Main landing gear wheel failure during taxi involving Boeing 737, VH-VUH, at Brisbane Airport, Queensland, on 4 January 2017
Final report
Safety summary
What happened
On 4 January 2017, a Boeing 737-8FE, registered VH-VUH (VUH) and operated by Virgin Australia Airlines Pty Ltd (Virgin) was holding on B3 taxiway at Brisbane Airport, Queensland, when the crew heard a loud noise from what they thought was a burst tyre on the left main landing gear wheel. The crew attempted to return the aircraft to the gate, but were held short of the gate when an attending engineer observed that the number one main wheel assembly (left hand outboard wheel) had failed.
What the ATSB found
The ATSB found that the number one main wheel ruptured due to tie bolt assemblies that had loosened while in service. This allowed the two wheel halves to move relative to each other, resulting in a fatigue crack and eventual wheel rupture. The loosening was most likely due to the presence of anti-seize compound between the wheel halves, which affected the clamping forces.
The ATSB also found that while tie bolt assemblies on this wheel-type (single-web) were more prone to in-service loosening than dual-web wheels, there were no mandated inspections suitable for detecting such loosening. There were also no mandated risk controls to prevent loosening or subsequent rupture.
What's been done as a result
Virgin advised that following this occurrence, regular inspections were implemented to identify and prevent the loosening of tie bolt assemblies.
The wheel manufacturer updated the wheel’s component maintenance manual with more detailed instructions for applying anti-seize compound.
Boeing has advised the 737 NG fleet of the issue and suggested two possible courses of action. These were based on two optional service bulletins that the manufacturer had in place prior to the occurrence:
- incorporation of a new inner half-wheel that allows for safe deflation if tie bolt assemblies loosen (Service Bulletin C20626-32-014)
- the addition of lockwire to the tie bolt nuts, to prevent loosening in the first place (Service Bulletin C20626-32-016).
Safety Message
This incident highlights the importance of compliance with all aspects of manufacturers’ maintenance procedures, including the appropriate application of anti‑seize. This is especially important if, as in this case, there is no simple means of detecting the effect that such excess product can have on fastener security.
The occurrence
What happened
On 4 January 2017, a Boeing 737-8FE, registered VH-VUH (VUH) and operated by Virgin Australia Pty Ltd (Virgin), was scheduled to fly from Brisbane, Queensland to Melbourne, Victoria. Prior to take off, at approximately 1710 Eastern Standard Time,[1] VUH was holding on B3 taxiway when one of the main wheels experienced what was believed to be a burst tyre. The flight crew began to taxi the aircraft back to the gate. An attending engineer instructed the flight crew to stop the aircraft before reaching the gate, as they noticed the number one main wheel assembly (left‑hand outboard wheel) had failed (Figure 1).
Figure 1: Damage to the number one main wheel assembly on VUH

Source: Virgin Australia
The flight was cancelled and passengers disembarked, however, the aircraft could not be jacked and towed via the axle due to the damaged wheel. Instead, wing jacks were sourced and a double wheel change performed on the tarmac. The aircraft was then towed to a maintenance facility for examination.
An inspection at the maintenance facility found that the inner half of the wheel assembly had fractured (see the section titled Wheel design). The tie bolt assemblies that connected the two halves of the wheel were all present with mating faces intact, however some of the bolts were found to be loose.
__________
Context
Wheel design
This particular wheel-type was designed for use on Boeing 737 NG aircraft. At the time of publication, the wheel manufacturer, Safran Landing Systems, estimated that approximately 2,000 aircraft were using the wheel globally. The wheel assembly used an asymmetric single-web[2] design, with both axle bearings contained within the outer half-wheel (Figure 2). Eighteen tie bolt assemblies connected wheel halves together, with the inner half-wheel attached to the axle only via the tie bolts and outer half-wheel. This asymmetric design allowed for larger brake assemblies to fit within the wheel, unlike dual-web designs where each half-wheel contains an axle bearing.
As a result of the asymmetry, the tie bolts were exposed to a more cyclic load profile (compared with a more symmetrical design). The forces in the bolt could potentially oscillate with the rotation of the wheel while in service.
In this incident, the failed wheel was one of the outboard wheels on the aircraft and a hubcap normally covered the tie bolt assemblies.
Figure 2: Cross section of the main wheel showing the fracture initiation point
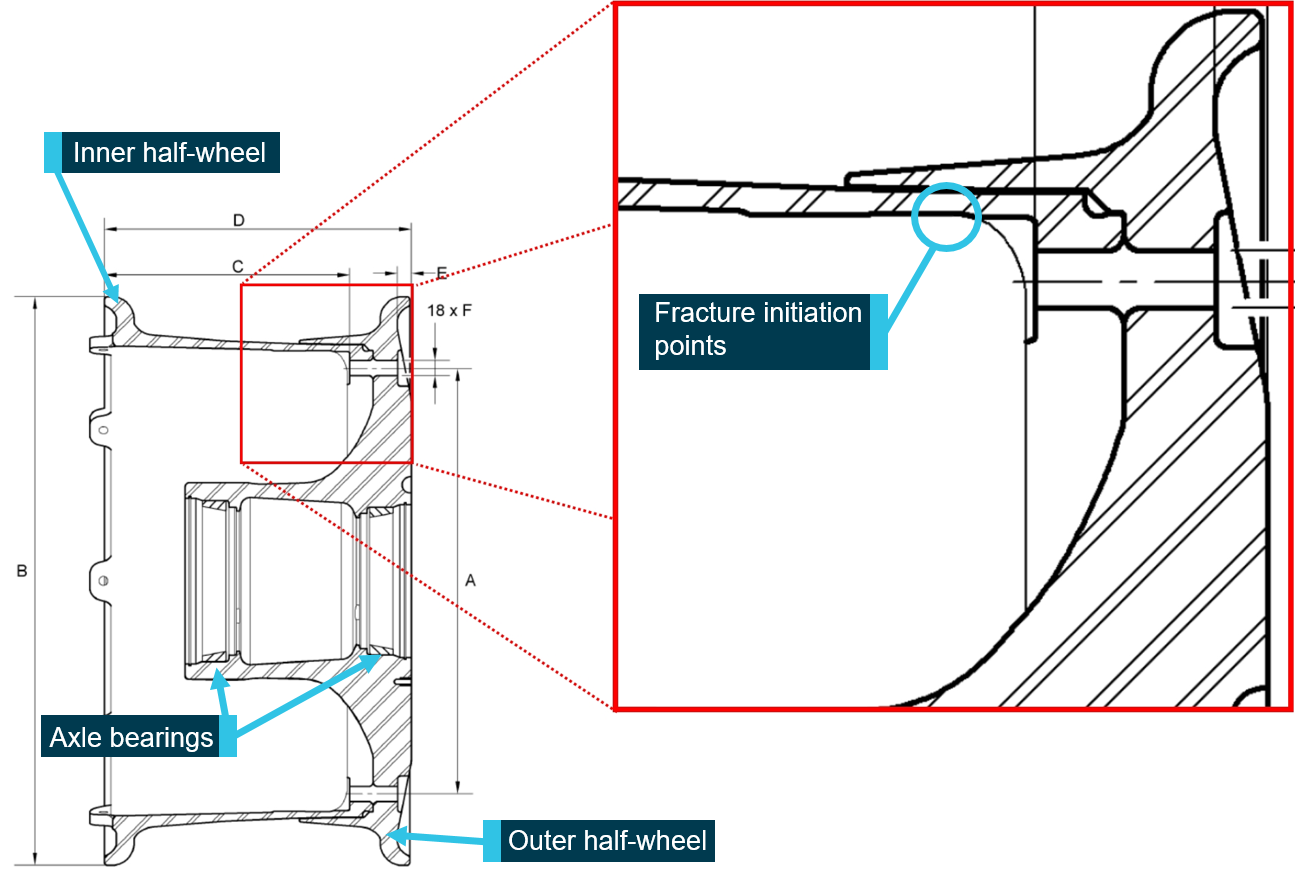
Source: Manufacturer, modified by the ATSB
The fracture location was coincident with a region of high stress during service. As seen in Figure 2, the cross section of the inner half-wheel reduced in thickness from left to right. The fracture occurred at the point where its cross section was thinnest, and near a change in geometry (tie bolt hole).
ATSB examination
The wheel halves from the ruptured assembly were initially sent to the ATSB for examination, where the following was found:
- Twelve of the 18 tie bolt assemblies could be twisted by hand.
- Several of the nuts had noticeably backed off the thread, with only three of the remaining six nuts above the minimum torque of 163 Nm.
- The breakaway torque[3] of each nut was tested, and four of the 18 nuts were below the acceptable value of 3.61 Nm.
- The tie bolt assemblies were visually inspected and found to be the correct part in every instance, with no evidence of damage.
- A region of the fracture surface near one of the tie bolt holes exhibited fatigue crack progression (beach) marks radiating away from several initiation points (Figures 3 and 4). The remainder of the fracture was consistent with shear overstress. There was no visual indication of material defect at the fatigue crack initiation sites.
Figure 3: Outboard fracture surface on the inner half-wheel, with a fatigue region
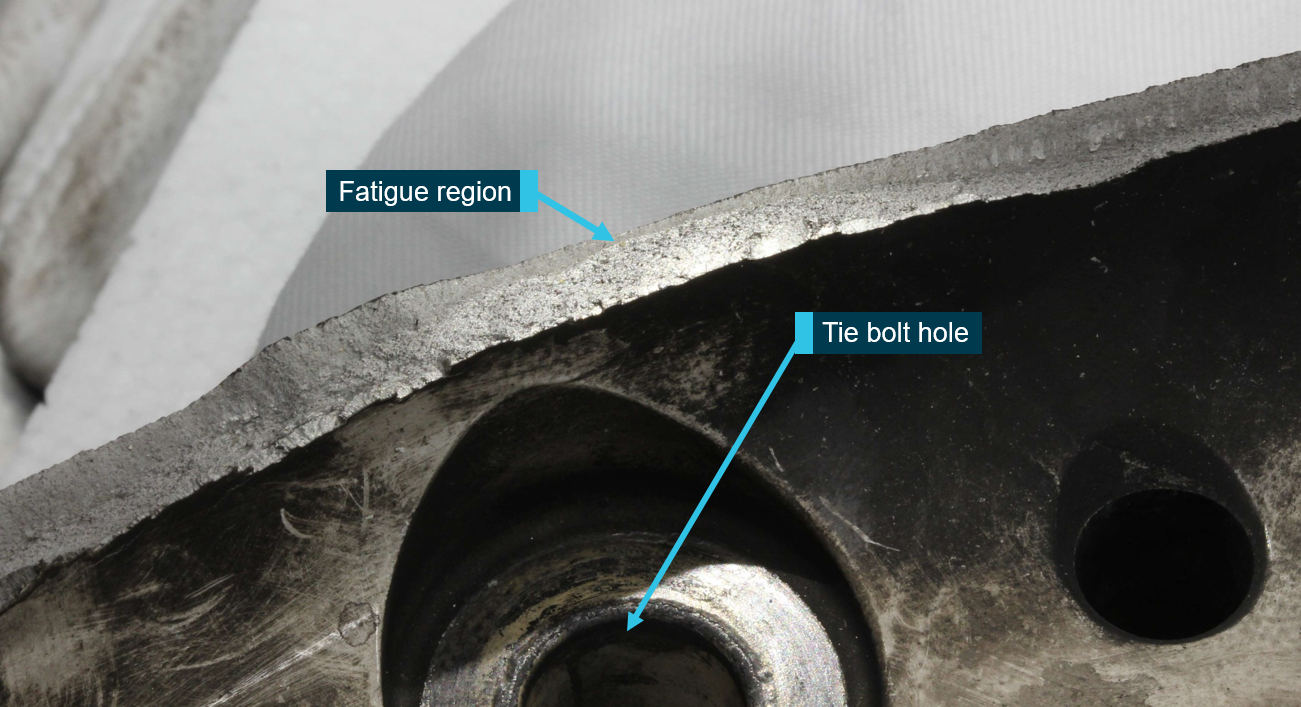
Source: ATSB
Figure 4: Fracture morphology of one of the fatigue cracks through the fractured inner half-wheel
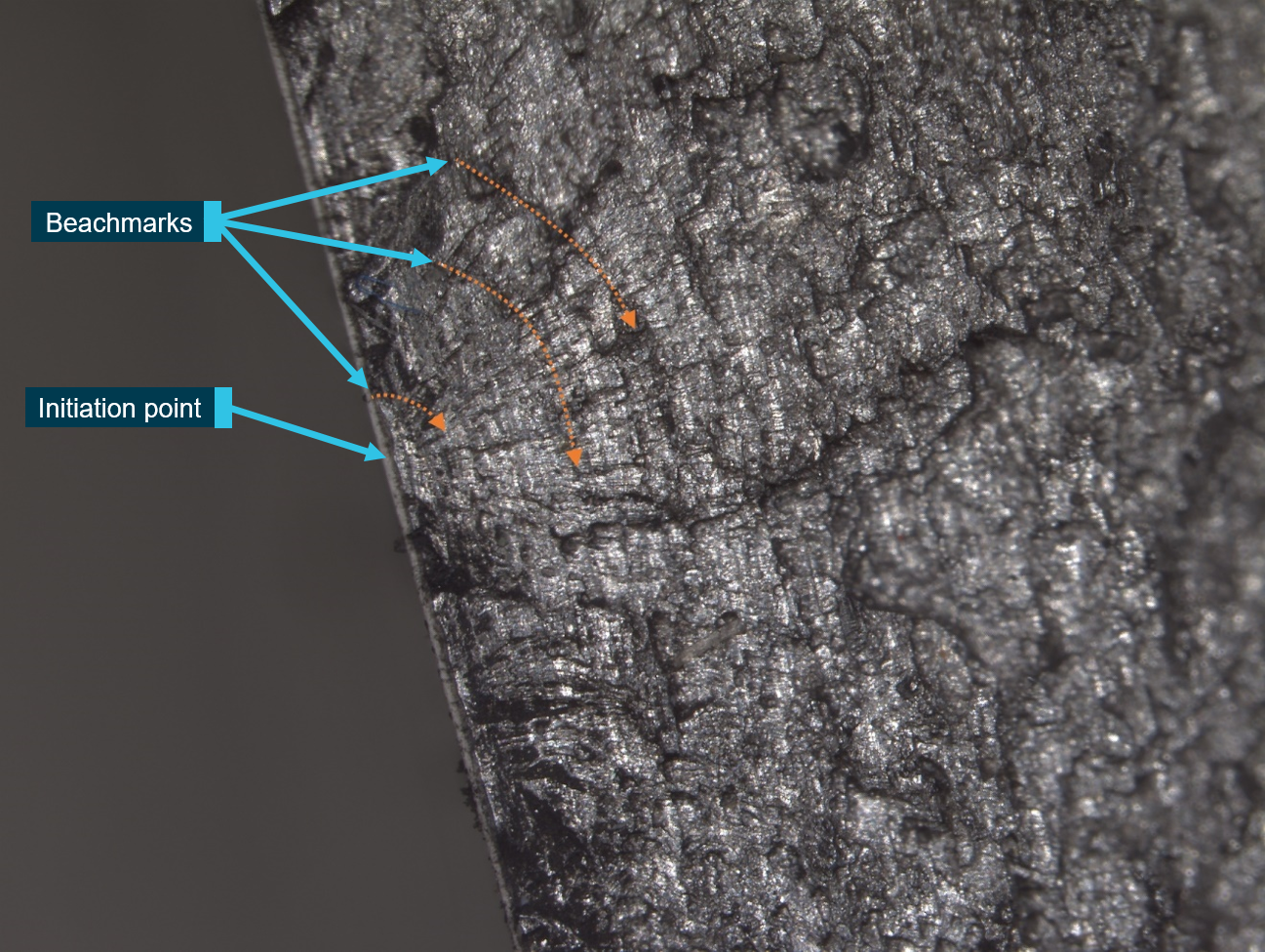
Source: ATSB
Manufacturer’s examination
The wheel manufacturer conducted a further examination of the failed main wheel, including a detailed analysis of the fracture morphology. They concluded that the wheel failed as a result of the observed fatigue cracks propagating into a mixed fatigue/ductile rupture mode. A small crack was also detected within the adjacent tie bolt hole, although this did not appear to have contributed to the wheel failure.
The manufacturer verified that the material composition and dimensions of the wheel were within specifications. Their report did not speculate on possible causes or factors contributing to the initiation or propagation of the observed fatigue cracking. However, they subsequently indicated that there was excessive ‘interposition product’ (anti-seize compound in this case) at the mating face of the occurrence wheel halves and that:
The presence of interposition product could lead to loss of bolt tension and then wheel rupture.
Specifically, it was believed that this interposition product prevented the wheel halves from abutting squarely against each other during assembly. Relative movement of the halves during service then resulted in loosening of the tie bolt assemblies and ultimately failure of the wheel. The manufacturer advised that the same mechanism was believed to have caused wheel failure in this type of wheel in two other instances (see the section titled Previous occurrences).
In March 2018, the wheel manufacturer visited the two different maintenance facilities responsible for Virgin’s 737 NG fleet to examine how the wheels were being maintained. Both facilities were following the tightening technique recommended by the manufacturer. However, at one facility the manufacturer reported seeing silicone grease on the mating faces of some of the wheel halves. This facility did not perform any maintenance on the occurrence wheel, and a subsequent visit by the manufacturer in September 2019 found that the grease was being applied appropriately.
Wheel history and maintenance
The occurrence wheel had undergone three tyre changes since its initial assembly in January 2016. It had operated for 173 cycles (47 days) since its last tyre change. According to one of the maintenance facilities responsible for the work, tie bolt assemblies generally lasted about three to four tyre changes before the lock nuts failed their breakaway torque tests and needed to be replaced. A tyre generally lasted approximately 40 days in service before needing replacement.
When reassembling the wheel after a tyre change, the tie bolt assemblies were tightened using a two-stage process, starting with an automatic dual spindle wrench. This device automatically torqued diametrically opposing nuts to a pre-set value of 70 Nm. In the second stage, the maintenance facility would use a single electronic torque/angle wrench for the final tightening. This involved rotating the nuts 100 degrees, as prescribed in the component maintenance manual (CMM). The wrench then indicated with a coloured light whether each nut was in the acceptable torque range.
This second stage was a relatively new tightening method introduced in 2014 via an optional service bulletin (SB C20626-32-007), to ‘improve wheel tie bolt clamping forces… and improve prevention against corrosion’. The service bulletin also recommended a new type of anti-seize compound, which was adopted by the maintenance facility prior to the occurrence. Following the occurrence, this new tightening method was made mandatory.
Prior to the occurrence, the manufacturer had updated the CMM to explicitly prohibit the application of any product to the mating faces of the wheel halves. Illustrations were included to demonstrate the proper application of anti-seize compound. A warning message regarding lubricant on the mating faces was also engraved on the wheels themselves. Since the occurrence, one of the maintenance facilities reported a change in nut design had resulted in fewer nuts failing their breakaway torque check.
Eddy current inspections[4] of the outer and inner wheel halves were mandated every tyre change. However, the CMM indicated that these were localised to the bead seat area of the wheel. These inspections would therefore not identify the fatigue cracks observed in this occurrence, which were at a different location. General inspections of Virgin wheels were performed every six tyre changes. These inspections included a visual inspection of each wheel half and dye penetrant inspection. It is not clear whether these tests would have revealed cracking such as that found in this occurrence. Regardless, the wheel ruptured after three tyre changes, so the inspection had not yet been performed.
Operator inspections for loose tie bolts
Following the main wheel failure, Virgin performed a fleet-wide inspection on this wheel-type. Two other wheels in service at that time had tie bolts loose enough to be moved by hand. One of these wheels was relatively new, and had not yet required a tyre change.
As another post-incident preventative safety measure, the maintenance facilities applied torque seal to all tie bolt assemblies after each tyre change. The torque seal provided a visual indication of loosening tie bolt assemblies without any additional equipment. All wheels were also inspected at regular intervals, with the longest time between inspections being 28 days in service. This interval was selected so that the majority of wheels would be inspected at least once before a tyre change (approximately 40 days in service).
When a wheel was found with broken torque seals, the wheels and tie bolt assemblies were visually inspected for damage and their breakaway torques were tested. Nuts were replaced if they failed their torque check and undamaged assemblies were put back into service. No other loose tie bolts were found following the initial fleet inspections until July 2017. From July 2017 to August 2018, the wheel inspections found:
- ten more wheels with at least one broken torque seal, including six with multiple broken torque seals
- broken torque seals on wheels that had come from each of Virgin’s maintenance facilities
- three wheels exhibiting tie bolts with broken torque seal, despite being above the minimum allowable torque
- one instance where a tie bolt with unbroken torque seal was below the minimum allowable torque.
The bolt with unbroken torque seal could indicate that not all tie bolt assemblies left the maintenance facilities with the appropriate torque. Conversely, the broken torque seals on correctly torqued nuts serve as confirmation the tie bolt assemblies loosened in service despite being appropriately tightened.
Since September 2018, there have been no more broken torque seals found during Virgin’s inspections.
Boeing advice on tie bolts loosening in service
In 2018, Boeing released a bulletin to its fleet, recognising several wheel failures involving this type of wheel and acknowledging that it was the result of tie bolt assemblies loosening in service. The publication stated:
As the nuts unscrew from the bolts, the wheel halves start to separate under the influence of tire pressure and ground loads. Eventually the wheel halves flex to a sufficient amount that the wheel ruptures…
The bulletin also stated:
The mechanism that causes the nuts to unscrew is not well understood and has been difficult to reproduce on a dynamometer during lab testing.
The bulletin described wheel-types from two different manufacturers, however both wheels had a similar single-web design, with the axle bearings contained within one wheel half. Boeing believed that the issue was unique to these two wheel-types. The bulletin stated that if the preload was ‘less-than-optimal, the nuts may start backing out, or ’unscrew’ from the bolts as the wheel rolls under load.’ Boeing identified two issues that were associated with loosening. From the digest:
Bolt preload. Strict adherence to the bolt/nut tightening procedures has been shown to minimize the likelihood of bolt loosening.
Bolt thread lubricant. Testing and in-service experience has shown that certain thread lubricants are more likely than others to result in nut loosening.
Wheel manufacturer service bulletins
The wheel manufacturer released two optional service bulletins that mitigated the likelihood or consequence of tie bolts loosening in service.
The first bulletin was released prior to the occurrence in July 2016, to ‘ease main wheel deflation in case of broken or missing tie bolts’ (SB C20626-32-014). This had not been implemented on the ruptured wheel. The service bulletin introduced a replacement for the inner half-wheel. The new part included grooves along the mating face of the half-wheel, so that any movement between the two halves would allow air to escape and result in the gradual deflation of the wheel. Based on estimations from the manufacturer, the new half-wheel currently has a 55-60 per cent adoption rate, on a global stock of approximately 12,000 in-service wheels.
The second service bulletin added lockwire on to the tie bolt assemblies to prevent any loosening while in service (SB C20626-32-016). This bulletin was released on 4 January 2018, however the wheel manufacturer advised that bulletin was not released in response to this occurrence.
Previous occurrences
The wheel manufacturer advised that globally, there have been three other cases in which this type of wheel has fractured, and in each case the manufacturer assessed that the fracture initiated from a loss of bolt tension. In two of those three cases, the manufacturer believed the loss of bolt tension was caused by interposition product (grease or anti-seize compound) between the mating faces of the wheel. VUH was the first and only occurrence in Australia (noting that Virgin and Qantas use this wheel-type on their 737 NG fleet).
While the number of wheel failures is known, the number of instances of loosening tie bolt assemblies could not be determined or accurately estimated. CMM instructions for disassembling the wheel did not include any instruction on recording bolt torque or inspecting for loose bolts. Instances of loosening tie bolts in Virgin’s fleet have been recorded since the occurrence, but in the global fleet the numbers are unknown.
__________
- The manufacturer described the design as single-web, because the web region connecting the axle bearings to the rim is only contained in the outer half-wheel. Dual-web designs have a web between the bearing and rim on both wheel halves.
- Breakaway torque measures the locking force of the nut. It is the torque required to loosen a nut that has been run onto a tie bolt.
- Eddy current testing involves using a magnetic field to induce a current in the material being inspected. This is known as an eddy current. Defects or cracks in this material can then be identified, as they may manifest as a measurable change in the eddy current.
Safety analysis
Occurrence event
The location of fatigue crack initiation in the wheel was coincident with areas of high service stress and there was no evidence of corrosion or manufacturing defect. A majority of the tie bolt assemblies on the fractured wheel were found to be loose, and nuts were found to be backing off on appropriately-torqued tie bolt assemblies on other wheels during service. Previous occurrences of wheel fracture have also been associated with loss of bolt tension. It was therefore most likely that tie bolt assemblies loosening in service resulted in the fatigue cracking and rupture of VUH’s left main wheel.
The loose tie bolt assemblies were likely a result of interposition product (grease or anti-seize compound) on the mating faces of the wheel halves. This prevented the halves from abutting squarely against one another when tightening the tie bolt assemblies. The wheel halves were then able to move relative to one another while in service, causing the tie bolt assemblies to loosen, reducing the clamping forces and inducing cyclic stresses.
Prevention or detection of tie bolt loosening
All of the possible reasons Boeing and the wheel manufacturer provided for the wheel ruptures related to having a suboptimal clamping force between the two hub halves, resulting in the failure mechanism described above. Prior to this occurrence, the wheel manufacturer had updated the component maintenance manual to explicitly prohibit interposition product between wheel halves. That update did not prevent this occurrence and the operator had 12 further instances of tie bolts loosening in service. However, since the manufacturer visited both of the organisations maintaining Virgin’s wheels, they have had no additional occurrences.
While actively preventing interposition product between the wheel halves appears to have been effective at reducing instances of loose tie bolts, there are other mechanisms that could reduce wheel clamping force. For example, since the occurrence there has been at least one instance of a wheel entering service with a bolt that was below the minimum required torque. Clamping force will also be affected by broken or missing tie bolts, which was the hazard addressed by the manufacturer through the introduction of hub grooves for safe tyre deflation.
At the time of publication there were no mandatory inspections capable of reliably detecting loose or missing tie bolt assemblies in service, between tyre changes. Those on the outer main wheels would not be readily observable due to the presence of a hubcap. In the absence of inspections, the two optional service bulletins (grooves for safe deflation, and lockwire on the tie bolt nuts) existed to prevent wheel ruptures and subsequent adverse outcomes, however their optional nature reduced the service bulletins’ effectiveness as risk controls.
Findings
From the evidence available, the following findings are made with respect to the main landing gear wheel failure of Boeing 737-8FE, registered VH-VUH, at Brisbane Airport, Queensland on 4 January, 2017. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
- A majority of the wheel's tie bolt assemblies loosened while in service, likely due to grease or anti-seize compound between the mating wheel halves. This resulted in fatigue cracking and ultimately, wheel rupture.
- The tie bolt assemblies on this wheel-type (single-web) were more prone than dual-web wheels to loosening during service, however there were no inspections for detecting loose tie bolt assemblies in service and no effective mandated risk controls to prevent wheel rupture.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Virgin Australia Airlines Pty Ltd
- Ground crew at Brisbane Airport
- Airservices Australia
- Main landing gear wheel manufacturer
- Wheel maintenance providers.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to Virgin Australia Airlines Pty Ltd, the main landing gear wheel manufacturer, the wheel maintenance providers, Boeing, the Civil Aviation Safety Authority (CASA), the French Bureau of Enquiry and Analysis for Civil Aviation Safety (BEA), and the National Transportation Safety Board (NTSB).
Submissions were received from the main landing gear wheel manufacturer, the wheel maintenance providers, CASA, and the BEA. The submissions were reviewed and, where considered appropriate, the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2020
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |

Occurrence summary
| Investigation number | AO-2017-003 |
|---|---|
| Occurrence date | 04/01/2017 |
| Location | Brisbane Airport |
| State | Queensland |
| Report release date | 30/03/2020 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Landing gear/indication |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 737-8FE |
| Registration | VH-VUH |
| Serial number | 34440 |
| Aircraft operator | Virgin Australia Airlines |
| Sector | Jet |
| Operation type | Air Transport High Capacity |
| Departure point | Brisbane, Queensland |
| Destination | Melbourne, Victoria |
| Damage | Minor |