Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
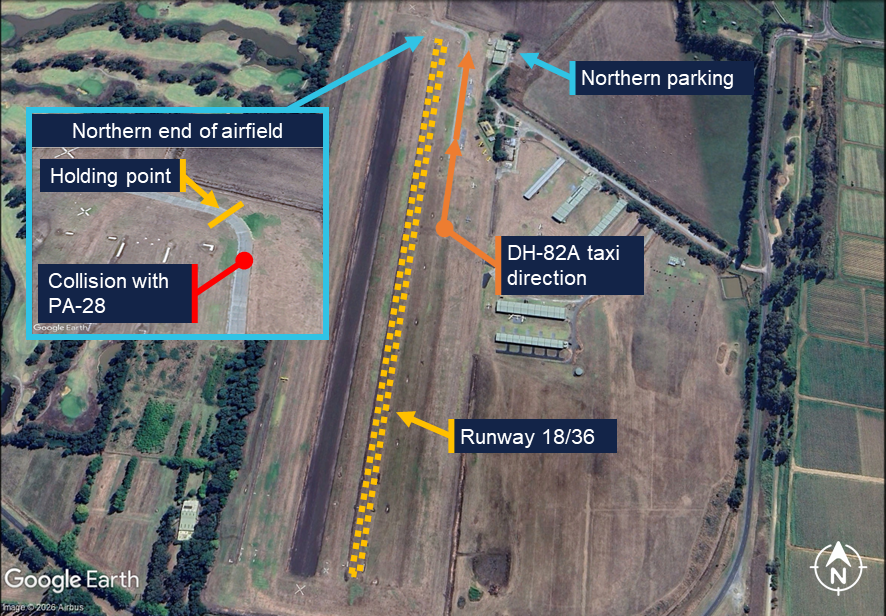
On 27 December 2025 at approximately 1015 local time, an instructor and student operating a Piper PA-28 were preparing to depart Lilydale Aircraft Landing Area (ALA), Victoria, for circuit training. After completing the pre-take-off and run-up[1] checks, the crew taxied to the holding point of runway 18 behind another aircraft. The instructor reported sighting a de Havilland DH-82A Tiger Moth taxiing from the southern end of the airfield.
The DH-82A, having returned from a joy flight with a pilot and passenger on board, exited runway 18 at approximately midfield and began to taxi back to parking at the northern end of the airfield (Figure 1).
Figure 1: Lilydale ALA
Source: Google Earth, annotated by the ATSB with information from operator
The pilot of the DH-82A reported that they did not observe the PA-28 during the taxi, with the nose-high characteristic of tailwheel aircraft likely limiting forward visibility. As the preceding aircraft entered the runway and began its take-off roll, the PA-28 crew were preparing to move forward to the holding point when the DH-82A’s left wing section collided with the rear of the PA-28. The impact resulted in damage to the PA-28’s right elevator trim tab, tail cone and beacon light (Figure 2).
Figure 2: Piper PA-28 damage
Source: Operator, annotated by the ATSB
The damage to the DH-82A was limited to the upper and lower wings (Figure 3). No injuries were sustained by the occupants of either aircraft.
Figure 3: de Havilland DH-82A damage
Source: Operator, annotated by the ATSB
Safety message
Maintaining situational awareness is crucial to ensure safe separation while operating in the vicinity of other aircraft and obstacles. When manoeuvring on the ground it is important that pilots maintain an effective lookout and communicate with other traffic when necessary. These risk controls help mitigate the risk of a taxi collision if a pilot is unsure of the surrounding hazards at any point. This is particularly applicable to pilots operating tailwheel aircraft due to their inherent nose-high attitude which limits forward visibility.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Run-up: a high‑power run-up check is carried out in a piston-engine aircraft to check the aircraft’s ignition and other systems before commencing an initial take‑off.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2026-003
Occurrence date
27/12/2025
Location
Lilydale Aircraft Landing Area
State
Victoria
Occurrence class
Serious Incident
Aviation occurrence category
Taxiing collision/near collision
Highest injury level
None
Brief release date
10/02/2026
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-28-151
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Damage
Minor
Aircraft details
Manufacturer
de Havilland Aircraft
Model
DH-82A
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 21 July 2025, at approximately 1000 Eastern Standard Time, a Cessna 152, with an instructor and student on board, taxied for circuit training operations on runway 35R at Moorabbin Airport, Victoria. While stationary at holding point A, a privately-operated Piper PA-32R-300 taxied into position behind the Cessna 152, awaiting departure for a flight to Broken Hill, New South Wales. After a brief pause, the PA-32R began rolling forward until the propeller contacted the 152’s tail structure. The collision resulted in minor damage to the PA-32R’s propeller and substantial damage to the 152’s tailplane structures, including the rudder, vertical stabiliser and right elevator (Figure 1). With the force from the propeller contact, debris was also spread along the taxiway. Neither of the 152 crew nor the PA-32R pilot sustained any injuries.
The PA-32R pilot reported that immediately prior to the collision, they had been conducting preparatory navigation-related tasks inside the cockpit and had not held sufficient pressure on the aircraft brakes to prevent the aircraft from moving. With their attention inside the cockpit, they had not realised the aircraft had begun to slowly move forward until the collision occurred.
Figure 1: Post‑incident damage to the Cessna 152
Source: Aerodrome operator
Safety message
This incident highlights the importance of pilots maintaining vigilance and situational awareness throughout all phases of flight – including ground operations and taxiing. While manoeuvring in proximity to other aircraft or obstacles, attention must remain outside the aircraft, with ancillary activities such as navigational preparation limited to periods where inadvertent aircraft movement would not create a collision risk.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
On 23 August 2024, a Bombardier Dash 8-300 was being operated as a ferry flight, departing Perth Airport, Western Australia to Onslow Airport before refuelling and continuing on to Minderoo aircraft landing area (ALA). On board was a captain, first officer and 2 cabin crew. The aircraft was then operated as a non-scheduled air transport passenger flight on the return leg from Minderoo ALA to Perth Airport.
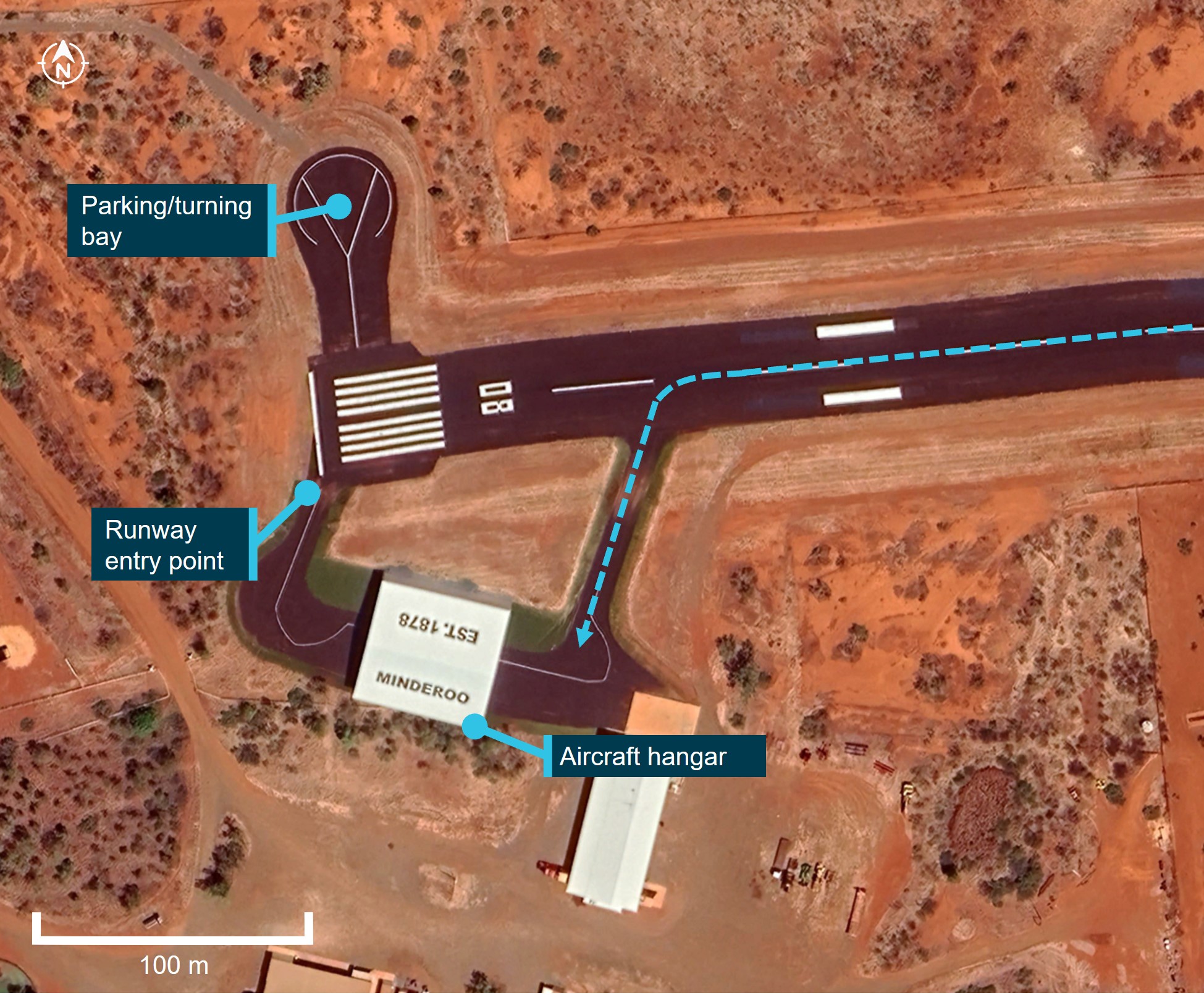
The aircraft departed Onslow at approximately 1402 local time for the 17-minute flight to Minderoo ALA. On approach to Minderoo, the captain made contact with another aircraft which was positioned on the taxiway near the threshold of runway 08, awaiting departure. The crew of this second aircraft instructed the captain to taxi into an open-ended hangar after landing to allow their aircraft to depart on runway 08, as the only other parking bay was occupied by a helicopter. The first officer, who was pilot flying, landed the aircraft on runway 26 and vacated at the first taxiway into a large hangar located on the south side of the runway (Figure 1).
At approximately 1446, the crew completed boarding of 24 passengers for the return leg to Perth inside the hangar. The captain assumed the role of pilot flying, started the engines and began to taxi following the taxi guideline markings[1] painted on the ground through the hangar.
During taxi, both pilots felt a slight drop, which they believed was the right main wheel moving off the taxiway onto the grass. The cabin crew member at the rear of the cabin thought the wing tip may have contacted the hangar as the jolt was greater in the rear of the aircraft. They inspected the wings out of the windows and noted nothing out of the ordinary. The captain continued to taxi towards the entry point of runway 08.
After entering and backtracking on runway 26, the crew aligned the aircraft for departure and final pre-take-off checks. At this time, the captain received a phone call from the operator’s head of flying operations who informed them that a witness reported that the aircraft may have made contact with the hangar during the initial taxi.
The crew shut down the aircraft on the runway and conducted an inspection. The inspection revealed damage to the aircraft’s left elevator (Figure 2). There were no reported injuries, the passengers were disembarked, and the aircraft was moved to the parking bay.
Following the event, the operator commenced an investigation into the occurrence using a third‑party investigator. The hangar was inspected, and no damage was identified (Figure 3).
Since the completion of the independent investigation on the occurrence, the operator has taken the following safety action:
A formal risk assessment for each new port is conducted prior to any operation being conducted regardless of the length of contract. This risk assessment also applies to ad hoc charters.
A risk assessment classification has been included into the aerodromes and routes procedure.
Charter briefs have been updated to include a triple signature sign‑off process to ensure that the head of flying operations (HOFO), head of safety and quality, and operations team lead have conducted all required risk assessments and briefs prior to the flights taking place.
Human factors training has been updated to include new materials related to this accident. This includes a requirement for all flight crew to undertake this training on initial employment and every 2 years thereafter.
The head of safety and quality has conducted a review of the risk assessment and change management process to ensure it is fit for purpose.
Safety message
The ATSB reminds pilots to exercise caution when operating near hangars and avoid taxiing aircraft directly inside. Hangars are confined spaces with limited clearances, increasing the risk of collisions with walls, equipment, or other aircraft. Visibility from the cockpit is often restricted, making it difficult for pilots to accurately judge distances or detect hazards. These factors significantly increase the likelihood of damage to the aircraft or surrounding structures.
To ensure safety, pilots should either stop the aircraft outside the hangar and allow trained ground personnel to tow or manually manoeuvre it into position or organise for a wing walker or marshal to be available during the taxi. This practice provides greater precision and reduces the potential for accidents. In this case, the use of a tug to tow the aircraft through the hanger or the use of a wing walker or marshal would have alleviated these risks.
Operators are also reminded that, even if they have previously used an ALA before, it is important to obtain all relevant information about the ALA prior to flight. ALAs located in remote or rural locations may vary significantly in their condition, dimensions, and available facilities. Operators should ensure they have up-to-date details about the runway surface, obstacles and likely restrictions within the ALA. Additionally, knowledge of available ground support equipment, parking, and turning areas is important for safe operations. Thorough pre-flight planning and communication with the airstrip operator or local contacts can help identify potential hazards and ensure that the aircraft and operation are suitable for the destination.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]A taxi guideline marking consists of a single conspicuous yellow or white line delineating a path for the aircraft to follow.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-004
Occurrence date
23/08/2024
Location
Minderoo Aircraft Landing Area, Western Australia
State
Western Australia
Occurrence class
Accident
Aviation occurrence category
Taxiing collision/near collision
Highest injury level
None
Brief release date
11/02/2025
Aircraft details
Manufacturer
Bombardier Inc
Model
DHC-8-315
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
On 4 November 2024, a Pilatus Aircraft PC-12/47E, registered VH-FXJ, and operated by the Royal Flying Doctor Service as Flydoc 543, taxied for departure at Adelaide Airport to conduct a medical transport flight to Pinnaroo Airport, South Australia. On board were a pilot and a flight nurse.
During taxi, after being incorrectly cleared to enter a NOTAMed closed section of taxiway, the pilot did not question the clearance, and the aircraft entered the taxiway and struck an unserviceability light used to identify the closed section. The pilot then continued with the departure.
There was no damage to the aircraft and no injuries as a result of this incident.
What the ATSB found
The ATSB found that, although both the air traffic controller and pilot were aware that the taxiway was closed, the aircraft was cleared and entered the area and consequently struck the light. Additionally, while there were indications via radio transmissions that an unserviceability light had been damaged, the pilot incorrectly assessed that the aircraft had not struck it and continued the flight without an inspection.
The ATSB also found that the lighting used to identify the entrance to the closed taxiway was insufficient to draw the pilot’s attention and the markers, required by the method of working plan, had not been used. In addition, the method of working plan, while stating that the closed area needed to be defined in accordance with the Civil Aviation Safety Regulations (CASR) Part 139 (Aerodromes) Manual of Standards 2019 (MOS), did not specify how many lights were required to denote the closed area.
In addition, the ATSB identified The Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019 section relating to the temporary closure of a taxiway at night did not:
provide a recommendation that when operating on an aerodrome with significant obscuring background lighting, consideration be given to increasing the span of unserviceability lights, similar to the recommendation provided for markers to cross the entire closed area
specify that both markers and unserviceability lights were required.
What has been done as a result
CASA is currently writing Advisory Circular (AC) 139.C-15 v1.0 - Safe planning and conduct for aerodrome works and has undertaken to include guidance on the use of both unserviceability cones and lights to designate closed taxiways at night. That guidance will include consideration of the detrimental effect background lighting can have on identifying closed infrastructure.
As a result of this incident, Airservices Australia released a standardised directive to Adelaide Tower air traffic controllers to clarify the occurrence management and reporting requirements following this incident. Operational command authority escalation was added to the Airservices focus area questions for initial and renewal assessments completed in October 2024.
Safety message
This incident highlights the importance of effective communication and potential for expectation bias. If flight crews receive a clearance that contradicts a NOTAM or current ATIS information, they should question the clearance before continuing.
Additionally, although the CASR Part 139 MOS did not specify a minimum number of lights to identify closed ground movement areas, it did state they should be identified as clearly as possible. When considering the adequacy of unserviceability lighting, operators should consider any obscuring background lighting and consider increasing the span of lighting if required.
Finally, if there is a possibility that an object has been struck by an aircraft, it should be checked for damage before continued flight.
The occurrence
On 4 November 2024, a Pilatus Aircraft PC-12/47E, registered VH-FXJ and operated by the Royal Flying Doctor Service as Flydoc 543, taxied for departure at Adelaide Airport to conduct a medical transport flight to Pinnaroo Airport, South Australia. On board the aircraft were a pilot and a flight nurse.
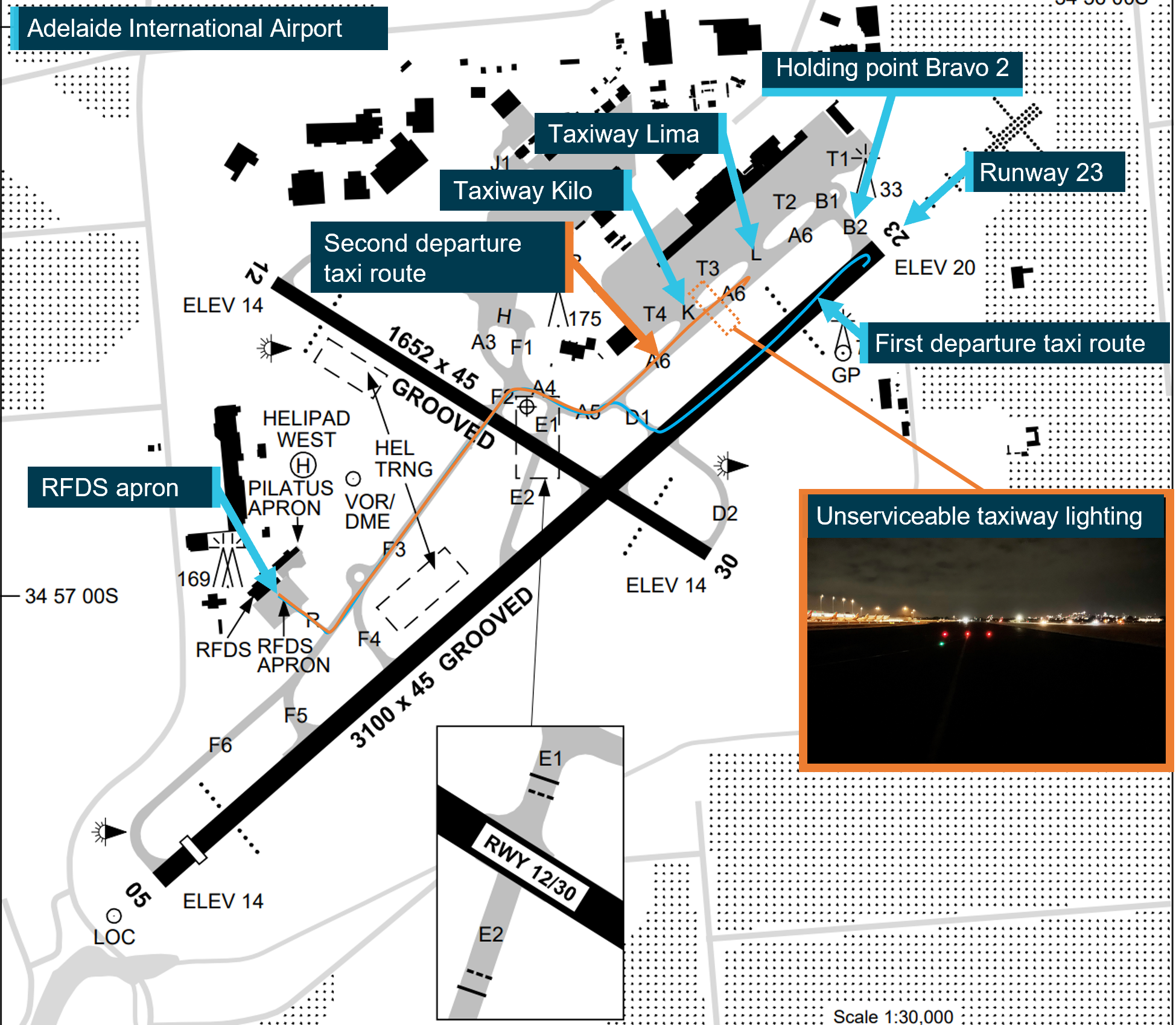
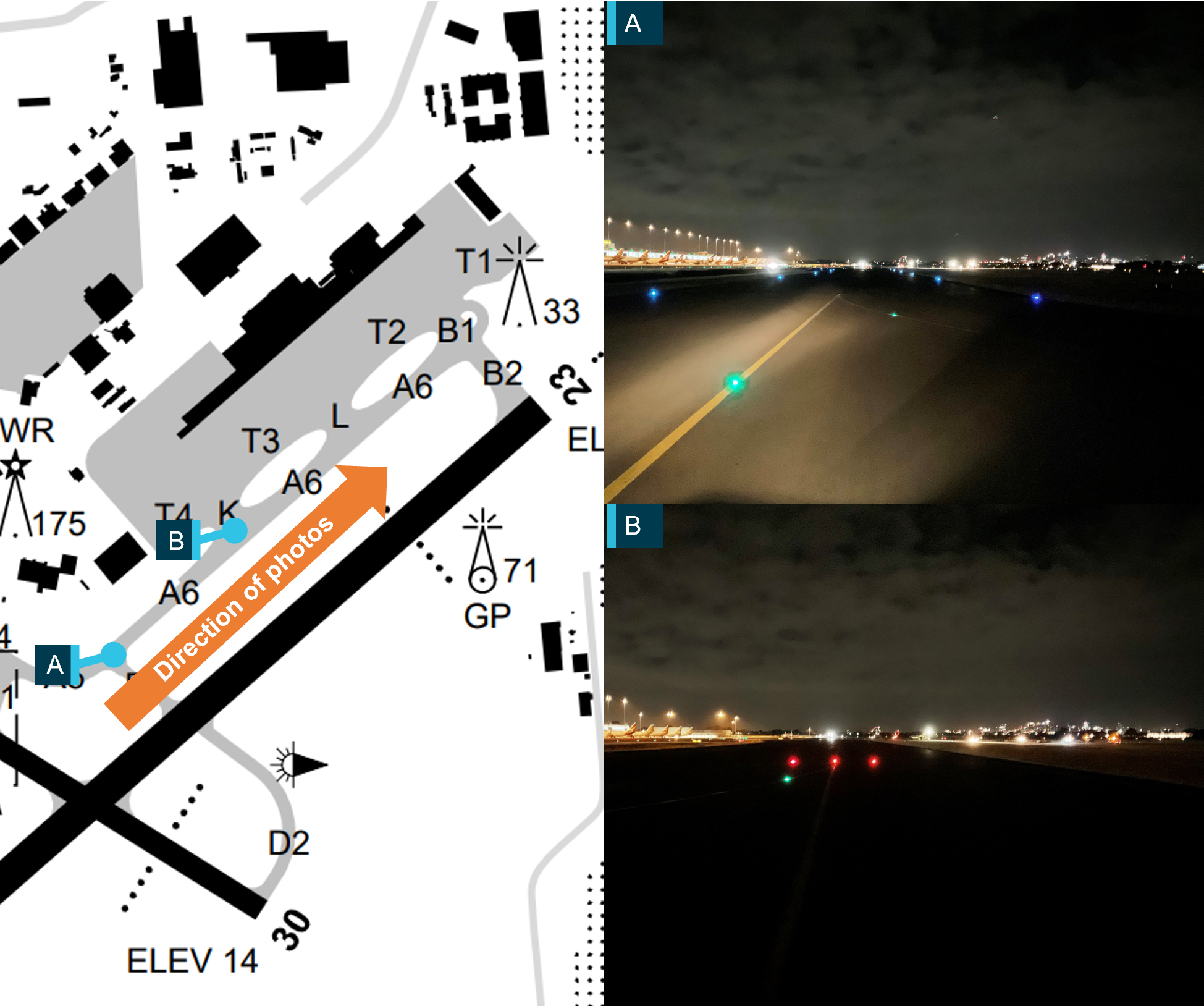
At the time of departure there was an active NOTAM[1] for multiple taxiway closures, including an area on taxiway A6 between taxiway K and holding point B2, due to work in progress on the grass beside the taxiway (Figure 1). The same information was broadcast on the Adelaide ATIS.[2] The closed section of taxiway was marked as unserviceable by 3 red lights across the taxiway at multiple entrances to the taxiway. The pilot reported being aware of the taxiway closures.
This was the pilot’s second flight from Adelaide during their duty period that night. On the first flight, the pilot had received the expected taxi clearance from the Adelaide ground air traffic service operator (controller) to taxi via taxiway D1, before entering and backtracking runway 23.[3] This taxi clearance avoided the unserviceable areas of the taxiway.
Figure 1: Adelaide Airport
The image shows both taxi routes taken by Flydoc 543 and the position of the unserviceable taxiway lights. The blue line is the taxi route for the first flight, the orange line is the taxi route for the incident flight. The view of the unserviceable taxiway lights was taken on 14 November 2024. It is an exemplar image of the lights on the night the incident took place. Source: Airservices Australia, Adelaide Airport, and Flightradar24; annotated by the ATSB
At 0309, the pilot taxied for departure on the incident flight. They expected to receive the same taxi clearance for the planned departure on runway 23. However, the clearance received was:
Flydoc 543 on Foxtrot cross runway 12 taxi holding point Bravo 2 runway 23.
This clearance required the aircraft to taxi through the unserviceable area. The pilot did not question the clearance, assuming that the works had ended early.
The pilot later reported that they did not detect the red lights across the taxiway. As they entered the closed section, unknown to the pilot, the aircraft most likely struck the centre unserviceability light. Shortly after, the controller advised the pilot they had entered the closed taxiway and requested they stop and conduct a 180° turn:
…Flydoc 543 that taxiway’s closed, apologies, can you do a 180 there?
A works safety officer, in a nearby aerodrome safety car, offered to remove the red lights on the taxiway before the aircraft taxied back through them. When they entered the taxiway, they detected debris and advised the controller via the ground radio frequency that this would need to be removed:
Adelaide Ground, Works 60, there is debris on taxiway, sorry taxiway Alpha 6 from the red light, I just need a moment to pick that up…
advising a short time later:
Adelaide Ground, Works 60, the debris has been picked up as well as the red lights on Alpha 6.
The controller then asked the pilot if they wished to continue and, after confirming with the flight nurse that they had not felt anything, the pilot advised the controller that they would continue with the departure.
After the operator was advised of the incident the aircraft was grounded, pending an inspection. The post-incident inspection found no damage to the aircraft associated with striking the taxiway light. There were no injuries.
Context
Aircraft information
VH-FXJ was a Pilatus Aircraft PC-12/47E which was manufactured in 2015 and issued serial number 1541. On 10 August 2015, it was registered in Australia with the operator. It was powered by a Pratt & Whitney PT6A-67P turbine engine driving a four-bladed, variable-pitch Hartzell propeller.
Pilot information
The pilot held a commercial pilot licence (aeroplane), an instrument rating and a class 1 aviation medical certificate. They had about 6,375 hours of flight experience at the time of the incident. A total of 1,650 hours had been accrued in PC‑12 aircraft, of which 128 were in the previous 90 days.
The pilot later reported that, at the time of the occurrence, they were fully alert and wide awake. They had been on duty for 5 hours when the incident occurred and awake for approximately 6 hours. In the previous 48 hours, the pilot had received 18 hours of sleep.
They also stated that if they thought they had hit something, they would have returned to the apron to have the aircraft checked by maintenance personnel.
Adelaide Airport
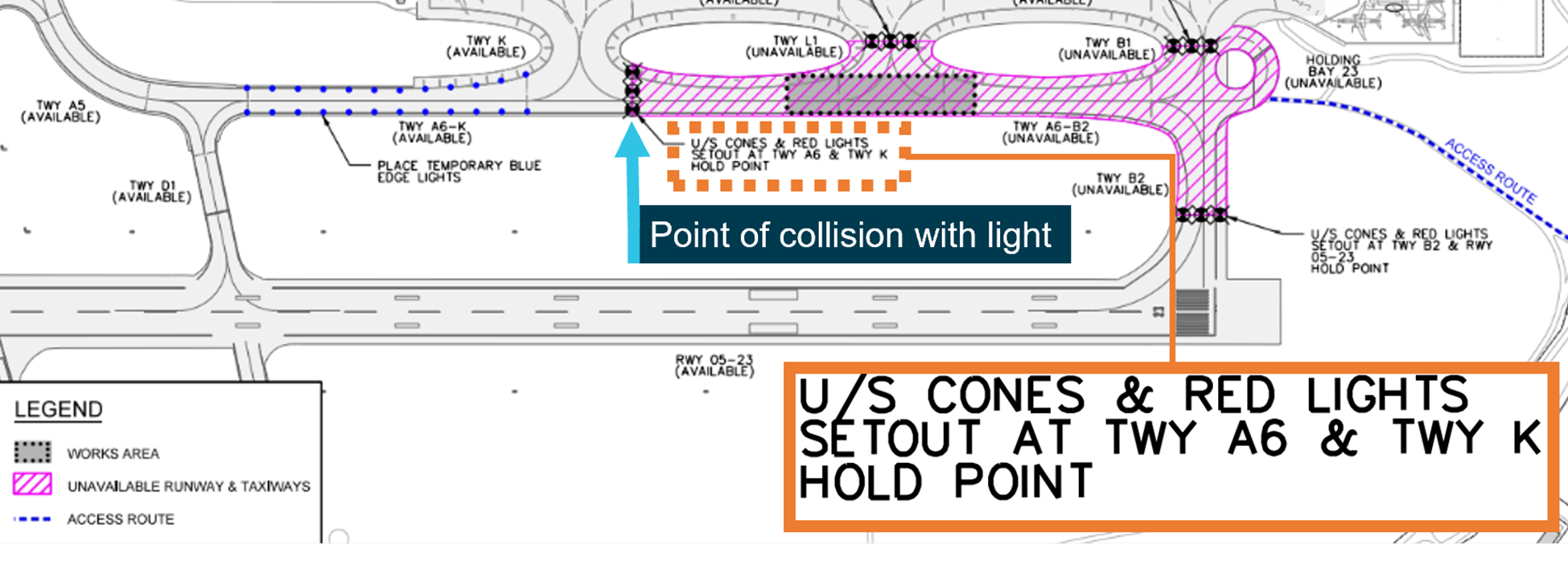
At the time of the incident, NOTAM C0661 was active at Adelaide Airport. It stated, from 3–9 November, between 2300 and 0600 local time, taxiway A6 north of taxiway K, taxiway B1, taxiway B2, taxiway L, and holding bay 23 were closed due to work in progress (Figure 2). This meant that an aircraft departing from runway 23, was required to enter the runway at taxiway D1 and backtrack on the runway to the threshold.
Figure 2: Method of working plan
Source: Adelaide Airport, annotated by the ATSB
The NOTAM was accompanied by information on the ATIS that was broadcast from 0218 and valid at the time of departure. The ATIS stated that runway 23 was in use and taxiways B1, B2, L, A6 north of K, and the 23 holding bay were not available due to works.
The ATIS also stated the wind was from 200 degrees at 8 kt, visibility was greater than 10 km, temperature 16°C, and cloud cover was few[4] at 4,000 ft.
The method of working plan stated that the closed areas ‘will be defined by works limit markers in accordance with Civil Aviation Safety Authority Part 139 (Aerodromes) Manual of Standards’. The method of working plan required that both cones and lights were used and showed on a diagram where the works limit markers needed to be placed (Figure 2). However, it did not provide guidance regarding how many markers or lights should be used to identify the area.
Parts of the aircraft movement area that are unserviceable as a result of the works being carried out will be defined by unserviceability cones and red lights. These will be positioned as described below:
• Taxiway A6 – on the hold point to Taxiway K…
Adelaide Airport later advised the ATSB that 3 lights placed across the entrance to the taxiway, at 3 m intervals, was its standard practice. Additionally, the ATSB was informed that on the night of the incident the unserviceability cones, required by the method of working plan, had not been put in place, and this was its general practice for night works.
Taxiway A6 was approximately 35 m in width. The lights used were steady red lights and were designed to break into fragments when struck, minimising damage to aircraft.
Taxiway A also normally had green centreline taxi lights. While not outlined as a safety measure in the method of working plan, at the time of the incident, the green centreline taxi lights were extinguished in the closed section, to assist in identifying this area.
Air traffic control
The controller
The controller had been employed by Airservices Australia since 2005 and held the required ratings to provide air traffic services at Adelaide Airport. They held operational command authority (OCA), which designated them as the final decision-making authority within the tower when a tower supervisor was not available. They reported having previously completed night shifts as the only controller. In addition, they advised that there was a period of no aircraft movements prior to the pilot requesting taxi clearance, and during this period, they were completing company computer‑based training and felt alert and awake.
The controller also stated that, unless there was an emergency, the use of the runway for aircraft backtracking should be limited. They also stated that the operator required that their aircraft use the full runway length for departures. This meant, under normal circumstances, when runway 23 was in use, a taxi clearance would include taxi on A6 to holding point B2.
Further, the controller advised that there was no actual work being done to the taxiway, it was closed to provide clearance for the workers working on the grass adjacent to the taxiway. They stated that they did not think there would be anything on the taxiway that could damage the aircraft.
Airservices also advised that the controller had completed the following:
assessment of renewal for its Adelaide tower endorsements – completed September 2024
examination requirements for renewal of Adelaide tower endorsements – completed October 2024.
Airservices had identified OCA refresher training to be included in the financial year 2024/2025 mandatory training plan. However, at the time of the incident, the controller had not completed this training.
Airport communication facilities
Adelaide Airport’s control tower was operating at the time of the incident and was occupied by a single controller. Due to the low level of activity, the controller was operating as Adelaide Delivery (providing airway clearances), Adelaide Ground (providing surface movement and control), and Adelaide Tower (aerodrome controller). Although the positions operated on different frequencies, while the tower was occupied by a single controller, all communications were re-transmitted across all 3 frequencies.
Control tower systems
The integrated tower automation suite (INTAS) was in use by controllers at Adelaide Airport. The INTAS was capable of selecting a runway as closed. When activated, the INTAS workstation would highlight this on the status bar for the runway label, which changed the runway designator from grey (normal) to red. Additionally, an alert was also generated based on the runway status.
In the context of this occurrence, INTAS did not facilitate marking a taxiway as unserviceable or provide an alert if an aircraft was cleared onto an unserviceable taxiway.
The controller reported they were aware of the airport taxiway closures. As they had no available tools to mark a taxiway or region as restricted or closed, they had created a custom text box on their display to help remind them of the closure. The text box did not provide any visual change to the closed taxiway or provide an alert if an aircraft was cleared into the area.
Post-incident procedures
Regarding required action following an occurrence, the NAAM stated:
5.1.1.5 Relief from operational duty
Whenever practicable, relieve the ATSO[5] from operational duty following any potential ATS occurrence for which there may be an ATS attribution.
5.1.1.6 Risk assess continued operation
If the ATSO cannot be relieved from operational duty following a potential ATS occurrence, conduct a risk assessment to determine if the affected ATSO can continue operational duties.
If there is any degree of, or doubt about, ATS attribution and the ATSO will continue duty, record the outcome of the risk assessment in the ATS Risk Assessment and Management Record…
Post-incident actions
After the incident, the controller remained on duty and submitted an internal report and logged the incident in the tower’s physical logbook. The controller advised the ATSB that they were unaware that a risk assessment was required to be completed following an incident or that they were required to contact the Air Traffic Management Director, based in Melbourne.
At approximately 1030, after their scheduled shift was completed, the controller contacted the on-duty tower supervisor to ensure they were aware of the incident. They were then informed that their air traffic services approval had been temporarily withdrawn.
Airservices Australia later reported that if a risk assessment had been completed as soon as practicable after the incident occurred, the controller would probably have been found suitable to continue operation:
the risk assessment outcome would have likely resulted in the controller involved in the incident being able to remain on console with additional controls until the next scheduled controller arrived at 0530, had it been completed at the time.
The risk assessment controls likely would have focused on the following:
welfare checks to ensure fatigue management
assessment of the pending scheduled traffic.
Recorded data
Images
Several days after the incident, Adelaide Airport provided photographs of the unserviceability lights on taxiway A6, taken in similar conditions to those at the time of the incident. The images identified that the red unserviceability lights were difficult to see while on the southern end of taxiway A6 due to bright works lights beyond the unserviceable area (Figure 3). However they became more noticeable as the aircraft approached the closed area.
Figure 3: Approaching unserviceability lights
Image shown is an exemplar of the lighting on the night of the incident. The photo shown was taken several days after the incident occurred. Source: Adelaide Airport, annotated by the ATSB
Video imagery
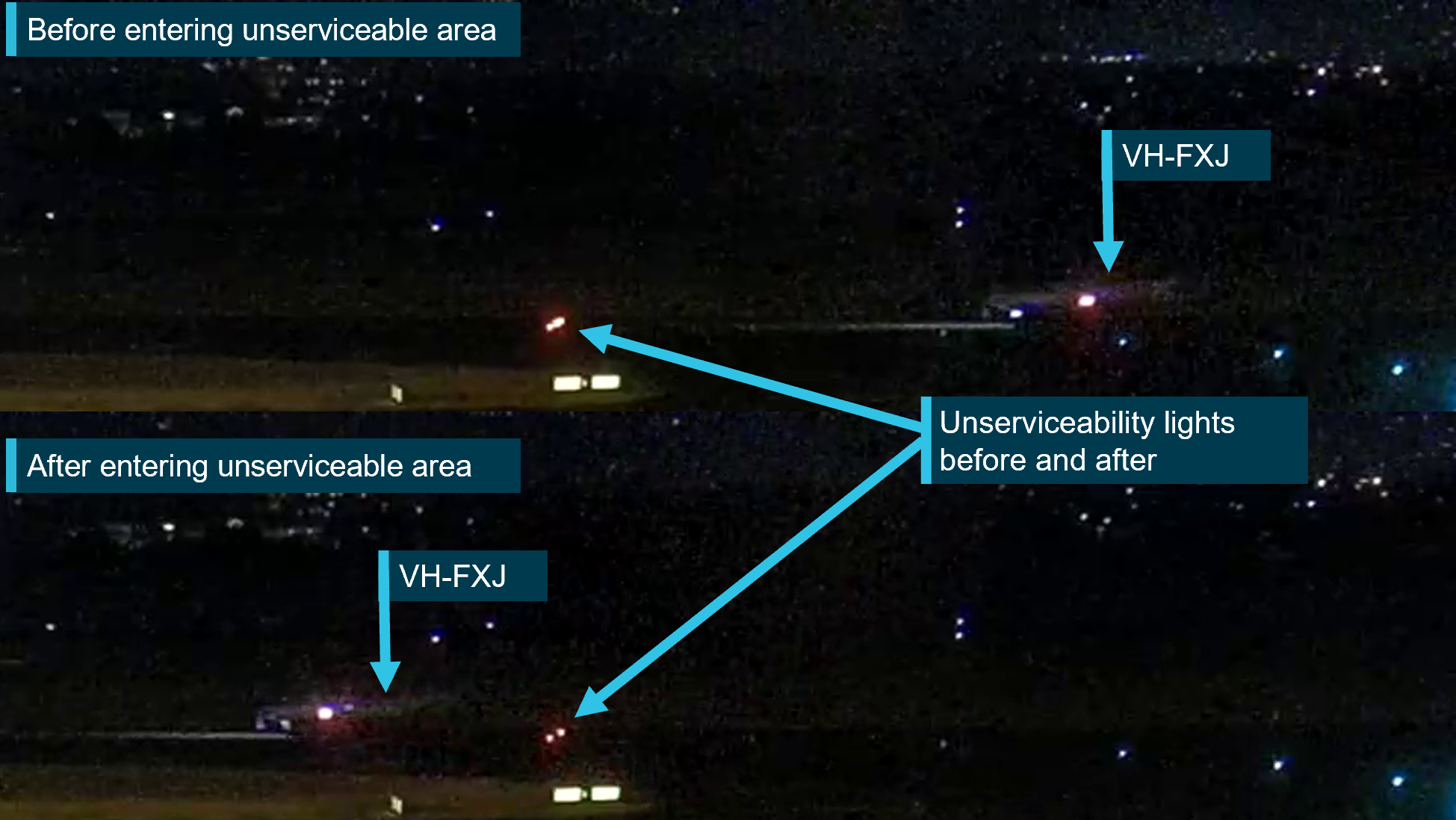
Adelaide Airport also provided the ATSB with video footage of the incident. This showed the unserviceability lighting before and after the aircraft entered the area (Figure 4). It also showed that after completing a 180° turn and coming to a stop facing the 2 remaining red unserviceability lights, the aircraft remained stationary for approximately 4 minutes while ground personnel cleared the remaining lights and debris.
Figure 4: A6 unserviceability lighting before and after the occurrence
Source: Adelaide Airport, annotated by ATSB
Regulatory requirements
Unserviceability lights and markers
The Civil Aviation Safety Regulations (CASR) Part 139 (Aerodromes) Manual of Standards 2019 (MOS) Chapter 8 - Visual aids provided by aerodrome markings, markers, signals, signs, wind direction indicators etc stated:[6]
Division 2 - Markers
8.06 Introduction
(1) A marker must be lightweight and frangible…
8.108 Use of unserviceability markers…
(1) Unserviceability markers must consist of a white standard cone:
(a) with a horizontal red stripe 25 cm wide around its centre halfway up the cone so as to provide 3 bands of colour, namely, white-red-white
(2) Unserviceability markers must be placed at the entrance to, and across, any part of the movement area of an aerodrome (including a runway) that is not to be used by aircraft.
(3) At least 3 unserviceability markers must be displayed across the centreline of any portion of a taxiway, apron or holding bay that is unserviceable, whether or not it is possible for aircraft to safely taxi past the area that is unserviceable.
Note: CASA recommends that additional unserviceability markers be displayed, 3 m apart, continuously across the entire width of the runway, taxiway, apron or holding bay.
Regarding unserviceability lighting, Chapter 9 - Visual aids provided by aerodrome lighting Division 14 Works and unserviceable area lighting stated:
9.127 Lighting associated with closed and unserviceable areas
(1) If a runway or taxiway, or a portion of a runway or taxiway, is closed (a closed facility), all aerodrome lighting on the closed facility, and any visual aids leading a pilot into the closed facility, must be extinguished or obscured except the lighting for visual aids used to warn pilots of the closed facility.
(3) For a partial or complete closure of a manoeuvring area for less than 5 days, the aerodrome lights for the closed area must be:
(a) obscured with an opaque cover ….
(b) if not so obscured — electrically isolated or disabled to prevent their inadvertent activation.
9.131 Movement area access in the vicinity of unserviceable areas
(1) If a closed runway or taxiway, or a portion of a closed runway or taxiway (the closed area) is intersected by a runway or taxiway which is used at night, unserviceability lights must be placed across the entrance to the closed area at intervals not exceeding 3 m.
9.132 Characteristics of unserviceability lights
Unserviceability lights must:
(a) be steady red lights; and
(b) have:
(i) an intensity that is sufficient to ensure conspicuity considering the intensity of the adjacent lights and the general level of illumination against which they would normally be viewed; and
(ii) an average output of red main beam light not less than 10 cd.
CASA also later advised that markers and lights should be used at night to delineate an unserviceable area:
… the Part 139 MOS does not state that markers are only required during the day, therefore they are required at all times.
CASA also published Advisory Circular 139.C-09v1.0 - Visual Aids, Markings, Signals and Signs, which did not provide any further clarification for how to identify a temporary unserviceable taxiway. This AC advised that ‘Visual aids required for the management of works on the aerodrome are outside the scope of this AC and are addressed in AC 139.C-15 Safe planning and conduct of aerodrome works however, at the time of writing, AC 139.C-15 had not been published.
The International Civil Aviation Organization (ICAO) - Annex 14 Aerodromes section 7.1 Closed runways and taxiways or parts thereof subsection 7.1.1 provided the minimum standard for identifying a temporary closed taxiway, which stated that:
‘a closed marking shall be displayed on a runway or taxiway or portion thereof which is permanently closed to the use of all aircraft.’
7.1.3 stated that
‘…on a taxiway a closed marking shall be placed at least at each end of the taxiway or portion thereof closed.’
Note 1. — When an area is temporarily closed, frangible barriers or markings utilizing materials other than paint or other suitable means may be used to identify the closed area.
Annex 14 did not provide a definition of a frangible barrier.
In addition, 7.1.7 stated that:
In addition to closed markings, when the runway or taxiway or portion thereof closed is intercepted by a usable runway or taxiway which is used at night, unserviceability lights shall be placed across the entrance to the closed area at intervals not exceeding 3 m…
In section 7.4 Unserviceable areas subsection 7.4.1 stated
Unserviceability markers shall be displayed wherever any portion of a taxiway, apron or holding bay is unfit for the movement of aircraft but it is still possible for aircraft to bypass the area safely. On a movement area used at night, unserviceability lights shall be used.
Note 1.— Unserviceability markers and lights are used for such purposes as warning pilots of a hole in a taxiway or apron pavement or outlining a portion of pavement, such as on an apron, that is under repair. They are not suitable for use when a portion of a runway becomes unserviceable, nor on a taxiway when a major portion of the width becomes unserviceable. In such instances, the runway or taxiway is normally closed.
Safety analysis
Introduction
On the night of the incident, Adelaide Airport had temporary taxiway closures in place. These closures were broadcast on the ATIS and published in the Adelaide Airport NOTAMs. Although, both the pilot and the controller were aware of the temporary closures, the aircraft was cleared to and entered a temporary unserviceable area and collided with an unserviceability light, before proceeding to take-off.
Clearance to enter taxiway
Although, the occurrence time was early in the morning, the controller reported feeling alert. They were experienced in working as the sole controller in the tower and remained active by completing company computer-based training.
As the operator’s aircraft were required to use the full runway length for departure, it is likely that the controller gave the commonly-used taxi clearance, while momentarily forgetting about the taxiway closures. Furthermore, while the controller had created a custom text box on their display to help remind them of the closure, it was ineffective and there was no built-in alerting system if an aircraft was cleared onto the closed taxiway.
Contributing factor
The controller issued a clearance for the aircraft to taxi through a temporarily closed movement area.
Aircraft entered closed taxiway
The pilot was aware of the taxiway closures and planned their taxi route to avoid them. However, as they assumed the clearance indicated the works were no longer active, they did not question the clearance.
The pilot reported they did not see the red unserviceability lights before entering the closed section of taxiway and the aircraft struck one of the temporary lights.
Contributing factor
On receipt of a clearance that required taxiing through a known temporarily closed area, the pilot did not question the clearance as they assumed the works had ceased. Additionally, they did not observe the identifying closure lights and, during entry to the closed movement area, the aircraft struck a temporary taxiway light.
Insufficient lighting and markers to denote the closed area
Three lights had been placed across the closed section of taxiway which was 35 m wide. Photographs, taken along the taxiway, showed that with the background lighting, it was difficult to identify the lights, although they were more noticeable close to the closed section. In any event, the lighting in place on the night was insufficient to alert the pilot that the taxiway was still closed. In addition, the markers required to denote the unserviceable area, were not in position.
Contributing factor
The lighting in place on the night was insufficient to draw the pilot's attention and avoid entering the temporary unserviceable area. Additionally, the required markers were not in place.
Continued departure
The pilot was made aware they had entered an unserviceable taxiway, and they waited while the taxiway lights were removed prior to exiting the area. During that time, comments by the works safety officer that they were removing debris from a broken light was rebroadcast on all frequencies, including the one being used by the pilot.
While the controller did not specifically state that there was debris on the taxiway, they did question the pilot about if they wanted to continue. The pilot, after checking with the flight nurse whether they had felt anything, assessed the aircraft had not struck a light and continued the departure. Regardless of whether the aircraft struck the light, due to the possibility of damage, an inspection should have been completed prior to continued flight.
Other factor that increased risk
Despite indications that an unserviceability light had been damaged by the aircraft, the pilot assessed that the aircraft had not struck it and continued the flight, without getting an inspection.
Method of working plan
While the method of working plan stated that the closed movement areas needed to be marked in accordance with the Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019 (MOS) and showed where the markers were to be placed, it did not specify a minimum number to be used. As it was Adelaide Airport’s general practice not to use cones to identify night works, this did not contribute to this incident.
In addition, 3 symbols were used to represent the unserviceability markers and red lights. It is likely that this influenced the Adelaide Airport’s general practise to use 3 lights to identify temporary unserviceable areas, as was the case on the night of the occurrence.
Contributing factor
Despite Adelaide Airport’s method of working plan stating that the markers used to identify the closed areas needed to comply with the Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019, it did not specify the number of unserviceability markers required. However, these were regularly not being used to denote the closed area at night. The plan also did not specify the number of lights to be used, and it was the general practise to use 3 red lights. This resulted in reduced prominence of unserviceable movement areas.
Clarity of regulations
The Civil Aviation Safety Regulations (CASR) Part 139 (Aerodromes) Manual of Standards 2019 (MOS) stated that a minimum of 3 markers were required to denote a temporary unserviceable movement area and while not mandatory, it recommended that markers cover the entire width of the taxiway at 3 m spacing.
The requirements in the MOS for identifying a temporary closed taxiway during daylight hours exceeded the Annex 14 – Aerodromes requirements.
For night closures, the regulations stated that unserviceability lights needed to be placed across the entrance at 3 m spacing but did not recommend that the lights should cover the entire width. While CASA had a requirement for lights to have an intensity that was sufficient to ensure conspicuity against the background which they would normally be viewed, as was the case in this occurrence, background lighting at busy airports can make it difficult to detect unserviceability lights.
Increasing the span of unserviceability lights, in circumstances where there is significant obscuring background lighting, would make a closed area much more distinguishable. As done for the markers, a recommendation would encourage operators to consider their circumstances to assess the number of lights required to clearly identify the area.
In addition, CASA advised that as the MOS did not state that markers were only required during daylight, therefore, they were required at night. Although implied by the MOS, there was no statement that clarified that at night both unserviceability lights and markers were required. This explicit requirement was contained within the wording of Annex 14.
Contributing factor
The Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019 section relating to the temporary closure of a taxiway at night did not:
provide a recommendation that when operating on an aerodrome with significant obscuring background lighting, consideration be given to increasing the span of unserviceability lights, similar to the recommendation provided for markers to cross the entire closed area
specify that both markers and unserviceability lights were required. (Safety issue)
Controller continued duty
After the incident took place, while the Air Traffic Service (ATS) controller entered an internal report and entered the incident into the physical tower logbook, they did not believe the incident required contacting the Air Traffic Management Director (ATMD), located in Melbourne. Although, the Airservices Australia’s records showed the controller had completed their annual renewal for the Adelaide tower endorsements, the controller reported they were unaware that a risk assessment was required for them to continue operating.
If contact had been made with the ATMD, the risk assessment would likely have found the controller suitable to continue operating, requiring extra welfare checks and an assessment of pending traffic.
As the risk assessment was not completed, the controller continued operations without additional risk controls in place.
Other finding
Following the occurrence, the controller continued operating as the sole tower operator without completing the required risk assessment. If conducted, such an assessment would probably have resulted in the controller completing their duty period with additional risk controls in place.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the entry to a closed taxiway involving Pilatus PC-12, VH-FXJ at Adelaide Airport, South Australia on 4 November 2024.
Contributing factors
The controller issued a clearance for the aircraft to taxi through a temporarily closed movement area.
On receipt of a clearance that required taxiing through a known temporarily closed area, the pilot did not question the clearance as they assumed the works had ceased. Additionally, they did not observe the identifying closure lights and, during entry to the closed movement area, the aircraft struck a temporary taxiway light.
The lighting in place on the night was insufficient to draw the pilot's attention and avoid entering the temporary unserviceable area. Additionally, the required cone markers were not in place.
Despite Adelaide Airport’s method of working plan stating that the markers used to identify the closed areas needed to comply with the Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019, it did not specify the number of unserviceability markers required. However, these were regularly not being used to denote the closed area at night. The plan also did not specify the number of lights to be used, and it was the general practise to use 3 red lights. This resulted in reduced prominence of unserviceable movement areas.
The Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019 section relating to the temporary closure of a taxiway at night did not:
provide a recommendation that when operating on an aerodrome with significant obscuring background lighting, consideration be given to increasing the span of unserviceability lights, similar to the recommendation provided for markers to cross the entire closed area
specify that both markers and unserviceability lights were required. (Safety issue)
Other factors that increased risk
Despite indications that an unserviceability light had been damaged by the aircraft, the pilot assessed that the aircraft had not struck it and continued the flight, without getting an inspection.
Other finding
Following the occurrence, the controller continued operating as the sole tower operator without completing the required risk assessment. If conducted, such an assessment would probably have resulted in the controller completing their duty period with additional risk controls in place.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019 section relating to the temporary closure of a taxiway at night did not:
provide a recommendation that when operating on an aerodrome with significant obscuring background lighting, consideration be given to increasing the span of unserviceability lights, similar to the recommendation provided for markers to cross the entire closed area
specify that both markers and unserviceability lights were required.
Additional safety action taken by Airservices Australia
As a result of this incident, Airservices Australia released a standardised directive to Adelaide tower to clarify the occurrence management and reporting requirements following this incident. In addition, operational command authority escalation was added to the Airservices focus area questions for initial and renewal assessments completed in October 2024.
Glossary
AC
Advisory Circular
ATMD
Air traffic management director
ATS
Air traffic services
ATIS
Automatic terminal information service
ATSO
Air traffic services officer
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
ICAO
International Civil Aviation Organization
INTAS
Integrated tower automation suite
MOS
Manual of Standards
NAAM
National ATS administration manual
NOTAM
Notice to airman
OCA
Operational control authority
Sources and submissions
Sources of information
The sources of information during the investigation included:
International Civil Aviation Organization (ICAO) - Annex 14 Aerodromes
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot and operator
the controller
Adelaide Airport
Airservices Australia
Civil Aviation Safety Authority
Submissions were received from:
the operator
Airservices Australia
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Notice to Airmen (NOTAM): a notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[2]Automatic terminal information service: the provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is prefixed with a unique letter identifier and is updated either routinely or when there is a significant change to weather and/or operations.
[3]Runway number: the number represents the magnetic heading of the runway.
[4]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered.
On the morning of 12 August 2024, a Fairchild SA227-DC was being operated by Skippers Aviation on a non-scheduled air transport passenger flight from Forrestania to Perth, Western Australia. Close to the top of descent into Perth, the crew experienced a complete loss of pressure in the aircraft’s hydraulic system. The crew coordinated with air traffic control for a holding pattern to allow for time to troubleshoot the failure and prepare for an appropriate approach and flapless landing. Ground inspection vehicles were requested to ascertain post-landing if fluid was visibly leaking onto the runway and a tow vehicle was requested to recover the aircraft after landing.
After successfully landing and stopping on the taxiway, the captain was unable to establish contact with the tow vehicle and then decided to continue to taxi to the operator’s apron. As the aircraft approached the operator’s apron, a slight downhill slope caused an increase in speed. However, when the crew applied the brakes, they were ineffective. In an effort to avoid collision with a hangar, the captain applied reverse thrust. However the aircraft continued to roll forward, the captain shut down the engines and feathered the propellors before impacting the hangar. The aircraft sustained damage to the right-side wingtip and propellor, there were no injuries to crew or passengers.
What the ATSB found
During the flight, the captain was supervising the cadet-entry first officer’s flying when a crack in a hydraulic line led to a hydraulic fluid leak and in-flight failure of the hydraulic system.
Consistent with the first officer’s minimal experience, their ability to contribute to the in-flight emergency management was limited, requiring the captain to manage the emergency. The captain was required to take on both the pilot flying and pilot monitoring roles, which reduced their ability to effectively manage the emergency.
The first officer's inexperience limited their ability to contribute to managing the hydraulic system failure. This negatively impacted crew resource management and increased the captain's workload.
After stopping on the taxiway, the captain mistakenly assumed the brakes were functioning. Unable to locate or contact the tow tug, and influenced by self-imposed pressure, they continued the taxi to the apron.
On arrival at the operator’s apron, the aircraft had minimal braking capacity and the crew was not able to stop the aircraft. Due to the proximity of the hangar, the captain had limited opportunity to take corrective action and a collision occurred.
What has been done as a result
The operator has advised it is reviewing maintenance practices for tube repairs and replacements for the fleet. In addition, the following actions have been advised to the ATSB by the operator:
The flight crew received refresher training in human factors, standard operating procedures, workload management and decision‑making. Additionally, the captain has completed remedial training on decision‑making.
The captain has completed a series of simulator exercises to confirm all procedures are followed in accordance with the aircraft quick reference handbook (QRH) and company standards.
During their fleet meeting, all fleet pilots were made aware of the incident and the lessons learnt to prevent reoccurrence.
All fleet pilots have completed theory training and examination on the hydraulic system.
Safety message
This occurrence highlights the necessity for accurate assessment of system functionality following an in-flight system failure and the need to follow standard operating procedures. Vigilance when assessing aircraft performance and an objective assessment of system status are vital to minimise opportunities for error and avoid relying on potentially misleading indicators.
Flight crews are advised to prioritise procedural compliance in uncertain circumstances, especially when perceived pressure is heightened to continue to operate an aircraft in non‑normal situations.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
At about 0900 local time on 12 August 2024, a Fairchild SA227-DC Metroliner (Metro) aircraft, registered VH-WAJ and operated by Skippers Aviation, was conducting a non‑scheduled air transport flight with 2 crew and 4 passengers on board from Forrestania to Perth, Western Australia. The first officer (FO), who was completing supervised line flying, was the pilot flying and the captain was in the pilot monitoring role.
At about 1000, the aircraft was close to the top of descent into Perth (Figure 1), when the right hydraulic system low-pressure annunciator light flickered and then subsequently remained solid, which indicated a system failure.
Figure 1: Flightpath and location of VH-WAJ at the time of hydraulic failure
Source: Google Earth and QAR data, annotated by the ATSB
The flight crew consulted the aircraft quick reference handbook (QRH) and followed the standard checklist procedures to manage the indicated hydraulic system failure. The crew identified that the hydraulic pressure remained between 1,700 and 2,100 psi and as per the QRH instruction, the flight should be continued as originally planned. The crew reported following the planned route until, a short time later, the left hydraulic low-pressure annunciator light illuminated. The captain checked the main pressure gauge which displayed 0 psi and identified that there was a total failure of the hydraulic system.[1] The captain requested vectors[2] from air traffic control (ATC) for a holding pattern to allow time to determine the appropriate speed and extra distance required to conduct a flapless landing. This also provided time for the captain to instruct the FO on how to conduct a manual extension of the landing gear using the hand pump, as this was the first time the FO had undertaken this task.
ATC provided vectors for holding, while the captain recalled trying to contact the company maintenance watch directly, however, was unable to find the correct frequency and instead was able to advise other company representatives of the situation.
The captain considered but elected not to broadcast a PAN PAN[3] call to ATC, instead advising them that a tow vehicle (tug) would be required to tow them from the runway to the apron. The captain also requested ATC to provide a vehicle to follow the aircraft after landing for an inspection of any fluid visibly leaking onto the runway.
After finalising details for landing, the captain and first officer swapped ‘pilot flying’ roles due to the limited experience of the FO. The captain then took control of the aircraft and conducted the flapless landing on runway 24 at Perth Airport.
After a successful landing, they exited the runway and stopped on taxiway ‘A’. The captain reported looking for the tow vehicle but could not visually locate it and was unable to establish direct communication with the tug. The captain recalled that at this time the hydraulic system pressure gauge showed a positive pressure and so they elected to test the brakes and found that some braking pressure was evident.
An airport vehicle following the aircraft reported to ATC that no fluid was observed on the runway. ATC requested the crew’s intentions, and the captain informed them that they would continue the taxi back to the operator’s apron without the assistance of a tug.
As the aircraft approached the operator’s apron and turned toward the hangar, the aircraft’s speed increased due to a slight downhill gradient. The captain and FO applied full braking, but neither of their systems responded.
Figure 2: VH-WAJ shown stationary after collision with operator’s hangar
Source: Operator
In an attempt to avoid collision with the hangar, the captain momentarily used reverse thrust, then shut down the engines and feathered[4] the propellers. However, the aircraft’s right wingtip collided with the hangar at low speed, before the right propeller made contact. The impact resulted in minor damage to the right propeller and wingtip (Figure 2). All of the occupants disembarked safely, with no injuries to the crew or passengers.
Context
Aircraft information
VH-WAJ, a Fairchild Industries SA227-DC Metroliner was manufactured in the United States in 1995. The 19-seat aircraft was fitted with 2 Garrett TPE331-12 turboprop engines.
The flight log for the morning of the incident showed that the aircraft was considered serviceable. Maintenance documentation identified the successful repair of a hydraulic leak in April 2024, with no known hydraulic deficiencies prior to the incident flight.
Flight crew
The crew was composed of a training captain and FO. Each pilot held a commercial pilot licence (aeroplane) and a class 1 medical certificate.
The captain had about 3,620 hours total flying experience of which about 1,120 hours were on the Metro.
The FO had 325 hours total flying experience and was a cadet in training, with about 34 hours experience on the Metro.
Cadet training
Skippers Aviation partnered with a training organisation, accepting cadets with little prior aviation experience and providing a training captain for them while conducting Part 121 operations.[5] For this scheme, the operator had identified that new cadet FOs may have little prior aeronautical experience and so may be near capacity in normal operations of the aircraft and possibly unable to effectively handle emergency situations or support other crew during such an event.
The operator confirmed that significant training is conducted with training captains to ensure that pilots’ skills are developed in live operational environments while ensuring safety through operational oversight. Supervised line flying, line training and line checks were used to expose cadets to the operator’s procedures and to enable them to gain real time experience conducting authorised activities on the aircraft over the operator's network. Additional training requirements for cadet FOs included increased simulator training sessions and expanded line oriented flight training to 100 hours from 50 hours to improve preparedness for both routine and emergency scenarios.
Civil Aviation Safety Regulation 119 (Australian air transport operators, certification and management) Subpart 119.E (Training and checking for operational safety‑critical personnel) details how an approved company exposition assesses the competence of a flight crew member and the training and checking system.
Airport information
Perth Airport is the major international aerodrome in Western Australia. The main runway 03/21 is 3,444 m in length and the secondary runway 06/24 is 2,163 m in length; both runways are 45 m wide (Figure 3).
A system of interconnected taxiways connects runways with terminals, aircraft aprons and hangars. The captain reported using asymmetric power to taxi (as nose wheel steering was not functional due to the hydraulics failure) at walking pace via taxiways D and H to the operator’s apron.
Figure 3: Aerial view of Perth Airport showing the route used by VH-WAJ after landing
Source: Google Earth and QAR data annotated by the ATSB. Metro model not to scale.
Meteorological conditions
The terminal forecast for Perth Airport on the day of the occurrence was for intermittent rain showers and scattered low cloud. The wind was mainly from the west at 15–25 kt and visibility was reduced to 5,000 m at times with low cloud down to 1,500 ft.
Recorded information
The aircraft was fitted with a Fairchild model A200S cockpit voice recorder (CVR) which was transported to the ATSB technical facilities in Canberra for download. The recovered audio data contained 5 channels of high-quality audio with about 32 minutes recorded which included the descent, landing and taxi.
The recorded audio is consistent with the crew’s recollection at interview of the event and their discussions with ATC for the descent, landing and taxi.
Hydraulic system
The main hydraulic system on the Metro provides hydraulic pressure for actuation of the landing gear, flaps and nose wheel steering. Without the hydraulic system, the flaps, nose wheel steering and landing gear were inoperable and aircraft braking had limited functionality.
The nose wheel steering system provides directional control while taxiing, however the nose wheel casters move freely when the system is not engaged. Additionally, there is a self‑contained hydraulic power system for brake operation.
The main hydraulic system is pressurised by two engine‐driven hydraulic pumps (EDPs) and there is one manually‑operated hand pump. The hand pump draws reserve hydraulic fluid from the same reservoir as the EDPs and provides pressure for the emergency landing gear extension.
Normal system pressure is 2,000 psi. Two warning lights on the annunciator panel warn of low pump pressure or pump failure and a pressure gauge on the instrument panel is used to monitor the hydraulic system.
The brake hydraulic system is completely independent of the main hydraulic system used for landing gear and wing flap actuation. The power brake system includes master cylinders, brake accumulators and a pressure gauge. The brake accumulators, pre-charged with nitrogen (to 650 psi) and hydraulic fluid (from the aircraft main landing gear extension lines to 2,000 psi), provide back-up to the main hydraulic system in case of hydraulic pressure loss. The brake accumulators allow multiple brake applications without anti-skid protection until the pressure depletes to a minimum level. A pressure gauge monitors the hydraulic pressure in the accumulators showing normal levels during operation and residual pressure in the case of hydraulic fluid loss. When the accumulators bleed down to their minimum pressure, the brakes become unavailable.
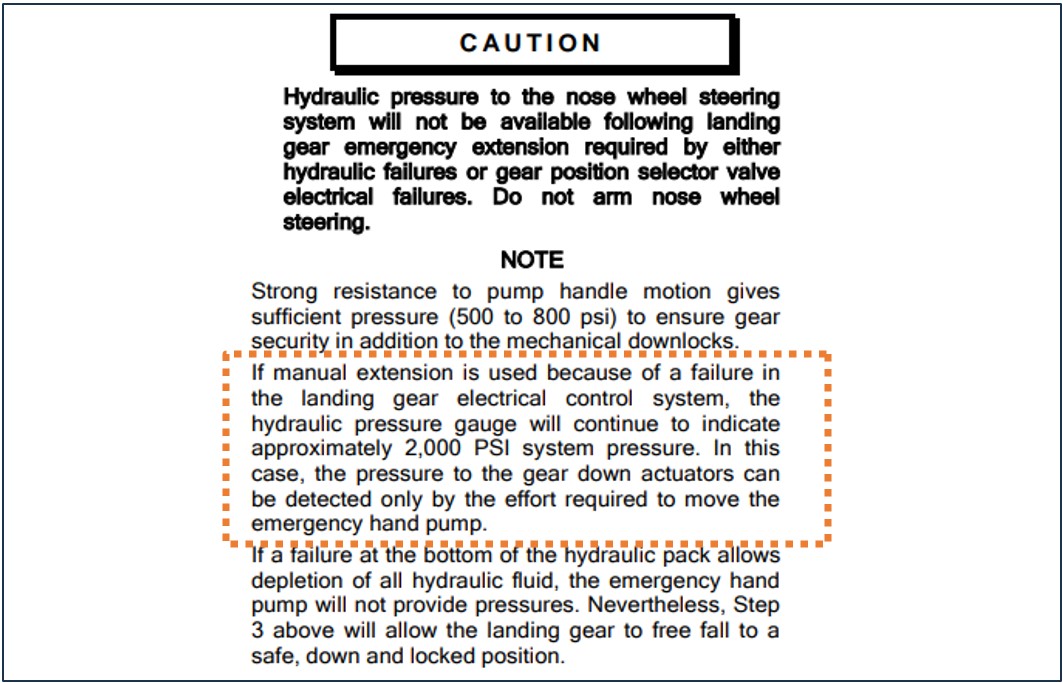
If an emergency manual extension of landing gear is needed, the main hydraulic pressure gauge will continue to indicate approximately 2,000 psi system pressure (Figure4). The captain recalled identifying that the hydraulic pressure read about 2,100 psi after landing.
Figure 4: Extract from operator’s QRH describing the pressure reading after landing gear emergency extension
Source: Operator’s Quick Reference Handbook, annotated by the ATSB
QRH procedure for hydraulic pressure loss
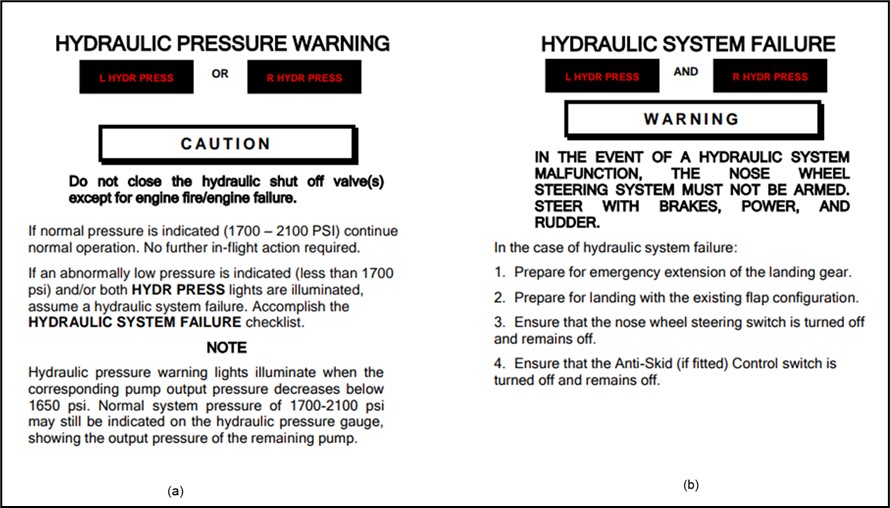
The crew reported that they followed the checklist procedures from the operator’s QRH to manage the hydraulic system failure. Figure 5 shows extracts from the QRH detailing the procedure for management of a hydraulic system failure.
Figure 5: Partial extracts from the operator’s QRH for hydraulic failure management
Source: Operator’s Quick Reference Handbook
The QRH also indicated that after landing with hydraulic system failure, the aircraft should have sufficient accumulator pressure to taxi clear of the runway.
Post‑event maintenance inspection
A post‑event maintenance inspection, conducted by the operator, indicated that the hydraulic system failure was due to a stress crack in the hydraulic pipe's union flare (located in the left landing gear wheel well). This crack allowed fluid loss, which then depleted the remaining hydraulic fluid and caused the warning lights to illuminate.
Flight crew workload
Descent, approach and landing phases are periods of high workload during normal operations due to the increase in task demand. In non-normal operations, such as equipment malfunction, workload levels escalate significantly for the crew who must assess and manage the abnormal conditions, complete additional tasks and make timely decisions under pressure.
At interview, the crew reported that the captain’s workload was very high at the time.
Research that has examined unexpected changes in workload during flight indicate that pilots who face abnormal or emergency situations experience a higher workload and increased number of errors, compared to pilots who do not encounter the same scenarios (Johannsen and Rouse, 1983).
During this time the captain was trying to involve the FO in the handling of the emergency situation by instructing them on the manual release of the landing gear.
Crew resource management
Crew resource management (CRM)[6] plays an important role in workload management and communication in the cockpit, particularly during non-normal situations. For the captain, who had to monitor the FO’s actions and provide instruction, this dual role led to task saturation and increased the likelihood of errors. The normal benefits of CRM to load-shed and delegate tasks can be unrealised when supporting flight crew have minimal experience in the aircraft type and low aeronautical experience.
Confirmation bias
Cognitive biases are mental shortcuts used to aid decision-making. Research points to most incidents of cognitive bias in flight operations happening during landing and at the end of their journey, with over 55% of incidents occurring in this phase (Nadri and others, 2024). A common bias is confirmation bias which describes a tendency for people to seek information and cues that confirm a tentatively held belief and not seek (or avoid) information that supports an opposite conclusion (Wickens & Hollands, 2000). Under high cognitive load this is amplified and individuals tend to focus on familiar or expected information reducing their openness to consider all relevant information (Liden, 2023).
Self-imposed pressure
Pilots may experience self-imposed pressure, for a range of reasons, that can form a desire to meet operational expectations. This pressure can manifest as a feeling to expedite tasks to avoid impacting schedules or inconveniencing other operators. The captain described that, after landing and bringing the aircraft to a stop on taxiway A, there was self-imposed pressure to clear the taxiway for incoming and outgoing aircraft.
Safety analysis
During a non-scheduled air transport flight from Forrestania to Perth, the crew of VH-WAJ experienced a complete loss of pressure in the hydraulic system. Without the hydraulic system, the flaps, nose wheel steering, and landing gear were not functional, however limited braking was available from a reserve pressure accumulator. The captain conducted a flapless landing and after stopping on the taxiway for a short moment, opted to continue the taxi to the operator’s hangar, mistakenly believing the hydraulic pressure had returned and that the brakes were functioning. In close proximity to the operator’s hangar, the crew applied the brakes to stop the aircraft while on a slight slope, but they were ineffective and the aircraft collided with the hangar, damaging the right wingtip and right propellor.
The complete loss of hydraulic pressure was identified post-flight as a result of a fluid leak from a hydraulic pipe crack in the union flare in the left main landing gear wheel well.
The training captain ordinarily had an increased physical and cognitive workload due to oversight of the aircraft and providing guidance for the novice FO. However, their workload surged considerably when the illumination of both hydraulic system warning lights required immediate management of the in-flight emergency. In addition to conducting the checklist procedures, the captain had the added responsibilities of all the radio communications and guiding the FO through the emergency task of the manual extension of the landing gear. Additionally, the captain assumed the role of pilot flying from the FO for the approach and landing at Perth. This contributed to the captain’s decision to continue taxiing to the apron after exiting the runway, as the demands of the emergency likely disrupted the typical task prioritisation for post-landing procedures after this event, which would have been to have the aircraft towed.
The FO’s inexperience and low number of hours on the Metro, while completing supervised line‑flying, reduced their capacity to contribute to decision-making, workload and task‑sharing in the same manner as a more experienced FO during the emergency. The FO’s unfamiliarity with non-normal procedures outside of the simulator meant that they were unable to anticipate the needs of the captain to help distribute the workload after the hydraulic system had failed. As a result, this limited their ability to fully support the captain, which negatively impacted CRM and further increased the captain’s workload.
The captain reported that they did not check the brake accumulator gauge after landing. It was likely that after using the brakes during landing, the reserve accumulator pressure became depleted, although this was not obvious based on the feel of the brakes when tested after stopping.
Both the in-flight positive pressure indication observed on the main hydraulic pressure gauge (due to the manual extension of the landing gear) and the report of no fluid on the runway mistakenly supported the captain‘s understanding that the pressure had returned to the aircraft and that the brakes were functional. The absence of establishing contact with a tow vehicle and being aware of other traffic requiring access to the taxiway, it is likely that the captain felt self-imposed pressure to continue to move the aircraft. This likely influenced the captain’s decision to continue to taxi to the hangar.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the hydraulics system failure involving Fairchild SA227-DC, registered VH-WAJ, at Perth Airport, Western Australia, on 12 August 2024.
Contributing factors
A crack in a hydraulic line in flight resulted in a loss of hydraulic pressure and required the crew to manage the emergency.
Following the hydraulic system failure, the captain was required to take-on both the pilot flying and pilot monitoring roles. This reduced the ability to effectively manage the emergency.
The first officer's inexperience limited their ability to contribute to managing the hydraulic system failure. This negatively impacted crew resource management and increased the captain's workload
After stopping on the taxiway, the captain mistakenly assumed the brakes were functioning. Unable to locate or contact the tow tug and influenced by self-imposed pressure, continued the taxi to the apron. Approaching a hangar, the crew applied the brakes, but they were ineffective and resulted in the right wingtip and propellor colliding with the hangar.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence
Safety action by the operator
The flight crew received refresher training in human factors, standard operating procedures, workload management and decision‑making. Additionally, the captain has completed remedial training on decision‑making.
The captain has completed a series of simulator exercises to confirm all procedures are followed in accordance with the QRH and company standards.
During their fleet meeting, all fleet pilots were made aware of the incident and the lessons learnt to prevent reoccurrence.
All fleet pilots have completed theory training and examination of the hydraulic system.
Skippers Aviation is carrying out a review of maintenance practices for tube repairs and replacements for the fleet.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the captain and first officer
Skippers Aviation safety manager
video footage of the accident flight and other photographs taken on the day of the accident
cockpit voice recorder.
References
Johannsen, G & Rouse, WB, (1983). Studies of planning behaviour of aircraft pilots in normal, abnormal, and emergency situations. Systems, Man and Cybernetics, IEEE Transactions on, (3), pp.267-278.
Nadri, C., Regalado, J., Ferris, T., & Zahabi, M. (2024). Cognitive Biases in Commercial Aviation: Empirical Review of Accident Reports. Proceedings of the Human Factors and Ergonomics Society Annual Meeting.
Wickens, C. D., & Hollands, J. (2000). Engineering psychology and human performance
(3rd ed.). Upper Saddle River, NJ: Prentice Hall.
Liden, M. (2023). Confirmation bias in criminal cases. Oxford University Press.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
captain and first officer
Skippers Aviation (the operator)
the Civil Aviation Safety Authority
Airservices Australia
There were no submissions received.
[1]The hydraulic system controls movement of external components including flaps and landing gear.
[2]Specific directions to sequence an aircraft for the safe and efficient movement of aircraft in controlled airspace.
[3]PAN PAN: an internationally recognised radio call announcing an urgency condition, which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[4]Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[5]Part 121 of Civil Aviation Safety Authority (CASA) regulations cover air transport rules for larger aeroplanes.
[6]Crew resource management (CRM) refers to the effective use of all available resources: human resources, hardware, and information to achieve safe and efficient operation.
The Tonga Civil Aviation Office (TCAO) commenced an investigation into a loss of control during taxi, and a subsequent ground collision involving a SAAB 340B, registered A3-PUA, at Fua'amotu International Airport, Tonga, on 8 December 2023. The TCAO requested assistance and the appointment of an accredited representative from the ATSB.
To facilitate this support and to provide the appropriate protections for the information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of the International Civil Aviation Organization Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
On 26 June 2025, the TCAO released its final report into this accident. Accordingly, the ATSB has concluded its involvement in the investigation.
Any enquiries relating to the accident investigation should be directed to the TCAO.
On 30 July 2019, a British Aerospace BAe146-RJ85 aircraft, registered VH-NJW and operated by National Jet Express (Cobham), was being prepared for a charter flight from Perth Airport to Granny Smith, Western Australia. During the pre-flight checks, the flight crew did not identify that there was no pressure in the braking system and did not pressurise this system prior to engine start.
Around the time of the start of the final engine in the starting sequence, the aircraft began to roll forward.
The dispatcher noticed the aircraft rolling and alerted the crew. The crew attempted to use their foot brakes and the park-brake, however, there was no brake pressure. Around 18 seconds after the aircraft started to roll, it collided with objects at the edge of the apron.
What the ATSB found
The ATSB found that the flight crew did not effectively check the brake pressure during pre-flight checks. Procedures required that the captain check brake pressure during two separate checklists, which provided two opportunities to pressurise the hydraulic system before engine start. There was also a shared responsibility for the first officer to monitor and cross-check. These checks were not done effectively and as a result, the crew did not identify that there was no available pressure prior to engine start.
The operator's dispatch practices did not involve placing chocks on the nose-wheel once the main wheel chocks were removed for engine start. At engine start, there was no brake pressure restraining the aircraft, nor was there any chock to prevent an inadvertent roll forward. The combined thrust of the four aircraft engines at idle and the slight apron slope caused the aircraft to inadvertently roll forward.
The absence of braking pressure also meant that the crew were not able to stop the aircraft with the aircraft brakes. The crew had a very limited opportunity to take corrective action before the aircraft collided with infrastructure. It is likely that the short distance to the terminal and the influence of surprise combined to reduce the pilots' ability to respond.
What's been done as a result
Cobham have sent a notice to check and training captains reminding them of the importance of vigilance during checklists.
Cobham have also reported that they plan to revise procedures to include the requirement to use nose-wheel chocks when dispatching from stand-off bays and to align all applicable procedures to capture this requirement.
Safety message
This investigation highlights the importance of ensuring all checklist items are addressed.
As highlighted in this accident, individuals can be vulnerable to omit checklist items and this can lead to accidents. Aviation safety relies on a resilient safety system involving multiple defences. In the context of multi-crew operations, one of the key defences against this type of accident is the other pilot. Monitoring and cross-checking can provide a last line of defence to trap individual errors.
Although safety systems should seek to reduce the development of errors, where possible engineering defences should also be used to reduce error consequences. Simple mechanical barriers, such as chocks, can be an effective defence.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the flight crew, the engineer, Cobham Aviation Services, BAe Systems via the accredited representative the UK Air Accidents Investigation Branch, the Civil Aviation Safety Authority,
Submissions were received from Cobham Aviation Services, BAe Systems, and the first officer. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Findings
From the evidence available, the following findings are made with respect to the Ground collision with airport infrastructure involving British Aerospace AVRO 146-RJ85, VH-NJW at Perth Airport, Western Australia on 30 July 2019. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The crew did not effectively check the brake system pressure during either the originating checklist or the starting checklist. As a result, the crew did not identify that there was no brake pressure prior to engine start.
After engine start, the aircraft inadvertently rolled forward and collided with objects at the edge of the apron. The absence of brake pressure, the slope of the apron and the absence of a nose-wheel chock were contributory to the aircraft rolling forward.
The operator's dispatch practices did not involve placing chocks on the nose-wheel for engine start. Although some ground handling procedures indicated nose-wheel chocks should be used, the operator’s training did not involve a step to place chocks on aircraft nose-wheels. The absence of a nose-wheel chock fore of the aircraft reduced the defences against the aircraft rolling forward.
The crew had a very limited opportunity to take corrective action before the aircraft collided with objects at the edge of the apron. It is likely that the short distance to the edge of the apron and the influence of surprise combined to reduce the crew’s ability to respond.
Safety analysis
Hydraulic systems not pressurised
The flight crew did not effectively check the brake system pressure during the originating checklist or the starting checklist. The captain did not identify that the pressure was less than required and consequently, did not pressurise the system prior to engine start. This was contrary to the checking requirements during these checklists.
Due to the low pressure, it is very likely that the BRK ACC LO PRES warning was current throughout the pre-flight sequence. However, the flight crew reported they had pulled the test and Ground Operation into the ground operation (mute) position, which would mean no attention-getting glare-shield lamps would flash and no aural chime would sound.
Furthermore, it is likely that this warning was generated at an early stage of the pre-flight. It would be common for flight crews to receive a low accumulator pressure warning at aircraft power-on since accumulator pressure would likely have decayed and pumps not yet activated. Consequently, flight crew would likely acknowledge the warning with the expectation that normal procedures would subsequently pressurise the accumulator. In such circumstances, the warning would not be effective at alerting the crew that the hydraulic system was not pressurised prior to engine start. The implication is that the safety system is reliant on effective checking by the operating crew.
Research has found that checklist deviations occur relatively frequently, compared to other forms of procedural deviation. Common forms of checklist deviation include responding without checking and performing flow-check procedures as read-do (Dismukes and Berman, 2010).
Flight crews are particularly vulnerable to checklist errors during the pre-flight sequence. During pre-flight, flight crews are faced with many competing requirements and can experience perceived or explicit pressure to make on-time departure requirements. Line observation research has found that the pre-flight stage of flight presented many and varied events that distracted and interrupted flight crews (Loukopoulos, Dismukes and Barshi, 2001).
None of the factors identified in the research were particularly prevalent in the development of this accident. The flight crew were not experiencing significant time pressure and there were no identifiable disruptions during the pre-flight checklists. Although the busyness of the airport due to the impending arrival of a new aircraft was consistent with there being a distraction for the crew, there was no evidence that the crew were distracted in a way that affected their performance of the checklists. On board recorders showed that the crew did not have any non-pertinent conversations while completing the checklists.
Overall, the missed pre-flight checks in this accident are indicative of the general vulnerability to omissions during checklists, particularly in the pre-flight sequence. Checklist performance is imperfect, and as such, resilient systems utilise redundant defences in order to reduce the likelihood of error and to minimise error consequence. The ATSB notes that the development of this accident required two separate omissions from checklist procedures. The safety system therefore did have some redundant controls, but these relied on vigilant checklist performance.
In multi-crew flight operations, one defence against individual checklist failures is the role of the other pilot. Monitoring and cross-checking is a key recovery defence in the multi-crew safety system and deficiencies in cross-checking has been implicated in the development of major accidents (Sumwalt, Thomas and Dismukes, 2002). Dismukes and Berman (2010) suggest that captains should explicitly brief the FO that they (the captain) will make mistakes and it is the job of the FO to detect mistakes and point them out.
While it may be challenging to monitor the other pilot for the entirety of flight preparation and into the flight, it is critical that this monitoring does occur during checklists. The design of checklist procedures reflects the criticality of the checklist items for ensuring safe flight. Checklists are limited to only those items that are critical and checklist procedures are designed so that flight crews have no other tasks to perform while doing the checklist.
In the development of this accident, the initial and primary missed checks related to the captain not performing the checklist items as required to identify no brake pressure. However, there was also a shared responsibility for the FO to monitor and cross-check. The FO did not monitor the checking actions of the captain and did not independently check the pressure systems. Because neither crew member effectively checked the pressure system, there was no braking pressure available during engine start.
Chocking procedures
The dispatcher’s decision to not reposition chocks to the nose-wheel of NJW was consistent with the training provided to ground handling personnel and the normative practice at Cobham. The training provided to dispatchers did not mention a requirement to reposition chocks to the nose-wheel. Prior to the accident, Cobham personnel were not repositioning chocks to the nose-wheel of departing aircraft.
Cobham procedures and training materials did not provide clear instructions regarding the use of nose-wheel chocks during dispatch. One of the manuals did state that dispatchers should reposition a chock to the nose-wheel, while another manual did not specify this requirement.
The absence of a clear requirement to reposition a chock to the nose-wheel of departing aircraft prior to engine start reduced the available defences against uncontrolled roll-forward.
Roll-forward and response
The combined forces of idle thrust from the four engines, and the slight slope of the apron, acted to overcome the inertia of the parked VH-NJW. In the absence of chocks, NJW rolled forward from its parking position. While it is likely that the park-brake was set prior to the start-up sequence, the lack of brake pressure would have made braking ineffective. Similarly, the crew’s attempt to use the foot brakes and the park-brake after the aircraft was rolling had no effect since there was no brake pressure.
After the confirmed stable start of the final engine (engine one), the next step in the normal pre-flight sequence included activating the engine driven pumps as part of the after-start scans. However, the ground handler alerting the crew, and the observation that the aircraft was rolling, meant that the pilots’ attention was diverted away from the normal pre-flight sequence, and toward responding to the perceived emergency situation. As such, the development of the accident meant that the pilots did not conduct the after-start scans.
The parking position NJ1 was close to the edge of the apron. It took around 18 seconds from when the aircraft started to roll to when it struck objects at the edge of the apron. Consequently, there was limited time to identify the problem and take action to recover from the unintended roll-forward.
The dispatcher attempted to alert the crew that the aircraft was rolling shortly after the roll commenced. However, the crew did not hear the initial alert and did not identify that the aircraft was rolling until around four seconds after that alert. It is possible that this delayed alert was associated with the crew listening to the ATIS. The delay in the crew identifying that the aircraft was rolling may have reduced the likelihood of them taking effective recovery actions to pressurise the hydraulic system.
In this case, the crew had around 10 seconds from the time they were alerted that the aircraft was rolling, to when the aircraft struck objects at the edge of apron. In that time, the crew had to confirm that the aircraft was rolling, attempt to use the braking system, identify that there was no pressure, pressurise and then apply the brakes. Time would also be required for the brakes to arrest the movement of the aircraft. The ATSB concluded that there was a very limited opportunity for the crew to take action to avoid the collision.
The crew were surprised when they heard that the aircraft was rolling, which further reduced their ability to respond. Research has shown that responses to unexpected and surprising situations are slower and more variable. For example, simulator research with experienced pilots has shown that upset recovery performance is much worse when pilots are surprised by the onset of the upset (Landman, 2017).
The nature of the crew’s response to the rolling aircraft is consistent with the effects of surprise. The crew reported that they were shocked and confused when they heard the aircraft was rolling and took steps to confirm that themselves. The psychological effects of surprise can include freezing, a loss of situational awareness and not remembering appropriate operating procedures (Rivera, Talone, Jentsch and Yeh, 2014; Burki-Cohen, 2010); the captain’s action of reaching to the overhead panel, then not completing this action, is also consistent with him being surprised by the unfolding accident.
As the crew did not take the necessary steps to pressurise the hydraulic system, they were not able to stop the aircraft rolling forward. As a result of the roll-forward, the aircraft collided with the objects at the edge of the apron.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Cobham reported that following this accident, the internal safety team reminded Check and Training captains that there is a responsibility to observe and verify responses to checklist items, that it is not acceptable to take a checklist response as given. The head of training and checking also sent a notice to check and training pilots which highlighted the requirement of vigilance during checklists. This notice also directed check and training pilots to threat and error management guidelines. As additional actions, Cobham reported that the occurrence will be incorporated into the Cobham Human Factors Training, and that there has been an enhanced focus placed on Line Operations and Safety Auditors to monitor checklist performance.
Cobham reported that they are undertaking several actions related to chocking procedures. This includes updating the procedures OM-A6 and OM-B6 to include the use of nose-wheel chocks for dispatches from stand-off bays. Cobham reported that they are reviewing other procedures relating to chocking and will align all procedures to include the use of nose-wheel chocks. Cobham also reported they have commenced spot checks of chocking during aircraft start, and that these spot checks are ongoing.
The occurrence
What happened
Aircraft preparation
On 30 July 2019, a British Aerospace AVRO 146-RJ85, registration VH-NJW (NJW), operated by National Jet Express (Cobham) was being prepared on Cobham bay NJ1, Perth Airport, for a charter flight to Granny Smith, Western Australia. The flight crew comprised the captain and the first officer (FO). In addition, there were 62 passengers and two cabin crew on board.
The flight crew signed on for duty at around 1330[1] for a scheduled departure time of 1430. The captain and the FO arrived at the aircraft and commenced pre-flight duties at around 1345.
While the captain and the FO completed the pre-flight checks, they remarked that the apron and the hangar were busy. A new aircraft was arriving later that afternoon and there were many people positioned around the apron to observe its arrival.
At around 1415, the dispatching engineer took position at the right side of the aircraft to operate the aircraft headset. He contacted the flight crew and requested clearance to remove chocks, which were at that stage installed on the outboard wheels of the left and right main landing gear.
After the captain gave the engineer clearance to remove the chocks, the engineer proceeded to walk around the outside of the aircraft, removing the left and right main wheel chocks. At around 1416, the engineer dragged both chocks away from the aircraft, off to an equipment bin at the edge of the apron.
Around this time, as part of the pre-start preparations, the flight crew conducted the originating checklist.
Engine start
At 1419, the engineer returned to the headset position on the side of NJW. The captain called the engineer, who confirmed that the chocks had been removed and the doors and panels had been secured, and that the crew were clear to start all engines. The engineer remained plugged in to the headset while he observed the engine starts.
After receiving the clearance from the engineer, the crew conducted the starting checklist.
After completing the starting checklist, the captain commenced starting the aircraft’s four engines, in the normal 4-3-2-1 sequence, from right outboard engine to left outboard engine. The captain and the FO monitored engine indications to confirm the stable start of each engine. The FO monitored the engine light for each engine to confirm when the starter motor had disengaged and called ‘starter cut-out’ for each of engines four, three and two, as each completed a stable start.
NJW rolls forward
At about 1424, NJW started moving forward. The engineer, who was still connected to the aircraft via the headset, noticed that NJW was moving and alerted the crew. The engineer alerted the crew at about the time the FO called ‘starter cut-out’ for the stable start of engine one.
The crew said that they were confused and alarmed when they heard the engineer and took a moment to confirm that they were in fact moving forward. The crew recalled that their actions following this were:
The captain’s first action was to apply his foot brakes, only to observe that they had no brake-line pressure. The FO tried his foot brakes at around this time, which was also ineffective.
The captain also recalled that he tried using the park-brake, which was ineffective.
The FO heard a loud bang, which he said was consistent with the sound of the park-brake releasing upon application of the foot brakes. The FO recalled this was shortly after he tried using the foot brakes.
With the aircraft rolling towards objects at the edge of the apron, the captain reached up to the overhead panel where the hydraulic pump switches are located. The captain said he could not recall what his intention was for this action, but said that he did not complete whatever that action was supposed to be.
About 18 seconds after the start of the roll-forward, NJW collided with movable aircraft stairs, which were in front of the Cobham terminal. The stairs struck the front of the aircraft, beneath the right pilot seat. Shortly after, NJW collided with a bollard in front of a light pole, then with the light pole itself. The roll-forward and collision with airport infrastructure was captured on Cobham CCTV (images shown in Figure 1).
Figure 1: CCTV showing start of roll-forward (top) and collision with infrastructure (bottom)
Source: Cobham, Original image cropped and annotated by ATSB
The aircraft was substantially damaged by the accident (see Figure 2). One cabin crew member was thrown from a standing position into a door handle during the collision with the light pole, but was not injured. There were no injuries to the other crew or the passengers.
Figure 2: VH-NJW following collision with airport infrastructure
The accident occurred on the Cobham apron at Perth Airport. VH-NJW was parked at bay NJ1, which is directly in front of the Cobham terminal buildings in the north-west corner of that apron.
Bay NJ1 is close to the edge of the apron with a slight slope from the parking position towards the terminal. Documentation supplied by Perth Airport indicated that the apron and aircraft parking positions were designed and approved in accordance with the Civil Aviation Safety Authority (CASA) Manual of Standards (MOS) part 139, Aerodromes.
Aircraft information
The BAe 146 is a four-engine turbofan aircraft, manufactured by British Aerospace (BAe). NJW was an Avro RJ85, a variant of the BAe 146. Because NJW routinely operated on gravel runways, metal deflectors (gravel kits) had been fitted to the aft of the nose landing gear.
A detailed mechanical inspection was conducted of the aircraft’s braking systems after the accident. There was no indication that any defects or anomalies were contributory to the collision.
BAe 146/ RJ85 braking system
The braking system consists of the foot brakes and a park-brake. The brakes are powered by the aircraft hydraulic system which has two subsystems: yellow and green. Only the yellow system powers the parking brake while both systems power the foot brakes. A selector switch on the centre console controls which system (yellow or green) supplies power to the wheel brakes.
Two reservoirs store fluid, one for each system. Pumps draw fluid from the reservoirs, pressurise that fluid and in doing so provide power to operate the brakes. Accumulators store fluid under pressure and provide reserves of hydraulic power. A schematic diagram of the hydraulic system is provided in Figure 3 below.
Figure 3: BAe 146/RJ85 hydraulic system schematic
Source: BAe
Systems for supplying brake pressure
The main pumps for providing hydraulic power are the engine driven pumps (EDPs). These pumps require engine power to operate. Without engine power, the yellow system can be pressurised by an AC electrical pump. When the AC pump is activated, it supplies pressure to the brake system almost instantaneously.
During a normal pre-flight sequence, the yellow system would only be pressurised using the AC pump. This would be done on an as-needs basis following the check of the park-brake during the originating checklist and of the brake pressure during the before start checklist. The EDPs will only supply pressure after they are selected on during the After start checks.
Power for the green system is primarily supplied by the number 3 engine EDP. Without engine power, the green system is pressurised by Power Transfer Unit, which is mechanically powered by the yellow system. Therefore, prior to engine start, without accumulated pressure or yellow system power, the green system will not be pressurised.
Yellow system brake accumulator
The brake accumulator is a secondary reservoir in the yellow system that supplies emergency and park-brake pressure. No pump is needed to supply pressure to the yellow system if the brake accumulator has been charged. The brake accumulator can be charged through the AC pump or using the emergency DC pump.
The accumulator, once charged, stores pressure. The pressure stored in the accumulator decays, however, the decay rate is normally low enough to ensure adequate park-brake pressure for around 150 minutes. The rate of decay increases if the park-brake valves are in poor condition.
A specific inspection was conducted on the pressure decay rate of the brake accumulator from NJW, which complied within the manufacturer’s specification of 150 minutes. Prior to the scheduled flight to Granny Smith, the aircraft had returned at 0847. Therefore, it had been well over 150 minutes since the aircraft was powered.
Controls and Instruments
Gauges on the captain’s instrument panel indicate the pressure available in the yellow and green hydraulic systems (hydraulic pressure). Gauges in front of the left-side (captain’s) control column indicate the level of pressure being supplied by the yellow and green systems (brake pressure).
The foot brakes are located in front of each pilot, as they sit in their flight seats.
The park-brake handle is located on the centre console. The park-brake can be released by depressing the right-hand seat brake pedal or by moving the handle. Disengagement of the park-brake on the RJ85 tends to produce a ‘bang’ sound, unless the park-brake handle is guided down to the un-activated position.
Low accumulator pressure warnings
When the brake accumulator pressure is less than 2500 psi, a BRK ACC LO PRESS annunciator light illuminates on the hydraulics panel, overhead the left-hand seat. The activation of the warning on the hydraulics panel triggers the illumination of the HYD↑ caption on the Master Warning Panel (MWP), which will cause amber attention-getting lamps on the glare-shield to flash and a single chime sound.
By pressing the attention-getting lamps on the glare-shield, pilots can acknowledge the warning light on the hydraulics panel, which will have the effect of dimming the light. Acknowledging warnings means that existing warnings are no longer displayed at full brightness, however, if triggered, new warnings will be displayed at full brightness.
The MWP also has a Test and Ground Operation switch. The BAe 146 Aircraft Maintenance Manual describes the function of this switch, when pulled into the ground operation (mute) position:
the light intensity on the MWP is set to a level sufficient to have seen under average daylight conditions, the bright-up function, the triple and single-chime inputs to the audible warning system and the red warning and amber caution lamp flasher circuits are inhibited. The switch has an integral red warning light to indicate that the mute system is in operation.
The pilots reported that they did not recall seeing or hearing any alerts or warnings during the accident sequence. The FO stated that the Test and Ground Operation switch had been pulled (to ground operation) prior to power on. This switch had been pushed in (to the normal position) prior to engine start, as per the operator’s Power-on Checklist procedures. The FO also stated that it was normal practice to see the hydraulic caption on the MWP activated prior to engine start.
Pre-flight procedures
The ATSB examined the pre-flight procedures used by Cobham crews, particularly as they relate to setting and pressurising the aircraft brake system. The primary document for these procedures was the Cobham manual OM-B2-146, BAe146 Aircraft Operating Manual (The operating manual). The other source was the British Aerospace Flight Crew Operating Manual (FCOM) for the BAe146/RJ series aircraft. The operating manual states that it takes precedence over the FCOM.
In terms of the use of checklists, the operating manual states:
The Checklists allow the development of ‘scans’ which can be accomplished before the checklist is read… The checklist then becomes the means to verify that items have not been forgotten…
The ‘Challenge and Response’ method shall be used, which requires the pilot reading the checklist to call the ‘Challenge’, after which both pilots shall, if physically possible, visually verify that the required action has been completed, and then the pilot nominated on the checklist as the respondent (usually the pilot who completed the action) shall reply with the required response.
Regarding the guidance for both pilots to visually verify each response item, the FO said that he found this difficult. The FO reported that he found it challenging to provide an additional verification of the captain’s checks since he was focussed on performing the duties allocated to him as the first officer. The FO said he thought verifying all of the captain’s actions would result in delays to getting the aircraft away on time.
Originating checklist
The flight crew conduct the Originating checklist (or the equivalent Transiting checklist) prior to engine start for all flights. The originating checklist contained the following checks:
Park-brake. Captain’s responsibility. Select the park brake on and check that the pressure is not less than 1,500 psi.
This checklist item provided an opportunity to check that there was sufficient brake pressure being applied, and to charge the brake accumulators, if required. The captain reported that it was normal to charge the hydraulics using the AC pump during the originating checklist.
The flight crew performed the originating checklist during the pre-flight sequence. The first officer called the item ‘park-brake’ and the captain responded ‘on, pressure checked’.
The captain reported to the ATSB that he recalled performing the originating checklist, but did not have a recollection of performing the check of the park-brake or the pressure gauge. The FO said he could not recall if he looked at the pressure gauge during the originating checklist, to cross-check the captain’s responses.
Starting checklist
The flight crew conduct the Starting checklist after receiving clearance to start the engines from the dispatcher. The first checklist item is ‘Brake Pressure’. The operating manual described this check as ‘ensure the brake pressure is at least 2500 psi immediately before push back or start.’
The crew conducted the starting checklist. For the brake pressure item, the first officer called ‘brake pressure’ and the captain responded ‘check’.
The captain stated he could not recall checking the brake pressure gauge during the starting checklist. The FO reported he could not recall whether he looked at the pressure gauge during the starting checklist.
After start scan
During the start of each engine, the FO monitors the starter operating light and calls ‘starter cut-out’ when the light extinguishes, to indicate stable start. The after-start scans are performed after stable start is confirmed for the final engine in the starting sequence (engine 1). Item 2 of the after-start scan is completed by the captain and included the following:
Select ENG 2 PUMP and ENG 3 PUMP ON and observe YELLOW and GREEN system pressures increase to normal (3100 +/- 50psi). Select PTU on only after GREEN system pressure has been checked.
The crew did not perform the after-start scans because of the development of the accident. This is described in the analysis section following.
Cobham procedures for chocking aircraft
Chocks are routinely fitted fore and aft of aircraft wheels to reduce the risk of the aircraft inadvertently rolling forwards or backwards. The following summarises Cobham procedures for chocking 146/RJ85 aircraft.
Cobham Ground Operations manual, OM-A6
Manual OM-A6 contained higher-level procedures for Cobham ground operations personnel, not specific to aircraft type. These procedures stated that prior to dispatch, ground handling personnel were to remove all chocks from the main landing gear and ensure that a chock was repositioned 150 mm ahead of the nose-wheel. The procedure did not specify any specific requirement, related to nose-wheel chocks, for gravel-kitted aircraft.
Cobham BAe 146 Ground Operations manual, OM-B6
Manual OM-B6 provided type-specific instructions for ground operations on BAe 146/RJ85 aircraft. The manual stated that chocks should be placed fore and aft all wheels, including nose-wheels. The procedures further stated that nose-wheel chocks should be used in windy conditions, or when the parking area was on a slope.
The manual provided limited instructions for the removal and repositioning of chocks in the section describing dispatch duties for aircraft on standoff bays using the intercom. The manual described the sequence of communications that should be made between the captain and the ground, being:
Captain: ‘Brakes parked, clear to remove chocks’
Ground: ‘Chocks removed’
This procedure indicated ground personnel removed all chocks at this stage. It did not specify the requirement to reposition chocks ahead of the nose-wheel, as stated in manual OM-A6.
Cobham BAe 146/RJ85 dispatch training
Cobham dispatch training materials described the steps involved in preparing a 146/RJ85 aircraft for dispatch as including the following:
Remove chocks from the main outboard wheels.
There was no step relating to repositioning chocks to the nose-wheel.
Procedures ‘as done’
The ATSB sought to determine the ‘as-done’ and ‘as-taught’ procedures for using chocks by Cobham dispatchers, to see if there was any variance from the ‘as-written’ procedures. A senior ground handler at Cobham, who was responsible for training dispatchers, advised that normal practice was for dispatchers to remove chocks during dispatch and not reposition chocks to the nose-wheel of any aircraft. Dispatchers were taught to remove chocks in a manner consistent with the dispatch training materials.
The dispatching engineer for NJW indicated he understood the procedures to be that chocks were not fitted to the nose-wheels of gravel-kitted aircraft.
Recorded data
Personnel from Cobham secured a copy of the quick access recorder (QAR) data for analysis and provision to the ATSB. The flight data recorder (FDR) and cockpit voice recorder (CVR) were also removed and dispatched to the ATSB laboratory in Canberra for analysis.
The QAR file provided a record of the entire pre-flight sequence. It shows the engines powering up in sequence (4-3-2-1). Soon after engine 1 began to power-up, the QAR shows an increase in longitudinal acceleration, consistent with the aircraft beginning to move forward. About 18 seconds later, a spike in longitudinal acceleration likely indicates the collision with objects at the end of the apron. All four engines are then shut-down. The QAR shows that there was insufficient hydraulic pressure available in the brake system to provide effective braking throughout the entire pre-flight sequence.
The FDR started recording about 7 seconds before the collision, after which it then stops recording. An examination of FDR data from a previous NJW flight indicated the FDR began recording after all engines had been started and the park-brake was released for taxiing. This would suggest that for this accident, the start of FDR data coincided with the release of the park-brake handle. This is consistent with the FO’s recollection of hearing the park-brake handle release (loud bang) during the rolling sequence.
The ATSB concluded that the park-brake was likely set to ON prior to engine start. However, without sufficient hydraulic pressure, the brakes were not effective.
Ground-cockpit communications
The ATSB considered what each crew member and the dispatcher recalled about what they heard and what they said during the time the aircraft was rolling towards the terminal. The following summarises these recollections:
The dispatcher recalled that when he saw the aircraft was moving, he said words to the effect of ‘brakes parked’ into his headset. He repeated this several times, with an increasingly urgent tone. The dispatcher said the flight crew did not acknowledge any of these messages.
The captain recalled hearing the dispatcher say the aircraft was moving via intercom. The captain reported hearing one such alert from the dispatcher and that the dispatcher’s tone was urgent.
The FO recalled he heard the dispatcher say ‘brakes, brakes’ on his headset, at around the time he (the FO) called ‘starter cut-out’ for engine one. The FO recalled then saying ‘brakes’ himself.
The CVR captured audio relating to the communications between the cockpit and the dispatching engineer. The following table summarises relevant communication:
Dispatcher: BRAKES BRAKES BRAKES! GROUND TO COCKPIT! BRAKES PARKED!
The recorded audio is generally consistent with the dispatcher’s recollection. The combined evidence suggests that the crew may not have heard the dispatcher’s initial warning about the aircraft rolling. It also indicates that the flight crew were not aware that the aircraft was rolling until four seconds after the initial warning and around ten seconds prior to the eventual impact.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 29 June 2019, at about 1249 Eastern Standard Time, an amphibious Cessna 208 aircraft, registered VH-ZWH, was travelling from Rose Bay to Berowra Waters, New South Wales (NSW). After the aircraft landed and was slowing down to taxi speed, the front left float of the aircraft bumped into a small stationary boat. There was no damage to the aircraft or boat, and one person in the boat sustained minor injuries.
What the ATSB found
The ATSB found that the pilot did not see the boat, due to a combination of factors including the weather conditions on the day as well as the colour, size, lack of movement and location of the boat as it was positioned in the aircraft’s direct path.
What's been done as a result
The aircraft operator has introduced the requirement for company pilots to manoeuvre towards the right side of the river to reduce the risk of a blind spot near the area of the collision. Also, as a standard operation, company pilots are to reduce the speed of the aircraft to an idle power taxi speed after landing, 100 m before the start of the 4-knot zone at Berowra. In addition, the company’s safety management system was updated to reflect additional post incident response requirements.
Safety message
This incident is a reminder of the importance of scanning and assessing landing areas for any potential hazards, and of the joint responsibility of both aircraft and marine vessels to see and avoid other aircraft/vessels operating on the water. When choosing an operating speed for any vessel or aircraft on the water, consideration should be given to any potential blind spots and areas where other vessels could emerge.
The occurrence
What happened
On 29 June 2019, at about 1230 Eastern Standard Time,[1] an amphibious Cessna 208 Caravan aircraft, registered VH-ZWH (ZWH) operated by Sydney Seaplanes, departed from Rose Bay on a charter flight to Berowra Waters, New South Wales (NSW). On board were the pilot and eight passengers.
At about the same time that the aircraft took off from Rose Bay, two adults and two children departed from the Berowra Waters Marina in a hired small aluminium boat, which the marina reported as being about 4.8 metres in length. The boat hirer (boat operator) did not have a boat licence, nor was one required to operate the boat. The children were wearing lifejackets and the adults were not wearing lifejackets, nor were they required to in the circumstances in accordance with NSW Marine Safety Regulation (2016).[2] After about 15 minutes, the boat operator stopped the boat near the middle of Berowra Creek to have lunch, and turned off the motor.[3]
About 5 minutes after the boat had stopped, ZWH approached the landing area on Berowra Creek (located in Berowra Waters). The pilot assessed that the wind conditions were suitable for landing and positioned the aircraft to land on Berowra Creek in a south-westerly direction (Figure 1). After landing, because of the long distance to taxi to the restaurant, the pilot kept the aircraft’s speed up, maintaining the aircraft ‘on the step’ (see Seaplane positions) for some time. At the same time, the pilot was also monitoring a large white boat that was heading south out of Calabash Bay, ensuring that it continued moving away from the aircraft and was not going to present a hazard. As the aircraft approached the 4-knot zone of the creek (Figure 1), the pilot reduced the speed and the aircraft moved from the step to the taxiing position.
The boat operator saw the aircraft land and travel towards their stationary boat. As the aircraft approached, the boat operator became concerned that the aircraft was not going to stop. Because the boat appeared to be in the aircraft’s direct path, the boat operator started the motor and began turning the boat away from the aircraft. As the aircraft was slowing to taxi the pilot felt a bump while at a speed of about 6 to 7 knots.[3] The pilot looked around the nose of the aircraft (which was obstructing part of the forward field of view) and saw that the front left float had contacted the boat, which the pilot had not seen until then. The silver hull of the boat had been motionless on the calm, glassy surface of the creek and its dark blue canopy and dark clothing worn by the adults in the boat had blended into the surrounding area.
The aircraft is powered by a PT6 series gas turbine engine with a full reversing propeller. After seeing the boat, the pilot reported selecting full reverse thrust and the aircraft moved away from the boat. There was no damage to the aircraft or the boat and one person on board the boat sustained minor injuries.
The boat operator subsequently reported previously hiring a boat in the same area once before but was unaware that seaplanes operated in the area. The previous time, the boat operator had not seen or heard any aircraft in the area, and therefore was not expecting to see one operating nearby.
Figure 1: Image of the Berowra Waters area showing the location of the collision, the landing direction of VH-ZWH and significant landmarks
Source: Google earth annotated by the ATSB.
Seaplane positions
When moving on the water, the aircraft had two states it could be in, either ‘on the step’ or in the taxiing position (Figure 2). On the step most of the weight of the aircraft is being supported by hydrodynamic lift rather than the buoyancy of the floats, and it is the take-off and landing position.
Figure 2: Diagram of the difference between being ‘on the step’ and being in the taxiing position
Source: FAA Seaplane, skiplane, and float/ski equipped helicopter operations handbook - annotated by the ATSB.
Safety analysis
Due to a combination of factors the pilot did not see the boat prior to the collision. The factors included the weather conditions on the day, as well as the colour, size, lack of movement and location of the boat as it was positioned in the aircraft’s direct path. The colour of the boat blended into the surrounding environment.
The actions of the boat operator of starting the engine and attempting to move out of the aircraft’s direct path likely reduced the risk to the boat occupants due to the change in the angle of impact as the aircraft struck the boat.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
While slowing to taxi speed, the aircraft collided with a small boat that was motionless in the middle of the creek and in the aircraft’s direct path. The boat’s lack of movement, silver hull and dark blue canopy reduced the pilot’s ability to discern it from the background environment.
After the boat operator realised the aircraft was travelling directly towards them, the boat operator started the motor and attempted to manoeuvre the boat out of the direct path of the aircraft.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Proactive safety action
Aircraft operator
As a result of this occurrence, the aircraft operator has advised the ATSB that they have taken the following safety actions:
Company pilots where possible are to manoeuvre on the right-hand side of the river to reduce the risk of a blind spot near the area of the incident.
As standard operations, company pilots are to reduce the speed of the aircraft to an idle power taxi speed after landing, 100 m before the start of the 4-knot zone at Berowra.
The company safety management system was updated to reflect additional post incident response requirements.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
At about 1830 Eastern Daylight‑saving Time[1] on 14 October 2017, the flight crew of a Qantas Airways (Qantas) Boeing 737 boarded the aircraft at Sydney Airport, New South Wales. The aircraft was scheduled to operate a passenger flight to Melbourne, Victoria, with two flight crew, five cabin crew, and 174 passengers.
After boarding, the flight crew found the aircraft had no battery power, as the battery switch had inadvertently been left on. Consequently, another Boeing 737 aircraft, registered VH-VZZ (VZZ) was assigned for the flight. Catering had already been loaded on the originally assigned aircraft so a catering crew (driver and marshaller) were tasked to transfer the catering to VZZ.
At about 1910, a dispatch engineer (engineer) was assigned to the departure of VZZ, which was scheduled for 1930.
At about 1921, the engineer arrived at the aircraft, and received a handover from the other engineer who had been in attendance. The engineers discussed the aircraft status under the aerobridge as it had just started to rain. At this time, the catering vehicle (truck) was loading the forward galley through the right forward main entry door (Figure 1). The pushback vehicle’s (tug) towbar was already connected to the aircraft.
Figure 1: Catering truck loading via the aircraft’s right forward main entry door
Source: Qantas, annotated by the ATSB
At about 1922, the catering crew completed loading the forward galley. They then moved the truck to the right rear main entry door and began loading the rear galley.
The engineer completed his walk around of VZZ and stood under the wing waiting for the catering crew to complete loading. He saw the catering crew close the main entry door and then visually checked that the aircraft door was closed.
The engineer then proceeded towards the front of the aircraft. He put on his headset, which was connected to an external jack point, and contacted the flight crew who confirmed they were ready to depart. As it was still raining, the engineer entered the right side of the tug and sat in its cabin.
Meanwhile, the catering crew retracted the truck’s loading platform and began lowering the truck’s body.
At about 1930, air traffic control cleared VZZ for pushback, and its captain informed the engineer accordingly.
When the aerobridge had been retracted, the engineer leaned out of the tug cabin and completed a visual check of the left forward main entry door.
At 1932:23, the catering truck body had finished lowering and the stabilisers began to raise. The crew exited the truck body.
A few seconds later, the flight crew turned on the aircraft’s anti-collision light.
At 1932:43, the engineer looked left and right from the tug cabin to check for vehicles. He then gave the ‘thumbs up’ signal to the tug driver to commence pushback. When VZZ began reversing, the engineer approved the flight crew to start the right engine. The crew selected the engine start switch and the engine began rotating. The catering truck driver began reversing the truck at this time.
A few seconds later, the catering truck’s marshaller identified that VZZ was moving and tried to alert the truck driver. At the same time, the engineer saw that the catering truck was not clear and ‘yelled’ at the tug driver to stop. The tug driver immediately applied the brakes. The tug stopped but the pins in the towbar sheared and it separated from VZZ (Figure 2).
Figure 2: The catering truck behind the aircraft’s wing when the towbar separated
Source: Qantas, annotated by the ATSB
The flight crew heard a loud ‘bang’ and then saw VZZ moving away from the tug. The catering truck was reversing but still 5-7 m behind the aircraft’s right engine so the engineer asked the flight crew to apply the aircraft’s brakes. The captain applied the brakes as firmly as possible. The aircraft slowed but continued rolling back 3-4 m.
At 1932:53, the aircraft’s right wing collided with the truck (Figure 3) before it came to a stop. The flight crew then engaged the aircraft’s park brake and turned the right engine switch to OFF and the engine wound down as fuel had not been introduced.
Figure 3: Location of catering truck after the collision
Source: Qantas
By 2012, a new towbar was connected to VZZ and it was towed back to the bay. No one was injured in the incident and the passengers disembarked. The aircraft was inspected and found to have substantial damage to its right outboard flaps, wing structure between the flaps and aileron, and the aileron (Figure 4).
Figure 4: Damage to the aircraft’s right wing
Source: Qantas, annotated by the ATSB
Operator’s investigation
An investigation of this incident by Qantas included reconstructing the view of the catering truck from the tug’s location (Figure 5).
Figure 5: View of the catering truck (circled) from the tug in daylight
Source: Qantas, annotated by the ATSB
The investigation also reviewed the engineering dispatch procedures. The procedures stated that the dispatch engineer could conduct the pushback from the tug cabin or walking clear of the aircraft and tug. The procedures included the requirement to confirm that all ground equipment was clear of the aircraft, the aerobridge was retracted, the pushback path was clear and all doors and panels were secured and locked. Once those requirements were met, the engineer could then signal the tug driver to commence the pushback.
The investigation also looked at the sequence and the time usually taken for various ground support operations, such as catering and baggage loading. The baggage belt loader was normally the last ground support equipment to clear the aircraft before pushback, and typically that took less than 30 seconds. A catering truck took longer to move clear (as in this case) but was normally clear before the belt loader.
Safety analysis
The engineer made some checks before signalling the pushback to start. He thought the catering truck was clear but did not visually confirm that it was. In part, the engineer’s assumption that the truck was clear was based on the incorrect expectation that the time required for it to move away would be similar to the short time taken by a baggage belt loader. Additionally, the catering truck was not usually the last equipment to move clear.
There were a number of physical reasons why the engineer did not see the catering truck. He did not have his wet weather gear and, as it was raining, decided to sit in the tug’s cabin for pushback. Seated in the tug, the engineer’s view of the truck was largely obstructed by the aircraft’s wing and a panel door (Figure 5). These obstructions were white, the same colour as the truck and blended with the small, unobstructed parts of the truck. Additionally, these parts blended into white hangars in the background. The trucks lighting and reflective strips were not in view. The dark and rainy conditions with lights reflecting off the wet tarmac also made it difficult to see the truck.
By the time the engineer saw the catering truck a few seconds after pushback started, it was too late to stop it safely. Emergency action was taken but the towbar failed, and the aircraft rolled back and collided with the truck. Other than the truck’s marshaller, no one else was in a position, or had the opportunity, to identify the conflict.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The dispatch engineer assumed that the catering truck was clear and did not visually confirm it was before he cleared VH-VZZ for pushback. In part, this assumption was based on an incorrect expectation of the time required for the truck to move clear.
The engineer’s view of the truck from the pushback tug’s cabin was largely obstructed by the aircraft. The dark and rainy conditions also made it difficult to see the truck, and the engineer saw it too late to prevent the collision.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Qantas
As a result of this occurrence, Qantas advised the ATSB that it has taken, or proposed, the following safety action:
Issued a safety information notice to all staff involved in aircraft dispatch activities highlighting the specific visual limitation issues associated with B737 aircraft pushback operations, and the importance of physically ensuring the pushback path is clear.
Provided relevant training to the dispatch engineer involved in this occurrence.
The engineering aircraft receipt and dispatch-training package will be revised to highlight the visual limitations and the risks which may be present during aircraft pushback operations.
Lessons learned from aircraft pushback occurrences will be included in the human factors training program.
Initiated a trial of cordless headsets to improve visibility during aircraft pushback.
Conducted an assessment of the risk associated with the engineer sitting inside the tug during aircraft pushback.
Safety message
This accident illustrates the busy and dynamic environment of airport aprons with various visual limitations. While there is currently no substitute for visually confirming a clear pushback path for aircraft, aids to support available visual means in the complex environment can help reduce risk.
The ATSB conducted a study into Ground operations occurrences at Australian airports, which occurred over a 10-year period. Pushback occurrences represented about 26 per cent of the total, and the most frequent ones involved tug connection/disconnection. The report concluded that there were a variety of reasons for the occurrences, but the main theme was communication between the dispatcher, flight crew and pushback tug driver. Communication and a common understanding is vital between involved persons operating in the dynamic environment of an airport apron.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 25 January 2017, a Jetstar Airways Airbus A320-232, registered VH-VGJ (VGJ), taxied for a scheduled passenger transport flight from Newcastle (Williamtown) Airport, New South Wales, to Brisbane Airport, Queensland. There were six crewmembers and 165 passengers on board the aircraft. The captain was the pilot monitoring and the first officer was the pilot flying.[1]
The aircraft parked at bay 4 at the Newcastle Airport terminal for passenger disembarkation and boarding (Figure 1). Bay 4 was a ‘pushback’ bay, which means that when the aircraft is ready for departure, the aircraft is pushed backwards from the parking bay by a tug under the supervision of a dispatcher. Another operator’s aircraft was parked on bay 5, to the left of VGJ. Bay 5 was a ‘power-out’ bay which means that on departure, aircraft taxi from the bay under their own power by turning sharply away from the terminal.
At about 1836 Eastern Daylight-savings Time (EDT), the crew of VGJ received a clearance from the surface movement controller to pushback, which placed VGJ to the right rear quarter of the aircraft parked on bay 5, and facing towards taxiway H (Figure 1). The dispatcher was walking beside the aircraft and was connected to the nose of VGJ by a headset for communications with the flight crew. The flight crew started the engines during the pushback in accordance with standard procedures. After the pushback was completed, the flight crew set the brakes, the tug disconnected and the dispatcher removed the nose wheel steering pin. [2] The flight crew then started their ‘after start flows’ (see: After start flows). After the tug disconnected from VGJ, the tug driver moved it to a position adjacent to the left wingtip of VGJ, facing towards the aircraft on bay 5.
At about 1838, the crew of the aircraft on bay 5 requested a clearance to taxi for departure. The surface movement controller questioned whether the aircraft could taxi to taxiway J and avoid VGJ.[3] The flight crew responded that they could. At this stage, the flight crew on board VGJ interrupted their ‘after start flows’ to monitor the other aircraft. The captain, seated in the left seat of VGJ, did not believe there was sufficient clearance for the other aircraft to turn around for taxiway J without a collision. The aircraft started to taxi from bay 5 in a right power-out turn, but stopped within a few metres.
When the tug driver observed the aircraft on bay 5 move towards them,[4] they moved the tug away from VGJ over to the terminal side of the apron, near bay 4, to remain clear of the other aircraft. Meanwhile the dispatcher assisting the aircraft on bay 5, had also moved from bay 5 towards bay 4 in order to monitor and signal wingtip clearance for the left wing of the aircraft conducting the power-out from bay 5.
Figure 1: Newcastle Airport apron
Source: Google earth, annotated by ATSB
Radio communications continued between air traffic control and the aircraft departing from bay 5, until it was confirmed that the aircraft would wait for VGJ before taxiing any further. The captain of VGJ, who was looking out the left window of the flight deck towards the bay 5 aircraft and the terminal, sighted their tug and a dispatcher near bay 4. They assumed that the dispatcher near bay 4 was their dispatcher, who had disconnected from their aircraft while they were monitoring the bay 5 aircraft movements and radio communications. At about 1840, the flight crew on board VGJ requested and received a clearance to taxi for runway 12 via taxiway H. The flight crew selected their taxi lights on, released the brakes and increased power.
The dispatcher for VGJ was still connected to the aircraft nose with their headset and waiting for their clearance from the flight crew to disconnect. They observed the taxi lights for VGJ illuminate, then they heard the engine noise increase, and then the aircraft started to taxi. They immediately disconnected their headset from the aircraft and moved clear to the left of the aircraft towards the terminal with the headset and the nose wheel steering pin. Once the dispatcher was clear of the aircraft, they turned around to display the nose wheel steering pin to the flight crew, but the captain was not looking towards them.
After start flows
On completion of starting both engines, the flight crew conduct their ‘after start flows’, which are memory item checks split between the pilot flying and pilot monitoring (Figure 2). The second-to-last item for the pilot flying is the announcement to the dispatcher that they are clear to disconnect. After the dispatcher disconnects their headset from the aircraft, they walk clear of the aircraft and provide a ‘thumbs-up’ signal to the flight crew while holding up the nose wheel steering pin for the flight crew to sight. During the ‘after start flows’, the attention of the flight crew on board VGJ was diverted to the radio communications between the aircraft parked on bay 5 and the surface movement controller.
Figure 2: After start flows
Source: Operator
The last item on the ‘after start flows’ is for the flight crew to complete the challenge and response ‘after start checklist’, which is as follows:
ANTI ICE…AS RQRD
ECAM STATUS…CHECKED
PITCH TRIM…SET
RUDDER TRIM…ZERO
DISP CLRNCE…SIGHTED
The last item on the ‘after start checklist’ is confirmation that the dispatcher was sighted clear of the aircraft. The left seat or right seat pilot reports to the other pilot ‘dispatch clearance sighted’. In this serious incident, the terminal was on the left side of VGJ and therefore it was expected that the captain, in the left seat, would sight the dispatcher. The captain reported remembering sighting a dispatcher, but could not recall what was communicated on the flight deck between the flight crewmembers.
On completion of the ‘after start checklist’, the flight crew request taxi clearance and turn on the taxi light.
Tug movements
After the tug disconnected from the aircraft, the tug driver moved the tug clear of the aircraft and initially waited for the dispatcher near the left wingtip. The tug normally waited beside the aircraft to offer the dispatcher a lift and because the nose wheel steering pin is stowed in the tug when removed from the aircraft. However, when the bay 5 aircraft started to move, the tug moved from the left wingtip to the terminal building near parking bay 4.
Safety analysis
After VGJ was pushed-back from bay 4 and the flight crew had started their ‘after start flows’, their attention was diverted to a potential risk of collision associated with the taxi instructions and movement of an aircraft parked on bay 5. Following confirmation between the conflict aircraft and surface movement control that they would wait for VGJ, the captain of VGJ misidentified the dispatcher for the bay 5 aircraft as their own dispatcher. At this time, the tug, which would normally wait beside the departing aircraft for the dispatcher, had moved away from VGJ towards the terminal to avoid a conflict with the bay 5 aircraft. Therefore, the dispatcher sighted by the captain, was next to the tug used for the pushback of VGJ. This potentially provided an association between the tug and the dispatcher in the mind of the captain, who assumed the dispatcher had removed the nose wheel steering pin and moved away from the aircraft. The diversion of the flight crew’s attention away from their ‘after start flows’ probably resulted in the pilot flying not completing their memory items. This was not detected in the ‘after start checklist’ because the captain had misidentified the dispatcher for the bay 5 aircraft as the dispatcher for VGJ. Consequently, the dispatcher connected to VGJ was not cleared to disconnect prior to VGJ starting to taxi.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The flight crew on board VGJ were distracted during their ‘after start flows’ by the radio communications between an aircraft parked on bay 5 and surface movement control, and the subsequent movement of that aircraft which had a potential risk of collision with VGJ.
The captain on board VGJ misidentified the dispatcher for the bay 5 aircraft as their own dispatcher, which resulted in VGJ starting to taxi without clearing the dispatcher to disconnect.
Safety message
Following this serious incident the captain reported that their most important lesson was distraction management. They considered either slowing down the ‘after start flows’ or re-starting the ‘flows’, before the ‘after start checklist’, as the most practical risk mitigation strategies.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.