Propeller failure involving de Havilland DH-82, VH-ARU, near Shute Harbour ALA, Queensland, on 2 July 2016
Final report
What happened
On 2 July 2016, at about 1420 Eastern Standard Time (EST), a de Havilland DH-82A aircraft, registered VH-ARU, departed Shute Harbour aircraft landing area (ALA), Queensland, for an aerobatic joy flight. On board were a pilot and one passenger.
When the aircraft reached about 4,500 ft over water, the pilot advised air traffic control (ATC) that they were commencing aerobatic operations. The pilot reported that they then raised the aircraft nose and reduced the throttle to idle. The aircraft then pitched nose-down and the pilot initiated a rotation to the left. After about one and a half rotations, the pilot levelled the aircraft wings and stopped the rotation. As the airspeed was then about 110 kt, which was the entry speed for the next manoeuvre (a loop), the pilot raised the aircraft nose and applied full power as the nose passed the horizon.
The aircraft was then passing about 3,500 to 4,000 ft on climb, when the pilot and passenger heard a bang. The pilot saw a small object fly past to their left in close proximity, and the passenger saw that the on-board camera had been knocked.
The pilot discontinued the manoeuvre and stabilised the aircraft in a glide attitude. As the aircraft continued to descend, the pilot elected to return to Shute Harbour ALA. The pilot reported that the aircraft was not vibrating and the tachometer was indicating maximum RPM. The pilot also assessed that the engine was not producing any thrust, regardless of the throttle position. The pilot advised ATC that they had completed operations and were returning to Shute Harbour. At no time did the pilot inform ATC that there was an emergency.
As the aircraft passed the highest terrain en route to Shute Harbour ALA, the pilot assessed that they were not going to be able to reach the ALA (Figure 1). The pilot then turned the aircraft to land on the beach at Funnel Bay, but sighted boats moored on the beach. The pilot therefore aimed to land the aircraft at Funnel Bay on the mudflats. The pilot conducted a forced landing onto the mud and the aircraft continued onto some rocks. After landing, as the pilot inspected the aircraft, they noticed that the propeller was missing.
Figure 1: Shute Harbour ALA and Funnel Bay
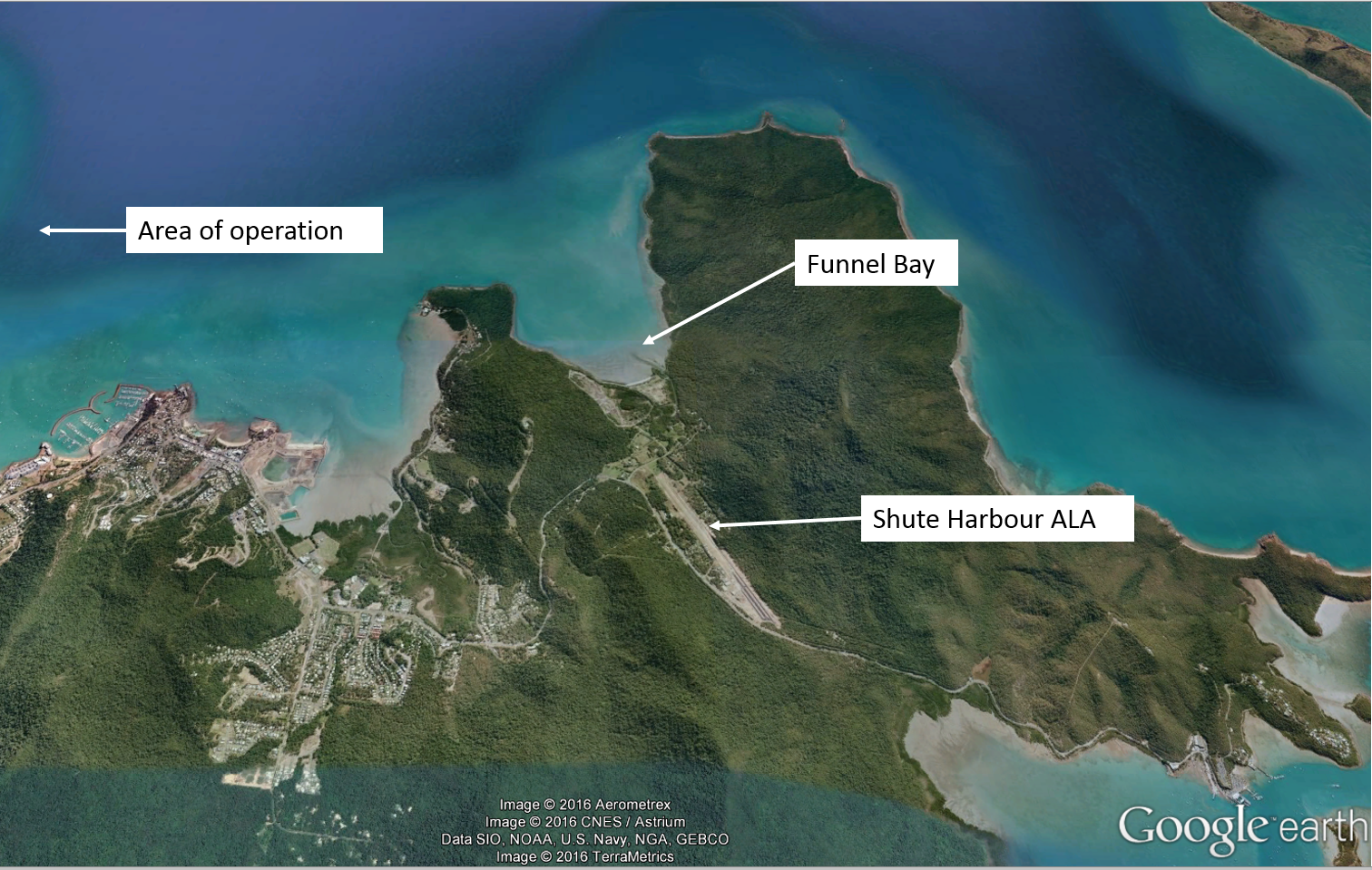
Source: Google earth – annotated by ATSB
The pilot was uninjured, and the passenger sustained minor injuries. The aircraft sustained substantial damage (Figure 2).
Figure 2: Accident site showing damage to VH-ARU

Source: Aircraft owner – modified by ATSB
Pilot comments
The pilot had completed a daily inspection of the aircraft earlier in the day and had subsequently flown it for about 6 minutes to assess the weather conditions. The incident flight was the first commercial flight of the day. During the pre-flight inspection, the pilot reported having made a visual check of the propeller for defects, gravel rash and any chips, but had not detected anything abnormal.
The pilot had asked the passenger their weight prior to the flight, and although they did not complete a weight and balance calculation, assessed that the aircraft was within its weight and balance limitations for aerobatic flight.
At the time of the incident, they were operating about 4 to 5 NM from the ALA, and over water. The pilot thought that the aircraft probably struck a bird resulting in the propeller failing.
When they realised that the aircraft was unable to reach the runway at Shute Harbour, the pilot had a secondary plan to land on the beach at Funnel Bay. They commented that their training helped to deal with the situation by being aware of their surroundings and having a series of plans in case of emergency.
Engineering report
The aircraft maintenance engineer assessed the aircraft after the incident and sent the remnants of the (timber) propeller that had remained attached to the aircraft to the ATSB. The engineer also spoke to the manufacturer of the propeller and was able to trace its history. The manufacturer suggested the propeller failure was indicative of a propeller overspeed, although they did not inspect the propeller remnants. The propeller was not retrieved as it failed when the aircraft was over water.
ATSB analysis
Video footage
The ATSB analysed the data card from the on-board camera. The camera was facing rearwards and no evidence of a birdstrike was visible on the footage when viewed frame-by-frame. Analysis of the sound component of the recording was conducted to determine the engine frequency at the time of the propeller failure, but the results were inconclusive due to background noise including a radio transmission.
From the video footage, it was evident that the aircraft entered a spiral manoeuvre that involved substantial rudder and aileron input such that the aircraft was in balance (not skidding or slipping sideways). The wings were then levelled and the aircraft pulled out of the dive. The propeller failed just as the aircraft nose passed back up through the horizon at the start of the next manoeuvre and power was applied. The propeller was under substantial load at this stage.
Propeller remnants
The ATSB examined two fragments of the propeller that were identified as parts of the hub section. An area of interest, depicted in Figure 3, showed evidence of bending consistent with the blade breaking away from the hub while under load. No bird remains were found on the fragments. The factors contributing to the propeller failure could not be determined from the timber fragments.
Figure 3: Propeller remnants
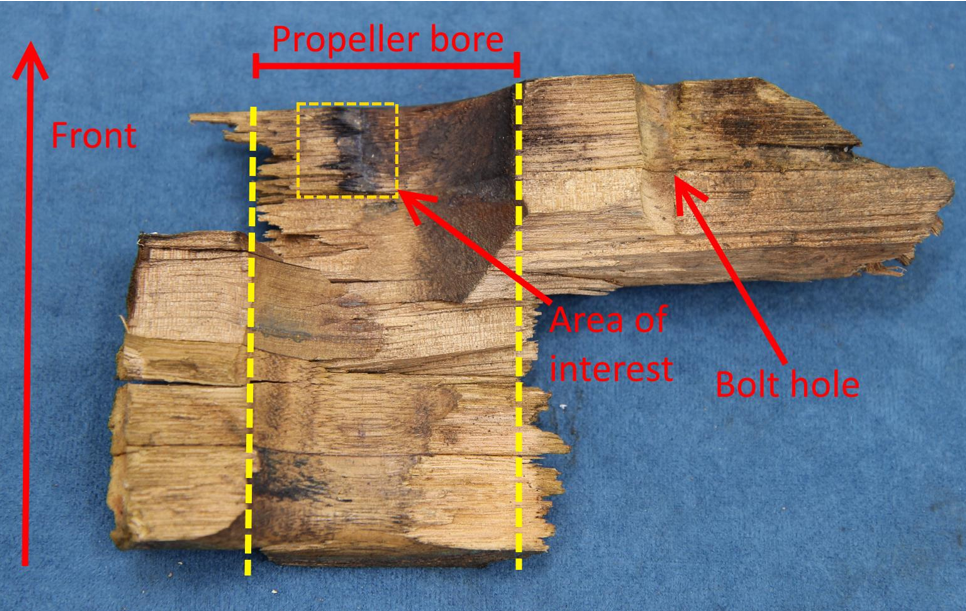
Source: ATSB analysis
ATSB comment
One of the findings of ATSB investigation AO-2013-226, In-flight break-up involving de Havilland DH82A Tiger Moth, VH-TSG, 300 m E of South Stradbroke Island, Queensland, 16 December 2013, was that ‘publicly-available video recordings showed that some Australian commercial Tiger Moth operators conducted aerobatic flick (otherwise known as ‘snap’) rolls and tailslide manoeuvres, which were prohibited by the Type Design Organisation’. However, the on-board video recording showed that the types of aerobatic manoeuvres conducted during the accident flight were all permitted for the aircraft type.
The ATSB cautions commercial vintage aircraft operators about the risks associated with aircraft age and the importance of understanding the originally-intended use of the design before commencing their operations.
Safety message
This incident highlights the value of always having a consideration of landing areas available in case a forced landing is required. Alerting air traffic control as emergencies arise enables them to provide the necessary and appropriate assistance.
Aviation Short Investigations Bulletin - Issue 54
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2016

Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
Occurrence summary
| Investigation number | AO-2016-071 |
|---|---|
| Occurrence date | 02/07/2016 |
| Location | near Shute Harbour (ALA) (Funnel Bay) |
| State | Queensland |
| Report release date | 22/11/2016 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Propeller/rotor malfunction |
| Occurrence class | Accident |
| Highest injury level | Minor |
Aircraft details
| Manufacturer | de Havilland Aircraft |
|---|---|
| Model | DH-82A |
| Registration | VH-ARU |
| Serial number | AM237 |
| Sector | Piston |
| Operation type | Charter |
| Departure point | Shute Harbour, Qld |
| Destination | Shute Harbour Qld |
| Damage | Substantial |