The ATSB is investigating a weather event involving a balloon display of multiple tethered balloons at Wangaratta Racecourse, Victoria, on 11 April 2026.
During a static balloon display, multiple tethered balloons encountered a sudden change of wind conditions.
One of the tether ropes for an Amateur-built GUS-69, registered VH-XUP, failed and the balloon became airborne before colliding with terrain resulting in injuries to a person on the ground.
The tether rope on a Kavanagh Balloons D-77, registered VH-CZX, was placed under extreme tension and the basket became briefly airborne before landing hard, resulting in injuries to an additional person on the ground.
The ATSB has commenced the examination and analysis of the initial evidence collected. To date, the ATSB investigation has included interviewing witnesses and involved parties, reviewing recorded data, and the collection of other relevant information. The continuing investigation will include examination of operational documentation and components from the site.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2026-070
Occurrence date
11/04/2026
Occurrence time and timezone
19:15 Australian Eastern Standard Time
Location
About 6.5 km north-north-west of Wangaratta Airport
State
Victoria
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Cabin injuries, Collision with terrain, Ground operations - Other, Hard landing, Turbulence/windshear/microburst
Occurrence class
Accident
Highest injury level
None
Aircraft details
Manufacturer
Amateur Built Aircraft
Model
GUS-69
Registration
VH-XUP
Serial number
GUS-01
Sector
Balloon
Operation type
Part 131 Balloons and hot air airships
Activity
General aviation / Recreational-Sport and pleasure flying-Other sport and pleasure flying
Departure point
Near Wangaratta Racecourse, Victoria
Injuries
None
Aircraft details
Manufacturer
Kavanagh Balloons
Model
D-77
Registration
VH-CZX
Serial number
D77-549
Sector
Balloon
Operation type
Part 131 Balloons and hot air airships
Activity
General aviation / Recreational-Sport and pleasure flying-Other sport and pleasure flying
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 22 November 2025, 3 balloons took off at dawn from a launch site near Mareeba, Queensland, to conduct scenic hot air balloon flights. The weather had light southerly surface winds, moderate north-easterly winds in the mid layers and stronger south‑easterly winds in the higher altitudes.
As the morning progressed, the surface winds died down while the mid layers became less consistent, resulting in the pilots conducting steeper descents into their landing areas.
One of the balloons, a Kavanagh Balloons G-450, landed moderately hard resulting in injury to an elderly passenger. Initially the passenger did not seek medical attention but later in the day X-rays were conducted, and it was determined that the passenger sustained fractures to both tibias with the left tibia becoming displaced.
Safety message
The ATSB recently published a Safety study into Australian balloon transport operation occurrences from 2014 to 2022 (AS-2023-002) which found that injuries, serious incidents and accidents were all more likely to occur during landing than any other phase of flight. For the period 2014–2022, the ATSB occurrence database recorded 58 minor injuries and 18 serious injuries sustained in commercial ballooning with layover and hard landings having contributed to the largest number of serious injuries. These resulted from balloon passengers being unrestrained within the basket and, in some occurrences, adopting an incorrect landing position. Wind was the most common factor reported to have contributed to these occurrences.
Balloon pilots are encouraged to use all available resources including passenger demonstrations and safety briefing cards to ensure that every passenger understands the landing position and its importance, and approved Bureau of Meteorology products, to ensure they understand the weather, particularly the wind, and its influence on flight safety.
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
On 4 May 2024, a Boeing 737, operated by Qantas Airways Limited, departed Sydney, New South Wales for a scheduled passenger carriage flight to Brisbane, Queensland. In the latter stages of descent, the aircraft entered a band of approaching cloud. While the flight crew expected some turbulence associated with the entry to cloud, after passing 11,400 ft about 36 km south‑east of Brisbane, the aircraft experienced unanticipated severe turbulence. Three cabin crew were unrestrained and suffered various injuries during the occurrence. Two received minor injuries, including a facial injury and concussion, whilst the third was seriously injured with a fractured ankle.
What the ATSB found
The ATSB found that the captain did not inform the cabin crew about the expected turbulence during descent, likely due to not being aware of its severity. This resulted in 3 unrestrained cabin crew being injured during severe turbulence.
Following the turbulence, the captain instructed all passengers and crew to return to their seats and fasten seatbelts. However, 2 cabin crew and 2 passengers remained unrestrained in the rear galley to assist the seriously injured crew member during landing. When the flight crew were informed of this, the captain repeated the instruction that everyone besides the injured crew member was to return to their seats for landing. Assuming the cabin would be secured after the repeated instruction, the flight crew proceeded with the landing, unaware that 4 crew and passengers remained unrestrained. Qantas 737 standard operating procedures relied on the customer service manager to inform the flight crew if the cabin crew had not secured the cabin for landing.
A crew member who had sustained a concussion returned to work before seeking medical treatment. The ATSB found that the operator did not have a procedure to ensure that crew were assessed for fitness for duty after a significant injury.
What has been done as a result
Qantas has updated the integrated operation control procedures for requesting medical assistance for cases where any crew member or passenger is significantly injured. Updated protocols now mandate that a doctor will immediately be required to assess the fitness of cabin crew members prior to commencing any further work‑related duties. Additionally, the operator will arrange immediate medical assessment following any turbulence or unplanned aircraft movement classified as moderate or severe with injuries or unrestrained crew.
Safety message
Effective coordination and communication among all crew members is critical in managing turbulence and ensuring cabin safety. This coordination should extend beyond pre‑flight briefings to include continuous communication throughout the flight, particularly during periods of increased workload and operational complexity.
Collaboration between the flight and cabin crew helps ensure the timely completion of service‑related tasks while minimising the risk of injury during known or anticipated encounters with turbulence.
Flight crew rely on clear and timely communication from the cabin crew to maintain awareness of the condition in the cabin. When there is a different understanding of the state of the cabin, there is an increased risk delayed responses or misaligned decision‑making which may lead to safety being compromised.
Aircraft are more likely to experience the effects of weather and wake turbulence during the descent, approach, and landing phases of flight, highlighting the importance of effective communication procedures to promote cabin safety and minimise the risk of injury to passengers and crew.
The occurrence
On 4 May 2024, a Boeing 737, registered VH‑VYK, being operated by Qantas Airways Limited as QF520, departed Sydney, New South Wales on a scheduled flight to Brisbane, Queensland. The aircraft departed Sydney at 1202 local time and was scheduled to arrive in Brisbane at 1335. On board was the flight crew, comprised of the captain and first officer (FO), a customer service manager (CSM) supported by 3 cabin crew members, and 143 passengers.
Prior to departing Sydney for Brisbane, the captain recalled briefing the CSM about leaving the seatbelt sign on for the departure from Sydney due to weather, however neither the captain nor the CSM could recall any specific details regarding the weather conditions in Brisbane.
Descent into Brisbane
At about 1300, the flight crew commenced their descent into Brisbane while approaching Lismore, New South Wales. As the aircraft continued descent towards Coolangatta, Queensland, the captain visually observed cloud over Moreton and Stradbroke islands, but recalled no weather radar indications that identified precipitation normally associated with increased turbulence.
After passing 30,000 ft above mean sea level (AMSL) at 1303, the captain, who was pilot monitoring, recalled performing the ‘prepare cabin’ public announcement (PA), and the cabin crew commenced securing the cabin for landing. About 6 minutes later, the captain contacted the CSM to enquire about the amount of time the cabin crew required to complete their cabin preparations. At about 15,000 ft AMSL, the aircraft entered a thick layer of stratiform[1] cloud with minimal turbulence observed initially by either the flight or the cabin crew. The CSM advised the captain the preparations would take about 2 minutes. About 2 minutes later, the captain turned on the seatbelt sign and announced the ‘seatbelts PA’.
Immediately after the captain turned on the seatbelt sign, the CSM and the 2 cabin crew members in the aft galley completed their duties as per the procedures. The CSM made a PA while standing in the forward galley, then checked and locked their assigned lavatory. The 2 cabin crew members in the rear galley got out of their jump seats to verify that the lavatories were vacant before locking them.
At about this time, the captain observed a cumulus[2] cloud embedded in the stratiform layers. However, there was no radar return consistent with increased turbulence, and the cloud did not appear to be overly concerning in terms of turbulence risk from their shape or size.
After descending below 12,000 ft AMSL at 1311, the aircraft encountered a severe turbulence event less than one minute after the seatbelt sign was illuminated, while 3 cabin crew were unrestrained. The CSM recalled observing the right 2 primary (R2P) cabin crew member at the rear galley rising off the floor and colliding with the aircraft's ceiling. They immediately fell back to the floor, landing on their right ankle. The R2P felt a crushing sensation as they landed on their ankle and experienced intense pain and was unable to move.
Events in the cabin
The CSM contacted the captain to inform them that the R2P was injured and that some passengers were standing. The captain responded with instructions that all passengers and cabin crew must remain seated. Following this interaction, the CSM made a public announcement to remind passengers to stay seated and to request assistance from the cabin crew if needed. The captain contacted the operator’s Brisbane airport coordinator to advise that there was an injured cabin crew member and medical assistance would be required on arrival in Brisbane. Queensland Ambulance service records showed that a request for an ambulance was received at 1315.
Although being instructed to remain seated, the CSM immediately moved to the rear of the aircraft to assist the injured R2P in the aft galley. There, they observed the injured R2P lying on the floor while a passenger was holding their leg. Another passenger, who identified themselves as a doctor, offered to assist with providing first aid. Meanwhile, another cabin crew member, the left two primary (L2P), was supporting the R2P’s head.
At this point, the CSM advised the L2P and the passengers that the captain had instructed everyone to return to their seats. However, they were unwilling to leave the R2P unattended. The CSM instructed the L2P to advise the captain of the situation. The CSM then retrieved the physician's kit from the front of the cabin. At this point, the passenger seated in 3F advised the CSM that they were a travelling cabin crew member and were able to assist.
The L2P contacted the captain to advise that all the occupants located in the rear galley were still unrestrained. However, the captain did not recall receiving requests for additional time to address the situation. The captain reiterated that all uninjured occupants must return to their seats as the aircraft was in the final stages of the approach and would be landing soon.
The CSM subsequently returned to the rear galley with the physician’s kit and the off‑duty cabin crew from 3F, who subsequently relieved the passenger who was holding the R2P’s leg. While the CSM was attempting to provide first aid and preparing a splint with the assistance of the travelling doctor, a passenger seated in 30D yelled, ‘we’re about to land’. Shortly after at 1322, the aircraft landed in Brisbane with 4 unrestrained passengers and cabin crew in the rear galley. The flight crew taxied the aircraft to its assigned gate, arriving at 1328, with paramedics in attendance at 1338.
Context
Flight crew information
Captain
The captain held an Airline Transport Pilot (aeroplane) Licence with an instrument rating and a Class 1 aviation medical certificate. They had 23,177 flight hours, including 15,005 hours on the Boeing 737, and had logged 165 hours on the 737 in the last 90 days.
The captain reported sleeping 7 hours the night before the occurrence. They were awake for 8 hours and 45 minutes at the time of the occurrence and reported feeling ‘responsive, but not at peak’.
First officer
The first officer held an Airline Transport Pilot (aeroplane) Licence with an instrument rating and a Class 1 aviation medical certificate. They had 10,163 flight hours, including 1,717 hours on the Boeing 737, and had logged 152 hours on the 737 in the last 90 days.
The first officer reported sleeping 7 hours the night before the occurrence. They were awake for 8 hours and 45 minutes at the time of the occurrence and reported feeling ‘somewhat fresh’.
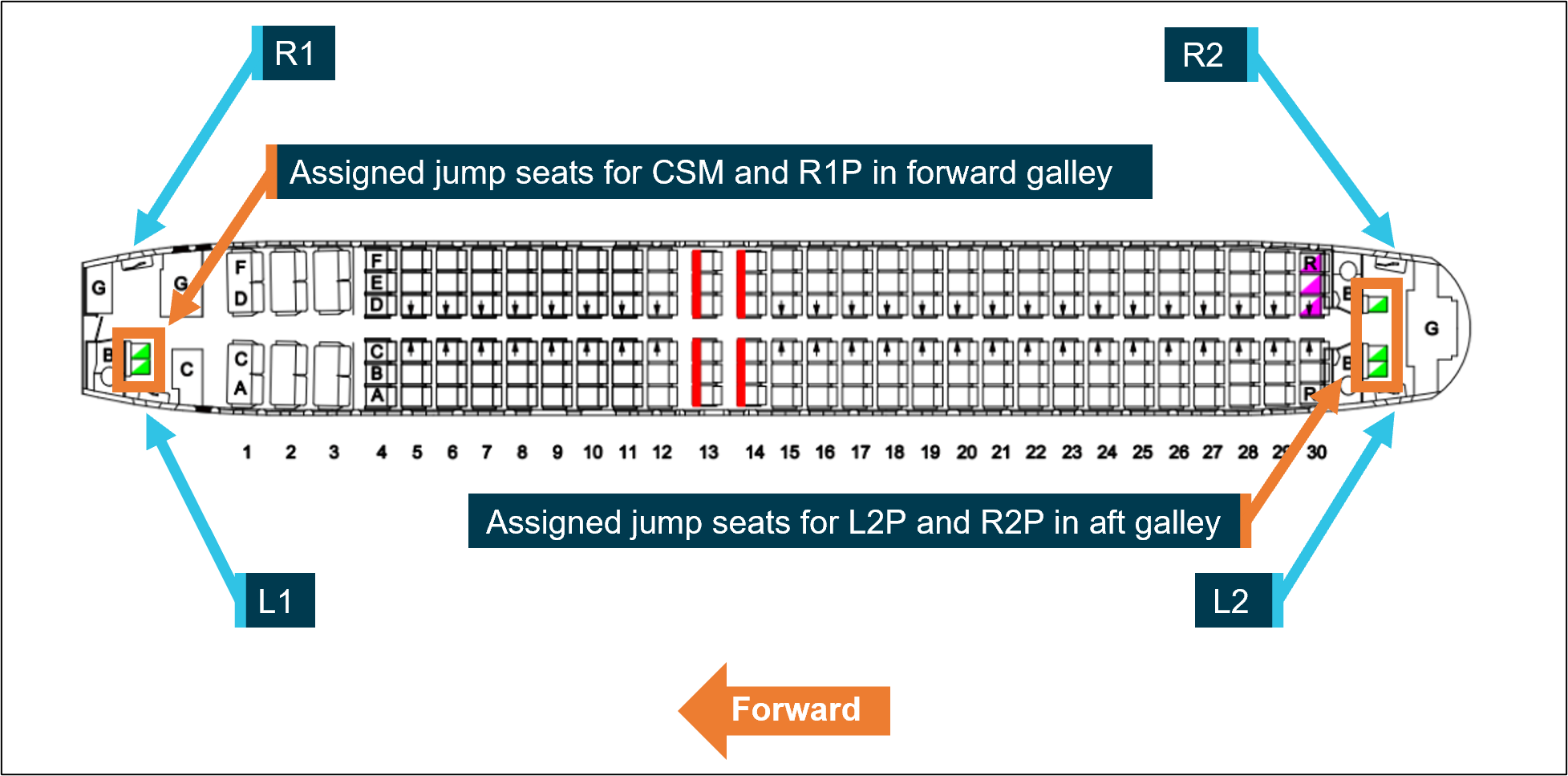
Cabin crew
The cabin crew on board was comprised of a complement of 4 members, with their assigned jump seats located in the forward and aft galleys. Each cabin crew member was responsible for one of the 4 main cabin doors (Table 1) during critical phases of flight, with their assigned jump seat (Figure 1) located immediately next to their assigned door. The cabin crew were under the supervision of the customer service manager (CSM) who was responsible to the captain for administration of in‑cabin service and liaison with the crew for all service and safety related matters.
Table 1: Cabin crew door assignment
Cabin Door
Cabin crew assignment
Left one (L1)
Customer service manager (CSM)
Right one (R1)
Right one primary (R1P)
Left two (L2)
Left two primary (L2P)
Right two (R2)
Right two primary (R2P)
Figure 1: 737 Cabin layout, doors and assigned jump seats for cabin crew
Source: Qantas, annotated by the ATSB
Cabin crew injuries
R2P
The R2P had been in the process of taking their seat when the turbulence occurred. They rose into the air during the turbulence, struck their head on the ceiling, and landed heavily on their feet. R2P immediately fell to the galley floor and told L2P that they were injured, possibly with a broken bone. They were later diagnosed in the hospital with a fracture involving 2 breaks in the ankle and another break in the leg, which required surgery.
CSM
The CSM sustained minor injuries due to striking aircraft fixtures while standing unsecured during the turbulence. The CSM self‑assessed their injuries and applied first aid the following day after noticing minor pain, including discomfort in their lower back and right shoulder blade. They also became aware of facial pain 2 days after the event.
L2P
The L2P sustained a head injury, due to striking the ceiling or other aircraft fixtures during the event but did not initially believe they were injured. They had several rostered days off after the event. They returned to work on 11 and 12 May and were made aware by co‑workers that they were displaying symptoms of possible injury. On 16 May, 12 days after the turbulence event, they were diagnosed with concussion after a consultation with their general practitioner.
Aircraft
The aircraft was registered as VH‑VYK in Australia on 11 January 2006, serial number 34183. The Boeing 737‑800 is a twin‑engine, narrow‑body commercial aircraft in the 737 Next Generation series, used for short to medium‑haul routes. It had a seating capacity of 174 passengers, with Qantas configuring its aircraft with 12 business class seats in a 2‑2 layout and 162 economy class seats. It is powered by two CFM56‑7B turbofan engines.
The passenger address system broadcasts announcements throughout the cabin, and the interphone facilitates communication between the flight and cabin crew.
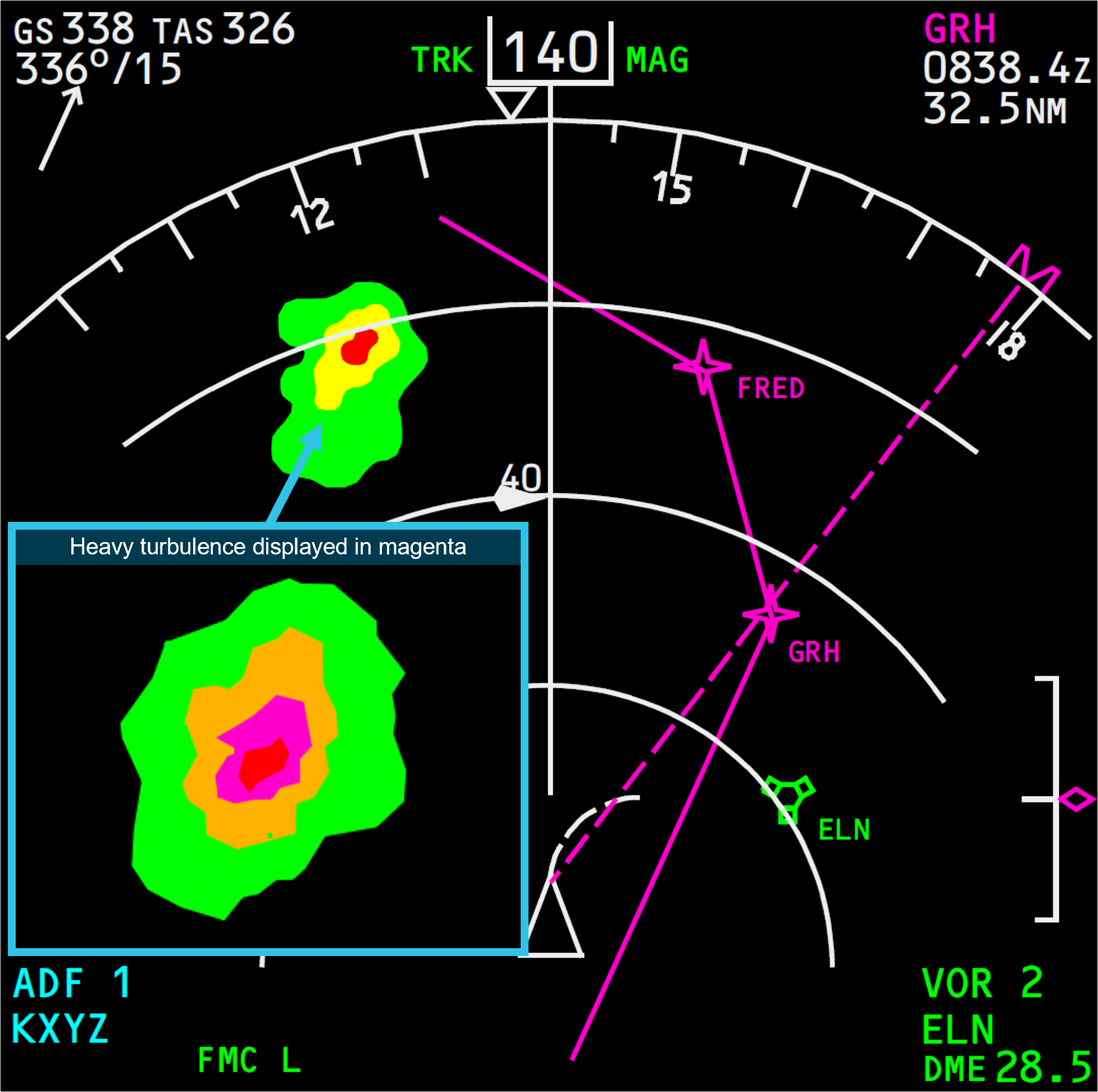
Weather radar
The weather radar system fitted to the Boeing 737 detects and locates various types of precipitation bearing clouds along the flight path of the aircraft and gives the pilot a visual indication in colour of the cloud’s intensity. The radar antenna sweeps a forward arc of 180°. The radar indicates a cloud’s rainfall intensity by displaying colours contrasted against a black background. Areas of heaviest rainfall appear in red, the next level of rainfall in amber, and the least rainfall in green (Figure 2).
Figure 2: Example depiction of 737 weather radar returns on pilot's navigational display
Source: Qantas, annotated by the ATSB
The turbulence mode displays normal precipitation and precipitation associated with turbulence. When the radar detects a horizontal flow of precipitation with velocities of 5 or more metres per second toward or away from the radar antenna, that target display becomes magenta. These magenta areas are likely associated with heavy turbulence.
The captain did not recall identifying areas of turbulence on the weather radar on descent or report that they were experiencing any difficulties operating the weather radar. Neither the captain nor the operator reported that the weather radar fitted to the aircraft was unserviceable during this occurrence.
Post‑event maintenance
Aircraft data was collected for use by the operator’s maintenance operations control, and engineering. The aircraft health monitoring (AHM) section collected and analysed data from aircraft components and systems post‑event to assess their condition and identify any potential overstressing of components. The operator’s AHM and flight data analysis showed that the event did not exceed tolerances, and no additional inspections were required.
Meteorological information
Brisbane Airport weather
The TAF for Brisbane Airport predicated winds from 100° at 10 kt with visibility more than 10 km in light rain showers and scattered cloud at 3,500 ft from 1200–2000 local time. Table 2 shows the automatic terminal information service (ATIS)[3] report at the time of departure.
Table 2: Brisbane Airport automatic terminal information service (abridged)
The TAF for Gold Coast Airport predicted winds from 100° at 10 kt with visibility more than 10 km in light rain showers and scattered cloud at 2,000 ft. There was a significant intermittent variation from the prevailing conditions from 1300–2200 local time. For up to 30 minutes at a time during this period, the visibility was forecast to reduce to 4 km in rain showers with broken[5] cloud at 1,500 ft.
Graphical area forecast
The flight transited through a region contained in the graphical area forecast for Queensland south, covering subdivisions A and A2 (Figure 3). Table 3 shows the forecast conditions for the duration of the descent into Brisbane Airport which was issued at 0815 local time.
Figure 3: Graphical area forecast Queensland south
Source: Australian Bureau of Meteorology, annotated by the ATSB
Table 3: Graphical area forecast Queensland south
Area
Surface visibility and weather
Cloud
Turbulence
A
Visibility greater than 10 km
Scattered[6] cumulus/stratocumulus clouds between 2,500–8,000 ft AMSL
Scattered altocumulus/altostratus clouds from 8,000 ft to above 10,000 ft
Broken cumulus cloud between 2,000–9,000 ft
Moderate turbulence associated with stratocumulus and altocumulus clouds
A2
Visibility 3 km in scattered showers of rain
Visibility 1 km in isolated thunderstorms with rain showers
Isolated towering cumulus cloud from 2,000 ft to above 10,000 ft
Broken stratus cloud between 800–2,000 ft
Broken cumulus cloud from 2,000 ft to above 10,000 ft
Moderate turbulence associated with cumulus cloud
Severe turbulence associated with thunderstorms, cumulonimbus and towering cumulus clouds
Turbulence reporting
In accordance with the requirements of regulation 91.675 of CASR (Civil Aviation Safety Regulations 1988) and instructions contained in the Aeronautical Information Publication Australia, a special air report must be provided to air traffic control whenever turbulence meeting the following specifications is encountered:
Moderate: Changes to accelerometer readings of between 0.5 g and 1.0 g at the aircraft’s centre of gravity. Moderate changes to aircraft attitude and/or altitude may occur but aircraft remains under positive control. Usually small changes in airspeed. Difficulty in walking. Loose objects moved about.
Severe: Changes to accelerometer readings greater than 1.0 g at the aircraft’s centre of gravity. Abrupt changes to aircraft attitude and/or altitude may occur; aircraft may be out of control for short periods. Usually large changes of airspeed. Loose objects tossed about.
The flight crew could not recall whether a special air report was provided to air traffic control and the turbulence event was classified as moderate in a post‑flight conference call between the captain and Qantas personnel. The operator defined moderate turbulence as ‘causing rapid bumps or jolts without appreciable changes in aircraft altitude or attitude.’ The description elaborated that unsecured objects are dislodged, and walking is difficult.
Recorded data
The operator’s internal investigation report detailed flight data and showed that over a 4‑second period, at an altitude of approximately 11,100 ft, the aircraft recorded:
vertical G went from +1.2G to -0.06G (negative) to +1.35G to +0.61G to +1.59G.
pitch attitude changed from -2.4deg to -0.7deg over 1 sec.
Operator procedures
Dispatch weather briefing
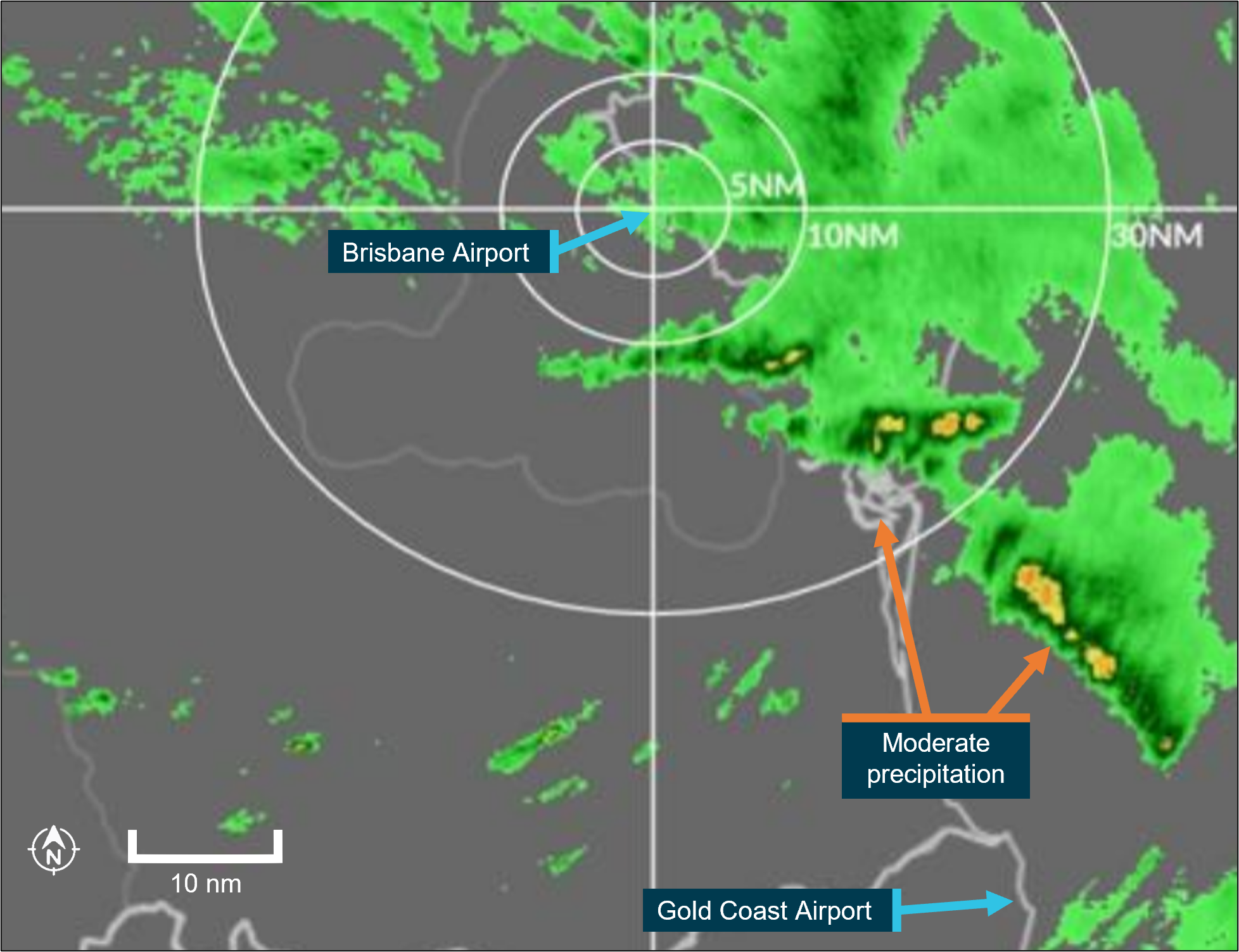
For the operator’s domestic sectors, a flight plan, textual weather, and notice to airmen (NOTAM)[7] were provided in a briefing package to flight crew via an electronic application installed on their iPads. The briefing information included graphical area forecasts, additional weather, turbulence information and weather radar overlay imagery. Figure 4 shows a weather radar overlay issued at the time of departure. For operator domestic flights under 90 minutes, the crew did not receive a flight watch service[8] from the operator’s flight dispatch during the flight and consequently, any hazard alerts or amended terminal forecasts (TAF)[9] were only provided by air traffic control.
Prior to departure from Sydney, the flight crew conducted their pre‑flight planning and reviewed the weather briefing package. The crew recalled that the weather briefing package contained forecast light showers and some cloud in the vicinity of Brisbane and that the forecast weather for departure at Sydney was worse.
Figure 4: Brisbane Airport weather radar overlay on 4 May at 1200 local time (time of departure)
Source: Qantas, annotated by the ATSB
Cabin preparation for landing
The Qantas Flight administration manual (FAM) specifies that the flight crew make the ‘prepare cabin’ public announcement (PA) for cabin crew to commence cabin preparations at 20,000 ft or no lower than 10,000 ft above the destination airport. This PA can be performed at a higher altitude when considering descent profile, arrival procedures, weather and workload management. The customer service manager will then confirm receipt of the PA by directly contacting the flight crew.
The Qantas Cabin crew operation manual (CCOM) states the timing of this announcement should provide the cabin crew at least 10 minutes to secure the cabin and occupants for landing prior to the illumination of the seatbelt sign. After receipt of the ‘prepare cabin’ PA, all activity by the cabin crew shall be safety‑related only and no new service duties may be initiated.
Additionally, the FAM stated, ‘should contingencies occur that impact on the planned preparation time, every effort should be made to advise the cabin crew of these changes.’
In the case of the occurrence, the CSM recalled that the captain advised them that they would prepare the cabin earlier for a ‘bit of weather’. The prepare cabin PA was performed after passing 30,000 ft and the seatbelt sign was illuminated less than 10 minutes later following a further discussion with the CSM relating to the progress of the cabin preparations.
Anticipated turbulence on descent
In the event that turbulence is anticipated on descent, the Qantas FAM stated that:
Where turbulence is anticipated during descent, the flight crew should consider the 10 minutes requirement to prepare the cabin for landing. Cabin crew are to be alerted to anticipated turbulence as early as possible to enable them to complete their duties.
Any time the seatbelt signs are illuminated for turbulence, a PA must be made by the crew.
Securing cabin for landing
Cabin secured for landing
The CCOM specified that when the seatbelt sign is illuminated at the conclusion of the 10 minutes, the CSM will make the following PA:
All customers and crew must now be seated for landing with their seatbelt fastened
The cabin crew will subsequently perform the following procedures:
• ensure passengers are seated
• verify lavatories are vacant
• conduct a simultaneous galley secure check
• return to jump seats and secure within one minute
• after one minute, the CSM initiates a callback from their jump seat to the other cabin crew, to advise that the cabin was secure
• perform silent [safety] review.
Cabin unsecured for landing
Approximately one minute after the seatbelt sign is illuminated, the CSM will initiate a callback from their designated jump seat. Each cabin crew member will respond with ‘door number, name, cabin secured for landing’. If the cabin is not secured for landing, the CSM will inform the flight crew. In this case, the CCOM stated the ‘the CSM will assess the situation and inform the flight crew regarding the status of the cabin.’ This allows alternative actions before the no contact period, which commences when the landing gear is extended for landing. The cabin crew are not to contact the flight deck under any circumstances during this period.
In this case, the captain stated they would have ensured that passengers and cabin crew assisting the injured member were seated before landing had they been informed the cabin was not secure.
Use of cabin secure notifications in Australian airlines
The ATSB also reviewed the cabin secure procedures of 7 similar Part 121 passenger air transport operators in Australia. Of those, 4 operators employed a positive signal to confirm cabin security during normal operations, while 3 did not.
In the past 20 years, the ATSB identified 26 occurrences involving unrestrained occupants on landing, based on historical occurrence data. None of these resulted in fatalities, serious injuries, or minor injuries. Of these 26 occurrences, only 4 could potentially be linked to the absence of a positive cabin secure signal.
Anticipated turbulence procedure
If the flight crew anticipates turbulence, the following procedure from the CCOM will apply:
When the flight crew become aware of anticipated turbulence, they will liaise with the CSM advising the time and likely duration of the anticipated turbulence.
The CSM will relay this information to the members of the cabin crew to enable them to prioritise their duties by securing carts, galleys, items of service equipment, cabin and galley curtains, and the passenger cabin, based on time available.
A PA may be made by the flight crew to the passengers and cabin crew advising that cabin service is to cease as there is a likelihood of turbulence and the following actions will be initiated (Table 4):
Table 4: Crew actions during anticipated turbulence
Action
Description
Seatbelt sign illumination
Must be illuminated by the flight crew no later than one minute prior to anticipated turbulence.
Cabin crew seated
Cabin crew to be seated in their jump seat within one minute of seatbelt signs illumination
Seatbelt announcement
Flight crew announces, ‘all passengers and crew to be seated and fasten seatbelts.’
Call back procedure
CSM initiates call back to ensure all cabin crew are seated and have assessed the cabin condition.
Cabin crew call back response
Cabin crew respond to CSM with, ‘door number, name, seated and secured,’ or if cabin or crew are not secure, cabin crew report this to CSM during the call back.
Confirming security
If secure, CSM calls flight crew via interphone to confirm, ‘passengers and crew are secure’, as well as any other relevant information
Unanticipated turbulence
Unanticipated light turbulence
If it is deemed necessary to illuminate the seatbelt signs for unanticipated light turbulence, the flight crew will perform the ‘seatbelts’ PA announcing, ‘all passengers and crew must be seated and fasten seatbelts.’
The CCOM states the following will then apply:
Cabin crew are to prioritise their duties by securing carts, galleys, items of service equipment and the passenger cabin and initiate crew actions for anticipated turbulence…..
When the captain illuminated the seatbelt sign prior to the turbulence encounter, they performed the ‘seatbelts’ PA. They stated they did this as a precautionary measure as this was their normal practice if there is the possibility of some turbulence.
Unanticipated turbulence posing an immediate hazard
In the event of unanticipated turbulence that poses an immediate safety hazard, the flight crew must select the seatbelt signs on and announce the ‘turbulence’ PA:
All passengers and crew be seated and fasten seatbelts immediately.
Following this announcement, the CCOM issues the following instructions:
Cabin crew will lock carts in position and secure themselves in the nearest seat or wedge themselves in the aisle.
If circumstances permit, the CSM will initiate the call back procedure, ascertain the condition of the cabin and relay this information to the flight crew.
Cabin crew incapacitation
In the event of a cabin crew member’s incapacitation, the CCOM calls for first aid to be administered, and the CSM and captain to be notified as soon as practicable. The CSM would then reassign the duties of the incapacitated crew member to an assist crew member, if available. If the incapacitation results in a crew complement less than the minimum required, the CSM, in consultation with the captain, will determine whether any additional off‑duty crew members are available to assume the role of the incapacitated cabin crew for landing.
The timing of the incapacitation placed concurrent procedural demands on the CSM and disrupted the cabin secure procedures. The CCOM procedures were sequential instructions designed to achieve consistent performance and reduce the potential for miscommunication and non‑conformances.
Injury response tool
The Qantas Group injury response tool specified the actions the crew must follow if an injury has occurred inflight. In this case, the injury response tool directed crew to seek immediate doctor advice via telephone for a turbulence event and for a head blow or head strike which fell under the classification as a ‘specific circumstance’. Consequently, the crew would be required to cease work immediately.
However, as neither co‑workers nor the injured crew recognised the symptoms of a concussion in the L2P or a facial injury in the CSM, they were not triaged according to the Group injury response tool. The operator stated that this likely occurred due to the injury response tool process relying on the self‑assessment of injuries which may not be immediately apparent.
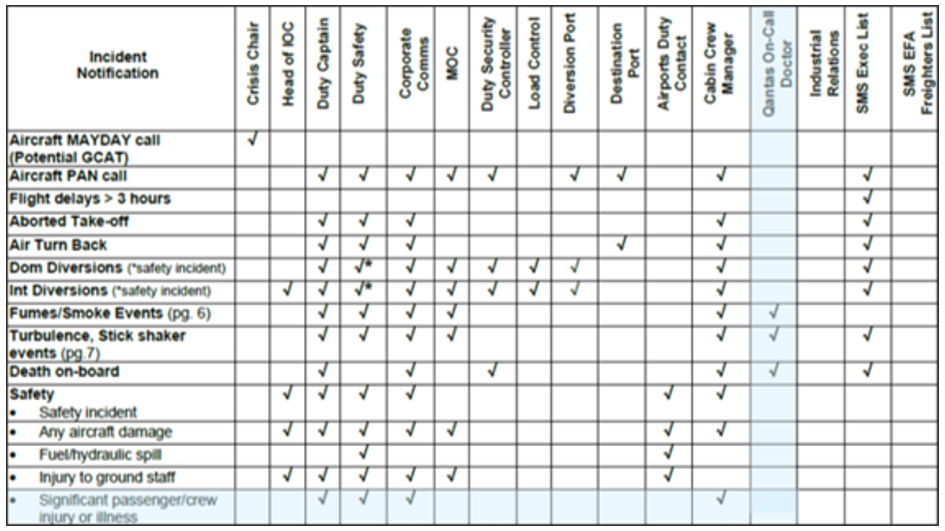
Integrated operations controls procedures
The integrated operations control (IOC) was the central point of contact during any kind of disruption or incident on a Qantas aircraft. At the time of this occurrence, the IOC incident notification communications protocol contained in the operations control procedure (Figure 5) included contact with the on‑call doctor in cases of severe turbulence regardless of whether there were reported injuries. The IOC notification process for a ‘significant passenger/crew injury or illness’ event did not include contact with the Qantas on‑call doctor.
As the turbulence in this event was deemed post‑event by flight crew as moderate, contact with the on‑call doctor was not required under the process.
Figure 5: Qantas incident notification communications protocol version 11, March 2024
Source: Qantas
Research into turbulence detection
There are occasions where it can be challenging to identify turbulence. The US National Transportation Safety Board conducted 10 case studies (National Transportation Safety Board, 2021) of accidents between 2019–2020 that involved turbulence and embedded convection and determined that:
Embedded convection may not be easily detected by onboard or ground‑based weather radar, and when not visible outside the aircraft windows, this class of convective activity can act as a hidden source of severe turbulence encounters within an otherwise benign‑looking cloud mass.
Research into turbulence related injuries
From 2009 through 2018, the US National Transportation Safety Board (NTSB)[10] found that turbulence‑related accidents accounted for more than a third of all Part 121 accidents. The accident data revealed that the most common phase of flight associated with turbulence‑related accidents in Part 121 operations was during the en route descent, which accounted for 36.0% of accidents.
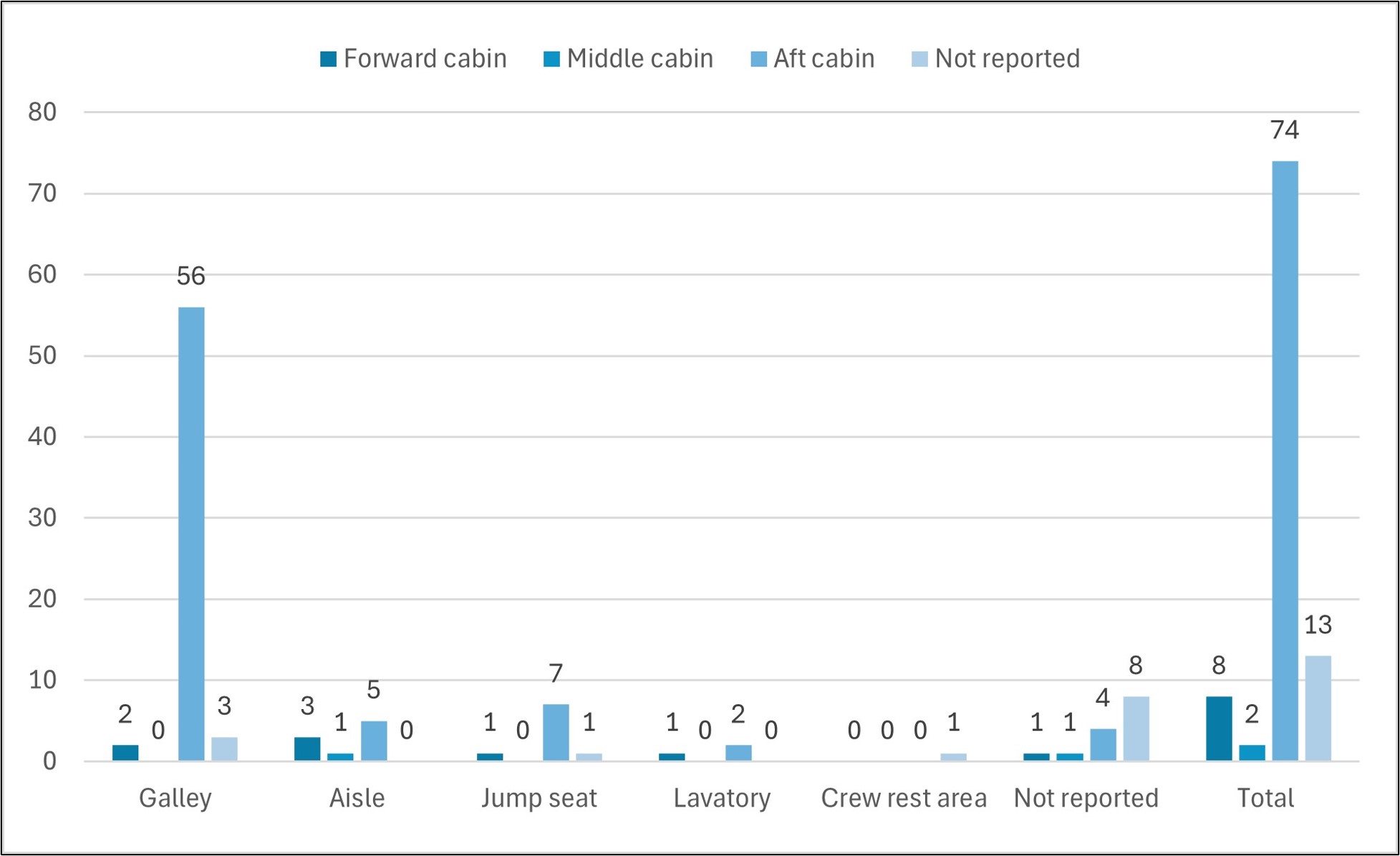
Further analysis indicated that cabin crew accounted for 78.9% of serious injuries, with the majority occurring in the aft section of the aircraft cabin. Passengers accounted for 21.1% of serious injuries, while no flight crew members were seriously injured (National Transportation Safety Board, 2021).
The distribution of cabin crew injuries found most occurring in or near an aft galley (Figure 6), which likely reflects that the service‑related duties of cabin crew often require them to spend more time working unrestrained in the galley area. The most commonly reported cabin crew activities at the time of serious injury were:
preparing the cabin for landing (39.2%)
conducting cabin service (13.4%)
preparing for cabin service (9.3%).
During this occurrence, the R2P and L2P sustained the most severe injuries while unrestrained in the aft galley as they prepared the cabin for landing, which is consistent with research on turbulence‑related injuries.
Figure 6: Location of cabin crew at time of turbulence‑related serious injury, 2009–2018
Source: National Transportation Safety Board
Safety analysis
Crew communication
During the descent into Brisbane, the captain commenced cabin preparations earlier than usual, using standard protocols to account for known weather conditions en route. Although the graphical area forecast indicated the possibility of moderate to severe turbulence, the captain did not observe weather radar returns or receive any other pilot reports indicating the presence of moderate to severe turbulence during the descent.
Approximately 5–6 minutes after initiating cabin preparations, the aircraft entered stratiform cloud and the captain contacted the customer service manager (CSM) to check on the cabin crew’s progress. The purpose of this communication was to provide the captain with information to guide the timing of the seatbelt sign illumination. However, the captain did not provide any weather‑related information to the CSM during this interaction, leaving the cabin crew unaware of any increased likelihood of turbulence.
Two minutes later, the seatbelt sign was illuminated, accompanied by the ‘seatbelt’ public announcement (PA). The captain then observed an approaching cumulus cloud along the flight path but determined it did not pose an immediate hazard based on a visual assessment and the lack of radar indications. As a result, the captain did not perform the ‘turbulence’ PA, which would have prompted the cabin crew to immediately secure themselves in the nearest seat or wedge themselves in the aisle to prepare for the turbulence encounter.
Although the captain contacted the CSM to confirm the time remaining to prepare the cabin, the absence of indications to the subsequent severity of the turbulence limited the captain's perception of the possible threat. Therefore, additional precautions were not considered. The captain followed normal descent procedures, however, did not discuss any additional weather‑related information in communications with the CSM.
As a result, the cabin crew, who relied on information from the flight crew, were unprepared for the turbulence encounter. This situation underscores the difficulties posed by unexpected turbulence, as the procedures for managing in‑flight turbulence rely on the flight crew's ability to predict or avoid these situations.
Contributing factor
The captain did not communicate to the cabin crew about the expected turbulence, likely as a result of the captain not knowing the severity of the turbulence.
Crew unrestrained during severe turbulence
When the seatbelt sign was illuminated during the descent, cabin crew members were required to perform several duties whilst being unrestrained. In the moments immediately preceding the turbulence encounter, the CSM and R2P recalled checking their assigned lavatories as part of securing the cabin for landing.
Cabin crew were required to complete their assigned duties within one minute of the seatbelt sign being illuminated, which was also the case for unanticipated light turbulence. The captain performed the ‘seatbelts’ PA when the seatbelt sign was illuminated, which indicated unanticipated light turbulence to the cabin crew members. However, the cabin crew did not recall hearing this PA and remained unaware of the increased risk of turbulence as the aircraft approached a cumulus cloud.
Because the turbulence event occurred less than one minute after the illumination of the seatbelt sign, which was accompanied by the ‘seatbelt’ PA, the cabin crew did not have sufficient time to ensure they were seated and restrained prior to the aircraft being affected by turbulence. The injuries sustained during the encounter reflect research showing that cabin crew members face a higher risk of turbulence‑related injuries, especially during the descent phase of a flight when they are preparing for landing (National Transportation Safety Board, 2021).
Contributing factor
Three cabin crew were unrestrained while performing duties during unanticipated severe turbulence resulting in all 3 receiving injuries.
Cabin management
After the turbulence event, the CSM and left 2 primary (L2P) turned their attention to the right 2 primary (R2P) who was laying on the floor of the aft galley and was unable to move due to their injury. The turbulence event occurred in the latter stages of the descent, which meant there was little time to provide first aid to the R2P and complete the required preparations for landing. The CSM, L2P and the passengers assisting the R2P were reluctant to return to their assigned seats despite the clear instructions from the captain to do so.
The situation in the aft galley disrupted the procedural flow and meant that the CSM and L2P became focused on providing first aid rather than returning to their seats to complete the callback and silent review prior to landing. Interruptions often lead people to forget to resume their tasks, while multitasking can further complicate the situation by increasing the overall workload within a limited timeframe (Loukopoulos & Barshi, 2009). In this case, the CSM and L2P had to balance providing first aid and securing the cabin. High stress levels are also known to cause errors(Kim & Hyun, 2022), which likely contributed to the CSM prioritising providing first aid over securing themselves and the cabin for landing.
The CSM subsequently lost situational awareness with respect to the phase of flight and the sequence of the standard operating procedures. As a result of being situated in the aft galley, the CSM likely missed audible cues, such as the extension of the landing gear.
The captain did not recall receiving any requests for more time to prepare the cabin for landing. Additionally, the single aisle cabin configuration of the Boeing 737 offered limited options for accommodating the R2P anywhere other than the aft galley. After repeated instructions for everyone to be seated for landing, the captain was confident that all uninjured occupants had complied.
The decision of the CSM and L2P to remain unrestrained in the aft galley during a critical phase of flight increased the risk of incapacitation to additional cabin crew, which could have further compromised their ability to manage a landing‑based emergency effectively if one was to happen. Additionally, the 5 occupants in the aft galley created a potential obstruction to emergency exits, increasing the likelihood of delays or complications if they needed to enact an emergency evacuation.
Other factor that increased risk
Although the captain had instructed that the uninjured passengers and crew needed to be seated, 3 cabin crew and one passenger were unrestrained for landing due to being preoccupied with administering first aid to the injured cabin crew member. This increased the risk of injury to the unrestrained occupants and had the potential to compromise a safe emergency evacuation if required.
The aircraft landed with the CSM, L2P, R2P and 2 passengers unrestrained in the aft galley. The flight crew was made aware by the CSM that the injured cabin crew member was unsecured and unable to be made secured for landing and instructed the CSM to ensure everyone else was secure for landing. While this instruction was communicated to those people unsecure in the cabin, the instruction was not followed as described above. The CSM attempted to inform the flight crew by instructing the L2P to communicate with them. However, the captain again instructed that everyone who could be secured needed to be, as they were landing. As such, the flight crew assumed all cabin occupants would be secure apart from the injured R2P crew. At this stage, the cabin crew operating procedures requiring the CSM to inform the flight crew if the cabin was not secure broke down as there was no further communication that the cabin was not secure.
The captain stated that if they had known that 4 uninjured occupants were still unrestrained in the aft galley, they would have taken appropriate action to ensure they had returned to their seats prior to the final approach to land. The lack of a positive signal increased the likelihood that flight crew would be unaware of unrestrained occupants during the approach and landing phases of flight.
While the lack of a positive cabin secure signal played a role in this occurrence, the available data does not indicate it as a significant ongoing risk.
Other factor that increased risk
The Qantas 737 procedures did not require flight crew to receive positive confirmation that the cabin was secure for landing. This increased the risk that occupants and objects were not secure for landing.
Post‑flight medical assessment
Shortly after arrival at the gate at Brisbane airport, the R2P was attended to by ambulance personnel. However, the CSM and L2P, who were also injured during the event, did not receive any follow‑up medical assessments or treatment. This situation arose due to procedural gaps, which relied on crew members to self‑assess and report a significant injury to receive a medical assessment.
While the CSM self‑diagnosed a minor injury and reported it the following day, the L2P was unaware of their injury. As a result, the L2P operated on multiple flights while experiencing symptoms of an undiagnosed concussion, until some days later when co‑workers noticed signs of a possible injury.
Other factor that increased risk
A crew member with undiagnosed concussion from the accident flight operated on subsequent flights without receiving appropriate medical attention.
The Qantas integrated operations control protocols did not mandate contacting the on‑call doctor in cases where a passenger or crew member was significantly injured. Although the protocol required consultation with the on‑call doctor in cases of severe turbulence, this turbulence event was classified as moderate, and no medical consultation was either required or requested. Additionally, the Qantas group injury response tool also relied on crew members self‑assessing their injuries to determine if medical treatment would be required, but an injured crew member may not realise the extent of their injury at the time.
In the cases of a concussion, symptoms may include impairments in neurocognitive functioning, primarily affecting attention, concentration, memory, and judgment or problem‑solving (Ryan & Warden, 2003). Returning to work with an undiagnosed concussion likely compromised the L2P’s ability to perform safety‑critical tasks. A subtle incapacity due to an undiagnosed injury could negatively impact operational safety, particularly during emergencies.
Other factor that increased risk
Qantas lacked a procedure to ensure cabin crew fitness was assessed after a significant injury. This increased the risk that a crew member could continue to operate while being unfit for duty. (Safety issue)
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the turbulence event and cabin crew injury involving Boeing 737, VH‑VYK, 36 km south‑east of Brisbane Airport, Queensland, on 4 May 2024.
Contributing factors
The captain did not communicate to the cabin crew about the expected turbulence, likely as a result of the captain not knowing the severity of the turbulence.
Three cabin crew were unrestrained while performing duties during unanticipated severe turbulence resulting in all 3 receiving injuries.
Other factors that increased risk
Although the captain had instructed that the uninjured passengers and crew needed to be seated, 3 cabin crew and one passenger were unrestrained for landing due to being preoccupied with administering first aid to the injured cabin crew member. This increased the risk of injury to the unrestrained occupants and had the potential to compromise a safe emergency evacuation if required.
The Qantas 737 procedures did not require flight crew to receive positive confirmation that the cabin was secure for landing. This increased the risk that occupants and objects were not secure for landing.
A crew member with undiagnosed concussion from the accident flight operated on subsequent flights without receiving appropriate medical attention.
Qantas lacked a procedure to ensure cabin crew fitness was assessed after a significant injury. This increased the risk that a crew member could continue to operate while being unfit for duty. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Qantas lacked a procedure to assess cabin crew fitness after a serious injury. This increased the risk that a crew member could continue to operate while being unfit for duty.
Glossary
AHM
Aircraft health monitor
AMSL
Above mean sea level
ATIS
Automatic terminal information service
CCOM
Cabin crew operations manual
CSM
Customer service manager
FAM
Flight administration manual
IOC
Integrated operations control
L1
Left one
L2
Left two
L2P
Left two primary
NOTAM
Notice to airmen
NTSB
National Transportation Safety Board
PA
Public announcement
R1
Right one
R1P
Right one primary
R2P
Right two primary
TAF
Terminal area forecast
Sources and submissions
Sources of information
The sources of information during the investigation included:
the captain of the accident flight
the customer service manager on the accident flight
the R2 primary cabin crew member on the accident flight
Kim, J. Y., & Hyun, S. (2022). Study on Factors That Influence Human Errors: Focused on Cabin Crew. International Journal of Environmental Research and Public Health, 19(9), 5696.
Loukopoulos, L. D., & Barshi, I. (2009). The multitasking myth : Handling complexity in real-world operations. Taylor & Francis Group. Taylor & Francis Group.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the captain of the accident flight
the customer service manager on the accident flight
the L2 primary cabin crew member on the accident flight
the R2 primary cabin crew member on the accident flight
Qantas Airways Limited
Civil Aviation Safety Authority
Bureau of Meteorology.
Submissions were received from:
the L2 primary cabin crew member on the accident flight
the R2 primary cabin crew member on the accident flight
Qantas Airways Limited
Civil Aviation Safety Authority
Bureau of Meteorology
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Stratiform: clouds that exhibit extensive horizontal development (in contrast to the vertical development of cumuliform clouds).
[2]Cumulus: a principal cloud type, forming in the low levels of the troposphere, characterised by flat bases and dome or cauliflower‑shaped upper surfaces. Small, separate cumulus are associated with fair weather but may grow into towering cumulus or cumulonimbus.
[3]Automatic terminal information service (ATIS): the provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts.
[4]Few is a meteorological term used in aviation to describe cloud coverage that occupies 1 to 2 oktas (eighths) of the sky.
[5]Broken cloud is a meteorological term used in aviation to describe cloud coverage that occupies 5 to 7 oktas (eighths) of the sky.
[6]Scattered cloud is a meteorological term used in aviation to describe cloud coverage that occupies 3 to 4 oktas (eighths) of the sky.
[7]NOTAM: Notice to Airmen (NOTAM) is a notice containing information or instructions concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to persons concerned with flight operations.
[8]Flight watch service: a flight watch service provides updated weather information to pilots en route.
[9]Terminal forecast (TAF): a TAF is a coded statement of meteorological conditions expected at an aerodrome and within a radius of 8 kilometres of the aerodrome reference point.
[10]National Transportation Safety Board. (2021). Preventing Turbulence‑Related Injuries in Air Carrier Operations Conducted Under Title 14 Code of Federal Regulations Part 121.
Occurrence summary
Investigation number
AO-2024-032
Occurrence date
04/05/2024
Location
36 km south-east of Brisbane Airport
State
Queensland
Report release date
27/05/2025
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Cabin injuries, Turbulence/windshear/microburst
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
The Boeing Company
Model
737-838
Registration
VH-VYK
Serial number
34183
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 11 April 2024, a Cessna 404 Titan was being operated on an aerial survey flight north of Emerald, Queensland, with 3 crew members onboard. During the survey run, the crew was affected by fumes inside the cabin and chose to return to Emerald. At 1538, the aircraft landed successfully at Emerald Airport, where all 3 crew members received medical treatment for impairment symptoms. The aircraft was temporarily withdrawn from service for examination.
What the ATSB found
The ATSB found that operating crew members were all affected by fumes in the cabin and, possibly due to the associated impairment, the pilot returned the aircraft to Emerald rather than diverting and landing at a closer alternate airport. Despite extensive ground and in‑flight examination after the occurrence, the source of the fumes could not be established.
What has been done as a result
On 30 April 2024, the operator issued a mandatory requirement for all pilots on all flights – including those below flight levels – to secure the onboard oxygen equipment within seated reach of the pilot-in-command. As an additional risk control, the operator also required photographic evidence of this to be forwarded to the Head of Flight Operations (HOFO) prior to departure.
On 2 May 2024, the operator issued guidance to all pilots via Notices to Aircrew (NOTACs) regarding the circumstances in which oxygen should be used in‑flight. The operator recommended that supplementary oxygen be used in the following circumstances:
discharge of a fire extinguisher in aircraft cabin
smoke or fumes in cabin
suspected CO in cabin
any other occasion where oxygen may assist the health or wellbeing of a crew member.
Pilots were also advised to follow existing standard operating procedures and conduct a precautionary landing as soon as possible in the event of smoke, fumes, or gas in the cabin. This guidance was also incorporated into the operator’s emergency training modules.
Safety message
Fumes and airborne contaminants can result in the rapid onset of incapacitation that significantly affects crew decision‑making, communication and aircraft handling ability. The degree of physical or cognitive incapacitation can also vary widely between individuals, which may make it difficult to detect and respond to fume events.
Operating crews should therefore be alert to the potential hazards posed by odours and fumes and not hesitate to use supplemental oxygen and all other available means to ventilate the cabin. It is also important to be aware of alternate airports en route, and consider diverting to reduce the airborne exposure time. Crews should also communicate the presence of fumes, and any symptoms being experienced, to air traffic control at the first available opportunity as this will maximise the assistance available to crews both in the air and on the ground.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 11 April 2024, a Cessna 404 Titan was being operated by Aero Logistics on an aerial survey flight north of Emerald, Queensland. The flight was being operated under visual flight rules,[1] with one pilot and 2 task specialists operating the survey equipment. At 1317 local time, the aircraft departed Emerald Airport to the north-east before turning towards Moranbah and climbing to an altitude of 5,000 ft (Figure 1).
Figure 1: Survey area location and recorded flight path between Emerald and Moranbah
Source: Google Earth and operator ADS-B data, annotated by the ATSB.
At around 1349, the aircraft approached the Moranbah area and was descended to 4,000 ft to begin the first survey run. This required the aircraft to maintain a constant altitude and speed while travelling along specific parallel ‘lines’ overhead the target area as instructed by the task specialists. Approximately 20 minutes into this run, all 3 crew members started to notice a sporadic smell in the cabin, although their recollection of the smell differed.
The pilot advised that, as the flight progressed, they noticed that they had increasing difficulty setting the aircraft up and aligning it correctly. One of the task specialists also began to feel affected by the fumes, and at 1449 the pilot cancelled the survey and commenced a return to Emerald Airport. The first task specialist moved to the rear of the aircraft due to the extent of their respiratory symptoms. The second task specialist was not experiencing any symptoms at this stage, and repositioned to the cockpit to assist the pilot if needed.
Return to Emerald
During the return to Emerald, the crew opened the windows, vents, and cabin door to ventilate the cabin. They also disconnected the survey equipment and checked several aircraft systems, including ensuring that the autopilot was selected off, in an attempt to control or reduce the fumes. None of these measures resulted in any improvement, and the pilot and task specialists reported experiencing worsening symptoms as the flight progressed, but the nature and extent of these symptoms varied between each person. Although several diversionary airports were available en route, the pilot chose to continue to the base at Emerald.
Approximately 15 minutes from Emerald, the pilot considered conducting a precautionary landing in a field, due to worsening symptoms. They initiated a descent, and made a broadcast to Brisbane Centre, advising they were ‘landing somewhere in a field hopefully’.
Recorded flight data showed that, during this descent, the aircraft reached a maximum descent rate of 2,664 ft/minute. The pilot levelled the aircraft off at around 2,200 ft, approximately 14.5 km north‑east of Capella Airport. However, the pilot did not consider a diversion to Capella at that time. The pilot advised that they had managed to get some fresh air and decided to continue.
Several minutes later the pilot observed that the trim wheel started what they assessed as an uncommanded nose down input, and that ‘the autopilot was actually now trying to push us into the ground.’ In response, the pilot asked the task specialist seated beside them to hold the trim wheel, which rectified the issue. The task specialist confirmed that the trim wheel was moving but that they did not require significant force to stop it. They also advised that it was possible the pilot accidently activated the electric trim switch on the control column.
Landing
The pilot advised air traffic control that they were experiencing fumes in the cabin, but they did not mention any control issues with the aircraft. They declined an offer for emergency services on arrival, and no MAYDAY[2] or PAN PAN[3] calls were heard or recorded by air traffic controllers at any point during the flight. The pilot continued to Emerald where, after confirming the wind direction on their electronic flight bag, and informing other traffic of their intentions, tracked for a right base leg of the circuit for runway 24,[4] and landed at 1538.
Although the pilot had not requested emergency services, the Brisbane Centre controller called the aerodrome reporting officer (ARO) at Emerald Airport to advise them of the aircraft’s approach. The ARO then called emergency services at around 1530, and several Queensland Fire and Emergency Service (QFES) appliances were waiting at the parking bay when the aircraft landed. The crew was able to disembark unassisted, but one task specialist exited the aircraft and lay down on the grass next to the aircraft due to nausea. The second task specialist reported having a headache towards the end of the flight.
The ARO did not detect any fumes or smoke when they opened the rear door of the aircraft. The operator’s chief engineer entered the aircraft and similarly could not identify any smells, fumes, or smoke inside the aircraft. QFES crews then attended the aircraft, conducting a thermal scan and gas sampling of the interior with nil results. All of the internal panels and the flooring were removed for inspection and the QFES crews did not detect any fluid leaks internally or externally, but the aircraft was isolated overnight as a precaution.
The crew was attended to by paramedics at the scene before being transported to Emerald Hospital. They were given several hours of high-flow oxygen as a standard treatment and cleared to leave hospital later that evening. Blood samples were not taken from the crew as Emerald Hospital did not have the equipment required for blood gas testing. The aircraft was temporarily withdrawn from service for additional examination and testing.
Context
Crew information
Pilot
The pilot was experienced with piston and turboprop aircraft, and possessed the relevant qualifications and competencies for the work being conducted. The pilot had several decades of experience conducting freight, passenger, and recreational flights with a number of operators across Australia and overseas. The pilot had recently joined the operator to operate their piston aircraft. The pilot had passed their most recent aviation medical examination in July 2023.
Task Specialist 1
Task specialist 1 (TS1) was experienced with aerial survey work, having worked for a number of years with the owner/operator of the aerial survey equipment installed on the aircraft. Most of their experience had been in Cessna 404 and 406 series aircraft, and they had not previously experienced fumes or smells inside the cabins of these aircraft.
Task Specialist 2
Task specialist 2 (TS2) had limited experience on the Cessna 404 and had spent most of their time on Cessna 406 and 441 series aircraft. At the time of the occurrence, they were in the process of obtaining an aeroplane pilot licence, with several hours of flight time already logged. TS2 had experienced fumes in another aircraft several years earlier caused by a fault in the air conditioning system, but had not encountered anything similar in the Cessna 404.
Response to fumes and symptoms
When the crew decided to cancel the survey run, the aircraft was around 37 km north‑west of Moranbah Airport and Emerald was around 200 km south. The pilot advised that they would have had to declare an emergency to land at Moranbah Airport, as it was a private airport, and at that stage they did not consider there was an emergency. They had also experienced a flap issue the day before with resultant fumes in the cockpit and they considered this to be a similar event.
The pilot had completed emergency response and hypoxia awareness training in November 2023 and had been issued a pulse oximeter as part of the operator’s standard induction process. The aircraft had oxygen equipment onboard and the pilot and both task specialists were trained in how to use this equipment. The task specialists confirmed that the pilot had given an emergency briefing prior to departure. They could not recall whether the onboard oxygen equipment had been mentioned specifically, however there had been no plan to fly above 10,000 ft.
The crew confirmed that during the return to Emerald, they used a supplied pulse oximeter to assess the oxygen saturation levels in their blood several times – however, none of the crew considered using the onboard oxygen equipment.
Aircraft information
The aircraft was a Cessna Aircraft Company 404 Titan, manufactured in 1978 and equipped with 2 Teledyne Continental GTSIO-520-M engines. It was one of 7 such aircraft in the operator’s fleet. The operator told the ATSB that these aircraft were not modified from the original Cessna 404 design apart from the floor cutouts for the survey equipment unit. This unit was placed above the fuselage cutout at the rear of the cabin and secured to the floor with the cameras and sensors facing downwards.
The survey operators would usually place aluminium tape or cardboard around the unit to seal any gaps between the unit and the cutout in the floor. The operator also confirmed that the cable routing and electrical harnesses for the equipment and aircraft systems had been arranged and routed in a standard configuration around the cutouts in the fuselage.
Maintenance information
On 10 April, the day prior to the incident, the same aircraft with the same crew was conducting similar survey runs north of Emerald. The pilot said that during this flight they experienced an uncommanded extension of the flaps to the full-down position after the flaps were extended to Flap 10. The pilot attempted to troubleshoot the problem by moving the flap lever back and forth, but the flaps did not respond to movements of the flap lever. The pilot also began to notice a smell in the cabin when the flap issue commenced, and that their airspeed was lower than expected. The pilot decided to return to Emerald, but did not advise the maintenance personnel of the presence of fumes.
An engineering inspection found that the wires on the micro-switch had detached from the flap select lever. The operator said that this inspection also found that ‘the wire hadn't touched any surrounding areas, hadn't tripped, hadn't burned or anything like that’. The wires were checked and reconnected on the morning of 11 April, and the flap lever was tested before the aircraft was released back into service that day. No flap issues were detected after this repair was made.
Following the incident flight, the operator undertook flight tests, scheduled maintenance, and strip‑down examinations of aircraft wiring and componentry, including inspections and testing of:
panels and flooring, which were removed to inspect for electrical wiring damage
the autopilot and electrical trim systems
around and underneath the cockpit dash and pilot side electrical panel and relay boxes
the battery and lighting systems
the heater and ventilation systems
the engines, including alternators and electrical looms
the hydraulic system
the nose and main landing gear bays and wiring
the tail interior and flight controls
the left and right inner wings
the flap coves and flight controls
the nose locker and wing lockers including interior lighting.
No mechanical or wiring issues that could have been related to fumes were detected. The survey operator found no wiring defects or component faults in their survey equipment unit, which was then reassembled and installed on a different aircraft. The operator also confirmed that there was a card-based carbon monoxide and a digital aural CO detector on the aircraft, and that neither of these detectors had activated during the incident flight or the test flights conducted after the occurrence. Additionally, neither the pilot nor task specialists recalled either CO monitor activating during the occurrence flight.
Environmental
Weather
Weather data was requested from the Bureau of Meteorology (BOM) for winds aloft and automated METARs[5] in the area between Emerald and Mackay. This data confirmed that visual meteorological weather conditions[6] existed, with temperatures around 25 ˚C and cloud cover[7] ranging between few and scattered up to altitudes of around 5,000 ft. These conditions were consistent for the duration of the flight.
Bushfires and mining activity
The crew did not observe any blast fumes or mining activity in the Moranbah area during the incident flight. BOM data also confirmed no known plumes and smoke in the area. Queensland government data on mining activity and blast fumes was requested but this was not provided. The pilot did not indicate the presence of any bushfires or smoke that could have generated fumes, and TS2 stated that there were some minor grass fires in the area, but these were not in the immediate vicinity of the flight path.
The operator confirmed through post-flight testing that ground-based fumes and smells could ‘be picked up within the cabin with the environmental settings open in the venting configuration’. The operator also described a smoke smell in the cabin during the post-incident test flight when the aircraft flew directly overhead a local grass fire. However, this smell was only temporary and limited to the specific fire area and was markedly different to the smell described by the crew.
Safety analysis
During the return flight to Emerald following the onset of impairment symptoms, the crew could not identify the source of the fumes inside the cabin. Based on the available evidence, no definitive cause or source for the fumes could be established. There were no visible signs of smoke or leaks, and there were no environmental conditions that could have consistently generated fumes inside the cabin. The onboard CO detectors did not activate, and post-incident testing by QFES did not identify noxious gases or thermal hotspots. The operator was also unable to identify any faults or defects in the wiring or componentry of the onboard systems and could not replicate the fumes in test flights.
Although the decision to cancel the survey run was prudent, flying back to Emerald, rather than diverting to closer suitable airports exposed the crew to the fumes for longer than necessary and may have worsened the impact. However, this decision may have been influenced by the flap‑related incident on the previous day. In addition, although the crew was trained to use the supplemental oxygen equipment onboard, and repeatedly used the pulse oximeters, the crew did not consider using the available oxygen.
It is probable that all the crew members were affected by the fumes, although these symptoms presented differently in each crew member. TS1, sitting at the rear of the aircraft, reported nausea and respiratory symptoms. TS2 reported experiencing a headache. The pilot did not experience any physical symptoms but may have been experiencing cognitive impairment in terms of their decision-making and aircraft handling, even though the pilot navigated and controlled the aircraft as per the established procedures and communicated effectively on the radio.
The pilot’s decision not to declare a MAYDAY or PAN PAN, or to have emergency services in attendance for the landing, may have been a result of their impaired decision‑making. Fortunately, the controller proactively initiated the emergency response by alerting the ARO.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fumes event involving Cessna 404, VH-LAD, near Moranbah, Queensland on 11 April 2024.
Contributing factors
The operating crew was affected by fumes in the cabin and the pilot returned the aircraft to Emerald rather than landing at a closer suitable alternate airport.
Other findings
Despite extensive post‑occurrence ground and in‑flight examination, the source of the fumes could not be established.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Aero Logistics
Prior to the commencement of the ATSB investigation, the operator proactively took several steps in response to the incident.
Placement of oxygen equipment
On 30 April 2024, the operator issued a mandatory requirement for all pilots on all flights – including those below flight levels – to secure the onboard oxygen equipment within seated reach of the pilot-in-command. As an additional risk control, the operator also required photographic evidence of this to be forwarded to the Head of Flight Operations (HOFO) prior to departure.
Use of oxygen equipment
On 2 May 2024, the operator issued guidance to all pilots via Notices to Aircrew (NOTACs) regarding the circumstances in which oxygen should be used in‑flight. The operator recommended that supplementary oxygen be used in the following circumstances:
discharge of a fire extinguisher in aircraft cabin
smoke or fumes in cabin
suspected CO in cabin
any other occasion where oxygen may assist the health or wellbeing of a crew member.
Pilots were also advised to follow existing standard operating procedures and conduct a precautionary landing as soon as possible in the event of smoke, fumes, or gases in the cabin. This guidance was also incorporated into the operator’s emergency training modules.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the operating crew
Aero Logistics
Airservices Australia
Bureau of Meteorology
recorded data from the ADS-B unit on the aircraft.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the operating crew
Aero Logistics
the Civil Aviation Safety Authority.
No submissions were received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2]MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
[3]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[4]Runway number: the number represents the magnetic heading of the runway.
[5]METAR: a routine report of meteorological conditions at an aerodrome. METAR are normally issued on the hour and half hour.
[6]Visual Meteorological Conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[7]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky.
On 12 April 2012, a Cessna Aircraft Company 310R, registered VH-JOF, departed Jabiru aerodrome on a charter flight. On board the aircraft were one pilot and two passengers.
While on final approach to Marlgawo Aircraft Landing Area the aircraft encountered suspected sudden and severe windshear at approximately 50 ft above ground level. The aircraft landed heavily and was seriously damaged. One passenger sustained minor injuries, the other occupants were uninjured.
The Flight Safety Foundation's Approach and Landing Accident Reduction tool kit provides guidance on avoiding, recognising and recovering from windshear. The tool kit reinforces the importance of following the windshear recovery technique recommended in the aircraft operating manual and flying a stabilised approach.
On 24 December 2011 an Agusta Westland AW139 helicopter departed Bankstown Airport in response to an emergency personal locator beacon in the Budderoo National Park, about 16 km west-south-west of Wollongong Airport, New South Wales. On board the helicopter were a pilot, an air crewman, two paramedics and a doctor.
On locating the emergency beacon, the crew identified a seriously injured person on a rock ledge near the bottom of a waterfall. They assessed that it would not be possible to winch emergency personnel directly to the patient. In response, the crew landed at a nearby clear area and devised a plan to access and retrieve the patient. During the retrieval, the patient and one of the paramedics hit rocks at the base of the waterfall. The paramedic died from the impact. The patient was subsequently transported to hospital for treatment.
What the ATSB found
The Australian Transport Safety Bureau (ATSB) identified that, due to reduced light, the paramedic and patient were accidentally pulled from the rock ledge as the helicopter was manoeuvred in preparation to lift them out using its winch.
The ATSB also identified several safety issues relating to training and use of the helicopter’s lighting and radios. A number of organisational issues that could adversely influence the way crews act in similar circumstances were also identified.
What has been done as a result
In response to this accident, the Ambulance Service of New South Wales and the helicopter operator took safety action in respect of the operating scope applied to retrieval operations and procedures used by helicopter emergency crews. In addition, paramedics, in their role as ambulance rescue crewmen, are now required to conduct annual night winching currency training. Finally, proactive safety action was taken by these parties in the areas of general crew training and operational risk assessment.
Safety message
This accident highlights the dangers associated with modifying established procedures in order to complete a difficult, and potentially not previously experienced, rescue task. Specifically, the use of procedures that are neither documented nor trained for by crews makes it difficult to identify hazards and manage the related risks.
Inquest
ATSB Response to Findings
On 16 September 2014, NSW Deputy State Coroner Forbes released findings into the fatal helicopter winching accident involving an Agusta Westland AW139 Helicopter (VH-SYZ) 16km WSW of Wollongong airport which occurred on 24 December 2011. The accident was the subject of ATSB Investigation AO-2011-166.
The ATSB summary explains that a paramedic died during the retrieval operation for an injured person at the base of waterfall. The paramedic and the injured person swung into rocks after coming off a ledge during the retrieval.
With respect to findings of fact, the Coroner was unable to make a finding as to how the paramedic and injured person came off the ledge, with some uncertainty as to the evidence at the inquest. For the reasons set out in its report, the ATSB found that the paramedic and injured person were accidentally pulled from the ledge in low light conditions.
There were no significant differences in views between the findings of the Coroner and the findings of the ATSB with respect to the manner in which safety could be improved. This included the ATSB’s key safety message that dangers associated with modifying established procedures in order to complete a difficult, and potentially not previously experienced, rescue task. Specifically, the use of procedures that are neither documented nor trained for by crews makes it difficult to identify hazards and manage the related risks.
The Coroner canvassed additional recommendations relating to the coordination and planning of the rescue which can be reviewed in the Coroner’s findings.
ATSB investigations and coronial investigations
Coronial investigations are separate to ATSB investigations. In this matter the respective authorities are largely in accord as to the factors that contributed to the development of the accident involving VH-SYZ.
The ATSB's report can be downloaded by clicking on the link: Final Report.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation.
What happened
On 22 March 2018, an Airbus A320-232 was on descent into Cairns, Queensland (Qld) when it encountered severe turbulence. A cabin crew member in the rear of the aircraft sustained a broken ankle as a result.
The aircraft was flying in and out of cloud at the time of the occurrence and the pilot reported that the weather radar only showed green patches, indicating nil significant turbulence. The seat belt signs were therefore not illuminated.
The pilot reported that no turbulence was forecasted or expected. No encounters with turbulence had been reported prior to the occurrence.
Safety message
The ATSB research report Staying safe against in-flight turbulence (AR-2008-034) details that while turbulence is normal and occurs frequently, it can be dangerous. It is rarely a threat to passenger aircraft or to pilot control of the aircraft. In a typical turbulence incident, 99% of people on board receive no injuries. The report discusses what you can do to stay safe.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation.
What happened
On 1 February 2018, at about 1631 Eastern Daylight-saving Time (EDT), an Airbus A330-202 was pushing back[1] from the gate for a scheduled departure from Sydney, New South Wales (NSW) to Melbourne, Victoria (Vic.).
During the pushback, the tow was disconnected and an aircraft engineer instructed the flight crew to apply the park brake. The brakes were applied by the flight crew while the aircraft was still moving. The aircraft stopped suddenly and the nose subsequently pitched upwards, resulting in multiple minor injuries and one serious injury to cabin crew who were standing at the time.
, identified individual actions as the most common contributing factor to ground operations incidents, highlighting the importance of risk controls, such as standard operating procedures and communication between ground and flight crews.
Ground and flight crews need to maintain situational awareness and communication during pushback procedures to ensure the most appropriate actions are taken.
Operators should ensure cabin crew are made aware of the hazardous nature of conducting duties while the aircraft is moving on the ground.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.