COVERS IS RECOMMENDED WHENEVER THE CO-PILOT QUICK-DISCONNECT DUAL CONTROL STICKS ARE REMOVED.
Another Operations Safety Notice, issued by Bell Helicopter in 1984, highlighted that a fatal helicopter accident resulted from a loss of lateral cyclic control due to an improperly-installed copilot’s quick-disconnect dual cyclic stick (or control).
Ballast bag
There was no manufacturer-specified ballast bag, or method or procedure for securing ballast in the helicopter in the aircraft flight manual. However, the manufacturer advised that was common industry practice to secure any ballast using a seatbelt assembly. Given the right front seat is the primary control position in the Bell 206L-1 helicopter, this suggests that the ballast would be secured with the left front seatbelt.
It was reported by the pilot that whenever a passenger occupied the left front seat, they had their feet on the ballast bag on the floor during flight. There were no passengers on board for the repositioning flight and the bag was not secured to the airframe. This explained the bag being ejected through the copilot’s front window during the rollover, as shown in a sequence of rapid photographs that were taken by a witness to the accident ().
Figure 3: Ballast bag and exposed cyclic control stub (at inset)
Source: ATSB
Wreckage and helipad information
Wreckage examination
Examination of the wreckage and surrounding area indicated that the helicopter was orientated in a westerly direction and the right landing skid was located along the right edge of the helipad landing mat (Figure 4). The right side of the helicopter sustained significant damage and was resting on the ground.
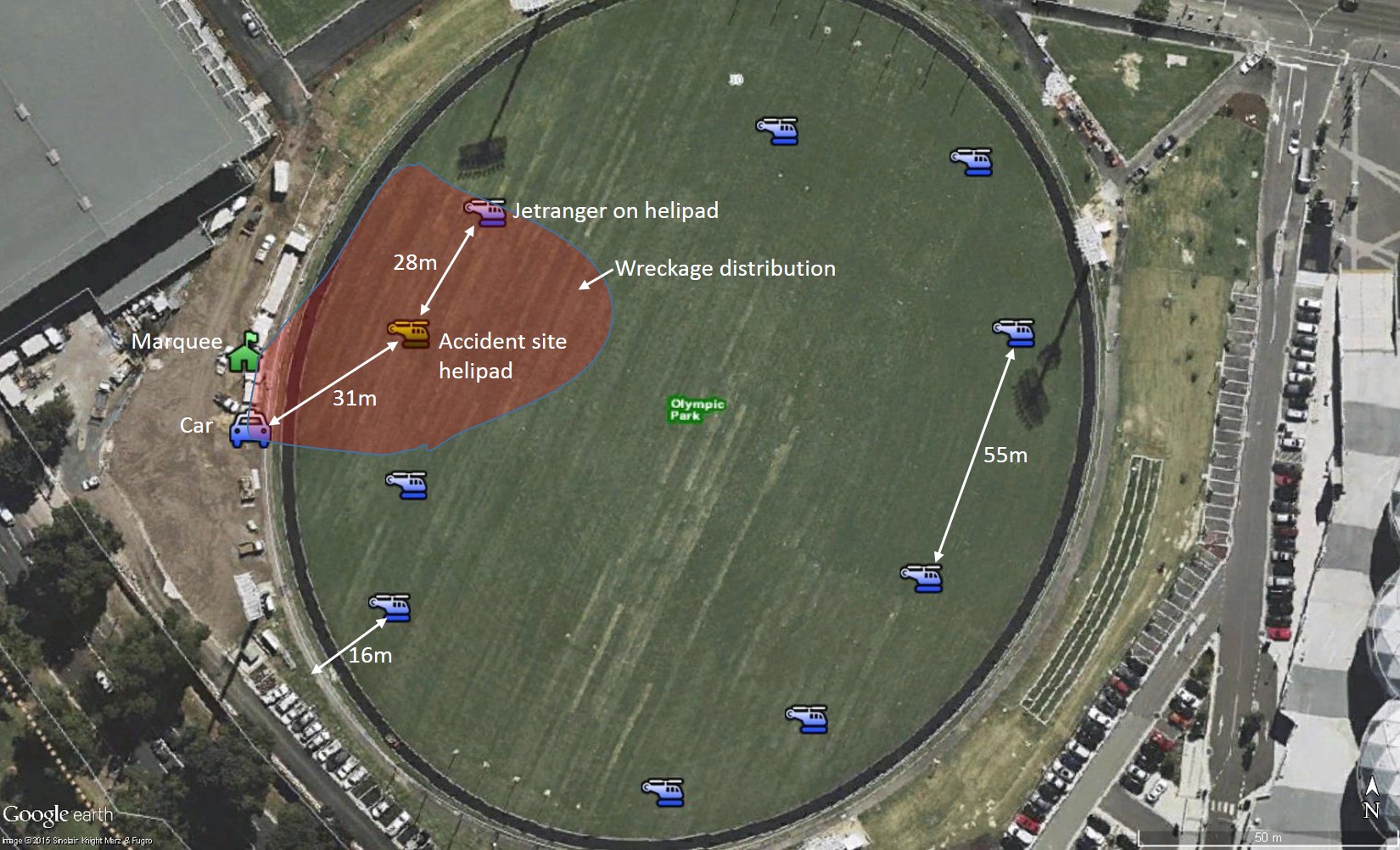
The engine was generating significant power when the main rotor blades impacted the ground as the main rotor transmission and engine were torn from the fuselage and large amount of debris was strewn about the area (Figure 5). Of note, a 1 m section of main rotor blade travelled about 40 m before lodging into a parked car and another section of rotor blade entered the passenger marquee about 30 m from the helipad (Figure 6 and Figure 7). The marquee was not occupied at the time of the rollover and there were no reports of injuries sustained as a result of the flying debris. The furthest piece of debris was located 44 m from the helipad landing mat.
On-site examination of VDZ confirmed the continuity of the flight control system. No mechanical defects were identified that would have precluded normal flight.
Helipad landing mat
The helipad landing mat was secured to the ground by small metal retaining pegs. These pegs were located at various intervals around the edge of the matting and along the midline where two sections of the matting adjoined. All retaining pegs were in place and, when examined, required a small amount of force to dislodge them from the grass and sandy loam subsurface. The charterer had reportedly used the semi-flexible meshed plastic matting on numerous previous occasions without incident. Witness photographs recorded the helicopter positioned with both skids on the landing mat immediately prior to the accident.
Figure 4: Helipad landing mat and right landing skid (looking east)
Source: ATSB
The helipad for VDZ was about 28 m from the perimeter of the oval where plastic bunting and a fence provided a barrier between the public access areas and the helicopter landing site. Distances from other helipads to the perimeter fencing varied, and in some instances were observed to have been closer than that of VDZ. The spacing between each of the helipads varied from about 24 m to 55 m (Figure 5).
Although the distance of some helipads to the perimeter fence or persons was less than the recommended 30 m, there were no reports of issues with rotor downwash or the operation of helicopters from the Olympic Park or Flemington venues.
A helicopter that was operating from the helipad adjacent to VDZ sustained some minor damage from the debris that required an engineering inspection before it departed Olympic Park. It was reported that the passengers on board that helicopter had not yet commenced disembarkation when the accident occurred.
Figure 5: Accident site and wreckage distribution showing the car and marquee that were struck by main rotor blade debris
Source: Google earth, modified by the ATSB
Figure 6: Main rotor debris imbedded in the marquee in the passenger staging area
Source: ATSB
Figure 7: Main rotor debris imbedded in the nearby car
Source: ATSB
Related occurrences
A review of the ATSB’s aviation occurrence database from 2005 to 2014 identified that although a total of 324 helicopter accidents were recorded, only five involved injuries or fatalities to persons located on the ground. Interestingly, 15 occurrences involved some form of helicopter rollover, of which eight were considered to have resulted from dynamic rollover. No fatalities resulted from the dynamic rollover occurrences.
As a comparison, a presentation by the National Transportation Safety Board as part of the NTSB’s 2015 Most Wanted List titled Remarks at Helicopter Association International Industry Government Forum, Alexandria, VA included a review of United States general aviation helicopter accident data. The presentation highlighted that, although there were a proportionally larger number of helicopter accidents, a small percentage were non-fatal dynamic rollover occurrences.
The ATSB has investigated several occurrences involving dynamic rollover. Two are reviewed in the following sections and are available from the ATSB website at www.atsb.gov.au.
On 13 June 2014, at about 0810 Western Standard Time[9], the pilot of a Bell 206 helicopter, registered VH-KSV, departed Mitchell Plateau campground, Western Australia, on a flight to a remote landing site about 30 NM (56 km) away to collect passengers.
As the pilot lowered the helicopter towards the rear of a rocky, sloped sandstone platform, he looked out of the pilot side window to select the best position to touch down. The front portion of the right landing skid touched down first and the right skid was sitting on a rock. The pilot was concerned about the suitability of the landing site and attempted to lift back into the hover. As the pilot raised the collective lever, the helicopter start to roll. The pilot assessed that this may have been an ‘incipient dynamic roll’ and lowered the collective lever. Although the pilot’s action recovered the helicopter from the roll, the helicopter tipped backwards off the edge of the rocky platform and slid about 2 m down the slope before coming to a halt.
On 7 October 2014 at about 0800 Eastern Standard Time[10], the pilot of a Bell 206B3 helicopter, registered VH-CLR, departed Cairns, Queensland with one passenger on board. The purpose of the flight was to conduct a charter flight to Mount Cook, about 9 km south-east of Cooktown Airport, Queensland.
As the pilot had not used the landing area previously, he conducted an aerial reconnaissance of Mount Cook landing area prior to arriving at Cooktown Airport to pick up the remaining passengers. The landing area was a rocky ledge near the top of Mount Cook. To assess the conditions in the area, the pilot made 3–4 practice approaches and a practice landing, touching down with the right skid on the ledge. The pilot assessed that stabilising the helicopter with the right skid on the ledge for embarking and disembarking the passengers was preferable to the previously-decided method of placing both skids on the uneven surface.
During the approach to land, the pilot reported feeling that the helicopter was stable and appeared unaffected by the increased wind. Guidance into the landing area was provided by the charter client’s ground coordinator, who was in radio contact with the pilot.
Just prior to stabilising the helicopter and touching down, the pilot felt it momentarily lift, most likely from a gust of wind, and drift to the right. The right skid scraped along the rock ledge and the helicopter rolled rapidly onto its right side and slid a short distance forward, prior to coming to rest.
The ATSB found that the occurrence was consistent with dynamic rollover.
On 2 November 2013, the pilot of a Bell 206L-1 helicopter, registered VH-VDZ (VDZ), was conducting passenger-carrying charter operations between Olympic Park oval and Flemington Racecourse (Flemington), Melbourne, Victoria. At about 1830 Eastern Daylight-saving Time[1] the pilot prepared to reposition the helicopter from one of the temporary landing pads (helipad) on the western side of the oval, to a position that would facilitate a departure for Flemington (Figure 1). The helicopter was orientated on a westerly heading.
Figure 1: Previous flight path of VH-VDZ from Flemington Racecourse to Olympic Park. Yarra River passing through the imagec
Source: Google earth, modified by the ATSB
Before the pilot could lift off and taxi the helicopter for departure, another helicopter approached the oval to land at an adjacent helipad. As the landing helicopter approached from a position that was beyond the view of the departing pilot, a marshaller, who was positioned in front of VDZ, signalled to the pilot of VDZ to hold their position on the helipad. Once the approaching helicopter landed on the adjacent helipad, the pilot of VDZ was given a visual signal by the marshaller to indicate that there were no conflicting aircraft or obstructions and that the pilot was clear to commence taxiing.
As the pilot began to lift VDZ into a hover, witnesses observed the helicopter’s skids lift slightly and drift to its right before the helicopter commenced rolling about the right skid. The pilot did not observe any right drift of the helicopter but affirmed that the right skid seemed to remain ‘stuck’ to the ground.
In rapid succession the left skid continued to rise and the helicopter rolled further right. Reported efforts by the pilot to recover from the roll were ineffective and the helicopter’s main rotor blades struck the ground. A large amount of high energy main rotor and other debris was released from the helicopter and impacted a nearby marquee, a number of vehicles and the helicopter on the adjacent helipad.
The helicopter was extensively damaged. Although witness photographs showed smoke after the rollover, there was no fire. This would suggest that the smoke was a result of escaping oil or hydraulic fluid coming into contact with hot aircraft parts or components.
The pilot sustained minor injuries and was able to exit the wreckage through the damaged front windscreen. Passengers disembarking from the adjacent helicopter, bystanders, company personnel, and others situated at a nearby marquee were not injured by any of the high energy debris.
During the conduct of passenger-carrying charter flights between Olympic Park oval and Flemington Racecourse, Melbourne, Victoria on 2 November 2013, Bell 206L-1 helicopter, registered VH-VDZ, collided with terrain as the pilot prepared to depart from the helipad.
There was no evidence of a mechanical or other helicopter system failure that contributed to the occurrence. In addition, there was no evidence that the helipad landing mat impacted on, or interfered with the helicopter during the pick-up procedure.
This analysis discusses a number of operational considerations in the development of the occurrence, including:
dynamic rollover
the potential for a flight control obstruction to have been a factor
the safety considerations when operating in close proximity to public access areas and gatherings.
Helicopter operations
Dynamic rollover
The lift-off was attempted with a left crosswind and a lateral centre of gravity that was to the right of the helicopter’s centre-line. Together with the helicopter’s normal tendency to drift right during lift-off, had the right landing skid been in contact with the ground and acted as a pivot point, each of these factors increased the tendency of the helicopter to roll right during lift-off.
The pilot recalled that the right landing skid seemed to remain ‘stuck’ to the ground during the attempted lift-off. In contrast, the marshaller reported observing both of the helicopter’s landing skids lift from the ground slightly before the helicopter drifted to the right and the right landing skid again contacted the ground. In either case, an in-contact right skid would have acted as a pivot point as the pilot continued the take-off, increasing the risk of dynamic rollover.
The degree of cyclic input and rate of collective application by the pilot could not be determined. However, the reported rapid rise of the left landing skid from the ground and right roll of the helicopter was consistent with the application of collective lever without appropriately coordinated cyclic input to control any roll. Coordinated control inputs would have allowed the pilot more time to detect and address the roll. In any event, the speed of the roll rapidly reduced the critical angle, increasing the likelihood of rollover.
The most effective means to recover from dynamic rollover is to smoothly lower the collective in coordination with appropriate cyclic input to control any roll and re-establish the helicopter’s weight evenly on the ground. The reported attempt by the pilot to lower the collective lever in response to the rapid roll was ineffective in stopping the roll before the helicopter passed the static rollover angle, after which recovery was not possible.
Helicopter landing sites
While the operation of helicopters near public areas carries a degree of risk, a review of ATSB occurrence data for the period 2005–2014 indicated that the risk of injury or death to people on the ground from helicopter operations was low. Guidance provided in Civil Aviation Advisory Publication (CAAP) 92-2(1) was intended to minimise the potential for injury while operating helicopters from helicopter landing sites and the charterer adopted elements of this guidance in its operations manual. Although the separation between most of the helipads at the Olympic Park oval was at least 24 m, other helipads were located within 15 m of the perimeter fence and nearby public walking tracks. These distances were less than the recommended 30 m in the CAAP, increasing the risk of injury to bystanders from rotor downwash.
The suggested perimeter distance of 30 m from a hovering or taxiing helicopter was intended to address the hazards associated with those operations. This is consistent with the inherent flexibility of a helicopter and its ability to access small landing, winching and other areas as measured by the widespread use of helicopters for search and rescue and aeromedical operations. However, the associated risk of this operational flexibility and utility is that, in the case of an accident during those operations, high energy main rotor and other debris can travel beyond the 30 m distance.
It is therefore prudent that, where possible and operational and/or safety imperatives dictate, operators consider increasing the recommended distance from their helipads to public access areas. This will further reduce the potential for injury in the event of an accident during helicopter operations.
Emergency response and first aid equipment
As the charterer had included an emergency procedure brief in the document suite issued to operational personnel, there was an expectation that those procedures would be followed in the event of an emergency. This included in case of injury to passengers or personnel or the containment of a fire relating to the operation of the helicopter.
Apart from the mandatory first aid and fire extinguishing equipment on board the helicopters, no ground-based fire extinguishing or first aid equipment was available at the Olympic Park basic helicopter landing site. In the case of an accident, the availability of those resources would have provided for a more effective and timely first aid response and offered an immediate response in the case of a minor fire until emergency services arrived. However, had there been a serious fire as a result of the rollover, it could be expected that the intensity of the fire would have been difficult to suppress, no matter what handheld device was used. It is likely that an immediate response by something approaching the Aerodrome Rescue & Fire Fighting Service normally associated with a major airport would be required to extinguish a serious fire.
In this case there was no fire. However, the amount of fuel and hydraulic fluid dispersed around the accident site increased the potential for a fire when combined with an ignition source. Potential ignition sources included the helicopter’s exhaust or other hot components or an electrical spark.
The pilot was the only occupant and was able to escape the smoke by exiting the helicopter through the damaged front windscreen, sustaining minor injuries. The severity of the occurrence may have increased if passengers were on board at the time and a fire erupted. With minimal available means to contain a fire, and a potentially more difficult exit from the rear of the helicopter, the risk of post-accident injury was increased.
Carriage of ballast
Despite the helicopter’s flight manual requirement for supplemental ballast with a combined front seat weight less than 77 kg, there was no indication of the ballast type to be used or method for securing it in the helicopter. As such, the pilot had no guidance as to whether the ballast bag was fit for purpose, though it was reported by the manufacturer as common practice to secure a heavy flight bag or ballast bag in the copilot’s seat using the existing seat harness.
Placing the unrestrained ballast bag on the front left floor was convenient and catered for the high frequency, short duration passenger- and non-passenger-carrying flights. However, it increased the risk that in the event of an emergency or turbulent flight, occupants may be injured by unintended movement of the bag about the cockpit/cabin. In addition, positioning any unrestrained object close to an unprotected control stub, such as the cyclic control, or collective lever increases the risk of control fouling and damage to the control stubs. Steps to mitigate those risks include the installation of the control stub covers.
Dual flight controls
Helicopters are often required to be reconfigured depending on the type of operation. The removal and installation of dual flight controls required a specific maintenance authorisation, often with appropriate conditions such as the completion of relevant training. This authorisation was not held by the either the charterer’s chief pilot or the pilot of the helicopter. Removal of the helicopter’s dual flight controls in those circumstances increased the risk of fouling of the flight controls during the subsequent passenger carrying charter-operations.
Findings
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving Bell 206L-1 helicopter, registered VH-VDZ, which occurred 13 km south-east of Essendon Airport, Victoria on 2 November 2013. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
Given the left crosswind and right lateral centre of gravity, which would have increased the tendency of the helicopter to roll right during liftoff, the pilot did not react to the developing right roll in sufficient time to prevent the dynamic rollover of the helicopter.
Other factors that increased risk
The helicopter’s dual flight controls were removed after the familiarisation flight by a person without the training or authorisation to conduct the maintenance procedure, increasing the risk of fouling of the flight controls during the subsequent passenger-carrying charter operations.
The pilot positioned an unsecured ballast bag on the left front floor of the helicopter, which increased the risk of a control restriction as a result of the exposed cyclic control stub and injury to the aircraft occupants in the case of an accident.
There was limited availability of fire extinguishers and first aid equipment at the Olympic Park basic helicopter landing site, which had the potential to inhibit an effective emergency response.
The proximity of the helipad to the perimeter fence and public access areas of the Olympic Park basic helicopter site increased the risk of injury to bystanders during the passenger-carrying charter operations.
Safety issues and actions
Proactive safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this accident.
Charterer of the helicopter
The charterer of the helicopter advised that for subsequent operations during the 2013 Spring Racing Carnival, portable fire extinguishers were located close to each helipad and first aid equipment was made available nearby. In addition, the helipads were repositioned further from the passenger marquee and passengers were not loaded or unloaded if helicopters were in the process of landing or taking off from adjacent helipads.
Operations at the Olympic Park oval ceased following the 2013 carnival.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
At about 1415 Eastern Daylight Time on 25 October 2013, an amateur-built Lancair Legacy aircraft, registered VH-ICZ, with the pilot and one passenger on-board, took off from Shepparton Airport, Victoria, for a flight to Yarrawonga, Victoria. Witnesses reported that the take-off and initial climb appeared normal, however shortly after, the aircraft’s pitch angle increased, after which it entered a descending right turn. The turn and descent continued until the aircraft collided with terrain alongside the airport boundary, fatally injuring the occupants and destroying the aircraft.
What the ATSB found
The ATSB found that shortly after take-off, and for reasons which could not be determined, the aircraft entered a steep climb, likely entered an aerodynamic stall, and began a descending right turn that continued until the aircraft collided with terrain.
The ATSB’s investigation was limited by the degree of damage to the aircraft and the presence of burnt carbon fibre. However, there was no evidence of any pre-existing mechanical fault with the aircraft and engine that could have contributed to the accident. A number of other possible contributing factors were considered and could not be completely discounted; those included sudden pilot incapacitation, aircraft handling, or the aircraft’s weight and balance being outside the design limits.
The aerodynamic characteristics of the aircraft design were such that it could enter a partial or completely stalled condition with little warning. The aircraft was not required to be (and was not) fitted with an angle-of-attack indicator or stall warning device.
The ATSB’s investigation found a number of instances where the regulatory requirements relating to the maintenance and operation of the aircraft had not been appropriately complied with. While the ATSB found no evidence that those non-conformances had brought about, or directly contributed to the accident, they did individually and collectively increase the risks associated with the aircraft’s operation.
Safety messages
Although amateur-built aircraft operated in the Experimental category are not required to be fitted with a stall warning device, owner-pilots should consider the benefits of such devices as a further defence against the inadvertent approach to, or entry into an aerodynamic stall.
While amateur-built experimental aircraft are not required to comply with the full range of safety regulations that are applicable to commercially-manufactured aircraft, the regulations that do apply are fundamentally important and have been introduced to control and reduce (as much as possible) the risks associated with the operation of this category of aircraft.
The ATSB research report AR-2007-043(2) makes numerous conclusions on the higher accident and fatality rates associated with amateur built aircraft operations. Pilots and passengers need to remain cognisant of the increased risks when flying in this category of aircraft.
On 23 September 2013, the pilot of a De Havilland DH-82 Tiger Moth aircraft, registered VH-RAY, taxied at Sandy Beach aeroplane landing area (ALA), New South Wales to conduct circuits in visual meteorological conditions. The pilot was the only person on board.
The pilot taxied to the end of the runway and applied the brakes to conduct engine run up checks. The pilot released the brakes and lined up on the runway heading and then applied full power for take-off. The aircraft accelerated down the runway. As the airspeed increased the tail rose to the take-off position, at about 200 meters down the runway and at about 30 knots indicated air speed the nose of the aircraft dropped very rapidly, and the aircraft flipped onto its back.
The aircraft was inspected by the maintenance organisation and it was determined that the left main landing gear brake drum had evidence of corrosion, and the brake operating rod was found stiff to operate. When the brakes were applied and released the left brake did not release fully. After the brake was cleaned and lubricated the brake operated normally. The maintenance organisation suspects that the left brake was partially engaged on take-off. The maintenance organisation determined that the aircraft was last flown on 12 February 2013 and the aircraft was normally stored in a high corrosion environment.
This accident is a timely reminder of the work that the Civil Aviation Safety Authority (CASA) is conducting on the safety of ageing aircraft in Australia.
On 23 October 2013, the pilot of a Cessna 182Q aircraft, registered VH-KKM and operating under the visual flight rules, departed Moruya Airport, New South Wales on a private flight to Mangalore Airport, Victoria. The flight route encompassed the Alpine National Park, where the forecast and actual weather included extensive thick cloud and severe turbulence.
Shortly after passing Mount Hotham Airport, Victoria, the aircraft collided with terrain on the eastern side of Mount Blue Rag, at about 5,000 ft above mean sea level. The pilot sustained fatal injuries and the aircraft was destroyed.
What the ATSB found
The ATSB found that the visual flight rules-qualified pilot had minimal total and recent flying experience and departed Moruya with less than visual meteorological conditions forecast along the planned route. It was very likely that these conditions were encountered shortly after passing Mount Hotham Airport, while flying over the Alpine National Park. From the evidence available it was likely that the pilot encountered reduced visibility to the extent that terrain avoidance could not be assured, resulting in the aircraft colliding with terrain in controlled flight.
Safety message
This accident highlights the risks associated with operating under the visual flight rules in adverse weather, particularly when flying in a challenging environment such as in mountainous terrain.
Thorough pre-flight planning is essential for avoiding weather. It is not only important to obtain the relevant weather forecasts to develop a mental picture of the conditions that may be encountered, but also to assess this information and understand how it relates to the planned flight. In forecast marginal weather, this involves consideration of alternative options such as diverting or turning back and pilots assessing their skills and/or aircraft’s suitability for the task in the conditions.
During flight, pilots must continuously assess the weather for conditions that may adversely affect the safety of the flight and be prepared to use an alternative course of action if conditions deteriorate. This can include seeking assistance, such as that available from air traffic control.
The ATSB is concerned about the frequency of accidents – many fatal – that involve pilots flying with reduced visual cues. This has been highlighted on the ATSB website as a SafetyWatch priority, along with a number of strategies to help manage the risk and links to relevant safety resources.
On 18 October 2013, the pilot of an Ayres Corporation S2R Thrush, registered VH-JAY, was conducting aerial agricultural spraying activities on a property near Hyden, Western Australia. At about 1330, following the completion of a number of spray runs and a break for lunch, the pilot departed to complete further spraying. Following the failure of the aircraft to return, a search was initiated. The aircraft wreckage was found a short time later about 1,700 m from the departure airstrip. The aircraft was destroyed, and the pilot was fatally injured.
What the ATSB found
The ATSB found that the aircraft departed controlled flight from which the pilot was unable to recover, leading to the collision with terrain. On the basis of the available evidence, it was not possible to determine the reasons for the loss of control.
The ATSB identified two aspects of the aircraft’s operation which had the potential to adversely affect safety. These were the use of an unapproved fuel mix and operation of the aircraft above its published maximum take-off weight.
Safety message
Operators and pilots are reminded of the dangers of operating aircraft engines on an unapproved fuel mix as this increases the likelihood of engine damage which could affect the safety of operations. Pilots and operators are also reminded of the need to adhere to an aircraft’s maximum take-off weight to ensure the on-going safety of the aircraft and operations.
Inquest
ATSB response to Findings
The Coroner’s Court of Western Australia (WA), without holding an inquest, recently made findings into a 2013 fatal accident involving an Ayers Corporation S2R Thrush.
The ATSB summary explains that on 18 October 2013, the pilot of an Ayres Corporation S2R Thrush, registered VH-JAY, was conducting aerial agricultural spraying activities on a property near Hyden, Western Australia. At about 1330, following the completion of a number of spray runs and a break for lunch, the pilot departed to complete further spraying. Following the failure of the aircraft to return, a search was initiated. The aircraft wreckage was found a short time later about 1,700 m from the departure airstrip. The aircraft was destroyed, and the pilot was fatally injured.
The Coroner adopted the sequence of events as set out in the Australian Transport Safety Bureau (ATSB) final report in relation to the circumstances that led up to the occurrence.
Safety message
Operators and pilots are reminded of the dangers of operating aircraft engines on an unapproved fuel mix as this increases the likelihood of engine damage which could affect the safety of operations. Pilots and operators are also reminded of the need to adhere to an aircraft’s maximum take-off weight to ensure the on-going safety of the aircraft and operations.
Proactive safety action
CASA advised that on 16 May 2014 they wrote to all operators of Thrush aircraft, informing them of exemption CASA EX01/12 – Maximum Take-off Weight – Restricted Category aircraft and aeroplanes engaged in aerial application operations. This letter reminds operators that there is no provision in the exemption to exceed whichever is the highest applicable MTOW specified in:
the aircraft flight manual or approved flight manual supplement;
an approved placard in the aircraft approved by CASA; or
the Type Certificate or Type Certificate Data Sheet for the aircraft.
The letter further advises about weight related airworthiness requirements and time-in-service recording and that the continuing airworthiness instructions for aircraft often include airworthiness limitations that apply to specified components of the aircraft. For safety reasons CASA has mandated compliance with airworthiness limitations via a direction in Civil Aviation Order 100.5. If such requirements apply to an aircraft, then the operator must ensure that the time in service for the aircraft and its components is properly calculated to ensure that airworthiness limitations are not exceeded.
Inquests are separate to ATSB investigations
Coronial investigations are separate to ATSB investigations.
The ATSB's report can be downloaded by clicking on the link:
The Coroner's report can be obtained from the Coroner's Court of WA. Contact details are available at: www.coronerscourt.wa.gov.au Queries regarding the Coroner's findings should be directed to the WA Coroner’s Court