The flight was a dual training exercise for a type endorsement. Some upper air work had been completed in the training area before the aircraft was flown to Camden for circuits and landings.
The instructor reported that during the third touch and go sequence, after a normal landing, the student had applied take-off power but then inadvertently selected the landing gear up, instead of the flaps. The instructor immediately closed the throttles as the right main landing gear collapsed. The aircraft slewed through 180 degrees before coming to rest on the flight strip. Both occupants vacated the aircraft without injury.
The pilot reported that after a normal landing and landing roll, whilst watching for the next exit from the runway, he accidentally raised the gear switch instead of the flap switch. The gear retracted and the aircraft slid to rest on the runway.
The aircraft was being operated as a scheduled passenger service from Singapore to Sydney, with the co-pilot as the handling pilot. Whilst cruising at flight level (FL) 370 over the centre of the Australian continent, turbulence was encountered. A diversion of about 30 NM to the right of track was carried out to avoid local storms, before returning to the original track. The seat belt signs had been on for some time and the cabin crew needed to resume the meal service which had been in progress. The pilot in command (PIC) requested a clearance to climb to FL390, which was approved. Conditions were smooth and clear at the higher level so the seat belt signs were turned off and the meal service resumed. The aircraft was being controlled by the number two autopilot.
Later, prior to reaching the top of descent, the co-pilot commenced the pre-descent review and briefing, which included a review of the aircraft fuel status. When the fuel system synoptic display was selected on the electronic centralised aircraft monitor (ECAM), a lateral fuel imbalance was observed, with the left inner fuel tank about 800 kg heavier than the right. The PIC elected to correct the situation and the fuel imbalance checklist was reviewed. The checklist required that the four fuel crossfeed valves be opened by depressing the four fuel crossfeed valve switches on the centre overhead panel, then turning off the fuel pumps in the lighter tank. The valve positions are monitored by observing the fuel system synoptic on the ECAM screen on the centre instrument panel.
The engine driven hydraulic pump push button switches are also located on the centre overhead panel, immediately above the fuel crossfeed valve switches. These switches are similar to the fuel crossfeed valve switches and are activated by the same push-button switching action. The engine driven hydraulic pump push button switches are not guarded to prevent inadvertent activation. All valve positions are monitored on the respective fuel or hydraulic system synoptic displays on the ECAM, on the centre instrument panel. Standard operating procedures require that, when a switch is manually activated, the respective valve position is monitored on the ECAM before any further switching actions are performed. This procedure is to confirm that the correct selection has been made.
The PIC reported that he raised his hand and placed his right index finger on a fuel crossfeed valve switch. Before depressing the switch, the co-pilot remarked that the fuel management was under automatic control, and in the forward transfer configuration at the time. The PIC removed his finger from the switch to refer back to the fuel system synoptic on the ECAM but then decided to continue with the fuel imbalance procedure. He then depressed what he thought was the number one fuel crossfeed valve switch, then the remaining switches in succession, leaving his finger on the last switch. He observed the white switch lights illuminate as each switch was activated but neither of the crew monitored the valve positions on the fuel system synoptic on the ECAM. After depressing the last switch, the PIC observed the green hydraulic system low pressure warning on the ECAM, heard one warning chime, together with the master caution light and alarm, and also heard the auto-pilot disconnect warning. He looked up and saw that he had inadvertently pushed all four engine driven hydraulic pump push button switches off and immediately switched them all back on.
When the autopilot disconnected automatically, due to the reduction in hydraulic pressure, the aircraft began to pitch up and the stall warning sounded twice. The PIC advised the co-pilot that he was taking control of the aircraft and gave a nose-down command to his side stick control, but did not utilise his side stick priority push button. At the same time the co-pilot also gave a momentary nose-down command to his side stick control before realising that the PIC had control. The aircraft pitched down, then up, before level flight was regained and the auto-pilot was re-engaged. During the event the aircraft climbed about 350 ft before returning to FL390.
The loss of hydraulic pressure to the hydraulically powered flight controls and the prevailing aerodynamic forces acting on the airframe, resulted in the aircraft pitching nose up. This configuration could not be reversed until hydraulic power was restored. However, during this period both crew had instinctively moved their respective side stick controls to a nose-down command. As the side stick inputs are summed, this action resulted in a rapid pitch reversal as hydraulic pressure was restored, and required a further nose-up correction before level flight was regained.
The resulting negative and positive vertical accelerations which occurred caused unrestrained passengers and cabin crew in the rear of the aircraft to be thrown about and injured.
ANALYSIS
The investigation identified a safety deficiency in that there were several factors which increased the potential for the inadvertent activation of the engine driven hydraulic pump push button switches. The switches were not guarded; they were similar in appearance to the fuel crossfeed valve switches; and were activated by the same push button switching action. They were also located immediately above the fuel crossfeed valve switches on the centre overhead panel.
The PIC had initially placed his finger on a fuel crossfeed valve switch. However, before he activated it, his attention was drawn to the ECAM fuel system synoptic on the centre instrument panel, when co-pilot commented that the fuel system was in automatic forward transfer. Whilst his attention was drawn to the ECAM his finger moved slightly higher and was then positioned over an engine driven hydraulic pump push button switch. Deciding that he would continue with the fuel imbalance procedure, the PIC looked up to the centre overhead panel to what he thought was the fuel panel and depressed the switch to the off position. He then continued to depress the remaining three engine driven hydraulic pump push button switches to the off position. Neither of the crew were alerted to the incorrect selection at that time as the ECAM fuel system synoptic was still displayed.
As the aircraft was relatively new, there would have been minimal internal hydraulic system leakage. The aircraft was flying in still air so there was little demand on auto-pilot input to the various flying control hydraulic actuators. The hydraulic system accumulators continued to provide some residual pressure whilst the main hydraulic pressure was bleeding off, so it took some time before the hydraulic pressure depleted sufficiently to trigger the hydraulic system low pressure warning, though the hydraulic pump low pressure warnings had occurred. This time allowed the PIC time to switch off all the hydraulic pumps before a warning was observed and corrective action taken.
SIGNIFICANT FACTORS
1. The four engine driven hydraulic pump push button switches were not guarded to prevent inadvertent activation.
2. Inadvertent selection of the four engine driven hydraulic pump switches to the off position resulted in the loss of hydraulic system pressure to the hydraulically powered flight controls. The autopilot disengaged automatically due to the reduced hydraulic pressure.
3. The crew did not monitor the fuel crossfeed valve positions on the ECAM fuel system synoptic, following each switching action, in accordance with standard operating procedure.
SAFETY ACTION
As a result of the investigation into this accident, the Bureau of Air Safety Investigation issued the following safety advisory notice SAN960163:
"Airbus Industrie, Civil Aviation Authority (Singapore), Bureau Enquetes-Accidents (France), Civil Aviation Authority (UK), Transportation Safety Board (Canada), Federal Aviation Administration (USA) and the Civil Aviation Safety Authority (Australia) should note the circumstances surrounding this occurrence and the safety deficiency identified by BASI's investigations."
SAFETY ACTION BY MANUFACTURER
Airbus Industrie, as a result of this advisory notice, and subsequent investigations by their own staff, undertook the following safety actions:
1. Issued a notification to all operators of the aircraft type of the details surrounding the occurrence.
2. As an additional precautionary measure, Airbus Industrie has decided to develop a modification introducing a guard on each engine driven hydraulic pump push button switch.
When the aircraft landed, there was a crosswind from the right at about 10 kts. After a ground roll of about 300 m, the pilot elected to retract the flaps before commencing braking. Because of the crosswind, he was looking ahead of the aircraft to maintain directional control and inadvertently selected the landing gear control to the UP position. The landing gear retracted, and the aircraft slid on its belly for a further 300 m.
On 12 October 2014, at about 1517 Central Daylight-saving Time, the flight crew operating a Qantas Airways B737 aircraft, registered VH-XZI, were preparing for the approach and landing into Adelaide, South Australia. The aircraft had departed about one and a half hours earlier from Alice Springs, Northern Territory, with the captain as the pilot flying (PF) and the first officer as the pilot monitoring (PM).
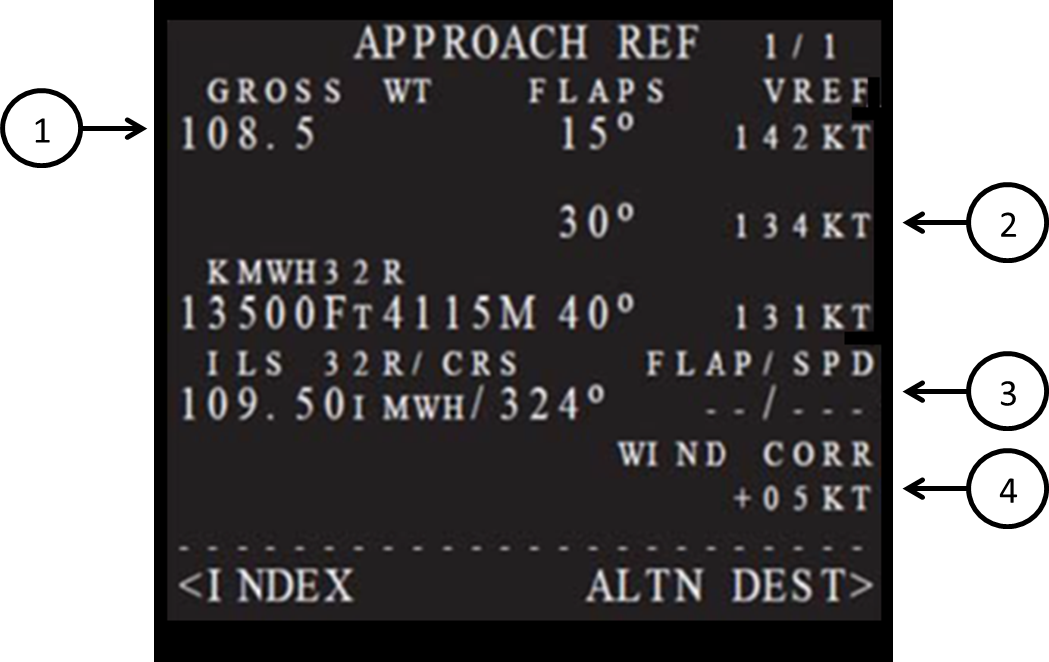
During descent preparations, air traffic control (ATC) issued arrival instructions which the crew loaded into the flight management computer (FMC)[1] via the control display unit (CDU)[2] (Figure 1). In accordance with company procedures, the PM calculated the expected landing weight. After obtaining confirmation from the PF that his calculations were valid, he entered this figure into the aircraft gross weight (Gross WT) section of the approach reference page, (Figure 1). However, according to the post-flight data obtained from the quick access recorder (QAR), a figure of 52 tonne (T) had been inadvertently entered instead of the predicted landing weight of 62 T.
To complete the manual selections, the PM stated he verbalised, and then selected the flap 30 field on the CDU (Table 1).
Figure 1: An example of a CDU Approach Reference page
Source: Qantas Flight Crew Training Manual
Table 1: Approach reference page expanded information
No.
Item
Function / notes
Detail
1
Aircraft Gross WT
Normally displays the FMC calculated aircraft Gross WT.
Manual entry of Gross WT is allowed. Leaving and returning to this page replaces a manually entered weight with FMC computed Gross WT.
2
Vref
FLAPS – VREF
Displays landing Vref for three flap settings as computed by the FMC. Speeds are based on displayed gross weights. Vref once selected, will not be updated. To obtain an updated speed, the current speed must be deleted, or a different Vref selected or entered.
3
Flap/Speed (FLAP/SPD)
Displays selected approach reference flap and speed setting.
Manual input of desired flap and/or speed settings may be made.
4
Wind Correction
Displays current wind correction for approach.
Default is +5 kt
Source: Qantas
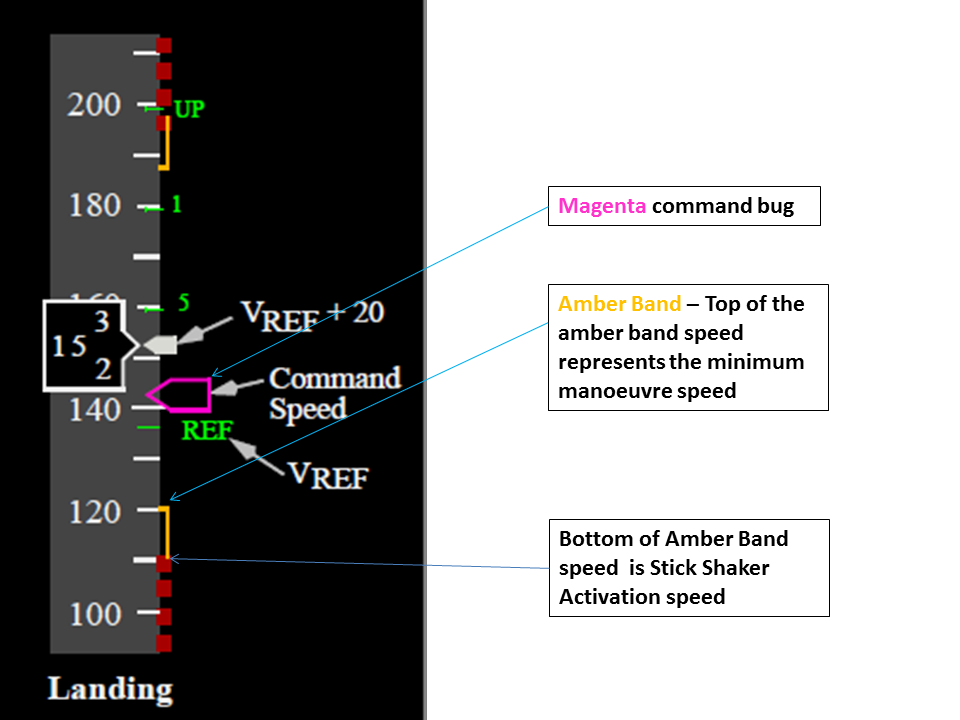
Following the inadvertent landing weight data entry error, the FMC calculated the flap speed schedule and the landing reference speed (Vref), based on this lower weight. With each stage of flap selection, the magenta bug[3] moved and pointed to the new command speed on the airspeed indicator. With the selection of flap 30, the command speed became Vref plus any wind correction factor entered by the crew[4] (Figure 2).
The captain briefed, then flew the arrival and approach onto runway 23 in clear conditions and mild, westerly winds. At about 1,500 ft above mean sea level, the aircraft was fully configured for landing with the gear down and flap 30. The captain disconnected the autopilot and hand flew the remainder of the approach and landing.
During the approach, the PM made a verbal reference about the airspeed being ‘wrong’. The PF reported he did not clearly hear what the PM had said, nor did he understand what message the PM was trying to convey. The captain assumed that the PM may have been making a comment in relation to a relatively new company procedure[5] used to calculate the approach speed. All the instrumentation presented to him looked normal, so he made the assumption that it was not something critical, and continued to focus on aircraft flight path management.
The PF continued to make adjustments to the thrust levers to allow for changes in wind. As was their normal procedure, the PF used the head-up guidance system (HGS) during the flight.[6] The PF reported that after the Flap 30 selection, he noted that the speed bug (‘magenta’ bug) moved a greater distance down the speed tape than normal, but he was not unduly concerned and continued to focus on flight path management.
At a height of about 200 ft, the PM reported he called “speed’ when he noticed the magenta speed bug on the primary flight display (PFD) airspeed indicator (ASI) reduce to within close proximity of the top of the amber band (Figure 2); however, the PF reported not hearing this call.
During touchdown, both crew noted that the aircraft’s pitch attitude was higher than usual. The aircraft had a nose-up pitch of 7.5°; whereas a normal nose-up pitch was 3.5-3.75°. The remainder of the landing was normal and there were no injuries and no damage to the aircraft.
The captain commented that with a non-VNAV approach, the crew set the approach speed into the mode control panel speed window (MCP). However, as in this case with a VNAV approach, the speed window is blank, the FMC selects the speed bug as the crew select the flap. This removed an opportunity for the crew to detect the speed mismatch.
The captain stated that in hindsight the aircraft nose attitude must have been higher than normal on the approach,[7] however he did not notice it during the occurrence.
First officer (PM) comments
When the PM noted that the magenta bug was closer than normal to the manoeuvring margin amber band on the PFD airspeed indicator, he thought the ‘moving’ amber band may have reached a higher airspeed due to the increased g loading in the gusty conditions, until he also noted the discrepancy on the CDU from the flaps 30 Vref calculated earlier during the preparation for descent phase.
The PM reported that when he made a reference about the airspeed being ‘wrong’, to the PF, he believed the call was clear and concise; he also added the instruction to fly a certain airspeed. He believed this was a safer option that going “head down” and reselecting the landing vref on the CDU.
As noted in Table 1 – note 1, once the crew left the approach reference page on the CDU and then returned to it, the page defaulted back to the FMC calculated (higher) GW and (higher) Vref for Flap 30. This realisation prompted the PM to say that the ‘speed’s wrong’ to the captain. When the PM saw the captain advance the thrust levers (for the gusty conditions) he thought this was a response to his comment.
Operator report
The operator conducted an investigation into the incident. Their report detailed the following:
The data entry error was made when entering the expected landing weight into the FMC Approach Reference page; this figure was not reconciled against the final load sheet
As the PM had only just started to comprehend the speed disparity, this led to the non-assertive comment. [note PM comment under First Officer comments regarding this aspect]
The Boeing Speed Calculation method may have contributed to a reduced level of recognition by the Captain of the significance of the position of the magenta bug and the amber band. This method varied from the previous Reference Ground Speed (RGS) method used to allow for changes in wind between when the aircraft was on approach and the wind experienced during touchdown
It is likely that the advancement of the thrust levels at the time the PM started to recognise a speed disparity led to a level of confirmation bias that the speed disparity was being addressed
The predicted landing weight was printed on the final load sheet given to the flight crew just prior to departure, however this figure did not allow for variations in fuel burn experienced in flight. The load sheet estimated landing weight was often used as a gross error check by flight crew, but it was not part of the company standard operating procedures. On this occasion, the crew did not conduct a gross error check using the load sheet figure, nor were they required to do so.
Non-technical skills training (NTS)
The operator reported that ‘flight crews undergo extensive non-technical skills training and recurrence during initial and cyclic training sessions. As part of this training, various levels of assertion are regularly highlighted in the event that a disparity in aircraft performance is recognised. Key indicators of uncertainty were observed in this occurrence around error recognition and confirmation. It is likely that this uncertainty resulted in a breakdown of the expected levels of assertion and a reduction in the preventative control’.
Recovery controls
The operator also noted that recovery controls would have been effective had the speed reduced to a critical amount. The head up guidance system provides visual caution/warning to the captain in the event that a tail strike pitch angle or rate is approaching, or has been exceeded. The head-up guidance system also indicates the angle of attack and normal angle of bank as a visual cue to the captain.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Flight operations
As a result of this occurrence, Qantas has advised the ATSB that they are taking the following safety actions:
Action taken by Qantas
As a result of this incident, the operator intends to revise the flight crew operations manual (FCOM) descent procedures. The procedures will include an item requiring the PM to compare the landing weight entered into the Approach Reference page during descent preparation, with the load sheet estimated landing weight.
Safety message
Data entry errors
Although having a primary focus on data input errors in preparation for take-off, the message is common. Errors can occur irrespective of pilot experience, operator, aircraft type, location and take-off [or landing] performance calculation method.
An ATSB research study titled Take-off performance calculated and entry errors: A global perspective is a research paper which focused on such incidents and accidents in the 20 years prior to 2009. A consistent aspect was the apparent inability of flight crew to perform ‘reasonableness checks’ to determine when parameters were inappropriate for the flight.
This research article is available at the ATSB website.
Also the ATSB have produced a short YouTube video on Safety concerns in regard to data input errors. This can be viewed at the ATSB website.
Crew communication
This incident highlights the importance of effective crew communication. The PM attempted to communicate his uncertainty to the PF, but the PF did not understand the specific nature of the PM’s concerns.
Non-technical skills (NTS) previously known as cockpit resource management (CRM) training has developed over many years to promote teamwork among pilots and to lead to a reduction in human error. Two studies conducted by Fischer, U., and Orasanu, J., published in 1999 looked at language and communication strategies between two groups of captains and first officers from three major US airlines. Of interest, the studies found that the strategies pilots indicated they would use to mitigate pilot errors, may not be the most effective ones. Also, there was a considerable difference between the captains’ and the first officers’ communication strategies.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
During a touch and go landing, the pilot inadvertently selected the landing gear up instead of the flap while the aircraft was still on the runway. The landing gear retracted, and the aircraft slid to a stop.
The aircraft was the second to take off in a stream of six on a night flight from the Tangalooma Resort strip to Coolangatta aerodrome. Shortly after take-off it struck the ground, nosed over, and was consumed by a fuel-fed fire.
The take-off run appeared normal, but the initial climb was shallow according to the witnesses, some of whom were pilots waiting their turn to take off. At about 150 ft above ground level the aircraft entered a descent which continued until ground impact, 164 m beyond the departure end of the strip. The nose gear collapsed at impact, but the aircraft remained upright and skidded along the ground on its main gear and front fuselage. It traversed a low sand dune, fell 10 ft to the beach and overturned. The aircraft came to rest 112 m beyond the first ground contact. All four passengers were able to evacuate the aircraft which had started to burn. The pilot was rescued by her passengers.
1.2 Weather and visibility
The weather was fine with some cumulus cloud over Moreton Bay to the west of the strip. It was a dark night with only stars visible. The wind was almost calm but slightly favoured a take-off towards the north. The northern take-off path extended over north-eastern Moreton Bay. Except for a possible light from a fishing trawler or house at Cowan township, there was no surface illumination and no discernible horizon. A take-off to the south on the other hand was available with a distinct horizon reference due to an illuminated Tangalooma Resort some 5 km south and the very bright lights of the Brisbane Port facilities at Fisherman Islands some 40 degrees to the right of runway heading.
1.3 Personnel information
1.3.1 Pilot in command
The pilot was a Grade 2 instructor, employed by the flying school where she learnt to fly. She had a current command multi-engine instrument rating and was endorsed to fly the aircraft type. The pilot was required to wear spectacles when flying and she did on this occasion.
On 14 September 1995, the pilot was checked on the route by the chief pilot. The route check included a night take-off at Tangalooma strip. Her most recent flights in the aircraft were on 15 October and 2 November 1996. Both flights were return flights between Coolangatta and Tangalooma, with a night take-off from the Tangalooma strip. The night take-off on 2 November was conducted towards the south.
1.3.2 Previous 72-hours history
The weather on the two days before the accident precluded any flying duties. During this period, the pilot worked at the flying school office and brought her book-keeping duties up to date. On the two nights prior to the accident, she had retired to bed at 2030 hours and 2130 hours local time, respectively. Prior to then she had been off duty for 9 days. On the day of the accident, the pilot commenced duties at 1400 hours, planning the afternoon flight to Tangalooma and the night return. Between her arrival at Tangalooma and the night take-off, she rested and had dinner at the resort.
1.3.3 Information from the pilot
The pilot was hospitalised with serious leg injuries. She had also suffered a blow to the head. She was interviewed in hospital and said that she could not remember the take-off and subsequent flight into terrain. The pilot said that the aircraft carried a printed checklist on a single sheet of paper which her employer required company pilots to use in normal aircraft operations. However, for reasons not established, the pilot did not use the checklist after landing at the island strip or during the subsequent night departure.
1.4 Passenger action
The four passengers were foreign nationals and were seated in rows 2 and 3. They were not injured in the crash and were able to crawl out through the open cabin doorway. A fuel-fed fire had started almost immediately, and the aircraft was well alight by the time they cleared the aircraft. They soon realised that the pilot was still in the cockpit. Some of the passengers crawled back inside and pulled the semi-conscious pilot clear of the aircraft. Other people arrived on the scene soon afterwards and moved the passengers and pilot further away from the burning aircraft.
1.5 Wreckage examination
The aircraft had come to rest upside down on a beach. The front of the cockpit was crushed during the nose-over. The cabin was completely destroyed by a post-impact fire which also damaged the right engine.
Examination of the wreckage found that the flaps were retracted and that the elevator trim was set about halfway between the take-off setting and the fully forward position. Both engines were removed for specialist bulk strip examination. This examination did not discover any defect which could have prevented the engines from developing rated power. This evidence supports witness information that the engines' note did not change during the entire flight sequence. Due to the high wing configuration, neither propeller contacted the ground until the aircraft nosed over. Examination showed significant torque twisting and bending to both propellers indicating that the engines were still developing significant power when the aircraft nosed over.
1.6 Aircraft flight characteristics and flight test
1.6.1 Flap retraction
Discussions with pilots experienced on the aircraft type indicated that during initial climb, the take-off flap must be retracted in stages, trimming the elevator at the same time. Their opinion was that if the flap was retracted in one movement instead of stages, the nose-down trim change would be significant.This would result in a lower nose attitude unless the pilot held back pressure on the control column.
1.6.2 Flight test
At the Bureau's request a flight in a Partenavia was undertaken by a Grade 1 instructor with the view to establishing elevator control forces under specific conditions. The aircraft was flown on a final approach with full flap selected. The elevator was trimmed so that there was no residual force on the elevator control. This resulted in a trim indication halfway between neutral and a fully nose-down position. A take-off was conducted with the elevator trim and flap in the previous position. The pilot reported that a medium-to-heavy rearward elevator force was required to rotate the aircraft and establish a positive rate of climb. At a safe height, the flaps were retracted. This procedure was accomplished twice with the following result:
If the indicated airspeed and rate of climb were maintained the elevator force increased to the point of being very heavy.
If the elevator force was not increased, the aircraft settled into a 400 ft per minute rate of descent.
The pilot conducting this test commented that unless a pilot was prepared, the high elevator force required to maintain a positive rate of climb was excessive and well outside the normal experience range of an average pilot.
1.7 Dark night take-off research
Bureau research has shown that dark night take-offs can present a number of special problems for pilots, particularly when departing from aerodromes in areas with little or no ground lighting. Specifically, the somatogravic illusion has been suggested as being a contributing factor in the majority of these accidents. A somatogravic or false climb illusion occurs when a pilot who is deprived of outside visual cues attempts to maintain a desired pitch attitude without reference to instruments whilst the aircraft is accelerating. Under such conditions, pilots can experience a sensation of excessive pitch-up. The sensation is thought to exist primarily at take-off, go-around and during visual flight into cloud. At take-off, pilots who attempt to correct for this sensation by relaxing the backward pressure on the elevator control, may fly the aircraft into the ground.
2. ANALYSIS
2.1 The checklist
The pilot said that she did not use the checklist following the daylight landing at the Tangalooma strip, nor did she use it prior to the night take-off. The pilot could not give an explanation for this omission. A checklist written on loose paper can be difficult to handle during busy periods of operation such as circuit work or in low-light conditions, specifically at night. This could explain the lack of use in this case. If a checklist is not used, the pilot must commit all checks to memory.
2.2 Elevator trim
The elevator trim was found in a position consistent with the trimmed position for a full-flap landing. It is highly likely that the pilot missed the trim item off her memorised checklist both following the daylight landing and during pre-take-off checks at night.
2.3 Evidence from the test flight
The test flight pilot reported that the elevator force induced by an incorrectly set elevator trim would overpower a pilot who was not prepared for this predicament. The shallow take-off witnessed by others was probably the result of the pilot encountering such an unexpected down-elevator force. The pilot probably retracted the take-off flap in one movement rather than in a staged retraction since she would have needed both hands on the control column. Such an action could only have exacerbated the downward force on the elevator.
2.4 Dark night take-off
In addition, the pilot was faced with a dark night take-off. Unless the pilot's attention was focussed almost solely on the correct climb attitude, it was likely that the nose attitude would be lowered inadvertently. Because of the unexpected elevator force, she was probably distracted from her proper instrument scan. Under these circumstances, an illusion of a false climb would have resulted in her not maintaining the high load needed on the control column. This would have resulted in the aircraft descending back onto the ground. That this came as a totally unexpected event is borne out by the lack of any action in correcting the aircraft attitude, reducing descent, or reducing power.
The collective decision by the pilots to conduct take-off operations towards the north was unwise, considering that a useful visual horizon was available for take-offs towards the south.
3. CONCLUSIONS
3.1 Findings
The pilot was fully qualified to undertake the flight.
The night was dark and the area beyond the departure end of the runway was devoid of any useful lighting.
A southerly take-off direction was available, with a visible horizon.
The pilot did not make use of the written checklist carried in the aircraft.
The elevator trim was set halfway between neutral and fully forward.
The flaps were fully retracted at impact.
The aircraft impacted wings-level and in a shallow descent.
Full power was maintained throughout the take-off and accident sequence.
3.2 Significant factors
The take-off direction was dark and had no visible horizon.
The elevator trim was not set for take-off.
The elevator load on take-off was high.
The pilot did not monitor the aircraft attitude after lift-off.
The flap was retracted in one movement, increasing the elevator load.
The pilot may have been affected by somatogravic illusion to the extent that she thought the climb attitude was adequate.
The pilots reported that the aircraft was being used for dual night circuits training. The student pilot inadvertently selected the gear up instead of the flaps while on the ground during the third touch and go landing. The instructor immediately took over and selected the gear down. The aircraft slid down the runway and came to a stop.
At about 1324 Eastern Standard Time on 28 July 2014, the flight crew of an Airbus A320 aircraft, registered VH-VFU, was preparing the aircraft for the return leg from Sydney, New South Wales, to Adelaide, South Australia.
ATC issued the crew with a departure clearance for runway 16L. A Configuration 2 (flap and slat setting) was required for take-off. Shortly after, ATC advised the crew that the clearance was cancelled and re-issued a new departure clearance for runway 34L.
As a Configuration 1 + F would now be required for take-off, the FMGC was updated. The crew then briefed on the new departure, however neither crew member recalled specifically briefing on the changed take-off configuration.
The PM inadvertently selected the originally calculated Flap 2 take-off setting. He then checked the flap position on the upper ECAM. As he believed he needed to set flap 2, the flap 2 setting displayed on the ECAM confirmed what he believed to be correct.
Despite carrying out all the required flows and checklists, as they taxied the aircraft to the runway 34L holding point, neither of the crew detected the incorrect configuration setting. The aircraft departed normally, and at about 800 ft the crew detected and managed the error and continued to Adelaide.
Jetstar has advised the ATSB they are taking the following Safety Actions.
Jetstar has decided to undertake a detailed review of the results from their Flight Safety Integration Audit (FSIA) program. This is a continuous safety audit program targeted toward identifying specific operational threats and risks associated with failed/erroneous Human-Machine Interface activities. The airline will then develop action plans to address any identified themes.
Jetstar will also incorporate a summary of the incident in the next edition of the company flight crew Technical Newsletter. This will include suggestions on how to mitigate against similar occurrences.