
Final report
Report release date: 14/07/2026
Investigation summary
What happened
On 15 and 23 November 2025 respectively, the pilots of the Robinson Helicopter Company R22 helicopters, registered VH-8H8 and VH-HFQ, each experienced abnormal in-flight indications immediately ahead of a rapid decay in main rotor speed.
Each pilot initiated autorotation and both aircraft subsequently landed hard. This resulted in significant damage to the helicopters, one of which was subsequently destroyed by post-impact fire after dry grass under the helicopter ignited. However, none of the occupants of either helicopter were seriously injured. Both occurrences were reported to the ATSB as suspected rotor drive belt (v-belt) failures.
What the ATSB found
The ATSB found that the occurrence involving VH-8H8 was consistent with drive belt failure. It was very likely that the forward belt became incorrectly engaged (misaligned) in the drive sheaves on startup, leading to rapid wear and failure, which then likely impacted and contributed to failure of the rear belt. The factors contributing to the belt misalignment were not determined.
The occurrence involving VH-HFQ was also likely to have been the result of failure of the drive belts. However, due to an absence of evidence the mechanism of failure was not determined.
Prior to the occurrences, both maintainers reported several instances of Robinson R22 drive belts requiring replacement at low hours due to stretching beyond allowable limits. While this appeared to be the case, any reasons for it were not determined, and the ATSB was unable to identify a broader issue.
Safety message
While the factors contributing to these occurrences were not fully determined, pilots should remain vigilant with pre-flight inspections, particularly around drive belt slack and alignment prior to startup.
Pilots should be prepared to take appropriate precautionary or emergency actions per the pilot operating handbook in the event of abnormal clutch light indications, and/or unusual noise, vibrations or smells that may precede drive belt failure, or if one or both belts fail with limited warning. The instruction for pilots to ‘immediately lower collective to enter autorotation’ is of prime importance in low-inertia rotor systems, such as that in the R22. Main rotor RPM can rapidly decay, and any delay in initiating emergency actions could significantly affect the pilot’s ability to conduct an effective autorotation landing, particularly at low altitudes where there is limited rotor recovery time.
The ATSB continues to encourage aircraft operators and maintainers to report technical component or system issues through the Civil Aviation Safety Authority defect reporting service (DRS). Doing so will assist authorities in understanding the magnitude of any issues and to take action where appropriate.
The investigation
| The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrences
Overview
In November 2025, the ATSB received 2 notifications of suspected rotor drive belt (v‑belt) failures involving Robinson Helicopter Company (RHC) R22 helicopters, registered VH-8H8 and VH-HFQ. Both resulted in hard landings, however none of the occupants were seriously injured. The helicopters had different operators and different maintainers.
VH-8H8, 15 November 2025
On the morning of 15 November 2025, the pilot of VH-8H8 was preparing for a flight around Argadargada Station, Northern Territory, to check on bores and stock.
The pilot conducted the pre-flight checks, which included a physical assessment of the drive belt slack, per the R22 pilot operating handbook (see Pre-flight and startup checks). The pilot expressed a concern to the operator’s senior pilot that the belts may have been slightly loose. The senior pilot then also conducted a physical inspection of the belts and assessed that the belt tension was acceptable and consistent with their other helicopters.
At approximately 0820, the helicopter took off with the pilot and a passenger on board. The pilot reported that the helicopter was operating normally. They noted that the clutch light flickered briefly during the flight, but nothing that they considered to be irregular or abnormal.
Around 10 to 15 minutes after take-off, while the helicopter was in cruise flight at a height of around 300 ft, the pilot smelled burning rubber. About 2 seconds later, they heard a ‘bang’. The pilot’s attention was immediately drawn to a sharp increase in engine RPM, and was initially focused on that, before noticing that the main rotor RPM had decayed to about 90%. On recognising that, the pilot lowered the collective1 to initiate autorotation,2 during which the main rotor RPM began to recover.
The pilot manoeuvred the helicopter from its initial downwind heading, back into the wind and towards an open space for landing. The helicopter impacted the ground with significant forward speed, and the skid on the pilot side dug into the ground, which caused the helicopter to roll over before coming to a stop (Figure 1). There was no post‑impact fire.
Figure 1: VH-8H8 accident site

The pilot shut down the engine before extracting themself and assisting the passenger from the wreckage. The pilot then radioed for assistance, before turning off the emergency locator beacon, which had activated during the accident. The pilot observed that the skids had spread significantly from the ground impact and that the passenger’s seat base had compressed. Additionally, the pilot noted that one drive belt had snapped and the other was separated into several pieces.
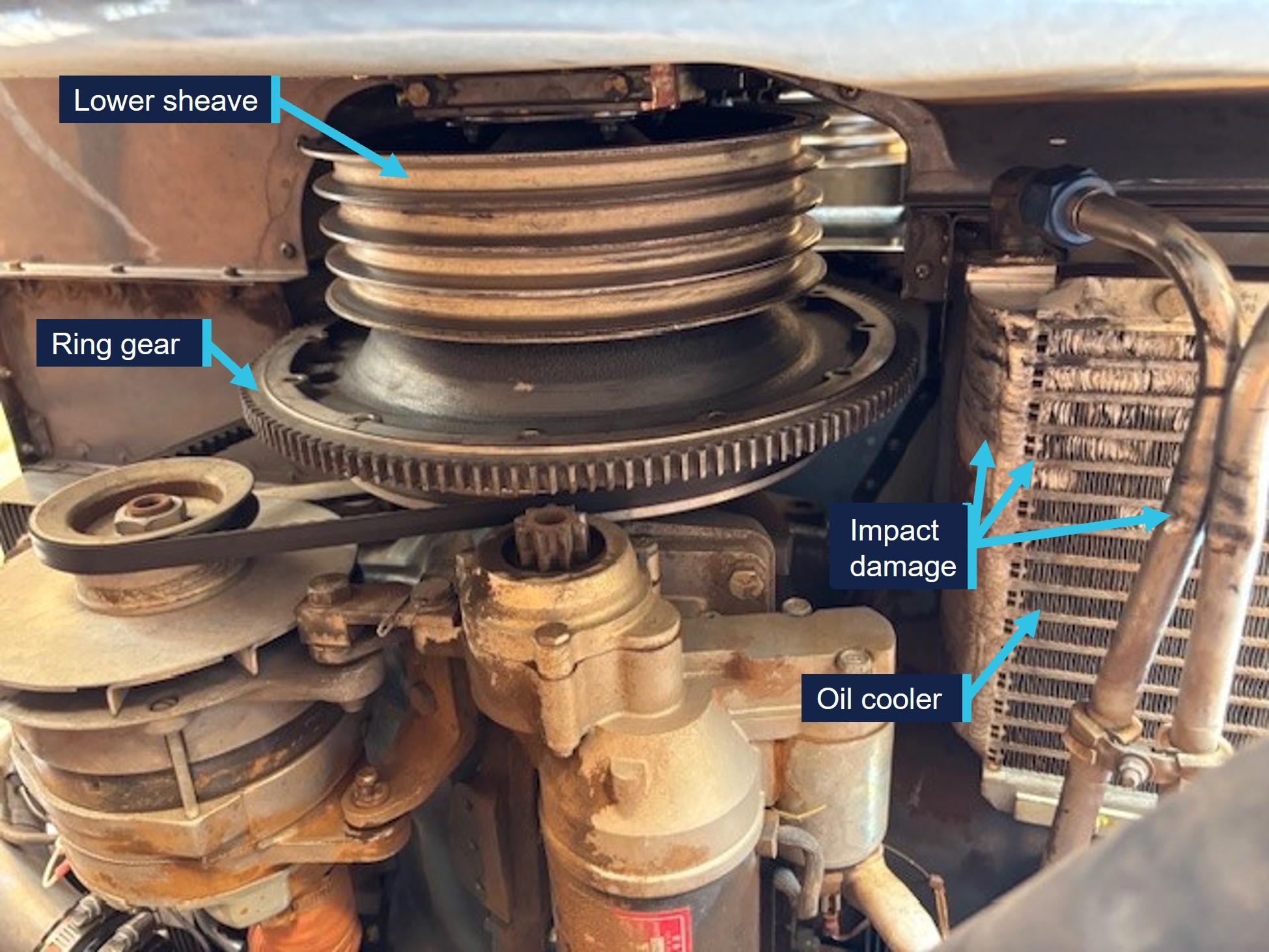
Subsequent examination of the helicopter by the operator showed additional evidence of in-flight drive belt failure, including an accumulation of black dust on the engine starter ring gear support (to which the lower drive sheave is connected), and rubber marks and impact damage to the oil cooler and feed lines adjacent to the belt drive (Figure 2).
Figure 2: VH-8H8 post-accident, viewed from underneath, showing oil cooler damage
VH-HFQ, 23 November 2025
On 23 November 2025, at around 1030, the pilot and sole occupant of VH-HFQ departed on a point-to-point flight from Mount Surprise to Chillagoe Aerodrome, Queensland. Prior to departing, the pilot conducted a pre-flight inspection of the helicopter, including an inspection of the drive belts. No defects were observed. The pilot reported that it was a very hot day, at around 37°C.
Approximately 30 minutes into the flight, while the helicopter was cruising at around
550 ft, the pilot heard a loud slapping noise, felt a significant vibration from the rear of the helicopter, and observed a rapid decay in main rotor RPM. The pilot lowered the collective to initiate autorotation and targeted a suitable landing site. The pilot did not recall hearing the low RPM horn.3
Just above tree height, about 30 to 40 feet above the ground, the pilot reported that they attempted to slow the helicopter and, because the engine was still running, momentarily applied collective to confirm the loss of drive. The helicopter dropped quickly and the pilot tried to cushion the landing. The landing caused the skids to spread horizontally and compress the base of the pilot’s seat. The helicopter remained upright.
The pilot was uninjured in the impact and was able to extract themself from the helicopter. As they did so, they noticed the remains of one of the drive belts hanging free of the drive train. The other drive belt was not observed. The pilot also observed that the fuel tanks appeared to be intact.
Shortly afterwards, a fire ignited in long, dry grass around the engine and exhaust. The fire subsequently destroyed the helicopter (Figure 3).
Figure 3: VH-HFQ post-accident

Context
Pilot information
The pilot of VH-8H8 had 1,488 hours total helicopter experience, including 1,132 hours on the R22. The pilot’s most recent biennial flight review was on 30 September 2025, which covered all emergency procedures, including multiple autorotations.
The pilot of VH-HFQ reported having accumulated approximately 9,000 hours total aeronautical experience over 20 years, and that they were up to date with their flight reviews.
Helicopter information
The Robinson Helicopter Company (RHC) R22 is a lightweight, 2-seat, 2-blade helicopter, powered by a Lycoming 4-cylinder piston engine.
VH-8H8 was an R22 Beta II, serial number 3293. It was manufactured in 2002 and first registered in Australia in 2023. The airframe had accumulated 2,943.8 hours total time in service.
VH-HFQ was an R22 Beta II, serial number 4279. It was manufactured in 2007 and first registered in Australia in 2008. The airframe had accumulated approximately 5,750 hours total time in service.
Rotor drive system
The R22 used a matched pair of banded, double-v, reinforced rubber drive belts (also known as v-belts) running on grooved aluminium sheaves (pulleys) to transmit power from the horizontally-mounted piston engine to the main and tail rotor clutch shaft (Figure 4 and Figure 5).
Figure 4: Diagram of the Robinson R22 rotor drive system
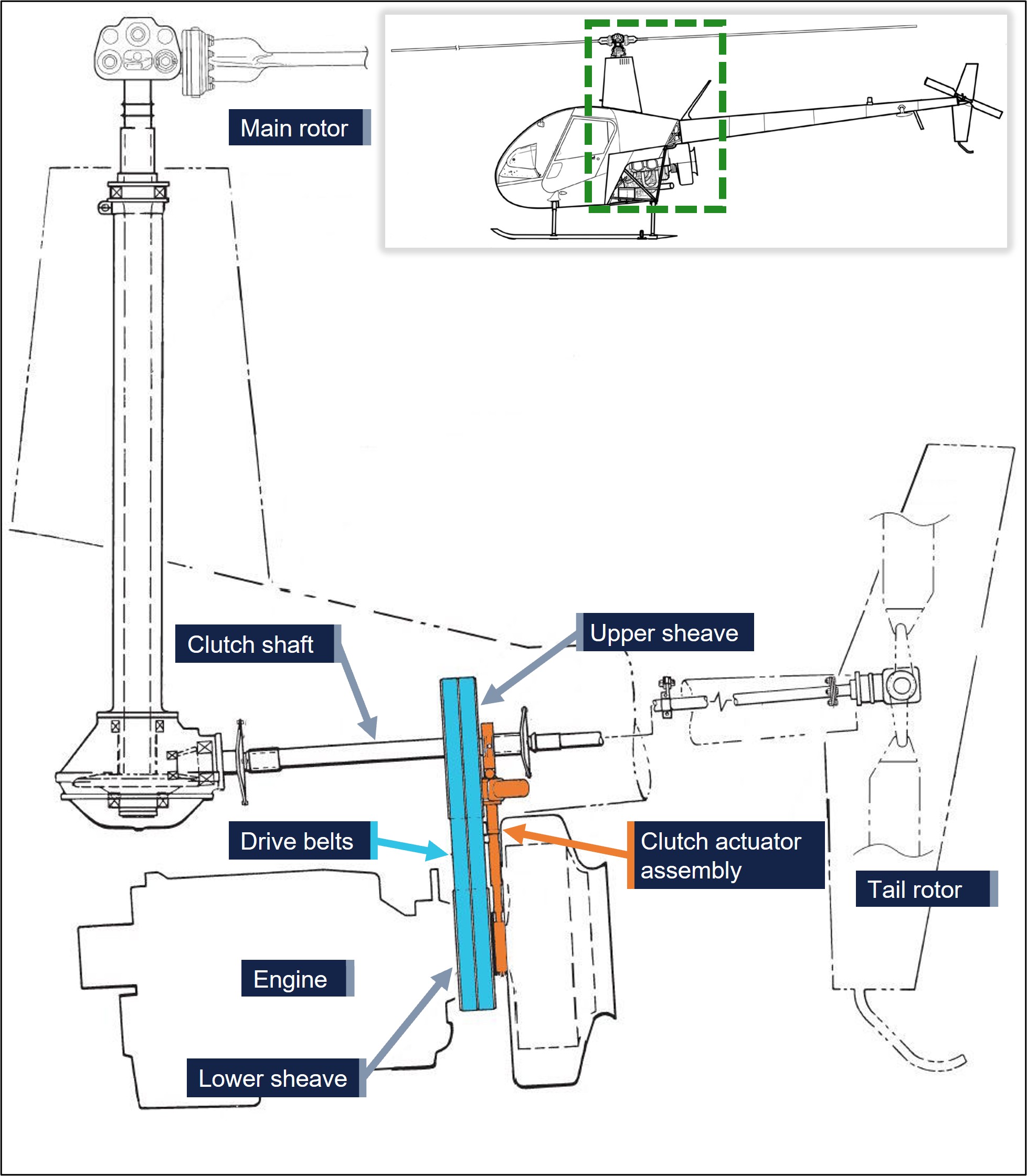
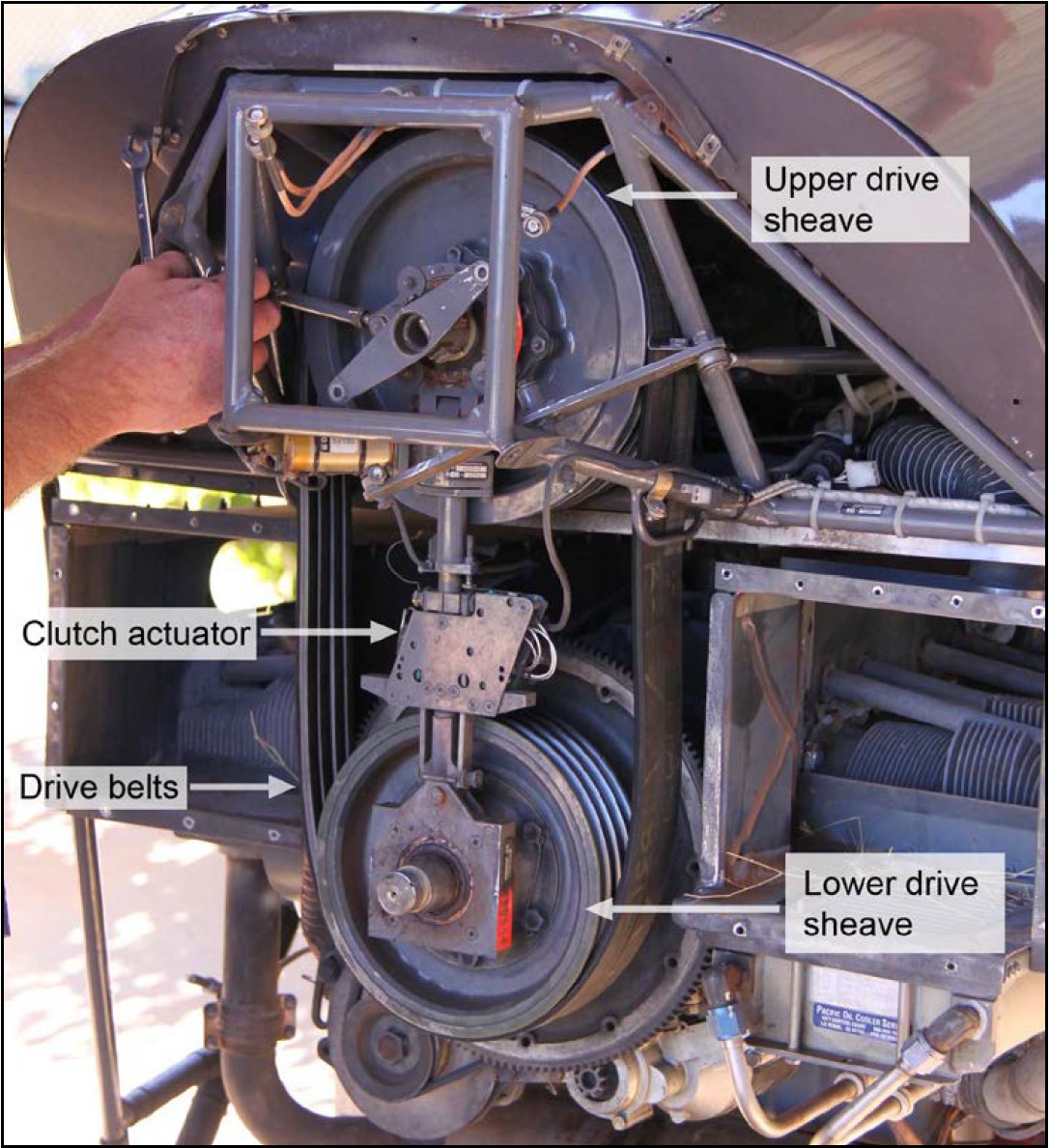
Figure 5: Typical mechanical arrangement of the R22 drive system (viewed from the rear with tailcone and cooling fan assembly removed)
The lower sheave is bolted to the output flange of the engine crankshaft and is connected to the upper sheave by an electrically-driven clutch actuator. The upper sheave incorporates a free-wheeling clutch that allows the clutch shaft (and the rotors) to continue turning when the engine is not driving the system.
The engine is started with the clutch actuator retracted so that the drive belts are retained in their grooves, but with enough slack to allow the engine to start without the excessive load of driving the rotor system. After engine start the pilot selects the clutch switch to ENGAGE, which gradually raises the upper sheave to tension the drive belts to a pre-set load, at which point the actuator ceases driving. A clutch caution light, located in the cockpit directly in front of the pilot, illuminates when the clutch motor is operating.
During normal operation the clutch switch is left in the engaged position until the helicopter is being prepared for shutdown on the ground. In operation, the drive belts become warm and can stretch slightly, lowering tension. When the belt tension reaches a lower threshold, the clutch motor automatically engages to restore the requisite tension.
If one or both belts fails with the clutch engaged, the clutch motor should begin driving to achieve the requisite load, illuminating the clutch caution light until it stops. If only one belt fails, this could lead to the other belt failing due to over-tensioning. If both belts fail, the actuator will extend to the maximum (until the limit switch is activated).
Drive belt monitoring and maintenance
Pre-flight and startup checks
The RHC R22 pilot’s operating handbook (POH) included daily or pre-flight checks of the drive belt condition and slack with the clutch actuator retracted. The slack was tested by applying inward lateral force to one belt at a time, at a specific location (just above the fan scroll wheel on the right-hand side of the helicopter) to measure deflection relative to the other belt. A maximum deflection of 1.5 inches (4 cm) was specified.
Additionally, the POH run-up checklist required pilots to verify that the rotor blades should begin turning within 5 seconds of clutch engagement on startup. A longer clutch engagement time could indicate excessively slack belts or a defective clutch actuator.
RHC safety notice SN-33, included in the POH, stressed the importance of pilots ensuring belts do not have excessive slack during engine start by completing the above checklist items. Measurements exceeding the prescribed limits increased the risk of the drive belts jumping out of the drive sheave grooves on clutch engagement after startup.
In addition to the above, the ATSB discussed with RHC other mechanisms for ensuring the belts were not excessively slack prior to startup. RHC offered that, as the drive belts were relatively accessible on an R22, it was possible for a pilot to attempt to physically dislodge the belts from their respective sheave grooves while the clutch was disengaged. The inability to do so would provide some indication that the belts were not excessively loose, although is not considered by RHC to be a replacement for the published test.
The clutch actuator could be adjusted to correct excessive belt slack on clutch retraction, with the POH noting that periodic adjustment by an aircraft maintenance engineer may be required as the belts wear in service. The actuator down‑limit stop screw on VH‑8H8 was adjusted to correct belt slack approximately one week (10 flight hours) after the previous 100‑hourly inspection.
Clutch caution light
Regarding illumination of the clutch caution light, the POH stated:
Clutch light may come on momentarily during run-up or during flight to re-tension belts as they warm-up and stretch slightly. If, however, the light flickers or comes on in flight and does not go out within 10 seconds, pull CLUTCH circuit breaker and land as soon as practical.4 Reduce power and land immediately if there are other indications of drive system failure5 (be prepared to enter autorotation). Have drive system inspected for a possible malfunction.
Maintenance requirements
In addition to the daily inspections and actuator adjustment to correct excessive belt slack, the RHC R22 maintenance manual required periodic maintenance inspection of the drive belt system at 12‑month or 100‑operating‑hour intervals, whichever came first.
The periodic maintenance included inspection of the physical condition of the drive belts. With the clutch engaged, the amount of drive belt stretch was assessed through a relative measurement of the clutch shaft angle. The belts were required to be replaced if the clutch shaft angle was outside of predefined limits.
The condition and horizontal alignment of the drive sheaves needed to be assessed as part of the periodic inspection and also during the procedure for drive belt installation. The sheaves were required to be replaced if they displayed any corrosion, pitting, flaking, roughness, sharp ridges, wear through the anodised coating, or blistering of the optional metallised coating at the time of inspection. Otherwise, the clutch assembly, incorporating the upper sheave, was required to be replaced when it had accumulated 2,200 hours in service.
Maintenance history
VH-8H8
The helicopter’s drive belts were fitted on 4 September 2025 at the most recent 100‑hourly inspection (2,856.2 hours). The installed belt set was part number A190‑2 revision Z, lot number6 2412130031. The reason for the belt replacement was not recorded.
The drive sheaves were not replaced with the belts. The maintainer reported that the intent was to replace the existing anodised aluminium upper sheave with the steel‑coated (metallised) type, as they had improved durability when exposed to dust and grit in harsh operating environments. However, the maintainer was unable to source a steel‑coated sheave at the time of the 100‑hourly inspection. The maintainer subsequently assessed that the condition of the existing upper sheave was acceptable for continued operation.
VH-HFQ
VH-HFQ had accumulated 5,720 hours total time in service at the time of the most recent maintenance. The helicopter maintenance release was destroyed in the accident, however the operator estimated that the helicopter had operated for approximately 30 hours since this time.
Maintenance records indicated the machine had recently had 2 A190‑2 revision Z belt sets replaced at low time, prior to the accident set. The reason recorded in each case was that the belts were ‘stretched to limits’ (Table 1).
Table 1: VH-HFQ drive belt maintenance history
| Date | Maintenance | Time in Service | Notes |
| 13 June 2025 | 100-hour inspection | 5,597.0 | Drive belts installed. Belt set lot number: 2410170331. |
| 29 August 2025 | 100-hour inspection | 5,691.8 | Drive belts replaced at 94 hours. Belt set lot number: 2412130031. |
| 23 September 2025 | Unscheduled maintenance | 5,720.0 | Drive belts replaced at 28.2 hours. Belt set lot number: 2412130031. |
Low-time belt replacements
Maintainer reports
The maintainers of the occurrence helicopters expressed a concern to the ATSB about a recent observed general increase in low-time belt replacements due to overstretching. This was identified through clutch shaft angle measurements exceeding limits during maintenance inspections.
The maintainer of VH-8H8 advised that for a similar number of helicopters serviced each year, they had replaced 61 sets of drive belts in the 12 months prior to the occurrence. This compared to 50 in the year prior and 30 sets the year before that. In addition, the maintainer reported that they had received 10 sets of belts with the same lot number as the failed belts. From the helicopters with those sets fitted, 2 had been removed at the first 100‑hourly inspection due to the clutch shaft angle measurement exceeding the maintenance manual limit.
The maintainer of VH-HFQ reported having installed 80 sets of belts in the 12 months prior to the accident, compared to 51 in the 12 months prior, and 32 belt sets in the year prior to that. There was also no significant change in the number of helicopters serviced. The maintainer advised that, along with the increase in belt replacements, they had observed variability in the texture of the new belts received, noting that some of the belts were comparatively softer and more rubbery when compared with others.
Defect reports
The ATSB reviewed the Civil Aviation Safety Authority (CASA) DRS (defect report service) reports from the previous 5 years (from January 2020).
From January 2022 to April 2026 there were 16 instances of drive belt issues in RHC R22 and R44 helicopters in Australia. Of those, 15 related to R22 Beta helicopters, and included:
- 8 reports of drive belts stretched beyond limits. All of the occurrences were found during scheduled maintenance. All were reported in 2025 or 2026.
- 3 reports of delaminated or cracked belts, found during pre-flight inspections.
- 1 report of abnormal vibrations, attributed to lumps found on the drive belts.
- 3 reports of the drive belts failing in flight.
The 3 occurrences of the drive belts failing in flight were not investigated by the ATSB. Two of the reports included the following details:
• 23 January 2024: Pilot reported failed drive belt in flight. There was report of a loud bang followed by a vibration and illumination of the clutch light. After 6 seconds, pilot pulled the CB [clutch circuit breaker] and directed the aircraft into wind. A second loud bang followed (2 seconds after pulling the CB) at which point the pilot entered auto-rotation to the ground. Forward belt was found missing. Rear belt was still on both sheaves but running in the forward belt position.
• 18 August 2022: Pilot reported clutch light flickering more than normal followed by a burning rubber smell and a bang. Clutch light on continuously. Pilot landed aircraft and shut down. On inspection [they] noted that the front drive belt had departed the aircraft and the rear belt had jumped one pulley groove.
There were no reports of stretched drive belts between November 2021 and May 2025. From May 2020 to November 2021, there were 20 reports of drive belt issues, 11 of which were for stretched belts and 2 for in-flight failures, and the remainder for defects found during routine inspections or maintenance.
The ATSB contacted one of the major Australian distributors of RHC Helicopters and spare parts, who indicated that they were not aware of any recent increase in drive belt defects or concerns.
RHC reported a total of 7 drive belt warranty claims worldwide for 2025. RHC also advised that it had surveyed some local service centres in the United States, which reported that they were not experiencing any premature belt stretching.
Component examination
VH-8H8
The ATSB did not attend the VH-8H8 accident site. The drive belt remains from the helicopter were examined at the ATSB technical facilities (Figure 6).
Figure 6: VH-8H8 drive belts as-recovered

The rear belt had a single tensile break through both vees in the same location and showed no abnormal wear or defect.
The forward belt was separated into multiple pieces. The front vee of the forward belt had entirely delaminated from the backing strap and was fractured at several places. The rear vee was still largely attached to the backing but was also separated in more than one location along the length.
The largest piece of the forward belt had taken on a curve, indicating that the vees had been subjected to non-uniform stretching. Where still continuous, the centre of the backing strap (between the vees) had deformation consistent with running on the crest of a sheave groove. A cross‑section through the belt showed significant wear of the rear vee (Figure 7).
The abnormal, non-uniform wear and stretching was consistent with the belt running while misaligned, with the belt having pushed forward and one of the vees not running in the drive sheaves. RHC advised that in this configuration, the belts might last 10–20 minutes before failure. RHC also advised that the belts would have to be very loose for this to occur, particularly as the outer sheave groove is raised to reduce the likelihood of such an event.
Figure 7: VH-8H8 forward belt cross‑section (left) and new rev-Z belt (right)

VH-HFQ
The ATSB did not attend the VH-HFQ accident site and no physical evidence was obtained from the destroyed helicopter.
Operational considerations
The R22 POH includes the following under ‘emergency procedures’:
A power failure may be caused by either an engine or drive system failure and will usually be indicated by the low RPM horn. An engine failure may be indicated by a change in noise level, nose left yaw, an oil pressure light or decreasing engine RPM. A drive system failure may be indicated by an unusual noise or vibration, nose right or left yaw, or decreasing rotor RPM while engine speed is increasing.
In the case of power failure, immediately lower the collective to enter autorotation.
The pilot of VH-8H8 reported that their initial distraction by the sharp rise in engine RPM delayed, by a few seconds, their observation of main rotor RPM decay and action to lower the collective to enter autorotation. The pilot reflected that this event reinforced the need for them to instinctively and immediately enter autorotation at the first indication of a power failure.
When conducting autorotations, the POH cautions:
The R22 has a light, low-inertia rotor system. Most of the energy required for an autorotation is stored in the forward momentum of the aircraft, not in the rotor. Therefore, a well-timed cyclic flare is required and rotor RPM must be kept in the green until just before ground contact.
The main rotor will deplete its stored energy quickly once power is removed, which will lead to a rapid decay in rotor RPM. The POH lists the minimum R22 power off main rotor speed limit as 90% and, in the section on practice autorotations, cautions that ‘catastrophic rotor stall could occur if the rotor RPM ever drops below 80%, plus 1% per 1000 feet of altitude [above sea level].’
The ATSB enquired with RHC about operation of drive belts stretched to the limits of the clutch actuator. RHC advised that the actuator would stop driving after triggering the upper limit switch, which could result in under-tensioned belts that slip on the sheaves. In this case, the clutch light should illuminate and remain on, requiring pilots to land as soon as possible in accordance with the POH instructions.
Injuries and damage
Spreading of the helicopter skids and compression of the seat base in each helicopter were features of the helicopter’s energy absorption design to reduce impact forces on the helicopter occupants during a hard landing or collision with terrain. In each occurrence, nothing was stored under the seat base. This ensured energy absorption functionality of the seat, minimising the risk of injury to the occupants.
Related occurrences
Hamilton Island, Queensland, 3 February 2021 (AO-2021-007)
While cruising at 1,500 ft, approximately 15 minutes into the flight, the pilot of an RHC R44 Clipper II, VH-SXC, smelled burning rubber and saw the clutch warning light flicker briefly. The pilot then heard what sounded like ‘a rubber band smacking against the cowling’, at which point the clutch warning light illuminated and remained on. The pilot identified a rise in engine RPM and a slow decline in main rotor RPM. The pilot pulled the clutch circuit breaker in response to the warning light and conducted a successful emergency landing with minimal damage to the helicopter and no injuries.
Of the 4 drive belts7 in the helicopter’s drive system, it was found that the forward 2 drive belts had dislodged and moved forward of the upper sheave. They then lodged against the sheave and clutch shaft, leading to damage to the drive belts and surrounding components. The other 2 drive belts remained intact but had shifted forward from their original sheave positions and were not effectively engaged within the grooves of the sheaves. Consequently, there was a loss of effective drive of the rotor system.
Outside of the occurrence event, the helicopter had experienced 2 instances of over‑stretched drive belts, which were replaced after 76.1 hours and 8.6 hours, respectively. The overstretching was attributed to a static belt‑stretching procedure that was introduced for new belts that were overly tight. RHC removed the belt‑stretching procedure in July 2021.
Julia Creek, Queensland, 9 May 2011 (AO-2011-060)
The pilot of an RHC R22 Beta II helicopter, VH-DSD, was conducting mustering operations and while the helicopter was operating in close proximity to the ground, drive to the rotor system was lost, resulting in a high rate of descent at the point of impact. The pilot was fatally injured.
The ATSB found that both drive belts had failed prior to the collision with terrain. The rear drive belt was found severed and wrapped around the drive sheaves. Almost all of the forward belt was found in 2 adjacent locations about 60 m from the main wreckage. Black rubber marks, consistent with a flailing drive belt, were found on the sides and lower surface of the engine. The forward drive belts showed significant abnormal wear of the forward vee, indicating that the belt had rolled forward over the front edge of the drive sheave. The ATSB was unable to establish the factors that contributed to the dislodgement.
The final investigation report noted the necessity of flying at very low level when conducting helicopter mustering, but also the potential risk of doing so. The pilot would have had limited time to recognise the condition, respond accordingly, and for the autorotation to develop before attempting to land. As a result, the report stressed the importance of pilot proficiency in responding to emergency situations resulting from aircraft malfunction.
Safety analysis
Drive belt failures
The VH-8H8 pilot report of a burning rubber smell, followed shortly afterwards by the ‘bang’, the significant reduction in main rotor RPM and sudden increase in engine RPM, was all consistent with failure of the helicopter’s drive belts. The short (10 to 15 minute) duration of flight, rubber smell, and uneven belt wear, was consistent with the forward belt not being correctly seated in the drive sheave grooves. This belt misalignment most likely occurred during startup, as the flight duration was consistent with RHC’s experience of belt longevity when operated in this configuration. The abnormal wear indicated that the forward belt most likely failed first and, noting the very brief time interval between the 'bang' and the main rotor RPM decay, the forward belt probably interfered with the rear belt, which then fractured, resulting in the complete drive train disconnect.
The VH-HFQ pilot report similarly indicated a rapid decay in main rotor RPM, consistent with the drive belt separation subsequently observed by the pilot on the ground. However, the mechanism of failure in this case was not determined. The drive belts were not available to the investigation, and the recounted circumstances of the occurrence were slightly different. Specifically, the significantly longer (30-minute) flight time and the absence of any reported burning rubber smell preceding the event. This may be indicative of a different failure mechanism, although the presence of any rubber smell would be dependent on local conditions and not necessarily detected.
In each of the occurrences the helicopters had recently been inspected, the drive belts were relatively new, and pilots reported conducting the required pre-flight checks without observing any issues. It is worth noting that, although the pilot of VH-8H8 sought a second opinion on the belt tension, ultimately it was assessed as acceptable by 2 pilots and therefore unlikely to have been excessively slack. Otherwise, there were no obvious operational factors reported or identified that might have led to the drive belts becoming unseated from the sheaves or that would otherwise contribute to a belt failure.
Pilot responses
In both occurrences, the initial indications of drive train failure were reported as being almost coincident with the main rotor RPM decay. There was no prolonged or abnormal clutch light illumination, or any other timely indications preceding the failure, and therefore no opportunity to conduct any kind of power-on landing.
As it was, both pilots had to assess the condition as an engine or drive system failure (noting the emergency procedure for both is the same), and immediately lower the collective to enter autorotation. Both pilots did this after observing the rapid main rotor RPM decay. The pilot of VH-8H8 later reflected on the few seconds delay in diagnosing the condition before lowering the collective and entering autorotation. In those few seconds the rotor speed decayed to the minimum allowable level, beyond which increased the risk of an adverse outcome, particularly at low level where time and altitude may be insufficient to recover low rotor RPM.
Aside from rotor RPM, there are a number of variables that can influence the success of an autorotation landing (including, airspeed, weight, density altitude, manoeuvring, and the timing and magnitude of pilot control inputs), and because of this, the specific factors that contributed to the hard landings in these events were not explored in detail. Nevertheless, these occurrences serve as a reminder that power loss events may occur with limited prior warning. They reinforce that pilots should be intimately familiar with the POH emergency procedures and be prepared to act immediately in the event of any abnormal in-flight indications.
Drive belt failure rates
Reports and records provided to the ATSB by both of the helicopter maintainers indicated a relatively recent increase in low-time drive belt replacements. The reported issues were similar to those captured in the CASA defect reporting scheme database around 2020–21 which was also reflected in the occurrence involving VH-SUX (AO‑2021‑007).
The occurrence belt sets, as well as the August low-time replacement on VH-HFQ and 2 other low-time replacements recorded by the maintainer of VH-8H8 were from the same lot number. This suggested the possibility that there was a manufacturing anomaly with a particular batch of belts that pre-disposed them to stretching. This would infer that the occurrence belts also had stretching issues, which was possible but could not be confirmed. There were also no reports to indicate that other belts, out of the 150 sets from the same lot number, had been replaced for a similar reason.
Moreover, the increase in belt replacements had been occurring over the previous few years, which might suggest a more significant manufacturing anomaly than a single batch. Despite this, there was no evidence of a more widespread, corresponding increase in reporting of recent, similar belt failures or stretching at a greater rate than usual.
The ATSB considered the operational risk if there were a broader issue involving excessive drive belt stretching. If not carefully monitored, belt stretch could lead to excessive slack on startup, which would increase the risk of the belts jumping out of the sheave grooves. However, vigilance around the existing pre-flight checks and monitoring of the 5-second clutch engagement time should mitigate that risk. It is also noted that, due to the way the clutch system operates, gradual belt stretching by itself should not create a safety issue during flight without warning.
The ATSB continues to encourage reporting of aircraft component failures or issues through the CASA DRS system to give a clearer indication of concerning defects or trends that may warrant further investigation.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the rotor drive belt failures resulting in collisions with terrain, involving Robinson R22s, VH-8H8 and VH-HFQ, near Argadargada Aerodrome, Northern Territory, and Chillagoe Aerodrome, Queensland, on 15 and 23 November 2025.
Contributing factors
- The forward drive belt on VH-8H8 probably became incorrectly engaged in the drive sheaves on startup, for reasons that could not be determined. This led to failure of the forward drive belt, which then likely impacted the rear drive belt and contributed to its failure.
- The forward drive belt on VH-HFQ likely failed in-flight, for reasons that could not be determined.
Other findings
- Prior to the occurrences, there were several reported instances of Robinson R22 drive belts requiring replacement at low hours due to stretching beyond allowable limits. It was not able to be determined whether the subject occurrences were influenced by reported concerns.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot of VH-8H8
- the pilot of VH-HFQ
- the station manager for VH-8H8
- the maintenance organisation for VH-8H8
- the maintenance organisation for VH-HFQ
- Robinson Helicopter Company
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the pilot of VH-8H8
- the pilot of VH-HFQ
- the station manager for VH-8H8
- the maintenance organisation for VH-8H8
- the maintenance organisation for VH-HFQ
- Robinson Helicopter Company
- the Civil Aviation Safety Authority
Submissions were received from the Civil Aviation Safety Authority. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
- ^ Collective is a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
- ^ Autorotation is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
- ^ An audio alert that sounds when the main rotor speed is below a certain level. In the Robinson R22, the threshold is 97% and is accompanied by the ‘LOW RPM’ caution light. The horn and light are muted when the collective is fully down.
- ^ The Robinson R22 POH defines: Land as soon as practical as ‘landing site is at the pilot’s discretion, based on the nature of the problem and available landing areas.’ Whereas, Land immediately means ‘land on the nearest clear area where a normal landing can be performed.’
- ^ Safety notice SN-28 in the POH notes these indications as the ‘smell of hot rubber, noise, or vibration.’
- ^ When individual belts are received by RHC, they are tensioned in a simulated sheave system, measured and subsequently matched into a set (of 2 for a R22 and 4 for a R44). RHC advised that the lot number for drive belt sets is applied by RHC as part of this process. As such, the lot number does not directly relate to a manufacturing batch or date, although belts being matched into sets would likely be manufactured around the same time. Lot number 2412130031 comprised 150 belt sets.
- ^ The Robinson R44 drive train has a matched set of 4 drive belts, as opposed to the set of 2 in the R22.
Occurrence summary
| Investigation number | AO-2025-069 |
|---|---|
| Occurrence date | 15/11/2025 |
| Occurrence time and timezone | 0830 Australian Eastern Standard Time |
| Location | Near Argadarga Aerodrome, NT, and Chillagoe Aerodrome, Qld |
| State | Northern Territory |
| Report release date | 14/07/2026 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Collision with terrain, Forced/precautionary landing, Transmission and gearbox |
| Occurrence class | Accident |
| Highest injury level | Minor |
Aircraft details
| Manufacturer | Robinson Helicopter Co |
|---|---|
| Model | R22 Beta |
| Registration | VH-8H8 |
| Serial number | 3293 |
| Aircraft operator | Georgina Pastoral Company Pty Ltd |
| Sector | Helicopter |
| Operation type | Part 138 Aerial work operations |
| Activity | General aviation / Recreational-Aerial work-Observation and patrol |
| Departure point | Argadargada, Northern Territory |
| Destination | Argadargada, Northern Territory |
| Injuries | Crew - 1 (minor), Passengers - 1 (minor) |
| Damage | Substantial |
Aircraft details
| Manufacturer | Robinson Helicopter Co |
|---|---|
| Model | R22 Beta |
| Registration | VH-HFQ |
| Serial number | 4279 |
| Aircraft operator | Sunrise Helicopters Pty Ltd |
| Sector | Helicopter |
| Operation type | Part 91 General operating and flight rules |
| Activity | General aviation / Recreational-Own business travel |
| Departure point | Mount Surprise Aerodrome, Queensland |
| Destination | Chillagoe Aerodrome, Queensland |
| Injuries | None |
| Damage | Destroyed |