On 26 June 2014, a Tecnam P96 Golf aircraft, recreational registration 24-4470, collided with terrain near Krondorf, Barossa Valley in South Australia.
Recreational Aviation Australia (RA-Aus) is responsible for investigating this accident. As part of its investigation, RA-Aus requested technical assistance from the Australian Transport Safety Bureau (ATSB) in the examination of physical components and recovery of data from a GPS unit being used by the pilot. To protect the information supplied by RA-Aus to the ATSB and the ATSB's investigative work to assist RA-Aus, the ATSB initiated an investigation under the Transport Safety Investigation Act 2003.
Results of a visual examination of the physical components were provided to RA-Aus on 7 August 2014.
Following examination of the GPS, a download of its data was attempted using the manufacturer's procedures. The GPS unit could not be powered and it was determined that the GPS unit had sustained circuitry damage sufficient to prevent its download by conventional means. Subsequently, the discrete device (chip) containing the track memory was identified, removed, and a raw data file downloaded using specialised techniques. Decoding of the raw information showed that there was no available data relevant to the investigation. A report detailing the download procedure was provided to RA-Aus on 19 September 2014.
On 14 September 2014, the pilot of a Bell 206 helicopter, registered VH-FHX, conducted a charter flight from Myra mine camp, Northern Territory with 3 passengers on board. After arriving overhead a specified location, the pilot conducted an orbit at about 500 ft above ground level (AGL) to assess the area for a suitable landing site. The pilot then conducted a second orbit at about 100 ft AGL and noted the hazards including a tree stump to the left of the target landing area and a tall tree to the right.
The pilot then conducted an approach and a vertical descent into the selected landing site. When at about 1 ft AGL, a passenger alerted the pilot to the tree stump on the left. The pilot immediately manoeuvred the helicopter up and to the right, resulting in the helicopter striking a tree.
The pilot conducted a climb away from the site, an orbit and a second approach to land. After landing, the pilot shut down the helicopter and conducted an external inspection. The pilot assessed the damage to be minor and unlikely to affect the safety of the flight. After completing the charter flight and returning to Jabiru, the pilot inspected the helicopter and found the damage to the main rotor blade had worsened significantly. An engineer subsequently determined that the main rotor blade and tail rotor blade had sustained substantial damage and required replacement.
This incident highlights the challenges of operating in confined areas and the risks posed by distractions. It is also a reminder to ensure an aircraft is fully serviceable prior to flight, particularly following an incident.
On the morning of 14 September 2014, the pilot and passenger of an amateur-built Van's Aircraft RV-6, two-seat aeroplane, registered VH-TXF and operated in the ‘Experimental’ category, approached Mudgee Airport. The aircraft had departed Dubbo Airport, New South Wales about 25 minutes earlier.
The pilot approached from the north-west and conducted a non-standard circuit entry including an orbit to the south of the airport. Prior to turning onto the downwind leg of the circuit, the aeroplane descended to about 600 ft above ground level. Witnesses stated that the pilot conducted a tight left turn onto final approach at a slow speed and low height. The witnesses also recalled hearing the aeroplane’s engine ‘splutter’ and then silence during the turn, followed by a ‘rev’ followed again by silence.
The aeroplane continued its high angle of bank left turn and, at about 1053, collided with terrain about 300 m south-west and short of the runway threshold. The pilot and passenger were fatally injured, and the aeroplane was substantially damaged.
What the ATSB found
The ATSB found that during the turn onto final approach to land, the aeroplane’s engine ceased operating. The aeroplane’s airspeed before the engine failure was within about 0.5 kt of the estimated stall speed during the high-bank turn. After the engine failure, it is likely the aeroplane entered an aerodynamic stall. The associated loss of control was not recovered, and the aircraft continued in the turn until it collided with terrain.
The ATSB also found that the engine failure was probably due to carburettor icing. No defects were identified that would have precluded normal engine operation prior to the accident, and uncontaminated fuel was being supplied to the engine at that time. However, the environmental conditions at the time of the accident were conducive to serious carburettor icing at descent power, and the pilot-operated carburettor heat control was found in the OFF position.
Analysis of the aeroplane’s global positioning system data showed that it was common for this pilot to fly approaches at lower than recommended circuit heights and at speeds close to the aircraft’s stall speed. On the turn to final approach on the accident flight, any loss of airspeed would have left a very short time before the aeroplane reached the stall speed.
The ATSB also found that the aeroplane’s weight was higher than the design limits. However, the effect of this weight on aircraft performance was not considered to have contributed to the accident.
The aeroplane was not required to be, and was not fitted with an angle-of-attack indicator or stall warning device.
Safety message
All pilots of aircraft fitted with a carburettor are advised to check the forecast weather conditions and consider the risk of carburettor icing as a result of those conditions prior to each flight.
Although amateur-built aeroplanes operated in the Experimental category are not required to be fitted with a stall warning device, owner-pilots should consider the benefits of such devices as a last line of defence against the inadvertent approach to, or entry into an aerodynamic stall.
Source: ATSB
The occurrence
At about 1024 Eastern Standard Time[1] on Sunday 14 September 2014, the pilot and passenger of an amateur-built Van's Aircraft RV-6 aeroplane, registered VH-TXF, departed Dubbo Airport on a private flight to Mudgee Airport, New South Wales.
At about 1049 the pilot approached Mudgee Airport from the north-west and conducted a nonstandard circuit entry. This included an orbit to the south of the airport. Airport audio recordings of aircraft broadcasts show that throughout the arrival at Mudgee, the pilot made all of the standard radio calls, including traffic advice of joining crosswind, base leg, and final approach for runway 04.[2] The pilot did not make any broadcasts suggesting any problems with the aircraft.
Prior to turning onto the downwind leg of the circuit, the aeroplane descended to about 600 ft above ground level. Witnesses stated that they saw the aeroplane turn left at about 45° angle of bank onto final approach at a slow speed and at a lower height than usual. The witnesses also recalled hearing the aeroplane’s engine ‘splutter’ and then silence during the turn, followed by a ‘rev’ followed again by silence.
The aeroplane continued its high angle of bank left turn beyond the final approach heading and, at about 1053, collided with terrain about 300 m south-west and short of the threshold of runway 04(Figure 1 and Figure 2). No witnesses reported seeing the aeroplane impact the terrain.
The pilot and passenger were fatally injured, and the aeroplane was substantially damaged.
Figure 1: Aerial view of the accident site on the day, showing the threshold of runway 04 and direction of travel prior to impact
Source: NSW Police Force, modified by the ATSB
Figure 2: Accident site, looking east-south-east and showing the airport boundary fence
The pilot held a Private Pilot (Aeroplane) Licence and the appropriate ratings and endorsements to operate the Van's Aircraft RV-6 (RV-6). The pilot also held a valid Class 2 Aviation Medical Certificate, which was sufficient for the pilot to exercise the privileges of their licence.
The last recorded entry in the pilot’s logbook was on 14 June 2014. A review of the pilot’s logbook and aircraft maintenance release for VH-TXF (TXF) indicated that the pilot had accrued a total of about 764 hours flight time. The pilot’s most recent biennial aeroplane flight review was on 9 June 2014.
A flying instructor who had flown with the pilot stated that the pilot was very aware of the risk of carburettor icing, and was in the habit of using carburettor heat at lower power settings.
Recent history
The only recorded flying by the pilot in the week prior to the accident was a 2.9-hour flight from Traralgon, Victoria, to Dubbo on 12 September 2014. Friends of the pilot reported that, on the evening before the accident, the pilot retired at about 2200, and was observed outside the hotel room the next morning at about 0800. There was no evidence that fatigue contributed to the accident.
Aircraft information
General information
TXF was a two-seat Van's Aircraft RV-6 aeroplane, and was manufactured by the pilot from a kit. It was first registered in Australia on 10 July 2001 and the kit was completed in 2006 (serial number 24677). TXF had accumulated about 425 hours total time in service at the time of the accident.
The aircraft was operated in the ‘Experimental’[3] category.
Maintenance history
Examination of the aeroplane’s maintenance records indicated that it was maintained to a day visual flight rules[4] standard in the experimental category. The last periodic inspection was completed on 16 December 2013, and a maintenance release was issued at that time. At the time of the accident, all of the required maintenance had been completed and there were no outstanding recorded defects.
Weight and balance
The aircraft kit manufacturer-published recommended gross weight for the RV-6 was 727 kg. This was also detailed on the aircraft’s data plate.[5] The pilot had generated their own weight and balance calculation paperwork, which detailed a maximum allowable gross weight of 748 kg. This paperwork, which the pilot carried in the aeroplane, indicated that the aeroplane’s gross weight on departure from Dubbo was 740 kg and was planned at about 731 kg on arrival at Mudgee.
The ATSB calculated that the aeroplane was about 4 kg over the manufacturer-recommended gross weight on arrival at Mudgee. However, according to the pilot’s paperwork, the aeroplane was within the pilot’s calculated flight envelope. The ATSB could not identify any data to indicate how the pilot determined the new gross weight for the aircraft. A calculation was performed by the ATSB to examine the effects of the weight increase on the aeroplane’s aerodynamic stall speed.[6] This calculation indicated that the aeroplane’s stall speed would have increased by about 0.5 kt.
Meteorological information
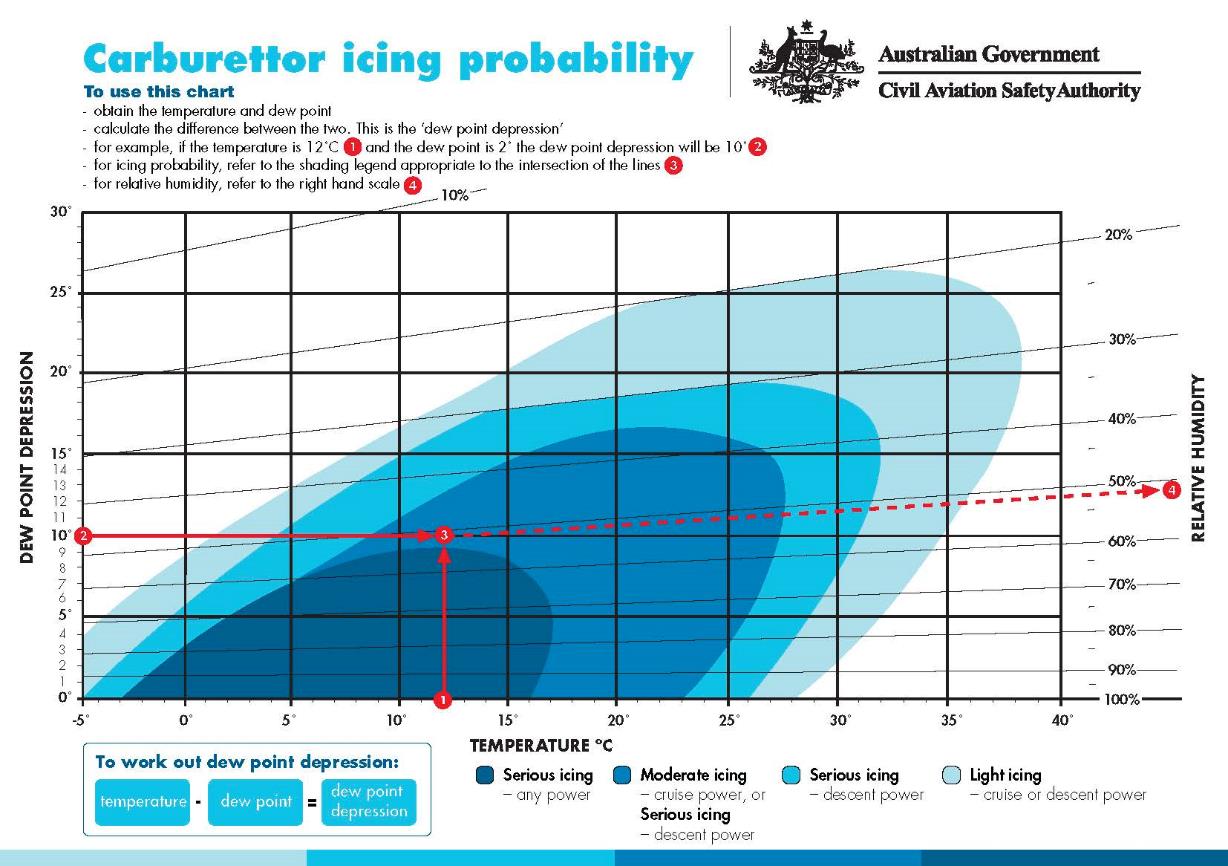
The observed weather at Mudgee Airport at the time was fine with a 6 kt breeze from the north and no cloud in the vicinity. The recorded temperature at about the time of the accident was 17 °C, with a dew point[7] of 11 °C. Given those temperatures, the probability of carburettor icing was calculated to be in the serious icing range for descent power, and moderate icing with cruise power selected (see appendix A – Carburettor icing-probability chart, available from the Civil Aviation Safety Authority (CASA) website).
Wreckage examination
Overview
The aeroplane struck the ground in a north-westerly direction, coming to rest about 18 m beyond the initial impact point. The impact collapsed the aeroplane’s fixed landing gear, damaged the engine, carburettor and air filter and ruptured the left wing fuel tank. The damage to the aeroplane and surrounding area indicated that the aeroplane impacted the ground in an upright, slightly leftwing low and nose-down attitude. All of the aeroplane’s major components were accounted for at the site. No evidence of fire or pre-impact damage was observed and flight control continuity was verified.
One blade of the aeroplane’s two-bladed wooden propeller was broken off at the root and shattered (Figure 3). The other blade remained attached to the hub. The unbroken blade and metal spinner that covered the propeller hub exhibited no evidence of rotational scratch marks or power at impact.
Figure 3: Broken two-bladed propeller blade and metal spinner, showing the reconstructed detached/shattered blade
Source: ATSB
The engine and a number of other items and components from TXF were recovered for technical examination at an approved engine overhaul facility and at the ATSB’s technical facilities in Canberra, Australian Capital Territory. This included a portable Garmin GPSMAP 296 global positioning system (GPS) receiver.
Fuel
The left fuel tank was breached along a rivet line, consistent with impact forces. Witnesses reported fuel running from the rivet line before being plugged by the attending fire service.
On examination by the ATSB, about 20 L of fuel remained in the left fuel tank and about 65 L in the right fuel tank. The fuel tank selector in the cockpit was selected to the right tank. Fuel was observed:
throughout the fuel system through to the engine-driven fuel pump
to run from the damaged carburettor bowl and its filter screen
to be free of debris and water throughout the aeroplane’s fuel system, and of a colour and odour that was consistent with aviation gasoline.
The ATSB concluded that fuel starvation or contamination did not contribute to the loss of engine power.
Survivability
The aeroplane was fitted with a 5-point harness for each seating position and both occupants were wearing their harness. The lap belts and crotch straps remained anchored to the floor and the shoulder harnesses were appropriately anchored to the fuselage structure behind the occupant’s seats and luggage area. ATSB analysis based on estimates of aircraft speed, impact angle, and energy absorption indicated that the impact forces imparted to the occupants would normally be expected to result in serious to fatal injuries.
During the impact sequence, the sides of the cockpit buckled, reducing the liveable space and allowing the fuselage behind the pilot and passenger to move forward (Figure 4). As a result, both occupants’ shoulder harnesses slackened and the occupants were no longer adequately restrained. Together with the effect of the estimated impact forces imparted to the occupants, this reduction in liveable space meant that the accident was considered not survivable.
Figure 4: Cockpit region showing buckling alongside the left and right seats
Source: ATSB
Engine and associated components examination
The aeroplane’s engine and associated components were removed and taken to an approved engine overhaul facility for disassembly and detailed examination under the supervision of the ATSB. No evidence was found to suggest abnormal engine operation prior to the impact with terrain. The engine’s two magnetos[8] and associated spark plugs performed correctly when examined and operationally tested on their respective test rigs.
Recorded data
Recorded data from the aircraft’s portable Garmin GPSMAP 296 GPS, including of the accident flight, was successfully downloaded at the ATSB’s technical facilities. This data included a series of points indicating the aeroplane’s latitude and longitude, altitude and the respective dates and times of those records.
The data for the day of the accident commenced at about 1019 and showed the path taken by the pilot from start-up at Dubbo Airport to the approach at Mudgee Airport. ATSB analysis of this data determined the aircraft’s height above ground, ground speed and heading at the various data points. This included the circuit entry at Mudgee, a southerly, figure eight-like orbit prior to the aeroplane joining the downwind leg of the circuit and the turn onto final approach to land as described by witnesses (Figure 5).
Figure 5: ATSB analysis of the recorded GPS data for the flight showing the aircraft’s heading, height above ground, and ground speed at various data points. The area of the southerly, figure eight-like orbit is indicated by a dashed blue border
Source: Google earth, modified by the ATSB
Data recovered from the aircraft’s Garmin GPSMAP 296 GPS also provided the flight path details for a number of previous flights, up to, and including the accident flight. Circuit entry procedures were compared between flights carried out in 2014 to better understand the pilot’s usual handling of the aeroplane from entering the circuit, through to the landing. None of the approaches analysed displayed a similar figure eight-like orbit prior to joining the crosswind leg as was done on arrival at Mudgee (Figure 5).
A review of the accident and 22 previous final approaches was performed using the recorded GPS data and wind information from the aerodromes visited by the aircraft during those flights. The review found that on 18 occasions, the aeroplane was below 500 ft at the beginning of the final approach and, on 11 of the 22 final approaches, below the target approach speed of 63 kt (see Aeroplane approach speed considerations) on joining the final leg of the circuit. On 10 of the 18 occasions when the aeroplane was below 500 ft at the beginning of the final approach, it was also below the target approach speed of 63 kt.
At the estimated arrival gross weight of 731 kg the aircraft had a stall speed of 48 kt. Turning onto the final leg of the circuit at Mudgee, as derived from the GPS data, the aircraft had:
a bank angle of about 48°
a descent rate of 1,770 ft/min
an airspeed of 59 kt (4 kt below the target approach speed)
an accelerated stall speed of 58 kt.
In combination these findings indicated that the aeroplane’s airspeed was about 1 kt above the calculated accelerated stall speed, or within about 0.5 kt when considering the aeroplane’s increased weight, which was above the kit manufacturer’s recommended gross weight.
Additional information
Carburettor icing
Carburettor icing[9] can occur in temperatures up to about 38 °C, and is less likely in very cold climates. Increased humidity increases the likelihood of icing. If ice continues to accumulate within the carburettor, the flow of air into the engine reduces and eventually, if the process is allowed to continue, the engine will stop.
Carburettor icing is more pronounced if the engine is operating at a low power setting. In this case, the airflow through the carburettor is partially-impeded by the throttle butterfly valve. This valve provides more area on which the ice can accrete and increases the partial vacuum downstream of the valve. This causes further chilling of the air and the water droplets, further increasing the likelihood of ice accretion.
For aircraft with fixed pitch propellers, as ice forms there is typically a small decrease in engine RPM but the engine may continue to run smoothly. As ice continues to accumulate, the reduction in RPM continues and the engine will begin to run rough. If the icing conditions are severe enough, and the pilot takes no remedial action, the engine will eventually fail.[10]
A carburettor heat control was available in TXF. If selected, warm air was directed from a heat muff[11] installed on the exhaust system to the carburettor inlet, melting any ice in the venturi.
During the on-site examination, the carburettor heat control was identified in the OFF position (pushed in). It is possible that the impact sequence may have depressed the carburettor heat control. However, surrounding push/pull controls were undisturbed in their pulled-out positions.
The environmental conditions and time between the accident and the ATSB’s examination of the wreckage meant that any icing in the carburettor throat would have melted and not been detectable during that examination.
On 24 October 2014, the aeroplane kit manufacturer released a notification to RV-6 owners to inspect their heat muff installations for the correct installation of a vent screen. If placed in the wrong position, there was a chance that the screen may obstruct warm airflow to the carburettor, hindering the ability to remove carburettor ice and/or reduce engine performance. Examination of the exhaust system in TXF confirmed that the heat muff installation was a different type to that specified in the notification, which was therefore not applicable.
Aerodrome circuit entry procedures
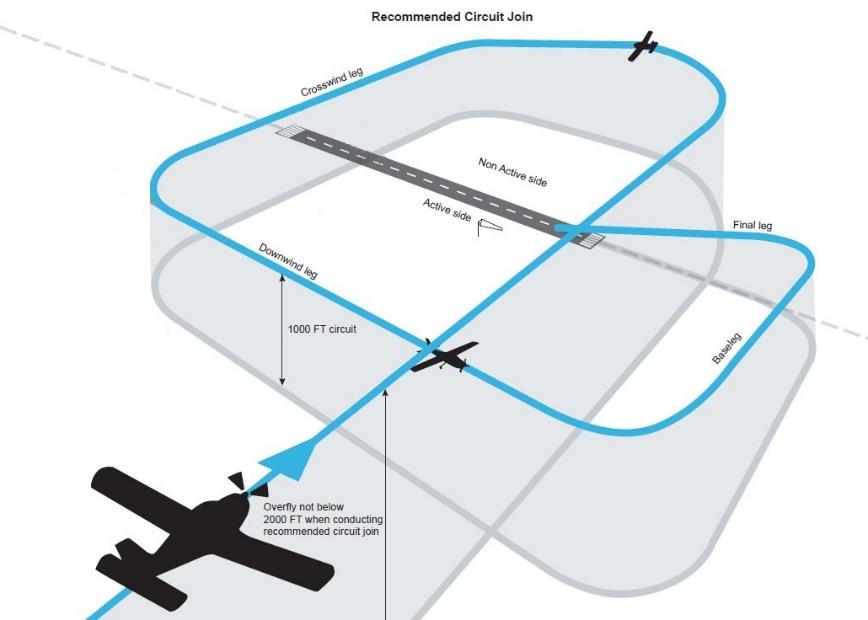
Among other guidance, CASA Civil Aviation Advisory Publication (CAAP) 166-1(3) Operations in the vicinity of non-controlled aerodromes strongly recommended the use of standard circuit procedures at all noncontrolled aerodromes.[12] Standard traffic circuit procedures were designed to facilitate orderly flow of aircraft traffic. Given these standard traffic circuit procedures, other aircraft operating in the vicinity of the aerodrome would have a reasonable expectancy of where to locate other joining and circuit traffic, informing affected pilots’ ‘see and avoid’ procedures (Figure 6). The traffic entry procedure generally consisted of overflying the aerodrome to ascertain the wind direction and which runway was in use by other aircraft, before joining a circuit pattern for landing.
Approach speeds are based on the aeroplane’s aerodynamic stall speed. A safety margin of generally 1.3 times the aeroplane’s aerodynamic stall speed in the landing configuration is applied to determine an aircraft’s approach speed.
The kit manufacturer’s published stall speed for the RV-6 at 1 g[13] and a gross weight of 727 kg was 48 kt. Therefore, in an RV-6 at the recommended gross weight, the calculated approach speed would have been about 63 kt. As the g load is increased, as it generally would in a turn, the stall speed also increases. This is known as an accelerated stall.
Stall warning devices
Certified aeroplanes were required to have a stall warning. This could be satisfied by either the inherent aerodynamic qualities of the aeroplane, or by the installation of a technical device that gives clearly distinguishable indications of an aerodynamic stall under the expected conditions of flight.[14]
The Unites States Federal Aviation Administration issued InFo[15] 14010 on 14 July 2014. This document recommended the installation and use of angle of attack (AoA)-based systems to reduce the risk of inadvertent aerodynamic stall that may result in a loss of control accident. The kit manufacturer did not produce a stall warning kit specific to the RV-6, but did encourage builders and owners to consider installing AoA indicators.
TXF was not fitted with a stall warning device or an AoA indicator, nor was it required to be as it was not a certified design. This meant that the only stall warning available to the pilot was via the aircraft’s aerodynamic qualities.
The stall characteristics for each individual aeroplane of an amateur-built type depend to an extent on the precision of the aeroplane build. This necessitates the completion by the pilot of stall testing for the aeroplane and recording the results in the aircraft’s flight manual. The flight manual for TXF was not able to be located to verify the stall speed characteristics as compared to those of the kit manufacturer.
From witness information and examination of the accident site, it is evident that during the turn onto final approach, the pilot lost control of the aeroplane and was unable to recover before impacting the ground. The observed departure from controlled flight was consistent with an aerodynamic stall.
This analysis will consider the factors with the potential to have contributed to the loss of control.
Interpretation of the flight path
The ATSB did not identify any issues that would have required the pilot to orbit to the south of the aerodrome as shown on the global positioning system (GPS)-derived flight path profile. Although unable to be confirmed, it was possible that the pilot manoeuvred to view their accommodation, which was just to the south of the runway. Whatever the reason for the orbit, the ATSB believes that it was unrelated to the accident.
Engine operation
The witness accounts of the engine being silent during the turn onto final approach, and the lack of rotational signatures on the propeller, indicates that the engine was not operating when the aeroplane collided with terrain. No defects were identified that would have precluded normal engine operation prior to the accident, and uncontaminated fuel was being supplied to the engine at that time.
Conditions around the time of the accident were conducive to serious carburettor icing at descent power, such as during the circuit and approach onto final. In combination, the as-found positions of the carburettor heat control in the depressed OFF position, and of the surrounding push/pull controls in the pulled-outed positions, were consistent with the carburettor heat control being in the OFF position before impact. In this case, it is probable that the air temperature in the carburettor was in the icing range and that carburettor ice would have formed. Although the pilot was reported in the habit of using carburettor heat at lower power settings, it is possible they forgot on this occasion, or were not aware of the suitability of the environmental conditions for carburettor icing.
Witnesses reported only hearing unusual engine sounds during the pilot’s turn from downwind onto final approach. It is considered unlikely that there was a detectable performance issue prior to that turn because, had that been the case, the pilot would probably have modified their circuit to attempt an earlier forced landing on either of the available runways. Recovery from an engine failure at greater height allows for increased landing options. However, the witness reports of the pilot’s apparent attempt to restart the engine on final approach would suggest that any carburettor icing remained undetected throughout the join and initial legs of the circuit.
In the absence of contradicting evidence, and considering the witness observations, ambient conditions that were conducive to carburettor icing and lack of any indication of propeller rotation at impact, the ATSB concluded that it was probable the engine failed during the final turn due to carburettor icing.
Weight and balance
The evidence indicated that the pilot was operating the aeroplane above the kit manufacturer’s recommended gross weight and above the gross weight as stated on the aeroplane’s data plate. The use of extrapolated data outside the recommended flight envelope is not considered accurate, precluding a full understanding of the effect on the aircraft’s performance. However, using the gross weight figure recorded on the pilot’s flight planning documentation to estimate the aircraft’s centre of gravity suggested that the aircraft was within the kit manufacturer’s recommended limits.
Given the aircraft was being operated above its limiting gross weight, wreckage examination found no evidence of an in-flight structural failure. As a result, the most probable effects of the operation outside the kit manufacturer’s recommended maximum gross weight were a slightly increased stall speed and likely increased difficulty during recovery from a loss of control.
Approach speed consideration
Based on the recorded GPS flight data, the pilot commonly flew their approaches at lower than recommended circuit heights and at speeds close to the aircraft’s stall speed. On the accident flight, the stall margin was significantly reduced throughout the last 48° angle of bank turn, being within about 0.5 kt of the aircraft’s stall speed.
Any loss of airspeed in those conditions left a very short time before the aeroplane reached its stall speed. Given that the engine failed during the steep angle of bank and low speed turn onto final approach, it is probable that the aeroplane entered an accelerated aerodynamic stall soon after the engine failure, from which the pilot was unable to recover before colliding with terrain.
Findings
From the evidence available, the following findings are made with respect to the collision with terrain involving a Van's Aircraft RV-6, registered VH-TXF that occurred near Mudgee Airport, New South Wales on 14 September 2014. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
As the aircraft was turned on to the final approach to land, the engine ceased operating.
The meteorological conditions at the time of the accident were conducive to carburettor icing, which probably led to the engine stopping.
The steep turn onto the final approach at low airspeed probably resulted in an accelerated aerodynamic stall shortly after the loss of engine power from which the pilot was unable to recover before impacting terrain.
Other factors that increased risk
The aeroplane was not fitted with a stall warning device or angle of attack indicator, increasing the risk of inadvertent aerodynamic stall.
The aeroplane was being operated at weights above the kit manufacturer’s recommended gross weight.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot’s previous flying instructors
aircraft kit manufacturer
Civil Aviation Safety Authority
United States Federal Aviation Administration
New South Wales State Coroner
New South Wales Police Force.
References
Australian Transport Safety Bureau, 2001, Melting Moments: Understanding Carburettor Icing, Educational fact sheet.
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Civil Aviation Safety Authority.
No submissions were received.
Appendices
Appendix A – Carburettor icing-probability chart
Source: Civil Aviation Safety Authority
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 5 September 2014, the pilot of a Mooney M20J aircraft, registered VH-JDY, conducted a solo training flight from Jandakot Airport to Northam aeroplane landing area (ALA), Western Australia. After a touch-and-go on runway 14 at Northam, the pilot conducted a second circuit with a missed approach from about 600 ft on final. The pilot then intended to conduct a third circuit with a touch-and-go. When on final, the pilot trimmed the aircraft in the approach configuration with full flaps (33°) and airspeed at about 70 kt.
The pilot flared the aircraft for landing and touched down about one third of the way along the runway. As the aircraft slowed, the pilot selected the flaps to 15° and applied full throttle along with right rudder to counteract the aircraft’s tendency to yaw left. As the airspeed increased to about 65 kt, the pilot rotated the aircraft for take-off and applied forward pressure against the control column as the aircraft nose tendency was to pitch up due to the combination of trim, flap and power settings.
When at about 50 ft above ground level, the aircraft had drifted to the right of the runway centreline and the pilot reduced the right rudder input. Soon afterwards, the aircraft nose pitched up. The stall warning sounded and the pilot applied full right rudder and pushed forward on the control column in an attempt to level the aircraft wings and recover from the stall. The left wing dropped as the aircraft stalled, and it collided with a hangar. The aircraft pivoted about the left wing and came to rest wedged between two hangars resulting in substantial damage.
On the afternoon of 25 August 2014, the pilots of two Robinson R22 helicopters were ferrying the helicopters from Yeeda to Springvale via a refuelling stop at Leopold Downs, within the Kimberley region of Western Australia. The pilot who was ahead by about 10 NM (18 km) arrived at Springvale about 40 minutes after last light but the pilot of the second helicopter, registered VH‑YPC, did not arrive as expected.
A search using helicopters began early the next morning and the overdue helicopter was soon found in a seriously damaged state, close to the intended track and 25 NM (46 km) west of Springvale. The pilot had been fatally injured.
What the ATSB found
The ATSB found that the pilot of VH-YPC, who did not hold a night visual flight rules (VFR) rating or instrument rating, continued flying towards the destination after last light (end of civil twilight), then in dark night conditions without local ground lighting, inadvertently allowed the helicopter to descend into terrain.
Safety message
This accident highlights the inherent high risk of night flying in remote areas due to the absence or degradation of the visual references for establishing an aircraft’s attitude and position. This risk is increased to unacceptable levels when night flying is attempted by pilots without night VFR or instrument flying qualifications. To avoid the usually fatal consequences of disorientation, day VFR pilots need to plan to arrive at their destination at least 10 minutes before last light and to have a realistic ‘Plan B’ to use when it becomes apparent that an intended flight cannot be completed in daylight. It is important, also, for operators and others involved in the operation of aircraft to actively support safety-first pilot decision making.
The ATSB is concerned about the frequency of accidents – many fatal – that involve pilots flying with reduced visual cues. This has been highlighted on the ATSB website as a SafetyWatch priority along with a number of strategies to help manage the risk and links to relevant safety resources.
On 2 August 2014, the pilot prepared the C206, VH-TND for the first of three scenic flights. As the aircraft departed from runway 03, the wind was from the east at about 8 knots.
On return to Rawnsley Park, the pilot conducted a straight in approach onto runway 21. The pilot did not compensate for the crosswind during the flare and touchdown, and after landing retracted all stages of flap, and applied light pressure to the brakes.
The aircraft then began to veer to the left. The pilot applied right rudder, but was unable to correct the situation, so initiated a go-around. During the go-around the horizontal stabiliser struck a shrub, causing significant damage to the aircraft. The pilot lowered the aircraft nose. After clearing a small tree, the pilot raised the aircraft’s nose in an attempt to clear the windsock.
Moments later, the aircraft spun rapidly to the left and collided with the ground. The pilot shut down the aircraft and assisted the passengers to exit. One passenger sustained serious injuries and another sustained minor injuries. The pilot was not injured. The aircraft was substantially damaged.
It appears that an incorrect technique was applied during the crosswind landing and subsequent go-around. The suddenness of the unexpected events during an otherwise routine exercise caught the pilot unprepared, resulting in a loss of situational awareness.
The Civil Aviation Safety Authority (CASA) has available on their website a booklet and DVD looking at situational awareness. Chapter 6 specifically looks at Losing Situational Awareness.
This is available through CASA’s online store: www.casa.gov.au
The European General Aviation Safety Team (EASA) published a Safety Promotion Leaflet on Decision Making for General Aviation Pilots. This leaflet suggests that many accidents are the result of pilot action, including the decisions that they make.
On 13 June 2014, the pilot of a Bell 206 helicopter, registered VH-KSV, conducted a flight from Mitchell Plateau campground, Western Australia, to a remote site about 30 NM away to collect passengers.
Approaching the site, the pilot conducted an orbit of the area at about 300 ft above ground level (AGL) to assess the landing area. As the helicopter descended over trees, the pilot observed that the helicopter was slightly higher than optimal for the approach. From a high hover, at about 10 ft AGL, the pilot continued to lower the helicopter slowly and elected to land towards the rear of a rocky sandstone platform to remain clear of the waiting passengers.
The right landing skid touched down first and only the front portion of the landing skids was in contact with the platform, with the right skid was sitting on a rock. The pilot attempted to raise the helicopter back into the air to relocate to a better landing position, but as he raised collective, he felt the helicopter start to roll and he quickly lowered the collective. The helicopter tipped backwards off the edge of the rocky platform and slid about 2 m down the slope before coming to a halt.
After shutting down the engine, the pilot inspected the helicopter and found substantial damage to the landing skid, a hole in the main rotor blade where it had struck the wirestrike cutter, and damage to the tail boom.
This incident highlights the importance of assessing a landing site thoroughly and conducting the approach to land so as to optimize the opportunity of sighting any potential hazards.
On 13 July 2014, the pilot of a Cessna 172 aircraft, registered VH-EEC, conducted a private flight from The Lily to Narrikup aeroplane landing areas (ALA), Western Australia, with two passengers on board.
At about 1320 Western Standard Time, the pilot broadcast an inbound call when about 10 NM north-east of Narrikup at about 6,500 ft above mean sea level (AMSL). The pilot elected to conduct an approach to runway 06 and overflew the runway at about 1,900 ft AMSL. He observed the windsock which did not indicate any significant crosswind. The aircraft then descended to circuit height and joined on the crosswind leg for runway 06.
When established on final for runway 06, the pilot reported that he had selected two stages of flap and had the aircraft stabilised at about 65 kt. When about 50 ft above ground level, the pilot reported that the aircraft encountered a wind gust which carried the aircraft about 30 m to the right. The pilot moved the aileron controls into wind and applied full power to commence a go-around; however, the aircraft’s right wing collided with trees on the right side of the landing area. The pilot reported that the right wing may have stalled as he applied full right aileron. The aircraft fell to the ground resulting in substantial damage.
This incident highlights the importance of being ready to conduct an early go-around when a pilot is not completely satisfied that a safe landing can be made.
On 12 July 2014, a pilot was undergoing training for mustering approval by a supervising pilot in a Robinson R22 helicopter, registered VH-ZZM. After completing about 7 hours of mustering, the helicopter was returning to a homestead near Dingo, Queensland, when about 1,000 ft above ground level (AGL) the supervising pilot instructed the pilot to conduct a practice autorotation turning through 180°, which the pilot completed, increasing power when at about 5 ft AGL.
During the subsequent climb, when at about 450 ft AGL, the supervising pilot took control of the helicopter and initiated a second autorotation. The supervising pilot initially observed the airspeed at about 65 kt, the rotor rpm in the green arc and the autorotation ‘looking good’, and assumed at this stage that he had handed control of the helicopter to the other pilot. At about 100 ft AGL, the pilot detected the rotor rpm decaying and a rapid rate of descent, but still assumed that the supervising pilot had control of the helicopter. When at about 20-40 ft AGL, the supervising pilot observed the vertical speed increasing and the rotor rpm decreasing and rapidly lowered the collective and increased the throttle. Just prior to the helicopter contacting the ground, the supervising pilot flared then levelled the helicopter and raised the collective.
The helicopter landed hard, bounced once and rotated through about 180° before coming to rest. The pilot sustained serious injuries and the supervising pilot minor injuries. The helicopter was substantially damaged.
This incident highlights the importance of good communication between a flight instructor and their student and the use of handover/takeover techniques to clarify who has control of the aircraft at any time.
On 4 July 2014, the pilot/owner of a Cessna Aircraft Company T210N aircraft, registered VH-ZFW, and two passengers were conducting a private flight from Inverell Airport to Bankstown Airport, New South Wales.
Shortly after take-off, oil appeared on the windscreen and the pilot rejected the take-off with the intent of landing back on the runway. As the oil temporarily obscured the pilot’s forward visibility, they looked to the left to assess their position along the runway. The pilot realised that they were a lot further along the runway than expected and that there was insufficient runway distance remaining to land safely. A go-around was commenced but the pilot reported that the engine did not respond. During the subsequent forced landing, the aircraft impacted a shrub beyond the end of the runway overrun and flipped, before coming to rest inverted.
The pilot and a passenger were hospitalised with serious injuries and the second passenger received minor injuries. The seriously-injured passenger later succumbed to their injuries. The aircraft was destroyed by the impact forces and a post-impact fuel-fed fire.
What the ATSB found
Examination of the aircraft found the engine oil filler cap detached from the oil filler tube but hanging by its chain. Further examination of the tube and cap determined that it was most likely the cap was not secure before the flight commenced. The Cessna T210N pilot’s operating handbook advised pilots to check the engine oil level during a pre-flight inspection but not the security of the separate oil filler cap. The ATSB could not establish the extent to which a specific checklist item about oil filler cap security would have assisted in identifying the unsecured cap in this case, although it would probably have increased the likelihood of detection.
Witness observations and the pilot’s assessment of the aircraft’s position along the runway during the rejected take-off indicated that the take-off was longer than normal. The reason for this could not be determined.
Examination of the engine and turbocharger found no mechanical defect or failure that would have precluded normal operation. While it was possible that a temporary issue occurred, resulting in the reported lack of engine response during the go-around, this could not be established.
The ATSB also determined that the engine manufacturer’s oil change interval had been exceeded by 3 months but it was very unlikely that this had any effect on the operation of the engine.
Safety message
This accident highlights that, prior to take-off, pilots should have in mind a go/no-go decision point along the runway by which time the aircraft should become airborne. If at that point the aircraft is not airborne, the pilot should reject the take-off. Having such a point assists pilot decision making during a critical phase of flight. This is particularly important when operating in conditions that may affect aircraft performance, such as tailwind conditions.
In addition, the ATSB highlights the importance of being aware of the daily inspection requirements when operating aircraft under a CASA maintenance schedule. In particular, how this may differ from the aircraft manufacturer’s pre-flight inspection procedure.
Photograph of VH-ZFW
Source: John Newby
The occurrence
On 4 July 2014, at about 1230 Eastern Standard Time,[1] the pilot/owner of Cessna Aircraft Company T210N aircraft, registered VH-ZFW (ZFW), and two passengers arrived at Inverell Airport to conduct a private flight to Bankstown Airport, New South Wales.
In preparation for the flight, the pilot removed the aircraft from the hangar and conducted a pre-flight inspection. The pilot could not initially recall adding engine oil to the engine during the inspection but later believed that was the case. Witnesses reported being aware of the pilot carrying out the pre-flight inspection but none observed the entire pre-flight, including whether the pilot added any engine oil. The two passengers remained some distance from the aircraft until the pilot completed the inspection. The pilot and passengers boarded the aircraft. The pilot started the engine and completed the pre-take-off checks, which were reported as normal.
The pilot recalled that there was a tailwind of less than 5 kt on runway 16.[2] Therefore, to allow for an immediate departure to the south, the take-off was planned from that runway. The pilot was aware that the minimal tailwind might prolong the take-off roll.
Just prior to taxiing, the pilot of ZFW conversed with the pilot of an inbound aircraft who was intending to land on runway 34. The pilot of ZFW then taxied to the threshold of runway 16 and waited for the other aircraft to land. After that aircraft vacated the runway, the pilot of ZFW commenced the take-off at about 1309. Ten degrees of wing flap was reported set for the take-off.
The pilot indicated that initially the take-off proceeded normally. However, shortly after becoming airborne, when at an estimated 200–300 ft above the ground, engine oil appeared on the windscreen, predominantly on the left. The pilot initiated a rejected take-off by reducing engine power to idle and lowering the nose of the aircraft. In response to the temporarily-obscured forward vision, the pilot looked out to the left of the aircraft to assess their position. Shortly after, the pilot realised that they were a lot further along the runway than expected as they[3] could see the threshold of the reciprocal runway 34 ahead (Figure 1). The pilot determined that there was insufficient distance remaining to land safely and commenced a go-around. The intent was to return to the airport for an immediate landing. However, the pilot reported that when full power was applied, the engine did not respond. The pilot initiated a forced landing.
The pilot was aware of the need to clear the boundary fence and ensure that the aircraft’s airspeed remained above the stall[4] speed. The pilot identified a cleared area to the right and turned the aircraft toward that area. The pilot reported having no further recollection of the forced landing until after the impact when the aircraft was on fire.
The pilot exited the aircraft and assisted the passengers. Shortly after, a number of people arrived and found the occupants clear of the burning wreckage. They moved the occupants further away and provided assistance until emergency services personnel arrived.
The pilot and front seat passenger were hospitalised with serious injuries. The second passenger, who was sitting in the middle row of seats, received minor injuries. The front seat passenger later succumbed to their injuries. The combined effects of the impact forces and post-impact fuel-fed fire destroyed the aircraft (Figure 2).
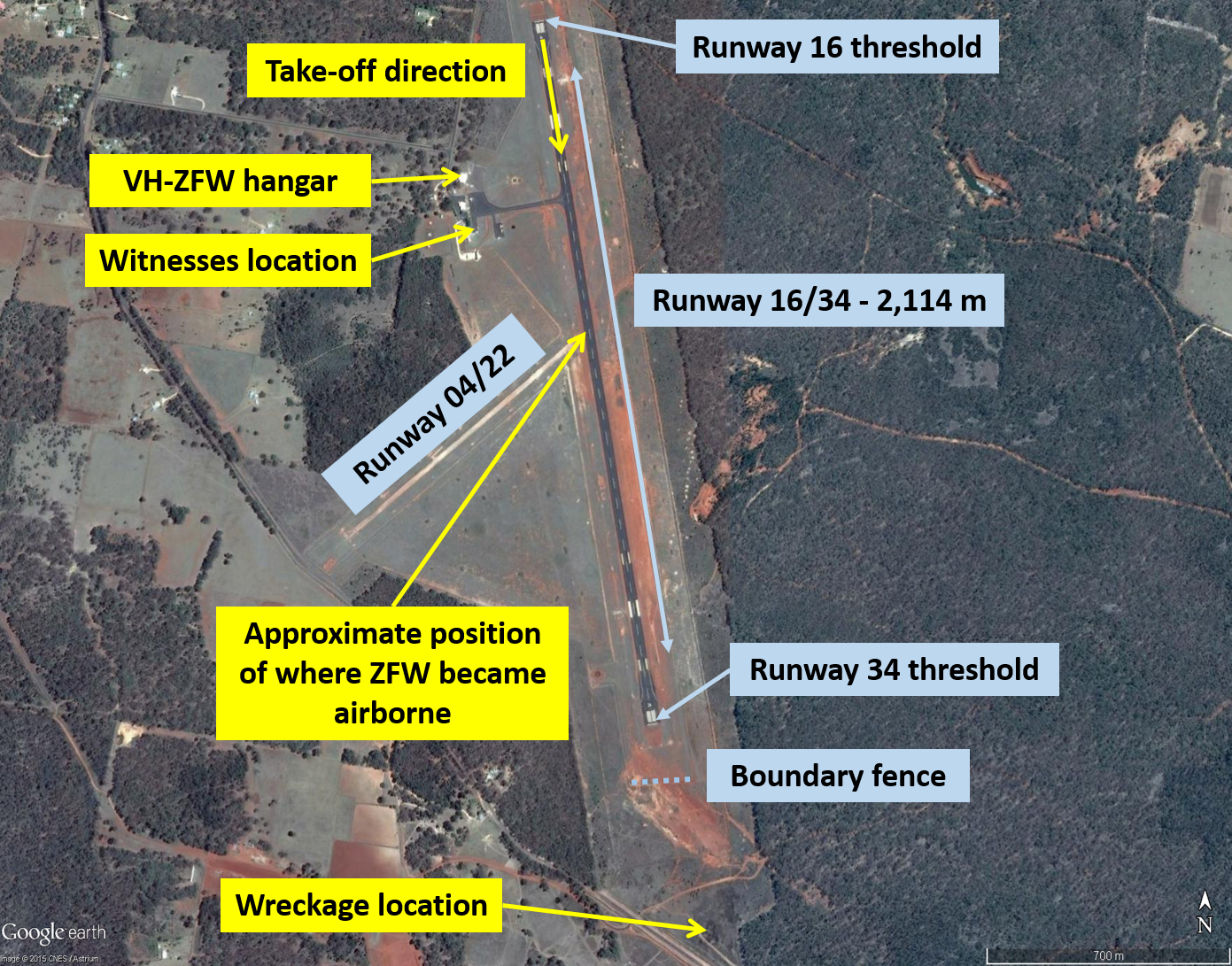
Figure 1: Runways at Inverell Airport, showing the location of the witnesses, approximate position that VHZFW became airborne and wreckage location
Source: Google earth, modified by the ATSB
Passenger observations
The passenger seated in the middle row reported that the engine sounded normal until some way down the runway when they started to notice something was wrong. The passenger reported removing their headset and noting that the engine sounded ‘weak’. At that time, the aircraft’s wheels were slightly above the ground and the aircraft about 10 m from the airport boundary fence. Shortly after, the passenger observed the pilot applying rearward pressure on the control column. The passenger felt the aircraft bounce before going over the fence. The aircraft then went to the right and flipped before coming to rest inverted. A fire commenced shortly thereafter. The passenger exited the aircraft and went to the main road to seek assistance.
The passenger did not observe any oil on the windscreen.
Witness observations
Witness 1
A witness who was familiar with ZFW and had observed the aircraft take-off from Inverell Airport on numerous occasions was positioned near a hangar overlooking runway 16/34 (Figure 1). The witness reported hearing ZFW start up and observed it taxi to the runway end and, soon after, commence the take-off. The witness indicated that during the initial stages of the take-off, the aircraft’s acceleration along the runway and engine sound appeared normal.
When in-line with their position, the witness was expecting the nose of the aircraft to lift but instead the aircraft continued along the runway. The witness indicated that if the nose did in fact lift from the runway, it would have only been centimetres above the ground. The witness became concerned and notified his colleagues.
As the aircraft passed runway 04/22, which is about 1,000 m along runway 16 and just before the depression in this runway (see the section titled Operational information - Airport information), it became airborne to about 10–13 ft (3–4 m). The witness reported that it looked like there was a slight crosswind as the aircraft’s tail moved to the right. The witness believed the pilot then rejected the take-off, as the aircraft appeared to settle back onto the runway. However, due to the depression in the runway, the witness could only see the aircraft’s wings. By this time, a second witness came of out of the hangar.
Witness 2
The second witness, who was also familiar with the aircraft, heard ZFW start up and the engine and other sounds associated with the pre-take-off checks. All were reported as sounding normal. The witness further indicated that, dependent on a number of conditions, ZFW would normally become airborne when about 500–800 m along the runway. By the upwind end of the runway, it would typically be about 200–300 ft above the ground.
Approaching the upwind end of the runway
Shortly after, as the aircraft neared the upwind end of the runway, both witnesses observed the aircraft suddenly climb to about 100–150 ft. Both commented that the aircraft appeared to be ‘labouring’. Neither witness could recall hearing the engine operating at that time, but the second witness believed that they should normally have been able to hear the engine from their position. The aircraft then turned right and descended below the rising terrain. Shortly after, the witnesses observed smoke in the area of the descent and went to assist.
The ATSB could not reconcile the discrepancy between the pilot’s recollection of the height gained after becoming airborne to that observed by the witnesses. However, it was possible that the accident and/or subsequent medical treatment affected the pilot’s recall.
Figure 2: Aerial view of the accident site showing VH-ZFW (looking west-north-west)
Source: New South Wales Police Force, modified by the ATSB
The pilot held a Private Pilot (Aeroplane) Licence that was issued on 10 June 2011 and a valid Class 2 Aviation Medical Certificate. The pilot’s logbook showed a total flying experience of 231.1 hours to the last entry dated 25 May 2014. Of these, about 118 hours were in ZFW. The pilot reported that, in the intervening period, they carried out a return flight to Archerfield Airport, Queensland and a local flight in ZFW in the weeks prior to the occurrence.
The pilot last completed a flight review on 8 November 2012.
Aircraft information
General
The Cessna T210N is a high-wing, single-engine aircraft with a retractable landing gear. The aircraft was manufactured in the United States (US) in 1980 and imported into Australia by the current owner/pilot. The aircraft was registered as VH-ZFW on 26 September 2012.
The aircraft was fitted with a six-cylinder, horizontally-opposed Teledyne Continental Motors TSIO-520-R9B engine. The engine drove a three-bladed McCauley Propeller Systems constant-speed propeller.
A review of the aircraft’s records indicated that ZFW was maintained in accordance with the approved Civil Aviation Safety Authority (CASA) maintenance schedule. The last periodic inspection was on 11 October 2013, at a total time in service of 3,973.6 hours. This included the last recorded engine oil change. Since that time, the aircraft accumulated about 40 hours. The maintenance records did not identify any defects or unserviceability with the aircraft prior to the occurrence.
Engine oil system
Oil for engine lubrication, propeller governor operation and turbocharger system control was supplied from a sump located on the bottom of the engine. The engine sump capacity was 10 quarts (about 10 L). Looking from the rear of the aircraft, the oil dipstick was located at the rear-left of the engine. The oil filler tube and cap was on top of the crankcase, near the front of the engine. Both the oil dipstick and filler tube were accessible through separate doors on the engine cowling.
The engine manufacturer advised that the oil filler cap fitted to the engine had been used on a large range of their engines since 1973. They further advised that the design of the cap was simple but effective and that they did not foresee a need to change the design.
The engine manufacturer’s recommended interval between oil changes was 50 hours or 6 months, whichever occurred first. The Cessna T210N pilot’s operating handbook (POH) also recommended changing the oil at least every 6 months, even though this may be less than the 50 hours accumulated. The POH further advised to reduce the interval when conducting short flights and during operations that involve long periods at idle revolutions per minute to avoid oil ‘sludging’. The term oil sludge refers to viscous deposits or gelling of the oil, which can lower the effectiveness of the lubrication system.
Turbocharger system
The aircraft was fitted with a Kelly Aerospace 400 series turbocharger. The function of the turbocharger was to maintain a desired manifold pressure at a given throttle setting, regardless of the ambient air temperature and pressure. A butterfly-type waste gate regulated the amount of exhaust gas fed to the turbocharger turbine wheel. The waste gate actuator and controller used engine oil pressure to operate. In the event of a turbocharger failure, the waste gate would move to the open position to prevent an overboost situation (excessive manifold pressure). The engine manufacturer stated that:
Rapid throttle movements may cause undershooting or overshooting of the desired manifold pressure, necessitating a subsequent adjustment once the turbocharger has stabilized. Gradual throttle movement will permit the turbocharger to keep pace with the change in power.
Speedbrakes
Precise Flight speedbrakes were installed on the aircraft to reduce shock engine cooling and allow for accelerated descents without decreasing engine power. The speedbrakes were located on the upper surface of each wing and were electrically actuated by an electric clutch. If the aircraft experienced a loss of electrical power, the clutch would automatically retract the speedbrakes. The speedbrakes took between 1.8–2.3 seconds to deploy.
Operational information
Meteorological information
The aerodrome forecast[5] for Inverell Airport indicated the wind would be from 300° (west-north-west) at 10 kt (19 km/h) with a temperature at the time of 15 °C. The pilot reported that, at the time of take-off, there was a tailwind of less than 5 kt on runway 16. This was consistent with witness observations of conditions including light and variable winds, with about a 5 kt tailwind on runway 16.
Airport information
Inverell Airport had two runways aligned 16/34 and 04/22. Runway 16/34 was the main runway and was 2,114 m long, with a 1 per cent upslope on runway 16. Runway 04/22 was to the west of and about 1,000 m along the main runway (Figure 1). Just beyond that point, there was a distinct depression in the main runway. Due to this variation in runway level, aircraft may not be sighted on opposite ends of the runway. The Airservices Australia Aerodrome Chart for the airport included a caution to this effect.
There was a 2 m high airport boundary fence about 160 m beyond the end of runway 16. Outside this fence was a semi-cleared area covered in low-lying shrubs and tall grasses.
Estimation of take-off and landing distances
An estimation of the aircraft’s expected take-off and landing distance (ground roll) that day was undertaken using the Cessna T210N POH. Taking into account the runway characteristics, the calculations were based on information from the aerodrome forecast and the pilot’s and witness recollections (Figure 3).
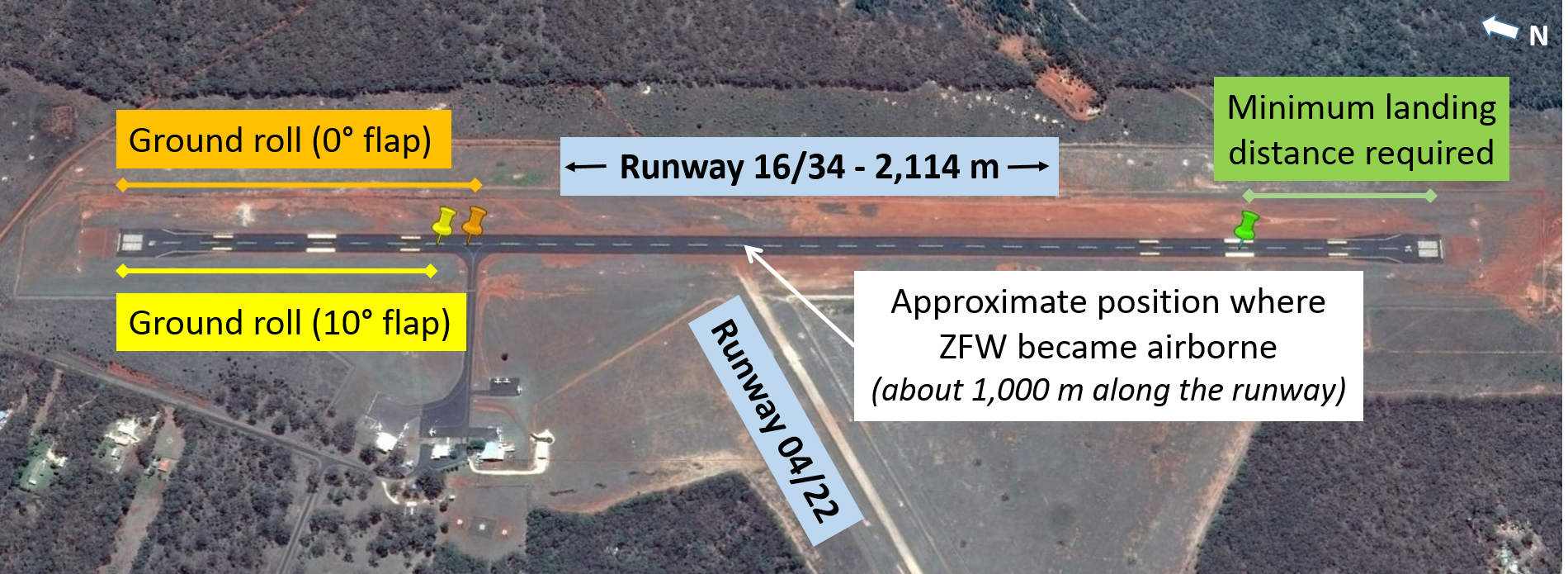
The POH indicated that a normal take-off was possible using a 0°–10° wing flap setting. However, 10° wing flap was preferred as it resulted in an earlier nose wheel lift-off and a 10 per cent reduction in ground run compared with 0° flaps. Based on the manufacturer’s preferred configuration, the take-off ground roll distance for the occurrence flight with a 10° flap setting and 5 kt tailwind was estimated to have been about 485 m. With a 0° flap setting, the estimated distance was about 535 m. The pilot reported that they would normally select 10° flap for take-off and be airborne well before passing runway 04/22.
The landing distance was also estimated from information in the POH and was based on a flap setting of 30°, engine power at idle and the application of maximum braking. Given these conditions, depending on the aircraft’s actual configuration at the time, the minimum distance required for landing and braking to a complete stop would have been at least 320 m (Figure 3). However, the actual runway distance remaining when the pilot rejected the take-off was unable to be determined.
Figure 3: Estimated take-off distances with 10° (in yellow) and 0° (in orange) of wing flap set, the observed lift-off position along runway 16 and the minimum estimated landing distance (in green)
Source: Google earth, modified by the ATSB
Take-off considerations
The pilot could not recall when the aircraft became airborne but reported that the take-off was normal until the oil appeared on the windscreen. However, after initiating the rejected take-off, the pilot realised that they were a lot further along the runway than expected. The pilot indicated that the aircraft would normally be about 500 ft above the ground by the runway end (runway 34 threshold). The pilot did not know why the aircraft was lower than normal at that time.
The pilot reported that they did not have a specific go/no-go decision point along the runway. In respect of the application of such decision points, the US Federal Aviation Administration (FAA) Airplane Flying Handbook stated that:
Prior to take-off, the pilot should have in mind a point along the runway at which the airplane should be airborne. If that point is reached and the airplane is not airborne, immediate action should be taken to discontinue the take-off.
Pre-flight inspection procedure
The Cessna T210N POH advised pilots to check the engine oil quantity during a pre-flight inspection walk-around but did not require a check of the security of the oil filler cap. In contrast, the Cessna service manual, which provided the recommended procedures and instruction for ground handling, servicing and maintaining the aircraft, included a requirement to check that the filler cap was tight and the oil filler cap was secure. A review of other handbooks for a range of aircraft types found that inclusion of that check in the pre-flight inspection process was inconsistent.
The daily inspection requirements, under the CASA maintenance schedule to which the aircraft was maintained, included a check of the oil level and that the oil dipstick and cap were secure and locked. The CASA Maintenance guide for pilots stressed the importance of the daily inspection in terms of it being:
…the only thorough inspection between periodic inspections and is the last opportunity to inspect the aircraft to ensure that it is airworthy and fit to fly…and must be carried out prior to the first flight of each day the aircraft is flown.
and the purpose of the pre-flight inspection being:
…to inspect the aircraft to ensure that it is safe, that nothing untoward has occurred since the daily inspection, and to determine if flight requirements can be met.
The pilot reported that they used the memorised flow pattern for each pre-flight inspection based on the checklist published in the POH. Consistent with this checklist, they checked the oil quantity on every pre-flight inspection. The pilot indicated that they were not aware of the CASA maintenance schedule daily inspection requirements, and would only check the security of oil filler cap after adding engine oil.
The pilot reported that on one previous occasion they had double-checked the oil filler cap and found it unsecured.
Wreckage and impact information
An examination of the wreckage found that the aircraft approached terrain in a relatively level attitude, with the nose and left wing slightly down. The nose wheel contacted the ground first and detached from the aircraft. The right wing then impacted a shrub, sustaining significant impact damage and the aircraft flipped, before coming to rest inverted. A post-impact, fuel-fed fire destroyed most of the fuselage (Figure 4).
The wreckage examination also found:
That the damage to the propeller blades and strike marks on the ground were consistent with the engine producing some power at impact, but not full power.
That the left side of the engine sustained more fire and heat damage then the right. After placing the engine in an upright position, the oil filler cap was found detached from the oil filler tube but hanging by its chain. There was evidence of oil around the oil filler tube and on the ground. The separate oil dipstick remained secured in position.
Small amounts of oil spotting on the rear of the left empennage and on the underside of the left horizontal stabiliser. There were also oil droplets on several windscreen fragments around the accident site.
A small amount of oil sludge inside the propeller hub shaft.
The propeller governor control was in a low pitch, high revolutions per minute position, consistent with the propeller pitch setting required for take-off.
The wing flaps were in the fully-retracted position (0°).
The speedbrake on the left wing was partially-deployed, while the speedbrake on the right wing was in the retracted position.
The engine was recovered from the wreckage and transported to an approved overhaul facility for technical inspection under the supervision of the ATSB. The speedbrake assembly from each wing was also removed for further examination at the ATSB’s technical facilities in Canberra, Australian Capital Territory.
Figure 4: Aircraft wreckage showing the tail empennage inverted to the right and the propeller visible on the left (looking south-south-west)
Source: ATSB
Test and research
Engine examination
The engine examination found that, while less than 2 L of oil was collected from the engine, there was no damage consistent with oil starvation. Overall, there was no evidence of internal mechanical failure that would have prevented normal operation of the engine prior to the occurrence. Externally, the engine was impact- and fire-damaged.
The turbocharger waste gate was in the open position and the turbine wheel assembly could not be rotated within its housing. The turbocharger assembly and the engine oil filler cap and tube were removed from the engine for further examination.
Engine oil filler cap and tube examination
The engine oil filler cap and gasket, which was located at the underside of the cap rim, showed evidence of significant fire damage. However, the cap did not appear distorted or damaged. The locking tangs used to secure the cap into the oil filler tube showed no contact marks to indicate the forcible removal of the cap from the filler tube during the impact sequence. There was evidence of oil on the outer surface of the oil filler tube. The physical appearance of the interacting cap and filler tube surfaces showed no deformation or mechanical damage. Therefore, it was considered very unlikely that the cap came off during the impact sequence.
Turbocharger examination
The turbocharger assembly sustained extensive heat damage from the post-impact fire. Examination of the waste gate determined that the valve was fixed in the open position, consistent with fire damage and the build-up of debris from exposure to water during the firefighting activities. There was evidence of oil residue on the bearings, which were in good condition and showed no signs of damage or distortion. Examination of the turbocharger assembly found no evidence to suggest that it was not operational prior to the occurrence.
Speedbrake examination
Both speedbrakes showed signs of post-impact fire damage and their spring mechanisms and wiring were compromised. Heat markings on the right speedbrake indicated that it was not in the open position during the fire. Discolouration from heat damage to the left speedbrake showed that it was extended to an angle of 30° during the fire. However, it was determined that the left speedbrake was released by the impact and there was no evidence to suggest that it deployed inflight.
Pilot reaction times
In 1999, the United Kingdom Civil Aviation Authority commissioned a simulator-based study into helicopter pilot reaction times in response to an emergency. The study determined that the mean total reaction time (time taken to detect and respond) generally ranged between 2–4 seconds, with 4–6 seconds typical of a longer but acceptable reaction time. The US FAA Airplane Flying Handbook also stated that the typical time for a pilot to react to an emergency situation was about 4 seconds.
Related occurrences
A review of the ATSB occurrence database identified eight occurrences in the period 2005 to 2014 where pilots reported oil on the windscreen or engine cowl in flight. Specifically, these involved single-engine aircraft and occurred because of an unsecured engine oil filler cap or dipstick. Below is a selection of these occurrences:
During the take-off, at about 30 ft above the runway, the pilot observed oil leaking from the engine cowl. The pilot rejected the take-off. After shutdown, the pilot found that the oil filler cap was not secured correctly (ATSB occurrence 201311271).
During the initial climb, the airspeed indicator failed and a large quantity of oil flowed onto the windscreen. The pilot returned for landing and inadvertently landed with the landing gear retracted. An inspection revealed that the oil filler cap was not secured prior to departure (ATSB occurrence 201106695).
At about 300 ft after take-off, the flight instructor noticed oil splatter on the windscreen. After shutdown, the student pilot realised that they replaced the oil cap but did not lock it in place (ATSB occurrence 201103050).
At about 1,500 ft after take-off the pilot noticed a small amount of oil on the windscreen. The aircraft was returned for an immediate landing. The pilot realised that the oil filler cap was not secured after adding oil during the pre-flight inspection (ATSB occurrence 201102652).
The following is a selection of similar international occurrences:
During the pre-flight inspection, the pilot added engine oil and placed the oil filler cap on top of the battery box. Subsequently, the pilot became distracted by the flight instructor. After departure, the pilot noticed oil on the windscreen and realised that they did not secure the cap. After landing, the filler cap was found still resting on top of the battery box (US Aviation Safety Report System occurrence 581462).
During the climb, the pilot noticed oil droplets that shortly after covered the left side of the windscreen. The pilot had not secured the oil filler cap after adding engine oil during the preflight inspection. The pilot reported that the aircraft manufacturer’s pre-flight inspection procedure as detailed in the POH called for a check of the oil level, but not the fitment of the oil filler cap (US Aviation Safety Report System occurrence 784956).
After take-off, the aircraft was climbed to about 100–200 ft before the pilot turned back toward the runway. The pilot reported obscuration of the windscreen by a layer of oil as the oil filler cap was mistakenly left off. The aircraft descended into terrain about 274 m beyond the runway in a wings level, 20° nose-down attitude. The pilot reported no pre-impact mechanical issues (US National Transportation Safety Board (NTSB) investigation LAX04LA225).
The pilot reported oil on the windscreen shortly after take-off and returned to the airport. Witnesses observed the aircraft level off at 300 ft, slow down and turn toward the airport. During the turn, the right wing dropped and the aircraft subsequently impacted terrain. The oil filler tube was found without the cap. The cap was attached to the neck by a chain and was found between cylinders No. 4 and 6. No preimpact anomalies were found with the aircraft that would have affected its performance (US NTSB investigation SEA04F165).
Shortly after becoming airborne, the pilot observed oil streaming from the engine compartment, severely impairing their visibility. The pilot had inadvertently left the oil filler cap off (United Kingdom Air Accidents Investigation Branch investigation EW/G2012/07/02).
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the pilot of VH-ZFW, the Licenced Aircraft Maintenance Engineer for VH-ZFW, witnesses, the aircraft manufacturer, the Civil Aviation Safety Authority and the United States National Transportation Safety Board.
Submissions were received from the aircraft manufacturer and a witness. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Findings
From the evidence available, the following findings are made with respect to the collision with terrain and subsequent post-impact fuel-fed fire involving a Cessna Aircraft Company T210N, registered VH-ZFW, which occurred near Inverell Airport, New South Wales on 4 July 2014. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
In response to oil on the windscreen, the pilot initially rejected the take-off, but deemed the remaining available runway insufficient to land safely and commenced a go-around. During the go-around, the engine did not respond as expected, resulting in a forced landing off the airport.
The oil filler cap was not secured, which resulted in oil being expelled onto the windscreen and temporarily obscuring the pilot's visibility during a critical phase of flight.
For reasons undetermined, the take-off was longer than normal, which reduced the distance available for the pilot to reject the take-off after detecting and responding to engine oil on the windscreen.
Other factors that increased risk
The aircraft manufacturer's pilot operating handbook advised pilots to check the engine oil level during a pre-flight inspection, but not the security of the oil filler cap.
The oil change interval exceeded the engine manufacturer's recommended period of 6 months.
Other findings
The reason for the reported lack of engine response during the go-around could not be established.
Safety analysis
Shortly after take-off, oil appeared on the windscreen, temporarily obscuring the pilot’s visibility. The pilot initiated a rejected take-off but then assessed that there was insufficient landing distance remaining to continue the rejected take-off safely. The pilot reported commencing a go-around by applying full power; however, the engine did not respond. The pilot then initiated a forced landing into a semi-cleared area beyond the airport boundary. During the landing, the aircraft impacted a shrub and flipped before coming to rest inverted. A post-impact, fuel-fed fire injured the occupants and destroyed most of the aircraft fuselage.
This analysis will examine the security of the oil filler cap, the longer-than-normal take-off distance and the oil change interval requirements and their potential influence on the development of the occurrence. It will also consider the pre-flight inspection checklist with regard to the security of the oil filler cap and the reported lack of engine response during the go-around.
Oil filler cap security
The pilot could not initially recall adding engine oil during the pre-flight inspection, nor did any of the witnesses observe this action. However, the pilot reported later that they believed they replenished the engine oil. The pilot’s injuries and medical treatment may have affected their memory during the ATSB’s initial interview. Subsequently, increased understanding of the circumstances of the occurrence, including potentially from media or other reports, friends and so on may have enhanced or otherwise affected the pilot’s recollection.
Following the occurrence, the oil filler cap, which was located on the left or pilot’s side of the engine, was found unsecured. This was consistent with the pilot’s recollection of oil appearing on the left side of the windscreen and oil spotting on that side of the aircraft wreckage. The oil temporarily obscured the pilot’s visibility during the take-off and climb.
Technical examination of the oil filler cap and tube determined that it was very unlikely that the cap came off during the impact sequence. Therefore, it was most likely that the cap was not secure before the flight commenced.
Prolonged take-off
A witness who was familiar with the aircraft’s operation at Inverell Airport saw it become airborne about 1,000 m along runway 16. This roughly aligned with being abeam the threshold of runway 22 at lift-off. ATSB estimations of the take-off ground roll distance that day indicated that the aircraft should have become airborne at about 500 m, which was consistent with the witness’s previous observations.
The pilot could not recall where the aircraft became airborne but believed that the take-off was normal until the oil appeared on the windscreen. The pilot further indicated that the aircraft would normally be airborne well before passing runway 04/22. A longer-than-normal take-off roll was consistent with the unexpected position of the aircraft as observed by the pilot after initiating the rejected take-off.
The ATSB considered a number of factors that may have prolonged the take-off roll. This included the aircraft’s configuration, meteorological conditions, runway characteristics, possible effect of any mechanical issues and pilot distraction. However, none of these factors was identified as contributory and the reason for the longer-than-normal take-off was not established. Despite this, pilots should be aware of such factors and how they degrade aircraft performance during a critical phase of flight, including the effect of tailwind conditions.
Discontinuation of the take-off at the position the aircraft was observed getting airborne should have allowed sufficient distance remaining to safely reject the take-off. However, the time taken for the oil to appear and the pilot to react to the loss of forward visibility compounded the already longer-than-normal take-off. In combination with the estimated minimum landing distance needed of 320 m, by the time the oil leak appeared, and the pilot reacted to the associated loss of forward visibility, it was very likely that there was insufficient runway remaining for the pilot to continue the rejected take-off. This was consistent with the pilot and passenger’s assessment of the aircraft’s position at that time.
Emergency or abnormal situations during take-off may require a pilot to reject the take-off. The decision to reject a take-off may appear simple but becomes critical under certain conditions. Further, the decision may be more complex when compared to the conditions under which the procedure was trained (Kaempf and Orasanu 2014). Therefore, prior to take-off, pilots should have in mind a go/no-go decision point along the runway by which time the aircraft should become airborne. The decision point should provide for sufficient runway distance remaining to allow the pilot to safely stop the aircraft by the end of the runway. If the aircraft is not airborne by the decision point, the pilot should reject the take-off.
It could not be determined if having a decision point would have changed the outcome of the flight. However, the occurrence emphasises the benefit of having such a point to assist pilot decision making during a critical phase of flight.
Oil change interval
The engine manufacturer’s oil change interval was 6 months. This was exceeded in ZFW by 3 months. However, there was insufficient evidence to determine if this contributed to the small amount of oil sludge found in the propeller hub. Despite this sludge, given the results of the examination of the engine and associated components, the overdue oil change had no effect on the operation of the engine.
Pre-flight inspection checklist
The pilot’s previous identification of an unsecured oil filler cap was the result of self-checking, not from following a checklist. Therefore, it could not be established if a specific checklist item would have resulted in the pilot identifying the unsecured cap prior to the occurrence flight. However, as documented in the United States Federal Aviation Administration Airplane Flying Handbook:
Checklists have been the foundation of pilot standardization and cockpit safety for years. The checklist is an aid to the memory and helps to ensure that critical items necessary for the safe operation of aircraft are not overlooked or forgotten.
The pilot’s pre-flight inspection, carried out from memory based on the checklist in the pilot’s operating handbook (POH), was a daily inspection as it was the first flight of the day. In this respect, the pilot was not aware of the CASA daily inspection requirements for the aircraft. The POH checklist required pilots to check the engine oil level during their pre-flight inspection. However, unlike the CASA daily inspection requirements for the aircraft, it did not require a check of the security of the separate oil filler cap. In the absence of any other safety mechanisms, the inclusion of this check in the POH pre-flight checklist may have increased the likelihood of the pilot identifying the insecure cap.
This occurrence highlights the importance of being aware of the daily inspection requirements when operating aircraft under a CASA maintenance schedule and how these requirements may differ from the aircraft manufacturer’s pre-flight inspection procedure. Had the pilot carried out the CASA daily inspection they likely would have identified the insecure engine oil cap.
Reported lack of engine response
Examination of the engine and turbocharger found no mechanical defect or failure that would have precluded normal operation prior to the occurrence. However, it was possible that the reported lack of engine response during the go-around was the result of a temporary issue. For example, the turbocharger may not have had sufficient time to stabilise because of a rapid sequence of throttle movements in this case. These included setting full power for the take-off, idle power for the rejected take-off and then full power again for the go-around. However, there was insufficient evidence to establish if a temporary issue occurred and the reason for the reported lack of engine response was not established.
In addition, a search of various aviation occurrence databases found only one occurrence where rapid throttle movement led to a temporary turbocharger issue. In that occurrence, the pilot of a Piper PA-31 aircraft advanced the throttle rapidly during the take-off, which resulted in the turbocharger surging. The pilot successfully rejected the take-off (ATSB occurrence 197504806). Of note, pilots may not report temporary issues if they are resolved without further concern.
Similar occurrences of oil dipstick or filler cap insecurity and oil being expelled onto the aircraft have led to varying outcomes but mostly resulted in a safe landing. However, the longer-than-normal take-off roll, the time taken for the oil to appear and the pilot to react, and the reported lack of engine response limited the options available to the pilot. From a low height, the pilot conducted a forced landing into unfavourable terrain, resulting in a collision with terrain and a post-impact fire.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.