Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
At about 1000 local time on 6 December 2024, a Leonardo Helicopters AW139, departed Bankstown Airport, New South Wales, on a visual flight rules (VFR) flight to respond to a search and rescue incident at Bondi Beach. The weather was clear departing from the airport, however on arrival at the scene, and at about 500 ft above mean sea level, a thin layer of fog was present. After the rescue operation was conducted using the helicopter’s rescue winch, the helicopter was requested to land at a pre-arranged site north of Bondi. In preparation for landing, the crew opened and secured the left side door. As the helicopter continued in a northerly direction, the weather deteriorated and the landing at the arranged site was no longer possible. To avoid the worsening weather, the pilot turned the aircraft eastward over the ocean toward clear skies. During this time, the crew planned for another landing site at the Sydney Children’s Hospital, however, as they continued in an easterly direction, the fog thickened considerably, and the pilot unintentionally entered instrument meteorological conditions (IMC). The pilot momentarily lost perception so added power and used the autopilot to climb to 1,000 ft where they became clear of cloud and visual.
The recorded flight data indicated that the helicopter maintained a climb rate of approximately 1,000 ft per minute with a 5° nose-up attitude. Between 400–500 ft, the pitch attitude gradually reduced to a nose-down attitude of 3° momentarily, resulting in a temporary reduction in the rate of climb to 500–600 ft per minute. The helicopter resumed a 5° nose-up attitude and continued climbing at a rate of approximately 1,000 feet per minute. This sequence occurred gradually over 10 seconds.
The helicopter continued to climb to 1,500 ft. At about this time, the pilot remembered the left side door was still open and realised that the 80-knot maximum airspeed limit had been exceeded while they were in IMC. The pilot immediately reduced the airspeed and the crew closed the door. After landing and shutting down at the hospital helipad, the helicopter was secured and taken out of service for a maintenance inspection to ensure airworthiness. The crew returned to base by alternate transport.
Safety message
The ATSB encourages all pilots, no matter what their experience levels, to develop the knowledge and skills required to avoid unintentional operations in IMC. This includes having alternate plans in case of unexpected changes in weather, and making timely decisions to turn back, divert or hold in an area of clear weather. The use of a ‘personal minimums’ checklist can also be a strong mitigator against the risk of flying into bad weather. Checklists can help pilots more clearly identify risk factors.
To increase the chances of safely recovering from an inadvertent entry into IMC, VFR pilots are encouraged undertake recovery training and basic instrument flying competency checks during their operator proficiency checks or other training.
ATSB booklet Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions (AR-2011-050) provides for guidance on avoiding VFR into adverse weather. Further specific information for helicopter pilots is also available on the ATSB website.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2024-051
Occurrence date
06/12/2024
Location
11 km east-north-east of Sydney Airport
State
New South Wales
Occurrence class
Serious Incident
Aviation occurrence category
VFR into IMC
Highest injury level
None
Brief release date
08/01/2025
Aircraft details
Manufacturer
Leonardo Helicopters
Model
AW139
Sector
Helicopter
Operation type
Part 138 Aerial work operations
Departure point
Bankstown Airport, NSW
Destination
Sydney Children’s Hospital Helicopter Landing Site, NSW
On 2 August 2024, a Leonardo Helicopters AW139, registered VH‑EXK, departed Longford Heliport, Victoria, for a hoist training exercise conducted under visual flight rules near Golden Beach, Victoria. During the training, the crew faced difficulties retrieving a waterborne training aid, but due to encroaching fog the instructor (Pilot Flying) elected to depart for Longford. They initiated a climb with the aid of the radar height hold function before ensuring the helicopter was correctly configured for departure. The helicopter then inadvertently entered instrument meteorological conditions (IMC) and the altitude and airspeed began to fluctuate. The enhanced ground proximity warning system then triggered as a result of increased airspeed and the helicopter’s flight path descending below 150 ft above sea level. The captain (Pilot Monitoring) took control and initiated a climb, allowing for a safe return to Longford Heliport without further incident.
What the ATSB found
Due to encountering fog the instructor conducted a hastened departure from the training area before securing the hoist, the cabin door and occupants. At the time, the captain, who was acting as pilot monitoring, was still occupied with recording the training aid position. During the initial climb, the helicopter inadvertently entered the encroaching fog, and the instructor, who was the pilot flying, lost visual references and became spatially disoriented.
The disoriented instructor attempted to exit instrument meteorological conditions but applied control inputs that resulted in the helicopter entering an unstable state. This triggered a terrain alert, and airspeed exceedances with the main rotor RPM at 102% and operations with the door open and the hoist extended.
Following the terrain warning, the captain took control of the helicopter prior to gaining situational awareness or conducting an appropriate control handover, increasing the risk of control conflict between the 2 crew members. Additionally, the operator had no defined procedures for inadvertent instrument meteorological conditions recovery during hoist operations or for responding to enhanced ground proximity warning system alerts and advisories.
Despite not gaining situational awareness and bypassing handover protocols, the captain’s control inputs immediately arrested vertical descent and initiated a climb, reducing the risk of collision with terrain.
What has been done as a result
Following this incident, Esso Australia conducted an internal investigation and has identified several actions to be taken.
A standardised procedure has been developed to ensure a controlled entry into instrument meteorological conditions from a low hover, including scenarios where aircrew may be connected to the hoist beneath the aircraft.
Flight crews will undergo further training during low-level operations in the helicopter and simulator to reinforce techniques for handling degraded visual environments.
Briefings for search and rescue and hoisting training operations will emphasise the importance of maintaining a safe distance from visibility-reducing conditions.
Crew resource management courses will also be updated to focus on upset training scenarios and flight crew responses.
Safety message
The ATSB encourages pilots to take proactive measures to manage the risks associated with inadvertent entry into instrument meteorological conditions. Loss of visual references can lead to spatial disorientation, reduced situational awareness and loss of control, particularly for pilots operating under visual flight rules. Pilots rated for instrument flight rules should prioritise the use of rehearsed recovery procedures, referencing flight instruments to safely regain visual meteorological conditions.
This incident shows the importance of establishing and monitoring operational safety margins, adherence to documented procedures, maintaining situational awareness and fostering effective crew resource management during high-workload scenarios like hoisting and search and rescue operations. The challenges presented by degraded visual environments, such as inadvertent entry to instrument meteorological conditions, increase the likelihood of spatial disorientation and loss of control in flight.
These proactive steps can significantly enhance safety and improve outcomes during low‑level operations in demanding conditions.
The occurrence
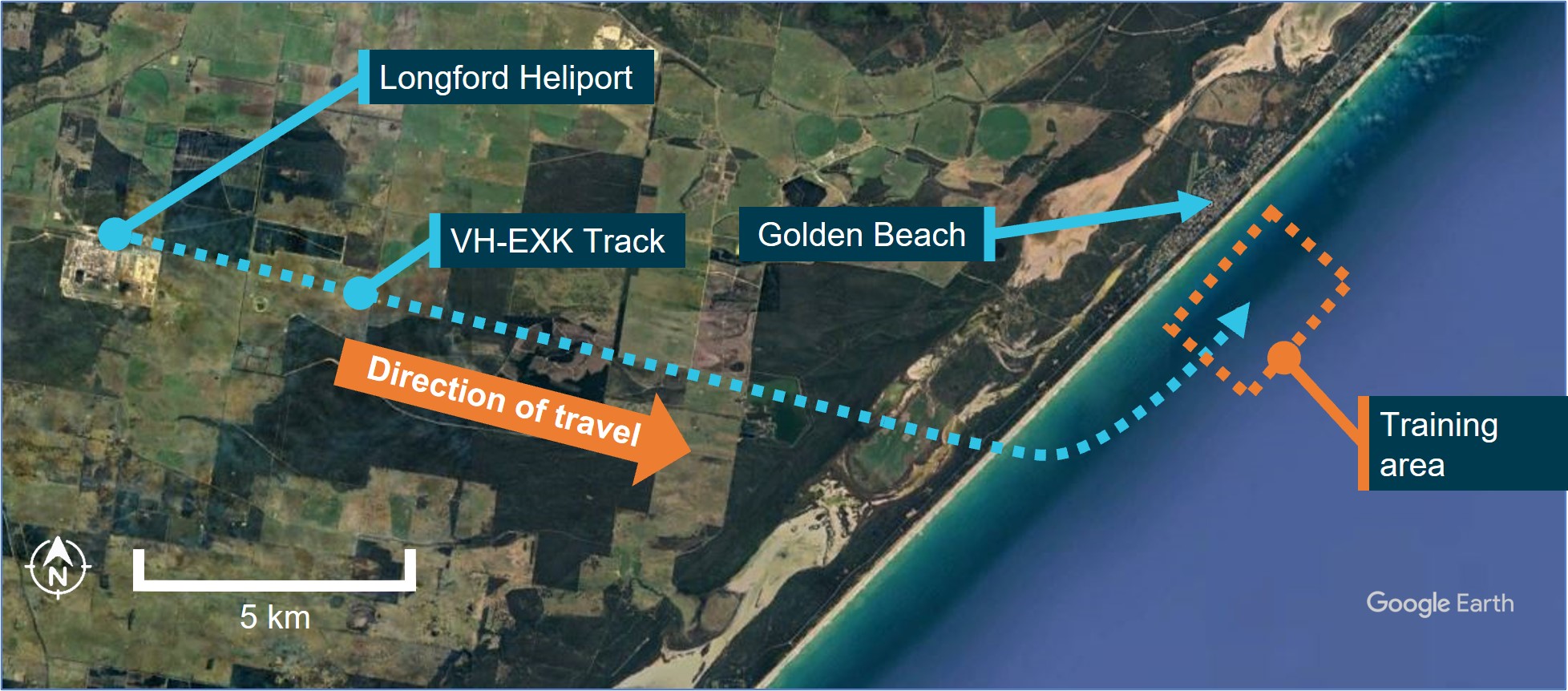
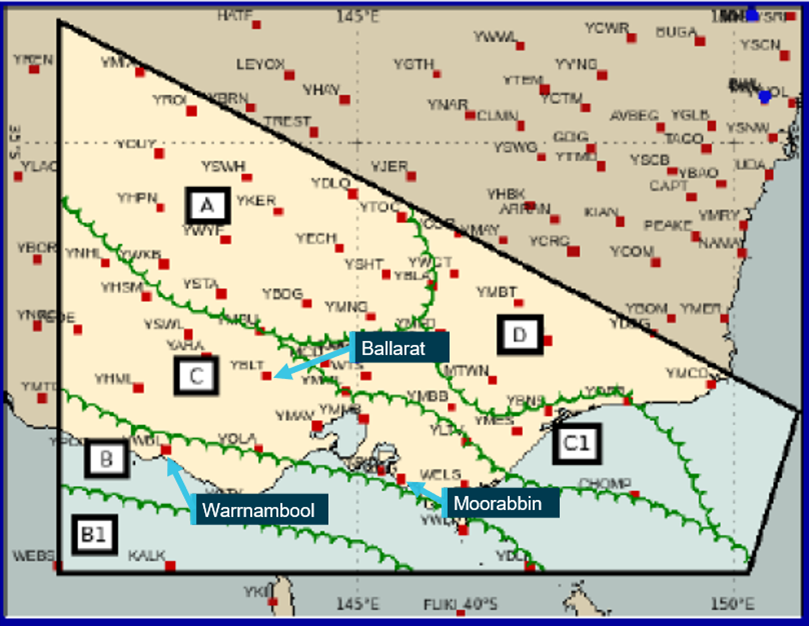
On 2 August 2024, a Leonardo Helicopters AW139, registered VH-EXK and operated by Esso Australia, departed Longford Heliport, Victoria at 0816 local time for a hoisting training exercise. The crew consisted of the captain, a flight instructor, a check aircrewman, and a hoist operator. The captain was initially the pilot flying (PF)[1] and was under the supervision of the instructor who was acting as pilot monitoring (PM).[2] The hoisting exercise took place near Golden Beach, Victoria (Figure 1) and was conducted under visual flight rules (VFR).[3] The crew crossed the coastline at 0821 and selected a training area approximately 2 km offshore. The exercise involved retrieving a training aid amidst large swells, sea spray and encroaching fog from the north-west. The training aid was deployed, and the exercise commenced at about 0825.
Figure 1: EXK track and key locations
Source: Google Earth, annotated by the ATSB
As the training progressed, the helicopter's proximity to the fog on the left side, where the instructor was seated, was observed to be decreasing. The flight crew noted that the skies were clear to the north and northeast of their position on the instructor’s side of the helicopter.
After conducting training for approximately 40 minutes, the instructor assumed control as PF and the check aircrewman assumed the role of hoist operator to retrieve the training aid. This involved hovering in a stationary position approximately 40 ft above the water's surface to retrieve a training aid, which was a wooden cross with ropes attached, designed to simulate a search and rescue scenario.
However, the attempt was unsuccessful, and due to the encroaching fog, the instructor immediately elected to depart and announced they would climb to avoid fog.
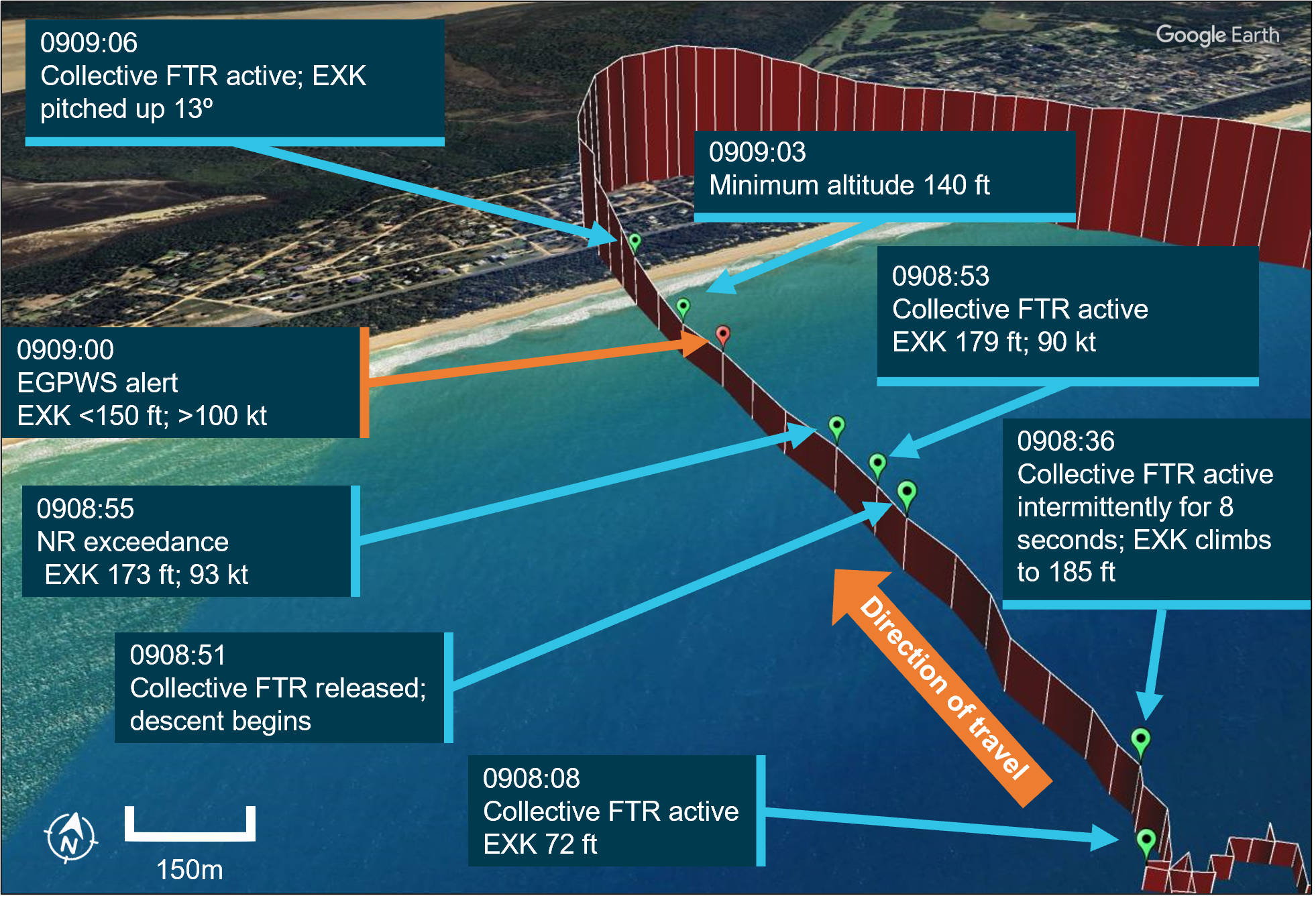
At 0908, the instructor manoeuvred the helicopter onto a north-westerly heading (Figure 2) and engaged the radar height hold (RHT) system while climbing using a combination of the collective[4] beep trim and force trim release (FTR).[5] At this time, the captain, acting as the PM, was focused on marking the GPS position of the training aid. This facilitated its retrieval in a subsequent training exercise later that day, as the large swells and fog disrupted the current exercise. During the departure climb, the right cabin door was open and approximately 40 ft of the hoist cable was extended.
Figure 2: EXK flight track and enhanced ground proximity warning system alert
Source: Google Earth, annotated by the ATSB
At about this time, the helicopter inadvertently entered instrument meteorological conditions (IMC),[6] and the instructor announced their intention to move forward to depart. The check aircrewman objected via the intercom to departing with the hoist still extended, as the post‑hoist procedures requiring the aircrew to secure the hoist cable and cabin had not yet been completed. Despite their objection, the instructor proceeded with the departure to regain visual meteorological conditions (VMC).
The instructor accelerated and continued to climb, reaching an altitude of 185 ft and an airspeed of 72 kt before beginning a shallow descent. The instructor who was PF noticed the increasing airspeed but took no actions to arrest this trend. As the helicopter continued accelerating, the captain observed on the primary flight display (PFD) a nose-down attitude and airspeed increasing through 80 kt, which exceeded the operational speed for the hoist operation. The captain announced ‘80 kt’ to draw the attention of the instructor to the increasing airspeed. The airspeed continued to increase above 90 kt, which resulted in an airspeed exceedance with the RPM (NR) at 102%, despite the captain’s attempt to set the RPM switch[7] to 100% to avoid this exceedance. As the helicopter accelerated through 100 kt it exceeded the maximum airspeed for the right main cabin door in the open and locked position.
At 0909, the helicopter had descended to 147 ft above sea level with an airspeed of 101 kt, triggering caution and warning alerts from the enhanced ground proximity warning system (EGPWS). In the 10-second period preceding the EGPWS warning, the collective FTR was active for 5 seconds while it was engaged and disengaged 3 times. The instructor recalled climbing and using the collective beep trim and collective FTR. However, they did not recall engaging the collective FTR after the negative vertical speed developed. The captain later noted that the collective FTR could be activated instinctively while manipulating the collective due to the switch's position, requiring discipline to avoid unintentional activation.
Responding to the increasing speed and ground proximity alert on the PFD, the captain reactively assumed control, reduced the helicopter’s speed, and initiated a climb by pulling back on the cyclic.[8] The check aircrewman suggested cutting the hoist cable for safety and indicated that the cable was trailing behind the aircraft. This was not actioned after consultation with the instructor, who stated they were satisfied that the cable did not pose a danger, and they lacked visual reference to the ground. The instructor decided not to cut the cable because they were unsure of what was underneath the helicopter at the time.
During the recovery, the captain climbed on a north‑westerly heading and reduced the helicopter’s airspeed and the instructor resumed control after a brief exchange with the captain. The flight crew regained VMC shortly after the recovery was initiated, recovered the cable and the helicopter was flown in an easterly direction away from the shoreline. The crew configured the helicopter for departure from the training area and returned to Longford Heliport. The helicopter landed without further incident at 0936 local time.
Context
Pilot information
Instructor
The instructor held an Airline Transport Pilot Licence (helicopter) with an instrument rating and a Class 1 aviation medical certificate. They had 11,129 flight hours, including 3,695 hours on the AW139, they had also logged 114 hours on the AW139 in the last 90 days. They were approved for training and checking duties with the operator, Esso Australia, including hoisting operational proficiency checks.
The instructor reported sleeping 7 hours the night before the occurrence. They were awake for 4 hours and were on duty for 2 and a half hours at the time of the occurrence, they stated they felt ‘alert but not at peak performance’.
Captain
The captain held an Airline Transport Pilot Licence (helicopter) with an instrument rating and a Class 1 aviation medical certificate. They had 15,402 flight hours, including 2,603 hours on the AW139 and had logged 81.9 hours on the AW139 in the last 90 days. They were approved as a line supervisory pilot with the operator.
The captain reported sleeping 7 and a half hours the night before the occurrence. They were awake for 4 hours and were on duty for 2 and a half hours at the time of the occurrence. They reported feeling ‘somewhat fresh’.
Helicopter information
The Leonardo Helicopters AW139, serial number 31886, was registered as VH-EXK in Australia to the operator, Esso Australia, on 8 January 2020. The helicopter was certified for day and night VFR, IFR,[9] offshore/elevated helideck[10] operations, and external load[11] operations.
Powerplant
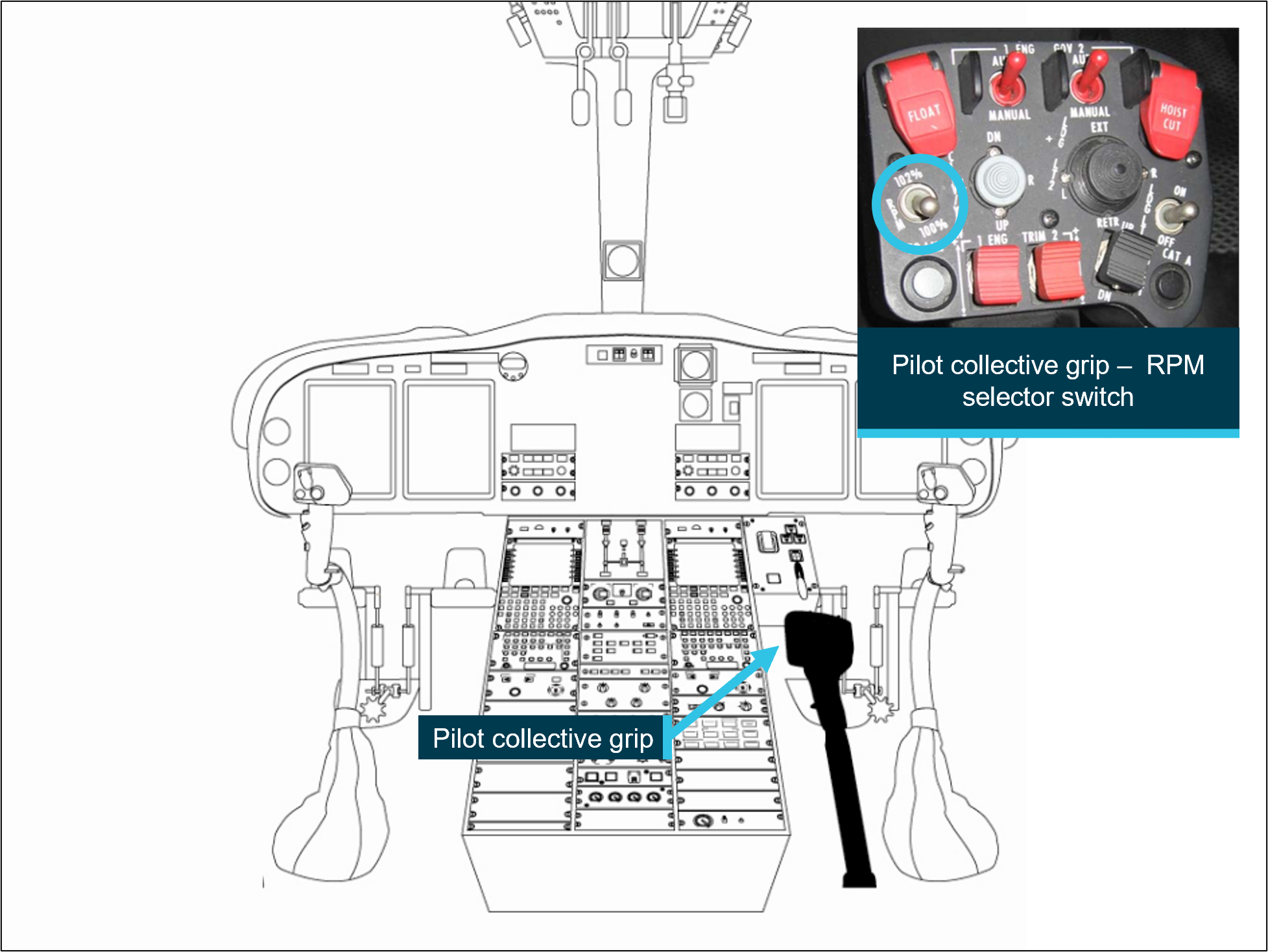
The AW139 is equipped with two Pratt & Whitney PT6C‑67C engines. The main rotor power can be set to 100% or 102% using the RPM selector switch (Figure 3) on the pilot’s (right seat) collective grip.
For Category A[12] operations below 80 kt, rotor RPM (NR) is set to 102%, enabling optimal performance in the event of an engine failure, allowing for either continued safe flight or a controlled landing. Real‑time rotor RPM is monitored on the multi‑function display with the maximum airspeed set to 90 kt at 102% NR to protect the rotor system from excessive stress.
Crew alerting system (CAS) messages are not triggered during RPM adjustments, allowing for changes without distracting alerts.
Figure 3: Pilot RPM selector switch
Source: Leonardo Helicopter file photo, annotated by the ATSB
Autopilot and radar height hold
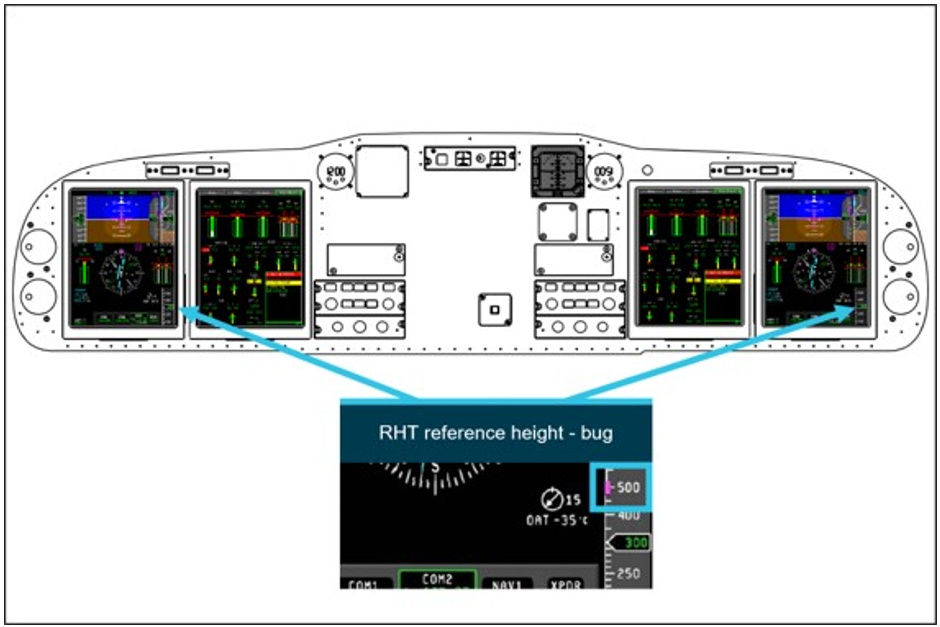
The AW139 is fitted with a 4‑axis autopilot system coupled with a 3‑cue flight director (FD), which controls the helicopter’s pitch, roll, yaw, and vertical axis. The radar height hold (RHT) mode maintains the helicopter at the radar height at the time of engagement. The RHT reference height is presented on a magenta bug (Figure 4) on the radar altimeter tape with a digital readout.
The helicopter flight manual stated that during hoist operations, that pilots should consider the effect of the use of the RHT function in flight and to monitor the helicopter performance closely when used.
Figure 4: RHT reference height
Source: Operator, annotated by the ATSB
The RHT reference height is adjustable using the following methods:
Collective force trim release (FTR): the ‘push and hold’ collective lever trim release button (Figure 5 left insert) is depressed to disengage the spring feel mechanism which enables the collective to be moved freely. When the button is released, the spring feel[13] is reset to zero force and the reference height is reset.
Collective beep trim switch: crews make incremental height adjustments using the collective beep trim switch, moving it aft to increase height and forward to decrease it (Figure 5 right insert). Adjustments occur at a rate of ±50 ft/second down or up, with audio tones (beep) signalling changes.
While RHT is designed to assist in stable altitude hold, crews are required to actively monitor and control the flight path.
Source: Leonardo Helicopters file photos, annotated by the ATSB
Cabin doors and hoist system
The sliding cabin doors fitted to VH‑EXK allowed for in‑flight hoisting operations, with speed limitations in place to prevent damage from slipstream pressure. The door could be locked open during hoist use. The operator required that the airspeed not exceed 80 kt when opening or closing the cabin sliding door and 100 kt when the door was locked open. The helicopter’s hoist system, located on the right side of the cabin, was equipped with an electric hoist motor, winch, and safety features including the primary quick release system, accessible to both flight crew and the hoist operator.
Enhanced ground proximity warning system
The helicopter was equipped with a Honeywell MK XXII‑30 enhanced ground proximity warning system (EGPWS), which displays terrain and obstacles. It is designed to provide alerts about nearby terrain or obstacles approximately 30 seconds ahead of the aircraft, giving warning of potential conflicts.
The functionality of the terrain awareness display and the ‘look ahead’ alerting and warning function was detailed in the AW139 rotor flight manual as:
This function uses information from the GPS and other sources on the aircraft to calculate horizontal position and vertical altitude. This data provides a three-dimensional position for the aircraft. This position is then compared to the terrain database and if a conflict with terrain or a known obstacle is imminent the system provides an alert.
Offshore mode
The EGPWS system fitted to the operator’s AW139 fleet included a dedicated offshore mode, which could be activated by the flight crew. Offshore mode is recommended for operations over water, as it adjusts terrain awareness boundaries to minimise nuisance alerts. This mode inhibits certain alerts and warnings in specific flight conditions. However, offshore mode is unsuitable for conventional IFR procedures, as it modifies terrain alerting parameters essential for standard instrument approaches and departures.
Operator information
Esso Australia operated from its headquarters in Longford, Victoria, supporting gas platform operations in Bass Strait. On 11 June 2024, the operator was issued with an air operator’s certificate (AOC), authorising Australian air transport operations and a Part 138 aerial work certificate, authorising aerial work operations.
Esso Australia operated a single helicopter type, the Leonardo AW139 helicopter, primarily for passenger transport, cargo transport and specialist aerial work operations, including external load and dispensing tasks. Its personnel were authorised to conduct both VFR and IFR flights.
Meteorological information
On the morning of 2 August 2024, the flight crew stated they conducted a weather briefing at the Esso Australia heliport base in Longford, Victoria. They recalled the presence of fog which delayed the departure by about an hour. While the crew prepared for departure, they received a report from another Esso Australia helicopter crew that the fog had sufficiently dissipated in the aera. Following a routine job safety analysis (JSA)[14] and final weather review, the crew assessed that the remaining fog posed no significant concern and proceeded with the flight.
Graphical area forecast
The flight to the training area and back was within the graphical area forecast for Victoria (GAF VIC), covering subdivisions A and A1. For the duration of the flight, the forecast conditions indicated:
visibility greater than 10 km, with broken stratus clouds between 100 and 1,000 ft above mean sea level (AMSL) in A1.
isolated freezing fog over land, with scattered fog south‑east of Mangalore and Wangaratta airports, reducing visibility to as low as 300 m.
Terminal forecast and special weather report East Sale (YMES)
The terminal forecast for East Sale predicted calm winds from 320° at 3 kt, with visibility reduced to 200 m in freezing fog, early in the morning.
By 0930 local time, conditions were expected to improve to greater than 10 km visibility with light winds. A 30% chance of mist, reducing visibility to 1,000 m was also forecast between 0900 and 1000. A special report (SPECI) at 0800 recorded calm conditions, with freezing fog reducing visibility to 200 m with scattered clouds at 100 ft.
Figure 6: Weather reporting locations
Source: Google Earth, annotated by the ATSB
Inflight weather observations
After a routine departure, the crew recalled observing a bank of fog along the coastline as the helicopter approached the training area. The instructor estimated that the fog bank was less than one kilometre from shore at the time. As the exercise began the flight crew reported that the fog began to obscure the shoreline near Golden Beach. However, clear skies were visible to the north and north‑east, while a large easterly swell created rough sea conditions below.
During the exercise, the flight crew reported that the helicopter was manoeuvred closer to the fog, which was situated on the left side of the helicopter, where the instructor was seated.
Operator procedures
Hoisting
Hoisting operations require coordination between all crew members and adherence to procedures and safety protocols. The hoist system, equipped with a cable and hook, facilitates the controlled retrieval of individuals or equipment, sometimes in challenging environments, such as water or rugged terrain.
Esso Australia hoisting crew compliment
Esso Australia hoist operations required a minimum crew of two flight crew, a hoist operator, and a wireman, each with defined roles (Table 1).
Table 1: Crew member location and roles
Crew member
Location
Role
Captain
Right side pilot seat
Oversees all aspects of the flight, especially during rescue operations, and briefs all crew members prior to departure.
Copilot
Left side pilot seat
Manages flight planning, navigates, monitors radios and helicopter systems, and assists with hoist operations as necessary.
Hoist operator (HO)
Cabin
Prepares rescue equipment, conducts pre-hoist checks, ensures cabin security, operates the hoist, and guides the pilot during hoisting.
Wireman
Cabin
Assists the HO, manages personal safety, and is prepared to descend on the hoist cable if needed.
The flight crew reported that the instructor and check aircrewman acted as copilot and wireman during the occurrence.
Hoist patterns and limitations
When conducting hoist exercises, helicopters typically follow a structured racetrack pattern approach, initially at 60 kt about 200–500 ft above obstacles. After approaching the site, the crew hover at a height below 100 ft over the target area to facilitate a stable hoisting environment.
The AW139 rotorcraft flight manual outlined the following operational limitations for hoist operations:
maximum 80 kt maximum forward flight speed during hoist operations
maximum 80 kt for opening/closing cabin door or 100 kt when door is locked open
fly manually or attentively when RHT mode is engaged.
The flight data from the occurrence revealed that the helicopter exceeded airspeed limitations for hoisting and the main door in the locked open position (See section titled Recorded information).
Post hoist procedures
Following a hoisting task, the hoist operator (HO) would secure the cabin and equipment, complete a post‑hoist checklist with the pilot monitoring (PM) using the challenge and response methodology,[15] and confirm the completion of the checklist items. The PM then completes the post‑hoist checks with the HO using the same checklist methodology (Table 2).
Table 2: Post hoist procedure and checks
Procedure
Actions
Post-hoist procedure
HO stows the equipment and closes the right main cabin door
HO announces, ‘cabin secure, post-hoist checks’
at this point the PF can climb.
Post-hoist check
PF safely establishes helicopter in the climb out
PM powers off the hoist and confirms circuit breakers are out
HO announces, ‘post hoist checks complete, clear to rotate’
PM initiates after take-off check.
After take-off check
PM checks NR set to 100% >80 kt
PM checks landing gear up >200 ft.
The crew recalled that before they departed the exercise site, the post‑hoist procedures and checks had not been performed.
Automation use
The use of automation for day VFR offshore flights, was detailed in the operator’s exposition stated as follows:
The advanced avionics suite in the AW139 promotes a high level of safety and crew situational awareness when used correctly. When not used correctly or understood, the opposite can occur allowing dangerous deviations and loss of situational awareness to quickly manifest.
ESSO Australia policy is for the flight management systems, multi-function control display units and avionics to be operated at a level that provides optimum navigation, communication and traffic awareness to the crews without drawing too much attention ‘inside the cockpit’. At all times, it is the responsibility of the PF to maintain effective control of the helicopter and its flight path/situation.
Handover and takeover procedures
Handover procedures in the operator exposition detailed the protocols flight crews must follow when transferring control to another pilot. The relinquishing pilot is required to state, ‘handing over,’ and the receiving pilot confirm by stating ‘taking over’ while placing their hands and feet on the controls. The first pilot then removes their inputs, ensuring clear role delineation. Handover drills must incorporate an active flight director, with no alternative transfer methods allowed.
The flight crew recalled that there was no verbalisation of the transfer of control during the recovery following the EGPWS alert.
The handover procedure was intended to ensure clear communication and role clarity by requiring the relinquishing pilot to state, 'handing over,' with the flying pilot to respond 'taking over' while actively taking control. These structured procedures are critical for maintaining operational safety and minimising risks during complex or dynamic situations. Neither pilot recalled referencing any rehearsed procedures in response to the inadvertent entry to IMC during the recovery. Additionally, they did not recall specific training in the helicopter or the simulator for EGPWS recovery.
Enhanced ground proximity warning procedures
As part of the pre‑flight checks, flight crews were required to test the EGPWS to confirm the serviceability of the system. The operator exposition also required that flight crews must respond to EGPWS cautions and warnings in marginal weather.
Neither pilot recalled any prescribed operator procedures that were referenced during the recovery following the EGPWS warnings during the occurrence.
Offshore operations
Standard procedures required crew to activate offshore mode once established beyond the coastline and to deactivate once established onshore. This selection of the offshore mode is verified by the PM and PF using the ‘coast check’ contained in the AW139 normal checklist.
Both flight crew recalled that offshore mode was activated on the EGPWS for the duration of the hoisting exercise.
Operator training
The operator’s exposition described the training and checking policies and procedures, and the regulatory requirements of the applicable Civil Aviation Safety Regulations (CASR). The operator maintained a training and checking organisation authorised by an instrument issued by the Civil Aviation Safety Authority (CASA). This training was conducted by nominated personnel put forward by the operator.
Upon completion of induction training, crews were required to complete recurrent training which included an operational proficiency check (OPC) for each type of operation.
Crew hoisting training
Crew hoisting training was provided by the operator as part of the combined search and rescue (SAR)/hoisting OPC. Additionally, a standalone hoisting OPC was conducted at 6‑monthly intervals. While the check events alternated every 6 months, they remained valid for 12 months from the date of completion.
The hoisting OPC assessed theoretical and practical aspects of hoisting, encompassing all phases of flight, with technical and non‑technical skills being assessed by approved personnel.
The instructor and captain conducted their hoisting OPC on 4 December 2023 and 23 October 2023 respectively. The instructor also conducted the captain’s combined SAR/hoist OPC on 16 May 2024, which included the same hoisting elements of the training that took place during the occurrence.
Scenarios involving a recovery from the hover with a prescribed low‑level inadvertent instrument meteorological conditions (IIMC) operating procedure were not included in the biannual SAR/hoist syllabus at the time of the occurrence.
Recurrent simulator training
Esso Australia conducted emergency OPC check every 6 months, in accordance with CASR 61 requirements in an AW139 full flight simulator. The emergency OPC satisfies the requirements for the type rating and low-level flight reviews.
All sequences flown were in a reduced visual cueing environment to mimic weather conditions that are regularly encountered when conducting flight operations in the Bass Strait.
Flight crews would encounter a simulated technical failure in reducing visibility at ‘low‑level’ below 500 ft leading to IIMC. This scenario would lead to either a ditching, or recovery in IIMC. In the case of the latter, this scenario required the flight crew to recover to a safe altitude, which the instructor and captain completed as a crew pairing on 18 September 2023.
Flight crew also received briefings on the 4 ‘Cs’ (Control, Climb, Course and Communicate) IIMC recovery technique (International Helicopter Safety Team).
Scenarios involving a recovery from the hover in IIMC conditions with a prescribed operating low‑level IIMC procedure were not included in the biannual simulator training syllabus at the time of the occurrence.
Esso Australia crew resource management training
Esso Australia conducted annual crew resource management (CRM) training every 12 months, in accordance with CASR 119 and CASR 133 requirements. The training modules covered:
human performance and limitations
situational awareness
decision-making
teamwork and communication
threat and error management
workload management and automation.
EGPWS training
The operator training requirements required that crew completed training specific to the Honeywell MK XXII‑30 EGPWS system installed on its AW139 fleet. The EGPWS training was incorporated into the AW139 differences training, which all flight crew had to complete during their initial entry into the Esso Australia check and training system. This included both theoretical knowledge and practical exercises to ensure proficiency in managing system operations. The training covered:
general overview of the system
normal procedures including setup for flight operations, functionality, general actions during an alert, and a demonstration of the self-test
limitations of the system
emergency and malfunction procedures.
The operator stated that EGPWS training events in the simulator had ceased in 2021 due to inaccuracies of the simulator‑generated warnings and alerts. As a result, Esso Australia flight crew underwent technical refresher ground training, which included a module dedicated to EGPWS. The instructor and captain conducted their EGPWS refresher training on 19 September 2023.
Recorded information
The AW139 helicopter is equipped with a multipurpose flight data recorder (MPFDR). The MPFDR combines both a flight data recorder (FDR) and a cockpit voice recorder (CVR), capturing helicopter data and audio.
Personnel from Esso Australia secured a copy of the FDR data for analysis and provided a copy of that data to the ATSB. The files were downloaded and confirmed to have contained flight data recorded during the EGPWS occurrence on 19 August 2024 from the MPFDR fitted to AW139 VH‑EXK. Although FDR data was available, no CVR data was retrieved for this occurrence due to the helicopter operating multiple flights in the days following the occurrence.
The recorded flight data captured parameters such as altitude, airspeed, control inputs and the activation of systems such as the RHT, FTR and EGPWS alerts. This data enabled a detailed reconstruction of the flight, providing insights into the helicopter’s performance and crew actions leading up to the event.
Recorded data
Just prior to the EGPWS event, an airspeed exceedance was identified, with the NR at 102% when the airspeed was above 90 kt. This persisted for a period of 3 seconds and occurred 2 seconds prior to the activation of the EGPWS system.
The EGPWS event trigger was identified as a combination of the radar altitude reducing below 150 ft as the airspeed exceeded 100 kt. The minimum radar altitude reached was 140 ft.
The MPFDR data revealed multiple key events during the event (Table 3).
Key events
Table 3: VH-EXK flight data
Local time
Event
Radio Height feet AGL
Pitch
+/- °
Groundspeed
knots
Computed airspeed
knots
Vertical speed
+/- fpm
0908:08
Collective beep AFT active; collective FTR active
72
5.976
0
0
-32
0908:18
Groundspeed begins increasing collective beep AFT active collective FTR active
85
5.625
2
0
128
0908:38
Computed airspeed above 0, helicopter climbing
Collective FTR active; over the next ten second period, the collective FTR is active for 8 seconds
154
0.176
28
38.5
192
0908:50
Rad alt peak 185, airspeed increasing through 75 kt collective FTR active
185
-5.976
66
75.5
-64
0908:51
Collective trim engaged
negative vertical speed begins developing
183
-6.855
70
79.5
-128
0908:55
Collective trim disengaged NR exceedance - >90 kt at 102% for 3 second duration
173
-2.109
82
93.75
-224
0908:59
Collective trim engaged; negative vertical speed is reducing
153
-1.406
90
99.5
-224
0909:00
Collective FTR active; EGPWS alert is activated for one second, followed by the EGPWS warning for 5 seconds
147
-0.879
90
101.5
-64
0909:03
Collective FTR active; minimum altitude reached
140
10.019
88
99.5
832
0909:07
Collective FTR active; following this, the collective FTR is active for 41 seconds of the following 54 seconds, as the helicopter climbs through 680 ft.
215
13.007
76
89.75
2048
Source: Operator supplied flight data recorder, tabulated by the ATSB
The recorded pitch changes during 60 seconds of flight data, showing a pitch range of up to 19°, coupled with fluctuating airspeed above limitations and unstable vertical speed, demonstrate an unstable aircraft profile during departure.
Operator internal investigation
Following the occurrence, Esso Australia conducted an internal investigation, concluding that inadequate procedures and work standards were the primary factors contributing to the incident. The internal investigation identified the root cause as:
Deficiencies in procedures regarding Search and Rescue (SAR) Training in the vicinity of fog.
Related occurrences
The following 2 ATSB investigations highlight the risks of inadvertent IMC encounters at close proximity to the ground and demonstrate the importance of rehearsed recovery drills in these situations. In both instances, the flight crew were IFR rated, and the helicopters were also IFR equipped.
These occurrences emphasise the effects of spatial disorientation[16] due to powerful and misleading orientation sensations during times of reduced visual cues, which can affect any pilot, no matter what their level of experience.
On 21 October 2016, the crew of a BK 117‑C2 were returning to their home base from Crookwell, New South Wales, after carrying out an emergency medical service mission. The flight was conducted under night visual flight rules with the aid of a night vision imaging system.
Conditions were marginal and, on departure, the helicopter entered low cloud. The aircrew officer declared loss of visibility on take‑off. The pilot had poor visibility ahead yet could see well to the right. The pilot thought visibility would improve as they passed ground lighting that was reflecting in raindrops on the canopy.
The visibility did not improve, and the pilot slowed the aircraft to maintain visual meteorological conditions. The low‑speed manoeuvre resulted in an undesired aircraft state and an EGPWS warning activated. The pilot conducted an inadvertent IMC drill, restabilised control, and continued the flight before landing safely.
On 13 May 2018, the crew of a Leonardo Helicopters AW139 departed Darwin, Northern Territory, to search for an active emergency position‑indicating radio beacon. The crew flew under night visual flight rules with support of a night vision imaging system.
During an approach to a potential target, smoke from nearby bushfires affected visibility and the helicopter developed an uncommanded high rate of descent. The aircrew officer, in the rear of the helicopter, called ‘Climb! Climb! Climb!’, and the pilot regained control with a rehearsed recovery drill.
During the recovery procedure, the power demand exceeded airframe limitations. This exceedance went undetected, and the helicopter was flown on a second sortie that same evening.
Safety analysis
Introduction and background
After concluding hoist training exercises near Golden Beach, Victoria, a Leonardo Helicopters AW139, registered VH‑EXK and operated by Esso Australia, inadvertently entered instrument meteorological conditions (IMC), which resulted in an enhanced ground proximity warning system (EGPWS) alert.
This analysis will examine factors contributing to the occurrence, including:
crew decision‑making
the transition from visual meteorological conditions (VMC) to IMC
the effects of spatial disorientation
control inputs during the event
operator procedures
crew response to the EGPWS alert.
Departure
During the hoisting exercise, both flight crews observed clear skies on the captain’s side of the helicopter to the north and north‑east of their position. Meanwhile fog approached from the north‑west on the instructor’s side and the instructor elected to depart and announced their intention to climb. Climbing immediately in the vicinity of fog may not have been necessary, as manoeuvring to the north or north‑east would have increased the distance from the fog. However, as the helicopter climbed, it encountered fog and the instructor immediately elected to depart, attempting to climb above the fog while tracking north‑west toward the shoreline.
As the instructor departed the training area for Longford at the conclusion of the exercise, the helicopter remained in a hoisting configuration. This meant the hoist was extended approximately 40 ft below the helicopter, the main cabin door was locked open and the helicopter’s main rotor RPM was set to 102%.
After hoisting exercises, the post‑hoist procedure required the hoist operator (HO) to stow the hoist, secure the cabin and advise the pilot monitoring (PM) prior to climbing. The PM would assist the HO in completing the post‑hoist check, confirming the crew actioned the appropriate items. However, due to the encroaching fog, the instructor elected to climb, lost visual references and reactively began to accelerate and climb the helicopter before completing the post‑hoist check.
These procedures ensure the helicopter is properly configured for departure, including securing the cabin, stowing the hoist and adjusting the main rotor RPM to 100%, once the helicopter accelerates through 80 kt.
As the helicopter accelerated the check aircrewman voiced their concern about departing, likely due to the present configuration not being suitable for forward flight.
Completing the post‑hoist procedure before departing would have removed the risk associated with potential interference from the extended hoist cable and exceeding the flight envelope limitations with the helicopter in the hoisting configuration. Additionally, by completing these procedures in a stationary position, the captain could have more effectively monitored the flight path during departure.
At the time of departure, the captain, who was the PM, was focused on marking the GPS position of the training aid in the flight management system (FMS) to facilitate retrieval during the next exercise. While this task had operational value, it distracted the captain from monitoring the helicopter’s dynamic state and assisting the instructor with flight path management, navigation and maintaining situational awareness. However, the captain was unaware of the instructor’s intention to depart, likely due to the expectation that the completion of the post‑hoist procedure had not been completed as a prerequisite to climb away.
Contributing factor
The instructor hastily departed the training area, due to encountering fog, before the hoist was secured with the door open, and while the captain as pilot monitoring was still occupied recording the training aid position.
Spatial disorientation
The instructor departed the training area on a north‑westerly heading, toward the shoreline and the previously observed fog. The instructor achieved a relatively stable climb, albeit with a steadily increasing forward airspeed. The helicopter's altitude peaked at 185 ft at 72 kt; however, as the climb progressed, the helicopter inadvertently entered IMC, depriving the crew of external visual references.
Both flight crew recall being in VMC when the climb commenced with the instructor verbalising their intention to climb above the fog toward an area of VMC. According to the instructor the helicopter entered fog as the helicopter began to climb while the captain was looking down and didn’t observe the transition to IMC.
The flight data recorder (FDR) captured altitude and airspeed fluctuations, consistent with flight control inputs from the pilot flying being uncertain of the flight path, including a nose‑down attitude and airspeed increasing through 80 kt. Therefore, without visual cues, the instructor likely became subject to the effects of spatial disorientation. This condition significantly impairs a pilot's ability to accurately interpret attitude, altitude and airspeed.
Contributing factor
After inadvertently entering instrument meteorological conditions, the instructor (pilot flying) became spatially disorientated.
Operating in degrading visibility creates ambiguity, stalling decision‑making as flight crew face conflicting situational cues (Orasanu, Martin, & Davidson, 2001). Continued reliance on visual cues in these scenarios can draw attention away from critical instrument readings (Summerfield & Enger, 2009). Coupled with the inherent instability of medium‑sized helicopters, these cognitive tendencies further increase the risks associated with spatial disorientation in degraded visibility environments.
Unstable flight
Frequent engagement and disengagement of the collective force trim release (FTR) when the radar height hold (RHT) was active further destabilised the helicopter, causing altitude and airspeed fluctuations. The operator exposition highlighted the potential risks by stating that the incorrect use of the AW139's automation systems can lead to dangerous deviations and loss of situational awareness. Additionally, the AW139's rotorcraft flight manual (RFM) stated that the helicopter must be attentively flown during hoisting operations using the RHT function. The FTR switch demands disciplined use, as its unintentional instinctual engagement can lead to unintended control inputs. As a result, crews must carefully monitor their inputs and selections when using the RHT and FTR functions. Pilots tend to overestimate their ability to continue to control the aircraft when visual references are lost (Wiggins, Hunter, O'Hare, & Martinussen, 2012). During the periods of high crew workload, the interactions of these systems added to the difficulties in sustaining stability in the degraded visual environment.
The combination of spatial disorientation, intermittent collective FTR use, flight control inputs and an overall impaired situational awareness of the crew, culminated in the helicopter being still in the hoisting configuration, whilst descending below 150 ft above sea level and exceeding 100 kt.
This resulted in flight envelope exceedances of:
operation with the hoist cable extended
the right cabin door in the open position
operation with the main rotor RPM at 102%.
This posed additional risks, including potential aircraft damage as a result of the hoist cable interfering with the tail rotor, damage to the aircraft due to slipstream pressure on the door. The situation reached a critical point when the EGPWS issued a terrain alert, signalling the imminent risk of collision with terrain.
Contributing factor
The instructor's attempt to leave IMC, while being spatially disorientated, resulted in control inputs that led to the helicopter entering an unstable state while still in IMC, triggering a terrain alert below 150 ft, and airspeed exceedances for operations with the main rotor RPM at 102%, the door open and hoist extended.
Recovery
Immediately following the EGPWS alert, the captain took control of the helicopter without a formal handover from the instructor by reactively pulling back on the cyclic. Prior to assuming control, the captain was occupied with entering GPS coordinates into the flight management system (FMS), which diverted their attention from monitoring the helicopter's flight path. This meant they were not able to actively observe changes to the dynamic state of the helicopter and missed the early indications of loss of spatial orientation by the PF due to the degrading visibility.
Due to a lack of visual cues, the captain was unsure of their altitude and reactively pulled back on the cyclic to arrest the helicopter's forward momentum and gain altitude. After the helicopter was established in a climb and following a brief exchange, control of the helicopter was transferred back to the instructor.
The captain bypassed handover protocols, likely due to the receipt of the EGPWS warning and perceived rapidly escalating events. Operator procedures also mandate that flight crews respond promptly to EGPWS warnings.
Reactive assumption of control by the non‑flying pilot had the potential to introduce further distractions, conflicting control inputs or further inappropriate control inputs in an already dynamic and demanding environment. Although the captain bypassed standard handover procedures, the absence of a structured handover also highlights the difficulties of managing dynamic situations under pressure and balancing conflicting demands.
Other factor that increased risk
Prior to gaining situational awareness and without an appropriate control handover, the captain reactively assumed control of the helicopter after the terrain warning, increasing the risk of control conflict between the 2 crew.
Operator procedures
Esso Australia did not provide crew with structured procedures for managing inadvertent entry into IMC and EGPWS alerts during hoist operations. Although the Esso Australia exposition required a pilot response to EGPWS alerts, this did not include specific guidance for managing such alerts. While training covered general EGPWS functionality, it did not include scenario‑based drills for complex situations involving degraded visibility or low-level operations.
Consequently, responses to alerts were reactive, with the crew relying on instinct rather than following a predefined recovery procedure. The absence of predefined inadvertent IMC‑specific recovery actions also exposed the crew to the cognitive effects and demands of operating in degraded visual environments.
The related occurrences further demonstrate the effectiveness of structured recovery protocols and crew resource management (CRM) in stabilising helicopters during degraded visual conditions. The absence of similar predefined procedures that the crew could have utilised, underscores the need for enhanced training and clear protocols to manage scenarios involving inadvertent IMC and EGPWS alerts.
Other factor that increased risk
Esso Australia did not have a procedure for a helicopter recovery from inadvertent IMC during hoist operations or recovery procedures for EGPWS alerts or advisories. (Safety issue)
Captain’s decision‑making
In a matter of seconds following the initial EGPWS caution, the captain arrested the rate of descent and transitioned into a climb while reducing the forward airspeed of the helicopter. The captain’s intervention immediately reduced the risk of a collision with terrain.
Before assuming control, the captain was able to identify and vocalise the increasing airspeed in an attempt to illicit corrective action from the instructor. A progressive intervention strategy is initiated by communicating a flightpath deviation (alert), then suggesting a course of action (advocacy and assertion) and then directly intervening, if necessary (Civil Aviation Safety Authority 2020). Despite bypassing Esso Australia handover protocols, the captain effectively recognised and responded to the EGPWS alerts and the reduced proximity to terrain.
Although the captain’s initial degraded situational awareness and lack of visual cues limited their initial understanding of the situation, their decision to establish control of the aircraft during a critical situation was sound.
Their decision to prioritise scanning the instruments to regain situational awareness during the event contributed to a successful recovery. The decisive nature of their intervention further underscores the importance of training and rehearsed recovery actions to mitigate the risks of spatial disorientation in degraded visual environments.
Other finding
The captain's control inputs stopped the vertical descent and established the helicopter in a climb, which reduced the risk of collision with terrain.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of control in flight involving Leonardo Helicopters AW139, VH‑EXK, 19 km east of Longford Heliport, Victoria, on 2 August 2024.
Contributing factors
The instructor hastily departed the training area, due to encountering fog, before the hoist was secured with the door open, and while the captain as pilot monitoring was still occupied recording the training aid position.
After inadvertently entering instrument meteorological conditions, the instructor (pilot flying) became spatially disorientated.
The instructor's attempt to leave IMC, while being spatially disorientated, resulted in control inputs that led to the helicopter entering an unstable state while still in IMC, triggering a terrain alert below 150 ft, and maximum airspeed exceedances for operations with the main rotor RPM at 102%, the door open and hoist extended.
Other factors that increased risk
Prior to gaining situational awareness, and without an appropriate control handover, the captain reactively assumed control of the helicopter after the terrain warning, increasing the risk of control conflict between the 2 crew.
Esso Australia did not have a procedure for a helicopter recovery from inadvertent IMC during hoist operations or recovery procedures for EGPWS alerts or advisories. (Safety issue)
Other findings
The captain's control inputs stopped the vertical descent and established the helicopter in a climb, which reduced the risk of collision with terrain.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Esso Australia did not have a procedure for a helicopter recovery from inadvertent IMC during hoist operations or recovery procedures for EGPWS alerts or advisories.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by Esso Australia
In addition to developing training and procedures for inadvertent IMC recovery from a search and rescue and hoisting scenario, the operator identified several actions to be taken which included:
discussing the weather phenomena and the possibility for sudden loss of visibility with crews
updating pre-flight training brief to highlight the need to maintain a safe distance to fog or cloud
developing training focusing on the radar height hold function of the AW139
including upset recovery training in CRM.
Glossary
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CRM
Crew resource management
CVR
Cockpit voice recorder
EGPWS
Enhanced ground proximity system
FDR
Flight data recorder
FTR
Force trim release
FMS
Flight management system
HO
Hoist operator
IIMC
Inadvertent IMC
IMC
Instrument meteorological conditions
JSA
Job safety analysis
MPFDR
Multi-purpose flight data recorder
NR
Rotor speed
OPC
Operational proficiency check
PF
Pilot flying
PFD
Primary flight display
PM
Pilot monitoring
RFM
Rotor flight manual
RHT
Radar height hold
SAR
Search and rescue
SPECI
A special report of meteorological conditions, issued when one or more elements meet specified criteria significant to aviation
VMC
Visual meteorological conditions
VFR
Visual flight rules
Sources and submissions
Sources of information
The sources of information during the investigation included:
Airservices Australia
Bureau of Meteorology
captain and instructor of VH-EXK
Civil Aviation Safety Authority
flight data from VH-EXK.
References
Australian Transport Safety Bureau. (2007). An overview of spatial disorientation as a factor in aviation accidents and incidents. ATSB Aviation Research and Analysis Report B2007/0063. Retrieved from/publications/2007/b20070063
Hoh, R. (1990). The effects of degraded visual cueing and divided attention on obstruction avoidance in rotorcraft, Report prepared for the United States Federal Aviation Administration (DOT/FAA/RD-90/40). Retrieved fromhttps://apps.dtic.mil/sti/citations/ADA380260
International Helicopter Safety Team. (n.d.). Training Fact Sheet – Inadvertent Entry Into Instrument Meteorological Conditions (IIMC). Retrieved from https://ushst.org/IIMC/Bulletin%20IIMC.doc
L, O. J. (1998). Errors in aviation decision making: A factor in accidents and incidents. In Proceedings of the Workshop on Human Error, Safety, and Systems Development. 100-107.
Orasanu J., Martin, L., & Davidson, J., (2001). Cognitive and contextual factors in aviation accidents, Linking expertise and naturalistic decision making, 209–226.
Summerfield C & Enger T. (2009). Expectation (and attention) in visual cognition, Trends in Trends in Cognitive Sciences. 13(9). 403-409.
United Kingdom Civil Aviation Authority. (2007). Helicopter flight in degraded visual conditions (Paper 2007/03). Retrieved fromwww.caa.co.uk.
Wiggins, M. W., Hunter, D. R., O’Hare, D., & Martinussen, M. (2012). Characteristics of pilots who report deliberate versus inadvertent visual flight into instrument meteorological conditions’, Safety Science. 50(3). 472-477.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
captain and instructor of VH-EXK
Esso Australia
Bureau of Meteorology
Civil Aviation Safety Authority
Submissions were received from:
Esso Australia
Bureau of Meteorology
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot flying (PF): focuses on handling the helicopter during hoisting operations.
[2]Pilot monitoring (PM): manages non-hoist communications, logs positions, monitors performance, and completes in‑flight checks, especially for height and potential obstructions.
[3]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[4]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[5]See Helicopter information, Autopilot and radar height hold
[6]Instrument meteorological conditions (IMC): weather conditions that require crews to fly primarily by reference to instruments, and therefore under instrument flight rules (IFR), rather than by outside visual reference.
[8]Cyclic: helicopter control mechanism for periodically varying the blade angle of each rotor blade, producing a tilt in the tip-path plane and effecting motion in a desired direction
[9]Instrument flight rules (IFR): rules which allow properly equipped aircraft to be flown under instrument meteorological conditions (IMC)
[10]Helideck: A heliport located on a fixed or floating offshore facility such as an exploration and/or production unit used for the exploitation of oil or gas.
[11]External load: carrying or towing a load outside an aircraft in flight and includes training for such an operation.
[12]Category A: In relation to rotorcraft, means a multi-engine rotorcraft that is capable of operation using take-off and landing data scheduled under a critical engine failure concept, which assures adequate designated ground or water area and adequate performance capability for continued safe flight, or safe rejected take-off in the event of engine failure, as mentioned in the rotorcraft’s flight manual.
[13]A dual action spring permits force‑feel hands on flying while the force trim is engaged. A pilot moving the flight controls without releasing the force trim results in full hands‑on controllability with control force feedback to the pilot. As the pilot releases the control to resume hands‑off flying, the spring returns the collective to its neutral position against the force trim.
[14]JSA: job safety analysis – crew briefing review of operational data, tech log details and rotor flight manual aircraft performance.
[15]Challenge and response procedures apply to multi‑crew operations, where checklist items are called by one crew member and either checked or completed by another.
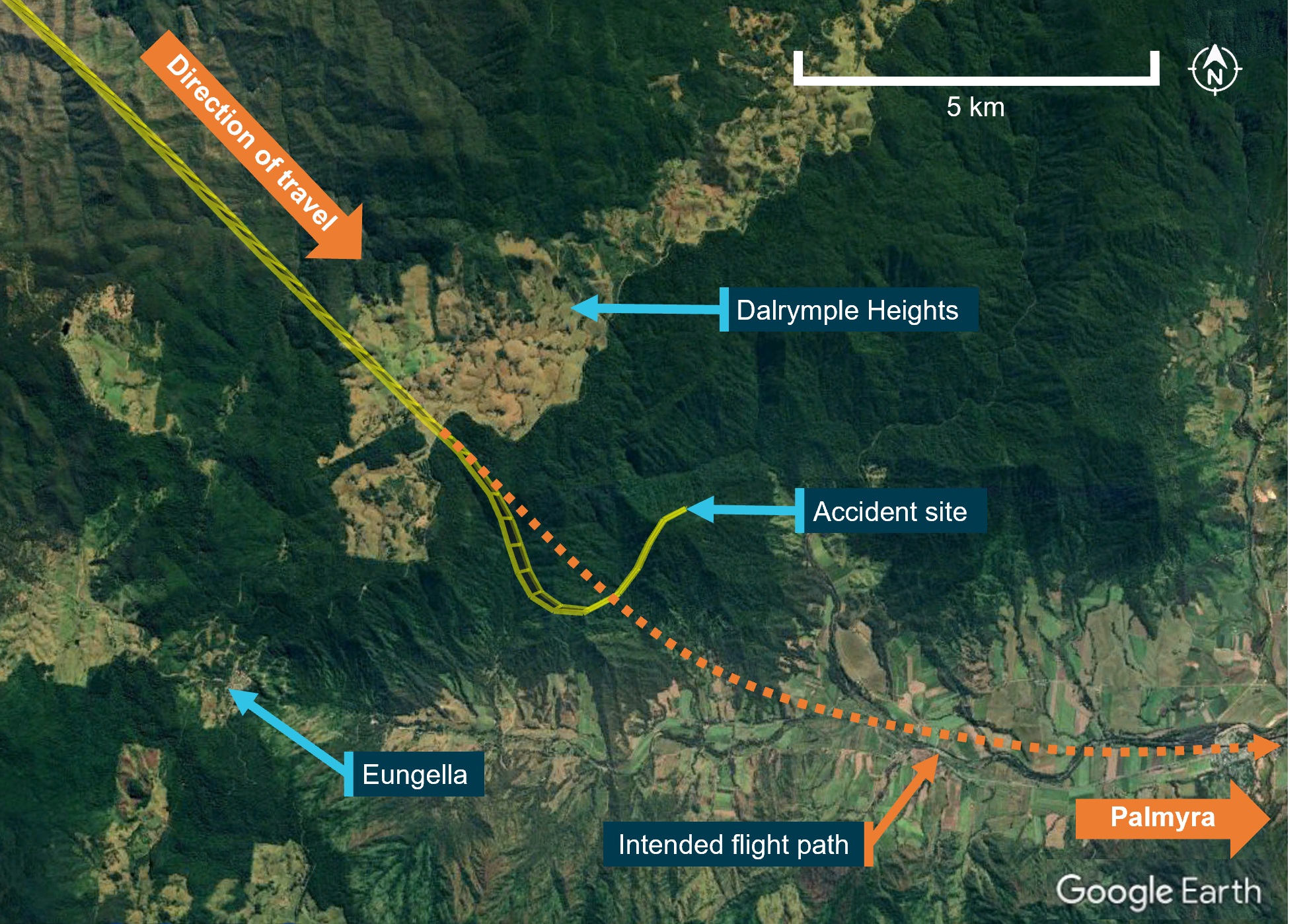
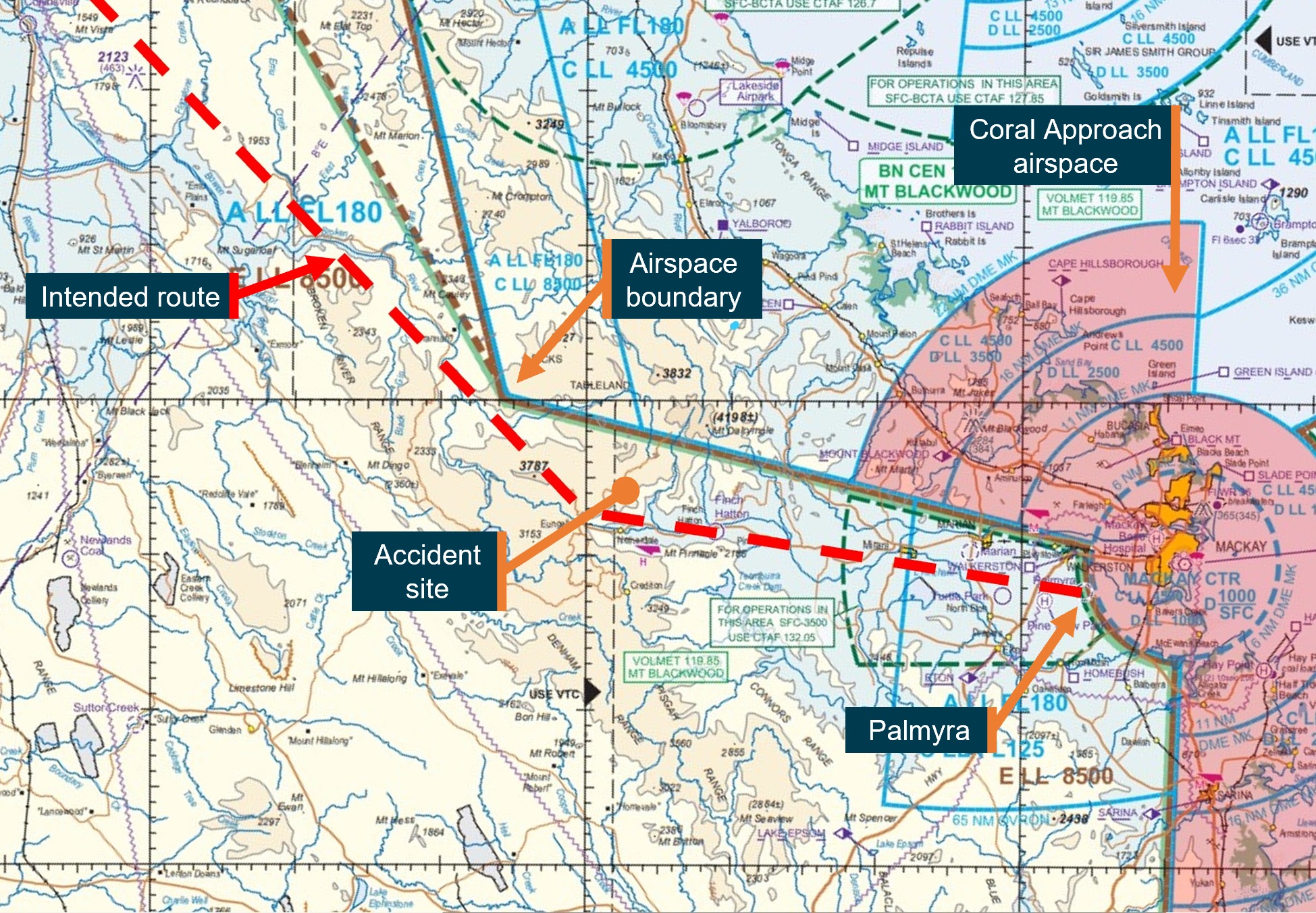
On the morning of 28 October 2023, a SOCATA-Groupe Aerospatiale TB-20, registered, VH-JTY, departed Montpelier aircraft landing area, Queensland, for a visual flight rules private flight to Palmyra aircraft landing area, Queensland. The flight was to be just over one hour duration and the pilot and their passenger were familiar with the route.
During the flight, the pilot contacted a friend at the destination for an appreciation of the weather. After the friend advised them of the prevailing conditions including cloud, the pilot replied that they would need to go through some cloud before arriving.
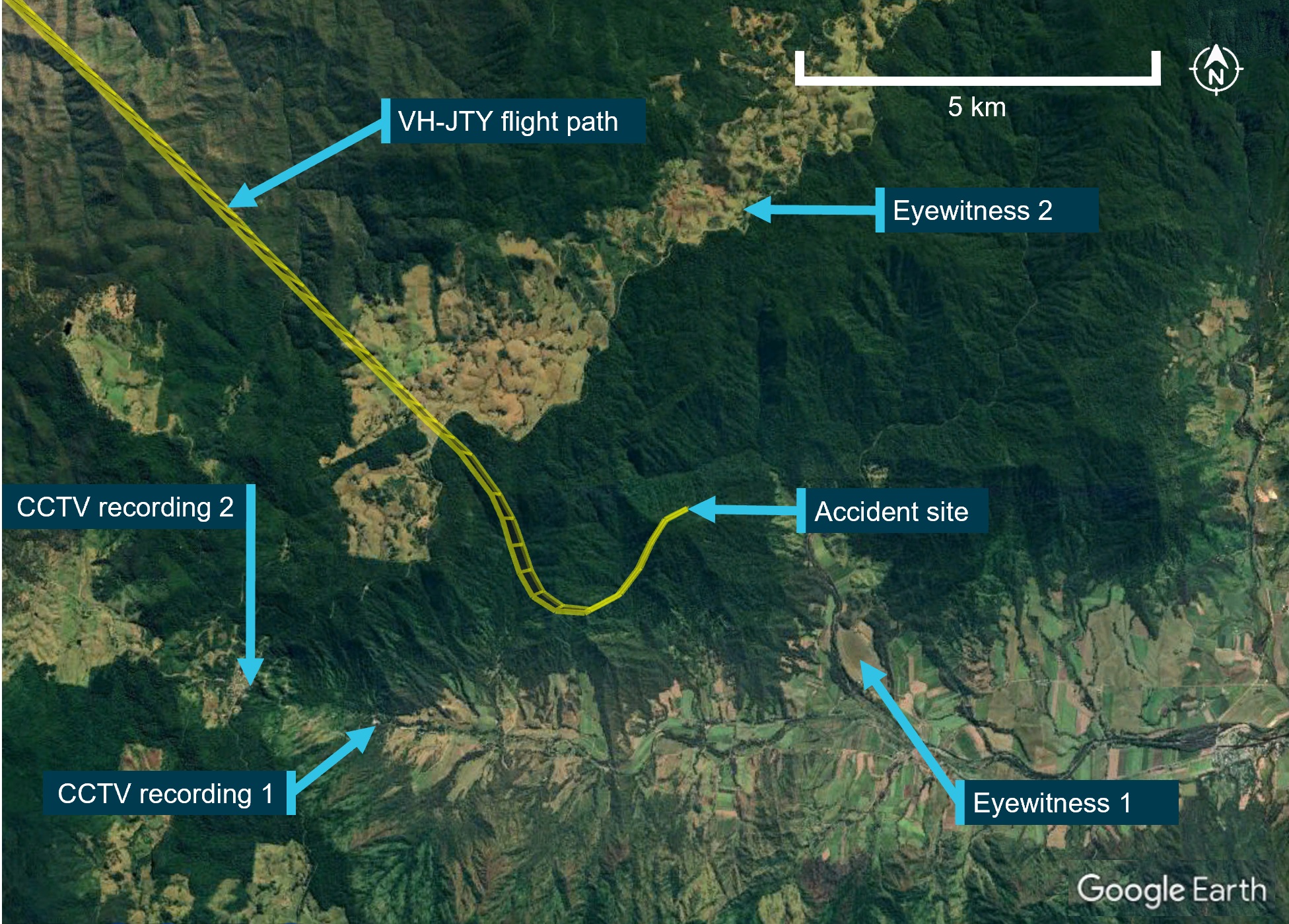
Around 30 NM from the destination, shortly after commencing descent for the intended landing, the aircraft began a steep descending turn to the left towards mountainous terrain. During this descent, the aircraft exceeded the airframe’s designed maximum airspeed before pitching up and passing over the top of Bull Mountain. The aircraft then entered a second steep descending turn, this time to the right, before the recorded flight path data ceased.
The wreckage was located nearby in dense forest on the north-east face of Bull Mountain. The accident site indicated that the aircraft had collided with terrain at a steep angle, and with significant forward velocity. The aircraft was destroyed and both occupants received fatal injuries.
What the ATSB found
The ATSB found that, after encountering cloud en route, the pilot elected to continue along the intended flight path through cloud instead of diverting around or remaining on top of it. Shortly after, it is very likely the pilot entered weather conditions not suitable for visual navigation, leading to spatial disorientation and a descent into mountainous terrain.
Safety message
One of the key risk controls for a visual flight rules (VFR) pilot to avoid entering instrument meteorological conditions (IMC) is appropriate pre-flight preparation and planning. Pilots should always obtain up-to-date weather information before and during flight. While forecasts will assist in selecting the route to be flown, pilots should plan an alternate or be prepared to make necessary deviations from the planned route should actual weather conditions indicate the possibility of not being able to comply with the VFR.
For a non-instrument rated pilot, even with basic attitude instrument flying proficiency, maintaining control of an aircraft in IMC by reference to the primary flight instruments alone entails a very high workload that can result in narrowing of attention and loss of situational awareness. While autopilot can be used to reduce workload, it is not infallible and should not be relied upon or used by VFR pilots as a risk mitigator to decide to fly into unsuitable conditions.
Unapproved mobile devices displaying charts and data from an approved data service provider are a useful supplement to navigation, but they cannot be used as a navigation device, and must not be the sole means of navigation when operating under the VFR. Pilots should use navigation equipment approved for aviation and maintain skills in navigating by reference to approved charts.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
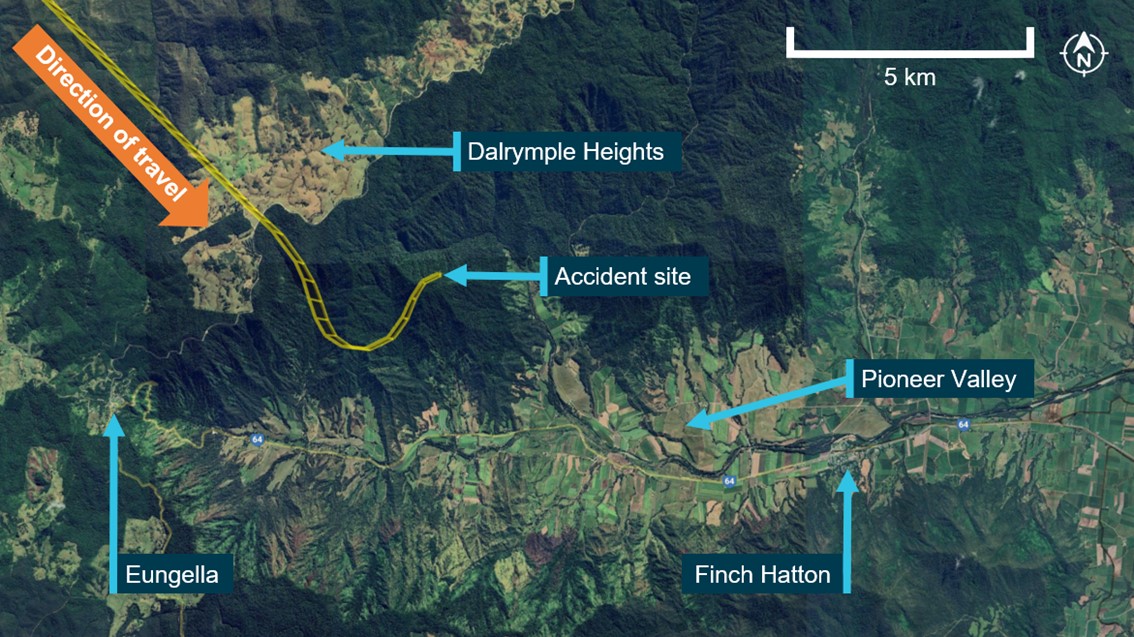
On 28 October 2023, at about 0735 local time, a SOCATA-Groupe Aerospatiale TB-20 (TB-20) registered VH-JTY, departed from Montpelier (Antill Plains) aircraft landing area,[1] Queensland, for a private flight to Palmyra aircraft landing area,[2] Queensland. The flight was to track via Dalrymple Heights, near Eungella before descending into the Pioneer Valley to the west of Mackay, and then track direct to Palmyra (Figure 1). On board were the pilot and a passenger, who was also a licenced pilot.
Figure 1: VH-JTY fight path
Source: Google Earth and OzRunways, annotated by the ATSB
OzRunways[3] data showed the aircraft was flown to 5,500 ft above mean sea level (AMSL) where it maintained a steady track without any significant deviations during the cruise phase of flight.
At 0814, approximately 20 minutes prior to commencing descent for the intended landing at Palmyra, the pilot made a phone call to a friend, another licenced pilot, in Mackay. It was reported that the pilot enquired about the weather at the destination. The friend recalled advising of the presence of cloud at Palmyra and blue sky to the south of the landing area. The pilot replied that they would have to go through some cloud.
The same friend called the pilot at 0833 to confirm their estimated time of arrival so they could meet the pilot in Palmyra. They stated that the pilot reported being over Eungella at 5,500 ft and was about to commence their descent. The friend reported ending the phone call so as not to cause any distraction.
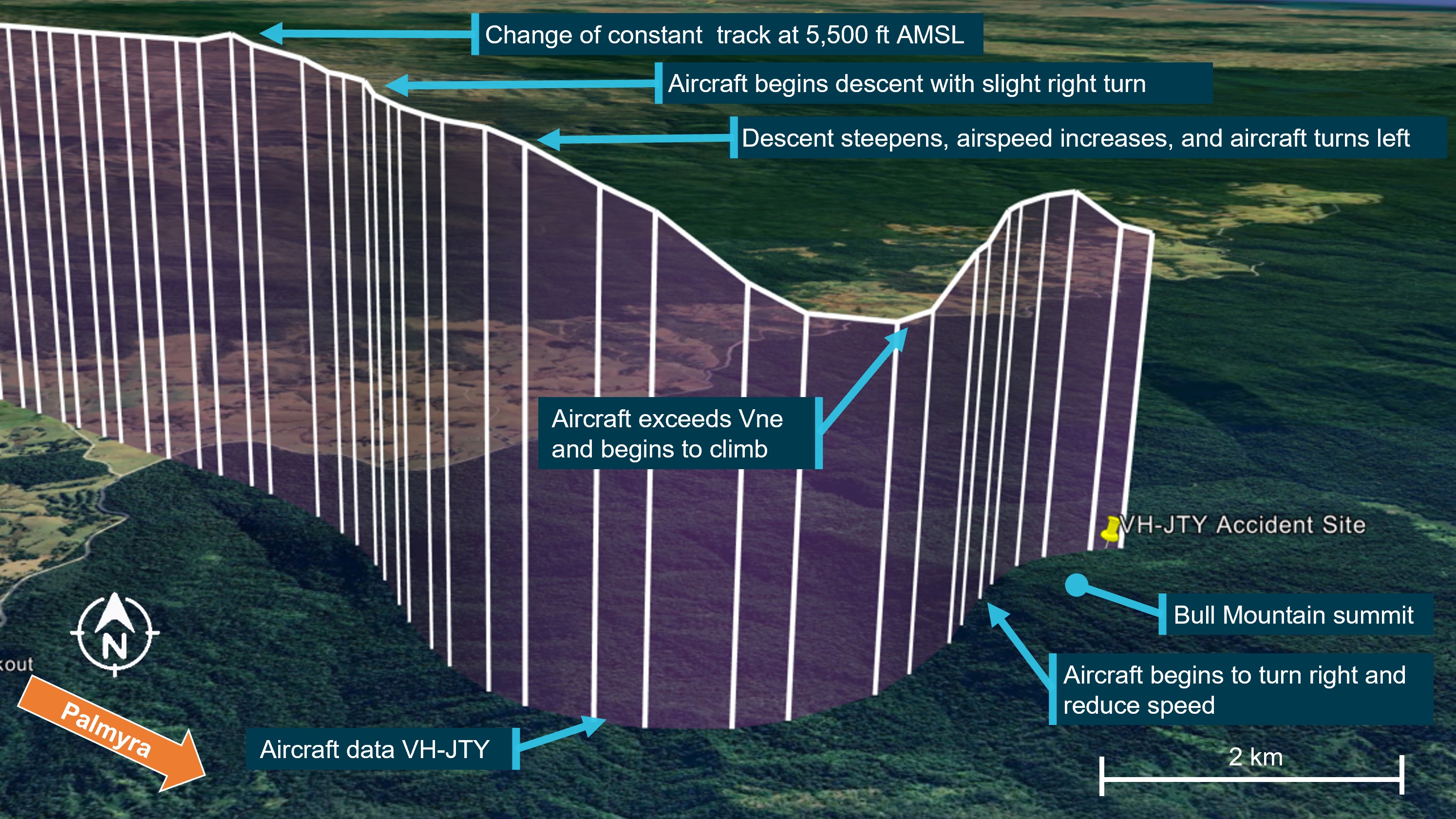
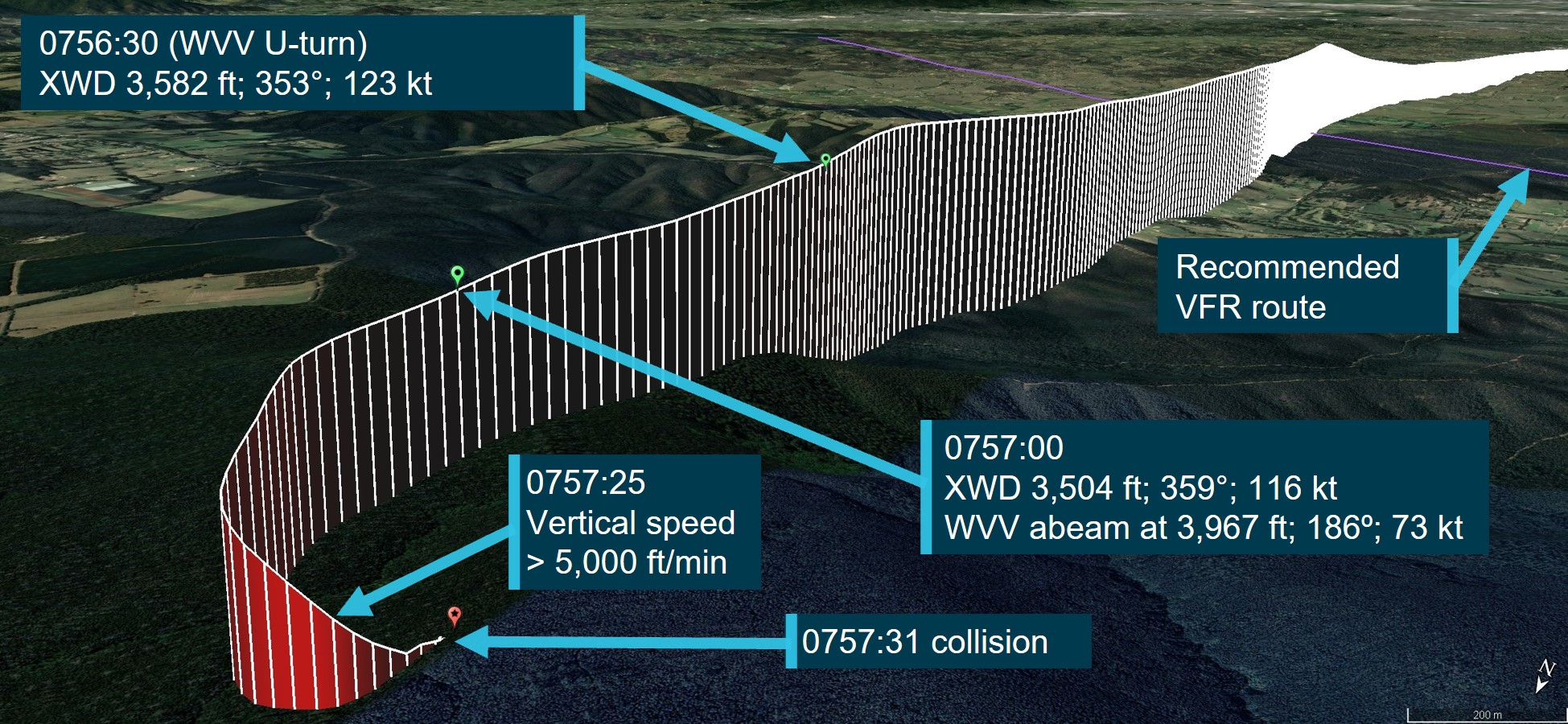
At 08:34, there was a change to the previously stable flight path. The aircraft initially climbed about 100 ft and entered a slight right turn before turning left towards Bull Mountain in a shallow descent. As the turn continued, the aircraft’s descent rate increased, descending about 1,600 ft in 13 seconds (average descent rate of 7,400 ft/min) (Figure 2).
Figure 2: VH-JTY descent
Source: Google Earth with overlaid OzRunways data, annotated by the ATSB
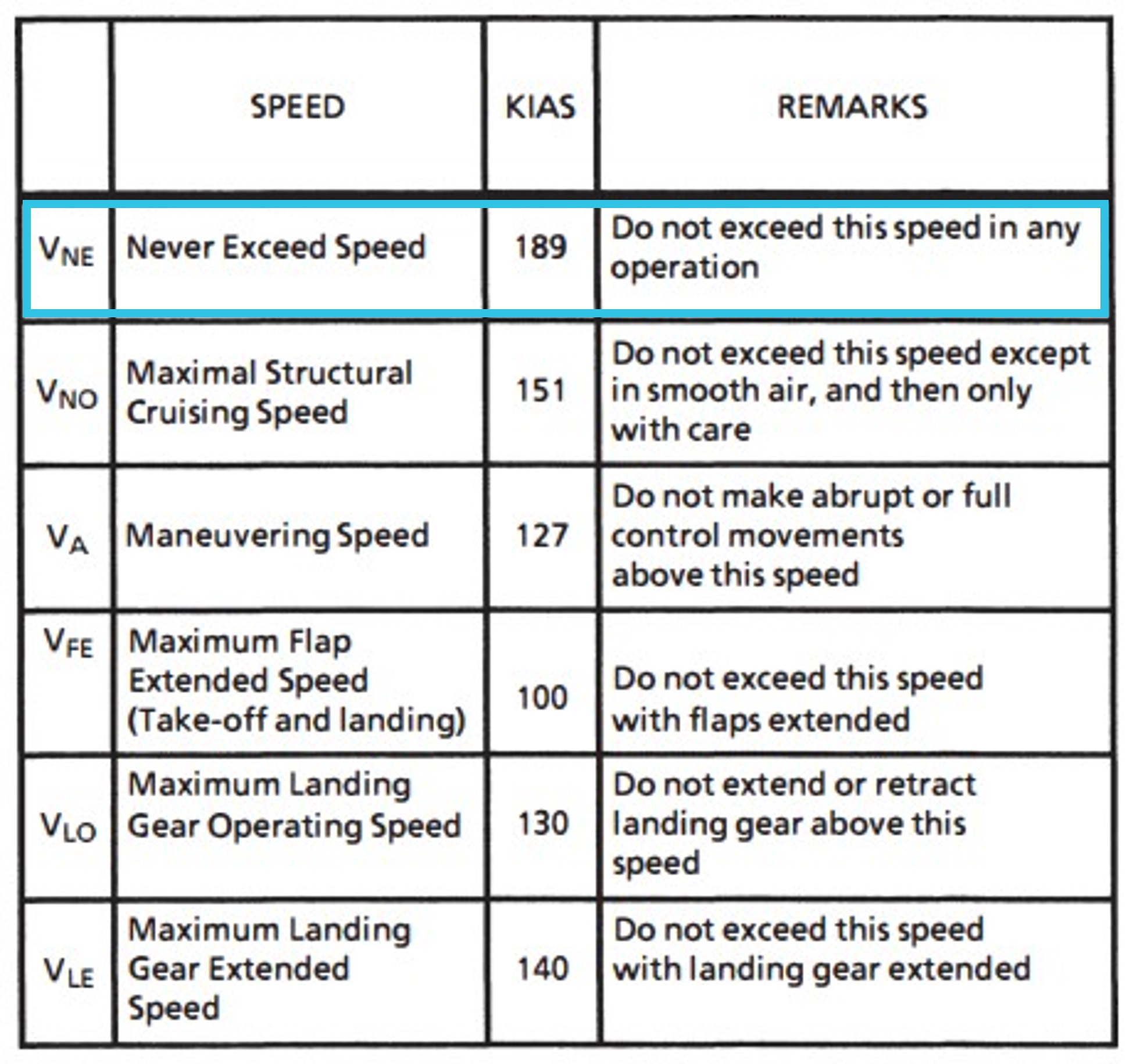
During this descent, the aircraft accelerated to about 218 kt, 29 kt above the aircraft’s published VNE[4] (velocity never exceed) of 189 kt (Figure 3).
Figure 3: TB-20 airspeed limitations
Source: Aircraft manufacturer, annotated by the ATSB
In the 10 seconds that followed, the aircraft pitched up steeply, climbed approximately 600 ft, and passed overhead Bull Mountain at 4,200 ft AMSL. The aircraft then slowed to 132 kt before entering a steep descending right turn to the east. The recorded data stopped at 0835, 3,655 ft AMSL with the aircraft estimated to be descending at around 6,000 ft/min in a right turn with 36° angle of bank and increasing roll angle.
The aircraft collided with terrain in dense forest on the north-east face of Bull Mountain 1,900 ft AMSL, not far from where the recorded data stopped. The aircraft was destroyed, and the pilot and passenger were fatally injured.
Context
Pilot information
The pilot was qualified and authorised to fly VH-JTY. They held a valid Private Pilot Licence (Aeroplane), issued on 4 May 2004. In addition, the pilot held a single engine aeroplane rating, and endorsements for manual propeller pitch control and retractable undercarriage. Their last flight review was conducted in July 2023 and valid to 30 September 2025. At the time of the accident the pilot had about 2,100 hours total aeronautical experience of which about 1,500 hours were in VH-JTY.
The pilot held a valid class 2 medical certificate that was issued on 12 December 2022 and valid to 7 October 2024. The class 2 was issued with the restrictions that both distance and reading vision correction was available during flight. A review of the pilot’s medical records showed that a chronic medical condition was being appropriately managed by the pilot and their designated aviation medical examiner (DAME). It required annual review and there were no additional restrictions placed on the pilot’s class 2 medical certificate.
A copy of the coroner’s toxicology and pathology reports were not available to the ATSB at the time of publishing this report.
Passenger information
The passenger was familiar with VH-JTY. While a licensed pilot, they had not renewed their medical certification for flight and had not conducted a recent flight review.
Aircraft information
General information
The TB-20 is an all-metal, 5-place, single engine aircraft with fully retractable landing gear. It was powered by a 6-cylinder Lycoming IO-540 fuel-injected engine, driving a 3-blade constant-speed propeller and equipped[5] for visual flight rules (VFR)[6] (Day) flying only. VH-JTY was manufactured in France in 1985 and was first registered in Australia in April 1987. The pilot had owned VH-JTY since April 2008 (Figure 4).
Figure 4: VH-JTY
VH-JTY as it appeared in 2015. The yellow lines and wingtips were later painted dark red.
Source: Simon Coates, modified by the ATSB
Maintenance history
The aircraft was maintained in accordance with the CASA system of maintenance defined in Civil Aviation Regulations 1988 - Schedule 5 and the last periodic inspection was conducted on 14 December 2022. A review of the maintenance records and history for VH-JTY did not show any outstanding defects. The active maintenance release was not recovered from the accident site.
The aircraft was equipped with a Bendix/King KLN 90 GPS navigation system and a Bendix/King KAP 150 2-axis (pitch and roll) autopilot system that had been installed since the aircraft was manufactured. A review of the maintenance history and comments of the approved maintenance organisation showed minor issues with the autopilot consistent with its age. The faults were reported to have resulted in the uncommanded disconnection of the autopilot in flight. The unit was repaired in March 2022 and there were no records of any further maintenance on the autopilot after this date.
In January 2023, a ground handling incident damaged VH-JTY’s vertical fin and rudder. Structural repairs were carried out and following inspection of the flight controls, the aircraft returned to service on 25 May 2023. At the time of the accident, VH-JTY had a total time in service of about 5,233.4 hours and had flown about 35 hours since return to service.
King KAP 150 Autopilot
The pilot information manual supplement for the autopilot did not provide a minimum activation airspeed for the TB-20 but did contain a maximum airspeed limitation of 175 kt for autopilot use. Automatic flight could be activated by pressing the AP ENG (autopilot engage) button on the control panel and disengaged by pressing the AP ENG button again, or by pressing the AP DISC (autopilot disconnect) button on the pilot’s control wheel. When the autopilot is disengaged, an aural alert sounds for 2 seconds to alert the pilot.
The supplement also provided maximum altitude losses that may be encountered following an autopilot malfunction. In a cruise, climb or descent configuration, the maximum altitude loss would be 450 ft.
Recorded data
ADS-B
The aircraft was equipped with a SkyEcho portable automatic dependant surveillance broadcast (ADS-B) antenna capable of receiving information from ADS-B equipped aircraft and transmitting positional information to nearby stations. A review of available flight track history revealed that this antenna did not transmit any positional information during the accident flight.
Mobile devices
There were almost certainly 2 iPads and 2 telephones onboard the aircraft. Queensland Police located and recovered one telephone from the accident site. ATSB data recovery specialists determined that the phone was too heavily damaged to recover the data from the phone’s internal memory. At least 2 mobile devices were running the OzRunways app.
OzRunways data
OzRunways is an electronic flight bag (EFB) provider in Australia that also provides a ‘TX’ service that tracks device location and uploads it to OzRunways servers over the cellular network every 5 seconds. This service displays the device’s location on a user‑selected chart and also plots location data from other aircraft utilising OzRunways. The pilot used the OzRunways application on an iPad for en route planning and navigation. The pilot’s passenger also carried a second iPad with OzRunways when they flew together.
OzRunways is an approved source of aeronautical charts, but it must not be used as a primary means of navigation. The iPad GPS does not meet technical standard order[7] (TSO) specifications for aviation use (OzRunways, 2022). Additionally, there are limitations to the data provided via OzRunways. Altitude information has a resolution of 100 ft, a change in altitude from 190 ft to 210 ft will be displayed as a change from 100 ft to 200 ft. Additionally, filtering applied to smooth the data can affect the accuracy of analysis of small sections of data.
Tracking data obtained from OzRunways provided latitude and longitude as well as time, speed and heading. The last data point was at an altitude of about 1,700 ft above ground level in the vicinity of the accident site (Figure 2). When the OzRunways data ended, the aircraft was shown heading east in a steep descending right turn. The lack of any further data points was probably due to a loss of cellular signal among the mountains.
Accident site
The aircraft wreckage was located in heavily vegetated steep mountainous terrain, north-east of Bull Mountain (Figure 5). A Central Queensland Rescue helicopter located the wreckage at 1113 on 28 October and first accessed the site by winch at about 1400 on the day of the accident. The rescue crew confirmed that both occupants were deceased and took preliminary photographs of the wreckage.
The ATSB was unable to access the accident site. ATSB investigators provided a briefing to Queensland Police Service (QPS) forensic officers prior to them attending site on 27 November. With the support of specialists trained in high angle rescue operations the QPS officers collected evidence and provided it to the ATSB.
Figure 5: Accident site terrain
Source: Central Queensland Rescue, annotated by the ATSB
Wreckage examination
The ATSB’s review of the accident site photographs, and evidence provided by QPS, showed that the aircraft impacted the terrain at a steep angle while tracking 036° (close to north-east). The aircraft was destroyed by the impact and consumed by a post-impact fuel‑fed fire. Several components were buried by shifting soil after the accident.
Figure 6: Propeller damage
Source: Queensland Police Service, annotated by the ATSB
The following observations were made from the wreckage examination:
Impact marks on engine and propeller components indicated that the propeller was turning with power applied when it impacted terrain, indicating the engine was almost certainly operational at that time (Figure 6).
The extremities of the aircraft, the wing tips and stabilator were found at the accident site indicating that the aircraft was complete at the time of collision.
Communications
Police contacted Mackay air traffic control tower following the report of a missing aircraft. The controller confirmed that they did not hear a radio transmission from VH-JTY and that aircraft operating in the area at the time did not hear a distress call from the aircraft.
Operational information
General
Peers of the pilot reported that the pilot would often climb to operate VFR over the top of cloud. The pilot would generally fly the cruise portion of the flight on autopilot and would use the autopilot if they ever had to fly through cloud. While VFR over the top of cloud is permitted under the VFR, a minimum separation from cloud is required when flying under the VFR (see section Visual meteorological conditions).
The Civil Aviation Authority of New Zealand safety publication Vector contained an article called Who’s really flying your aircraft?The article discussed the potential downfalls of relying on automation in the cockpit, and its prevalence in VFR into instrument meteorological conditions (IMC) accidents.
VH-JTY was fitted with an approved GPS. The pilot was not known to program flight plans into the unit, instead relying on OzRunways for navigation. The CASA Visual Flight Guide provided the following note to VFR pilots utilising GPS in their aircraft:
An approved GNSS system may be used under the VFR:
• to supplement map reading and other visual navigation techniques
• to derive distance information for enroute navigation and traffic separation.
The positioning and navigational tools featured in the OzRunways application rely on equipment such as mobile phones or iPads that do not meet the required standard for operational use in aircraft. OzRunways acknowledges this limitation and advises users that the OzRunways application shall not be used as a primary means of navigation. It can, however, be used to supplement traditional visual navigation methods such as map reading.
Previous flights
Data obtained for the previous 3 months showed a number of previous flights between the two locations consistent with logged flight records (Figure 7). Each flight took about 1.2 hrs depending on the route taken.
Flights would often depart Palmyra, tracking inland towards Townsville where they would descend outside the Townsville control zone steps and land at Montpelier Airfield. On return to Palmyra, the pilot routinely flew inland past Collinsville and would descend down the Pioneer Valley approaching Palmyra from the west below the Mackay control zone steps.
Figure 7: Previous flight data
Source: Google Earth and OzRunways, annotated by the ATSB
Selection of route
The pilot and their passenger were familiar with the route between Montpelier and Palmyra, completing the return journey as often as once a fortnight for the last few years. When they considered the weather unsuitable for flight, they would make the trip by car, and had a vehicle at their disposal in both locations.
The pilot was known to plan routes that were outside controlled airspace (Figure 8). Witnesses interviewed advised this was common practice among local pilots due to the potential of encountering delays in access to controlled airspace in that region.
Figure 8: Intended flight path
Source: Visual Navigation Chart, annotated by the ATSB
Visual meteorological conditions
Visual meteorological conditions (VMC) are expressed in terms of in-flight visibility and distance from cloud (horizontal and vertical) and are prescribed in the Civil Aviation Safety Regulations (CASR) Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 2.07 VMC criteria. A VFR flight can be conducted above cloud provided VMC can be maintained for the entire flight, including climb, cruise, and descent.[8] The CASA Visual Flight Rules Guide included the following notes for VFR flight:
Pilots should not initiate VFR flight on top of more than SCT [scattered][9] cloud when weather conditions are marginal. Before committing to operate VFR flight on top of more than SCT cloud, pilots should be confident that meteorological information used is reliable and current, and clearly indicates that the entire flight will be able to be conducted in VMC.
And:
When navigating by visual reference to the ground or water, you must positively fix the aircraft’s position by visual reference to features marked on topographical charts at intervals not exceeding 30 minutes.
Figure 9, taken from the CASA Visual Flight Rules Guide, provides a visual depiction of the VMC criteria for aeroplanes below 10,000 ft.
Figure 9: VMC criteria below 10,000 ft
Source: Civil Aviation Safety Authority
Weather reports obtained by the pilot
According to CASR Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 7.02 Forecasts for flight planning, an authorised weather forecast must cover the whole period of the flight, and include a wind and temperature forecast and, for a flight at or below 10,000 ft AMSL, a general aviation meteorological area forecast (GAF).
Airservices Australia conducted a review of the pilot’s national aeronautical information processing system (NAIPS)[10] account activity. Two accounts were linked to the pilot. On the day of the flight, one account had expired, and the other had not been accessed since a password update 2 months earlier. Weather requests through OzRunways use the user’s NAIPS login credentials to retrieve the requested information. A third account, linked to the passenger, was last accessed through OzRunways 5 days prior to the flight to obtain an area briefing.
While other third party information such as weather radar overlays, satellite imagery and wind observations are available without an NAIPS login,[11] NAIPS is the only source through which OzRunways obtains weather forecasts for flight planning.
Notwithstanding the requirement of a forecast for flight planning, CASR Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 7.03 Flights unable to obtain an authorised weather forecast before departure states that a flight can still depart without an authorised forecast provided other conditions are met. These include:
The pilot in command reasonably considers that the weather conditions at the departure aerodrome will permit the aircraft to return and land safely at the departure aerodrome within 1 hour after take-off.
The pilot in command of a Part 91 flight must return to the departure aerodrome if:
(a) the authorised weather forecast required for the planned destination aerodrome is not obtained within 30 minutes after take-off; and
(b) the pilot in command has not nominated a destination alternate aerodrome if required to do so by subsection 8.04 (3).[12]
CASA defined what constituted an approved weather report and a list of who could provide one.[13] Licenced pilots were included in the list. The pilot obtained a weather update for the destination from their friend en route. While the accuracy of the information could not be verified, as a licenced pilot, the weather report provided by the pilot’s friend would have been considered an approved weather report for the destination. Based on the pilot’s phone records, this report was obtained about 39 minutes after departure.
Meteorological information
Forecast weather
The planned flight from Montpelier to Palmyra was within the QLD north (QLD-N) Graphical Area Forecast (GAF)[14] region. Forecast weather conditions in the GAF, valid from 0300 to 0900 on 28 October 2023, included average conditions of greater than 10 km visibility with areas of scattered stratocumulus clouds between 2,000 and 4,000 ft. The cloud was forecast to lift and become scattered cumulus and stratocumulus between 4,000 and 8,000 ft with moderate turbulence below 8,000 ft in thermals later in the day.
The Bureau of Meteorology aerodrome forecast (TAF)[15] for Mackay Airport, issued at 0435 and valid at the time of the accident showed an expected visibility of greater than 10 km, few cloud at 3,000 ft and a wind of 17 kt from the south-east.
Based on the forecasts, local pilots interviewed by the ATSB described the conditions as being conducive to mechanical turbulence around the ranges.
Actual weather
The meteorological aerodrome report (METAR)[16] for Mackay Airport reported wind from the east at 17 kt (100°), visibility greater than 10 km and cloud scattered at 3,300 ft and broken[17] at 5,500 ft. There was no rainfall recorded in the previous 24 hours.
The ATSB requested an assessment of the weather from the Bureau of Meteorology who provided the following observations for the morning of the accident:
• Cloud extended from the coast to the ranges and was clear west of ranges.
• South easterly winds persisted which often bring cloud between 2,000 – 3,000 ft, being lower earlier in the day and climbing as the day warms up.
• Over the accident site, cloud was overcast to broken.
• Cloud extended 25 NM south of accident site.
• Eungella Dam was visible to the west on satellite images.
• Closer to the coast cloud was scattered to broken.
Bureau of Meteorology satellite images showed cloud building in the Pioneer Valley east of the ranges from 0600, covering the mountains to the north of the Pioneer Valley by 0800. Figure 10 shows cloud cover at 0830, 3 minutes before the accident.
Figure 10: Satellite image showing cloud formation on 28 October at 0830 local time
Source: Source: Bureau of Meteorology, annotated by the ATSB
Figure 11 shows the location of witnesses and CCTV recorded at the time of the accident.
Eyewitness 1 located near Bull Mountain heard a low flying aircraft that stopped suddenly. They stated that the top of the mountain was visible around the time of the accident.
Eyewitness 2 described the cloud as being very thick that morning from when they woke at 0500. The cloud started to rise around 0800 but still produced limited visibility of their paddock until around 1000. They also described a ‘good breeze’ on the ground during the morning with occasional gusts but did not recall strong winds on the day. CCTV footage from that location showed low cloud close to where the pilot commenced their descent (Figure 12).
CCTV recording 1 obtained from a business 5 km south-west of the accident site showing diffuse light indicating cloud cover at the time of the accident.
CCTV recording 2 facing north from an elevated position at the head of the valley. That footage showed low cloud to the east and tree movement equivalent to a fresh breeze.
Additionally, a large bushfire around 70 km to the south-east had filled the Pioneer Valley with smoke which was yet to dissipate. The pilot of the rescue helicopter advised that during the search for VH-JTY at around 1000, the cloud base was scattered at 3,000 ft with poor visibility in smoke haze.
Figure 11: Witness locations
Source: Google Earth, annotated by the ATSB
Figure 12: Closed circuit footage from Dalrymple Heights
Source: Supplied
Decision making
Flight under the VFR requires minimum conditions of visibility and distance from cloud. Variation from the expected weather conditions en route may prevent a pilot from reaching their destination under this ruleset. Flying into instrument meteorological conditions[18] (IMC) can occur in any phase of flight. However, a 2005 ATSB research publication – General Aviation Pilot Behaviours in the Face of Adverse Weather (B2005/0127) – concluded that the chances of a VFR into IMC encounter increased as the flight progressed, with the maximum chance occurring during the final 20 per cent of the planned flight. It stated:
This pattern suggests an increasing tendency on the part of pilots to ‘press on’ as they near their goal. To turn back or divert when the destination seemed ever closer became progressively more difficult.
The CASA Resource Booklet 7 Decision making contained the following:
A non-instrument rated pilot who proceeds with a flight in marginal weather and ends up in instrument meteorological conditions (IMC) decides to firstly, proceed with the flight and secondly, not turn back when the weather indicated visual flight rules were not able to be maintained
Dejoy (1992, cited in Hunter, 2002) suggests that a person’s propensity to engage in risky behaviour is the result of lower perceived risk in the outcome. Studies have shown that pilots who do not perceive the risks with adverse weather are more likely to engage in higher risk activities when dealing with weather (Cooper, 2003).
A Transportation Safety Board of Canada report A23O0028 into a VFR into IMC accident looked at pilot decision making and the acceptance of unsafe practices.
Pilot decision making is a cognitive process used to select a course of action between alternatives. Several factors, circumstances, and biases can affect pilot decision making, including the flight objective or goal, and the pilot’s knowledge, experience, and training. These factors can lead to situations where pilots might prioritize the achievement of the goal over the management of threats, likely resulting in a reduced safety margin.
A focus on achieving a goal or outcome may lead to a reduced sensitivity to risk, especially when high-risk activities repeatedly result in no negative outcomes. Flight crew members may grow accustomed to these risks, altering their perception and acceptance of such risks over time (Hollenbeck and others 1994).
In conditions where visual cues are poor or absent, such as in poor weather, up to 80 per cent of the normal orientation information is missing. Humans are then forced to rely on the remaining 20 per cent, which is split equally between the vestibular system and the somatic system. Both of these senses are prone to powerful illusions and misinterpretation in the absence of visual references, which can quickly become overpowering.
Pilots can rapidly become spatially disoriented when they cannot see the horizon. The brain receives conflicting or ambiguous information from the sensory systems, resulting in a state of confusion that can rapidly lead to incorrect control inputs and resultant loss of aircraft control.
For non-instrument rated pilots, statistics show they may not be able to recover at all. Research has shown the pilots not proficient in maintaining control of an aircraft with sole reference to the flight instruments will typically become spatially disoriented and lose control of the aircraft within 1 to 3 minutes after visual cues are lost.
The FAA Advisory Circular FAA AC60-4A Pilot’s spatial disorientation discussed the challenges associated with recovering from spatial disorientation. The results of a test conducted with qualified instrument pilots found that it took as much as 35 seconds to establish full control by instruments after the loss of visual reference with the ground or surface.
The ATSB report AR-2011-050 was updated in 2019 and found that in the 10 years prior, there were 101 VFR into IMC occurrences in Australian airspace reported to the ATSB. Of these, 9 were accidents resulting in 21 fatalities. An almost 10% chance of the encounter ending in a fatal accident.
A search of the ATSB Aviation Occurrence Database shows that in the 5 years since 2019, there have been 56 VFR into IMC occurrences reported to the ATSB. Of these, 10 resulted in accidents with 16 fatalities. The dangers of spatial disorientation following a loss of visual cues remains one of the most significant causes of concern in aviation safety.
Similar Occurrences
The risks of visual flight rules (VFR) pilots flying from visual meteorological conditions (VMC) into instrument meteorological conditions (IMC) are well documented, and have been the focus of numerous ATSB reports and publications. VFR pilots flying into IMC is a significant cause of aircraft accidents and fatalities.
AO-2022-016 – VFR into IMC, loss of control and collision with terrain involving Airbus Helicopters EC130 T2, VH-XWD, near Mount Disappointment, Victoria, on 31 March 2022
On 31 March 2022, at about 0741 local time, 2 Microflite Airbus EC130 helicopters, registered VH‑WVV and VH-XWD, departed the Batman Park helicopter landing site in Melbourne, for the town of Ulupna, Victoria. Both helicopters were operated in accordance with the VFR and departed in VMC conditions. Cloud was forecast along the route, but the pilots elected to continue to the destination. The helicopters encountered instrument meteorological conditions (IMC) over Mount Disappointment and VH-WVV conducted a U-turn to avoid entering cloud. While also attempting to conduct a U-turn, VH-XWD entered cloud, developed a high rate of descent, and collided with terrain. The helicopter was destroyed, and the 5 occupants were fatally injured.
AO-2021-017 – VFR into IMC and in-flight break-up involving Van's Aircraft RV-7A, VH-XWI 90 km south of Charters Towers, Queensland, on 23 April 2021
On 23 April 2021, a Van’s Aircraft RV-7A, registered VH-XWI, was being operated on a private flight under the visual flight rules (VFR) from Winton to Bowen, Queensland. During the flight, the pilot most likely entered IMC and lost control of the aircraft several times. This led to the airspeed limitations for the aircraft being exceeded and the aircraft sustained an in-flight break-up. The pilot was fatally injured, and the aircraft was destroyed.
VFR into IMC resources
The 2011 ATSB publication, Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions, updated in 2019, includes a selection of weather-related general aviation accidents and incidents that show weather alone is never the only factor affecting pilot decisions that result in inadvertent IMC encounters. The documented investigations consistently highlight that conducting thorough pre-flight planning is the best defence against flying into deteriorating weather.
CASA also released a collection of resources related to this type of occurrence on its website titled Preventing VFR into IMC and other related resources on its pilot safety hub under Weather and forecasting.
For more information on VFR into IMC occurrences, recognising inadvertent entry into IMC, and what to do to recover, refer to the following publications:
Civil Aviation Authority United Kingdom: Safety sense booklet VFR flight into IMC
Data collected by the OzRunways electronic flight bag (EFB) application indicated that shortly after commencing descent from 5,500 ft, VH-JTY made a series of turns that displayed excessive sink and climb rates before colliding with terrain. This manoeuvring indicates that the autopilot was not being used during this part of the flight. Site and wreckage examination indicated that the aircraft was complete, had significant forward velocity, a high angle of entry and the engine was producing power. Those items of evidence indicated that the aircraft was most likely in an uncontrolled state when it collided with terrain.
The analysis considers the limited evidence available and discusses possible explanations for the departure from controlled flight:
pilot incapacitation
technical failure or malfunction
decision making
spatial disorientation.
Pilot incapacitation
Pilot incapacitation following a medical event was considered unlikely based on the short timeframe between ending the phone conversation prior to descent and the apparent departure from controlled flight. Medical records indicated that the pilot’s pre-existing condition was being appropriately managed and in the absence of any additional evidence, that was excluded.
Additionally, the passenger was also a pilot, although not current at the time, and they would have been capable of assuming control if the pilot had a medical episode.
Technical malfunction
Structural failure was considered as a possible explanation for the departure from controlled flight. The propeller, wing tips, stabilator, and vertical stabiliser/rudder were all located in site photographs. This was significant in determining that the recent repair to the vertical stabiliser had not failed. With the main components identified at the accident site, the possibility of an in-flight break‑up was excluded. Further, the damage to the engine and propeller indicated the engine was producing power at the time of the accident, eliminating engine malfunction as a possible explanation for the rapid descent.
The autopilot was installed in the aircraft from new and the pilot had owned the aircraft for close to 15 years. The pilot was almost certainly familiar with basic operation of the autopilot. The design of the autopilot servos that moved flight control surfaces incorporated a clutch so a pilot could override the autopilot in the event of a malfunction. The unit also incorporated a design whereby the autopilot would disengage if excessive pitch or roll rates were encountered. The autopilot had been repaired almost a year prior with no record of any additional maintenance, and the nature of the previous autopilot failures would not induce a loss of control.
If a technical malfunction occurred that would have affected the immediate safe continuation of the flight, it is very likely the pilot would have made a radio call declaring an emergency. No radio call was detected.
With no evidence of a failure or malfunction that would have induced uncommanded control inputs, it is considered unlikely that the autopilot contributed to a loss of control.
Pilot decision making
After excluding pilot incapacitation and technical failure, the ATSB considered pilot decision making and the flight path through cloud during the final minutes of the flight.
There was no record that the pilot obtained relevant aviation weather forecasts prior to the flight, and it could not be determined if additional weather information was obtained from other non‑approved sources. However, as the flight was a relatively short distance, and the pilot was very familiar with the route and destination, it is almost certain that they had knowledge and experience of weather behaviour and conditions to be expected. Additionally, the weather report obtained over the telephone while en route provided an accurate assessment of the prevailing conditions along the intended flight path.
Weather observations showed that at the cruising altitude of 5,500 ft, VH-JTY would have been in VMC above cloud before commencing descent. While there was variation in the witness reports concerning the lower level of the cloud, evidence showed there was significant cloud present, and that the pilot planned to pass through it. Witness statements related that it was common practice for the accident pilot to intentionally fly through cloud with the autopilot on. While this action would represent intentional non-compliance with aviation regulations, the main advantage of doing so would be to avoid loss of control following loss of visual references. The hazard being that if the autopilot or any of its input sensors failed or were inadvertently disengaged, loss of control would reasonably ensue.
This behaviour without previous consequence may have affected their perception of the associated risk of continuing through cloud and influenced their decision to continue along the intended flight path instead of diverting around the cloud en route (Cooper, 2003). Personal bias and misperception of the risks associated with VFR flight into IMC (Hollenbeck and others, 1994) is a factor frequently seen in aircraft accidents (Hunter, 2002).
The Bureau of Meteorology assessment of the conditions and analysis of satellite imagery matched the report of the pilot’s friend on conditions at the destination. While cloud existed around to the east of Mackay and around the mountains of the Pioneer Valley, the west and south of the destination were clear of cloud. It was determined that in this context, it is highly likely that the pilot chose to fly through cloud rather than continue visual flight over the top of cloud, divert around weather, or plan flight through controlled airspace.
Spatial disorientation
The flight path from Montpelier to top of descent was compared to previous flights. It was determined to be consistent with the way the pilot would normally conduct cross-country flights in VH-JTY and was almost certainly being flown on autopilot during cruise. The sudden change in flight path prior to descent indicated disconnection of the autopilot and resumption of hand flying.
The weather on the day of the flight was conducive to poor or absent visual cues and turbulence, factors which are known to contribute to spatial disorientation. The pilot was not trained or experienced in flying in low visibility. In these conditions, the pilot would have been required to reference the aircraft’s flight instruments to maintain control. In this case the aircraft was not equipped with the instruments required for flight in IMC.
The accident site showed that the aircraft collided with terrain tracking north-east, indicating that the turn to the right continued after the flight path recording ended. The instability of the flight path with excessive rates of descent and climb are markers commonly observed in spatial disorientation occurrences where pilots are aware of a departure from controlled flight and attempt to correct the unusual flight attitude.
Due to the limited information available, it is not known whether the autopilot disconnect was intentional or why the pilot’s reported strategy of using autopilot when flying through cloud failed on this occasion. Following the commencement of the turn to the left, the significant deviation of pitch attitude during the turn was likely unintentional. The high rate of descent was consistent with the pilot becoming spatially disoriented after flying into weather conditions not suitable for visual navigation. As a result, the aircraft collided with terrain.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the VFR into IMC, loss of control and collision with terrain involving SOCATA-Groupe Aerospatiale TB-20, VH‑JTY, 65 km west of Mackay Airport, Queensland, on 28 October, 2023.
Contributing factors
The pilot made the decision to descend through cloud rather than remain VFR over the top or divert around weather.
The visual flight rules pilot very likely entered weather conditions not suitable for visual navigation, leading to spatial disorientation and collision with terrain.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Queensland Police Service
accident witnesses
recorded data from the OzRunways navigation application
CCTV video footage and other photographs taken on the day of the accident
Cooper D. (2003). Psychology, Risk and Safety: Understanding how personality & perception can influence risk taking. Professional Safety. Journal of the American Society of Safety Engineers, November 2003, 39-46.
Hunter DR. (2002), Risk Perception and Risk Tolerance in Aircraft Pilots. Federal Aviation Administration, DOT/FAA/AM-02/17, 2002.
Hollenbeck, J. Ilgen, D. Phillips, J. Hedlund J. (1994) Decision risk in dynamic two-stage contexts: beyond the status quo. Journal of Applied Psychology, Vol.79, Issue 4, pp. 592–598.
OzRunways. (2022). How can OzRunways be used for navigation? On-line, Retrieved 19 August
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
maintenance organisation for VH-JTY
aircraft manufacturer
Civil Aviation Safety Authority
Airservices Australia
Bureau of Meteorology
OzRunways.
Submissions were received from:
the aircraft manufacturer.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Montpelier aircraft landing area is located about 20 km south-south-east of Townsville Airport and is the site of the former military airfield Antill Plains.
[2]Palmyra aircraft landing area is located about 12 km west-south-west of Mackay Airport.
[3]OzRunways is an electronic flight bag app that provides planning, briefing, flight plan filing and moving map navigation services.
[4]VNE (Never Exceed Speed): the speed limit that may not be exceeded at any time. The calculation of this speed is driven by structural or aerodynamic limitations; however, control system flutter is typically one limitation that factors heavily into the calculation of VNE.
[5]The aircraft is equipped with the flight and navigation equipment listed in the aircraft’s flight manual and any additional equipment required for the type of operation in accordance with Civil Aviation Order 20.18.
[6]Visual flight rules (VFR): regulations that permit a pilot to operate an aircraft in conditions whereby navigation and orientation of the aircraft by visual reference is possible.
[7]Technical Standard Order (TSO) – a TSO is a minimum performance standard for specified materials, parts, and appliances used on civil aircraft.
[8]VFR flight above more than 4/8 cloud cover is known as ‘VFR over the top’, as the phrase ‘VFR on top’ is a clearance provided to an instrument flight rules flight to operate at a VFR level in visual conditions.
[9]Scattered: describes cloud covering three or four eighths (oktas) of the sky.
[10]The National Aeronautical Information Processing System (NAIPS) is a multi-function, computerised, aeronautical information system. It processes and stores meteorological information and operational notices and enables the provision of briefing products and services to pilots and the Australian Air Traffic Control platform.
[11]Radar weather overlays and satellite imagery is downloaded from the Bureau of Meteorology. Wind observations obtained through the private company Windy.com are obtained from publicly available weather databases produced by worldwide weather agencies (including the BoM).
[12]CASR Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 8.04 Destination alternate aerodromes — weather.
[13]CASR Part 121 Chapter 9 Division 2 –Dictionary.
[14]GAF (Graphical Area Forecast): provides information on weather, cloud, visibility, icing, turbulence and freezing level in a graphical layout with supporting text.
[15]TAF (Aerodrome Forecast): a statement of meteorological conditions expected for the specified period of time in the airspace within 5 nautical miles (9 km) of the aerodrome reference point.
[16]METAR (Meteorological Aerodrome Report) is a routine aerodrome weather report issued at half hourly time intervals. The report ordinarily covers an area of 8 km radius from the aerodrome reference point.
[17]Broken: used to describe an amount of cloud covering the sky of between 5 and 7 oktas (eighths).
[18]Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules (IFR), rather than by outside visual reference. Typically, this means flying in conditions of limited visibility.
Preliminary report
Report release date: 14/12/2023
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 28 October 2023, at about 0735 local time, a SOCATA-Groupe Aerospatiale TB-20 (TB-20) registered VH-JTY, departed from Montpellier aircraft landing area,[1] Queensland, for a private flight to Palmyra aircraft landing area[2] (Figure 1). On board was the pilot and a passenger, who was also a pilot.
A friend of the pilot stated that they made a phone call to the pilot at 0814. The pilot stated that they were at 5,500 ft above cloud and asked about weather conditions at Palmyra airfield. The pilot stated they were passing Dalrymple Heights and on descent and that their intentions were to fly along the Pioneer Valley to Palmyra airfield.
At about 0834, the OzRunways[3] flight track (Figure 1) showed that the pilot made a right turn, followed by a left turn before colliding on the northern side of Bull Mountain, at about 1,900 ft above mean sea level. The aircraft was destroyed, and the pilot and passenger were fatally injured.
Figure 1: VH-JTY flight track
Source: Google Earth, OzRunways, annotated by the ATSB
Context
Pilot information
The pilot held a valid Private Pilot Licence (Aeroplane) and a Class 2 aviation medical certificate, valid until October 2024. The pilot held a single engine aeroplane rating, and endorsements for manual propeller pitch control and retractable undercarriage. Their last flight review was conducted in July 2023, and at the time of the accident the pilot had about 2,100 hours total aeronautical experience of which about 1,500 hours were in VH-JTY.
Aircraft information
General information
The TB-20 is an all-metal, 5-place, single engine aircraft with fully retractable landing gear. It was powered by a 6-cylinder Lycoming IO-540 fuel-injected engine, driving a 3-blade constant-speed propeller. VH-JTY was manufactured in France in 1985 and was first registered in Australia in April 1987. The pilot had owned VH-JTY since April 2008 (Figure 2).
The last periodic inspection was conducted on 14 December 2022. In January 2023, VH-JTY sustained rudder and vertical fin damage in a ground handling incident. Structural repairs were carried out and the aircraft returned to service on 25 May 2023. At the time of the accident, it had accrued a total time in service of about 5233.4 hours and had flown about 35 hours since the repairs were carried out.
Figure 2: VH-JTY
Source: Simon Coates, modified by the ATSB
Site and wreckage information
The aircraft wreckage was located in steep mountainous terrain with heavy vegetation, to the north-east of Bull Mountain.
The aircraft fuselage sustained a heavy impact initially with vegetation and then terrain before becoming significantly disrupted with some components sliding downhill and being consumed by fire.
Wreckage examination
Due to the remote location, extreme terrain, and degradation of the accident site, ATSB has not been able to attend the site. However, Queensland Police Service specialist forensic officers have provided detailed on-site photographic evidence. This has assisted the ATSB with gaining an understanding of the accident site location and layout, as well as an appreciation of the level and type of damage to the aircraft’s structure and components.
Photographic evidence review of engine and propeller components indicated that the propeller was under a significant level of power when it impacted with terrain, indicating the engine was almost certainly operational at that time.
Further investigation
To date, the ATSB has:
examined photographs of the aircraft wreckage
conducted witness interviews
examined the maintenance history of the aircraft
reviewed historic flight data
reviewed air traffic control recordings.
The investigation is continuing and will include:
further review of recorded data and recovered components from the accident site
analysis of available flight data
analysis of aircraft maintenance and repairs.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB would like to acknowledge the assistance provided by the Queensland Police Service who provided site information and photographs in the course of the on-site phase of this investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Montpellier aircraft landing area is located about 20 km south-south-east of Townsville Airport.
[2] Palmyra aircraft landing area is located about 12 km west-south-west of Mackay Airport.
[3] OzRunways is an electronic mobile application, utilising approved data for electronic maps, and used for navigation.
Occurrence summary
Investigation number
AO-2023-052
Occurrence date
28/10/2023
Location
65 km west of Mackay Airport
State
Queensland
Report release date
02/10/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Loss of control, VFR into IMC
On 31 March 2022, at about 0741 local time, 2 Microflite Airbus EC130 helicopters, registered VH‑WVV and VH-XWD, departed the Batman Park helicopter landing site in Melbourne, for the town of Ulupna, Victoria. The helicopters encountered instrument meteorological conditions (IMC) over Mount Disappointment and VH-WVV conducted a U-turn to avoid entering cloud. While also attempting to conduct a U-turn, VH-XWD entered cloud, developed a high rate of descent, and collided with terrain. The helicopter was destroyed and the 5 occupants were fatally injured.
What the ATSB found
The ATSB found that, while visual meteorological conditions (VMC) prevailed at the departure point, the pilots of the helicopters planned and commenced a route for which IMC was forecast. The pilots continued the flight as conditions deteriorated below VMC until a rapid change of course was required to avoid entering cloud. The accident pilot did not maintain adequate control of the pitch attitude during the attempted U-turn and a high rate of descent developed resulting in a collision with terrain. This pilot had no instrument flying experience, and the helicopter was not equipped with any form of artificial stabilisation, nor was either required by the regulations.
The operator had not mandated several of the risk controls available to them for their day visual flight rules pilots, which included inadvertent IMC recovery training and basic instrument flying competency checks during operator proficiency checks, nor were they required to by the regulations. The operator had also not introduced an inadvertent IMC recovery procedure for their air transport operations or a pre-flight risk assessment to trigger an escalation process for marginal weather conditions identified at the pre‑flight planning stage.
The operator had identified poor weather conditions as a risk. However, their management of that risk was limited to the regulatory requirements and did not consider an inadvertent IMC event. The Civil Aviation Safety Regulations Part 133 for rotorcraft air transport only required the risk of a visual flight rules inadvertent IMC event to be managed through avoidance. While important, avoidance of inadvertent IMC has and will fail on occasion, but Part 133 did not address the risk of recovery from such an event.
The ATSB also found that the standby artificial horizon in VH-XWD was not powered on during the flight and erroneously indicated an unusual attitude as the helicopter approached the cloud. The pilot was momentarily distracted by this indication immediately before executing the U-turn. In addition, the helicopter was scheduled to be modified with the latest service bulletins to prevent a turbine blade shedding event but they were not accomplished at the time of the accident. These 2 factors were not considered contributory but increased the risks of spatial disorientation and a post-impact fire respectively.
What has been done as a result
As a result of this accident, the operator has taken the following actions:
drafted a dedicated risk assessment addressing visual flight rules into IMC
upgrading their fleet of EC130 and AS350 helicopters with the Garmin G500H primary flight display and multifunction display incorporating synthetic vision and a terrain alerting functionality
modifying their AS350 helicopters with the Garmin GFC 600H helicopter flight control system (approved data for the EC130 was not available at the time of the investigation)
acquired ICARUS (instrument conditions awareness recognition and understanding system) instrument flying training hoods
introduced basic instrument flying training and inadvertent IMC recovery training
updated their operator proficiency check syllabus to include knowledge and practical skills checks for avoiding and recovering from inadvertent IMC
added the Helicopter Association International online academy ‘56 Seconds to Live’ inadvertent IMC avoidance course to their pilot training program
introduced a pre-flight risk assessment tool
introduced a company ‘Task rejection’ policy statement into their operations manual
obtained an Airbus Helicopter Training Centre approval.
The ATSB has issued a safety recommendation to the Civil Aviation Safety Authority to take further safety action to address the risk to rotorcraft air transport (Part 133) passenger safety from a visual flight rules inadvertent instrument meteorological conditions event.
Safety message
Helicopter inadvertent IMC occurrences result in a higher proportion of accidents and a similar proportion of fatal accidents as those involving aeroplanes. The ATSB encourages all pilots to develop the knowledge and skills required to manage the risk of inadvertent IMC, which can be assisted with educational material from regulators and industry bodies directed at flight planning and weather assessments. Decision-making in marginal weather conditions can be supported with the use of a pre-flight risk assessment tool.
At an organisational level, the risk of helicopter inadvertent IMC should be considered within the context of a company’s operations. The effective management of this risk relies on multiple layers of controls to reduce the risk of single-point of failure accidents. This includes training and procedures for avoidance and recovery, which can be enhanced with equipment, such as autopilots to reduce the risk of loss of control, and terrain awareness and warning systems to reduce the risk of controlled flight into terrain.
Summary video
The occurrence
Overview
On 31 March 2022, 2 Airbus Helicopters EC130 T2 helicopters, registered VH-WVV (WVV) and VH-XWD (XWD), and operated by Microflite under the visual flight rules, departed the Batman Park helicopter landing site (HLS), Melbourne, Victoria, for the destination of Ulupna, Victoria. Each helicopter had a pilot and 4 passengers on board. While tracking overhead Mount Disappointment towards Ulupna, the pilots of both helicopters encountered instrument meteorological conditions. The pilot of WVV was in the lead and called for a U-turn and exited from the conditions. The pilot of XWD attempted to follow WVV with a U-turn but entered cloud and lost control of the helicopter, which resulted in a collision with terrain that fatally injured the 5 occupants and destroyed the helicopter.
Positioning flight to Batman Park helicopter landing site
At about 0709 local time, XWD departed Moorabbin Airport for Batman Park HLS about 10 seconds behind another company helicopter, WVV.[1] Their task was to transport a charter group from the Batman Park HLS in the city, north to Ulupna on the border with New South Wales.
The pilot of WVV later recalled that the weather forecast had been a concern the night before and again on the morning of the accident as the forecast for Melbourne Airport included scattered[2] cloud at 1,500 ft above the aerodrome from 0700. This was 30 minutes before their scheduled departure time from Batman Park and indicated that they would not be able to transit through the ranges to the north below cloud. The recommended visual flight rules (VFR)[3] route, for a track north outside controlled airspace, was through Kilmore Gap, which had an elevation of 1,200 ft. The pilot of WVV believed the Melbourne Airport forecast would not allow them to maintain their minimum legal height if they attempted to track via Kilmore Gap below cloud. Therefore, they planned to take a more direct track to their destination, over Mount Disappointment (elevation of 2,605 ft), about 12 NM (22 km) to the east of Kilmore Gap. Figure 1 depicts the key locations.
Note: The 2 purple pins depict the ends of the recommended VFR route. Source: Google Earth and OzRunways, annotated by the ATSB
The recording from the Appareo[4] camera fitted onboard XWD showed that, after start at Moorabbin Airport, the pilot erected the main artificial horizon (AH)[5] on the helicopter’s instrument panel but did not turn on and erect the standby AH. Therefore, the standby AH presented the helicopter’s attitude as a 90° roll to the left with a red off flag in the top right corner.
After take-off from Moorabbin, the pilots assessed the weather and observed the forecast cloud was not yet established over the ranges (refer to section titled Meteorological information). Therefore, they considered the route over Mount Disappointment would be suitable for the planned charter flights and continued to Batman Park to collect their passengers. At about 0717, the helicopters landed at Batman Park and were shut down (Figure 2). The pilots then proceeded to the operator’s HLS office to meet their charter group of 8 passengers for their business trip to Ulupna. They escorted the passengers to the helicopters where they were divided into 2 smaller groups of 4 passengers for each helicopter and provided a safety briefing.
Figure 2: XWD (left) and WVV (right) at Batman Park HLS
Source: Operator, through Victoria Police
Departure from Batman Park helicopter landing site
At about 0741, XWD departed from Batman Park 30 seconds behind WVV. The standby AH in XWD remained off and continued to indicate a 90° left roll attitude (Figure 3). Both helicopters were operating VFR outside controlled airspace without a flight plan.[6] The helicopters initially headed east to remain outside controlled airspace before turning north toward Ulupna. As they tracked east and then north, the lower limit of controlled airspace increased,[7] and the helicopters climbed from 1,500 ft above mean sea level to 2,500 ft and then to 3,500 ft. The pilots reportedly discussed the weather over the radio and noted the conditions to the west were consistent with the forecast, but that the conditions to the north had not deteriorated, and they continued to track northbound.
While tracking north towards Mount Disappointment, the helicopters climbed above a layer of scattered cloud that the pilot of WVV estimated to have a top of about 2,500-3,000 ft and below a layer of broken cloud with an estimated base of about 4,500 ft. The pilot of WVV later recalled that they could see areas of sunlight striking the ground ahead of them, and therefore considered the weather ahead suitable to climb on top of the scattered layer of cloud, rather than attempt to cross Mount Disappointment underneath the cloud layers.
As they approached Mount Disappointment, XWD was about 1.5 NM (3 km) behind WVV, and the helicopters were cruising at an altitude of about 3,500 ft with a 120 kt ground speed. At this time, the pilot of WVV noted the layer of scattered cloud below them was becoming broken, that the tops were rising, and that the base of the cloud above them appeared to be lowering, resulting in the 2 layers of cloud appearing to converge ahead of them. They tracked around a rising cloud top, that otherwise would have forced them to climb into controlled airspace. Once around that cloud top, the pilot of WVV could still see spots of sunlight striking the ground ahead. Therefore, they were confident to continue.
Mount Disappointment
Before they crossed Mount Disappointment, the pilot of WVV was confronted with a ‘wall of cloud’ in front, and to the left and right of their intended track, and so broadcast to XWD their intention to turn around. The pilot of WVV knew that XWD was nearby and wanted to ensure that the pilot of XWD understood WVV would be making a U-turn. The pilot of WVV reported that the pilot of XWD was initially confused as to why WVV was turning around and might have thought the conditions were suitable to continue. The pilot of WVV then broadcast ‘U-turn, U-turn, U-turn’ to XWD. At 0756:30 (Figure 5), the pilot of WVV conducted a sharp left turn onto a southerly track at 3,635 ft. At that time, XWD was at 3,582 ft, with 100 kt indicated airspeed (KIAS), and a first limit indicator (FLI)[8] power setting of about 5.
At 0756:54, while maintaining 3,600 ft with FLI 5, the Appareo camera recording showed that the cloud through the windscreen of XWD appeared to change from broken to overcast. Over the next 5 seconds, the FLI reduced to 2 and XWD started to descend at about 500 ft/min.[9] The pilot also started actively scanning to the left and above.
At 0757:00, WVV had turned onto a southerly track (186°), climbed to 3,967 ft with a ground speed of 73 kt, and was close to passing abeam XWD, which was at 3,504 ft tracking north (359°), with a ground speed of 116 kt. The pilot and passengers onboard WVV sighted XWD when they passed above and abeam the left-side of XWD. This was the last visual contact with XWD. Figure 4 depicts the meteorological conditions from XWD shortly after the helicopters passed abeam each other at 0757:09.
Figure 4: Footage of weather conditions from XWD at 0757:09
Source: ATSB (from the Appareo)
At 0757:10, XWD briefly rolled left about 30° with a FLI indication of 2, before returning to a level attitude. Three seconds later, the pilot looked across to the right side of the instrument panel. At that time, the helicopter was pitched 10° nose down, wings level, at 70 KIAS and 3,500 ft, and with a FLI indication of 4. The pilot then reached across the instrument panel, grasped the standby AH knob momentarily and then released it, with no change to it indicating a 90° left roll with the off flag still visible in the top right corner.
At 0757:20, at an altitude of about 3,300 ft at 75 KIAS with a FLI indication of 1 and while descending at 1,300 ft/min, XWD rolled left to about 60° angle of bank with the nose pitched 5° down. One second later, the nose down attitude had reached 15°, the airspeed had reduced to about 70 KIAS, and the rate of descent increased to 1,400 ft/min with FLI 1.5. Within 3 seconds, the horizon disappeared off the top right corner of the main AH, such that only ground was visible on the instrument, with a 1,500 ft/min rate of descent and FLI 2.
At 0757:26, the vertical speed indicator reached the full-scale descent deflection of 3,000 ft/min. The main AH still displayed full ground nose down attitude, but the angle of bank had reduced to about 30° left. The airspeed was about 85 KIAS with a FLI indication of 1. The Appareo global positioning system data indicated the helicopter’s rate of descent exceeded 5,000 ft/min from 0757:23 to 0757:28 and peaked at about 5,700 ft/min at 0757:25 (Figure 5.).
At 0757:29, at an altitude of about 2,700 ft, with a low FLI setting and the vertical speed indicator still at full-scale deflection, trees became visible in the cloud. In the last second of footage, the helicopter pitched significantly nose up while the altimeter continued to decrease from 2,700 ft to 2,600 ft. The vertical speed indicator remained at full-scale deflection, the airspeed decayed by 20 KIAS, there was no significant change in the FLI indication, and the LIMIT[10] caution light activated twice. The Appareo cabin area microphone also detected the rotor overspeed warning activate and the sound of the rotor blades striking the trees. The collision with tree occurred at 0757:31. The flight track for XWD is presented in Figure 5.
Source: Google Earth and OzRunways, annotated by the ATSB
After WVV completed the U-turn onto a southerly heading, the pilot found a clearing through the cloud and turned back northbound with a clearance from air traffic control to climb to not above 5,000 ft after reporting they were in instrument meteorological conditions. After a few minutes, the pilot and passengers onboard WVV attempted to contact the pilot and passengers onboard XWD, initially with the helicopter radio, then with their mobile phones, with no success. The pilot then contacted the Microflite operations manager, which started the search and rescue process. WVV diverted to Mangalore Airport and landed without further incident.
The emergency locator transmitter fitted to XWD did not activate after the accident and low cloud in the area initially hampered the search. The wreckage site was located at about midday at an elevation of 2,359 ft (719 m). The 5 occupants were fatally injured and the helicopter was destroyed.
VH-WVV passenger reports
The passenger in the front middle seat had flown regularly with the pilot of WVV and considered the pilot to be very cautious regarding the weather. The passenger recalled that, during the flight, the pilot radioed XWD about the approaching weather. A ‘wispy cloud then went past us, and it felt like a heavy white cloud came down and dumped on us’.
The passenger in the front right seat had flown in helicopters for about 30 years. The passenger recalled that, as they crossed Mount Disappointment, heavy cloud rolled in resulting in ‘a white‑out[11] with ground visibility no longer evident’. The pilot radioed XWD and said words to the effect of ‘U-turn, U-turn, U-turn’. Then the pilot of WVV immediately completed a U-turn. The pilot of XWD radioed back with words to the effect ‘aren’t we going to cut through?’ The passenger then saw XWD pass just below them.
The passenger seated behind the pilot had flown once previously with the pilot of WVV and found them to be very professional and relaxed. During the flight, the passenger was reading emails, but noted as they approached Mount Disappointment that the pilot’s body language had changed, which gave the passenger the feeling that something was not right. The passenger looked outside and saw cloud in front and to the left, and then heard the pilot announce they were going ‘hard left’. When the passenger next looked outside, they ‘could not see anything, it was like a white‑out’. The passenger then felt the helicopter in a hard left turn.
Context
Pilot information
Qualifications and experience
The pilot of VH-XWD (XWD) held a Commercial Pilot Licence (Helicopter) (CPL(H)), issued 22 February 2016, with a single-engine helicopter class rating and a Class 1 Aviation Medical Certificate with an expiry date of 28 February 2023. In addition, the pilot held an aerial application rating and a low-level rating with a sling endorsement. The Civil Aviation Safety Authority (CASA) had no record of the pilot holding a gas turbine endorsement[12] but noted that the pilot had conducted several flight reviews with an authorised instructor in turbine-powered helicopters since being issued with the CPL(H) in 2016.
The pilot was initially employed as a line pilot conducting scenic flights in the Northern Territory from March 2016 until April 2019. The pilot then moved to another employer in south-east Queensland from May 2019 before joining Microflite in December 2019.
The pilot received company approval by Microflite to conduct visual flight rules (VFR) charter operations on 22 December 2019. According to the operator’s records, the pilot had accumulated 3,005.8 flying hours on helicopters, which included 330.6 hours on the EC130, 2,507.3 hours total turbine, and 2,866.8 hours in command. Their records indicated the pilot had no instrument flying,[13] simulated instrument flying or night flying experience.
Since joining Microflite, the pilot had completed operator VFR proficiency checks[14] on 21 December 2019 (EC130), 21 April 2020 (EC120),[15] 14 October 2020 (AS350),[16] 25 May 2021 (EC120), and 31 October 2021 (AS350) to a pass standard with no remedial training required. According to the operator’s training manual, the proficiency checks included ‘flight planning, refuelling, aircraft weight and balance, passenger briefing, forced landings and all emergency operations.’ The instrument flying unit of competency was optional and not tested on any of the checks.
The pilot had completed the following ground school courses with Microflite:
Microflite fatigue management policy questionnaire – 4 December 2019
Controlled flight into terrain / Approach and landing accident reduction – 23 December 2019
Wire and obstacle environment awareness – 10 July 2020
Drug and alcohol management plan awareness – 12 August 2020
Human factors training for helicopter flight crew – 5 September 2020
Dangerous goods by air – 7 January 2022
Pilot maintenance approval – 23 February 2022.
Flight and duty period limits
According to the Microflite operations manual, the company operated to Civil Aviation Order 48.1 Instrument 2019 (Appendix 4) for their air transport operations, which provided prescriptive flight and duty period limits. A review of the pilot’s flight and duty periods from 1 March 2022 up to, and inclusive of 30 March 2022, found the pilot recorded 169.2 hours of duty with 47.8 flight hours and had 11 rostered days off. In the previous 90 and 365 days, the pilot accumulated 108.5 and 274.5 flight hours respectively. On 30 March 2022, the day prior to the accident, the pilot was on duty from 1030 to 1825 (7.9 hours) and recorded 2.2 flight hours. On the day of the accident, the pilot’s duty started at 0630. There was no evidence to indicate that the pilot had exceeded any of the flight or duty period limits set in appendix 4.
Pilot of VH-WVV
The pilot of VH-WVV (WVV) was issued with a CPL(H) in 2016 and held a low-level rating. At the time of the accident, the pilot had reportedly accumulated about 2,500 hours, which included about 1,500 hours on the EC130, EC120 and AS350 single-engine turbine helicopters. The pilot joined Microflite as a day VFR line pilot in 2019 with about 3 years prior experience of charter operations in Victoria and Queensland and had no instrument or night flying experience. The pilot of WVV reportedly paired with the pilot of XWD about 10 times in the previous 2 years, noting that tasks for 2 helicopters were the exception and single helicopter taskings were the norm.
The chief pilot noted that while the pilot of XWD had slightly more flying hours experience and qualifications than the pilot of WVV, the pilot of WVV started with Microflite before the pilot of XWD. Therefore, the chief pilot considered the 2 pilots to be of equivalent experience for the task and there was no operator appointed hierarchy or ‘lead’.
Helicopter information
General information
The accident helicopter was an Airbus Helicopters EC130 T2 manufactured in France in 2017 and equipped with a Safran Helicopter Engines Arriel 2D turboshaft engine, 3-bladed main rotor and Fenestron[17] tail rotor (Figure 6). The helicopter was registered VH-XWD in Australia in August 2019 in the night VFR operational category. At the time of the accident, XWD was owned by and registered to Asian Pacific Building Corporation Pty Ltd and operated by Microflite under a cross‑hire agreement. The helicopter was in a 7-seat configuration, with 3 seats in the front row and 4 seats in the rear row. Dual flight controls were fitted. The flight controls operated in the conventional sense with hydraulic assistance. No stability augmentation system or autopilot was fitted (refer to section titled The stabilisation problem).
The supporting Manual of Standards for the Civil Aviation Safety Regulations (CASR) Part 133 Air transport operations-rotorcraft stipulated that rotorcraft operating under VFR by day were required to be fitted with the following flight instruments: indicated airspeed, pressure altitude, magnetic heading, time, slip, and outside air temperature. Additional instruments such as attitude and standby attitude (artificial horizon (AH)) were required for night VFR and IFR operations. XWD was approved for night VFR operations.
The instrument panel had a conventional layout with analog flight instruments on the left, a vehicle and engine multi-function display (VEMD) in the middle, and a standby AH on the right. The pilot’s seat was on the left side and the centre console was fitted with a Garmin GTN 750 touch-screen global positioning system, which was used for navigation and communications.
The AHs were electrically powered. The main AH was powered on when the battery was turned on, but the red off flag would not clear until generator power (28 V) was supplied. After power on, the pilot was required to erect the gyro with a cage knob to align it with local gravity. The standby AH had a push-button switch located on the centre console to provide power. The red off flag would not clear unless it was powered on, at which stage the pilot could erect the gyro as per the main AH.
Setting each of the AHs after start for flight was not specifically stated in the checklist. There was a step for: ‘all necessary instruments…on – tested’ after engine start. Therefore, which instruments were set for flight would depend on the specific helicopter configuration, regulatory requirements, and pilot’s requirements for the planned role.
Weight and balance
The helicopter weight and balance were calculated for the accident flight at the time of take-off and at the top of the final descent, and it was determined to be within the published limits. Therefore, helicopter performance was not considered to be a factor in this accident.
Following a request from the ATSB to analyse the development of the nose low attitude in the final turn, Airbus Helicopters conducted an aerodynamic analysis of the helicopter’s response to lateral cyclic input for a 60° angle of bank turn to the left, and provided the following comments:
With respect to control positions in level flight (0° bank angle), in order to maintain a trimmed attitude in a coordinated turn at 60° left bank angle in the same conditions, the pilot has to apply significantly more collective[18] pitch and push the longitudinal cyclic[19] stick slightly further forwards.
Response to a lateral cyclic input:
Starting from the above conditions but with a "conventional" pitch attitude (-6° nose down), we consider a single lateral cyclic input to the left (with no other action on controls) such as to bring the helicopter to a 60° bank angle to the left. In these conditions we can expect that:
• Bank angle will increase.
• The descent rate will increase: indeed, if the collective pitch is not adjusted, the vertical component of the rotor lift will diminish with the bank angle whereas the force of gravity will remain the same.
• Given the general instability of the helicopter, it is difficult to predict with either certainty or accuracy whether or not the aircraft will pitch down.
• What we can say, is that a change of pitching attitude will affect the inclination of the rotor disk and the longitudinal component of the rotor lift and cause the helicopter to accelerate or decelerate. In other words, with no other actions on the controls (on collective control in particular), if the helicopter pitches down, we can expect the helicopter to accelerate. If the helicopter pitches up, we can expect the helicopter to decelerate.
Emergency locator transmitter
The emergency locator transmitter (ELT) was a KANNAD 406 INTEGRA transmitter, factory fitted to a mounting bracket in the rear baggage bay, left side, aligned with the normal axis. It is set in the ARM position for flight so that the G-switch[20] will provide impact-activation. The G-switch orientation is 45° below the longitudinal axis, so that it will detect a component of longitudinal and normal accelerations. After the G-switch is activated, the ELT will conduct a self-test before the first transmission is made about 65 seconds after activation. If the ELT or its antennae connection are destroyed within the initial 65 second period, no signal will be transmitted. According to Airbus Helicopters, the shock accelerations qualification defined in the regulations (for ELT) are consistent with a survivable impact and typically different than cockpit voice and flight data recorder equipment, which is by design more robust to an impact. There was no ELT activation detected.
Engine overspeed protection
According to Safran Helicopter Engines, a power turbine overspeed[21] may occur if the engine is delivering power and there is a rupture in the power transmission chain at the reduction gearbox, or transmission shaft, or the engine to main gearbox driveshaft. To avoid a power turbine disc bursting from an overspeed condition, the engine incorporates a power turbine blade-shedding system. This is set by the design of the power turbine blades to occur below the disc burst speed with a safety margin. The engine is designed to contain the energy from blade-shedding, but not a disc burst. It is also a certification requirement for aircraft engines to prevent disc burst.
Safran published a service bulletin (SB 292 73 2210), applicable from January 2019, on the subject: Electronic Engine Control Unit (EECU). Modification of software (V603). Application of modification TU 210. The SB applied to the Arriel 2D engine and included the following warning:
Failure to apply this service bulletin can lead to an uncommanded in-flight engine shut-down which, on a single-engine helicopter, can lead to an emergency autorotation landing.
The purpose of modification TU 210 was to modify the engine control software to:
improve detection of a slow decrease in performance of the fuel low pressure pump
signal a sudden interruption of the fuel supply at engine inlet
limit damage associated with a power turbine overspeed.
According to the SB, if the engine speed exceeded 120%, the engine control system would send an activation command to the engine stop electro-valve. This would allow engine shut‑down provided the associated Airbus Helicopters hardware SB modification had been incorporated.
On 22 August 2019, the European Union Aviation Safety Agency issued safety information bulletin (SIB) 2019-10 on the subject: Power turbine over-speed protection on Arriel 2D engines. The SIB explained that the extra thermal energy released from the engine during blade-shedding was a potential source of ignition for a post-impact fire. While the ignition source for post-impact fires was not always determined, the introduction of an electronic overspeed protection (TU 210) aimed to limit blade-shedding and reduce the potential for post-impact fire.
At the time of the release of the SIB, the concern was not considered to warrant airworthiness directive action.[22] However, the SIB recommended operators incorporate the engine and helicopter modifications into their affected helicopters.
A review of the maintenance records for XWD revealed the EECU was manufactured, and software downloaded in May 2016. The EECU was installed in August 2016 and the records indicated there had been no modifications incorporated since manufacture. On review, Safran confirmed the TU 210 modification was not embodied in the accident EECU.
The operator reported that they had complied with the relevant SBs from Safran and Airbus Helicopters. The operator’s helicopters with a build date prior to 2019 received the EECU software update in May 2019 when a Safran technician attended their facility (the hardware and training required to comply with the SB was not available in Australia prior to the date of the accident). XWD was assembled in September 2019 and therefore not available for that modification at the time of the Safran visit but was scheduled for a later update within the compliance period for the Safran and Airbus SBs. Their helicopters with a build date from 2021 received the update in the factory.
Wreckage and impact information
Accident site
The ATSB’s site survey established that XWD had impacted a large old growth tree, which broke the upper tree trunk and significantly disrupted the cabin. Cabin debris, including the overhead panel with the rotor-brake handle, was littered around the base of this tree. The helicopter then descended at an angle of about 45° on a southerly trajectory to the ground. Figure 7 and Figure 8 depict the old growth tree break from overhead the main wreckage site.
Figure 7: Overhead view of old growth tree break and main wreckage site
Source: ATSB
Figure 8: View to the north of old growth tree break from overhead the main wreckage site
Source: ATSB
The vegetation surrounding the accident site comprised of 2 distinct levels of growth. A new growth canopy with a height of about 24 m, and old growth trees with a height of about 70 m, as measured by a remotely piloted aircraft system. The elevation of the base of the old growth tree was 718 m, which indicated that the elevation of the top of the tree was about 788 m. The tree break was 41 m above ground level at an elevation of 759 m. Therefore, the tree impact very likely occurred at an altitude of 2,490–2,585 ft (759–788 m).
General crash survival requirements include maintaining a liveable volume, keeping occupants restrained and the impact loads within human tolerance, and providing the means and time to escape (Fox, 1989). Given the breakup of the cabin on impact with the old growth tree and associated height above ground level, this was not considered to be a survivable accident.
Wreckage examination
The helicopter was subject to a post-impact fire, resulting in the destruction of some components. However, from the components available there was no evidence of any pre-existing defect that would have prevented normal operation.
The engine had disconnected from both the main rotor and Fenestron driveshafts. The Fenestron driveshaft exhibited significant scoring damage, which indicated it was rotating at high speed during the accident sequence. Damage to the leading edges of the engine compressor blades was also characteristic of high-speed rotation (Figure 9) and the power turbine exhibited blade shedding. The rupture of the engine to main gearbox transmission drive shaft and flexible coupling,[23] with its screws sheared on the main gearbox side, was consistent with a sudden over‑torque. Overall, the damage observed indicated that the engine was producing power at the time of impact.
The centre console push-button switch for the standby AH was found in the off position (push‑button out). The other push-button switches on the same row as the standby AH were in the correct position for flight – off (out) for the fuel pump (the electric fuel pump is a booster pump for engine start and is switched off after start), off for the dome light, and on (in) for the avionics.
The ATSB retrieved the pilot’s electronic flight bag (iPad), an Appareo cabin-mounted camera, the vehicle and engine multi-function display (VEMD), a Garmin GTN 750 global positioning system, the EECU, and the central warning panel for further analysis. The engine data recorder was not able to be recovered due to fire damage.
Recorded information
The pilot’s iPad, Appareo camera and VEMD were successfully downloaded by the ATSB. The pilot’s iPad contained 1-second flightpath data and the Appareo memory included the positioning flight to the Batman Park HLS, the accident flight, and some footage of flights on the previous day. There were 2 audio channels on the Appareo for the intercom system and cabin area microphone. However, only the cabin area microphone successfully recorded.
A review of the available logs on the VEMD indicated there were no faults, failures or limits reached until the beginning of the impact sequence when a high rotor speed value of 410 rotor revolutions per minute was recorded, which was consistent with the Appareo download. The EECU and Garmin GTN750 global positioning system were not attempted to be downloaded due to significant fire damage and it was considered unlikely that they would have provided additional information. The central warning panel did not contain a memory module and did not provide any evidential data.
Medical and pathological information
A full post-mortem examination of the pilot was conducted. No soot was found in the airways and the cause of death was recorded as ‘Multiple injuries sustained in a helicopter incident (pilot)’. Further, the pilot’s toxicological results did not identify any substances that could have impaired their performance.
An external examination with computed tomography scan was performed on the passengers. The post-mortem reports for the passengers stated, ‘A reasonable cause of death would appear to be: Multiple injuries and effects of fire sustained in a helicopter incident (passenger)’. However, the forensic pathologist assisting the Victorian Coroner confirmed to the ATSB that the pilot’s cause of death, which did not include the effects of fire, was the most reliable indicator for all the occupants.
Meteorological information
Graphical area forecast
According to the Bureau of Meteorology, the graphical area forecast (GAF) is designed primarily to meet the needs of pilots flying in the airspace between the surface and 10,000 ft above mean sea level (AMSL). They provide information on weather, cloud, visibility, icing, turbulence, and freezing level in a graphical layout with supporting text.
The GAF for Victoria, current at the time of the departure from the Batman Park HLS, was issued at 0321 on the morning of 31 March 2022 and was valid from 0400-1000. The GAF divided the state into 4 areas, identified as A, B, C and D, with sub-divisions in areas A, B and C, separated by green scalloped lines (Figure 10). The flight was planned to start in area C2, transit area C1 (including Mount Disappointment), A1 and end in area A. The destination of Ulupna is located 8 NM (15 km) west of Tocumwal (YTOC in Figure 10).
Figure 10: GAF with direct track from Melbourne to Ulupna west of Tocumwal (YTOC)
Source: Bureau of Meteorology, annotated by ATSB
For the flight route, from departure to the planned destination, the GAF specifically stated that:
All of area C was forecast to have a broken layer of stratus cloud from 2,000-3,000 ft and a broken layer of cumulus/stratocumulus cloud from 3,000-8,000 ft with visibility greater than 10 km. In addition, area C included scattered showers of rain with cloud tops up to 10,000 ft.
Kilmore Gap, identified as a critical location on the GAF, was in area C1. The cloud forecast for Kilmore Gap was for a broken layer of cumulus/stratocumulus at 3,000 ft with TEMPO (temporary) conditions from 0600-1000 for a broken layer of stratus at 1,200 ft with the note ‘CLD ON GND’ [cloud on the ground].
Area A was forecast to have few cumulus/stratocumulus cloud from 3,000-5,000 ft.
The grid point wind and temperature forecast, valid from 0500, indicated the wind was 13 kt from 180° at 2,000 ft and 32 kt from 140° at 5,000 ft.
Melbourne Airport forecast
Melbourne Airport was north of the departure point and nearby the intended route (Figure 10). It has an elevation of 434 ft, and as an international airport, it provides a 24-hour aerodrome forecast. An aerodrome forecast is valid for a radius of 5 NM (9 km) from the aerodrome reference point. It includes cloud bases, visibility, weather, and surface wind. However, it does not include the height of cloud tops.
The forecast valid for the departure of the accident flight included wind from 180º at 10 kt, visibility greater than 10 km, light showers of rain, scattered cloud with a base of 1,500 ft above the aerodrome and broken cloud with a base of 2,500 ft. The forecast scattered cloud base of 1,500 ft above the aerodrome was 1,934 ft AMSL. This was consistent with the 2,000 ft cloud base on the GAF. The forecast for broken cloud at 2,500 ft above the aerodrome (2,934 ft AMSL) was consistent with the 3,000 ft cloud base on the GAF.
Kilmore Gap weather station and camera
The Bureau of Meteorology Kilmore Gap weather station and web camera was located 19 km west-north-west of the accident site (Figure 11). At 0750, 8 minutes prior to the accident, the camera depicted cloud overhead Mount Disappointment (Figure 12). Shortly after the accident, at 0800 and 0810, the camera showed extensive development of low cloud in the area (Figure 13 and Figure 14).
Figure 11: Kilmore Gap webcam view looking east on 3 May 2022
Source: Bureau of Meteorology, annotated by the ATSB
Figure 12: View towards Mount Disappointment at 0750 (8 minutes before the accident)
Source: Bureau of Meteorology, annotated by the ATSB
Figure 13: View towards Mount Disappointment at 0800 (2 minutes after the accident)
Source: Bureau of Meteorology, annotated by the ATSB
Figure 14: View towards Mount Disappointment at 0810 (12 minutes after the accident)
Source: Bureau of Meteorology, annotated by the ATSB
The weather station recorded a relative humidity of 93-95% from 0730-0830. From 0730 until 0741, the time the accident flight departed the Batman Park HLS, the lowest cloud at Kilmore Gap was 590 ft above ground level and the coverage was fluctuating between scattered and broken. At about 0758, the temperature and dewpoint were 9.7 °C and 8.9 °C respectively, and the wind was 17 kt from 171°. There was few cloud at 394 ft and broken cloud at 3,510 ft above ground level. At about 0811, 13 minutes after the accident, the cloud became broken at 394 ft and 3,510 ft. The cloud conditions continued to deteriorate through to 0830, at which time the cloud was broken at 295 ft.
Accessing weather forecasts
The National Aeronautical Information Processing System (NAIPS) is a multi-function, computerised, aeronautical information system that allows users, such as pilots, to obtain weather information and submit flight plans into the air traffic system. The pilots of XWD and WVV were using a NAIPS mobile app developed by OzRunways.[24] This app included a location briefing, area briefing and a chart selection icon. According to the app developer, only the first person to request a specific chart via the chart icon (such as the GAF) will be recorded by the NAIPS system as the requestor. The chart is then saved to cache memory on their server and all subsequent requests to view that chart via the app chart icon will result in retrieval of the chart from their server, rather than the NAIPS server. Therefore, while the submission of a location and/or area briefing request would be recorded on the NAIPS system, the selection of an area forecast via the chart icon would not necessarily be recorded on NAIPS.
Interpretation of the forecast
The pilot of WVV reported that the weather was a concern both the night before and in the morning. From the Melbourne Airport forecast, there was scattered cloud at 1,500 ft at 0700. As they were scheduled to depart 30 minutes after that, they were concerned that the weather was ‘already going to be established’ and they would not be able to get over the range. They elected to assess the actual conditions on their way to the Batman Park HLS.
The pilot further stated that the flight was planned as a VFR flight outside controlled airspace, which did not require a flight plan, and none was submitted. Consequently, they intended to remain below the controlled airspace steps that surrounded Melbourne Airport on their route from the HLS to Ulupna. The pilot of WVV also indicated that they were concerned about the cloud height above ground level at Kilmore Gap, where the terrain is at 1,200 ft AMSL. The forecast cloud at 1,500 ft indicated to the pilot that they would not be able to transit Kilmore Gap at their minimum height above ground of 500 ft.
Operational information
Visual meteorological conditions
Visual meteorological conditions (VMC) are expressed in terms of flight visibility and distance from cloud (horizontal and vertical) and are prescribed in the Civil Aviation Safety Regulations (CASR) Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 2.07 VMC criteria. In addition to visibility and distance from cloud, VMC may also be subject to operational requirements. There are a variety of criteria for the different altitudes and airspace that a VFR flight is operating in.
For aircraft operating below 10,000 ft in class G airspace (uncontrolled airspace), the VMC criteria were a minimum flight visibility of 5,000 m, horizontal distance from cloud of 1,500 m and vertical distance from cloud of 1,000 ft. For aircraft operating in class G airspace below 3,000 ft AMSL, or 1,000 ft above ground level, whichever is higher, the distance from cloud is reduced to ‘clear of cloud’, provided the aircraft is operated in sight of ground or water. For a helicopter operating below 700 ft above ground level, the visibility can be reduced to 800 m.
A VFR flight can be conducted above cloud provided VMC can be maintained for the entire flight, including climb, cruise, and descent.[25] The CASA Visual Flight Rules Guide included the following note for VFR flight above cloud:
Pilots should not initiate VFR flight on top of more than SCT [scattered] cloud when weather conditions are marginal. Before committing to operate VFR flight on top of more than SCT cloud, pilots should be confident that meteorological information used is reliable and current, and clearly indicates that the entire flight will be able to be conducted in VMC.
The accident flight was conducted in class G airspace and climbed to about 3,500 ft AMSL, which was above 1,000 ft above ground level, before reaching Mount Disappointment. Therefore, while the minimum visibility remained at 5,000 m, the distance from cloud increased from ‘clear of cloud’ while they were below 3,000 ft and in sight of the ground, to 1,000 ft vertical and 1,500 m horizontal distance as soon as they climbed above 3,000 ft. Figure 15 provides a visual depiction of the VMC criteria below 10,000 ft (excludes helicopter VMC below 700 ft) from the CASA Visual Flight Rules Guide.
According to CASR Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 7.02 Forecasts for flight planning, an authorised weather forecast must cover the whole period of the flight, and include a wind and temperature forecast and, for a flight at or below 10,000 ft AMSL, a GAF or general aviation meteorological[26] area forecast. In addition, CASR Part 133 Air transport operations-rotorcraft, subpart 133.130: Flight preparation requirements, stated:
A rotorcraft operator’s exposition[27] must include procedures for complying with the following for a flight of the rotorcraft:
(a) the flight preparation (weather assessments) requirements;
(b) the flight preparation (alternate aerodromes) requirements.
Microflite requirements
The Microflite operations manual section 2B1.1: Planning and briefing materials, detailed the pre‑flight requirements for a pilot in command, which included the following:
An appropriate route is selected, consistent with safety and ATC [air traffic control] requirements and available facilities; and having regard for weather, navigational accuracy and suitable en route emergency airfields.
If leaving the vicinity [local area] (30 minutes at cruise speed), the current weather reports and en-route, departure and destination forecasts issued by Airservices Australia are valid and satisfactory for the type of operation.
Section 2B1.7: Minimum safe altitudes / lowest safe altitude (LSALT), provided the following advice for their day VFR pilots:
For day VFR flights over unfamiliar or raised terrain pilots should make themselves aware of relevant LSALT. It is recommended that pilots be aware of and take into consideration LSALT.
Section 2C3.3 Diversions due weather, provided the following guidance for handling deteriorating weather in-flight:
A diversion due to weather (either enroute or from a destination) is a contingency which can occur on virtually any flight. If the weather conditions are known to be marginal, such diversions should be allowed for during planning. However the weather can deteriorate rapidly and unexpectedly, and unplanned diversions may become necessary. The primary consideration in such a situation is the safety of the aircraft and its occupants, and communications are an important aspect. When in controlled airspace, Pilots in Command are to request an amended clearance to enable clearance to be granted before diversion is necessary. When remaining OCTA [outside controlled airspace], Pilots in Command are to keep the ATS [air traffic service] and other traffic informed of their intentions.
Chief pilot’s expectation
The chief pilot reported that the pilots had a company issued iPad (electronic flight bag) that provided them with up‑to‑date access to the booking information on the company calendar. In addition, they were issued with a credit card, which could be used to purchase their flight planning apps subscriptions. The chief pilot provided the following explanation for the flight planning sequence:
Flight planning starts with the booking, which captures the planned departure, destination, number of passengers and weights. From this, the pilots can calculate their fuel load and weight and balance. Most pilots will look at the weather the day prior so that clients can be notified if there might be weather issues and provide them with the option to cancel or hold their booking. On the day of the service, they should check the various weather information available, including the GAF and any webcams en route, the briefing document(s) for the landing site(s) and contact the client if there are any concerns. The client contact details are in the work calendar, which will include a lead person their pilot can talk directly to about any issues, including if it is a no-go or delay to wait for changes.
If the company knows the weather is marginal the day prior to the service, then client services staff will call the clients, rather than the pilots, to see if they wish to change their booking. However, the pilots have full authority to proceed or delay the flight, they do not have to escalate the decision to delay to anyone else in the company. One of the passengers on board WVV during the accident flight was the lead client for the charter group and was a regular client for the company. The pilot of WVV was one of the client’s regular pilots.
The chief pilot acknowledged the client on board WVV was an important client, being a regular client, but that this should not have changed the conduct of the flight. The chief pilot also recognised that perceived pressure to deliver for a client was normal within the industry and it was not limited to charter, it could also occur in aerial work operations. However, from a company management perspective, they attempted to provide support for their pilots by not applying pressure to conduct a flight, using client services staff to liaise with clients, and organising alternate transport (road vehicles) for clients if a flight cannot proceed or a pilot decides their planned destination cannot be reached. The chief pilot had not flown with the client for the accident charter group, and therefore did not know the client as well as the pilot of WVV. From their own interactions with the client, they did not believe they would have pressured the pilots to proceed on the accident flight.
Accident pilot
The accident pilot accessed NAIPS on 30 March 2022 (the day prior to the accident flight) at 1506,[28] via the OzRunways app and requested meteorological and notice to airmen[29] information for Melbourne Airport. At this time, the pilot was at Warragul, from where a return flight was conducted to Moorabbin Airport via Lancefield and the Batman Park HLS. The request was limited to a location briefing for Melbourne Airport and did not include an area briefing (GAF) request. This was the only request recorded on NAIPS for the 24 hours prior to the accident.
The pilot did not submit any NAIPS location requests on 31 March 2022. Examination of the pilot’s iPad found that the OzRunways and WillyWeather[30] apps were running at the time of the accident. The pilot accessed the WillyWeather app at 0633 and it continued to run. The WillyWeather app support reported that they did not offer any features specific to aviation, but did offer most of the data required, such as cloud cover, wind, temperature, and predicted rainfall. When selecting a location, the app also provided a link to the nearest weather radar station feed.
In the week prior to the accident, the pilot submitted a location briefing request for Melbourne Airport at 2212:46 on 24 March 2022. The following day, the pilot conducted a passenger transport return flight in XWD between Moorabbin Airport and the Cathedral Lodge Golf Course, which is about 55 NM (102 km) north-east of Moorabbin and 32 NM (59 km) east-north-east of the accident site, on the north side of the ranges. The outbound flight was 0836-0910 and the return flight was 1612-1650. There was no record of a briefing request submitted either on the morning prior to departure, or in the afternoon prior to the return flight. However, as described earlier, it was possible the pilot viewed a GAF chart without it being recorded by the NAIPS system.
Pilot of VH-WVV
According to the pilot of WVV, the 2 pilots accessed the weather information independently on 30 and 31 March 2022, but then discussed it together. The pilot of WVV accessed NAIPS via OzRunways on 30 March 2022, the day before the accident, to submit a meteorological and notice to airmen request for the locations Moorabbin, Essendon, Melbourne, Avalon, and Coldstream. This occurred at 1103, 1111, 1118 and 1124, and they departed from Moorabbin Airport at about 1219 to collect their charter group from the Batman Park HLS. The same request was made at 1242 before departure from Batman Park, at 1506 before departure from Warragul, at 1602 and 1618 before departure from Lancefield, at 1751 before departure from Batman Park for the return flight to Moorabbin, and at 1950 after arrival.
On the morning of the accident, the pilot resubmitted the request for the locations Moorabbin, Essendon, Melbourne, Avalon, and Coldstream at 0545, 0559 and 0628. At interview, the pilot reported that they would have checked the GAF but not the grid-point wind and temperature chart, and demonstrated to the ATSB how they used their NAIPS app to check the current GAF.
The pilot stated that the Melbourne Airport forecast would be consulted the evening before a client services flight as it provided a 24-hour forecast, and therefore, provided an indicator of the potential conditions for the next day. Normally, the company operations staff would consult one of the pilots at about 1630 to check on the likelihood of weather cancellations the following day. If the weather looked unsuitable, then client services would contact the client and confirm if they wished to hold their booking, noting the risk that it could be cancelled, or arrange alternative transportation.
The pilot reported that the client on the day of the accident had never pressured them to conduct a flight in marginal weather and that there were numerous occasions when a service was cancelled due to weather. The pilot could not provide a specific example of a weather cancellation, but explained that, due to the elevation of Melbourne and the built-up area, they would cancel a client pick-up from the city [Batman Park HLS] if the cloud was forecast to be below 1,400 ft AMSL or there was reduced visibility, and that ‘it happens a lot’.
Former company pilot
The ATSB spoke to a former Microflite pilot during the investigation. This pilot provided similar information to that provided by the pilot of WVV and the company’s chief pilot. They reported that for flight planning, they would look at the Melbourne Airport forecast the night before to get an indication of the weather for the Melbourne Basin[31] the next day. The company operations staff might ask a pilot at the close of business if the weather was going to be acceptable the next day for client liaison purposes. For operations around the basin, the pilot would use the location forecasts and weather radar, but if they planned to fly over the ranges, then they would ‘get everything’ including location forecasts either side of the ranges, the GAF, grid point wind and temperature chart, and check the web cameras.
The pilot reported that, if conditions were marginal or even instrument meteorological conditions (IMC),[32] then pilots might take-off if the weather at Mangalore was clear. There were several areas that they would go to assess the actual weather and if it was possible to pass through the ranges, which included Kilmore Gap to the north.
The pilot confirmed that the company would stand between their pilots and the clients if required, provided they were aware of marginal weather the evening prior to the service. They reported that the company has clients whose businesses could be negatively impacted if they missed a meeting due to a flight cancellation, which is why the operations staff proactively checked the risk of a weather cancellation. The pilot was able to recall an instance of rejecting a task due to weather while working for the operator.
Weather cancellations
The operator provided a copy of their flight cancellation records for the period 1 January 2021 to 31 March 2022. There were 895 cancellations recorded and they reported that 1,917 flights were conducted. This indicated that 32% of their planned flights were cancelled during this period. Of these flights, 331 (37%) were cancelled for COVID-related reasons. A total of 145 flights (119 charter flights) were cancelled due to weather-related reasons, which was about 16% of all cancellations and 5% of the planned flights. However, it was noted that 20% of the cancellations did not have a code, and therefore, it was possible that the actual percentage of weather-related cancellations was higher than recorded.
Organisational information
Microflite
The operator, Microflite Pty Ltd, trading as Microflite Helicopter Services, was founded in 2000 and purchased by the current owners in 2004, with company headquarters at Moorabbin Airport. The company structure included a Chief Executive Officer, Executive General Manager, Head of Flying Operations (chief pilot), Head of Operations (chief flying instructor) and Head of Aircraft Airworthiness and Maintenance Control. They conducted flight training, passenger transport (charter), special aerial work operations and commercial freight operations with their fleet of 18 single and twin-engine turbine helicopters. Their operations included day and night VFR (including aided night VFR with night vision imaging system), and IFR. They were also an approved maintenance organisation.
Safety risk management
Microflite was re-issued with their Air Operator’s Certificate, that included charter operations, on 25 May 2020 with an expiry date of 31 May 2022. With the transition from Civil Aviation Regulations to the Civil Aviation Safety Regulations (CASR), helicopter charter operations became CASR Part 133–Australian air transport operations–rotorcraft, on 2 December 2021. While the Part 133 regulations did not require an operator to have a safety management system at the time of the accident, the Microflite manual suite included an Integrated Management System Manual, which contained the elements of safety and quality management. This included a section on risk management with the following introduction:
Identified hazards should be recorded objectively in the company Risk register in the SERA [safety event reporting and analysis] system.
Some risks are acceptable, some can be eliminated, and others can be reduced to the point where they are acceptable.
For each identified and reported hazard, a representative of the Quality and Safety Team, in conjunction with suitably qualified and experienced other personnel where necessary, will assess the likelihood and potential consequences to calculate a risk.
Risk management of adverse weather
On 1 September 2015, Microflite raised a risk assessment for air transport operations - Risks associated with general charter operations from Company known and frequently used locations. The risk assessment included the following weather threat:
Weather - poor weather conditions including low cloud (cloud base below 1000' AGL), fog, thunderstorms, hail, or strong winds (over 50 kts) may compromise safety of operations. Risks include hail damage to aircraft, loss of VMC, strong wind shear, which may lead to loss of airframe.
The initial risk assessment, without controls, was assessed as ‘high’ risk. According to their manual, this level of risk was unacceptable and required a treatment plan to reduce it to at least a tolerable level (medium risk). It was treated with the following controls:
In the event that actual or forecast weather conditions fall below company set minima, all operations are to be cancelled. If this occurs with aircraft away from base, the aircraft will be grounded and alternative ground based transport will be arranged by Operations team. All Microflite aircraft have dedicated iPads with the NAIPS app loaded so that pilots have access to current weather and flight information and can make informed decisions.
The controls were assessed as ‘effective’ and ‘fully implemented’, which reduced the likelihood of the risk to ‘rare’, thereby lowering the risk from ‘high’ to ‘low’. The result was an acceptable level of risk that required no further action from the management team. The consequence for this risk was ‘catastrophic’, which was consistent with a loss of VMC accident for a VFR pilot. However, the definition for ‘unlikely’ (one level above ‘rare’) included that it ‘has happened before in the industry’. Use of ‘unlikely’ would have elevated the risk from ‘low’ to ‘medium’ but would not have required any further action as the risk was assessed as low as reasonably practicable.
The ATSB found that the operator’s pilots were issued with iPads and each had a budget to purchase the flight planning app of their choice. In addition, the ATSB received evidence that flights were routinely cancelled due to weather and an instance when their helicopters could not proceed due to weather, landed out-field, and ground transport was arranged for their clients. This was consistent with their documented risk controls.
Their risk of ‘loss of VMC’ was managed by cancelling operations. While the controls did not refer to how this would be managed in-flight, the company had published several procedures in their manual suite relevant to this risk. They included controls that could mitigate the risk of ‘loss of VMC’ through prevention and recovery, such as section 2B1.7 Minimum Safe Altitudes / Lowest Safe Altitude (LSALT), section 2C3.3 Diversions due weather, and in their training and checking manual Inadvertent Entry into IMC Recovery Training:
Inadvertent Entry into IMC recovery training is conducted in Microflite’s FSTD (Flight Simulator training Device), and is recommended (but not required) training for all company pilots. Training is to be recorded in the pilots personnel file.
The accident pilot and pilot of WVV had not conducted the Inadvertent Entry into IMC Recovery Training. In addition, the lowest safe altitude instructions for day VFR flights were published as a ‘should’ rather than a ‘shall’, indicating that it was not mandatory.
The Microflite operations manual volume 2C5: Adverse weather operations, did not include any reduced VMC operating procedures or inadvertent IMC recovery procedures. The company did have a procedure for inadvertent IMC under volume 2D1.18: Formation flying. The goal of this procedure was to ensure safe separation of the formation aircraft after an inadvertent IMC entry and was therefore not applicable as a risk control for their day VFR charter pilots.
Assessing pre-flight risk
The risk assessment performed at an operator’s management level is by design a high-level assessment that does not necessarily capture the circumstances for each particular flight. In a multi-crew airline environment, there are multiple checks in the system and the junior flight crewmembers will spend years learning decision-making from senior flight crewmembers before they progress to the role of pilot in command. This system of learning and oversight is generally not available in the single-pilot sector by the nature of the task. Consequently, there has been a growing adoption of easy-to-use pre-flight risk assessment tools, which can help inform pilots of the cumulative level of risk to their operation at the planning stage and can be employed in the commercial sector to escalate decision-making to management for oversight. In 2014, this was introduced by the United States Federal Aviation Administration (FAA) into their helicopter air ambulance regulations under Code of Federal Regulations 135.617: Pre-flight risk assessment. Later, in 2016, the FAA Safety Team released their flight risk assessment tool, based on scoring predefined criteria, with the introduction:
Because every flight has some level of risk, it is critical that pilots are able to differentiate, in advance, between a low risk flight and a high risk flight, and then establish a review process and develop risk mitigation strategies. A FRAT [flight risk assessment tool] enables proactive hazard identification, is easy to use, and can visually depict risk. It is an invaluable tool in helping pilots make better go/no-go decisions and should be a part of every flight.
Civil Aviation Safety Authority requirements
The ATSB reviewed the CASR Part 133 and the corresponding Manual of Standards to determine the regulatory expectation on operators for managing the risk of VFR into IMC and any subsequent loss of control or controlled flight into terrain. While the ATSB was unable to identify any CASR Part 133 specific requirements for managing the risk of VFR into IMC that were additional to what would already be expected for all pilots under CASR Part 91, including private/pleasure flights, it was noted that CASA can stipulate additional conditions to manage specific risks through the safety regulations and standards. For example:
CASR Part 133 required operators to include risk assessments in their expositions, for CASA approval, for any planned performance class 2 with exposure operation (a Category A rotorcraft flight where failure of an engine or system does not permit continued safe flight and does not ensure a forced landing into a suitable forced landing area).
To reduce the risk of controlled flight into terrain, larger rotorcraft being operated on passenger or medical transport flights under IFR were required to be fitted with a terrain awareness and warning system.
CASR Part 135 (air transport operations – smaller aeroplanes) operators were required to include procedures for low-visibility operations and stabilised approach criteria in their exposition to mitigate the risk of approach and landing accidents.
Civil Aviation Safety Authority oversight
In 2023, the ATSB requested a copy of the last 5 CASA surveillance activities of Microflite, which included a:
September 2022 surveillance report for passenger and cargo air transport operations in single‑engine helicopters
29-30 March 2022 surveillance report for flight training operations
November 2018 surveillance report for passenger handling at the Batman Park HLS
March 2018 surveillance report for low flying operations
2017 investigation report for an alleged breach of low flying at a sport event.
There were no reports of ramp checks provided, which would have captured flight planning activities.
The November 2018 surveillance of passenger handling started as an unannounced event and the CASA inspector reported that all flying was initially cancelled due to the weather in the morning. When flying commenced, the inspector noted the operator maintained positive control of the passengers and positive separation between the helicopters. There was only one safety finding from the 4 surveillance reports, which was for training records. The September 2022 surveillance activity was a follow-up to this accident to determine if any changes had been made. The inspector recorded that the operator reported an increased focus on instrument flying during training and proficiency checks, and the implementation of a flight risk assessment tool.
Basic instrument flying standards
Microflite pilot proficiency checks
Proficiency checks are intended to assess a pilot’s flying skills and operational knowledge in carrying out normal, abnormal, and emergency procedures. This ensures the pilot is competent to conduct the flights the operator has assigned that pilot. According to the chief pilot, the accident pilot’s initial check to line as a charter pilot would have covered general handling, and emergency procedures for flying around Melbourne, Yarra Valley, and coastal scenic routes. The chief pilot reported that instrument flying would only be conducted during proficiency checks for night and instrument rated pilots, and that for their day VFR pilots, the flight review could be completed without an instrument flying component.
According to the pilot of WVV, the operator’s proficiency checks included a ground theory component, and they were required to obtain a detailed weather briefing, including location forecasts, GAF and grid-point wind and temperature forecasts. They were then checked to ensure they understood all the information they were presented with. The pilot of WVV and a former Microflite pilot both reported that they were never trained or checked for instrument flying because it was not a requirement.
The chief pilot reported that when the accident pilot’s aerial application rating for fire-fighting training was done in October 2021, they would have conducted training in the hills around Melbourne. This would have included dealing with mountain flying in adverse weather conditions. The chief pilot could not confirm if any specific exit manoeuvres for adverse weather were included and reported that they had discussions about the subject previously within the company but could not provide a specific procedure for all situations that might be encountered. They did not believe there was any ‘one-size-fits-all’ rule being taught by their instructor staff and that it was a matter of their pilots adapting to the circumstances and ensuring they always have an exit route.
International Civil Aviation Organization
The International Civil Aviation Organization’s (ICAO) Annex 1: Personnel Licensing foreword stated:
Annex 1 contains Standards and Recommended Practices adopted by the International Civil Aviation Organization as the minimum standards for personnel licensing.
Section 2.4 described the general requirements for the issue of a commercial pilot licence. Under the specific requirements for the helicopter category, section 2.4.4.1.1.1 (c) stated the applicant shall have completed, in helicopters, not less than 10 hours of instrument instruction time of which not more than 5 hours may be instrument ground time. Section 2.4.4.2 stated the instructor shall ensure that the applicant has operational experience in at least the following areas to the level of performance required for the commercial pilot: (i) basic flight manoeuvres and recovery from unusual attitudes by reference solely to basic flight instruments.
ICAO Annex 6 Part III – International Operations – Helicopters (July 2016), section 7.4.3 Pilot proficiency checks stated:
The operator shall ensure that piloting technique and the ability to execute emergency procedures is checked in such a way as to demonstrate the pilot’s competence on each type or variant of a type of helicopter. Such checks shall be performed twice within any period of one year.
Civil Aviation Safety Authority
Integrated and non-integrated training programs
There were two types of commercial pilot licence training courses:
intensive integrated courses, through Part 142 flight training operators
non-integrated courses, through Part 141 flight training operators.
The Integrated training meant an intensive course of training:
(a) that is designed to ensure that a course participant receives ground theory training integrated with practical flight training; and
(b) for which:
(i) the ground theory training and practical flight training are conducted by the same operator; or
(ii) the operator that conducts the practical flight training engages another person or organisation to conduct the ground theory training on behalf of the operator; and
(c) that is conducted according to a syllabus that satisfies the knowledge and flight standards specified in the Part 61 Manual of Standards for the grant of a private or commercial pilot licence; and
(d) that is designed to be completed within a condensed period of time.
According to CASR Part 61(Flight crew licensing), instrument flying training is a requirement for a CPL(H) under an integrated training program. The aeronautical experience required under Part 61.595 (Aeronautical experience requirements for grant of commercial pilot licences—helicopter category) was 10 hours instrument time with a minimum of 5 hours instrument flight time in a helicopter. The instrument flight time included full panel (IFF)[33] and limited panel (IFL).[34] Both IFF and IFL included basic instrument flight manoeuvres and recovery from unusual attitudes and inadvertent IMC (IIMC). However, under a non‑integrated training program for a CPL(H), there was no instrument flying training required. Both IFF and IFL were required for an aeroplane CPL. In addition to recovering from unusual attitudes and IIMC, on 21 November 2023, in response to the draft report, CASA reported:
Instrument flying training for day VFR pilots is to give the pilot exposure to the difficulty associated with low flight experience instrument pilot skills requirements, the frailty of human systems in DVE [degraded visual environment], the errors associated with flight instruments and to achieve a flight crew licencing competency requirement. It is also notably to encourage the pilot to develop strategies not to enter IIMC.
The pilot’s CPL(H) flight test report recorded the IFF and IFL units of competency as ‘not tested’ and CASA confirmed the flight test form indicated it was a non‑integrated training program. The pilot of WVV stated that they did not do any instrument flying training as it was not required for their licence. Another former Microflite pilot also reported that they did not do any instrument flying training, but that they were advised to complete the instrument rating theory examination after completing their CPL(H) training in case they ever had ambition to work in the offshore helicopter industry. That pilot completed their theory examination but no instrument flying.
The Part 61 Manual of Standards single-engine helicopter flight review competency standards indicated instrument flying was ‘optional’. In comparison, the flight review competency standards for single and multi-engine aeroplane, and multi-engine helicopter, all required basic instrument flying sequences. However, under CASR Part 133 Air transport operations-rotorcraft, subpart 133.370: Composition, number, qualifications and training, it stated the following:
(e) if the flight is a VFR flight at night that is a passenger transport operation or a medical transport operation—at least one of the flight crew members must hold an instrument rating;
In addition, according to CASR Part 133.370(4), the Part 133 standards may prescribe requirements related to training and checking that must be completed by a flight crew member for a flight. However, the Part 133 standards Chapter 12 – Flight crew member training and checking, did not require an operator’s proficiency check of a day VFR pilot to include any instrument flight or IIMC recovery exercises.
History of the integrated and non-integrated syllabi
With the commencement of CASR Part 61 – Flight Crew Licensing in 2014, CASA introduced a requirement for applicants of a CPL with a helicopter category rating, to complete flight training and basic instrument flight, to comply with the standards specified by ICAO Annex 1: Personnel licensing.
To give industry time to develop the capability to conduct such training, transitional regulation CASR 202.277B provided relief from the new requirements by continuing to recognise the previous requirements for the grant of a CPL(H) as specified under Civil Aviation Regulation 5.127. This did not require instrument flying training until 31 August 2017. A subsequent amendment to the CASR in 2017 extended the time for transition until the end of August 2018. The accident pilot’s training was completed prior to the end of this transition period.
Prior to the end of the transitional period, CASA undertook a review of the instrument flight time experience requirements, which resulted in an amendment to CASR Part 61 in 2018. The amendment to CASR 61.615 continued the previous requirements specified for the grant of a CPL(H). An explanation of that amendment was included in the Explanatory Statement associated with that amendment: Civil Aviation Safety Amendment (Flight Crew Licensing Measures No. 1) Regulations 2018 (legislation.gov.au)
The review undertaken by CASA included a survey of the helicopter industry. The Explanatory Statement rationale for making the instrument flight time experience requirements optional for a non-integrated training course was in response to the survey results and as follows:
The measure responds to concerns raised by the helicopter flight training sector about the availability of suitably equipped flight training aircraft, and flight instructors capable of conducting basic instrument flying training. This measures also addresses safety concerns raised about newly qualified pilots being tempted to fly in marginal conditions in aircraft that lack basic flight instruments. A CPL(H) granted on this basis would not comply with the standards and recommended practices published by the International Civil Aviation Organization; however, this is not a significant matter for Australian pilots and safety is not compromised.[36]
ATSB review of CASA industry survey
The ATSB requested a copy of the 2018 helicopter industry survey responses and noted that 87% (55/63) of respondents opposed basic instrument flying training when asked about the introduction of this for ICAO compliance purposes. The reasons provided included the rationales listed in the following Table 1.
Table 1: Rationales for opposing basic instrument flying training
Rationale
No. of respondents
Percentage of total
No requirement/not relevant
20
32%
Inadequate flight instruments
16
25%
No safety benefit
11
18%
Could lead to overconfidence
10
16%
Unnecessary financial burden on flight schools
10
16%
Better to teach avoidance
7
11%
Perishable skill
7
11%
Won’t make the licence transferable
7
11%
Excessive flying hours required for the training
4
6%
Instructional staff not qualified
3
5%
Several respondents indicated that they did not believe CASA had made a safety case for the introduction of this requirement. Some supporters and opponents indicated that 2-3 hours of flying training to teach recovery from unusual attitudes should be sufficient. One opponent indicated that if the requirement was to teach recovery from unusual attitudes on instruments, instead of compliance with ICAO licencing requirements, they might have supported the proposal. One supporter of the requirement indicated that as the rules allow helicopter flight in visibility reduced to 800 m, some basic instrument flying skills are required.
In consideration of the industry objections published by CASA in their Explanatory Statement:
The ATSB reviewed a manufacturer’s website for one of the most popular piston-engine training helicopters and noted they were offered for sale without an attitude indicator in their most basic configuration. This was consistent with 25% of respondents reporting that a lot of training helicopters in use at the flying schools were not fitted with the minimum instruments required to teach instrument flying.
While 5% of respondents indicated there were insufficient instructional staff qualified to teach instrument flying, a 4-year transition period was provided to upgrade instructional staff.
Throughout the course of this investigation, the ATSB found no research to demonstrate a link between basic instrument flying training and overconfidence resulting in VFR into IMC accidents.
Foreign jurisdictions
United States
The US Code of Federal Regulations, Part 61.129 prescribed the aeronautical experience required for a CPL. The instrument flying required for the helicopter rating under Part 61.129 (c)(3)(i) stated:
Five hours on the control and maneuvering of a helicopter solely by reference to instruments using a view-limiting device including attitude instrument flying, partial panel skills, recovery from unusual flight attitudes, and intercepting and tracking navigational systems. This aeronautical experience may be performed in an aircraft, full flight simulator, flight training device, or an aviation training device.
Commercial helicopter pilots, employed for commuter and on demand operations (CASR Part 133 equivalent), operate under Part 135. Subpart 135.293 initial and recurrent pilot testing requirements stated:
Each competency check given in a rotorcraft must include a demonstration of the pilot's ability to maneuver the rotorcraft solely by reference to instruments. The check must determine the pilot's ability to safely maneuver the rotorcraft into visual meteorological conditions following an inadvertent encounter with instrument meteorological conditions. For competency checks in non-IFR [instrument flight rules]-certified rotorcraft, the pilot must perform such maneuvers as are appropriate to the rotorcraft's installed equipment, the certificate holder's operations specifications, and the operating environment.
European Union and United Kingdom Civil Aviation Authority
The European Union Aviation Safety Agency and United Kingdom Civil Aviation Authority content for their skill test for the issue of a CPL(H) included instrument flying training. Their recurrent training and checking syllabus for operator proficiency checks in accordance with the Organisational Requirements for Air Operations – Flight Crew – ORO.FC.230 (b) Operator proficiency check, included ‘(1) Each flight crew member shall complete operator proficiency checks as part of the normal crew complement to demonstrate competence in carrying out normal, abnormal and emergency procedures.’ Their acceptable means of compliance (AMC1 ORO.FC.230) included (1) recovery from unusual attitudes, and (2) IMC autorotation[37] techniques.
Canada
The Transport Canada aviation regulations flight test requirements for issuing a CPL(H) (Schedule 6 of Standard 428) included instrument flying in the airwork section of the syllabus and minimum safe altitude operations in the navigation section. In addition, air taxi (Standard 723.28) and commuter (Standard 724.24) (CASR Part 133 equivalent) helicopter pilots who operated to the reduced VFR visibility limits in uncontrolled airspace were to receive initial and annual recurrent flight training in reduced visibility procedures specified in the company operations manual. The manual was to contain low visibility operational procedures and pilot decision-making considerations, which included weather and the potential for white-out. However, Transport Canada had not introduced basic instrument flight sequences into their flight review requirements.
Research into VFR into IMC accidents
Introduction
Accidents from VFR into IMC are normally the result of either controlled flight into terrain or loss of control. Loss of control events can be the result of spatial disorientation, which is the inability of a pilot to correctly interpret aircraft attitude, altitude, or airspeed in relation to the Earth or other points of reference. This can lead to a pilot making incorrect control inputs or responding incorrectly to attitude changes. If flight path information is available it may be possible to conclude whether the aircraft was on a controlled or erratic path prior to the accident, indicating either controlled flight into terrain or loss of control occurred, respectively. However, flight data information is generally required to determine if an aircraft attitude change either preceded or followed pilot input in a loss of control event.
United States Helicopter Safety Team
In 2021, the US Helicopter Safety Team published a study that examined 221 fatal helicopter accidents that occurred between 2009 and 2019 in the US. An analysis of these events found that unintentional IMC events were one of the top causes of fatal accidents. Notably, they determined that a helicopter pilot operating under VFR who unintentionally continued flight into IMC would very likely lose control and collide with terrain within an average of 56 seconds. They have also released a video showing how rapidly a pilot could lose control when attempting to continue visual flight into IMC. They have also developed a ‘56 Seconds to Live Course’, which provides pilots with scenario-based training designed to teach them to employ pre-flight risk assessments and en route weather minima decision points to reduce the chance of an inadvertent IMC accident.
Transportation Safety Board of Canada Aviation Safety Study 90-SP002
A 1990 Transportation Safety Board (TSB) of Canada safety study on VFR into adverse weather (report 90-SP002) was prompted by the disproportionately high number of fatalities each year from these accidents. Their study identified 352 accidents in Canada between 1976 and 1985, which accounted for 6% of the total number of recorded accidents, but 23% of all fatal accidents. While 12.7% of the total accidents in this period were fatal, VFR into IMC accounted for a significantly higher proportion of fatal accidents (50.2%). The TSB report noted that in uncontrolled airspace in Canada, reduced visibility of 1 statute mile (1,609 m) was allowed, which ‘implicitly assume that orientation by other than reference to a natural horizon may be required to maintain control during VFR flight’.
The report also explored VFR into IMC specifically for the category of commercial helicopter pilots. Of the 33 helicopter accidents, they found that 27 were the result of white-out conditions in which the pilots were unable to maintain visual reference to the ground. Only 1 of the pilots held an instrument rating, and of the remaining, only 2 had acquired some instrument flying experience, but this was less than 20 hours for each of them.
The report noted that, from July 1987, the commercial helicopter pilot licence required 20 hours of actual and simulated instrument flying training, but before this, no instrument flying training was required. Consequently, the accidents identified in the study involved pilots who were not required to have instrument training to have obtained their helicopter licence. Therefore, the lack of instrument flying experience among the general population of commercial helicopter pilots was ‘expected to lead to a continuation of weather-related accidents in whiteout conditions’. This was also evident in the comparison between Canadian and US pilots with the following finding:
Both Canadian and American pilots with instrument flying experience were less likely to be involved in VFR-into-IMC accidents; and U.S. commercially-licensed pilots (who generally possessed instrument ratings) were less apt to be involved in VFR-in-IMC accidents compared to their Canadian counterparts (who generally did not possess an instrument rating).[38]
In addition, at the time of the TSB (1990) report, there was no requirement for commercial helicopter pilots to conduct recurrent basic instrument flying training as a condition of their licence. Therefore, the TSB noted that recently licenced pilots ‘will find that their instrument flying skills will deteriorate if not practised.’ They concluded that an evaluation of basic instrument flying skills during a pilot’s annual proficiency check would ensure commercially-employed helicopter pilots demonstrated ‘proficiency in skills necessary for coping with the major cause of VFR helicopter accidents in adverse weather.’ Noting that the annual proficiency checks for commercially‑employed pilots focussed on aircraft handling skills and technical knowledge, the TSB made the following finding and recommendation:
Technical piloting skills were seldom found wanting in the accidents examined in this study, suggesting that the present method of evaluating pilots' skills do not address the root causes of most commercial VFR-into-IMC accidents. The study indicates that without some means of evaluating pilots' decision-making skills, professional inadequacies will go undetected until after an accident has occurred…Accordingly, the Board recommends that: The Department of Transport devise and implement a means of regularly evaluating the practical decision-making skills of commercially-employed pilots engaged in small air carrier operations.
They also recommended to the Canadian Department of Transportation that all commercially‑operated helicopters be equipped with appropriate instrumentation, specifically an attitude indicator, for the conduct of basic instrument flying.
United States National Transportation Safety Board SS-05/01
In 2005, the US National Transportation Safety Board published a safety study into the Risk factors associated with weather-related general aviation accidents, highlighting that:
…the goal of instrument flight training for VFR-only pilots is to enable them to maintain control of an aircraft while making a course reversal or diversion if they inadvertently enter clouds.
The study examined 72 general aviation accidents that occurred between August 2003 and April 2004 (report NTSB/SS-05/01). When an accident occurred, they contacted pilots of flights operating in the vicinity at the same time as the accident, which added 135 non-accident flights to their study for statistical comparison. One of their findings was that not having an instrument rating was associated with significantly higher accident risk. Specifically, ‘pilots who did not hold an instrument rating were found to be 4.8 times more likely than instrument-rated pilots to be involved in a weather-related accident.’
The stabilisation problem
Introduction
The prevalence of loss of control helicopter accidents in degraded visual environments (DVE) has resulted in several research studies into helicopter handling qualities and the associated pilot effort and performance in DVE. They include the US FAA (Hoh, 1990), the United Kingdom Civil Aviation Authority (2007) and Crognale & Krebs (2011), detailed below. A helicopter cannot be certified for instrument flight rules unless it complies with the airworthiness stability criteria for helicopter instrument flight, which is generally achieved with a stability augmentation system (artificial stabilisation). The success of these certification standards and the continued loss of control accidents in the light helicopter sector led to the US Helicopter Safety Team publishing a white paper on this issue (Oltheten & Trang, 2021). For the purposes of this section, the tasks requiring pilot attention are divided into control (managing the attitude), guidance (managing the flight path), and navigation (managing the route).
The effects of degraded visual cueing and divided attention on obstruction avoidance in rotorcraft
Hoh (1990) reported that a deterioration in the effective rotorcraft flying qualities[39] occurred in DVE. The pilot workload in such conditions was observed to be very high for aircraft control. This left the pilot with very little excess attentional capacity to maintain situational awareness.[40] The US Army experiments reported by Hoh (1990) found that the addition of artificial stabilisation improved flying qualities in DVE, which increased the pilot’s available capacity to maintain situational awareness.
Helicopter flight in degraded visual conditions
The United Kingdom Civil Aviation Authority (2007) reported that the inherent instability of many small and some medium helicopters can rapidly lead to excessive pilot workload when attempting to fly in DVE. Their performance study found that a key factor was the division of attention between the guidance and stabilisation [control] tasks, and there was a strong interdependency between handling qualities and visual cues. They also established that ‘attitude command‑attitude hold’ stabilisation systems were essential for safer operations in DVE. Their conclusions from simulator trials included the following:
The underlying argument on which the framework is based is that ACAH [attitude command-attitude hold] response types confer reduced workload through minimising the effort required for closed-loop stabilisation. In DVE conditions, this can free critical attention to enable the pilot to concentrate on the guidance aspect of flight management.
The Level 3 characteristics[41] of the Basic[42] type are likely to present a serious flight safety hazard in inadvertent DVE situations such as IIMC.
Test cases flown without instruments were intended to emulate the situation where instruments are referred to infrequently, or ignored altogether, and resulted in loss of control in the case of the Turn manoeuvre.
Performance of Helicopter Pilots During Inadvertent Flight Into Instrument Meteorological Conditions
Crognale & Krebs (2011) tested 20 commercial instrument rated helicopter pilots on a US FAA approved flight simulator running a program for a Bell 206 helicopter that they were all qualified to fly. Each participant conducted 5 runs at varying altitudes and speeds and their results depicted a distinct change in pilot control inputs when external visual references were lost, indicating an increase in pilot workload to maintain control of the helicopter. The only accident during the study was a controlled flight into terrain when one of the participants was given a simulated air traffic control radar vector towards a mountain.
Figure 16 depicts the raw data for bank angle (left panel) and lateral cyclic[43] control movements (right panel) for a participant with 7,600 hours experience on their first run. The arrows at the bottom of each panel in the figure indicate where the visibility was reduced to 1 mile and then zero to simulate entering cloud. The right panel depicts large changes in lateral cyclic control input when the visibility reduced to zero, with associated bank angle changes on the left panel.
Figure 16: Bank angle (left) and lateral cyclic movement (right)
Source: Crognale and Krebs (2011)
Loss‐of‐control in‐flight mitigation through installation of stability augmentation and autopilot systems in light helicopters
In 2021, Oltheten and Trang published their report for the US Helicopter Safety Team’s helicopter safety enhancement number 70, output number 3. The purpose of the report was to encourage the use of technologies to reduce the risk of fatal helicopter accidents.
The report specifically stated that helicopters are generally more susceptible to loss of control accidents than aeroplanes due to their inherent instability and lack of mechanical trim. The need for inherent stability and trim are not as essential when operating in VMC. However, as conditions deteriorate, this need becomes increasingly essential to assist pilots with maintaining positive control during a temporary loss of visual cues or if they become disorientated.
Therefore, many loss of control accidents could be avoided if all helicopters were designed to meet some of the instrument flight rules stability requirements. They noted that the systems used in the transport category[44] sector have proven their effectiveness and safety for flight in IMC over 30 years but most of them were too heavy or complex to integrate into light helicopters. However, emerging technologies reduce the weight, complexity, and cost of these systems, which are now available for the light helicopter industry. Therefore, their paper advocated for industry and the US FAA to encourage the development and installation of these systems in light helicopters.
Civil Aviation Safety Regulations Part 133
Under CASR Part 133 rotorcraft air transport, an automatic pilot or automatic stabilisation system was required for instrument flight rules or single pilot night VFR without external visual references. While the accident helicopter was not in the instrument flight rules category, Airbus Helicopters reported there was a stability augmentation and autopilot system available for the EC130 T2 helicopters, which provided attitude stabilisation, altitude hold and heading fly‑to and maintain capability.[45]
ATSB database review
Occurrence data
A review of the ATSB accident and incident (occurrence) database for the period 2008-2022 was conducted to identify helicopter VFR into IMC and engine failure or malfunction events. The category of ‘engine failure of malfunction’ was selected for comparison as managing engine failures is a licencing and flight review requirement for helicopter pilots. In contrast, recovery from VFR into IMC requires instrument flying skills that were not required under the previous Civil Aviation Regulation 5 and not required on the current non-integrated syllabus.
The results, provided in Table 2, were consistent with findings from other jurisdictions that helicopter accidents from VFR flight into adverse weather have a high proportion of fatalities. In this period, engine failures (13%) accounted for a greater proportion of the total helicopter accidents (all categories) compared with VFR into IMC (1.3%). However, there were nil fatal accidents for engine failure or malfunction. In contrast, most VFR into IMC accidents resulted in a fatal outcome (83%), accounting for 14% of all helicopter fatalities for this period. If VFR dark night collision with terrain accidents were included in the VFR into IMC category, together they would represent 3.2% of all helicopter accidents and 29% of all helicopter fatalities.
Another comparison (Table 3) was made between helicopter and aeroplane VFR into IMC accidents for the period 2008-2022. The comparison noted that the fatal outcome of a VFR into IMC accident was similar for both aircraft categories. However, of significance was that there was a notably lower percentage of VFR into IMC occurrences that resulted in an accident for aeroplanes, when compared with helicopters.
Table 3: VFR into IMC comparison between helicopters and aeroplanes
Aircraft category
Total occurrences
Accidents (N)
Accidents (%)
Fatalities (N)
Fatal accidents (N)
Fatal accidents (%)
Helicopter
12
6
50
13
5
83
Aeroplane
135
13
10
22
10
77
A Fisher’s exact test[46] was applied to the helicopter and aeroplane VFR into IMC occurrences for accident and non-accident outcomes. The association between the groups (helicopter and aeroplane) and their outcomes (accident and non-accident) was found to be statistically significant, which indicated the difference in the proportion of accident outcomes between these 2 groups was not due to chance.[47] The previously cited research indicated to the ATSB that the 2 main issues likely contributing to the difference between these groups, in their ability to recover from IIMC, were a lack of instrument flying training for helicopter pilots and the control difficulties associated with operating helicopters without stabilisation. As day VFR helicopters and aeroplanes are not required to be equipped with an artificial horizon, and they are not required to plan a lowest safe altitude, these were not identified as differences between the 2 groups.
Accident summaries
A more detailed breakdown of the 6 helicopter accidents is provided in Table 4.
* Although classified as a private flight, this was the transport of the helicopter owner by a pilot employee.
The pilot involved in AO-2009-077 survived the accident and stated that he did not consider using the flight instruments as a means of recovering from being in cloud as the pilot was a VFR pilot and did not feel adequately trained to use them. Following the accident, the New South Wales National Parks and Wildlife Service proposed introducing requirements for helicopters to be in the night VFR category, pilots to be night VFR rated, and for operators to demonstrate that they have provided guidance to pilots for ‘action to take if inadvertent instrument conditions are encountered’. However, at an industry forum held on 27 July 2010, ‘feedback was very negative and overwhelmingly indicated that this would not only be practically unachievable but would likely significantly decrease safety levels.’ Therefore, the proposal was not actively pursued.
Likewise, the pilot of AO-2010-076 survived the accident. The pilot reported that, after inadvertently entering IMC while attempting to turn away from the weather ‘he became spatially disoriented and attempted to level out and fly through the cloud with the aid of the helicopter’s flight instruments.’ The helicopter exited the base of the cloud with about 41° left wing-low and 4,300 ft/min rate of descent. The pilot had time to flare the helicopter and reduce airspeed before it collided with trees.
The pilot of AO-2011-085 overcontrolled the helicopter after inadvertent IMC, which resulted in loss of control and inflight break-up. The ATSB’s investigation report specifically noted that ‘...The pilot was not trained or qualified for instrument flight, nor was the helicopter equipped with the required instruments, such as an artificial horizon. In those circumstances the pilot probably became spatially disoriented, leading to inappropriate control inputs…’.
In AO-2015-131, there was no flight tracking data available immediately prior to the collision with terrain. Therefore, it could not be determined if it was a loss of control or a controlled flight into terrain event. However, the ATSB found that the pilot likely encountered reduced visibility conditions leading to loss of visual reference leading to the collision with terrain.
In AO-2022-017, the ATSB found that, having encountered forecast low cloud and reduced visibility conditions, the pilot landed the helicopter at an interim landing site. Later that day, the helicopter then departed into cloud and visibility conditions unsuitable for visual flight. During the flight, recorded data showed that the helicopter had commenced a rapid climb and shortly after, entered a left turn descent that exceeded 3,800 ft/min followed by a collision with terrain. It was highly likely the cloud and visibility conditions resulted in the pilot experiencing a loss of visual reference and probably becoming spatially disoriented.
Non-accident occurrences
The 6 non-accident occurrences were reviewed for how the pilots exited IMC. Two reported climbing above cloud and in one of those cases it was to the lowest safe altitude in accordance with the operator’s IIMC procedure. In three cases they reported a descent below the cloud, and in one of those cases the helicopter was VFR over the top of cloud and had to descend through the cloud layer that was overcast below them. The last occurrence received assistance from air traffic control but the reporter did not describe how the helicopter exited from IMC.
Geographical distribution
The geographical distribution of the accidents was consistent with the east coast ranges through Victoria and New South Wales. Orographic uplift cloud from a moist maritime airmass at these locations can produce cloud bases at or near ground level. The Appendix figures depict the geographical distribution of accidents and reported occurrences for helicopters and all aircraft types for the 15-year period 2008 to 2022.
Intervention strategies
Many recommendations have been made to reduce the risk of VFR into IMC accidents from various accident investigation, regulatory and industry bodies. This section presents 2 industry papers that capture a significant number of the recommendations, including the key historical themes for how to reduce the risk of an inadvertent IMC encounter and accident.
Helicopter pilots in inadvertent IMC situations
The International Helicopter Safety Team has published several fact sheets about IIMC that are available from the US Helicopter Safety Team website. Their fact sheet, Helicopter pilots in inadvertent IMC situations, acknowledges that these encounters are the ‘most demanding, disorienting, and dangerous conditions a pilot can experience’ and result in the highest percentage of fatal injuries from helicopter accidents. Therefore, the combined use of flight simulators and ground instruction to improve instrument flying skills and proficiency is emphasised. This provides an opportunity to apply policies and procedures, and practice IIMC recovery, noting that these skills are considered perishable.
The fact sheet explained the immediate actions required by pilots in IIMC stating that:
A pilot’s immediate actions after encountering inadvertent IMC will determine the outcome of the entire event. Pilots who possess a plan of action prior to encountering it are more likely to experience a successful outcome (staying alive) than those who are less trained and proficient in the recognition and recovery procedures.
If IIMC occurs, helicopter pilots can follow the 4 ‘Cs’: control, climb, course, and communicate, which need to be immediate memory recall items for a pilot who encounters IIMC:
Control: Fly the aircraft. Refocus the scan inside the cockpit to the primary flight instruments – airspeed, altitude, and attitude.
Climb: As soon as the aircraft is under control by reference to the instruments, a controlled climb should be initiated. Inadvertent IMC encounters often occur at low altitudes where rising terrain poses a serious threat. The pilot should initiate a straight ahead controlled climb to an altitude that will provide obstruction clearance in the area of operation…
Course: After the aircraft is in a controlled climb, the pilot can elect to turn to a new heading if known obstacles are ahead and/or divert to a different location with better known or forecast weather conditions.
Communicate: After the pilot has control of the aircraft, initiated a climb, and on course, they should communicate with ATC regarding their intentions and need for assistance. Careful preflight planning will allow a pilot to focus their attention on maintaining control of the aircraft and reduce the distraction of having to formulate a complete plan in the midst of a dangerous situation. Pilots must be prepared to deal with (recognize & accept) such inadvertent IMC encounters whenever they occur in a reliably disciplined and practiced manner.
In addition to recovering from IIMC, their fact sheet provided the following preparations for avoiding IIMC:
• Get a good forecast for departure, en route, and arrival.
• Avoid flight in Marginal VFR (MVFR).
• Check weather ahead of you en route, use ATC [air traffic control] & Flight Watch.
• Use planned En Route Decision Points (EDPs).[49]
• Recognize signs of deteriorating weather, obscured hills, fog, visual precipitation, and descent below planned altitude.
• Assess the situation and if the signs back up the warnings, decide to land or turn around before you get to inadvertent IMC.
Helicopter accident trends in 8 ISASI [International Society of Air Safety Investigators] countries and how we might improve the fatal accident even further
Matthews, Alexander, and Stone (2017) conducted an analysis of fatal helicopter accidents across 8 jurisdictions with large helicopter fleets for the period 2001 to 2015. Their analysis of VFR into IMC accidents included the following:
VFR into IMC involves both a lack of pre-flight planning and risk. A lack of pre-flight planning or proper risk assessment in turn can reflect self-imposed pressure to perform a mission, or continuing to press ahead even as a pilot recognizes that weather is deteriorating.
Reducing these accidents must rely on establishing, adhering to and training to good SOPs [Standard Operating Procedures] and risk assessment programs, with particular emphasis on currency of experience, pre-flight planning and go/no-go decision making.
When discussing the importance of IIMC recovery training, the report emphasised that ‘one-off training efforts’ had little or no effect as instrument flying skills are perishable. Instead, to be effective, repeated training reflecting an operator’s procedures and risk assessments was required. Further, regulators can contribute by increasing their surveillance of an operator’s procedures or helping in the development of these procedures and risk assessment programs. Their paper concluded with a comprehensive list of recommended training, process, and technology interventions with an accompanying explanation for each.
Safety analysis
Introduction
On the morning of 31 March 2022, 2 Airbus Helicopters EC130 helicopters, operated by Microflite, commenced a passenger transport flight from the company’s Batman Park helicopter landing site in Melbourne to Ulupna on the northern border of Victoria. Recorded data and interviews established that the first helicopter, VH-WVV (WVV) performed a U-turn overhead Mount Disappointment to avoid entering cloud. The second helicopter, VH-XWD (XWD), entered a high rate of descent and collided with terrain while attempting to follow WVV with the U-turn. The 5 occupants were fatally injured and the helicopter was destroyed.
This analysis will discuss the circumstances leading to the collision with terrain, including the route planning, entry into cloud, loss of control, instrument flying experience of the pilot, benefits of autopilot and artificial stabilisation, and the state of the standby artificial horizon. It will also examine how the risk of an inadvertent instrument meteorological conditions (IIMC) encounter was being managed in terms of recovery training, proficiency checks, a pre-flight risk assessment, and the operator’s risk management approach to adverse weather. Further, it will discuss the need for the regulator to provide greater safety assurance for passengers in the rotorcraft air transport sector.
The terms ‘VFR into IMC’ and ‘IIMC’ are used interchangeably in the analysis to reflect the nomenclature used by the respective references.
Route planning
The weather forecast for the Mount Disappointment area indicated broken stratus cloud at 2,000‑3,000 ft above mean sea level (AMSL) and a mixture of broken cumulus/stratocumulus cloud at 3,000-8,000 ft. The peak of Mount Disappointment is 2,605 ft and the upper limit of uncontrolled airspace was 3,500-4,500 ft. This indicated that cloud was forecast to develop below visual meteorological conditions (VMC) from ground level up into controlled airspace. This made the route over Mount Disappointment under the controlled airspace steps unsuitable for visual flight rules (VFR) planning purposes. Further, there were scattered showers of rain with cloud up to 10,000 ft forecast over the ranges, but north of the ranges was forecast to be clear.
The forecast for Kilmore Gap, the recommended VFR route to the north, included broken cloud at 3,000 ft with temporary periods of cloud on the ground from 0600-1000. This indicated a route via Kilmore Gap was an option with the caveat that the forecast included periods that it could be impassable. This option would have kept the pilots in sight of ground, which would have provided them with visual references for a turn-back and potential emergency landing sites if they could not proceed or turn-back. However, it was the Melbourne Airport forecast of cloud at 1,500 ft above that aerodrome that resulted in the pilots’ assessment that they might not be able to transit through Kilmore Gap below cloud. Instead, they selected a more direct route over Mount Disappointment above the lower layer of cloud. This plan was confirmed during their flight into the city from Moorabbin where they observed that the forecast cloud was not established over the ranges.
From interviews, it was reported to be common practice to use the 24-hour forecast for Melbourne Airport to assess the suitability of conditions for the following day’s taskings. While this forecast was useful for the Melbourne basin, it did not provide the height of the cloud tops (as available on the graphical area forecast) and was not valid for a cross-country flight. Although the pilot of WVV reported that they would have checked the graphical area forecast, the information provided on the Melbourne Airport forecast was a deciding factor in the pilots’ route selection. The ATSB was unable to determine why the Melbourne Airport forecast was more influential than the graphical area forecast for their assessment of the Kilmore Gap route. The fact that the pilot of WVV had made multiple location requests for weather and had concerns regarding the Melbourne Airport forecast, and the accident pilot had the WillyWeather app running from 0633 indicated that both pilots were conscious of the weather but were not able to associate the risk of their plan with the forecast conditions.
Entry into cloud
After departing the Batman Park helicopter landing site, with WVV in lead and XWD in trail about 30 seconds behind, the pilot of WVV could see the ranges and sunlight striking the ground ahead, indicating to them the cloud cover ahead was scattered. Consequently, they elected to proceed over the top of the cloud rather than divert via the recommended VFR route. On reaching 3,500 ft, the cloud coverage below gradually increased from scattered to broken but the pilot could still see patches of sunlight striking the ground and continued. The pilot’s repeated references to sunlight striking the ground ahead as they approached Mount Disappointment suggested that this visual indicator supported their plan.
The increasing cloud cover was starting to concern the pilot of WVV as the layer below was starting to rise towards their upper limit of uncontrolled airspace at 3,500 ft. There was also a layer above at about 4,500 ft, and these 2 layers appeared to be converging ahead over Mount Disappointment. The Appareo footage from XWD was consistent with the description of the conditions provided by the pilot of WVV and the forecast for the Mount Disappointment area.
As the minimum vertical clearance from cloud had increased from ‘clear of cloud’ to 1,000 ft when the helicopters climbed to the 3,500 ft upper limit, it was likely shortly after this that they encroached the criteria for VMC. However, the changing conditions had not yet triggered a decision for the pilots to divert.
As the cloud ahead continued to deteriorate, the pilot of WVV was eventually confronted with a wall of cloud, consistent with the passenger observations of white-out conditions. As they could not manoeuvre around the cloud while remaining outside controlled airspace, they advised the pilot of XWD they were turning around. The query from the pilot of XWD about the need for a U‑turn suggested the conditions had also not yet triggered a decision for them to divert. The pilot of WVV broadcast the U-turn manoeuvre so that the pilot of XWD would know to do the same. However, the pilot of XWD started a descent and waited to visually sight WVV pass abeam before attempting the turn. It could not be determined why the pilot of XWD delayed the turn, but it was possible they were either concerned about a mid-air conflict or were waiting to follow WVV.
As the pilot and passengers onboard WVV reported that they sighted XWD after the U-turn, the helicopters were not in cloud at this stage. However, shortly after the helicopters passed abeam each other, the footage showed that the main artificial horizon (AH) on XWD started to wander 10º in pitch and 30º in roll, which indicated the pilot had very likely lost external visual references at this stage.
Loss of control
After WVV passed abeam XWD, the footage showed that the pilot of XWD encountered IIMC. For the U-turn, the pilot attempted a steep left turn at about 60° angle of bank with low power, as indicated by the low FLI setting. While a steep turn would have facilitated exiting the cloud conditions quicker, it also required more significant changes to the flight control inputs than a small angle of bank turn for the pilot to maintain control of the vertical profile (climb, descent or level as necessary). After rolling into the left turn, the nose down pitch attitude increased, such that the main AH indicated ground only. The rate of descent subsequently increased significantly with at least a 3,000 ft/min full scale deflection observed on the vertical speed indicator and a peak of about 5,700 ft/min from the global positioning system data. This was about 10 times the normal descent rate stipulated by the operator for passenger charter operations. The significant deviation of the pitch attitude during the turn was likely unintentional and the result of inadequate pilot control due to a lack of instrument flying training and artificial stabilisation.
The pilot’s setting of the main AH before take-off and control of the angle of bank to enter the final turn, during the turn and exit from the turn, indicated they had developed some ability to read the bank angle on the AH. However, the loss of control and high rate of descent was consistent with other helicopter VFR into IMC accidents.
The pilot reversed the roll to about 10º angle of bank to the right as the helicopter reached its reciprocal heading, at which point the trees became visible in the cloud. A significant pitch-up was applied but could not prevent the collision.
Instrument flying experience
An IIMC event presents the risk of either controlled flight into terrain or loss of control and collision with terrain. The goals of instrument flying training for day VFR pilots include recovering from unusual attitudes and recovering to visual conditions after an IIMC event. Their ability to do this is dependent on receiving initial and recurrent training.
As the pilot had completed the non-integrated Commercial Pilot’s Licence (Helicopter) (CPL(H)), they had not been trained in basic instrument flying, which was supported by their flight test report. Likewise, the operator’s copy of the pilot’s logbook showed that the pilot had accumulated about 3,000 hours total experience but had not recorded any actual or simulated instrument flying. This was consistent with the pilot’s operator proficiency checks, which indicated instrument flight sequences were not assessed, in-line with the operator’s requirements for the day VFR pilots. Consequently, there was no recorded evidence that the pilot had ever been trained to manage or demonstrated an ability to safely recover a helicopter from an IIMC event. The pilot of WVV and a former company pilot also reported no instrument flying experience and therefore this was not unique to the accident pilot.
Autopilot and stabilisation
The accident helicopter, XWD, was not equipped with an autopilot or stability augmentation system and had an excessive rate of descent during the attempted U-turn in cloud when the nose down pitch attitude increased significantly after the turn entry. As established through tests and research, the handling qualities of helicopters without artificial stabilisation deteriorated in degraded visual environments to the extent that the pilot’s full attentional resources were required to maintain control of the helicopter. Consequently, a pilot may not have spare attentional capacity for either the guidance (managing the flight path) or navigation (managing the route) of the helicopter in IMC. Conversely, if their attention is diverted to guidance, they may not have sufficient capacity to maintain control (managing the attitude).
Consequently, helicopter certification for instrument flight rules includes stability characteristics, which can be met with a stability augmentation system. In addition, the Civil Aviation Safety Regulations (CASR) Part 133 for rotorcraft air transport require either an autopilot or automatic stabilisation system for helicopters engaged in instrument flight rules or single-pilot night VFR operations without external visual references.
In this case, if the helicopter had been equipped with an autopilot or stability augmentation system, and the pilot was trained to use the equipment, the attitude control and guidance provided by these systems would have reduced the risk of the loss of control. As emphasised by Oltheten and Trang (2021), many loss of control accidents could have been avoided if the helicopters met some of the instrument flight rules stability requirements. Therefore, the ATSB encourages the adoption of these systems wherever feasible.
Standby artificial horizon
Video footage showed that the pilot erected the main artificial horizon (AH) on start up at Moorabbin Airport but did not erect the standby AH. Likewise, the footage showed that the standby AH remained off on departing the Batman Park Airport, which was consistent with the position of the corresponding push-button switch found in the wreckage.
Immediately after WVV had completed the U-turn due to the deteriorating weather conditions and passed abeam XWD, the pilot of XWD looked across the cockpit at the standby AH that had a red ‘OFF’ flag visible and was indicating a 90º roll to the left. The pilot reached across and attempted to erect the standby AH and then released it with no change in the indications. As the pilot had not switched the power on to the instrument, the AH could not be erected. Consequently, this would have presented conflicting attitude information to the pilot, which they were unable to correct at about the same time they lost external visual references. Conflicting attitude information increases the risk of a pilot experiencing spatial disorientation. However, while the pilot was temporarily distracted by the standby AH, as they did not appear to scan this instrument during the accident turn, it was not considered to be a contributing factor.
Engine service bulletin
In 2019, the European Union Aviation Safety Agency issued a safety information bulletin describing the blade shedding design of the Arriel 2D engine for preventing turbine disc burst from an overspeed condition. The purpose of the bulletin was to explain the risk of thermal energy being released during blade shedding potentially contributing to post-crash fires and that Safran Helicopter Engines and Airbus Helicopters were working on the introduction of a fuel shut-off modification to prevent blade shedding events. They had introduced service bulletins for the hardware (Airbus) and software (Safran) requirements.
At the time a representative from Safran attended the operator’s facility to incorporate the software modification for their fleet, XWD was not available. In addition, the Airbus hardware modification had not yet been embodied for their fleet. However, both modifications were scheduled to be embodied within their respective compliance periods. Consequently, blade shedding as the design control for overspeed conditions still applied to XWD. This likely occurred when the engine to main gearbox drive shaft ruptured during the collision. However, the accident was of a severity that was not considered survivable, and the damage associated with the tree and ground impacts suggested a fire was likely to occur irrespective of the blade shedding. Therefore, the absence of the service bulletin was not considered to be a contributing factor.
Inadvertent instrument meteorological conditions recovery procedure and training
The International Helicopter Safety Team fact sheet – Helicopter Pilots in Inadvertent IMC Situations explained that it is the immediate actions after an IIMC encounter that will usually determine the outcome of the event. Furthermore, this emphasised that ‘pilots who possess a plan of action prior to encountering it are more likely to experience a successful outcome than those who are less trained and less proficient in the recognition and recovery procedures.’ The 4 immediate actions they advocated were control, climb, course, and communicate.
These actions represent the emergency procedure steps required following an IIMC encounter, which need to be immediate memory recall items. Without a published procedure for passenger operations, Microflite was reliant on individual pilots to identify the need and develop their own procedure. In contrast, the operator had published an IIMC procedure for formation flying, which was part of their formation pre-flight briefing. This indicated that the operator recognised IIMC as a potential in-flight risk and that immediate memory recall was required to minimise the likelihood of it being mishandled during a formation flight.
The operator had also published in their training manual that IIMC recovery training was available and conducted in their simulator. However, it was only a recommended sequence and neither the pilot of XWD or WVV had undergone this training. Statistics have shown that a loss of control and collision with terrain from IIMC could occur in about 56 seconds. In this accident, the pilot rolled the helicopter to a 60° angle of bank after encountering IMC, followed by a significant nose down attitude and rate of descent. This resulted in a collision with terrain in less than 30 seconds.
Successful recovery from an emergency requires a pilot to recognise what the problem is and what decisions and actions are required in response. In the IIMC avoidance and recovery scenarios the pilot needs the recognition, decision-making and basic instrument flying skills to handle degraded visual conditions. As noted by the United States Helicopter Safety Team, having standardised procedures ensures an enhanced level of safety by providing structure and preparing pilots to respond to normal and abnormal situations.
While the operator had a system that could have delivered training to their pilots for IIMC avoidance and recovery in accordance with a published procedure, they had not developed a procedure or mandated the training. If the pilot had received the technical and procedural training to recover from IIMC, this would have reduced the risk of this accident.
Operator proficiency checks
The Civil Aviation Safety Authority CPL(H) was divided into 2 syllabi, identified as the integrated syllabus and the non-integrated syllabus of training. The non‑integrated syllabus did not require instrument flying training, as was required for an aeroplane licence. Therefore, while the flight review for the aeroplane licence required an assessment of instrument flying, this was only optional for a helicopter flight review. Consequently, the operator did not conduct any basic instrument flying skills checks on their pilots who were employed as day VFR charter pilots.
The first action required to recover from IIMC is to control the helicopter with reference to the flight instruments, which requires the pilot to transition from an external visual scan to an internal scan of the primary flight instruments. Initial training is required for the pilot to develop the understanding and skill for how to control the helicopter by sole reference to instruments. However, instrument flying skills, like engine failure handling skills, are perishable skills and therefore regular practice and competency checks are required to maintain and assure proficiency.
The 6 previous helicopter IIMC accidents reviewed in this investigation found none of the pilots were likely proficient in basic instrument flying, having had no recent experience or no experience at all. This was supported by the report from one pilot with basic instrument flying training 18 months prior to their accident that they did not feel adequately trained to use their flight instruments. Proficiency checks provide operators with the opportunity to assess if their pilots have the decision-making and handling skills to perform their normal and emergency procedures to the required standard. Likewise for the pilot under assessment, feedback from the assessor can confirm if their decision-making and actions were appropriate.
While the operator’s decision not to assess instrument flying skills was consistent with regulations and the helicopter industry’s historical opposition to basic instrument flying training, research into IIMC accidents has shown that these encounters often result in fatalities from a loss of control or controlled flight into terrain. Therefore, as noted by the International Helicopter Safety Team, those pilots who are trained and proficient in IIMC recognition and recovery procedures are more likely to experience a successful outcome. As the accident pilot had neither been trained or subjected to a basic instrument flying skills check, this increased the risk of a loss of control while attempting to recover from the IIMC encounter over Mount Disappointment.
Pre-flight risk assessment
As noted by Matthews, Alexander, and Stone (2017), VFR into IMC accidents can involve a lack of pre-flight planning and/or risk assessment. The accident flight was a Part 133 rotorcraft day VFR passenger air transport operation with the pilots conducting their flight planning and preparation independent of direct oversight. While neither of the pilots were inexperienced, this sector of the industry is predominantly a single-pilot operational environment (the pilot’s flying experience indicated about 95% of flight time as pilot in command). Therefore, pilots have significantly less opportunity to learn operational decision-making from more experienced pilots than they would in a multi-crew environment.
In the Transport Safety Board of Canada’s safety study of IIMC accidents, they noted that technical piloting skills were not found to be deficient in the history of accident pilots’ check flights. Rather, the problem was with their decision-making in situations not traditionally assessed. In this case, the accident pilot had passed several proficiency checks with the operator and expanded their technical flying skills and qualifications with a low-level rating with sling endorsement and an aerial application rating.
The single-pilot passenger transport environment poses the challenge to operators for how to manage the oversight of planning activities conducted by their line pilots and afford them the decision-making learning experience from senior pilots that is available in the multi-crew environment. A tool that can assist with this is a pre-flight risk assessment that provides an escalation process commensurate with the level of risk. Weather is one of the key elements of a pre-flight risk assessment and provided the tool is designed to trigger an escalation if conditions are marginal for a VFR flight, then it will provide an operator with a risk-based approach to oversight flight planning. This process has been extensively used throughout the helicopter emergency medical services sector.
The operator did not have a process in place for independent checks of their line pilots’ flight planning activities. However, an oversight process could be made available with the use of a fit‑for-purpose pre-flight risk assessment tool with the records saved for verification and validation purposes. In this case, if a conversation had taken place with a manager or instructor pilot prior to the accident flight there likely would have been more scrutiny of the graphical area forecast and the recognition that a route via the Kilmore Gap was a lower risk option.
Risk management of inadvertent instrument meteorological conditions
In 2015, the operator had raised a risk assessment for air transport operations for the purpose of identifying the risks associated with their general charter operations from company known and frequently used locations. This included the threat of poor weather conditions, such as the risk of loss of VMC. The controls associated with this threat were cancelling operations if the forecast weather was below company minima, the arrangement of ground transport, and that all their pilots were issued with an iPad to access and assess the weather. During the investigation, the ATSB found evidence that the operator’s controls for the threat of poor weather conditions were being practiced and that charter flights had been routinely cancelled due to weather. However, the risk assessment did not consider how this threat would be managed in-flight.
The ATSB identified several recommended controls in the operator’s manual suite that could have been employed to mitigate the in-flight risk of IIMC. These included the use of minimum safe altitudes and recovery training for IIMC. However, they were not mandatory and therefore they were not effective risk controls. The operator’s client services management process and procedure for diversions due to weather were also missing from their risk assessment. Combined, this indicated the loss of VMC preventive controls were incomplete.
Despite the published preventive controls, the accident flight was planned and continued along a route forecast to be below VMC. This highlighted that a pilot’s weather assessment and diversions would not necessarily prevent a route planning mistake escalating into IIMC. The various optional and existing controls indicated the operator understood the risk, but that the regulatory environment for day VFR helicopter pilots likely meant that no further action was considered necessary as their published risk controls were in accordance with these requirements.
The operator’s approach to the risk of IIMC was consistent with the 2018 CASA helicopter industry survey, where most respondents opposed basic instrument flying training. However, this did not recognise that air transport safety has built and relied on multiple layers of controls to reduce the risk of single-point of failure accidents.
Civil Aviation Safety Regulations Part 133
The day VFR helicopter and aeroplane industry sectors typically range from private flying, flying training, aerial work activities, to air transport operations, which includes scheduled and non‑scheduled passenger transport, scenic flights and medical transport. The regulatory framework and expectations of the level of safety across these categories is graduated with separate rule sets, which facilitates the development of regulations that can be tailored to each specific sector. In the passenger air transport sector, there is a public and industry expectation that the flights will be operated to a higher safety standard than other sectors of the aviation industry. However, this distinction is not always captured within the regulations and standards for known risks, such as VFR into IMC.
In terms of a comparison between aircraft categories, helicopters and aeroplanes both had a high percentage of fatal VFR into IMC accidents, consistent with other jurisdictions, but helicopters were more likely to be involved in an accident following a VFR into IMC occurrence. Despite this, there was a notable difference between helicopter and aeroplane licencing and training requirements. The aeroplane CPL syllabus included a requirement to teach basic instrument flying (as did the integrated CPL(H) syllabus), which included recovery from IIMC as one of the units of competency. These perishable skills were required to be checked on flight reviews for aeroplane pilots. In contrast, the training was optional for the non-integrated CPL(H) and consequently the instrument flying flight review requirements were optional for all CPL(H). As such, it was very likely that VFR pilots from the non-integrated syllabus conducting passenger air transport operations would not have been trained to recover from IIMC.
There is a variety of risk controls that could be implemented to reduce the risk of an IIMC accident. They include equipment, such as artificial stabilisation and autopilots, warning devices, such as terrain awareness and warning systems, IIMC recovery training, pre-flight risk assessments, flight plan reviews, minimum safe altitudes, and supporting procedures. Noting these risk controls and the training differences described above, the ATSB reviewed the regulations and standards to determine how the Civil Aviation Safety Regulations (CASR) Part 133 air transport passenger operators were expected to manage the risk of a day VFR pilot experiencing IIMC.
The CASR Part 133 (air transport operations - rotorcraft) and associated Part 133 Manual of Standards set the helicopter air transport specific requirements for operators to prepare their exposition, to demonstrate how they intend to comply with the legislative requirements and how they will manage safety. This may include risk assessments, procedures, and equipment for the various categories of flight. Therefore, while operational risk identification is traditionally the domain of the operator, CASA can require the assessment of specific risks through the safety regulations and then audit against them for safety assurance purposes.
Further, in terms of the primary flight instruments required for controlling an aircraft when experiencing IIMC, this would include instruments providing airspeed, altitude, and attitude information. The requirements stipulated in the Part 133 Manual of Standards for day VFR operations included flight instruments for indicated airspeed and pressure altitude, but there was no reference to having attitude (artificial horizon) or standby attitude instruments. Additional flight instruments were required for night VFR and instrument flight rules (IFR) operations.
Likewise, an autopilot or automatic stabilisation system that would assist with controlling the helicopter in normal flight and reduce the risk of loss of control in IIMC was only required for IFR and some night VFR operations. A terrain awareness and warning system, alerting pilots when in hazardous proximity to terrain to reduce the risk of controlled flight into terrain, was only required for larger rotorcraft conducting passenger flights or medical transport operations, both operating under IFR.
The ATSB often finds that optional risk controls related to the occurrence under investigation were not implemented at the time of the occurrence. The pilots involved in this accident completed the non-integrated syllabus and therefore optional basic instrument flying training was not done. The operator’s risk controls for loss of VMC met the regulatory requirements. Hence, their IIMC recovery training was optional, and the pilots involved had not done it.
Part 133 does include some procedural controls, such as fatigue management, minimum flight crew experience for the pilot in command and additional training and checking requirements that are in addition to the general requirements of Part 91. However, the investigation found that the controls being employed to manage the risk of IIMC within the context of a Part 133 operation were broadly aligned with the requirements of Part 91 for a weather assessment and compliance with VMC criteria and found no evidence of any stricter criteria for forecasts of marginal VMC or recovery controls from an IIMC event. Hence, the regulations for day VFR rotorcraft air transport did not offer a higher level of passenger safety than a private flight for this specific risk. While voluntary guidance and educational resources are useful for both private and commercial pilots, they will not provide assurance for passenger safety.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the VFR into IMC, loss of control and collision with terrain involving a Microflite Airbus Helicopters EC130 T2, registered VH-XWD, near Mount Disappointment, Victoria, on 31 March 2022.
Contributing factors
The pilots of the two helicopters selected a route that was forecast to be unsuitable for visual flight. This was based on an incorrect assessment of the weather before and while in-flight.
The pilots of both helicopters continued flight towards deteriorating cloud and into reduced visual cues, below the required visual meteorological conditions. These conditions were consistent with the area forecast for the Mount Disappointment area.
While conducting a 180 degree turn without visual cues to exit from instrument meteorological conditions, the pilot could not maintain adequate control of the pitch attitude of the helicopter, which resulted in the development of a high rate of descent and collision with terrain.
The pilot was not trained to fly the helicopter by sole reference to the instruments and almost certainly did not have any instrument flying experience, nor was it required by the regulations.
The helicopter was not equipped with an autopilot or stability augmentation system, nor was it required to be. This equipment would have reduced the risk of a loss of control when the pilot attempted to exit from instrument meteorological conditions.
Microflite had not published an inadvertent instrument meteorological conditions (IIMC) recovery procedure for their day visual flight rules pilots and their IIMC recovery training was not mandatory, nor were they required by the regulations. The provision of this procedure and training would have reduced the risk of a loss of attitude control following an IIMC encounter. (Safety issue)
The Microflite Operator Proficiency Checks did not include a mandatory instrument flight component for their day visual flight rules pilots, nor was it required by the regulations. This would have reduced the risk of a loss of control event following an inadvertent instrument meteorological conditions encounter. (Safety issue)
Microflite did not provide, nor require, their pilots to complete a pre-flight risk assessment for their taskings. A pre-flight risk assessment would have provided pre‑defined criteria to ensure consistent and objective decision-making and reduced the risk of them selecting an inappropriate route. (Safety issue)
The Microflite air transport operations risk assessment for poor weather conditions did not consider the risk controls required for inadvertent instrument meteorological conditions. Rather, it relied on their pilots using the actual or forecast conditions to cancel their operations to manage the threat of poor weather. (Safety issue)
The Civil Aviation Safety Authority's Part 133 (air transport - rotorcraft) exposition requirements did not adequately address the risk to passenger safety from a visual flight rules inadvertent instrument meteorological conditions event. (Safety issue)
Other factors that increased risk
The standby artificial horizon was not turned on and presented conflicting information to the main artificial horizon. This resulted in a momentary distraction to the pilot when visual cues were reduced and increased the risk of spatial disorientation.
The operator was in the process of modifying their fleet of helicopters in accordance with the service bulletins for overspeed protection to reduce the likelihood of blade shedding. However, this was not accomplished for the accident helicopter at the time of the accident, which increased the risk of a post-impact fire.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The Microflite Operator Proficiency Checks did not include a mandatory instrument flight component for their day visual flight rules pilots. This would have reduced the risk of a loss of control event following an inadvertent instrument meteorological conditions encounter.
Inadvertent instrument meteorological conditions recovery procedure and training
Safety issue description: Microflite had not published an inadvertent instrument meteorological conditions (IIMC) recovery procedure for their day visual flight rules pilots and their IIMC recovery training was not mandatory. The provision of this procedure and training would have reduced the risk of a loss of attitude control following an IIMC encounter.
Safety issue description: Microflite did not provide, nor require, their pilots to complete a pre-flight risk assessment for their taskings. A pre-flight risk assessment would have provided pre‑defined criteria to ensure consistent and objective decision-making and reduced the risk of them selecting an inappropriate route.
Risk management of inadvertent instrument meteorological conditions
Safety issue description: The Microflite air transport operations risk assessment for poor weather conditions did not consider the risk controls required for inadvertent instrument meteorological conditions. Rather, it relied on their pilots using the actual or forecast conditions to cancel their operations to manage the threat of poor weather.
Civil Aviation Safety Regulations Part 133 requirements
Safety issue description: The Civil Aviation Safety Authority's Part 133 (air transport - rotorcraft) exposition requirements did not adequately address the risk to passenger safety from a visual flight rules inadvertent instrument meteorological conditions event.
Safety recommendation description: The Australian Transport Safety Bureau recommends that the Civil Aviation Safety Authority takes safety action to further address the risk to rotorcraft air transport (Part 133) passenger safety from a visual flight rules inadvertent instrument meteorological conditions event.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by Microflite
During the investigation, Microflite advised the ATSB they had initiated the following proactive safety action.
Introduction of autopilots
Microflite are modifying their AS350 and EC130 helicopters with the Garmin GFC 600H helicopter flight control system. The AS350 has approved data for this modification but approval for the EC130 was not available at the time of the investigation.
Flight instrument upgrades to the fleet
Microflite are upgrading their fleet of EC130 and AS350 helicopters with the Garmin G500H primary flight display and multifunction display, incorporating synthetic vision and a terrain alerting functionality to improve pilot situational awareness in a degraded visual environment.
ICARUS flying hoods
Microflite has acquired 2 ICARUS (instrument conditions awareness recognition and understanding system) instrument flying training hoods, one for the left-seat of the EC130 and one for the right-seat of the AS350, to enhance the transition training from visual to instrument flight conditions.
Inadvertent instrument meteorological conditions avoidance training
Microflite required all their pilots to complete the Helicopter Association International online academy ’56 Seconds to Live’ training. The stated goal of this course was for pilots to ‘Recognize and avoid the trap of departing into, or continuing VFR flight into deteriorating weather conditions’.
Task rejection policy
Microflite introduced a company ‘Task rejection’ policy statement into their operations manual. The policy requires their pilots to cancel VFR flights if it is determined that VMC cannot be assured for the planned flight. It also provides management support to their pilots for cancelling their flights if the risk profile is deemed unsafe by the pilot in command.
Airbus helicopter training centre approval
Microflite obtained an Airbus Helicopter Training Centre approval. This approval provides them with greater access to the manufacturer’s technical resources for training their staff and operating and maintaining their helicopter fleet.
Glossary
ACAH
Attitude command-attitude hold
AH
Artificial horizon
ATC
Air traffic control
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
DVE
Degraded visual environment
EDP
Enroute decision point
EECU
Electronic engine control unit
ELT
Emergency locator transmitter
FAA
Federal Aviation Administration of the United States
HLS
Helicopter landing site
ICAO
International Civil Aviation Organization
ICARUS
Instrument conditions awareness recognition and understanding system
IIMC
Inadvertent IMC
IMC
Instrument meteorological conditions
ISASI
International Society of Air Safety Investigators
MVFR
Marginal VFR
NTSB
National Transportation Safety Board of the United States
SB
Service bulletin
SIB
Safety information bulletin
TSB
Transportation Safety Board of Canada
US
United States
VEMD
Vehicle engine multifunction display
VMC
Visual meteorological conditions
VFR
Visual flight rules
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Bureau of Meteorology
chief executive officer, chief pilot, head of training and checking and safety manager of Microflite
pilot of VH-WVV
Civil Aviation Safety Authority
closed circuit television camera footage from Moorabbin and Batman Park HLS
flight track data
former company pilot
French Bureau of Enquiry and Analysis for Civil Aviation Safety
Airbus Helicopters
Safran Helicopter Engines
forensic pathologist assisting the Victorian Coroner
recorded data from the helicopter’s Appareo camera and vehicle and engine multifunction display.
Australian Transport Safety Bureau (2018) Collision with terrain involving Airbus Helicopters EC135 T1, VH-GKK, 10 km NNW Cooranbong, New South Wales, 7 November 2015 (AO-2015-131). Retrieved from /publications/investigation_reports/2015/aair/ao-2015-131
Australian Transport Safety Bureau (2011) Visual flight into instrument meteorological conditions Dorrigo, New South Wales 9 December 2009 VH-MJO, Bell Helicopter Company 206L-1 LongRanger (AO-2009-077). Retrieved from /publications/investigation_reports/2009/aair/ao-2009-077
Crognale MA & Krebs WK 2011, ‘Performance of helicopter pilots during inadvertent flight into instrument meteorological conditions’, The International Journal of Aviation Psychology, 21:3, 235-253. Retrieved from https://www.researchgate.net/publication/233000179
European Union Aviation Safety Agency 2019, Power turbine over-speed protection on Arriel 2D engines (SIB 2019-10).
Fox RG 1989, Helicopter crashworthiness – part one, Report prepared for the Flight Safety Foundation’s Helicopter Safety Vol.15, No.6, November/December 1989. Retrieved from https://flightsafety.org/
Hoh RH 1990, The effects of degraded visual cueing and divided attention on obstruction avoidance in rotorcraft, Report prepared for the United States Federal Aviation Administration (DOT/FAA/RD-90/40). Retrieved from https://apps.dtic.mil/sti/citations/ADA380260
International Helicopter Safety Team (n.d.) Helicopter Facts – Follow the Four “C’s”: Helicopter Pilots in Inadvertent IMC Situations. Retrieved from https://ushst.org/iimc/
Matthews RC, Alexander R & Stone RB 2017, Helicopter accident trends in 8 ISASI countries and how we might improve the fatal accident even further. Technical paper prepared for the 2017 seminar of the International Society of Air Safety Investigators. Retrieved from https://www.isasi.org/Library/technical-papers
Oltheten E & Trang J 2021, Loss‐of‐control in‐flight mitigation through installation of stability augmentation and autopilot systems in light helicopters. Report prepared for the United States Helicopter Safety Team. Retrieved from https://ushst.org/h-se-details/
Transport Safety Board of Canada 1990, Aviation safety study:Report of a safety study on VFR flight into adverse weather (90-SP002). Retrieved from www.bst-tsb.gc.ca.
United Kingdom Civil Aviation Authority 2007, Helicopter flight in degraded visual conditions (Paper 2007/03). Retrieved from www.caa.co.uk.
United States National Transportation Safety Board 2005, Safety study: Risk factors associated with weather-related general aviation accidents (NTSB/SS-05/01). Retrieved from www.ntsb.gov.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
chief executive officer, chief pilot and head of training and checking of Microflite
pilot of VH-WVV
Civil Aviation Safety Authority
former company pilot
French Bureau of Enquiry and Analysis for Civil Aviation Safety
Airbus Helicopters
Safran Helicopter Engines
forensic pathologist assisting the Victorian Coroner.
Submissions were received from the operator, Microflite, and the Civil Aviation Safety Authority, and, where considered appropriate, the text of the draft report was amended accordingly.
Appendix
Geographic distribution of VFR into IMC incidents and accidents
Figure 17: Helicopter VFR into IMC accidents, 2008-2022
Source: ATSB
Figure 18: Helicopter VFR into IMC reported occurrences (accidents in orange and incidents in blue), 2008-2022
Source: ATSB
Figure 19: VFR into IMC accidents for all aircraft types, 2008-2022
Source: ATSB
Figure 20: VFR into IMC reported occurrences for all aircraft types (accidents in orange and incidents in blue), 2008-2022
Source: ATSB
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] The flight data for VH-XWD was OzRunways, which provided data at 1-second intervals with the altitude rounded to the nearest 100 ft. The flight data for VH‑WVV was TracPlus, which provided data at 15-second intervals with the altitude to the nearest foot.
[2] Cloud cover: cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that cloud is covering less than a quarter of the sky, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[3] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[4] The APPAREO Vision 1000 device is used to record video imagery and audio data from inside the aircraft cabin. The system also records global positioning system inertial and positioning data. The data from the camera fitted to WVV could not be retrieved due to a technical fault with the camera.
[5] A flight instrument that informs the pilot of the aircraft’s orientation relative to the Earth’s horizon. The miniature aircraft and horizon bar show the relationship of the aircraft relative to the actual horizon. It is a primary instrument for flight in instrument meteorological conditions.
[6] This was in accordance with their company operations manual, which stated: The primary method of flight following for company aircraft is through the TracPlus satellite tracking system. Alternatively, the pilot in command shall ensure that either a FLIGHT PLAN is submitted to Air Traffic Services, or a SARTIME is nominated to a Company representative and flight details are left with home base in the office.
[7] The lower limit of controlled airspace increased progressively along the planned track from 1,500 ft to 4,500 ft. The increase from 3,500-4,500 ft occurred in the vicinity of Mount Disappointment.
[8] On start-up, the multi-function display presents the engine temperature, torque, and gas generator speed. After start, these 3 parameters are combined into a single indicator called the FLI, which displays information relating to a value of a limiting parameter of the engine. The limiting parameter is the engine parameter that is the closest to its limit. Engine power output and the FLI reading are derived from the collective lever position. Therefore, changes to the FLI indirectly indicate movement of the collective lever – a lower FLI indicates the collective lever has been lowered.
[9] The Microflite operating procedures for flight planning and preparation (Flying Operations Manual, Volume 2, Aircraft Operations) stated that ‘Pilots on passenger charter operations are to plan for cabin descent rates of no more than 500 feet per minute’.
[10] The LIMIT caution light indicates excessive load factor and the Appareo recorded 3.63 G in the last second of data. (G load is the nominal value for acceleration. In-flight, g load represents the combined effects of flight manoeuvring loads and turbulence and can have a positive or negative value).
[11] External visibility totally obscured by environmental factors, in this instance by cloud.
[12] The ATSB considered this was likely an outstanding administrative error and not contributory.
[13] Flight by reference to the aircraft’s flight instruments.
[14] Proficiency checks are intended to assess a pilot’s flying skills and operational knowledge in carrying out normal, abnormal, and emergency procedures. This ensures the pilot is competent to conduct the flights the operator has assigned that pilot.
[17] A Fenestron is an enclosed helicopter tail rotor.
[18] Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[19] Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[20] G load: the nominal value for acceleration. In flight, g load represents the combined effects of flight manoeuvring loads and turbulence and can have a positive or negative value.
[21] An exceedance of the maximum authorised speed of rotation.
[22] An airworthiness directive contains mandatory instructions to carry out work on an aircraft, engine, propeller or component in order to address an unsafe condition which exists, or is likely to exist, or could develop.
[23] The flexible couplings deform to absorb the small misalignments between the engine drive shaft and the main gearbox input pinion. They transmit the engine torque to the main gearbox and are subject to high loads.
[24] OzRunways is an electronic flight bag app that provides planning, briefing, flight plan filing and moving map navigation services.
[25] VFR flight above more than 4/8 cloud cover is known as ‘VFR over the top’, as the phrase ‘VFR on top’ is a clearance provided to an instrument flight rules flight to operate at a VFR level in visual conditions.
[26] General aviation meteorological (GAMET) area forecast: An area forecast in abbreviated plain language for low-level flights for a flight information region or sub-area thereof, prepared by the meteorological office designated by the meteorological authority concerned and exchanged with meteorological offices in adjacent flight information regions, as agreed between the meteorological authorities concerned.
[27] CASA AC 1-02 v3.2 Guide to the development of expositions and operations manuals, para 3.1.1 states: Fundamentally, the terms 'exposition' and 'operations manual' mean the same thing; that is, a means to describe how an organisation will comply with all applicable legislative requirements, and how they will manage the safety of their operations. This objective may be achieved with a single document, or a set of documents.
[28] All references to NAIPS access times were retrieved from NAIPS.
[29] A notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[30] The WillyWeather app was privately run and displayed information produced by external organisations including the Bureau of Meteorology and the National Oceanic and Atmospheric Administration.
[31] The Melbourne Basin is a 16,000 square kilometre area, which spans the Port Philip and Westernport region.
[32] Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[33] Full panel (IFF) is an exercise that does not simulate the failure of any flight instruments.
[34] Limited panel (IFL) is an exercise that simulates the failure of one or more flight instruments before or after inadvertently entering cloud.
[35] To exercise the privileges of a rating, a pilot must have completed a flight review for the rating within the last 2 years. Pilots conducting flights for an operator will likely be subject to operator proficiency checks (OPC) to determine their competency. While a flight review can incorporate training to achieve competency, the OPC does not include training and is conducted to a pass/fail standard. Completion of an OPC may satisfy the flight review if the OPC includes all the review requirements.
[36] Australia has filed a state difference with the ICAO Standards and Recommended Practices for licencing as follows: ‘Licences that are not compliant with Annex 1 paragraph 2.4.4.1.1.1 include an appropriate remark.’ The difference level is described as ‘Less protective or partially implemented not implemented’.
[37] Autorotation is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
[38] In the TSB study, about 35% of the accidents involved aircraft engaged in commercial operations, compared to about 23% in the US. About 15.5% of Canadian commercial pilot licence holders possessed instrument ratings, compared to about 83.3% in the US.
[39] The Cooper-Harper handling qualities rating and visual cue rating scale were used for the assessment. The Cooper‑Harper scale assesses the adequacy of the aircraft characteristics for a selected task or operation, which may be adequate, deficiencies warrant improvement, deficiencies require improvement or improvement mandatory. The visual cue scale was developed to quantify the ability of a pilot to make attitude and translational rate cues for stabilisation.
[40] Situational awareness was defined as awareness of the helicopter’s position and movement with respect to the ground or obstructions.
[41] Level 3 characteristics refers to the Cooper-Harper handling qualities ratings 7-9, which indicated ‘Major handling qualities deficiencies, adequate performance cannot be achieved with tolerable pilot workload.’
[42] The ‘Basic’ type referred to the helicopter model used without artificial stabilisation.
[43] Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[44] Transport category: an airworthiness categorisation that applies to multi-engine aircraft primarily intended for regular public transport and/or cargo for hire or reward.
[45] This system had an advertised 2023 list pricing of $92,560 USD plus installation for the EC130 T2. The product is certified for a variety of small piston and turbine helicopters.
[46] Fisher's exact test is a statistical test used to determine if there are non-random associations between 2 categorical variables.
[47] The two-tailed P-value was 0.0012. A P-value of 0.05 or lower is generally considered statistically significant and a smaller P-value means that there is stronger evidence in favour of the alternative hypothesis.
[48] The HeliSAS unit provided a stability augmentation system for attitude control and autopilot for flight path guidance.
[49] En Route Decision Points are based on weather conditions.
Preliminary report
Report release date: 12/05/2022
Preliminary report released 12 May 2022
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 31 March 2022, at about 0709 Eastern Daylight-saving Time,[1] an Airbus Helicopters EC130 T2, registered VH-XWD (XWD) and operated by Microflite, departed Moorabbin Airport for Batman Park Heliport, Melbourne City, Victoria, with one pilot on board. XWD departed Moorabbin Airport in trail,[2] 10 seconds behind another company EC130 helicopter, registered VH-WVV (WVV).[3]
At about 0717, the helicopters landed at Batman Park and were shut down (Figure 1). The pilots then proceeded to the operator’s heliport office to meet a charter group of 8 passengers for a business trip. They provided the passengers with a safety briefing and escorted them to the helicopters where they were divided into 2 smaller groups of 4 passengers for each helicopter.
Figure 1: VH-XWD (left) and VH-WVV (right) at Batman Park Heliport
Source: Operator, through Victoria Police
At about 0741, WVV departed from Batman Park with XWD in a 30 second trail. Both were operating as visual flight rules (VFR)[4] outside controlled airspace. They initially headed east to remain outside controlled airspace before turning north towards their planned destination, Ulupna, in the north of Victoria. As they tracked east and then north, the lower limit of uncontrolled airspace increased, and the helicopters climbed from 1,500 ft above mean sea level (AMSL) to 2,500 ft and then to 3,500 ft.
At interview, the pilot on board WVV recalled that there was scattered[5] cloud at 1,500 ft on the forecast that would not allow them to track below cloud via the recommended VFR route to Kilmore Gap (elevation 1,200 ft AMSL). Therefore, they elected to take a more direct track to their destination, which took them over Mount Disappointment, to the east of Kilmore Gap (Figure 2). While tracking north towards Mount Disappointment, the helicopters were above a layer of scattered cloud with an estimated top of 2,500-3,000 ft and below a layer of broken cloud with an estimated base of about 4,500 ft. The pilot of WVV reported that they could see areas of sunlight striking the ground ahead of them, and therefore considered the weather ahead suitable to continue.
Figure 2: VH-XWD flight track and key locations
Source: Google Earth and OzRunways, annotated by the ATSB
As they approached Mount Disappointment, XWD was in a 1.5 NM (3 km) trail behind WVV, and the helicopters were cruising at an altitude of about 3,500 ft and 120 kt ground speed. At this stage, the pilot of WVV noted the layer of scattered cloud below them was becoming broken, that the tops were rising, and that the base of the cloud above them appeared to be lowering, resulting in the 2 layers of cloud appearing to converge ahead of them.
Before they could cross Mount Disappointment, the pilot of WVV reported they were confronted with a ‘wall of cloud’ in front, and to the left and right of their track, and broadcast to XWD their intention to turn around. The pilot of WVV reported that the pilot of XWD may have been confused by this broadcast and thought the conditions were suitable to continue. The pilot of WVV reported they then broadcast ‘U-turn, U-turn, U-turn’ to XWD. At about 0756:30, the pilot of WVV conducted a sharp left turn onto a southerly track at 3,635 ft. At about 0757:00, XWD passed below and to the left of WVV, with XWD continuing to track north at about 3,500 ft and 115 kt. This was the last visual contact the occupants of WVV had with XWD.
At 0757:15, the pilot of WVV found a clearing through cloud and turned back northbound at 3,957 ft, with a clearance from air traffic control to climb to not above 5,000 ft. At the same time, the flight data for XWD indicated a track of 333° at 3,300 ft and 100 kt. At 0757:20, XWD was on a track of 297° at about 3,100 ft and 91 kt. The last recorded data point was at 0757:25, at which time XWD had a track of 213° at about 2,800 ft and 54 kt (Figure 3). XWD collided with terrain about 250 m south of the last recorded data point. The elevation of the main wreckage site was about 2,359 ft (719 m). The 5 occupants were fatally injured, and the helicopter was destroyed.
Figure 3: VH-XWD flight track and accident site
Source: Google Earth and OzRunways, annotated by the ATSB
Context
Helicopter information
The accident helicopter was an Airbus Helicopters EC130 T2 manufactured in 2017 and equipped with a Safran Arriel 2D turboshaft engine, 3-bladed main rotor and Fenestron[6] tail rotor. The helicopter was registered VH-XWD in Australia in August 2019 in the night VFR operational category. It was configured with 3 seats in the front row and 4 seats in the rear row. The pilot’s seat was front left.
Wreckage and impact information
The ATSB’s site survey established that XWD had impacted a large old growth tree (Figure 4), which broke the upper tree trunk and severely disrupted the cabin. The helicopter then descended on a southerly trajectory at an angle of about 45° to ground impact. The vegetation surrounding the accident site was comprised of 2 distinct levels of growth. A new growth canopy that had an average height of 24 m, and old growth trees that had an average height of about 70 m. The old growth tree break was about 41 m above ground level (elevation of 759 m). The elevation of the base of this tree was 718 m, which indicated that the elevation of the top of the tree was likely about 2,585 ft (788 m). Therefore, the tree impact very likely occurred between 2,490–2,585 ft (759–788 m).
Figure 4: Overhead view of old growth tree break and main wreckage site
Source: ATSB
The helicopter was subject to a post-impact fire, resulting in the destruction of some components. However, from the components available there was no evidence to indicate any pre-existing defect that would have prevented normal operation. The engine had disconnected from both the main rotor and Fenestron driveshafts. The Fenestron driveshaft exhibited significant scoring damage, which indicated it was rotating at high speed during the accident sequence. Damage to the leading edges of the engine compressor blades was also characteristic of high-speed rotation (Figure 5). In addition, the power turbine exhibited blade shedding.
Figure 5: Damage to the engine compressor blades
Source: ATSB
The ATSB retrieved the pilot’s electronic flight bag (iPad), an Appareo camera, the vehicle and engine multi-function display, a Garmin GTN 750 global positioning system, the engine electronic control unit, and the central warning panel. The engine data recorder fitted to the helicopter was not found within the wreckage.
Meteorological information
The graphical area forecast for Victoria, current at the time of the departure, was issued at 0321 on the morning of the accident and was valid from 0400-1000. The forecast divided the state into 4 areas, identified as A, B, C and D. The flight was planned to start in area C and end in area A. The forecast for cloud in area C was for a broken layer from 2,000-3,000 ft and a broken layer from 3,000-8,000 ft. Area A was forecast to have few cloud from 3,000-5,000 ft.
Kilmore Gap was in area C and identified as a critical location.[7] The cloud forecast for Kilmore Gap was for a broken layer at 3,000 ft with TEMPO[8] conditions from 0600-1000 for a broken layer at 1,200 ft with the note ‘CLD ON GND’ [cloud on the ground].
The Bureau of Meteorology Kilmore Gap web camera was located 19 km west-north-west of the accident site and depicted cloud overhead Mount Disappointment prior to the time of the accident. At 0758, at Kilmore Gap, the relative humidity was 95% and the wind was 17 kt from 171°. The cloud cover was few at 394 ft and broken at 3,510 ft above ground level. At 0811 the cloud had become broken at 394 ft above ground level.
VH-WVV passenger reports
The passenger in the front middle seat had flown regularly with the pilot of WVV and considered the pilot to be very cautious regarding the weather. The passenger recalled that, during the flight, the pilot radioed XWD about the approaching weather. A ‘wispy cloud then went past us, and it felt like a heavy white cloud came down and dumped on us’.
The passenger in the front right seat had flown in helicopters for about 30 years. The passenger recalled that, as they crossed Mount Disappointment, heavy cloud rolled in resulting in ‘a white-out with ground visibility no longer evident’. The pilot radioed XWD and said words to the effect of ‘U‑turn, U-turn, U-turn’. Then the pilot of WVV immediately completed a U‑turn. The pilot of XWD radioed back with words to the effect ‘aren’t we going to cut through?’ The passenger then saw XWD pass just below them.
The passenger seated behind the pilot had flown once previously with the pilot of WVV and found them to be very professional and relaxed. During the flight, the passenger was reading emails but noted as they approached Mount Disappointment that the pilot’s body language had changed, which gave the passenger the feeling that something was not right. The passenger looked outside and saw cloud in front and to the left, and then heard the pilot announce they were going ‘hard left’. When the passenger next looked outside, they ‘could not see anything, it was like a white‑out’. The passenger then felt the helicopter in a hard left turn.
Further investigation
To date, the ATSB has examined the accident site and wreckage; collected meteorological data from the Bureau of Meteorology; visited the operator to conduct interviews, and collect operational and maintenance data; and liaised with Victoria Police, and the French Bureau of Enquiry and Analysis for Civil Aviation Safety (BEA) as the accredited representative for the helicopter and engine manufacturers.
The investigation is continuing and will include:
download and analysis of the electronic items retrieved from the accident site
analysis of the meteorological data
analysis of the wreckage examination
helicopter maintenance history
evaluating witness information
review of the pilot’s qualifications, experience, and medical information
review of the operator’s management systems
review of commercial helicopter pilot training and flight review requirements
similar occurrences.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB acknowledges the assistance provided by Victoria Police, Victoria State Emergency Services, the operator, and the French Bureau of Enquiry and Analysis for Civil Aviation Safety.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 25 February 2021, a Piper Aircraft PA-28, registered VH-FPS, operated by Moorabbin Aviation Services, departed Warrnambool Airport for Moorabbin Airport, Victoria. The flight crew were conducting a training flight under the visual flight rules (VFR). There was an instructor, student pilot and a passenger on board.
During the cruise, the weather deteriorated and the aircraft was returned to Warrnambool. As the aircraft approached Warrnambool, the visibility reduced and the instructor initiated a climb into cloud. They contacted air traffic control and received navigation assistance to an area free from cloud. The flight then proceeded to Moorabbin Airport where the aircraft landed safely.
What the ATSB found
The ATSB found that although the flight crew had conducted a pre-flight briefing, they did not detect the forecast deteriorating weather in the Warrnambool area. In addition, they did not assess the aerodrome forecast for both Moorabbin and Warrnambool to ensure they were suitable destination airports. The aircraft departed Warrnambool in visual flight conditions however, as forecast, the weather subsequently deteriorated and the flight crew initiated a return to Warrnambool. During the return, the conditions reduced below that required for visual flight resulting in the VFR certified aircraft entering instrument meteorological conditions (IMC).
After entering IMC, the pilot requested assistance from the controller and maintained control of the aircraft.
What has been done as a result
As a result of this occurrence, the operator advised that they have developed a:
weather information board, which displays the synoptic charts, relevant TAFs and grid point wind and temperature charts for the day at the Moorabbin base.
Warrnambool PowerPoint presentation for dual and solo flight exercises, to emphasis the prevailing weather in that region of Victoria and Bass Strait.
supervision policy in the Training Management Manual to facilitate varying supervision based on the experience level and proven competency of the junior instructors and other circumstances which may challenge the junior instructor’s skill set.
company policy to provide organisational support for flight crew required to stay away from base overnight due to adverse weather, aircraft unserviceability or pilot incapacity/fatigue, including arrangement and payment of transport and accommodation if required. This policy will be promoted through both staff and student levels.
program on effective decision making to be delivered to all staff.
Safety message
Weather related incidents continue to be a significant concern in aviation safety. As stated in the ATSB publication Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions,1 in 10 VFR into IMC events result in a fatal outcome. This report highlights that ‘thorough pre-flight preparation is the best defence against flying into deteriorating weather’.
The ATSB encourages pilots, of all experience levels, to develop the knowledge and skills required to avoid unintentional operations in IMC. However, if a VFR‑rated pilot does find themselves in marginal weather, they should seek whatever assistance is available, including contacting air traffic services.
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 25 February 2021 the flight crew of a Piper Aircraft PA-28-161 aircraft, registered VH-FPS (FPS) and operated by Moorabbin Aviation Services, arrived at Moorabbin Airport to prepare for a VFR training flight.[1] The flight crew consisted of an instructor and student pilot (student), with a second student pilot observing the flight. The flight was part of the navigation training for the student’s integrated commercial pilot licence training course.
The student obtained the weather forecast and completed the planning for the training flight, which was to depart Moorabbin Airport and overfly Bacchus Marsh, Ballarat, Ararat, Horsham, and then to Warrnambool, where they [2] planned to land before 1400. At Warrnambool, they planned to refuel, before returning to Moorabbin Airport (Figure 1).
Once the planning was complete, the student briefed the instructor on the forecast weather and the procedures for the flight. They identified that at the time of their arrival at Warrnambool, the aerodrome forecast (TAF) was forecasting the visibility to be greater than 10 km with scattered[3] cloud at 3,000 ft above ground level (AGL). However, at 1500 a forecast INTER[4] was due to commence, with the visibility decreasing to 5,000 m in showers of rain and the cloud cover increasing to broken[5] and the cloud base lowering to 1,000 ft AGL. The student pilot did not brief the instructor on deteriorating weather in the Warrnambool area which was forecast on the graphical area forecast (see the section titled Weather forecasts) and the instructor did not detect this omission. The instructor later advised that they did not put enough emphasis on considering the weather forecast during this briefing.
Figure 1: Flight planned track and diversion
The red full line shows the flight track, which was planned and flown, the red broken line shows the intended flight planned track and the blue line shows the track flown after the diversion from Lake Goldsmith, near Ballarat, to Warrnambool.
Source: Google earth, annotated by the ATSB
The flight departed Moorabbin Airport at around 1200 Eastern Daylight-saving Time,[6] an hour later than planned, with the student flying the aircraft from the left seat. After passing Ballarat at 4,500 ft above mean sea level (AMSL), the instructor put the student under the hood,[7] to practise flying with reference to instruments only. After flying for about 14 minutes, the hood was removed and the instructor asked the student to identify the location of the aircraft. The student correctly identified the aircraft’s position and the instructor then tasked them to divert directly to Warrnambool, which they did successfully.
The instructor advised that the aircraft landed at Warrnambool at around 1400. The weather was clear however, as they parked the aircraft, the wind strength increased. As an air ambulance helicopter was due to land and refuel, the student and passenger took a short break in the terminal. While the helicopter was refuelling, the cloud cover increased and it began to rain. The flight crew waited until the rain stopped before commencing refuelling their aircraft.
The instructor advised that while waiting for the weather to improve, they checked the weather from various sources using their mobile phone. They observed that the TAF for Warrnambool had been amended and was now forecasting a TEMPO[8] with the visibility reducing to 4,000 m in showers of rain and the cloud had increased to broken with the base at 800 ft AGL. They could not recall how much of the graphical area forecast (GAF)[9] was reviewed and whether they checked the TAF for Moorabbin Airport at this time.
The instructor then contacted two senior pilots at their Moorabbin base and advised them that they were delayed at Warrnambool as the weather had deteriorated. Both of these pilots advised the instructor to wait until the weather had cleared and the senior base pilot advised them to remain at Warrnambool overnight if required.
The instructor reported that the cloud level subsequently lifted and the aerodrome weather information service (see the section titled Warrnambool airport observations) stated that the cloud was scattered at 1,900 ft AGL. A decision was made to depart, with the plan that they would return to Warrnambool if the weather deteriorated. The instructor advised that at the time of departure, while there were some clouds, there were also patches of blue sky and the visibility to the east was clear. However, they noted that there was an increased amount of cloud to the north-west of the airport.
It was reported that, during the initial cruise, the visibility was good but the cloud base lowered as the flight progressed. The student stated that during the cruise they were maintaining about 1,200 ft above mean sea level (AMSL) with the cloud base lowering to 1,300 ft. The instructor advised they were continually checking behind them to ensure they had clear weather to return to Warrnambool if required.
Due to the deteriorating weather, the instructor decided to divert to Cobden Airport to land and wait until the weather cleared. As the aircraft approached Lake Elingamite, about 5 km south-west of Cobden (see Figure 1), the visibility reduced significantly in rain. As a result, the instructor, in the right seat, took control of the aircraft. They stated they could no longer see Cobden Airport and a decision was made to return to Warrnambool.
Figure 2: Photograph taken en route to Cobden Airport
Source: supplied
The flight crew reported that during the initial stages of the return, the visibility was good. As they got closer to Warrnambool however, the visibility reduced, and they had to descend as the cloud base again began to lower. The instructor advised they were continuously listening to the AWIS during the return. At about 1615, while approaching Warrnambool township, at approximately 450 ft AGL, the instructor slowed the aircraft and extended two stages of flap. The visibility reduced significantly and the instructor, not wanting to descend further, made the decision to climb into cloud.
Figure 3: Photograph taken at 1613 during the return to Warrnambool Airport
Source: supplied
The instructor advised that they unsuccessfully attempted to contact air traffic control (ATC) to report that they were a VFR aircraft changing category to instrument flight rules (IFR).[10] They reported that they were having radio difficulties and this call may not have been received. Despite that, ATC responded to a call where the instructor advised they were in cloud and were requesting assistance. After clarifying the aircraft’s location and the pilot’s intentions, ATC assisted with information on the local weather, the lowest safe altitude and subsequently provided advice to keep the wings level, maintain a constant speed and to trust their instruments.
Initially the instructor maintained a shallow climb and a low angle of bank turn to remain within an area around Warrnambool known to be clear of obstacles. When they reached 3,000 ft, they turned north to ensure they did not track over water. They advised that in an attempt to fix the apparent radio problems they also switched between the two radio units in the aircraft and exchanged headsets with the student pilot. They continued the climb to 4,500 ft.
ATC identified the aircraft on radar and issued the flight crew with a heading to Avalon Airport as the pilot of a helicopter in that area had reported operating clear of cloud. During the cruise, the instructor became concerned that they would enter controlled airspace and requested a clearance at 4,500 ft, which was approved.
The aircraft exited cloud about 10 NM south-west of Avalon Airport, where the instructor requested, and was cleared for, descent to 2,500 ft. The flight then continued to Moorabbin Airport for an uneventful landing.
Context
Personnel information
Instructor
The grade three instructor held a valid Commercial Pilot Licence (Aeroplane), with a class 2 aviation medical certificate. They held an instrument rating with multi-engine aeroplane (IR-MEA), IAP 2D and IAP 3D endorsements.[11] They had completed an instrument proficiency check in March 2020 but had not conducted any instrument flying since that date.[12] In addition, they had never conducted instrument flying from the right seat of the aircraft.
They had accrued a total of 1,241 flying hours, having flown approximately 62 hours in the previous 90 days.
At the time of the incident, the pilot had a self-assessed fatigue level[13] of ‘2: very lively. Responsive, but not at peak’.
Student pilot
The student pilot held a recreational pilot licence and was training for their commercial pilot licence. They had accumulated approximately 81 hours of flying with approximately 17 hours in the previous 90 days.
Aircraft
The Piper PA-28-161 is a single engine, low wing, four seat aircraft. FPS was certified for day and night VFR operations only. The main aircraft flight instruments are located on the left side of the cockpit (Figure 4).
Figure 4: PA-28 cockpit
Source: supplied
Weather forecasts
The student received the graphical area forecast (GAF)[14] at 0910. It was valid until 1600. The GAF was split into six different areas on the day (Figure 5). The flight was planned to traverse two of these areas: B and C.
Area C
The initial section of the flight from Moorabbin Airport was planned in area C. This area was forecast to have greater than 10 km visibility and scattered cloud between 1,600 and 3,000 ft AMSL. From 1500, cloud was forecast to increase to broken between 3,000 and 8,000 ft AMSL.
Area B
The flight was then planned to enter area B, which included Warrnambool. From 1400, the visibility in this area was forecast to reduce to 3,000 m in scattered rain with broken stratus[15] cloud between 500 and 2,000 ft AMSL and broken stratocumulus[16] clouds between 2,000 and 9,000 ft AMSL.
Grid Point Wind and Temperature forecast
The Grid Point Wind and Temperature forecast valid at the time of the flight, forecast the wind to be at 27 kt from 249˚ in the Ballarat area and 11 kt from 249˚ in the Warrnambool area.
No AIRMETs[17] or SIGMETs[18] were issued during the validity period.
Figure 5: Graphical area forecast valid for flight
Source: Bureau of Meteorology, annotated by the ATSB
Warrnambool aerodrome forecast
The TAF for Warrnambool was issued at 0445 and was valid when the student received the information at 0938. It was forecasting visibility greater than 10 km and scattered cloud with a base at 3,000 ft AGL. An INTER was forecast from 1500, where the visibility was forecast to reduce to 5,000 m in showers of rain with broken cloud at 1,000 and 2,500 ft AGL.
The Bureau of Meteorology released an amended TAF at 1243, after the aircraft had departed Moorabbin Airport. It forecast that at the time of their arrival the visibility would be greater than 10 km, with showers of rain and few[19] cloud with a base of 1,500 ft AGL. The forecast INTER was due to commence at 1600 with visibility reducing to 5,000 m in showers of rain and a broken cloud base at 1,000 ft AGL. The crew did not receive this forecast.
At 1500, a second amended TAF was released that forecast visibility to remain greater than 10 km with showers of rain and scattered cloud with bases at both 1,000 and 2,000 ft plus broken cloud at 3,000 ft AGL. There was also a TEMPO associated with this TAF which commenced at 1500, forecasting the visibility to reduce to 4,000 m in showers of rain and broken cloud at 800 and 2,000 ft AGL.
Warrnambool airport observations
An automatic weather station (AWS) recorded actual weather conditions at Warrnambool Airport. The cloud base and amount is measured by a ceilometer, which is a device that uses a laser, or other light source, to determine the height of the cloud base. As such, it measures the cloud in one direction only and this may not give an accurate interpretation of the surrounding conditions.
The AWS recorded a SPECI[20] report about 5 minutes before the aircraft departed Warrnambool that showed the visibility was greater than 10 km with scattered cloud at 1,100 ft and broken cloud at 1,900 ft AGL.
While the aircraft was returning to Warrnambool, the AWS recorded that the visibility was fluctuating between 5,000–9,000 m, with cloud at 900 ft AGL, varying between broken and scattered.
Moorabbin Airport forecast
The TAF current at the time of departure from Moorabbin Airport, issued at 0505, was valid for the entire flight. It forecast CAVOK conditions at the time of departure and for the return to Moorabbin.[21] However, a new TAF was issued at 1032, before the flight departed Moorabbin, which was valid from 1100 to 2300. It also forecast conditions to be CAVOK during the flight, with deteriorating conditions associated with an INTER due to commence at 1900.
Flight planning
Civil Aviation Regulations (CAR), 239Planning of flight by pilot in command, stated that ‘before beginning a flight, the pilot in command shall study all available information appropriate to the intended operation, and in the cases of flights away from the vicinity of an aerodrome…current weather reports and forecasts for the route to be followed and at the aerodromes to be used’.
Aeronautical Information Publication (AIP) Enroute 1.10 Flight planning stated that the forecast information must include an airport forecast for the destination and, when required, the alternate airport. It also stated that if the pre-flight information is obtained more than 1 hour prior to the estimated departure time, updated information is required.
In addition, AIP Enroute 1.1 10.7.2 Weather conditions stated that when planning a day VFR flight in a fixed wing aircraft, an alternate airport is required when conditions at the destination airport are forecast to be cloud greater than scattered below 1,500 ft or visibility less than 8 km. If a TEMPO is associated with the forecast, which reduces conditions below this requirement, then the pilot is required to plan an alternate airport or to have enough fuel to hold for 1 hour.
Visual flight rules
Civil Aviation Regulations 1988 (CAR), 172Flight visibility and distance from cloud, outlined that flight under the VFR can only be conducted in visual meteorological conditions (VMC).[22] Additionally, when operating at or below 2,000 ft above the ground or water, the pilot must be able to navigate by visual reference to the ground or water.
In addition to minimum visibility and distance from cloud, a pilot is also required to maintain a minimum height above the ground. CAR 157Low flying, directs that a pilot in command must not fly the aircraft over:
any city, town, or populous area at a height lower than 1,000 ft; or
any other area at a height lower than 500 ft.
This does not apply if ‘through stress of weather or any other unavoidable cause it is essential that a lower height be maintained’.
Similar occurrences
Between 2011 and 2021, the ATSB was notified of 106 occurrences, where a VFR flight entered IMC. Of these, there were 13 accidents that resulted in 26 fatal injuries.
Safety analysis
Both the instructor and the student pilot advised that they assessed the weather forecasts during the pre-flight planning. They also both advised that they planned to land at Warrnambool before 1400, which was before the deteriorating weather was forecast to commence on the Warrnambool TAF. However, they did not assess the forecast deteriorating weather in area B on the GAF, which was also due to commence at 1400.
Additionally, as the flight left more than 60 minutes after the pre-flight weather forecasts were obtained, updated weather forecasts were required. However, the weather information had not changed significantly. The delayed departure and the time spent on the ground in Warrnambool both added to the likelihood of the aircraft encountering the forecast deteriorating weather.
The instructor advised that they checked the weather for the return flight while they were on the ground at Warrnambool. However, they used the TAF for Warrnambool and the surrounding airports, rather than the area forecast and Moorabbin TAF, to provide an indication of the likely weather to be encountered on return to Moorabbin. This was a missed opportunity to identify the forecast reduced visibility and low-level cloud subsequently encountered during the flight.
In addition, as the instructor planned to return to Warrnambool Airport if conditions deteriorated, they should have considered the forecast in relation to its use as a destination. As the TAF forecast a TEMPO with conditions deteriorating below the alternate minima requirements, they were required to plan for an alternate airport or have enough fuel to hold for 1 hour.
The flight crew had refuelled at Warrnambool, so the aircraft had sufficient endurance for the required holding. However, when planning to hold for 1-hour, consideration should also be given to the likely weather conditions – in this case, the conditions were forecast to have visibility reducing to 4,000 m and broken cloud at 800 ft AGL. The flight crew had experienced the rapidly changing weather environment, and consideration should have been given to how they were going to hold for 1‑hour in potentially poor weather conditions.
The instructor also did not adequately reassess the conditions at Moorabbin prior to departure from Warrnambool, however the conditions were suitable for the return flight.
Although the conditions on departure from Warrnambool were suitable for VFR flight, they soon deteriorated resulting in the decision to return. During the return to Warrnambool, the aircraft encountered forecast conditions which were no longer suitable for VFR flight and the instructor climbed the aircraft and entered cloud. The instructor had an instrument rating however, they had not practiced this skill in eleven months. In addition, the aircraft was not certified for instrument flight.
After making the decision to enter cloud, the instructor was conscious that they were not current and had never flown with reference to instruments from the right seat, which required them to use the instruments on an angle across the cockpit. Consequently, they ensured that they minimised control movements to maintain control of the aircraft. They also contacted ATC at the earliest opportunity to advise of their situation and request assistance. This ensured the instructor could concentrate on flying and maintaining control of the aircraft and also expedite the return to visual flight conditions.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the VFR flight into IMC involving Piper Aircraft PA-28, VH-FPS, near Warrnambool, Victoria on the 25 February 2021.
Contributing factors
While conducting preparation for the flight, neither the instructor nor the student pilot identified the forecast deteriorating weather in the Warrnambool area.
Prior to departure from Warrnambool, the instructor did not analyse either the Warrnambool or Moorabbin aerodrome forecasts for their suitability as destination airports. This probably resulted in them selecting Warrnambool as an alternate airport, despite the forecast temporary deterioration, and encountering poor weather conditions during the return to Warrnambool.
Conditions reduced below that required for visual flight resulting in the VFR‑certified aircraft entering instrument meteorological conditions.
Other findings
After entering instrument meteorological conditions (IMC), the instructor maintained control of the aircraft and requested assistance from air traffic control.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future.
Safety action by Moorabbin Aviation Services
As a result of this occurrence, the operator have developed a:
weather information board which displays synoptic charts, relevant TAFs and grid point wind and temperature (GPWT) chart for the day at the Moorabbin base
Warrnambool PowerPoint presentation for dual and subsequent solo exercises to emphasis weather in that region of Victoria and Bass Strait
supervision policy in the Training Management Manual to facilitate varying supervision based on the experience level and proven competency of the junior instructors and other circumstances which may challenge the junior instructor’s skill set
company policy to provide organisational support for flight crew required to stay away overnight due to adverse weather, aircraft unserviceability or pilot incapacity/fatigue, including arrangement and payment of transport and accommodation if required. This policy will be promoted through both staff and student levels
program on effective decision making to be delivered to all staff.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
flight crew
Moorabbin Aviation Services
Bureau of Meteorology
Airservices Australia
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
flight crew
Moorabbin Aviation Services
Bureau of Meteorology
Civil Aviation Safety Authority
Airservices Australia
Submissions were received from:
the instructor
Moorabbin Aviation Services
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the afternoon of 12 January 2020, the pilot of an amateur-built Wittman Tailwind aircraft, registered VH-TWQ (TWQ), departed Evans Head Airport, New South Wales, with one passenger on board. The pilot was conducting a private flight under the visual flight rules from Evans Head, to Boonah, Queensland.
The pilot flew in a north-north-westerly direction towards Boonah via the Richmond River valley. At 1353, the pilot commenced a 180° turn overhead the township of Kyogle and diverted, due to the weather, south back down the valley to Casino Aerodrome, landing at 1406.
At 1454, the pilot took off from Casino and flew in a west-north-westerly direction. At 1512 TWQ commenced a series of rapid descents and climbs followed by a descending left turn. The turn and descent continued until TWQ collided with terrain. The pilot and passenger were fatally injured, and the aircraft was destroyed.
What the ATSB found
The ATSB found that the pilot departed an interim landing site for Boonah under the visual flight rules with a high risk of encountering forecast cloud. En route to Boonah, the aircraft entered an area of reduced visibility and the pilot likely became spatially disorientated resulting in a loss of control and collision with terrain.
Safety message
Weather-related accidents remain one of the most significant causes of fatal accidents in general aviation and continues to be a focus of the ATSB’s SafetyWatch initiative. SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns relates to inflight decision making, particularly involving pilots flying with reduced visual reference. SafetyWatch provides information about each safety concern, and strategies to help manage risk areas, along with links to safety resources. In relation to visual flight rules (VFR) pilots flying into areas of reduced visibility, some key messages are:
Pilots should avoid deteriorating weather by conducting thorough pre-flight planning. They should ensure they have alternate plans in case of an unexpected deterioration in the weather and make timely decisions to turn back, divert or hold in an area of good weather.
VFR pilots should use a ‘personal minimums’ checklist to help control and manage flight risks through identifying risk factors that include marginal weather conditions and only fly in environments that do not exceed their capabilities.
Pilot’s should consider reducing speed and/or altering the configuration of the aircraft to allow more time for decision making and manoeuvring in areas of deteriorating or marginal weather conditions
Pressing on into instrument meteorological conditions without a current instrument rating carries a significant risk of severe spatial disorientation due to powerful and misleading orientation sensations with reduced visual cues. Disorientation can affect any pilot, no matter what their level of experience.
If VFR pilots find themselves in marginal weather and becoming disoriented or lost, they should seek whatever help is available. Air Traffic Services (ATS) may be able to provide assistance, especially if the aircraft is in ATS surveillance coverage. There have been a number of reported occurrences where this simple action has averted potential disaster.
The occurrence
On Friday, 10 January 2020 the pilot of an amateur-built Wittman Tailwind aircraft, registered VH‑TWQ (TWQ), departed Toowoomba, Queensland, and flew via Boonah, to Evans Head, New South Wales. The purpose of the flight was to pick up a passenger at Boonah and then attend the Great Eastern Fly-In (Fly-In) at Evans Head. The Fly-In was planned for the weekend of 11‑12 January. However, due to poor weather, the event program was significantly disrupted.
On the morning of 12 January 2020, the pilot attended the Fly-In event briefing which included the meteorology for the day. The event was cancelled at 0830 due to the cloud base at Evans Head being approximately 1,000 ft above ground level (AGL) with a reduction to 600 ft AGL forecast during the day. Due to the cancellation of the event the pilot elected to return to Toowoomba and contacted relatives there for an update on the weather. They sent photos of the local conditions and said the cloud at Toowoomba was not really low, there was no wind and there had been some rain. At 1336 Eastern Daylight-saving Time,[1] the pilot departed Evans Head Airport , with one passenger on board. The pilot was conducting a private flight under the visual flight rules[2] to Toowoomba via Boonah (Figure 1).
Figure 1 - Accident flight departure, destination and accident locations
Source: Google Earth, annotated by the ATSB
The pilot flew in a north-north-westerly direction towards Boonah via the Richmond River valley (Figure 2). The aircraft reached a maximum altitude of 1,950 ft above mean sea level[3] just prior to reaching Kyogle. At 1353, the pilot commenced a 180° turn overhead the township of Kyogle and diverted, likely due to low cloud on their intended flight path. At 1357 a family member contacted the passenger as they had seen the turnaround overhead Kyogle on OzRunways.[4] The passenger replied to say they were ‘going home due low cloud’. The pilot flew south back down the valley to Casino Aerodrome, landing at 1406.
During the time on the ground at Casino, the pilot contacted a friend in the area and left a voice message. The message stated they could not get past Kyogle due to the weather, so they had landed at Casino. (refer to the section titled Meteorological information below.)
Figure 2 - Flight tracks for VH-TWQ on 12 January 2020
Source: Flightradar24 and Google Earth, annotated by the ATSB
At 1454, the pilot took off from Casino and flew in a west-north-westerly direction. At 1510 TWQ commenced a series of rapid descents and climbs, between 3,100 and 4,000 ft, followed by a left descending turn. Shortly afterwards TWQ collided with terrain. The pilot and passenger were fatally injured, and the aircraft was destroyed. There were no witnesses to the accident.
The pilot held a Private Pilot Licence (Aeroplane) issued in July 1982 and was qualified to fly by day under the visual flight rules. The pilot also held a single-engine aeroplane class rating. The pilot last conducted a single-engine aeroplane flight review in June 2018 that was valid until June 2020. The pilot had about 1,200 hours flying experience recorded in the pilot’s logbook with a total of about 140 hours on the Wittman Tailwind. In the 90 days prior to the accident, the pilot had flown 12.4 hours total, of which 11.2 hours were in TWQ.
The pilot’s logbook showed a total of 8.4 hours instrument flying experience. Of these, 5 hours were accumulated between 1982 and 1983. The remaining 3.4 hours were accumulated from 1986 to 2015. The pilot did not hold an instrument rating.
Medical information
The pilot held a Class 2 aviation medical certificate that was valid until October 2021 with two restrictions noted. One restriction required distance vision correction be worn and the other required reading correction to be available during flight.
The pilot was reported to be in good health and not taking any medications at the time of the accident.
Due to the pilot being away from home for the days preceding the accident, a detailed 72-hour history could not be obtained. From the limited information available there were no fatigue‑related concerns identified.
A limited post-mortem examination and toxicological screening was performed. There was nothing found to support incapacitation.
Aircraft information
Overview
VH-TWQ (TWQ) was a Wittman Tailwind, an amateur-built aircraft in the experimental category. TWQ had a two seat, side-by-side seating arrangement. The structure was a combination of tubular steel frames and fabric covering on the fuselage. Wooden wing ribs had a bonded plywood skin covering. The flight controls consisted of push-pull type control tubes. All flight controls and flaps were fabric covered. The Wittman had a fixed undercarriage in a taildragger configuration.
TWQ was fitted with a Lycoming XIO-320[5] four cylinder, horizontally opposed piston engine and was fitted with a ground adjustable Whirlwind two-bladed composite propeller.
Entries in the logbook indicated that the owner-pilot commenced construction of the aircraft as an amateur builder in January 2006. The aircraft was completed in August 2018. A CASA authorised person issued a special certificate of airworthiness in the experimental category on 25 December 2018.
On 28 June 2019, the pilot issued a maintenance release that was valid for 12 months. This allowed the aircraft to be operated privately under the day visual flight rules. The aircraft flew for 33.3 hours between 28 June 2019 and the day of the accident. No defects or unserviceable equipment endorsements were recorded on the maintenance release.
The last entry in the aircraft’s maintenance records was the change, by the pilot, of the engine oil and filter in October 2019. The pilot changed the engine oil filter in accordance with the maintenance schedule.
Operating limitations
Aircraft operating limitations were contained within the flight manual for the aircraft and relevant limitations are detailed in Table 1 and Table 2.
Table 1 – Airspeed limitations
Speed
Knots indicated airspeed (KIAS)
Remarks
Vne – Never exceed
174
Do not exceed this speed in any operation
Vno – Max structural cruising
155
Do not exceed this speed except in smooth air, then only with caution
Va – Manoeuvring
155
Do not make full or abrupt control movement above this speed, because under certain conditions the aircraft may be overstressed.
Table 2 - Stall speeds
Configuration
Power off (KIAS)
Power on (KIAS)
Clean
52
49
Flaps Land
47
40
Navigation / cockpit instruments
The aircraft was fitted with a Garmin G3X (G3X) flight display, capable of displaying the engine monitoring instruments, primary flight instruments and navigation information.
The pilot was reported to navigate primarily by using paper maps, using the main Garmin screen to display attitude and heading information as well as engine parameters. The pilot had an iPad mounted beside the G3X unit running the OzRunways application. It was reported that the pilot’s use of OzRunways navigation and flight planning features was limited to using the direct to function which plotted a track from the aircraft’s current location to a desired destination. The pilot was also reported to use the weather radar overlay function on OzRunways. This overlay displayed rain when detected by radar but did not display the presence of clouds.
Wreckage and accident site information
Accident site
The accident site was located in dense rainforest, about 72 km west-north-west of Casino, within the Tooloom National Park (Figure 2). The New South Wales Police Rescue and Bomb Disposal Unit assisted ATSB investigators to access the site on foot.
The accident site was on the eastern side of a ridgeline at an elevation of 3,170 ft. The highest ground in the immediate area of the accident site was approximately 3,200 ft.
Wreckage examination
The aircraft’s structure was substantially disrupted (Figure 3). The wreckage trail was about 120 m long on a bearing of approximately 270°. All major aircraft components were located at the accident site. ATSB investigators did not identify any signs of pre-existing airframe damage. Due to the disruption of the airframe, the aircraft’s attitude when it entered the tree canopy could not be determined. There was no evidence of fire. Site and wreckage examination did not identify any defects or anomalies that might have contributed to the accident.
Figure 3 - VH-TWQ’s empennage at the accident site
Source: ATSB
Engine and propeller
On-site examination of the engine and propeller did not identify any defects that could have contributed to the accident. Damage noted to the propeller, during this examination, were consistent with the engine producing significant power at the time of the accident.
Flight control system
All primary and secondary flight controls were located on-site. An examination of the flight control systems did not identify any faults that could have contributed to the accident.
Fuel
The fuel tank was located toward the end of the wreckage trail. It was torn from the fuselage and had ruptured. Rain had entered the tank post-accident, therefore the fuel that remained in the tank was not tested.
Weight and balance
The on-site examination found a small amount of lightweight cargo. It was reported that the occupants took minimal cargo with them when they departed for the weekend. Weight and balance was calculated using full fuel and maximum baggage on departure out of Toowoomba and was calculated to be within limits. The aircraft did not refuel again after departing Toowoomba. Weight and balance was also calculated for the expected fuel remaining at the time of the accident and was also within limits.
Emergency locator transmitter
The aircraft was not fitted with an ELT, nor was it required to be. An Emergency Position Indicating Radio Beacon was located in the wreckage and had not been activated. This unit was tested on-site and functioned as required.
Operational Information
The flight from Evans Head to Boonah required the pilot to cross the McPherson Range (Figure 4). The McPherson Range is a spur of the Great Dividing Range, heading in an easterly direction from near Wallangarra, Queensland, to the coast. It also forms part of the border between New South Wales and Queensland.
Figure 4 - Accident site and McPherson Range
Source: Google Earth and Flightradar24, annotated by the ATSB
Terrain across the range varies in altitude with several areas above 3,000 ft and some peaks above 4,000 ft.
The initial flight from Evans Head to Casino, indicated that the aircraft was attempting to cross the ranges via a route known as the ‘border loop’. The border loop is a route commonly used by VFR pilots to transit the range. Tracking is north up the Richmond River valley, past the town of Kyogle, then over the ranges where the railway cuts through the high ground.
Another common route over the ranges is to fly via the Toonumbar Dam, then Killarney to Warwick, which is similar to the track of the second flight. Another pilot who attended the Fly‑In reported that when attempting to fly over the ranges they use a minimum of 4,000 ft, and normally fly over the range at about 5,000 ft.
Meteorological information
Bureau of Meteorology forecast
The planned flight from Evans Head to Boonah traversed two Graphical Area Forecast (GAF)[6] areas. The accident site was located on the border of the GAF NSW East (NSW-E) and the GAF QLD South (QLD-S).
Forecast weather conditions in the GAF for NSW-E, valid from 1000 to 1600 on 12 January 2020, that potentially affected the flight included:
Average conditions of greater than 10 km visibility with areas of broken[7] stratocumulus clouds between 3,000 and 6,000 ft
Widespread smoke reducing visibility to 8,000 m
Isolated showers of rain reducing visibility to 4,000 m with associated cloud including broken stratus 1,000 to 2,000 ft and broken cumulus, stratocumulus 2,000 to 8,000 ft
Isolated thunderstorms and rain reducing visibility to 2,000 m with associated cloud including isolated cumulonimbus 6,000 to above 10,000 ft, broken stratus 500 to 2,000 ft and broken stratocumulus 2,000 to 6,000 ft
Isolated smoke over land reducing visibility to 1,000 m
Moderate turbulence is implied in cumulous, stratocumulus and altocumulus cloud. Severe turbulence is implied in thunderstorms, cumulonimbus and towering cumulus
The GAF for QLD-S was valid from 0900 to 1500. Forecast conditions that potentially affected the flight included:
Average conditions of greater than 10 km visibility with areas of scattered stratus 1,500 to 3,000 ft, scattered cumulus and stratocumulus 2,500 to 7,000 ft, and further cloud layers above 8,000 ft
Isolated dust and smoke reducing visibility to 7,000 m and 5,000 m respectively
Scattered rain reducing visibility to 5,000 m with associated broken stratus 1,200 to 4,000 ft, broken stratocumulus 5,000 to 8,000 ft and broken altocumulus and altostratus 8,000 to above 10,000 ft
Scattered showers of rain reducing visibility to 3,000 m with associated occasional towering cumulus 5,000 to above 10,000 ft and broken stratus 1,200 to 3,000 ft
Isolated thunderstorms and rain reducing visibility to 2,000 m with associated isolated cumulonimbus 4,000 to above 10,000 ft, broken stratus 1,500 to 4,000 ft and broken stratocumulus 4,000 to 6,000 ft
Moderate turbulence is implied in cumulous, stratocumulus and altocumulus cloud. Severe turbulence is implied in thunderstorms, cumulonimbus and towering cumulus
Neither of the GAFs were corrected and no SIGMETs or AIRMETs affecting the QLD-S area were issued during the validity period. An AIRMET was issued for the NSW-E GAF region, however this was for an area to the west of the flight path and did not affect the conduct of this flight.
The Bureau of Meteorology (BoM) Grid Point Wind and Temperature forecast valid at the time of the flight, forecast the wind to be 20 kt from 160° at 2,000 ft and 19 kt from 130° at 5,000 ft.
The BoM also provided an aerodrome forecast (TAF)[8] for Ballina and Lismore. Lismore Aerodrome was the closest aerodrome to the flight path with a TAF available. TWQ flew within 9.7 km of Lismore aerodrome on the flight from Evans Head to Casino. Lismore is located 20 km east north east of Casino with an elevation of 35 ft. The amended Lismore TAF, issued at 1145 on 12 January 2020, was valid from 1300 on the day of the accident. The TAF forecast 14 kt winds from 160°, visibility greater than 10 km and light showers of rain. Cloud was forecast to be scattered with a base of 2,000 ft above the aerodrome and broken with a base 3,000 ft above the aerodrome. The forecast indicated that between 1300 and 1700 there would be temporary periods, greater than 30 minutes but less than 60 minutes in duration, of deteriorating weather conditions. These conditions included visibility reducing to 4,000 m, showers of rain and broken cloud with a base of 1,000 ft above the aerodrome.
Great Eastern Fly-In event meteorology
On the morning of 12 January 2020, the pilot of TWQ attended the Fly-In pilot’s briefing which included the meteorology for the day. The briefing, delivered by event staff, included weather information based on forecasts available from the BoM for Evans Head, the surrounding airfields and the GAF NSW-E. The display was cancelled at 0830 during the briefing due to the cloud base at Evans Head being approximately 1,000 ft above ground level (AGL) with a reduction to 600 ft AGL forecast during the day.
Bureau of Meteorology observations and analysis
The BoM reported that there were no observations of the actual conditions at the location of the accident. The BoM commented that the winds south of the McPherson Range, below 5,000 ft, would have been south-west to south-easterly. The generally southerly wind flow, heading towards the range, would be consistent with orographic cloud[9] formation. The BoM noted that the forecast broken cloud at 3,000 ft was likely to be a reasonable representation of the conditions. The BoM also stated that the summits of Wilsons Peak at 4,030 ft and Mount Barney 4,430 ft are higher than the bases of the cloud forecast in this area. No thunderstorm activity was detected near the flight path from Casino.
Lismore airport observations
Half hourly observations[10] were recorded at Lismore Airport on the day of the accident. At 1500, the wind was from 170° at an average speed of 11.1 kt, with a gust of 15.9 kt recorded. The temperature was 23.2 °C and the mean seal level pressure was 1014.4 hectopascals (hPa). Cloud was overcast with a base of 3,300 ft.
Casino aerodrome weather recordings
The Casino Automatic Weather Station (AWS) recorded several weather parameters on the day of the accident. At 1500, the wind at Casino Aerodrome was from 170° at an average speed of 6 kt and the temperature was 23.6 °C. No cloud data is available for Casino AWS, as no ceilometer is installed at this location.
Witness observations of weather
Local residents
Residents in the vicinity of the accident location confirmed that the top of the ridgeline, where the accident site was located, was in cloud on the afternoon of the accident. Several of the witnesses commented they could see about three quarters of the way up the ridgeline, which was calculated to be approximately 2,800 ft. These residents commented that it was an overcast day and it had been raining on and off throughout the day.
Tooloom fire tower weather observations
The Forestry Corporation of New South Wales has several observation towers positioned in the region of the flight. The Tooloom tower is located closest to the flight path from Casino, at an elevation of 2,619 ft (Figure 5).
An observer was positioned in the tower on 12 January from 0900 to 1500 and recorded weather conditions on the hour. Throughout the day, visibility remained at 0 km, with the cloud recorded as 8 oktas. In addition, the relative humidity was recorded at 98 per cent or above throughout the day. The wind was from the south-south-east around 9 kt with an average gust of 19 kt.
Figure 5 – Tooloom fire tower location and proximity to flight track
Source: Google Earth and Flightradar24, annotated by the ATSB
Flight track proximity to Tooloom Fire Tower
At 1509, TWQ, at its closest, passed 4.23 km to the west-south-west of the Tooloom Fire Tower (Figure 5). The aircraft was tracking from the south-east to the north-west. At 1509 the aircraft was at 3,575 ft, with a ground speed of 141 kt and tracking 332°. Tooloom Fire Tower has an elevation of 2,619 ft, and was in cloud at 1500, as it had been since 0900.
Pilot access to weather information
On the morning of the accident, the pilot attended the Fly-In event briefing which included weather for the event and the area. There was no log recorded indicating that the pilot accessed the weather information through the National Aeronautical Information Processing System (NAIPS) on the day of the accident. However, it is possible that the pilot obtained additional weather information from other sources.
Recorded data
Overview
The aircraft was fitted with a Mode S transponder that broadcast ADS-B[11] data which included the position and altitude of the aircraft. The data was received by Flightradar24 and provided to the ATSB. Also on-board was a mobile device with the OzRunways electronic flight bag (EFB) application installed. The application had an option enabled for live flight tracking by transmitting the device’s position and altitude. OzRunways information was also obtained by the ATSB. This data had a sampling rate of every 5 seconds.
The ATSB compared the data from both sources and they were found to be consistent. The flight data from OzRunways was plotted for the accident flight along with the terrain elevation. (Figure 6).
Figure 6 - OzRunways data and terrain elevations for the final flight of TWQ
Figure 5 shows the aircraft’s flight data from OzRunways. Groundspeed is annotated in red, altitude in light blue and track in black. The altitude of Tooloom fire tower is also marked in blue. This line starts from the time where TWQ was abeam the fire tower. Terrain directly underneath the flight path is marked in green.
Source: OzRunways, US National Aeronautics and Space Administration Shuttle Radar Topography Mission data and ATSB
The first climb on the graph is part of the departure from Casino aerodrome. On a track generally to the north-west. The aircraft reached 3,000 ft and then descended to 2,200 ft.
The climb that commenced at approximately 1502 corresponded with the first range of high ground en route. A groundspeed of about 145 kt was maintained during this climb. The climb commenced at 2,200 ft and reached a peak of 4,100 ft.
The following descent from 4,100 ft to 3,100 ft, corresponded to a ground speed increase from 145 kt to 173 kt and a rate of descent of about 600 feet per minute. The altitude of TWQ at the bottom of this descent was above the altitude of Tooloom Fire Tower (Figure 6).
Over the last 4 minutes of the flight, the aircraft’s recorded groundspeed, rate of climb/descent and altitude oscillated significantly over short periods with the aircraft’s:
ground speed varying rapidly between 109 and 175 kt,
rate of climb and descent being between maximum values of +2,400 ft per minute and -2,400 ft per minute,
altitude oscillating between 4,000 and 3,100 ft.
At approximately 1512 the final descent and turn towards the high ground commenced. The descent commenced from 4,000 feet with the aircraft travelling at 133 kt groundspeed and tracking 316°.
The last data point was recorded at 1512:49. The aircraft was passing 3,100 ft with an 1,800 feet per minute rate of descent. It was travelling at 172 kt groundspeed and tracking 276°.
Of note, during the last few minutes of flight, prior to the collision with terrain, TWQ maintained more than 1,000 ft clearance with the ground and in most places more than 2,000 ft above the ground.
G3X flight display
The G3X unit can log flight and engine data on a removable SD card, or additionally to an internal Flight Log. The G3X unit was badly damaged in the accident sequence. The SD card and a number of circuit boards from the G3X unit were recovered from the accident site. The SD card was found in the read only mode and therefore did not contain any data from the accident flight. While some flight data was able to be recovered from the internal memory, the last recovered flight data was from 30 December 2019.
Air Traffic Control
TWQ was operating outside controlled airspace at the time of the accident. The Brisbane Centre audio recording was obtained from Airservices for the New England area, which covered the accident flight path. There were no radio calls recorded from TWQ, however, they were not required to make any routine radio calls on this frequency.
Additional information
Visual Flight Rules
The CASA Visual Flight Rules Guide outlined that flight under the visual flight rules (VFR) can only be conducted in Visual Meteorological Conditions (VMC).[12] Additionally, when operating at or below 2,000 ft above the ground or water, the pilot must be able to navigate by visual reference to the ground or water.
The flight, and the location of the accident, were in (non‑controlled) Class G airspace. The following conditions were stipulated for flight under the VFR in Class G airspace when below 10,000 ft and above 3,000 ft or 1,000 ft above ground level (whichever is higher):
a flight visibility of 5,000 m
a minimum vertical distance of 1,000 ft and horizontal distance of 1,500 m from cloud.
In the case of aeroplane operations in Class G at or below 3,000 ft or 1,000 ft above ground level (whichever is higher), the following minimum conditions were stipulated:
a flight visibility of 5,000 m
that the aeroplane shall be maintained clear of cloud and in sight of the ground or water
In addition to minimum visibility and distance from cloud, a pilot is also required to maintain a minimum height above the ground. CAR 157 details that a pilot in command must not fly the aircraft over:
any city, town, or populous area at a height lower than 1,000 ft; or
any other area at a height lower than 500 ft.
This does not apply if through stress of weather or any other unavoidable cause it is essential that a lower height be maintained.
Risks of flying in areas of reduced visual cues
The safety risks of VFR pilots flying from VMC conditions into instrument meteorological conditions (IMC)[13] are well documented. This has been the focus of numerous ATSB reports and publications, as VFR pilots flying into IMC represents a significant cause of aircraft accidents and fatalities. In 2013, the ATSB Avoidable Accidents series was re-published. Of these publications, the booklet titled Accidents involving pilots in Instrument Meteorological Conditions outlined that:
In the 5 years 2006–2010, there were 72 occurrences of visual flight rules (VFR) pilots flying in instrument meteorological conditions (IMC) reported to the ATSB…About one in ten VFR into IMC events result in a fatal outcome.
In another occurrence investigation,[14] the ATSB has found that the ‘continuation of flight towards an area of low cloud and rain was likely influenced by the inherent challenges of assessing low visibility conditions, particularly without instrument flying proficiency.’ This finding was based on the following references.
The United States National Transportation Safety Board (NTSB) (2005) found that ‘reduced-visibility weather represents a particularly high risk to [general aviation] operations’ and that ‘weather may…test the limits of pilot knowledge, training, and skill to the point that underlying issues are identified.’ The NTSB study also outlined that historically, about two-thirds of all general aviation (GA) accidents that occur in IMC are fatal, a rate much higher than the overall fatality rate for GA accidents.
Wiegmann and Goh (2000) explained that pilots may make errors in assessing the deteriorating weather conditions and decide to continue to VFR flight into the adverse weather. The previously mentioned NTSB report (2005) added that in these cases, pilots who might appear to intentionally engage in risky behaviour may actually be making choices that they mistakenly believe to be safe by underestimating the risks associated or overestimating their ability to handle the risks.
Wiggins and O’Hare (1995) further explained how errors in assessment can take place, acknowledging that weather-related decision making can be highly complex and therefore more prone to errors:
Because of the variable nature of operations in the aviation environment, weather-related decision making is often considered a skill that cannot be prescribed during training. Rather it is expected to develop gradually through practical experience. However, in developing this type of experience, relatively inexperienced pilots may be exposed to hazardous situations with which they are ill‑equipped to cope.
ATSB Aviation Research and Analysis Report B20070063, An overview of spatial disorientation as a factor in aviation accidents and incidents, stated that pilots should not attempt to fly into instrument meteorological conditions under the VFR. Pilots should develop a plan prior to take-off on what to do if the weather en route is different from that expected or deteriorates. This plan should consider a requirement to divert or turn back prior to entering instrument meteorological conditions. However, this depends on a pilot correctly assessing the weather conditions. The NTSB (2005) noted that targeted weather-related training programs have had some success in teaching pilots to recognise and respond to deteriorating weather conditions.
A cue-based training system called Weatherwise, was made available to pilots by the Civil Aviation Safety Authority (CASA). Additionally, CASA produced a Weather to Fly education program which focuses on topics such as the importance of pre-flight preparation, making decisions early, and talking to ATC.
One of the ATSB’s SafetyWatch priorities concerns in-flight decision making in relation to VFR flight in environments with reduced visual references. One of the key messages is for pilots to avoid deteriorating weather by conducting thorough pre-flight planning and to have alternate plans in case of an unexpected deterioration in the weather and making timely decisions to turn back or divert.
Spatial disorientation
Spatial disorientation is a type of loss of situation awareness, and is different to geographical disorientation, or incorrectly perceiving the aircraft’s distance or bearing from a fixed location. Spatial disorientation occurs when pilots do not correctly sense their aircraft’s attitude, airspeed or altitude in relation to the earth’s surface. In terms of an aircraft’s attitude, spatial disorientation is often described simply as the inability to determine ‘which way is up’, although the effects can often be more subtle than implied by that description.
Spatial disorientation occurs when the brain receives conflicting or ambiguous information from the sensory systems. It is likely to happen in conditions in which visual cues are poor or absent, such as in adverse weather or at night.[15] Spatial disorientation presents a danger to pilots, as the resulting confusion can often lead to incorrect control inputs and resultant loss of aircraft control.
Research on spatial disorientation indicates that, for pilots who are not instrument rated, loss of control will likely occur between about 60 seconds (Benson, 1988 in Gibb, Gray and Scharff, 2010) and 178 seconds on average (Bryan, Stonecipher, & Aron, 1954) after the loss of visual reference. These studies led to the FAA’s and CASA’s ‘178 seconds to live’ educational campaigns. Gibb, Gray and Scharff (2010) also stated that ‘spatial disorientation accidents have fatality rates of 90–91 percent, which indicates how compelling the misperceptions can be.’
Related Occurrences
There have been a number of accidents relating to VFR pilots flying into reduced visibility conditions. Many of these occurrences have been summarised in the research reports previously mentioned (B2005/0127 and AR-2011-050) as well as in ATSB accident reports (for example, AO‑2015-131 and AO-2016-006). Of particular interest are those occurrences where pilots have avoided an accident outcome by seeking assistance from other aircraft or from ATC. Of note are two occurrences that occurred on the same day in a similar location but with a very different outcome. See below for details.
On 16 June 2017, a Cessna Aircraft Company C172M, registered VH-FYN, was being operated on a private flight from Southport Mason Field, Queensland to Ballina Airport, New South Wales. The purpose of the flight was to ferry the aircraft to Ballina for scheduled maintenance. Enroute, near the town of Bangalow New South Wales, the aircraft entered an area of reduced visibility, including low cloud, fog and drizzle. The aircraft diverted off the initial track and was last seen disappearing into cloud heading inland. A short time later the aircraft collided with terrain and the pilot was fatally injured.
ATSB occurrence 201702740
On 16 June 2017, the pilot of a light aircraft was flying under VFR from Taree, New South Wales, to Southport, Queensland. While near Ballina, New South Wales the weather suddenly deteriorated and the pilot attempted to turn back to land at Coffs Harbor, New South Wales. However, the weather continued to close in, at which point the pilot reported to ATC that he was now flying in instrument meteorological conditions (IMC). ATC observed a sporadic radar return in the position described by the pilot and advised that the pilot gain altitude, which assisted with radar identification. ATC then guided the aircraft to Evans Head, New South Wales where the weather had cleared sufficiently for the aircraft to land safely.
While en route from Evans Head, New South Wales, to Boonah, Queensland, the pilot of amateur-built Wittman Tailwind aircraft, registered VH-TWQ (TWQ), diverted to Casino, New South Wales, due to low cloud on the McPherson range. The pilot then took off after approximately fifty minutes on the ground and attempted to reach Boonah via a different route across the range. During the flight TWQ entered an area of reduced visibility. Approximately fifteen minutes after take-off TWQ commenced a series of rapid climbs and descents followed by a descending left turn which continued until TWQ collided with terrain.
Site and wreckage examination did not identify any defects or anomalies that might have contributed to the accident. Additionally, there was no evidence to support the pilot being incapacitated. Therefore, this analysis will focus on the examination of the factors that led to a visual flight rules (VFR) pilot entering an area of reduced visibility and losing control of the aircraft.
Decisions to depart Evans Head and Casino
After the Fly-In was called off due to the poor forecast weather the pilot and passenger elected to fly home to Boonah and Toowoomba. The pilot had attended the Fly-In event briefing that morning and was therefore aware of the local weather conditions and forecast. Neither the pilot’s nor the passenger’s family could identify a time pressure for the aircraft to return to Boonah and Toowoomba that day.
The relevant Graphical Area Forecasts did not preclude a departure under the VFR from Evans Head via Boonah to Toowoomba. However, they indicated the possibility of encountering areas of cloud, dust and rain in which visibility would reduce below that required for VFR flight. The inland route to Boonah, required the aircraft fly across the McPherson Range. Several of the peaks along this range are greater than 3,000 ft and a few are greater than 4,000 ft.
The generally south-south-easterly wind flow, heading towards the range, would have had the effect of pushing the weather up against the McPherson Range and reducing the visibility. So, while it was possible to depart under the VFR, the forecast conditions would have indicated that it was likely there would have been cloud on the ranges and have necessitated planning for an alternate route or diversion to avoid the area if the actual conditions reflected the forecast.
The pilot’s decision to depart the interim landing site can be interpreted as likely taking advantage of acceptable conditions at Casino with the notion that the weather further inland may have allowed for VFR flight over the ranges.
Once airborne, the pilot would have been in a position to assess the in-flight visibility and cloud and rain in the intended direction of travel. However, as discussed in the United States National Transportation Safety Board report (2005), it is possible that the continuation of flight towards the area of low cloud was influenced by the inherent challenges of assessing low visibility conditions.
The ATSB was unable to determine the pilot’s understanding of the weather conditions ahead of the aircraft prior to entering an area of low visibility conditions. However, the pilot had demonstrated an awareness of the risk posed by the weather and the need to maintain visual reference by diverting from the original track and turning back from the first attempt to cross the Ranges.
Development of the accident
Flying into an area of reduced visibility
The majority of the flight from Casino was conducted between 2,000 and 4,000 ft. Approximately 30 km north-west of Casino the aircraft began a climb over the first area of high ground. Terrain in this area is approximately 1,800 ft high. At about 1506, the aircraft reached a maximum altitude of 4,100 ft then entered a 600 ft/min descent where the groundspeed rapidly increased from 145 kt to 173 kt. It is likely that the pilot initiated the climb to clear terrain and then descended when the cloud conditions became unsuitable. This climb took TWQ above the forecast and observed cloud heights in the area, which indicated a cloud base of around 2,600 - 2,800 ft. The descent levelled out at 3,100 ft, and the terrain underneath was about 1,430 ft, allowing the pilot to continue the descent a further 1,670 ft and remain clear of the terrain, if the pilot was visual with terrain. It is possible that the pilot entered an area of deteriorating visibility at this time leading to the rapid descent and level off well above terrain.
From this point on, the pilot flew no lower than 3,100 ft, which was around the height of the some of the ridge lines in the area. It is therefore possible that the pilot was aware of the spot heights of terrain in the area and was attempting to stay above them.
At about 1508, in the vicinity of the Tooloom Fire Tower, the pilot commenced another climb. As the fire tower was in cloud, it is likely that the pilot entered an area of cloud during this climb. Flight data showed that the final turn and descent of TWQ was towards the high ground. The accident site was located near the top of the ridgeline. Either side of this ridgeline were areas of low ground, which the pilot could have manoeuvred towards if visual with terrain. The direction of turn as well as the descent and acceleration towards the terrain indicate the pilot was not visual with terrain at the time of the accident.
Spatial disorientation resulting from a loss of visual cues
Flight data from the last 4 minutes of the flight recorded the aircraft’s groundspeed speed varying between 109 and 175 kt. The aircraft’s rate of climb and descent varied between +2,400 ft/min and -2,400 ft/min. The aircraft’s altitude varied between 4,000 and 3,100 ft.
Of note, the speed recorded by the data is ground speed. Forecast winds for the area were up to 20 kt in the direction of travel of TWQ and could be considered all tail wind. If the actual winds were as forecast, the aircraft was being operated above the published manoeuvring speed limit of 130 kt indicated airspeed KIAS and likely up to the maximum structural cruising speed at some points.
The final data point showed the aircraft descending through 3,100 ft and travelling at 172 kt groundspeed. The aircraft was descending at 1,800 ft/min and was tracking towards the high ground.
The flight data from the last 4 minutes of flight was not consistent with normal operations of a Wittman Tailwind. The abrupt speed and altitude reversals and the operation of the aircraft over and near these speed limitations are indicative of a loss of control.
It is therefore likely that within 4 minutes of flying into conditions of reduced visibility, without adequate visual reference to the horizon, the pilot of TWQ became spatially disorientated leading to a loss of control and collision with terrain. It is possible that the pilot of TWQ was able to maintain some control initially upon entering cloud due to the pilot’s previous instrument flying experience. However, without recent experience and the training and qualification of an instrument rating the pilot was unlikely to have been able to maintain control in cloud for an extended period of time.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving Wittman Tailwind, VH-TWQ, which occurred in Tooloom National Park, New South Wales, 12 January 2020.
Contributing factors
The pilot departed an interim landing site for Boonah under the visual flight rules with a high risk of encountering forecast cloud that reduced conditions below that required for visual flight.
It is likely the pilot encountered conditions of reduced visual cues and became spatially disorientated which led to a loss of control and collision with terrain.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Benson, AJ, 1999a, “Spatial disorientation – general aspects”, in J Ernsting, AN Nicholson & DJ Rainford (Eds.), Aviation Medicine (3rd ed.), Oxford, England, Butterworth Heinemann, pp. 419-436.
Gibb, R, Gray, R and Scharff, L, 2010, Aviation Visual Perception: Research, Misperceptions and Mishaps, Ashgate Publishing Limited, Surrey, United Kingdom.
Wiegmann, D and Goh, J, 2000, Visual Flight Rules (VFR) Flight into Adverse Weather: An Empirical Investigation of Factors Affecting Pilot Decision Making, Federal Aviation Administration research DTFA 00-G-010, Illinois, United States.
Wiggins, M and O’Hare, D, 1995, “Expertise in Aeronautical Weather-Related Decision Making: A Cross-Sectional Analysis of General Aviation Pilots”, Journal of Experimental Psychology: Applied Vol. 1 No. 4, pp. 305-320.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Family of the pilot
Civil Aviation Safety Authority
Fly-In Event Organiser
Fly-In Chief Marshall
Bureau of Meteorology
Coroner’s representative
Submissions were received from:
Bureau of Meteorology.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Preliminary report
Report release date: 11/03/2020
What happened
On 12 January 2020, at 1336 Eastern Daylight-saving Time,[1] the pilot of an amateur-built Wittman Tailwind aircraft, registered VH-TWQ (TWQ), departed Evans Head Airport, New South Wales, with one passenger on board (Figure 1). The pilot was conducting a private flight under the visual flight rules[2] from Evans Head, New South Wales to Boonah, Queensland.
The pilot flew in a north-north-westerly direction towards Boonah via the Richmond River valley. At 1353, the pilot commenced a 180° turn overhead the township of Kyogle and diverted south back down the valley to Casino aerodrome, landing at 1406.
At 1454, the pilot took off from Casino and flew in a west-north-westerly direction. At 1511, TWQ commenced a left turn and, shortly afterwards, collided with terrain. The pilot and passenger were fatally injured, and the aircraft was destroyed.
Figure 1: Flight tracks of VH-TWQ 12 January 2020
Source: Flightradar24 and Google annotated by the ATSB
Recorded data
The aircraft was fitted with a Mode S transponder that broadcast ADS-B data. This information included the position and altitude of the aircraft and was received by Flightradar24 and provided to the ATSB. Also on board was a mobile device with the OzRunways application installed. This application provides the option for live flight tracking by transmitting the device’s position and altitude and that option was enabled for this flight. OzRunways information was also obtained by the ATSB. The data indicated that the aircraft was travelling at approximately 170 kt ground speed and in a descending left turn just prior to the collision with terrain.
Wreckage examination
The accident site was located in rainforest, about 72 km west-north-west of Casino, within the Tooloom National Park. Examination of the wreckage indicated that the aircraft collided with a number of trees before coming to rest on the rainforest floor at an elevation of 996 m (3,169 ft) (Figure 2).
Figure 2: VH-TWQ’s empennage at the accident site
Source: ATSB
The aircraft’s structure was substantially disrupted, with the wreckage trail on an approximate east to west heading and covering a length of about 120 metres. All major components were located at the accident site. Due to the disruption of the airframe, the aircraft’s attitude when it entered the tree canopy could not be determined. There was no evidence of fire.
Pilot details
The pilot held a Private Pilot (Aeroplane) Licence and was qualified to fly by day under the visual flight rules. The pilot also held a single-engine aeroplane class rating. The pilot last conducted a single-engine aeroplane flight review in June 2018 that was valid until June 2020. His logbook indicated he had a total of about 1,200 hours flying experience. The pilot held a Class 2 aviation medical certificate that was valid until October 2021.
Weather conditions
Forecast meteorological conditions valid for the accident flight included visibility of 10 km or greater and broken[3] cloud from 3,000 to 6,000 ft above mean sea level. Isolated rain and thunderstorms were also forecast, with associated reduced visibility and lower cloud bases. Widespread smoke was also forecast due to bush fires in the area, reducing visibility to 1,000‑8,000 m.
Ongoing investigation
The investigation is continuing and will include examination of:
meteorological conditions and pre‑flight preparation
pilot qualifications, experience
recovered wreckage, aircraft performance characteristics and recorded flight data
aircraft maintenance documentation and operational records.
Acknowledgement
The ATSB acknowledges the significant assistance provided by the New South Wales Police Force during the on-site phase of this investigation.
The information contained in this update is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this update. As such, no analysis or findings are included.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 29 March 2016, the pilot of a Piper PA-28-181 aeroplane, registered VH-BDB, conducted a private flight from Aldinga, South Australia, to Hay, New South Wales (NSW), under the visual flight rules (VFR).[1] After refuelling in Hay, the pilot planned the next VFR flight to Bankstown, NSW.
The pilot obtained the latest weather forecast for the area, and for Bankstown and Bathurst airports. As the weather forecast for Bankstown indicated conditions would be marginal for VFR flight, the pilot planned for an alternate landing at Bathurst.
The aircraft departed Hay and tracked towards Katoomba, NSW. When about 30 minutes from Katoomba, the pilot, who was the only person on board, contacted a flight instructor who was on the ground at Bankstown Airport for an appraisal of the current weather conditions. Based on the forecast and the instructor’s comments, the pilot continued an indirect track towards Glenbrook via Katoomba and then planned to track to Bankstown (Figure 1).
Figure 1: Radar image annotated with approximate track of VH-BDB and relevant locations
Source: Airservices Australia – annotated by the ATSB
At about 1511, the pilot saw the cloud appear to be closing in on the planned track ahead. The pilot scanned from the left to the right and assessed that it would not be possible to continue on their current track and remain clear of cloud, so commenced a right turn. The aircraft then entered cloud.
At about 1512, the pilot contacted Bankstown Tower air traffic control and declared a mayday.[2] By the time the pilot had completed the transmission, the aircraft had flown clear of the cloud. About 90 seconds later, the pilot advised the tower controller that they had stabilised flight and that the aircraft was then at 3,000 ft tracking into the Richmond restricted airspace without a clearance, to remain clear of cloud. According to the radar data, the aircraft entered Richmond airspace at about 1515, on climb passing 3,800 ft. The tower controller coordinated with Sydney Approach to provide the pilot with a clearance, then advised the pilot to contact Sydney Approach for assistance.
At about 1516, the approach controller assigned the aircraft a discrete transponder code, and asked the pilot to advise their current situation regarding visibility, and their intentions. The pilot responded that they were then on top of cloud and unable to find a way down. The pilot elected to continue tracking to the north where the weather was clearer and away from the rising ground to the west. The aircraft tracked north and then north-east (Figure 1).
The pilot then advised that the aircraft’s current altitude was 5,000 ft and climbing. The controller responded with a clearance to continue on their current heading at 5,000 ft, which was well above the radar lowest safe altitude[3] on that track, and to advise if a change in level or heading was required. The controller subsequently advised the pilot to remain in visual meteorological conditions[4] (VMC) and to deviate around cloud if necessary.
At about 1519, the controller contacted Richmond and Williamtown air traffic control to obtain updated weather information to assist the pilot. The controller at Williamtown responded that it was hard to tell what the cloud was like due to the rain, but that there was a lower cloud band to the west than to the north-east.
About 2 minutes later, the pilot advised the controller that they could see the ground and were assessing their options to get down under the cloud. The controller asked the pilot to confirm that they could maintain separation from the cloud and terrain while descending through the gap.
The pilot then advised that they required a left turn to remain clear of cloud, and the controller asked the pilot to confirm they were maintaining 5,000 ft as the transponder was not displaying altitude. The pilot realised that they had inadvertently selected the altitude mode on the transponder off and switched it on, then advised the controller they were now maintaining 5,500 ft and required further left turn.
The aircraft was then heading west, and the pilot stated to the controller that their best option would be to get over the escarpment and divert to Bathurst. The controller asked the pilot what the aircraft’s remaining fuel endurance was, but the pilot was unable to calculate the endurance due to the high workload to remain clear of cloud.
At about 1525, the aircraft was 10 NM north of Richmond aerodrome. The pilot advised that there was a large opening to their right and advised that they were turning onto a heading of 050° and shortly after, advised they were commencing a descent. The controller responded that the radar lowest safe altitude in the area was 3,500 ft and asked the pilot to confirm they were able to maintain visual contact with terrain on descent. The pilot confirmed they could maintain VMC through the gap in the cloud and was then cleared to descend visual with terrain.
At about 1527, the controller advised that they had confirmation of visual conditions towards Bathurst. The pilot stated that they would assess over the next 5 miles. In response to a request for their endurance, the pilot stated that they were busy keeping clear of cloud, and would get back with the endurance shortly. The aircraft was then tracking north-east at 5,000 ft, and descended to 4,200 ft by about 1529. The controller then advised that the radar lowest safe altitude on the aircraft’s track was now 2,500 ft and confirmed the pilot was still visual with terrain. A minute later, the aircraft had descended to about 3,500 ft, and the controller advised that the radar lowest safe altitude was 2,700 ft on the aircraft’s current heading, and again asked the pilot to confirm they were still visual with terrain and that at their current rate of descent, they had plenty of space to remain in VMC. The pilot responded that they were still visual with terrain but needed a left turn to remain clear of cloud. The controller responded that the pilot could turn as required, and advised the pilot that the main thing was to maintain in VMC. The aircraft descended to 3,000 ft during the left turn.
At about 1532, the pilot stated that Bathurst was ‘starting to look good’. The controller again reminded the pilot to maintain VMC at all times. The pilot responded that the gaps were closing up every time they approached one. The aircraft climbed and tracked west-south-west. The controller asked whether the pilot was using carburettor heat. Then the controller advised that the weather was CAVOK[5] at Bathurst and probably just climbing above the cloud, maintaining VMC and tracking to Bathurst would be the best plan from the information available at that stage. Again, the controller stated that the main thing was to stay in VMC.
The pilot then turned the aircraft onto a heading direct to Bathurst. The controller advised that they were now well above the lowest safe altitude in the area, and requested the fuel endurance. The pilot advised that they had sufficient fuel endurance to Bathurst with 45 minutes reserve and at present, were focused on flying the aircraft but could work out the actual endurance once clear of the cloud.
At about 1538, the controller advised that the aircraft had about 56 miles to run to Bathurst and was heading in a good general direction. The pilot reported that they had 5 km terrain visibility and were going to be doing a bit of cloud dodging to maintain the altitude (the aircraft was still at 6,700 ft).
At 1542, the controller asked whether they were visual with terrain in any direction and the pilot responded that they were visual with terrain directly below and behind, and bits ahead through quite a large gap in the cloud. The controller advised that there was report of overcast at Bathurst at 9,500 ft. Three minutes later, the controller asked how the weather directly in front looked, and whether the pilot had seen anywhere they might be able to descend to Bathurst. The pilot responded that everything was opening up ahead.
The aircraft exited controlled airspace at about 1546 tracking direct to Bathurst at 6,700 ft. At about 1550, the pilot reported they were commencing descent into Bathurst. The controller confirmed that the pilot would be able to maintain visual with terrain and advised the pilot to contact air traffic control on the area frequency.
The aircraft landed on runway 17 at Bathurst without further incident.
Weather information
Aerodrome terminal information service
The aerodrome terminal information service (ATIS)[6] current at Bankstown around the time of the incident included that pilots were to expect an instrument approach, the runways were wet, visibility was 5,000 m in rain, and there were layers of cloud with bases at 1,500 and 2,000 ft.
Forecast
The relevant area forecasts valid for the flight included Area 20 and Area 21. The forecast weather was for multiple layers of cloud, including low cloud with a base of 1,000 ft AMSL. The visibility included reducing to 4,000 m in showers of rain. At Mt Victoria, about 9 NM north-northwest of Katoomba, there was a forecast of cloud on the ground and showers of rain.
The forecast for Bankstown Airport included showers of rain with cloud bases at about 2,000 ft, with the chance of lower cloud at 1,000 ft. Bathurst Airport forecast included precipitation and the chance of low cloud 800 ft above the aerodrome.
Pilot comments
The pilot provided the following comments:
The aircraft was only in cloud for about 3 to 5 seconds, and the pilot felt confident in using the instruments to maintain control of the aircraft.
When the aircraft entered cloud, instead of turning right, in hindsight the pilot thought they should have moved the aircraft to the right of the corridor between clouds and then turned left to remain clear of cloud.
Air traffic control was ‘brilliant’ – the pilot did not feel alone, and was looked after. The controller provided the radar lowest safe altitude in the location, and the pilot found it reassuring. The visibility was about 5–6 km, and it was helpful to know that the weather was more open ahead.
The weather conditions were in accordance with the forecast to Katoomba, but around Glenbrook, the pilot was expecting a cloud base of about 1,500 to 2,000 ft above ground level (AGL), but it was more like 500 ft AGL.
Based on the forecast, the pilot assessed that the weather conditions were marginal, but it may be possible to land at Bankstown. The pilot had planned to divert to Bathurst if it did not look possible to get to Bankstown in VMC.
Safety message
This incident highlights the benefits of seeking assistance from ATC when a pilot is in difficulty. It enabled ATC to provide appropriate assistance including clearance into controlled airspace, and to prioritise their resources. Airservices Australia commented that under the circumstances, it would have been more effective for the pilot to broadcast a MAYDAY on the area frequency than on Bankstown Tower frequency. On the area frequency, ATC would have been able to provide more immediate and direct assistance.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. Flying with reduced visual cues such as in this occurrence remains one of the ATSB’s major safety concerns.
Avoiding deteriorating weather or instrument meteorological conditions (IMC)[7] requires thorough pre-flight planning, having alternate plans in case of an unexpected deterioration in the weather, and making timely and decisions to turn back or divert.
Pressing on into IMC with no instrument rating carries a significant risk of severe spatial disorientation due to powerful and misleading orientation sensations in the absence of visual cues. Disorientation can affect any pilot, no matter what their level of experience.
VFR pilots are encouraged to use a personal minimums checklist to help identify and manage risk factors that include marginal weather conditions.
Also available from CASA’s online store are:
Weather to Fly DVD – highlights the dangers of flying in cloud and ways to avoid VFR into IMC.
Flight Planning – always thinking ahead. A flight-planning guide designed to help you in planning and conducting your flight. This guide includes a personal minimums checklist.
A similar incident occurred on 21 April 2016, and the pilot advised ATC they had entered cloud and requested assistance. The controller identified the aircraft using ADS-B and provided heading and turn guidance to the pilot. The aircraft landed safely.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 19 March 2016, a student pilot prepared for their first solo navigation training exercise in Cessna 172, registered VH-EOV (EOV). The flight was planned from the Gold Coast Airport, Queensland (Qld), overhead Casino, and onto Grafton Airport, New South Wales (NSW). The return leg plan was from Grafton Airport direct to the Gold Coast Airport (Figure 1 blue lines).
Prior to departure, the pilot and their instructor checked the flight plan and discussed the weather forecast. They both then checked the live weathercam[1] at Lismore Airport, NSW, as Lismore is close to Casino. The weathercam showed some fog and low cloud, with clear skies above. As a final assessment, the pilot and instructor walked outside and visually assessed the conditions.
Source: Airservices Australia Armidale World Aeronautical Chart annotated by ATSB
The instructor was satisfied that the low cloud at Lismore would soon burn off and the pilot would be able to complete the visual flight rules (VFR)[2] navigation exercise at the planned level of 6,500 ft above mean sea level. The instructor then prepared to depart on another flight. About thirty minutes later, the instructor taxied past EOV in another aircraft and noted that the pilot was still preparing EOV for the flight.
At about 1012 Eastern Standard Time (EST), EOV departed on runway 14, about 1.5 hours after they were approved by the instructor to depart. Due to jet traffic, the Gold Coast Tower controller instructed the pilot to make a right turn after take-off (on to their planned track) and climb to 2,500 ft. About two minutes later, the Tower controller cleared EOV to climb to 3,000 ft. As the pilot initiated the right turn, they assessed that the weather conditions on their intended track were worse than they had expected, with the visibility ahead reduced by haze and cloud.
Part way through the right turn, the pilot unintentionally stopped the turn and started to track in a southerly direction, instead of south-westerly toward Casino. Noting that the aircraft was not tracking as expected, the Tower controller asked the pilot to confirm their current heading. The pilot asked the controller to ‘standby’. With no further response from the pilot, the controller then instructed them to turn right onto a heading of 250°. However, the pilot continued to track about 40° left of track (Figure 2). To assist the pilot, the controller advised them of their current position, cleared the aircraft from that position direct to Casino, and as per normal procedure, and instructed the pilot to change frequency to contact Brisbane Approach.
Figure 2: Flight planned track to Casino in yellow. EOV (green) tracking to the east of Murwillumbah Airport (YMUR, white circle) in a southerly direction
Source: Airservices Australia – annotated by ATSB
The aircraft was now very close to cloud and the pilot had turned all their attention to this threat. At 1020, the pilot contacted the Approach controller to request a climb to not above 5,500 ft, as this would give them flexibility to climb or descend as required to avoid entering cloud. The Approach controller advised the pilot there would be a short delay prior to this request being approved. During this period, EOV entered cloud.
The pilot spent the next few minutes focussed solely on the flight instruments but did not inform the controller that they were in cloud. The Approach controller then approved the pilot to climb to 5,000 ft. While still in cloud, the pilot began the climb, and inadvertently started to turn left. The Approach controller questioned what heading the pilot was on and when the pilot could not answer correctly, they suggested a heading for Casino. The pilot turned on to the suggested heading. The pilot then observed a break in the cloud below them and requested a descent. The Approach controller approved the descent and asked the pilot to confirm that operations were normal. The pilot replied that all their instruments were working correctly. The pilot then descended to 1,500 ft and exited the cloud. The pilot later estimated that they were in cloud for approximately three minutes.
The pilot had a brief radio discussion with their instructor, who was flying in a different aircraft in the vicinity. Their instructor advised them that Casino Airport was closed. Making the decision to discontinue the navigation exercise and to return to the Gold Coast along the coast, the pilot turned EOV to the east. At 1100, the pilot advised Brisbane Centre (Centre) air traffic control (ATC) that they were about 3 NM east of Lismore, and were now tracking to the coast. At 1105, Centre ATC identified EOV on radar 4 NM south of Ballina, NSW.
The pilot of EOV did not change the radio frequency to the common traffic area frequency (CTAF) as required when transiting within 10 NM of Ballina. At 1108, as a regular public transport jet aircraft was inbound to Ballina, the Centre controller attempted to call the pilot of EOV to advise them of the conflicting traffic. However, the pilot did not respond. The Centre controller then issued a safety alert to the pilot of EOV advising the jet traffic was now at 1,100 ft (the same level as EOV). The pilot in EOV acknowledged this alert advising that they had the jet traffic sighted. The two aircraft passed within 1.7 NM of each other at a similar level.
As EOV tracked north along the coast toward the Gold Coast (red line in Figure 1), the Centre controller advised the pilot of a conflicting aircraft tracking southbound. The pilot acknowledged this call and advised they were looking for this traffic. The two aircraft passed without incident. The pilot then continued to the Gold Coast and landed without incident.
Pilot experience and comments
At the time of the incident, the pilot had logged about 46 flying hours. Three hours of this was instrument[3] flight training.
The pilot provided the following comments:
The weather had changed very quickly, and that it was different to that expected.
They felt no pressure to conduct the flight. They had been briefed to ‘turn back’ to the Gold Coast if at any time they felt uncomfortable with the weather.
They did not specifically alert ATC that they had entered cloud. They had however, advised ATC that they were uncertain of the aircraft’s position, and accepted assistance in that regard.
They had attempted to program the “Direct To” function on the KLN89B GPS installed in the aircraft, but had not been able to get this to work. They were not confident in the use of the navigation aids (VOR and ADF).
The pilot reported that the level of stress they were under after entering cloud had added to the normal stress level of conducting a first solo navigation exercise. This had made processing information much more difficult, but they remained focussed on keeping the aircraft level using their limited experience relying solely on the flight instruments.
The pilot had sat the Private Pilot Licence theory test the day prior to the flight, and therefore the week before the flight had been busy.
The pilot advised the best safety message to convey to other pilots with limited experience was to stay aware of the terrain around you. If the weather is not as expected, make an early decision to turn back.
Instructor experience and comments
The instructor held a Commercial Pilot’s Licence with a grade 2 training endorsement.
This instructor had been the pilot’s regular instructor and had conducted all the previous dual navigation exercises with them. The instructor reported that the student had previously experienced some difficulty with departures from the Gold Coast, but this had been addressed with training.
The instructor provided the following comments:
They were surprised when the pilot had not departed until about 1.5 hours after being authorised to depart.
They also found the weather worse than forecast and were surprised how much cloud was still around.
By the time the pilot did depart, a safer cruising level would have been about 2,500 ft.
All students at the flying school are exposed to basic use of the navigation aids at this stage of their training. Loading a flight plan into the GPS is demonstrated, but it is not expected that the student would be proficient in the use of these aids at this stage.
While on another flight in the Casino area, they had advised the pilot by radio that Casino Airport was unserviceable.
The student had done well in the instrument flight component of their training.
They felt comfortable with the decision to let the pilot depart on the solo exercise that day.
Flying School comments
The flying school reported that the student departed with the intention of reaching the planned altitude of 6,500 ft with broken cloud at 3,500 ft without carefully considering alternative altitudes.
The school also advised that the student incorrectly used the VHF Omnidirectional Radio Range (VOR) for establishing the departure track and did not identify the cloud ahead in a timely manner.
The student did not clarify with ATC that a climb was required in order to remain in VMC and when they entered cloud, they did not follow the procedure to ensure they returned to VMC as quickly as possible.
Weather
Initial weather reports indicated that the conditions would be suitable for the solo flight. The Gold Coast Airport Aerodrome Forecast was for scattered cloud at 2,000 ft above ground level, with broken cloud at 3,500 ft. The Area Forecast pertinent to the planned flight indicated that the broken low cloud would lift by 0900.
ATSB comment
Pilots are encouraged to make conservative decisions when considering how forecast weather may affect their flight. If poor weather is encountered enroute, timely and conservative decision making may be critical to a safe outcome. It is advisable to make a positive decision to turn back if the weather is not as planned and outside the capability of their experience level.
The ATSB also encourages pilots to seek assistance from ATC as soon as they find themselves in difficulty, or preferably, before the situation escalates to that point, so that ATC can provide timely assistance.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Operator – flying school
As a result of this occurrence, flying school has advised the ATSB that they are taking the following safety actions:
A formalised brief will be given to all students prior to their first training area solo flight.
This brief will have an emphasis on:
maintaining situational awareness when weather conditions are less than optimal
the importance of maintaining VMC at all times will be re-addressed
the importance of conducting a 180° turn on instruments if a pilot does inadvertently find themselves in cloud
when encountering cloud, to include the phrase ‘due cloud’ in transmissions with ATC
the importance of seeking early assistance from ATC, rather than letting the situation deteriorate
when to use ‘request’ and when to use ‘require’ when seeking a clearance from ATC
be clear on phraseology like ‘not above’ when requesting altitudes from ATC.
Safety message
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry.
Number 4 in the Avoidable Accident series published by the ATSB titled ‘Accidents involving pilots in Instrument Meteorological Conditions’ lists three key messages for pilots:
Avoiding deteriorating weather or IMC requires thorough pre-flight planning, having alternate plans in case of an unexpected deterioration in the weather, and making timely decisions to turn back or divert.
Pressing on into IMC conditions with no instrument rating carries a significant risk of severe spatial disorientation due to powerful and misleading orientation sensations in the absence of visual cues. Disorientation can affect any pilot, no matter what their level of experience.
VFR pilots are encourage to use a ‘personal minimums’ checklist to help control and manage flight risks through identifying risk factors that include marginal weather conditions.
Available from CASA’s online store are:
Weather to Fly – This DVD highlights the dangers of flying in cloud, and how to avoid inadvertent VFR into IMC.
Flight Planning – always thinking ahead. A flight-planning guide designed to help you in planning and conducting your flight. This guide includes a ‘personal minimums checklist.
SKYbrary have published an informative article looking at pre-flight risk management / and practical measures to maintain control for a limited period if a pilot had inadvertently flown VFR into IMC.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the morning of 8 September 2015, a pilot planned a navigation exercise from Moorabbin Airport, overhead Yarram aircraft landing area (ALA), and then on to Bairnsdale Airport, Victoria (Figure 1). The return flight from Bairnsdale to Moorabbin was to be via Latrobe Valley Airport, Victoria. The pilot had recently passed their Private Pilot Licence, and this solo navigational exercise was part of the training toward a Commercial Pilot Licence.
Figure 1: Planned route for the navigation exercise
Source: Airservices Australia Melbourne World Aeronautical Chart (WAC)
The pilot reviewed the Area 30 weather forecast, including the terminal area forecasts (TAFs)[1] and METARs[2] for Moorabbin, Latrobe Valley, and Bairnsdale, to assess the suitability of the conditions for the planned visual flight rules (VFR) flight.
The Area 30 Forecast (ARFOR) overview, issued at 0805 Eastern Standard Time (EST), which covered the time of the flight, predicted isolated scattered showers, and snowfalls above 4,000 ft. Low cloud with precipitation particularly on the windward slopes was also forecast. It was expected that this low cloud would contract to the north-east section of Area 30 by 1200, and clear by 1400. The wind below 5,000 ft was forecast as south-westerly and between 20 and 25 kt. A note stated that winds up to 5,000 ft were forecast to be 10-20 kt stronger in the east (including the Bairnsdale region).
Confident that the flight could be safely conducted under the VFR, the pilot then discussed the planned route, and associated weather forecasts with a senior instructor at the flying school. During this discussion, the pilot and instructor decided that due to the METAR at Bairnsdale Airport indicating strong winds of up to 35 kt, the pilot should make an assessment upon arrival there. If the pilot did not assess the wind as suitable/safe for landing, the brief was to overfly the airport and commence the return leg to Latrobe Valley. They also decided to delay the flight’s departure time from Moorabbin, so that the planned arrival time back into Latrobe Valley fell outside the INTER/TEMPO[3] period for this airport.
Pilot recollection of the flight
The pilot prepared a Piper PA28 (Warrior) aircraft, registered VH-TAU (TAU), and then departed Moorabbin at the delayed time of 1239. The pilot reported that both the departure and initial climb went as planned.
To maintain separation from the cloud, the pilot levelled the aircraft at about 3,000 ft above mean sea level (AMSL) and conducted a crosscheck of their calculations. They visually confirmed the aircraft’s location, noting this on the flight plan.
About 15 NM into the initial leg of the flight (Figure 2), the pilot reported noticing some cloud on the ranges around the aircraft, with the base at about 3,000 ft. Still with the mindset that the weather was suitable for the flight, and wanting to continue, the pilot elected to fly around the lower patches of cloud. At this stage, they were confident that they could ‘push on’. The pilot reported that they had accompanied a friend on the same navigation exercise the previous week, in similar weather conditions. The pilot’s friend had had been successful in negotiating the weather and completing the flight.
Figure 2: Initial leg of flight planned track, from Moorabbin Airport to overhead Yarram ALA
Source: Airservices Australia – Melbourne Visual Navigation Chart annotated by ATSB
In hindsight, the pilot reported an unawareness of how thick and widespread the cloud ahead really was, and how it was different to what had been expected. After manoeuvring around several patches of cloud, the pilot made a decision to conduct a 180° turn onto the reciprocal track, and return to Moorabbin. After logging the diversion time on the flight plan, the pilot initiated a turn to the left. Almost instantly, the pilot realised that the aircraft was now completely engulfed in cloud, and had entered instrument meteorological conditions (IMC). The pilot was not instrument rated, nor was the aircraft approved for flight in IMC. The aircraft was equipped with a Very High Frequency Omnidirectional Range (VOR), but the pilot had not been trained to operate this navigational aid.
Although having completed the mandatory basic instrument flight requirements during earlier training, the pilot had not been in cloud before; and reported feeling totally overwhelmed by such an unfamiliar environment. While trying to control the aircraft solely by reference to the instruments, the pilot reported having an escalating concern about the aircraft’s altitude, the height of the surrounding terrain, and the total loss of visual cues to be able to ascertain the aircraft’s position.
The request for assistance
At about 1313, the pilot reported stopping the turn at a heading of about 300 °M, levelling the wings, and called Melbourne Centre for assistance (see Table 1).
Melbourne Centre clarified the aircraft’s position, and placed an uncertainty phase (INCERFA[4] ) on the aircraft. The air traffic controller (ATC) then contacted the instructor in an instrument flight rules (IFR) Cirrus S22, VH-QQT (QQT), who was conducting dual IFR training at nearby Latrobe Valley Airport. The controller at Melbourne Centre confirmed the in-flight conditions with the instructor in QQT, who advised that the cloud tops were about 6,500 ft. Both the instructor and controller then focussed on assisting the pilot in TAU.
Assistance provided by instructor in QQT
The experienced instructor in QQT began providing assistance over the radio to the pilot in TAU. After establishing the facts, and the pilot’s level of experience, the instructor in QQT began to ‘mentor’ the pilot in TAU. The instructor was concerned about the current altitude, which was below the lowest safe altitude (LSALT) of 3,400 ft in the area, and the possibility of icing. Therefore, the instructor talked the pilot through maintaining a focus on keeping the aircraft wings level (to prevent a turn), while initiating a climb through the thick layer of cloud.
The instructor in QQT was able to work methodically with the pilot in TAU, focusing on reducing the pilot’s workload and keeping them calm. The instructor requested all the required airspace clearances for both aircraft from ATC; and ATC assisted in arranging and expediting these. The pilot in TAU reported clear of cloud at about 6,400 ft, some 15 NM north of the original flight planned track (Figures 3 and 4).
ATC then provided vectors to the instructor in QQT to locate TAU, which was now some distance from the Cirrus. The instructor advised that the transponder paint of TAU on the traffic collision avoidance system (TCAS) in QQT had kept ‘dropping out’.
The instructor in QQT continued to work closely with ATC who again arranged all required clearances for both aircraft in tandem, back to Moorabbin. As part of this assistance, ATC advised the instructor that there was a large break in the cloud over Port Phillip Bay west of Moorabbin. The two aircraft travelled to this area and once the instructor had confirmed that the pilot in TAU was orientated, and able to manage the descent, approach and landing back into Moorabbin, the two aircraft parted and TAU landed uneventfully some minutes later.
Figure 3: Surveillance image at about the time VH-TAU first broke clear of cloud. Note distance from intended waypoint of Yarram
Source: Airservices Australia annotated by the ATSB
Figure 4: Google earth representation of where TAU broke clear of cloud
Source: Google earth annotated by ATSB
Actual flight path
The ATSB was provided with surveillance data from Airservices Australia. Table 1 presents a summary of what the surveillance data showed.
Table 1: Surveillance data - main points
Source: Compiled by ATSB from Airservices Australia surveillance data
Relevant Terminal Area Forecasts (TAFs)
In addition to the overview of the Area 30 forecast mentioned previously, the relevant TAFs covering the period of the flight are as follows:
Moorabbin: Issued at 0907: Scattered cloud at 3,000-4,000 ft, with deteriorating conditions from 1800.
Bairnsdale: Issued at 1027: Wind from 250°T at 14 kt; 10 km visibility; light rain showers and scattered cloud at 3,000 ft, with broken cloud at 4,000 ft.
Latrobe Valley: Issued at 1030: 10 km visibility, light rain showers. Cloud few at 2,500 ft and scattered at 3,500 ft.
Safety message
The importance of seeking assistance from ATC as soon as a pilot is in difficulty, or preferably before they reach that point, cannot be overstated. This is a common and important message in most of the educational material on VFR into IMC scenarios. It almost certainly led to a good outcome in this occurrence. ATC could prioritise resources and gain assistance from a nearby aircraft. In this occurrence, good teamwork between the pilots of both aircraft and air traffic control ensured a successful outcome.
The ATSB and CASA publications listed below highlight the importance of really understanding the weather you may encounter at the planning stage, making good decisions, knowing your aircraft and all its equipment, and using a personal minimums checklist.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. Flying with reduced visual cues such as in this occurrence remains one of the ATSB’s major safety concerns.
Avoiding deteriorating weather or IMC requires thorough pre-flight planning, having alternate plans in case of an unexpected deterioration in the weather, and making timely decisions to turn back or divert.
Pressing on into IMC conditions with no instrument rating carries a significant risk of severe spatial disorientation due to powerful and misleading orientation sensations in the absence of visual cues. Disorientation can affect any pilot, no matter what their level of experience.
VFR pilots are encouraged to use a ‘personal minimums’ checklist to help control and manage flight risks through identifying risk factors that include marginal weather conditions.
Available from CASA’s online store are:
Weather to Fly – This DVD highlights the dangers of flying in cloud, and how to avoid VFR into IMC.
Flight Planning – always thinking ahead. A flight-planning guide designed to help you in planning and conducting your flight. This guide includes a ‘personal minimums checklist.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
The aircraft departed the base airstrip to fly to the treatment area but did not arrive. The pilot and wreckage were located after first light by search aircraft. The aircraft had collided with trees and crashed into an empty paddock. The pilot has not provided a report. However, information provided by other sources suggests that he inadvertently entered low cloud and during an attempt to turn back collided with the trees.