
Aero Commander 680F, VH-SPP, 33 km south of Cloncurry, Queensland, on 9 November 1994
Summary
Synopsis
VH-SPP departed Cloncurry on a low level aero-magnetic survey flight at the estimated time of 0730 EST with an endurance of about 7 hours. The aircraft was due to return to Cloncurry by 1230 but failed to arrive. Attempts were made to contact the aircraft throughout the afternoon before it was declared overdue at about 2030. The burnt-out wreckage of the aircraft was found by search aircraft the following morning about 9 km north of the survey area and 30 km south of Cloncurry.
The aircraft had struck the ground in a nose-down, inverted attitude. It bounced from this position and came to rest upright, facing the opposite direction. At impact, the left propeller was in the feathered position and fuel to this engine had been shut off. The right engine was operating normally at impact, with fuel being fed from the centre tank.
The investigation revealed that, apart from a 2-hour flight the previous day, the pilot had no other experience in SPP. It was also revealed that there were two significant differences between the fuel system in SPP and that of other Aero Commander models the pilot had flown. These differences concerned the time taken for the outboard fuel tanks to empty and the orientation of the cockpit fuel selector switches.
The analysis concludes that these differences probably led to mismanagement of the fuel system by the pilot and to failure of the left engine due to fuel starvation, followed a short time later by failure of the right engine, also due to fuel starvation. It is possible that the pilot realised what had happened and was able to restart the right engine but not before the performance of the aircraft had deteriorated to such an extent that control of the aircraft with one engine operating could not be maintained.
1. FACTUAL INFORMATION
1.1 History of the flight
The aircraft was engaged in aero-magnetic survey operations in an area which extended from approximately 40–130 km south of Cloncurry. The task involved flying a series of north-south tie lines spaced 2 km apart at a height above ground of 80 m and a speed of 140 kts. At this speed, each tie line occupied about 20 minutes of flight time. The flight was planned to depart Cloncurry at 0700–0730 EST and was to return by 1230 to prepare data collected during the flight for transfer to the company’s head office.
An employee of the operating company saw the crew (pilot and equipment operator) preparing to depart the motel for the airport at about 0500. No person has been found who saw the crew at the aerodrome or who saw or heard the aircraft depart.
At about 1000, three witnesses at a mining site in the southern section of the survey area saw a twin-engine aircraft at low level heading in a northerly direction. One of these witnesses, about 1.5 hours later, saw what he believed was the same aircraft flying in an easterly direction about 1 km from his position. Between 1000 and 1030, two witnesses at a mine site some 9 km north of the survey area (and about 5 km west of the accident site) heard an aircraft flying in a north-south direction, apparently at low level.
On becoming aware that the aircraft had not returned to Cloncurry by 1230, a company employee at Cloncurry initiated various checks at Cloncurry and other aerodromes in the area, with Brisbane Flight Service, and with the company’s head office later in the afternoon. At about 2030, the employee advised the company chief pilot that the aircraft was overdue. The chief pilot contacted the Civil Aviation Authority Search and Rescue organisation at about 2045, and search-and-rescue action was initiated. The burnt-out wreckage of the aircraft was found early the following morning approximately 9 km north of the survey area.
1.2 Injuries to persons
| Crew | Passengers | Other | Total | |
| Fatal | 2 | – | – | 2 |
| Serious | – | – | – | – |
| Minor | – | – | – | – |
| None | – | – | – | – |
| Total | 2 | – | – | 2 |
1.3 Damage to aircraft
The aircraft was destroyed by impact forces and post-impact fire.
1.4 Other damage
No other damage was reported.
1.5 Personnel information
Pilot Equipment operator
| Sex | Male | Male |
| Age | 60 years | 47 years |
| Licence category | ATPL | N/A |
| Medical certificate | Class 1 | N/A |
| Total hours | Approx. 11400 | N/A |
| Total on type | Approx. 710 (see note below) | N/A |
| Total last 90 days | Approx. 82 | N/A |
| Total last 24 hours | Approx. 2 | N/A |
Note. As far as could be ascertained, all 710 hours on type were flown in 500 Series Aero Commander aircraft. No record was found of the pilot having flown a 680F model Aero Commander until he flew SPP for about 2 hours on the day before the accident.
Two of the 500 Series aircraft the pilot had flown (VH-KAC and VH-FGS) were 500S models which had been modified by the fitment of long-range (outboard) tanks. Operation of the fuel systems in these aircraft was similar to that in SPP (see 1.17.4).
Pilot’s recent flying experience
Company records showed that, between 7 July and 7 October 1994, the pilot flew approximately 113 hours on overwater low-level survey tasks in a Ted Smith 601-P aircraft.
There was evidence that the pilot next flew on 4 November 1994 when he conducted endorsement training on an Aero Commander 500S aircraft for a pilot from another survey company. According to this pilot, the endorsing pilot said that he was not very practised in asymmetric flight or in asymmetric operations and that he would leave all the flying to the pilot undergoing the endorsement. Notwithstanding this information, the pilot had extensive check-and-training experience in Aero Commander aircraft.
During the flight, aircraft speed was reduced towards VMCA but not to VMCA.
Pilot’s previous 72-hour history
The pilot travelled from Perth to Cloncurry on 7 November arriving at approximately 2100. On the afternoon of 8 November he conducted a survey flight in SPP which was restricted to approximately 2 hours because of problems with the on-board sensor equipment. After dining at about 2000 and retiring to his motel room at about 2200 on 8 November, the pilot, along with the equipment operator, was observed preparing to depart the motel at about 0500 on 9 November. Neither crew member was supplied any breakfast by the motel.
1.6 Aircraft information
1.6.1 Significant particulars
| Registration | VH-SPP |
| Manufacturer | Aero Commander Division |
| Model | 680-F |
| Serial no. | 680F-1128-74 |
| Country of manufacture | USA |
| Year of manufacture | 1961 |
| Engines | 2 Avco Lycoming IO-720-BIBD |
| Propellers | Harzell 3-blade, variable pitch |
| Certificate of airworthiness | Issued 2 Feb. 1979 |
| Maintenance release | No. 226763 Issued 3 Nov. 1994 |
| Total airframe hours | 7,546 (at 3 Nov. 1994) |
| Maximum take-off weight | 3,630 kg |
| Basic weight (survey configuration) | 2,914 kg |
No outstanding maintenance requirements were identified concerning the aircraft.
1.6.2 Weight and balance
| Basic weight (survey configuration) | 2,914 kg |
| Fuel load | 669 kg (956 L, see 1.6.5) |
| Pilot, equipment operator | 172 kg (standard weight 86 kg x 2) |
| Take-off weight | 3,755 kg |
| Maximum take-off weight | 3,630 kg |
| Exceedance | 125 kg or 3.4% |
1.6.3 Single-engine rate of climb
The aircraft flight manual lists single-engine rate of climb figures for the aircraft using maximum continuous power on the operating engine, landing gear and flaps up, and the inoperative engine feathered. In this configuration, at an aircraft gross weight of 3,630 kg, a pressure altitude of 2,000 ft and an outside air temperature of 37 degrees C, a rate of climb of 160 ft/min should be achieved at a best climb speed of 102 kts.
1.6.4 Cabin environmental control
The operator advised that cockpit/cabin cooling in the aircraft was via ram air only. The aircraft was not equipped with air-conditioning or blower fans as electrical motors interfered with the survey equipment. Fresh (ram) air was available through the normal aircraft system which included vents in the cockpit. Additional ram air ducts had been installed to provide supplementary outside air to both the cockpit and the survey equipment rack.
1.6.5 Fuel load for the flight
Information from the operator indicated that the aircraft fuel load for the flight was approximately 956 L, including a full centre tank, full outboard tanks, and 90 L useable fuel in the boot tank. This estimate was based on the flight time for the previous day’s flight.
1.6.6 Fuel usage rate
The aircraft flight manual indicated that, at sea level, 24 degrees C, 21 inches MAP, 2,100 RPM and 137 KIAS, the aircraft would have been using 112 L fuel per hour. Fuel consumption at rated power was 256 L/h. According to the operator, based on actual fuel usage, SPP had been using 112 L fuel per hour on low-level survey at 140 KIAS.
1.7 Meteorological information
The following information was recorded at Mt Isa on 9 November 1994:
| Time (EST) | Ambient temperature (degrees C) |
| 0600 | 23 |
| 0700 | 26 |
| 0800 | 29 |
| 0900 | 32 |
| 1000 | 34 |
| 1100 | 34 |
| 1200 | 36 |
The sky was clear throughout the period and the relative humidity was around 10%. The low-level winds were from the south-east at about 10 kts. There was moderate thermal and mechanical turbulence at low level.
No weather observations were taken at Cloncurry, which is situated approximately 104 km east of Mt Isa. It is likely, however, that weather conditions at Cloncurry were similar to those at Mt Isa.
1.8 Aids to navigation
Not relevant.
1.9 Communications
No record was found of any communications from the aircraft to any Air Traffic Services agency. See also 1.15.2 (‘SAR activities’).
1.10 Flight recorders
The aircraft was not equipped with a flight data recorder or a cockpit voice recorder, nor were these required by regulation.
1.11 Wreckage and impact information
The aircraft struck the eastern slope of a 200-ft high ridge running approximately northsouth. At impact, the aircraft was heading in a westerly direction, was banked left in excess of 120 degrees, and was in a nose-down attitude of about 35 degrees. Initial impact occurred when the left engine and forward fuselage struck embedded rocks, causing severe airframe disruption. The aircraft then bounced up the hill a short distance, coming to rest right way up and pointing east. Most of the aircraft was destroyed by the subsequent fire, although some components, including the engines and propellers, were recovered for later examination.
1.11.1 Left engine
A strip examination of the left engine did not reveal any fault which might have precluded normal operation. Examination of a section of damaged exhaust pipe from the engine confirmed that the damage occurred when the pipe was cold.
1.11.2 Right engine
A strip examination of the right engine did not reveal any fault which might have precluded normal operation. Examination of a section of damaged exhaust pipe from the engine confirmed that the damage occurred when the pipe was hot.
1.11.3 Propellers
Both propellers were dismantled. Inspection confirmed that the left propeller was in the feathered position and the right propeller in or near the fine pitch position. There was no pre-existing fault evident in either propeller mechanism.
1.11.4 Fuel tank selector valves
Inspection of the fuel tank selector valves (see 1.17.2) at the accident site revealed the following:
- For the left engine, both the centre and outboard tank selector valves were in the closed position.
- For the right engine, the centre tank selector valve was in the open position while the outboard tank selector valve was in the closed position.
1.12 Medical and pathological information
Post-mortem examination was unable to confirm the medical condition of the pilot at the time of the accident. However, the pilot held a current Class 1 medical certificate issued by the CAA.
1.13 Fire
The impact caused the fuel tanks to be disrupted, releasing a substantial quantity of
aviation gasoline. Ignition probably resulted from electrical arcing and/or contact with high-temperature engine components.
1.14 Survival aspects
The accident was not survivable due to both impact forces and fire.
1.15 Search and rescue
1.15.1 Company procedures
The company operations manual stated that all operational flights were to be the subject of prior flight plan notification on the minimum basis of a SARTIME for the end of the last flight of the day. The manual also stated that, when an operation from any temporary base was likely to continue for more than a few days, application might be made to the appropriate airways operations unit for the acceptance of a standard plan to cover daily flying activities.
No flight plan had been submitted for the flight. Another company pilot participating in the survey indicated that no plan was submitted because the operation was only scheduled for a few days and local company SAR was being maintained by the other company personnel at Cloncurry.
1.15.2 SAR activities
No information was held by the CAA concerning the flight prior to the initial telephone call from a company employee at Cloncurry at about 1640. During the progress of this conversation, attempts were made by Brisbane Flight Service to contact SPP through another aircraft in the Cloncurry area. At 1641, the pilot of this aircraft advised Flight Service that he was in contact with SPP. He was asked by Flight Service to request an estimate for when SPP would return to Cloncurry. A short time later, the pilot of the other aircraft advised that he was no longer in contact with SPP. (The pilot later advised that radio communications on the day of the accident were very scratchy.) Flight Service advised the company employee that contact with SPP had been lost, at which stage he terminated the call. At 1826, the company employee again called Brisbane Flight Service, asking if there was any contact with SPP. Flight Service advised that there had been no contact with the aircraft. At 2043, the company chief pilot called Flight Service and advised that SPP was overdue. He was then transferred to SAR, whereupon search action was initiated.
1.16 Human performance aspects
1.16.1 Heat stress
Heat stress, or hyperthermia, occurs when the body’s temperature regulation mechanisms fail. In extreme conditions, heat stress can lead to an inability to control body temperature and result in mental impairment and collapse. Individual responses to heat stress are influenced by factors such as age, lack of sleep, the amount and rate of work being performed, and acclimatisation to environmental conditions.
Heat stress not only causes physiological changes but also results in performance impairment. Even a slight increase in body temperature can impair an individual’s ability to perform complex tasks such as those required to operate an aircraft safely. Some of the known effects of heat stress on individuals are that:
- error rate increases;
- short-term memory becomes less reliable; and (c) perceptual motor skills slow.
Importantly, the affected individual may not recognise a decrease in efficiency but may feel perfectly normal and able to continue operations.
1.16.2 Time zone change
When the pilot travelled from Perth to Cloncurry two days before the accident, he moved into the Eastern Standard Time zone, which is 2 hours ahead of Western Standard Time. In other words, 0500 EST is equivalent to 0300 WST.
1.16.3 Food and water
The operator advised that two flasks containing 7–8 L water were on board the aircraft for the flight. Food was generally not carried on survey flights. Whether any food was carried on this flight could not be determined but the crew did not request that the motel provide any food for the flight.
1.17 Aircraft fuel systems
Among the various Aero Commander models that have been produced, aircraft fuel systems have differed. Long-range models of the aircraft were fitted with integral wing tanks (called outboard tanks), and in some cases boot tanks in the rear fuselage, in addition to the main, or centre tank. In some aircraft, additional tanks were incorporated during manufacture, while in others, they were fitted as a modification after manufacture.
1.17.1 Fuel system Aero Commander 680F Series aircraft
The Aero Commander 680F fuel system comprises four tanks: the centre tank, the boot tank, and two outboard tanks. The centre tank consists of five interconnected cells having a total capacity of 601 L (592 useable). This tank supplies fuel to both engines. Tank contents are indicated on a cockpit gauge. The boot tank has a capacity of 439 L (419 L useable). Fuel is transferred from this tank to the centre tank by the activation of a switch on the cockpit instrument panel. This is normally conducted in cruise, in stages, when the centre tank level has reduced to 90 US gallons indicated (340 L) or below. The left and right outboard tanks each have a capacity of 127 L (254 L total useable). The contents of these tanks are indicated on gauges in the cockpit. The total fuel capacity of the aircraft is 1,294 L (1,265 useable).
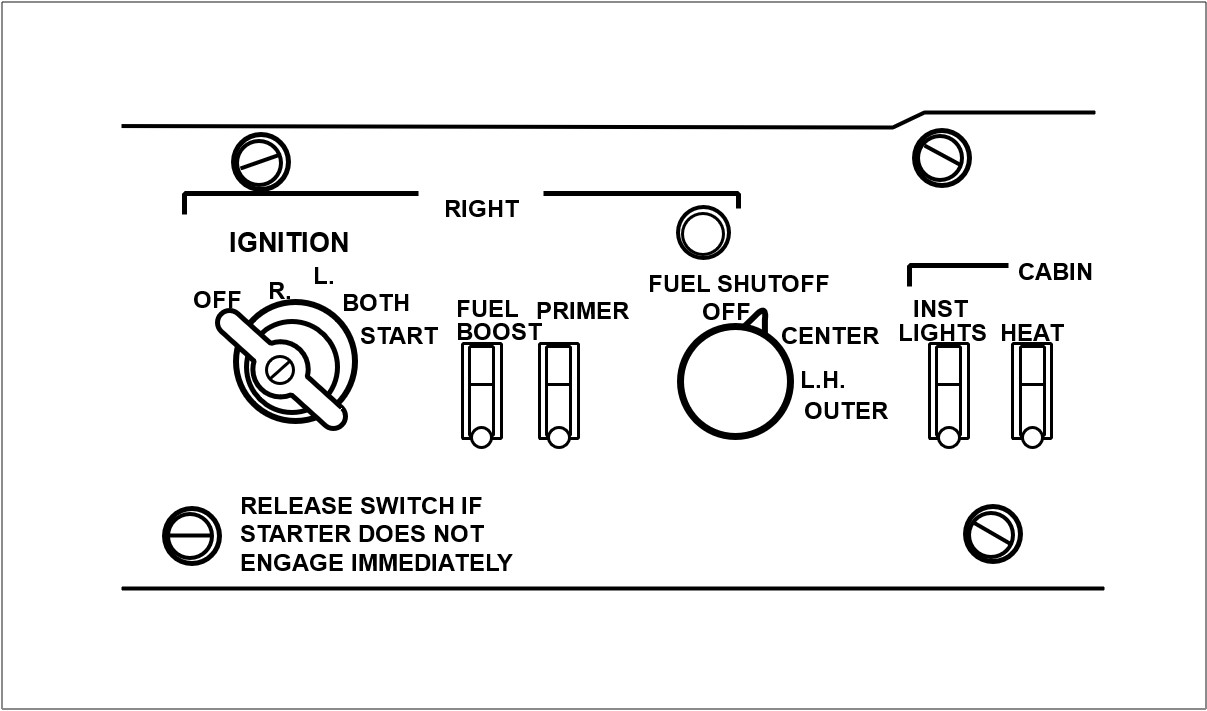
Rotary fuel selector switches located on the cockpit overhead switch panel control the flow of fuel to the engines from either the centre tank or the outboard tanks by way of electrically operated shut-off valves located in each main landing-gear wheel well. Rotating the switches to the right and left OUTBOARD positions (three o’clock and nine o’clock positions respectively) allows fuel from the outboard tanks to flow to the respective engine. At the same time, fuel flow from the centre tank is shut off. Fuel vapour return from the fuel injector pumps is fed to the centre tank.
Switching the selector switches to the CENTRE position (half-past ten o’clock position on the left switch and half-past one o’clock position on the right switch) allows fuel to flow from the centre tank to the respective engine and shuts off flow from the outboard tanks. Selecting the switch to OFF (twelve o’clock position on both switches) closes both shut-off valves and cuts off fuel flow to the engines. A sketch of the right fuel control selector panel is shown below.
The aircraft flight manual, section 4 (‘Normal Procedures’) contained a caution note which stated (emphasis theirs):
CAUTION. Burn centre tank first. When 100 gallons is shown on centre tank gauge, switch to outboard tanks. Do not allow engine to be starved of fuel when outboard tanks run dry. Select centre tank at first indication of fuel pressure loss. Fuel boost pumps must be on when switching tanks.
Anecdotal evidence obtained during the investigation indicated that, should a tank run dry and air enter the fuel lines, up to 2–3 minutes were required to restore normal engine operation following selection to another tank. It was not uncommon for there to be substantial engine power surges during this period.
1.17.2 Fuel selector valves
The centre and outboard tank fuel systems each have their own electrically operated shutoff valve. Electrical power is required to both open and close the valves. Placing the fuel selector switch in the OFF position closes both shut-off valves controlled by that selector.
Control of the valves is lost in the event of a total loss of electrical power in the aircraft.
1.17.3 VH-SPP fuel system and modification
According to the aircraft logbook, in October 1963 the six-cylinder IO-540 engines which were standard fitment for the aircraft were replaced with eight-cylinder Lycoming IO-720 engines. As part of this conversion, bypassed fuel from the engine-driven pump was returned to the pump inlet instead of being fed to the centre tank. The engines were later fitted with turbochargers.
In 1981, apparently to overcome fuel pump cavitation problems, the fuel system was modified to incorporate a pressure relief return line. According to the aircraft logbook, the modification was completed on 25 May 1981 to approved Engineering Order DFS-AC-08. No reference could be found in the (then) CAA Aircraft History File concerning the modification. Further, the approved flight manual for the aircraft contained no flight manual supplement or other reference to the modification However, a copy of the engineering order cover sheet was obtained from the operator. This indicated that the order had been approved by the then Department of Transport on 11 May 1981. The delegate of the Secretary, Department of Transport, who approved the modification, was unable to recall, other than in a very broad sense, the events surrounding approval of the modification. In particular, he was unable to recall what consideration might have been given to including detail of the modification as an approved supplement to the approved flight manual for the aircraft. (The then ANO (now CAO) 100.6 addresses ‘Administration and Procedure – Design Approval of Modifications, Repairs and Replacement Components’. The order indicates, among other things, that the Secretary may require the (approved) flight manual to be amended upon an approved modification being installed in an aircraft.)
The operator advised that the modification fed bypassed fuel to the centre tank. Advice from pilots who had flown SPP was that, during typical low-level survey operations, outboard tank transfer was complete in about 20 minutes. In other words, in excess of 5 L of fuel per minute was bypassed from each outboard tank to the centre tank. These pilots also indicated that the left outboard tank fed at a slightly higher rate than the right outboard tank so that, during typical low-level survey flight, it emptied 3–5 minutes quicker than the right tank.
1.17.4 VH-SPP fuel system management
Information from the operator indicated that its fuel system management procedures, and those probably followed by the pilot of SPP, were as follows:
- Start, taxi, and take-off with centre tank selected.
- After approximately 1 hour, when centre tank contents indication falls to about 80 US gallons, transfer boot tank fuel to centre tank.
- When centre tank contents again indicates about 80 US gallons, select both outboard tanks.
- Re-select centre tank as each outboard tank indication approaches empty.
During survey operations, tank changes were only made during turns between line runs because operation of the boost pumps (which was part of the tank change procedure) caused electrical interference in the survey equipment.
1.17.5 VH-SPP briefing
Another company pilot at Cloncurry, who was experienced on SPP, briefed the accident pilot on the operation of the aircraft prior to the 2-hour flight he conducted on 8 November 1994. The briefing was conducted in a motel room. Matters covered included the aircraft fuel system. The briefing pilot indicated that he told the accident pilot that the outboard tanks were normally selected when the centre tank contents were indicating about 80 gallons and that they emptied in 15–20 minutes. He recalled some discussion on the latter point as the accident pilot had thought it would take about 60 minutes for the outboard tanks to empty. (This belief was probably based on his experience in 500S Series Aero Commander aircraft in which outboard tank transfer during low-level survey flight took approximately 60 minutes.) During this discussion, the accident pilot indicated that his habit was to select the left and right outboard tanks so that both were feeding at the same time.
1.17.6 Alternative outboard tank transfer procedure
Discussions with other Aero Commander pilots during the investigation revealed an alternative outboard tank transfer procedure. This involved selecting the outboard tank for one engine and leaving the other engine to continue to receive fuel from the centre tank. When the outboard tank neared empty, the procedure was reversed. The advantage of this procedure was that it ensured centre tank fuel was always available to at least one engine, thus providing a safeguard against failure of the aircraft electrical system (which rendered the fuel selector valves inoperative).
1.17.7 Flight in VH-SPP by pilot on 8 November 1994
The flight in SPP conducted by the pilot on the day before the accident was limited to 2 hours due to survey equipment malfunction. According to the operator, the aircraft fuel load on departure was 844 L, this being a full centre tank (590 L) and full outboard tanks (254 L). The boot tank was empty. Approximately 290 L fuel was used during the flight, all from the centre tank. The outboard tank fuel was reported not to have been used.
1.17.8 Fuel system 500S Models VH-KAC and VH-FGS
500S Model Aero Commander aircraft KAC (Aircraft Serial No. 3185) and FGS (Aircraft Serial No. 3315) were fitted with long-range (outboard) tanks shortly after leaving the factory. According to the relevant documentation, KAC was modified in July 1974 in accordance with STC SA 973SW, and FGS was modified in August 1978 in accordance with STC SA-2826-SW. A check revealed that the STCs were identical except that, in SA-2826-SW, figures 24 and 24.1 (‘Overhead Switch Panel Cover Rework’) contained the following: ‘NOTE: 500 B, U, S, thru s/n 3075 only’.
The modification involved the fitment of outboard wing tanks and associated system work. The capacity of the outboard tanks was 254 L, the same as in SPP. Part of the modification involved the installation of rotary fuel selector switches to the cockpit overhead switch panel.
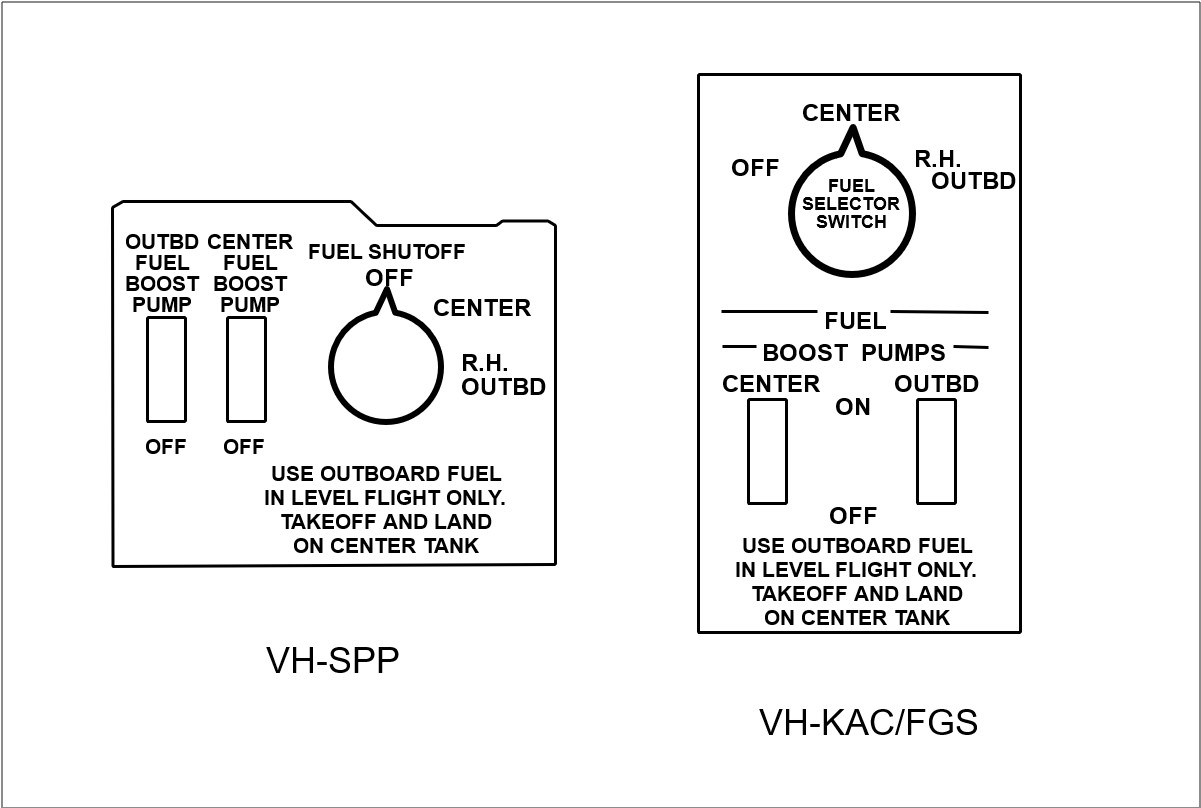
A physical check of the fuel selector panels on KAC and FGS revealed that, in these aircraft, the CENTRE tank selections were at the 12 o’clock position. In turn, this meant that the left and right OFF positions were at half-past one/half-past ten o’clock, while the OUTBOARD positions were at half-past ten/half-past one o’clock. In other words, the orientation of the selector switches was different to that in SPP. The holder for STC SA-2826-SW advised that to maintain the selector switch OFF position at twelve o’clock would have required considerable rework.
A sketch comparison of the fuel control panels for SPP and KAC/FGS is shown below.
1.18 Class endorsement
CAO part 40, section 40.1.0, subsection 4, para. 4.1 states:
A class endorsement specified in Part 1, Part 2 or Part 3 of Appendix IA authorises the holder of the endorsement to fly an aeroplane included in that class as pilot in command.
The notes to this sub-section state:
NOTE 1: The holder of a class endorsement should not act as pilot in command of any aeroplane included in the class on any flight unless he or she is familiar with the systems, the normal and emergency flight manoeuvres and aircraft performance, the flight planning procedures, the weight and balance requirements and the practical application of take-off and landing performance charts of the aeroplane to be flown and has sufficient recent experience or training in the aeroplane type, or in a comparable type, to safely complete the proposed flight.
NOTE 2: The owner and the operator of a type of aeroplane included in a class of aeroplane should ensure that any person who proposes to fly as pilot in command of the aeroplane complies with the requirements set out in Note I and should, where necessary, require the pilot to provide evidence of recent experience or training in the aeroplane type, or in a comparable aeroplane type.
Part 2 of appendix IA (‘Class Endorsements’) includes Aero Commander as a class.
Appendix IB (‘Classes of Aeroplanes’) includes, among other things, Aero Commander 680F and various Aero Commander 500 models (including Aero Commander 500S) in the Aero Commander class.
1.19 Time/event information
The operator provided information concerning pre-flight preparation and in-flight activities, which enabled the following time/event sequence to be developed. This information was based on the experience of other company pilots and was, therefore, an estimate only.
| Time | Event |
| 0515 | Depart motel |
| 0520 | Arrive airport |
| 0630 | Survey equipment ground calibration complete |
| 0700 | Refuelling complete |
| 0710 | Taxi |
| 0720 | Airbourne |
| 0745 | Survey equipment airborne tests complete |
| 0750 | Commence survey |
The estimated amount of fuel used from engine start to commencement of survey at 0750 was 160 L.
2. ANALYSIS
2.1 Impact and wreckage information
The factual information obtained from examination of the accident site and the wreckage enabled a number of deductions to be made concerning the accident sequence.
Fire damage to the wreckage indicated that there was substantial fuel on board the aircraft at impact.
The extreme, unusual attitude of the aircraft at impact indicated that the pilot lost control of the aircraft prior to impact. The respective propeller positions and engine operating conditions at impact imply that, with the right engine operating and the left propeller feathered, such an impact attitude could have resulted from the aircraft developing an uncontrollable roll left as a result of aircraft speed reducing below VMCA.
No mechanical fault was identified in the left engine which might have been reason for the left propeller to have been feathered. The closed position of both selector valves implied deliberate movement of the fuel selector in the cockpit to the OFF position.
The right engine was operating at impact and the aircraft performance charts indicated that the aircraft had sufficient single-engine performance at its estimated operating weight to climb from the survey operating height and return to Cloncurry. This leaves the following questions:
- Why was the (serviceable) left engine shut down?
- Why did the pilot apparently lose control of the aircraft?
2.2 Hypothesis
In the absence of any recorded or witness information, the answers to these questions are necessarily speculative. However, after consideration of the factual evidence, the following hypothesis is considered a plausible explanation of the accident sequence.
Background relevant to the hypothesis centres on the accident flight being only the second time the pilot had flown SPP but the first time he had cause to feed fuel from the outboard tanks. Significant differences between SPP and other Aero Commander aircraft the pilot had flown involved the orientation of cockpit fuel tank selector switches and outboard tank fuel transfer time.
With respect to the fuel selectors, in the 500 Series aircraft the centre tank selection was at the twelve o’clock position. This compared with SPP where the twelve o’clock position was OFF. Fuel transfer from the outboard tanks took approximately 1 hour in the 500 Series aircraft, while it took some 20 minutes in SPP. Also, the left outboard tank emptied 3–5 minutes more quickly than the right outboard tank.
Assuming that the aircraft commenced survey at about 0750 (see 1 .17.2) and had, at that time, used 160 L fuel, the following time/event sequence is hypothesised (based on a fuel usage rate of 112 L/h on survey):
| Time | Event | Fuel Situation |
| 0750 | Commence survey | 160 L used from centre tank 432 L remaining in centre tank 776 L remaining total (432 + 90 (boot) + 254 (outboard)) |
| Time | Event | Fuel situation |
| 0859 | Commence boot tank transfer | Reduce centre tank to 80 US gallons (303 L) = 129 L used in 69 minutes |
| 0947 | Centre tank again at 80 US gallons commence outboard tank transfer | 90 L boot tank fuel used in 48 minutes |
| 1007 | Outboard tanks empty in approx. 20 minutes | Total fuel remaining = 530 L |
If the pilot followed his normal habit of selecting both outboard tanks at about the same time but forgot that the tanks emptied in about 20 minutes in SPP instead of at least 60 minutes as he was accustomed to from his experience in other Aero Commander aircraft, then at about 1007, the left engine would have ceased operating as the tank ran dry. The expected reaction to such an event would be for the pilot to reselect the centre tank and switch the boost pump on. However, in the stress of the moment, he may have regressed to previously learned behaviour and placed the cockpit selector in the twelve o’clock position, forgetting that this was OFF in SPP, even though this involved passing the centre tank detent and greater angular rotation of the knob than from the OUTBOARD to CENTRE position. When normal left engine operation was not restored, it would have been reasonable for the pilot to have increased power on the right engine, feathered the left propeller, and commenced a climb from survey height. Within a short time, however, the right engine would have begun to run roughly as the right outboard tank became empty. The resultant power loss would have caused the aircraft to lose performance rapidly. Now with similar malfunctions in both engines, the pilot might have realised that he had made an incorrect fuel selection for the left engine and positioned the right selector correctly at the centre tank (half-past one o’clock) position. Given that these events would take time and could have resulted in air entering the right engine fuel line, the aircraft could have lost both performance and altitude by the time the fuel supply to the engine was restored. The sudden power increase as fuel flow was restored could have been sufficient to yaw and roll the aircraft uncontrollably to the left and result in the impact attitude found at the accident site.
The location of the wreckage north of the survey area could mean that the aircraft was heading towards Cloncurry at the time of the accident. It could also indicate that the pilot selected outboard tanks prior to commencing a south-north survey run, and that those tanks emptied around the time that run was completed (20 minutes later).
Apart from the possible sighting of the aircraft by one witness at about 1130, there is consistency between the time of the accident deduced above (1002–1007 EST) and the other witness sightings. That the 1130 sighting was a possible sighting could be reason enough to discount this report.
There is a disparity between the deduced time of the accident and the reported radio contact established with SPP by the other aircraft at 1641. However, as the aircraft endurance was only some 7 hours, fuel exhaustion would have occurred before 1500. It would appear, therefore, that, perhaps due to the poor radio conditions existing at the time, the pilot of the other aircraft may have misidentified the transmission from another aircraft as being from SPP. The possibility that SPP had landed at a remote strip for some reason and later taken off again to continue the survey task was considered. However, as the crew were aware of the requirement to return to Cloncurry by 1230, it would be reasonable to expect that they would have contacted the company if this requirement could not be met. No such contact was made.
2.3 Aircraft single-engine climb performance
Assuming the aircraft weight at take-off was 3,735 kg, then 105 kg (153 L) of fuel had to be used before weight reduced to maximum take-off weight (3,630 kg). Given that approximately 160 L fuel was used by 0750 EST when the survey proper was estimated to have begun, it follows that, at any later time, the aircraft should have been able to achieve a single-engine rate of climb of at least 160 ft/min (see 1.6.2).
2.4 Fuel system modification
It is arguable that the fuel system modification to SPP (1.17.3) did warrant inclusion in the approved flight manual because of its effect on outboard tank transfer time, not only with respect to SPP, but also in comparison to other Aero Commander models with similar fuel systems. However, given that the pilot was briefed on the operation of the SPP fuel system the day before the accident (including specific reference to the outboard tank transfer time), it is debatable whether flight manual reference to the fuel system modification could be considered a factor in the accident.
2.5 Fuel system briefing
CAO part 40 places responsibility on the operator and the pilot for ensuring that the pilot is familiar with the aircraft systems. It seems clear that a briefing took place and that the unique features of the SPP fuel system were discussed with the pilot. However, the briefing may have been more effective had it been conducted in the aircraft.
2.6 Human performance
There are a number of human performance aspects which could have affected the pilot’s ability to operate the aircraft safely. These include:
- The high ambient temperatures and the non-airconditioned cockpit could have resulted in the pilot experiencing some degree of heat stress. The longer the flight continued, the more serious this would have become.
- There was no evidence of the pilot having consumed any food before or during the flight. Thus, the pilot had probably not eaten for up to 14 hours before the accident.
- Low-level survey flying is both physically and mentally demanding on the pilot. High temperatures and turbulence increase these demands.
- The pilot had been at Cloncurry for less than 40 hours at the time of the accident. He therefore had only limited opportunity to adjust to the local weather conditions and the 2-hour time change from Perth.
- The pilot’s ability to cope with the above influences could have been limited by his age.
2.7 Other aspects
In analysing this accident, other possibilities such as pilot incapacitation and bird strike were considered. However, given the engine, propeller, and fuel selector valve configurations at aircraft impact, and the deliberate actions by the pilot these configurations imply, neither of these possibilities was considered realistic.
3. CONCLUSIONS
3.1 Findings
- The pilot held a valid ATPL, was appropriately endorsed, and held a current medical certificate at the time of the accident.
- The pilot had substantial experience on 500-S Series Aero Commander aircraft but minimal experience on VH-SPP.
- A modification to the fuel system of VH-SPP reduced the time taken for the outboard tanks to empty to approximately 20 minutes compared to about 60 minutes in some 500 Series Aero Commander models.
- The approved flight manual for the aircraft contained no reference to the fuel system modification.
- The pilot’s fuel system management technique involved feeding fuel from the left and right outboard tanks simultaneously.
- An alternative fuel system management technique, as used by some other pilots, was to feed fuel from one outboard tank at a time.
- On the day before the accident, the pilot was briefed by another company pilot on the aircraft fuel system and its operation, including reference to the outboard tank transfer time. The briefing was not conducted in the aircraft.
- The aircraft maintenance release was valid and no outstanding maintenance requirements were identified.
- The aircraft departed Cloncurry at a weight which exceeded the MTOW by about 125 kg; however, this was not considered to have been a factor in the accident.
- There was no indication that either engine or either propeller had suffered any mechanical failure.
- The aircraft impacted the ground inverted, in a steep nose-down attitude.
- Both fuel selector valves for the left engine were closed and the left engine was not operating at impact.
- The left propeller was in the feathered position at impact.
- The outboard tank selector valve for the right engine was closed, while the centre tank selector valve was open.
- The right engine was operating at impact.
- Water, but no food, was carried on the aircraft.
- The pilot had been in the Cloncurry area for less than 40 hours at the time of the accident.
- The flight was conducted in very hot, dry, conditions with moderate thermal turbulence.
- During the 2-hour flight on the day before the accident, the pilot did not operate the outboard tank fuel-feed system.
3.2 Significant factors
- For reason(s) which could not be conclusively established, the pilot shut off the fuel supply to the left engine and feathered the left propeller.
- For reason(s) which could not be conclusively established, the pilot lost control of the aircraft.
Occurrence summary
| Investigation number | 199403314 |
|---|---|
| Occurrence date | 09/11/1994 |
| Location | 33 km S Cloncurry |
| Report release date | 01/03/1997 |
| Report status | Final |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Fuel starvation |
| Occurrence class | Accident |
| Highest injury level | Fatal |
Aircraft details
| Manufacturer | Aero Commander |
|---|---|
| Model | 680 |
| Registration | VH-SPP |
| Serial number | 680F-1128-74 |
| Sector | Piston |
| Operation type | Aerial Work |
| Departure point | Cloncurry, QLD |
| Destination | Cloncurry, QLD |
| Damage | Destroyed |