Sequence of events
At about 1215 eastern summer time on 30 October 2004, the pilot of Bell Helicopter Company 206B, registered VH-JVW, was conducting aerial work in support of the Forbes area Plague Locust Control Campaign (campaign) that was being administered by the NSW Department of Primary Industries (DPI). Also on board the helicopter were the local Rural Lands Protection Board (RLPB) senior ranger, who was seated in the left front seat of the helicopter, and one RLPB and one DPI staff member who were seated in the rear cabin of the helicopter.
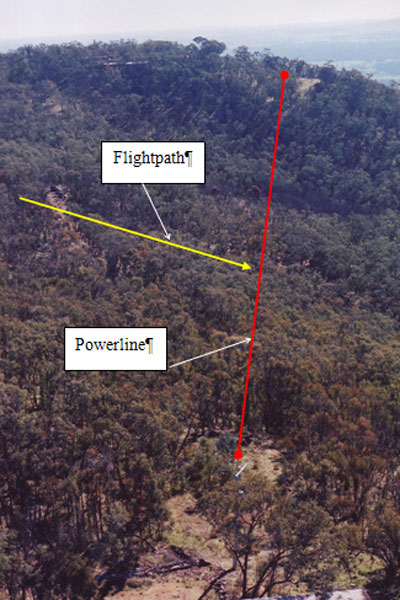
The senior ranger requested the pilot to land in a paddock in order to examine a previously unidentified band1 of locusts. The pilot reported conducting two orbits of the proposed landing area prior to commencing the approach to land in a north-easterly direction. During those orbits, the pilot asked all the occupants of the helicopter to keep a look out for power cables and other potential hazards in or around the landing area. However, one of the rear seat occupants reported the understanding of not being required to call or report power cables unless it was felt that the pilot had not seen a cable. While neither of the rear seat occupants reported the presence of any power cables to the pilot, the pilot and senior ranger saw a north to south running power cable located on the western boundary of the paddock. They also noted a westerly spur line emanating from a power pole located abeam the intended landing point. That power pole was also supporting the north to south power cable. No-one aboard the helicopter identified a second spur line emanating from that same power pole, and tracking to the east and overhead the intended touchdown point.
The pilot reported that, when at 'low airspeed' and passing through an estimated 25 ft above ground level (AGL) on the final stages of the approach to land, a previously unidentified power cable became caught between the skids and underbelly of the helicopter. The pilot indicated that he attempted to manoeuvre the helicopter free from the cable, but that the helicopter pitched 90 degrees nose down and impacted the ground heavily on its nose before rolling onto its roof. The helicopter came to rest on its right side, facing back along the direction of approach, and was extensively damaged. There was no fire. The senior ranger suffered minor injuries, and the pilot and rear cabin occupants were not injured.
Personnel information
The pilot was appropriately qualified for aerial work operations in the helicopter, and reported being medically fit, feeling well and adequately rested. The pilot was not required to wear or carry any vision correction spectacles, although he reported that he was wearing tinted sunglasses at the time of the accident. He had about 300 hours low flying experience2 at the time he was nominated by the operator for employment in the plague locust survey task. The pilot indicated that he had:
- most recently been operating in the Kununurra area
- not previously operated in the Forbes area, or with the operator
- no experience in plague locust survey or other operations.
The senior ranger indicated that he had flown in a helicopter once prior to the 2004 campaign. However, he had carried out an estimated 15 to 20 plague locust survey flights in helicopters during the 20 to 25 days preceding the accident. He had attended in-class locust control training courses that were administered by the DPI earlier in the year, but had received no experiential training in accordance with the requirements of DPI Standard Operating Procedure (SOP) for Australian Plague Locust Control in NSW number 15.16. Among other requirements, that SOP required that all DPI and RLPB staff assigned to fly in survey aircraft should have appropriate experience in detecting bands and directing spray aircraft. The senior ranger reported that, during the occurrence flight, his responsibilities included managing the survey task and acting as an observer.
One of the rear seat occupants had been involved in two previous survey flights during the campaign, and reported being responsible for spotting and recording locusts during the flight. That spotter had attended two brief, in-class training courses conducted by the DPI shortly before the campaign, but had been given no experiential training in the detection of bands or direction of spray aircraft.
The second rear seat occupant had been airborne in a helicopter once previously during the campaign and had minimal aviation experience. During the flight, that occupant shared responsibility for spotting and recording locust infestations. That spotter reported having attended a DPI workshop prior to participating in the campaign that examined the identification of plague locusts, but that no experiential training in relation to the detection of bands of direction of spray aircraft had been provided.
Aircraft information
Based on the evidence provided to the investigation, the aircraft was certified, equipped and maintained in accordance with the regulations and approved procedures. The windscreen was reported to have been clean, and there was no damage to the windscreen, or any obstruction that might have adversely affected visibility from the cockpit. The aircraft was not fitted with, and neither was there a regulatory requirement for the installation of a wire-strike protection system3 (WSPS). The Chief Pilot indicated that he felt WSPS might not have had any effect in this instance because the helicopter struck the power cable at low speed.
One spotter reported an intermittently operating intercom system, requiring communication with the remainder of the helicopter occupants through the second rear seat occupant. The rear seat belts installation included four-point lap and shoulder harness seatbelts for each occupant.
Meteorological information
No evidence was found to suggest that the weather conditions influenced the circumstances of the occurrence.
Survival aspects
Civil Aviation Order (CAO) 20.11 included the requirement for pilots to orally brief all passengers before each take-off. The pilot reported that, while he had briefed the passengers in accordance with that requirement, the actions in the event of an emergency and a reliable method for reporting power cables, or other hazards by the senior ranger and spotter were not discussed. For example, …wire right 3 o'clock, 300 m, travelling front to rear (of survey helicopter), etc.
The pilot indicated that he had been wearing a helmet at the time of the occurrence, and that the helmet visor was in the raised position. There was no regulated requirement for the senior ranger or rear seat spotters to be similarly equipped, and no stipulated minimum standard of flying or personal clothing for those persons for airborne operations in accordance with DPI or RLPB requirements. Such requirements might typically include full-cover clothing, safety boots, etc.
Administration of the 2004 plague locust infestation
In NSW, the Rural Lands Protection Act 1998 (RLPB Act) and Pest Control Order Number 6 under that Act declared the Australian Plague Locust to be a pest and imposed obligations on the occupiers of controlled land to report locusts on their lands to their local RLPB and to destroy those locusts. Assistance could be provided by the relevant RLPB, DPI or Australian Plague Locust Commission when the destruction of the locusts became beyond the capability of the individual land owner(s). In addition, the RLPB Act established a State Council as a corporate body with responsibility for ensuring implementation by RLPBs of:
- the general policies for the protection of rural lands
- operations in accordance with determinations made from time to time at State Conferences or by postal ballot.
The State Emergency and Rescue Management Act 1989 (SERM Act) required the DPI to coordinate the response to agricultural or animal emergencies with the support of relevant participating and supporting organisations. The State Agricultural and Animal Services Supporting Plan Memorandum of Understanding (MOU) established the DPI and State Council responsibilities for the preparedness for, and response to agricultural or animal emergencies. That MOU enabled the DPI to approach the State Council in order to seek technical expertise, personnel support and other assistance from RLPBs in agricultural emergencies.
At the time of the accident, there were 48 RLPBs throughout NSW. Each Board was a statutory authority under the RLP Act and was constituted for each rural lands protection district. Legislated RLPB responsibilities included those functions affecting the protection of rural lands, including the surveying and monitoring of plague locust infestations on pastoral lands. Should an infestation be considered to reach a defined density, the relevant RLPB and DPI determined the appropriate control measure. That was the case in 2004, when the locust infestation reached plague proportions in certain regions of NSW.
In response to the expected magnitude of the locust outbreak in the spring of 2004, the DPI requested through the State Emergency Management Committee (SEMC) that the locust outbreaks should be recognised as an emergency under the SERM Act, with DPI as the lead agency in any emergency response. That was supported by the SEMC and allowed the DPI to access relevant emergency management systems and resources. That included a request for assistance from the State Council to RLPBs from throughout NSW.
In response, RLPBs sought volunteers from among their staff who: were willing to be involved; could be released from their own Boards for the agreed period; and had the requisite skills or experience for the necessary tasks. During the campaign, those volunteer personnel were under the control of the relevant Local (locust) Control Centre, while administratively remaining a responsibility of their respective RLPB.
Aerial control of the 2004 locust infestation was coordinated by the Australian Plague Locust Commission, with responsibility for the area west of the Newell Highway and the DPI, east of that highway. The DPI responsibility included:
- monitoring locust populations and levels of infestation
- implementing particular aerial control measures for application in specific areas
- contracting for the provision of aeroplane and helicopter services in response to aerial spraying and survey requirements
- the purchase and supply of chemicals for airborne and ground-based application.
Contractual information
In response to the unpredictable nature of the requirement for aerial support to assist in activities related to the control of Australian plague locust and other species, the DPI sought Expressions of Interest (EOI) from aircraft operators to become 'prequalified service providers' of that aerial support. Successfully pre-qualified operators were placed on an approved pre-qualified applicant list, indicating operators' agreement that their aircraft, pilots and crewmembers would assist with locust control activities on a 'call when needed' basis.
The submission of an EOI by an operator indicated the operator's agreement with the Conditions of Contract as set out in section three of the EOI. Those conditions included that:
- The operator was required to notify the DPI of any variation in respect of aircraft and/or pilot information and obtain DPI approval in writing for that variation.
- The operator and its employees were suitably trained and able to demonstrate current competency. In that regard, an operator's Chief Pilot was required to certify that each pilot was rated, endorsed and competent to complete plague locust tasking.
- No pilot may undertake any task for the DPI unless approved in writing. That was reflected in the contract clauses, requiring an operator to obtain that written approval before allowing a pilot to undertake aerial support in connection with locust control services.
In respect of the operator's interaction with the DPI under those conditions:
- In response to a post-accident request by DPI, the operator provided the pilot's information by facsimile on 17 December 2004. There was no measure in place at the Forbes or other local control centres to allow local staff to check variations in pilot information against a DPI master list of approved pilots prior to a pilot commencing locust control work. That was the case with the occurrence pilot.
- The Chief Pilot certified the pilot's ratings, endorsements and competence for employment in the plague locust task on 29 October 2004. That certification was not forwarded to DPI until 17 December 2004.
- There was no control measure in place at local control centres to ensure that written approval was given by the DPI prior to the occurrence, or other pilots undertaking locust survey tasks.
In addition, the EOI allocated responsibility for the training of DPI and RLPB staff, and any other person involved in airborne operations, to the operators of those aircraft. The minimum requirements for applicants for pre-qualification included that 'pilots engaged or to be engaged by the Applicant must have at least 50 hours plague locust spraying and/or survey experience as appropriate' and 'Low Flying approval with at least 500 hours experience'. In the case of aerial spraying of locusts, pilots were required to hold a Grade 1 Agricultural Rating and be Spray Safe-accredited by the Aerial Agricultural Association of Australia (AAAA). In addition to requiring defined flying experience in agricultural operations, that rating included an examination to confirm a pilot's knowledge of the content of the CASA Aerial Agricultural Pilot's Manual, which stressed the importance of an agricultural pilot to carry out his or her own airborne inspection of an area to be sprayed. That was because it was the spray pilot's last critical opportunity to confirm their hazard map and other planning details. In the case of locust survey aircraft:
…the pilot must have a general permit for low flying ("Low Flying approval") in accordance with Regulation 157 of the Civil Aviation Regulations 19884.
During the evaluation of the response to the EOI that was submitted by the operator, DPI staff identified that, of the two company pilots initially nominated for the plague locust survey task, one certified having 18 hours locust survey experience and, the second pilot, no locust survey experience. Notwithstanding, the operator was contracted by the DPI as a Pre-Qualified Service Provider, Locust Control on 13 October 2004.
The Chief Pilot reported having an agreement with an operator located in the north of WA for the cross-hire of helicopters between the companies, and short notice cross-employment of pilots. That was to allow for the movement of those resources in response to seasonal up and downturns in each company's workload. The occurrence pilot commenced plague locust survey support work in the Forbes area while remaining an employee of the WA-based operator.
NSW DPI / RLPB Standard Operating Procedures for Locust Control - Effective 16 July 2004
The NSW DPI / RLPB Standard Operating Procedures (SOPs) for Locust Control established the requirements for aircraft operations involved in the 2004 campaign. Knowledge of the content of the SOPs varied amongst those aboard the helicopter. One DPI / RLPB staff member indicated having read the SOPs, although being unsure of the requirements placed on locust survey aircraft, while another confirmed that there were SOPs, but indicated having not read them comprehensively.
All DPI and RLPB staff assigned to fly in locust survey aircraft were required to '…have SLC [State Locust Controller] approval to fly and appropriate training and experience in detecting bands and directing spray aircraft'. During the investigation a previously unknown error in the SOP was identified by DPI concerning that approval. That error included that approval for DPI and RLPB staff to undertake locust survey flights had always been at the local level. DPI advice was that at the Forbes Control Centre, employees were allocated to locust survey aircraft on a weekly basis, and that allocation was notified to staff on a whiteboard. No written record was available to confirm staff allocation to the occurrence helicopter. Subsequent advice from the DPI included that, due to the nature of the 2004 locust campaign, the SOPs 'were seen as "living" documents which could be changed if required'. In that regard, the change in the approval process for employees to fly in survey helicopters had been conveyed to local control centres verbally, although the text of the SOPs had not been modified.
The SOP included the potential for helicopter survey of widespread and sparsely concentrated young (nymphs) or adult locusts. In the case of nymphs, the initial survey was required to be conducted at about 1,500 feet AGL. The location of significant infestations was marked using Global Positioning System (GPS) equipment and the number and size of the nymphs estimated in order to identify 'blocks' for subsequent aerial control, including aerial spraying of identified infestations to complement the ground spraying campaign.
The SOP included that onboard DPI / RLPB observer(s) 'may require the helicopter to land so that [they can] verify their observations' if the nymphs were not 'banding as normal5', or there was extensive ground cover. It was reported that had been the case during the occurrence flight, when the senior ranger had decided that the pilot should land the helicopter in order to prioritise target bands for spraying the following day. The senior ranger indicated that there had been recent discussion between local and other RLPB / DPI staff regarding the need to land a survey helicopter in order to prioritise bands for subsequent spraying. The senior ranger was unable to confirm the outcome of that consideration.
When conducting searches for adult locusts, and in the expectation that the adult locusts would flush up ahead or around the manoeuvring helicopter, the SOP required pilots to:
…fly along tree and creek lines and in localised areas of green vegetation approximately 12 ft (3 m) above ground level and at 30 knots (60 km/h).
Once a target group of locusts had been identified for aerial spraying, the SOP required the Local Locust Controller (LLC) or ranger aboard the locust survey aircraft to direct the spray aircraft to the target using GPS coordinates. The LLC or ranger was then required to:
- Relay the boundaries of the target to the pilot of the spray aircraft. That entailed either:
- the survey pilot flying the boundaries, and the LLC or ranger confirming the spray pilot's understanding of the boundaries via radio communication; or
- the LLC or ranger verbalising the boundaries via radio communication, then observing the spray pilot flying around those boundaries. - Identify and highlight any sensitive areas and hazards to the spray pilot. That included environmental and physical hazards, such as farm dams and power lines.
The Airfield Controller (controller) was responsible for coordinating aircraft operations at an airfield or landing area, compiling and managing Search and Rescue (SAR) logs, etc. That controller complied with the SOP requirement for the completion of a SAR - Aircraft Information Sheet for the occurrence helicopter task. In addition, the SOP required the controller to follow laid down, incremental search procedures should an aircraft fail to make a planned radio broadcast indicating normal aircraft operations or to return to base. The pilot indicated that he had been transmitting scheduled Operations Normal radio broadcasts at regular intervals to indicate normal helicopter operations, and the expected time of the next such transmission by the pilot. The pilot reported that he did not transmit a distress call upon striking the power cable. Notification of the occurrence was via a combination of telephone calls by the pilot and DPI / RLPB staff once clear of the wreckage.
Regulatory framework
In accordance with Civil Aviation Regulations (CAR) 157, flight is authorised below 500 ft when clear of any city, town or populous area and the aircraft is conducting aerial work operations that:
…require low flying, and the owner or operator of the aircraft has received from CASA either a general permit for all flights or a specific permit for the particular flight to be made at a lower height while engaged in such operations;…
The operator held a Low Level Flying Permit that authorised air work operations below a height of 500 ft AGL. Those operations were specified in the company Operations Manual and included aerial spotting and/or counting of wildlife and other similar tasks on behalf of landowners or Government Departments/Agencies/Instrumentalities. In addition, the company Operations Manual included that pilots in command of company aircraft carrying out low-level aerial spotting operations must:
(b) hold an appropriate agricultural rating or mustering approval or have satisfactorily completed the dual training specified for the appropriate kind of aircraft in CAO 29.10, Appendix 1;
CAR 206 lists aerial spotting and agricultural operations as operations conducted for aerial work purposes. Agricultural operations are defined as:
…the broadcasting of chemicals, seeds, fertilizers and other substances from aircraft for agricultural purposes of pest and disease control.
CAO 40.6 defines the requirements of Agricultural Pilot Rating Grades 1 and 2. Those requirements include completion of a period of ground training and a written exam, before carrying out initial and operational flying training. The operational flying training is followed by a period under supervision, before the newly rated agricultural pilot is able to conduct unrestricted agricultural operations. The Grade 1 rating required a helicopter pilot to hold, or have held a Grade 2 rating, and to have logged a minimum of 500 hours experience on helicopter agricultural operations.6
Aerial stock mustering is defined in CAO 29.10 as 'the use of aircraft to locate, direct and concentrate livestock whilst flying below 500 feet above ground level'. The aeronautical experience requirements for a pilot to engage in mustering operations include that the pilot must complete 5 hours low flying training7 and an exam to confirm pilot proficiency, followed by 10 hours operational training. The occurrence pilot completed the low flying training component of that requirement in March 1999.
Pilot induction
The Chief Pilot indicated that the pilot's preparation for the conduct of plague locust survey support included that:
- On 29 October 2004, the pilot signed as having read the company Operations Manual. That indicated the pilot's agreement to operate the helicopter in accordance with that manual
- The Chief Pilot conducted a pre-flight brief followed by a 0.3 hour check flight with the pilot on the morning of the accident. The content and duration of that flight was reported to be based on the pilot's recency with the helicopter type, and the high degree of commonality between the Bell 206B helicopters being operated by the company in support of the locust control campaign, and by the pilot's company in the north of WA. The primary differences between the helicopters included the radio installation and associated switches.
The Chief Pilot reported placing heavy emphasis on identification and avoidance of power cables and other hazards during the pre-flight brief, and stressing the particular dangers associated with operating below the tree tops. That was in recognition of the majority of the pilot's experience being in the Kununurra area, where the Chief Pilot felt there were not as many wires compared with the Forbes area. There was no practical application or review in the check flight of means available to a pilot to identify power cables and their orientation, or to demonstrate the difficulties affecting that identification.
In addition, the Chief Pilot indicated that he preferred steeper landing approaches and departures, because that increased the likelihood that any power cables might be seen during the approach or departure. In order to increase the power margin8 available for that steeper landing approach and departure technique, the Chief Pilot's preference was to restrict the number of passengers carried to no more than two. Those considerations were developed by the Chief Pilot during the campaign, and were not passed on to the pilot during the pre-flight brief or check flight.
Risk management
Australian/New Zealand Standard AS/NZS 4360:2004 Risk Management (the Standard) defined risk as:
the chance of something happening that will have an impact upon objectives.
NOTE 1: A risk is often specified in terms of an event or circumstance and the consequences that may flow from it.
NOTE 2: Risk is measured in terms of a combination of the consequences of an event … and their likelihood…
NOTE 3: Risk may have a positive or negative impact.
The Standard described risk management as 'the culture, processes and structures that are directed towards realizing potential opportunities whilst managing adverse [or negative] effects'. Residual risk is that 'risk remaining after implementation of risk treatment'. Options for modifying or treating identified risks with negative outcomes included:
- influencing the likelihood of a risk, in order to reduce the probability of a negative outcome
- changing the consequence(s) of an event to minimise the extent of any losses.
RLPBs were required to satisfy themselves that adequate arrangements were in place to manage risks associated with aerial survey operations before allowing their employees to undertake work-related tasks in support of the locust control campaign. There was no evidence of any guidance, such as the Standard having been provided to RLPBs to allow their confirmation of the adequacy of those arrangements. The State Council indicated that, while low-level survey by any aircraft was a high risk activity, the adoption of appropriate risk control measures had the potential to reduce the probability of an adverse incident to acceptable levels. However, the Council recognised that, even with such risk controls in place, there remained the residual risk of a serious incident or accident.
Wire density and the requirement to mark overhead power cables
The pilot stated that there were virtually no power cables in the Kununurra area when compared with his locust survey support experience in the Forbes area. The investigation determined that the density of the known power cables within a 100 km radius of Kununurra, excluding in the townships of Kununurra and Wyndham was one known power cable per 10,476 square kilometres. That represented three power cables that tracked between the two towns, and from Kununurra to the Ord River Dam and on to the site of the Argyle Diamond Mine.
In the Forbes area, that wire density, excluding in any townships was estimated to approach one known power cable per 10 square kilometres. The pilot indicated that the cable struck by the helicopter had not been marked on the World Aeronautical Chart used to navigate to the nominated survey area. He felt that the power cable had been difficult to see because of the extended spacing between the poles supporting that cable when compared with the spacing of the poles supporting the north to south power cable that was identified on the western boundary of the intended landing area.
The requirements for the mapping and marking of power cables and their supporting structures are published in Australian Standards AS 3891.1 1991 Part 1: Permanent marking of overhead cables and their supporting structures, and AS 3891.2 - 1992 Part 2: Marking of overhead cables for low level flying. The general requirements of those standards were discussed in ATSB investigation report BO/200404286 and include that, in general, there is no requirement for the marking of power cables with a height above terrain or obstacles of less than 90 m. The power cable that was struck by the helicopter did not require marking in accordance with either standard.
Technical committees are formed by Standards Australia to develop and review relevant standards, and comprise a balance of interested and affected parties that are nominated by generally national organisations. The aim is that the standards should include consideration of the views of large, common interest groups. Organisations that consider they represent a valid, previously unrepresented interest group are able to nominate for consideration for inclusion in a committee. A number of aviation industry associations and other bodies were involved in the development of the Australian Standards affecting the marking of overhead power cables and their supporting structures. That did not include some of the groups and associations normally associated with a number of agricultural and other low-level operations.
1 A 'band' was described by a ranger to indicate the presence of immature, ground-limited locusts. Bands appear as dark, ribbon-like or patchy marks, somewhat like a tide mark or stain.
2 The pilot indicated that his experience included bird control, some power line work and telecommunication equipment survey and support work in the Kununurra area in the north of WA.
3 Equipment installed on an aircraft to reduce the lethality of an impact with power or other cables.
4 CAR 157 placed a requirement on an operator; it did not directly affect qualifications required to be held by a pilot.
5 One of the rear seat occupants indicated that, on a hotter day, the locusts were more active. In that case, the band would be more dispersed and therefore difficult to interpret from the air in terms of density, size, etc.
6 Experience for the award of an Agricultural Pilot (Aeroplane) Rating Grade 1 included 1,000 hours agricultural flight time, of which 250 hours experience was required on spraying operations.
7 Including: avoidance of obstacles; aerial reconnaissance and operational planning; and the effect of obstacles on operational procedures.
8 The surplus of power between that produced by the helicopter engine compared to the power required by the helicopter and its systems during the approach in the ambient conditions.