The ATSB is investigating an occurrence where a tool was located inside the left wing of a Qantas Airbus A380, registered VH-OQK, on 9 January 2026. The aircraft had flown 2 sectors prior to the tool being located.
In the course of the investigation, the ATSB has identified potential limitations in risk controls relevant to the occurrence. Examination of these factors represent an increase in the scope of this investigation, and it has been upgraded from Short to Defined as a result (the ATSB's different levels of investigation are detailed here).
The draft report internal review process has been completed. The draft report has been distributed to directly involved parties (DIPs) to check factual accuracy and ensure natural justice. Any submissions from those parties will be reviewed and, where considered appropriate, the draft report will be amended accordingly.
Following the external review process, any submissions and amendments to the draft report are internally reviewed. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2026-004
Occurrence date
09/01/2026
Occurrence time and timezone
15:00 Australian Eastern Daylight Time
Location
Sydney Airport
State
New South Wales
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Final report: Internal review
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Foreign object damage / debris
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Airbus
Model
A380-842
Registration
VH-OQK
Serial number
0063
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
Activity
Commercial air transport-Scheduled-International
Departure point
Dallas/Fort Worth International Airport, United States of America
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 18 February 2025, an Airbus A330‑303 was undergoing a scheduled aircraft maintenance check at Brisbane Airport, Queensland. Multiple tasks were completed by engineers throughout the aircraft’s inspection. Engineers used lock wire to complete various tasks underneath the engine cowl. Once completed, the engineers signed off the aircraft as ‘safe for flight’ and it was released to service. The aircraft was subsequently flown on 51 international flights.
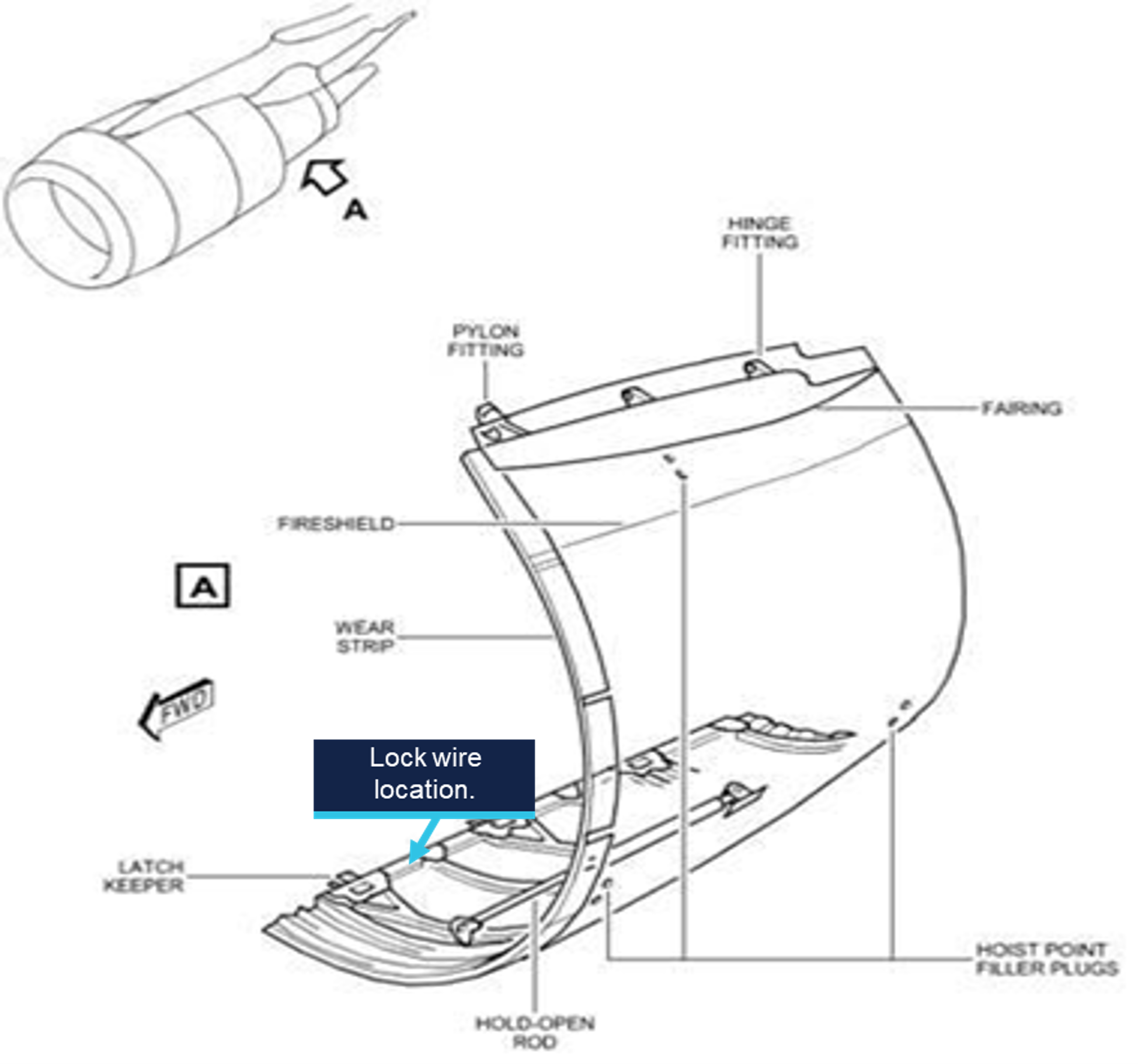
On 17 March 2025, the aircraft was due to undergo further routine aircraft maintenance checks. Engineers removed the engine cowl and a roll of lock wire (Figure 1) was discovered on the inward layer of the outboard section (Figure 2). The operator advised that the roll of lock wire had inadvertently not been removed during the first maintenance inspection that occurred on 18 February 2025. There was no effect on the aircraft during subsequent international flights.
Figure 1: Roll of lock wire
Source: Operator, annotated by the ATSB
Figure 2: Engine diagram
Source: Operator, annotated by the ATSB
Safety action
The operator has communicated with its maintenance crews, in the form of a quality alert, the importance of a clearance inspection post‑aircraft maintenance. Any existing loose lock wire across the business has also been returned to a controlled point of issue, and lock wire without clear identification information has been discarded.
Safety message
This incident demonstrates the importance of extensive crosschecks and accuracy when declaring an aircraft is ‘safe for flight’ and subsequently returned to service.
Checklists are an essential tool for overcoming memory item mistakes and assumptions. While their value may seem redundant or may not be obvious for frequently performed tasks like routine maintenance inspections, in this occurrence it is likely that if checklist items had been completed, the presence of the lock wire would have been detected. A visual confirmation check prior to declaring the aircraft safe for flight should always be best practice.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow‑up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-016
Occurrence date
17/03/2025
Location
Brisbane Airport
State
Queensland
Occurrence class
Incident
Aviation occurrence category
Foreign object damage / debris, Ground Operations
Highest injury level
None
Brief release date
22/05/2025
Aircraft details
Manufacturer
Airbus
Model
A330-303
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 6 December 2023, an Airbus A380-842 aircraft, registered VH‑OQI and operated by Qantas Airways Limited, was undergoing a 3-day scheduled maintenance check at Los Angeles International Airport (LAX), United States.
On day one of the maintenance check, during a scheduled borescope inspection of the outboard left engine, a tool was left in the engine inlet. On the evening of 8 December, the aircraft was released to service and departed for Melbourne, Victoria.
On 1 January 2024, the aircraft returned to the LAX maintenance facility for a 3-day scheduled maintenance check, where the missing tool was discovered in the outboard left engine low‑pressure compressor. The aircraft had flown 34 cycles totalling 293.74 hours with the tool in the outboard left engine.
What the ATSB found
The ATSB found that the tool was not located during the end of task foreign object inspections, which resulted in it remaining in the engine. The Qantas Engineering lost tool procedure was not commenced prior to the aircraft being released to service and the certifying engineer did not follow up on the lost tool, prior to releasing the aircraft to service.
What has been done as a result
On 2 January 2024, a Qantas Engineering internal incident report was raised with an immediate action to brief staff on the importance of ensuring that all tooling is returned and actioned by tool store personnel. A Qantas Engineering internal investigation was completed and on 4 March 2024, the executive manager for Qantas Engineering released an internal safety directive for immediate action requiring all Qantas Engineering employees to meet the company tooling control requirements without exception.
Safety message
Foreign object debris and damage poses a significant threat to the safe operation of aircraft. Regulations, procedures, and training have been put in place and refined to limit the risk of foreign object damage, especially from introduced objects during maintenance. As a result, the correct application of tool control is an important, fundamental, and necessary aspect of the maintenance process to mitigate any human errors that may arise.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 6 December 2023, an Airbus A380-842 aircraft, registered VH-OQI and operated by Qantas Airways Limited, was inducted into the Qantas Engineering[1] Los Angeles Line Maintenance facility for scheduled maintenance at Los Angeles International Airport (LAX), United States.
The scheduled maintenance was to be carried out over 3 days and included a borescope inspection of the left outboard engine’s intermediate-pressure compressor. The borescope inspection was to be conducted on day one and was estimated to take approximately 6 hours. The aircraft was located outside of the maintenance hangar, on the hardstand, for the duration of the scheduled maintenance.
Day 1 – 6 December 2023
0700 local time
A licenced aircraft maintenance engineer (LAME 1) assigned 2 aircraft maintenance engineers (AME 1 and AME 2) to the engine borescope inspection task. A support engineer was also assigned to assist AME 1 and AME 2. AME 2 and the support engineer were both unfamiliar with the borescope task and were provided guidance by AME 1.
AME 1 and AME 2 collected the required managed tooling[2] from the hangar tool store[3], which included a 1.25 m long by 2.5 cm wide nylon rod, known as a turning tool[4] (Figure 1). The tooling was signed out by AME 1. The engineers placed access stands around the left outboard engine and commenced the task. The support engineer entered the engine inlet via the access stand and rotated the engine’s intermediate-pressure compressor, as required, using the turning tool. AME 1 and AME 2 remained underneath the engine, operating the borescope.
1300
AME 1 left work early for a medical appointment and then proceeded onto 3 rostered days off. The borescope task was only partially completed at this time and the turning tool remained assigned to AME 1.
After the departure of AME 1, AME 2 asked LAME 1 if the tools used on the borescope task required returning to the tool store. LAME 1 advised AME 2 to leave the tools with the aircraft as the afternoon shift, commencing at 1500, would complete the remainder of the task. AME 2 and the support engineer were then reassigned onto other tasks by LAME 1.
1500
The hangar tool store personnel ran a scheduled daily tooling report, [5] which identified that the turning tool was assigned to AME 1 and had not been returned.
Due to the borescope task being unfinished, LAME 1 decided to remain at work until the task was completed and certified in the aircraft’s computer‑based maintenance log (Maintenix).[6]
The afternoon shift, which consisted of 2 aircraft maintenance engineers (AME 3 and AME 4), commenced the remaining steps of the borescope task. AME 3 was experienced in the use of the borescope procedure and AME 4 had not conducted the procedure before.
The support engineer briefly returned to the task and provided guidance to AME 4 on the use of the turning tool prior to departing work for 3 rostered days off. AME 3 operated the borescope and AME 4 operated the turning tool.
AME 3 completed the inspection operating the borescope and asked AME 4 if they wanted to view the images prior to reinstalling the borescope access plugs on the engine. AME 4 left the turning tool in the inlet, as they believed it would be used again later, and proceeded out of the inlet down to the ground to view the borescope images. Neither AME 3 nor AME 4 re‑entered the engine inlet for the remainder of the shift.
1700
Tool store personnel emailed the scheduled daily tooling report, which was run at 1500, to all LAX service engineers, LAMEs, managers, and tooling personnel.
LAME 1 requested AME 2, the only AME remaining at work from the initial borescope tasking, to return the tooling used for the borescope task to the hangar tool store. AME 2 proceeded up to the inlet cowl to visually inspect that all tools were removed. AME 2 identified that an inlet cowling protective mat was still on an access stand. AME 2 removed the mat and conducted a brief visual inspection of the inlet to ensure no foreign objects remained. AME 2 did not use a torch and did not observe the turning tool.
The borescope equipment was returned to the hangar tool store and AME 2 then left work for the day. AME 2 was unaware that the turning tool was still in the low-pressure compressor case.
1830
LAME 1 conducted the first inspection[8] of the completed borescope task, and also conducted a foreign object debris check of the inlet using a torch but did not detect the turning tool. LAME 1 then certified the required tasks in Maintenix prior to proceeding on to 3 rostered days off, unaware that the turning tool had not been returned.
2100
Another licenced aircraft maintenance engineer, LAME 2, conducted the required second independent inspection.[9] LAME 2 inspected the security of the engine borescope access plugs and the engine lower area. They did not conduct an inspection of the inlet cowl.
2130
A third LAME, LAME 3, who was not involved in the task, while performing end-of-shift task closure duties, became aware of the missing turning tool identified in the tooling report. As the turning tool was assigned to AME 1, who was no longer at work, LAME 3 contacted AME 1 who advised that they had finished work at 1300 and that the turning tool was still in use at that time. LAME 3 then informed tool store personnel that the turning tool was still in use by the second shift when the daily tooling report had been run. LAME 3 took no further action.
Day 2 – 7 December 2023
1500
Tool store personnel conducted the daily scheduled tooling report. The report identified that the turning tool was still unaccounted for. The tooling report was not emailed to LAX service engineers, LAMEs, managers, or tooling personnel at this time.
Day 3 – 8 December 2023
1500
The hangar tool store personnel conducted the daily scheduled tooling report, which identified that the turning tool was still unaccounted for.
1840
Tool store personnel emailed the tooling report to all LAX service engineers, LAMEs, managers, and tooling personnel to remind them of the missing turning tool, noting that the aircraft was scheduled to depart at 2235 that night.
1845
The operations manager sent an email to the service engineer, who was certifying the Certificate of Release to Service (CRS)[10] for VH-OQI, reminding them that if the turning tool was still unaccounted for, to ensure that the Qantas Engineering lost tool procedure was carried out prior to aircraft departure (see Context section titled Lost toolprocedure).
2012
The service engineer, aware that the tool had been missing since 6 December and believing that the tool could not be still fitted to the aircraft, replied to the email from the operations manager and the on-duty tool store personnel acknowledging that VH-OQI was leaving at 2235 but also noted that the tool had been missing since 6 December 2023. The service engineer did not view the tooling report and continued with their certification of the CRS for VH-OQI (see the section titled Service engineer comments).
2336
VH-OQI departed LAX for Melbourne, Victoria.
10 December 2023
0700
LAME 1 returned to work after 3 rostered days off and was made aware of the missing turning tool. LAME 1 conducted a search of stores, engine stands, the hardstand (where VH-OQI’s maintenance was conducted) and the hangar, for the missing turning tool. The turning tool was not located.
1700
LAME 1 raised a missing tool report in Maintenix against VH-OQI. Although, the required follow-up process was not commenced and the associated administrative task, UTL-1, was not raised (see the Context section titled Lost tool procedure).
11 December 2023
0758
VH-OQI returned to LAX from Melbourne, on a scheduled passenger flight, but was not inducted into maintenance. The aircraft was not searched for the missing turning tool.
The aircraft returned to LAX on 19 December and again on 28 December. No scheduled maintenance was conducted at either time.
27 December 2023
Qantas engineers in Sydney, Australia, requested that Sydney tool store personnel remove the missing tool report against VH-OQI as it was affecting the issue of a CRS.
28 December 2023
1424
Sydney tool store personnel changed the status of the turning tool in Maintenix to ‘Ready for Issue’. They then sent an email to LAX tool store personnel requesting to change the status of the tool in the LAX tool store to ‘Quarantined’.
1530
LAX tool store personnel set the missing tool to ‘Quarantined’ and created a Maintenix task UTL‑2. As noted above, UTL-1 was not created in Maintenix, as procedurally required, after the missing tool report was raised on 10 December (see the Context section titled Lost tool procedure).
1 January 2024
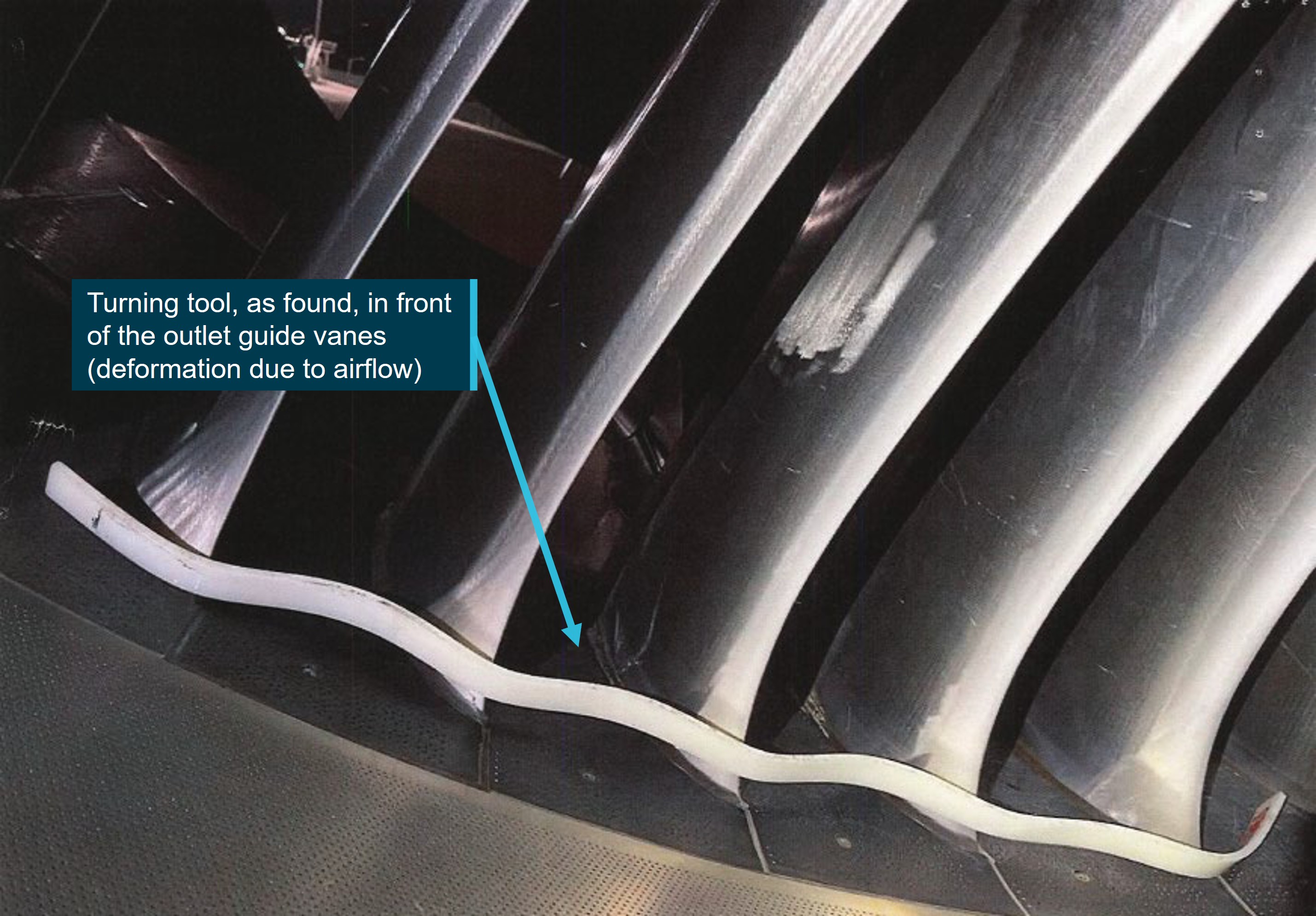
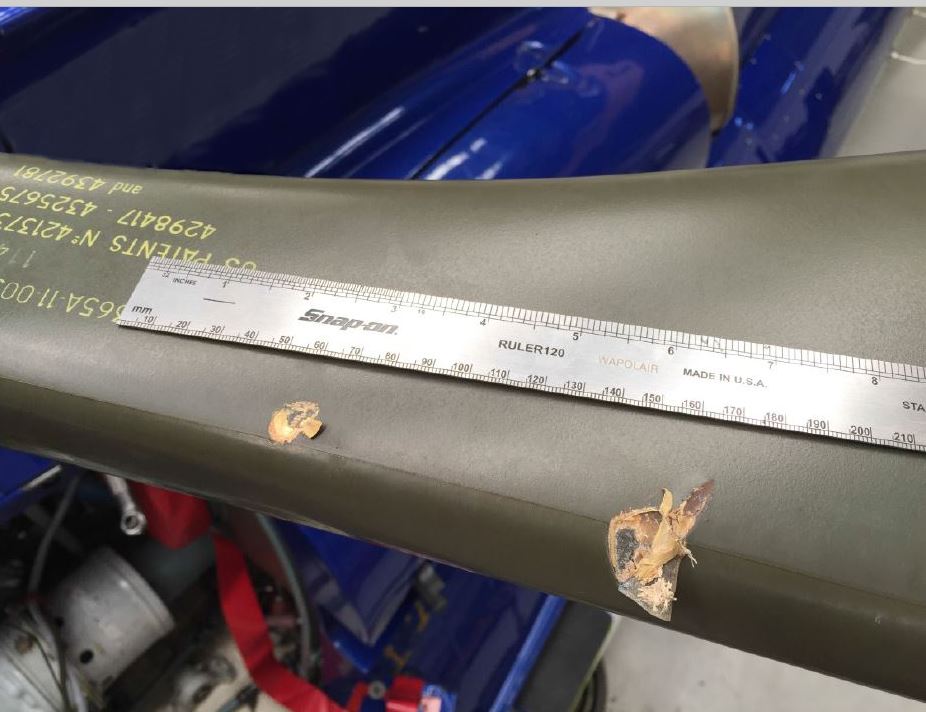
VH-OQI returned to LAX on 1 January 2024, for a fourth time since the tool was reported missing and was inducted into scheduled maintenance. This scheduled maintenance included a detailed inspection of the low-pressure compressor blades on all 4 engines. During this inspection, the engineers located the missing turning tool in the outboard left engine in the low-pressure compressor and in front of the outlet guide vanes (Figure 1). The turning tool was removed from the engine and returned to the hangar tool store where it was physically placed in quarantine.[11]
Figure 1: Location of the turning tool as found in front of the low-pressure compressor outlet guide vanes
Source: Qantas Airways Limited, annotated by the ATSB
2 January 2024
1420
LAX tool store personnel closed UTL-2 in Maintenix.
Context
Borescope task
The intermediate-pressure compressor inspection task is a routine maintenance procedure in which the condition of the internal components of the engine are visually inspected and recorded using a portable borescope. The engine casing has a series of removable access ports known as borescope access blanking plugs. Once removed, these plugs allow an engineer to insert a borescope camera into the internals of the engine while a second engineer reaches between the low-pressure compressor blades and rotates the intermediate‑pressure compressor with the turning tool. This allows the borescope operator to inspect the rotating components of the engine as they pass by the borescope camera lens.
One of the final procedural steps of the intermediate-pressure compressor borescope inspection is to remove all inspection equipment from the engine.
Turning tool location
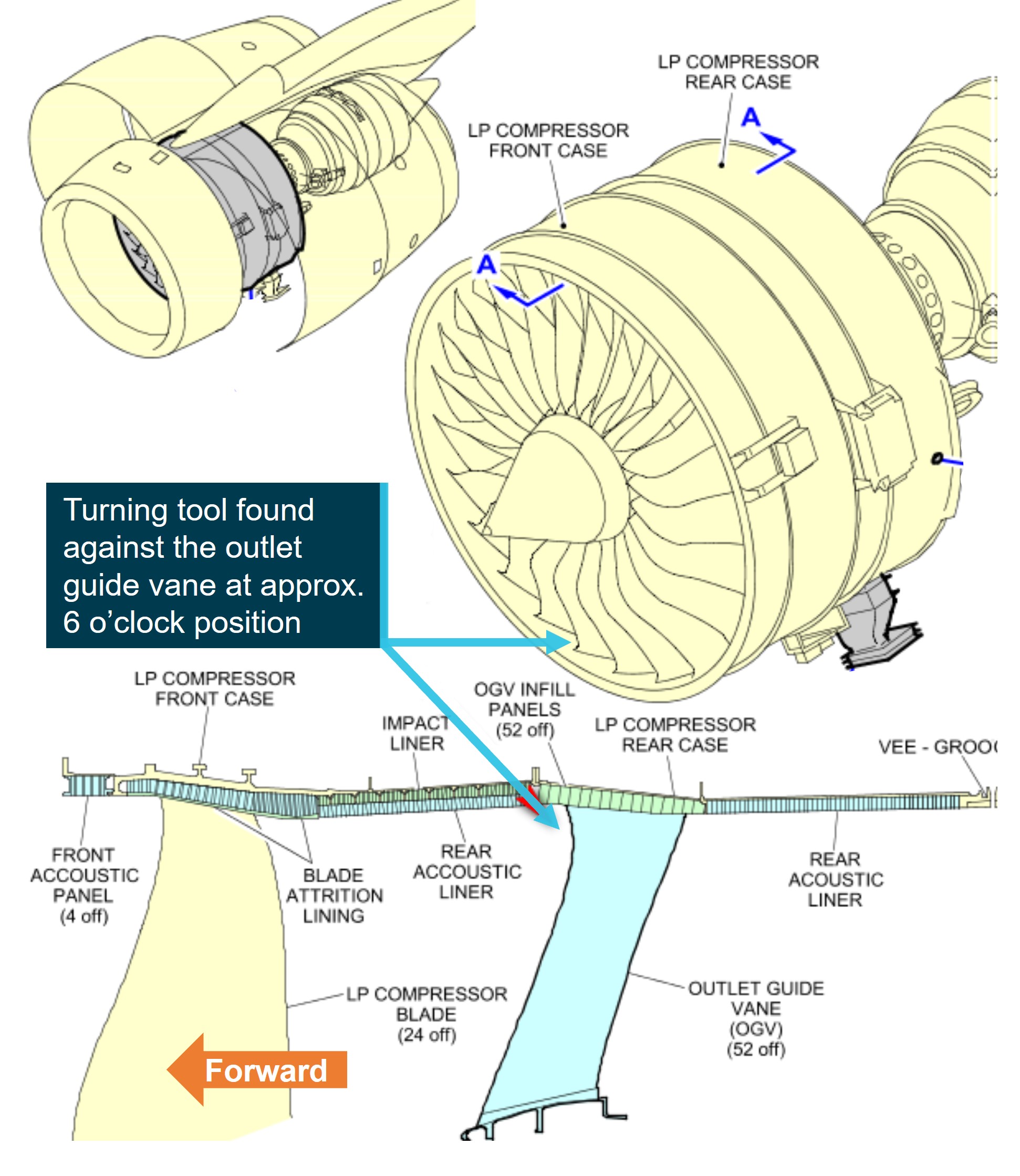
The turning tool was found behind the rotating low-pressure compressor blades, in approximately the 6 o’clock position (Figure 1 and Figure 2). It had been deformed by high energy airflow around the low-pressure compressor outlet guide vanes (non-rotating). There was no damage observed to any engine components.
Figure 2: Schematic of the Rolls Royce Trent 972-84 engine identifying the location of the turning tool
Source: Qantas Airways Limited, annotated by the ATSB
Tool issue and control
To facilitate turnaround times, Qantas, like other operators of large, complex aircraft, ran around‑the‑clock maintenance facilities, with teams of engineers working shifts. A single task, such as the borescope task, can take multiple workers and shifts to complete, and required specific tools for the duration. As no personal tools were used in the Qantas Engineering Los Angeles Line Maintenance facility, all tooling was kept in a hangar tool store and was issued to individual maintenance engineers for tasks.
Procedures to control these tools were in place and designed to track where the tool was, what aircraft it was being used on, and who was using it. This was from the time it was issued until it was returned. Any tools then unaccounted for, became ‘lost tools’, and another procedure commenced, this was to reduce the likelihood of tools being inadvertently left in an aircraft (see the Context section titled Lost tool procedure).
Before the end of a shift, or prior to an aircraft departure, tool store personnel conducted a scheduled daily tooling report. This tooling report was a snapshot of the tool store inventory and captured tooling that had not been returned and was still assigned to an individual. If the report identified any unaccounted for tools, the report was sent via email to LAX service engineers, LAMEs, managers, and tooling personnel. The report was also loaded against the aircraft in Maintenix. The on-shift service engineer would determine if that individual was still at work and take the appropriate action.
In interview with the service engineer from day 3, it was stated that no tools were to be passed onto the next shift but, rather, returned and re-issued to the AME continuing the task.
Lost tool procedure
Qantas Engineering tooling and equipment loss procedure outlined actions to be taken when a tool loss had been identified. This procedure was to be commenced before the end of a shift and prior to the certification of the CRS.
Upon identification of a tool loss, a comprehensive search for the tool was to be initiated and the supervisor immediately notified. The loss was then raised in Maintenix against the aircraft. The supervisor /duty maintenance manager would then determine if the tool was lost in a critical[12] or non-critical[13] area.
If the tool was lost in a critical area and unable to be located, the DMM / supervisor in conjunction with the service engineer, were to decide if the aircraft CRS was to be certified and released to flight once the area was thoroughly searched, or if the aircraft should be grounded until the tool was located. The follow-up process was then to be commenced.
If the tool was lost in a non-critical area and was unable to be located, the follow-up process was to be commenced and a CRS was then able to be certified.
The follow-up process was an administrative task, which was entered against the aircraft in Maintenix. The intent of this task was to act as an advisory to any engineer, worldwide, conducting maintenance on that aircraft of the unaccounted tool. The task, titled UTL-1, was renewed monthly, for a maximum of 3 months becoming UTL-2 and UTL-3 respectively. If the tool was still unaccounted for after 3 months, the tool was considered lost, and then the tool was electronically archived from the Maintenix system. If the tool was found the task would be signed off from Maintenix.
Certification responsibilities
To meet the Civil Aviation Safety Regulations for the conduct and certification of maintenance, Qantas Engineering’s internal procedures detailed maintainer responsibilities when maintenance was being certified. This included ensuring all tooling and equipment was located and removed from an aircraft, engine, or component upon task completion.
The documents also detailed the following requirements for the issue of a CRS:
The issuer is to verify[14] that all tools and equipment have been removed from the aircraft and accounted for. Tooling and equipment removal can be confirmed by viewing the tooling report that has been completed daily by tool store personnel. This tooling report is available in Maintenix and should be used. It is not necessary to physically re-inspect a task.
If there is any tooling listed as unaccounted for on the tool store tooling report, then the whereabouts of this tooling needs to be confirmed as not posing a risk. Raise a missing tool report and if the tooling cannot be located then Tooling and Equipment Loss Policy procedure shall be followed.
Service engineer comments
In interview with the ATSB, the service engineer stated that, prior to their certification of the CRS, and upon receiving the email from the operations manager regarding the missing turning tool, they were aware that the tool was identified as missing on day one of the servicing. They further advised that they believed the tool was a larger, gearbox turning tool that required physical fitment to the engine and could not possibly be fitted to the aircraft without being visible. Therefore, the tool could not be on the aircraft. With this incorrect belief, the service engineer certified the CRS and released the aircraft for flight.
Safety analysis
On 6 December 2023, an Airbus A380-842 aircraft, registered VH-OQI and operated by Qantas Airways Limited, underwent a 3-day scheduled maintenance check at Los Angeles International Airport (LAX), United States. During the maintenance check, a 1.25 m long nylon turning tool was left in the outboard left engine. The aircraft flew 34 cycles, totalling 293.74 hours, with the tool in the engine prior to it being discovered on 1 January 2024.
Tool location and visibility
The turning tool was last used by engineering staff to turn the compressor during a borescope inspection and found wedged against the low-pressure compressor outlet guide vanes and deformed by engine airflow. It is likely that this is where the tool was left as, if the turning tool was left in front of the low-pressure compressor, it would likely have displayed more damage from passing through the rotating low-pressure compressor blades during engine operation and been more visible to AME 2 and LAME 1 during their foreign object inspections.
After dark, AME 2 returned the borescope tools to the tool store and inspected the inlet area but did not use a torch and did not observe the turning tool. LAME 1 conducted a foreign object inspection of the inlet area with a torch but did not observe the turning tool either.
The combination of:
AME 2, the support engineer, and AME 4’s unfamiliarity with the task
the requirement of AME 1 to leave the task early with the turning tool assigned to them
the re-tasking of AME 2 and the support engineer to other duties
LAME 1’s advice to leave the tools on the task without a return and re-issue of tooling to the next shift
likely affected all the involved maintainers’ sense of ownership and accountability for the turning tool.
Lost tool procedure
LAME 3 became aware of the turning tool being unaccounted for by the daily tooling report during their end-of-shift task closure actions. After contacting AME 1 at home and being informed that the turning tool was still in use when they had left work for the day, LAME 3 did not check to see if the tool had been returned to the tool store. If LAME 3 had discovered that the tool was still unaccounted for, it is likely that the lost tool procedure would have been commenced at this time.
As this did not occur, the next opportunity to identify that the tool was unaccounted for was the daily tooling report that was conducted on day 2. It could not be determined why this report was not emailed to the required staff, but this action, in conjunction with the LAME and AME that had the initial ownership of the turning tool being on leave, likely resulted in the lost tool procedure not being commenced at this time either.
The email received by the service engineer from the tool store on day 3, along with the prompt from the operations manager, should have flagged that the tool was still unaccounted for, as this was the purpose of the email. The service engineer did not view the tooling report, incorrectly believing it was a larger, more noticeable tool requiring physical fitment to the aircraft, and, as the turning tool was unaccounted for since day one of the servicing, the tool must not be on the aircraft.
If the lost tool follow-up procedure had of been commenced and the tool was unaccounted for, there would have been a UTL-1 entry into Maintenix which would have been visible to the service engineer during their certification of the CRS. The lack of a UTL-1 entry in Maintenix further supported the service engineer’s belief that the tool was not on the aircraft.
The aircraft returned to LAX the day after departure, and as lost tool proceedings had not commenced, the aircraft was not searched. Aside from the tool store having a record of the tool unaccounted for at this time, it is unknown if any other engineering staff were aware that the tool was missing. The lost tool procedure was not commenced until LAME 1 returned to work, 2 days after the aircraft had departed.
Although the task procedure was followed and certified, neither AME 2 nor LAME 1 observed the tool during their foreign object inspections. Upon the initial instance that the tool was identified as missing, the lost tool procedure should have been commenced. The individuals that were directly involved in the task proceeded onto rostered days off without returning the tools; ownership of the tooling and subsequent responsibility for initiating the lost tool procedure did not occur until their return to work.
The service engineer, as required by the internal procedure for the issue of a CRS, was to verify the whereabouts of any tooling listed on the tooling report and, if the tool could not be located, they were to conduct the lost tool procedure. The service engineer did not review the tooling report during CRS certification and did not commence the lost tool procedure.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the foreign object debris event involving Airbus Industrie A380-842, VH-OQI, at Los Angeles International Airport, United States, on 1 January 2024.
Contributing factors
An aircraft maintenance engineer and a licenced maintenance engineer did not observe an engine turning tool that was left in the low-pressure compressor case during their foreign object inspections after maintenance on the engine.
The lost tool procedure was not commenced by the involved aircraft maintenance engineers when the tool was identified as missing.
The service engineer certified a certificate of release (CRS) with the tool unaccounted for. As a result, the aircraft flew 34 cycles and 293.74 hours with the turning tool in the outboard left engine low-pressure compressor.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Qantas Engineering
Consistent with the application of its safety management system, Qantas advised that the following actions were taken following this incident.
On 2 January 2024, a Qantas Engineering internal incident report was raised. This advised that staff were briefed on the importance of ensuring that all tooling is returned and actioned by the tool store personnel.
On 4 March 2024, the executive manager for Qantas Engineering released an internal safety directive for immediate action requiring all Qantas Engineering employees to meet the requirements of tooling control without exception.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Qantas Airways Limited engineering staff.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Qantas Airways Limited
service engineer
Civil Aviation Safety Authority.
A submission was received from Qantas Airways Limited.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Qantas Engineering is the engineering department of the Qantas group.
[2]An item that is administratively allocated to an individual and an aircraft to track its location when in use.
[3]A storage location in the hangar where task specific and specialist tooling is kept and managed by tool store personnel.
[4]A tool designed to pass through the low-pressure compressor blades from the front of the engine allowing the maintainer to manually rotate the intermediate-pressure compressor.
[5]This report is a snapshot of the tool store inventory at the end of the shift, and captures tooling that has not been returned, to whom that tool is assigned and to what aircraft it is assigned to.
[6]A computer-based maintenance management system that is used to schedule and track all aspects of maintenance conducted on company aircraft, including managed tooling.
[7]Last light at Los Angeles on 6 December 2023 was 1710.
[8]Due to the critical nature of certain aircraft systems, such as engine and flight control systems, an inspection is required from a suitably qualified and authorised person.
[9]A second inspection is applied as a further risk control for critical system maintenance from a suitably qualified and authorised person that has not been directly involved in the conduct of the task.
[10]A coordination certification that verifies that any maintenance conducted since the last flight was completed and that the aircraft is ready for flight.
[11]The tool is accounted for but not available for use pending investigation.
[12]An area vital to the conduct of flight, such as flight control areas, engines and landing gear wheel wells. Any tool remaining in that area may impact the safety or controllability of the aircraft.
[13]An area that is not vital to the conduct of flight, such as cabin area and cargo holds. Any tool remaining in that area will not affect the safety or controllability of the flight.
[14]Verify is listed in the procedure as meaning: to confirm that tasks have been completed by sighting evidence, such as certified technical logbooks, electronic logbooks, or task card entries.
Occurrence summary
Investigation number
AO-2024-006
Occurrence date
01/01/2024
Location
Los Angeles International Airport
State
International
Report release date
14/11/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Foreign object damage / debris, Powerplant/propulsion - Other
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Airbus
Model
A380-842
Registration
VH-OQI
Serial number
55
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 17 November 2022, the flight crew of a Beech 1900D aircraft, registered VH-NYA, refuelled then boarded passengers at Fortnum Aerodrome for a flight to Perth, Western Australia. On the gravel-surface apron, there were pieces of conveyor-belt matting fixed to the ground to allow engines to be operated with minimal propeller damage.
The crew started both engines and taxied the aircraft to an adjacent parking area to allow another aircraft to access the refuelling truck. The crew positioned the aircraft propellers over the matting to complete pre-flight checklists. On completion of the checklists, the crew applied engine power to taxi to the runway.
Immediately there was a loud bang and severe vibration. The captain observed that the left propeller was damaged and shutdown the engines. The passengers were disembarked and escorted of the apron. There were no injuries.
What the ATSB found
As the flight crew was conducting pre-take-off checks, the end of conveyer belt matting under the left propeller was drawn into the propeller arc, resulting in a sheared propeller blade and vibration damage to the aircraft.
The conveyer belt matting installed on the aerodrome apron was a non-standard method to prevent propeller damage and was not subject to any installation specifications or inspection requirements.
What has been done as a result
The aircraft operator requested that the aerodrome operator remove the conveyor belt strips from the aerodrome apron, which was carried out.
Safety message
As this occurrence demonstrates, the consequences of a propeller strike can be serious, and operators of aircraft and aerodromes are advised to review the use of any non-standard surfaces for aircraft movement areas.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 17 November 2022, Penjet was operating 2 Beech 1900 aircraft on mine personnel transfer flights from Perth, Western Australia to Fortnum Aerodrome and return.
Fortnum Aerodrome has a gravel runway, taxiways, and parking area. In the parking area, there were designated parking areas with pieces of conveyor-belt matting fixed to the ground to allow engines to be operated with minimal propeller damage from loose gravel.
VH-NYA was the first to arrive at Fortnum and the flight crew parked the aircraft near the fuel truck to allow refuelling. After refuelling and boarding the passengers, the crew started both engines and taxied the aircraft to one of the designated parking areas to allow a following aircraft to access the fuel truck.
The crew positioned the aircraft propellers over the matting to complete pre-flight checklists. This was in accordance with operator instructions to prevent stone damage to the propeller blades. On completion of the checklists, the crew applied engine power to taxi to the runway.
Immediately there was a loud bang and severe vibration. The captain observed that the left propeller was damaged and shutdown the engines. The passengers were disembarked and escorted off the apron. There were no injuries.
The aerodrome manager, who witnessed the event, advised that the propeller picked up a corner of the matting and one propeller blade was ejected about 50-100 m in the air. The blade landed on the apron about 10 m in front of the other aircraft parked near the fuel truck.
Figure 1: Damaged aircraft and dislodged matting
Source: Westgold Resources Ltd (cropped by the ATSB)
Figure 2: Dislodged inner matting
Source: Penjet (cropped by the ATSB)
Context
Aerodrome information
Fortnum Aerodrome was operated by Westgold Resources Limited in support of their nearby gold mining operation. The aerodrome had been renovated in 2019 under the supervision of an aerodrome consultant. Although the aerodrome was uncertified, the operator had processes for daily and weekly aerodrome inspections by trained aerodrome reporting officers (AROs).
On the morning of 17 November 2022, the ARO conducted a daily inspection of the aerodrome and completed the associated checklist form. All of the apron (parking and movement area) items were annotated as meeting the standard.
The daily apron assessment items included, ‘no loose material or debris on apron or flanks’ but did not include reference to the mats. There was also no reference to the mats in the weekly inspection checklist.
The mats had been installed by the aerodrome operator about 3 years previously in response to a request from the aircraft operator. There was no record of any technical consideration of mat security. The matting involved in this occurrence was in 3 sections and held down by large nails between 200–250 mm length. The outer belt was newer than the inner belt and its end was nailed down at the corners and the middle (Figure 2). The end of the inner belt had been nailed only at the corners. A white line had been applied to the centre of the matting, which was used by the crew to position to the aircraft.
According to the aerodrome operator, there was no record of any communication between the aircraft operator and the aerodrome operator about the condition of the mats. The aerodrome manager recalled that on one occasion a mat was dislodged by twisting associated with aircraft wheel movement. The captain of VH-NYA advised that previously mats had been reported coming loose and these had been resecured.
The aerodrome operator engaged the aerodrome consultant to conduct annual aerodrome audits. In the audit prior to the occurrence, on 11 February 2022, the consultant found that the aerodrome was in a safe and serviceable condition, and the apron was in good condition. There was no reference to the presence of the mats or their condition.
The consultant advised that conveyer belts had been used in a similar way on the movement areas of other aerodromes of comparative size to Fortnum Aerodrome and some certified aerodromes where larger aircraft had been operated. Although the consultant had heard that incidents had occurred, no record of a similar occurrence was found and the mat coming loose to strike the propeller was a surprise.
In the Fortnum aerodrome risk assessment compiled by the aerodrome operator, foreign object damage was identified as a hazard that was controlled through the daily/weekly inspections, restricted airside access, and monitoring during aircraft movements.
For reference, the regulatory guidance for inspection of certified aerodromes (AC 139.C-03v1.0) specified that serviceability inspection of the apron should check the surfaces, including the aircraft parking positions for surface break up and foreign object debris (FOD).
Aircraft damage
In addition to the detached propeller blade (Figure 3), other damage included:
another propeller blade snapped approximately 250 mm from the blade tip
left engine propeller governor control arm fracture, with associated damage to top forward cowling
buckling to the left engine firewall
cracking to the nacelle structure adjacent to the left engine mount.
Figure 3: Propeller hub and detached propeller
Source: Westgold Group
Aircraft operator information
The aircraft operator advised they had been operating 6 weekly flights into Fortnum Aerodrome for about 3 years and pilots had been instructed to park with the propellers over the matting to prevent foreign object damage to the propellers. There was no record provided of any communications between the aircraft operator and the aerodrome operator related to the condition of the matting. The apron matting had not been identified as a risk in the operator’s safety management system.
Other occurrences
A search of the ATSB database was conducted for events between 2012 and 2022 involving mats or conveyor belt used on aircraft movement areas. This identified 3 other occurrences involving a helicopter that resulted in contact between matting and the main rotor blades and 2 aeroplanes that resulted in propeller strikes.
Safety analysis
The operator had been conducting flights into Fortnum aerodrome for about 3 years without any adverse consequences related to the conveyer belt matting on the apron. The flight crew of VH‑NYA were following the operator’s guidance to park over the matting to reduce stone damage to the propellers.
By aligning the centreline of the aircraft with the central white line, the aircraft was positioned with the left propeller disc located above the intersection of two conveyor belts. It is evident that the airflow produced at the propeller tips produced a lifting force on the matting and the corner nails of the inner belt were not sufficiently secured to hold it. As a result, the corner of the belt was drawn into the propeller arc and one propeller blade was sheared off near the hub and another blade was damaged. With one blade detached the propeller was severely unbalanced and generated significant engine vibration that damaged the aircraft.
Although it is not possible to establish the condition of the inner belt before the accident, the aerodrome reporting officer and flight crews did not notice anything amiss. If other crews were also using the central white line to position aircraft over this matting, on those occasions one propeller would generally be placed over the intersection of the belts and there might have been progressive degradation of mat security. The crew did not have the opportunity to look at the matting as they might have done before an engine start in the same position.
Additionally, the aerodrome operator’s risk assessment did not identify the matting as a potential propeller strike hazard, nor did the previous audit by the aerodrome consultant. This was probably related to the absence of specifications and specific inspection requirements for the non-standard apron surface. It is also possible that the matting security had deteriorated since the risk assessment and audit were carried out.
As this occurrence demonstrates, the consequences of a propeller strike can be serious, and operators of aircraft and aerodromes are advised to review the use of any non-standard surfaces for aircraft movement areas.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the foreign object damage involving Beech 1900D, VH-NYA on 17 November 2022.
Contributing factors
As the flight crew was conducting pre-take-off checks, the end of conveyer belt matting under the left propeller was drawn into the propeller arc, resulting in a sheared propeller blade and vibration damage to the aircraft.
Other factors that increased risk
The conveyer belt matting installed on the aerodrome apron was a non-standard method to prevent propeller damage and was not subject to any material specifications, installation instructions, or maintenance requirements.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Penjet
Penjet requested that the aerodrome operator remove the conveyor belt strips from the aerodrome apron.
Safety action by Westgold Resources Limited
Westgold Resources Limited advised that the conveyer belt strips, and fixing nails were removed from the Fortnum Aerodrome apron.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
aircraft captain
Fortnum Aerodrome manager
aerodrome operator – Westgold Resources Ltd
aircraft operator – Penjet Pty Ltd
aerodrome consultant
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
aircraft captain
Westgold Resources Ltd
Penjet Pty Ltd
aerodrome consultant
Submissions were received from:
aircraft captain
aerodrome consultant
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Occurrence summary
Investigation number
AO-2022-059
Occurrence date
17/11/2022
Location
Fortnum Aerodrome
State
Western Australia
Report release date
30/05/2023
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Foreign object damage / debris
Occurrence class
Accident
Aircraft details
Manufacturer
Beech Aircraft Corp
Model
1900D
Registration
VH-NYA
Serial number
UE4
Aircraft operator
Penjet Pty Ltd
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
On 27 October 2017, at about 1900 Co-ordinated Universal Time,[1] a Jetstar Airways Airbus A320 aircraft, registered VH-VGY, was being prepared for a scheduled passenger service from Auckland International Airport, New Zealand to Sydney, Australia. The captain was designated as the pilot flying and the first officer was the pilot monitoring.[2]
At about 1909, the leading hand had finished loading the last container into the aircraft hold and was organising his paperwork. As it was raining, he decided to put the clipboard in the right engine (No. 2) cowling to stop his paperwork from becoming wet and blown by the wind, with the intention to retrieve it later. The leading hand went to the flight deck, gave some paperwork to the flight crew, and returned to the ground to organise the aircraft’s push back.
At about 1919, the dispatcher cleared the ground and servicing equipment from the aircraft and conducted the ‘duty of care’ walk-around. During the walk-around, she noticed the clipboard in the right engine and thought that the leading hand would return for it, so she continued with the walk-around. Soon after, the engines reportedly started normally.
At about 1925, when the aircraft was taxiing, the leading hand realised his clipboard with the paperwork was missing and thought the dispatcher had the paperwork. The leading hand asked the dispatcher about the clipboard and she mentioned she saw it in the right engine during the walk-around. The ground crew returned to where they were preparing the aircraft and noticed paper debris on the ground. The ground crew organised for their operations area to contact the flight crew.
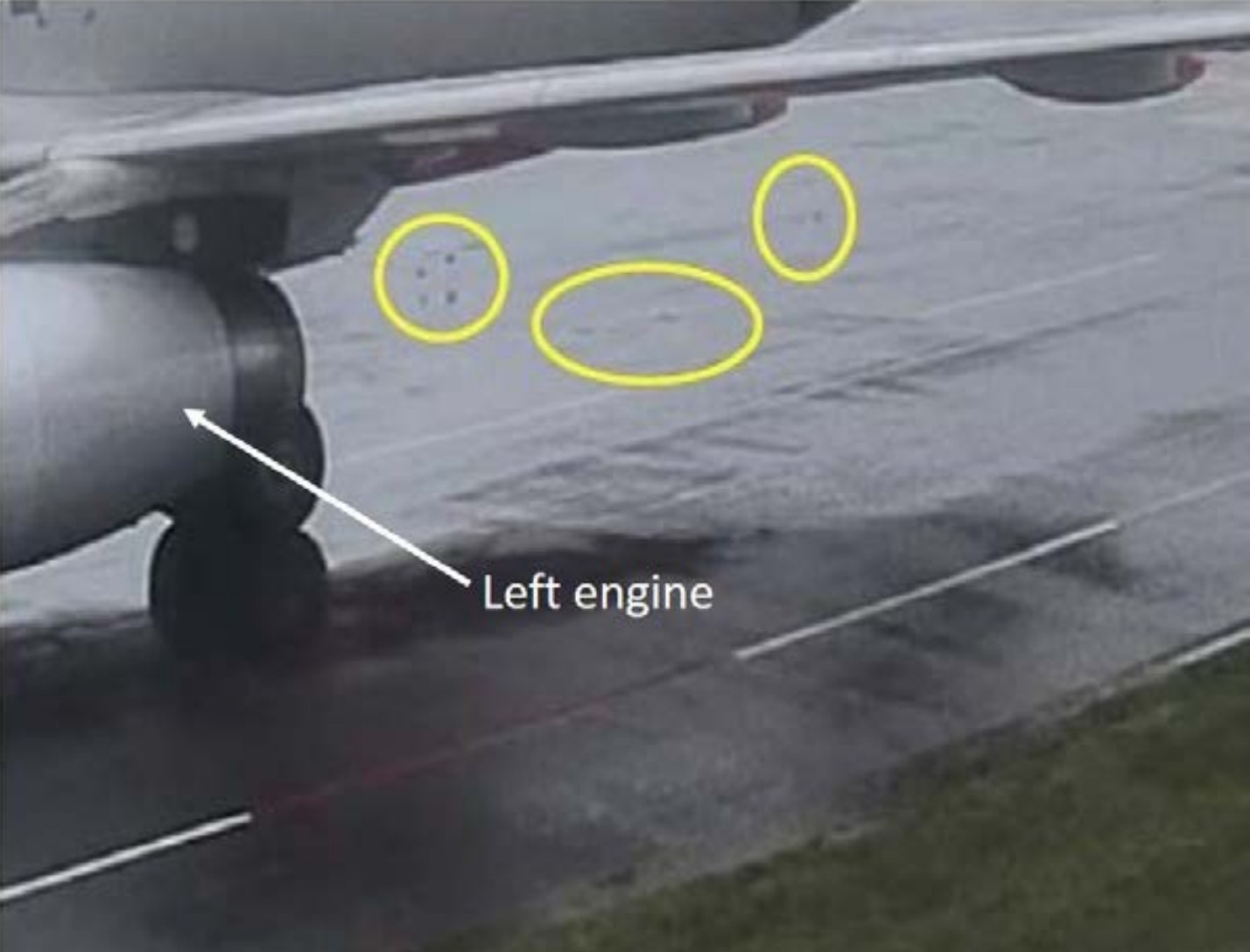
At about 1937, the aircraft departed. Shortly after, when on climb through flight level[3] 150, the flight crew received a radio call from the Auckland Approach air traffic controller to contact the surface movement controller. The captain handed control of the aircraft to the first officer and contacted the surface movement controller who advised that the ground crew had lost their paperwork and it may have been placed on the engine. The captain requested further information about the paperwork, specifically whether the paper was on top of the engine or inside the inlet. The flight crew checked the engine instruments and there were no abnormal indications. The surface movement controller confirmed that the paperwork was placed within the inlet and paper debris was found on the tarmac (Figure 1). The captain then contacted the company engineer at the airport and asked whether it was just paperwork or a clipboard with a metal clip. The engineer advised that a piece of sheared metal had been found. The flight crew decided to return to Auckland.
After landing at about 2048, the engine was inspected by engineers and paper was found throughout the engine. They also found minor damage to an engine fan blade and attrition liner.[4]
Figure 1: Foreign object debris on the ground behind the aircraft (circled)
Source: Aerocare, modified by the ATSB
Additional comments
The leading hand stated that, due to the wind and rain, he felt the need to shelter the paperwork. Normally, staff use the pushback tractor for shelter during adverse weather and to prepare paperwork for the flight. There is a metal box on the loader to store the folder. However, as the pushback tractor was not yet present at the bay, he used the engine cowling. He recalled that he did not feel pressured to rush the departure.
The dispatcher stated that she did not view the clipboard as a foreign object as it belonged to the leading hand and had the paperwork for the flight. She assumed that the leading hand would retrieve it later, prior to engine start-up.
The captain stated that, to obtain more information about the incident, numerous calls were made to other agencies, which took considerable time. Further, due to poor communications, he was unable to contact the operator’s maintenance controller to discuss the engine’s status.
Procedures
The internal investigation into the incident by the ground handling operator, Aerocare, noted that the Jetstar Airways operational manual detailed the responsibilities of the dispatcher when conducting the ‘duty of care’ walk-around and provided a table of the steps involved for this process. While there was no specific requirement to check the engine cowlings/intakes for foreign objects, the manual stated that all staff operating near the aircraft were to be constantly observant for abnormalities and to report these to the leading hand or supervisor prior to the aircraft departing.
The investigation also noted that there was no procedure for the ground crew to establish communications with the flight crew in the event of a non-normal or emergency situation, either prior to or after the aircraft had departed. Further, there was no guidance on how paperwork was to be prepared and managed by ground crew during adverse weather conditions.
Previous occurrences
A search of the ATSB database found the following occurrence where a foreign object has been left on an aircraft:
On 3 November 2015, the pilot conducted a maintenance test flight in a Eurocopter AS365 N3 helicopter, registered VH-WPX, at Jandakot Airport, Western Australia (ATSB investigation AO-2015-127). During the post-flight inspection, following this test flight, a licenced aircraft maintenance engineer noticed two large gouges to the leading edge of one of the main rotor blades. A spanner that had been used during the track and balance related adjustments could not be located. It was later located on an adjacent taxiway about 43 m from the hangar. Due to the scuff marks and scratches found on the spanner, it was determined that it had been left in the rotor head area and was likely ejected during engine start up.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
While preparing the aircraft for departure, the leading hand placed a clipboard in the right engine, which was subsequently ingested during start-up.
During the walk-around, the dispatcher noticed the clipboard in the right engine, but believing it would be retrieved prior to the aircraft departing, the dispatcher did not notify the leading hand or supervisor of the foreign object debris as per company procedures.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety notices
Both Jetstar Airways and Aerocare have released a notice, which outlines that foreign object debris also includes items accidentally left behind. It further states that engines are not to be touched or used for the placement of items, and emphasises the responsibilities of ground crew to manage foreign object debris by clearing them and reporting their presence to other crew.
Updated procedures
As a result of this incident, Jetstar Airways released an updated aircraft dispatch procedure, which included:
a specific warning about not placing items in the engine cowling
improved detail around checks and responsibilities
a section on emergency and non-normal procedures
detailing methods for re-establishing communications between ground crew and flight crew such as visually gaining the attention of the flight or contacting them via radio.
Safety message
The presence of foreign object debris poses a significant threat to aircraft safety. It has the potential to cause aircraft damage during critical phases of flight, costing airlines and airports millions of dollars each year. This incident demonstrates the effect foreign object debris has on aircraft operations and emphasises the importance of not placing objects in aircraft engines. It further highlights that all staff operating near aircraft are responsible for reporting any non-normal events they encounter. It should not be assumed that others will perform a task where a hazard has been identified. Assuming other people will undertake a task, such as removing a hazard increases the risk of the task not being completed.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 3 November 2015, at about 1400 Western Standard Time (WST), a pilot of a Eurocopter AS365 N3 (Dauphin), registered VH-WPX, conducted a maintenance test flight at Jandakot Airport, Western Australia.
The test flight was the third that day, to conduct track and balancing of the main rotor, following reports of vibration.
During the post-flight inspection following this test flight, one of two Licenced Aircraft Maintenance Engineers (LAMEs) involved in the test flight, noticed two large gouges to the leading edge of one of the main rotor blades (Figure 1).
A spanner that had been used during the third track and balance related adjustments could not be located. It was later located on an adjacent taxiway about 43 m from the hangar. Due to the scuff marks and scratches found on the spanner, it was determined that it had been left in the rotor head area and was likely ejected during the aircraft start up.
Figure 1: Damage to leading edge of a main rotor blade on VH-WPX
Source: Aircraft operator
Events leading up to the foreign object damage
Prior to the event, the main rotor head bolts (bolts) had approached their scheduled life limit. So on 26 October the maintenance organisation replaced the bolts, in accordance with the Airbus Helicopters AS365[1] Maintenance Manual. The maintenance manual required that a main rotor blade track and balance be performed following this replacement.
Helicopter vibration was automatically monitored using the Honeywell Chadwick Helmuth Vibration Expert (VXP), which was installed in the helicopter. The VXP data generated was automatically sent to an external diagnostics organisation for trend monitoring. Additionally, LAMEs could access this data for rotor track and balancing requirements.
The operator advised that when the bolts were replaced, a work pack[2] was generated for the task.[3] Prior to the required track and balancing flights, one of the two LAMEs tasked with the job (LAME 2), transferred the main rotor blade track and balancing procedure to the aircraft technical log[4] and ground run/test flight sheet.[5]
However, due to non-availability of flight crew, the test flights were not conducted until 28 October. The ground run/test flight record indicated that the results of the track and balance procedure were satisfactory, and the aircraft was returned to service the same day.
The aircraft continued in service, and flew about 14 hours between 28 October and 3 November. During this period, the maintenance organisation reported that a 4P vibration[6] (within manufacturer tolerance) was being monitored and a pilot advised of a vibration. However, this information was not formally recorded on technical documentation.
On 2 November, the external diagnostics company that monitored the aircraft VXP data, advised the operator of a rising vibration trend. This rising vibration trend was still within tolerance, and supported the pilot reported vibration that was being monitored by the maintenance engineers. At this time, the Chief Engineer advised the other LAME (LAME 1) to conduct further main rotor track and balancing during the following few days, subject to pilot availability.
Further track and balancing, and smoothing, was conducted on 3 November. The two LAMEs’ recollections and observations of the task are detailed below.
LAME 1
Reported that a work pack had not been created for the subsequent track and balancing job, however, they (LAME 1) endorsed the ground run/test flight sheet and annotated the corresponding number on the technical log prior to the test flights.
Reported that the Chief Engineer had discussed the required maintenance with them.
Reported that although not formally assigned the role, thought they were most likely the Job Coordinator.
LAME 1 had tagged out a socket and a screwdriver. Prior to each test flight, LAME 1 placed the tools being used into a metal tray, and then placed the tray on top of the toolbox. As the job was ongoing, there had been no documented requirement to place the tools back into their assigned location. LAME 1 had visually checked the tools in the metal tray prior to the third test flight, but did not use the tag procedure (refer Tool Control Procedure).
LAME 1 had performed adjustments to the main rotor pitch links and blade weights, and had asked LAME 2 to perform an independent inspection[7] of the work after the second test flight. LAME 1 reported that the request had been for LAME 2 to both perform the independent inspection, and to check that no tools had been left on the helicopter.
LAME 1 was not aware that the spanner that they had been using had been left on top of the main rotor blades.
LAME 2
Also reported that a work pack had not been created for the job.
Stated that prior to the third test flight, they (LAME 2) had completed an independent inspection of the maintenance tasks, performed by LAME 1.
LAME 2 did not notice that the spanner had been left on top of a main rotor blade. They noted that the blade was very flat, and that it would not be possible to see it on top of the rotor blade from the ground.
LAME 2 had tagged the spanner and several other tools out earlier in the day. The tools had not been returned to the toolbox during the day, as it was expected that further adjustments would be required.
Pre-flight inspection
The daily inspection had been certified in the aircraft technical log by an engineer prior to the first flight. Additionally, the pilot reported conducting a ‘walk-around inspection’ in accordance with the flight manual procedures. The pilot was aware that flight control maintenance had been conducted by the engineering group. The pilot signed the aircraft technical log and ‘accepted’ the aircraft prior to each of the three test flights.
The pilot reported that the aircraft handled normally throughout the three test flights.
Tool control procedure
While there was a practice of tool control in place prior to the incident, formal procedures had not been documented and incorporated in the maintenance organisation manual (MOM).
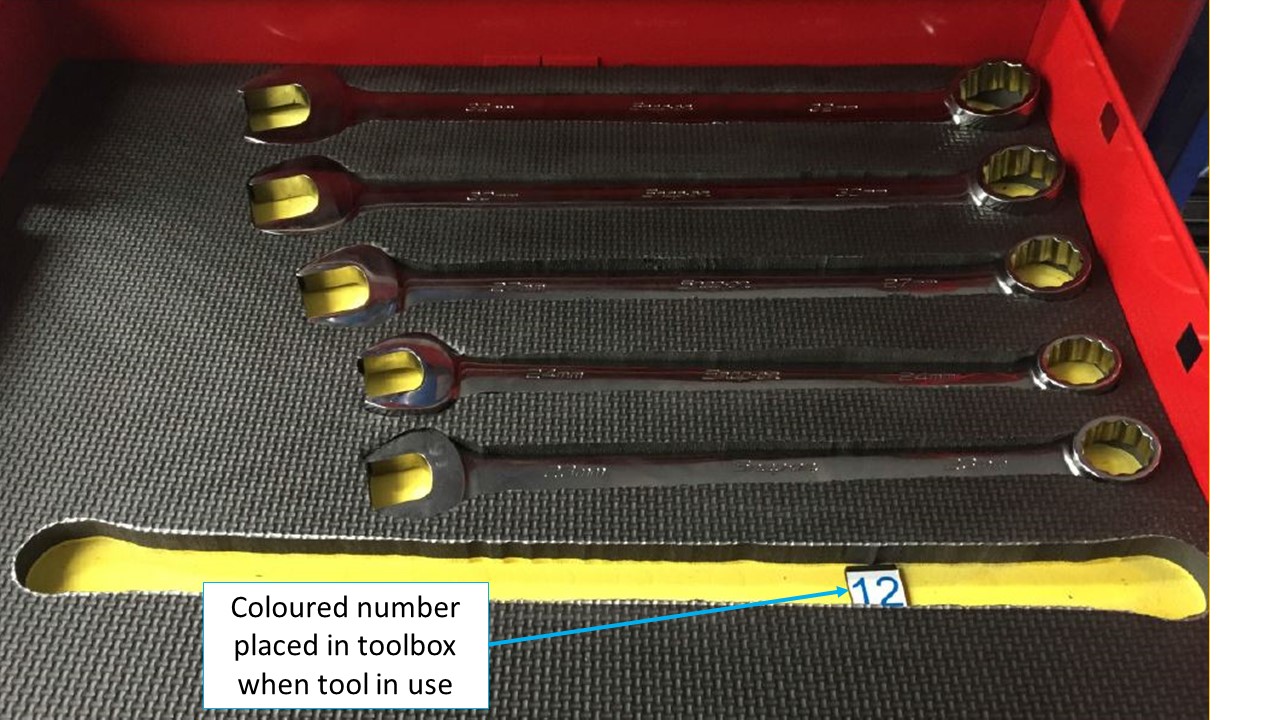
The tool control practice in place, prior to this incident, required that that each tool removed from the toolbox be tagged out by the person removing the tool. Each engineer was assigned a series of numbered tags of a certain colour, and the tag was placed into the ‘empty’ location (cut out) of the tool being used (Figure 2). A review of both the toolbox and the engineer’s assigned tags would quickly identify if any tools were still in use.
Figure 2: Tool control procedure showing coloured number replacing tool in use by the engineer assigned the blue coloured tags
Source: Operator
Operator procedures
The MOM stated that induction training of all staff shall be carried out on all new maintenance staff. This training was to provide staff with sufficient information to enable them to integrate into the company and to ensure compliance with the policies and procedures of the organisation. However, there was no written record of any such induction training having taken place.
ATSB comment
The organisation involved conducted a thorough internal investigation after this occurrence. There were a range of other issues identified in regard to training and documentation procedures, and the company have initiated remedial action in all these areas. These other issues do not fall within the scope of this investigation.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
The operator
As a result of this occurrence, the aircraft operator has advised the ATSB that they are taking the following safety actions:
Tool control procedure
A tool control procedure was in place at the time of the incident, however, the procedure had not been documented in the MOM. Additionally, there was no documented procedure requiring the tools to be returned to the toolbox prior to the aircraft being started.
The operator will incorporate the tool control procedure into the MOM. This procedure requires that all tools used during any aircraft maintenance are returned to the tool storage location prior to any of the company aircraft being started.
A tool control procedure will be implemented for any maintenance that occurs away from the main base. Additionally, a tool control procedure will be implemented to ensure external maintenance providers (for example avionics specialists) adopt the company tool control procedure.
Training for maintenance personnel
All maintenance personnel be provided with sufficient training and information to enable them to understand the workings of the organisation, its policies, manuals, procedures and their individual responsibilities.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
The Australian Transport Safety Bureau did not conduct an on scene investigation of this occurrence. The information presented below was obtained from information supplied to the Bureau.
The crew of a Boeing 737, registered VH-TAH, reported that, on 15 May 2004, during the take-off roll on runway 34 Left at Sydney Kingsford Smith Airport, they felt shuddering from the nose wheel. The crew of a subsequent landing aircraft reported debris on the runway. An inspection found tyre segments and pieces of aircraft structure. The 737 crew were notified and elected to return for a landing.
An investigation by the operator found that the 737 struck a Boeing 747 thrust reverser blocker door that had fallen from an aircraft that had previously used the runway. That door damaged the 737 nose landing gear tyre and gashed the aluminium skin of the fuselage. The investigation was unable to identify the 747 and whether the loss of the door occurred during take-off or landing.
This was the second reported occurrence of a blocker door falling from a 747 aircraft. At least two 747 operators (one Australian and one international) are known to have found that an earlier 747 blocker door modification had a deficient metal/composite bond. The Australian 747 operator has initiated a project to scope and implement a new modification program to repair or replace all blocker doors.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation.
What happened
On 20 June 2021, the Eurocopter AS350 helicopter was involved in lifting operations transporting materials to a worksite on Mount Difficult, approximately 38 km south-east of Horsham, Victoria. The lift operations were conducted by a single pilot, using a 100 ft line, and supported by a second pilot acting as ground crew. The ground crew member was also an experienced long line pilot. The two crew had swapped roles and worked extensively together throughout the project.
The pilot had completed eight lifts that day and at 1350 local time, after all required lifts had been completed, the helicopter returned to the Mount Difficult Helicopter Landing Site (HLS) near the worksite. The landing site was a confined area on the edge of a rock ledge with trees and shrubs nearby (Figure 1). The established procedure was to lower the remote hook and line to the ground before releasing the line from the belly of the aircraft at the lowest safe height. The helicopter would then reposition for an approach. This allowed the helicopter to approach the HLS without the 100 ft line attached.
The pilot placed the line to the south of the HLS and re-positioned to land. Most of the line was lying on the ground, but a small section of the line was suspended in a sapling 10–12 ft right front of the aircraft nose. The aircraft landed clear of the line, and after receiving confirmation from the ground crew member that the landing position looked safe, the helicopter was shut down.
As the engine spooled down the ground crew member commenced sorting and coiling the line into the back of the aircraft. This placed tension on the line between the coiled section in the helicopter and the looped section in the tree, thereby bringing the line into the path of the rotor disc. This was caught by a blade and subsequently entangled the rotor head. The line pulled the ground crew member’s arm upwards, snared their lower leg and body, before pulling them sideways along the ground.
The crew member sustained minor bruising to their face, right elbow, left leg and foot and was later cleared of concussion or serious injury. The line was later found to have wrapped around the mast, resulting in minor damage to the swashplate, mast, rotor head and main rotor blades.
Figure 1: Mount Difficult HLS
Source: Supplied by operator, annotated by the ATSB
Safety action
The ATSB has been advised the operator has implemented the following safety action in response to this occurrence:
A safety briefing was conducted with all company pilots, which included an incident analysis, review of procedures and safety measures. A new requirement was introduced that now states that objects should not be raised above shoulder height while under the rotor disc.
The Flying Operations Manual and relevant Aircraft Operations Plans (including Daily Safety Briefing and Emergency Plan) were updated to specifically clarify that:
movement of equipment, including aerial work equipment, into and out of aircraft should be conducted while the rotor is stationary unless strictly necessary; and
coiling of lines and the assembly of equipment must be completed outside the rotor disc unless the rotor is completely stationary.
Safety message
Despite having produced detailed safety assessments and extensively documented operating procedures, an unintentional decision error resulted in a serious incident. Operators involved in complex operations need to remain vigilant when monitoring potential hazards around the area of operations, especially when equipment is to be stored or positioned close to operating aircraft.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation.
What happened
On 27 March 2020 at around 1822 Eastern Daylight-saving Time, a Diamond DA 40 was being prepared for a training flight. There was a student and instructor on board.
During the pre-flight inspection, while the student was conducting the flight controls free and correct movement check, he observed abnormal elevator movement. The elevator required more force than usual to move, and was unable to be deflected through its full and normal operating range. The student notified the instructor of the issue, the flight was cancelled and the aircraft was deemed unserviceable.
Engineering inspection
The engineers removed the right pilot seat to examine the flight control mechanism. They found a plastic navigation ruler lodged within the elevator push rod mechanism, which was restricting the movement of the elevator. It was determined that the ruler fell between the seat and the centre console in the cockpit.
Figure 1: Navigation ruler lodged in elevator push rod mechanism
Source: Operator’s engineering department
Operator comments
It is important that Diamond DA 40 and DA 42 operators and pilots are alerted to the fact that items and equipment placed on the seat or between the seat and centre console can, in some instances, work their way down through the narrow gap between the inner seat edge and the centre console (Figure 2). This could allow thin items and equipment to find their way into the area under the seat which contains the elevator and aileron control push-rods.
Figure 2: Narrow gap between front seats and centre console
Source: Operator’s engineering department
Safety action
As a result of this occurrence, the operator has advised the ATSB that it is taking the following safety actions:
Providing a briefing and the publication of photos to all instructors for awareness.
Placing a renewed emphasis in pre-flight briefings to solo students on objects taken into and out of the aircraft, to reduce the instances of foreign object debris (FOD) being left in the cockpit.
Requiring that all navigation equipment and similar items carried in aircraft be labelled with the owner's name. This will increase accountability and source tracing when FOD is located and help to ensure pilots place the aircraft unserviceable for a FOD inspection if an item is missing at the end of a flight.
Safety message
This incident highlights the importance of ensuring that all pre-flight checks and procedures are carried out comprehensively and systematically. It also serves as a reminder for flight crew to ensure that any misplaced or missing items from their flight bag be identified and located. If unable to locate any missing items, this information should be reported promptly so an aircraft inspection can be carried out.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation.
What happened
On 22 March 2020 at about 1030 Western Standard Time, a privately chartered de Havilland DH-82 Tiger Moth commenced take-off for a local flight. As the aircraft became airborne, the aircraft’s attitude pitched up with the high take-off power setting and the pilot was unable to move the elevator control forward. The pilot performed a precautionary landing on the remaining available runway by adjusting power to control aircraft pitch attitude.
The aircraft was taxied back to the parking bay and secured. Upon examination, the pilot observed a hand-held inspection mirror lodged between the elevator control and the frame of the aircraft.
Figure 1: Hand-held inspection mirror lodged in elevator control
Source: Operator
Operator’s investigation
The mirror was not visible during a normal pilot pre-flight inspection and the elevator had full and free movement during both the pre-flight inspection and the pre-take-off checks. The operator concluded that the mirror was therefore inside the cockpit in a position not easily visible prior to the flight. It appeared to have moved during the take-off run into the position inhibiting elevator control.
The operator held a workshop safety briefing into the incident but was unable to confirm how the mirror got into the aircraft.
Safety message
This incident highlights the importance of effective tool control and ensuring any items that are unaccounted for are located. Loose items must also be secured to prevent interference with aircraft controls.
The presence of foreign object debris can pose a significant threat to aircraft safety and has the potential to result in damage during critical phases of flight.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.