Correctly fitted, secured and maintained flight helmets can save lives
Safety Advisory Notice
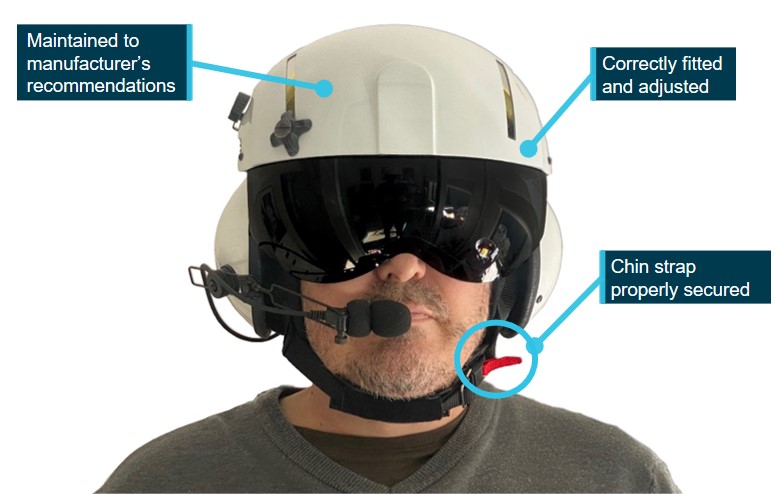
A correctly fitted and secured flight helmet can significantly reduce injuries and save lives in the event of a serious incident or accident. But a helmet is only fully effective if it is fitted correctly, retained securely on the wearer’s head, and maintained in accordance with the manufacturer’s instructions.
Source: ATSB
What happened
On 31 July 2020, the pilot of a Robinson R44 helicopter was conducting aerial spraying along a property fence line. During the fifth spray load, as the helicopter descended from above trees to recommence spraying, it struck a powerline about 5 metres above the ground. The helicopter subsequently collided with terrain resulting in substantial damage. The pilot sustained fatal injuries.
Survivability
The pilot was not adequately restrained by the seat belt’s shoulder sash resulting in the pilot’s head impacting on the left side of the helicopter. This resulted in non-survivable head injuries.
The pilot was wearing a helmet during the initial impact. While it could not be determined if the accident impact forces were survivable, the helmet may not have been fully effective as it came off during the accident sequence.
There was also no evidence that the helmet had been maintained or serviced, including after it had likely been worn in a previous accident.
Helmet regulations and standards
For all pilots conducting low-level operations, a helmet is an essential component of personal protective equipment required to be worn under work, health and safety guidelines. Wearing a helmet is not mandated by the Civil Aviation Safety Authority, and there is no Australian Standard for flight helmets. However, many commercially available helmets meet or exceed military and US and European civilian standards, some of which are designed specifically for helicopter operations.
To work as designed, a helmet must be adjusted to fit the head and the chin strap must be fastened securely. The helmet must be serviced regularly, routinely inspected for damage, and replaced immediately if it has sustained a major impact.
Safety advisory notice
- fit for purpose
- custom fitted to the pilot’s head
- properly secured by using the chin strap
- maintained in accordance with the manufacturer’s recommendations.
Read more about the ATSB’s investigation: Wirestrike and collision with terrain involving Robinson R44, VH-HNF, 69 km south-east of Hay Airport (Steam Plains), New South Wales, on 31 July 2020
Publication details
| Investigation number | AO-2020-040 |
|---|---|
| Publication type | Safety Advisory Notice |
| Publication mode | Aviation |
| Publication date | 04/03/2022 |