
Final report
Report release date: 19/06/2026
Investigation summary
What happened
On the morning of 17 August 2022, 2 freight trains were planned to cross at Oonoomurra station on the Mount Isa line, Queensland. The Mount Isa line was a single bi-directional rail line with designated stations to allow trains to cross or pass.
The network control officer (NCO) authorised the crew of freight train 9227, operated by Qube, to depart Cloncurry station, travel east, and stop at Oonoomurra station. After stopping, the driver notified the NCO that train 9227 was in-clear and complete then released the ownership of the block section between the Cloncurry and Oonoomurra stations to the NCO.
The NCO then contacted the driver of freight train 9M48, operated by Aurizon, to extend their authority. The authority permitted the driver to continue west through the Oonoomurra station and toward the Cloncurry station, without stopping.
The driver of train 9M48 entered Oonoomurra station and continued at a speed of about 23 km/h. As they rounded a sweeping left curve at the western end, they saw several freight wagons from the rear of train 9227 obstructing the track ahead. The driver made an emergency brake application but was unable to avoid a collision.
The lead locomotive of train 9M48 subsequently derailed, uncoupled from the trailing locomotive and rolled onto its side. Several wagons on train 9227 were also damaged and zinc concentrate spilled onto the track. There was a minor injury to the driver of 9M48. The crew of train 9227 were not injured.
What the ATSB found
The ATSB found that the stopping point of train 9227 was about 317 m from the limit of authority at the eastern end of Oonoomurra station. The Qube competency procedures had not verified the driver of train 9227 was familiar with the operation of the on-board electronic distance counter device. The driver, unsure of its operation, did not use it to check the locomotive, when stopped at the chosen location, had travelled a sufficient distance within the station, for all wagons of the train to have cleared the block section between the Cloncurry and Oonoomurra stations.
The block section was obstructed by several wagons from the rear of train 9227. However, the driver determined train 9227 was within the limits of the Oonoomurra station and erroneously passed ownership of the block section between the Cloncurry and Oonoomurra stations to the NCO.
It was also established that there was limited functionality available for the NCO to independently verify the physical availability of a block section before issuing an authority, in this case, the extension of authority to train 9M48. The driver of 9M48, in receipt of an extension, proceeded with the expectation that train 9227 had cleared the block ahead. The track alignment with the left curve meant the driver did not see the obstructed track at a distance sufficient to enable them to stop and avoid a collision.
After the collision, the lead locomotive on 9M48 came to rest on its side. The driver was in darkness and unable to readily locate safety equipment, make an emergency radio call to network control or exit the cab without the assistance from members of the public. The driver, operating the train as a driver-only service, was exposed to several known evacuation hazards due to the overturned locomotive. As identified in previous ATSB investigations, the emergency exit pathway through a side window, and the emergency equipment available in the enclosed cab of an Aurizon 2800 class locomotive were inadequate to ensure a prompt escape by the crew. This also potentially limited access by emergency services in the event of a locomotive overturning.
What has been done as a result
Queensland Rail issued a formal letter to Qube requesting demonstration of the effectiveness of its compliance with the controls in the interface risk management plan and the direct traffic control standard MD-10-113. Qube confirmed the existing measures within its safety management system and interface risk management plan were effective and provided controls sufficient to mitigate recurrence of this type of event by Qube. Additionally, Queensland Rail commenced projects to provide notification to network control should a trailable point not return to the normal position within a defined time and where there was an obstruction at the clearance points of a directional travel station.
Aurizon continued to implement its access and egress compliance program to ensure the locomotive fleet met the revised requirements detailed in AS7522 and associated standards. Additionally, Aurizon progressed implementation trials of prototype window assemblies for the 2800 class locomotive together with other improvements to emergency lighting and safe egress arrangements in the locomotive cab.
Safety message
In the direct traffic control system of safeworking, it is incumbent on the crew of the first train to arrive at a directional travel station to validate their train was complete and in‑clear before releasing the block section to the rear of their train. Additionally, the crew of the second train to arrive who were in receipt of authority to continue, must not expect the block section ahead to be physically available for the passage of their train and should remain vigilant to conditions that may affect the network.
This accident also highlighted the importance of equipping locomotive rolling stock with systems to mitigate evacuation hazards that crew may encounter following the derailment and rollover of a locomotive. In particular, when operating as driver‑only and in remote locations where assistance may not be readily available.
Summary video
The occurrence
Overview
On 17 August 2022, train 9227 operated by Qube was on a scheduled freight service between Mount Isa and Stuart Yard (near Townsville), Queensland. The train, operated by 2 crew, had stopped at their limit of authority at Oonoomurra station to wait for freight train 9M48 to arrive, travelling in the opposite direction.
Train 9M48, operated by Aurizon, was on a scheduled freight service between Stuart Yard and Mount Isa. The train was crewed by a single driver who had received an authority from Queensland Rail network control to travel to Oonoomurra station, cross1 train 9227, and continue toward Cloncurry station.
As train 9M48 approached the points at the western end of the Oonoomurra station to complete the cross, the driver saw several of the wagons from the rear of train 9227 were not clear of the single line block section ahead. The driver applied emergency braking, however, train 9M48 collided with the stationary wagons at about 17 km/h.
At 0637 local time, the lead locomotive of train 9M48 derailed, uncoupled and rolled onto its side. The driver sustained minor injuries. Several wagons of train 9227 were also damaged in the collision, spilling zinc concentrate onto the track. The crew of train 9227 were uninjured.
Precursor events
On 16 August 2022, train 9M48 was travelling in a westerly direction toward Nonda station on the Queensland Rail Mount Isa line. The train was running late and would not arrive on time for a scheduled crew change.
At about 2115, Aurizon operations personnel contacted the relief driver for train 9M48 to defer their shift start time until 2245. The driver subsequently signed on at Cloncurry station then drove by road to Nonda station, to meet train 9M48 and take control for the journey toward Cloncurry station. Due to recurring issues with the automatic train protection (ATP)2 system on the lead locomotive of train 9M48, it was running further behind schedule.
On 17 August 2022, at about 0120, train 9M48 arrived at Nonda station. The incoming and relief drivers conducted the handover, and the relief driver took control of the train. They radioed the far west network control officer (NCO) at the Queensland Rail Townsville network control centre to exchange direct traffic control (DTC) codes3 and obtain an authority to proceed.4 At about 0127, train 9M48 departed Nonda station to travel in a westerly direction.
Concurrently, Qube train 9227 was travelling in an easterly direction on the Mount Isa line to Stuart Yard. At about 0525, train 9227 arrived at Cloncurry station where the incoming and relief crews conducted the handover. The relief crew, comprising of 2 drivers, took control of the train.
At about 0550, the driver at the controls of train 9227 radioed the NCO to exchange DTC codes in preparation to receive their authority to proceed east. The NCO instructed them to wait at Cloncurry station for the arrival of train 9M48.
Around that time, train 9M48 was approximately 40 km from Cloncurry station and travelling toward Pymurra station. The NCO was aware5 the train was running further behind schedule due to the recurring issue with the ATP system.
At about 0551, the NCO radioed the driver of train 9M48 and informed them their current authority to travel to Cloncurry station would be reduced to Oonoomurra station, where they would now cross train 9227 (Figure 1). The driver acknowledged the instruction, exchanged the DTC codes, and read back the authority to the NCO to confirm its content. The authority permitted the driver to travel to the block limit board OA 18, located on the up track6 at the western end of Oonoomurra station (see Safeworking system).
At about 0552, the NCO radioed the driver of train 9227 and exchanged DTC codes before the driver read back the authority to the NCO to confirm its content. The authority permitted them to travel to the block limit board OA 25 located on the down track at the eastern end of Oonoomurra station where they would stop and wait for train 9M48 to cross. At 0557, train 9227 departed Cloncurry station. The 20-minute trip from Cloncurry to Oonoomurra stations was uneventful.
Figure 1: Locations and stations on the Mount Isa line
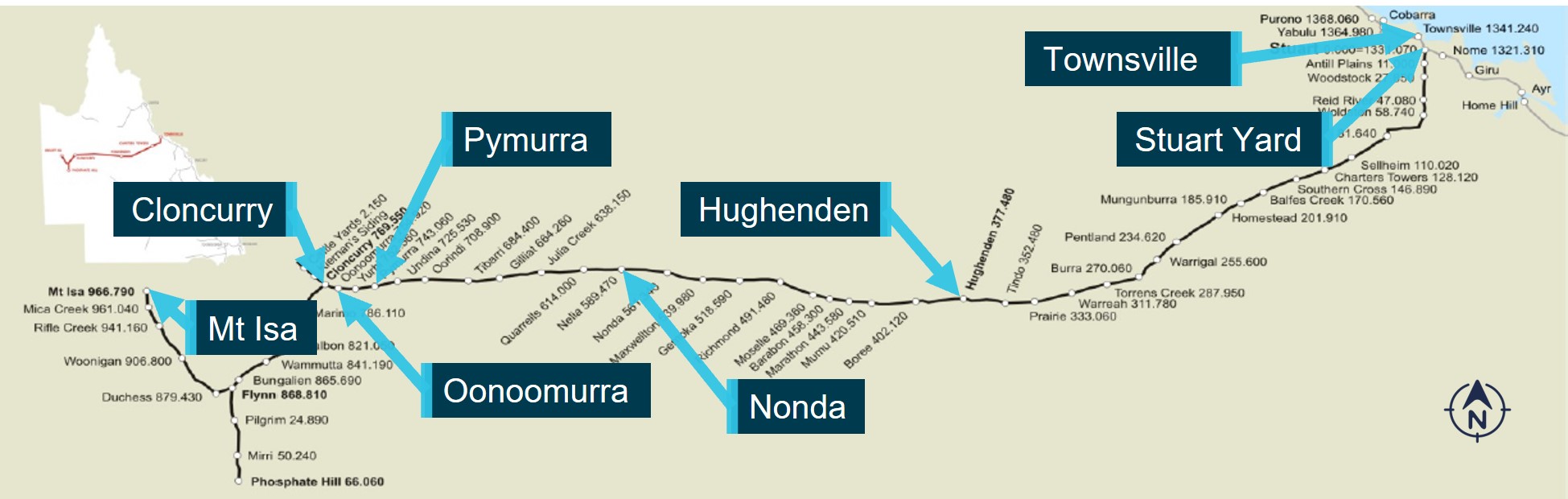
Source: Queensland Rail, annotated by the ATSB
Events at Oonoomurra station
Arrival of train 9227
As train 9227 neared the Landsborough Highway level crossing at the western end of Oonoomurra station, the driver slowed their train. Shortly after, the driver and second driver confirmed the correct position of the trailable points7 at the entrance to Oonoomurra station. The train was travelling at about 25 km/h when it passed over the points and entered the western end of the station. At about 0619, the driver radioed the NCO to report they were nearing their limit of their authority for the cross with train 9M48.
The driver recalled it was their first stop at Oonoomurra station in years, since they usually did not need to cross a train there. On arrival at the station, the driver recalled the glare from the rising sun made it hard to see the track, and their limit of authority ahead. The driver also said they typically controlled the train speed with the objective of stopping a locomotive around 50 m from the limit of authority at a station. However, they were concerned the reduced visibility increased the risk of misjudging the stopping point and passing their limit of authority, which would result in a signal passed at danger.8 The driver decided to use the ‘Oonoomurra’ sign, located adjacent to the down track, as a reference point to stop the lead locomotive prior to OA 25. The driver recalled they typically used the sign as a landmark where they would release the dynamic brake9 while managing the train's speed when passing straight through the Oonoomurra station.
At about 0621, the locomotive data logger recorded the driver made a brake application, with the train coming to a stop at about 0622. After stopping, the driver recalled the track alignment, and surrounding vegetation obscured their view of the train’s rear in the locomotive rearview mirror. However, they could see road traffic crossing the Landsborough Highway level crossing behind the train. The driver remarked that seeing vehicles crossing, along with their understanding the train was shorter than usual, and belief that it would be in buff10 led them to conclude the end of train 9227 had cleared the block limit board OA 16.
The driver then radioed the NCO to provide the release code for the section11 between Cloncurry and the Oonoomurra block limit board OA 16. The NCO responded to confirm the block release and their understanding that train 9227 was intact and in‑clear12 of block limit board OA 16 on the down track at Oonoomurra station. The driver confirmed to the NCO that information was correct.
After the block was released, the second driver recalled that they felt uneasy about the stopping point, which was around midway along the station, as the Qube procedure for the management of trains in safety‑critical zones13 nominated a target stopping point 50 m short of the block limit board (see Train working). They subsequently asked the driver if they were sure the train was in-clear, as they understood the train was typically 900 m long.
The driver stated the train length was 824 m as they understood 3 wagons had been removed due to a load imbalance and assured the second driver the train should be in‑clear. Despite these assurances, the second driver recalled they still felt uneasy as their comparison of the stopping point, length of the train, and available standing room14 between block limit boards at either extremity of the station created doubt that the train was in‑clear. The second driver, however, did not insist the driver move the train further along the track towards block limit board OA 25.
Arrival of train 9M48
At 0626, the driver of 9M48 informed the NCO that they were moving again after another issue with the ATP, which had stopped the train about 10 km from Oonoomurra station. The driver reported that Aurizon had authorised the disconnection of the ATP system for the rest of the trip to Cloncurry station. The NCO acknowledged the ATP disconnection and then exchanged DTC codes to issue the next authority to the driver.
The driver read back the authority, which permitted them to cross train 9227 and continue through Oonoomurra toward Cloncurry stations. The authority no longer required the driver of train 9M48 to stop at the block limit board OA 18 at the western end of Oonoomurra station. The driver later said they believed the receipt of an authority was like ‘a green light’ and they had exclusive possession of the block section ahead. At about 0635, train 9M48 was travelling at about 23 km/h when it entered the eastern end of Oonoomurra station and proceeded along the up track toward train 9227. The driver of train 9M48 recalled that train 9227 appeared to have stopped short of its limit of authority but was unsure whether to contact its crew to confirm their stopping point. Earlier, the driver of 9M48 had passed 10 wagons parked at Pymurra station, presumed they belonged to Qube, and that train 9227 was likely shorter than usual and was planning to couple with those wagons.
As train 9M48 continued along the up track at a steady speed of 23 km/h, the driver recalled starting to enter the DTC codes in readiness to release the block section to the rear of their train. On passing, they waved to the crew of 9227, turned the locomotive headlight back on15 then continued toward the western end of Oonoomurra. The driver recalled the morning sky was beginning to brighten, but that it was still dark at ground level.
As train 9M48 entered a left curve at the western end of Oonoomurra, the driver recalled looking ahead to check the Landsborough Highway active level crossing, located about 200 m from the station, was free of road traffic. The driver was mindful that they had limited visibility of the crossing and approaching road traffic due to the track curvature, height of the wagons on the adjacent train and trackside vegetation.
As train 9M48 continued around the curve, the driver recalled picking up the radio handset to contact the NCO to complete the exchange of DTC codes for the return of the block when they saw wagons from train 9227 were not in-clear.16
The collision
At 0637, train 9M48 was travelling at about 23 km/h when the driver, having identified wagons from train 9227 were obstructing the track, moved the automatic brake handle to the emergency position and the throttle to idle to stop the train. The braking continued for around 30 m when, at about 17 km/h, the lead locomotive (2808) collided with the side of wagons GOAF 0060 and GOAF 0059 from train 9227. Locomotive 2808 subsequently derailed, uncoupled from the trailing locomotive and rolled onto its side (Figure 2).
Figure 2: Collision damage to trains 9M48 and 9227

Source: Aurizon, annotated by the ATSB
Post‑collision
The driver of train 9M48 recalled that they were shocked by the collision and rollover and that they sustained a cut to their hand during the accident sequence. The cab was in darkness, and they were unable to see anything. They could not reach the side window on the upper side of the overturned cab and tried unsuccessfully to kick out the windscreen. The driver further recalled they tried to make an emergency radio call to the NCO, however, the train borne radio had ceased working. The equipment within the cab was disarranged and they were unable to locate the emergency window breaking hammer or their kit bag containing a handheld radio.
At 0639, while still within the cab, the driver telephoned17 the NCO to report their train had collided with the rear wagons of train 9227 and that the lead locomotive had overturned onto its side. Shortly after, the driver became aware that 2 bystanders18 had climbed onto the side of the upturned locomotive, opened the side window and called to the driver to check on their condition. They assisted the driver’s egress by reaching down and lifting the driver through the side window of the cab. They then jumped from the locomotive and noted that it was leaking diesel fuel.
Shortly after, the NCO telephoned the driver of train 9227 asking of their awareness of the accident and to appoint them the on-site coordinator until the arrival of support personnel. The driver confirmed they were aware of an accident and that the second driver was on their way to check with the driver of 9M48. Queensland emergency services19 arrived at the accident site at 0725.
The Mount Isa line remained closed between Cloncurry and Oonoomurra stations until being reopened to rail traffic on 21 August 2022.
Context
Train crew information
Aurizon crew
Roles and experience
Train 9M48 was crewed as a driver-only operation.20 The driver had a total of 21 years experience driving locomotives at various locations in Queensland. They had a current health assessment and met the fitness for duty criteria according to the national standard of health assessment for rail safety workers. In April 2022, the driver successfully completed an off-the-job assessment in safeworking competencies for the Queensland Rail network that included the direct traffic control system. In May 2022, the driver successfully completed an on‑the‑job assessment for locomotive driver. This assessment included sections on train operations and safeworking.
Recent history
Over the 7 days prior to the accident, the driver had worked 4 consecutive duty periods. The driver had recently operated train services through Oonoomurra.
On 16 August 2022, they completed a shift at 0230 and were next rostered to commence work at 2100 later that same evening. The driver was contacted by Aurizon operations staff at around 211521 to delay their start time to 2245. At 2210, the driver undertook a self-test for the presence of alcohol prior to starting their shift at the Cloncurry depot, which returned a zero result.
The driver recalled they obtained around 4–5 hours sleep and napped for around 2 hours before the telephone call from Aurizon operations staff. From commencement of their shift on 16 August 2022, the driver was on duty for approximately 8 hours. During the ATSB interview, the driver self-assessed against the Samn-Perelli fatigue scale22 that they felt ‘OK somewhat fresh’. They further described, when they were crossing another train, in this case 9227, ‘you are alert’ due to the increased task requirements they were undertaking at that time.
Qube crew
Roles and experience
Driver at the controls
Train 9227 was crewed by 2 drivers. The driver had a total of 25 years experience driving locomotives at various locations in Queensland. In February 2022, they commenced employment with Qube. They were assessed by a mentor driver/assessor in locomotive preparation and operation as well as the safeworking competencies over multiple trips for the Hughenden to Cloncurry route. The locomotive used in the assessment was recorded as a PRL class (see Train 9227). The driver was signed off as competent in all train handling and safeworking tasks including:
- stop the train in the correct mode (compressed or stretched) to suit the track gauge
- operate the train in accordance with the applicable safeworking rules and procedures.
The driver had a current health assessment and met the fitness for duty criteria according to the national standard of health assessment for rail safety workers.
Second driver
The second driver23 had a total of 21 years of experience driving locomotives at various locations in Queensland. In July 2022, they commenced employment with Qube and were assessed in locomotive preparation and operation, as well as the safeworking competencies for the Cloncurry to Mount Isa and Cloncurry to Hughenden routes. The second driver had a current health assessment and met the fitness for duty criteria according to the national standard of health assessment for rail safety workers.
The second driver was not normally rostered to work with the driver (at the controls) and had swapped a shift to work train 9227 on 17 August 2022. They stated they felt comfortable working with the driver and together they had discussed arrangements for sharing the driving and safeworking duties throughout the trip.
Recent history
Driver at the controls
Over the 7 days prior to the accident, the driver had worked 3 duty periods, which included afternoon and night shifts, broken by full days off. After completing their overnight shift on 16 August 2022, at 0750 they retired to a motel in Cloncurry to rest. They reported usually having difficulty obtaining sleep at the motel, due to lighting and road noise. The driver recalled waking at about 0400 on the morning of the accident and reported feeling ‘OK but not lively’. They commenced work at 0545 and had been on duty for about 40 minutes before reaching Oonoomurra station.
Second driver
For the same period, the driver had worked 4 consecutive duty periods, which included an afternoon and a day shift with a full day off prior to the accident. The driver said they typically went to bed at 2200 and slept 5–6 hours. They had slept at home and recalled having good quality sleep, were rested and not feeling fatigued.
Train information
Train 9M48
General
Aurizon freight train 9M48 consisted of locomotive 2808 in the lead and locomotive 2831 trailing, hauling a combination of 59 GSZY, GZSC and GSZZ class wagons. Train 9M48 provided a bulk ore freight service between Mount Isa and Stuart Yard (near Townsville) and was on the return journey to Mount Isa, with empty ore wagons. The train measured 759 m in length24 with a gross weight of 1,278 t.
2800 class locomotive
The lead locomotive was a CM30-8 diesel electric locomotive (built by A Goninan & Co.), measuring 20.4 m long, 2.87 m wide and 3.68 m high. The hood-type locomotive design featured full width cabs at both ends. Access to the locomotive was provided via fixed steps on either side of the frame and exterior walkways along both sides of the locomotive.
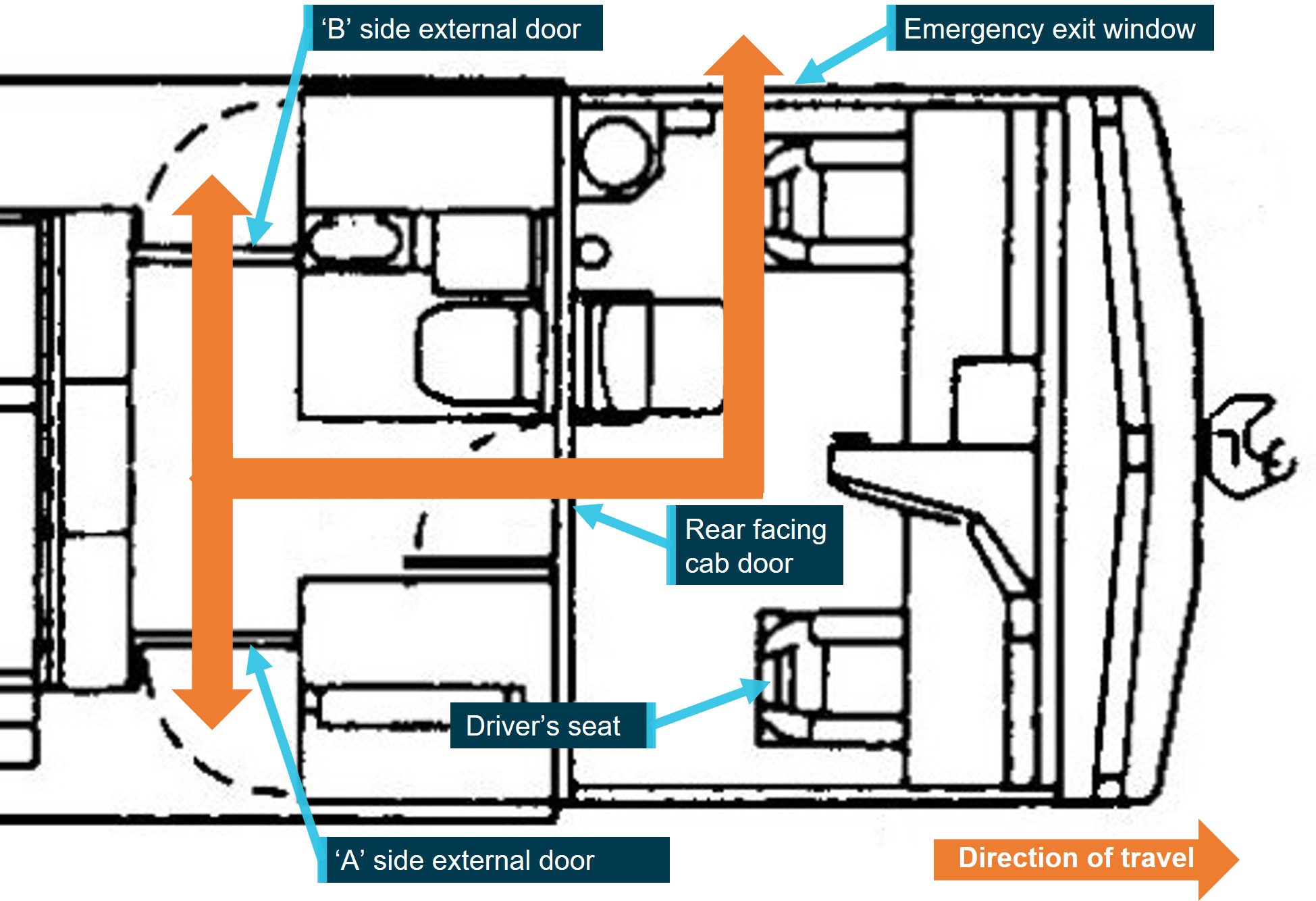
Access and egress for the No 1 end operator's cab was through a rear facing internal door that opened into a vestibule. External doors provided access/egress to the walkways on both sides next to the engine hood. The No 2 end operator's cab was accessed through a rear facing external door that led directly to the walkway on the ‘B’ side of the engine hood only. The locomotive was designed to be operable in either direction from the respective operator's cab. At the time of the derailment, the driver was operating the locomotive from the No 1 end (Figure 3). These access and egress pathways were also the primary emergency escape paths.25
The locomotive windscreens were made of laminated glass and not fitted with release handles to remove the windscreen in the event of an emergency. Aurizon designated the side windows of the cab as the alternate pathway for emergency egress from the enclosed space by either sliding open the window or using a glass hammer to break out the window.
The locomotive also incorporated internal and external lighting systems that included access lights and cab lighting to create a safe working environment for operating staff. The cab lighting comprised of several individually switched circuits for overhead lights, timetable lights, gauge lights and panel lights. Three overhead fluorescent lights were fitted in each cab. The lights were operated either from a cab light switch on the driver’s overhead console or a switch on the assistant driver’s console. An eyeball light and rocker switch were located over the train inspector’s seat.26
The Aurizon 2800 class locomotives, including 2808, were not fitted with emergency lighting or a back-up power supply in the event of a main battery failure.
Figure 3: Top view of the Goninan CM30-8 diesel electric locomotive
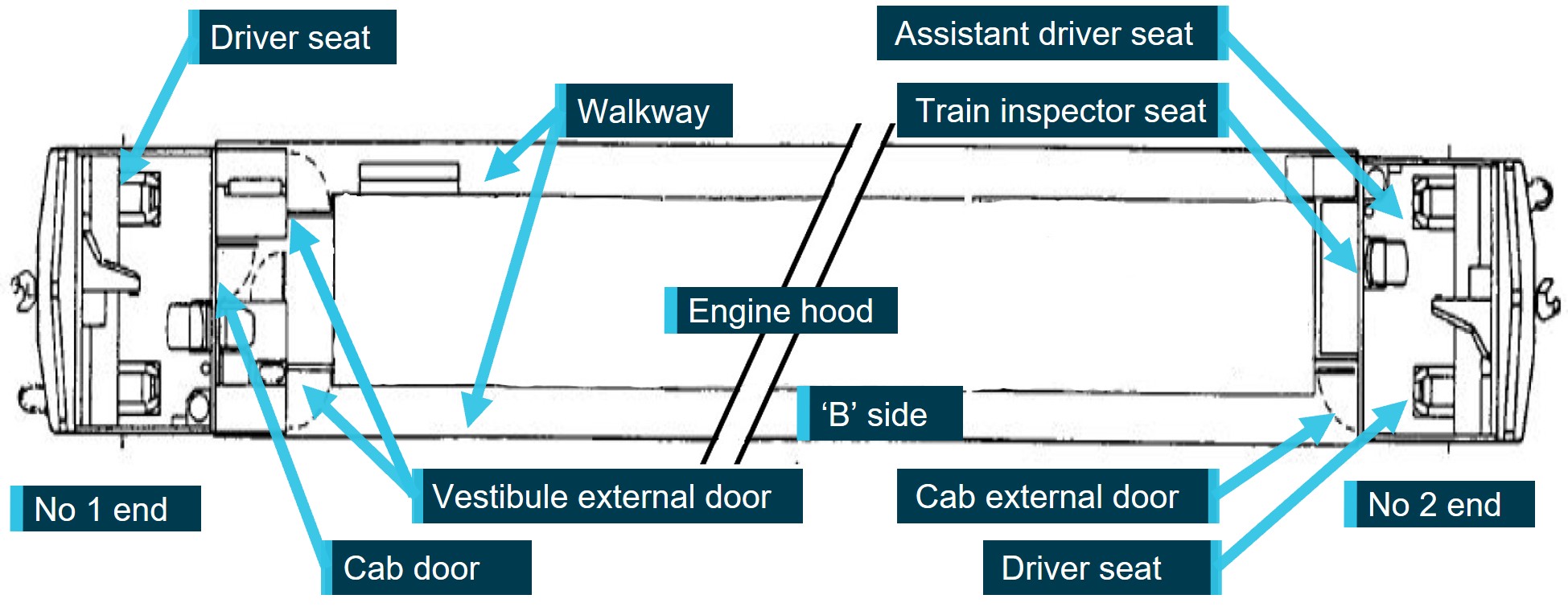
Source: Goninan & Co Ltd 1998, annotated by the ATSB
Train 9227
General
Qube freight train 9227 consisted of locomotive PRL201 in the lead and PRL202 and PRL204 trailing, hauling a combination of 68 GQGY and GOAF class wagons27 loaded with ore. Train 9227 provided a bulk ore freight service between Mount Isa and Stuart Yard. The train length was recorded as 824 m28 and trailing mass of 5,274 t. Each PRL class locomotive weighed approximately 110 t providing a gross mass of about 5,500 t.
Locomotive PRL201
The locomotive was a GT22C-3 diesel electric locomotive (originally built by Clyde Engineering). The locomotive was equipped with a single driver’s cab at the short hood end. The driver’s console featured a control stand beside the driver and a gauge console in front of the driver (Figure 4).
Figure 4: Driving position control stand and console arrangement

Source: Progress Rail, annotated by the ATSB
The gauge console was fitted with an analogue-style digital speedometer that incorporated a distance counter function. The electronic distance counter function provided a driving aid where, once activated, it displayed the distance the locomotive subsequently travelled. This device could be used by the driver to accurately determine the distance travelled by the locomotive after activation. For example, this measurement, used in conjunction with known train and station lengths could be used by train crew to calculate whether the chosen stopping location meant the rear of the train had cleared a block section.
A variety of counter models, each with different methods of operation may be fitted to the PRL locomotive. The method of operation may be as simple as dedicated on/off buttons on the ME-149 model (Figure 5, right) or more complex requiring a level of programming via additional inputs from the driver to pre-select the correct function, as with the ME-250 model (fitted to locomotive PRL201) (Figure 5, left).
Figure 5: Models of speedometer and distance counter fitted to PRL class locomotives
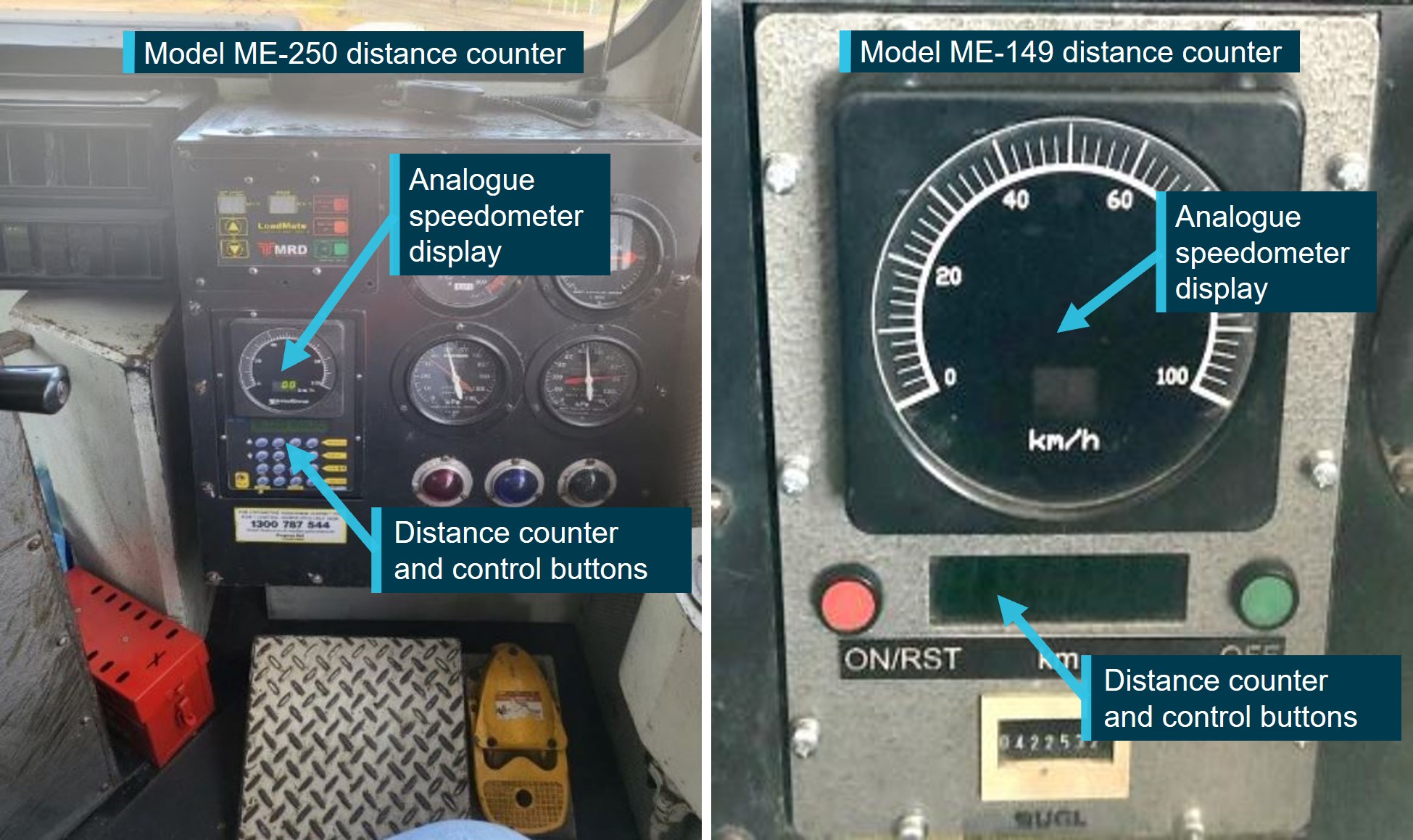
Source: Qube, annotated by the ATSB
The PRL class locomotive operational features and procedures were documented in an operator’s manual.29 The manual included a brief description of the controls and indications used by the operating crew. Information was provided for the ME-149 type speedometer and distance counter device. However, other than a mention of the ME-250 as an option, no information was provided on its operation.
Qube advised that training in the operation of the PRL locomotive was provided ‘holistically’. They stated that, although the speedometer/distance counter device was identified during training, specific instructions on the operation of the 2 types of counters were not provided. The driver of train 9227 identified they were unfamiliar with the operation of the more complex distance counter device and therefore did not use it as an aid during their arrival at Oonoomurra.
Environmental conditions
The driver of train 9227 recalled that the morning sun was starting to rise above the horizon upon their arrival at Oonoomurra station. They further stated that the resultant glare impeded their vision of the track toward their typical stopping point, located 50 m prior to the limit of authority. As a result, the driver chose a different stopping point. The second driver of train 9227 also recalled that the sun was just starting to rise. They described the sunrise as a ‘yellow glare’ and were required to turn their head to the side to avoid looking directly at the sun.
The twilight and sunrise times were calculated30 for 17 August 2022 at Oonoomurra and are shown in Table 1. At the time train 9227 had stopped at the station (0622), the calculations indicated that the position of the sun was 9.34° below the horizon and the ambient light was transitioning between nautical and civil twilight.
Table 1: Twilight and sunrise times at Oonoomurra
| Event | Time |
| Local time of astronomical twilight | 0544 |
| Local time of nautical twilight | 0610 |
| Local time of civil twilight | 0636 |
| Local time of sunrise | 0659 |
Source: Geoscience Australia
Geoscience Australia defined nautical and civil twilight as:
Nautical twilight
Is defined as the instant in the morning, when the centre of the Sun is at a depression angle of twelve degrees (12°) below an ideal horizon.31 At this time in the absence of moonlight, artificial lighting or adverse atmospheric conditions, it is dark for normal practical purposes. For navigation purposes at sea, the sea horizon is not normally visible.
Civil twilight
Defined as the instant in the morning, when the centre of the Sun is at a depression angle of six degrees (6°) below an ideal horizon. At this time in the absence of moonlight, artificial lighting or adverse atmospheric conditions, the illumination is such that large objects may be seen but no detail is discernible. The brightest stars and planets can be seen and for navigation purposes at sea, the sea horizon is clearly defined.
Queensland Rail information
Mount Isa line
The Queensland Rail Great Northern Railway, more commonly known as the Mount Isa line, extended from Stuart Yard (south of Townsville) at the eastern end to Mount Isa in the west. The single line, narrow gauge32 system was 1,032 km in length, including the Phosphate Hill Branch and was constructed with 46 stations where trains could cross/pass.
The Mount Isa line was operated by remote control signalling between Stuart Yard and Antill Plains and direct traffic control (DTC) with automatic train protection (ATP) between Antill Plains and Mount Isa/Phosphate Hill. Train movements between Stuart Yard and Mount Isa were controlled from the Queensland Rail Townsville Network Control Centre.
The stations between Townsville and Mount Isa ranged between 1,100–1,040 m in length and were equipped with trackside location boards (block limit boards [BLBs]) that marked the limit of the respective station for trains travelling in either the up or down direction.
Oonoomurra station
Oonoomurra was a directional travel station33 extending for 1,033 m and equipped at each end with a trailable point. The points were set to divert an approaching train to the right-side track alignment in the direction of travel (Figure 6).
The track alignment was primarily tangent and the terrain relatively flat with low open woodland vegetation trackside. Approximately 280 m prior to the western end point the track transitioned from tangent through an 805 m radius curve, before returning to tangent track at the Landsborough Highway.
Figure 6: Oonoomurra station track alignment

Source: Google Earth, annotated by the ATSB
Safeworking system
Direct traffic control
The Mount Isa line used the DTC safeworking system. The system governed the movement of rail traffic on the bi‑directional single track and through the stations. DTC operated on the principle of absolute block working and was managed by instructions contained in DTC authorities issued by the network control officer (NCO) to the rail traffic crew (driver) of each rail traffic movement. The system provided that only one rail traffic movement would be authorised to travel on any one block section, at any one time.
The DTC territory was divided into distinct block sections. Directional travel stations, such as Oonoomurra, were equipped with trackside location boards (BLBs) that marked the limit of the respective block and station track sections (Figure 7).
Figure 7: Oonoomurra block limit boards
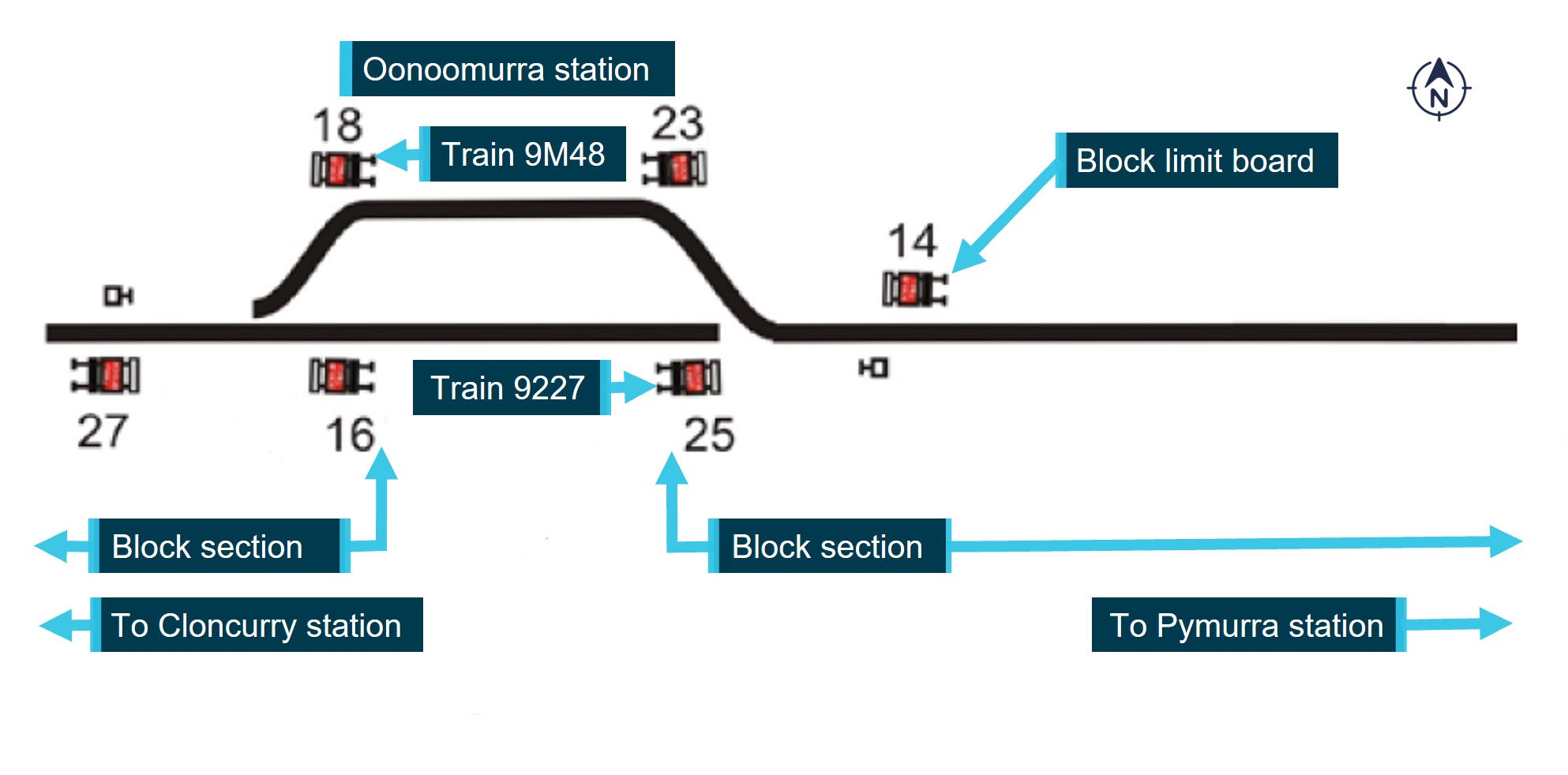
Source: Queensland Rail, annotated by the ATSB
The NCO issuing a DTC authority up to a nominated BLB effectively transferred ownership of the affected block(s) from the NCO to the driver. After exiting a block, the driver could transfer ownership back to the NCO with the provision of a release code.
The transfer of block ownership was primarily through numerical codes communicated verbally between the NCO and driver. In addition, the DTC system software supplied an oversight function when generating and validating the codes. It compared the GPS location of the locomotive against the selected block(s) to be released, and those that would remain in the authority when the release was finalised. This occurred through a combination of functionality in the DTC driver workstation equipment in the locomotive cab and the controller workstation equipment in the network control centre.
The driver workstation calculated whether the current locomotive GPS location was within the block(s) that would remain in the authority after the release and, if not, triggered an alarm requiring confirmation of the release. The driver workstation functionality detected the position of the locomotive only, and did not hold information on the train length, so it could not prove the location of the rear vehicle of the train when calculating the release.
On receipt of the release code from the driver, the NCO selected the rail traffic and entered the code into the control workstation. The control workstation calculated whether the current GPS location was within the blocks that would remain in the authority after the release and, if not, displayed a prompt requiring confirmation of the release. The control workstation did hold information on the train length and used this information to confirm that the length of the train would fit within the blocks still in the authority. The control workstation did not calculate whether the train was in‑clear and therefore did not provide an alert to the NCO.
Queensland Rail standard MD-10-113 Direct traffic control manual34 summarised limitations of the DTC system. It stated that, although the system design created and validated authorities for issue by the NCO, it could not:
• detect if blocks that were currently occupied, or to be occupied, were released by the rail traffic crew or by the NCO
• detect if a block that was available to the NCO was physically unavailable for traffic for any reason such as a track defect.
Procedure for crossing rail traffic at a DTC station
DTC station working
For a cross at a directional travel station, such as Oonoomurra, the NCO relied on the rail traffic crew at the station to confirm their train was complete and in-clear within the block section being occupied. For train 9227, the crew were to confirm the rear if the train had passed BLB OA 16 at Oonoomurra. This meant the train effectively no longer occupied the Cloncurry to Oonoomurra block section.
Following receipt of confirmation and the release code from the crew, the NCO could then issue the next electronic authority, or extend an existing authority, for the opposing rail traffic to proceed and occupy the vacated block. For train 9M48, the authority would allow it to pass BLB OA 18 and occupy the Oonoomurra to Cloncurry block section.
To facilitate this, the DTC manual required rail traffic crew of rail traffic arriving at the station to:
• check the points indicator is in the normal position
• if necessary, stop the rail traffic clear of the points and reset them to the correct position
• enter the station, on the road indicated on the DTC Authority, at a maximum speed 25 km/h
• stop the rail traffic within the clearance point boards35
• make sure the rail traffic is complete
• report to Network Control Officer the rail traffic is in clear and complete and release unoccupied blocks
• check the points, and if necessary, correctly set them for the opposing rail traffic
The opposing rail traffic crew arriving at the station were to:
• check the opposing rail traffic is clear and complete
• tell the opposing rail traffic crew their rail traffic is clear and complete, or otherwise
• obtain an Authority to proceed
• proceed in accordance with the Authority
• release unoccupied blocks when clear and complete
Speed of rail traffic
The DTC manual stated that, when approaching a station, the driver was to reduce rail traffic speed to a ‘controlled speed’. The Queensland Rail standard MD‑10‑107 General operational safety manual36 defined controlled speed as:
…a speed that allows rail traffic to stop short of an obstruction within half the distance of clear line that is visible ahead.
Arriving at a station where the driver was to stop at a limit of authority, such as BLB OA 18, the driver was to travel at a maximum speed of 25 km/h through the points at the entrance then manage the train speed to stop at the limit of authority. If travelling through the station in accordance with the authority, the driver was to travel at a maximum speed of 25 km/h until the whole rail traffic had passed through the points and turnout curve both at the arrival and departure of the station.
Procedure for checking rail traffic in-clear and complete
MD-10-107 required that, when rail traffic was stopped at a station in single line bi‑directional territory (such as the Mount Isa line) to cross other rail traffic, its crew must check the rail traffic was complete and in-clear by:
• verbal confirmation of another who can see the rear of train signals, or
• visually determining the correct rail vehicle is at the rear of the rail traffic, or
• the correct number of rail vehicles are on the rail traffic, or
• carrying out a brake pipe leakage test
Note: A rail traffic driver may assume the rail traffic is complete if the Brake Pipe Leakage Test is successful.
• make sure the rail traffic is in clear by comparing the length of the rail traffic with the capacity of the main line or loop
• if rail traffic is not in clear, tell Network Control Officer and rail traffic crew of opposing rail traffic
• protect the rail traffic, if necessary.
For an unattended directional travel station, such as Oonoomurra, the driver of the first rail traffic to arrive could satisfy the requirements for ensuring their train was complete by conducting a brake pipe leakage test. For checking the train was in‑clear, they could:
- compare the stopping point, train length and the available track length at the station, or
- count the distance travelled by the locomotive after entering the station and compare the available track length at the station.
The crew of the second rail traffic to arrive could satisfy the requirement for checking their train was in‑clear and complete through the receipt of verbal confirmation from the first rail traffic crew indicating that they had sighted the end of train marker on the second rail traffic.
If the crew of the second rail traffic to arrive found the first rail traffic not to be in-clear of the track ahead, the crew were to:
• stop clear of other rail traffic
• tell rail traffic crew of other rail traffic their rail traffic is not in clear.
The crew of the first rail traffic were to then pull in-clear of the opposing track, if possible. There was no requirement for the rail traffic crew of either train to advise the NCO.
If the second crew found the first rail traffic to arrive was not complete, they were to tell the other crew and notify the NCO. The NCO was then to check the location of all rail vehicles and make sure the section was clear. The second crew were not to proceed until authorised by the NCO.
There was also no requirement in the procedure for train crew to use the reading from a distance counter device to crosscheck that the locomotive had travelled a sufficient distance to ensure the rear of the train was in‑clear. In the absence of an accurate measurement of the distance travelled by a locomotive on entering a station, a variety of alternative methods were available to a driver to confirm their train was in-clear including:
- selecting a stopping point as close as practicable to their limit of authority
- using a familiar landmark that worked previously for a train of similar length
- a calculation using the estimated distance travelled after entering the station or the estimated distance remaining to the limit of authority in conjunction with the train and station track lengths.
Qube information
Train working
The Qube crew of train 9227 were required to follow the applicable Queensland Rail safeworking rules, such as ensuring a train was in-clear and complete at a station, as well as other instructions implemented by Qube when stopping their train at a limit of authority.
Qube procedure, PCE-216 Two-person train crewing, described the responsibilities and authorities applicable to the train crew.
The train driver operating the train service was responsible for:
• Delegating duties to the train driver’s assistant and ensuring that these duties are performed to the required standard.
• Carrying out their activities in accordance with all QLRS [Qube], track access provider [in this instance Queensland Rail] and legislative requirements.
The train driver’s assistant was responsible for:
• Carrying out their activities in accordance with the train driver’s instructions and all QLRS [Qube], track access provider [in this instance Queensland Rail] and legislative requirements.
• Completing safe working documentation if qualified to do so
• Communicating with the track access provider and CSC [Qube Customer Service Centre] when required and efficient to do so – this allows the train driver to concentrate on operating the train.
The procedure highlighted that both members of the train crew had shared, and equal responsibility for the safe operation of the train including:
• The communication and implementation of safeworking requirements
• The communication of information about route conditions, signalling aspects and limits of authority.
• Ensuring that the train is managed in accordance with proceed authorities, gradients and speed signs.
• Ensuring that safeworking documentation is completed including recording authority numbers.
Each member of the train crew was authorised to challenge the other if they believed that approved procedures were not being followed. If resolution could not be achieved and safe operations implemented, the Qube Customer Service Centre was to be contacted immediately.
The importance of communication between crew was highlighted, particularly for the safe operation of trains within the safety‑critical zone approaching a limit of authority, to prevent a signal passed at danger incident.
Approaching a location board, such as BLB OA 25 at Oonoomurra station where there was a planned stop, the crew were to:
- crosscheck the limit of authority
- agree where the train was to stop
- prioritise the task of stopping the train at the stopping location
- ensure the train was operated in a manner to guarantee the train would stop at the desired location.
To ensure the train stopped at the desired location, the train crew were to reduce train speed to not more than 15 km/h at a minimum of 200 m in advance of the stopping point. The train was then to be advanced at no more than 15 km/h until the stopping point was reached.
The stopping point was defined as:
A stopping point is a point 50 metres in advance of a signal, track circuit, clearance point, yard [or station] limit board, etc that indicates that a stop is required.
After the crew stopped the train at the desired location, they were to continue to implement the procedural requirements detailed in the Queensland Rail safeworking rules for DTC territory to ensure the train was in-clear and complete before returning ownership of the block section to the rear of the train, in this instance the Cloncurry to Oonoomurra block section. There was no requirement for the train crew to use the distance counter device to verify the locomotive had stopped with sufficient distance for the rear of the train to have cleared a control point.
After returning the ownership of the block section to the NCO, the crew had discussed the stopping point and whether the train was in‑clear. Although the second driver remained unsure, there was no discussion on moving the train forward toward the limit of authority or contact made with the Qube Customer Service Centre.
Rail safety worker competency
The procedure for rail safety worker assessment and certification37 defined the method for maintaining competence and certification to meet Qube, regulatory and track access provider standards. The training requirements for each grade of driver were detailed in a training plan. The plan included accredited Australian Quality Framework requirements and recognition of prior learning of competencies gained through formal study and work experience. Each stage of training included:
• off job training and off job training assessment
• on job training exercises
• a period of on job application
• assessment of competence.
Competence was assessed against a train operations performance checklist38 that listed a range of tasks that checked the knowledge and skills of the worker against the competencies required for the rail safety work being undertaken.
The checklist included the DTC system of safeworking,39 which encompassed driver knowledge of the rules and procedures contained in MD-10-107 and PCE-216.
Aurizon information
Train working
The Aurizon driver working 9M48 was required to follow the applicable Queensland Rail safeworking rules, as well as other instructions implemented by Aurizon. The driver had an authority to travel through Oonoomurra and was to implement the procedural requirements detailed in the safeworking rules for DTC territory to affect the cross with train 9227.
Emergency response
The Aurizon emergency response guide40 provided rail traffic crew with information for their response to an emergency, such as a collision or derailment. A key element was to immediately report the emergency to the NCO and to provide sufficient information to enable an appropriate and timely response. After alerting the NCO, the crew were to contact the Aurizon live run operations centre to report the emergency.
The guidance reinforced that, in an emergency the primary responsibility of the crew was to protect their own safety, and, within the limits of their safety and training, that of any other person, followed by the rail traffic that they were responsible for. In the event of an emergency, such as a fire or locomotive rollover, the guidance noted that emergency egress may not be possible by the normal route. Alternative exits varied between locomotive classes as some may be fitted with glass breakout hammers for the side windows, while others were fitted with release handles for front windscreen removal. The guidance noted that in some classes of locomotive (such as the 2800) the windscreen was not an alternative exit path due to it being toughened laminate with no release handles.
Accident site information
The lead locomotive of train 9227 stopped about 317 m before the limit of authority at BLB OA 25 (Figure 8). The last 8 ore wagons of the train consist (extending approximately 86 m in length) did not clear BLB OA 16. The Cloncurry to Oonoomurra block section remained occupied and the trailable points at the western end (adjacent to the ‘trailable point indicator’ in Figure 9) of the station were fouled by the wagons from train 9227.
Figure 8: Stopping location of the lead locomotive from train 9227 from the limit of authority at BLB OA 25

Source: Aurizon, annotated by the ATSB
Figure 9: Rear portion of train 9227 showing the wagons were not in-clear of BLB OA 16

Source: Aurizon, annotated by the ATSB
The leading corner of the modular cab and chassis of the lead locomotive (2808) on train 9M48 collided with the wagons of train 9227. The 65th wagon (GAOF 0060) was first impacted, approximately mid-way along its length, damaging the side bolsters. The convergence in the track alignment toward the trailable points increased the force of the collision until the leading corner of wagon GOAF 0059 was impacted. The side of the wagon was breached and some of the contained zinc concentrate spilled onto the track. None of the wagons on train 9227 derailed.
During the collision, the lead locomotive (2808) of train 9M48 derailed, uncoupled from the trailing locomotive and rolled onto its ‘A’ side coming to a stop on the right side of the track in the direction of travel (Figure 10). The locomotive diesel fuel tank was ruptured and fuel was spilled. There was no post‑impact fire.
Figure 10: Derailed and overturned lead locomotive 2808 of train 9M48

Source: Aurizon, annotated by the ATSB
Survivability aspects
Post‑accident egress from locomotive 2808 of train 9M48
The driver was ejected from their seat onto the ‘A’ side wall/window. The diesel engine had shut down, and electrical power was supplied from the locomotive main battery bank only. The driver reported that the cab was in darkness, was disarranged, the train borne radio was not working, and they were unable to locate the handheld radio. The survivable space within the modular cab was not compromised and the cab remained attached to the locomotive subframe.
The escape paths available to the driver at the No 1 end of the locomotive were via the rear‑facing internal door (the normal access and egress route) that led to the internal vestibule area, then through the external door leading to the walkway on the ‘B’ side of the engine hood. An alternative emergency exit was located at the assistant driver’s side sliding window. The side windows were the designated emergency evacuation points from the enclosed cab of a 2800 class locomotive. An additional path may be available via the vestibule and external door on the ‘A’ side of the engine hood, however, this egress point was located under the overturned locomotive (Figure 11).
Figure 11: Locomotive 2808 emergency exit pathways
Source: Goninan, annotated by the ATSB
The driver reported they did not attempt to egress via the rear facing door into the vestibule area but initially attempted unsuccessfully to kick out the windscreen. They then considered egress via the assistant driver’s side window (alternative pathway) that was situated on the high side of the overturned locomotive cab. However, they were unable to reach the alternative pathway. Following the arrival of bystanders, the driver was able to egress via the side window with their assistance. The driver and bystanders then jumped from the side of the locomotive onto a ballast mount located at the front of the locomotive (Figure 12).
Figure 12: Overturned lead locomotive of train 9M48

Source: Aurizon, annotated by the ATSB
The lead locomotive of train 9M48 (2808) was fitted with window breaking hammers for the train crew to access the outside of the vehicle in an emergency. Hammers were fitted to the overhead console above the driver and assistant driver positions. Each hammer was attached by a short tether to the mount.
The 2800 class locomotive was not fitted with any purpose-built footholds or climbing arrangements either internal or external to the cab to assist rail traffic crew egress via the alternative pathway or to assist with descending the outside of the locomotive.
Locomotive emergency egress standards
Overview
Rolling stock operators, as the risk owner, were to provide for the effective management of safety risks associated with their railway operations through the implementation of a safety management system. The system encompassed the identification of hazards and the assessment of risk, and the implementation of risk control measures to address those risks. Control measures included the application of standards, codes of practice, guidelines and rules that were either developed individually to address the organisation’s unique operations or operational requirements, adopted from Rail Industry Safety and Standards Board (RISSB) products, or a combination of both.
RISSB was the accredited standards development organisation for the rail industry in Australia. RISSB collaborated with its rail industry members to promote best practices by the provision of a catalogue of publications including standards, codes of practice, guidelines and rules.
To develop publications, RISSB relied on input from the rail industry to ensure the products best reflected the needs of stakeholders. RISSB sought nominations from rail industry subject matter experts to form development groups, tasked to deliver the products. Standards were developed following an 8-step process, and in compliance with the requirements of Standards Australia SG-003: Standards & Other Publications.
RISSB also published a hazard register that was available to member organisations for reference when undertaking their organisation’s risk assessment process. RISSB noted that it did not own the hazards/risks and therefore could not mandate associated controls or actions, as the responsibility was with the relevant organisation using the product.
The RISSB hazard register broadly grouped content under rolling stock, infrastructure and operational‑related hazards. Further subgrouping defined the source, precursors and related factors. An identified source associated with rolling stock was ‘evacuation hazards’. Several precursors were listed against this source including derailment, track failure, track obstructions or environmental impact. There were 44 related factors (hazardous events/publishable consequences) associated with evacuation hazards including:
- evacuation capacity of exit(s) being inadequate
- no instructions being provided, so persons do not know how to evacuate
- exits being out of reach (for example, overturned vehicle) preventing safe exit
- no exit being available
- being unable to operate exits.
Each of these factors was linked to an evacuation not being successfully initiated or unable to successfully evacuate.
Australian industry standards
Railway rolling stock access and egress
The purpose of the rolling stock Access and Egress (AS 7522:2021) standard was to describe:
…the requirements for access and egress of workers and passengers on locomotives, freight, passenger, and infrastructure maintenance (track machines) rolling stock.
The main purpose of the requirements is to provide safe, efficient, equitable and dignified access and egress, and to minimize risks to passengers and workers associated with access and egress, emergency evacuations, and requirements for people with disabilities.
The scope was expanded from the previous version (AS 7522:2012), to make the standard applicable to existing rolling stock as well as modified and new locomotives, freight, passenger and infrastructure maintenance rolling stock. Compliance with the standard referenced the 4 types of provisions (requirements, recommendations, permissions and constraints) typically contained within the Australian Standards developed by RISSB.
The adoption of all requirements (identified by the term ‘shall’) was mandatory for claiming full compliance with the standard. Recommendations (identified by the term ‘should’) was a preferred option but did not exclude other possibilities. The standard also stated:
For compliance purposes, where a recommended control is not applied as written in the standard it could be incumbent on the adopter of the standard to demonstrate their actual method of controlling the risk as part of their WHS or Rail Safety National Law obligations. Similarly, it could also be incumbent on an adopter of the standard to demonstrate their method of controlling the risk to contracting entities, or interfacing organisations where the risk may be shared.
RISSB Standards address known hazards within the railway industry. Hazards, and clauses within this Standard that address those hazards, are listed in Appendix B.
The hazardous events/publishable consequences controlled by the standard (listed in Appendix B of the standard) were related to fires and slips, trips or falls. None of the listed hazardous events related to the evacuation hazards from locomotives or passenger rolling stock.
The section titled Emergency evacuation contained requirements and recommendations relevant to locomotive, freight, passenger and infrastructure maintenance rolling stock. For locomotives, several requirements were stated including:
Enclosed cabs of rolling stock shall be fitted with sufficient emergency exits to provide escape paths to the vehicle exterior when the vehicle is upright and when overturned on the side.
In the previous version (AS 7522:2012), when discussing egress from new and modified rolling stock, the standard stated that:
A suitable solution is for emergency exit windows on each side and another emergency exit either in the front or rear of the compartment.
This reference was removed from the 2021 version of the standard.
The section titled Emergency exits recommended emergency exit windows should have a built-in lever, handle or another device such as a breakout hammer. The section also included a recommendation that:
Emergency exit performance shall be verified in a type test.
Lighting and visibility
The purpose of the Lighting and Visibility (AS 7531:2015) standard was to describe the requirements for lighting and rolling stock visibility. The scope was applicable to new and existing locomotive, freight, passenger and infrastructure maintenance rolling stock. The adoption of requirements and recommendations was the same as other RISSB rolling stock standards if claiming compliance.
The standard defined the requirements for normal and emergency interior lighting. For emergency interior lighting, the standard stated:
Spaces (cabins, rooms, vestibules, aisles etc.) on locomotives, passenger rolling stock, and infrastructure maintenance rolling stock where people may be enclosed in during operation, shall have emergency lighting.
Emergency lighting was defined as:
Lighting, powered from a separate source (e.g. battery) to the vehicle's main power source, providing illumination for evacuation purposes.
Several additional emergency lighting requirements were specified, however, they were only applicable to new and modified locomotives, and not existing locomotives.
The hazardous events/publishable consequences (listed in Appendix A of the standard) controlled by the standard were related to poor visibility of train and work health and safety hazards due to inadequate illumination. One of the listed hazardous events related to an evacuation hazard arising from an inability to locate exits and being unable to reach an exit safely or unable to successfully evacuate.
After the accident, on 21 December 2023, RISSB published AS 7531:2023, Rolling stock lighting and visibility, superseding AS 7531:2015. The objective was similar to the previous version. Notably, the scope was amended to be applicable to new and modified self-propelled locomotive, freight, passenger, road rail vehicles and infrastructure maintenance rolling stock. Reference to ‘existing’ rolling stock was deleted. Like the previous version of the standard, hazardous events controlled by the standard were listed (Appendix A of the standard). However, none of the listed events related to hazardous events associated with an emergency evacuation.
Aurizon rolling stock standards
General
Aurizon developed a catalogue of rolling stock standards to address its unique operations and risk management programs. The standards detailed the requirements to attain the desired performance and to manage hazards that might arise during operation of the rolling stock. The standards referenced related documents including the Australian industry standards published by RISSB.
The requirements to manage hazards that rail traffic crew may be exposed to when egressing a locomotive in an emergency were contained in several Aurizon standards including:
- 07-STD-003-RSK Emergency equipment carried in rolling stock
- 07-STD-004-RSK Rolling stock interior environment
- 07-STD-009-RSK Rolling stock structural requirements
- 07-STD-013-RSK Rolling stock fire performance.
Emergency equipment carried in rolling stock 07-STD-003-RSK
Aurizon standard 07-STD-003-RSK, published with an effective date of 3 October 2017, defined the key requirements for the emergency equipment that must be carried to manage risk in the event of an accident, obstruction or mechanical failure involving rolling stock. The equipment was to facilitate the provision of protection for the train when stopped on the track, first aid, fire suppression and evacuation.
The standard included a list of required equipment and included flags, audible track warning devices, signal lamp, hand torch, wheel chocks and clips, and specifications of the equipment. For example, the hand torch was specified as an electric waterproof torch capable of maintaining one candela of white light continuously for 5 hours.
For an evacuation, the requirements specified:
On existing rolling stock, a window breaking hammer shall be accessible for every worker occupied glassed area that does not have emergency access to the outside of the vehicle as per AS 7522, Railway Rolling Stock, Access and Egress.
At the time of publication of the Aurizon standard, AS 7522:2012 Railway Rolling Stock Access and Egress – Part 1 Locomotive Rolling Stock, was current. This standard was superseded, and the 2021 version was current at the time of the derailment of train 9M48. The construction of the 2800 class locomotives occurred prior to the publication of both 07‑STD‑003‑RSK and AS 7522:2021.
Rolling stock interior environment 07-STD-004-RSK
Aurizon standard 07-STD-004-RSK defined the interior environment requirements for locomotives related to noise, vibration, air quality and non-ionising radiation, and magnetic fields. Under the heading ‘air quality’, the standard identified:
Interior lighting systems shall comply with applicable parts and sections of AS 7531 Railway Rolling Stock - Lighting and Rolling Stock Visibility.
Standard 07-STD-004-RSK was published with an effective date of 3 October 2017. At the time of publication, AS 7531:2015 Lighting and Visibility, was current.
The construction of the 2800 class locomotives occurred prior to the publication of 07‑STD‑004‑RSK and AS 7531:2015.
Rolling stock structural requirements 07-STD-009-RSK
Key requirements of standard 07-STD-009-RSK were for the structure and attachments of rolling stock to withstand normal train forces and the minimisation of risk of injury during a collision and derailment. In a derailment, the locomotive was, as far as practicable, to remain coupled, upright and resist jack-knifing. In the event of a rollover onto its side, the cab structure design was to maximise protection to the train crew by:
…..supporting the weight of the locomotive (including the bogies) in the situation when the locomotive is resting on its side without exceeding the critical design stress in the main supporting members, assuming the locomotive is supported on the edge of the underframe and at the cantrail of the cab.
Rolling stock fire performance 07-STD-013-RSK
Aurizon standard 07-STD-013-RSK, published with an effective date of 3 October 2016, described that fire safety performance of rolling stock was not solely determined by the fire resistance of materials used but included vehicle design, occupant response, ease of evacuation, and detection and suppression. The standard applied to existing rolling stock that was proposed to be operated under changed operational conditions, that was to be modified, and any new rolling stock introduced into operation. A key goal of the standard was to assist staff and emergency service operations in response to a fire.
The vehicle design methods considered fire prevention, suppression/retardation and the protection of people. For the protection of people, the standard detailed 25 requirements including:
• Exit design to have adequate capacity to evacuate all persons onboard within a suitable time….
• Adequate normal and emergency lighting levels be provided - refer AS 7531.1 Railway Rolling Stock - Lighting and Rolling Stock Visibility – Locomotive Rolling Stock and AS 2293.3, Emergency Escape Lighting and Exit Signs for Buildings - Emergency Escape Luminaries and Exit Signs
• Emergency lighting to be provided along exit paths and at all emergency exits.
• Back-up power supplies to have adequate capacity to provide required power output for suitable period of time.
• Assist staff and emergency service operations
• Provide emergency exits accessible from outside the vehicle for use by emergency service personnel to gain entry to the vehicle
• Communication systems to have back-up power supply.
Existing locomotives that complied with recognised national and international rolling stock fire standards (such as AS 5062 Fire Protection for Mobile and Transportable Equipment) were deemed to comply with the standard, subject to certain qualifications contained in the appendix. The qualification related to the provision of emergency lighting stated:
Emergency lighting to comply with the requirements of 07-STD-004-RSK, Rolling Stock Interior Environment, instead of the prescribed requirements
There were no qualifications related to emergency exits or backup power supplies for emergency lighting or communication systems.
Standard 07-STD-013-RSK included a reference to the superseded Australian Standard AS 7531.1. The content of AS 7531.1 had been consolidated into standard AS 7531:2015 Lighting and Visibility, which was the current standard at that time.
Risk management
In order to ensure the safety of operations, the Office of the National Rail Safety Regulator’s Guideline, Safety Management System (2019) stated that:
…an RTO [rail transport operator] must eliminate or minimise risks to safety SFAIRP [so far as is reasonably practicable]…Risk management is a critical activity and the SMS [safety management system] supports the management of risk to ensure that risks are identified, assessed, eliminated or controlled.
Specifically, risk assessments should:
- identify all reasonably foreseeable risks to safety arising from railway operations, under both normal and abnormal conditions
- analyse the identified risks, including specification of the control measures to be used to manage those risks
- evaluate whether the identified risks have been managed so far as is reasonably practicable, or whether further treatments are required.
Aurizon had a risk management framework as part of its safety management system. However, it was unable to provide risk assessments or other documentation that evaluated the effectiveness of the emergency exit and equipment arrangements provided in the 2800 class locomotive in addressing the known evacuation hazards to workers egressing from an overturned locomotive in an emergency.
Similar occurrences
The ATSB has investigated several occurrences that identified common safety factors associated with the application of the DTC system of safeworking and crew survivability following the derailment and rollover of a locomotive. The crew survivability safety factors pertained to the access and egress arrangements following an emergency, particularly the associated hazards to rail traffic crews, from the derailment and rollover of locomotives.
ATSB investigation RO-2015-028
On 27 December 2015, Aurizon train 9T92 derailed on the Mount Isa rail line near Julia Creek, Queensland, after entering a section of track where floodwaters had overtopped the track and scoured the ballast and formation. Locomotive 2814 (a 2800 class locomotive) derailed and rolled onto its ‘A’ side. The train was crewed by 2 drivers. A third driver was also travelling in the locomotive cab to obtain route knowledge along various track sections. Following the derailment and rollover, the train borne radio failed and communications with network control were lost.
To exit the locomotive cab crewmembers initially tried to smash the windscreens using the breakout glass hammer. After this failed, the crew assisted each other to climb from the locomotive cab through the assistant driver’s side window and onto the ‘B’ side of the locomotive cab.
The ATSB’s investigation identified that the Aurizon emergency egress arrangements for rail crew from the 2800 class locomotive were not effective in all foreseeable circumstances. In response, Aurizon advised that it continued to reassess the emergency evacuation procedures, locomotive windscreens and secondary communication options/opportunities.
ATSB investigation RO-2018-006
On 27 February 2018, Pacific National train 9221 and Aurizon train 9T66 collided while completing a scheduled train cross at the western end of the Oonoomurra station on the Mount Isa line, Queensland. Train 9221, travelling in an easterly direction toward its limit of authority at BLB OA 25, had stopped on the down track at Oonoomurra station. The driver then released the rear block section to the NCO.
The NCO subsequently extended the authority of train 9T66, travelling in a westerly direction, to continue through Oonoomurra toward Cloncurry station. Train 9T66 was travelling at about 25 km/h as it rounded a sweeping left curve at the western end. The crew then sighted 3 empty container wagons at the rear of train 9221, with the last wagon obstructing the single line track section ahead.
The driver made an emergency brake application but was unable to avoid a collision. The collision caused minor damage to the lead locomotive of train 9T66 and the last wagon of train 9221. There was no injury to the rail traffic crew of either train.
The ATSB’s investigation identified the on-board information system (distance counter) on the lead locomotive of train 9221 was faulty and displayed an incorrect measurement to the driver. The driver relied solely on the readout to determine whether the train was clear of the track block section to its rear. The crew of train 9T66 were, as they passed train 9221, observing the wagons on the adjacent train, but it was not until the track alignment transitioned to straight that the crew sighted the wagons obstructing the track ahead. Despite making an emergency brake application, a collision was unavoidable.
In response, Pacific National undertook several actions related to the verification of on‑board systems and reinforced procedures associated with the active identification of a stopping location (stopping point).
ATSB investigation RO-2020-014
On 28 July 2020, a planned cross was to occur between Aurizon train 9261 and road rail vehicle ZH42 at Sellheim station on the Mount Isa line, Queensland. Train 9261, travelling in an easterly direction toward its limit of authority at BLB SM23 stopped at an information sign location, as required by local procedures. The driver then released the block section to the train’s rear to the NCO.
The NCO subsequently extended the authority of ZH42, travelling in a westerly direction, to continue through Sellheim station toward Charters Towers.
The driver of ZH42 advised the release code was available but that they were stationary at BLB SM16, as the rear of train 9261 was not in-clear. The driver of ZH42 estimated that 2 and a half wagon lengths (at the rear of 9261) were occupying the block section ahead.
In response, Queensland Rail undertook a risk assessment of the information signs at Sellheim station and subsequently moved the signs approximately 134 m east of the first location. Queensland Rail also started a program of works to find locations on the Mount Isa line and other lines where inconsistencies existed between the trackside infrastructure and the information contained in route maps, signalling arrangement diagrams and the DTC software.
ATSB investigation RO-2022-003
On 23 February 2022, Aurizon train Y279 derailed on the North Coast rail line near Traveston, Queensland, after entering a section of track where floodwaters had overtopped the track and scoured the ballast formation. Locomotive 2811 (a 2800 class locomotive) derailed and rolled onto its ‘A’ side. The train was crewed by a single driver. During the derailment and overturning, the driver was ejected from their seat, fell across the cab to the assistant driver’s side and landed on their back in water that had entered the cab. The cab was in darkness and equipment disarranged. The driver was able to self-extricate from the locomotive cab via the rear facing door but due to widespread flooding, there was a significant delay before the arrival of emergency services to assist the driver.
The ATSB’s investigation identified that Queensland Rail weather‑related alarm response procedures were ineffective in providing network operations personnel with timely notification of a flood event. Additionally, although the driver did not use an emergency exit following the derailment and rollover of locomotive 2811, the Aurizon emergency egress arrangements for rail crew from the 2800 class locomotive were not effective in all foreseeable circumstances. The ATSB subsequently provided a safety issue to Aurizon (RO-2022-003-SI-04).
In response to this safety issue, on 25 April 2025, Aurizon advised the ATSB that it had developed an access and egress compliance strategy to outline the steps it was taking to align its diverse locomotive fleet to the requirements of the RISSB Australian Standard Access and Egress (AS 7522:2021). Aurizon further advised it was actively participating as a member of the RISSB development group to review AS 7522. Additionally, per Aurizon's compliance strategy, when the standard has been agreed and published, Aurizon reported it would review and update its engineering standards as relevant, assess rolling stock compliance, and implement agreed solutions.
Safety analysis
Introduction
On 17 August 2022, 2 freight trains were planned to cross at Oonoomurra station. The driver of the first train to arrive stopped their train at the station and reported to the network control officer (NCO) it had arrived and was clear of the block section to its rear. However, several wagons from the train still occupied the block section.
The NCO then contacted the driver of the second train and extended their authority. The authority allowed the driver to continue through Oonoomurra station. As the driver rounded a sweeping left curve at the western end, they saw wagons from the other train were obstructing the block section ahead. The driver made an emergency brake application but was unable to avoid a collision with the side of the wagons. The lead locomotive derailed, uncoupled from the trailing locomotive and overturned. The driver sustained a minor injury.
This analysis will discuss factors associated with selection of the stopping point by the driver of the first train to arrive, local environmental conditions at the western end of Oonoomurra station and the application of the direct traffic control procedures. It will then discuss other factors identified during the investigation that increased safety risk to the crew following the derailment and rollover of a locomotive.
Stopping point
The cross between trains 9227 and 9M48 was initially planned to occur at Cloncurry station but was changed due to the late running of train 9M48. This change meant the driver of 9227 was now required to stop at Oonoomurra station.
The driver stated that, when undertaking a cross, they would typically aim to stop the locomotive around 50 m from the limit of authority. However, sun glare had reduced their visibility of the track ahead, and the limit of authority block limit board (BLB) OA 25. Although both crew of train 9227 commented on the presence of sun glare on arrival, this was inconsistent with the observations of the ambient light conditions by the driver of train 9M48 and the Geoscience Australia calculations of the sunrise time at that location.
Regardless of the extent of the ambient environmental conditions present at that time, the driver was concerned they could misjudge the available braking distance to the limit of authority, potentially leading to a signal passed at danger. The driver chose an alternative trackside landmark (Oonoomurra location sign) for their stopping point reference. The sign was a familiar landmark to the driver (prior to BLB OA 25) and was situated adjacent to the track on the driver’s side of the locomotive, and likely relatively visible to the driver.
After stopping and providing the release to the network control officer (NCO), the crew of 9227 then discussed the train length and the assistant driver’s concern that the stopping point meant the train may not be clear of the single line block section to the rear. The driver could not see the rear of the train in the locomotive mirrors due to the track alignment and surrounding vegetation but could see road traffic travelling over the level crossing. Although the level crossing was located approximately 200 m from the western end of the Oonoomurra station, the driver believed sighting the road traffic supported their conclusion that the train was in-clear.
This, combined with the belief the train was shorter than usual, likely influenced the driver’s decision to not move the train closer to their typical stopping point within a station, around 50 m from the limit of authority. Although the assistant driver was uneasy about the stopping point, they did not insist the driver move the train closer to the limit of authority.
On this occasion, the driver based their decision on whether the train was in-clear on several assumptions. These were not verified by other means, particularly as the distance travelled after entering the western end of Oonoomurra was not measured or estimated. The locomotive remained stopped at a point about 317 m from the limit of authority with the rear of train 9227 occupying the block section between Cloncurry and Oonoomurra.
Contributing factor To mitigate the potential of exceeding their limit of authority, the driver stopped train 9227 at a location about 317 m from block limit board OA 25. However, they then erroneously determined their complete train had passed block limit board OA 16. This resulted in the block section between Cloncurry and Oonoomurra remaining occupied by the rear of the train when they passed ownership of the block section to the network control officer, which was not in accordance with the procedure for when crossing rail traffic. |
Driver expectation
When the driver of train 9M48 was advised that the location of the cross with train 9227 had changed from Cloncurry to Oonoomurra stations, they received an authority to stop at OA 18 at the western end of Oonoomurra station. However, prior to their arrival, they received an extension to their authority to continue through the station. This meant that the driver was no longer required to stop at OA 18 and they would be controlling their train speed through the station to satisfy the specified applicable maximum speed of 25 km/h.
The method of safeworking on the Mount Isa line was direct traffic control (DTC). Under the DTC system the ownership of block section resided either with the NCO or the rail traffic crew. The system specified that only one train movement would be authorised to travel on any one block section, at any one time.
The driver of 9M48 had an authority to enter the Oonoomurra to Cloncurry block section and held the belief that they had exclusive possession. Although this understanding was consistent with the absolute block working method of safeworking on the Mount Isa line, it did not mean that the track within the block was physically available and clear from any fault or obstruction. That is, an authority under the DTC system was not a ‘green light’ for the availability of the track.
To address a potential obstruction from rail vehicles, the rules required the driver of train 9M48 to check that all vehicles of the other rail traffic had cleared the block section, before they entered.
The driver was cognisant of the need to check the rear of train 9227 and advise its crew that it was in-clear and complete. The driver recalled that, when approaching train 9227 at 23 km/h, the train seemed to have stopped short of its limit of authority, but rather than contacting the opposing train crew they assumed the train was shorter than normal. While the driver recognised an anomaly with the location of train 9227, they discounted it and likely continued with the expectation that having received their authority all the rail vehicles from train 9227 were in-clear, the train continued at a speed below the specified maximum in the DTC rules.
When the track alignment transitioned from the left curve to straight on approaching the Landsborough Highway level crossing, the driver sighted the rear wagons of train 9227 obstructing the track. On identifying the obstruction, the driver applied emergency braking but there was insufficient distance available for them to stop the train and avoid a collision.
Contributing factor The driver of 9M48 in receipt of an authority expected the track ahead to be clear and continued through the Oonoomurra up track at a speed of 23 km/h. Local geographic and ambient conditions meant the driver did not see the occupied track section ahead at a distance sufficient to enable them to stop their train and avoid a collision. |
Direct traffic control train cross procedures
When undertaking a cross, the Queensland Rail procedures for DTC method of safeworking required the crew of the first train to arrive to approach the station at a controlled speed and then proceed at a maximum of 25 km/h until their train had completely traversed the points. Once stopped just prior to the limit of authority, they were to ensure their train was positioned in-clear and complete at the location. Similarly, for the second rail traffic to arrive, the crew were required to approach at a controlled speed, then proceed at 25 km/h and stop at their limit of authority. When stopped, the crews of both trains had time available to check the opposing train was in‑clear and complete, and communicate with its crew, before contacting the NCO to pass ownership of the applicable block section. This likely addressed the collision hazard from the first train not being in-clear and complete.
However, requiring both trains to stop when crossing at every location would likely be impractical, as it could introduce additional time delays and operating costs to train services. Therefore, to facilitate traffic flow, the procedures enabled the NCO to extend a limit of authority, allowing the driver of the second train to continue through the station at 25 km/h without stopping. Although, the procedure still required them to check the opposing train was in-clear and complete.
It was noted that the DTC workstations did not have functionality to trigger an alarm for the NCO if the rear of the first rail traffic was not clear when the block section was released to them. This meant, an error by one crew in providing a release code when their rail vehicle was not in-clear increased reliance on the second (opposing) crew checking the other rail traffic to detect the occupied block section in sufficient time to avoid a collision. Therefore, correct implementation of the DTC procedures by the first crew to arrive was important, as the NCO had limited information available to independently verify a train or portion of a train was in-clear before transferring ownership of a block section to the second crew to arrive.
While the second rail traffic travelling at 25 km/h reduced the potential for a collision, it did not eliminate the risk. Situations arising from adverse environmental conditions or track alignment could reduce a driver’s opportunity to sight the vehicle(s) of the opposing train in sufficient time to avoid a collision. This was the case for this, and a similar accident that occurred on 27 February 2018 at the western end of Oonoomurra.
Further reducing speed by requiring the second train to then travel at a controlled speed toward the western end of Oonoomurra station would likely be operationally impractical, given the sighting distance available, and the effective response times of a train’s braking system. The controlled speed required would likely be so low the crew would effectively be required to stop, negating any benefit from the extension of their authority.
In summary, the Queensland Rail DTC system provided limited functionality for the NCO to verify the physical availability of a released block section prior to issuing an authority to the second rail traffic crew to arrive. With an extension of authority, this limitation placed increased reliance on the ability of the crew on the second train to detect the obstructed track at a distance sufficient to avoid a collision. This may not always be achievable, particularly at locations such as the western end of Oonoomurra station.
Contributing factor There was limited functionality for a Queensland Rail network control officer to physically verify the availability of a released section block prior to issuing an authority in the direct traffic control system. With an extension of authority, increased reliance was placed on the second train crew detecting the section was obstructed at a distance sufficient to avoid a collision, which may not be achievable in all situations. (Safety issue) |
On board information
The Queensland Rail DTC procedures for arriving at a station required the crew to stop their train within the clearance point boards, in this instance between BLB OA 16 and BLB OA 25. Locomotive PRL201 from train 9227 was fitted with an electronic distance counter measurement device, which, when used in combination with the known train and station lengths, could have assisted the crew with verifying the train was within these limits. However, there was no specific requirement in either the DTC or Qube procedures that required the driver to use the counter to confirm the rear of the train was in-clear. Also, the driver reported they were unfamiliar with the operation of that type of counter and did not use it during their arrival at Oonoomurra station.
Alternative methods for confirming the train was in-clear included selecting a stopping point close to the limit of authority, using a familiar landmark that worked previously for a train of similar length, and/or estimating the distance travelled after entering the station or remaining to the limit of authority, accounting for the train and station track lengths. In this instance, the driver stopped the train about 317 m prior to the limit of authority and had not previously used the location sign as a landmark to stop a similar length train. Instead, they selected the stopping point based on a landmark rather than estimating the distance travelled or remaining, relied on their assumption the train was shorter than normal, and a visual check of the level crossing to confirm the train was in-clear of BLB OA 16.
Regardless of the method used to determine the stopping location, it was the responsibility of the crew to confirm that the locomotive had travelled sufficient distance to ensure the block to the rear of the train was no longer occupied before contacting the NCO to pass ownership of a block section.
If conditions were such that the crew were unsure whether the rear of their train was in‑clear they could opt to retain ownership of the block section and communicate their concern to the NCO and crew of the second train to arrive. However, the discussion between the crew of train 9227 on whether the train was in‑clear occurred after reporting to the NCO that the rail traffic was in-clear and complete, leading to the release of the Cloncurry to Oonoomurra block section. Given ownership of the block section had been transferred it was unlikely that the crew would then revisit their decision as to whether the train was in-clear without opposing information that could have been provided by the distance counter.
Other factor that increased risk The driver of 9227 did not use, nor were they familiar with the operation of, the on‑board electronic measurement device fitted to the PRL201 locomotive. This would have provided another mechanism to confirm that, at the chosen stopping point, the rear of the train was in-clear at Oonoomurra. |
Worker competency
The Qube rail safety worker competency assessments for train crew was a performance‑based assessment. The train operations performance assessment included items related to the DTC safeworking system and tasks associated with operating a Qube train service. This encompassed the correct application of rules and procedures for undertaking a train cross.
The assessment of the driver of train 9227 was undertaken exclusively by a mentor driver/assessor observing the driver’s on-the-job application of the required procedures and related tasks while operating a train service over a series of trips between Cloncurry and Hughenden and return. The final assessment recorded the locomotive used was a PRA/PRL class. The assessment did not record which specific locomotive class was leading nor the type of distance counter device fitted.
Qube advised the training provided on the PRL class locomotive included the crew being shown the counter device as part of their instruction. However, there was no specific training on both types of devices (analogue and electronic). Similarly, while the locomotive operations manual referred to the analogue counter, there was no information provided on the use of the electronic counter. Rather, information on the operation of the electronic device was reported to be captured holistically within the overall locomotive competency training.
The driver of train 9227 was aware of the distance counter devices and had used the analogue type previously. However, they stated they were not shown how to operate the more complicated electronic device fitted to locomotive PRL201.
Following the completion of the competency assessment, the driver had operated train services for 6 months, which would have involved completing numerous crosses with other trains. The driver was likely familiar with stopping at those stations and targeted a stopping point closer to the limit of authority.
However, without training and instruction on how to use the more complex electronic device fitted to PRL locomotives, it was unlikely it would be used. This removed an alternative means for drivers to confirm that the rear of the train was in‑clear at a location, thereby increasing the potential for the ownership of a block section to be erroneously released to the NCO.
Other factor that increased risk The competency procedures for Qube train crew did not verify that drivers attained the required skills, knowledge or ability to operate the electronic distance counter device installed on some PRL locomotives. This increased the likelihood that drivers, uncertain in the operation of the device, may not use it to confirm the rear of the train was in-clear. |
Emergency egress
After derailing to the right side of the track in the direction of travel, the locomotive rolled onto the right side (‘A’ side). The driver was ejected from their seat and was standing on the wall/window in darkness.
The train borne radio communication system ceased operating following the collision and rollover and the locomotive was not fitted with an emergency lighting system. The disarrangement of equipment within the darkened cab hindered the driver’s ability to assess their situation or readily locate emergency equipment such as the handheld radio or emergency hammer.
The driver did find their personal mobile telephone and contacted the NCO to notify them of the emergency. The NCO checked on the driver’s welfare while other network control personnel arranged for the emergency response.
A crew member from 9227 had alighted from the train and was making their way back to check the welfare of the driver of 9M48. In this instance, 2 members of the public accessed the rail corridor from the Landsborough Highway level crossing, climbed onto the overturned locomotive and lifted the driver free of the cab before the crew member arrived.
The driver of 9M48 sustained a minor injury during the accident sequence. Due to the rollover, they were unable to reach the emergency exit provided by the assistant driver’s side window that was now overhead. They did not attempt to egress the cab via the rear facing door to the vestibule area, opting instead to try to kick out the windscreen of the locomotive. This was unsuccessful as the windscreen was not designed to be removed therefore was not available as an alternative exit.
Crewing the train as driver-only operation meant the driver had no other crew to assist in alerting network control of the emergency, assessing/treating injury, or aiding in egress from the overturned locomotive cab. The driver experienced conditions in the locomotive cab following the collision and derailment that increased risk to their welfare. On exiting the overturned locomotive cab, and jumping from height, the driver observed diesel leaking from the ruptured tank on the lead locomotive.
In this instance, it was fortunate that bystanders, who were prepared and able to provide timely assistance, were close by and there was no post-accident fire. This may not always be the case.
Other factor that increased risk After the collision, the lead locomotive came to rest on its side. The driver was in darkness and unable to readily locate safety equipment, make an emergency radio call to network control or exit the cab without the assistance from members of the public. |
Collision survivability – locomotive
Emergency equipment – lighting and communications
The Aurizon rolling stock standards cross‑referenced relevant Australian Standards published by the Rail Industry Safety and Standards Board (RISSB). The RISSB standards were developed to broadly address rolling stock related hazards across multiple rail transport operators. Aurizon standards were developed to address hazards specifically applicable to the Aurizon operations and rolling stock fleet (including locomotives). As the standards were developed by Aurizon and RISSB independently, variance between the version dates and specified requirements contained in the respective standards were likely.
Additionally, for older locomotive classes such as the 2800, which were constructed prior to the published date of referenced RISSB standards, variance between the existing locomotive construction or equipment fit out and the requirements of the standard may also arise. Variances were typically addressed through the scope of RISSB standards being applicable only to new or modified locomotives.
Both the Aurizon standard for rolling stock fire performance and interior environment referred to requirements contained in the RISSB lighting and rolling stock visibility standard. To protect people, the Aurizon fire performance standard specified rolling stock was to have adequate capacity to evacuate within a suitable time, adequate normal and emergency lighting (with reference to AS 7531) and back-up power supplies with adequate capacity. The back-up power supplies applied to both lighting and communications systems. As there was no distinction between the communication systems fitted to locomotive or passenger rolling stock, this indicated that the train borne radio communication system should have a back-up power supply in the event of a main battery failure.
The scope of standard AS 7531 applied to existing locomotives and included requirements for spaces (cabins, rooms, vestibules, aisles) to be fitted with emergency lighting. The Aurizon 2800 class locomotive, including 2808, was not fitted with an emergency lighting system or back-up power supplies. Rail traffic crew (including driver‑only operations) responding to an emergency during the hours of darkness were then reliant on locating, in the disarranged cab of an overturned locomotive, a hand-held torch carried as part of rolling stock emergency equipment.
Similarly, in the event of damage to the train borne radio or failure of the main battery, rail traffic crew were also reliant on locating a serviceable 2-way radio or mobile telephone, if issued to the locomotive and mobile service was available, to notify network control of an emergency and for ongoing welfare communications during an emergency response.
Egress pathways
Locomotive 2808 was being operated from the No 1 end when it overturned. Although the driver was ambulatory, they realised they would not be able to readily reach the alternative emergency exit, which was the assistant driver’s side window that was now on the high side of the overturned 2.87 m wide locomotive cab. In the darkness, they instead attempted to kick the windscreen out, which would have allowed them to exit the cab at ground level. However, the laminated windscreen in the 2800 class locomotive could not be broken out using the window breakout hammer and was not designed to be removed from inside the locomotive cab.
On this occasion, 2 bystanders had witnessed the collision from the Landsborough Highway, entered the rail corridor and climbed onto the side of the locomotive to assist the driver. The bystanders were able to slide open the assistant driver’s side window and reach in to lift the driver from the enclosed cab. The rigidity of the side window glass and frame to withstand the forces applied by a rail traffic crew member, or responders, using this pathway was unknown.
Should the driver (and other crew) be required to self-extricate they may be required to use the window breakout hammer to remove the window glass above their head. Their pathway would likely be difficult due to the hammer being fixed by a short tether to the overhead console, the necessity to climb and the layout of the console, and other fixtures and contents within the cab that are likely disarranged. The crew members may also have incurred injuries that potentially affect their mobility.
As the 2800 class locomotive cab did not have any footholds or climbing arrangements to aid crew egress via the alternative pathway, this potentially increased their exposure to known evacuation hazards. This was particularly relevant to driver-only operations where no other train crew, or responders, were immediately available to provide assistance to egress the overturned locomotive cab in an emergency.
Once the crew members had exited to the high side of the overturned locomotive, they then had to descend safely to the surrounding ground level. Similar to the above, there were no external footholds or climbing arrangements to assist in descending from the locomotive to the ground level. Unless emergency services were present with a ladder, the crew would likely need to climb down onto the locomotive bogie, if attached, or jump. In this case, the driver and bystanders jumped to the ground level, exposing them to the additional hazard of falling from height.
Similarly, ATSB investigations RO-2015-028 and RO-2022-003 found the Aurizon emergency egress arrangements for rail crew from the 2800 class locomotive were not effective in all foreseeable circumstances. In response to the RO-2022-003 safety issue, Aurizon advised it had developed an access and egress compliance strategy to outline the steps it was taking to align its diverse locomotive fleet to the requirements of the RISSB Access and Egress (AS 7522:2021) standard. The proactive safety action identified by Aurizon is ongoing.
As previously acknowledged in ATSB investigation RO-2022-003, a collision or derailment can result in structural damage to the cab and/or result in the locomotive rolling onto its side. This can hinder egress pathways normally used to access the cab and expose rail traffic crew to a range of evacuation hazards. This exposure is increased when operating the locomotive in the driver-only configuration, where no immediate support is readily available to assist a potentially injured driver to egress from an overturned locomotive.
Risk management
This and previous ATSB investigations have identified findings related to the adequacy of egress pathways and emergency equipment, such as lighting and back-up power supplies, on the 2800 class locomotive. While Aurizon had an established risk management framework, neither a risk assessment or other supporting documentation was available to sufficiently demonstrate to the ATSB that the emergency exit and equipment arrangements for this locomotive class were assessed. Consequently, exposures to foreseeable evacuation hazards may remain.
Other factor that increased risk The emergency exit pathway through a side window, and the emergency equipment available in the enclosed cab of an Aurizon 2800 class locomotive were inadequate to ensure a prompt escape by crew and potentially limited access by emergency services in the event of a locomotive overturning. Aurizon provided limited assurance the risk controls implemented to mitigate these known evacuation hazards were sufficient to reduce the potential of further injury to the crew. (Safety issue) |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision between Aurizon train 9M48 and Qube train 9227, Oonoomurra, Queensland, on 17 August 2022.
Contributing factors
- To mitigate the potential of exceeding their limit of authority, the driver stopped train 9227 at a location about 317 m from block limit board OA 25. However, they then erroneously determined their complete train had passed block limit board OA 16. This resulted in the block section between Cloncurry and Oonoomurra remaining occupied by the rear of the train when they passed ownership of the block section to the network control officer, which was not in accordance with the procedure for when crossing rail traffic.
- The driver of 9M48 in receipt of an authority expected the track ahead to be clear and continued through the Oonoomurra up track at a speed of 23 km/h. Local geographic and ambient conditions meant the driver did not see the occupied track section ahead at a distance sufficient to enable them to stop their train and avoid a collision.
- There was limited functionality for a Queensland Rail network control officer to physically verify the availability of a released section block prior to issuing an authority in the direct traffic control system. With an extension of authority, increased reliance was placed on the second train crew detecting the section was obstructed at a distance sufficient to avoid a collision, which may not be achievable in all situations. (Safety issue)
Other factors that increased risk
- The driver of 9227 did not use, nor were they familiar with the operation of, the on‑board electronic measurement device fitted to the PRL201 locomotive. This would have provided another mechanism to confirm that, at the chosen stopping point, the rear of the train was in-clear at Oonoomurra.
- The competency procedures for Qube train crew did not verify that drivers attained the required skills, knowledge or ability to operate the electronic distance counter device installed on some PRL locomotives. This increased the likelihood that drivers, uncertain in the operation of the device, may not use it to confirm the rear of the train was in‑clear.
- After the collision, the lead locomotive came to rest on its side. The driver was in darkness and unable to readily locate safety equipment, make an emergency radio call to network control or exit the cab without the assistance from members of the public.
- The emergency exit pathway through a side window, and the emergency equipment available in the enclosed cab of an Aurizon 2800 class locomotive were inadequate to ensure a prompt escape by crew and potentially limited access by emergency services in the event of a locomotive overturning. Aurizon provided limited assurance the risk controls implemented to mitigate these known evacuation hazards were sufficient to reduce the potential of further injury to the crew. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Rail industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Train cross procedures
Safety issue number: RO-2022-010-SI-01
Safety issue description: There was limited functionality for a Queensland Rail network control officer to physically verify the availability of a released section block prior to issuing an authority in the direct traffic control system. With an extension of authority, increased reliance was placed on the second train crew detecting the section was obstructed at a distance sufficient to avoid a collision, which may not be achievable in all situations.
Collision survivability – locomotive
Safety issue number: RO-2022-010-SI-02
Safety issue description: The emergency exit pathway through a side window, and the emergency equipment available in the enclosed cab of an Aurizon 2800 class locomotive were inadequate to ensure a prompt escape by crew and potentially limited access by emergency services in the event of a locomotive overturning. Aurizon provided limited assurance the risk controls implemented to mitigate these known evacuation hazards were sufficient to reduce the potential of further injury to the crew.
Glossary
| ATP | Automatic train protection |
| BLB | Block limit board |
| DTC | Direct traffic control |
| GPS | Global positioning system |
| NCO | Network control officer |
| RISSB | Rail Industry Safety and Standards Board |
| RTO | Rail transport operator |
| SFAIRP | So far as is reasonably practicable |
| SMS | Safety management system |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the train crew of train 9227
- the train crew of train 9M48
- Qube Logistics
- Aurizon
- Queensland Rail
- recorded data from train 9227 and train 9M48
- Geoscience Australia
- Rail Industry Safety and Standards Board.
References
National Transport Commission. (2017). National standard for health assessment of rail safety workers. https://www.ntc.gov.au/codes-and-guidelines/national-standard-health-assessment-rail-safety-workers
Office of the National Rail Safety Regulator. (2019). ONRSR Guideline Safety Management System.
Rail Industry Safety and Standards Board. (2012). Australian Standard AS 7522:2012 – Railway Rolling Stock Access and Egress – Part 1 Locomotive Rolling Stock.
Rail Industry Safety and Standards Board. (2023). Australian Standard AS 7531:2023 – Lighting and Visibility.
Rail Industry Safety and Standards Board. (2024). Code of Practice - Risk Management for Driver Only Operation.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the train crew of train 9227
- the train crew of train 9M48
- Qube Logistics
- Aurizon
- Queensland Rail
- Office of the Rail Safety Regulator.
Submissions were received from:
- Qube Logistics
- Aurizon
- Queensland Rail
- Office of the Rail Safety Regulator.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
- ^ To go past another rail traffic travelling in the opposite direction.
- ^ The ATP system supervises train speed and target speed, alerts driver of the braking equipment, and enforces braking when necessary. The system may be intermittent, semi-continuous or continuous according to its track-to-train transmission updating characteristics.
- ^ An absolute block safeworking system used to control the movement of trains in non-signalled territory. This prevents more than one train being authorised into a defined section or block at any one time. Central to DTC is a computer within the locomotive cab that displays authorities to train crew stored in its database. The relevant authority is activated by the train crew following an exchange of codes between the crew and NCO. Codes are exchanged verbally using the train control radio.
- ^ An instruction displayed on a computer screen, or on a prescribed form issued for rail traffic movement.
- ^ Rail traffic crew are required to report the time through each station location to the NCO.
- ^ Trains travelling east to Stuart Yard were in the down direction, while trains travelling west to Mount Isa were travelling in the up direction.
- ^ Trailable points were designed to permit a trailing movement through points closed against the intended move. The points are mechanically locked in position for a facing move but can be thrown to the reverse position by the wheel flanges of a train travelling in the trailing direction, which spring back to the normal position after the wheelset is through. The points are not controlled by the NCO.
- ^ Unauthorized passing of a signal displaying a stop indication as follows: 1. completely missed 2. driver misjudged 3. restored as train approached 4. other.
- ^ Braking that uses the momentum of the locomotive and train to cause a braking effect. The traction motors are in effect turned into generators and the power is dissipated as heat through fan blown grids on the locomotive.
- ^ When a train comprised of more than one vehicle coupled together is in compression.
- ^ The line between the departure end yard limit of one location and the arrival end yard limit of another location. A section consists of one or more blocks.
- ^ Term in-clear means all vehicles were located between the block limit boards at either end of the station. Term complete means the last vehicle is coupled to the rail traffic, indicated by an attached end of train marker.
- ^ A safety‑critical zone is the area forward of a restrictive signalling aspect, is 2,500 m from a known stopping location, and starts from a location where the next signal aspect cannot be confirmed.
- ^ The distance along the track between points of minimum allowable clearance where rolling stock is permitted to stand.
- ^ Drivers typically dim/extinguish headlights when approaching to avoid glare for the opposing train crew.
- ^ Wagons GOAF 0016, 0052, 0050, 0060, 0059, 0102, 0012 and 0017 totalling about 85 m of train 9227 were not in-clear of block limit board OA 16.
- ^ The driver used their personal mobile telephone.
- ^ Bystanders (members of the public) had accessed the rail corridor from the Landsborough Highway level crossing.
- ^ Emergency services included the Queensland ambulance, police, and fire and emergency services.
- ^ Operation of a rail traffic by a driver without another driver or other person in the driver’s cabin or rail traffic who is qualified in, and has suitable experience in, the operation of the rolling stock and the safeworking system that form part of the network rules (Rail Industry Safety and Standards Board, 2024).
- ^ The drivers could arrange for Aurizon operations to provide a wake-up call prior to the commencement of their rostered shift. The driver in this instance requested a wake-up call 1.5 hours prior to the commencement of their shift.
- ^ The Samn-Perelli 7-level fatigue scale was a subjective method for evaluating fatigue state. Where level 1 was assessed as fully alert and level 7 completely exhausted.
- ^ Seated at the assistant driver’s position in the locomotive cab.
- ^ The effective train crossing loop length was also recorded as 809.33 m, which included an allowance for train slack and handling safety (comparison length).
- ^ The locomotive manufacturer’s Operators manual 2800 class did not provide any guidance on emergency egress pathways. The manual was to be used only for the servicing and maintenance of the locomotive.
- ^ The train inspector’s seat was a small fold‑down seat located on the rear wall of the locomotive cab.
- ^ GQGY and GOAF wagons were respectively 13.63 m and 10.33 m in length.
- ^ Qube records the effective train crossing loop length, which included an allowance for train slack and handling safety (comparison length).
- ^ Progress Rail GT22C-3 Operators manual PRL class locomotives, M2022-07-004 revision 1.0, July 2022.
- ^ Australian Government Geoscience Australia, geodetic calculator application.
- ^ An ideal horizon exists when the surface forming the horizon is at a right angle to the vertical line passing through the observer's position on the Earth.
- ^ Queensland narrow track gauge measures 1,067 mm.
- ^ A station at which the points are normally set to allow simultaneous entry and exit of trains through the up and down lines.
- ^ Queensland Rail Standard MD-10-113 Direct traffic control Manual, version 3.1, dated 28 October 2019.
- ^ Clearance point boards were typically not provided at directional travel stations on the Mount Isa Line.
- ^ Queensland Rail Standard MD-10-107 General operational safety manual, version 5.2, dated 13 September 2021.
- ^ Qube PCE-217 Rail safety worker assessment and certification, version 8.0 dated 7 December 2021.
- ^ Qube FM-780 Train operations performance checklist, version 3.0, dated 10 October 2017.
- ^ Performance checklist tasks were generic, conditions/variables (weather, route complexity, traffic density, safeworking system and vehicle class) present at the time of assessment were recorded individually.
- ^ Aurizon Emergency and abnormal situation response for rail traffic crew, version 1.1 dated 29 April 2022.
Occurrence summary
| Investigation number | RO-2022-010 |
|---|---|
| Occurrence date | 17/08/2022 |
| Occurrence time and timezone | 06:37 Australian Eastern Standard Time |
| Location | Oonoomurra |
| State | Queensland |
| Report release date | 19/06/2026 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Rail |
| Rail occurrence category | Collision, Derailment |
| Occurrence class | Accident |
| Highest injury level | Minor |
Train details
| Train operator | Qube |
|---|---|
| Train number | 9277 |
| Track operator | Queensland Rail |
| Type of operation | Freight |
| Rail vehicle sector | Freight |
| Departure point | Mount Isa, Queensland |
| Destination | Stuart Yard (near Townsville), Queensland |
| Persons on board | Crew – 2, Passengers – 0 |
| Injuries | Crew – 2, Passengers – 0 |
| Train damage | Substantial |
Train details
| Train operator | Aurizon |
|---|---|
| Train number | 9M48 |
| Track operator | Queensland Rail |
| Type of operation | Freight |
| Rail vehicle sector | Freight |
| Departure point | Stuart Yard (near Townsville), Queensland |
| Destination | Mount Isa, Queensland |
| Persons on board | Crew – 1, Passengers – 0 |
| Injuries | Crew – 1 (minor), Passengers – 0 |
| Train damage | Substantial |