Accident experience has provided substantial evidence that the use of upper torso restraints reduces the risk of serious injuries to the head, neck, and upper torso of aircraft occupants, and they reduce the rate of fatalities for occupants involved in otherwise survivable aircraft accidents.
What happened
On 10 January 2017 a Cessna 172M, registered VH‑WTQ, departed Agnes Water aeroplane landing area (ALA), Queensland on a passenger charter flight to a beach ALA on Middle Island. While the pilot was conducting an airborne inspection of the beach, at a height of about 60 ft, the aircraft had a total engine power loss.
The aircraft impacted the beach and was destroyed. One of the rear-seat passengers was fatally injured and the other three occupants sustained serious injuries.
Wreckage of VH-WTQ (Source: ATSB)
Identified safety issue
The ATSB identified that the rear seats of VH-WTQ were not equipped with upper torso restraints (UTRs). An UTR is a shoulder strap or harness, and when fitted in addition to a lap belt makes an aircraft’s passenger restraint similar to a normal seat belt in a car. Had such restraints been fitted, the rear-seat passengers’ injuries would very likely have been less severe.
A substantial body of research has demonstrated that wearing UTR in small aircraft significantly reduces the severity of injuries compared to wearing only a lap belt. In particular, UTRs reduce the risk of head, neck and upper body injuries, associated with the person’s upper body flailing forward, and potentially striking seats, the side of the aircraft or other objects.
Currently, small aeroplanes manufactured after 12 December 1986 and helicopters manufactured after 17 September 1992 are required to have UTRs fitted for all seats. Based on the substantial body of research, there have been many recommendations over the years for UTRs to be fitted for all seats in small aeroplanes and helicopters manufactured before these dates (rather than just the front seats). These recommendations have been made by investigation agencies in the United States, Canada, the United Kingdom and Australia.
In addition, some aircraft manufacturers have published safety information letters and service bulletins, encouraging the fitment of UTRs to passenger seats that did not have UTRs fitted when the aircraft were manufactured. Options for retrofitting UTRs are available for many models of small aircraft.
: The Australian Transport Safety Bureau strongly encourages operators and owners of small aeroplanes manufactured before December 1986 and helicopters manufactured before September 1992 to fit upper torso restraints to all seats in their aircraft (if they are not already fitted).
Pilotsmust learn to recover from an incipient spin and demonstraterecovery from the manoeuvreduring flight tests. Evidence suggests that in some cases, this trainingis being performed in aircraft that are not approved forintentional spins. Depending on the aircraft type, the manufacturer may not have specified whether that restriction applies to an incipient spin or only a developed spin.
What happened
On 26 September 2017, an instructor and student conducted a training flight in a Diamond Aircraft Industries DA40 aircraft, registered VH-MPM, from Archerfield Airport, Queensland. The purpose of the flight was a simulated Recreational Pilot Licence flight test to prepare the student for an upcoming flight test.
Factors uncovered during the investigation
The ATSB identified concerns relating to the conduct of incipient spin training in aircraft types not approved for intentional spinning.
The DA40 aircraft type is certified to recover from a one-turn spin or a three-second spin (whichever takes longer), and is not proven or certified to be recoverable from a longer spin. The aircraft’s manuals state that intentional spins are prohibited. During the ATSB investigation, the aircraft manufacturer clarified that this limitation prohibits any action that is intended to induce a spin, even if the aircraft is immediately recovered.
Aircraft types with similar limitations are currently in use throughout the world for flying training. In Australia, the Civil Aviation Safety Authority requires the demonstration of recovery from an incipient spin during flight tests. However, there is no clear and consistent definition of the point at which a manoeuvre becomes a spin (or incipient spin) for the purposes of flying training.
Crucially, the ATSB found that there can be varying interpretations of an ‘incipient spin’, and this has led to aircraft not approved for intentional spins being used for incipient spin training and assessment.
: Operating an aircraft within the stated limitations is essential to the safe conduct of a flight. Training organisations are required to conduct incipient spin recovery training, which includes intentionally inducing a spin and recovering before it fully develops. Some organisations may be conducting this training in aircraft not approved for intentional spinning. The ATSB advises these training organisations to clarify with aircraft manufacturers the extent to which the intentional entry into the early stages of a spin, including an incipient spin, is permissible.
The standard industry practice of re-using self-locking nuts on Robinson helicopters may inadvertently result in the omission to replace MS21042L or NAS1291-series nuts with D210-series corrosion resistant (CRES) nuts on critical fasteners.
Safety advisory notice
The Australian Transport Safety Bureau advises all maintenance personnel for Robinson helicopters to ensure that before re-using a self-locking nut, that the correct part number is fitted, and that the D210-series corrosion-resistant nuts are used for reassembly of critical fasteners in accordance with the Robinson Helicopter Company instructions for continued airworthiness.
What happened
On 2 August 2017, a Robinson R22 Beta helicopter impacted terrain about 7 km north-north-west of Cloncurry Airport, Queensland. The pilot, who was the only person on board, was fatally injured and the helicopter was destroyed. The accident flight was the first commercial flight post the helicopter’s second 2,200-hour overhaul.
Finding of increased risk
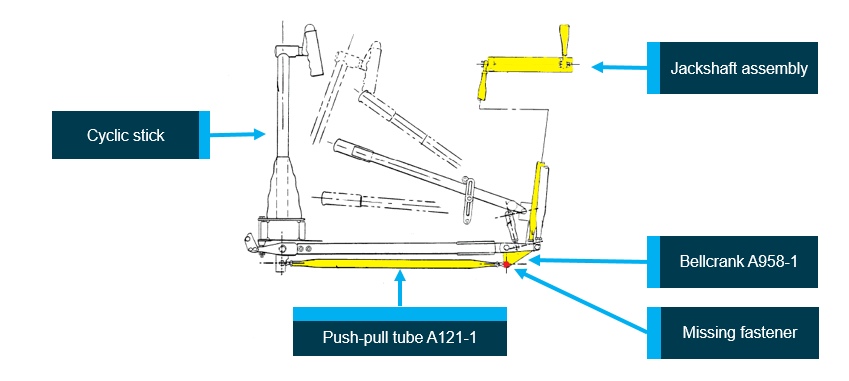
During the review of on-site accident photographs to verify the flight control joints, the ATSB noted an anomaly with the helicopter’s bellcrank (part number A958-1) in the cyclic control system. The fastener, which attached the horizontal push-pull tube (part number A121-1) to the bellcrank, was missing. The bellcrank’s remaining fasteners were all attached. The bellcrank and missing fastener bolt were recovered, but the reason for the separation of the nut from the bolt has not yet been determined.
The missing fastener was part of the longitudinal cyclic pitch control system, which controls the fore-aft tilt of the main rotor disc (Figure 1).
Figure 1: Robinson R22 helicopter cyclic control system
Robinson R22 helicopter cyclic control system schematic: The horizontal push-pull tube, bellcrank, vertical push-pull tubes and jackshaft are highlighted in yellow. The location of the missing fastener is highlighted in red. Source: Robinson Helicopter Company, modified by ATSB
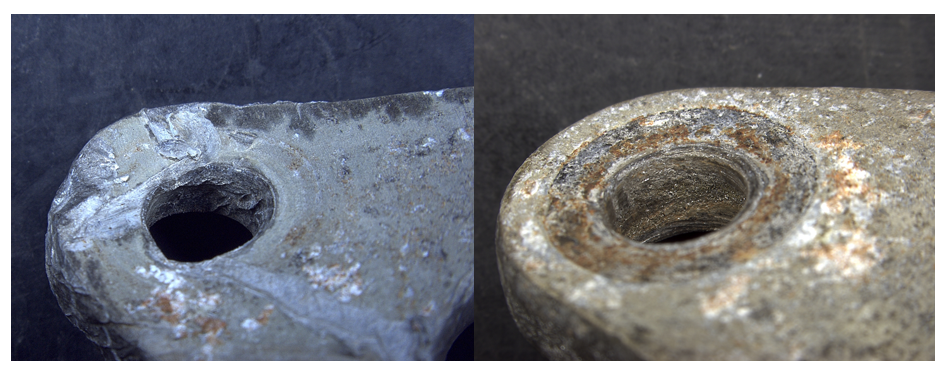
The examination of the bellcrank found that the bolt-holes for the missing fastener exhibited heat damage different to that of the bolt-holes for the remaining fasteners (Figure 2). In addition, the deformation of the bellcrank prevented the installation of a bolt where the fastener was missing, but did not prevent the removal of the remaining fasteners. This indicated that the bolt was not in-situ at the time of the post-impact fire.
Figure 2: Comparison of the bellcrank bolt-holes
Left: bolt-hole for the missing fastener. Right: bolt-hole for a removed fastener. Source: ATSB
Re-use of self-locking nuts
Cracking from hydrogen embrittlement of the type of nuts fitted to Robinson helicopters has been previously identified.[1] In October 2014, the Robinson Helicopter Company (RHC) published service letters for the R22 (SL‑64), R44 (SL-50) and R66 (SL-09) helicopters on the subject of D210 Corrosion-Resistant (CRES) Nuts. The service letters stated that, whenever maintenance that involves the disassembly and reassembly of a critical fastener is performed, the MS21042L or NAS1291 nut should be replaced with a D210-series nut.[2] The R22 maintenance manual was amended in October 2014 to incorporate what was stated in SL-64. For specific instances of cracked nuts, RHC have published service bulletins for their replacement within a compliance period.[3]
The R22-series maintenance manual included the following information under section 1.300 Fastener Torque Requirements:
D. Critical Fastener: A critical fastener is one which, if removed or lost, would jeopardize safe operation of the helicopter. This includes joints in the primary control system, and non-fail-safe structural joints in the airframe, landing gear, and drive system.
CAUTION: D210-series nuts, which supersede MS21042L-series and NAS1291-series nuts, are required on critical fasteners.
In the course of interviewing personnel employed by the maintenance organisation, the ATSB noted a low level of awareness of the need to replace MS21042L/NAS1291-series nuts with the D210-series nuts when critical fasteners were reassembled. In accordance with the R22 maintenance manual, critical fasteners include a self-locking nut in their assembly. It is a standard practice within sectors of the aviation industry to re-use self-locking nuts provided the nut cannot be turned onto the bolt thread by hand and the published torque value for the fastener is achieved.
During the course of the investigation the ATSB spoke with another maintenance organisation, who reported they employ the same practice of re-using self-locking nuts, and the helicopter manufacturer confirmed this was an acceptable practice. The United States National Transportation Safety Board reported on this practice as accepted by the manufacturers of light helicopters in their aircraft accident report AAR-13/01.[4] They noted that guidance on the re-use of self-locking nuts was provided by Eurocopter (now Airbus Helicopters), Sikorsky, Bell and the United States Federal Aviation Administration.
In December 2018, the ATSB received the accident helicopter’s jackshaft, which had the fasteners attached. The jackshaft was one of a number of parts within the flight control system that was disassembled and sent for non-destructive inspection during the 2,200-hour overhaul. The bellcrank was not subject to non-destructive inspection and therefore not required to be disassembled. In late January 2019, the ATSB completed semi-quantitative chemical analysis of the nuts fitted to the jackshaft and found they were consistent with a carbon/alloy steel, and therefore not consistent with D210-series stainless steel corrosion-resistant nuts. The nuts fitted to the jackshaft had similar markings to the nuts fitted to the bellcrank, which were consistent with MS21042L/NAS1291-series nuts.
At the time of the reassembly of the accident helicopter, the current R22 Illustrated Parts Catalog detailed the part number D210-4 for the nuts fitted to the jackshaft, and RHC confirmed there was no alternate part number to the D210-series nuts.
In consideration of the evidence, the ATSB concluded that the industry practice of re-use of self‑locking nuts on Robinson helicopters may result in the omission to install D210-series nuts when critical fasteners are reassembled.
The ATSB advises that this finding of increased risk applies to all approved maintenance organisations for Robinson helicopters and at present has not been identified as a contributing factor to this accident.
Brisbane Airport Corporation and the Civil Aviation Safety Authority have both previously recommended that operators use covers on their aircraft’s pitot probes during turnarounds to mitigate the risk of insects building nests in them and significantly affecting the reliability of airspeed indications. In addition to using pitot probe covers, rigorous processes need to be in place to ensure that covers are removed prior to flight.
What happened
During a take-off roll at Brisbane Airport on 18 July 2018, the flight crew of an Airbus A330 (international operation) detected an airspeed anomaly including red speed (SPD) flags on both primary flight displays. The flight crew continued the take-off and climb and carried out several checklists before returning to Brisbane Airport.
A subsequent inspection after the aircraft landed identified that pitot probe covers were fitted to the aircraft’s three pitot probes, which made the probes ineffective for flight.
Why did it happen
The ATSB investigation is continuing, and the full reasons and context associated with the pitot probe covers not being removed prior to flight, and the take-off being continued with unusable airspeed information, are still being examined.
In recent years there have been several reports of insect activity disrupting aircraft systems at Brisbane Airport. These included blocked pitot probes, mainly from nests built by mud-dauber and other wasps, resulting in airspeed discrepancies and other effects.
The international operator did not routinely use pitot probe covers for turnarounds at Brisbane Airport or other locations. Shortly after the previous flight on 18 July, covers were placed on the aircraft’s three pitot probes by a local engineering support person. Due to miscommunication, the operator’s certifying engineer was not aware of their fitment, and subsequent inspections during the turnaround by personnel from the operator and the ground handling service provider did not identify that they had been fitted.
: The Australian Transport Safety Bureau advises all operators that conduct flights to Brisbane Airport to consider the use of pitot probe covers and, if covers are used, ensure there are rigorous processes for confirming that covers are removed before flight.
Read more about this ATSB investigation: AO-2018-053
Reconstruction of pitot probe covers on 9M-MTK, showing pitot cover damage and rub marks on aircraft skin from the streamer
The current legislation does not require commercial operators of aircraft not greater than 5,700 kg maximum take-off weight (MTOW) to provide instructions and procedures for crosschecking the quantity of fuel on board before and/or during flight. This increases the risk that operators in this category will not implement effective fuel policies and training to prevent fuel exhaustion events.
What happened
On 17 July 2016, at about 1039 Central Standard Time, a McDonnell Douglas Corporation 369D helicopter, registered VH-PLY, experienced fuel exhaustion and a collision with terrain while performing powerline inspections 36 km north-west of Hawker, South Australia. There were three crew on board the helicopter. One pilot in the front left seat, one line-worker in the front right seat and one line-worker in the rear left seat. The three crew members were seriously injured and the helicopter was substantially damaged.
Why did it happen
The ATSB found that the pilot was mistakenly told by ground staff that the aircraft had been refuelled and through distraction, omitted a crosscheck of the fuel quantity before flight. The pilot’s monitoring of the fuel in-flight was based on anticipated endurance, which resulted in him not detecting a low fuel level. The ATSB also found the requirements for the development of fuel policy by operators were dispersed throughout the aviation legislation—14 legislative and three guidance material requirements were found—but they did not require the operator to publish procedures for determining fuel on board before and during flight for commercial operators of aircraft not greater than 5,700 kg MTOW.
: From 2003 to 2017, the ATSB has received 26 reports of fuel exhaustion events from Air Operator Certificate holders operating aircraft not greater than 5,700 kg MTOW. Two key contributing factors from these reports are pilots not crosschecking the fuel on board before and/or during flight. Aircraft greater than 5,700 kg MTOW are not represented in the ATSB fuel exhaustion reports. In accordance with CAO 20.2, operators of these aircraft are required to publish instructions and procedures in their operations manuals for the pilot in command to verify the fuel on board before flight. Additionally, CAAP 215-1(2) Appendix B includes guidelines for publishing operations manual procedures for inflight fuel management.
CASA 29/18 – Civil Aviation (Fuel Requirements) Instrument 2018, which contains proposed changes to the current fuel regulations and guidance material is scheduled to commence 8 November 2018. The ATSB considers that the implementation of these changes should address this safety issue.
Until the proposed changes to the current fuel regulations and guidance material are implemented, the ATSB advises Air Operator Certificate holders for aircraft not greater than 5,700 kg MTOW, to consider this safety issue and take action where appropriate.
Read more about this ATSB investigation: AO-2016-078.
Research of accidents into water has shown that occupants who survive the initial impact will likely have to make an in-water or underwater escape, as helicopters usually rapidly roll inverted post-impact. The research has also shown that drowning is the primary cause of death following a helicopter accident into water.
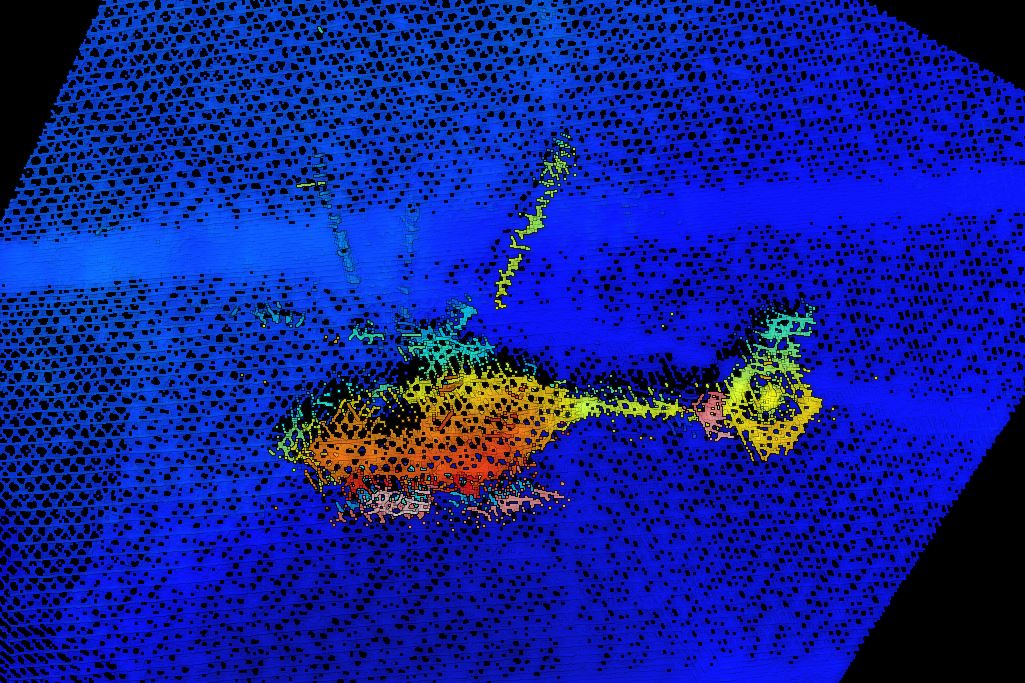
Sonar image of helicopter on seabed
Source: Pilbara Ports Authority and contractors working on their behalf
What happened
On 14 March 2018, at about 2330 Western Standard Time, an Eurocopter EC135 helicopter, registered VH‑ZGA departed Port Hedland Heliport, Western Australia to collect a marine pilot from a departing ship.
The flight was conducted at night under the Visual Flight Rules. A pilot, recently employed by the operator, was flying the helicopter, under the supervision of a training and checking pilot.
At about 2348, the helicopter was operating in vicinity of the ship when it descended and collided with the water. The training and checking pilot escaped from the helicopter and was rescued a short time later. The location of the other pilot was unknown, and a search commenced.
On 17 March 2018, the helicopter wreckage was located on the seabed and the missing pilot was found inside.
Why did it happen
The ATSB investigation is continuing. The ATSB emphasises that it is too soon to conclude factors involved in the pilot under check not surviving the accident.
Notwithstanding, HUET (helicopter underwater escape training) is considered to provide individuals with familiarity with the crash environment and confidence in their ability to cope with the emergency situation. Interviews with survivors from helicopter accidents requiring underwater escape frequently mention they considered that HUET had been very important in their survival. Training provided reflex conditioning, a behaviour pattern to follow, reduced confusion, and reduced panic.
The training and checking pilot had completed a HUET course within the previous 3 years. Although the pilot under check had completed a HUET course, that training was conducted 9 years ago.
Safety advisory notice
AO-2018-022-SAN-001: The Australian Transport Safety Bureau advises helicopter operators involved in overwater operations of the importance of undertaking regular HUET for all crew and regular passengers to increase their survivability in the event of an in-water accident or ditching.
Regular training can assist survivability
Regular HUET courses can assist occupants following a ditching or water impact. That training enables them to practice the techniques to make an in-water or underwater escape from a cockpit or cabin.
Detecting an unsecured canopy prior to take-off could prevent in-flight control issues resulting in injury or aircraft damage.
What happened
On 14 October 2014, a Van’s Aircraft Inc. (Van’s) RV-6A departed Moorabbin Airport, Victoria on a local flight. Shortly after reaching 2,900 ft, the aircraft descended rapidly and a witness reported observing objects falling from the aircraft. The aircraft collided with the ground next to a house 8 km south of Moorabbin. The pilot was fatally injured and the aircraft was destroyed. Members of the public found a number of items away from the accident site that belonged to the pilot.
Tip-up canopy open
(Source: Supplied)
Why did it happen
The liberation of the items from the aircraft’s interior indicated that the tip-up (forward-hinged) canopy likely opened in‑flight. While the ATSB was unable to determine how the canopy opened and the effect on aircraft control, there were indications the pilot was attempting to respond to the situation. However, for reasons undetermined, recovery did not occur before the impact with the ground. The ATSB found that, in a number of Van’s models, the in-flight opening of a tip-up canopy may potentially result in a significant pitch down tendency that may affect aircraft control.
: The consequences when an aircraft canopy opens in-flight, including on other than Van’s aircraft types, can vary from being relatively benign to significant, such as a sudden pitch down. In any event, in the first instance, pilots should expect an element of startle and distraction. The detection of an unsecured canopy prior to take-off could prevent in-flight control issues resulting in injury or aircraft damage. The ATSB advises pilots to be vigilant and to confirm the security of their aircraft’s canopy prior to take-off.
Check the security of your canopy
The in-flight opening of canopies in a number of Van’s aircraft models highlights the varying consequences in the case of such occurrences. The result can vary from being relatively benign to significant. While this investigation focused on Van’s aircraft, the implications are applicable to all aircraft fitted with a canopy, in particular, a tip-up canopy. Such occurrences serve as a reminder for pilots to check the security of their aircraft’s canopy prior to take‑off. Additional measures, such as the incorporation of a specific pre-flight checklist item, and/or the installation of a canopy-open warning device, have the potential to assist pilots detect an unintentionally-open canopy.
The ATSB encourages pilots who experience a canopy opening in-flight to notify the aircraft manufacturer and, in the case of difficulty controlling their aircraft, the ATSB in accordance with the reporting requirements of the Transport Safety Investigation Act 2003. This will allow for a greater understanding of the safety implications of these types of occurrences.
Read more about this ATSB investigation: AO-2014-164
In the early hours of 14 July 2015, the offshore support vessel (OSV) Skandi Pacific was loading cargo from an oil rig about 165 km off Australia’s north-west coast. As the weather deteriorated, cargo operations were stopped and the OSV moved a short distance from the rig. Two crewmembers then began securing the cargo on the vessel’s aft deck.
While securing the cargo, the crewmembers slackened the securing chain they had used to secure the containers on the starboard side to better secure the entire stow. Shortly after, two large waves came over Skandi Pacific’s open stern, shifting the unsecured containers forward. One crewmember was trapped between the moving containers, chains and a skip and suffered fatal crush injuries.
Skandi Pacific's aft deck
Source: DOF Management
Why did it happen
The deteriorating weather conditions had resulted in the cargo operations being stopped. After the crewmembers had lashed the cargo they found two mini-containers forward were not properly secured. To secure the containers, they decided to use a secondary chain, by securing it to the crash barrier then to the primary chain. When tightened, this chain would bring the primary chain in tight against the mini-containers. Their plan required slackening the primary chain to secure the secondary.
However, the sequence of working exposed them to high risk if water was shipped on Skandi Pacific’s aft deck. The crewmember attempting to fasten a securing chain forward of the two unsecured mini-containers was in a position of danger when waves came over the vessel’s open stern.
The Australian Transport Safety Bureau (ATSB) found that vessel’s managers had not adequately assessed the risks associated with shipping seas over the vessel’s stern while securing cargo on this type of vessel (the OSV had an open stern). Further, there were no clearly defined limits for excessive water on deck that necessitated stopping operations, leaving individuals to make difficult, and necessarily subjective, decisions about whether or not to stop work.
The ATSB investigation also identified that the vessel’s safety management system procedures did not contain clearly defined weather limits for working or securing cargo in adverse weather.
: The Australian Transport Safety Bureau advises the masters, owners and operators of all offshore support vessels to ensure that the risks associated with working on the aft deck of vessels with open sterns are adequately assessed.
Effective coordination and communication between airside crews could help prevent or detect mistakes that led to a collision between an Airbus A330 and aerobridge during boarding.
What happened
On 31 March 2016, an Airbus A330 was being boarded at Melbourne Airport, Victoria. Seeing that the parking brake was on, a maintenance engineer removed the main chocks early. The crews removed the nose gear chocks to dock the towbarless tractor without checking the main gear chocks. The captain, unaware that no chocks were in place, released the park brake and the aircraft rolled back, striking the aerobridge. There were no injuries and the aircraft door and aerobridge were damaged.
Why did it happen
The ATSB found that the ground and flight crew procedures were not harmonised, reducing cohesion between the crews. In the absence of clear guidance or instruction on coordinating activities during pushback, and based on incorrect assumptions, key steps involving the chocks and parking brake were performed out of sequence and without being communicated between tractor, engineering and flight crews.
Damaged forward-left door
Source: Melbourne Airport, modified by the ATSB
Safety advisory notice
Effective coordination and communication between airside crews can prevent or detect mistakes that could otherwise lead to damage or injury. The ATSB advises organisations that work airside to ensure that ground and flight crew activities are harmonised, and to foster active communication and coordination between working crews.
Communicate and coordinate airside activities
An aircraft is attended at a terminal bay by people carrying out a wide range of concurrent tasks. Typically, they and their respective organisations work alongside many others, each operating with different processes and to varying contractual arrangements. Defining a set of processes that can apply across such varied situations and aligning them well with the other activities can be difficult. In practice, mechanical malfunctions and honest mistakes can rarely be completely eliminated. An effective procedure will include steps to ensure that activities are appropriately aligned with other procedures. One way to achieve this is to pause and check if the situation is as it should be, and to inform others of activities that could affect them.