On 23 November 2007, a Boeing Company 767-338, registered VH-OGG, was being operated on a scheduled passenger service between Sydney, NSW and Melbourne, Vic. On board were two flight crew, seven cabin crew and 255 passengers. The aircraft departed Sydney at 1426 Eastern Daylight-saving Time (EDT).
At about 1455, a passenger reported to a flight attendant that he could smell fumes coming from the gasper air vent above his seat. The passenger later reported that the fumes smelled like jet exhaust. The passenger became unconscious and was administered oxygen. He regained consciousness within a few seconds of being administered oxygen. A second passenger, seated in the area, also reported feeling nauseous at the time.
The flight crew declared a state of urgency to air traffic control and began performing the 'Smoke or Fumes - Air Conditioning' checklist. The aircraft landed at Melbourne Airport at 1529.
There were no other reports of adverse effects from any of the other passengers or crew on board the flight. The two affected passengers had travelled extensively by air with no previous adverse reactions. The investigation could not determine whether the passengers' symptoms were as a result of fumes in the aircraft cabin, or whether there were other unidentified medical conditions that may have contributed to the symptoms exhibited by the two passengers.
The investigation identified a non-contributory safety issue related to adherence to curing times following application of corrosion inhibiting compounds in the aircraft's cargo bays. The report details safety action taken by the operator to address this safety issue.
On 5 August 2007 at 1407 Eastern Standard Time, a Saab Aircraft AB 340B, registered VH-RXX, was being operated on a scheduled passenger service from Sydney to Albury, NSW. It was the aircraft's first flight of the day and the first flight after a routine compressor wash carried out on the engines.
An odour, which had been apparent inside the aircraft during the preflight procedure and taxi, and which was described as 'similar to curry', became much stronger from just before rotation until about two minutes after take-off. Believing the fumes were caused by compressor wash fluid and would dissipate, the flight crew elected to continue the flight.
The manufacturer of the compressor wash fluid confirmed that, when heated, it would produce an odour similar to curry.
The operator reported that their compressor wash procedure had been followed and was unable to explain the subsequent ingress of fumes to the cockpit and cabin of the aircraft.
On 5 June 2009, during a scheduled passenger service from Melbourne, Victoria (Vic.) to Coolangatta, Queensland (Qld), the cabin crew of a Boeing Company 737-800 aircraft, registered VH-VBL, detected a strong intermittent smell in the rear of the cabin. An inspection by the cabin crew did not detect the source of the smell.
On descent prior to landing, cabin crew presented various symptoms. Two of the cabin crew used oxygen before recovering sufficiently to resume their duties. No passengers were affected.
The airport rescue and fire fighting service attended the aircraft at the arrival gate. Paramedics conducted medical checks on the cabin crew. Both the cabin crew and flight crew were taken to the local hospital for further examination and later released.
The cargo holds were opened prior to a precautionary inspection for the source of the fumes. The source and nature of the fumes was not identified.
As a result of the incident, the operator initiated and completed a number of safety actions to improve communications and processes in relation to air contamination events.
While it was not possible to determine the nature or source of the reported fumes, the incident highlights the potential for crew incapacitation from exposure to toxic smoke and fumes.
Occurrence summary
Investigation number
AO-2009-025
Occurrence date
05/06/2009
Location
En route Melbourne, Victoria to Coolangatta, Queensland
On 25 February 2008, at about 2128 Eastern Daylight-saving Time, the flight crew of a Boeing Company 747-338 (747) aircraft, registered VH-EBY, detected a smell that slowly increased in intensity. At that time, the aircraft was cruising at 37,000 ft and was about 275 km west south-west of Sydney, NSW.
The flight crew donned their emergency oxygen equipment and transmitted a PAN call to air traffic control. The aircraft was cleared direct to Sydney for landing and was escorted to the terminal by the airport fire services for disembarkation.
An inspection by the operator determined that loose terminal connections to the left windshield heat element resulted in electrical arcing and fumes on the flight deck.
The aircraft manufacturer has a programme to replace the windshields in the 747 with an enhanced windshield heater wiring connection that should address the risk of electrical arcing in that component.
The Australian Transport Safety Bureau did not conduct an on-scene investigation of this occurrence. The report presented below was prepared principally from information supplied to the Bureau.
REPORTED INFORMATION
On 15 January 2005, at about 0915 eastern summer time, an Airbus A320 aircraft, registered ZK-OJA, with a crew of six and 135 passengers, departed Christchurch, New Zealand on a scheduled passenger service to Melbourne, Victoria.
During descent, the flight crew noticed a strong, sweet, solvent smell. They immediately advised the purser who reported that there was a strong smell in the forward cabin similar to that being experienced on the flight deck. No abnormal smells were evident in the main cabin, but there was a strong smell in the rear cabin similar to that in the forward cabin. A crew member in the rear cabin reported feeling unwell and nauseous. The flight crew donned oxygen masks and broadcast a Pan-Pan transmission1 to air traffic control.
The flight was completed without further incident.
The aircraft was returned to service following an engineering examination that found no environmental, mechanical or operational factors that could have influenced the circumstances of the occurrence.
1A Pan-Pan transmission is made in the case of an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
On 2 September 2004, the aircraft manufacturer reported that it was reviewing the following:
failure conditions that can affect lavatory hand basin water shutoff mechanisms
design, panel assembly and installation of 717 aft cabin interphones
electrical installations associated with 717 aircraft lavatory modules
lavatory faucet reliability data.
Operator
On 5 December 2004, the aircraft operator reported that its 717 flight simulator landing gear `down' indication during flight on emergency electrical power was incorrect. As a consequence, the aircraft manufacturer made software changes to 717 flight simulators to correct that anomaly.
Factual Information
FACTUAL INFORMATION
At 1435 Eastern Standard Time on 10 August 2004, a Boeing Company 717-200 aircraft, registered VH-VQA, was climbing to cruise altitude on a scheduled passenger service from Melbourne, Vic. to Hobart, Tas. with six crew and 52 passengers on board. As the aircraft passed through flight level (FL) 110, the crew heard a loud bang, with a corresponding increase in indicated left engine vibrations. The left engine began to spool down and the turbine gas temperature (TGT) indications began to increase significantly.
The crew initially brought the left engine power lever back to idle. However, the TGT continued to increase, indicating a maximum of 1,149oC, before they shut the engine down and discharged a fire bottle into the cowling area in accordance with the operator's procedures. They then notified Melbourne air traffic control (ATC) of the engine failure and returned to Melbourne.
The operator examined the left engine and found metal fragments in the exhaust area and some metallisation1 of the exhaust duct.
At the time of the failure, the BR700-715 engine, serial number 13148, had completed 10, 321 hours and 8,888 cycles since new, and 6,474 hours and 5,417 cycles since repair.
Engine investigation
The operator removed the engine and forwarded it to the engine manufacturer in Germany for detailed investigation, under the supervision of a representative of the German Federal Bureau of Aircraft Accident Investigation (BFU2), on behalf of the Australian Transport Safety Bureau (ATSB).
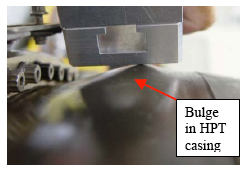
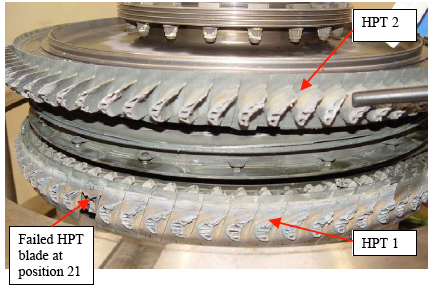
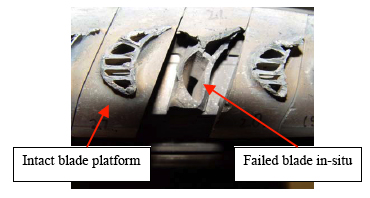
The manufacturer conducted a visual inspection of the engine's exterior, noting a bulge around most of the circumference of the high-pressure turbine (HPT) casing (Figure 1), in line with the Stage-1 HPT (HPT 1). A borescope examination of the engine interior showed that one HPT 1 blade was almost completely missing, with the remaining HPT 1 blades separated just above the blade platforms (Figure 2). There was also significant damage to the subsequent HPT and low-pressure turbine stages. Examination of the engine's compressor assembly revealed no significant damage. All of the high energy debris from the failure had been fully contained3.
A detailed examination of the engine revealed that the reason for the engine failure was the release of a single HPT 1 blade. The blade failed following the development of low-cycle fatigue4 (LCF) cracking in its internal cooling passages. All other engine damage was considered to be a consequence of the initial HPT 1 blade failure.
Figure 1: Bulged HPT casing
Figure 2: Damage to HPT 1 and HPT 2 rotors
Blade design considerations
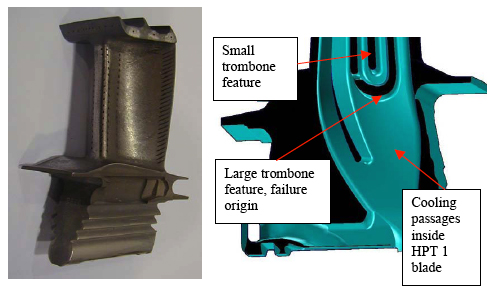
The failed HPT 1 blade (Figure 3) was a life improvement package5 (LIP) blade. The blade was a shrouded-tip aerofoil design, with multi-passage internal cooling (Figure 4). There was a vapour aluminised coating on the blade's external aerodynamic surfaces and internal cooling passages.
The manufacturer indicated that there have been four similar failures of LIP HPT blades in the BR700-715 engine type, with another engine failure still under investigation. One failure occurred prior to this event in November 2003. The remainder occurred after this incident.
Figure 3: The failed HPT 1 blade (position 21)
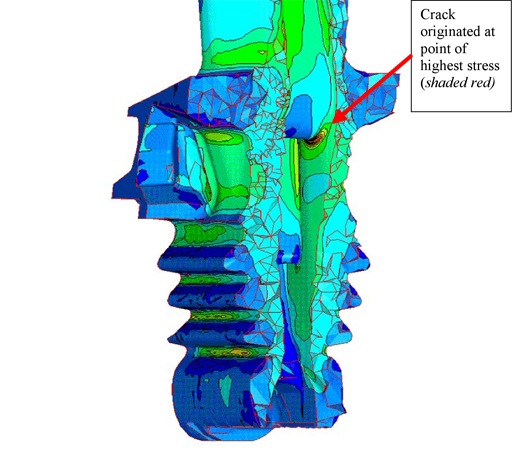
Following those failures, the manufacturer conducted additional computer stress modelling on the LIP blades. That modelling found that there were stress levels in the larger trombone radius feature, within the blade's cooling passages (Figure 4) that were potentially in excess of the manufacturer's original design intent. The manufacturer also found that the thickness of the vapour aluminised coating inside the blade's internal cooling passages was variable and difficult to predict. In certain operational conditions, dependent upon high strains in areas of stress concentration and local temperature, the coating could crack with the possibility of subsequent growth into the coated (parent) material. The area from which the failure occurred was confirmed to be the most susceptible to this behaviour (Figure 5).
Figure 5: Computer generated stress diagram from the manufacturer indicating the point of potentially excessive stress and crack origin
Flight data recorder information
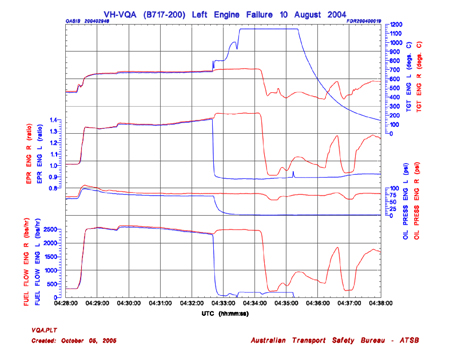
The ATSB's examination of the aircraft's flight data recorder (FDR) for the occurrence flight found that the left engine had surged as the aircraft passed through 10,240 ft. The engine pressure ratio (EPR) and engine rotational speed indications decreased abruptly, while the turbine gas temperature (TGT) for the engine began to increase. HPT vibration values for the engine increased from a level of 0.5 units before the failure to a maximum of 6.3 units over a three-second period. The manufacturer's high-limit for vibrations was 4.0 units.
The FDR readout indicated that the TGT for the engine continued to increase following the engine failure and remained at an indicated maximum of 1,149oC for 1 minute and 46 seconds before decreasing (Figure 6). It is likely that the maximum TGT reached during the failure was higher than 1,149oC, however the aircraft systems do not record above that temperature.
The FDR report indicated that there were no anomalies observed in the performance of the left engine prior to the failure.
Figure 6: FDR data plot of key engine parameters at the time of the failure
1 Metal pulverised by the turbine becomes molten and flows rearward attaching to the subsequent turbine and exhaust assemblies (US Department of the Air Force (1987). Safety Investigative Techniques (AF Pamphlet 127-1, Volume II. Washington DC: Author). 2 Bundesstelle für Flugunfalluntersuchung (BFU). 3 FAA AC 33-5, paragraph 5.c. definitions state '…Contained means that no fragments are released through the engine structure, but fragments may be ejected out of the engine air inlet or exhaust'. 4 Fatigue that occurs at relatively small numbers of cycles. Brooks, C. (1993). Metalurgical Failure Analysis. USA: McGraw-Hill, Inc. 5 The Life improvement Package 3 (LIP3) was a suite of HP Turbine modifications that included the HPT blade P/N BRH20351. The manufacturer introduced the package by SB-BR700-72-100801.
Summary
Sequence of events
On 26 July 2004, as the Boeing 717 (717), registered VH-VQA, was being prepared a scheduled passenger service between Brisbane and Hamilton Island Qld, the cabin crew noticed water spilling from the hand basin in the aircraft's aft left lavatory, and notified the flight crew. The leakage was cleaned up, and the aircraft was dispatched from Brisbane with the aft lavatory locked and placarded to prevent its use during the flight, in accordance with the provisions of the CASA-approved aircraft minimum equipment list.
During the cruise at flight level 320, when the aircraft was about 60 NM south of Mackay, the cabin crew noticed a faint `electrical smell' in the aft area of the passenger cabin. The cabin manager notified the flight crew, and about 1 minute later advised the flight crew that the aft cabin interphone hand piece located on the outside wall of the aft left lavatory was very hot, and that the smell was becoming stronger. Shortly after, the cabin manager notified the flight crew that the aft cabin interphone handset flexible-wiring loom was `melting'.
The flight crew conducted the aircraft quick reference handbook (QRH) `Electrical Smoke/Fumes of Unknown Origin' non-normal checklist. They both donned their oxygen masks, and selected emergency electrical power, as per the checklist. The 717 QRH non-normal checklist procedure dictated that a flight crew should plan to land at the nearest suitable airport. At that stage, the aircraft was about 30 NM south of Mackay. The flight crew broadcast a PAN1 to air traffic control, and advised the controller that they required a clearance for an immediate descent and diversion to Mackay. The flight crew notified the cabin crew of their intentions, and the cabin crew prepared the passenger cabin for the landing at Mackay.
The controller in receipt of the PAN call notified the Mackay tower controller, who activated the aerodrome emergency plan and notified the emergency response services. The aircraft landed safely at Mackay about 9 minutes after the flight crew first notified air traffic control of the problem. After the aircraft landed, the flight crew confirmed with the aerodrome rescue and fire fighting service that there was no smoke at the rear of the aircraft. The flight crew also confirmed with the cabin manager that the electrical smell had abated and that the cabin interphone had cooled down. The aircraft was taxied to the terminal, and a normal disembarkation was conducted through the forward door of the aircraft. Eight of the occupants were treated for smoke/fumes inhalation after they had left the aircraft. There were no other reported injuries.
Following the occurrence, the flight crew reported to the operator that during the landing approach at Mackay, the landing gear `down' indication in the aircraft was different from that indicated in the 717 flight simulator during training sessions for flight on emergency electrical power. The operator conducted an investigation into the matter, and determined that the simulator landing gear `down' indication for flight under those conditions was incorrect. That was confirmed by the aircraft manufacturer.
During the subsequent engineering inspection of the aircraft, the B1-778 `Miscellaneous Cabin & Lavatory Occupied Aft' electrical circuit breaker was found to have popped, and could not be reset. The fault was traced to a short circuit in a connector plug located under the aft left lavatory hand basin. Water from the overflowing hand basin had seeped into the connector plug. The short circuit within the connector plug resulted in several pins within the plug becoming welded together. As a consequence, the aft cabin interphone handset flexible-wiring loom was overheated from a 115 VAC over-current within the loom and resulted in the in-flight `electrical smell' and overheating of the handset. The damaged components were replaced, and the aircraft was returned to service.
1 PAN is a radio broadcast indicating uncertainty or alert. It is a general broadcast to the widest area, but not yet the level of a MAYDAY, which is the international broadcast for urgent assistance.
The Boeing 747-400 aircraft, registered 9M-MPE, was conducting an international scheduled passenger flight from Kuala Lumpur, Malaysia to Melbourne. During cruise at flight level 390, the cabin crew reported an electrical smell near doors 1, 2 and 4. The flight crew immediately completed the "Smoke, Fumes, Fire, Electrical" checklist actions and the smell dissipated. Approximately one hour later, a similar smell became evident in the cockpit and the flight crew elected to divert the aircraft to Adelaide as a precaution.
After landing at Adelaide, an engineering inspection of the aircraft was conducted by the operator's engineers. This inspection revealed that the air conditioning right overhead recirculation fan had seized and the left overhead recirculation fan was causing the circuit breaker to trip. Both overhead recirculation fans were isolated electrically in accordance with the requirements of the aircraft's Minimum Equipment List and the aircraft was returned to service.
Summary
The Boeing 747-400 aircraft, registered 9M-MPE, was conducting an international scheduled passenger flight from Kuala Lumpur, Malaysia to Melbourne. During cruise at flight level 390, the cabin crew reported an electrical smell near doors 1, 2 and 4. The flight crew immediately completed the "Smoke, Fumes, Fire, Electrical" checklist actions and the smell dissipated. Approximately one hour later, a similar smell became evident in the cockpit and the flight crew elected to divert the aircraft to Adelaide as a precaution.
After landing at Adelaide, an engineering inspection of the aircraft was conducted by the operator's engineers. This inspection revealed that the air conditioning right overhead recirculation fan had seized and the left overhead recirculation fan was causing the circuit breaker to trip. Both overhead recirculation fans were isolated electrically in accordance with the requirements of the aircraft's Minimum Equipment List and the aircraft was returned to service.
Preliminary investigation was undertaken into a category 4
occurrence where fumes were detected in an Airbus A330-300 fare
paying passenger flight and the crew diverted to Adelaide.
Subsequent inspection by maintenance personnel showed no evidence
of fire or burning and there have been no reports during subsequent
flights.
Status: Downgraded the occurrence to category 5
and investigation discontinued.
On 23 January 2003, CASA airworthiness directive AD/BAe 146/102 became effective, requiring all operators of BAe 146 aircraft to action the requirements of BAE Systems (Operations) Limited, Inspection Service Bulletin (ISB) 21-156. That ISB relates to inspections of air-conditioning ducts. It has been found that the sound attenuating material used in the air-conditioning ducts can absorb oil and become a source of persistent air contamination.
On 10 July 2003, CASA airworthiness directive AD/BAe 146/105 became effective, requiring all operators of BAe 146 aircraft to carry out a modification in accordance with BAE Systems Service Bulletin SB. 49-036-36019E. That modification provides an improved seal at the aircraft - APU interface, reducing the likelihood of contamination of cabin air due to ingestion of oil from the APU bay.
Operator
The operator of the aircraft involved in this incident previously incorporated various modifications to the cabin air system, APU and engines and introduced improved maintenance practices in an effort to minimise the occurrence of cabin fumes events.
More recently, the operator has undertaken to go beyond the requirements listed in CASA AD/BAe 146/102, by fully replacing the sound attenuating ducts of their entire BAe 146 fleet. On 30 April 2003 the operator advised that during the period since August 2002, when the first duct replacement was completed, there has been a reduction in safety reports received. It has not stopped air quality events occurring but has removed the occurrence of lingering odours.
The operator has also:
commenced trials of a new bearing seal that has realised positive results during recent bench testing by the engine manufacturer
refined a flowchart for use by engineering personnel that ensures that every regulatory aspect is completed during the maintenance investigation and certification process
developed a stand-alone Cabin Air Quality Safety Report, as an adjunct to the Safety Occurrence/Incident Report currently in use. This allows the operator to focus on the specifics of air quality and what symptoms crews are experiencing
employed a coordinator to be the company's single point of contact for liaison with external agencies such as CASA and the ATSB, regarding all air quality matters.
Analysis
It is likely that the copilot's initial attempt to clear the fumes on 2 December was unsuccessful because the problem involved more than just an air conditioning pack. An oil mist forming in the APU bay as a result of the faulty generator drive seal could have resulted in the contamination of the air supply to both air conditioning packs. The maintenance engineers believed that they had identified the source of the fumes and had taken appropriate action. It is considered likely that their assessment was correct and that the report of fumes during the following flight was due to residual contamination of the air conditioning packs.
When checking for fumes during the ground test of the air conditioning packs, the engineers used bleed air from engines 1 and 4 and consequently missed an opportunity to identify engines 2 or 3 as the possible source of the contamination. The difficulty in positively identifying the origin of the contamination was highlighted by the smell reported by the operating crew on 6 December. It could not be discounted that the cabin fumes were a result of the intermittent leak of oil in the number 3 engine, that was identified ten days after the original incident, instead of, or as well as, the APU.
Summary
The British Aerospace 146-100A (BAe 146) was being prepared for a regular public transport service from Perth to Newman, WA. As the copilot boarded the aircraft to conduct pre-flight checks he detected strong fumes in the cabin and the flight deck. He noted that the auxiliary power unit (APU) was supplying bleed air to one of the aircraft's two air conditioning packs that in turn supplied conditioned air to the flight deck and cabin. In an attempt to clear the fumes, he directed the bleed air supply to the alternate pack.
Bleed air from the APU was generally used when air conditioning was required during ground operations or during the take-off and landing phases. During flight, the air conditioning packs receive bleed air from the engines.
As the copilot continued the pre-flight checks, he noticed the cabin fumes becoming stronger and so shut down the air conditioning pack and opened the flight deck windows.
Maintenance engineers were requested to investigate the source of the fumes and subsequently discovered an oil leak in the APU generator drive adaptor pad. Rectification work, including the replacement of a carbon seal, was carried out 11 days later, on 13 December. To enable the aircraft to continue in service on the day of the incident, the APU was isolated from the air conditioning system in accordance with the terms of the aircraft's Minimum Equipment List (MEL) that permitted operation of the aircraft in non-standard configurations. The operator reported that the maintenance engineers then addressed the defect in accordance with the Civil Aviation Safety Authority (CASA) airworthiness directive AD/BAe146/86, effective 3 April 2001, and the British Aerospace Systems Inspection Service Bulletin (ISB) 21-150. That ISB called for certain actions to be performed whenever a cabin air quality problem was identified, which was suspected of being associated with oil contamination of the air supply from the air conditioning packs. No oil contamination was found. The engineers then operated both packs using bleed air from engines 1 and 4 until they were satisfied that there were no fumes and the aircraft was then released for service.
The copilot had been exposed to the fumes for approximately 30 minutes. The two cabin crew, who boarded the aircraft shortly after the copilot, were exposed to the fumes for approximately 20 minutes. All three were eventually affected by the fumes, became unwell, and were removed from flight duty. In accordance with company standard practice they underwent medical examinations. The pilot in command was exposed to the fumes for less than 5 minutes and was not affected. Impaired performance due to the inhalation of contaminated air is considered a potential threat to flight safety. For that reason, company procedures emphasise the importance of flight crew donning oxygen masks if poor air quality is suspected during flight.
The pilot in command and a replacement crew subsequently departed in the same aircraft for the flight to Newman. The cabin crew reported a slight smell of fumes toward the rear of the aircraft during the first sector. On the return sector, both cabin crew reported feeling unwell, with symptoms consistent with fumes inhalation.
Follow-up inspections of the air conditioning system, engines and APU were carried out in accordance with the CASA airworthiness directive and no contamination was evident. On 6 December, the operating crew indicated that a smell was apparent and it appeared to be consistent with the operation of the APU. As the APU was still isolated, engineers doubted that it could be contaminating the air conditioning system. All four engines and the regenerative ducts were again checked, with no contamination evident. Follow up inspections were scheduled in accordance with the ISB.
A further cabin air quality event occurred on 12 December, when the flight deck crew detected fumes shortly after departure. The flight crew proceeded to identify the source of the fumes using a contamination source location schedule. That schedule involved selecting different combinations of engine air and air conditioning packs. The fumes were traced to the number 3 engine, which was isolated, and the flight continued as planned. Subsequent inspection revealed oil wetness in the number 3 engine high-pressure compressor; the result of a worn number 1 bearing seal. Trend monitoring had not indicated abnormal oil consumption for that engine. The engine was replaced and airworthiness directive AD/BAe146/86 was complied with. No further contamination was evident and fumes were not reported during subsequent flights.
Evidence from previous incidents of air system contamination on this aircraft type had indicated that fume events were often intermittent in nature and were associated with engine or APU oil contamination of the air conditioning system. The air supplied to the air conditioning packs was protected from contamination by oil seals in the engines and APU. A defect in one of those seals could result in oil entering the cabin air conditioning system, with the first sign of the defect being an awareness of fumes by passengers or crew members.
The investigation of cabin fumes incidents on BAe 146 aircraft has typically been characterised by a difficulty in precisely locating the original source of the oil leak that led to the creation of the fumes. That has been especially so if there was more than one engine/APU leak combination. The failure of oil seals has been a common factor in the majority of those incidents.
The operator has undertaken to raise awareness among flight crew about the risks of possible crew incapacitation from fumes and the importance of not delaying the donning of oxygen masks during emergency checklist actions. This notice should include reiteration of the primacy of any immediate recall emergency checklist actions over other operator documentation. This will be achieved by a re-write of the procedures detailed in the operator OM-2 operations manual.
The ATSB expressed concern to the operator about the lack of advice provided to medical staff as to what medical tests should be carried out on crew after possible exposure to fumes. The operator undertook to introduce a procedure to communicate a list of prescribed minimum tests, published by the airframe manufacturer in SIL 21/45, to medical practitioners whenever crewmembers require testing for fume exposure. This would ensure that the attending doctor would have the latest testing information available at the time of the test. It was agreed that the information should, as a minimum, cover the appropriate medical tests for such exposure as listed on Pages 10 and 11 of BAe SIL 21/45 Issue Number 1 dated January 2001 (or as amended).
With regard to the concern about appropriate use of the diluter type masks and portable oxygen bottles by cabin crew in heavy smoke or fumes situations, the operator has undertaken to issue a flight attendant safety memo (FASM). This FASM will raise awareness among cabin crew of the limitations of the portable oxygen bottle and diluter type masks when used in a fumes contaminated environment.
Analysis
The aircraft type has been the subject of recurring fume incidents throughout its operating life as commented on by the PIC. It has been subject to intense investigations by both operators and the manufacturer. These investigations have resulted in the promulgation of several service information letters, bulletins, airworthiness directives and NOTOP troubleshooting requirements.
Because of this history, the fume events may have become `routine' in the thinking of some operating crew and awareness of the possible risks may have diminished as a result. This familiarity was a concern to the manufacturer as evidenced by the wording in the AOM to the operator. Familiarity may have led the PIC to delay the donning of his oxygen mask. The imperative to ascertain the source of contamination as soon as practicable in accordance with the operator's NOTOP directive may have also influenced the PIC's decision making.
Although the PIC felt that there was no need for him to don his oxygen mask, this action was contrary to the operator's emergency procedures. The completion of the NOTOP diagnostic action should be accomplished after any emergency checklist actions. By choosing to remain exposed to potentially contaminated air, the PIC might have risked degradation of his faculties, which then may have reduced his ability to correctly determine if there was a flight hazard and respond appropriately. This increased exposure may also have long term or cumulative effects that are not yet understood.
If the emergency checklist had been performed first, both pilots should have donned oxygen masks and the subsequent occasional removal of an oxygen mask by one pilot for air sampling would have likely had minimal safety consequences. This is further reinforced by the fact that both pilots experienced some after-effects that required stand down from flight duties even though one, the copilot, had donned an oxygen mask early in the event.
The PIC's request to the FAs and their subsequent actions in opening the flight deck door were contrary to procedures. The smoke/fumes procedures in both cockpit and cabin are safety of flight defences designed to minimise the potential for flight crew incapacitation by isolating the flight deck from cabin hazards. Again the possible perception that fume events are a `routine' part of the environment in which the crews operate may have led both flight and cabin crew to believe that the action was appropriate under the circumstances.
The oxygen bottle used by the cabin crew was fitted with a diluter or therapeutic type mask. This design does not provide protection from smoke or fumes as most of the air mixture provided is ambient air. Under certain circumstances involving heavy contamination by fumes, the use of this type of mask might mislead the user into a false sense of protection and lead to the possibility of being overcome by the fumes. The limited protection afforded by this type of mask should be brought to the attention of cabin crew.
Summary
The crew carried out the take-off in the British Aerospace Plc BAe 146 (BAe 146) with number 4 engine air bleed selected on, and engine numbers 1, 2 and 3 and the auxiliary power unit air bleeds selected off in compliance with an item in the discrepancy log. Shortly after take-off, at approximately 700 ft above ground level, the copilot switched on the remaining engine air bleeds and both air conditioning packs. Shortly after selecting engine anti-ice on, the pilot in command (PIC) asked the copilot if he could smell fumes. The copilot agreed that he too had detected a smell. The engine anti-ice system was then switched off.
A short time after commencing the cabin service, a flight attendant (FA) called the flight deck and informed the PIC of fumes in the cabin and that they were particularly bad near the rear of the cabin where another FA had donned an oxygen mask. This mask was of the diluter type that supplies a mixture of the incoming oxygen with the ambient air that is then delivered to the user. The copilot then indicated to the PIC that `he felt he should go onto oxygen' and donned an oxygen mask, but the PIC did not feel he needed to perform the same action at that time.
The PIC later stated that he did not don his oxygen mask at this time, as he was considering if the fumes were oil related in accordance with a notice to pilots (NOTOP) from the operator. This NOTOP required the PIC to make a diagnosis as to the source of contamination `wherever it is safe and practicable to do so'. The PIC's findings were required by the operator to determine the level of response required to later rectify the problem and return the aircraft to service.
The PIC stated that the aircraft type had a history of fumes related problems and not donning his oxygen mask was a normal practice for himself and, he believed other aircrew employed by the operator. He said `most smells and odours were considered the normal environment of the day to day operation of the BAe 146' and he would have discontinued his NOTOP diagnostic action if he perceived a flight hazard issue and would have reverted to the emergency checklist action. He also stated that the copilot, being on oxygen, could confirm a successful isolation procedure by occasionally removing his mask and comparing pure air with the ambient air of the flight deck.
This was at variance with the emergency checklist for SMOKE/FUMES/FIRE IN COCKPIT/CABIN. This list takes priority over any other action. The first item on the checklist is `Oxgen masks and goggles...Flight crew don, check 100%'. The imperative in relation to fumes events was also highlighted in an all operator message (AOM) from the manufacturer, which states in part `pending the definition of any necessary corrective actions, oil leaks and cabin/flight deck smells must be regarded as a potential threat to flight safety and not just a nuisance'.
The copilot completed fault isolation checks that appeared to improve the air quality on the flight deck. The PIC then asked the FAs if they could come to the flight deck so that he could better assess the situation in the cabin. The FAs came forward in turn, opened the flight deck door and entered. This action was at variance with the operations manual actions for flight attendants in the event of smoke/fumes in the cabin. The manual stated that, in the event of smoke/fumes, the FAs were to inform the PIC via the intercom and were not to open the flight deck door.
In his original report, the PIC stated that `each time when they opened the flight deck door, we noticed that the odour intensified'. The FAs' cabin crew reports to the operator also stated that the odour and fumes were still evident in the passenger cabin during the remainder of the flight. The PIC described the odour to be unlike any odour previously encountered and then decided the safest option was to return to the departure airport.
The incident operating crew underwent medical examinations that evening as directed by the operator after the event. The PIC stated that the medical practitioner they visited told him she knew very little about the effects of odours on crew and was unaware of any specific blood testing requirements for such an event. Medical testing information printed by the aircraft manufacturer in Service Information Letter (SIL) 21/45 Issue Number 1, dated January 2001, details specific test requirements. The PIC stated that it was sometimes difficult to find a medical practitioner at short notice (especially late at night) who was familiar with the required testing procedures.
After advising the medical practitioner that he was unsure if he would be able to work the following day, the PIC was given a medical certificate excusing him from flight duties for the following 24 hours. Even though he donned his oxygen mask, the copilot was similarly affected and was also excused from flight duties for the same period as the PIC. The operator reported that the remaining crew did not exhibit any residual effects from the incident.
A maintenance investigation by the operator included compliance with the latest airworthiness directive and service bulletins. All engines and the auxiliary power unit were checked. The airconditioning regenerative ducting and the delivery ducting to the rear cabin were also dismantled and inspected. That investigation determined that the number-3 engine was the likely source of the fumes and the engine was changed. The aircraft was returned to service with subsequent operating crews reporting no further fumes problems.