Collision with terrain involving Socata TB-10 Tobago, VH-YTM, near Mount Gambier Airport, South Australia, on 28 June 2017
Preliminary report
Preliminary report released 1 August 2017
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
At about 0800 Central Standard Time[1] on 28 June 2017, a SOCATA TB-10 aircraft, registered VH-YTM (YTM), departed Murray Bridge Airport for Mount Gambier Airport, South Australia.
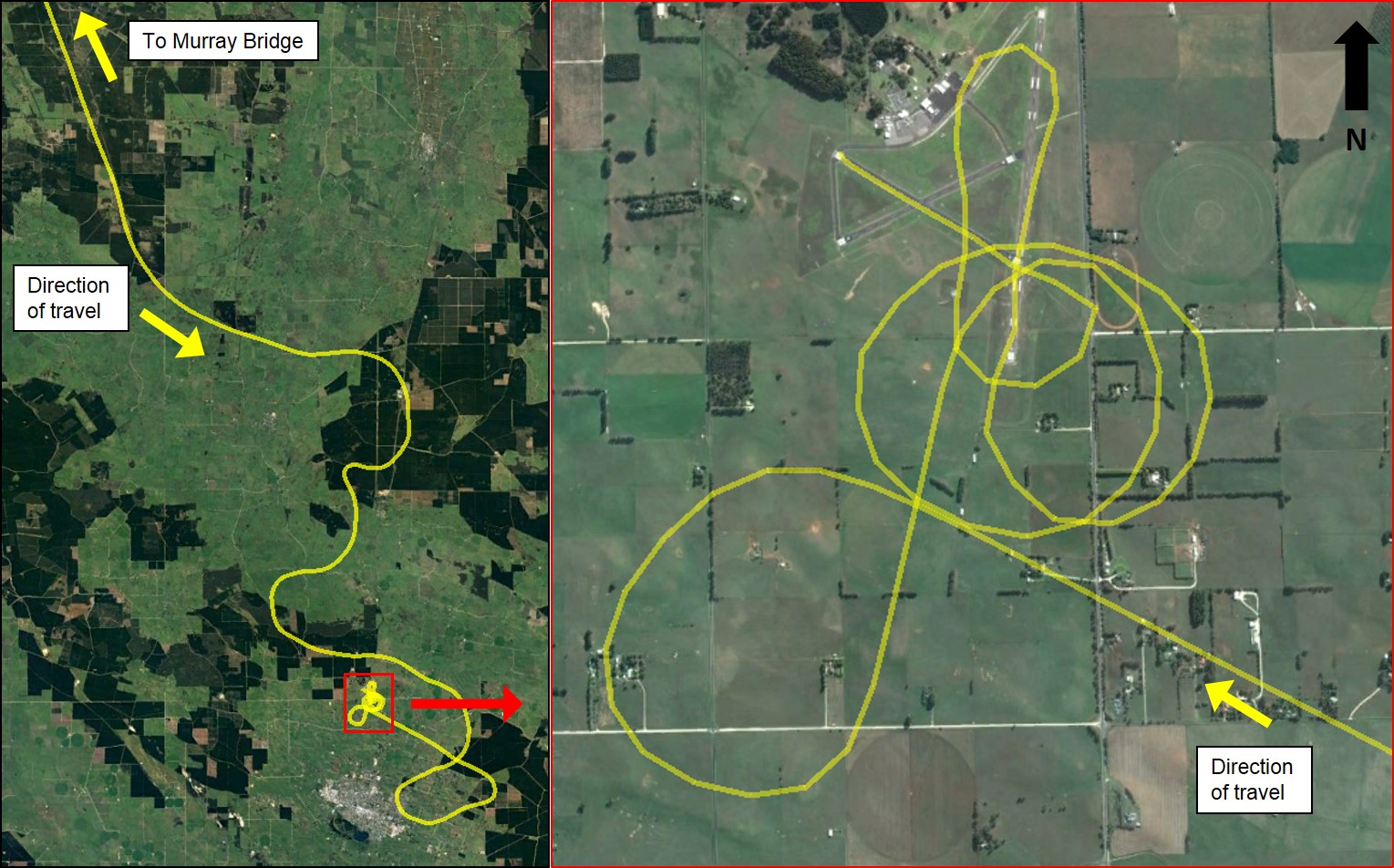
Position and altitude information obtained from OzRunways[2] showed that the aircraft’s inbound path (Figure 1) from Murray Bridge was straight and at an altitude of about 4,500 ft. At about 42 km north-north-west of Mount Gambier Airport, the altitude decreased and there was a significant deviation from the direct route. Several manoeuvres were then made at low altitude in the vicinity of the airport, including a possible attempted landing on runway 36. After a series of low-level turns, the aircraft landed on runway 29 at about 1008.
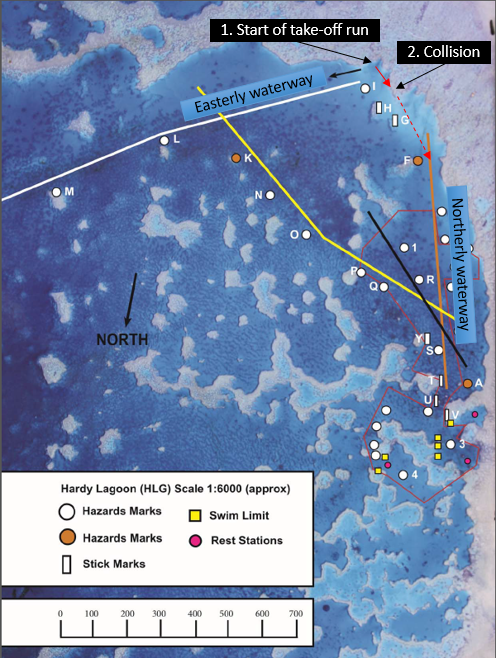
Figure 1: Approach path of VH-YTM showing the initial deviations from the direct flight path on the left, and the series of low level turns prior to landing on runway 29 on the right
The pilot then refuelled the aircraft and boarded two passengers, to conduct a flight to Adelaide arranged by the charity Angel Flight Australia.[3] The flight was to be conducted as a private flight under visual flight rules (VFR).
Witnesses in the vicinity of Mount Gambier Airport reported fog in the area at the time of landing and take-off. Similarly, CCTV footage showed the fog and reduced visibility conditions at the airport at the time of landing and take-off.
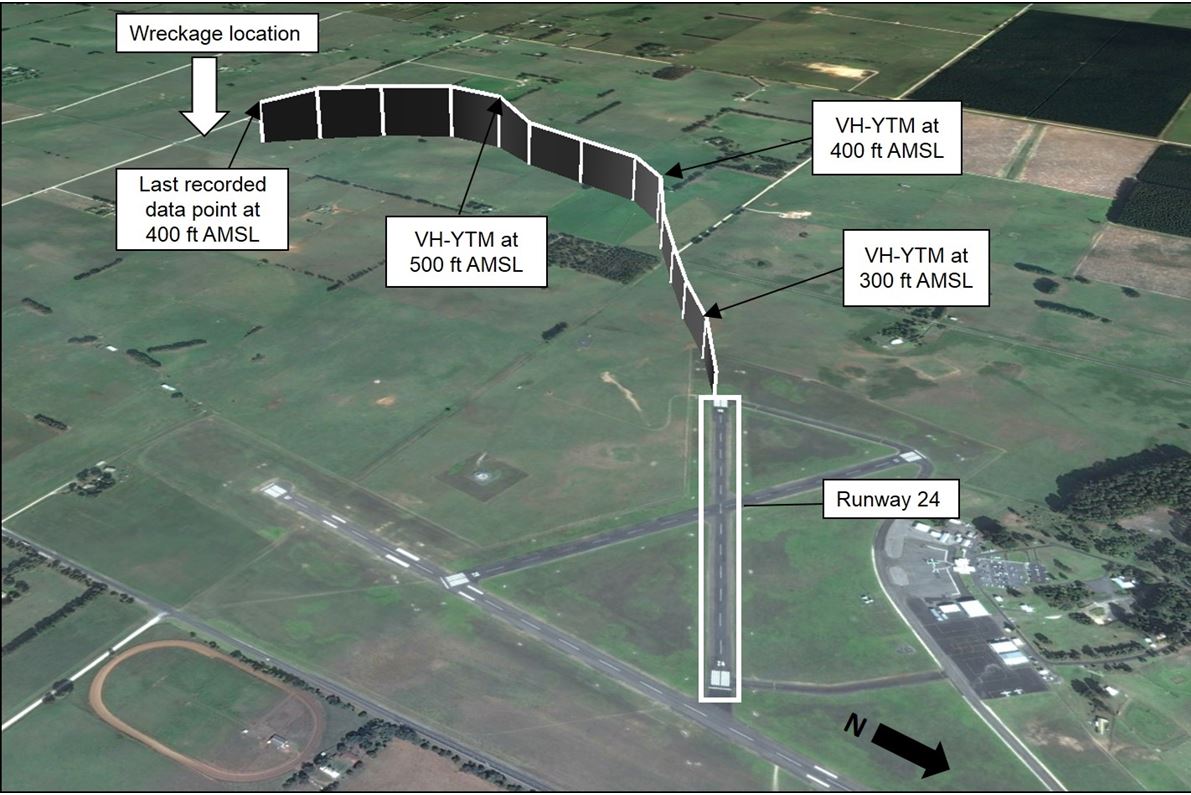
OzRunways data (Figure 2) and CCTV footage showed the aircraft took off from runway 24 at about 1020. Just after take-off, YTM veered to the left of the runway, at an altitude of approximately 300 ft above mean sea level (AMSL). The aircraft reached a maximum altitude of about 500 ft, 45 seconds after take-off. The last recorded information, about 65 seconds after take-off, showed the aircraft at an altitude of 400 ft.
A number of witnesses heard a loud bang, consistent with the aircraft’s impact with terrain.
Figure 2: Flight path of VH-YTM after departing runway 24 at Mount Gambier Airport, where each vertical line represents 5 seconds, and an indication of the wreckage location
Transmissions from the pilot of YTM on approach and take-off were recorded on the common traffic advisory frequency for Mount Gambier Airport. However, no emergency call was recorded. The aircraft was not equipped with a flight data recorder or cockpit voice recorder, nor was it required.
Minutes after impact the aircraft was found by witnesses passing the accident site, and emergency services responded to the scene shortly thereafter. The aircraft wreckage was located 212 m south of the last recorded position, just over 2 km from the departure runway (Figure 2). The pilot and two passengers were fatally injured, and the aircraft destroyed.
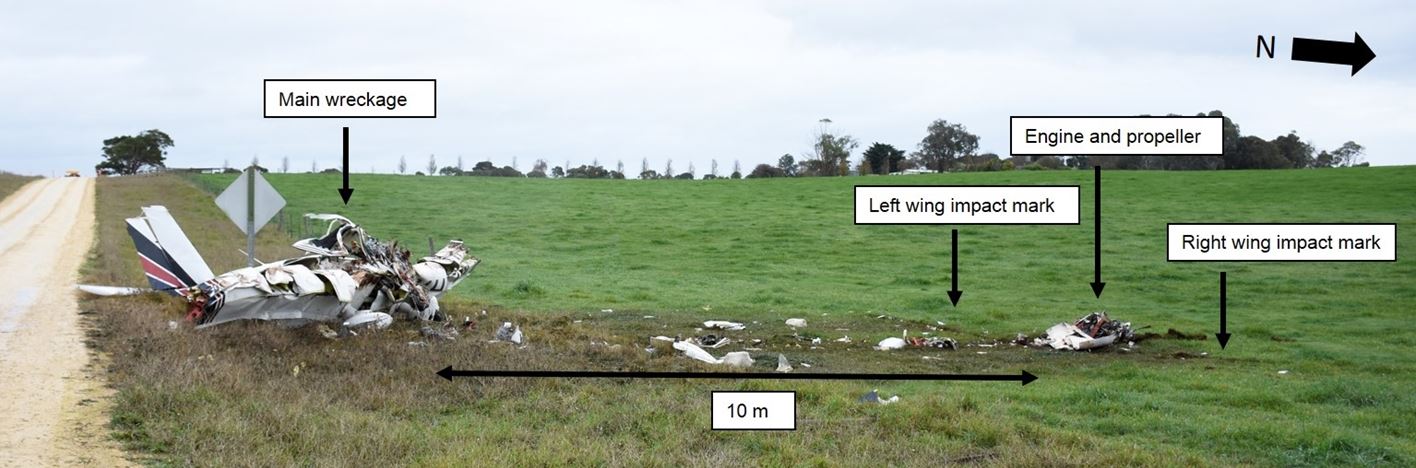
On-site examination of the wreckage and surrounding ground markings (Figure 3) indicated that the aircraft impacted terrain at approximately 30° from vertical, in an inverted attitude. The engine and propeller were located at the initial impact point. The fuselage and remainder of the aircraft had detached from the engine at the firewall, and came to rest in an upright position about 10 m beyond the engine, with the tail and wings attached. The wings had sustained significant impact damage to the leading edge. A strong smell and presence of fuel was evident at the accident site, however there was no evidence of fire. The aircraft did not have an emergency locator transmitter fitted, nor was it required. A portable locator beacon was found in the cockpit, but had not been activated.
Figure 3: Accident site looking north-west, showing the engine and propeller location alongside the left- and right-wing impact marks, about 10 m from the main wreckage, which is upright and facing in a north-north-easterly direction
Several components and documentation were removed from the accident site for further examination by the ATSB.
The investigation is continuing and will include examination of the following:
- recovered components and available electronic data
- aircraft maintenance documentation
- weather conditions
- pilot qualifications and experience
- coordination and planning of the charity flight
- the use of private flights for the transfer of passengers for non-emergency medical reasons
- similar occurrences.
____________
The information contained in this web update is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this web update. As such, no analysis or findings are included in this update.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2017
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |

__________
- Central Standard Time (CST) was Co-ordinated Universal Time (UTC) +9.5 hours.
- OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight planning information.
- Angel Flight Australia is a charity that coordinates non-emergency flights to assist people to access specialist medical treatment.
Final report
Safety summary
What happened
On 28 June 2017, the pilot of a SOCATA TB-10 Tobago aircraft, registered VH-YTM, was conducting a community service flight from Mount Gambier Airport, South Australia, to Adelaide, South Australia. The flight was organised by the charity Angel Flight to transport a passenger for medical treatment and an accompanying family member. The aircraft took off at 1020 Central Standard Time as a private flight operating under visual flight rules. After reaching a height of 300 ft, the aircraft descended and impacted terrain about 70 seconds after take-off. The pilot and both passengers were fatally injured, and the aircraft was destroyed.
What the ATSB found
The ATSB found that the pilot took off in low-level cloud without proficiency for flight in instrument meteorological conditions. Shortly after take-off, the pilot likely lost visual cues and probably became spatially disorientated, resulting in loss of control of the aircraft and collision with terrain.
The ATSB has previously established that the fatal accident rate of private operations is substantially higher than commercial passenger transport (eight times higher than charter and 27 times higher than low-capacity regular public transport, with no fatal accidents on high capacity RPT). This ATSB investigation further established that community service flights conducted on behalf of Angel Flight Australia (Angel Flight) had substantially more occurrences, accidents and fatal accidents per flight than other private operations (including that the fatal accident rate was more than seven times higher per flight than other private flights).
It is almost certain this higher occurrence rate is due to community service flights being exposed to different operational risk factors when compared to other private operations. The ATSB found two aspects in particular likely contributed to this higher rate. These were the potential for some pilots to experience perceived or self-induced pressure by taking on the responsibility to fly ill, unknown passengers, at scheduled times to meet predetermined medical appointments, often with an expected same day return; and the required operation to unfamiliar locations, and limited familiarity with procedures in controlled airspace (associated with larger aerodromes). These factors were consistent with lessons learned from the US experience, the occurrence data analysis of Angel Flight organised flights, and submissions made to a Civil Aviation Safety Authority (CASA) public consultation on changes to community service flights.
The types of occurrences where flights organised by Angel Flight were statistically over-represented (as a rate per flight) compared to other private operations were consistent with these operational differences. In particular, occurrences which involved pre- and in-flight planning and decision-making errors were over-represented, which was a factor in this accident as well as in a previous fatal accident in 2011 which involved an Angel Flight organised passenger flight. The higher occurrence rate in particular types of occurrences indicated an elevated and different risk profile in Angel Flight organised private community service flights compared with other private operations.
Angel Flight had insufficient controls in place, and provided inadequate guidance to pilots for addressing the additional operational risks associated with community service flights. Furthermore, the ATSB found that there were limited opportunities for Angel Flight to be made aware of any safety related information involving flights conducted on its behalf, restricting its ability to identify and manage organisational risks.
It was identified that Angel Flight did not consider the safety benefits of commercial flights when suitable flights were available. While Angel Flight arranged and paid for commercial flights (18 per cent of all flights) for capital city transfers, or when private pilots cancelled, it was estimated that nearly two-thirds of the private flights conducted for Angel Flight had a commercial regular public transport option available, which offered considerable safety benefits when compared to private operations. Of these, at least 22 per cent had suitable same day return flights four or five days a week, with at least two-thirds of these regular public transport flights being of comparable cost to Angel Flight when compared with the volunteer costs. The ATSB acknowledges that there will be passengers who cannot travel on regular public transport flights, and that there are times and locations where this option is not available or suitable. However, Angel Flight should still consider the use of suitable commercial flights as a primary option when arranging and paying for flights to assist financially disadvantaged people. On the day of the accident, suitable and cost-comparative commercial passenger flights were available.
CASA did not have a system to differentiate between community service flights and other private operations that would allow for ongoing oversight and review of the safety of these flights. Differentiation would allow for the identification of areas of specific concern through evidence-based analysis, and consideration of appropriate risk controls to be applied to all organisations offering community service flights. The lack of this differentiation limited CASA’s ability to identify and manage risks associated with community service flights.
What's been done as a result
Angel Flight Australia advised it had received permission for all registered pilots to access the community service pilot education online course Public Benefit Flying: Balancing safety and compassion, developed in the United States by the Aircraft Owners and Pilots Association Foundation’s Air Safety Institute, while an Australian course is developed. It also indicated it was facilitating the sharing of all CASA safety seminar schedules, with a request for feedback on attendance and the content presented, and engaging a volunteer to develop systems and processes to manage its safety risks. Additionally, pilot, passenger and health referrer guidelines had also been updated. The ATSB will monitor the progress of these safety actions.
The ATSB has issued a safety recommendation to Angel Flight Australia to take action to consider the safety benefits of using commercial flights where they are available to transport its passengers.
The ATSB was advised CASA had implemented a new safety standard regarding the conduct of community service flights. These requirements commenced on 19 March 2019 and included:
- A flight notification (full flight notification or SARTIME) that identifies the flight as a community service flight to be submitted to Airservices Australia.
- Pilots to annotate that the flight conducted was a community service flight in their personal logbook.
These changes will allow CASA to conduct ongoing identification and monitoring of risks associated with community service flights to be able to manage and control those risks.
CASA has also promoted its updated human factors education package to the industry broadly, including the community service flight sector, and refers to it on the community service flight landing page on its website. CASA also intends to release targeted guidance information to further assist the community service flight sector in the coming months.
Safety message
Organisations conducting community service flights and their pilots should be aware of the additional operational risks present. It is important that organisations have appropriate operational controls in place, and ensure pilots have access to guidance and education regarding the risks, to enable them to make objective decisions.
The occurrence
On 28 June 2017 at about 0800 Central Standard Time,[1] the pilot of a SOCATA TB-10 aircraft, registered VH-YTM (YTM), departed Murray Bridge Airport, South Australia (SA), for Mount Gambier Airport, SA. The charity Angel Flight Australia (Angel Flight) had arranged for the pilot to conduct a private flight for two passengers from Mount Gambier Airport at 1000, to facilitate the passengers’ access to specialist medical services in Adelaide, SA. Both trips were conducted as private flights under the visual flight rules (VFR).[2]
Position and altitude information obtained from OzRunways[3] showed that the aircraft initially tracked directly from Murray Bridge toward Mount Gambier, at an altitude of about 4,500 ft above mean sea level (AMSL). About 23 NM north-north-west of Mount Gambier Airport, the aircraft descended to approximately 1,000 ft AMSL and there was a significant deviation from the direct route (Figure 1).
Figure 1: Track of VH-YTM approaching Mount Gambier Airport from Murray Bridge, the track deviation and approximate locations when initial CTAF calls were made, and inset, a map of South Australia showing the relative positions of Adelaide, Murray Bridge and Mount Gambier
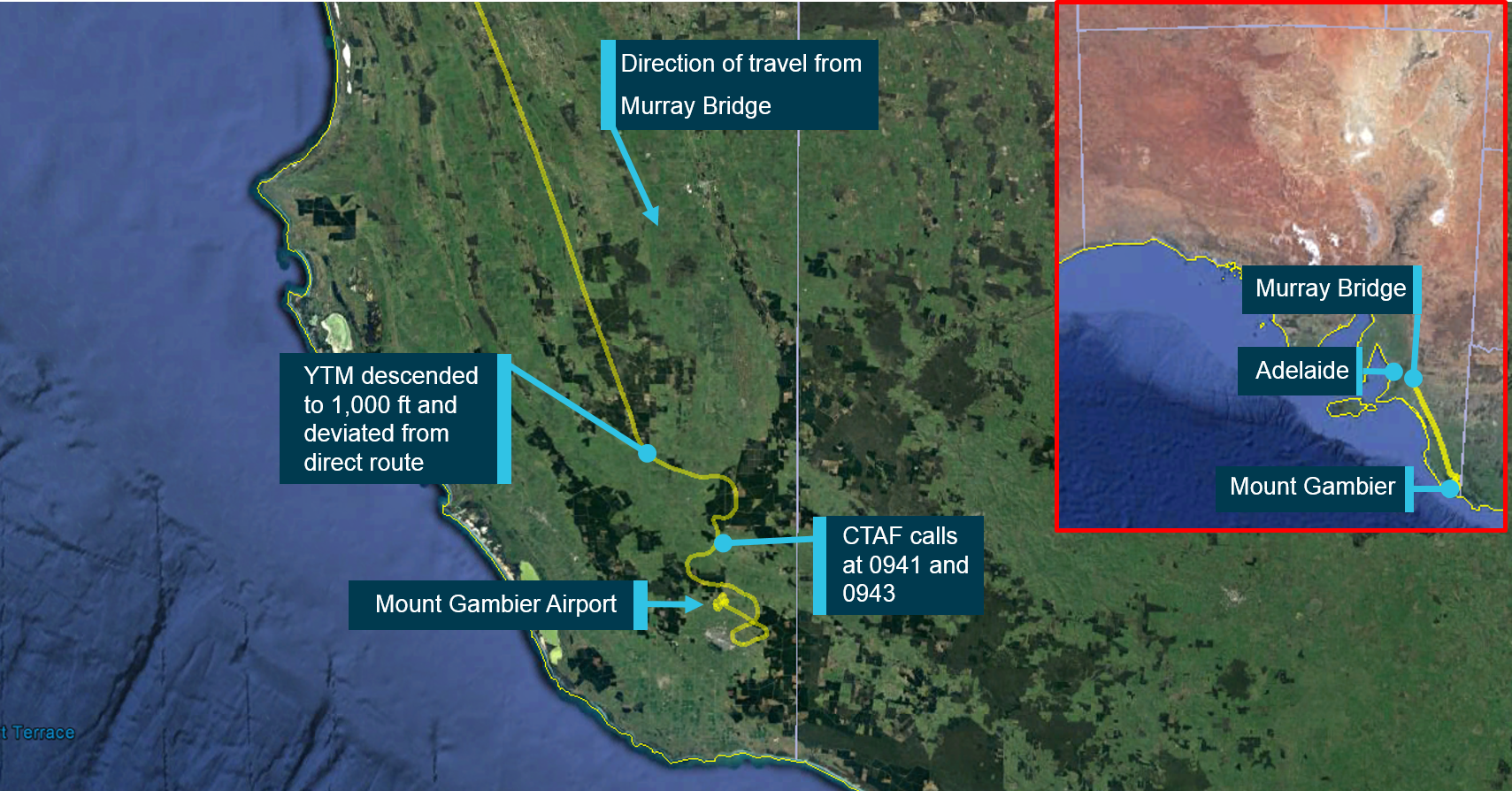
Source: Google Earth and OzRunways, annotated by ATSB
At 0941, the pilot of YTM broadcast on the common traffic advisory frequency (CTAF)[4] that the aircraft was 7 NM from the aerodrome at an altitude of 1,000 ft. This was followed by a second broadcast 2 minutes later, about 5 NM to the north-west of the aerodrome in which the pilot requested the cloud base over the airport. The pilot of an aircraft operating under the instrument flight rules (IFR)[5] that was taxiing out at Mount Gambier Airport, responded that the ‘cloud base is at the minima…we’re departing out to the east where it’s a bit clearer…it’s fairly well fogged in to the west and to the south…you should get in.’ The pilot of YTM replied to this asking the pilot to confirm that he could get in from the south or west, and the pilot of the IFR aircraft indicated possible better visibility to the north-west.
After approaching the airport from the south-east, the aircraft made several manoeuvres at a low height, including a series of turns at about 200 ft above ground level (AGL) (Figure 2). Witnesses near the airport reported hearing an aircraft, but due to the low, thick cloud, the aircraft was not visible.
At 1003, as YTM passed over the top of runway 36 in a westerly direction, the pilot made a CTAF broadcast ‘lining up for 36’, indicating that he intended to land on runway 36. Witnesses reported that the pilot then conducted a go around after initially touching down on runway 36, and witnesses reported then seeing the aircraft climb back into cloud. The pilot then broadcast on the CTAF ‘going around for runway 24’. After another two low-level turns over the airport, in which the aircraft was captured emerging from the cloud on closed‑circuit television (CCTV) at low altitude, the aircraft landed on runway 29 at about 1008.
Figure 2: Track of YTM approaching Mount Gambier Airport, low-level manoeuvres, and location of CTAF calls
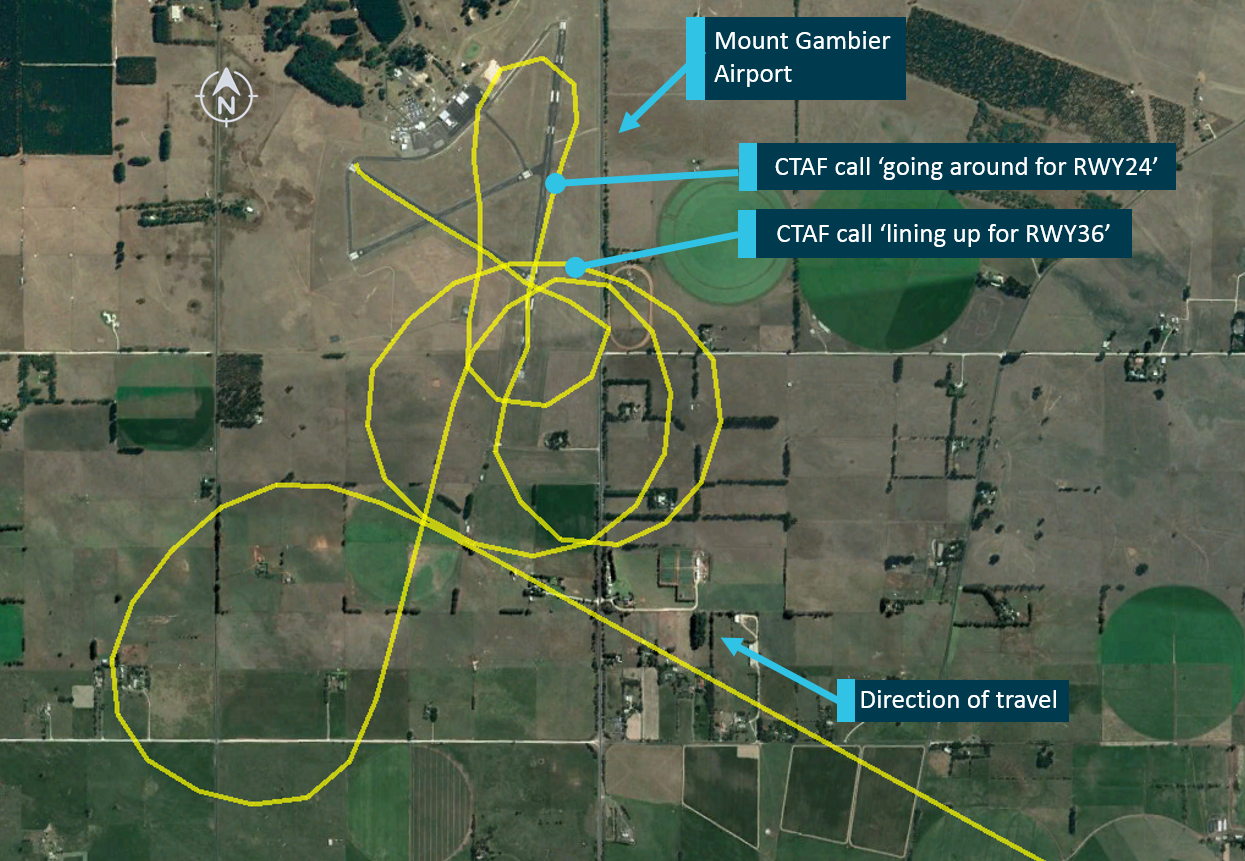
Source: Google Earth and OzRunways, annotated by ATSB
The pilot then boarded the two passengers to conduct the flight to Adelaide. The pilot broadcast that he was lined up and rolling on runway 24, and the aircraft took off from Mount Gambier Airport at 1020, approximately 20 minutes later than the intended departure time. At the time YTM departed, CCTV footage and Bureau of Meteorology (BoM) live weather cameras showed the presence of low cloud and reduced visibility conditions.
The OzRunways data showed that, just after take-off at an altitude of about 100 ft AGL, YTM’s track veered slightly to the left of the runway. The aircraft reached a maximum altitude of about 300 ft AGL, 45 seconds after take-off. The last recorded position, about 65 seconds after take-off, showed the aircraft at an altitude of 200 ft AGL (Figure 3). Soon after, the aircraft impacted terrain. A number of witnesses heard a loud bang, consistent with the ground impact.
Figure 3: Flight path of VH-YTM after departing runway 24 at Mount Gambier Airport. Each vertical line represents 5 seconds

Source: Google Earth and OzRunways, annotated by ATSB
The aircraft wreckage was located just over 200 m south of the last recorded position, approximately 2 km from the departure runway (Figure 3). Minutes after impact the aircraft was found by witnesses passing the accident site (Figure 4), and emergency services responded to the scene shortly thereafter. The pilot and two passengers were fatally injured, and the aircraft was destroyed.
Figure 4: Accident site, showing the engine and propeller location, the left- and right-wing impact marks and the main wreckage

Source: South Australia Police, annotated by ATSB
__________
- Central Standard Time (CST) was Coordinated Universal Time (UTC) + 0930 hours.
- Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
- OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight planning information. Mount Gambier Airport’s elevation is 212 ft above mean sea level.
- Common Traffic Advisory Frequency (CTAF): A designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled aerodrome.
- Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft to operate in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR).
Context
Pilot information
The pilot obtained a Private Pilot (Aeroplane) Licence in December 2014, and held the appropriate aircraft endorsements required to operate YTM. His logbook showed a total aeronautical experience of approximately 530 hours. In the 90 days prior to the accident flight, he had conducted the three take-offs and landings required by Civil Aviation Safety Regulation (CASR) 61.395 to permit the carriage of passengers. At the time of the accident, he held a valid Class 2 Aviation Medical Certificate renewed on 6 June 2017. This included a requirement for reading vision correction to be available while exercising the privileges of the licence.
The pilot commenced training for a Night Visual Flight Rules (VFR) rating in December 2015; this included about 3.5 hours recorded as instrument flight time. The pilot completed a total of 12 hours of training in flight under night VFR between December 2015 and May 2016, however he did not obtain this qualification. The pilot did not hold an instrument rating and his logbook recorded a total of 7 hours of instrument flight time, the latest of which was 0.1 hours in simulated flight conditions during an aeroplane flight review on 29 November 2016.
The ATSB assessed whether the pilot may have been experiencing a level of fatigue known to have an effect on performance. Consideration was made of the pilot’s sleep obtained, time awake at the time of the occurrence, time on task, potential workload and environmental factors. Based on the available evidence, the pilot was very unlikely to have been experiencing a level of fatigue known to affect performance.
Medical and pathological information
The pilot’s medical records, postmortem examination and toxicological analysis identified no acute or pre-existing medical conditions that may have contributed to the accident.
Aircraft information
General
YTM was a SOCATA TB-10 five-seat, low-wing, all-metal, unpressurised aircraft designed and manufactured in France, with a fixed undercarriage. Power was provided by a Lycoming O-360-A1AD four-cylinder piston engine, rated at 180 horsepower, through a McCauley three-bladed constant-speed propeller.[6]
Maintenance release
The aircraft maintenance release was issued on 4 May 2017 for 12 months or 100 hours flight time, whichever occurred first. The aircraft had flown for approximately 44 hours since the maintenance release at the time of the accident. The maintenance release was issued in the IFR category[7] and the aircraft was appropriately equipped. The documentation did not identify any unserviceable equipment or defects at the time of the accident.
The maintenance release indicated that a ‘portable emergency locator transmitter’ was required to be carried to satisfy the requirements of Civil Aviation Regulation (CAR) 252A requiring the installation of a 406 MHz emergency locator transmitter. A personal locator beacon was found in the cockpit, but had not been activated. The aircraft was not fitted with a flight data recorder or cockpit voice recorder; nor were either required.
Weight and balance
Seating positions, and approximate passenger and baggage weight were known at the time of the accident. From this information, and taking into account any fuel loading, it was calculated that the aircraft’s centre of gravity would have been within the manufacturer’s permitted range when departing Mount Gambier Airport. The aircraft weight was also calculated to be below the maximum take-off weight at the time of the accident.
Wreckage and impact information
Ground scars and evidence from the wreckage indicated that the aircraft impacted the ground nose down in an inverted attitude, approximately 30° from vertical, and that the engine was producing power at the time of impact. A strong smell and presence of fuel was evident at the accident site, however, there was no evidence of a pre- or post-impact fire. The impact sequence was not survivable.
On-site examination of the wreckage established continuity of all flight controls, and that all of the primary structural components were in the immediate area of the accident site. No pre-impact damage or failure of the primary structural components or the aircraft flight control system were identified.
A number of instruments and other components were recovered from the accident site for further technical examination at the ATSB facilities in Canberra. It was determined that there was no pre‑impact damage or failure of any of the components.
Carburettor icing
The conditions recorded at Mount Gambier Airport at the time of the accident were applied to a Civil Aviation Safety Authority (CASA) carburettor icing probability chart. Based on this chart, the probability of carburettor icing at any power setting was serious.
Due to accident damage, the carburettor heat control settings could not be determined. However, the recorded flight path, witness statements, the impact sequence, ground markings and wreckage analysis indicated the engine was performing normally before the accident. It was therefore concluded that carburettor icing was not a factor.
Airport information
Mount Gambier Airport is located about 8 km to the north of the city of Mount Gambier. It was a non‑controlled aerodrome, in Class G airspace. As shown in Figure 5, it has three runways, aligned 18/36, 11/29 and 06/24. Instrument approaches were only available on runways 18/36.
Different minima[8] apply for aircraft depending on whether they are landing or departing, conducting flight under Instrument Flight Rules (IFR) or VFR, and the category of aircraft being flown.
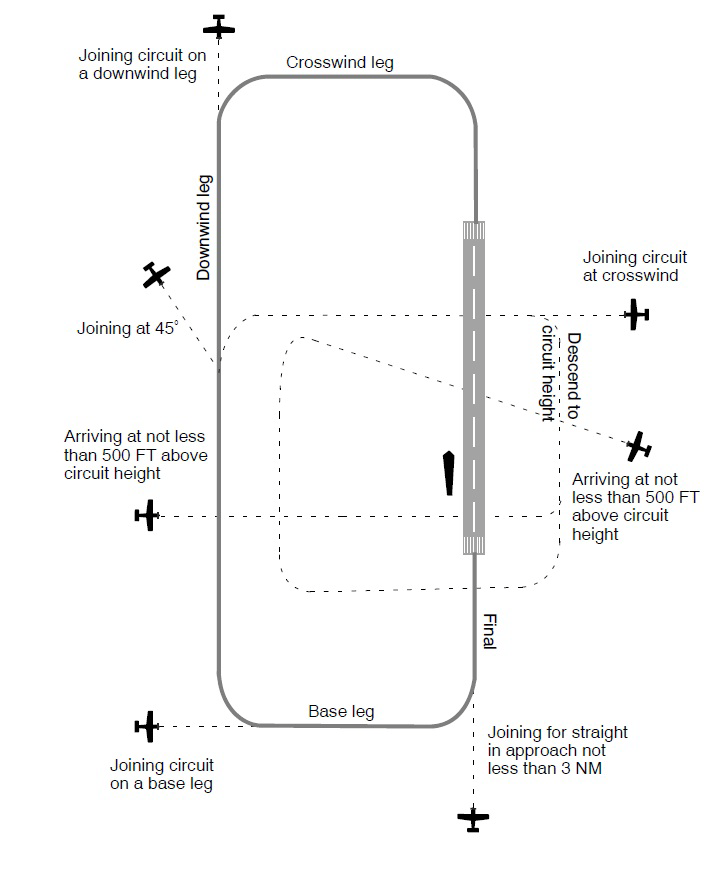
As outlined in CASA’s Visual Flight Rules Guide, standard circuit procedure is normally a left‑circuit pattern (as shown in Figure 5). For aircraft such as YTM, the standard circuit height is 1,000 ft above the aerodrome elevation (Mount Gambier Airport elevation is 212 ft above mean sea level (AMSL)). To allow the aircraft to be stabilised for approach, the turn onto the final leg should be completed by not less than 500 ft above the aerodrome elevation.
For pilots operating under VFR, as was the case for YTM, for both landings and departures, they are required to remain clear of cloud, and have a visibility of at least 5,000 m.
Figure 5: A standard circuit approach is shown on the left, and alignment of Mount Gambier Airport runways is shown on the right
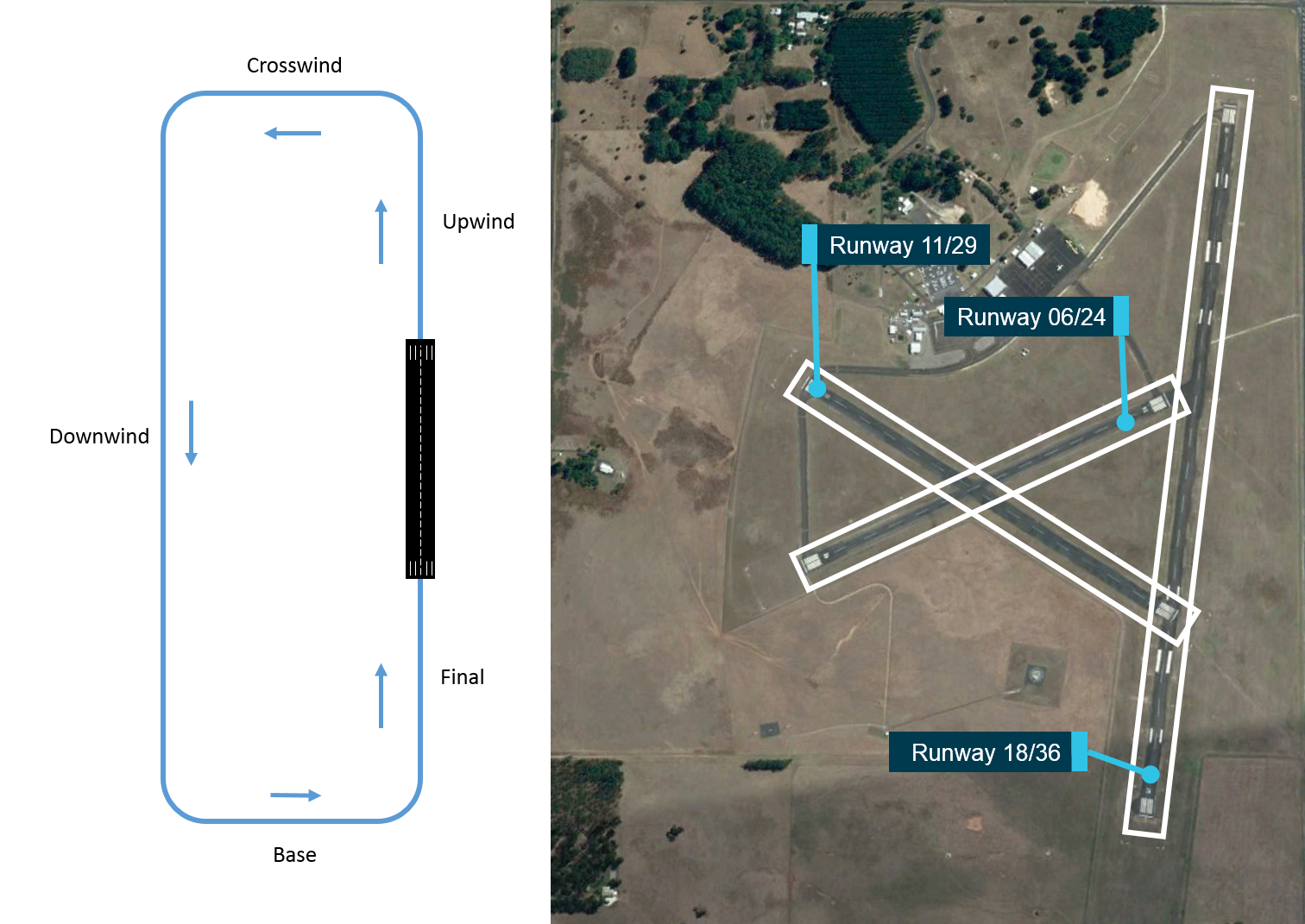
Source: Google Earth with ATSB annotations
For Category A,[9] Category B and Category C aircraft conducting an RNAV GNSS instrument approach,[10] the lowest approach minima was 518 ft AGL with a required visibility of 2,900 m. For aircraft conducting an approach using either non-directional beacon or VHF omnidirectional radio range the approach minima was 668 ft with a required visibility of 2,400 m (for Category A and B aircraft), or 768 ft AGL with a required visibility of 4,000 m for Category C aircraft.
For aircraft conducting a single engine IFR departure, a cloud ceiling of 300 ft and visibility of 2,000 m was applicable.
Meteorological information
Visual flight rules
CASA’s Visual Flight Rules Guide outlined that flight under VFR may only be conducted in visual meteorological conditions (VMC). For Class G airspace, as at Mount Gambier Airport, these conditions included:
- For aircraft operating at or below 3,000 ft AMSL or 1,000 ft AGL (whichever is higher), a minimum visibility of 5,000 m, remaining clear of cloud and in sight of ground or water.
- For aircraft operating below 10,000 ft, a minimum flight visibility of 5,000 m and a vertical and horizontal distance from cloud of 1,000 ft and 1,500 m respectively is required.
Forecast weather
The Bureau of Meteorology (BoM) provides observations, forecasts, warnings and advisories for aviation operations. For flight planning purposes, pilots are required to obtain the relevant information for the flight from Airservices Australia, the official provider of aeronautical information services.
Area forecasts (ARFOR)[11] for the proposed route included Area 50 and Area 30; Area 50 covered the proposed route from Murray Bridge to Mount Gambier Airport, and return to Adelaide, with Mount Gambier Airport located on the border of Area 50 and Area 30.
The ARFOR for Area 50 valid at the time of the pilot’s departure from Murray Bridge was issued by BoM at 0605 and was valid to 1730. The forecast included scattered showers, isolated thunderstorms and broken[12] low cloud until 1030, with isolated fog and mist forecast until 0930.
The ARFOR for Area 30 valid at the time of the pilot’s departure from Murray Bridge was issued by BoM at 0700 and was valid to 2030. The forecast included isolated to widespread showers, fog patches and broken low cloud.
The aerodrome forecast (TAF)[13] for Mount Gambier issued at 0744 included a forecast of fog, visibility of 500 m and broken low cloud at 300 ft AGL until 0930. It also included an INTER[14] from 0930 to 1230 for showers with associated visibility of 5,000 m and broken low cloud at 1,000 ft AGL.
An amended Mount Gambier TAF was released at 0942 while YTM was en route to Mount Gambier. The amended TAF included showers of rain, scattered cloud at 1,000 ft AGL, visibility of greater than 10 km, and included the same INTER as the previous TAF.
Shortly after 1030, a pilot operating in the vicinity of Mount Gambier telephoned the BoM aviation forecaster, to advise conditions at Mount Gambier Airport were worse than indicated by the TAF. In response to that call, at 1039 the TAF was again amended to include a forecast of fog and broken low cloud at 200 ft AGL with visibility of 800 m, from 1030.
From the evidence available, the ATSB could not determine if the pilot accessed the available weather forecasts or observations prior to departing Murray Bridge, or at any point en route.
Actual weather conditions
Weather recordings
Live weather observations were available to the pilot through the Automatic Weather Information System. Weather observations at Mount Gambier Airport were issued as a SPECI[15] every half an hour on the morning of the accident flight with the information seen in Table 1.
Table 1: Visibility and cloud height observation reports
| Time of issue | Visibility (m) | Cloud (height AGL) |
| 0730 | 350 | Overcast at 200 ft |
| 0800 | 350 | Overcast at 200 ft |
| 0830 | 450 | Overcast at 200 ft |
| 0900 | 1,500 | Overcast at 200 ft |
| 0930 | 1,800 | Overcast at 200 ft |
| 1000 | 3,400 | Overcast at 200 ft |
| 1030 | 4,000 | Overcast at 200 ft |
These observations indicated that visibility between 1000 and 1030 was still below the minimum required for VFR flight but was generally increasing as the morning progressed. The overcast (complete sky cover) cloud height observations also indicated that an aircraft would almost certainly not be able to remain clear of cloud or to keep the ground in sight above 200 ft AGL.
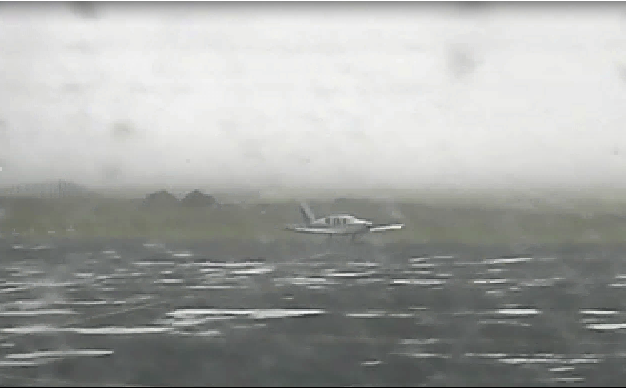
Observational weather data from the aerodrome automatic weather station (AWS) were recorded at 1-minute intervals, as were images from the live weather cameras. These were located near the runway junction, with images captured in four directions—north-east, north-west, south-east, and south-west. The AWS data and the weather camera images (Figure 6) indicated that low visibility conditions, with clouds broken or overcast at a ceiling of 200 ft, were present at the airport at the time of YTM’s approach and subsequent departure.
Figure 6: An image from the BoM weather camera at 1020, showing the direction of take-off

Source: Bureau of Meteorology, annotated by ATSB
An analysis of the local weather at the time of the accident flight was provided by BoM. The analysis concluded that:
…areas of patchy fog persisted until mid-morning then lifted into a mix of mist/haze and low cloud which persisted til late morning… It is considered likely that around the time of the incident conditions would have included broken low cloud and visibility reducing at times in mist.
Witness and camera observations
Airport closed‑circuit television (CCTV) footage of the approach, taxiing, and departure of YTM showed the aircraft passing in and out of cloud at low levels (Figure 7).
Figure 7: Mount Gambier Airport CCTV images of YTM conducting a low level manoeuvre on approach over the airport at 1006 with aircraft highlighted (top), and taxiing out to runway 24 at 1018 (bottom)

Source: Mount Gambier Airport, annotated by ATSB
A number of witnesses heard the aircraft in the vicinity of the airport (both when arriving and departing), however, due to low cloud, the aircraft was not visible. The cloud base was estimated by witnesses to the west of the airport be at about 200 ft AGL. Witnesses located at the airport observed the aircraft pass in and out of cloud during the low level manoeuvring on approach, and again on departure.
Pilots operating in the area at the time YTM approached, landed and took off, reported the weather was clearing to the east, but was below the required IFR minima (see Airport information section for minima) to the north and to the west. Due to the prevalent weather conditions at Mount Gambier Airport being below the VFR minima, witnesses assumed that YTM was operating under IFR, and the pilot responses on the CTAF referred to IFR criteria. The pilot of an aircraft that departed under IFR on runway 06 prior to YTM approaching the airport reported being in cloud with no visibility between 500 ft and 1,000 ft AGL.
Two regular public transport (RPT) flights were due to arrive at Mount Gambier Airport about the time YTM arrived and departed. Based on the forecast and observed weather conditions, one flight delayed its departure for Mount Gambier by approximately two hours, as the weather was below IFR minima for landing. The other aircraft, having attempted an approach to Mount Gambier Airport at 1030, conducted a missed approach, and remained in a holding pattern to the south of the airport for 50 minutes until the conditions cleared sufficiently to land. Both these RPT aircraft were operating under IFR. Another aircraft operating under IFR from Adelaide to Mount Gambier delayed its 0830 departure for two hours due to the forecast and observed weather. On approaching Mount Gambier Airport at approximately 1120, due to the weather present, the pilot was unable to sight the runway by the required minimum descent altitude and elected to divert to an alternate aerodrome.
Flight in low visibility conditions
Risks of flying in areas of reduced visual cues
The safety risks of VFR pilots flying from visual meteorological conditions (VMC) into instrument meteorological conditions (IMC)[16] are well documented. This has been the focus of numerous ATSB investigations and publications, as VFR pilots flying into IMC has been identified as a contributing factor in a considerable number of aircraft accidents and fatalities. The ATSB Avoidable Accidents series booklet (AR-2011-050) titled Accidents involving pilots in Instrument Meteorological Conditions outlines that:
In the 5 years 2006–2010, there were 72 occurrences of visual flight rules (VFR) pilots flying in instrument meteorological conditions (IMC) reported to the ATSB…About one in ten VFR into IMC events result in a fatal outcome.
Additionally, a study conducted by the United States’ National Transportation Safety Board (NTSB, 2005) found that reduced-visibility weather represents a particularly high risk to general aviation pilots, testing ‘the limits of pilot knowledge, training, and skill to the point that underlying issues are identified.’
The NTSB study also outlined that historically, about two-thirds of all general aviation accidents that occur in IMC are fatal; a rate much higher than the overall fatality rate for general aviation accidents. A study by Newman (2007) conducted for the ATSB titled An overview of spatial disorientation as a factor in aviation accidents and incidents outlined that there was a four times greater chance of fatality in a VFR flight into IMC accident than any other sort of accident (quoting Batt and O’Hare, 2005 and NTSB, 1989).
In the context of this accident, it is therefore important to outline why the risk of entering IMC is so high, which is linked directly to how and why pilots experience spatial disorientation when entering areas of low visibility.
Experiencing spatial disorientation
The ATSB Avoidable Accident booklet outlines that there are three sensory systems used by pilots to establish or maintain orientation relative to the environment. The visual system is by far the most important system, providing 80 per cent of orientation information. The remaining 20 per cent is split equally between the vestibular system, which obtains its information from the balance organs in the inner ear, and the somatic system, which uses the nerves in the skin and proprioceptive senses in our muscles and joints to sense gravity and other pressures on the body. In the absence of visual references, both the vestibular and somatic senses can be misinterpreted and are prone to illusions.
Spatial disorientation is defined by Benson (1999) as where ‘the pilot fails to sense correctly the position, motion or attitude of the aircraft or of him/herself’ with respect to the ground. For pilots flying under VFR, seeing the horizon is crucial for orientation of both the pilot’s sense of pitch and bank of the aircraft (Gibb and others, 2010). In conditions of low visibility, where the horizon may not be visible to the pilot, they can become rapidly disorientated.
Benson (1999) outlined that spatial disorientation would typically occur within 60 seconds of all visual cues being removed, while another United States study showed a loss of control by non-instrument rated pilots within an average of 178 seconds after the loss of all visual cues (Bryan, Stonecipher, and Aron, 1954).
Spatial disorientation presents a danger to pilots as the resulting confusion can often lead to incorrect control inputs and resultant loss of aircraft control. Gibb and others (2010) state that spatial disorientation accidents have a fatality rate of about 90 per cent, indicating how compelling the misperceptions can be.
A range of factors can influence the extent to which a pilot may experience or be able to recover from spatial disorientation. Common factors include limited or ambiguous visual cues outside the cockpit, not directing sufficient attention to the flight instruments due to workload or distraction, and not being proficient in instrument flying skills. The risk of experiencing spatial disorientation can be managed effectively in the absence of external visual cues by reference to suitable aircraft instrumentation. However, controlled flight by sole reference to cockpit instruments is a separate and complex learned skill from those skills associated with flight in visual conditions.
In the absence of visual information, a pilot’s perception (or lack of perception) of movement obtained from their vestibular system (inner ear) can lead to spatial disorientation. Two vestibular‑based illusions are the somatogravic and somatogyral illusions.
Somatogravic illusion
The vestibular illusion known as somatogravic illusion is associated with acceleration, particularly at take-off. Any vehicle that accelerates will push a forward-facing occupant backward in their seat. This generates a vestibular sense that is very similar to the sensation of tilting back. In the absence of supporting visual cues, it is possible for pilots to mistake this vestibular sense when accelerating (such as for take-off) with a sense of a pitch-up change in attitude. It is more pronounced with greater acceleration during the take-off run. A greater take-off speed, particularly if the aircraft continues to accelerate after take-off, can further amplify the illusion in the absence of significant external visual cues.
The risk of somatogravic illusion is that the pilot responds by pitching down, which is particularly dangerous soon after take-off. The illusion can be mitigated by pilots being aware of it and understanding it, and by effective use of flight instruments to control the aircraft in the seconds after take-off. This illusion is most prevalent and hazardous immediately after take-off in fixed wing aircraft, but can also occur when the aircraft is longitudinally accelerated.
Somatogyral illusion
This illusion relates to a pilot’s incorrect understanding of an aircraft’s angle of bank. The pilot’s vestibular system will register an angular acceleration (above a threshold level) when the aircraft’s angle of bank is changed. Once the aircraft is in a constant turn, the pilot’s vestibular system will stop registering any input because there is no angular acceleration. In the absence of any other sensory information or vestibular input a pilot may experience a sensation that the aircraft is no longer turning.
This sensation is normally overridden by the visual system that is influenced by seeing the world rotating as the turn continues. However, in the absence of external visual cues, successful orientation relies on the use of the information available from the aircraft’s flight instruments. The perceived conflict of information between the vestibular and the visual cues requires a pilot to disregard vestibular sensations in preference to flight by reference to the flight instruments alone.
If a roll movement occurs gradually, it may be below the level that a pilot can detect through the vestibular senses. The human threshold for detecting a short duration roll movement (5 seconds or less) is about 2° per second, and for longer durations, it is about 0.5° per second (Cheung, 2004). When flying, these sensory thresholds are often higher, particularly when a pilot’s attention is directed elsewhere (Benson, 1999). With limited or no external visual information, gentle rolls can continue unnoticed unless detected through the monitoring of instruments.
However, if noticed from instruments and corrected, the return roll to straight flight often occurs faster and is therefore perceived by the vestibular senses. The pilot may end up with the sensation that the aircraft is now in a turn (in the opposite direction). This can also occur in longer turns when the initial sense of roll stops during the turn. Commonly known as ‘the leans’, this sensation will wear off in time each occasion it is experienced, but unless the aircraft is flown solely by instruments, it has the potential to disorientate the pilot.
Instrument flying proficiency
Entering IMC conditions with no instrument rating carries a significant risk of severe spatial disorientation (Frederick, 2002; Batt and O’Hare, 2005; Transportation Safety Board of Canada, 1990; NTSB, 1989). Furthermore, Groff and Price (2006) found that the risk of an accident in reduced visibility increases nearly five-fold for pilots that did not hold an instrument rating.
When there are no external visual cues, the ability to fly on instruments is essential. The NTSB (1988) also noted that ‘tests and experience have shown that non-instrument-trained pilots or non‑proficient pilots are rarely successful in overcoming spatial disorientation’. Gibb and others (2010) add that a visual-only general aviation pilot encountering weather or night conditions is severely at risk because of their total inexperience, education, and training in using instruments.
Although instrument flying proficiency is a very important defence against spatial disorientation, many studies have shown overall flying hours has little, if any, influence on spatial disorientation accident rates (Gawron, 2000). Importantly, Gawron (2000) stated that the level of training and recency of the training to be factors, with those inexperienced in instrument flight, or with a lack of recent instrument flying, being at higher risk of spatial disorientation. In an effort to communicate how pilots can reduce the risk, Newman (2007) outlined:
It is advisable for pilots to undertake regular instrument flight exposures, preferably with an experienced instructor. This can be combined with some inflight disorientation demonstrations and upset/unusual attitude recovery practice (Braithwaite, 1997; Collins, Hasbrook, Lennon, & Gay, 1978).
Weather-related pilot decision making
A study by Wiegmann and Goh (2000) suggested a number of possible factors that contribute to instances of VFR flight into adverse weather conditions. These included:
- situation assessment (an inaccurate assessment by a pilot of the conditions)
- risk perception (a pilot may not appreciate the risks involved with continuing the flight)
- motivational factors (‘get-home-itis’ or personal/social pressures to complete the flight).
That is, pilots are seen to engage in VFR flight into IMC because they do not accurately assess the hazard (that is, the deteriorating weather conditions).
Specifically, one of the reasons why pilots may decide to continue a VFR flight into adverse weather is that they make errors when assessing the situation. However, pilots are often simply trying to make decisions to the best of their ability. The NTSB (2005) outlined that:
Even if pilots are able to correctly assess current weather conditions, they may still underestimate the risk associated with continued flight under those conditions, or they may overestimate their ability to handle that risk.
When outlining how weather-related decision making could be improved, Wiggins and O’Hare (1995) stated:
Because of the variable nature of operations in the aviation environment, weather-related decision making is often considered a skill that cannot be prescribed during training. Rather it is expected to develop gradually through practical experience. However, in developing this type of experience, relatively inexperienced pilots may be exposed to hazardous situations with which they are ill‑equipped to cope.
Wiggins and O’Hare (2003) also evaluated the effectiveness of a cue-based training system, which was designed to equip VFR pilots with the skills to recognise and respond to the cues associated with deteriorating weather conditions during flight. VFR pilots were more likely to use the cues following the training, with subsequent improvements in their weather-related decision‑making. CASA produced a Weather to Fly[17] education program which focuses on topics such as the importance of pre-flight preparation, making decisions early and talking to air traffic control, along with initiatives to help pilots establish personal minimums.
Related occurrences
The US NTSB investigated four accidents involving community service flights[18] in 2007 and 2008, which resulted in three Safety Recommendations being issued (see Identified community service flight risks below).
The ATSB has investigated one other fatal accident and one incident involving flights organised by Angel Flight Australia, which are summarised below. Additionally, a number of recent ATSB investigations examined VFR into IMC accidents.[19] Of these, two are summarised below, as is the ATSB research report AR-2008-045 Improving the odds: Trends in fatal and non-fatal accidents in private flying operations.
ATSB investigated Angel Flight Australia occurrences
ATSB investigation AO-2011-100
On 15 August 2011, the pilot of a Piper PA-28-180 Cherokee aircraft, registered VH-POJ, was conducting a private flight arranged by Angel Flight Australia, transporting two passengers from Essendon to Nhill, Victoria under VFR. The flight was arranged to return the passengers to their home location after medical treatment in Melbourne.
Global Positioning System data recovered from the aircraft indicated that when about 52 km from Nhill, the aircraft conducted a series of manoeuvres followed by a descending right turn. The aircraft subsequently impacted the ground at 1820 Eastern Standard Time, fatally injuring the pilot and one of the passengers. The second passenger later died in hospital as a result of complications from injuries sustained in the accident.
The ATSB found that the pilot landed at Bendigo and accessed a weather forecast before continuing towards Nhill. After recommencing the flight, the pilot probably encountered reduced visibility conditions approaching Nhill due to low cloud, rain and diminishing daylight, leading to disorientation, loss of control and impact with terrain.
ATSB investigation AO-2011-162
On 9 December 2011 a SOCATA TBM 700 aircraft, registered VH-VSV, departed Bankstown Airport for a private flight arranged by Angel Flight Australia to Merimbula, New South Wales. Onboard the aircraft were the pilot and one passenger.
The pilot was cleared to depart Bankstown control zone on a downwind departure from runway 11 left, however, the pilot mistakenly conducted an upwind departure. The aircraft penetrated Sydney controlled airspace by 2.3 NM and came within 1.2 NM horizontally with no vertical separation of another aircraft on approach into Sydney Airport and a loss of separation occurred.
The investigation highlighted the importance of developing a technique to ensure a clearance is processed, understood and actioned correctly. It is also important to clarify a clearance if any ambiguity exists. Finally, pre-flight planning is essential to ensure safe flight.
ATSB investigated VFR into IMC occurrences
ATSB investigation AO-2015-131
At about 1730 on 7 November 2015, the owner-pilot of an Airbus Helicopters (Eurocopter) EC135 T1, registered VH-GKK, departed Breeza, New South Wales, on a private flight to Terrey Hills, New South Wales. The flight was conducted under VFR and there were two passengers on board.
About 40 km to the south-west of the Liddell mine, the pilot diverted towards the coast, probably after encountering adverse weather conditions. Witnesses in the Laguna area observed the helicopter overfly the Watagan Creek Valley in the direction of higher terrain. The helicopter was then observed to return and land in a cleared area in the valley.
After 40 minutes on the ground, the pilot departed to the east towards rising terrain in marginal weather conditions. About 7 minutes later and approximately 9 km east of the interim landing site, the helicopter collided with terrain. The pilot and two passengers were fatally injured.
The ATSB found that the pilot departed an interim landing site under VFR in marginal weather conditions. The pilot likely encountered reduced visibility conditions leading to loss of visual reference leading to the collision with terrain.
ATSB investigation AO-2016-006
On the morning of 29 January 2016, a Piper PA-28-235 aircraft, registered VH-PXD, was on a private flight from Moorabbin Airport, Victoria to King Island, Tasmania. After passing over Point Lonsdale, the aircraft entered an area of low visibility. The pilot conducted a 180° turn and initially tracked back towards Point Lonsdale, before heading south over the ocean. After about 2 minutes, the aircraft was again turned right before entering a rapid descent. The aircraft impacted the water 6.6 km south-west of Point Lonsdale. All four occupants of the aircraft were fatally injured.
The ATSB found that continuation of the flight beyond Point Lonsdale, and towards an area of low visibility conditions, was likely influenced by the inherent challenges of assessing those conditions.
The ATSB also found that due to the presence of low cloud and rain, the pilot probably experienced a loss of visual cues and became spatially disorientated, leading to a loss of control and impact with the water. The risk of a loss of control in the conditions was increased by the pilot’s lack of instrument flying proficiency.
ATSB research report AR-2008-045
The ATSB research report Improving the odds: Trends in fatal and non-fatal accidents in private flying operations found that 44 per cent of all accidents and over half of fatal accidents between 1999 and 2008 were attributed to private operations.[20] These figures far surpassed the proportions for any other flying category, even though private operations contributed to less than 15 per cent of the hours flown in that decade.
Problems with pilots’ assessing and planning were identified as contributing factors in about half of fatal accidents in private operations, and about a quarter involved problems with aircraft handling. Other contributing factors associated with fatal accidents to a smaller extent were visibility, turbulence, pilot motivation and attitude, spatial disorientation, and monitoring and checking. Non-fatal accidents were just as likely to involve aircraft handling problems, but had fewer contributing factors than fatal accidents.
Action errors and decision errors were both common to fatal accidents. Violations, while less frequently found, were mostly associated with fatal accidents.
In light of the contributing factors that were associated with fatal accidents in private operations, the report provides advice to pilots for improving the odds of a safe flight. Pilots are encouraged to make decisions before the flight, continually assess the flight conditions (particularly weather conditions), evaluate the effectiveness of their plans, set personal minimums, assess their fitness to fly, set passenger expectations by making safety the primary goal, and seek local knowledge of the route and destination as part of their pre-flight planning. In addition, becoming familiar with the aircraft’s systems, controls and limitations may alleviate poor aircraft handling during non-normal flight conditions. Finally, pilots need to be vigilant about following rules and regulations that are in place—they are there to trap errors made before and during flight. Violating these regulations only removes these ‘safety buffers’.
Organisational information
Angel Flight Australia
Background
Angel Flight Australia (Angel Flight) is a charity that assists financially disadvantaged people who cannot readily access financial assistance from other sources, to access medical services that are not available locally. It was established in 2003 and was based on the model operating in the United States at the time. The Angel Flight website described the operation as:
a charity which coordinates non-emergency flights to assist country people to access specialist medical treatment that would otherwise be unavailable to them because of vast distance and high travel costs. All flights are free and may involve travel to medical facilities anywhere in Australia.
The Australian Charities and Not-for-profits Commission (ACNC) lists Angel Flight’s constitution. The objects in that constitution stated that Angel Flight:
… assists financially disadvantaged people throughout Australia by:
a) Arranging carriage of financially disadvantaged people with medical conditions, in non-emergency circumstances;
b) Arranging carriage of such people in aircraft which contain no specialised medical fittings or equipment;
c) Arranging carriage of such people in aircraft without any requirement for medically trained personnel to be on board;
d) Arranging carriage of such people on the condition that they are sufficiently fit to undertake normal travel without assistance, and in the case of children or persons with a disability, to travel with a carer who can render any assistance required;
e) Arranging carriage of such people without any charge being made and without any form of reward being received by the pilot, aircraft owner or the Company [Angel Flight] in respect of that carriage, provided however, that the Company [Angel Flight] may, from time to time, authorise reimbursement of the cost of fuel for flights;
f) Arranging, where possible, free air transportation of blood and blood products and transplant organs to needy recipients; and
g) Arranging further support, monetary or otherwise, to financially disadvantaged people in need of medical treatment in Australia.
h) Arranging ground transport at city venues for transportation of such people to and from medical or treatment centres, either by commercial taxi service or volunteer drivers/vehicle owners, and in the case of private volunteer drivers/vehicle owners, that no charge be made or reimbursement being received by the driver/vehicle owner, provided however, that the Company [Angel Flight] may, from time to time, authorise appreciation gift cards to be provided to drivers/vehicle owners.
For passengers (a patient and their travelling companion—if any) to be considered for a flight, a formal request must be submitted by a health professional registered with Angel Flight. In submitting the request, the health referrer certifies the patient and any travelling companion meet Angel Flight’s criteria of requiring financial assistance to travel for medical treatment that is not available locally.
Most flights co-ordinated by Angel Flight are conducted using volunteer pilots on flights classified as private operations, and Angel Flight did not hold an Air Operator’s Certificate (see Civil Aviation Safety Authority below). However, about 18 per cent of the passenger flights co-ordinated by Angel Flight were conducted on commercial RPT flights, with the cost of these flights covered by Angel Flight.
To enable the private flights to be provided to the passengers free of charge, Angel Flight negotiated waivers of the Airservices Australia landing and air navigation charges, and reimburses pilot fuel costs. As at June 2017 Angel Flight had co-ordinated the conduct of about 20,000 passenger carrying flights, referred to as ‘missions’, and had 3,180 registered pilots. A handbook provided to Angel Flight pilots specified that ‘it is the objective of this organisation to assist as many people as possible that need our services, within the scope of the Angel Flight charter and standards.’
Pilot and aircraft requirements
To volunteer for Angel Flight, pilots needed to have a minimum of 250 hours as pilot in command (PIC), with either 5 hours as PIC on the aircraft type for flight to be conducted under VFR, or 10 hours on aircraft type for flights to be conducted under IFR. They also needed access to a VH‑registered aircraft,[21] with public liability insurance. Pilots need to provide copies of their licence, aviation security identification card, and any required flight reviews, proficiency checks and medical certificate. Prior to being assigned to any planned flight, pilots have to re-confirm their license and currency requirements were met, that the aircraft was insured for public liability and all maintenance complied with relevant statutory provisions.
For this accident, consistent with Angel Flight requirements the pilot of YTM was appropriately licensed for the planned private VFR flight, had maintained currency and recency on the TB10 aircraft, and had undertaken numerous Angel Flight missions in the recent past, including flying the passengers involved in the accident flight. The aircraft was appropriately insured and maintained to complete the planned flight.
Pilot documentation
Once the minimum criteria were satisfied and a pilot was registered to conduct flights on its behalf, Angel Flight would send pilots a number of documents including a pilot handbook, a pilot affirmation form, its code of conduct, and information regarding work health and safety for volunteers.
The pilot handbook contained guidelines on how to complete a flight successfully on behalf of Angel Flight. It contained advice relating to the safety of the flight such as:
- Ability to cancel the flight: the pilot was responsible for the conduct of the flight and could cancel the mission for any reason. ‘No flight will be for time-critical or emergency situations…The passengers will be aware that the flight may be cancelled should the pilot have any safety concern.’
- Pilot competency: ‘Be competent. The release form signed by your passengers will show that they recognise the gains and risk. Act in a reasonable manner and be able to show that you know what you are doing.’
- Prepare alternate plans: ‘Even the best plans go astray. Develop a ‘Plan B’. For example, an alternate airport due to a NOTAM[22] being issued or a change in the weather’, and ‘get a full weather briefing immediately before flying the flight.’ ‘There are always alternatives, such as: waiting until later in the day, waiting until the next day…or even cancelling the flight.’
- Regulatory compliance: ‘CASA regulations must be adhered to for the flight to be legal…Angel Flight does not attempt to cover this issue. ... All pilots volunteering for Angel Flight are required by law to prepare for a flight in accordance with CARs and CASRs including but not limited to flight planning, weather briefing, pre-flight, airworthiness inspections, licensing etc. These subjects will not be addressed in this document.’
Additionally, when applying online for a flight, the following comment was displayed:
‘Please Remember: Never compromise safety in any way in order to complete a flight. Cancelling a flight is considered a demonstration of good judgement and will never be criticized.’
Flight planning requirements
Guidance provided by Angel Flight to its volunteer pilots stated that the PIC was wholly responsible for the planning, operation and management of the flight. Any topics considered to be part of PIC responsibilities, including flight planning, weather briefing, pre-flight, airworthiness, and licensing requirements, were explicitly not addressed in any Angel Flight documentation.
Pilots and passengers were made aware that if a flight could not be completed, that Angel Flight would do its best to make alternative provisions for the passengers. Additionally, passengers were aware that they may be required to make their own alternative travel arrangements.
Flight requests and pilot assignment
To initiate an Angel Flight mission, a flight request would be submitted by an Angel Flight registered health professional, along with a referral regarding the passenger’s medical condition, and all required signed passenger documents (see Passenger documentation). Angel Flight mission co-ordinators then posted the request details on an e-bulletin board, accessible to registered pilots and drivers. Flight details included origin, destination, date and details of the proposed flight, number and weights of passengers, passenger medical condition, and baggage requirements. Pilots then registered their interest in a flight, and once all required passenger and pilot documentation were confirmed, the flight was assigned. If no applications were made and the flight date was approaching, mission co-ordinators contacted pilots based in the area via email in an attempt to assign the flight. Where the flight could not be assigned, or the pilot cancelled at short notice, RPT flights would then be considered as an alternative.
For this accident, consistent with the Angel Flight processes, an initial flight request and all required forms were submitted by the health referrer about 2 weeks prior to the passengers’ first Angel Flight in May 2017. Following this, a subsequent trip request for regular flights was submitted to Angel Flight. Based on the passenger’s needs and the frequency of the flights it was determined that return flights once a fortnight could be supported. Four private flights had been successfully completed, with one of these flights being conducted by the pilot involved in the accident.
On being assigned the accident flight, additional information provided to the pilot of YTM included passenger contact details, information regarding the ground transport to and from the medical facility, and return flight details. For the two passengers involved in the accident flight, one was accessing medical services in Adelaide, and the other was a family member.
Pilot and passenger communication
On being assigned a mission, pilots were advised to contact all parties involved and confirm the schedule.
On the day of the accident, between 0850 and 0900, text messages were sent between the pilot and passengers. A further message was sent by the passengers just prior to the arrival of YTM into Mount Gambier at 1006. The ATSB was unable to establish the content of the messages.
Passenger documentation
Passengers acknowledged, through a Patient Guidelines Form, that the flight was not a charter or ambulance flight, and that the pilots and aircraft did not meet commercial standards relating to qualifications, training or maintenance requirements, as they were not a commercial flying operation. The documents also stated that it is important the pilot stay on schedule as set by the appointment time, location of the passengers and location of the appointment, and the presence of connecting pilots or drivers at each destination.
Passengers were also required to sign a liability waiver noting acceptance of aviation related risks; however, there was no information provided in the documentation package outlining the comparative risks between flight operation types (see Safety comparison between private operations and commercial air transport), nor guidance or direction to where this information could be found. The Angel Flight briefing paper stated ‘our volunteer pilots’ flight credentials exceed the requirements of the Civil Aviation Safety Authority and the aircraft meet specified CASA and insurance minimums.’ This referred to the minimum number of PIC hours required, including at least 5 hours on the aircraft type for VFR flight and at least 10 hours on type for an IFR flight.
Reporting of flight safety occurrences
Air Operator’s Certificate (AOC) holders are required by CASA to have a safety management system (SMS). One standard aspect of an SMS is for the operator to maintain a record of incidents and accidents (occurrences)[23] and safety hazards which are reported to them by its pilots and others. The organisation must examine and investigate these occurrences and hazards where necessary, find ways of reducing risks identified, and/or provide awareness education for pilots, in order to improve the on-going safety of its operation.
As Angel Flight is a charity and not an aviation organisation, it is not required to hold an AOC. Therefore there was no regulatory requirement for pilots to report to Angel Flight any safety hazards or occurrences that took place during a flight operated for it. Angel Flight only required its pilots to notify them if a withdrawal or suspension of its licence, ratings or endorsements occurred.
Angel Flight had implemented a voluntary fuel report, through which pilots submitted fuel records for subsequent reimbursement, which also included a comment section. This section was predominantly used to comment on the fuel usage; there was no request for any safety related information.
In response to the ATSB investigation AO-2011-100 into the 2011 fatal accident of an Angel Flight organised flight (see Related occurrences above), Angel Flight provided information in June 2013 that showed that it was aware of three accidents (including AO-2011-100) and two incidents that had occurred during the conduct of Angel Flight missions. These occurrences had been communicated to Angel Flight through a variety of informal channels. In response to two of the four non-fatal occurrences, Angel Flight requested the pilots involved provide further information and documentation in relation to the occurrences and, in one case, required that the pilot undergo remedial training and provide evidence of its satisfactory completion prior to undertaking further missions. These responses were additional and separate to any regulatory action taken by CASA in response to these incidents.
Civil Aviation Safety Authority
CASA is an independent statutory authority with the primary function of conducting the safety regulation of civil air operations in Australia and the operation of Australian aircraft overseas.
Under the Australian civil aviation regulations there were four separate classes of operations:
- regular public transport (RPT)
- charter
- aerial work
- private.
Different regulatory requirements apply to each class of operation, with RPT operations having the highest minimum standards and regulatory oversight, and private operations having the most limited.
Previous CASA advice, in relation to ATSB investigation AO-2011-100, outlined flights conducted on behalf of Angel Flight were classified as private operations. For flights conducted under private operations, all operational responsibility for the flight remained with the pilot in command (PIC). This was consistent with advice received from Angel Flight that it was not (and never had been), an AOC holder or operator.
CASA completed a regulatory review of the safety requirements outlined in the Civil Aviation Regulations and Civil Aviation Orders in 1996, with the revised legislation to be termed Civil Aviation Safety Regulations (CASRs). Following this review CASA identified the change in the operation classification, from the current four-tier system to a three-tier system, where all passenger carrying operations (RPT and charter) are to be combined into the same tier. This created an issue in relation to how Angel Flight operations could continue as private operations while carrying passengers as a service.
Discussion paper DP1317OS: Safety standards for community service flights
As part of CASA’s ongoing regulatory reform process, for each of the areas affected by the regulatory development, stakeholders were identified and consulted. Part of the consultation included the publication of a discussion paper DP1317OS – Safety standards for community service flights conducted on a voluntary basis’ in August 2014, for industry consideration and input regarding community service flights, and how they should be regulated under the new CASRs. The discussion paper considered the concept of community service flights as:
flights that are provided on a voluntary basis for public benefit. The term refers only to non-emergency flights provided as part of an organised voluntary or charitable activity and does not include the ‘one-off’ type of flight in which a pilot provides a flight to a friend or family member.
Prior to this discussion paper being published, CASA held preliminary consultation meetings with two charities identified as operating community service flights, which included Angel Flight, in which the proposed CASR operational regulations were discussed, along with their potential impact on established practices.
The discussion paper was to ‘stimulate discussion and invite comment’ from the industry and public. It outlined the objectives, background, key risks, and potential regulatory options under the proposed regulatory framework. The discussion paper acknowledged the valuable societal benefits provided by community service flights. The paper noted that full compliance with the proposed new regulations could result in community service flights becoming untenable, and therefore sought to establish an appropriate safety standard. Some of the key regulatory risks identified were varying pilot qualifications and experience, aircraft certification and maintenance standards, and pilot and aircraft selection for each flight. It was recognised that as the use of community service flights increased, these risk factors would become more significant without regulatory oversight.
At the time (2003) Angel Flight was established, it indicated to CASA that there was an expectation that 250-300 pilots would be conducting approximately 800 flights per year when fully operational. As these flights were being conducted as private flights, and were expected to constitute a small percentage of this regulated sector, CASA considered the overall risk impact was negligible, and a formal risk assessment was not conducted. In the period 2008-2017, an average of 1,686 flights per year were being conducted, and as at June 2017 a pool of 3,180 volunteer pilots were registered. Since that time (2003) other operators providing similar flights have also been established.
The paper identified that there was a lack of visibility of the conduct of community service flights, which in turn prevented a more informed view for evidence‑based decision making in this sector of the industry. It proposed 10 main options for consideration, ranging from administrative options through operational requirements, with the potential to combine a range of the proposed options, or consider additional options suggested through the consultation process.
The submissions received in response to the discussion paper highlighted strong opposition to the prospect of any regulatory involvement in the sector, indicating that community service flying would no longer be financially viable if any of the options were applied. Based on the submissions received, no regulatory changes were initiated, with the flights remaining as private operations with no additional regulatory requirements and no additional organisational-based risk controls.
Guidance material
CASA has developed numerous publications, videos and other education material to highlight and address the flight safety risks in private operations. Some of these included video series’ such as Weather to fly and Out ‘n’ Back, personal minimums checklists, online e-learning modules through AviationWorx, the Flight Safety Australia magazine, and safety seminars and workshops. Further, based on investigation outcomes and research studies, the ATSB also developed the Avoidable Accident series, which outlines common contributing factors to fatal accidents, and how to minimise the risks associated with these factors. Additionally, both the Aircraft Owners and Pilots Association (AOPA) Australia and United States AOPA provide education materials and training courses to their members addressing flight safety risks in private operations. The US AOPA also has material which directly addresses community service flight risks.
While no material in Australia has been specifically developed for pilots conducting community service flights, information regarding many of the flight safety risks and potential mitigating strategies is contained in information available to all private pilots.
Community service flights in the United States
Numerous organisations in the United States, generally referred to as volunteer pilot organisations, provided community service flights similar to Angel Flight Australia. All community service flights in the US are conducted as private flights. Each organisation was administered separately and operated within different geographical areas.
Regulator
United States regulations required volunteer pilot organisations to apply for exemptions if the flights included reimbursement of some or all of the flight costs incurred.[24] These exemptions relate to the fact that these community service flights are conducted as private flights, but compensation is received, resulting in the pilot paying less than their pro rata share of the operating expenses for that flight. They allowed the volunteer pilot of a charity organisation to be reimbursed some or all of the costs associated with the private flight. In doing so, these exemptions added operational limitations to manage risks associated with these types of flights.
Having assessed the volunteer pilot organisation submissions and identified regulatory risks, the United States aviation regulator, the Federal Aviation Administration (FAA), issued exemptions that contained conditions and limitations intended to raise the level of safety for these flights. Additional clarification of the FAA position was provided through the publication of a policy on community service flights (charitable flights) in February 2013. The policy outlined that this activity can be conducted safely by applying limits to organisations, pilots and aircraft, with the limitations outlined in the exemptions issued to each organisation. The requirements and operational considerations differ to some extent for each organisation, however all impose additional requirements in the following areas:
- pilot qualification and training programs
- minimum pilot qualifications
- documentation for each pilot and mission flown
- mandatory passenger briefings
- higher aircraft airworthiness requirements
- higher instrument flight rules operational minima (where applicable).
The FAA continuously updates these exemptions for each charity as necessary to best ensure these operations meet the required level of safety.
Identified community service flight risks
The United States NTSB investigation of four accidents in 2007 and 2008, which occurred during community service flights, resulted in three safety recommendations addressed to the Air Care Alliance (ACA)[25] in 2010. The safety recommendations[26] addressed the following aspects:
- The need to verify pilot currency prior to each flight.
- A requirement to inform passengers that the flight would not be conducted under the same standards that apply to a commercial flight.
- To develop, disseminate and implement written safety guidance, best practices, and training material addressing, at a minimum, aeronautical decision making, proper pre-flight planning, pilot qualification, training and currency, and self-induced pressure.
These areas were identified by the NTSB as increasing the risk of incidents and accidents involving community service flights.
While it was acknowledged that there was some constraint in the ability to address safety issues that are the responsibility of the PIC, it was also recognised that volunteer pilot organisations could provide tools to assist with making better decisions. In correspondence regarding the NTSB safety recommendation A-10-104, the ACA stated:
ACA seeks to strike that balance between leaving all decision making in the hands of the pilot in command, while still providing the tools through the [Volunteer Pilot Organisations] to assist them to make better decisions. The intent is to rely on the [Federal Administration Regulations] for requirements but also to provide the pilots with the tools to assess what is reasonable for their level of proficiency and the demands of the flight to be undertaken.
In response to these recommendations, and in conjunction with the Aircraft Owners and Pilots Association (AOPA) Foundation’s Air Safety Institute (ASI),[27] the online training course Public benefit flying: Balancing safety and compassion was developed. The course focused on pressures and risks associated with these flights, and included mitigation strategies to manage them. Some of the potential additional risks to flight safety when operating community service flights identified in this course were:
- managing passengers and passenger expectations
- proper pre-flight planning
- perceived or self-induced pressure.
For a period of time, this course, and various tools developed alongside it, were included specifically in the conditions and limitations listed in the FAA issued exemptions. However, more recently, as the FAA was not responsible for the content or quality control of the course, it has removed references to the course and tools, but added specific areas in the training program to address the identified risks. While it has been removed as a regulatory requirement, many organisations still require their pilots to complete the course, in addition to the minimum requirements contained within the relevant exemption.
The United States AOPA training course highlighted some of the areas pressure can arise from, and outlined some objective decision making strategies to assist pilots with recognising and managing these risks. A summary of each of these risks as identified in the training course is outlined below.
Managing passengers: Passengers often have limited knowledge and experience with light aircraft used in general aviation. For nervous or first time flyers, the pilot needs to be aware of and manage anxiety levels of the passengers, to ensure this does not become a distraction, particularly at critical stages of flight. For all passengers, and particularly those with little exposure to general aviation, a thorough passenger briefing can assist by outlining the forecast and expected flight conditions, discussing general aircraft safety and expected sounds during the flight, such as engine changes and gear extension/retraction, and the need for a sterile cockpit at various points in the flight. Periodically reviewing the passenger’s needs during the flight and informing them of progress can also assist in managing a passenger’s anxiety levels. If they are nervous or concerned this allows an opportunity to identify and discuss the concerns, and allows for appropriate deviations or breaks if required. Pilots should also outline go/no go decisions points and explain any back-up plans. This enables determination of suitable alternatives that meet the passenger’s needs, while not compromising flight safety. Conservative planning will help reduce any time pressures associated with delays or passengers requiring breaks during the flight. If delays are unacceptable, ensure passengers have a plan B, and maintain contact with trip co-ordinators, as they can assist in determining alternatives and help alleviate any stress felt by pilots from cancellations or delay.
Pre-flight planning: Proper pre-flight planning in the context of community service flights takes into account the additional considerations and pressures associated with this type of flying. An assessment of a pilot’s current state of physical and mental health, and their own capabilities and proficiencies is important in regard to the expected flight conditions. Development and implementation of personal minimums,[28] with requirements beyond the specified regulatory minimums, can assist in making safe, objective decisions in marginal conditions. Conservative time planning can avoid hurried passenger briefings and additional stress when delays occur. It is important to travel prepared for unexpected layovers, which may be due to unexpected weather, or passenger related instances, so that objective decision making is not influenced by a lack of preparation. Flights into unusual environments such as busy terminal areas, or less familiar airports with different procedures require thorough pre-flight planning to ensure familiarity with requirements, and for remote airports, obtaining local knowledge of weather patterns, runway layout and conditions can assist with safe decision making at times of higher workload. Pre-flight planning minimises in-flight decision errors because it removes the unforeseen element from situations that arise during the flight. Failure to carry out this prior planning can result in decisions being made under a situation of considerable stress and increases the likelihood of poor or incorrect decision making.
Perceived pressure: Perceived pressure was identified in the course as one of the biggest issues facing volunteer pilots. The pressure was often self-induced and motivated by the desire to please passengers and complete an agreed trip. Additionally, knowledge of a patient’s condition can put additional psychological pressure on the pilot, and needed to be recognised as a negative influence on objective decision making. The language used, including ‘missions’ in the context of these flights can also be interpreted that it is imperative the flight be completed. Pilots must remain aware that the volunteer flight is not an emergency. Maintaining contact with trip co-ordinators during times of delay or cancellation can help alleviate any pressure felt by the pilot in these situations.
Australian evidence of perceived pressures
In Australia, from December 2018 to January 2019, CASA sought public comment on proposed changes to community service flights. A summary of the submissions was provided in Summary of consultation on proposed safety standard – community service flights, and some submissions are available on the CASA website. The responses came from both the community and pilots, so not all respondents could comment on operational matters.
The CASA summary noted that while 10 per cent of respondents (22) commented that they believed community service flights were far more complex than other private flights, 19 per cent (42) considered there was no difference in complexity between community service flights and other private operations.
While not a specific question, some respondents discussed their views on operational pressures. Of the publically available submissions, 18 respondents, at least 12 of who were pilots who had conducted community service flights, identified that there were additional pressures and operational differences associated with this type of flying, when compared with other private flights.
Twelve respondents, including pilots who had conducted community service flights, commented that they did not believe there were any operational differences between community service flights and other private flights. For example:
Why is a community service flight different to any other private flight? The fact that a passenger may or may not know the pilot prior to the flight is irrelevant.
If I can fly people privately and the regulations deem that as being safe, I see no difference when it comes to CSFs [community service flights].
There is no difference between a PPL [private pilot licence] pilot transporting passengers from A to B for charitable purposes, and a PPL pilot transporting passengers from A to B for recreational travel.
I totally reject the suggestion that these volunteer community flights are different to any other private flight.
Why is it different to any other flight a passenger is a passenger in the non-commercial way. Also long as the pilot in command obeys the rules of there [sic] endorsements and is current.
However, as discussed above, other pilots provided submissions that show evidence that perceived pressures from community services flights do affect some pilots:
Having flown both critical EMS [emergency medical service] operations and pressured CSF flights,…. the pressures involved with CSF flights can be as great or even greater than full EMS operations, as the aircraft are usually single engine, the operation is single pilot, crewed by less competent and lower time pilots and at times, it is obvious that the passengers on the CSF flights are critically ill.
There have been too many incidents involving flights where passengers are in need to arrive at a medical appointment by a certain deadline which imposes the need to get them there by the pilot. These pressures can force pilots to fly in conditions that they would normally not operate in, and inexperienced pilots can and do find themselves in situations they should not be in. As a charter pilot ….
I think the nature of this flying - the transport of medically fragile patients and dealing with emotive relatives could benefit from a training package. It should cover special considerations for the transport of people with differing conditions in the aviation environment, medical divert considerations, mission pressures (patient having an episode etc).
Managing non aviation strangers with medical needs and often in less than perfect weather is an order of magnitude of difference from typical private ops with family when you choose to fly in perfect VFR weather, and have the option to change or cancel the flight if the weather deteriorates - and your family understands that. Saying no to strangers who need to get to medical treatment is hard.
Carrying pax [passengers] who are not your friends is a huge change for the average PPL.
The psychological factors for the pilot of you must not let vulnerable people down and of doing good work, helping sick disadvantaged people... The irresistible conclusion is that any CSF flight involving long distance transport of ill patients and patient family member has a complexity beyond any normal private flight.
There is an increased sense of responsibility carrying people who you may have never met before and a possible self imposed pressure to meet what might be seen as a commitment. It could be argued that the reason for VFR into IMC is the pressure of ‘having’ to get someone somewhere at a particular time. I would agree that is possible.
Although it is almost certain that at least some pilots at least some of the time have experienced operational pressures from community service flights that were beyond what is usually experienced during other private operations, the extent of this is difficult to determine. The ATSB considered conducting a survey of Angel Flight pilots to determine the extent of perceived operational pressure on Angel Flight pilots. However, this was not conducted for the following reasons:
- Obtaining accurate responses to questions designed to elicit insights into a pilot having experienced implicit social pressures depends on their awareness of it having happened. In that case, the validity of answers pilots give will be limited as some will only indicate an absence of awareness of their susceptibility to these influences rather than an absence of these influences.
- The social desirability of admitting to have been influenced by goals other than those of safety may be a challenge for some pilots.
- Due to publicity surrounding potential regulatory changes for community service flights after this accident (described above), there was a potential for some responses to be biased, either in an attempt to protect the reputation of Angel Flight, or to advocate for additional oversight or regulation.
- A large number of responses would need to be gained across a representative sample of Angel Flight pilots to allow for valid statistical tests to be conducted.
Safety occurrences during flights organised by Angel Flight Australia
The per flight risks associated with Australian community service flights[29] had not been established prior to this investigation. Two fatal accidents occurring on passenger-carrying flights organised by Angel Flight suggested that further understanding of the nature of non-fatal occurrences was necessary, to identify if differences with other private operations existed. Similarly, it would also identify if any differences could provide context to potential systemic safety concerns that may be present during Australian community service flights.
The risk to passengers on community service flights was a particular focus of this analysis. This is because the ATSB’s focus is on the risk to travelling public[30] and Angel Flight passengers are regarded by the ATSB as being consistent with this statement, as supported by Recommendation 2 of the Australian Senate Inquiry completed 23 May 2013.[31] However, an additional assessment of non-passenger carrying repositioning flights (flights to or from the pilot’s base prior to and following passenger carrying flights) was conducted to provide further context to the risk profile of these operations.
The analysis presented in the following section was focused on establishing a baseline of the safety risks associated with these flights. As noted above, twice the number of respondents believed that community service flights have no additional complexity to other private operations than respondents who believed they introduced additional complexities. However, Angel Flight stated that there are differences in the operational environments for many Angel Flight organised flights compared to other private operations. This analysis was intended to establish if there were differences and identify if there are any areas where Angel Flight organised flights are exposed to additional safety risks. This was conducted in order to direct efforts to improve safety, rather than to attribute blame or liability.
Safety comparison between private operations and commercial air transport
As Angel Flight conduct community service flights as private operations, an evaluation of private operations against commercial air transport (RPT and charter)[32] operations was conducted to compare the relative risk per flight. In addition to community service flights, such as Angel Flight, private operations include flights for pleasure and personal transport, parachuting operations and aerobatics. Non‑commercial flights for business are also included in this analysis. Although there are large differences between the types of flying conducted in private operations, the regulatory regime is the same, and as such, all of these operations were included to provide a holistic context of the relative risk of an accident occurring during an Angel Flight organised flight.
An ATSB research investigation published in 2010 (AR-2008-045 Improving the odds: Trends in fatal and non-fatal accidents in private flying operations) reviewed trends in accidents in private flying operations in Australia. This research found that 44 per cent of all accidents, and over 50 per cent of fatal accidents in the ten years 1999-2008 were attributed to private operations, even though they accounted for less than 15 per cent of hours flown in VH-registered aircraft in Australia.
This is consistent with data used in this analysis from 2008-2017 showing that private and business operations (including flights conducted on behalf of Angel Flight) in Australia have a disproportionate number of accidents compared to commercial air transport operations relative to the number of flights conducted (Figure 8). This shows that despite conducting only 21 per cent of flights, private and business operations had 77 per cent of accidents, and 84 per cent of fatal accidents from 2008 to 2017. Further data for the number of occurrences, flights and flight hours in each category are in Table B1 of Appendix B – Additional data.
Figure 8: Number of flights and accidents in private and air transport operations as a percentage of all air transport and private operations in Australia, 2008-2017
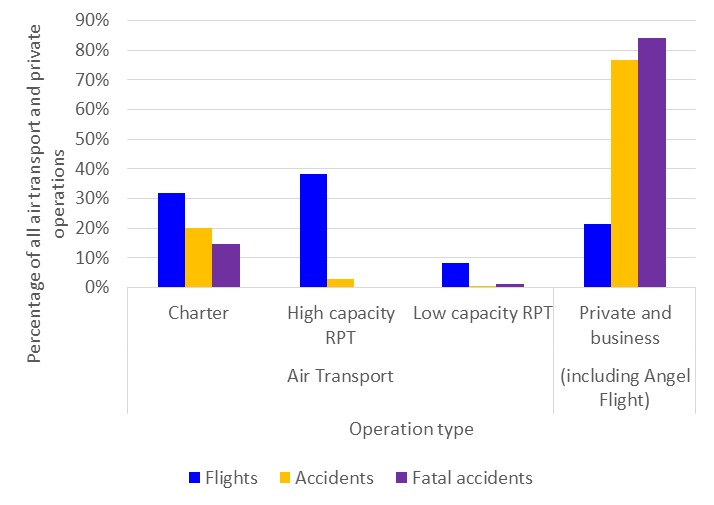
On average, flights conducted for private or business were at least:
- five times more likely to end in an accident when compared to charter operations
- more than 46 times more likely than high capacity RPT
- 69 times more likely than low-capacity RPT.
Furthermore, when considering fatal accidents, private and business operations were eight times more likely on average to end in a fatal accident compared to charter operations, and about 27 times more likely than low-capacity RPT. Note that there were no reported fatal accidents for high capacity RPT, and the single low capacity RPT accident (AO-2010-019) was during training with no fare-paying passengers on board.
Identification of Angel Flight related safety occurrences
Safety accidents and incidents (occurrences) must be reported by pilots and others to the ATSB in line with the Transport Safety Investigation Act and Regulations. It was unknown how many safety occurrences related to Angel Flight operations prior to this analysis, because safety occurrences were not always reported as involving a flight conducted for Angel Flight (nor were these required to be). To enable a safety comparison between Angel Flight and other types of operations, Angel Flight related occurrences needed to be identified. To achieve this, the ATSB obtained flight records from Angel Flight, which included departure and arrival locations, date and time of departure, and aircraft registrations covering the period between 2005 and 2017. Flights hours were not provided. Only data for the passenger carrying flights was provided, and Angel Flight was unable to provide data from 2003 and 2004.
Identification of occurrences relating to flights prior to, during and following privately conducted passenger carrying flights was performed by comparing the records provided by Angel Flight Australia and ATSB safety occurrence records. The identification process is described in Appendix A – Data analysis methods. A summary of each occurrence is located in Appendix C – Angel Flight occurrence summaries.
Through comparison with the ATSB aviation occurrence database, Angel Flight records served two primary purposes, to:
- identify safety accidents and incidents that occurred on passenger carrying flights (and repositioning flights) organised by Angel Flight
- calculate the likelihood of accidents and incidents per flight organised by Angel Flight.
A total of four accidents and 52 incidents were identified as occurring on 16,451 passenger carrying private flights conducted on behalf of Angel Flight between 2005 and 2017. A further 21 incidents prior to the passenger carrying flight and 28 incidents following passenger carrying flights were also identified.
For the purpose of the analysis, data from the most recent 10 years was used, from 2008-2017.[33] During this time, there were 47 Angel Flight occurrences identified from a total of 13,389 flights conducted as passenger carrying private flights. Of the 47, four were accidents (two of which resulted in fatalities, including this accident), and 43 were reportable safety incidents. This equated to about one occurrence every 2 and a half months between 2008 and 2017. Furthermore, during repositioning flights, 16 incidents and one serious incident were identified in flights prior to, and 21 incidents were identified in flights following passenger carrying flights conducted for Angel Flight during this period.
Normalisation for comparison of Angel Flight operations with others
The number of safety occurrences per 10,000 flights was used as the primary means for comparison of Angel Flight safety occurrences and other operations. Referred to as normalisation, dividing the number of occurrences by flights allows for comparisons between groups even when the overall level of activity differs between the groups.
As stated in the ATSB’s annual Aviation occurrence statistics report,[34] aircraft flights (or departures) are widely used as a measure of exposure, that is, the opportunity for an event to occur within a certain amount of flying activity. Flights were the appropriate normaliser for this analysis, as the focus was on the likelihood a passenger would encounter a safety occurrence during a flight. The number of flights are also generally considered a more appropriate normaliser measure than hours flown, as most accidents occur either during the approach and landing or departure phases of flight.[35] As such, flights are usually used for operational safety analysis by the ATSB and others (for example, the annual International Civil Aviation Organization Safety Report[36]). A further description of the rationale behind this selection can be found in Appendix A – Data analysis methods.
To allow comparison against other operations, data on flight hours and the number of flights in each operation was obtained from the Bureau of Infrastructure, Transport and Regional Economics (BITRE). The number of flights for private (including business), and charter operations was calculated by combining reported data from 2014 to 2017, and estimated data between 2008 and 2013. BITRE data between 2008 and 2013 was only available in-flight hours for each operation, with only an aggregated number of flights per year known for each aircraft. The estimation process for the earlier data is detailed in Appendix A – Data analysis methods.
Accident rates: Passenger carrying Angel Flight operations
For the purposes of this analysis, accidents involving passenger carrying[37] community service flights organised by Angel Flight were considered separately to accidents involving other private operations. The objective of this analysis was to understand the risk to passengers per flight.
Figure 9 shows the number of accidents, fatal accidents and fatal injuries per 10,000 flights for privately conducted passenger carrying flights organised by Angel Flight, commercial air transport, and remaining private operations. The number of flights in each category were used to identify the relative likelihood of accidents occurring per flight. Further data for the categories shown in Figure 9 can be found in Table B1 of Appendix B – Additional data.
Based on the two fatal accidents[38] occurring within 13,389 privately conducted passenger carrying Angel Flights between 2008 and 2017, statistical analysis showed it is very likely[39] that there is an increased likelihood of a fatal outcome during a community service flight conducted on behalf of Angel Flight compared to other private operations, and almost certainly higher than all commercial air transport. This indicates that it is almost certain that the nature of passenger carrying Angel Flight operations differ from the other operations, and that these differences have resulted in the higher likelihood of a fatal accident per flight. The average likelihood of a fatal accident involving an Angel Flight organised passenger carrying flight was more than seven times higher than other private flights (purple bars in Figure 9).
The accident rate per 10,000 flights in Angel Flight passenger carrying operations was likely39 to be greater than other private operations, with almost three accidents per 10,000 flights for Angel Flight operations compared to about 1.5 accidents per 10,000 flights in other private operations (yellow columns in Figure 9).38 The accident rate per 10,000 flights for both private operations for Angel Flight and other private operations were considerably higher than commercial air transport.
Figure 9 shows further comparisons between the different operational categories of the accident and fatal accident rates.
Figure 9: Total accidents, and fatal accidents and injuries, by type of operation per 10,000 flights in Australia between 2008 and 2017
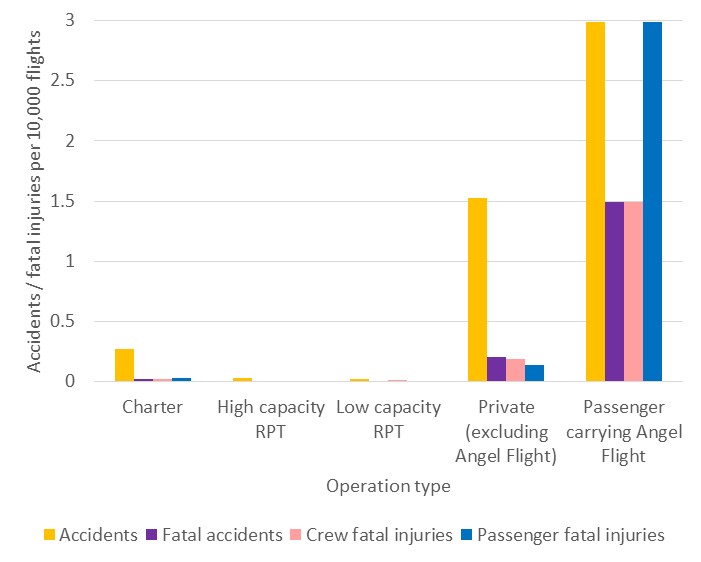
Passenger carrying community service flights organised by Angel Flight always carried at least one passenger. Consequently, more people were likely to be exposed to the risk of a fatal injury during an accident involving an Angel Flight compared to other private operations (pink bars of Figure 9). As the two fatal accidents involving Angel Flight were not survivable, the four passenger fatal injuries between 2008 and 2017 presented a higher risk of fatal injury per flight than all other operations compared (blue bars of Figure 9). The average exposure to passenger fatality per flight was 98 times higher than charter operations, and there were no fatal injuries recorded for passengers in high or low capacity RPT.
Compared to other private flights, the passenger fatal injury rate per flight was 21 times higher for flights conducted on behalf of Angel Flight. This was driven by both the higher average occupancy of Angel Flight fatal accidents (2 passenger fatal injuries in each fatal accident) compared to other private flights (0.7 passenger fatal injuries per fatal accident) and higher fatal accident rate compared to other private operations, and is expected to represent an ongoing increased risk.
Characteristics of passenger carrying Angel Flight occurrences
All safety occurrences reported to the ATSB are classified in accordance with the ATSB’s three-tiered safety occurrence taxonomy.[40] Due to the relatively smaller number of Angel Flight occurrences, the statistical analysis conducted focussed on the second tier types of occurrences. The number of occurrences in each occurrence type category were calculated for Angel Flight and other private occurrences for comparison. Further details can be found in Appendix A – Data analysis methods.
Privately conducted passenger carrying community service flights organised by Angel Flight had an average likelihood of 35 occurrences23 per 10,000 flights based on the 47 safety occurrences (4 accidents and 43 incidents) between 2008 and 2017. This was considerably higher than other private operations with an average of seven occurrences per 10,000 flights.
Due to the disproportionate average rate of safety occurrences per flight in comparison to other private operations, an in-depth analysis was conducted. The aim was to identify if any systemic trends existed within Angel Flight operations that may provide opportunities for safety improvement, by identifying and explaining the more common types of occurrences contributing to the higher rate of safety occurrences.
To aid this process, statistical comparisons between passenger carrying Angel Flight operations and other private operations were conducted for the different types of occurrences.[41] Figure B1 in Appendix B – Additional data shows the main groups of reported occurrences for Angel Flight passenger carrying flights between 2008 and 2017. A complete list of results showing all differences in types of occurrences between reported Angel Flight occurrences and other private operations are shown in Appendix B – Additional data tables B2 to B7.
The following areas were identified where Angel Flight occurrences were disproportionately higher[42] than other private operations per flight, and are displayed in Figure 10:
- runway events – incursions and landing/departing on the wrong runway
- operational non-compliance
- communications breakdowns
- Air Navigation Service Provider (ANSP) errors
- flight preparation/navigation
- aircraft separation
- airframe-related issues - landing gear/indications
- airspace infringement
Figure 10 illustrates the rate of each category of reported occurrences per 10,000 flights for Angel Flight flights (shown in blue), and other private operations (shown in red). Numbers above each column are the total number of occurrences identified for each operation category.
Figure 10: Largest statistical differences between occurrence type categories where passenger carrying Angel Flight operations were greater than other private operations, 2008-2017, as a rate per 10,000 flights (numbers indicate number of occurrences)
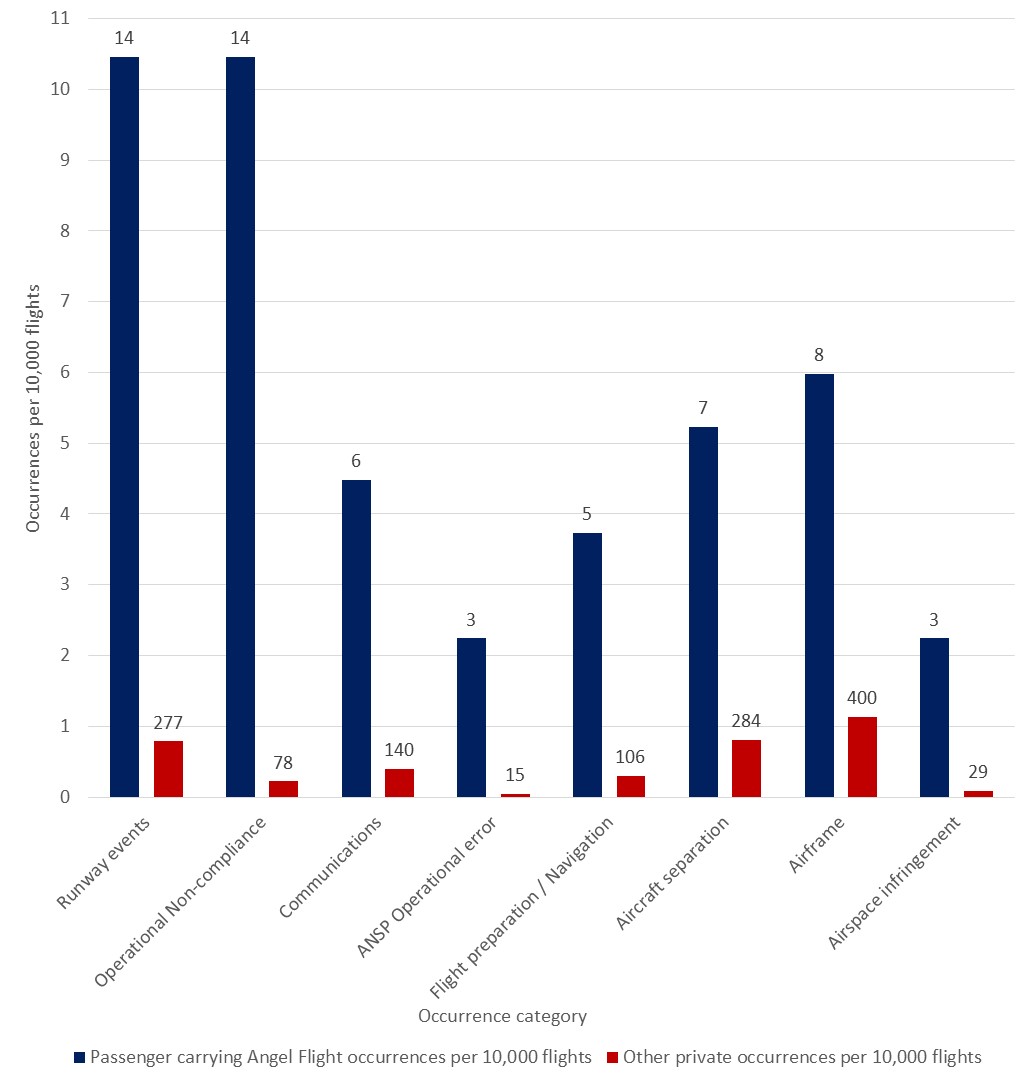
Runway events included runway incursions, and landing, departing or approaching the wrong runway, at times resulting in consequential missed approaches for other aircraft.
Communication breakdown occurrences included incorrect read backs, not using the correct frequency and misinterpreting verbal instructions. These occurrences resulted in loss of communication, and additional co-ordination requirements for ATC to ensure required aircraft separation is maintained.
Air Navigation Service Provider errors were also elevated in comparison to other private operations. This probably relates to flights conducted on behalf of Angel Flight entering controlled airspace relatively more often per flight compared to the collective average of other private operations. However, while elevated, the Angel Flight rate is lower in contrast to other occurrences more likely to be reported in controlled airspace, such as operational non-compliance, runway events and communications. This probably indicates that the other elevated rate of other occurrence types cannot be explained by the increased frequency of flights into these locations alone, and that other factors are likely to be present.
Flight preparation and navigation occurrences during Angel Flight passenger carrying flights included VFR into IMC, being lost or unsure of position, and flight below minimum altitude. These types of occurrences were notable due to being identified in both fatal Angel Flight accidents. Further, VFR into IMC accidents result in a fatal accident in a quarter of the instances reported to the ATSB. Air traffic control (ATC) provided assistance in other cases, to assist in vectoring aircraft out of cloud or to provide navigational assistance. The risks to flight safety for these types of occurrences are significant, and discussed in Risks of flying in areas of reduced visual cues above.
Airspace related occurrences included entering controlled airspace without a clearance (airspace infringements), not maintaining assigned altitudes or headings and not complying with published procedures or verbal instructions (operational non-compliance), and flying too close to other aircraft (aircraft separation). Operational non-compliance and airspace infringement occurrences all resulted in an additional safety event, such as an additional workload for ATC to maintain separation standards, loss of separation, and diversion of other traffic.
Airframe‑related issues predominantly involved landing gear indications and included mechanical faults resulting in landing gear not retracting, landing gear failure to extend, and gear indication failures or misinterpretation. One of these occurrences resulted in the collapse of the undercarriage on touchdown, and substantial damage to the aircraft.
Although Figure 10 shows occurrence type categories where flights conducted on behalf of Angel Flight were statistically more likely compared to other private operations, there were a number of occurrence categories that were similar or less likely. Most notably, powerplant and propulsion issues, in particular engine failures or malfunctions, were considerably lower in flights conducted on behalf of Angel Flight compared to other private operations. Fuel related occurrences were also relatively lower in flights conducted on behalf of Angel Flight compared to other private operations, driven mainly by the absence of fuel starvation. All areas of comparison are shown in Appendix B – Additional data tables B2 through to B7 and are grouped by categories shown in Figure B1.
The considerably higher rate of safety occurrences during passenger carrying flights organised on behalf of Angel Flight compared to other private operations is likely indicative of a different overall operational environment. The occurrence category comparison indicated that it is almost certain that additional operational risk factors are present in Angel Flight community service flights. In particular, this is shown by relatively more occurrences related to runway events, airspace related issues, communications, flight preparation and navigation and airframe issues. Analysis of the occurrences indicated that they were not attributed to a small number of pilots, rather, that the occurrences are spread across the volunteer group, with many pilots having similar, single occurrences, and therefore probably due to broader systemic issues, rather than a small subset of pilots within the Angel Flight group.
Angel Flight repositioning flights occurrences
While passenger carrying Angel Flight occurrences were the focus of the analysis, the elevated occurrence categories identified in the repositioning flights analysis were consistent with the passenger carrying flight analysis, with the comparative data presented in Appendix B – Additional data.
While the occurrence rate was not as elevated as the passenger carrying flights, the repositioning flights were elevated in comparison to other private operations. The passenger carrying rate of occurrences per 10,000 flights was more than twice as high as the non-passenger carrying rate. Furthermore, the non-passenger carrying Angel Flight occurrence rate was more than twice as high as the average of other private operations, with passenger carrying Angel Flights being more than four times higher. This indicates that each of the three groups have a different safety risk profile, with Angel Flight passenger carrying flights having the highest likelihood of a safety occurrence per flight. Results of this comparison is shown in Table B2 of Appendix B.
Consideration of alternative options
The investigation identified that on the day of the accident, there was an RPT service on the same sector (Mount Gambier to Adelaide), scheduled to depart within 15 minutes of the planned private Angel Flight. As outlined in Safety comparison between private operations and commercial air transport, RPT flights have a lower relative safety risk than private operations.
In the overview section of Angel Flight’s Health professionals flight request forms document, there is acknowledgement that regular public transport (RPT) flights between capital cities are much more economical than using light aircraft:
For long haul or capital city to capital city transfers Angel Flight does not engage our volunteer pilots as commercial flights are much more economical. Angel Flight Australia does save some funds available to cover the cost of commercial flights however we reserve these funds for use when weather conditions prevent the flight of light aircraft and the travel date is imperative.
Angel Flight did not actively consider RPT flights as a primary option where they were available, unless the flights were for capital city transfers. This was confirmed by Angel Flight, who further stated that it considered using RPT flights, other than as a back-up or for long distance compassionate flights, as inappropriate and not aligned with the model for which the charity was constituted. Angel Flight stated that its ‘policy is to use volunteer pilots wherever possible;’ RPT flights are only considered if the pilot cancels the private flight, and the passengers are located at an RPT base, the RPT flights are available, and the times suitable.
Identification of alternative options
Considering the lower relative safety risk of RPT flights, the ATSB undertook further examination of RPT alternatives and comparative sector costs. A review of all completed Angel Flight private flights was conducted to determine how often an alternative option was available. Using Angel Flight records, the review identified that between 2005 and 2017,[43] 3,669 flights were conducted using RPT (18 per cent), and 16,356[44] as private flights (82 per cent) (inner circle Figure 12). Private flights were mainly conducted in south-eastern Australia, covering the states of Victoria, south-eastern Queensland, eastern New South Wales and the south-east of South Australia (Figure 11).
Figure 11: Passenger carrying private flights flown on behalf of Angel Flight 2005-2017

Figure 12: Breakdown of regular public transport options for flights flown on behalf of Angel Flight in 2005-2017
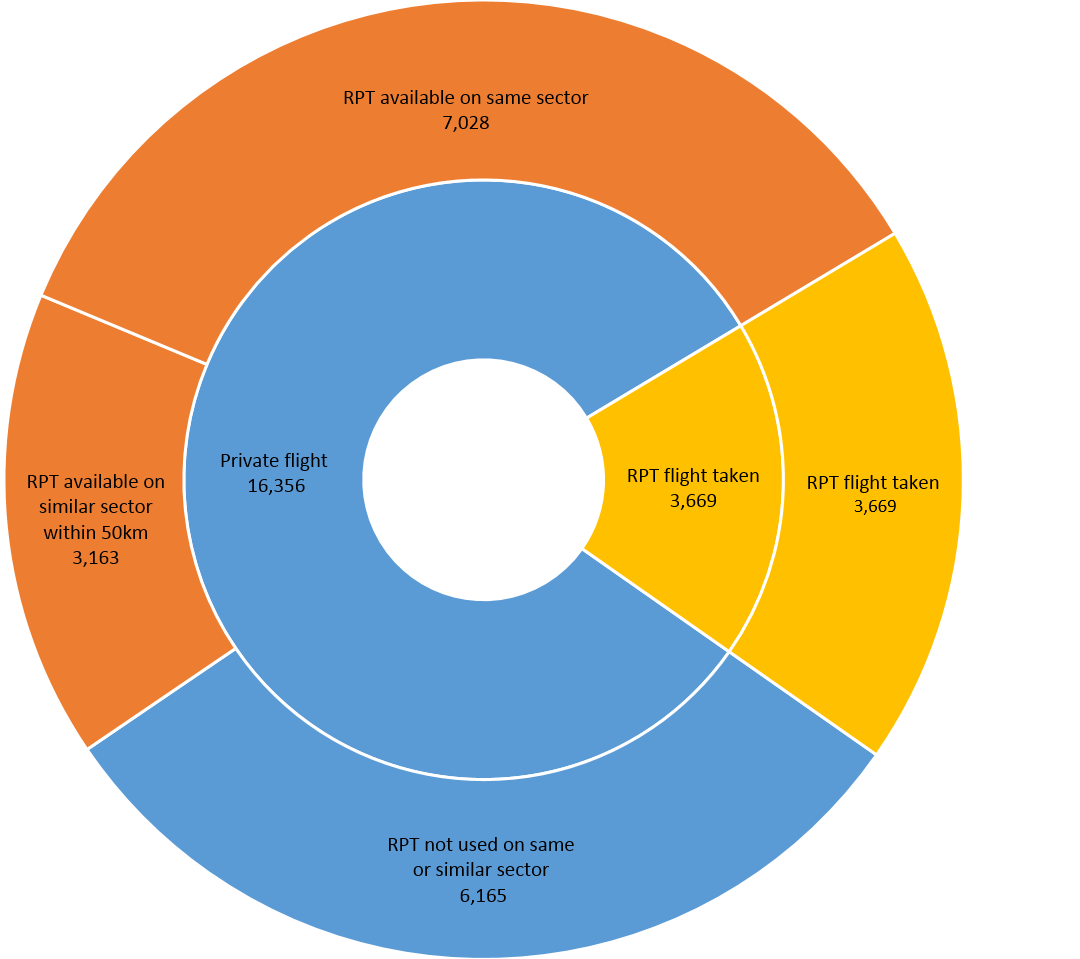
Financial considerations of RPT use
The Angel Flight constitution quoted above determined that passengers would not have to pay for their own flights. Further, although the Angel Flight constitution allowed for pilots to be reimbursed for fuel costs ‘from time to time’, Angel Flight reported that pilots did not claim for fuel costs for between 10 and 15 per cent of completed flights. As such, at least 85 per cent of privately-operated flights on behalf of Angel Flight have come at a cost to the charity.
It was evident that RPT options were available for a considerable percentage of flights (over two-thirds of all conducted flights). However, since the service is funded by a charity, the costs involved are relevant when considering the choice between RPT and private operations. The ATSB conducted a cost-analysis of available RPT flight costs compared to the estimated fuel cost of a light aircraft (which Angel Flight provide the volunteer pilots) for the accident sector. This was determined using data provided by Angel Flight.
The two passengers involved in the accident had been flown from Mount Gambier to Adelaide (return) on two previous occasions. For each of those four flights, fuel costs had been claimed by the pilots.[45] The total fuel costs claimed of the four flights was $2,021. Angel Flight documents also included information related to ground transport times. That is, the time required to travel from the airport to the appointment and the planned return to the airport for the return flight. A review of the available RPT schedules showed that suitable return flights were available on both of those days, accounting for the additional time requirements associated with RPT travel. According to the publically available costs, economy flights on these sectors were between $175 and $250 per person per flight. For two people for two return flights, the RPT option would have cost Angel Flight between $1,400 and $2,000, comparable to the privately claimed fuel costs.
The pilot flying the accident flight had previously flown these passengers, on the same sector (one way from Mount Gambier to Adelaide), using the same aircraft with similar repositioning flights, and had claimed $361 in fuel costs. On the morning of the accident flight, two RPT departures from Mount Gambier would have had the passengers arrive in time for the scheduled medical appointment, and this had been nominated as a backup in the case of the private pilot cancelling the flight. For two passengers on the RPT flight, the potential costs would have been between $350 and $500.
As this accident sector analysis demonstrated that suitable RPT flights were available for a comparable cost for this route, the analysis was extended to other sectors flown on behalf of Angel Flight. The purpose of the analysis was to provide a generalised indication of an RPT alternative being available where data analysis had confirmed that these services had been historically utilised by Angel Flight. Where an RPT option was available, the potential costs were compared with the estimated theoretical fuel costs.
To estimate the potential fuel costs for a private flight, the Angel Flight fuel reimbursement guidelines were used. Consistent with the evidence provided, a multiplier for the repositioning flights was included in calculating the total distance flown. This was a conservative estimate, with the distance between the departure and destination pairs based on a direct route, which did not consider IFR waypoints and approaches.[46] Fuel costs were based on the average June 2017 price per litre.
RPT costs were estimated by using publically available sources, planned for a same day return trip. The daily return trip was calculated as if purchased between 4 and 7 days ahead of the planned departure, consistent with the Angel Flight required notice. These return trips were then averaged to provide an average return cost per person.
To compare the costs between an RPT and private flight it was assumed two passengers (a patient and a companion) were travelling. The cost of a private flight was then compared to the cost for two people to fly that same sector using the averaged RPT option. This analysis was conducted using the 22 sector pairs, which accounted for the highest proportion of private flights flown where Angel Flight had previously used an RPT flight. This analysis showed that for two-thirds of the assessed sectors, the average RPT costs were cheaper than the potential fuel costs for a private flight. This conservatively indicated that of the 62 per cent of private flights where RPT options had previously been used, at least an additional 15 per cent of flights could have been conducted using RPT operations for a comparable or cheaper cost than a private flight.
Other considerations regarding the suitability of RPT
Angel Flight outlined the following reasons that it considered made the use of RPT unsuitable to assist its clients to attend appointments:
- The Angel Flight constitution and its policy to use volunteer pilots in private aircraft.
- The volunteer drivers’ ability to assist with carry-on luggage to and from the aircraft is limited at RPT ports.
- Many passengers are not located nearby commercial airports.
- Many regional locations only have RPT operating on certain days, and flights may not be available on required dates.
- The RPT timetabling does not allow for lengthy cross-city travel.
- Additional travel time for RPT flights – check in, luggage collection (if needed), ground transport delays.
- Private flights allow passengers to travel to their appointment and return home in one day, avoiding accommodation costs in major cities.
- Additional parking costs apply for volunteer drivers at RPT ports.
- Passenger cancellation at last minute, with associated non-refundable RPT costs.
- Not all passengers are recommended to travel RPT (e.g. immunocompromised).
- Number of passengers travelling.
While Angel Flight stated its objective was to use volunteer pilots in private aircraft, this policy was not documented, nor was it a requirement in its constitution. Additionally, Angel Flight’s constitution indicated that commercial taxi services could be used for ground transport. Health referrer information and passenger guidelines indicated that Angel Flight did not automatically arrange for ground transportation at the destination, and that passengers and health referrers must endeavour to arrange ground transport before requesting this service from Angel Flight. Further, this transport was only to and from the treatment facility, and did not include assistance between the passengers’ home and the originating aerodrome. Passengers were also requested to keep their luggage requirements to a minimum, due to the limited space and weight requirements of light aircraft.
As outlined in Identification of alternative options, analysis of the flight sectors indicated 62 per cent of private flights were over sectors that had previously used an RPT option, either on the same sector or with 50 km. This implied that many passengers were located near commercial airports. Additionally, 43 per cent of those flights conducted privately were conducted on an identical sector to an RPT service, indicating that there would not be additional travel requirements for the passengers. The 22 per cent of private flights reviewed had suitable daily return RPT flight options 4 or 5 days a week. Moreover, Angel Flight passenger carrying sectors were required to be completed in daylight hours; with delay at any point risking the return flight not being completed in daylight hours—a constraint that does not apply to commercial flights.
From the evidence provided approximately 35 per cent of completed flights were for passengers travelling alone, with two travellers (patient and one companion) accounting for a further 31 per cent, and about one-third of organised flights carrying three or more travellers. Of the flights flown, about 45 per cent of aircraft used by Angel Flight had a maximum capacity of three passengers, and with limited aircraft size and weight restrictions, baggage was also limited.
There was no available evidence that indicated the rate of short-notice cancellation by passengers. While short-notice cancellation may result in non-refundable RPT costs, this is dependent on the cancellation policy in place. With respect to a private flight, a potential fuel cost may be associated with the repositioning flights of a late cancellation.
__________
- A propeller system that incorporates a governor to maintain the selected engine speed.
- Aircraft in this category are appropriately equipped to be operated in instrument meteorological conditions under instrument flight rules.
- Approach minima refers to the height and distance at which the runway must be visible to the pilot to continue the approach to landing. If the runway environment is not in sight, a missed approach must be initiated. Departure minima refers to cloud ceiling and visibility requirements.
- Aircraft approach categories refer to the speed at which an aircraft approaches a runway for landing. Category A approach speeds are less than 91 kt, Category B approach speeds are between 91-120 kt, and Category C are between 121-140 kt.
- Available instrument approaches to Mount Gambier airport consisted of RNAV (GNSS), NDB and VOR. These different approaches refer to the navigation aids (ground based, aircraft equipment and/or space based) required to conduct the approach.
- Area forecast (ARFOR): routine forecasts below 10,000 ft AMSL for designated areas and amendments when prescribed criteria are satisfied. Australia is subdivided into a number of forecast areas.
- Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
- Aerodrome forecasts (TAF) are a statement of meteorological conditions expected for a specified period in the airspace within a radius of 5 NM of the aerodrome reference point.
- INTER: an intermittent deterioration in the forecast weather conditions, during which a significant variation in prevailing conditions is expected to last for periods of less than 30 minutes duration.
- Special reports (SPECI) are aerodrome weather reports issued whenever weather conditions fluctuate about or are below specified criteria.
- Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under Instrument Flight Rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
- The weather to fly education program is also available in DVD format via the CASA website.
- Variously referred to as charitable medical transport, public benefit or humanitarian flights in the United States. For clarity in this report, all such flights will be referred to as community service flights.
- All of the following investigation reports are available on the ATSB website at www.atsb.gov.au
- This is consistent with the statistics for the period 2008-2017, which are presented in Safety comparison between private operations and commercial air transport
- VH aircraft are registered with the Civil Aviation Safety Authority. In Australia, some light aircraft can be registered with various recreational aviation organisations.
- Notice(s) to Airmen (NOTAM): A notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
- Occurrences consist of accidents and incidents. Accidents are defined as an occurrence involving an aircraft where a person dies or suffers serious injury, or the aircraft is destroyed or seriously damaged. Incidents are defined as an occurrence, other than an accident, associated with the operation of an aircraft which affects or could affect the safety of operations (ICAO Annex 13).
- Those charity organisations where pilots donate all costs are not required to have exemptions.
- The ACA is a league of nationwide humanitarian flying organisation and is the primary forum for volunteer pilot organisations in the US. The four accident flights were organised by three separate charities, all who were members of the ACA.
- National Transportation Safety Board Safety Recommendation A-10-102 through 104. See www.ntsb.gov for more information.
- AOPA ASI provides free educational resources and supports initiatives to improve general aviation safety through AOPA members.
- Personal minimums refer to a pilot’s personal set of rules and criteria for deciding if and under what conditions to fly or to continue flying based on their knowledge, skills and experience (adapted from Parson, 2006). They act as a ‘safety buffer’ between the demands of the situation and the extent of the pilot’s skill.
- While other organisations have been established which conduct community service flights in Australia, Angel Flight has been the longest established, and has operated in excess of 90% of the completed community service flights.
- Minister’s statement of expectations for the ATSB 1 July 2017 to 30 June 2019 states that the ATSB will continue to give priority to transport safety investigations that have the potential to deliver the best safety outcomes for the travelling public, 30 May 2017. www.atsb.gov.au/about_atsb/ministers-statement-of-expectations/
- Recommendation 2: The committee recommends that the minister, in issuing a new Statement of Expectations to the ATSB, valid from 1 July 2013, make it clear that safety in aviation operations involving passengers (fare paying or those with no control over the flight they are on, for example, air ambulance) is to be accorded equal priority irrespective of flight classification. Inquiry into Aviation accident investigations, 23 May 2013, Australian Senate.
- Commercial air transport refers to scheduled and non-scheduled commercial operations used for the purposes of transporting passengers and/or cargo for hire or reward. This includes:
- RPT, or Regular Public Transport operations are conducted in accordance with fixed schedules to and from fixed terminals over specific routes – this is divided into High Capacity RPT, for larger aircraft with more than 38 seats, or having a maximum payload capability exceeding 4,200 kg, and Low Capacity RPT for all other (relatively smaller) aircraft less than either of the aforementioned limits.
- Charter operations involve the carriage of passengers and/or cargo on non-scheduled flights by the aircraft operator or operator’s employees for trade or commerce. - The most recent 10 year period was used to evaluate the contemporary safety of operations, as is routinely done in ATSB analysis such as the annual Aviation occurrence statistics report.
- For example, Aviation Occurrence Statistics 2008 to 2017, (AR-2018-030)
- The ATSB Aviation Occurrence Statistics only normalises by hours flown (rather than flights) when: the number of flights is unknown (due to historical data collection limitations); or the analysis relates to general aviation operations that are exposed to greater risk outside of take-offs and landing such as agricultural and search and rescue aircraft performing low flying as part of normal operations.
- International Civil Aviation Organization (2018). ICAO Safety Report 2018 Edition, Montréal, Canada
- The repositioning flights for the purpose of an Angel Flight organised passenger carrying flight were not included in this analysis, however, a separate analysis was performed for reference including these flights.
- There were no accidents recorded for repositioning flights prior to or following passenger carrying Angel Flights: results for repositioning flights combined with passenger carrying Angel Flights are shown in Appendix B – Additional data Tables B1 and B2.
- Monte-Carlo methods using 1,000,000 samples from beta distributions using Haldane Prior (nil prior information, a0=b0=0) generated from the number of occurrences and flights from 2008 to 2017: - 1. All accidents: Passenger carrying Angel Flight, Beta(4,13385) > other Private operations, Beta(539,3526540), P = 0.85
2. Fatal accidents: Passenger carrying Angel Flight, Beta(2,13387) > other Private operations, Beta(72,3527007), P = 0.97. - The occurrence type taxonomy is the coding scheme for recording ‘What’ happened in a safety occurrence, and can be found on the ATSB’s website: www.atsb.gov.au/avdata/terminology.
- Due to differences in reporting requirements in the Transport Safety Investigation Regulations for commercial air transport (compared to private operations) and nature of commercial air transport, these were not included in the following analysis.
- Monte-Carlo methods were adopted using 1,000,000 samples from beta distributions generated from the number of occurrences in each category and total flights using Haldane Prior (nil prior information -a0=b0=0) testing Angel Flight operations > other private operations from 2008 to 2017. Results shown in descending order of probability from left to right – P > 0.999 for results from the left up to airspace infringements. A complete list of all test results (including those not shown) can be found in Appendix B – Additional data Tables B2-B7
- This analysis used all flight data Angel Flight provided to the ATSB, covering 13 years. This differs from the safety occurrence analysis which only used the most recent 10 year period.
- Eighty-four private flights were excluded from the analysis – see Appendix A – Data analysis methods: Flight records used in RPT analysis for further information.
- Fuel reimbursements included fuel for repositioning flights from and return to the pilot’s home aerodrome as well as the passenger carrying flights.
- Angel Flight determined the acceptable fuel use using IFR waypoints and approaches, with diversions factored in; this would increase the allowable fuel costs for a private flight.
Safety analysis
Introduction
The ATSB identified that there were no mechanical defects present, and that the aircraft was serviceable at the time of the accident. A review of the pilot’s medical records and postmortem examination results did not identify any acute or pre-existing medical conditions that may have contributed to the accident. In that context, the safety analysis will examine the factors that led a visual flight rules (VFR) pilot to fly into instrument meteorological conditions, land, and subsequently depart in similar conditions. In addition, identified flight safety risks related to community service flights, Angel Flight Australia risk controls, and regulatory aspects of community service flights will be discussed.
Pilot decision to depart Mount Gambier
As part of the investigation, careful consideration was given to the possible reasons behind the pilot’s decision to depart Murray Bridge, and to then land and depart from Mount Gambier Airport in instrument meteorological conditions (IMC). On departure from Murray Bridge at about 0800, the weather forecasts indicated marginal visual meteorological conditions (VMC) at Mount Gambier, but with conditions expected to improve from 0930, with the pilot’s planned arrival between 0930 and 1000. The Mount Gambier aerodrome forecast (TAF) released at 0942 also indicated marginal but improving conditions compared with the previous TAF. However, the SPECI and live weather observations available to the pilot en route indicated that the observed conditions, while improving, were not suitable for VFR. While it could not be determined if the pilot accessed this information en route, weather-related diversions were noted in the recorded flight path, and radio calls requesting the cloud base at Mount Gambier were made.
It is not known if the pilot fully comprehended the unsuitability of the weather conditions for visual flight on approach to and at Mount Gambier, or if any other options were considered. However, the following are some of the possible reasons for deciding to continue to land, rather than divert or hold, and subsequently depart. These have been outlined to highlight the risks to others, and are based on the three factors listed by the Wiegmann and Goh (2000) empirical study of factors affecting pilot decision-making relating to VFR flight into adverse weather: situation assessment, risk perception and other motivational factors.
Situation assessment
The ability to assess a situation accurately depends on a number of factors, in particular; domain knowledge based on learning, training received, flying hours, and expectations based on exposure to a variety of situations (Gawron, 2000). Wiggins and O’Hare (1995) also stated that pilots with greater practical experience were able to make more informed decisions. In this case, the ability to assess the situation accurately would have been limited by the pilot not having an instrument rating, having had limited exposure to instrument flight conditions in training, and only holding his licence for about four years at the time of the accident.
Decisions are usually made with an individual’s best intentions and based on the information they have to conduct an assessment. In this case, the pilot may have interpreted information from pilots of other aircraft on the Mount Gambier common traffic advisory frequency to indicate that a landing was plausible, when in fact the conditions were observed to be marginal even for flight under the instrument flight rules (IFR). After conducting a non-standard, high-risk approach and landing, in conditions not suitable for VFR flight, the pilot should have had enough evidence available to assess that a departure soon after would very likely result in flight in the same conditions despite his limited flying experience and training. However, there is insufficient evidence to establish whether the pilot accurately assessed the conditions.
The pilot’s assessment of the conditions prior to departure could also have been informed by checking the forecast and reported actual weather conditions, but the short duration between landing and take-off (considering passenger loading occurred in this timeframe) indicated a limited opportunity to do so.
Risk perception
A United States National Transportation Safety Board (NTSB) study (2005) outlined that ‘even if pilots are able to correctly assess current weather conditions, they may still underestimate the risk associated with continued flight under those conditions, or they may overestimate their ability to handle that risk’.
In this case, the pilot’s perception of the risk associated with departure from Mount Gambier is not known. It is known that en route to Mount Gambier, the pilot conducted weather-related track diversions, which indicated an awareness of the adverse weather in the area. However, he then conducted a non-standard approach and landed into Mount Gambier in low visibility conditions, in which he encountered difficulty in sighting and selecting a runway. He then elected to depart 12 minutes later in conditions similar to that which he arrived. It is possible he perceived that being able to land was a positive indicator for being able to depart.
Given the significant risks associated with entering IMC as a VFR pilot, it was considered unlikely that the pilot willingly flew into IMC without some assurance that he was able to handle it. However, the ability to do so depends on pilots possessing instrument proficiency. It was considered very unlikely in this case that the pilot possessed the instrument proficiency to sustain flight in the conditions encountered on the day of the accident. The ability to underestimate these risks is not exclusive to this one case; it is prevalent throughout the industry, particularly in general aviation.
Motivational factors
In addition to an assessment of the weather conditions, and perception of risk associated with this, it is possible that the pilot was influenced in his decision to take off by other motivational factors (Wiegmann and Goh, 2000). After landing in Mount Gambier and loading the passengers, the pilot was about 20 minutes later than his initial flight plan indicated. It is possible that inherent pressures associated with the purpose of the flight increased the perceived need to get to Adelaide (as outlined in the Context, Identified community service flight risks, and discussed further below in Potential for perceived pressures). Angel Flights are only offered to those who require financial and medical assistance. The pilot was aware of the medical condition of the passenger and the timing of the medical appointment, and having flown these passengers previously had knowledge of the family.
As stated at the start of this section, it is not known what influenced the pilot’s decision to approach, land and depart into IMC. The widespread nature of VFR into IMC accidents show that it is a common error in judgement, and one that should not indicate inherent failings of someone’s overall abilities as a pilot. It should be noted, however, that community service flights have a disproportionately high rate of flight preparation and navigation occurrences when compared to private operations.
Pilot proficiency for flight in instrument meteorological conditions
Although the pilot’s experience and recency were appropriate for the planned VFR flight, he was not qualified or experienced in conditions requiring instrument flying proficiency, which was what the conditions on departure from Mount Gambier required for safe flight. It was unlikely that a VFR pilot could overcome the risks posed by low visibility conditions when climbing into thick cloud (including a lack of a horizon and a loss of visual cues), and avoid experiencing spatial disorientation.
Spatial disorientation resulting from a loss of visual cues
The aircraft track recorded a departure on runway 24 and YTM entered an area of low visibility almost immediately. The recorded aircraft track then showed the aircraft slowly turning left while continuing to climb to a height of 300 ft above ground level. The last recorded position of the track indicated that the aircraft had started to descend whilst in a left turn. The aircraft wreckage indicated that just prior to impact the aircraft had been inverted.
On entry into low cloud, the pilot of YTM would have lost visual cues, in particular the horizon and visual reference to the ground. It is well established that a loss of visual cues significantly increases the risk of spatial disorientation.
The time between departure (which is also approximately the same time as entering the low cloud) and the aircraft’s impact with the ground was about 70 seconds. This is consistent with the range of times indicated by research between the loss of visual cues, experiencing spatial disorientation and a subsequent loss of control. Further evidence that the pilot of YTM experienced spatial disorientation due to the lack of visual cues included:
- the aircraft’s track and height were not consistent with the expected track if a pilot were departing for Adelaide
- the aircraft had started to descend while in a left turn suggesting the pilot had lost reference to the horizon
- inverted state of the aircraft prior to impact indicated a loss of control.
In summary, the ATSB found that shortly after take-off, while in low level cloud, the pilot likely experienced a loss of visual cues and probably became spatially disorientated, resulting in loss of control of the aircraft and collision with terrain.
Considerations of the use of alternative options
It was established that commercial passenger flights, consisting of charter and regular public transport (RPT) have a lower risk of adverse safety outcomes than private operations. The ATSB considered whether RPT options were available for the passengers of the accident flight to travel between Mount Gambier and Adelaide for the specialist medical appointment they were attending and return home on the same day. It was determined that there were RPT options that would have the passengers arrive at their appointment in a similar timeframe, and allow them to return home on the same day. It was also determined the costs to Angel Flight to cover the fuel component for a private flight (which it did for most private flights) were comparable to the costs for two people to fly on a commercially available RPT flight.
While Angel Flight noted that RPT flights between capital cities were more economical, RPT flights were not considered as a primary option where they were available on other sectors. From the evidence available, and confirmed by Angel Flight, its ‘policy is to use volunteer pilots in private operations wherever possible’, and RPT options were only explored when there were no private pilots available to conduct the flight.
However, while Angel Flight agrees that RPT flights were not considered as a primary means of transporting passengers, it has stated that this was because such considerations would be against its constitution. The primary stated objective of the constitution was ‘Arranging carriage of financially disadvantaged people with medical conditions, in non-emergency circumstances’. This appears to be independent of whether volunteer private pilots or commercial flights were used.
The constitution’s objectives made no reference to the safety of passengers. If Angel Flight considered the safety of passengers was an important consideration to take into account, then consideration could be expected to be given to the safety benefits of using commercial passenger transport, taking into account availability, passenger suitability, and comparative costs.
The ATSB acknowledges that there will be passengers who cannot travel on RPT, and that there are times and locations where RPT is not available or suitable for the reasons outlined previously. However, where those flights are available and suitable, using the safer transport option would reduce the overall safety risk, while still achieving the stated constitutional objective of assisting people to attend medical appointments where they are not available locally.
In relation to the accident flight, while an RPT option was identified as a backup, this would only be used if the private pilot cancelled. The RPT option was not selected because the policy was to use private pilots wherever possible. No consideration was given to the safety benefits of using the available RPT, nor were the comparative costs considered. It is unlikely that any of the considerations outlined previously would have prevented the use of a commercial flight.
Risks associated with community service flights
During this investigation, the ATSB determined that per flight, the likelihood of a safety occurrence during an Angel Flight community service flight was higher than flights conducted in other private operations. Furthermore, there was an increased risk of fatal injuries in passenger carrying flights conducted by Angel Flight. This was driven by both the expected average higher occupancy of these flights compared to other private operations, and the very likely higher fatal accident rate. There was an increased prevalence of flight preparation and navigation errors in Angel Flight community service flights, compared with other private operations. This is a known precursor to fatal accidents, and was identified in both fatal accidents involving Angel Flight. It is almost certain that the risk profile associated with flights conducted on behalf of Angel Flight are not the same as other private operations. The identified occurrence type categories show that other events or conditions that increase risk are present during Angel Flight community service flights which are either not present or are effectively mitigated during other private flights.
It was considered that there would be no notable differences in the pilot skills, recency and experience, or the aircraft equipment, maintenance and reliability, as both groups are licensed and regulated in the same way.
Therefore, the ATSB considered the potential for Angel Flight pilots being exposed to factors different to other private operations associated with the key differences between the flights conducted for Angel Flight and most other private operations. The key differences are:
- the carriage of ill, unrelated (and often unknown) passengers, rather than friends and family
- flying at times to meet scheduled medical appointments rather than times chosen by the pilot
- flying to and from pre-arranged locations, generally requiring cross country navigation and often into controlled airspace
- operational costs (fuel and landing fees) of the private flight are covered by a third party.
These factors included considerations such as:
- Implicit (rather than explicit) pressures of flying a ‘mission’ where the pilot is responsible for transporting unrelated passengers to necessary medical appointments.
- Flying in and out of locations with which they may have limited familiarity, including small aerodromes in areas outside of ones they perhaps routinely use, and limited familiarity with procedures in controlled airspace.
Per flight, Angel Flight pilots were shown to be more likely to make operational errors (particularly associated with flight preparation and navigation, airspace, runway events, and communications breakdowns) when compared to other private operations. This required further consideration, and therefore the above topics have been explored in more detail below.
Potential for perceived pressures
The safety investigations and research conducted in the United States, and highlighted in the Aircraft Owners and Pilots Association training course Public Benefit Flying: Balancing Safety and Compassion, identified that pilots conducting community service flights may be exposed to factors that are detrimental to safe decision making. This included the identification of the potential for perceived or self-induced pressure due to the nature of the flight being undertaken, and the impact this could have on objective decision making. Key areas identified by the US research and investigations included the terminology used, feelings of personal obligation to provide a service on an assigned trip, knowledge of passenger’s condition, and managing passengers and their expectations.
Perceived or self-induced pressure is specific to each pilot, may come from a range of sources, and may not be evident or easily identifiable by the pilot. Not every flight will result in potential for pilots to experience pressure; some pilots may not have experienced pressure due to the flights they have been involved in, and some pilots may not feel pressure in circumstances where other pilots do. This is evident from submissions about personal experiences made to Civil Aviation Safety Authority (CASA) by Australian pilots during the 2018-2019 consultation on proposed changes to community service flights. Some pilots indicated they saw no differences to other private flights, while others indicated that there were significant pressures associated with community service flights consistent with the above United States investigations and research. The ATSB consider the following aspects of community service flying will likely be sources of potential pressure perceived by some pilots:
- The terminology used in this sector, including referring to the flights as ‘missions’ and pilots as ‘heroes.’
- Desire to complete the trip, having been assigned a ‘mission,’ when completion of such flights can lead to ‘satisfaction that cannot be described.’
- Knowledge of the patient’s condition may motivate the pilot to continue when other factors may otherwise have them altering their plans.
- Managing passenger expectations, when passenger briefing notes indicate an on time flight according to the scheduled times to meet the medical appointment.
- Belief that there are limited other options for the passengers to attend their medical appointments.
- Passenger requirement to travel to the appointment and return home in one day.
While it could be demonstrated that most of the elements outlined above were present in the accident flight, there was insufficient evidence available to determine the influence of each of these on the pilot’s decision to continue to land, and subsequently depart, rather than diverting or holding, or delaying or cancelling the flight.
It was evident through interviews with key organisational staff, and in documentation such as the Pilot Handbook, that Angel Flight does not pressure pilots to complete assigned missions. However, pilots undertaking these flights do not necessarily have the benefit of education and exposure to compelling evidence of how motivational factors can override other safety considerations when they are making decisions. They are also alone in their decision making for a ‘go/no go’ situation, unlike in other sectors where support staff and other crew influence the outcomes, and tools and procedures have been implemented to manage the identified risks.
Flight preparation and navigation
According to Angel Flight documentation, the flight times and locations of community service flights are determined by the passenger’s needs. This generally means the pilot will be flying into a small aerodrome near the passenger’s home, and then to a major city centre, with time requirements that align with the passenger’s specialist appointments.
The pilot may not be familiar with, or may not have flown to either of the locations previously, and may have limited exposure to flying into controlled airspace surrounding larger airports, as many private pilots flying recreationally are not necessarily exposed to these circumstances on a regular basis. This results in pilots flying through controlled airspace and into airports with unfamiliar layouts, while carrying passengers, which can lead to an increased workload when compared with recreational flying.
Flight in unfamiliar airspace requires additional pre-flight planning. This includes knowledge and familiarity with established procedures, radio communication protocols, the limits of restricted and controlled airspace, and airport runway and taxiway layouts. Pre-flight planning minimises in-flight decision errors because it removes the unforeseen element from situations that arise during the flight. Failure to carry out this prior planning can result in decisions being made under a situation of considerable stress and increases the likelihood of poor or incorrect decision making.
The training to obtain a private pilot licence and the aeroplane flight review conducted biannually included the operational requirements and knowledge to conduct these flights. However, while pilots may demonstrate knowledge satisfactorily during the biennial flight review, not all of these areas are tested under the flight review, and not all these skills are practiced regularly during recreational flying, potentially resulting in reduced proficiency in these skills.
In summary, the increased occurrence and fatal accident rates were almost certainly a result of community service flight pilots being exposed to a range of operational differences because of the task being undertaken. These operational differences included the carriage of passengers according to a scheduled time, with specific location requirements involving cross country navigation and flight into controlled airspace, and often with a same day return expectation. As a result of the operational differences present in these flights, some of the factors identified which may impact decision making, and consistent with the occurrence categories where the Angel Flight occurrence rate was higher, included the potential for perceived pressures, and flying in unfamiliar locations, with a resulting impact on flight safety.
Angel Flight organisational controls
The community could reasonably expect that a provision of services such as the community service flight organised by Angel Flight would have at least a level of safety commensurate with other private operations, if not higher. However, this investigation has showed that they are actually less safe than other private operations, and previous research has shown that private operations are also less safe than charter and regular public transport. When compared with private operations, this indicates that there are risk factors which are not currently being managed. Analysis of the occurrence types where the greatest differences were identified between private flights and community service flights were predominantly operational.
As community service flights are exposed to additional operational risks, it is important that those organising these flights have appropriate operational controls in place, and these pilots have access to guidance and education in what these risks are, and how to avoid adverse influences.
In the United States, in response to the NTSB recommendations, guidance related to the identified safety risks in the community service flight sector was developed to help pilots identify and minimise the flight safety risks. Additionally, for those community service flights conducted privately but with reimbursement from a volunteer pilot organisation, the Federal Aviation Administration determined these flights could be safely conducted by applying operational limitations on each organisation through their exemption process. This required organisations to ensure minimum pilot qualifications were applied, increased recency requirements and required additional training to be undertaken, and increased required flight rule minimums above the minimum required for private flights. Documentation must also be maintained for each pilot and mission flown, including in some cases a pre-flight risk assessment tool, which reinforced the organisational applied minima, to assist pilots with decision making in marginal conditions. The United States model shows that organisations like Angel Flight can sustain operations with additional operational risk controls in place to address the specific risks associated with community service flights, and which are ongoing and apply to individual flights.
At the time of this accident, similar guidance and educational material to that developed in the United States had not yet been developed for the Australian context. Although there has been material developed by CASA and the ATSB for private pilots which addressed some of the flight safety risks, these did not target pilots conducting community service flights, nor address the different operational factors present.
Angel Flight operational controls were limited to 250 hours as pilot in command, VH-registered aircraft, and 5/10 hours on aircraft type for VFR/IFR flights respectively. These are basic measures for a base line level of entry for registration as a pilot with Angel Flight. There is limited evidence flying hours alone are sufficient to make informed decisions. As outlined by Gawron (2000) and Wiggins and O’Hare (1995), pilots with greater practical experience, particularly made up of domain knowledge based on learning, training received (and its recency) and expectations based on exposure to a variety of situations, make more informed decisions. While the current licensing and endorsement requirements for private pilots ensures the flight related knowledge and skills are taught, it is also valuable for them to receive regular education, training and practice to maintain many of the skills needed to safely conduct community service flights.
In addition, the Angel Flight Pilot Handbook included comments outlining a pilot’s ability to cancel a flight for any reason. It also stated that any subjects related to pilot in command responsibilities would not be covered, and that the flight must be conducted legally.
During this investigation, the ATSB found that community service flights had a higher occurrence rate, and a different risk profile than other private operations, almost certainly due to exposure to different operational factors which influence decision making. This higher occurrence rate indicated that insufficient organisational controls had been implemented to address the risks to flight safety.
Under the current regulatory framework, there is no specific oversight of community service flights. Therefore, organisational controls to address the areas of elevated risk can only be implemented by the community service flight organiser. Similarly, only the community service flight organiser can undertake the targeted promotion of relevant material to its pilots.
The ATSB acknowledges that Angel Flight cannot be responsible for the pilots’ preparation and conduct of flights, and is limited in its ability to address decisions that are the responsibility of the pilot in command. However, the ATSB considers that Angel Flight is in a position to implement organisational requirements and controls, and to facilitate access to material and relevant information that can assist pilots to identify risk factors associated with these flights. Pilots would then have an increased opportunity to develop and implement appropriate mitigation strategies to address these risks.
Availability of safety information to Angel Flight
It is well-understood in the aviation industry that ‘the effective management of safety is highly dependent on the effectiveness of safety data collection [and] analysis...’ and that ‘reliable safety data and safety information is needed to identify trends, make decisions and evaluate safety performance…and to assess risk’ (International Civil Aviation Organisation (ICAO), 2018). Identifying and collecting this data should be aligned with the organisations’ role and scope of influence.
The nature of safety information in this context relates to any hazards or occurrences that arise during a pilot’s Angel Flight mission. The utilisation of safety information by an organisation like Angel Flight will differ significantly from aviation operators responsible for the management of flight operations. By identifying these hazards or occurrences, it can inform decisions about future pilot requirements, any guidance or educative material that could be helpful, or any other risk treatment measures possible within the scope of Angel Flight’s role.
At the time of the accident, occurrence notifications from pilots, air traffic control and aerodrome personnel received by the ATSB and CASA were reported as private flights, and generally were not further identified as community service flights; nor were they required to be. As these notifications were not identified as community service flights, neither CASA nor the ATSB had awareness of the incidents as occurring during community service flights, and further, the ATSB public database could not differentiate these occurrences from other private operations, and so community service flight organisations did not have visibility of these occurrences.
Angel Flight did not request or require any information regarding flight safety related incidents from its pilots. Therefore, the only way for Angel Flight to be aware of a safety occurrence apart from when the organisation was formally investigated as part of an ATSB investigation, was for the pilot, passenger(s) or other involved person to report it directly. This informal system was limited in the ability to capture safety related information because:
- the passengers likely have limited knowledge or exposure to general aviation regulations or knowledge of flight safety
- in the absence of an established just culture policy[47] in relation to reporting of safety occurrences, pilots may be reluctant to report a safety occurrence to Angel Flight as they may perceive it would have implications for being considered for future missions
- other involved persons may not be aware the private flight is a community service flight
- if pilots are not specifically asked or required to provide information on safety matters, there is a reduced likelihood that they will consider it necessary to do so.
Where Angel Flight had been notified of incidents or accidents, further information had been requested, and in some cases, additional action taken for specific pilots. However, this was limited to the known incidents which constituted less than 10 per cent of occurrences identified during this investigation. If Angel Flight had sought to identify and understand systemic risks relating to flights conducted on behalf of the charity, the limited availability of safety related information to Angel Flight would have prevented this. However, it must also be noted that where punitive action has been known to be taken, this increases the risk of non-reporting to the organisation. This is due to well recognised concerns amongst pilots that reporting errors results in subsequent punitive action. It also does not allow for identification of, or address the broader systemic risks, which are present in all privately conducted flights on behalf of Angel Flight. This in turn prevented Angel Flight from identifying and applying appropriate risk controls to manage the safety risks associated with these flights.
Regulatory differentiation between community service flying and private operations
In order to identify risks and monitor safety performance of any one sector of the industry, it is necessary to have systems to differentiate the sector from other similar activities. In Australia, the regulator facilitates this.
CASA had previously identified key regulatory risks applicable to community service flights and outlined potential mitigation methods, which were communicated to the public and industry through a discussion paper in 2014. Many responses to the discussion paper indicated there was no evidence to support the need for additional oversight; however, as identified in the discussion paper, there was a lack of visibility of the conduct of community service flights (as they were considered private operations). Due to the predominantly negative responses, no regulatory changes were initiated, and the flights remained as private operations. This prevented a more informed view for decision making in this sector of the industry, as lack of identification or differentiation of the flights from other private operations prevented the regulator identifying ongoing areas of sector specific concern.
At the time of the accident, there were no legislated minimum qualifications or experience requirements for community service flights. While not required by regulation, organisations providing community service flights are able to apply their own risk controls; for example, Angel Flight applied requirements of minimum pilot in command hours and VH‑registered aircraft. Other organisations coordinating community service flights also specified minimum requirements for their volunteer pilots, which differed substantially between each organisation. However, these risk controls were voluntary and unregulated, and were applied by each organisation to address organisational identified risks. Where organisations are not aviation operators, organisational controls required to identify or address flight safety risks associated with these flights, and they can be altered or removed with no reference to external parties or the regulator.
A system to differentiate these flights would allow for ongoing oversight and review of the safety of these flights. This would allow for the identification of areas of specific concern through evidence-based analysis, and consideration of appropriate risk controls to be applied to all organisations offering community service flights.
A previous fatal accident involving Angel Flight in 2011 was as a result of VFR flight into low visibility conditions. The lack of visibility of community service flights in occurrence data made quantifying the risk by Angel Flight, CASA and the ATSB not possible. However, analysis from data obtained under the Transport Safety Investigation Act 2003 for this investigation shows that flight preparation and navigation related occurrences are over‑represented in Angel Flight operations relative to other private operations. If community service flights could have routinely been identified in the ATSB occurrence database, this analysis could have been part of routine safety analyses by CASA. Such analysis could have demonstrated that there were ongoing additional risks faced by Angel Flight pilots beyond those faced by other private pilots, and provided the justification for mitigating those risks. As discussed, the additional risks such as perceived pressure to complete missions can have a strong influence on pilot decision making, resulting in decisions to operate in marginal weather conditions. Decisions made by the pilot of YTM that resulted in VFR flight into IMC leading to this fatal accident were consistent with risks apparent in the data.
__________
- The concept of a ‘just culture’ refers to an environment where pilots and others are not blamed or punished for actions, omissions or decisions which are commensurate with their experience and training, but they are held accountable for negligence, wilful violations and destructive acts.
Findings
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving a SOCATA TB-10 Tobago aircraft, registered VH-YTM, that occurred near Mount Gambier Airport, South Australia, on 28 June 2017. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
- The pilot took off from Mount Gambier into low-level cloud without proficiency for flight in instrument meteorological conditions.
- Shortly after take-off, while in low-level cloud, the pilot likely experienced a loss of visual cues and probably became spatially disorientated, resulting in loss of control of the aircraft and collision with terrain.
- Angel Flight did not consider the safety benefits of commercial passenger flights when suitable flights were available. [Safety Issue]
Other factors that increased risk
- Community service flights conducted on behalf of Angel Flight had considerably more occurrences per flight than other private operations. It is almost certain this higher occurrence rate is due to exposure to different operational factors as a result of the task being undertaken.
- Angel Flight had insufficient controls in place, and provided inadequate guidance to pilots to address the additional operational risks associated with community service flights. [Safety Issue]
- There were limited opportunities for Angel Flight to be made aware of any safety related information involving flights conducted on its behalf. [Safety Issue]
- The Civil Aviation Safety Authority did not have a system to differentiate between community service flights and other private operations, which limited its ability to identify risks. This hindered the Civil Aviation Safety Authority's ability to manage risks associated with community service flights. [Safety issue]
Safety issues and actions
The safety issues identified during this investigation are listed in the Findings and Safety issues and actions sections of this report. The Australian Transport Safety Bureau (ATSB) expects that all safety issues identified by the investigation should be addressed by the relevant organisation(s). In addressing those issues, the ATSB prefers to encourage relevant organisation(s) to proactively initiate safety action, rather than to issue formal safety recommendations or safety advisory notices.
Depending on the level of risk of the safety issue, the extent of corrective action taken by the relevant organisation, or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue safety recommendations or safety advisory notices as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, it had carried out or were planning to carry out in relation to each safety issue relevant to its organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Angel Flight Australia consideration of commercial flights
Safety issue number: AO-2017-069-SI-01
Safety issue description: Angel Flight did not consider the safety benefits of commercial passenger flights when suitable flights were available.
Safety recommendation description: The Australian Transport Safety Bureau recommends that Angel Flight Australia takes action to enable it to consider the safety benefits of using commercial flights where they are available to transport its passengers.
Insufficient organisational risk controls implemented by Angel Flight Australia
Safety issue number: AO-2017-069-SI-02
Safety issue description: Angel Flight had insufficient controls in place, and provided inadequate guidance to pilots to address the additional operational risks associated with community service flights.
Availability of safety information to Angel Flight Australia
Safety issue number: AO-2017-069-SI-03
Safety issue description: There were limited opportunities for Angel Flight to be made aware of any safety related information involving flights conducted on its behalf.
Regulatory differentiation between community service flying and private operations
Safety issue number: AO-2017-069-SI-04
Safety issue description: CASA did not have a system to differentiate between community service flights and other private operations, which limited its ability to identify risks. This hindered the Civil Aviation Safety Authority's ability to manage risks associated with community service flights.
Additional safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Civil Aviation Safety Authority
A legislative instrument imposing conditions on pilots conducting certain non-emergency medical community service flights arranged by third party organisations (CASA 09/19 — Civil Aviation (Community Service Flights — Conditions on Flight Crew Licences) Instrument 2019) was made on 12 February 2019 and came into force on 19 March 2019.
The instrument sets out new minimum licence, experience and recency standards for pilots operating community service flights that are conducted by volunteer pilots and coordinated by a charity or for a charitable or community service.
Community service flights are flights:
- where patients and their families or carers are transported
- to a destination for non-emergency medical treatment or services; or
- from the treatment destination back to the place from which they departed or to a destination where they reside; and.
- medical treatment is not provided on board a community service flight, passengers can receive medication and treatment for an unexpected medical emergency; and
- no more than five passengers can be carried, including the patient; and
- cannot be operated under the visual flight rules (VFR) at night.
In addition to the above requirements, community service flight requirements include:
- licence must be PPL CPL or ATPL (not RPL)
- for a multi-engine aeroplane, at least 25 hours of flight time as pilot in command of a multi-engine aeroplane
- for PPL holders only, at least 400 hours of flight time and at least 250 hours of flight time as pilot in command (does not apply to CPL/ATPL holders)
- a current class 1 or 2 medical certificate
- for a flight conducted under the VFR, pilots must have at least 10 hours of flight time in an aeroplane of the same type as being used for the Community Service Flight
- for a flight conducted under the IFR, pilots must have at least 20 hours of flight time in an aeroplane of the same type as being used for the CSF
- landed the same class rated or type rated aeroplane within the previous 30 days
- aircraft maintained to the CASA maintenance schedule must have a current maintenance release with a periodic inspection conducted every 100 hours or 12 months (whichever is earlier).
A community service flight cannot be flown in:
- an amateur-built aircraft accepted under an Amateur Built Aircraft Acceptance
- a limited category aircraft
- an aircraft with an experimental certificate
- an unregistered aeroplane.
Further information: www.casa.gov.au/licences-and-certification/standard-page/community-service-flights.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Angel Flight Australia
- The Civil Aviation Safety Authority
- Witnesses
- The Bureau of Meteorology
- Airservices Australia
- Bureau of Infrastructure, Transport and Regional Economics
- Federal Aviation Administration
- Air Care Alliance
- National Transportation Safety Board
References
ATSB 2011, Avoidable Accidents No. 4 Accidents involving pilots in Instrument Meteorological Conditions, Australian Transport Safety Bureau, Aviation Research and Analysis publication AR-2011-050.
Batt, R and O’Hare, D 2005, General aviation pilot behaviours in the face of adverse weather, Australian Transport Safety Bureau, Aviation Research and Analysis Report B2005/0127
Benson, A (1999) Spatial disorientation – general aspects. In J Ernsting, AN Nicholson, DJ Rainford (Eds.) Aviation medicine (pp.419-436). London: Butterworths & Co. Ltd.
Bryan, L., Stonecipher, J., & Aron, K. (1954). 180-degree turn experiment (Vol. 54(11), pp. 1-52): University of Illinois Bulletin.
Cheung, B. (2004). Nonvisual spatial orientation mechanisms, in FH Previc & WR Ercoline (Eds.) Spatial disorientation in aviation, Lexington MA, American Institute of Aeronautics and Astronautics, pp. 37-94.
Frederick, M 2002, AOPA Air Safety Foundation. 2002 Nall report: Accident trends and factors for 2001: AOPA Air Safety Foundation.
Gawron, V 2000, ‘Psychological factors’, in FH Previc & WR Ercoline (Eds.) Spatial disorientation in aviation, Lexington MA, American Institute of Aeronautics and Astronautics, Inc, pp. 145-195.
Gibb, R, Gray, R and Scharff, L 2010, Aviation Visual Perception: Research, Misperceptions and Mishaps, Ashgate Publishing Limited, Surrey, United Kingdom.
Groff, LS & Price, JM 2006, ‘General aviation accidents in degraded visibility: A case control study of 72 accidents’, Aviation, Space, and Environmental Medicine, vol. 77, pp. 1062–7.
International Civil Aviation Organization, 2018, Doc 9859 Safety Management Manual, Fourth Edition (advance), Montreal, Canada.
International Civil Aviation Organisation, 2018, ICAO Safety Report 2018 Edition, Montreal, Canada
Newman, DG, 2007, An overview of spatial disorientation as a factor in aviation accidents and incidents, Australian Transport Safety Bureau, Aviation Research and Analysis Report B2007/0063.
NTSB 1988, Commercial emergency medical service helicopter operations, National Transportation Safety Board Safety Study NTSB/SS-88-01, Washington DC, United States.
NTSB 1989, Safety report: General aviation accidents involving visual flight rules flight into instrument meteorological conditions, National Transportation Safety Board NTSB/SR-89-01, Washington, DC, United States
NTSB 2005, Risk Factors Association with Weather-Related General Aviation Accidents, National Transportation Safety Board Safety Study NTSB/SS-05/01, Washington DC, United States.
Parson, S. (2006, May/ June). Getting the Maximum from Personal Minimums. FAA Aviation News, 1-8.
Transportation Safety Board of Canada. (1990). Report of a safety study on VFR flight into adverse weather (90-SP002.). Gatineau, Canada: Transportation Safety Board of Canada.
Wiegmann, D and Goh, J 2000, Visual Flight Rules (VFR) Flight into Adverse Weather: An Empirical Investigation of Factors Affecting Pilot Decision Making, Federal Aviation Administration research DTFA 00-G-010, Illinois, United States.
Wiggins, M and O’Hare, D 2003, Weatherwise: Evaluation of a cue-based training approach for the recognition of deteriorating weather conditions during flight, The Journal of Human Factors and Ergonomics Society, pp.337-345.
Wiggins, M and O’Hare, D 1995, Expertise in Aeronautical Weather-Related Decision Making: A Cross-Sectional Analysis of General Aviation Pilots, Journal of Experimental Psychology: Applied Vol. 1 No. 4, pp. 305-320.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Civil Aviation Safety Authority, Angel Flight Australia, the Bureau of Meteorology, the National Transportation Safety Board, and Bureau of Infrastructure, Transport and Regional Economics.
Submissions were received from the Civil Aviation Safety Authority, Angel Flight Australia, the Bureau of Meteorology, the National Transportation Safety Board, and Bureau of Infrastructure, Transport and Regional Economics. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Data analysis methods
Identification of Angel Flight occurrences
The ATSB undertook a data matching exercise between Angel Flight Australia (Angel Flight) records and the ATSB’s aviation occurrence database to find safety occurrences that occurred during an Angel Flight organised private flight. A number of techniques were employed to identify Angel Flight occurrences recorded as other operations, and provide assurance that the occurrence data was related to passenger carrying Angel Flights.
A total of 4,434 ATSB occurrence records were identified as having a registration match with Angel Flight used aircraft. To identify those records that occurred during flights conducted on behalf of Angel Flight, the following techniques were applied. Twenty-four ATSB occurrence records already identified as a flight operated for Angel Flight were also validated using these techniques and removed from analysis if a positive match could not be identified.
Flight pair matching (passenger carrying flights only)
- An evaluation was conducted by matching Angel Flight and ATSB occurrence records on the following parameters: departure aerodrome, arrival aerodrome, aircraft registration (country and registration mark), within the same day. The time difference between the Angel Flight recorded departure time and the occurrence time was recorded and used for ranking and assessment purposes. Ninety-two distinct occurrence records were identified using this technique.
Occurrence location name matching
- A probable airport for each of the 4,434 potential occurrence locations were identified. Matches were performed on the following parameters: departure and arrival aerodrome with occurrence location name according to aircraft phase of flight and flight plan details; time within 6 hours. The time difference between the Angel Flight time and occurrence time was recorded for validation. Twenty-four distinct occurrences were identified for further review.
Spatio-temporal matching of flight paths
- The location of occurrences compared to the great circle flight path between the departure and arrival airport for Angel Flight records was evaluated. These were considered for occurrences within 50 NM of the flight path and up to 1 day between the recorded occurrence time and Angel Flight record. A significant benefit of this approach was where the specific departure and arrival airports were not known for the ATSB occurrence and where the occurrence was not recorded relative to the departure or arrival airport. One hundred and fifty-five records were identified in addition to Angel Flight records identified using the aforementioned techniques.
A total of 271 distinct Angel Flight records were matched with 233 reported occurrences using the techniques described above. Included in these occurrences were probable passenger carrying flights and re-positioning flights. Each Angel Flight record combined with occurrence records were ranked where more than one match was found. A probable match weighting was assigned to each match based on the reported proximity of the occurrence to the flights, time between the reported occurrence and the nominated flight time in the Angel Flight dataset, and location name matches. These weighting techniques were also used to exclude records where a match could not be identified.
This was calculated according to the following priorities:
- Matched flight pairs – these were prioritised because the flight legs matched exactly with those recorded in the ATSB occurrence.
- Records identified using flight path proximity were calculated next by multiplying ratios of distance and time together. A higher (more favourable) weighting was assigned to records that were nearest the reported time and distance.
- The small number of location name matched-records were weighted by time.
All paired Angel Flight records and ATSB occurrences were manually verified using the calculated metrics to assist in the assessment. This also allowed a review of a reasonable expected time difference between the reported Angel Flight departure times and the time of the safety occurrence, given the distance from the departure. Occurrence times preceding the Angel Flight time were noted as likely to be the flight prior if a positive match could not be established for the aerodromes of arrival and/or departure. In other cases, the destination airport for Angel Flight was recorded as the origin for the ATSB occurrence at some time after the Angel Flight time. These were recorded as the flight after the Angel Flight. Both flights prior and following Angel flights were excluded from the primary analysis, but have been documented in the following appendices for reference.
Further use of Angel Flight records in analyses
Flight records used as normalisers
All flights not specifically labelled by Angel Flight as ‘regular passenger transport (RPT)’ were used as the primary normaliser for Angel Flight safety occurrences. This ensured the largest, and most conservative result with respect to occurrences and accidents per 10,000 flights analyses. A total of 13,389 flight records were identified as privately conducted flights on behalf of Angel flight between 2008 and 2017. One record was excluded as the label ‘NonPaxFlight’ was recorded in the Registration field.
Flight records used in RPT analysis
All non-standard aircraft registrations with the exception of flights labelled as ‘RPT’ were excluded from the analysis of private compared to RPT flight utilisation. A total of 20,025 records were used in this case, with 3,669 recorded as RPT, and 16,356 as private. 85 flight records were excluded from private operations. This was performed to provide a conservative count of private flights, and did not have any significant effect on results.
Number of flights as primary normaliser
Although the number of flights and flight hours are both commonly used as normalisers in aviation safety analysis, each provide different benefits. The total number of flights in each category were selected as the primary normaliser in this case for the following reasons:
- To provide an indication of the likelihood that an Angel Flight community service flight is involved in a safety occurrence. In other words the likelihood of a passenger being exposed to a reduced level of safety during a flight.
- To help identify systemic factors related to the conduct of Angel Flight community service flights.
Flight hours were considered by the ATSB as a normaliser, however were assessed as more limited in answering the safety objectives of the analysis, in particular where the duration of a flight may be a factor in a safety occurrence. Additionally, the number of flights for passenger carrying Angel Flights was known providing more confidence in the calculated rate compared to the number of flight hours, which required estimation. However, for reference, a comparison of the overall occurrence and accident rates is presented in Table B1 of Appendix B – Additional data.
Normalising by the number of flights around towered airports was also considered by the ATSB for analysis. This was not considered appropriate for the holistic, non-attribution based focus of the analysis. While this may provide an indication of the likelihood of pilot versus air traffic control errors around these airports, a comparison would not be possible between occurrences away from these locations. Furthermore, the primary objective of identification of relatively more likely occurrences relating to airspace related occurrences may be mis-represented in comparison to other private operations. Put in another way, even if Angel Flight airspace occurrences are elevated because they fly into these locations relatively more often, this represents an elevated safety risk, explained in part by them flying into these locations.
Estimation of Private, Business and Charter landings: 2008 to 2013
As of 2014, BITRE collected landing data in each operation category for each registration. Prior to this, the number of flights in charter, private and business operations required estimation due to landings data being collected by BITRE in aggregate form for each aircraft registration. Landing data (for example, number of flights conducted) for 2008 to 2013 was required due to the number of flights being known and flight hours being unknown for flights conducted on behalf of Angel Flight. The following process described how this was estimated using the known number of flight hours for private, business and charter operations and the ratio of these flight hours to total landings for each operation where there was a high proportion of a single operation category.
The objective was to approximate the typical flight length in each operation category, with the aim being to determine the number of landings given the number of hours flown in each operation category. This model was applied to each aircraft record individually based on ratios generated from the entire set of data given the breakdown of hours for each operation type. This model has three main assumptions based on a fixed proportion of operation category hours to landings.
The subscripts below denoted as x, y and z represent different operation types such as private, business and charter. For example, Hoursx denotes hours for operation type x.
Assumption 1: Within each operation category, there is the same ratio of hours to departures within the category which remains constant over all aircraft. That is,

Since individual hours are known for each operation type, and the constant can be derived for each from the sole operation types for some aircraft, the approximate departures can be derived for each operation type. The fixed ratio of departures to hours is defined as the average from those aircraft where the hours flown belong to one operation type.
Assumption 2: All aircraft conducting a particular operation, conduct similar length flights to those only conducting that operation. For example, those aircraft only conducting charter flights would have a similar flight length to those conducting charter flights 10% of the time.
Thus, the total departures for operation types x, y and z could be represented as:
Due to uncertainty and inherent variability in aircraft flying hours, and the likelihood that aircraft flying hours will change over time and for different aircraft operators, this model will have a high level of uncertainty.
Assumption 3: These flights follow the same model derived, and therefore the same proportion will apply to the original departures as per the ratio of the derived departures within each operation type.
The final calculation against each individual aircraft registration means that the total of the estimated departures always equals the total actual departures. To account for large differences between airframes, four groups were created and calculated separately for the combinations of fixed and rotary wing aircraft, and single and multiple engines, and were derived from aircraft that solely performed each operation type. For example, the landings per hour rate for fixed wing single engine private operations was derived from aircraft only used for private operations.
Note that Angel Flight landings were subtracted from the estimated total of private flights for analysis purposes, accounting for Angel Flight community service flights being a sub-set of private operations.
Estimation of city flight pairs
An analysis was conducted comparing known regular public transport (RPT) flight routes to privately conducted Angel Flight routes to provide a general indication of RPT as an alternative. To achieve this, the flight sector pairs of sponsored Angel Flight RPT flights were compared to the sectors of privately conducted Angel Flights.
Due to some private and RPT flights using different airports in similar regions, it was desired to identify regions rather than the specific airports. This is because it is expected that it may be practical to travel to and from different airports in the same region. To account for this, airports within 50 kilometres of the published Angel Flight departure and arrival airport were considered as viable options. This is illustrated in Figure A1.
Figure A1: Diagram of the region identification for determining availability of RPT options
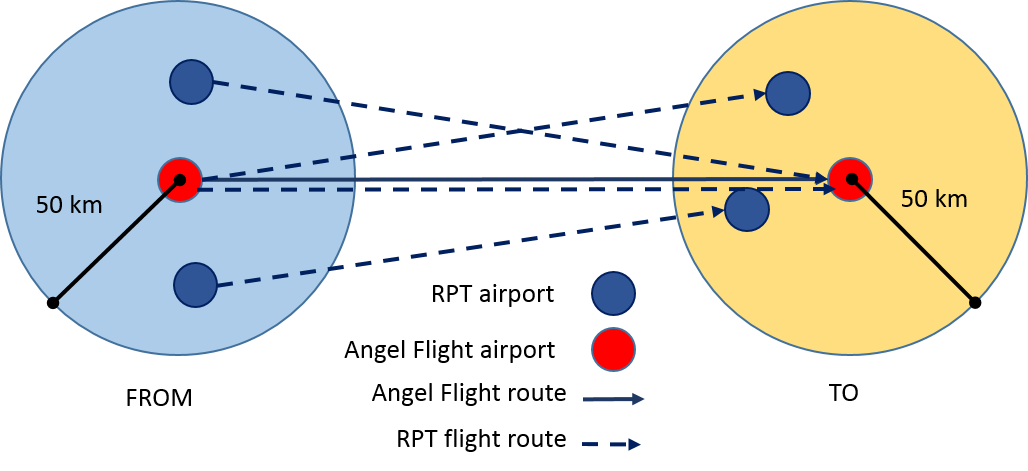
A list of flight routes using direct RPT flights was developed based on records of RPT flights used by Angel Flight. Each privately operated community service flight was classified into the following categories: no RPT option used, exact RPT match or RPT within 50 kilometres. A limitation of this approach is that the availability of RPT flights has not been quantified for the day of travel – and as such, there may not have been availability (or indeed the conduct of an RPT flight) on that day. In contrast, it is possible that RPT flights may have available for use in some regions, however, have not been previously utilised. Due to this analysis relying on RPT routes historically used by Angel Flight, sectors never used by Angel Flight are not identified using this approach. As such, it should be noted that the purpose of this analysis is to provide a generalised indication of an RPT alternative being available where it is confirmed that these services have been historically utilised by Angel Flight Australia.
Estimation of repositioning flight totals
A supplementary analysis was conducted to evaluate safety occurrences on repositioning flights – that is, those flights occurring prior to and following privately conducted passenger carrying flights on behalf of Angel Flight Australia, for the purposes of flying from the pilot’s location to the passenger meeting point, and return. This occurrence data required normalisation to compare and combine this with other analyses. As the number of these repositioning flights was unknown, they required estimation based on the passenger carrying flight information provided by Angel Flight Australia.
Analysis of the passenger carrying flights revealed cases where passenger carrying flights using the same aircraft would be conducted in consecutive segments within a relatively short period of time. This was assumed to be cases where Angel Flight passengers were transported to medical aid, followed by the medical appointment and transport back to their homes. For example, a flight from Port Lincoln to Adelaide, SA would be conducted followed 5 and a half hours later by a return flight from Adelaide to Port Lincoln. In these cases, it was considered probable that repositioning flights were not required in between these passenger carrying legs when the same aircraft was being used.
Passenger carrying flights with the same aircraft registration and matching arrival / departure location were grouped when the recorded departure times were within 24 hours. The total number of groups were calculated and used as the estimated figure for the number of repositioning flights, as illustrated by Figure A2. This shows two hypothetical groups of Angel Flights covering a scenario where a pilot and their aircraft conduct a single Angel Flight leg requiring a flight from a home base to the passengers’ location, the repositioning flight prior, followed by the passenger carrying leg from A to B, and a possible return home to C, if B is not the home-base location. The second scenario in Figure A2 covers the potential where a prior repositioning leg is flown to location A to collect Angel Flight passengers to location B. Followed by a break, and then a return flight from B to A. In this case, the pilot may not need to return home between flights. Consequently, there would be only two repositioning flights, rather than four.
Figure A2: Estimation of repositioning flight legs using known passenger carrying flights
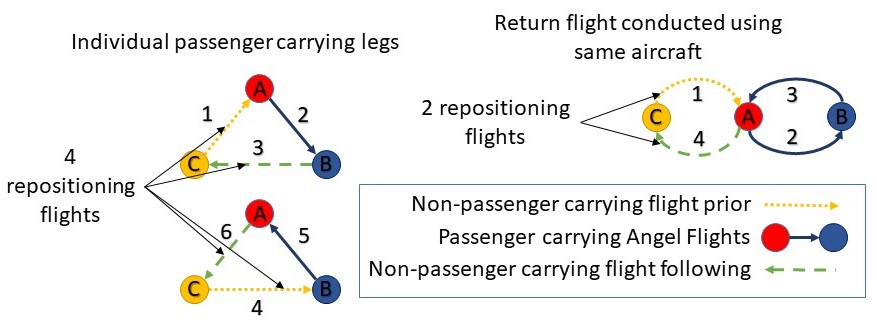
The estimations performed are expected to have two main conflicting limitations. It may be possible that pilots would return or fly to another location between legs, however, noting that although a maximum of 24 hours was used, the median time taken between flights was 5 hours and a half hours from the first departure time – this is expected to be around the time taken for a medical appointment, including return ground transport to the medical centre from the airport. Furthermore, the home base for the pilot may actually be located at one of the locations. For example, there may be pilots based at a metropolitan airport used for the passenger ground transport to the medical centre. This would mean only one repositioning flight per leg, rather than two. As such, these factors are expected to provide some balance, however, the precise breakdown is not known.
The analysis conducted revealed 1,246 consecutive flight pairs, and 38 flight triplets. Summation of the groups with single legs revealed a total of 12,068 groups. Therefore, 12,068 flights were attributed to both the prior repositioning and post repositioning flights, a total of 24,136 flights.
Occurrence data set comparisons
The entire sets of both Angel Flight and other private safety occurrences were used for the analysis. Comparisons between subsets of the same category were conducted between Angel Flight organised flights and other private operations, normalised by the respective number of flights in each group. For example, a comparison of the total number of flight preparation and navigation occurrences or fatal accidents. All remaining private occurrences excluding those associated with Angel Flight operations were used as the main comparison group to allow focus on the safety outcomes, rather than attribution to specific parties. For example, safety occurrences related to runway events are identified in the study as being disproportionately higher per flight for Angel Flight organised flight compared to the private average, revealing that this is an area of safety concern for Angel Flight. Although the explanation of why this is the case is likely to be due to a combination of factors, such as exposure to the particular airports that Angel Flight pilots are flying to or other operational factors, the likelihood of this safety occurrence happening is of primary concern.
The reasons why specific safety indicators were elevated for Angel Flight were outside the scope of the investigation. This was because the safety baseline for Angel Flight community service flights was unknown, and the ATSB’s primary concern being the identification of the most prevalent areas of safety concern, regardless of attribution. The rational of the ATSB’s safety focus is discussed in depth in ATSB report AR-2007-053.[48] However, the areas of safety concern identified in this analysis are encouraged to be used as drivers for further analysis. In these cases, each safety indicator could be evaluated against various confounding factors which may include normalising by the number of flights into specific airports, or case-control type studies to isolate and control for known factors. However, it is important to note that controlling for these factors in the first case was expected to bias the data and may have prevented these safety risks from being identified.
Quantification of uncertainty and probability based assessments
The calculated average rate of safety occurrences per flight allows the quantitative comparison of the likelihood of a safety occurrence between different operational groups, revealing elevated safety risks in one operational group compared to another, and the overall probability of a safety occurrence per flight within a group. To assess the likelihood that observed differences in the rate of occurrences per flight were unlikely to occur through random chance, statistical analyses were performed. All statistical assessments were performed in the R programming language[49] using base level functions unless specified. The main objectives were to indicate the probability, or chances of different types of safety occurrences being more likely during flights conducted for Angel Flight Australia compared to flights in other operational groups, and to quantify the uncertainty in the difference between occurrence rates.
The main statistical test used assesses the probability that Angel Flight occurrences are more prevalent per flight compared to other private operations and other operations in various categories. Additionally, the assessment uses credible intervals of the difference in proportions to show the possible magnitude of these differences.
Thresholds used for statistical assessment
Using the same rationale as the ATSB’s approach to the identification of potential safety issues, statistical thresholds in this report use burdens of proof in line with ATSB’s safety focussed approach to identify potential safety issues. This is to allow problems to be solved, thereby assisting in improving safety and the prevention of further loss of life. As such, the statistical assessments described below were conducted using the thresholds of greater than 67%, and greater than 95%. In the same way as for the evaluation of a single occurrence, it is expected that the mid-range standard of 67% used in this analysis will produce a reasonable, useful and appropriately qualified picture of the nature of Angel Flight safety occurrences (AR-2007-053 section 6.3)48. Note also that this threshold is the same as applied in most civil court proceedings in Australia. Descriptions to a 95% probability or credible interval were included to provide reference to traditional statistical analyses.
The ATSB uses IPCC definitions to communicate uncertainty regarding technical information, as noted in section 2.6.3 of ATSB report AR-2007-05348. In the case of this quantitative data analysis, probability and credible intervals are described against these specific thresholds. These are presented as where the data probably lies, within a 67% probability, and also where it is highly likely that the rate difference lies, to a 95% probability. It should also be noted that these statistical tests are not used in isolation, and in many cases, the results meet traditional ‘significance’ levels.
Calculation of probability
All assessments of safety occurrences were conducted using the Bayesian model for a Binomial proportion to calculate the probability of the relevant Angel Flight occurrence category being greater than private or other operations. The Binomial model was assumed to represent the probability of an occurrence, given the number of flights in each group.
The test was performed using Monte-Carlo methods, randomly sampling and comparing binomial distributions representing the rate of occurrences for private or other operations rate with the binomial distribution from the relevant Angel Flight operation category. One-million paired samples were taken from each of the two distributions and assessed. If the sample from the Angel Flight binomial distribution x-axis value had a lower proportion (representing the rate), a 0 was recorded against the paired sample, and if higher, a 1 was recorded. The probability was calculated by taking the proportion of values recorded as one from the one-million paired samples. This is equivalent to summing the right side of the distribution greater than 0 generated by calculating the difference between the binomial distributions for Angel Flight and comparison operation. This represents a right-tailed statistical assessment alternate hypothesis Angel Flight greater than comparison operation.
Throughout this report the rate of all safety occurrences was derived from the probability of an occurrence (per flight) using prior beta distribution with the Haldane prior. The Haldane prior beta (0,0) is the most appropriate prior for minimising the influence of prior data on the posterior distribution for a beta binomial model.[50] Probability is presented as a calculated ‘point value’, indicating the overall confidence that Angel Flight operations were greater or smaller in the tested category. A value of 50% indicates confidence that it is about as likely as not that Angel Flight had a higher likelihood of this occurrence group per flight compared to the comparison group.
Calculation of uncertainty between rates – credible intervals
The magnitude of the difference in occurrence rates per 10,000 flights between Angel Flight and other operations is presented in terms of credible intervals (CIs). These are calculated from the difference in binomial proportions, from the upper and lower bounds of the Highest Density Interval of the binomial proportions from each operational group. These were calculated using Markov Chain Monte Carlo (MCMC) within R.[51] The Highest Density Interval (HDI) is the shortest interval which a specified proportion of the data is contained. Alternatively, it can be defined as the interval in which there is a specified probability that the mode of the data resides.
The thresholds used for credible intervals were 67% and 95%, as described in Thresholds used for statistical assessment. As the distribution being assessed is the difference between Angel Flight and a comparison operational group, if the lower bound of the 95% credible interval is above 0, this indicates where a traditional two-tailed statistical test would be labelled as ‘significant’. The 67% CI indicates the range where the rate difference between the Angel Flight and comparison operation probably lies. However, it should be noted that as this is a safety focussed analysis, the calculation of probability is a right-tailed assessment driven by the primary hypothesis of the likelihood of Angel Flight having more safety occurrences per flight compared to other operations.
Appendix B – Additional data
Occurrences and injuries across operations
Table B1 outlines the occurrences and accidents by operation over the ten-year period from 2008 to 2017. The calculated rate of total occurrences, accidents and fatal accidents is also shown per 10,000 flights and per 10,000 flight hours. The number of flights and flight hours used to calculate the rates required estimation in some operational categories. These processes are documented in Appendix A – Data analysis methods, and are annotated against relevant figures in Table B1. Safety occurrences for both passenger carrying and non-passenger carrying repositioning Angel Flights are also included in the table below.
Table B1: Occurrences, accidents and injuries by operation, 2008 to 2017
| Category | Private on behalf of Angel Flight | Commercial air transport | ||||||
| Passenger carrying | Non-passenger carrying flight prior | Non-passenger carrying flight following | Other private | Charter | High capacity air transport | Low capacity air transport | ||
| Occurrences | Incidents | 43 | 16 | 21 | 1,711 | N/A[52] | N/A[52] | N/A[52] |
| Serious incidents | 0 | 1 | 0 | 280 | 146 | 106 | 43 | |
| Total accidents | 4 | 0 | 0 | 539 | 141 | 21 | 3 | |
| Fatal accidents | 2 | 0 | 0 | 72 | 13 | 0 | 1 | |
| Fatal injuries | Crew fatalities | 2 | 0 | 0 | 66 | 11 | 0 | 2 |
| Passenger fatalities | 4 | 0 | 0 | 49 | 16 | 0 | 0 | |
| Total fatalities | 6 | 0 | 0 | 115 | 27 | 0 | 2 | |
| Rate per 10,000 flights | Occurrence rate | 35.1 | 14.09 | 17.4 | 7.17 | N/A | N/A | N/A |
| Accident rate | 2.99 | 0 | 0 | 1.53 | 0.27 | 0.03 | 0.02 | |
| Fatal accident rate | 1.49 | 0 | 0 | 0.2 | 0.02 | 0 | 0.01 | |
| Total flights | 13,389 | 12,067[53] | 12,067[53] | 3,527,079[54] | 5,277,429[54] | 6,352,077 | 1,368,131 | |
| Rate per 10,000 flight hours | Occurrence rate | 27.53 | 11.05 | 13.65 | 7.48 | N/A | N/A | N/A |
| Accident rate | 2.34 | 0 | 0 | 1.59 | 0.35 | 0.02 | 0.02 | |
| Fatal accident rate | 1.17 | 0 | 0 | 0.21 | 0.03 | 0 | 0.01 | |
| Total hours flown | 17,070[55] | 15,387[55] | 15,387[55] | 3,381,998 | 3,994,207 | 13,128,430 | 1,306,556 | |
Table B2 shows results of statistical analyses using the approach documented in Appendix A – Data analysis methods: Quantification of uncertainty and probability based assessments. Comparisons between private flights on behalf of Angel Flight Australia compared to all other private operations are shown. The data in the table is grouped by the occurrence categories where statistical analysis was performed for all occurrences, accidents and fatal accidents.
Statistical tests were performed for the number of safety occurrences for all three types of Angel Flight legs, including aggregated totals. However, due to no accidents being identified in non-passenger carrying repositioning flights, only the passenger carrying and combined Angel Flight rate was calculated based on the aggregate of all calculated passenger carrying and repositioning Angel Flights.
The first six columns of data show the number of occurrences, number of flights and rate of occurrences per 10,000 flights in pairs for Angel Flight (labelled AF), and other private (labelled PV) operations in each group. Data for each specific Angel Flight operation is shown in the column Angel Flight Operation Category as follows:
- Pax Angel Flight – Passenger carrying private flights on behalf of Angel Flight
- Prior AF Non-Pax – Non passenger carrying repositioning flights prior to passenger carrying Angel Flights
- Post AF Non Pax – Non passenger carrying repositioning flights following passenger carrying Angel Flights
- All Non Pax AF – All non passenger carrying repositioning flights prior to and following passenger carrying Angel Flights
- AF Combined – All non passenger carrying repositioning flights prior to and following passenger carrying Angel Flights, and passenger carrying Angel Flights
The columns labelled ‘Probable rate differences: Angel Flight – Other private’ toward the right side of Table B2 show results from the calculation of difference in binomial proportions between the labelled Angel Flight Operational category and other private operations, as described further in Appendix A – Data analysis methods: Quantification of uncertainty and probability based assessments. The data in columns 67% CI and 95% CI show the credible intervals calculated from the difference in the binomial proportions of Angel Flight compared to other private operations. This indicates the expected difference in the rate of Angel Flight occurrences compared to private occurrences per 10,000 flights providing an indication of where the rate difference probably (67%) lies, and where it is very likely (95%) to lie.
For example, from the first row of data, there are probably (67%) between 22.4 and 32.3 more safety occurrences per 10,000 flights for passenger carrying Angel Flights compared to other private operations.
The column ‘Probability (Angel Flight > Other Private)’ shows the calculated binomial probability that Angel Flight has more occurrences per flight compared to other private operations. These calculations are also discussed further in Appendix A – Data analysis methods: Quantification of uncertainty and probability based assessments. The probability presented represents the statistical expected likelihood Angel Flight occurrences per flight were greater than other private operations in each occurrence grouping.
For example, from the first row of data, a probability greater than 99.9% was calculated that safety occurrences were more common per flight for passenger carrying Angel Flight operations combined compared to other private operations. This statistical calculation accounted for the number of flights (13,389 for private passenger carrying flights conducted on behalf of Angel Flight, and approximately 3.5 million flights for private operations) to provide confidence, maximising the use of the data available.
Table B2 shows that the rate of total occurrences per 10,000 flights is almost certainly (>99%) higher for all Angel Flight operation categories compared to other private operations. It is highly likely that there are between 18.1 and 38.0 more safety occurrences per 10,000 flights for passenger carrying Angel Flights compared to the average of other private flights. This was a much larger difference compared to both prior and post non-passenger carrying Angel Flight operations. The combination of all non-passenger carrying Angel Flights were expected to have 3.7 to 13.6 more occurrences per 10,000 flights compared to other private flights.
The passenger carrying Angel Flight accident rate was probably higher (P=84.9%) compared to other private operations. When combining this with the estimated number of non-passenger carrying repositioning flights, it is unlikely (P=17.8%) that the accident rate was higher. In contrast, the fatal accident rate was calculated to be probably higher (P=82.0%) for Angel Flight operations when taking into account non passenger carrying repositioning flights, and very likely (P=96.8%) when considering passenger carrying flights alone. It is highly likely that the Angel Flight passenger carrying fatal accident rate ranges from -0.2 fewer to 3.4 more fatal accidents per 10,000 flights compared to other private operations.
Table B2: Comparison of Angel Flight occurrences with private operations flights prior to and following passenger carrying Angel Flights, 2008 to 2017
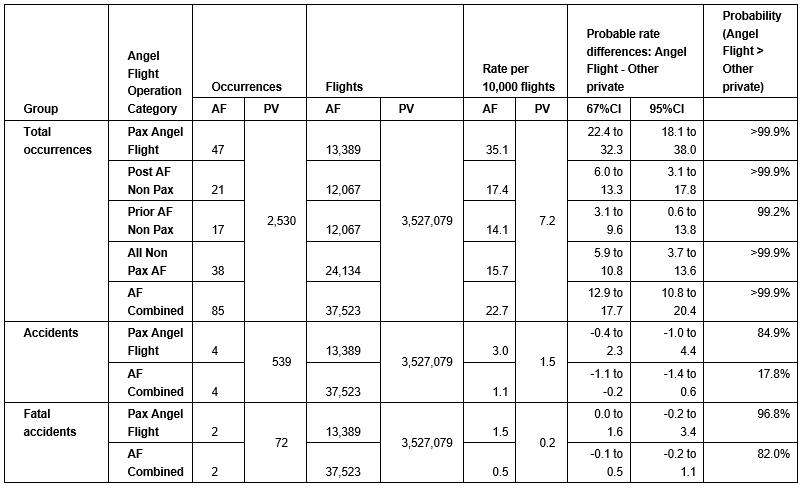
Angel Flight occurrence type analysis results
The following data displays the analysis results of the types of reportable safety occurrences (occurrence types) during flights conducted on behalf of Angel Flight in comparison to other private operations. A full list of occurrence types, along with their definitions, is available on the ATSB website Terminology page associated with the national aviation occurrence database.
Figure B1 displays the relative number of occurrences involving passenger carrying flights conducted on behalf of Angel Flight in five main categories, as shown in the inner ring. Secondary groupings shown in the outer ring of Figure B1 further refine the classification of these occurrences. It is common to have multiple occurrence types reported for each occurrence, therefore, these occurrences should not be aggregated by each sub-category. However, the total number of occurrences in each grouping are displayed in the left side column of tables B3 through to B7 below, with the grand-total occurrences in each table displayed in the title of each.
Figure B1: Passenger carrying Angel Flight safety occurrence groups, 2008 to 2017
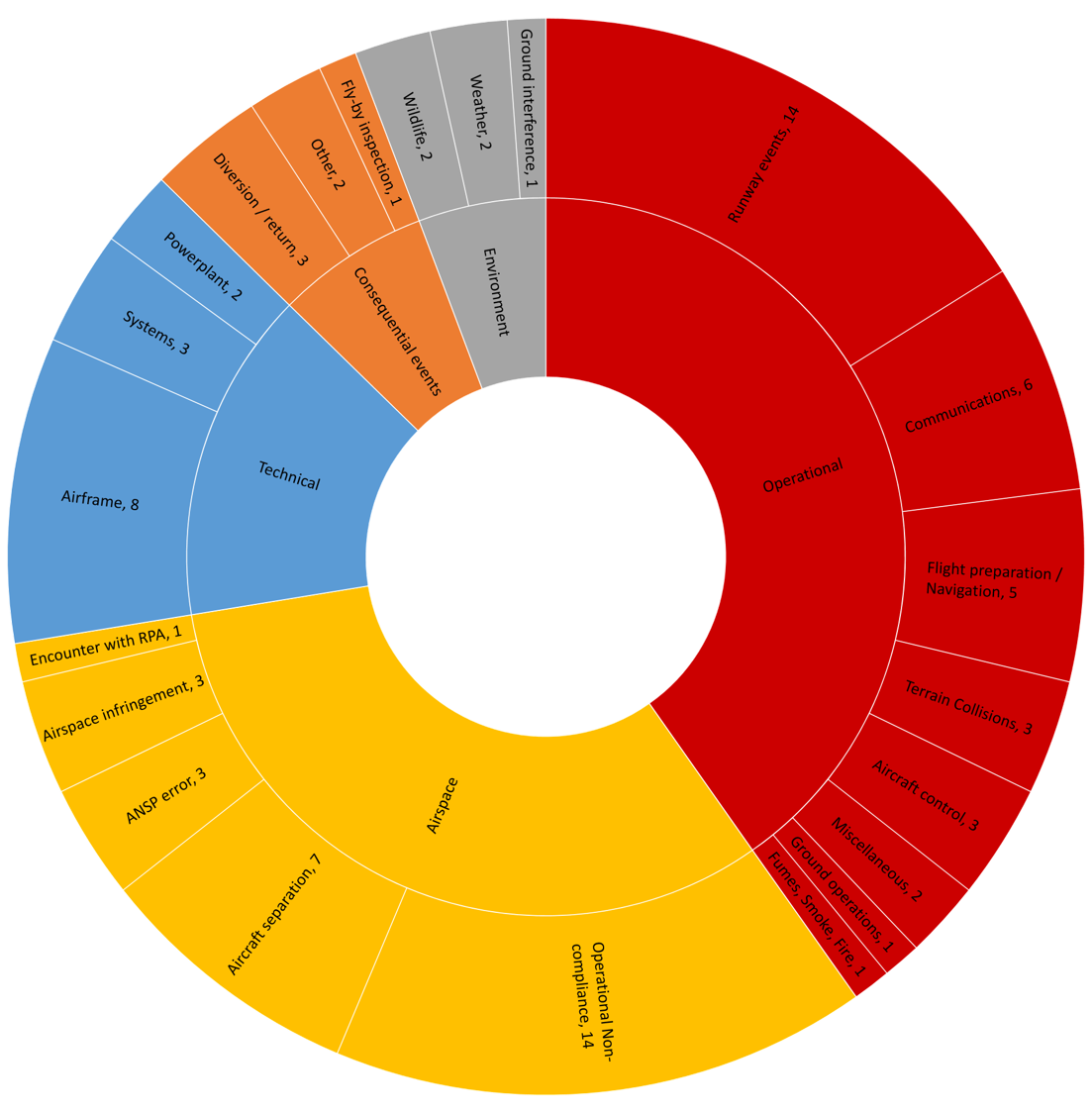
Relative proportions of occurrence groups in Angel Flight and other private operations (Figures B3 – B6)
Figures B3 – B6 show the proportion of occurrence types against the total occurrences in each operational category (as displayed in the legend). These figures are indicated as a pictorial illustration to complement the percentage difference column (labelled “PD”) in Tables B3 – B7 below, being the calculated difference of the percentages in each category.
This provides an indication of the relative prevalence of an occurrence group compared to all other safety occurrences between passenger carrying and non-passenger carrying Angel Flight operations, and other private operations. Numbers above each column show the total number of safety occurrences in each occurrence group. As for Figure B1, these occurrence groups should not be aggregated due to the possibility of multiple occurrence grouping per safety occurrence, however, the overall total presented in the legend can be used for this purpose. Note that the occurrence categories presented align with the outer ring in Figure B1, and in Tables B3 – B7 on the left side “Minor occurrence grouping” column.
For example, the total of five flight preparation and navigation forms about 10.6% (5/47) of all passenger carrying Angel Flight operations, compared to 4.2% (106/2530) of other private operations, equating to a percentage difference of 6.5% (rounded) as shown in Table B3. Note that non-passenger carrying flights are separated from passenger carrying Angel Flights in Figures B3 – B6 to compare and contrast these to each other and other private operations in each occurrence grouping. In contrast, Tables B3 – B7 present passenger carrying and the combined (passenger and non-passenger carrying total) for the statistical analysis due to the analysis focus on passenger carrying flights, and to reduce uncertainty in results.
Results of statistical analysis between Angel Flight and other private operations ordered by largest differences (Tables B3 to B7)
The five tables below B3 through to B7 display similar information to Figure B1, and compare the types of occurrences involving flights conducted on behalf of Angel Flight to all other private operations. Each table contains aggregates for each of the five major occurrence types, as shown in the inner circle of Figure B1. The left side of each table shows groupings of similar types of occurrences, as shown in Figure 10, the outer circle of Figure B1, and the horizontal axis categories of Figures B3-B6. This contains the number of occurrences (in brackets under the name), the rate of occurrences per 10,000 flights and two statistical measures – the beta-binomial probability, and the percentage difference between Angel Flight and other private operations. The occurrence groupings are ordered by the largest statistical differences where Angel Flight had more occurrences per flight compared to private operations.
Figure B2: Extract from Table B3 – Flight preparation and navigation safety occurrences
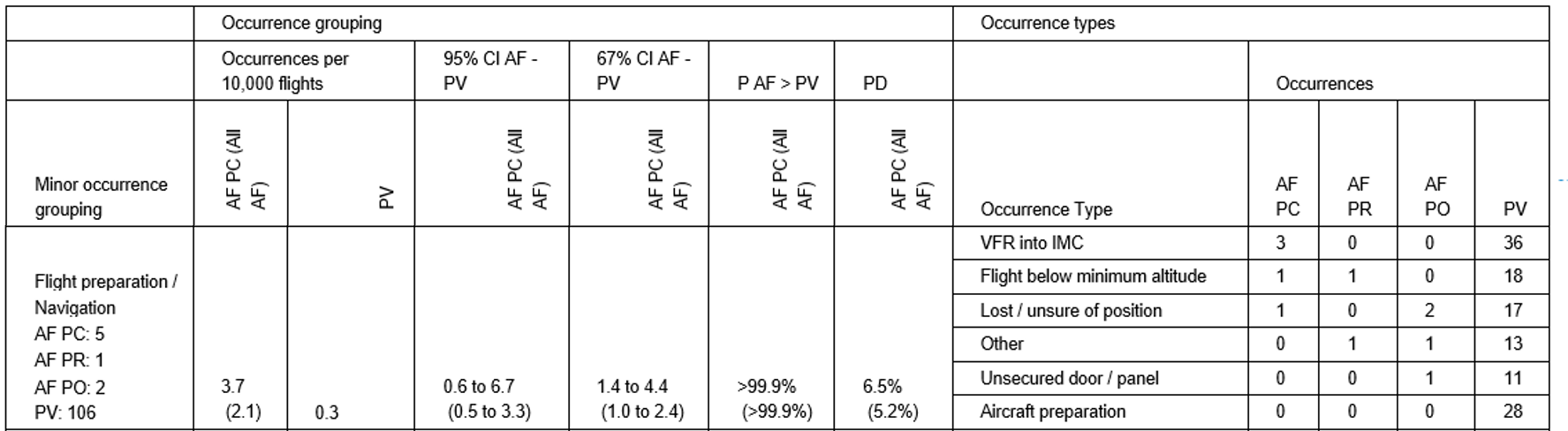
The following abbreviations are used in the column headings of Tables B3 – B7:
- AF PC: Private passenger carrying flights on behalf of Angel Flight
- AF PR: Repositioning flights prior to passenger carrying flights on behalf of Angel Flight
- AF PO: Repositioning flights following passenger carrying flights on behalf of Angel Flight
- All AF: All Angel Flight combined
- PV: Other private flights
- 67%CI / 95%CI: Credible intervals – Probable range (67%) and Highly likely range (95%)
- AF – PV: Angel Flight (Generalised) minus other Private
- P AF > PV: Probability Angel Flight (Generalised) greater than other private
- PD: Percentage difference between Angel Flight categories and other private operations.
The following describes the data under each column in Tables B3 – B7. To aid use of these tables, a sample interpretation using the known fatal accident pre-cursor flight preparation and navigation is also presented below. Reference data for the sample is contained in Figure B2.
Minor Occurrence Grouping: Description of the occurrence grouping containing similar occurrences. This shows the name of the occurrence grouping, for example “Flight preparation / navigation”, and shows the total number of occurrence in this group for each operational category, in this case, 5 passenger carrying, 1 prior and 2 post repositioning Angel Flights had flight preparation or navigational issues compared to 106 private flights.
AF PC (All AF): The five columns labelled AF PC (All AF) indicate where results of two parallel analyses are presented for Angel Flight occurrences; the primary passenger carrying analysis, labelled AF PC, and the combined analysis for all privately operated passenger and non-passenger carrying flights conducted on behalf of Angel Flight, presented in brackets.
Occurrences per 10,000 flights: The rate of nominated occurrences per 10,000 flights for Angel Flight, labelled AF PC (All AF), and all other private operations, labelled PV. In the example above: 3.7 (2.1), indicates the Angel Flight passenger carrying rate of 3.7 flight preparation or navigation safety occurrences per 10,000 flights, with a combined rate of 2.1 safety occurrences per 10,000 flights. For comparison, the private rate in this example is 0.3.
67%CI / 95%CI: The data in columns 67% CI and 95% CI show the credible intervals calculated from the difference in the binomial proportions of Angel Flight compared to other private operations. Further explanation of these can be found in the descriptions for Table B2, and Appendix A – Data analysis methods: Quantification of uncertainty and probability based assessments.
P AF > PV: Shows the calculated binomial probability that Angel Flight has relatively more occurrences per flight compared to other private operations. These calculations are discussed further in Appendix A – Data analysis methods: Quantification of uncertainty and probability based assessments, with other discussions explained for Table B2. In the example, a probability greater than 99.9% was calculated that flight preparation and navigation was more common per flight for both passenger carrying and all Angel Flight operations combined compared to other private operations.
Conversely, note also that a result of 37.2%, as shown in table B5 for occurrences relating to powerplant and propulsion, indicates a 62.8% chance that other private operations were greater. Records marked as N/A indicate where there were no Angel Flight occurrences identified producing an invalid statistical result with the techniques used. Statistical parameters used are discussed in Appendix A – Data analysis methods.
PD: Percentage differences shown indicate differences in each occurrence category between Angel Flight and other private operations against the total occurrences in each type of operation. This is calculated by subtracting the percentage of each operation in Angel Flight from Private operations percentage. It is also useful to provide an indication of the relative frequency of these occurrences where no Angel Flight occurrences were identified in a category (and no statistical result exists). For example, there were no reported fuel related occurrences for passenger carrying flights conducted on behalf of Angel Flight and this was 4.7% lower than fuel related occurrences in other private operations.
It is important to note that all percentages were calculated from the total of all occurrences in each operational group, for example, 47 occurrences from passenger carrying Angel Flights and 2,530 other private operations safety occurrences, shown in Table B1.
Further description for this calculation using the example of flight preparation and navigation can be found in the description for Figures B3-B6, where this is shown pictorially.
Occurrence types: Occurrence types shown on the right side of tables B3 to B7 display more specific information relating to the occurrence grouping. These are ordered by types of occurrence with the largest number of Angel Flight occurrences. This is shown for all four operational categories. For example, Flight preparation or navigation – VFR into IMC was recorded in three passenger carrying Angel Flights, 36 cases for private flights with no cases being recorded in either operational categories of non-passenger carrying Angel Flights.
Sample interpretation of data analysis – flight preparation and navigation
Tables B3-B7 are intended to be used as a tool to identify occurrence groups that are most different between the two types of operations, to drive safety actions in areas most likely to reduce the increased rate of occurrences for during flights conducted on behalf of Angel Flight. The following paragraph provides a brief interpretation of a comparison between Angel Flight and other private operations using the tabled data for the flight preparation and navigation occurrence grouping using the specific figures published. This rationale could be applied across all other occurrence groupings.
For both passenger carrying and the combination of all Angel Flight operations, there was a very high probability (more than 999 in 1,000 chance) that flight preparation and navigation occurrences were more likely to occur in comparison to other private operations. For every 10,000 flights conducted in each operational category, is very likely (95%CI) there would be at least 0.6 more flight preparation and navigation occurrences during passenger carrying Angel Flights compared to other private operations, probably (67%CI) ranging between 1.4 and 4.4. As the lower bound of the 95%CI is above zero, this also indicates statistical significance in this case.
Figure B3: Operational related safety occurrence groups by total proportion of operation category, 2008 to 2017
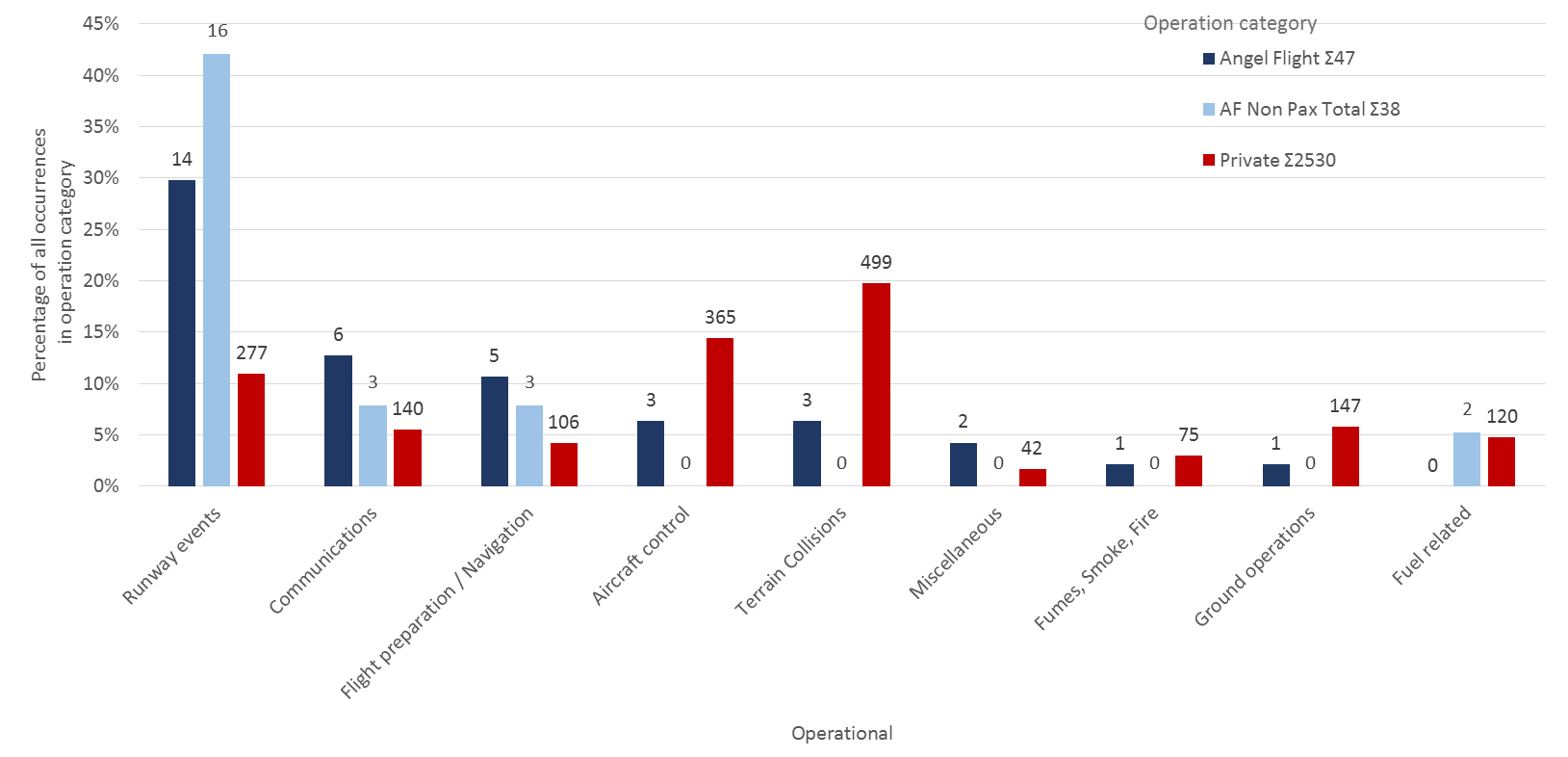
Table B3: Operational Angel Flight (Passenger carrying and combined) occurrences ordered by largest statistical differences to other private operations, 2008 to 2017 (Total occurrences: AF PC: Σ25, AF PR Σ7, AF PO: Σ13, PV Σ1,344)
| Occurrence grouping | Occurrence types | ||||||||||
| Occurrences per 10,000 flights | 95% CI AF - PV | 67% CI AF - PV | P AF > PV | PD | Occurrences | ||||||
| Minor occurrence grouping | AF PC (All AF) | PV | AF PC (All AF) | AF PC (All AF) | AF PC (All AF) | AF PC (All AF) | Occurrence Type | AF PC | AF PR | AF PO | PV |
| Runway events AF PC: 14 AF PR: 7 AF PO: 9 PV: 277 | 10.5 (8.0) | 0.8 | 4.5 to 15.3 (4.5 to 10.1) | 6.5 to 11.8 (5.6 to 8.4) | >99.9% (>99.9%) | 18.8% (24.3%) | Runway Incursion | 11 | 5 | 8 | 72 |
| Depart / App / Land Wrong Runway | 3 | 2 | 1 | 20 | |||||||
| Runway Excursion | 1 | 0 | 0 | 182 | |||||||
| Runway undershoot | 0 | 0 | 0 | 6 | |||||||
| Other | 0 | 0 | 0 | 4 | |||||||
| Communications AF PC: 6 AF PR: 2 AF PO: 1 PV: 140 | 4.5 (2.4) | 0.4 | 0.9 to 7.7 (0.6 to 3.6) | 1.9 to 5.2 (1.1 to 2.6) | >99.9% (>99.9%) | 7.2% (5.1%) | Air-ground-air | 6 | 2 | 1 | 128 |
| Other | 0 | 0 | 0 | 8 | |||||||
| Transponder related | 0 | 0 | 0 | 4 | |||||||
| Flight preparation / Navigation AF PC: 5 AF PR: 1 AF PO: 2 PV: 106 | 3.7 (2.1) | 0.3 | 0.6 to 6.7 (0.5 to 3.3) | 1.4 to 4.4 (1.0 to 2.4) | >99.9% (>99.9%) | 6.5% (5.2%) | VFR into IMC | 3 | 0 | 0 | 36 |
| Flight below minimum altitude | 1 | 1 | 0 | 18 | |||||||
| Lost / unsure of position | 1 | 0 | 2 | 17 | |||||||
| Other | 0 | 1 | 1 | 13 | |||||||
| Unsecured door / panel | 0 | 0 | 1 | 11 | |||||||
| Aircraft preparation | 0 | 0 | 0 | 28 | |||||||
| Miscellaneous AF PC: 2 AF PR: 0 AF PO: 0 PV: 42 | 1.5 (0.5) | 0.1 | -0.1 to 3.5 (-0.1 to 1.2) | 0.1 to 1.7 (0.0 to 0.5) | 98.8% (92.4%) | 2.6% (0.7%) | Other | 2 | 0 | 0 | 15 |
| Security related | 0 | 0 | 0 | 1 | |||||||
| Unauthorised low flying | 0 | 0 | 0 | 4 | |||||||
| Warning Devices | 0 | 0 | 0 | 22 | |||||||
| Aircraft control AF PC: 3 AF PR: 0 AF PO: 0 PV: 365 | 2.2 (0.8) | 1.0 | -0.8 to 3.8 (-1.0 to 0.7) | -0.4 to 1.8 (-0.8 to 0.0) | 83.6% (25.7%) | -8.1% (-10.9%) | Loss of control | 3 | 0 | 0 | 143 |
| Other | 0 | 0 | 0 | 21 | |||||||
| Stall warnings | 0 | 0 | 0 | 1 | |||||||
| Unstable approach | 0 | 0 | 0 | 3 | |||||||
| Wheels up landing | 0 | 0 | 0 | 62 | |||||||
| Airframe overspeed | 0 | 0 | 0 | 1 | |||||||
| Control issues | 0 | 0 | 0 | 32 | |||||||
| Hard landing | 0 | 0 | 0 | 99 | |||||||
| Incorrect configuration | 0 | 0 | 0 | 17 | |||||||
| In-flight break-up | 0 | 0 | 0 | 4 | |||||||
| Fumes, Smoke, Fire AF PC: 1 AF PR: 0 AF PO: 0 PV: 75 | 0.7 (0.3) | 0.2 | -0.3 to 2.0 (-0.3 to 0.6) | -0.2 to 0.6 (-0.2 to 0.1) | 75.3% (45.2%) | -0.8% (-1.8%) | Fumes | 1 | 0 | 0 | 22 |
| Smoke | 1 | 0 | 0 | 43 | |||||||
| Fire | 0 | 0 | 0 | 22 | |||||||
| Terrain Collisions AF PC: 3 AF PR: 0 AF PO: 0 PV: 499 | 2.2 (0.8) | 1.4 | -1.2 to 3.4 (-1.3 to 0.3) | -0.7 to 1.4 (-1.2 to -0.4) | 70.5% (10.3%) | -13.3% (-16.2%) | Collision with terrain | 3 | 0 | 0 | 319 |
| Ground strike | 1 | 0 | 0 | 149 | |||||||
| Wirestrike | 0 | 0 | 0 | 30 | |||||||
| Controlled flight into terrain | 0 | 0 | 0 | 11 | |||||||
| Ground operations AF PC: 1 AF PR: 0 AF PO: 0 PV: 147 | 0.7 (0.3) | 0.4 | -0.5 to 1.8 (-0.5 to 0.4) | -0.4 to 0.4 (-0.4 to -0.1) | 57.3% (21%) | -3.7% (-4.6%) | Collision on ground | 1 | 0 | 0 | 100 |
| Foreign object damage / debris | 0 | 0 | 0 | 13 | |||||||
| Ground handling | 0 | 0 | 0 | 2 | |||||||
| Ground prox | 0 | 0 | 0 | 1 | |||||||
| Injury | 0 | 0 | 0 | 2 | |||||||
| Jet blast / Prop / Rotor wash | 0 | 0 | 0 | 2 | |||||||
| Other | 0 | 0 | 0 | 7 | |||||||
| Taxiing collision / Near collision | 0 | 0 | 0 | 64 | |||||||
| Ground proximity alerts / warnings AF PC: 0 AF PR: 0 AF PO: 0 PV: 1 | 0.0 (0.0) | 0.0 | 0.0 to 0.0 (0.0 to 0.0) | 0.0 to 0.0 (0.0 to 0.0) | N/A (N/A) | 0.0% (0.0%) | Ground proximity alerts / warnings | 0 | 0 | 0 | 1 |
| Regulations and SOPs AF PC: 0 AF PR: 0 AF PO: 0 PV: 2 | 0.0 (0.0) | 0.0 | 0.0 to 0.0 (0.0 to 0.0) | 0.0 to 0.0 (0.0 to 0.0) | N/A (N/A) | -0.1% (-0.1%) | Other | 0 | 0 | 0 | 1 |
| Standard Operating Procedures | 0 | 0 | 0 | 1 | |||||||
| Aircraft loading AF PC: 0 AF PR: 0 AF PO: 0 PV: 4 | 0.0 (0.0) | 0.0 | 0.0 to 0.0 (0.0 to 0.0) | 0.0 to 0.0 (0.0 to 0.0) | N/A (N/A) | -0.2% (-0.2%) | Dangerous goods | 0 | 0 | 0 | 1 |
| Loading related | 0 | 0 | 0 | 3 | |||||||
| Significant event AF PC: 0 AF PR: 0 AF PO: 0 PV: 14 | 0.0 (0.0) | 0.0 | -0.1 to 0.0 (-0.1 to 0.0) | 0.0 to 0.0 (0.0 to 0.0) | N/A (N/A) | -0.6% (-0.6%) | Other | 0 | 0 | 0 | 14 |
| Crew and cabin safety AF PC: 0 AF PR: 0 AF PO: 0 PV: 19 | 0.0 (0.0) | 0.1 | -0.1 to 0.0 (-0.1 to 0.0) | -0.1 to 0.0 (-0.1 to 0.0) | N/A (N/A) | -0.8% (-0.8%) | Depressurisation | 0 | 0 | 0 | 5 |
| Flight crew incapacitation | 0 | 0 | 0 | 12 | |||||||
| Unrestrained occupants / objects | 0 | 0 | 0 | 2 | |||||||
| Warning device AF PC: 0 AF PR: 0 AF PO: 0 PV: 27 | 0.0 (0.0) | 0.1 | -0.1 to 0.0 (-0.1 to 0.0) | -0.1 to -0.1 (-0.1 to -0.1) | N/A (N/A) | -1.1% (-1.1%) | Landing gear unsafe indication | 0 | 0 | 0 | 27 |
| Fuel related AF PC: 0 AF PR: 0 AF PO: 2 PV: 120 | 0.0 (0.5) | 0.3 | -0.4 to -0.3 (-0.3 to 0.9) | -0.4 to -0.3 (-0.3 to 0.3) | N/A (63.6%) | -4.7% (-2.4%) | Contamination | 0 | 0 | 0 | 16 |
| Exhaustion | 0 | 0 | 0 | 12 | |||||||
| Leaking or venting | 0 | 0 | 0 | 14 | |||||||
| Low fuel | 0 | 0 | 0 | 6 | |||||||
| Other | 0 | 0 | 1 | 4 | |||||||
| Starvation | 0 | 0 | 1 | 70 | |||||||
Figure B4: Airspace related safety occurrence groups by total proportion of operation category, 2008 to 2017
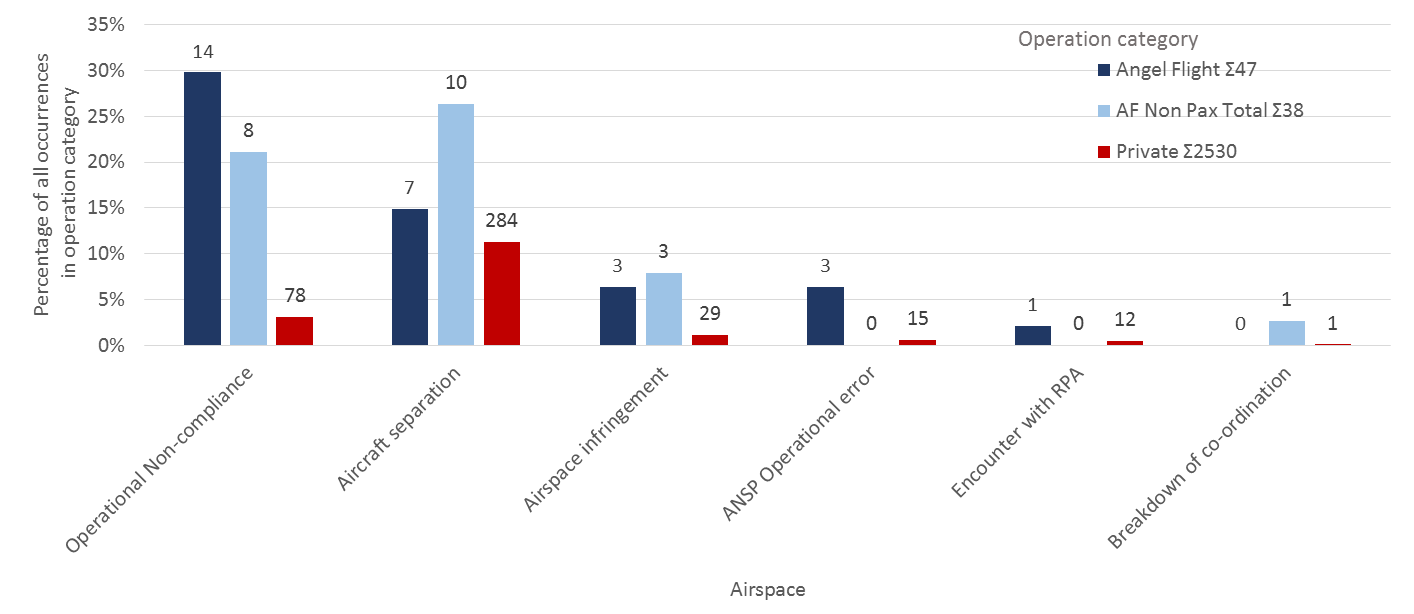
Table B4: Airspace related Angel Flight (Passenger carrying and combined) occurrences ordered by largest statistical differences to other private operations, 2008 to 2017 (Total occurrences: AF PC: Σ20, AF PR Σ9, AF PO: Σ8, PV Σ369)
| Occurrence grouping | Occurrence types | ||||||||||
| Occurrences per 10,000 flights | 95% CI AF - PV | 67% CI AF - PV | P AF > PV | PD | Occurrences | ||||||
| Minor occurrence grouping | AF PC (All AF) | PV | AF PC (All AF) | AF PC (All AF) | AF PC (All AF) | AF PC (All AF) | Occurrence Type | AF PC | AF PR | AF PO | PV |
| Operational Non-compliance AF PC: 14 AF PR: 4 AF PO: 4 PV: 78 | 10.5 (5.9) | 0.2 | 5.1 to 15.8 (3.3 to 8.1) | 7.1 to 12.4 (4.3 to 6.7) | >99.9% (>99.9%) | 26.7% (22.8%) | Operational Non-compliance | 14 | 4 | 4 | 78 |
| Verbal instruction | 9 | 3 | 3 | 22 | |||||||
| Published information | 3 | 0 | 0 | 13 | |||||||
| ANSP Operational error AF PC: 3 AF PR: 0 AF PO: 0 PV: 15 | 2.2 (0.8) | 0.0 | 0.2 to 4.7 (0.0 to 1.7) | 0.6 to 2.8 (0.2 to 1.0) | >99.9% (>99.9%) | 5.8% (2.9%) | Information / procedural error | 3 | 0 | 0 | 14 |
| Failure to pass traffic | 0 | 0 | 0 | 1 | |||||||
| Aircraft separation AF PC: 7 AF PR: 5 AF PO: 5 PV: 284 | 5.2 (4.5) | 0.8 | 1.0 to 8.4 (1.7 to 5.9) | 2.1 to 5.8 (2.5 to 4.6) | >99.9% (>99.9%) | 3.7% (8.8%) | Loss of separation | 6 | 3 | 0 | 46 |
| Issues | 1 | 2 | 3 | 152 | |||||||
| Airborne collision alert system warning | 0 | 1 | 0 | 12 | |||||||
| Collision | 0 | 0 | 0 | 3 | |||||||
| Loss of separation assurance | 0 | 0 | 2 | 7 | |||||||
| Near collision | 0 | 0 | 0 | 74 | |||||||
| Airspace infringement AF PC: 3 AF PR: 1 AF PO: 2 PV: 29 | 2.2 (1.6) | 0.1 | 0.1 to 4.7 (0.4 to 2.8) | 0.6 to 2.8 (0.7 to 1.9) | >99.9% (>99.9%) | 5.2% (5.9%) | Airspace infringement | 3 | 1 | 2 | 29 |
| PRD | 2 | 0 | 1 | 2 | |||||||
| Controlled airspace | 1 | 0 | 1 | 13 | |||||||
| Encounter with RPA AF PC: 1 AF PR: 0 AF PO: 0 PV: 12 | 0.7 (0.3) | 0.0 | -0.1 to 2.2 (-0.1 to 0.8) | 0.0 to 0.8 (0.0 to 0.3) | 95.6% (88.1%) | 1.7% (0.7%) | Near encounter with RPA | 1 | 0 | 0 | 12 |
| Breakdown of co-ordination AF PC: 0 AF PR: 0 AF PO: 1 PV: 1 | 0.0 (0.3) | 0.0 | 0.0 to 0.0 (0.0 to 0.8) | 0.0 to 0.0 (0.0 to 0.3) | N/A (99%) | 0.0% (1.1%) | Breakdown of co-ordination | 0 | 0 | 1 | 1 |
| Other AF PC: 0 AF PR: 0 AF PO: 0 PV: 4 | 0.0 (0.0) | 0.0 | 0.0 to 0.0 (0.0 to 0.0) | 0.0 to 0.0 (0.0 to 0.0) | N/A (N/A) | -0.2% (-0.2%) | Other | 0 | 0 | 0 | 4 |
Figure B5: Technical failure safety occurrence groups by total proportion of operation category, 2008 to 2017

Table B5: Technical failures related to Angel Flight (Passenger carrying and combined) occurrences ordered by largest statistical differences to other private operations, 2008 to 2017 (Total occurrences: AF PC: Σ13, AF PR Σ3, AF PO: Σ3, PV Σ1,139)
| Occurrence grouping | Occurrence types | ||||||||||
| Occurrences per 10,000 flights | 95% CI AF - PV | 67% CI AF - PV | P AF > PV | PD | Occurrences | ||||||
| Minor occurrence grouping | AF PC (All AF) | PV | AF PC (All AF) | AF PC (All AF) | AF PC (All AF) | AF PC (All AF) | Occurrence Type | AF PC | AF PR | AF PO | PV |
| Airframe AF PC: 8 AF PR: 1 AF PO: 0 PV: 400 | 6.0 (2.4) | 1.1 | 1.1 to 9.0 (-0.2 to 2.9) | 2.4 to 6.3 (0.3 to 1.8) | >99.9% (96.9%) | 1.2% (-5.2%) | Landing gear / Indication | 6 | 1 | 0 | 320 |
| Objects falling from aircraft | 1 | 0 | 0 | 31 | |||||||
| Other | 1 | 0 | 0 | 7 | |||||||
| Windows | 1 | 0 | 0 | 13 | |||||||
| Rotors / tail rotor | 0 | 0 | 0 | 1 | |||||||
| Control surface | 0 | 0 | 0 | 2 | |||||||
| Doors / Exits | 0 | 0 | 0 | 20 | |||||||
| Furnishings and fittings | 0 | 0 | 0 | 3 | |||||||
| Fuselage / Wings / Empennage | 0 | 0 | 0 | 4 | |||||||
| Landing gear | 0 | 0 | 0 | 64 | |||||||
| Systems AF PC: 3 AF PR: 2 AF PO: 0 PV: 291 | 2.2 (1.3) | 0.8 | -0.6 to 4.0 (-0.5 to 1.7) | -0.2 to 2.0 (-0.2 to 0.9) | 90% (79.9%) | -5.1% (-5.6%) | Avionics / Flight Instruments | 1 | 0 | 0 | 98 |
| Electrical | 1 | 2 | 0 | 90 | |||||||
| Other | 1 | 0 | 0 | 8 | |||||||
| Fire protection | 0 | 0 | 0 | 1 | |||||||
| Flight controls | 0 | 0 | 0 | 27 | |||||||
| Flight instruments | 0 | 0 | 0 | 3 | |||||||
| Fuel | 0 | 0 | 0 | 32 | |||||||
| Hydraulic | 0 | 0 | 0 | 16 | |||||||
| Air / Pressurisation | 0 | 0 | 0 | 13 | |||||||
| Anti-ice protection | 0 | 0 | 0 | 3 | |||||||
| Avionics | 0 | 0 | 0 | 17 | |||||||
| Powerplant / propulsion AF PC: 2 AF PR: 0 AF PO: 3 PV: 509 | 1.5 (1.3) | 1.4 | -1.4 to 2.1 (-1.1 to 1.1) | -1.2 to 0.4 (-0.8 to 0.3) | 42.5% (37.2%) | -15.9% (-14.2%) | Engine failure or malfunction | 2 | 0 | 2 | 411 |
| Partial power loss / rough running | 1 | 0 | 1 | 120 | |||||||
| Propellers / Rotor malfunction | 0 | 0 | 0 | 17 | |||||||
| Total power loss / engine failure | 0 | 0 | 0 | 107 | |||||||
| Transmission and gearboxes | 0 | 0 | 0 | 9 | |||||||
| Abnormal engine indications | 0 | 0 | 1 | 74 | |||||||
| Other | 0 | 0 | 0 | 27 | |||||||
Figure B6: Environmental related safety occurrence groups by total proportion of operation category, 2008 to 2017
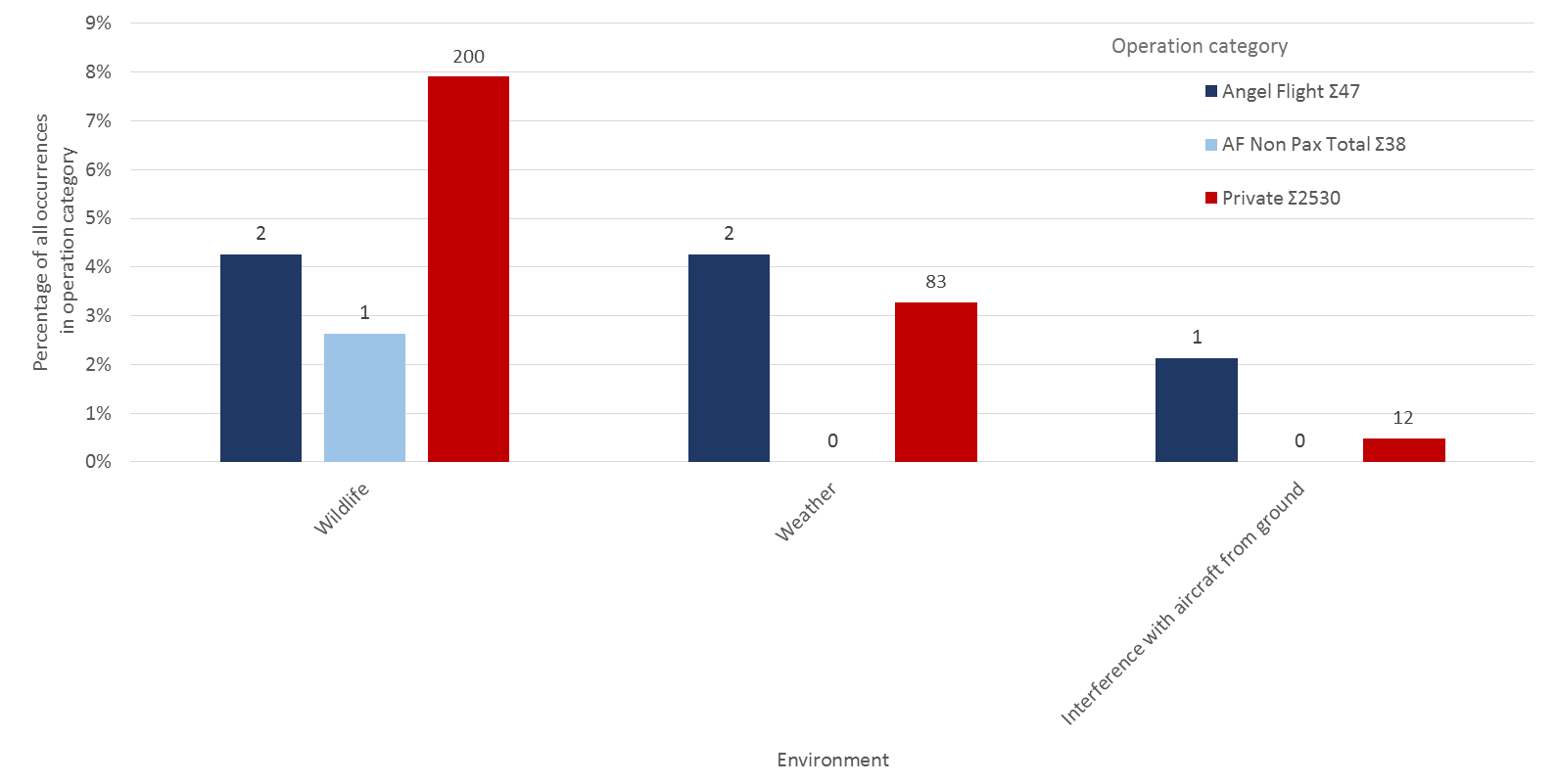
Table B6: Environment related Angel Flight (Passenger carrying and combined) occurrences ordered by largest statistical differences to other private operations, 2008 to 2017 (Total occurrences: AF PC: Σ5, AF PR Σ0, AF PO: Σ1, PV Σ296)
| Occurrence grouping | Occurrence types | ||||||||||
| Occurrences per 10,000 flights | 95% CI AF - PV | 67% CI AF - PV | P AF > PV | PD | Occurrences | ||||||
| Minor occurrence grouping | AF PC (All AF) | PV | AF PC (All AF) | AF PC (All AF) | AF PC (All AF) | AF PC (All AF) | Occurrence Type | AF PC | AF PR | AF PO | PV |
| Weather AF PC: 2 AF PR: 0 AF PO: 0 PV: 83 | 1.5 (0.5) | 0.2 | -0.2 to 3.3 (-0.2 to 1.1) | 0.0 to 1.6 (-0.2 to 0.4) | 95.9% (77.8%) | 1.0% (-0.9%) | Other | 1 | 0 | 0 | 37 |
| Unforecast weather | 1 | 0 | 0 | 9 | |||||||
| Windshear / microburst | 0 | 0 | 0 | 7 | |||||||
| Turbulence / Windshear / Microburst | 0 | 0 | 0 | 19 | |||||||
| Icing | 0 | 0 | 0 | 7 | |||||||
| Lightning strike | 0 | 0 | 0 | 7 | |||||||
| Interference with aircraft from ground AF PC: 1 AF PR: 0 AF PO: 0 PV: 12 | 0.7 (0.3) | 0.0 | -0.1 to 2.2 (-0.1 to 0.8) | 0.0 to 0.8 (0.0 to 0.3) | 95.6% (88.1%) | 1.7% (0.7%) | Interference with aircraft from ground | 1 | 0 | 0 | 12 |
| Wildlife AF PC: 2 AF PR: 0 AF PO: 1 PV: 200 | 1.5 (0.8) | 0.6 | -0.5 to 3.0 (-0.5 to 1.2) | -0.4 to 1.3 (-0.3 to 0.5) | 82.3% (64.2%) | -3.7% (-4.4%) | Birdstrike | 2 | 0 | 1 | 165 |
| Other | 0 | 0 | 0 | 10 | |||||||
| Animal strike | 0 | 0 | 0 | 26 | |||||||
| Other AF PC: 0 AF PR: 0 AF PO: 0 PV: 1 | 0.0 (0.0) | 0.0 | 0.0 to 0.0 (0.0 to 0.0) | 0.0 to 0.0 (0.0 to 0.0) | N/A (N/A) | 0.0% (0.0%) | Other | 0 | 0 | 0 | 1 |
Table B7: Infrastructure related Angel Flight (Passenger carrying and combined) occurrences ordered by largest statistical differences to other private operations, 2008 to 2017 (Total occurrences: AF PC: Σ0, AF PR Σ0, AF PO: Σ0, PV Σ14)
| Occurrence grouping | Occurrence types | ||||||||||
| Occurrences per 10,000 flights | 95% CI AF - PV | 67% CI AF - PV | P AF > PV | PD | Occurrences | ||||||
| Minor occurrence grouping | AF PC (All AF) | PV | AF PC (All AF) | AF PC (All AF) | AF PC (All AF) | AF PC (All AF) | Occurrence Type | AF PC | AF PR | AF PO | PV |
| Runway lighting AF PC: 0 AF PR: 0 AF PO: 0 PV: 4 | 0.0 (0.0) | 0.0 | 0.0 to 0.0 (0.0 to 0.0) | 0.0 to 0.0 (0.0 to 0.0) | N/A (N/A) | -0.2% (-0.2%) | Runway lighting | 0 | 0 | 0 | 4 |
| Aerodrome related AF PC: 0 AF PR: 0 AF PO: 0 PV: 7 | 0.0 (0.0) | 0.0 | 0.0 to 0.0 (0.0 to 0.0) | 0.0 to 0.0 (0.0 to 0.0) | N/A (N/A) | -0.3% (-0.3%) | Other | 0 | 0 | 0 | 7 |
| Other AF PC: 0 AF PR: 0 AF PO: 0 PV: 10 | 0.0 (0.0) | 0.0 | 0.0 to 0.0 (0.0 to 0.0) | 0.0 to 0.0 (0.0 to 0.0) | N/A (N/A) | -0.4% (-0.4%) | Other | 0 | 0 | 0 | 10 |
Appendix C – Angel Flight occurrence summaries
The following tables show the summaries of each reported incident or accident identified as occurring on either a passenger carrying flight (Table C1), a repositioning flight prior to a passenger carrying flight (Table C2) or a repositioning flight post a passenger carrying flight conducted on behalf of Angel Flight Australia (Table C3). These incidents were identified using the techniques described in Appendix A, and all were reviewed manually to positively confirm the records related to Angel Flight organised flights.
Table C1: Summaries of reported safety occurrences during private passenger carrying flights conducted on behalf Angel Flight, 2005 to 2017
| ATSB Reference Number | Occurrence Category | Fatal Injuries | Occurrence Date | Location | Occurrence Types | ATSB Summary |
| 200506303 | Incident | 0 | 22 Nov 2005 | 46km S Nowra, Aerodrome | Systems: Electrical; Diversion / return: Diversion / return | While the aircraft was en route at 7,500 ft in IMC, the alternator failed. The pilot elected to divert to Nowra for a landing without incident. |
| 200506574 | Incident | 0 | 10 Dec 2005 | 19km E Chinchilla | Systems: Electrical | While en-route, the aircraft's alternator failed. The pilot advised ATC that the radio equipment had to be shut down due to the problem. They issued the pilot with a discreet transponder code and the aircraft proceeded to Archerfield without further incident. |
| 200506905 | Incident | 0 | 27 Dec 2005 | Coffs Harbour, Aerodrome | Runway events: Runway Incursion | While taxiing after landing, the aircraft crossed runway 10 without clearance. |
| 200601354 | Incident | 0 | 12 Mar 2006 | Archerfield, Aerodrome | Airframe: Landing gear; Airframe: Landing gear / Indication | During the landing roll, the right main tyre deflated. The pilot stopped the aircraft on the runway strip and the wheel fairing was removed before the aircraft was towed clear. |
| 200602983 | Incident | 0 | 12 May 2006 | Bankstown, Aerodrome | Aircraft separation: Issues; Aircraft separation: Issues | The pilot reported that shortly after turning onto the assigned SID heading within the GAAP CTR, his aircraft was overflown by another aircraft in close proximity. |
| 200605074 | Incident | 0 | 29 Aug 2006 | Cooma, Aerodrome | Diversion / return: Diversion / return; Warning device: Landing gear unsafe indication; Airframe: Landing gear / Indication | When the landing gear was selected down, the pilot received an unsafe landing gear indication and diverted to Canberra. ATC declared a local standby for the aircraft's arrival. |
| 200705246 | Incident | 0 | 11 Aug 2007 | Bankstown Aerodrome | Runway events: Runway Incursion | The aircraft entered the runway without clearance. ATC instructed an aircraft on final approach to go around. |
| 200707377 | Incident | 0 | 23 Oct 2007 | Essendon Aerodrome, 050° M 15Km | Missed approach / go-around: Missed approach / go-around; Communications: Air-ground-air; Aircraft separation: Loss of separation assurance | While the aircraft was on approach, ATC could not establish communication with the pilot. A green light was displayed for a landing clearance, but the aircraft conducted a go-around. Communications were subsequently re-established. |
| 200707648 | Incident | 0 | 5 Dec 2007 | Bankstown Aerodrome | Runway events: Runway Incursion | The aircraft entered the runway without a clearance. |
| 200800346 | Incident | 0 | 20 Jan 2008 | Bankstown Aerodrome | Wildlife: Birdstrike | During final approach, the aircraft struck a bird that impacted the left main windscreen. |
| 200802093 | Incident | 0 | 30 Mar 2008 | Bathurst Aerodrome, 210° M 56Km | Airframe: Other; Diversion / return: Diversion / return | During the cruise, the pilot reported diverting to Bathurst due to a vibrating aircraft. The aircraft landed safely. |
| 200803172 | Incident | 0 | 11 May 2008 | Bankstown Aerodrome | Runway events: Depart / App / Land Wrong Runway; Operational Non-compliance: Verbal instruction; Operational Non-compliance: Operational Non-compliance | The aircraft was cleared to join final for runway 11, but was subsequently observed on downwind for runway 29. |
| 200804895 | Incident | 0 | 25 July 2008 | KAMBA (IFR) | Operational Non-compliance: Verbal instruction; Communications: Air-ground-air; ANSP Operational error: Information / procedural error; Operational Non-compliance: Operational Non-compliance | During the climb, the pilot incorrectly readback the assigned level. The trainee and supervising controller did not detect the incorrect readback. As the aircraft climbed through the assigned level the CLAM activated. |
| 200806888 | Incident | 0 | 20 Oct 2008 | Williamtown Aerodrome, N M 4Km | Aircraft separation: Loss of separation; Operational Non-compliance: Verbal instruction; Operational Non-compliance: Published information; Operational Non-compliance: Operational Non-compliance; ANSP Operational error: Information / procedural error | The pilot of the PA-28 was instructed to maintain runway heading after departure, but was subsequently observed to turn left. This resulted in an infringement of separation standards with a formation of F/A-18s operating in activated airspace 2 NM to the north. To avoid further conflict, the pilot of the PA-28 was given a heading away from the airspace, resulting in the aircraft operating below the minimum safe altitude in IMC. |
| 200807761 | Incident | 0 | 1 Dec 2008 | Benalla Aerodrome, E M 15Km | Interference with aircraft from ground: Interference with aircraft from ground; Encounter with RPA: Near encounter with RPA | During cruise at 7,000 ft, the pilot sighted a model aircraft at the same altitude. When the model aircraft turned towards the PA-34, the pilot took immediate evasive action. |
| 200905403 | Incident | 0 | 2 Sept 2009 | Gladstone Aerodrome | Operational Non-compliance: Published information; Runway events: Runway Incursion; Operational Non-compliance: Operational Non-compliance | During works on the runway 10 strip, the safety vehicle and the workers were located within the runway strip while an aircraft took off on runway 10. The safety officer did not hear the required taxi broadcast from the pilot. |
| 200905594 | Incident | 0 | 13 Sept 2009 | Bankstown Aerodrome | Operational Non-compliance: Verbal instruction; Runway events: Depart / App / Land Wrong Runway; Operational Non-compliance: Operational Non-compliance | While inbound, the pilot was instructed to join crosswind for runway 29R. The pilot read back the instruction correctly, but the aircraft was subsequently observed to be on a left downwind for runway 29L. |
| 200906755 | Incident | 0 | 1 Nov 2009 | Bankstown Aerodrome, 210° M 7Km | Operational Non-compliance: Verbal instruction; Communications: Air-ground-air; Operational Non-compliance: Operational Non-compliance | While inbound, the pilot reported at Prospect Reservoir and was issued tracking and circuit joining instructions relevant to the reported position. The aircraft was subsequently observed by ATC to be approximately 4 NM SSW of Prospect. |
| 200907403 | Accident | 0 | 29 Nov 2009 | Tara (ALA) | Aircraft control: Loss of control; Weather: Other; Ground operations: Collision on ground; Runway events: Runway Excursion; Terrain Collisions: Ground strike; Terrain Collisions: Collision with terrain | On touchdown, the aircraft encountered a small whirlwind which caused the aircraft to lift, rotate, and depart the runway. The aircraft subsequently collided with a drain and the propeller struck the ground. The aircraft was seriously damaged. |
| 200907574 | Incident | 0 | 2 Dec 2009 | Moorabbin Aerodrome | Runway events: Runway Incursion | After landing on runway 35R, the aircraft entered runway 31L without a clearance. |
| 201000279 | Incident | 0 | 13 Jan 2010 | Brewarrina Aerodrome, E M 19Km | Airframe: Windows; Airframe: Objects falling from aircraft | While on descent, the right emergency exit window detached from the aircraft. |
| 201002067 | Incident | 0 | 20 Mar 2010 | near Inverell Aerodrome | Systems: Other | During cruise, the vacuum pump failed. The pilot reported operations were normal and continued to Inverell. |
| 201005862 | Incident | 0 | 17 Aug 2010 | Albury Aerodrome, 215° M 24Km | Aircraft separation: Issues; Operational Non-compliance: Verbal instruction; Operational Non-compliance: Operational Non-compliance; Aircraft separation: Issues | The Cessna 210 (C210) was cleared outbound on the 200 omni radial and the SF-340 was cleared inbound on the 219 omni radial. The C210 tracked right and approached the 215 radial conflicting with the SF-340. Vertical separation was maintained throughout. |
| 201102242 | Incident | 0 | 29 Mar 2011 | Moorabbin Aerodrome, S M 15Km | Fumes, Smoke, Fire: Smoke; Systems: Avionics / Flight Instruments; Fumes, Smoke, Fire: Fumes | During the cruise, the pilot reported smoke in the cockpit. The engineering inspection revealed a faulty GPS unit. |
| 201103299 | Incident | 0 | 10 May 2011 | Bankstown Aerodrome, 340° M 65Km | Airspace infringement: PRD; ANSP Operational error: Information / procedural error; Airspace infringement: Airspace infringement | The controller inadvertently assigned the aircraft an altitude which placed it in restricted airspace. |
| 201103508 | Incident | 0 | 18 May 2011 | Parafield Aerodrome | Runway events: Runway Incursion; Operational Non-compliance: Verbal instruction; Operational Non-compliance: Operational Non-compliance | During taxiing, the crew did not comply with an instruction to hold position and the aircraft entered the runway without a clearance. |
| 201103806 | Incident | 0 | 29 May 2011 | Bankstown Aerodrome | Aircraft separation: Loss of separation; Aircraft separation: Loss of separation | The Cessna 550 was cleared to land while the Piper PA-28 was still partially within the runway strip resulting in a loss of runway separation. |
| 201105079 | Accident | 3 | 15 Aug 2011 | Horsham Aerodrome, 352.5° M 31Km | Flight preparation / Navigation: VFR into IMC; Terrain Collisions: Collision with terrain; Aircraft control: Loss of control | During the flight, the aircraft collided with terrain. The three occupants were fatally injured and the aircraft was destroyed. It was determined that the pilot probably encountered reduced visibility conditions approaching Nhill due to low cloud, rain and diminishing daylight, leading to disorientation, loss of control and impact with terrain. |
| 201106395 | Incident | 0 | 13 Sept 2011 | Bankstown Aerodrome | Operational Non-compliance: Verbal instruction; Runway events: Runway Incursion; Runway events: Depart / App / Land Wrong Runway; Operational Non-compliance: Operational Non-compliance | The aircraft landed on an incorrect runway without a clearance. |
| 201108462 | Incident | 0 | 9 Dec 2011 | Sydney Aerodrome, 250° M 9Km | Aircraft separation: Loss of separation; Aircraft separation: Loss of separation; Airspace infringement: Controlled airspace; Airspace infringement: Airspace infringement; Operational Non-compliance: Operational Non-compliance | A S.O.C.A.T.A. Groupe Aerospatiale TBM 700 aircraft, registered VH-VSV (VSV) on a private flight was cleared to depart Bankstown control zone on a downwind departure from runway 11 left, however mistakenly conducted an upwind departure. The aircraft penetrated Sydney controlled airspace by 2.3 NM and came within 1.2 NM with no vertical separation of another aircraft on approach into Sydney Airport and a breakdown of separation occurred. This incident highlights the importance of developing a technique to ensure a clearance is processed, understood and actioned correctly. It is also important to clarify a clearance if any ambiguity exists. Finally, pre-flight planning is essential to ensure safe flight. CASA has published a Visual Pilot Guide for Archerfield, Jandakot, Melbourne, Parafield and Sydney areas to provide detailed assistance for operating in these areas. |
| 201204836 | Incident | 0 | 14 May 2012 | near Bankstown Aerodrome | Diversion / return: Diversion / return; Airframe: Landing gear / Indication | During approach, the nose landing gear failed to extend and the aircraft returned to Moree. Engineers replaced an o-ring. |
| 201206658 | Incident | 0 | 5 July 2012 | Mangrove Mountain (ALA), 340° T 20Km | Powerplant / propulsion: Partial power loss / rough running; Powerplant / propulsion: Engine failure or malfunction | During the cruise, the left engine began to run roughly and the pilot shut down the engine. An inspection found a broken exhaust valve in the number two cylinder. |
| 201300547 | Incident | 0 | 20 Jan 2013 | Bankstown Aerodrome | Runway events: Runway Incursion | The aircraft entered a runway without a clearance. |
| 201300955 | Incident | 0 | 31 Jan 2013 | Sydney Aerodrome, 297° M 39Km | Flight preparation / Navigation: Lost / unsure of position; Airspace infringement: PRD; Airspace infringement: Airspace infringement | The aircraft entered controlled airspace without a clearance. ATC subsequently provided the crew with navigational assistance. |
| 201301172 | Incident | 0 | 6 Feb 2013 | Essendon Aerodrome, 130° M 9Km | Operational Non-compliance: Verbal instruction; Communications: Air-ground-air; Operational Non-compliance: Operational Non-compliance | During climb, the pilot did not adhere to an ATC communication instruction. |
| 201302684 | Incident | 0 | 20 Mar 2013 | Oakey Aerodrome, W M 56Km | Flight preparation / Navigation: VFR into IMC | During cruise, the cloud layer became unbroken below the aircraft operating under VFR and the crew requested assistance from ATC to find a safe location to commence a descent. The aircraft subsequently descended through cloud with the assistance of ATC and the crew of a military helicopter operating in the area. |
| 201303014 | Accident | 0 | 29 Mar 2013 | Bankstown Aerodrome | Airframe: Landing gear / Indication; Diversion / return: Diversion / return | During the initial climb, the landing gear failed to retract. The crew conducted troubleshooting before returning to Bankstown. On short finals, the tower advised HPR to ‘check wheels’, the pilot confirmed that the green down and locked light was still illuminated and that the gear selector was in the down position. On landing, the landing gear collapsed and the aircraft sustained substantial damage. The landing gear mechanism was visually inspected and the worm drive was almost to the full retraction position, indicating the gear was retracted electrically. The reason for this electrical retraction despite the gear selector being in the down position was not determined. |
| 201304154 | Incident | 0 | 1 May 2013 | Bankstown Aerodrome | Miscellaneous: Other; Operational Non-compliance: Published information; Communications: Air-ground-air; Operational Non-compliance: Operational Non-compliance | During the approach, the pilot was instructed to join downwind for runway 29 L but was observed joining downwind for runway 11 R. |
| 201307472 | Incident | 0 | 31 July 2013 | near Merimbula Aerodrome | Airframe: Landing gear / Indication; Fly-by inspection: Fly-by inspection; Other: Other | During the approach, the pilot received unsafe landing gear indications and conducted a fly-by. Ground observers advised that the landing gear appeared to be down and locked. An investigation did not find any faults with the landing gear system and it was established that the three green indication lights were not visible due to the automatic dimming of the cockpit navigation lights. |
| 201308964 | Incident | 0 | 16 Sept 2013 | Moorabbin Aerodrome | Airframe: Landing gear / Indication | During approach, the crew recieved an unsafe nose landing gear indication. The engineering inspection revealed that a microswitch was not engaging due to a bent bracket. |
| 201311746 | Incident | 0 | 27 Nov 2013 | Jandakot Aerodrome | Airframe: Landing gear / Indication | During landing, a tyre deflated. |
| 201401148 | Incident | 0 | 28 Jan 2014 | near Jandakot Aerodrome | Systems: Electrical; Other: Other | During the cruise, the alternator failed. The pilot conducted a fly-by inspection to confirm that the landing gear was extended. |
| 201407749 | Incident | 0 | 26 Aug 2014 | Bankstown Aerodrome | Wildlife: Birdstrike | Passing 50 ft on final approach, the aircraft struck a bird. |
| 201409556 | Incident | 0 | 4 Nov 2014 | Bankstown Aerodrome | Aircraft separation: Loss of separation; Operational Non-compliance: Operational Non-compliance; Aircraft separation: Loss of separation | The inbound Piper PA-30 did not track as instructed by ATC which resulted in a loss of separation with the departing Beech 35. |
| 201500555 | Incident | 0 | 22 Jan 2015 | Cowra Aerodrome, WSW M 37Km | Powerplant / propulsion: Engine failure or malfunction | During cruise, the pilot detected abnormal engine indications and a loss of power from the right engine. The engineering inspection revealed a faulty inlet valve in the No. 1 cylinder. |
| 201501241 | Incident | 0 | 13 Feb 2015 | Adelaide Aerodrome | Missed approach / go-around: Missed approach / go-around; Runway events: Runway Incursion | The Piper PA-34 entered the runway without a clearance and the controller instructed the crew of the Bombardier DHC-8 on final approach to conduct a missed approach. |
| 201502089 | Incident | 0 | 12 Mar 2015 | Bankstown Aerodrome | Runway events: Runway Incursion; Communications: Air-ground-air | While taxiing, the aircraft entered the runway without a clearance. |
| 201505821 | Incident | 0 | 7 July 2015 | Moorabbin Aerodrome | Runway events: Runway Incursion; Operational Non-compliance: Operational Non-compliance | While taxiing, the aircraft entered and crossed the runway without a clearance. |
| 201506291 | Incident | 0 | 25 July 2015 | Bankstown Aerodrome | Runway events: Runway Incursion; Missed approach / go-around: Missed approach / go-around; Runway events: Runway Incursion | The Cessna 210 entered runway 29 without a clearance. The controller instructed the crew of the Alpha Aviation R2160 on approach to the same runway to conduct a missed approach. |
| 201508190 | Incident | 0 | 25 Nov 2015 | Williamtown Aerodrome | Aircraft separation: Loss of separation; Aircraft separation: Loss of separation | The controller cleared the Raytheon B200 to descend to FL 110 while the Beech 35 was in cruise at 10,000ft AMSL. This resulted in a loss of separation due to the QNH transition level at the time. |
| 201505886 | Incident | 0 | 9 Dec 2015 | Bankstown Aerodrome | Airframe: Landing gear / Indication; Miscellaneous: Other | During the descent, the landing gear extended uncommanded and the pilot conducted a fly-by inspection prior to landing. The engineering inspection revealed the pressure line to the undercarriage pressure switch had failed. |
| 201600355 | Incident | 0 | 17 Mar 2016 | Bankstown Aerodrome | Flight preparation / Navigation: Flight below minimum altitude; Communications: Air-ground-air; Weather: Unforecast weather | During approach in IMC, the aircraft descended below the lowest safe altitude on several occasions and ATC had difficulty contacting and maintaining communications with the pilot. |
| 201602694 | Incident | 0 | 19 May 2016 | Moorabbin Aerodrome | Runway events: Runway Incursion | During taxi, the aircraft entered runway 31L without a clearance. |
| 201700715 | Incident | 0 | 9 Feb 2017 | Adelaide Aerodrome | Airspace infringement: Airspace infringement; Aircraft separation: Loss of separation; Aircraft separation: Loss of separation | During cruise, the Diamond DA40 infringed controlled airspace resulting in a loss of separation with the Piper PA-32. |
| 201702311 | Incident | 0 | 15 May 2017 | Adelaide Aerodrome | Runway events: Runway Incursion | After landing, the pilot did not contact ATC for clearance and subsequently entered runway 12 without a clearance. |
| 201702907 | Accident | 3 | 28 June 2017 | Mount Gambier Aerodrome, 202.37° T 5Km (Suttontown) | Terrain Collisions: Collision with terrain; Flight preparation / Navigation: VFR into IMC; Aircraft control: Loss of control | The aircraft collided with terrain and the pilot and two passengers were fatally injured. The investigation is continuing. |
Table C2: Summaries of reported safety occurrences during private flights prior to passenger carrying flights conducted on behalf Angel Flight, 2005 to 2017
| ATSB Reference Number | Occurrence Category | Fatal Injuries | Date | Location | Occurrence Types | ATSB Summary |
| 200502940 | Incident | 0 | 21 June 2005 | Tamworth, Aerodrome | Flight preparation / Navigation: VFR into IMC | During the aircraft's arrival, ATC observed the VFR aircraft frequently fly through cloud in IMC. The pilot advised being IFR capable but did not change the flight category to IFR. |
| 200504035 | Incident | 0 | 11 Aug 2005 | 28km E Orange, Aerodrome | Systems: Avionics; Systems: Avionics / Flight Instruments | While the aircraft was en route, the transponder failed. |
| 200605438 | Incident | 0 | 14 Sept 2006 | Essendon, Aerodrome | Runway events: Runway Incursion | The aircraft was taxied for takeoff and entered runway 35 without a clearance. |
| 200706488 | Incident | 0 | 15 Oct 2007 | Mansfield (ALA), 217° M 20Km | Diversion / return: Diversion / return; Powerplant / propulsion: Partial power loss / rough running; Powerplant / propulsion: Engine failure or malfunction | While on climb passing FL130, the engine failed. Power was restored during the enforced descent. The aircraft diverted to an adjacent airfield and landed safely. Engineering inspection revealed a faulty waste gate controller and actuator. |
| 200803246 | Incident | 0 | 14 May 2008 | Moorabbin Aerodrome | Runway events: Runway Incursion | While taxiing for takeoff, the aircraft entered runway 35L without a clearance. |
| 200803532 | Incident | 0 | 26 May 2008 | Inverell Aerodrome, S M 8Km | Systems: Electrical; Diversion / return: Diversion / return | While the aircraft was en route, the electrical system failed. The pilot diverted the aircraft to Tamworth for a landing. |
| 200808252 | Incident | 0 | 20 Dec 2008 | Moorabbin Aerodrome | Runway events: Runway Incursion; Aircraft separation: Loss of separation; Aircraft separation: Loss of separation | The Cessna 172 was observed by ATC to have crossed the holding point for runway 17R without a clearance, resulting in an infringement of separation standards with a Cessna 182 departing from that runway. |
| 200907176 | Incident | 0 | 19 Nov 2009 | Sydney Aerodrome, 282° M 48Km | Airspace infringement: Controlled airspace; Aircraft separation: Loss of separation; Airspace infringement: Airspace infringement; Aircraft separation: Loss of separation | The Piper PA-28 was observed by ATC to have entered controlled airspace without a clearance, resulting in an infringement of separation standards with a Mooney M20J. |
| 201002038 | Incident | 0 | 19 Mar 2010 | Bankstown Aerodrome | Airframe: Landing gear / Indication; Missed approach / go-around: Missed approach / go-around | During the approach, the crew received an unsafe landing gear indication and conducted a missed approach. The subsequent engineering inspection revealed a sticking squat switch. |
| 201100938 | Incident | 0 | 9 feb 2011 | Richmond (NSW) Aerodrome | Systems: Electrical; Diversion / return: Diversion / return | Shortly after takeoff, the alternator failed. The aircraft was returned for a landing. An investigation revealed a failed alternator belt. |
| 201105577 | Incident | 0 | 10 Aug 2011 | near Bankstown Aerodrome | Operational Non-compliance: Verbal instruction; Communications: Air-ground-air; Operational Non-compliance: Operational Non-compliance | The aircraft descended without a clearance. The pilot failed to reply to several readback requests from ATC, and used non standard terminology. |
| 201106856 | Incident | 0 | 2 Oct 2011 | Moorabbin Aerodrome | Operational Non-compliance: Verbal instruction; Runway events: Runway Incursion; Operational Non-compliance: Operational Non-compliance | The aircraft failed to comply with taxi instructions, and entered the runway without a clearance. |
| 201107318 | Incident | 0 | 21 Oct 2011 | near Archerfield Aerodrome | Operational Non-compliance: Verbal instruction; Runway events: Depart / App / Land Wrong Runway; Operational Non-compliance: Operational Non-compliance | The pilot did not comply with the ATC circuit joining instructions and the aircraft joined downwind for the wrong runway without a clearance. |
| 201401115 | Incident | 0 | 28 Jan 2014 | near Amberley Aerodrome | Flight preparation / Navigation: Flight below minimum altitude; Flight preparation / Navigation: Other | It was reported that the aircraft was in IMC below LSALT during the climb. |
| 201407227 | Incident | 0 | 7 Aug 2014 | Moorabbin Aerodrome | Runway events: Runway Incursion; Operational Non-compliance: Operational Non-compliance | After landing on runway 35R the aircraft vacated onto runway 31R without a clearance. |
| 201501073 | Incident | 0 | 5 Feb 2015 | Gold Coast Aerodrome, 230° M 6Km | Runway events: Depart / App / Land Wrong Runway | The aircraft did not track in accordance with ATC instructions and joined the circuit for an incorrect runway. |
| 201502590 | Incident | 0 | 13 May 2015 | Archerfield Aerodrome, 260° M 24Km | Aircraft separation: Loss of separation; Aircraft separation: Loss of separation; Airspace infringement: Airspace infringement | The outbound Beech A36 entered controlled airspace without a clearance resulting in a loss of separation with the inbound Beech B200. |
| 201505500 | Incident | 0 | 26 Nov 2015 | near Armidale Aerodrome | Aircraft separation: Airborne collision alert system warning; Aircraft separation: Issues; Aircraft separation: Airborne collision alert system warning; Aircraft separation: Issues | During the approach, ATC advised the crew of the SAAB 340 of an aircraft on a conflicting track, that was subsequently identified at the Piper PA-28. The 340 crew established communication and mutual separation with the PA-28 crew. The 340 crew subsequently received a TCAS RA on the PA-28 and manoeuvred to ensure that separation was maintained. |
| 201600947 | Serious Incident | 0 | 14 Jan 2016 | Dubbo Aerodrome | Aircraft separation: Issues; Aircraft separation: Issues | The Robinson R22 was observed to pass below the Cirrus SR20 within the circuit area. |
| 201700302 | Incident | 0 | 6 Jan 2017 | Adelaide Aerodrome | Runway events: Runway Incursion; Communications: Air-ground-air | During taxi, the aircraft entered runway 12 without a clearance. |
| 201700806 | Incident | 0 | 15 Feb 2017 | Adelaide Aerodrome | Runway events: Runway Incursion | After landing on runway 23, the aircraft vacated the runway onto runway 12 without a clearance. |
Table C3: Summaries of reported safety occurrences during private flights following to passenger carrying flights conducted on behalf Angel Flight, 2005 to 2017
| ATSB Reference Number | Occurrence Category | Fatal Injuries | Date | Location | Occurrence Types | ATSB Summary |
| 200503504 | Incident | 0 | 21 July 2005 | Essendon, Aerodrome | Runway events: Runway Incursion | While it was taxiing for departure, ATC observed the aircraft to cross the holding point and enter the runway strip without a clearance. |
| 200602754 | Incident | 0 | 1 May 2006 | 7km W Moorabbin, Aerodrome | Fumes, Smoke, Fire: Fumes | While the aircraft was on approach, the pilot detected electrical fumes in the cabin. The aircraft was landed without incident and submitted for maintenance. |
| 200603630 | Incident | 0 | 17 June 2006 | 30km SSW Port Macquarie, Aerodrome | Powerplant / propulsion: Abnormal engine indications | While the aircraft was en route, the pilot reported a loss of oil pressure and considered returning the aircraft for a landing. The pilot subsequently reported that all systems seemed normal and the flight would continue to Bankstown. The pilot also reported that the fault could have been an electronic monitoring problem rather than a mechanical problem. |
| 200606137 | Incident | 0 | 14 Oct 2006 | 56km E Albury, Aerodrome | Operational Non-compliance: Published information; Operational Non-compliance: Verbal instruction; Operational Non-compliance: Operational Non-compliance; Flight preparation / Navigation: Flight below minimum altitude | The aircraft was observed on radar descending without clearance to below LSALT. The pilot did not respond to calls from ATC until the aircraft passed 7,800 ft on descent to 7,000 ft in VMC. The pilot reported that the immediate descent was to escape severe turbulence. The pilot had received the SIGMET forecasting severe turbulence. |
| 200700766 | Incident | 0 | 14 Feb 2007 | Camden Aerodrome, SW M 28Km | Aircraft separation: Issues; Aircraft separation: Issues | On 14 February 2007 at about 1127 Eastern Daylight-saving Time, the pilot of a Cessna Aircraft Company 182T (182) was positioning to conduct a sector entry for an area navigation (RNAV) global navigation satellite system (GNSS) arrival procedure to runway 06 at Camden Aerodrome, NSW. The aircraft was approaching the aerodrome from the east. At the same time, the pilot of a Cessna Aircraft Company 210L (210) was approaching Camden from the south-west with the intention of conducting a Camden runway 06 straight-in RNAV (GNSS) approach. The two aircraft had similar estimated times of arrival at the approach commencement waypoint. They were both being operated under the instrument flight rules (IFR), in Class G airspace. The air traffic controller provided the pilots with mutual radar based traffic information. The pilot of the 210 contacted the controller and was provided with traffic information about the 182. The pilot of the 182 climbed the aircraft to minimise the risk of a collision as he was unsure of the intentions of the pilot of the 210. Recorded radar data showed that, when the aircraft passed, there was 500 ft vertically and 2.1 NM laterally between them. |
| 200702530 | Incident | 0 | 21 April 2007 | Moorabbin Aerodrome, 37Km 025° M | Operational Non-compliance: Operational Non-compliance; Flight preparation / Navigation: Other | The aircraft was inbound to Moorabbin from the north-east. ATC advised the pilot to expect an NDB approach due low cloud at 800 ft and visibility 6 km in rain. The pilot replied that he could not fly the approach due to his documentation and approach charts being in the back of the aircraft. With IMC prevailing and the aircraft only having approximately 60 minutes fuel remaining, ATC declared an Alert Phase. When the aircraft was overhead Moorabbin, the pilot advised he had the airport in sight and could descend visually. The aircraft landed safely. |
| 200705087 | Incident | 0 | 3 Aug 2007 | Stawell Aerodrome, 020° M 27Km | Powerplant / propulsion: Abnormal engine indications; Powerplant / propulsion: Other; Systems: Fuel | During cruise, the pilot found that the throttle could not be moved. The pilot declared a PAN and continued to Moorabbin. During descent, the engine was shut down due to excessive power at lower altitude. While on downwind the pilot restarted the engine and the aircraft landed safely. |
| 200802722 | Incident | 0 | 24 April 2008 | Bankstown Aerodrome | Wildlife: Birdstrike | During the landing roll, the aircraft struck a plover. |
| 200802738 | Incident | 0 | 24 April 2008 | Griffith Aerodrome, E M 37Km | Powerplant / propulsion: Partial power loss / rough running; Diversion / return: Diversion / return; Powerplant / propulsion: Engine failure or malfunction | During the cruise, the crew reported a rough running engine. The aircraft was returned to Griffith. |
| 200805056 | Incident | 0 | 4 Aug 2008 | Moorabbin Aerodrome | Runway events: Runway Incursion | The aircraft was observed by ATC to have entered the runway 35L strip without a clearance. |
| 200806797 | Incident | 0 | 20 Oct 2008 | Essendon Aerodrome | Runway events: Runway Incursion | The aircraft was observed by ATC to have entered the runway 17 strip without a clearance. |
| 200900479 | Incident | 0 | 27 Jan 2009 | Bankstown Aerodrome | Runway events: Runway Incursion | The aircraft entered the runway 29R strip without a clearance. |
| 200900560 | Incident | 0 | 28 Jan 2009 | near Essendon Aerodrome | Operational Non-compliance: Verbal instruction; Airspace infringement: Controlled airspace; Flight preparation / Navigation: Lost / unsure of position; Operational Non-compliance: Operational Non-compliance; Airspace infringement: Airspace infringement | The pilot did not comply with the route clearance direct to Essendon. ATC issued a visual heading to assist the pilot. |
| 200906344 | Incident | 0 | 16 Oct 2009 | Moorabbin Aerodrome | Runway events: Runway Incursion | The aircraft entered runway 22 without a clearance. |
| 201007041 | Incident | 0 | 6 Oct 2010 | Essendon Aerodrome | Operational Non-compliance: Verbal instruction; Runway events: Runway Incursion; Aircraft separation: Loss of separation assurance; Operational Non-compliance: Operational Non-compliance; Aircraft separation: Loss of separation assurance | The Beech 35 crossed runway 35 without clearance when the Beech 200 was on 1 NM final for the runway and had been cleared to land. ATC cancelled the Beech 200's landing clearance until the Beech 35 had vacated the runway. |
| 201106398 | Incident | 0 | 13 Sept 2011 | Moorabbin Aerodrome | Operational Non-compliance: Verbal instruction; Runway events: Runway Incursion; Operational Non-compliance: Operational Non-compliance | After landing, the aircraft taxied across two runways without a clearance. |
| 201106955 | Incident | 0 | 6 Oct 2011 | near Essendon Aerodrome | Airspace infringement: PRD; Flight preparation / Navigation: Lost / unsure of position; Flight preparation / Navigation: Unsecured door / panel; Diversion / return: Diversion / return; Flight preparation / Navigation: Other; Airspace infringement: Airspace infringement | The pilot had requested navigational assistance from the controller prior to aircraft entering restricted airspace without a clearance. The aircraft was returning to Essendon due to an open door. |
| 201203086 | Incident | 0 | 28 Mar 2012 | Moorabbin Aerodrome | Operational Non-compliance: Verbal instruction; Aircraft separation: Issues; Operational Non-compliance: Operational Non-compliance; Aircraft separation: Issues | The Cessna 172 pilot did not adhere to the circuit sequence instructions. |
| 201204445 | Incident | 0 | 4 May 2012 | Moorabbin Aerodrome | Runway events: Runway Incursion | The aircraft entered the runways without a clearance. |
| 201301134 | Incident | 0 | 6 Feb 2013 | Bankstown Aerodrome | Runway events: Runway Incursion | The aircraft entered the runway without a clearance. |
| 201306609 | Incident | 0 | 12 July 2013 | near Moorabbin Aerodrome | Powerplant / propulsion: Abnormal engine indications | During approach, the crew detected abnormal engine indications. An inspection revealed a low engine oil level. |
| 201404949 | Incident | 0 | 4 July 2014 | Essendon Aerodrome | Powerplant / propulsion: Engine failure or malfunction; Fuel related: Starvation | During taxi after landing, the engine failed due to fuel starvation. |
| 201502184 | Incident | 0 | 21 May 2015 | near Parafield Aerodrome | Aircraft separation: Issues; Aircraft separation: Issues | The inbound Piper PA-32 did not adjust track to pass behind the outbound SOCATA TB-10 on a crossing track. The TB-10 turned to maintain separation. |
| 201502918 | Incident | 0 | 29 June 2015 | Chinchilla Aerodrome | Runway events: Depart / App / Land Wrong Runway; Fuel related: Other; Diversion / return: Diversion / return | During cruise, the pilot diverted to Chinchilla due to low fuel indications and subsequently landed on a closed runway. |
| 201504794 | Incident | 0 | 29 Oct 2015 | Wollongong Aerodrome | As the Piper PA-34 was landing on runway 08, the Jabiru J170 started crossing the runway. The PA-34 crew applied heavy braking and stopped the aircraft short of the J170's position. The J170 crew subsequently reported that they had assumed that the PA-34 was landing on runway 34. | |
| 201603962 | Incident | 0 | 25 Aug 2016 | East Sale Aerodrome | Aircraft separation: Loss of separation assurance; Breakdown of co-ordination: Breakdown of co-ordination | ATC cleared the military aircraft to climb into the adjacent sector before coordinating with the sector controller. As a result, a loss of separation assurance occurred with the Piper PA-32 in the adjacent sector. |
| 201702322 | Incident | 0 | 15 May 2017 | Adelaide Aerodrome, 0° M 9Km | Communications: Air-ground-air | The aircraft was not in normal communication with ATC. |
| 201704435 | Incident | 0 | 14 Sept 2017 | Amberley Aerodrome | Aircraft separation: Issues; Operational Non-compliance: Operational Non-compliance | During approach, the aircraft descended below its assigned level, resulting in ATC issuing a safety alert to a formation of super hornets on approach. The aircraft climbed back to its assigned level to maintain separation. |
__________
- Australian Transport Safety Bureau (2008). AR-2007-053 Analysis, Causality and Proof in Safety Investigations, Canberra, Australia. This can be found on the ATSB’s website www.atsb.gov.au.
- R Core Team (2017). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL www.R-project.org/.
- Puza, B. (2015). Bayesian Methods for Statistical Analysis, ANU eView: Acton, ACT
- Martyn Plummer, Nicky Best, Kate Cowles and Karen Vines (2006). CODA: Convergence Diagnosis and Output Analysis for MCMC, R News, vol 6, 7-11
- Due to different reporting requirements, incidents are not comparable between private and commercial air transport.
- Non-passenger carrying repositioning flights required estimation by the ATSB based on privately conducted passenger carrying Angel Flights. This process is described in Appendix A – Data analysis methods: Estimation of repositioning flight totals.
- Number of flights 2008 to 2017 for Private (including Business), and Charter operations was calculated by combining reported data from 2014 to 2017, and estimated data between 2008 and 2013. The estimation process for the earlier data is detailed in Appendix A – Data analysis methods: Estimation of Private, Business and Charter landings: 2008 to 2013.
- Hours estimated for Angel Flight based on ratio reported community service flight hours to the number of flights as recorded by BITRE between 2014 and 2017.
Purpose of safety investigations & publishing information
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2019
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
Occurrence summary
| Investigation number | AO-2017-069 |
|---|---|
| Occurrence date | 28/06/2017 |
| Location | 2 km south-west of Mount Gambier Airport |
| State | South Australia |
| Report release date | 13/08/2019 |
| Report status | Final |
| Investigation level | Systemic |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Collision with terrain |
| Occurrence class | Accident |
| Highest injury level | Fatal |
Aircraft details
| Manufacturer | SOCATA-Groupe Aerospatiale |
|---|---|
| Model | TB-10 |
| Registration | VH-YTM |
| Serial number | 1518 |
| Aircraft operator | Private Pilot |
| Sector | Piston |
| Operation type | Private |
| Departure point | Mt Gambier, South Australia |
| Destination | Adelaide, South Australia |
| Damage | Destroyed |