Loss of control in flight involving Leonardo Helicopters AW139, VH-YHF, near Adelaide River mouth, 38 km east-north-east of Darwin, Northern Territory, on 13 May 2018
Final report
Report release date: 16/04/2020
Safety summary
What happened
At 2000 Central Standard Time on 13 May 2018, the crew of a Leonardo Helicopters AW139, registered VH-YHF, departed Darwin, Northern Territory, to search for an active emergency position-indicating radio beacon (EPIRB). The crew flew under night visual flight rules with support of a night vision imaging system.
During an approach to a potential EPIRB target, smoke from nearby bushfires affected visibility and the helicopter developed an uncommanded high rate of descent. The Aircrew Officer, in the rear of the helicopter, called ‘Climb! Climb! Climb!’, and the pilot regained control with a rehearsed recovery drill. During the recovery procedure, the power demand exceeded airframe limitations. This exceedance went undetected, and the helicopter was flown on a second sortie that same evening.
What the ATSB found
The pilot entered instrument meteorological conditions during approach, and lost control of vertical speed. The helicopter descended to 31 ft above ground level during the event. Reversion to standard patter and practiced drills allowed the crew to recover the situation and avert an accident.
Two layers of protection available to the crew of the helicopter were not used. Flight instruments were not referred to in the incident approach, and a crewmember trained to support the pilot in monitoring the approach was required to be in the rear of the aircraft.
A main gearbox over-torque of 159.5 per cent occurred during the recovery. The crew could not determine the magnitude of the potential over-torque after the event. Subsequently the aircraft remained in service in a condition of uncertain airworthiness.
What has been done as a result
CareFlight has established three main controls aiming to prevent reoccurrence:
- Stabilised Approach Criteria was written into standard operating procedures, requiring an immediate go-around if the aircraft leaves a prescribed range of approach parameters.
- Controlled flight into terrain (CFIT) avoidance training was incorporated into the ground-based training syllabus.
- Improved advice on use of auto hover functions was written into aircraft handling standard operating procedures. This included a requirement that the function was not to be engaged while the helicopter was descending.
Safety message
Pilots must be aware of the human factors hazards associated with loss of visual references. Pilots can protect themselves by maintaining the use of instrument scans in approaches at night, and making use of monitoring by trained and available crewmembers.
Flight planning should include assessment of the risk of a degraded visual environment. Operators should document their minimum acceptable levels of illumination and levels of tolerable risk. Where the risk exists, predetermined responses should be readily available.
Instrument flight rules (IFR) pilots in IFR-rated aircraft should prioritise use of inadvertent instrument meteorological conditions drills and pre-planned exit routes over recovery of visual meteorological conditions.
Flight crew and engineering teams should not rely solely on indicators, or absence of indicators, to determine airworthiness. If there is any reason to suspect exceedance of aircraft limits, operators should run diagnostics to determine the airworthiness of the aircraft beyond doubt.
People have a responsibility to aid their own rescue. Up-to-date registration of an EPRIB, and correct use of an EBIRB and other signalling equipment, simplifies a rescue of people in need. Australian Maritime Safety Authority guidelines exist to help people prepare for onshore and offshore remote area travel.
The occurrence
Incident flight
On the evening of 13 May 2018 at 1943 Central Standard Time,[1] the Rescue Coordination Centre (RCC) tasked the crew of a Leonardo Helicopters AW139, registered VH-YHF, to locate an active emergency position-indicating radio beacon[2] (EPIRB) 38 km north-east of Darwin Airport, Northern Territory. The EPIRB had been activated within the vicinity of a waterway called Salt Water Arm (Figure 1).
Figure 1: Map showing Darwin take-off point, search area, and location of incident event
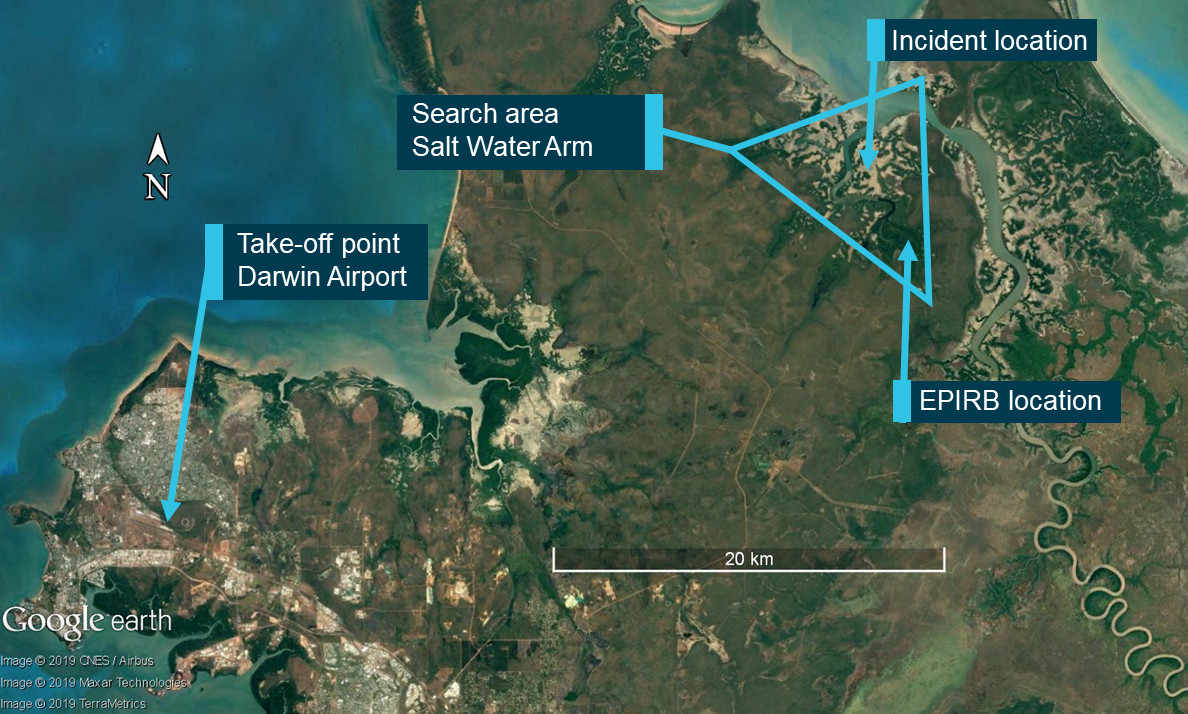
Source: Google Earth annotated by the ATSB
The area was popular with recreational anglers, so the crew of VH-YHF anticipated responding to a boating event. They also determined that such a response would likely require use of the aircraft’s winch.
The crew configured the aircraft with the pilot on night vision goggles[3] (NVG) in the front right seat, the aircrew officer (ACO) with NVG in the rear cabin by the right hand door, and the flight nurse in the rear cabin without NVG. Lighting within the cockpit and cabin was NVG-compatible. Two steerable searchlights mounted to the front, one steerable searchlight mounted to the right side of the aircraft, a handheld light operated by the ACO, and LED light bars at the front and rear of the helicopter supported the Night Vision Imaging System[4] (NVIS).
At about 2000, the crew departed Darwin Airport with good visibility. At that time, a five-metre tide was receding from Salt Water Arm. There was little illumination as the moon had set at 1653, and the sun had set at 1830. There was limited celestial light available through the gaps in the clouds which were forecast as scattered[5] cumulus and stratocumulus clouds at 2,000 ft, with cloud tops to 10,000 ft. Smoke from outlying grass fires drifted across the search area below 7,000 ft, reducing visibility to 4 km in places. The crew could not easily detect the smoke due to low illumination.
As the crew descended into the search area and commenced the search, smoke became evident as the task progressed. The ACO described visibility as 5 km but dropping in and out due to large amounts of smoke. These conditions are common for the region, and recent check flights for the crew had been conducted in similar conditions.
During the flight, the beam of the search light would reflect off smoke and ash. Backscatter from the beam was affecting visibility, reducing NVG image quality, and reducing peripheral vision. As a result, the beam required frequent adjustment. The ACO contacted the RCC and advised that limited visibility may hamper the operation.
The helicopter was fitted with direction-finding equipment (DF) which enabled the crew to locate the source of a 121.5 MHz beacon signal, such as the EPIRB. The crew found that readings from the DF were erratic and unreliable. This added a level of complexity to the operation, making it difficult to locate the beacon. As a result, the crew conducted a visual search for potential targets from a safe working height of above 800 ft above ground level (AGL).
While the use of NVG allowed the crew to detect targets, the image quality was not high enough to verify the targets from this safe working height. The crew had to fly the aircraft down to 400 ft AGL to verify whether their target was one requiring rescue. The crew flew the descent to the target visually, using searchlights to ensure the approach and departure paths were clear of obstacles. The intent was to decrease rate of descent and airspeed before activating auto-hover (HOV) mode at 400 ft AGL.
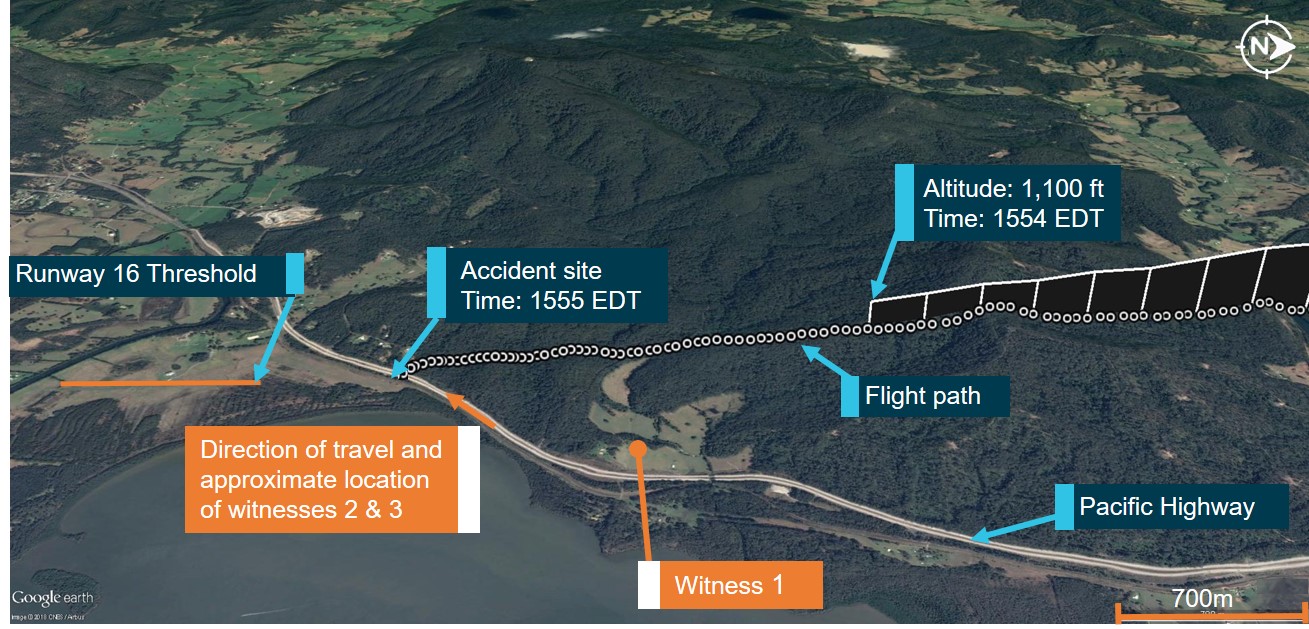
At 2110:30, the crew commenced an approach from the north to a point of interest in Salt Water Arm. The pilot reported visibility on approach to the target as good to the north-west, and dark to the north and east. During this approach, the pilot lost visual references. At 2110:40, the pilot activated HOV mode. At this time, the helicopter had already developed an undesired high rate of descent (Figure 2).
Figure 2: Flight path of VH-YHF during the event
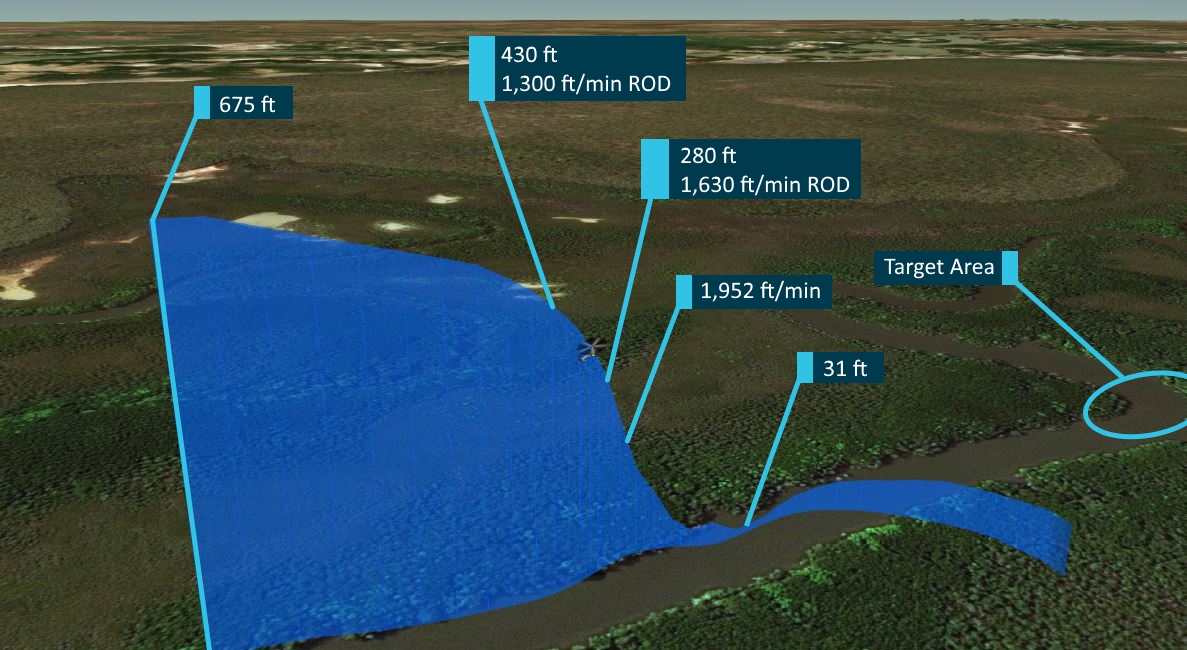
Source: Leonardo interpretation of data from the Flight Data Recorder, annotated by ATSB
At the point of activation of HOV mode, the aircraft was at 430 ft, pitched 19.7 degrees nose-up, and descending at over 1,300 ft/min with a ground speed of 14 kt. The autopilot increased collective[6] pitch to 48 per cent to arrest the rate of descent.
Due to the lighting installed on the aircraft, and prioritisation of peripheral vision, the ACO could see the ground below and advised the pilot of a high rate of descent. The ACO provided advice twice more to the pilot before transitioning to an emergency call of ‘Climb! Climb! Climb!’ The pilot was by now receiving clear visual cues and detected a rapid rate of closure with the ground.
At 2140:46, at a height of 280 ft with a rate of descent of 1,630 ft/min, in a reversion to drilled emergency procedures, the pilot overrode aircraft automatics and used forward cyclic[7] and collective to reverse the rate of descent. The pilot directed his attention to the attitude indicator and the picture outside. The pilot increased collective pitch to 77 per cent. At this point, the rate of descent increased to 1,952 ft/min, indicative of onset of vortex ring state[8].
Maintaining forward cyclic, the pilot was aware of engine temperature limits and made a small reduction in collective to avoid exceeding the limits, before increasing collective again to 84 per cent.
At 2140:50, a yellow caution light illuminated and a crew alert system (CAS) message appeared on the display. Occupied with the recovery procedure, the pilot flew solely through the outside picture and the attitude indicator. The aircraft descended to a height of 31 ft AGL before attaining a positive rate of climb. As the pilot’s recovery manoeuvre ceased and control inputs returned to normal, the warning self-extinguished at 2140:57. The pilot noticed the warning, but could not read it before it extinguished.
It is likely that any further delay in conduct of the recovery drill would have led to an impact with terrain.
Return to base
The crew advised the RCC that they would end the flight and return to base. The crew landed the helicopter back at base at 2158. The pilot found that ash had accumulated on the fuselage of the helicopter, confirming flight through streams of smoke. During the flight through smoke, visibility was reduced below the visual minima.
A crew debrief took place and it was thought that a main gearbox overtorque could have occurred. There is no capacity in the aircraft for the crew to check for overtorque without the presence of an aircraft maintenance engineer (engineer). As a precaution, and as per Operations Manual requirements, the crew called a duty engineer to explain the situation and seek advice.
The duty engineer asked the crew to check the CAS system for messages. If an overtorque occurred, a white status message saying ‘maintenance’ would be present. This would signal a requirement to download and analyse data from the aircraft’s central maintenance computer (CMC).
The pilot estimated the extent of a potential overtorque to be within operational limits. The crew did not detect a maintenance message. With this information, the duty engineer advised that no maintenance activity was required.
Subsequent mission flight
Prior to the mission’s second flight, the crew thoroughly discussed the event. They developed a different strategy for the search to prevent reoccurrence, including the use of topography over the DF.
At 2254, the crew departed for the second flight to locate the source of the EPIRB transmission. The crew flew the arms of the river system at 1,000 ft using the autopilot, with the pilot flying with reference to instruments, and the ACO visually searching from the back.
The EPIRB was successfully located and noted to be in the bottom of a 14 ft metal-hulled recreational fishing boat. The boat carried two people and was in total darkness. As the vessel was unlit, the ACO could see the EPIRB flashing in the bottom of the boat. The position of the EPIRB had most likely resulted in the sporadic readout of the DF.
The helicopter crew directed a nearby Northern Territory Water Police vessel to the scene. The Water Police were then able to assist.
Detection of main gearbox overtorque
The following day, the crew related the experience to an engineer in the hangar and requested a download of the CMC data to check for potential issues. An overtorque of the main gearbox is recorded when a torque limit is exceeded. The limits for all engines operative are 110 per cent for five minutes, or 121 per cent for 5 seconds.
The engineer downloaded and analysed the data. An overtorque in excess of 125 per cent requires grounding of the aircraft, and analysis of the data by the engine and airframe manufacturers. He found that a main gearbox overtorque to 159.5 per cent had occurred during the first flight. The extent of the overtorque was such that the helicopter should not have been flown until the engine and airframe manufacturers declared the helicopter serviceable.
The engineer grounded the helicopter and sent data to the manufacturers of the engines and airframe for analysis. This meant that the crew had departed for their second flight of the previous evening in an aircraft of uncertain airworthiness.
Five days later, the engine manufacturer confirmed that the engines were undamaged and suitable for service. The helicopter manufacturer advised that the helicopter’s main gearbox was serviceable and required inspection of oil for metal contamination at 50 flight-hour intervals. The engineers carried out the necessary actions, and subsequently returned the helicopter to service.
__________
- Central Standard Time (CST): Coordinated Universal Time (UTC) + 9.5 hours.
- EPIRB: Emergency Position-Indicating Radio Beacon. A distress beacon which, when activated, broadcasts a 406 MHz signal to a network of satellites, and a 121.5 MHz signal for homing in on by search and rescue assets.
- Night Vision Goggles (NVG): A helmet mounted binocular device that intensifies ambient light, providing flight crew with improved vision at night.
- Night Vision Imaging System (NVIS): a system of internal and external lighting, combined with night vision goggles, which provides enhanced vision to crew for operation at night.
- Scattered clouds cover between three eights and one half of the visible sky.
- Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
- Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
- Vortex Ring State: an undesirable state of powered flight where the helicopter settles in its own downwash.
Context
Personnel
Pilot
The pilot had over thirty-seven years’ experience in flying helicopters. He held an Airline Transport Pilot Licence (Helicopter) and instrument rating (Helicopter), authorising him to conduct night visual flight rules[9] (NVFR) and instrument flight rules[10] (IFR) operations as pilot. The pilot had gained experience around the world in military helicopter operations, onshore and offshore resource support, mountain flying, search and rescue, and ambulance helicopter operations. He held a current Class 1 Aviation Medical Certificate.
Table 1: Pilot’s rotary-wing hours accumulated
| Total Time Rotary Wing | 9,800 |
| Instrument Flight | 327.5 |
| Night Flight | 833.0 |
| AW139 | 724.9 |
Source: Pilot
The pilot had more than 100 hours’ experience in command with night vision imaging systems (NVIS) and held a grade 1 NVIS rating. The operator’s training and checking system evaluated the pilot as level 2 night vision goggles (NVG).
The pilot achieved currency with an NVIS proficiency check on 9 May 2018. Notes on file advised the pilot to seek practice opportunities in order to consolidate skills for future upgrade to a level 1 NVG pilot. The report also noted that a lack of opportunity to practice was preventing the pilot from making best use of the aircraft’s automated systems.
The pilot’s roster pattern was week-on, week-off, performing 24-hour standby while rostered on. The most recent pattern started on 09 May 2018. In the 4 days prior to the incident, the pilot had accumulated 27.3 hours of duty and 5.8 hours of flight time. Within the Operator’s Fatigue Risk Management System[11] (FRMS), scores of 75 or less were considered consistent with safe working practices. The pilot’s score was 51. He reported feeling well and alert.
Aircrew Officer
The Aircrew Officer (ACO) had 23 years’ experience in crewing Search and Rescue (SAR) and Emergency Medical Services (EMS) helicopters as winch operator and down the wire rescue crewmember. He also held a Commercial Pilot Licence (Helicopter). His total experience in crewing helicopters was over 3,500 hours.
The ACO was NVIS and winch current, having undergone currency and proficiency flights on 10 and 12 May 2018. The Operator’s AW139 crewmembers all completed a pilot’s ground school course for the AW139. The ACO was trained and competent in front seat support and rear cabin activities. The ACO was rated as a Level 1 NVG crewmember within the operator’s system. He had over ten years’ NVIS experience, and he was part of a team that first integrated NVIS into company operations.
The ACO worked on a week-on, week-off, 24-hour standby roster. The ACO reported feeling well and rested at the time of the incident. The ACO’s score of 32 in the Operator’s FRMS supported this.
Flight Nurse
The Flight Nurse (FN) was a medical crewmember responsible for patient care, and not expected to be involved in the operation of the aircraft in flight.
Flight crew configuration
Exemption to operate with crewmember in rear cabin
The Civil Aviation Safety Authority (CASA) provided the Operator with an exemption to Supplement 60 of the AW139 rotorcraft flight manual. The exemption allowed the ACO to operate from the rear cabin of the aircraft during flight below 300ft and for landing at unimproved sites.
The Operator provided a risk analysis for landing at unprepared helicopter landing sites (HLS) under NVG to CASA in support of the exemption. For the descent and final approach phases, the identified risks were concerned with unintentional interference from the ground, obstacles, and loose objects. The helicopter manufacturer had no technical objection to the exemption on the provision that, amongst other things, the crewmember focussed on ensuring identification of obstacles.
Focussing on flight below 300 ft, the risk analysis provided for the initial exemption did not consider risks in the approach phase of flight relating to monitoring and the need for a single pilot to transition from outside goggle vision to instruments to supported peripheral vision. This exemption was later rendered unnecessary by an amendment to Supplement 60 in revision 22 of the AW139 rotorcraft flight manual on 19 October 2017. The manufacturer stated that they addressed risks during transition phase in the initial NVIS certification of the aircraft.
Climb-through
The Operator listed the responsibilities of an ACO in their operations manual as:
Under direction of the pilot assist with the operation of all aircraft equipment and systems during the conduct of VFR, NVG and IFR operations;
and
… operate the winch, dispatch, and recovery of personnel and assist the pilot in maintaining clearance from obstacles by lookout and reporting over the intercom.
Company ACOs could not carry out all of their duties from one location in the aircraft. The ACO had to climb between the front and back as operational requirements demanded. CASA’s position was that they supported the role of the ACO in the front left seat and did not support the transfer of the ACO from the front to rear of the cabin and vice versa in flight. CASA preferred operators to land for the ACO transfer through the aircraft to take place.
When responding to an emergency, the ACO would ordinarily begin the flight in the front and assist the pilot, then climb through to the rear to operate the winch as required. When an ACO used the climb-through, the company required the crew to file a report for data collection and analysis of the procedure.
On this flight, with no available landing sites on scene, and a short flight to the search area with anticipated use of the winch, the ACO began the flight in the back of the helicopter.
Aircraft information
General
Leonardo Helicopter’s AW139 is a medium-sized twin-engine helicopter powered by two Pratt & Whitney PT6C-67C engines (Figure 3). Each engine is capable of producing take-off power of 1,252 kW. Each engine produces enough power for the aircraft to climb in the event of one of the engines failing. The main gearbox’s maximum limit for power from both engines is 1,641 kW. Therefore, overtorque of the transmission can occur when a pilot demands excessive engine power with both engines operative.
VH-YHF
AW139 serial number 31108 was registered in Australia on 18 February 2008 as VH-YHF, and at the time of the occurrence had flown 3,423 hours. The helicopter was certified and maintained for IFR and NVIS operations.
The helicopter’s autopilot was a 4-axis system with enhanced 3-cue flight director (FD). The FD is capable of controlling the helicopter’s movement in the pitch, roll, yaw, and vertical axis. The installed version of the FD had auto-hover functionality (HOV) mode, yet did not offer SAR modes that can mark, return, and transition down to a selected target.
Figure 3: AW139 helicopter VH-YHF

Source: Careflight
Auto-hover
HOV mode incorporates two systems to hold the aircraft at a point in space selected by the pilot. The first system controls the pitch and roll of the aircraft to maintain a zero ground speed in all directions. The second uses the barometric altitude or the radio altimeter[12] (RADALT) information and control of height to maintain the altitude selected by the pilot.
Aside from the panel-mounted autopilot controller, the pilot can activate both systems with the centre of the pitch/roll beep trim selector switch on the cyclic (Figure 4). With the airspeed below 75 kt, ground speed below 60 kt and altitude between 15 ft and 2,000 ft above ground level the system can be engaged. Engaging the system instructs the autopilot to make control inputs to bring the aircraft to a hover at the height showing on the RADALT at the time the pilot presses the switch. There was no vertical speed limit to engage HOV mode. The manufacturer did not intend for HOV mode to be engaged with a high vertical speed, though it did not preclude a pilot from doing so.
If engaged with a high vertical speed, the system would show as engaged and the autopilot would make adjustments necessary to attain the height designated by the pilot. This would induce a magnitude of overshoot relative to the vertical speed at time of engagement. A difference between the reference height and actual height would trigger a warning once large enough. For example, at a reference height of 500 ft, a message ‘HTLM’ appears on the PFD and ‘ALTITUDE, ALTITUDE’ sounds when the actual height passes below 430 ft.
Figure 4: Exemplar AW139 Cyclic and PFD showing HOV Mode engaged
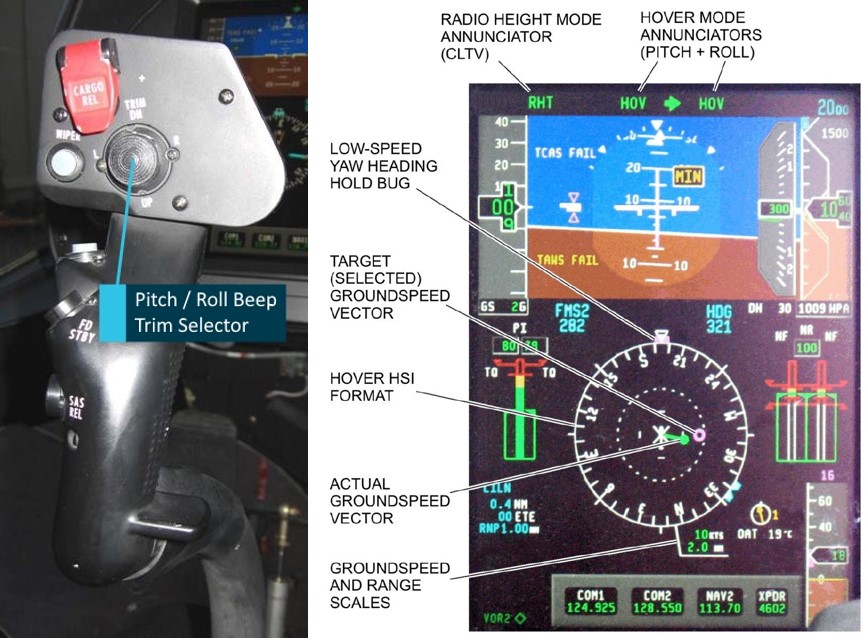
Source: Leonardo Helicopters, annotated by the ATSB
Crew Alert System
The primary flight display (PFD) and the multi-function flight display (MFD) present instrumentation to the pilot (Figure 5). The PFD displays FD modes selected, and their status. The MFD displays engine and aircraft system data and the crew alert system (CAS). The CAS displays messages pertaining to the operation and condition of the aircraft to the crew for information and action.
Figure 5: Exemplar AW139 cockpit displays
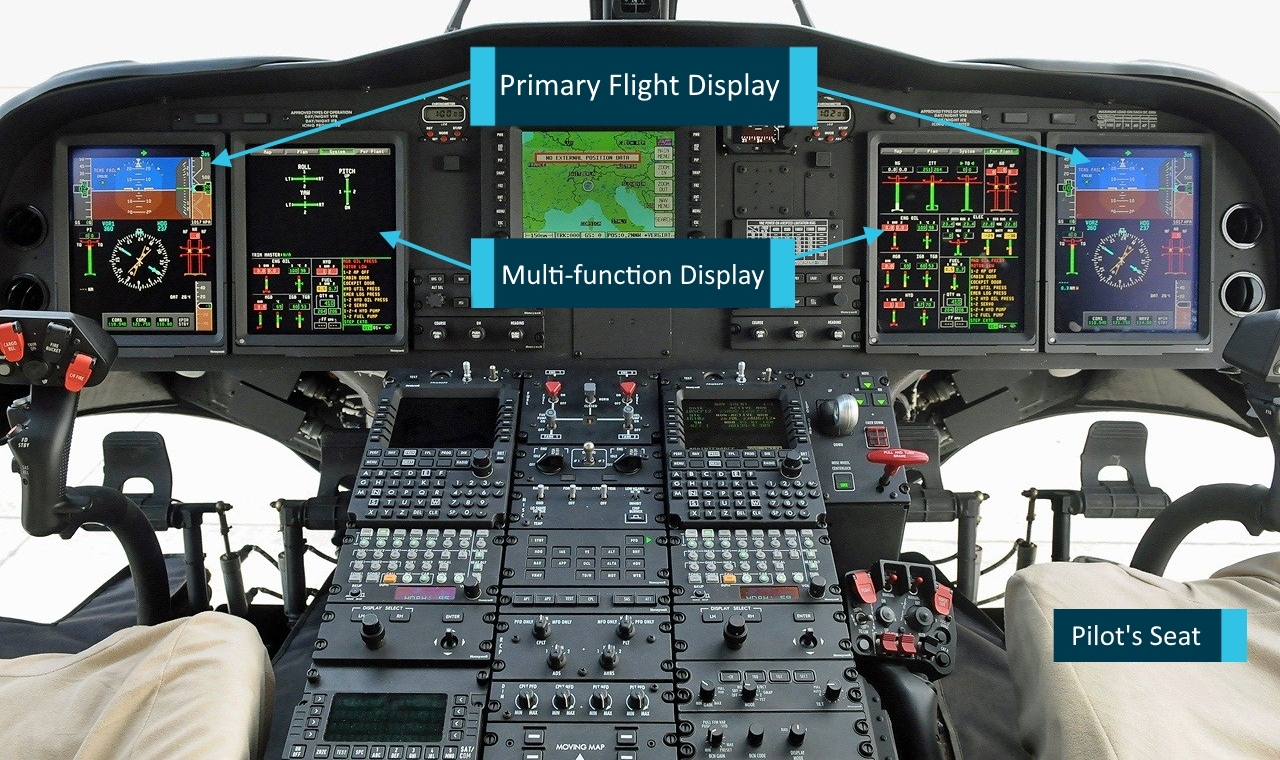
Source: Leonardo Helicopters file photo, annotated by the ATSB
The CAS messages appear in order of priority. Red warnings appear at the top of the list, next are yellow caution messages, third are green advisory messages, and fourth are white status messages. The final line in the list is white text stating ‘END.’ Each page shows twelve lines and crew can scroll through pages. When scrolling, red warnings cannot be hidden and remain at the top of the list on each page.
A warning or caution message will show with a coloured background until acknowledged. Once acknowledged, it appears as coloured text on a black background. Some messages such as “XMSN OVTQ” (main transmission overtorque) will disappear when the condition causing them has passed. White status messages will only show on the ground with weight on wheels (Figure 6).
The “MAINTENANCE” message is significant because following exceedance of a limit such as torque, it will illuminate after landing. The presence of the “MAINTENANCE” message is a cue to an aircraft maintenance engineer (engineer) to investigate and rectify the cause of the message before cancelling the message.
Figure 6: Exemplar caution light and maintenance message on CAS
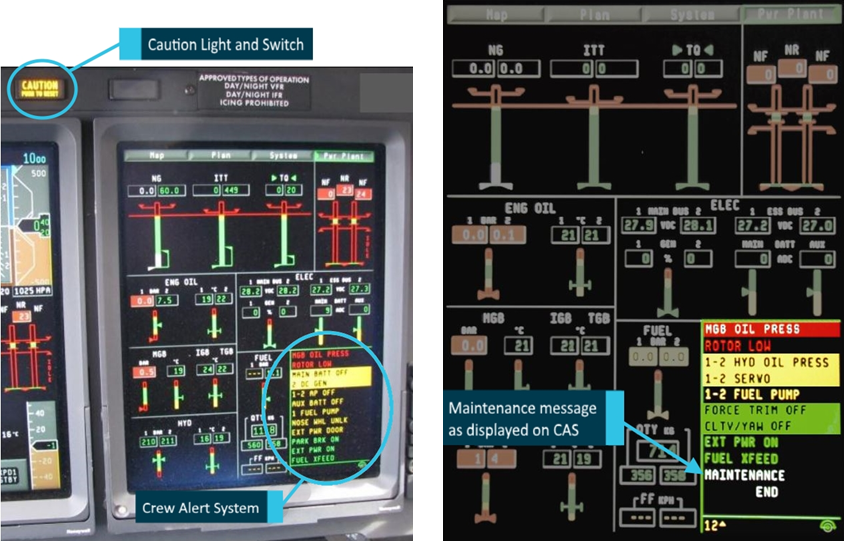
Source: Leonardo Helicopters, annotated by the ATSB.
Night vision imaging system
To improve vision during night operations, the helicopter crew utilised an NVIS. The operator was experienced in application of these technologies. They trained their own crews and offered NVIS training to other operators.
The operator’s NVIS comprises:
- AN/AVS-9 green phosphor Night Vision Goggles (NVG)
- NVG-compatible cockpit lighting
- NVG-compatible cabin lighting
- 2 x 450 W incandescent forward facing steerable search lights
- 1 x 450 W incandescent steerable search light by winch
- White flood lights at the front and back of the aircraft.
The operator mandated the use of NVIS for all visual flight rules (VFR) flights at night.
Goggle position
The human eye carries two sets of light-sensitive receptors: rods and cones. The cones are packed into the fovea, the central part of the retina responsible for focal vision. The rods populate the area of the retina used for peripheral vision. The way in which information from the focal regions and information from the peripheral regions is processed differs significantly (Miller & Tredici, 1992).
Peripheral vision is processed automatically and quickly. Humans utilise peripheral information to orientate themselves within their environment without even noticing. Focal vision requires conscious processing, which happens slowly and takes up cognitive resources (RTCA, 2001). The information delivered to the user through NVG is largely within the focal region. The cognitive resources required take away from other tasks requiring focal vision, such as interpretation of instruments (Salazar et al, 2003).
NVG offer a field of view (FOV) of 40° vertically and horizontally, much narrower than the 200° horizontally and 120° vertically most humans experience (Morawiec and others, 2007). Goggles are normally adjusted to a point where the central image is sharp, and the edge of the picture is slightly blurred yet becomes sharp when focussed upon. This puts the eyepiece approximately 25 mm from the eye.
This operator advised that they extend the NVG further away from the eye again. This reduces the FOV by a couple of degrees and increases the amount of peripheral vision available. This, in combination with copious white light, provides for increased peripheral vision when looking around the goggles below 400 ft in the obstacle environment.
This provides benefit in spatial orientation in low-level hover operations. The effect will be lost if peripheral cues become unreliable and obscure the target, such as happens with backscatter from obscurants like smoke.
White light
The use of white light is fundamental to this operator’s NVIS usage strategy. NVG-friendly[13] searchlights do not help in obstacle clearance as the NVG do not detect the light reflected by obstacles in the vicinity. White light (detectable by NVG) is amplified by the goggles and provides a clear image of where obstacles are. The crew moves the lights in a ‘scan and pause’ pattern with a wide swath either side of the planned approach and departure paths looking for obstacles.
The combination of peripheral vision and white light likely aided the ACO in his assessment of rate of closure and enabled his timely use of emergency phase Crew Resource Management (CRM).
NVIS approach procedure
Overhead the HLS or point of interest, the pilot marks the target on the GPS. The pilot then flies a circuit at 1,000 ft to set up an approach to the spot. Since the visual acuity afforded by the goggles does not provide ground cover detail until a height of 400 ft, the pilot must use instruments to monitor the progress of the aircraft, as per normal night flight procedures. The company operations manual highlights three critical instruments for the initial stage of the approach:
- attitude indicator, to avoid incorrect attitude adversely affecting airspeed and rate of descent
- vertical speed indicator, to make up for the reduced visual cues for rate of descent
- radio altimeter, to incorporate a visual and audible warning that is set at 400 ft as a defence against unexpected rates of terrain closure
The pilot manually flies to a datum point of 400 ft above ground level (AGL) to attain the visual acuity required to identify the target. It is common to come to a hover at 400 ft to complete the reconnaissance and crew brief. The pilot can select HOV mode to pause. If there is a need to descend to winching height, the crew scans the approach and departure paths with searchlights using a ‘stop, scan, move’ process.
Once clear, the crew agrees to continue and the pilot eases the aircraft forward and down with the autopilot. ACO and pilot will work together to bring the aircraft to the best hover reference.
Meteorological information
During the shift, the pilot monitored weather reports and weather forecasts from sources at Darwin and surrounding airports, and the Bureau of Meteorology (BoM). The Aerodrome Forecast (TAF) for Darwin airport, valid for the duration of the flight, forecast wind as 6 kt from the south‑east, visibility of 10 km or greater, nil significant weather, and nil significant cloud below 5,000 ft. The aerodrome report matched the forecast precisely with the exception of showing wind to be 5 kt.
The BoM issued a Graphical Area Forecast (GAF) at 1332 Central Standard Time (CST), which carried a validity from 2030 CST for six hours. The planned operation was within area B2, and the operations were close to the boundary with B1. The GAF forecast scattered cloud with base 2,000 ft and tops to 10,000 ft in the area of B1. The forecast for the area B2 was visibility over 10 km reducing to 5,000 m with isolated areas of smoke below 7,000 ft. The crew reported that some of the conditions associated with B1 existed in their area of operation.
At 1923 CST, BoM published a new GAF. The new GAF showed visibility of 10 km reducing to 4,000 m with isolated areas of smoke below 7,000 ft in B2. Pilots utilising NVG must maintain visibility of 5,000 m at or above 500 ft above terrain or obstacles (Civil Aviation Order 82.6). In areas of smoke, visibility could be expected to be below that required for VFR flight at night.
Environmental conditions
On the night of the incident, there was very little celestial illumination. The moon had set at 1653 CST, and the sun had set at 1830 CST. The only light was starlight. Clouds obscured much of the starlight available.
Grass fires had been burning to the southeast of the region for several days. Smoke from the outlying grass fires drifted across the search area below 7,000 ft, reducing visibility in places. The operations manual mentioned smoke as a common cause of loss of visual reference, and pilots were required to memorise loss of visual reference drills.
The crew reported that these conditions had prevailed for a week. Training notes from a flight three days prior described similar conditions. The report stated:
…this flight was conducted on an especially difficult NT typical night – no moon, very low illumination, and smoke contamination.
Where operationally viable, the crew flew the helicopter above the smoke inversion, which they reported to be at around 1,000 ft.
Risk management of deteriorating weather and loss of visual references
The operator’s risk management profile recognised the risk of deteriorating weather and loss of visual references during a SAR operation. Among the potential consequences was loss of control leading to an aircraft accident. The management of the risk included controls for prevention of an occurrence, and for recovery should the event occur.
Prevention controls
Documented controls for the prevention of loss of visual references were:
- Training and checking, to ensure that crews have relevant experience of similar conditions, all crew know how to assist in the approach and landing phase, and that procedures are being correctly followed.
- Maintenance of good CRM, to ensure effective mission management and decision making aboard the aircraft.
- Keeping the ACO current to assist the pilot with management of the flight.
Recovery controls
Recovery controls covered four aspects of operation:
- Equipment fit, ensuring that the aircraft is appropriately equipped and has a functioning RADALT and Attitude Indicator.
- Sound knowledge of procedures and limits for visual illusions and inadvertent instrument meteorological conditions (IIMC).
- Crew preparedness: Use of simulator training to ensure crews have exposure to implementing correct technique in recovery procedures.
- Crew Resource Management: Ensuring unambiguous and timely communication in situations requiring urgent action.
Beacon activation
Activating an emergency position-indicating radio beacon (EPIRB) begins a distress signal transmission on the 406 MHz frequency, which is detected by satellites. The transmission contains a code that identifies the registered owner of the EPIRB in a database. The Rescue Coordination Centre (RCC) can use the registration details to source information on the activation of the beacon, and contact the owner or a nominated emergency contact.
In this case, the EPIRB belonged to a Queensland-registered vessel, which was sold some time before without re-registration of the EPIRB. As a result, the RCC had no current contact details or information for the current owner of the EPIRB.
EPIRBs in Australia also transmit on the 121.5 MHz frequency. Search and Rescue Assets carry direction-finding (DF) equipment to home in on 121.5 MHz signals. When the beacon is correctly deployed, the DF shows the crew the direction the signal is coming from.
Similar occurrences
AO-2007-028
On 22 July 2007, the crew of a Bell 412 were searching for the source of an EPIRB transmission. The pilot was IFR-rated and the aircraft IFR-equipped. The crew were operating on a dark night with searchlights without NVG. There was smoke from active bushfires in the area.
During the approach, the pilot lost visual references due to the haze from smoke and dust in the atmosphere. The helicopter entered a high rate of descent. The aircrew officer called ‘zero airspeed.’ The pilot initiated recovery actions and the main gearbox was over-torqued in the recovery.
There was a landing site available and the pilot continued the approach from 200 ft AGL and inspected the helicopter after landing. The Bell 412 had a physical indicator that clearly indicated to the crew that overtorque had occurred.
AO-2009-077
In December 2009, the crew of a Bell 206L was conducting aerial work on a fire ground. The pilot was not IFR-rated and helicopter was not IFR-equipped. On take-off, the helicopter entered low cloud. The pilot lost control and the aircraft collided with the ground; the pilot was seriously injured and the passenger was fatally injured. There was no option for the pilot to conduct an IIMC drill to stabilise the aircraft and attain a safe profile.
AO-2016-160
On 21 October 2016, the crew of a BK 117-C2 were returning to base from carrying out an EMS mission. The pilot was IFR-rated and the aircraft was IFR-equipped. The flight was conducted under NVFR with NVIS. Conditions were marginal, and on departure, the helicopter entered low cloud.
The ACO declared loss of visibility on take-off. The pilot had poor visibility ahead yet could see well to the right. The pilot thought visibility would improve as they passed ground lighting that was reflecting in raindrops on the canopy.
The visibility did not improve, and the pilot slowed the aircraft to maintain visual meteorological conditions. The low-speed manoeuvre resulted in an undesired aircraft state and a terrain awareness warning activated. The pilot conducted an IIMC drill, restabilised control, and continued the flight before landing safely.
Aeromedical flights in the United States
In an analysis of aeromedical flights in the US, Aherne and others (2016) found that between 1995 and 2013, the US aeromedical industry had 32 fatal accidents resulting in 100 deaths. These flights were all single-pilot operations at night. All flights were operated under VFR, and two thirds of the fatal accidents occurred in instrument meteorological conditions (IMC).
__________
- Night Visual flight rules (NVFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going, at night.
- Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft to operate in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
- Fatigue Risk Management System (FRMS): defined by ICAO as "a data-driven means of continuously monitoring and maintaining fatigue related safety risks, based upon scientific principles and knowledge as well as operational experience that aims to ensure relevant personnel are performing at adequate levels of alertness".
- Radio Altimeter: a device that detects phase shift between a transmitted and a reflected radio signal, to calculate the height of the aircraft from terrain directly below it. Also known as Radar Altimeter.
- NVG-friendly: a light system that excludes frequencies detected by the NVG. The intent is for a light to be available for crews that does not dazzle the NVG wearer.
Safety analysis
Introduction
During an approach to a potential search and rescue target, smoke from nearby bushfires affected the visibility for the flight crew. The helicopter developed an uncommanded high rate of descent, and the aircrew officer in the rear alerted the pilot, at which point a recovery was enacted. The recovery manoeuvre resulted in an airframe limitation exceedance, which went undetected for the subsequent flight.
This analysis will examine the operator’s risk management, degraded visual environments, single pilot operations, and airframe limitation exceedance management.
Operator’s risk controls
On this occasion, prevention controls failed and recovery controls worked to save the aircraft and crew. There were, however, gaps in the implementation of all of the documented controls:
- Training and checking achieved the aim of creating relevant experience, yet an identified limited practice opportunity reduced efficacy.
- Crew resource management (CRM) lapsed in a missed announcement of loss of visual references. CRM was, however, restored to good effect in recovery.
- The aircrew officer (ACO) was trained yet not positioned to assist the pilot in managing the approach.
There were no preventative controls that helped crews to define limits of visibility beyond the description of visual flight rules (VFR) minima.
The operations manual stated:
Illumination levels are significantly affected by moon position and strength, cloud presence, and cultural lighting and during NVG operations; illumination levels have a profound effect on the ability of the NVG to clearly discern terrain at distance. Visibility is also affected by the usual day time issues of dust, snow, moisture, bushfire smoke and other atmospheric obscurants.
However, the operations manual offered no guidelines on interpretation of factors affecting visibility or definition of acceptable limits. This meant the crew had to interpret marginal conditions during operations and decide if the minima were sufficient. This meant that the organisation did not set its own tolerance for risk in this regard.
During the event, CRM, the well-rehearsed recovery drill, and use of the attitude indicator were all vital in recovering control of the aircraft. The documented and implemented recovery controls worked as intended.
Contribution of night vision imaging system
Studies have shown that night vision goggles’ (NVG) performance can lead pilots to revert to a daytime model of operation (Rash, 2010), leading them to overlook the threats and complexities of operating with NVG. The operator’s operations manual clearly reminded crew that NVG does not turn night into day, and that the use of NVG carries limitations and risk.
Low-contrast Terrain
The search area was an area of low-contrast terrain for night vision imaging systems (NVIS) operations. This meant that elements of the terrain reflected similar amounts of celestial light, creating a low-quality image in the NVG. This lack of detail reduced visual cues. The reduction in visual cues most likely led to difficulty in perceiving the aircraft’s attitude and estimation of terrain clearance (Parush et al., 2011).
Obscurants
Airborne particles affect the image that NVG produce. The cues that would normally be relied upon for loss of visual meteorological conditions (VMC)[14] may not be present. Operating unaided, light sources begin to disappear as obscurants increase. Under NVG, as obscurants reduce the light energy reaching the goggles, NVG will continue to amplify the light signal, disguising the worsening visibility (see CAAP 174-01 11). There will be steady reduction in image quality outside of the bright spots as signal to noise ratio reduces. Scintillation[15] in the image will occur.
Sighting pinpoints of bright light over long distances does not mean that visibility is in excess of 5 km. Visibility must be measured by the distance detail can be seen on the ground. If a pilot using NVG can see lights but no ground detail, they may be in or very close to instrument meteorological conditions (IMC).[16] An early decision to use a recovery drill if visual references are lost is also vital to ensure entry into IMC does not develop into a loss of control or controlled flight into terrain.
Degraded visual environment
Conditions of degrading visibility create ambiguity. This ambiguity can stall decision-making, as two contextually different situations are faced (Orasanu and others, 2001). Either the approach continues and the target is assessed, or the approach is aborted and the mission is delayed.
Pilots rely on appropriate visual cues to assess quickly and accurately the aircraft’s current and future situation. Darkness, even while utilising a NVIS, reduces availability of these cues. No one is immune to these phenomena and strict adherence to an instrument scan on night approach is the primary protection available.
Pilots tend to underestimate the likelihood of loss of control and overestimate their ability to continue to control the aircraft if visual references are lost (Wiggins and others, 2012). The cues for IMC are an absence of those for VMC. The search area for cues to resolve the ambiguity is external to the aircraft, and as such, attention can be drawn outside (Summerfield & Egner, 2009).
Humans also often incorrectly believe that changes will be easy to detect in their environment. Unless someone observes a change while it is taking place, there is a good chance it will not be picked up (Wickens & McCarley, 2008). While searching outside for cues, changes on instruments can be missed. These missed changes can lead a pilot to believe that their knowledge of their position and trajectory in space is accurate. This belief leads to a reduction in the search for new information or information to the contrary (Wickens & McCarley, 2008).
Above 400 ft, the approach should be predominantly made with reference to instruments (see CAAP 174-01 D.3). The pilot was primarily using goggle vision and looking outside. The narrow field of view of the NVG’s requires a demanding and deliberate scan pattern to integrate the outside with instruments. As the pilot slowed to below 45 kt with reducing visual cues, the picture outside was not giving enough information to manage the closure rate of the aircraft. This resulted in a loss of the ability to recognise, with any accuracy, the aircraft’s position and trajectory.
Single-pilot operation
Monitoring is a fundamental tool to boost threat and error management (Flight Safety Foundation, 2014). Furthermore, inadequate monitoring is related to a high number of approach and landing accidents. While there is a clear benefit to multi-crew operations, there is no requirement for multi-crew in Australian search and rescue (SAR), and emergency medical services (EMS). SAR/EMS Operators in Australia tend to perform reduced crew flight operations, whereby extra crewmembers are called upon only for periods of vulnerability.
Crew in the back of an AW139 cannot hear alarms from the cockpit. The 400 ft warning from the Radio Altimeter (RADALT) and the 150 ft warning from the aircraft are only available to front seat crew. The aircraft descended through 400 ft at 1,430 ft/min. The pilot resumed manual control at the time of the emergency climb call as the aircraft passed through 280 ft, 3.5 seconds later.
Had there been a second person in the cockpit monitoring the approach, their first indication of a loss of visual reference, if not announced by the pilot, would most likely be an unusual combination of attitude and vertical speed. The aircraft had developed an unusually high 900 ft/min rate of descent 12 seconds before passing through 400 ft. This information may take a monitoring Aircrew Officer (ACO) a second or two to process. Once processed, however, the aircrew officer (ACO) is in a position to call for a go-around, and to provide accurate information to the pilot regarding the aircraft state much sooner in the sequence.
While facing a high risk of encountering a degraded visual environment, the requirement to have the ACO in the rear cabin for winch operations degraded the crew’s defences against loss of control. The addition of another trained crewmember would be an ideal risk control for operations in potentially degraded visual environments.
Caution and maintenance messages
There is no option for the crew to review caution messages once the message has self‑cleared, or to interrogate the system to discover the extent of any exceedance. As the main transmission torque limit exceedance message (XMSN OVTQ) was missed because it appeared during a time of high workload in flight, the crew could not know of the nature and extent of the exceedance without the support of an aircraft maintenance engineer (engineer).
The crew and the engineer who downloaded the data the following day reported that no maintenance message was detected on the crew alert system (CAS). Analysis of the central maintenance computer (CMC) log showed that eight minutes before the incident flight, a maintenance message activated for 41 seconds. A maintenance message again illuminated four minutes after landing for 31 seconds until shutdown.
The crew reported that the maintenance message was overly generic and related to a host of issues, ranging from critical to inconsequential. The only way to determine the meaning of the message was for an engineer to access the CMC through a laptop. Given the remote locations and 24‑hour nature of operations, engineer access was often impractical, and some telephone diagnosis had to take place.
Additionally, a software update had previously caused issues by instructing the aircraft that equipment it did not have was fitted. As a result, numerous maintenance messages related to the failure of the non-existent equipment were seen. This nuisance message issue was resolved 6 months prior to the event.
These nuisance alerts and generic nature of the message could combine to dilute the significance of the maintenance message and reduce the likelihood that crews would seek out and respond to genuine alerts.
Automatic hover mode use
The autopilot’s automatic hover (HOV) mode fitted to the helicopter could be engaged while the helicopter had a high rate of descent. If this system was not explicitly understood, the pilot may believe that HOV mode had adequate control of the aircraft upon activation. It would display as engaged even though it could be subject to a considerable overshoot, outside of the system’s capacity to recover before impact with terrain. At the height engaged, the mismatch between reference height and actual radar height would have triggered a PFD message ‘HTLM’ and an aural callout of ‘ALTITUDE, ALTITUDE’ after about 2.5 s, as the aircraft passed through a point between 39 ft and 70 ft below the reference height. The pilot input came 4.2 s after engagement of automatic hover. Without the correct mental model of HOV mode operation, time taken to interpret autopilot performance may have delayed manual recovery actions.
Beacon registration and placement
When the vessel was located, the crew saw the emergency position-indicating radio beacon (EPIRB) laying in the bottom of the boat and not deployed as per Australian Maritime Safety Authority guidance. This resulted in a scattered signal and created inaccuracies in the operation of the Direction Finder (DF). The crew could not resolve the direction of the beacon.
The lack of accurate registration details and sporadic output of the DF caused distraction to the crew and increased their time to find the target. The result for the crew was that they were required to identify a number of targets and make approaches to them for visual identification. This increased the complexity and time taken to complete the operation.
Figure 7: Correct EPIRB placement following activation
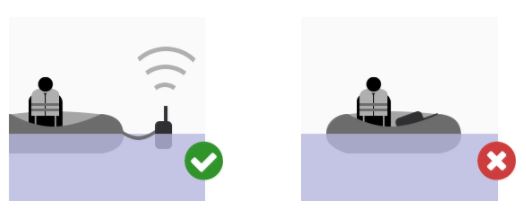
Source: Australian Maritime Safety Authority
__________
- Visual Meteorological Conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
- Scintillation: rapid changes in brightness at random points which to the viewer looks like a sparkling effect across the image.
- Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under Instrument Flight Rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
Findings
From the evidence available, the following findings are made with respect to the loss of control of a Leonardo Helicopters AW139, registered VH-YHF, on 13 May 2018, and the subsequent release of the aircraft without a required inspection. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
- During the search for a transmitting beacon, the helicopter crew planned to approach to a hover near a target. However, low celestial illumination and drifting smoke created a high risk of encountering a degraded visual environment. This resulted in a loss of visual references on approach.
- During the approach to hover in a degraded visual environment, searching outside for visual cues drew the pilot’s attention away from the flight instruments. This resulted in flight instruments not being referenced when they were needed.
- The required position of the aircrew officer in the rear of the helicopter prior to descent negated the benefit of having a trained and competent crewmember to assist the pilot, resulting in a degraded monitoring capability in the approach to hover.
- While on approach in a degraded visual environment, without the protections of flight instrument use or monitoring, the helicopter entered an uncommanded, undetected high rate of descent, resulting in a transmission overtorque during recovery.
Other factors that increased risk
- Auto hover had no design limit on vertical speed for engagement, which permitted overshoot following engagement with high rate of descent.
- As the aircrew could not confirm the existence of an exceedance, and a maintenance message was not detected on the Crew Alert System, the aircraft was operated despite requiring an inspection.
Other findings
- Application of good Crew Resource Management and practiced recovery techniques supported the crew in restoring control.
- The emergency position-indicating radio beacon was not registered to the current owner, and was incorrectly placed in the boat. The placement scattered the beacon's signal, leading to loss of accuracy in direction-finding equipment. As a result, mission complexity and time taken to rescue were increased.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot and crew
- Careflight
- Aviation Specialities Unlimited
- the Bureau of Meteorology
- Airservices Australia
- Leonardo Helicopters
- the Civil Aviation Safety Authority.
References
Aherne BB and others, 2016, Pilot Domain Task Experience in Night Fatal Helicopter Emergency Medical Service Accidents, Aerospace Medicine and Human Performance. 87(6). 550-556.
Arthur W and others, 1998, Factors That Influence Skill Decay and Retention: A Quantitative Review and Analysis, Human Performance. 11(1), 57-101.
Australian Transport Safety Bureau, 2004, ASR B2004/0152, Night Vision Goggles in Civil Helicopter Operations
Bailey RE and others, 2017, An Assessment of Reduced Crew and Single Pilot Operations in Commercial Transport Aircraft Operations, 2017 IEE/AIAA 36th Digital Avionics Systems Conference, St Petersburg
Biggs AT and others, 2015, Examining perceptual and conceptual set biases in multiple-target visual search, Atten Percept Psychophys. 77. 844-855.
Civil Aviation Authority, 2013, CAP 739, Flight Data Monitoring
Civil Aviation Safety Authority, 2017, CAAP 174-01 v2.1, Night vision imaging – helicopters
Dismukes RK & Berman B, 2010, Checklists and Monitoring in the Cockpit: Why Crucial Defenses Sometimes Fail, National Aeronautics and Space Administration, Moffett Field
Ersting J & King P, 1995, Aviation Medicine, 2nd ed., Butterworth-Heinemann Ltd, Oxford.
Flight Safety Foundation, 2014, A Practical Guide for Improving Flight Path Monitoring, Washington.
Flight Safety Foundation, 2018, Position Paper: Pilot training and competency, Alexandria.
Miller RE & Tredici TJ, 1992, Night Vision Manual for the Flight Surgeon, Armstrong Laboratory, AL-SR-1991-0002
Morawiec G, Niall KK & Scullion K, 2007, Distance estimation to flashes in a simulated night vision environment, Defence R&D Canada, TR 2007-143
Orasanu J & Martin L, (1998). Errors in aviation decision making: A factor in accidents and incidents. In Proceedings of the Workshop on Human Error, Safety, and Systems Development. 100-107.
Orasanu J, Martin L & Davison J, (2001). Cognitive and contextual factors in aviation accidents, in Salas E and Klein G (Eds.) Linking expertise and naturalistic decision making, Lawrence Erlbaum Mahwah NJ. 209–226.
Parush A, Gauthier M, Arseneau L & Tang D, (2011). ‘The Human Factors of Night Vision Goggles Perceptual, Cognitive, and Physical Factors’, Reviews of Human Factors and Ergonomics. 7. 238-279.
Previc FH & Ercoline WR, 2004, Spatial Disorientation in Aviation, American Institute of Aeronautics and Astronautics, Inc., Reston.
Rash CE, 2010, ‘Lighting Up the Night’, Aero Safety World. August 2010. 14-18.
Robson D, Night Flight, 2008, Aviation Theory Centre, Cheltenham.
RTCA 2001, Concept of Operations: Night vision imaging systems for civil operators, RCTA/DO-268, RTCA, Washington, D.C.
Salazar G and others, 2003, Civilian use of night vision goggles, Aviation Space and Environmental Medicine. 74. 79-84.
Summerfield C & Enger T, 2009, Expectation (and attention) in visual cognition, Trends in Cognitive Sciences. 13(9). 403-409.
Wickens CD & McCarley JS, 2008, Applied Attention Theory, CRC Press, Boca Raton
Wiggins MW and others, 2012, ‘Characteristics of pilots who report deliberate versus inadvertent visual flight into instrument meteorological conditions’, Safety Science. 50(3). 472-477.
Wiggins MW and others, 2014, ‘Cue-utilisation typologies and pilots’ pre-flight and in-flight weather decision-making’, Safety Science. 65. 118-124.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Civil Aviation Safety Authority, the Bureau of Meteorology, Leonardo Helicopters, the crew of VH-YHF, engineers for VH-VHF, and Careflight.
Submissions were received from the Civil Aviation Safety Authority, the Bureau of Meteorology, Leonardo Helicopters, the crew of VH-YHF and Careflight. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
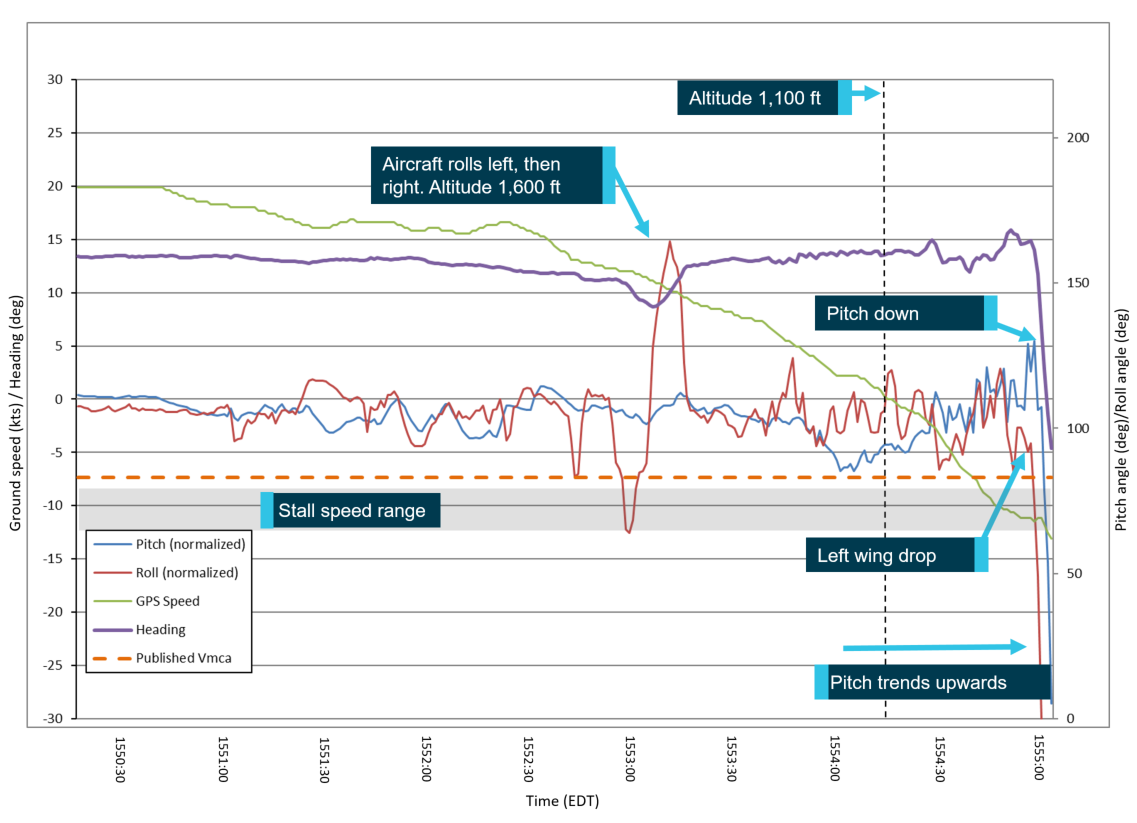
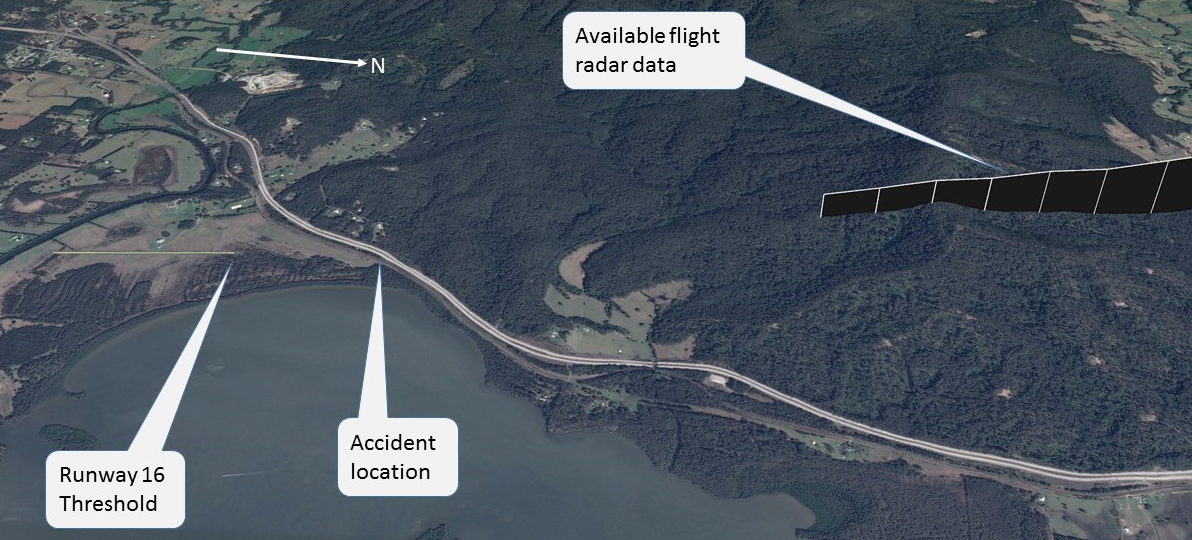
Appendix A: Flight data
Figure 8: Incident flight data
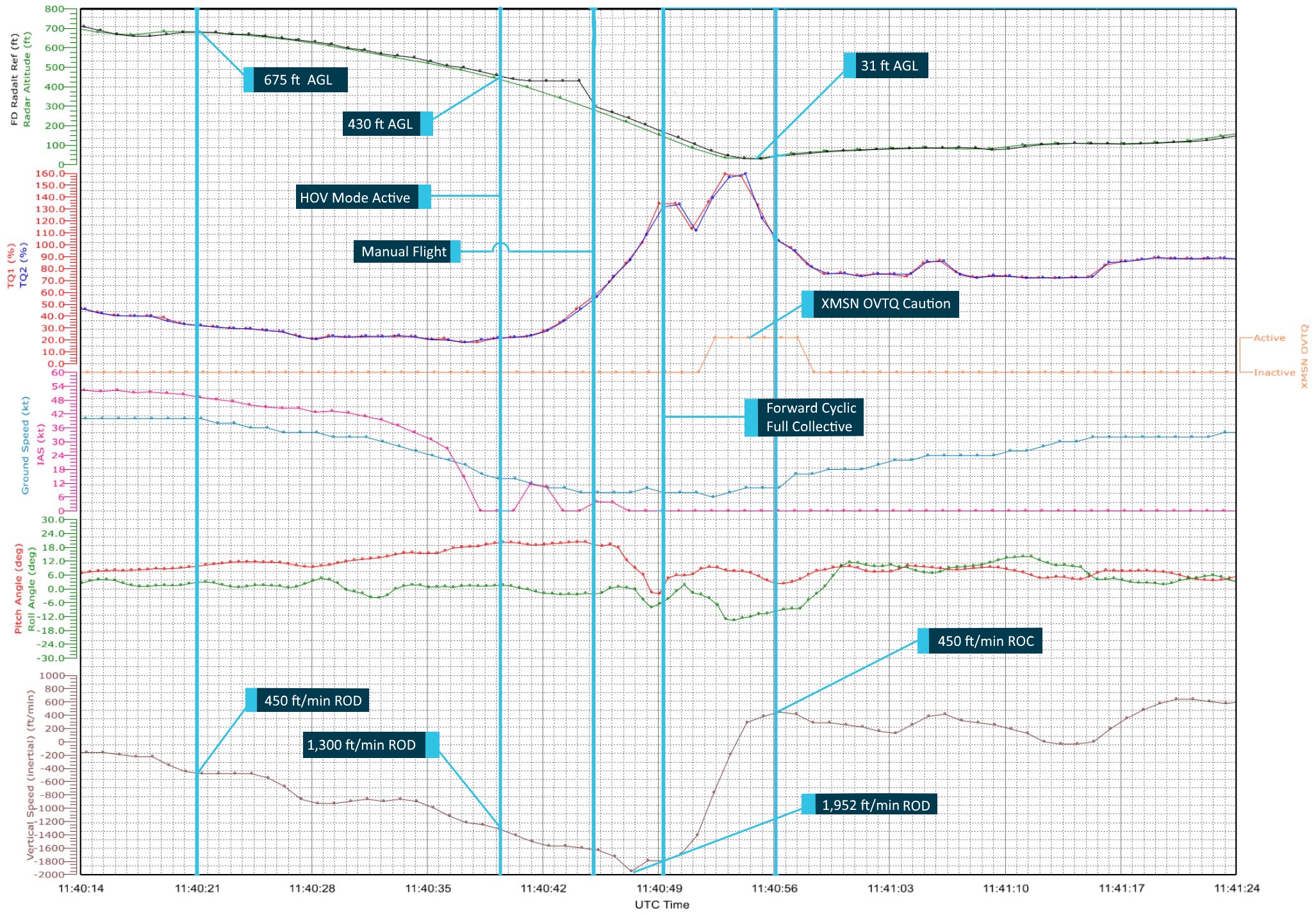
Source: Operator / Leonardo Helicopters, annotated by the ATSB
Figure 9: Incident flight data
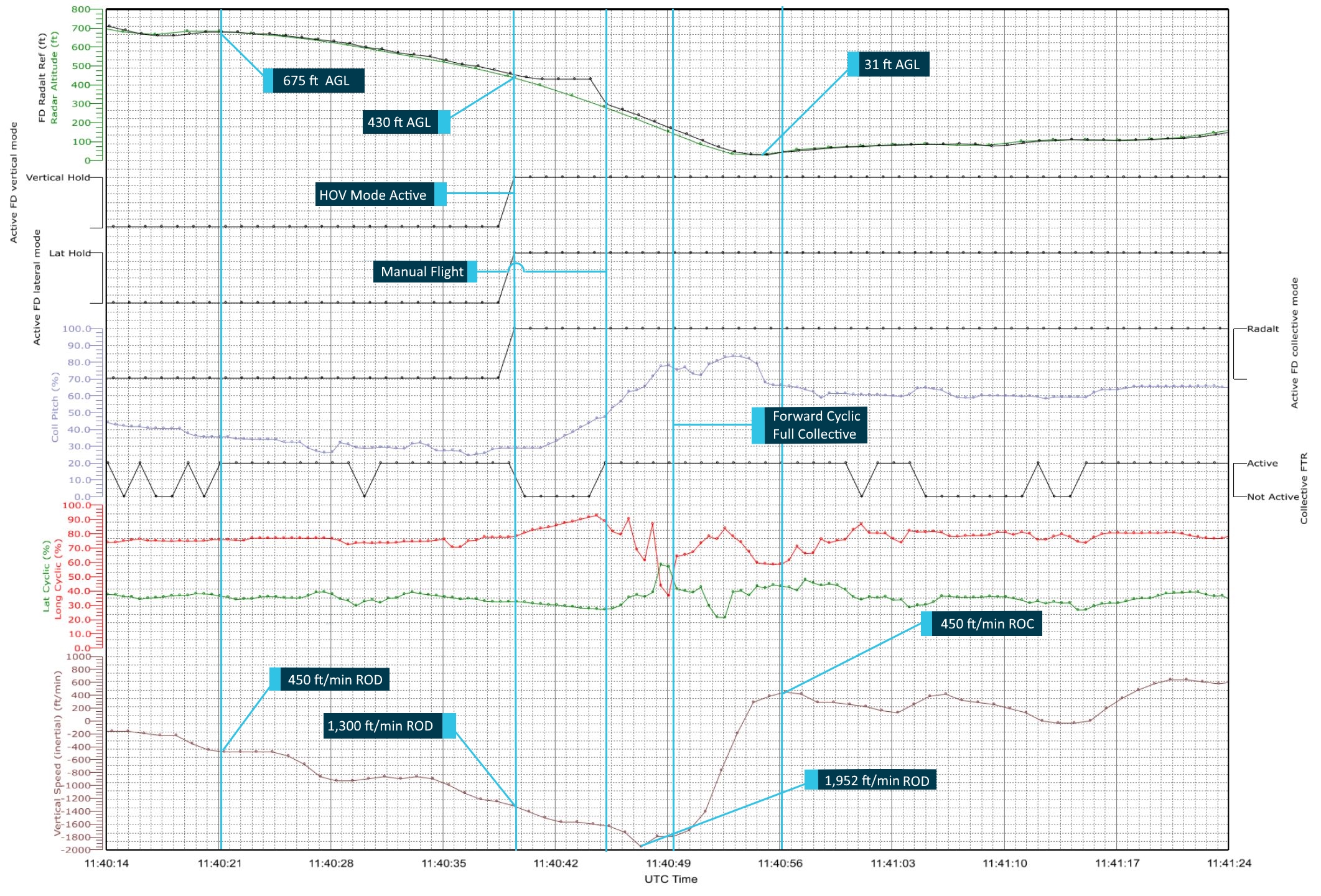
Source: Operator / Leonardo Helicopters, annotated by the ATSB
Purpose of safety investigations & publishing information
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2020 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
Occurrence summary
| Investigation number | AO-2018-039 |
|---|---|
| Occurrence date | 13/05/2018 |
| Location | 38 km east-north-east of Darwin |
| State | Northern Territory |
| Report release date | 16/04/2020 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Loss of control |
| Occurrence class | Serious Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Leonardo Helicopters |
|---|---|
| Model | AW139 |
| Registration | VH-YHF |
| Serial number | 31108 |
| Aircraft operator | Careflight |
| Sector | Helicopter |
| Operation type | Aerial Work |
| Departure point | Darwin, Northern Territory |
| Destination | Darwin, Northern Territory |
| Damage | Nil |