The aircraft departed Harrison's Pocket for Redcliffe. It was seen to enter cloud and subsequently impacted the mountain range. The aircraft fell through the trees to the ground and came to rest inverted.
On 10 April 2015, at about 1120 Central Standard Time (CST), the pilot of a Robinson R44 helicopter, registered VH‑LOL (LOL) was engaged in herbicide dispensing operations near Marion Bay on the Yorke Peninsula in South Australia.
Also on board were client representatives who were directing the noxious weed management operation and manually dispensing the chemical into each bush. In the course of traversing the field at low level in search of the weed, the helicopter struck a previously unidentified power line. The helicopter’s main rotor blade made initial contact with the power line and during the avoidance manoeuvre, the tail rotor blades also made contact, severing the blade tips (Figure 1). The pilot landed the helicopter safely. The helicopter was substantially damaged but the occupants were uninjured.
Figure 1: Tail rotor blade damage to VH-LOL
Source: Maintenance organisation
Power line identification
In preparation for the herbicide operations, the pilot conducted an aerial survey of the area. The aerial survey was a standard operating procedure to confirm the powerlines as previously advised by local sources. This survey identified main power lines running parallel to a boundary road and a secondary power line running parallel to the main lines (Figure 2). The secondary line effectively dissected the target area and operations were concentrated on sectors to the north and south of the secondary line. The location of the power lines were also mapped on the data logger that was being used to track the progress of the herbicide dispensing.
The unidentified powerline was a single wire that was strung between the poles supporting the main and secondary powerlines and traversed, unsupported, through the southern boundary of the operational area. It was not mentioned by the locals, nor marked on the data logger map. It was not readily discernible from the air although additional support poles did lead the wire away from the secondary power line towards a distant building.
Figure 2: Powerlines and boundary fencing
Source: Google Earth and modified by ATSB
Pilot comment
The pilot stated that the aerial survey of the powerlines confirmed the accuracy of the local knowledge and created a sense of confidence in him that all obstructions had been identified and accordingly mapped. In hindsight, a fully independent assessment by the pilot in command for the presence of powerlines in the target area may have located the single wire. The pilot had in excess of 14,000 hours operating at low level but not necessarily in powerline congested areas.
Risk management
The helicopter operator had documented a risk assessment of the planned operation, addressing aircraft operational considerations, environmental impacts, required personal protective equipment and herbicide management. The cabin occupants were also provided with a helicopter safety brief and formal induction prior to commencement of flight operations. Risk assessment outcomes and operational requirements were included in a specific job plan that was discussed in briefings with ground and flight crews at the beginning of the campaign. Briefings were also conducted with crews prior to the commencement of each day’s flying.
Wire awareness, detection and avoidance techniques were also documented in the company operations manual in various sections along with specific references to aerial agriculture publications where mitigation for such hazards are addressed.
ATSB comment
This accident provides a reminder to flight crews of the need for consistency in aerial surveys for powerlines, the establishment of standardised procedures for their identification and the need for independent assessment of their presence.
Single wires can be difficult to see and occur in the most unexpected places in rural areas. ATSB research article ‘Avoidable accidents No. 1 - Low level flying’ provides additional information on wire hazards associated with flight below 500’. The report is available at the ATSB website.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Aircraft operator
As a result of this occurrence, the aircraft operator has advised the ATSB that they are taking the following safety actions:
The operator has reviewed the risk assessment and moved to standardise procedures and now place greater emphasis on employee inductions with a focus on hazards and published information relating to high-risk activities. Whilst the published information was generally available to company pilots, a greater focus on promulgating this information was recognised as beneficial. The use of non-permanent staff was to be reconsidered along with the dissemination and acknowledgement of receipt of safety critical information specific to the contracted flying program.
Operator client
Following a separate, internal investigation into the accident, the client updated its procurement processes. This update was to further ensure that contractor and project sponsor responsibilities were clearly defined in contracts and operational plans, with respect to:
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 11 April 2015, the student pilot of a Piper PA-28 aircraft, registered VH-TXH (TXH), prepared to conduct a solo, local flight, from Moorabbin Airport, Victoria. The flight was to be the pilot’s second solo to the training area, where he was to practice simulated forced landings. The pilot inspected the aircraft, including checking the oil quantity and colour. He noted that the dipstick indicated 5.5 L of oil and the oil appeared to be of a golden colour. After completing the pre-flight checks, the pilot of TXH taxied the aircraft to the run-up bay and performed engine run-ups. He noted that all indications were normal and within the required performance limits.
At 11:29:06 Eastern Standard Time (EST), the pilot made a radio call to the Moorabbin surface movement controller (SMC) on the Ground frequency, advising that he was conducting a solo flight to the training area and requested a departure from runway 35 Right (35R). The SMC cleared TXH to taxi via taxiway A for a departure from runway 35R. TXH then taxied to the holding point for runway 35R, and, at 11:36:37, the pilot of TXH contacted the aerodrome controller – east (ADC1) on the Tower East frequency. He reported ready for take-off, and ADC1 cleared TXH for take-off.
At 11:37:08, the pilot of a Cessna 172 aircraft, registered VH-EUU (EUU), contacted the SMC and requested a clearance to taxi for a local private flight, with three passengers on board. The SMC cleared EUU to taxi to runway 35R via taxiway A, and the pilot commenced taxiing.
The pilot of TXH reported that the take-off run was normal, with the engine indications in the normal range. After rotation, when about 150 ft above ground level (AGL), the engine began to run roughly. The pilot lowered the aircraft nose slightly and within 2-3 seconds, the engine regained full power and the aircraft continued to climb. When approaching 500 ft AGL, the engine again ran roughly and partially lost power. The pilot suspected a fuel issue to be the cause of the rough running, and, as the fuel pump was still on, changed the selected fuel tank. The engine returned to producing full power and the pilot initiated a right climbing turn, leaving the fuel pump switched on. As the aircraft climbed, the engine lost power again.
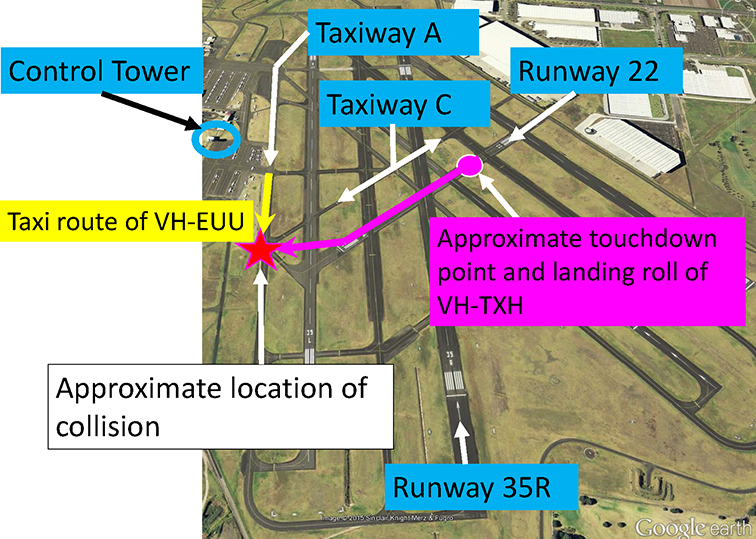
At 11:37:58, the pilot advised ADC1 that he had a ‘spluttering engine’ and requested a return to land. ADC1 had observed TXH in the initial climb and noted that it did not appear to be climbing out normally and was then quite low, at an estimated 300 ft AGL. ADC1 initially responded that TXH was number one for runway 35R and then offered runways 22 or 31 if required. The pilot responded that he would use runway 22 (Figure 1).
ADC1 gave TXH priority to land over all other aircraft, advised the SMC of an aircraft with engine trouble, requested runway 22, and coordinated with the SMC for release of runway 22 (see section: Air traffic control). The SMC checked the crossing taxiways, helicopter traffic and for any works in progress that may have conflicted with the use of runway 22, then handed ADC1 the green runway strip for runway 22. ADC1 then placed the strip in the runway bay on the console. ADC1 also coordinated with the aerodrome controller – west (ADC2), who instructed a couple of aircraft in the circuit for runway 35 Left (35L) to go-around to ensure they remained clear of the crossing runway. ADC1 instructed the pilots of two aircraft that were in the circuit for runway 35R to go-around and another to conduct a full stop landing. The SMC reported then focusing on checking the runways and taxiways crossing runway 22. Taxiway A did not cross runway 22, and as the SMC remained seated, was unable to see EUU on taxiway A as it was obstructed by the tower console.
Figure 1: Moorabbin Airport, aircraft tracks and collision point
Source: Google earth annotated by the ATSB
At 11:39:06, ADC1 cleared TXH to land on runway 22. The pilot of TXH conducted a tight right turn towards runway 22 and as he was concerned about clearing the buildings on the approach to runway 22, he did not select any flap. After passing over the buildings, the pilot reduced the power to idle. He reported that the aircraft touched down about one third of the way along runway 22. ADC1 observed that TXH appeared to land about half way along the runway and did not decelerate normally after touching down. The SMC observed that TXH appeared very low on final approach to runway 22 and crossed the threshold travelling very fast. The ADC1 stated to the SMC and ADC2 controllers ‘he’s landed long’ and ‘gee he’s quick’.
The pilot of TXH assessed that he was not going to be able to stop the aircraft prior to the end of the sealed runway, but that there was a suitable grassed overshoot area beyond it, and maintained the aircraft on the runway centreline. ADC2 was standing up, and sighted EUU on taxiway A. ADC2 alerted the SMC to the Cessna (EUU) on taxiway A. ADC1 observed that EUU was then still north of the extended centreline of runway 22 on taxiway A.
As TXH approached the end of runway 22, the pilot of TXH sighted EUU taxiing on taxiway A to his right, and was unsure whether it was going to stop or not. He veered TXH to the right in an attempt to pass behind EUU and avoid a collision. At 11:39:25, the SMC directed EUU to ‘hold position, STOP, STOP’. The pilot of EUU braked immediately and as his body moved forward in response to the aircraft braking, he sighted TXH in his left peripheral vision. The pilot of TXH saw EUU brake suddenly.
The pilot of EUU assessed that if he stopped there, TXH would collide squarely with EUU, so he released the brakes and progressed forwards. The left wing of TXH then struck the tail of EUU and spun EEU around through about 180°. TXH continued veering to the right for about 20 m further before coming to rest on a grassed area (Figure 2).
Figure 2: Accident site
Source: Airport Operator
The pilot of TXH observed fuel spilling from the ruptured fuel tank and immediately exited the aircraft and reported that he was not injured. The pilot of EUU reported that he momentarily lost consciousness at the time of the collision, but came to within seconds. He then observed fuel leaking, and although feeling disoriented, he conducted a normal aircraft shut down, including switching off the aircraft electrics and fuel. He and the passengers disembarked and were treated for minor injuries. Both aircraft sustained substantial damage (Figures 3 and 4).
Figure 3: Damage to VH-TXH
Source: Airport operator
Figure 4: Damage to VH-EUU
Source: Airport Operator
Pilot comments
The pilot of TXH provided the following comments:
He did not declare an emergency as he assessed that he would be able to land the aircraft safely. He remained calm and focused on his approach to, and landing on, runway 22.
He wanted to ensure that if the engine failed completely he would have sufficient height to clear the buildings in the approach path of runway 22.
He did not have sufficient altitude to continue a circuit and land on 35R.
He was unable to stop the aircraft before the end of runway 22, but if there had not been an aircraft on the taxiway, he would have been able to stop safely in the overshoot area.
The pilot of EUU commented that as he was on Ground frequency and the pilot of TXH was on Tower frequency, he was not aware of TXH until he sighted it immediately prior to the collision. He reported that if he had been directed to stop earlier, it may have averted the collision.
Controller comments
The ADC1 controller provided the following comments:
The ADC1 offered the pilot of TXH the choice of runways to land on, but did not know what was achievable for the pilot or aircraft.
The ADC1 and ADC2 controllers both stood up when the pilot of TXH reported engine trouble.
The incident was a good example of how quickly things happen; about 90 seconds after an aircraft took off it was back on the ground and at least two aircraft had to be sent around in the interim.
The SMC reported checking the works strip under the runway designators in the console. The SMC scanned the eastern helicopter area, checked the taxiways that crossed runway 22 – ‘F’, ‘B’ and ‘C’ for any aircraft waiting to taxi, and did not see anything that may pose a risk to an aircraft landing on runway 22. Taxiway A was not a crossing taxiway for runway 22. The SMC reported that these scans were performed multiple times after the pilot of TXH advised of engine trouble. The SMC further commented that if TXH had maintained the runway centreline, the aircraft would not have collided.
Moorabbin Airport and weather conditions
Runway 22 at Moorabbin was 571 m in length, runway 35R was 1335 m. The wind was from 030° at about 7 kt, resulting in a tailwind on runway 22.
Air traffic control (ATC)
There were three ATC positions active at the time; a combined surface movement controller / coordinator position (SMC), an aerodrome controller – east (ADC1), and an aerodrome controller – west (ADC2). The three controllers were seated in the tower in that order from north to south facing towards the east, and were the only people in the control tower at the time. Runways 35L and 35R were the runways in use prior to the pilot of TXH reporting engine trouble. A runway in use is a runway under the control of an aerodrome controller. All runways are considered ‘active’ and a clearance is required to cross or enter any runway. The runways other than those in use, were held by the SMC. The ADC1 therefore required the release of runway 22 from the SMC prior to clearing TXH to land. The controller places the runway strips of the runways for which they hold responsibility, in the runway bay of the console.
Engineering inspection
A post-accident inspection of the engine of TXH found a small quantity of oil on the cylinders and some fouling of the spark plugs which may have led to the rough running.
Safety message
The ATSB publication Avoidable Accidents No. 3 – Managing partial power loss after take-off in single-engine aircraft, found causes of partial power loss after take-off include fuel starvation, spark plug fouling, carburettor icing and pre-ignition conditions. A pre-flight safety brief that considers actions to take following a partial power loss after take-off, gives pilots a much better chance of maintaining control of the aircraft and of responding immediately. Such actions include landing immediately within the aerodrome, landing beyond the aerodrome, and conducting a turn back towards the aerodrome.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 29 March 2015, an Aeronavics SkyJib 8 remotely piloted aircraft (RPA) (Figure 1) was being used to assist with media coverage of the International Cricket Council World Cup Final, at the Melbourne Cricket Ground (MCG), Melbourne, Victoria. The RPA was being operated from the top of the south-western scoreboard of the MCG. The operating team consisted of:
a flight controller, who piloted the RPA
a ground station controller, who performed a range of functions including monitoring the position of the RPA and providing a back-up control for the flight controller
a camera gimbal controller, who controlled the camera mounted beneath the RPA.
Figure 1: RPA prepared for flight with camera mounted beneath
Source: RPA operator
The accident flight followed four earlier uneventful flights that day. The crew completed all pre-flight checks[1] and made broadcasts on appropriate air traffic frequencies, then launched the RPA at about 1430 Eastern Daylight-saving Time. On this particular flight, the operator intended to capture footage of the MCG and surrounds as the competing teams entered the MCG and during the pre-match ceremonies. The RPA’s take-off and departure were normal. The RPA was flown slowly southward toward Hisense Arena (Figure 2), climbing to a height of about 300 ft above ground level. The route was similar to that flown during earlier flights, without incident. All three control systems (flight control, ground station control and camera gimbal control) appeared to be functioning normally during the departure and transit to Hisense Arena.
About 2 minutes into the flight and soon after the competing teams entered the MCG, with the RPA over the northern roof of Hisense Arena, the camera gimbal operator lost control of the gimbal. The gimbal operator reported the loss of control to the other team members. Several seconds later, the ground station controller also lost communication with the RPA. At that point, with the RPA moving slowly southward over Hisense Arena, the flight controller made a decision to discontinue the flight and return the RPA to the top of the scoreboard. The flight controller made appropriate control inputs but found that the RPA was unresponsive, and it continued to move slowly southward.
Having lost normal control of the RPA, the flight controller commenced alternate RPA recovery procedures. The flight controller switched from GPS to attitude mode,[2] but was still unable to control the RPA. The flight controller then activated the ‘return to home’ function, but this was also ineffective. The flight controller then reverted to manual control,[3] in an attempt to recover control of the RPA, but the RPA remained unresponsive. Throughout this time, the ground station controller continued attempts to re-establish communication with the RPA, also without success.
About 20 seconds after the initial control problems, the RPA commenced travelling at medium speed in a westerly direction, and began slowly descending. The flight controller continued attempts to re-establish control by switching between control modes and again activating the ‘return to home’ function, but all attempts were unsuccessful. When the RPA reached a point south of Rod Laver Arena, it appeared to cease lateral movement and stabilise just above treetop level. Continued attempts by the flight controller to regain control were unsuccessful, and the RPA descended beneath the treetops, out of sight of the controlling crew.
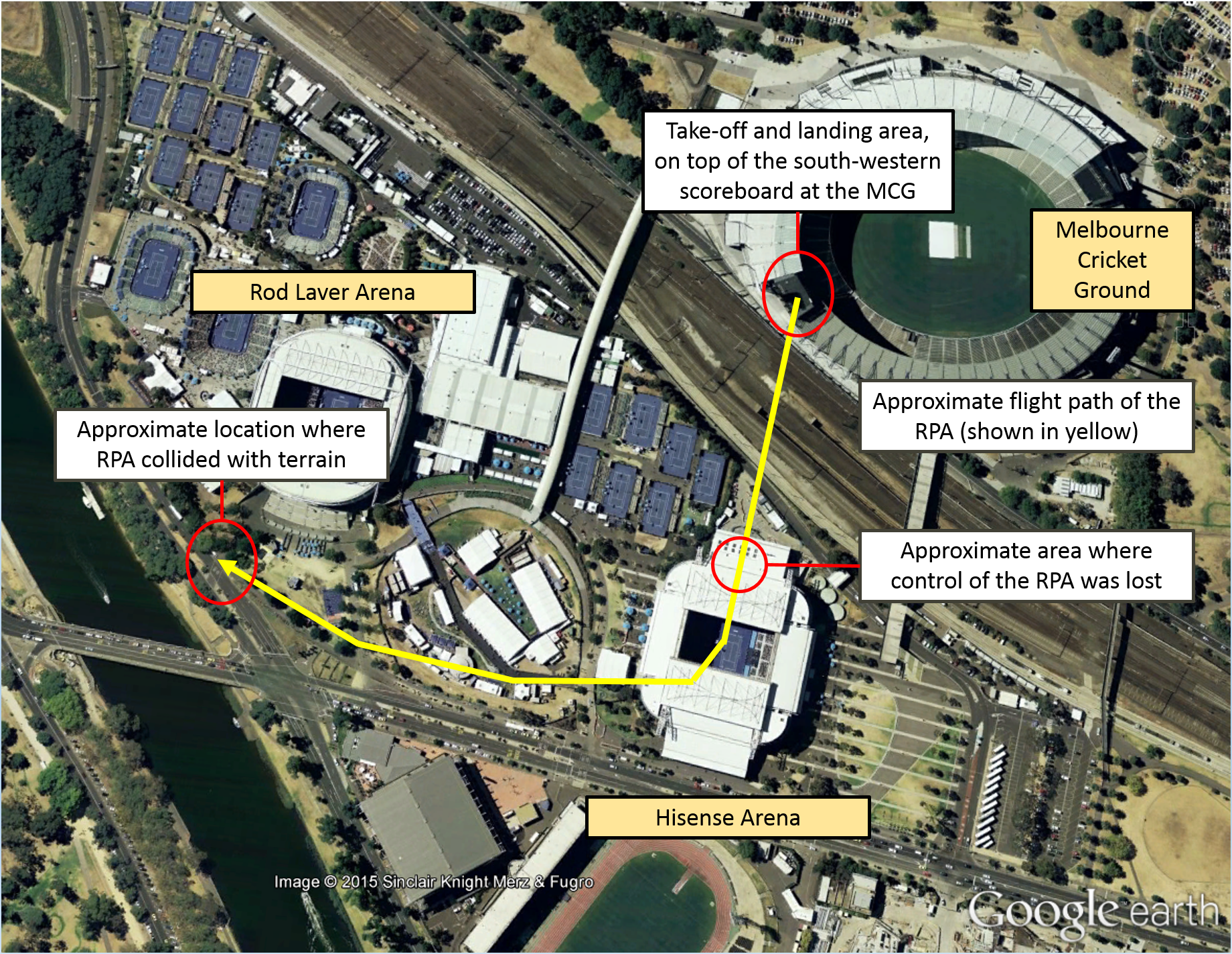
The RPA collided with terrain on the median strip on Batman Avenue to the south of Rod Laver Arena, a little over 3 minutes after the flight had commenced. The operating crew had maintained line of sight with the RPA until it descended beneath the treetops. Initial control difficulties were experienced when the RPA was just over 200 m from the position of the operating crew. The collision with terrain was about 450 m from their position (Figure 2).
There were no injuries to people on the ground, and no damage to other property, but the RPA and associated equipment were substantially damaged during the collision.
Figure 2: Approximate flight path of the RPA, from the take-off location on top of the south-western scoreboard at the MCG, to where control was lost over Hisense Arena and the collision location on Batman Avenue
Source: Google Earth with additions by the ATSB
Operator’s approval and risk assessment
The operator had approval from the Civil Aviation Safety Authority to operate the RPA near people and over populous areas while taking aerial photography during the event. The approval included a number of conditions related to such things as RPA control capabilities, the operating area and the operating environment. The operator had also conducted a risk assessment relevant to the flight during which the accident occurred. This assessment included consideration of a range of environmental factors, and outlined a number of risk mitigation measures. Among other things, the risk assessment included consideration of:
weather conditions that may affect control of the RPA
light conditions that may affect the ability of the operating crew to maintain visual contact with the RPA
the intended flight path with respect to the location of people and property
the location of structures, other obstacles and other air traffic that may affect the flight
the adequacy of emergency procedures and possible equipment failure modes
the operating environment in terms of noise and possible distractions (operating crew and members of the public).
Operator’s investigation
The operator investigated the accident, with a particular focus of establishing the reasons for which control of the RPA was lost. The investigation included consideration of a number of system-related and environmental factors, and the behaviour of the RPA following the loss of control.
The operator’s report concluded that radio frequency interference was the most likely cause of the accident. The volume of radio frequency traffic at the time of the accident was probably substantial, and perhaps sufficient to override RPA control signals. Numerous fixed telecommunications facilities and mobile broadcast vehicles in the vicinity of the MCG were probably transmitting at the time of the accident. Over 93,000 people attended the event, many of whom were probably using personal mobile communication devices at about the time of the accident. Furthermore, the use of portable communication devices by event management personnel (such as security and emergency services personnel) may also have contributed to the volume of radio frequency traffic.
The operator considered that the behaviour of the RPA was consistent with signal interference or confusion, rather than signal loss. In the event that the signal was lost, the RPA would have entered a fail-safe mode. In fail-safe mode, if the RPA had a valid GPS signal it would have returned to the starting point and landed. Without a valid GPS signal, the RPA would have held position, then descend slowly in that position, until touch down. Additionally, the operator found no evidence that there was any fault with the RPA control systems or any hardware issues, which may have resulted in the loss of control.
The operator’s investigation report commented that very similar operations had been conducted without incident prior to the accident flight. On this particular flight, the scale of the event, and probably the amount of associated radio frequency traffic, were more substantial. The operator’s report also acknowledged that further testing and analysis was required before the primary cause of the accident could be confirmed beyond doubt.
Safety action
As a result of this occurrence, the RPA operator has advised the ATSB that they are planning further tests to better understand the nature of the loss of control of the RPA. A better understanding of the nature of the problem may allow identification of engineering measures to reduce the risk associated with the possibility of radio frequency interference.
The operator also intends to review procedures and update risk assessments considering the circumstances surrounding this accident.
Safety message
On this occasion, the available evidence suggests that a high volume of radio frequency traffic compromised RPA control and communication functions. This accident highlights the need for careful consideration of ‘what might be different this time’ during risk assessments, including the identification of appropriate risk mitigation strategies. Although the operator had conducted a risk assessment for the accident flight, the possible effects of a substantial increase in the volume of radio frequency traffic had not been specifically considered.
In a broader sense, this accident highlights the ongoing importance of appropriate RPA operational controls and procedures. These are particularly important where operations are intended in the vicinity of populated areas or other air traffic. The careful application of operational controls and procedures, underpinned by robust risk assessment, will become increasingly important as relevant technologies develop further and new RPA applications continue to emerge.
Important information for RPA operators, including information about relevant regulations, operational approval requirements and RPA associations, is available on the CASA website.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 20 March 2015, at about 1140 Eastern Standard Time (EST), a Robinson R22 helicopter, registered VHHUA, departed from Stanbroke Station for a private flight to Devoncourt Station, Queensland. On board were a pilot and one passenger. The main fuel tank was filled to capacity prior to departure, with 68 L of fuel. While en route between the two stations, the pilot was assessing the water available for stock by overflying water holdings.
At about midday, while about 500 ft above ground level, the helicopter approached a gorge. To assess the water quantity in the gorge, the pilot conducted a descent to about 100 ft and slowed the helicopter to a hover. As the pilot shifted his focus outside, the rotor revolutions per minute (RPM) decreased, the low rotor RPM warning horn sounded and the helicopter commenced descending. The pilot immediately lowered the collective[1] and turned the helicopter away from the higher gorge walls in an attempt to increase forward speed and rotor RPM. He was unable to regain sufficient rotor RPM and the helicopter continued to descend.
The right skid landed heavily on uneven ground, followed by the left skid. The main rotor then collided with a rock and the helicopter rolled onto its right side. The pilot and passengers exited the helicopter and were not injured. The helicopter sustained substantial damage (Figure 1).
Figure 1: Damage to VH-HUA
Source: Aircraft operator
Local conditions
The temperature at the time was about 42 °C and the elevation of the area was about 1,000 ft above mean sea level. The pilot reported the wind was southerly at about 10-15 kt, but the gorge was sheltered and the wind in the vicinity of the accident was calm.
Pilot comments
The pilot reported that his attention was momentarily diverted outside checking the water, when he would normally be watching the gauges and monitoring the rotor RPM. He usually operated without a passenger on board, so the extra weight of the passenger had reduced the helicopter’s performance, particularly its ability to maintain a hover out of ground effect.
Power required and power available
A number of factors related to the power required and the power available may have contributed to the decaying main rotor RPM during a hover out of ground effect.[2] These factors include density altitude, take-off weight and the wind component.
Density altitude. Increasing density altitude adversely affects helicopter performance through the combined effects of reducing the power available and increasing the power required. Considering elevation and temperature, and barometric pressure in the area, the density altitude at the accident site would have been around 4,000 ft. High relative humidity would have had the effect of further increasing the density altitude.
Operating weight. Increasing the helicopter weight increases the power required. The greater lifting force demanded of the main rotor, and the requirement to counter the associated increased torque effect[3] with the tail rotor, both contribute to an increased power requirement. The weight of the helicopter at the time of the accident was less than the maximum permitted operating weight, but reduced the ability to hover out of ground effect.
Wind component. A nil wind component increases the power required because of the diminished or delayed influence of translational lift.[4]
The following references discuss factors affecting helicopter performance, and provide some guidance to pilots regarding the associated considerations:
A ‘Good Aviation Practice’ booklet titled Helicopter Performance, produced by the Civil Aviation Authority (CAA) of New Zealand. The booklet is available via the CAA website.
The Federal Aviation Administration (FAA) Helicopter Flying Handbook (chapter 7 deals with helicopter performance). The handbook is available on the FAA website.
Safety message
The Robinson R22 Pilot’s Operating Handbook includes a number of important safety tips and notices. Pilots (particularly those who fly Robinson helicopters) are encouraged to carefully reflect on these safety tips and notices – the tips are intended to improve safety, while the notices have been issued as a result of various accidents and incidents. The R22 Pilot’s Operating Handbook – Section 10 Safety Tips and Notices is available at Robinson Helicopter website.
The Robinson Helicopter Company Safety Notice SN-10: Fatal accidents caused by low rpm rotor stall, advised that a ‘primary cause of fatal accidents in light helicopters is failure to maintain rotor RPM. To avoid this, every pilot must have his reflexes conditioned so he will instantly add throttle and lower collective to maintain RPM in any emergency’.
Three other ATSB investigation reports that identified helicopter performance and low main rotor RPM as possible factors include AO-2013-203, 200600979 and 199900833. These investigation reports are available on the ATSB website.
This incident provides a reminder of the effect of density altitude, weight, and wind on helicopter performance. Pilots are encouraged to carefully and accurately assess these factors to ensure that an adequate performance margin is maintained. When performance is likely to be adversely affected by a combination of these factors, extreme caution is warranted.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the morning of 20 March 2015, the pilot of a Piper PA 25-235/A9 Pawnee aircraft, registered VH-NLP, departed a private airstrip near Derrinallum to conduct insect baiting operations on a property near Darlington, Victoria. Shortly after commencing that task, the aircraft collided with terrain and was destroyed by impact forces and a post-impact fire. The pilot, who was the sole occupant, was fatally injured.
What the ATSB found
The ATSB found that while positioning the aircraft for a baiting run, the pilot inadvertently descended below the normal application height over an adjacent paddock. While recovering from this loss of height and avoiding terrain, the aircraft probably stalled and entered an incipient spin at a height from which recovery was not possible before colliding with terrain.
There was no evidence of any pre-existing mechanical defect with the aircraft or engine that could have contributed to the accident. However, the aircraft was being operated outside the flight envelope as it exceeded the design maximum take-off weight. In addition, the conditions were conducive for the formation of carburettor icing.
Safety message
Operators and pilots are reminded of the hazards associated with agricultural low-level flying and the increased risk of collision with terrain. The ATSB highlights the importance to pilots and operators of ensuring that their aircraft’s weight and balance is within specified limits, and understanding the effects of operating outside the flight envelope on the aircraft’s flying characteristics. This accident is also a reminder of the importance of monitoring environmental conditions and the associated risk of carburettor icing.
Photograph of VH-NLP
Source: The operator
Findings
From the evidence available, the following findings are made with respect to the collision with terrain involving Piper Aircraft Corporation PA-25/A9 Pawnee, registered VH-NLP, which occurred 10 km west of Darlington, Victoria, on 20 March 2015. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
While positioning the aeroplane for a baiting run, and for reasons that could not be determined, the pilot inadvertently descended below the normal application height over an adjacent paddock before climbing and then losing control.
The aircraft probably stalled and entered an incipient spin at a height from which the pilot was unable to regain control before colliding with terrain.
Other factors that increased risk
The pilot took off with the aircraft about 102 kg over its approved maximum take-off weight, which can affect the aircraft’s handling characteristics.
Other findings
The weather at the time of the accident was conducive to carburettor icing, but the time between the accident and examination of the wreckage meant that any ice, if present, had melted.
The occurrence
On 20 March 2015, a Piper Aircraft Corporation PA-25-235/A9 Pawnee aircraft, registered VH‑NLP (NLP), was being prepared for an agricultural flight from a private airfield near Derrinallum, Victoria. A witness reported observing an estimated total of about 100–120 l of fuel on board, and load of about 450 kg of insect bait. The witness observed that the pilot appeared to be well rested and enthusiastic about the task.
The planned flight was an insect baiting operation, consisting of spreading a poison-infused wheat product. This was to be carried out on a farming property near Darlington, Victoria, over three adjoining paddocks in an east-west direction. The plan was for the pilot to conduct the bait application in a left racetrack pattern,[1] at about treetop level.
At about 0850 Eastern Daylight-saving Time,[2] NLP departed for the 10-minute flight to Darlington. The operator considered the wind to be calm at the time NLP departed Derrinallum. A witness at the accident site indicated that the conditions were calm at about 0900–0915, when they heard the aircraft. They noticed that the wind did come up later in the morning. Bureau of Meteorology weather observations were available for Mortlake, about 15 km to the west of the farming property. At about the time of the bait application operation, the Mortlake recorded weather indicated that the wind was from the west at 7 kt, the temperature was 12.3 °C and that the dewpoint[3] temperature was 10 °C.
Several witnesses observed and heard the aircraft operating in the area of the three paddocks between about 0900 and 0915. One witness, who was travelling along a nearby highway to the south-east of the three paddocks, observed NLP at treetop height, heading west. They then observed it rolling left and right before suddenly descending. Black smoke was seen by witnesses coming from a paddock in the area where NLP had been operating. The aircraft impacted terrain, out of sight of the witnesses, at about 0915.
The pilot, who was the sole occupant, was fatally injured and the aircraft was destroyed by impact forces and a post-impact fire. The accident was not considered survivable.
Operational aspects
Pilot information
The pilot was appropriately qualified for the flight, holding a Commercial Pilot (Aeroplane) Licence, a Class 2 Agricultural Rating (Aeroplane), and a Class 1 Aviation Medical Certificate. The pilot completed their agricultural rating on 9 April 2014, which included their 2-yearly flight review. The pilot had a total aeronautical experience of about 281 hours, about 17 hours of agricultural flying and about 15 hours in NLP.
After obtaining an agricultural rating in Victoria, the pilot was employed for about 4 months by an operator in Queensland. Although the pilot performed a number of training and general flights with that operator, there were no recorded agricultural flights during that period. The pilot returned to Victoria in August 2014, and performed various duties. These included agricultural operations and aerial work through until November 2014.
The pilot’s most recent aerial agricultural operations occurred about 5 months prior to the accident in October 2014. That involved three baiting flights and two flights spraying liquid chemical. The pilot then completed three general flights in January 2015. Of these, the last entry in the pilot’s logbook was for a flight on 26 January 2015. The pilot’s logbook did not include a ferry flight undertaken in NLP on the day prior to the accident.
An aerial agriculture instructor who had flown with the pilot stated that, although the pilot was conscientious and deemed safe for flying agricultural operations, there were particular situations where the pilot’s lower level of experience became evident. These situations, which were reported to sometimes be observed in other ‘junior’ agricultural pilots, included difficulty managing the aeroplane’s attitude during turns and anticipation of a pending aerodynamic stall.[4]
Aircraft information
Piper Aircraft Corporation PA-25-235 Pawnee NLP was manufactured as a single-seat aircraft in the United States in 1965, and certified in the normal category. It was converted to an ‘A9’ variant in Australia in 1983 under a Civil Aviation Safety Authority Supplemental Type Certificate, and certified the normal and agricultural categories. This conversion included the installation of a second seat, replacement of the fabric-covered wings with metal wings and a larger chemical hopper.
The last periodic inspection was carried out on 5 August 2014 at 8,762.8 flying hours.
The Supplemental Type Certificate for the PA25-235/A9 detailed a maximum take-off weight of 1,315 kg. Based on the reported fuel and insect bait on board for the flight, the ATSB estimated that the aircraft departed at about 102 kg over the approved maximum take-off weight at take-off. Similarly, based on a planning fuel use of 60 l/hr and a ‘best guess’ metered bait application rate of 15 kg/hectare, it was estimated that the aircraft was about 39 kg over its maximum take-off weight after the first bait application run. Exceeding operational limitations can affect an aircraft’s handling and performance, reducing the normal operational safety margins. Depending on the magnitude of the exceedance, it can also impose significant structural loads in excess of the aircraft’s design loads. In turn, this can reduce the aircraft’s effective service life and potentially cause structural failure.
Preparation for the operation
Several days prior to the accident, the operator contacted the property owner to discuss the planned baiting job. The operator reported also taking the opportunity to carry out an airborne survey of the paddocks that were to be baited by the pilot. The operator recalled meeting with the pilot for a briefing on the afternoon before the planned flight. The briefing was reported to include a discussion of the boundaries of the paddocks that were to be baited, the powerlines and on the pre‑programming of the aircraft’s global positioning system equipment.
On-site examination
Accident site
The wreckage was located in the eastern-most paddock of the three to be baited. Examination of the accident site indicated that NLP impacted terrain nose-down, in an almost vertical orientation. The aircraft came to rest about 7 m from the initial impact point. The forward fuselage and cockpit sustained significant damage as a result of the initial impact, and a post‑impact fire consumed the the internals of the aircraft’s global positioning system equipment, the majority of the fuselage and the inboard wing sections (Figure 1). Damage to the leading edge of each wing also indicated a vertical impact. ATSB analysis based on estimates of the aircraft’s speed, the almost vertical impact angle and the energy absorbed by the aircraft indicated that the impact forces imparted to the pilot would normally be expected to result in fatal injuries.
Examination of the propeller, along with evidence from the impact crater, indicated that the propeller was rotating under a level of power at the time of impact. Flight control continuity was confirmed. Due to the level of damage, the flap position could not be determined.
No pre‑existing anomalies were identified at the accident site that would have precluded normal operation of the aircraft.
Figure 1: Aircraft wreckage (looking east), showing the lower surface of the aeroplane. Note the significant damage to the forward fuselage and cockpit area and the extent of the fire damage to the fuselage and inboard wing sections
Source: ATSB
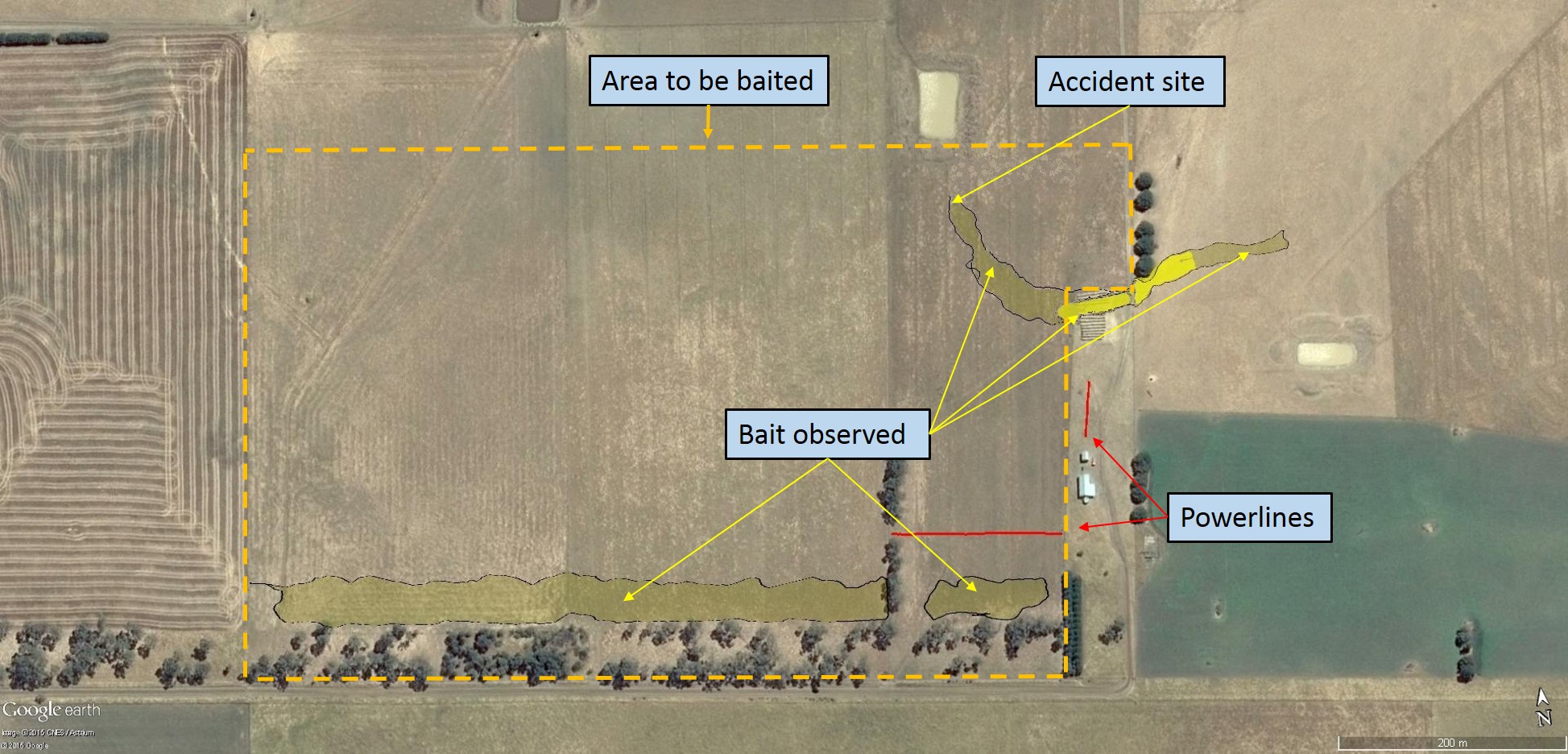
Insect bait was found in a straight and regular swathe along the southern fence line of the paddock, consistent with a bait application run (Figure 2). This swathe ran for the entire length of the planned baiting area and was about 36 m wide. Additionally, a bait swathe of varying width and density from the middle of the adjacent paddock was observed outside and to the top‑right of the baiting area. This continued in an arc to the initial impact point. This swathe initially decreased from about 16 m down to 7 m wide, then increased to 30 m wide before tapering off towards the accident site.
Figure 2: Area to be baited (outlined by the yellow dashed line), with dispensed bait shaded in yellow and higher-concentration bait shown as bright yellow
Source: Google earth, modified by the ATSB
Survivability and post-mortem results
The forensic pathologist who conducted the pilot’s post-mortem examination concluded that the pilot succumbed to the effects of fire and impact-related injuries. No abnormalities were identified that could have led to pilot incapacitation. Toxicology results did not identify any substances that could have impaired the pilot’s performance.
The sources of information during the investigation included the:
operator of VH-NLP
maintainer of VH-NLP
pilot’s aerial agriculture flying instructor
Bureau of Meteorology
Civil Aviation Safety Authority
Supplemental Type Certificate holder.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the pilot’s aerial agriculture flying instructor, the operator of VH-NLP, the Bureau of Meteorology and the Civil Aviation Safety Authority.
Submissions were received from the operator and the Civil Aviation Safety Authority. The submissions were reviewed and where considered appropriate, the text of the draft report was amended accordingly.
Safety analysis
Introduction
From witness information and examination of the accident site, it is evident that during the turn onto the second bait application run, the pilot lost control of the aircraft and was unable to recover before impacting the ground. The observed wing rock and descent was consistent with an aerodynamic stall and wing drop.
Examination of the aircraft and engine did not identify any anomalies that would have precluded normal operation, or that would have required the pilot to jettison the hopper load to the east of the intended bait application area. The wind at the time was not considered significant to the baiting operation.
This analysis will consider the factors with the potential to have contributed to the loss of control, including the potential influence of the aeroplane weight and loss of engine power due to carburettor icing.
Interpretation of the flight path
Set-up for and initiation of the second bait application run
Following the first bait application run, the pilot repositioned the aircraft for the next swathe along the paddocks, which was intended from east to west. The location and orientation of the bait application outside the intended area was consistent with its commencement prior to the beginning of the planned baiting run, as the pilot was finalising the repositioning turn. The spread width of the bait (see the following discussion) was consistent with the aircraft being at a lower height than for the previous run. The ‘track’ of the bait appeared to indicate that the pilot may have been attempting to avoid the tree line at the north‑eastern corner of the area to be baited. The increased bait concentration in the vicinity of those trees was consistent with the pilot jettisoning the load, as opposed to a normal application, which is at a metered rate.
Examination of the second bait application run
The spread width of the bait throughout the initial application run was about 36 m. Consistent with the aircraft owner’s standard bait application height of between treetop height and 100 ft (30 m), a witness observed VH- NLP (NLP) conducting runs at treetop height, or about 50 ft (15 m) above ground level. This reported height, and the known spread width on the first run, was used as a basis for determining the approximate height of NLP between the grain release in the adjacent paddock through to the accident site.
The spread width decreased from 16 m to 7 m, before increasing again to a width of 30 m. This indicates that NLP was below the previous application height, and continued to descend before climbing until about 70 m from the accident site. From this position the aircraft descended and impacted the ground. This is consistent with an attempt by the pilot to regain height after descending in the latter stages of the repositioning turn.
Reason for the height loss and jettison of the load
In an effort to understand the reason for the commencement of the bait application before entering the intended baiting paddock, the ATSB considered whether the pilot may have been momentarily confused by the apparent similarity of the respective tree lines immediately east of the area to be baited, or concerned with the powerlines on and near the south-eastern boundary of the area. The tree lines were each outside the area and the pilot had correctly ceased the first application run before passing over and east of the south-eastern tree line. In addition, the first application run passed close to the powerlines, and the pilot could be expected to have been aware of their location. On this basis, the ATSB concluded that it was unlikely the pilot misinterpreted the relevance of the location of the north‑eastern tree line, or would have been overly concerned with the location of the powerlines, when setting up for the application run.
In respect of the jettison of the bait, the ATSB considered whether the pilot may have unintentionally descended lower than planned or mishandled the repositioning turn. The pilot had relatively low total aeronautical experience and low and interrupted experience in agricultural operations. In addition, an aerial agricultural instructor advised that, similar to the instructor’s experience with other less-experienced agricultural pilots, the pilot at times had difficulty maintaining attitude in turns and anticipating an impending aerodynamic stall. The instructor reported that this was a particular risk when low-experience pilots were not current in agricultural‑type operations. It is not possible to quantify the effect of the pilot’s more recent, non‑agricultural flights in January 2015 on their handling of the aircraft in the baiting operation.
Another reason for the pilot to jettison the load was a loss of engine power. In this regard, although there were no engine anomalies identified that would have precluded normal operation, the ambient conditions were conducive to serious icing at any power setting. Carburettor icing can lead to a loss of engine power (see the subsequent discussion). However, the time between the accident and examination of the wreckage allowed sufficient time for any ice, if present, to have melted.
Aerodynamic stall and loss of control
Flying at low-level gives very little or no margin to recover from unexpected events, such as aerodynamic stalls or other losses of control. Height loss from a stall in general aviation aeroplanes, assuming correct recovery technique and expectancy of the pending stall, is generally 100–350 ft (30–107 m). Therefore, stall prevention (including maintaining airspeed) is essential at low heights.
One of the limitations of stall training and practice is that stalls are generally expected by students and follow a routine pattern. For unexpected or non-routine situations, a pilot will be focussed on the task at hand or perhaps a developing situation and potentially miss the available cues. In this accident, this could have included the pilot focussing on the unintended loss of height during the repositioning turn. Pilot knowledge and skill in recognising a developing stall situation, and responding effectively, is an essential element of flight safety in any operation.
NLP travelled a relatively short 70 m across the ground after the apparent attempt to regain height until impacting the ground. The physical evidence at the site indicated that the aircraft was inverted in an almost vertical, nose-down attitude at impact. The short distance between the initial point of impact with the ground and location of the main wreckage indicated low speed at that time.
Loss of control as a result of an aerodynamic stall could not be definitively proven. However, the low-level flight and manoeuvring by the pilot leading up to the loss of control increased the risk that they might miss any cues of an impending stall. The orientation of, and damage to the aircraft at impact, and low speed at that time indicated that the most probable scenario was an aerodynamic stall and subsequent right wing drop, consistent with an incipient spin. The height of the aircraft at that time was insufficient for the pilot to regain control before impacting the ground.
Weight and balance
Although the aircraft was being operated above its maximum take-off weight by about 102 kg at take‑off, and by about 39 kg at the time the pilot jettisoned the load, there was no evidence of an in-flight structural failure. There was insufficient evidence to determine what, if any, effect the overweight operation of the aircraft had on the flight characteristics or the development of the accident. Despite the overweight operation not being found to be contributory, operators and pilots are reminded that operations within the approved weight and balance envelop provide for known handling and performance characteristics.
Carburettor icing
The recorded temperature at about the time of the accident was 12.3 °C, with a dewpoint[5] of 10 °C. Given these temperatures, the probability of carburettor icing was calculated to be in the serious icing range at any power setting (see the Carburettor icing-probability chart that is available from the Civil Aviation Safety Authority website.
Increased humidity increases the likelihood of carburettor icing. If ice continues to accumulate in the carburettor, the flow of air to the engine reduces. If the process is allowed to continue, it will result in a power reduction, and eventually the engine will stop. Examination of the wreckage indicated that the engine was still operating, however, the level of power being produced was not able to be determined.
A carburettor heat control was available in NLP. If selected, warm air was directed from a heat muff[6] installed on the exhaust system to the carburettor inlet, melting any ice in the carburettor. Due to the level of damage, the ATSB could not determine the position of the carburettor heat control at the time of the accident.
As previously discussed, given the time between the accident and examination of the wreckage, there was insufficient evidence to conclude that carburettor icing occurred or affected normal engine operation.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 10 February 2015, a Drifter and a Thruster ultralight aircraft, recreational registration 25-0452 and 10-0339 respectively, both collided with terrain approximately 7km south of Donnington Airpark, near Townsville, QLD.
Recreational Aviation Australia (RA-Aus) is the organisation responsible for investigating this accident. As part of its investigation, RA-Aus requested technical assistance from the Australian Transport Safety Bureau (ATSB) in the examination of physical components from the involved aircraft. To protect the information supplied by RA-Aus to the ATSB and the ATSB's investigative work to assist RA-Aus, the ATSB initiated an investigation under the Transport Safety Investigation Act 2003.
Results of a visual examination of the physical components were provided to RA-Aus on 8 April 2015.
On the morning of 28 February 2015, an instructor and student were conducting a training flight in a Robinson R22, registered VH-CMK, at Archerfield Airport, Queensland. The objective of the flight was to teach the student how to manage jammed anti-torque pedal[1] and jammed collective[2] emergencies. Conditions were fine and clear with a light and variable wind.
The flight commenced with the instructor flying the helicopter in a set direction, demonstrating how to effectively control the helicopter with the pedals jammed in position. The jammed pedal condition was simulated by holding the pedals in a set position with foot pressure, then manipulating the other flight controls and adjusting engine power and airspeed to control the helicopter. Satisfied that the key elements of the demonstration had been effectively addressed and nearing the boundary of the area in which the helicopter had been cleared to operate, the instructor turned the helicopter through about 180 degrees and commenced a similar demonstration travelling in the opposite direction.
During the second demonstration, the helicopter was established in forward flight around 15 ft above the ground at an airspeed of about 40 kt. The instructor simulated a jammed pedal condition, setting the left pedal slightly forward of the neutral position. As the demonstration progressed, the instructor elected to complete the exercise by conducting a simulated jammed pedal run-on[3] landing. The helicopter touched down on a grass surface near the northern boundary of the airport, just outside the runway strips associated with runways 22R/04L and 22L/04R. The grass in the area where the helicopter touched down was slightly longer than the grass on the runway strips, but the instructor was comfortable continuing with the run-on landing, noting that it was not uncommon to operate helicopters on that surface.
The demonstration went as expected up until the point that the helicopter touched down. Still travelling forward at about 10 to 15 kt, the helicopter bounced slightly and yawed to the left. The instructor discontinued the demonstration at that moment, allowing himself full use of the pedals, but he was unable to correct the yaw before the helicopter touched down again. When the helicopter touched down a second time after a very short and shallow bounce, even though the helicopter was level, the forward part of the right skid dug into a surface undulation. The right skid then effectively acted as a pivot, tipping the helicopter to the right. The instructor fully lowered the collective, but the roll continued. The instructor then applied left cyclic[4] but he was unable to stop the helicopter rolling onto its right side.
Aware that a fuel leak had developed, the instructor closed the fuel shut-off valve and turned the master electrical switch off. The instructor and student moved to a safe distance following which the instructor contacted air traffic control (who alerted emergency services). The instructor and student suffered minor injuries and the helicopter was substantially damaged.
Instructor comment
The instructor made the following comments in relation to the accident:
The nature of the surface (outside the runway strips) probably contributed to the accident, given the manner in which the right skid dug into a surface undulation. There was a current NOTAM[5] at the time of the accident stating that grass areas were soft and wet, but the reason the skid dug in rather than skipped forward, seemed to relate more directly to the slightly undulating nature of the surface, rather than how firm the surface was. During future similar exercises involving run-on landings on unprepared surfaces, the instructor intends to inspect the surface for suitability beforehand.
The instructor was mindful of the possibility of dynamic rollover[6] under the circumstances, so consciously avoided applying power and collective as the helicopter tipped.
The instructor had invited the student to place his hands and feet lightly on the controls during the demonstration, to maximise the training benefit of the exercise. The instructor commented that the student may have inadvertently applied some pressure on the pedals during the accident, which could have reduced the effectiveness of the instructor’s attempt to correct the yaw after the initial bounce.
Safety message
This accident highlights the manner in which some hazards may not be immediately obvious. Helicopter training organisations are encouraged to consider the quality of the landing area surface during hazard identification and risk assessment processes associated with training operations, particularly those that involve run-on landings.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.