The Piper Tomahawk aircraft was being used to conduct a series of touch-and-go landings during a dual instructional flight. During the climb after the second take-off, and when the aircraft was at a height of about 200 ft, the engine failed without warning. The instructor manoeuvred the aircraft to avoid landing in a lake located just beyond the end of the runway and landed in an adjacent paddock. Although the aircraft hit some low bushes during the landing roll, the pilots were not injured, and the aircraft was not damaged.
The aircraft was moved to a maintenance facility and, prior to conducting any maintenance or inspections, the engine was started and ground-run without any obvious problems. The maintenance inspection revealed a contact mark had been worn through the Teflon coating of the wear area of the carburettor float needle. When the carburettor was reassembled and tested, it was found that the carburettor float needle would stick in the valve seat and prevent fuel flowing into the carburettor bowl. The float needle and seat were replaced, and the aircraft test-flown without further incident.
The student pilot hired a Cessna 150L aircraft to undertake a local training flight with an instructor. The aircraft departed Canberra airport at approximately 1705 Eastern Summer Time and proceeded directly to the training area. The aircraft entered the circuit area for a landing at Canberra about 1.2 hours later. At that time, the pilot was instructed by air traffic control to track the aircraft in order to position it on a left downwind leg for a landing on runway 12. However, the controller observed the aircraft positioning for a right downwind leg. The controller instructed the pilot to turn left onto a heading of 090 degrees to reposition for a left circuit. Following the turn, the student pilot and instructor observed a decrease in engine power. The instructor resumed control of the aircraft and attempted to diagnose the loss of power. The engine surged a number of times and then lost power entirely, including stoppage of the propeller. The instructor transmitted a mayday message, and was cleared by the controller to track for the closest runway. When it became apparent that the aircraft would not reach the runway, the instructor changed heading and was manoeuvring to land in a field when the aircraft struck a tree and impacted the ground.
Both occupants were injured in the accident, but vacated the aircraft through the left door. There was no post-impact fire. The instructor died seven days later as a result of complications associated with injuries suffered in the accident.
Before the flight, the instructor had dipped the fuel tanks and ascertained that the aircraft contained 40 L of useable fuel, with 4 L more in the right tank than the left tank. The fuel tanks are interconnected and are intended to allow fuel to self-level. It is not possible to select fuel from individual tanks during flight.
Examination of the wreckage indicated that the aircraft had impacted the ground in a nose-down attitude. The engine was not operating at the time of the impact and the propeller was stationary. The aircraft was considered to have been capable of normal operation before impact.
The fuel tanks were found to be intact. However, the fuel and cross-vent plumbing on the right tank was disrupted during the impact sequence. That disruption would have prevented fuel from transferring between tanks following the accident. There was no indication of a fuel spill at the accident site. The left fuel tank was found to contain no fuel, and the right tank was found to contain 12 L. Advice from the manufacturer and the owner's manual indicated that the unusable fuel for that aircraft was 11.4 L, which is spread throughout the fuel system (including the two tanks). No defect was found in the fuel system that would have caused a difference in the quantity in the fuel tanks or the engine power loss. Nor were any defects found in the fuel gauges or their respective sender units.
At the time of the engine failure, the aircraft had been airborne for about 1.2 hours. During the exercise, the instructor and student engaged in steep turning exercises at 45 and 60 degrees bank angle, and in spiral dive and incipient spin recovery. The instructor also demonstrated how to configure the aircraft to commence a loop, which was conducted at 5,500-6,000ft. Much of the lesson would have required the use of full power to achieve the desired performance.
The owner's manual indicated the fuel consumption for a 75% power setting to be 22 L/h. Company policy was to plan for 22 L/h. An engine manufacturer's representative indicated that a fuel consumption of 33.4 L/h could be expected when operating the aircraft at the full-power setting.
An aircraft manufacturer publication titled "Pilot Safety and Warning Supplements" cautions pilots regarding uncoordinated flight for longer than 30 seconds when the fuel tanks are less than one-quarter full. The publication indicates that the aircraft is considered to be in uncoordinated flight when the balance "ball" on the turn coordinator instrument is displaced more than one quarter from its centre position. Uncoordinated flight may result in an interruption of the fuel supply to the engine.
The instructor held a commercial pilot licence and a valid medical certificate. The instructor's licence was endorsed with a Grade 3 instructor rating. The student pilot held a student pilot licence. ANALYSIS The investigation could not determine the reason for the engine failure, although the circumstances were consistent with fuel starvation. The aircraft departed Canberra with 40 L of useable fuel. The instructor and student had planned for a fuel consumption of 22 L/h, consistent with operations at 75% power and equating to an endurance of 1.8 hours flight time. However, much of the lesson would have required using full power with a fuel consumption rate of about 33 L/h. The aircraft had been operating for 1.2 hours when the engine lost power. It is possible that training manoeuvres resulted in fuel transferring from the left to the right tank, and may explain the fuel quantity imbalance noted during the post-accident examination of the fuel system. While the aircraft may have had sufficient fuel to complete the flight, an uncoordinated turn to position the aircraft for the correct approach may have resulted in the remaining fuel in the right fuel tank being displaced away from the fuel pick-up pipe, disrupting the fuel supply to the engine.
The aircraft was flown before necessary certification processes were completed.
The aircraft performed a barrel roll or similar manoeuvre for reasons undetermined, and the engine stopped during the manoeuvre.
The engine stoppage was most probably due to fuel starvation.
The pilot lost control of the aircraft and was unable to regain control before the aircraft struck the ground.
Analysis
The investigation established that the aircraft performed a barrel roll or similar manoeuvre to the right, followed immediately by a series of flick rolls or a spin to the left. (A barrel roll is a manoeuvre where the nose of the aircraft is made to travel around a spiral path which is some distance from the axis of the roll. A flick roll is a manoeuvre where the aircraft is induced into a stall at a higher than normal speed and the aircraft rotates or rolls rapidly about its longitudinal axis. A spin is characterised by the same rotational movement but the axis of a spin is usually vertical.) The investigation could not establish any reason for the manoeuvre. During the course of the roll, the engine noise was heard to cease, and this was most probably due to fuel starvation. The investigation established that the centre of gravity may have been near the aft limit and this would have accentuated the uncontrolled manoeuvre and reduced the chances of recovery by the pilot. During the recovery from the rolling manoeuvre, the aircraft then stalled and rolled rapidly left two or three times before ground impact.
The engine was estimated to have been running for approximately 50 minutes before the accident. As a result, the fuel quantity remaining may have been insufficient to allow continued fuel supply to the engine when the aircraft was banked steeply, and may have caused the engine to cease operating due to fuel starvation.
Summary
The homebuilt aircraft had been completed over a period of about 22 years and was in flying condition. The aircraft, known as the Smyth Model S Sidewinder, was designed in the USA in 1958. The designer was aiming to produce a sporting monoplane that was reasonably easy to build, easy to fly, stressed to 9g for aerobatics, and economical in operation. The first flight of this aircraft type was made on 21 February 1969 and it received the Outstanding Design Award at the 17th Experimental Aircraft Association Fly-in that year. Plans became available to amateur constructors and in 1973 the plans for the accident aircraft were purchased by the owner.
By 1978, the fuselage construction was well advanced and the initial inspection was carried out. The project proceeded slowly and in 1985 the owner moved from NSW to live in Qld. The aircraft was nearing completion in 1994 when the owner made an application to the then Civil Aviation Authority (CAA) to reserve the registration VH-LKV. The aircraft was a first of type in Australia, and the necessary certification processes were incomplete. At the time of the accident, the aircraft was unregistered and did not have a certificate of airworthiness or a permit to fly. However, the pilot on the accident flight had flown the aircraft some weeks earlier on its first flight.
It had not been the intention of the owner to fly the aircraft on the day of the accident. The pilot arrived at the aerodrome and found the owner and his friend working on the aircraft. After some discussion, the pilot suggested to the owner that they should take the aircraft for a flight. The owner initially declined the offer but the pilot persuaded him to accede to the suggestion. Subsequently, the pilot added 20 L of fuel to the main fuel tank, which had contained about 6 L of residual fuel. The pilot then assisted the owner and his friend to replace panels and cowling and to prepare the aircraft for flight.
The weather was fine with a light south-easterly wind. Witnesses observed the aircraft taking off from runway 06. After take-off, the aircraft initially flew low down the runway with a tail-down attitude, and then began a shallow climb. A flight of about 30 minutes was conducted, during which the pilot demonstrated some of the handling characteristics to the owner. The pilot also carried out circuits and landings during this period. The aircraft was then landed and taxied back to the hangar. While the engine was running and the owner was getting out of the aircraft, the pilot motioned to the owner's friend to come over to the aircraft. The friend indicated to another person he was with at the time, that he did not wish to go flying as he would be late getting home. However, he boarded the aircraft and the pilot taxied out for another take-off.
The aircraft became airborne, again from runway 06, and headed north-east for about 2 km before turning left and heading back towards the aerodrome. When the aircraft was over the aerodrome at about 1,000 ft, witnesses saw the aircraft descend in a shallow dive and then perform what appeared to be a steeply banked manoeuvre or barrel roll to the right. One witness said he remembered seeing the belly of the aircraft faced towards him. Another witness said the aircraft rolled completely over in what appeared to be a controlled manoeuvre. During this manoeuvre, a third witness heard the engine noise increase and then completely cease. The aircraft recovered to a level attitude but immediately flick-rolled to the left and adopted a steep nose-down attitude. The aircraft continued to flick-roll or spin and struck the ground. The aircraft was descending almost vertically at impact with a 30-degree nose-down attitude. There was no fire and the impact was not survivable.
Aircraft particulars
This was the first aircraft of its type to be constructed in Australia. Another builder in WA had commenced construction of a Sidewinder at about the same time, but the project was not completed. The aircraft was powered by a Lycoming Model 0-290-D2B engine which had a take-off power rating of 140 h.p. at 2800 r.p.m. The aircraft was designed with a fixed tricycle landing gear but the subject aircraft had been fitted with retractable gear. The gear was not retracted on the accident flight because the alternate gear extension system was not operative. The main fuel tank had a capacity of 65 L. The two wing tanks each had a capacity of 49 L, and were empty on the accident flight. The fuel consumption quoted by the engine specifications was 6.5 US gal or 24.6 L/h for economical cruise. Fuel consumption for the pre-accident flights could not be determined but would have been significantly higher than the economical cruise consumption because of the nature of the flights.
The aircraft was fitted with fully functioning dual controls and side-by-side seating for two persons. The constructor's manual quoted a stalling speed of 48 kts and a maximum speed (Vne) of 174 kts. The flight characteristics of this aircraft were unknown as a flight test schedule had not been carried out. The empty weight of the aircraft was approximately 477.5 kg but a final weighing of the aircraft had not been carried out as was required for certification of type. The aircraft had been test flown in December 1996 by the accident pilot. After that flight, the pilot had expressed his dissatisfaction with the aircraft's stalling characteristics, and said that he would not fly it again. It was discovered that the aircraft had 26 L of fuel in the left-wing tank and no fuel in the right tank. This may have affected the stalling characteristics.
Damage to aircraft
The aircraft impacted the ground whilst rotating to the right with a nose-down attitude of approximately 30 degrees. The cockpit area was destroyed by the impact. The engine was embedded in the ground to a depth of about 0.5 m. One propeller blade was sheared off and fragmented by impact. The fractured surface indicated no powered rotational movement at the time of impact. The remaining propeller blade was intact and undamaged. The cockpit structure and floor had been compressed forward against the rear of the engine. The force of impact against the rear of the engine had fractured the engine gear housing. The throttle was found in the fully open position, the mixture fully rich and carburettor heat control in the cold position. However, the position of the cockpit controls before impact could not be positively determined due to the extent of damage. The main fuselage fuel tank had disintegrated and there was no evidence of fuel at the accident site immediately after the accident.
Wreckage examination
Examination of the airframe did not reveal any failure or defect which might have contributed to the accident. The engine exhaust pipe was metallurgically tested and was at less than operating temperature at impact. The engine was bulk stripped and no defects or failures were discovered other than those caused by impact damage. The retractable landing gear was in the extended position at impact. During the investigation the possibility of propeller or spinner failure was considered, but there was no evidence to support this hypothesis. The possibility of a bird strike was also considered, but again there was no evidence found during the wreckage examination to support this theory.
Weight and balance
The aircraft had been weighed on 10 January 1994 to determine the empty weight and centre of gravity. A final weighing was required after fitting of the radio and other equipment but this had not been carried out. The actual weight and balance at the time of the accident could not be determined. However, based on the initial weight and balance determination, the aircraft was within the weight and balance envelope and the centre of gravity near the prescribed aft limit. The summary showed that with two persons on board and no fuel, the centre of gravity was 0.55 inches forward of the aft limit.
Personnel information
The pilot was the holder of a senior commercial pilot licence (aeroplane) and was qualified and endorsed on the aircraft category. He had flown the aircraft on one other occasion some three weeks before the accident, but otherwise had no experience on the particular aircraft type. He was, however, widely experienced with over 38 years as a flying instructor, airline pilot and general aviation pilot. He had previously test flown a home-built aircraft for the passenger on the accident flight. The passenger held a student pilot licence and had accumulated about 267 hours aeronautical experience.
Medical information
The pilot was medically fit and qualified to perform the flight. He had a current class one medical certification status. There was no evidence found to indicate that there were any physiological or medical factors which may have contributed to the accident. The passenger was medically fit and held a valid medical certificate for his licence category.
Meteorological conditions
Witnesses reported conditions at the time of the accident as fine with a light easterly breeze. There was an insignificant amount of high-level cloud and the temperature was 24 degrees C.
Communications
The aircraft was fitted with a VHF radio. The Caboolture aerodrome is outside controlled airspace but within the Caloundra/Redcliffe Common Traffic Advisory Frequency area. The frequency is used for inter-aircraft and advisory communication and is not recorded. There was no other known flying activity in the vicinity of Caboolture aerodrome at the time of the accident, and it is not known if there were any transmissions made from the aircraft immediately before the accident.
Aerodrome information
The Caboolture aerodrome is unlicensed. The grass runways are 06/24 and 12/30, and are 900 m and 1,350 m in length respectively. The aerodrome is 40 ft above sea level. The aircraft impacted the aerodrome on the southern side the runway 06 flight strip near the north-eastern end of the runway.
This report outlines the circumstances surrounding a fatal accident involving a Cessna 337 aircraft near Albany, in Western Australia on 13 March 1996. The aircraft crashed during a low-level inspection of a bay on the coastline to the east of Albany.
The accident occurred after the pilot lost control of the aircraft at low level. Loss of control was precipitated by a loss of power on both engines whilst the aircraft was being flown in a maximum-performance turn.
Loss of power on the rear engine was the result of fuel starvation, probably caused by un-porting of the fuel supply line during prolonged unbalanced flight. The reason for loss of power on the front engine could not be determined although it is possible that the pilot inadvertently selected the front engine to off whilst attempting to change the fuel selection on the rear engine from the main to the auxiliary fuel tank.
History of the flight
Witness evidence indicates the aircraft and pilot were hired so the passengers, Federal and State officers, could complete an aerial inspection of some unidentified drums located in a small bay 45 km east of Albany. An attempt to reach the drums on foot had failed because of dense undergrowth.
The pilot's post-flight report form shows the flight departed Albany Airport at 0901. Passengers' watches indicate the accident occurred between 0920 and 0925. There were no witnesses to the route flown or the accident.
The aircraft was reported missing at 1500, and the wreckage was located at 1615, on the edge of the bay containing the drums.
Pilot information
The pilot held a current commercial pilot licence with a Cessna 337 type rating. He was approved to conduct low-level operations. He was experienced in low-level operations, having worked as an agricultural and whale-spotting pilot for many years. He should also have been familiar with the coastline in the area of the crash, having operated in the area as a whale spotter.
The pilot held a Class 1 medical certificate. Post-mortem examination did not disclose any medical condition that may have been a factor in the accident.
Aircraft information
Cessna 337C VH-FAM was manufactured in the USA in 1968 and placed on the Australian register on 16 October 1968. The aircraft had completed 5,390 hours time in service. The rear engine, Serial Number IO-360-C-10344, had completed 393 hours of its 1,500-hour service life. The front engine, Serial Number IO-360-C-10014, had completed 1,726 hours of its 1,800-hour service life. The additional 300 hours available on the front engine were the result of earlier maintenance which extended the service life of that engine. An inspection of the aircraft's logbooks revealed that it had been maintained in accordance with the manufacturer's and regulatory requirements. A valid maintenance release was in force and no unserviceable items were recorded prior to the final flight.
The Cessna 337 is a twin-engine aircraft with the engines located fore and aft on the main fuselage. The rear engine is reported by the manufacturer to be the critical engine. Single-engine performance is less with only the front engine operating rather than the rear. In addition, the front engine is positioned below the total thrust line and the rear engine above it. Any loss of power in the rear engine will result in a nose-up pitching moment.
The estimated weight of the aircraft at the time of the accident was 1,927 kg. Maximum allowable weight was 1,996 kg. The pilot and one passenger were seated in the front row. The other two passengers were seated in each of the other two rows. The centre of gravity was within the defined envelope.
Meteorological information
The surface wind at 0900 at Albany was recorded as coming from 080 degrees at 16-18 kts. Meteorological advice indicates that the terrain around the crash site is conducive to the formation of small-scale eddies or rotors which cause turbulence. The pilot of the search helicopter reported that, 7 hours after the crash, conditions in the bay at low level were very turbulent. Wind conditions appeared to be significantly affected by the surrounding terrain. It was reported that the average wind conditions tended to push any aircraft operating in the bay towards the hills around the bay.
Communications
A review of the air traffic service recording tapes indicates that no radio transmissions from the pilot were recorded before or during the flight. There was no requirement for the pilot to contact an air traffic service agency. Wreckage and impact information
On-site inspection
It was apparent from aircraft and foliage damage that the aircraft impacted at a nose-down angle of approximately 60 degrees with the wings level. The left wingtip contacted the ground first, because of the slope of the terrain, followed by the lower, forward fuselage. Damage to the cockpit/cabin area was extensive. The fuselage section, aft of the wings, exhibited only moderate damage. The wreckage remained upright and mostly intact after the impact. There was no wreckage trail.
The direction of the impact indicated that the aircraft was flying towards the north, following the coastline in the bay, when it crashed.
The front engine was torn from the fuselage and suffered considerable impact damage to the crankcase, cylinders, and accessories. Engine oil was found on the ground under the engine. The rear engine suffered minor damage only, although the engine mounts fractured on impact.
The front propeller drive shaft fractured during the crash. Whilst both blades on the front propeller and one blade on the rear propeller were bent, neither propeller exhibited damage consistent with being under power at impact.
The landing gear was retracted.
The position of the flap motor worm drive indicated the flaps were extended to half travel.
All control surfaces were present, and all systems appeared to be working correctly prior to the accident. All damage was consistent with being caused by the impact.
Both wings were destroyed. The main fuel tanks, two in each wing, were split at the seams and exhibited severe distortion caused by the movement of fuel. The auxiliary fuel tanks, one in each wing, were intact although each had been breached. They also exhibited severe distortion caused by the movement of fuel. The distortion made it possible to determine that the main tanks were almost full and the auxiliary tanks half full, at impact. The right auxiliary was the only wing tank still containing fuel (3 L) at the time of the inspection. All other wing fuel had drained from the damaged areas. Both fuel sumps, one in each tail boom, were intact and undamaged. Only the left sump contained fuel.
The fuel lines running from the main and auxiliary tanks to their respective engine fuel filters were intact (right tanks to the rear engine and left tanks to the front engine). The fuel supply line from the filter to the rear engine was intact. The line on the front engine had been severed although fuel in the line was trapped by crimping adjacent to the fracture and the angle at which the wreckage was lying. No pre-existing blockages were found in the fuel system.
Approximately 50 mL of fuel was removed from the fuel supply line, filter, and engine-driven fuel pump for the rear engine. This amount is representative of residual unusable fuel. The right fuel sump was empty although beach-marks indicated that it contained approximately 1.25 L of fuel at impact. Approximately 250 mL of fuel was recovered from the lines and filter for the front engine, the amount expected from a fully charged system. The left fuel sump contained 1.3 L of fuel and beach-marks indicated that it had been full at the time of impact. No water was evident in any of the fuel recovered. The fuel colour and smell indicated it was 100/130 avgas. The difference in the amount of observed fuel and fuel at the time of the crash was probably the result of evaporation. The on-site wreckage inspection took place 5 weeks after the crash (due to the unavailability of a suitable winching helicopter). Both fuel sumps were open to the atmosphere as a result of main tank damage and were lying at an angle which placed open lines above the fuel. The amount of evaporation was about the same for each sump.
Despite the damage to the main fuel tanks, the wreckage situation was such that it was possible for fuel to pool in the leading edge of the inboard left main tank following the accident. This fuel could have recharged the left fuel supply lines after the crash, leading to the fuel found during the post-crash investigation. A similar situation did not exist on the right side of the wreckage.
Although the cockpit/cabin area was destroyed, the engine control panel was recovered intact. The throttles, propellers and mixture levers were found set at a cruise power setting. There was evidence they had been locked in their pre-crash position by the impact. The ignition and battery switches were on, and the auxiliary fuel pump switches were off. The flap selector was set to just below the first detent. This corresponded with the position of the flap motor drive shaft.
The fuel selector panel indicated that the front engine was selected to the left main tank and the rear engine to the right auxiliary tank. The left fuel selector valve was also set to the left main tank: the cable was intact and exhibited little damage. The fact that the selected position corresponded with the valve position and that cable stretch was minimal indicates that the control position was probably the selected position. The right selector valve was set between the main tank and off positions. The cable was severely stretched and kinked. The centre wire had been pulled from a clamp on the actuating arm at the fuel selector panel. Stretching of the right fuel selector cable could move the selector valve from the auxiliary position, through the main tank and towards the off position. There was some restriction to movement of the right selector valve.
Propeller examination
The fractured drive shaft from the front propeller was examined in detail. No evidence was found in either the mode of failure (bending) or in the nitride coating on the shaft, to indicate the propeller was under any power at impact.
The rear propeller was still attached to the engine. There was no evidence of any rotational damage on the blades. There was some evidence that the rear of the spinner had rubbed against the engine cowl during the crash. The rub marks were minor, indicating that, whilst the propeller was rotating, it was not under power. The rear propeller was lying across one tail boom following the crash. There were no strike marks on the boom.
Engine examination
The engines were examined at an engine overhaul facility. The inspection indicated that both engines should have been capable of normal operation prior to the crash. No faults were found with the engine's electrical and fuel systems.
Aircraft fuel system
Fuel contents
The aircraft was refuelled to full main tanks 1 month prior to the final flight. At that time, the auxiliary tanks were estimated to be half full. The aircraft was kept locked in a hangar when not in use. The distortion of the fuel tanks during the crash confirmed that there was sufficient fuel on board at the time. There were no witnesses to the pilot's pre-flight inspection; therefore, it could not be confirmed that he had completed a fuel check, including a check for water. Fuel recovered at the crash site did not contain any water and there was no other evidence that fuel contamination was a factor.
Fuel caps
All fuel caps were fitted with vents and the vents were clear.
Fuel selector panel
The Cessna 337C fuel selector panel is mounted in the cockpit/cabin roof. There are separate selector knobs for the front and rear engines. The knobs are the same shape and size and are mounted longitudinally, with the knob for the rear engine at the rear.
To move the rear engine fuel selector from the main to the auxiliary tank position, the knob is turned one notch to the right. Moving the front engine fuel selector one notch to the right from the left main tank position, turns the fuel off. There is no bar to prevent accidental selection to the off position on either selector, as the knob must be moved through off to select crossfeed.
Selection of auxiliary on either selector depresses a button which changes the fuel gauge indication from main to auxiliary tank. The button is depressed as the lever moves and does not need to be depressed to move the lever. The normal method of fuel selection in the Cessna 337 is to operate the front engine from the left fuel system and the rear engine from the right fuel system.
The selector panel was dismantled and inspected. As was noted above, the operating cable for the rear engine/right fuel selector had been pulled from a clamp at the selector end of the cable. There were marks on the selector actuator arm which indicated that it had been pulled hard against the pinion gear shaft before the cable was pulled from the clamp. It was apparent that separation occurred during the crash process. Although the rear selector knob was set to the auxiliary tank position, it was free to move as a result of the separated cable. This, coupled with the witness marks on the selector actuator arm, indicates that the final knob position was not the selected position.
Fuel selector valves
The fuel selector valves were examined. Both valves appeared capable of normal operation. The restriction to movement reported in the right valve was determined to be excessive friction caused by a build-up of corrosion. It could not be determined if the corrosion was present prior to the crash.
The selector operation had been checked during the periodic servicing which took place 41 flying hours prior to the crash. Evidence was also available that the fuel selector controls and valves had operated correctly two flights prior to the final one. The selector had not been moved on the penultimate flight.
Fuel tanks
In the Cessna 337C the auxiliary fuel tanks, mounted inboard of the tail booms, feed directly to the engines via their respective selector valves.
The main fuel tanks, mounted outboard of the tail booms, feed the engines via a fuel sump located in each tail boom. Each sump has a capacity of 2.7 L and is gravity-fed from the main tanks. Fuel is drawn through an outlet, located in the top of the sump, by the engine-driven fuel pump. The outlet is displaced to the inboard side of the sump centreline. As a result, the unusable fuel, in a 45-degree banked turn, varies from 1 L to 1.25 L, depending on the direction of the turn. The unusable fuel in the right sump in a right turn is 1.25 L. The unusable sump fuel, in level flight, was measured at 500 mL. An auxiliary fuel pump is provided in the event of engine-driven pump failure.
Under normal conditions (balanced flight), unusable fuel is not a consideration as the fuel system is designed to keep the sumps full. In some circumstances (unbalanced flight), it is possible that gravity feed to the sump may cease. For example, in an unbalanced turn to the right, if the pilot introduces left rudder to help keep the nose up as bank angle is increased, gravity feed from the main fuel tanks to the right fuel sump will stop. The sump is above the main tanks and gravity and centrifugal force will tend to move the fuel downwards and away from the main tank outlet. Fuel will continue to feed to the left sump as the situation is reversed. Selection of the right auxiliary tank will overcome this problem as it bypasses the sump, and the outlet is on the lower part of the tank in a right turn.
At cruise fuel consumption rates (37.5 L/hour/engine), it will take just over 2 minutes for the rear engine to use the 1.45 L of useable fuel available in the right sump in an unbalanced turn. If the fuel selector is selected off or moved to a position were fuel supply is interrupted, tests indicate power loss will occur after approximately 9 seconds, as fuel supply is stopped downstream from the sump.
In the Cessna 337D and later models the auxiliary fuel tank is interconnected with the main tank and also feeds the sumps. This arrangement overcomes any possible fuel feed problems that might occur during an unbalanced turn.
Survival aspects
The crash was not considered survivable. Crashworthiness information indicates that aircraft occupants are unlikely to survive an impact at 60 degrees to the horizontal if the airspeed is more than 55 kts. As the stalling speed was probably in excess of 80 kts, impact speed would have exceeded 55 kts.
Although no evidence was found that the pilot had left a formal flight note with a responsible person, an associate of one of the passengers raised the alarm when the aircraft had not returned. Initial concerns were expressed to the manager of Albany Airport at 1330. A formal search was started by the Melbourne Search and Rescue Centre at 1500, once local attempts to establish the whereabouts of the aircraft had failed. The wreckage was located at 1615 by aircraft from the Western Australian Police Air Wing. The search aircraft initially flew over the wreckage without sighting it. The crew were directed back to the site by the signal from the emergency locator transmitter.
The aircraft was fitted with a fixed installation emergency locator transmitter that complied with TSO C91a. The transmitter was activated by the crash. However, its signal was not received by the search-and-rescue satellite until the day after the accident and therefore did not provide an early indication that a crash had occurred. The coaxial cable from the transmitter to the fixed aerial had been severed at the aerial. Movement of the coaxial cable during recovery of the bodies probably led to the signal being received by the satellite.
Organisational and management information
The operator held an appropriate air operators’ certificate. No organisational or management issues were identified as contributing directly to the accident. The drums were later found underneath bush on the edge of the bay. They were not visible from the air. A State Police helicopter was operating in the area of the crash site at the time but was not used in the search for the drums.
Terrain
The bay in which the accident occurred is open to the south-east and surrounded by hills up to 1,843 ft high. The average ground slope, which starts at the waterline, is 33 degrees. The bay is rectangular in shape and 300 m wide and 400 m deep. Calculation based on the manufacturer-supplied performance figures indicates a Cessna 337 cannot out-climb the terrain from inside the bay with only one engine operating.
Stalling speeds
The Cessna 337 owner’s manual details the expected stalling speeds for various configurations. At 1,905 kg the stalling speeds are:
At 0 degrees of bank: 65 kts with flap up, 60 kts with flap at one-third and 55 kts with full flap.
At 30 degrees of bank: 69 kts with flap up, 64 kts with flap one-third and 59 kts with full flap.
At 60 degrees of bank: 91 kts with flap up, 85 kts with flap one-third and 78 kts with full flap.
Thus, stalling speed reduces with the application of flap but increases significantly with increasing bank angles. The estimated stalling speed for the aircraft configuration was between 80 kts and 85 kts.
Post-accident inspection flights and other operational information
During the investigation, flights were conducted in a twin- and a single-engine aircraft over the bay area. The pilot of the twin-engine aircraft reported he could not remain inside the bay in a right turn with less than 60 degrees of bank selected. He was operating at a higher speed (120 kts) than the Cessna 337's assumed operating speed. The investigator in charge inspected the bay in a Cessna 182. His pilot flew a pattern which he thought was the best way to view the bay: this consisted of commencing an orbit over the bay at 900 ft (clear of the terrain and turbulence). When the drums were not sighted, he descended in a continuous 30–45-degree banked turn, at 75 kts with flap set, to 500 ft (the limit because of turbulence and safety).
Discussion with experienced pilots indicates that during low-level inspections it is not unusual for a pilot to introduce top rudder in a turn to allow bank angle to be increased and thereby improve the view below the aircraft without losing altitude in the process.
Flight tests and calculations indicate that to operate a maximum-weight Cessna 337 with half flap set, with both engines operating at cruise power, in nil-wind conditions and at low level in the bay area, requires a steep turn of more than 51 degrees of bank and an airspeed of no more than 90 kts. Once committed to the turn inside the bay, a pilot would have no option but to continue the turn to exit. Any adverse wind conditions would cause an increase in the bank angle required.
Experience indicates that operations at low level in confined situations place pilots in a high workload environment where they need to concentrate their attention outside the cockpit. In previous investigations it has been determined that this type of operation often leads to poor airspeed control. It can also lead to the unsighted operation of ancillary controls such as fuel selectors, particularly if the pilot is experienced on the aircraft type and does not need to look at the control to confirm where it is or how it operates.
Information from fuel starvation occurrences indicates that an engine will usually start surging rather than just stop when the fuel quantity available is low, particularly when operating in turbulent conditions. Usually, the first action by the pilot in the event of a sudden and unexpected power loss in cruise flight is to move the fuel selector to another tank that has fuel in it. If there is no response, this action is usually followed by selection of the auxiliary fuel pump. Fuel pump selection varies, depending on aircraft type.
Tests and research
BASI Report 87-116 (Australian Aviation Occurrences Involving Fuel Starvation & Exhaustion 1969-1986) concludes that pilot factors were involved in 89% of fuel exhaustion occurrences and in 45% of the fuel starvation occurrences reviewed. It goes on to report that 71% of the factors involved mismanagement of the fuel system. The report looked at all types of general aviation aircraft, both single and multi-engine.
To further refine the information obtained from Report 87-116, the air safety occurrence databases of the Bureau and the US National Transportation Safety Board were reviewed to determine the types of events that led to loss of power to both engines in twin-engine aircraft in general and to loss of power in one or both engines in the Cessna 337.
The following are explanations of some of the terms used.
Fuel exhaustion occurs when all the useable fuel in the aircraft has been consumed. Pilot miscalculation is often the main factor, although there are some occasions where problems with the fuel system may give the pilot false information or fuel is lost overboard.
Fuel starvation occurs when there is still adequate fuel on board the aircraft, but it is not being supplied to the engine(s) for some reason. Mismanagement of the fuel system is often the main factor. However, there are occasions where such problems as fuel contamination or fuel blockage may be factors.
Un-porting occurs when the fuel tank outlet is uncovered, and air enters the system. A low fuel state or unusual manoeuvres can lead to un-porting.
Mechanical failure/malfunction includes failure of an engine component or accessory, low oil pressure, low fuel pressure, fouled spark plugs and rough running.
"Undetermined" covers those factors which could not be or were not determined by the investigating authority.
The events listed as "other" include one-off occurrences such as icing conditions.
The review of the Bureau's database covered the years 1969-1996 and included power-loss occurrences (accidents and incidents) in all types of aircraft and the Cessna 337 in particular.
Fifty-nine occurrences involving loss of power in both engines in all types were identified. Of these, 31 were the result of fuel exhaustion, 20 of fuel starvation, six for other reasons and two were of undetermined origin. Sixty-five percent of the fuel starvation occurrences involved pilot factors.
There were 67 occurrences involving a loss of power on one engine in the Cessna 337. Of these, 52 were the result of mechanical failure/malfunction, 12 were due to fuel starvation and three were for undetermined reasons. There were seven occurrences where there was a loss of power on both engines in a Cessna 337. Four were the result of fuel exhaustion and three involved fuel starvation. Two of the three involved pilot factors. The factors in the third were undetermined.
The review of the National Transportation Safety Board's database covered the years 1985-1995 and Cessna 337 accidents involving a loss of power on one or both engines.
There were 12 accidents involving loss of power on one engine and 23 accidents involving loss of power on both engines. Four single-engine accidents resulted from mechanical failure/malfunction, four were for undetermined reasons, two were from fuel starvation and two occurred for other reasons. The records for the multiple-engine failure accidents indicate 11 resulted from fuel exhaustion, eight from fuel starvation, three were for undetermined reasons and one was the result of un-porting of the fuel supply lines. A breakdown of factors in the National Transportation Safety Board's recorded accidents could not be determined from the information available.
No occurrences were identified, in either database, where a loss of power in both engines resulted from mechanical failure/malfunction.
The one report of un-porting in a Cessna 337 involved a pilot entering a wings-level, steep descent whilst there was minimum fuel in the tanks. Both engines stopped during the descent as a result of un-porting of the fuel lines.
The manufacturer reported that a military version of the Cessna 337C was used extensively as a forward air control aircraft in Vietnam without any similar fuel feed problems being reported. Forward air control often results in extreme flight attitudes.
Anecdotal evidence indicates that the rear engine of early model Cessna 337s occasionally stopped without warning during varying phases of flight. Some of these stoppages led to accidents when the loss of power was not identified early enough by the pilot. A common reason for these stoppages was not formally identified.
Overview
It is evident from information provided on the purpose of the flight, the location of the crash, the impact direction, and the damage, that the pilot was conducting a low-level inspection of the bay area in an attempt to find the drums. To complete this task, he had to fly the aircraft in a steep, right turn at a slow speed. During the turn both engines lost power. The loss of power led to a loss of control and the pilot was unable to recover the situation prior to impact.
Engine power loss
The lack of rotational damage to either propeller indicates that both engines had lost power prior to impact.
The lack of fuel in the system supplying the rear engine suggests fuel starvation contributed to its loss of power. The fact that the sump was depleted indicates that the fuel supply to it was interrupted. As no blockages were found, the most probable reason is that a prolonged, unbalanced, right turn stopped fuel feed to the right fuel sump from the right main tank. In less than 3 minutes, all useable fuel in the sump had been consumed and the engine stopped.
One flight conducted during the investigation indicated that the accident aircraft probably commenced an orbit over the bay area at a higher altitude than that used for the final circuit. When unable to see the drums, the pilot probably descended until he entered the bay on the final orbit at low level. As a result, the turning-time required to deplete the useable fuel in the sump could have been exceeded.
No direct evidence was available to establish why the front engine was not producing power. The investigation found that fuel was available and that all the engine systems were probably serviceable. The engine controls were all selected to the operating position at impact.
The research indicates there are no recorded occurrences where a loss of power to both engines resulted from mechanical failure/malfunction of the engines. The most common reasons for loss of power to both engines in a twin-engine aircraft (and in particular the Cessna 337) are either fuel exhaustion or fuel starvation. There was adequate fuel on board the aircraft; therefore, fuel exhaustion is not a consideration. As a result, fuel starvation is considered to be the most likely reason for the loss of power to the front engine. Pilot factors were identified in 45% of fuel starvation occurrences in all types of aircraft and in 65% of those involving twin-engine aircraft. In the absence of any evidence indicating a problem with the aircraft systems, pilot factors are considered the most probable contributors to loss of power to the front engine.
As it is common practice to select a different fuel tank following sudden power loss, it is possible that the pilot inadvertently selected the front engine off whilst he was attempting to restart the rear engine by changing the fuel tank selection. The design of the fuel selector switches and the pilot's concentration outside the cockpit may have contributed to his action. Fuel supply to the engine was probably re-established when the pilot realised his mistake and reversed the selection. Fuel then flowed backed into the lines, but the engine had insufficient time to restart.
Loss of control
The pilot had extended the flaps to reduce the stalling speed and increase his safety margin. Evidence indicates the aircraft was probably flying at 85-90 kts. This speed gave the pilot a small margin above the stall and allowed the aircraft to remain inside the bay. Under the circumstances, any interruption to engine power would have resulted in a sudden reduction in flying speed. This may have been sufficient to cause the aircraft to stall. If the rear engine lost power first, the nose-up pitching moment would have exacerbated the situation. The tendency for the prevailing wind to push the aircraft towards the hills could have resulted in an unconscious action by the pilot to increase bank and tighten the turn, thereby further reducing the safety margin. Turbulence may also have been a factor.
Impact sequence
The steep nose-down attitude indicates the aircraft was probably in an aerodynamically stalled condition for some time prior to impact. Considering the pilot's experience, the stalled condition probably resulted from a loss of control at inspection height. In a more controlled situation, the pilot would have attempted to manoeuvre the aircraft to a crash landing, and any last-minute stall would have been less severe. The relatively intact nature of the wreckage and the lack of severe damage to the aft fuselage indicates the loss of control occurred at low altitude.
Summary
As the right sump fuel contents approached the unusable level, it is likely the rear engine began to surge rather than just lose all power immediately. Re-establishment of fuel supply from the auxiliary tank would have corrected the situation and prevented complete power loss. The pilot probably attempted to change the tank selection. The lack of fuel in the rear fuel supply lines indicates that this did not occur. Although there is no substantive evidence to explain the loss of power to the front engine, it is possible the pilot inadvertently selected it off instead of selecting the rear engine to the auxiliary tank.
Failure of the rear engine alone may have been sufficient to cause the loss of control, particularly if the pilot was distracted from flying the aircraft by the engine/fuel situation. Failure of both engines at a critical point in a maximum-performance turn in a confined area will almost certainly lead to loss of control.
The low operating altitude probably prevented recovery from the loss of control situation before impact.
The task requirements and the terrain conditions meant the pilot had to fly the aircraft in a continuous maximum-performance right turn at low level. Whilst they approached the limits, these conditions were still within the aircraft's and the pilot's capabilities. As the aircraft was operating at or near the limits, there was little margin for error. The margin available was insufficient to prevent loss of control when the situation changed unexpectedly.
To improve visibility, the pilot probably introduced left rudder and increased the angle of bank, thereby creating an out-of-balance condition.
A prolonged, unbalanced turn probably led to fuel starvation and loss of power to one engine.
A sudden, unexpected loss of power during a maximum-performance turn resulted in loss of aircraft control.
The loss of power and control occurred at low altitude and there was insufficient height to effect recovery.
VH-SPP departed Cloncurry on a low level aero-magnetic survey flight at the estimated time of 0730 EST with an endurance of about 7 hours. The aircraft was due to return to Cloncurry by 1230 but failed to arrive. Attempts were made to contact the aircraft throughout the afternoon before it was declared overdue at about 2030. The burnt-out wreckage of the aircraft was found by search aircraft the following morning about 9 km north of the survey area and 30 km south of Cloncurry.
The aircraft had struck the ground in a nose-down, inverted attitude. It bounced from this position and came to rest upright, facing the opposite direction. At impact, the left propeller was in the feathered position and fuel to this engine had been shut off. The right engine was operating normally at impact, with fuel being fed from the centre tank.
The investigation revealed that, apart from a 2-hour flight the previous day, the pilot had no other experience in SPP. It was also revealed that there were two significant differences between the fuel system in SPP and that of other Aero Commander models the pilot had flown. These differences concerned the time taken for the outboard fuel tanks to empty and the orientation of the cockpit fuel selector switches.
The analysis concludes that these differences probably led to mismanagement of the fuel system by the pilot and to failure of the left engine due to fuel starvation, followed a short time later by failure of the right engine, also due to fuel starvation. It is possible that the pilot realised what had happened and was able to restart the right engine but not before the performance of the aircraft had deteriorated to such an extent that control of the aircraft with one engine operating could not be maintained.
1. FACTUAL INFORMATION
1.1 History of the flight
The aircraft was engaged in aero-magnetic survey operations in an area which extended from approximately 40–130 km south of Cloncurry. The task involved flying a series of north-south tie lines spaced 2 km apart at a height above ground of 80 m and a speed of 140 kts. At this speed, each tie line occupied about 20 minutes of flight time. The flight was planned to depart Cloncurry at 0700–0730 EST and was to return by 1230 to prepare data collected during the flight for transfer to the company’s head office.
An employee of the operating company saw the crew (pilot and equipment operator) preparing to depart the motel for the airport at about 0500. No person has been found who saw the crew at the aerodrome or who saw or heard the aircraft depart.
At about 1000, three witnesses at a mining site in the southern section of the survey area saw a twin-engine aircraft at low level heading in a northerly direction. One of these witnesses, about 1.5 hours later, saw what he believed was the same aircraft flying in an easterly direction about 1 km from his position. Between 1000 and 1030, two witnesses at a mine site some 9 km north of the survey area (and about 5 km west of the accident site) heard an aircraft flying in a north-south direction, apparently at low level.
On becoming aware that the aircraft had not returned to Cloncurry by 1230, a company employee at Cloncurry initiated various checks at Cloncurry and other aerodromes in the area, with Brisbane Flight Service, and with the company’s head office later in the afternoon. At about 2030, the employee advised the company chief pilot that the aircraft was overdue. The chief pilot contacted the Civil Aviation Authority Search and Rescue organisation at about 2045, and search-and-rescue action was initiated. The burnt-out wreckage of the aircraft was found early the following morning approximately 9 km north of the survey area.
1.2 Injuries to persons
Crew
Passengers
Other
Total
Fatal
2
–
–
2
Serious
–
–
–
–
Minor
–
–
–
–
None
–
–
–
–
Total
2
–
–
2
1.3 Damage to aircraft
The aircraft was destroyed by impact forces and post-impact fire.
1.4 Other damage
No other damage was reported.
1.5 Personnel information
PilotEquipment operator
Sex
Male
Male
Age
60 years
47 years
Licence category
ATPL
N/A
Medical certificate
Class 1
N/A
Total hours
Approx. 11400
N/A
Total on type
Approx. 710 (see note below)
N/A
Total last 90 days
Approx. 82
N/A
Total last 24 hours
Approx. 2
N/A
Note. As far as could be ascertained, all 710 hours on type were flown in 500 Series Aero Commander aircraft. No record was found of the pilot having flown a 680F model Aero Commander until he flew SPP for about 2 hours on the day before the accident.
Two of the 500 Series aircraft the pilot had flown (VH-KAC and VH-FGS) were 500S models which had been modified by the fitment of long-range (outboard) tanks. Operation of the fuel systems in these aircraft was similar to that in SPP (see 1.17.4).
Pilot’s recent flying experience
Company records showed that, between 7 July and 7 October 1994, the pilot flew approximately 113 hours on overwater low-level survey tasks in a Ted Smith 601-P aircraft.
There was evidence that the pilot next flew on 4 November 1994 when he conducted endorsement training on an Aero Commander 500S aircraft for a pilot from another survey company. According to this pilot, the endorsing pilot said that he was not very practised in asymmetric flight or in asymmetric operations and that he would leave all the flying to the pilot undergoing the endorsement. Notwithstanding this information, the pilot had extensive check-and-training experience in Aero Commander aircraft.
During the flight, aircraft speed was reduced towards VMCA but not to VMCA.
Pilot’s previous 72-hour history
The pilot travelled from Perth to Cloncurry on 7 November arriving at approximately 2100. On the afternoon of 8 November he conducted a survey flight in SPP which was restricted to approximately 2 hours because of problems with the on-board sensor equipment. After dining at about 2000 and retiring to his motel room at about 2200 on 8 November, the pilot, along with the equipment operator, was observed preparing to depart the motel at about 0500 on 9 November. Neither crew member was supplied any breakfast by the motel.
1.6 Aircraft information
1.6.1 Significant particulars
Registration
VH-SPP
Manufacturer
Aero Commander Division
Model
680-F
Serial no.
680F-1128-74
Country of manufacture
USA
Year of manufacture
1961
Engines
2 Avco Lycoming IO-720-BIBD
Propellers
Harzell 3-blade, variable pitch
Certificate of airworthiness
Issued 2 Feb. 1979
Maintenance release
No. 226763 Issued 3 Nov. 1994
Total airframe hours
7,546 (at 3 Nov. 1994)
Maximum take-off weight
3,630 kg
Basic weight (survey configuration)
2,914 kg
No outstanding maintenance requirements were identified concerning the aircraft.
1.6.2 Weight and balance
Basic weight (survey configuration)
2,914 kg
Fuel load
669 kg (956 L, see 1.6.5)
Pilot, equipment operator
172 kg (standard weight 86 kg x 2)
Take-off weight
3,755 kg
Maximum take-off weight
3,630 kg
Exceedance
125 kg or 3.4%
1.6.3 Single-engine rate of climb
The aircraft flight manual lists single-engine rate of climb figures for the aircraft using maximum continuous power on the operating engine, landing gear and flaps up, and the inoperative engine feathered. In this configuration, at an aircraft gross weight of 3,630 kg, a pressure altitude of 2,000 ft and an outside air temperature of 37 degrees C, a rate of climb of 160 ft/min should be achieved at a best climb speed of 102 kts.
1.6.4 Cabin environmental control
The operator advised that cockpit/cabin cooling in the aircraft was via ram air only. The aircraft was not equipped with air-conditioning or blower fans as electrical motors interfered with the survey equipment. Fresh (ram) air was available through the normal aircraft system which included vents in the cockpit. Additional ram air ducts had been installed to provide supplementary outside air to both the cockpit and the survey equipment rack.
1.6.5 Fuel load for the flight
Information from the operator indicated that the aircraft fuel load for the flight was approximately 956 L, including a full centre tank, full outboard tanks, and 90 L useable fuel in the boot tank. This estimate was based on the flight time for the previous day’s flight.
1.6.6 Fuel usage rate
The aircraft flight manual indicated that, at sea level, 24 degrees C, 21 inches MAP, 2,100 RPM and 137 KIAS, the aircraft would have been using 112 L fuel per hour. Fuel consumption at rated power was 256 L/h. According to the operator, based on actual fuel usage, SPP had been using 112 L fuel per hour on low-level survey at 140 KIAS.
1.7 Meteorological information
The following information was recorded at Mt Isa on 9 November 1994:
Time (EST)
Ambient temperature (degrees C)
0600
23
0700
26
0800
29
0900
32
1000
34
1100
34
1200
36
The sky was clear throughout the period and the relative humidity was around 10%. The low-level winds were from the south-east at about 10 kts. There was moderate thermal and mechanical turbulence at low level.
No weather observations were taken at Cloncurry, which is situated approximately 104 km east of Mt Isa. It is likely, however, that weather conditions at Cloncurry were similar to those at Mt Isa.
1.8 Aids to navigation
Not relevant.
1.9 Communications
No record was found of any communications from the aircraft to any Air Traffic Services agency. See also 1.15.2 (‘SAR activities’).
1.10 Flight recorders
The aircraft was not equipped with a flight data recorder or a cockpit voice recorder, nor were these required by regulation.
1.11 Wreckage and impact information
The aircraft struck the eastern slope of a 200-ft high ridge running approximately northsouth. At impact, the aircraft was heading in a westerly direction, was banked left in excess of 120 degrees, and was in a nose-down attitude of about 35 degrees. Initial impact occurred when the left engine and forward fuselage struck embedded rocks, causing severe airframe disruption. The aircraft then bounced up the hill a short distance, coming to rest right way up and pointing east. Most of the aircraft was destroyed by the subsequent fire, although some components, including the engines and propellers, were recovered for later examination.
1.11.1 Left engine
A strip examination of the left engine did not reveal any fault which might have precluded normal operation. Examination of a section of damaged exhaust pipe from the engine confirmed that the damage occurred when the pipe was cold.
1.11.2 Right engine
A strip examination of the right engine did not reveal any fault which might have precluded normal operation. Examination of a section of damaged exhaust pipe from the engine confirmed that the damage occurred when the pipe was hot.
1.11.3 Propellers
Both propellers were dismantled. Inspection confirmed that the left propeller was in the feathered position and the right propeller in or near the fine pitch position. There was no pre-existing fault evident in either propeller mechanism.
1.11.4 Fuel tank selector valves
Inspection of the fuel tank selector valves (see 1.17.2) at the accident site revealed the following:
For the left engine, both the centre and outboard tank selector valves were in the closed position.
For the right engine, the centre tank selector valve was in the open position while the outboard tank selector valve was in the closed position.
1.12 Medical and pathological information
Post-mortem examination was unable to confirm the medical condition of the pilot at the time of the accident. However, the pilot held a current Class 1 medical certificate issued by the CAA.
1.13 Fire
The impact caused the fuel tanks to be disrupted, releasing a substantial quantity of
aviation gasoline. Ignition probably resulted from electrical arcing and/or contact with high-temperature engine components.
1.14 Survival aspects
The accident was not survivable due to both impact forces and fire.
1.15 Search and rescue
1.15.1 Company procedures
The company operations manual stated that all operational flights were to be the subject of prior flight plan notification on the minimum basis of a SARTIME for the end of the last flight of the day. The manual also stated that, when an operation from any temporary base was likely to continue for more than a few days, application might be made to the appropriate airways operations unit for the acceptance of a standard plan to cover daily flying activities.
No flight plan had been submitted for the flight. Another company pilot participating in the survey indicated that no plan was submitted because the operation was only scheduled for a few days and local company SAR was being maintained by the other company personnel at Cloncurry.
1.15.2 SAR activities
No information was held by the CAA concerning the flight prior to the initial telephone call from a company employee at Cloncurry at about 1640. During the progress of this conversation, attempts were made by Brisbane Flight Service to contact SPP through another aircraft in the Cloncurry area. At 1641, the pilot of this aircraft advised Flight Service that he was in contact with SPP. He was asked by Flight Service to request an estimate for when SPP would return to Cloncurry. A short time later, the pilot of the other aircraft advised that he was no longer in contact with SPP. (The pilot later advised that radio communications on the day of the accident were very scratchy.) Flight Service advised the company employee that contact with SPP had been lost, at which stage he terminated the call. At 1826, the company employee again called Brisbane Flight Service, asking if there was any contact with SPP. Flight Service advised that there had been no contact with the aircraft. At 2043, the company chief pilot called Flight Service and advised that SPP was overdue. He was then transferred to SAR, whereupon search action was initiated.
1.16 Human performance aspects
1.16.1 Heat stress
Heat stress, or hyperthermia, occurs when the body’s temperature regulation mechanisms fail. In extreme conditions, heat stress can lead to an inability to control body temperature and result in mental impairment and collapse. Individual responses to heat stress are influenced by factors such as age, lack of sleep, the amount and rate of work being performed, and acclimatisation to environmental conditions.
Heat stress not only causes physiological changes but also results in performance impairment. Even a slight increase in body temperature can impair an individual’s ability to perform complex tasks such as those required to operate an aircraft safely. Some of the known effects of heat stress on individuals are that:
error rate increases;
short-term memory becomes less reliable; and (c) perceptual motor skills slow.
Importantly, the affected individual may not recognise a decrease in efficiency but may feel perfectly normal and able to continue operations.
1.16.2 Time zone change
When the pilot travelled from Perth to Cloncurry two days before the accident, he moved into the Eastern Standard Time zone, which is 2 hours ahead of Western Standard Time. In other words, 0500 EST is equivalent to 0300 WST.
1.16.3 Food and water
The operator advised that two flasks containing 7–8 L water were on board the aircraft for the flight. Food was generally not carried on survey flights. Whether any food was carried on this flight could not be determined but the crew did not request that the motel provide any food for the flight.
1.17 Aircraft fuel systems
Among the various Aero Commander models that have been produced, aircraft fuel systems have differed. Long-range models of the aircraft were fitted with integral wing tanks (called outboard tanks), and in some cases boot tanks in the rear fuselage, in addition to the main, or centre tank. In some aircraft, additional tanks were incorporated during manufacture, while in others, they were fitted as a modification after manufacture.
1.17.1 Fuel system Aero Commander 680F Series aircraft
The Aero Commander 680F fuel system comprises four tanks: the centre tank, the boot tank, and two outboard tanks. The centre tank consists of five interconnected cells having a total capacity of 601 L (592 useable). This tank supplies fuel to both engines. Tank contents are indicated on a cockpit gauge. The boot tank has a capacity of 439 L (419 L useable). Fuel is transferred from this tank to the centre tank by the activation of a switch on the cockpit instrument panel. This is normally conducted in cruise, in stages, when the centre tank level has reduced to 90 US gallons indicated (340 L) or below. The left and right outboard tanks each have a capacity of 127 L (254 L total useable). The contents of these tanks are indicated on gauges in the cockpit. The total fuel capacity of the aircraft is 1,294 L (1,265 useable).
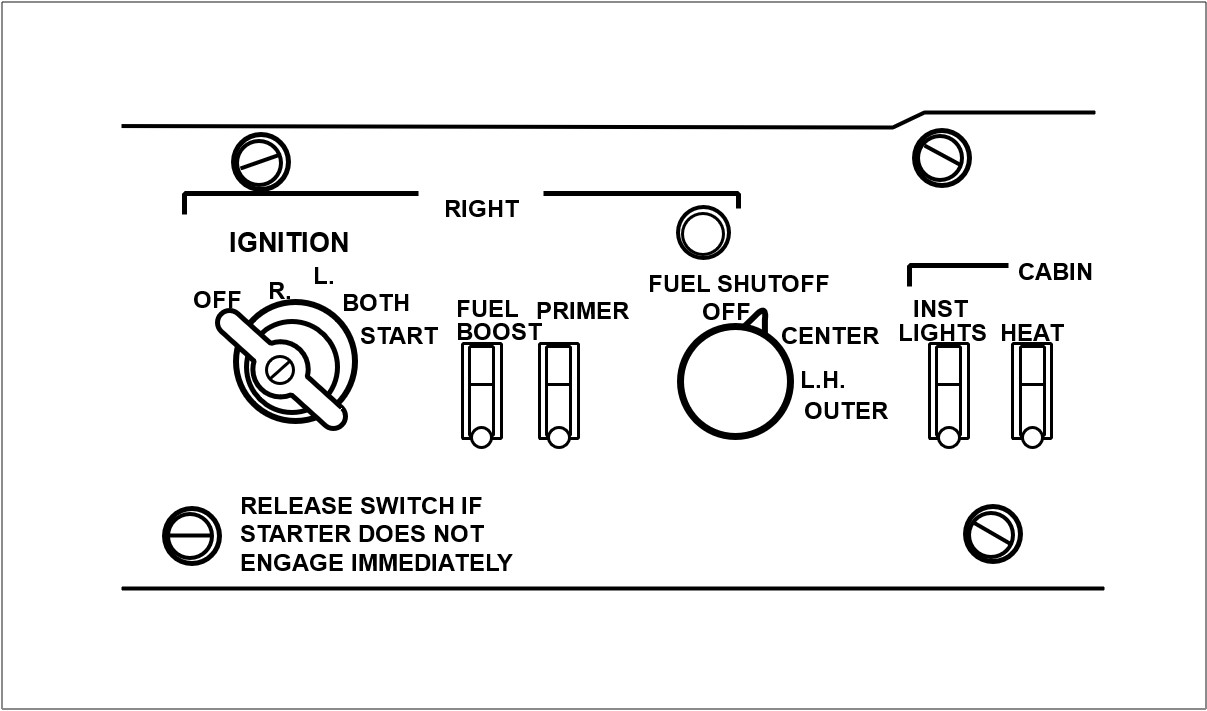
Rotary fuel selector switches located on the cockpit overhead switch panel control the flow of fuel to the engines from either the centre tank or the outboard tanks by way of electrically operated shut-off valves located in each main landing-gear wheel well. Rotating the switches to the right and left OUTBOARD positions (three o’clock and nine o’clock positions respectively) allows fuel from the outboard tanks to flow to the respective engine. At the same time, fuel flow from the centre tank is shut off. Fuel vapour return from the fuel injector pumps is fed to the centre tank.
Switching the selector switches to the CENTRE position (half-past ten o’clock position on the left switch and half-past one o’clock position on the right switch) allows fuel to flow from the centre tank to the respective engine and shuts off flow from the outboard tanks. Selecting the switch to OFF (twelve o’clock position on both switches) closes both shut-off valves and cuts off fuel flow to the engines. A sketch of the right fuel control selector panel is shown below.
The aircraft flight manual, section 4 (‘Normal Procedures’) contained a caution note which stated (emphasis theirs):
CAUTION. Burn centre tank first. When 100 gallons is shown on centre tank gauge, switch to outboard tanks. Do not allow engine to be starved of fuel when outboard tanks run dry. Select centre tank at first indication of fuel pressure loss. Fuel boost pumps must be on when switching tanks.
Anecdotal evidence obtained during the investigation indicated that, should a tank run dry and air enter the fuel lines, up to 2–3 minutes were required to restore normal engine operation following selection to another tank. It was not uncommon for there to be substantial engine power surges during this period.
1.17.2 Fuel selector valves
The centre and outboard tank fuel systems each have their own electrically operated shutoff valve. Electrical power is required to both open and close the valves. Placing the fuel selector switch in the OFF position closes both shut-off valves controlled by that selector.
Control of the valves is lost in the event of a total loss of electrical power in the aircraft.
1.17.3 VH-SPP fuel system and modification
According to the aircraft logbook, in October 1963 the six-cylinder IO-540 engines which were standard fitment for the aircraft were replaced with eight-cylinder Lycoming IO-720 engines. As part of this conversion, bypassed fuel from the engine-driven pump was returned to the pump inlet instead of being fed to the centre tank. The engines were later fitted with turbochargers.
In 1981, apparently to overcome fuel pump cavitation problems, the fuel system was modified to incorporate a pressure relief return line. According to the aircraft logbook, the modification was completed on 25 May 1981 to approved Engineering Order DFS-AC-08. No reference could be found in the (then) CAA Aircraft History File concerning the modification. Further, the approved flight manual for the aircraft contained no flight manual supplement or other reference to the modification However, a copy of the engineering order cover sheet was obtained from the operator. This indicated that the order had been approved by the then Department of Transport on 11 May 1981. The delegate of the Secretary, Department of Transport, who approved the modification, was unable to recall, other than in a very broad sense, the events surrounding approval of the modification. In particular, he was unable to recall what consideration might have been given to including detail of the modification as an approved supplement to the approved flight manual for the aircraft. (The then ANO (now CAO) 100.6 addresses ‘Administration and Procedure – Design Approval of Modifications, Repairs and Replacement Components’. The order indicates, among other things, that the Secretary may require the (approved) flight manual to be amended upon an approved modification being installed in an aircraft.)
The operator advised that the modification fed bypassed fuel to the centre tank. Advice from pilots who had flown SPP was that, during typical low-level survey operations, outboard tank transfer was complete in about 20 minutes. In other words, in excess of 5 L of fuel per minute was bypassed from each outboard tank to the centre tank. These pilots also indicated that the left outboard tank fed at a slightly higher rate than the right outboard tank so that, during typical low-level survey flight, it emptied 3–5 minutes quicker than the right tank.
1.17.4 VH-SPP fuel system management
Information from the operator indicated that its fuel system management procedures, and those probably followed by the pilot of SPP, were as follows:
Start, taxi, and take-off with centre tank selected.
After approximately 1 hour, when centre tank contents indication falls to about 80 US gallons, transfer boot tank fuel to centre tank.
When centre tank contents again indicates about 80 US gallons, select both outboard tanks.
Re-select centre tank as each outboard tank indication approaches empty.
During survey operations, tank changes were only made during turns between line runs because operation of the boost pumps (which was part of the tank change procedure) caused electrical interference in the survey equipment.
1.17.5 VH-SPP briefing
Another company pilot at Cloncurry, who was experienced on SPP, briefed the accident pilot on the operation of the aircraft prior to the 2-hour flight he conducted on 8 November 1994. The briefing was conducted in a motel room. Matters covered included the aircraft fuel system. The briefing pilot indicated that he told the accident pilot that the outboard tanks were normally selected when the centre tank contents were indicating about 80 gallons and that they emptied in 15–20 minutes. He recalled some discussion on the latter point as the accident pilot had thought it would take about 60 minutes for the outboard tanks to empty. (This belief was probably based on his experience in 500S Series Aero Commander aircraft in which outboard tank transfer during low-level survey flight took approximately 60 minutes.) During this discussion, the accident pilot indicated that his habit was to select the left and right outboard tanks so that both were feeding at the same time.
1.17.6 Alternative outboard tank transfer procedure
Discussions with other Aero Commander pilots during the investigation revealed an alternative outboard tank transfer procedure. This involved selecting the outboard tank for one engine and leaving the other engine to continue to receive fuel from the centre tank. When the outboard tank neared empty, the procedure was reversed. The advantage of this procedure was that it ensured centre tank fuel was always available to at least one engine, thus providing a safeguard against failure of the aircraft electrical system (which rendered the fuel selector valves inoperative).
1.17.7 Flight in VH-SPP by pilot on 8 November 1994
The flight in SPP conducted by the pilot on the day before the accident was limited to 2 hours due to survey equipment malfunction. According to the operator, the aircraft fuel load on departure was 844 L, this being a full centre tank (590 L) and full outboard tanks (254 L). The boot tank was empty. Approximately 290 L fuel was used during the flight, all from the centre tank. The outboard tank fuel was reported not to have been used.
1.17.8 Fuel system 500S Models VH-KAC and VH-FGS
500S Model Aero Commander aircraft KAC (Aircraft Serial No. 3185) and FGS (Aircraft Serial No. 3315) were fitted with long-range (outboard) tanks shortly after leaving the factory. According to the relevant documentation, KAC was modified in July 1974 in accordance with STC SA 973SW, and FGS was modified in August 1978 in accordance with STC SA-2826-SW. A check revealed that the STCs were identical except that, in SA-2826-SW, figures 24 and 24.1 (‘Overhead Switch Panel Cover Rework’) contained the following: ‘NOTE: 500 B, U, S, thru s/n 3075 only’.
The modification involved the fitment of outboard wing tanks and associated system work. The capacity of the outboard tanks was 254 L, the same as in SPP. Part of the modification involved the installation of rotary fuel selector switches to the cockpit overhead switch panel.
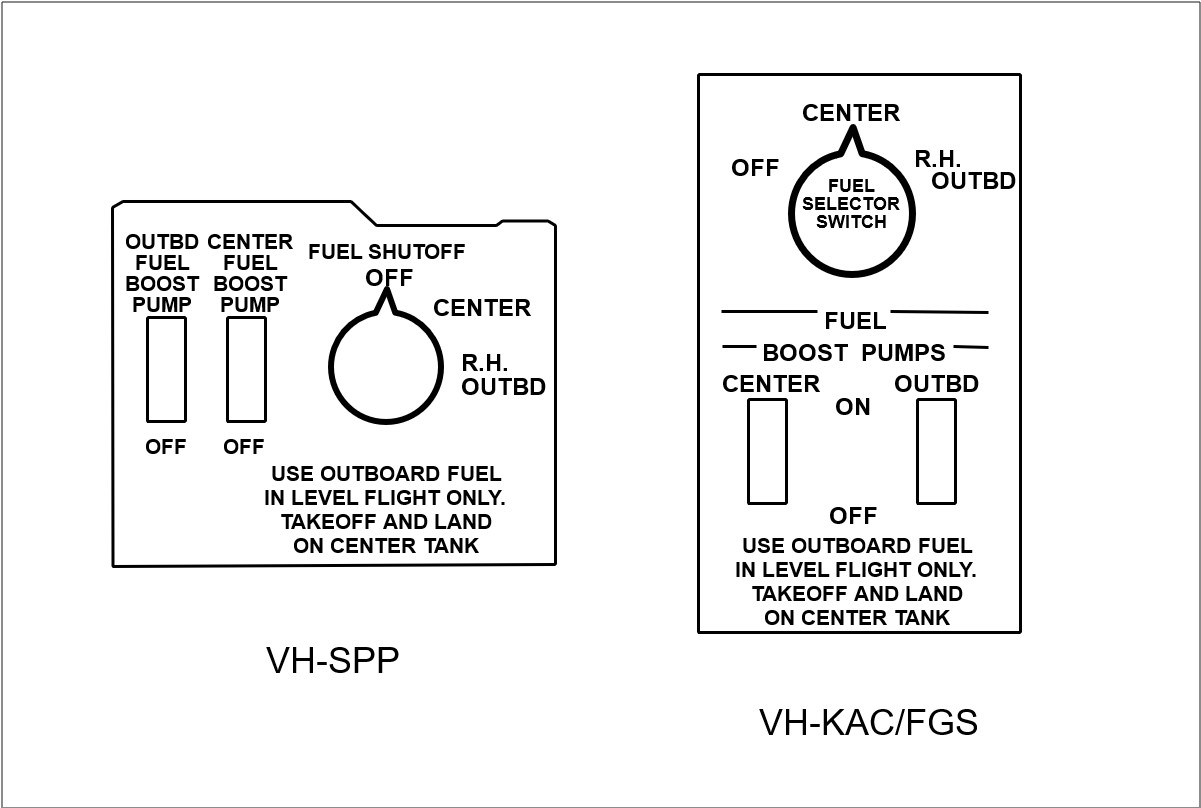
A physical check of the fuel selector panels on KAC and FGS revealed that, in these aircraft, the CENTRE tank selections were at the 12 o’clock position. In turn, this meant that the left and right OFF positions were at half-past one/half-past ten o’clock, while the OUTBOARD positions were at half-past ten/half-past one o’clock. In other words, the orientation of the selector switches was different to that in SPP. The holder for STC SA-2826-SW advised that to maintain the selector switch OFF position at twelve o’clock would have required considerable rework.
A sketch comparison of the fuel control panels for SPP and KAC/FGS is shown below.
1.18 Class endorsement
CAO part 40, section 40.1.0, subsection 4, para. 4.1 states:
A class endorsement specified in Part 1, Part 2 or Part 3 of Appendix IA authorises the holder of the endorsement to fly an aeroplane included in that class as pilot in command.
The notes to this sub-section state:
NOTE 1: The holder of a class endorsement should not act as pilot in command of any aeroplane included in the class on any flight unless he or she is familiar with the systems, the normal and emergency flight manoeuvres and aircraft performance, the flight planning procedures, the weight and balance requirements and the practical application of take-off and landing performance charts of the aeroplane to be flown and has sufficient recent experience or training in the aeroplane type, or in a comparable type, to safely complete the proposed flight.
NOTE 2: The owner and the operator of a type of aeroplane included in a class of aeroplane should ensure that any person who proposes to fly as pilot in command of the aeroplane complies with the requirements set out in Note I and should, where necessary, require the pilot to provide evidence of recent experience or training in the aeroplane type, or in a comparable aeroplane type.
Part 2 of appendix IA (‘Class Endorsements’) includes Aero Commander as a class.
Appendix IB (‘Classes of Aeroplanes’) includes, among other things, Aero Commander 680F and various Aero Commander 500 models (including Aero Commander 500S) in the Aero Commander class.
1.19 Time/event information
The operator provided information concerning pre-flight preparation and in-flight activities, which enabled the following time/event sequence to be developed. This information was based on the experience of other company pilots and was, therefore, an estimate only.
Time
Event
0515
Depart motel
0520
Arrive airport
0630
Survey equipment ground calibration complete
0700
Refuelling complete
0710
Taxi
0720
Airbourne
0745
Survey equipment airborne tests complete
0750
Commence survey
The estimated amount of fuel used from engine start to commencement of survey at 0750 was 160 L.
2. ANALYSIS
2.1 Impact and wreckage information
The factual information obtained from examination of the accident site and the wreckage enabled a number of deductions to be made concerning the accident sequence.
Fire damage to the wreckage indicated that there was substantial fuel on board the aircraft at impact.
The extreme, unusual attitude of the aircraft at impact indicated that the pilot lost control of the aircraft prior to impact. The respective propeller positions and engine operating conditions at impact imply that, with the right engine operating and the left propeller feathered, such an impact attitude could have resulted from the aircraft developing an uncontrollable roll left as a result of aircraft speed reducing below VMCA.
No mechanical fault was identified in the left engine which might have been reason for the left propeller to have been feathered. The closed position of both selector valves implied deliberate movement of the fuel selector in the cockpit to the OFF position.
The right engine was operating at impact and the aircraft performance charts indicated that the aircraft had sufficient single-engine performance at its estimated operating weight to climb from the survey operating height and return to Cloncurry. This leaves the following questions:
Why was the (serviceable) left engine shut down?
Why did the pilot apparently lose control of the aircraft?
2.2 Hypothesis
In the absence of any recorded or witness information, the answers to these questions are necessarily speculative. However, after consideration of the factual evidence, the following hypothesis is considered a plausible explanation of the accident sequence.
Background relevant to the hypothesis centres on the accident flight being only the second time the pilot had flown SPP but the first time he had cause to feed fuel from the outboard tanks. Significant differences between SPP and other Aero Commander aircraft the pilot had flown involved the orientation of cockpit fuel tank selector switches and outboard tank fuel transfer time.
With respect to the fuel selectors, in the 500 Series aircraft the centre tank selection was at the twelve o’clock position. This compared with SPP where the twelve o’clock position was OFF. Fuel transfer from the outboard tanks took approximately 1 hour in the 500 Series aircraft, while it took some 20 minutes in SPP. Also, the left outboard tank emptied 3–5 minutes more quickly than the right outboard tank.
Assuming that the aircraft commenced survey at about 0750 (see 1 .17.2) and had, at that time, used 160 L fuel, the following time/event sequence is hypothesised (based on a fuel usage rate of 112 L/h on survey):
Time
Event
Fuel Situation
0750
Commence survey
160 L used from centre tank
432 L remaining in centre tank
776 L remaining total
(432 + 90 (boot) + 254 (outboard))
Time
Event
Fuel situation
0859
Commence boot tank transfer
Reduce centre tank to 80 US gallons
(303 L) = 129 L used in 69 minutes
0947
Centre tank again at 80 US gallons commence outboard tank transfer
90 L boot tank fuel used in 48 minutes
1007
Outboard tanks empty in approx.
20 minutes
Total fuel remaining = 530 L
If the pilot followed his normal habit of selecting both outboard tanks at about the same time but forgot that the tanks emptied in about 20 minutes in SPP instead of at least 60 minutes as he was accustomed to from his experience in other Aero Commander aircraft, then at about 1007, the left engine would have ceased operating as the tank ran dry. The expected reaction to such an event would be for the pilot to reselect the centre tank and switch the boost pump on. However, in the stress of the moment, he may have regressed to previously learned behaviour and placed the cockpit selector in the twelve o’clock position, forgetting that this was OFF in SPP, even though this involved passing the centre tank detent and greater angular rotation of the knob than from the OUTBOARD to CENTRE position. When normal left engine operation was not restored, it would have been reasonable for the pilot to have increased power on the right engine, feathered the left propeller, and commenced a climb from survey height. Within a short time, however, the right engine would have begun to run roughly as the right outboard tank became empty. The resultant power loss would have caused the aircraft to lose performance rapidly. Now with similar malfunctions in both engines, the pilot might have realised that he had made an incorrect fuel selection for the left engine and positioned the right selector correctly at the centre tank (half-past one o’clock) position. Given that these events would take time and could have resulted in air entering the right engine fuel line, the aircraft could have lost both performance and altitude by the time the fuel supply to the engine was restored. The sudden power increase as fuel flow was restored could have been sufficient to yaw and roll the aircraft uncontrollably to the left and result in the impact attitude found at the accident site.
The location of the wreckage north of the survey area could mean that the aircraft was heading towards Cloncurry at the time of the accident. It could also indicate that the pilot selected outboard tanks prior to commencing a south-north survey run, and that those tanks emptied around the time that run was completed (20 minutes later).
Apart from the possible sighting of the aircraft by one witness at about 1130, there is consistency between the time of the accident deduced above (1002–1007 EST) and the other witness sightings. That the 1130 sighting was a possible sighting could be reason enough to discount this report.
There is a disparity between the deduced time of the accident and the reported radio contact established with SPP by the other aircraft at 1641. However, as the aircraft endurance was only some 7 hours, fuel exhaustion would have occurred before 1500. It would appear, therefore, that, perhaps due to the poor radio conditions existing at the time, the pilot of the other aircraft may have misidentified the transmission from another aircraft as being from SPP. The possibility that SPP had landed at a remote strip for some reason and later taken off again to continue the survey task was considered. However, as the crew were aware of the requirement to return to Cloncurry by 1230, it would be reasonable to expect that they would have contacted the company if this requirement could not be met. No such contact was made.
2.3 Aircraft single-engine climb performance
Assuming the aircraft weight at take-off was 3,735 kg, then 105 kg (153 L) of fuel had to be used before weight reduced to maximum take-off weight (3,630 kg). Given that approximately 160 L fuel was used by 0750 EST when the survey proper was estimated to have begun, it follows that, at any later time, the aircraft should have been able to achieve a single-engine rate of climb of at least 160 ft/min (see 1.6.2).
2.4 Fuel system modification
It is arguable that the fuel system modification to SPP (1.17.3) did warrant inclusion in the approved flight manual because of its effect on outboard tank transfer time, not only with respect to SPP, but also in comparison to other Aero Commander models with similar fuel systems. However, given that the pilot was briefed on the operation of the SPP fuel system the day before the accident (including specific reference to the outboard tank transfer time), it is debatable whether flight manual reference to the fuel system modification could be considered a factor in the accident.
2.5 Fuel system briefing
CAO part 40 places responsibility on the operator and the pilot for ensuring that the pilot is familiar with the aircraft systems. It seems clear that a briefing took place and that the unique features of the SPP fuel system were discussed with the pilot. However, the briefing may have been more effective had it been conducted in the aircraft.
2.6 Human performance
There are a number of human performance aspects which could have affected the pilot’s ability to operate the aircraft safely. These include:
The high ambient temperatures and the non-airconditioned cockpit could have resulted in the pilot experiencing some degree of heat stress. The longer the flight continued, the more serious this would have become.
There was no evidence of the pilot having consumed any food before or during the flight. Thus, the pilot had probably not eaten for up to 14 hours before the accident.
Low-level survey flying is both physically and mentally demanding on the pilot. High temperatures and turbulence increase these demands.
The pilot had been at Cloncurry for less than 40 hours at the time of the accident.He therefore had only limited opportunity to adjust to the local weather conditions and the 2-hour time change from Perth.
The pilot’s ability to cope with the above influences could have been limited by his age.
2.7 Other aspects
In analysing this accident, other possibilities such as pilot incapacitation and bird strike were considered. However, given the engine, propeller, and fuel selector valve configurations at aircraft impact, and the deliberate actions by the pilot these configurations imply, neither of these possibilities was considered realistic.
3. CONCLUSIONS
3.1 Findings
The pilot held a valid ATPL, was appropriately endorsed, and held a current medical certificate at the time of the accident.
The pilot had substantial experience on 500-S Series Aero Commander aircraft but minimal experience on VH-SPP.
A modification to the fuel system of VH-SPP reduced the time taken for the outboard tanks to empty to approximately 20 minutes compared to about 60 minutes in some 500 Series Aero Commander models.
The approved flight manual for the aircraft contained no reference to the fuel system modification.
The pilot’s fuel system management technique involved feeding fuel from the left and right outboard tanks simultaneously.
An alternative fuel system management technique, as used by some other pilots, was to feed fuel from one outboard tank at a time.
On the day before the accident, the pilot was briefed by another company pilot on the aircraft fuel system and its operation, including reference to the outboard tank transfer time. The briefing was not conducted in the aircraft.
The aircraft maintenance release was valid and no outstanding maintenance requirements were identified.
The aircraft departed Cloncurry at a weight which exceeded the MTOW by about 125 kg; however, this was not considered to have been a factor in the accident.
There was no indication that either engine or either propeller had suffered any mechanical failure.
The aircraft impacted the ground inverted, in a steep nose-down attitude.
Both fuel selector valves for the left engine were closed and the left engine was not operating at impact.
The left propeller was in the feathered position at impact.
The outboard tank selector valve for the right engine was closed, while the centre tank selector valve was open.
The right engine was operating at impact.
Water, but no food, was carried on the aircraft.
The pilot had been in the Cloncurry area for less than 40 hours at the time of the accident.
The flight was conducted in very hot, dry, conditions with moderate thermal turbulence.
During the 2-hour flight on the day before the accident, the pilot did not operate the outboard tank fuel-feed system.
3.2 Significant factors
For reason(s) which could not be conclusively established, the pilot shut off the fuel supply to the left engine and feathered the left propeller.
For reason(s) which could not be conclusively established, the pilot lost control of the aircraft.
The aircraft had been flown from Brisbane to Luskintyre to carry out a series of joy flights over the weekend. At the completion of those flights, it was configured for a wing-walking demonstration in which, during flight, a person would stand strapped to a demountable frame installed above the fuel tank on the upper wing centre section.
The aircraft was refuelled during the morning prior to the accident. Two local flights were flown before the wing-walking frame was installed. The wing-walker, who was also a Tiger Moth pilot and was experienced with this routine, was strapped into the frame. After starting the engine, the pilot boarded the aircraft, taxied to the eastern end of the airfield, turned, and commenced a take-off to the west.
After lift-off, a climb was made at a low airspeed. At approximately 150 ft above the ground, the aircraft's engine lost power. The aircraft commenced a turn to the left, the turn continuing to develop until the aircraft's nose dropped. The aircraft then descended steeply into the ground, caught fire, and was destroyed. Both pilot and passenger were fatally injured.
The accident occurred within the confines of the airfield, and no other property was involved.
1.2 Crew information
The pilot held a commercial pilot licence. He had 1,200 hours flight time, of which 570 were on Tiger Moth aircraft. Both his pilot licence and medical certificate were valid.
The wing-walker also held a pilot licence and was endorsed on the Tiger Moth aircraft.
Both crew members were experienced with the wing-walking routine.
1.3 Site, aircraft and wreckage information
The weather was fine with a light breeze from the north-west. Weather was not considered to be a factor in the accident.
There were no known unserviceabilities with the aircraft prior to the flight. The aircraft was properly certificated, and the maintenance release was valid. The last periodic maintenance inspection was performed in December 1993 and was valid for 12 months or 100 hours, whichever was the sooner. The aircraft had flown approximately 30 hours since that inspection.
The airframe was extensively burned and had suffered impact and heat distortion. It was not possible to definitely establish pre-accident serviceability. However, the wreckage examination disclosed an apparent anomaly with the flight control system in that the right rudder control horn was fractured. Specialist metallurgical examination determined that the fracture had occurred after the horn was affected by the post-accident fire.
The engine was extensively damaged by impact and fire. There was no evidence of power interruption from water contamination or mechanical damage, and evidence of sufficient fuel supply was obtained.However, during a strip inspection it was found that an unmodified fuel needle valve was fitted to the carburettor.
1.4 Engine examination
The carburettor contained a fuel needle valve of a design that the manufacturer had declared obsolete in 1957. The needle fitted to the carburettor was Part Number CH 28696 and should have been replaced by Part Number CH 46155 in accordance with Gipsy Major Modification G1136. The modified needle was introduced to obviate sticking of the needle. This was accomplished by increasing the side clearance between the needle and the housing to 12-15 thousandths of an inch (0.012-.015 in). The original had a maximum clearance of two thousandths of an inch (0.002 in). The British manufacturer of the carburettor had declared the modification to be "highly desirable and strongly recommended to be embodied not later than the next complete overhaul provided parts are available". Existing needles were able to be modified, and new needles were manufactured.After consideration, the Australian regulatory authority at that time did not make compliance mandatory for Australian-registered aircraft.
The engine was last overhauled in Griffith, NSW during 1982. There was no record of the fuel needle valve modification being incorporated nor was a mandatory requirement in force in 1982 for the modification to be incorporated. Since this accident, other engines in service on Australian-registered Tiger Moth aircraft have been found fitted with the obsolete fuel needle valves.
The carburettor needle and the needle valve seat exhibited signs of particulate contamination which appeared to be compacted dust or dirt.
There were no defects found in the remaining component parts of the engine or its accessories.
1.5 Video recording
A visitor to the airfield filmed both the preparation for the flight and the flight itself on a hand-held video camera. The video recording (with sound) revealed that the engine was operating normally during the take-off and initial climb but then lost power. The engine continued to run with the spluttering, staccato beat typical of an engine of this type at idle power. The recording also showed that right aileron and left rudder were applied for much of the period after the engine lost power.
Information was provided to the investigation team suggesting that an independent examination of the video recording had found evidence that the pilot's arm could be seen waving out of the cockpit, and that he was probably trying to grab flailing rudder cables. It was also reported that the recording indicated that the rudder was jammed to the left by the tail skid.
However, the video recording showed that the aircraft was normal in all respects as it taxied and lined up and took off. Had the rudder jumped over the skid keepers and been jammed, the pilot would not have been able to effect a straight take-off. The wreckage examination did not show any marks on the skid or the rudder to indicate that the rudder was restricted, and the skid itself was free to rotate in its tube housing. Because the skid was free to rotate in its housing, even if the rudder had jumped over the keepers, the rudder would still have been able to travel side to side had the pilot applied pressure to the control bar. However, total movement in one direction would have been slightly reduced.
The flailing rudder cables were supposedly from the failed right rudder control horn. Metallurgical examination did not support this hypothesis, and the wreckage examination did not show any other areas of distress within the rudder control system.
The video recording was digitised to aid enhancement. The images in the early part of the accident sequence, purported to be of the pilot's arm, were found to be images of the cowl-mounted air cleaner scoop and the propeller. An image adjacent to the fuselage in the area of the left wing root, noticeable on frames immediately prior to impact, was found to be the left cockpit door which was open throughout the flight. Both images were affected by pixel flare. (Pixel flare is the merging of the dots that make up the screen picture and is very evident in an image that is fast-moving on a screen.)
Specialist examination determined that the recording of the accident was of such a quality that even with enhancement it was not possible to detect the control cables.
1.6 Wing-walking
Wing-walking was prohibited in Australia until 1989 when Civil Aviation Regulation 250 was amended to relax this total prohibition. Regulations were drafted to allow wing-walking stunts in special circumstances under vigorously controlled conditions. Flying Operations Instruction 27-2, Issue 1, dated 21 April 1989, was raised to specify those circumstances and conditions.
Flying Operations Instruction 27-2 approved wing-walking stunts only at the following venues:
an Authority-approved air display as detailed in Flying Operations Instruction 27-1;
a commercial film production; or
practice sessions for either of the above.
The wing-walking stunt on the day of the accident was for the benefit of a welfare group with whom the pilot and wing-walker were associated. The event was not an Authority-approved air display, nor was commercial filming undertaken. The Flying Operations Instruction did not contain guidance for approving the event as a practice session and there was no evidence that the pilot had been granted blanket approval to use this sort of event as a practice session.
The Flying Operations Instruction contains a requirement that the flying display be previewed and approved by the Authority. The preview is to be an assessment of the display sequence flown by the display pilot, with the aircraft fitted with the approved wing-walking structure containing a dummy of equivalent weight to the intended wing-walker. Although there has been verbal advice to the Bureau that an assessment was made, the Civil Aviation Authority files available to the investigation did not contain evidence that the Authority had formally assessed and approved the sequence flown by the pilot. There is no evidence that an assessment had been made of the performance and handling characteristics of VH-UNA when configured for wing walking. The Flying Operations Instruction required such an assessment to be made.
Neither the Civil Aviation Authority files nor those files held by the pilot contained any evidence that the pilot had applied to the Authority for permission to install the frame assembly and carry out wing-walking. Accordingly, there was no evidence that the pilot had been formally apprised by the Authority of its requirements. Although there was no formal record of the stunt being assessed and approved, the stunt had been incorporated into some airshow programs approved by the Authority.
1.7 Aircraft performance
The Tiger Moth is a low powered, high drag aircraft. During the investigation it was found that a wing-walker would increase the drag by 27%. This increased drag would reduce the aircraft's maximum cruise speed from 75 kts to 58 kts.
The wing-walking frame fitted to the accident aircraft was manufactured for and fitted to Tiger Moth VH-GVA in January 1990. This aircraft was subjected to flight tests (supervised by the Civil aviation Authority) to assess, in accordance with Flying Operations Instruction 27-2, its performance and handling characteristics. The investigation found no evidence that any performance calculations were made prior to the flight tests.
During the initial flight test, VH-GVA was fitted with a propeller having a 4 ft 6 in pitch. On a subsequent flight, with a 4 ft 2 in pitch propeller fitted, the rate of climb improved, and it was established that the particular aircraft/engine/propeller/pilot combination achieved a best initial climb speed of 53 kts. The maximum attainable straight and level speed was 63 kts. The normal climb and cruise speeds are 59 kts and 75 kts respectively. The accuracy of the test results could not be determined as there was no requirement to calibrate the instrument system on the aircraft prior to the tests.
The flight tests found that before being fitted with the frame, VH-GVA accelerated from 50 kts to 70 kts in 12 seconds. With the frame fitted and a dummy installed, the aircraft took 24 seconds to accelerate from 50 kts to its maximum straight and level speed of 63 kts. There was also a noticeable rudder buffet that was later found to be reduced if the wing-walker stood with feet apart.
The wing-walk frame was later sold to the pilot of VH-UNA, who fitted it to his aircraft in February 1992, in accordance with an engineering order approved by the design engineer involved with the original installation on VH-GVA.
Along with the engineering order, the pilot received a copy of Civil Aviation Authority letter V131/24/34, dated 28 March 1990, which required among other things that for all wing-walking flights the propeller fitted to the aircraft should be of 4 ft 2 in pitch. The propeller fitted to the aircraft at the time of the accident was Part Number
DH5220/H/26 and of 4 ft 11 in pitch. There was no record of a fine-pitch propeller having been fitted to VH-UNA since the wing-walking frame was initially fitted in 1992.
There is no regulatory requirement for the owner of an aircraft to inform the Authority of any approved modification being fitted to an aircraft. Also, for this particular modification, there was no requirement for the flight manual to be amended to detail the conditions surrounding the installation of the modification. Consequently, the Authority's file for the aircraft did not contain details of the fitting of the frame to the aircraft.
The first entry in relation to the wing-walking equipment occurred one year after installation when an airworthiness survey of the aircraft found irregularities in the procedures used during installation. Certification for manufacture of the frame had not been made, and weight and balance considerations had not been addressed. The Authority's file did not contain a copy of the Authority's own letter that required a fine-pitch propeller to be fitted, nor did the survey disclose that an incorrect propeller was installed.
The design engineer who completed the original work on VH-GVA and authorised the installation onto VH-UNA is based at Bankstown, and his file was held in the Bankstown, NSW office of the Authority. The aircraft was based at Archerfield, Qld and its file was accordingly held in the Archerfield office of the Authority. There is no system within the Authority requiring that modifications approved by a design engineer be reflected on the file for the aircraft concerned.Accordingly, there was no opportunity for the Archerfield-based officer carrying out the survey on the aircraft to check the configuration requirements prior to conducting a survey.
The first flight of VH-UNA after it was modified was conducted with the accident pilot in the frame. The pilot on that flight stated that he had difficulty climbing out of ground effect and that he was only able to attain a climb speed of 45 kts. The accident pilot is reported to have later stated that he had developed a slow flying technique that gave a climb performance acceptable to him. This technique is evident from videos taken at previous airshow performances which show the attitude difference between the accident aircraft and another Tiger Moth during take-off.
1.8 Incorporation of modifications
The carburettor manufacturer recommended that the modified fuel needle be introduced at the next overhaul after 29 April 1957, and parts were made available to accomplish that requirement.The manufacturer's recommendation was not made mandatory by the then Australian Department of Civil Aviation. From 1957 to 1988, aircraft owners and operators were required to incorporate only those modifications made mandatory by airworthiness directives promulgated by the Department and its successor organisations.
Changes to the Civil Aviation Regulations initiated in 1988 made the aircraft owner responsible for deciding what modifications should be carried out. The regulator still retained the capacity to issue airworthiness directives.
Civil Aviation Regulations current at the time of the accident required that aircraft maintenance be carried out in accordance with the applicable provisions of the aircraft's approved maintenance data; that is, in accordance with the manufacturer's instructions specifying how maintenance should be carried out.
The Authority's airworthiness officers interviewed during the investigation disagreed as to whether the effect of that requirement would mean that Modification G1136 would need to be incorporated at next overhaul. One view was that it is impractical to catch up with 50 years of modifications on old aircraft such as the Tiger Moth and that "ancient" modifications could be ignored. A contrary view was that although many older aircraft could be grounded by the requirement, all modifications required by the manufacturer should be incorporated, regardless of the age of the aircraft.
1.9 Pilot reaction time
The time between the first engine splutter and the aircraft commencing a left turn was 3.5 seconds. The time between that first splutter and ground impact was 5.8 seconds. If VH-UNA was climbing at 50 kts, the rate of loss of airspeed after an engine power interruption is estimated to be 5 kts per second. The aircraft has a stall speed of approximately 40 kts. Therefore, the pilot would have had just two seconds to apply corrective action before the aircraft stalled. There is evidence that the aircraft had on at least one occasion attained only 45 kts, which would allow even less time to react to an unexpected emergency situation.
The Royal Air Force Institute of Aviation Medicine, Farnborough, UK carried out two experiments on pilot response times to emergencies presented in flight simulators. The experiments were conducted in the wake of an airliner accident in which the pilot took 5 seconds to react to an unanticipated emergency situation.
The first experiment involved a measure of the time taken to apply brakes after presentation of locked controls at rotation of a fixed wing aircraft. The second involved the time taken for helicopter pilots to depress the collective lever after the presentation of a double engine failure.
The mean reaction time was 3.4 seconds in the first experiment and 3.08 seconds in the second. Although these response times appear long, the fact that they were measured in a simulator in which pilots were expecting emergencies, makes them, if anything, conservative estimates of the response times likely to occur in actual flight. Even in this simulation some pilots took 7 seconds to react to an emergency they would have been anticipating.
2. ANALYSIS
2.1 Introduction
Shortly after the aircraft became airborne the engine lost power, possibly because the carburettor fuel needle became jammed in the housing sometime during taxi prior to take-off. If this had occurred, when the pilot applied take-off power the jammed needle would have limited the amount of fuel able to flow into the fuel chamber to replace fuel being used for take-off power (that is, the needle would have remained in its pre-take-off, idle power position). With the fuel being used at a rate greater than it was being replaced, it would only be a matter of time before the engine lost power. Possibly contributing to the event was a fuel needle valve of obsolete design coupled with the presence of some particulate contaminant.
Although the manufacturer had recommended the fitment of a different fuel needle valve, it was not mandated at the time by the Australian regulatory authority. At the time of the accident there was some confusion as to whether legislation required the installation of the modified valve.
2.2 Aircraft handling
It has been established that the pilot had developed a procedure to fly the aircraft at a very slow speed to obtain a rate of climb that was acceptable to him. The investigation was not able to establish precisely what speed was used, nor what rate of climb was attained. With the very high drag occasioned by the wing-walker, the high-nose attitude and the low forward speed, any loss of power such as occurred on this flight would have led to a very rapid loss of airspeed to a point where control would have been lost unless almost instant corrective action were taken. The most effective corrective action would have been to immediately lower the nose to maintain airspeed. It is not known why this was not accomplished.
The video recording showed that a substantial left rudder deflection and an application of right aileron occurred immediately after power was lost. The left rudder deflection occurred almost simultaneously with the wing-walker adopting the crouched position.
On a previous flight in VH-GVA, it was found that the position of the wing-walker could effect the airflow over the tail of the aircraft, which resulted in rudder buffet if the wing-walker did not stand with feet apart. The investigation was unable to determine whether the position adopted by the wing-walker after the loss of power resulted in the left rudder deflection. The effect of the wing-walker adopting a crouching position is not known but it could be that some airflow disturbance was generated that may have caused the left rudder deflection.
Another possibility is that left rudder was applied by the pilot in an attempt to execute a flat turn back towards the airfield. Yawing the aircraft in this manner would have rolled it to the left, a secondary effect which the pilot may have attempted to counteract by applying right aileron.
The Tiger Moth is fitted with differential aileron control which reduces the yaw effect of aileron application. Flying at slow speed, and thus at a high angle of attack, the down going left aileron would, even with differential aileron control, still increase the effective angle of attack of that wing beyond the stall angle, resulting in the rapid roll to the left, further yaw and nose-down attitude as seen on the video recording. The control positions seen on the video were those which, given low airspeed, could be expected to result in the aircraft entering a spin to the left.
2.3 Aircraft performance
The propeller fitted to VH-UNA had a pitch of 4 ft 11 in, a standard cruise propeller for that aircraft. The initial test on VH-GVA showed the aircraft to be performance-limited when fitted with a 4 ft 6 in pitch propeller. It was necessary to fit a fine-pitch propeller of 4 ft 2 in pitch to obtain a climb performance acceptable to that pilot. With a coarse pitch propeller fitted, VH-UNA would have been even more severely performance-limited than VH-GVA.
The pilot of VH-UNA possessed a copy of a Civil Aviation Authority letter that detailed the requirement to fit a fine-pitch propeller. It is not known why he did not comply with the requirement. However, had he fitted a fine-pitch propeller prior to departure from Brisbane, his cross-country cruise capability would have been degraded.
The Authority's procedures for recording that the wing-walking frame had been installed onto VH-UNA were deficient. Although the details were held on file in the Authority's Bankstown office in relation to the design engineer who approved the installation, they were not required to be copied to the aircraft file for VH-UNA which was held at Archerfield. The Queensland-based officer carrying out the survey on the aircraft would not have been aware from the data held on the aircraft file that the modification had been carried out some 12 months prior to the survey. Nor would he have been aware of the conditions surrounding the installation and operation of the wing walking frame.Accordingly, the chance to detect the incorrect propeller installation was missed.
2.4 Organisational factors
The aviation system has a number of built-in defences which are designed to detect any hazards before they lead to an accident. In this case, when the regulations were altered to allow activities such as wing-walking, instructions were issued by the Authority to regulate the conduct of the activity. These instructions were, in effect, aircraft and event specific in that they required approval on an individual basis.
The pilot of VH-UNA had acquired the wing-walk frame which he subsequently fitted to his aircraft under the approval of an authorised person.There was no evidence that the Authority was aware of the fitment of the frame other than when the pilot was approved to take part in certain air displays.Accordingly, the Authority did not carry out, as required by the Flying Operations Instruction, an airworthiness inspection, nor an assessment of the aircraft's performance.
Similarly, there was a requirement that the wing-walking stunt be previewed and approved by the Authority. Although the investigation received anecdotal evidence that this was done, no formal evidence of the preview having taken place was found. If the preview did take place, it was apparently of a cursory nature in that it did not detect that there had not been an airworthiness inspection, nor an assessment of VH-UNA's performance.
Moreover, surveillance conducted by the Authority on the aircraft did not detect that the fitment of the wing-walking frame had not been completed as required and that the aircraft was fitted with an incorrect propeller of a coarser pitch.
When the pilot purchased the frame, he obtained a copy of the engineering order relating to the fitment of the frame and an Authority letter that required the fitment of a fine-pitch propeller to the aircraft for wing-walk activities. He apparently chose not to fit the propeller. In so doing, he circumvented the protection afforded by the fitment of a fine-pitch propeller which would have improved the climb performance.
Following the poor climb performance obtained on the initial flight with the frame fitted, the pilot apparently developed a flying technique which involved operating at a slower climb speed. By using a lower climb speed, the pilot had almost entirely removed any margin of performance to allow adequate reaction time in an emergency.
3. CONCLUSIONS
3.1 Findings
The pilot held a current commercial pilot licence, and his medical certificate was valid.
Both crew members had previous experience with wing-walking activities.
The performance of the aircraft was significantly degraded when carrying a wing-walker.
The extent of the performance degradation was not calculated during the initial approval process.
The calculations made as a part of this investigation showed that the Tiger Moth was probably not an appropriate aircraft for carrying out wing-walking stunts.
The processes involved in approving the stunt, and in approving the pilot to carry out the stunt, were ineffectively controlled and poorly documented by the Civil Aviation Authority.
The pilot did not carry out this particular flight under the conditions specified by the Civil Aviation Authority.
The aircraft was not fitted with the required fine-pitch propeller.
The incorrect propeller installation was not detected during an airworthiness survey of the aircraft.
The fuel needle installed in the carburettor was of an obsolete configuration and a modification, to increase the fuel needle to housing clearance to preclude jamming, had not been carried out.
The fuel needle and housing showed evidence of particulate contamination which would have increased the probability of the needle jamming.
The manufacturer introduced the modification in 1957 for incorporation at the next overhaul. The Australian regulatory authority did not list the modification for mandatory incorporation.
The engine lost power suddenly, possibly because of a jammed fuel needle valve.
The loss of power occurred shortly after take-off while the aircraft was climbing at slow speed in a nose-high, high-drag configuration.
The aircraft's speed rapidly decayed to a point where control was lost.
The video recording showed that, following loss of power, the nose of the aircraft was not effectively lowered, and the controls were in a pro-spin configuration (i.e. left rudder and right aileron applied).
When control was lost there was insufficient height to effect a recovery before the aircraft impacted the ground.
3.2 Significant factors
The following factors were considered relevant to the development of the accident.
The performance of the Tiger Moth was such that the aircraft was probably inappropriate for carrying outwing-walking stunts.
The flight was not carried out in accordance with the conditions for wing-walking prescribed by the Civil Aviation Authority.
The aircraft suffered a power loss while in the climb.
Immediate, appropriate control inputs were not applied, and control was consequently lost at a height insufficient to effect a recovery.
4. SAFETY ACTION
4.1 Recommendations
As a result of this investigation the Bureau, on 14 June 1994, issued Interim Recommendation IR940146, which stated:
The Bureau of Air Safety Investigation recommends that the Civil Aviation Authority review all approvals granted for high drag installations fitted to aircraft to ensure that the particular aircraft has been proven to have a satisfactory performance. This should meet, as a minimum, the manufacturer's climb speed, and take regard of common emergency conditions that could arise.
The Civil Aviation Safety Authority response, dated 30 August 1995, stated:
The Authority does not maintain a central register of approvals issued for high drag installations. However, the number of such approvals is small, and most are issued for reasons unrelated to high drag or low performance. I am therefore confident that the problem highlighted by this accident is confined to "wing walking" situations.
The Authority formally accepts your recommendation and will review any further applications for "wing walking" flights to take account of the performance parameters outlined in the recommendation.
4.2 Safety advisory notices
As a result of the investigation into this occurrence, The Bureau of Air Safety Investigation issues the following Safety Advisory Notice.
SAN960062
The Bureau of Air Safety Investigation suggests that the Civil Aviation Safety Authority advise all owners of Gipsy Major-powered aircraft to expedite the incorporation of Gipsy Major modification G1136.
On the day before the accident, the aircraft flew from Aurukun to Weipa with the chief pilot occupying the left pilot seat and the pilot involved in the accident occupying the right pilot seat. At Weipa the chief pilot left the aircraft, instructing the other pilot to fly some practice circuits before returning the aircraft to Aurukun. Before commencing the circuits and the return flight to Aurukun, the aircraft's two main tanks each contained 100 L of fuel and the two wing tip tanks each contained about 90 L of fuel.
On the day of the accident the pilot added 200 L of fuel at Aurukun to the aircraft's tanks and then flew the aircraft and the passengers to Weipa. About 50 minutes before sunset, the aircraft taxied for departure from runway 30 for the 25-minute return flight to Aurukun.
When the aircraft was about 300 ft above ground level after take-off, a witness reported that all engine sounds stopped and that the aircraft attitude changed from a nose-high climb to a more level attitude. A short time later, the noise of engine power surging was heard. The aircraft rolled left and entered a spiral descent. It struck level ground some 350 m beyond the departure end of runway 30 and 175 m to the left of the extended centreline.
Wreckage examination
The aircraft had impacted the ground in a 30-degree nose-down attitude with 45 degrees of left bank. The left wing was broken at mid-span. The cockpit and forward cabin were totally crushed back to the leading edges of the wings.
The right propeller had gouged a deep hole in the soil and the propeller blades were bent both against the direction of rotation and rearwards toward the engine, indicating that this engine was producing considerable power at impact. The right fuel distributor valve contained fuel.
The left propeller was in fine pitch. One blade was bent rearwards toward the engine and the other blade was undamaged. Part of the spinner was crushed and part of it was almost intact. This damage pattern indicates that the left engine had stopped before impact. The left fuel distributor valve contained little fuel.
The left engine was removed from the aircraft and dismantled. No pre-impact damage that would have prevented the engine from operating was found.
Inspection of the airframe and other systems did not reveal any faults which might have contributed to the accident.
Fuel system
The aircraft had been fitted with the manufacturer's wing tip tank modification. Each tip tank had a useable capacity of 104.5 L and each main tank a useable capacity of 240 L. A flight manual supplement detailing the operation of this fuel system had been issued and incorporated in the flight manual. The fuel management section of this supplement indicates that, for structural reasons, fuel from the tip tanks must be used last, and that 50 L should be retained in each tip tank unless the fuel is needed for holding or diversion to another airfield. There is a warning in the flight manual supplement that take-offs and landings on main tanks are prohibited when the gauges read less than three gallons (about 14 L). There is no corresponding warning for the tip tanks.
Examination of the tip tanks showed that the fuel feed line was located centrally at the inboard tank baffle/outer wing rib near the bottom of the tank. The two main fuel selectors in the cockpit had moved from main fuel cock selection when the cockpit area was crushed during the main impact. However, examination of the fuel system confirmed that the main fuel cocks were open.
Toggle switches which control the main/tip tank selection were destroyed during impact. However, the light globes from the fuel tank indicators were examined and these indicated that the tip tanks were selected at the time of impact. Further inspection of the fuel supply system confirmed that the electrically actuated tip tanks fuel cocks were selected to draw fuel from the tip tanks.
The left tip tank was ruptured and separated from the wing. It contained about 5 L of fuel. The right tip tank was partially separated and did not contain any fuel. Reports from people at the scene immediately after the accident indicated that a large amount of fuel from the ruptured main tanks was present at the site.
The pilot
Six weeks before the accident, the pilot completed his endorsement training on an Islander aircraft which was not fitted with the tip tank modification. However, the endorsing instructor had briefed the pilot on the various fuel systems encountered in the Islander family of aircraft, including the particular wing tip tank modification fitted to VH-JUU. After his endorsement the pilot flew VH-JUU for a total of 3.6 hours until the day before the accident. The duration of the flight on the day before the accident, together with that of the passenger flight to Weipa on the day of the accident, was approximately one hour and twenty minutes. Therefore, at the time of the accident, the pilot had a total of 6.7 hours on the aircraft type.
Passengers and freight
The purpose of the flight was to collect cartons of beer from Weipa. The Aurukun Community had a policy of allowing a maximum of ten cartons to be carried on any one charter flight. However, sometimes passengers would insist on carrying more. The aircraft wreckage contained 30 cartons of beer and two bottles of rum, the latter being totally prohibited by the community. The cartons had been packed on and around seat rows four and five. The load had not been tied down. The aircraft gross weight was calculated to have been 47 kg below the limit for this take-off. The centre of gravity was within limits.
Checklist
The endorsing instructor had given the pilot an Islander checklist. The aircraft usually carried a normal procedures checklist on a clipboard, but this was inadvertently left at Aurukun. A checklist for normal procedures was not found in the wreckage although an emergency procedures checklist was found incorporated in the flight manual carried on board.
Fuel management
For planning purposes on this flight, the flight manual indicated a fuel consumption rate of 135 L per hour. The chief pilot reported that when he handed the aircraft over to the pilot at Weipa on the day before the accident there was about 90 L in each tip tank and that the tip tanks were probably selected to provide fuel to each engine.
2. ANALYSIS
If the tip tanks were selected since the previous day, the tip tank fuel contents should have been exhausted at about the time of the final take-off from Weipa. With a low quantity of fuel in each tip tank, the fuel lines from each tank probably became unported as the aircraft climbed after take-off, resulting in engines losing power from fuel starvation. When the pilot changed the attitude of the aircraft after the loss of power, some fuel probably became available to the right engine which then regained power.
Other factors include the pilot's low level of experience in the aircraft type, the absence of a normal procedures checklist and pressure from the passengers to complete the return flight with the excess alcohol. This pressure may also have accounted for the freight not being correctly secured.
A double, simultaneous engine failure was probably outside the pilot's experience level. A forced landing option was available which would have necessitated the closing of both throttles and landing on the Weipa-Coen road, which cut across the extended centreline of the runway at an angle of about 30 degrees. However, once the aircraft entered a spiral descent at low speed and with asymmetric power, recovery was not possible in the height available.
3. CONCLUSIONS
Findings
The aircraft was being operated within weight and centre-of-gravity limits.
No defects that were likely to have contributed to the occurrence were found with the aircraft.
The aircraft's wing tip tanks were selected to feed fuel to the engines.
The right engine was producing considerable power at impact.
The left engine had stopped before ground impact and the propeller was not feathered.
The pilot did not operate the aircraft fuel system in accordance with flight manual instructions.
Both engines were starved of fuel during the initial climb after take-off.
The pilot had probably operated the aircraft exclusively on fuel from the wing tip tanks, which were near empty at take-off.
A suitable forced landing option was available.
There was no warning in the aircraft flight manual to alert the pilot to the danger of operating with near empty wing tip tanks.
Following the entry into the spiral there was insufficient height available for a recovery to controlled flight. Significant factors
The pilot mismanaged the aircraft fuel system.
Both engines suffered a total power loss due to fuel starvation.
The right engine regained power probably as a result of a change in aircraft attitude.
The pilot lost control of the aircraft.
Recovery was not possible in the height available.
4. SAFETY ACTION
During the course of this investigation Interim Recommendation IR 940193 was issued. It stated:
The Bureau of Air Safety Investigation recommends that the Civil Aviation Authority review the approval for the Flight Manual Supplement pertaining to wingtip fuel tanks on BA-2A-21 aircraft. Consideration should be given to adding suitable warnings that the use of partially filled wingtip tanks during take-off, landing and manoeuvring may lead to fuel starvation.
The following response, dated 8 November 1994, was received from the CAA:
"The Interim Recommendation on the aircraft has been reviewed and action in line with the BASI recommendation is being taken to update the aircraft flight manual."
The aircraft, with only the pilot on board, was being flown from Archerfield to Caboolture via the light aircraft lane to the west of Brisbane in company with another aircraft. About five minutes after departing Archerfield, the pilot radioed that he was experiencing problems with both engines and that he was in an emergency situation. The pilot of the other aircraft advised him that there were suitable forced landing areas in and around a nearby golf course. However, the aircraft continued and slowly lost altitude before rolling inverted and diving steeply into the ground.
Ground witnesses reported hearing loud backfiring and fluctuating engine RPM from the aircraft. These sounds were accompanied by erratic rolling and yawing of the aircraft before it rolled to the left and inverted. The right wing was severed outboard of the engine as the aircraft impacted a large tree before crashing onto a road.
Wreckage examination revealed that the fuel selectors for both engines were set at the auxiliary tank positions, causing fuel for each engine to be drawn from the corresponding auxiliary tank in each wing. It was established that the aircraft had been refuelled to full main tanks prior to the flight. Further, the pilot had advised in a telephone conversation with an engineer before the flight that the contents of both auxiliary tanks was 60 litres or less. All fuel tanks except the left auxiliary tank were ruptured during the impact sequence. About one litre of fuel was recovered from this tank.
Examination of the aircraft engines indicated that the right engine was under power at impact while the left engine was not. The mechanical condition of the engines indicated that they were capable of normal operation.
The PA-31 pilot's operating handbook states that the main fuel tanks must be selected for take-off. However, the behaviour of the aircraft, the position of the fuel selectors, and the information concerning the contents of the auxiliary tanks suggest that the pilot probably commenced the flight with the auxiliary tanks selected. As the flight progressed and fuel was used, intermittent un-porting of the fuel outlet lines occurred. This caused temporary fuel starvation, resulting in engine surging. These interruptions to engine power would have caused the aircraft to lose altitude, as described by witnesses, and airspeed. The event in which the aircraft rolled to the left and inverted is consistent with the right engine suddenly surging to high power when the aircraft was flying at a low airspeed while the left engine was delivering little or no power.
The pilot gained a PA-31 type endorsement in July 1992. At the time of the accident, he had logged a total of 37.8 hours flying multi-engine aircraft, including 35 hours on this aircraft type.
It was established that the pilot did not use a written checklist. Had such a checklist been used, the incorrect fuel tank selection may have been detected. Notwithstanding this, fuel system management is a basic and essential aspect of aircraft operation. In particular, fuel tank selection is a standard check item in the event of engine malfunction during flight. The pilot's apparent failure to select the main fuel tanks may be explained, at least in part, by his relatively low level of aeronautical experience, both overall and on type. Additionally, the pilot's information processing capacity may have been affected by the stressful situation in which he found himself. There were indications from the radio transmissions made by the pilot that he was in a highly anxious state when he reported that he was experiencing difficulties.
There were areas beneath the aircraft's flight path upon which a forced landing could have been conducted, albeit with probable aircraft damage. The pilot's failure to conduct a forced landing is considered a factor in the severity of the accident.
Evidence obtained during the investigation and the circumstances surrounding this occurrence suggest that the pilot did not have an adequate understanding of the aircraft systems.
Significant Factors
The following factors are considered relevant to the development of the accident:
1. The pilot did not use a written checklist.
2. The pilot operated the aircraft with the auxiliary tanks selected when the fuel contents of these tanks was low.
Pilot transmitted a Mayday call stating the aircraft engine had failed 10 miles NW Aurukun and that he was conducting a forced landing into trees. Nothing further was heard from the aircraft, and the burnt-out wreckage was found some hours later in a densely treed, inhospitable area 44 km north of Aurukun.
The investigation determined that the engine fuel mixture control cable end had become detached from the mixture control arm on the fuel control unit. This allowed the control arm to move to the 'idle cut-off' position, causing the engine to fail because of fuel starvation.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation.
What happened
On 1 May 2022, at about 1558 local time, the pilot of a Quest Kodiak 100 departed Orange Airport, on a private flight, to Mittagong, New South Wales.
At 1620, while cruising at 9,500 ft, the pilot observed the ‘reservoir fuel’ warning light illuminate. They immediately put the fuel pump on, checked both fuel cocks were on, checked the fuel quantity and balance and reduced the power to preserve fuel. Shortly after, the pilot then received a fuel starvation imminent warning followed by low fuel pressure warnings.
At the time of the warnings, the aircraft was overflying a remote sandstone escarpment region that contained deep gorges and large cliff lines, and was approximately 30 NM (56 km) away from any open land. Due to limited options to conduct a precautionary landing, the pilot continued to cycle the fuel pump, further reduced the power and turned towards an area suitable for a forced landing. During this time, the pilot heard multiple loud bangs.
The pilot continued to cycle the fuel pump and after a few minutes the fuel messages stopped. When the pilot was satisfied that the engine had enough fuel, they tracked direct to Mittagong and landed the aircraft safely at about 1651.
Engineering inspection
Following the incident, the pilot conducted a post-flight inspection and observed the upper skin on the right wing had crumpled and collapsed. To relieve the vacuum in the wing, the pilot attempted to open the fuel cap by forcing a piece of laminate under the cap. After partly opening the cap, a large amount of air was sucked into the tank and the upper skin of the wing popped back out once the pressure was relieved. However, there was still a large depression of about 11 mm (Figure 1).
Figure 1: Fuel tank depression on the right wing
Source: The pilot, annotated by ATSB
An engineering inspection of the right wing revealed the ribs and stringers had failed and the wing was no longer airworthy. Further inspection of the fuel tank vent line inlet recess also revealed mud wasp nests deep inside the vent lines for both wings, which were unable to be inspected or seen visually during the pre-flight inspection (Figure 2 and Figure 3).
Figure 2: Fuel tank vent line NACA inlet recess on the wing
Source: The pilot
Figure 3: Diagram of the fuel tank vent line within the wing
Source: Pilot, annotated by ATSB
Fuel tank vents are used to ensure the pressure inside the tank is maintained when fuel is being used by the engine. If a fuel tank vent becomes blocked while fuel is being pumped out, it will create a vacuum due to the inability of air not being vented in to replace the fuel, which can cause the tank to collapse.
Pilot comments
The pilot advised:
The aircraft was parked in a hangar and had been flown on the Thursday and Friday prior to the occurrence. No abnormalities during those flights were detected.
They would typically only fill the fuel tanks halfway, but while at Orange they had filled them up to the top. They postulated that the vacuum occurred in this flight because there was less air in the tank compared to when the tanks are half full.
Safety action
As a result of this occurrence, the pilot advised the ATSB that they made a protective plug for the fuel tank vent lines to prevent wasps from building nests (Figure 4). The plug consists of a clear plastic tube that is long enough to be inserted into the vent line, which can be used to detect an obstruction in the line if resistance is felt. At the end of the tube is a masonry plug with a screw to seal the tube and streamers to ensure the plug is not missed during the pre-flight inspection. In addition to this, the pilot has also informed other operators at the aerodrome of the potential hazard.
Figure 4: Devised plug to protect the vent line inlet recess
Source: Pilot
Safety message
Blocked, or even partially blocked, pitot tubes and fuel tank vents can compromise the safety of the flight. Wasps can begin to build a nest rapidly and significantly block a fuel vent line or pitot tube within 30 minutes. Regardless of whether an aircraft has a short turn-around time or is parked overnight, protective covers and screens should be used on both fuel vent lines, fuel caps and pitot tubes. In addition to visually inspecting pitot tubes during pre-flight inspections, pilots should also inspect fuel vent lines. Moreover, operators and aerodrome personnel should monitor and remove any wasp nest sites in the general area of where the aircraft is stored and maintained to further reduce the risk.
For further information on wasp nest infestations please refer to the CASA Airworthiness Bulletin AWB-02-052.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.