Australia celebrates three decades of independent transport safety investigations.
On 7 June 1982, the Bureau of Air Safety Investigation (BASI) was created as an operationally independent agency, marking the start of a new era in transport safety for Australia.
Now operating as the Australian Transport Safety Bureau (ATSB), Australia's national transport safety investigator has earned its reputation for excellence, both at home and abroad.
More than 4,000 investigations later, the ATSB has become a world-leader in transport safety investigations. It is internationally acknowledged for its excellence as a transport safety investigator based on its reputation in the field of human factors, operational independence, objectivity, and technical expertise.
Whether investigating aviation, marine or rail incidents and accidents, the ATSB is committed to safer transport for industry and the travelling public.
The use of mobile phones and other electronic devices is restricted as they could interfere with vital aircraft navigation systems. Current regulations give aircraft crew the power to prohibit the use of any device which can threaten the safety of an aircraft. It is very important that passengers listen to and comply with announcements from the cabin crew when these restrictions apply.
The ATSB recently received a confidential report from an airline passenger concerned that passengers were using their 3G mobile devices onboard a flight from Sydney to Melbourne. The report below outlines the passenger's concerns along with the ATSB's response and advice to the travelling public.
Report narrative: The reporter expressed a safety concern about the use of 3G mobile devices onboard a Syd-Melb flight. The reporter, who is a regular traveller, observes that passengers are using these devices more and more frequently, texting and using internet connectivity during flight. The reporter believes that cabin crew do not take this safety matter seriously and often do not adequately warn passengers to turn off electronic devices or that the devices should be in flight mode.
Responses/received: REPCON supplied the operator with the de-identified report. The following is a version of their response:
Cabin safety has advised that a review of our occurrence database from 01/01/11 shows that on over 500 occasions cabin crew have reported the hazard of passengers using their mobile phones and personal electronic devices (PEDs) onboard. It is felt that the sheer volume of reports received in relation to passenger non-compliance with our PED policy illustrates that cabin crew are very aware of the regulatory requirements and company policies on this matter and are very vigilant in ensuring compliance, particularly during the pre-departure preparations as the cabin is being secured for take-off.
In addition, it's quite possible that onboard passengers writing text messages are constructing them whilst their phones are in flight mode. It is also not possible for cabin crew to manage passenger use of PEDs during takeoff and/or the descent phase as the cabin crew must be seated. The reports we receive also highlight passenger reluctance and attitudes towards PED usage and the belief it is the operator's policy and not a regulatory requirement. However, the operator honestly believes the hundreds of reports that come through each year show that our cabin crew take passenger use of PEDs at inappropriate times very seriously.
In addition, the PED policy is currently part of the cabin crew recurrent emergency procedures curriculum and is covered in the "Standard Operating Procedures" section of the training day. The proliferation of PEDs has made the potential much higher for non-compliance but it is not possible for cabin crew to check that all PEDs are switched to flight mode and then off. In this respect cabin crew act in good faith that passengers are compliant, responsible and accountable themselves.
REPCON supplied CASA with the deidentified report and a version of the operator's response. The following is a version of the response that CASA provided:
CASA has reviewed this matter with internal subject matter experts and has examined the operator's procedures, CASA is satisfied with the operator's response.
ATSB comment: The use of mobile phones and other electronic devices is restricted as they could interfere with vital aircraft navigation systems. Current regulations give aircraft crew the power to prohibit the use of any device which can threaten the safety of an aircraft. It is very important that passengers listen to and comply with announcements from the cabin crew when these restrictions apply.
REPCON allows any person who has an aviation safety concern to report it to the ATSB confidentially. All personal information regarding any individual (either the reporter or any person referred to in the report) remains strictly confidential, unless permission is given by the subject of the information.
The goals of the scheme are to increase awareness of safety issues and to encourage safety action by those best placed to respond to safety concerns.
REPCON would like to hear from you if you have experienced a 'close call' and think others may benefit from the lessons you have learnt. These reports can serve as a powerful reminder that, despite the best of intentions, well-trained people are still capable of making mistakes. The stories arising from these reports may serve to reinforce the message that we must remain vigilant to ensure the ongoing safety of ourselves and others.
What may be reported with REPCON? Any matter may be reported if it endangers, or could endanger the safety of an aircraft. These matters are reportable safety concerns.
Examples include: • unsafe scheduling or rostering of crew; or • crew or aircraft operator bypassing safety procedures because of commercial pressures; or • non-compliance with rules or procedures.
To avoid doubt, the following matters are not reportable safety concerns and are not guaranteed confidentiality: • matters showing a serious and imminent threat to a person's health or life • terrorist acts • industrial relations matters • conduct that may constitute a serious crime.
Submission of a report known by the reporter to be false or misleading is an offence under section 137.1 of the Criminal Code.
The ATSB is investigating the accident involving cargo ship Tycoon at Christmas Island on 8 January 2012.
Update 13 January The ATSB investigation team has finished interviewing the crew and other witnesses. The team is now liaising with the salvors, who are on the island, to arrange the recovery of documents and other evidence from the wreck.
They are also making arrangements to inspect the port's mooring arrangements.
Updates to the ATSB investigation will be published here as significant information comes to hand.
12 January 2012 The ATSB investigation team on Christmas Island will today be interviewing eyewitnesses including some stevedores and mine workers. The team will also be liaising with other agencies including the Port Authority, AFP, Customs and the Navy to gather other evidence.
10 January 2012 The ATSB investigation team arrived at Christmas Island at around midday today (WA time) to begin the on-site investigation. The team comprises a Master Mariner and an experienced marine Chief Engineer.
The team will spend the afternoon talking to relevant people including the Harbour Master, the harbour pilot and members of the ship's crew.
The team will also make arrangements to either board the wreck of the vessel when it is safe to do so, or for the evidence on board to be otherwise protected.
Further updates on the ATSB's investigation will be made available here as information comes to hand.
10 January 2012 Two ATSB investigators are en route to Christmas Island to begin the on-site phase of the investigation. The team is due to arrive around midday Western Australia time, however they may be delayed due to bad weather on the Island.
As part of the investigation, the ATSB investigators will:
board the ship (when it is safe) to gather evidence such as shipping documentation and inspect relevant equipment
interview the ship's crew as well as any witnesses to the accident
examine weather conditions during the time of the accident
look at the harbour facilities.
The ATSB preliminary investigation report, presenting factual information about the of the incident and the investigation, will be available within 30 days.
Updates to the ATSB investigation will be published here as information comes to hand.
Check out our latest avoidable accidents booklet on aviation fuel management.
Starved and exhausted: Fuel management aviation accidents highlights the importance of fuel management through real cases involving fuel-related accidents and incidents. The book also provides helpful advice on good fuel management practices and procedures.
The booklet is available on the ATSB website along with the rest of the Avoidable Accidents series.
With the Holiday season upon us, the Australian Transport Safety Bureau (ATSB) has encouraged air travellers to keep their seat belts fastened at all possible times.
The call coincides with the release of the ATSB report into an in-flight upset that occurred on-board a Qantas A330 aircraft en-route from Singapore to Perth in October 2008. At least 110 of the 303 passengers and 9 of the 12 crew members were injured. Of these, 51 received hospital medical treatment.
The Chief Commissioner of the ATSB, Mr Martin Dolan, said that the accident provided a salient reminder about the importance of seat belts, and he urged passengers to keep their seat belts fastened during flight whenever they are seated.
'At least 60 of the passengers were seated without their seat belts fastened. Although some of those wearing a seat belt were also injured, most of the injuries occurred when unrestrained occupants were thrown into the aircraft's ceiling. The rate and severity of injuries was much greater for those who were not wearing a seat belt.'
'Although passengers are routinely reminded on each flight to wear their seat belts when seated during a flight, some passengers do not follow this advice,' Mr Dolan said.
The in-flight upset that occurred on-board a Qantas A330 aircraft was a unique event and extremely unlikely to happen again according to the ATSB. During the flight, approximately 154 kilometres west of Learmonth, WA, the aircraft suddenly pitched down, due to a combination of problems involving two aircraft systems; the flight control computers and one of the aircraft's three air data inertial reference units (ADIRUs).
Due to a limitation in software design, the flight control computers commanded the aircraft to pitch down in response to a very rare pattern of incorrect angle of attack data from one of the ADIRUs.
Mr Dolan said that Airbus had taken prompt action to reduce the likelihood of another similar accident.
'Very soon after the accident, the manufacturer issued new pilot procedures to manage the effects of any future cases of a similar ADIRU failure,' Mr Dolan said.
'The aircraft manufacturer then redesigned its software. Passengers, crew and operators can be confident that the same type of accident will not happen again.'
An extensive investigation into what triggered the ADIRU failure mode concluded that it was very unlikely to have been caused by electromagnetic interference from the Harold E. Holt Naval Communications station at Exmouth or from a personal electronic device such as a laptop or mobile phone. A range of other possible mechanisms were also discounted.
Mr Dolan stated that the ATSB investigation covered a range of complicated issues, including some that had rarely been considered in depth by previous accident investigations.
'Given the increasing complexity of aircraft systems, this comprehensive investigation has offered an insight into the types of issues that will become increasingly relevant for future investigations. It identified a number of specific lessons for the manufacturers of new, complex, safety-critical systems,' Mr Dolan says.
The Australian Transport Safety Bureau (ATSB) has been advised of the unintentional entry of a Qantas A380 aircraft, registered VH-OQG and operating as QFA094, into a forecast area of potential volcanic ash. The aircraft was en route from Los Angeles in the United States to Melbourne Airport, Victoria via a route that was previously forecast to be clear of volcanic ash.
It was reported that, while cruising at flight level (FL)[1] 400 and approaching position 27° south and 177° east, the flight crew were advised by air traffic services (ATS) personnel of the release of an updated SIGMET[2]. That SIGMET indicated that an ash cloud had moved further north than previously advised.
The flight crew requested and were cleared by ATS to climb to FL 410 and to deviate from track to clear the area. It was estimated that the aircraft spent about 15 minutes in the revised area of potential volcanic ash. The flight crew advised that there was no visual or other indication of their encountering any ash.
On arrival in Melbourne, the aircraft was subjected to an engine inspection with no fault found. The aircraft was released to service.
The initial reports of this incident indicate a routinely reportable matter under the Transport Safety Investigation Act 2003. The ATSB's initial examination of the circumstances of the occurrence does not disclose any issues that might affect the future safety of aviation operations.
On that basis, the initiation of a transport safety investigation is unlikely. However, the ATSB will consider the aircraft operator's more detailed formal notification of the occurrence before any final determination of whether to initiate an investigation.
[1] Level of constant atmospheric pressure related to the datum of 013.25 hPa, expressed in hundreds of feet. FL 400 equated to 40,000 ft above mean sea level.
[2] Information that concerns the occurrence or expected occurrence, in an area over which a meteorological watch is being maintained, of any of a number of prescribed phenomena. Those phenomena included a volcanic ash cloud.
The ATSB is investigating an occurrence involving a Qantas A380 aircraft that experienced an uncontained engine failure over Batam Island, Indonesia on 4 November 2010. The aircraft landed safely in Singapore having returned with the aircraft's No 2 engine shut down. There were no injuries.
Update 19 January 2012 The investigation team is being led by the Australian Transport Safety Bureau (ATSB). With the assistance of accredited representatives from the Bureau d'Enquêtes et d'Analyses (BEA), the Air Accidents Investigation Branch of the United Kingdom (UK AAIB), the Air Accident Investigation Bureau of Singapore (AAIB Singapore), the National Transportation Safety Committee of Indonesia (NTSC), and advisors to those investigation bodies including Rolls-Royce, Airbus, SAFRAN Sagem, Honeywell (USA and UK), Aerolec UK and Singapore Aero Engine Services Private Limited, the data gathering phase of the investigation is complete and the team has commenced analysing that data.
During the period July to August 2011, accredited representatives from the BEA and UK AAIB and advisors from Airbus met with ATSB investigators in Canberra, Australia to ratify relevant A380 technical data in respect of the structural and systems damage sustained by the aircraft as a result of the uncontained engine failure. The examination of relevant Rolls-Royce Trent 900 engine data and a number of engine manufacturing processes is nearing completion.
The ATSB has met with Rolls-Royce and Qantas Airways to update those parties on the progress of the investigation. In accordance with international protocol and ATSB policy and procedures, those and other relevant stakeholders will be involved in the development of the investigation findings and final report.
In conjunction with the UK AAIB and Rolls-Royce, the ATSB is continuing its examination of the circumstances and missed opportunities with the potential to have detected the reduced wall thickness and offset counter bore of the oil feed pipe prior to, during and after the manufacture of the module 51 assemblies. The ATSB has also reviewed the quality audits undertaken, and quality assurance system affecting the module 51 design and manufacturing process, and their effectiveness in detecting deficiencies in that process.
In the interim, Rolls-Royce has conducted a number of major internal investigations into its processes including the:
manufacture of oil pipes with reduced wall thickness
management of retrospective concessions of manufactured components
failure mode, effects and criticality analysis (FMECA) of previous component failures.
As a result of those investigations, Rolls-Royce has:
revised procedures for new structures that include feature verification and risk assessment during the design and manufacture process
introduced a revised, standalone procedure with appropriate supporting training to better manage the application of retrospective manufacturing concessions
revised its FMECA procedures to provide 'best practice' numerical justification for any assumptions made.
The investigation will monitor the progress of those initiatives.
Aircraft response to the disc failure
The examination of airframe and systems damage that resulted from the engine disc burst has been completed. That examination did not reveal any significant or critical safety issues.
The continuing repair of the aircraft in Singapore has allowed the examination of relevant removed/replaced aircraft components at the ATSB's technical facilities in Canberra. Those components have included a number of wiring looms, elements of the aircraft's airframe and a number of sub-components.
Airbus proactive safety action
As part of its ongoing examination of this event, Airbus has commenced working with a number of airport and rescue and firefighting agencies to develop an agreed safe means for those agencies to externally shut down engines on Airbus aircraft - as became necessary in this case. Any agreed procedures will be incorporated in the Airbus Aircraft Rescue and Fire Fighting Chart and be made available to airports and fire crews on line in document and poster form.
Ongoing investigation activities
The investigation is continuing and has progressed to the analysis of the large amount of complex factual information that has been gathered during the investigation. The drafting of the investigation report has commenced and will include extensive liaison with domestic and international stakeholders. In accordance with international protocol, that will include a 60-day consultation period for international parties to the investigation.
The final report is anticipated for public release in the third quarter of 2012.
The information contained in this web update is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this web update. As such, no analysis or findings are included in this update.
Update 3.00pm - 18 May 2011 An interim ATSB investigation report has confirmed the sequence of events that led to the 4 November 2010 uncontained engine failure on board a Qantas A380 aircraft over Batam Island, Indonesia.
The investigation team has inspected the damaged engine and components and determined the sequence of events that led to the failure of the engine disc.
The investigation is also examining the airframe and systems damage that resulted from the engine disc burst to understand its effect on those systems and the impact on flight safety. That includes their effect on the aircraft's handling and performance and on crew workload. A flight simulator program was used to conduct a number of tests in a certified A380 flight simulator. Analysis of the flight simulation test data is ongoing.
Update 3.30pm - 23 December 2010 The ATSB investigation into the in-flight uncontained engine failure that occurred over Batam Island, Indonesia on 4 November 2010 is continuing. Two ATSB investigators have recently returned to Australia from meetings with the European Aviation Safety Agency (EASA), Rolls-Royce plc and Airbus. During these meetings the progress and findings of the investigation to date were reviewed and the scope of the ongoing investigation discussed.
In the United Kingdom (UK), Rolls-Royce plc is continuing the examination of the engine HP/IP structures at their facility in Derby, under the supervision of the UK Air Accident Investigations Branch. Rolls-Royce plc is also working with European airworthiness authorities to facilitate the return to service of all affected A380 aircraft.
Work to characterise the oil feed pipe fracture surfaces has identified that the location of the fatigue fracture appears to be associated with the thinnest pipe wall section, consistent with the previously-identified counter-bore eccentricity.
Since early in the investigation, an inspection regime has been in place to detect any abnormal leakages in key parts of Trent 900 engines. Based on recent engine inspections, manufacturing data and stress analysis work, Rolls-Royce plc has revised the threshold for inspection and the intervals at which inspection should be completed.
The ATSB will continue to report significant progress in the investigation as information comes to hand.
Update 3.30pm - 8 December 2010 Results from safety inspections of engines On 2 December 2010, the ATSB issued a safety recommendation that identified a potential manufacturing defect with an oil tube connection to the high-pressure (HP)/intermediate pressure (IP) bearing structure of the Trent 900 engine installed in some A380 aircraft.
As a result of the safety recommendation, Rolls-Royce plc immediately issued revision 1 to the non-modification service bulletin (NMSB) 72-G595 incorporating assessment and engine rejection criteria for the measurement of potential oil feed stub pipe counter-bore misalignment, and a tightening of the compliance time frame from 20 to 2 flight cycles.
Since the issue of that bulletin, 45 Trent 900 engines have been inspected, and of those engines:
29 engines were installed on operating aircraft
8 engines were not installed on aircraft
4 engines were due to be delivered on a new aircraft
4 engines were on a flight test aircraft.
Three engines failed the inspection and were removed from service for further examination. All Qantas aircraft engines currently flying had no defects recorded and remain in service.
In addition, the European Aviation Safety Agency (EASA) approved software updates to the Rolls-Royce plc change to the engine electronic control system has now been incorporated in all operating aircraft. The software upgrade predicts intermediate turbine overspeed events and shuts the engine down before a turbine disc failure occurs.
Update 10.30am - 3 December 2010 Manufacturing problem potential factor in QF32 engine failure In a preliminary investigation report released today, the ATSB outlines safety actions that have already been taken in response to an uncontained engine failure on board a Qantas A380 aircraft over Batam Island, Indonesia on 4 November 2010.
"The investigation highlights Australian and international cooperation in the interests of aviation safety," said the ATSB's Chief Commissioner, Martin Dolan. "The ATSB is the lead investigator, but many others are involved and their cooperation has been essential".
"We're still in the early stages of investigation," Mr Dolan added, "but significant action has already been taken to minimise the risk of a recurrence". Full media releasemore...
Update 1.00pm - 2 December 2010 Manufacturing problem potential factor in QF32 engine failure The ATSB has issued a safety recommendation about potential engine problems in some Airbus A380 aircraft.
The safety recommendation identifies a potential manufacturing defect with an oil tube connection to the high-pressure (HP)/intermediate-pressure (IP) bearing structure of the Trent 900 engine installed in some A380 aircraft.
The problem relates to the potential for misaligned oil pipe counter-boring, which could lead to fatigue cracking, oil leakage and potential engine failure from an oil fire within the HP/IP bearing buffer space.
In response to the recommendation Rolls Royce, affected airlines and safety regulators are taking action to ensure the continued safe operation of A380 aircraft. The action involves the close inspection of affected engines and the removal from service of any engine which displays the suspected counter-boring problem.
The ATSB will hold a media briefing tomorrow (Friday 3 December 2010) at 10.30am to accompany the release of its preliminary factual investigation report into the QF32 occurrence. ATSB Chief Commissioner Mr Martin Dolan will present the known facts gathered from the investigation and highlight the key safety issues that have resulted from the investigation to date.
The full safety recommendation is available via the ATSB website at AO-2010-089.
Update 11.00am - 1 December 2010 Media Briefing On Friday 3 December 2010, the ATSB will hold a media briefing to accompany the release of its preliminary factual investigation report into the 4 November 2010 engine failure onboard Qantas Flight QF32 over Batam Island, Indonesia.
Update 4.40 pm - 22 November 2010 Engine examination ATSB investigators examining the engine in Singapore are expected to return to Australia on Wednesday 24 November. The parts of interest from the failed No 2 engine have been removed. This includes the Low Pressure Turbine (Figure 1) module and the Intermediate Turbine module and drive shaft. The Intermediate Pressure components have been photographed and are being shipped to Rolls-Royce in the UK for detailed examination by Rolls-Royce, under the supervision of the UK Air Accidents Investigation Branch.
Figure 1: Low Pressure Turbine module removed from the No 2 engine
Aircraft examination The examination of the aircraft damage is continuing with a focus on the hydraulic, mechanical and electrical systems affected by debris strikes. ATSB investigators involved in this examination are expected to return to Australia on Friday 26 November.
On-going investigation activities The ATSB is continuing to analyse the recorded data recovered from the aircraft systems.
The next update on this investigation will coincide with the release of the preliminary factual report on 3 December 2010.
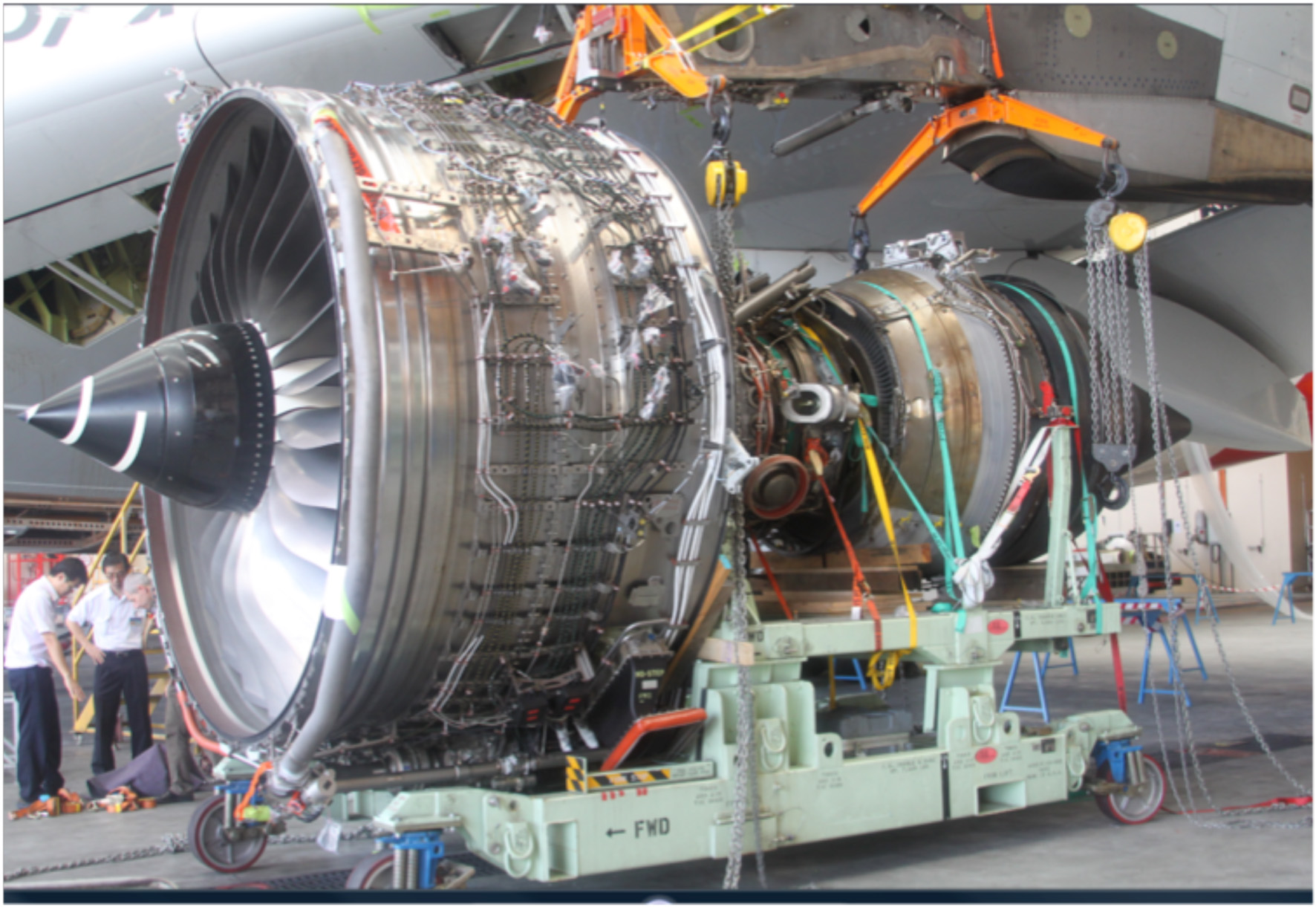
Update 4.00 pm - 17 November 2010 Engine examination The No 2 engine has been successfully removed from the aircraft in Singapore (Figure 1), and is being progressively dismantled in a local engine workshop. The Low Pressure Turbine module has been removed to allow access to the damaged Intermediate Pressure Turbine area for examination. The disassembly and examination of the remainder of the engine should be completed by the end of this week.
The examination of the recovered No 2 engine turbine disk segment at the Rolls-Royce facility in Derby, United Kingdom has been completed. The two ATSB investigators who supervised that examination have returned to Australia. The ongoing examination of relevant No 2 engine components and of any material subsequently recovered from Batam Island, Indonesia will be carried out at the Rolls-Royce, Derby facility. This will be done under the supervision of investigators from the United Kingdom Air Accident Investigation Branch.
ATSB investigators will continue their oversight of activities in the United Kingdom in cooperation with the Rolls-Royce engineering staff in Derby, and with the supervising Air Accident Investigation Branch investigators.
Figure 1: No 2 engine being removed from aircraft
Source: ATSB
Aircraft examination The examination of the aircraft in Singapore is also continuing. A number of wing and body fairing panels have been removed from the aircraft to facilitate the examination of the underlying structure and systems affected by the engine failure.
This work is expected to continue for at least the remainder of this week.
Locating aircraft components The search for the remaining engine debris on Batam Island, Indonesia was concluded by the Indonesian National Transportation Safety Committee and ATSB investigators on Saturday 13 November 2010. A number of small engine components were recovered during the search, including some turbine blades and blade attachments; however, other significant parts of the liberated No 2 turbine disk have not been located.
If anyone on Batam Island finds anything that resembles the remainder of the turbine disk or other engine components, they are requested to contact the local authorities.
On-going investigation activities ATSB investigators are also reviewing:
the recorded Singapore Air Traffic Control radio and radar data
the flight and cabin crew interviews
the downloaded flight and other data from the aircraft.
Relevant information from these sources will be included in the ATSB preliminary factual report that is planned for public release by 3 December 2010.
Update: 4.00pm - 13 November 2010 Aircraft examination continuing In Singapore, the No 2 engine has been successfully removed from the aircraft and is being prepared for transport to a local engineering facility for technical examination under ATSB supervision. The removal of the engine will also facilitate closer examination of the damage to the surrounding wing and other structures and systems.
Locating aircraft components The search for the remaining engine and debris on Batam Island by the Indonesian National Transportation Safety Committee and ATSB investigators and local authorities is ongoing. After initial success, the search is becoming increasingly difficult as a result of the local terrain, which includes virgin jungle (Figure 1).
Figure 1: Indication of the some of the terrain on Batam Island
On board recorded flight and other data The retrieval and analysis by ATSB investigators of the recorded flight, cockpit voice, engine monitoring and other data is continuing. The aircraft's 'black box' flight data and cockpit voice recorders were removed from the aircraft and returned to Australia immediately after the occurrence.
The aircraft's flight data recorder provided extensive flight and engine data, including from the entire occurrence flight (Figure 2). That data was forwarded to the aircraft and engine manufacturers through the relevant accredited representatives to allow a full understanding by the various parties of the event as the physical and other examinations were taking place.
Figure 2: Aircraft's flight data recorder
The cockpit voice recorder was transported to the ATSB's technical facilities in Canberra, Australia for download and analysis. Over 2 hours of cockpit audio was recovered. However, due to the failure of the No 1 engine to shutdown in Singapore, and therefore continuing power supply to the recorder, the audio at the time of the engine failure well over 2 hours before the No 1 engine could be shut down, was overwritten. That said, elements of the available audio are expected to be of assistance to the investigation.
Figure 3: Aircraft's cockpit voice recorder
A number of other data recorders, such as the aircraft's wireless quick access recorder have also been recovered by the ATSB for download (Figure 4). Those recorders offer a record of additional engine and other parameters to those recorded by the aircraft's flight data recorder. This information is particularly valuable in gaining a full understanding of this type of event, more specifically during the lead up to and during the engine failure.
Despite initial difficulties as a result of damage to the aircraft's electrical system, the ATSB, in collaboration with Airbus, Qantas, the Air Accident Investigation Bureau of Singapore and the aircraft condition monitoring system manufacturer, have successfully recovered all pertinent data. That data has been shared with Rolls-Royce and other participants in the investigation.
Conclusion The integration, examination and analysis of the data from the various recorders is continuing, and will supplement the evidence obtained from the examination of the No 2 engine turbine disk segment at the Rolls-Royce facility in Derby, United Kingdom and the disassembled No 2 engine and damaged aircraft in Singapore.
Update: 6.55pm - 12 November 2010 Engine investigation The examination under ATSB supervision of the No 2 engine turbine disk segment at the Rolls-Royce facility in Derby, United Kingdom is continuing. Boroscopic and other examination of the engine itself continues in Singapore.
EASA Airworthiness Directive (AD) On 10 November 2010 (European time), the European Aviation Safety Agency issued EASA AD No: 2010-0236-E in respect of the operation of the Rolls-Royce PLC RB211 Trent 900 series engines. The airworthiness directive introduced a requirement for the periodic inspection of the high pressure/intermediate pressure engine structure for any abnormal oil leakage. If any discrepancy is identified, the further operation of that engine is prohibited.
The action by the European Aviation Safety Agency was based on a preliminary analysis of the circumstances of the engine failure by the European Aviation Safety Agency, which the agency said showed that an oil fire in the high pressure/low pressure structure cavity may have caused the failure of the intermediate pressure turbine disc.
Rolls-Royce announcement This evening, Rolls-Royce announced that its own investigations had led it to draw two key conclusions:
'First, as previously announced, the issue is specific to the Trent 900. Second, the failure was confined to a specific component in the turbine area of the engine. This caused an oil fire, which led to the release of the intermediate pressure turbine disc.'
At this stage, the ATSB does not have enough information to comment on the first conclusion. The second conclusion is not inconsistent with the ATSB's work to date in Derby and Singapore. The ATSB supports any proactive safety action that is undertaken in response.
Ongoing ATSB investigation The effort by the ATSB and investigation team to fully understand the nature and implications of the engine failure and its consequences is ongoing. The search for additional engine and other components on Batam Island, Indonesia enjoyed initial success, with the recovery of a small engine part. The search continues and it is hoped that additional large portions of the No 2 engine turbine disk will be located.
Preparations for the removal of the No 2 engine from the aircraft are nearing completion and it appears that the engine may be able to be removed from the aircraft somewhat earlier than initially planned. Once safely removed from the aircraft, the engine will be transported to a local engine repair facility for disassembly and technical examination under ATSB supervision.
In Australia, the flight crew interviews have been finalised and collated. Qantas has invited ATSB investigators to attend the cabin crew post-incident de-brief.
Update: 12.55pm - 12 November 2010 Locating aircraft components ATSB investigators will arrive in Batam Island this morning to assist Indonesian National Transportation Safety Committee investigators search for the remaining engine and debris on Batam Island. The mapping of the damage to the aircraft is complete and has meant that the search will concentrate to the right of the aircraft's track (Figure 1). Assistance from the local authorities on Batam Island and a number of Rolls Royce staff is being coordinated by National Transportation Safety Committee investigators. Any recovered engine components will be forwarded to the Rolls Royce facility in Derby, United Kingdom for technical examination under ATSB supervision.
Figure 1: Search area of interest (aircraft tracking from top to bottom)
click photo for larger version
Cabin crew interviews ATSB investigators are gaining an understanding of how the cabin crew managed the cabin safety during the recovery of the engine failure as well as during the landing and exit of passengers at Singapore. Initial planning is to interview the cabin manager and relevant cabin services staff. A survey of the remaining cabin services staff is also being planned.
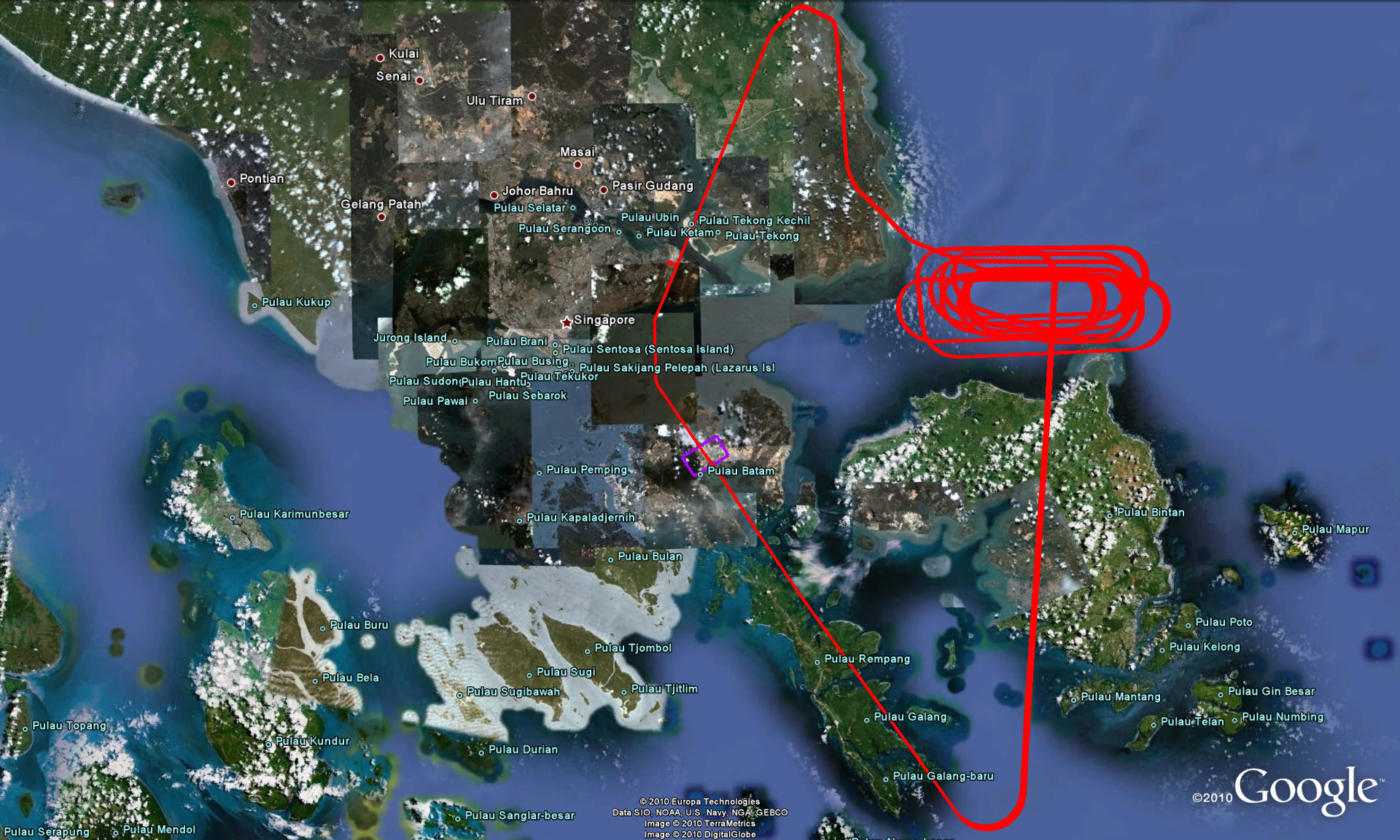
Figure 2:Aircraft track showing the departure from Singapore, the holding pattern as the crew managed the emergency and reduced the aircraft's landing weight and the recovery to Singapore
click photo for larger version
Aircraft examination continuing Internal examination of the on-wing No 2 engine has been carried out via borescope and a specialist lifting cradle is en route to Singapore from Germany to facilitate the removal of the engine from the aircraft. That removal is planned for this weekend. A number of electronic engine control and other components have been removed from the engine and sent to the Rolls Royce facility in Derby, United Kingdom for examination and possible recovery of recorded data.
Turbine disk examination Technical examination of the sectioned No 2 engine turbine disk at the Rolls Royce facility in Derby, United Kingdom is ongoing. Additional areas of the disk are being sectioned before cleaning for closer examination. If located on Batam Island, the remainder of the turbine disk and other engine components will be subjected to similar examination.
Update: 2.50pm - 11 November 2010 Safety action in response to the engine failure On 10 November 2010 (European time), the European Aviation Safety Agency issued airworthiness directive EASA AD No: 2010-0236-E in respect of the operation of the Rolls-Royce PLC RB211 Trent 900 series engines. The airworthiness directive introduces a requirement for the periodic inspection of the high pressure/intermediate pressure engine structure for any abnormal oil leakage. If any discrepancy is identified, the further operation of that engine is prohibited.
This action is based on a preliminary analysis of the circumstances of the engine failure by the European Aviation Safety Agency, which the agency says shows that an oil fire in the high pressure/low pressure structure cavity may have caused the failure of the intermediate pressure turbine disc.
While the investigation is ongoing, and may take some time to fully understand the nature and implications of the engine failure, the action by the European Aviation Safety Agency to issue AD No: 2010-0236-E represents proactive safety action to minimise risk. That safety action will be reflected in the ATSB preliminary factual report that will be released to the public no later than 3 December 2010.
Update: 10.15am - 11 November 2010 Flight crew interviews ATSB investigators have completed their interviews of the flight crew, which began in Sydney yesterday, assisted by a senior Airbus A380 test pilot. The flight crew interviews have provided an understanding of the aircraft's performance during the emergency, the effect on the aircraft's systems during that time, and of the flight crew's actions to recover from the emergency. It is anticipated that the examination of the management of the emergency will identify valuable insights into the handling of future emergencies in the A380.
Aircraft examination continuing Qantas engineers have developed a number of technical orders and work sheets to prepare for the removal of the No 2 engine from the aircraft. It is anticipated that the removal of the engine for disassembly and further examination will occur later in the week.The examination will take place in a Singapore engineering facility under ATSB supervision.
Locating aircraft components The mapping of the damage to the aircraft is complete. It has been integrated with the relevant recorded flight data to localise the search for the remaining engine and other debris on Batam Island. The results of that integration are encouraging, markedly reducing the potential search area. Investigators from the Indonesian National Transportation Safety Committee are presently returning to Batam Island to coordinate the search with the authorities on the island. ATSB and Singapore Air Accident Investigation Bureau investigators will travel from Singapore to Batam Island to assist with the search.
Turbine disk examination The initial technical examination of the recovered portion of the No 2 engine turbine disk at the Rolls Royce facility in Derby, United Kingdom has concluded. The disk will be sectioned into more manageable parts. The relevant surfaces and areas will be forensically 'cleaned' before anadditional, more detailed examination.
Failure of the No 1 engine to shut down after landing at Singapore The ATSB is working with engineering advisors from Airbus, Rolls Royce, the European Aviation Safety Agency and other members of the investigation team to understand the nature and implications of the failure of the No 1 engine to shut down after landing.
Timeframe The ATSB has begun planning for the release of a preliminary factual report via the ATSB website at www.atsb.gov.au by 3 December 2010. The investigation is anticipated to be completed within 1 year of the occurrence. However, should any critical safety issues emerge, the ATSB will immediately bring those issues to the attention of the relevant authorities or organisations and publish them as required.
Update: 4.50pm - 9 November 2010 Flight crew interviews The ATSB today commenced interviews in Sydney with the flight crew, and are being assisted by an Airbus A380 test pilot. The flight crew interviews will provide an understanding of the aircraft's performance during the emergency, and of the flight crew's actions to recover from that emergency. The flight crew will also be able to advise what went well during their management of the emergency. This will provide highly useful safety lessons for managing similar incidents in the future.
Aircraft examination continuing The aircraft has now been moved to a hangar at Changi Aerodrome. An initial internal examination of the No 2 engine has been carried out using a slender optical periscope (borescope). The engine is expected to be removed from the aircraft's wing for technical examination during the next few days.
Locating aircraft components The ATSB has mapped the damage to the aircraft. This map is being used with relevant recorded flight data to localise the search on Batam Island for the remaining engine and other debris. The ATSB is working with the Indonesian Transportation Safety Committee and Batam Island authorities to recover those components. ATSB investigators are particularly interested in recovering the remainder of the fractured turbine disk. The ATSB advises Batam island residents to avoid handling any of the aircraft components due to potential health risks.
Turbine disk examination ATSB investigators have arrived at the Rolls Royce facility in Derby, the United Kingdom to examine the recovered portion of the No 2 engine turbine disk. A copy of the recorded flight data has been provided to the engine and aircraft manufacturers by the respective accredited representatives. This will allow the manufacturers to assist with a full understanding of the data and its implications for the investigation. An investigation of this complexity can take up to a year to complete. However, should any critical safety issues emerge, the ATSB will immediately bring those issues to the attention of the relevant authorities.
Update: 12.15pm - 8 November 2010 The portion of the recovered engine component has arrived in the United Kingdom under the ATSB's custody. The component is being transported to the engine manufacturer's premises in Derby for a detailed technical examination under ATSB supervision. That examination is planned to commence when additional ATSB technical expertise arrives in Derby on Tuesday 9 November 2010.
The examination of the aircraft in Singapore is continuing. This involves mapping the damage to the aircraft as a result of the uncontained engine failure. Once finalized, that damage map may assist the investigation, the Indonesian National Transportation Safety Committee and Batam Island authorities to localize the search for the remainder of the engine component on the island.
In addition, the No 2 engine and surrounds were prepared for the engine's removal from the aircraft. A comprehensive plan for that removal was developed with expert assistance from the engine and aircraft manufacturer members of the investigation team.
An Airbus A380 test pilot will arrive in Canberra today to assist Operations Group investigators. The Operations Group will examine the cockpit indications leading up to the engine failure, and the aircraft operational aspects of the failure and subsequent recovery to Singapore.
It is anticipated that interviews will take place with the flight crew in the next few days.
Update: 9.15am - 7 November 2010 The ATSB has requested any residents of Batam Island that might have recovered additional aircraft items, in particular similar to the portion of what looks like a geared disk at Figure 1, to forward those items to the local police for retention. The recovery of that disk could be crucial to a full understanding of the nature of the engine failure, and may have implications for the prevention of future similar occurrences.
The Indonesian Transportation Safety Committee has assisted the ATSB with the recovery of a number of items of debris from the QANTAS A380 aircraft that sustained an engine failure overhead Batam Island, Indonesia on Thursday, 4 November 2010. The recovered items arrived in Singapore on 6 November, and a portion of a recovered engine component has been prepared for on forwarding to the United Kingdom in the custody of the ATSB. On arrival in the United Kingdom, that item will be examined by the engine manufacturer and other expert parties under the supervision of ATSB investigators.
Additional ATSB investigators will depart Australia on 7 November 2010 for the United Kingdom to oversight the examination of the recovered engine component, and to Singapore to assist the in-place investigation team with the ongoing examination of the aircraft, and of the remaining debris that was recovered from Batam Island.
Figure 1: Portion of recovered turbine disk
At Changi International Airport, Singapore the damage to the aircraft as a result of the engine failure is being mapped by investigators in order to understand the nature of the uncontained engine failure, and the failed number two engine and surrounds is being readied for removal from the aircraft. Once removed from the aircraft, the engine will be transported to an appropriate engineering facility for disassembly and technical examination.
A highly-experienced and technically-qualified international team of accredited representatives and advisors has assembled in Singapore to assist the ATSB investigation. Those representatives and advisors are being overseen by the ATSB and include personnel from the aircraft and engine manufacturers, the aircraft operator, the United Kingdom Air Accident Investigation Branch, the Indonesian National Transportation Safety Committee, the Singapore Aircraft Accident Investigation Bureau and the French Bureau d'Enquêtes et d'Analyses pour la sécurité de l'aviation civile (BEA). Personnel from those organizations and agencies can also be expected to partake in the examination of the recovered engine component in the United Kingdom.
Update: 3.00pm - 5 November 2010 General Manager, Aviation Safety Investigations, Mr Ian Sangston conducted a media briefing today on known factual aspects of the investigation. • Media Release
Update: 11.30am - 5 November 2010 ATSB investigators arrived in Singapore last night to examine the Qantas A380 aircraft. Flight data recorders have arrived in Australia and are currently being downloaded in Sydney. The Australian Transport Safety Bureau is working with international counterparts, including the UK AAIB, Rolls Royce, the French BEA, Airbus, Singapore AAIB and the Indonesian NTSC.
Update: 5:55pm - 4 November 2010 The ATSB has confirmed, following consultation with Singaporean and Indonesian officials that the ATSB will lead the investigation into the incident. Singaporean and Indonesian investigation officials can expect to be invited to be involved in the ATSB investigation in accordance with international protocols.
Indonesian representatives are currently supervising the collection and preservation of physical evidence on Indonesian territory. The ATSB has quarantined a number of aircraft components for later technical examination.
A team of four ATSB investigators are expected to arrive in Singapore early Friday, 5 November.
Update: 4:30pm - 4 November 2010 The ATSB is investigating the incident involving Airbus A380 aircraft operating as flight QF32 near Singapore today and is dispatching a team of four investigators to Singapore tonight. The ATSB is already working closely with its Indonesian and Singaporean colleagues and anticipates commencing its examination of the aircraft tomorrow, Friday 5 November.
Further investigation updates from on-site will be promulgated as they come to hand. A preliminary factual report is anticipated for public release on the ATSB web site www.atsb.gov.au no later than 3 December 2010. Readers can ensure advice of the release of that report by subscribing to the ATSB web site.
The ATSB is investigating the 30 March 2011 fatal aircraft accident involving a Piper Turbo Saratoga SP at Moree in NSW.
Update 1 April 2011 The ATSB investigation team arrived in Moree yesterday afternoon.
This morning, they interviewed many of the witnesses staying in the adjacent caravan park. Because many of the witnesses are tourists, it is important that the ATSB gets their statements before they move on.
The team have begun examining the site including the surrounding area for additional evidence such as ground scars or broken tree branches.
Further updates will be made available as significant information comes to hand.
Update 31 March 2011 Four ATSB investigators, three from Canberra and one from Brisbane, will arrive at Moree later this afternoon. Over the next few days they will examine the wreckage site, interview witnesses and collect maintenance records.
The ATSB will also conduct a media briefing on its investigation at the accident site on Blueberry Road, Moree on 1 April 2011 at 11.00am (AEDT).
Further updates will be made available as information comes to hand.
The ATSB is investigating the 5 February accident involving a Cessna 310R on Bathurst Island in the Northern Territory. The aircraft collided with terrain shortly after taking off from Bathurst Island Aerodrome. Last updated 3.05pm - 8 February 2011
Update 3.05pm - 8 February 2011
The ATSB investigation team commenced investigation of the Bathurst Island accident site on Monday morning. Access to the site has been difficult, with dense undergrowth and very wet conditions hampering activities. The investigation team has mapped the wreckage distribution and is proceeding to examine key aircraft systems and structures in closer detail.
Ongoing activities will include interviews with witnesses and aircraft operational and maintenance personnel. Maintenance, training and operation records have been quarantined and will be reviewed as part of the ongoing investigative process.
Update 1.10pm - 7 February 2011
The ATSB is investigating the 5 February accident involving a Cessna 310R on Bathurst Island in the Northern Territory. The aircraft collided with terrain shortly after taking off from Bathurst Island Aerodrome. The pilot (the only person on board) sustained fatal injuries.
The ATSB deployed a team of four investigators to the accident site on Sunday morning - two officers from the ATSB Canberra central office and two from the Brisbane office. The team arrived in Darwin early Sunday afternoon and commenced investigations by contacting police, Air Services Australia and the aircraft operator. The team will be travelling to Bathurst Island early Monday morning to commence the on-site phase of the investigation.
A preliminary report, containing a summary of factual information gathered during the ATSB's initial investigation, will be issued within 30 days.
More information on the investigation is available on the investigation page AO-2010-017
The ATSB is investigating an accident involving a Robinson R44 helicopter, registered VH-HFH. The helicopter crashed into the ground at Cessnock Airport in New South Wales and burnt as a result. Of the three occupants, two were fatally injured and one sustained serious injuries.
Update 12.10pm - 7 February 2011
The ATSB team of investigators completed their on-site examination of the wreckage on Sunday, 6 February. They have retained several components of the Robinson R44 helicopter, which will be brought back to the Canberra laboratories for examination and analysis.
Today, the investigators will continue to collect other documentation in Newcastle, including training and maintenance records. They will also be interviewing witnesses and other relevant parties.
Further updates will be posted as information comes to hand.
Update 3.10pm - 5 February 2011
The ATSB is investigating an accident involving a Robinson R44 helicopter, registered VH-HFH. The helicopter crashed into the ground at Cessnock Airport in New South Wales and burnt as a result. Of the three occupants, two were fatally injured and one sustained serious injuries.
The ATSB has dispatched a team of four investigators to the site. They will arrive tonight and be on-site for a number of days. During that time, the team will:
examine the site
interview witnesses and the surviving crew member
collect training, maintenance and relevant operator records and documentation.
More information on the investigation is available on the investigation page AO-2011-016
Further updates will be posted as information comes to hand.