The pilot reported that shortly after take-off, at approximately fifteen feet above ground level, the aircraft yawed to the right and collided with some low scrub. The aircraft came to a stop clear of the right hand side of the strip. It was also reported that the strip met all requirements and that there were no apparent control malfunctions.
The reason for the loss of control was not determined.
The owner pilot and his wife flew to Cape Naturaliste where a water landing was carried out and the aircraft was taxied on to the beach. On departure the aircraft was positioned for a water take-off into a 10-knot southerly breeze on a slight sea. The pilot reported that the aircraft lifted off after a few bounces at the end of the water run and was held level to build up climb speed. Shortly thereafter the aircraft appeared to yaw violently to the right, rolling to the vertical. The right wing entered the water, and the aircraft cartwheeled coming to rest nose down and inverted. The pilot was flung clear, and his wife was able to extricate herself from the wreckage. Both were supported in the water by their life jackets while awaiting rescue. The aircraft sank and was not recovered.
A number of agricultural aircraft were operating on fire suppression work from Snowy Range airfield which is situated in the Victorian Alps at an elevation of 5300 feet. The airfield has two grass strips. The north/south strip is 900 metres long and the east/west strip is 550 metres long. VH-DRO was based at Wangaratta and its pilot had never been to Snowy Range airfield. Because of this, when he arrived at the airfield, he made a touch and go landing on each strip prior to making a full stop landing. The pilot said the wind was a 12-knot westerly. The crosswind limit for the aircraft is 15 knots.
After taking on a load of fire-retardant chemical, the pilot taxied for take-off into the west using the short strip. The aircraft became airborne a short distance before the end of the strip and the pilot estimated it got to a height of about 10 feet. It then sank back towards the strip, clipped a fence at the end of the strip and shortly afterwards hit a dirt mound. The pilot said he realised then that the aircraft was not going to fly so he closed the throttle and let the aircraft slide to a stop over the rough ground.
The landing gear was torn out and the aircraft sustained substantial damage in the ground slide. After the pilot evacuated the aircraft, he noted the wind had dropped to completely calm conditions. This was verified by ground crew at the scene. Aircraft performance data indicated that under the conditions prevailing at the time of the attempted take-off, the aircraft would take about a 450 metre ground roll before becoming airborne which is approximately the distance taken on this occasion. The take-off distance required to a height of 50 feet was about 870 metres.
The pilot said that when the aircraft started to sink, he tried to dump the load, but his attempt was not successful.
A report from the pilot indicated that he made a steeper than normal approach to a private strip. The aircraft landed some distance in from the threshold before bouncing back into the air. The pilot elected to apply power and go around for a further circuit. Despite application of full power, the aircraft did not clear obstacles beyond the end of the runway, and the pilot was forced to land in an adjacent paddock. The aircraft landed heavily.
The flight was planned as a fire spotting flight. All systems were normal during the pre-flight, start and after start checks. The aircraft took off towards the east. The wind was reported as blowing from a southerly direction at approximately 10 knots. Witnesses reported that, after liftoff, the aircraft climbed at a very steep angle and very slow airspeed to approximately 300 feet above ground level. At that point the aircraft entered a flat spin to the left and completed four turns prior to impact 110 metres to the left of the runway centreline and 300 metres from the start of the take-off role. The engine ran at a high-power setting throughout the flight.
A post-accident inspection of the wreckage did not disclose any aircraft failure that might have contributed to the accident. The inspection did determine that the aircraft was not fitted with an aural stall warning device, similar to those fitted to all the other PA18 aircraft used by the Operator.
A row of trees, designed to act as a wind break, is located along the southern side of the flight strip. These trees may cause some turbulence when a southerly wind is blowing.
The pilot advised that he was concerned about possible turbulence from the trees and the crosswind effect on the aircraft. As a result, he attempted to climb the aircraft above the trees as soon as possible after liftoff. During the climb the pilot was distracted by the aircraft's proximity to the trees, and he did not monitor the airspeed closely. He allowed the airspeed to reduce and at approximately 300 feet above ground level the aircraft stalled and entered a flat spin to the left.
The pilot had no warning of the stall. There was no pre-stall buffet, and the aircraft was not fitted with an aural stall warning device.
The pilot attempted to recover from the stall, but the aircraft impacted the ground before his attempt had any effect.
It is possible that had an aural stall warning been fitted to the aircraft it would have alerted the pilot in sufficient time to prevent the loss of control.
On the afternoon of 14 October 2014, the pilot/owner of an amateur-built Van’s Aircraft Inc. RV-6A aircraft, registered VH-JON and operated in the ‘experimental’ category, departed Moorabbin Airport, Victoria on a local flight.
Shortly after reaching a cruise altitude of 2,900 ft, the aircraft descended to 2,500 ft. After that time, no further air traffic control radar returns were received from the aircraft. The aircraft descended rapidly and a witness reported observing objects falling from the aircraft. The aircraft subsequently collided with the ground next to a house in the suburb of Chelsea, 8 km south of Moorabbin. The pilot was fatally injured, and the aircraft was destroyed.
Following the accident, members of the public found a number of aviation-related items away from the accident site that belonged to the pilot.
What the ATSB found
The liberation of the items from the aircraft’s interior indicated that the canopy likely opened in‑flight. However, this was based on the assumption that the items were initially inside the cabin.
Examination of the primary and secondary canopy locks found varying degrees of damage and one component was missing. Therefore, the state of the locking mechanisms prior to the impact could not be established.
It was possible that the pilot was startled and distracted after the canopy opened due to the severe cockpit wind, noise and debris flying about. Though, the extent to which this contributed to the occurrence was unknown.
Also, while the ATSB was unable to determine how the canopy opening would have affected aircraft control, there were indications that the pilot was attempting to respond to the situation. However, for reasons undetermined, recovery did not occur.
Finally, the ATSB identified a safety issue regarding the potential for the in‑flight opening of a tip‑up, forward-hinged canopy to result in a significant pitch down tendency in a number of Van’s Aircraft Inc. models that may affect aircraft control.
What’s been done as a result
Van’s Aircraft Inc. developed a service letter for distribution to builders and operators highlighting the varying consequences of a canopy opening in-flight, in particular, involving a tip-up canopy. The letter recommends inspecting the canopy locking mechanism to confirm that it operates as designed and to ensure the mechanism fully engages when closed, and highlights the need to secure the secondary latch at the top-rear of the canopy in the RV-6/7/9 design prior to take-off.
Additionally, the ATSB has issued a safety advisory notice to all owners of Van’s aircraft to highlight the findings of this investigation.
Safety message
This accident and other reported experiences highlight the varying consequences when a canopy opens in-flight from no effect to a sudden pitch down. The result can vary from being relatively benign to significant, but pilots could expect an element of startle and distraction. Additionally, the ATSB reminds pilots to check the security of the canopy prior to take-off.
Shortly after reaching 2,900 ft, Vans Aircraft Inc. RV-6, registered VH-JON (JON), descended rapidly and collided with the ground next to a house. The pilot was fatally injured, and the aircraft was destroyed. Following the accident, members of the public found a number of aviation-related items belonging to the pilot at distances of up to 3 km north of the accident site.
The recorded engine data showed that the engine was operating normally prior to the impact. This was consistent with the engine examination, which identified no internal mechanical failure or abnormality that would have precluded normal operation. In addition, the integrity of the aircraft structure and the flight controls was also established.
This analysis will examine why the aircraft’s canopy likely opened in flight, how this may have occurred and the possible consequences for continued safe flight.
Canopy opening in flight
Timing of the canopy opening
A witness reported observing items falling from the aircraft during the aircraft’s descent. This was consistent with the location of some of the pilot’s belongings found external to the aircraft and away (up-track) from the accident site. With no other place for the items to exit the cockpit, the liberation of the items from the aircraft’s interior indicated that the canopy likely opened in flight. While based on the assumption that the items were initially inside the cockpit, this conclusion was similar to that by the United States National Transportation Safety Board’s (NTSB) investigation into an RV‑6 accident on 20 June 2014 (see NTSB report CEN14FA306).
The ATSB considered the possibility that the pilot’s flight bag containing the items was inadvertently left on the aircraft’s wing during the departure from Moorabbin Airport. However, as the bag would most likely slide off the wing during the take‑off, this was the least probable scenario.
The ATSB also examined the possibility that the pilot deliberately opened the canopy for a particular reason such as experiencing smoke, fire or fumes in the cockpit. While there was insufficient evidence to support this scenario one way or the other, given the results of the pilot’s post‑mortem, it was deemed unlikely.
Canopy locking mechanism
Damage to the primary locking lever mechanism suggested that it was initially closed but forced open during the impact. However, anecdotal reports from RV-6 pilots indicated that, under some circumstances, it was possible for the canopy in these aircraft to open when the lever was in the closed position. Furthermore, the ATSB could not discount that the pilot of JON may have manipulated the lever in attempt to lock the canopy during the descent.
There was no damage to the two hooks and their respective receptacles at the rear of the canopy whereas, if engaged at the time of impact, some level of damage to these components would be expected. While it was possible that the primary lock was open prior to the impact, the aircraft sustained significant damage, which may have affected the state of the mechanism. Also, the locking catch and spring were not found and could not be examined.
The secondary lock was found in the unlocked position and showed no signs of damage. However, as this lock is readily moved by turning the associated handle, it could not be discounted that it moved on impact. Also, it was possible that the lock was initially closed prior to take-off and worked its way open during the flight.
In summary, there was insufficient evidence to establish if either of the locking mechanisms remained unlocked since prior to take-off, or if they failed in flight.
Because upsets that occur in normal flight operations are unplanned and inadvertent, pilots may be startled or surprised, adversely impacting recognition or recovery.
Martin and others (2012) also stated that, if pilots were not expecting things to go wrong, the level of startle or surprise they experience could be significant and may last between 0.3 and 1.5 seconds. The rapid capture of attention due to a startling event can distract a pilot from the primary task of flying.
The NTSB investigation report into the fatal RV-6 accident in the United States on 20 June 2014 recognised that there may be a tendency for pilots to experience ‘shock and chaos’ with an open canopy due to the severe cockpit wind, noise and debris flying about. This was similar to reports from a number of RV-6 pilots who cited lots of wind noise and distraction when their canopy opened in flight. Van’s also indicated that an open canopy could be distracting.
The recorded engine data showed that, about 7 seconds after the oil pressure began to fluctuate, the pilot reduced the engine power to idle. This was slightly above the typical reaction time of 4‑6 seconds for pilots responding to an emergency situation.[8] However, it was unknown if the pilot conducted any other actions prior to this time.
The ATSB concluded that it was possible that the pilot of JON was startled and distracted after the canopy opened. The extent to which this contributed to the occurrence could not be established.
Aircraft control
Reports from a number of RV-6 pilots who had experienced an in-flight opening of a tip-up canopy showed varying results. Some reported no consequences while others experienced a sudden pitch down. In these cases, the aircraft was reported to remain controllable. In contrast, the NTSB concluded that the likely in-flight opening of an RV-6 canopy resulted in a loss of pitch control and collision with terrain. Similarly, the pilot of an RV‑12 reported experiencing a pitch down after their aircraft’s canopy opened in flight to the full vertical position shortly after take-off. That pilot also reported that there was no response from the elevator or rudder after the canopy opened.
Van’s advised that an in-flight canopy opening would generally not cause any problems. However, while not tested, they theorised that a forward pitching moment may occur at higher airspeeds due to a disruption in the airflow over the aircraft’s horizontal stabiliser. Given the variability in consequences reported, and without flight testing, the ATSB was unable to establish how the canopy opening on JON would affect its controllability, and if this directly resulted in the loss of control. Nonetheless, other reported experiences after an in-flight canopy opening suggest that, under some circumstances, in-flight opening of the tip-up canopy on some Van’s aircraft can result in a sudden pitch down with related controllability issues.
The reduction by the pilot of engine power to idle and witness observations of the aircraft banking and the wings then coming level, suggest that the pilot was attempting to respond to the in-flight canopy opening. However, for reasons undetermined, the pilot was unable to recover the situation before impacting terrain.
Summary
While the ATSB was unable to establish how the canopy likely opened, this accident and other reported in-flight canopy openings in a number of Van’s aircraft models highlight the varying consequences when such occurrences take place. The result can vary from being relatively benign to significant, but pilots can expect an element of startle and distraction. Additionally, such occurrences serve as a reminder for pilots to check the security of their aircraft’s canopy prior to take‑off. Of note, Van’s advised the ATSB that the RV‑12 and RV‑14 models now have a ‘canopy open’ warning switch incorporated into the kit design. Other pilots who have experienced an in‑flight canopy opening have included an additional checklist item to confirm the canopy was locked before departing.
On the afternoon of 14 October 2014, the pilot/owner of an amateur-built Van’s Aircraft Inc. (Van’s) RV-6A aircraft, registered VH-JON (JON) and operated in the ‘experimental’ category, departed Moorabbin Airport, Victoria on a local flight.
The aircraft departed at about 1323 Eastern Daylight-saving time[1] and was identified on Airservices Australia surveillance radar tracking southbound toward the coast. The wind conditions at the time were 17 kt from the south‑south‑east. At about 1325, the aircraft reached an altitude of 2,900 ft. Shortly after, at 1326, the aircraft descended to 2,500 ft. After that time, no further radar returns were received from the aircraft.
A witness reported observing the aircraft banking and seeing objects falling, like ‘packages’ were being ‘dropped’. The aircraft’s wings then became level. Another witness also reported sighting the aircraft banking and then becoming level. Both reported that the aircraft was descending rapidly. The aircraft subsequently collided with the ground in a laneway next to a house in the suburb of Chelsea, 8 km south of Moorabbin (Figure 1).
The pilot was fatally injured, and the aircraft was destroyed. A number of small post-impact fires were extinguished and a number of houses and cars sustained damage.
Members of the public reported finding a number of aviation-related items belonging to the pilot. These items were recovered at distances of up to 3 km north of the accident site.
Examination of the recorded air traffic control radio frequencies revealed no emergency broadcast from the pilot.
Figure 1: Accident site from the initial impact point on the left, looking south down the laneway
The safety issues identified during this investigation are listed in the Findings and Safety issues and actions sections of this report. The ATSB expects that all safety issues identified by the investigation should be addressed by the relevant organisation(s). In addressing those issues, the ATSB prefers to encourage relevant organisation(s) to proactively initiate safety action, rather than to issue formal safety recommendations or safety advisory notices.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are repeated separately on the ATSB website to facilitate monitoring by interested parties. Where relevant the safety issues and actions will be updated on the ATSB website as information comes to hand.
Potential adverse effects of a tip-up canopy opening in-flight
In‑flight opening of the tip-up canopy in a number of Van’s Aircraft Inc. models has resulted in varying consequences, including a significant pitch down tendency, increasing the risk of a loss of control.
From the evidence available, the following findings are made with respect to the collision with terrain involving an amateur-built Van’s RV-6A, registered VH-JON, which occurred 8 km south of Moorabbin Airport, Victoria on 14 October 2014. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
Shortly after levelling off in the cruise, the tip-up canopy in VH-JON likely opened, resulting in a loss of control from which the pilot was unable to recover before impacting terrain.
Other factors that increased risk
In‑flight opening of the tip-up canopy in a number of Van’s Aircraft Inc. models has resulted in varying consequences, including a significant pitch down tendency, increasing the risk of a loss of control. [Safety issue]
Other findings
The reason for the canopy opening in VH-JON could not be determined.
Sources and submissions
Sources of information
The sources of information during the investigation included:
a number of witnesses
Van’s Aircraft Inc.
the Van’s Airforce Forum
Airservices Australia
the Civil Aviation Safety Authority
Victoria Police.
References
Federal Aviation Administration 2004, Airplane Flying Handbook, United States Department of Transportation.
Federal Aviation Administration 2015, Upset Prevention and Recovery Training (Advisory Circular 120-111), United States Department of Transportation.
Flight Safety Foundation 1999, ‘Simulator-based study of emergencies yields insights into pilots’ reaction times’, Helicopter Safety, March-April 1999, vol. 25, no. 2.
Martin, WL, Murray, PS & Bates, PR 2012, The Effects of Startle on Pilots During Critical Events: A Case Study Analysis, Brisbane, Griffith University.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to Van’s Aircraft Inc., the Civil Aviation Safety Authority and the United States National Transportation Safety Board.
A submission was received from Van’s Aircraft Inc. The submission was reviewed and where considered appropriate, the text of the report was amended accordingly.
Context
Pilot information
The pilot held a Private Pilot (Aeroplane) Licence that was issued on 24 September 1985.[2] As at 2 October 2014, the pilot had a total flying experience of 1,659 hours.
The pilot held a valid Class 2 Aviation Medical Certificate and was required to wear distance vision correction and have vision correction available for reading. The pilot was reported to have been well rested and in good health prior to the accident.
The pilot’s post-mortem examination found amyloid deposition[3] in the heart, which was often considered age‑related. However, the role of this and any other natural disease in the development of the occurrence could not be established. Furthermore, there was no evidence to suggest that fumes, smoke, or fire had affected the pilot prior to the impact. The pilot’s clothing did not show any obvious evidence of grease or foreign materials such as bird feathers from a birdstrike.
Aircraft information
The Van’s Aircraft Inc. (Van’s) RV-6A is a kit-built aircraft with a low-wing and fixed undercarriage. VH-JON (JON) was constructed by the pilot and registered with the Civil Aviation Safety Authority on 4 July 2003 (Figure 2). A review of the aircraft’s logbook and other related documentation indicated that JON was maintained in accordance with an approved Civil Aviation Safety Authority maintenance schedule. The last periodic inspection was conducted on 1 July 2014, at which time the total time in service was about 338 hours for the airframe and 201 hours for the engine. The last oil change occurred on 30 September 2014. At the time of the occurrence, all of the required maintenance had been completed and there were no defects recorded.
Figure 2: JON showing the tip-up canopy in the open position
Source: Supplied
Tip-up canopy
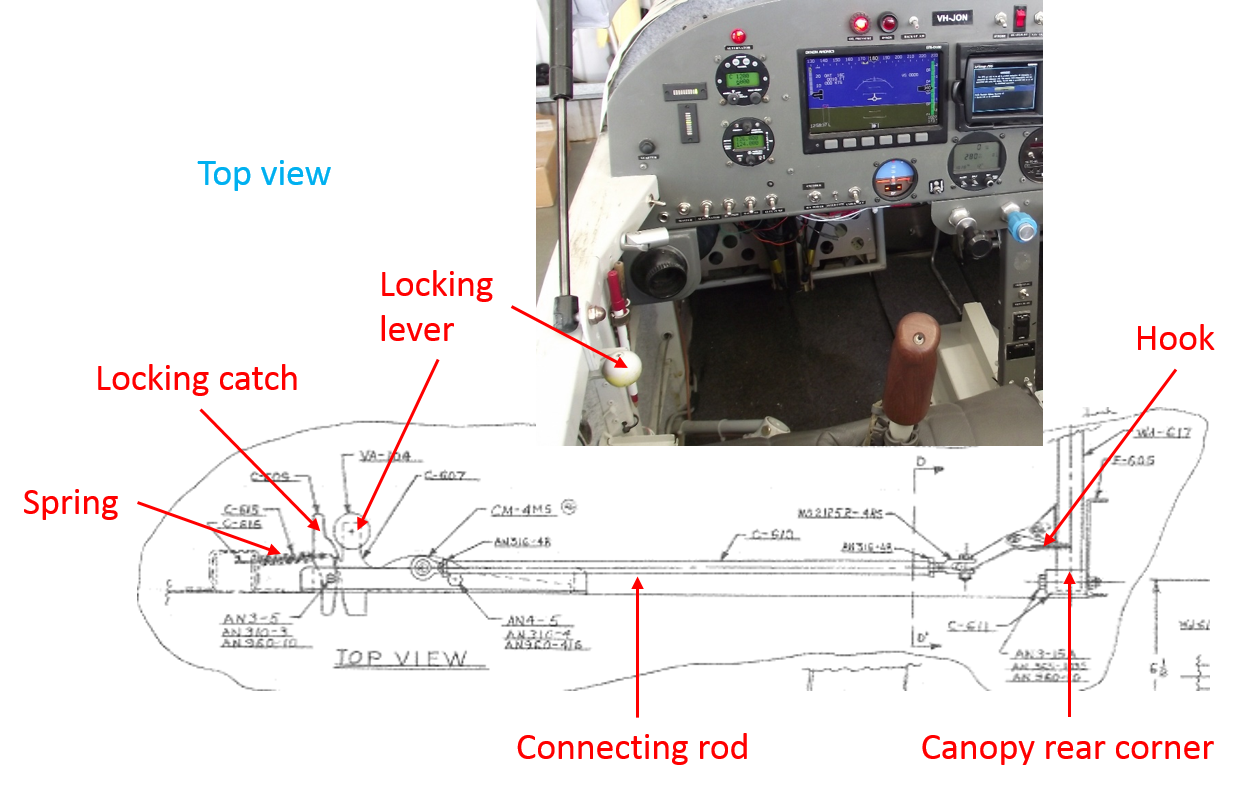
Although the Van’s RV-6 could be installed with aft- and forward-hinged canopies, JON was fitted with a forward-hinged ‘tip-up’ canopy (Figure 2), which had two locking mechanisms. The primary locking mechanism was operated by a locking lever located on the left side of the fuselage, adjacent to the pilot’s seat. When placed into the locked position, a connecting rod from the lever latched two hooks into corresponding receptacles in the two rear corners of the canopy. The lever was then locked by a spring-loaded locking catch (Figure 3 and Figure 4).
Figure 3: Van’s Aircraft Inc. diagram showing the primary canopy locking mechanism from the top view in the locked position (labelled in red). The locking lever in JON is shown in the photograph at inset
Source: Van’s Aircraft Inc. and supplied, both modified by the ATSB
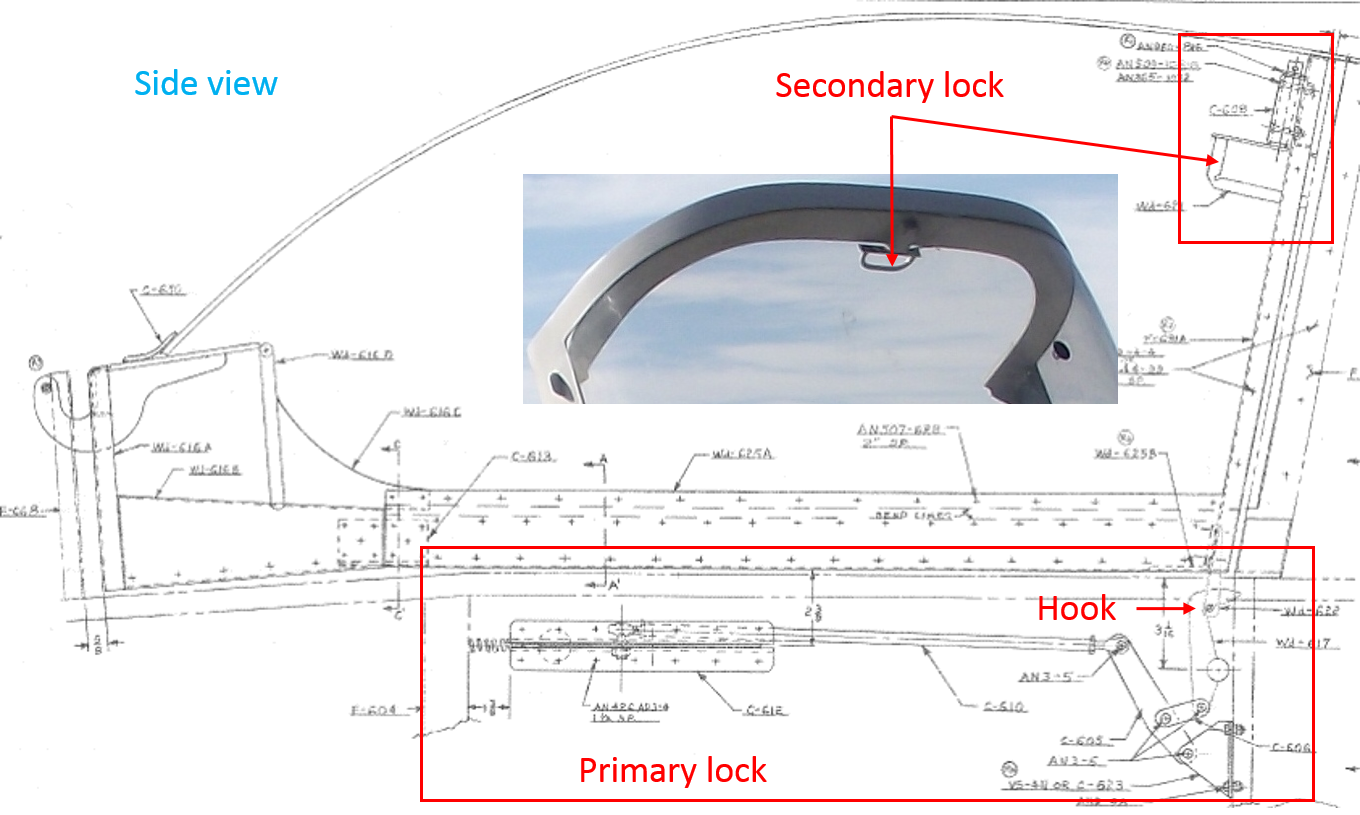
The secondary mechanism was a handle attached to the centre of the canopy frame, which was also used to assist with closing (Figure 4). Once closed, the handle was turned 90° so that a tang on the end of the handle extended under the adjacent fuselage frame. This provided redundancy in the event the main locking mechanism malfunctioned.
Figure 4: Van’s Aircraft Inc. diagram from the side view showing the primary and secondary locking mechanisms. The secondary lock attached to JON is shown in the photograph at inset
Source: Van’s Aircraft Inc. and supplied, both modified by the ATSB
Previous occurrences involving JON
A search of the ATSB’s occurrence database revealed that JON was involved in two previous landing accidents. One in 2007 and in 2010. On both occasions, the engine was replaced, the damage repaired and the aircraft returned to flying status.
The aircraft was also involved in an incident about 1 month prior to the October 2014 accident. It was reported that a minor engine fire occurred on the ground at Moorabbin due to over priming the engine for a ‘hot start’.[4] The fire was extinguished with the assistance of ground personnel. The pilot reportedly conducted an inspection of the engine and associated area, with nil damage found. Several flights were conducted since that time and it could not be established if the fire contributed to the occurrence south of Moorabbin Airport on 14 October 2014.
Recorded information
The aircraft was fitted with two Garmin global positioning system (GPS) units, a Dynon EMS‑D120 engine monitoring system and a Dynon EFIS-D100 electronic flight information system. The aircraft’s track on the day was recovered from recorded data from one of the GPS units and was consistent with the Airservices Australia surveillance radar track (Figure 5).
The Dynon D100 system did not provide any recorded data, but the D120 system recorded a number of engine parameters and the fuel level in each wing. The data was downloaded by the ATSB and captured the accident flight up until 1326:09, several seconds before the impact with terrain. Specifically, the data showed:
Up until 1325:52, the engine data appeared stable and the oil pressure remained normal at around 75 pound per square inch (psi). After this, the pressure fluctuated to as low as 34 psi (Figure 5). By the last second of the recorded data, the pressure increased to 72 psi. The fluctuations likely resulted from a sudden change in aircraft attitude temporarily disrupting the oil supply in the oil sump.
An analysis of the recorded fuel levels indicated that, at around the same time the oil pressure began to fluctuate, the fuel levels diverged at a rate higher than previously recorded. This was possibly due to an abrupt roll[5] to the left or acceleration in yaw.[6]
Until 1326:00, the propeller revolutions per minute (RPM) was relatively constant at 2,405 RPM. Immediately after, it reduced for 1 second and then increased to 3,069 RPM over the next 3 seconds. From 1326:05 until the recording ceased, the RPM stabilised, indicating that the propeller governor was functioning as required. The variation in RPM was also likely the result of a change in the aircraft's attitude.
At 1326:00, the engine manifold pressure was recorded as 26.625 inches Hg. After this, it reduced to as low as 4.6875 inches Hg. This coincided with a reduction in fuel pressure and was representative of the pilot reducing the engine power to idle (Figure 5).
The exhaust gas temperatures were stable, but decreased with the reduction in manifold pressure, which would be expected.
Figure 5: Downloaded GPS track, and the position of the first oil pressure fluctuation and reduction in engine manifold pressure
Source: Google earth, modified by the ATSB
Wreckage and impact information
Examination of the wreckage found that the aircraft initially impacted a house fence at a descent angle of about 35° and slightly left wing down. Images recovered from a nearby closed‑circuit television camera showed the last seconds of the flight and confirmed a steep nose-down flight path (Figure 6). The ATSB estimated that, based on the video footage, the aircraft’s speed at that time was about 200 kt (370 km/h).
Figure 6: Composite image of the aircraft’s descent. The image was developed from sequential video frames to show the aircraft’s descent and was used to estimate the aircraft’s speed within a 1‑second timeframe
Source: Victoria Police, modified by the ATSB
The left wing and top section of the canopy remained at the initial impact point and the remainder of the aircraft continued along the laneway. The propeller, engine, and tail surface also separated from the remainder of the wreckage and were located along the wreckage trail. The right wing and fuselage came to rest about 90 m from the initial impact point. Items associated with the aircraft were located in the laneway up to 130 m away.
A number of fires occurred along the wreckage trail. A number of small, localised fires on the engine were captured by the closed-circuit television footage. The wreckage examination also:
Identified all flight controls and major aircraft components and established control continuity. The aircraft damage was consistent with the impact.
Identified parts of the aircraft’s canopy at the beginning and along the wreckage trail. The secondary canopy locking mechanism was found in the unlocked position.
Found evidence of propeller rotation.
Established that the engine oil hoses and oil filler cap/dipstick were secure, though the dipstick housing had fractured from the impact. Oil was observed over the engine, consistent with impact damage to the crankshaft.
Found that all fuel hoses were secure; however, a localised area of burning was observed on the fuel hose. The firewall and in-cockpit soundproofing foam also showed evidence of burning.
Established that the exhaust muffler, air filter and induction system were clear of debris or restriction.
Established continuity of the engine and propeller cockpit controls.
Found an oil coating on some sections of the aircraft, including the tail, right wing, fuselage and canopy Perspex. This was likely due to the significant disruption to the aircraft.
The engine was recovered from the wreckage and transported to an approved overhaul facility for detailed inspection under the supervision of the ATSB. The ATSB also conducted further examinations of the engine fuel hose, the engine firewall and part of the canopy locking mechanism at the ATSB’s technical facilities in Canberra, Australian Capital Territory.
Recovered items
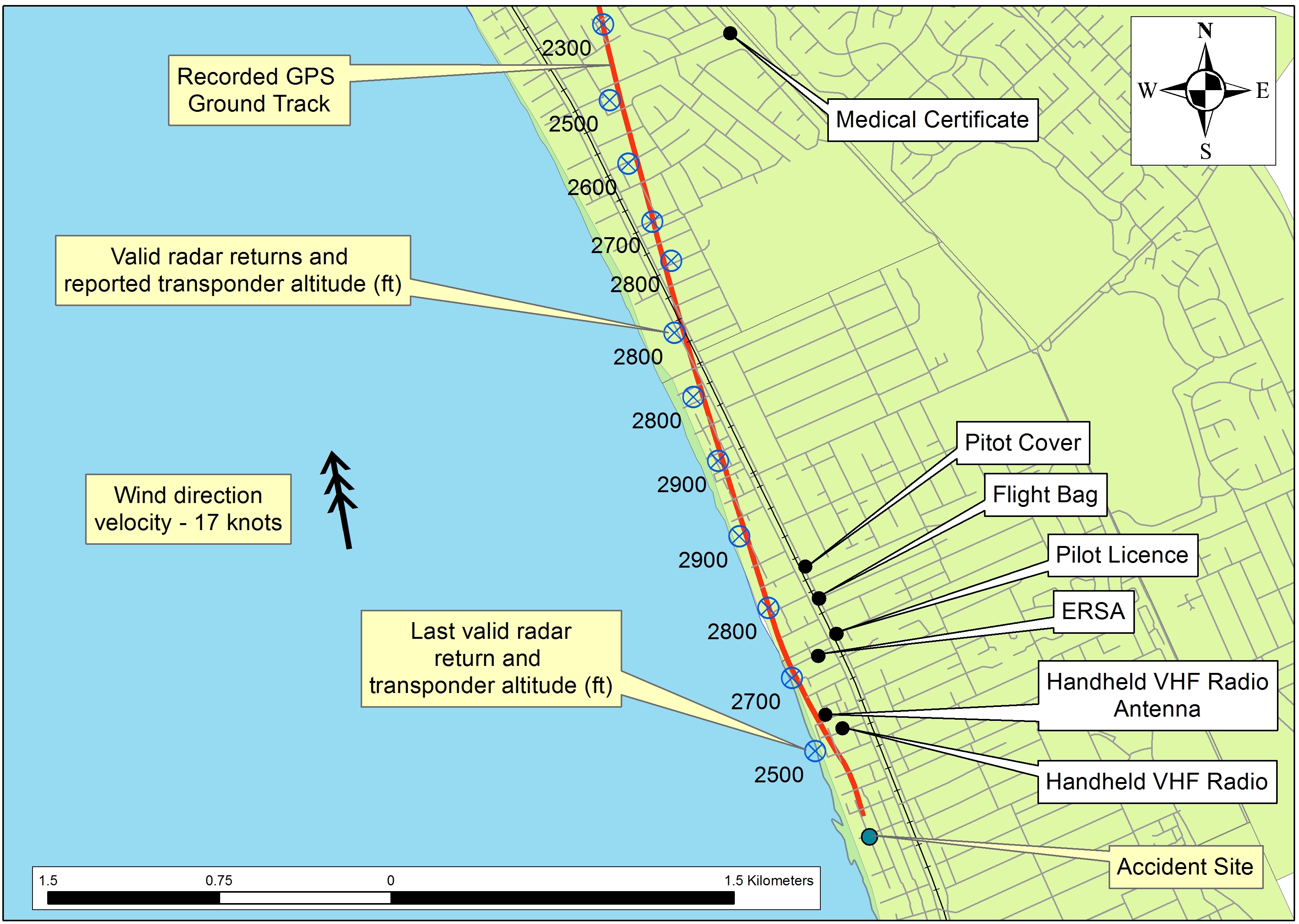
A number of aviation-related items were found by members of the public at distances up to 3 km north of the accident site (Figure 7). These items included the pilot’s Civil Aviation Safety Authority flight crew licence and aviation medical certificate, an aircraft pitot tube cover and warning flag, a flight bag, an En Route Supplement Australia and a very high frequency handheld transceiver and antenna. None of these items displayed evidence of fire damage.
Figure 7: Location of recovered aviation-related items relative to the accident site
Source: ATSB
Test and research
Engine examination
The engine examination found no evidence of internal mechanical failure that would have prevented normal operation prior to the occurrence. Any damage observed was consistent with impact forces.
Fuel hose and engine firewall
Examination of the fuel hose determined that the localised scorching and sooting was limited to the outer fire sleeve. The inner steel braiding and hose showed no evidence of heat or fire damage. A very small breach was observed in the inner hose; however, its position suggested that this was caused by deformation of the hose from impact forces.
Heat testing of a piece of undamaged firewall and in-cockpit soundproofing foam showed that, if a fire was present in the engine bay near the firewall, some smoking could be expected in the cockpit. However, the results of the heat testing indicated that the extent of the fire damage was more likely from the post‑impact fire.
Canopy locking mechanism
An inspection of the canopy locking mechanism found that the secondary lock was in the unlocked position. There was no evidence to indicate that the lock was forced open.
The primary locking lever was found in the unlocked position, however, the surrounding airframe structure was damaged and deformed. The locking catch and spring were not located, but the corresponding bolt was in place. The two hooks and hook receptacles on the rear corners of the canopy were not damaged or deformed.
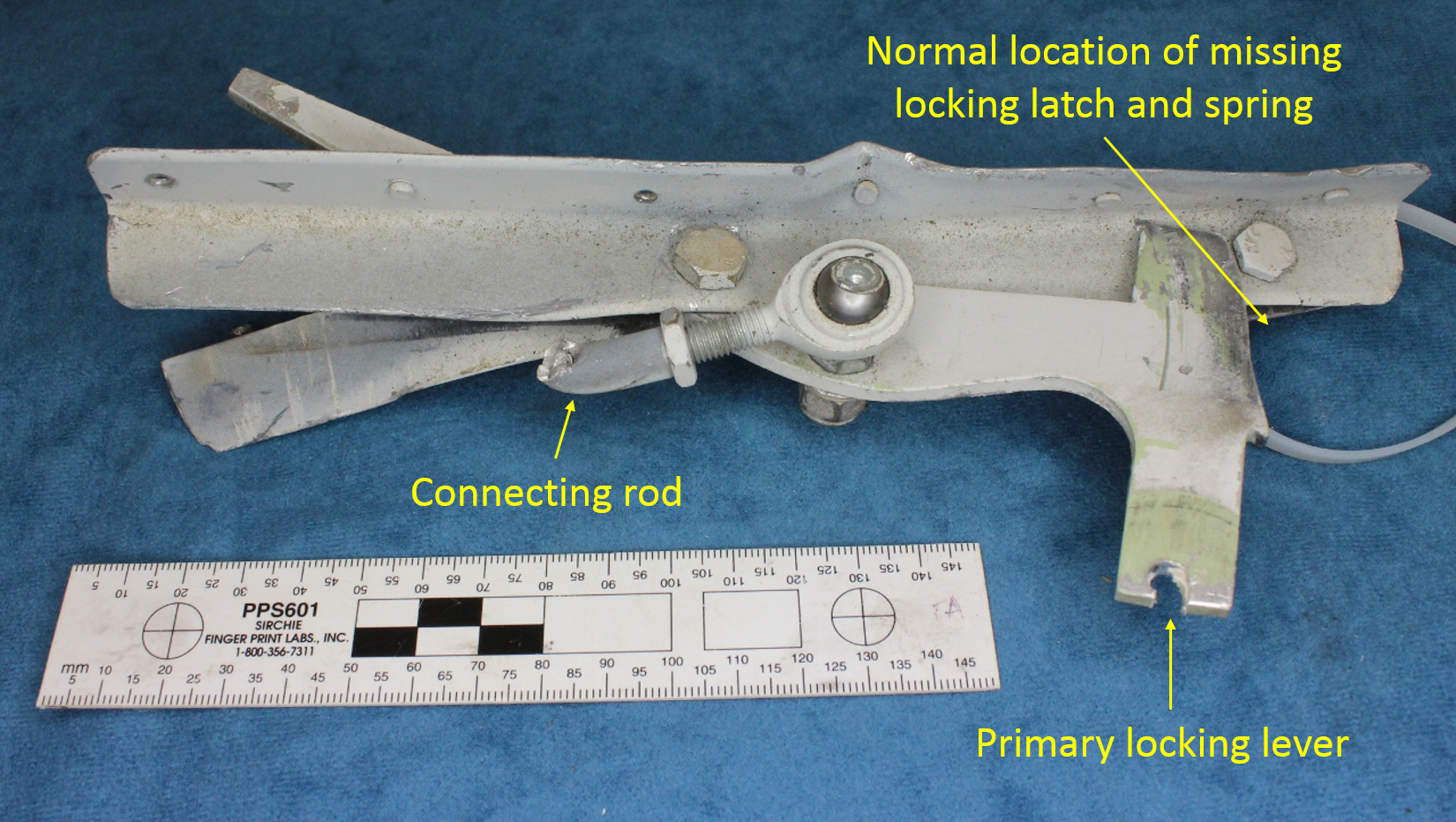
Examination of the primary locking lever found that (Figure 8):
The damage and deformation of the lever suggested that it was initially closed, but was forced out of its housing into a partially-open position at some point during the impact sequence.
While the locking catch and spring were not found, the attaching bolt was intact. It could not be determined whether the catch fractured during the impact sequence or was not previously in position.
The locking lever connecting rod fractured in overstress, likely due to the impact. It could not be determined whether those impact forces caused the lever to open.
Figure 8: Primary locking lever, normal location of the missing locking catch and spring, and the fractured connecting rod
Source: ATSB
Related occurrences
ATSB occurrence database
A review of the ATSB’s aviation occurrence database identified a range of reports where an aircraft’s canopy opened in flight. None of these reports involved the RV‑6/6A, RV‑7/7A or RV‑9/9A model aircraft.
Overseas investigations
On 20 June 2014, a Brumwell (Van’s) RV-6 aircraft impacted a house in the United States after departure from cruise flight. A witness reported observing a jet aircraft flying east and a small aircraft flying north. The small aircraft’s wings then started ‘rocking back and forth’ before the ‘nose went down’. That witness also reported seeing two objects come from the aircraft. The objects were later found near the accident site. The effects of wake turbulence from the jet aircraft, if any, could not be determined. However, the United States National Transportation Safety Board determined that the exit of the objects from the aircraft’s interior indicated that the canopy likely opened in-flight, which led to a loss of pitch control. The safety board was unable to establish the reason for the canopy opening due to fire damage (NTSB report CEN14FA306).
The pilot of an RV-12 aircraft reported that, as the aircraft became airborne, the tip-up canopy opened to about 3 inches (7.6 cm). The pilot reported grasping the canopy and simultaneously lowering the nose of the aircraft and partially reducing engine power in an attempt to land on the remaining runway. As the aircraft pitched down, the pilot lost grip of the canopy and it opened to the full vertical position. This reportedly caused the nose of the aircraft to pitch over further and, when the pilot applied back pressure on the control stick, there was no response from the elevator. The pilot also reported that there was no response from the rudder. The pilot was able to level the aircraft’s wings prior to landing hard. The pilot indicated that the canopy latch was hard to latch and they most likely did not secure it properly. Van’s commented on the accident, stating that they had not conducted any testing on the aerodynamic effects of the RV-12 canopy opening in flight. Therefore, they could not contest the pilot’s claims that the canopy opened to the full vertical position. Van’s indicated that they had a reasonable amount of field experience with tip‑up canopies opening in flight on the RV-6/6A, RV-7/7A, RV-9/9A models and other incidents involving the RV-12 where no loss of control was reported. They further stated that, while the extent that a canopy opens tends to vary with the aircraft’s airspeed, from their experience, the canopy typically opens to a point of aerodynamic equilibrium. At this point, the canopy’s position stabilises. This accident was the first reported where the aircraft’s pitch authority was affected by a tip-up canopy opening in flight on a Van’s aircraft (NTSB report CEN13LA340).
The pilot of an RV-12 aircraft did not secure the canopy latch after entering the cabin. After take‑off, the pilot noticed that the canopy was unsecured. The pilot became distracted with securing the canopy as the aircraft descended toward the runway. The aircraft collided with the runway as the pilot attempted to re-establish a level flight attitude. The pilot indicated that the accident could have been prevented had they focused on flying the aircraft instead of attempting to secure the unlatched canopy (NTSB report CEN11LA601).
Pilot forum reports
Anecdotal reports from a number of Van’s RV-6 pilots detailed varying consequences from an open canopy in flight. These included:
An instance when the aircraft was in the cruise at 4,500 ft and about 155 kt. After several minutes, the pilot heard a loud noise or pop and determined that the canopy had opened. The pilot noted that the primary locking lever was in the locked position. The pilot reported that the aircraft ‘had a definite pitch down attitude’ but was controllable. The pilot reduced the airspeed to about 85–105 kt before closing and re-locking the canopy. The pilot could not recall if the secondary latch was locked, though this would normally be double-checked before take-off.
A case where the pilot reported not double-checking the secondary latch prior to take-off, but indicated that the primary latch was locked. As the aircraft was climbed through 3,000 ft at 100 kt, the canopy opened. The aircraft was reported to instantly pitch 45°down with lots of wind noise in the cockpit. The pilot reduced power to idle and commenced arresting the descent. The pilot reported a 1,000 ft altitude loss. With the aircraft slowed to 60 kt, the two occupants closed the canopy. The pilot reported that, as a result of this occurrence, they included an additional checklist item to check that the canopy was locked.
A report from one pilot that they intentionally flew an RV-6A and an RV-7A with the tip-up canopy open during flight testing. The pilot indicated nil effect on the aircraft’s handling, other than a high noise level. This pilot further suggested that, from testing, the canopy could be used in place of a non‑usable elevator. The pilot indicated that, once their aircraft was slowed and trimmed for level flight, pushing the canopy up caused the aircraft’s nose to lower and closing the canopy caused the nose to rise.
A report of an RV-6A tip-up canopy that came open during cruise at 4,000–5,000 ft and 155‑170 kt. When the canopy opened it reportedly 'jerked the stick’ out of the pilot’s hand and the aircraft began a rapid descent. The pilot attempted to close the canopy but it did not move until the aircraft was under control and slowed down to near the stall[7] speed. The aircraft was recovered after descending through several thousand feet.
An instance where an RV-6 aircraft’s tip-canopy was reported to have opened twice during flight. The pilot reported that in the first incident they forgot to close and lock the canopy after leaving it open during taxi. During climb-out, the canopy gradually opened as the aircraft’s airspeed increased. The pilot reported slowing the aircraft and securing the canopy. On the second occasion, the aircraft was in a ‘dive’ at about 185 kt when the canopy suddenly opened ‘violently’ resulting in a pitch down. The canopy was reported to have lifted up before settling at a height of about 18 inches (45.7 cm). The pilot reduced the power to idle and arrested the descent until approaching the stall speed. With some effort, the pilot closed the canopy. After landing, the pilot determined that the secondary lock had been secured, but the primary mechanism had not been completely locked. The pilot felt that with in-flight vibrations, the primary mechanism released and that, due to the descent, the secondary latch had worked its way open.
Van’s comments
Van’s, the manufacturer of the aircraft kit advised that they were aware of incidents where the tip‑up canopy opened on RV-6 aircraft. They reported that this typically happened when the primary and/or secondary locking mechanisms were not engaged. Van’s also indicated that:
While not normal, it may be possible for the primary locking mechanism to not engage completely if the aircraft was not built accurately.
When the primary lock was not engaged or was ineffective due to build issues, the secondary lock may be sufficient to hold the canopy until the aircraft’s speed built up. As the aircraft’s speed built and the amount of suction on the canopy increased, there was the risk that the secondary lock would twist, allowing the canopy to open.
The suction holding the canopy open could make it difficult for pilots to overcome.
Generally, the canopy opening did not result in any control issues. The main risk was the pilot becoming distracted, particularly when close to the ground.
Some pilots have reported a pitch down, while others have not.
Theoretically, it is possible that at higher airspeeds, an open canopy may disrupt the airflow over the aircraft’s horizontal stabiliser. If this occurred, a forward pitching moment results. However, this had not been tested.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Safety Advisory Notice
Detecting an unsecured canopy prior to take-off could prevent in-flight control issues resulting in injury or aircraft damage.
On 16 October 2014, the pilot of a Cessna 206 aircraft, registered VH-KRR, conducted a solo training flight from Bankstown to Cootamundra, New South Wales and return. At about 0800 Australian Eastern Daylight Time, the aircraft departed Bankstown Airport with full fuel and landed at Cootamundra Airport at about 0943.
After taxiing to the parking bay and shutting down the engine, the pilot dipped the fuel tanks. He reported that 100 litres remained in the right tank and 85 litres in the left. This indicated an actual fuel consumption rate of about 67-70 litres/hour, and about 12 litres less fuel remaining in the tanks than the pilot had expected.
At about 1022, the aircraft departed Cootamundra on a planned track to Bankstown via Rugby and Bindook. At about 1100, the pilot observed that the aircraft had deviated from the planned track and attempted to track direct to Bindook, however took up a heading of about 120°, which resulted in a further deviation from the planned track.
At about 1114, and at 5,500 feet above ground level, the aircraft’s engine surged and then stopped. The pilot conducted some emergency checks and sighted a suitable landing area. The aircraft collided with trees about 50 metres short of the intended landing site and was substantially damaged. The pilot sustained a minor injury.
The aircraft owners attended the accident site and reported that about 7 litres of fuel (unusable) remained in the right tank and none in the left. This incident highlights the importance of thorough pre-flight planning and monitoring and reassessing actual versus planned flight tracks and aircraft fuel consumption.
On 20 September 2014, a de Havilland Canada DHC-6-300 aircraft, registered P2-KSF, collided with terrain 12 km north-east of Jacksons International Airport, Port Moresby, Papua New Guinea. Four of the 9 occupants were fatally injured.
An investigation into the circumstances of the accident was conducted by the PNG Accident Investigation Commission (AIC). The AIC requested assistance from the Australian Transport Safety Bureau (ATSB) with the download and analysis of information from various components including a cockpit voice recorder (CVR), forward-looking cockpit video camera and an enhanced ground proximity warning system (EGPWS) computer. To facilitate this support and to provide the appropriate protections for the CVR information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of ICAO Annex 13 and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
The PNG AIC published its final investigation report (AIC 14-1005) on 3 August 2015.
The report is available from the AIC website: www.aic.gov.pg.
Occurrence summary
Investigation number
AE-2014-155
Occurrence date
20/09/2014
Location
12 km north-east of Jacksons International Airport, Port Moresby, PNG
State
International
Report release date
15/10/2015
Report status
Final
Investigation level
Defined
Investigation type
External Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
De Havilland Canada/De Havilland Aircraft of Canada
On 7 October 2014, the pilot of a Bell 206B3 helicopter registered VH-CLR, departed Cairns, Queensland with one passenger on-board to conduct a charter flight to Mount Cook, about 9 km south-east of Cooktown Airport, Queensland.
To assess the landing area at Mount Cook, the pilot made 3-4 practice approaches and a practice landing prior to continuing to Cooktown to pick up the remaining passengers. The landing area was a rocky ledge jutting out from the south-eastern side near the top of Mount Cook.
The pilot conducted two flights to drop off a total of five passengers. He reported that the wind during these two flights was about 10 knots from the south-east. When he returned to pick up the first load of passengers, the wind had increased to about 14-15 knots.
During the approach to land, the pilot reported that he felt the helicopter was stable and appeared unaffected by the increased wind. As the helicopter prepared to touch down, both the ground co-ordinator and a passenger moved closer to it. Just prior to touching down on the right skid, the pilot felt the helicopter momentarily lift, most likely from a gust of wind, and drift to the right. The helicopter rolled rapidly onto its right side and slid a short distance forward, prior to coming to rest.
The helicopter fell onto the ground controller and nearby passenger. The ground controller sustained serious injuries. The pilot and passenger received minor injuries and the helicopter was substantially damaged.
The roll onto the right side by the helicopter is consistent with the phenomenon known as dynamic rollover. When a helicopter rests on one skid, the aircraft may begin rolling, and under certain circumstances it cannot be controlled.
The operator has advised the ATSB that they have taken several Safety Actions since the occurrence. These are detailed in the report.
On 23 September 2014, at about 1500 Central Standard Time, a Robinson R44 helicopter, registered VH-HLB, departed Bulman camp, Northern Territory, to conduct gravity survey operations. On board were a pilot and a geophysical field technician. The operation involved flying to specified locations 2 km apart and selecting a suitable landing site within 400 m of the location.
At about 1630, after completing landings at about 30 sites, the helicopter arrived overhead a specified location. The pilot identified a potential landing site, overflew it to more closely assess the site and then entered an out-of-ground-effect hover just above treetop height to determine whether the selected site was suitable for landing. The pilot decided the site was unsuitable as trees prevented sufficient clearance for the main and tail rotors.
As the pilot attempted to depart the area, the helicopter started to sink and the pilot observed the rotor revolutions per minute (RRPM) decaying. He lowered the collective and rolled on throttle in an attempt to increase the RRPM. The outside air temperature gauge indicated about 40 °C and the pilot reported that increasing the throttle did not provide any detectable increase in power. The pilot then eased forward on the cyclic. The helicopter continued to descend and the main rotor blade collided with multiple tree branches. When at about 6 ft above ground level, the helicopter rotated about 180° and landed hard with the left skid touching the ground first. The helicopter sustained substantial damage and the pilot and passenger were uninjured.
This incident highlights the effect of air temperature on aircraft performance. Understanding the controllability issues at the limits of the normal operating envelope can assist pilots in recognising the symptoms of reduced aircraft performance.