On 7 May 2023, the pilot of a Diamond Aircraft Industries Inc. DA 40, registered VH-ERE and operated by Flight Training Adelaide, was conducting a solo training flight from Sunshine Coast Airport, Queensland to Brisbane West Wellcamp Airport, Queensland.
At about 1328 local time, the DA 40 entered the runway 31 strip without a clearance resulting in a Boeing 737 aircraft that had been cleared to land conducting a go around.
What the ATSB found
The ATSB found that the pilot incorrectly thought they were holding at a taxiway intermediate holding position due to the distance from the holding point to the threshold and this was reinforced due to misunderstanding of a required instruction from the air traffic control to hold short at runway 31. As a result, they crossed the holding point in anticipation of there being a second holding point closer to the runway.
The ATSB also found that due to the angle of the taxiway in relation to the runway, it would have been difficult for the pilot to have seen the 737 aircraft on final. It is also likely that the crew of the 737 would not have seen the aircraft cross the holding point as it was obscured. Further, although not required to, the information in the Airservices Australia Departure and Approach Procedure charts and the Enroute Supplement did not indicate the holding point locations. Finally, while the Civil Aviation Safety Authority Manoeuvring map for the Sunshine Coast Airport did include the occurrence holding point, neither it nor the runway were accurately depicted.
What has been done as a result
The operator conducted an internal investigation into the runway incursion and has taken the following safety actions:
a NOTAC[1] was issued to address landings in controlled zones, at airports other than home base, and solo flights to controlled zones
a qualified flight instructor (QFI) meeting was conducted to communicate the importance of students understanding the signs, markings, lights and phraseology particularly when at a controlled aerodrome
a student meeting was conducted to reiterate the points outlined in the QFI meeting.
the results of class G and class C & D airspace quizzes appear in the monthly students reports to QFIs
existing tutorials for class D, class C, Sunshine Coast Airport, Archerfield Airport, and Gold Coast Airport were reviewed and updated
an exam and quiz specifically for Sunshine Coast Airport has been created
quizzes for Sunshine Coast Airport, Archerfield Airport, and Gold Coast Airport have been made mandatory for all students before visiting these airports.
The operator is also in the process of reviewing the:
requirements for solo flights to controlled zones, including the requirement for dual flight before any solo flight to any of the training controlled zones
forms used by QFIs for issuing flight plans in controlled zones.
Sunshine Coast Airport, through its safety management process, carried out a review of the occurrence and has undertaken the following safety actions:
Requested an update to the CASA manoeuvring map to correctly identify the runway length, location of displaced threshold and holding point Foxtrot.
The airport has changed the information provided to Airservices Australia in relation to the Aeronautical Information Package (AIP) Enroute Supplement (ERSA) and the Departure and Approach Procedure (DAP) to reflect the runway 31 available take-off distance. Additionally, they have added the distance between holding point Foxtrot and the runway to the additional information section in the ERSA.
The Civil Aviation Safety Authority (CASA) will provide further clarification on the terminology and definition of runway starter extensions and clarity around the runway shading on ERSA and DAP diagrams. CASA has also recommended and supported a runway hotspot depiction at taxiway Foxtrot at the Sunshine Coast Airport to be added to the ERSA and DAP. Finally, the Sunshine Coast manoeuvring map, produced by CASA, has been upgraded to accurately reflect the airport layout.
Safety message
Runway incursions and other runway separation issues are one of the most significant risks to safe aviation operations and are a key global safety priority. This occurrence serves as a reminder to pilots that they should study the most up to date airport information using all available resources if they plan to land at an unfamiliar airport.
In addition, they should never hesitate to ask ATC for clarification if they are unsure or confused about instructions, as it helps prevent potential errors or worse. Common contributory factors and methods of safety controls have been published by Air Services Australia in Runway Incursions at Metro D Aerodromes.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 7 May 2023, a pilot of a Diamond Aircraft Industries Inc. DA 40, registered VH-ERE (ERE) and operated by Flight Training Adelaide, was conducting a solo training flight from Sunshine Coast Airport, Queensland to Brisbane West Wellcamp Airport, Queensland.
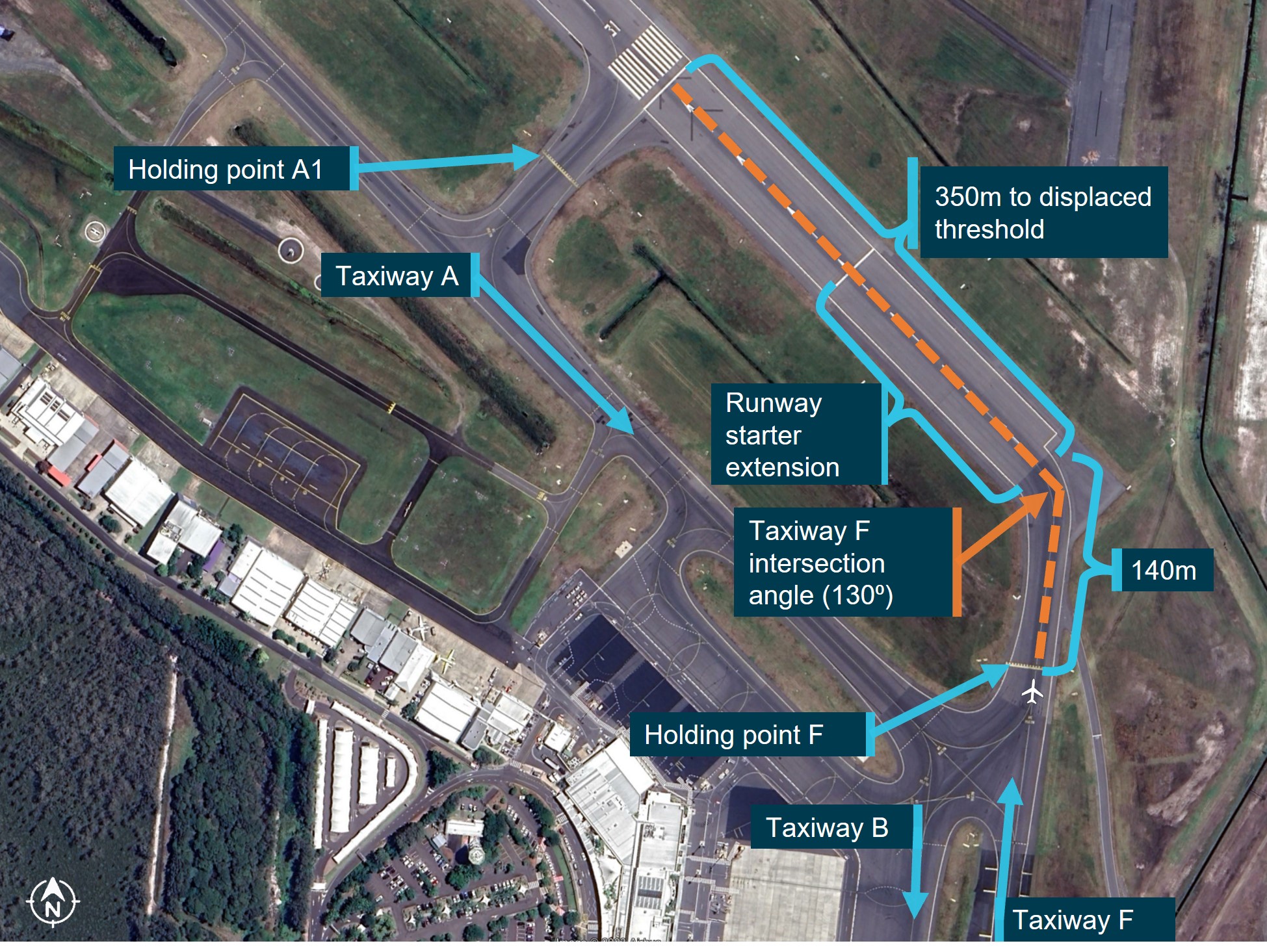
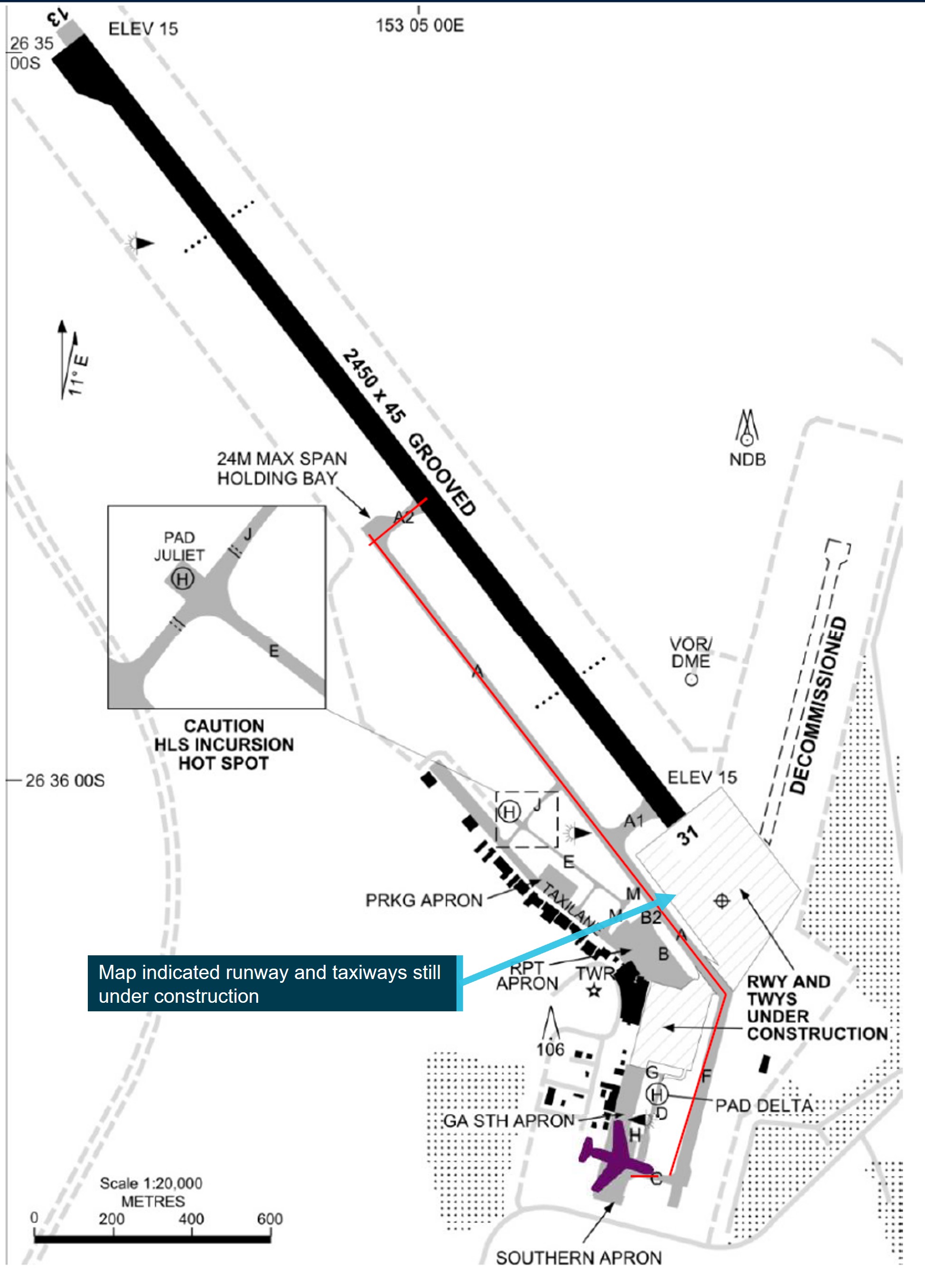
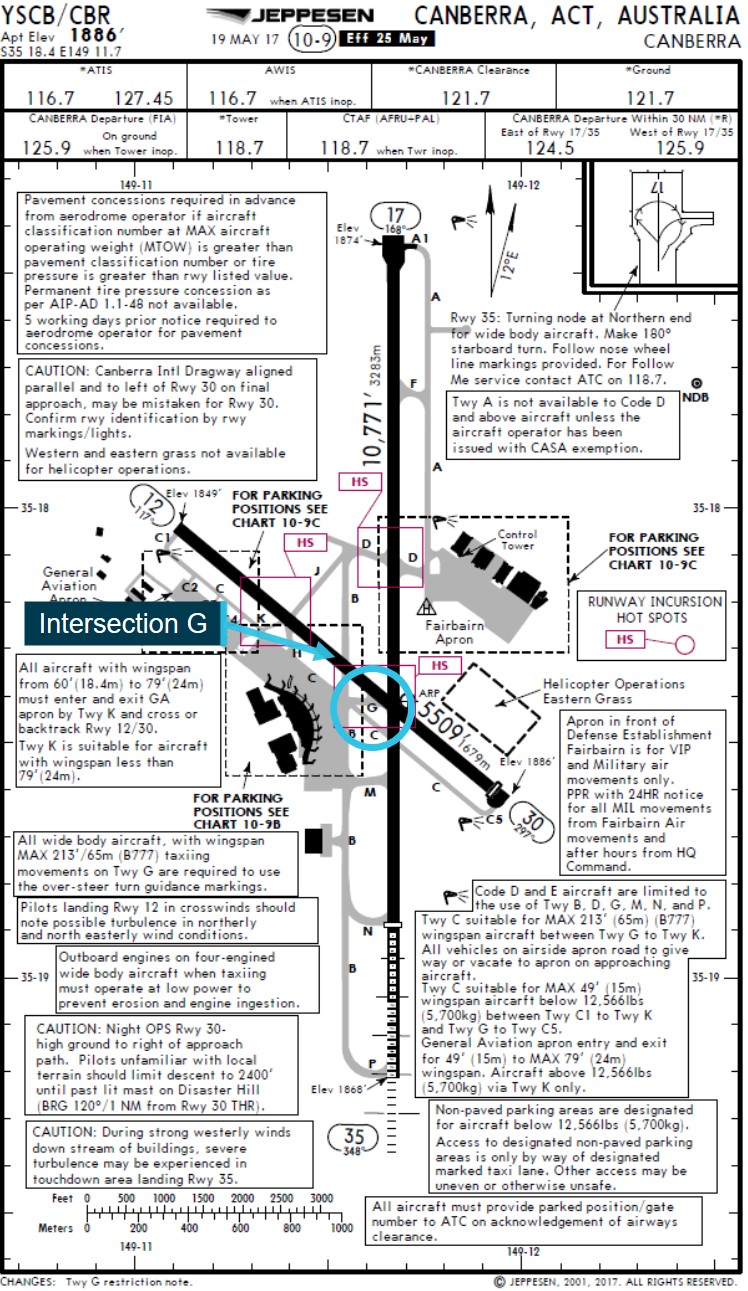
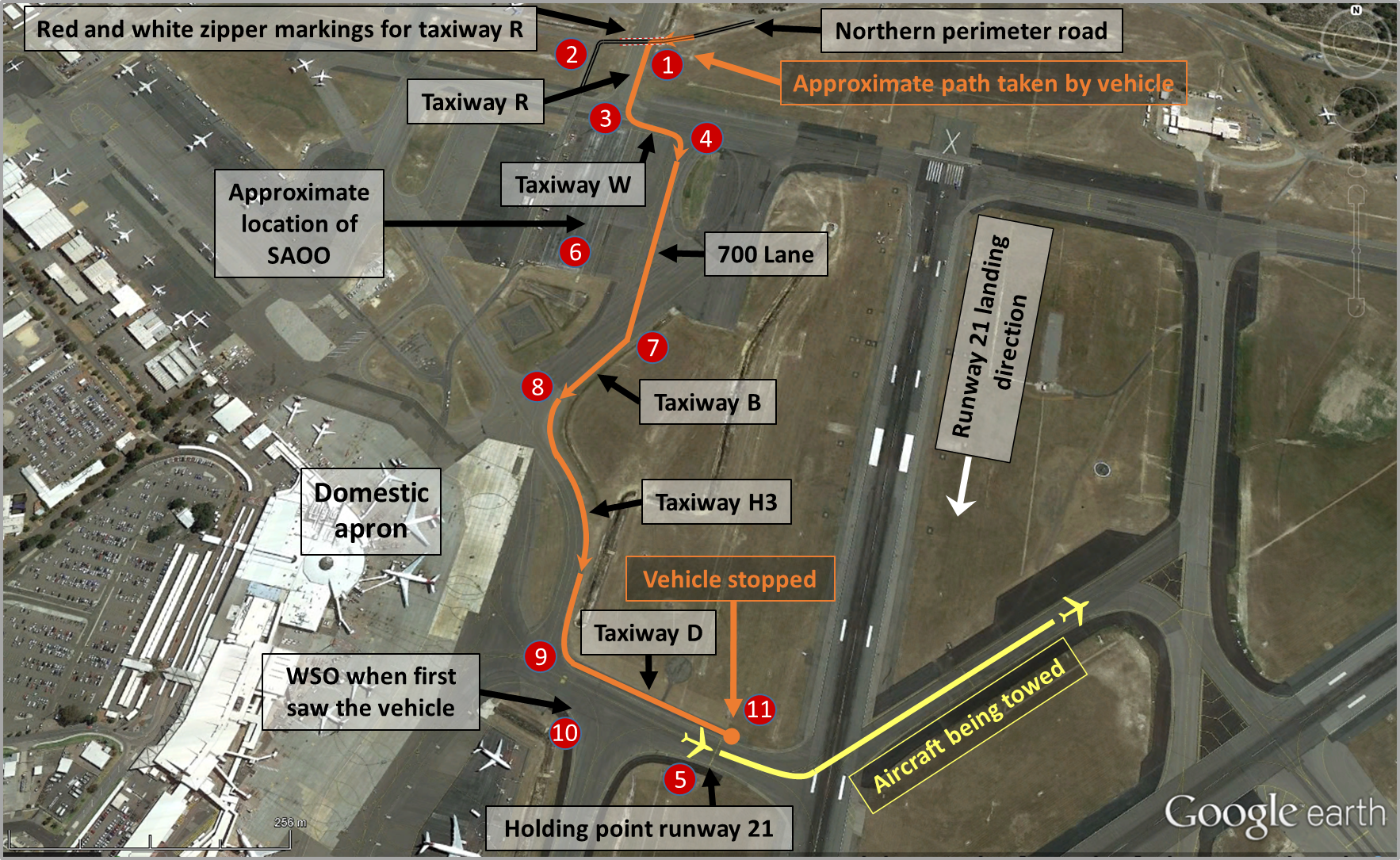
At 1322 local time, while parked at the general aviation area on the airport, the pilot contacted air traffic control (ATC) requesting a departure to the south‑west. ATC instructed the pilot to ‘taxi via Foxtrot to holding point[2] Foxtrot runway 31’[3] (Figure 1) and cleared them to depart for Wellcamp via Esk at 4,500 ft. The pilot readback ‘taxi via Foxtrot, use runway 31 and cleared to Esk at 4,500’. ATC reiterated ‘taxi to holding point Foxtrot’ to which the pilot apologised after reading back ‘taxi to holding point Foxtrot’.
Figure 1: VH-ERE taxi path
Source: Google Earth annotated by the ATSB
ATC then turned their attention to a Boeing 737 (737), which was on final for runway 31, and an airport safety car that was escorting an aircraft under tow to the general aviation parking area. At 1327:25, while the 737 was on final approach, ATC cleared it to land on runway 31.
At 1327:40, ERE stopped at holding point Foxtrot and 20 seconds later the pilot radioed ATC and advised ‘holding short of Foxtrot’. ATC observed ERE stationary at the holding point and instructed the pilot to ‘hold short runway 31’ to which the pilot responded ‘Wilco’. ATC then requested a specific readback of the instruction to hold short runway 31 however, the pilot did not respond. Following a second request from ATC, the pilot responded with ‘Hold short runway 31’.
Ten seconds later, while ATC was completing a departure clearance for another aircraft on the ground and updating flight progress strips,[4] ERE proceeded to cross the holding point without a clearance. The pilot later advised misunderstanding the instruction to hold short of runway 31 as they thought they were holding short of taxiway Foxtrot and that there was a second holding point closer to the runway. The driver of the safety car, who could see ERE and had heard the exchange between the pilot and ATC, notified ATC that ERE had ‘gone onto the runway’ as soon as there was a break on the radio. ERE had travelled approximately 74 m in this time.
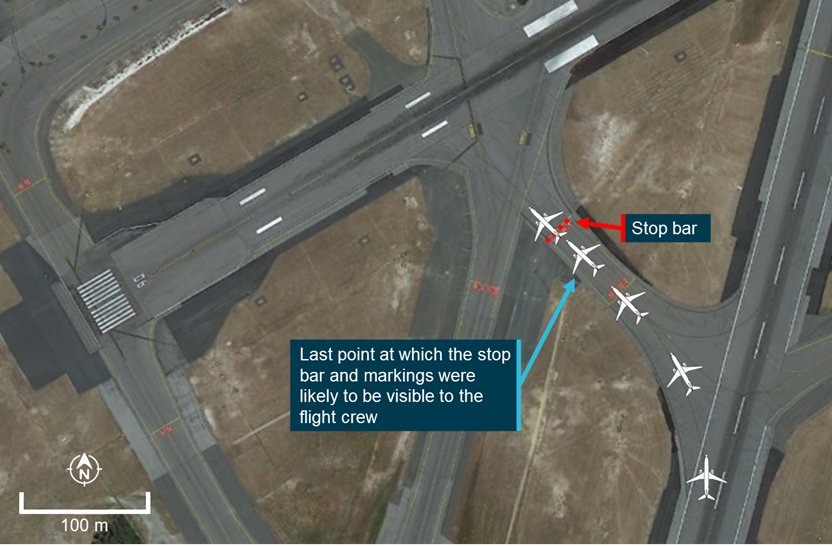
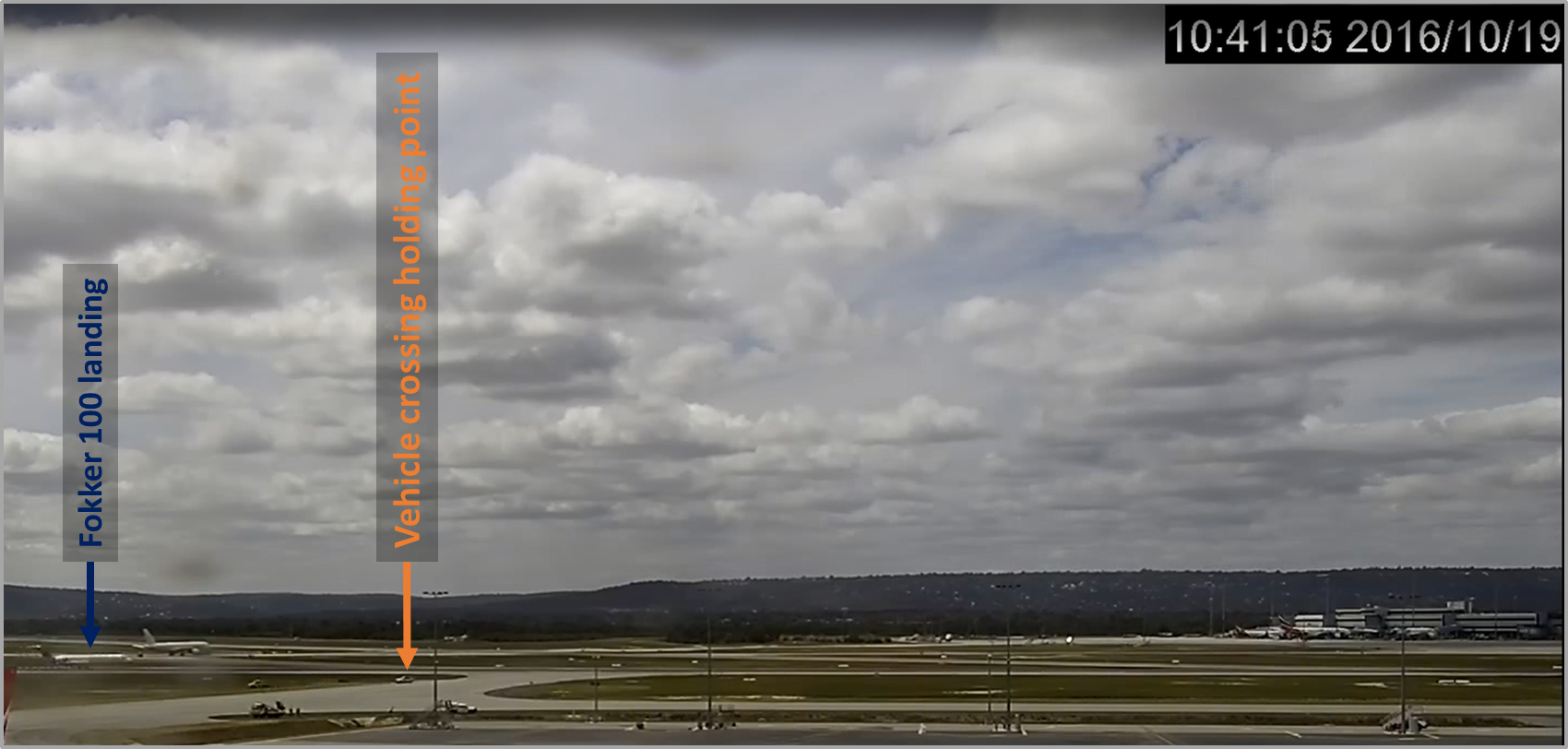
Figure 2: Location of VH-ERE to inbound aircraft
Source: Sunshine Coast Airport annotated by the ATSB
The controller immediately instructed the 737, which was now on late final about 250 ft above the runway, to conduct a go around. One second after the go around instruction was given, ERE stopped. The pilot advised that as they were nearing the intersection with the runway and after hearing ATC instruct the approaching aircraft to go around, they stopped as they could not see a second holding point. The crew of the 737 advised that they had seen ERE stationary at holding point Foxtrot, however due to the high nose attitude of the aircraft, they lost sight of it under the aircraft’s nose as they continued the approach.
At 1329, ATC advised the 737 to make a left circuit and 20 seconds later instructed ERE to make a right turn and vacate the runway at Foxtrot. The pilot turned the aircraft around and taxied back on taxiway Foxtrot and after passing the holding point, was instructed by ATC to turn around and hold position. The 737 landed on runway 31 uneventfully 6 minutes later.
At 1337, ATC advised ERE to taxi ahead and hold short of runway 31 on Foxtrot. The pilot taxied on Foxtrot and just prior to reaching the holding point, ATC advised the pilot that they were at the holding point and described the markings.
At 1341, ATC instructed ERE to line up on runway 31, however, before they entered the runway ATC confirmed with the pilot that they were okay to continue the flight, to which the pilot replied, ‘all good’. ATC then cleared ERE for take-off and the pilot conducted an uneventful take-off and flight to Brisbane West Wellcamp Airport.
Context
Pilot
The pilot held a student pilot licence. They commenced training on 12 September 2022 at Brisbane West Wellcamp Airport. At the time of the occurrence, they had a total flying experience of 132.5 hours, of which 33.7 hours had been in the previous 30 days.
Runway and taxiway information
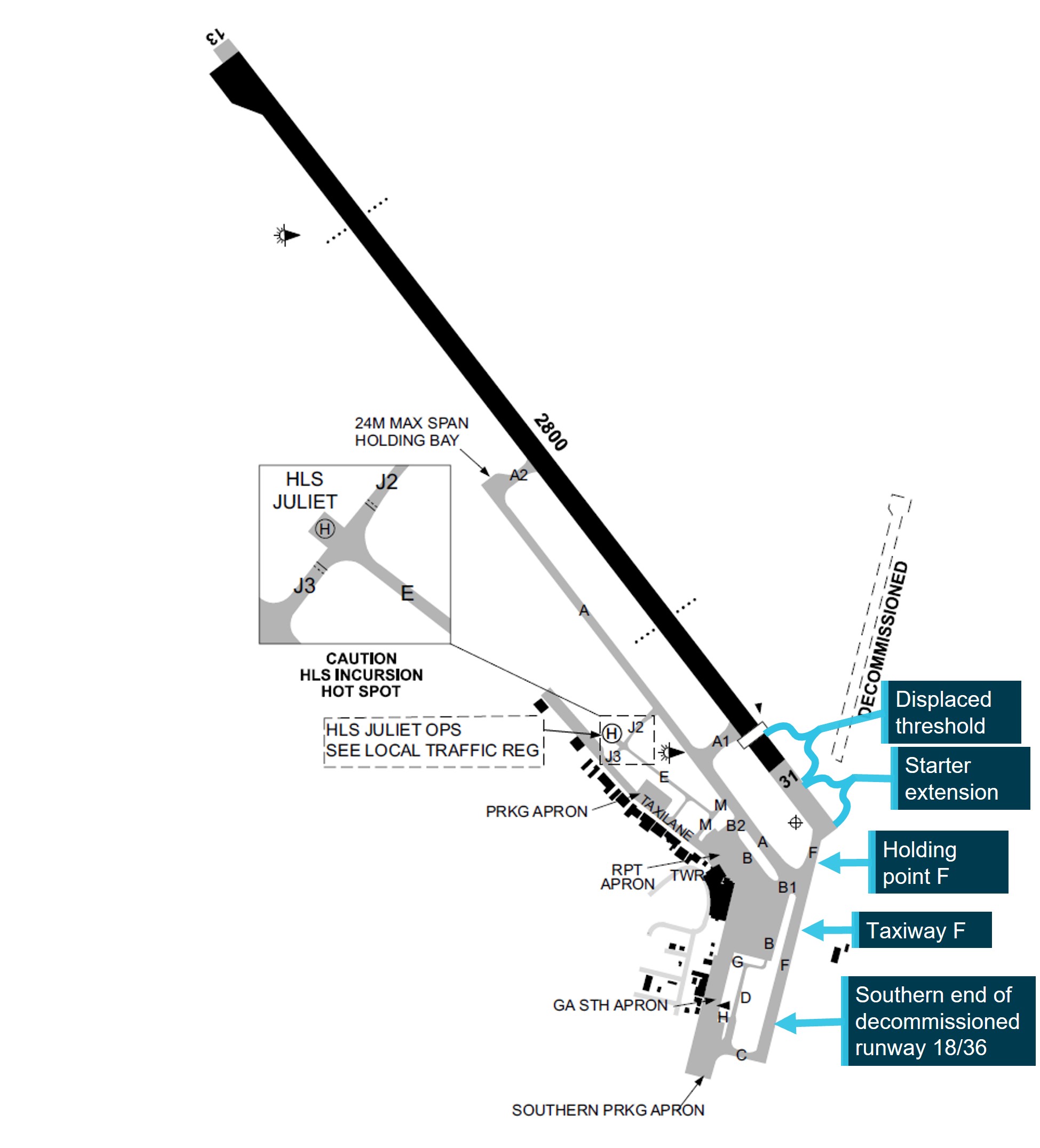
In June 2020, stage 1 construction of a new runway was completed and officially handed over to the Sunshine Coast Airport for operation. Stage 2, which included the completion of the displaced threshold, was completed in December 2020. The runway has an orientation of 128 degrees/308 degrees magnetic, giving the runway its 13/31 designation. The runway length is 2,800 m, which includes a 175 m permanently displaced threshold for runway 31 and a 170 m starter extension.[5] The airport operates within Class D airspace.
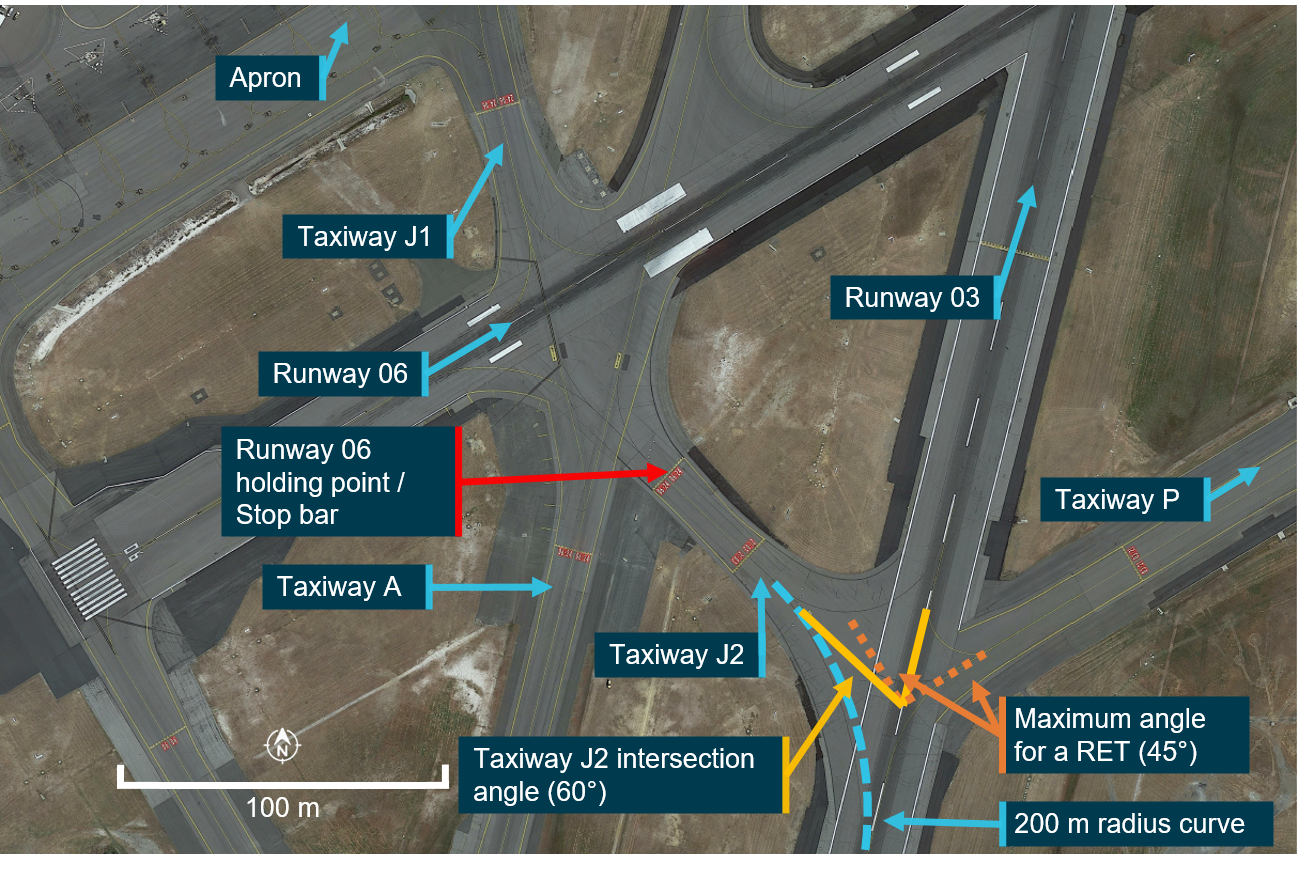
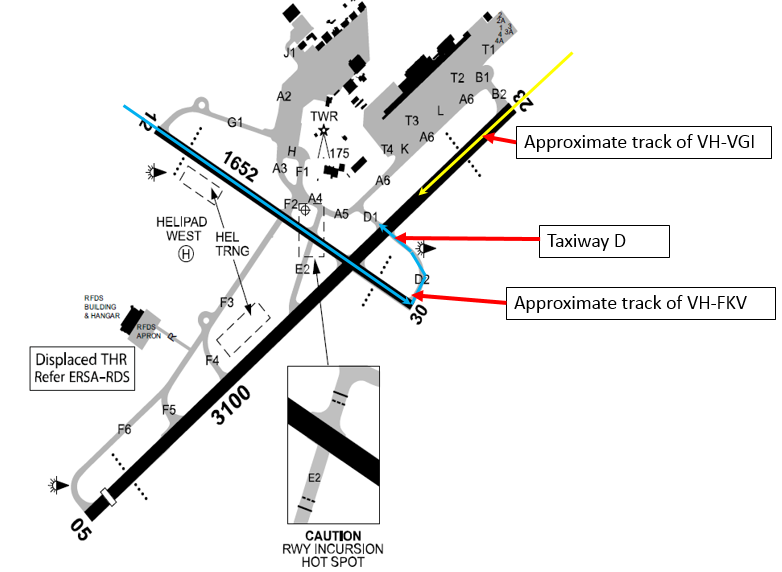
Taxiway Foxtrot is the repurposed southern end of the decommissioned runway 18/36. Due to the angle between the taxiway and runway 31 (approximately 130⁰ - Figure 3), there is approximately 140 m of taxiway from holding point Foxtrot to the intersection with runway 31 required to ensure that the holding point remained outside of the runway strip. Once reaching the intersection, there is approximately 350 m to the displaced runway threshold.
Figure 3: Taxiway Foxtrot in relation to the runway and other taxiways
Source: Google Earth annotated by the ATSB
Airport diagrams
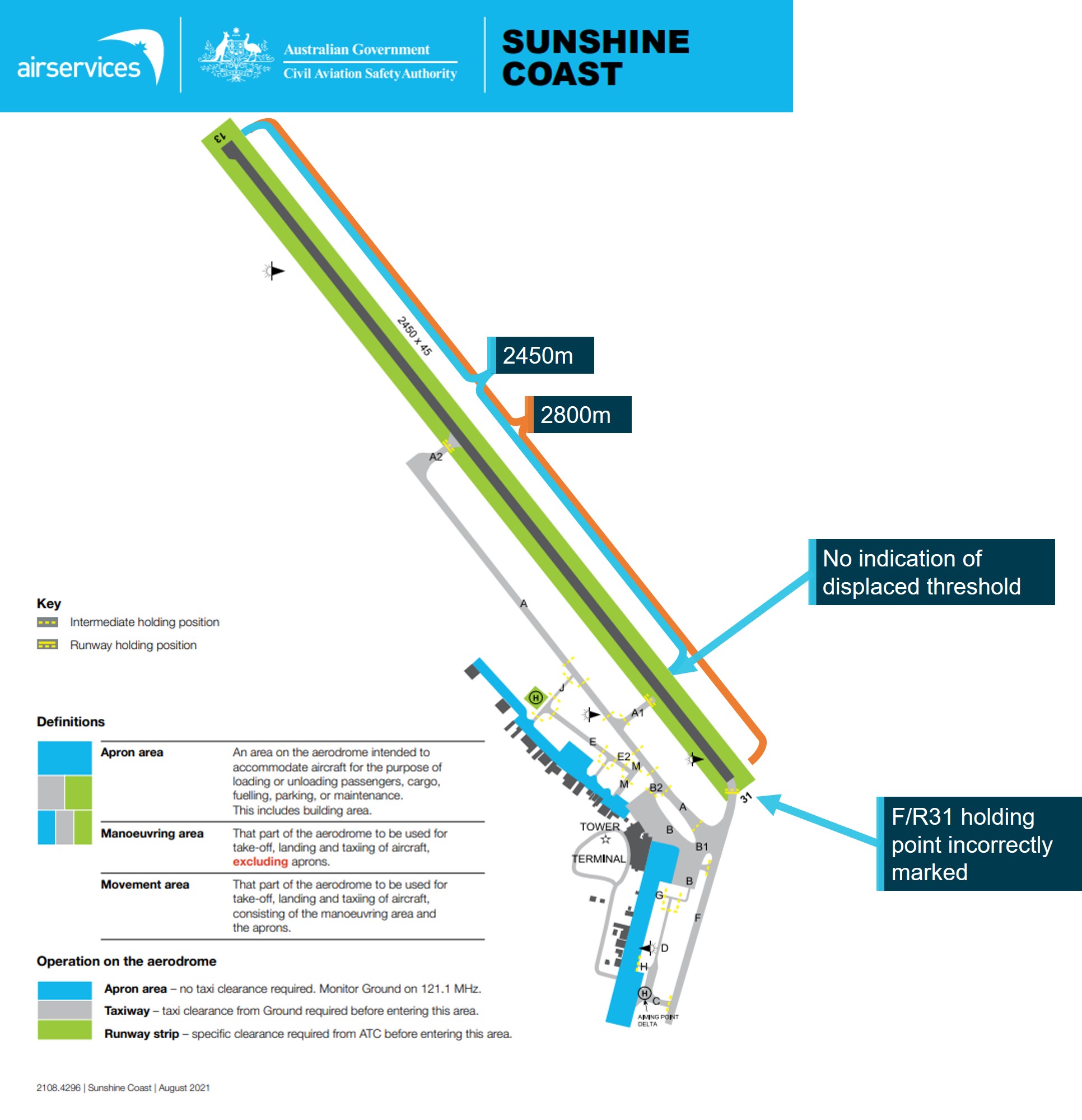
The airport diagram for the Sunshine Coast Airport in the Aeronautical Information Publication (AIP) Enroute Supplement (ERSA) (Figure 4) and the Departure and Approach Procedure (DAP) chart did not indicate any specific holding point locations. In the additional information section in the ERSA, it did not indicate the distance from the holding point to the runway junction. In addition, the ERSA did not indicate the full length of the runway (2800 m) in black shading, which is used to depict the length of runway available for take-off.
The information in these charts is supplied to Airservices Australia as the publishing body, by the Airport owner. The Civil Aviation Safety Regulations Part 139 Manual of Standards (MOS) Chapter 5 Division 2 Standards for information stipulates what information is required to be presented in the AIP documents. This did not require that holding points be depicted in the diagrams. However, International Civil Aviation Organisation Annex 4 Aeronautical charts section 13.6 (g) required that runway holding positions be marked. Australia had filed a difference with ICAO in relation to this requirement.
In addition, Part 139 MOS did not have a definition of a runway starter extension and did not outline the runway shading requirements when a runway starter extension was present.
Figure 4: ERSA Sunshine Coast airport diagram
Source: Airservices Australia annotated by the ATSB
The Civil Aviation Safety Authority (CASA) aerodrome manoeuvring map for Sunshine Coast Airport (Figure 5) indicated that the entire length of the runway was 2,450 m and did not display the extra 350 m of displaced threshold. Additionally, the placement of holding point Foxtrot was not accurately depicted, with it being shown approximately 110 m closer to the intersection of the taxiway and extended runway. The map did not show the decommissioned runway.
Figure 5: Aerodrome Manoeuvring Map for Sunshine Coast
Source: CASA Aerodrome Manoeuvring Map for Sunshine Coast annotated by the ATSB
Holding point Foxtrot
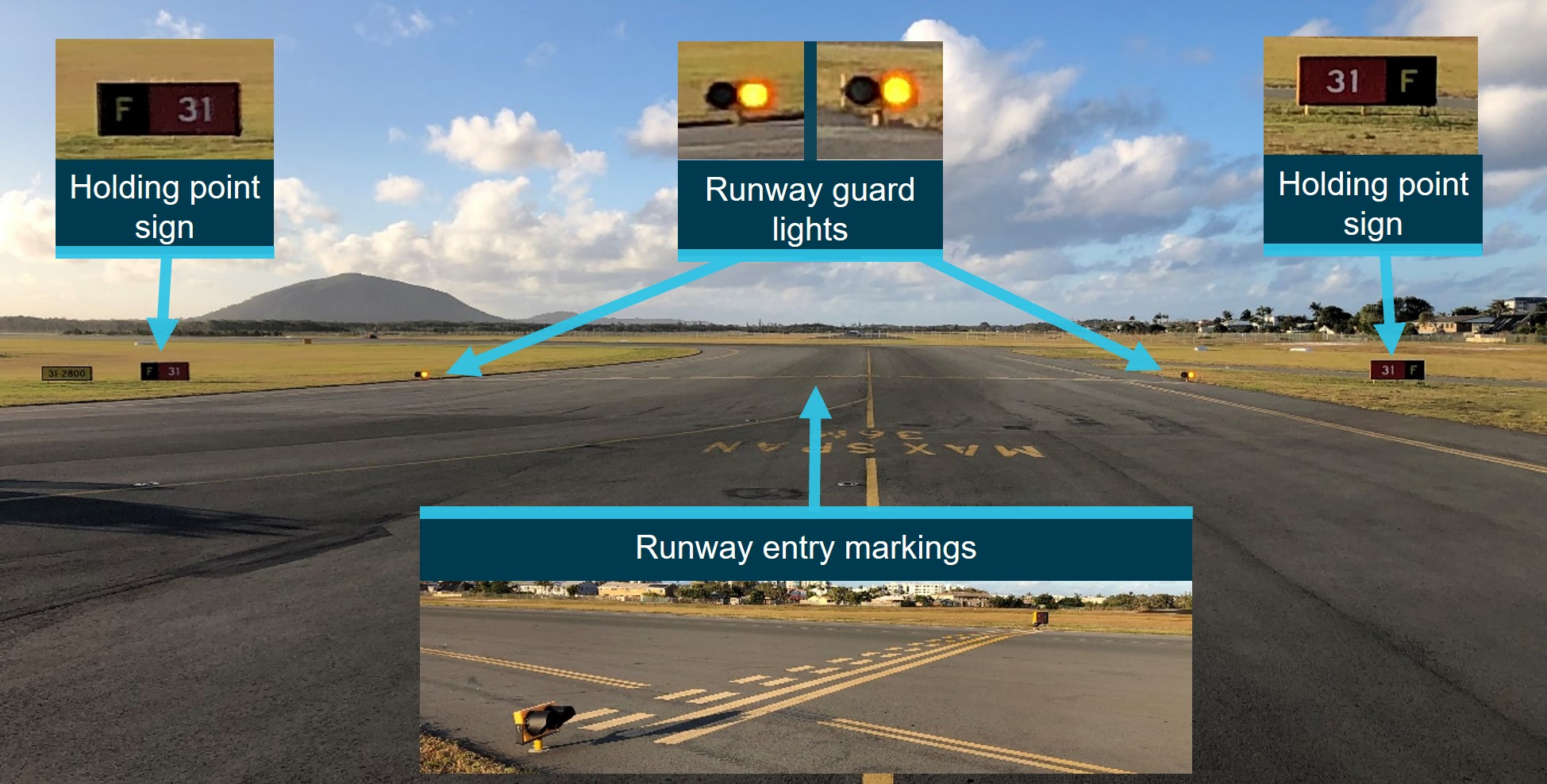
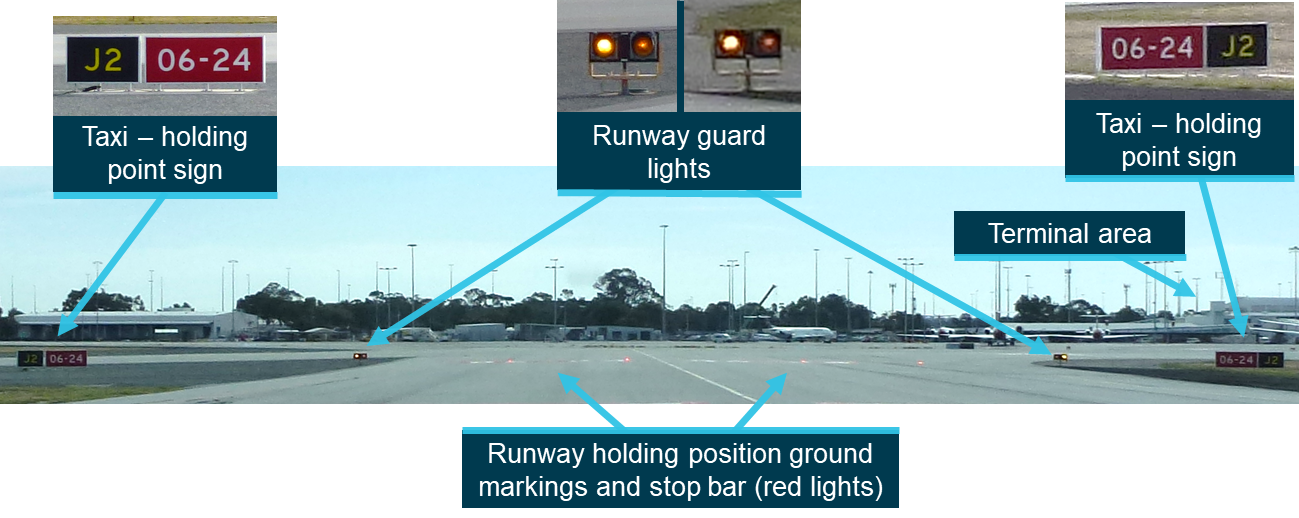
Holding point Foxtrot was equipped with signage and ground markings to provide flight crews with visual cues indicating their position and proximity to the runway strip (Figure 6). The holding point was also equipped with runway guard lights which sat 30 cm above the ground on either side of the taxiway. These were bright yellow, and flashed when the runway was in operation.
The gable markers at the intersection between taxiway Foxtrot and runway 31 were in an irregular configuration to delineate the extent of the graded runway strip. Due to the location of the taxiway intersecting at the corner of the runway strip, flush rather than raised gables were provided at the taxiway shoulder. The gable that would be within the taxiway has been omitted. These differences were conducted under CASA approval.
Figure 6: Holding point markings, signage and lights
Source: Sunshine Coast Airport annotated by the ATSB
From the control tower, which is approximately 400 meters from holding point Foxtrot, the entire length of taxiway Foxtrot, the holding point and the displaced threshold of runway 31 are visible.
Figure 7: View of holding point Foxtrot from the Sunshine Coast Airport control tower
Source: Air Services annotated by the ATSB
Training and briefings
The operator had multiple training documents on runway markings and signs. Students were also taught ground basics at the commencement of their training. Prior to flying solo to any airport in Class D airspace, the operator required that they complete a competency check. They also had a guidance section which included that ‘the student must first have demonstrated competence on two visits to the same aerodrome without instructor takeover’.
The training school records indicated that the pilot had completed the required competency check for operating to a Class D airspace on 18 April 2023, flying into Archerfield Airport, Queensland. The pilot had also completed 3 training flights to Sunshine Coast Airport, 2 flights with an instructor on 28 March and 4 April 2023, and a solo flight on 5 May 2023. None of these flights had required the use of holding point Foxtrot.
The operator had a briefing for Sunshine Coast Airport that contained:
communication frequencies for the airport and surrounds
reference points for training flights
inbound and outbound information
ground information.
The information relating to the runways and taxiways contained a graphic of the runway and taxiways at Sunshine Coast Airport (Figure 8) prior to the runway extension and taxiway Foxtrot completion in 2021. The map showed only 2 runway holding points: A1 and A2.
Figure 8: Sunshine Coast Airport map used in the operator airport briefing for students.
Source: Flight Training Adelaide annotated by the ATSB
Pre-flight briefing
On the occurrence flight, the student used the current ERSA for planning and runway information, and the departure and approach procedures (DAP) available at the time for ground information while taxiing at the airport. The student’s instructor reported that prior to the flight, when a briefing of the airport layout was conducted with the student, only holding points A1 and A2, and the location of general aviation parking were discussed.
Other occurrences
The ATSB has investigated previous runway incursions at various locations throughout Australia, including:
Runway incursion involving Beech Aircraft Corp. 58, VH-NSK Bankstown Airport, New South Wales, on 26 October 2021 (AO-2021-046)
Runway incursion involving a SAAB 340B, VH-ZRH Carnarvon Airport, Western Australia, on 31 August 2020 (AO-2020-045)
Runway incursion involving Sling 2, VH-ZSD Moorabbin Airport, Victoria, on 23 July 2020 (AO‑2020-037)
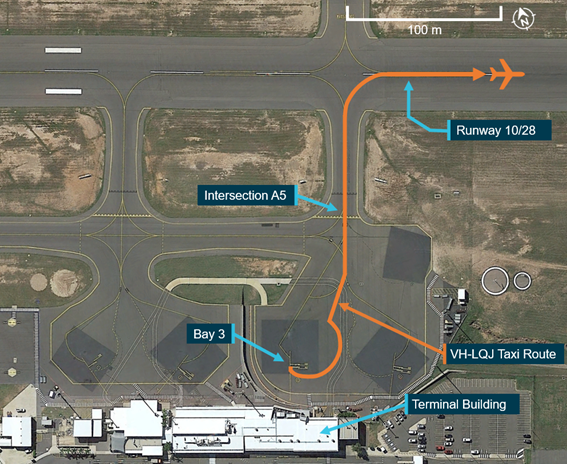
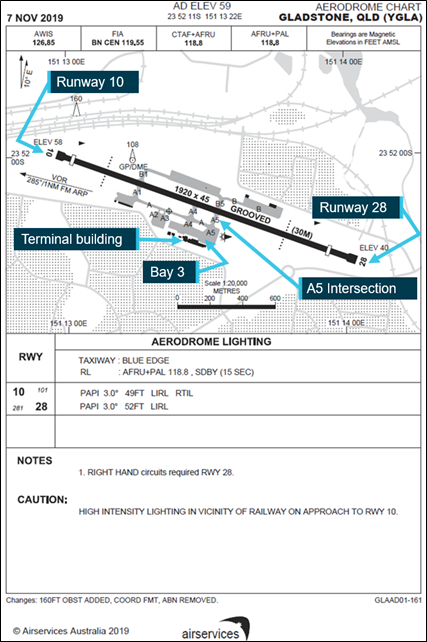
Runway incursion and communication issues involving Bombardier Dash 8, VH-LQJ, Gladstone, Queensland, on 17 March 2020 (AO-2020-019)
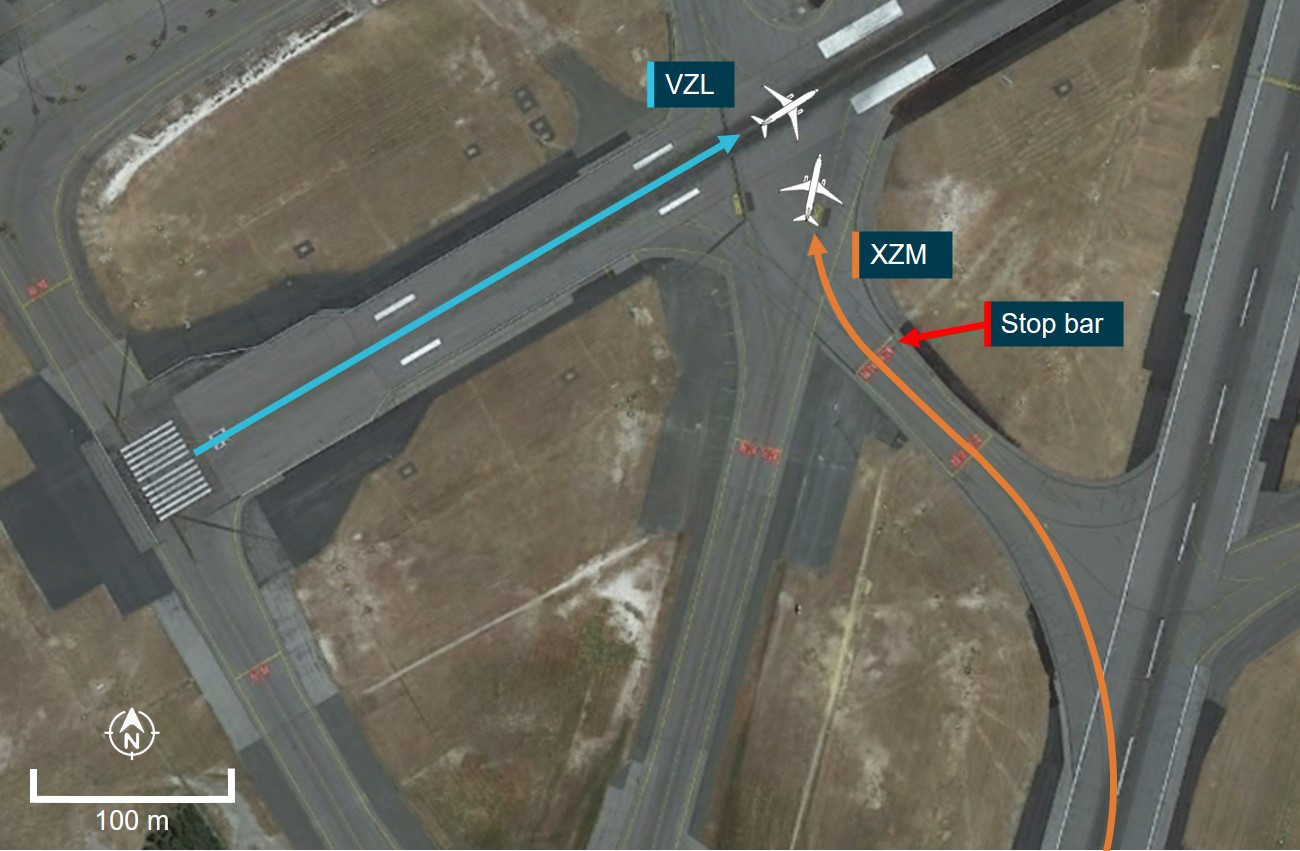
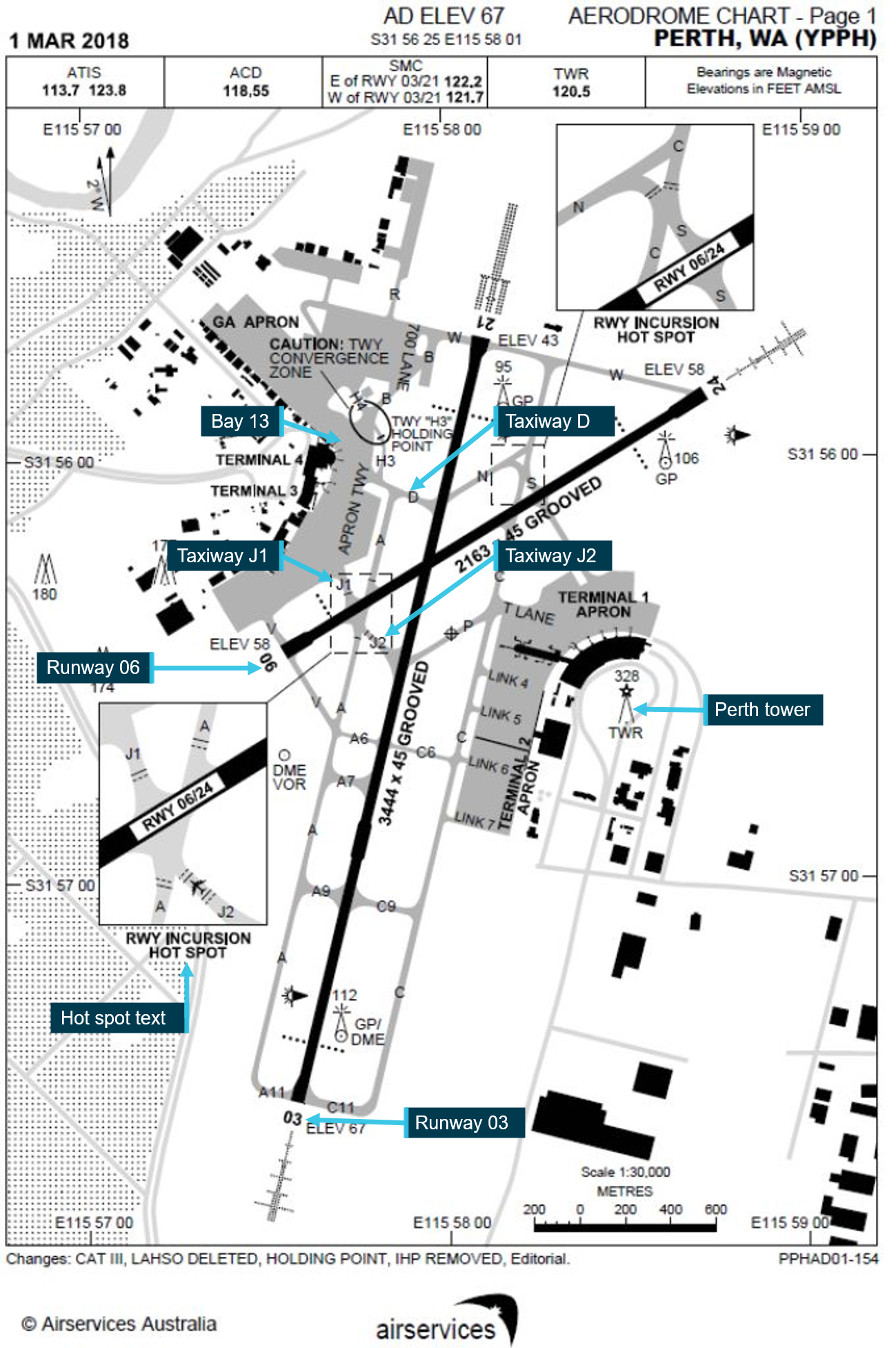
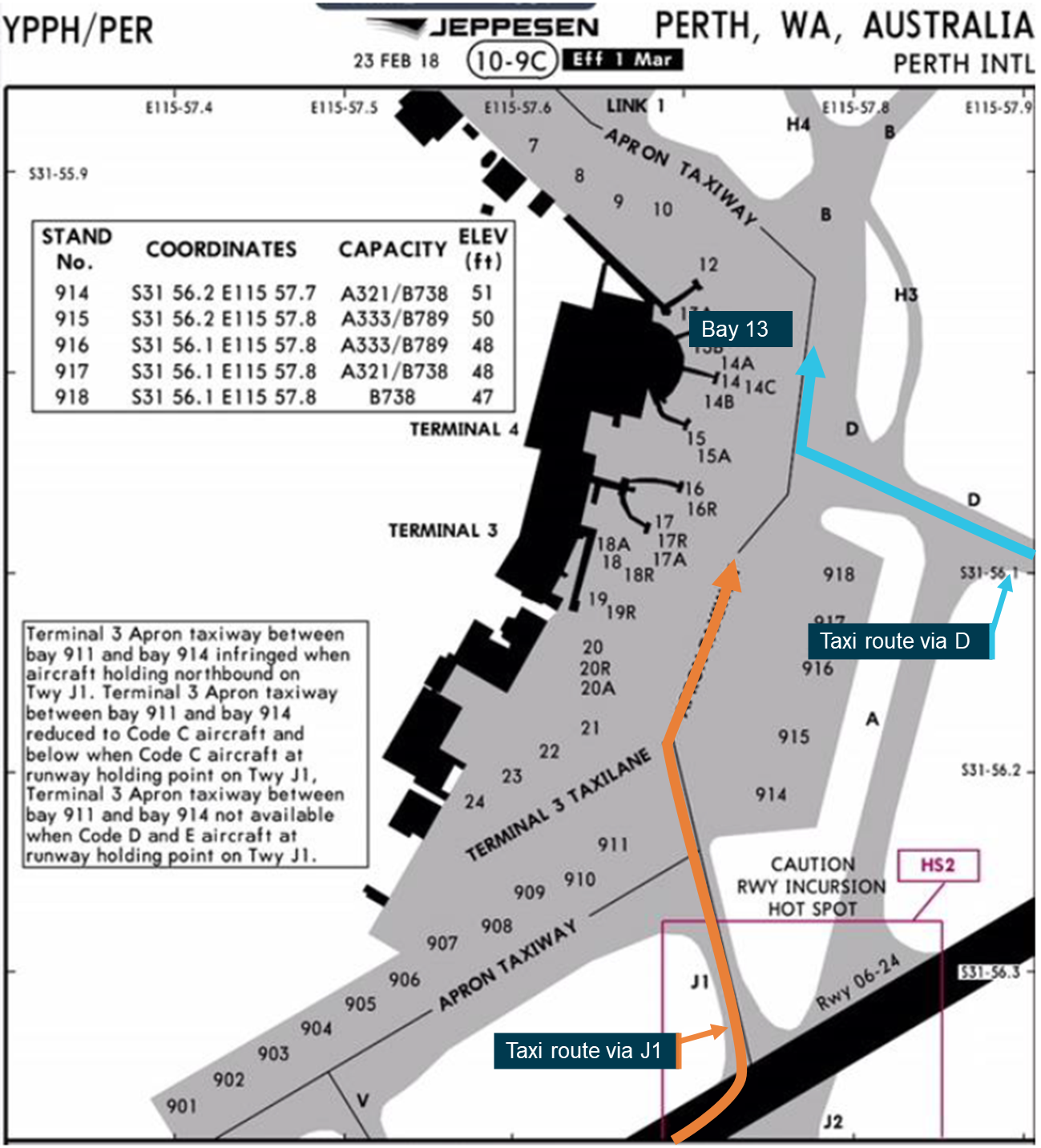
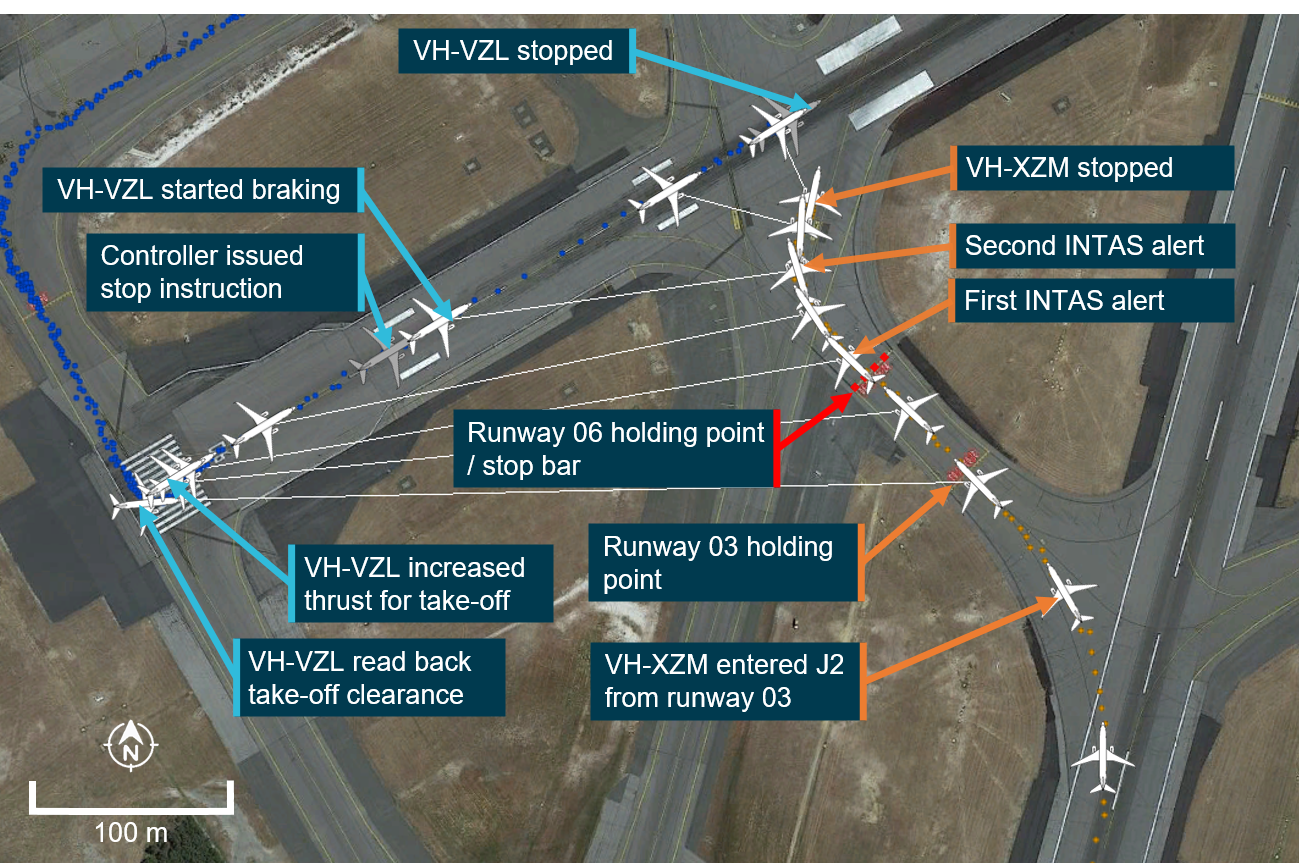
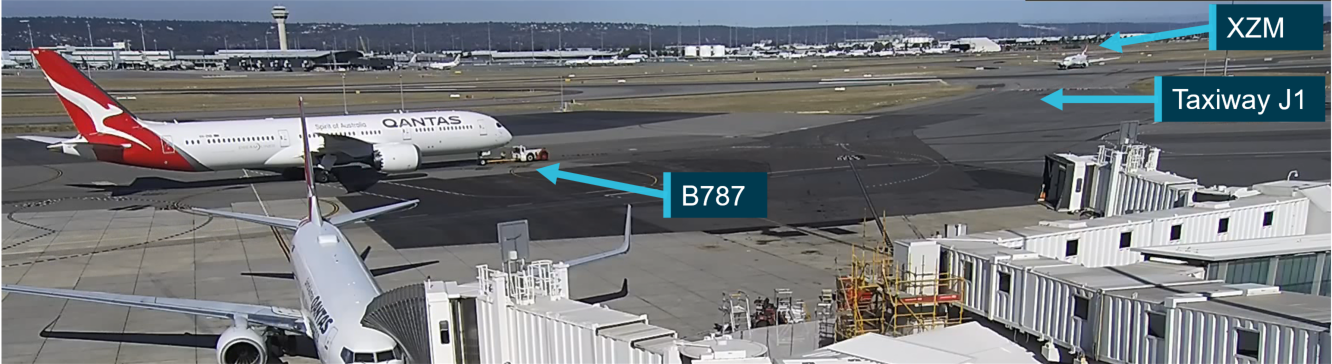
Runway incursion involving Boeing 737, VH-XZM, resulting in a rejected take-off involving Boeing 737, VH-VZL, Perth Airport, Western Australia, on 28 April 2018 (AO-2018-032)
Safety analysis
The pilot was familiar with the runway configurations at Sunshine Coast Airport having flown to the airport previously. However, having never used taxiway Foxtrot, they were unfamiliar with the length of taxiway from holding point Foxtrot to the intersection with the runway associated with the oblique angle between them, and the displaced threshold on runway 31. Due to this distance of almost 500 m, they incorrectly assessed that they were holding at a taxiway intermediate holding position, despite the visible difference between the marking of runway and intermediate hold points and the correct lighting and signage at the holding point. This error was reinforced when the pilot received instructions to ‘hold short runway 31’, as the change in terminology from ATC led them to believe there was an additional holding point closer to the runway. At this point, and while unsure where any additional holding point might be located, the pilot did not ask ATC for clarification on the instructions and instead proceeded to cross the holding point. As the pilot did not expect to enter the runway strip, they did not scan for incoming aircraft. While they had heard an aircraft being cleared to land, they were unaware of the aircraft’s proximity to the runway.
The controller had given the 737 clearance to land prior to ERE reaching the Foxtrot holding point. At that stage, the landing path for the 737 was clear. The controller visually confirmed ERE had stopped at the holding point and had ensured they had read back that they were to ‘hold short runway 31’ prior to turning their attention to another aircraft. The controller was not required to check the landing path for the 737 again until immediately before the aircraft crossed the threshold.
Due to the angle of taxiway Foxtrot to the runway, a pilot in the left seat of an aircraft would need to scan for landing aircraft at an angle of 125–130⁰ from directly ahead. As explained in ATSB report AS-2022-001, a normal field of view is approximately 190° (95° either side of the forward view). This would have placed the approaching 737 outside the normal field of view of the pilot of ERE. It is also likely that the pilot was concentrating to the front of the aircraft as they were looking for a holding point. In addition, the pilot was sitting on the left side of the aircraft and so their view would also have been blocked by aircraft structure. This would have required them to move forward in the seat to have visibility of an aircraft on final approach.
The crew of the 737 did not know ERE had crossed the holding point as their view was obscured by the nose of the aircraft. As such, they were unaware of the runway incursion and would likely not have taken evasive action if they had not been instructed to conduct a missed approach. The aerodrome reporting officer (ARO) proactively alerted ATC to the incursion and reduced the likelihood of a serious incident.
The ERSA and the DAP diagrams for the Sunshine Coast Airport did not include holding point locations. While the ERSA was not required to show the locations of holding points, inclusion of this information reduces the potential for confusion or ambiguity around their position. Also, the marking used on the runway diagram to depict the take-off distance available was not accurate. Additionally, the CASA aerodrome manoeuvring map for Sunshine Coast Airport did not give an accurate representation of the holding points or the runway and, if compared to the ERSA, would increase confusion for pilots.
The operator’s briefing documentation on the layout of Sunshine Coast Airport was also not current and did not provide the correct information to students. However, this was found not to have contributed to the pilot’s lack of understanding of the airport taxiway layout and markings as the pilot was using the ERSA for pre-flight planning and the DAP as a location reference while at the airport, and so had the latest available information about the runway layout at the airport.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the Runway incursion involving Diamond Aircraft Industries Inc. DA 40, VH-ERE that occurred at the Sunshine Coast Airport, Queensland on 7 May 2023.
Contributing factors
The student misinterpreted the instruction given by ATC and their location in relation to the runway, resulting in their aircraft entering the runway strip while a Boeing 737 was on final approach.
The Airservices Australia‑published Departure and Approach Procedure chart (DAP) for the Sunshine Coast Airport did not indicate the position of the holding point on taxiway Foxtrot, which added to the confusion of the pilot when instructed to hold short of runway 31.
Other factors that increased risk
The oblique angle of the taxiway to the runway meant that the pilot of the DA 40 would not have had the Boeing 737 within their normal field of view and the 737 pilots on final would not have seen the Diamond as it was obscured under the nose of the aircraft while on final approach. This limited both crew's ability to react without intervention from a third party.
The Civil Aviation Safety Authority (CASA) Sunshine Coast manoeuvring map did not accurately depict the position of holding point Foxtrot and the large runway displacement.
Other factors
The aerodrome reporting officer (ARO) proactively alerted ATC to the incursion and as such reduced the likelihood of a serious incident.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Flight Training Adelaide
Flight Training Adelaide conducted an internal investigation into the runway incursion and has actioned the following safety actions:
A notice to crew (NOTAC) was issued to address landings at controlled zones, airports other than home base, and solo flights to controlled zones.
A qualified flight instructor (QFI) meeting was conducted to communicate the importance of students understanding the signs, markings, lights and phraseology, particularly when at a controlled aerodrome.
A student meeting was conducted to reiterate the points outlined in the QFI meeting.
The results of class G and class C & D airspace quizzes appear in the monthly students reports to QFIs.
Existing tutorials for class D, class C, Sunshine Coast Airport, Archerfield Airport, and Gold Coast Airport were reviewed and updated.
An exam and quiz specifically for Sunshine Coast Airport has been created.
Quizzes for Sunshine Coast Airport, Archerfield Airport, and Gold Coast Airport have been made mandatory for all students before visiting these airports.
The operator is also in the process of reviewing the:
requirements for solo flights to controlled zones, including the requirement for dual flight before any solo flight to any of the training controlled zones
forms used by QFIs for issuing flight plans in controlled zones.
Safety action by Sunshine Coast Airport
Sunshine Coast Airport, through its safety management process, carried out a review of the occurrence and has undertaken the following safety actions:
Figure 9: New runway holding point markings at Sunshine Coast Airport
Source: Sunshine Coast Airport
Requested an update to the CASA manoeuvring map to correctly identify the runway length, location of displaced threshold and holding point Foxtrot.
Changed the Aeronautical Information Publication (AIP) Enroute Supplement (ERSA) and the Departure and Approach Procedure (DAP) to reflect the full length of runway 31. Additionally, the distance between holding point Foxtrot and the runway has been added to the additional information section in the ERSA.
Safety action by the Civil Aviation Safety Authority
The Civil Aviation Safety Authority (CASA) has taken the following safety actions:
provided clarity around the runway shading on ERSA and DAP diagrams
upgraded the Sunshine Coast manoeuvring map to accurately reflect the airport layout.
recommended and supported the addition of a runway hotspot depiction at taxiway Foxtrot at the Sunshine Coast Airport to the ERSA and DAP.
CASA further advised that clarification on the terminology and definition of runway starter extensions will be added to the Part 139 MOS. They are also in the process of transferring the Aeronautical Information Package to digital form, which includes transferring all runway maps to digital versions. This will allow a more detailed map to be available.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the involved pilots and air traffic controller
Airservices Australia
Flight Training Adelaide
References
Australian Transport Safety Bureau (2022). AS-2022-001 - Aircraft performance and cockpit visibility study supporting investigation into the mid-air collision involving VH-AEM and VH-JQF near Mangalore Airport, Victoria on 19 February 2020. Canberra: Australian Transport Safety Bureau
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the involved pilots and air traffic controller
Sunshine Coast Airport
Flight Training Adelaide
Qantas
Civil Aviation Safety Authority
Airservices Australia
Submissions were received from:
the air traffic controller
Sunshine Coast Airport
Flight Training Adelaide
Civil Aviation Safety Authority
Airservices Australia
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] NOTAC: The purpose of the NOTAC is to communicate information on new or changed policies and procedures and matters of an urgent or safety related nature affecting the proper and legal flying operations of the operator.
[2] Holding point: Signifies the entry to the runway environment.
[3] Runway number: the number represents the magnetic heading of the runway.
[4] Flight progress strip: Controllers use fight progress strips to maintain situation awareness of ATC operations and traffic. Standard annotations (such as recording the departure runway/location) provide information to assist with the correct execution of the controller’s plan and the early detection of any errors that may occur.
[5] Starter extension: an additional runway length made available for take-off, prior to the normal runway end at the commencement of the take-off run.
Occurrence summary
Investigation number
AO-2023-023
Occurrence date
09/05/2023
Location
Sunshine Coast Airport
State
Queensland
Report release date
27/10/2023
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Runway incursion
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Diamond Aircraft Industries
Model
DA40
Registration
VH-ERE
Serial number
40.736
Aircraft operator
Flight Training Adelaide Pty Ltd
Sector
Piston
Operation type
Part 142 Integrated and multi-crew pilot flight training
Departure point
Sunshine Coast Airport, Queensland
Destination
Wellcamp Airport, Toowoomba, Queensland
Damage
Nil
Aircraft details
Manufacturer
The Boeing Company
Model
737-838
Registration
VH-VYD
Serial number
33992
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On the 26 October 2021, a Beech Aircraft Corp. 58, registered VH-NSK, operated by Little Wings Limited, was prepared for a private flight from Bankstown Airport, New South Wales. The purpose of the flight was to test the stall warning system following maintenance. The pilot was the sole person on board.
The aircraft was cleared to enter and line up on runway 29 right (29R) however, the pilot crossed the runway and entered occupied runway 29 centre (29C) without a clearance. As the pilot was cleared to take-off, the controller identified the error and instructed the pilot to hold position on the runway. At the same time, the pilot detected an Embraer 190, which was conducting high power engine runs on the upwind end of runway 29C and did not commence the take‑off.
What the ATSB found
The ATSB found that the pilot typically departed Bankstown from the centre runway, under the instrument flight rules procedures. This likely created an expectation that they were using this runway, despite reading back the correct runway to the controller. This resulted in them crossing runway 29R and entering runway 29C without a clearance.
Additionally, while the air traffic controller watched the aircraft enter 29R, due to subsequent focused attention on two helicopters in the vicinity of the airport, they did not identify its continued movement on to the occupied runway 29C.
Safety message
This incident illustrates the importance of pilots focusing on the specific instructions given by air traffic controllers. In 2012, the United States Federal Aviation Administration Safety Team (FAASTeam) released notice NOT4214 Pilot safety tip – Expectation biasstating that ‘analysis of runway incursion data shows that expectation bias is one of the most common causal factors for pilot deviations’.
The notice went on to say that pilots ‘need to understand that expectation bias often affects the verbal transmission of information. When issued instructions by air traffic control, pilots should “focus on listening and repeat to yourself exactly what is said in your head — and then apply that information actively”.’
Runway incursions remain an ongoing safety concern globally. In October 2016, Airservices Australia released A pilot’s guide to Runway Safety. This guide focused on seven important areas in surface operations and identified safety measures to help reduce the errors that lead to runway incursions. In addition, Airservices Australia have released specific guidance for pilots flying at Bankstown Airport Tips for flying at Bankstown, along with tips for flying at other metropolitan airports: Moorabbin, Parafield, Jandakot and Archerfield.
The investigation
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 26 October 2021, a Beech Aircraft Corp. 58, registered VH-NSK and operated by Little Wings Ltd, was prepared for a private flight under the visual flight rules (VFR) from Bankstown Airport, New South Wales (Figure 1). The purpose of the flight was to test the aircraft’s stall warning system following maintenance. The pilot was the sole person on board.
Figure 1: VH-NSK
Source: JETPHOTOS, Gavin Louis, modified by the ATSB
The operator had requested that the pilot conduct the test flight prior to conducting an instrument flight rules (IFR) flight, later that day. The pilot advised that they had not flown under the VFR or to the Bankstown training area for over 40 years. As such, they prepared themselves by researching the airspace around Bankstown Airport and revising the procedures for the flight test.
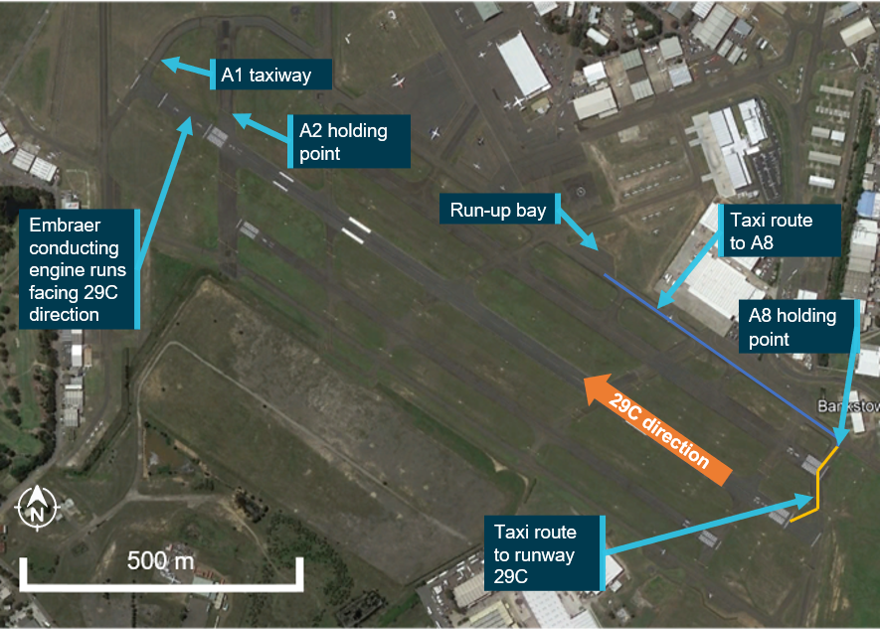
The next morning, the pilot conducted their normal pre-flight checks and started the engines. As the pilot taxied across the apron, they contacted the Bankstown surface movement controller (SMC), to obtain their taxi clearance. The SMC instructed them to taxi to holding point A8 for runway 29R[1] (Figure 2). This clearance automatically included an approval for the aircraft to enter a run-up bay to conduct the pre-flight engine checks and then taxi to the runway holding point. The pilot was not aware of this and advised the SMC that they needed to taxi to the run-up bay, which the SMC advised they were cleared to do. During this exchange, the pilot advised the SMC that they had not been to the Bankstown training area for over 40 years.
As the pilot was conducting their engine checks in the run-up bay, the crew of an Embraer 190 (Embraer) requested, and received, clearance to taxi to holding point A2 (Figure 2), the upwind end of runway 29C, to conduct high power engine runs for maintenance purposes.
When the pilot of NSK completed their checks in the run-up bay, they clarified with SMC that they were approved to taxi to holding point A8. The SMC confirmed they were approved and instructed them to contact Bankstown Tower at the holding point.
Figure 2: Bankstown Airport showing the route NSK took to the holding point
Source: Google Earth, annotated by ATSB
At 1114, the crew of the Embraer contacted Bankstown Tower and was cleared to enter runway 29C.
On reaching holding point A8, the pilot of NSK changed frequency to Bankstown Tower. At 1117, they contacted the Tower controller and advised they were ‘on A8 holding short of runway 29R ready for an upwind departure’. The Tower controller instructed them to hold position.
At 1118, the Tower controller instructed ‘NSK runway 29R line up and wait’. The pilot read back ‘line up and wait right NSK’. The Tower controller advised that aircraft would initially taxi along the same path if they were crossing runway 29R or lining up on that runway to depart.
After watching NSK commence taxiing, the Tower controller directed their attention to two helicopters. One helicopter was operating north of Bankstown Airport, with a second departing to the north. The Tower controller passed traffic information to both helicopter pilots, to assist them to identify each other. During the period the Tower controller’s attention was diverted, NSK crossed runway 29R, then entered and lined up on runway 29C.
At 1119:23, after the helicopter pilots advised they had each other sighted, the Tower controller instructed ‘NSK runway right clear for take-off’. As they were finishing the instruction, they detected that NSK was on 29C and immediately instructed ‘NSK hold position, hold position you are lined up on Centre, hold position’. The controller then instructed NSK to ‘Stop, hold position’. At 1119:35 the controller again instructed ‘NSK Stop, hold position’ and 5 seconds later stated ‘NSK Stop, stop, stop, hold position’.
At this time, the Bankstown tower frequency had at least one occasion, where a pilot over transmitted while the controller was broadcasting on the radio.
The pilot of NSK advised that as they were turning to line up on the runway, the controller cleared them to take-off. They immediately detected an Embraer at the other end of the runway and reported they advised the controller that there was a jet on the runway and they would hold position, however this was not heard by the controller. This was likely the over transmission on the frequency. At 1119:42 the pilot of NSK read back ‘NSK Stop, stop, stop, holding position’.
At 1121, after giving instructions to a number of other aircraft in the area, the controller instructed the pilot of NSK to hold short of runway 29R. The pilot of NSK responded by stating ‘I am holding at the threshold 29’. The controller then advised ‘NSK you are currently lined up on 29C hence why I told you to hold position. Vacate to the right and hold short of runway 29R’. NSK responded ‘Roger, vacating to the right hold short of 29R, NSK’.
The Embraer completed their engine runs and exited the runway onto taxiway A1, taxiing around runway 29R (Figure 2).
The controller then cleared NSK to enter and take off from runway 29R. The pilot advised they observed the Embraer taxiing at the end of the runway, but they were unsure if the Embraer was on the runway or was on the taxi way behind the runway. They advised that they waited until the Embraer had cleared the take-off overrun, before commencing the departure. The test flight and return to Bankstown were conducted without issue.
Context
Pilot
The pilot held an Air Transport Pilot’s Licence (Aeroplane) with over 23,500 hours of aeronautical experience.
They were volunteering their time to fly for the operator while they were stood down from an airline which had reduced international flights due to COVID 19 restrictions. The pilot had been flying the Beech Aircraft Corp. 58 regularly on IFR flights for the previous 18 months, with their most recent flight being circuits on the night before the incident.
They advised that they felt uncomfortable doing a VFR flight to the training area due to the different procedures and had never departed from runway 29R prior to that day. They reported that they thought the controller had instructed them to use runway 29C and had no recollection of reading back 29R.
They advised they had slept well and were fit and healthy.
Air traffic controller
The controller had almost 20 years experience, with around 14 years at Bankstown Airport. They advised they were feeling ‘fine’ at the time, having received their normal amount of sleep over the previous days. They had been operating as the tower controller for about 15 minutes prior to the occurrence and advised that they did not consider the workload to be high.
Bankstown Airspace
Bankstown Airport uses Class D airspace procedures. It has three parallel runways aligned in the 29/11 direction (Figure 2). When runway 29 was the operational runway:
runway 29R was used for departing and arriving VFR aircraft
29C was used for departing and arriving IFR aircraft and overflow if 29R was busy
29L was used mainly for circuits.
When the airport was busy, 29L was controlled by one controller and 29 R and C were controlled by a second controller. When it was quiet, a single controller controlled all three runways.
On this morning, the tower controller was controlling all three runways. There were two aircraft in the circuit area, two aircraft inbound, a helicopter operating north of the airport and another helicopter departing to the north.
Safety analysis
The experienced pilot had been conducting IFR flights for the operator on a regular basis over the previous 18 months. On these flights, they had only conducted IFR departures using the centre runway. This most likely led to them having an expectation they were going to depart from runway 29C. According to Skybrary Flight crew expectation bias:
Expectation bias occurs when a pilot hears or sees something that he or she expects to hear or see rather than what actually may be occurring. That expectation often is driven by experience or repetition. For example, if a pilot is regularly cleared to cross a particular runway during operations at a familiar aerodrome, he/she may come to “expect” the clearance. This could cause a potentially dangerous situation if on a particular day, the pilot actually is instructed not to cross the runway in question due to another aircraft landing or taking off.
Despite confirming the instruction to line up and wait on runway 29R, the pilot reported no recollection of this. It is likely the pilot was thinking ahead to conducting the VFR departure, narrowing their focus to their actions after the departure. Consequently, their attention was probably not on the clearance to enter the runway, rather reverting to what they had done previously.
The controller had no indication from the pilot’s readback that the pilot had a different understanding of what was instructed. Therefore, when the aircraft commenced taxiing as expected, they diverted their attention to other tasks.
Both the pilot and the controller detected an issue and stopped the departure prior to the aircraft commencing the take-off run, although at this stage the pilot was still unaware, they were not on their cleared runway.
The air traffic control system is dependent on radio communication which requires both pilots and controllers to clearly and accurately articulate what they are doing. An analysis of runway incursion data conducted by the United States Federal Aviation Administration Safety Team in 2012, found that expectation bias is one of the most common contributing factors to pilots deviating from a clearance instruction.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the runway incursion involving Beech Aircraft Corp. 58, VH-NSK at Bankstown Airport, New South Wales, on 26 October 2021.
Contributing factors
Despite correctly acknowledging the clearance to enter and line up on runway 29R, the pilot crossed runway 29R and entered runway 29C without a clearance, probably due to expectation bias associated with previous operation only from 29C.
The controller watched VH‑NSK enter 29R however, due to subsequent focused attention on two helicopters in the vicinity of the airport, they did not identify its continued movement on to the occupied runway 29C.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot
controller
Airservices Australia
Little Wings Limited
No submissions were received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 31 August 2020, a Regional Express (REX) SAAB 340B, registered VH-ZRH, and a Shine Aviation Piper PA-31, registered VH-ITF, were both being prepared for their respective passenger transport flights at Carnarvon, Western Australia.
At about 1704 local time, VH-ZRH entered runway 22 just after VH-ITF had commenced its take-off roll on the same runway. The pilot of VH-ITF immediately advised the crew of VH-ZRH that they were rolling and then rejected the take-off. VH-ZRH stopped just inside the runway strip.
What the ATSB found
The ATSB found that, although the crews of both aircraft were aware that they were mutual traffic, their expectations led to an incorrect understanding of the other’s position and/or intentions. This situation led to them not recognising the potential conflict and therefore not directly communicating with each other.
The lookout conducted by the flight crew of VH-ZRH prior to entering the runway was not effective and likely to have been influenced by the crew’s expectation that VH-ITF had already departed.
What has been done as a result
REX advised that the incident was discussed amongst its checking and training organisation for future training events. The operator also published related policy items in an operations notice to highlight the requirements for operating in non-controlled environments. REX also reviewed its human factors and non-technical skills training specifically in relation to communication.
Shine Aviation planned for the incident to be used as a learning tool in order to promote discussion of behaviours and best practice with respect to communications in CTAF environments.
Safety message
This incident highlights the potential effects that expectations can have on how a flight crew perceives information. It is important that flight crew remain vigilant while maintaining situational awareness to counter any expectation bias. Pilots should not hesitate to contact another aircraft if there is any uncertainty as to their position and/or intentions.
The ATSB’s SafetyWatch highlights the broad safety concerns that come out of the bureau’s investigation findings and from occurrence data reported by industry. One of those safety concerns is that insufficient communication between pilots operating in the same area is the most common cause of safety incidents near non-controlled aerodromes. The ATSB booklet A pilot’s guide to staying safe in the vicinity of non-controlled aerodromes outlines many of the common problems that occur at non-controlled aerodromes.
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 31 August 2020, a Regional Express (REX) SAAB 340B, registered VH-ZRH, and a Shine Aviation Piper PA-31, registered VH-ITF, were both being prepared for their respective passenger transport flights at Carnarvon, Western Australia. VH-ITF was flying to Geraldton with one pilot and two passengers. VH-ZRH was flying to Perth with three crew (two pilots and one flight attendant) and 30 passengers. Both flights were being conducted under instrument flight rules (IFR).
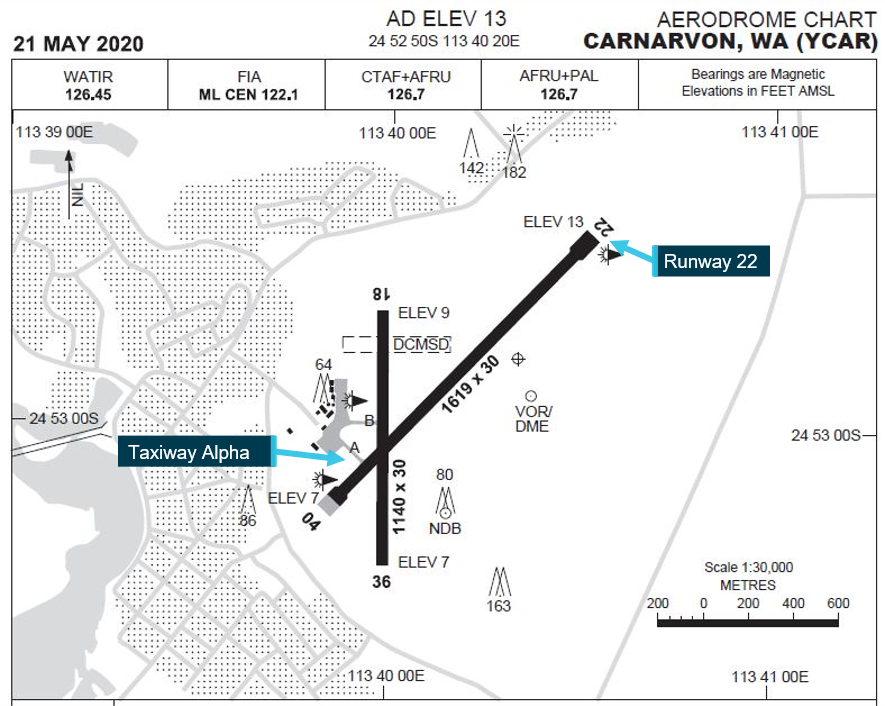
At 1659:10 Western Standard Time,[1] the pilot of VH-ITF contacted Melbourne centre air traffic control and advised them that they were taxiing at Carnarvon for runway 22 (Figure 1). Melbourne centre advised the pilot that there was no other IFR traffic. Shortly after, the pilot broadcast on the Carnarvon common traffic advisory frequency (CTAF) that they were taxiing for runway 22. At about 1700, the pilot broadcast on the CTAF that they were entering and backtracking runway 22.[2]
While on the aerodrome apron, the flight crew of VH-ZRH observed VH-ITF taxi past. The first officer was outside the aircraft conducting external inspections and the captain was on the flight deck at the time. The CTAF was not yet being monitored (nor was it required to be at that stage), and therefore VH-ITF’s radio calls during this period were not heard by the pilots of VH-ZRH.
At 1702:51, the crew of VH-ZRH contacted Melbourne centre to advise taxi details. Melbourne centre advised the crew to stand by. While waiting for Melbourne centre, the captain directed the first officer to broadcast on the CTAF that they were about to taxi. Although the pilot of VH-ITF heard this taxi call, they did not respond, nor was there any other response to VH-ZRF’s CTAF broadcast. The crew of VH-ZRH then commenced taxiing for runway 22.
At 1703:16 Melbourne centre advised the crew of VH-ZRH that IFR traffic for them was VH-ITF. Melbourne centre stated that VH-ITF was taxiing at Carnarvon for Geraldton and had planned the same route (as VH-ZRH) at 9,000 ft. The crew of VH-ZRH acknowledged the traffic information at 1703:36.
At 1703:44 Melbourne centre contacted the pilot of VH-ITF to confirm they had received the information about VH-ZRH taxiing. The pilot of VH-ITF confirmed they had. At this time, VH-ITF was approaching the threshold of runway 22 and about to turn around and line up. VH-ZRH was approaching the holding point[3] for runway 22. The flight crew of VH-ZRH subsequently reported that they did not hear the exchange between Melbourne centre and the pilot of VH-ITF.
As they approached the holding point, the crew of VH-ZRH completed a lookout for traffic. The first officer stated they were not able to see left (towards the runway threshold) due to their seat position and the aircraft window configuration and therefore they only cleared to the right and front. The captain cleared to the left and front, observing the runway, runway threshold and approach areas. The captain stated that they did not see VH-ITF on the runway.
At about this time, the pilot of VH-ITF broadcast on the CTAF they had lined up and were rolling on runway 22. The flight crew of VH-ZRH did not hear this transmission. Since they believed the runway to be clear, the first officer of VH-ZRH broadcast that they were entering and backtracking runway 22, just prior to passing the holding point at about 1704.
By this time the pilot of VH-ITF had advanced the throttles to about three quarters (of full travel) and they had commenced the take-off roll. The pilot heard and observed VH-ZRH enter the runway and they immediately advised VH-ZRH they were rolling on runway 22. Shortly after, the Carnarvon aerodrome reporting officer (ARO) also advised the crew of VH-ZRH that VH-ITF was on the runway. The pilot of VH-ITF subsequently rejected their take-off and commenced backtracking on runway 22.
The flight crew of VH-ZRH did not hear the pilot VH-ITF’s full transmission but did realise what had occurred and immediately stopped a few metres past the holding point (Figure 1) and prior to crossing the edge of the runway. They then advised the pilot of VH-ITF that their transmissions were readability two[4] and quite scratchy.
The flight crew of VH-ZRH then vacated runway 22, repositioned on taxiway alpha and advised VH-ITF that they would hold short of runway 22. VH-ITF then departed before VH-ZRH continued with their flight.
Figure 1: Aircraft positions at the time of the runway incursion
Source: Google Earth, annotated by the ATSB
Context
Personnel information
The captain of VH-ZRF had a total of 3,088 flight hours, with 2,851 hours on type. They commenced with REX in 2015 and had been a captain since mid-2019.
The first officer had a total of 1,976 flight hours, with 577 hours on type. They had previously worked as a flight instructor and charter pilot (single and multi-engine aircraft) before commencing flying at REX in 2019.
The pilot of VH-ITF had a total of 1,476 flight hours, with 265 hours on type. Their previous experience included flight instruction and charter flying with about 15 months flying multi-engine aircraft.
All three pilots indicated that they were not tired or fatigued prior to commencing their flights.
Aircraft information
VH-ZRH was a SAAB 340B, serial number 340B-392. The SAAB was a twin turboprop engine aircraft capable of carrying up to 36 passengers. It is normally crewed by two pilots and a flight attendant.
VH-ITF was a Piper PA-31 Navajo, serial number 31-7812014. The Navajo was a twin piston-engine aircraft capable of carrying up to 8 passengers. It is normally operated by a single pilot.
Operations at non-controlled aerodromes
Civil Aviation Regulation 166 C (Responsibility for broadcasting on VHF radio) stated that, when operating at non-controlled aerodromes, a pilot was to make a broadcast whenever ‘it is reasonably necessary to do so to avoid a collision, or the risk of a collision’. A civil aviation advisory publication[5] provided further guidance on this as follows:
Whenever pilots determine that there is a potential for traffic conflict, they should make radio broadcasts as necessary to avoid the risk of a collision or an Airprox event. Pilots should not be hesitant to call and clarify another aircraft’s position and intentions if there is any uncertainty.
Both aircraft had been provided traffic advice by Melbourne centre, which clearly indicated that the other aircraft was taxiing at Carnarvon at the same time. Considering the aerodrome configuration (Figure 2), it was reasonable to assume that a potential conflict existed.
Although the crews of both aircraft made appropriate common traffic advisory frequency (CTAF) broadcasts of their position and intentions, they did not communicate directly with one other.
Figure 2: Carnarvon aerodrome chart
Source: Airservices Australia, annotated by the ATSB
Traffic awareness
Although the crew of VH-ZRH had acknowledged the traffic information provided by Melbourne centre, both pilots did not realise that VH-ITF was still taxiing at Carnarvon.
Both pilots believed that VH-ITF had already departed by the time they were ready to taxi. They stated that this belief was due to multiple factors, including:
The pilots estimated at least 10 minutes elapsed between observing VH-ITF taxi past and the incident. They believed this should have been more than sufficient time for VH‑ITF to have already departed. Based on the recorded radio transmissions, the ATSB estimated that the incident occurred at about 1704, 5 minutes after VH-ITF’s taxi call to Melbourne centre and about 1 minute after VH-ZRH commenced taxiing.
They did not receive a response to their CTAF taxi call at 1703 from VH-ITF’s pilot.
They did not observe any traffic on their aircraft’s traffic collision avoidance system (TCAS). The operator subsequently conducted an operational check of the aircraft’s TCAS and no technical faults were identified.
When VH-ITF taxied past them on the apron, the flight crew of VH-ZRH were not yet monitoring the CTAF, nor were they required to do so at that point. The crew were using COM 1 for company communications and COM 2 was not used until ground power was connected, which was sometime after VH-ITF had taxied past. ATSB estimated that this was likely to be after VH-ITF had commenced backtracking on runway 22. Therefore, the crew of VH-ZRH would not have heard VH-ITF’s taxi call or entry/backtracking call on the CTAF and were not able to maintain awareness of VH-ITF’s position.
When providing traffic information to the crew of VH-ZRH, the Melbourne centre clearly stated that the VH-ITF was ‘taxiing at Carnarvon for Geraldton’. The crew of VH-ZRH advised that, in their experience, ATC will provide the same information about another aircraft until they receive a departure call from that aircraft, which can occur sometime after the aircraft has become airborne.
The crew of VH-ZRH did not hear Melbourne centre pass traffic information to VH-ITF, nor did they hear VH-ITF’s CTAF transmission that they were lining up and rolling. The crew stated that, at about the same time as those transmissions, they were confirming the assigned transponder code. Due to an error in the initial readback, the code had to be read back again, which delayed the code’s input. This possibly diverted their attention long enough to not hear the transmissions.
The pilot of VH-ITF believed that VH-ZRH was aware of their position on the runway and would hold short until they had departed. This belief was developed because they had heard Melbourne centre providing VH-ZRH with traffic information. It was then reinforced once VH-ITF had turned around on runway 22 and they had VH-ZRH visual, and thus assumed the crew of VH-ZRH also had them visual.
Visibility from taxiway alpha holding point
Although the captain of VH-ZRH did not see VH-ITF prior to entering the runway, immediately after the incident the captain and first officer were able to see VH-ITF. Upon repositioning at the holding point, the captain noted that the background buildings and terrain made it difficult to identify VH-ITF on the runway threshold.
The ATSB reviewed images of the runway threshold from the holding point on taxiway alpha. Although the images did support the captain’s view of potential difficulty in identifying an aircraft on the threshold, it was noted that the aerodrome reporting officer (ARO), who was positioned on the apron adjacent to taxiway alpha, had VH-ITF in sight.
The pilot of VH-ITF stated that there were no impediments to visibility and, although they were looking from the opposite direction, had VH-ZRH in sight.
VHF transmission quality
The flight crew of VH-ZRH recalled that the transmissions from VH-ITF were faint and quite scratchy. This was supported by the ARO. The ATSB reviewed the CTAF recording and noted that VH-ITF’s transmissions were distinctly weak in comparison to those from VH-ZRH or the ARO but they were still audible and understandable. There was no indication that VH-ITF’s transmissions to Melbourne centre were degraded in any way.
Following the incident, Shine Aviation noted a history of issues relating to VH-ITF’s VHF radio COM 1, all of which were in 2018 and had been already actioned. On 30 September 2020 (after this incident), VH-ITF again experienced an issue with VHF radio COM 1 and maintenance action was commenced to ascertain the cause. The ATSB noted that COM 1 was being used for CTAF transmissions at the time of the incident on 31 August 2020.
VH-ITF’s initial CTAF transmissions were not heard by the crew of VH-ZRH since they were not yet monitoring the CTAF. VH-ITF’s lining up and roll call was probably missed by the crew of VH‑ZRH due to a combination of VH-ITF’s weak CTAF transmission and VH-ZRH’s crew having diverted their attention to transponder code confirmation and entry. However, the ATSB noted that the crew of VH-ZRH also did not perceive the exchange between VH-ITF and Melbourne centre, which was on a radio for which no communications difficulty was identified.
While the crew of VH-ZRH described VH-ITF’s transmissions as faint and difficult to hear, the ATSB noted that, immediately after the incident, communications between VH-ITF and VH-ZRH were established and continued without issue.
There were multiple radio transmissions regarding the movement of VH-ITF, between various parties, over two radio channels (COM 1 and COM 2). It was evident that the crew of VH-ZRH had received (and acknowledged) at least one of these communications advising that VH-ITF was traffic for them, so it was reasonable to assume that a potential conflict existed. Considering the crew’s diverted attention towards their transponder code input at the time of these communications, VH-ITF’s weaker transmissions alone were not considered contributory to the incident.
Safety analysis
In this incident, the crews of both aircraft were provided with sufficient information to aid their situational awareness and be alerted to traffic relevant to them. However, the pilots did not fully comprehend the traffic picture and/or did not recognise the potential conflict that existed.
Although the flight crew of VH-ZRH believed VH-ITF to have departed, the traffic information provided to them by Melbourne centre clearly stated that VH-ITF was still taxiing at Carnarvon. Although it is possible that a controller could provide such information in cases where an aircraft had departed and the crew had not yet made a departure call, the statement that VH-ITF was taxiing (and was therefore a potential conflict) should have been assumed to be true until the crew could confirm otherwise.
Expectations strongly influence where a person will search for information and what they will search for (Wickens and McCarley 2008), and they also influence the perception of information (Wickens and others 2013). In simple terms, people are more likely to see or hear what they expect to see or hear, and less likely to see or hear things they do not expect. Expectations are more likely to have an influence when some of the available cues are not salient. In this case, the flight crew had developed an expectation that VH-ITF had already departed, and it is likely that this expectation then strongly influenced their perception of subsequent information.
In particular, this expectation bias likely influenced the flight crew’s ability to visually scan for traffic prior to entering the runway. As they were not expecting traffic to be there, the captain looked but did not see VH-ITF on the threshold. The ATSB notes that although the background potentially masked VH-ITF from the captain’s scan, the ARO was able to see VH-ITF from a similar position.
The pilot of VH-ITF was fully aware that VH-ZRH was taxiing and, having heard all of that crew’s transmissions, assumed they were equally aware of VH-ITF. The pilot expected VH-ZRH would hold short and, therefore, a potential conflict did not exist. Consequently, the pilot did not believe there was a need for direct radio contact with the other crew to clarify their intentions.
As the pilot of VH-ITF had VH-ZRH visual, they were able to quickly reject the take-off when VH‑ZRH entered the runway.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the runway incursion involving a SAAB 340B, VH-ZRH at Carnarvon Airport, Western Australia, on 31 August 2020.
Contributing factors
The flight crew of VH-ZRH were not aware, as they entered the runway, that VH-ITF had commenced its take-off roll. As a result, a potential conflict existed that required the pilot in command of VH-ITF to reject their take-off.
The lookout conducted by the flight crew of VH-ZRH before entering the runway was not effective in identifying VH-ITF on the runway threshold. This was likely influenced by the crew’s expectation that VH-ITF had already departed.
Although both flight crews were aware that they were mutual traffic, they both had an incorrect understanding of the other’s position and/or intentions, which led to them not recognising the potential conflict and therefore not directly communicating with each other.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Regional Express
Regional Express (REX) reported that the flight crew had been debriefed on all aspects of the incident. The incident was also discussed amongst the REX checking and training organisation for consideration in future training outcomes.
REX also published an operations notice (for pilots) that included related policy items to highlight the requirements for operating in non-controlled environments. It also reviewed its human factors and non-technical skills training specific to communication.
REX advised that operations at non-towered aerodromes continues to be a focus of its safety promotion activities, with recent articles being published in its September 2021 Group Safety Newsletter.
Safety action by Shine Aviation
Shine Aviation’s internal investigation recommended this incident be used as a learning tool to promote discussion of behaviours and best practice with respect to communications in CTAF environments.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew of VH-ZRH
the pilot of VH-ITF
Regional Express
Shine Aviation
the Carnarvon Shire Council
the Civil Aviation Safety Authority
Airservices Australia.
References
Wickens CD, Hollands JG, Banbury S & Parasuraman R 2013, Engineering psychology and human performance, 4th edition, Pearson Boston, MA.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the captain and first officer of VH-ZRH
the pilot of VH-ITF
Regional Express
Shine Aviation
the Civil Aviation Safety Authority.
Submissions were received from:
the captain of VH-ZRH
the first officer of VH-ZRH
Regional Express.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the afternoon of 23 July 2020, five aircraft were operating in the runway 17 Left (L) circuit at Moorabbin Airport, Victoria. A Piper PA-28 aircraft, VH-TAX (TAX), was lined up in the displaced threshold area of runway 17L. A Sling 2 aircraft, VH-ZSD (ZSD), then on the base leg of the circuit approaching the occupied runway, passed above TAX and conducted a touch and go landing. The runway incursion by ZSD removed the required runway separation between the aircraft.
What the ATSB found
The ATSB found that the student pilot of ZSD sighted TAX but decided to conduct the touch and go landing due to an incorrect belief that the controller had provided a landing clearance. The ATSB identified that the student pilot’s training had not been effective in conveying that a go‑around must be initiated if the runway was occupied.
The investigation also found that the air traffic controller did not identify the developing conflict as ZSD approached runway 17L. Additionally, the controller did not recall the aircraft passing above TAX and conducting a touch and go landing, and remained unaware of the incident until after it was reported over an hour later.
What has been done as a result
Royal Victorian Aero Club, the flight training school operating ZSD, has made changes to its student training program including educational, procedural and recurring activities. The school updated instructor and student educational materials, procedural guidance and examination content.
Safety message
Runway incursions and other runway separation issues are one of the most significant risks to safe aviation operations and a key global safety priority. Airport operators and air navigation service providers are strongly encouraged to identify and mitigate risk areas, especially at locations with inexperienced pilots or unusual airport configurations, such as displaced thresholds. The Airservices‑published safety bulletin Preventing the risk of a runway incursion and the runway safety article Tips for flying at Moorabbin provide relevant guidance.
Pilots are strongly encouraged to identify potential conflicts or runway incursions that may develop during circuits early and to attend carefully to air traffic control communications. It is important that flight training schools reinforce training regarding occupied runways and go‑arounds to students. Air traffic controllers are encouraged to monitor all aircraft and provide clear and unambiguous instructions to their flight crew to avoid runway incursions and related occurrences.
The occurrence
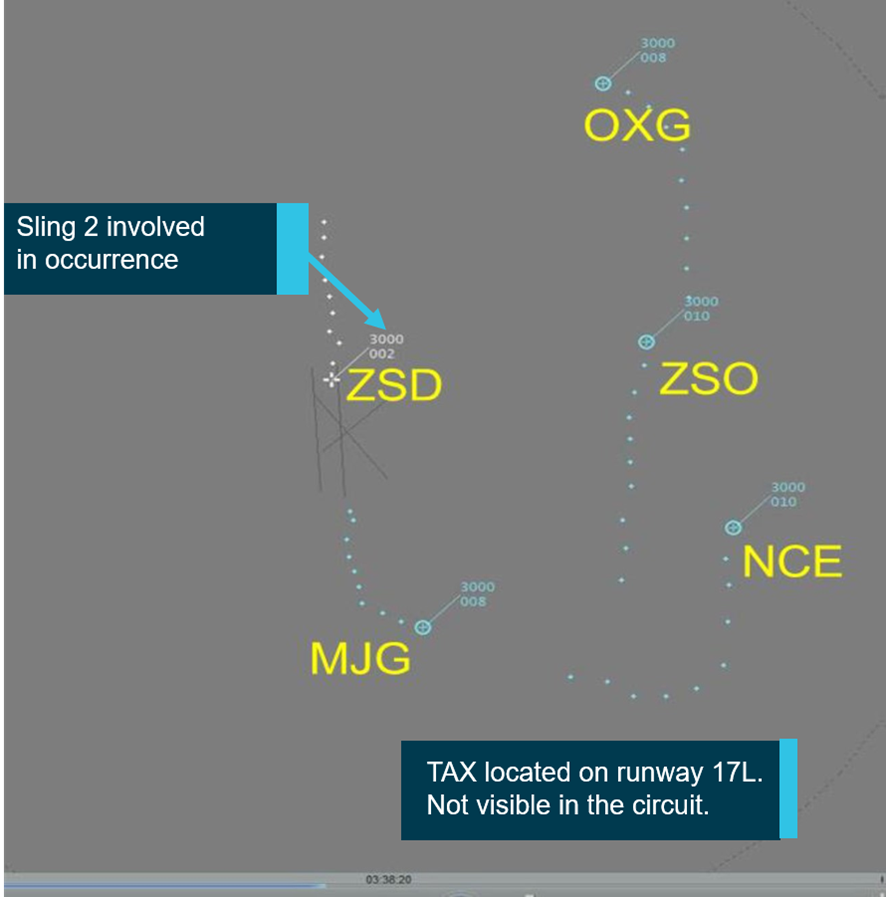
At about 1334 Eastern Standard Time[1] on 23 July 2020, five aircraft were operating in the runway 17 left (17L) circuit at Moorabbin Airport, Victoria (Figure 1). They included a Sling 2, registered VH-ZSD (ZSD), operated by the Royal Victorian Aero Club (RVAC) with a student pilot on a second, solo flight. The pilot conducted a touch and go landing on runway 17L a few minutes earlier.
Figure 1: Runway 17L circuit traffic situation display screen shortly before the occurrence
Source: Airservices Australia
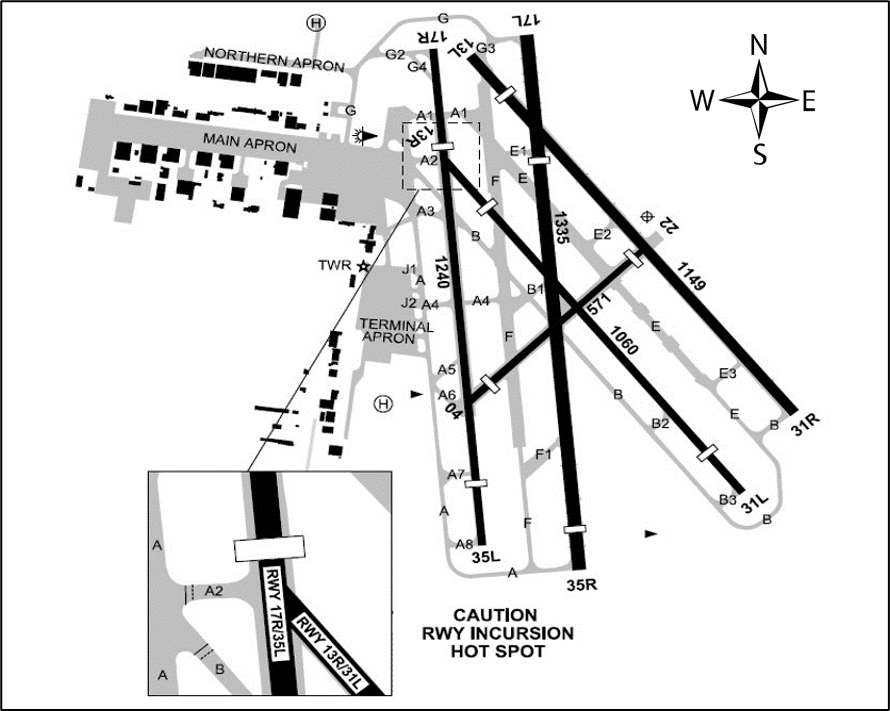
In addition to the circuit traffic, a Piper PA-28, registered VH-TAX (TAX), operated by Moorabbin Flying Services, with an instructor and student pilot on board, was at the holding point of taxiway G for 17L (Figure 2). The aircraft was in the final stages of preparation for a local training flight.
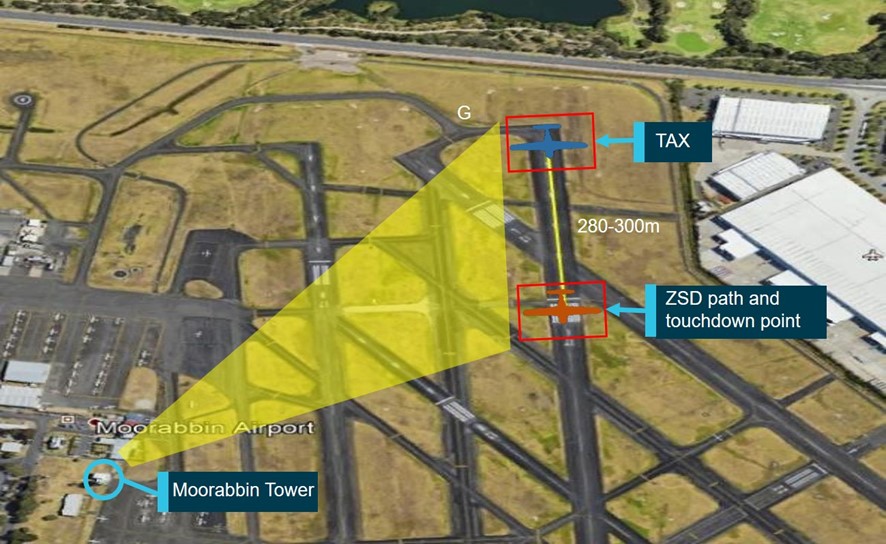
Figure 2: Overview of Moorabbin Airport showing key locations
The shaded yellow area indicates the tower perspective of the part of the runway when ZSD overflew the lined-up TAX.
Source: Airservices Australia, annotated by ATSB
At 1334:49, the Moorabbin Tower (tower) air traffic controller instructed the pilot of ZSD: ‘Zulu Sierra follow Cessna late downwind'.[2] The pilot responded: ‘Zulu Sierra Delta’, and shortly after began preparing for a touch and go landing on runway 17L. The pilot of ZSD also mistakenly thought that the controller had issued a landing clearance. There was no further communication with the controller during that circuit.
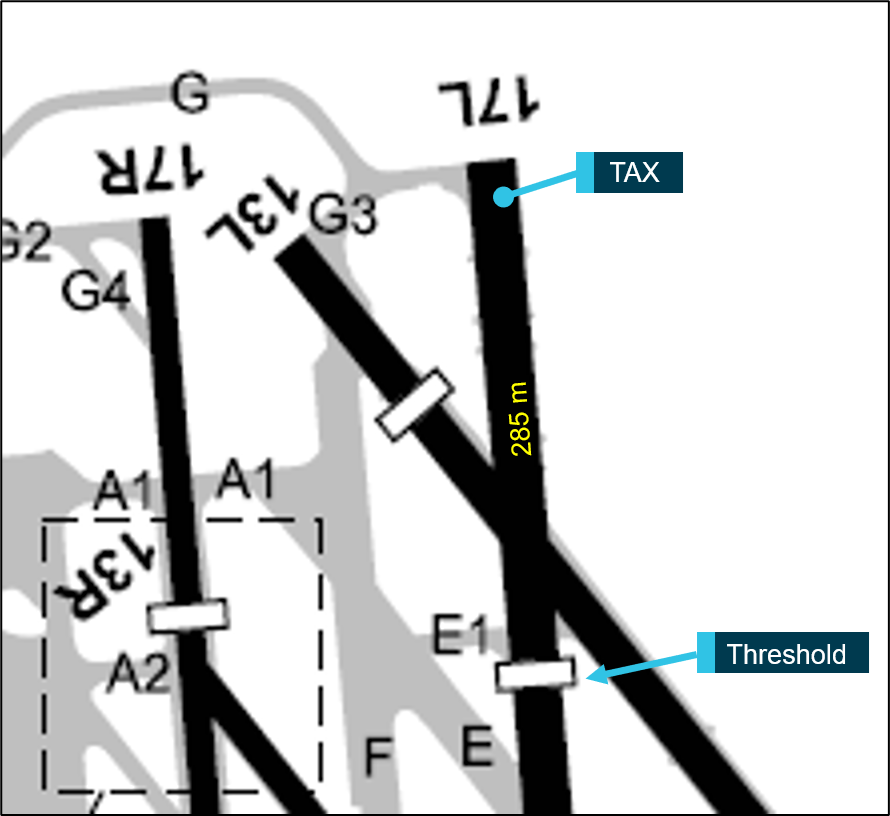
At 1336:49, the controller instructed the pilot of TAX to line up on runway 17L. One minute later, TAX was still waiting in the lined-up position about 280 m behind the displaced threshold. The pilot of ZSD sighted TAX on the runway during the approach for landing. Just as the instructor was about to contact the tower to ask about the take-off clearance, ZSD passed above TAX and conducted a touch and go landing.[3]
The instructor was surprised by the unusual event of an aircraft overflying another but did not immediately report the runway incursion, deciding instead to focus on TAX and its flight, and deal with incident-related matters in the post-flight debrief. At 1338:43, the controller (unaware of the incident) issued a take-off clearance and shortly after, TAX departed for the training area.
The pilot of ZSD did not believe any incident had occurred and continued conducting circuits, landing shortly after 1349.
At about 1440, after TAX completed the training flight, the instructor reported the incident to the flight training school’s head of operations and then phoned the tower. The tower supervisor was informed and, in turn, advised the incident controller.
Moorabbin Airport has five runways (Figure 3) and the vast majority of operations at the airport involve training activities. Runway 17L is 1,335 m in length and has an unusually long (285 m) displaced threshold (Figure 4). The airport operates within Metro Class D airspace and Airservices Australia (Airservices) provides the air traffic services (see Air traffic services section).
Figure 3: Moorabbin Airport
Source: Airservices Australia
Figure 4: Runway 17L section showing the position of TAX behind the displaced threshold
Source: Airservices Australia annotated by ATSB
Air traffic services
Moorabbin Class D airspace
Moorabbin Airport’s Class D terminal airspace is controlled by controllers situated in the Moorabbin control tower. The Class D airspace extended to the north and south-west from ground level to a 3 NM boundary.
Staffing
Airservices determines a minimum number of full time equivalent (FTE) staff (referred to as the mature requirement) to adequately staff a control tower. Moorabbin Tower’s mature requirement at the time of the incident (and for a number of years prior) was 11 FTE, but actual FTE numbers had been higher. The staff in excess of the mature requirement (the surplus) were available to assist in the tower.
In 2019, an informal ‘spotter’ position was created to utilise surplus staff. There was no licensing requirement for a ‘spotter’ nor a job description or procedure for utilising the position, but it was included in the roster. In practice, the ‘spotter’ was an additional resource to assist controllers in performing their duties.
In the months before the incident, however, there were some changes to staffing levels. One change was the removal of the ‘spotter’ position from the roster due to Airservices’ pandemic management plan,[4] which introduced isolation rosters to mitigate virus spread by physically distancing controllers.
At the time of the incident on 23 July 2020, all three control positions in the tower were staffed. Four controllers were present: the operating Aerodrome Controller West (ADC-W), the outgoing controller handing over the ADC-W position, the Surface Movement Controller-Coordinator (SMC-COORD) and the Aerodrome Controller East (ADC-E). The ADC-E (the controller involved in this incident) controlled the runway and airspace in the eastern part of the airport area using radio frequency 118.1 MHz while the ADC-W performed those functions for the western part on 123.0 MHz.
According to the tower supervisor, a request to Airservices to reinstate the ‘spotter’ position was under consideration at the time with the intention to formally introduce the position when staffing numbers allowed. During the course of this investigation, a proposal to increase the mature requirement to 12.5 FTE was submitted to Airservices in November 2020. A reason given to support the proposal was that traffic levels and complexity at Moorabbin Airport were at a level where there was a risk of missing conflicts. At the time of publication of this report, the request was being considered with a view to allowing the SMC-COORD position to be de-combined during busy periods, but not to provide any additional resource for a formal or informal ‘spotter’ position.
Traffic movements
Under routine conditions, the training environment at Moorabbin Airport includes the workload demands of students learning to fly. In addition to this workload, the controller involved in this incident perceived that there had recently been a 20 to 25 per cent increase in movements at the airport. The tower supervisor also noted the increase in traffic over the previous 5 months and observed that traffic levels were quite saturated with the workload becoming challenging.
These perceptions were supported in part by objective data. Airservices Australia records indicated that monthly traffic movements at Moorabbin Airport had, on average, increased by 8.74 per cent between February and July 2020 (from 19,943 to 21,686 movements). A possible reason for the increase in movements was that pilots who could no longer fly for major airlines (due to the impact of the Coronavirus pandemic) and held an instructor rating, were working at flight training schools and this contributed to increased student flight training activities.
The instructors of both student pilots involved indicated that it had been busier for them over the past 15 months and that they had noticed reduced staffing in the tower. Overall, there appeared to have been an increase in the amount of traffic management work for controllers at Moorabbin Airport.
Traffic during the event
The incident controller assessed that traffic conditions at the time of the event were moderate to high. The airspace contained two aircraft with very similar callsigns, Zulu Sierra Delta (ZSD) and Zulu Sierra Oscar (ZSO). The presence of aircraft with similar callsigns operating in the same area and especially on the same frequency often gives rise to potential and actual flight safety incidents. This hazard is usually referred to as ‘callsign confusion’.
At 1334:49, the controller instructed the pilot of ZSD: ‘Zulu Sierra follow Cessna late downwind', without including ‘Delta’ to avoid potential confusion with ZSO (which was also in the circuit and conducted four landings before the occurrence and two subsequently). Two downwind calls were made by ZSO and November Charlie Echo (NCE), with the first call from ZSO coinciding with the approximate time that take-off clearance for TAX would have been expected for its immediate departure following Mike Juliet Golf (MJG). After the conflict occurred, the controller had a pause in communications (prior to an instruction at 1340:09 'Zulu Sierra Delta follow Cessna late downwind') and only after the conflict, at 1340:30, emphasised the word 'Oscar' in an instruction ('Zulu Sierra Oscar cleared touch and go').[5]
Traffic control errors
In June 2020, Airservices conducted an operational safety study of Moorabbin Tower incidents from January 2013 to July 2018. The study provided an overview of the nature and frequency of Air Traffic Control (ATC) conflicts. The purpose of the study was to support operational managers in understanding the unit’s safety performance based on results derived from submitted safety occurrence reports.
The study showed that 5 per cent of the total coded occurrences were ATC attributable with six occurrences (3 per cent of the total) resulting in the system entering an undesired state (incorrect presence of at least one aircraft on a runway). The occurrences related to ATC inducing tactical conflicts (occurrences that are pilot attributed) with the tactical planning-related failures being resolved prior to entering the undesired state. The study showed that ATC attributable errors do occur, albeit with a low level of incidence of ATC induced tactical conflicts.
Landing clearances
Airservices provide landing clearance requirements directly relevant to the airspace in which this incident occurred. The Airservices Aeronautical Information Publication En-route (AIP ENR) 1.1 states that a pilot in command must not land unless they receive specific clearance ‘Cleared to land’.
AIP ENR 1.1 provides the following separation standards for Class D controlled airspace:
A landing aircraft will not be permitted to cross the threshold of the runway on its final approach until:
- a preceding departing aircraft using the same runway:
- is airborne and
- has commenced a turn; or
- is beyond the point on the runway at which the landing aircraft could be expected to complete its landing roll and there is sufficient distance to manoeuvre safely in the event of a missed approach;
- is at least 1,000 m from the runway threshold, and has commenced the take-off run, and
- in the opinion of the controller, no collision risk exists
The controller was working in the ADC-E position at Moorabbin tower. The controller was first rated in August 2003, achieved a rating for all tower positions in March 2007, and was qualified to conduct training and assessment in July 2010. There was also an endorsement to provide relief staffing at Avalon tower when needed. The controller successfully passed a renewal check in April 2020 and had been operating on an approved leave reduction program, of 4 days on, followed by 12 days off duty since early 2020. This level of recency, however, met Airservices’ requirements.
There was no evidence to suggest any likelihood of reduced controller performance due to fatigue, distractions or general health. The weather conditions and visibility were also not considered to have influenced the controller’s actions.
Tools available
In addition to visual observations from the Moorabbin tower and using voice communications, controllers use other tools to assist with performing their duties.
The controller was using a traffic running sheet to record aircraft movement data and to assist in sequencing aircraft. The traffic running sheet provides a back-up memory prompt to the primary function of visual monitoring of traffic. The running sheet that the controller used contained many changes, corrections and annotations, reflecting the level of activity and traffic complexity, which increased the likelihood of making an error (see Appendix – Traffic Running Sheet). The sheet also indicated that the controller remained unaware of the incident between ZSD and TAX.
Moorabbin Tower also utilises a support tool called the Traffic Situation Air Display (Figure 5). This display provides awareness of aircraft higher than about 200 ft, which is higher than ZSD was operating at the time of the incident.
Flight progress strips (FPS)[6], a tool that has the same functional objective as traffic running sheets, are not used at Moorabbin Airport. According to Airservices, FPS are generally not required for visual flight rules (VFR) flights.
Figure 5: View and perspective from controller position towards runway 17L
Source: Airservices Australia annotated by ATSB
Air traffic communications
Table 1 provides the air traffic communications between the tower and ZSD and TAX in the lead up to the runway incursion. A large number of communications were also made between the controller and various other aircraft. Significant items are highlighted in the table.
Table 1: Communications and events leading up to the time of the incident
Time
Communications and events
Notes
1334:46
‘Zulu Sierra follow Cessna late downwind’
1334:49
‘Zulu Sierra Delta’
Pilot’s response to instruction for turning downwind (Last radio call before incident).
1334:52
‘Oscar X-Ray Golf is going around’
1334:54
‘Oscar X-Ray Golf’
1335:15
‘Moorabbin Tower November Charlie Echo is ready runway 17 Left circuits’
1335:21
‘November Charlie Echo line up’
1335:23
‘Line up November Charlie Echo’
1335:42
‘November Charlie Echo follow the Sling upwind. Cleared for takeoff’
1335:45
‘Copy traffic. Cleared for takeoff November Charlie Echo’
1336:27
‘Mike Juliet Golf follow the twin upwind cleared touch and go’
1336:30
‘Cleared touch and go Mike Juliet Golf’
1336:33
‘Oscar X-Ray Golf turning downwind touch and go’
1336:36
‘Oscar X-Ray Golf follow the Sling on base’
1336:39
Oscar X-Ray Golf
1336:41
‘Moorabbin Tower Tango Alpha X-Ray is ready, one, runway 17 left for oblique crosswind departure to the training area’
1336:49
‘Tango Alpha X-Ray line up’
TAX given clearance to line up, ZSD is on base and sights TAX below
1336.51
‘Lining up Tango Alpha X-Ray’
TAX gives radio call about lining up
1337:15
‘Sierra Oscar follow the twin late downwind’
Tower talks to ZSO
1337:20
‘Zulu Sierra Oscar follow the twin late downwind’
Tower talks to ZSO
1337:22
‘Zulu Sierra Oscar’
1337:44
‘November Charlie Echo turning downwind touch and go’
1337:48
‘Charlie Echo follow the Sling mid downwind’
1337:51
‘November Charlie Echo’
1337:51
ZSD does touch and go over the top of TAX
The incident
1338:41
‘Tango Alpha X-Ray cleared for take-off’
TAX given clearance for take-off
1338:43
‘Cleared for take-off Tango Alpha X-Ray’
TAX reads back the take-off clearance and departs for the training area
1340:09
'Zulu Sierra Delta follow Cessna late downwind'
Controller pause in communications
1340:30
'Zulu Sierra Oscar cleared touch and go'
Controller emphasises ‘Oscar’
Student pilot information
The student pilot commenced training on 9 June 2020, with the first flying lesson on 23 June. Records showed a total flying experience of 18.5 hours to the last recorded flight (the occurrence flight) on 23 July, all on the Sling 2 aircraft type. Of that total experience, 17 hours had been in the previous 30 days. The student was not required to, and did not, hold a flight crew licence.
The pilot was an international student and had completed the General English Language Proficiency (GELP) test on 14 July 2020. On 23 July, the pilot was operating a second session of solo circuits and stated ‘feeling very nervous’ because English was not their first language. The incident occurred during the final leg of the fourth circuit, prior to a full stop landing.
The training school records indicated that the student pilot had completed the required training (as per the lesson entry reports) approved by the school’s instructors. The student was familiar with the runway configurations at Moorabbin, including the unusually long displaced threshold of runway 17L. The training school manual had a requirement about occupied runways and directed that students undertake specific training, including missed approaches/go‑arounds.
If for any reason, it is judged that an approach cannot be continued to a successful landing, a missed approach (go-around) will be conducted.
The operator’s training manual also provided runway descriptions and airport markings (including displaced thresholds). This incident was the first time that the student pilot had experienced another aircraft on the runway when approaching to land. The pilot also expressed a belief that it was permitted to have another aircraft lined up on the runway when landing. The pilot also believed that a landing clearance had been issued, observed that TAX was stationary and thought that it would not take off until the tower issued a take-off clearance.
After the incident, the instructor debriefed the student pilot and explained the requirement to conduct a go around if an aircraft was lined up on the runway. The instructor did not think this had been specifically discussed with the student previously although it may have been covered otherwise in training (during theory classes or briefings). Following that debrief, the pilot reported having a correct understanding of what to do in the event of an occupied runway.
There was no evidence that fatigue risk, distractions or other personal health aspects were likely to have been present. The weather conditions and visibility were also not considered to have influenced the pilot’s actions.
Monitoring regulations
The Civil Aviation Safety Authority (CASA) requirements for instructors monitoring students on their second solo flight are contained within Civil Aviation Safety Regulation (CASR) Part 61.112(3). These requirements state that a flight is suitably supervised if the instructor:
(a) provides guidance to the person in relation to the flight,
(b) during the flight is at the aerodrome from which the flight began and
(c) can be contacted during the flight by radio or other electronic means.
CASR Part 142.340 details the required exposition content for operators conducting integrated and multi-crew flight training. This states that the exposition must contain a description of the procedures by which the operator conducts and manages the activities, including the supervision of instructors and persons participating in activities.
Additionally, the CASR Part 142 Technical Assessor handbook details how the above requirements are to be documented in an organisation’s exposition. Section C3.1.1 (k) of the handbook ‘Procedures for Conduct and Management of Training - Supervision of Student Pilot Solo Flight’ outlined the documented expectations that are to be contained within an exposition with respect to the supervision of student pilots. While not a regulatory requirement, CASA inspectors are advised to check the following.
-The process should include provision for active monitoring of each solo flight by a flight instructor. As well as active monitoring, the supervising instructor should provide flight following, operational control and the rendering of assistance if necessary.
-For solo circuit operations, the applicant should ensure that a competent instructor is assigned to visually monitor circuit operations. The supervising instructor may be provided with two-way radio communication with circuit aircraft for the purpose of exercising operational control over solo flights, if necessary.
-For training area and navigation solo flight operations, an application should ensure that an instructor is assigned to monitor radio frequencies when possible, to provide assistance if necessary, and maintain a search and rescue watch.
Visual monitoring
The instructor usually monitored students by listening to the ATC frequency via radio from the RVAC operations room, as was the case at the time of the incident. There was no CASA requirement to visually monitor operations, and CASA advised that while the instructor needs to be available, it would not be appropriate to intervene in operations at a controlled airport such as Moorabbin. Hence, CASA considers the first knowledge a training school would have of such an incident at a controlled airport is similar to the way this incident unfolded, or the tower would inform the school by telephone.
In any case, from the operations room, the instructor was unable to visually monitor aircraft, as per the suggested guidance in the assessor handbook. The view was also partially obstructed by parked aircraft and the instructor was dividing attention between monitoring the radio and administrative work.
At 1337 on 23 July 2020, the PA-28 aircraft, VH-TAX (TAX), was lined up on the threshold of runway 17L at Moorabbin Airport, awaiting take-off clearance. The Sling 2 aircraft, VH-ZSD (ZSD) was on the base leg of the circuit and its student pilot believed (incorrectly) that a clearance for a touch and go landing had been provided. The student pilot saw the lined-up aircraft but continued the approach, passed above TAX about a minute later and conducted a touch and go landing.
The air traffic controller in the Moorabbin Tower (tower) managing the movements of the two aircraft did not identify the developing conflict as ZSD approached the runway or the aircraft passing above TAX and conducting a touch and go landing, and remained unaware of the incident until advised about an hour later.
Decision to continue the approach and landing
The student pilot’s decision to continue the approach and conduct a touch and go landing on the occupied runway was based on an incorrect belief that a landing clearance had been provided, and a misconception that landing on a runway with another aircraft lined up was permitted. The belief that a clearance had been provided may have been influenced by the following factors:
callsign confusion
expectation bias
cognitive tunnelling
authority gradient and pilot inexperience.
As discussed, aircraft with similar callsigns operating in the same area and, especially, on the same frequency often gives rise to flight safety incidents. At the time of the incident, ZSD and ZSO were in the circuit at the same time and conducting touch and go landings on runway 17L. It is possible that the downwind calls made by ZSO prior to the event may have been mistakenly heard as a clearance by the student pilot of ZSD.
The student pilot misperceived the tower communications and assumed the expected clearance had been provided by the controller. There may have been an expectation to hear this clearance, where the student pilot filled in the gaps in the communication. Expectation bias can occur when an individual's expectations about an outcome influence perceptions of one's own or others’ behavior.[7] The student pilot may have been experiencing this bias (expecting the landing clearance to be provided), which could explain why the pilot made the decision to conduct the touch and go, and later recalled hearing a clearance.
There may also have been a degree of cognitive tunnelling for the student pilot. It has long been established that cognitive tunnelling is an inattentional blindness where one becomes overly‑focused on some variable other than the present environment.[8] It can occur under periods of high stress or workload, which student pilots experience due to high demands on their attentional resources in the training environment.
During this occurrence, the student pilot may have been so focussed on the landing and avoiding a collision with TAX on the runway, that attentional resources were not focussed on tower communications. Hence, the student pilot incorrectly assumed a verbal clearance by the tower had been provided.
Finally, the student pilot’s belief that the controller had provided a landing clearance and deciding to land on an occupied runway may also have been influenced by a steep authority gradient between the student and the controller, as well as the student’s lack of experience.
Authority gradient refers to the established and/or perceived command and decision-making power hierarchy in a team, crew or group situation and how balanced the distribution of this power is experienced within the team, crew or group (Hawkins 1993). A steep gradient occurs when a role appears dominant over another and leads to others being less likely to express concerns, question decisions or even clarify instructions.
As the student pilot was conducting a second solo flight and had English as a second language there may have been a steep authority gradient, which could explain why the student would not have clarified the (assumed) landing instruction.
The evidence shows the student pilot decided to continue the touch and go landing due to an incorrect belief that a clearance had been provided, and a misconception that landing on a runway with an aircraft lined up was permitted. Exact reason(s) for believing a clearance had been provided could not be established, but factors that may have contributed to that belief include callsign confusion, expectation bias, cognitive tunnelling, authority gradient and pilot inexperience, or a combination of these factors.
Occupied runway training
The student pilot of ZSD conducted the touch and go after seeing TAX lined up behind the runway threshold. According to the training instructions and AIP procedures, the approach should not have continued, as the runway was occupied, and a landing clearance had not been received. The instructor did not think this had been specifically discussed with the student previously although it may have been covered otherwise in training. The pilot later stated understanding what to do in future in the event of an occupied runway.
While the training documentation contained occupied runway requirements and Airservices’ safety publications provide further guidance, interview evidence, as well as the student's actions, indicate that learning in this aspect had not been effective.
Unidentified conflict
The controller did not see ZSD approaching to conduct a touch and go landing with TAX lined up and, therefore, took no action to avoid the runway incursion. Normally, pilots report that they are on short final (for example, OXG and NCE in the circuit that day). However, the pilot of ZSD did not contact the tower when approaching for that touch and go landing. Based on the available evidence, the controller’s ability to identify the conflict may have been influenced by the following factors:
traffic density
workload and communications
callsign confusion.
Evidence from the interviews of the controller, the tower supervisor and the involved pilots; as well as the recorded traffic movement data, suggest that traffic movements increased in the months leading up to the time of the event. A controller’s ability to detect a conflict can depend on the traffic load and more controllers miss more potential conflicts when traffic density is high, compared to when it is low.[9]
The changing traffic movements may also have affected the controller’s workload level. The following research-based observation is relevant to this relationship with workload.
Workload reflects the interaction between a specific individual and the demands imposed by a particular task and represents the cost incurred by the human operator in achieving a particular level of performance. An individual has a finite set of mental resources they can assign to a set of tasks and will seek to perform at an optimum level of workload by balancing the demands of their tasks.[10]
Both the controller and the supervisor indicated that workload was influenced by traffic movements. Additionally, the number of communications leading up to the event and the many changes to the traffic running sheet suggest high workload. It is probable that an increased level of mental workload because of increased traffic density, resulted in the controller having less opportunity to identify the conflict. Airservices’ safety study data referred to earlier also shows that ATC‑attributable errors have occurred at Moorabbin Airport.
It is also possible that callsign confusion played a part in the controller not identifying the conflict. There was significant communication at the time, both ZSD and ZSO had similar communications with the tower while operating in the same area on the same frequency. At 1334:49, the controller also omitted ‘Delta’ in the instruction ‘Zulu Sierra follow Cessna late downwind' giving potential for confusion between ZSD and ZSO. The first two phonetics of these callsigns (that is, ZS) were the same. Further, they had visually similar shapes that can be easily mixed up as they only differ by their last designator (for example, on a traffic running sheet). The controller’s pauses are indicative of some level of confusion and only emphasising the phonetic ‘Oscar’ after the occurrence, suggests the controller may not have recognised the potential for confusion in time.
Overall, the evidence shows that the controller did not identify the conflict between ZSD and TAX, but the exact reason(s) could not be established. This may have occurred due to the high traffic density and resulting communications workload or the similar aircraft callsigns operating in the same circuit on the same frequency, or a combination of these factors. While it is possible some other factors may have had an influence (for example, runway confusion or not following standard operating procedures), there was no evidence to justify considering such factors.
Other considerations
As the informal ‘spotter’ position was no longer used, the controller was the only person that could have identified the developing conflict because, as explained, the student pilot’s instructor could not have done so. Further, as the instructor in TAX (who had reasons to delay it) did not report the incident immediately, the corrective action taken to address the immediate operational risks by relieving the controller was delayed by more than an hour.
Single person controller operations where a position/sector is operated by one person are unsuitable during busy periods, as they can lead to high task loads, distraction, failure to detect threats and not recognising errors. Monitoring each other’s actions (also known as the ‘four-eye principle’) reduces the likelihood of this error by increasing situation awareness. This was probably the main safety-related reason for rostering an informal ‘spotter’ in Moorabbin Tower.
Airservices’ safety study provides an indicative level of risk that it can use to assess the level of acceptable risk for single person controller operations at Moorabbin, including situations involving student pilot errors or non-compliance with ATC instructions. The ATSB did not find any additional information, such as incident trend data or studies into optimal workload levels (for Moorabbin or similar towers) to make findings with respect to tower staffing levels.
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the runway incursion involving The Airplane Factory Sling 2, VH-ZSD at Moorabbin Airport, Victoria, on 23 July 2020.
Contributing factors
While the Piper PA-28, VH-TAX, was in the lined-up position (behind the displaced threshold) on runway 17L, the Sling 2, VH-ZSD, passed overhead and conducted a touch and go landing.
The student pilot of ZSD sighted TAX but decided to conduct the touch and go landing due to an incorrect belief that it was permitted to have another aircraft lined up on the runway when landing, and that the controller had provided a landing clearance.
The student pilot’s training had not been effective in conveying that a go-around must be initiated if the runway, including its displaced threshold, was occupied.
The air traffic controller did not identify the runway incursion developing, see ZSD pass above TAX or its touch and go landing and remained unaware of the incident until advised about 1 hour later.
Safety actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are provided separately on the ATSB website, to facilitate monitoring by interested parties. Where relevant, the safety issues and actions will be updated on the ATSB website as further information about safety action comes to hand.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by Royal Victorian Aero Club
The Royal Victorian Aero Club advised the ATSB that it has taken the following actions.
Flight crew and student education
Briefings for circuits and circuit emergencies have been updated.
Instructor training now includes being trained on checking essential knowledge for the lesson.
New manuals have been provided to all instructors and have been signed as acknowledged.
The pre solo exam and pre area solo exam have been updated to cover the scenario of runway occupied/no clearance provided.
Procedural actions
The recreational pilot licence training manual has been updated to include essential knowledge to be checked before solo flights.
Instructors were briefed and have acknowledged the updated manual.
Proactive action
Solo flights have been reviewed, ensuring that instructors comply with the training manual including supervision requirements and checking essential knowledge.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Pilot and instructor for VH-ZSD
the instructor of VH-TAX
Airservices Australia
The air traffic controller
The tower supervisor
Royal Victorian Aero Club
Moorabbin Flying Services
Bureau of Meteorology.
References
Hawkins FH 1993, Human Factors in Flight 2nd ed, Ashgate Aldershot UK.
Mack A & Rock I 1998, Inattentional blindness, MIT Press Cambridge MA.
Metzger U & Parasuraman R 2001, The role of the air traffic controller in future air traffic management: An empirical study of active control versus passive monitoring, Human Factors, vol. 43, pp.519-528.
Most SB 2010, What's "inattentional" about inattentional blindness?, Consciousness and Cognition, vol. 19, pp.1102-1104.
Orlady HW & Orlady LM 1999, Human factors in multi-crew flight operations, Ashgate Publishing Ltd Hants England.
Williams JB, Popp, D, Kobak KA & Detke MJ 2012, The power of expectation bias, European Psychiatry, vol. 27, pp.1
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot and instructor for VH-ZSD
the instructor of VH-TAX
Airservices Australia
the air traffic controller
Royal Victorian Aero Club
Moorabbin Flying Services
Civil Aviation Safety Authority
Submissions were received from:
Airservices Australia
the air traffic controller
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix – Traffic running sheet
Source: Airservices Australia
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the morning of 17 March 2020, a QantasLink Bombardier Dash-8-402, registered VH-LQJ (LQJ), was being taxied for a scheduled flight from Gladstone Airport, Queensland to Brisbane Airport, Queensland. There were two flight crew, two cabin crew and 34 passengers on board. At the same time, an ATEC Faeta 321, registered 24-8279 (Faeta 8279), with one instructor and student on board, was conducting circuit training at Gladstone Airport.
At about 0645, as Faeta 8279 was on approach to conduct a touch-and-go on runway 10, LQJ entered and taxied along the runway in front of Faeta 8279. The instructor on board Faeta 8279 conducted a go-around to avoid an incident on the occupied runway.
What the ATSB found
The ATSB found that the flight crew of LQJ set the incorrect common traffic advisory frequency and did not select the appropriate traffic collision avoidance system/transponder mode during the before start checks. These errors were likely influenced by increased workload and time pressures experienced during before start preparations.
The errors went undetected during the taxi phase of flight. As a result, the flight crew’s situational awareness was significantly degraded and caused the captain and first officer to form the shared belief that no other traffic was operating in the vicinity of Gladstone Airport. This shared incorrect mental model likely impacted the efficacy of the visual scan conducted prior to entering the runway, with neither flight crew member sighting the approaching aircraft.
What has been done as a result
Following this incident, QantasLink undertook a review of operating procedures at non-controlled airports. The procedural review included transponder activation and introduced a requirement to contact Air Traffic Control prior to entering the runway. QantasLink also provided internal communications to flight crew detailing the importance of standard operating procedures and threat management when dealing with distractions and workload.
Safety message
This incident illustrates the human factors implications associated with the combination of increased workload and time pressures. Flight crews can guard against similar outcomes by applying effective threat and error management strategies that recognise when such threats may arise and set in place suitable actions that minimise error potential. These actions include strict adherence to standard operating procedures and increased cross-checking of system inputs and mode changes.
The investigation
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
At about 0600 Eastern Standard Time,[1] on 17 March 2020, the crew of a QantasLink Bombardier Dash-8-402 aircraft, registered VH-LQJ (LQJ), commenced pre-flight preparations for a scheduled regular public transport flight from Gladstone Airport, Queensland to Brisbane Airport, Queensland. The crew comprised the captain, first officer (FO) and two cabin crew.
It was the first flight of the day for LQJ and the scheduled departure at 0645 meant that the crew had about 45 minutes to prepare the aircraft. Shortly after arriving at the aircraft, the captain started the auxiliary power unit (APU),[2]while the FO conducted the aircraft walk around. The captain then commenced the ‘originating’ and ‘before start’ checks, which included selecting APU bleed air ‘ON’ to provide air-conditioning to the cabin. At this point the APU failed, so the captain completed the automatic APU shutdown actions.
At about 0610 during the walk around, the FO noticed a small aircraft taxi behind LQJ. This aircraft was an ATEC Faeta 321, registered 24-8279 (Faeta 8279), that was being taxied for circuit training with one instructor and one student on board. The FO made a mental note of the taxiing aircraft, finalised the walk around, and returned to the flight deck to complete the remainder of the pre-flight preparations.
The captain and FO then restarted the APU, but it failed for a second time when APU bleed air was selected ‘ON’. At about the same time, a ground crew member attended the flight deck to inform the captain and FO that a ‘person in custody’[3]and their police escort would be travelling on the flight. The captain left the flight deck to review the person in custody paperwork and brief the cabin crew on the custody arrangements. The person in custody and their escort then boarded the aircraft, with the remainder of the flight’s 34 passengers boarding a short time later.
At about 0622, Faeta 8279 commenced circuit training using runway 28. The occupants of Faeta 8279 made regular positional broadcasts on the Gladstone Airport common traffic advisory frequency (CTAF) [4]throughout the training activity.
Meanwhile, on board LQJ, the captain returned to the flight deck and elected to apply the Minimum Equipment List (MEL)[5] to the APU system. The captain and FO then actioned the procedures required to apply the MEL with remote support provided by QantasLink maintenance engineers. Completing this task took the crew 5-10 minutes.
Once the MEL had been finalised, the captain and FO undertook the remainder of the before start checks, but omitted to set the traffic collision avoidance system (TCAS)[6]/transponder[7] to ‘ON ALT’ and to select the Gladstone CTAF in VHF COM 2.[8]The CTAF omission was identified by the FO during the departure briefing and subsequently addressed. However, the FO entered the incorrect frequency of 126.7 MHz instead of 118.8 MHz, which was the correct frequency for the Gladstone CTAF.
At 0643, a pilot in Faeta 8279 made a CTAF broadcast advising traffic that the aircraft would be changing runway direction for a touch-and-go on runway 10. The captain and FO of LQJ did not receive this broadcast as they were monitoring the incorrect frequency.
The weather at the time was reported as being a wind from 201 degrees magnetic at 6 knots, no cloud, and a visibility of 43 km. As the wind did not favour either runway, the flight crew of LQJ elected to use runway 28 to avoid departing towards the rising sun. This required a short taxi from bay 3 to the A5 intersection, and a right turn to enter and backtrack runway 28 (Figure 1 and Figure 2).
Figure 1: Overview of VH-LQJ taxi routing
Source: Google Earth, annotated by the ATSB
Figure 2: Gladstone aerodrome chart
Source: Airservices Australia, annotated by ATSB
At 0643:38, the FO made a broadcast on the incorrect CTAF using VHF COM 2 and LQJ was taxied from its parked position on bay 3.
At 0644:23, the FO made a second broadcast on the incorrect CTAF as the aircraft taxied towards the A5 intersection.
At 0644:29, a pilot in Faeta 8279 made a broadcast on the Gladstone CTAF advising traffic that the aircraft was on short final for a touch-and-go on runway 10. The flight crew of LQJ did not receive this broadcast either.
The captain and FO conducted a visual scan as LQJ neared the A5 intersection, but neither flight crew sighted Faeta 8279 on approach for runway 10. At about 0645, LQJ was taxied onto the runway in front of the approaching Faeta 8279. In response, the instructor on board Faeta 8279 commenced a go-around and attempted, unsuccessfully, to contact LQJ on the Gladstone CTAF.
At 0645:02, as LQJ backtracked along the runway, the FO made a taxi report to Brisbane Centre[9] using VHF COM 1. A secondary surveillance radar transponder code[10] was provided to LQJ and the captain entered it into the transponder. Shortly afterwards, the captain identified that the TCAS/transponder was not appropriately set and selected it to ‘ON ALT’.
At 0645:42, the TCAS presented the flight crew with a traffic advisory[11] indicating climbing traffic above LQJ. The traffic – Faeta 8279 – was subsequently sighted by the captain and FO climbing in an easterly direction overhead the airport.
The captain and FO checked the frequency set in VHF COM 2 and identified the incorrect frequency selection. The frequency was changed to the correct frequency of 118.8 MHz and the FO made a broadcast at 0646:29 advising that LQJ was ‘entering and backtracking’ runway 28.
At about 0646:36, a pilot in Faeta 8279 replied to LQJs broadcast, but the flight crew of LQJ did not respond to Faeta 8279’s transmission. A short time later, the instructor in Faeta 8279 broadcast the intention to manoeuvre for runway 28 to allow LQJ to depart. At about 0648, LQJ commenced its take-off from runway 28.
Context
Air Traffic Control communications
The captain and FO elected to delay the taxi report to Brisbane Centre until LQJ had entered the runway. This was due to the shared understanding that the Gladstone Airport terminal buildings shield VHF transmissions and prevent contact being made with Brisbane Centre when parked on bay 3. QantasLink procedures permit an aircraft to be moved to an alternate location when communications with air traffic services are not possible on the bay.
Human factors
The same crew had flown LQJ into Gladstone Airport the evening prior, arriving at about 1900 on 16 March 2020. The crew then stayed overnight in local hotel accommodation. Both the captain and FO reported no fatigue issues associated with the overnight stay, and an assessment of the flight crew’s previous 14-day roster did not identify any significant fatigue risk factors.
During pre-flight preparations, the captain and FO encountered a number of unanticipated events and distractions, including two APU failures, boarding of a person in custody, and application of a MEL to the APU system. The additional actions, due to these events, increased their workload.
On the morning of the incident, neither the captain nor the FO recalled listening for an aerodrome frequency response unit (AFRU)[12] reply to the two broadcasts made on the incorrect frequency. The first broadcast took place when both flight crew members recall increased workload associated with the turn off bay 3. The second CTAF broadcast was made mid-way through the short taxi to the runway intersection.
Prior to entering the runway, the captain recalled believing there was no other aircraft in the vicinity of Gladstone Airport as the crew had not heard any broadcasts on VHF COM 2 and there was no traffic indicating on the TCAS display. The FO recalls making reference to the small aircraft that had been sighted during the walk around checks. However, given the elapsed time since the sighting, combined with the lack of transmissions received on VHF COM 2, the FO concluded that the traffic was no longer in the vicinity of the airport.
Safety analysis
This was the first flight of the day for LQJ and the crew had about 45 minutes to complete all pre‑flight preparations prior to the scheduled departure time of 0645. During this period, the captain and FO encountered several unanticipated events and distractions, including the APU failure and person in custody paperwork, that required additional actions to be performed within the allocated timeframe. These interruptions and additional actions within a defined time period added workload and time pressures.
The combination of increased workload and time pressures is known to result in degraded information processing, increased errors, the tunnelling of attention, and an increased reliance on familiar strategies or actions (Staal, 2004). This response to workload and time pressures likely resulted in the flight crew’s omission of the two ‘before start’ checklist items and the selection of the incorrect frequency in VHF COM 2.
The frequency selection error was further compounded by the flight crew not recognising an absence of AFRU reply when making radio calls on the incorrect frequency. As a result, the captain and FO were not aware that they were monitoring and broadcasting on the incorrect CTAF.
The flight crew’s inadvertent omission of the TCAS/transponder selection resulted in the captain and FO incorrectly believing the TCAS would alert them to the presence of any transponder equipped aircraft that were operating in the vicinity of Gladstone Airport.
As a result of the frequency selection and TCAS/transponder errors, the flight crew’s situational awareness was significantly degraded resulting in the captain and FO forming the shared belief that no other traffic was operating in the vicinity of Gladstone Airport. This shared incorrect mental model likely impacted the efficacy of the visual scan conducted by the flight crew as they neared the A5 intersection. Consequently, neither flight crew member identified the approaching aircraft and LQJ was taxied onto the runway in front of Faeta 8279. The instructor on board Faeta 8279 conducted a go-around to avoid an incident on the occupied runway.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the runway incursion involving Bombardier Dash-8-402, registered VH-LQJ, at Gladstone Airport, Queensland, on 17 March 2020.
Contributing factors
The flight crew of VH-LQJ were not aware that light aircraft 24-8279 was on approach and taxied onto the runway in front of it. Consequently, the pilot of 24-8279 had to conduct a go‑around.
The visual scan by the flight crew of VH-LQJ before entering the runway did not identify the approaching 24-8279, probably because of their degraded situational awareness.
Increased workload and distractions while preparing VH-LQJ for departure led to the crew not setting the correct radio frequency and the appropriate mode on the traffic collision avoidance system/transponder. Without these essential aids to situational awareness, neither pilot developed an accurate mental model of the traffic.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by QantasLink
Following this incident, QantasLink undertook a review of operating procedures at non-controlled airports. The procedural review included transponder activation and introduced a requirement to contact Air Traffic Control prior to entering the runway. QantasLink also provided internal communications to flight crew detailing the importance of standard operating procedures and threat management when dealing with distractions and workload.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew of VH-LQJ
the pilot in command of 24-8279
QantasLink
Avdata
Civil Aviation Safety Authority
Airservices Australia.
References
Staal MA 2004, Stress, cognition, and human performance: A literature review and conceptual framework, National Aeronautics and Space Administration Technical Memorandum NASA/TM-2004-212824.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the crew of VH-LQJ, the pilot in command of 24-8279, QantasLink, and the Civil Aviation Safety Authority.
Submissions were received from QantasLink and the captain of VH-LQJ.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On the evening of 25 September 2019, the flight crew of a GIE Avions de Transport Régional ATR72 aircraft, registered VH-VPJ and operated by Virgin Australia Airlines, received a clearance to line‑up on runway 35 from intersection ‘Golf’ at Canberra Airport, Australian Capital Territory. While taxiing to the runway, the flight crew inadvertently lined-up on runway 30. Almost immediately after commencing the take-off roll, and at about the same time air traffic control instructed them to ‘stop’, the flight crew rejected the take‑off. The aircraft was re‑positioned for a departure from runway 35.
What the ATSB found
The ATSB found that the flight crew elected to depart from intersection ‘Golf’ for runway 35. Due to the close proximity of the aircraft’s parking bay to the ‘Golf’ runway holding point, the selection of this intersection reduced the distance, and therefore the amount of time available for the flight crew to complete their pre-departure checks. After passing through the holding point, the captain taxied the aircraft onto runway 30, following the lead-on lights for that runway, while the first officer’s attention was focussed on completing procedures and checklists. This likely resulted in the flight crew having reduced awareness of the runway environment and aircraft orientation.
The lead-on lights to runway 30 were active with the taxiway lighting and the lead-on lights to runway 35 were activated when the holding point stop bar at intersection ‘Golf’ was turned off by air traffic control. Therefore, both runway lead-on lights were active. This increased the risk of an aircraft being manoeuvred onto the incorrect runway, particularly at night and/or in low visibility conditions. In this case, the captain, who recalled being focused on the lead-on lights, followed the first set of lights that led to runway 30.
The ATSB also established that Virgin Australia Airlines’ ATR72 Before take-off procedure did not specify when ‘ready [for take-off]’ was to be communicated to air traffic control. This increased the risk of procedures and checklists being completed while the aircraft was taxiing onto the runway, at a time when monitoring was critical. Virgin Australia Airlines’ procedures applicable to all the aircraft in their fleet did not include a runway verification check using external cues, including runway markings, signs and/or lights.
What has been done as a result
After the incident, Virgin Australia Airlines discontinued the use of intersection ‘Golf’ for departure at Canberra Airport during the day and night. Subsequent action included a proposal to amend the ATR72 Before take-off procedure to ensure it was completed at a time when the flight crew’s attention was not diverted to other tasks. However, ATR72 operations ceased before this was implemented. In addition, Virgin Australia Airlines have developed a runway verification procedure to be included in their Flight Crew Operating Manual for the Boeing 737, their current fleet.
Safety message
The design of airport runways and taxiways vary from relatively simple to more complex layouts. This can be exacerbated by reduced visual cues, such as night-time or poor weather, which can easily increase confusion. It is important for all flight crew to familiarise themselves with these layouts, particularly any unique designs, and ensure effective flight crew co-ordination is employed to minimise the risk of a runway incursion.
Operators should ensure the design of their operating procedures minimises the risk of human error. Clearly delineating procedural steps may reduce the likelihood of flight crews’ heads down activities at critical moments throughout the flight.
The occurrence
What happened
On the night of 25 September 2019, at about 1840 Eastern Standard Time (EST),[1] the flight crew of a GIE Avions de Transport Régional ATR72-212A (ATR72) aircraft, registered VH‑VPJ and operated by Virgin Australia Airlines, were preparing for a scheduled passenger service from Canberra, Australian Capital Territory, to Sydney, New South Wales. The flight was planned to depart at 1900 and the captain recalled they were running ahead of schedule.
As part of their pre-flight planning, the flight crew elected to depart from intersection ‘Golf’ (G) for runway 35 (refer to section titled Canberra Airport information). The flight crew reported they based this decision on the aircraft’s performance, taking into account the weight and environmental conditions at the time, and the proximity of intersection G to their parking bay.
At about 1855, after the flight crew completed their pre-flight briefing, they requested a pushback clearance from air traffic control (ATC), which was approved. Several minutes later, the flight crew requested a taxi clearance to the holding point at intersection G, which was also approved. At around the same time, the flight crew of two other aircraft also requested clearances for pushback and taxi.
At about 1858, the captain commenced taxiing the aircraft. While taxiing to intersection G, the flight crew completed their departure review, which included checking the departure runway and intersection, take-off performance speeds and the flap setting. Before departure, there was no mention of the departure’s complexity or its designation as a hotspot. Just prior to reaching the holding point, the first officer (FO) advised ATC that they were ‘ready’ [to take-off] and then commenced the Before take-off procedure (refer to section titled Take-off performance).
At about 1859, ATC instructed the flight crew to line-up on runway 35 and about a minute later, they were cleared for take-off, with both instructions read back correctly by the FO. After the stop bar was deactivated by ATC, the aircraft crossed the holding point and the captain commenced turning through the intersection, inadvertently aligning with the centreline of runway 30.
During the turn, the FO was completing the final Before take-off checks and therefore, only looked up after the aircraft was lined-up on the runway. The captain recalled focusing on taxiing the aircraft to follow the lead-on lights (refer to section titled Airport lighting) and trying not to go too far into the intersection. Both flight crew recalled ‘the picture didn’t look right’ when they were lined-up on what they thought was the departure runway (runway 35). They also reported the runway (runway 30) appeared shorter than expected and that there was no centreline lighting (Figure 1). Neither of the flight crew could recall if they cross-checked the aircraft’s heading or position by available means as per the operator’s Before take-off procedure when they were in the lined-up position.
Figure 1: Night comparison of runway 30 and runway 35 from intersection Golf
Note: The vehicle lights were turned on in the runway 35 photograph (right).
Source: Canberra Airport, annotated by the ATSB
Air traffic control reported noticing the aircraft moving on runway 30 and immediately instructed the flight crew to ‘stop stop’ as they ‘seemed to be taking off on [runway] 30’. About 6 seconds later, the FO advised ATC they were ‘stopping’. The flight crew reported that take-off power[2] had not been applied, nor the take-off roll commenced, and no braking was required. However, recorded flight data showed an immediate increase in torque for both engines from 4-6 per cent during taxi to 17.7 per cent, as well as a decrease in brake pressure to 16 pounds per square inch (psi) after the turn onto runway 30 (Figure 2). About 4 seconds later, the engine torque reached 28.1 per cent, indicating the power levers had been advanced to commence the take-off. At about this time, ATC instructed the flight crew to stop, after which, the data showed a decrease in the power lever positions to flight idle and an increase in brake pressure to 1,686 psi.
The flight data was consistent with airport closed-circuit television footage. This footage showed the aircraft cross the holding point and line-up on runway 30, followed by a brief pause, then a short acceleration before a sudden braking. The aircraft then remained stationary on the runway for a few seconds before it was taxied forward along the runway and vacated at the next exit.
Air traffic control provided further instructions to the flight crew to taxi off runway 30 and reposition for a departure from intersection ‘November’ for runway 35. The flight continued to Sydney without further incident.
Figure 2: Flight data showing the aircraft’s turn onto runway 30 with key events
Note: The green line from taxiway golf onto runway 30 indicates the aircraft track.
Source: Virgin Australia Airlines, annotated by the ATSB
The captain held an Air Transport Pilot (Aeroplane) Licence, multi-engine command instrument rating and a Class 1 Aviation Medical Certificate. At the time of the incident, the captain had a total of 6,500 hours of aeronautical experience, of which 2,375 hours were on the ATR72.
The captain was based in Brisbane and scheduled to travel on the 2130 service from Sydney to Brisbane on arrival in Sydney. However, during the turn‑around in Canberra, the captain contacted the airline’s crewing department to reschedule the commute to an earlier flight that departed Sydney at 2000, 10 minutes after the incident flight’s scheduled arrival time in Sydney.
First officer
The FO held a Commercial Pilot (Aeroplane) Licence, multi-engine instrument rating and a Class 1 Aviation Medical Certificate. At the time of the incident, the FO had a total of 6,700 hours of aeronautical experience, of which 6,100 hours were on the ATR72.
Experience in Canberra
Both the captain and the FO reported regularly operating from Canberra Airport over a number of years during both the day and night and being familiar with the airport’s layout. However, they could not recall previously using intersection G for departure at night but had used it for departure at least once during the day.
Fatigue considerations
A review of the sleep and roster information obtained found there was a low likelihood the flight crew were experiencing a level of fatigue known to have an adverse effect on performance.
Canberra Airport information
Canberra Airport has two runways, 17/35,[3] with a length of 3,283 m and width of 45 m; and 12/30, with a length of 1,679 m and width of 30 m. At the time of departure, both runway 30 and 35 were active.
The intersection departures available for runway 35 were from taxiways ‘Golf’ (G), ‘Mike’, ‘Papa’, and ‘November’ (Figure 3). Taxiway G leads to the intersection of the two runways 17/35 and 12/30 and is listed as a runway incursion hotspot due to this complex layout (refer to section titled Runway incursions). There are few airports in Australia where a taxiway led to the intersection of two runways.
Figure 3: Canberra Airport chart
Source: Virgin Australia Airlines, annotated by the ATSB
Airport signs
Canberra Airport had runway and taxiway signs as per the Civil Aviation Safety Authority’s Part 139Manual of Standards for Aerodromes and International Civil Aviation Organization’s Annex 14: Aerodromes. However, these documents do not include standards for signs at taxiways that lead to the intersection of two runways. Intersection G had a red runway sign for 12/30 on the left and a runway sign for 17/35 on the right of the taxiway when viewed from the cockpit (Figure 4). Adjacent to the holding point lights on the left side of the taxiway was the yellow runway distance remaining board for runway 35.
Figure 4: View of intersection G at Canberra Airport
Source: Canberra Airport, annotated by the ATSB
In comparison, the United States Federal Aviation Administration Aeronautic Information Manual stated that if a sign was located on a taxiway that intersects the intersection of two runways, the designation for both runways should be shown on the sign along with arrows showing the approximate runway alignment of each runway. In addition to showing the approximate runway alignment, the arrow indicates the direction to the threshold of the runway whose designation is immediately next to the arrow (Figure 5).
Figure 5: Federal Aviation Administration standards for signs at holding points with two runways
Source: Federal Aviation Administration
While intersection G was a complex layout, the runway signs were consistent with the applicable standards. Although other signs could be used at taxiways that lead to the intersection of two runways, such as those shown above, there were no other incidents reported for Canberra Airport where an aircraft had been inadvertently taxied onto the wrong runway from intersection G.
Airport lighting
The lighting system at Canberra Airport included runway lighting and taxiway lighting (Figure 6). Runway lighting consisted of white lights on the edges of the runway, and green and red lights positioned at the ends of the runway landing and departure thresholds respectively. Taxiway lighting consisted of green centreline lighting. There were also red stop bar lights at all the holding points for both runways. Only runway 17/35 had white centreline lighting.
Stop bars are installed at runway entry points to prevent an aircraft inadvertently entering the runway without a clearance. The lead-on lights for runway 35 from intersection G were linked with the stop bar so that when the stop bar was deactivated by ATC, the green centreline lighting beyond the stop bar activated. The lead-on lights for runway 30 were on the same circuit as the taxiway lighting, and therefore already active irrespective of the state of the stop bar. Therefore, it was possible for the lead-on lights to both runway 30 and 35 to be illuminated at the same time.
Figure 6: Canberra Airport lighting
Source: Canberra Airport, annotated by the ATSB
Operational information
Aircraft performance
From intersection G, there was 1,810 m of take-off run available[4] and 1,870 m of take-off distance available[5] for departure from runway 35. For runway 30 there was 1,030 m of take-off distance available. Factoring the aircraft’s weight and environmental conditions, about 1,700 m was required for the take-off. The accelerate stop distance[6] required for either runway was about 1,650 m.
Given the shorter length of runway available for take-off from intersection G, the aircraft’s limitations for using this intersection was a maximum take-off weight of 20,541 kg and maximum air temperature of 31 °C. At the time of the incident, the aircraft’s actual take-off weight was 20,000 kg and the ambient air temperature was recorded as 11 °C.
As part of an internal review following the incident, Virgin Australia Airlines examined the ATR72 specific departure data from Canberra Airport for the 9 months prior to the incident. The data showed that 4 per cent of all ATR72 departures were from intersection G during both the day and night. Less than 1 per cent of all departures were from intersection G at night.
Simulator session
To assess the outcome of a take-off from runway 30, Virgin Australia Airlines conducted a simulator session. The same data as the incident flight was loaded into the simulator and the flight crew briefed an intersection G departure from runway 35. When the flight crew reached the intersection of runway 30 and 35, they were instructed to keep turning until they were lined-up on runway 30. Since the aircraft was lined-up near the intersection of the runways, the course deviation bar was observed to be centred.
The flight crew conducted the take-off, applying full torque of 90 per cent. The aircraft reached a height of 50 ft at the upwind threshold and continued without any terrain warnings. The scenario was repeated with an engine failure after take-off, which resulted in the flight crew receiving a terrain warning. Based on the results from these sessions, it was assessed that the take-off could have been successful if the departure was continued from runway 30. However, a runway overrun would have likely occurred if these was an engine failure at around their selected V1[7] speed, or if there was any mishandling of the take-off. The operator’s flight technical specialists reviewed the flight data and conditions on runway 30 on the night of the incident and estimated around 980 m was required for the aircraft to become safely airborne using a minimum rotate/unstick airspeed.
Operator procedures
Take-off performance
At the time of the incident, Virgin Australia Airlines did not publish ATR specific performance charts for departure using runway 12/30. Therefore, the flight crew were restricted to using runway 17/35 only.
Before take-off procedure and checklist
In preparation for departure, the flight crew were required to complete the Before take-off procedure and checklist specified in Virgin Australia Airlines’ ATR72 Standard Operating Procedures. This procedure was to be completed after the cabin was secure and the departure review had been conducted. The procedure did not include a step for when ‘ready’ [for take-off] should normally be reported to ATC, and the flight crew recalled they would often report ‘ready’ [for take-off] prior to commencing the Before take-off procedure. By comparison, calling ‘ready’ was placed at the end of Virgin Australia Airlines’ Boeing 737 Before take-off procedure.
The ATR72 procedure referred to flight crew member 1 (CM1) as the pilot in the left seat (the captain) and flight crew member 2 (CM2) as the pilot in the right seat (the FO). Each flight crew member was assigned specific tasks to complete, which were applicable to all flights. Table 1 lists the tasks to be completed as part of the Before take-off procedure. Of note, the second to last item was required to be performed prior to entering the runway for take-off and the last item was to be completed on the runway. On the evening of the incident, the flight crew allowed themselves less than 90 seconds to complete this procedure while taxiing to the intersection. In comparsion, taxiing to the other intersections closer to the runway end would have taken several minutes, allowing more time to complete this procedure.
Table 1: Virgin Australia Airlines ATR72 Before take-off procedure
CM1 (captain)
CM2 (FO)
Call ‘cabin secure’ and turn over the CABIN SECURE card to display the green lettering ‘secure’.
Conduct the take-off review, which involves verifying their assigned runway and calculated speeds.
Call ‘gust lock’, check for unrestricted rudder travel, and check rudder cam is centred.
Release gust lock and check for unrestricted aileron and elevator travel in all directions and check spoiler lights.
Set the bleed valves in accordance with performance data calculations and check airflow is selected to NORM.
Call ‘before take-off checklist’
Check the flight controls and confirm the bleed valves/airflow were set. Then call ‘before take-off checklist’ complete.
Immediately prior to entering the runway for take-off or when back tracking the runway (as appropriate) cycle the NO DEVICE switch to achieve the two audible chimes.
When on the runway both the flight crew are required to verify they are lined up on the centreline by checking the flight director lateral bar is centred when in the lined-up position.
Note: This table combined the Before take-off procedure and checklist provided by Virgin Australia Airlines.
The Before take-off procedure also specified that flight crew were required to verify the aircraft had lined-up on the correct runway using internal cues within the cockpit such as those provided by the horizontal situation indicator.[8] Specifically, the procedure stated:
Use all available information such as heading and [flight management system] course indication [primary flight display],[9] lateral profile [multi-function display][10] and departure runway [multi‑function control and display unit][11] to ensure the aircraft is at the assigned runway and correct intersection for take-off.
Virgin Australia Airlines’ procedures applicable to all fleet did not include the use of external cues to verify the aircraft’s position prior to entering the runway and/or commencing the take-off roll at all times. The only reference to checking the take-off runway was during low visibility operations. External cues include runway markings, lights, and signs. An informal review of other operators’ procedures found they included a runway verification check, which was conducted prior to take‑off. This procedure required the flight crew to confirm the runway entry point prior to entry, and the departure runway prior to commencing take-off, with reference to both internal and external cues. This procedure would be conducted by both flight crew, and it required them to verbalise the identification and verification.
Runway incursion prevention
Virgin Australia Airlines’ Operations Manual: Operating Policies and Procedures applicable to all aircraft in their fleet described strategies to assist flight crew to manage the risk of runway incursions. These strategies included:
To avoid a runway incursion, flight crew must maintain a high level of situational awareness and vigilance during taxi, both before take-off and after landing. The following will assist flight crew in achieving this:
1. The Pilot Flying (PF) should brief the anticipated taxi route during the departure or approach briefing, as applicable, when:
a. Complex taxi routing is expected; or
b. Advice including NOTAMs affect taxiway routing or runways; or
c. Active runways will be crossed; or
d. Runway incursion 'hotspots' are identified on airport charts.
Ensure the aircraft location and that of other proximate traffic is known at all times by use of airport signage and reference to the airport diagram chart. Navigation displays should be used to aid orientation whenever practicable. During complex taxiing the [pilot monitoring] may assist awareness by verbal confirmation of taxiway passage or clearances.
Administrative tasks and checklists should be accomplished at the appropriate time, with due consideration to active runway or ‘hotspots’ on the taxi route.
Prior to crossing a runway or entering a runway for take-off the flight crew must:
a.) Verify the correct runway.
b.) Confirm that there is no conflicting traffic on the runway or on approach. Use of Traffic Collision Avoidance System may assist in the display of traffic but does not preclude visual verification.
Runway incursions
The International Civil Aviation Organization (2007) define runway incursions as:
Any occurrence at an aerodrome involving the incorrect presence of an aircraft, vehicle or person on the protected area of a surface designated for the landing and take-off of aircraft.
Incident reports show runway incursions are often clustered at particular runway holding points and/or intersections. These are known as ‘hotspots’. Specifically, a runway incursion hotspot is defined as ‘a location on an aerodrome movement area with a history or potential risk of collision or runway incursion, and where heightened attention by pilots/drivers is necessary’ (International Civil Aviation Organization 2007). These hotspots are included on charts provided by Airservices Australia and Jeppesen. Virgin Australia Airlines provided their flight crew with Jeppesen charts for their flight planning.
According to Airservices Australia’s Pilot’s Guide to Runway Safety (2016) a reason why runway incursions occur was due to runway confusion, which is when pilots enter, take-off, or land on the incorrect runway. The risk increases at airports with multiple runways, complex layouts or during night operations. One countermeasure to avoid runway confusion was to visually identify the correct runway before you enter or land on it using available cues such as signage, orientation, and runway markings.
An ATSB research report Factors influencing misaligned take-offs at night reviewed Australian and international occurrences where aircraft lined up on runway edge lighting or departed from closed/incorrect runways or taxiways. Common themes identified in these occurrences were flight crew divided attention/distraction/eyes inside (including due to workload and lack of familiarity with runway or airport) and confusing runway/taxiway entry/lighting.
The Pilot’s guide to runway safety also provided the following considerations to avoid runway incursions (not limited to):
plan the taxi using available airport charts
minimise heads down activity while the aircraft is moving
resist the pressure to take short cuts.
Similar occurrences
A review of the ATSB’s occurrence database did not find any other incidents where an aircraft entered runway 30 instead of 35 at Canberra Airport while taxiing from intersection G in the previous 5 years. The following incidents were identified where aircraft had been lined-up on the incorrect runway or intersection:
On 21 January 2017, the flight crew of an Airbus A320 aircraft, registered VH-VNC, prepared to conduct a regular passenger service from Cairns to Brisbane, Queensland.
At about 1511, ATC cleared the flight crew to taxi to holding point ‘B5’, which was the clearance they had expected and briefed. The aircraft was then taxied behind another aircraft along taxiway B. However, as that aircraft entered the runway from taxiway ‘B4’, the FO of VH-VNC inadvertently also taxied to holding point B4. At about 1515, the captain advised ATC that they were ready for take-off. Air traffic control cleared the flight crew to line up on the runway. The FO taxied the aircraft onto the runway and the flight crew completed the pre-take-off checks.
About 1 minute later, ATC cleared the flight crew to take-off. Immediately after, the captain read back the take-off clearance and ATC advised the flight crew that they were lined up at the B4 (not B5) intersection. The take-off clearance was cancelled. The aircraft subsequently took off from the B5 intersection and the flight continued without incident. Intersection B4 was 403 m shorter than B5.
The investigation noted that the pre-take-off checklist required the flight crew to verbally confirm that they were on the correct runway. However, reference to an intersection was not part of the verbal check/response. The FO commented that confirming the intersection as well as the runway during the pre-take-off checks may prevent a similar incident occurring.
On 25 November 2007, a Gulfstream Aerospace Corporation G-IV aircraft, registered HB-IKR, was being operated on a charter flight from Brisbane, Queensland to Sydney, New South Wales. At about 2225, the pilot in command of the aircraft commenced a take-off run on taxiway Alpha, adjacent to the active runway 01. Air traffic control instructed the pilot to cancel the take-off clearance. The flight crew stopped the take-off and ATC instructed them to taxi to the end of the runway for a take-off using the full runway length.
The investigation identified various factors that contributed to the attempted take-off on the taxiway, including the take-off being conducted at an intersection departure from taxiway A7, which did not have normal runway threshold markings. Further, there was increased workload for the captain and possible self-imposed time pressure.
On the evening of 25 September 2019, the flight crew of a GIE Avions de Transport Régional ATR72 aircraft, registered VH‑VPJ and operated by Virgin Australia Airlines, received a clearance to line-up on runway 35 from intersection ‘Golf’ (G) at Canberra Airport, Australian Capital Territory. The aircraft was inadvertently taxied onto runway 30 and the take-off roll was commenced. The flight crew rejected the take-off about the same time as air traffic control (ATC) issued them an instruction to ‘stop’.
This analysis will discuss the flight crew’s actions and responsibilities prior to take-off, and the runway lighting characteristics. It will further discuss Virgin Australia Airlines’ Before take-off procedures and the cues used to verify an aircraft’s position in relation to the runway environment.
Line-up on incorrect runway
Shortly after the flight crew were cleared for take-off on runway 35 at night by ATC, the captain inadvertently taxied the aircraft onto runway 30. After lining-up on runway 30, the engine power increased and brake pressure decreased, which was consistent with commencing the take-off roll. The recorded flight data was consistent with the airport closed-circuit television footage of the aircraft’s movements on the taxiway and runway 30.
While the flight crew did not recall commencing the take-off roll, they did notice there were differences in the runway environment to what they were expecting and discussed it with each other. Specifically, there was no centreline lighting and the runway appeared shorter than expected. The abrupt rejection of the take-off at about the same time ATC issued the ‘stop’ instruction was consistent with the flight crews’ reported awareness of a problem with the runway environment.
Time pressure before take-off
The flight crew elected to depart from intersection G for runway 35 primarily due to its proximity to their parking bay and this departure was within the performance limits. Although there were no delays on the night of the incident and the flight was reported to be running early, it was possible that the flight crew were also attempting to depart ahead of the other two aircraft, particularly given the captain’s rescheduled flight to Brisbane. However, neither flight crew recalled these factors influenced their decision to use intersection G for departure.
By selecting intersection G, the flight crew only allowed themselves around 90 seconds to complete their preparatory tasks before arrival at the holding point. These tasks included the departure review and Before take-off procedure. If they had selected another taxiway entry to runway 35, they would have had several additional minutes before arrival at the respective holding point in which to complete their checks.
This self-imposed time pressure led to the First Officer (FO) calling ‘ready’ as the aircraft taxied to the holding point for intersection G and prior to completing the Before take-off procedure. This procedure should have been completed before entering the runway, with the exception of the last item in the procedure to confirm that they were lined-up on the runway’s centreline. This resulted in the FO’s attention being diverted to the procedure when entering the runway environment.
Reduced awareness of the runway environment
On the night of the incident, the flight crew elected to depart from intersection G for runway 35. Although they operated routinely to Canberra Airport, they both reported they could not recall having departed from this intersection at night. After pushback and while taxiing towards intersection G, the flight crew briefed the departure, but did not specifically include the layout of the intersection in their brief.
As they approached intersection G, the FO reported focusing on the Before take-off procedure and was therefore not monitoring the external environment. The captain reported being focussed on the lead-on lights. However, the Before take-off procedure was a challenge and response procedure, and therefore would have required some of the captain’s attention. This likely resulted in the captain taxiing the aircraft through the intersection with divided attention while the FO’s attention was focussed inside the cockpit. Barshi and others (2009) reported that during busy periods, it is easy for attention to be absorbed in one task, which can divert attention from other important tasks, such as monitoring.
Neither flight crew could recall if they checked the aircraft’s heading after line-up. As they subsequently commenced the take-off roll, they had not identified they were lined-up on the incorrect runway. This indicated the flight crew had a reduced awareness of their position within runway environment.
Lead-on lights from intersection ‘Golf’
Taxiway G led to the intersection of runway 12/30 and runway 17/35. This intersection was identified as a hotspot, which could potentially be confusing to flight crew, particularly at night. When ATC issued the line-up clearance to the flight crew from this intersection, the stop bar was selected off by ATC and the lead-on lights for runway 35 illuminated. The lead-on lights for runway 30 were already illuminated with the taxiway lighting, which resulted in the lead-on lights for both runways illuminated at the same time. As the lead-on lights for runway 30 were the first set encountered when entering the intersection, these lights likely drew the captain’s attention, resulting in the aircraft being manoeuvred to follow them.
A risk when operating at an airport with a complex layout at night and/or low visibility conditions is runway confusion, where pilots enter, take-off, or land on the incorrect runway (Airservices Australia 2016). This can occur when features of the taxiway or runway, such as lighting are misidentified. While there were no other known incidents at Canberra Airport, the simultaneous activation of the lead‑on lights at intersection G increased the risk of an aircraft being manoeuvred onto the incorrect runway.
ATR72 before take-off procedure
The flight crew called ‘ready’ prior to commencing the Before take-off procedure on the night of the incident, which they reported they had done frequently. However, the Virgin Australia Airlines ATR72 Standard Operating Procedure did not specify a particular time when the flight crew were to make this call to ATC. By comparison, calling ‘ready’ was specified as the final item in the operator’s Boeing 737 Before take-off procedure, meaning that there were no further tasks to be completed until the flight crew received their take-off clearance from ATC.
Degani and Weiner (1993) as well as Barshi and others (2016) research into checklist design concluded that checklists should be designed in such a way that their execution will not be integrated with other tasks. They suggested countermeasures could include carefully examining the content and timing of procedures and checklists, such as specifying the tasks that must be completed at specific points in each phase of flight. Specifically, the timing of the procedure and checklist should minimise the risk of interruptions, distractions, and concurrent tasks. Similarly, Virgin Australia Airlines and Airservices Australia provide general guidance to consider the timing of tasks, such as avoiding heads down activity while the aircraft is moving.
For the incident flight, the timing of the ‘ready’ call resulted in the aircraft crossing the holding point and entering the runway with the FO focussed on checklist items. Consequently, the FO was unable to monitor the environment as the aircraft entered the runway to line-up.
Therefore, the omission of a step in the ATR72 Before take-off procedure for the ‘ready’ call, increased the risk of flight crews actioning this procedure while entering the runway. In turn, diverting their attention to checklist items at a time when monitoring and verifying the runway environment was critical.
Runway verification cues procedure
Virgin Australia Airlines’ ATR72 Standard Operating Procedure and fleet-wide policy and procedures draw reference to the importance of verifying the aircraft is on the correct runway. However, the only cues listed in the ATR72 Before take-off procedure to achieve this related to internal cues such as the cockpit instruments, including the horizontal situation indicator. The only other reference to external runway verification cues was in specific reference to low visibility operations.
The external cues available to the flight crew at the intersection G holding point prior to runway entry included the airport chart and runway marker boards. The cues to indicate they were on runway 30, in addition to the aircraft instruments, were the absence of centreline lighting, the presence of the apron lighting and the proximity of the runway end lights.
Other operators, particularly those operating into airports with complex layouts, include a runway verification procedure. This procedure would require the flight crew to verbalise their identification and verification of the runway entry point prior to entry, and the departure runway prior to commencing take-off using available internal and external cues. Making use of all available external cues at an airport, including signs, lighting, and markings will improve awareness of the environment and reduce the risk of runway incursions (Federal Aviation Administration 2016).
To avoid a runway incursion or overrun event, operators and flight crew need to ensure the aircraft enters the correct runway from the correct holding point and is then lined-up on the correct runway for take-off. The inclusion of a published procedure could promote a habit of directing attention to both internal and external cues, to verify the aircraft’s position in the runway environment.
Detection of incorrect runway
When the flight crew lined-up and commenced the take-off roll on runway 30, ATC immediately issued a stop instruction. At around the same time, the flight crew rejected the take-off and commenced braking. The ATSB’s calculations based on the runway length and the aircraft’s performance data showed that there was insufficient distance available on runway 30 for the aircraft to take-off. Virgin Australia Airlines conducted simulator sessions that demonstrated a successful take-off was possible if there were no abnormal conditions.
Therefore, had neither the flight crew nor ATC detected the aircraft was lined-up on the incorrect runway, it was possible that the take-off would have been achieved. However, if an engine failure occurred near V1, or if the take-off was mishandled, there was a risk of a runway overrun due to the shorter runway length.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the take-off being commenced on the wrong runway involving GIE Avions de Transport Régional, ATR72, VH‑VPJ, Canberra Airport, Australian Capital Territory, on 25 September 2019.
Contributing factors
At night, the flight crew inadvertently lined-up and commenced the take-off roll on runway 30, rather than the assigned runway 35. The flight crew and air traffic control noticed the error about the same time and the take-off was rejected.
The runway intersection selected reduced the taxi time, resulting in the flight crew announcing they were 'ready' before completing the 'before take-off' procedure.
While taxiing onto the runway, the captain was focused on following the runway lead-on lights while the first officer was completing the Before take-off procedure and checklist. This likely resulted in them having a reduced awareness of the runway environment and aircraft orientation.
When the runway holding point stop bar at intersection Golf was turned off, the lead-on lights to both runway 30 and 35 were illuminated. This increased the risk of an aircraft being manoeuvred onto the incorrect runway, particularly at night and/or in low visibility conditions.
The Virgin Australia Airlines Before take-off procedure did not include a stepto report ‘ready’ to air traffic control. This increased the risk of flight crews completing this procedure while entering the runway, diverting their attention to checklist items at a time when monitoring and verifying was critical (Safety issue).
Virgin Australia Airlines did not require flight crew to confirm and verbalise external cues such as runway signs, markings, and lights to verify an aircraft’s position was correct prior to entering and lining up on the runway (Safety issue).
Other findings
The immediate response of air traffic control and the flight crew with rejecting the take-off, reduced the risk of a runway overrun.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Virgin Australia Airlines did not require ATR flight crews to complete the Before take-off procedure prior to reporting ‘ready’ to air traffic control. This increased the risk of flight crews completing this procedure while entering the runway, diverting their attention to checklist items at a time when monitoring and verifying was critical.
Safety issue description: Virgin Australia Airlines did not require flight crew to confirm and verbalise external cues such as runway signs, markings, and lights to verify an aircraft’s position was correct prior to entering and lining up on the runway.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Discontinuation of departures from intersection G
After the incident, Virgin Australia Airlines issued a flight notice to all flight crew advising departures using intersection G at Canberra Airport would be discontinued. All performance platforms on the ATR72 were updated and the Canberra ‘TWY G’ intersection departure was removed.
Proposed changes to the ‘Before take-off’ procedure
Virgin Australia Airlines approved changes to the ATR72 standard operating procedure to include an additional statement highlighting the checklist must be completed before entering the runway. However, ATR72 operations ceased prior to the implementation of this change.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew
Virgin Australia Airlines
Airservices Australia
Canberra Airport.
References
Airservices Australia 2016, A pilot’s guide to runway safety. Airservices Australia.
Barshi, I, Loukopoulos, LD & Dismukes, RK 2009. The multitasking myth: Handling complexity in real-world operations. Ashgate Publishing Aldershot.
Barshi, I, Mauro, R, Degani, A. & Loukopoulou, L 2016, Designing flightdeck procedures, National Aeronautics and Space Administration Technical Memorandum NASA/TM—2016–219421
Civil Aviation Safety Authority 2017, Manual of Standards Part 139 - Aerodromes. Canberra: CASA.
Degani A & Wiener EL 1993, ‘Cockpit checklists: Concepts, design, and use’, Human Factors, vol. 35(2), pp.345–59.
Federal Aviation Administration 2016, Pilot’s handbook of aeronautical knowledge FAA-H-8083-25B. US Department of Transportation, Federal Aviation Administration, Flight Standards Service.
Federal Aviation Administration 2020, Aeronautical Information Manual. US Department of Transportation, Federal Aviation Administration.
International Civil Aviation Organization 2007, Manual for the prevention of runway incursions (Doc 9870), Montreal: ICAO.
International Civil Aviation Organization 2018, Aerodromes - Volume 1: Aerodrome design and operations (8th edition), International Civil Aviation Organization.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties: the captain, first officer, the tower controller, Airservices Australia, Virgin Australia Airlines, Canberra Airport, and Civil Aviation Safety Authority.
Submissions were received from Virgin Australia Airlines, Canberra Airport, and the first officer. The submissions were reviewed and where considered appropriate, the text of the draft report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 28 April 2018, a Qantas Boeing 737 (VH-XZM) landed on runway 03 at Perth, Western Australia. The aircraft exited the runway onto taxiway J2, which led to a holding point for crossing runway 06. The aircraft did not stop at the holding point and crossed an illuminated stop bar without an air traffic control clearance.
At that time, a second Qantas Boeing 737 (VH-VZL) had commenced take-off from runway 06. An automated warning alerted the aerodrome controller (ADC) of the stop bar violation and the controller issued an instruction for the departing 737 to stop immediately. Soon after, the flight crew of VH‑XZM became situationally aware of their position and stopped just before crossing the edge of runway 06. VH-VZL’s wingtip passed about 15 m from VH-XZM’s nose at low speed.
What the ATSB found
The captain of VH-XZM developed an incorrect mental model of the exit taxiways off runway 03, believing the aircraft would not have to cross runway 06 after exiting onto either of the potential taxiways (J2 or D). Due to this incorrect mental model, and a combination of workload and distractions at key times, the flight crew did not detect the runway crossing issue until their aircraft had almost reached the edge of runway 06.
Taxiway J2 was the preferred runway exit for jet aircraft landing on runway 03. However, the location and design of the taxiway significantly increased the risk of a runway incursion onto runway 06/24. In particular, it had a relatively shallow intersection angle with the runway and a relatively wide turn radius, leading to higher taxi speeds, and a short distance to the holding point for runway 06/24.
Although the junction around taxiway J2 was identified as a ‘hot spot’, there was no detailed information about the reasons why it was a hot spot on aerodrome charts, and Qantas did not specifically require pilots to brief hot spots during departure and approach briefings.
What's been done as a result
In response to the runway incursion, Airservices Australia made taxiway J2 unavailable for use. Subsequently, Perth Airport removed taxiway J2 from aerodrome charts.
In addition, Airservices Australia changed the settings of an alerting system to ensure tower controllers at Perth Airport performing multiple roles received appropriate aural and visual alerts at their workstation.
Qantas published a safety information notice to all pilots containing information about the background of runway incursions, details of two recent runway incursion occurrences and safety educational information related to influencing factors, stop bar techniques and strategies to avoid a runway incursion. Qantas also updated its Flight Administration Manual to include a requirement for pilots to brief relevant airport hot spots and their contingency planning to mitigate against the possibility of collision or runway incursion.
Safety message
Runway incursions are one of the most significant risks to safe aviation operations and a key global safety priority. Airport operators and local runway safety teams are strongly encouraged to identify and mitigate the risk of hot spots, especially those that involve short distances between runways, complicated junctions, and the potential for higher taxi speeds.
Pilots are strongly encouraged to identify runway hot spots during departure and approach briefings, and discuss the actions they will take to reduce the risk of a runway incursion at such hot spots.
Air traffic controllers are strongly encouraged to provide safety alerts and/or clear instructions (such as ‘stop immediately’) to the flight crews of all aircraft involved in runway incursions and related occurrences.
Safety analysis
Introduction
After landing on runway 03, VH-XZM vacated onto taxiway J2 and crossed the runway 06 holding point, with an illuminated stop bar, without an air traffic control (ATC) clearance. The aircraft continued to taxi toward runway 06. The aerodrome controller (ADC) received aural and visual alerts and instructed the crew of another aircraft (VH-VZL) taking off from runway 06 to stop immediately. The flight crew of the departing aircraft rejected their take-off, preventing further escalation of the occurrence.
This analysis will firstly discuss flight crew situational awareness, mental models and approach briefings associated with VH-XZM’s incursion onto runway 06. It will then discuss the design characteristics of taxiway J2 that increased the risk of incursion into runway 06/24. Finally, it will discuss a range of other safety factors identified during the investigation.
Flight crew situational awareness and mental model
The captain’s mental model of the expected taxi route from landing on runway 03 to the parking bay was incorrect. Instead of having to cross runway 06 on taxiway J2, the captain expected to be on a taxiway that connected straight to the apron and did not have cross the other active runway.
This incorrect mental model developed due to a combination of factors:
The captain’s prior experiences landing at Perth had not used taxiway J2, instead generally landing on runway 03 and vacating at taxiway D or, more commonly, landing on runway 24 and vacating at taxiway J1. Both of these taxiways led directly onto the apron area with no runway crossing.
The captain’s intention on this occasion was to use taxiway D, expecting they would be using taxiway D up until after they landed on runway 03.
When taxiways were discussed during the approach briefing, the captain was referring to the apron chart rather than the full aerodrome chart, and this smaller chart did not include runway 03 or the full length of taxiway J2. When the first officer (FO) briefed that taxiway J2 needed to cross runway 06, the captain believed the FO was referring to crossing runway 06 while still on runway 03 and did not discuss this different (and incorrect) understanding with the FO.
The approach briefing did not include a discussion of the airport’s known hot spots, including the hot spot associated with taxiway J2 (see also Approach briefing).
After landing, the captain realised that the request for taxiway D had not been made and quickly re-planned an exit onto taxiway J2, although continuing to have the same expectation that they not need to cross an active runway to reach the apron.
The runway holding point markings and warning lights would normally provide enough cues that an aircraft was approaching a runway holding point. In this case these cues were also supplemented by the very salient illuminated stop bar. However, although the captain saw the stop bar, it was not identified as a problem and no revision was made to the mental model of the taxiways, instead rationalising in a time-compressed situation that the stop bar had been installed incorrectly.
This behaviour is consistent with confirmation bias, or the tendency for people to seek information that confirms their hypotheses, interpret ambiguous evidence as supporting their hypotheses, and either discount or not seek information that contradicts their hypotheses (Wickens and others 2013). Confirmation bias is an inherent aspect of human decision-making and has been demonstrated to occur in a wide range of contexts.
Workload and distraction
High workload and time pressure lead to a reduction in the number of information sources a person will search, and the frequency or amount of time these sources are checked (Staal 2004). They also result in people conducting tasks with simpler strategies, relying on responses or strategies with which they are familiar, and persevering with a response or strategy even when it has proven to be unsuccessful (Staal 2004, Wickens and others 2013). In addition, people are likely to miss important cues and experience difficulty integrating disparate pieces of information and making sense of them (Burian and others 2005). Associated with the reduced search of information sources and increased perseverance, the influence of confirmation bias will be enhanced (Wickens and others 2013).
The flight crew’s overall workload during the approach and landing was not abnormally high. However, workload and distraction at key points in time combined together to result in a situation where the problem with the captain’s mental model was not detected and corrected.
During the approach phase, the captain's workload as pilot monitoring was increased due to the FO’s low level of experience and air traffic control's (ATC’s) request for a high-speed descent. This workload contributed to an omission of routine secondary tasks prior to landing, such as requesting a taxiway D exit from the tower and pre-setting the surface movement control (SMC) frequency in the radio’s standby frequency position.
These omissions were examples of prospective memory errors. Prospective memory relates to an intention to perform an action at a later time, and a delay between forming the intention and acting on it. It is known to be vulnerable to failure and has been associated with many aviation accidents and incidents (Dismukes 2006). Conditions that increase this vulnerability include the delay between the intention to do a task and the execution of the task being filled with other activities, an interruption to a task sequence, and the cues or prompts to retrieve the intention from memory not being explicit. Neither of these tasks was associated with a specific checklist item (and by themselves were not important enough to be checklist items), and their omission was not detected until after landing.
After landing, when the captain realised the omission in not requesting taxiway D, the normal workload associated with landing was increased, associated with replanning the exit onto taxiway J2 while taking over control of the aircraft.
During the taxi phase, there was less time than would normally be the case to detect the problem. As the aircraft was crossing the runway edge, the runway 06 holding point was only about 176 m away. The captain’s delayed realisation that they needed to exit on taxiway J2, and misidentification of taxiway J2 as a rapid exit taxiway (RET), meant the aircraft entered J2 at a higher groundspeed than usual. The relatively high exit speed and relatively short distance to the runway 06 holding point meant that the flight crew only had limited time after leaving runway 03 to identify the problem before reaching the holding point.
During this period, a series of distractions occurred. More specifically:
After vacating runway 03, the FO focussed attention inside the flight deck for a period of time to select the SMC frequency, instead of performing the more safety critical task of monitoring the aircraft's taxi path as it approached a known runway incursion hot spot. The FO assumed the captain would be stopping at the holding point and, focused on changing frequency and contacting the SMC, did not see that they had passed the holding point until about the time the captain was braking to stop.
When approaching the holding point, the captain briefly went heads down to gain an understanding for the delay in changing to the SMC frequency and then advised the FO of the applicable SMC frequency. This reduced the time available to notice and comprehend the holding point signs, warning lights and stop bar lights ahead.
After passing the holding point, the presence of runway 06 ahead still provided an indication of a potential problem. However, the captain was distracted by the presence of another aircraft on the apron. This focused attention on the distant apron area and reduced the ability to visually identify the runway immediately in front of the aircraft. The FO was still primarily focused inside the flight deck during this period.
Approach briefing and approach briefing guidance
The approach briefing was the best opportunity for the flight crew to have established a shared and correct understanding of the requirements for the remainder of the flight, including the taxiway options. However, as already noted, they did not specifically discuss the taxiway J2 hot spot during the approach briefing, even though the FO had identified it on the aerodrome chart. Had the topic of the hot spot been raised and discussed in the briefing, as well as the main reason why it was a hot spot (that it led to another runway), the captain’s mental model of the taxiway J1/J2 layout would probably have been enhanced.
The International Civil Aviation Organization (ICAO) has emphasised that flight crews should prepare well in advance for departure and arrival at any airport, including reviewing hot spots before taxiing from the gate and prior to beginning descent. Accordingly, departure and approach briefings should contain a complete review of not just the expected taxi routes but potential routes as well, with special attention to any hot spots.
Qantas provided detailed guidance to flight crews on the content of approach briefings. Hot spots should have been considered a threat under the threat and error management section of the briefing guidance. However, since that briefing guidance contained no specific requirement to brief hot spots or runway incursion threats, it is likely that the presence of hot spots on a taxi route would not always be noted by a flight crew.
Although the aerodrome chart for Perth identified that the area around taxiway J2 was a runway incursion hot spot, it did not provide specific information about the nature of the threat or why it was a hot spot. Such information would better enable flight crews to understand how the hot spot may affect them. If flight crews are to effectively identify and plan mitigating actions to avoid runway incursions, they should be provided with detailed information to assist their understanding of the common reasons why previous flight crews have incurred a runway at particular locations.
Taxiway location and design
Airservices Australia data identified that the rate of runway incursions at Perth Airport was significantly higher than other major airports across Australia. A significant proportion of the Perth incursions occurred on taxiway J2 and, accordingly, it was designated as a hot spot. To assist with minimising the risk of incursions, stop bars and CASA approved runway identifier markings (in addition to other holding point markings and lights) had recently been introduced.
In addition to providing salient or conspicuous markings and cues about the position of a holding point, it is also important to ensure flight crews are provided sufficient time during a high workload period after landing to identify and comprehend runway holding point visual cues and to allow for ATC to intervene, if required, before an aircraft incurs a runway.
Taxiway J2 was not a rapid exit taxiway (RET), but it had some similar qualities: a relatively shallow intersection angle and a relatively wide curve radius. These characteristics led some pilots to use higher speeds when exiting runway 03. Although the intersection angle was not acute enough to actually be a RET, the angle would be difficult to judge while approaching it from the runway.
Flight data showed VH-XZM entered taxiway J2 at about 35 kt, which was slightly higher than the taxiway design limit of 31 kt. Flight data analysis of other flights provided by Qantas showed its aircraft commonly vacated runway 03 onto taxiway J2 at a relatively high speed.
In addition, taxiway J2 had a relatively short distance from the exit from runway 03 to the runway 06 holding point. This meant that flight crews had less time to see the holding point markings and an illuminated stop bar, especially if taxiing at higher speeds.
Taxiway J2 also led to a relatively complicated runway crossing point, with other taxiways intersecting at the same point. A complicated intersection can be difficult for crews to navigate and can draw their attention.
Overall, the location and design of taxiway J2 significantly increased the risk of a runway incursion on runway 06/24 for aircraft landing on runway 03. In particular, the following features made taxiway J2 problematic:
a relatively shallow intersection angle from runway 03
a wider than usual entry curve radius
a relatively short distance from the turn to the runway 06 holding point
the next intersection leading directly to a runway rather than a parallel taxiway
the next intersection being relatively complicated
the intersection adjoining the first two-thirds of runway 06.
In addition, the risk associated with taxiway J2, and runway incursions was exacerbated by it being made the preferred exit for landing off runway 03. Although many flight crews elected to use taxiway D instead, this required the crew to proactively make that request.
The introduction of stop bars in March 2018 would certainly have reduced the risk but, depending on the situation, not eliminated the risk. Although the exact sequence of events associated with this particular occurrence would have been difficult to predict beforehand, there was undoubtedly an increased risk of runway incursions that needed to be managed, and a range of scenarios that could have resulted in a high-risk runway incursion given the inherent limitations of the taxiway J2 location and design.
As previously noted, taxiway J2 had some features that would have made it appear similar to a RET. Flight crews would normally become aware of the existence of a RET from tables of information about an airport in the aerodrome charts. However, a flight crew may forget or may not brief the existence or absence of a RET among the potential taxiways that could be used. At the time of the occurrence there was no requirement in Australia for airports to use indicator lights at RETs to distinguish them from other taxiways, so there was no immediate way to identify a taxiway as a RET or otherwise during the landing. However, unless all RETs were equipped with the appropriate indicator lights, the absence of indicator lights at a particular taxiway may not be that effective as a cue. Overall, unless briefed otherwise, it would be generally safer for a flight crew to assume that a taxiway was not a RET and adjust the aircraft’s speed appropriately.
Air traffic control response
The ADC became aware of the problem on receipt of the first integrated tower automation suite (INTAS) alert. The ADC considered that, as VH-XZM had vacated and was clear of runway 03, the flight crew would most likely have changed over to the SMC frequency and therefore would have been unable to hear any safety alert instructions on the ADC frequency. Instead, an instruction was issued to VH-VZL to stop immediately.
A research study showed that the average time for tower controllers to act in response to a system alert was 4.6 seconds with a mean response duration of 2.3 seconds, with maximum response times being 8.1 seconds and 5.3 seconds respectively (Sanchez and others 2009). In this occurrence, the ADC transmitted the stop immediately instruction to the flight crew of VH-VZL about 7 seconds after the first alert, a time which included a period of blocked frequency from another aircraft transmitting.
The ADC’s action was effective in mitigating the consequence of the runway incursion. The ‘stop immediately’ instruction was simple and easily comprehended by the captain of VH-VZL, who was actively monitoring the developing situation and responded promptly to the ADC’s instruction.
However, although VH-VZL’s flight crew received a timely and clear instruction from ATC, VH‑XZM’s flight crew did not receive any communication from ATC during the period after the first INTAS alert (1442:04) until 1442:26, when the SMC asked the flight crew if they were on the SMC frequency. This was after the captain had commenced braking (1442:19), and 10 seconds after the FO made initial contact with the SMC (when the FO was unaware of the problem).
The exact reasons why the SMC did not issue an alert and instruction to the flight crew of VH‑XZM are unclear. In response to the first INTAS alert, the SMC was aware of the developing problem. However, at that stage there may have been some doubt regarding whether the flight crew had switched over to the SMC frequency. In addition, the SMC was in the progress of providing a pushback clearance to another aircraft. The SMC had received training in issuing stop instructions as well as compromised separation recovery training.
The second INTAS alert at 1442:16 was broadcast on the ADC workstation’s speaker at the same time as the VH-XZM FO’s first transmission on the SMC frequency, to which the SMC did not reply. The SMC may have focussed on the more relevant event—the second INTAS alert—at this time and as a result did not process VH-XZM’s transmission. Nevertheless, even after hearing the ADC provide the other aircraft with a stop instruction (1442:11), a prompt instruction to VH-XZM was warranted to further minimise any potential collision risk. A stop immediately instruction over any frequency that the flight crew might be using would have led to a more rapid response from that flight crew.
Although not directly related to this occurrence, the investigation identified some limitations with ATC processes that increased the potential risk of other occurrences:
Due to the way INTAS was configured at Perth, the SMC’s workstation did not directly receive INTAS alerts if the SMC position was combined with other positions. This meant that an SMC may not have received a salient warning that an aircraft under their control was at risk of collision. In this case, the SMC’s awareness of the runway incursion was raised as a result of the INTAS aural alert played through a speaker on the ADC’s workstation, but in other situations an SMC may not identify such an alert.
Communication practices for runway crossings at Australian airports differed from those recommended by ICAO and used in some countries overseas. According to ICAO, runway crossings should be managed by the ADC, which ensured that flight crews of aircraft crossing a runway were aware of any instructions being issued to aircraft using that runway. In Australia (and some other countries), runway crossings were handled by the SMC and not the ADC. Having two aircraft on a runway at the same time but not requiring them to be on the same frequency does create the potential for flight crews not to be aware of the presence of the other aircraft at a critical point in time. However, Airservices Australia reported that it trialled a version of the ICAO-recommended approach and determined it did not reduce the risk of runway incursions and instead it introduced new safety issues and concerns in the Australian environment, including a potential reduction in controller situational awareness.
Depending on how it was implemented, the ICAO-based approach could have required a flight crew to transfer to the SMC frequency, before the SMC then transferred them back to the ADC frequency prior to crossing the runway, which would have increased the complexity of communications at a location such as Perth Airport for aircraft landing on runway 03 and exiting on taxiway J2. One option that could have assisted with managing the unique problems associated with taxiway J2 was for the ADC to require flight crews landing on runway 03 and vacating on taxiway J2 to remain on the ADC frequency until after they crossed runway 06. However, introducing a unique approach to managing radio frequencies at one specific location in Australia could also increase risk. Alternatively, local procedures could have included advising a flight crew landing on runway 03 and exiting at taxiway J2 of the crossing runway hazard ahead.
The occurrence
Overview
On 28 April 2018, a Boeing 737-838 (737) aircraft, registered VH-XZM, was being operated by Qantas Airways Limited (Qantas) on a regular public transport flight from Sydney, New South Wales to Perth, Western Australia. The aircraft landed on runway 03 and exited using taxiway J2 (Figure 1). The aircraft did not stop at the runway 06 holding point and crossed an illuminated stop bar without an air traffic control (ATC) clearance.
VH-XZM’s incursion into the flight strip of runway 06 resulted in a rejected take-off of another Qantas Boeing 737 aircraft (VH-VZL), which was taking off from runway 06. VH-VZL’s wingtip passed about 15 m from the nose of VH-XZM at low speed before stopping.
Figure 1: Overview of the runway incursion
Source: Google Earth, modified by ATSB
Events prior to the occurrence
VH-XZM departed Sydney at 1033 Western Standard Time[1] on the scheduled flight to Perth. During their review of NOTAMs,[2] the flight crew noted the recent installation of stop bars at Perth Airport.
On this sector the captain was pilot monitoring and the first officer (FO) was pilot flying.[3] Prior to descent, the approach controller cleared the flight crew for an area navigation (RNAV-X) runway 03[4] approach. Weather conditions for the descent and approach were good.
Prior to descent, the FO conducted an approach briefing, noting taxiway J2 (Figure 2) was the preferred exit and they would need to get an ATC clearance to cross runway 06. The FO recalled being aware that taxiway J2 was a designated ‘hot spot’ but did not brief it as a hot spot or state that runway incursions happened there. The captain expressed a preference to request taxiway D, which was closer to the terminal building. At the completion of the briefing, the FO believed that the captain understood they would vacate runway 03 onto taxiway J2 unless they had a clearance to exit at taxiway D.
The captain recalled the briefing as professional and very thorough, but did not fully absorb all of the FO’s briefing points (due to the level of detail in the briefing). The captain also recalled, that when discussing the taxi route to their assigned parking bay (13), being mainly focussed on vacating onto taxiway D, which led directly onto the apron, with taxiway J2 being the secondary plan. Having referenced the smaller apron chart (Figure 3) and not the larger aerodrome chart, the captain’s mental model of the taxiway J layout was that if they used taxiway J2 they would vacate the landing runway 03 directly on taxiway J1, which led directly to the apron area. The captain interpreted the FO’s point about a requirement to cross runway 06 as being during the landing roll on runway 03.
During the approach phase, another aircraft, also on approach to land on Perth runway 03, was following VH-XZM. It had been slowed down by ATC to coordinate the two arriving aircraft. ATC requested the flight crew of VH-XZM to maintain a high speed descent, which they accepted.
Figure 2: Perth aerodrome chart
Source: Airservices Australia, annotated by ATSB
Figure 3: Perth apron chart showing captain’s mental model of taxi routes to bay 13
Source: Qantas, annotated by ATSB
Final approach and landing
The RNAV-X runway 03 approach required a descending right turn from about 2,180 ft to 790 ft. The FO recalled the captain commenting that, when flying the RNAV-X runway 03 approach, it could be difficult to slow the aircraft down and they would need to conservatively configure the aircraft for the arrival.
At 1438:55, the captain made first contact with the aerodrome controller (ADC) on the Perth ADC (tower) frequency. The captain recalled that the radio call was made during a period of high workload while closely monitoring the FO, the aircraft speed and the approach profile, and that the aircraft was not slowing down as quickly as desired.
The aircraft descended through 1,600 ft, configured with gear down and flaps 15 set, and the airspeed about 175 kt. As that speed was the flaps extension limit speed for flaps 30 (the intended flaps setting for landing), the captain suggested to the FO they select flaps 25 (a non-normal setting) to decelerate to enable selection of flaps 30, which they did once the aircraft slowed.
The captain recalled being ‘totally focused’ on the FO flying an accurate approach profile and descending turn. Due to this high workload, the request to take taxiway D after landing was forgotten. The captain also forgot to pre-set the Perth ground frequency in the radio’s standby frequency position, a routinely performed task.
The captain started actioning the landing checklist. At 1439:28, that process was interrupted by the ADC issuing them a clearance to land on runway 03. At that time the aircraft was passing approximately 1,100 ft and still in a descending right turn to final approach. The flight crew completed the landing checklist and continued the approach within the requirements of the Qantas stabilised approach criteria.
During this time, VH-VZL was taxiing to runway 06 for departure and its flight crew were monitoring the Perth surface movement controller (SMC/ground) frequency. At 1440:59, that flight crew changed to the ADC frequency and advised the ADC they were ready. At 1441:02, the ADC cleared them to line up and wait on runway 06.
At 1441:21, VH-XZM landed on runway 03 and the FO selected idle reverse thrust. While the aircraft was decelerating, the captain realised that an egress onto taxiway D had not been requested from the ADC and believed they were now committed to vacate via taxiway J2. At about 60 kt, the captain took control of the aircraft from the FO (consistent with normal procedures)[5] and applied heavier braking so the aircraft could make taxiway J2.
Approaching taxiway J2 for the first time, the captain thought it appeared to be a rapid exit taxiway (RET). The aircraft’s groundspeed was about 53 kt when, at 1441:42, the captain started to turn off the runway centreline towards taxiway J2, continuing to slow throughout the turn and passing over the left edge of runway 03 at 1441:47 at 35 kt.
Taxi and runway incursion
At 1441:51, once certain that VH-XZM would vacate runway 03 onto taxiway J2, the ADC issued VH‑VZL’s flight crew a take-off clearance on runway 06, which was then read back by the crew of VH-VZL. At 1441:59, another aircraft, which had been following VH-XZM and was now on final approach to runway 03, also made a transmission on the ADC frequency.
The captain of VH-XZM recalled hearing the ADC issue a take-off clearance to another Qantas aircraft but did not recall hearing the words ‘runway 06’ and did not associate it with a potential threat at the time. The FO did not recall hearing any ATC transmission at that time.
The SMC reported being aware that VH-XZM was on taxiway J2, and the flight crew would soon be calling on the SMC frequency to report they were at the holding point. However, when the ADC gave VH-VZL a take-off clearance, the SMC switched attention to other aircraft on the apron area, knowing that VH-XZM would not be able to cross runway 06 for a while.
Figure 4 shows the relative positions of VH-XZM and VH-VZL during the remainder of the occurrence sequence.
Figure 4: Overview of the runway incursion
White aircraft symbols show the aircraft positions at 5-second intervals. White lines show the angle between the two aircraft at some of those times. Labels show events that occur within 1 second of the aircraft’s position illustrated.
Source: Google Earth, modified by ATSB
At 1441:55, VH-XZM passed over the holding point for runway 03 at a groundspeed of about 22 kt. At about this time, the FO assessed that the captain was still slowing the aircraft at a rate to stop at the runway 06 holding point; the FO was aware that they needed an ATC clearance to cross runway 06 and assumed that the captain would stop.
The FO then refocused their attention inside the flight deck and noticed that the Perth SMC frequency had not been pre‑set as the radio’s standby frequency. As a result, reference was made to the aerodrome chart to find the frequency to set. This led to a delay in contacting the SMC to receive taxi instructions. The captain recalled also briefly looking down to understand the reason for the delay and telling the FO the required frequency.
Although being aware that stop bars had recently been installed at Perth, the captain recalled being surprised to see an illuminated stop bar ahead on the taxiway and thought it strange that a stop bar would be positioned at that location. The captain believed they were on taxiway J1, which did not require a runway crossing, and rationalised that the stop bar had been mistakenly constructed with omnidirectional lighting[6] and that it was for aircraft taxiing from the opposite direction entering runway 03. The captain also thought that, given their current taxi speed and how quickly it appeared after exiting the runway, the stop bar could not be meant for their aircraft. The captain did not recall noticing any markings that identified runway 06. Consequently, they taxied over the illuminated stop bar and through the runway 06 holding point.
At 1442:01, the nose of VH-XZM passed the runway 06 holding point (with an illuminated stop bar) at a groundspeed of 17 kt. At 1442:04, in the tower, the integrated tower automation suite (INTAS) made the first of two aural and text alerts on the ADC’s workstation. The aural alert comprised a synthetic voice stating ‘warning runway zero six stop bar violation’. The alert was designed to trigger when the aircraft was registered to be 8 m past the stop bar. At this time, the aircraft was travelling at about 14 kt.
Due to default settings within INTAS, no aural or text alert was provided on the SMC’s workstation. The SMC later reported hearing the aural alert through a speaker on the ADC’s workstation, and then saw VH-XZM entering the runway and VH-VZL rolling for take-off. At this time the SMC was part way through providing a pushback clearance to another aircraft and the flight crew of that aircraft then read back the clearance details on the SMC frequency.
At the time of the first INTAS alert, the flight crew of VH-VZL had just commenced rolling for take-off on runway 06 and were setting engine thrust. The ADC recalled having communication with VH-VZL and considered that, as VH-XZM had vacated runway 03, it should have transferred to the SMC frequency. Initially, a radio transmission from another aircraft prevented the ADC from transmitting on the ADC frequency. As soon as it stopped, at 1442:11, the ADC instructed VH-VZL’s flight crew to ‘stop immediately, stop immediately, runway incursion ahead’.
The captain of VH-VZL subsequently reported being aware of the other aircraft when it was taxiing on taxiway J2. When the stop instruction from the ADC was received, the captain was just starting to have an element of doubt as to whether the other aircraft would stop, and during the instruction initiated a rejected take-off by bringing the thrust levers back and braking. At that time the aircraft’s groundspeed was 58 kt.
As VH-XZM’s flight crew had transferred to the SMC frequency at some point before 1442:11, they did not hear the stop instruction issued to VH-VZL and were unaware of that aircraft’s presence and proximity. The captain continued taxiing towards runway 06 at about 10 kt, and then observed another aircraft (a Boeing 787) ahead on the apron (Figure 5). It had recently pushed back and was now blocking taxiway J1. The captain reported being distracted by the aircraft on the apron as it blocked their intended route on taxiway J1 and now required their aircraft to turn onto taxiway A.
Figure 5: Aircraft on the apron as XZM taxis toward runway 06
Source: Perth Airport
At 1442:16, the second INTAS aural (‘warning runway zero six occupied’) and text alert activated while the flight crew of VH-VZL was rejecting the take-off. As with the previous alert, the second alert was not presented at the SMC’s workstation. As the first INTAS alert was still active, the controllers now had multiple warnings sounding, which increased the noise level in the tower.
At the same time as the second INTAS alert, VH-XZM’s FO contacted the SMC advising they were taxiing for bay 13. The SMC did not respond to that transmission, and subsequently could not recall whether that transmission was heard.
The captain of VH-XZM recalled seeing (in peripheral vision) an aircraft (VH-VZL) going faster than would be expected on a taxiway, then applying the brakes to stop the aircraft. The FO recalled that, when looking up, probably about the time the captain began braking, they realised they were in a different position to that expected and called ‘stop, stop, stop’.
The captain applied VH-XZM’s brakes at 1442:19, when the speed was 9 kt, and the aircraft came to a full stop at 1442:25. At 1442:29, VH-VZL came to a stop on runway 06, having just passed ahead of VH-XZM. The wingtip of VH-VZL passed about 15 m from the nose of VH-XZM at low speed.
At 1442:26, just before VH-VZL stopped, the SMC asked if VH-XZM was ‘on this frequency’ and the FO responded with ‘affirm’, their callsign, and the intended bay. The SMC advised VH-XZM’s crew that they had crossed a stop bar and had a runway incursion, and to hold position. The flight crew of VH-VZL were subsequently cleared to taxi back to runway 06 for departure. The flight crew of VH-XZM were cleared to taxi to bay 13.
From the evidence available, the following findings are made with respect to the runway incursion involving a Boeing 737, registered VH-XZM, which resulted in a rejected take-off involving a Boeing 737, registered VH-VZL, at Perth Airport, Western Australia on 28 April 2018. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safetyissues, orsystemproblems, arehighlightedinboldtoemphasisetheirimportance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
The captain developed an incorrect mental model of the exit taxiways off runway 03, believing the aircraft would not have to cross runway 06 after exiting on either of the potential taxiways (J2 or D). As a result, the captain did not expect to cross a runway holding point or stop bar and, upon seeing the stop bar was illuminated, incorrectly thought that it must only apply to aircraft coming from the other direction.
During the approach phase, the captain's workload as pilot monitoring was increased due to the first officer's low level of experience and air traffic control's request for a high-speed descent. This workload contributed to the omission of routine secondary tasks, such as requesting a taxiway D exit from the tower and pre-setting the surface movement control frequency.
After vacating runway 03, the first officer focused inside the flight deck for a period of time to select the surface movement control frequency, instead of performing the more safety critical task of monitoring the aircraft's taxi path as it approached a known runway incursion hot spot.
When approaching the holding point for runway 06, the captain briefly focused inside the flight deck to gain an understanding for the delay in changing to the next frequency. This reduced the time available to notice the holding point signs and lights ahead.
The captain taxied passed the runway 06 holding point (with an illuminated stop bar) without an air traffic control clearance.
After taxiing passed the illuminated stop bar, the captain was distracted by the presence of another aircraft on the apron. This focused the captain’s attention on the distant apron area, reducing the likelihood of visually identifying the runway immediately in front of the aircraft.
During the approach briefing, the flight crew discussed taxiway J2 and taxiway D, but the flight crew did not discuss the potential threat of the hot spot associated with taxiway J2.
Although some aerodrome navigational charts in Australia had identified hot spot locations, they generally provided limited explanatory information to enhance flight crew understanding or awareness of why the hot spot was there and what actions they could take to mitigate the associated risk.
The location and design of taxiway J2 at Perth Airport significantly increased the risk of a runway incursion on runway 06/24 for aircraft landing on runway 03. Taxiway J2 was published as the preferred exit taxiway for jet aircraft and, although mitigation controls were in place, they were not sufficient to effectively reduce the risk of a runway incursion. [Safety issue]
Although the flight crew of VH-VZL taking off on runway 06 were provided with an instruction to stop immediately to reject their take-off, no safety alert or instruction was provided to the flight crew of VH-XZM during the period between when the controllers received a stop bar violation alert (1442:04) and the captain applied the brakes at 1442:19.
Other factors that increased risk
Airservices Australia’s configuration of the integrated tower automation suite (INTAS) at Perth Airport had resulted in a situation where controllers performing some combined roles had the INTAS aural and visual alerts inhibited at their workstation. As a result, controllers performing such combined roles would not receive a stop bar violation alert or runway incursion alert at their workstation. [Safety issue]
Other findings
The stop bar alert and the aerodrome controller’s high level of situational awareness led to a timely instruction to the flight crew of VH-VZL to stop immediately.
The high level of situational awareness of the VH-VZL flight crew significantly aided their immediate action to reject their take-off on runway 06 following the controller’s instruction.
Safety issues and actions
The safety issues identified during this investigation are listed in the Findings and Safety issues and actions sections of this report. The Australian Transport Safety Bureau (ATSB) expects that all safety issues identified by the investigation should be addressed by the relevant organisation(s). In addressing those issues, the ATSB prefers to encourage relevant organisation(s) to proactively initiate safety action, rather than to issue formal safety recommendations or safety advisory notices.
All of the directly involved parties are provided with a draft report and invited to provide submissions. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Depending on the level of risk of the safety issue, the extent of corrective action taken by the relevant organisation, or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue safety recommendations or safety advisory notices as part of the final report.
Operator guidance for flight crew briefing of aerodrome hot spots
Safety issue description: Although Qantas provided detailed guidance to flight crews about the content of departure and approach briefings, it did not specifically require aerodrome hot spots to be briefed.
Location and design of taxiway J2 at Perth Airport
Safety issue description: The location and design of taxiway J2 at Perth Airport significantly increased the risk of a runway incursion on runway 06/24 for aircraft landing on runway 03. Taxiway J2 was published as the preferred exit taxiway for jet aircraft and, although mitigation controls were in place, they were not sufficient to effectively reduce the risk of a runway incursion.
Inhibition of safety alerts for combined air traffic control roles
Safety issue description: Airservices Australia’s configuration of the integrated tower automation suite (INTAS) at Perth Airport had resulted in a situation where controllers performing some combined roles had the INTAS aural and visual alerts inhibited at their workstation. As a result, controllers performing such combined roles would not receive a stop bar violation alert or runway incursion alert at their workstation.
Additional safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Qantas Airways advised that on 17 September 2019, following a runway incursion subsequent to this occurrence, it published a safety information notice to all pilots, which contained information about failure to comply with taxi clearances and details of the recent runway incursion occurrence. It also contained safety educational information related to influencing factors, mitigation techniques and strategies to avoid non-compliance with air traffic control ground clearances.
Airservices Australia and Qantas Airways advised they were in discussions to ascertain if there was merit in the conduct of a new trial of the ICAO-recommended approach to runway crossings, with the crossing aircraft on the ADC frequency,
The Civil Aviation Safety Authority (CASA) advised that in September 2019, CASR Part 139 (Aerodromes) Manual of Standards introduced guidance for rapid exit taxiway indicator lights (RETILs). The guidance stated ‘RETIL may be provided on a runway intended for use in RVR conditions less than 350 m or where the traffic density is heavy’. CASA advised the ‘optional’ application of subsection 9.89 (1) was consistent with ICAO SARPs (see Annex 14 volume I para 5.3.15.1), which set the application of RETIL as a Recommendation.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew of VH-XZM
the captain of VH-VZL
the aerodrome controller
the surface movement controller
flight data recordings from VH-XZM and VH-VZL
closed-circuit television recordings
Qantas Airways Limited
Airservices Australia
Perth Airport Pty Ltd.
References
Burian BK, Barshi I & Dismukes K 2005, The challenge of aviation emergency and abnormal situations, National Aeronautics and Space Administration Technical Memorandum NASA/TM-2005-213462.
Dismukes, K 2006. ‘Concurrent task management and prospective memory: pilot error as a model for the vulnerability of experts’. Proceedings of the Human Factors and Ergonomics Society 50th Annual Meeting, pp. 909–913.
Sanchez J, Smith EC & Chong RS 2009, Controller and Pilot Response Times to Runway Safety Alerts, MTR090237, The MITRE Corporation, McLean, VA.
Staal MA 2004, Stress, cognition, and human performance: A literature review and conceptual framework, National Aeronautics and Space Administration Technical Memorandum NASA/TM-2004-212824.
Wickens CD, Hollands JG, Banbury S & Parasuraman R 2013, Engineering psychology and human performance, 4th edition, Pearson Boston, MA.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the flight crew of VH-XZM, the captain of VH-VZL, Qantas Airways Limited, the aerodrome controller, the surface movement controller, Airservices Australia, Perth Airport and the Civil Aviation Safety Authority.
Submissions were received from the captain of VH-XZM, Qantas Airways Limited, the aerodrome controller, Airservices Australia, Perth Airport and the Civil Aviation Safety Authority. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Context
Personnel information
Flight crew of VH-XZM
The captain held an Airline Transport Pilot (Aeroplane) Licence (ATPL) and was appropriately qualified to conduct the flight. Having flown 737s since 2007, the captain had operated into Perth Airport many times, including three to four times in the last 4–5 months. Most of the landings at Perth were on runway 21 or 24, using taxiway J1 from runway 24. The captain had rarely landed on runway 03 and only recalled using taxiway D off that runway and had not previously used taxiway J2. Although aware that stop bars had been installed at Perth Airport, and having encountered them at other airports, the captain had not previously encountered them at Perth.
The first officer (FO) held an ATPL and was appropriately qualified to conduct the flight. The occurrence flight was the third set of flights since completing FO training on the 737, having previously operated as an Airbus A330 second officer. The FO had landed at Perth on five previous occasions, including two landings on runway 03 (which had exited on taxiway D). The occurrence flight was the first time the FO had landed on runway 03 and vacated via taxiway J2.
Both flight crew were based in Brisbane. They both had 3 days off duty during 24–26 April 2018, then on 27 April they commenced a 3-day trip together. On 27 April they signed on at 0530 Eastern Standard Time (EST)[7] and flew a series of flights, ending their duty time at about 1530 EST. On 28 April, they signed on for duty at Gold Coast Airport about 0725 EST, then operated a flight from the Gold Coast to Sydney. Following a transit in Sydney they then commenced the flight to Perth. At the time of the occurrence both of them had been on duty for 10.3 hours. They described the workload during the day as not being significant or unusual. They departed Sydney about 1 hour behind schedule due to connecting aircraft and reported not feeling any commercial pressure.
The flight crew’s roster provided both flight crew with sufficient sleep opportunity in the nights prior to the occurrence. The captain reported having about 7 hours sleep the night before the occurrence and normal sleep in the nights before. The FO reported having a normal amount of sleep the night before the occurrence and the nights before that. Both flight crew reported being a little tired at the time of the occurrence. However, given the other available information, there was insufficient evidence to suggest they were experiencing a level of fatigue that has been demonstrated to adversely influence performance.
Air traffic controllers
At the time of the occurrence, Perth tower was staffed by two air traffic controllers:
the aerodrome controller (ADC), who was responsible for controlling all aircraft and vehicle movements on all runways
the surface movement controller (SMC), who was performing the combined duties of SMC (responsible for controlling all aircraft and vehicle movements on the airport aprons and other manoeuvring areas) and airways clearance delivery controller (responsible for issuing airways clearances to departing aircraft).
Both controllers were correctly endorsed for their roles. The ADC on duty at the time of the occurrence had over 30 years’ experience and was fully endorsed for all roles in the Perth tower. The SMC had 3 years’ experience at Perth tower (and prior experience overseas) and was endorsed for all roles in the Perth tower.
The controllers reported that aircraft movements had been ‘quiet’ in the period leading up to the occurrence, with only 4 or 5 aircraft movements occurring at intermittent times.
The ADC reported having about 8 hours sleep the night before the occurrence and normal sleep in the nights before. On 28 April, the ADC signed on for duty at 0730 WST and had several rest periods during the shift. At the time of the occurrence, the ADC had been on duty for 7.2 hours, due to sign off at 1530.
The SMC reported having a normal sleep the night before the occurrence and normal sleep in the nights before. On 28 April, the SMC signed on for duty at 1345, and had been performing the role for about 45 minutes prior to the occurrence.
Both of the controllers recalled feeling alert at the time of the occurrence and had sufficient sleep opportunity in the nights prior to the occurrence. There was no evidence to suggest they were experiencing a level of fatigue that has been demonstrated to adversely influence performance.
Meteorological information
At the time of the occurrence, the Perth automatic terminal information service (ATIS) broadcast the wind was variable at 5 kt with a maximum tailwind on runway 03 of 5 kt. The conditions were CAVOK[8] and the temperature was 28 °C. The ATIS also advised that stop bars were active at all runway holding points.
The flight crew of VH-XZM reported the weather conditions as fine with light winds and good visibility. The captain stated there was no tailwind during landing on runway 03. There were no reported concerns with sun glare or other factors affecting visibility for the flight crew of VH‑XZM. The controllers stated the weather conditions were fine with no restrictions on visibility from the tower.
Closed-circuit television footage at the terminal verified all recollections of weather and visibility conditions made by flight crews and controllers.
Recorded information
On-board recordings
Both 737 aircraft involved in the occurrence (VH-XZM and VH-VZL) were fitted with a flight data recorder (FDR) and cockpit voice recorder (CVR) as required by the applicable legislation.
Qantas downloaded both FDRs and sent the digital files to the ATSB. Both FDRs included data over the period of the occurrence. This information has been included in this report where relevant.
Each CVR was capable of recording 2 hours of data, which would have included communications between the flight crew, communications with air traffic control and various flight deck sounds, alerts and warnings. The CVR for VH-XZM was not preserved before being overwritten during ground activities.[9]
There were no reported defects associated with VH-XZM.
Air traffic control recordings
Air traffic control (ATC) audio recordings and integrated tower automation suite (INTAS) data records were obtained from Airservices Australia. The audio recordings provided all relevant radio communications between controllers and flight crews, and the synthetic voice INTAS warnings. INTAS data records provided aircraft position information that could be compared with other sources of recorded data.
Flight crew briefing requirements
Operator information
The Qantas FlightAdministrationManual (FAM) outlined standard operating procedures and detailed guidance to flight crew on the conduct of briefings.
The FAM stated:
The objective of a briefing is to ensure all Flight Crew understand and share a common mental model for the proposed plan of action.
Furthermore, it stated that for the briefings to remain effective they should be:
Interactive – engaging all Flight Crew members and ensuring a practical understanding of what is proposed.
ThreatandErrorManagementBased – briefing points should include identification and assessment of threats. Plans for dealing with identified threat should be discussed. The depth of the briefing content should be commensurate with the assessed threat environment.
ConciseandRelevant – content must serve to refresh knowledge considered necessary for crew coordination. It is unnecessary to reiterate standard operating procedures or discuss every detail of published procedures as each Flight Crew member must review pertinent information and FMS [flight management system] setup in preparation for the briefing.
Briefing emphasis should be directed to plans or requirements which vary from those routinely used.
On a multi-sector tour of duty involving Australian ports, there is no requirement for repetition of items previously briefed for the same departure or arrival, provided that the Pilot In Command is satisfied that the pertinent information is understood by all Flight Crew.
TimelyandLogical – to assist delivery and understanding, briefings must be scheduled so as not to interfere with operational tasks and the content should follow a logical sequence based on phase of flight. The briefing framework must conform to the following structure and sequence:
– Considerations with emphasis on threat identification, assessment and implementation of management strategies.
– Normal operations with emphasis on sharing plans of action.
– Contingency and non-normal aspects with emphasis on contingency planning.
For approach and arrivals at an airport, it was standard practice for the briefing to be completed prior to commencing the descent.
The FAM section 21.2.4.4 gave flight crew the following guidance:
Considerations – identify and assess the threats and considerations that may affect the arrival plan which may include but not necessarily be limited to terrain, adverse weather, airport conditions, NOTAMs, aircraft maintenance status, RMS [route manual supplement] or specific state requirements, traffic, ATC, ground support and fuel conservation opportunities.
NormalOperations
– ArrivalandApproach – brief chart page number, together with relevant charted requirements. For runways where there is no published instrument procedure the anticipated arrival plan should be briefed. Nominate planned approach procedures.
– NavigationandAltimetry – brief the relevant navigation and altimetry requirements.
– Automation – brief the planned level of automation to be used and the transition to manual flight.
– Landing – brief landing flap configuration, level of reverse thrust and auto-brake setting for planned runway exit.
– ContingencyPlanning – brief contingency plans for all threats assessed as requiring crew management.
The FAM guidance did not specifically require flight crews to brief hot spot locations or describe how runway incursion threats would be mitigated.
Other guidance for flight crew briefings
International Civil Aviation Organization (ICAO) document 9870 ManualonthePreventionofRunwayIncursions stated:
The “before start” and “descent” briefings should also contain a complete review of the expected taxi routes with special attention to the hot spots.
Guidance from the United States Federal Aviation Administration (FAA) in 2012 called for operators to develop and implement specific procedures to prevent runway incursions. The FAA advisory circular AC 120-74B (Parts 91, 121, 125, and 135 Flight crew procedures during taxi operations) emphasised that a thorough taxi briefing should include a review of the airport diagram and identify critical locations on a taxi route, including, but not limited to, hot spots, complex taxiway intersections and runway crossing points. In addition, the circular called for procedures that would require flight crews to describe how runway incursion threats would be mitigated: by briefing the timing and execution of checklists and communications, so that no flight crew member was preoccupied or head-down when approaching an active runway.
There was no CASA guidance regarding the inclusion of runway hot spots or incursion threats in pre-flight or in-flight briefings. The ATSB reviewed the documentation of two other Australian airlines and found that one specified a mandatory requirement for flight crews to verbally brief runway hot spots, and the other provided detailed guidance material regarding runway hot spots and recommended that flight crews verbally brief them.
Airport information
General information
Perth Airport had two runways. The main runway was oriented 03/21 and the cross runway 06/24 (Figure 2). Both were 45 m wide and had a 150-m wide flight strip.[10]
Preferred taxiway
Since 2014, the Aeronautical Information Publication (AIP) entry for Perth Airport stated the preferred exit taxiways for arriving aircraft on each runway and for different types of aircraft. The preferred taxiway for jet aircraft landing on runway 03 was J2 and for turboprop aircraft it was A6. The AIP stated that the preferred taxiways were to ‘ensure minimum runway occupancy time and support optimum spacing on final [approach]’.[11]
Data provided by Airservices Australia indicated that, from May 2017 to April 2018, about 24 per cent of all aircraft landing on runway 03 exited via J2. Data provided by Qantas showed that, of its 737 fleet landings on runway 03, about 44 per cent vacated runway 03 at taxiway J2. Qantas noted that its pilots preferred to exit runway 03 at taxiway D as it resulted in a shorter and more direct route to the terminal.
The AIP stated that, unless specified otherwise by ATC, an aircraft must promptly vacate the runway after landing without backtracking. There was no requirement under the AIP for an aircraft to use the first available taxiway.
Taxiway J2
Arrangement
Taxiway J2 was located approximately 1,911 m from the threshold of runway 03. It led to a 6-way intersection comprising runway 06/24 and three other taxiways (Figure 6).
Taxiway J2 intersected runway 03 at a 60° angle. The straight distance from the edge of runway 03 to the runway 06 holding point was approximately 176 m, and the distance from the runway 03 holding point and the runway 06 holding point was about 70 m. The distance from the runway 06 holding point to the edge of runway 06 was about 102 m.
Figure 6: Taxiway J2 in relation to runways and other taxiways
All annotations are approximate and for illustration purposes only.
Source: Google earth annotated by ATSB
The Civil Aviation Safety Authority (CASA) outlined Australian requirements for aerodromes in Civil Aviation Safety Regulation (CASR) Part 139 and the associated Manual of Standards (MOS). As an airport operator licensed by CASA, Perth Airport was responsible for the safety of the aerodrome in accordance with those requirements.
The MOS section 6.3.3 Taxiway Curves defined the minimum curve radius required for taxiway design speeds, which are listed in Table 1. For taxiway J2, with a curve radius of 200 m, the taxiway design speed was about 31 kt. VH-XZM’s turn from the runway onto the taxiway was made at an average speed of 34 kt.
Table 1: Taxiway design speed for minimum radius of curve
Taxiway design speed
Curve radius
20 km/h (11 kt)
24 m
30 km/h (16 kt)
54 m
40 km/h (22 kt)
96 m
50 km/h (27 kt)
150 m
60 km/h (32 kt)
216 m
70 km/h (38 kt)
294 m
80 km/h (43 kt)
384 m
90 km/h (49 kt)
486 m
100 km/h (54 kt)
600 m
Runway holding point markings
Perth Airport runway holding points (or runway-holding positions) were equipped with signage and ground markings to provide flight crews with visual cues indicating their position and proximity to a runway. Those markings identified the location where an aircraft was required to stop when it did not have an ATC clearance to proceed onto or to cross a runway.
For flight crew vacating runway 03 on taxiway J2, the holding point for runway 06/24 was marked with red and white ground markings identifying the runway ahead,[12] taxi-holding point signs and location signs. The runway holding point was also equipped with unidirectional[13] runway guard lights, which flashed continuously, and a stop bar (Figure 7).
Figure 7: View of the runway 06/24 holding point on taxiway J2
The central panoramic image was taken from the entrance to taxiway J2 from runway 03/21. The other images were taken from close to the runway holding point. All images were taken at a height lower than that of the flight crew of a Boeing 737.
Source: ATSB
Stop bars
Stop bars were intended to provide additional protection of runway/taxiway intersections to prevent runway incursions. They were a series of unidirectional lights at right angles to a taxiway centreline (Figure 8). The lights were spaced 3 m apart and located 0.3 m before a holding point. Stop bars showed red in the direction of approach to the stop bar. They were controlled by ATC and were independent of the runway guard lights. Additional raised lights at each end of the stop bar were not installed, nor were they required to be.[14]
Figure 8: Runway identifier (red and white markings) and stop bar (red lights) installed on taxiway J2
Source: ATSB
When seated in the normal position, the flight crew of a Boeing 737-800 cannot see the ground that is less than 11.5 m ahead of the aircraft’s nose (due to the obstruction of the flight deck glareshield). Consequently, the VH-XZM flight crew’s last opportunity to see the stop bar on taxiway J2 was at 1442:00, about 5 seconds after completing the turn onto the taxiway and 1 second prior to crossing the stop bar (Figure 9).
Figure 9: Last point when stop bar was visible from flight deck of VH-XZM
Source: Google Earth, modified by ATSB.
The AIP required flight crew to stop and hold their aircraft at all illuminated stop bars. Flight crew could only proceed to taxi an aircraft further once an ATC clearance to enter or cross a runway had been received and the stop bar lights had been switched off.
Stop bars were implemented at Perth on 30 March 2018. At the time of the occurrence (28 April 2018), all stop bars were reported to be operating correctly.
Other taxiways
In terms of the other taxiways off runway 03 (see Figure 2):
Most taxiways intersected at 90° with a curve radius of about 100 m.
Taxiway D intersected at 80° with a curve radius of about 60 m.
Taxiways P intersected at 45° with a turn radius of 100 m, with 318 m between the edge of runway 03 and the next (taxiway) holding point.
Taxiway N intersected at 45° with a turn radius of 100 m. In addition to taxiway J2, it was the only taxiway at Perth with a single holding point and a relatively short distance between the two runways. It led to a somewhat complicated four-way intersection. Two of the taxiways crossed runway 06/24 and shared a single holding point from taxiway N, set back about 120 m from the runway 06/24 flight strip. Both required a turn after the holding point to cross the other runway. The distance between the edge of runway 03 and the runway 06/24 holding point was about 350 m (with the first 280 m being a straight line).
Flight data analysed by Qantas indicated that the average exit speed of Qantas aircraft onto taxiway J2 over a 2-year period was 28 kt, compared with the average exit speed of 17 kt onto the tighter, near-right angle exit at taxiway D. The exit speed of VH-XZM was about 35 kt, and about 20 per cent of the landings over the 2-year period had an exit speed of 35 kt or higher (and about 5 per cent having an exit speed of over 40 kt).
Qantas reported that the distance between the runway 03 exit and the holding point for runway 06 on J2 at Perth was much shorter than any other runway exit taxiway leading directly to another runway on its 737 route network. The next shortest was about 397 m at Sydney Airport (for taxiway A2 off runway 34L that led to runway 25).
Rapid exit taxiway information
Requirements for rapid exit taxiways
As noted in The occurrence, the captain of VH-XZM thought that, when approaching taxiway J2 during the landing roll, the taxiway was a rapid exit taxiway (RET). Accordingly, the ATSB considered the design requirements for RETs.
The MOS defined a rapid exit taxiway (RET) as:
A taxiway connected to a runway at an acute angle, designed and intended to allow landing aeroplanes to turn off the runway at higher speeds than are achieved on exit taxiways, thereby minimizing runway occupancy times.
It additionally noted:
The provision of rapid exit taxiways is a financial decision for the aerodrome operator. The aerodrome operator should seek specialist advice on the geometric design of rapid exit taxiways.
The International Civil Aviation Organization (ICAO) specified standards and recommended practices (SARPs) for international aviation operations in a series of Annexes. ICAO Annex 14 (Aerodromes, Volume 1 AerodromeDesignandOperations) defined a taxiway as:
A defined path on a land aerodrome established for the taxiing of aircraft and intended to provide a link between one part of the aerodrome and another, including:
…c) Rapid exit taxiway. A taxiway connected to a runway at an acute angle and designed to allow landing aeroplanes to turn off at higher speeds than are achieved on other exit taxiways thereby minimizing runway occupancy times.
Annex 14 recommended that a RET should be designed with a curve radius of at least 550 m for certain types of runway (including those in Perth) to enable 93 km/h (50 kt) taxi under wet conditions. It also recommended that a RET should have a straight distance after the turn-off curve sufficient for an exiting aircraft to come to a full stop clear of any intersecting runway. There was no guidance regarding appropriate taxiway lengths, turn angles or curve radii.
ICAO also published other guidance about aerodrome taxiways. ICAO document 9157 (Aerodrome Design Manual Part 2 Taxiways, Aprons and Holding Bays) stated that the intersection angle of a RET with the runway should not be greater than 45° and preferably be 30°.
Neither the CASA MOS nor ICAO's Annex 14 provided restrictions or recommendations on direct access from one runway to another without an intermediate, transitional taxiway. The European Organisation for the Safety of Air Navigation (EUROCONTROL) in its November 2017 version of the EuropeanActionPlanforthePreventionofRunwayIncursions, recommended:
A RET should meet with a parallel taxiway, and never end directly onto another active runway (that is used for take-off/landing).
Similarly, the United States Federal Aviation Administration (FAA) Advisory Circular 150/5300 stated:
Do not provide direct access from a high speed exit to another runway.
The Airports Council International RunwaySafetyHandbookFirstEdition 2014 identified key elements to eliminate runway incursions, including:
• Rapid Exit Taxiways should be designed in such a way that crossing another runway via a rapid exit taxiway is not possible. A rapid exit taxiway should never be used for entry to a runway; and
• Complicated Taxiway Layouts linking adjacent runways – such as multi-taxiway intersections, Y-shaped taxiways, taxiways crossing high speed exits and taxiways connecting to V-shaped runways – should be avoided in the design. If any of these are unavoidable, mitigation measures for runway incursion should be included in the design.
Rapid exit taxiway identification
At airports equipped with RETs, aerodrome charts provided flight crews with information such as RET location, maximum design exit speed and lighting systems, if fitted. This information was included in text in the airport efficiency procedures section rather than annotated on a map of the aerodrome.
ICAO Annex 14 recommended aerodrome operators install rapid exit taxiway indicator lights (RETILs). RETILs consisted of six yellow lights adjacent to the runway centreline and configured in a three/two/one pattern spaced 100 m apart; the single light was 100 m from the start of the turn for the RET.
The Australian AIP detailed differences between Australian national aviation legislation and those specified by ICAO as SARPs. With regard to RETILs, Australia notified ICAO of a difference to the SARPs under the level of ‘less protective, partially implemented or not implemented’. Accordingly, at the time of this occurrence, CASR Part 139 and the MOS did not require or recommend aerodrome operators to install RETILs.
Rapid exit taxiways in Australia
Taxiway J2 was not designated as a rapid exit taxiway (RET) and it did not meet the design requirements of CASA MOS or ICAO Annex 14 for a RET. There were no RETs at Perth.
RETs were provided at several other airports in Australia, including Brisbane, Melbourne and Sydney. None of these RETS had RETILs.
Runway incursion hot spots
Recommended practices for identification of hot spots on aerodrome charts
ICAO defined a runway incursion as ‘any occurrence at an aerodrome involving the incorrect presence of an aircraft, vehicle or person on the protected area of a surface designated for the landing and take-off of aircraft’.
ICAO document 9870 (ManualonthePreventionofRunwayIncursions) defined a hot spot as:
A location on an aerodrome movement area with a history or potential risk of collision or runway incursion, and where heightened attention by pilots/drivers is necessary.
The document stated that, once hot spots have been identified, suitable strategies should be implemented to either remove the hazard or to manage and mitigate the risk to be as low as reasonably practicable.
ICAO recommended that the local generation of AIP aerodrome charts show runway hot spots (see for example Figure 2). The criteria used to establish a hot spot on an aerodrome chart and the symbols to be used were contained in ICAO Annex 4 (Aeronautical charts), with more guidance provided in Annex 14 and document 9870.
Aerodrome charts for Perth
Aerodrome charts were published by Airservices Australia in the AIP. Jeppesen charts, used by Qantas, provided details similar to the AIP about the airport and taxiway layout and associated information, such as warnings and runway incursion hot spots.
Jeppesen charts identified the location of hot spots and marked the area of risk with a magenta box in accordance with the ICAO recommendation. Text on the aerodrome chart stated ‘HS2 – Caution Runway Incursion Hot Spot’. No text or specific information was provided to explain the risk and reasons why previous runway incursions had occurred at those locations (in either the Airservices Australia or the Jeppesen charts).
Study of aerodrome chart effectiveness
In 2016, EUROCONTROL published a safety study report that examined how AIP hot spot information was transposed to commercially-produced aerodrome charts and promoted practices to help improve the accessibility, visibility and quality of the information. The study collected samples of AIP and commercial aerodrome diagrams for 64 European airports and a small number of samples from Australia, China and the United States for comparison purposes. It stated:
Of those airports that did have Hot Spot information on their AIP charts, only 39% were judged to be effective or very effective. Effectiveness, in this case, being a combination of presentational clarity and usefulness of the information. However 45% of airport AIP charts were judged to be of no or low effectiveness.
The Australian samples included Adelaide, Darwin, Sydney and Perth. The report judged all of these AIP charts to be of low effectiveness, stating:
The expanded graphic of the runway incursion Hot Spots are useful, but there is no text to enhance the pilot’s understanding other than to use caution. Since it is not unreasonable to assume that pilots do exercise caution when taxying, the effectiveness of the Hot Spot information is low.
The report noted that in many countries, including Australia, there was variation in the manner in which hot spot information was presented at different airports.
The report also noted the following presentation styles that ‘seemed to provide clarity and effectiveness’ of hot spot information to flight crew:
• Each Hot Spot depicted by a clear bright red circle and joined to a red label box e.g. HS1
• Large tabulated textual information elaborating the action required of pilots in and around the Hot Spot. This may be on the main aerodrome diagram or on the obverse page if clarity is best served.
• The use of additional graphical boxes depicting the Hot Spots in greater detail. These additional boxes should be physically linked by lines or arrows to the Hot spot on the main diagram, if possible.
• Where the aerodrome diagram would otherwise be too cluttered to present Hot Spots effectively, the use of specific Hot Spot pages can be effective.
• The use of a colour-coded format which assists the depiction of runways, Hot Spot areas and normal taxiways.
In 2017, the FAA issued Safety Alert for Operators 17012 (High collision risk during runway crossing) that warned pilots of high-risk runway incursions and potential collisions in the first two-thirds of an active runway (with many such events occurring in the first third of the active runway). At Perth, the junction between taxiway J2 and runway 06 was within the first third of runway 06.
Runway incursions at Perth Airport
Airservices Australia recorded 44 runway incursions at Perth Airport between July 2015 and the day of the occurrence (Table 2). That equated to a rate of 11.6 incursions per 100,000 movements – higher than other major airports in Australia, including Sydney (2.0) and Melbourne (0.3).
Table 2: ICAO classification of the severity of runway incursions at Perth Airport, 1 July 2015 to 28 April 2018
ICAO severity classification
ICAO severitydescription
Numberof runwayincursions atPerth
Numberof runwayincursions ontaxiwayJ2 atPerth
A
A serious incident in which a collision is narrowly avoided.
0
0
B
An incident in which separation decreases and there is significant potential for collision, which may result in a time-critical corrective/evasive response to avoid a collision.
1[a]
1[a]
C
An incident characterized by ample time and/or distance to avoid a collision.
10
4
D
An incident that meets the definition of runway incursion, such as the incorrect presence of a single vehicle, person, or aircraft on the protected area of a surface designated for the landing and takeoff of aircraft but with no immediate safety consequences.
31
10
E
Insufficient information or inconclusive or conflicting evidence precludes a severity assessment.
2
1
[a] Including the investigation occurrence.
Source: Airservices Australia
Of the 44 incursions, 16 involved taxiway J2 on both runway 03/21 and runway 06/24. For that reason, the taxiway intersection of J2, J1 and A with runway 06/24 was marked as a runway incursion hot spot on aerodrome charts.
The ATSB’s occurrence database recorded 52 runway incursions at Perth involving turbine-engined aircraft (not under tow) over a 5-year period up to and including the 28 April 2018 occurrence. Exposure data was not available. Of these 52 incursions, the following types of incursion were excluded:
14 incursions that involved apparent ATC clearance errors (mostly not turning off stop bars after clearance was issued)
5 incursions involving a closed runway
2 incursions due to aircraft not departing the runway fully after landing.
Of the remaining 31 incursions, there were:
14 incursions on the cross runway via a taxiway immediately after landing (similar to the 28 April 2018 occurrence)
9 incursions that involved aircraft turning onto the cross runway instead of a taxiway
8 other incursions (general taxiing incursions).
Figure 10 shows the approximate location of incursions in these three groups, with most of the incursions on a cross runway via a taxiway happening near taxiway J2.
Figure 10: Selected types of runway incursion at Perth in a 5-year period
Source: Airservices, annotated by ATSB
Runway safety activities
ICAO have recognised runway safety as one of its highest priorities given it is currently one of the most significant threats to global aviation safety. In response, in 2011 the ICAO Runway Safety Programme (RSP) promoted the establishment of runway safety teams (RSTs) at airports as an effective means to reduce runway related accidents and serious incidents.
As part of Australia’s State Safety Programme, a National Runway Safety Group (NRSG) was established to perform a national advisory and coordination role, and promote the establishment and effectiveness of local runway safety teams (LRSTs). It utilised intelligence from these forums and other sources to develop and implement national strategies to improve runway safety and reduce runway related accidents and incidents.
An LRST consisted of local representatives addressing local runway safety issues. The purpose of an LRST was to identify current and potentially emerging issues related to runway safety and implement initiatives to assure the continuing safety of operations at their aerodrome.
Perth Airport had an LRST which met biannually and included the aerodrome operator, Airservices Australia, airline operators and other stakeholders operating at the airport.
Air traffic control information
Air traffic control at Perth Airport
Airservices Australia provided a 24-hour air traffic service at Perth Airport. The controllers responsible for all aircraft and vehicle movements on taxiways, runways and in the immediate vicinity of the airport were located in a tower on the eastern side of runway 03/21 (Figure 2).
The distance from the tower to the runway 06/24 holding point on taxiway J2 was about 1,200 m, and from the tower to the runway 06 threshold was about 3,000 m.
At the time of the occurrence the airport traffic flow was operating in a North flow. This permitted the most efficiency and therefore achieved the most operating capacity at Perth. A North flow traffic pattern had departures from both runway 03 and 06 and arrivals on runway 03.
Runway crossing procedures
The Australian AIP provided flight crew of domestic aircraft with procedures to follow when taxiing after landing. It stated:
2.16.2 After landing, unless specified otherwise by ATC, an aircraft must comply with the following:
a. Promptly vacate the runway without backtracking.
b. Change from the aerodrome frequency to the SMC frequency (where established) when vacating the runway strip and obtain an ATC taxi instruction.
c. Not cross any runway that intersects the taxi route unless in receipt of a taxi instruction and a “CROSS RUNWAY (number)” instruction from ATC…
The ICAO Manual on the Prevention of Runway Incursions outlined best practice for radio transmission guidelines and techniques. It stated:
Communication with any aircraft using the runway for the purpose of taxiing should be transferred from the ground controller to the aerodrome controller prior to the aircraft entering/crossing a runway.
The requirement for domestic aircraft to automatically[15] transfer to the SMC frequency when vacating the runway strip had been in place since prior to 2003. In June 2010 Airservices Australia commenced a trial of aircraft and vehicles being on the ADC frequency when crossing runways in line with the ICAO recommendation. The trial was conducted at Sydney, Cairns, Brisbane, Coolangatta, Perth, Adelaide and Broome.[16]
A post implementation review found no evidence that the trial procedures reduced the risk associated with runway incursions. It also identified a number of safety issues and concerns, including the reduction in ADC and SMC situational awareness at airports where crossing of active runways was required (including crossing runway configurations such as at Perth). Airlines involved in the trial agreed at that time that the trial should be ceased. Consequently, Airservices Australia returned the procedures to the pre-trial requirements of the AIP (as stated above).
Qantas advised that the ICAO-recommended approach to runway crossings, with the crossing aircraft on the ADC frequency, was used overseas in countries such as the United Kingdom and the United States. The ATSB identified that other countries such as New Zealand used a similar approach to that specified in the Australian AIP, with aircraft required to automatically transfer to the SMC frequency after landing.
Integrated tower automation suite
Tower controllers were responsible for separating aircraft visually but used a range of systems at their workstations to assist with performing that task. Each station in Perth tower was fitted with the integrated tower automation suite (INTAS), which included the advanced surface movement guidance and control system (A-SMGCS).
The INTAS provided controllers with electronic flight and operational information to enhance airport efficiency. The system combined flight and operational data, surveillance and voice communications into a single integrated, control tower-specific layout. Controller workstations were equipped with four customisable touch screens that displayed electronic flight strips, operational information, weather, terminal area radar displays, and, where available, surface surveillance data through the A-SMGCS.
The A-SMGCS provided automatic identification of all aircraft and transponder-equipped vehicles at Perth Airport. Using the collection of that surveillance data from multiple sources, the system provided controllers with an electronic picture of what was happening on the ground at any time. Additionally, the system added to a controller’s situational awareness by predicting potential conflicts between vehicles and aircraft, and multiple aircraft movements, before they could occur. Those protections included runway incursions by aircraft or vehicles. Visual and aural alarms alerted controllers to potential problems, enabling them to take early corrective action.
During the implementation of INTAS in the Perth tower, the system was configured with associated alert settings assigned to each controller’s position. The selection of a role (including combined position roles) by the tower shift manager automatically triggered the associated system alert settings that were assigned to each role in the INTAS adaptation settings.
At the time of the occurrence, due to the configuration of the Perth tower INTAS, when an SMC was operating the combined workstation roles of SMC, airways clearance delivery (ACD) and shift manager, the A‑SMGCS alerts were off. This inhibited the SMC from receiving an aural and visual stop bar violation alert (and runway occupied alert) at their workstation.
Emergency response actions
The Australian ManualofAir Traffic Standards (MATS) defined a safety alert as:
The provision of advice to an aircraft when an ATS Officer becomes aware that an aircraft is in a position which is considered to place it in unsafe proximity to terrain, obstructions or another aircraft.
The manual also stated:
Unless the pilot has advised that action is being taken to resolve the situation or that the other aircraft is in sight, issue a Safety Alert prefixed by the phrase ‘SAFETY ALERT’ when you become aware that an aircraft is in a situation that places it in unsafe proximity to:
a) terrain; b) obstruction; c) active restricted or prohibited areas; or d) other aircraft.
In addition, the manual stated:
Do not assume that because another Controller has responsibility for an aircraft that an unsafe situation has been observed and a Safety Alert or avoidance advice has been issue.
The MATS procedures for aerodrome controllers stated that, for cancelling a take-off clearance:
Only cancel a take-off clearance once an aircraft has commenced take-off roll in circumstances where an aircraft is in imminent danger e.g. ‘STOP IMMEDIATELY (repeat aircraft callsign) STOP IMMEDIATELY (reason)’. Accompany any instruction to cancel take-off with a description of the nature of the emergency.
Compromised separation recovery training
Separation between aircraft is considered to be compromised when separation standards have been infringed, or where separation assurance is absent to the extent that a breakdown of separation is imminent.
In order to help ensure controllers provided effective response actions when separation is compromised, they undertook compromised separation recovery (CRT) training. The ATSB has previously noted limitations with the provision of such training by Airservices Australia and the Department of Defence to their controllers in several investigation reports. In 2014 and in 2016, Airservices undertook a series of actions to improve its CRT training.[17]
The ATS Training Operations Manual stated in 2014:
Compromised separation recovery training must be included in all ATC endorsement training courses, and in particular, skills-based training in the simulator. The training must be assessed for competency…
EGM [Executive General Manager] ATC has determined that all operational staff must successfully complete annual training and assessment in compromised separation recovery training. It is a mandatory requirement that all controllers are assessed in skills-based simulator Compromised Separation Recovery training at intervals not exceeding three years.
In September 2020, Airservices Australia confirmed that, since 2012, all endorsed controllers were required to complete the knowledge-based component of compromised separation recovery training as part of the annual refresher training program. It also advised:
The skills-based component [of CRT training] only applies to tower controllers that hold the ADC endorsement. Given the role and responsibilities of a surface movement controller this continues to be appropriate. Separation on the manoeuvring area is a joint pilot controller responsibility and there are no defined separation standards.
The skills based compromised separation training scenarios do not align with the responsibilities of an SMC. All SMC endorsed controllers are trained and assessed at recognising ground conflicts and taking action as required commensurate with the risk of the situation using standard phraseology and taking into consideration aspects of the local operational context. The records of such training is maintained in individual training files.
In addition, all controllers that complete a tower course do destination specific CSR exercises as a part of the aerodrome control course element.
… all SMC endorsed controllers are trained and assessed at recognising ground conflicts and taking action as required commensurate with the risk of the situation using standard phraseology, as such no further rationale is required.
As noted in Air traffic controllers, both of the controllers involved in the 28 April 2018 occurrence sequence held an ADC endorsement, and therefore had undertaken skills-based as well as knowledge-based CRT training. The ADC reported the most recent training included a stop bar violation and runway incursion at Perth.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 19 September 2017, the pilot of a Cessna C208 aircraft, registered VH-SJJ, was operating from Toowoomba, Queensland to Ballina, New South Wales (NSW) then onwards to Nambucca Heads, NSW. The C208 pilot landed at Ballina Byron Gateway Airport (YBNA) and was clear of the runway at 1055 Eastern Standard Time (EST). Two Robinson R22 helicopters were also operating at YBNA at this time.
YBNA is a certified, non-controlled aerodrome utilising Common Traffic Advisory Frequency (CTAF) procedures[1]. A Certified Air/Ground Radio Service Operator (CA/GRO)[2] had been on duty since around 1030.
At 1104, the C208 pilot transmitted to the Brisbane Centre Air Traffic Control, announcing his intention to taxi to the runway for departure. Brisbane Centre advised that traffic was an inbound Airbus A320 aircraft due at YBNA at 1109 with additional VFR traffic[3] in the circuit. The C208 pilot responded: ‘copied the inbound Airbus and helicopters in the circuit.’
At about the same time, one of the R22s, registered VH-JKH (JKH), was operating clear of the runway strip in an area known as the southern grass (Figure 1). The other R22, registered VH-MFH (MFH), was being used for circuit training on runway 06 with approach and landing to a point about two thirds along the runway. At 1105, the instructor in MFH broadcast on the CTAF that they were on a left base for runway 06 to the runway.
At 1106:24, the C208 pilot broadcast on the CTAF that they were taxiing for departure on runway 06. The CA/GRO acknowledged that the C208 pilot already had traffic information on the inbound Airbus and advised, ‘…on your right-hand side there is helicopter JKH, also…’ and following a four-second pause, ‘…conducting operations runway 06, helicopter MFH’. At 1106:55, the C208 pilot responded ‘thanks for that and SJJ is entering and rolling runway 06’.
At this time, MFH was on short final for runway 06 at approximately 200 ft above the runway and approaching a point that was about two thirds of the way along runway 06. The instructor realised that the C208 was departing and transmitted that MFH was ‘runway 06 for the runway’. That call partly over-transmitted on the C208 pilot’s response to the CA/GRO. The instructor took control of the helicopter and vacated the runway to the north followed by a call to advise their location at the ‘northern grass.’
The C208 pilot continued the take-off and departure to Nambucca Heads.
Figure 1: Approximate location of aircraft when the C208 pilot called entering and rolling
Source: Google Earth, annotated by the ATSB
Operational aspects
Certified Air/Ground Radio Service (CA/GRS)
A CA/GRS is an aerodrome radio information service providing traffic, weather and other operational information to all pilots. Its primary purpose is to enhance the safety of air transport operations by the provision of relevant traffic information. A CA/GRO is to maintain a vigilant watch on the changing positions of aircraft so that relevant traffic information can be provided. When the CA/GRS is operating, pilot procedures are unchanged from the standard non-controlled aerodrome operating and communication procedures.
In this case, the CA/GRO immediately responded to the C208 pilot‘s taxi broadcast but the traffic advice was broken by a four-second pause. He recalled that he hesitated as he attempted to relocate MFH in the circuit area to provide a specific position. The CA/GRO had lost sight of MFH after it turned onto the final approach due to the eaves of the cabin partially obscuring his view, requiring him to move from his desk to the cabin window. The CA/GRO was still able to advise that MFH was conducting operations to runway 06. The CA/GRO sighted MFH as it vacated the runway, which was moments after the C208 pilot called ‘entering and rolling’.
C208 pilot comments
The C208 pilot had operated at YBNA for the last 14 years and had always known the helicopters to operate on the grass areas. Although he stated he had a good view of the runway from the holding point, he did not see nor hear the helicopter. The C208 pilot could not recall all traffic information he had received except for the inbound Airbus A320, which was his focus due to a desire to depart prior to its arrival.
ATSB comment
The CA/GRO provided traffic information to the C208 pilot in accordance with standard procedures. This is an advisory service only and a pilot is expected to use that information to supplement standard operating and communication procedures.
The C208 pilot did acknowledge the traffic information provided but had not developed a complete traffic picture prior to entering the runway. This was probably due to his focus on departing prior to the arriving Airbus A320 and based on previous experience, not expecting the helicopters to be on the runway.
The instructor on MFH recognised the potential traffic conflict and took appropriate action.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The pilot of the C208 entered and rolled on the runway prior to positively identifying the helicopter on short final for the same runway.
Safety message
Pilots are reminded to apply effective see-and-avoid principles when operating at or near non-controlled aerodromes. While broadcasting on and monitoring of the CTAF is the key way for pilots to establish situational and traffic awareness, it is also important to maintain a constant visual lookout to validate any operating assumptions and avoid traffic conflicts.
One of the safety concerns relates to communication and self-separation in non-controlled airspace.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 19 October 2016, at about 1037 Western Standard Time (WST), a vehicle was travelling along the northern perimeter road at Perth Airport, Western Australia. The vehicle had a driver and three passengers who were going to conduct a customs inspection on an aircraft, which was scheduled to depart Australia.
The driver had been advised that the aircraft would be parked on the international apron in preparation for the inspection. When the vehicle arrived at the international apron, the aircraft was not there, so the driver decided to show the other passengers some different areas of the airport while they waited for the aircraft to arrive.
As they drove towards the domestic apron, an area unfamiliar to the driver, the driver observed the aircraft that they were to meet, stationary in a position different to what was expected. They thought the aircraft was on the domestic apron, and instead of continuing along the northern perimeter road to the domestic apron, the driver turned left (Figure 1 item 1) and crossed the red and white zipper markings[1] that denote the road is crossing taxiway R (Figure 2). About another 50 m past taxiway R, was a left turn (item 2) for vehicles to access the domestic apron.
Figure 1: Airport map showing the path of the vehicle
Source: Google earth, modified by the ATSB
Figure 2: Photo showing stop sign and red and white zipper markings that denote a taxiway like that for taxiway R
Source: Airport operator
Rather than being parked as assumed by the driver, the aircraft was actually being towed in company with two safety vehicles and was stationary at taxiway D holding point, waiting for clearance to cross-runway 21. The vehicle then turned left onto taxiway W (item 3) and then right onto the 700 lane (item 4). At about 1038, the surface movement controller (SMC) cleared the aircraft that was being towed (item 5), to cross runway 21. At about the same time, a senior airport operations officer (SAOO), who was in a vehicle and parked near the 700 lane (item 6), noticed the vehicle traveling along the 700 lane but was not able to identify it. The vehicle turned right onto taxiway B (item 7) and then left onto taxiway H3 (item 8).
At about 1040, the tower air traffic controller cleared a Fokker Aircraft F28 MK 100 aircraft (Fokker 100) that was on final approach, to land on runway 21.
At about the same time, the SAOO contacted the SMC to determine the identity of the vehicle that was just turning onto taxiway D (item 9). The SMC advised that they assumed that the vehicle was associated with works being conducted at the intersection of taxiways A and D. The vehicle was not fitted with a transponder. A transponder was not required for operating in the non-manoeuvring area of the airport, but the vehicle was displayed intermittently on the surface movement control system.[2]
A work safety officer (WSO), who was supervising a work site at the intersection of taxiways A and D heard this exchange and observed the vehicle in the rear-view mirror (item 10). They turned their vehicle around, and followed the unidentified vehicle that was traveling along the paved edge of taxiway D, towards the runway 21 holding point. As the vehicle should not have been there and did not appear to be stopping, the WSO used their vehicle’s siren, horn and loudspeaker to alert the driver, and informed them that they were about to enter the runway and to stop immediately.
The vehicle passed over the holding point for runway 21 before it stopped. The vehicle stopped about two to three car lengths past the holding point (item 11). The WSO stopped about 5 m before the holding point and over the loudspeaker instructed the driver to go no further and to turn around. The WSO also advised the SMC that they were talking with the driver. The vehicle had stopped about 20 m before the white gable markers that denote the runway strip. The vehicle did a hard right turn and crossed back over the holding point at about 10:41:05 (Figure 3). About 3 seconds later, the Fokker 100 aircraft that had just landed on runway 21, passed the vehicle position. At this time, the estimated distance between the vehicle and the Fokker 100 was about 100 m. The crew of the Fokker 100 did not notice the vehicle.
Figure 3: Location of Fokker 100 aircraft landing on runway 21 and vehicle as it crossed back over the taxiway delta holding point for runway 21
Source: Airport operator, modified by ATSB
Vehicle driver comment
The vehicle driver indicated that the three passengers were new to the airside area of Perth Airport and they had used the delay to show the passengers the charter area that was on the same side of the airport as the domestic terminal. As they were traveling back to the international terminal, the driver saw, in the distance, the aircraft that they were to meet. The driver indicated that they were not familiar with the domestic area of the airport where the incident occurred, and they were focused on the aircraft that they needed to meet to complete their job, which also had time constraints.
The driver reported that as they approached the runway, they had stopped to allow the landing aircraft to pass before they saw the flashing lights of the WSO vehicle.
The driver reported that during the training to obtain the authority to drive airside (ADA), they would take every opportunity to gain more experience but would generally go to the same places.
The vehicle was not fitted with a VHF radio to communicate on or hear any of the air traffic control frequencies, nor was it required to be, as it was only authorised to travel on the perimeter road and apron areas.
The driver advised that there was no airport map or airside driving manual located in the vehicle.
Work safety officer comment
The WSO advised that the vehicle did not seem to be slowing down as they crossed the holding point and only seemed to start to slow when the WSO commenced calling on the loudspeaker.
The driver seemed confused and was focused on getting to the aircraft to complete their inspection, rather than where they were on the airport.
Airport operator comment
The airport operator conducted an investigation into the incident and determined that:
The vehicle was not fitted with a transponder, as the vehicle was not permitted to access the airport manoeuvring area.
The vehicle driver was issued with a category 2 authority to drive airside (ADA) in April 2016, which included approval to drive on all aprons and roadways but was not permitted on any taxiways or runways.
The actions of the vehicle driver in leaving the marked perimeter roadway, traversing several taxiways and then crossing a marked runway holding point, were the actions of an individual confused with their location on the airport.
The lost procedures for Perth Airport are promulgated in the airport driver-training programme and the Airside drivers pocketbook.
Safety analysis
The driver observed the aircraft they were scheduled to inspect and thought they were stationary on the domestic apron. They did not realise that the aircraft was being towed and was stopped at the holding point for runway 21. The driver entered the taxiways without a clearance and without having authorisation to do so. They became confused and crossed the holding point for runway 21. The WSO used their vehicle’s siren, horn, and loudspeaker to alert the driver, and informed them that they were about to enter the runway and to stop immediately.
The driver was focused on completing a time critical activity in an area of the airport that they were not familiar with. These probably combined to affect the driver’s ability to recognise that the aircraft they were to meet was being towed and stationary on a taxiway and not parked on the apron. The driver also did not identify that they had turned off the perimeter road and traversed several taxiways before crossing a holding point and entering an active runway.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The driver incorrectly assumed that the aircraft was parked on the domestic apron and in an effort to save time, entered several taxiways without the required approval and authorisation.
The driver was confused with their location, as they were unfamiliar with that area of the airport, and continued traveling down taxiway D and crossed the holding point for runway 21 before the WSO stopped the vehicle.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Airport operator
As a result of this occurrence, the airport operator has advised the ATSB that they are taking the following safety actions:
A review of the zipper markings will be conducted in areas where taxiways cross roadways to provide an enhanced level of identification to airside drivers.
The incident and lessons regarding airfield familiarity, lost procedures and general situational awareness will be communicated in an incident alert.
Explore the option to implement an authority to drive airside (ADA) ’zoning system’, to include a review of all organisations and their requirement to access different areas of the airport.
Review the system of ADA categories to determine if there is scope to implement a system that controls the access of particular organisations to prevent them from entering areas that they do not have a requirement to regularly access.
Safety message
The International Civil Aviation Organisation (ICAO) has identified runway safety as one of its priorities and has been working with countries and aviation organisations globally to reduce runway safety accidents. ICAO has developed a runway safety website, which offers a range of information and products to assist the aviation community to improve runway safety.
and this is available from the ICAO website. The manual includes information on the prevention of runway incursions. The manual discuses that deficiencies in design, training, technology, procedures, regulations and human performance can result in a system break down and safety being compromised. It is important in a complex and dynamic airport environment that all people working in that environment remain vigilant, maintain open communications, and use the systems in place to minimise the risk of a system break down.
Additional information on runway safety is also available from the Airservices Australia webpage Runway safety.
In addition, Airservices Australia has published a guide for airside drivers, The Airside Drivers Guide to Runway Safety, which focuses on four aspects of operating safely on an aerodrome:
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 17 August 2016, at about 0926 Central Standard Time (CST), an Alliance Airlines Fokker F27 MK 50 aircraft (Fokker 50), registered VH-FKV (FKV), and operating with callsign ‘Unity 3201’, landed on runway 12 at Adelaide Airport, South Australia (SA) after a flight from Olympic Dam, SA. The flight crew consisted of a captain seated in the left seat and a check captain seated in the right seat acting as the first officer. Also on board were two cabin crewmembers and 49 passengers.
Air traffic control (ATC) audio recordings showed that at 0926:53, after FKV had rolled through the intersection with runway 23, the aerodrome controller (ADC) cleared an aircraft for take-off on runway 23 (Figure 1).
Figure 1: Adelaide Airport
Source: Airservices Australia – annotated by ATSB
At the end of runway 12, FKV then exited runway 12 onto taxiway D2. After vacating the runway, the check captain switched the aircraft radio from the ATC Tower frequency to Ground frequency and reconfigured the aircraft in accordance with standard operating procedures after landing. The check captain was unable to immediately contact the surface movement controller (SMC) due to congestion on the Ground frequency. The SMC position had combined SMC and airways clearance[1] delivery responsibility.
At 0927:46, the ADC cleared a Jetstar Airbus A320 aircraft, registered VH-VGI (VGI), to land on runway 23. At that stage, the ADC sighted the A320 about 3 NM away on final approach. The flight crew of FKV did not hear that clearance.
Shortly after entering taxiway D2, the check captain, seated on the right of FKV looked outside and sighted an aircraft in the take-off roll on runway 23 and also sighted the A320 on final approach. They estimated that the A320 was 5 to 6 NM away. Based on that estimate, the check captain assessed that they would probably be cleared to cross runway 23 behind the departing aircraft and in front of the landing A320, and then turned their attention inside the cockpit to complete their after-landing checks.
As FKV approached holding point D2, the flight crew had not received an ATC clearance to cross runway 23, and the flight crew therefore assumed they were going to stop at the holding point. The check captain was still waiting for a break in transmissions to make their initial contact with the SMC to advise ‘Adelaide Ground, Unity 3201 for bay 50 golf’.
The SMC was issuing a clearance to another aircraft when they sighted FKV taxiing on taxiway D2 towards the direction the controller was facing. At 0927:49, the SMC told the flight crew of an aircraft awaiting an airways clearance to standby, then immediately said ‘Unity 3201 hold short of runway 23, I’ve got you going to 50 golf’.
The check captain of FKV reported that the start of the transmission from the SMC was over-transmitted and what they heard was ‘runway 23 and I’ve got you for bay 50 golf’. As the instruction included the parking bay, the check captain thought the SMC had instructed them to ‘cross runway 23…’ and read back ‘cross runway 23 to 50 golf, Unity 3201’. The SMC thought the pilot read back ‘short runway 23...’ and assumed that the word ‘hold’ had been ‘clipped’. Both flight crewmembers of FKV thought they had received a clearance to cross runway 23.
The ADC sighted FKV on taxiway D2 and heard the SMC say ‘hold short’, but did not hear the response from the flight crew. The ADC scanned runway 23 to check it was still clear for the landing A320, which was then over buildings and less than 30 seconds from touchdown, and then commenced a handover of the ADC position to another controller.
At 0928:10, the SMC coordinated[2] with the ADC and cleared a vehicle to cross runway 12.
The captain (in the left seat) of FKV then looked to their left and stated ‘clear left’ and taxied the aircraft onto runway 23 to cross. The check captain then looked to their right and sighted the A320 and reported that it was a lot closer than they had expected.
The SMC had looked down at their screen to check the flight strip for the aircraft awaiting a clearance. As the controller looked up, they saw FKV crossing the holding point.
At 0928:21, the SMC called ‘hold short’ and immediately realising that was not the correct instruction, said ‘Unity expedite expedite Unity’. The SMC could then see the A320 in the go-around. The ADC heard the SMC call ‘expedite’ and looked up to see the A320 about 100 ft above the runway – already in the go-around. At 0928:25, the ADC directed the A320 crew to go around.
The captain of FKV continued to taxi the aircraft across the runway and onto taxiway D1 and did not sight the A320 at any time. The A320 (VGI) returned to land without further incident.
Flight crew (FKV) comments
Check captain acting as first officer
The check captain commented that a crossing instruction fitted with their judgment of the situation when they first sighted the A320 while taxiing on D2. They were close to the holding point when they received the initial (hold short) instruction from ATC, and assessed that there was a level of urgency in the SMC’s voice which indicated to them that it was a crossing instruction.
The sun was behind the A320 on final approach to runway 23, which may have affected the check captain’s initial estimate, when they first entered taxiway D2, of how far away the A320 was. However, it was not a factor when FKV taxied onto the runway. At that time, the check captain estimated that the A320 was about 1.5 NM away at about 200 ft above the runway. The check captain decided not to advise the left-seat captain then of the A320 as they had already entered the runway.
There was no confusion in the flight deck over whether they had been instructed to cross the runway or not, they both thought that was the clearance.
The clearance was clipped or over-transmitted and led them to believe it was ‘cross’ not ‘hold short’. In hindsight, the pilot commented that maybe they should have reconfirmed the clearance to cross because the words were clipped, but they expected the readback would give the SMC confirmation that what they understood was correct and the opportunity to detect any misunderstanding. They did not hear anything that sounded like ‘hold short’. It was possible that the check captain had pushed their transmit (push-to-talk (PTT)) button which had momentarily over-transmitted the SMC’s call.
If the check captain had sighted the A320 later in the taxi and closer to the holding point, they would probably have expected to hold short rather than cross in front of it.
The controller’s addition of the bay information to the instruction was not consistent with a hold short instruction. The standard clearance is either hold short (with no further instructions), or cross and taxi to your bay or with additional taxiing instructions.
It was possibly a professional courtesy so the pilot did not have to respond with their bay number, but it added to their expectation that it was a crossing instruction. The flight crew had contacted their company personnel about 100 NM prior to their arrival and were issued with parking bay 50G. It was standard procedure to advise the SMC of their bay number on first contact with the SMC. The SMC presumably gets the bay allocation from the airport ground personnel, and provided that information to the flight crew to save a radio transmission. However, its addition to the end of the hold short instruction misled the pilots.
In the absence of any communication with the SMC prior to reaching the holding point, they would have stopped at the holding point rather than enter the runway.
When discussing the incident afterwards, the captain told the check captain that they had not been aware of or sighted the A320 at any time. The check captain commented that maybe they should have told the captain ‘there is one rolling and one on final’ when they first saw the two aircraft to increase the captain’s situational awareness.
Captain
The captain was normally based in New Zealand and commented that to cross an active runway there, pilots are required to contact the ADC on the Tower frequency for a clearance.
The captain was intending to stop at the holding point, but proceeded to cross when they thought they got the clearance to do so. They had to increase power to accelerate, having slowed ready to stop.
The bay number was a non-normal addition to a taxi instruction, possibly provided as the check captain had not yet been able to give the normal transmission with their bay allocation after exiting the runway.
Controller comments
The air traffic controllers provided the following comments.
Aerodrome controller
It was a quiet and routine traffic sequence and the weather at the time was benign.
The voice equipment was fitted in 2013 to Adelaide Tower. The Tower was a ‘quiet tower’, which means that the controllers can only hear the transmissions on the frequency they are controlling, in their own headsets. Although the ADC could hear the SMC give the instruction to hold short, they could not hear any response from flight crew on the Ground frequency.
Prior to the implementation of the quiet tower, controllers could hear transmissions on the other frequencies on speakers in the Tower. The ADC commented that this improved their situational awareness, particularly from a coordination perspective.
The ADC commented that since the incident, in a similar situation, they would wait for the aircraft to land before commencing a handover.
The ADC commented that following the incident there would be a greater focus among the controllers, not just on the instructions controllers give, but that it is not complete until you get adequate readback that responds to all the components of the clearance. In addition, there should be no taxi instruction beyond a hold short instruction.
Controller taking over from aerodrome controller
The controller in the process of a handover/takeover with the ADC was looking at the weather display and listening to the ADC handing over, when they heard the SMC say ‘hold short’ and then ‘expedite’. The controller looked across and sighted FKV half way across the runway and the A320 in the go-around.
The controller commented that before the ‘quiet tower’ they could all hear each other’s radio, which improved their situational awareness.
The controller also commented that when they receive a call from a pilot, they sometimes miss the first part of the transmission. The controller reported that this is a known fault that the controllers have reported via the Airways systems issues reporting scheme (see below). They also advised that they have become desensitised to hearing only part of the readback, which negates the effectiveness of the readback.
The controller advised that there were a number of things that could have prevented the incident:
if the SMC had heard the readback correctly
better scanning by air traffic controllers and pilots of aircraft approaching and crossing runways
stop bars[3] could have been an effective risk control even without hearing the readback or effective scanning.
The controller commended the actions of the A320 flight crew.
Surface movement controller
The SMC was confident they had given the hold short instruction clearly.
The SMC thought that the Unity flight crew would be expecting to hold short because there was no way they were going to be cleared to cross in front of the landing A320. The SMC commented that if they had not contacted Unity 3201 as they were approaching the holding point, they would have stopped. Because the aircraft was taxiing towards the runway and it is difficult to tell if the aircraft is slowing down, the SMC issued the hold short instruction to be sure they would stop.
They commented that they added the bay number to the hold short instruction to save a transmission, as another aircraft was waiting for their clearance. They were not sure why they did not pick up the incorrect readback, but they did not hear the first word.
The SMC asserted that in most of the transmissions in Adelaide, the initial second of a readback is clipped, for example they only hear ‘short’ instead of ‘hold short’. The controller thought the readback was ‘short runway 23’ not ‘cross runway 23’. As they thought the pilot would be expecting to hold short, the controller was expecting the readback to be ‘hold short’ and that expectation affected what the controller heard.
In Adelaide Tower, it is difficult to tell when a controller’s PTT button is released and whether the frequency is open or closed. Normally for a ‘hold short’ readback, you would be expecting two words but they get used to looking for one word. If you are not certain of a readback, you are meant to ask again, but if they don’t get the first word every time, it can lead to a lot of additional transmissions. Maybe if radio operators push the PTT button and then wait two heartbeats before they start talking, that technique may prevent transmissions being clipped.
The pilots may not hear the controllers’ instructions clearly either as they are also not listening in a perfect environment.
The airport ground staff provide the ADC with bay allocations, which the ADC then put on the flight strip. When the pilots first make contact with the SMC, they state the bay allocated by their company and the SMC checks that matches the bay number on the strip.
The SMC did not hear the ADC clear the A320 to land (or the other aircraft to take off) because they were issuing a clearance at the time.
If the A320 had landed and FKV had crossed the runway, they may have just got across in front of it but it would have been close.
If the airport had stop bar lights, the incident would more than likely not have occurred.
Manual of air traffic services
In the Manual of air traffic services (MATS), under section 12.3.1.11 Taxiing across runways, section 12.3.1.11.1 Intermediate holding points, stated: ‘Do not include positions beyond required intermediate holding points in taxi instructions.’
Airways systems issues database report
Airservices Australia provided the ATSB with a copy of the relevant Airways systems issues database (ASID) report. In June 2013, the ASID report from Adelaide ATC stated that inbound calls from pilots were clipped at the beginning of calls. This could be heard on recorded audio from the tower transmissions and was compared with transmissions recorded prior to the implementation of the new radio system. Following ATC transmissions, when the controller releases the PTT, the voice communications control system switch remains in the transmit state for 200 milliseconds, known as the guard period. During this period, receive audio is blocked, therefore the audio from pilots is dropped.
In August 2014, the report was updated to state that the clipping issue had been incorporated into the voice system training manual. On 17 December 2015, the comment added was ‘Vendor has advised that this defect will be addressed in the next software release which is currently scheduled for delivery in June 2016’. There was no indication what, if anything, was delivered in that release to address the issue.
On 25 August 2016, a comment was added to the report indicating that rather than a system defect, the cut-off responses could be ‘mostly attributed to poor radio technique by pilots or ATC’. Furthermore, ‘it is also important that controllers release PTT as soon as possible to ensure that the receiver is unmuted’.
The ASID entry dated 17 December 2015 was based on information received from the vendor. Airservices sought input from the vendor on whether they believed the reported issue was a defect and whether the guard period could be adjusted.
Airservices received a response from the vendor with a list of issues which the vendor aimed to address in the next release and the guard period issue was included in this list. Airservices has investigated this issue and has determined it is not a system issue, given that the guard period of 200 milliseconds is less than other voice communication systems used by Airservices and the same as used in other Integrated Tower Automation Suite (INTAS) towers where there has been no observed replication of this issue. It was instead concluded that this issue was due to controller actions related to extended engagement of the foot PTT beyond the end of their transmissions. Airservices considers that the issue was not prevalent in the occurrence as was communicated by the interviewees.
Airservices Australia comment
Airservices Australia provided the following comments in response to the ATSB draft report.
Quiet tower
Although some controllers prefer speakers to increase their situational awareness, it may also result in considerable noise when all three positions are open during periods of increased traffic. Such noise is particularly distracting for controllers that have transitioned from an enroute environment where headsets are used and speakers are not permitted.
Additionally, ATC procedures are designed to ensure controllers can perform their duties safely without reliance on speakers. The use of speakers does not always increase situational awareness and should not be relied upon as an effective threat barrier.
Clipped transmissions
The recorded audio leading up to, during and after the occurrence did not contain any clipped transmissions related to the ‘fault’ reported.
Adelaide Tower Line Manager's and Shift Manager's regular monitoring of the controller's air ground communications have observed that pilot transmissions may occasionally be missing the first part of the call (clipped transmissions are less than one second in duration). This typically occurs when the pilot commences their response prior to the controller releasing the press to talk (PTT) button. However, clipping of this nature does not occur frequently and not to a point where controllers would become desensitised to only hearing part of the readback.
Existing ATC procedures require the controller to obtain a correct readback of instructions (in accordance with per AIP GEN 3.4 -12). In the absence of the correct and complete readback, the controller must challenge the readback until they are satisfied it is correct.
Audio sample
Airservices randomly sampled 90 minutes of audio from 1 August 2016 at Adelaide and did not identify any calls which had a clipped the transmission.
On 12 September, Airservices reviewed the radio technique of a controller in the tower using a foot PTT and noted that there was a significant (0.5-1 second) delay from the end of the delivery of the instruction by the controller to the time when the controller disengaged the foot PTT. This anomaly in the controller's technique resulted in a number of clipped pilot transmissions due to them starting the readback whilst the foot PTT was still engaged. The controller's error was rectified by using the in-line PTT which decreased the delay of the controller releasing the foot PTT.
Additionally, the Voice Communications and Control System (VCCS) enables controllers to view the status of the transmitter and receiver.
ATSB comment
The A320 crew are to be commended for their actions in preventing a potentially more serious incident occurring.
The flight crew of FKV thought they were cleared to cross the runway probably because of the bay allocation at the end of the hold short instruction. An effective sighting of the aircraft on final approach may have led them to query their understood instruction to cross the runway.
The SMC heard one word in response and mis-heard it as ‘short’ rather than ‘cross’ and that assumed ‘hold’ had been clipped from the transmission. The SMC did not question the pilots about the missing word as they had some previous experiences of the beginning of transmissions being clipped. As there was a ‘quiet tower’ communications system, there was no opportunity for the ADC to hear this pilot read-back to the SMC and notice the misunderstandings before the runway incursion.
The ADC was in the process of handover/takeover and was not watching the landing A320 or the runway as they assumed FKV would hold short and that the runway was clear.
Safety message
The risk of runway incursions and other separation events can be minimised through good communication. This incident highlights the importance of:
controllers and flight crews using correct phraseology
controllers and pilots challenging instructions which they have not heard or understood fully
pilots looking carefully for aircraft or other hazards before entering an active runway.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.