Prior to commencing a charter flight from Launceston to Flinders Island the pilot made a visual check of the
fuel tanks and assessed that they were full. He was not aware that since the aircraft had been refuelled it
had made a flight of 1 hour 45 minutes duration. On the return flight, approaching Launceston, the pilot
was given landing instructions and when the aircraft was established on a visual descent, the engine failed.
As he was only 1, 000 feet above unsuitable terrain, he turned towards the only suitable field in the area and
attempted to restart the engine. Being unable to do so the pilot gave his attention to the forced landing and
requested a wind velocity from Launceston Tower. Because of his position and altitude he elected to land
downwind in the 15 knot wind, in the field previously selected. The aircraft touched down and rolled for a
considerable distance before the pilot began a ground loop to avoid striking a fence across his path. This
manoeuvre was only partly successful because of the damp grass and the aircraft struck a fence post and
damaged the tail plane and rear fuselage.
The pilot had completed three aerial seeding flights over areas In timbered and mountainous terrain In
a light northerly wind. On the fourth flight he was making runs down a slope from north-east to south-west
and, after each run, was repositioning his aircraft at the top of the slope by flying a right hand circuit.
At the end of one run and with only a small area to complete, the pilot decided to make a left turn and a
finishing run up the slope and to leave the area by turning left again. During the final run he became aware
there was Insufficient space to permit the Intended manoeuvre so he turned right toward a lower spur line
but realised he was unlikely to clear this. The pilot operated the dump lever, the aircraft settled Into the
trees with full power applied and fell to the ground, coming to rest Inverted.
During the day the pilot, who was inexperienced in agricultural
operations, had completed the spreading of superphosphate while
under the supervision of a Class 1 agricultural pilot. The strip
used, though adequate in length, was substantially below the
prescribed minimum in width, it was bordered by rough, rutted
ground and targe rocks and the transverse gradient was in excess of
the specified maximum. In the late afternoon the pilot returned to
the strip to load some equipment. The wind was calm and shortly
after making a normal landing the aircraft diverged approximately
12 feet to the right of the strip centre line. Due to the rough
ground and downslope the pilot was unable to regain the central
strip and the main wheels struck some large rocks tipping the
aircraft on to its nose.
Prior to landing on a strip which is aligned in a southerly direction, the pilot estimated that he would be subject to a cross wind of from 10 to 12 knots from the left. However, he was not aware that the topography adjacent to the strip threshold could considerably influence the ambient wind and, during the landing flare -out, the aircraft encountered a strong wind gust from the left. On touchdown the aircraft commenced to turn to the left and, although the pilot took remedial action, he was unable to maintain directional control. In the latter stages of the landing run, the aircraft swung further into wind and the nose landing gear strut bent.
The aircraft was engaged in superphosphate spreading in hilly
country and, after commencing operations at approximately 1400
hours, had completed seven sorties. The runs were made in
predominantly easterly and westerly directions and the eastern end
was close to the main north-south ridge of the Brawboy Range. The
aircraft had been observed turning at the eastern end of the runs
by proceeding out through gaps in the ridge and then returning
across the crest of the range to spread in a westerly direction. At
the termination of the last completed run to the east the aircraft
was seen to pull up high and turn inside the face of the ridge
before descending and disappearing from the view of the witness.
Smoke was seen to rise from the area immediately and the burning
wreckage was sighted shortly afterwards by searching aircraft.
The pilot and an assistant had rigged a launching device which
utilized a bungee assembly of motor tyre tubes, and a vehicle and
cable to launch a glider over the slope of Big Talbingo Mountain.
It was intended that when the glider was released, sustained
acceleration was to be obtained by the vehicle and cable moving
away from the glider. The weather conditions were favourable with
the glider facing into a wind of 10-15 knots. The assistant
positioned the vehicle such that the slack in the system was taken
up before he spoke to the pilot who was now in the cockpit and who
briefed him again on the required procedure. The vehicle was driven
away, stretching the bungee assembly, but at a speed too slow to
sustain acceleration of the glider after automatic release. The
pilot was aware of the situation, but was committed to the launch
and when further movement of the vehicle automatically released the
cable retaining the glider, the launch commenced and the glider
moved forward without continuing to accelerate and rolled over the
edge of the clearing. The left wing dropped and the aircraft
continued to sink until it struck the rocky cliff face. The
launching system, modified from one used previously by the pilot,
was untried and the procedures to be used had not been
practised.
On the morning of the accident the pilot flew the aircraft from
Glenrelgh Station to Hughenden, a distance of 63 nautical miles and
arrived at approximately 1000 hours. During the course of the day
he consumed a quantity of alcohol. The pilot, who was not qualified
for instrument flight, planned to return to Glenreigh that evening
but, although last light at Glenrelgh was at 1844 hours, he did not
depart Hughenden until 1810 hours and made a planned landing at
Peronne Station some 10 minutes later. At about 1825 hours the
pilot departed on the 43 nautical mile flight to Glenreigh Station
and arrived over the airstrip at about the end of daylight. The
aircraft was seen to circle over the strip and make an approach
Into the south east with the landing lights Illuminated. A vehicle
had been positioned at the side of the north western end of the
strip so as to Illuminate the landing area with Its headlights.
When the aircraft was almost at the touch down point at the north
western end of the strip, the engine power increased and the
aircraft climbed away. It made a left hand turn as though to
continue around and make another approach. However, when flying
above the almost featureless terrain In a position some 2700 feet
to the north east of the strip, the aircraft entered a steep dive,
crashed to the ground and immediately caught fire. The pilot had
been undergoing medical treatment involving tranquilislng and
sedative drugs and the possibility exists that this medication
interacted with the alcohol consumed to further impair the ability
of the pilot.
While cruising in level flight the engine, without warning,
commenced to vibrate severely. Engine instrumentation remained
normal and a magneto check was satisfactory. The vibration
increased rapidly to such a degree that the pilot had no
alternative but to close the throttle fully and carry out a forced
landing. The aircraft was over very rough terrain and the only
field available was 1,580 feet in length with trees to 70 feet high
at one end and to 20 feet high at the other. The approach was made
towards the taller timber, with the wheels down and half flap in a
cross wind of about 10 knots from the left. After touching down the
pilot realized that the aircraft would overrun the available area
and he immediately initiated a turn to the right. Because of the
speed and the rough surface, the aircraft skidded sideways and the
undercarriage collapsed. The aircraft performance chart indicates
that an actual distance of 1,740 feet is required to stop the
aircraft from a height of 50 feet when using full flap under the
conditions existing at the time of the landing.
When the aircraft arrived over Hughenden it descended to a
height of about 400 feet over houses on the southern and
north-eastern areas of the town, then climbed slightly and flew at
a low height across the town towards the golf course. The aircraft,
on two occasions, flew at a height of about 300 feet over the golf
course, in the vicinity of the club house, then climbed, circled to
the left and descended to a very low height over a group of people
who were playing golf. The aircraft then climbed steeply to
approximately 200 feet at which height the pilot apparently lost
control of the aircraft and it stalled, yawed sharply and dived to
the ground. The Initial impact was taken on the nose and starboard
main wheel and the aircraft skidded for a distance of 169 feet
before coming to rest.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation.
What happened
On 28 April 2021, at 0830 Eastern Standard Time,[1] a flight instructor and student pilot were conducting circuit training in a Guimbal Cabri G2 helicopter at Redcliffe Airport, Queensland.
The student completed one circuit before the instructor took over control of the helicopter to demonstrate another circuit. The instructor reported the controls felt slightly unusual and initially thought that may be due to the crosswind or their own control inputs at the time. The instructor turned the helicopter onto the crosswind then downwind legs of the circuit, before levelling off at 800 ft.
When the instructor attempted to level the helicopter, it did not respond to cyclic inputs and initially maintained the angle of bank (about 20° to the right), before a small increase in angle of bank and a significant nose-down pitch. The cyclic was full aft and left and the helicopter did not respond to instructor inputs.
The helicopter entered a nose-down descending right turn and the instructor broadcast a MAYDAY[2] call. While moving the cyclic, the instructor regained control of the helicopter and conducting a shallow approach back to the airfield with no further control issues.
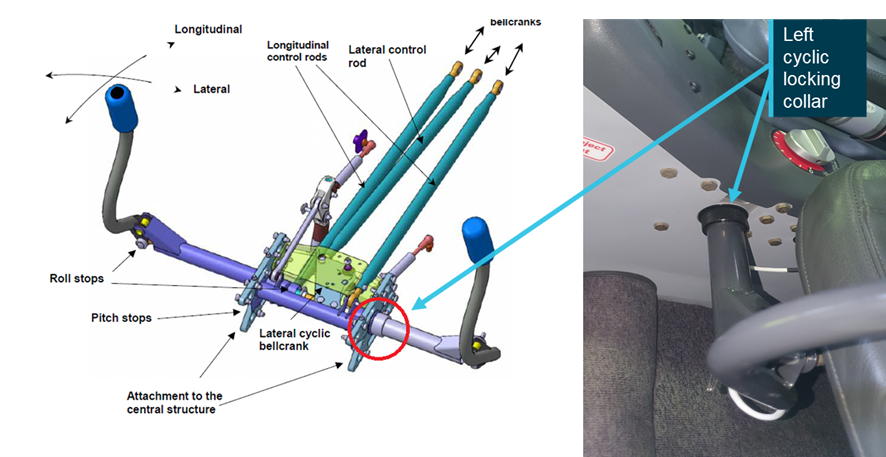
Post-flight inspection of the helicopter revealed the left cyclic locking collar was not secure, allowing the cyclic to disengage (Figure 1). The dual controls had been removed and reinstalled the previous day for a private flight. The position of the left cyclic locking collar was not noted prior to the flight and the right side cyclic was serviceable throughout.
Figure 1: Dual controls showing the left cyclic control locking collar
Source: Aircraft operator
Safety action
As a result of this occurrence, the aircraft operator advised the ATSB of the following proposed safety action:
removal and installation of dual controls by engineers instead of pilots
redesign of the dual control sign in/out register to mitigate confusion
consider dual check sign-off for installation of dual controls
raising a company safety alert to highlight the importance of removing distraction while engaged in safety critical tasks.
The operator assessed that the pilot installing the dual controls may have been distracted, as they were concurrently explaining the installation process to another pilot.
Safety message
This occurrence reinforces the importance of a thorough inspection of all visible flight control components and attachment points following maintenance and before flight.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.