On 7 September 2014 at about 1303 Australian Eastern Standard Time, a Piper Arrow, registered VH-KGP was completing a private, visual rules flight (VFR) from Orange to Wollongong, New South Wales. On board were a pilot and one passenger.
At about 10 NM north of Wollongong, the pilot broadcast an inbound call on the common traffic advisory frequency (CTAF). At the time, an instructor and student in an Evektor Sportstar registered 24-4467 were one of two aircraft conducting circuit training on runway 34.
The pilots of both KGP and 4467t communicated their respective position and intentions, and at 1306, the pilot of KGP called joining an extended downwind for runway 34.
When 4467 was on the crosswind leg for runway 34, the crew noted KGP on their left, about 100 metres ahead and at about the same level as them.
The instructor in 4467 initiated a climbing turn and shortly after, KGP passed underneath and just behind 4467.
This incident highlights the importance of using standard phraseology, and making extra calls when there is any uncertainty regarding another aircraft’s position when operating at non-controlled airports. As well as a requirement, it is good airmanship given the limitations of the See-and-Avoid Principle.
On 6 June 2014, a Grob G-115CD aircraft, registered VH-ZYM departed Merredin for Jandakot, Western Australia, on a dual navigation exercise.
After arriving at Jandakot, and having a lunch break, another instructor briefed the student on circuit procedures at Jandakot. A third instructor then conducted a session of circuits with the student. The student then taxied back to the apron where the instructor egressed. The student then conducted 3-4 solo circuits prior to returning to the southern apron for parking.
As the aircraft arrived at the company parking area, the student saw the fuel truck operator refuelling an aircraft on the left side of the taxiway. He assessed that there was sufficient room to taxi past the vehicle, and entered the taxiway with the vehicle on his left.
Shortly after, the aircraft’s left wing struck the vehicle and it then swung rapidly around facing the diesel fuel tank. The student applied the brakes, and the aircraft propeller stopped within centimetres of the tank.
The fuel vehicle operator had seen the aircraft taxi in and had hit the emergency stop button as the aircraft struck the vehicle.
The student was not injured, however the aircraft and fuel truck sustained minor damage.
As a Safety Action the flying college have temporarily ceased to use the taxiways into the parking lines. Operational staff have been briefed and trained on safe aircraft manoeuvring in this area.
Also, as agreed with the fuel company, all new students will participate in a Fuel Hazards training course conducted by the fuel company. Students will have to complete all relevant training modules before commencing flying training.
The fuel company are considering the use of cone markers around the vehicle during refuelling operations.
A collaborative Safety Action between the flying college, the refuelling company and the airport operator have changed refuelling and taxying procedures on the southern apron.
On 31 December 2013, at about 0945 Western Standard Time (WST), the driver of an ambulance received a telephone call from the State Operations Centre to meet a rescue helicopter at the Jurien Bay aeroplane landing area (ALA), Western Australia.
At about 0950, the pilot of a Cessna 208 aircraft, registered VH LNI (LNI), landed at Jurien Bay (ALA) and parked at the northern apron, in front of the Royal Flying Doctor Service (RFDS) terminal, with the engine running, in preparation for the arrival of parachutists. At about 0955, the ambulance arrived at the aerodrome at the RFDS gate. The driver stopped the ambulance and unlocked the gate and cut rope barriers that had been erected and were blocking ambulance access to the RFDS terminal.
The ambulance entered the airport and proceeded via the RFDS apron towards the runway. The driver reported that the ambulance deviated past the standing aircraft leaving about 14 m distance from the aircraft propeller. The pilot of LNI estimated the distance to be about 3 m.
The ambulance then entered the runway and drove towards the helipad, about 300 m south of the RFDS apron. While driving along the runway, the ambulance driver received a call from the Operations Centre advising that the helicopter was at the Jurien Bay marina awaiting the ambulance for patient transfer. He made a U turn and returned via the same route, and reported again deviating around the stationary aircraft maintaining a safe distance. The pilot of LNI reported that the ambulance passed within about 2 m of the aircraft wingtip.
This incident highlights the importance of understanding local procedures around non-controlled aerodromes, in particular having agreements between users of a facility.
On the evening of 8 October 2013 a Dornier DO228 aircraft, registered VH-VJN (VJN) was taxiing to the company hangar at Brisbane Airport, Queensland after the completion of a charter flight.
As the flight crew turned right onto the Hotel 2 South taxiway, two vehicles were travelling along the designated movement area along Hotel 2 South from the opposite direction.
This incident did not involve an on-site investigation by the ATSB and the investigation includes differing recounts of the event from the flight crew and the driver of the second vehicle.
Aircraft movements at Brisbane Airport have increased from 123,000 in 2004 to 222,000 in 2013. At the time of the incident there were about 1,700 vehicles approved to access the taxiway hotel system.
The ATSB published a research paper on ground operation occurrences at Australian Airports over a 10 year period. Of the 282 ground occurrences reported to the ATSB between 1 January 1998 and 31 December 2008, about 37 per cent of those incidents occurring as the aircraft approached a gate, were attributed to near collisions with vehicles. This report is available at: www.atsb.gov.au/publications/2009/ar2009042.aspx.
On 26 August 2013, a Qantas Airways Boeing 737 aircraft, registered VH-VZA (VZA) was completing a scheduled passenger flight from Cairns, Queensland to Sydney, New South Wales.
After landing, at about 2010 Eastern Standard Time, VZA was cleared by air traffic control (ATC) to taxi to Bay 6 of the Domestic 1 (DOM 1) apron area at Sydney Airport. At about the same time, the captain observed the lights of a white security vehicle approaching from about 50 m away and about 90° to the right of the aircraft.
As the vehicle approached the intersection of the airside road and taxiway ‘Bravo 2’ the driver reported slowing to between 25 to 30 km/h. He looked to his left, but did not see the lights of VZA. Assuming the area was clear; he directed his attention to the parking bay area to the right.
The captain thought the vehicle would continue along the airside road, however, as the car continued in a northerly direction across the intersection the captain believed it was on a collision course with VZA. Realising the vehicle driver had not seen VZA the captain immediately stopped the aircraft.
The security vehicle continued toward the aircraft then came to an abrupt stop about 10 m to the right of the aircraft’s nose.
The ATSB published a research paper on ground operation occurrences at Australian airports over a 10-year period. This publication highlighted ground operations as potentially being one of the most dangerous areas of aircraft operation. Of the 282 ground occurrences reported to the ATSB between 1 January 1998 and 31 December 2008, 11 per cent happened when the aircraft was approaching the gate. About 37 per cent of the approaching the gate phase occurrences were attributed to near collisions with vehicles. These occurrences required immediate braking action by the flight crew or vehicle driver in order to avoid a collision.
On 2 August 2013, at 1400 Eastern Standard Time, the student of a Cessna 172R aircraft, registered VH‑IMS (IMS), conducted a solo navigation flight from Archerfield to Sunshine Coast via Caboolture, Queensland. After landing at Sunshine Coast Airport, the student taxied the aircraft to the general aviation apron.
Other aircraft were operating in the area and the pilot wanted to ensure he remained clear of them. The pilot noted a fence and power pole on his left, and then focused on an aircraft taxiing in front of IMS. While the pilot was watching the other aircraft taxiing, he advised that IMS may have rolled forward unnoticed. When the pilot commenced a right turn, the aircraft was past the end of the fence and as he turned the aircraft, the left wing collided with a power pole.
The pilot reported that he had learnt a valuable lesson from the accident, in that the flight is not over until the aircraft has been shut down and secured. This incident also highlights the need to keep a good look out during taxi as well as in flight.
On 10 August 2013, an Airbus A320-232, registered VH-VGR (VGR) and operated by Jetstar Airways Pty Ltd was holding short of gate D2 at Melbourne Airport, Victoria. At the same time, a Boeing B737-800, registered VH-YID (YID) and operated by Virgin Australia Airlines Pty Ltd. (Virgin) was approved by air traffic control for a pushback from bay E1 once VGR was on the gate at bay D2. The dispatcher for YID assessed VGR was on the gate and commenced the pushback. During the pushback, the left wingtip of YID collided with the tail cone of VGR, damaging both aircraft. There were no injuries.
What the ATSB found
The ATSB found that the dispatcher for YID could not visually confirm the position of VGR relative to gate D2 and assessed that because the aircraft hadn’t moved, it was on the gate. The pushback ground staff followed the normal practice for a pushback from bay E1. However, this practice did not allow for visual monitoring of the left side of the aircraft, such as by using a wing walker. This meant it was not possible for the dispatcher to identify the collision risk in time to prevent the collision.
What's been done as a result
Virgin advised that following this occurrence, they issued a local instruction to ground staff, mandating the use of wing walkers from certain bays at Melbourne Airport, including bay E1.
Safety message
This occurrence highlights the importance of ensuring that adequate clearance exists prior to commencing pushback. This includes using sufficient personnel to ensure visibility of each side of the aircraft at all times.
Findings
From the evidence available, the following findings are made with respect to the collision during pushback between Boeing B737-8FE, registered VH-YID, and Airbus A320‑232, registered VH‑VGR, at Melbourne Airport, Victoria on 10 August 2013. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
The dispatcher of the B737 could not visually confirm the position of the A320 relative to its assigned gate and incorrectly assessed that, as the aircraft was stationary, it was at the gate.
The pushback of the B737 was commenced with insufficient clearance from the A320, which was not identified prior to the collision as the dispatcher's position to the right-front of the B737 prevented observation of its left wing.
Appendices
The occurrence
On 10 August 2013, Airbus A320, registered VH-VGR (VGR) and operated by Jetstar Airways Pty Ltd (Jetstar), was flown from Sydney, New South Wales to Melbourne, Victoria. Upon arrival, the crew of VGR were cleared by the air traffic control surface movement controller (ground controller) to taxi to gate D2.
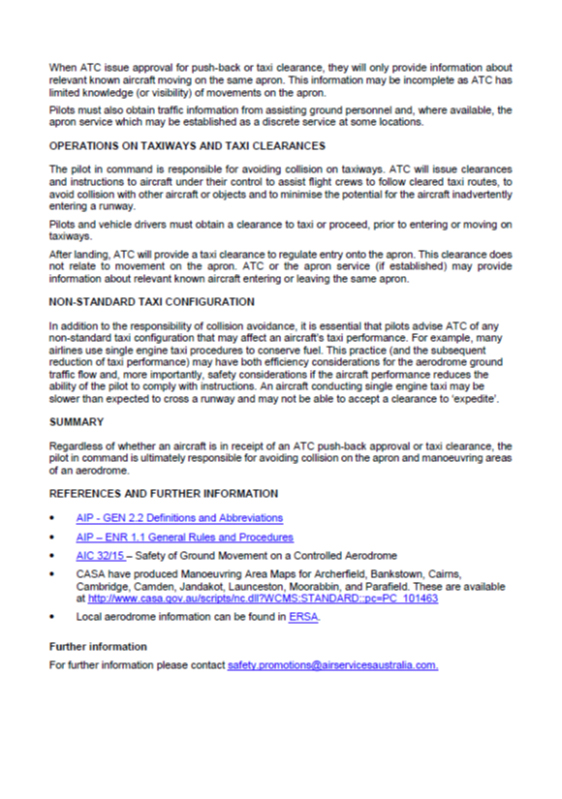
At 0930 Eastern Standard Time[1], VGR entered the apron en route to gate D2, when a Boeing B737-800, registered VH-YID (YID), requested pushback approval from gate E1 (Figure 1). YID was being operated by Virgin Australia Airlines Pty Ltd. on a flight to Maroochydore, Queensland. The controller advised the crew of YID that a Jetstar A320 was entering the apron behind them for bay D2 and that when that traffic was ‘on the gate’[2], pushback from bay E1 was approved.
The flight crew of YID reported that they saw VGR (the Jetstar A320) pass behind them from the reflection in the terminal window in front of their parked aircraft. The captain of YID relayed the pushback approval to the dispatcher, including that it could only commence once the A320 was on the gate. The dispatcher was standing to the right of the aircraft’s nose.
At 0931:34, as VGR approached the gate on bay D2, the automatic nose-in guidance system (NIGS) displayed a message ‘STOP-WAIT’. In response the flight crew stopped the aircraft short of the gate. The dispatcher on YID reported looking under the aircraft and observing that VGR was stopped. The dispatcher reported then waiting for about 15–20 seconds to confirm the aircraft remained stationary. As it did, the dispatcher was satisfied that VGR was on the gate and the pushback of YID could commence. Pushback began at 0931:46.
At 0931:58, the crew of VGR transmitted to the controller that they were holding short of the bay because of the NIGS. However, that message was over‑transmitted by another aircraft. Forty seconds later, the crew re‑transmitted the same message. The message was acknowledged by the controller, who requested to be advised when the aircraft was at the gate.
Neither the crew of VGR nor the controller mentioned the gate number during the transmissions. The crew of YID later reported they did not hear these transmissions.
At 0933:03, the left wingtip of YID contacted the tail cone of VGR immediately aft of the operating auxiliary power unit. The tail cone of VGR immediately aft of the auxiliary power unit separated from the aircraft and fell to the ground. The left wingtip of YID was damaged during the collision.
Following the collision, YID was towed back to gate E1 and VGR was marshalled to gate D2.
There were no injuries as a result of the collision.
Figure 1: Position of A320 VGR (in green), holding short of gate D2, and B737 YID (in grey) during pushback from Bay E1 at the time of the collision. The position of the dispatcher and tug for YID are also shown
The collision between the two aircraft occurred when the B737, VH-YID (YID) was being pushed back from gate E1. At that time the A320, VH-VGR (VGR) was holding short of gate D2 due to a STOP-WAIT indication from the guidance system. The following analysis will examine the factors leading to the collision.
Pushback approval and commencement
The ground controller issued a pushback approval to YID that required VGR to be on gate D2 before commencement. While this was accurately conveyed to the dispatcher by the captain of YID, from the dispatcher’s position at the front-right of YID, there were insufficient visual cues for the dispatcher to accurately determine that VGR had stopped at gate D2. While VGR was actually holding short of the gate, the dispatcher formed the opinion that the aircraft was on the gate based on the observation that it had been stationary for a period of time. This was consistent with their experience and as a result, they did not move to a position from where they could accurately assess VGR’s location.
After observing that VGR was stationary for a period of time, the dispatcher signalled the pushback driver to commence YID’s pushback. From the dispatcher’s walking position, it was not possible to see the clearance lines for bay D2 marked on the apron. It was also not possible for the dispatcher to see VGR’s fuselage or its position in relation to the gate. From the dispatcher’s perspective, YID obscured most of VGR. The operator’s standard operating procedures required the dispatcher to have ‘clear visibility of the aircraft wingtips or wing walkers and potential obstructions at all times’.
As was reported to be normal practice, a wing walker was not used in this case for a pushback from bay E1. In the absence of a wing walker, the dispatcher was not able to ensure the aircraft would not collide with potential obstructions during the pushback as there was no visibility of the left side of YID. Following this occurrence, Virgin Australia Airlines Pty Ltd. provided a local instruction to Melbourne Airport ground staff that stipulated the gates that required the presence of a wing walker prior to push back. Gate E1 was included in that list of gates.
Communication
The flight crew of YID did not recall hearing the transmissions between VGR and the ground controller. There were a number of factors that may have affected the crew being alerted by the communication:
the surface movement control radio frequency was very congested in the time leading up to the occurrence, being in use for about 96 per cent of the time
during the 2 minutes and 20 seconds between issuing pushback approval and the collision, the ground controller participated in sequences of transmissions between seven different aircraft and one ground tug
VGR’s transmissions were abbreviated and fast, likely as a result of the frequency congestion discussed above
VGR’s crew did not mention the gate number in their holding short transmission, nor were they required to as it was included in the ground controller’s initial contact with the crew
the pilots’ expectation that in the radio environment, messages would be directly addressed between the controller and a specific aircraft, and not broadcast generally. Pilots will therefore pay more attention to transmissions directed to their aircraft.
Given these factors, it is not reasonable to expect that the transmission from VGR could have alerted the crew of YID to the collision risk. In addition, in the lead up to the collision, the crew of VGR were communicating with their company to resolve the issue with the nose‑in guidance system at the gate. This limited their ability to identify and therefore react to the collision risk.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew of YID and VGR
the dispatch ground staff for YID
recorded data from both aircraft
recorded data from Melbourne Airport
Virgin Australia Airlines Pty Ltd. (Virgin)
Airservices Australia.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to Airservices Australia, flight crew and ground staff from Virgin, flight crew from Jetstar Airways Pty Ltd and the Civil Aviation Safety Authority.
Submissions were received from the captain of VGR, the dispatcher of YID and Virgin. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Context
Communications
During the pushback from Bay E1, the dispatcher of YID communicated with the aircraft captain via a headset that was plugged into the nose of the aircraft on the first officer’s (FO) (right) side. The dispatcher communicated with the tug driver by hand signal.
When the ground controller issued the conditional approval for a pushback to the crew of YID, it was acknowledged by the FO. The captain heard the transmission and relayed it to the dispatcher. In turn, once the dispatcher was satisfied of VGR’s location at Bay D2, they communicated the commencement of the pushback to the tug driver using hand signals.
The surface movement control radio frequency was used for communication between the ground controller and aircraft. This frequency was not normally used for direct communication between aircraft. During this period, the crew of YID were also monitoring other communication channels, including the cabin interphone, the company radio frequency and the dispatcher.
When VGR had to hold short of the gate at bay D2, the flight crew notified the ground controller. While not required to do so, this displayed good judgement and communication in an effort to ensure a common understanding of their situation.
Aerodrome information
Control of aircraft during airport ground operations
While flight crew need a clearance from the ground controller to be allowed to move their aircraft on the apron, responsibility for separation between a moving aircraft and any obstacles rests with the flight crew and supporting company staff (see Appendix A).
There are taxi lines marked for aircraft to follow when entering or departing from any bay/gate. Guidance lines also show pushback limits and where to disconnect from a tug after a pushback.
Clearance lines indicate the limit of an area on the apron where an aircraft may park and, once located ‘on the gate’, be assured of adequate clearance. An aircraft holding short of a designated gate may not be wholly beyond the clearance line and may therefore present a collision risk.
Nose-in guidance system
A nose-in guidance system (NIGS) is an automatic system for accurately guiding aircraft to the gate. The NIGS at bay D2 had a function that identified the shape of an approaching aircraft. Using this feature, the NIGS only provided guidance to the specific aircraft type that was programmed into the NIGS at that time.
If the NIGS did not identify an approaching aircraft as the correct type, it would not provide guidance. Instead, it would display a message ‘STOP-WAIT’ when the aircraft was about 20 m short of the gate.
Recorded information
Recorded flight data was obtained from both aircraft. The cockpit voice recording was available from VGR; however, the recorded audio from YID had been overwritten.
Audio recordings of the surface movement control radio frequency and data from the surface movement radar were also obtained.
Wreckage and impact information
The left wingtip of YID was damaged during the collision (Figure 2).
Figure 2: Damage to the left wingtip of YID
Source: ATSB
The tail cone of VGR aft of the auxiliary power unit (APU) and the APU exhaust duct separated from the aircraft (Figure 3). The bulkhead aft of the APU was buckled and there was also minor localised damage to the external skin.
Figure 3: Damage to the tail cone of VGR aft of the APU, looking from left to right of the aircraft
Source: ATSB
No other damage was identified on either aircraft.
Pushback procedures
Dispatcher
Under Virgin Australia Airlines Pty Ltd. (Virgin) operating procedures, the dispatcher was responsible for the guidance of the aircraft and for the avoidance of obstructions when the aircraft was under tow. They were responsible from the time that voice communications were first established with the cockpit, until the flight crew indicated the aircraft was clear to start taxiing under its own power.
The standard operating procedures stated:
The aircraft dispatcher is to stand in a position that gives clear visibility of aircraft wingtips or wing walkers and potential obstructions at all times.
From the dispatcher’s position to the front-right of YID on the day of the occurrence, it was not possible to see the left side of the aircraft during the pushback (Figure 4). During the ATSB’s observation of operations at Bay E1 the following day, it was similarly noted that the dispatcher’s position meant that the dispatcher could not see the left side of the aircraft (Figure 5).
Figure 4: Screenshot of YID during pushback,5 seconds before thecollisionwith VGR and showing the position of the tug and the dispatcher
Source: Melbourne Airport, modified by the ATSB
Figure 5: Pushback of the same Virgin flight from bay E1 on the next day
Source: ATSB
Once YID was pushed back from bay E1 on the day of the occurrence, it was turned slightly ‘tail left’ from the pushback driver’s point of view. The geometry of the aircraft and the tug meant the pushback driver was positioned well to the right of the aircraft’s nose. The dispatcher reported they could not safely change from one side of the aircraft to the other while the aircraft was moving. However, the dispatcher could walk on the side that gave a bigger field of view during any expected turn. In this occurrence, the dispatcher could have walked on the left side of the aircraft during the pushback.
The dispatcher reported that it was normal practice to walk on the side of the aircraft where the headset sockets were located, which for the 737 was the right side. The dispatcher reported they had never walked on the other side of the aircraft during a pushback before. It was also reported as being normal for the 737 to be pushed back from bay E1 without using a wing walker. This meant that normally only one wingtip could be monitored visually during pushback.
Before starting a pushback, dispatchers normally visually assessed the area for potential obstacles behind the aircraft. In this occurrence, the dispatcher did this by looking under and around the engines.
Pushback driver
The pushback driver reported that their attention was focussed on controlling the aircraft and the tug. As such, they were not concentrating on any collision potential during the pushback.
Wing walkers
The dispatcher was required to use a wing walker if they did not have clear visibility of the aircraft wingtips.
If a wing walker was used, the wing walker was responsible for monitoring the wingtip and tail clearances on that side of the aircraft.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 22 April 2013, the flight crew of a United Airlines Incorporated Boeing 747-422, registered N119UA, flew from Sydney, New South Wales to Melbourne, Victoria. At Melbourne, the crew taxied to gate D5 and stopped, applying the parking brake. Shortly after stopping, the aircraft started to move forward again slowly. The flight crew realised the aircraft was moving and re-applied the brakes. The aircraft’s left wing collided with the aerobridge before the movement had stopped. No one was injured during the occurrence and the aircraft sustained minor damage.
What the ATSB found
After stopping at the gate, the aircraft parking brake was likely inadvertently released before the nose wheels were chocked and the engines shut down. The flight crew’s attention was inside the cockpit, focused on shutting down the engines. As such they were not actively monitoring aircraft movement, nor was that required at this stage. In addition, the parking guidance system at the gate was set to emergency stop mode by ground personnel when the aircraft first arrived, removing the possibility of an alert for the flight crew that the aircraft had moved. The flight crew became aware of the movement when the captain detected motion through peripheral vision. The very slow acceleration, combined with a lack of visual cues available to the flight crew made it difficult for the crew to detect the movement in time to prevent the collision.
Safety message
This occurrence highlights the importance of flight crew remaining aware of the possibility of aircraft movement whenever the engines are running as aircraft movement, particularly if it is slow, is difficult to detect. Additionally, ground support crew are reminded of the need to leave the parking guidance system in normal mode, unless an emergency stop is required.
Boeing 747 N119UA
Source: Benedikt Mathweis
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew of N119UA
United Airlines Incorporated (United)
ground staff
Melbourne airport
data from the flight recorders on N119UA.
References
Dismukes, K 2006, ‘Concurrent task management and prospective memory: pilot error as a model for vulnerability of experts’ Proceedings of the Human Factors and Ergonomics Society 50th Annual Meeting – 2006, pp.909-913.
Monaco, W & Kalb, J 2007, Motion detection in the far peripheral visual field, U.S. Army Research Laboratory, Maryland, United States.
Reason, J 1990 Human Error, Cambridge University Press, Cambridge, United Kingdom.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to United, the flight crew of N119UA and the Civil Aviation Safety Authority.
A submission was received from United. The submission was reviewed and where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A - Selected parameters from the recorded flight data when the aircraft arrived at gate D5
Source: ATSB
Explanation
Recorded data
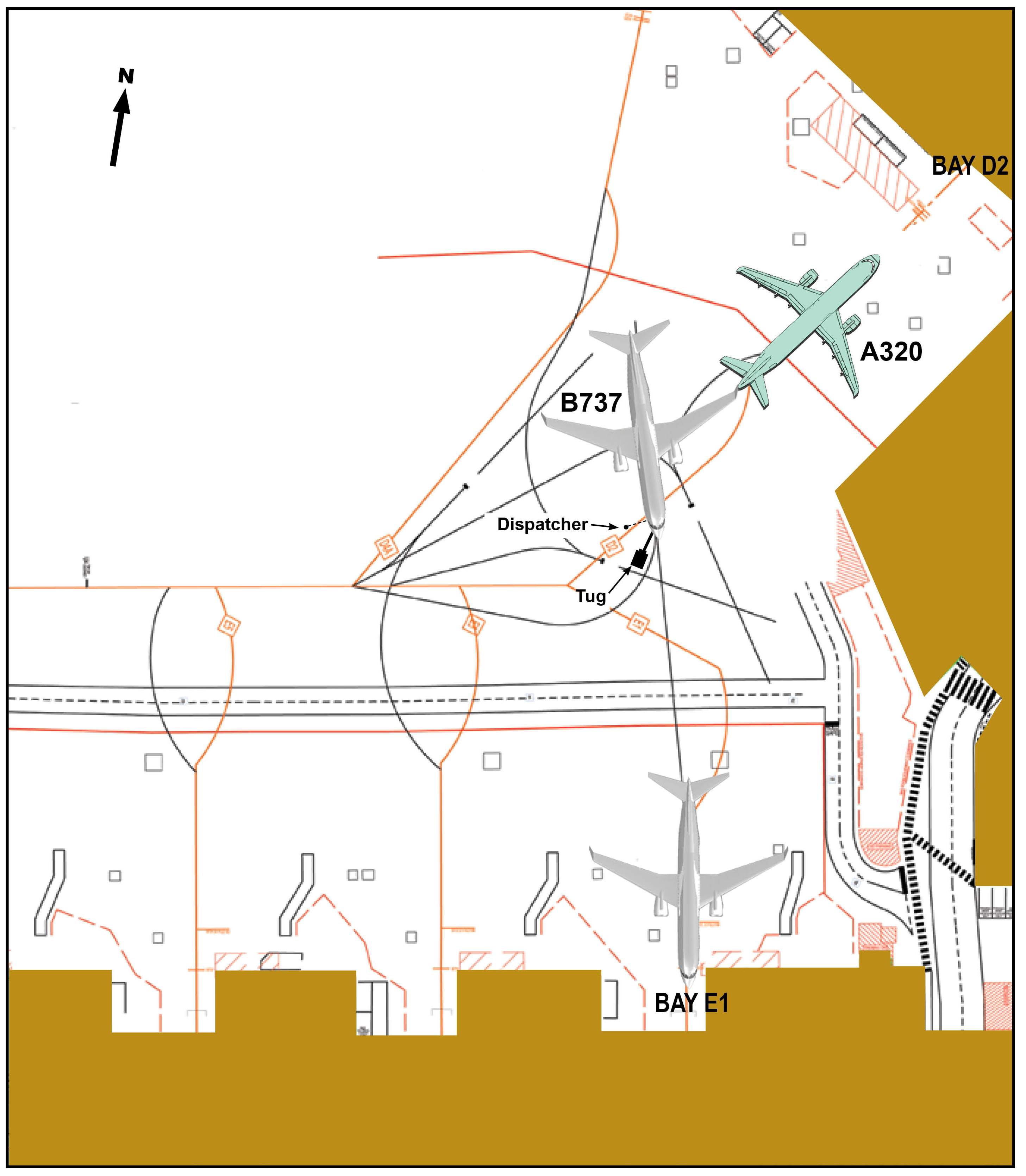
In accordance with the normal aircraft shut down procedures, the digital flight data recorder ceased recording shortly after the engines were shut down. The digital aircraft condition monitoring system recorder is normally switched off later in the shut down sequence. Therefore, the digital monitoring system recorder continued to record information including the longitudinal g[12] parameter. The plot of recorded data above shows data from both flight recorder systems and indicates the sequence of events beginning with the aircraft turning into the parking bay.
Movement
The ATSB derived the aircraft’s speed from variations in longitudinal g, correlated with video recordings from the airport terminal. This showed that:
From 0024:24, the aircraft turned into the parking bay, turning slightly right. As the aircraft approached the parking bay, there were variations in rudder pedal position and longitudinal g.
At 0024:52, there was an increasing negative longitudinal g, or deceleration, which reduced as the aircraft stopped at 0024:54. About 4 seconds later, a positive change of about 0.02 longitudinal g indicated that the aircraft began to move forward again.
The aircraft gradually decelerated as the engines were shut down by the fight crew actioning the fuel cut-off for each engine, although a video recording indicated the aircraft continued to move forward.
At 0025:13, a sharp deceleration indicated the aircraft was being stopped.
Rudder pedal position
Rudder pedal position has no influence on the aircraft when taxying at slow speed. At this speed, the aircraft is steered by a separate control, the tiller, which controls nose wheel steering. However, while taxying an aircraft, the handling pilot’s feet rest on the rudder pedals. This is done so the pilot can operate the wheel brakes by applying force to the tops of the respective rudder pedals. The continuous slight movement in the rudder pedals between when the aircraft came to a stop until the aircraft started to move again is consistent with someone having their feet resting on the rudder pedals until that time.
Speed brake position
The speed brakes are hinged panels on the upper surface of the wing that may be extended to reduce aerodynamic lift from a wing. A speed brake may also be called a spoiler, as can be seen in this plot. The spoiler handle position was moved from 100 per cent to 0 per cent, commanding a retraction of the spoilers at the same time as the aircraft started to move.
The captain had about 28,000 hours aeronautical experience with 15 years flying Boeing 747 aircraft.
The first officer (FO) had about 10,000 hours aeronautical experience and had recently completed training for the Boeing 747 type rating, having 16 hours experience on this aircraft type. The flight from Sydney to Melbourne was part of the initial operating experience[4] requirement and was the FO’s first flight as pilot monitoring under the captain’s supervision.
Fatigue
Both crew reported that they were well rested after having about 25 hours rostered time off prior to commencing duty for the 1.5 hour flight from Sydney to Melbourne. They had been rostered together for the previous 3 days. The FO’s roster and reported sleep during that period indicated that fatigue should not have been an issue.
The captain’s sleep history was not obtained. However, as they had been working to the same rostered schedule as the FO, there was nothing to indicate that fatigue would have been an issue.
Workload
The captain reported feeling that there was a slight increase in their workload because this was the FO’s first flight as pilot monitoring. That workload increase was expected and the captain reported no problem in handling it.
Aircraft information
Wheel brake system
The Boeing 747 has independent left and right side, hydraulically-powered wheel brakes to all the main landing gear wheels.
The wheel brakes are controlled by applying force at the top of the captain’s or FO’s rudder pedals. The rudder pedals for each pilot are mechanically interconnected. Therefore, either pilot can apply input to all wheel brakes as required.
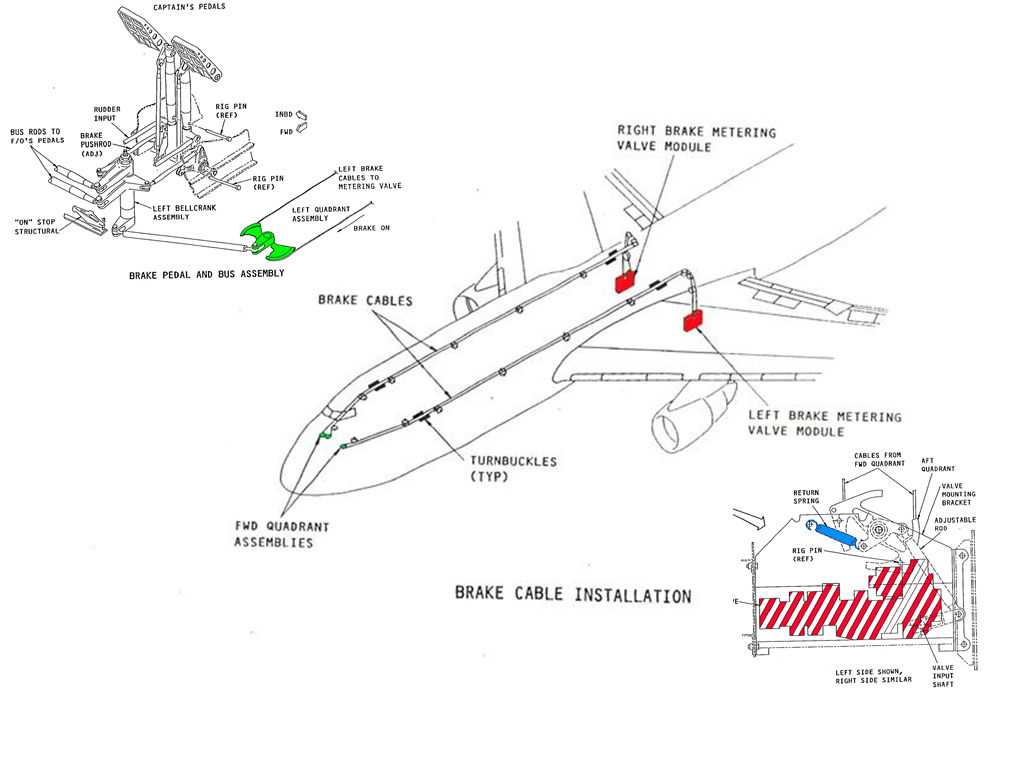
Activating the brakes allows the brake metering valves to supply hydraulic pressure to the wheel brakes. Removing the force from the tops of the rudder pedals returns the metering valves to neutral through the action of the return springs (Figure 2). This relieves the hydraulic pressure to the wheel brakes.
Flight crew normally position their feet to operate the rudder with their heels on the floor. In that position, the height of the rudder pedals above the floor makes it necessary for them to slide their feet up the rudder pedals to apply the wheel brakes.
Figure 2: Boeing B747-400 wheel brake system schematic. The upper-left image shows the mechanical interconnection between depressing the top of the rudder pedal and the movement of the brake cables, the centre image the wheel brake cables’ layout and the lower-right image a hydraulic metering valve (the return spring is shown in blue)
Source: Boeing, modified by the ATSB
Parking brake
The 747-400 wheel brake system incorporates a parking brake function that retains hydraulic pressure in the wheel brakes. The parking brake is used during:
the installation or removal of chocks after an aircraft stops or is about to move in the bay
taxi manoeuvres, when the aircraft must wait for other traffic to clear
short-term parking.
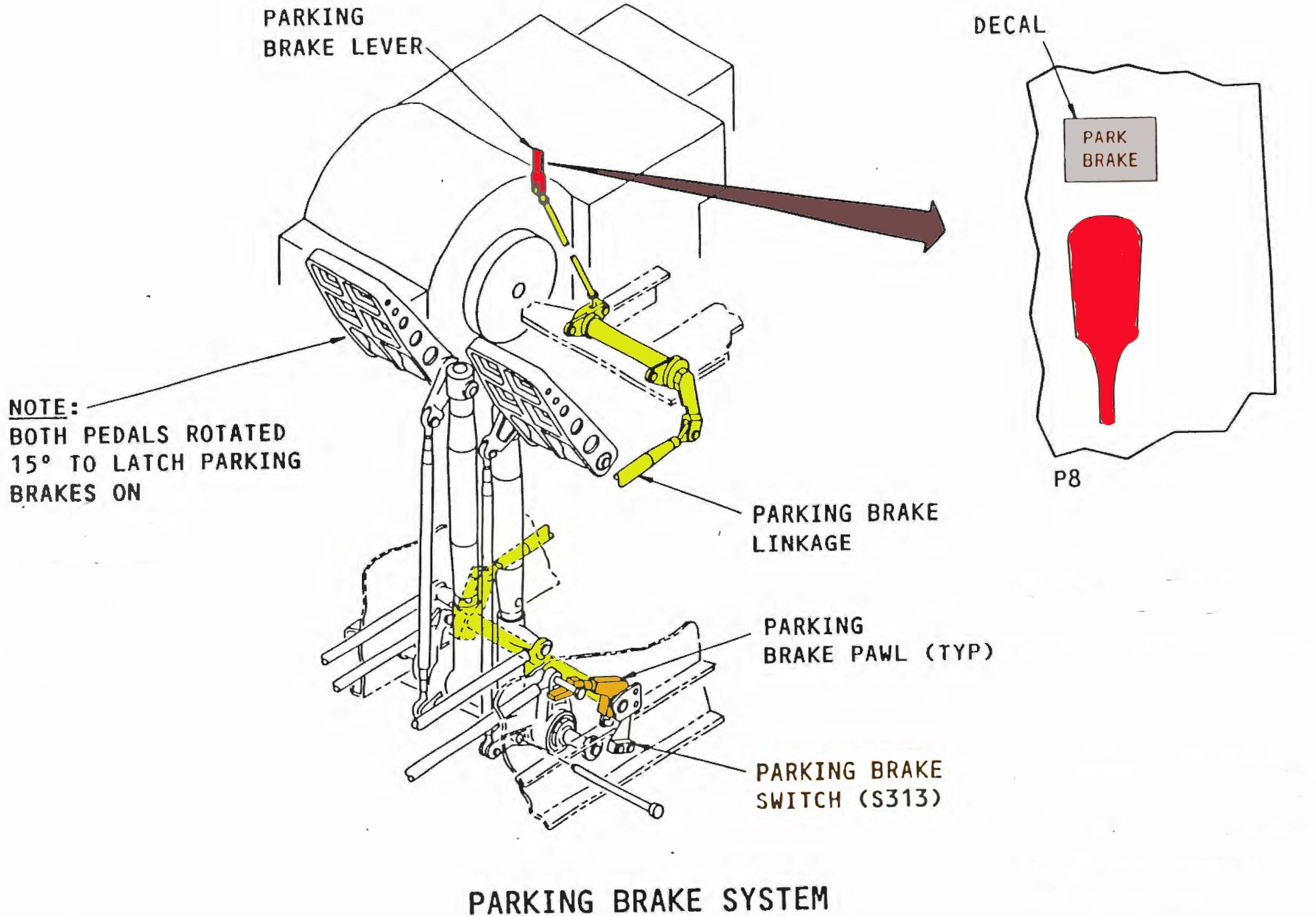
The parking brake system is controlled using a parking brake lever situated on the left (captain’s) side of the flight deck centre console. The lever is connected mechanically to a pawl at the rudder pedals (Figure 3). Once the tops of either pilot’s rudder pedals are pressed to at least 15°, the lever can be raised allowing engagement of the pawl. The pawl retains the rudder pedals in this position and the metering valves allow continued supply of hydraulic pressure to the brakes.
The pawls are themselves held in position by the force applied by the metering valve return springs. Applying additional force to the tops of the rudder pedals results in the pawls moving away from the ‘locked’ position, releasing the wheel brakes.
The parking brake also activates an isolation valve to trap the hydraulic pressure in the brake lines at the wheel brakes. As a result, once the parking brake is set, fluctuations in hydraulic system pressure do not have an effect on the wheel brakes.
Figure 3: Boeing B747-400 Parking brake system, showing the mechanical interconnection (in yellow) between the parking brake lever (in red) and the parking brake pawl (in orange) and the location of parking brake switch (switch S313)
Source: Boeing, modified by the ATSB
Parking brake engagement activates the parking brake switch that in turn annunciates the ‘Park brake set’ message on the engine indicating and crew alerting system (EICAS)[5]. The captain reported seeing this message when the parking brake was engaged.
Aircraft wheel brake system examination
Following the occurrence, a review of data recorded on the aircraft’s central maintenance computer found no defects for the aircraft’s wheel brake system.
United Airlines Incorporated (United) inspected the aircraft’s wheel brake system and conducted a number of functional tests in accordance with the manufacturer’s maintenance manual. No anomalies or defects were found in the aircraft’s wheel brake and parking brake systems.
Airport information
Visual docking guidance system
Gate D5 was equipped with a visual docking guidance system (VDGS). The VDGS provided guidance for crew in terms of aircraft centre-line position and nose wheel position.
Crew use the guidance system to bring the aircraft to a stop at the correct point for an aerobridge disembarkation of passengers. After the aircraft has stopped, the aerobridge is moved forward to the aircraft fuselage.
The normal sequence of operation for the VDGS is as follows:
prior to an aircraft’s arrival, a ground engineer selects the aircraft type on the VDGS control panel
the VDGS starts scanning for the aircraft
the VDGS matches the approaching aircraft with the selected aircraft type and:
- if correct, the VDGS guides the aircraft using directional and speed arrow messages
- if incorrect, the VDGS displays STOP and the aircraft is stopped short (up to about 20 m).
at the correct stop position, the VDGS displays STOP and:
- if the aircraft stops in time, the VDGS waits for 5 seconds and then signals OK, alerting flight crew that parking is complete
- if the aircraft does not stop in time or moves forward more than 30 cm within 5 seconds, the VDGS displays TOO FAR, alerting flight crew that the aircraft has overshot the stop position.
The VDGS control panel includes an emergency stop button that can be activated by ground crew at any time. Once the emergency stop button is activated, the VDGS displays the STOP signal and ceases monitoring the aircraft’s position and movement.
The displayed STOP signal is the same for normal and emergency stopping conditions. However, the STOP signal is displayed for more than 5 seconds for an emergency selection.
Flight crew procedures for use of the VDGS
The VDGS instructions available to the flight crew stated that the OK signal indicated that the aircraft was parked in the correct position but did not provide information about the TOO FAR signal display. The flight crew’s procedures also stated that once the aircraft was chocked, ground staff would manually change the display to CHOCK ON. However, the CHOCK ON message was not available at gate D5. This meant that any communication about the position of the chocks would be verbal.
Ground procedures and actions for use of the VDGS
The ground standard operating procedures (SOP) applicable to gate D5 stated that ground personnel could initiate the emergency stop signal if required. Under those circumstances, once the emergency had been addressed, the ground engineers would marshal the aircraft to complete the parking procedure manually.
As an aircraft approaches the relevant gate, one of the ground crew stands near the VDGS control panel, ready to press the emergency stop button if the need arose. In this occurrence, the VDGS equipment log recorded that, almost immediately after the normal STOP signal was displayed, the emergency stop button was pressed. As a result, the STOP message remained displayed, even though the aircraft started to move again shortly after and collided with the aerobridge about 15 seconds later.
The ground engineers stated that they sometimes pressed the emergency stop button to ensure the STOP message was displayed in good time.
Flight Recorders
Cockpit voice recorder
The aircraft’s cockpit voice recorder[6] continued to record for some time after the aircraft collided with the aerobridge as it remained powered. As a result, the recorder had recorded over the events from the time of the aircraft’s arrival at gate D5, until the collision.
Recorded flight data
The aircraft was equipped with a digital flight data recorder, and a digital aircraft condition monitoring system recorder[7]. Analysis of data from those media showed:
slight movement of the rudder pedals while the aircraft was stopped at the gate
all four engines were running at idle thrust while the aircraft was stopped at the gate
the aircraft was stationary for 4 seconds before commencing forward movement
the forward movement commenced at the same time as the speed brakes were stowed
once the aircraft started to move, there was hardly any further movement on the rudder pedals
all engines were shut down about 5 seconds after the aircraft started to move
about 15 seconds after the aircraft commenced moving, it collided with the aerobridge
at the same time as the aerobridge collision, the wheel brakes were applied.
Flight recorder sampling of the parking brake lever position data occurred once every 64 seconds. At the time the aircraft started to move, the parking brake lever was recorded as being ‘not on’. However, as the occurrence happened between two recorded samples, the actual position of the parking brake lever for the 4 seconds between when the aircraft stopped and commenced movement again, could not be determined.
Additionally, the recorded data indicated that sufficient hydraulic pressure was available to the aircraft wheel brake systems throughout the occurrence.
Selected parameters from the recorded flight data are at appendix A.
Wreckage and impact information
Damage to the aircraft
The left wing inboard leading edge was damaged by the collision with the aerobridge (Figure 4). A landing light cover was also damaged. Before the aircraft was ferried to United’s home base, the leading edge and landing light covers were temporarily repaired. Permanent repairs were carried out in the United States.
Figure 4: Close up of the damage to the left wing inboard leading edge and landing light cover
Source: United
Organisational and management information
Ground handling
Another airline was contracted to provide ground handling services to United at Melbourne Airport. There were three ground engineers awaiting the arrival of the aircraft at gate D5. They included a licenced aircraft maintenance engineer (LAME) and two unlicensed aircraft maintenance engineers. Other ground crew were located outside the aircraft’s designated parking area. Additionally, ground staff were positioned at the entrance and halfway along the aerobridge.
The SOP for ground personnel actions upon arrival of an aircraft contained the following steps (in part):
…
4.When meeting an arriving aircraft the person who is assigned to communicate with the flight
crew on the headset must ensure:
a. The aircraft has stopped and brakes are on before connecting the headset.[[8]]
b. All engines are shut down and no abnormal conditions exist (such as tail pipe fire, wheel
or brake fire etc) before disconnecting from the headset.
c .Chocks are placed just Fwd and Aft of the tires on the nose landing gear once the park
brake has been set.
Place chocks Fwd and Aft of the outboard (or inboard) set of tires of each main landing
gear.
…
The engineers stated that they provided ground handling services for a number of different operators and aircraft types. They stated that some operators were proactive with communicating to the ground crew on arrival while others were not.
The LAME reported that the aircraft came to a stop at the designated parking location. The two aircraft mechanical engineers then moved into a position to place a chock at the rear of the nose wheel.[9] After placing the rear chock, they moved to place the forward chock in position. At that moment, the aircraft started to move forward. The engineers expected the aircraft to stop again quickly, but it did not. They became aware of the aircraft’s engines nearing their positions and abandoned any further attempt to chock the wheels.[10] Instead, they rapidly moved clear of the aircraft.
The LAME also reported that they had not spoken to the flight crew before the aircraft started to move again. The LAME stated they had insufficient time or opportunity[11] to connect ground communications to the aircraft.
Flight crew after landing procedures
According to United’s procedures, the after landing flow can be conducted any time after landing, when time permits. The flight crew indicated that it was usually conducted as soon as the aircraft had exited the runway. The procedures stated that the captain’s first action was to stow the speed brake by moving the speed brake lever to the forward stowed position (see the section titled Additional information).
Recorded flight data indicated that all the after landing flow actions were completed by the crew soon after landing, except for retracting the speed brakes. The speed brakes were retracted by the captain after the aircraft stopped at the gate.
The concept of prospective memory is described as ‘remembering to perform an action that cannot be executed when the intention is formed’ (Dismukes, 2006), and is typified by:
an intention to perform an action at some later time when circumstances permit
a delay between forming and executing the intention, typically filled with activities not directly related to the deferred action
the absence of an explicit prompt indicating that it is time to retrieve the intention from memory.
The crew reported that after landing, their focus was on remaining clear of ground traffic and on specific aircraft parking requirements. This focus on different activities may have distracted the crew from retracting the speed brakes until the aircraft arrived at the gate. The captain’s retraction of the speed brake after arriving at gate D5 was consistent with a lapse in prospective memory.
Flight crew parking procedures
The flight crew parking procedures required that once the aircraft had stopped at its intended parking position, the flight crew were to start the parking flow sequence of actions. In this sequence, the captain conducted 11 actions and the FO conducted nine actions. A notice at the start of the actions stated that:
Ground personnel expect the right engines to be shut down, or ready for immediate shut down, upon arrival at the parking location.
The captain’s first action was to set the parking brake lever. The procedure for setting the parking brake stated:
The parking brake lever is pulled to set the brakes, after both pedals are fully depressed.
The captain stated that when applying the parking brake they feel for the ‘click’ in the parking brake lever, and felt that had occurred in this case. In order to feel a click in the parking brake lever, the parking brake lever would already have to be pulled when the brake pedals were pressed. This would have meant that the engaging pin was in contact with the pawl as the pin was moved by pedal depression. That action may have influenced the likelihood of an incomplete parking brake engagement.
To minimise the likelihood of the parking brake not being engaged, the procedure incorporated the following verification actions:
The captain was to check:
- the parking brake lever position - an EICAS memo message PARK BRAKE SET was displayed - the BRAKE SOURCE light was off - there was no aircraft movement.
The FO’s second action was to verify:
- the parking brake lever position - there was no aircraft movement.
Aside from the status of the BRAKE SOURCE light, which was not mentioned at interview, the crew stated that they conducted all of these actions to verify that the parking brake was set and the aircraft was not moving.
The remaining actions directed both pilots’ attention inside the cockpit. They mostly involved the overhead control panel or the centre console between the pilots’ seats. None related to aircraft movement, brake or chock status. Despite both crew having their attention inside, the captain did notice aircraft movement through peripheral vision and the FO reported that the VDGS STOP indication appeared closer, although any change was insidious. In the event, the captain’s perception of the aircraft’s movement did not occur in sufficient time to prevent the collision.
Additional information
Parking brake and speed brake controls
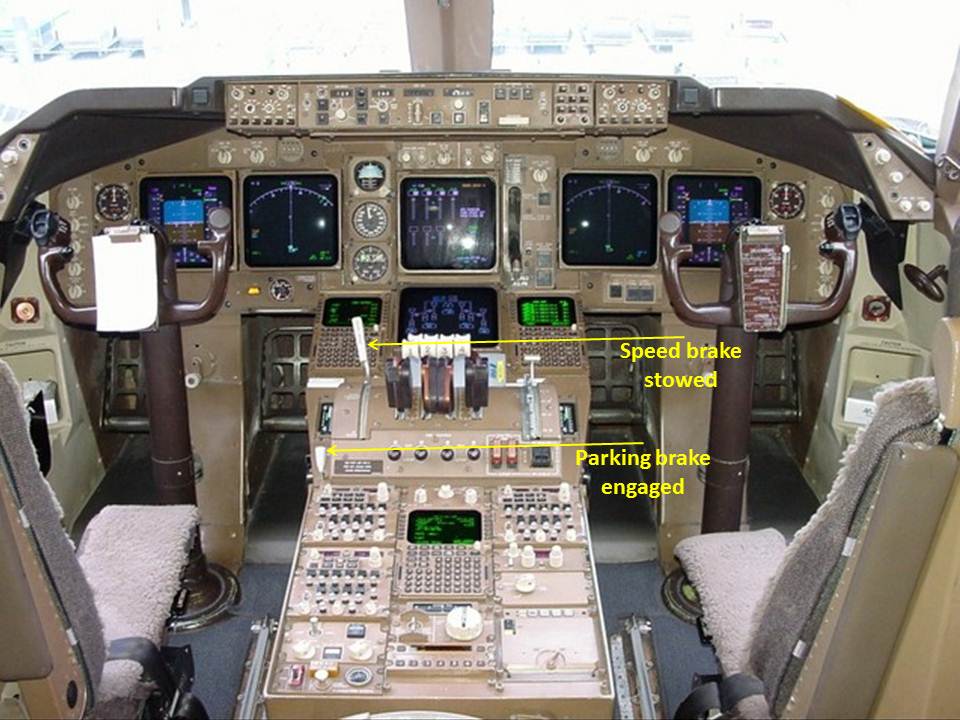
The speed brake lever and the parking brake lever are in the same area of the flight deck, however they are different in size and shape (Figure 5). While the speed brake lever can be moved without any additional action, the parking brake lever only operates in coordination with pressing the brake pedals.
The FO reported paying specific attention to the captain setting the parking brake in Melbourne because of the unintended wheel brake disengagement at Sydney. The FO recalled the parking brake lever remained raised (brake engaged) after the captain removed their hand from the lever.
Figure 5: Cockpit control layout, showing the location of the speed brake and parking brake controls
Source: Boeing, modified by the ATSB
Other occurrences
The aircraft manufacturer reported that it had been notified of an occurrence when a Boeing 747‑400 aircraft started to move after the parking brake had been incompletely engaged. No defect was identified in the aircraft.
A review of the ATSB occurrence database identified seven reported occurrences between 2008 and 2013 in which jet aircraft moved after coming to a stop during parking. Of these:
In one occurrence, the park brake was reportedly set and the aircraft rolled forward on a downslope during engine shutdown. No fault was found with the brake system.
Another occurrence involved a mechanical issue with the park brake, which led to it disengaging.
The remaining five occurrences involved the wheels not being chocked prior to park brake release or having the chocks in the incorrect position.
There were no occurrences relating to inadvertent park brake release.
From the evidence available, the following findings are made with respect to the collision between an aerobridge and a Boeing Company B747-422, registered N119UA, at Melbourne Airport, Victoria on 22 April 2013. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
A likely inadvertent disengagement of the parking brake, prior to the aircraft being chocked and while the engines were operating at idle thrust, allowed the aircraft to recommence moving forward.
While the crew were conducting the parking flow, procedural task requirements drew both flight crew members’ attention inside the flight deck. This, combined with the limited visual cues available, reduced their ability to detect the aircraft’s movement in time to prevent the collision.
Other factors that increased risk
The activation of the Visual Docking Guidance System emergency stop function inhibited display of a 'TOO FAR' message, reducing the cues available to crew and increasing the risk that any aircraft movement would not be detected.
Safety analysis
Introduction
A review of past occurrences showed that undetected movement following inadvertent disengagement of the parking brake is a rare event. In this occurrence, the aircraft started moving 4 seconds after it was stopped at the gate.
The flight crew reported that the parking brake was set after stopping and an inspection of the aircraft’s wheel brake system and a number of functional checks by United Airlines Incorporated found no anomalies or defects with the aircraft’s wheel or parking brake systems to explain the unintended aircraft movement. The application of the wheel brakes by the captain on detecting the movement would have disengaged the park brake. This was consistent with the as-found position of the park brake handle after the aircraft collided with the aerobridge.
This analysis will examine the defences in place to prevent such an occurrence and the human performance factors identified during the investigation as having influenced the flight crew’s actions and ability to detect the aircraft movement.
Parking brake
When parking at an aerobridge, the wheel brakes are applied and locked on with the parking brake system. The parking brake is the primary means of restraint for the aircraft and is regularly used when the engines are operative.
The captain’s parking brake engagement technique was not entirely consistent with the documented procedure. Despite this, the crew’s subsequent verification checks should have identified if the parking brake did not engage properly. The crew reported that the engine indication and crew alerting system indicated that the parking brake had engaged and both crew reported verifying visually that the aircraft was not moving. As such, it is likely the parking brake had engaged correctly.
The reason why the parking brake disengaged could not be determined. However, recorded data showed rudder pedal movement when the aircraft started to move after the parking brake was initially set. A properly-engaged parking brake cannot be released unless force is applied to the brakes at the top of the rudder pedals. However, the recorded flight data does not record brake pedal movement, preventing confirmation of this action from the recorded data.
Sufficient force to disengage the parking brake is more likely to be applied if a crew member has their feet positioned on the top of the rudder pedals. The captain would have had their feet in this position a short time before, in order to apply the parking brake on arrival at the gate.
The speed brakes were lowered at the same time as the aircraft started to move and this action would have put a demand on the hydraulic system. However, recorded data indicated that sufficient hydraulic pressure remained available to operate the wheel brakes. The parking brake system was independent of the hydraulic supply system, therefore changes to hydraulic pressure would not have affected the parking brake engagement.
Reason (1990) stated that ‘a necessary condition for the occurrence of a slip of action is the presence of attentional “capture” associated with either distraction or preoccupation. This means that wherever else the limited attentional resource is being directed at that moment, it will not be focused on the routine task at hand’. Reason outlined that there are two conditions necessary for a slip of action: the performance of some largely automatic task in familiar surroundings, and a marked degree of attentional capture by something other than the job in hand. The concept of ‘automatic’ action refers to the way that certain tasks can be executed without conscious oversight, thereby limiting the use of processing resources.
Stowing the speed brake was not part of the captain’s usual actions after stopping at the gate. However, this out of sequence action may have been sufficiently distracting to result in the captain’s slip of action to unintentionally activate the wheel brake pedals and release of the parking brake. At other times (such as when setting the parking brake), activating the wheel brake pedals would be intentional.
Aircraft movement
Installation of the wheel chocks
Ground staff normally installed the nose wheel chocks once the aircraft stopped and the parking brake was set. They were in the process of placing them in position when the aircraft moved forward, preventing installation of the forward chock.
The only means of communication between the ground and flight crews on the status of the wheel chocks was via hand or other visual signals, or after the ground crew plugged in their headset. The height of the pilots’ seating, and position of the ground crew generally below the aircraft, meant that visual signalling was generally not practicable in the busy/congested tarmac environment because:
one of the ground crew would need to move away from underneath the nose of the aircraft and into one of the pilot’s view
that pilot would need to establish and maintain visual contact with the ground crew member.
The ground crew’s headset could not be plugged into the nose wheel landing gear intercom socket to allow communication with the flight crew until the aircraft stopped and the parking brake was engaged. The movement of the aircraft before the forward chock was in place prevented ground crew from establishing the intercom link with the crew. This lack of communication, and therefore flight crew understanding of the status of the wheel chocks, emphasised the flight crew’s reliance on the parking brake and on comprehending any subsequent aircraft movement should that brake fail or disengage.
If the ground crew had been able to complete the installation of the nose wheel chocks before the aircraft recommenced moving, the chocks may have prevented that movement. Alternately, if the chocks were unable to prevent the aircraft’s movement, the ‘bump’ as the aircraft rolled up or over the forward chock would likely have alerted the flight crew of the movement.
Flight crew focus
After commencing the parking flow actions, the flight crew’s focus was predominantly inside the flight deck. These actions involved shutting down the engines, which at that stage remained at idle but, until shut down:
given the aircraft’s weight, provided sufficient thrust to move the aircraft if unrestrained
prevented ground crew from approaching the main landing gears and installing the associated wheel chocks.
Therefore, although not inherently conducive to looking outside the flight deck, shutting down the engines was a priority task for the flight crew.
The captain first detected movement via peripheral vision when moving their attention from the overhead panel down to the centre console. One of the main functions of peripheral vision is to detect motion (Monaco and Kalb, 2007). This ability depends on the velocity and duration of the movement, the size of the moving object and its location in the peripheral vision.
Consistent with the first officer’s report of the insidious nature of any movement when glancing out of the cockpit and seeing the VDGS, there was no salient visual stimulus when looking forward from the flight deck. The aircraft’s movement was too slow for the terminal wall to appear to move and, as a result of the ground crew activating the emergency stop function on the visual docking guidance system (VDGS), the VDGS displayed the same STOP message as when the crew first stopped the aircraft.
Utility of the VDGS
Activation of the emergency stop button on the VDGS by the ground crew provided a means for the ground crew to instruct the flight crew to stop immediately. This function was only available until the aircraft stopped at its intended parking position.
In this case, the emergency stop button was pressed immediately after the aircraft stopped the first time. As a result, in addition to the ongoing display of the STOP message, display of the TOO FAR message in the case of the aircraft recommencing moving was inhibited. This meant that, although the first officer reported periodically glancing outside the flight deck and seeing the VDGS, its display would not have assisted the crew identify any aircraft movement.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 21 July 2011, at 1630 Central Standard Time, the crew of a Super Puma helicopter, registered VH-LAG (LAG), was taxiing in the vicinity of two parked aircraft on the apron at Port Keats Airport, Northern Territory when the main rotor blades contacted a light pole. As the main rotor disintegrated, the helicopter was propelled towards the pole and rolled onto its left side. The aircraft was seriously damaged including significant disruption to the cockpit area.
The two crew members and three of the four passengers sustained minor injuries. Three bystanders also sustained minor injuries and one of the parked aircraft and four parked vehicles were damaged by flying debris.
As a result of this accident, the helicopter operator conducted an internal investigation that produced a number of recommendations addressing operations to remote airfields, obstacle separation standards and emergency management.
On 29 May 2006, an Australian registered and operated Boeing Co. 747-400 was taxiing at New York, John F Kennedy (JFK) Airport. During the aircraft's final turn into its allocated parking bay, the right wingtip contacted a blast fence, resulting in damage to the outboard end of the right wing. An investigation was conducted by the US Federal Aviation Administration in conjunction with the US National Transportation Safety Board and the Australian Transport Safety Bureau.