Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 12 April 2026, a student pilot, the sole occupant of a Cessna 172R, was conducting solo circuits at Archerfield Airport, Queensland. Prior to this, dual training (with an instructor) was conducted for about half an hour. The flight was the third time the student had flown solo, and an instructor was responsible for supervising their flight. There was a quartering headwind at about 8 kt.
The solo circuits were initially conducted on runway 28L prior to the pilot requesting a ‘full-stop landing’1 to complete the flight. At this point the air traffic controller (tower) changed the runway assignment to runway 28R.
The pilot then conducted three unsuccessful landing attempts to runway 28R. Each of these attempts resulting in the aircraft either ‘bouncing’2 or ‘porpoising’3 followed by the student conducting a go-around. The student pilot reported that during one of the attempted landings a significant ‘bounce’ occurred.
The controller reported to the operator that the second landing attempt involved the aircraft porpoising, resulting in a tail strike and what appeared to be a possible propeller strike.
The supervising instructor reported observing that the third landing was a hard landing. noting the nose wheel came into contact with the runway first. The earlier landing attempts were not fully visible by the instructor due to them not having a clear line of sight.
After the third attempt to land, the supervising instructor contacted the air traffic control tower and communicated directly with the student, via the tower frequency, to provide the student verbal assistance, helping to facilitate a safe landing on the fourth attempt.
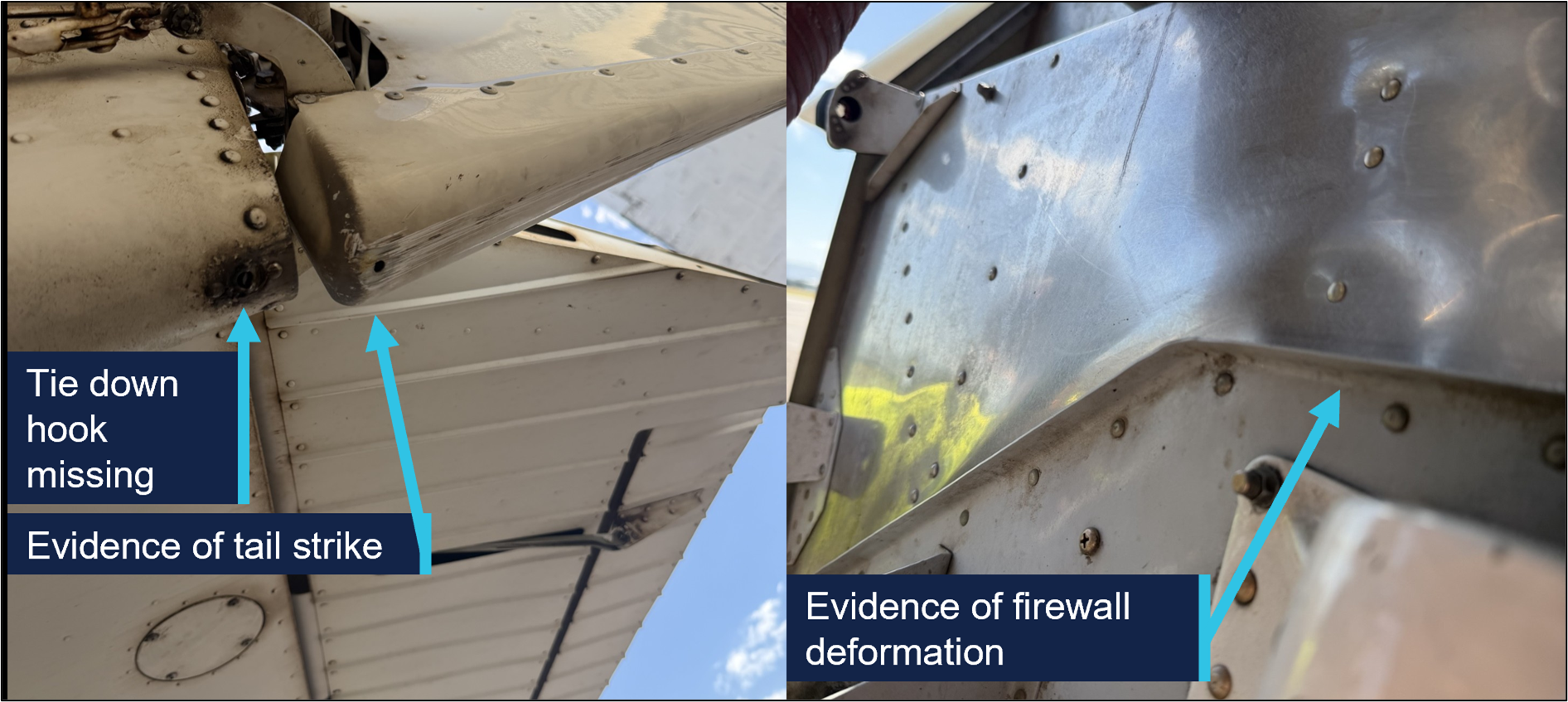
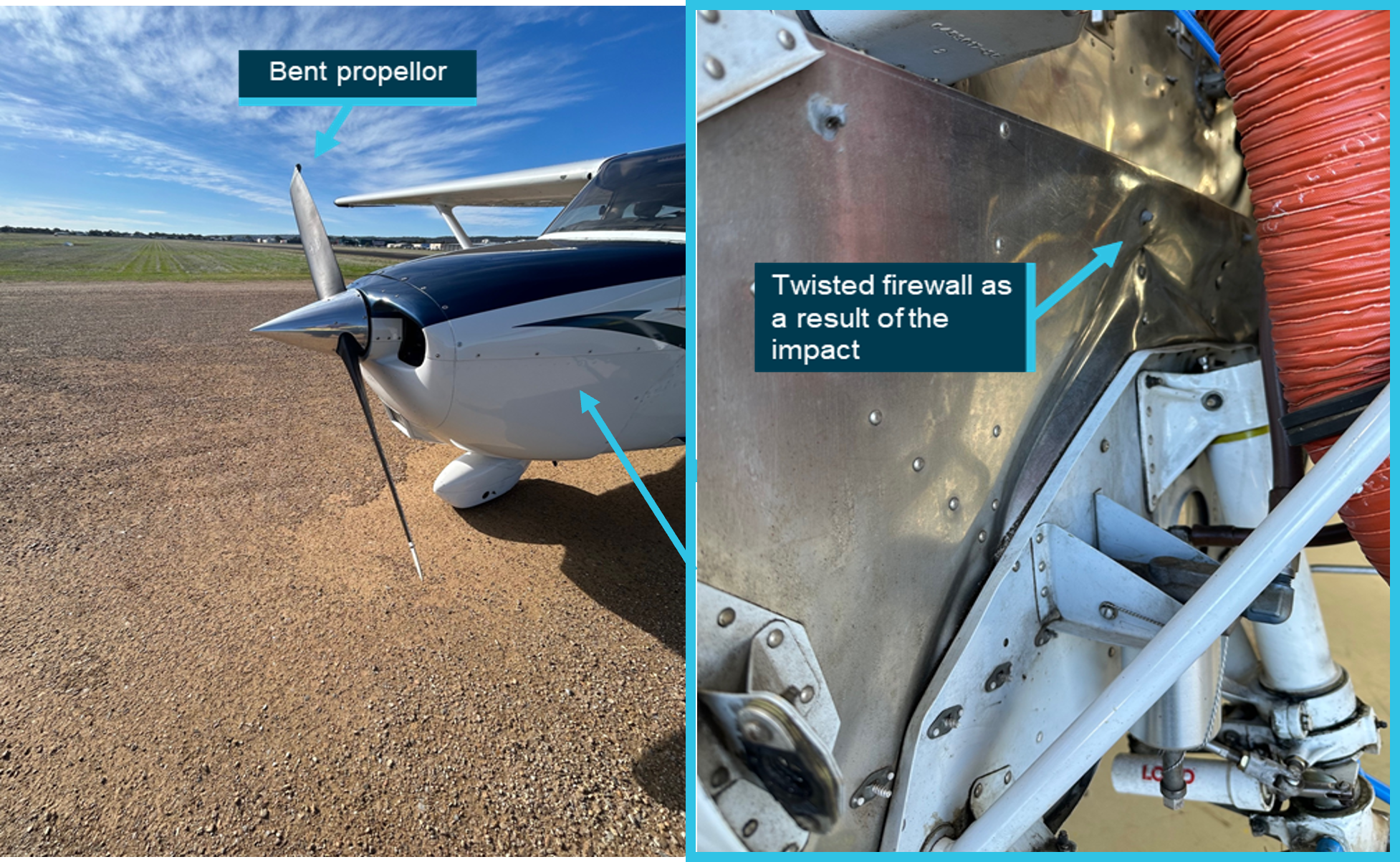
A post-flight inspection of the aircraft by the operator revealed the tail tie-down hook was missing, with evidence of a tail strike and firewall deformation (Figure 1).
Figure 1: Damage to aircraft
Source: Operator, annotated by the ATSB
Safety message
While conducting training flights, students can experience a high workload, particularly during solo flights and landing. Maintaining a calm mindset is important in order to adjust the aircraft’s profile and airspeed accordingly and determine if a go‑around is necessary.
All pilots, regardless of their experience levels, should be prepared to undertake a go‑around rather than continuing if they are not confident that a successful landing can be achieved. This occurrence also serves as a reminder that after any hard landing or other related incident where the integrity of the airframe or structure may be compromised, an engineering inspection can detect damage that may not be immediately apparent.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
^A ‘full-stop landing’ in pilot training means the pilot does not intend to take off again immediately.
^A bounced landing is a condition where the aircraft lands on the runway, but instead of rolling on the surface after touchdown, it rebounds/bounces off the ground.
^‘Porpoising’ refers to the manoeuvre that can occur after a bounced landing that is improperly recovered, in which the aeroplane comes in nose first setting off a series of cyclic vertical motions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2026-024
Occurrence date
12/04/2026
Location
Archerfield Airport
State
Queensland
Occurrence class
Accident
Aviation occurrence category
Control issues, Hard landing, Missed approach
Highest injury level
None
Brief release date
22/05/2026
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
172R
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Activity
General aviation / Recreational-Instructional flying-Instructional flying - solo
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 16 April 2026, a pilot and passenger on board a Van’s RV-7 departed Archerfield Airport on a private flight to Fig Tree Aircraft Landing Area (ALA), Queensland. The Fig Tree ALA had a 400 m unsealed grass runway at an elevation of 1,600 ft AMSL. The pilot noted that they were conscious of the increased risk of operating into an airstrip with a short runway and had conducted short field landing practice at Archerfield the day prior.
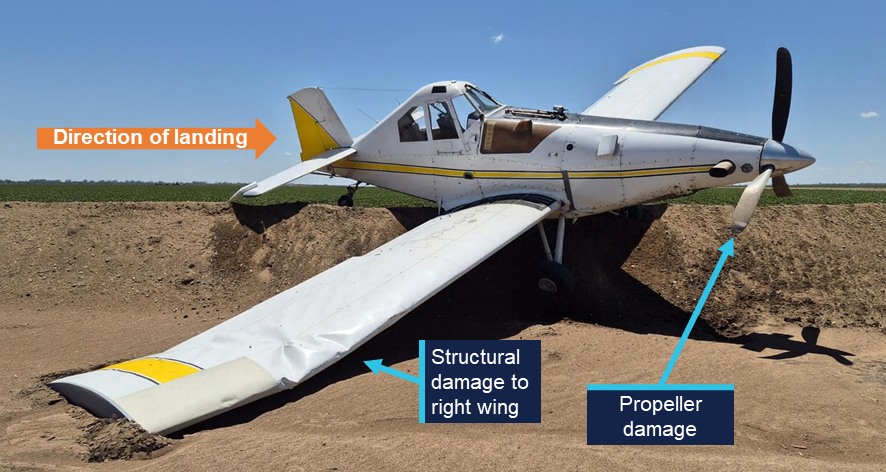
After arriving overhead Fig Tree airfield, a standard field inspection and a go-around was conducted to gain familiarity with the runway characteristics, as was required by the field operator. At 1110 local time, the aircraft commenced an approach and landing on runway 16. As the aircraft touched down midfield on the runway, the pilot determined that with the remaining landing distance available and the aircraft’s high speed, a go-around was required. During the go-around at approximately 20 ft AGL, the aircraft encountered sink and failed to climb as expected. The pilot made the decision to reduce the power to idle and attempted to conduct an off-field landing. The aircraft subsequently collided with thick shrubbery off the end of runway 16, resulting in substantial structural damage. (Figure 1). Both occupants were uninjured and extricated themselves from the aircraft.
After the occurrence, the pilot recalled that the accident approach was faster than anticipated. The operator determined there were no technical faults with the engine that affected the reduced climbing performance.
Figure 1: Fig Tree ALA
Source: Operator, annotated by the ATSB
Safety message
The margin for error while operating at airfields with short runways is limited and requires pilots to conduct the appropriate short field take-off and landing technique. In the case when an approach becomes unsuitable for a safe landing to occur, it is vital that pilots conduct a go-around as soon as practical.
The occurrence also highlights the importance for all pilots to have a personal minimums checklist that aligns with their individual flying experience. If at any time the conditions exceed these minimums or doubt is experienced, pilots should not continue to land and consider using alternative runways, alternative airfields or returning to the departure location if the available fuel permits.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2026-026
Occurrence date
16/04/2026
Location
Fig Tree Aircraft Landing Area
State
Queensland
Occurrence class
Accident
Aviation occurrence category
Collision with terrain, Control issues, Missed approach
Highest injury level
None
Brief release date
21/05/2026
Aircraft details
Manufacturer
Van's Aircraft
Model
RV-7
Sector
Piston
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational – Sport and pleasure flying – Pleasure and personal transport
Departure point
Archerfield Airport, Queensland
Destination
Irongate/Fig Tree Aircraft Landing Area, Queensland
The ATSB is investigating a flight control issue involving a Beech Aircraft Corp 35-B33, registered VH-NEW, at Griffith Airport, New South Wales, on 11 May 2026.
It was reported that, during the initial climb the instructor and student on board the aircraft detected a reduction of aileron and elevator effectiveness. The student held the control yoke stable while the instructor controlled the aircraft with elevator and rudder inputs and conducted a successful return to Griffith Airport. An engineering inspection later revealed a bolt had been liberated from the control torque link due to a missing split pin.
The evidence collection phase of the investigation will involve examining the recovered components, interviewing witnesses and involved parties, examination of maintenance records, retrieving and reviewing recorded data, and the collection of other relevant information.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Occurrence summary
Investigation number
AO-2026-078
Occurrence date
11/05/2026
Occurrence time and timezone
14:30 Australian Eastern Standard Time
Location
Griffith Airport
State
New South Wales
Report status
Pending
Anticipated completion
Q4 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Evidence collection
Investigation status
Active
Aviation occurrence category
Control issues, Flight control systems
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Beech Aircraft Corp
Model
35-B33
Registration
VH-NEW
Serial number
CD-615
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Activity
General aviation / Recreational-Instructional flying-Instructional flying - dual
The ATSB is investigating a runway excursion and collision with tree involving a GippsAero GA8 Airvan, VH-WSU, at Lindeman Island, Queensland, on 8 March 2026.
During landing on soft and wet ground, the wheels slid and the pilot applied full power to conduct a go-around. The aircraft became airborne after the end of the runway and the landing gear contacted a tree, resulting in substantial damage. The aircraft was flown with reduced performance to Shute Harbour due to the runway condition at Lindeman Island being deemed unsuitable.
The ATSB has completed the evidence collection and analysis phases of the investigation and is drafting the final report.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2026-065
Occurrence date
08/03/2026
Occurrence time and timezone
14:35 Eastern Australia Standard Time
Location
Lindeman Island
State
Queensland
Report status
Pending
Anticipated completion
Q4 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Drafting
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Control issues, Diversion/return, Missed approach, Stall warning
Occurrence class
Accident
Highest injury level
None
Aircraft details
Manufacturer
Gippsland Aeronautics Pty Ltd
Model
GA8
Registration
VH-WSU
Serial number
GA8-17-244
Aircraft operator
Wave Air
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Activity
Commercial air transport-Non-scheduled-Joyflights / sightseeing charters
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 9 December 2025, an Ayres Thrush S2R-T34was being used to conduct agricultural spraying, which involved multiple circuits and landings to pick up and disperse approximately 40 loads.
During landing, before picking up the final load for the day, the pilot observed a vehicle approaching the landing strip towards the loading area. The pilot applied additional braking to avoid a possible collision with the vehicle and the aircraft subsequently veered towards a drainage channel adjacent to the landing strip.
While the pilot monitored the approaching vehicle, the aircraft continued towards the end of the landing strip and the drainage channel. The pilot subsequently attempted to correct the aircraft to remain on the strip however there was insufficient distance and time, and the aircraft entered the channel. There were no injuries to the pilot, and the aircraft was substantially damaged.
Figure 1: Aircraft damage
Source: operator, edited by the ATSB
Safety message
In this occurrence the distraction of the vehicle approaching the landing strip diverted the pilot’s attention from monitoring the landing roll, resulting in a loss of situational awareness.
This type of distraction is more likely to impact performance due to the cognitive demands of one spatial visual scanning task (i.e. monitoring landing roll) being interrupted by another spatial task (i.e. a vehicle moving towards the aircraft’s projected path), particularly during a critical phase of flight where there is very little time to assess the situation.
Concurrent task management depends on the pilot’s ability to effectively prioritise tasks and appropriately time share tasks by rapid switching, whereby attention quickly shifts between tasks. This is essential when the pilot is dealing with multiple tasks, which are all critical to flight safety.
The ability to appropriately prioritise and use rapid switching may be affected by workload and fatigue, which can be a factor during operations involving large numbers of short, similar flights in quick succession. Effective use of rapid switching can also be improved through experience as well as specific task management training.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
The ATSB is investigating abnormal engine indications and ditching involving Bell 206L-3, VH-LMW, 6.5 km west of Horn Island Airport, Queensland, on 6 January 2026.
During climb, the pilot observed uncommanded yaw and fluctuating torque indications. The pilot received a low rotor alert and conducted an autorotation before activating the floats and ditching the helicopter.
The ATSB has commenced the examination and analysis of the initial evidence collected.
To date, the ATSB investigation has included interviewing the flight crew, examination of maintenance and pilot records and other relevant documentation.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Preliminary report
Report release date: 16/04/2026
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 6 January 2026, at about 1406 local time, a Bell B206L-3 helicopter, registered VH‑LMW and operated by Fortescue Helicopters, was returning to Horn Island (Ngurupai) from Sadie’s Beach Helipad, Thursday Island (Waiben), Queensland, after transporting 2 passengers between the outer Torres Strait Islands.
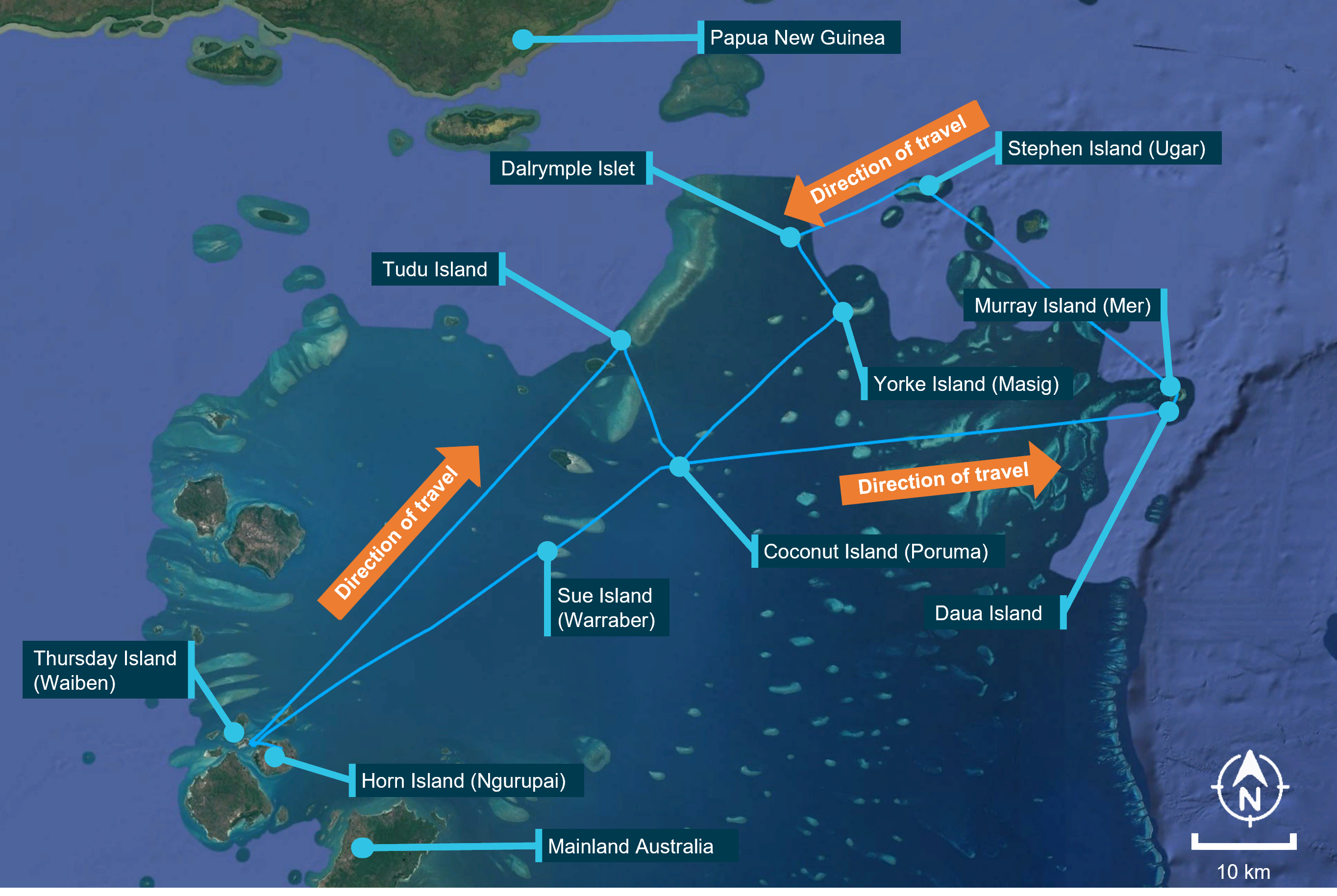
VH-LMW operations that day included 11 sectors, beginning from Horn Island Airport before embarking passengers at Thursday Island at about 0800. Following the departure from Thursday Island, the helicopter tracked and landed briefly at Tudu Island, Coconut Island (Poruma), Daua Island, Murray Island (Mer), Stephen Island (Ugar), Dalrymple Islet, Yorke Island (Masig), Coconut Island and Sue Island (Warraber), before returning the passengers to Thursday Island at about 1400 (Figure 1). The helicopter had completed about 3.2 hours of flying that day prior to the accident flight.
Figure 1: VH-LMW flight track
Source: Google Earth, annotated by the ATSB
On each of the 2 stops at Coconut Island, about 130 km north-east of Thursday Island, the helicopter was refuelled from a company intermediate bulk container (IBC). The pilot reported that after disembarking the passengers at Sadie’s Beach Helipad, Thursday Island (Figure 2), before the re-positioning flight to Horn Island, about 200 lb (114 L) of fuel remained on board.
Figure 2: Location of Sadie’s Beach, Thursday Island
Source: Google Earth, annotated by the ATSB
Following a normal take-off, at about 300 ft over the water, the pilot reported the helicopter made several sudden and violent yawing[1] movements of about 60° to each side, accompanied by a reduction in both engine RPM and rotor RPM. An immediate scan of the engine gauges indicated that the torque gauge was fluctuating between 10–90%. The pilot partially reduced the collective[2] to recover rotor RPM, estimating they had lost about 5–6% rotor RPM at this time, however it continued to decay until the low rotor RPM warning light illuminated.
The pilot initiated an autorotation[3] and activated the pop-out floats at about 100 ft above the water. The pilot reported that the engine had stopped before the aircraft landed on the water.
After landing on the water, the helicopter remained afloat and upright for about 15 seconds, during which time the pilot transmitted a MAYDAY call. They recalled the helicopter then rolled about 120 degrees onto the right side. Images of the inverted helicopter showed the rear right float had detached from the skid tube and the front right float had also partially detached. The pilot reported that the float had pushed against their door which prevented egress from their nearest exit, requiring the pilot to egress through the front left (passenger) door. They then swam away from the helicopter before inflating their lifejacket. The helicopter continued to roll in the water until it became inverted.
A private boat nearby, followed by a police boat, arrived within about 5 minutes to rescue the pilot.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Helicopter) single-engine class, with a low‑level rating. At the time of the occurrence, the pilot’s total flying experience was 1,144 hours with about 300 hours on the Bell 206. The pilot’s last flight review was a proficiency check on 30 October 2025, valid for 2 years.
The pilot completed helicopter underwater escape training (HUET) on 25 September 2025 and held a Class 1 medical certificate valid until 14 January 2026. They had been employed by the operator since September 2025.
Aircraft information
VH-LMW was a Bell 206L-3, single-engine turbine powered helicopter, serial number 51120, constructed in the United States in 1984. A Rolls-Royce Allison 250-C30P engine was fitted to the helicopter and was registered to Fortescue Helicopters Pty Ltd, on 19 April 2023. VH‑LMW was fitted with emergency pop‑out floats for short‑term stability in the event of a ditching.
Meteorological information
Meteorological information recorded at Horn Island Airport at 1400 indicated:
The operator was contracted to transport employees of an organisation that regularly conducted inspections on islands throughout the Torres Strait.
The previous day, VH-LMW had flown 2.3 hours conducting similar inspections on islands in the north of the Torres Strait. Prior to that the helicopter had not been flown since 22 December 2025 when it had returned from Atherton, Queensland, following scheduled maintenance.
Wreckage and post-impact information
The helicopter ditched shortly after take-off from Sadie’s Beach Helipad, about 6.5 km from Horn Island Airport. Following the pilot’s rescue, the police and pilot anchored the helicopter to prevent it drifting in the current while the operator was making recovery arrangements.
The operator subsequently arranged recovery of the helicopter and commissioned an independent engineering report. The results of the engineering report were not available to the ATSB at the time of writing.
Fuel
The pilot’s flight plan showed the intended fuel for departure at the commencement of their day from Horn Island Airport was 800 lb (363 L).
The helicopter used Jet A-1 fuel that was stored in static tanks on Horn Island and an intermediate bulk container (IBC) on Coconut Island which was supplied via Horn Island as part of a broader distribution network. The pilot reported the IBC had been refilled in early December 2025.
Fuel quality and contamination
Free water[6], if present in aviation fuel, can result in filter blockages and, in more severe cases, engine failure through fuel starvation. In tropical climates, it can also create conditions that support algal growth in fuel tanks, which can degrade fuel quality and further contribute to filter obstruction. Water contamination is commonly checked in fuel using a water detecting tablet or paste which indicates the presence and level of water.
Microorganisms that can be found in aviation turbine fuel can include bacteria, yeasts and fungi. As these organisms develop, they form solid residues that can block and damage fuel filters. Some microorganisms also generate acids that can accelerate corrosion of metal components. Because most microbial growth depends on the presence of free water, this kind of contamination is most commonly found anywhere fuel meets water, particularly in high humidity environments.
The CASA advisory circular AC 91-25 v1.2 Fuel and oil safety stated that:
Fuelling in remote locations exposes operators to increased risk in various areas, such as:
multi-transfer fuelling cycles,
contamination of fuelling equipment whilst in transit and during aircraft arrival
At the completion of the scheduled maintenance in December 2025, the pilot reported they had a discussion with the maintenance provider about algal growth which the pilot had identified in the helicopter’s fuel tanks. The pilot subsequently began an algal preventative treatment for VH-LMW. That involved adding an algal preventative to the full fuel tank while the helicopter remained on the ground between 22 December and 5 January.
Operator refuelling process
The operator’s procedure for drum stock refuelling required that fuel be sourced from approved drums and subjected to a series of quality checks prior to use. The procedure detailed that:
Drum stocks of fuel should be:
Stored under cover;
Stored with minimal ground contact (using wooden slats or equivalent);
Stored horizontally with bungs at the 3 and 9 o'clock position, or stored vertically with drum tops covers in place;
Refueling pumps must be fitted with a Go/No-Go filter;
Drum seals are checked that they are tight and not broken prior to use;
Drum-stock fuel is to be consumed within the specified Aviation Release Note certification date - Check the release note for the fuel to confirm it is from an approved source and within date;
Before fuelling an aircraft, a small amount of fuel is to be pumped into a container to be visually checked for colour, clarity and freedom from dirt and/or visible water;
Prior to opening the drum stand the drum upright and leave for a minimum of 30 minutes for AVGAS and one hour for JET A1 (or as long as practical);
Before commencing fuelling operation’s, the following earthing procedures should be carried out prior to opening the fuel cap: a. Drum to ground; b. Aircraft to ground; c. Nozzle to aircraft (disconnect by reversing this procedure);
Check fuel pump and associated equipment for contamination – should the pump not be fitted with an aviation grade filter the fuel should be checked for contamination using water detector capsules, or an approved equivalent;
Full or partly used drums should be stored when not under cover by tilting the drum so that the bungs are clear of any pooled water, or by laying the drum on its side.
The pilot reported they had taken a fuel sample from VH-LMW prior to their departure from Horn Island that morning and reported that the fuel drain looked normal. Prior to refuelling VH-LMW from the IBC at Coconut Island, the pilot had also reported they took 2 fuel samples from the IBC, an initial large sample that, in their experience, often contained contaminants, followed by a second smaller sample which they used to assess the quality of the fuel before refuelling the helicopter. They also stated they were conscious that the presence of water within the IBC was possible and therefore did not place the fuel hose toward the bottom of the IBC where water was likely to settle.
A Go-No-Go absorptive cartridge (filter) can be fitted to a fuel pumping device to absorb water from the fuel and remove any solids.
The pilot reported that during their time with the operator they had not used a filter when refuelling from an IBC. However, they had previously used filters during their employment with other operators within the Torres Strait. The pilot reported they were unaware the operator had a filter and were advised after the occurrence the filter was stored at the company‑owned pilot accommodation on Thursday Island.
Survival aspects
The pilot conducted an autorotation and ditched the helicopter which remained stable for a brief time before rolling onto its right side. The pilot, who had completed helicopter underwater escape training (HUET), was able to egress and swim clear of the helicopter. However, the effectiveness of the emergency pop-out flotation system was limited. Images of the helicopter after impact showed the right rear float detached from the skid tube and the right front float displaced and the pilot reported the float obstructed their door and required an egress via the front left door. This may have impeded egress in a multi-occupant scenario or for occupants who had not completed HUET training.
HUET involves a replica of a helicopter cabin and fuselage being lowered into a swimming pool to simulate the ditching of a helicopter. The cabin can rotate upside down and focuses participants on bracing for impact, identifying primary and secondary exit points, opening an exit, releasing harness, egressing the wreckage and surfacing. HUET is normally part of a program of graduated training that builds in complexity, with occupants utilising different seating locations, exits and visibility. This training is conducted in a controlled environment with safety divers in the water.
The pilot recalled that HUET assisted them to quickly determine their primary exit was blocked by the float and identified the front left door as a secondary exit and successfully egressed the overturned and partially submerged helicopter.
Further investigation
To date, the ATSB has:
collected records from the aircraft operator and Civil Aviation Safety Authority
collected fuel source records and quality control documentation
collected recorded data
interviewed the pilot, passengers and operator.
The investigation is continuing and will include:
further interviews relating to fuel quality monitoring
analysis of the survivability of the accident post-water impact
analysis of the independent engineering investigation report
review of operator’s fuel management process for mobile storage facilities and quality control
review of pilot induction training and procedures.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Yawing: a yaw rotation is a movement around the yaw axis of an aircraft that changes the direction the vehicle is facing.
[2]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[3]Autorotation is a condition of helicopter flight during which the main rotor of a helicopter is driven only by aerodynamic forces with no power from the engine. It is a means by which a helicopter can be landed safely in the event of an engine failure.
[4]Scattered: 3–4 okta of cloud cover. An okta is a unit of measurement used to describe the extent of cloud cover (1–8).
[5]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
[6]Water in aviation fuel exists in a dissolved form, in solution and as free water that is separated from the fuel and may be present as droplets or settled at the base of storage systems.
Occurrence summary
Investigation number
AO-2026-003
Occurrence date
06/01/2026
Occurrence time and timezone
14:08 Australian Eastern Standard Time
Location
6.5 km west of Horn Island Airport
State
Queensland
Report release date
16/04/2026
Report status
Preliminary
Anticipated completion
Q4 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Control issues, Ditching, Engine failure or malfunction
Occurrence class
Accident
Highest injury level
None
Aircraft details
Manufacturer
Bell Helicopter Co
Model
206L-3
Registration
VH-LMW
Serial number
51120
Aircraft operator
Fortescue Helicopters Pty Ltd
Sector
Helicopter
Operation type
Part 133 Air transport operations - rotorcraft
Activity
General aviation / Recreational-Other general aviation flying-Ferry flights
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 22 December 2025 at 1640, a pilot was conducting circuit operations with one passenger on board a Cessna 150H at West Sale Airport, Victoria.
In contrast to the recorded weather conditions, the pilot identified a left-hand crosswind via the aerodrome windsock for the one runway available. Alternate grass runways were unavailable due to rain in the preceding 24 hours.
During landing in the crosswind on runway 27, the pilot ‘crabbed’ by yawing[1] the nose of the aircraft into the wind to prevent the aircraft from drifting off the centreline. The pilot assessed that the approach was stable and proceeded to touch down. During rollout, after the flare, the aircraft encountered a gusting wind, resulting in the aircraft ballooning[2] and yawing to the right. In response, the pilot attempted to counteract with a left yaw. However, the conditions exceeded the aircraft’s capabilities and the aircraft was carried to the right, and the right wheel contacted the runway surface. The right main landing gear collapsed, and the right wing tip struck the ground before the aircraft veered off the runway.
The pilot and passenger exited the aircraft without injuries, and the aircraft was substantially damaged (Figure 1).
Figure 1: Damage to the Cessna 150H right landing gear
Source: Aircraft owner
Safety message
Crosswind gusts during the later stages of landing can present challenges for pilots. Depending on the magnitude and direction of the gust, there may be insufficient time to apply corrective controls before the aircraft deviates from the intended path.
Once the aircraft wheels touch down, it's important to remain focused and use your rudder to keep the aircraft straight, even after you have touched down, to retain control and stability.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Yawing: the motion of an aircraft about its vertical or normal axis.
[2]Coequally a sudden unwanted gain in height of aircraft that can occur on approach and landing.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 8 November 2025, at approximately 1315 local time,[1] a Boeing A75N1 (Stearman), with one pilot on board, departed a privately-owned runway near Dochra, New South Wales.
The pilot conducted a 30-minute private flight, before returning to the 500 m-long grass runway, orientated almost north-south. The pilot reported that the shorter runway required them to use a ‘short field’ landing technique and that the wind was westerly at less than 10 kt and variable near the ground.
The pilot conducted 3 consecutive landings and take-offs on the southern facing runway. During their third approach, the pilot recognised that the aircraft was about 200 feet higher than normal on final approach, however continued the approach.
They reported touching down in a 3-point attitude, too far down the runway and applied hard braking which caused the tail to lift once elevator effectiveness reduced. This resulted in the aircraft slowly tipping forward, striking the propeller and then flipping over onto its back and rudder (Figure 1).
Figure 1: Aircraft post-occurrence
Source: Operator
The aircraft sustained damage to its rudder, propeller, wing and strut. The pilot was uninjured.
Safety message
Good landings are made from stable approaches and conducting a go-around is normally the safest course of action if a pilot is not entirely comfortable with the approach.
Pilots should also consider the required approach performance for short field landings of their aircraft when assessing their approach to land with limited runway length. Heavy braking in high centre-of-gravity, tailwheel aircraft increases the risk of loss of control on landing, which places greater importance on ensuring the approach is conducted appropriately.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]All times referred to in this report are local time, Coordinated Universal Time (UTC) + 11 hours.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-060
Occurrence date
08/11/2025
Location
near Dochra
State
New South Wales
Occurrence class
Accident
Aviation occurrence category
Collision with terrain, Control issues, Ground strike
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 17 October 2025, at 1413 local time, an American Champion Aircraft Corp 8GCBC (Scout), with 2 pilots on board, had conducted aerial observation operations before landing at Busselton Airport, Western Australia.
The pilot reported that during the crosswind landing, after touching down with the tailwheel still clear of the ground, the aircraft left wing lifted due to a gust and the right wing struck the runway.
The pilot also believed that whilst they were recovering using the rudder controls, the toe brakes may have been inadvertently applied. This likely caused the aircraft to pitch forward, resulting in propellor impact with the ground and the aircraft coming to rest in a nose-over position (Figure 1).
Figure 1: Aircraft post-occurrence
Source: Photo supplied by operator
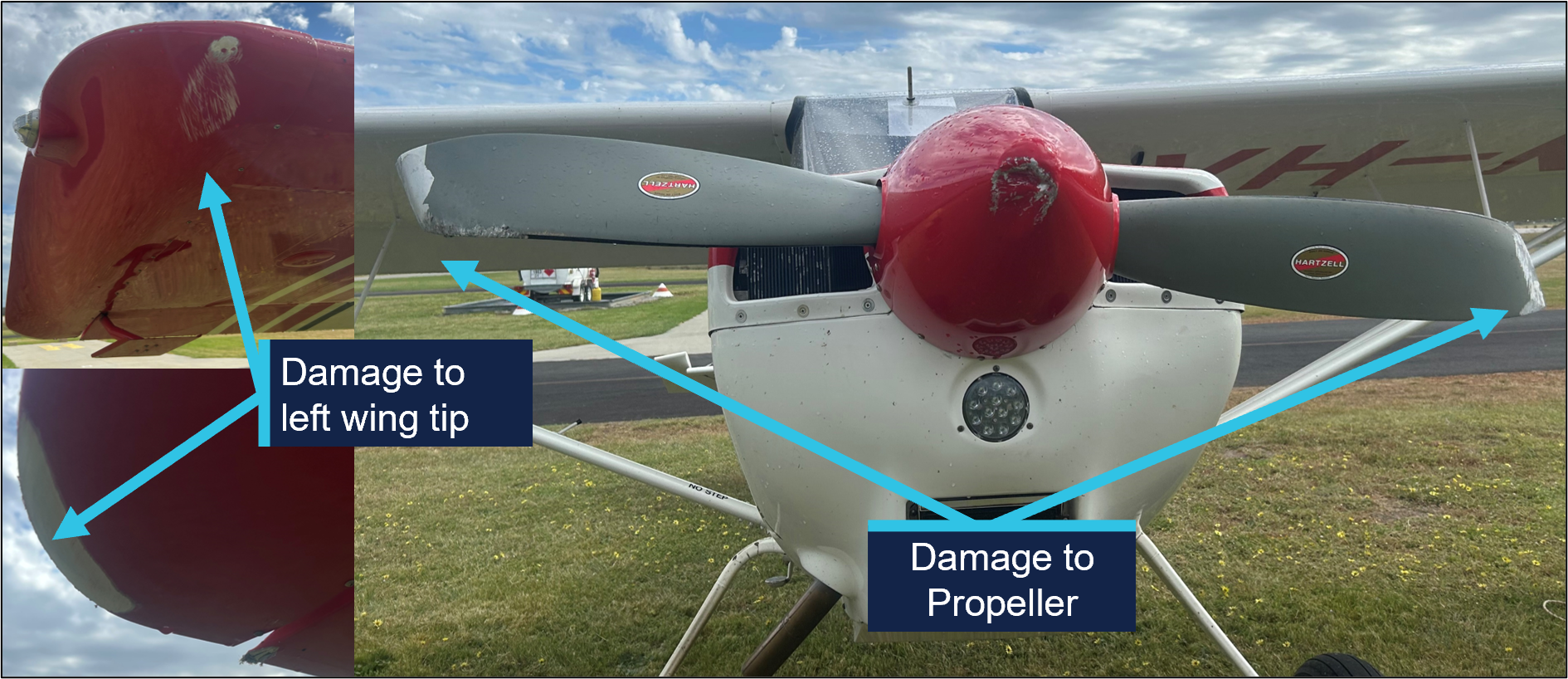
Inspection of the aircraft post‑event noted damage to the aircraft, that included the right wing and the propeller (Figure 2). One of the pilots incurred minor injuries.
Figure 2: Aircraft damage
Source: Photo supplied by operator, annotated by the ATSB
The landing was on runway 03 (Figure 3). The recorded weather conditions at the time was wind at 332° at 12 kt, gusting to 15 kt.
Figure 3: Approach orientation Busselton Airport
Note: aircraft not to scale. Source: Google Earth, annotated by the ATSB
The pilot operating manual for the Scout notes a crosswind limit of 17 kts. The variable wind strength of the gusting crosswind may have been close to the maximum demonstrated limit for the aircraft.
The operator reported that the pilot flying had previously demonstrated competency in crosswinds during landing. Furthermore, in this instance, the senior pilot in the back seat did not attempt to take over control during the landing, as they felt the conditions well within both the aircraft and the pilot flying’s capabilities.
The manual describes that the technique is to place the control stick into the wind (up‑wind aileron up) and assume a tail high attitude with the elevator to prevent drift.
Safety message
This occurrence highlights the importance of exercising caution when operating in conditions that have the potential to exceed the maximum demonstrated crosswind speed of an aircraft.
It also illustrates the need for pilots to establish a personal minimums checklist that is commensurate with the flying experience of the individual. If the conditions do not meet these criteria, or if there is any doubt, pilots should not attempt the landing, consider conducting a go-around, change runways or hand control to a more experienced pilot.
Tailwheel aircraft can be susceptible to crosswind gusts during the later stages of landing. Depending on the magnitude and direction of the gust, there may be insufficient time to apply corrective controls before the aircraft deviates from the intended path.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-055
Occurrence date
17/10/2025
Location
Busselton Airport
State
Western Australia
Occurrence class
Serious Incident
Aviation occurrence category
Control issues, Ground strike
Highest injury level
Minor
Brief release date
17/11/2025
Aircraft details
Manufacturer
American Champion Aircraft Corp
Model
8GCBC
Sector
Piston
Operation type
Part 138 Aerial work operations
Departure point
Margaret River Aircraft Landing Area, Western Australia
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 3 July 2025 at 1147 local time, a student pilot, the sole occupant of a Cessna 172S, was conducting circuit operations at Parafield Airport, South Australia.
During the seventh touch-and-go of the circuit training, the aircraft encountered a gust of wind as it crossed the runway threshold, resulting in a yaw to the right. In response, the pilot advised that they pushed forward on the control column and overcorrected, resulting in the aircraft landing hard, ballooning[1] and striking the runway a second time. A propellor strike occurred during the second impact with the runway. The aircraft sustained substantial damage to the fuselage and landing gear.
Figure 1: Damage to Aircraft
Source: Operator
Safety message
Wind gusts can be unpredictable. Gusty wind conditions present a challenge for all pilots, but in particular, less experienced student pilots. Maintaining a calm mindset is important in order to adjust the aircraft’s profile and airspeed accordingly and determine that a go‑around is necessary.
The ATSB reminds pilots that as soon as landing conditions become unfavourable, or the approach unstable, initiating a go-around will allow time to reconfigure the aircraft and conduct a safe landing.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Ballooning occurs when the pilot flares and the aircraft climbs instead of descending onto the runway.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-050
Occurrence date
03/07/2025
Location
Parafield Airport
State
South Australia
Occurrence class
Accident
Aviation occurrence category
Control issues, Hard landing
Highest injury level
None
Brief release date
30/10/2025
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
172S
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training