On 6 January 2021, loaded Pacific National freight train 3YN2 was operating between Broken Hill and Newcastle, New South Wales. Just before 0914, a contractor working near the rail line, noticed a wagon on train 3YN2 was dragging on the rail. This was reported to representatives from the rail infrastructure manager and the crew of 3YN2 were directed to stop their train. The train stopped between Euabalong West and Kiacatoo with a crack found through the underframe of the 32nd wagon. The air tank was resting on the rail and it was later found that three level crossings had been struck by the wagon. There was superficial damage at the level crossings and no reported injuries.
What the ATSB found
Train 3YN2 departed Broken Hill with an existing crack in the underframe of wagon NDHX14836G. This crack progressed during the journey with the underframe of the wagon striking three level crossings. The underframe of NDHX14836G likely fractured due to a fatigue crack at a weld on the lower edge of the sill. This defect was likely detectable for a period of time prior to the occurrence. The train had undergone the required maintenance inspections however these were not sufficient to identify the cracking at a location of known risk prior to the structural failure.
What has been done as a result
Following the occurrence Pacific National released a rolling stock safety notice detailing the failure and requiring an inspection of all affected wagons within the class wagon.
Pacific National advised the following actions have been planned to prevent recurrence:
Develop a lifecycle asset management strategy for affected class of wagons (NDHX/ICX) with a butt weld.
Complete a risk assessment to assess the limitations of NDHX wagons and requirements for ongoing use.
Review the wagon maintenance manual associated with the inspection of the wagon underframe to include details for ICX class wagons.
Review and adjust the current non-destructive strategy applied across Pacific National’s fleet of wagons.
Safety message
The incident highlights the importance of managing ageing assets to ensure continued safe operation through the lifecycle of the asset. Rolling stock operators should ensure that their maintenance and inspection regimes effectively monitor and detect conditions that might escalate and contribute to accidents.
The investigation
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 5 January 2021, two Pacific National (PN) train drivers (crew 1 and crew 2) were assigned to shunt and attach 17 wagons from within the CBH Resources - Rasp Mine at Broken Hill to the rear of freight train 3YN2.
During the shunting movement, a roll-by inspection[1] was performed by crew 1. Between 1905[2] and 2020, crew 1 completed a general examination (GX) of the 17 wagons. The inspection was completed without incident and a brake certificate was issued.
On 6 January 2021, train 3YN2 departed Broken Hill bound for Newcastle, New South Wales. The train consisted of three locomotives and 44 wagons with a total length of 977 m. The train departed Broken Hill at 0149 and a roll-by inspection was performed from both sides by crew 1 and crew 2 without incident.
Just before 0914, a contractor working near the rail line noticed a broken wagon on 3YN2 was dragging on the rail. This was reported to a track worker located at Parkes, who passed the message on to the network controller at Junee. At 0915, the network controller contacted the crew of train 3YN2 and directed them to stop and inspect their train.
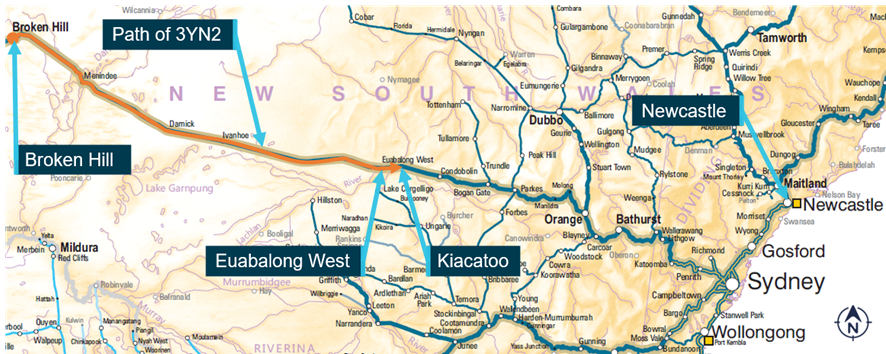
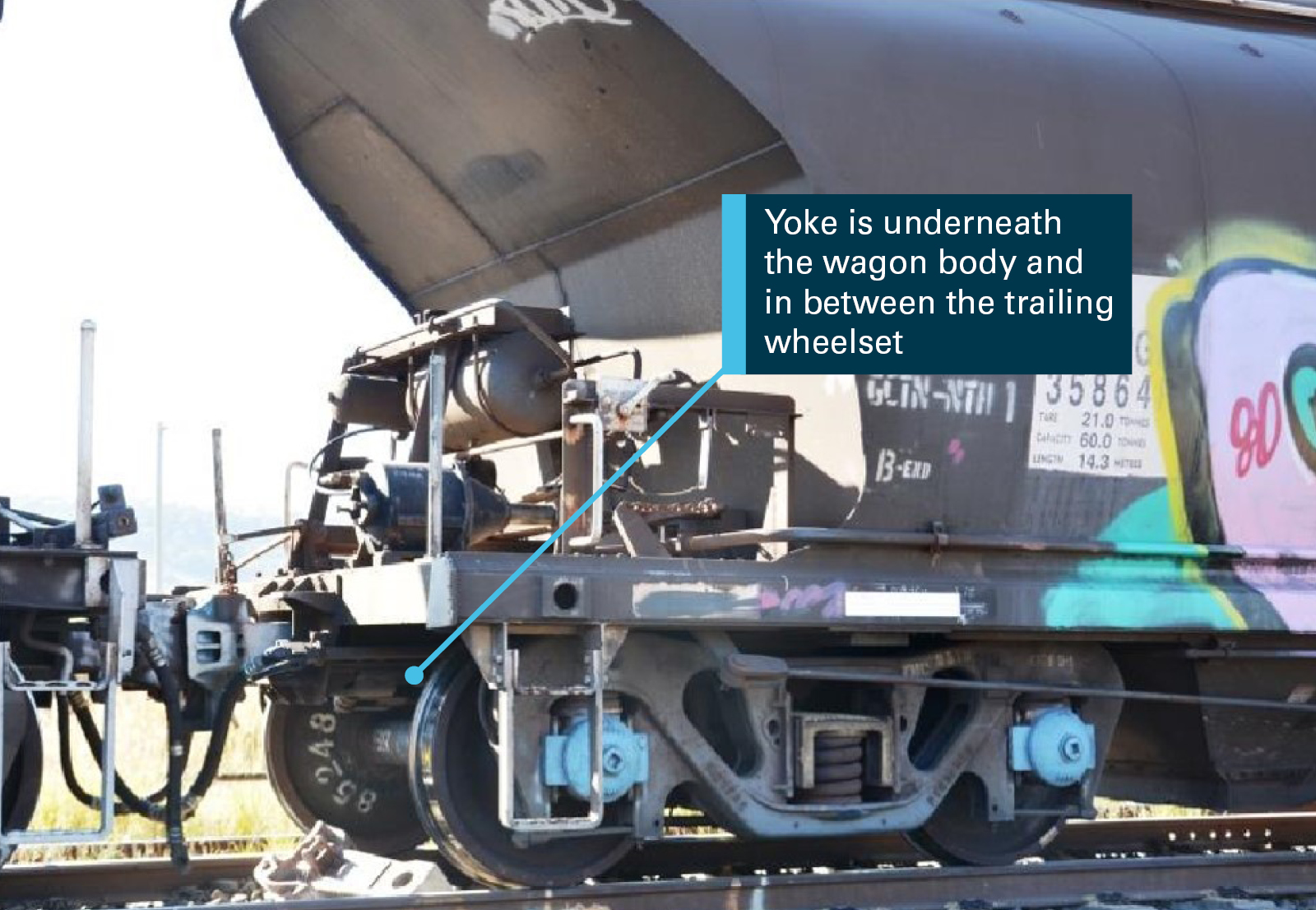
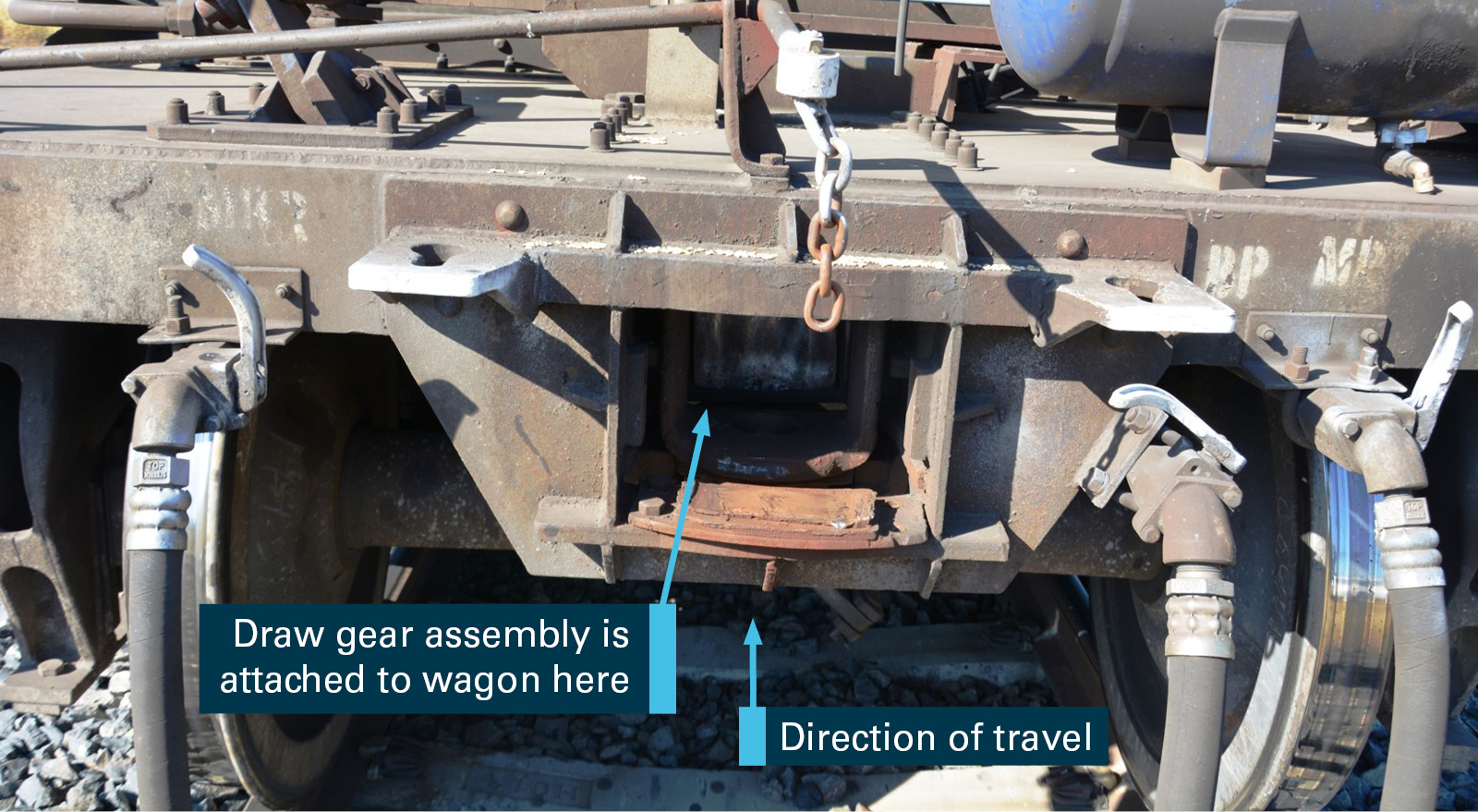
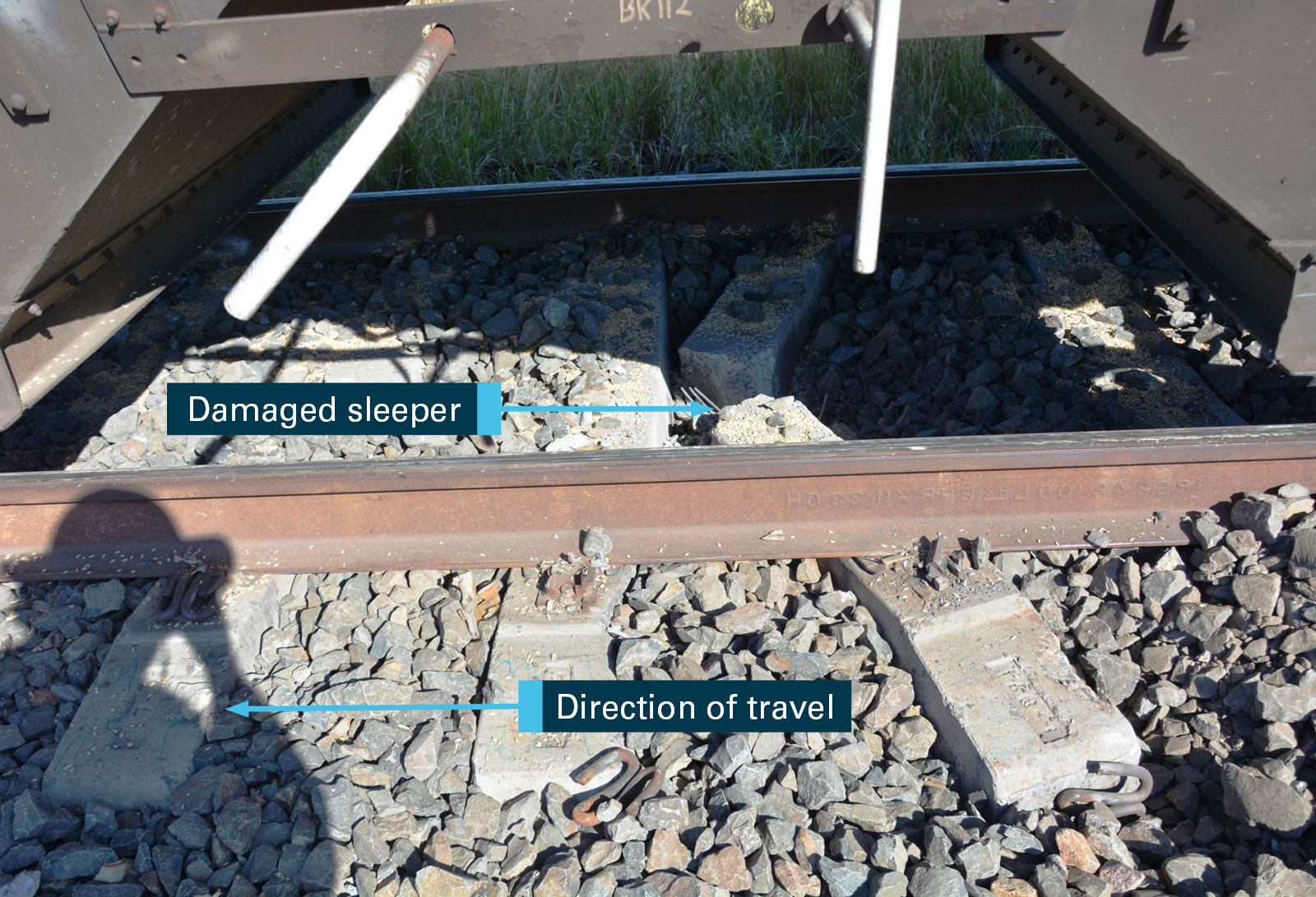
The crew stopped to inspect the train between Euabalong West and Kiacatoo. The crew identified that the wagon frame on the 32nd wagon (NDHX14836G) had failed and the air tank was resting on the rail near 583.900 km[3] (Figure 1 and Figure 2). The wagon was loaded with two containers carrying zinc (Zn) concentrate at the time which remained secured to the wagon.
Inspection post incident identified superficial scrape marks on the rail and at three level crossings between 595.518 km and 583.900 km. There was no reported damage to the sleepers or rail fasteners from the failed wagon. There were no reported injuries.
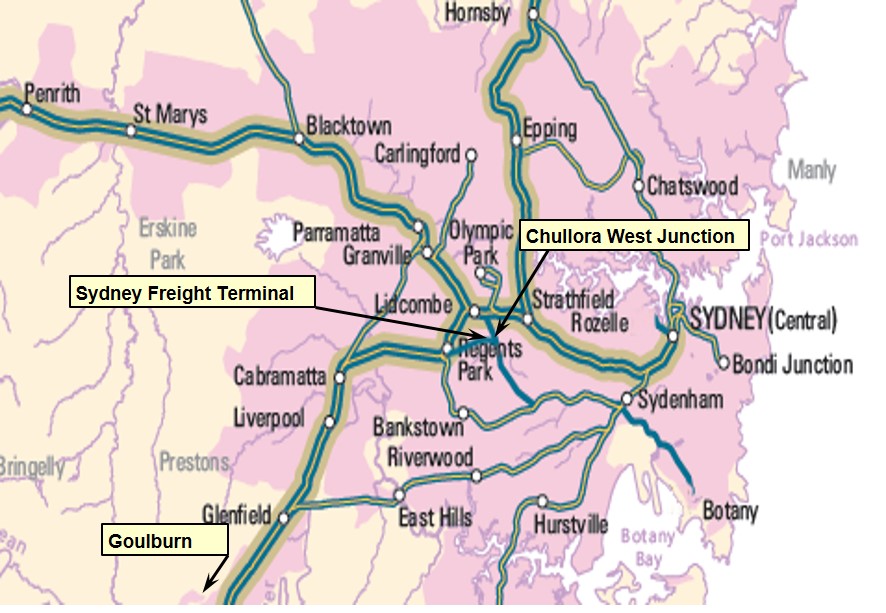
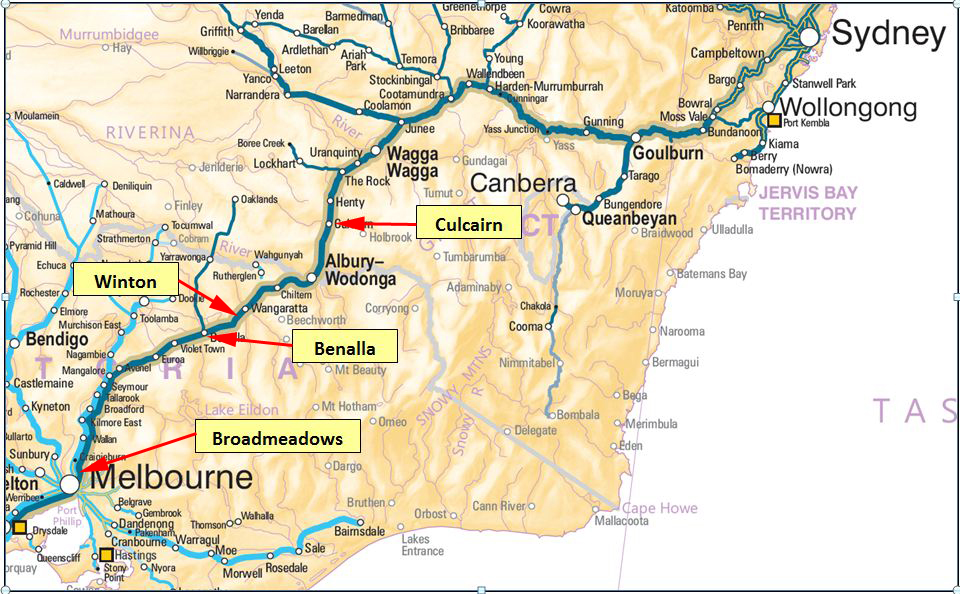
Figure 1: Path of 3YN2
Source: Geoscience Australia, modified and annotated by OTSI
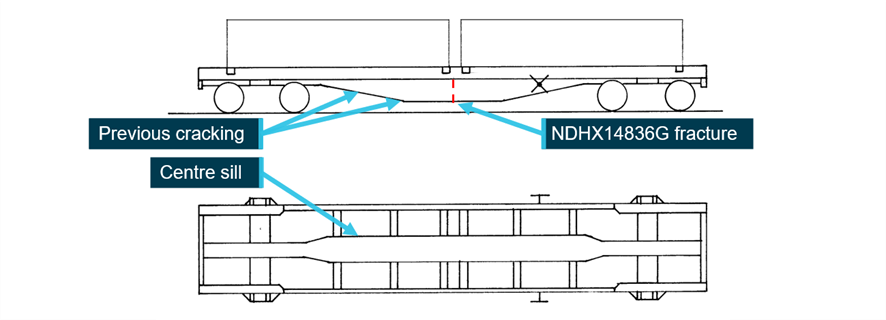
Figure 2: Rolling stock irregularity
Wagon NDHX14836G shown with centre of the wagon sagging under the load of the 20 ft containers. Inset image shows the fracture in the underframe and an air tank resting on the rail.
Source: Pacific National, modified and annotated by OTSI
Context
Wagon
Wagon NDHX14836G was designated as a sleeper carrying wagon with a tare mass of 20 t and a maximum capacity of 60 t. Previously the wagon was designated NQHX (container flat wagon)[4] before it was converted to a sleeper carrying wagon in 2009. In 2010 this modification was reverted and the wagon returned to original use, however, this was not communicated effectively to the various rail infrastructure managers.
The wagon was manufactured as an ICX class wagon with the centre sill forming the load bearing structure (Figure 3). This class of wagon was manufactured from approximately 1968 onwards and PN had a total of 136 ICX class wagons in operation at the time of the incident (Table 1).
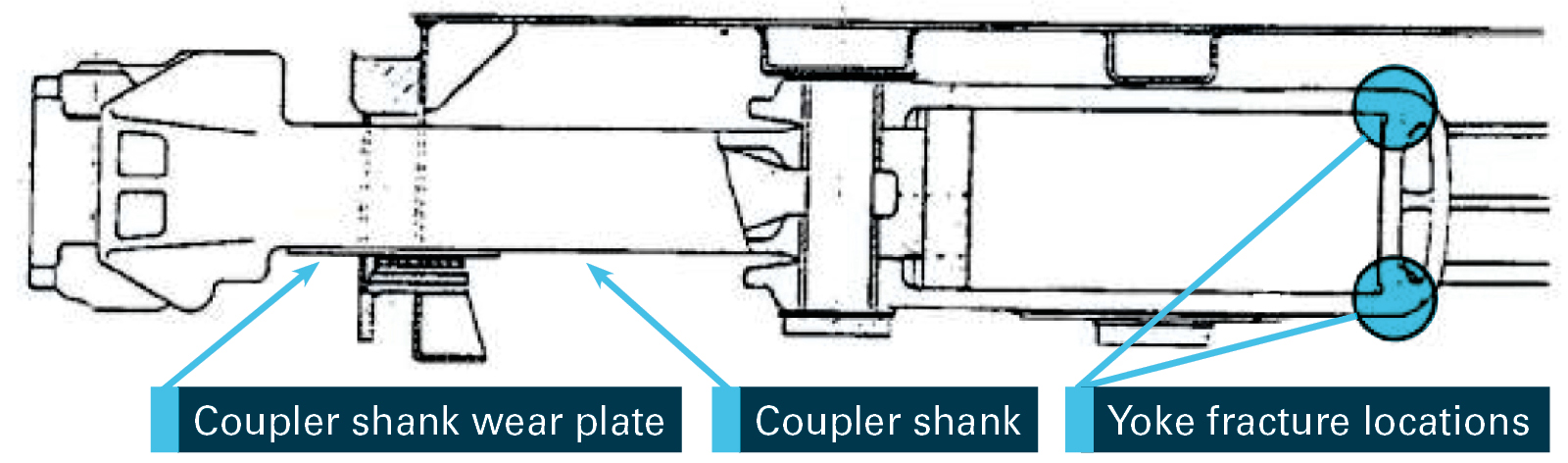
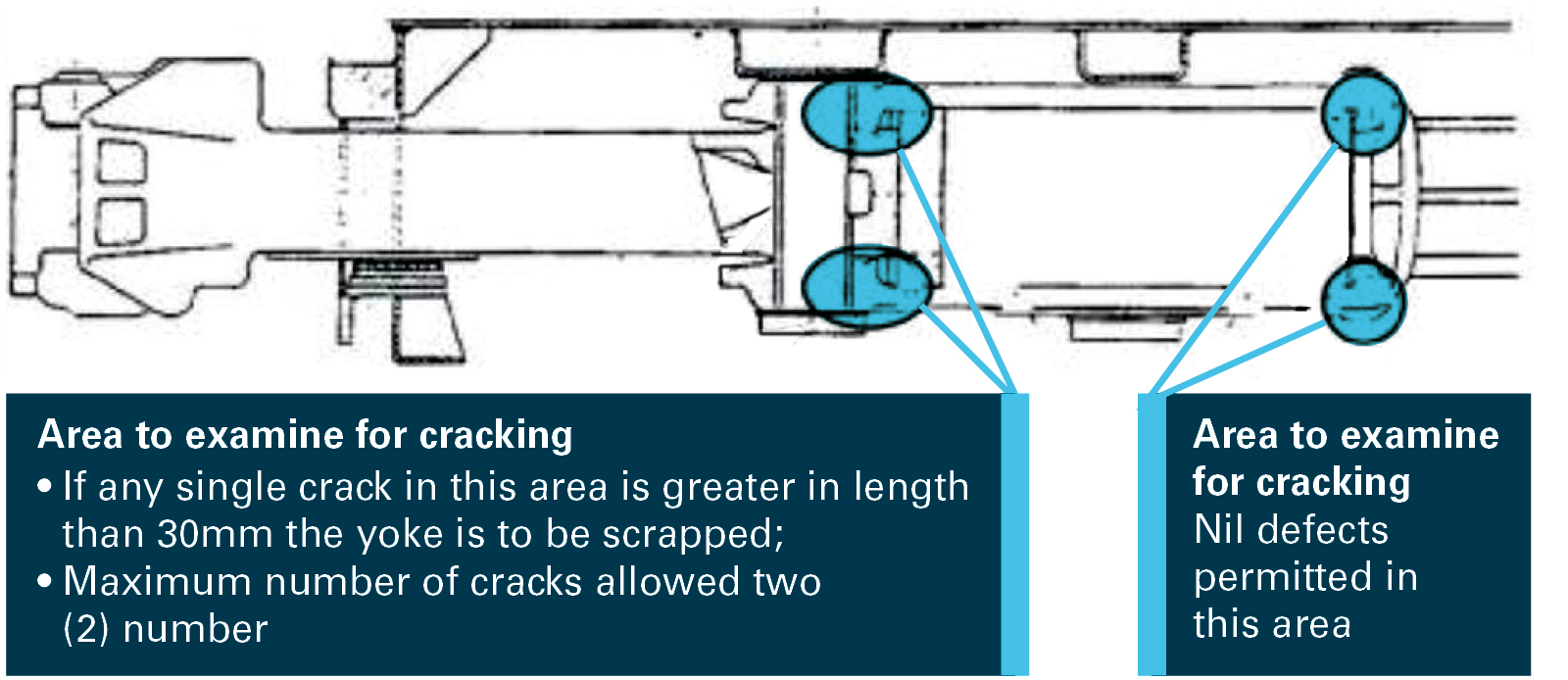
Figure 3: ICX class wagon underframe and cracking locations
A side and top down view of the wagon and underframe structure. The centre sill runs the length of the wagon and supports the load.
Source: Pacific National, modified and annotated by OTSI
Table 1: ICX class
Wagon code
Wagon Type
Quantity
Comment
NDHX
Sleeper carrying wagon
36
Previously NQHX container wagon
NQHX
Container
76
Previously NQIX container wagon
NQIX
Container
24
Historically, cracking had been detected on some ICX class wagons at butt welds along the centre sill lower flange at a change in material thickness (Figure 3). Repair procedures had been developed with doubler plates[5] fitted if cracking was detected.[6] The location of the previous cracking was along the centre sill but not at the location of the fracture on NDHX14836G.
Maintenance
Wagon NDHX14386G was under a unit train maintenance (UTM) regime requiring the wagon to be inspected every 56 days (maximum 7-day tolerance) in accordance with the Wagon Maintenance Manual (WMM 01-01 and WMM 01-18).
Additionally, the wagon required inspection at intervals of 150,000, 450,000 and 900,000 km. Both the 56 day on train inspection and kilometre-based inspection referred to the same work instruction for the inspection of the underframe (Underframes, Body Work and Load Supports WMM 04-02).
The most recent maintenance records are shown in Table 2. The wagon had operated for 51 days since the last 56 day on train inspection and was not overdue at the time of the occurrence.
Table 2: Maintenance history
Date
Inspection type
Comments
07/07/2020
56 day on train maintenance
Completed 70 days between previous inspection
24/09/2020
56 day on train maintenance
Completed 79 days between previous inspection
16/11/2020
56 day on train maintenance
Completed 53 days between previous inspection
Train examination
Prior to departure the 17 wagons underwent a GX as required by the Train Inspection Manual (TIM 01-03). The examination was limited to the major components of the wagon but included checking the wagon body for structural damage. The GX was performed by crew 1 who held the required qualifications and had three years’ experience. There were no defects noted with wagon NDHX14836G.
Crew 2 who assisted with the roll-by inspection, held the appropriate qualifications and had approximately eight years’ experience.
Loading
The containers were loaded on to the 17 wagons at CBH Resources - Rasp Mine. The train consist and records for container mass indicated all wagons were within the permitted loading limits (60 t).
Loading records indicated wagon NDHX14836G was loaded with two 20 ft concentrate containers with a total mass of 59.54 t. Post occurrence the mass of the containers were weighed at 59.9 t,[7] closely matching the loading records.
On 21 April 2018, Pacific National intermodal freight train 6MP4 derailed near Glenalta, South Australia. It was found that there was a pre-existing structural crack on platform 2 of wagon RRYY01X that had not been identified during multiple train examinations and maintenance inspections. A combination of the pre-existing structural crack, in-train forces (compression and tension) and tight curves on a descending grade likely resulted in the derailment. A contributing factor and safety issue of this occurrence was:
Pacific National’s inspection processes did not identify key structural points for inspection on RRYY class wagons, including the susceptibility to cracking in the junction between container loading outriggers, pull rod boxed opening, and the bottom centre sill sections. This reduced the likelihood of cracks being detected. (Safety issue)
This wagon was of a different design and class to NDHX14836G, although, both were operated and maintained by Pacific National. The same work instruction was also utilised for the inspection of the underframes of RRYY and NDHX (ICX) class wagons (WMM 04-02). This inspection procedure was revised as part of the safety action to address the safety issue.
On 5 December 2012, crew performing a roll-by inspection of a SQYD wagon near Gulgong, New South Wales, detected a wagon sagging in the middle and almost dragging on the ground. The wagon struck and damaged the road surface on several level crossings before it was detected.
It was found that the underframe of wagon SQYD0060G failed at a transverse butt weld at the mid-point of the centre sill. The failure was the result of poor weld design, welding practices/techniques and inadequate non-destructive testing at the time of the weld.
The SQYD wagon was similar in design to the ICX class wagon but the two wagon classes were at different ends of the asset lifecycle. The SQYD wagons entered service in the 12 months prior to the occurrence while ICX class wagons were approaching end of life.
Safety analysis
Train 3YN2 travelled approximately 530 km before wagon NDHX14836G struck a level crossing at 595.518 km. The wagon struck two more level crossings before the train was stopped at 583.900 km. The actions of the contractor reporting the defect prevented the escalation of this occurrence.
The wagon was found with a fracture extending across the bottom flange (underside) and up both vertical plates (web) at the mid-point of the centre sill. The lower portion of the fracture face was damaged by ballast strikes, particularly on the trailing edge (in the direction of travel) of the fracture.
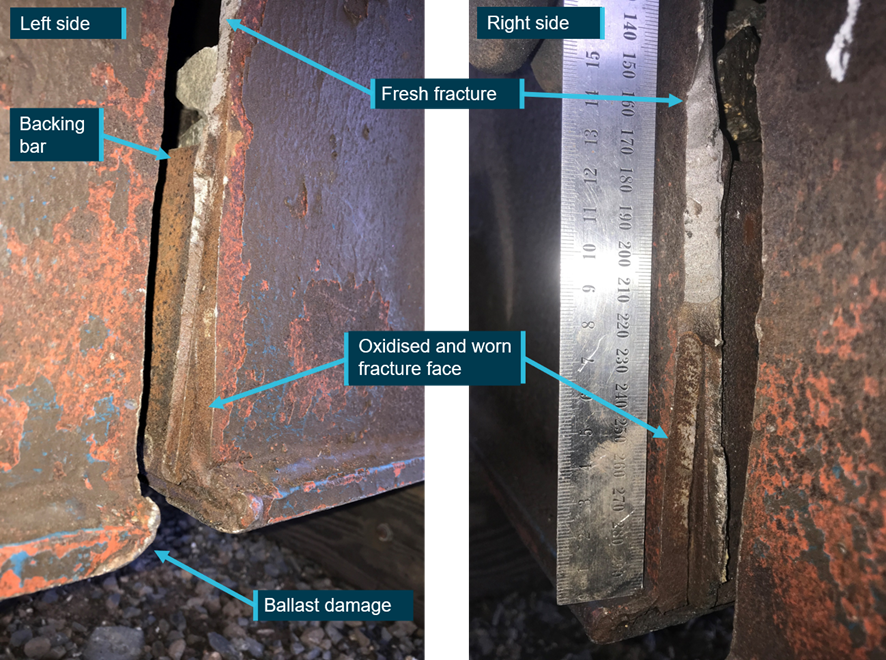
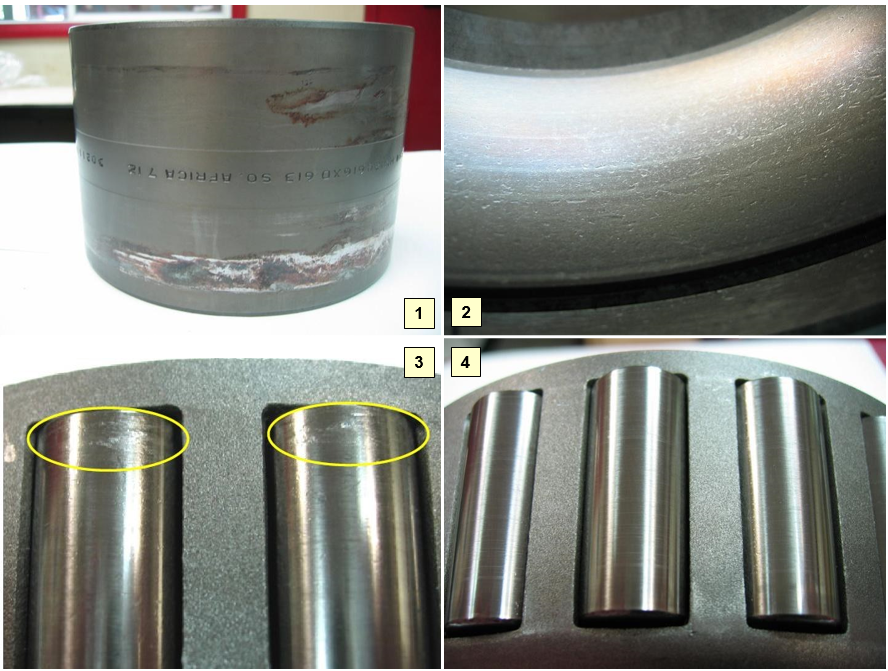
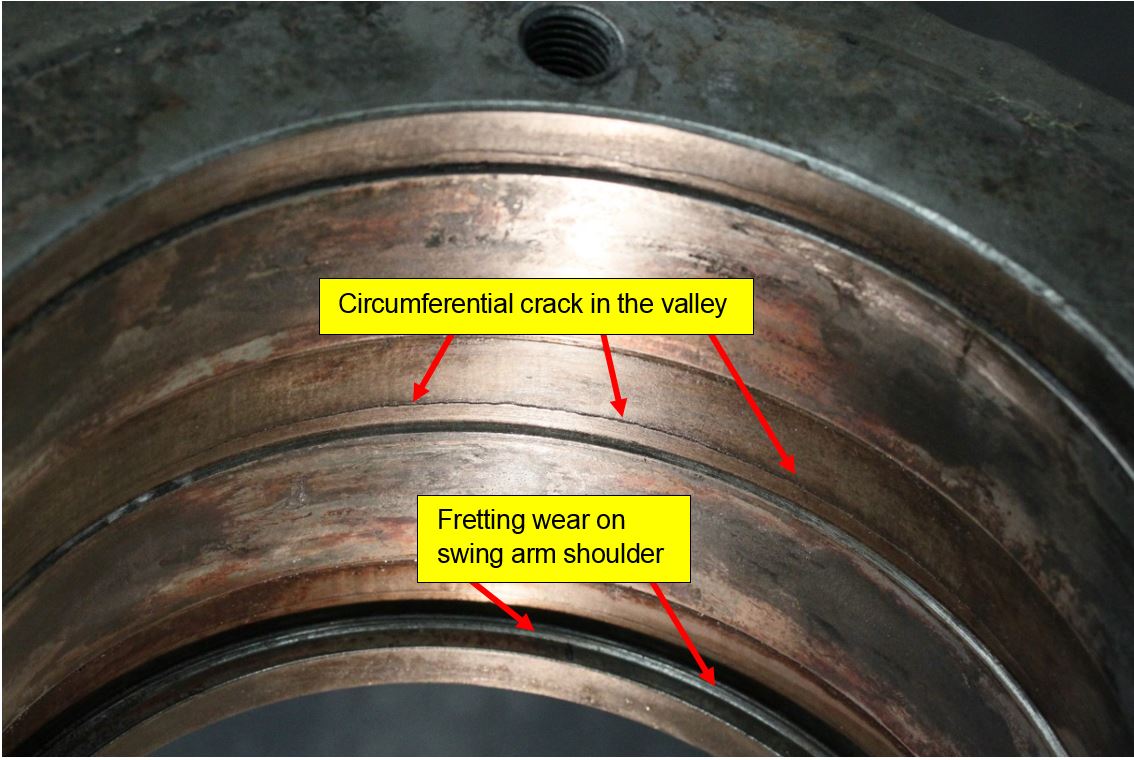
Assessment of the fracture indicated that the fracture was at the mid-point of the centre sill transverse weld. A backing bar[8] was present along the length of the weld although there was no obvious weld penetration. Oxidation was visible on the lower section of both vertical plates and the fracture face was worn (Figure 4). The presence of both oxidation and wear is consistent with fatigue cracking however there were no beach marks[9] observed in this region. The remaining fracture face was free from oxidation and likely progressed quickly.
Figure 4: Wagon NDHX14836G fracture
Photograph shows the left and right sides of the centre sill.
Source: Pacific National and OTSI, annotations by OTSI
Train 3YN2 underwent the required maintenance inspection prior to departing Broken Hill on 6 January 2021. These inspections did not detect the existing fracture on the frame of NDHX14836G.
The GX inspection scope was limited although the partial fracture would likely have been visible during close inspection of the centre sill vertical plates (web). The investigation was unable to determine when the frame was partially fractured, the oxidation indicates a fracture was almost certainly present during numerous GX and roll-by inspections.
Maintenance records (Table 2) showed two of the three most recent 56 day on inspections (UTM) were completed in exceedance of the 7-day tolerance. The UTM maintenance plan was associated with the rake[10] of wagons rather than individual wagon. If a wagon was moved from the rake it could have operated in exceedance of the maintenance plan, increasing the likelihood of a rolling stock irregularity progressing without detection.
Wagon maintenance manual WMM-04-02 provided guidance for the inspection of various wagon classes although did not specifically detail inspections of NQHX (NDHX) wagons. The guidance for inspecting the underframe was general and did not highlight the location of cracking as found on NDHX14836G. Additionally, there was no requirement for more detailed inspections of ageing assets.
The design and construction of the ICX class wagons varied with some wagons having a centre sill transverse weld at the mid-point on the lower edge of the sill. Design drawing provided as part of the investigation did not indicate the presence of the weld or provide details for the original weld specification. A weld at this location of high stress increases the risk of fatigue cracking and presented different risk profiles within the same wagon class.
Non-destructive testing consisting of magnetic particle inspection (MPI) was only required if a crack was visually detected. Without more advanced non-destructive testing, a crack would need to propagate to be visibly detectable on the surface before it may be addressed.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the rolling stock irregularity involving freight train 3YN2.
Contributing factors
3YN2 departed Broken Hill with an undetected crack on wagon NHDX14836G; the crack progressed and the wagon sagged under the load striking three level crossings.
The centre sill of wagon NDHX14386G likely fractured due to fatigue cracking initiating at a transverse weld on the lower edge of the sill.
Pacific National's maintenance and inspection regime was not sufficient to identify cracking at a location of known risk before the structural failure of wagon NDHX14836G.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Pacific National
Maintenance and inspection
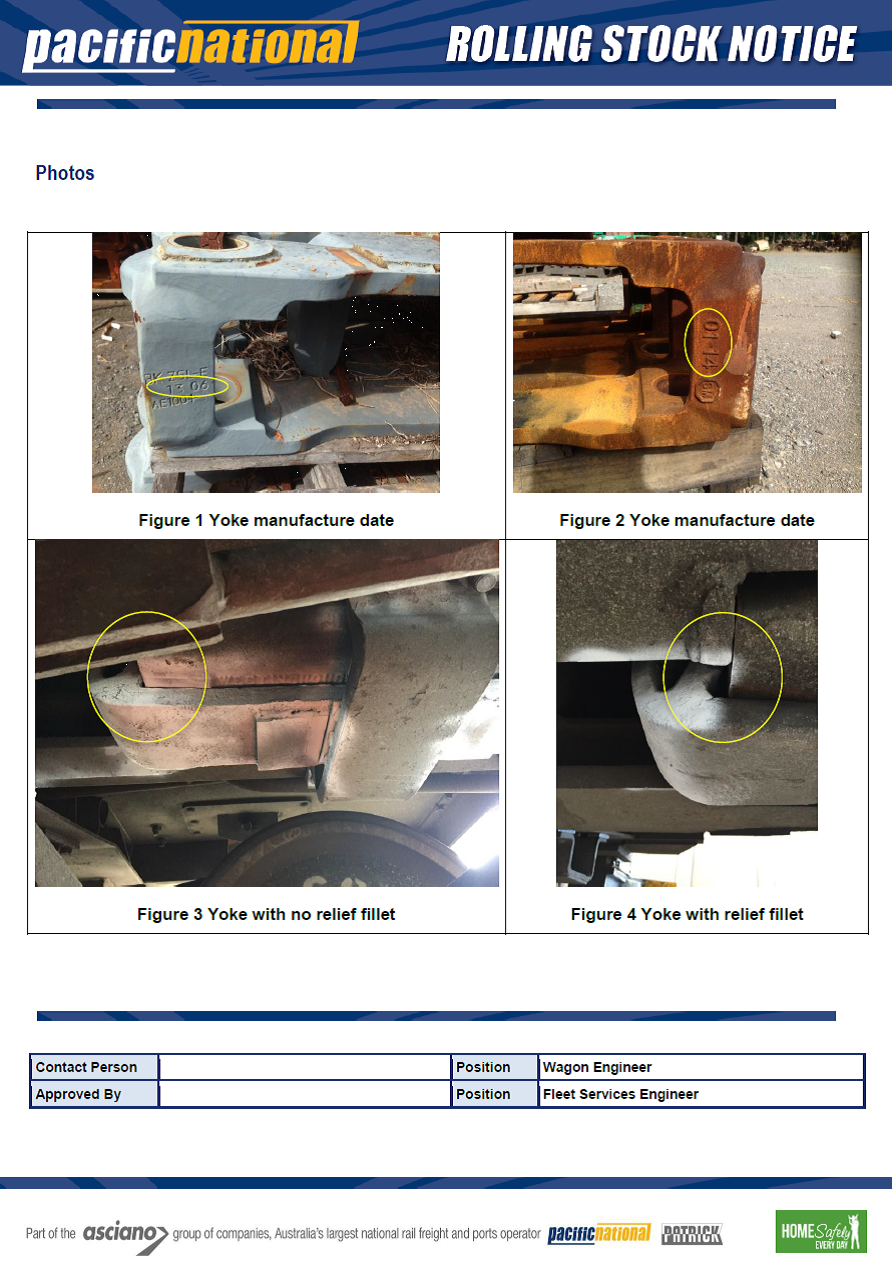
On the day of the occurrence, Pacific National issued a Rolling Stock Notice (RSN E 21-002) requiring an underframe crack inspection on NDHX, NQHX and NQIX wagons. The visual inspection required:
checking if there was a butt weld at the midpoint of centre sill
checking for cracks on the underside of the centre sill at the location of the butt weld
checking the vertical web plate for the presence of crack propagation
confirming the presence of doubler plates and any cracking associated with the doubler plates.
A total of 134 wagons were inspected as of 21 January 2021 with no cracks identified at the centre sill. The last wagon was inspected on 27 May 2021 with no cracks identified. Wagon NDHX14836G was to be scrapped, reducing Pacific National’s number of ICX class wagons to a total of 135.
Pacific National advised that they have completed a risk assessment to determine the NDHX wagon limitations and ongoing monitoring program requirements and plans for ongoing use. The following actions are also planned in relation to this occurrence:
Broken Hill maintenance depot to conduct a risk assessment associated with the inspection of underframe of ICX class wagons during time based and kilometre based inspections.
Review facilities available at Broken Hill to provide maintenance personnel easier access to complete underframe inspections.
Develop a lifecycle management strategy for NDHX/ICX wagon classes with a butt welds.
Develop an asset management strategy for the identification and implementation of the appropriate wagon lifecycle strategies.
Review wagon maintenance manual WMM 04-02 to include details for ICX class wagons.
Review and adjust the current non-destructive strategy applied across Pacific National’s fleet of wagons.
Compliance with maintenance standards
In relation to the management of trains under unit train maintenance (UTM) strategies, a Rolling Stock Notice (RSN E 21-003) was issued on 18 January 2021. The notice advised of the transition from unit train maintenance (UTM) at the rake level (group of wagons) to the individual wagon level. This notice was distributed to asset management and maintenance personnel and detailed actions to be taken. This change was to ensure that wagons receive the correct inspection when required. Pacific National's maintenance management system was updated to reflect these changes and wagons with overdue maintenance activities were identified and prioritised for inspection.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Australian Rail Track Corporation
Pacific National.
References
Pacific National (2015), Train Inspection Manual, General Train Inspection Procedure, TIM 01-03_05, 14 December 2015
Pacific National (2017), Wagon Maintenance Manual, Maintenance of Freight Wagons, WMM 01-01_05, 26 June 2017
Pacific National (2020), Wagon Maintenance Manual, UTM/ Block/ OK Spare/PM Inspection, WMM 01-18_07, 21 October 2020
Pacific National (2020), Wagon Maintenance Manual, Underframes, Body work and Load Supports, WMM 04-02_05, 1 July 2020
Rail Industry Safety and Standards Board (2021), Glossary of Terms. Accessed at: www.rissb.com.au/glossary/
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Australian Rail Track Corporation
Office of the National Rail Safety Regulator
Pacific National
Transport for NSW.
Submissions were received from:
Australian Rail Track Corporation
Office of the National Rail Safety Regulator
Pacific National.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the ATSB to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation. The statement is published as a report in accordance with section 25 of the TSI Act, capturing information from the investigation up to the time of discontinuance.
Overview of the investigation
The occurrence
On 2 October 2020, at about 1117 Eastern Standard Time,[1] a SCT Logistics freight train 3PG1 travelling from Port Germain, South Australia to Parkes, New South Wales, began to lose brake pipe air, resulting in the application of the brakes. The train subsequently came to a stand with the leading locomotive at about 904 track km, 90 km west of Ivanhoe, New South Wales.
In response to the loss of air, the driver and driver assistant (both employed by Momentum Rail) commenced an inspection of the wagons. However, they stopped before arriving at the back of the train as the driver considered the issue to be a computer error. They returned to the lead locomotive and the driver tried to restore the brake pipe air by resetting the electronic air brake system, which was unsuccessful. The driver assistant re‑inspected the wagons, finding and closing an open brake pipe tap on the back of the last wagon (ABSY2792Y). They reported this to the driver, but for differing reasons, the end of train marker was not checked or the number of the last wagon was not confirmed.
The train’s brake pipe air was restored, allowing the brakes to release. The driver reported to train control that the loss was due to an animal strike and the trip resumed. On arrival at the Darnick yard limit board (YLB), the previously issued train order (Kaleentha loop to Trida YLB) was cancelled and a new train order from Darnick YLB to Ivanhoe YLB was issued. The crew of 3PG1 did not check whether their train was complete at this location and the train controller did not request confirmation, as required by the Australian Rail Track Corporation train order working procedure.
However, due to concerns with not having checked the end of train marker, the driver assistant conducted a roll-by inspection as the train proceeded into the Ivanhoe loop. At that time, they identified that the train consist was incomplete and the last 4 wagons were missing. The crew concluded that the missing wagons were likely left behind at the point where the train had lost brake pipe air pressure, about 2 hours prior. The section of track with the 4 parted wagons was left without protection with another train waiting at Darnick to enter the occupied section.
Investigation activities
During the investigation, the ATSB:
interviewed the train crew and network controller
conducted analysis of data from the locomotive’s event recorder
reviewed recorded communications between train control and the crew
reviewed the track access and labour agreements in place between the involved parties
reviewed the experience, training and competencies held by the train crew
conducted analysis of possible contributors to the parting, including a review of the wagon inspection results and maintenance history
analysed the practical actions required, including actioning applicable rules and procedures when train crews respond to a loss of brake pipe air event
reviewed the tasks conducted post-occurrence to recover the lost wagon.
ATSB observations
From the investigation, the ATSB determined:
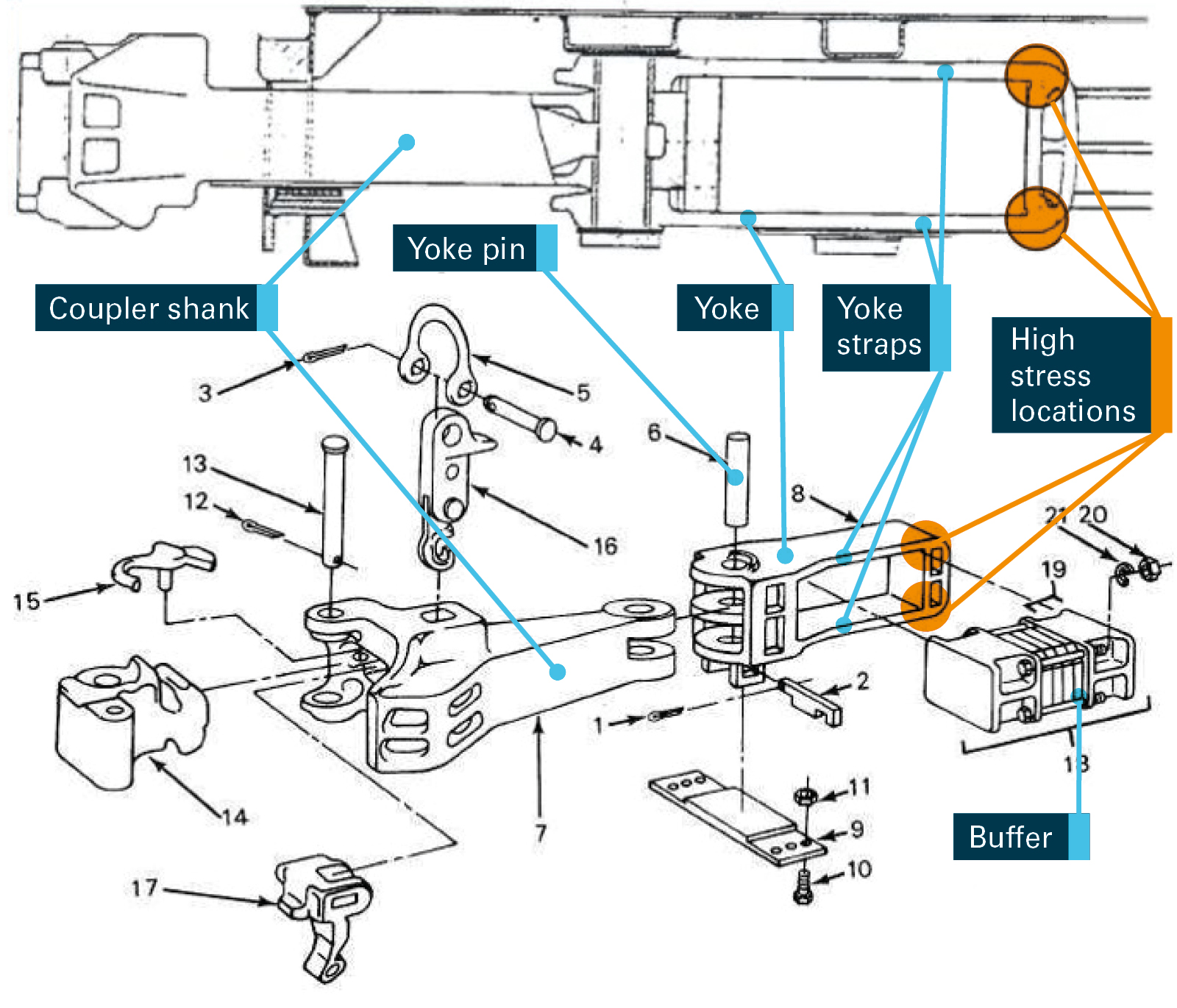
The coupler locking block and knuckle on the leading end of wagon ABSY2792Y were worn, which very likely resulted in 4 rear wagons parting, and train 3PG1 subsequently loosing brake pipe pressure.
The crew did not identify that the end of train marker was not present on the last coupled wagon or otherwise identify that the 4 rear wagons had parted. Instead, during an inspection of the train, the driver assistant closed an open brake pipe air tap on the back of the last coupled wagon, which allowed all the wagon brakes to release. Consequently, the train resumed the journey incomplete.
The 4 parted wagons were left occupying the track section when the protection on the section of track (Kaleentha to Darnick) was removed. The crew of 3PG1 cancelled the existing train order without conducting a further inspection.
The driver assistant was not experienced in the role they were undertaking. This, combined with having only partially completed the relevant driver qualification, contributed to them not recognising the potential reasons for an open air tap on the back of the last wagon, which included the risk that the train had parted. This likely compromised the crew's understanding of the occurrence and led them to incorrectly attribute the problem to a known cause.
The lock blocks on three couplers, including the coupler that initiated the parting, were not replaced at previous 'B' inspections. However, the replacement was a requirement in SCT Logistics’ maintenance provider’s (Gemco Rail) procedures. Subsequently, the component was in use past its intended service life when the parting occurred.
Reasons for the discontinuation
The ATSB gives priority to transport safety investigations that have the potential to deliver the greatest public benefit through systemic improvements to transport safety.
Given the ATSB’s constrained resources, the ATSB considered it was unlikely that further investigation would identify systemic safety issues or identify opportunities for the enhancement of transport safety. Consequently, the ATSB has discontinued this investigation.
The ATSB has briefed SCT Logistics and Momentum Rail about its observations and potential learnings. However, it considered that broader communication of this information would not be of significant benefit to other parties.
The evidence collected during this investigation remains available to be used in future investigations or safety studies. The ATSB will also monitor for any similar occurrences that may indicate a need to undertake a further safety investigation.
This investigation was conducted under the Transport Safety Investigation Act 2003 (Commonwealth) by the Office of Transport Safety Investigations (NSW) on behalf of the ATSB in accordance with the Collaboration Agreement. Released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Safety summary
What happened
On 13 October 2020, TrainLink passenger service SN68, was operating from Moss Vale to Campbelltown, New South Wales with approximately 20 passengers on board.
The train driver stopped the train at Yerrinbool Station after being alerted to a small fire at the rear of the train. The fire was identified as coming from the vicinity of an axle bearing on the rear wheelset of the train. The passengers were evacuated onto the platform and the driver attempted to extinguish the fire using an on-board fire extinguisher.
The fire was subsequently extinguished by Fire and Rescue NSW. As a result of the fire, parts of the axle box were heat affected and sustained significant damage to the speed sensor and rubber suspension components. There were no reported injuries.
What the ATSB found
The investigation determined that the fire was the result of a collapsed axle bearing on wheel 8 on the trailing bogie on car 2811, the end of the train. The axle bearing failed when the axle end cap bolts loosened and one fractured which caused the collapse of the bearing and frictional heat to be generated. The resulting fire was fuelled by grease, oil and rubber suspension components in the immediate vicinity of the axle box.
It is likely that during the last overhaul of bogie NJA31, the locking plate tabs retaining the axle end cap bolts were not fitted correctly against the sides of the bolts. The axle bearing installation process was not sufficient to ensure the tabs on the locking plate were installed correctly during a refurbishment three months before the incident.
A wayside monitoring system at Burradoo on the Down Main line detected an elevated temperature on one bearing, but the temperature recorded was below the threshold for an alarm to be sent to network control.
What has been done as a result
Following the occurrence Sydney Trains, which is the maintenance provider for NSW Trains, initiated an inspection of similar axle boxes in the fleet and undertook an audit of the contracted maintainer’s practices.
Sydney Trains have advised the following actions have taken place to prevent a recurrence:
Improvements have been made to the contracted maintainer’s quality assurance processes to ensure that bolts and locking tabs are correctly installed.
An improved process was implemented to review and retain the contracted maintainer’s certificate of completion checklists.
Safety message
Bearing failures continue to occur within the Australian rail network. This occurrence emphasises the significance of having adequate bearing installation processes and ensuring that axle bearings are correctly maintained and monitored throughout their operational life.
The Occurrence
On Tuesday 13 October 2020, TrainLink passenger service SN68, operated by NSW Trains,[1] departed Moss Vale at 1757.[2] The two-car Endeavour train was crewed by a driver in the front cab and a guard in the rear cab. There were approximately 20 passengers on board the train as it departed Moss Vale (Figure 1). The train was to make 11 stops before being scheduled to arrive at Campbelltown at approximately 1900.
The train stopped at Burradoo and Bowral before departing Mittagong at approximately 1809. The train crew said they had experienced no problems with the train before Yerrinbool.
At 1820, as the train was slowing to stop at Yerrinbool Station, the guard, from inside the cab at the rear of the train, heard a loud noise and noticed smoke outside the window. The guard used the train’s bell system to ask the driver to stop. The driver brought the train to a stand at Yerrinbool Station.
Figure 1: Incident location and path of SN68
Source: Geoscience Australia, annotated by OTSI
Once the train stopped at Yerrinbool Station, the guard used the trains’ public address system to ask the passengers to move to the front of the train. The guard made a second announcement shortly afterwards, requesting passengers disembark onto the platform. The driver walked along the platform to the rear of the train and observed a flame and dark smoke coming from the last wheelset of the train, wheel 8 on axle 4 under the bogie of car 2811.
The driver spoke to an Australian Rail Track Corporation (ARTC) network controller at Junee requesting permission to go down onto the track to attempt to extinguish the fire. The network controller applied signal blocking to prevent rail traffic in both directions and then gave permission for the driver to access the track. Another passenger service, SN61, was stopped by the signaller at a signal before the platform at Yerrinbool. This provided protection on the adjacent line so the driver could go onto the track. The driver went onto the track and used the on-board fire extinguisher to attempt to put out the fire. The fire continued to smoulder/burn as the heat source remained.
Fire and Rescue NSW arrived on site at approximately 1828 and ensured the fire was extinguished before departing at 1850. Train passengers were transferred to buses which replaced train services between Campbelltown and Moss Vale in both directions. There were no reported injuries as a result of this incident.
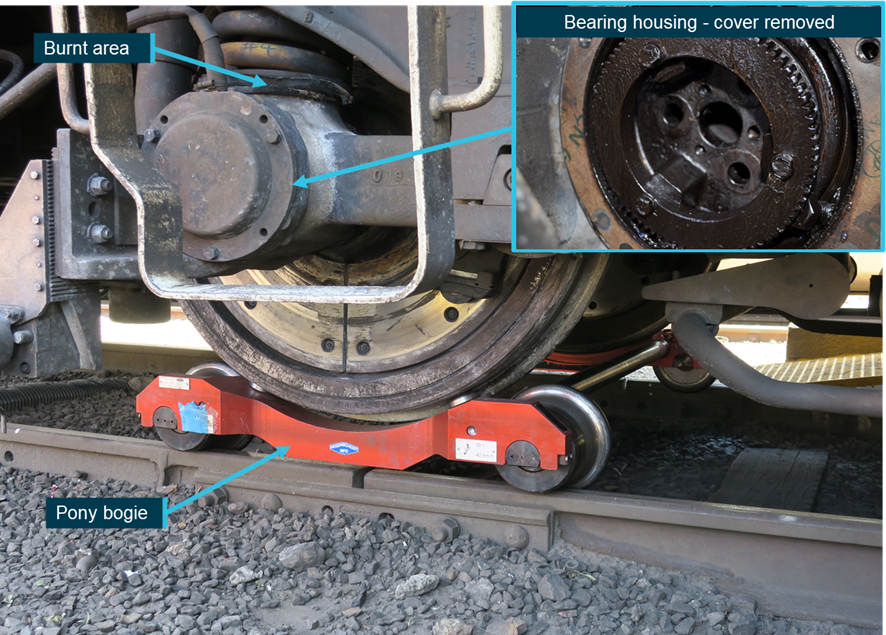
The maintenance shift manager at Eveleigh Maintenance Centre organised for the Rail Emergency Recovery Unit to arrange pony bogies (Figure 2) to be fitted under all wheels of bogie NJA31 and the train was worked back to Eveleigh over the next two nights. Under the supervision of Office of Transport Safety Investigations (OTSI) investigators, Office of the National Rail Safety Regulator representatives and Sydney Trains engineering staff a partial disassembly of the axle end cap and removal of bolts from the affected bearing was undertaken. A further strip down inspection of the axle bearing assembly was conducted at bogie maintainer United Group Limited Unipart (UGLU) at Auburn, also under the supervision of OTSI investigators and Sydney Trains engineering staff.
Figure 2: Heat affected area and pony bogie fitted under NJA31
The inset image shows the axle cover removed. Two bolts were found to be missing from the end cap and one bolt was broken. All three bolts remained within the axle housing.
Source: OTSI
The damage was contained to this localised area around the trailing axle of the rear bogie. Parts of the axle box were heat affected and the speed sensor and rubber suspension components were significantly damaged.
The Bureau of Meteorology (BOM) automatic weather station at Moss Vale, recorded the temperature as 24.4 °C at 1500 on 13 October 2020. Yerrinbool is approximately 30 km north-east of Moss Vale. Weather conditions were fine and clear.
Location
Yerrinbool Station is on the Main South line in the Southern Highlands of New South Wales (Figure 3). Yerrinbool is located at 116.310 km.[3]
Figure 3: South-bound Endeavour two-carriage set at Yerrinbool Station
The figure shows south-bound (Down) Endeavour set at Yerrinbool Station. Image of car 2811 inset
Source: railgallery.wongm.com, annotated by OTSI
Train crew
The train was crewed by a driver, operating the train in the front driver’s compartment, and a guard located in the rear drivers’ compartment. The train crew were appropriately qualified and held the required route qualifications.
Train information
Train SN68
The passenger train involved in the incident, SN68, was an Endeavour railcar two-carriage set. This diesel-powered multiple unit train was operated by TrainLInk and built by ABB Transportation in Dandenong, Victoria. There were 14 Endeavour sets in service at the time of the incident and they first entered service in March 1994. Twenty-three Xplorer cars which have the same bogie types and axle bearings were also in service at the time of the incident.
The leading car of SN68 was LE2861, with TE2811 being the trailing car. The LE carriages feature a dedicated luggage space and can seat 95 passengers. The TE carriages feature a wheelchair accessible toilet and can seat 82 passengers.
The drivers’ cab, positioned at each end of the train, is a full width driving compartment with the driver's seat offset to the left-hand side. Passengers enter and exit through power activated doors operated and controlled by the driver or the guard. Dry chemical fire extinguishers are fitted in the drivers’ compartment.
Bogies
The bogies fitted to the Endeavour and Xplorer sets are NJA and PJA bogies. The bearing collapse occurred on an NJA bogie, the rear trailing bogie on car 2811. The NJA bogie is the trailer bogie (Figure 4), as opposed to the PJA powered bogie. Built for the State Rail Authority in 1994, the bogie involved in this incident was designated as NJA31. This bogie was installed on car 2811 on 7 July 2020 and had travelled approximately 66,087 km since installation.
Figure 4: NJA31 bogie
Source: OTSI
Axle bearing installation
The maintenance and installation processes for critical components holding the axle bearing were examined as part of the investigation.
Each bogie has two wheelsets which have an axle bearing at each end of the axle (four bearings per bogie). The axle bearings were Timken SP130 type bearings. Securing the axle end cap were three different brands of bolts with the head markings showing: NLGS, JDF and HEC (Figures 5 and Figure 6). The axle end cap bolts were hexagonal head, metric 16 mm diameter (M16), 40 mm length (fully threaded), 2 mm pitch, and class 8.8. There are two types of end caps used, a standard or combined end cap suitable for mounting a phonic wheel. The phonic wheel is used as part of the train’s on-board system for recording speed and detecting wheel slide during braking, this end cap was the phonic wheel type.
Figure 5: Three types of axle end cap bolts removed from hub following incident
Source: OTSI
Figure 6: Side view of three axle end cap bolts, including broken NGLS bolt
Source: OTSI
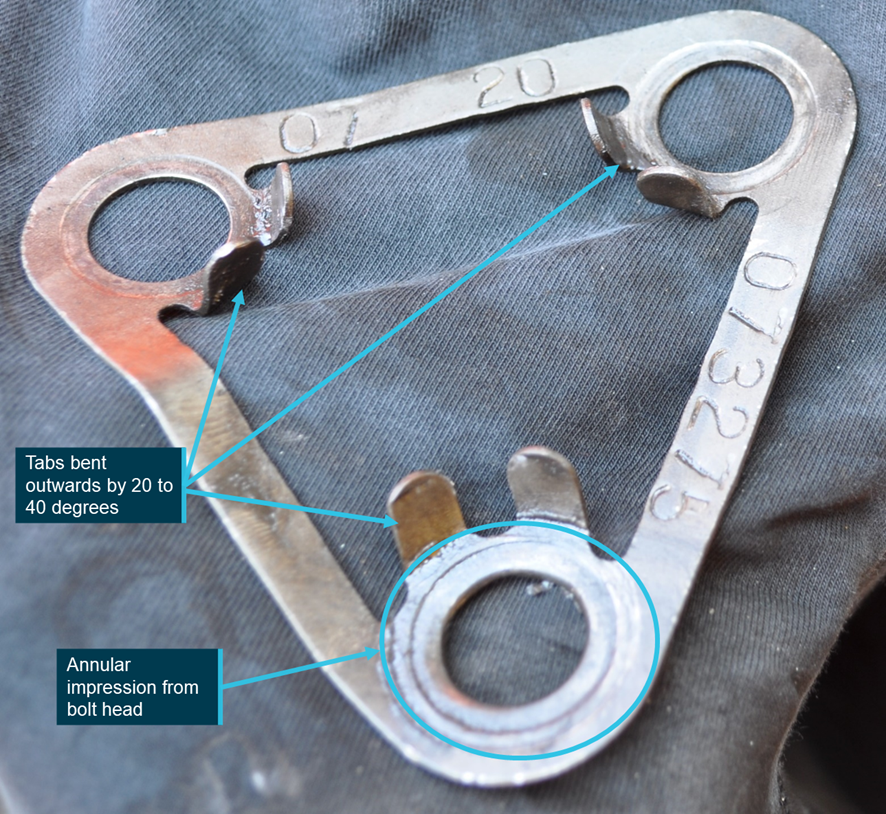
The locking plate was a Timken brand K-422091 R.S 120-130. Stamped on the plate was the axle number (073275) and installation date (07 20 – July 2020) (Figure 7).
Figure 7: Locking plate
Source: OTSI
The requirements for installing the SP130 bearings onto the axles is documented in a Sydney Trains Standard Instruction.[4] This instruction provided maintenance workers with the details for installing the end cap, torque requirements for bolts and installing the locking tabs. There was a wheelset certificate of completion used by the maintenance workers to show that bogie NJA31 was refurbished. This work was completed on 1 July 2020. There are check boxes on a form that the maintenance workers complete when each task is done. These were all checked as completed and the installation tolerances for the bearing were correct at the time of installation.
The axle bearing installation process commences with the bearing being pressed onto the axle journal before being retained on the journal by an end cap. The end cap is secured by three M16 bolts with a new locking plate positioned underneath the bolt heads. The bolts are screwed in threaded holes and using a calibrated torque wrench are finally torqued to 80 – 100 Nm.
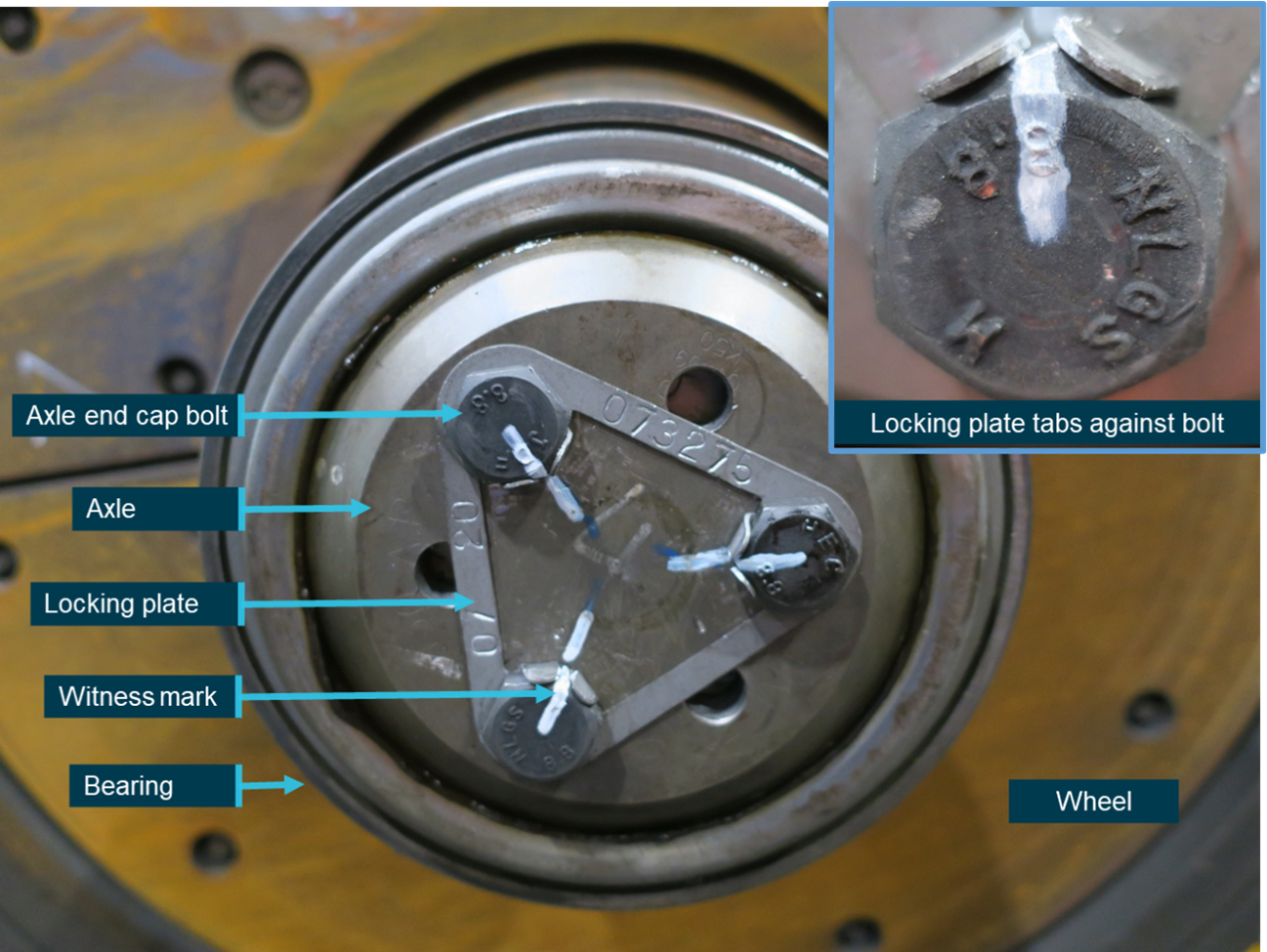
The bolts are torqued in sequence until there is no further movement of the bolt resulting from the application of the specified torque. It may be necessary to further tighten the bolt to align the head with the locking plate tabs. The tabs on the locking plate are then bent up to engage with the sides of the bolt head to form a tight fit. After the process is complete a witness mark is applied to the bolt head and adjacent area to show the original position of the bolts (Figure 8). Movement can be visibly determined during any subsequent inspections.
Figure 8: Correct bolt and locking tab installation bolt
Inset image shows a close of the locking tabs correctly bent up and in contact with the head of the bolt as well as the witness mark (white paint pen).
Source: OTSI
Involved parties
The Australian Rail Track Corporation (ARTC) is the rail infrastructure manager that manages the Main South Line from Macarthur on the outskirts of Sydney to Melbourne, including the wayside monitoring device.
NSW TrainLink provides rail services in NSW and also operates some interstate services to Victoria and Brisbane.
Sydney Trains is responsible for maintenance activities on the trains operated by Sydney Trains and NSW TrainLink.
United Group Limited Unipart (UGLU) are contracted maintenance providers to Sydney Trains and serviced the bogies of the Endeavour and Xplorer fleet. UGLU is a joint venture between United Group Limited and Unipart.
Track and infrastructure information
The section of track at Yerrinbool was standard gauge (1435 mm). It consisted of an Up Main line and a Down Main line. At the time of the incident SN68 was travelling towards Sydney on the Up Main line.
ARTC maintains operational control for this area from Network Control Centre South at Junee.
Wayside detectors
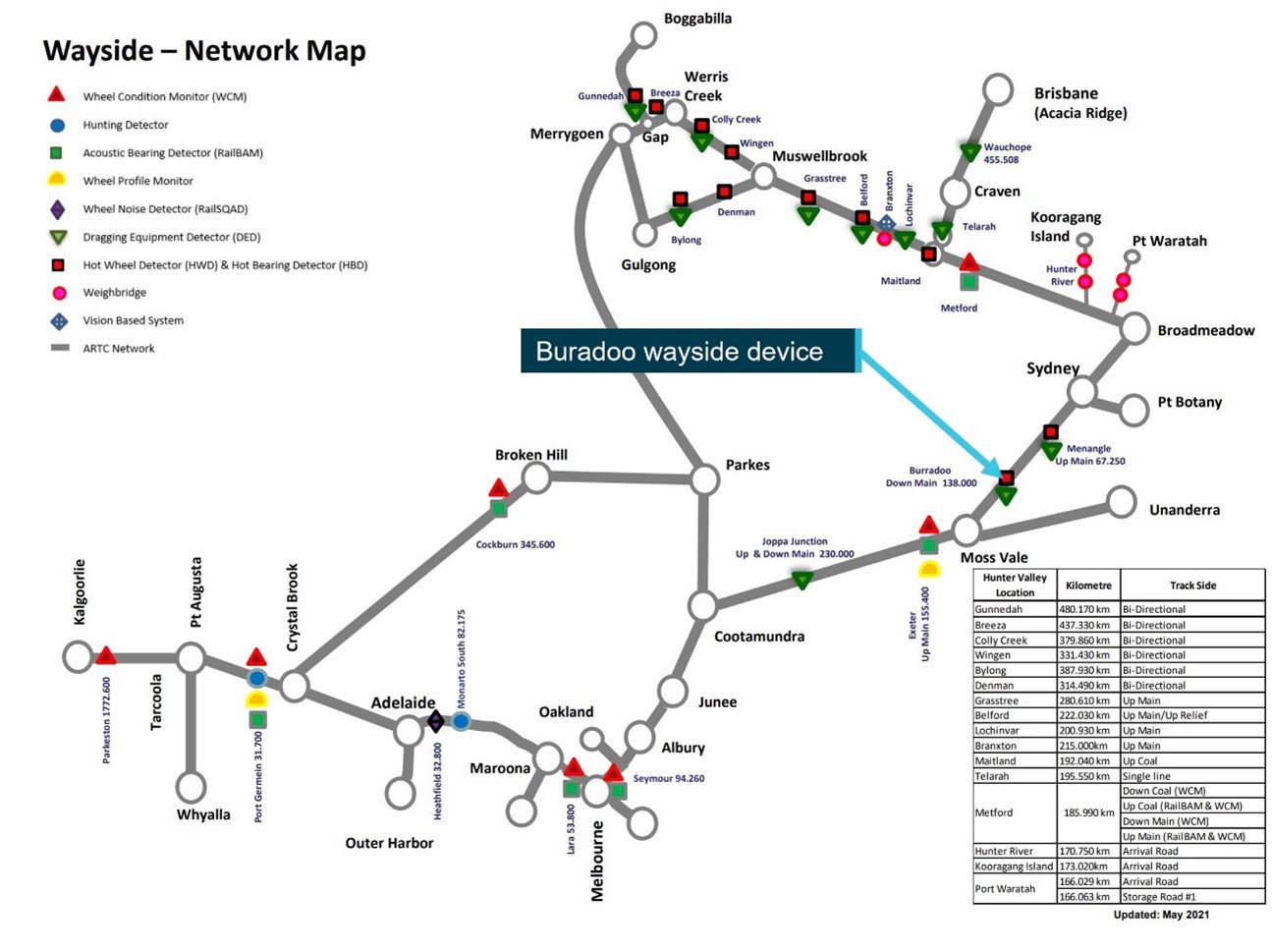
The ARTC, operates and maintains the wayside monitoring systems in the vicinity where this incident occurred. There are different types of wayside devices including but not limited to detectors for hot bearings, wheel impact loads, acoustic wheel monitoring, and dragging equipment (Figure 10).
At Burradoo, 138.000 km, on the Down Main line, an operational wayside device detected an elevated bearing temperature as SN68 as it passed, in the Down direction, on the way to Moss Vale. This occurred at 1703 when the elevated temperature was recorded on car 2811 (wheel 8 on axle 4), the location of the subsequent collapsed bearing. The temperature was recorded as 84°C, below the threshold to trigger an alarm. The temperature of the other bearings on the bogie were recorded as 73°C, 65°C and 69°C.
The ARTC has two threshold categories for hot bearing detector alarms.[5] When a threshold temperature is exceeded an alarm is sent to the network controller who must ensure the category of alarm condition is understood by the driver and is responded to according to the required action outlined below (Figure 9).
Figure 9: Wayside Device Alarm Categories
Temperature Alarm
Required Action
Hot Alarm
100°C
The temperature has passed the critical level and there is a possibility of bearing damage. Trains to be stopped immediately and vehicle inspected. Rail operator notified and Train Control Report (TCR) is raised.
Warm Alarm
90°C at 20°C ambient varied by 80% for the actual threshold.
The temperature is higher than normal and the bearing may need attention. Train to be stopped immediately and vehicle inspected. Rail operator to be notified and TCR raised.
Source: ARTC
The other wayside monitoring system between Campbelltown and Moss Vale was located at Menangle on the Up Main at 67.25 km. It is likely that the hot bearing would have been detected here, 50 km past Yerrinbool.
Sydney Trains also checked previous passes by car 2811 over wayside monitoring systems and did not identify any other warm bearing temperature for this wheelset for the period 5 July 2020 to the incident date on 13 October 2020.
Figure 10: ARTC Network wayside detectors
Source: ARTC, annotated by OTSI
Related occurrence
On 1 December 2020, less than two months after the incident at Yerrinbool, a related incident occurred when a hot bearing on an Xplorer train was detected by a Sydney Trains wayside detector on the Up Main at Wyee, NSW. TrainLink passenger service, NP24, travelling from Armidale to Sydney was stopped at Wyee after the driver was notified of a hot bearing. After inspection, the train proceeded at a low speed (under 25 km/h) to Wyong where the passengers were disembarked. There was no injury or damage.
The Xplorer was subsequently examined at Eveleigh Maintenance Centre where it was found that two axle end cap bolts on car 2508 (wheel 8) had moved from their original position. It was also found that the locking plate tabs were incorrectly bent up. The last refurbishment of the wheelset was 22 months before the incident on 1 March 2019.
The investigation determined that the fire in the wheel area of SN68 at Yerrinbool was caused by a collapsed bearing on wheel 8 on the trailing bogie on car 2811. This led to frictional heat to be generated and a fire started. The fire was fuelled by grease, oil, and rubber suspension components in the immediate vicinity of the axle box. The fire did not spread to other parts of the train.
The likely precipitating events to the bearing collapse was the loosening of two of the three axle end cap bolts which placed higher loading on the remaining bolt which then started to fracture. During every cycle of the bearing there are micro movements within the system. The locking plate tabs, if positioned correctly against the face of the bolts, assist in retaining the bolts in position. The two bolts, inadequately restrained by the locking plate, continued to loosen and fell out and the remaining bolt then fractured completely (Figure 11). With the end cap unsecured the outer cone of the bearing was able to move on the axle. Wayside data indicated that once the bolt fractured it took approximately 15-20 minutes for the failure to be identified.
Figure 11: Axle end with protruding failed bolt
Insert image showing the inside collapsed axle box and failed bolt protruding.
Source: OTSI
An initial inspection of the axle bearing and components was conducted following the incident at Eveleigh Maintenance Centre. All three bolts and the locking plate were recovered and, although damaged, were able to be examined. There were three different brands of bolts used and the failed bolt was identified as a NLGS bolt. A further inspection at UGLU Auburn Maintenance Centre was conducted when the bogie was disassembled. Present at these inspections were representatives from OTSI, Sydney Trains and UGLU. Measurements were taken and recorded for critical items, such as bearing end float, end cap installation torque and axle diameters on the other three undamaged bearings. These measurements were all were consistent and within specification.
Torque values were also measured on the other three undamaged bearing axle end cap bolts. Four out of the nine torqued bolts remaining on the bogie exceeded the 80‐100 Nm torque range and two bolts were recorded at 180 Nm and 200 Nm. The differing torque amounts was attributed to bolts being tightened further to achieve the alignment with the locking tabs. This torque was the breaking torque, not the original application torque.
An independent metallurgical examination was also conducted on the bolts and the locking plate, as well as a sample of other similar bolts. The scope of this analysis included: examination and fractography, hardness testing on all bolts, microscopy analysis of the grain structure, tensile testing and compliance to applicable standards. A report was produced following this examination.[6]
The metallurgical examination showed that the bolts had no material or surface defects and complied with the requirements of the Australian Standard.[7] The use of differing bolt brands was initially identified as a concern but was later ruled out as an issue as all brands complied with the requirements of the standard. The metallurgical examination also showed the locking plate to be without issue. Other results from the metallurgical examination were:
- Damage was most severe on the first two bolts which loosened and fell out. These bolts were damaged after being tumbled around inside the case.
- The third bolt had the least damage as it had fractured after the first two bolt had fallen out.
- The third bolt had partially unscrewed about 4-5 mm before failure.
- The third bolt failure occurred progressively over a period of approximately one to two hours.
- The locking plates were made of low hardness steel which provided less resistance to loosening if the stresses in the system were sufficient to unscrew the bolts.
- The locking plate showed heavy damage and bent arms at the hole where the third bolt fractured.
The metallurgical report stated: ‘A potential factor in the failures was insufficient tensioning of the bolts on installation, however, annular impressions around the locking plate holes were mostly similar, which is a rough indication that torqueing of the bolts had been similar. This observation is very subjective, and the conclusion of similar torqueing may be erroneous.’ The investigation could not verify what torque level was applied to the axle end cap bolts that came loose.
Bearing installation process
An inspection of the processes undertaken at UGLU Auburn Maintenance Centre demonstrated that standard processes were in place, marked components were used, and calibrated torque wrenches available to be used by appropriately qualified personnel. Despite this, the physical evidence shows that it is likely that during the last refurbishment of the wheelset, on 1 July 2020, just over three months before the incident, the locking tabs were not sufficiently bent up against the face of the bolts.
There was completed documentation showing the processes had been checked off by a qualified maintenance person. The relevant checkboxes for all items were completed, this included:
- checking the bolt torque (new bolts used)
- tabs locked flat on the screw head face
- torque marking of screws.
However, at the time of the refurbishment there was no additional quality assurance check once this process was completed.
The subsequent Sydney Trains investigation report into this incident at Wyee on 1 December 2020 showed strong similarities with the incident at Yerrinbool. The detection of the locking plate tabs not being bent up supports the same findings for Yerrinbool.
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collapsed bearing on passenger train SN68 at Yerrinbool, New South Wales on 13 October 2020.
Contributing factors
The fire that occurred on SN68 was the result of excessive heat generated from a collapsed bearing on the trailing bogie of locomotive TE2811.
The bearing collapse was the result of two axle end cap bolts becoming loose and the remaining bolt fracturing due to the increased load. Once the three bolts were no longer holding the end cap in position the bearing rapidly collapsed.
It is likely that during the last NJA31 bogie overhaul the tabs on the locking plate were not installed correctly. This enabled the two axle end cap bolts to loosen.
The axle bearing installation process was not sufficient to ensure the tabs on the locking plate were installed correctly. (Safety Issue)
Other (key) finding
The brake and bearing temperature alarm detected an elevated temperature on an axle bearing at Burradoo as SN68 passed over it approximately 60 minutes before the fire was noticed at Yerrinbool. The temperature recorded was below the threshold for an alarm to be sent to network control.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the [aviation, marine, rail] industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are provided separately on the ATSB website, to facilitate monitoring by interested parties. Where relevant, the safety issues and actions will be updated on the ATSB website as further information about safety action comes to hand.
Safety issue description: The axle bearing installation process was not sufficient to ensure the tabs on the locking plate were installed correctly (Safety Issue).
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Australian Rail Track Corporation
NSW Trains
Sydney Trains
United Group Limited Unipart.
References
Australian Standard AS 4291.1 / ISO 898.1 Mechanical properties of fasteners made of carbon steel and alloy steel.
Rail Industry Safety and Standards Board (2021), Glossary of Terms.
Sydney Trains (2020), Systemic Safety Investigation Report Collapsed bearing on car 2811 at Yerrinbool on 13 October 2020.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Australian Rail Track Corporation
NSW Trains
Office of the National Rail Safety Regulator
Sydney Trains
Transport for NSW
Submissions were received from:
Office of the National Rail Safety Regulator
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the Australian Transport Safety Bureau (ATSB) to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation.
The ATSB commenced an investigation into a train runaway operated by Genesee & Wyoming Australia (GWA), which occurred on 31 July 2019. The train was operating within the Liberty Primary Steel complex at Whyalla, South Australia.
Within the steelworks, GWA operated trains using a single driver. The driver controlled the locomotive through a combination of cab controls and remote control equipment depending on the task (transiting, loading, unloading).
At about 0815 (Central Standard Time) on 31 July 2019, a driver was connecting a pair of locomotives to an empty rake of wagons using the remote control equipment. The driver was in the process of transferring control from the remote control to the locomotive cab. At about 0824, while in the locomotive cab, the driver noticed that the train was beginning to move backwards, towards the steelworks. At that time, the removable locomotive control handles were not in their normal location, so the driver was unable to operate the train’s airbrakes. The driver attempted to stop the train by applying the mechanical handbrake outside the locomotive cab, but this had no effect. With the train accelerating, the driver chose to jump off while the train was moving at low speed, and alert train control.
For about 11 minutes, the empty train rolled through the steelworks yard, reaching a maximum speed of 51 km/h over track with a permitted speed of 15 km/h. The train passed over eight level crossings and crossed a railway track used to move rail wagons carrying molten iron. As the track levelled out, the train slowed by itself and stopped on the steelworks balloon loop. The train travelled about 6 km without a driver in control.
Initial information from GWA suggests that while transferring control from the remote equipment to the locomotive cab, a pneumatic connection was closed before the brake pipe had been exhausted. This condition, combined with an undetected fault on one locomotive, resulted in all brakes releasing and the subsequent train runaway.
The Government of South Australia funds the ATSB, through a charging agreement, to undertake safety investigations for incidents that occur on intra-state rail networks in South Australia. At the time of this incident, the funding agreement had expired, although the Government of South Australia is committed to working with the ATSB to draft the terms for a future agreement. While the ATSB initiated a safety investigation under the TSI Act, the Government of South Australia informed the ATSB that they considered additional investigatory effort would not provide any increased understanding of the root cause of the incident, and had decided not to fund any ongoing activities. Consequently, the ATSB has discontinued this investigation.
_____________
The information contained in this update is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence.
A six-car Metro Trains Melbourne (MTM) passenger train travelling from Flinders Street Station to Lilydale Station uncoupled shortly after leaving Croydon Station. The train consisted of two 3-car units and uncoupled at the mid-coupling. The train was travelling at about 78 km/h when the 3-car units uncoupled. The trailing car unit came to a stop under automatic emergency braking. Once the train driver noticed that the trailing car unit had uncoupled, he applied emergency braking and brought the lead unit to a stop about 300 m from the trailing car unit. There were no injuries in the incident.
What the ATSB found
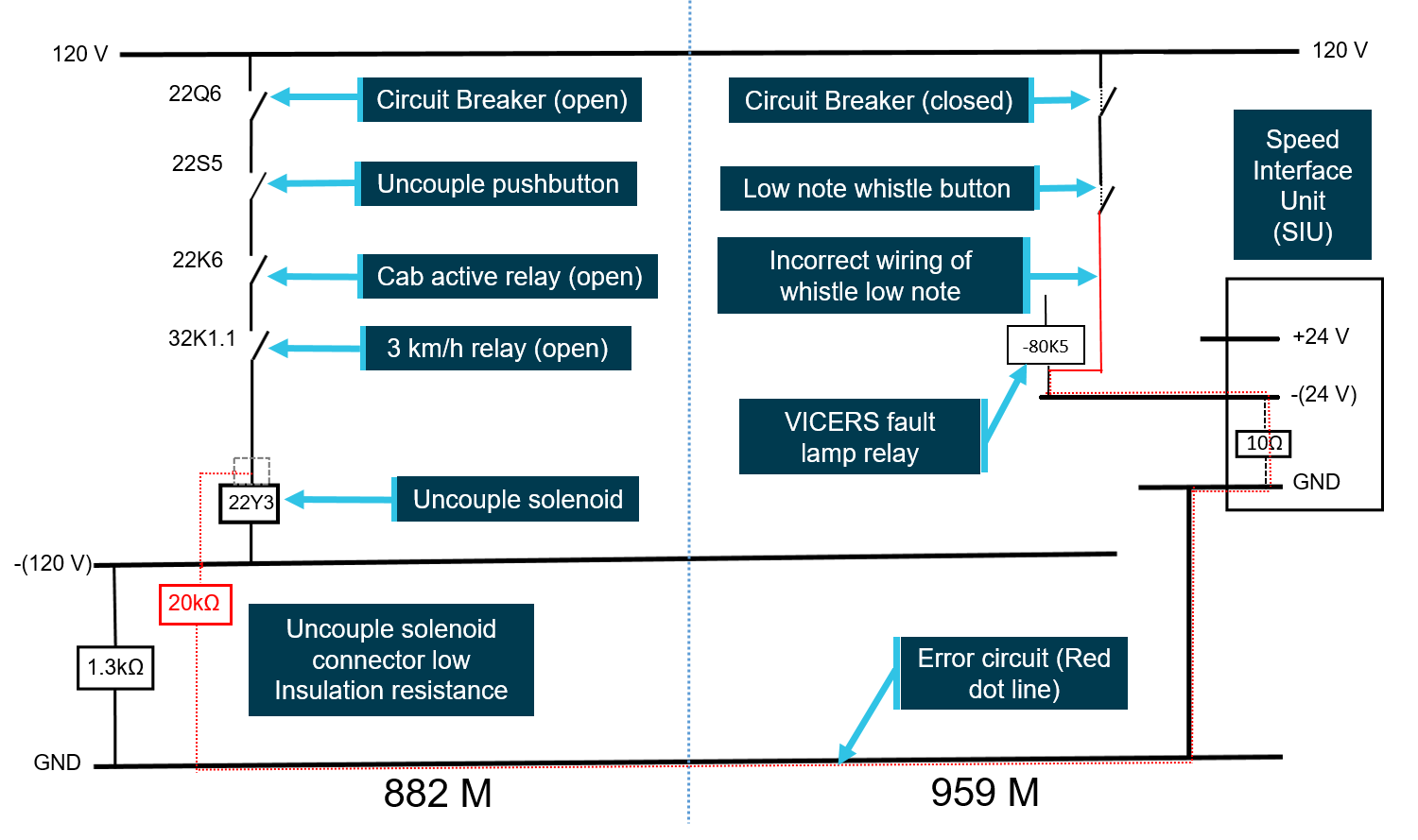
It was found that two technical faults had combined to cause the uncoupling. Inspection and testing conducted by MTM revealed that a wiring error was made during a modification to the train’s low-note whistle on the lead car of the train. Further, there was a deterioration of insulation resistance in the uncouple solenoid connector of the lead car of the trailing car unit. The low insulation resistance of the uncouple solenoid combined with the incorrect wiring of the low-note whistle resulted in an error circuit forming to energise and actuate the uncouple solenoid. This resulted in the unintended uncoupling.
What's been done as a result
The X’Trapolis fleet was inspected by MTM. Eleven of the motor cars were found to have the low-note whistles wired incorrectly and these were rectified. The low-note whistle wiring document has been updated to provide further clarity and to prevent future wiring errors with respect to this modification. In addition, maintainers involved in low-note whistle modification work have been briefed and re-trained on the modification method statements. Further, completed modification work will require self-checks and supervisor checks.
MTM advised that it has implemented a program of mandatory insulation resistance testing of the uncoupling solenoid connectors. The information from the testing will be provided to the original equipment manufacturer in order to assist with determining the root cause for the failure and take appropriate remedial action.
MTM further advised that it is reviewing the scope for improving negative to ground testing during depot based scheduled maintenance and exploring a design for a system for monitoring common negative to ground potential.
Safety message
This incident highlights the importance of ensuring that a verification program is incorporated into quality assurance systems to mitigate the risk of errors during installation or modification of electrical systems.
The occurrence
On the afternoon of 9 November 2018, two empty 3-car X’Trapolis units[1] were coupled at the Camberwell sidings in preparation for operating the 1607 Metro Trains Melbourne (MTM)[2] passenger service from Flinders Street Station to Lilydale Railway Station (Figure 1). Car 959M was designated the lead car of the train and operated as a non-revenue service from Camberwell sidings to Flinders Street Station.
Analysis of the VICERS[3] data logger indicated that at 1552, just prior to departure from Camberwell, the driver sounded the low-note whistle and there was a momentary loss of electrical signals between the leading and trailing 3-car units. At 15:52:15, the train departed from Camberwell sidings for Flinders Street Station.
On arrival at Flinders Street Station at about 1606, a driver exchange occurred. The new driver conducted the prescribed safety checks, entered the train describer number (TD 3817) and departed Flinders Street Station at about 1608. The train stopped at Southern Cross Station and Flagstaff Station before arriving at Melbourne Central Station at about 1615.
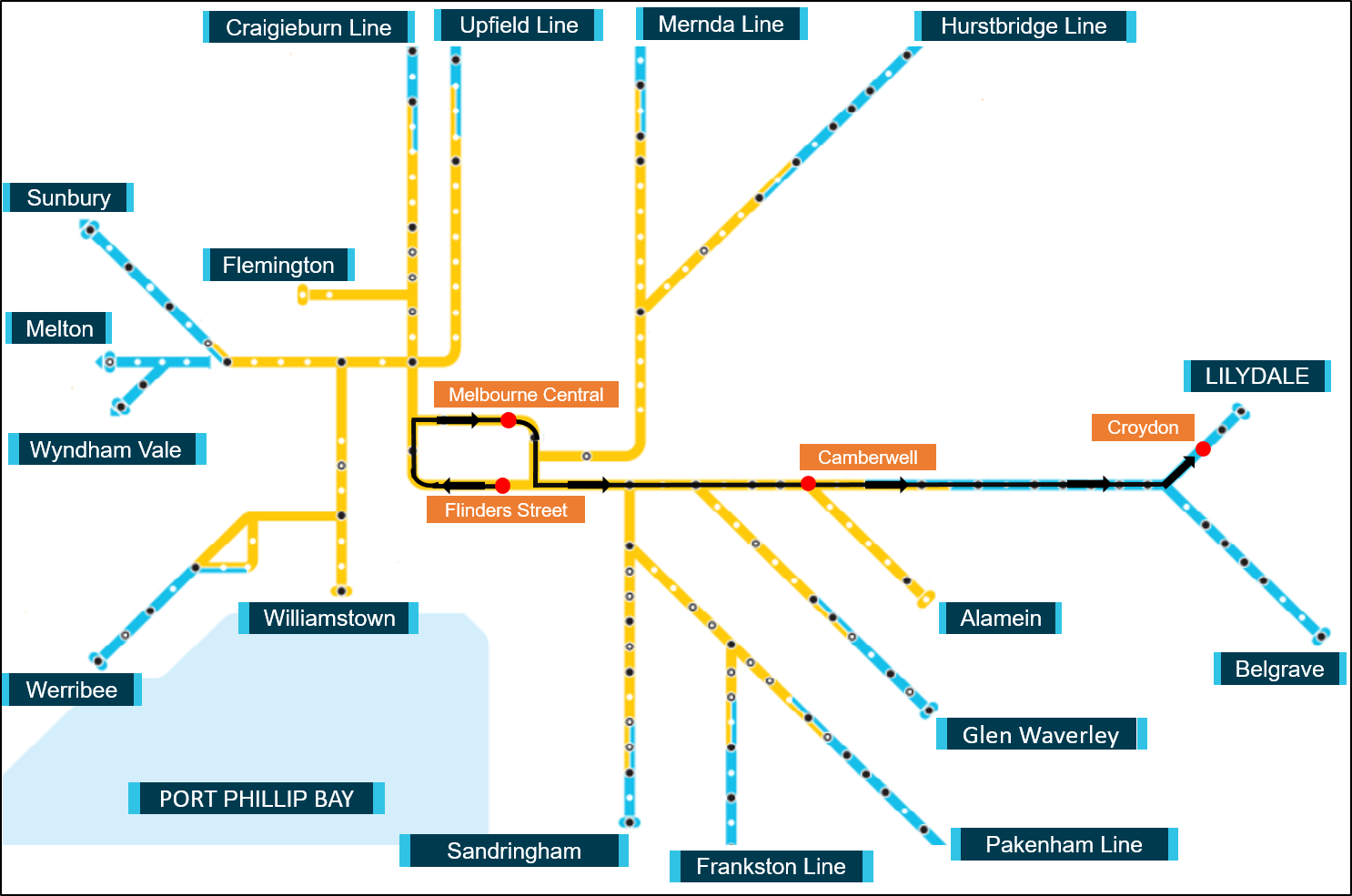
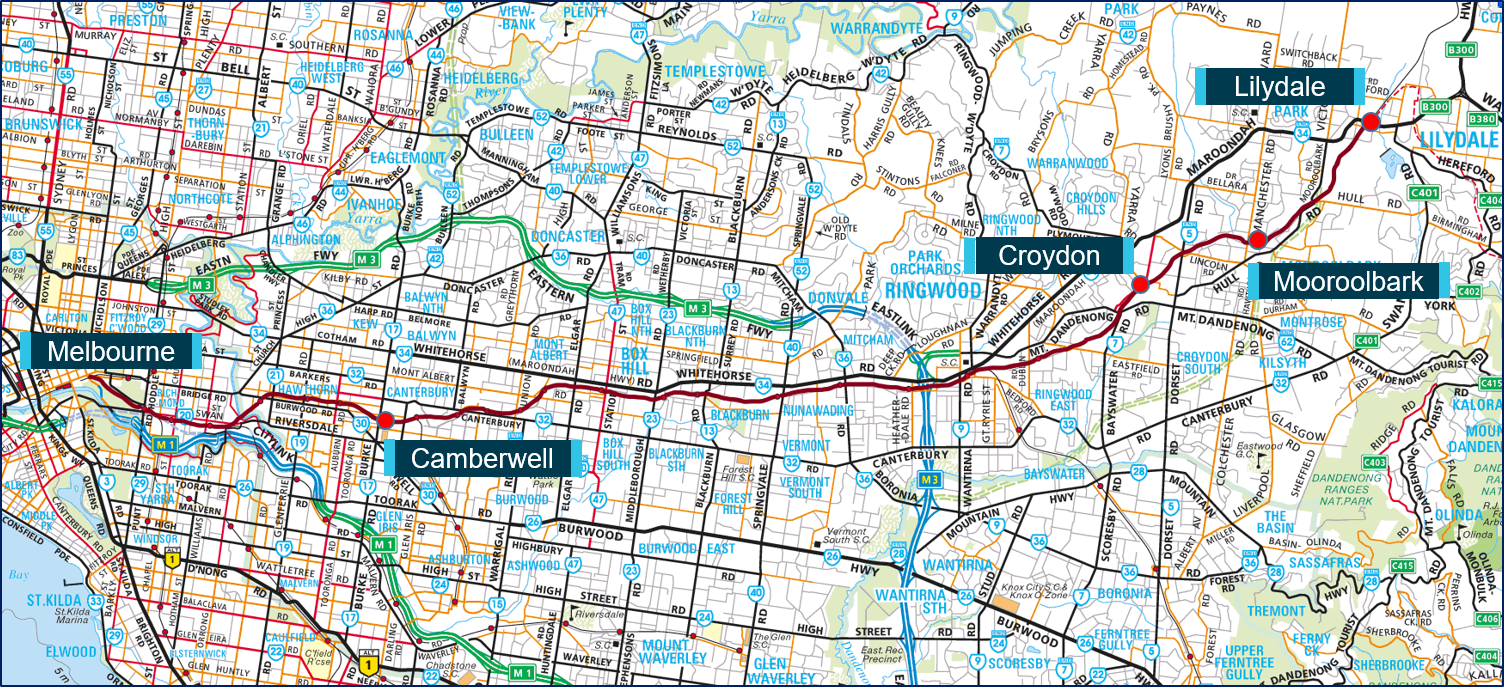
Figure 1: Melbourne train network showing train TD 3817 route on Lilydale Line
Source: Metro Trains Melbourne with annotations by Chief Investigator, Transport Safety (Vic)
The driver reported that at Melbourne Central Station, the message ‘Decoupling/Re-coupling’ appeared on the Driver’s Display Unit (DDU). He reported this to the Train Services Officer (TSO) at Metropolitan Train Control (METROL) who advised him that it could be the coupler pins not aligning in the centre coupler (coupler between the two 3-car sets). The driver reported that after a few seconds, a new message ‘PIDS[4] Inoperative’ appeared and then after a short period the normal screen was restored. He then re-entered the Train Describer number into the DDU.
Analysis of the data from the VICERS indicated an electrical disconnection lasting about 7 seconds at Melbourne Central Station. At about 1616, the electrical signal was re-connected, the emergency brake safety loop re-established and the train departed Melbourne Central Station.
The train stopped at several stations before arriving at Croydon Station at about 1656. Although the DDU did not indicate any further irregularities, the VICERS data download traces between Melbourne Central Station and Croydon Station indicated three further electrical disconnections. These electrical disconnections did not disrupt the operation of the train.
The train departed Croydon Station at about 1657, with about 150 passengers on board. After leaving Croydon Station and on the approach to Coolstore Road level crossing (about 200 m from the station) the driver sounded the low-note whistle. The train then entered a left-hand curve, about 800 m from Croydon Station. About half way through the curve, the driver looked back through the rear-view mirror and noticed that the train consist had only three cars and the trailing unit had uncoupled (Figure 2). He immediately applied emergency braking and brought the three-car set to a stop.
Figure 2: Coupled cars 960M and 882M of X’Trapolis train that uncoupled
Source: Metro Trains Melbourne annotated by Chief Investigator, Transport Safety
The VICERS data download indicated that about 30 seconds after departing Croydon Station, an emergency brake application was made on cars 882M and 881M, and the trailing 3-car set came to a stop at about 1658. The download further indicated a momentary brake application on cars 959M and 960M (the motor cars of the leading 3-car set), but this brake application was not sustained and the car set continued moving. The VICERS download indicated an emergency brake application at about 1658 and shortly after, the leading car set 959M came to a stop about 371 m from the lead car 882M of the trailing car set. The train was travelling at about 78 km/h when the 3-car sets uncoupled. The trailing car set travelled under emergency braking for about 196 m before coming to a stop.
Events after uncoupling of 3-car units
After the leading car set came to a stop, the train driver made a priority radio call to advise METROL of the uncoupling of the trailing car set. METROL despatched an empty train (under extreme caution[5]) from Lilydale Station towards Croydon Station to locate the 3-car set that had detached from the lead car set. Victoria Police, the Melbourne Fire Brigade (MFB) and the Ambulance Services arrived soon after and detrained about 150 passengers from the two detached 3-car sets.
The parting of the two 3-car units of train TD 3817 occurred about 500 m from Croydon Station. Croydon Station is on the Lilydale rail line and is located about 32 rail km from Flinders Street Station, Melbourne (Figures 1 and 3).
Figure 3: Location of Croydon on Lilydale train line
Source: Copyright Melway Publishing 2018, with annotations by the Chief Investigator, Transport Safety (Vic)
The environment and track
At the time of the incident, the weather was fine with light winds and the temperature was about 190 C.
The rail track from Croydon Station to the location of the train parting was concrete sleepered. From Croydon Station there were a number of left and right hand curves between 31.2 km and 32 km marks. The track slopes down at a slight gradient from 31.2 km to about 31.5 km and then is flat until about the 32 km mark.
Train driver
The train driver was employed by MTM for over 9 years and was qualified to drive Electrical Multiple Units (EMU). His driving performance was audited regularly by MTM driver supervisors and was last audited in July 2018. No non-conformances were recorded during these audits. Medical certification for the driver was valid and current at the time of the incident. No alcohol or drugs were detected during post-incident tests conducted on the driver.
The train
The X’Trapolis EMU is operated as a 3-car or 6-car set. The car body modules were designed and constructed in France and assembled at Alstom Australia, in Ballarat, Victoria. Each 3-car set is coupled in motor-trailer-motor configuration. They are coupled by auto-couplers between motor cars and semi-permanent couplers between the motor and the trailer cars, with rubber bellows inter-car canopy walkways.
TD 3817 was a 6-car set and consisted of 959M-1680T-960M-882M-1641T-881M passenger cars.[6] A Scharfenberg automatic coupler connected the two 3-car units of TD 3817 between 960M and 882M. A 6-car train set has the total effective capacity for 752 passengers and this train was carrying 150 passengers at the time of the uncoupling.
The motor units are 24.46 m in length and the trailer units are 22.76 m in length. Each 3-car set is 71.68 m in length and a 6-car set is 143.36 m in length. The average mass of a 6-car set is about 244 t. Each car has six doorways, located at the front, middle and rear of the cars and the nominal floor height of the car is 1185 mm above top of the rail. The EMU is capable of a maximum speed of 130 km/h.
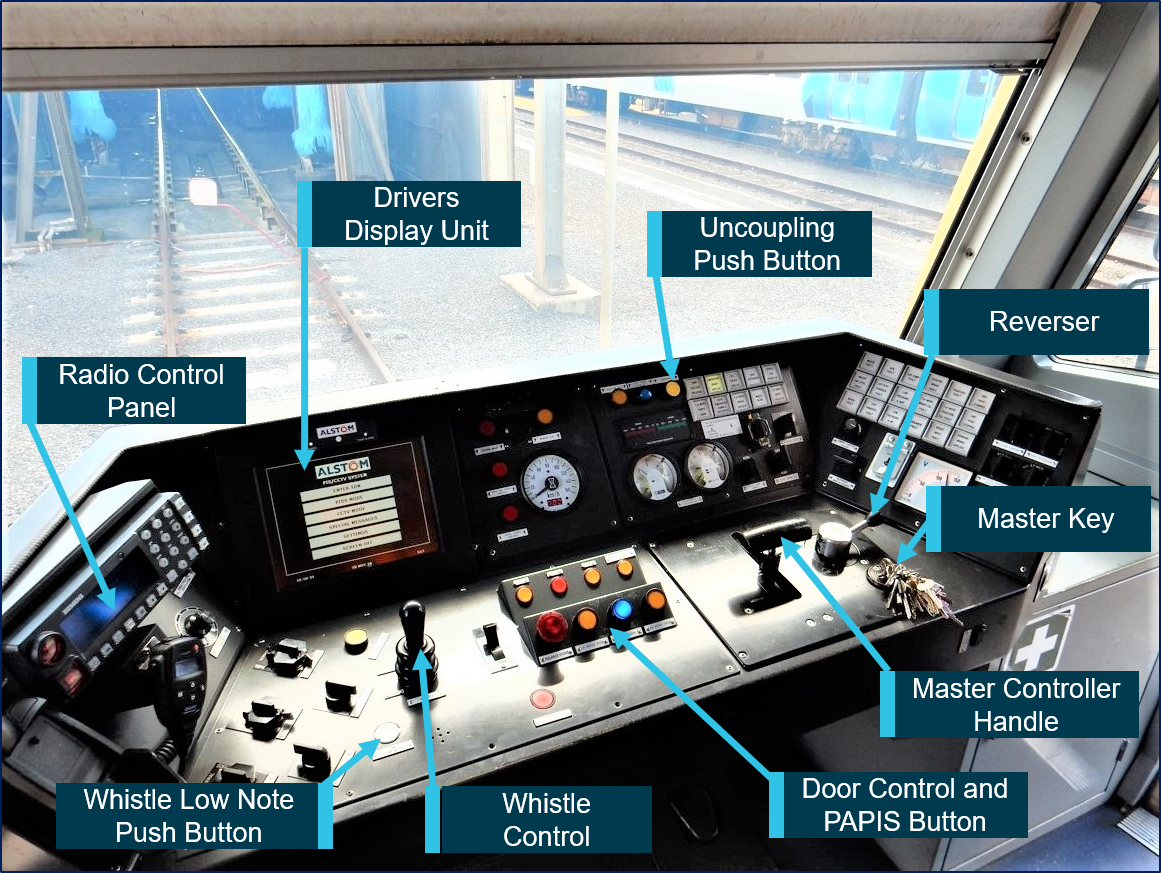
Master Controller and Operations
In order to prepare the train for operation, the driving cab must be made electrically operational by inserting and switching on the Master Key making it the cab-in-service. The driver then enters the Train Describer number into the radio control unit. The Master controller handle is moved back and forth between four positions—motor, coast, brake and emergency brake. The Reverser is a three-positon switch that can be moved to forward, neutral and reverse positions. In order to get forward traction, the Reverser must be moved to the forward position and the master controller moved from the brake to coast to the motor position. The position of the Master controller between the coast and motor positions dictates the tractive effort. The console and controls are accessible from the driving position (Figure 4).
Figure 4: Master Controller Panel
Source: Chief Investigator, Transport Safety (Vic)
Vigilance, Control and Event Recording System (VICERS)
The X'Trapolis fleet is fitted with a Vigilance Control Event Recorder System (VICERS). The vigilance component monitors task-linked activities and in the absence of any such activities provides intervention by applying the train’s brakes. It also incorporates an event recorder system, which monitors a number of on board systems including the operation of a number of driver control functions. The system records a comprehensive range of operational parameters including control equipment status, train speed, traction and braking and location.
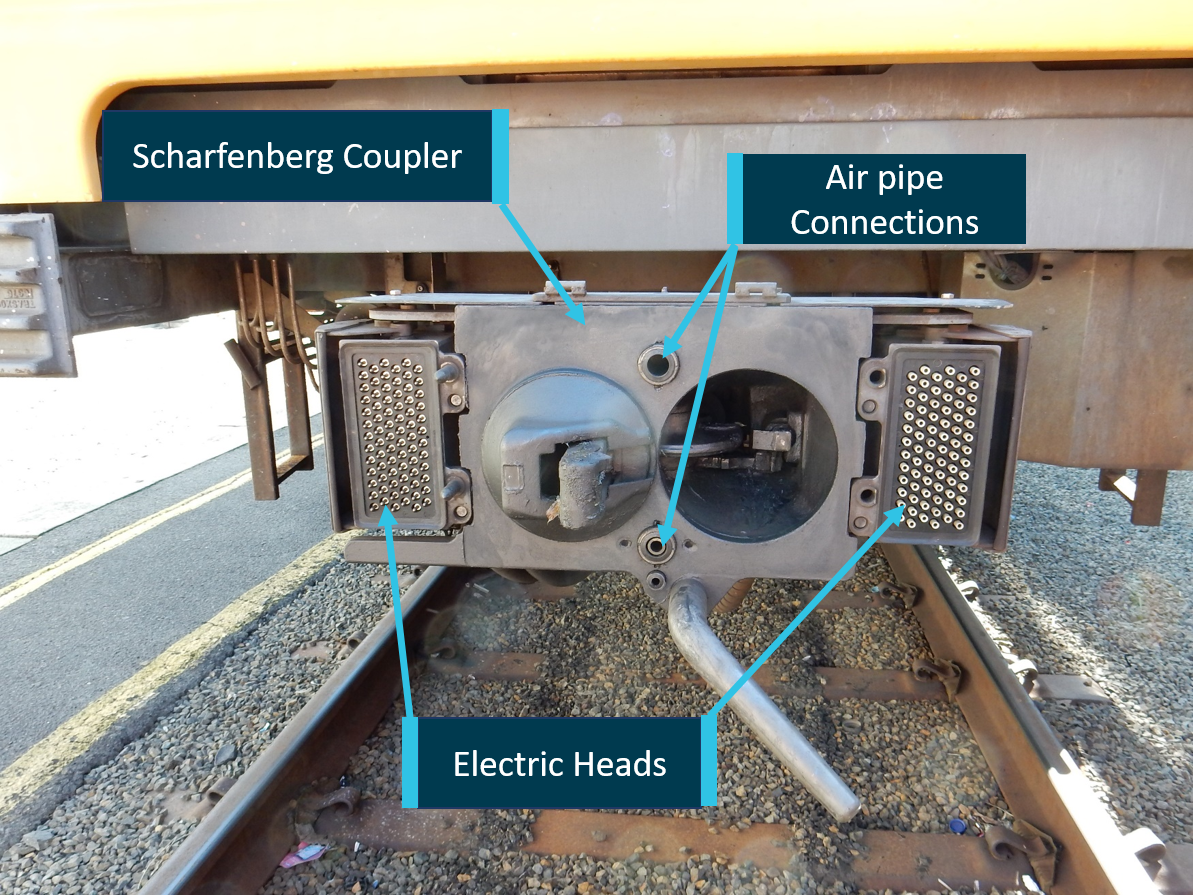
Coupling and Uncoupling of Scharfenberg Coupler
Each end of the 3-car units were equipped with an automatic Scharfenberg coupler that enabled mechanical, pneumatic and electrical coupling of two 3-car units (Figures 5 and 6).
Figure 5: Mechanical, pneumatic and electrical components of Scharfenberg coupler
Source: Chief Investigator, Transport Safety (Vic)
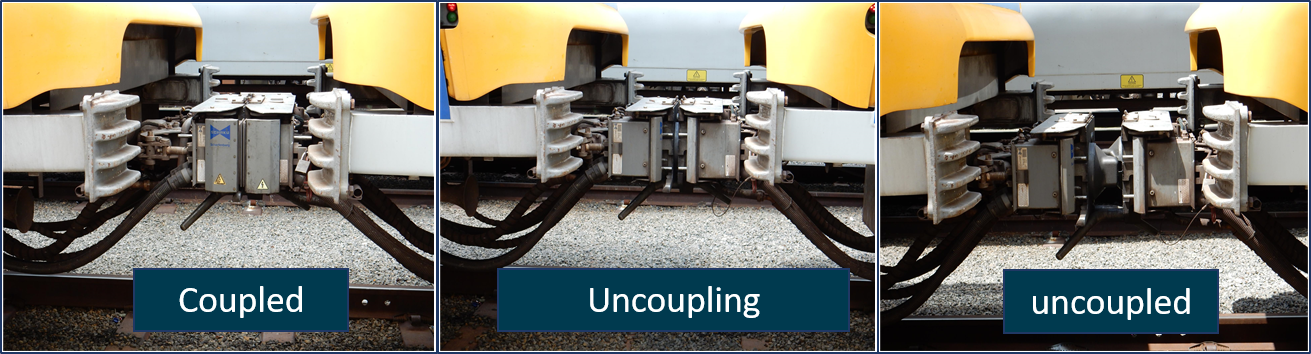
Figure 6: Scharfenberg coupler between cars shown uncoupling
Source: Chief Investigator, Transport Safety (Vic)
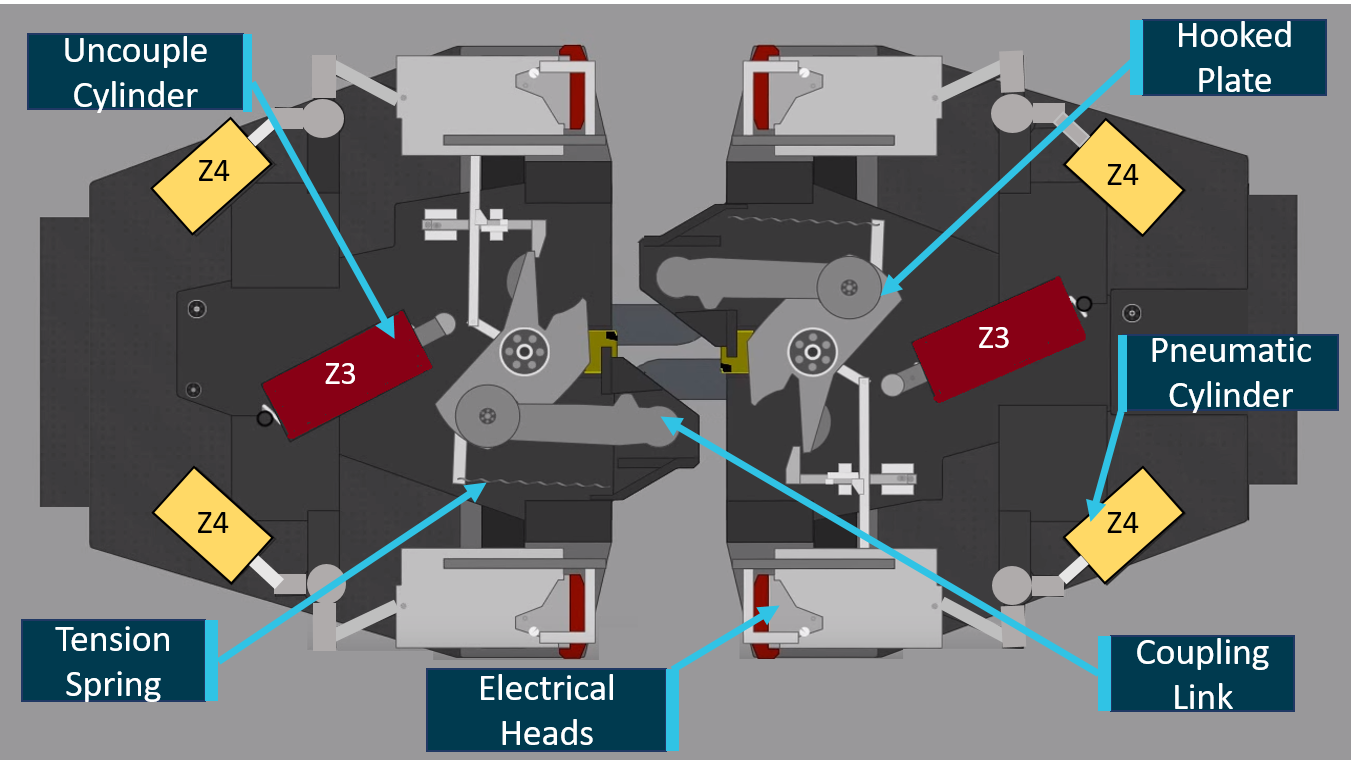
The Scharfenberg coupler has a coupler lock that consists of a rotating hooked plate, a coupling link and tension springs (Figure 7). During coupling, the coupling link of one coupler engages the hooked plate of the mating coupling and locks in the indentations on the hooked plates. The cone and funnel shape design of the coupler front plates establishes a rigid and slack-free connection. During the coupling, the electric heads and the air pipe connections engage to ensure connectivity between the two car units. The coupler has a flexible buffer assembly that allows movement of the cars when negotiating vertical and horizontal curves.
Figure 7: Illustration of uncoupled Scharfenberg coupler
Source: Voith Group, annotated by Chief Investigator, Transport Safety (Vic)
The units can be coupled or uncoupled remotely from the driver’s cab or manually from trackside. The automatic coupling process involves moving one 3-car unit against a stationary 3-car unit.
X’Trapolis electrical and pneumatic systems for uncoupling
The Melbourne metropolitan electrified rail network operates on 1,500 V direct current (DC), supplied to the train via a roof-mounted pantograph that is in contact with the overhead wire. Two power inverters (static) convert the 1500 V DC to 400 V, 3-phase or 230 V single-phase alternating current (AC) to supply the various loads on the train. The 400 V AC supply is rectified and transformed to provide 120 V DC through a battery charger system.
The 120 V DC power supply is distributed to three lines; the permanent LV line, prepared LV Line and the prepared and cab operative line, each corresponding to an operational state of the train.
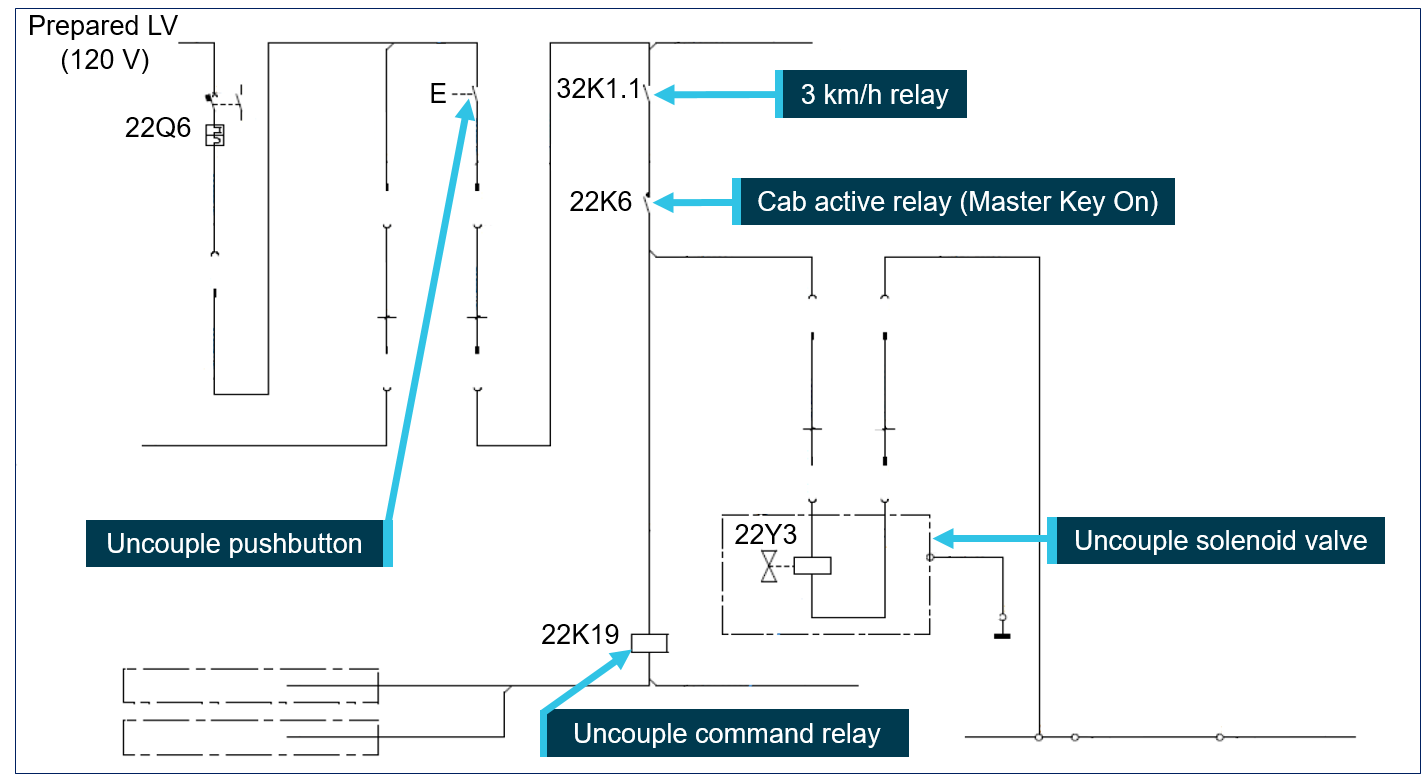
The prepared LV line supplies the uncoupling system (Figure 8). An intended uncoupling operation requires the train to be stationary and local cab active. The uncouple pushbutton (Figure 4 and 8) is pressed to energise and actuate the uncouple solenoid valve (VS). The energised uncouple solenoid valve directs supply air to the uncouple cylinders (Z3) on both couplers
Figure 8: Wiring diagram for uncoupling system
Source: Alstom Drawing AX00000263675, simplified and annotated by Chief Investigator, Transport Safety (Vic)
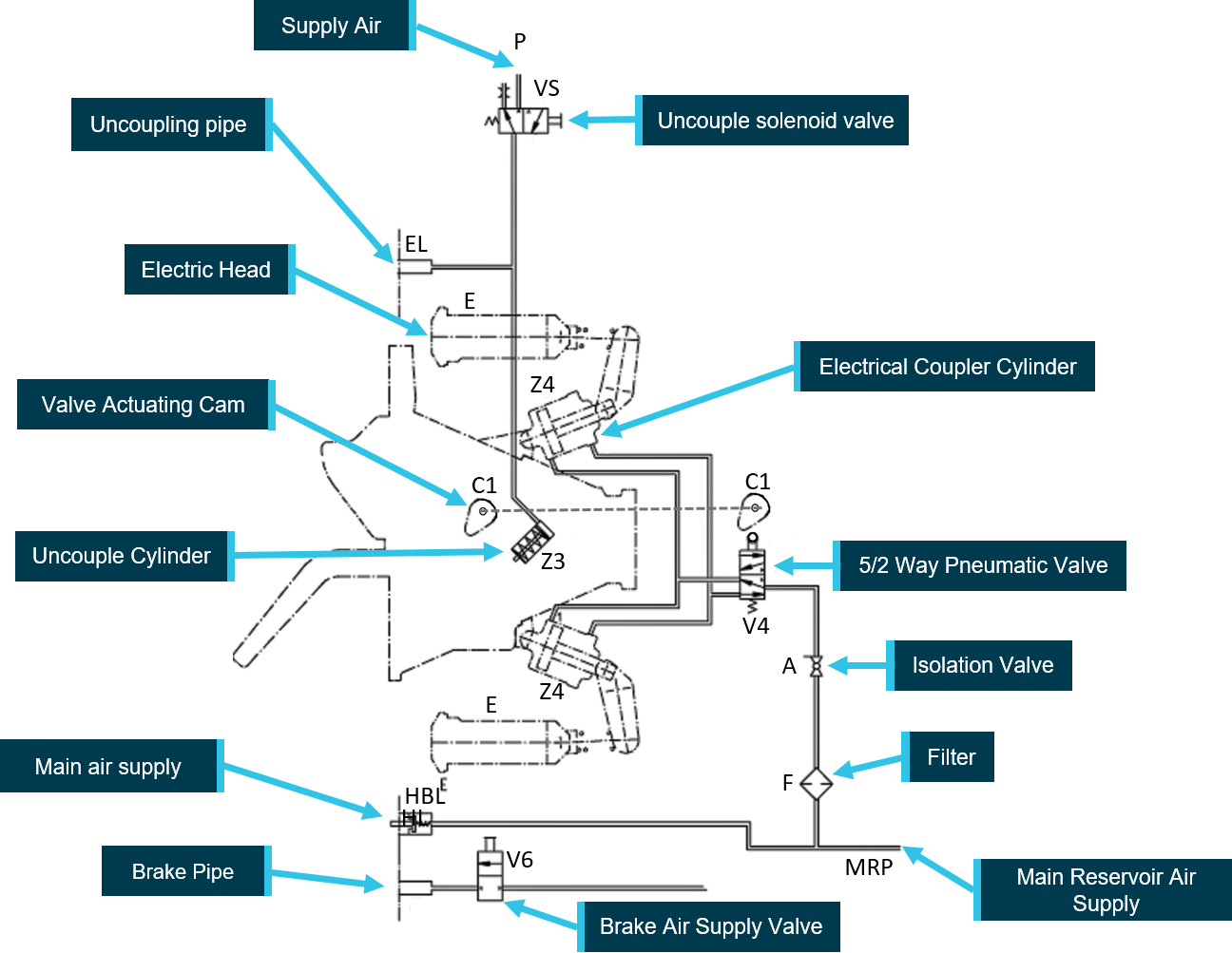
The uncouple cylinder (Z3) actuating piston rotates the hooked plates of the coupler against the force of the tension springs (Figure 7 and 9). The coupling links slip out of the indentations on the hooked plates and the couplers can then be separated. The uncouple cylinder actuating piston also rotates the cam (C1) that actuates the 5/2 way pneumatic valve (V4). Actuation of the 5/2 way pneumatic valve allows air to be directed to the pneumatic cylinders (Z4) that retract the electrical heads (E).
For the uncouple pushbutton to activate the uncouple solenoid valve, the cab has to be in-service (cab active) and the train speed has to be below 3 km/h (Figure 8). Pressing the uncouple pushbutton from the active cab energises the uncouple command relay which deactivates the coupling detection contactor relays. These in turn disconnect the traction and braking signals across the coupler electrical heads prior to uncoupling.
Figure 9: Pneumatic schematic for uncoupling of Scharfenberg coupler
Source: Scharfenbergkupplung GmbH & Co. (annotated by Chief Investigator, Transport Safety (Vic)
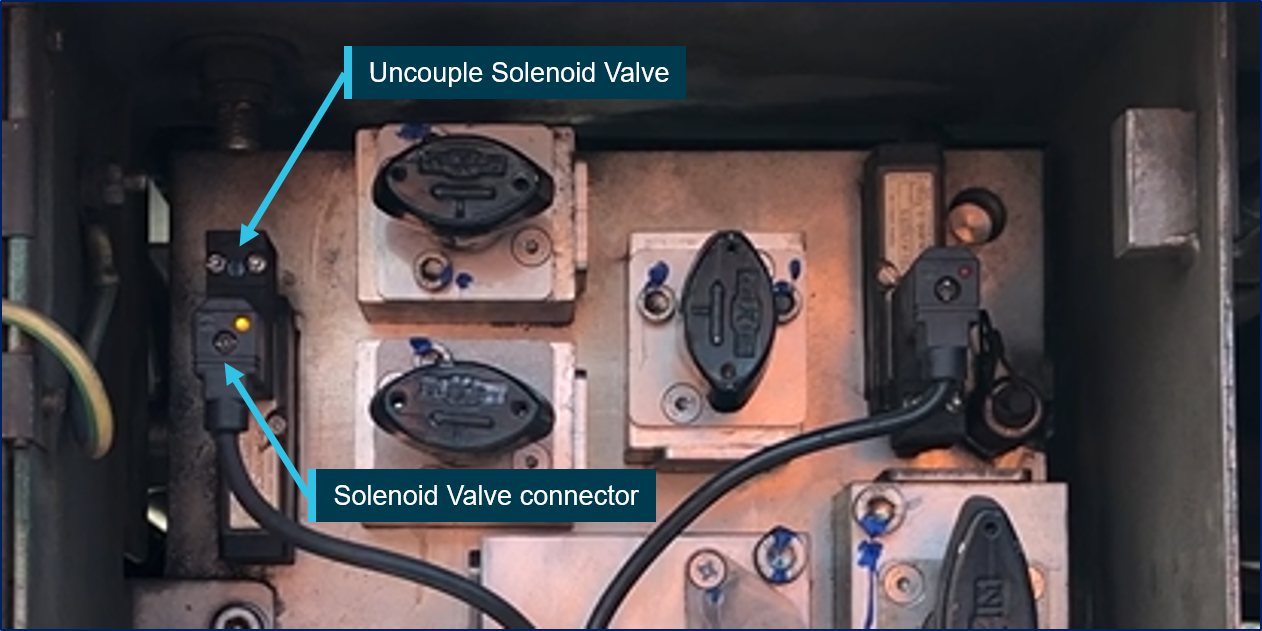
Metro Trains Melbourne (MTM) conducted multiple dynamic tests of the train in an attempt to replicate the fault, without success. The Scharfenberg coupler and associated mechanical and pneumatic components were inspected and no fault was identified. The Scharfenberg coupler can be manually uncoupled by actuating the automatic coupler manual release handle. Examination of the manual release mechanism did not indicate that it had been used. It was concluded that the most likely initiator for an uncoupling event was via the activation of the uncouple solenoid (22Y3).
Insulation resistance testing of uncouple solenoid
Uncouple solenoid connectors of the coupled motor cars (959M and 882M) were tested for insulation resistance (IR)[7] to ground (vehicle body/frame). The IR value for the uncoupling solenoid connector of car 882M was found to be 20 kΩ, when the typical IR is required to be over 100 MΩ. However, the low IR would not result in unintentional energising of the uncoupling solenoid valve without a power source to the solenoid.
Source: Chief Investigator, Transport Safety (Vic)
Further, testing indicated that both the uncoupling solenoid and the uncouple relay picked-up and actuated at a minimum voltage of about 50 V, which was not unusual.
Insulation resistance testing carried out on all the uncoupling solenoid connectors of the X’Trapolis fleet revealed that 15 uncoupling solenoid connectors measured low insulation resistance. In addition, 19 trip re-set connectors[8] and 15 trip raise connectors[9] also indicated low insulation resistance.
Low-note whistle wiring error
MTM conducted test runs of the 3-car set with car 959M as the lead cab-active car. Normally, zero voltage should exist between a power supply common negative and ground (earth/vehicle body). However, during the tests on car 959M, an oscilloscope measured an intermittent 120 V between the common 120 V negative and ground. Examination of the VICERS download trace indicated that the voltage spike coincided with the use of the low-note whistle (Figure 4). Further, static testing confirmed that activation of the low-note whistle resulted in the application of 120 V supply between common negative to ground.
Examination of the low-note whistle wiring indicated that a relay on car 959M was installed incorrectly and a cable was connected to a wrong terminal. This error resulted in the low-note whistle’s 120 V supply being connected to the negative (24 V) of the Speed Interface Unit (SIU), which is an interface between the car’s speed detector and the VICERS unit (Figure 11).
MTM’s investigation of the wiring error revealed that although the electrical circuit diagrams were accurate, the technician carrying out the modification had made a cable connection error. Inspection of the X’Trapolis fleet indicated that 11 low-note whistles were wired incorrectly by the same technician. A function test would not reveal the wiring error, as pushing the low-note whistle button would complete the circuit to actuate the low-note whistle. In this instance, an assurance program involving a secondary and independent check of the wiring modification may have been the only means of detecting this error.
Figure 11: Electrical schematic showing incorrect wiring of low-note whistle
Source: Chief Investigator, Transport Safety (Vic)
Speed Interface Unit (SIU) design
The SIU converts the speed signal (0-20 mA) to a pulse train output to the VICERS unit. It provides isolation between the train circuits and VICERS unit. The negative of the SIU was connected to ground providing an electrical ground for the 24V system and the circuit path to actuate the uncoupling solenoid valve.
The safety loop circuit and uncoupling
The safety loop is a control circuit passing through each carriage within the trainset and is closed during operation under normal conditions. When the safety loop is opened due to an abnormal operating condition, the emergency brake solenoid valve is de-energised causing a maximum brake application.
In this instance, the uncoupling function was activated through an electrical circuit that was created by a wiring error in car 959M and the low IR of the uncouple solenoid of car 882M. This error resulted in the cab active relay, push button and the 3 km/h relay interlock devices being bypassed and allowing the unintended activation of the uncoupling circuit. The safety loop circuit on the lead car unit maintained the closed safety loop, hence emergency braking was not applied and it continued its journey until the driver realised that the trailing car unit had uncoupled, and brought the lead 3-car unit to a stop. As there were no active cabs in the trailing 3-car unit, the safety loop was opened, de-energising the emergency brake solenoid valves, resulting in the application of the emergency brakes on the trailing car unit bringing it to a stop.
The following findings are made with respect to the parting of a passenger train TD 3817 at Croydon, Victoria on 9 November 2018. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
A wiring error was made during a modification to the trains low-note whistle on car 959M.
The wiring error was not detected by Metro Train Melbourne’s verification program. [Safety Issue]
There was a deterioration of insulation resistance in the uncouple solenoid connector of car 882M.
The connection between the negative and ground via the Speed Interface Unit provided a path that created the circuit to actuate the uncoupling solenoid valve.
Safety issues and actions
The safety issues identified during this investigation are listed in the Findings and Safety issues and actions sections of this report. The Australian Transport Safety Bureau (ATSB) expects that all safety issues identified by the investigation should be addressed by the relevant organisation(s). In addressing those issues, the ATSB prefers to encourage relevant organisation(s) to proactively initiate safety action, rather than to issue formal safety recommendations or safety advisory notices.
Depending on the level of risk of the safety issue, the extent of corrective action taken by the relevant organisation, or the desirability of directing a broad safety message to the rail industry, the ATSB may issue safety recommendations or safety advisory notices as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Safety issue description: The wiring error was not detected by Metro Train Melbourne’s verification program.
Additional safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
MTM advised that it has implemented a program of mandatory insulation resistance testing of the uncoupling solenoid connectors. The information from the testing will be provided to the original equipment manufacturer in order to assist with determining the root cause for the failure and take appropriate remedial action.
MTM further advised that it is reviewing the scope for improving negative to ground testing during depot based scheduled maintenance and exploring a design for a system for monitoring common negative to ground potential.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Metro Trains Melbourne Pty Ltd.
SNC-Lavallin Rail & Transit Pty Ltd.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
Submissions were received from Metro Trains Melbourne Pty Ltd and the Office of the National Rail Safety Regulator. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Occurrence summary
Investigation number
RO-2018-019
Occurrence date
09/11/2018
Location
Croydon, 32 km from Flinders Street Station, Melbourne
On the morning of 12 December 2017, train TM78A operated by Pacific National (PN) was unloading coal at the Kooragang Coal Terminal (KCT).[1] At the time, a maintenance worker was conducting a roll-by inspection[2] after the train moved through the unloading bay. The worker visually identified a crack on the lead bogie of wagon NHBH 42954J, this was the 35th wagon in the direction of travel. The train was stopped and the wagon was removed to allow for inspection.
The train operated between KCT to Clarence on the 10 December, before returning to Newcastle Infrastructure Coal Group (NCIG). On 11 December the train operated empty from NCIG to Tahmoor before returning loaded to KCT (Figure 1). During these journeys, the trackside condition based monitoring equipment recorded elevated bearing temperatures on axle 4 of wagon NHBH 42954J, as well as an increased angle of attack (AoA).[3] These recordings did not generate an alert at the time of passing the various detection sites and the train continued to operate until the fractured bogie was visually identified by the maintenance worker.
Figure 1: Incident location
Source: Geoscience Australia, annotated by OTSI
Safety analysis
A PN maintenance worker was located inside the unloading bay at NCIG on 11 December, this worker’s primary function was to observe the wagon doors close. It was not clear if this worker was deemed to additionally be conducting a roll-by inspection. The worker was positioned on the opposite side (to the bogie fracture) of wagon NHBH 42954J and did not report any defects. The bogie was probably visibly fractured at the time based on the increased AoA.
The roll-by inspection completed on 12 December was completed by a single worker, with the worker positioned on the same side as the fractured bogie and the defect was identified. The axle showed signs of rotating forward and up relative to the frame as the fracture opened under the weight of the wagon (Figure 2). As the fracture opened the effective axle spacing changed, lengthening the wheelbase on the side of the cracked frame. PN maintenance standards permit roll-by inspections being completed by a single worker. The defect was detected during a roll-by inspection, however could have been missed if the worker was positioned on the opposite side.
Figure 2: Fractured bogie frame NDCA 1199
Source: Pacific National, annotated by OTSI
The train underwent unit train maintenance (UTM) and a full train examination (FX) on 8 December 2017 at the PN Lithgow maintenance depot. During this inspection, there were no defects reported in relation to bogie NDCA 1199. Prior to identifying the fractured bogie, the train was compliant with the PN technical maintenance plan.
Bogie NDCA 1199 underwent schedule maintenance in July 2015. The bogie frame was subjected to non-destructive testing (NDT) consisting of magnetic particle inspection (MPI) and tested in accordance with PN procedure WMM 11-08_06 One Piece Bogie Inspection. There were no defects detected at the time of testing and the location of the fracture was at the extremity of the area subjected to NDT. Evidence of remnant MPI marker paint was present on the outboard plate, but there was no apparent marker paint on the inboard plate at the region of the fracture.
Fatigue cracking has historically been identified in the NDCA bogies at the welded junction joining the vertical plate and bottom plate section due to the design and manufacturing process used to build this class of bogie at the time. The NDCA bogie is comprised of welded steel plates to form a single piece box section bogie frame.
Prior to this occurrence, a derailment occurred in 2011 at Leigh Creek, South Australia. This derailment was reportedly the result of a fractured NDCA bogie. The bogie fracture increased the wheelbase on the side of the fractures, likely placing additional loading on the axle bearing as the axle tracked abnormally, this led to the bearing overheating and failing.
Post-occurrence inspection of the bogie NDCA1199 showed a fatigue crack most likely initiated at the toe of the weld on the inboard corner of the bogie side frame before progressing across the lower plate and inboard vertical plate (Figure 3). The inboard fracture face was smooth and displayed beach marks (slow progression), while the outboard face was jagged in appearance indicative of rapid progression.
Figure 3: NDCA 1199 fracture analysis
The image shows the bogie fracture from the underside of the bogie to show the three fracture faces. Source: OTSI
The trackside condition based monitoring equipment recorded increased bearing temperatures from 10 December after departing Clarence, as well as an increased AoA on 11 December. Analysis of this recorded data following the event, indicates that the change was likely the result of the bogie frame fracture progressing. As the fracture progressed, the wheelbase (spacing between the axles) increased between axle 3 and 4, affecting the AoA and placing additional loading on the bearing.
At the time of passing through the various trackside condition based monitoring sites, the recorded bearing temperatures did not trigger an automatic alarm to notify the rail infrastructure manager (RIM) or PN. The track side detection equipment utilises algorithms to determine critical levels[4] that trigger automatic alarms to advise the RIM or operator. In relation to bearing temperature, only warm or hot bearing alarms will trigger an automatic alarm that requires immediate attention. Low bearing temperature alerts and AoA are recorded by the system but do not generate automatic alarms.
The wagon loading for the previous journeys was reviewed and indicated, that between 10 December and 12 December, the wagon operated within the allowable 100 t gross limit. The operation of the train and wagon loading does not appear to have contributed to this occurrence.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
A fatigue crack likely originated at the toe of a weld on the inboard lower plate of the bogie frame that was not identified during the preventative maintenance activities, prior to the structural failure of the frame. The fatigue cracking most likely progressed across the full face of the lower plate and inboard side plate before rapidly progressing across the outboard side plate.
The NDCA bogie design has a history of fatigue cracking which increases the risk of derailment if the cracking is not identified. Pacific National had processes in places to identify fatigue cracking but this crack was likely not detected due to the location of the defect.
Trackside condition based monitoring equipment recorded elevated bearing temperature and increased angle of attack in the days prior to the fractured bogie being identified. This was likely a result of the bogie fracture progressing. The recorded temperature did not trigger an automatic alert to advise the rail infrastructure manager or operator.
Safety action
The ATSB has been advised of the following safety action in response to this occurrence.
Pacific National
As a result of this occurrence, Pacific National has advised the ATSB that they have taken the following safety actions:
Bogie Survey
Pacific National undertook a visual inspection of all NDCA bogie frames for evidence of cracking as directed by Office of the National Rail Safety Regulator (ONRSR).
Revised Maintenance Standard
Pacific National revised maintenance standard WMM 11-08_06 One Piece Bogie Inspection to increase the area subjected to NDT testing during schedule overhauls. The entire side frame is now tested on the inboard and outboard plates as well as the underside of the bogie frame through the horn cheek area.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 22 April 2017, Qube Logistics (Qube) grain train 8960, travelling from Bogan Gate to Inner Harbour, Port Kembla, New South Wales, ranaway as it descended the Illawarra Mountain between Dombarton and Unanderra. After passing Dombarton, the driver realised he had lost control of the train. At 1248, the driver contacted the ARTC network controller who, in conjunction with Sydney Trains’ train controller, cleared a pathway for 8960. The maximum allowable speed for the Dombarton to Unanderra section was 30 km/h; however, the train reached a maximum speed of 107 km/h. At 1255, the train stopped, assisted by a shallower gradient near Unanderra station. There were no injuries or damage because of the incident.
What the ATSB found
The ATSB’s investigation found that as train 8960 was operated down the Illawarra Mountain, the train management actions by the driver did not conform to train handling procedures. After passing Summit Tank, the driver made ten brake applications and in doing so did not allow the train’s pneumatic brake system to fully recharge. This resulted in a loss of necessary braking capability to be able to control the train’s speed on the steep continuous descent. The incident was further compounded when the driver’s actions caused the locomotive’s dynamic braking system to be rendered inoperative, further reducing control of the train.
The braking system was operating within specification and were loaded below the maximum allowable payload. However, the train was loaded by approximately 10% more than that recorded on the train’s consist record. It is probable that the additional mass placed an extra load on the braking system and affected the handling characteristics of the train.
After the incident, the train controller in Sydney directed the driver of train 8690 to move the train from the rail network to Inner Harbour Terminal without any formal inspection following the runaway event. The Pacific National yard train controller in Inner Harbour did not alert ground personnel of the emergency event or of a runaway train being directed into their terminal.
What's been done as a result
Immediately following the incident, Qube withdrew the QBX locomotives and CGSY wagons from this route pending testing and inspections. They have since been cleared to return to operate on this route. Qube also changed the requirements for competency assessment on the Moss Vale to Unanderra section, from a single initial assessment to every six months. If a train driver has not been rostered over the corridor within six months he or she must be reassessed on this route. Qube also implemented other more stringent requirements for the training of drivers and weekly auditing of train operations between Moss Vale and Inner Harbour.
A review between the various rail infrastructure managers was conducted regarding the plans and procedures enacted in emergency events, and the decision-making process to move trains from the rail network to Inner Harbour.
Safety message
In order to minimise the risk of runaway events, freight operators should ensure that train drivers receive regular training and competency assessment for steep continuous gradient routes. The standards that apply to these routes should ensure that the locomotive and wagon braking ratios are suitable for the terrain the train will encounter on its route. Contingency plans and procedures to accommodate runaway trains in this area should be continually reviewed and tested by rail infrastructure managers.
Safety analysis
The investigation determined that the runaway event between Dombarton and Unanderra was the result of the train management actions made by the driver of train 8960. Despite concerns raised by train crew and another driver about the effectiveness of the train’s braking system, it was found to be within the specified standards.
It also analysed train management, braking performance, train loading, and risk management by the train operator and rail infrastructure managers.
Train management
Train management is a critical aspect of driving a train, especially loaded trains on a route that includes a long steep descent. Besides an understanding of the train performance itself, drivers need to have route knowledge over each rail section they travel over. Some aspects of route knowledge include gradients, train behaviour, location of signals, location of speed boards, brake release points and any changes to train operating conditions.
Drivers are trained and assessed in the operation of each locomotive type. This training consists of classroom instruction, in-field instruction and operation of the light engine working. The driver was assessed as competent in the operation of QBX locomotives on 3 September 2016.
The driver of 8960 had driven this route 31 times previously since the start of the year. The driver had also operated a further 20 different grain train configurations on this same route. The second person had also previously accompanied this driver and other drivers on this route. He said that he had done the trip between 15 to 20 times since 1 January 2017.
Neither crew member had previously experienced a runaway train incident. During interview, the driver said ‘you have to give that mountain a lot of respect’. Both crew members stated they understood the risks and were not complacent about the task of operating a loaded train down the Illawarra Mountain.
Qube restricted the speed of its freight services down the Illawarra Mountain to a maximum of 30 km/h. It stated in a work instruction[9] that ‘the 65 km/h and 45 km/h speed boards between Mount Murray and Dombarton must be disregarded. The Sydney Trains speed board approaching Unanderra must also be disregarded. Train speed must not exceed 30 km/h’. Specific instructions and driving techniques were also detailed in this work instruction. This instruction states that ‘if the brake pipe pressure reduction needs to exceed 100 kPa in order to control the speed then you must:
stop the train and apply the locomotives’ independent brakes
apply sufficient handbrakes if required, before recharging the train brake
fully recharge the train’s air brake system before releasing the independent brake.
In this case, the driver did not get the chance to follow this instruction as he only became aware there was a problem after the train had started running away. By this time, the train was travelling at 46 km/h and its speed was increasing. The window of opportunity to take action by completely stopping the train and applying the handbrakes on the wagons had passed.
The critical sequence of train management actions occurred after Summit Tank. The driver made ten air brake applications, which did not allow a full recharge of the train’s air brake system. This resulted in a loss of necessary braking capability to control the train’s speed on the steep descent.
When the driver applied the independent brake, at 12:46:41, it also deactivated the dynamic brake via a power knockout switch. When, ten seconds later, the driver applied the automatic brake controller to the full emergency this did not increase the braking effort as, by this time, the train air braking system was already fully applied. At this stage there was nothing further the train crew could do to reduce the speed of the train.
The driver understood that when he applied the independent brake the locomotive’s dynamic braking system would become inoperative. He stated that ‘it is the golden rule that you never put it into emergency on this mountain.’ When questioned at interview why he did so, he said that he panicked.
A few weeks after the incident, on 9 June 2017, an operational test was performed of the braking capabilities of a similar train between Moss Vale and Inner Harbour. This test was done with a similarly configured train—40 loaded CGSY wagons hauled by two QBX locomotives. However, this train was 3179 t, compared to 3680 t on the runaway train. There was no information provided in the test report regarding the condition of the brake slack adjustors and other braking components on the test train on 9 June 2017.
This test assessed the effectiveness of the current work instruction for the operation of freight services on this route. A representative of The Instruction Company, a training organisation responsible for the production of the Qube work instructions, was present and supervised the actions of the train crew. The train was operated according to the Qube work instruction. The train completed the journey without issue over the test route.
Brake performance
The locomotives, wagons and wagon brake system components were examined and tested a number of times both before and following the incident. While a number of minor faults were identified, overall, the train braking system complied with standards. Some of these checks and examinations are discussed below.
The train had undergone a number of inspections on its braking system before the incident.
A qualified train examiner inspected the train at Bogan Gate the day before the incident.
The train crew at Bogan Gate inspected the train after it was loaded and operated the train to Goobang Junction.
Another train crew operated this train between Goobang Junction and Goulburn without problem.
A qualified train examiner inspected the train at the Goulburn depot on the morning of departure without problem.
The driver tested the brake pipe continuity in the Goulburn depot.
The train crew conducted a roll by inspection as the train departed Goulburn.
The train crew conducted a running brake test between Goulburn and Mt Murray.
The train crew conducted a performance test of the train’s air brakes just past Summit Tank.
No issues or concerns were raised about the braking performance of 8960 on the day of the incident or the day before the incident when it was operated from Bogan Gate to Goulburn. The train examiners certificates, issued at Bogan Gate and Goulburn, indicated that the examined wagons were within specification.
Following the incident, the train was inspected a number of times. The summary of these tests are described below.
The second person conducted a visual inspection immediately after the incident. A wagon with an extended brake piston travel, and worn brake shoes were noted (these were within the allowable metrics). The end of train marker was also confirmed as being in place.
The Office of Transport Safety Investigations (OTSI) inspected the train approximately four hours after the incident. The brakes were still hot. No problems were identified with the exception of two wagons, which had worn brake blocks and excessive piston travel. There was no evidence of overheated brakes or wear.
On the day after the incident, 23 April 2017, an independent brake engineer tested the brake retention time, brake pipe leakage rate and brake pipe continuity. All were within specification.[10]
As well as testing the train’s brakes, the brake cylinder piston travel lengths were measured on all 40 CGSY wagons. It found that seven piston lengths exceeded the Asset Standard Authority (ASA) criteria relating to piston travel. Qube stated in their report that as the train had been manually regulated the piston travel was not considered a contributing issue.
On 1 May 2017, a single car air test (SCAT) was carried out on three randomly chosen wagons: CGSY 4502, CGSY 4507 and CGSY 4510. This test was conducted by an independent contractor. The tests found that the slack adjusters were ineffective. This can cause irregular braking forces if the piston lengths increase outside tolerances and they fail to take up or let out the slack. The issue with the slack adjusters was known to the operator and ‘due to their design have never been effective.’[11] The slack adjusters have since been re-engineered but at the time they were manually inspected and regulated prior to every train journey between Goulburn and Unanderra.
On 4 May 2017, the train was inspected by an independent railway bogie and braking engineer. The inspection found that apart from the known problem with the slack adjusters there were no other braking issues that may have affected the performance of the train. It found that the slack adjuster operation would not have contributed to the incident as adequate mitigation strategies had been put in place by CFCL Australia (CFCLA) and Qube.[12]
On 18 May 2017, an independent contractor measured the actual mass of a CGSY wagon. The total tare mass of a wagon (CGSY 4502V) was found to be 23.096 t. At this time, the Net Brake Ratio was calculated.[13] The ASA standard stated that for composite brake blocks a fully loaded wagon should have a net brake ratio of 13 per cent minimum. The net brake ratio calculated for this wagon complied with ASA standards.[14]
On 23 May 2017, a brake control valve from CGSY 4502 was tested by an independent contractor to determine its operational suitability. The test found that the valve was able to make repeatable minimum and normal brake applications and hold applied pressure for 15 minutes. It was considered satisfactory for normal use.[15]
On 9 June 2017, a simulated braking performance test was conducted at Goulburn Workshops. This test was conducted by an independent brake engineer, an independent driver trainer, and an independent wagon maintenance expert. Other staff from Qube and CFCLA assisted. The test involved two QBX locomotives (QBX 4 and QBX 5) with 42 loaded CGSY wagons. Pressure gauges were fitted to the brake cylinder and auxiliary reservoir on three test wagons. A test gauge was also fitted to the brake pipe of the 42nd wagon. The purpose of the test was to simulate the brake applications and release made before the runaway to assess the train braking performance. The result was that the train braking system performed satisfactorily. It also showed that the brake applications made by the driver on the day of the incident may have been ‘less than optimal to ensure full recharge of the brake system’.
The investigation noted that there were anecdotal reports from drivers that train 8960 did not handle consistently. The braking performance of the train was criticised by the train crew during the interview. The driver said ‘normally it is not a very good braking train. Most of the other trains you take down the hill when you use balanced braking they go down nice and sweet. This one, it doesn’t do anything the same on each particular day it is always different. It is a lot different actually.’
The second person was also critical of the braking performance of the train. He said ‘I have been down there (Illawarra Mountain), with that train, same wagons, a different driver, I’ve had to wind ten handbrakes on it, we’ve pulled it up, it hadn’t stopped, we wound five (handbrakes) on and it didn’t make much difference. So when we did pull up eventually the second time, I went and put another five on.’
Another driver from Qube came forward and was interviewed. This experienced driver said that this train did not brake consistently. ‘One time I can’t fault it; next time I’m flat out stopping it.’
Despite the criticism of the train braking performance by the train crew and another driver, the testing found that the train’s braking system was operating and adjusted to within the specified standards current at the time of the incident.
Since the runaway incident, the ASA has modified the braking ratios for bulk type commodity wagons across the rail network. This change was not made as a result of this incident but, rather, due to the introduction of new coal hopper wagons, and testing that identified brake performance deficiencies.
At the time of the incident, the net brake ratio was specified as a minimum of 13 per cent for high friction composite brakes on freight vehicles. From 1 January 2018 this specification was raised to 16 per cent for bulk commodities. The minimum level of 13per cent is still permitted, provided the brake performance can be confirmed by a stopping distance test.
The standard states: ‘From 1 January 2018 for all new bulk commodity type wagons, such as grain hopper, coal hopper, ore hopper, and wagons that are commonly marshalled in unit train consist at their fully loaded condition (for example, container wagons used to haul grain), the higher figure of 16% net brake ratio should be used as the minimum. Figures of less than 16%, down to 13% net brake ratio as a minimum, may be accepted; however, the wagons will require a dynamic brake test in the loaded condition in a comparable consist to confirm that the train consisting of these wagons is able to stop within the brake performance curves applicable for the operating corridor. Generally these will be the GW16, GW30, and GW40 brake performance curves; refer to T HR RS 00830 ST.’ [16]
The ATSB has been informed, that since the incident Qube has not experienced any significant braking incidents with grain trains operating from Moss Vale to Port Kembla. This provides some evidence that the changes made since April 2017 have, to a large extent been positive. The changes have included both procedural changes to the operation of the train, as well as a design change refinement to the braking system on the CGSY wagons. It has been noted by the ATSB that whilst the component level checks have been made and procedure specific train loading and setup as per the April 2017 incident has not been recreated exactly, commercial logistics have precluded this to date.
Train loading
There were discrepancies between the recorded train load and the actual mass of the train. The train consist recorded gross tonnage for the 40 wagons as 3360 t (84 t per wagon). It appeared that the mass for each wagon was originally recorded as 92 t with a gross tonnage of 3680 t however this had been hand written over. The changes to the consist should have been signed or initialled by the train crew, but this was not done.
The mass recorded on the train consist was 10 per cent lighter than the actual mass of the load. While the total mass was within the allowable limits of the track infrastructure, the heavier load impacted on the braking performance of the train. The train crew, that took over at Goulburn, said that they noticed the consist had been altered, they also noticed the extra load as the train was coming out of Goulburn. This indicated that the train crew was aware of the extra load and its potential to affect train performance.
The tare (unloaded) mass of each wagon was designated as 22.2 t with a loading capacity of 68.8 t. The actual tare mass of a wagon (CGSY 4502V) was measured after the incident. It was 23.1 t, 900 kg over the tare mass of 22.2 t stencilled on the side of the wagon and that designated by the manufacturer. Typically, the greater the payload (up to the allowable limit) loaded into the wagon the better the economic return on the trip.
When the train was discharged at the Quattro facility at Inner Harbour, the wheat load was weighed at the facilities as 2784 t in total. The heaviest wagon contained 73.91 t and the lightest 45.49 t. The average was 69.6 t per wagon (see Figure 9). This meant that the wagon mass was 3708 t, an average of 92.7 t per wagon. When the extra wagon mass and the extra grain mass was added together there was an extra 349 t or 10 per cent more than what the consist recorded.
As specified in the Qube work instruction, a calculation that should be performed by train crew before departing is the Tonnes per Operative Brake (TOB).[17] This will determine the braking effort required to control the train on the downward sections of the route. It is calculated by adding the mass of the locomotives to the total mass of the wagons, then dividing this by the number of wagons. In the case of 8960, it was the addition of locomotive 1 (134 t) with locomotive 2 (134 t) and the mass of consist (3360 t). This gives 8960 a TOB of 90.7. The work instruction states: ‘grain trains with a TOB that exceeds 80 generally require higher brake cylinder pressures to bring the train to a stop or to control the train speed. Train drivers need to be mindful of this requirement when operating down steep grades’.[18]
The train crew were aware of the extra load of the train, the driver said ‘we ran the train at 80 km/h that day, you can tell as soon as you get out of Goulburn, an extra 300 t is a heavy weight. It felt heavy pulling along the flat.’ The extra mass placed an additional load on the braking system and affected the handling characteristics of the train.
Figure 9: Wagon mass
This figure shows the recorded and actual loading of the 40 wagons in the train consist. Source: Qube Logistics and Quattro grain facility. Calculations by ATSB
Risk management
The track section where the runaway occurred had a ruling gradient of 1 in 30. Unlike the Blue Mountains, west of Sydney, there are no relief sections of shallow gradients to allow for the recharging of the air brake system.
Until the mid-1990s, a dead-end siding was available near Dombarton to divert an uncontrolled train in the event of a runaway. This siding was a part of the former Dombarton crossing loop. Though not originally placed as a risk mitigation measure, it could act as such if required. The siding was subsequently removed on the basis that the brakes on modern rollingstock were more effective.
Other issues
The train was moved on soon after coming to a stand despite not being formally inspected for any faults by a suitably qualified person. This was after a request from Sydney Trains Wollongong Signalling Complex to move the train from the Sydney Trains network to Arrival Road 3 in Inner Harbour. The request was made to keep the passenger line open.
The driver said that he should probably have refused to move the train but ‘wanted to do the right thing’. It was probable the driver was still affected by the incident. While the train was operated safely at a low speed into Inner Harbour, after such a runaway event it would have been prudent to ensure the train was safe to be moved and have an alternative crew to operate the train.
In addition, the Pacific National Train Controller at Inner Harbour did not inform any ground personnel, in particular the Pacific National Illawarra shift leader, of the emergency event of a runaway train being directed into the terminal. The original joint decision by Sydney Trains and Pacific National was to route the train into the Number 1 Departure Road. This road is adjacent to fuel storage and office buildings and other options were not discussed or considered. The option of routing the train into Number 1 Departure Road was not used as the train came to a stand outside the terminal.
Remedial actions
Qube have undertaken a number of changes since the incident. These include the following changes:
The QBX locomotives and CGSY wagons were initially suspended from service on the Goulburn to Inner Harbour route. After testing the QBX locomotives and the CGSY wagons were returned to service on the Goulburn to Inner Harbour route.
QUBE train drivers are now competency assessed on the Moss Vale to Unanderra section of track every 6 months. If a train driver has not been rostered over the corridor within 6 months he or she must be reassessed on the corridor.
All driver trainers are now competency assessed by an external Registered Training Organisation (RTO) on the Moss Vale to Unanderra section of track.
Trainee train drivers are now briefed to the same level as a train driver before being rostered on the Moss Vale to Unanderra section of track.
A training audit for assessing train handling strategies on the corridor has been conducted. This has resulted in the instruction being amended.
The recommencement of diesel and air brake refresher training for train crew was undertaken.
An RTO was engaged to develop an improved training package. The first train crew to be trained were the train crew on the Goulburn to Unanderra line.
An RTO was engaged to review QUBE Work Instruction WI-540 Train Management Moss Vale to Inner Harbour.
A QUBE investigation officer, since the incident, has conducted weekly audits of trains operating between Moss Vale and Inner Harbour.
Regular scheduled datalogger downloads have commenced for trains between Moss Vale and Unanderra.
As a result of this incident, Pacific National have undertaken a number of changes since the planned movement of 8960 into its facilities. These include the following changes:
Review with Sydney Trains the plans and procedures enacted in emergency events, and the decision making process to move Qube Trains from Sydney Trains network to Inner Harbour.
Review training for Train Controllers to ensure the protocols for an emergency event are followed, and risks are managed, for example: depot evacuation, and escalation process is followed.
From the evidence available, the following findings are made with respect to the runaway incident involving train 8960, between Dombarton and Unanderra, New South Wales on 22 April 2017. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
The train was loaded by approximately 10 per centmore than that recorded on the train’s consist, it is probable that the additional mass placed an extra load on the braking system and affected the handling characteristics of the train.
Train 8960 was not operated down Illawarra Mountain in accordance with the operator’s work instructions. After passing Summit Tank the driver made ten brake applications and the brake system was never permitted to fully recharge again before the brakes were reapplied. This resulted in a loss of control of a train on a steep descent. The incident was further compounded when the driver’s actions caused the locomotive’s dynamic braking effort to be deactivated, further reducing control of the train.
Other factors that increased risk
The Sydney Trains’ train controller directed the driver of train 8690 to move the train from the Sydney Trains network to Inner Harbour without any formal inspection of the train following the runaway event.
The Pacific National Train Controller did not inform Inner Harbour ground personnel of the emergency event of a runaway train being directed into the terminal.
Other findings
The train crew of 8960 was experienced and fully qualified. The crew had travelled this route down the Illawarra Mountain on numerous occasions.
The train braking system was operating within the required specifications.
Context
Incident location
The runaway incident occurred between Dombarton and Unanderra on the Moss Vale – Unanderra line. Unanderra is in the Illawarra district, 88 rail km south of Sydney’s Central station (Figure 5).
Figure 5: Location of incident
This map shows the incident location and the path of 8960 (shown in red).
Source: Geoscience Australia, annotated by ATSB
Train information
The train, designated as 8960, was a loaded wheat service operating from Bogan Gate to Port Kembla. It consisted of two QBX-type locomotives (Figure 6), QBX003 and QBX002 and 40 loaded CGSY wagons.
Qube Logistics (Qube) owned the diesel-electric locomotives and the wagons were leased from CFCL Australia (CFCLA). The train was 664 m long and had a gross trailing load of approximately 3360 tonnes (as recorded on the train consist).
The wagons were a CGSY grain hopper-type wagon (Figure 7). The wagons were designed and built in China in 2015.
Figure 6: QBX locomotive
This figure shows the side elevation of a QBX locomotive.
Source: Qube Logistics
Figure 7: CGSY wagon
This figure shows CGSY wagon CGSY451F.
Source: ATSB
Braking system
The automatic brake, the independent brake and the dynamic brake are sub-systems of the train’s braking system.
Automatic brake
This brake is the normal service brake on the train and applies the brakes in balance when brake pipe pressure is reduced. When the train’s brake pipe is charged to 500 kPa, the train brakes are released. Maximum braking effort is achieved when the brake pipe pressure is reduced to 350 kPa. There is no increase in braking effort between 340 kPa and 0 kPa.
The brakes on the train do not apply simultaneously. The brake on the leading wagon will apply first and the other wagons sequentially. It may take 30 seconds for all the wagons brakes to fully apply. When the train’s air brakes are applied and released it may take 40 seconds for the air pressure to be fully restored to 500 kPa or to a level where the brakes can be effectively reapplied.
The train automatic brake controller has five positions:
Release – provides 500 kPa of air pressure in the brake pipe and releases the automatic brake and independent brake on the locomotive (if the independent brake controller is in release as well).
Minimum (or lap) – reduces the brake pipe pressure from 500 kPa to 430 kPa, this also initiates a minimum application of the train brakes and the locomotives brakes.
Service zone – allows the brake pipe pressure to be progressively reduced from 430 kPa to 350 kPa.
Full service – reduces the brake pipe pressure to 350 kPa and fully applies the locomotive brakes and train brakes.
Emergency – reduces the brake pipe pressure faster than other brake applications so that the train brakes and the locomotive independent brakes are quickly applied. This turns off the dynamic braking system.
Independent brake
This brake applies air brakes to the locomotive and works independently of the train brake system. The locomotive’s brakes are applied when the locomotive independent brake controller is operated separately from the train brake system. This turns off the dynamic braking system.
Dynamic brake
Dynamic braking is a function on locomotives designed to reduce wear and heat in the friction type braking equipment on the train. Being a supplementary system, it provides an additional means of train-speed control but is not a substitute for the train air brakes. Dynamic braking operates through the electrical traction motors that drive the locomotive wheels by reversing the function, from a motor using electrical current, to a generator producing electrical current. When using dynamic braking, the current generated by the traction motors dissipates out through an electrical resistor bank on the locomotive’s roof as heat. Increasing or decreasing the amount of electrical resistance varies the retardation or braking effect on the rotating locomotive wheels and thereby train.
Control of the braking system
The QBX-type locomotive is fitted with a Wabtec braking system. ‘The Wabtec system is an electro-pneumatic interface between the operation of the driver’s automatic and independent brake controller stands and the brake computer. This interface provides the various braking functions on the locomotive and the train as is required.’[5]
The position of the brake controller is to the driver’s left when seated (Figure 8). The movement of either brake controller transmits electronic signals to the brake computer, which in turn, responds to give the required brake application. The train control display shows pressure representations in numeric values on the driver’s screen.
The train control display shows the following air brake settings:
brake pipe pressure
equalising reservoir pressure
main reservoir pressure
brake cylinder pressure
brake pipe flow meter
end of train brake pipe setting (where fitted).
Figure 8: QBX locomotive driver’s control area
This figure shows the various controls and display areas for the driver’s position on a QBX-type locomotive.
Source: ATSB
Train crew
The train was crewed by a driver and a second person based at Qube’s Goulburn Depot. The driver was qualified for the rollingstock and the Goulburn to Port Kembla route. The driver had 17 years’ experience as a freight train driver and had previously worked in the rail industry as a shunter.
The second person was in training and qualified to drive a train under the supervision of the driver. Both the driver and second person held current competencies and medical certification.
Track information
The line on the Illawarra Mountain between Moss Vale and Unanderra is mostly a single track with crossing loops at Mt Murray. The section between Summit Tank and Unanderra, where the train ranaway, has a posted track speed of 30 km/h. At Dombarton, the line reverts to a double line. The track between Summit Tank and Unanderra has a ruling gradient of 1 in 30.
The posted track speed varies from 115 km/h from Goulburn to Moss Vale to 30 km/h from Summit Tank to Unanderra.
This standard gauge railway line was built in 1932. It provides a direct route linking Wollongong and Port Kembla to the Main South line. It carries mostly freight services (intermodal, coal and grain) and occasionally heritage passenger services.
No evidence exists to support that track conditions contributed to the incident.
Train control information
As 8960 progressed from Goulburn to its ultimate destination to the grain terminal at Port Kembla Inner Harbour, it came under three separate train control entities: ARTC, Sydney Trains and Pacific National.
Train movements on the Main South line from Goulburn to Moss Vale, and then between Moss Vale and Unanderra (at 91.080 km) are controlled from the ARTC Network Control Centre South at Junee under network rule ANSY 500 Rail Vehicle Detection System.
For trains travelling in the ‘Up’[6] direction, once a train passes the network interface boundary at 91.080 km the train enters the Sydney Trains network. Sydney Trains direct train movements in their network from the Rail Management Centre in Sydney. These movements are controlled in conjunction with Wollongong Signalling Complex.
The Quattro grain unloading facility is located in the Port Kembla Inner Harbour terminal. Once trains are routed into the terminal controlled by Pacific National Inner Harbour Train Control. Movements in and out of this terminal are controlled in conjunction with the Wollongong Signalling Complex.
Environmental conditions
Weather conditions at the time of the incident were dry and fine. The Bureau of Meteorology recorded a maximum temperature of 23.3°C, at Bellambi, approximately 15 km from Unanderra.
It was determined that environmental conditions did not contribute to the incident.
Related occurrences
On 7 February 2011, a loaded El Zorro Transport grain service travelling to Port Kembla ranaway down the Illawarra Mountain. The driver was unable to control the speed of the train towards the end of the descent. The 2988 tonne train was 691 metres in length.
After passing Summit Tank, the driver made a number of progressively larger brake applications on the descent into Unanderra. As the train approached the bottom of the Illawarra Mountain, braking effort was at its maximum. The train then proceeded uncontrolled through Unanderra Station and signal WG 1014 at Stop, before coming to a stand on the slight uphill gradient 527 metres beyond the signal.
When the crew realised they were in difficulty, the driver told the co-driver to contact the signaller to have signal WG 1014 cleared for them. The co-driver stated that he tried to do so on nine occasions using a mobile telephone but was unsuccessful. The signaller at Wollongong explained that he was busy on other calls at the time.
The Office of Transport Safety Investigations (OTSI) conducted an investigation[7] into this incident and found that the grain service became uncontrolled during its descent of the Illawarra Mountain because the train was not managed in accordance with current train management procedures.
The investigation also found that the company had no documented policies or procedures for the control of trains descending the Illawarra Mountain. Instead, drivers were instructed to use the rail infrastructure managers’ Train Operating Condition (TOC) manuals. It also found, despite being issued with TOC waivers that classified the wagons as single pipe wagons[8], the company operated the grain train services under differing dual pipe conditions from the time of introduction of the wagons into service. This anomaly was not identified by the rail infrastructure managers.
The train was loaded by approximately 10 per cent more than that recorded on the consist, it is probable that the additional mass placed an extra load on the braking system and affected the handling characteristics of the train.
The occurrence
Events leading up to the occurrence
On 22 April 2017, a Qube Logistics (Qube)[1] train crew, comprising a driver and second person, signed on at Goulburn, New South Wales, depot at 0800[2]. The crew were rostered to operate a loaded grain train, 8960, to Inner Harbour at Port Kembla where it was to be unloaded at the Quattro facility. The train had been loaded with wheat the previous day at Bogan Gate and was operated to Goulburn where it arrived at 2130 and was stabled overnight. The next day, a qualified train examiner inspected the train and no defects were reported.
Before departure, the train crew performed an inspection of the train. The driver instructed the second person to apply the brakes while the driver walked to the rear of the train to ensure that the brakes applied and there was brake pipe continuity on the train. He then radioed to the second person to release the brakes. The driver walked back to visually ensure that the brakes released and that all brake pipe and main reservoir pipe hoses were connected, and isolating cocks were in the open position.
At 0910, train 8960 departed Goulburn with the second person operating the train under the supervision of the driver. As the train departed Goulburn yard, a roll by inspection was performed to ensure that there were no visible or audible defects. The train then travelled on the Up Main line to Moss Vale where it branched off towards Unanderra and Inner Harbour. The train passed through Moss Vale at 1045. The second person continued to drive the train, under the supervision of the driver, from Goulburn to Robertson. At Robertson, the driver took over the controls from the second person in order to operate the train down the Illawarra Mountain (Figure 1).
Figure 1: Gradient diagram Moss Vale to Robertson
Source: Qube Logistics, annotated by ATSB
Between Goulburn and Mt Murray, the driver made a number of running brake applications using the train’s air brake system to gauge the train’s braking capability. There were no issues found with the train’s braking capability. This is known as a running brake test and it is a standard driving practice that train crews conduct this test.
The train passed Mt Murray and then, at 1216 it was brought to a stand just past Summit Tank, as required by a Qube work instruction.[3] Here, the driver conducted a performance test of the brakes. The driver was satisfied with the braking performance and resumed the journey.
The track gradient between Summit Tank and Unanderra is one of the steepest in the New South Wales rail network and runs for approximately 18 km with a ruling gradient of 1 in 30. There is only one short intermediate shallow grade of 1 in 120 as the track passes through the Number 2 Tunnel (Figure 2). This means that once a train passes Summit Tank there are no rest points along the section where the train’s brake system can be fully recharged.
On departing Summit Tank, at 1216, event recorders indicated that the train increased speed to 28 km/h before the driver made a brake application, which reduced the train’s speed to 15 km/h. With dynamic brake engaged, the driver then made a further nine brake applications, and on each occasion, did not allow the air brake system to fully recharge prior to the next brake application.
Figure 2: Gradient diagram Mt Murray to Unanderra
Source: Qube Logistics, annotated by ATSB
The occurrence
The driver said the first indication that he had a problem was past signal WG 1058 (100.500 km), at Dombarton. The time was 1242. He said that the signal was at full clear with the train travelling at 20 km/h.
At 1242:07, the driver made a release of the train’s air brake for approximately 30 seconds. He then reapplied the air brakes with a 50 kPa reduction in the brake pipe pressure. The dynamic brake was delivering 229 kN of braking force. The independent brake handle was in the release position and there was 0 kPa in the locomotive brake cylinders.
At 1242:28, the train’s speed had increased to 30 km/h. At this point, the train brake air that had been venting to atmosphere was stopped by the movement of the automatic brake handle by the driver to the release position. The driver reduced the brake pipe pressure to 420 kPa. However, despite this, the train’s speed continued to increase. The driver continued to reduce the brake pipe pressure in order to slow the train. The driver again reduced the brake pipe pressure to 344 kPa and the train’s speed reached 46 km/h. The dynamic brake was still delivering 229 kN of force.
As the train approached a 20 km/h curve, at 1246:41, the driver applied the locomotive’s independent brake, which activated the dynamic brake power knockout switch. This eliminates the dynamic braking effort and is a feature that is designed to prevent skidded wheels from excessive braking effort. The train was travelling at 44 km/h at the time.
At 1246:52, the driver moved the automatic brake handle to the full emergency position. When the automatic brake handle is placed into the emergency position, the brake pipe pressure is reduced to zero. The brake pipe pressure took 25 seconds to reduce to 0 kPa, the locomotive independent brake cylinder pressure increased to 482 kPa. The maximum amount of available braking effort was applied however, the train’s speed increasing to 46 km/h.
The action of applying the automatic brake controller to the full emergency position by the driver did not increase the braking effort as the train brake was already fully applied. It also meant that the dynamic braking system was deactivated. At this stage there was nothing further the train crew could do to reduce the speed of the train.
At 1248:37, the driver alerted ARTC train control at Network Control Centre South (NCCS) via the train radio that the train was running away.
NCCS: ‘8960 received. Over.’
Driver: ‘Yeah mate, we are in emergency braking running away down the hill. Over.’
NCCS: ‘You are running away there? Over.’
Driver: ‘That is correct.’
The ARTC network controller[4] at NCCS remained in constant communication with the driver throughout the runaway. This communication was effective in gaining information about the train’s speed, location, and informing the driver about the route settings.
The ARTC network controller at 1249 notified Sydney Trains South Coast Control (STSCC) that Qube service 8960 was running away and that the train was in the ARTC controlled Dombarton to Unanderra section, but heading towards Sydney Trains’ network. The train controller from STSCC also communicated with the driver and NCCS throughout the runaway.
At 1250, STSCC confirmed to NCCS and the driver that 8960 had the ‘full road’—meaning that the route had been cleared for the train and that there was no rail traffic in its path. Around the same time, Sydney Trains Wollongong Complex contacted Pacific National’s Inner Harbour train control to confirm that the route was clear of rail traffic. Number 1 Departure Road was confirmed as the final destination, in the event that the train ran that far.
At 1252:11, the train reached a maximum speed of 107 km/h as it rounded a curve approaching Unanderra station. The track speed at this location was 100 km/h. The train passed through Unanderra railway station where it was captured on CCTV camera (Figure 3). At 1252:21, the train started to reduce speed once it had reached the rising gradient at Unanderra north junction. The ARTC network controller expressed his concern to STSCC train controller that the driver had been unable to get the train under control. Just as he was saying this, the driver announced that the speed had reduced to 95 km/h.
Figure 3: Runaway train passing Unanderra station
Source: Sydney Trains
Post occurrence
As the train was coming to a stand the ARTC network controller asked the driver about his condition, the driver responded that apart from a few nerves he was good. He said, “I am just coming to a stand there now, I don’t know what my engine brakes are like but there is a lot of smoke behind me on the train, over.” The train controller from STSCC, who was also connected into the conversation along with the area controller from the Sydney Trains Wollongong complex, informed the driver that Wollongong complex would take control of their route once the train had come to a stand.
At 1255:03, train 8960 came to a stand at 85.225 km, on the Up Inner Harbour South Fork line. The train had come to a stand on the Sydney Trains network. It was approximately 13 minutes from the time the runaway event commenced and during that time the train had travelled 14 km.
At 1259, under instructions from the area controller at Sydney Trains Wollongong Complex, the train driver moved 8960 from the main line into Inner Harbour. However, despite the runaway, no formal inspection was made on the train before it was moved.
At 1306, the area controller then requested that the train crew ensure that the end of train marker (EOTM) was still present. The driver then moved the train at reduced speed forward while the second person conducted a roll by inspection of the train. After inspecting the train and confirming that the EOTM was intact at its rear, the second person called the driver on the radio to confirm that everything was in order. The driver then stopped the train and walked back to meet the second person approximately halfway along the train. They discussed what problems they had identified and noted that one wagon had an extended brake piston travel and that several brake shoes were worn below limits. Under direction from the Pacific National Inner Harbour train controller, the driver moved 8960 into the Number 3 Arrival Road in Inner Harbour and waited for the train to be examined (Figure 4).
Figure 4: Inner Harbour track diagram
Source: Asset Standard Authority NSW, annotated by ATSB
At 1436, Sydney Trains inspected the track from the ARTC interface boundary at 91.080 km to Unanderra. No defects were found and the track was certified for use.
As well, ARTC organised a track inspection, from Mt Murray (118.800 km) to its boundary at 91.080 km. This was to observe if there was any:
damage to the track or track infrastructure
mechanical components that may have fallen from any train
contamination (such as curve wear grease) on the rail head
grease pots over greasing
grain spills on or around the track.
At 1615, ARTC reported internally that there was no evidence of damage to the track or infrastructure. The track was certified for use.
At 1632, the train crew were drug and alcohol tested. They returned negative test results.
Six days later, on 28 April 2017, the train departed the Number 3 Arrival Road and discharged its load of wheat at the Quattro facility in Inner Harbour, Port Kembla and the mass of each wagon was measured.
The sources of information during the investigation included:
Australian Rail Track Corporation
CFCL Australia
Pacific National
Office of National Rail Safety Regulation
Qube Logistics
Sydney Trains
Transport for NSW
References
AR Ball Rolling Stock Maintenance Pty Ltd. CGSY Braking System Incident Moss Vale to Unanderra line. 22 April 2017.
Asset Standards Authority NSW. T HR RS 00400 ST RSU 400 Series – Minimum Operating Standards for Rolling Stock – Freight Vehicle Specific Interface Requirements. Version 2.0. Issued 24 August 2017.
Australian Wheat Board (AWB) Wagon loading instructions. Issued by El Zorro No. 002 31 October 2010.
CFCL Australia. CGSY Wagon data sheet. Issue No. 1.
Lacterus Verus Pty Ltd. Report into the braking system performance of QBX 003 locomotive on 22 April 2017. 23 May 2017.
Office of National Rail Safety Regulator. Guideline for the top event classification of notifiable occurrences – OC-G1. 2008.
OTSI Investigation Report 04505 (2011) Uncontrolled movement of El Zorro grain service 3996 Unanderra 7 February 2011.
Pacific National Incident Report – Dombarton to Unanderra, to Inner Harbour. 31 August 2017.
QUBE Logistics. Initial Investigation Report FM-512. Version 1. 1 June 2017.
Qube Logistics. Work InstructionWI-540Moss Vale to Inner Harbour Train Management. Version 3.0. 14 September 2016.
SNC-Lavalin Rail & Transit Pty Ltd. Principal author Bruce Sismey. 10 May 2017 amended on 1 Nov 2017.
Sydney Trains. Incident Information System Management - Incident Report 43. 24 April 2017.
The Instruction Company. QLRS Train Braking Procedures Moss Vale to Inner Harbour – Participants Workbook. Version 1.0. 10 June 2017.
The Instruction Company. Report on 9 June 2017 test run Goulburn to Inner Harbour. 15 June 2017.
Wayne Clift Consulting Pty Ltd. Test report for train braking simulation on 9 June 2017. 26 May 2017.
Wayne Clift Consulting Pty Ltd. Test report for auxiliary reservoir fill times on CGSY 4502. 26 May 2017.
Wayne Clift Consulting Pty Ltd. Test report for control valve from CGSY 4502. Issued 25 May 2017.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Australian Rail Track Corporation, CFCL Australia, Pacific National, the Office of National Rail Safety Regulation, Qube Logistics, Sydney Trains, and Transport for NSW.
Submissions were received from the Office of National Rail Safety Regulator and CFCL Australia.
The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 6 April 2016, Pacific National (PN) grain train 5422N parted at Parkville on the Main North Line. A fractured yoke on the trailing end of the fifth wagon allowed the yoke pin to fall out and the coupler shank to disengage from the wagon. The coupler shank fell into the four foot of the track and damaged the underbelly discharge doors on 10 wagons as the train progressed over the coupler. Approximately 10 tonnes of barley was released from the wagons as a result. The trailing wheelset on the thirteenth wagon was derailed, then ran in a derailed state for approximately 45 metres causing damage to several track sleepers before the train came to a stop. Regular services were able to continue under caution past the incident site via the adjacent crossing loop. Wagon recovery and track repairs was completed without any further incident.
What the ATSB found
A draftgear component (the yoke), that was not compliant with a PN maintenance standard, was not identified during a maintenance inspection and re-entered service undetected. The yoke was an earlier design and susceptible to fatigue failure. PN had identified the issue and completed a programme to replace this yoke design across their grain wagon fleet however, the yoke on this wagon had been overlooked.
What's been done as a result
PN issued an additional Rolling Stock Notice to their maintenance teams to advise of the incident and to mandate that all yokes in the grain wagon fleet were checked to ensure no yoke of this design remained in service.
Safety message
Maintenance systems must ensure that when a non-compliant component is identified as needing replacement, all such units are located and replaced.
Figure 1: 5422N at Parkville
Source: ATSB
Safety issues and actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety actions in order to reduce their safety risk. The ATSB has been advised of the following safety actions in response to this occurrence.
The presence of the earlier design of yoke on wagon NGKF 35898X was not detected during preventative maintenance activities.
The occurrence
At 0230 on 6 April 2016 PN grain train 5422N parted at Parkville (approximately 322.350 km[1]) on the Main North Line, Hunter Valley, NSW. The train parted due to a fractured yoke (in the draw gear assembly) on the trailing end of the fifth wagon (NGKF 35898X). The crew of 5422N comprised of a driver and second person.
The fractured yoke allowed the yoke pin to fall out and the coupler shank to disengage from the wagon. The coupler shank fell into the four foot of the track and damaged the underbelly discharge doors on 10 wagons as the train progressed over the coupler. Approximately 10 tonne of barley was released from the wagons as a result.
The trailing wheelset on the thirteenth wagon was derailed when the fallen coupler struck the wagon’s fourth axle. The wheelset ran in a derailed state for approximately 45 metres before both parts of the train came to a stop. A number of track sleepers were damaged during the incident.
The driver notified the Network Control Officer Upper Hunter 2 (NCO) that 5422N was stopped approximately 80 m from signal 06-12M. The driver told the NCO, he had experienced a sudden loss of air from the train which led him to believe the train had parted.
The second person conducted a walking inspection of the train and radioed the driver that the train had parted behind the sixth wagon and he could not see the remainder of the train.
The driver advised the NCO that an adjacent train in the Parkville crossing loop was not to move as he could not confirm the location of his detached train. The NCO told the driver of 5422N that he would warn the other train of the incident. The NCO also advised the driver that based on his indicator board, the two portions of the train were between the two yard signals and the line was clear for the other train to come out of the crossing loop.
With that knowledge, the NCO cleared the signal for the other train to depart from Parkville crossing loop. The second person continued his inspection and found the detached portion of 5422N and the flashing tail light marker[2] on the final wagon, confirming the train was clear of the yard signals.
The driver asked the NCO for confirmation of track protection for 5422N. The NCO confirmed that protection of the train was being provided by the yard signals being blocked[3].
The second person secured the detached portion of 5422N by applying the handbrakes on all wagons. The driver secured the locomotives and the front wagons of the train.
At approximately 0400 the NCO informed the driver that a Condition Affecting the Network (CAN) had been issued.
The driver and second person were post incident drug and alcohol tested and ceased duties for the rest of their shift in accordance with PN procedures. Both crew members returned a negative result from the post incident testing.
Site clean up started at approximately 1500. PN arranged for the damaged wagons and the spilled barley to be cleared from the site. PN then shunted the two portions of 5422N and re-railed the derailed wagon.
At 0210 on 7 April 2016 Australian Rail Track Corporation (ARTC) track maintainers were able to commence emergency track repairs and were completed by 0600. In accordance with ARTC procedures, a temporary speed restriction of 40 km/h was placed on the main line through Parkville to allow operations to continue.
From the evidence available, the following findings are made with respect to the derailment of grain train 5422N at Parkville, NSW on 6 April 2016. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
The yoke was an earlier design prone to failure through fatigue cracking.
The presence of the earlier design of yoke on wagon NGKF 35898X was not detected during preventative maintenance activities.
Other factors that increased risk
Nil
Safety analysis
The ATSB found that a draftgear component (an older design yoke), that was not compliant with a Pacific National (PN) maintenance standard, and not identified during a periodical wagon maintenance inspection and the yoke re-entered service undetected.
PN had a system in place to remove this early design yoke from their grain wagon fleet and replace it with a later design yoke better suited to the application. However, this yoke had been overlooked by the wagon maintainers and consequently continued in service up until its failure on 6 April 2016.
The yoke fitted on the rear of the fifth wagon, NGKF 35898X, was of an early design and was known to be susceptible to fatigue failure. The undetected older style yoke eventually failed in-service and led to the train parting and the subsequent derailment (see Figure 10).
While the train data logger information indicated that some brake applications on 5422N did not comply with PN procedures, ATSB concluded train handling did not contribute to the incident. After the yoke pin fell out of the assembly, the downhill operation most likely kept the two portions of the train together until the train negotiated a slight uphill gradient at Parkville. Here the train experienced a longitudinal tensile load that allowed the two portions of the train to separate.
The track leading to the incident site was inspected by a track specialist on behalf of PN. It was concluded there were no track defects or anomalies that could have contributed to the incident.
Figure 10: Event sequence
Source: ATSB
Yoke failure
The yoke from wagon NGKF 35898X had a manufacture date stamp ‘10/71’. NGKF wagons were manufactured in 1976. The yoke was approximately five years older than the wagon itself. It was therefore, likely that this yoke was the original yoke fitted to this wagon.
The yoke design had recently been identified by PN as having a finite life due to a propensity to fatigue failure. The tensile strength of the parent metal and the lack of internal rounded relief fillets in high stress areas of the yoke contributed to this issue.
The yoke had fractured at the rear section where the top and bottom longitudinal straps connected with the backing face (see Figure 11).
Figure 11: Fractured yoke
Source: Bureau Veritas, annotated by ATSB
PN commissioned Bureau Veritas (BV) to conduct a metallurgical examination to identify the nature of yoke’s failure mechanism. The examination identified that the yoke had failed due to fatigue cracking which had initiated at multiple points on the inner face of the top yoke strap (see Figure 12). Fatigue cracking had progressed through approximately 85 per cent of the material’s cross-section before the ductile failure of the remaining material. The bottom yoke strap subsequently failed with approximately 10 per cent of the material’s cross-section subject to fatigue cracking before the ductile fracture, failing after the top arm failed.
The BV report stated that:
‘it was suspected that the fracture may be due to a material with low toughness properties[6] being in service for a long time, which was exposed to cyclic stress.’
The BV metallurgical examination focussed on the material properties and while it did not review the design of the component, the report did note that “stresses are concentrated at the critical regions (e.g. radius relief groove, curves, thickness change)”.
Figure 12: Fracture faces of yoke
Source: Bureau Veritas including annotation
Fatigue cracking in yokes
Other research has been conducted into fatigue cracking and stresses in yokes in heavy haul services[7]. Cookson et al 2013, identified a propensity for fatigue cracking in yokes due to the vertical oriented bending of the draft system. This vertical oriented bending in yokes was considered most likely due to misalignment in the draft system. As such, identifying misalignment in the draft system was considered important as it could affect the overall service life of the yoke.
It was noted that PN’s Wagon Maintenance Manual (WMM) 07-02_09 (dated 7 May 2009) Couplers and Draft Gear Maintenance makes reference to checks for alignment when inspecting varous parts of the draft system, including; the knuckle, coupler shank, the yoke strap and drawgear carriers.
Wagon maintenance
The periodic maintenance program in place for PN’s grain wagons was developed to ensure reliable and safe operation of the wagons.
WMM 07-02_09 sets out the maintenance requirements for wagon couplers and draft gear. Section 1.9 deals with yokes and it includes the following:
Yoke straps are to be inspected for cracking
Where video/borescopes are available these shall be used to detect cracking in yoke straps.
If cracking is found (in the internal radius locations) the yoke shall be scrapped
Further, Section 1.9.4 makes specific reference to earlier design yoke straps:
‘Wagons manufactured before 1980 used lower grade steel in the draft gear castings and do not have a relief fillet in the rear top and bottom inside corners as identified in the picture below (see Figure 13) (i.e. sharp radius). Replace these when found.’
Additionally, while wagons with a draft capacity of less than 1.3 MN were excluded from this last requirement, NGKF 35898X had a draft capacity of 1.8 MN.
These requirements specified in PN’s WMM suggests the yoke on wagon NGKF 35898X should have been identified and replaced at the last maintenance intervention.
Figure 13: Yoke inspection areas
Source: PN WMM 07-02
It is worth noting the task requirements on wagon maintainers when required to inspect a unit train consist[8]. When a unit train consist is scheduled for maintenance, such as the B inspection[9], the consist is scheduled into a maintenance centre for usually 24 hours before being scheduled onto its next service.
In this time the wagon maintainer would need to attend to a list of items and either, test, service or lubricate, replace, adjust, gauge, measure or inspect each of these items on each wagon (for grain unit train consists, 40 wagons). The list of items to attend to on the B inspection sheet is 92 items.
Additionally, the location of the yoke in situ makes it challenging for the wagon maintainer to identify cracking in the yoke. As pictured in Figure 14, the wagon maintainer is required to inspect the highlighted areas. As Figure 15 shows, the access to view these areas while the yoke is in situ is difficult and potentially restricted by time constraints in the maintenance opportunity.
Figure 14: Yoke inspection areas
Source: PN WMM 07-02
Figure 15: Yoke in situ
Source: ATSB
Train handling
The yoke pin was found nearly 6 km before Parkville. There was a constant falling grade towards Parkville and the train driver was using dynamic braking to control train speed. Therefore, the wagons of the train generally remained in a compressed state ensuring the train did not part.
On account from the driver, there is a slight incline after Wingen just prior to the downhill into Parkville. At this point the driver allowed the train to roll freely through the section of track to maintain speed. This coincides with a releasing of the buffering or compressive forces in the draw gear. The yoke pin most likely fell from the train at this point which is where it was found during inspection post incident (see Figure 16).
The train was able to continue without a mechanical connection through to Parkville as compressive forces kept the train and brake air hoses together on the downhill into Parkville. However, as the train rolled into Parkville at approximately 60 km/hr, the driver reduced dynamic braking to account for the slight incline to the middle of the yard which is when the train parted, seperating the air hoses. This enabled the brakepipe to vent to atmosphere, triggering an emergency brake application which brought both parts of the train to a stop.
The train handling in the lead-up to the incident was not considered a contributing factor to the incident.
Figure 16: Yoke pin lying in the four foot
Source: ARTC including annotation
Previous incidents
PN reported that, over the five years preceding the incident, there were 14 incidents of trains parting due to defective yokes. These incidents occurred between 2011 and 2016. There were a further 13 wagons that had their yokes replaced during maintenance between 2011 and 2012. No older style yokes were detected after that date until this incident in 2016.
Pacific National investigation
PN conducted a safety investigation into the incident at Parkville. PN’s internal Investigation Report (Form PN-FOR-SAF) dated 10 May 2016 identified that the incident wagon (NGKF35898X)
‘underwent regular maintenance and inspection as per WMM 01-01b_05 Bulk Services Division Services Schedule of Inspections; however, the early model yoke strap on this wagon was not identified or replaced (as per WMM 07-02_09).’
Two of the preventative actions in the report were:
To develop and issue a Rolling Stock Notice (RSN) to all wagon maintenance and engineering teams to reiterate required inspections on early model yokes on wagons and replacement of specified parts.
Develop a safety alert detailing the contributing factors for derailment and distribute to NSW/Vic operations.
ATSB requested PN to demonstrate that the actions had been completed. PN notified the ATSB that the first two items had been closed out by issuing a single RSN (see Appendix A) to wagon maintainers.
Appendix A – Pacific National Rolling Stock Notice
Sources and submissions
Sources of information
The sources of information during the investigation included:
The Australian Rail Track Corporation Ltd.
Office of the National Rail Safety Regulator
Pacific National
Submissions
Nil
Context
Incident location
Parkville is located between Scone to the south and Murrurundi to the northwest (see Figure 2). Train 5422N was travelling from Werris Creek to Carrington Grain Terminal near Newcastle on the Main North Line. The incident occurred adjacent to the township of Parkville in the Upper Hunter region of NSW.
Figure 2: Incident location map
Source: Geoscience Australia, annotated by ATSB
Rail infrastructure information
There are two tracks at Parkville, namely a main line and a crossing loop. A single, bidirectional line connects Parkville and Murulla to the north. The track from Murulla to Parkville is predominantly on a falling grade or downhill (see figure 3). Murulla sits between Murrurundi and Parkville at approximately 339.4 km.
Figure 3: Curve and Gradient diagram of track between Murulla and Parkville
Source: ARTC, annotated by ATSB
Safeworking system
The safeworking system in place was Centralised Traffic Control (CTC). In this system, lineside signals and associated track circuits allow the NCO, from the control centre at Broadmeadow, see the location of any given train operating along the Main North Line.
Train information
5422N was a loaded grain train consisting of 40 wagons and hauled by three locomotives. It was approximately 636 m long with a mass of 3040 tonne excluding the locomotives. It was typical of many grain trains working throughout NSW.
The yoke and draw gear assembly
The yoke is an integral component of a wagon’s draw gear assembly. While a number of different designs are in service, they are all designed to retard the train’s longitudinal draft and buffering[4] forces. The major components of a draw gear assembly are typically: coupler shank, buffer package, yoke and yoke pin (see Figure 4).
The yoke houses the buffer and is connected to the coupler by a pin or key (in this case a pin). The yoke is a part of the draw gear and transmits draft and buffering forces between wagons. Under compression, the force is transferred between the back-strap of the yoke and the wagon. In operation, the back-strap is subjected to repetitive loads. To mitigate against this effect, later yoke designs (post-1980) have internal rounded smooth radius fillets at high stress locations which are better able to withstand the cyclic stresses that are imposed on these areas. The later yokes are manufactured from a higher tensile steel.
The yoke in this incident was a pre-1980 design made from a lower tensile steel and without rounded smooth radius fillets in the high stress locations.
PN has maintenance systems in place to manage it’s total wagon fleet of approximately 15,000[5] wagons, across several locations in Australia.
PN was aware that the early design yokes (in grain wagons manufactured before 1980) needed to be removed from their fleet and replaced with later design yokes made from higher tensile steel and with internal rounded smooth radius fillets.
As such, specific instructions in PN’s Wagon Maintenance Manual (WMM) had been developed to provide instruction to PN’s wagon maintainers to identify and change out the early-design yokes as the wagons came in for preventative maintenance.
Site observations
ATSB observed the train had parted five wagons behind the locomotive (see Figure 1). The draw gear assembly was missing from the rear of the fifth wagon, NGKF 35898X (see Figure 5). The coupler shank was found under the rear axle of the rear bogie of the sixteenth wagon, NGKF 35864R (see Figure 6).
Figure 5: Location for draw gear assembly
Source: ATSB
Figure 6: Coupler shank in four foot
Source: ATSB
The bottom discharge doors on 10 wagons had been damaged. Approximately 10 tonne of barley had spilled from the wagons (see Figure 7).
Figure 7: Wagon doors and spilled grain
Source: ATSB
The coupler shank struck the axle of the trailing wheelset on the thirteenth wagon, NGPF 36032J. This resulted in the wheelset derailing near the crossing loop (see Figure 8). The wheelset travelled in a derailed state for approximately 45 m, damaging a number of concrete sleepers, before coming to a stop. (see Figure 9).
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 23 September 2015, two Pacific National terminal operators and the train crew were completing a shunt of train 4MW2 at the Sydney Freight Terminal. After detaching the remaining wagons, the train crew moved the five locomotives toward the end of the stabling road, where a shunt driver was waiting trackside to take over. After stopping, the train crew exited the cab and alighted from the lead locomotive. The train crew had left the locomotive independent brake handle fully applied but did not operate the park brake prior to leaving the cab.
The shunt plan required two of the five locomotives to be uncoupled and stabled. In readiness to uncouple, one of the terminal operators entered between the locomotives and isolated the air taps, disconnected the train hoses and lifted the coupling pin to the two trailing locomotives. Neither the train crew nor shunt driver realised that the rear two locomotives had been uncoupled. Shortly after, the shunt driver boarded the lead locomotive and in conjunction with the other terminal operator moved the front three locomotives to another area of the terminal. The two trailing locomotives remained at the end of the road, unattended by a qualified worker.
Shortly before 1751, sufficient air had bled from the brake cylinders to allow locomotives NR24 and NR12 to begin to roll away. The locomotives continued to roll uncontrolled through the Sydney Freight Terminal before exiting into the Australian Rail Track Corporation network. The locomotives travelled a short distance on the Down South Fork before coming to rest at Chullora West Junction. There were no injuries or damage due to the run away.
What the ATSB found
The ATSB found that a combination of individual action and ambiguous radio communications resulted in a breakdown of controls to prevent an uncontrolled movement of rolling stock. The interface coordination arrangements at the eastern interface between Pacific National and the Australian Rail Track Corporation were ineffective in capturing an uncontrolled movement before exiting the Sydney Freight Terminal.
What's been done as a result
The Australian Rail Track Corporation have issued instructions for the restoration of points at the interface following each movement and commenced investigation into the feasibility of automatic resetting of the points at that location.
Pacific National undertook toolbox briefings and issued Business Safety Notices restricting terminal operators from uncoupling locomotives and reinforcing the importance of applying communications and shunting procedures.
Safety message
Rail transport operators and rail safety workers must ensure the correct and consistent application of communication protocols and procedures when undertaking safety critical work, such as detaching and securing unattended locomotives.
Safety analysis
Planning and coordination of a shunt
In planning a shunt, the PN standard required the communication of the shunt plan to the shunting team (terminal operators) and locomotive driver to ensure:
the identification of the shunter in control and responsible for coordinating shunting movements
the identification of the roles of each shunter involved in the shunt
the planning to complete the shunt in the safest number of moves
the informing of locomotive driver and the shunt team about the planned shunt moves
confirming the shunt sequence and rolling stock to be moved
On 23 September 2015, the communication of the shunt plan commenced when a terminal operator advised the inbound train crew via radio that they would be operating the locomotives to shunt from the EPA1 road onto the EPA3 and EPA4 roads, before heading to the number 9 road.
The terminal operators then commenced uncoupling wagons in accordance with the shunt plan. The terminal operators communicated between each other to transfer the role of shunter in control. The shunter in control communicated instructions to the train crew for the movement of the train. The train crew did not have a copy of the shunt plan to facilitate clear understanding of shunt sequence and the rolling stock that would be uncoupled.
After detaching the remaining wagons on the number 9 road, the last entry in the shunt plan indicated ‘to bed’ against locomotives NR12 and NR24. There was a series of communications:
between the shunter in control at that time and the train crew
between the two terminal operators, and
between one of the terminal operators and the SFT shift manager.
Each conversation contained information related to the intended actions to address the shunt plan for locomotives NR12 and NR24. However, the communications did not ensure that there was a clear understanding among all parties of what was to occur.
Communication protocols
The PN voice radio protocols promoted effective spoken radio communications to be:
clear and unambiguous
relevant to the task at hand
agreed as to its meaning before being acted upon
The communication protocols and shunting procedures required the locomotive driver and terminal shunter to reply to each communication to indicate that they have complied with the request or to acknowledge the previous communication. The protocols contain a warning that qualified workers must not assume that a receiver has understood a message before the receiver confirms that the message has been understood.
The sequencing of radio exchanges between the parties that occurred during the preparation for the final shunt of the locomotives resulted in essential information being misunderstood or lost. This was particularly pertinent to the application of the three-step protection process.
The application of these processes to ensure protections were in place before the terminal operator entered between rolling stock may have alerted the train crew of the intention to uncouple the locomotives.
Procedures for uncoupling locomotives
Following the request from a terminal operator, the driver moved the locomotives forward to the entrance of number 9 road and applied braking using the independent brake lever.
The independent brake valve was self-lapping, meaning the degree of braking effort was proportional to the positioning of the lever by the driver. The valve regulated the air pressure applied to the brake cylinders of the lead locomotive, and through the train pipe and interconnecting hoses to the brake cylinders of the four trailing locomotives to stop the train.
Once stationary, the driver left the independent brake handle in the full application position, which maintained the air pressure to the brake cylinders holding the locomotives with maximum braking effort. The train crew then gathered their gear and vacated the cab in preparation to leave the locomotive.
The train crew did not apply the locomotive park brake prior to vacating the cab. The implementation of the park brake requirements in the procedure for securing locomotives would almost certainly have prevented the runaway from occurring.
When on the ground, a short conversation occurred between the crew and the SFT shunt driver, which included a briefing on the set up of the locomotives in the train on arrival at the SFT. During this time, the terminal operator entered between locomotives AN8 and NR24 and uncoupled the locomotives. The terminal operator on completing this task assumed that the locomotive drivers were aware of the intention to undertake a task, and had made the rolling stock safe in accordance with the three-step process. The terminal operator did not subsequently contact the drivers to arrange the removal of protections to enable the operation of locomotives.
Terminal operators were only authorised by PN to undertake the task of uncoupling wagons. The task of uncoupling and securing locomotives was the responsibility of the locomotive crew or SFT shunt driver. It was apparent however that some terminal operators, who during their employment with other rail operators, had received training in undertaking this task and would on occasion assist a locomotive driver to uncouple locomotives.
Although PN undertook compliance and safety audit monitoring programs, these had not identified the practice of terminal operators assisting locomotive drivers existed, or that variances in the application of the radio communication protocols, such as the three-step process, were occurring at the SFT.
Interface risk assessment
The ARTC Engineering (Signalling) Standard[22] includes the option of providing self-normalisation[23] of catch points on sidings to protect the main line. Where self-normalisation is provided in the signalling arrangement, the catch point sets to normal (open position) when the signalling interlocking system indicates that the catch point has been continuously free to move for a period not less than 45 seconds. The self-normalisation principle could also apply for power-operated points on a turnout (as installed at each end of the SFT).
The design of the ARTC interlocking at Chullora did not include the functionality to self-normalise either the catch point or points at the interface between PN and ARTC.
The PN assessment of risk from an unauthorised movement exiting the SFT relied on the effectiveness of a series of engineering and administrative controls. The assessment identified the automatic operation of the points at either end of the SFT toward a dead end track section, when the associated signals were at red as an engineering control. The assessment assigned responsibility for this control to the ARTC.
As the interlocking design at Chullora did not include automatic operation of the points, PN’s reliance on automatic operation as an engineering risk control was therefore incorrect at this location.
The signalling at Chullora operated as an ‘Entrance – Exit’ system. To set a route the NCO operated controls to select the required entrance and exit signals along the desired route. The interlocking set the points (if free to move) to the required orientation before clearing the required signals along the route. If required, the system also enabled the NCO to operate the point machines individually to set the desired orientation.
The interface coordination required liaison between the SFT Shift Manager and NCO to progress movements through the interface area. Signalled routes were set to enable train services to enter or exit the SFT. If required, signalled routes could also be set to enable PN to shunt long trains from the SFT through the interface area and onto the main line. The point machines within the selected route would lie in the orientation set for the previous movement until the operation of another set of entrance and exit signals to request a new route.
The draft interface agreement identified the Chullora operational boundaries at ED 288 signal and the clearance point at the back of 361B turnout. The agreement identified the ARTC and PN as responsible for operations within their respective territory, and jointly responsible for the management of risk at the interface. The correct orientation of the ARTC controlled point machine 361B situated between the interface boundary of the PN Sydney freight terminal and PN dead end track section, was essential to ensure the preferred routing of an uncontrolled movement toward the dead end (that is, away from the main line).
The administrative process associated with the interface coordination between the PN Shift Manager and the NCO did not ensure that, on the completion of PN rail movements, the motorised point machine adjacent signal ED288 diverted any uncontrolled rolling stock movement toward a dead end track section and away from the ARTC network.
The Interface Agreement IA1919 was in draft since mid-2014. Neither ARTC nor PN had endorsed the interface coordination arrangements for the joint management of risk at the ARTC/PN boundary. The absence of a self-normalising turnout or a finalised agreement on responsibilities for the coordination at the interface, likely increased risk to the ARTC corridor.
On 23 September 2015, the points at the eastern interface toward Chullora West Junction remained set from a previous PN rail movement through the interface area. This allowed locomotives NR24 and NR12 to exit the PN controlled SFT and onto the ARTC network.
On 23 September 2015, Pacific National (PN) freight train 4MW2 departed Melbourne and travelled along the Interstate Main Line via Junee and Goulburn toward Sydney. Within the Sydney area, 4MW2 traversed sections of the Australian Rail Track Corporation (ARTC) Southern Sydney Freight Line and the Metropolitan Freight Network en route to, the PN Sydney Freight Terminal (SFT) at Chullora (Figure 1). Train 4MW2 consisted of five locomotives hauling 76 wagons.
Figure 1: Location of Pacific National Sydney Freight Terminal
Map of Sydney area showing various passenger and freight rail lines. Train 4MW2 travelled along the rail line from Goulburn through Cabramatta then toward the Pacific National Sydney Freight Terminal at Chullora. Source: Geoscience Australia, annotations by ATSB
At about 1657,[1] as train 4MW2 approached Chullora, the co-driver contacted staff at the SFT by radio seeking instruction on the final destination road[2] for the train within the terminal. A terminal operator waiting for the arrival of 4MW2 informed the train crew that it was to enter the EPA1[3] road in preparation for shunting.
At about 1658, train 4MW2 arrived at the EPA1 road where the terminal operator further advised the train crew that there were no local relief train crew available, and that they would need to assist in the shunt of train 4MW2. The train crew, in conjunction with two terminal operators then commenced a series of shunt movements onto the various EPA roads. The terminal operators coordinated with each other to control the shunt and to uncouple and secure the required wagons in accordance with the shunt plan for that train.
After completing the shunt movements to the EPA roads, a terminal operator instructed the train crew to push the remainder of the train to the number 9 road. Number 9 road was located adjacent to the gantry crane roads in another section of the SFT.
The train crew, with the assistance of the terminal operators, moved the five locomotives and remaining wagons to the gantry crane area and toward the dead end of the number 9 road. The terminal operators again coordinated with each other to position the shunt movement along the road.
Around this time, a SFT shunt driver was working on number 6 road testing the air brake system of a rake of wagons in the gantry crane area. On completing the testing, the SFT shunt driver moved the shunt locomotive to the entrance of the number 6 road, secured it and took a short rest break.
At about 1734, a terminal operator (TO1) uncoupled and secured the remaining wagons from the locomotives. The same terminal operator also contacted the train crew to ask where they wanted to leave the back two locomotives (NR24 and NR12), as the shunt plan had also listed them to be detached, but did not specify the final road. The locomotive driver replied that they wanted to leave all five locomotives and get off. Shortly after, the other terminal operator (TO2) who was at the opposite end of the wagons situated at the dead end of number 9 road interrupted, suggesting that the locomotives be moved to the entrance of number 9 road where the SFT shunt driver could take over from the train crew and finish the shunt of the locomotives.
The train crew subsequently moved locomotives (NR91, NR82, AN8, NR24, and NR12) forward toward the entrance to the number 9 road. The driver applied the independent brake[4] fully, stopping the locomotives adjacent to the SFT shunt driver. The SFT shunt driver on returning from the rest break overheard a conversation between the terminal operators and train crew that he was to take over the locomotives on number 9 road. The SFT shunt driver then waited trackside adjacent to number 9 road.
As the terminal operator (TO1) continued to secure the detached wagons, the other terminal operator (TO2) moved from the dead end of number 9 road to meet the five locomotives that were now stationary at the entrance of number 9 road. The terminal operator (TO2) knew that the back two locomotives were to be detached but did not know the final road for stabling. The SFT shift manager and terminal operator briefly discussed arrangements for the two locomotives and decided to leave them on number 9 road where a local train crew would attend to them when available, about 30 minutes later.
Once adjacent the locomotives, the terminal operator (TO2) went between locomotives AN8 and NR24, disconnected the air hoses to the main reservoir and brakes, and lifted the pin in the coupler. Immediately after completing this task, the terminal operator departed the area to take a meal break. There was no direct communication between the terminal operator and train crew or SFT shunt driver, so the drivers were unaware that the terminal operator had entered between the locomotives and undertaken this task.
About the same time, the train crew were in the process of alighting from the lead locomotive and meeting with the SFT shunt driver, who was standing on the ground adjacent to the locomotives. After discussing the operational state of the five locomotives, the train crew departed and the SFT shunt driver boarded the lead locomotive.
Shortly after, the terminal operator (TO1), who had completed securing the wagons that were detached earlier, joined the SFT shunt driver. The terminal operator and SFT shunt driver then moved locomotives NR91, NR82, and AN8 from number 9 road. Neither the shunt driver nor terminal operator was aware the locomotives had been uncoupled. Locomotives NR24 and NR12 remained on the number 9 road and unattended by a qualified worker.
About 8 minutes later, sufficient air had leaked from the brake cylinders to allow locomotives NR24 and NR12 to commence rolling away. The locomotives continued an uncontrolled movement through the SFT traversing a number of roads and trailable points[5], reaching a maximum speed of about 21 km/h within the yard.
The locomotives continued toward the eastern interface point between the SFT and the ARTC network. While signal ED288 was set to stop, the points at the interface were set to direct rail traffic toward the ARTC Chullora West Junction.
At about 1751, locomotives NR24 and NR12 passed signal ED288 at stop. This generated a Signal Passed at Danger (SPAD) alarm at the ARTC Network Control Centre South (NCCS) in Junee. About a minute later, the locomotives passed a further signal (ED278), generating another SPAD alarm.
The NCCS NCO contacted the SFT shift manager to identify the train movement that triggered the SPAD alarms. The SFT shift manager confirmed that there was no shunting operation occurring in that area, but would investigate the source of the SPAD alarms. At about 1759, the SFT shift manager confirmed to the NCO that two locomotives (NR24 and NR12) had run away and exited the SFT. The locomotives came to rest with the front of the lead locomotive (NR24) located at about the 17.407 km point[6] on the Down South Fork of the Chullora West Junction.
The SFT shift manager dispatched Pacific National staff from the SFT to take control and secure the locomotives. The locomotives remained at that location until ARTC and Pacific National staff had inspected the track sections traversed by the locomotives. There was no damage identified to either the locomotives or track.
At about 2035, locomotives NR24 and NR12 cleared from the ARTC main line to the interface area and back towards the SFT.
From the evidence available, the following findings are made with respect to the uncontrolled movement (runaway) of locomotives NR24 and NR12 from the Pacific National Sydney Operations yard onto the ARTC main line at Chullora, NSW on 23 September 2015. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
A terminal operator entered between locomotives AN8 and NR24 disconnecting the air hoses to the main reservoir and brakes, and lifted the pin in the coupler.
The train crew did not apply the locomotive park brake prior to vacating the cab.
Power operated point machines at Sydney Freight Terminal eastern interface were not set to direct rolling stock toward the dead end track section.
The implementation of communication protocols and procedures for the planning and coordination of the shunt was ineffective in ensuring that the shunt plan was clear and unambiguous and that adequate protections against the unintended movement of rolling stock were in place.
Other factors that increased risk
The engineering control listed in the Pacific National risk assessment SFT SHT-01 incorrectly identified the availability of an automatically operated point machine at the interfaces to the Australian Rail Track Corporation network to mitigate risk from an uncontrolled rolling stock movement.
Context
The location
The SFT was located at Chullora in Sydney, NSW at about the 19.828 km point on the ARTC Sydney Metropolitan Freight Network (Figure 2). Rail access from the Sydney Metropolitan Freight Network (MFN) to the western and eastern extremity of the SFT was available via turnouts located at Enfield West and the Chullora West Junction respectively. The ARTC Network Control Centre South (NCCS) at Junee controlled rail operations along the MFN and at the interface with the private sidings at Chullora.
Figure 2: ARTC Sydney Rail Freight Corridors
Figure illustrates the various main line track arrangements in the Sydney area and relative location of Chullora and the Chullora West Junction. Source: Australian Rail Track Corporation, annotations by ATSB
Train and train crew information
Train 4MW2 consisted of five locomotives (NR91 leading, NR82, AN8, NR24 and NR12) and 76 wagons. The train was 1501 m long and had a trailing mass of 3132 t. The trailing mass included the locomotives AN8 and NR24 because they were setup as ‘off line’. Train 4MW2 was crewed by a driver and co-driver.
In conjunction with the train crew, two terminal operators and an SFT shunt driver also undertook various activities in the shunting of 4MW2 within the terminal. Post incident, the train crew of 4MW2, two terminal operators and the SFT shunt driver underwent preliminary testing for the presence of alcohol or a drug[7]. The result of this testing was negative.
The locomotive drivers and terminal operators held PN qualifications for shunting rolling stock and using communications systems. An examination of the health assessment records confirmed that their health assessments were current and that each satisfied the standards prescribed by the National Standard for Health Assessment of Rail Safety Workers.
Chullora – Private Sidings
The Chullora area contained four private sidings[8] that interfaced with the ARTC MFN at five locations (Figure 3).
The PN Sydney Operations Yard was a private siding with an eastern and western interface to the ARTC network. Motorised point machines on the turnout at each interface may be set to direct an uncontrolled movement (runaway) toward a dead end track section. The NCO controlled the points and signals at the interface locations remotely from the NCCS.
The NCO also controlled rail movements at the interface with the other private sidings by providing a release from the NCCS. The release enabled a qualified employee to set the points by operating the associated local ground frame[9].
A motorised catch point[10] was located at the eastern boundary of the Chullora interface area to protect the ARTC network from an uncontrolled rolling stock movement (runaway) from the private sidings entering the Down south fork and Down Main line. The ARTC controlled the signals, catch-point, and all other motorised point machines at the Chullora West Junction remotely from the NCCS.
Figure 3: Track arrangement at Chullora West Junction
Figure illustrates the main line track arrangement at Chullora Junction including the interface connections to the Pacific National Sydney Operations Yard and other private sidings. Source: Australian Rail Track Corporation annotations by ATSB
ARTC/PN Interface coordination – Sydney Freight Terminal
An interface agreement[11] stipulated the arrangements for the joint management of the operational risk at the ARTC/PN boundary. The interface agreement was in draft, dated 23 April 2015. The risk assessment of operational hazards in the draft agreement identified no site-specific risk factors that raised the generic ARTC corridor risk rating above low.
The PN risk assessment for the SFT[12] access and egress through the interface boundary identified the hazard of unauthorised entry or exit of a train to/from the SFT. An unauthorised movement may take the form of a train operated by a driver or rolling stock (locomotive or wagon) that is uncontrolled. The risk assessment identified various controls requiring the driver to comply with signal indications and approval protocols that permitted access/egress through the interface. For an uncontrolled rolling stock movement approaching the interface, the risk control relied on diverting the rolling stock away from the interface area.
At the eastern end of the SFT, motorised points adjacent signal ED288 provided the control mechanism to divert rolling stock toward a dead end track section (shunt neck) and away from the ARTC network (Figure 4). The signalled route selected determined the orientation of the motorised points. At the time of the uncontrolled movement, the route was set to allow access between the ARTC network and the SFT.
Figure 4: PN Sydney Freight Terminal eastern interface point and dead end road
Interface point at the eastern end of the PN Sydney Freight Terminal. Signal ED288 and the motorised point machine were controlled by the ARTC from the Junee control centre. The points should be positioned as shown to route any uncontrolled movement toward the dead end and away from the roads of the other private sidings and main lines at Chullora West Junction. Source: Australian Transport Safety Bureau
Pacific National Sydney Freight Terminal
The SFT encompassed the EPA, Gantry, Shed, and Transfer rail marshalling areas (Figure 5). The PN Shift Manager controlled the incoming and outgoing rail movements in conjunction with the other routine internal shunting operations. The standby train crew or a terminal shunt driver in coordination with terminal operator ground staff undertook the rolling stock shunting operations for the marshalling of trains within the various areas of the SFT.
Within the SFT areas, the terminal operator ground staff manually operated (hand throw) points to route the rolling stock between the various roads of each area. The design of a number of these manually operated points enabled a trailing movement[13] through the point assembly by the rolling stock.
The track grade from the entrance to of the Gantry road area toward Chullora West Junction started with a falling grade of about 0.70% before increasing to 1.166% through the Arrivals road area. The falling grade then reduced to around 0.060% through the Transfer road area before transitioning to a rising grade of around 0.26% through the interface area with the ARTC.
At the top of the grade in the Gantry area, four of the roads (#5, 6, 7 and 8) were equipped with a manually operated derail mechanism to prevent unauthorised access into or to capture an uncontrolled movement from the respective road. Road #9 was not equipped with a derail mechanism.
Figure 5: Pacific National Sydney Freight Terminal
View of the Pacific National Sydney Freight Terminal showing the relative location of the EPA and Gantry road areas. The uncontrolled movement of locomotives NR24 and NR12 commenced at the #9 road in the gantry area before travelling through the transfer road area and toward Chullora West Junction. Source: Google, annotated by ATSB
Pacific National shunting procedures
The Pacific National standard[14] and procedure[15] outlined the safe practices established for the movement of rolling stock. Both documents were applicable to operations undertaken on the main line, a terminal or a yard.
The standard identified PN’s obligation relating to the assessment of shunting risks and defined the responsibilities for the PN staff involved. In a terminal or yard, the terminal operator in charge of a shunt was responsible for providing instructions to the locomotive driver to facilitate the placement of rolling stock. The terminal operator was also responsible for detaching or coupling wagons.
Rolling stock - Wagons
The PN procedure detailed the specific processes and communication exchange protocols required when undertaking a shunt movement. A key component of the procedure was the implementation of a three-step protection process before a qualified worker (terminal operator or locomotive driver) entered between rolling stock to detach or couple wagons.
The intention of the three-step protection process was to ensure clear communications between the driver and qualified worker (in the case of 4MW2, the terminal operator) of the intention to enter in between rolling stock to undertake a task. The process was reliant on a sequential exchange of instruction and acknowledgement between the two parties to ensure the driver had undertaken actions to secure the rolling stock from moving.
To implement the thee-step protection, the driver was required to:
fully apply the locomotive’s independent brake and if required the automatic brake[16]
position the throttle to idle
move the reverser lever to the centre position
Once the driver confirmed these protections, the qualified worker could then enter between the rolling stock. On completing the required task, further communication between the terminal operator and the driver was to occur before removal of the protections and the locomotives operated.
Where a wagon or number of wagons were uncoupled and left unattended for any period, the qualified worker was also responsible for ensuring the application of the park brake. A PN generic procedure[17] for securing trains with park brakes specified the minimum number of park brakes required to hold the rolling stock. The number of park brakes required varied depending on the location where stabled and local track grade.
Rolling stock - Locomotives
The safe practices contained in the standard and procedure were similarly applicable to the shunting of locomotives. Where a locomotive or locomotives were to be left unattended[18], the locomotive driver (whether operating as a two-man crew or as Driver Only Operation) was responsible for the uncoupling of locomotives and ensuring that the park brake was correctly applied. A PN generic procedure[19] for securing locomotives with park brakes specified the required actions to ensure the correct application of the park brake.
The park brake on the NR locomotives was a spring-operated device held off by the application of air pressure sourced from the main reservoir. When selected, by the operation of a pushbutton in the locomotive cab, the device released the air pressure and the spring applied the brake to the wheels. The park brake selection relayed electrically to other similarly equipped locomotives coupled in the train via the Multiple Unit interconnector cable.
Previous occurrences
Several incidents have occurred of the uncontrolled movement of rolling stock (run away) in New South Wales. None was directly comparable to the runaway incident at the SFT on 23 September 2015. That is, they did not involve runaway locomotives.
The previous incidents principally related to the securing of wagons that were uncoupled from locomotives or stabled. The incidents prompted the Independent Transport Safety Regulator (ITSR) to issue a Transport safety alert on 13 April 2011[20] to address the effective securement with handbrakes and stop block functionality.
The Office of Transport Safety Investigations (OTSI) also investigated a runaway of rolling stock at Enfield Yard on 3 May 2011[21]. A rake of 28 wagons loaded with aggregate (total mass in excess of 2500t) ran away from North Road No. 1 in Enfield Yard and through the yard before colliding with a rake of 15 empty fuel tanker and three flatbed wagons stabled in South Road No. 1. The investigation identified the immediate cause of the incident was that, during maintenance activities, the air brakes were released on a wagon and the rake ran away due to the rake’s remaining brakes being insufficient to hold it stationary on the prevailing grade.
Pacific National proposed a number of safety actions in response to the Transport safety alert and investigation into the runaway at the Enfield yard.
The sources of information during the investigation included the:
Australian Rail Track Corporation
Pacific National
Pacific National Sydney Freight Terminal staff
Office of the National Rail Safety Regulator
Office of Transport Safety Investigations
RISSB Glossary of Railway Terminology – Guideline Version 1, December 2010
References
Australian Rail Track Corporation ESD-05-01 Common Signal Design Principles S1 – Signalling Locking and Train Dynamics, Version 3.0 Dated 13 October 2015
Australian Rail Track Corporation, Interface Agreement IA1919, Version 8 - draft, dated 23/04/2015
Independent Transport Safety Regulator, Transport Safety Alert, TSA no. 36, Dated 13 April 2011, Effective securement with handbrakes and stop block functionality
Office of Transport Safety Investigations, Rail Safety Investigation Report, Runaway of Rolling Stock, Enfield Yard, 3 May 2011, Investigation reference 04514
Pacific National, Safety Standard Form risk assessment, SFT SHT-01, Revision 4
Pacific National, PN-STD-SAF Shunting Standard, Version 1, 1 June 2015
Pacific National, PN-PRO-SAF Shunting Procedure, Version 1, 1 June 2015
Pacific National, GPR_6_10 Securing Trains with Park Brakes – R02, Dated 1 July 2015
Pacific National, GPR_6_12 Securing Locomotives with Park Brakes R02, Dated April 2009
Rail Safety National Law National Regulations 2012
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Australian Rail Track Corporation, Pacific National, the Office of the National Rail Safety Regulator and the relevant Sydney Freight Terminal staff involved in the shunt of 4MW2.
Submissions were received from the Australian Rail Track Corporation, Pacific National, the Office of the National Rail Safety Regulator. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Safety actions
Additional safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action taken by Australian Rail Track Corporation
On 28 October 2015, the Australian Rail Track Corporation issued an instruction to all Network Control Officers at the Network Control Centre South (NCCS), Junee requiring:
The restoration of the points at the eastern end interface of the Sydney Freight Terminal to the normal position (toward the dead end track section) following each rail movement. There was no exception to this requirement, even when following train movements were to occur.
The Australian Rail Track Corporation also advised the commencement of an investigation into the feasibility of modifications to the signalling control systems to restore the points at the interface automatically and the provision of a catch point alarm on the NCO’s control panel at Junee.
Additional safety action taken by Pacific National
Pacific National post incident actions included:
Toolbox meetings involving all train crew and terminal operators at the Sydney Freight Terminal briefing on the incident and reinforcing the importance of correct communications and the need to follow procedures.
Issue a Business Safety Notice, BSN 15-29 to outline the restrictions on terminal operators uncoupling locomotives, reiterate the application of the three-step protection, and the shunting procedures.
The provision of a manually operated derail situated at the entrance to the Number 9 road in the Gantry road area.
The review and update of the shunting procedures used at the Pacific National Sydney Freight Terminal. The revised procedure includes instruction prohibiting Terminal Operators from uncoupling locomotives from other locomotives.
The locomotive crew undertook re-training in the relevant procedures for securing locomotives and in radio protocols.
Pacific National monitors, on a random basis, the orientation of turnouts at the interface. Where found to be incorrectly set, the ARTC control centre at Junee is requested to set the points for the correct orientation.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 24 October 2014, the Melbourne to Sydney XPT service ST24 was approaching Culcairn station when there was a severe vibration. The driver stopped at the station and upon inspecting the train found that the axle had broken adjacent to the bearing box on the fourth passenger carriage. There were no injuries to passengers or crew. The passengers continued their journey to Sydney on chartered buses.
What the ATSB found
The ATSB found that the axle bearing had failed and completely seized, probably due to cage failure.
The probable cage failure caused the rollers to misalign and seize. This seizure of the rollers generated friction and excessive amounts of heat into the bearing journal. The heat applied to the bearing journal caused it to go ‘plastic’ and separate from the axle (commonly referred to as a screwed journal). In this case, much of the evidence was either lost or damaged beyond useful examination. Consequently, there was insufficient evidence available to determine why the bearing cage may have failed.
The ATSB also identified that ARTC train control, despite receiving reports of trackside fires, made contact with NSW Trains operations, rather than directly with the driver. It is unlikely that direct communication with the driver of ST24 would have resulted in a different outcome in this case because, by the time the potential cause of fires was known, ST24 was already on its way to Culcairn. However, in some scenarios, communicating directly with the train driver would likely ensure a more timely response to issues that may affect the safety of the network.
What's been done as a result
ARTC will ensure that all matters relating, or potentially relating to, the safety of a train operating on the network will be advised in the first instance to the driver of the involved train by the relevant Network Control Officer.
Safety message
Any issues with train services that can compromise the integrity and safety of the network must be communicated directly to the train driver. Communicating through a third party can compromise a timely response.
Source: Sydney Trains
Appendices
Appendix A – Condition monitoring systems
Hot-box detectors
Hotbox detectors are a reactive method of condition monitoring. They usually detect the infrared signature of bearing components and alarm if the temperature exceeds a predetermined setting. However, there are a number of variables that can affect their performance on a mixed freight/passenger rail corridor. These variables include but are not limited to:
train loading
train speed
weather conditions.
Consequently, hotbox detection is usually used as a ‘last line of defence’ to protect railway infrastructure assets critical to production processes such as coal and ore carrying railways.
Due to the potentially unreliable performance of hotbox detectors under mixed freight/passenger conditions, more effort has been directed towards predictive condition monitoring of railway rolling stock travelling on the interstate main lines.
Bearing Acoustic Monitoring
Bearing Acoustic Monitoring (BAM) is a predictive condition monitoring system that ‘listens’ to the acoustic signature of bearings and can detect faults as they develop. It is the primary method for detecting potential bearing faults on rolling-stock travelling on the interstate main line. Recorded data from each train is stored in a database allowing evaluation, trending, and maintenance scheduling of rolling-stock based on predicted bearing condition.
BAM uses sensitive acoustic arrays to record the sounds emanating from wheels and bearings passing through the monitoring site. The recordings are processed for the sound characteristics that are unique to specific types of bearing faults. BAM is best at detecting faults on rolling surfaces such as the inner and outer raceways, and rollers in rolling-stock bearings. BAM can also detect looseness or fretting faults and ‘noisy’ wheels (flanging and wheel flats).
BAM systems are usually installed and maintained by infrastructure managers. However, the data is made available to rolling stock operators through a web interface. The BAM database categorises potential bearing faults in the form of levels of severity (1, 2, and 3 with level 1 being the most critical). The database allows operators to analyse bearing fault history and trends in order to plan their preventative maintenance strategies.
As for any monitoring system, there are some limitations. For example, BAM is a system that ‘listens’ for bearing noises, and under some conditions, other noises (rubbing equipment, tread defects or flanging wheels) may affect the results. However, being a predictive condition monitoring system, multiple passes of potentially defective bearings allows true fault trends to be clearly identified and actioned before a defect reaches a critical level.
It is evident that predictive condition monitoring and a pro-active approach by train operators has become an integral tool for managing the risk of bearing defects on freight rolling stock, especially in relation to rolling surface defects. For example, the ARTC BAM site at Nectar Brook showed a reduction in the number of level 1 rolling surface faults from about 0.5% in 2002 to about 0.05% in 2010. However, Level 1 looseness or fretting (LF1) faults have not experienced the same improvement. In 2002, LF1 faults were about 1.2%, reducing down to about 0.6% in 2005 before rising back to 1.0% in 2009 and 2010.
On-board condition monitoring
In the past, condition monitoring of rolling-stock has been the realm of trackside equipment (Hotbox, RailBAM, etc.), usually fixed at a specific geographical location. While predictive systems may provide a broader level of protection, reactive systems are limited to protection of equipment and infrastructure in the immediate vicinity.
The next evolution of condition monitoring would be one that continuously monitored each wagon for developing faults (predictive) and immediately communicated any critical conditions to the train drivers (reactive). This type of system is referred to as an on-board condition monitoring system. While various limitations (functional and economic) have prevented these systems being widely used on railway freight operations in the past, recent technological developments have now made the concept more attractive. However, at the time of this incident, only limited developmental work had been started within Australia.
Findings
From the evidence available, the following findings are made with respect to the axle failure on XPT ST24 on 24 October 2014 at Culcairn NSW. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
The XPT axle failed when the bearing seized, generating enough heat for the bearing journal to go ‘plastic’ and separate from the axle, a condition commonly referred to as a ‘screwed journal’
In the absence of any evidence to the contrary, the most probable cause of bearing seizure was failure of the bearing cage. This likely allowed the rollers to misalign and jam, resulting in slippage of the inner bearing ring on the journal.
Other findings
There was insufficient evidence available to determine why the bearing cage may have failed.
It is likely that a progressively failing bearing on ST24 caused the trackside fires reported to the ARTC train control.
On receipt of the initial advice of the fire at Winton ARTC promptly communicated with the NSW Trains Operations Manager. However, direct contact with the Driver of ST24 would have been more appropriate.
The grease used by the bearing manufacturer in the new supplied bearings was not an approved grease as documented in ESR 0400 Engineering Standard for bearing grease.
The Hasler data logger in lead power car XP2001 was defective in that it was not recording brake cylinder pressure or distance.
The occurrence
At about 0700[1] on October 24 2014, TrainLink[2] Sydney to Melbourne passenger service ST21, operated by NSW Trains,[3] arrived at Broadmeadows[4] Victoria (Figure 1). At Broadmeadows, there was to be a crew change and passengers disembarking the service.
As ST21 arrived at Broadmeadows, the relief driver, who was waiting on the platform, noticed what the driver described as a strong smell of brakes. During the handover briefing, the two drivers discussed the smell coming from the train. Although a smell coming from the brakes was common on long trips, the relieving driver, now in charge of the train, decided that he would undertake further inspection at McIntyre. McIntyre is located between Broadmeadows and Southern Cross station and was where refuelling of the return service to Sydney occurred.
At McIntyre, the train was re-fuelled and cleaned in readiness for the return journey to Sydney, with a new train identification number of ST24. While re-fuelling, the driver also examined the area of the train thought to be the source of the smell, paying particular attention to the brakes. While he again noticed the brake smell, he did not consider it unusual for a train having just completed a trip from Sydney. He then readied the train, departed McIntyre and arrived at Broadmeadows at about 0835 to pick up passengers. At about 0855, train ST24 departed Broadmeadows for Sydney with 125 passengers and crew on-board.
Figure 1: Location of Broadmeadows, Benalla, Winton, and Culcairn.
Source: Geoscience Australia annotated by the ATSB
At about 1041, ST24 arrived at Benalla station, stopping briefly to set down and pick up passengers. At about 1106, ST24 undertook another passenger stop at Wangaratta before continuing on to its next scheduled stop at Albury.
At about 1123, the Emergency Service Telecommunications Authority (ESTA known as ‘000’) received a phone call from a member of the public, advising of a fire between the Hume Hwy and the railway line about 5 km north of Benalla. After confirming the location, the operator dispatched the Country Fire Authority (CFA) to attend the scene. For the next 20 minutes, passing motorists and members of the public in the Benalla Winton area, reported more spot fires to 000.
At about 1143, the Australian Rail Track Corporation (ARTC) Train Transit Manager (TTM) at Junee Train Control Centre, NSW received a call from the CFA. The CFA reported that a fire in the Winton area was adjacent to the railway line.
Soon after, ST24 arrived at Albury station to set down and pick up passengers, then departed Albury for Culcairn at about 1153.
At about the same time, the ARTC TTM received another call from the CFA reporting that crews were attending the trackside fires. The CFA suggested that the last train through the area (about 30-45 minutes prior) had started the fires. The TTM advised that, at about 1100, a northbound passenger train (ST24) had passed through that area. The CFA re-affirmed their belief that this train had started the fire, as no other fires had been reported anywhere other than the Winton area. The TTM advised that he would contact TrainLink operations in Sydney and get them to make enquiries with the driver of ST24 about its possible connection with the Winton fires.
The TTM contacted the NSW Trains Daily Operations Continuity Centre (DOCC) Operations Manager and informed him of the fire in the Winton area. The TTM explained that the only train through that area in the last 50 minutes was the XPT Melbourne to Sydney service ST24 and that this train may have caused the fire. The Operations Manager informed the TTM that he would contact the driver of ST24 and make further enquiries regarding any problems with the train.
At around 1200, the NSW Trains Operations Manager contacted the driver of ST24 to inform him of a fire in the Winton area. He told the driver that the TTM in Junee had contacted him after they had received a report from the CFA regarding a fire adjacent to the track in the Winton-Benalla area. He told the driver that they believed his train had started it and asked if he had any issues with his train. The driver reported that everything seemed to be okay, but would inspect his train at his next scheduled stop.
The DOCC Operations Manager then contacted the TTM and informed him that he had spoken directly to the driver of ST24 and the driver reported nothing wrong with his train. He also advised that the driver would check it at the next scheduled stop.
At about 1213, the driver of ST24 experienced what felt like a run-in,[5] which he considered unusual for the approach into Culcairn. At about the same time, the driver heard (over the radio) the Passenger Attendant (PA) report to the Passenger Services Supervisor (PSS) of a severe vibration in the first class passenger car. Shortly thereafter, the PSS contacted the driver and advised that something was wrong with the first class passenger car. The PSS described it as a severe vibration, as if the passenger car was running over something.
At this stage, ST24 was approaching Culcairn. The driver determined that the train was still coupled and on the rails, so he decided to continue on the short distance to Culcairn.
At about 1216, the driver stopped the train at the station and notified Train Control (TC) that he was in clear[6] at Culcairn. He also advised that he was going to inspect the train, as the PSS had reported vibration in a passenger car. He asked for the departure signal to be placed at stop and asked for permission to access the track to inspect the train.
After inspecting the train, the driver notified TC that the trailing axle on car B (XL2235) had sheared off (Figure 2). He informed TC that the train was unable to continue its journey and alternative arrangements would be required for passengers to continue their journey. During the conversation, TC informed the driver of other reported fires in the Albury and Gerogery areas.
Figure 2: Failed axle and swing arm hanging down.
The image shows the failed axle journal, commonly referred to as a ‘screwed journal’. As the bearing housing no longer supports the axle, the swing arm has dropped. Source: NSW Trains, annotated by the ATSB
Events post-derailment
Passengers continued their journey on buses. The Australian Rail Track Corporation (ARTC) and NSW Trains examined options for moving the train to a siding at Culcairn. Once a suitable solution was identified, the damaged car was moved to the siding where it remained until arrangements could be made to replace the defective bogie. The remainder of the train then continued to Sydney.
It is likely that a progressively failing bearing on ST24 caused a number of fires beside the track. The fire services attended the fires, while the police attended the scene at Culcairn.
The ARTC arranged for an inspection to ensure the track had not been damaged by the dragging swing-arm. There was no damage to the track infrastructure.
Sydney Trains XPT Inspection Schedule & TMP Inspection Timetable
ASM Handbook, Volume11, Failure Analysis and Prevention
State Rail Authority Engineering Instruction EIDSS 5152 22 November 2004 issue 2
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to Transport for NSW, Sydney Trains, the driver of train ST24, NSW Trains, Bearing Engineering Services, the Australian Rail Track Corporation, and The Office of National Rail Safety Regulator (ONRSR).
Safety actions
Additional safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action taken by ARTC
ARTC will ensure that all matters relating, or potentially relating to, the safety of a train operating on the network will be advised in the first instance to the driver of the involved train by the relevant Network Control Officer.
Context
Location
The failed axle occurred near Culcairn (NSW), about 357 km [7] from Melbourne (Figure 1). The line, referred to by Train Control Junee as Main Line South, forms a main arterial link between Sydney and Melbourne.
The first reported fire occurred near Winton in Victoria (Figure 1) located at about the 207 km point.
Train information
The Express Passenger Train (XPT) is a ‘push-pull’ configured train with a power car at each end of the consist. The XPT was introduced in 1982 and is based on the InterCity 125/Class 43 design used in Britain.
Figure 3: XPT TrainLink power car XP2001.
The image shows an XPT power car and passenger car. ST24 consisted of five passenger cars, identified by the letters A-E, with a power car both leading and trailing. Source: ATSB
Sydney Trains owns the XPT fleet. NSW Trains is the operating agency providing passenger services through country NSW and to Brisbane, Canberra, and Melbourne.
The XPT train (ST24) consisted of a 5-car set with power car XP2001 leading and XP2016 trailing.
Train crew information
At the time of the incident, there were seven train crew on board, including the train driver. The driver of ST24 had over 13 years driving experience with 7 years driving XPT trains. The driver was tested for drugs and alcohol, and returned zero readings.
Train handling
The XPT power cars are fitted with Hasler tape data logging devices. Hasler data loggers record:
time, speed, distance
throttle position (power/idle)
vigilance acknowledgement
brake cylinder pressure.
Of the two devices, the data logger in XP2016 (trailing car) was fully functioning. The recording for the leading power car, XP2001 was incomplete in that it did not record distance or brake cylinder pressure correctly.
The data logged from XP2016 was validated against train control graphs for distance travelled. The brake cylinder pressure could not be validated against XP2001 data logger. However, the recorded brake cylinder pressures changes indicate a consistent deceleration pattern with similar changes seen in the recorded BCP during all braking sequences on XP2016.From the evidence available, it was determined that the train handling was generally consistent with common train handling practices.
Refuelling
The XPT trains require mid-journey refuelling for the service from Sydney to Melbourne and return. During the re-fuelling at McIntyre, the driver of ST24 also looked for any issues that may have caused the brake smell observed at Broadmeadows.
Due to the train’s position, it was not safe to check its left hand side (in the direction of travel to Sydney) because of the adjacent live track. However, the driver did check the right hand side of the train, checking cars A, B, and C (Melbourne end - last three carriages). During these checks, the driver did not see any signs of the journals or bearing boxes being abnormal but noted that there was a smell and the brakes were warm. However, the driver did not think it was out of the ordinary, as the train had just completed a journey of over 1000 km.
Track information
The Main Line South track is a standard gauge track[8] consisting of continuously welded rail on concrete sleepers, fastened by resilient clips.
The ARTC lease and manage the track. Control for the Main Line South signalling is from the ARTC Train Control Centre at Junee.
Track speed approaching Culcairn station is 160 km/h for XPT services. The service only stops at Culcairn when passengers are scheduled to disembark or board the service.
Bearings
The bearings used on the XPT fleet are Timken SP120 package tapered roller bearing. Package bearings consist of two tapered bearing assemblies (commonly referred to as cones, and includes the inner rings, rollers and cage). Between the two bearing assemblies is a spacer ring of specific width, correctly positioning the two cones when the bearing is assembled. Outside each bearing assembly is a seal wear ring, over which the grease seal is positioned. When installed in the wheel-set, a backing ring is mounted on the inboard side of the axle journal and an end-cap is bolted onto the outer end of the bearing journal (Figure 4).
Figure 4: Package bearing components
Source: ATSB
The Engineering Instruction for TrainLink wheelsets requires the bearings to be put into service within two years of manufacture or requalified date. If the date is more than two years, the bearings are required to have the grease replaced.[9]
Package bearings are installed as fully greased sealed units and are press fitted onto the journal at Unipart UGL in Auburn. The bearings do not require in-service regreasing, which reduces the risk of inadequate, excessive, or contaminated lubricant during operation.
Bearing history
Timken bearings supply new SP120 bearings to Bearing Engineering Services[10] (BES), which then supply UGL Unipart bearings for the XPT fleet. BES also service and requalify bearings for reinstallation.
Combinations of new and requalified bearings were installed on passenger car XL2235. The new bearings were manufactured in South Africa in 2012. These bearings were supplied to UGL with Renolit MP3 grease, as installed by the manufacturer. The requalified bearings were overhauled in 2013 (by BES) and supplied to UGL with Timken premium railroad grease.
The bearing installed into position 3 (Figure 5) on bogie NHA-8B in June 2014 was a new bearing. The serial number of the bearing was 302379 with a manufacture date of July 2012.
At the time of its failure, the bearing was well within its service life of 375,000 km.[11]
Figure 5: Bearing position on bogie NHA-8B
Source: ATSB
Bearing and axle examination
The bogie was taken to the UGL Unipart in Auburn for examination. Preliminary examination of the failed bearing components by the ATSB indicated that the bearing had seized. The remains of the bearing and the accompanying swing arm were taken back to ATSB laboratory for further analysis. The remains of the axle journal were not recovered.
It was evident that the bearing had seized while the axle was still turning. The heat generated by the failed bearing was sufficient to heat the journal, to make it ‘plastic’ (Figure 6) and cause it to separate from the axle (commonly referred to as a screwed journal).
Figure 6: Swing-arm bearing housing
The XPT bogie swing-arm bearing housing, viewed from the inboard side. The heat damage is evident and the remaining bearing components can be seen inside the housing. Source: ATSB
The ATSB failure analysis specialists conducted an examination of the failed bearing. Witness marks at the interface between the bearing and the swing-arm bearing housing could not be examined due to the extensive damage to the bearing.
There were a number of flat rollers on the inboard (Figure 7-1) and the outboard (Figure 7-3) bearings. Markings on the flattened rollers indicate that the rollers seized and misaligned in the bearing cage while the axle was rotating.
The inboard raceway showed evidence of full-width spalling[12] fatigue (Figure 7-2). The spalling fatigue began from the 6 o’clock position and continued in the direction of rotation to the 9 o’clock position. There was also some fracturing of the shoulders on the unworn surfaces of the track.
The outboard raceway showed a full-width area of galling[13] and deposited metal (Figure 7-4). Galling is usually associated with a lack of lubrication, resulting in the two metal surfaces welding together for brief periods.
The investigation also examined the partner bearing from the opposite end of the axle.
The partner bearing was removed from the journal and the end cap bolt torque measured. The torque values were consistent with the maintenance requirement. Initial observations indicated that the partner bearing was generally in good condition.
Partner bearing examination by BES
BES conducted an examination of the partner bearing, with the ATSB present.
The bearing was weighed and grease samples from the inner, outer and spacer (centre) of the bearing was taken and sent for analysis. The BES examination found that the bearing showed uneven adaptor fretting[14] marks on the cup exterior (Figure 8-1). There was also wear and damage to the inboard raceway (Figure 8-2) and outside edges of the inboard cone rolling elements (Figure 8-3). Conversely, the raceway and rolling elements of the outboard cone (Figure 8-4) were in good condition.
Based on the amount of fretting on the bearing cup BES concluded that the bearing was probably misaligned (unevenly loaded) from when the bogie was put into service.
Figure 8: Partner bearing
Image 1: Uneven fretting marks on the exterior of bearing cup indicating uneven contact pressure between the bearing cup and the swing-arm bearing housing.
Image 2: Indentation damage to the inboard raceway.
Image 3: Peeling damage to the rolling elements of the inboard cone, predominately on the outside edges due to uneven loading.
Image 4: Undamaged rolling elements from the outboard cone. Source: BES
During the BES examination, ATSB investigators took grease samples from the partner bearing for analysis. After the BES examination was completed, ATSB investigators retained the partner bearing for further analysis.
Partner bearing examination by the ATSB
An ATSB failure analysis specialist examined the partner bearing components using an illuminated magnifier and with a stereomicroscope.
Outer cone
The outer cone had limited wear with fine brinelling,[15] scoring and polishing. This wear was also evident in the analysis of the grease samples. The samples contained iron but not chromium from alloy steel (the rollers, cup, and cone). The wear had mostly come from the soft, plain-carbon steel cage.
Inboard cone
The results of the inboard cone analysis contrasted with that of the outboard cone, with significantly higher presence of chromium from the alloy steel cup, cones and rollers.
The examination found evidence of metal loss to the bearing spacer and inner rear enclosure. The wear on the spacer would likely have resulted in some loss of preload on the bearings resulting in excessive end float. Increased end float would have placed uneven loading on the bearing, in particular the back-face end of the inner cone/double cup. It is possible that this point on the partner bearing acted as a fulcrum when the axle journal failed and the opposite end of the axle became unsupported.
The rollers of the inboard cone showed evidence of adhesive wear, but only at the back-face end. This corresponded with the inboard raceway, which exhibited a worn shoulder with several bright areas of spalling.
Swing-arm Bearing Housing
The swing-arm bearing housing showed heavy fretting wear that corresponded with asymmetric fretting wear on the bearing cup (Figure 9). Also observed, was the crack in the upper half of the bearing housing (Figure 10).
Figure 9: Partner bearing (position 4) serial number 302111
The corresponding fretting marks found on the partner-bearing cup was also evident on the partner swing arm. Source: ATSB
Figure 10: Swing arm assembly with exploded view of the bearing housing bore below
Figure 10 is of the partner swing arm (from the same axle). The exploded view shows the fretting wear on the swing arm shoulder evident by the shiny marks as annotated. As illustrated, there is also a crack in the valley of the housing. Source: ATSB
These wear patterns provided further evidence of uneven loading, possibly due to the axle misaligning when the axle journal failed and the opposite end of the axle became unsupported.
When matching the bearing cup witness marks to those in the swing-arm bearing housing, the marks ranged from a 9-3 o’clock position and were asymmetric in nature. This indicated that there might have also been some misalignment in the horizontal plane (Figure 11).
Figure 11: Bearing position on bogie NHA-8B
Figure 11 is for illustrative purposes and not a direct representation of an XPT bogie. The black dotted line on the trailing axle represents the centreline of the axle when running true. The red line illustrates a misalignment of the trailing axle, in the horizontal plane. Source: ATSB
The ATSB concluded that there was evidence of uneven loading. However, there was insufficient evidence to determine if the misalignment was predominantly in the horizontal or vertical planes.
When considering the physical evidence and examinations by both BES and ATSB specialists, the most likely conclusion is there was a misalignment in the axle. However, there was insufficient evidence to determine if this was a pre-existing condition or if it occurred because of the bearing failure.
There were no conditions associated with the partner bearing (position 4) that would suggest a possible cause for the failure of the bearing in position 3.
Grease analysis
The type of grease used by Timken in the new bearings is Renolit MP3 grease. The operator’s Engineering Standard for grease used in journal bearings for seal and package units requires that the grease be approved by the Association of American Railroads (AAR). Renolit MP3 grease is not approved by the AAR in this application. However, the grease has almost identical properties to that of an AAR approved grease type such as Timken premium railroad grease. There is no evidence that the use of Renolit MP3 grease contributed to the failure.
Partner bearing grease analysis
The partner bearing grease samples were sent to the ALS Laboratory Group for analysis. The results showed a mid-range content of silicon (contaminant) and higher levels of iron from the centre (spacer ring) grease sample, mid-range chromium and silicon with higher levels of iron from the inboard sample and low levels of chromium with mid-range levels of silicon and higher levels of iron from the out-board sample.
The chromium levels from the inner and outer grease samples indicate that it was liberated most likely from the inner and outer cup and because of the peeling damage from the inboard cone roller faces. Indentation marks on the inner and outer race was evident from the BES report and ATSB analysis.
The iron found in all three samples is likely to be from the roller cage as a result of the axle failure placing more stress on the partner bearing.
Although the grease analysis showed high levels of contaminants and iron it is likely this is due to the failed axle.
Examination of the partner bearing grease found no condition or anomaly that could be directly related to a potential issue with the corresponding failed bearing.
Bearing failure types
The recovered bearing components were examined in relation to the common failure modes for railway bearings.
A loss of interference fit between the bearing and axle journal often occurs later in the failure sequence. That is, other faults may combine to cause progressive loss of interference fit. Initial slippage may be small, but as the journal wears, the amount of slippage increases.
However, if a bearing seizes, slippage of the inner ring on the journal can suddenly occur.
Lubrication failure
The function of a lubricant is to separate the rolling contact surfaces at the point of high-pressure contact. The lubricant film between the surfaces acts to reduce wear, friction and corrosion such that the bearing should achieve its predicted fatigue life; assuming that no other factors exist that may cause premature failure. Lubrication failure can occur due to an inappropriate grade of lubricant, insufficient lubricant or contamination of the lubricant.
Cage failure
The bearing cage is designed to retain the rollers within the bearing in a consistently spaced and correctly aligned position. The cage has no role in the transmission of forces. The cages in bearings used in the railway industry are usually pressed out of metal plate.
The purpose of roller bearings is to avoid sliding friction. However, sliding at the cage surfaces cannot be avoided. Consequently, the softer material of the cage (when compared to other components) is likely to be the first area to wear when lubrication becomes inadequate or foreign material causes abrasion. Once wear occurs, the cage loses the ability to align the rollers correctly and leads to a rapidly deteriorating cage resulting in a complete failure of the cage. Once the cage fails, material jams the rollers, generating heat and the bearing inevitably fails.
Bogie NHA-8B maintenance
UGL Unipart, located in Auburn NSW, is the contracted maintenance provider for XPT bogie refurbishments. XPT carriage bogies are overhauled every 750,000 km with the wheelsets overhauled every 375,000 km. New or requalified[16] bearings are fitted with the changed out wheelsets.
The ATSB examined the maintenance records of bogie NHA-8B. The records show that during the assembly and overhaul of the bogie, all components and relevant measurements meet the requirements of the XPT carriage NHA Bogie Overhaul Specification RX01_0200_123MP.
In June 2014, passenger car XL2235 had the overhauled bogie NHA-8B fitted to the B end of the passenger car. The failed axle of the bogie set (the trailing axle in this case) had new bearings installed. The lead axle assembly had requalified bearings.
In-service inspection and maintenance
XPT carriages undergo trip inspections either at 2-day intervals or at 3000km, and maintenance every 90 days.[17] Both inspection intervals include the testing of axle box temperatures (by feel) as the train is being fuelled and decanted.
Axle boxes are also inspected for:
loss of lubricant at rear axles seals
discolouration indicating overheating.
During the operation of carriage XL2235 on 15 August 2014, a defect was noted on bogie NHA-8B on the power car logbook[18]. The defect was reported as a ‘whirring’ noise from beneath the car and the axle boxes were warm to touch. The defect was inspected on the next scheduled service on 16 August 2014 and no issue was found. The carriage was returned to service without any further noted defect regarding whirring noises or warm axle boxes.
The last documented trip inspection was on 23 October 2014 with no issue recorded. Analysis of the maintenance documentation including the defect history and inspection records indicated that there were no pre-existing maintenance issues identified with bogie NHA-8B.
Condition monitoring systems
Condition monitoring systems can be split into two generic types, reactive and predictive. These are akin to reactive and preventative maintenance. A reactive approach requires an immediate action after a serious condition develops or equipment failure occurs, whereas a predictive/preventative approach identifies the requirement for future action before a serious condition develops.
Reactive condition monitoring, such as hotbox detectors, are usually used as a ‘last line of defence’ to protect significant or critical railway infrastructure assets. They are usually used on track associated with production processes such as coal and ore carrying railways, but less common on mixed freight/passenger tracks such as the interstate main lines (refer to appendix A).
In this case, there were no reactive condition monitoring systems in place that could have detected the imminent failure of the bearing on XPT service ST24.
Infrastructure managers and rolling stock operators have directed more effort towards predictive condition monitoring of railway rolling-stock travelling on the interstate main lines. With regards to bearing condition monitoring, the predictive systems adopted are Bearing Acoustic Monitoring (BAM) systems (refer to appendix A).
Being a predictive condition monitoring system, multiple passes of potentially defective bearings are required for trends to be clearly identified and actioned before a defect reaches a critical level. Consequently, the systems are positioned throughout the interstate network based on major rail corridors. For the Sydney-Melbourne corridor, the BAM system was located on the Main South up line at Exeter, NSW (about 155 km from Sydney).
Examination of the BAM data for XPT passenger car XL2235 found no evidence of acoustic signatures to suggest the onset of a bearing failure.
In this case, much of the evidence that may have indicated the cause of its failure was either lost or damaged beyond useful examination. However, the absence of BAM data indicating a developing bearing fault would suggest that the bearing on XL2235 experienced a relatively quickly developing fault resulting in catastrophic failure. Consequently, failure modes such as metal fatigue, rolling surface defects and loose bearing components are less likely to have been failure initiators.
Examination of the partner bearing provided no clear indication of a failure mode that may have resulted in the failure of the bearing on XL2235. However, some iron particles where found in the grease indicating wear on the bearing cage. There was also evidence of uneven loading due to misalignment of the axle. However, there was insufficient evidence to determine if this was a pre-existing condition or if it occurred because of the bearing failure.
As most failure modes were considered less likely, the most probable cause of the bearing failure was a cage failure. The cage failure caused the bearing rollers to become misaligned and subsequently seize in the bearing housing. The seizure then caused friction resulting in excessive heat to build up in the bearing housing within the swing arm and journal. This generated enough heat into the bearing journal to cause it to go ‘plastic' and separate from the bearing journal.
Bearing cages may fail due to lack of lubrication, bearing misalignment (uneven loading), shock loading (wheel impacts), or a combination of these conditions. In this case, there was insufficient evidence available to determine why the bearing cage may have failed.
Reports of trackside fires
While in Melbourne, the driver of XPT train ST24 noticed a strong smell typical of hot brakes. The driver inspected the train before departure, but found nothing of concern. The investigation found no other precursor events or conditions that might suggest imminent failure of a bearing on XPT car XL2235 prior to its departure from Melbourne. However, there were events reported during the journey that may have suggested a potential problem with XPT train ST24.
After the passage of ST24, several fires were reported to the fire authorities, which required fire crews to attend.
The first report to the ARTC train control centre was of a fire in the Benalla-Winton area. Soon after, train ST24 arrived at Albury, set down and picked up passengers, then departed Albury for Culcairn. At about the same time, the Country Fire Authority made a second call to the ARTC.
The reported fires were all in close proximity to the track, suggesting that a train had started them. The timing and sequence of the reports suggested that train ST24 had started the fires, as it was the last train to have travelled through that area. It is likely that the failing bearing liberating hot components that consequently started the fires.
Following the second call from the Country Fire Authority, the ARTC TTM contacted the NSW Trains operations manager to advise that there may be a problem with their TrainLink service ST24, and requested them to check their train.
County Link operations contacted the driver of ST24 as he was travelling through the Table Top area advising him of the fire in the Benalla-Winton area. About 15 minutes had passed between the first report to train control and the request for the driver to check the condition of train ST24.
The North Albury and Gerogery fires were reported to train control when ST24 was already at Culcairn. There were no other fires reported on the Main Line South between Winton/Benalla and Sydney for that period.
It is likely that heat generated by a progressively failing bearing on ST24 had started a number of trackside fires. While the fires were reported to train control, there was no direct communication with the driver of ST24.
Communications between train control and ST24
TrainLink XPT trains have mobile phones fitted to every power car that use the Telstra mobile network.
An examination of phone records show that the calls made to the lead power car of ST24 were from the NSW Trains Daily Operations Continuity Centre (DOCC) in Sydney. Phone records obtained from ARTC and Sydney Trains confirm that at no stage prior to the axle failure did ARTC train control contact the driver of ST24.
ARTC Emergency Management
ARTC has an emergency management procedure (TA44) which outlines the management of emergencies within the ARTC rail network. The procedure addresses trackside fires and the management of the network and trains that may be affected by that fire. In short, the Train Transit Manager (TTM) or nominated representative takes the role of the Incident Response Coordinator, responsible for advising the relative parties such as emergency services and train operators of the incident.
In this case, the TTM assumed the incident response coordinator’s role when advised of the fire in the Benalla-Winton area. The TTM then liaised with the CFA control centre to ascertain the position of the fire and if CFA officers were on or near the track.
With respect to a fire in or near the rail corridor, it was evident that the procedures documented in procedure TA44 were intended to manage potential damage to infrastructure, and to manage the risks associated with fire crews working near the rail track. The procedure did not include consideration of the potential cause of a fire.
Requirements under Network Rule ANTR 402
Network rule ANTR 0402 ‘Inspecting trains’ covers inspecting of trains during travel in NSW. The Inspection during travel rule states that:
If unsafe conditions or defects are reported to Network Control, a Network Control Officer must:
Tell the affected Train Crew about unsafe conditions and defects, and
Follow the requirements of Rule ANGE 206 Reporting and responding to a Condition Affecting the Network
An equivalent requirement is not specifically documented in the rules applicable to Victoria.
In this case, the ARTC received advice from the CFA that they believed a train that had started the fires at Winton. By this time, ST24 had just departed Albury and was travelling towards Culcairn. The ARTC contacted a third party (DOCC) requesting a check of train ST24, rather than directly contacting the train crew.
It is unlikely that direct communication with the driver of ST24 would have resulted in a different outcome in this case because, by the time the potential cause of fires was known, ST24 was already on its way to Culcairn. However, in some scenarios, communicating directly with the train driver would likely ensure a more timely response to issues that may affect the safety of the network.
The ATSB identified a similar issue during another investigation.[19] In that incident, it was apparent that the use of a third party was common for facilitating communication between Network Control Officers and train drivers.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.