On 27 February 2015, the pilot of a Liberty XL-2 aircraft registered VH-CZT, conducted circuits at Moorabbin Airport, Victoria. At the completion of the first circuit, the pilot flared the aircraft to land on runway 17 Left (17L). The main landing gear contacted the runway and the aircraft bounced into the air. The pilot immediately applied full power and conducted a go-around.
The pilot then conducted a second circuit and established the aircraft on final approach to the runway about 3-4 kt slower than the previous approach. The aircraft touched down normally and the pilot then performed a touch-and-go and continued the circuit.
On the third approach to runway 17L, as the pilot flared the aircraft for the landing, it collided with the runway. The aircraft then bounced into the air and the pilot initiated a go-around by applying full power and slight forward pressure on the control stick. Instead of climbing away, the aircraft struck the runway again and veered to the left. The pilot applied right rudder in an attempt to counteract the left yaw and the aircraft again became airborne before colliding with the runway and skidding towards the grass to the left of the runway.
During the accident sequence, the main landing gear collapsed and the propeller and left wingtip struck the runway, resulting in substantial damage. The pilot was not injured.
This incident highlights how different aircraft types and configurations can affect the approach profile and landing characteristics. The visual cues and the control inputs required to conduct safe landings vary depending on many factors including aircraft design and performance, weight and balance, and environmental conditions including wind strength and direction.
The pilot obtained and studied relevant meteorological forecasts and submitted to Townsville Air Traffic Control a flight plan for a flight Townsville-Julia Creek-Townsville, operating in accordance with the Visual Flight Rules (VFB). He did not hold an instrument rating and was therefore restricted to VFR operations. The planned route was via Thornton Gap and Wando Vale on each sector and the nominated cruising altitudes were 8000 feet outbound and 7000 feet on the return sector. The forecasts indicated that VFR flight in accordance with the flight plan would be possible but, over the eastern section of the route, scattered stratus cloud base 1000/2000 feet and visibility decreasing to 5000 metres was expected in rain showers. The forecast for Townsville indicated that, between 1200 and 1800 hours for periods not exceeding 30 minutes, there would be heavy rain showers with 5/8 stratus cloud base 1000 feet and visibility decreasing to 4000 metres.
The flight from Townsville to Julia Creek was completed without known incident and with only the pilot on board. Four passengers boarded at Julia Creek and the return flight to Townsville commenced.
Shortly after the aircraft departed Julia Creek, the pilot was advised of amended forecast cloud conditions for the eastern section of the route. The amended forecast included scattered stratus cloud base 1000/2000 feet, scattered cumulus cloud base 2000 feet to 4000 feet and scattered strato-cumulus. At 1439 hours the pilot reported his position as abeam of Richmond and that his amended cruising altitude was 9,000 feet.
At about 1445 hours weather conditions in the Townsville Control Zone began to deteriorate with rain and reduced visibility. A Special weather report issued at Townsville at 1500 hours indicated visibility 6000 metres in heavy showers with 2/8 stratus cloud base 600 feet. This report and subsequent special weather reports issued at 1510 hours and 1530 hours were not communicated to VH-ROC. At 1520 hours the pilot reported his position to Townsville Flight Service Unit (FSU) as Wando Vale, on descent to 5000 feet, and his estimated time of arrival at Townsville at 1600 hours. He was advised that the Townsville Control Zone was then closed to VFR operations, the Thornton Gap was closed and that Townsville Air Traffic Control considered his most suitable route to be via Charters Towers.
At 1528 hours the pilot asked if it seemed that Thornton Gap was "going to clear in the near future or not" and he was advised that advice from the Control Tower was "your best chance would be below two via the Charters Towers railway line. It doesn't look as though Thornton Gap will clear. We are open now VFR to the north through east to south but still closed to the west and south-west". The pilot replied that he would be tracking via Charters Towers.
By 1533 hours the Control Zone was opened to VFR operations but Thornton Gap, which is outside the Zone, appeared to be still in an area of adverse weather. At 1539 hours the pilot asked for an appraisal of the weather at Thornton Gap adding that "from my present position I can see the western side and it appears to be fairly good". He was informed that the tower controllers could not see much past Mount Bohle (some 7 km west of the airport) in that direction. The pilot then advised that "west of the ranges the cloud base is approximately three thousand and only broken cumulus".
At 1541 hours the pilot reported "from my position I can see most of Thornton Gap. I'd like a clearance to track via Thornton Gap". The aircraft was then operating outside controlled airspace and the pilot was instructed to call Townsville Approach Control approaching Thornton Gap. The pilot established communication with Townsville Approach Control at 1548 hours and advised "approaching Thorntons Gap at three thousand. Request clearance through Thorntons Gap. From the western side Thorntons Gap looks quite okay. The shower activity just between Thorntons Gap and the City". The aircraft was given a clearance to make a visual approach via Thornton Gap and was requested to "report one five DME". At 1550 hours, on request, the pilot advised he was 23 miles by DME from the airport and at 1554 hours, again on request, reported DME distance as "one six and we're approaching one thousand". He was instructed to continue a visual approach, given information on traffic in the circuit area and requested to report again when 10 miles by DME. The pilot did not acknowledge this instruction and information and there was no response to subsequent calls directed to the aircraft by Approach Control. The Alert Phase of Search and Rescue procedures was declared at 1605 hours and an Army helicopter operating in the area commenced search action.
The helicopter checked the eastern side of the Thornton Gap area and the pilot advised that the cloud was "right on the ground". The Distress Phase was declared at 1615 hours and, at this time, the helicopter pilot estimated the cloud base as 750 feet, some 300 feet below the level of the Gap. There was drizzling rain in the area. Soon after 1630 hours, the wreckage of VH-ROC was located on the south-eastern side of Mount Cataract, some 8 km north-east of Thornton Gap and 4 km north of the track bearing 062 magnetic from Thornton Gap to Townsville.
The aircraft had struck trees near the crest of the hill on the heading of about 015 in a slightly right wing low attitude, climbing on a 5° gradient. It was severely damaged by contact with the trees and dived steeply to the ground while rolling to the left. Detailed examination of the aircraft did not reveal any evidence of unserviceability or malfunction which might have contributed to the accident.
Evidence of persons on the ground in the vicinity of Thornton Gap and the accident site indicates that there was drizzle, rain periods, low cloud and reduced visibility in the area throughout the day.
On 28 December 2014, an Indonesia Air Asia Airbus A320 aircraft, registered PK-AXC, was conducting a regular public transport flight from Juanda International Airport, Surabaya to Changi International Airport, Singapore. Radar contact with the aircraft was lost while it was en route over the Karimata Strait, Indonesia. The aircraft impacted into water shortly after radar contact was lost. During the search and rescue operation, items of wreckage were found floating about 30 NM southeast of the aircraft’s last known radar position.
The National Transportation Safety Commission of Indonesia (NTSC) is the agency responsible for investigating this occurrence. The NTSC requested the ATSB to provide a flight recorder specialist to assist in the download and analysis of the flight recorders from the aircraft. The ATSB provided this assistance as part of the Australian Government Indonesia Transport Safety Assistance Package (ITSAP).
In accordance with clause 5.23 of Annex 13 to the Convention on International Civil Aviation (ICAO Annex 13), the ATSB appointed an Accredited Representative to assist the NTSC and initiated an investigation under the Australian Transport Safety Investigation Act 2003.
On 1 December 2015, the NTSC published the final report into this investigation.
The National Transport Safety Committee of Indonesia is responsible for releasing the investigation report.
National Transportation Safety Committee Ministry Of Transportation Republic Of Indonesia Transportation Building 3rd Floor Jalan Medan Merdeka Timur No. 5 Jakarta Pusat 10110 Indonesia
On 2 January 2015 a Schempp-Hirth Nimbus 2 glider, registered VH-GOV, collided with terrain near Benalla, Victoria. The pilot, the sole occupant, was fatally injured.
The Gliding Federation of Australia (GFA) requested the technical assistance from the ATSB in the recovery of flight data from a damaged data-logging device to assist with the investigation into the occurrence. To facilitate this assistance and protect the information received from the GFA, an external investigation was initiated under the provisions of the Australian Transport Safety Investigation Act 2003.
The ATSB successfully downloaded the damaged data-logging device on 23 January 2015 and provided the GFA with a copy of the data.
Further information may be obtained by contacting the Gliding Federation of Australia.
At about 0525 Western Standard Time on 11 February 2015, the pilot of a Robinson R22 helicopter, registered VH-APP, departed from a camp site north of Kalbarri, Western Australia, with a passenger on board. The purpose of the flight was to conduct a reconnaissance of the area where goats were to be mustered that day. The role of the passenger was to point out landmarks relevant to the mustering operation. There was some confusion about the landmarks, but the pilot and passenger completed their reconnaissance then landed at another site (the goat yards) where the passenger disembarked.
From the goat yards, the pilot was to return to the muster area to commence the mustering operation. The passenger was himself also involved in the mustering operation, and had a ground vehicle pre-positioned at the goat yards.
When they landed at the goat yards, the passenger disembarked the helicopter under the supervision of the pilot, but the pilot still had some important points that he needed to clarify with the passenger. Rather than shut down the engine, the pilot elected to leave the helicopter running. After applying cyclic and collective control friction,[1] he disembarked the helicopter to follow the passenger. Having caught up with the passenger about 30 m from the running helicopter, they then engaged in a conversation to clarify the points of concern to the pilot.
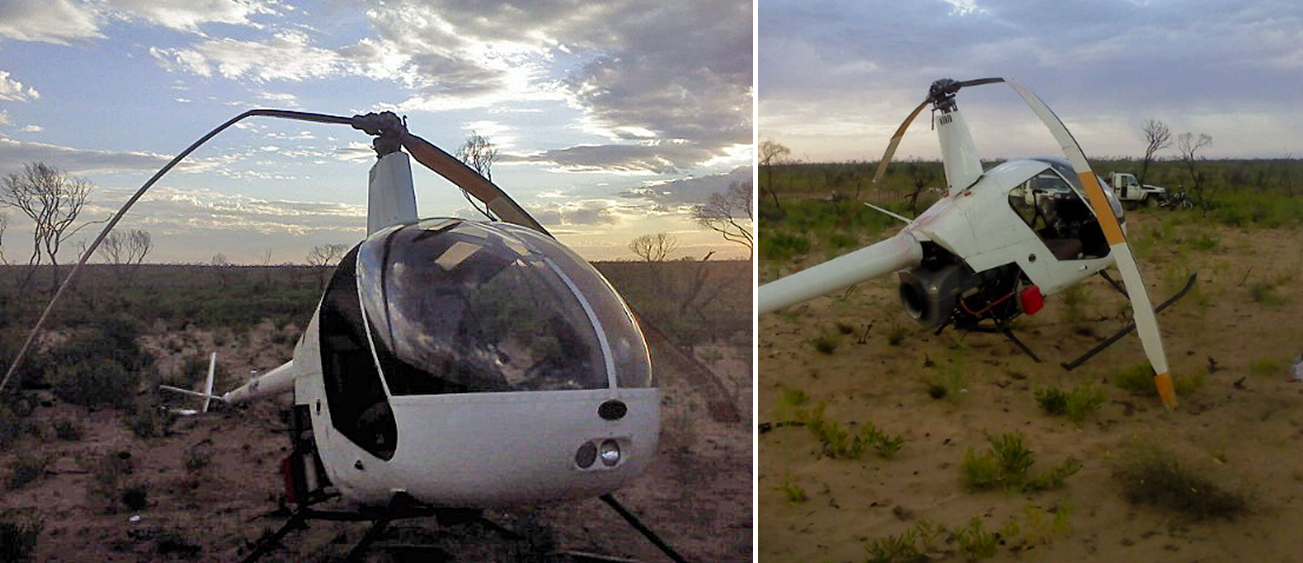
The pilot was unable to recall the exact length of time, but sometime in excess of about 2 minutes later, just as the pilot and passenger had concluded their conversation, the pilot heard the helicopter engine RPM increase and almost simultaneously, noticed that the helicopter was lifting clear of the ground. The helicopter climbed to a height of about 3 to 4 m above the ground and yawed through about 80 degrees to the left. The helicopter travelled backwards for a distance of about 8 m, remaining laterally level, and sank back to the ground with a significantly nose-high attitude. The tail of the helicopter struck the ground first, followed by the rear end of the skids. The tail rotor blades separated from the helicopter as the tail struck the ground and the rear part of the left skid broke away during the impact. The helicopter settled upright but during the accident sequence, the main rotor blades struck the ground and stopped abruptly. When the pilot was satisfied that it was safe to approach the helicopter, he moved forward and shut the engine down. Although the helicopter remained upright, it was substantially damaged (Figure 1). The pilot and passenger were both uninjured.
Figure 1: Helicopter damage
Source: Pilot
Pilot comments
The pilot believed that despite the application of control frictions, the vibration of the helicopter over the following couple of minutes (as he was engaged in conversation with the passenger) was enough to allow the collective to vibrate up with a commensurate application of engine power. He also commented that he was surprised at how quickly the accident happened. From the moment he heard the engine RPM begin to increase to the collision with terrain, was only a few seconds.
The pilot noted that he was possibly distracted at the time of the accident. Although he was an experienced mustering pilot, he had not mustered goats for some time. He was anxious to commence mustering as soon as possible that morning, mindful that in hot conditions goats were often more difficult to muster than cattle. Added to the distraction of perceived time pressure, the pilot had limited sleep during the evening prior to the accident and was generally mindful that it was likely to be a challenging day ahead. The pilot considered that with the benefit of hindsight, these distractions may have combined to influence his judgement in managing the circumstances surrounding the accident.
Robinson R22 Pilot’s Operating Handbook
The Normal Procedures in the R22 Pilot’s Operating Handbook (POH) includes the caution: ‘Never leave helicopter flight controls unattended while engine is running.’[2] The POH also includes a number of important safety tips and notices. One Safety Notice with relevance to this accident is Safety Notice 17, which includes the following text:
NEVER EXIT HELICOPTER WITH ENGINE RUNNING
Several accidents have occurred when pilots momentarily left their helicopters unattended with the engine running and rotors turning. The collective can creep up, increasing both pitch and throttle, allowing the helicopter to lift off or roll out of control.
Along with a range of important reference information about Robinson Helicopters, the R22 POH is available on the Robinson Helicopter Company website under the Publications tab.
Company Operations Manual
The company Operations Manual permitted pilots to leave a company helicopter unattended with the engine running for a period not exceeding 5 minutes, under specific conditions. Those conditions related primarily to the operational circumstances and the operating environment. The conditions also required the pilot to lock the controls and ensure that passengers and any other personnel in the vicinity of the helicopter were appropriately managed. The pilot believed that he was operating in accordance with those conditions at the time of the accident.
Safety message
Leaving any vehicle unattended with the engine running carries considerable risk. Even where appropriate approvals are in place, pilots are encouraged to exercise extreme caution when considering the circumstances, and not allow perceived time pressures or other external factors to affect their judgement.
CASA Flight Safety Australia magazine Issue 91 (March/April 2013) includes an article titled Don’t Walk Away which discusses regulatory issues surrounding leaving a helicopter unattended with the engine running. Pilots and operators are encouraged to ensure that they are familiar with the relevant regulations and the conditions attached to any associated exemptions. Furthermore, operators are encouraged to seek advice from CASA where any doubt exists regarding application of the regulations or associated exemptions. The article also provides a summary of some accidents that resulted when pilots left helicopters unattended with the engine running. A copy of the March/April 2013 edition of the CASA Flight Safety Australia magazine is available on the CASA website.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 10 February 2015, at about 1145 Eastern Daylight-saving Time (EDT), an instructor and student were conducting an in-ground-effect[1] hover lesson in a Robinson R22, registered VH-YLP (YLP) at Orange Airport, New South Wales.
The lesson had covered individual effect and use of the pedals, the collective[2] and the cyclic[3] and included student practice immediately after each instructor demonstration. Throughout the lesson, the student had progressed from individual use of each control separately, to coordinating combinations of the three controls.
The instructor reported that at times during the student practice, the student allowed the helicopter to hover sideways or forwards, and instead of easing the cyclic or pushing the cyclic in the opposite direction to counter this movement, the student incorrectly pushed it in the direction of movement. Hence on a couple of occasions, the instructor re-briefed the correct procedure.
In the last few minutes of the hour long lesson, the student requested a little more time to practice the new sequences. A few moments into this practice, at about 3 ft above ground level (AGL), with the student controlling the cyclic and the instructor lightly controlling the pedals and collective, the helicopter began to roll to the right and move rearwards. The student reacted quickly, but moved the cyclic further backwards and to the right, which resulted in an increase in the rearward speed in this direction. The instructor attempted to regain control, but due to the sudden rearward movement of the cyclic, his thumb had bent back behind his wrist. The instructor managed to ‘grab’ the collective and lift it up a small amount, but by the time any significant control input could be applied, the right skid had struck the ground (Figure 1). The helicopter rolled further to the right, and fell onto the ground. The manner in which the helicopter had pivoted around the right skid and fallen onto its side was described by both the instructor and operator as dynamic rollover[4].
The student and instructor exited the helicopter and moved clear. The instructor was not injured, however the student received minor injuries and the helicopter was substantially damaged.
Instructor experience and comments
The instructor had about 735 hours of helicopter flying experience, with the majority of their commercial experience working as an instructor.
Prior to the lesson, the instructor had conducted a 45-minute pre-flight briefing with the student. This covered the aims, objectives and sequences to be covered in the flight lesson, and also looked at preventative measures to assist in mitigating against any potential threats and errors, including dynamic rollover.
During the flying component of the lesson, the in-ground-effect hover had been practiced at about 3ft. The instructor also reported that with the high temperature and density altitude on the day, the helicopter had limited excess power available.
Figure 1: VH-YLP showing initial contact point
Source: Operator
At the time of the accident, the instructor reported that the student was using all three controls and the instructor was lightly on the collective and pedals, monitoring the student’s performance.
Due to the hot and dry conditions in the previous few weeks, the ground was very hard and dry and caused the helicopter to bounce when the skid first impacted the ground. This further exacerbated the helicopter’s instability.
The instructor felt that as soon as the helicopter tilted to the right, the blades probably struck the ground; the instructor also commented how quickly the whole event happened.
In hindsight, the instructor felt that as the student had progressed so well throughout the lesson, this had possibly influenced the decision for a little less intense instructor engagement, with a belief that with direction, the student would be able to recover the helicopter from the rearward motion. This allowed critical moments of delay when attempting to regain control when it was required.
Student experience and comments
The student had a total of about 5 flying hours, all on helicopters. This was the student’s first lesson in hovering and fifth lesson overall. The student reported that, with the intense instruction throughout the session, it is possible that they both lost situational awareness in relation to proximity to the ground. The student reported that at the time of the loss of control, the instructor had control of the collective and the pedals while they retained control of the cyclic.
The student commented that they felt it would be advantageous to practice sequences such as effects of controls at a higher altitude, gradually moving closer to the ground with increased competence.
The student also noted that they often felt quite tired at the end of an hour long lesson, as there was so much new information to understand and put into practice.
Figure 2: Detached right door and damaged rotor blades
Source: Operator
Operator comments
During the last ten minutes of the dual lesson, the heel of the right skid contacted the ground and the helicopter moved approximately 4 m to the right before coming to rest on its right side.
It is most likely that applied collective pitch may have been the reason for the movement laterally. When the helicopter moved rearward, the student was instructed to correct the unwanted movement. Initially the student applied incorrect aft cyclic, which increased the velocity of the unwanted movement and a subsequent sink off the ‘ground cushion’ created by the downwash from the rotor blades.
The company also identified that the hover height for the sequence was too low.
ATSB Comment
As noted by the instructor and the operator, the pivoting roll by the helicopter to the right, around the skid in contact with the ground, and subsequent loss of control is consistent with the phenomenon known as dynamic rollover.
A helicopter is susceptible to this later roll, but some factor must first cause the helicopter to roll or pivot around a skid until its crucial rollover angle is reached. This angle is around 5° to 8 ° dependent on the type of helicopter, winds and loading.
Once started, dynamic rollover cannot be stopped by application of opposite cycle control alone. Even with full left cyclic applied, the main rotor thrust vector and its moment follows the aircraft as it continues rolling to the right. Quickly reducing collective pitch is the most effective way to stop dynamic rollover from developing.
The role of the instructor as pilot in command is a dynamic and complex one. There remains a fine balance between providing an interesting and beneficial learning experience for your student and keeping the situation safe.
A manual produced by the Civil Aviation Safety Authority (CASA) Australia and the Civil Aviation Authority (CAA) New Zealand for helicopter instructors has many useful tips and tools relating to the principles and methods of flight instruction. It includes 28 chapters on flying sequences from ab initio through to mountain flying awareness.
The manual discusses the need to always closely supervise student practice sequences and to not allow students to make mistakes. It also highlights the necessity of using the correct handing over and taking over model, so there is never any doubt as to who has control at any one time.
In relation to the hovering sequence, it notes that this exercise demands a high degree of coordination and should not be taught until the student has acquired a reasonable state of competence in the first five lessons. An alternative technique is to use slow flight to introduce hovering. This procedure take the form of low, slow flight into the wind across a suitable clear area. Speed and height are progressively reduced in successive passes until the helicopter is creeping forward at a walking pace in ground effect and is then momentarily halted before transitioning into forward flight again. These momentary pauses are in fact periods of hovering, and are gradually extended as competency improves.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Operator
As a result of this occurrence, the aircraft operator has advised the ATSB that they are taking the following safety actions:
Flight training operations
Since the accident, the company has advised that the hover height should not be below about 1.5 – 2.0 m (5.0 – 6.5 ft) of skid height, particularly in the first or second hover lesson
Instructor’s hand position must be kept closer to the cyclic during a student’s early training and control should be taken as soon as an unwanted movement starts; do not allow rearward movement of the helicopter at this stage of training
Care should be taken to adhere to the power limits in the pilot operating handbook and guidance in the operations manual. Caution should be applied to monitor the helicopter’s height above the ground.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 1 February 2015, the pilot of a Robinson R44 helicopter, registered VH-YYF, prepared for a local flight at Warwombie Station, near Hughenden, Queensland. The pilot did not observe any abnormalities during the pre-flight inspection, with oil quantity within the normal range, about 80 L of fuel on board, and no water or other contaminants found during a fuel drain and check. The helicopter was loaded within the normal operating weight and balance limitations. The temperature was 20 °C, the sky clear of cloud and the wind was calm.
At about 0800 Eastern Standard Time (EST), the helicopter lifted off normally. At about 20 ft above ground level, the pilot lowered the nose of the helicopter in attempt to gain forward speed and transition from hover to forward flight. The helicopter then sank quickly and the rotor rpm decayed. The pilot pulled back on the cyclic[1] control in an attempt to flare and reduce the rate of descent, prior to contacting the ground. The left skid contacted the ground first and then the helicopter spun to the right. The rear of the right skid dug into the ground and the helicopter rolled onto the right side. The pilot selected the master switch off before exiting the helicopter uninjured. The helicopter sustained substantial damage (Figure 1).
Pilot comments
The pilot had about 9,000 hours total helicopter aeronautical experience. He had practiced autorotations often and believed that his experience enabled him to escape uninjured. The incident had happened very quickly and he was unsure what had caused the helicopter to sink and lose rotor rpm.
Figure 1: Damage to VH-YYF
Source: Daniel Cook
Safety message
The Robinson Helicopter Company Safety Notice SN-24 stated that rotor stall due to low RPM causes a very high percentage of helicopter accidents. These mostly occur close to the ground during take-off and landing. Safety Notice SN-10 reminds pilots to have their ‘reflexes conditioned so they will instantly add throttle and lower collective to maintain RPM in any emergency’.
The pilot in this incident had completed significant number of practice autorotations. The avoidance of injury highlights the benefits of practice. The following links provide information regarding practice autorotations:
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 23 January 2015, the pilot of a Robinson R22 helicopter, registered VH-ZBH, prepared for a private flight to inspect a property at Herbertvale, Queensland, with one passenger on board. Nothing abnormal was found during the pre-flight inspection of the helicopter. About 35 L of fuel was on board the helicopter, and the pilot conducted a fuel drain with nil contaminants found. At about 0600 Eastern Standard Time (EST), the pilot started the engine. All indications were normal throughout the run-up checks.
The pilot then increased the power to 104% for take-off and the helicopter lifted off into a low hover. The pilot reported that the helicopter responded normally and he turned the helicopter 90° to the north to depart. The helicopter transitioned from the hover to forward flight, moving about 10 m forwards and climbed to about 20 ft above ground level. The engine then lost power and the pilot detected vibration. He observed the rotor rpm decreasing and the low rotor rpm warning sounded.
The pilot immediately wound on throttle and lowered the collective[1] in an attempt to increase the rotor rpm and to ensure the helicopter cleared a fence. He then prepared for an emergency landing. The rear of the skids touched down first and the helicopter skidded forwards. As the helicopter still had forward momentum, the pilot then pulled back on the cyclic[2] to prevent the helicopter rolling over forwards, and it became airborne, moved forwards and yawed right, and bounced again before coming to rest upright (Figure 1).
The helicopter was substantially damaged due to the impact on the skids, and the pilot and passenger were uninjured.
Engineering inspection
A post-accident engineering inspection did not reveal any cause of the engine loss of power.
Figure 1: Damage to VH-ZBH
Source: Owner
Safety message
The pilot in this incident had recently completed a check flight including practice autorotations. The avoidance of injury and handling of the autorotation highlights the benefits of practice. The following links provide information regarding practice autorotations:
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 16 January 2015, at about 0930 Eastern Standard Time (EST), the pilot of a Robinson R22 helicopter, registered VHSSD, was conducting aerial mustering operations on a property 23 km north-east of Roma, Queensland.
The helicopter was about 100 ft above ground level (AGL), with a low forward airspeed of about 5-10 kt and the cattle moving slowly uphill, when the pilot observed the cattle start to move back down the side of the hill towards a creek. The wind was light and blowing across the path of the helicopter from the left. The pilot elected to descend along the side of the cattle and turned the helicopter towards the right.
As he did that, the helicopter turned downwind with a high-power setting and low forward speed. The pilot realised he had turned downwind and started to raise the nose of the helicopter and raise collective.[1] He then detected a high rate of descent and an incipient vortex ring state, as the helicopter started to settle into its own downwash. He attempted to fly out of the situation, lowered the collective and wound the throttle on, but had insufficient forward speed and low rotor rpm. The low rotor rpm horn sounded at about 15-20 ft AGL. The pilot tried to regain rotor rpm but the helicopter sank quickly.
The pilot then ensured the skids were level and the helicopter collided with the ground. Due to the rough surface, the helicopter bounced into the air. The pilot pulled back on the cyclic[2] control, which resulted in the tail of the helicopter being chopped off by the main rotor. The helicopter then spun around and came to rest on its side (Figure 1). The helicopter was substantially damaged, and the pilot was uninjured.
Figure 1: Damage to VH-SSD
Source: Operator
Vortex ring state
The United States Federal Aviation Administration (FAA) handbook www.faa.gov/regulations_policies/handbooks_manuals/ describes the vortex ring state or settling with power, as an aerodynamic condition in which a helicopter may be in a vertical descent with 20% to maximum power applied and little or no climb performance.
The following combination of conditions is likely to cause settling in a vortex ring state in any helicopter:
1. A vertical or nearly vertical descent of at least 300 feet per minute (fpm). The actual critical rate depends on the gross weight, rpm, density altitude, and other pertinent factors.
2. The rotor system must be using some of the available engine power, between 20-100%.
3. The horizontal velocity must be slower than effective translational lift.
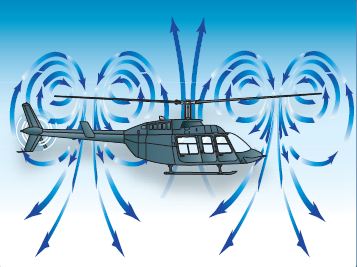
A fully developed vortex ring state is characterized by an unstable condition in which the helicopter has uncommanded pitch and roll oscillations, little or no collective authority, and a descent rate that may approach 6,000 fpm, if allowed to develop (Figure 2).
Figure 2: Vortex ring state
Source: FAA
Safety message
The pilot involved in this incident was highly experienced, with over 10,000 hours total flying (helicopter) time and over 6,000 hours in Robinson R22 aircraft. He stated that the fundamental message was to always have forward airspeed before turning downwind.
This incident highlights the importance of continually assessing and reassessing the prevailing conditions and their effect on aircraft performance. The Airbus Helicopters (formerly Eurocopter) publication, Decision Making for Single-Pilot Helicopter Operations, explains some of the factors that affect pilots’ decision making.
In the ATSB investigation AO-2013-099, the pilot of the helicopter lost situational awareness during a night approach and the helicopter developed a high rate of descent with a low forward airspeed. This resulted in the onset of an incipient vortex ring state in the final stages of flight.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
During the morning of 9 January 2015, the pilot of VH-YMD was operating in support of the Northern Territory Police. As part of the operation, the pilot conveyed two passengers to a site on the Todd River, just north of Alice Springs. The pilot landed on the sandy surface of the river bed where the passengers disembarked, then flew the helicopter from that location to a local landmark known as the Telegraph Station, about 3 km away. The pilot then conveyed another two passengers from the Telegraph Station to the site, and again landed on the sandy surface of the river bed, facing in a westerly direction (Figure 1).
Figure 1: VH-YMD landing site on the river bed
Source: Northern Territory Police
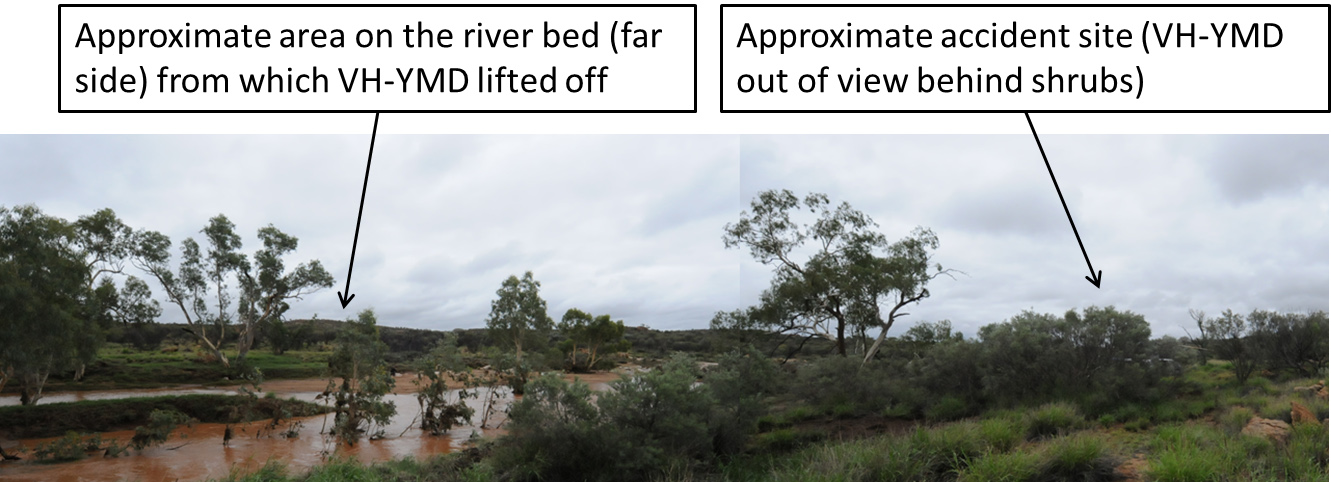
Soon after, the pilot was asked to convey three passengers back to the Telegraph Station, as a continuing part of the police operation. When all three passengers had boarded the helicopter, the pilot lifted off from the river bed. Lift-off was normal, and the pilot commenced departure in a southerly direction over the river (Figure 2) to follow what he assessed to be the most clear and suitable departure route from the river bed. As the helicopter climbed away from the river bed, the pilot became aware that the main rotor RPM was decaying. In response, he overrode the governor and applied full throttle.
The pilot needed to maintain height to clear the rocks and shrubs on the southern side of the river, but was acutely aware that rotor RPM would be further compromised by the application of more collective.[1] The pilot carefully managed the collective and the helicopter cleared the rocks and shrubs, but with decaying rotor RPM, he realised that continued climb was not possible. The pilot steered the helicopter toward a flat area, just above the river bed on the southern side of the river, and conducted a run-on landing[2] (Figure 3).
Figure 2: Photograph taken from left side of VH-YMD as it crossed the river
Source: Northern Territory Police
Figure 3: Take-off and landing area
Source: Northern Territory Police (two photographs joined and edited by the ATSB)
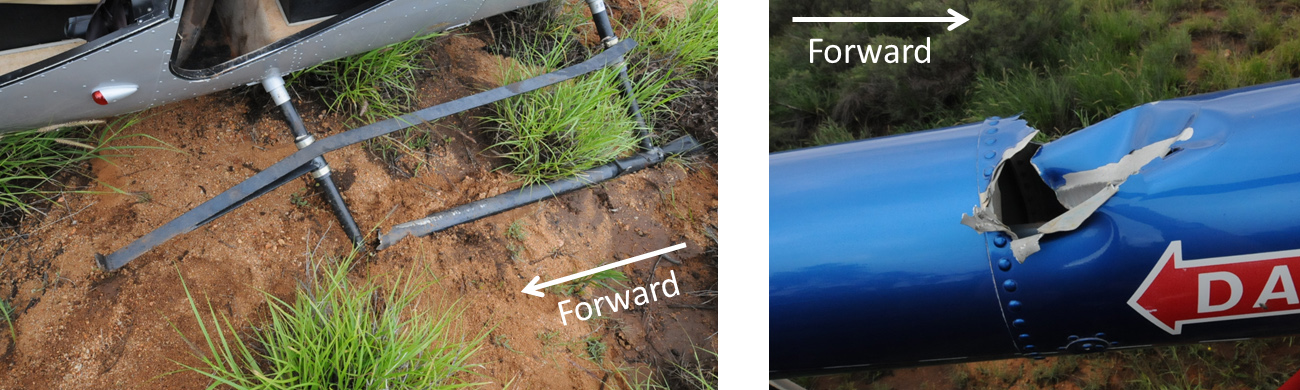
During the run-on landing, the left skid sank into mud and struck a rock. The left skid was substantially damaged by the impact (Figure 4) and the helicopter tipped precariously. As the helicopter came to a stop, it was on a substantial lean. The pilot reported that he considered the situation to be unsafe, so he immediately lifted off again and repositioned the helicopter on the ground with a level attitude. During the second lift off, a passenger recalled that the main rotor of the helicopter struck the limb of a tree, and that this was when damage to the tail boom occurred[3] (Figure 4). The pilot then shut down the engine and the passengers evacuated the helicopter.
Figure 4: Damage to VH-YMD skid (left) and tail boom (right)
Source: Northern Territory Police (edited by the ATSB)
Weather conditions
At the time of the accident, weather conditions were overcast, with showers in the area and a temperature of about 25 ºC. The wind at Alice Springs Airport (about 18 km to the south) was from the north-west at about 15 kt, and the QNH[4] was about 1003 hectopascals. While the pilot was aware that the wind was generally a north-westerly, he assessed the wind at the site as relatively light and variable. The relative humidity at Alice Springs Airport was around 80 per cent, and the pilot reported humid conditions at the accident site.
Pilot comment
The pilot commented that he believed that the accident resulted from a combination of a relatively heavy take-off weight, the prevailing conditions, and limited departure options because of surrounding terrain and obstacles. The pilot indicated that, with the benefit of hindsight, he should have taken two trips to move the three passengers, rather than attempt to take off with three passengers on board. He believed that he would have been able to complete the departure safely at a lower take-off weight.
Power required and power available
A number of factors related to the power required and the power available warrant consideration in understanding the probable reasons for which the pilot experienced decaying main rotor RPM during departure from the river bed, as the helicopter moved out of ground effect[5] and transitioned into forward flight. These factors include density altitude, take-off weight and the wind component.
Density altitude. Increasing density altitude adversely affects helicopter performance through the combined effects of reducing the power available and increasing the power required. Considering elevation and temperature, and barometric pressure in the area, the density altitude at the accident site would have been around 4,000 ft. High relative humidity would have had the effect of further increasing the density altitude.
Take-off weight. Increasing the take-off weight increases the power required. The greater lifting force demanded of the main rotor, and the requirement to counter the associated increased torque effect[6] with the tail rotor, both contribute to an increased power requirement. The pilot estimated the weight of the helicopter at the time of the accident to be less than the maximum permitted take-off weight, however subsequent calculations by the operator using actual data, indicated that the take-off weight was marginally above the maximum permitted take-off weight.
Wind component. Taking off with a tailwind component increases the power required because of the diminished or delayed influence of translational lift.[7] Additionally, a tailwind or crosswind component may require greater tail rotor force to maintain directional control during departure, which places an increased power demand on the engine. Although the pilot commented that the wind seemed light and variable prior to departure, the helicopter may have encountered a tailwind component as it climbed away from the river bed during the accident flight.
The following references discuss factors affecting helicopter performance, and provide some guidance to pilots regarding the associated considerations:
A ‘Good Aviation Practice’ booklet titled Helicopter Performance, produced by the Civil Aviation Authority (CAA) of New Zealand. The booklet is available via the
The Federal Aviation Administration (FAA) Helicopter Flying Handbook(chapter 7 deals with helicopter performance). The handbook is available on the FAA website.
Safety message
The Robinson R44 Pilot’s Operating Handbook includes a number of important safety tips and notices. Pilots (particularly those who fly Robinson helicopters) are encouraged to carefully reflect on these safety tips and notices – the tips are suggestions intended to improve safety, while the notices have been issued as a result of various accidents and incidents. The safety tips and notices are available in the R44 Pilot’s Operating Handbook on the Robinson Helicopter Company website under the Publications tab. Two Safety Notices with relevance to this accident are Safety Notice 10 (Fatal accidents caused by low RPM rotor stall) and Safety Notice 24 (Low RPM rotor stall can be fatal). One safety tip with particular relevance to this accident is:
Never allow rotor RPM to become dangerously low. Most hard landings will be survivable as long as the rotor is not allowed to stall.
Three other ATSB investigation reports that identified helicopter performance and low main rotor RPM as possible factors include AO-2013-203, 200600979 and 199900833. These investigation reports are available on the ATSB website.
This accident provides a reminder of the effect on helicopter performance of density altitude, weight, and possibly wind. Pilots are encouraged to carefully and accurately assess these factors before committing to any departure. Careful assessment of these factors is essential to ensure that an adequate performance margin is maintained, particularly under high density altitude conditions, when the helicopter is near its maximum take-off weight, or where the direction of departure is downwind. When performance is likely to be adversely affected by a combination of these factors, extreme caution is warranted.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.